
Maternal Cardiac Dysfunction and Remodeling in Women With Preeclampsia at Term
30
ISSN: 1524-4563 Copyright © 2010 American Heart Association. All rights reserved. Print ISSN: 0194-911X. Online 72514 Hypertension is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX DOI: 10.1161/HYPERTENSIONAHA.110.162321 published online Nov 22, 2010; Hypertension Basky Thilaganathan Karen Melchiorre, George Ross Sutherland, Aigul Baltabaeva, Marco Liberati and Term Maternal Cardiac Dysfunction and Remodeling in Women With Preeclampsia at http://hyper.ahajournals.org/cgi/content/full/HYPERTENSIONAHA.110.162321/DC1 Data Supplement (unedited) at: http://hyper.ahajournals.org located on the World Wide Web at: The online version of this article, along with updated information and services, is http://www.lww.com/reprints Reprints: Information about reprints can be found online at [email protected] 410-528-8550. E-mail: Fax: Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters http://hyper.ahajournals.org/subscriptions/ Subscriptions: Information about subscribing to Hypertension is online at by on November 28, 2010 hyper.ahajournals.org Downloaded from
Transcript of Maternal Cardiac Dysfunction and Remodeling in Women With Preeclampsia at Term
ISSN: 1524-4563 Copyright © 2010 American Heart Association. All rights reserved. Print ISSN: 0194-911X. Online
72514Hypertension is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX
DOI: 10.1161/HYPERTENSIONAHA.110.162321 published online Nov 22, 2010; Hypertension
Basky Thilaganathan Karen Melchiorre, George Ross Sutherland, Aigul Baltabaeva, Marco Liberati and
TermMaternal Cardiac Dysfunction and Remodeling in Women With Preeclampsia at
http://hyper.ahajournals.org/cgi/content/full/HYPERTENSIONAHA.110.162321/DC1Data Supplement (unedited) at:
http://hyper.ahajournals.org
located on the World Wide Web at: The online version of this article, along with updated information and services, is
http://www.lww.com/reprintsReprints: Information about reprints can be found online at
[email protected]. E-mail:
Fax:Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters
http://hyper.ahajournals.org/subscriptions/Subscriptions: Information about subscribing to Hypertension is online at
by on November 28, 2010 hyper.ahajournals.orgDownloaded from
Maternal Cardiac Dysfunction and Remodeling in WomenWith Preeclampsia at Term
Karen Melchiorre, George Ross Sutherland, Aigul Baltabaeva, Marco Liberati, Basky Thilaganathan
Abstract—Preeclampsia is a disease associated with significant cardiovascular morbidity during pregnancy and in later life.This study was designed to evaluate cardiac function and remodeling in preeclampsia occurring at term. This was aprospective case–control study of 50 term preeclampsia and 50 normal pregnancies assessed by echocardiography andtissue Doppler analysis. Global diastolic dysfunction was observed more frequently in preeclampsia versus controlpregnancies (40% versus 14%, P�0.007). Increased cardiac work and left ventricular mass indices suggest that leftventricular remodeling was an adaptive response to maintain myocardial contractility with preeclampsia at term.Approximately 20% of patients with preeclampsia at term have more evident myocardial damage. Diastolic dysfunctionusually precedes systolic dysfunction in the evolution of ischemic or hypertensive cardiac diseases and is of prognosticvalue in the prediction of long-term cardiovascular morbidity. The study findings also have significant implications forthe acute medical management of preeclampsia. (Hypertension. 2011;57:00-00.) ● Online Data Supplement
Key Words: diastolic dysfunction � echocardiography � left ventricular remodeling � preeclampsia � pregnancy� strain rate � tissue Doppler
Preeclampsia (PE) is a pregnancy complication of placen-tal etiology with acute onset of predominantly cardiovas-
cular manifestations.1 The pathological changes in this disor-der are primarily ischemic in nature and are known to affectthe placenta, kidney, liver, and brain, whereas there is scantand conflicting information about the impact on the heart.1–7
Cardiopulmonary morbidity is seen in a significant propor-tion of preeclamptic cases8 and autopsy data have demon-strated that preeclamptic women have a 10-fold higherprevalence of myocardial contraction band necrosis thandeaths in pregnancy from other causes.9 Epidemiological datahave also highlighted the strong relationship between pre-eclampsia and premature morbidity and mortality from car-diovascular disease10,11 thought to be related to shared car-diovascular risk factors.12 All these data suggest thatpreeclampsia may be associated with the potential for signif-icant myocardial damage. Tissue Doppler (TD) velocity anddeformation indices are highly sensitive at detecting evenmild myocardial damage.13–18 The aim of this study is to testthe hypothesis that PE provokes significant myocardial dam-age/dysfunction by using both conventional echocardiogra-phy and TD analysis in women with and without PE.
MethodsStudy SubjectsThis was a prospective case–control study carried out over a 2-yearperiod from January 2008. All women with singleton pregnancy and
PE at term (37 to 42 completed weeks of gestation) were recruitedconsecutively as cases after informed consent and with local insti-tutional review committee approval. Only women without comor-bidities, nonsmokers, and before starting any medication were askedto take part in the study. PE and nonproteinuric gestational hyper-tension (GH) were defined according to the International Society forthe Study of Hypertension in Pregnancy guidelines.19 Normotensivehealthy, nonsmoking control subjects matched for maternal age,gestation, and ethnicity and women diagnosed with GH at term werealso recruited as control subjects from the routine antenatal clinic.
EchocardiographyAll subjects were studied by standard 2-dimensional and Dopplertransthoracic echocardiography at rest. Patients were studied in theleft lateral decubitus position and data acquired at end expirationfrom standard parasternal/apical views using a GE Vivid 9 scan-ner.20,21 For each acquisition, 3 cardiac cycles of noncompresseddata were stored in cine-loop format and analyzed without blindingoffline by 1 investigator (K.M.). Cardiac indices were normalized forbody surface area, height, and end-diastolic left ventricle long orshort axis lengths, as appropriate.22–24 TD, strain, and strain rateindices are given as absolute values.
Heart RemodelingChamber quantification and left ventricular (LV) geometric patternwere estimated using M-mode as previously described.20 Proximalseptal bulging was assessed in the parasternal long-axis and apical4-chamber views.25
Systolic FunctionLV volumes and ejection fraction were derived from Simpson’smodified biplane method from apical 4-chamber and 2-chamber
Received September 2, 2010; first decision September 25, 2010; accepted October 25, 2010.From the Fetal Maternal Medicine Unit (K.M., B.T.), Department of Obstetrics and Gynecology and the Department of Cardiology and Cardiothoracic
Surgery (K.M., G.R.S., A.B.), St Georges Hospital, University of London, London, UK; and the Department of Obstetrics and Gynecology (K.M., M.L.),University of Chieti, Chieti, Italy.
This study was approved by the Wandsworth Local Research Ethics Committee (Ref No. 01.78.5).Correspondence to Basky Thilaganathan, Fetal Maternal Medicine Unit, St George’s University of London, Cranmer Terrace, London SW17 0RE, UK.
E-mail [email protected]© 2010 American Heart Association, Inc.
Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.110.162321
1 by on November 28, 2010 hyper.ahajournals.orgDownloaded from

views.20 Maternal blood pressure was measured following therecommendation of the National High Blood Pressure EducationProgram Working Group on High Blood Pressure in Pregnancy.1
Hemodynamic and systolic cardiac indices were calculated asdescribed before26 (see supplementary material; available at http://hyper.ahajournals.org). Longitudinal and radial systolic functionwere assessed both globally and regionally using color and pulsedTD velocity indices and color TD-encoded strain and strain rateindices as previously described.17,18
Diastolic FunctionGlobal diastolic dysfunction was graded using a diagnostic algorithm(Figure 1) based on the recommendations of European Associationof Echocardiography and American Society of Echocardiography21
with the following adjustments: (1) age is a primary factor indefining normal velocity and time interval indices.21 Indices wereonly considered as abnormal if they were �2 SDs from the expectedmean for the age group; (2) circulating volume in pregnancy isincreased.1 Emphasis was therefore given to those cardiac indicesthat are least affected by loading conditions (left more than septalmitral annulus TD indices)23; and (3) the acute nature of PE on apreviously normal cardiovascular system.1 Specific importance wasgiven to indices that reflect diastolic function at the time ofassessment (transmitral, pulmonary and TD velocities, time inter-
vals, and regional deformations) rather than indices of left atrialremodeling, which commonly reflect the cumulative effect of fillingpressure in chronic conditions such as longstanding essentialhypertension.21
Regional longitudinal diastolic function was assessed by measur-ing color TD early and late diastolic velocity and strain rate indicespositioning the sample at the level of the basal and midsegments ofthe inferoseptal and anterolateral LV walls in 4-chamber view.Early/late diastolic myocardial TD index ratio of �1 was taken as anindex of altered segmental relaxation (segmental diastolic dysfunc-tion) as previously proposed.27,28
Statistical AnalysisData were analyzed using SPSS 12 software (SPSS, Chicago, Ill).Variables were compared using Mann-Whitney U or �2 tests, asappropriate. Paired group comparisons were only undertaken ifKruskal-Wallis testing indicated significant differences. A samplesize of 22 in each group was calculated to observe a �20%difference in early diastolic mitral wave velocity/average lateral andseptal diastolic myocardial velocities ratio between cases and controlsubjects with 85% power and a 5% Type I risk.29 Stepwise multipleregression analysis was used to assess the influence of cardiacparameters, demographic variables (ethnicity, maternal age, bodymass index), and pregnancy characteristics on indices of cardiac
Normal diastolic function
E/A<0.73 DT>194 ms IVRT>83 ms
Val ∆ E/A<0.5 ±Av E/E1<=8
E/A: 0.73-2.33 DT: 138-194 ms IVRT: 51-83 ms ±AR-A>=30 ms ±Val ∆ E/A>0.5 ±Av E/E1: 9-12
E/A>2.33 DT<138ms
IVRT<51 ms ±AR-A>=30 ms ±Val ∆ E/A>0.5 ±Av E/E1>=13
Impaired myocardial relaxation with normal
left ventricular end diastolic pressure
(GRADE I)
Impaired myocardial relaxation with increased left
ventricular end diastolic pressure
(GRADE Ia)
Lateral E1 >=14 cm/sec
Lateral E1<14 cm/sec
ARdur-Adur<30 ms ARdur-Adur>=30 ms
ARdur-Adur Pseudonormal filling pattern
(GRADE II)
Restrictive pattern (GRADE III)
EF>50%
Figure 1. Diagnostic algorithm for the classification of diastolic dysfunction. EF indicates ejection fraction; Lateral E1, pulsed wave tis-sue Doppler peak early diastolic velocity at the left side of mitral valve annulus; E, peak early diastole transmitral wave velocity; A, peaklate diastole transmitral wave velocity; E/A, early to late diastole peak transmitral velocity ratio; DT, deceleration time of E wave; IVRT,isovolumetric relaxation time; Adur, mitral A wave duration; Val � E/A, percentage of decrease in the mitral E/A ratio with Valsalvamaneuver; Av E/E1, E to average of lateral and septal E1 velocities; AR, peak retrograde late diastolic pulmonary wave velocity; ARdur,AR duration.
2 Hypertension January 2011
by on November 28, 2010 hyper.ahajournals.orgDownloaded from
function and remodeling. A value of P�0.05 was consideredstatistically significant and all tests were 2-sided. To test interob-server and intraobserver reproducibility, 2 independent operators(K.M. and A.B.) undertook offline analyses on the cine loops from10 randomly selected women and repeated this after 1 month. The95% limits of agreement, coefficients of variation, within-subjectSDs, and repeatability coefficients were calculated.
ResultsA total of 50 women with PE and 50 women with normalpregnancy were recruited during the study period. Thesecases were closely matched (Table 1) for age, ethnicity, andgestational age.
Diastolic FunctionTwenty women with PE (40%) met the criteria for the diagnosisof global diastolic dysfunction compared with 7 (14%) in thecontrol group (P�0.007; Table 2; Figures 2 and 3). In thewomen with PE, there were 13 with Grade I, 4 with Grade Ia,and 3 with Grade II diastolic dysfunction. PE cases with normalglobal diastolic function still had evidence of regional diastolicdysfunction compared with control subjects (Table 3; Figure 4).PE women with global diastolic dysfunction had significantlyhigher end-systolic left atrial volume index than control subjectswith 12 women having a left atrial volume index above thecutoff value of 34 mL/m2 (Table 2). The only demographicdifference was that PE women with global diastolic dysfunctionwere significantly older than those without.
Remodeling and HemodynamicPE women had significantly higher LV mass and cardiac workindices compared with control subjects with no significantdifference in LV end-systolic wall stress index (Table 4). PEwomen with global diastolic dysfunction, but not those withnormal global diastolic function, had significantly higher totalvascular resistance index compared with control subjects (Table4). The proportion of patients with LV geometric remodelingwas significantly higher in the PE group (36 of 50 [72%]) versusthe control group (12 of 50 [24%]; P�0.0001; Table 4; Figure5). There were 10 cases of LV concentric hypertrophy amongpatients with PE. LV remodeling was asymmetrical with thepresence of basal septal bulge seen (n�7) only in the womenwith PE with global diastolic dysfunction (P�0.001).
Systolic FunctionThere were no significant differences in indices of global (radialand longitudinal) systolic function between the groups both byconventional and TD assessment. Regional systolic function wasalso similar between PE with normal global diastolic functionand control subjects. PE women with global diastolic dysfunc-tion had significantly reduced regional (basal septal) end-systolicstrain and peak-systolic strain rate indices compared with controlsubjects. The amplitude of basal septal postsystolic shorteningindex was well above 25% in 5 of 20 (25%) PE women withglobal diastolic dysfunction compared with none of the controlsubjects (P�0.002; Figure 6).
