The Influence of Aristide Cavaillé-Coll on French Romantic Organ Building and Organ Music
Upload
independentCategory
view
5download
0
Lymphocytic Infiltrates and Subclinical Epithelial TumorExtension in Patients With Chronic Leukemia andSolid-Organ TransplantationKHOSROW MEHRANY, MD, DAVID R. BYRD, MD, RANDALL K. ROENIGK, MD, ROGER H.WEENIG, MD, P. KIM PHILLIPS, MD, TRI H. NGUYEN, MD, AND CLARK C. OTLEY, MD
Division of Dermatologic Surgery, Mayo Clinic, Rochester, Minnesota
BACKGROUND. Dense infiltrates in association with squamouscell carcinoma (SCC) or basal cell carcinoma (BCC) in patients
with underlying chronic lymphocytic leukemia (CLL) maycomplicate pathologic interpretation of histologic margins.
OBJECTIVE. The study was conducted to determine the
frequency of identifying dense inflammatory infiltrates in frozenhistologic sections during Mohs operation for BCC or SCC inpatients with CLL and organ-transplant recipients, to char-
acterize the infiltrate (reactive versus leukemic) in CLL, and toestimate the subclinical tumor extension in patients with CLL,transplant recipients, and control subjects undergoing Mohs
procedure.
METHODS. Frozen sections of head and neck BCC and SCCobtained during Mohs procedures in patients with CLL, organ
transplant recipients, and a control group were reviewedretrospectively. Biopsy specimens of CLL with dense infiltrates
were assessed with immunohistochemical stains. Subclinicaltumor extension (postoperative defect size minus preoperativetumor size) was evaluated in each group.
RESULTS. Dense infiltrates were found in tumors of 20 of 55patients with CLL (36%), 1 of 8 transplant recipients (13%),and 1 of 105 controls (1%). In patients with CLL, 75% of the
dense infiltrates were B-cell leukemic. Compared with controls,the mean subclinical tumor extension was larger in patientswith CLL (P5 0.029) and in transplant recipients (P5 0.55).
CONCLUSION. Dense leukemic infiltrates associated with BCCor SCC in CLL may complicate pathologic interpretation of
Mohs surgical histologic margins and may be associated withlarger postoperative defects relative to preoperative clinicaltumor appearance. In patients with CLL, as in transplantrecipients, SCC seems more likely to develop than BCC.
K. MEHRANY, MD, D. R. BYRD, MD, R. K. ROENIGK, MD, R. H. WEENIG, MD, P. K. PHILLIPS, MD, T. NGUYEN, MD,AND C. C. OTLEY, MD HAVE INDICATED NO SIGNIFICANT INTEREST WITH COMMERCIAL SUPPORTERS.
CHRONIC LYMPHOCYTIC leukemia (CLL) is themost frequent form of leukemia in adults of Westerncountries, accounting for 25% of all leukemias.1 Therisk for development of CLL progressively increaseswith age and is two times higher in men than inwomen.2 The estimated annual incidence of CLL inthe United States ranges from 7,300 to 12,500 newcases, and the overall incidence rate is 2.3 per100,000.3
Because immune function is impaired in CLL,patients have an increased risk for development ofother malignant neoplasms. Skin cancer is the mostfrequently associated malignancy in CLL, and squa-mous cell carcinoma (SCC) predominates over basalcell carcinoma (BCC).4 Lymphoma- and leukemia-associated SCCs are unusually aggressive and have
substantially higher rates of recurrence and metasta-sis.5,6 Microscopically controlled excisions of BCCand SCC therefore may represent the optimal tech-nique for management of patients with CLL.5,6
For surgeons who perform the Mohs operation,dense lymphocytic infiltrates associated with non-melanoma skin cancers may pose an intraoperativechallenge for interpretation of histologic sectionsbecause they obscure possible residual tumor. If theinfiltrate represents inflammation caused by tumor,then further resection may be indicated, whereasleukemic infiltrates that do not imply tumor wouldnot require further resection.7 Leukemic infiltrates alsocomplicate the pathologic findings by camouflagingtumor cells or trapping collagen in a manner thatdisguises tumor islands.
