Long-term follow-up after liver transplantation for autoimmune hepatitis: evidence of recurrence of...
11
Journal of Hepatology 1999; 30:131-141 Printed in Denmark • All rights reserved Munksgaard. Copenhagen Copyright © European Association for the Study of the Liver 1999 Journal of Hepatology ISSN 0168-8278 Long-term follow-up after liver transplantation for autoimmune hepatitis: evidence of recurrence of primary disease Vlad Ratziu l, Didier Samuel 1, Myl6ne Sebagh 3, Olivier Farges 1, Faouzi Saliba l, Philippe Ichai l, Hocine Farahmand 2, Mich~le Gigou 1, Cyrille F6ray l, Michel Reyn6s3 and Henri Bismuth 1 I Centre H~pato-Biliaire, 2Banque du Sang and 3Service d'Anatomie Pathologique, Hdpital Paul Brousse, Villejuif UniversitO Paris-Sud, UPRES Virus HOpatotropes et Cancer, France Background~Aims: After liver transplantion for auto- immune hepatitis, the long-term results and the inci- dence of recurrence of primary disease are unknown. Methods: In this retrospective study we reviewed the clinical course of 25 patients transplanted for autoim- mune hepatitis and followed for a mean of 5.3 years (2-8.5 years). Results: The actuarial 5-year patient and graft sur- vival rates were 91% (-+6%) and 83% (---8%). The actuarial 1-year rate of acute rejection was 50% (-10.2%), which was comparable to that of patients transplanted for primary biliary cirrhosis and pri- mary sclerosing cholangitis. Autoantibodies persisted in 77% of patients, at a lower titer than before liver transplantation. Ten patients were excluded from the study of autoimmune hepatitis recurrence, one be- cause of an early postoperative death and nine because of hepatitis C virus infection acquired before or after liver transplantation. In the remaining 15 patients, who were free of hepatitis C virus infection, 5-year patient and graft survivals were 100% and 87%, re- spectively. Despite triple immunosuppressive therapy, three patients (20%) developed chronic hepatitis with histological and serological features of autoimmune hepatitis in the absence of any other identifiable cause. The disease was severe in two patients, leading to graft failure and asymptomatic in another, despite marked histological abnormalities. In one of these three patients, autoimmune hepatitis recurred on the second liver graft as well. Conclusions: Patients undergoing liver transplantation for autoimmune hepatitis have an excellent survival rate although severe primary disease may recur, sug- gesting the need for stronger post-operative immuno- suppressive therapy. Key words: Autoantibodies; Autoimmune hepatitis; Hepatitis C virus; Immunosuppression; Liver trans- plantation; Recurrence; Rejection. E fER TRANSPLANTATION is now routinely considered in patients with end-stage liver disease, mainly due to progress achieved in surgical techniques, im- munosuppression therapy, management of post-operat- ive complications and better patient selection. Since survival in transplanted patients is longer, recurrence of primary disease has become a major concern. Autoimmune hepatitis (AIH) is a relatively rare indi- cation for liver transplantation, accounting for 2.6% of liver transplants in Europe (1). The long-term prognosis Received 24 April; revised 3 August; accepted 6 August 1998 Correspondence: Didier Samuel, Centre H6pato-Biliaire, H6pital Paul Brousse, 12 Av. Paul Vaillant Couturier, 94804 Villejuif, France. Tel: 33 1 45 59 31 99. Fax: 33 1 45 59 38 57. and the patient and graft survival rates are not well known. Moreover, the issue of disease recurrence is still controversial. Disease recurrence has either been re- ported in isolated cases (2,3) or not fully documented (4), whereas conflicting data have been reported by other investigators (5). The pathogenesis of AIH remains ob- scure since the initial event that triggers the autoimmune response is unknown. In addition, a specific liver auto- antigen has not been identified and pathogenic liver-spe- cific autoantibodies have not been recognized (6). Hepa- titis adoptive transfer in experimental animal models has suggested a pathogenic role for cell-mediated im- munity (7), whereas an impaired immunoregulation due to decreased T cell suppressor function has been demon- strated in patients with AIH (8). Whether these abnor- malities persist after liver replacement is not known but 131
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Long-term follow-up after liver transplantation for autoimmune hepatitis: evidence of recurrence of...

Journal of Hepatology 1999; 30:131-141 Printed in Denmark • All rights reserved Munksgaard. Copenhagen
Copyright © European Association for the Study of the Liver 1999
Journal of Hepatology ISSN 0168-8278
Long-term follow-up after liver transplantation for autoimmune hepatitis: evidence of recurrence of primary disease
Vlad Ratziu l, Didier Samuel 1, Myl6ne Sebagh 3, Olivier Farges 1, Faouzi Saliba l, Philippe Ichai l, Hocine Farahmand 2, Mich~le Gigou 1, Cyrille F6ray l, Michel Reyn6s 3 and Henri Bismuth 1
I Centre H~pato-Biliaire, 2Banque du Sang and 3Service d'Anatomie Pathologique, Hdpital Paul Brousse, Villejuif UniversitO Paris-Sud, UPRES Virus HOpatotropes et Cancer, France
Background~Aims: After liver transplantion for auto- immune hepatitis, the long-term results and the inci- dence of recurrence of primary disease are unknown. Methods: In this retrospective study we reviewed the clinical course of 25 patients transplanted for autoim- mune hepatitis and followed for a mean of 5.3 years (2-8.5 years). Results: The actuarial 5-year patient and graft sur- vival rates were 91% (-+6%) and 83% (---8%). The actuarial 1-year rate of acute rejection was 50% (-10.2%), which was comparable to that of patients transplanted for primary biliary cirrhosis and pri- mary sclerosing cholangitis. Autoantibodies persisted in 77% of patients, at a lower titer than before liver transplantation. Ten patients were excluded from the study of autoimmune hepatitis recurrence, one be- cause of an early postoperative death and nine because of hepatitis C virus infection acquired before or after liver transplantation. In the remaining 15 patients, who were free of hepatitis C virus infection, 5-year
patient and graft survivals were 100% and 87%, re- spectively. Despite triple immunosuppressive therapy, three patients (20%) developed chronic hepatitis with histological and serological features of autoimmune hepatitis in the absence of any other identifiable cause. The disease was severe in two patients, leading to graft failure and asymptomatic in another, despite marked histological abnormalities. In one of these three patients, autoimmune hepatitis recurred on the second liver graft as well. Conclusions: Patients undergoing liver transplantation for autoimmune hepatitis have an excellent survival rate although severe primary disease may recur, sug- gesting the need for stronger post-operative immuno- suppressive therapy.