Interdependency of IndicesMultiple regression analysis showed that hemodynamic indi-ces were the only independent predictors of LV mass indices(R�0.50; P�0.0001). Hemodynamic and LV remodelingindices were independent predictors of global diastolic func-tion. TD indices of myocardial relaxation and filling pres-sures appeared to be independently determined by afterload,longitudinal systolic function, and LV mass indices. Therewas a strong and independent relationship between longitu-dinal systolic and diastolic functional indices. Demographicand pregnancy characteristics did not independently contrib-ute to echocardiographic findings.
Gestational HypertensionWomen with GH (n�20) who were also matched for age,gestation, and ethnicity, demonstrated equivalent changes inLV geometry/remodeling to women with PE but did not haveany evidence of significant global diastolic or systolic dys-function (Table 5).
Repeatability and ReproducibilityThe intraobserver and interobserver coefficients of variationranged between 1.7% and 12%. The intra- and interobserveragreements were good for all indices. Please refer also to listof supplementary material.
DiscussionThe study data indicate that most women with PE undergoadaptive responses with significant heart remodeling, but asubgroup of approximately 20% of women demonstrate moreevident myocardial damage and overt global diastolic dysfunction.
Table 1. Demographic Characteristics and PregnancyOutcome of Cases With Preeclampsia and Control Subjects*
Control Subjects(n�50)
Cases(n�50) P
Recruitment
Maternal age, years 31.5 (26–36) 32.0 (29–37) 0.6
Nulliparous 32 (64) 34 (68) 0.8
White 32 (64) 32 (64) 0.9
Afro-Caribbean 11 (22) 11 (22) 0.8
Asian 7 (14) 7 (14) 0.8
Prepregnancy BMI, kg/m2 23.9 (21.2–27.5) 25.9 (24.1–31.1) 0.0001
Prepregnancy BSA, m2 1.5 (1.3–1.8) 1.8 (1.4–2.1) 0.1
SBP at booking visit,mm Hg
120 (110–125) 120 (110–130) 0.5
DBP at booking visit,mm Hg
60 (60–70) 60 (60–70) 0.2
Assessment
BMI, kg/m2, atassessment
27.7 (24.4–33.1) 30.1 (27.9–35.8) 0.005
BSA at assessment, m2 1.7 (1.5–2.1) 2.1 (1.7–2.5) 0.024
Gestational age atassessment, weeks
37 (37.2–38.5) 37 (37.5–39) 0.1
SBP at assessment,mm Hg
110 (100–120) 150 (140–160) 0.0001
DBP at assessment,mm Hg
70 (60–80) 95 (90–100) 0.0001
*Values are given as median (interquartile range) or no. of subjects(percentage).
BMI indicates body mass index; BSA, body surface area; SBP, systolic bloodpressure; DBP, diastolic blood pressure.
Melchiorre et al Cardiac Impairment in Preeclampsia at Term 3
by on November 28, 2010 hyper.ahajournals.orgDownloaded from
Diastolic FunctionThis is the first study to use an evidence-based algorithm21 todiagnose and grade diastolic dysfunction in women pres-enting with PE. This global approach to the interpretation ofcardiac indices demonstrates impaired myocardial relaxationand normal global systolic function in almost half of the
women with PE. Studies in patients with ischemic andhypertensive cardiac disorders have also demonstrated simi-lar findings, termed “isolated diastolic dysfunction.”30 Previ-ous studies of cardiac function and remodeling in PE havefailed to identify a consistent pattern of diastolic dysfunctionpossibly due to the inadequacy of the conventional cardiac
S1S1S1
1 E1 E1
A1
E
A1 A1
15
10
5
-5
5
-10
-15
10-.16
-2.0 -1.5 -1.0 -0.5 0.087HR100 mm/s
[cm/s]
.16
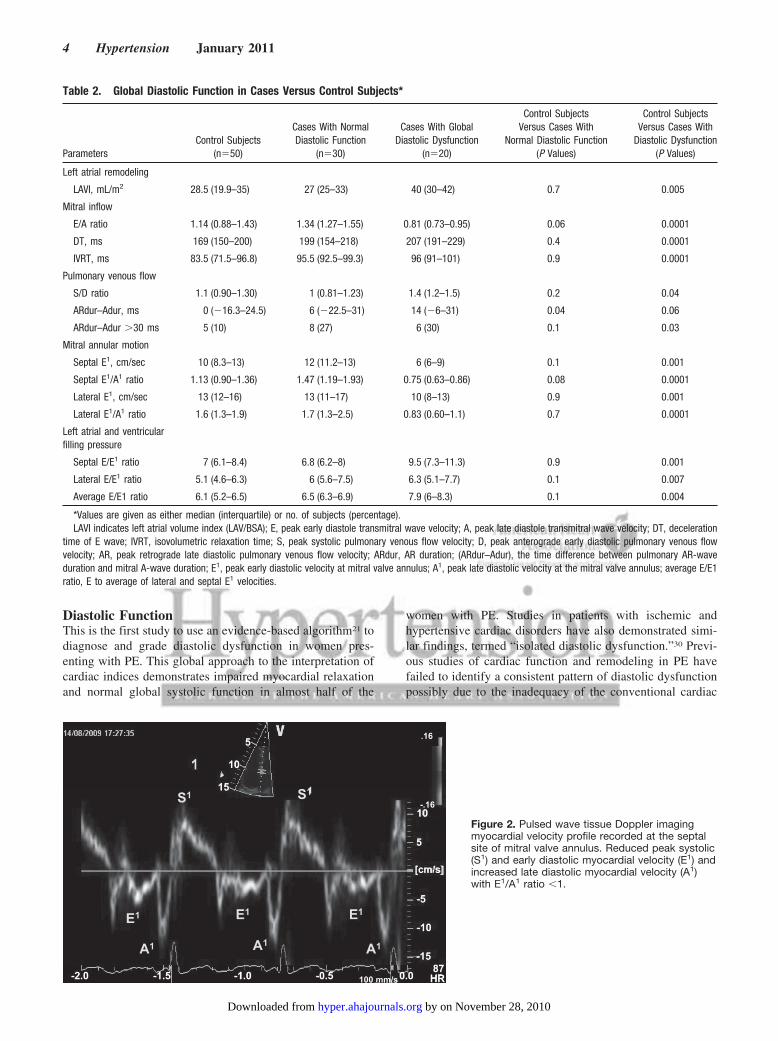
Figure 2. Pulsed wave tissue Doppler imagingmyocardial velocity profile recorded at the septalsite of mitral valve annulus. Reduced peak systolic(S1) and early diastolic myocardial velocity (E1) andincreased late diastolic myocardial velocity (A1)with E1/A1 ratio �1.
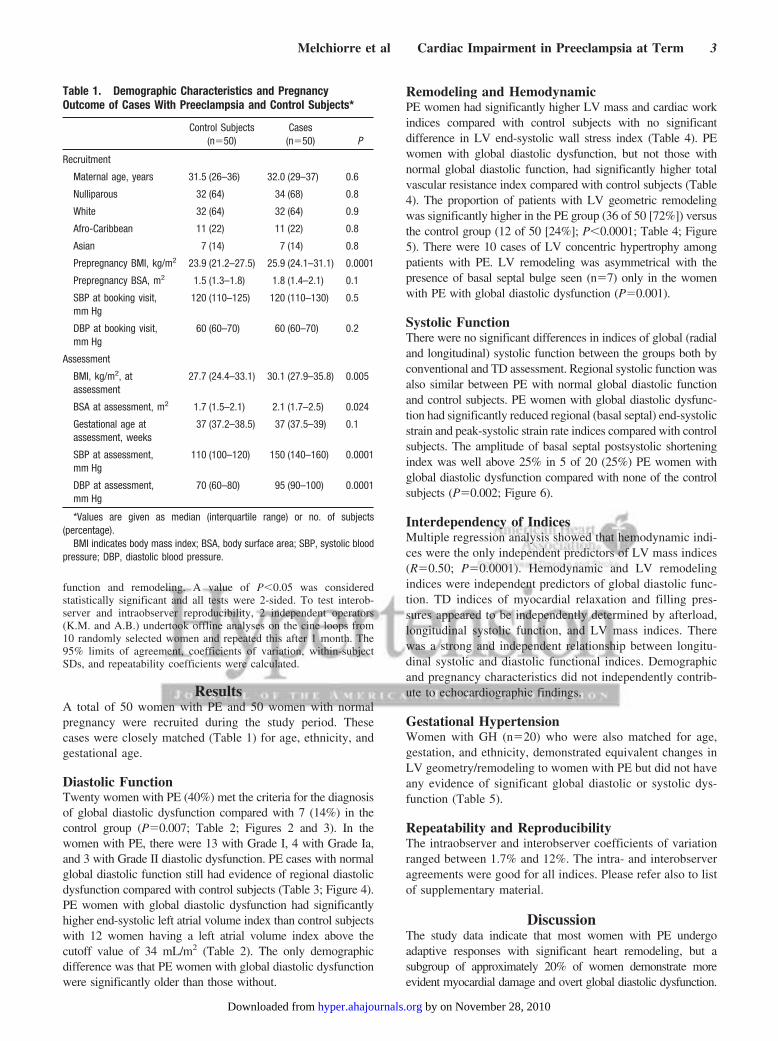
Table 2. Global Diastolic Function in Cases Versus Control Subjects*
ParametersControl Subjects
(n�50)
Cases With NormalDiastolic Function
(n�30)
Cases With GlobalDiastolic Dysfunction
(n�20)
Control SubjectsVersus Cases With
Normal Diastolic Function(P Values)
Control SubjectsVersus Cases With
Diastolic Dysfunction(P Values)
Left atrial remodeling
LAVI, mL/m2 28.5 (19.9–35) 27 (25–33) 40 (30–42) 0.7 0.005
Mitral inflow
E/A ratio 1.14 (0.88–1.43) 1.34 (1.27–1.55) 0.81 (0.73–0.95) 0.06 0.0001
DT, ms 169 (150–200) 199 (154–218) 207 (191–229) 0.4 0.0001
IVRT, ms 83.5 (71.5–96.8) 95.5 (92.5–99.3) 96 (91–101) 0.9 0.0001
Pulmonary venous flow
S/D ratio 1.1 (0.90–1.30) 1 (0.81–1.23) 1.4 (1.2–1.5) 0.2 0.04
ARdur–Adur, ms 0 (�16.3–24.5) 6 (�22.5–31) 14 (�6–31) 0.04 0.06
ARdur–Adur �30 ms 5 (10) 8 (27) 6 (30) 0.1 0.03
Mitral annular motion
Septal E1, cm/sec 10 (8.3–13) 12 (11.2–13) 6 (6–9) 0.1 0.001
Septal E1/A1 ratio 1.13 (0.90–1.36) 1.47 (1.19–1.93) 0.75 (0.63–0.86) 0.08 0.0001
Lateral E1, cm/sec 13 (12–16) 13 (11–17) 10 (8–13) 0.9 0.001
Lateral E1/A1 ratio 1.6 (1.3–1.9) 1.7 (1.3–2.5) 0.83 (0.60–1.1) 0.7 0.0001
Left atrial and ventricularfilling pressure
Septal E/E1 ratio 7 (6.1–8.4) 6.8 (6.2–8) 9.5 (7.3–11.3) 0.9 0.001
Lateral E/E1 ratio 5.1 (4.6–6.3) 6 (5.6–7.5) 6.3 (5.1–7.7) 0.1 0.007
Average E/E1 ratio 6.1 (5.2–6.5) 6.5 (6.3–6.9) 7.9 (6–8.3) 0.1 0.004
*Values are given as either median (interquartile) or no. of subjects (percentage).LAVI indicates left atrial volume index (LAV/BSA); E, peak early diastole transmitral wave velocity; A, peak late diastole transmitral wave velocity; DT, deceleration
time of E wave; IVRT, isovolumetric relaxation time; S, peak systolic pulmonary venous flow velocity; D, peak anterograde early diastolic pulmonary venous flowvelocity; AR, peak retrograde late diastolic pulmonary venous flow velocity; ARdur, AR duration; (ARdur–Adur), the time difference between pulmonary AR-waveduration and mitral A-wave duration; E1, peak early diastolic velocity at mitral valve annulus; A1, peak late diastolic velocity at the mitral valve annulus; average E/E1ratio, E to average of lateral and septal E1 velocities.
4 Hypertension January 2011
by on November 28, 2010 hyper.ahajournals.orgDownloaded from

indices used.3,4 The current study used color and pulsed TDvelocity and deformation indices, which are well correlatedwith invasive indices of myocardial relaxation/filling pres-sures and long-term cardiovascular risk.31–33 Furthermore,previous studies disregarded the interdependency of cardiacevents by assessing differences in cardiac indices in isola-tion,3–6 but rather evaluating global diastolic and systolicindices using a validated diagnostic algorithm. LV myocar-dial relaxation is paradoxically an energy-dependent processthat results in a rapid decrease in LV pressure after the end ofcontraction and during early diastole.21 Hence, the process ofmyocardial relaxation is more vulnerable than contractionand is apparently compromised in both early-stage cardiovas-cular disorders30 and in PE. Multiple regression analysisdemonstrated that in PE, diastolic dysfunction was signifi-cantly related to both increased afterload and/or increased LVmass as seen in nonpregnant subjects.32,33 Longitudinal sys-
tolic and diastolic function indices were also independentlyrelated, highlighting the importance of simultaneously assess-ing systolic/diastolic function and remodeling and their syn-ergic contribution toward altered cardiac function. Womenwith PE and normal global diastolic function also hadregional diastolic abnormalities more often than controlpregnancies. These findings suggest that regional diastolicdysfunction may be an antecedent event, leading to globaldiastolic dysfunction as additional segments become affected.It is possible that women with PE and regional diastolicdysfunction may have developed global dysfunction if thepregnancy had not been delivered.