Our objective was to clarify the issues surroundinginfiltrates in histologic sections from patients withCLL and to compare the findings with those incontrols and in another immunosuppressed group
r 2003 by the American Society for Dermatologic Surgery, Inc. � Published by Blackwell Publishing, Inc.ISSN: 1076-0512/02/$15.00/0 � Dermatol Surg 2003;29:129–134
Address correspondence to: Randall K. Roenigk, MD, Division of
Dermatologic Surgery, Mayo Clinic, 200 First Street SW, Rochester,
MN 55905.
with severe skin cancers, namely, recipients of solid-organ transplants. We sought (1) to determine thefrequency of a dense inflammatory infiltrate duringMohs operation for BCC or SCC in patients with CLLand in organ transplant recipients, (2) to characterizethe infiltrate (reactive vs. leukemic) in patients withCLL, and (3) to estimate subclinical tumor extensionin patients with CLL, transplant recipients, andcontrols undergoing the Mohs procedure.
Methods
The study was approved by the Mayo FoundationInstitutional Review Board. The Mayo Clinic diag-nostic index was used to identify all patients with ahistory of CLL who had undergone the Mohsoperation. The 56 patients identified (48 males and 8females) had a total of 76 BCCs or SCCs of the headand neck. Eight representative patients (seven malesand one female) who had received solid-organtransplants and who underwent the Mohs procedurefor 53 BCCs or SCCs of the head and neck wererandomly selected for comparative purposes. Thecontrol group included 105 patients (70 males and35 females) with a total of 105 tumors. The controlgroup included sequential patients undergoing Mohsprocedure for BCCs or SCCs of the head and neck
without a diagnosis of CLL or a history of organtransplantation.
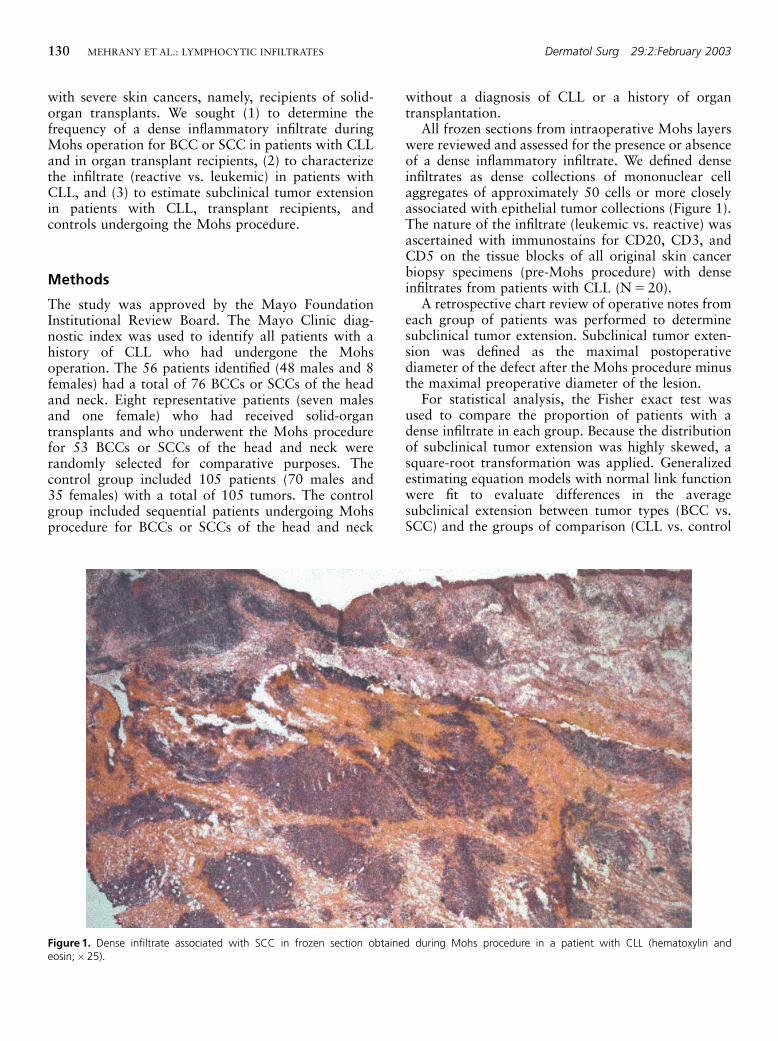
All frozen sections from intraoperative Mohs layerswere reviewed and assessed for the presence or absenceof a dense inflammatory infiltrate. We defined denseinfiltrates as dense collections of mononuclear cellaggregates of approximately 50 cells or more closelyassociated with epithelial tumor collections (Figure 1).The nature of the infiltrate (leukemic vs. reactive) wasascertained with immunostains for CD20, CD3, andCD5 on the tissue blocks of all original skin cancerbiopsy specimens (pre-Mohs procedure) with denseinfiltrates from patients with CLL (N5 20).