Key words: Autoantibodies; Autoimmune hepatitis; Hepatitis C virus; Immunosuppression; Liver trans- plantation; Recurrence; Rejection.
E fER TRANSPLANTATION is now routinely considered in patients with end-stage liver disease, mainly
due to progress achieved in surgical techniques, im- munosuppression therapy, management of post-operat- ive complications and better patient selection. Since survival in transplanted patients is longer, recurrence of primary disease has become a major concern.
Autoimmune hepatitis (AIH) is a relatively rare indi- cation for liver transplantation, accounting for 2.6% of liver transplants in Europe (1). The long-term prognosis
Received 24 April; revised 3 August; accepted 6 August 1998
Correspondence: Didier Samuel, Centre H6pato-Biliaire, H6pital Paul Brousse, 12 Av. Paul Vaillant Couturier, 94804 Villejuif, France. Tel: 33 1 45 59 31 99. Fax: 33 1 45 59 38 57.
and the patient and graft survival rates are not well known. Moreover, the issue of disease recurrence is still controversial. Disease recurrence has either been re- ported in isolated cases (2,3) or not fully documented (4), whereas conflicting data have been reported by other investigators (5). The pathogenesis of AIH remains ob- scure since the initial event that triggers the autoimmune response is unknown. In addition, a specific liver auto- antigen has not been identified and pathogenic liver-spe- cific autoantibodies have not been recognized (6). Hepa- titis adoptive transfer in experimental animal models has suggested a pathogenic role for cell-mediated im- munity (7), whereas an impaired immunoregulation due to decreased T cell suppressor function has been demon- strated in patients with AIH (8). Whether these abnor- malities persist after liver replacement is not known but
131

V. Ratziu et aL
may be of major relevance to the issue of disease recur- rence after liver transplantation.
The aim of this study was to determine the long- term outcome in patients undergoing liver transplan- tation for AIH, to evaluate the incidence of recurrence of pr imary disease and to determine its clinical, bio- chemical and histological characteristics on the en- grafted liver.
Patients and Methods Study population Twenty-five consecutive adult patients with an established diagnosis of AIH underwent orthotopic liver transplantation at our Center be- tween April 1985 and December 1992. These patients were part of a larger group consisting of 805 patients with severe chronic liver dis- ease, in whom 843 liver transplants were performed during the same time period. Diagnosis of AIH required the presence of at least three of the following diagnostic criteria (9,10): a) anti-nuclear antibodies (ANA), anti-smooth muscle antibodies (SMA), anti-liver-kidney- microsome type I antibodies (LKM0 or anti-liver cytosol (LC0 (11) at significant titers (>1150); b) female sex; c) gamma globulin level greater than 20 g/k d) concomitant non-hepatic immunologic dis- orders (other manifestations of autoimmune diseases) such as: auto- immune thyroiditis, Raynaud's syndrome, rheumatoid arthritis, or Sj6gren's syndrome; e) the presence of HLA B8DR3 haplotype or DR3 allotype; and f) a liver biopsy showing features compatible with chronic hepatitis (9). Type I AIH was defined by the presence of ANA and/or SMA and type lI AIH by the presence of anti-LKM~ and/or LCI (10).
There was no history of parenteral exposure to blood products, use of intravenous drug substances, exposure to hepatotoxic drugs or alcohol abuse in any of the patients. All patients included in this study after 1990 were negative for antibodies directed to hepatitis C virus (anti-HCV). Frozen stored sera of patients transplanted before 1990 were all retrospectively tested for anti-HCV antibodies. All pa- tients lacked HBsAg. Transferrin saturation and serum ferritin, al- pha- 1 antitrypsin, ceruloplasmin and serum and urinary copper levels were normal.
The duration of the disease was estimated from the first known episode of jaundice and/or abnormal levels of serum transaminases and/or histological signs of chronic hepatitis. Liver transplantation was performed if one or several of the following criteria were present: a) clinical and biochemical features of advanced liver disease: ascites, jaundice, encephalopathy or variceal hemorrhage; low albumin (<34 g/l) and low prothrombin level with factor V activity below 50% of the normal value; b) histologically proven cirrhosis; or c) no improve- ment after well-conducted immunosuppressive therapy.
During the same time period, 80 patients received a first liver trans- plant for primary biliary cirrhosis and 30 for primary sclerosing chol- angitis. These patients were compared to the study group with regard to survival and incidence of acute and chronic rejection.
Clinical biochemical and virological Jollow-up after liver transplantation Orthotopic liver transplantation was performed with an ABO-com- patible liver graft, using the same technique in all patients. After dis- charge from the hospital, the patients were followed weekly up to the 4th month, monthly up to 1 year, then on a quarterly basis. Follow- up consisted of physical examination, liver function tests including serum levels of alanine-aminotransferase (ALT), alkaline phospha- tase, gamma glutamyl transpeptidase, bilirubin, prothrombin level and gamma globulin, detection of autoantibodies (ANA, SMA and LKM0, HBsAg and second-generation ELISA for anti-HCV anti- bodies and hepatic Doppler ultrasonography. All patients received corticosteroids, azathioprine and cyclosporine as standard triple im- munosuppressive therapy. Cyclosporine doses were adjusted to main- tain whole-blood trough levels between 300-400 ng/ml in the first
132
month after liver transplantation, 200-300 ng/ml in the first 3 months and 100-200 ng/ml subsequently, as determined by a monoclonal radioimmunoassay. Treatment of acute hepatic rejection was decided on the basis of a histological score (12) and the extent of abnormali- ties of liver function tests. Treatment consisted of intravenous admin- istration of 1 g of methylprednisolone, which was repeated 48 h later if disturbances in liver function tests persisted. If this was inefficient, a 10-day course of OKT3 (Orthoclone ® Ortho Raritan, NJ. USA) 5 mg i.v. per day was administered. Chronic rejection and persistent acute rejection were treated with Tacrotimus (Prograf ~, Fujisawa, Japan).
