Measuring ambulation in adults with central neurologic disorders
17
Measuring Ambulation in Adults with Central Neurologic Disorders Karen J. Nolan, PhD a,b, *, Mathew Yarossi, MS a,c , Arvind Ramanujam, MS a INTRODUCTION Throughout rehabilitation medicine, there is an emphasis on the ability to ambulate as a functional outcome and as an overall indicator of quality of life. When ambulation is affected by central neurologic disorders (CND), it is typically as a result of a combina- tion of impairments and the compensatory strategies used to accommodate these impairments. Pathologic ambulation can result from impairments within a single Disclaimers: None. Grant Support: Supported by Kessler Foundation. Declaration of Interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper. a Human Performance and Engineering Laboratory, Kessler Foundation Research Center, 1199 Pleasant Valley Way, West Orange, NJ 07052, USA; b Department of Physical Medicine and Rehabilitation, University of Medicine and Dentistry of New Jersey - New Jersey Medical School, Newark, NJ 07103, USA; c Department of Rehabilitation & Movement Sciences, Graduate School of Biomedical Sciences, University of Medicine and Dentistry of New Jersey - New Jersey Medical School, Newark, NJ 07101, USA * Corresponding author. Human Performance and Engineering Laboratory, Kessler Foundation Research Center, 1199 Pleasant Valley Way, West Orange, NJ 07052. E-mail address: [email protected] KEYWORDS Ambulation Rehabilitation Measurement Gait analysis Walking speed Central neurologic disorder KEY POINTS Examine strategies for appropriate measurements of ambulation in individuals with central neurologic disorder within three distinct environments: 1) clinical; 2) laboratory; and 3) community. Discuss common challenges and solutions for clinicians and researchers when selecting appropriate outcomes for measuring ambulation. Description of technology-driven assessment tools for measuring ambulation to obtain objective, quantifiable outcomes. Explore techniques and research related to measurement of quantitative and qualitative ambulation in the community for persons with central neurologic disorder. Phys Med Rehabil Clin N Am 24 (2013) 247–263 http://dx.doi.org/10.1016/j.pmr.2012.12.001 pmr.theclinics.com 1047-9651/13/$ – see front matter Ó 2013 Elsevier Inc. All rights reserved.
-
Upload
kesslerfoundation -
Category
Documents
-
view
0 -
download
0
Transcript of Measuring ambulation in adults with central neurologic disorders

Measuring Ambulation in Adultswith Central Neurologic Disorders
Karen J. Nolan, PhDa,b,*, Mathew Yarossi, MS
a,c,Arvind Ramanujam, MS
a
INTRODUCTION
Throughout rehabilitation medicine, there is an emphasis on the ability to ambulate as
a functional outcome and as an overall indicator of quality of life. When ambulation is
affected by central neurologic disorders (CND), it is typically as a result of a combina-
tion of impairments and the compensatory strategies used to accommodate these
impairments. Pathologic ambulation can result from impairments within a single
Disclaimers: None.Grant Support: Supported by Kessler Foundation.Declaration of Interest: The authors report no conflicts of interest. The authors alone areresponsible for the content and writing of the paper.a Human Performance and Engineering Laboratory, Kessler Foundation Research Center, 1199Pleasant Valley Way, West Orange, NJ 07052, USA; b Department of Physical Medicine andRehabilitation, University of Medicine and Dentistry of New Jersey - New Jersey Medical School,Newark, NJ 07103, USA; c Department of Rehabilitation &Movement Sciences, Graduate Schoolof Biomedical Sciences, University of Medicine and Dentistry of New Jersey - New Jersey MedicalSchool, Newark, NJ 07101, USA* Corresponding author. Human Performance and Engineering Laboratory, Kessler FoundationResearch Center, 1199 Pleasant Valley Way, West Orange, NJ 07052.E-mail address: [email protected]
KEYWORDS
� Ambulation � Rehabilitation � Measurement � Gait analysis � Walking speed� Central neurologic disorder
KEY POINTS
� Examine strategies for appropriate measurements of ambulation in individuals with central
neurologic disorder within three distinct environments: 1) clinical; 2) laboratory; and 3)
community.
� Discuss common challenges and solutions for clinicians and researchers when selecting
appropriate outcomes for measuring ambulation.
� Description of technology-driven assessment tools for measuring ambulation to obtain
objective, quantifiable outcomes.
� Explore techniques and research related to measurement of quantitative and qualitative
ambulation in the community for persons with central neurologic disorder.
Phys Med Rehabil Clin N Am 24 (2013) 247–263http://dx.doi.org/10.1016/j.pmr.2012.12.001 pmr.theclinics.com
1047-9651/13/$ – see front matter � 2013 Elsevier Inc. All rights reserved.
system or within a combination of systems, such as musculoskeletal, neuromuscular,
sensory/perceptual, and cognitive/behavioral.1
Functional ambulation is the extent to which an individual is capable and willing to
move around in their environment.2 Measuring ambulation is a complex task involving
clinical expertise, laboratory technology, and the ability to translate information to
a community setting.
Measuring ambulation can be challenging, because walking occurs in multiple envi-
ronments and must be assessed at multiple time points to indicate improvement or
decline. There is an added complexity, because, in a traditional clinical environment,
a single numerical value or scale score is preferred to summarize a series of complex
movements,3 whereas in a laboratory environment, researchers typically prefer quan-
tifiable continuous data, which allow for complex analysis of multiple outcome vari-
ables. Measuring ambulation in a community also presents unique challenges and
often requires a combination of strategies to obtain valid outcomes.4 This review
examines strategies for appropriate measurements of ambulation in individuals with
CND within 3 distinct environments: (1) clinical, (2) laboratory, and (3) community.
The purpose of this article is not to provide an exhaustive list of the measures that
can be used to assess ambulation but rather to describe the most frequently used
measures and to discuss common challenges faced by clinicians and researchers
in establishing an accurate picture of an individual’s ability to ambulate.
MEASURING AMBULATION IN THE CLINICAL ENVIRONMENT
In a clinical environment, it is important to select measures that can evaluate changes
in impairment, function, and performance.3 Test selection is often dependent on
nonclinical criteria such as cost, time to administer, and available equipment.5 It is
also important for the patient to understand the test instructions, because unfamiliarity
with the test can alter performance and outcomes.5 Some examples of typical clinical
assessments commonly used for measuring ambulation can be found in Table 1.
The Functional Independence Measure (FIM) was designed to measure burden of
care in multiple rehabilitation populations.3 The scores are based on clinical observa-
tion of 18 items of activities of daily living (ADLs) (13 motor and 5 cognition items).6
Although there are motor items associated with this measure (including 1 item labeled
locomotion and 1 labeled stairs), the overall FIM score is often not sensitive enough to
reflect improvements in ambulation (particularly in situations in which walking perfor-
mance has improved without a change in the level of assistance needed). Previous
research also revealed a ceiling effect, and the FIM shows poor sensitivity to change
in individuals with better walking abilities.13 The FIM is typically used to determine
independence at admission and discharge from inpatient rehabilitation. Another
example of a frequently used clinical measure of motor deficits is the Fugl-Meyer
Motor Assessment, which has previously been shown to correlate with length of
stay in inpatient rehabilitation, and has been found to be predictive of discharge
FIM scores and performance in ADLs. The disadvantage of this measure is that it
assesses only gross limb movement and not fine or complex movements or coordina-
tion. Both the FIM and Fugl-Meyer Motor Assessment as a whole do provide reliable
information about the results of rehabilitation, but it is difficult to specifically determine
if, and how much, ambulation has improved using either of these assessment tools.