A retrospective chart review of operative notes fromeach group of patients was performed to determinesubclinical tumor extension. Subclinical tumor exten-sion was defined as the maximal postoperativediameter of the defect after the Mohs procedure minusthe maximal preoperative diameter of the lesion.
For statistical analysis, the Fisher exact test wasused to compare the proportion of patients with adense infiltrate in each group. Because the distributionof subclinical tumor extension was highly skewed, asquare-root transformation was applied. Generalizedestimating equation models with normal link functionwere fit to evaluate differences in the averagesubclinical extension between tumor types (BCC vs.SCC) and the groups of comparison (CLL vs. control
Figure 1. Dense infiltrate associated with SCC in frozen section obtained during Mohs procedure in a patient with CLL (hematoxylin andeosin;�25).
130 MEHRANY ET AL.: LYMPHOCYTIC INFILTRATES Dermatol Surg 29:2:February 2003
and transplant recipients vs. control). An exchangeablecorrelation structure was specified to model thecorrelation between multiple tumors within a patient.All calculated P values were two sided, and Pvalues less than 0.05 were considered statisticallysignificant.
Results
Patients with CLL were significantly more likely tohave a dense infiltrate than controls (Po0.001)(Table 1). Organ transplant recipients also were morelikely to have a dense infiltrate than controls, but thisdifference was not statistically significant (P50.14)(Table 1).
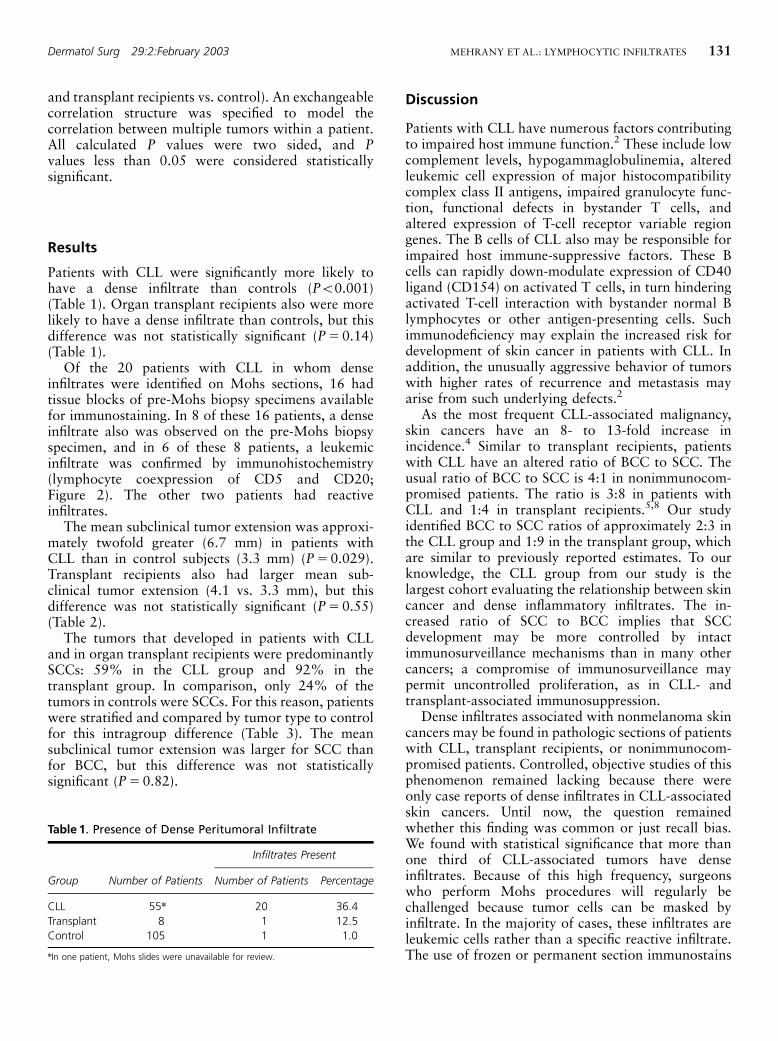
Of the 20 patients with CLL in whom denseinfiltrates were identified on Mohs sections, 16 hadtissue blocks of pre-Mohs biopsy specimens availablefor immunostaining. In 8 of these 16 patients, a denseinfiltrate also was observed on the pre-Mohs biopsyspecimen, and in 6 of these 8 patients, a leukemicinfiltrate was confirmed by immunohistochemistry(lymphocyte coexpression of CD5 and CD20;Figure 2). The other two patients had reactiveinfiltrates.