Histological follow-up Liver biopsies were systematically performed 1, 2 and 5 years after liver transplantation, as well as in cases of abnormal liver function tests. Histological sections were stained with hematein-eosin-safran, picrosirius for collagen and Perls staining for hemosiderin. Staining for HBsAg and HBcAg was performed in selected cases. Tissue anti- gen detection on the liver graft was performed by immunohistochem- istry using the following polyclonal antibodies and dilutions: anti- HBs 1/2000 (DAKO SA) and anti-HBc 1/2000 (DAKO SA). For the purpose of this study, reports were reviewed to identify all cases in which liver biopsies revealed a diagnosis other than normal or mini- mal changes. Those cases were reevaluated by a single staff pathol- ogist (MR). Acute hepatic rejection was defined according to well- established histological criteria (12). Evolution toward chronic rejec- tion was considered in the presence of a Joss of more than 50% of interlobular bile ducts on liver biopsy when more than 20 portal areas were present. The biopsy specimens were screened for features con- sidered to be consistent with AIH, i.e. aggressive piecemeal necrosis, lympho-plasmocytic infiltrate of portal tracts, lobular inflammation and lobular necrosis. Histological evaluation of chronic hepatitis was performed according to the recently described METAVIR score: ac- tivity (A) was scored on a scale of 0 to 3 and fibrosis (F) from 0 to 4 (13).
Etiologk:al evaluation #1 patients with chronk' hepatitis All patients presenting histological features of chronic hepatitis after liver transplantation underwent an extensive etiological evaluation consisting of: evidence for alcohol abuse or treatment with hepatotox- ic drugs; complete physical examination; liver function tests and whole blood cyclosporine dosage; ultrasonographic and Doppler ex- amination of the graft; liver biopsy with histological analysis as de- scribed above and staining for HBsAg and HBcAg; detection of anti- HCV antibodies by second-generation recombinant immunoblot as- say (RIBA), and polymerase chain reaction (PCR) in serum for HCV RNA; detection of HBsAg and anti-HBc antibodies and serum PCR for HBV DNA; detection of anti-CMV antibodies and ami-EBV anti- bodies and detection of auto-antibodies ANA, SMA, LKM~ and anti liver-cytosol.
Laboratoo, methods" HBsAg, HBeAg and anti-HBe antibodies were tested using a com- mercial kit (ELISA Murex Diagnostics limited, Kent, UK), as were anti-HBs and anti-HBc (Hoechst Boehring Diagnostics, Marburg Germany), anti-HCV (RIBA-2 Ortho Diagnostic, Raritan, N J, USA) and anti-HIV (ELISA Diagnostics, Pasteur, Marnes la Coquette, France). HBV DNA was detected by a standard molecular hybridiza- tion spot test before March 1993, and by a Digene Hybrid Capture System HBV DNA assay (Murex Diagnostics, Chatillon, France) afterwards. HBV-DNA was also detected by PCR through amplifi- cation of the preC/C region (14). HCV-RNA was detected by PCR through amplification of the 5' conserved region (15). Autoantibodies were detected by indirect immunofluorescence and titrated on a com- posite block of rat liver, kidney and stomach with fluorescein-conju- gated anti-human polyvalent immunoglobulin (16). HLA class I typ- ing was done by a microlymphocytotoxicity test with an automated reading and a double coloration. Class II typing was performed by DNA typing using Sequence Specific Oligonucleotide Probe Hybridi- zation (PCR-SSOPH).

Results Study population During the study period, 25 patients (24 females and one male) with AIH underwent liver transplantation at our institution. Of these, 18 were French, five Italian, one Greek and one Israeli. Clinical and biochemical data are presented in Table 1. HLA B8 haplotype was present in six patients, HLA DR 3 in eight patients and B8DR 3 in four patients. All but two patients received immunosuppressive treatment before referral for liver transplantation for a mean duration of 9 years (1-20 years). This immunosuppressive treatment consisted of corticosteroids in all patients, in association with aza- thioprine (50 mg/day) in 11 of them. By the time of referral for liver transplantation the mean dose of corticosteroids was 23 mg/day (5 to 40 mg/day). Subse- quently, the daily dose of corticosteroids was progress- ively tapered to a daily dose of 5 mg by the time of liver transplantation. In two patients, corticosteroid therapy was started after referral for liver transplantation and given for less than 2 months (4 and 6 weeks) before liver transplantation was performed. All patients ful- filled pre-established criteria for liver transplantation. As shown in Table 1, this was subsequently confirmed by the calculation of an aggregate score according to a scoring system recommended by an expert panel (de- finite AIH is defined by a score higher than 15 before treatment) (9). The two patients in whom immunosup- pressive therapy was started after referral for liver transplantation experienced a rapid deterioration that precipitated the need for a graft.
Autoimmune hepatitis recurrence after L T
Follow-up and survival Among the 25 patients who received a first liver trans- plant, one patient was retransplanted at day 2 for pri- mary non-function of the graft and died 21 days later of an overwhelming sepsis due to Acinetobacter. The remaining 24 patients were followed for a mean of 5.3 years (2 to 8.5 years). The actuarial 5-year patient sur- vival rate was 91% (___ 6%) which was not significantly different from patients transplanted for primary bili- ary cirrhosis (80%___4%) or primary sclerosing cholan- gitis (85.5%---7%) (p=0.43 n.s.). Causes of death were Acinetobacter sepsis in two patients (21 days and 6 years post-transplant), opportunistic infection in one patient with transfusion-acquired HIV infection (4.5 years post-transplant), and liver failure due to hepatitis C viral infection of the graft in one patient (5.5 years post-transplant). The actuarial 5-year graft survival was 83% (-+8%), which was not significantly different from patients transplanted for primary biliary cir- rhosis (76%--_5%) or primary sclerosing cholangitis (65%___9%). Five patients received a second graft for the following reasons: primary non-function of the graft at day 2, sclerosing cholangitis at 10 months (17), chronic hepatitis of unknown cause at 3 years, and hepatitis C viral cirrhosis at 6 and 8 years. One patient received a third liver transplant for hepatitis C recur- rence at 6 years.
The actuarial rate of acute rejection requiring ad- ditional immunosuppressive therapy (i.e. intravenous administration of methylprednisolone) was 50% (___10%) at 1 year, which did not differ from patients
TABLE 1
Study population
Total HCV negative HCV positive*
No. of patients 25 19 6 Sex ratio (M/F) 1/24 1/19 0/6 Age, mean (range) 27 (13-60) 28 (13-60) 28 (13-40) Autoimmune hepatitis
Type I 18 (ANA 9, SMA 16) 14 (ANA 6, SMA 12) 4 (ANA 3, SMA4) Type II 7 (LKM1) 5 (LKM 0 2 (LKMI)
Associated autoimmune conditions** 3/25 (12%) 3/19 (16%) none Aggregate score (median/range)*** 18.5 (12-33) 19.5 (16-23) 14.5 (12-16) Cirrhosis 25/25 (100%) 19/19 (100%) 6/6 (100%) Ascites 21/25 (84%) 16/19 (84%) 5/6 (83%) Jaundice 21/25 (84%) 17/19 (89%) 4/6 (67%) Prothrombin <50% of normal 15/25 (60%) 12/19 (63%) 3/6 (50%) Variceal hemorrhage 6/25 (24%) 4/19 (21%) 2/6 (33%) Gammaglobulin # 26.5 (9.7) 27 (8.9) 25 (7.2) Albumin ~ 30.5 (3.6) 30 (3.2) 32 (4.1) Bilirubin ## 84 (46.7) 88 (49.4) 71 (42.5) Mean duration of the disease before LT in years (range) 9 (1-20) 9.5 (1 15) 7.5 (1-20) Mean duration of immunosuppressive treatment before 9 (0-20) 8 (0-15) 12 (4-20)
LT in years (range)
*Liver transplantation (LT) performed before 1990; **Rheumatoid arthritis, IgA nephropathy, IgA deficiency; ***according to ref. (9); #: g/1 (mean-s.d.); ##: pmol/1.