The Ambulation Index (AI) is an ordinal rating scale designed to assess independent
mobility by evaluating the time and degree of assistance required to walk 7.62m (25 ft),
as well as the ability to transfer.8 Previous research has found the AI to be useful as
a grouping variable when measuring ambulation in individuals with stroke.14 The
Nolan et al248

Table
1
Outcomesformeasu
ringambulationin
aclinicalenvironment
NameofScale
Description
Measu
rement
FunctionalIndependence
Measure
6
A7-leve
lordinalscale
thatdescribesstagesofco
mplete
dependence
toco
mplete
independence
inperform
ance
of
basicactivitiesofdailyliving
Ordinalscoresbasedonclinicalobservation
Fugl-Meye
rMotorAssessment7
Eva
luatesmove
ment,reflexe
s,co
ordination,andspeed,derive
dfrom
theBrunnstrom
stagesofpoststrokereco
very.
Frequentlyusedto
measure
motordeficits
Ordinalscoresare
basedonclinicalobservation
andobservedmove
ments
AmbulationIndex8
Anordinalratingscale
designedto
assess
independentmobility
byeva
luatingthetimeanddegreeofassistance
requiredto
walk
7.62m
(25ft).Thescale
rangesfrom
0(asymptomaticand
fullyactive)to
9(restrictedto
wheelchair;unable
totransfer
independently)
Ordinalscoresare
basedonclinicalobservation,
includingobservedperform
ance,andtimed
walkingspeed
Emory
FunctionAmbulation
Profile,ModifiedEmory
FunctionalAmbulationProfile
9,10
Thetime(s)to
ambulate
through5co
mmonenvironmental
terrainswithorwithoutanassistive
device
ormanual
assistance
Thesum
ofthetime(s)requiredto
complete
the5tasks
WalkingTe
sts(2-m
inute,6-m
inute,
10-m
inute,and12-m
inute)3
Distance
walkedin
meters
inagiventimeismeasuredto
indicate
perform
ance
Distance
walked(m
)
Dyn
amic
GaitIndex1
1A
toolto
assess
gait,balance,andfallrisk.Eightabilitiesare
gradedona4-pointscale
(0–3
)from
norm
alperform
ance
toseve
rely
impaired.Theratingisbasedontheindividual’s
abilityto
maintain
ahealthygaitpattern
andpace,without
deviatingorstumbling
Ordinalscoresare
basedonclinicalobservation
andobservedperform
ance
Tim
edUpandGo12
Thetime(s)requiredto
rise
from
anarm
chair,walk
3m,turn,
walk
back,andsitdownagain
Acategoricalscale
basedonthetime(s)required
toaccomplish
thedescribedtask
10-m
Walk
Test,Tim
ed7.62m
(25-ft)
Walk
Test
3
Ameasure
ofambulationcapacity
includingthetime(s)to
walk
10m
or7.62m
(25ft)atmaximum
butsafe
gaitspeed
Tim
eanddistance
tocalculate
maximum
gaitspeed(m
/s)
GaitSp
eed3
Therate
(s)agivendistance
(m)isco
veredto
determ
ine
self-selectedorfastest
gaitspeed
Tim
eanddistance
tocalculate
speed(m
/s)
Adaptedfrom
Finch
E,B
rooksD,Stratford
PW,e
tal.Physicalrehabilitationoutcomemeasures.2ndedition.O
ntorio(Canada):Lippinco
ttW
illiams&W
ilkins;2002.
Measuring Ambulation in Central Neurologic Disorders 249

measure is useful in rehabilitation medicine, but it is not sensitive enough to measure
small changes in ambulation. Overall, the FIM, Fugl-Meyer, and AImeasure impairment
and function but have limited usefulness in describing and evaluating ambulation.
Whenmeasuring ambulation in a clinical environment, it is important to consider that
individuals with CND may have difficulty adapting to the demands of walking in the
community, such as rising from a chair, stepping over an obstacle, ascending stairs,
and navigating various terrains.9 The challenge is to select tasks and terrains that
mimic community ambulation that are easy to administer and provide relevant clinical
information. The Emory Functional Ambulation Profile (EFAP) and the modified EFAP
(mEFAP) were designed to provide quantitative information about ambulation by
measuring the time to walk over a standardized array of community obstacles and
surfaces, accounting for the use of assistive devices.9,10 The EFAP and mEFAP are
reliable and valid clinical tests of ambulation that are sensitive to changes in ambula-
tion speed.9,10 Research in individuals with stroke found that the mEFAP is sensitive to
changes in gait function during inpatient rehabilitation and therefore could be used to
supplement traditional subjective measures of clinical ambulation.15
Walking tests measure the distance walked in a given amount of time to indicate
walking performance. These tests are generally 2, 6, 10, or 12 minutes in duration and
are widely used in clinical and research applications for individuals with CND.3 These
measures are more quantitative and provide information directly related to ambulation,
including walking endurance. Previous research in this area suggests that individuals
must negotiate a distance of between 332 and 360 m to access goods and services
in the community.16,17 Walking distance is therefore a key indicator of ambulation.18
For individuals with CND, it is important to have clinical assessments that identify
individuals who are at risk for falling and may benefit from interventions designed to
improve balance.19 The Dynamic Gait Index (DGI) was developed as a clinical tool
to assess an individual’s ability to modify gait in response to changing task
demands.11 The limitation of the DGI is that scores are reduced for those individuals
using an assistive device, regardless of performance.20 The DGI has been applied to
individuals with CND as a reliable measure of dynamic balance and potential fall
risk.20,21 The Timed Up and Go (TUG) is a screening test of balance that is commonly
used to evaluate functional mobility.19 The time to complete the test is strongly corre-
lated to the level of functional mobility. Adults who complete the TUG in less than
20 seconds are considered to be independent in transfer tasks associated with
ADLs and can maintain walking speeds sufficient for community ambulation.12,22
In individuals with CND, alterations in gait mechanics, strength, and balance have
a direct effect on gait speed.5 The 10-m walk test and timed 7.62 m (25-ft) walk are
measures of ambulation capacity in which gait speed is the primary outcome variable.
