LINE - UNAIDS
93
ON THE FRONT LINE A review of programmes that address HIV among international peacekeepers and uniformed services 2005–2010 United Nations DEPARTMENT OF PEACEKEEPING OPERATIONS
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of LINE - UNAIDS

ON THE FRONT LINE
A review of programmes that address HIV among international peacekeepers and uniformed services 2005–2010
United Nations DEPARTMENT OF PEACEKEEPING OPERATIONS
United Nations DEPARTMENT OF PEACEKEEPING OPERATIONS

ON THE FRONT LINE
A review of programmes that address HIV among international peacekeepers and uniformed services 2005–2010

The adoption of United Nations Security Council Resolution 1308 in 2000 represented a water-shed moment in the global AIDS response. For the first time in its history, the United Nation’s highest decision-making body in charge of peace and security matters unanimously adopted a resolution addressing a public health concern and its implications for international peace and security. The resolution recognized that societal violence and instability exacerbate the spread of HIV and, left unchecked, could pose a threat to international peace and security. It called on the Joint United Nations Programme on HIV/AIDS (UNAIDS) and the United Nations Department of Peacekeeping Operations (DPKO) to develop HIV/AIDS-specific strategies and programmes within the context of United Nations peacekeeping operations.
This progress report comes at a time when the global AIDS response is at a cross-roads. It has been 30 years since the AIDS epidemic began and 10 years since the United Nations Security Council adopted resolution 1308 and the United Nations General Assembly adopted the Declaration of Commitment on HIV/AIDS. Significant progress has been made in providing access to HIV prevention, treatment, care and support ser-vices for all sections of society including peacekeepers and other uniformed services per-sonnel. Nevertheless, during the past 10 years, the evolving landscape of demographic crises and conflicts throughout the world has reshaped these challenges and underscored the need for a new response to AIDS in the context of United Nations actions to help prevent conflict, ensure security and build peace.
This report outlines the progress made and the obstacles encountered in implement-ing Resolution 1308. There are clearly new opportunities for consolidating the prog-ress and addressing new challenges. The imperative to further explore the relationship between AIDS and insecurity is also clear. Research during the past five years suggests that, although the pandemic does not make states fragile in the short term, it can erode the competence available to local and regional governments, including the management of conflict, which can undermine the economy and thus adversely affect security. We recognize that global, national and personal insecurity could undermine further success in achieving the UNAIDS vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths.
The deliberations on AIDS in June 2011 by both the United Nations General Assembly and the United Nations Security Council provide an opportunity to reinvigo-
FOREWORD

Foreword iii
Alain Le RoyUnder-Secretary-Generalfor United Nations Peacekeeping Operations
rate international commitments to achieve universal access to HIV prevention, treat-ment, care and support for peacekeepers, members of the uniformed services, their fami-lies and the communities they serve. This report makes a compelling case for doing this. It gives Member States the impetus to accelerate programmes for uniformed personnel as an integrated component of their broader national AIDS responses and in preparation for contributing troops and police for United Nations peacekeeping.
UNAIDS and DPKO remain committed to support the implementation of all relevant resolutions towards achieving universal access to HIV prevention, treatment, care and support among uniformed personnel and the populations they protect. United Nations Security Council actions provide unique opportunities for the international community to situate the AIDS response among uniformed services within the broader context of protection of civilians; social inequality and health; preventing violence against women and girls, including sexual violence in conflict situations; and all efforts to pre-vent conflict and build peace.
Michel SidibéExecutive DirectorUNAIDS

Cover photo
Credit and Caption
UNAIDS
20, Avenue Appia
CH-1211 Geneva 27, Switzerland
http://www.unaids.org
United Nations
Department for Peacekeeping Operations
380 Madison Avenue, 19th Floor
New York, NY 10017, USA
http://www.un.org/peacekeeping
© United Nations 2011 All rights reserved
All inquiries
Leo Kenny: [email protected]
Dr. Megh Gurung: [email protected]