133

V. Ratziu et al.
Autoantibody titers
1:1000
1:800
1:600
1:400
1:200
time after liver 0 4m 2y transplantation
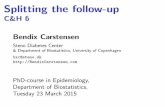
Fig. l. Titers of anti-SMA (0)andanti-LKM1 ((D) before and after liver transplantation in 15 patients without evi- dence of infection by HCV. Triangles represent patients with autoimmune hepatitis recurrence (all with anti-SMA ). The titers did not change significantly after the second year.
transplanted for primary biliary cirrhosis (52%+-6%) primary sclerosing cholangitis (50%-+9%) or HCV-cir- rhosis (48%+-3%) and was higher than in patients transplanted for alcoholic cirrhosis (29%+3%) and HBV-cirrhosis (21%-+4%) as previously reported (18).
Serum was available for autoantibody detection in 22 of 24 patients who survived more than 6 months after liver transplantation. Autoantibodies were de- tected in 17 of 22 patients (77%) and were of the same type, although at a lower titer than before liver trans- plantation (Fig. 1).
Hepatitis C virus infection Anti-HCV antibodies and/or HCV viremia were retro- spectively detected in the serum of six of the 24 pa- tients before liver transplantation. All were women, with two of them having anti-LKM1 antibodies (at ti- ters of 1/500 and 1/1000, respectively), whereas the other four had SMA and ANA (at titers of 1/500 and 1/250, respectively). Of the remaining 18 patients, three acquired HCV infection during surgery for liver trans- plantation or on subsequent follow-up. Of these three patients, one also acquired HIV infection during post- operative blood transfusions (19). In this total group of nine HCV-infected patients, the 5-year survival was 78% (+_ 11%). The cause of death was septic shock in one patient and was unknown in the other (4.5 and 5 years after liver transplantation). The 5-year graft survival was 78% (-+8%). Two patients underwent a second liver transplant, 6 and 8 years later for reinfec- tion of the graft by HCV (cirrhosis in one case, chronic
134
hepatitis with fibrosis in the other). At the last follow- up, two patients had developed HCV-related cirrhosis, three had developed HCV-related chronic hepatitis with fibrosis and four had normal graft histology. These nine patients with HCV infection as well as the patient who died 21 days after liver transplantation were not studied for the risk of autoimmune hepatitis recurrence.
Follow-up of patients without evidence of hepatitis C viral infection During follow-up, 15 patients repeatedly tested nega- tive for anti-HCV antibodies by ELISA II and serum HCV RNA by PCR (Table 2). There was no difference between this subgroup of patients and the remaining group of 10 patients in regard to age, duration of dis- ease before liver transplantation, duration and type of immunosuppressive treatment before liver transplan- tation and clinical features listed in Table 1. Ten pa- tients had type I AIH (median titer of ANA 1/200 and of SMA 1/360) and five had type II AIH (median titer of anti-LKM~ antibodies 1/500). Fourteen of these 15 patients received an immunosuppressive treatment be- fore referral for liver transplantation for a mean time of 8 years (1 20 years). The mean follow-up after liver transplantation was 4.8 years (2-8.5 years) with eight patients followed for more than 5 years. The 5-year patient survival was 100%. One patient died 6 years after liver transplantation from septic shock due to Ac- inetobacter. The other 14 patients were still alive at the last follow-up (mean 6.5 years (2.5-10) after the first graft). The 5-year graft survival was 87%. Two patients underwent a second liver transplantation, one for sclerosing cholangitis and the other for a chronic hepa- titis of unknown origin (due to AIH recurrence, see below) 10 months and 3 years after the first transplant, respectively.
Six months after liver transplantation, all patients were free of jaundice and their clinical condition im- proved. Liver function tests were normal in 10 patients and abnormal in five. Autoantibodies persisted in 12 of the 14 patients who where tested (86%). Their mean titer decreased in the first 4 months after liver trans- plantation, slightly increased over the next 2 years, reaching a lower titer than before liver transplantation and subsequently remained unchanged (Fig. 1). Auto- antibodies were of the same type before and after liver transplantation. Hypergammaglobulinemia persisted in 5 of 15 patients (33%) at the same level as before liver transplantation, whereas it resolved within 6 months in the other patients. Persistence of autoanti- bodies was not correlated to the persistence of hyper-

Autoimmune hepatitis recurrence after L T
o
"=o
0
0
.o
e.
.,d
g.
t',t
~d
¢,
0
. ,d
O0
t¢3
c q
-~ r4 ~1¢3
e~ 0
0
~~-~_ o
g ~ o
m ~ < ~
--.N~N ,~
0 ~ 0 ,- y , ,-,
0 r~
0
0 0 0
0 ~ 0
~ oo
o ~ ~ ~ . ~ "d
. ~ . . o =
=o ~.~"
0 ~ 0
y . o o . . ~-
o o o ~ ~.
~ =
o ~ ~
O ,~ ~ '~ ~.~
- e . P. ,- ~ , . = . ~ -
.'~ .~ ~
, ' , E - -
~ ' ~ - ~ =
"6
Z ~A
o
II
<
0
II
0
e~
"N
135

v. Ratziu et al.
gammaglobulinemia, liver function tests or liver his- tology.
Among these 15 HCV-negative patients, nine (60%) experienced at least one episode of biopsy-proven acute rejection that required specific immunosuppres- sire therapy (i.e. intravenous administration of methyl- prednisolone). Four patients received OKT3 (Ortho- clone ® Ortho Raritan, NJ, USA) for corticosteroid re- sistant acute rejection.