These tests have been widely used in populations with CND and are easy to administer
in a clinical environment.3 When measuring ambulation, it is important for clinicians to
select measures capable of detecting changes that reflect real life function.23 Gait
speed is an important and reliable measure of ambulation for individuals, because
safe navigation of community crosswalks mandates that an individual be able to
complete a prescribed distance in a defined time period.16,23 Previous research in
stroke found that when an ankle foot orthotic was worn on the paretic limb, individuals
gained the ability to modulate gait speed. The orthotic intervention provided individ-
uals with stroke with the functional ability to increase speed in the community, which
is essential for negotiating obstacles and safely crossing community streets.14,16 Gait
speed is used in clinical and research applications as the hallmark of recovery, it is
simple to implement, and it has robust psychometric properties.24 Several studies
have provided evidence to support the predictive validity of gait speed, and it has
Nolan et al250

been shown to be positively correlated with level of disability, function, and quality of
life in individuals with stroke.25–27 However, what represents a clinically meaningful
change in gait speed has not been defined in all patient populations.
MEASURING AMBULATION IN A LABORATORY ENVIRONMENT
In a laboratory, ambulation is measured using traditional clinical assessments in
conjunction with technology-driven mobility assessment tools, to create quantifiable
outcomes that can be used to describe mechanisms that may lead to improved ambu-
lation. For example, increased gait speedmay indicate improved ambulation, but does
not necessarily indicate improved gait mechanisms or functional recovery. The goals
of laboratory-based outcomes for measuring ambulation are to enhance traditional
clinical measures, or to become fully integrated into routine clinical care to help direct
treatment options and accurately measure changes in ambulation throughout the
rehabilitation process.
History and Evolution of Measuring Ambulation
Gait is the way ambulation is achieved using human limbs, and gait analysis is the
systematic evaluation of a person’s walking pattern.28 The origins of the science of
gait analysis began in the seventeenth century in Europe, when scientists and
researchers provided a solid scientific foundation of our current knowledge and the
understanding of human ambulation.29 Research in the twentieth century benefited
from technological advancements, including the development of three-dimensional
(3D) force plates, and kinesiological electromyography (KEMG), which moved the
measurement precision of gait analysis significantly forward.29Asummary of the evolu-
tion of these early techniques into the systems used today is described in Table 2.29–31
Although the early principles of gait analysis are recognized as the foundation of
measuring ambulation, the methods used were too labor-intensive for practical appli-
cation in a clinical setting.29 Technology-driven systems for measuring ambulation
continue to evolve in the laboratory, with the goal of translating these outcome
measures into the clinical and community setting.
Techniques for Measuring Ambulation in a Research Laboratory
Gait analysis is a widely used measurement technique to assess, plan, and treat indi-
viduals with conditions affecting their ability to walk. Gait analysis emerges from the
combined interaction of the human eye (image capture) and the human brain (image
processing) used for recognition and identification of changes in ambulation.32 A
complete gait analysis can be achieved using visual observation to interpret human
locomotion. Therapists frequently use observational gait analysis to evaluate patient
ambulation, because instrumented measurement systems are not feasible during
time-limited clinical visits. Observational gait analysis typically reveals compensations
or impairments from underlying diseases but it is limited by the experience of the
observer. Instrumented gait analysis is a more technical method that involves collec-
tion of quantifiable information through the use of cameras, force plates, electromyog-
raphy (EMG), pressure sensors, and computer analysis to objectively measure an
individual’s walking pattern.32 Quantitative state-of-the-art methods of analysis and
equipment offer greater precision, specificity, and sensitivity to change. It is within
the laboratory environment that the comparison of observational versus instrumented
gait analysis must continue to be explored to advance clinical outcomes.
Healthy walking is the standard against which disease is measured. The key gait pa-
rameters that the clinician needs to compare against disease are described in Table 3.1
Measuring Ambulation in Central Neurologic Disorders 251

Table 2
Techniques for gait analysis: evolution and history
KEMG J.R. Close, 1959 Studied the phasic action of muscles using a 16-mmmovie camera with a sound track and was able torecord single-channel muscle action potentials oncine film
R.W. Vreeland andD.H. Sutherland, 1961
Used a 16-mm movie camera mounted on a turntableabove an oscilloscope with a 3-channel EMG
J.V. Basmajian, 1962 Developed the technique of inserting 2 very fineelectrodes (50-mm) through a single small needle(fine-wire EMG)
J.U. Baumann, 1974 Obtained an 8-channel Honeywell tape recorder with6 channels for KEMG transmitted through telemetry
S.R. Simon, 1977 Electromyography permitted simultaneous recordingfrom 12 channels transmitted through a cable fromsubject to computer
Current Various commercially available multichannel surfaceand fine-wire EMG systems, including telemeteredand wireless EMG capability and integrated softwarefor comprehensive outcome analysis. Capable ofmeasurements inside (clinical or laboratory) andoutside (community) in various environments
Kinematics M.P. Murray, 1964 Attached reflective targets to anatomic landmarks ofsubjects walking in illumination of strobe light
P.V. Karpovich andG.P. Karpovich, 1959
Electrogoniometry
R. Linder, 1965 Vanguard motion analyzer: developed methods tomeasure yaw, pitch, and roll using mathematicalformulae, 2 or more cameras and a two-dimensionalcoordinate system
E.H. Furnee, 1967–1989 Primas system: TV/motion analysis systems withautomated recording of reflective marker positions
Current Multiple commercially available real-time opticalmotion capture systems with: (1) infrared HD cameras;(2) markerless motion capture; (3) active light-emitting diode technology; (4) wired and wirelesssystems and integrated software for comprehensiveoutcome analysis. Capable of measurements inside(clinical or laboratory) and outside (community) invarious environments
Kinetics M. Carlet, 1872 Developed and used air reservoirs to measure forceapplied to the heel and forefoot
E.J. Marey, 1894 Developed first true force plate, which measuredvertical component of ground reaction usinga pneumatic mechanism
J. Amar, 1916 Produced the world’s first 3-component (pneumatic)force plate, Trottoire Dynamique
J. Hawthorn, 1971 Dynamic force plate (piezoelectric force transducers)Current Several multichannel force (6! of freedom) and pressure
measurements systems. Capable of measurement invarious environments indoors, outdoors. and underwater
Adapted from Sutherland, DH, 2001, 2002, 2005 Refs.29–31
Nolan et al252

Measuring Ambulation Using Temporal-Spatial Characteristics
Temporal
Temporal parameters are calculated using the timing characteristics within a gait
cycle, where each gait cycle is further divided into individual gait phases to make
comparisons across several cycles. The complete gait cycle includes initial double
support (the time between foot contact and contralateral toe off), single support
(the time between contralateral toe off and contralateral foot contact), terminal double
support (the time between contralateral foot contact and ipsilateral toe off), and swing
(the time between ipsilateral toe off and ipsilateral foot contact).33
Spatial
Spatial parameters are measured using the linear measurements (displacement of
markers) during a gait cycle. They include step length (the forward linear distance
