
Linear and nonlinear analyses of EEG dynamics during non-painful somatosensory processing in chronic...
8
Linear and nonlinear analyses of EEG dynamics during non-painful somatosensory processing in chronic pain patients Carolina Sitges a , Xavier Bornas a , Jordi Llabrés a , Miquel Noguera b , Pedro Montoya a, ⁎ a University Institute of Health Sciences Research (IUNICS), University of Balearic Islands (UIB), Palma, Spain b Universitat Politècnica de Catalunya (UPC), Barcelona, Spain abstract article info Article history: Received 19 January 2010 Received in revised form 23 May 2010 Accepted 31 May 2010 Available online 9 June 2010 Keywords: Chronic pain Somatosensory ERP Multiscale entropy Fractal dimension FFT Affective modulation The aim of our study was to characterize brain dynamics of affective modulation of somatosensory processing in chronic pain. We hypothesized that chronic pain patients will show abnormal EEG activity under negative mood conditions compared to healthy controls. Nineteen patients with chronic pain and 21 healthy subjects participated in the experiment. Multiscale entropy, fractal dimension, event-related potentials, and fast Fourier transform were used to analyze EEG data. A significant enhancement of entropy was found in pain patients at P4 compared to P3. Analysis of fractal dimension also revealed significantly higher values at P4 than P3 when pain patients were viewing unpleasant pictures. By contrast, no significant differences due to hemisphere or affective condition were found on nonlinear measures for healthy controls. Analyses of somatosensory ERPs showed that P50 amplitudes elicited by pleasant pictures were more reduced in chronic pain patients than in healthy controls. Finally, we observed that EEG band power was lower in pain patients than in healthy controls, in particular for theta and beta bands over sensorimotor cortices and temporal regions when viewing pleasant images. These findings suggest that sustained pain seems to be accompanied by an abnormal activation and dynamic of brain networks related to emotional processing of somatosensory information in chronic pain. Furthermore, our findings suggest that both linear and nonlinear measures of EEG time series may contribute to the understanding of brain dysfunction in chronic pain. © 2010 Elsevier B.V. All rights reserved. 1. Introduction Although the pathophysiology of chronic pain is still unclear, it has been observed that altered brain processing of nociceptive information exists and that negative mood can modulate pain perception in these patients (Geisser et al., 2003; Staud et al., 2003). Moreover, it has been argued that chronic pain should be considered a cognitive state, which might interfere with other emotionally charged cognitive states (Apkarian et al., 2004). However, despite the fact that affective modulation of somatosensory brain activity has now been reported in chronic pain patients (Montoya et al., 2004, 2005b), the question of how emotion and processing of body information influence brain dynamics in chronic pain patients in comparison with healthy controls remains open. In the last years, the theory of nonlinear dynamical systems has been applied to electroencephalographic (EEG) and magnetoencephalographic (MEG) data in order to capture the macroscopic spatial and temporal dynamics of brain activity (Elbert et al., 1994; Lutzenberger et al., 1992a,b, 1995, 1997; Stam, 2005), and has provided suitable methods to understand how the brain works in healthy and pathological states (Stam, 2005). For instance, nonlinear measures such as fractal dimension and entropy have proved successful in quantifying the complexity (Liu et al., 2005) and the regularity of EEG time series (i.e., the predictability of future amplitude values of the EEG based on one or two previous amplitude values), providing information about the flexibility that the brain needs to respond to cognitive demands (Pincus, 1995; Costa et al., 2002; Abásolo et al., 2006). Thus, low EEG entropy (reflecting enhanced EEG regularity and low brain complexity) has been associated with several physiological and pathological states including sleep, anesthesia, schizophrenia, Parkinson's and Alzheimer's diseases (Stam, 2005; Abásolo et al., 2006). In a similar way, fractal dimension of the EEG has been related to the activity and extent of the neuronal cell assemblies underlying sensorimotor or cognitive processes (Lutzenberger et al., 1997; Liu et al., 2005). Moreover, previous research has shown that emotional processing is associated with enhancements in fractal dimension compared to neutral conditions, especially in posterior brain regions (Aftanas et al., 1994, 1997a,b, 1998). In addition, reduced fractal dimension has been associated with states of meditation (Aftanas and Golocheikine, 2002) and anesthesia (Klonowski, 2007). Although all these data seem to indicate that nonlinear measures may reflect specific changes on brain activity in pathological states, no information exists about brain complexity of somatosensory processing and the influence of mood in chronic pain patients. International Journal of Psychophysiology 77 (2010) 176–183 ⁎ Corresponding author. University Institute of Health Sciences Research (IUNICS), University of Balearic Islands, Carretera de Valldemossa km 7.5, 07122 Palma, Spain. Tel.: +34 971 172646; fax: +34 971 172309. E-mail address: [email protected] (P. Montoya). 0167-8760/$ – see front matter © 2010 Elsevier B.V. All rights reserved. doi:10.1016/j.ijpsycho.2010.05.010 Contents lists available at ScienceDirect International Journal of Psychophysiology journal homepage: www.elsevier.com/locate/ijpsycho
Transcript of Linear and nonlinear analyses of EEG dynamics during non-painful somatosensory processing in chronic...

International Journal of Psychophysiology 77 (2010) 176–183
Contents lists available at ScienceDirect
International Journal of Psychophysiology
j ourna l homepage: www.e lsev ie r.com/ locate / i jpsycho
Linear and nonlinear analyses of EEG dynamics during non-painful somatosensoryprocessing in chronic pain patients
Carolina Sitges a, Xavier Bornas a, Jordi Llabrés a, Miquel Noguera b, Pedro Montoya a,⁎a University Institute of Health Sciences Research (IUNICS), University of Balearic Islands (UIB), Palma, Spainb Universitat Politècnica de Catalunya (UPC), Barcelona, Spain
⁎ Corresponding author. University Institute of HealtUniversity of Balearic Islands, Carretera de ValldemossTel.: +34 971 172646; fax: +34 971 172309.
E-mail address: [email protected] (P. Montoya
0167-8760/$ – see front matter © 2010 Elsevier B.V. Adoi:10.1016/j.ijpsycho.2010.05.010
a b s t r a c t
a r t i c l e i n f oArticle history:Received 19 January 2010Received in revised form 23 May 2010Accepted 31 May 2010Available online 9 June 2010
Keywords:Chronic painSomatosensory ERPMultiscale entropyFractal dimensionFFTAffective modulation
The aim of our study was to characterize brain dynamics of affective modulation of somatosensoryprocessing in chronic pain. We hypothesized that chronic pain patients will show abnormal EEG activityunder negative mood conditions compared to healthy controls. Nineteen patients with chronic pain and 21healthy subjects participated in the experiment. Multiscale entropy, fractal dimension, event-relatedpotentials, and fast Fourier transform were used to analyze EEG data. A significant enhancement of entropywas found in pain patients at P4 compared to P3. Analysis of fractal dimension also revealed significantlyhigher values at P4 than P3 when pain patients were viewing unpleasant pictures. By contrast, no significantdifferences due to hemisphere or affective condition were found on nonlinear measures for healthy controls.Analyses of somatosensory ERPs showed that P50 amplitudes elicited by pleasant pictures were morereduced in chronic pain patients than in healthy controls. Finally, we observed that EEG band power waslower in pain patients than in healthy controls, in particular for theta and beta bands over sensorimotorcortices and temporal regions when viewing pleasant images. These findings suggest that sustained painseems to be accompanied by an abnormal activation and dynamic of brain networks related to emotionalprocessing of somatosensory information in chronic pain. Furthermore, our findings suggest that both linearand nonlinear measures of EEG time series may contribute to the understanding of brain dysfunction inchronic pain.
h Sciences Research (IUNICS),a km 7.5, 07122 Palma, Spain.
).
ll rights reserved.
© 2010 Elsevier B.V. All rights reserved.
