
Inflammation, Growth Factors, and Pulmonary Vascular Remodeling
10
Inflammation, Growth Factors, and Pulmonary Vascular Remodeling Paul M. Hassoun, MD,* Luc Mouthon, MD, PHD,† Joan A. Barberà, MD,‡ Saadia Eddahibi, PHD,§ Sonia C. Flores, PHD, Friedrich Grimminger, MD, PHD,¶ Peter Lloyd Jones, PHD,# Michael L. Maitland, MD, PHD,** Evangelos D. Michelakis, MD,†† Nicholas W. Morrell, MA, MD,‡‡ John H. Newman, MD,§§ Marlene Rabinovitch, MD, Ralph Schermuly, PHD,¶¶ Kurt R. Stenmark, MD,## Norbert F. Voelkel, MD,*** Jason X.-J. Yuan, MD, PHD,††† Marc Humbert, MD, PHD‡‡‡ Baltimore, Maryland; Paris, Créteil, and Clamart, France; Barcelona, Spain; Denver, Colorado; Giessen, Germany; Philadelphia, Pennsylvania; Chicago, Illinois; Edmonton, Alberta, Canada; Cambridge, United Kingdom; Nashville, Tennessee; Stanford and La Jolla, California; and Richmond, Virginia Inflammatory processes are prominent in various types of human and experimental pulmonary hypertension (PH) and are increasingly recognized as major pathogenic components of pulmonary vascular remodeling. Macrophages, T and B lymphocytes, and dendritic cells are present in the vascular lesions of PH, whether in idiopathic pulmonary arterial hypertension (PAH) or PAH related to more classical forms of inflammatory syndromes such as connective tissue dis- eases, human immunodeficiency virus (HIV), or other viral etiologies. Similarly, the presence of circulating chemo- kines and cytokines, viral protein components (e.g., HIV-1 Nef), and increased expression of growth (such as vascular endothelial growth factor and platelet-derived growth factor) and transcriptional (e.g., nuclear factor of activated T cells or NFAT) factors in these patients are thought to contribute directly to further recruitment of inflammatory cells and proliferation of smooth muscle and endothelial cells. Other processes, such as mitochondrial and ion channel dysregulation, seem to convey a state of cellular resistance to apoptosis; this has recently emerged as a necessary event in the pathogenesis of pulmonary vascular remodeling. Thus, the recognition of complex inflammatory distur- bances in the vascular remodeling process offers potential specific targets for therapy and has recently led to clinical trials investigating, for example, the use of tyrosine kinase inhibitors. This paper provides an overview of specific in- flammatory pathways involving cells, chemokines and cytokines, cellular dysfunctions, growth factors, and viral pro- teins, highlighting their potential role in pulmonary vascular remodeling and the possibility of future targeted therapy. (J Am Coll Cardiol 2009;54:S10–9) © 2009 by the American College of Cardiology Foundation Pulmonary arterial hypertension (PAH) constitutes a heterogeneous group of clinical entities sharing similar pathologies that have been subcategorized as idiopathic pulmonary arterial hypertension (IPAH), familial PAH, pulmonary hypertension (PH) associated with other dis- eases such as connective tissue diseases, (e.g., systemic sclerosis [SSc]), portopulmonary hypertension, and PH related to human immunodeficiency virus (HIV) infec- tion, drugs, and toxins (1). Although modifications to this classification are reviewed elsewhere in this series, this review focuses on inflammatory processes in PAH and other forms of PH, highlighting specific components of inflammation in the development of PH, as well as potential targets for therapy. From the *Division of Pulmonary and Critical Care Medicine, Department of Medicine, Johns Hopkins University, Baltimore, Maryland; †Department of Internal Medicine, Cochin Hospital, Paris-Descartes University, Paris, France; ‡Servei de Pneumologia, Hospital Clinic, Universitat de Barcelona, and CIBERES, Barcelona, Spain; §Departement de Physiologie, Hôpital Henri Mondor, Créteil, France; Division of Pulmonary Sciences & Critical Care Medicine, University of Colorado, Denver, Colorado; ¶Medical Clinic IV and V, University Hospital Giessen and Marburg GmbH, Giessen, Germany; #University of Pennsylvania, Penn/CMREF Center for Pulmonary Arterial Hypertension Research, Philadelphia, Pennsylvania; **Section of Hematology/Oncology, Department of Medicine and Committee on Clinical Pharmacology and Pharmacogenomics, University of Chicago, Chicago, Illinois; ††Pulmonary Hypertension Program, University of Alberta Hospital, Edmonton, Al- berta, Canada; ‡‡Pulmonary Vascular Diseases Unit, Department of Medicine, Univer- sity of Cambridge School of Clinical Medicine, Cambridge, United Kingdom; §§De- partment of Medicine, Division of Pulmonary/Allergy/Immunology, Vanderbilt Univer- sity Medical Center, Nashville, Tennessee; The Wall Center for Pulmonary Vascular Diseases, Stanford University School of Medicine, Stanford, California; ¶¶Department of Internal Medicine, Justus-Liebig University of Giessen, Giessen, Germany; ##Developmental Lung Biology Laboratory, University of Colorado at Denver and Health Sciences Center, Denver, Colorado; ***Pulmonary and Critical Care Division, Virginia Commonwealth University, Richmond, Virginia; †††Department of Med- icine, University of California San Diego, La Jolla, California; and the ‡‡‡Université Paris-Sud, Service de Pneumologie et Réanimation Respiratoire, Hôpital Antoine Béclère, Clamart, France. Please see the end of this article for each author’s conflict of interest information. Manuscript received February 6, 2009, accepted April 15, 2009. Journal of the American College of Cardiology Vol. 54, No. 1, Suppl S, 2009 © 2009 by the American College of Cardiology Foundation ISSN 0735-1097/09/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2009.04.006
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Inflammation, Growth Factors, and Pulmonary Vascular Remodeling

Phpppes
FMMPS�DMC*C†b
Journal of the American College of Cardiology Vol. 54, No. 1, Suppl S, 2009© 2009 by the American College of Cardiology Foundation ISSN 0735-1097/09/$36.00P
Inflammation, Growth Factors,and Pulmonary Vascular RemodelingPaul M. Hassoun, MD,* Luc Mouthon, MD, PHD,† Joan A. Barberà, MD,‡ Saadia Eddahibi, PHD,§Sonia C. Flores, PHD,� Friedrich Grimminger, MD, PHD,¶ Peter Lloyd Jones, PHD,#Michael L. Maitland, MD, PHD,** Evangelos D. Michelakis, MD,††Nicholas W. Morrell, MA, MD,‡‡ John H. Newman, MD,§§ Marlene Rabinovitch, MD,��Ralph Schermuly, PHD,¶¶ Kurt R. Stenmark, MD,## Norbert F. Voelkel, MD,***Jason X.-J. Yuan, MD, PHD,††† Marc Humbert, MD, PHD‡‡‡Baltimore, Maryland; Paris, Créteil, and Clamart, France; Barcelona, Spain; Denver, Colorado;Giessen, Germany; Philadelphia, Pennsylvania; Chicago, Illinois; Edmonton, Alberta, Canada;Cambridge, United Kingdom; Nashville, Tennessee; Stanford and La Jolla, California; and Richmond, Virginia
Inflammatory processes are prominent in various types of human and experimental pulmonary hypertension (PH) andare increasingly recognized as major pathogenic components of pulmonary vascular remodeling. Macrophages, T andB lymphocytes, and dendritic cells are present in the vascular lesions of PH, whether in idiopathic pulmonary arterialhypertension (PAH) or PAH related to more classical forms of inflammatory syndromes such as connective tissue dis-eases, human immunodeficiency virus (HIV), or other viral etiologies. Similarly, the presence of circulating chemo-kines and cytokines, viral protein components (e.g., HIV-1 Nef), and increased expression of growth (such as vascularendothelial growth factor and platelet-derived growth factor) and transcriptional (e.g., nuclear factor of activated Tcells or NFAT) factors in these patients are thought to contribute directly to further recruitment of inflammatory cellsand proliferation of smooth muscle and endothelial cells. Other processes, such as mitochondrial and ion channeldysregulation, seem to convey a state of cellular resistance to apoptosis; this has recently emerged as a necessaryevent in the pathogenesis of pulmonary vascular remodeling. Thus, the recognition of complex inflammatory distur-bances in the vascular remodeling process offers potential specific targets for therapy and has recently led to clinicaltrials investigating, for example, the use of tyrosine kinase inhibitors. This paper provides an overview of specific in-flammatory pathways involving cells, chemokines and cytokines, cellular dysfunctions, growth factors, and viral pro-teins, highlighting their potential role in pulmonary vascular remodeling and the possibility of future targetedtherapy. (J Am Coll Cardiol 2009;54:S10–9) © 2009 by the American College of Cardiology Foundation
ublished by Elsevier Inc. doi:10.1016/j.jacc.2009.04.006
rtttaop
spsDo#HViPB
ulmonary arterial hypertension (PAH) constitutes aeterogeneous group of clinical entities sharing similarathologies that have been subcategorized as idiopathiculmonary arterial hypertension (IPAH), familial PAH,ulmonary hypertension (PH) associated with other dis-ases such as connective tissue diseases, (e.g., systemicclerosis [SSc]), portopulmonary hypertension, and PH
rom the *Division of Pulmonary and Critical Care Medicine, Department ofedicine, Johns Hopkins University, Baltimore, Maryland; †Department of Internaledicine, Cochin Hospital, Paris-Descartes University, Paris, France; ‡Servei de
neumologia, Hospital Clinic, Universitat de Barcelona, and CIBERES, Barcelona,pain; §Departement de Physiologie, Hôpital Henri Mondor, Créteil, France;Division of Pulmonary Sciences & Critical Care Medicine, University of Colorado,enver, Colorado; ¶Medical Clinic IV and V, University Hospital Giessen andarburg GmbH, Giessen, Germany; #University of Pennsylvania, Penn/CMREFenter for Pulmonary Arterial Hypertension Research, Philadelphia, Pennsylvania;
*Section of Hematology/Oncology, Department of Medicine and Committee onlinical Pharmacology and Pharmacogenomics, University of Chicago, Chicago, Illinois;
†Pulmonary Hypertension Program, University of Alberta Hospital, Edmonton, Al-erta, Canada; ‡‡Pulmonary Vascular Diseases Unit, Department of Medicine, Univer-o
elated to human immunodeficiency virus (HIV) infec-ion, drugs, and toxins (1). Although modifications tohis classification are reviewed elsewhere in this series,his review focuses on inflammatory processes in PAHnd other forms of PH, highlighting specific componentsf inflammation in the development of PH, as well asotential targets for therapy.