between the heel markers from foot contact to subsequent contralateral foot contact),
stride length (the forward linear distance between the heel markers from foot contact
to ipsilateral foot contact), and step width (the linear medial-lateral distance between
heel markers from foot contact to contralateral foot contact).33
Symmetry
Symmetry measures are used to compare characteristics between the limbs.33
Temporal-spatial gait symmetry indices are calculated using mean swing (seconds)
and stance times (seconds) on both limbs to calculate the following variables: overall
temporal symmetry; temporal swing symmetry; temporal stance symmetry; temporal
swing stance symmetry; and spatial step symmetry (the ratio of step lengths on both
limbs in millimeters). A normative range for temporal-spatial symmetry is assumed to
be 0.9 to 1.1.33 This technique has been effectively used in stroke to assess the
Table 3
Outcomes for measuring ambulation in a laboratory environment
Spatial-temporalcharacteristics33
Spatial Step length, stride length, step width, velocity,cadence
Temporal IDS (initial double support time),SS (single support time), TDS (terminal doublesupport time), swing time
Symmetry Temporal-spatial symmetry ratios between limbs
Joint kinematics34–36 Rotations 3D joint angular rotationsAngular velocities Rate of change of 3D joint anglesCenter of mass Excursion of the 3D center of mass
Joint kinetics37 Forces 3D joint forces (effect of ground reaction forceson joint motions)
Torques 3D joint torques (a combination of jointrotations and forces)
EMG37 Muscle firing EMG analysis to assess muscle activation patterns(timing and amplitude) as it relates to jointkinematics
Co-contraction Simultaneous activation of agonist andantagonist muscles, if any
Pedobarography27,38,39 Plantar pressures Measuring the magnitude and timing ofpressure acting between the plantar surface ofthe foot and a supporting surface to quantifyloading, weight transfer, and area duringwalking
Measuring Ambulation in Central Neurologic Disorders 253

behavior of the paretic and nonparetic limbs during gait, where an overall temporal
symmetry value greater than 1 indicates a preference to rely on the nonparetic limb
during walking.33,40
Quantifying Ambulation with Kinematic and Kinetic Analysis
Kinematic
Kinematic data consist of temporal, linear, and angular variables. They quantify
the features of gait describing the movements of the body segments and joint
angles: temporal (timing), linear (displacement), and angular measurements. Temporal
data describe the stride duration and the limb coordination patterns. Distance data,
computed from the coordinates of the markers, describe the stride length, the
distances between limb placements, and the flight paths of the body parts. Angular
data describe the displacements, velocities, and accelerations of the body segments
and joints. Kinematic output from the motor control system is useful for measuring the
movement variance during walking and helps to classify gait diseases.36,41 Fig. 1
shows sagittal plane joint angles at the hip, knee, and ankle during healthy walking.42
Motion capture systems in a laboratory setting are routinely used to measure ambu-
lation by evaluating changes in gait kinematics. Reflective markers are placed on
selected anatomic landmarks and captured with the use of infrared cameras in a 3D
space. Data reduction and kinematic modeling can then be performed to calculate
linear and angular measurements. The data may then be displayed graphically for
presentation and report generation.1,43 Deviations or changes in kinematics can
help to identify and measure gait deficits, thereby initiating clinical interventions for
rehabilitation. In an individual with CND, gait analysis may show unilateral or bilateral
circumduction, abnormal pelvic movements, and a lack of ankle dorsiflexion during
Fig. 1. Sagittal plane gait kinematics, during healthy adults walking: (A) hip, (B) knee, and(C) ankle. Each plot represents the mean " standard deviation for 1 representative subjectover 10 consecutive trials. (Data from Ramanujam A, Forrest GF, Sisto SA. Methological vari-ability in evaluating gait dynamics: a comparative study. Gait and Clinical Movement Anal-ysis Society 13th Annual Meeting. Richmond, Virginia, April 2-5, 2008. p. 278–9.)
Nolan et al254

swing (foot drop). After physical therapy or assistive device intervention, further kine-
matic testing can precisely measure changes in ambulation to direct future treatment
strategies.44
Kinetic
Kinetic analysis measures forces, both external and internal to the body. Forces devel-
oped by muscles are transformed into rotations of the limb segments that produce
movement. The ground reaction forces (GRF) during locomotion can be recorded
using a force plate. Intrinsic joint forces and torques are then calculated from knowl-
edge of the GRFs using inverse dynamic calculations. When an individual steps on the
force plate, the force is detected by transducers or strain gauges and is converted to
an electrical signal that is amplified and recorded. Variables measured by the force
plate include the stance duration, the magnitude of the vertical, longitudinal (horizontal
craniocaudal), and transverse (horizontal mediolateral) forces, the time when the peak
forces occur, the impulses (area under the force time curves), and the point of appli-
cation of the force (center of pressure). Displacement of the center of pressure has
been evaluated for individuals with stroke and has been a robust measure to predict
gait velocity, a reliable indicator of both pathologic gait and general functional status in
rehabilitation.45–47
Normal forces plantar to the foot during walking can also be measured using pres-
sure sensor technology, such as insole sensors or pressure mats. Measuring changes
in loading during ambulation provides quantitative information that cannot be obtained
without instrumentation. This technology has been used to evaluate weight transfer,
an analytical method that quantifies linearity of loading and transfer of momentum
during gait. These outcome variables have been used to evaluate orthotic intervention
and are significant factors related to the improvement of ambulation.39
Use of EMG
EMG provides information on the state of activity of the motor neurons at rest, during
reflex contraction, and during voluntary contraction. During ambulation, muscular
contraction generates forces that stabilize and move the limbs. This process is
preceded by electrical activation, which can be detected and recorded as the EMG.
EMG signals are used in clinical and laboratory environments as a diagnostic tool to
identify neuromuscular diseases and disorders of motor control. When measuring
ambulation, the outcome variables obtained from EMG analysis provide quantifiable
information about the coordination of complex muscle movements and can show
mechanisms to compensate for muscle weakness.48 Recent research investigating
the use of a peroneal nerve stimulator in individuals with stroke found increased
muscle activation during gait. Use of EMG provided information about therapeutic
gains after intervention that extended beyond the ankle joint and the typically
measured increase in dorsiflexion angle.49
Measuring Energy Consumption in a Research Laboratory
Individuals with CND who experience difficulty with ambulation typically also have an
increased energy cost during walking. Decreased walking speed associated with CND
contributes to reduced gait efficiency by preventing efficient energy transfer.50
Previous research has suggested that faster walking speeds promote a more cost-
effective gait pattern.50,51 A straightforward method of evaluating the energy cost of
walking is the physiologic cost index (PCI). The PCI measures the effort involved in
walking as an increase in steady heart rate during movement (compared with a resting
state) divided by the velocity of that movement.52 Research has suggested a linear
Measuring Ambulation in Central Neurologic Disorders 255
relationship between heart rate during sustained walking and maximum oxygen
consumption.53 PCI can provide quantitative information of energy cost to anymobility
assessment by adding a device to measure heart rate and velocity.