1. Introduction
Although the pathophysiology of chronic pain is still unclear, it hasbeen observed that altered brain processing of nociceptive informationexists and that negative mood can modulate pain perception in thesepatients (Geisser et al., 2003; Staud et al., 2003). Moreover, it has beenargued that chronic pain should be considered a cognitive state, whichmight interferewithother emotionally charged cognitive states (Apkarianet al., 2004). However, despite the fact that affective modulation ofsomatosensory brain activity has now been reported in chronic painpatients (Montoya et al., 2004, 2005b), the question of how emotion andprocessing of body information influence brain dynamics in chronic painpatients in comparison with healthy controls remains open.
In the last years, the theory of nonlinear dynamical systems has beenapplied to electroencephalographic (EEG) andmagnetoencephalographic(MEG) data in order to capture the macroscopic spatial and temporaldynamics of brain activity (Elbert et al., 1994; Lutzenberger et al., 1992a,b,1995, 1997; Stam, 2005), and has provided suitable methods to
understand how the brain works in healthy and pathological states(Stam, 2005). For instance, nonlinear measures such as fractal dimensionand entropy have proved successful in quantifying the complexity (Liu etal., 2005) and the regularity of EEG time series (i.e., the predictability offuture amplitude values of the EEG based on one or two previousamplitude values), providing information about the flexibility that thebrain needs to respond to cognitive demands (Pincus, 1995; Costa et al.,2002; Abásolo et al., 2006). Thus, low EEG entropy (reflecting enhancedEEG regularity and low brain complexity) has been associated withseveral physiological and pathological states including sleep, anesthesia,schizophrenia, Parkinson's andAlzheimer's diseases (Stam, 2005;Abásoloet al., 2006). In a similarway, fractal dimensionof theEEGhasbeen relatedto the activity and extent of the neuronal cell assemblies underlyingsensorimotor or cognitive processes (Lutzenberger et al., 1997; Liu et al.,2005).Moreover, previous research has shown that emotional processingis associatedwithenhancements in fractaldimensioncompared toneutralconditions, especially in posterior brain regions (Aftanas et al., 1994,1997a,b, 1998). In addition, reduced fractal dimensionhasbeenassociatedwithstatesofmeditation(AftanasandGolocheikine, 2002)andanesthesia(Klonowski, 2007). Althoughall thesedata seemto indicate thatnonlinearmeasures may reflect specific changes on brain activity in pathologicalstates, no information exists about brain complexity of somatosensoryprocessing and the influence of mood in chronic pain patients.
Table 1Clinical and demographic characteristics of healthy controls and chronic pain patients.
Healthy controls(n=21)
Chronic pain patients(n=19)
Age (yrs)Mean (SD) 40.5 (16.7) 48.4 (6.9)Range 23–73 37–64
Medication, n (%)Antidepressants – 72.2%Analgesics / muscular relaxants/ NSAIDs
– 83.3%
Anxiolytics – 52.6%Duration of pain (yrs)
Mean (SD) – 6.2 (7.8)Range – 0.8–35.0
Pain intensity (VAS, 0–8 cm)Mean (SD) – 5.2 (1.4)Range – 2.8–8.0
State-trait anxiety Inventory (raw score)Mean (SD) 14.8 (9.5)⁎ 30.8 (14.7)Range 6–45 5–57
Beck depression inventory (raw score)Mean (SD) 6.2 (5.6)⁎ 19.3 (8.8)Range 0–20 7–40
McGill Pain Questionnaire (number of adjectives)Sensory – 9.0 (2.2)Affective – 1.9 (0.7)Miscellaneous – 2.4 (0.8)
West Haven-Yale Multidimensional Pain Inventory (0–6)Social support – 4.1 (1.8)Affective distress – 4.1 (1.1)Interference social activities – 4.1 (1.3)Interference daily activities – 5.1 (0.8)Pain intensity – 4.9 (1.0)Life control – 3.2 (1.7)Distracting responses – 3.9 (1.6)Solicitous responses – 2.6 (1.8)Punishing responses – 1.7 (1.7)Household chores – 3.2 (2.0)Activities away from home – 2.1 (1.1)Outdoor work – 1.3 (1.6)Social activities – 1.7 (1.1)
⁎ Significant group differences: p≤ .001.
Table 2Clinical details from chronic musculoskeletal (MSK) pain patients, including type ofpathology and years of evolution.
Patient # Diagnosis Years
1 Spondylosis (discarthrosis) at lumbar level 102 Polyneuritis, radiculopathy 23 Herniated disk 134 Herniated disk 105 Neck pain 156 Degenerative arthrosis 107 Herniated disk 18 Herniated disk 79 Herniated disk 810 Arthritis (hips, knees, feet, hands) 1611 Herniated disk 212 Herniated disk 313 Vertebral injury at cervical level 214 Neuralgia 115 Herniated disk 1516 Back pain 1317 Polyradiculopathy 418 Herniated disk, discarthrosis 119 Trigeminal neuralgia 4
177C. Sitges et al. / International Journal of Psychophysiology 77 (2010) 176–183
Research on EEGpower spectra has further suggested a link betweenpain perception and brain activity in healthy controls. Thus, for instance,lowered power in the alpha rhythmover primary somatosensory cortexhas been observed during the expectancy of predictable painfulstimulation (Babiloni et al., 2003, 2006). Early reports have also revealedthat chronic pain patients show less alpha asymmetry than healthysubjects (De Benedittis and De Gonda, 1985; Stevens et al., 2000), andthat neurofeedback training to increase alpha waves would be aneffective method to reduce pain perception (Melzack and Perry, 1975).There is, however, no information about the conjoint influence ofemotion and somatosensory processing on frequency bands of the EEGspectrum among chronic pain patients.
The present report aims at testing the existence of differencesbetween chronic pain patients and healthy controls in linear andnonlinear measures of EEG signals during a dual-task specificallydesigned to assess the affective modulation of somatosensory brainprocessing. Accordingwith previous results (Montoya et al., 2005b), wehypothesize that chronic pain patients as compared to healthy controlswill displaymore reduced entropy and fractal dimension, aswell as EEGalpha power and evoked responses to non-painful body informationunder negative mood conditions.
2. Materials and methods
2.1. Participants
Nineteen female patients (mean±SD: 48.37±6.90 years old), allright handed (except one), with a diagnosis of chronic musculoskeletal
(MSK) pain due to degenerative joint, intervertebrae disc, or inflam-matory diseases (e.g., arthrosis, herniated disk at different levels of thespinal cord, polyradiculopathy, polyneuritis, neuralgia, carpal tunnelsyndrome) for at least 6 months (mean±SD: 6.19±7.78 years) wererecruited from the PainManagement Unit of a tertiary care hospital andtheMedical Unit for Disability Assessment of the Spanish Social SecurityAgency in Palma (Spain) (Table 2). They had normal hearing, correctedvisual acuity, and no history of head trauma or drug abuse. All patientswere taking regular medication, including analgesic/myorelaxant/NSAID (83.3%), antidepressant (72.2%), and anxiolytic (52.6%) drugs(Table 1). Twenty-one female students (40.52±16.68 years old), allright handed (except one), enrolled in the Senior Learning Program orthe Psychology Graduate Program of the University of the BalearicIslands were recruited as healthy controls. At the moment of theexamination, eight chronic pain patients were involved in a litigationprocess for financial compensation due to disability. Subjects wereverbally informed about the details of the study during the recruitmentand noted that participation in the experiment was not linked to theirpossible litigation process. A specifically designed information leafletwas also given, and after agreeing to participate, subjects providedwritten consent. The studywas approvedby theEthics Committee of theUniversity of the Balearic Islands (Spain). Data from 15musculoskeletalchronic pain patients were already compared with a group offibromyalgia patients and published elsewhere (Montoya et al., 2005b).
2.2. Clinical pain assessment
All patients underwent an extensive medical and psychologicalassessment, including self-report questionnaires: the Spanish versionsof the Beck Depression Inventory (BDI) (Beck et al., 1961), the State-Trait Anxiety Inventory (STAI) (Spielberger et al., 1970), the WestHaven–YaleMultidimensional Pain Inventory (MPI) (Kerns et al., 1985),and the McGill Pain Questionnaire (MPQ) (Melzack, 1975) werecompleted.