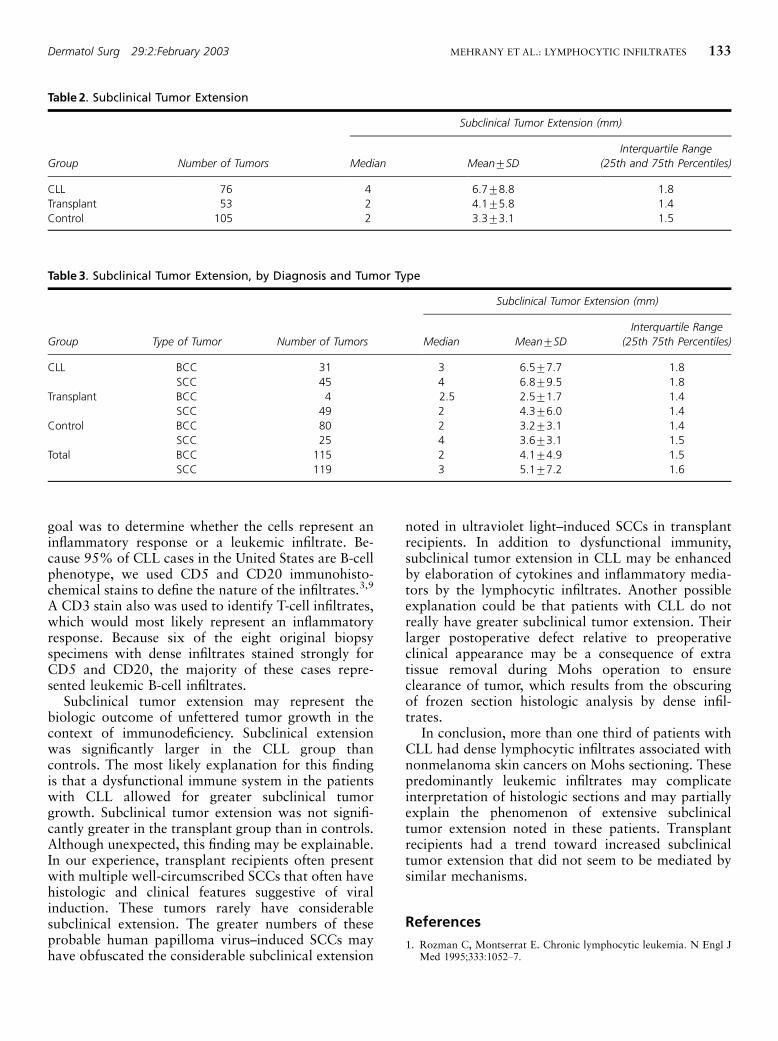
The mean subclinical tumor extension was approxi-mately twofold greater (6.7 mm) in patients withCLL than in control subjects (3.3 mm) (P50.029).Transplant recipients also had larger mean sub-clinical tumor extension (4.1 vs. 3.3 mm), but thisdifference was not statistically significant (P50.55)(Table 2).
The tumors that developed in patients with CLLand in organ transplant recipients were predominantlySCCs: 59% in the CLL group and 92% in thetransplant group. In comparison, only 24% of thetumors in controls were SCCs. For this reason, patientswere stratified and compared by tumor type to controlfor this intragroup difference (Table 3). The meansubclinical tumor extension was larger for SCC thanfor BCC, but this difference was not statisticallysignificant (P50.82).