Alternatively, VO2 peak can be used as an indirect measure of an individual’s peak
aerobic capacity. Aerobic capacity has been defined as the maximal amount of phys-
iologic work an individual can perform, measured by oxygen consumption.54
Measurements of walking economy can estimate the energy demands of an individual
and characterize physiologic capacity for exercise.55 In a laboratory environment,
measurement of VO2 and walking economy can be obtained using precise instrumen-
tation and a standard treadmill.56
MEASURING AMBULATION IN THE COMMUNITY
Reintegration into the community and maintenance of ADLs are the goal of rehabilita-
tion programs for persons with CND. In a free-living population, technology-driven
ambulation assessment measures often cannot be effectively used because of the
constraints of the home/community environment. Measurement of community ambu-
lation involves an individual’s interaction within their environment and therefore must
take into account the psychosocial aspects of that interaction as well as the physical
impairment.4,57 It is the patient’s home environment that sets the context for evalua-
tions of individual goals as they relate to quality of life. Complex measures that are
both qualitative and quantitative are required, making measurement of ambulation
in the community perhaps the most challenging environment in which to define mean-
ingful outcomes for measuring ambulation.58
Additional levels of complexity in measuring community ambulation are found in the
interaction with other impairments such as cognition that affect spatial recognition,
memory, and attention.59,60 In clinical and laboratory environments, there is diminished
attention paid to cognitive impairments, to focus on the effects of physical impairments
on ambulation. In the community, an individual must be able to ambulate in combina-
tion with cognitive tasks, therefore the cognitive and physical are interrelated when
measuring community ambulation.22,61,62 Although several clinical measures have
been developed to simulate community ambulation activities, such as those requiring
gait over uneven surfaces or dual task assessments requiring additional cognitive or
attentional involvement during gait, the ability to measure the interaction with other
impairments in real situations in the community are virtually nonexistent.
Previous research has concentrated on several areas related to measurement of
mobility impairment in the community such as measurement of impairment, activity,
participation, and quality of life.4 The following section highlights several of the impor-
tant techniques and findings related to measurement of ambulation in the community
for persons with CND.
Qualitative Measurements of Ambulation
Most often, qualitative measurements of community ambulation are obtained through
the use of self-report survey instruments that seek to categorize an individual’s ability
to ambulate in different situations. Measures of community ambulation and participa-
tion are often aimed at categorically identifying the ADLs that an individual is capable
of performing, as well as the level of assistance needed, in terms of use of assistive
devices and care from another person.
In the population with stroke, both Perry and colleagues46 and Lord and
colleagues61 have conducted studies in which participants rated their ability to
perform such tasks as getting to appointments or walking from their homes to the
Nolan et al256
mailbox. Based on their ability to accomplish such tasks independently, participants
were classified as noncommunity, limited community, or full community ambulators.
In a 2005 review, Lord and colleagues61 described many of the classification
schemes to assess community participation in stroke such as the Subjective Index
of Physical and Social Outcome,63 the Reintegration to Normal Living Index,64 the
Sickness Impact Profile,65 the Frenchay Activities Index,66 the Nottingham Extended
Activities of Daily Living Index,67 and the Stroke Impact Scale.68 The Unified
Parkinson’s Disability Rating Scale is the gold standard instrument used to measure
disease severity in Parkinson disease and includes questions about the ability to
successfully ambulate in various community environments.69 Although these scales
have been validated for the classification of community ambulation ability, few could
be considered measurement tools that can successfully assess the quantity or quality
of ambulation in the community. The Spinal Cord Injury-Functional Index measure-
ment system uses a 5-factor model, comprising basic mobility, ambulation, wheel-
chair mobility, self-care, and fine motor function, with the goal of comprehensively
assessing physical function for individuals with spinal cord injury.70
Although many of these classification systems are specific to 1 population, the
International Classification of Functioning (ICF) from the World Health Organization71
has been used across many populations with CND. The ICF has multiple compo-
nents that aim to assess the way an individual’s disability affects all aspects of
life. To assess the effect of limited community ambulation, as it relates to overall
quality of life, the ICF uses 3 domains: (1) body functions and structures (impair-
ment); (2) activity; and (3) participation.72 Using this framework, deficits in the ability
to ambulate in the community can be categorized as impairments of body functions
and structures (such as weakness or pain), environmental factors (including acces-
sibility of the home and available transportation), as well as personal factors
(including motivation and support). Included in this assessment are questions about
self-efficacy, which represents the individual’s perception of their own ability. Often
individuals avoid activities that they perceive are too difficult, and therefore it is
important to understand the perception of disability when evaluating the effect of
disability as a whole.71 The goal of the ICF is to provide a framework that considers
not only physical impairment but also social barriers to accurately classify commu-
nity ambulation.71,72
Other broadly used scales across multiple populations are the Ambulatory Self-
Confidence Questionnaire,73 aimed at specifically examining self-efficacy, which
has been used in patient populations with both Parkinson disease and multiple scle-
rosis. The Environmental Analysis of Mobility Questionnaire, developed in nonneuro-
logically impaired geriatric populations, has also been validated to study community
ambulation in persons with CND.62,74
Quantitative Measurements of Community Ambulation
Quantitative measurements of community ambulation provide more reliable
outcomes, compared with qualitative measures, when used in various populations
with CND. Many of the laboratory technologies described earlier cannot be used in
the community. Often, assessments of community ambulation must depend on
comparatively simple technologies that result in different outcomes/goals from those
of laboratory and clinical assessments. Unlike in the laboratory, where greater spec-
ificity and detail are paramount, community-based technologies must be able to
collect data for long periods and not impede ADLs.75 However, the need to under-
stand commonly used clinical and laboratory ambulation measures is essential to
effectively adapt quantitative measures to evaluate community outcomes.