At the most recent follow-up, nine out of these 15 patients (60%) had normal or near normal graft his- tology and liver function tests, whereas six (40%) had abnormal graft histology. Among these six patients, one had chronic rejection and two had ductopenia with jaundice, presumably related to chronic rejection. One of these two experienced histological improvement with a decline in serum bilirubin levels after treatment by Tacrolimus. The remaining three patients (20%) had abnormal histological findings compatible with chronic hepatitis of indeterminate cause. All these pa- tients underwent an extensive etiological evaluation as described in the Patients and Methods section, which was negative, and therefore they were thought to have autoimmune hepatitis recurrence as detailed below.
Follow-up o f patients with chronic hepatitis o f undetermined cause Clinical and biochemical characteristics of these three
patients are listed in Table 2 (Patients 1 to 3). They were all women transplanted for autoimmune type I hepatitis and had all received a long-term immunosup- pressive treatment before liver transplantation. At re- ferral for liver transplantation, all three patients had jaundice, ascites, and intense asthenia, and one of them had encephalopathy. All received an ABO blood group-identical orthotopic liver transplant and a stan- dard triple immunosuppressive regimen consisting of corticosteroids, azathioprine and cyclosporine. Thus pre-transplant history, clinical and biological features at liver transplantation as well as immunosuppression after liver transplantation were not different between these three patients and the remaining 12 patients who were not thought to have autoimmune hepatitis recur- rence.
Patient 1, a 60-year-old woman, received OKT3 dur- ing the first 8 days after liver transplantation because of early post-operative renal insufficiency, and subse- quently did not develop acute rejection. One year post- transplant she remained asymptomatic with normal liver function tests, but the routine follow-up liver bi- opsy showed chronic hepatitis with moderate activity and portal fibrosis (A2F1). There was an important portal inflammatory infiltrate (Fig. 2) made of
136
Fig. 2. Patient 1. Enlargement o f the portal tracts with marked infiltrate, fibrosis and without bridging. ( Picrosirius stain, G 30 : 1).
Fig. 3. Patient 2. Nascent cirrhosis on the graft, 3 years after the first liver transplantation. (Picrosirius stain, G 30 . 1).
lymphocytes, plasmocytes and scarce lymphoid nod- ules with disruption of the hepatocyte-limiting plate and scant areas of lobular necrosis. She was taking 15 mg of corticosteroids, 240 mg of cyclosporine and 50 mg of azathioprine daily. Four years later the histologi- cal lesions were almost identical. The patient was still asymptomatic with normal liver function tests, and therefore the immunosuppressive regimen remained unchanged. An extensive evaluation failed to reveal any cause for the histological findings. The patient was taking no medication other than the immunosuppres- sire regimen and was not consuming alcoholic bever- ages. Markers of HBV and HCV infection repeatedly tested negative in serum (HBsAg, anti-HBc antibodies, anti-HCV antibodies by second-generation ELISA, PCR for HBV and HCV) and histological HBsAg staining of the liver was negative. Doppler ultrasono- graphic examination of the graft was normal. Hyper- gammaglobulinemia persisted at 20 g/l, and auto-anti- bodies persisted at a slightly lower level than before

liver transplantation (anti-SMA 1/50, anti-nuclear antibodies at 1/100). A liver biopsy performed 6 years after the liver transplantation showed the persistence of the same lesions without further progression.
Patient 2, a 21-year-old woman who experienced an episode of acute rejection on the 4th post-operative day, was successfully treated with high dose i.v. methyl- prednisolone. Another episode of acute rejection was di- agnosed 18 months after liver transplantation. This epi- sode was accompanied by mild transient abnormalities of liver function tests that regressed without any specific treatment. Two and a half years after the liver transplan- tation, the patient became jaundiced and complained of intense asthenia. Total bilirubin was 51/~mol/1, conju- gated bilirubin 33/zmol/1, AST was 3 times the normal value (3 N) ALT 4N, alkaline phosphatase 2N and gamma glutamyl transpeptidase 12N. The prothrombin level was normal and albumin 34 g/1. Her only medi- cation was 10 mg of corticosteroids, 180 mg of cyclo- sporine and 50 mg of azathioprine daily. The liver bi- opsy showed a portal lymphocytic infiltrate with piece- meal necrosis and porto-portal fibrosis, and a lobular in- flammatory infiltrate with lobular necrosis (chronic hepatitis with moderate activity, A2F2). An extensive etiologic evaluation was negative. Serum gammaglobu- lin level was normal and autoantibodies persisted at ti- ters similar to those before liver transplantation (anti- SMA 1/100, anti-nuclear antibodies 1/640). Over the next few months, her clinical condition deteriorated with increasing jaundice (total bilirubin 510/zmol/l, con- jugated bilirubin 230 /xmol/1) and a decrease in pro- thrombin level below 45% of the normal value. A de- cision to retransplant was made and the patient received a second liver graft 3 years after the first one. The graft showed severe chronic hepatitis with mutilation of nor- mal architecture and nascent cirrhosis (A2F3) (Fig. 3). The post-operative course was uneventful except for an episode of acute rejection, diagnosed on a routine fol- low-up liver biopsy 5 months later. Liver function tests were normal and the doses of immunosuppressants were increased.
Eighteen months after the second liver transplan- tation, a regular follow-up liver biopsy showed a mild lympho-plasmocytic portal infiltrate. A two-fold in- crease in transaminases occurred 6 months later and the liver biopsy showed fibrotic portal spaces with por- to-portal fibrosis, a lympho-plasmocytic infiltrate with piecemeal necrosis and a mild lobular lymphocytic in- filtrate with hepato-cellular necrosis (A2F2). One year later at the last follow-up, the patient had mild jaun- dice, with bilirubin 54/tmol/1, ALT 4N, alkaline phos- phatase 3N and gammaglutamyl transpeptidase 8N. Liver histology showed bridging fibrosis with extensive
Autoimmune hepatitis recurrence after LT
Fig. 4. Patient 2. Bridging fibrosis and marked acttvlty on the liver graft, 1 year after the second transplantation. ( Hematoxylin-eosin-safran stain, G 100:1).
Fig. 5. Patient 3. Severe fibrotic lesions with bridging and nascent cirrhosis. (Picrosirius stain G30:1).
piecemeal necrosis (Fig. 4). Testing for HBV and HCV viruses was negative in the serum by PCR and serology and there was no evidence of biliary tract or arterial complications of the graft, nor for a drug-induced liver disease. The gammaglobulin level was normal. Anti- nuclear antibodies and anti-SMA antibodies persisted at a titer of 1/500 and 1/100, respectively. Other auto- antibodies were absent.