ity of Cambridge School of Clinical Medicine, Cambridge, United Kingdom; §§De-artment of Medicine, Division of Pulmonary/Allergy/Immunology, Vanderbilt Univer-ity Medical Center, Nashville, Tennessee; � �The Wall Center for Pulmonary Vasculariseases, Stanford University School of Medicine, Stanford, California; ¶¶Department
f Internal Medicine, Justus-Liebig University of Giessen, Giessen, Germany;#Developmental Lung Biology Laboratory, University of Colorado at Denver andealth Sciences Center, Denver, Colorado; ***Pulmonary and Critical Care Division,irginia Commonwealth University, Richmond, Virginia; †††Department of Med-
cine, University of California San Diego, La Jolla, California; and the ‡‡‡Universitéaris-Sud, Service de Pneumologie et Réanimation Respiratoire, Hôpital Antoineéclère, Clamart, France. Please see the end of this article for each author’s conflict
f interest information.Manuscript received February 6, 2009, accepted April 15, 2009.
I
Ihce[cbflAsrdamsPio
olspirocCtpC(crufTccpaC
sckgttewCP
adittii
gfmcmPtfllveratcaSmrSwtCcpemdtptIbnjhpiCPGtfge(h
S11JACC Vol. 54, No. 1, Suppl S, 2009 Hassoun et al.June 30, 2009:S10–9 Pulmonary Vascular Remodeling
nflammation in PAH
nflammation plays a significant role in various types ofuman PH, such as IPAH and PAH associated withonnective tissue diseases and HIV infection and inxperimental animal models (e.g., monocrotalineMCT]-induced PH). A subset of PAH patients haveirculating autoantibodies, including antinuclear anti-odies (2), and elevated circulating levels of the proin-ammatory cytokines interleukin (IL)-1 and IL-6 (3).lthough there are serologic and pathologic features
uggestive of inflammation in both IPAH and PAHelated to SSc (PAH-SSc) or other connective tissueiseases, it is likely that inflammatory pathways andutoimmunity are more pronounced in PAH-SSc. Thisight explain survival discrepancies and differential re-
ponse to therapy between the 2 syndromes (4). As such,AH-SSc might be considered the prototypic syndrome
n which to study inflammatory processes potentiallyperative in the pathogenesis of PAH.A role for inflammation in PAH is based on the finding
f inflammatory cells, including macrophages and T and Bymphocytes, and dendritic cells around the plexiform le-ions of PAH (5). Levels of macrophage inflammatoryrotein-1�, IL-1� and -6 (3,6), and P-selectin (7) arencreased in severe IPAH. Involvement of leukocytes, mac-ophages, and lymphocytes in the complex vascular lesionsf IPAH was initially described by Tuder et al. (8) andonfirmed in more recent studies by Dorfmüller et al. (9).ytokine- and chemokine-dependent mechanisms leading
o inflammatory cell recruitment in human PAH are alsorominent in PAH.ytokines and chemokines in PAH. Balabanian et al.
10) demonstrated that fractalkine (CX3CL1), a uniquehemokine that promotes the chemokine (C-X3-C motif)eceptor 1 (CX3CR1)-expressing leukocyte recruitment, ispregulated in circulating CD4� and CD8� T lymphocytesrom PAH patients as compared with control subjects.hese patients also have elevated soluble CX3CL1 plasma
oncentrations; their lung tissue samples demonstrate in-reased CX3CL1 messenger ribonucleic acid (mRNA) ex-ression as compared with control subjects, and pulmonaryrtery (PA) endothelial cells (ECs) from these lungs expressX3CL1 protein.Regulated upon Activation, Normal T cell expressed and
ecreted (RANTES, also known as CCL5) is an importanthemoattractant for monocytes and T-cells. CCL5 plays aey role in several vascular inflammatory processes such aslomerulonephritis, Kawasaki disease, and Takayasu’s ar-eritis. CCL5 might also play an indirect role in PAHhrough the induction of endothelin (ET)-convertingnzyme-1 and ET-1, a potent endothelium-derived factorith strong vasoconstrictive and mitogenic action. Indeed,CL5 mRNA expression is increased in lung samples from
AH patients as compared with control subjects and prob- mbly originates from ECs, asemonstrated by in situ hybrid-zation and immunohistochemis-ry (11). The exact relevance ofhese findings to the pathophys-ology of PAH requires furthernvestigation.
Two recent studies further sug-est that chemokines producedrom small PAs of PAH patientsight contribute to inflammatory
ell recruitment and PA smoothuscle cell (SMC) proliferation.erros et al. (12) demonstrated
hat CX3CL1 is expressed by in-ammatory cells surrounding PA
esions and that SMCs from theseessels have increased CX3CR1xpression. In addition, culturedat PA-SMCs express CX3CR1,nd CX3CL1 induces prolifera-ion but not migration of theseells. Therefore, fractalkine mightct as a growth factor for PA-MCs. The hypothesis that che-okines might play a role in PA
emodeling was further studied byanchez et al. (13). Comparedith control subjects, IPAH pa-
ients have elevated levels ofCL2, also known as monocyte
hemotactic protein (MCP)-1, inlasma and lung tissue. In additionlevated CCL2 release from pul-onary ECs or PA-SMCs was
emonstrated. Monocyte migra-ion was markedly increased in theresence of pulmonary ECs (par-icularly from patients withPAH) and significantly reducedy CCL2-blocking antibodies. Fi-ally, compared with control sub-
ects, PA-SMCs from patients ex-ibited stronger migratory androliferative responses to CCL2,n keeping with the finding thatCR2 was markedly increased inA-SMCs in these patients (13).rowth factors and inflamma-
ion in PAH. Several growthactors, including platelet-derivedrowth factor (PDGF) (14,15),pidermal growth factor (EGF)16), and vascular endothelial growth factor (VEGF) (17),ave been implicated in the abnormal proliferation and
Abbreviationsand Acronyms
AECA � anti-endothelialcell antibody
bcl � B-cell lymphoma
COPD � chronic obstructivepulmonary disease
EC � endothelial cell
EGF � epidermal growthfactor
ET � endothelin
HCV � hepatitis C virus
HHV � human herpes virus
HIV � humanimmunodeficiency virus
5-HT � serotonin
5-HTT � serotonintransporter
IL � interleukin
IPAH � idiopathicpulmonary arterialhypertension
Kv � voltage-dependentpotassium channel
MCT � monocrotaline
mRNA � messengerribonucleic acid
NFAT � nuclear factor ofactivated T cells
PA � pulmonary artery
PAH � pulmonary arterialhypertension
PCR � polymerase chainreaction
PDGF � platelet-derivedgrowth factor
PDGFR � platelet-derivedgrowth factor receptor
PH � pulmonaryhypertension
RV � right ventricular
SIV � simianimmunodeficiency virus
SMC � smooth muscle cell
SSc � systemic sclerosis
TGF � transforming growthfactor
TN � tenascin
TNF � tumor necrosis factor
VEGF � vascularendothelial growth factor
igration of PA vascular cells. The
y act as potent mitogens
ac
V
tsoVh(tatVie
P
dPatatbrapercdIPesPsmlicr
E
StTdir
S
iccm(
rpiS
wes5t5PcgStatgtP
aPPo(sdftScshgpIph5
S
mlshSrsatdtp
S12 Hassoun et al. JACC Vol. 54, No. 1, Suppl S, 2009Pulmonary Vascular Remodeling June 30, 2009:S10–9
nd chemoattractants for SMCs, fibroblasts, and ECs andause resistance to apoptosis.