Discussion
Patients with CLL have numerous factors contributingto impaired host immune function.2 These include lowcomplement levels, hypogammaglobulinemia, alteredleukemic cell expression of major histocompatibilitycomplex class II antigens, impaired granulocyte func-tion, functional defects in bystander T cells, andaltered expression of T-cell receptor variable regiongenes. The B cells of CLL also may be responsible forimpaired host immune-suppressive factors. These Bcells can rapidly down-modulate expression of CD40ligand (CD154) on activated T cells, in turn hinderingactivated T-cell interaction with bystander normal Blymphocytes or other antigen-presenting cells. Suchimmunodeficiency may explain the increased risk fordevelopment of skin cancer in patients with CLL. Inaddition, the unusually aggressive behavior of tumorswith higher rates of recurrence and metastasis mayarise from such underlying defects.2
As the most frequent CLL-associated malignancy,skin cancers have an 8- to 13-fold increase inincidence.4 Similar to transplant recipients, patientswith CLL have an altered ratio of BCC to SCC. Theusual ratio of BCC to SCC is 4:1 in nonimmunocom-promised patients. The ratio is 3:8 in patients withCLL and 1:4 in transplant recipients.5,8 Our studyidentified BCC to SCC ratios of approximately 2:3 inthe CLL group and 1:9 in the transplant group, whichare similar to previously reported estimates. To ourknowledge, the CLL group from our study is thelargest cohort evaluating the relationship between skincancer and dense inflammatory infiltrates. The in-creased ratio of SCC to BCC implies that SCCdevelopment may be more controlled by intactimmunosurveillance mechanisms than in many othercancers; a compromise of immunosurveillance maypermit uncontrolled proliferation, as in CLL- andtransplant-associated immunosuppression.
Dense infiltrates associated with nonmelanoma skincancers may be found in pathologic sections of patientswith CLL, transplant recipients, or nonimmunocom-promised patients. Controlled, objective studies of thisphenomenon remained lacking because there wereonly case reports of dense infiltrates in CLL-associatedskin cancers. Until now, the question remainedwhether this finding was common or just recall bias.We found with statistical significance that more thanone third of CLL-associated tumors have denseinfiltrates. Because of this high frequency, surgeonswho perform Mohs procedures will regularly bechallenged because tumor cells can be masked byinfiltrate. In the majority of cases, these infiltrates areleukemic cells rather than a specific reactive infiltrate.The use of frozen or permanent section immunostains
Table 1. Presence of Dense Peritumoral Infiltrate
Infiltrates Present
Group Number of Patients Number of Patients Percentage
CLL 55n 20 36.4
Transplant 8 1 12.5
Control 105 1 1.0
nIn one patient, Mohs slides were unavailable for review.
Dermatol Surg 29:2:February 2003 MEHRANY ET AL.: LYMPHOCYTIC INFILTRATES 131
may assist in assessing the presence of residual tumorwithin areas of dense infiltrate; we have not routinelyused these techniques.
Dense infiltrates were not significantly increased inour transplant group compared with controls. Thus,although both patients with CLL and transplantrecipients are immunosuppressed, the tendency for
development of nonmelanoma skin cancers in eachgroup may arise from a different underlying mechan-ism. In CLL, the immune response may be exaggeratedyet dysfunctional, whereas in the transplant setting,there is an iatrogenic immune defect.
In evaluating the dense infiltrates associated withnonmelanoma skin cancers in patients with CLL, our
Figure 2. Immunostains of pre-Mohs biopsy specimen of basal cell carcinoma leukemic infiltrate (� 100.) (A) CD20. (B) CD5. (C) CD3. Note theprominent lymphocyte coexpression of CD20 and CD5 in the setting of sparse CD3 positivity.
132 MEHRANY ET AL.: LYMPHOCYTIC INFILTRATES Dermatol Surg 29:2:February 2003
goal was to determine whether the cells represent aninflammatory response or a leukemic infiltrate. Be-cause 95% of CLL cases in the United States are B-cellphenotype, we used CD5 and CD20 immunohisto-chemical stains to define the nature of the infiltrates.3,9
A CD3 stain also was used to identify T-cell infiltrates,which would most likely represent an inflammatoryresponse. Because six of the eight original biopsyspecimens with dense infiltrates stained strongly forCD5 and CD20, the majority of these cases repre-sented leukemic B-cell infiltrates.
