
Mechanisms of immune dysfunction in stem cell transplantation
16
International Journal of Immunopharmacology 22 (2000) 1041 – 1056 Mechanisms of immune dysfunction in stem cell transplantation James E. Talmadge a, *, Rakesh Singh a , Kazuhiko Ino b , Ana Ageitos c , Suleyman Buyukberber d a Department of Pathology and Microbiology, Uni6ersity of Nebraska, 987660 Nebraska Medical Center, Omaha, NE 68198 -7660, USA b Department of Obstetrics and Gynecology, Nagoya Uni6ersity School of Medicine, Japan c Department of Oncology, Fundacion Jimenez Diaz Ser6icio de Oncologia, Spain d Department of Internal Medicine, Turgut Ozal Medical Center, Turkey Abstract High dose therapy (HDT) and stem cell transplantation (SCT) results in alterations in the immunologic network, thymic re-education and the induction of peripheral tolerance. The changes to the immunoregulatory cascade and tolerance induction associated with autotransplants have been investigated in a series of studies focused on leukocyte reconstitution and function following HDT and autologous SCT. In these studies, we observed a significant decrease in the CD4:CD8 T cell ratio post-transplantation compared to normal peripheral blood (PB) donors due to a decrease in CD4 + cells. In addition, T cell function (phytohemagglutinin (PHA) mitogenesis) was consistently depressed compared to samples obtained from normal PB donors. The loss of T cell function was associated with an increased frequency of circulating monocytes, their expression of Fas ligand (FasL) and a high frequency of apoptotic CD4 + T cells. Indeed, 28–51% of circulating CD4 + T cells were observed to be apoptotic during the first 100 days following HDT and SCT. These studies suggest that ‘primed’ or activated Fas + CD4 + lymphocytes interact with FasL + monocytes, resulting in apoptosis, leading to the preferential deletion of CD4 + T cells, a decrease in the CD4:CD8 T cell ratio and depressed T cell function. Further, as discussed herein, the T cells are activated with a predominantly type 2 phenotype, which may also contribute to the maintenance of the immunosuppressive condition. Therefore, there is the potential to regulate immune recovery by stem cell product manipulation or post-transplantation cytokine administration. © 2000 International Society for Immunopharmacology. Published by Elsevier Science Ltd. All rights reserved. Keywords: Peripheral tolerance; Immune regulation; T cell function www.elsevier.com/locate/ijimmpharm 1. Introduction HDT followed by SCT or bone marrow trans- plantation (BMT) is used to treat a variety of advanced malignancies [1 – 6]. We and others, ob- served immune dysfunction in the peripheral * Corresponding author. Tel.: +1-402-5595639; fax: +1- 402-5594990. E-mail address: [email protected] (J.E. Talmadge). 0192-0561/00/$20.00 © 2000 International Society for Immunopharmacology. Published by Elsevier Science Ltd. All rights reserved. PII: S0192-0561(00)00078-3
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Mechanisms of immune dysfunction in stem cell transplantation

International Journal of Immunopharmacology 22 (2000) 1041–1056
Mechanisms of immune dysfunction in stem celltransplantation
James E. Talmadge a,*, Rakesh Singh a, Kazuhiko Ino b, Ana Ageitos c,Suleyman Buyukberber d
a Department of Pathology and Microbiology, Uni6ersity of Nebraska, 987660 Nebraska Medical Center, Omaha,NE 68198-7660, USA
b Department of Obstetrics and Gynecology, Nagoya Uni6ersity School of Medicine, Japanc Department of Oncology, Fundacion Jimenez Diaz Ser6icio de Oncologia, Spain
d Department of Internal Medicine, Turgut Ozal Medical Center, Turkey
Abstract
High dose therapy (HDT) and stem cell transplantation (SCT) results in alterations in the immunologic network,thymic re-education and the induction of peripheral tolerance. The changes to the immunoregulatory cascade andtolerance induction associated with autotransplants have been investigated in a series of studies focused on leukocytereconstitution and function following HDT and autologous SCT. In these studies, we observed a significant decreasein the CD4:CD8 T cell ratio post-transplantation compared to normal peripheral blood (PB) donors due to a decreasein CD4+ cells. In addition, T cell function (phytohemagglutinin (PHA) mitogenesis) was consistently depressedcompared to samples obtained from normal PB donors. The loss of T cell function was associated with an increasedfrequency of circulating monocytes, their expression of Fas ligand (FasL) and a high frequency of apoptotic CD4+
T cells. Indeed, 28–51% of circulating CD4+ T cells were observed to be apoptotic during the first 100 days followingHDT and SCT. These studies suggest that ‘primed’ or activated Fas+ CD4+ lymphocytes interact with FasL+
monocytes, resulting in apoptosis, leading to the preferential deletion of CD4+ T cells, a decrease in the CD4:CD8T cell ratio and depressed T cell function. Further, as discussed herein, the T cells are activated with a predominantlytype 2 phenotype, which may also contribute to the maintenance of the immunosuppressive condition. Therefore,there is the potential to regulate immune recovery by stem cell product manipulation or post-transplantation cytokineadministration. © 2000 International Society for Immunopharmacology. Published by Elsevier Science Ltd. All rightsreserved.
Keywords: Peripheral tolerance; Immune regulation; T cell function
www.elsevier.com/locate/ijimmpharm
1. Introduction
HDT followed by SCT or bone marrow trans-plantation (BMT) is used to treat a variety ofadvanced malignancies [1–6]. We and others, ob-served immune dysfunction in the peripheral
* Corresponding author. Tel.: +1-402-5595639; fax: +1-402-5594990.
E-mail address: [email protected] (J.E. Talmadge).
0192-0561/00/$20.00 © 2000 International Society for Immunopharmacology. Published by Elsevier Science Ltd. All rights reserved.
PII: S0192-0561(00)00078-3
J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–10561042
blood (PB) of patients following HDT and SCTdespite restoration of T cell numbers [7–18]. Thisimmunologic dysfunction includes a decrease inthe CD4:CD8 T cell ratio and a depression of Tcell function [9,10,19]. Studies from our labora-tory and recently others, demonstrated a cell-me-diated suppression of T cell function in stem cellproducts and PB of cancer patients [12,13,20–30].This loss of function is associated with increasedT cell apoptosis [9,10,19,31–33] which occurs pre-dominantly with CD4+ T cell subpopulations.The induction of apoptosis is mediated, at least inpart, by FasL expression on monocytes, which arefound in significantly higher numbers followingSCT [32]. High levels of type 2-associated cytoki-nes are also found in the infused T cells andmonocytes as well as in the PB post-transplanta-tion [28,31,34].
Apoptosis is one mechanism for peripheralCD4+ T cell homeostasis. It is a highly regulatedcell process, dependent upon the expression of afamily of death-inducing ligands, including FasLand tumor necrosis factor-related apoptosis-in-ducing ligand (TRAIL) and their receptors [35–42]. Enhanced monocyte-dependent apoptosis ofuninfected CD4+ T cells is postulated to con-tribute to CD4+ T cell depletion in HIV-infectedindividuals, which leads to an inverted CD4:CD8T cell ratio [43,44]. Recent data from our labora-tory suggests that cancer patients undergoingHDT and SCT, similar to HIV-infected individu-als, have prolonged immune dysfunction, an in-verted CD4:CD8 T cell ratio and the induction ofperipheral tolerance [10,12,13,27,45,46].
In addition to the induction of peripheral toler-ance and resultant apoptosis, changes in cytokinelevels also can regulate immune function. Tlymphocytes express two distinct cytokine pat-terns: type 1 cells produce interleukin (IL)-2 andinterferon (IFN)-g; whereas, type 2 cells produceIL-4 and IL-10 [47,48]. Type 1 cytokines promotecell-mediated immune responses, while type 2 cy-tokines promote immunoglobulin production andmay also inhibit cell-mediated immunity [47–54].Similarly, monocytes produce IL-8, IL-10 andtumor necrosis factor (TNF)-a, which can alsomodulate the overall immune response [55]. Cur-rently, the differential expression of type 1/type 2
cytokines and monokine-specific mRNA tran-scripts and their significance in the regulation ofthe immune function of the cells in the peripheralblood (PB) from patients undergoing HDT andSCT remains unclear [34,56]. A type 2 immuneresponse may also have a role in tolerance, as wasrecently suggested by a study in which the prog-nostic significance of IL-10 production were stud-ied in patients prior to an allogeneic BMT [57].High levels of spontaneous IL-10 production werecorrelated with a subsequent low incidence ofgraft-versus-host disease (GVHD) and transplant-related mortality compared to patients with lowor intermediate levels of IL-10 [57]. Support forthe role of IL-10 is also provided by the observa-tion that increased IL-10 production by mononu-clear cells is associated with tolerance in severecombined immunodeficiency disease (SCID) pa-tients following haplotype identical BMT [58].The results reviewed in this manuscript examineimmunologic reconstitution following HDT andSCT and potential mechanisms that preclude therecovery of a functional immune response. Thegoals are to gain insight into the potential ofHDT and autologous SCT to serve as a therapeu-tic modality and to improve our understanding ofthe mechanisms of immune reconstitution.