EGF. Cool et al. (18) demonstrated intense expression ofhe VEGF receptor KDR, coupled with a reduced expres-ion of p27/kip1, a cell cycle inhibitory protein, in the ECsf plexiform lesions. Other markers of angiogenesis, such asEGF and hypoxia inducible factor-1 subunits � and �, areighly expressed in ECs of plexiform lesions in severe PAH19). In addition, expression of C-Src kinase (19), a proteinhat mediates VEGF-induced production of prostacyclinnd nitric oxide in ECs, is decreased in PAH. Takenogether, these findings suggest a central role in PAH forEGF, a mediator of angiogenesis but also a factor involved
n permeability and inflammatory processes in the vascularndothelium.
DGF. Platelet-derived growth factor is synthesized by manyifferent cell types including SMCs, ECs, and macrophages.DGF induces the proliferation and migration of SMCsnd fibroblasts and has been proposed as a key mediator inhe progression of several fibroproliferative disorders such astherosclerosis, lung fibrosis, and PH (14). As a result, novelherapeutic agents, such as tyrosine kinase inhibitors, haveeen tested in experimental models of PH (15) and moreecently in clinical trials. The rationale for use of thesegents is discussed in more detail in later sections. Theathogenic role of PDGF was demonstrated by increasedxpression of PDGF and platelet-derived growth factoreceptors (PDGFRs) by reverse transcription-polymerasehain reaction (PCR) performed on laser-captured micro-issected PAs from native lungs of patients with severePAH who underwent lung transplantation (20). TheDGF-A, PDGF-B, PDGF-R �, and PDGF-R � mRNAxpression is increased in small PAs from patients withevere IPAH as compared with control subjects. In smallAs, PDGF-B is mainly expressed in ECs, SMCs, and inome perivascular inflammatory cells, and PDGFR-� isainly expressed in SMCs. The PDGF-BB–induced pro-
iferation and migration of PA-SMCs is inhibited bymatinib (20). Taken together, these data support theoncept that PDGF is overproduced and promotes PAemodeling in PAH.
GF. The EGF-dependent proliferation and migration ofMCs is dependent on the extracellular matrix componentenascin C (TN-C). In addition, EGF colocalizes withN-C in PAH lesions (21), suggesting a direct role inisease progression. It is noteworthy that the EGF receptor
nhibitor PKI166 reverses established MCT-induced PH inats (16).
EROTONIN AND SEROTONIN TRANSPORTER. In addition tots vasoactive effects, serotonin (5-HT) exerts mitogenic ando-mitogenic effects on PA-SMCs. In contrast to theonstricting action of 5-HT on SMCs, which is mainlyediated by 5-HT receptors (5-HT 1B/D, 2A, and 2B)
22), the mitogenic and co-mitogenic effects of 5-HT t
equire internalization of indoleamine by serotonin trans-orter (5-HTT) (23). Accordingly, drugs that competitivelynhibit 5-HTT also block the mitogenic effects of 5-HT onMCs (24).Serotonin transporter is abundantly expressed in the lung,
here it is predominantly located in PA-SMCs (24). Directvidence that 5-HTT plays a key role in PA remodeling isupported by studies showing that mice with targeted-HTT gene disruption develop less severe hypoxic PHhan wild-type control subjects (25) and that selective-HTT inhibitors attenuate hypoxia- and MCT-inducedH (26). Conversely, increased 5-HTT expression is asso-iated with increased severity of hypoxic PH (27). Trans-enic mice with selective overexpression of 5-HTT inMCs spontaneously develop PH (28). Pulmonary hyper-ension seems to develop in these mice without any alter-tions in 5-HT bioavailability and as a sole consequence ofhe increased expression of 5-HTT in SMCs. Taken to-ether, these observations suggest a close correlation be-ween 5-HTT expression and/or activity and the extent ofA remodeling during experimental PH.Serotonin transporter expression is increased in platelets
nd in the media of thickened PAs in IPAH (24). TheA-SMCs from patients with IPAH grow faster thanA-SMCs from control subjects when stimulated by 5-HTr serum, as a consequence of increased 5-HTT expression24). In the presence of 5-HTT inhibitors, the growth-timulating effects of serum and 5-HT are markedly re-uced, and the difference between growth of PA-SMCsrom patients and control subjects was abolished. Takenogether, 5-HTT overexpression and/or activity in PA-MCs from IPAH patients seem responsible for the in-reased mitogenic response to 5-HT. The 5-HT is synthe-ized by ECs in the normal lung as a result of tryptophanydroxylase-1 enzyme activity and seems to be the mainrowth factor produced by ECs, acting on PA-SMCs in aaracrine fashion. In conclusion, PA-SMC hyperplasia inPAH seems to result from both dysregulation of 5-HTroduction by ECs due to overexpression of tryptophanydroxylase-1 and from an increased PA-SMC response to-HT due to overexpression of the 5-HTT (29).
URVIVIN. Survivin (16.5 kDa) is the smallest member of theammalian inhibitor of the apoptosis family. Several ma-
ignant processes have been linked to dysregulation ofurvivin expression. The normal absence of survivin fromealthy tissues suggests it is a potential target for therapy.urvivin is overexpressed in PAs from PAH patients and inats with MCT-induced PAH, compared with controlubjects (30). Wild-type survivin delivered via an inhaleddenovirus to normal rats causes PH. Conversely, geneherapy with an adenovirus carrying a phosphorylation-eficient survivin mutant with dominant-negative proper-ies (T34A survivin) reverses established MCT-PAH androlongs survival (30). Administration of the survivin mu-
ant reduces pulmonary vascular resistance, right ventricular
(vPoidosrpetTTndidf[pf(t
ilpPlvTt(c
cpCrPf(manPN
Pdodbie
ialItartTrea
V
Hbardoom
islduoScaDliRpppiidtrHoPrib
csp
S13JACC Vol. 54, No. 1, Suppl S, 2009 Hassoun et al.June 30, 2009:S10–9 Pulmonary Vascular Remodeling
RV) hypertrophy, and PA medial hypertrophy. Both initro and in vivo, inhibition of endogenous survivin inducesA-SMC apoptosis, depolarizes mitochondria, causes effluxf cytochrome c in the cytoplasm, translocates apoptosis-nducing factor into the nucleus, and increases voltage-ependent potassium channel (Kv) current, whereas thepposite effects are observed with gene transfer of wild-typeurvivin. Survivin also induces the production of the PDGFeceptor in human vascular SMCs (31). Therefore, the pro-osed causative role of survivin in PAH and the lack of itsxpression in normal PA wall and systemic vasculature makehis gene attractive for future targeted therapy in PAH.
ranscriptional factors: the nuclear factor of activatedcells in inflammation and vascular remodeling. The
uclear factor of activated T cells (NFAT), originallyescribed in T cells, is a master activator of T cells,
ncreasing the transcription of multiple inflammatory me-iators, including many interleukins and tumor necrosisactor (TNF)�, and activating T and B cells (32). IncreasedCa2�]i activates calcineurin, which dephosphorylates cyto-lasmic NFAT, allowing its entry to the nucleus, where itorms complexes with other important transcription factorse.g., GATA or activator protein-1) and regulates generanscription (32).
Several recent observations suggest that NFAT might benvolved in PAH. The NFAT activation causes downregu-ation of Kv1.5 (33), which plays a preponderant role inulmonary vasoconstriction. Second, ET (upregulated inAH) activates NFAT, which in turn increases B-cell
ymphoma (bcl)-2 expression, contributing to the prosur-ival and antiapoptotic effects of ET in the heart (34).hird, NFAT directly or indirectly regulates the transcrip-
ion of several genes that regulate mitochondrial functione.g., pyruvate decarboxylase and the electron transporthain enzyme cytochrome C oxidase) (35).