Patient 3, a 32-year-old woman, experienced a unique episode of acute rejection on day 24 after the transplant, which was successfully treated with intravenous methyl- prednisolone. One year later the liver biopsy was nor- mal. Two years after the liver transplant, while the pa- tient was asymptomatic and had normal liver function tests, a routine liver biopsy showed chronic hepatitis with moderate activity and porto-portal fibrosis (A2F2). Anti-SMA and anti-nuclear autoantibodies were detected at lower titers than before liver transplan- tation (1/160 and 1/80, respectively). Serum gamma- globulin was 29 g/l. The patient was taking daily doses of 10 mg corticosteroids, 200 mg cyclosporine and 50 mg
137

V. Ratziu et al.
azathioprine without other medications. She was asymptomatic for the next 2.5 years, then developed progressive jaundice and asthenia. Five years after the liver transplantation, a liver biopsy showed a dense lymphocytic and plasma cell infiltrate with piecemeal necrosis and progression of the fibrotic lesions. One year later, her condition further deteriorated with total bili- rubin at 518/2mol/1, AST 7N, ALT 3N, PAL 3.5N, and prothrombin level at 50% of the normal value. The liver biopsy showed cirrhosis with moderate activity (A2F4) (Fig. 5). An extensive etiological evaluation including HBV DNA and HCV RNA by PCR was negative, ex- cept for the persistence of anti-SMA and anti-nuclear autoantibodies at titers between 1/100 and 1/160. Gammaglobulin was at 27 g/1. Two months later the pa- tient died of overwhelming Ac ine tobac t e r sepsis while waiting for a second liver transplantation. No post-mor- tem examination was performed.
Discussion The aim of this study was to determine the long-term outcome of patients transplanted for autoimmune hepatitis and the incidence and characteristics of AIH recurrence. This study included patients with sympto- matic cirrhosis despite prolonged, well-conducted im- munosuppressive treatment with corticosteroids, either alone or in association with azathioprine. Two patients underwent liver transplantation after failing a short trial of immunosuppressive therapy. The actuarial pa- tient 5-year survival rate was 91%, comparable to the survival of patients transplanted for primary biliary cirrhosis and primary sclerosing cholangitis during the same period in our institution.
Among the initial 25 patients, six (25%) were in- fected with HCV prior to liver transplantation. Be- cause of the high titer of autoantibodies, young age and female sex, we believe that our patients had auto- immune hepatitis associated with HCV infection rather then HCV chronic liver disease with autoimmune fea- tures. However, this is controversial (20-22), and there- fore these patients were excluded from the study of AIH recurrence. Three other patients who acquired HCV infection after liver transplantation were also ex- cluded, since histological features of autoimmune hepatitis and of HCV infection are indistinguishable.
The main finding of this study is the occurrence of chronic hepatitis after liver transplantation in 3 of 15 patients (20%) without hepatitis C viral infection. We believe this is due to the recurrence of autoimmune hepatitis on the engrafted liver, for the following rea- sons. First, extensive evaluation failed to identify any other etiology. In particular, serological, molecular and histological markers of hepatitis B or C all repeatedly
1 3 8
tested negative, thus rendering viral infection of the graft highly improbable. Secondly, the histological fea- tures were characteristic of autoimmune hepatitis, namely the presence of periportal piecemeal necrosis and a lymphocytic portal infiltrate with abundant plasma cells (9,23). None of the patients displayed any biliary or vascular changes, granulomas, steatosis, sid- erosis or acidophilic bodies that might suggest a differ- ent etiology. Thirdly, serological markers of autoim- munity were present in all three patients (i.e. circulating autoantibodies of the same type as before the trans- plantation, and in two of them elevated serum gamma- globulin levels). The above-mentioned histological and immunological abnormalities in the absence of any alternative explanation are highly suggestive of recur- rence of autoimmune hepatitis. Moreover, in one pa- tient the same condition developed on the second liver graft, thus further supporting this diagnosis.
Recurrence of autoimmune hepatitis was first sug- gested by Neuberger et al. (2), in a 26-year-old female, 18 months after liver transplantation following a dra- matic reduction in the immunosuppressive therapy (the patient was receiving 5 mg of corticosteroids daily). The patient was symptomatic and exhibited histologi- cal abnormalities similar to those seen in our three cases, namely enlarged portal tracts with an abundant lymphocytic and plasma cell infiltrate and piecemeal necrosis. After an increase in immunosuppressive ther- apy, the clinical and biochemical abnormalities and the autoantibodies disappeared. There are several note- worthy differences between this case report and the three patients reported here. First, none of these three patients received reduced doses of immunosuppressive therapy. They were all under triple immunosuppressive therapy with a higher daily dose of corticosteroids than the patient described by Neuberger et al., and consist- ent with the doses that are used in the maintenance treatment of autoimmune hepatitis. While this suggests recurrence despite appropriate immunosuppressive treatment, one cannot exclude that on an individual basis these patients were receiving a less than optimal immunosuppression. Indeed, two of the three patients experienced an episode of acute rejection. There was no temporal correlation between acute rejection and AIH recurrence. Acute rejection occurred long before AIH recurrence and histological signs of rejection were absent when the recurrence was diagnosed.
A second difference between the studies is that in most of our cases, including the three patients with re- currence, the autoantibodies persisted after liver trans- plantation. This may suggest the persistence of an underlying autoimmune process despite the replace- ment of the liver, Similar findings can be found in the

long-term follow-up of patients transplanted for pri- mary biliary cirrhosis. Antimitochondrial antibodies persisted after liver transplantation at a lower yet sig- nificant titer in all patients in the study by Polson et al. (24), in 43 of 45 patients from Esquivel et al. (25), and in 56% of patients from our institution followed for more than 4 years (26). This seemed unrelated to the immunosuppressive therapy since in some patients antimitochondrial antibodies disappeared in the first few months following liver transplantation, and then reappeared in spite of only minor changes in the im- munosuppressive regimen (27). These findings suggest that the primary disease process reflects a dysfunction of the immune system rather than the consequence of pathological mechanisms primarily located in the liver. Interestingly, the autoantibodies also persisted in 82% (9/11) of our transplanted patients who did not develop AIH recurrence. There was no correlation between autoantibody persistence and the occurrence of liver dysfunction, long-term results of liver graft or survival. This is similar to findings from patients transplanted for primary biliary cirrhosis (26-29). This further sug- gests that the autoantibodies currently detected in AIH or primary biliary cirrhosis are not pathogenic but merely reflect an underlying autoimmune disorder.