CONTENTS
Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xi
A snapshot of progress . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xiFindings and recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xiii
Peacekeeping, peacebuilding and command-centred approaches . . . . . . . . . xiiiResolution 1308: contributing to United Nations efforts on peacebuilding and preventing violence against women . . . . . . . . . . . . . . . . . . . . . . . . . . . . xivPrevention programmes among uniformed services . . . . . . . . . . . . . . . . . . . xvAIDS and security. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xviPolice and other uniformed services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xviiOverall recommendation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xviii
Section One
A decade of United Nations and Security Council involvement with the AIDS response. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
United Nations Security Council Resolution 1308 . . . . . . . . . . . . . . . . . . . . . . . 3Declaration of Commitment on HIV/AIDS . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3United Nations Security Council Resolution 1325 . . . . . . . . . . . . . . . . . . . . . . . 4United Nations Security Council Resolution 1820 . . . . . . . . . . . . . . . . . . . . . . . 4United Nations Security Council Resolution 1888 . . . . . . . . . . . . . . . . . . . . . . . 4United Nations Security Council Resolution 1889 . . . . . . . . . . . . . . . . . . . . . . . 5United Nations Security Council Resolution 1960 . . . . . . . . . . . . . . . . . . . . . . . 5The changing global context of Resolution 1308 . . . . . . . . . . . . . . . . . . . . . . . . . 5
AIDS, health and security. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Changes since 2000 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
This report. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Section Two
HIV and Uniformed Services. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
International peacekeepers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13New mix of troop-contributing countries . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
HIV prevalence among international peacekeepers . . . . . . . . . . . . . . . . . . . . . . . 14HIV status and HIV-related repatriations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15HIV prevalence among uniformed services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Military personnel. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16National law enforcement officers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–2010vi
Section Three
Progress in implementation: preventing HIV infection among peacekeeping personnel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
New policy environment on HIV counselling and testing. . . . . . . . . . . . . . . . . . 23Increased HIV awareness and prevention training . . . . . . . . . . . . . . . . . . . . 25Increased number of peer educators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Progress in distributing condoms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Improvement in HIV-related services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29HIV and behaviour change. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Support for local communities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32Mainstreaming HIV into disarmament, demobilization and reintegration and security sector reform . . . . . . . . . . . . . . . . . . . . . . . . . 32Post-conflict peacebuilding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Section Four
Progress in implementation: preventing HIV among uniformed services personnel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Including HIV prevention for uniformed services in national AIDS strategies . . 39Increased HIV prevention. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Alignment of military HIV policies with national programmes . . . . . . . . . . 40HIV and behavioural change . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42Increased funding for HIV interventions for national uniformed services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44Other uniformed services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45Sexual violence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
Section Five
Increased partnerships and regional networks. . . . . . . . . . . . . . . . . . . . . . . . . . . 49
Partnerships . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51Global Task Force on HIV among Uniformed Services . . . . . . . . . . . . . . . . 51Global Task Force on HIV among Uniformed Services . . . . . . . . . . . . . . . . 51International Committee on Military Medicine . . . . . . . . . . . . . . . . . . . . . . 51International Centre for Technical Cooperation . . . . . . . . . . . . . . . . . . . . . . 52International Military HIV/AIDS Conference . . . . . . . . . . . . . . . . . . . . . . . 52Regional networks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52African initiatives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
Southern Africa . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53South African Development Community Military Health Services Committee on HIV and AIDS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
Latin America and the Caribbean . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54Asia and Pacific Regional Network on Police and AIDS . . . . . . . . . . . . . . . . . . . 54
Contents vii
Section SixConclusion and recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
Findings and recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59Peacekeeping, peacebuilding and command-centred approaches . . . . . . . . . 59Resolution 1308: contributing to United Nations efforts on peacebuilding and preventing violence against women . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60Prevention programmes among uniformed services . . . . . . . . . . . . . . . . . . . 62AIDS and security. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62Police and other uniformed services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63Overall recommendation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65Bibliography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
Tables
1 Knowledge about HIV prevalence in various military forces . . . . . . . . . . . 18 2 Comparison of KAPB surveys among peacekeepers in UNMIL, Liberia
(2004) and MINUSTAH, Haiti (2007) . . . . . . . . . . . . . . . . . . . . . . . . . . . 31 3 Main achievements of country projects in Latin America and the
Caribbean . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
Figures
Map of current DPKO missions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 1. Top 26 troop-contributing countries by the number of troops
contributed, January 2011. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14 2. National HIV prevalence (%) in troop-contributing countries with HIV
prevalence exceeding 1%. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14 3. Number of HIV-related repatriation by troop-contributing country
(TCC), October 2003 to June 2007 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
4. Number of HIV-related repatriation, evacuation and mortality cases by personnel group, 2005 to the end of 2009 (n = 110) . . . . . . . . . . . . . . . 16
5. HIV prevalence among military recruits in Myanmar and Thailand, 1989–2009 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
6. Total number of UN peacekeepers receiving HIV induction training by category and year, 2004–2010 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
7. Total number of peacekeepers inducted since inception of UN missions, end of 2010 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
8. Number of peacekeepers trained as peer educators, 2004–2010 . . . . . . . . . 27 9. Total number of condoms distributed to peacekeepers in all missions,
2004–2010 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29 10. Number of UN peacekeepers and civilians seeking HIV counselling and
testing, 2005–2010 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29 11. Percentage of countries reporting progress in HIV prevention,
treatment and care programmes among uniformed services, 2005, 2007 and 2009 (percent). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
12. KABP survey results by country: selected countries in South America and the Caribbean, 2005, 2007 and 2009 . . . . . . . . . . . . . . . . . . . . . . . . . 43

