
Neurologic Variant Laryngomalacia Associated with Chiari Malformation and Cervicomedullary...
6
Anmllxn/Ololiigy. Rhinology à t^iryngology I2()(2):'W-1O3. C> 2011 Annals Pubtishing Company. All rights reserved. Neurologic Variant Laryngomalacia Associated With Chiari Malformation and Cervicomedullary Compression: Case Reports Rajanya S. Petersson, MD; Nicholas M. Wetjen, MD; Dana M. Thompson, MD, MS Two infants presented with intermittent stridor and evidence of laryngomalacia on flexible Iaryngoscopy. The first was a 10month-old girl who had undergone 3 supraglottopla.sty surgeries at an outside institution, without long-term resolution 1)1 symptoms. She was found during our evaluation to have a Chiari malformation. Laryngomalacia symptoms resolved after suboccipital decompression and CI laminectomy, and the patient remained .symptom-free at 6-m()nth follow-up. The second infant was a 24-day-()ld boy with velocardiofacial syndrome who was found to have posterior cervicomcdul- huy junction compression at the level of CI. He underwent CI laminectomy for decompression of the brain stem, which resulted in immediate resolution of symptoms, and he remained symptom-free at 12-month follow-up. Neurologic ab- normalities have been reported in up to 50% of infants with laryngomalacia. As such, brain stem dysfunction should be considered among the causes of laryngomalacia during evaluation, especially in patients with failure of supraglottoplasty. Both of these infants had resolution of symptoms after their neurosurgical procedures. I Key Words: brain stem compression, Chiari malformation, laryngomalacia, stridor. INTRODUCTION Laryngomalacia is a condition of weak laryngeal tone resulting in dynamic prolapse of supraglottic tissue into the airway. This causes inspiratory stridor and airway obstruction. The diagnosis is suspected in the presence of symptoms of inspiratory stridor that worsens with agitation, supine positioning, feeding, and crying, and is confirmed by flexible Iaryngoscopy. Laryngoscopic findings may include prolapse into the airway of supra-arytenoid muco- sa or the arytenoid cartilages themselves, foreshort- ened aryepiglottic folds, and/or an omega-shaped or retroflexed epiglottis. In up to 20% of infants with laryngomalacia, there have been associated neuro- logic abnormalities.' ; Laryngeal stridor has been reported in associa- tion with Chiari II malformations (caudal displace- ment of the brain stem into the cervical spinal canal associated with myelomeningocele), with the stri- dor most often caused by vocal fold paralysis.2'^ In some of these cases, the actual laryngeal abnormal- ity was not discovered.-^'* We present 2 cases of in- fants with neurologic variant laryngomalacia. One infant was found to have an underlying Chiari I mal- formation, and the other was found to have cervi- comedullary compression by a Cl posterior arch. In both patients, laryngomalacia and associated symp- toms resolved after decompressive surgery. CASE REPORTS Case I. A 10-month-old girl with intermittent inspiratory stridor, episodes of cyanosis, and aspi- ration throughout infancy presented to our clinic. The stridor worsened with supine positioning. She had undergone supraglottoplasty 3 times at an out- side institution, with only temporary improvement in symptoms. After the first supraglottoplasty, the episodes of cyanosis resolved. She had temporary relief of other symptoms, but shortly after surgery she experienced worsening stridor and aspiration. This prompted a second supraglottoplasty 5 months later, from which she had relief of symptoms for only 2 days. Overall, the stridor was improved after her first surgery, but was still present during sleep and with agitation. A third supraglottoplasty was performed 1 month later, again with only 2 days of symptom relief. The patient presented to us 7 days after her last surgery. At presentation, she had inspiratory stridor dur- ing sleep without desaturations. The stridor was high-pitched during sleep, and the patient's breath- ing sounded raspy during the daytime while she was active. She was not experiencing cyanosis or retrac- tions. She was still aspirating thin liquids, and was From the Departments of Otorhinolaryngology (Petersson. Thompson) and Neurologic Surgery (Wetjen), Mayo Clinic, and the Divi- sion of Pédiatrie Otorhinolaryngology. Mayo Clinic and Mayo Eugenio Litta Children's Ho.spital (Thompson). Rochester, Minnesota. Presented at the meeting of the American Broncho-Esophagological Association. Las Vegas, Nevada. April 28-29. 2010. Correspondence: Dana M. Thompson, MD, Division of Pédiatrie Otorhinolaryngology, Mayo Clinic. 200 First St SW, Rochester, MN, 55905. 99
-
Upload
mayoclinic -
Category
Documents
-
view
0 -
download
0
Transcript of Neurologic Variant Laryngomalacia Associated with Chiari Malformation and Cervicomedullary...