2.3. Somatosensory stimulation task and recording of brain activity
Somatosensory stimulationwas applied to the indexfinger of the rightor the left hand using a pneumatic stimulator, which consisted of a smallmembrane attached to the digit by a plastic clip andfixatedwith adhesivestrips. During the somatosensory stimulation task, two types of stimuliwere presented in a random series such that one of themwas frequentlydelivered to the right hand (86% of the trials), and the otherwas delivered

178 C. Sitges et al. / International Journal of Psychophysiology 77 (2010) 176–183
to the left hand (14% of the trials) (oddball paradigm). One stimulationblock consisted of 560 stimuli (480 frequent and 80 deviant stimuli) of100 ms duration with a constant pressure of 2 bars, and a variable inter-stimuli interval of 550 ms±50ms. Participants received two stimulationblocks: onewhen theywere viewing forty pictureswith negative valence(unpleasant content), and other when they were viewing forty pictureswith positive valence (pleasant content). Each picture was presented for6 s and was followed by a 6-second blank screen. One deviant and sixfrequent tactile stimuli were delivered during each slide presentation, aswell as during the blank screen. All pictures were selected from theInternational Affective Picture System (IAPS)1 (Lang et al., 1997), andwere the sameasusedelsewhere (Montoya et al., 2005b). Theorder of thetwo stimulation blockswas counterbalanced between the subjectswithineach group.
Patients were instructed to ignore tactile stimulation and to payattention to the slides trying to imagine experiencing themselves inthe situations described by the pictures. Subjects were seated in frontof a computer screen in a sound attenuated room, and instructed tokeep eye movements and blinks to minimum during the experiment.
2.4. Recording of brain activity
Brain activity elicited by somatosensory stimulation was recordedunder two experimental conditions (each lasting about 8 min):viewing pleasant and unpleasant pictures. Electroencephalography(EEG) was recorded from 32 electrodes (10–20 International System)with linked-earlobe reference. An electrooculogram (EOG) channelwas also obtained using two electrodes placed above and below theleft eye. A ground electrode was placed anteriorly to Fpz. Electrodeimpedances were kept below 10 kΩ. The EEG and EOG were sampledwith a digitization rate of 1000 Hz and amplified with a 0.10–70 Hzbandpass filter and a 50 Hz notch filter.
2.5. Preprocessing analysis
For analysis purposes, EEG datawere preprocessed in three differentways. First, raw EEG datawere segmented in epochs of 700 ms duration(from 100 ms before to 600 ms after stimulus onset), and corrected foreye-movement artifacts (Gratton et al., 1983). Additionally, visualanalysis was followed by exclusion of epochs containing non-correctedeye-movement as well as other movement artifacts. Somatosensoryevoked potentials (SEPs) to frequent (tactile stimuli delivered to theright hand) and deviant stimuli (left hand) were separately averagedrelative to a 100 ms prestimulus baseline for both experimentalconditions (viewing unpleasant vs. pleasant pictures). Peak amplitudeswere computed for following SEPs components: P50 (20–80 ms afterstimulus onset at electrodes C3/C4), N80 (60–110 ms at C3/C4), andP200 (135–260 ms at Cz).
Second, raw EEG data were resampled offline at 500 Hz, segmentedin epochs of 512 data points (1024 ms), and corrected for eye-movement artifacts (Gratton et al., 1983). Visual analysis was alsofollowed by exclusion of epochs containing non-corrected eye-movement as well as other movement artifacts. To avoid artifacts atthe beginning and at the end of the recording session, only the twocentral minutes of the EEG time series (between 180 and 300 s afterrecording onset) were analyzed. Averaged power spectra ofthe following frequency bands were obtained using Fast Fourier
1 Pleasant: 4500, 4510, 4531, 4532, 4533, 4599, 4606, 4607, 4608, 4609, 4611, 4640,4651, 4652, 4653, 4659, 5260, 5470, 5480, 5621, 5623, 5626, 5628, 5629, 7330, 7502,8031, 8034, 8080, 8161, 8170, 8190, 8200, 8210, 8370, 8380, 8420, 8460, 8470, 8490(mean valence: 7.57±0.32; mean arousal: 6.11±0.49). Unpleasant: 2710, 2800, 3010,3030, 3051, 3053, 3060, 3071, 3080, 3100, 3102, 3110, 3120, 3130, 3140, 3150, 3170,3230, 3550, 6211, 6212, 6312, 6313, 6540, 6570, 6940, 8480, 9040, 9050, 9181, 9250,9252, 9400, 9404, 9410, 9420, 9421, 9611, 9910, 9920 (mean valence: 1.62±0.28;mean arousal: 7.30±0.36).
transform (FFT): delta (2–4 Hz), theta1 (4–6 Hz), theta2 (6–8 Hz),alpha1 (8–10 Hz), alpha2 (10–12 Hz), beta1 (12–18 Hz) and beta2 (18–22 Hz).
And third, a 2 min epoch of EEG (offline resampled at 500 Hz) wasselected in the time window from 180 to 300 s after recording onsetfor nonlinear analyses. In order to explore the nonlinearity of EEGtime series, we also obtained surrogate data using the AmplitudeAdjusted Fourier Transform (AFFT) with α=0,05 (Theiler et al., 1992;Hegger et al., 1999; Schreiber and Schmitz, 1996, 2000). Twoparameters of nonlinear complexity were computed on EEG timeseries: multiscale entropy and fractal dimension.
Multiscale entropy (MSE) has been shown to be useful in thecharacterization of EEG signal's complexity (Abásolo et al., 2006). MSEwas calculated using the algorithm developed by Costa et al. (2002).Briefly, the MSE analysis constructs consecutive coarse-grained timeseries by averaging a successively increasing number of data points innon-overlapping windows. For scale 1, the coarse grained time seriesis the original time series. For scale 2, the time series is made up of theaverage of consecutive pairs of data points, so that its length is thelength of the original time series divided by the scale factor (in thiscase 2), and so on. Then, sample entropywas calculated for each of thecoarse-grained time series, defined as the negative natural logarithmof the conditional probability that two sequences similar for m pointsremain similar at the next point.
Sampleentropy m; r;Nð Þ = − ln Am rð Þ= Bm rð Þ½ �;
where Bm(r) is the probability that two sequences will match for mpoints, and Am(r) is the probability that two sequences will match form+1 points.
Thus, MSE estimates the degree of irregularity (or disorder) of asequence of values process when such estimation is done atincreasingly longer time scales. Due to the multiscale approach oftheMSE algorithm, more complex time series, with features at variousscales, will exhibit entropy values that strongly depend on the timescale, while a less complex signal will show a constant entropy value.For calculation purposes, the parameter r of the MSE algorithm wasset to 20% of the standard deviation and the parameter mwas set to 2,values that are within the usual range suggested to measure this kindof entropy (Pincus, 1995). The series were coarse-grained up to scale20, so that the shortest time series had 3000 points.
Fractal dimension (FD) has been used as a sensitive index forquantifying complexity of EEG time series, reflecting the activation ofneuronal cell assemblies (Lutzenberger et al., 1992a,b, 1995, 1997; Liuet al., 2005). FD was calculated following the procedure described byLiu et al. (2005). For this purpose, data were first normalized to bewithin a unit square by rescaling the time axis and the EEG signal ofthe data space:
i′ = i =N; s′ i′� �
= s ið Þ–smin=smax−smin
where s(i) are the original EEG time series and s′(i′) are normalized ofthe ith data point; smax and smin are the maximal and minimal valuesof the signal; i=1, 2, 3,..., N is the serial number of the data points andi′ is the normalized one.
FD values were then calculated by implementing the Sevcikalgorithm (Liu et al., 2005) in Matlab (MathWorks Inc., versionR2008a):
FD = 1 + ln Lð Þ=ln 2 N � 1ð Þð Þ
where L is the total length of the data section in the normalizedcoordinate system.