The NFAT is upregulated and activated (i.e., translo-ated in the nucleus) in circulating inflammatory cells inatients with PAH, including IPAH and PAH-SSc. TheD3-positive cells with activated NFAT are also seen in
emodeled PAs. Intriguingly, NFAT is also activated in theA-SMCs of remodeled arteries. The PA-SMCs isolated
rom PAH patients maintain in culture a unique phenotypedownregulated Kv1.5, upregulated bcl-2, hyperpolarizeditochondria), which is associated with activated NFAT
nd resistance to apoptosis. The NFAT is not activated inormal lungs and PA-SMCs. The unique phenotype ofAH PA-SMCs is normalized by selective inhibition ofFAT.Inhibition of NFATc2 (predominant NFAT isotype in
AH) by VIVIT (a competitive peptide that inhibits theocking of NFAT to calcineurin) or cyclosporine (inhibitorf calcineurin), restores Kv1.5 expression and current andecreases [Ca2�]i, [K�]i, bcl-2, and mitochondrial mem-rane potential (��m), leading to increased apoptosisn vitro (36). In vivo, cyclosporine treatment decreases
stablished MCT-induced PAH in the rat (36). Intrigu- tngly, PA-SMCs exposed to chronic hypoxia display NFATctivation, hyperpolarized mitochondria, and downregu-ated Kv1.5, similar to the SMC phenotype of PAH.nhibition with VIVIT or cyclosporine reverses this pheno-ype, normalizing the mitochondrial membrane potentialnd level/function of Kv1.5 in these cells. There has beenecent interest in developing specific NFAT inhibitors forhe treatment of cardiac hypertrophy and failure (37).herefore, in PAH, NFAT inhibitors might contribute to
eversing RV hypertrophy and pulmonary vascular remod-ling through their effects on cardiomyocytes, PA-SMCs,nd inflammatory cells.
iral and Other Infectious Etiologies in PAH
ypothetically, PH is caused by latent viral infections,ecause associations between Epstein Barr virus infectionnd Hodgkin’s disease and parvovirus and cytomegalovi-us infection and SSc have been described (38); bothiseases have also been associated with PH. Infectiousrganisms can affect the lung circulation directly, bybliterating lung vessels, or indirectly, by causing andaintaining inflammation.However, there is little evidence for a “direct” role for
nfectious agents in the pathogenesis of severe PH. Even inchistosomiasis-associated PH, it is unclear to what extentiver disease and therefore portopulmonary hypertensionominate the pathobiology of PH. Schistosoma eggs mod-late regulatory T-cell activity and express a novel memberf the transforming-growth factor (TGF)-� superfamily,chistosoma mansoni inhibin/activin (SmInAct) (39). Re-ently a mouse model of pneumocystis-induced PH associ-ted with muscularized PAs has been reported (40), andaley et al. (41) reported a mouse model of highly muscu-
arized PAs after a regimen of aspergillus antigen (ag)mmunization.
ole of human herpes virus-8, HIV, and SHIV-Nef inulmonary vascular remodeling. Pulmonary arterial hy-ertension has a prevalence of 0.0002% in the generalopulation, but in HIV-infected individuals the prevalences 0.46% in France (42). The HIV-related PAH (HRPAH)s independent of CD4� T cell counts (43) and antiviralrug treatment. The clinical features of HRPAH are similaro PAH of other etiologies. Although highly active antiret-oviral therapy might have decreased the incidence of
RPAH and might partially reverse PH in a small numberf HIV-1–infected individuals only when combined withH-specific treatment such as bosentan (44), this disease
emains a significant clinical complication in the HIV-1–nfected population. Other studies showed no correlationetween viral load and right heart changes (45).Most of the pathways involved in virus pathogenesis
onverge on either prosurvival or proangiogenic signals, theame signals associated with PH. In the lung, HIV-1 infectsrimarily macrophages, providing a potential reservoir for the
ransmission of the virus to circulating T-cells, and is a source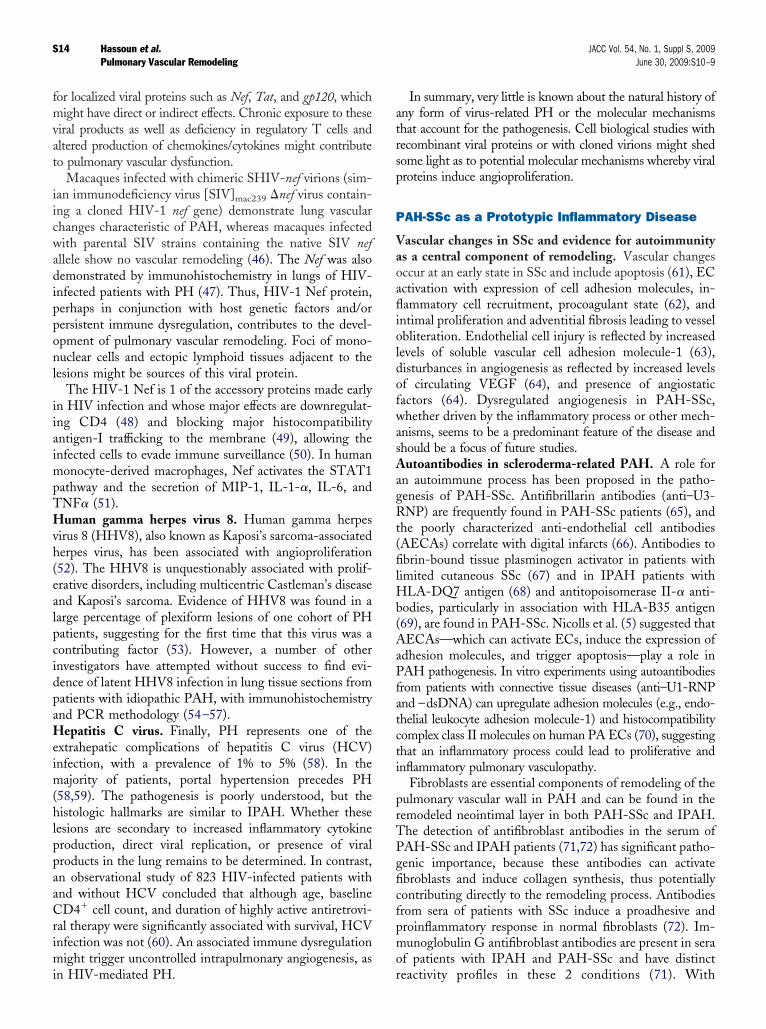
fmvat
iicwadipponl
iiaimpTHvh(ealpcidpaHeim(hlppaaCrimi
atrsp
P
VaoaflioldofwasAagRt(filHb(AaPfatcti
prTPgficfpmo
S14 Hassoun et al. JACC Vol. 54, No. 1, Suppl S, 2009Pulmonary Vascular Remodeling June 30, 2009:S10–9
or localized viral proteins such as Nef, Tat, and gp120, whichight have direct or indirect effects. Chronic exposure to these
iral products as well as deficiency in regulatory T cells andltered production of chemokines/cytokines might contributeo pulmonary vascular dysfunction.
Macaques infected with chimeric SHIV-nef virions (sim-an immunodeficiency virus [SIV]mac239 �nef virus contain-ng a cloned HIV-1 nef gene) demonstrate lung vascularhanges characteristic of PAH, whereas macaques infectedith parental SIV strains containing the native SIV nef
llele show no vascular remodeling (46). The Nef was alsoemonstrated by immunohistochemistry in lungs of HIV-
nfected patients with PH (47). Thus, HIV-1 Nef protein,erhaps in conjunction with host genetic factors and/orersistent immune dysregulation, contributes to the devel-pment of pulmonary vascular remodeling. Foci of mono-uclear cells and ectopic lymphoid tissues adjacent to the
esions might be sources of this viral protein.The HIV-1 Nef is 1 of the accessory proteins made early
n HIV infection and whose major effects are downregulat-ng CD4 (48) and blocking major histocompatibilityntigen-I trafficking to the membrane (49), allowing thenfected cells to evade immune surveillance (50). In human
onocyte-derived macrophages, Nef activates the STAT1athway and the secretion of MIP-1, IL-1-�, IL-6, andNF� (51).uman gamma herpes virus 8. Human gamma herpes
irus 8 (HHV8), also known as Kaposi’s sarcoma-associatederpes virus, has been associated with angioproliferation52). The HHV8 is unquestionably associated with prolif-rative disorders, including multicentric Castleman’s diseasend Kaposi’s sarcoma. Evidence of HHV8 was found in aarge percentage of plexiform lesions of one cohort of PHatients, suggesting for the first time that this virus was aontributing factor (53). However, a number of othernvestigators have attempted without success to find evi-ence of latent HHV8 infection in lung tissue sections fromatients with idiopathic PAH, with immunohistochemistrynd PCR methodology (54–57).
epatitis C virus. Finally, PH represents one of thextrahepatic complications of hepatitis C virus (HCV)nfection, with a prevalence of 1% to 5% (58). In the
ajority of patients, portal hypertension precedes PH58,59). The pathogenesis is poorly understood, but theistologic hallmarks are similar to IPAH. Whether these
esions are secondary to increased inflammatory cytokineroduction, direct viral replication, or presence of viralroducts in the lung remains to be determined. In contrast,n observational study of 823 HIV-infected patients withnd without HCV concluded that although age, baselineD4� cell count, and duration of highly active antiretrovi-
al therapy were significantly associated with survival, HCVnfection was not (60). An associated immune dysregulation
ight trigger uncontrolled intrapulmonary angiogenesis, as
n HIV-mediated PH. rIn summary, very little is known about the natural history ofny form of virus-related PH or the molecular mechanismshat account for the pathogenesis. Cell biological studies withecombinant viral proteins or with cloned virions might shedome light as to potential molecular mechanisms whereby viralroteins induce angioproliferation.