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–2010viii
Boxes
1. Training national staff as peer leaders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28 2. Involvement of command structure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28 3. HIV counselling and testing among military personnel
and their families in Mozambique . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32 4. Sudan: collaborative efforts in disarmament,
demobilization and reintegration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33 4. Armed forces and law enforcement agencies – Ukraine regional meeting. . 45 5. HIV, human rights and gender training . . . . . . . . . . . . . . . . . . . . . . . . . . . 47 6. Minimum standards relevant to HIV and AIDS in the military . . . . . . . . 53

Contents ix
ACRONYMS
AIDS Acquired Immune Deficiency SyndromeASCI AIDS, Security and Conflict InitiativeBINUB United Nations Integrated Office in BurundiCOPRECOS LAC Committee for the Prevention and Control of HIV/AIDS in the Armed
Forces and National Police of Latin America and the Caribbean
DFS United Nations Department of Field SupportDHAPP United States Department of Defence HIV/AIDS Prevention ProgrammeDPKO United Nations Department of Peacekeeping OperationsGFATM Global Fund to fight AIDS, Tuberculosis and MalariaHIV Human Immunodeficiency VirusMINURCAT United Nations Mission in the Central
African Republic and ChadMINURSO United Nations Mission for the Referendum in Western SaharaMINUSTAH United Nations Stabilization Mission in HaitiMONUC United Nations Organization Mission in the Democratic
Republic of the CongoPEPFAR United States President’s Emergency Plan for AIDS ReliefT/PCC Troop/police contributing countriesUNAIDS Joint United Nations Programme on HIV/AIDSUNAMA United Nations Assistance Mission in AfghanistanUNAMI United Nations Assistance Mission for IraqUNAMID African Union/United Nations Hybrid operation in DarfurUNDOF United Nations Disengagement Observer ForceUNDP United Nations Development ProgrammeUNESCO United Nations Educational, Scientific and Cultural OrganizationUNFICYP United Nations Peacekeeping Force in CyprusUNFPA United Nations Population FundUNHCR Office of the United Nations High Commissioner for RefugeesUNICEF United Nations Children’s FundUNIFEM United Nations Development Fund for WomenUNIFIL United Nations Interim Force in LebanonUNIPSIL United Nations Integrated Peacebuilding Office in Sierra LeoneUNMEE United Nations Mission in Ethiopia and EritreaUNMIL United Nations Mission in LiberiaUNMIM United Nations Mission in MexicoUNMIS United Nations Mission in the SudanUNMIT United Nations Integrated Mission in Timor-LesteUNMOGIP United Nations Military Observer Group in India and PakistanUNOCHA United Nations Office for Coordination of Humanitarian AffairsUNOCI United Nations Operation in Côte d’IvoireUNODC United Nations Office on Drugs and CrimeUNOMIG United Nations Observer Mission in GeorgiaUNTSO United Nations Truce Supervision OrganizationWFP World Food ProgrammeWHO World Health Organization

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–2010x
SPLA Commander testing for HIV (Sudan)