179C. Sitges et al. / International Journal of Psychophysiology 77 (2010) 176–183
2.6. Statistical design
Demographic and questionnaire data (STAI and BDI) were analyzedwith two-sample t-tests to examinemean differences between the twogroups (chronic pain patients vs. healthy controls). Moreover, multi-variate analyses of variance (MANOVAs) with the within-subjectsfactors emotional context (unpleasant vs. pleasant) and the between-subjects factor group (chronic pain patients vs. healthy controls) wereused to test differences on nonlinear (MSE and FD) and linear measures(FFT and SEP amplitudes) at following electrodes: F3, F7, C3, P3, T3, O1,F4, F8, C4, P4, T4, O2, Fz, Cz, and Pz. To further test topographical effectson linear and nonlinear measures, EEG electrodes were grouped intohemisphere (left vs. right) and brain location (frontal [F3/F4], fronto-lateral [F7/F8], central [C3/C4], parietal [P3/P4], temporal [T3/T4],occipital [O1/O2]). Finally, a within-subjects factor stimulus type(frequent vs. infrequent stimuli) was also included for the analyses ofSEP amplitudes to test the effects elicited by frequent and deviantstimuli. All post hoc analyses were based on pairwise comparisonswithBonferroni adjustment. Statistical analyses were conducted with SPSS(Statistical Package for the Social Sciences Inc., version 15.0).
3. Results
3.1. Demographic and clinical data
Pairwise comparisons between chronic pain patients and healthycontrols revealed that both groups were comparable in age.Significant group differences were found on the State-Trait AnxietyInventory (t[35]=3.913, p=.001) and on the Beck DepressionInventory (t[35]=5.405, pb .001). These results indicated thatchronic pain patients were more depressed and anxious than healthycontrols.
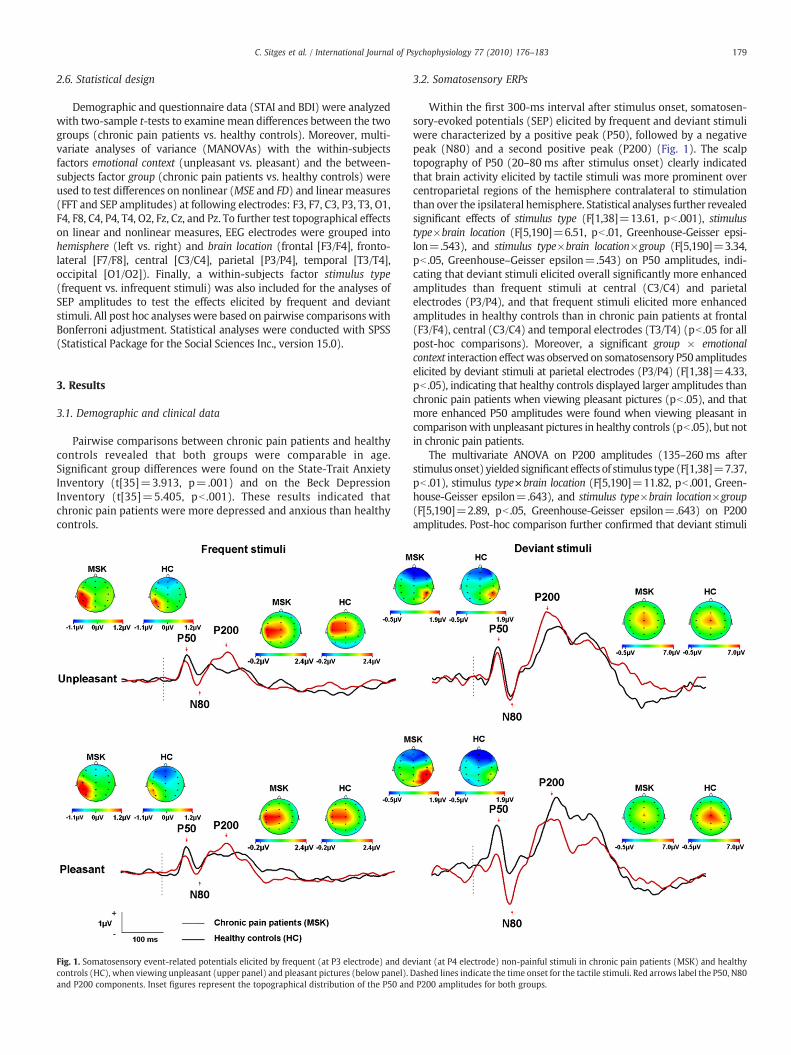
Fig. 1. Somatosensory event-related potentials elicited by frequent (at P3 electrode) and decontrols (HC), when viewing unpleasant (upper panel) and pleasant pictures (below panel).and P200 components. Inset figures represent the topographical distribution of the P50 and
3.2. Somatosensory ERPs
Within the first 300-ms interval after stimulus onset, somatosen-sory-evoked potentials (SEP) elicited by frequent and deviant stimuliwere characterized by a positive peak (P50), followed by a negativepeak (N80) and a second positive peak (P200) (Fig. 1). The scalptopography of P50 (20–80 ms after stimulus onset) clearly indicatedthat brain activity elicited by tactile stimuli was more prominent overcentroparietal regions of the hemisphere contralateral to stimulationthan over the ipsilateral hemisphere. Statistical analyses further revealedsignificant effects of stimulus type (F[1,38]=13.61, pb .001), stimulustype×brain location (F[5,190]=6.51, pb .01, Greenhouse-Geisser epsi-lon=.543), and stimulus type×brain location×group (F[5,190]=3.34,pb .05, Greenhouse–Geisser epsilon=.543) on P50 amplitudes, indi-cating that deviant stimuli elicited overall significantly more enhancedamplitudes than frequent stimuli at central (C3/C4) and parietalelectrodes (P3/P4), and that frequent stimuli elicited more enhancedamplitudes in healthy controls than in chronic pain patients at frontal(F3/F4), central (C3/C4) and temporal electrodes (T3/T4) (pb .05 for allpost-hoc comparisons). Moreover, a significant group × emotionalcontext interaction effectwas observed on somatosensory P50 amplitudeselicited by deviant stimuli at parietal electrodes (P3/P4) (F[1,38]=4.33,pb .05), indicating that healthy controls displayed larger amplitudes thanchronic pain patients when viewing pleasant pictures (pb .05), and thatmore enhanced P50 amplitudes were found when viewing pleasant incomparisonwith unpleasant pictures in healthy controls (pb .05), but notin chronic pain patients.
The multivariate ANOVA on P200 amplitudes (135–260 ms afterstimulus onset) yielded significant effects of stimulus type (F[1,38]=7.37,pb .01), stimulus type×brain location (F[5,190]=11.82, pb .001, Green-house-Geisser epsilon=.643), and stimulus type×brain location×group(F[5,190]=2.89, pb .05, Greenhouse-Geisser epsilon=.643) on P200amplitudes. Post-hoc comparison further confirmed that deviant stimuli
viant (at P4 electrode) non-painful stimuli in chronic pain patients (MSK) and healthyDashed lines indicate the time onset for the tactile stimuli. Red arrows label the P50, N80P200 amplitudes for both groups.
180 C. Sitges et al. / International Journal of Psychophysiology 77 (2010) 176–183
elicited significantlymore enhanced amplitudes that frequent stimuli atfrontal (F3/F4), central (C3/C4), parietal (P3/P4) andoccipital electrodes(O1/O2) in chronic pain patients, and at temporal (T3/T4), parietal (P3/P4) and occipital (O1/O2) in healthy controls (pb .05 for all post-hoccomparisons). No significant effects involving the factor emotionalcontext were observed on P200 amplitudes.
The multivariate ANOVA on N80 amplitudes (60–110 ms afterstimulus onset) yielded no significant effects involving the factorsstimulus type, emotional context or group.