Systolic Function and Heart RemodelingGlobal (radial and longitudinal) systolic function was pre-served in women with PE. The majority of women with PEshowed evidence of LV concentric remodeling and increased
Sm Sm SmSm
Em Em Em
Am Am Am
15
10
5
15
10
5
24
-24
cm/s
10
5
0
-5
-100.0 0.5 1.0 1.5
v7.49 cm/s t1.337 sv(cm/s) 5.48
AVO AVC AVO AVC AVO AVC AVO
87HR
Figure 3. Color-encoded tissue Doppler imagingmyocardial velocity profile recorded at the basalinferoseptal segment. Reduced peak systolic (Sm)and early diastolic myocardial velocity (Em) andincreased late diastolic myocardial velocity (Am)with Em/Am ratio �1. AVO and AVC denote aorticvalve opening and closure, respectively.
Table 3. Regional Diastolic Function Color Doppler Myocardial Velocities and Deformations of Preeclamptic Women With andWithout Global Diastolic Dysfunction and Control Subjects*
ParameterControl Subjects
(n�50)
Cases With NormalDiastolic Function
(n�30)
Cases With GlobalDiastolic Dysfunction
(n�20)
Control SubjectsVersus Cases WithNormal Diastolic
Function (P Values)
Control SubjectsVersus Cases With
Diastolic Dysfunction(P Values)
Inferoseptal wall
Basal Em/Am ratio 1.6 (1.3–2.5) 2.1 (1.2–2.5) 1 (0.6–1.2) 0.9 0.0001
Mid Em/Am ratio 1.8 (1.3–2.2) 2.2 (1.1–3.4) 0.9 (0.6–1.1) 0.6 0.0001
Basal SRE/SRA ratio �1 7 (14) 8 (27) 12 (60) 0.1 0.0001
Mid-SRE/SRA ratio �1 16 (32) 13 (43) 12 (60) 0.8 0.06
Anterolateral wall
Basal Em/Am ratio 2.8 (1.6–4.5) 1.7 (1.2–5.1) 1.5 (0.9–2.4) 0.5 0.003
Mid-Em/Am ratio 2.7 (1.5–4.2) 3.3 (1.5–4.2) 1.4 (0.6–2.3) 0.8 0.013
Basal SRE/SRA ratio �1 8 (16) 10 (33) 10 (50) 0.1 0.008
Mid-SRE/SRA ratio �1 7 (14) 5 (17) 7 (35) 1 0.09
Total no. of strain rate alteredsegmental myocardial relaxation
38/200 (19) 36/120 (30) 41/80 (51) 0.034 0.0001
*Values are given as median (interquartile) or no. of subjects (percentage).Em indicates peak early diastolic myocardial velocity; Am, peak late diastolic myocardial velocity; SRE, early diastolic myocardial strain rate; SRA, late diastolic
myocardial strain rate.
Melchiorre et al Cardiac Impairment in Preeclampsia at Term 5
by on November 28, 2010 hyper.ahajournals.orgDownloaded from

LV mass indices. These changes are likely to be an adaptiveresponse to reduce the wall stress associated with increasedafterload, thereby maintaining the balance between myocar-dial oxygen demand and supply. This inference is supportedby the finding that the LV end-systolic wall stress indexbetween PE and controls remains unchanged. Multiple re-gression analysis demonstrated strong independent associa-tions between LV mass indices and hemodynamic indices.These associations are consistent with a mechanically appro-priate response to increased afterload, thus preserving intrin-
sic myocardial contractility in PE. These assertions aresupported by the findings of other studies, which also showedthat the ratio between LV mass and cardiac work indices isunchanged in PE.3,7
LV concentric hypertrophy with a characteristic basalseptal bulge and markedly reduced regional (basal septal)longitudinal systolic function with high-amplitude postsystol-ic shortening was evident in approximately 20% of womenwith PE, who also demonstrated global diastolic dysfunction.These findings suggest that there is early myocardial impair-
SRE
SRA
SRESRE
SRA SRA
SRE SRE
PSSR PSSR PSSR
AVO AVC AVO AVC AVO AVC
10
5
10
5
1.5
1.0
0.5
0.0
-0.5
-1.0
-1.50.0 0.5 1.0 1.5
3.0 1/s
-3.0 1/s
1/s SR -1.02 1/s t 1.25 s
85HR
Figure 4. Color-encoded tissue Doppler longitudi-nal strain rate curve recorded at the basal infero-septal segment. Reduced myocardial lengtheningduring passive filling (SRE) and increased myocar-dial lengthening during atrial contraction (SRA) witha SRE/SRA ratio �1. AVO and AVC denote aorticvalve opening and closure, respectively.
Table 4. Hemodynamic and Remodeling Parameters of Cases With and Without Global Diastolic Dysfunction and Control Subjects*
ParameterControl Subjects
(n�50)
PE With NormalGlobal Diastolic Function
(n�30)
PE With GlobalDiastolic Dysfunction
(n�20)
Control SubjectsVersus Cases WithNormal Diastolic
Function (P Values)
Control SubjectsVersus Cases With
Diastolic Dysfunction(P Values)
Hemodynamic indices
HR, beats/min 82 (74.5–93) 80 (72–85) 83 (74–95) 0.4 0.6
MAP, mm Hg 83 (74–92) 112 (107–117) 112 (107–120) 0.0001 0.0001
CI, L/min/m2 3.2 (2.2–3.9) 3.2 (1.9–3.9) 2.9 (2.1–3.6) 0.3 0.7
SVI, mL/m2 39 (31–48) 36 (27–44) 38 (26–40) 0.8 0.8
TVRI, (dynes�s�1�cm�5)/m2 698 (577–876) 856 (583–1083) 922 (740–1105) 0.060 0.010
Left ventricle remodeling indices
RWT 0.34 (0.29–0.41) 0.44 (0.39–0.51) 0.43 (0.41–0.50) 0.0001 0.0001
LVMI, g/m2 70 (55–82) 73 (59–93) 80 (71–92) 0.028 0.0001
Cardiac work and wall stress indices
Meridian end systolic wall stress index,dyne/cm2/m2
43 (27–48) 42 (32–52) 52 (34–63) 0.9 0.3
Cardiac work index,mm Hg�L�min�1�m�2
262 (194–291) 312 (256–401) 360 (293–412) 0.0001 0.0001
Left ventricle geometric pattern
Normal 38 (76) 12 (40) 2 (10) 0.003 0.0001
LV concentric remodeling 11 16 8 0.009 0.2
LV eccentric remodeling 1 2 0 0.6 0.6
LV concentric hypertrophy 0 0 10 … 0.0001
*Values are given as median (interquartile) or no. of subjects (percentage).HR indicates heart rate; MAP, mean arterial pressure; CI, cardiac index; SVI, stroke volume index; TVRI, total vascular resistance index; LV, left ventricle; RWT,
relative wall thickness; LVM, left ventricular mass; LVMI, left ventricular mass index normalized for body surface area (BSA).
6 Hypertension January 2011
by on November 28, 2010 hyper.ahajournals.orgDownloaded from

ment, mainly localized at the level of the basal septum, inthese cases. The basal septum has the highest radius ofcurvature in the LV and is, hence, under higher local wallstress.14 The latter is usually compensated for by transseptalpressure from the right ventricle that acts to reduce wallstress.14,34 When this compensation becomes insufficient,local stress increases, leading to the development of thecharacteristic basal septal bulge and regional longitudinaldysfunction.14,25,34,35 LV concentric hypertrophy is known tobe accompanied by subendocardial fibrosis both in hyperten-sive subjects and from autopsy data.36,37 The coexistence ofLV hypertrophy and regional longitudinal systolic dysfunc-tion in PE suggests that there is regional subendocardialimpairment, presumably due to subendocardial ischemiaand/or fibrosis in the longitudinal myocardial fibers that aremainly distributed in the subendocardium.14,38 This assertionis supported by the autopsy finding of subendocardial ische-mia in severe PE with adverse outcome.9
Gestational HypertensionAlthough women with GH had similar hemodynamic and LVgeometric patterns as women with PE, they did not demon-strate global diastolic or regional systolic abnormalities. Thelatter finding suggests that some cardiac changes in PE arerelated to factors other than hypertension. Although highblood pressure is the sole cardinal feature of GH, hyperten-sion is only 1 of a cluster of signs used to define themultisystem disorder of PE.1 It is possible that coexistence ofoxidative stress and endothelial damage in PE could beresponsible for the diastolic and systolic dysfunction seen inthis condition. Alternatively, the cardiovascular stress pro-voked by PE may have exposed an independent underlyingmyopathic process.
Clinical Implications of the Study FindingsThe findings of this study have significant clinical implica-tions for peripartum intravascular volume management, be-cause the women with global diastolic dysfunction are theones most likely to sustain acute cardiopulmonary morbidity,most commonly from pulmonary edema.8,39–42 The latter maybe better predicted by the early diastolic mitral wave velocity/average lateral and septal diastolic myocardial velocities ratioin patients with global diastolic dysfunction, because it is abetter indirect index of pulmonary capillary wedge pressurethan central venous pressure.42,43 The study findings alsodemonstrate that PE is associated with heart remodeling andsignificant changes in cardiac function. Many of the alteredTD indices are known to be independently related to thelong-term risk of cardiovascular morbidity in nonpregnantsubjects.13,21,31–33,44 A better understanding of the relationshipof these indices and subsequent morbidity in the context ofpregnancy may provide an opportunity for early cardiovas-cular risk stratification and the introduction of prophylacticstrategies.
PerspectiveThe findings of this study indicate that cardiac changes inwomen with PE are mainly adaptive in nature, maintainingcardiac function at the same time as minimizing wall stress
10
5
10
5
15
15
20%
-20%
0
-5
-10
-15
0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0 2.285
HR
SR -6.9% t 1.25 sAVO AVC AVO AVC
Figure 6. Color-encoded tissue Doppler longitudi-nal strain curve recorded at the basal inferoseptalsegment. Segmental shortening (negative strain)throughout systole to an end-systolic maximumdeformation (yellow arrow) followed by a furtherpostsystolic shortening (light blue arrow) duringthe isovolumetric relaxation time. AVO and AVCdenote aortic valve opening and closure,respectively.
V
5
Figure 5. An apical 4-chamber view showing abnormal convex-ity and thickening of the basal septum (arrow) toward the leftventricular cavity in a preeclamptic patient.
Melchiorre et al Cardiac Impairment in Preeclampsia at Term 7
by on November 28, 2010 hyper.ahajournals.orgDownloaded from

and maintaining myocardial oxygen delivery. There wasevidence of myocardial damage in 20% of women with PE inthis study. These women are at highest risk of cardiovascularcomplications in the acute phase of PE and may manifestincreased cardiovascular morbidity and mortality later in life.Clarification of the latter is important from a public healthperspective, because early identification and intervention mayameliorate subsequent cardiovascular disease.
AcknowledgmentsWe are grateful to the midwives and sonographers of the FetalMaternal Medicine Unit, St George’s Hospital, for their invaluablehelp with patient recruitment.
Sources of FundingK.M. was funded for her PhD thesis research by the University ofChieti, Chieti, Italy.
DisclosuresNone.
References1. Report of the National High Blood Pressure Education Program Working
Group on High Blood Pressure in Pregnancy. National High BloodPressure Education Program Working Group on High Blood Pressure inPregnancy. Am J Obstet Gynecol. 2000;183:S1–S22.
2. Hibbard JU, Shroff SG, Lang RM. Cardiovascular changes in pre-eclampsia. Semin Nephrol. 2004;24:580–587.
3. Simmons LA, Gillin AG, Jeremy RW. Structural and functional changesin left ventricle during normotensive and preeclamptic pregnancy. Am JPhysiol Heart Circ Physiol. 2002;283:H1627–H1633.
4. Borghi C, Esposti DD, Immordino V, Cassani A, Boschi S, Bovicelli L,Ambrosioni E. Relationship of systemic hemodynamics, left ventricularstructure and function, and plasma natriuretic peptide concentrationsduring pregnancy complicated by preeclampsia. Am J Obstet Gynecol.2000;183:140–147.
5. Bamfo JE, Kametas NA, Chambers JB, Nicolaides KH. Maternal cardiacfunction in normotensive and preeclamptic intrauterine growth restriction.Ultrasound Obstet Gynecol. 2008;32:682–686.
6. Hamada RR, Larssonb A, Pernowc J, Bremmea K, Erikssond MJ.Assessment of left ventricular structure and function in preeclampsia byechocardiography and cardiovascular biomarkers. J Hypertens. 2009;27:2257–2264.
7. Lang RM, Pridjian G, Feldman T, Neumann A, Lindheimer M, BorowKM. Left ventricular mechanics in preeclampsia. Am Heart J. 1991;121:1768–1775.
8. Bauer ST, Cleary KL. Cardiopulmonary complications of pre-eclampsia.Semin Perinatol. 2009;33:158–165.
9. Bauer TW, Moore GW, Hutchins GM. Morphologic evidence forcoronary artery spasm in eclampsia. Circulation. 1982;65:255–259.
10. McDonald SD, Malinowski A, Zhou Q, Yusuf S, Devereaux PJ. Cardio-vascular sequelae of preeclampsia/eclampsia: a systematic review andmeta-analyses. Am Heart J. 2008;156:918–930.
11. Ray JG, Vermeulen MJ, Schull MJ, Redelmeier DA. Cardiovascular HealthAfter Maternal Placental Syndromes (CHAMPS): population-based retro-spective cohort study. Lancet. 2005;366:1797–1803.
12. Berends AL, de Groot CJ, Sijbrands EJ, Sie MP, Benneheij SH, Pal R,Heydanus R, Oostra BA, van Duijn CM, Steegers EA. Shared constitu-tional risks for maternal vascular-related pregnancy complications andfuture cardiovascular disease. Hypertension. 2008;51:1034–1041.