EXECUTIVE SUMMARY
This progress report serves as background for the United Nations Security Council, which will convene in June 2011 to consider progress on the implementation of United Nations Security Council Resolution 1308 (2000). It tracks progress and identifies gaps and chal-lenges in addressing the statement by the President of the Security Council on 18 July 2005 (S/PRST/2005/33) that underlines the responsibility of the Security Council for maintain-ing international peace and security as it relates to AIDS and international peacekeeping operations and that also expressed the Council’s continued readiness to further promote and support the implementation of Resolution 1308.
Between 2005 and 2011, 186 of the United Nations Secretary-General’s reports to the Security Council cite AIDS-related concerns and action taken to address them with respect to thematic concerns including the protection of civilians, children and armed con-flict, durable peace in Africa, women and peace and security and sexual violence in armed conflict.
The United Nations, Member States and partners have made important progress in implementing Resolution 1308 at the international, regional and national levels. During the past five years, UNAIDS, DPKO and partners have succeeded in moving the response to Resolution 1308 from a project to programme approach, integrating HIV interventions amongst uniformed services into the national response in countries. Nevertheless, the chang-ing landscape of threats to international peace and security and the evolving evidence on the relationship between AIDS and security have created new challenges and opportunities to further strengthen these actions and contribute to United Nations’ efforts to prevent conflict and build peace.
A snapshot of progress• Peacekeeper induction training on HIV awareness has increased almost seven-fold
between 2005 and the end of 2010. In the same period, the number of peacekeepers in field missions increased from 69,838 to nearly 100,000. In 2005, 11% had received HIV induction training. By the end of December 2010, this had increased to 55%. Action has focused on reducing risks for peacekeeping operations but also for host communities and on addressing the related challenges of sexual violence in armed conflict. Training modules have been developed on gender and sexual violence, sexual exploitation and abuse and child protection issues. These modules are also integrated into the compulsory United Nations Standardized Generic Training Module for United Nations Peacekeeping for countries contributing troops and police. More than 1500 peacekeeping officers were trained as HIV peer educators in 2010.
• DPKO has mainstreamed HIV into every United Nations peacekeeping mission and assigned 9 Chief HIV/AIDS officers/policy advisers, 78 support staff and 13 focal points to this task. Pre-deployment HIV training has become standard practice for all troop and police-contributing countries.
• The global advocacy efforts of UNAIDS, DPKO and their partners has resulted in dramatically increased recognition and commitments from top leadership that all uni-formed services should address AIDS. Creation of a Global Task Force on HIV among

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–2010xii
Uniformed Services has played a catalytic role in coordinating technical support and harmonization of guidance. Six regional networks of uniformed services have been cre-ated to foster partnerships and identify best practices as part of South–South regional collaboration on AIDS. With the support from the United States Government, mili-tary-to-military AIDS programmes have been established in more than 80 countries. More than 60% of national strategic plans on AIDS have articulated programmes for uniformed services, and development partners have increased their funding support.
• Evidence in this report suggests that the damaging impact of AIDS on the health of international peacekeeping personnel and uniformed services has been limited partly because of increased efforts in HIV prevention and care among the national uni-formed services and among United Nations peacekeeping personnel and partly by pre-recruitment national HIV testing policies. Important parts of military AIDS policy and programming remain poorly aligned with national or civilian policies, especially in Africa.
• As part of their national strategic plans, 60% of countries have integrated pro-grammes for military police and other uniformed personnel but often without bud-get allocation from domestic sources. In most regions, uniformed services have been recognized both as a key population at higher risk of HIV exposure and as important partners in the response to AIDS. Interventions addressing uniformed services are considered a major opportunity for promoting behavioural change, especially reduc-ing stigma and discrimination and preventing violence against the populations most vulnerable to HIV.
• Increased resources for HIV programming among uniformed services has been made available, notably through the United States President’s Emergency Plan for AIDS Relief and other development partners such as the European Union (EU) and the Global Fund to Fight AIDS, Tuberculosis and Malaria. United States programme funding for military-to-military assistance with HIV related activities has enabled a fivefold increase in the number of military programmes during the past decade. In 2010, the Global Fund approved an unprecedented US$ 58.8 million for a regional project for uniformed services in 15 countries in Latin America and the Caribbean.
• Increased prevention and care services have been provided to uniformed services and UN Peacekeeping personnel. These include peer education, access to voluntary coun-selling and testing, condom provision and antiretroviral therapy. The coverage and quality of HIV prevention and care services varies between peacekeeping missions and countries. Although interventions have increased HIV knowledge, their effects on high-risk sexual and drug-related practices are still very difficult to assess in the absence of effective monitoring and evaluation systems. Condom use is still inconsistent. The effectiveness of stand-alone peer education programmes has been questioned due to the high mobility of trained peers. Progress has clearly been made in implementing Resolution 1308. Nevertheless, major gaps and challenges still need to be addressed. These are often similar to the gaps and challenges faced by national AIDS responses in countries: a lack of budget allocation; the need to address stigma and discrimination; and insufficient emphasis on prevention.
• Many troop-contributing countries have national mandatory HIV testing policies for their uniformed personnel before and after deployment in DPKO peacekeeping opera-tions. Thirty-five of 52 countries surveyed have official or draft policies on pre-recruit-ment HIV testing, and 39 of 49 countries conduct either pre- or post-deployment HIV testing or both. A few countries allow recruits known to be living with HIV to serve in the military, and 11 of 34 countries surveyed deploy troops known to be living with HIV as peacekeepers.