3.3. EEG power spectra
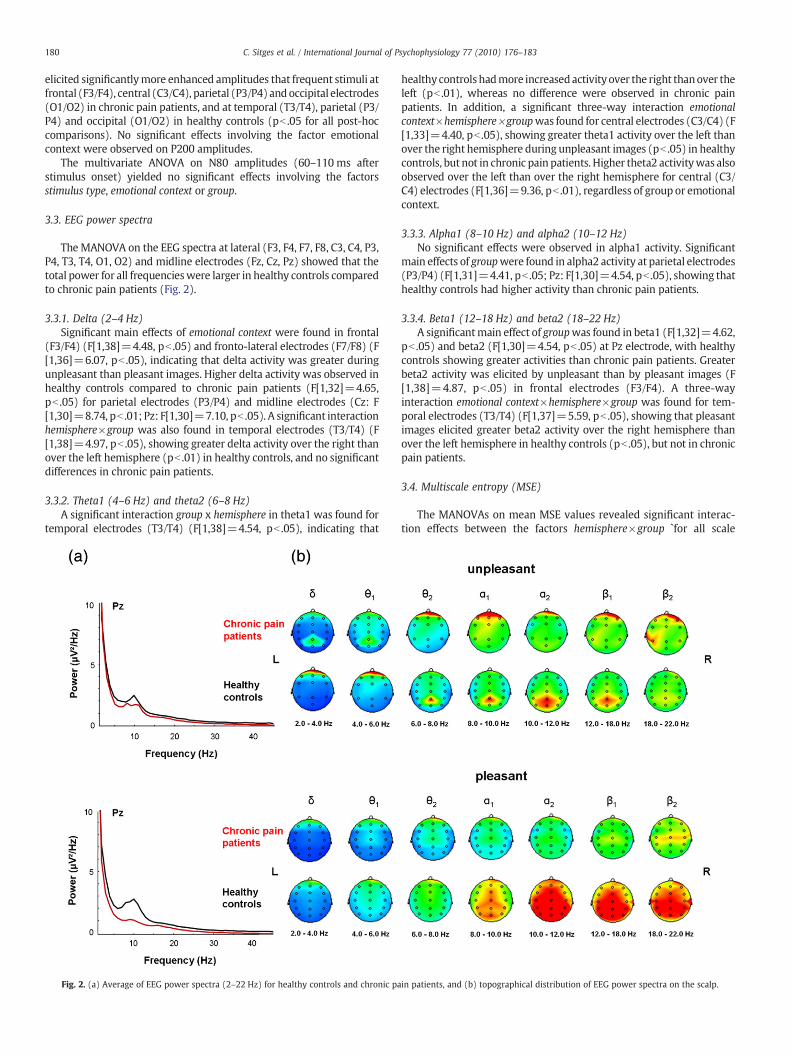
TheMANOVA on the EEG spectra at lateral (F3, F4, F7, F8, C3, C4, P3,P4, T3, T4, O1, O2) and midline electrodes (Fz, Cz, Pz) showed that thetotal power for all frequencieswere larger in healthy controls comparedto chronic pain patients (Fig. 2).
3.3.1. Delta (2–4 Hz)Significant main effects of emotional context were found in frontal
(F3/F4) (F[1,38]=4.48, pb .05) and fronto-lateral electrodes (F7/F8) (F[1,36]=6.07, pb .05), indicating that delta activity was greater duringunpleasant than pleasant images. Higher delta activity was observed inhealthy controls compared to chronic pain patients (F[1,32]=4.65,pb .05) for parietal electrodes (P3/P4) and midline electrodes (Cz: F[1,30]=8.74, pb .01; Pz: F[1,30]=7.10, pb .05). A significant interactionhemisphere×group was also found in temporal electrodes (T3/T4) (F[1,38]=4.97, pb .05), showing greater delta activity over the right thanover the left hemisphere (pb .01) in healthy controls, and no significantdifferences in chronic pain patients.
3.3.2. Theta1 (4–6 Hz) and theta2 (6–8 Hz)A significant interaction group x hemisphere in theta1 was found for
temporal electrodes (T3/T4) (F[1,38]=4.54, pb .05), indicating that
Fig. 2. (a) Average of EEG power spectra (2–22 Hz) for healthy controls and chronic pa
healthy controls hadmore increasedactivity over the right thanover theleft (pb .01), whereas no difference were observed in chronic painpatients. In addition, a significant three-way interaction emotionalcontext×hemisphere×groupwas found for central electrodes (C3/C4) (F[1,33]=4.40, pb .05), showing greater theta1 activity over the left thanover the right hemisphere during unpleasant images (pb .05) in healthycontrols, but not in chronic pain patients. Higher theta2 activitywas alsoobserved over the left than over the right hemisphere for central (C3/C4) electrodes (F[1,36]=9.36, pb .01), regardless of group or emotionalcontext.
3.3.3. Alpha1 (8–10 Hz) and alpha2 (10–12 Hz)No significant effects were observed in alpha1 activity. Significant
main effects of groupwere found in alpha2 activity at parietal electrodes(P3/P4) (F[1,31]=4.41, pb .05; Pz: F[1,30]=4.54, pb .05), showing thathealthy controls had higher activity than chronic pain patients.
3.3.4. Beta1 (12–18 Hz) and beta2 (18–22 Hz)A significantmain effect of groupwas found in beta1 (F[1,32]=4.62,
pb .05) and beta2 (F[1,30]=4.54, pb .05) at Pz electrode, with healthycontrols showing greater activities than chronic pain patients. Greaterbeta2 activity was elicited by unpleasant than by pleasant images (F[1,38]=4.87, pb .05) in frontal electrodes (F3/F4). A three-wayinteraction emotional context×hemisphere×group was found for tem-poral electrodes (T3/T4) (F[1,37]=5.59, pb .05), showing that pleasantimages elicited greater beta2 activity over the right hemisphere thanover the left hemisphere in healthy controls (pb .05), but not in chronicpain patients.
3.4. Multiscale entropy (MSE)
The MANOVAs on mean MSE values revealed significant interac-tion effects between the factors hemisphere×group `for all scale
in patients, and (b) topographical distribution of EEG power spectra on the scalp.
181C. Sitges et al. / International Journal of Psychophysiology 77 (2010) 176–183
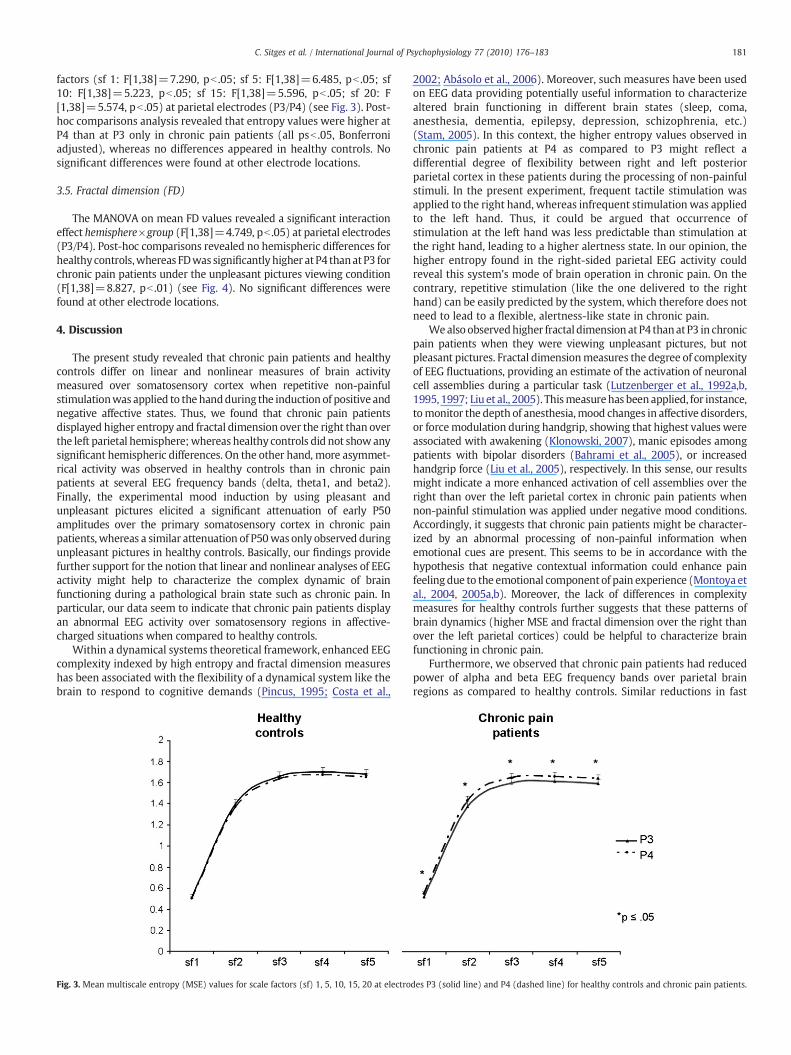
factors (sf 1: F[1,38]=7.290, pb .05; sf 5: F[1,38]=6.485, pb .05; sf10: F[1,38]=5.223, pb .05; sf 15: F[1,38]=5.596, pb .05; sf 20: F[1,38]=5.574, pb .05) at parietal electrodes (P3/P4) (see Fig. 3). Post-hoc comparisons analysis revealed that entropy values were higher atP4 than at P3 only in chronic pain patients (all psb .05, Bonferroniadjusted), whereas no differences appeared in healthy controls. Nosignificant differences were found at other electrode locations.