2. Materials and methods
2.1. Patients
High-risk breast cancer patients, who were can-didates for HDT and SCT (N=12) at the Univer-sity of Nebraska Medical Center (UNMC), wereentered into the mechanism study. Written in-formed consent for stem cell collection and au-tologous transplantation was obtained from eachpatient. All patients received an average of fourcycles of chemotherapy prior to HDT and SCTand all received Cytoxan, Thiotepa and Hydrea asthe HDT regimen. SCT patients were mobilizedwith granulocyte colony-stimulating factor (G-CSF) [59] and a target dose of 6.5×108 mononu-clear cells per kilogram body weight was collectedand cryopreserved. The samples were obtainedusing protocols approved by the Institutional Re-view Board (IRB) of UNMC. In the immune

J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–1056 1043
recovery studies, a total of 72 patients diagnosedwith primary refractory non-Hodgkin’slymphoma (NHL), relapsed NHL, high-risk NHLand first complete remission or partial remissionNHL, who had received multiple cycles ofchemotherapy, were included. PB samples wereobtained prior to mobilization and apheresis orBM harvest and on days 15, 30, 100 and 365post-transplantation. These samples were ob-tained using protocols approved by the IRB andfollowing written informed consent. Prior to thePSC collection in both studies, the patients re-ceived subcutaneous daily injections of 10 mg/kgper day G-CSF (Filgrastim, Amgen, ThousandOaks, CA) for 4–5 days. PSC apheresis wasstarted when the white blood cell (WBC) countreached 10 000 cells/ml (3–4 days after initiationof G-CSF administration). Leukapheresis wasperformed as an outpatient procedure with aCOBE spectra (COBE BCT Inc., Lakewood, CO).Each patient underwent three to 15 leukaphereses(median 4). The HDT regimen given to the NHLpatients varied based on histological diagnosisand previous tumor responses. Patients receivedcarmustine on day 1 (300 mg/m2) and cyclophos-phamide (2.5 g/m2) for 2 days, hydroxyurea (1.5g/m2) every 6 h for 12 doses and etoposide (150mg/m2) every 12 h for six doses (BECH), or theyreceived carmustine on day 1 (300 mg/m2) andcyclophosphamide (35 mg/kg) for 4 days,etoposide (100 mg/m2) every 12 h for eight dosesand cytarabine (100 mg/m2) every 12 h for eightdoses (BEAC). Following SCT, all patients re-ceived G-CSF until their absolute neutrophilcount was 1500/mm3 on 2 consecutive days.
2.2. Mononuclear cell isolation
The fresh, uncultured PSC products from pa-tients were diluted 1:2 in HBSS (Gibco BRL,Grand Island, NY), layered on Ficoll–Hypaque(Organon Teknika, Durham, NC), and cen-trifuged for 20 min at 400×g, using a BeckmanTJ6R centrifuge with swinging bucket rotor.Mononuclear cells from normal donors were usedas controls. The cells were washed twice withHank’s balanced salt solution (HBSS) and ad-justed to 4×106 cells/ml in RPMI-1640 contain-
ing 10% fetal bovine serum (FBS), 10 mMHEPES, gentamycin and L-glutamine.
2.3. Flow cytometric analysis
For phenotypic analysis, mononuclear cells iso-lated from PSC product and PB were counted andadjusted to 1×106 cells in phosphate bufferedsaline (PBS) (Gibco BRL) containing 2.5% FBSto maintain cell viability. Non-specific bindingwas blocked with human IgG and an aliquot of1×105 cells was stained for 30 min at 4°C witheach cocktail of monoclonal antibodies (at satu-rating concentrations) to various human leuko-cyte antigens. The antibodies used in this studywere purchased from Becton Dickinson (San Jose,CA) and Coulter Corporation (Hialeah, FL). Allthree-color data were acquired on a Becton Dick-inson FACStarPlus. Detailed three-color data anal-ysis was performed using the Attractors andCellQuest software from Becton-Dickinson, as de-scribed previously [27]. Each subpopulation wasgated using forward and side scatter and fluores-cence intensity for the specific markers, CD14,CD4 and CD8, CD95 (Fas) and CD95L (FasL).With the use of this technique, CD14+ monocyteswere defined as cells with intermediate side scatterand expressing high levels of CD14, which al-lowed us to distinguish them from lymphocytes,polymorphonuclear neutrophils and granulocytes.The lymphocyte population was distinguishedbased on lower side scatter and high expression ofCD4 and CD8.
2.4. Assay for apoptosis
A multicolor flow cytometric analysis includinga terminal TdT-mediated dUTP nick end labeling(TUNEL) assay for apoptosis was used to deter-mine the frequency of apoptotic T cells in the PBcells of the patients undergoing HDT and SCT, asdescribed previously [27]. Briefly, cell suspensionswere stained with either phycoerythrin (PE) orbiotin-antigen-presenting cells (APC), washedtwice in PBS, resuspended in ice-cold PBS/1%bovine serum albumin (BSA) (100 ml) and fixedwith 10% of buffered formalin. The cells werepermeabilized using 0.1% Triton X-100/0.1%
J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–10561044
sodium citrate solution by incubating at 0°C for 2min. After washing, the cells were resuspended in50 ml of TUNEL reaction mixture (0.03 g molFITC-UTP, 3 mmol dATP, 2 ml of 25 mM CaCl2and 25 U TdT) (Boehringer Mannheim, Indiana-polis, IN) and incubated for 60 min at 37°C. Thecells were washed and analyzed by flow cytome-try. A forward scatter by side scatter plot wasused to gate all the cells while excluding celldebris and aggregated cells. CD4+ and CD8+
cells were then individually backgated to deter-mine the frequency of cells undergoing apoptosis.
2.4.1. Mitogen response assayMononuclear cells from either BMT or SCT
patients or normal PBMC (1×105 cells/well) wereincubated in medium alone, medium containingPHA at 0.5 mg/ml, (DIFCO, Detroit, MI), ormedium containing pokeweed mitogen (PWM) ata 1:1600 dilution (Sigma, St. Louis, MO) in a96-well culture plate. After 72 h of culture, 1mCi/well 3H-thymidine was added and the cellsincubated for an additional 24 h. Cells were har-vested with a 96-well harvester onto fiberglassfilters and radioactivity counted in a Packard(Meriden, CT) multi-well b-counter. All experi-ments were performed in triplicate. The 3H-thymidine incorporation between BMT, SCT andnormal PBMC was compared with or withoutPHA or PWM, respectively and the stimulationindex calculated.
2.4.2. Cellular-dependent T cell inhibitory (CDTI)acti6ity
Normal Ficoll–Hypaque-purified PBMC (1×105 cells/well) from healthy donors were used asresponder cells and co-cultured with varying num-bers of irradiated (500 cGy) cells from BMT orSCT patients or normal PBMC at inhibitor toresponder (I:R) ratios of 4:1, 2:1, 1:1 and 0.5:1 inthe presence of PHA 0.5 mg/ml, as previouslydescribed [12,13,27,60–62]. Cells were then cul-tured at 37°C and 5% CO2 for 96 h. The mito-genic response by the responder population wasassayed by pulsing with 1 mCi/well of 3H-thymidine over the final 24 h of culture. Cellswere harvested with a multi-well harvester ontofiberglass strips and radioactivity counted in a
Packard multi-well b scintillation counter. All ex-periments were performed in triplicate. Percent Tcell inhibitory activity was calculated by compar-ing the 3H-thymidine incorporated in I+R co-culture with R alone.