In our patients, as in the King's College report (2), AIH recurrence was detected between 1 and 3 years after liver transplantation. The disease was clinically hetero- geneous. One patient exhibited an asymptomatic form with mild histological abnormalities, while two others presented a serious disease that resulted in graft failure, ultimately leading to death in one of them and to a sec- ond liver transplant in the other. Interestingly, in this lat- ter patient, the same lesions occurred on the second graft, resulting in a severe disease associating jaundice and hepatic insufficiency. Histologically, all patients had an aggressive piecemeal necrosis which has been iden- tified in autoimmune hepatitis as the main factor of pro- gression to cirrhosis (23). Serial biopsies showed an evo- lution toward porto-portal bridging fibrosis and eventu- ally cirrhotic nodules with persistence of inflammatory activity. In contrast to the patient reported by Neuberg- er et al., this occurred in the absence of a significant amount of necrosis, since lobular necrosis was minimal and bridging necrosis was absent. The significance of bridging necrosis in patients with chronic hepatitis is un- clear (30). It is considered by some an intermediate lesion and an important predictor of evolution toward cirrhosis (31). Our cases describing AIH occurrence on an engrafted liver support previous studies of AIH on native liver (32,33), suggesting that this lesion is not es- sential in the occurrence of cirrhosis.
Wright et al. also reported autoimmune hepatitis re-
Autoimmune hepatitis recurrence after L T
currence in 11 of 43 patients transplanted in Pittsburgh (4), a proportion that is close to our series. However, this population had a highly unusual serological pro- file, since all 11 patients had LKMI coexisting with SMA. The authors provide scant data about the histo- logical criteria used for defining the recurrence, the se- verity and evolution of autoimmune hepatitis on the liver graft and the doses of immunosuppressive drugs administered. HCV infection was ruled out as no anti- HCV antibodies were detected, but the absence of vi- remia was not assessed by PCR, a more sensitive marker in transplanted patients. Recurrence of the dis- ease appeared to be more frequent in HLA DR3-posi- tive recipients who received a DR3-negative graft. In contrast, in our cases we were unable to identify any correlation between the HLA status of the donor or the recipient and the recurrence (data not shown).
In contrast to the above-mentioned studies, no case of recurrence has been documented among 23 patients transplanted for autoimmune hepatitis at the Mayo Clinic (5). The reason for the difference from our study is unclear since most of the epidemiologic features were similar between the two populations: duration of ill- ness and of immunosuppressive therapy before liver transplantation, proportion of patients with cirrhosis, and the clinical and biological severity of the disease. Mean patient age at referral for liver transplantation was slightly older than in our patients (35 vs 27 years) and, although the disease seems to be more aggressive in younger patients, the significance of this difference is uncertain. Also, the follow-up was shorter than in our series, (3.3 vs 5.3 years), but it was probably long enough to diagnose a recurrence since in all above- mentioned reports, as well as in ours, it occurred in the first 3 years. Immunosuppressive therapy was also similar to our study except for higher doses of azathio- prine (100 vs 50 mg). There is one striking difference, however, which is the rapid disappearance of autoanti- bodies in all patients from the Mayo Clinic in the first year following liver transplantation, accompanied by normalization of gammaglobulin levels. In our study autoantibodies persisted in 79% of patients, of the same type but at a lower level than before liver trans- plantation. Two mechanisms may account for this dis- crepancy and for the difference in the incidence of re- currence. The first may be a stronger immunosuppres- sion achieved by the use of higher doses of azathio- prine. Azathioprine is a potent immunosuppressant that is efficiently used at high doses in AIH in case of failure of corticosteroids or relapse (10). The second explanation may be a difference in the evolution of the immunologic abnormalities after liver transplantation. Although hypothetical, such a difference could be ex-
139

V. R a t z h t e t al.
plained by the evolution of the disease before liver transplantation: patients transplanted for end-term liver disease who eventually escaped prolonged im- munosuppressive therapy may behave differently from those transplanted for advanced liver disease in whom immunosuppressive treatment was introduced too late or primarily failed. In the first case, the immunologic disorder may be less likely to be reversed or controlled by post-operative immunosuppressive therapy and re- moval of the target organ, whereas this may be achiev- able in the second case. Additional data concerning the evolution of immunological anomalies in patients transplanted for autoimmune hepatitis are needed in order to support this hypothesis.
Whether the recurrence should be treated by an in- crease in the immunosuppressive therapy is unknown. Interestingly, in the above-mentioned case reports the re- currence presented while immunosuppression was markedly reduced, consisting of low doses of cyclospor- ine alone in one patient (3) or in combination with 5 mg daily of corticosteroids in the other (2). In both it was treated with an increase in the dosage of corticosteroids and the introduction of azathioprine, which was fol- lowed within several weeks by the disappearance of clin- ical and biochemical abnormalities. In contrast, recur- rence presented in our patients while on triple immuno- suppressive therapy including azathioprine and cortico- steroids at daily doses higher than 10 mg. One of them had an asymptomatic form, the second experienced a rapid deterioration in clinical condition that justified a liver transplantation, whereas the last patient ultimately developed liver failure and died of septic complications before a second liver graft was available. In none of these patients was the immunosuppression increased, and therefore we do not know whether stronger immunosup- pression would have altered the course of the disease.
In summary, in patients with autoimmune hepatitis and without HCV infection, liver transplantation was associated with a 5-year survival rate of 100%. Auto- antibodies persisted in most patients, although at a lower titer than before transplantation. Recurrence of the primary disease occurred in 20% of patients with- out associated hepatitis C virus infection, despite a triple immunosuppressive treatment at standard doses. Clinically autoimmune hepatitis recurrence may be ex- tremely severe, leading to graft failure and death in the absence of retransplantation. Even asymptomatic forms may conceal serious histological lesions that may evolve to liver fibrosis. Considering the possibility of disease recurrence, a stronger post-operative im- munosuppression in these patients deserves consider- ation. The persistence of autoimmune markers and the recurrence of the primary disease suggest that in auto-
140
immune hepatitis the immunologic disturbances are not corrected by liver transplantation.
References 1. European Liver Transplant Registry Report: 5/1968-12/1994,
H6pital Paul Brousse, Villejuif, France 1995. 2. Neuberger J, Portmann B, Calne R, Williams R. Recurrence of
autoimmune chronic active hepatitis following orthotopic liver grafting. Transplantation 1984; 37: 363-5.
3. Devlin J, Portmann B, Heaton N, Tan K-C, Williams R. Recur- rence of autoimmune hepatitis following liver transplantation. Liver Transplant Surg 1995; 1:162 5.
4. Wright HL, Bou-Abboud CE Hassanein I", Block GD, Demetris A J, Starzl TE. et al. Disease recurrence and rejection following liver transplantation for autoimmune chronic active liver disease. Transplantation 1992; 53: 136-9.