13. Mogelvang R, Goetze JP, Pedersen SA, Olsen NT, Marott JI, Schnohr P,Sogaard P, Jensen JS. Preclinical systolic and diastolic dysfunctionassessed by tissue Doppler imaging is associated with elevated plasmapro-B-type natriuretic peptide concentrations. J Cardiac Fail. 2009;15:489–495.
14. Bijnens BH, Cikes M, Claus P, Sutherland GR. Velocity and deformationimaging for the assessment of myocardial dysfunction. Eur J Echo-cardiogr. 2009;10:216–226.
15. Citro R, Bossone E, Kuersten B, Gregorio G, Salustri A. Tissue Dopplerand strain imaging: anything left in the echo-lab? Cardiovasc Ultrasound.2008;30:6–54.
16. Greenberg NL, Firstenberg MS, Castro PL, Main M, Travaglini A, Oda-bashian JA, Drinko JK, Rodriguez LL, Thomas JD, Garcia MJ. Doppler-derived myocardial systolic strain rate is a strong index of left ventricularcontractility. Circulation. 2002;105:99–105.
17. Marciniak A, Claus P, Sutherland GR, Marciniak M, Karu T, BaltabaevaA, Merli E, Bijnens B, Jahangiri M. Changes in systolic left ventricularfunction in isolated mitral regurgitation. A strain rate imaging study. EurHeart J. 2007;28:2627–2636.
18. Baltabaeva A, Marciniak M, Bijnens B, Moggridge J, He FJ, AntoniosTF, MacGregor GA, Sutherland GR. Regional left ventricular defor-mation and geometry analysis provides insights in myocardial remod-elling in mild to moderate hypertension. Eur J Echocardiogr. 2008;9:501–508.
19. Brown MA, Lindheimer MD, de Swiet M, Van Assche A, Moutquin JM.The classification and diagnosis of the hypertensive disorders of preg-nancy: statement from the International Society for the Study of Hyper-tension in Pregnancy (ISSHP). Hypertens Pregnancy. 2001;20:IX–XIV.
20. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, PellikkaPA, Picard MH, Roman MJ, Seward J, Shanewise J, Solomon S, SpencerKT, St John Sutton M, Stewart W; American Society of Echocardiogra-phy’s Nomenclature and Standards Committee; Task Force on ChamberQuantification; American College of Cardiology Echocardiography Com-mittee; American Heart Association; European Association of Echocar-diography, European Society of Cardiology. Recommendations forchamber quantification. Eur J Echocardiogr. 2006;7:79–108.
Table 5. Summary Hemodynamic, Remodeling, Cardiac Function Indices for Control, Term Gestational Hypertension,and Term PE Pregnancies*
ParameterTerm Control
(n�50)GH
(n�20)PE
(n�50)
GH VersusControl
(P Values)
PE VersusControl
(P Values)PE Versus GH
(P Values)
MAP, mm Hg 83 (74–92) 109 (107–118) 113 (106–120) 0.0001 0.0001 0.4
CI, L/min/m2 3.2 (2.2–3.9) 2.8 (2.4–3.2) 2.9 (2.1–3.8) 0.6 0.6 0.5
TVRI, (dynes�s�1�cm�5)/m2 645 (570–840) 951 (756–1086) 716 (574–1036) 0.003 0.012 0.7
Global diastolic dysfunction 7 (14) 2 (15) 20 (40) 0.9 0.007 0.031
Regional diastolic dysfunction† 3 (7) 0 9 (30) 0.6 0.022 0.028
Total LV geometric abnormality 12 (24) 15 (75) 34 (68) 0.0001 0.0001 0.7
Septal bulge 0 0 7 (14) … 0.019 0.2
LV basal postsystolic shorteningindex �25%
1 (2) 1 (5) 9 (18) 0.9 0.011 0.2
*Values are given as median (interquartile) or no. of patients (percentage).†Regional diastolic dysfunction is computed among patients with normal global diastolic function.MAP indicates mean arterial pressure; CI, cardiac index; TVRI, total vascular resistance index.
8 Hypertension January 2011
by on November 28, 2010 hyper.ahajournals.orgDownloaded from

21. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA,Waggoner AD, Flachskampf FA, Pellikka PA, Evangelista A. Recom-mendations for the evaluation of left ventricular diastolic function byechocardiography. J Am Soc Echocardiogr. 2009;22:107–133.
22. Oxborough D, Batterham AM, Shave R, Artis N, Birch KM, Whyte G,Ainslie PN, George KP. Interpretation of two-dimensional and tissue Dopp-ler-derived strain and strain rate data: is there a need to normalize forindividual variability in left ventricular morphology? Eur J Echocardiogr.2009;10:677–682.
23. Batterham A, Shave R, Oxborough D, Whyte G, George K. Longitudinalplane colour tissue-Doppler myocardial velocities and their association withleft ventricular length, volume and mass in humans. Eur J Echocardiogr.2008;9:542–546.
24. Dewey FE, Rosenthal D, Murphy DJ, Froelicher VF, Ashley EA. Doessize matter? Clinical applications of scaling cardiac size and function forbody size. Circulation. 2008;117:2279–2287.
25. Lever HM, Karam RF, Currie PJ, Healy BP. Hypertrophic cardiomyop-athy in the elderly. Distinctions from the young based on cardiac shape.Circulation. 1989;79:580–589.
26. Poppas A, Shroff SG, Korcarz CE, Hibbard JU, Berger DS, Lind-heimer MD, Lang RM. Serial assessment of the cardiovascular systemin normal pregnancy. Role of arterial compliance and pulsatile arterialload. Circulation. 1997;95:2407–2415.
27. Pavlopoulos H, Nihoyannopoulos P. Abnormal segmental relaxationpatterns in hypertensive disease and symptomatic diastolic dysfunctiondetected by strain echocardiography. J Am Soc Echocardiogr. 2008;21:899–906.
28. Takemoto Y, Pellikka PA, Wang J, Modesto KM, Cauduro S, BelohlavekM, Seward JB, Thomson HL, Khandheria B, Abraham TP. Analysis ofthe interaction between segmental relaxation patterns and global diastolicfunction by strain echocardiography. J Am Soc Echocardiogr. 2005;18:901–906.
29. Innelli P, Sanchez R, Marra F, Esposito R, Galderisi M. The impact ofaging on left ventricular longitudinal function in healthy subjects: apulsed tissue Doppler study. Eur J Echocardiogr. 2008;9:241–249.
30. Yu CM, Lin H, Yang H, Kong SL, Zhang Q, Lee SW. Progression ofsystolic abnormalities in patients with ‘isolated’ diastolic heart failure anddiastolic dysfunction. Circulation. 2002;105:1195–1201.
31. Yu CM, Sanderson JE, Marwick TH, Oh JK. Tissue Doppler imaging. Anew prognosticator for cardiovascular diseases. J Am Coll Cardiol. 2007;49:1903–1914.
32. Wang M, Yip GW, Wang AY, Zhang Y, Ho PY, Tse MK, Lam PK,Sanderson JE. Peak early diastolic mitral annulus velocity by tissue
Doppler imaging adds independent and incremental prognostic value.J Am Coll Cardiol. 2003;41:820–826.
33. Wang M, Yip GW, Wang AY, Zhang Y, Ho PY, Tse MK, Yu CM,Sanderson JE. Tissue Doppler imaging provides incremental prognosticvalue in patients with systemic hypertension and left ventricular hyper-trophy. J Hypertens. 2005;23:183–191.
34. Heng MK, Janz RF, Jobin J. Estimation of regional stress in the leftventricular septum and free wall: an echocardiographic study suggestinga mechanism for asymmetric septal hypertrophy. Am Heart J. 1985;110:84–90.
35. Mone SM, Sanders SP, Colan SD. Control mechanisms for physiologicalhypertrophy of pregnancy. Circulation. 1996;94:667–672.
36. Huysman JA, Vliegen HW, Van der Laarse A, Eulderink F. Changes innonmyocyte tissue composition associated with pressure overload ofhypertrophic human hearts. Pathol Res Pract. 1989;184:577–581.
37. Vliegen HW, van der Laarse A, Cornelisse CJ, Eulderink F. Myocardialchanges in pressure overload-induced left ventricular hypertrophy. Astudy on tissue composition, polyploidization and multinucleation. EurHeart J. 1991;12: 488–494.
38. Voigt JU, Lindenmeier G, Exner B, Regenfus M, Werner D, Reulbach U,Nixdorff U, Flachskampf FA, Daniel WG. Incidence and characteristicsof segmental postsystolic longitudinal shortening in normal, acutely is-chemic, and scarred myocardium. J Am Soc Echocardiogr. 2003;16:415–423.
39. Young PF, Leighton NA, Jones PW, Anthony J, Johanson RB. Fluidmanagement in severe preeclampsia (VESPA): survey of members ofISSHP. Hypertens Pregnancy. 2000;19:249–259.
40. Benedetti TJ, Kates R, Williams V. Hemodynamic observations in severepreeclampsia complicated by pulmonary edema. Am J Obstet Gynecol.1985;152:330–334.
41. Clark SL, Greenspoon JS, Aldahl D, Phelan JP. Severe preeclampsia withpersistent oliguria: management of hemodynamic subsets. Am J ObstetGynecol. 1986;154:490–494.
42. Clark SL, Cotton DB. Clinical indications for pulmonary artery catheter-ization in the patient with severe preeclampsia. Am J Obstet Gynecol.1988;158:453–458.
43. Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, RedfieldMM, Tajik AJ. Clinical utility of Doppler echocardiography and tissueDoppler imaging in the estimation of left ventricular filling pressures: acomparative simultaneous Doppler–catheterization study. Circulation.2000;102:1788–1794.
44. Bhathia RS, Tu LV, Lee DS, Austin PC, Fang J, Haouzi A, Gong Y, LiuPP. Outcome of heart failure with preserved ejection fraction in apopulation-based study. N Engl J Med. 2006;355:260–269.
Melchiorre et al Cardiac Impairment in Preeclampsia at Term 9
by on November 28, 2010 hyper.ahajournals.orgDownloaded from
ONLINE SUPPLEMENT
MATERNAL CARDIAC DYSFUNCTION AND REMODELING IN WOMEN
WITH PREECLAMPSIA AT TERM
Short title: Cardiac impairment in preeclampsia at term
Karen Melchiorre1, 2, 3 MD, George Ross Sutherland2 MD, FRCP, Aigul
Baltabaeva2 MD, Marco Liberati3 MD, PhD, Basky Thilaganathan1 MD,
FRCOG
1Fetal Maternal Medicine Unit, Department of Obstetrics and Gynecology,
St George’s Hospital, University of London, London, United Kingdom
2Department of Cardiology and Cardiothoracic Surgery, St George’s Hospital,
University of London, London, United Kingdom
3Department of Obstetrics and Gynecology,
University of Chieti, Chieti, Italy
Correspondence: to Prof. Basky Thilaganathan
Fetal Maternal Medicine Unit
St George’s University of London
Cranmer Terrace
London SW17 0RE
Telephone: 020 8725 0071
Facsimile: 0208725 0079
E-mail: [email protected]
by on November 28, 2010 hyper.ahajournals.orgDownloaded from

2
Method Calculation of echocardiograhic indices 1. Left ventricle meridian end-systolic stress (ESS) was calculated using cuff
systolic blood pressure (SBP) taken at the end of the echocardiographic examination. ESS meridian = (1.35xSBPxLVESD)/[(4xLVPWs) x (1+{LVPWs/LVESD})], where LVESD is left ventricle end-systolic dimension and LVPWs is left ventricle posterior wall thickness in systole.
2. Stroke volume (SV) was calculated as the product of aortic Doppler flow velocity time integral (VTI) and cross-sectional area of the left ventricle outflow tract (CSA).
3. Cardiac output (CO) was obtained as the product of stroke volume and heart rate (HR) derived from ECG monitoring.
4. Total vascular resistance (TVR) was calculated in dynes x sec-1 x cm-5 according to the formula: TVR = (MAP in mmHg/CO in L/min) × 80.