2.5. Analysis of cytokine mRNA expression
Total cellular RNA was isolated from PBMCusing Trizol® reagent (Gibco BRL, Gaithersburg,MD) [63] and reverse-transcription based poly-merase chain reaction (RT-PCR) was performed,as described earlier [34]. First strand cDNA wassynthesized using total RNA (2 mg), oligo (dT)18
primer and superscript RT (Gibco BRL). A totalof 2 ml of first strand cDNA (1:10 dilutions) wereamplified using PCR primer sets [34] and DNAthermal cycler (Perkin–Elmer, Foster City, CA).Each cycle set used a denaturing temperature(94°C) for 60 s, annealing temperatures (55°C forb-actin, IL-4, IL-10, TNF and IL-8 and 53°C forIL-2 and IFN-g) for 90 s and extension tempera-ture (72°C) for 90 s for a total of 20 cycles forb-actin and 40 cycles for the other genes. PCRfragments were separated on a 2% agarose gelcontaining ethidium bromide (0.25 mg/ml) andvisualized and photographed using a UV trans-il-luminator (Kodak, Rochester, NY). For quantita-tive studies and to confirm the specificity of theamplified sequences, gels were blotted on GeneS-creen membrane (DuPont) and processed forSouthern blot analysis, as described earlier[32,56]. The membranes were hybridized with 32P-labeled specific oligonucleotide or cDNA probesfor 4 h, washed under stringent conditions foreach cytokine and analyzed by digital autoradiog-raphy (Phosphor-Imager, Molecular Dynamics,Sunnyvale, CA). Relative amounts of radioactiv-ity between samples blotted on each membranewere examined using the ImageQuant (MolecularDynamics) analysis system. Relative mRNA tran-scripts levels were obtained by using an equalnumber of cells with simultaneous amplificationwithin the linear range and by blotting and prob-ing the samples to be compared. Cytokine signalsare expressed as expression index, the ratio ofeach cytokine signal to the signal from the house-keeping gene b-actin.

J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–1056 1045
2.6. Statistical analysis
SPSS for Windows® (SPSS Inc., Chicago, IL)was used for the independent samples t-test (two-tailed) to compare means. The data presented area composite of all the patients analyzed in eachgroup.
3. Results
3.1. Functional analysis of PB cells post-SCTcompared to normal PB cells
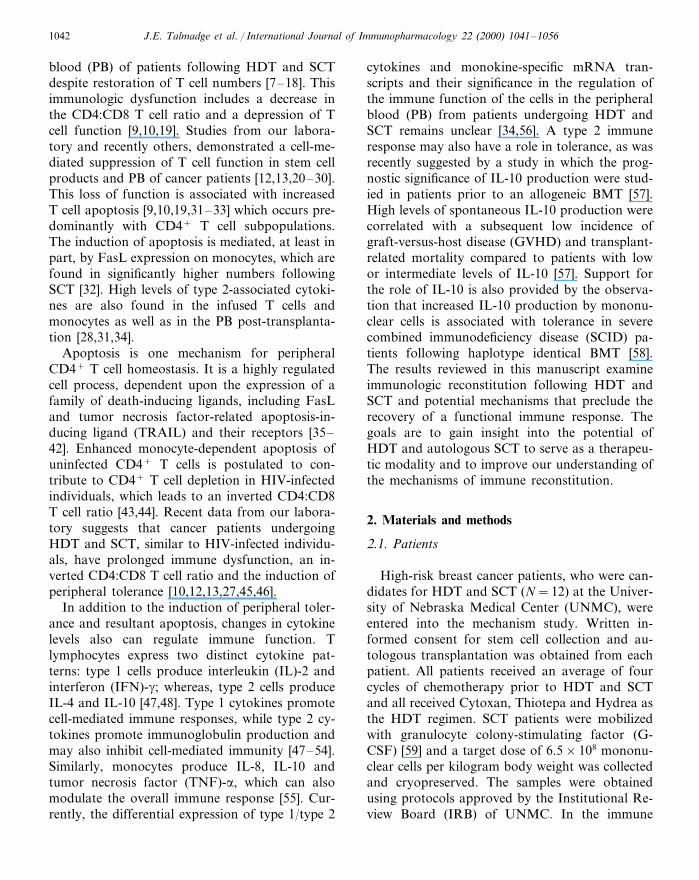
In a series of studies, we examined immunephenotype and function following HDT and au-tologous SCT for the treatment of NHL [12,13].The PBMC following SCT had a significantlydecreased phytohemagglutinin (PHA) mitogenicactivity during the first 365 days following HDTand transplantation compared to normal PBMC(P50.001) (Fig. 1). In agreement with the loss ofT cell mitogenic activity, PBMC had significantlyhigher levels of CDTI activity on days 15 and 30post-transplantation (Fig. 1) compared to normalPBMC. As previously demonstrated, the CDTIactivity is directly correlated with monocyte fre-quency [33] and can be partially blocked by estab-lishing the co-cultures in the presence ofneutralizing antibody to FasL (Fig. 2).
3.2. T cell reconstitutionDespite the loss of T cell function, the fre-
quency and absolute numbers of CD3+ andCD8+ were similar to pretransplant levels in thePB of NHL patients who were candidates forHDT and SCT, although CD4+ cell numberswere significantly depressed. The frequency andabsolute number of T lymphocyte subsets pre-mo-bilization and on days 15, 30, 100 and 365 post-transplantation are shown in Fig. 3. These studiesreveal that the frequency and absolute number ofCD3+ cells were significantly lower on day 15post-transplantation compared to normal PB andpretransplant levels. The frequency of CD3+ cellsreturned to pretransplant and normal values onday 30 post-SCT (Fig. 3). In contrast, no signifi-cant change in the frequency and absolute number
of CD8+ cells was observed post-SCT comparedto pretransplant. However, the frequency and ab-solute number of CD4+ cells was significantly
Fig. 1. Functional analysis of peripheral blood mononuclearcells (PBMC) from SCT compared to normal PBMC. Assaysinclude PHA mitogenesis and a co-culture assay of normalPBMC with irradiated effector cells from an apheresis productin a CDTI assay. cSignificantly different from normal PBMC(P50.005). Values represent the mean9S.E.M.
J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–10561046
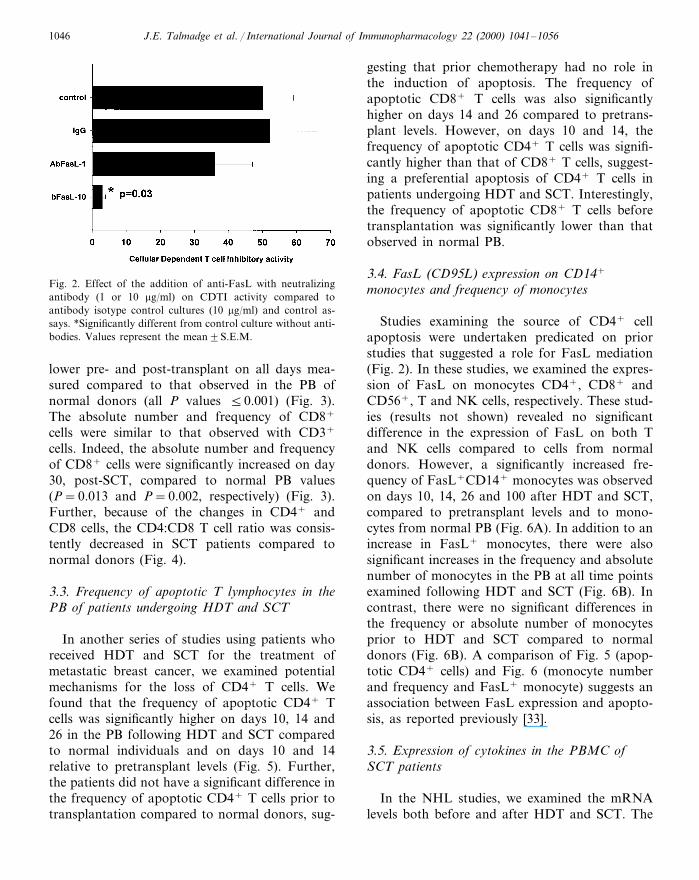
Fig. 2. Effect of the addition of anti-FasL with neutralizingantibody (1 or 10 mg/ml) on CDTI activity compared toantibody isotype control cultures (10 mg/ml) and control as-says. *Significantly different from control culture without anti-bodies. Values represent the mean9S.E.M.
gesting that prior chemotherapy had no role inthe induction of apoptosis. The frequency ofapoptotic CD8+ T cells was also significantlyhigher on days 14 and 26 compared to pretrans-plant levels. However, on days 10 and 14, thefrequency of apoptotic CD4+ T cells was signifi-cantly higher than that of CD8+ T cells, suggest-ing a preferential apoptosis of CD4+ T cells inpatients undergoing HDT and SCT. Interestingly,the frequency of apoptotic CD8+ T cells beforetransplantation was significantly lower than thatobserved in normal PB.