Measuring Ambulation in Central Neurologic Disorders 257
Common technologies used for quantitative assessment of community ambulation
include pedometers, accelerometers, and GPS (Global Positioning System)-based
devices.58,75 The goal of these instruments is to provide long-term, remote, unobtru-
sive monitoring of ambulatory activity.76,77 It is also important to provide data on
a timescale that allows the observation of changes in activity patterns.78
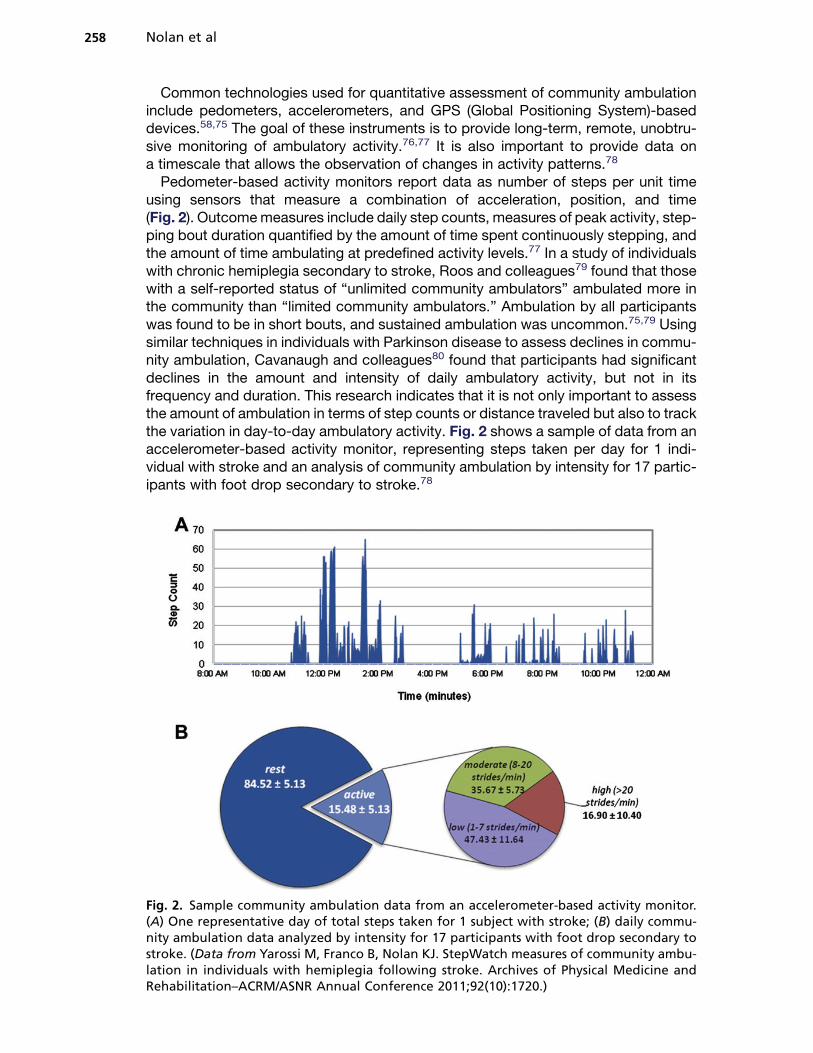
Pedometer-based activity monitors report data as number of steps per unit time
using sensors that measure a combination of acceleration, position, and time
(Fig. 2). Outcomemeasures include daily step counts, measures of peak activity, step-
ping bout duration quantified by the amount of time spent continuously stepping, and
the amount of time ambulating at predefined activity levels.77 In a study of individuals
with chronic hemiplegia secondary to stroke, Roos and colleagues79 found that those
with a self-reported status of “unlimited community ambulators” ambulated more in
the community than “limited community ambulators.” Ambulation by all participants
was found to be in short bouts, and sustained ambulation was uncommon.75,79 Using
similar techniques in individuals with Parkinson disease to assess declines in commu-
nity ambulation, Cavanaugh and colleagues80 found that participants had significant
declines in the amount and intensity of daily ambulatory activity, but not in its
frequency and duration. This research indicates that it is not only important to assess
the amount of ambulation in terms of step counts or distance traveled but also to track
the variation in day-to-day ambulatory activity. Fig. 2 shows a sample of data from an
accelerometer-based activity monitor, representing steps taken per day for 1 indi-
vidual with stroke and an analysis of community ambulation by intensity for 17 partic-
ipants with foot drop secondary to stroke.78
Fig. 2. Sample community ambulation data from an accelerometer-based activity monitor.(A) One representative day of total steps taken for 1 subject with stroke; (B) daily commu-nity ambulation data analyzed by intensity for 17 participants with foot drop secondary tostroke. (Data from Yarossi M, Franco B, Nolan KJ. StepWatch measures of community ambu-lation in individuals with hemiplegia following stroke. Archives of Physical Medicine andRehabilitation–ACRM/ASNR Annual Conference 2011;92(10):1720.)
Nolan et al258

Reports of agreement between self-report and objective measures of community
ambulation are mixed.61,81 Average daily steps were measured for individuals with
chronic incomplete spinal cord injury (n 5 50), and a significant difference was found
between self-reported community and noncommunity walkers.81 In contrast, a study
by Lord and colleagues61 concluded that persons with stroke showed greater activity
on self-report measures than what was measured objectively. Self-report measures
inherently depend on an individual’s perception of their own health and impairment
and are often useful only in the context of the individual and are difficult to evaluate
at the group level.
Understanding the strength of the relationship between commonly used clinical and
laboratory measures and ambulatory activity in the community is essential for the use
of clinical measurement to predict community outcomes. Research in chronic stroke
reported on correlation and predictive ability of several clinical measures of ambula-
tion including the Rivermead Mobility Index, Rivermead Motor Assessment, 6-minute
walk test (6MWT), 10-m walk test (10MWT), and data collected from step activity
monitors (SAM) worn in the community by participants with chronic stroke.77 Only
the 6MWT and the 10MWT were found to correlate with SAM data, and only the
6MWT was a significant predictor of step counts. In recent research in individuals
with stroke, step activity was analyzed by intensity (see Fig. 2), and no significant
relationships were found between clinical measurements of gait speed and endurance
(timed 7.62-m [25-ft] walk and 6MWT), the number of steps taken per day, or the
amount of the day spent active.78,82 Clinical measures were correlated to measures
of peak activity only during community ambulation, which indicated that individuals
with hemiplegia who were able to sustain activity greater than 20 steps per minute
walked more in the community.78 Future work to better understand and measure
community ambulation will have a valuable impact when evaluating individuals for
treatment, which will provide more independence in performing ADLs.
SUMMARY
The goal of most rehabilitation programs is successful reintegration into the commu-
nity. The ability to accurately measure ambulation, one of the most important metrics
used to show transition into a community environment, is essential to measure treat-
ment effectiveness and rehabilitation outcomes in populations with CND.
Measurements of ambulation in populations with CND should: (1) be predictive of
disease state or progression; (2) be useful for evaluating recovery or intervention; (3) be
diagnostic; (4) indicate the need for assistance in the community; (5) be able to provide
information related to quality of life; and (6) use state-of-the-art technology. In addition,
measurements of ambulation should be carefully examined for administration within
a particular environment (clinical, laboratory, or community). Even the most robust
measure of ambulation is affected by the environment in which it is implemented. Type
of measurement or environment selected depends on the clinical or research question
and the specificity of the hypothesis investigated.
REFERENCES
1. Perry J, Burnfield JM. Gait analysis: normal and pathological function. 2nd
edition. Thorofare (NJ): Slack; 2010.
2. Coleman KL, Smith DG, Boone DA, et al. Step activity monitor: long-term, contin-
uous recording of ambulatory function. J Rehabil Res Dev 1999;36(1):8–18.
3. Finch E, Brooks D, Stratford PW, et al. Physical rehabilitation outcome measures.
2nd edition. Ontario (Canada): Lippincott Williams & Wilkins; 2002.
Measuring Ambulation in Central Neurologic Disorders 259
4. Lord SE, Rochester L. Measurement of community ambulation after stroke:
current status and future developments. Stroke 2005;36(7):1457–61.
5. Jackson AB, Carnel CT, Ditunno JF, et al. Outcome measures for gait and
ambulation in the spinal cord injury population. J Spinal Cord Med 2008;31(5):
487–99.
6. Keith RA, Granger CV, Hamilton BB, et al. The functional independence measure:
a new tool for rehabilitation. Adv Clin Rehabil 1987;1:6–18.
7. Fugl-Meyer AR, Jaasko L, Leyman I, et al. The post-stroke hemiplegic patient. 1.
A method for evaluation of physical performance. Scand J Rehabil Med 1975;
7(1):13–31.