5. Sanchez-Urdazpal L, Czaja A J, Van Hock B, Krom RAE Wiesn- er RH. Prognostic features and role of liver transplantation in severe corticosteroid-treated autoimmune chronic active hepa- titis. Hepatology t991: 15: 215-21.
6. Mackay IR. Pathogenesis of autoimmune chronic active hepa- titis. In: Krawitt EL, Wiesner RH, editors. Autoimmune Liver Diseases. New York: Raven Press; 1991: p. 21-42.
7. Lohse AW. Experimental models of autoimmune hepatitis. Semin Liver Dis 1991: 11:241 7.
8. Mieli-Vergani G, Lobo-Yeo A, McFarlane BM, McFarlane IG, Mowat AE Vergani D. Different immune mechanisms leading to autoimmunity in primary sclerosing cholangitis and autoimmune active hepatitis of childhood. Hepatology 1989; 9: 198-203.
9. Johnson PJ, McFarlane IG. Meeting report: international auto- immune hepatitis group. Hepatology 1993; 18: 998-1005.
10. Czaja AJ. Diagnosis prognosis and treatment of classical auto- imune chronic active hepatitis. In: Krawitt EL, Wiesner RH, edi- tors. Autoimmune Liver Diseases. New York: Raven Press: 1991: p. 143-65.
11. Manns M, Gerken G, Kyriatsoulis A, Staritz M, Meyer zum B~is- chenfelde KH. Characterisation of a new subgroup of autoim- mune chronic active hepatitis by autoantibodies against a soluble liver antigen. Lancet 1987; 1: 2924.
12. Reynes M. Pathology of the liver graft. In: Herve P, Vuitton DA, Rile G, editors. Organ Transplantation and Tissue Grafting. Paris, London: Inserm/John Libbey, 1996:1126-38.
13. The French METAVIR Cooperative Study Group. Intraobserver and interobserver variations in liver biopsy interpretation in pa- tients with chronic hepatitis C. Hepatology 1994; 20:15 20.
14. Roche B, Samuel D, Gigou M, Feray C, Virot V, Schmets L, et al. De novo and apparent de novo hepatitis B virus infection after liver transplantation. J Hepatol 1997; 26:517 26.
15. Feray C, Gigou M, Samuel D, Paradis V. Wilber J, David ME et al. The course of hepatitis C virus infection after liver transplan- tation. Hepatology 1994; 20:1137M,3.
16. Roitt IM, Doniach D. Immunofluorescent test for the detection of antibodies. In: WHO Booklet of Immunological Studies, Ge- neva: World Health Organization; 1972: p. 1- 12.
17. Sebagh M, Farges O, Kalil A, Samuel D, Bismuth H, Reynes M. Sclerosing cholangitis following human orthotopic liver trans- plantation. Am J Surg Pathol 1995; 19: 81-90.
18. Farges O, Saliba E Farhamant H, Samuel D, Bismuth A, Reynes M, et al. Incidence of rejection and infection after liver transplan- tation as a function of the primary disease: possible influence of alcohol and polyclonal immunoglobulins. Hepatology 1996; 23: 240-8.
19. Bouscarat E Samuel D, Simon E Debar E Bismuth H, Saimot AG. An observational study of 11 French liver transplant recipi- ents infected with human immunodeficiency virus type 1. Clin Infect Dis 1994; 19: 854-9.
20. Lunel E Abuaf N, Frangeul L, Grippon E Perrin M, Le Coz Y, et al. Liver/kidney microsome antibody type I and hepatitis C virus infection. Hepatology 1992; 16: 630-6.

Autoimmune hepatitis recurrence after L T
21. Garson JA, Lenzi M, Ring C Casani F, Ballardini G, Briggs M, et al. Hepatitis C viraemia in adults with type 2 autoimmune hepatitis. J Med Virol 1991; 34: 223~.
22. Bellary S, Schiano T, Hartman G, Blach M. Chronic hepatitis with combined features of autoimmune chronic hepatitis and chronic hepatitis C: favorable response to prednisone and aza- thioprine. Ann Intern Med 1995; 123: 32-4.
23. Batts KP, Ludwig J. Histopatholoy of autoimmune chronic active hepatitis, primary biliary cirrhosis, and primary sclerosing chol- angitis. In: Krawitt EL, Wiesner RH, editors. Autoimmune Liver Diseases. New York: Raven Press; 1991: p. 75-92.
24. Poison R J, Portmann B, Neuberger J, Calne RY, Williams R. Evidence for disease recurrence after liver transplantation for pri- mary biliary cirrhosis. Gastroenterology 1989; 97: 715-25.
25. Esquivel CO, Van Thiel DH, Demetris AJ, Bernardos A, Iwatsuki S, Markus B, et al. Transplantation for primary biliary cirrhosis. Gastroenterology 1988; 94: 1207-16.
26. Dubel L, Farges O, Bismuth H, Sebagh M, Homberg J-C, Johanet C. Kinetics of anti-M2 antibodies after liver transplan- tation for primary biliary cirrhosis. J Hepatol 1995; 23: 674-80.
27. Haagsma EB, Manns M, Klein R, Grond J, Huizenga JR, Sloof
MJH, et al. Subtypes of antimitochondrial antibodies in primary biliary cirrhosis before and after orthotopic liver transplantation. Hepatology 1987; 7: 129-33.
28. Demetris A J, Markus B, Esquivel CO, Van Thiel DH, Saidman S, Gordon R, et al. Pathologic analysis of liver transplantation for primary biliary cirrhosis. Hepatology 1988; 8: 939-47.
29. Balan V, Batts KP, Porayko MK, Krom RAE Ludwig J, Wiesner RH. Histological evidence of recurrence of primary biliary cir- rhosis after liver transplantation. Hepatology 1993; 18: 1392-8.
30. Combes B. The initial morphologic lesion in chronic hepatitis, im- portant or unimportant? Hepatology 1986; 6:518-22.
31. Schalm SW, Korman MG, Summerskill WHJ, Czaja AJ, Baggen- stoss AH. Severe chronic active liver disease. Prognostic signifi- cance of initial morphologic patterns. Dig Dis 1977; 22: 973-80.
32. DeGroote J, Fevery J, Lepoutre L. Long term follow-up of chronic active hepatitis of moderate severity. Gut 1978; 19: 510- 3.
33. Davis GL, Czaja AJ, Ludwig J. Development and prognosis of histologic cirrhosis in corticosteroid-treated l'/epatitis B surface antigen-negative chronic active hepatitis. Gastroenterology 1984; 87: 1222-7.
141