3.4. FasL (CD95L) expression on CD14+
monocytes and frequency of monocytes
Studies examining the source of CD4+ cellapoptosis were undertaken predicated on priorstudies that suggested a role for FasL mediation(Fig. 2). In these studies, we examined the expres-sion of FasL on monocytes CD4+, CD8+ andCD56+, T and NK cells, respectively. These stud-ies (results not shown) revealed no significantdifference in the expression of FasL on both Tand NK cells compared to cells from normaldonors. However, a significantly increased fre-quency of FasL+CD14+ monocytes was observedon days 10, 14, 26 and 100 after HDT and SCT,compared to pretransplant levels and to mono-cytes from normal PB (Fig. 6A). In addition to anincrease in FasL+ monocytes, there were alsosignificant increases in the frequency and absolutenumber of monocytes in the PB at all time pointsexamined following HDT and SCT (Fig. 6B). Incontrast, there were no significant differences inthe frequency or absolute number of monocytesprior to HDT and SCT compared to normaldonors (Fig. 6B). A comparison of Fig. 5 (apop-totic CD4+ cells) and Fig. 6 (monocyte numberand frequency and FasL+ monocyte) suggests anassociation between FasL expression and apopto-sis, as reported previously [33].
3.5. Expression of cytokines in the PBMC ofSCT patients
In the NHL studies, we examined the mRNAlevels both before and after HDT and SCT. The
lower pre- and post-transplant on all days mea-sured compared to that observed in the PB ofnormal donors (all P values 50.001) (Fig. 3).The absolute number and frequency of CD8+
cells were similar to that observed with CD3+
cells. Indeed, the absolute number and frequencyof CD8+ cells were significantly increased on day30, post-SCT, compared to normal PB values(P=0.013 and P=0.002, respectively) (Fig. 3).Further, because of the changes in CD4+ andCD8 cells, the CD4:CD8 T cell ratio was consis-tently decreased in SCT patients compared tonormal donors (Fig. 4).
3.3. Frequency of apoptotic T lymphocytes in thePB of patients undergoing HDT and SCT
In another series of studies using patients whoreceived HDT and SCT for the treatment ofmetastatic breast cancer, we examined potentialmechanisms for the loss of CD4+ T cells. Wefound that the frequency of apoptotic CD4+ Tcells was significantly higher on days 10, 14 and26 in the PB following HDT and SCT comparedto normal individuals and on days 10 and 14relative to pretransplant levels (Fig. 5). Further,the patients did not have a significant difference inthe frequency of apoptotic CD4+ T cells prior totransplantation compared to normal donors, sug-

J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–1056 1047
mRNA expression of IL-2 and IFN-g was signifi-cantly higher in the PBMC obtained followingSCT compared to steady-state PBMC from nor-mal donors at all time points examined. The type
1 cytokine levels in the PBMC of SCT patients,prior to and 15, 30 and 100 days post-transplanta-tion, were similar to that observed in PHA-stimu-lated normal PBMC (Fig. 7). In contrast, the IL-2
Fig. 3. The frequency and absolute number of CD3+, CD4+ and CD8+ premobilization and days 15, 30, 100 and 365post-transplantation. cSignificantly different from normal peripheral blood leukocytes (P50.005). Values represent the meanpercent positive cells9S.E. of the mean (S.E.M.).

J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–10561048
Fig. 4. The CD4:CD8 ratio in SCT patients and normal PBL,premobilization and days 15, 30, 100 and 365 post-transplan-tation. Values represent the mean percent positive cells9S.E.M. cSignificant difference between lymphocyte levels inSCT patients and normal donors (P50.005).
Fig. 6. (A) The frequency of CD14+ monocytes in the PB ofpatients undergoing HDT and SCT was determined by three-color flow cytometry. Results are reported as the mean9S.E.M. *Significantly different from pretransplant levels(P50.05). cSignificantly different from normal PB (P50.05). (B) Flow cytometry analysis of FasL expression onCD14+ monocytes in the PB of breast cancer patients follow-ing HDT and SCT. The results are shown as frequency ofFasL+ cells in the total monocyte cell gate. Results arereported as the mean9S.E.M. *Significantly different frompretransplant levels (P50.05). cSignificantly different fromnormal PB (P50.05).
and IFN-g mRNA levels on day 365 were signifi-cantly lower than pretransplant levels (P=0.02)and that of PHA-stimulated normal PBMC (Fig.7). The expression of IFN-g mRNA transcriptlevels were insignificantly higher on day 30 follow-
Fig. 5. The frequency of apoptotic CD4+ or CD8+ T cells ina total cell gate of CD4+ or CD8+ T cells as determined usingthree-color flow cytometry. Results are reported as themean9S.E.M. *Significantly different from pretransplant lev-els (P50.05). cSignificantly different from normal PB (P50.05). $Significant difference in the frequency of apoptoticCD4 and CD8 T cells. (P50.05).
ing HDT and SCT compared to pretransplantlevels (Fig. 7).
Similarly, we observed significantly higher lev-els of IL-4 and IL-10 mRNA in the PBMC ofSCT patients compared to normal donors (Fig.8A,B). The IL-4 mRNA levels were higher (in-significantly) on day 100 following HDT and SCTcompared to pretransplant levels (Fig. 8A). Wealso observed a significant increase in the levels ofIL-10 mRNA transcripts on days 30 and 100post-transplantation (P=0.02) compared to thepretransplant levels. This increase in IL-10 mes-

J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–1056 1049
sage levels returned to pretransplant levels by day365 (Fig. 8B). At all time points examined follow-ing HDT and SCT, the levels of IL-10 mRNAtranscripts in SCT patients were similar to PHA-activated PBMC from normal donors (Fig. 8B).
4. Discussion
The loss of T cell function following transplan-tation appears to be due, in part, to both thefrequency of monocytes and monocytes express-ing FasL [32]. We suggest that the preferential
Fig. 8. (A,B) Expression of IL-4 and IL-10. The mRNAexpression for IL-4 and IL-10 was analyzed. The expressionindexes for IL-4 and IL-10 were calculated by comparing themwith the housekeeping gene b-actin. The values are mean9S.E. for each group. *Significantly different from normalPBMC (P50.05). cSignificantly different from pretransplan-tation (P50.05). $Significantly different from PHA activatednormal PBMC (P50.05).
Fig. 7. (A,B) Expression of IL-2 and IFN-g. The mRNAexpression of IL-2 and IFN-g was analyzed by RT-PCR.Expression indices were calculated by comparing the values ofIL-2 and IFN-g with the housekeeping gene b-actin. Thevalues are mean9S.E. for each group. *Significantly differentfrom normal PBMC (P50.05). cSignificantly different frompretransplantation levels (P50.05). $Significantly differentfrom PHA activated normal PBMC (P50.05).
deletion of the CD4+ T cells is due to theirincreased expression of Fas, s compared to CD8+
T cells which have a normal frequency of Fasexpression and a high frequency of monocytesexpressing FasL in the PB [32]. These studiessuggest a possible mechanism for the immunedysfunction, peripheral tolerance and decreasedCD4:CD8 T cell ratio that are observed followingHDT and SCT [7–10,12,13]. Further, we hypoth-esize that the high frequency of FasL expressionon monocytes is due to the secretion of high levels

J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–10561050
of monocyte-activating cytokines by the T cellsfollowing transplantation [34]. Ex vivo studiesreveal that monocytes in mobilized PSC products,as well as in PB following transplantation, inhibitT cell function [12,13,17,26,27] by inducing T cellapoptosis [26]. Although these studies do notprovide definite proof, the high frequency ofapoptotic CD4+ T cells following HDT and SCTmight contribute to the loss of abnormally acti-vated T cells resulting in the development oftolerance for epitopes critical to disease expres-sion. Reports by Donnenberg et al. [64,65] suggestthat T cell apoptosis parallels lymphopoiesis inpatients who have undergone BMT. An acceler-ated spontaneous and activation-induced T cellapoptosis is also observed in the PB of individualsinfected with HIV, which may occur by a similarmechanism [66]. In vitro studies using cells fromAIDS patients suggest that T cell apoptosis [67–70] is associated with T cell activation by eitherCD3+ cross-linking, PMA or PHA[12,13,21,26,27,29,60]. The requirement for T cellactivation appears to be a common feature ofmonocyte-dependent T cell apoptosis mediated byFas–FasL interaction [17,39,44,66]. Our previousresults suggest that T cells and monocytes in thePB of the HDT and SCT patients are highlyactivated based on the expression of immunoregu-latory cytokines [34,56,71], while the circulating Tlymphocytes from HIV-infected individuals areactivated [67], have an increased expression of Fason their membranes [68,69] and are more suscepti-ble to FasL-mediated killing [69]. Thus, we sug-gest that activated CD4+ T cells in the PB ofHDT and SCT patients undergo apoptosis afterencountering monocytes expressing FasL. How-ever, the circumstance and site(s) whereby a sus-ceptible CD4+ T cell encounters anapoptosis-inducing ligand remains unknown.