Anmllxn/Ololiigy. Rhinology à t^iryngology I2()(2):'W-1O3.C> 2011 Annals Pubtishing Company. All rights reserved.
Neurologic Variant Laryngomalacia Associated With ChiariMalformation and Cervicomedullary Compression: Case Reports
Rajanya S. Petersson, MD; Nicholas M. Wetjen, MD; Dana M. Thompson, MD, MS
Two infants presented with intermittent stridor and evidence of laryngomalacia on flexible Iaryngoscopy. The first was a10month-old girl who had undergone 3 supraglottopla.sty surgeries at an outside institution, without long-term resolution1)1 symptoms. She was found during our evaluation to have a Chiari malformation. Laryngomalacia symptoms resolvedafter suboccipital decompression and CI laminectomy, and the patient remained .symptom-free at 6-m()nth follow-up.The second infant was a 24-day-()ld boy with velocardiofacial syndrome who was found to have posterior cervicomcdul-huy junction compression at the level of CI. He underwent CI laminectomy for decompression of the brain stem, whichresulted in immediate resolution of symptoms, and he remained symptom-free at 12-month follow-up. Neurologic ab-normalities have been reported in up to 50% of infants with laryngomalacia. As such, brain stem dysfunction should beconsidered among the causes of laryngomalacia during evaluation, especially in patients with failure of supraglottoplasty.Both of these infants had resolution of symptoms after their neurosurgical procedures.
I
Key Words: brain stem compression, Chiari malformation, laryngomalacia, stridor.
INTRODUCTION
Laryngomalacia is a condition of weak laryngealtone resulting in dynamic prolapse of supraglottictissue into the airway. This causes inspiratory stridorand airway obstruction. The diagnosis is suspectedin the presence of symptoms of inspiratory stridorthat worsens with agitation, supine positioning,feeding, and crying, and is confirmed by flexibleIaryngoscopy. Laryngoscopic findings may includeprolapse into the airway of supra-arytenoid muco-sa or the arytenoid cartilages themselves, foreshort-ened aryepiglottic folds, and/or an omega-shaped orretroflexed epiglottis. In up to 20% of infants withlaryngomalacia, there have been associated neuro-logic abnormalities.' ;
Laryngeal stridor has been reported in associa-tion with Chiari II malformations (caudal displace-ment of the brain stem into the cervical spinal canalassociated with myelomeningocele), with the stri-dor most often caused by vocal fold paralysis.2'^ Insome of these cases, the actual laryngeal abnormal-ity was not discovered.- '̂* We present 2 cases of in-fants with neurologic variant laryngomalacia. Oneinfant was found to have an underlying Chiari I mal-formation, and the other was found to have cervi-comedullary compression by a Cl posterior arch. Inboth patients, laryngomalacia and associated symp-
toms resolved after decompressive surgery.
CASE REPORTS
Case I. A 10-month-old girl with intermittentinspiratory stridor, episodes of cyanosis, and aspi-ration throughout infancy presented to our clinic.The stridor worsened with supine positioning. Shehad undergone supraglottoplasty 3 times at an out-side institution, with only temporary improvementin symptoms. After the first supraglottoplasty, theepisodes of cyanosis resolved. She had temporaryrelief of other symptoms, but shortly after surgeryshe experienced worsening stridor and aspiration.This prompted a second supraglottoplasty 5 monthslater, from which she had relief of symptoms foronly 2 days. Overall, the stridor was improved afterher first surgery, but was still present during sleepand with agitation. A third supraglottoplasty wasperformed 1 month later, again with only 2 days ofsymptom relief. The patient presented to us 7 daysafter her last surgery.