5. Cardiac work (CW) was calculated using the formula: CW=CO x MAP.
by on November 28, 2010 hyper.ahajournals.orgDownloaded from
3
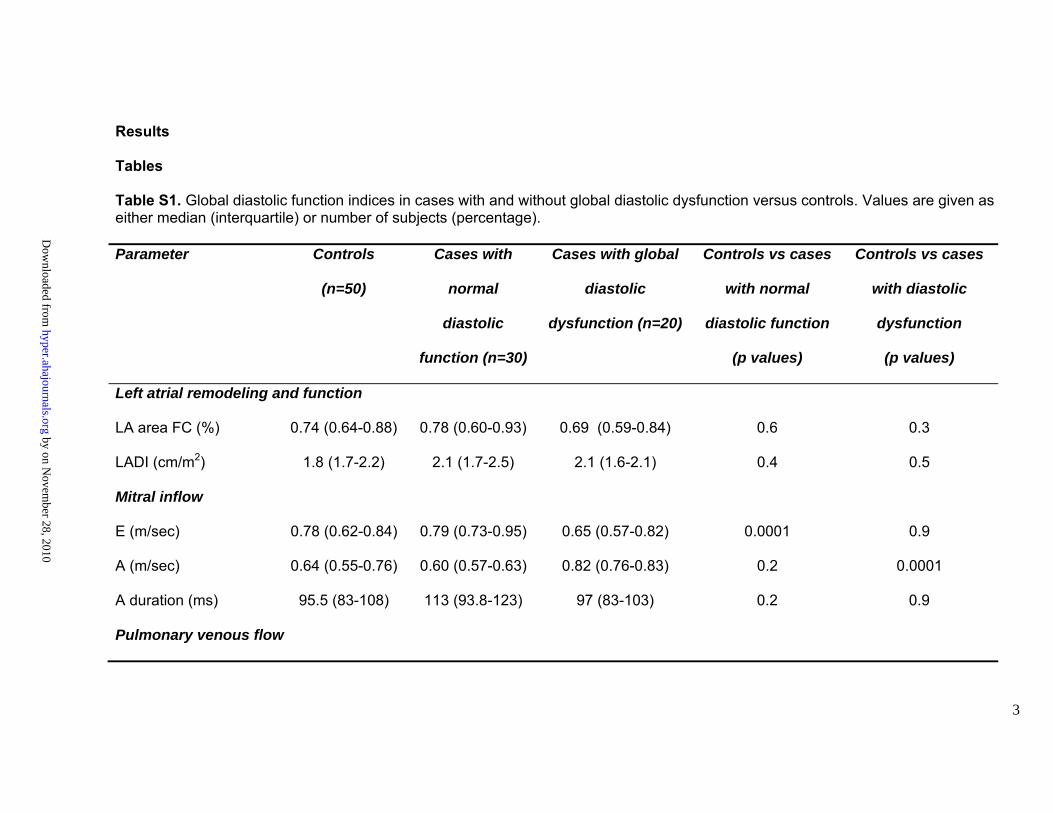
Results Tables Table S1. Global diastolic function indices in cases with and without global diastolic dysfunction versus controls. Values are given as either median (interquartile) or number of subjects (percentage). Parameter
Controls
(n=50)
Cases with
normal
diastolic
function (n=30)
Cases with global
diastolic
dysfunction (n=20)
Controls vs cases
with normal
diastolic function
(p values)
Controls vs cases
with diastolic
dysfunction
(p values)
Left atrial remodeling and function
LA area FC (%) 0.74 (0.64-0.88) 0.78 (0.60-0.93) 0.69 (0.59-0.84) 0.6 0.3
LADI (cm/m2) 1.8 (1.7-2.2) 2.1 (1.7-2.5) 2.1 (1.6-2.1) 0.4 0.5
Mitral inflow
E (m/sec) 0.78 (0.62-0.84) 0.79 (0.73-0.95) 0.65 (0.57-0.82) 0.0001 0.9
A (m/sec) 0.64 (0.55-0.76) 0.60 (0.57-0.63) 0.82 (0.76-0.83) 0.2 0.0001
A duration (ms) 95.5 (83-108) 113 (93.8-123) 97 (83-103) 0.2 0.9
Pulmonary venous flow
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from
4
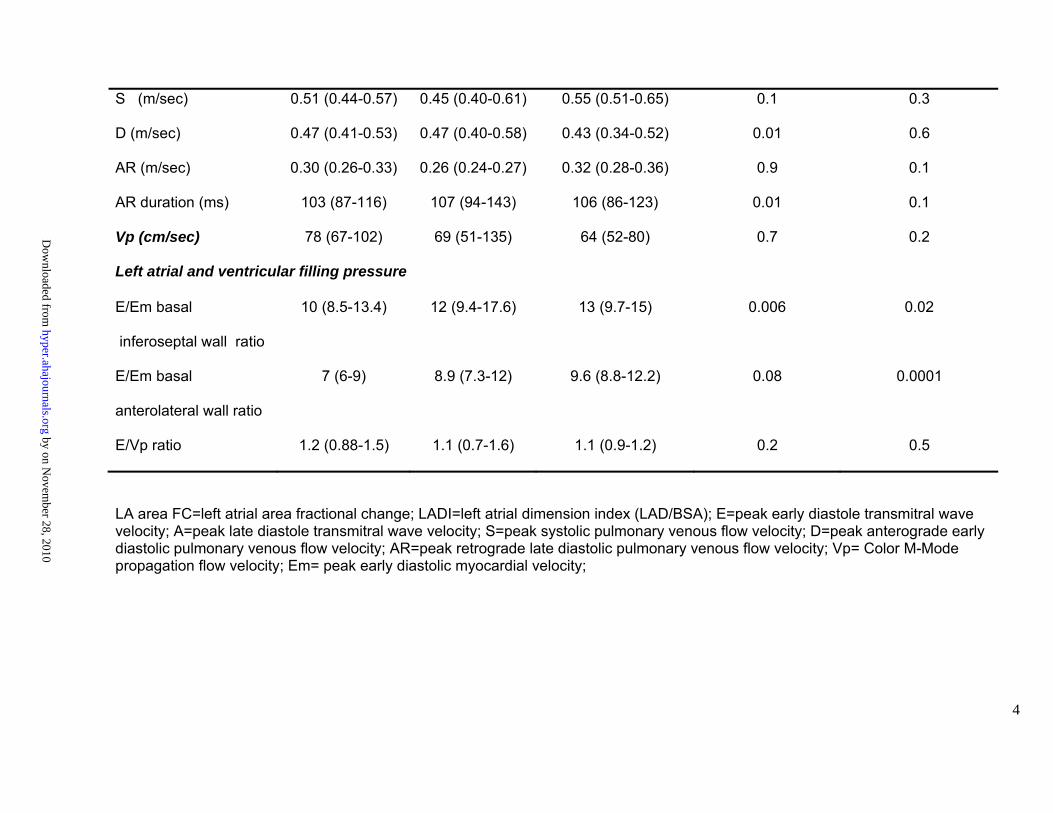
S (m/sec) 0.51 (0.44-0.57) 0.45 (0.40-0.61) 0.55 (0.51-0.65) 0.1 0.3
D (m/sec) 0.47 (0.41-0.53) 0.47 (0.40-0.58) 0.43 (0.34-0.52) 0.01 0.6
AR (m/sec) 0.30 (0.26-0.33) 0.26 (0.24-0.27) 0.32 (0.28-0.36) 0.9 0.1
AR duration (ms) 103 (87-116) 107 (94-143) 106 (86-123) 0.01 0.1
Vp (cm/sec) 78 (67-102) 69 (51-135) 64 (52-80) 0.7 0.2
Left atrial and ventricular filling pressure
E/Em basal
inferoseptal wall ratio
10 (8.5-13.4) 12 (9.4-17.6) 13 (9.7-15) 0.006 0.02
E/Em basal
anterolateral wall ratio
7 (6-9) 8.9 (7.3-12) 9.6 (8.8-12.2) 0.08 0.0001
E/Vp ratio 1.2 (0.88-1.5) 1.1 (0.7-1.6) 1.1 (0.9-1.2) 0.2 0.5
LA area FC=left atrial area fractional change; LADI=left atrial dimension index (LAD/BSA); E=peak early diastole transmitral wave velocity; A=peak late diastole transmitral wave velocity; S=peak systolic pulmonary venous flow velocity; D=peak anterograde early diastolic pulmonary venous flow velocity; AR=peak retrograde late diastolic pulmonary venous flow velocity; Vp= Color M-Mode propagation flow velocity; Em= peak early diastolic myocardial velocity;
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from
5
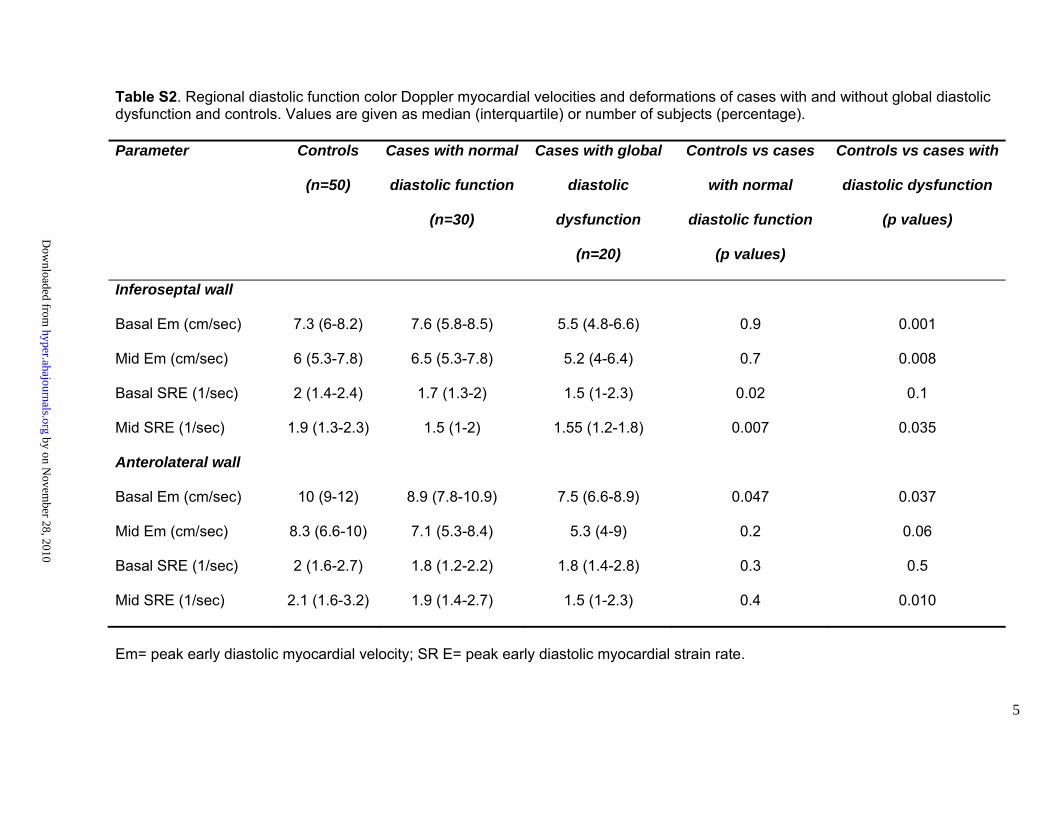
Table S2. Regional diastolic function color Doppler myocardial velocities and deformations of cases with and without global diastolic dysfunction and controls. Values are given as median (interquartile) or number of subjects (percentage). Parameter Controls
(n=50)
Cases with normal
diastolic function
(n=30)
Cases with global
diastolic
dysfunction
(n=20)
Controls vs cases
with normal
diastolic function
(p values)
Controls vs cases with
diastolic dysfunction
(p values)
Inferoseptal wall
Basal Em (cm/sec) 7.3 (6-8.2) 7.6 (5.8-8.5) 5.5 (4.8-6.6) 0.9 0.001
Mid Em (cm/sec) 6 (5.3-7.8) 6.5 (5.3-7.8) 5.2 (4-6.4) 0.7 0.008
Basal SRE (1/sec) 2 (1.4-2.4) 1.7 (1.3-2) 1.5 (1-2.3) 0.02 0.1
Mid SRE (1/sec) 1.9 (1.3-2.3) 1.5 (1-2) 1.55 (1.2-1.8) 0.007 0.035
Anterolateral wall
Basal Em (cm/sec) 10 (9-12) 8.9 (7.8-10.9) 7.5 (6.6-8.9) 0.047 0.037
Mid Em (cm/sec) 8.3 (6.6-10) 7.1 (5.3-8.4) 5.3 (4-9) 0.2 0.06
Basal SRE (1/sec) 2 (1.6-2.7) 1.8 (1.2-2.2) 1.8 (1.4-2.8) 0.3 0.5
Mid SRE (1/sec) 2.1 (1.6-3.2) 1.9 (1.4-2.7) 1.5 (1-2.3) 0.4 0.010
Em= peak early diastolic myocardial velocity; SR E= peak early diastolic myocardial strain rate.