8. Hauser SL, Dawson DM, Lehrich JR, et al. Intensive immunosuppression in
progressive multiple sclerosis. A randomized, three-arm study of high-dose intra-
venous cyclophosphamide, plasma exchange, and ACTH. N Engl J Med 1983;
308(4):173–80.
9. Wolf SL, Catlin PA, Gage K, et al. Establishing the reliability and validity of
measurements of walking time using the Emory Functional Ambulation Profile.
Phys Ther 1999;79(12):1122–33.
10. Baer HR, Wolf SL. Modified Emory Functional Ambulation Profile: an outcome
measure for the rehabilitation of poststroke gait dysfunction. Stroke 2001;32(4):
973–9.
11. Shumway-Cook A, Woollacott M. Motor control: theory and applications.
Baltimore (MD): Wilkins & Wilkins; 1995.
12. Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional
mobility for frail elderly persons. J Am Geriatr Soc 1991;39(2):142–8.
13. Cohen ME, Marino RJ. The tools of disability outcomes research functional status
measures. Arch Phys Med Rehabil 2000;81(12 Suppl 2):S21–9.
14. Nolan KJ, Savalia KK, Lequerica AH, et al. Objective assessment of functional
ambulation in adults with hemiplegia using ankle foot orthotics after stroke.
PM R 2009;1(6):524–9.
15. Liaw LJ, Hsieh CL, Lo SK, et al. Psychometric properties of the modified Emory
Functional Ambulation Profile in stroke patients. Clin Rehabil 2006;20(5):429–37.
16. Cohen JJ, Sveen JD, Walker JM, et al. Establishing a criteria for community
ambulation. Top Geriatr Rehabil 1987;3(1):71–7.
17. Lerner-Frankiel MB, Vargas S, Brown M, et al. Functional community ambulation:
what are your criteria? Clinical Management 1986;6(2):12–5.
18. Fulk GD, Echternach JL, Nof L, et al. Clinometric properties of the six-minute walk
test in individuals undergoing rehabilitation poststroke. Physiother Theory Pract
2008;24(3):195–204.
19. Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in
community-dwelling older adults using the Timed Up & Go Test. Phys Ther
2000;80(9):896–903.
20. Jonsdottir J, Cattaneo D. Reliability and validity of the dynamic gait index in
persons with chronic stroke. Arch Phys Med Rehabil 2007;88(11):1410–5.
21. McConvey J, Bennett SE. Reliability of the Dynamic Gait Index in individuals with
multiple sclerosis. Arch Phys Med Rehabil 2005;86(1):130–3.
22. Smulders K, van Swigchem R, de Swart BJ, et al. Community-dwelling people
with chronic stroke need disproportionate attention while walking and negotiating
obstacles. Gait Posture 2012;36(1):127–32.
23. Fulk GD, Echternach JL. Test-retest reliability and minimal detectable change of
gait speed in individuals undergoing rehabilitation after stroke. J Neurol Phys
Ther 2008;32(1):8–13.
Nolan et al260
24. Tilson JK, Sullivan KJ, Cen SY, et al. Meaningful gait speed improvement during
the first 60 days poststroke: minimal clinically important difference. Phys Ther
2010;90(2):196–208.
25. Goldie PA, Matyas TA, Evans OM, et al. Maximum voluntary weight-bearing by
the affected and unaffected legs in standing following stroke. Clin Biomech
(Bristol, Avon) 1996;11(6):333–42.
26. Schmid A, Duncan PW, Studenski S, et al. Improvements in speed-based gait
classifications are meaningful. Stroke 2007;38(7):2096–100.
27. Nolan KJ, Yarossi M. Preservation of the first rocker is related to increases in gait
speed in individuals with hemiplegia and AFO. Clin Biomech 2011;26(6):655–60.
28. Chambers HG, Sutherland DH. A practical guide to gait analysis. J Am Acad
Orthop Surg 2002;10(3):222–31.
29. Sutherland DH. The evolution of clinical gait analysis. Part I: kinesiological EMG.
Gait Posture 2001;14(1):61–70.
30. Sutherland DH. The evolution of clinical gait analysis. Part II: kinematics. Gait
Posture 2002;16(2):159–79.
31. Sutherland DH. The evolution of clinical gait analysis. Part III: kinetics and energy
assessment. Gait Posture 2005;21(4):447–61.
32. Whittle MW. Gait analysis an introduction. 4th edition. New York: Butterworth
Heinemann; 2007.
33. Patterson KK, Parafianowicz I, Danells CJ, et al. Gait asymmetry in community-
ambulating stroke survivors. Arch Phys Med Rehabil 2008;89(2):304–10.
34. Wu G, Siegler S, Allard P, et al. ISB recommendation on definitions of joint coor-
dinate system of various joints for the reporting of human joint motion–part I:
ankle, hip, and spine. International Society of Biomechanics. J Biomech 2002;
35(4):543–8.
35. Wu G, van der Helm FC, Veeger HE, et al. ISB recommendation on definitions of
joint coordinate systems of various joints for the reporting of human joint motion–
part II: shoulder, elbow, wrist and hand. J Biomech 2005;38(5):981–92.
36. Lee HJ, Chou LS. Detection of gait instability using the center of mass and center
of pressure inclination angles. Arch Phys Med Rehabil 2006;87(4):569–75.
37. Winter DA. Biomechanics and motor control of human movement. 4th edition.
Hoboken (NJ): John Wiley; 2009.
38. Soames RW. Foot pressure patterns during gait. J Biomed Eng 1985;7(2):120–6.
39. Nolan KJ, Yarossi M. Weight transfer analysis in adults with hemiplegia using
ankle foot orthosis. Prosthet Orthot Int 2011;35(1):45–53.
40. Esquenazi A, Ofluoglu D, Hirai B, et al. The effect of an ankle-foot orthosis on
temporal spatial parameters and asymmetry of gait in hemiparetic patients.
PM R 2009;1(11):1014–8.
41. Burnfield JM, Powers CM. The role of center of mass kinematics in predicting peak
utilized coefficient of friction during walking. J Forensic Sci 2007;52(6):1328–33.
42. Ramanujam A, Forrest GF, Sisto SA. Methodological variability in evaluating gait
dynamics: a comparative study. Gait and Clinical Movement Analysis Society
13th Annual Meeting. Richmond, Virginia, April 2-5, 2008. p. 278–9.
43. Bensoussan L, Viton JM, Barotsis N, et al. Evaluation of patients with gait abnor-
malities in physical and rehabilitation medicine settings. J Rehabil Med 2008;
40(7):497–507.
44. Nolan KJ, Savalia KK, Yarossi M, et al. Evaluation of a dynamic ankle foot orthosis
in hemiplegic gait: a case report. NeuroRehabilitation 2010;27(4):343–50.
45. Mizelle C, Rodgers M, Forrester L. Bilateral foot center of pressure measures
predict hemiparetic gait velocity. Gait Posture 2006;24(3):356–63.