3.5. Fractal dimension (FD)
The MANOVA on mean FD values revealed a significant interactioneffect hemisphere×group (F[1,38]=4.749, pb .05) at parietal electrodes(P3/P4). Post-hoc comparisons revealed no hemispheric differences forhealthy controls,whereas FDwas significantly higher at P4 thanat P3 forchronic pain patients under the unpleasant pictures viewing condition(F[1,38]=8.827, pb .01) (see Fig. 4). No significant differences werefound at other electrode locations.
4. Discussion
The present study revealed that chronic pain patients and healthycontrols differ on linear and nonlinear measures of brain activitymeasured over somatosensory cortex when repetitive non-painfulstimulationwas applied to the handduring the induction of positive andnegative affective states. Thus, we found that chronic pain patientsdisplayed higher entropy and fractal dimension over the right than overthe left parietal hemisphere;whereas healthy controls did not showanysignificant hemispheric differences. On the other hand, more asymmet-rical activity was observed in healthy controls than in chronic painpatients at several EEG frequency bands (delta, theta1, and beta2).Finally, the experimental mood induction by using pleasant andunpleasant pictures elicited a significant attenuation of early P50amplitudes over the primary somatosensory cortex in chronic painpatients, whereas a similar attenuation of P50was only observed duringunpleasant pictures in healthy controls. Basically, our findings providefurther support for the notion that linear and nonlinear analyses of EEGactivity might help to characterize the complex dynamic of brainfunctioning during a pathological brain state such as chronic pain. Inparticular, our data seem to indicate that chronic pain patients displayan abnormal EEG activity over somatosensory regions in affective-charged situations when compared to healthy controls.
Within a dynamical systems theoretical framework, enhanced EEGcomplexity indexed by high entropy and fractal dimension measureshas been associated with the flexibility of a dynamical system like thebrain to respond to cognitive demands (Pincus, 1995; Costa et al.,
Fig. 3. Mean multiscale entropy (MSE) values for scale factors (sf) 1, 5, 10, 15, 20 at electro
2002; Abásolo et al., 2006). Moreover, such measures have been usedon EEG data providing potentially useful information to characterizealtered brain functioning in different brain states (sleep, coma,anesthesia, dementia, epilepsy, depression, schizophrenia, etc.)(Stam, 2005). In this context, the higher entropy values observed inchronic pain patients at P4 as compared to P3 might reflect adifferential degree of flexibility between right and left posteriorparietal cortex in these patients during the processing of non-painfulstimuli. In the present experiment, frequent tactile stimulation wasapplied to the right hand, whereas infrequent stimulation was appliedto the left hand. Thus, it could be argued that occurrence ofstimulation at the left hand was less predictable than stimulation atthe right hand, leading to a higher alertness state. In our opinion, thehigher entropy found in the right-sided parietal EEG activity couldreveal this system's mode of brain operation in chronic pain. On thecontrary, repetitive stimulation (like the one delivered to the righthand) can be easily predicted by the system, which therefore does notneed to lead to a flexible, alertness-like state in chronic pain.
Wealso observedhigher fractal dimension atP4 thanatP3 in chronicpain patients when they were viewing unpleasant pictures, but notpleasant pictures. Fractal dimensionmeasures the degree of complexityof EEG fluctuations, providing an estimate of the activation of neuronalcell assemblies during a particular task (Lutzenberger et al., 1992a,b,1995, 1997; Liu et al., 2005). Thismeasurehas beenapplied, for instance,tomonitor the depth of anesthesia,mood changes in affective disorders,or forcemodulation during handgrip, showing that highest values wereassociated with awakening (Klonowski, 2007), manic episodes amongpatients with bipolar disorders (Bahrami et al., 2005), or increasedhandgrip force (Liu et al., 2005), respectively. In this sense, our resultsmight indicate a more enhanced activation of cell assemblies over theright than over the left parietal cortex in chronic pain patients whennon-painful stimulation was applied under negative mood conditions.Accordingly, it suggests that chronic pain patients might be character-ized by an abnormal processing of non-painful information whenemotional cues are present. This seems to be in accordance with thehypothesis that negative contextual information could enhance painfeelingdue to the emotional component of pain experience (Montoya etal., 2004, 2005a,b). Moreover, the lack of differences in complexitymeasures for healthy controls further suggests that these patterns ofbrain dynamics (higher MSE and fractal dimension over the right thanover the left parietal cortices) could be helpful to characterize brainfunctioning in chronic pain.
Furthermore, we observed that chronic pain patients had reducedpower of alpha and beta EEG frequency bands over parietal brainregions as compared to healthy controls. Similar reductions in fast
des P3 (solid line) and P4 (dashed line) for healthy controls and chronic pain patients.
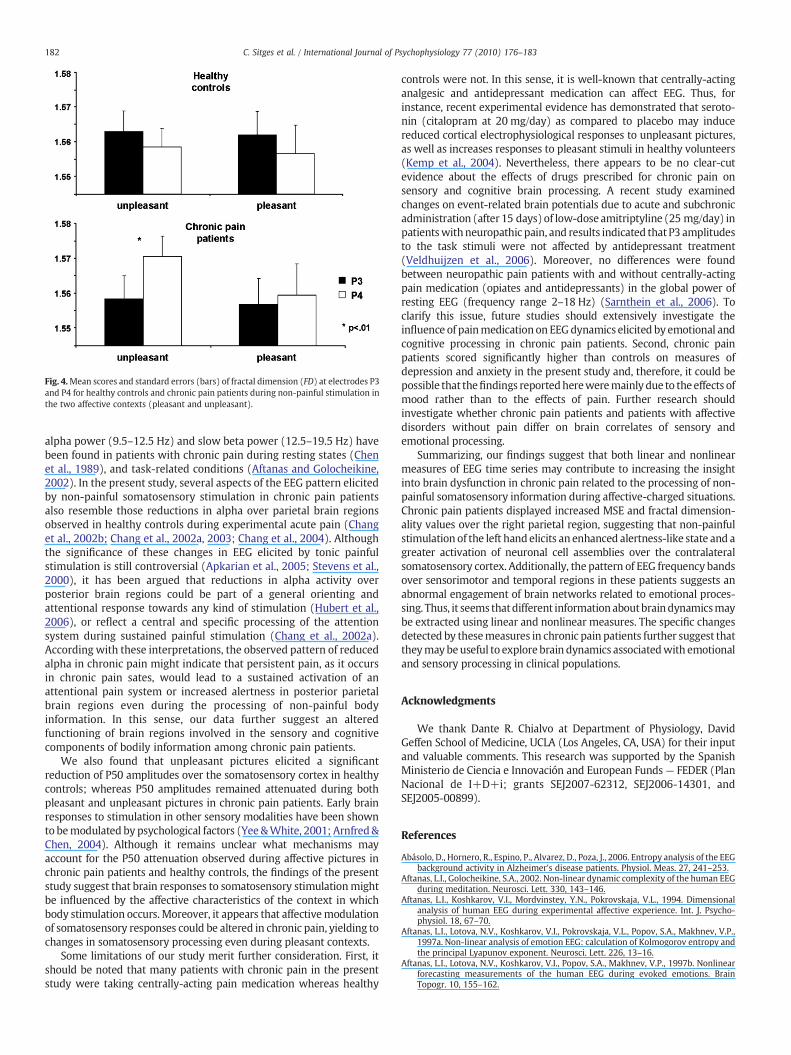
Fig. 4.Mean scores and standard errors (bars) of fractal dimension (FD) at electrodes P3and P4 for healthy controls and chronic pain patients during non-painful stimulation inthe two affective contexts (pleasant and unpleasant).