Recently, we reported that monocytes in mobi-lized PSC products, as well as PBL, after trans-plantation inhibit T cell function [12,13,26,27] byinducing T cell apoptosis [26]. Our present datademonstrate a higher frequency of apoptoticCD4+ T cells in the PB of patients followingHDT and SCT, possibly contributing to abnormalimmune reconstitution. Similar effects were re-ported following allotransplantation [7,9] where
abnormal CD4:CD8 ratios are also observed[9,45]. An accelerated spontaneous and activation-induced T cell apoptosis is also observed in thePB of individuals infected with HIV, which mayoccur by a similar mechanism [66–70].
Recent reports from our laboratory and otherssuggest that T cell apoptosis is associated with Tcell activation by either CD3+ cross-linking,PMA or PHA [12,13,21,26,27,29,60]. This occursthrough a major histocompatible complex (MHC)non-restricted monocyte-dependent mechanism[27]. The requirement for T cell activation appearsto be a common feature of monocyte-dependentapoptosis mediated by Fas–FasL interaction[39,44,66]. Our previous results suggest that Tcells and monocytes in the PB of HDT and SCTpatients are highly activated based on the expres-sion of immunoregulatory cytokines [34,56].These results are similar to the finding that circu-lating T lymphocytes from HIV-infected individu-als are activated [67], have an increased expressionof Fas on their membranes [68,69] and are moresusceptible to FasL-mediated killing [69]. Ourdata also suggest that CD4+ T cells in the PB ofHDT and SCT patients undergo apoptosis afterencountering monocytes expressing FasL.Whether this is predominantly a PB or lymphnode phenomenon is unknown. Thus, the circum-stance whereby a susceptible CD4+ T cell encoun-ters an apoptosis-inducing ligand remainsunknown.
Previous in vitro studies suggest a requirementfor cell-to-cell interactions in monocyte-dependentT cell apoptosis [27] and a role for a membrane-associated form of FasL, but do not eliminate arole for soluble FasL. A recent report demon-strated that human monocytic cells contain highlevels of intracellular FasL, which is rapidly re-leased following cellular activation [72], suggest-ing an additional FasL mechanism. Furthermore,results from preclinical [73,74] and clinical studies[75,76] suggest that cytokine mobilization can re-sult in a type 2 cytokine storm that also con-tributes to immune deficiency. Theimmunosuppression within the PSC products andPB post-transplantation, therefore, may also in-volve type 2 cytokines.

J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–1056 1051
As reported here, following HDT and SCT,NHL patients demonstrated significant increasesin the mRNA levels of all cytokines examined,compared to normal PBMC. This difference incytokine mRNA levels was not due to a decreasein the lymphocyte frequency of the PBMC, al-though the CD4:CD8 T cell ratio was significantlylower than that observed in the PB of normaldonors. Despite the increased cytokine expression,which suggests that the immune cells were acti-vated, the mitogenic (PHA) T cell response in thePB was significantly depressed. Earlier reportssuggest that defects in cytokine expression mightcontribute to the immune dysfunction in au-tologous BMT patients, including decreased IL-2levels [77–82] or increased IL-10 levels [83]. Thehigh levels of cytokine mRNA that we observedin the PBMC of NHL patients prior to transplan-tation suggest an abnormal activation of the im-mune cells, which may be associated withprevious cycles of chemotherapy or tumor bur-den. Recent reports support this hypothesis withthe demonstration that chemotherapeutic agentssuch as Taxol and adriamycin enhance the levelsof cytokine (IL-1, IL-8, TNF-a) mRNA frommonocytes in vitro and IL-8 expression in a sub-set of ovarian cancer cells in vivo [84,85]. In aprevious report, we demonstrated that the numberof prior chemotherapy cycles inversely correlatedwith the PHA response suggest an associationbetween prior chemotherapy and T cell function[13]. In addition, in hairy cell leukemia, tumorburden was reported to correlate with the plasmaor serum levels of IL-1a, IL-1b, IL-6 and solubleIL-2R [86]. Recent reports also suggest that pre-treatment of mice and humans with G-CSF polar-izes donor T lymphocytes towards a type 2cytokine production, induces T cell unresponsive-ness [73] and increases the frequency of myeloiddendritic cells, which also appear to have im-munosuppressed activity [31,74]. It remains un-clear whether chemotherapy, tumor burden, orboth, regulate cytokine gene expression in thePBMC of NHL patients undergoing HDT andSCT.
Studies on abnormalities in the cytokine net-work post-transplantation have focused on theproduction of T cell-derived cytokine and hema-
topoietic growth factors following allogeneic andautologous BMT with limited reports on cytokinegene expression following SCT [78–80,82,87–96].These studies demonstrated defects in the produc-tion of IL-2 [78], IL-3 and GM-CSF [96], IL-6[95], IL-10 [92] and IFN-g [81]. Results presentedhere are the first to detail cytokine gene expres-sion in the PBMC of patients undergoing HDTand autologous SCT. Recent reports from ourlaboratory suggest that despite high levels of cy-tokine mRNA expression, the function oflymphocytes from these patients remains de-pressed [27,32,56]. Recently, high levels of IL-2mRNA, but not IL-2 protein expression, wereobserved in leukocytes from breast cancer patients[97]. The lack of IL-2 translation and secretiondespite IL-2 mRNA transcription in tumor-infiltrating leukocytes (TIL) might be due to atranslational control that results in a T cell energy[97,98]. It is not clear from our studies if higherlevels of mRNA transcripts in the PBMC of thesepatients translates to increased cytokine produc-tion. Aberrant cytokine production may arisefrom defective transcription and/or instability ofthe cytokine mRNA transcript. Alternatively, de-fective translation and reduced cytoplasmicprotein half-life could result in decreased secre-tion. However, in our preliminary studies ofmononuclear cells from PSC products we foundthat the levels of cytokine mRNA transcriptsdirectly correlated with mitogen-stimulated cy-tokine secretion [34,56]. Additionally, a defect inthe signaling pathways might contribute to theinability of cytokines to function. One reportdemonstrates that BMT patients exhibited such adeficit that the signaling cascade downstream ofsecond messenger generation was effectively re-sulting in impaired cytokine production [79]. Al-ternative studies suggest that high IL-10 levels[28,83] or impaired co-stimulation [29] of cells inPSC products may also contribute to immunedysfunction.
In summary, our data suggest that ‘primed’Fas+ CD4+ lymphocytes interact with activatedmonocytes that express FasL, resulting in apopto-sis, which leads to preferential deletion of CD4+
T cells, a decrease in the CD4:CD8 T cell ratioand immune dysfunction. We suggest that this is
J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–10561052
one mechanism in the peripheral tolerance ob-served in cancer patients following HDT andSCT. The prevention of apoptosis in CD4+ Tcells and effective immune reconstitution by themanipulation of PSC products or cytokine/anti-body support post-transplantation may be an im-portant adjuvant therapeutic strategy in patientsundergoing HDT and SCT. Recovery of a func-tional immune system is essential for effectiveeradication of minimal residual disease and con-trol of opportunistic infections following HDTand SCT. A better understanding of the mecha-nism of cytokine gene transcription/translationand signaling events will allow us to effectivelymanipulate the graft product or design adjuvantimmunotherapy.
Acknowledgements
Source of support: JE Talmadge, NIH GrantRO1-CA61593.
References
[1] Appelbaum FR, Sullivan KM, Buckner CD, Clift R,Deeg HJ, Fefer A, Hill R, Mortimer J, Neiman P,Sanders J, Singer J, Stewart P, Storb R, Thomas ED.Treatment of malignant lymphoma in 100 patients withchemotherapy, total body irradiation, and marrow trans-plantation. J Clin Oncol 1987;5:1340–7.
[2] Kessinger A, Bierman PJ, Vose JM, Armitage JO. High-dose cyclophosphamide, carmustine, and etoposide fol-lowed by autologous peripheral stem cell transplantationfor patients with relapsed Hodgkin’s disease. Blood1991;77:2322–5 Published erratum appears in Blood 1991Dec 15;78(12) 3330.
[3] Ager S, Scott MA, Mahendra P, Richards EM, JesticeHK, Boraks P, Baglin TP, Marcus RE. Peripheral bloodstem cell transplantation after high-dose therapy in pa-tients with malignant lymphoma: A retrospective com-parison with autologous bone marrow transplantation.Bone Marrow Transplant 1995;16:79–83.
[4] Kessinger A. Is blood or bone marrow better? Stem Cells1993;11:290–5.