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from
6
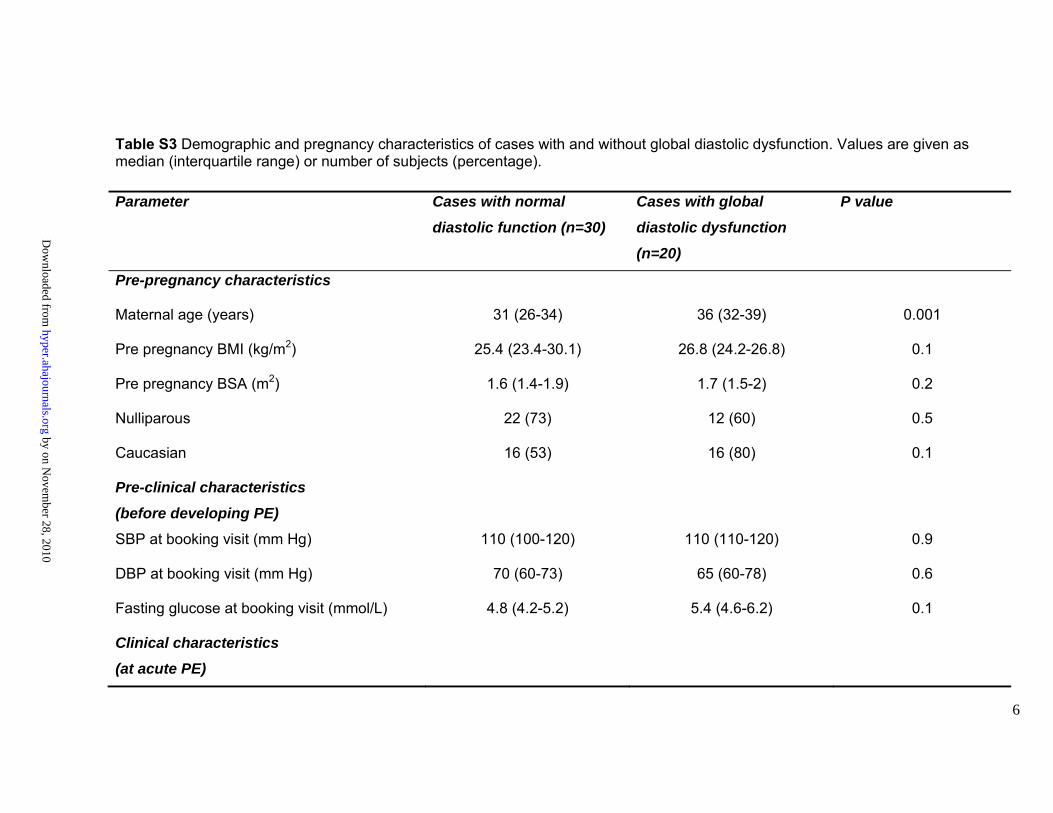
Table S3 Demographic and pregnancy characteristics of cases with and without global diastolic dysfunction. Values are given as median (interquartile range) or number of subjects (percentage). Parameter Cases with normal
diastolic function (n=30)
Cases with global
diastolic dysfunction
(n=20)
P value
Pre-pregnancy characteristics
Maternal age (years) 31 (26-34) 36 (32-39) 0.001
Pre pregnancy BMI (kg/m2) 25.4 (23.4-30.1) 26.8 (24.2-26.8) 0.1
Pre pregnancy BSA (m2) 1.6 (1.4-1.9) 1.7 (1.5-2) 0.2
Nulliparous 22 (73) 12 (60) 0.5
Caucasian 16 (53) 16 (80) 0.1
Pre-clinical characteristics
(before developing PE)
SBP at booking visit (mm Hg) 110 (100-120) 110 (110-120) 0.9
DBP at booking visit (mm Hg) 70 (60-73) 65 (60-78) 0.6
Fasting glucose at booking visit (mmol/L) 4.8 (4.2-5.2) 5.4 (4.6-6.2) 0.1
Clinical characteristics
(at acute PE)
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from
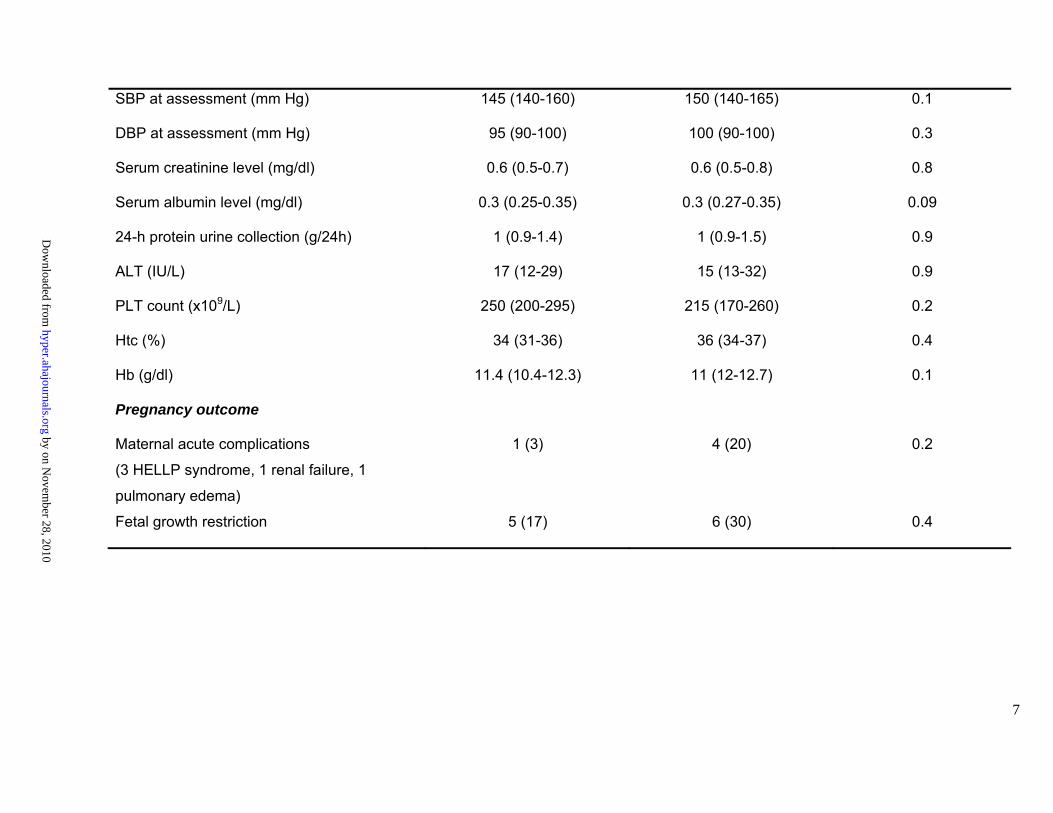
7
SBP at assessment (mm Hg) 145 (140-160) 150 (140-165) 0.1
DBP at assessment (mm Hg) 95 (90-100) 100 (90-100) 0.3
Serum creatinine level (mg/dl) 0.6 (0.5-0.7) 0.6 (0.5-0.8) 0.8
Serum albumin level (mg/dl) 0.3 (0.25-0.35) 0.3 (0.27-0.35) 0.09
24-h protein urine collection (g/24h) 1 (0.9-1.4) 1 (0.9-1.5) 0.9
ALT (IU/L) 17 (12-29) 15 (13-32) 0.9
PLT count (x109/L) 250 (200-295) 215 (170-260) 0.2
Htc (%) 34 (31-36) 36 (34-37) 0.4
Hb (g/dl) 11.4 (10.4-12.3) 11 (12-12.7) 0.1
Pregnancy outcome
Maternal acute complications
(3 HELLP syndrome, 1 renal failure, 1
pulmonary edema)
1 (3) 4 (20) 0.2
Fetal growth restriction 5 (17) 6 (30) 0.4
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from
8
BMI=body mass index; BSA=body surface area; SBP=systolic blood pressure; DBP=diastolic blood pressure; ALT=alanine transaminase; PLT=platelet count; Htc=hematocrit; Hg=hemoglobin; HELLP=hemolysis, elevated liver enzymes, low platelet count.
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from

9
Table S4. LV remodeling parameters of cases with and without global diastolic dysfunction and controls. Values are given as median (interquartile) or number of subjects (percentage). Parameter Controls
(n=50)
PE with normal
global diastolic
function (n=30)
PE with global
diastolic
dysfunction
(n=20)
Controls vs cases
with normal
diastolic function
(p values)
Controls vs cases
with diastolic
dysfunction
(p values)
IVSd (cm) 0.8 (0.7-0.9) 1 (0.9-1.1) 0.9 (0.8-1) 0.0001 0.0001
IVSs (cm) 1 (1-1.1) 1.3 (1.1-1.4) 1.1 (1.1-1.3) 0.0001 0.003
LVPWd (cm) 0.8 (0.7-0.9) 1 (0.9-1.1) 1 (0.9-1.1) 0.0001 0.0001
LVPWs (cm) 1.2 (1-1.3) 1.4 (1.3-1.6) 1.3 (1.2-1.4) 0.0001 0.02
LVEDDI (cm/m2) 2.5 (2.2-2.8) 2.4 (1.9-2.8) 2.1 (1.7-2.7) 0.09 0.019
LVESDI (cm/m2) 1.8 (1.5-2) 1.6 (1.1-1.9) 1.6 (1.2-2) 0.1 0.041
LVMI 1 (g/h2.7) 27.6 (24.1-36.2) 38 (31-45) 37 (34-44) 0.0001 0.0001
LV=left ventricle; IVSd=interventricular septum wall thickness at diastole; IVSs=interventricular septum wall thickness at systole; LVPWd=left ventricular posterior wall thickness at diastole; LVPWs=left ventricular posterior wall thickness at systole; LVEDDI=left ventricular end diastolic dimension index; LVESDI=left ventricular end systolic dimension index; LVMI 1=left ventricular mass index 1 (LVM normalized for height raised at 2.7).
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from

10
Table S5. LV global longitudinal systolic function indices of cases with and without global diastolic dysfunction and controls. Values are given as median (interquartile). Parameter
Controls (n=50)
PE with normal global
diastolic function (n=30)
PE with global diastolic
dysfunction (n=20)
Controls vs cases with normal
diastolic function (p values)
Controls vs cases with diastolic dysfunction (p values)
Mitral valve annulus septal siteMitral ring
displacement (mm) 11.7 (10.2-13.3) 14.2 (12.8-19.2) 10.7 (9-12) 0.4 0.6
S1 (cm/sec)
9 (7.3-9.8) 7 (6.3-7) 7 (6-8) 0.014 0.03
Long axis shortening (%)
1.4 (1.2-1.8) 1.9 (1.6-2.8) 1.4 (1.2-1.6) 0.09 0.8
S1/LAX (1/sec)
1.1 (0.9-1.2) 0.9 (0.88-0.93) 0.97 (0.85-1.1) 0.1 0.06
Mitral valve annulus lateral site
Mitral ring displacement (mm)
12.6 (11.1-14.5) 11.5 (9.9-13.6) 12.2 (9.7-15) 0.02 0.8
S1
(cm/sec) 8.5 (7-9.8) 7.5 (5.3-9) 7 (7-9) 0.5 0.2
Long axis shortening (%)
1.7 (1.3-1.9) 1.6 (1.3-1.8) 1.7 (1.3-1.9) 0.1 0.6
S1/LAX (1/sec)
1.1 (0.9-1.3) 1 (0.8-1.2) 1 (0.9-1.1) 0.2 0.1
Strain rate study (8 segments model)
Peak systolic strain rate index
(1/sec)
1.57 (1.34-1.66) 1.50 (1.34-1.58) 1.3 (1.10-1.75) 0.2 0.4
Peak systolic strain rate index/LV LAX
0.20 (0.17-0.23) 0.19 (0.17-0.23) 0.18 (0.14-0.24) 0.3 0.6
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from

11
(1/sec/cm) S1=pulsed wave Doppler peak systolic velocity; LV= left ventricle; LAX: end-diastolic LV long axis length; long axis shortening=mitral ring displacement normalized for LAX (expressed in mm). S1/LAX =pulsed wave Doppler peak systolic velocity normalized for LAX (expressed in cm).
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from
12
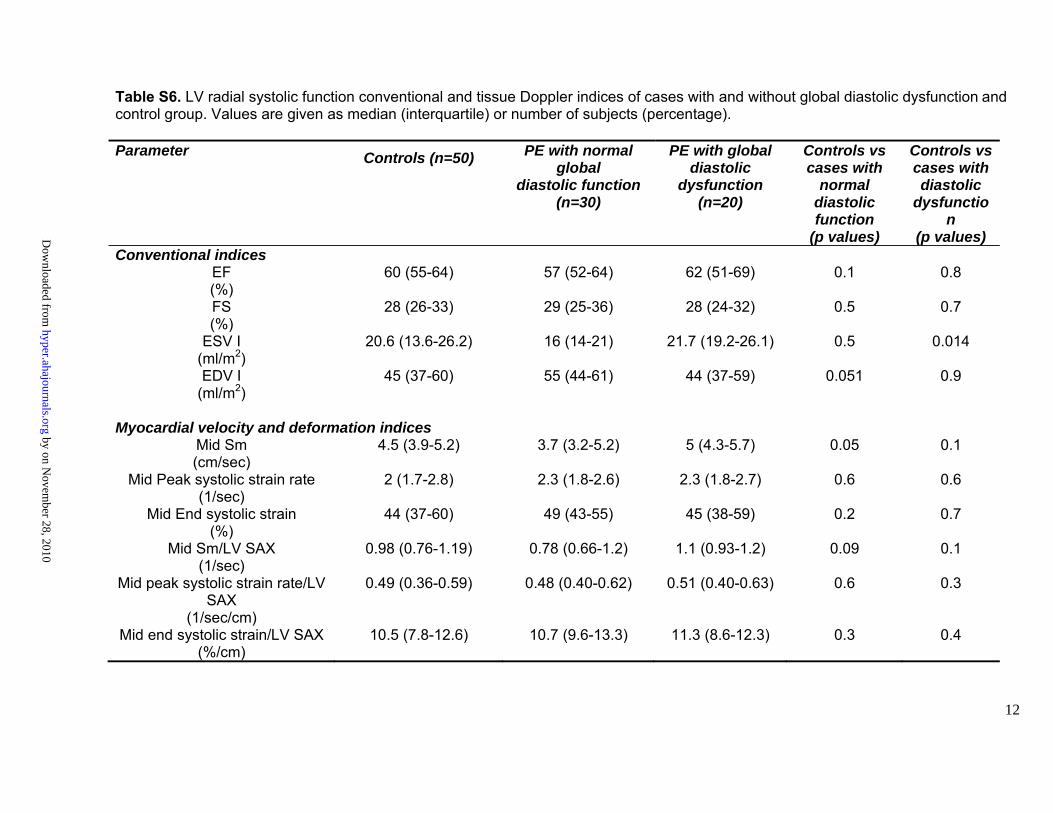
Table S6. LV radial systolic function conventional and tissue Doppler indices of cases with and without global diastolic dysfunction and control group. Values are given as median (interquartile) or number of subjects (percentage). Parameter Controls (n=50) PE with normal
global diastolic function
(n=30)
PE with global diastolic
dysfunction (n=20)
Controls vs cases with
normal diastolic function
(p values)
Controls vs cases with diastolic
dysfunction
(p values) Conventional indices
EF (%)
60 (55-64) 57 (52-64) 62 (51-69) 0.1 0.8
FS (%)
28 (26-33) 29 (25-36) 28 (24-32) 0.5 0.7
ESV I (ml/m2)
20.6 (13.6-26.2) 16 (14-21) 21.7 (19.2-26.1) 0.5 0.014
EDV I (ml/m2)
45 (37-60) 55 (44-61) 44 (37-59) 0.051 0.9
Myocardial velocity and deformation indices
Mid Sm (cm/sec)
4.5 (3.9-5.2) 3.7 (3.2-5.2) 5 (4.3-5.7) 0.05 0.1
Mid Peak systolic strain rate (1/sec)
2 (1.7-2.8) 2.3 (1.8-2.6) 2.3 (1.8-2.7) 0.6 0.6
Mid End systolic strain (%)
44 (37-60) 49 (43-55) 45 (38-59) 0.2 0.7
Mid Sm/LV SAX (1/sec)
0.98 (0.76-1.19) 0.78 (0.66-1.2) 1.1 (0.93-1.2) 0.09 0.1
Mid peak systolic strain rate/LV SAX
(1/sec/cm)
0.49 (0.36-0.59) 0.48 (0.40-0.62) 0.51 (0.40-0.63) 0.6 0.3
Mid end systolic strain/LV SAX (%/cm)
10.5 (7.8-12.6) 10.7 (9.6-13.3) 11.3 (8.6-12.3) 0.3 0.4
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from

13
EF=ejection fraction; FS=fractional shortening; BSA=body surface area; EDVI=left ventricular end diastolic volume index (EDV/BSA); ESVI=left ventricular end systolic volume index (ESV/BSA). Myocardial velocities and deformation indices: Sm =peak systolic myocardial fibers velocity; LV=left ventricle; SAX=end-diastolic short axis length in cm.