182 C. Sitges et al. / International Journal of Psychophysiology 77 (2010) 176–183
alpha power (9.5–12.5 Hz) and slow beta power (12.5–19.5 Hz) havebeen found in patients with chronic pain during resting states (Chenet al., 1989), and task-related conditions (Aftanas and Golocheikine,2002). In the present study, several aspects of the EEG pattern elicitedby non-painful somatosensory stimulation in chronic pain patientsalso resemble those reductions in alpha over parietal brain regionsobserved in healthy controls during experimental acute pain (Changet al., 2002b; Chang et al., 2002a, 2003; Chang et al., 2004). Althoughthe significance of these changes in EEG elicited by tonic painfulstimulation is still controversial (Apkarian et al., 2005; Stevens et al.,2000), it has been argued that reductions in alpha activity overposterior brain regions could be part of a general orienting andattentional response towards any kind of stimulation (Hubert et al.,2006), or reflect a central and specific processing of the attentionsystem during sustained painful stimulation (Chang et al., 2002a).According with these interpretations, the observed pattern of reducedalpha in chronic pain might indicate that persistent pain, as it occursin chronic pain sates, would lead to a sustained activation of anattentional pain system or increased alertness in posterior parietalbrain regions even during the processing of non-painful bodyinformation. In this sense, our data further suggest an alteredfunctioning of brain regions involved in the sensory and cognitivecomponents of bodily information among chronic pain patients.
We also found that unpleasant pictures elicited a significantreduction of P50 amplitudes over the somatosensory cortex in healthycontrols; whereas P50 amplitudes remained attenuated during bothpleasant and unpleasant pictures in chronic pain patients. Early brainresponses to stimulation in other sensory modalities have been shownto bemodulated by psychological factors (Yee &White, 2001; Arnfred&Chen, 2004). Although it remains unclear what mechanisms mayaccount for the P50 attenuation observed during affective pictures inchronic pain patients and healthy controls, the findings of the presentstudy suggest that brain responses to somatosensory stimulationmightbe influenced by the affective characteristics of the context in whichbody stimulation occurs. Moreover, it appears that affectivemodulationof somatosensory responses could be altered in chronic pain, yielding tochanges in somatosensory processing even during pleasant contexts.
Some limitations of our study merit further consideration. First, itshould be noted that many patients with chronic pain in the presentstudy were taking centrally-acting pain medication whereas healthy
controls were not. In this sense, it is well-known that centrally-actinganalgesic and antidepressant medication can affect EEG. Thus, forinstance, recent experimental evidence has demonstrated that seroto-nin (citalopram at 20 mg/day) as compared to placebo may inducereduced cortical electrophysiological responses to unpleasant pictures,as well as increases responses to pleasant stimuli in healthy volunteers(Kemp et al., 2004). Nevertheless, there appears to be no clear-cutevidence about the effects of drugs prescribed for chronic pain onsensory and cognitive brain processing. A recent study examinedchanges on event-related brain potentials due to acute and subchronicadministration (after 15 days) of low-dose amitriptyline (25 mg/day) inpatientswithneuropathic pain, and results indicated that P3 amplitudesto the task stimuli were not affected by antidepressant treatment(Veldhuijzen et al., 2006). Moreover, no differences were foundbetween neuropathic pain patients with and without centrally-actingpain medication (opiates and antidepressants) in the global power ofresting EEG (frequency range 2–18 Hz) (Sarnthein et al., 2006). Toclarify this issue, future studies should extensively investigate theinfluence of painmedication on EEGdynamics elicited by emotional andcognitive processing in chronic pain patients. Second, chronic painpatients scored significantly higher than controls on measures ofdepression and anxiety in the present study and, therefore, it could bepossible that thefindings reportedhereweremainly due to theeffects ofmood rather than to the effects of pain. Further research shouldinvestigate whether chronic pain patients and patients with affectivedisorders without pain differ on brain correlates of sensory andemotional processing.
Summarizing, our findings suggest that both linear and nonlinearmeasures of EEG time series may contribute to increasing the insightinto brain dysfunction in chronic pain related to the processing of non-painful somatosensory information during affective-charged situations.Chronic pain patients displayed increased MSE and fractal dimension-ality values over the right parietal region, suggesting that non-painfulstimulation of the left handelicits an enhanced alertness-like state and agreater activation of neuronal cell assemblies over the contralateralsomatosensory cortex. Additionally, the pattern of EEG frequency bandsover sensorimotor and temporal regions in these patients suggests anabnormal engagement of brain networks related to emotional proces-sing. Thus, it seems thatdifferent informationaboutbraindynamicsmaybe extracted using linear and nonlinear measures. The specific changesdetected by thesemeasures in chronic pain patients further suggest thattheymaybeuseful to explore brain dynamics associatedwith emotionaland sensory processing in clinical populations.
Acknowledgments
We thank Dante R. Chialvo at Department of Physiology, DavidGeffen School of Medicine, UCLA (Los Angeles, CA, USA) for their inputand valuable comments. This research was supported by the SpanishMinisterio de Ciencia e Innovación and European Funds — FEDER (PlanNacional de I+D+i; grants SEJ2007-62312, SEJ2006-14301, andSEJ2005-00899).
References
Abásolo, D., Hornero, R., Espino, P., Alvarez, D., Poza, J., 2006. Entropy analysis of the EEGbackground activity in Alzheimer's disease patients. Physiol. Meas. 27, 241–253.
Aftanas, L.I., Golocheikine, S.A., 2002. Non-linear dynamic complexity of the human EEGduring meditation. Neurosci. Lett. 330, 143–146.
Aftanas, L.I., Koshkarov, V.I., Mordvinstey, Y.N., Pokrovskaja, V.L., 1994. Dimensionalanalysis of human EEG during experimental affective experience. Int. J. Psycho-physiol. 18, 67–70.
Aftanas, L.I., Lotova, N.V., Koshkarov, V.I., Pokrovskaja, V.L., Popov, S.A., Makhnev, V.P.,1997a. Non-linear analysis of emotion EEG: calculation of Kolmogorov entropy andthe principal Lyapunov exponent. Neurosci. Lett. 226, 13–16.
Aftanas, L.I., Lotova, N.V., Koshkarov, V.I., Popov, S.A., Makhnev, V.P., 1997b. Nonlinearforecasting measurements of the human EEG during evoked emotions. BrainTopogr. 10, 155–162.

183C. Sitges et al. / International Journal of Psychophysiology 77 (2010) 176–183
Aftanas, L.I., Lotova, N.V., Koshkarov, V.I., Makhnev, V.P., Mordvinstev, Y.N., Popov, S.A.,1998. Non-linear dynamical complexity of the human EEG during evokedemotions. Int. J. Psychophysiol. 28, 63–67.
Apkarian, A.V., Sosa, Y., Krauss, B.R., Thomas, P.S., Fredrickson, B.E., Levy, R.E., Harden, R.N., Chialvo, D.R., 2004. Chronic pain patients are impaired on an emotionaldecision-making task. Pain 108, 129–136.
Apkarian, A.V., Bushnell, M.C., Treede, R.D., Zubieta, J.K., 2005. Human brainmechanisms of pain perception and regulation in health and disease. Eur. J. Pain9, 463–484.
Arnfred, S.M., Chen, A.C., 2004. Exploration of somatosensory P50 gating inschizophrenia spectrum patients: reduced P50 amplitude correlates to socialanhedonia. Psychiatry Res. 125, 147–160.
Babiloni, C., Brancucci, A., Babiloni, F., Capotosto, P., Carducci, F., Cincotti, F., Arendt-Nielsen, L., Chen, A.C.N., Rossini, P.M., 2003. Anticipatory cortical responses duringthe expectancy of a predictable painful stimulation. A high-resolution electroen-cephalography study. Eur. J. Neurosci. 18, 1692–1700.
Babiloni, C., Brancucci, A., Del Percio, C., Capotosto, P., Arendt-Nielsen, L., Chen, A.C.,Rossini, P.M., 2006. Anticipatory electroencephalography alpha rhythm predictssubjective perception of pain intensity. J. Pain 7, 709–717.