[5] Korbling M, Fliedner TM. The evolution of clinical pe-ripheral blood stem cell transplantation. Bone MarrowTransplant 1996;17:675–8.
[6] To LB, Haylock DN, Simmons PJ, Juttner CA. Thebiology and clinical uses of blood stem cells. Blood1997;89:2233–58.
[7] Chakraborty N, Bilgrami S, Maness L, Guo C, Perez-Diez A, Mukherji B, Tutschka P. Myeloablativechemotherapy with autologous peripheral blood stem celltransplantation for metastatic breast cancer: immunologicconsequences affecting clinical outcome. Bone MarrowTransplant 1999;24:837–43.
[8] Avigan D, Wu Z, Joyce R, Elias A, Richardson P,McDermott D, Levine J, Kennedy L, Giallombardo N,Hurley D, Gong J, Kufe D. Immune reconstitution fol-lowing high-dose chemotherapy with stem cell rescue inpatients with advanced breast cancer. Bone MarrowTransplant 2000;26:169–76 In Process Citation.
[9] Lin MT, Tseng LH, Frangoul H, Gooley T, Pei J, Bar-soukov A, Akatsuka Y, Hansen JA. Increased apoptosisof peripheral blood T cells following allogeneic hemato-poietic cell transplantation. Blood 2000;95:3832–9 In Pro-cess Citation.
[10] Mackall CL, Stein D, Fleisher TA, Brown MR, HakimFT, Bare CV, Leitman SF, Read EJ, Carter CS, WexlerLH, Gress RE. Prolonged CD4 depletion after sequentialautologous peripheral blood progenitor cell infusions inchildren and young adults. Blood 2000;96:754–62 In Pro-cess Citation.
[11] Verfuerth S, Peggs K, Vyas P, Barnett L, O’Reilly RJ,Mackinnon S. Longitudinal monitoring of immune recon-stitution by CDR3 size spectratyping after T-cell-depletedallogeneic bone marrow transplant and the effect ofdonor lymphocyte infusions on T-cell repertoire. Blood2000;95:3990–5 In Process Citation.
[12] Talmadge JE, Reed E, Ino K, Kessinger A, Kuszynski C,Heimann D, Varney M, Jackson J, Vose JM, Bierman PJ.Rapid immunologic reconstitution following transplanta-tion with mobilized peripheral blood stem cells as com-pared to bone marrow. Bone Marrow Transplant1997;19:161–72.
[13] Talmadge JE, Reed EC, Kessinger A, Kuszynski CA,Perry GA, Gordy CL, Mills KC, Thomas ML, PirruccelloSJ, Letheby BA, Arneson MA, Jackson JD. Immunologicattributes of cytokine mobilized peripheral blood stemcells and recovery following transplantation. Bone Mar-row Transplant 1996;17:101–9.
[14] Henon PR, Liang H, Beck WG, Eisenmann JC, LepersM, Wunder E, Kandel G. Comparison of hematopoieticand immune recovery after autologous bone marrow orblood stem cell transplants. Bone Marrow Transplant1992;9:285–91.
[15] Roberts MM, To LB, Gillis D, Mundy J, Rawling C, NgK, Juttner CA. Immune reconstitution following periph-eral blood stem cell transplantation, autologous bonemarrow transplantation and allogeneic bone marrowtransplantation. Bone Marrow Transplant 1993;12:469–75.
[16] Kiesel S, Pezzutto A, Korbling M, Haas R, Schulz R,Hunstein W, Dorken B. Autologous peripheral bloodstem cell transplantation: analysis of autografted cells andlymphocyte recovery. Transplant Proc 1989;21:3084–8.

J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–1056 1053
[17] Scambia G, Panici PB, Pierelli L, Baiocchi G, Rumi C,Menichella G, Foddai M, Serafini R, Arno E, BonannoG. Immunological reconstitution after high dosechemotherapy and autologous blood stem cell transplan-tation for advanced ovarian cancer. Eur J Cancer1993;29A:1518–22.
[18] Olsen GA, Gockerman JP, Bast RC, Jr, Borowitz M,Peters WP. Altered immunologic reconstitution afterstandard-dose chemotherapy or high-dose chemotherapywith autologous bone marrow support. Transplantation1988;46:57–60.
[19] Brugnoni D, Airo P, Pennacchio M, Carella G, MalagoliA, Ugazio AG, Porta F, Cattaneo R. Immune reconstitu-tion after bone marrow transplantation for combinedimmunodeficiencies: down-modulation of Bcl-2 and highexpression of CD95/Fas account for increased susceptibil-ity to spontaneous and activation-induced lymphocyte celldeath. Bone Marrow Transplant 1999;23:451–7.
[20] Mielcarek M, Roecklein BA, Torok-Storb B. CD14+ cellsin granulocyte colony-stimulating factor (G-CSF) mobi-lized peripheral blood mononuclear cells induce secretionof interleukin-6 and G-CSF by marrow stroma. Blood1996;87:574–80.
[21] Mielcarek MB, Martin PJ, Torok-Storb B. Suppression ofalloantigen-induced T-cell proliferation by CD14+ cellsderived from granulocyte colony-stimulating factor-mobi-lized peripheral blood mononuclear cells. Blood1997;89:1629–34.
[22] Beverly B, Kang SM, Leonardo MJ, Swartz RH. Reversalof in vitro T cell clonal anergy by IL-2 stimulation. Int JImmunol 1992;4:661–71.
[23] Oghiso Y, Yamada Y, Ando K, Ishihara H, Shibata Y.Differential induction of prostaglandin E2-dependent and-independent immune suppressor cells by tumor-derivedGM-CSF and M-CSF. J Leukocyte Biol 1993;53:86.
[24] Koyama S, Fukao K. Phenotypic analysis of nylon-wool-adherent suppressor cells that inhibit the effector processof tumour cell lysis by lymphokine-activated killer cells inpatients with advanced gastric carcinoma. J Cancer ResClin Oncol 1994;120:240.
[25] Farinas MC, Rodriguez-Valverde V, Zarrabeitia MT,Parra-Blanco JA, Sanz-Ortiz J. Contribution of mono-cytes to the decreased lymphoproliferative response tophytohemagglutinin in patients with lung cancer. Cancer1991;68:1279–84.
[26] Ageitos AG, Varney M, Bierman P, Vose J, WarkentinPI, Talmadge JE. Comparison of monocyte dependent Tcell inhibitory activity in GM-CSF vs. G-CSF mobilizedPSC products. Bone Marrow Transplant 1999;23:63–9.
[27] Ino K, Singh RK, Talmadge JE. Monocytes from mobi-lized stem cells inhibit T cell function. J Leukocyte Biol1997;61:583–91.
[28] Mielcarek M, Graf L, Johnson G, Torok-Storb B. Pro-duction of interleukin-10 by granulocyte colony-stimulat-ing factor-mobilized blood products: a mechanism formonocyte-mediated suppression of T-cell proliferation.Blood 1998;92:215–22.
[29] Tanaka J, Mielcarek M, Torok-Storb B. Impaired induc-tion of the CD28-responsive complex in granulocytecolony-stimulating factor mobilized CD4 T cells. Blood1998;91:347–52.
[30] Young MR, Wright MA, Pandit R. Myeloid differentia-tion treatment to diminish the presence of immune-sup-pressive CD34+ cells within human head and necksquamous cell carcinomas. J Immunol 1997;159:990–6.
[31] Arpinati M, Green CL, Heimfeld S, Heuser JE, AnasettiC. Granulocyte-colony stimulating factor mobilizes Thelper 2-inducing dendritic cells. Blood 2000;95:2484–90In Process Citation.
[32] Singh RK, Varney ML, Buyukberber S, Ino K, AgeitosA, Reed E, Tarantolo S, Talmadge JE. Fas-FasL-medi-ated CD4+ T-cell apoptosis following stem cell. CancerRes 1999;59:3107–11.
[33] Ino K, Bierman PJ, Varney ML, Heimann DG, Kuszyn-ski CA, Walker SA, Talmadge JE. Monocyte activationby an oral immunomodulator (bestatin) in lymphomapatients following autologous bone marrow transplanta-tion. Cancer Immunol Immunother 1996;43:206–12.
[34] Singh RK, Ino K, Varney M, Heimann D, Talmadge JE.Immunoregulatory cytokines in bone marrow and periph-eral blood stem cell products. Bone Marrow Transplant1999;23:53–62.
[35] Dhein J, Walczak H, Baumler C, Debatin KM, KrammerPH. Autocrine T-cell suicide mediated by APO-I/(Fas/CD95). Nature 1995;373:438–41.
[36] Brunner T, Mogil RJ, LaFace D, et al. Cell-autonomousFas (CD95)/Fas–ligand interaction mediates activationinduced apoptosis in T cell hybridomas. Nature1995;373:441–4.