AH-SSc as a Prototypic Inflammatory Disease
ascular changes in SSc and evidence for autoimmunitys a central component of remodeling. Vascular changesccur at an early state in SSc and include apoptosis (61), ECctivation with expression of cell adhesion molecules, in-ammatory cell recruitment, procoagulant state (62), and
ntimal proliferation and adventitial fibrosis leading to vesselbliteration. Endothelial cell injury is reflected by increasedevels of soluble vascular cell adhesion molecule-1 (63),isturbances in angiogenesis as reflected by increased levelsf circulating VEGF (64), and presence of angiostaticactors (64). Dysregulated angiogenesis in PAH-SSc,hether driven by the inflammatory process or other mech-
nisms, seems to be a predominant feature of the disease andhould be a focus of future studies.utoantibodies in scleroderma-related PAH. A role for
n autoimmune process has been proposed in the patho-enesis of PAH-SSc. Antifibrillarin antibodies (anti–U3-NP) are frequently found in PAH-SSc patients (65), and
he poorly characterized anti-endothelial cell antibodiesAECAs) correlate with digital infarcts (66). Antibodies tobrin-bound tissue plasminogen activator in patients with
imited cutaneous SSc (67) and in IPAH patients withLA-DQ7 antigen (68) and antitopoisomerase II-� anti-
odies, particularly in association with HLA-B35 antigen69), are found in PAH-SSc. Nicolls et al. (5) suggested thatECAs—which can activate ECs, induce the expression of
dhesion molecules, and trigger apoptosis—play a role inAH pathogenesis. In vitro experiments using autoantibodies
rom patients with connective tissue diseases (anti–U1-RNPnd –dsDNA) can upregulate adhesion molecules (e.g., endo-helial leukocyte adhesion molecule-1) and histocompatibilityomplex class II molecules on human PA ECs (70), suggestinghat an inflammatory process could lead to proliferative andnflammatory pulmonary vasculopathy.
Fibroblasts are essential components of remodeling of theulmonary vascular wall in PAH and can be found in theemodeled neointimal layer in both PAH-SSc and IPAH.he detection of antifibroblast antibodies in the serum ofAH-SSc and IPAH patients (71,72) has significant patho-enic importance, because these antibodies can activatebroblasts and induce collagen synthesis, thus potentiallyontributing directly to the remodeling process. Antibodiesrom sera of patients with SSc induce a proadhesive androinflammatory response in normal fibroblasts (72). Im-unoglobulin G antifibroblast antibodies are present in sera
f patients with IPAH and PAH-SSc and have distinct
eactivity profiles in these 2 conditions (71). With
2rPvtdmtcfigp
rpaspsfaIPraC3iv(IfkmP
(EpTtd
tofip
IC
Pchtv
iiCiwlpcVcnaiCeidllTnceiatpgp
TTi
TaAwteSmiehdwenfiIiWtD
S15JACC Vol. 54, No. 1, Suppl S, 2009 Hassoun et al.June 30, 2009:S10–9 Pulmonary Vascular Remodeling
-dimensional immunoblotting technique, several antigensecognized by serum immunoglobulin G from IPAH andAH-SSc patients were identified, including proteins in-olved in regulation of cytoskeletal function, cell contrac-ion, cell and oxidative stress, cell energy metabolism, andifferent key cellular pathways (73). Although the specificembrane antigens targeted by these autoantibodies remain
o be determined, it is likely that they react to membraneomponents, because they typically bind to unpermeabilizedbroblasts, and might mediate the release of cytokines androwth factors which in turn might contribute to theathogenesis of vascular remodeling in PAH (71).Taken together, particularly in light of the positive
esponse to immunosuppressive therapy for one-third ofatients with PAH associated with systemic lupus erythem-tosus and mixed connective tissue disease (74), thesetudies suggest that inflammation and autoimmunity couldlay a major role in the pathogenesis of PAH. Thus, aearch for specific biomarkers of inflammation could be aocus of future studies in IPAH, PAH-SSc, and otherutoimmune conditions associated with PAH.nflammatory genes in SSc and scleroderma-relatedAH. An increasing number of candidate genes have been
eported to be associated with SSc in different populations:variant in the promoter of MCP-1 (75); 2 variants inD19 (�499G�T, and a GT repeat polymorphism in the=-UTR region) (76); a promoter and coding polymorphismn TNF-� (TNF-� 238A�G, TNF-� 489A�G) (77); aariant in the promoter of the IL-1� gene (IL1-� �889T)78); and a 3-single nucleotide polymorphism haplotype inL-10 (79). Thus, compelling data support a genetic basisor SSc. Despite these recent advances in genetics, little isnown about genetic involvement in PAH-SSc. BMPR2utations have not been identified in 2 small cohorts ofAH-SSc patients (80,81).Recently, an association between an endoglin gene
ENG) polymorphism and PAH-SSc was identified (82).ndoglin, a homodimeric membrane glycoprotein primarilyresent on human vascular endothelium, is part of theGF-� receptor complex. The functional significance of
he ENG polymorphism in SSc patients remains to beetermined.Aside from the few examples cited in the preceding text,
he genes relevant to the pathogenesis and generally poorutcome associated with PAH-SSc have not been identi-ed. Their definition will require robust, well-characterizedatient populations to provide adequate power for analysis.
nflammation in PH Associated Withhronic Obstructive Pulmonary Disease
ulmonary vascular remodeling is a common finding inhronic obstructive pulmonary disease (COPD) and ineavy smokers with normal lung function (83). Inflamma-ory cells might contribute to the alterations of pulmonary
essels. Indeed, the extent of pulmonary vascular remodel- rng correlates with the severity of the inflammatory cellnfiltrate in small airways (84). Furthermore, patients withOPD have an increased number of inflammatory cells
nfiltrating the adventitia of muscular PAs, as comparedith nonsmokers (85). This inflammatory infiltrate is
argely constituted by activated T lymphocytes with aredominance of the CD8� T cell subset (85) withouthange in neutrophils, macrophages, and B-lymphocytes.EGF. Patients with mild-to-moderate COPD show in-
reased expression of VEGF in PAs compared with controlonsmokers (86). The VEGF expression correlates withrterial wall thickness, suggesting a potential role of VEGFn the pathogenesis of pulmonary vascular remodeling inOPD. In patients with advanced COPD and severe
mphysema, the expression of VEGF in PAs is lower thann patients with mild-to-moderate disease and does notiffer from control nonsmokers (86), suggesting downregu-
ation of VEGF in patients with emphysema that mightead to EC apoptosis.
GF-�. In COPD, TGF-� has been implicated in con-ective tissue deposition (87) and airway macrophage re-ruitment (88). In patients with very severe COPD, thexpression of type II receptor (TGF-� RII) but not TGF-�s increased in the tunica media and intima of PAs (89),long with a normal cell proliferation rate in both layers ofhe vessel wall, suggesting that TGF-� might exert arotective role (restraining cell proliferation) and thatrowth factors other than TGF-� might be involved inulmonary vascular remodeling (89).
argeting Signaling Pathways:he Role of Antineoplastic Drugsn the Control of Vascular Remodeling in PAH
he concept of “targeted” therapy holds popular appeal fordvancing cancer treatment. Imatinib, an inhibitor of Bcr-bl kinase, has dramatically changed prognosis for patientsith chronic myeloid leukemia (90). Although imatinib is
he archetype for targeted cancer therapeutics, it does notxclusively inhibit Bcr-Abl but also inhibits PDGFR (91).chermuly et al. (15) tested the effects of imatinib in rodentodels, on the basis of evidence that PDGF signaling is an
mportant process in the pathophysiology of PAH (92). Theffects of MCT on RV systolic pressure, cardiac index, RVypertrophy, and overall survival were reversed in dose-ependent fashion with administration of imatinib, alongith downregulation of phosphorylated PDGFR� and
xtracellular signal-related kinase in lung tissue homoge-ates. Clinical validation of imatinib as PAH therapy wasrst suggested in case reports (93–95). These led to a PhaseI trial to evaluate the safety, tolerability, and efficacy ofmatinib in patients with PAH that, at the time of the PH
orld Congress, was open to accrual at multiple centers inhe U.S. and Europe.
isrupting PDGF and VEGF signaling. Although the
ole for specific disruption of PDGFR signaling in cancer
tosiWrh
pngfp(I
S16 Hassoun et al. JACC Vol. 54, No. 1, Suppl S, 2009Pulmonary Vascular Remodeling June 30, 2009:S10–9
herapeutic regimens is still under investigation, the efficacyf 2 U.S. Food and Drug Administration-approved agents,unitinib and sorafenib, is attributed in part to their dualnhibition of VEGF and PDGF signaling pathways.
hereas PDGF is a validated specific target in PH, theationale for testing antiproliferative drugs in advanceduman PAH is also based on the presence of dysregulated
Figure 1 Mechanisms of Inflammation-Mediated Remodeling
This schematic features inflammatory mediators, cells, and mechanisms involvedcytokines and chemokines in remodeled vessels (e.g., plexiform lesions) or in themediate the influx of inflammatory cells (e.g., monocytes, T and B lymphocytes). Cmotor and growth mediators, activation of transcriptional factors (e.g., nuclear facThe net effect is a shift of balance in favor of cell proliferation and decreased apotherapeutic target sites include inhibition of growth factors with tyrosine kinase inhpolypeptide (a competitive peptide that inhibits the docking of NFAT to calcineurin)CCL2 � chemokine (C-C motif) ligand 2; CCL5 � chemokine (C-C motif) ligand 5 oCX3CL1 � chemokine (C-X3-C motif) ligand 1 (fractalkine); CX3CR1 � chemokineFGF � fibroblast growth factor; 5-HT � serotonin; HIV-1 � human immunodeficiennary arterial hypertension; PDGF � platelet-derived growth factor; PGI2 � prostacy
roliferation of microvascular ECs and SMCs, monoclo-al EC expansion (96), increased expression of secretedrowth factors such as VEGF and basic fibroblast growthactor (97), and the fact that this condition—with itsoor prognosis—is reminiscent of advanced solid tumors98). Also at the time of the PH World Congress, a Phaseclinical trial to determine the safety and tolerability of
onary vascular remodeling as well as potential therapeutic targets. Release oftion, from activated endothelial cells (ECs) and smooth muscle cells (SMCs),dysfunction (particularly involving EC and SMC) contributes to release of vaso-ctivated T lymphocytes [NFAT]), influx of calcium, and mitochondrial dysfunction.