Bahrami, B., Seyedsadjadi, R., Babadi, B., Noroozian, M., 2005. Brain complexityincreases in mania. NeuroReport 16, 187–191.
Beck, A.T., Ward, C.H., Mendelson, M., Mock, J., Erbaugh, J., 1961. An inventory formeasuring depression. Arch. Gen. Psychiatry 56, 561–571.
Chang, P.F., Arendt-Nielsen, L., Chen, A.C., 2002a. Differential cerebral responses toaversive auditory arousal versus muscle pain: specific EEG patterns are associatedwith human pain processing. Exp. Brain Res. 147, 387–393.
Chang, P.F., Arendt-Nielsen, L., Chen, A.C., 2002b. Dynamic changes and spatialcorrelation of EEG activities during cold pressor test in man. Brain Res. Bull. 57,667–675.
Chang, P.F., Arendt-Nielsen, L., Graven-Nielsen, T., Chen, A.C., 2003. Psychophysical andEEG responses to repeated experimental muscle pain in humans: pain intensityencodes EEG activity. Brain Res. Bull. 59, 533–543.
Chang, P.F., Arendt-Nielsen, L., Graven-Nielsen, T., Svensson, P., Chen, A.C., 2004.Comparative EEG activation to skin pain and muscle pain induced by capsaicininjection. Int. J. Psychophysiol. 51, 117–126.
Chen, A.C., Dworkin, S.F., Haug, J., Gehrig, J., 1989. Topographic brain measures ofhuman pain and pain responsivity. Pain 37, 129–141.
Costa, M., Goldberger, A.L., Peng, C.K., 2002. Multiscale entropy analysis of complexphysiologic time series. Phys. Rev. Lett. 89, 98–106.
De Benedittis, G., De Gonda, F., 1985. Hemispheric specialization and the perception ofpain: a task-related EEG power spectrum analysis in chronic pain patients. Pain 22,375–384.
Elbert, T., Ray, W.J., Kowalik, Z.J., Skinner, J.E., Graf, K.E., Birbaumer, N., 1994. Chaos andphysiology: deterministic chaos in excitable cell assemblies. Physiol. Rev. 74, 1–37.
Geisser, M.E., Casey, K.L., Brucksch, C.B., Ribbens, C.M., Appleton, B.B., Crofford, L.J., 2003.Perception of noxious and innocuous heat stimulation among healthy women andwomen with fibromyalgia: association with mood, somatic focus, and catastro-phizing. Pain 102, 243–250.
Gratton, G., Coles, M.G., Donchin, E., 1983. A new method for off-line removal of ocularartifact. Electroencephalogr. Clin. Neurophysiol. 55, 468–484.
Hegger, R., Kantz, H., Schreiber, T., 1999. Practical implementation of nonlinear timeseries methods: the TISEAN package. Chaos 9, 413–435.
Hubert, M.T., Bartling, J., Pachur, D., Woikowsky-Biedau, Sv., Lautenbacher, S., 2006. EEGresponses to tonic heat pain. Exp. Brain Res. 173, 14–24.
Kemp, A.H., Gray, M.A., Silberstein, R.B., Armstrong, S.M., Nathan, P.J., 2004.Augmentation of serotonin enhances pleasant and suppresses unpleasant corticalelectrophysiological responses to visual emotional stimuli in humans. Neuroimage22, 1084–1096.
Kerns, R.D., Turk, D.C., Rudy, T.E., 1985. The West Haven-Yale Multidimensional PainInventory (WHYMPI). Pain 23, 345–356.
Klonowski, W., 2007. From conformons to human brains: an informal overview ofnonlinear dynamics and its applications in biomedicine. Nonlinear Biomed Phys. 1, 5.
Lang, P.J., Bradley, M.M., Cuthbert, B.N., 1997. International Affective Picture System(IAPS): Technical Manual and Affective Ratings. The Center for Research inPsychophysiology, University of Florida, Gainesville.
Liu, J.Z., Yang, Q., Yao, B., Brown, R.W., Yue, G.H., 2005. Linear correlation betweenfractal dimension of EEG signal and handgrip force. Biol. Cybern. 93, 131–140.
Lutzenberger, W., Birbaumer, N., Flor, H., Rockstroh, B., Elbert, T., 1992a. Dimensionalanalysis of the human EEG and intelligence. Neurosci. Lett. 143, 10–14.
Lutzenberger, W., Elbert, T., Birbaumer, N., Ray, W.J., Schupp, H., 1992b. The scalpdistribution of the fractal dimension of the EEG and its variation with mental tasks.Brain Topogr. 5, 27–34.
Lutzenberger, W., Preissl, H., Pulvermüller, F., 1995. Fractal dimension of electroen-cephalographic time series and underlying brain processes. Biol. Cybern. 73,477–482.
Lutzenberger, W., Flor, H., Birbaumer, N., 1997. Enhanced dimensional complexity ofthe EEG during memory for personal pain in chronic pain patients. Neurosci. Lett.226, 167–170.
Melzack, R., 1975. The McGill Pain Questionnaire: major properties and scoringmethods. Pain 1, 277–299.
Melzack, R., Perry, C., 1975. Self-regulation of pain: the use of alpha-feedback andhypnotic training for the control of chronic pain. Exp. Neurol. 46, 452–469.
Montoya, P., Larbig, W., Braun, C., Preissl, H., Birbaumer, N., 2004. Influence of socialsupport and emotional context on pain processing andmagnetic brain responses infibromyalgia. Arthritis Rheum. 50, 4035–4044.
Montoya, P., Pauli, P., Batra, A., Wiedemann, G., 2005a. Altered processing of pain-related information in patients with fibromyalgia. Eur. J. Pain 9, 293–303.
Montoya, P., Sitges, C., Garcia-Herrera, M., Izquierdo, R., Truyols, M., Blay, N., Collado, D.,2005b. Abnormal affective modulation of somatosensory brain processing amongpatients with fibromyalgia. Psychosom. Med. 67, 957–963.
Pincus, S., 1995. Approximate entropy (ApEn) as a complexity measure. Chaos 5,110–117.
Sarnthein, J., Stern, J., Aufenberg, C., Rousson, V., Jeanmonod, D., 2006. Increased EEGpower and slowed dominant frequency in patients with neurogenic pain. Brain129, 55–64.
Schreiber, T., Schmitz, A., 1996. Improved surrogate data for nonlinearity tests. Phys.Rev. Lett. 77, 635–638.
Schreiber, T., Schmitz, A., 2000. Surrogate time series. Physica, D 142, 346–382.Spielberger, C.D., Gorsuch, R.L., Lushene, R.E., 1970. The State-Trait Anxiety Inventory
(STAI): Test manual. Consulting Psychologists Press, Palo Alto, CA.Stam, C.J., 2005. Nonlinear dynamical analysis of EEG and MEG: Review of an emerging
field. Clin. Neuropsychol. 116, 2266–2301.Staud, R., Robinson, M.E., Vierck Jr, C.J., Cannon, R.C., Mauderli, A.P., Price, D.D., 2003.
Ratings of experimental pain and pain-related negative affect predict clinical painin patients with fibromyalgia syndrome. Pain 105, 215–222.
Stevens, A., Batra, A., Kötter, I., Bartels, M., Schwarz, J., 2000. Both pain and EEG responseto cold pressor stimulation occurs faster in fibromyalgia patients than in controlsubjects. Psych. Res. 97, 237–247.
Theiler, J., Eubank, S., Longtin, A., Galdrikian, B., Farmer, J.D., 1992. Testing fornonlinearity in time series: the method of surrogate data. Physica, D 58, 77–94.
Veldhuijzen, D.S., Kenemans, J.L., van Wijck, A.J., Olivier, B., Kalkman, C.J., Volkerts, E.R.,2006. Acute and subchronic effects of amitriptyline on processing capacity inneuropathic pain patients using visual event-related potentials: preliminaryfindings. Psychopharmacology 183, 462–470.
Yee, C.M., White, P.M., 2001. Experimental modification of P50 suppression.Psychophysiology 38, 531–539.




