Measuring Ambulation in Central Neurologic Disorders 261

46. Perry J, Garrett M, Gronley JK, et al. Classification of walking handicap in the
stroke population. Stroke 1995;26(6):982–9.
47. Nolan KJ, Yarossi M. Changes in COP displacement with the use of a foot drop
stimulator in individuals with stroke 13th Emed Scientific Meeting (ESM). Aalborg,
Denmark, August 1–4, 2012.
48. Brunner R, Romkes J. Abnormal EMG muscle activity during gait in patients
without neurological disorders. Gait Posture 2008;27(3):399–407.
49. Yarossi M, Ramanujam A, Pilkar R, et al. Therapeutic gains after utilization of
a foot drop stimulator in stroke extend beyond the ankle joint: a case report.
Archives of Physical Medicine and Rehabilitation– ACRM/ASNR Annual Confer-
ence 2012;93(10):e19.
50. Lamontagne A, Stephenson JL, Fung J. Physiological evaluation of gait distur-
bances post stroke. Clin Neurophysiol 2007;118(4):717–29.
51. Hesse S, Werner C, Paul T, et al. Influence of walking speed on lower limb muscle
activity and energy consumption during treadmill walking of hemiparetic patients.
Arch Phys Med Rehabil 2001;82(11):1547–50.
52. MacGregor J. The evaluation of patient performance using long-term ambulatory
monitoring technique in thedomiciliaryenvironment.Physiotherapy1981;67(2):30–3.
53. Wieler M, Stein RB, Ladouceur M, et al. Multicenter evaluation of electrical stim-
ulation systems for walking. Arch Phys Med Rehabil 1999;80(5):495–500.
54. Resnick B, Michael K, Shaughnessy M, et al. Inflated perceptions of physical
activity after stroke: pairing self-report with physiologic measures. J Phys Act
Health 2008;5(2):308–18.
55. Macko RF, Smith GV, Dobrovolny CL, et al. Treadmill training improves fitness
reserve in chronic stroke patients. Arch Phys Med Rehabil 2001;82(7):879–84.
56. Michael K, Macko RF. Ambulatory activity intensity profiles, fitness, and fatigue in
chronic stroke. Top Stroke Rehabil 2007;14(2):5–12.
57. Donovan K, Lord SE, McNaughton HK, et al. Mobility beyond the clinic: the effect
of environment on gait and its measurement in community-ambulant stroke
survivors. Clin Rehabil 2008;22(6):556–63.
58. Gebruers N, Vanroy C, Truijen S, et al. Monitoring of physical activity after stroke:
a systematic review of accelerometry-based measures. Arch Phys Med Rehabil
2010;91(2):288–97.
59. Lord SE, Rochester L, Weatherall M, et al. The effect of environment and task on
gait parameters after stroke: a randomized comparison of measurement condi-
tions. Arch Phys Med Rehabil 2006;87(7):967–73.
60. Brauer SG, Morris ME. Can people with Parkinson’s disease improve dual tasking
when walking? Gait Posture 2010;31(2):229–33.
61. Lord SE, McPherson K, McNaughton HK, et al. Community ambulation after
stroke: how important and obtainable is it and what measures appear predictive?
Arch Phys Med Rehabil 2004;85(2):234–9.
62. Blennerhassett JM, Dite W, Ramage ER, et al. Changes in balance and walking
from stroke rehabilitation to the community: a follow-up observational study.
Arch Phys Med Rehabil 2012;93(10):1782–7.
63. Trigg R, Wood VA. The Subjective Index of Physical and Social Outcome (SIPSO):
a new measure for use with stroke patients. Clin Rehabil 2000;14(3):288–99.
64. Wood-Dauphinee SL, Opzoomer MA, Williams JI, et al. Assessment of global
function: the Reintegration to Normal Living Index. Arch Phys Med Rehabil
1988;69(8):583–90.
65. BergnerM, Bobbitt RA, CarterWB, et al. The Sickness Impact Profile: development
and final revision of a health status measure. Med Care 1981;19(8):787–805.
Nolan et al262

66. Holbrook M, Skilbeck CE. An activities index for use with stroke patients. Age
Ageing 1983;12(2):166–70.
67. Nouri FM, Lincoln NB. An extended activities of daily living scale for stroke
patients. Clin Rehabil 1987;1(4):301–5.
68. Duncan PW, Wallace D, Lai SM, et al. The stroke impact scale version 2.0. Eval-
uation of reliability, validity, and sensitivity to change. Stroke 1999;30(10):
2131–40.
69. Movement Disorder Society Task Force on Rating Scales for Parkinson’s Disease.
The Unified Parkinson’s Disease Rating Scale (UPDRS): status and recommenda-
tions. Mov Disord 2003;18(7):738–50.
70. Tulsky DS, Jette AM, Kisala PA, et al. Spinal cord injury-functional index: item
banks to measure physical functioning in individuals with spinal cord injury.
Arch Phys Med Rehabil 2012;93(10):1722–32.
71. Stucki G, Ewert T, Cieza A. Value and application of the ICF in rehabilitation
medicine. Disabil Rehabil 2003;25(11–12):628–34.
72. Jette AM. Toward a common language for function, disability, and health. Phys
Ther 2006;86(5):726–34.
73. Asano M, Miller WC, Eng JJ. Development and psychometric properties of the
ambulatory self-confidence questionnaire. Gerontology 2007;53(6):373–81.
74. Shumway-Cook A, Patla A, Stewart AL, et al. Assessing environmentally deter-
mined mobility disability: self-report versus observed community mobility. J Am
Geriatr Soc 2005;53(4):700–4.
75. Orendurff MS, Schoen JA, Bernatz GC, et al. How humans walk: bout duration,
steps per bout, and rest duration. J Rehabil Res Dev 2008;45(7):1077–89.
76. Halstead LS. Longitudinal unobtrusive measurements in rehabilitation. Arch Phys
Med Rehabil 1976;57(4):189–93.
77. Mudge S, Stott NS. Timed walking tests correlate with daily step activity in
persons with stroke. Arch Phys Med Rehabil 2009;90(2):296–301.
78. Yarossi M, Franco B, Nolan KJ. StepWatch measures of community ambulation in
individuals with hemiplegia following stroke. Archives of Physical Medicine and
Rehabilitation–ACRM/ASNR Annual Conference 2011;92(10):1720.
79. Roos MA, Rudolph KS, Reisman DS. The structure of walking activity in people
after stroke compared with older adults without disability: a cross-sectional study.
Phys Ther 2012;92(9):1141–7.
80. Cavanaugh JT, Ellis TD, Earhart GM, et al. Capturing ambulatory activity decline
in Parkinson’s disease. J Neurol Phys Ther 2012;36(2):51–7.
81. Saraf P, Rafferty MR, Moore JL, et al. Daily stepping in individuals with motor
incomplete spinal cord injury. Phys Ther 2010;90(2):224–35.
82. van de Port IG, Kwakkel G, Lindeman E. Community ambulation in patients with
chronic stroke: how is it related to gait speed? J Rehabil Med 2008;40(1):23–7.
Measuring Ambulation in Central Neurologic Disorders 263