At presentation, she had inspiratory stridor dur-ing sleep without desaturations. The stridor washigh-pitched during sleep, and the patient's breath-ing sounded raspy during the daytime while she wasactive. She was not experiencing cyanosis or retrac-tions. She was still aspirating thin liquids, and was
From the Departments of Otorhinolaryngology (Petersson. Thompson) and Neurologic Surgery (Wetjen), Mayo Clinic, and the Divi-sion of Pédiatrie Otorhinolaryngology. Mayo Clinic and Mayo Eugenio Litta Children's Ho.spital (Thompson). Rochester, Minnesota.Presented at the meeting of the American Broncho-Esophagological Association. Las Vegas, Nevada. April 28-29. 2010.Correspondence: Dana M. Thompson, MD, Division of Pédiatrie Otorhinolaryngology, Mayo Clinic. 200 First St SW, Rochester,MN, 55905.
99

100 Petersson et al. Neurologie Variant Laryngomalacia
Fig 1. (Case I) Magnetic resonance imaging. A) Preoperative scan shows Chiari I malfornuition with descent ofcerebellar tonsils below foramen magnum. B) Scan performed 6 months after neurosurgical decompression showsresoiution.
on a thickened formula diet. She was on twice-dai-ly proton pump inhibitor and nighttime histamine 2receptor antagonist therapy. Flexible laryngoscopyrevealed a slightly omega-shaped epiglottis with-out significant supra-arytenoid tissue prolapse; thelowest oxygen saturation was 90% during the ex-amination. Significant cobblestoning of the poste-rior pharyngeal wall was noted. A functional endo-scopie evaluation of swallowing study revealed la-ryngeal penetration of thickened formula with resul-tant cough, and occasional bolus passage withoutpenetration or aspiration; there was direct laryngealpenetration and aspiration with thin liquid.
As it is unusual for an infant to continue to havesymptoms of laryngomalacia after a third supra-glottoplasty, a thorough evaluation was planned.Computed tomography (CT) scans of the neck andchest showed no anatomic anomalies and no signsof chronic aspiration. Magnetic resonance imaging(MRI) of the head was scheduled to look for anyintracranial or skull base disorders as contributingfactors and did, in fact, reveal a Chiari I malforma-tion, with descent of the cerebellar tonsils below thelevel of the foramen magnum with significant com-pression within the foramen magnum (Fig 1 A). Thepatient was referred to the pédiatrie neurosurgerydepartment at this time, and further plans for a pHstudy and overnight polysomnography were put onhold.
She was taken to the operating room in conjunc-tion with our pédiatrie neurosurgery colleagues formicrolaryngoscopy and rigid bronchoscopy and for
suboccipital decompression and Cl laminectomy.Her airway examination revealed an omega-shapedepiglottis with the lateral surfaces folding into theairway and producing stridor and foreshortenedaryepiglottic folds, but no arytenoid prolapse. Rigidbronchoscopy revealed mucosal edematous chang-es but a widely patent airway. On postoperative day(POD) 1, the patient still had her baseline level ofinspiratory stridor, with some improvement on POD2, when she was discharged from the hospital. Byher 1-week follow-up appointment, her stridor hadresolved. She was still taking thickened formula, butwithout any symptoms of aspiration. Six months af-ter her decompressive surgery, she was completelyasymptomatic; she had no stridor or signs of aspi-ration with thin liquids, was tolerating table foods,was in the 95th percentile for weight, and was nolonger requiring proton pump inhibitors or hista-mine 2 receptor antagonists. Her postoperative MRIno longer showed descent of her cerebellar tonsils(Fig IB).