Subclinical tumor extension may represent thebiologic outcome of unfettered tumor growth in thecontext of immunodeficiency. Subclinical extensionwas significantly larger in the CLL group thancontrols. The most likely explanation for this findingis that a dysfunctional immune system in the patientswith CLL allowed for greater subclinical tumorgrowth. Subclinical tumor extension was not signifi-cantly greater in the transplant group than in controls.Although unexpected, this finding may be explainable.In our experience, transplant recipients often presentwith multiple well-circumscribed SCCs that often havehistologic and clinical features suggestive of viralinduction. These tumors rarely have considerablesubclinical extension. The greater numbers of theseprobable human papilloma virus–induced SCCs mayhave obfuscated the considerable subclinical extension
noted in ultraviolet light–induced SCCs in transplantrecipients. In addition to dysfunctional immunity,subclinical tumor extension in CLL may be enhancedby elaboration of cytokines and inflammatory media-tors by the lymphocytic infiltrates. Another possibleexplanation could be that patients with CLL do notreally have greater subclinical tumor extension. Theirlarger postoperative defect relative to preoperativeclinical appearance may be a consequence of extratissue removal during Mohs operation to ensureclearance of tumor, which results from the obscuringof frozen section histologic analysis by dense infil-trates.
In conclusion, more than one third of patients withCLL had dense lymphocytic infiltrates associated withnonmelanoma skin cancers on Mohs sectioning. Thesepredominantly leukemic infiltrates may complicateinterpretation of histologic sections and may partiallyexplain the phenomenon of extensive subclinicaltumor extension noted in these patients. Transplantrecipients had a trend toward increased subclinicaltumor extension that did not seem to be mediated bysimilar mechanisms.
References
1. Rozman C, Montserrat E. Chronic lymphocytic leukemia. N Engl JMed 1995;333:1052–7.
Table 3. Subclinical Tumor Extension, by Diagnosis and Tumor Type
Subclinical Tumor Extension (mm)
Group Type of Tumor Number of Tumors Median Mean7SD
Interquartile Range
(25th 75th Percentiles)
CLL BCC 31 3 6.577.7 1.8
SCC 45 4 6.879.5 1.8
Transplant BCC 4 2.5 2.571.7 1.4
SCC 49 2 4.376.0 1.4
Control BCC 80 2 3.273.1 1.4
SCC 25 4 3.673.1 1.5
Total BCC 115 2 4.174.9 1.5
SCC 119 3 5.177.2 1.6
Table 2. Subclinical Tumor Extension
Subclinical Tumor Extension (mm)
Group Number of Tumors Median Mean7SD
Interquartile Range
(25th and 75th Percentiles)
CLL 76 4 6.778.8 1.8
Transplant 53 2 4.175.8 1.4
Control 105 2 3.373.1 1.5
Dermatol Surg 29:2:February 2003 MEHRANY ET AL.: LYMPHOCYTIC INFILTRATES 133

2. Kipps TJ. Chronic lymphocytic leukemia. Curr Opin Hematol2000;7:223–34.
3. Kalil N, Cheson BD. Chronic lymphocytic leukemia. Oncologist1999;4:352–69.
4. Weimar VM, Ceilley RI, Goeken JA. Aggressive biologic behavior ofbasal- and squamous-cell cancers in patients with chronic lympho-cytic leukemia or chronic lymphocytic lymphoma. J Dermatol SurgOncol 1979;5:609–14.
5. Perez-Reyes N, Farhi DC. Squamous cell carcinoma of head andneck in patients with well-differentiated lymphocytic lymphoma.Cancer 1987;59:540–4.
6. Frierson HF Jr, Deutsch BD, Levine PA. Clinicopathologic features ofcutaneous squamous cell carcinomas of the head and neck in patients
with chronic lymphocytic leukemia/small lymphocytic lymphoma.Hum Pathol 1988;19:1397–402.
7. Albregts T, Orengo I, Salasche S., et al. Squamous cell carcinoma in apatient with chronic lymphocytic leukemia: an intraoperativediagnostic challenge for the Mohs surgeon. Dermatol Surg1998;24:269–72.
8. Berg D, Otley CC. Skin cancer in organ transplant recipients.epidemiology, pathogenesis, and management. J Am Acad Dermatol2002;47:1–17.
9. Jaffe ES. Pathology and Genetics of Tumours of Haematopoietic andLymphoid Tissues. Lyon: IARC Press, 2001.
134 MEHRANY ET AL.: LYMPHOCYTIC INFILTRATES Dermatol Surg 29:2:February 2003
Copyright © 2022 FDOKUMEN