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from
14
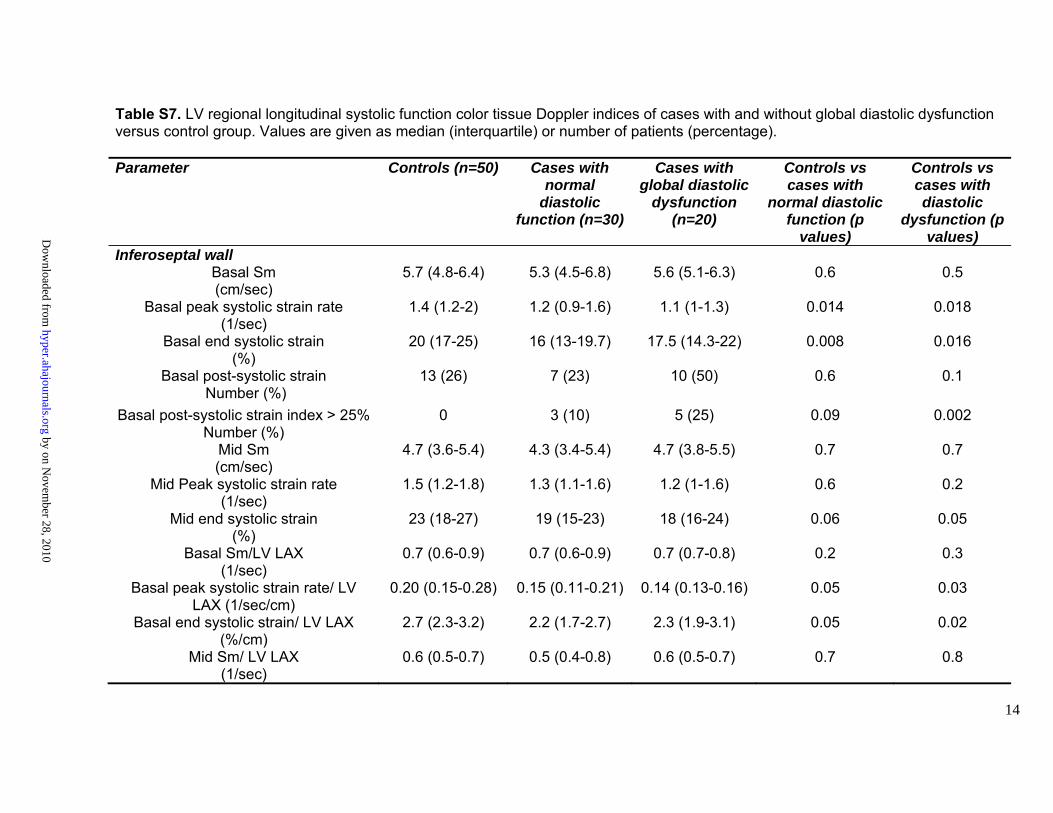
Table S7. LV regional longitudinal systolic function color tissue Doppler indices of cases with and without global diastolic dysfunction versus control group. Values are given as median (interquartile) or number of patients (percentage). Parameter Controls (n=50) Cases with
normal diastolic
function (n=30)
Cases with global diastolic
dysfunction (n=20)
Controls vs cases with
normal diastolic function (p
values)
Controls vs cases with diastolic
dysfunction (p values)
Inferoseptal wall Basal Sm (cm/sec)
5.7 (4.8-6.4) 5.3 (4.5-6.8) 5.6 (5.1-6.3) 0.6 0.5
Basal peak systolic strain rate (1/sec)
1.4 (1.2-2) 1.2 (0.9-1.6) 1.1 (1-1.3) 0.014 0.018
Basal end systolic strain (%)
20 (17-25) 16 (13-19.7) 17.5 (14.3-22) 0.008 0.016
Basal post-systolic strain Number (%)
13 (26) 7 (23) 10 (50) 0.6 0.1
Basal post-systolic strain index > 25% Number (%)
0 3 (10) 5 (25) 0.09 0.002
Mid Sm (cm/sec)
4.7 (3.6-5.4) 4.3 (3.4-5.4) 4.7 (3.8-5.5) 0.7 0.7
Mid Peak systolic strain rate (1/sec)
1.5 (1.2-1.8) 1.3 (1.1-1.6) 1.2 (1-1.6) 0.6 0.2
Mid end systolic strain (%)
23 (18-27) 19 (15-23) 18 (16-24) 0.06 0.05
Basal Sm/LV LAX (1/sec)
0.7 (0.6-0.9) 0.7 (0.6-0.9) 0.7 (0.7-0.8) 0.2 0.3
Basal peak systolic strain rate/ LV LAX (1/sec/cm)
0.20 (0.15-0.28) 0.15 (0.11-0.21) 0.14 (0.13-0.16) 0.05 0.03
Basal end systolic strain/ LV LAX (%/cm)
2.7 (2.3-3.2) 2.2 (1.7-2.7) 2.3 (1.9-3.1) 0.05 0.02
Mid Sm/ LV LAX (1/sec)
0.6 (0.5-0.7) 0.5 (0.4-0.8) 0.6 (0.5-0.7) 0.7 0.8
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from
15
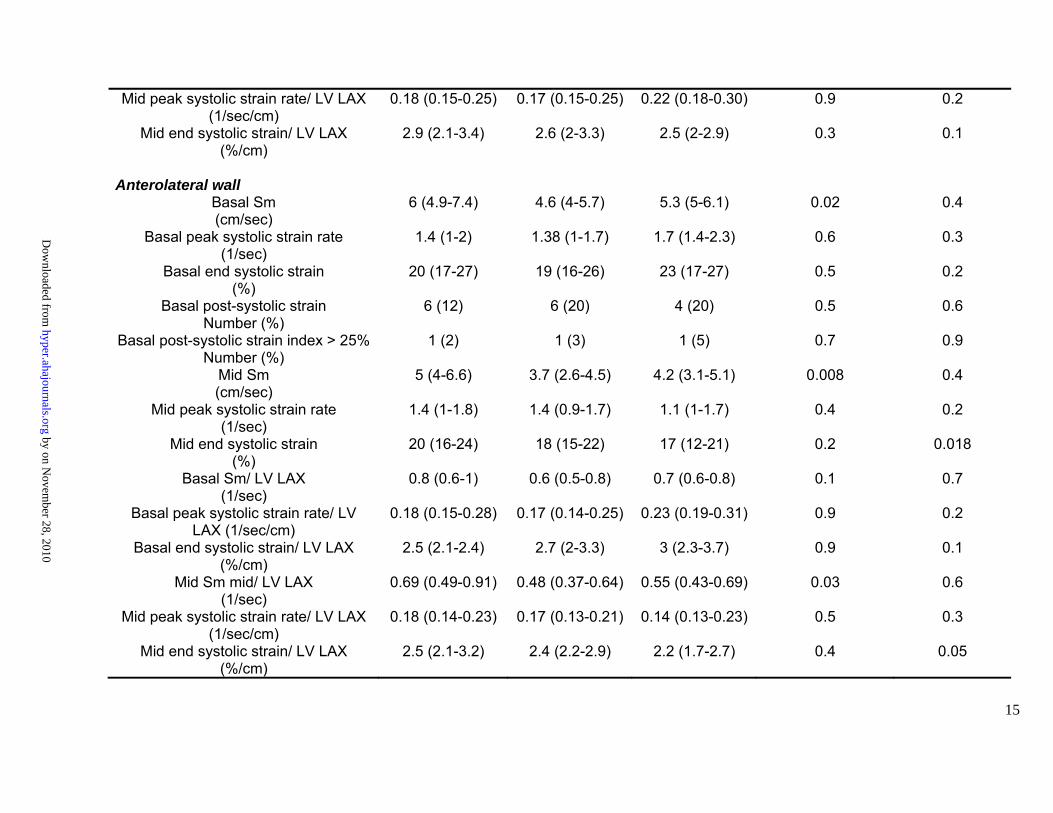
Mid peak systolic strain rate/ LV LAX (1/sec/cm)
0.18 (0.15-0.25) 0.17 (0.15-0.25) 0.22 (0.18-0.30) 0.9 0.2
Mid end systolic strain/ LV LAX (%/cm)
2.9 (2.1-3.4) 2.6 (2-3.3) 2.5 (2-2.9) 0.3 0.1
Anterolateral wall
Basal Sm (cm/sec)
6 (4.9-7.4) 4.6 (4-5.7) 5.3 (5-6.1) 0.02 0.4
Basal peak systolic strain rate (1/sec)
1.4 (1-2) 1.38 (1-1.7) 1.7 (1.4-2.3) 0.6 0.3
Basal end systolic strain (%)
20 (17-27) 19 (16-26) 23 (17-27) 0.5 0.2
Basal post-systolic strain Number (%)
6 (12) 6 (20) 4 (20) 0.5 0.6
Basal post-systolic strain index > 25% Number (%)
1 (2) 1 (3) 1 (5) 0.7 0.9
Mid Sm (cm/sec)
5 (4-6.6) 3.7 (2.6-4.5) 4.2 (3.1-5.1) 0.008 0.4
Mid peak systolic strain rate (1/sec)
1.4 (1-1.8) 1.4 (0.9-1.7) 1.1 (1-1.7) 0.4 0.2
Mid end systolic strain (%)
20 (16-24) 18 (15-22) 17 (12-21) 0.2 0.018
Basal Sm/ LV LAX (1/sec)
0.8 (0.6-1) 0.6 (0.5-0.8) 0.7 (0.6-0.8) 0.1 0.7
Basal peak systolic strain rate/ LV LAX (1/sec/cm)
0.18 (0.15-0.28) 0.17 (0.14-0.25) 0.23 (0.19-0.31) 0.9 0.2
Basal end systolic strain/ LV LAX (%/cm)
2.5 (2.1-2.4) 2.7 (2-3.3) 3 (2.3-3.7) 0.9 0.1
Mid Sm mid/ LV LAX (1/sec)
0.69 (0.49-0.91) 0.48 (0.37-0.64) 0.55 (0.43-0.69) 0.03 0.6
Mid peak systolic strain rate/ LV LAX (1/sec/cm)
0.18 (0.14-0.23) 0.17 (0.13-0.21) 0.14 (0.13-0.23) 0.5 0.3
Mid end systolic strain/ LV LAX (%/cm)
2.5 (2.1-3.2) 2.4 (2.2-2.9) 2.2 (1.7-2.7) 0.4 0.05
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from
16
Sm =peak systolic myocardial fibers velocity; LV= left ventricle; LAX=end-diastolic long axis length (expressed in cm).