Case 2. A 24-day-old boy with velocardiofacialsyndrome presented with intermittent biphasic stri-dor, nasopharyngeal régurgitation, spitting up, andbrief cyanotic episodes that occurred with feeding.Flexible laryngoscopy confirmed laryngomalaciawith supra-arytenoid tissue prolapse into the glot-tal inlet, foreshortened aryepiglottic folds, and aslightly omega-shaped epiglottis (Fig 2A); he expe-rienced desaturations into the mid-80% range dur-ing the examination. As such, overnight oximetrywas performed and revealed a mean oxygen satura-tion of 95% with a high of 100% but a low of 72%;
Petersson et al. Neurologie Variant Larvngomalacia 101
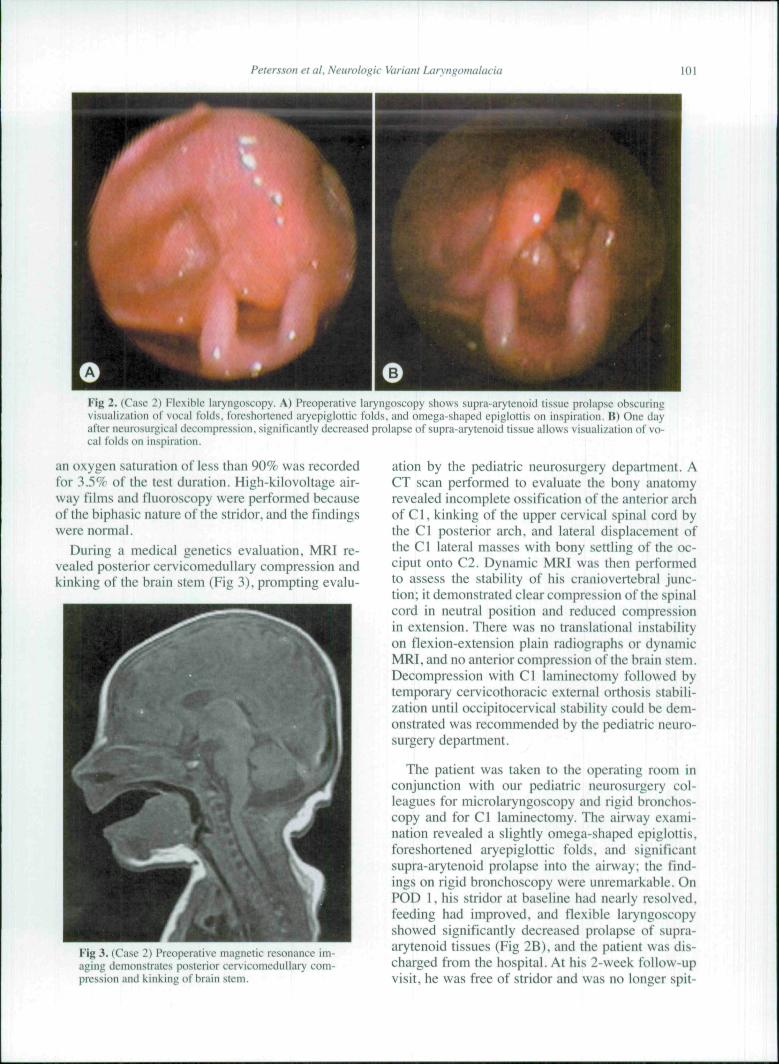
Fig 2. (Case 2) Flexible laryngoscopy. A) Preopcraiive laryngoscopy shows supra-arytenoid tissue prolapse t)bscuringvisualization of vocal folds, foreshortened aryepiglottic folds, and omega-shaped epiglottis on inspiration. B) One dayafter neurosurgical decompression, significantly decreased prolapse of supra-arytenoid tissue allows visualization of vo-cal folds on inspiration.
an oxygen saturation of less than 90% was recordedfor 3.5% of the test duration. High-kilovoltage air-way films and fluoroscopy were performed becauseof the biphasic nature of the stridor, and the findingswere normal.
During a medical genetics evaluation, MRI re-vealed posterior cervicomedullary compression andkinking of the brain stem (Fig 3), prompting evalu-
3. (Case 2) Preoperative magnetic resonance im-aging demonstrates posterior cervicomedullary com-pression and kinking of brain stem.
ation by the pédiatrie neurosurgery department. ACT scan performed to evaluate the bony anatomyrevealed incomplete ossification of the anterior archof C1, kinking of the upper cervical spinal cord bythe Cl posterior arch, and lateral displacement ofthe Cl lateral masses with bony settling of the oc-ciput onto C2. Dynamic MRI was then performedto assess the stability of his craniovertebral junc-tion; it demonstrated clear compression of the spinalcord in neutral position and reduced compressionin extension. There was no translational instabilityon flexion-extension plain radiographs or dynamicMRI. and no anterior compression of the brain stem.Decompression with Cl laminectomy followed bytemporary cervicothoracic external orthosis stabili-zation until occipitocervical stability could be dem-onstrated was recommended by the pédiatrie neuro-surgery department.