[37] Ju ST, Panka DJ, Cui H, Ettinger R, el Khatib M, SherrDH, Stanger BZ, Marshak RA. Fas (CD95)/FasL inter-actions required for programmed cell death after T cellactivation. Nature 1995;373:444–8.
[38] Ettinger R, Panka DJ, Wang JK, Stanger BZ, Ju S-T,Marshak-Rothstein A. Fas ligand mediated cytotoxicity isdirectly responsible for apoptosis of normal CD4+ T cellsresponding to bacterial superantigens. J Immunol1995;154:4302–8.
[39] Badley AD, Dockrell D, Simpson M, Schut R, LynchDH, Leibson P, Paya CV. Macrophage-dependent apop-tosis of CD4+T lymphocytes from HIV-infected individ-uals is mediated by FasL and tumor necrosis factor. JExp Med 1997;185:55–64.
[40] Krammer PH, Behrmann I, Daniel P, Dhein J, DebatinKM. Regulation of apoptosis in the immune system. CurrOpin Immunol 1994;6:279–89.
[41] Alderson MR, Tough TW, Braddy S, Davis-Smith T,Roux E, Schooley K, Miller RE, Lynch DH. Regulationof apoptosis and T cell activation by Fas-specific mAb.Int Immunol 1994;6:1799–806.
[42] Smith CA, Farrah T, Goodwin RG. The TNF receptorsuperfamily of cellular and viral proteins: activation, cos-timulation, and death. Cell 1994;76:959–62.

J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–10561054
[43] Badley AD, McElhinny JA, Leibson PJ, Lynch DH,Alderson MR, Paya CV. Upregulation of Fas ligandexpression by human immunodeficiency virus in humanmacrophages mediated apoptosis of uninfected Tlymphocytes. J Virol 1996;70:199–206.
[44] Wu MX, Daley JF, Rasmussen RA, Schlossman SF.Monocytes are required to prime peripheral blood T cellsto undergo apoptosis. Proc Natl Acad Sci USA1995;92:1525–9.
[45] Small TN, Papadopoulos EB, Boulad F, Black P, Castro-Malaspina H, Childs BH, Collins N, Gillio A, George D,Jakubowski A, Heller G, Fazzari M, Kernan N, Mackin-non S, Szabolcs P, Young JW, O’Reilly RJ. Comparisonof immune reconstitution after unrelated and related T-cell-depleted bone marrow transplantation: effect of pa-tient age and donor leukocyte infusions. Blood1999;93:467–80.
[46] Small TN, Avigan D, Dupont B, Smith K, Black P,Heller G, Polyak T, O’Reilly RJ. Immune reconstitutionfollowing T-cell depleted bone marrow transplantation:effect of age and posttransplant graft rejection prophy-laxis. Biol Blood Marrow Transplant 1997;3:65–75.
[47] Romagnani S. Human TH1 and TH2 subsets: regulationof differentiation and role in protection and im-munopathology. Int Arch Allergy Immunol 1992;98:279–85.
[48] Romagnani S. Human TH1 and TH2 subsets: doubt nomore. Immunol Today 1991;12:256–7.
[49] Paul WE, Seder RA. Lymphocyte responses and cytoki-nes. Cell 1994;76:241–51.
[50] Romagnani S. Type 1 T helper and type 2 T helper cells:functions, regulation and role in protection and disease.Int J Clin Lab Res 1991;21:152–8.
[51] Lederer JA, Liou JS, Todd MD, Glimcher LH, LichtmanAH. Regulation of cytokine gene expression in T helpercell subsets. J Immunol 1994;152:77–86.
[52] Spagnoli GC, Juretic A, Schultz TE, Dellabona P,Filgueira L, Horig H, Zuber M, Garotta G, Heberer M.On the relative roles of interleukin-2 and interleukin-10 inthe generation of lymphokine-activated killer cell activity.Cell Immunol 1993;146:391–405.
[53] Yamamura M, Modlin RL, Ohmen JD, Moy RL. Localexpression of antiinflammatory cytokines in cancer. J ClinInvest 1993;91:1005–10.
[54] Kharkevitch DD, Seito D, Balch GC, Maeda T, BalchCM, Itoh K. Characterization of autologous tumor-spe-cific T-helper 2 cells in tumor-infiltrating lymphocytesfrom a patient with metastatic melanoma. Int J Cancer1994;58:317–23.
[55] Nathan CF. Secretory products of macrophages. J ClinInvest 1987;79:319–26.
[56] Varney ML, Ino K, Ageitos AG, Heimann DG, Tal-madge JE, Singh RK. Expression of interleukin-10 inisolated CD8+ T cells and monocytes from growth fac-tor-mobilized peripheral blood stem cell products: amechanism of immune dysfunction. J Interferon CytokineRes 1999;19:351–60.
[57] Holler E, Roncarolo MG, Hintermeier-Knabe R, EissnerG, Ertl B, Schulz U, Knabe H, Kolb HJ, Andreesen R,Wilmanns W. Prognostic significance of increased IL-10production in patients prior to allogeneic bone marrowtransplantation. Bone Marrow Transplant 2000;25:237–41.
[58] Bacchetta R, Bigler M, Touraine JL, Parkman R, TovoPA, Abrams J, de Waal MR, de Vries JE, RoncaroloMG. High levels of interleukin 10 production in vivo areassociated with tolerance in SCID patients transplantedwith HLA mismatched hematopoietic stem cells. J ExpMed 1994;179:493–502.
[59] Pierelli L, Iacone A, Quaglietta AM, Nicolucci A,Menichella G, Panici PB, D’Antonio D, DeLaurenzi A,DeRosa L, Fioritoni G, Indovina A, Leone G, MajolinoI, Montuoro A, Scime R, Torlontano G. Haemopoieticreconstitution after autologous blood stem cell transplan-tation in patients with malignancies: A multicenter retro-spective study. Br J Haematol 1994;86:70–5.
[60] Mills KC, Gross TG, Varney ML, Heimann DG, ReedEC, Kessinger A, Talmadge JE. Immunologic phenotypeand function in human bone marrow, blood stem cellsand umbilical cord blood. Bone Marrow Transplant1996;18:53–61.
[61] Badger AM, King AG, Talmadge JE, Schwartz DA,Picker DH, Mirabelli CK, Hanna H. Induction of non-specific suppressor cells in normal Lewis rats by a novelazaspirane, SK&F 105685. J Autoimmun 1990;3:485–500.
[62] Bishop MR, Anderson JR, Jackson JD, Bierman PJ,Reed EC, Vose JM, Armitage JO, Warkentin PI,Kessinger A. High-dose therapy and peripheral bloodprogenitor cell transplantation: effects of recombinanthuman granulocyte-macrophage colony-stimulating factoron the autograft. Blood 1994;83:610–6.
[63] Chomczynski P, Sacchi N. Single-step method for RNAisolation by acid guanidinium thiocyanate-phenol-chloro-form extraction. Anal Biochem 1987;162:156–9.
[64] Donnenberg AD, Donnenberg VS, Margolick JB, BeltzLA. Apoptosis parallels lymphopoiesis in bone marrowtransplantation and HIV disease. Res Immunol1995;146:11–21.
[65] Donnenberg AD, Margolick JB, Donnenberg VS.Lymphopoiesis, apoptosis and immune amnesia. Ann NYAcad Sci 1995;770:213–26.
[66] Groux H, Torpier G, Monte D, Mouton Y, Capron A,Ameisen JD. Activation-induced death by apoptosis inCD4+ T cells from human immunodeficiency virus in-fected asymptomatic individuals. J Exp Med1992;175:331–40.
[67] Giorgi JV, Detels R. T-cell subset alterations in HIV-in-fected homosexual men: NIAID Multicenter AIDS co-hort study. Clin Immunol Immunopathol 1989;52:10–8.
[68] Debatin KM, Fahrig-Faissner A, Enenkel-Stoodt S,Kruez W, Benner A, Krammer PH. High expression ofAPO-1 (CD95) on T lymphocytes from human im-munodeficiency virus-1-infected children (letter). Blood1994;83:3101–3.

J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–1056 1055
[69] Katsikis PH, Wunderlich ES, Smith CA, Herzenberg LA.Fas antigen stimulation induces marked apoptosis of Tlymphocytes in human immunodeficiency virus-infectedindividuals. J Exp Med 1995;181:2029–36.
[70] Finkel TH, Tudor-Williams G, Banda NK, Cotton MF,Curiel T, Monks C, Baba TW, Ruprecht RM, Kupfer A.Apoptosis occurs predominantly in bystander cells andnot in productively infected cells of HIV- and SIV-in-fected lymph nodes. Nat Med 1995;1:29–134.