, leading to remodeling and narrowing of the pulmonary vascular lumen. Potential, calcineurin with cyclosporine, and prevention of NFAT activation with VIVITific mechanisms are further detailed in the text. bcl2 � B-cell lymphoma 2;ES (Regulated upon Activation, Normal T cell expressed and secreted);motif) receptor 1; DC � dendritic cells; ET1 � endothelin 1; FB � fibroblasts;
s 1; IgG � immunoglobulin G; MO � monocyte; NO � nitric oxide; PAH � pulmo-OK � Rho kinase; VEGF � vascular endothelial growth factor.
in pulmcirculaellulartor of aptosisibitors. Specr RANT(C-X3-Ccy viruclin; R

sdnTo
C
Icpisdt
A
D(HDAcScNhShf5PutEgbhGhNoGDa
RPMup
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
S17JACC Vol. 54, No. 1, Suppl S, 2009 Hassoun et al.June 30, 2009:S10–9 Pulmonary Vascular Remodeling
orafenib in PAH patients with stable clinical and hemo-ynamic status on prostacyclin-based therapy was open andow has since been completed at the University of Chicago.he results of these trials should help advance developmentf this therapeutic strategy in PAH.
onclusions
t has become clear that inflammatory processes involvingellular effectors, chemokines, cytokines, and growth factorslay a preponderant role in the vascular remodeling character-stic of PAH (Fig. 1). Recognition of these specific pathwayshould allow development of additional targeted therapy in thisisease, with the hope of altering a prognosis that has been alloo dismal in spite of significant recent progress.
uthor Disclosures
r. Hassoun has received research grants from ActelionCotherix), the National Institutes of Health, the National
eart, Lung and Blood Institute, and United Therapeutics.r. Mouton has received honoraria and research funds fromctelion, GlaxoSmithKline, and Pfizer. Dr. Barberà has re-
eived honoraria and research funds from Actelion, Bayerchering, GlaxoSmithKline, and Pfizer. Dr. Flores has re-eived grants from the National Institutes of Health and theational Heart, Lung and Blood Institute. Dr. Grimminger
as received honoraria and research funds from Actelion, Bayerchering, Novartis, and Pfizer. Dr. Jones has received anonorarium from Novartis. Dr. Maitland has received researchunding from Bayer and the National Cancer Institute,K23CA124802, and has consulted for Abbott, Astellasharma, and Takeda. He is co-inventor on a patent filing forse of sorafenib in the treatment of pulmonary arterial hyper-ension. Dr. Michelakis has received consultant fees fromncysive and Pfizer Inc. Dr. Morrell has received researchrant support from the British Heart Foundation, the Cam-ridge NIHR Biomedical Research Center, and Novartis, andas received honoraria for educational lectures from Actelion,laxoSmithKline, and Pfizer. Dr. Schermuly has received
onoraria and research funds from Actelion, Bayer Schering,ovartis, Pfizer, and Solvay. Dr. Humbert has received hon-
raria and research grants from Actelion, Bayer Schering,laxoSmithKline, Novartis, Pfizer, and United Therapeutics.rs. Eddahibi, Newman, Rabinovitch, Stenmark, Voelkel,
nd Yuan report no conflicts of interest.
eprint requests and correspondence: Dr. Paul M. Hassoun,rofessor of Medicine, Johns Hopkins University Department ofedicine, Pulmonary and Critical Care Medicine, 1830 East Mon-
ment Street, Room 530, Baltimore, Maryland 21287. E-mail:[email protected].
EFERENCES
1. Simonneau G, Galiè N, Rubin LJ, et al. Clinical classification ofpulmonary hypertension. J Am Coll Cardiol 2004;43:5S–12S.
2. Isern RA, Yaneva M, Weiner E, et al. Autoantibodies in patients withprimary pulmonary hypertension: association with anti-Ku. Am J Med1992;93:307–12.
3. Humbert M, Monti G, Brenot F, et al. Increased interleukin-1 andinterleukin-6 serum concentrations in severe primary pulmonary hy-pertension. Am J Respir Crit Care Med 1995;151:1628–31.
4. Fisher MR, Mathai SC, Champion HC, et al. Clinical differencesbetween idiopathic and scleroderma-related pulmonary hypertension.Arthritis Rheum 2006;54:3043–50.
5. Nicolls MR, Taraseviciene-Stewart L, Rai PR, Badesch DB, VoelkelNF. Autoimmunity and pulmonary hypertension: a perspective. EurRespir J 2005;26:1110–8.
6. Fartoukh M, Emilie D, Le Gall C, Monti G, Simonneau G, HumbertM. Chemokine macrophage inflammatory protein-1� mRNA expres-sion in lung biopsy specimens of primary pulmonary hypertension.Chest 1998;114:50S–1S.
7. Sakamaki F, Kyotani S, Nagaya N, et al. Increased plasma P-selectinand decreased thrombomodulin in pulmonary arterial hypertensionwere improved by continuous prostacyclin therapy. Circulation 2000;102:2720–5.
8. Tuder RM, Groves B, Badesch DB, Voelkel NF. Exuberant endothe-lial cell growth and elements of inflammation are present in plexiformlesions of pulmonary hypertension. Am J Pathol 1994;144:275–85.
9. Dorfmüller P, Humbert M, Perros F, et al. Fibrous remodeling of thepulmonary venous system in pulmonary arterial hypertension associ-ated with connective tissue diseases. Hum Pathol 2007;38:893–902.
0. Balabanian K, Foussat A, Dorfmüller P, et al. CX3C chemokinefractalkine in pulmonary arterial hypertension. Am J Respir Crit CareMed 2002;165:1419–25.
1. Dorfmüller P, Zarka V, Durand-Gasselin I, et al. Chemokine RANTESin severe pulmonary arterial hypertension. Am J Respir Crit Care Med2002;165:534–9.
2. Perros F, Dorfmüller P, Souza R, et al. Fractalkine-induced smoothmuscle cell proliferation in pulmonary hypertension. Eur Respir J2007;29:937–43.
3. Sanchez O, Marcos E, Perros F, et al. Role of endothelium-derivedCC chemokine ligand 2 in idiopathic pulmonary arterial hypertension.Am J Respir Crit Care Med 2007;176:1041–7.
4. Humbert M, Monti G, Fartoukh M, et al. Platelet-derived growthfactor expression in primary pulmonary hypertension: comparison ofHIV seropositive and HIV seronegative patients. Eur Respir J 1998;11:554–9.
5. Schermuly RT, Dony E, Ghofrani HA, et al. Reversal of experimentalpulmonary hypertension by PDGF inhibition. J Clin Invest 2005;115:2811–21.
6. Merklinger SL, Jones PL, Martinez EC, Rabinovitch M. Epidermalgrowth factor receptor blockade mediates smooth muscle cell apoptosisand improves survival in rats with pulmonary hypertension. Circula-tion 2005;112:423–31.
7. Sakao S, Taraseviciene-Stewart L, Cool CD, et al. VEGF-R blockadecauses endothelial cell apoptosis, expansion of surviving CD34�precursor cells and transdifferentiation to smooth muscle-like andneuronal-like cells. FASEB J 2007;21:3640–52.
8. Cool CD, Kennedy D, Voelkel NF, Tuder RM. Pathogenesis andevolution of plexiform lesions in pulmonary hypertension associatedwith scleroderma and human immunodeficiency virus infection. HumPathol 1997;28:434–42.
9. Tuder RM, Chacon M, Alger L, et al. Expression of angiogenesis-related molecules in plexiform lesions in severe pulmonary hyperten-sion: evidence for a process of disordered angiogenesis. J Pathol2001;195:367–74.
0. Perros F, Montani D, Dorfmüller P, et al. Platelet-derived growthfactor expression and function in idiopathic pulmonary arterial hyper-tension. Am J Respir Crit Care Med 2008;178:81–8.
1. Jones PL, Cowan KN, Rabinovitch M. Tenascin-C, proliferation andsubendothelial fibronectin in progressive pulmonary vascular disease.Am J Pathol 1997;150:1349–60.
2. MacLean MR, Herve P, Eddahibi S, Adnot S. 5-hydroxytryptamineand the pulmonary circulation: receptors, transporters and relevance topulmonary arterial hypertension. Br J Pharmacol 2000;131:161–8.