The patient was taken to the operating room inconjunction with our pédiatrie neurosurgery col-leagues for microlaryngoscopy and rigid bronchos-copy and for Cl laminectomy. The airway exami-nation revealed a slightly omega-shaped epiglottis,foreshortened aryepiglottic folds, and significantsupra-arytenoid prolapse into the airway; the find-ings on rigid bronchoscopy were unremarkable. OnPOD 1, his stridor at baseline had nearly resolved,feeding had improved, and flexible laryngoscopyshowed significantly decreased prolapse of supra-arytenoid tissues (Fig 2B), and the patient was dis-charged from the hospital. At his 2-vveek follow-upvisit, he was free of stridor and was no longer spit-

102 Petersson et al. Neurologie Variant Laryngomalacia
ting up with feeding. Flexible laryngoscopy revealeda normally shaped and placed epiglottis and onlymild supra-arytenoid prolapse; there was no audiblestridor, even with agitation. Supraglottoplasty wasnever required. The child remained symptom-freeat the 18-month follow-up, and cervical flexion-ex-tension radiographs demonstrated no occipital C1 -2instability.
DISCUSSION
Laryngeal stridor due to vocal fold paralysis as-sociated with Chiari II malformations (also knownas Amold-Chiari malformations) has been com-monly reported.2'^ There have been few reportedcases of laryngomalacia associated with Chiari mal-formations, and no reported cases of laryngomala-cia caused by Cl posterior arch compression of thecervicomedullary junction. Portier et al^ describeda case of an infant with a Chiari I malformation(elongation of cerebellar tonsils through the fora-men magnum) and laryngomalacia causing respira-tory obstruction that resolved 10 days after posteriorfossa decompression. Their study found that majorabnormal laryngeal dynamics, most often vocal foldparalysis, were found in 11% of infants with ChiariII malformations and less than 1% of those withChiari I malformations. Neither of our patients hadvocal fold paralysis in addition to laryngomalacia.
Neurologic disease of any type is a well-knowncomorbidity associated with laryngomalacia, withreported rates of 8% to 50%, and is known to con-tribute to supraglottoplasty failure.'-'0-17 Supraglot-toplasty in general carries a high success rate, andhas been reported to approach 94%, even when re-vision is required.'-'^ Thus, the fact that our firstpatient failed to have complete resolution of symp-toms after 3 supraglottoplasty procedures led us tobelieve that she may have had an underlying neuro-logic disorder. It is important to consider potentialcomorbidities and additional testing in infants withfailed supraglottoplasty, as it is an operation withhigh success rates in the absence of comorbidities.
Recognizing that our second patient had MRI evi-dence of cervicomedullary compression that couldbe decompressed by a neurosurgical procedure ob-viated the need for supraglottoplasty. This patient
might have undergone supraglottoplasty flrst, withpotential failure, if MRI had not been performed forevaluation of anomalies associated with velocardio-facial syndrome.
The pathophysiology of brain stem dysfunctionassociated with Chiari malformations has been at-tributed to either hydrocephalus or brain stem com-pression itself.̂ Our patient with the Chiari I tnalfor-mation did not have hydrocephalus, so we assutnethat the dysfunction was related to physical cotn-pression. Knowledge of the neurologic pathways re-sponsible for laryngeal function and tone is impor-tant in understanding how brain stern compressionmay contribute to development of laryngomalacia.There is a vagal nerve-mediated reflex called thelaryngeal adductor reflex,' which is activated whenmechanoreceptors and chemoreceptors of the supe-rior laryngeal nerve are stimulated, sending sensoryafferent information to the brain stem nuclei respon-sible for regulating respiration and swallowing. In-tegration between the nucleus tractus solitarius andthe nucleus ambiguus occurs in the brain stem. Ef-ferent signals are sent via the vagus nerve to the lar-ynx, causing vocal fold adduction and a swallow.These efferent signals are also responsible for laryn-geal tone.' Thus, brain stem compression may af-fect efferent vagal responses, leading to decreasedlaryngeal tone and laryngomalacia. Both of our pa-tients had complete resolution of symptoms associ-ated with laryngomalacia and no evidence of laryn-gomalacia on flexible laryngoscopy after their brainstem decompressive procedures. This outcome maybe further evidence supporting the neurologic theo-ry of laryngomalacia causation.