Executive Summary xiii
Findings and recommendationsPeacekeeping, peacebuilding and command-centred approachesThe prevalence of HIV infection among peacekeeping personnel tends to reflect the preva-lence among young men of similar age groups in their countries of origin. The HIV preva-lence in national uniformed services (including national police services) is similar to that of the general population, with some exceptions in countries in sub-Saharan Africa – but not, as was postulated in 2000, 2–5 times higher than in comparable civilian populations. The inci-dence of HIV infection tends to rise with increasing duration of deployment in a duty area. This underlines the need to intensify HIV prevention while personnel are deployed.
Some of the HIV prevention successes in military forces have been achieved through approaches that place responsibility for HIV policy and practice within the army command rather than on the health services alone. Research during the past five years indicates that command-centred approaches to HIV prevention are likely to be more effective in reduc-ing HIV risk among rank and file than solely relying upon education and training based on individual behavioural or medical approaches. A command-centred approach requires systematic assessment of HIV within an institution and the design and adoption of policies that address prevention, treatment, care and support for uniformed services personnel and their families. An essential element of the command-centred approach is the development of lines of accountability and enforcement of mechanisms to prevent sexual violence within military institutions. Also critical is to ensure that the needs of women living with HIV who experienced rape or other sexual violence committed by members of national, regional and multinational forces, be they civilian, police or military, are addressed comprehensively. The Military Institutional Audit and Force Capabilities Framework assessment, as outlined by Cranfield University for the AIDS, Security and Conflict Initiative, includes tools that can support this approach.
Integrating HIV prevention and response into the design and command of AIDS policies in international peace support operations, (which must address issues of pre- and post-deployment testing, including people living with HIV in the forces), should be aligned with the operational demands of the mission and the capacity of troop-contributing coun-tries. In all situations, testing should be accompanied by counselling and treatment refer-ral. Building on the operational tools of a command-centred approach to HIV prevention, DPKO and UNAIDS should consider developing a third tool specific to peace support missions: an HIV security risk assessment to be carried out as part of establishing a peace support mission, performed before deployment or on arrival at the mission area. The DPKO would be responsible for this, but it would be coordinated among actual or poten-tial troop-contributing countries. This tool would map findings from the Force Capabili-ties Framework and Military Institutional Audit tools in the particular operational mandate and locality. The mission would undertake measures to ensure the continuity of AIDS pro-grammes through troop rotations, for example, making sure that best practices are sustained.
For Member States and the United Nations
• Move to military command responsibility for HIV policy development and implemen-tation. This requires developing clear lines of accountability and enforcement mecha-nisms. Accountability for addressing sexual violence should be placed on command structures but also on peer co-responsibility through peer education programmes about sexual violence and human rights.
• The notion of zero tolerance for sexual abuse, both within peace support missions and between peacekeepers and the host population, should be coupled to the agendas of structural prevention and the command-centred approach. Zero tolerance should not