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from
17
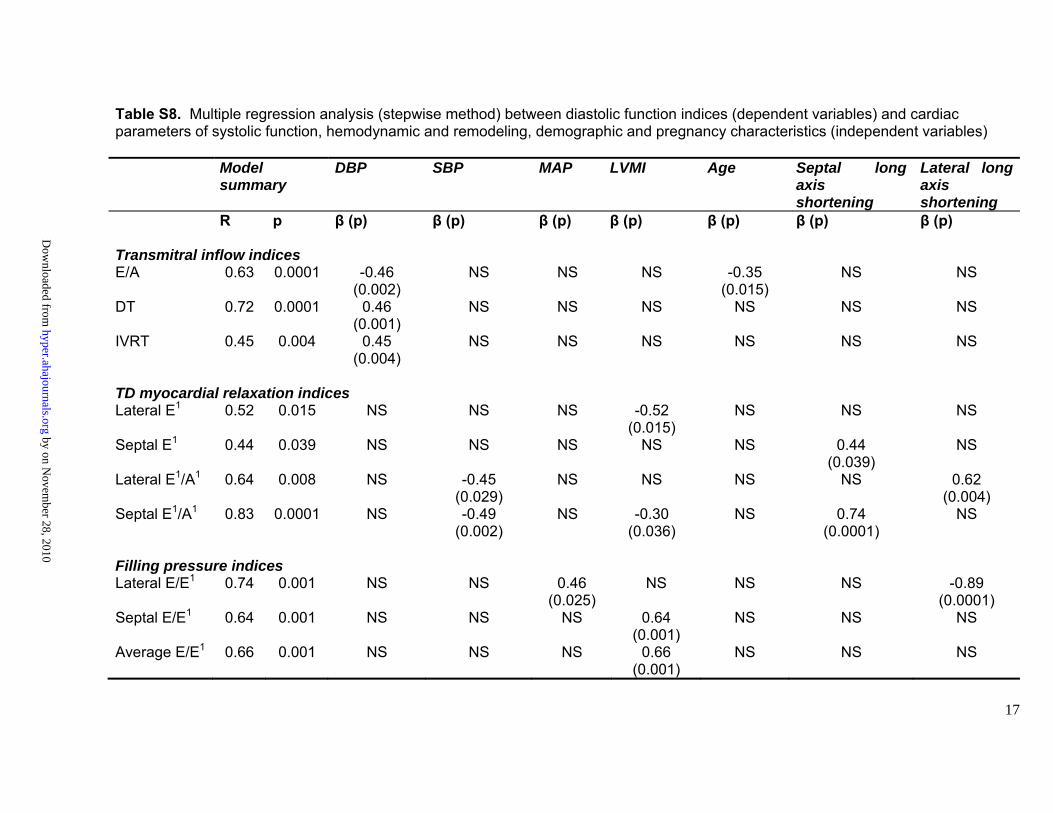
Table S8. Multiple regression analysis (stepwise method) between diastolic function indices (dependent variables) and cardiac parameters of systolic function, hemodynamic and remodeling, demographic and pregnancy characteristics (independent variables) Model
summary DBP SBP MAP LVMI Age Septal long
axis shortening
Lateral long axis shortening
R p β (p) β (p) β (p) β (p) β (p) β (p) β (p) Transmitral inflow indices E/A 0.63 0.0001 -0.46
(0.002) NS NS NS -0.35
(0.015) NS NS
DT 0.72 0.0001 0.46 (0.001)
NS NS NS NS NS NS
IVRT 0.45 0.004 0.45 (0.004)
NS NS NS NS NS NS
TD myocardial relaxation indices Lateral E1 0.52 0.015 NS NS NS -0.52
(0.015) NS NS NS
Septal E1 0.44 0.039 NS NS NS NS NS 0.44 (0.039)
NS
Lateral E1/A1 0.64 0.008 NS -0.45 (0.029)
NS NS NS NS 0.62 (0.004)
Septal E1/A1 0.83 0.0001 NS -0.49 (0.002)
NS -0.30 (0.036)
NS 0.74 (0.0001)
NS
Filling pressure indices Lateral E/E1 0.74 0.001 NS NS 0.46
(0.025) NS NS NS -0.89
(0.0001) Septal E/E1 0.64 0.001 NS NS NS 0.64
(0.001) NS NS NS
Average E/E1 0.66 0.001 NS NS NS 0.66 (0.001)
NS NS NS
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from
18
R=multiple correlation coefficient; β=Standardized beta coefficient. E/A=early diastole peak transmitral wave velocity to late diastole peak transmitral wave velocity ratio; DT=deceleration time of E wave; IVRT=isovolumetric relaxation time; E1=pulsed Doppler peak early diastolic velocity at mitral valve annulus; A1=peak late diastolic velocity at mitral valve annulus; SBP=systolic blood pressure; DBP=diastolic blood pressure; MAP=mean arterial pressure; LVMI=left ventricle mass index; long axis shortening=mitral ring displacement normalized for left ventricle end-diastolic long axis length. NS=not significant. Only indices found to be significantly independently correlated to diastolic function indices are shown in the table.
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from
19
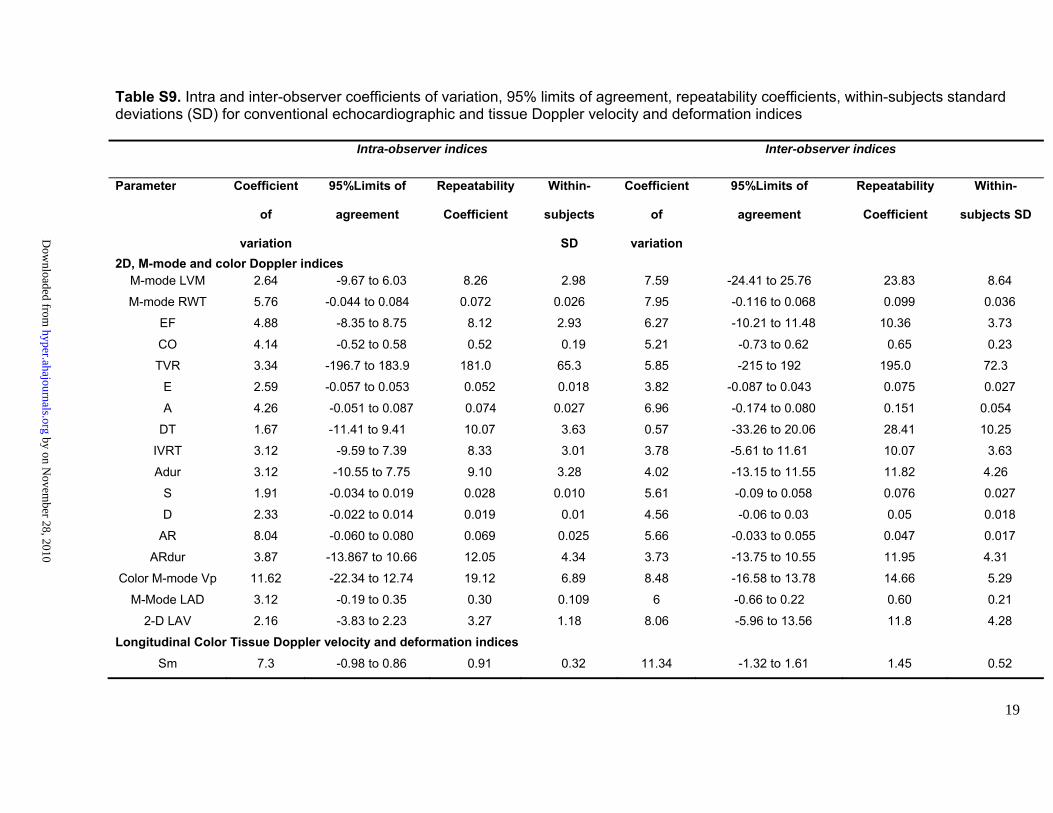
Table S9. Intra and inter-observer coefficients of variation, 95% limits of agreement, repeatability coefficients, within-subjects standard deviations (SD) for conventional echocardiographic and tissue Doppler velocity and deformation indices Intra-observer indices Inter-observer indices
Parameter Coefficient
of
variation
95%Limits of
agreement
Repeatability
Coefficient
Within-
subjects
SD
Coefficient
of
variation
95%Limits of
agreement
Repeatability
Coefficient
Within-
subjects SD
2D, M-mode and color Doppler indicesM-mode LVM 2.64 -9.67 to 6.03 8.26 2.98 7.59 -24.41 to 25.76 23.83 8.64
M-mode RWT 5.76 -0.044 to 0.084 0.072 0.026 7.95 -0.116 to 0.068 0.099 0.036
EF 4.88 -8.35 to 8.75 8.12 2.93 6.27 -10.21 to 11.48 10.36 3.73
CO 4.14 -0.52 to 0.58 0.52 0.19 5.21 -0.73 to 0.62 0.65 0.23
TVR 3.34 -196.7 to 183.9 181.0 65.3 5.85 -215 to 192 195.0 72.3
E 2.59 -0.057 to 0.053 0.052 0.018 3.82 -0.087 to 0.043 0.075 0.027
A 4.26 -0.051 to 0.087 0.074 0.027 6.96 -0.174 to 0.080 0.151 0.054
DT 1.67 -11.41 to 9.41 10.07 3.63 0.57 -33.26 to 20.06 28.41 10.25
IVRT 3.12 -9.59 to 7.39 8.33 3.01 3.78 -5.61 to 11.61 10.07 3.63
Adur 3.12 -10.55 to 7.75 9.10 3.28 4.02 -13.15 to 11.55 11.82 4.26
S 1.91 -0.034 to 0.019 0.028 0.010 5.61 -0.09 to 0.058 0.076 0.027
D 2.33 -0.022 to 0.014 0.019 0.01 4.56 -0.06 to 0.03 0.05 0.018
AR 8.04 -0.060 to 0.080 0.069 0.025 5.66 -0.033 to 0.055 0.047 0.017
ARdur 3.87 -13.867 to 10.66 12.05 4.34 3.73 -13.75 to 10.55 11.95 4.31
Color M-mode Vp 11.62 -22.34 to 12.74 19.12 6.89 8.48 -16.58 to 13.78 14.66 5.29
M-Mode LAD 3.12 -0.19 to 0.35 0.30 0.109 6 -0.66 to 0.22 0.60 0.21
2-D LAV 2.16 -3.83 to 2.23 3.27 1.18 8.06 -5.96 to 13.56 11.8 4.28
Longitudinal Color Tissue Doppler velocity and deformation indices
Sm 7.3 -0.98 to 0.86 0.91 0.32 11.34 -1.32 to 1.61 1.45 0.52
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from
20
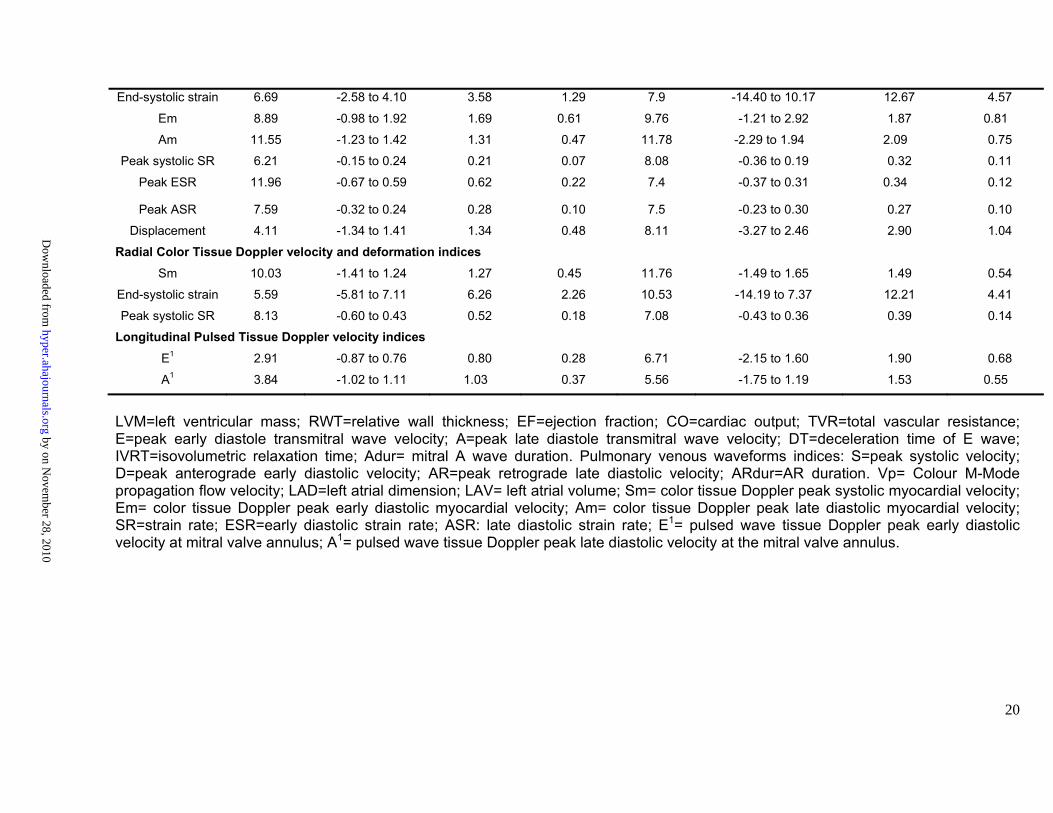
End-systolic strain 6.69 -2.58 to 4.10 3.58 1.29 7.9 -14.40 to 10.17 12.67 4.57
Em 8.89 -0.98 to 1.92 1.69 0.61 9.76 -1.21 to 2.92 1.87 0.81
Am 11.55 -1.23 to 1.42 1.31 0.47 11.78 -2.29 to 1.94 2.09 0.75
Peak systolic SR 6.21 -0.15 to 0.24 0.21 0.07 8.08 -0.36 to 0.19 0.32 0.11
Peak ESR 11.96 -0.67 to 0.59 0.62 0.22 7.4 -0.37 to 0.31 0.34 0.12
Peak ASR 7.59 -0.32 to 0.24 0.28 0.10 7.5 -0.23 to 0.30 0.27 0.10
Displacement 4.11 -1.34 to 1.41 1.34 0.48 8.11 -3.27 to 2.46 2.90 1.04
Radial Color Tissue Doppler velocity and deformation indices
Sm 10.03 -1.41 to 1.24 1.27 0.45 11.76 -1.49 to 1.65 1.49 0.54
End-systolic strain 5.59 -5.81 to 7.11 6.26 2.26 10.53 -14.19 to 7.37 12.21 4.41
Peak systolic SR 8.13 -0.60 to 0.43 0.52 0.18 7.08 -0.43 to 0.36 0.39 0.14
Longitudinal Pulsed Tissue Doppler velocity indices
E1 2.91 -0.87 to 0.76 0.80 0.28 6.71 -2.15 to 1.60 1.90 0.68
A1 3.84 -1.02 to 1.11 1.03 0.37 5.56 -1.75 to 1.19 1.53 0.55
LVM=left ventricular mass; RWT=relative wall thickness; EF=ejection fraction; CO=cardiac output; TVR=total vascular resistance; E=peak early diastole transmitral wave velocity; A=peak late diastole transmitral wave velocity; DT=deceleration time of E wave; IVRT=isovolumetric relaxation time; Adur= mitral A wave duration. Pulmonary venous waveforms indices: S=peak systolic velocity; D=peak anterograde early diastolic velocity; AR=peak retrograde late diastolic velocity; ARdur=AR duration. Vp= Colour M-Mode propagation flow velocity; LAD=left atrial dimension; LAV= left atrial volume; Sm= color tissue Doppler peak systolic myocardial velocity; Em= color tissue Doppler peak early diastolic myocardial velocity; Am= color tissue Doppler peak late diastolic myocardial velocity; SR=strain rate; ESR=early diastolic strain rate; ASR: late diastolic strain rate; E1= pulsed wave tissue Doppler peak early diastolic velocity at mitral valve annulus; A1= pulsed wave tissue Doppler peak late diastolic velocity at the mitral valve annulus.
by on Novem
ber 28, 2010 hyper.ahajournals.org
Dow
nloaded from




