[71] Varney ML, Ino K, Ageitos AG, Heimann DG, Tal-madge JE, Singh RK. Expression of interleukin-10 inisolated CD8+ T cells and monocytes from growthfactor-mobilized peripheral blood stem cell products: amechanism of immune dysfunction. J Interferon CytokineRes 1999;19:351–60.
[72] Kiener PA, Davis PM, Rankin BM, Klebanoff SJ, Led-better JA, Starling GC, Liles WC. Human monocytic cellscontain high levels of intracellular Fas ligand. Rapidrelease following cellular activation. J Immunol1997;159:1594–8.
[73] Zeng D, Dejbakhsh JS, Strober S. Granulocyte colony-stimulating factor reduces the capacity of blood mononu-clear cells to induce graft-versus-host disease: impact onblood progenitor cell transplantation. Blood1997;90:453–63.
[74] Pan L, Delmonte J, Jr, Jalonen CK, Ferrara JLM. Pre-treatment of donor mice with granulocyte colony-stimu-lating factor polarizes donor T lymphocytes towardType-2 cytokine production and reduces severity of exper-imental graft-versus-host disease. Blood 1995;86:4422–9.
[75] Rutella S, Rumi C, Lucia MB, Sica S, Cauda R, LeoneG. Serum of healthy donors receiving granulocyte colony-stimulating factor induces T cell unresponsiveness. ExpHematol 1998;26:1024–33.
[76] Rutella S, Rumi C, Testa U, Sica S, Teofili L, MartucciR, Peschle C, Leone G. Inhibition of lymphocyte blasto-genic response in healthy donors treated with recombi-nant human granulocyte colony-stimulating factor(rhG-CSF): possible role of lactoferrin and interleukin-1receptor antagonist. Bone Marrow Transplant1997;20:355–64.
[77] Shenoy S, Mohanakumar T, Todd G, Westhoff W, Dun-nigan K, Adkins D, Brown R, DiPersio J. Immune recon-stitution following allogeneic peripheral blood stem celltransplant. Bone Marrow Transplant 1999;4:335–46.
[78] Welte K, Ciobanu N, Moore MA, Gulati S, O’Reilly RJ,Mertelsmann R. Defective interleukin 2 production inpatients after bone marrow transplantation and in vitrorestoration of defective T lymphocyte proliferation byhighly purified interleukin 2. Blood 1984;64:380–5.
[79] Schneider LC, Antin JH, Weinstein H, Abrams JS, PearceMK, Geha RS, Vercelli D. Lymphokine profile in bonemarrow transplant recipients. Blood 1991;78:3076–80.
[80] Lum LG, Joshi ID, Smith MR, Ratanatharathorn V,Galoforo SC, Karanes C, Uberti JP, Sensenbrenner LL.Constitutive and mitogen-stimulated cytokine mRNA ex-pression by peripheral blood mononuclear cells from
most autologous and allogeneic bone marrow transplantrecipients is intact. Bone Marrow Transplant1994;13:187–95.
[81] Hanenberg H, Dilloo D, Laws H-J, Zessack N, Heyll A,Burdach S. Time course of interferon-g production defi-ciency after autologous and allogeneic stem cell transplan-tation for malignancies. Exp Hematol 1995;23:1543–52.
[82] Cayeux S, Meuer S, Pezzutto A, Korbling M, Haas R,Schulz R, Dorken B. T cell ontogeny after autologousbone marrow tranplantation: Failure to synthesize inter-leukin-2 (IL-2) and lack of CD2- and CD3-mediatedproliferation by both CD4+ and CD8+ cells even in thepresence of exogenous IL-2. Blood 1989;74:2270.
[83] Baker K, Roncarolo M-G, Peters C, Bigler M, DeFor T,Blazar B. High spontaneous IL-10 production in unre-lated bone marrow transplant recipients is associated withfewer transplant-related complications and early deaths.Bone Marrow Transplant 1999;23:1123–9.
[84] Asano T, Fujimaki W, McWatters A, An T, MatsushimaK, Kleinerman ES. Effect of Adriamycin on liposomalmuramyl tripeptide’s ability to up-regulate monocyte cy-tokine expression. Cancer Immunol Immunother1993;37:408–11.
[85] Lee LF, Schuerer MC, Lofquist AK, van-Haaften-Day C,Ting JP, White CM, Martin BK, Haskill JS. Taxol-depen-dent transcriptional activation of IL-8 expression in asubset of human ovarian cancer. Cancer Res1996;56:1303–8.
[86] Aguilar-Santelises M, Loftenius A, Ljungh C, SvensonSB, Andersson B, Mellstedt H, Jondal M. Serum levels ofhelper factors (IL-1 alpha, IL-1 beta and IL-6), T-cellproducts (sCD4 and sCD8), sIL-2R and beta 2-mi-croglobulin in patients with B-CLL and benign Blymphocytosis. Leukemia Res 1992;16:607–13.
[87] Kawano Y, Takaue Y, Saito S-I, Sato J, Shimizu T,Suzue T, Hirao A, Okamoto Y, Abe T, Watanabe T,Kuroda Y, Kimura F, Motoyoshi K, Asano S. Granulo-cyte colony stimulating factor (G-CSF), macrophage-CSF, interleukin-3, and interleukin-6 levels in sera fromchildren undergoing blood stem cell autografts. Blood1993;81:856–60.
[88] Cairo MS, Gillan ER, Weinthal J, Yancik S, van de VenC, Ho W, Shen V, Buzby J, Suen Y. Decreased endoge-nous circulating steel factor (SLF) levels following allo-geneic and autologous BMT: Lack of an inversecorrelation with post-BMT myeloid engraftment. BoneMarrow Transplant 1993;11:155–61.
[89] Miksits K, Beyer J, Siegert W. Serum concentrations ofG-CSF during high-dose chemotherapy with autologousstem cell rescue. Bone Marrow Transplant 1993;11:375.
[90] Haas R, Gericke G, Witt B, Caycux S, Hunstein W.Increased serum levels of granulocyte colony-stimulatingfactor after autologous bone marrow or blood stem celltransplantation. Exp Hematol 1993;21:109.
[91] Ho AD, Maruyama M, Maghazachi A, Mason JR, GluckS, Corringham RET. Soluble CD4, soluble CD8, solubleCD25, lymphopoietic recovery, and endogenous cytokines

J.E. Talmadge et al. / International Journal of Immunopharmacology 22 (2000) 1041–10561056
after high-dose chemotherapy and blood stem cell trans-plantation. Blood 1994;84:3550–7.
[92] Guillaume T, Sekhavat M, Rubinstein DB, Hamdan O,Leblanc P, Symann ML. Defective cytokine productionfollowing autologous stem cell transplantation for solidtumors and hematologic malignancies regardless of bonemarrow or peripheral origin and lack of evidence for arole for interleukin-10 in delayed immune reconstitution.Cancer Res 1994;54:3800–7.
[93] Testa U, Martucci R, Rutella S, Scambia G, Sica S,Benedetti PP, Pierelli L, Menichella G, Leone G, Man-cuso S. Autologous stem cell transplantation: Release ofearly and late acting growth factors relates with hemato-poietic ablation and recovery. Blood 1994;84:3532–9.
[94] Takamatsu Y, Akashi K, Harada M, Teshima T, Inaba S,Shimoda K, Eto T, Shibuya T, Okamura S, Niho Y.Cytokine production by peripheral blood monocytes andT cells during haemopoietic recovery after intensive
chemotherapy. Br J Haematol 1993;83:21–7.[95] Watts MJ, Jones HM, Sullivan AM, et al. Accessory cells
do not contribute to G-CSF or IL-6 production nor torapid haematological recovery following peripheral bloodstem cell transplantation. Br J Haematol 1995;91:767–72.
[96] Baiocchi GP, Scambia G, Benedetti G, et al. Autologousstem cell transplantation: Sequential production of hema-topoietic cytokines underlying granulocyte recover. Can-cer Res 1993;53:1297.
[97] Coventry BJ, Weeks SC, Heckford SE, Sykes PJ, BradleyJ, Skinner JM. Lack of IL-2 cytokine expression despiteIl-2 messenger RNA transcription in tumor-infiltratinglymphocytes in primary human breast carcinoma: selec-tive expression of early activation markers. J Immunol1996;156:3486–92.
[98] Garcia SJ, Lenig D. Translational control of interleukin 2messenger RNA as a molecular mechanism of T cellenergy. J Exp Med 1996;184:159–64.
.




