CONCLUSIONS
Neurologic abnormalities have been reported inup to 50% of infants with laryngomalacia. As such,brain stem dysfunction should be considered amongthe causes of laryngomalacia prompting furtherevaluation, especially in patients who have failedsupraglottoplasty or other underlying comorbidities(eg, genetic syndrome, congenital anomalies). Bothof these infants had resolution of laryngomalacia-associated symptoms after their brain stem decom-pression procedures.
1. Thompson DM. Abnormal sensorimotor integrative func-tion of the larynx in congenital laryngomalacia: a new theory ofetiology. Laryngoscope 2007;117(suppl 114):l-33.
2. Smith ME. The association of laryngeal stridor with me-ningo-myelocele. J Laryngol Otol 1959;73:188-90.
3. Fitzsimmons JS. Laryngeal stridor and respiratory ob-struction associated with meningomyelocele. Arch Dis Child
REFERENCES
1965;40:687-8.
4. Krieger AJ, Detwiler JS, Trooskin SZ. Respiratory func-tion in infants with Amold-Chiari malformation. Laryngoscope1976;86:718-23.
5. Cochrane DD, Adderley R, White CP, Norman M, Stein-bok P. Apnea in patients with myelomeningocele. Pediatr Neu-rosurgl990-1991;16:232-9.

Petersson et al. Neurologie Variant Laryngomalacia 103
6. Portier F, Marianowski R. Morisseau-Durand MP. ZerahM, Manac'h Y. Respiratory obstruction as a sign of brainstenidysfunction in infants with Chiari malformations. Int J PediatrOtorhinolaryngol 2(X)1;57; 195-202.
7. Morley AR. Laryngeai stridor, Amold-Chiari malforma-tion and medullary haemorrhages. Dev Med Child Neurol 1969;11:471-4.
8. Papasozomenos S, Roessmann U. Respiratory distressand Amold-Chiari malformation. Neurology 198I;31;97-IOO.
9. Holitiger PC. Holinger LD. Reichert TJ. Holinger PH.Respiratory obstruction and apnca in infants with bilateral ab-ductor vocal cord paralysis, mcningomyelocele, hydrocephalus,and Artiold-Chiari malformation. J Pediatr l978;92;368-73.
10. Hoff SR, Schroeder JW Jr, Rastatter JC, Holinger LD.Supraglottoplasty outcomes in relation to age and comorbidconditions. Int J Pediatr Otorhinolaryngol 2010;74;245-9.
11. Reddy DK, Matt BH. Unilateral vs bilateral supraglotto-plasty for severe laryngomalacia in children. Arch OtolaryngolHead Neck Surg 2001;127;694-9.
12. Olney DR. Greinwald JH Jr. Smith RJ, Bauman NM. La-ryngomalacia and its treatment. Laryngoscope 1999;109;1770-5.
13. Toynton SC. Saunders MW, Bailey CM. Aryepiglotto-plasty for laryngomalacia: 100 consecutive cases. J LaryngolOtol 2001 ;115;35-8.
14. Denoyelle F, Mondain M,Gresillon N, Roger G.ChaudreF, Garabedian EN. Failures and complications of supraglotto-plasty in children. Arch Otolaryngol Head Neck Surg 2003; 129:1077-80.
15. Roger G, Denoyelle F, Triglia JM, Garabedian EN. Se-vere laryngomalacia; surgical indications and results in 115 pa-tients. Laryngoscope 1995; 105:1111-7.
16. McClurg FL, Evans DA. La.ser laryngoplasty for laryn-gomalacia. Laryngoscope 1994;104;247-52.
17. Prescott CA. The current status of corrective surgery forlaryngoinalacia. Am J Otolaryngol 1991 ; 12;230-5.
18. Richter GT,Thompson DM. The surgical managetncnt oflaryngomalacia. Otolaryngol Clin North Am 2008;41:837-64,vii.

Copyright of Annals of Otology, Rhinology & Laryngology is the property of Annals Publishing Company and
its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for individual use.




