3. Eddahibi S, Fabre V, Boni C, et al. Induction of serotonin transporter
by hypoxia in pulmonary vascular smooth muscle cells. Relationshipwith the mitogenic action of serotonin. Circ Res 1999;84:329–36.
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
S18 Hassoun et al. JACC Vol. 54, No. 1, Suppl S, 2009Pulmonary Vascular Remodeling June 30, 2009:S10–9
4. Eddahibi S, Humbert M, Fadel E, et al. Serotonin transporteroverexpression is responsible for pulmonary artery smooth musclehyperplasia in primary pulmonary hypertension. J Clin Invest 2001;108:1141–50.
5. Eddahibi S, Hanoun N, Lanfumey L, et al. Attenuated hypoxicpulmonary hypertension in mice lacking the 5-hydroxytryptaminetransporter gene. J Clin Invest 2000;105:1555–62.
6. Guignabert C, Raffestin B, Benferhat R, et al. Serotonin transporterinhibition prevents and reverses monocrotaline-induced pulmonaryhypertension in rats. Circulation 2005;111:2812–9.
7. MacLean MR, Deuchar GA, Hicks MN, et al. Overexpression of the5-hydroxytryptamine transporter gene: effect on pulmonary hemody-namics and hypoxia-induced pulmonary hypertension. Circulation2004;109:2150–5.
8. Guignabert C, Izikki M, Tu LI, et al. Transgenic mice overexpressingthe 5-hydroxytryptamine transporter gene in smooth muscle developpulmonary hypertension. Circ Res 2006;98:1323–30.
9. Dempsie Y, Morecroft I, Welsh DJ, et al. Converging evidence insupport of the serotonin hypothesis of dexfenfluramine-induced pul-monary hypertension with novel transgenic mice. Circulation 2008;117:2928–37.
0. McMurtry MS, Archer SL, Altieri DC, et al. Gene therapy targetingsurvivin selectively induces pulmonary vascular apoptosis and reversespulmonary arterial hypertension. J Clin Invest 2005;115:1479–91.
1. Wang GJ, Sui XX, Simosa HF, Jain MK, Altieri DC, Conte MS.Regulation of vein graft hyperplasia by survivin, an inhibitor ofapoptosis protein. Arterioscler Thromb Vasc Biol 2005;25:2081–7.
2. Macian F. NFAT proteins: key regulators of T-cell development andfunction. Nat Rev Immunol 2005;5:472–84.
3. Rossow CF, Minami E, Chase EG, Murry CE, Santana LF.NFATc3-induced reductions in voltage-gated K� currents aftermyocardial infarction. Circ Res 2004;94:1340–50.
4. Kawamura T, Ono K, Morimoto T, et al. Endothelin-1-dependentnuclear factor of activated T lymphocyte signaling associates withtranscriptional coactivator p300 in the activation of the B cellleukemia-2 promoter in cardiac myocytes. Circ Res 2004;94:1492–9.
5. Bushdid PB, Osinska H, Waclaw RR, Molkentin JD, Yutzey KE.NFATc3 and NFATc4 are required for cardiac development andmitochondrial function. Circ Res 2003;92:1305–13.
6. Bonnet S, Rochefort G, Sutendra G, et al. The nuclear factor ofactivated T cells in pulmonary arterial hypertension can be therapeu-tically targeted. Proc Natl Acad Sci U S A 2007;104:11418–23.
7. McKinsey TA, Olson EN. Toward transcriptional therapies for thefailing heart: chemical screens to modulate genes. J Clin Invest2005;115:538–46.
8. Hamamdzic D, Kasman LM, LeRoy EC. The role of infectious agentsin the pathogenesis of systemic sclerosis. Curr Opin Rheumatol2002;14:694–8.
9. Freitas TC, Jung E, Pearce EJ. TGF-� signaling controls embryodevelopment in the parasitic flatworm Schistosoma mansoni. PLoSPathog 2007;3:e52.
0. Swain SD, Han S, Harmsen A, Shampeny K, Harmsen AG. Pulmo-nary hypertension can be a sequela of prior Pneumocystis pneumonia.Am J Pathol 2007;171:790–9.
1. Daley E, Emson C, Guignabert C, et al. Pulmonary arterial remod-eling induced by a Th2 immune response. J Exp Med 2008;205:361–72.
2. Sitbon O, Lascoux-Combe C, Delfraissy JF, et al. Prevalence ofHIV-related pulmonary arterial hypertension in the current antiretro-viral therapy era. Am J Respir Crit Care Med 2008;177:108–13.
3. Pellicelli AM, Barbaro G, Palmieri F, et al. Primary pulmonaryhypertension in HIV patients: a systematic review. Angiology 2001;52:31–41.
4. Zuber JP, Calmy A, Evison JM, et al. Pulmonary arterial hypertensionrelated to HIV infection: improved hemodynamics and survival asso-ciated with antiretroviral therapy. Clin Infect Dis 2004;38:1178–85.
5. Barbaro G, Lucchini A, Pellicelli AM, Grisorio B, Giancaspro G,Barbarini G. Highly active antiretroviral therapy compared withHAART and bosentan in combination in patients with HIV-associated pulmonary hypertension. Heart 2006;92:1164–6.
6. Marecki J, Cool C, Voelkel N, Luciw P, Flores S. Evidence forvascular remodeling in the lungs of macaques infected with simian
immunodeficiency virus/HIV NEF recombinant virus. Chest 2005;128:621S–2S.7. Marecki JC, Cool CD, Parr JE, et al. HIV-1 Nef is associated withcomplex pulmonary vascular lesions in SHIV-nef-infected macaques.Am J Respir Crit Care Med 2006;174:437–45.
8. Lundquist CA, Tobiume M, Zhou J, Unutmaz D, Aiken C. Nef-mediated downregulation of CD4 enhances human immunodeficiencyvirus type 1 replication in primary T lymphocytes. J Virol 2002;76:4625–33.
9. Swann SA, Williams M, Story CM, Bobbitt KR, Fleis R, Collins KL.HIV-1 Nef blocks transport of MHC class I molecules to the cell surfacevia a PI 3-kinase-dependent pathway. Virology 2001;282:267–77.
0. Collins KL, Chen BK, Kalams SA, Walker BD, Baltimore D. HIV-1Nef protein protects infected primary cells against killing by cytotoxicT lymphocytes. Nature 1998;391:397–401.
1. Olivetta E, Percario Z, Fiorucci G, et al. HIV-1 Nef induces therelease of inflammatory factors from human monocyte/macrophages:involvement of Nef endocytotic signals and NF-�B activation. J Im-munol 2003;170:1716–27.
2. Desrosiers RC, Sasseville VG, Czajak SC, et al. A herpesvirus ofrhesus monkeys related to the human Kaposi’s sarcoma-associatedherpesvirus. J Virol 1997;71:9764–9.
3. Cool CD, Rai PR, Yeager ME, et al. Expression of human herpesvirus8 in primary pulmonary hypertension. N Engl J Med 2003;349:1113–22.
4. Henke-Gendo C, Mengel M, Hoeper MM, Alkharsah K, Schulz TF.Absence of Kaposi’s sarcoma-associated herpesvirus in patients withpulmonary arterial hypertension. Am J Respir Crit Care Med 2005;172:1581–5.
5. Katano H, Ito K, Shibuya K, Saji T, Sato Y, Sata T. Lack of humanherpesvirus 8 infection in lungs of Japanese patients with primarypulmonary hypertension. J Infect Dis 2005;191:743–5.
6. Laney AS, De Marco T, Peters JS, et al. Kaposi sarcoma-associatedherpesvirus and primary and secondary pulmonary hypertension. Chest2005;127:762–7.
7. Bendayan D, Sarid R, Cohen A, Shitrit D, Shechtman I, Kramer MR.Absence of human herpesvirus 8 DNA sequences in lung biopsies fromIsraeli patients with pulmonary arterial hypertension. Respiration2008;75:155–7.
8. Moorman J, Saad M, Kosseifi S, Krishnaswamy G. Hepatitis C virusand the lung: implications for therapy. Chest 2005;128:2882–92.
9. Robalino BD, Moodie DS. Association between primary pulmonaryhypertension and portal hypertension: analysis of its pathophysiologyand clinical, laboratory and hemodynamic manifestations. J Am CollCardiol 1991;17:492–8.
0. Tedaldi EM, Baker RK, Moorman AC, et al. Influence of coinfectionwith hepatitis C virus on morbidity and mortality due to humanimmunodeficiency virus infection in the era of highly active antiretro-viral therapy. Clin Infect Dis 2003;36:363–7.
1. Sgonc R, Gruschwitz MS, Boeck G, Sepp N, Gruber J, Wick G.Endothelial cell apoptosis in systemic sclerosis is induced by antibody-dependent cell-mediated cytotoxicity via CD95. Arthritis Rheum2000;43:2550–62.
2. Cerinic MM, Valentini G, Sorano GG, et al. Blood coagulation,fibrinolysis, and markers of endothelial dysfunction in systemic scle-rosis. Semin Arthritis Rheum 2003;32:285–95.
3. Denton CP, Bickerstaff MC, Shiwen X, et al. Serial circulatingadhesion molecule levels reflect disease severity in systemic sclerosis.Br J Rheumatol 1995;34:1048–54.
4. Distler O, del Rosso A, Giacomelli R, et al. Angiogenic and angiostaticfactors in systemic sclerosis: increased levels of vascular endothelial growthfactor are a feature of the earliest disease stages and are associated with theabsence of fingertip ulcers. Arthritis Res 2002;4:R11.
5. Okano Y, Steen VD, Medsger TA Jr. Autoantibody to U3 nucleolarribonucleoprotein (fibrillarin) in patients with systemic sclerosis. Ar-thritis Rheum 1992;35:95–100.
6. Negi VS, Tripathy NK, Misra R, Nityanand S. Antiendothelial cellantibodies in scleroderma correlate with severe digital ischemia andpulmonary arterial hypertension. J Rheumatol 1998;25:462–6.
7. Fritzler MJ, Hart DA, Wilson D, et al. Antibodies to fibrin boundtissue type plasminogen activator in systemic sclerosis. J Rheumatol1995;22:1688–93.
8. Morse JH, Barst RJ, Fotino M, et al. Primary pulmonary hypertension,tissue plasminogen activator antibodies, and HLA-DQ7. Am J Respir
Crit Care Med 1997;155:274–8.
6
7
7
7
7
7
7
7
7
7
7
8
8
8
8
8
8
8
8
8
8
9
9
9
9
9
9
9
9
9
K
S19JACC Vol. 54, No. 1, Suppl S, 2009 Hassoun et al.June 30, 2009:S10–9 Pulmonary Vascular Remodeling
9. Grigolo B, Mazzetti I, Meliconi R, et al. Anti-topoisomerase II �autoantibodies in systemic sclerosis-association with pulmonary hyper-tension and HLA-B35. Clin Exp Immunol 2000;121:539–43.
0. Okawa-Takatsuji M, Aotsuka S, Fujinami M, Uwatoko S, KinoshitaM, Sumiya M. Up-regulation of intercellular adhesion molecule-1(ICAM-1), endothelial leucocyte adhesion molecule-1 (ELAM-1)and class II MHC molecules on pulmonary artery endothelial cells byantibodies against U1-ribonucleoprotein. Clin Exp Immunol 1999;116:174–80.
1. Tamby MC, Humbert M, Guilpain P, et al. Antibodies to fibroblastsin idiopathic and scleroderma-associated pulmonary hypertension. EurRespir J 2006;28:799–807.
2. Chizzolini C, Raschi E, Rezzonico R, et al. Autoantibodies tofibroblasts induce a proadhesive and proinflammatory fibroblast phe-notype in patients with systemic sclerosis. Arthritis Rheum 2002;46:1602–13.
3. Terrier B, Tamby MC, Camoin L, et al. Identification of targetantigens of antifibroblast antibodies in pulmonary arterial hyperten-sion. Am J Respir Crit Care Med 2008;177:1128–34.
4. Sanchez O, Sitbon O, Jaïs X, Simonneau G, Humbert M. Immuno-suppressive therapy in connective tissue diseases-associated pulmonaryarterial hypertension. Chest 2006;130:182–9.
5. Karrer S, Bosserhoff AK, Weiderer P, et al. The �2518 promotorpolymorphism in the MCP-1 gene is associated with systemic sclero-sis. J Invest Dermatol 2005;124:92–98.
6. Tsuchiya N, Kuroki K, Fujimoto M, et al. Association of a functionalCD19 polymorphism with susceptibility to systemic sclerosis. ArthritisRheum 2004;50:4002–7.
7. Tolusso B, Fabris M, Caporali R, et al. �238 and �489 TNF-alphaalong with TNF-RII gene polymorphisms associate with the diffusephenotype in patients with systemic sclerosis. Immunol Lett 2005;96:103–8.
8. Hutyrova B, Lukac J, Bosak V, Buc M, du Bois R, Petrek M.Interleukin 1alpha single-nucleotide polymorphism associated withsystemic sclerosis. J Rheumatol 2004;31:81–4.
9. Crilly A, Hamilton J, Clark CJ, Jardine A, Madhok R. Analysis of the5= flanking region of the interleukin 10 gene in patients with systemicsclerosis. Rheumatology (Oxford) 2003;42:1295–8.
0. Morse J, Barst R, Horn E, Cuervo N, Deng Z, Knowles J. Pulmonaryhypertension in scleroderma spectrum of disease: lack of bone morpho-genetic protein receptor 2 mutations. J Rheumatol 2002;29:2379–81.
1. Tew MB, Arnett FC, Reveille JD, Tan FK. Mutations of bonemorphogenetic protein receptor type II are not found in patients withpulmonary hypertension and underlying connective tissue diseases.Arthritis Rheum 2002;46:2829–30.
2. Wipff J, Kahan A, Hachulla E, et al. Association between an endoglingene polymorphism and systemic sclerosis-related pulmonary arterialhypertension. Rheumatology (Oxford) 2007;46:622–5.
3. Peinado VI, Barberà JA, Ramırez J, et al. Endothelial dysfunction inpulmonary arteries of patients with mild COPD. Am J Physiol Lung
Cell Mol Physiol 1998;274:L908–13. r4. Barberà JA, Riverola A, Roca J, et al. Pulmonary vascular abnormal-ities and ventilation-perfusion relationships in mild chronic obstructivepulmonary disease. Am J Respir Crit Care Med 1994;149:423–9.
5. Peinado VI, Barberà JA, Abate P, et al. Inflammatory reaction inpulmonary muscular arteries of patients with mild chronic obstructivepulmonary disease. Am J Respir Crit Care Med 1999;159:1605–11.
6. Santos S, Peinado VI, Ramırez J, et al. Enhanced expression ofvascular endothelial growth factor in pulmonary arteries of smokersand patients with moderate chronic obstructive pulmonary disease.Am J Respir Crit Care Med 2003;167:1250–6.
7. Vignola AM, Chanez P, Chiappara G, et al. Transforming growthfactor-� expression in mucosal biopsies in asthma and chronic bron-chitis. Am J Respir Crit Care Med 1997;156:591–9.
8. de Boer WI, van Schadewijk A, Sont JK, et al. Transforming growthfactor �1 and recruitment of macrophages and mast cells in airways inchronic obstructive pulmonary disease. Am J Respir Crit Care Med1998;158:1951–7.
9. Beghe B, Bazzan E, Baraldo S, et al. Transforming growth factor-�type II receptor in pulmonary arteries of patients with very severeCOPD. Eur Respir J 2006;28:556–62.
0. Druker BJ, Guilhot F, O’Brien SG, et al. Five-year follow-up ofpatients receiving imatinib for chronic myeloid leukemia. N EnglJ Med 2006;355:2408–17.
1. Carroll M, Ohno-Jones S, Tamura S, et al. CGP 57148, a tyrosine kinaseinhibitor, inhibits the growth of cells expressing BCR-ABL, TEL-ABL,and TEL-PDGFR fusion proteins. Blood 1997;90:4947–52.
2. Eddahibi S, Humbert M, Sediame S, et al. Imbalance between plateletvascular endothelial growth factor and platelet-derived growth factorin pulmonary hypertension: effect of prostacyclin therapy. Am J RespirCrit Care Med 2000;162:1493–9.
3. Ghofrani HA, Seeger W, Grimminger F. Imatinib for the treatmentof pulmonary arterial hypertension. N Engl J Med 2005;353:1412–3.
4. Patterson KC, Weissmann A, Ahmadi T, Farber HW. Imatinibmesylate in the treatment of refractory idiopathic pulmonary arterialhypertension. Ann Intern Med 2006;145:152–3.
5. Souza R, Sitbon O, Parent F, Simonneau G, Humbert M. Long termimatinib treatment in pulmonary arterial hypertension. Thorax 2006;61:736.
6. Yeager ME, Halley GR, Golpon HA, Voelkel NF, Tuder RM.Microsatellite instability of endothelial cell growth and apoptosis geneswithin plexiform lesions in primary pulmonary hypertension. Circ Res2001;88:e2–11.
7. Izikki M, Guignabert C, Fadel E, et al. Endothelial-derived FGF2contributes to the progression of pulmonary hypertension in humansand rodents. J Clin Invest 2009;119:512–23.
8. Adnot S. Lessons learned from cancer may help in the treatment ofpulmonary hypertension. J Clin Invest 2005;115:1461–3.
ey Words: growth factors y inflammation y pulmonary vascular
emodeling.


![Pulmonary Inflammation Induced by a Recombinant Brugia malayi [gamma]-glutamyl transpeptidase Homolog: Involvement of Humoral Autoimmune Responses](https://static.fdokumen.com/doc/165x107/631e10e40ff042c6110c2b14/pulmonary-inflammation-induced-by-a-recombinant-brugia-malayi-gamma-glutamyl-transpeptidase.jpg)
