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–2010xiv
be a pretext for a command to halt prevention measures, such as condom distribution, based on a policy of exclusive abstinence.
• The practices of national, regional and United Nations peace support missions should be aligned. The ultimate goal is a universal standard of HIV prevention, treatment, care and support across all troop/police-contributing countries, in accordance with universal access goals. An interim objective is sufficient alignment of policy and prac-tice to enable a common treatment protocol among the different contingents compris-ing a peace support operation. This requires involving commanders and also touches on the issue of mandatory testing. Member States should review their HIV testing and counselling policies to ensure confidentiality and referral to a continuum of care for personnel found to be living with HIV. Members of national uniformed services living with HIV should be deployed based on their fitness to perform duties, with competent medical authorities determining and documenting this fitness.
• The synergy between peacekeeping and peacebuilding should be addressed. There should be increased dialogue amongst partners and institutions with complementary mandates in this area – the United Nations Security Council, the United Nations Peacebuilding Commission, the African Union Peace and Security Council and other regional mechanisms – to address the heightened risks of HIV during post-conflict peacebuilding and to ensure the continuity of HIV prevention during post-conflict transitions, including disarmament, demobilization and reintegration.
Resolution 1308: contributing to United Nations efforts on peacebuilding and preventing violence against womenInsufficient progress has been achieved to ensure that implementing Resolution 1308 is also contributing to United Nations efforts on peacebuilding and preventing violence against women. In accordance with Security Council Resolutions 1325, 1820, 1888 and 1960, there is now an opportunity to scale up and focus these efforts. These efforts need to be aware of the Security Council’s framing of sexual violence as a core civilian protection concern. This view is reflected in successive Security Council resolutions: 1820 (2008), 1888 (2009) and 1960 (2010). These are historic resolutions: they recognize the relationship between prevent-ing and addressing wartime sexual violence and ensuring sustainable peace and security.
Although there is a better understanding of the conflict and post-conflict continuum as a period of heightened risk for sexual violence and acquiring HIV infection, there is a variance in the findings of the limited research on links between sexual violence and HIV. The AIDS, Security and Conflict Initiative research indicates three central explanations for the dissonance of findings about the reciprocal links between sexual violence and HIV: (1) the underestimation of physiological susceptibility and social risk factors in epidemiological and behavioural models of transmission risk; (2) the absence of reliable baseline and compara-tive data for the incidence and prevalence of both HIV and sexual violence before, during and after conflicts take place; and (3) the lack of agreement on definitions of sexual violence as measurement indicators. Nevertheless the combined effects of sexual violence against girls and women and increased risk of HIV transmission have profound implications for individual and possibly national security.
Recognition must be given to violence, and especially sexual violence, as a physiological and social factor in the risk of HIV transmission and in HIV, humanitarian, public health and security policies. The role of force or coercion should be made explicit in data linking HIV with social and behavioural factors. The prevention of sexual violence and prevention of HIV must be more closely aligned, and preventing sexual violence should be central to AIDS policies and strategies in conflict-affected environments.

Executive Summary xv
Although HIV prevention is often a first-line response to sexual violence by treating sexually transmitted infections, providing post-exposure prophylaxis and other measures, the prevention of sexual violence is rarely considered an entry point for HIV prevention in the context of security and humanitarian responses, including through disarmament, demo-bilization and reintegration programmes and reconstruction and early recovery programmes.
UNAIDS is working as part of United Nations Action against Sexual Violence in Con-flict and being supported by the United States National Institute of Health in convening a scientific research planning meeting to support advancing UNAIDS’ priority commitment to stop violence against women and girls and to align global, regional and national strategies for preventing sexual violence and AIDS. This expert group meeting of leading virologists, epidemiologists, mathematical modellers, social scientists and public health specialists will be convened with the aim of identifying new approaches for assessing the role of sexual violence in HIV risk transmission. The course of this debate, and its conclusions, will have significant implications for the global HIV response, security sector reforms and humanitarian action and should be considered a priority for future work on addressing conflict-related sexual violence and HIV.
For Member States and the United Nations
• HIV prevention strategies should be aligned with preventing and responding to sexual violence against women and girls (and sometimes, boys and men) in conflict.
• Measures and training for preventing sexual violence should be scaled up and inte-grated into policing and law enforcement practices – especially in relation to stig-matized and criminalized activities and populations at higher risk of HIV exposure. Much more work needs to be done as part of policing and law enforcement practices to address the nexus between sexual violence, trafficking of women and girls, trafficking of drugs and the heightened risk of HIV.
• The prevention of sexual violence should be considered an entry point for HIV preven-tion in the context of security and humanitarian responses, including through disar-mament, demobilization and reintegration programmes and reconstruction and early recovery programmes.
• Uniformed personnel and others should be trained to understand clearly the implica-tions and effects of sexual violence on victims and perpetrators alike.
For the United Nations
• The prevention of conflict-related violence should be better integrated into disarma-ment, demobilization and reintegration programmes. In so doing, care should be accorded to the specific needs of female combatants and girls and women associated with armed forces, including their reproductive health needs.
• Partnerships should be renewed between DPKO and other United Nations and non–United Nations partners to facilitate capacity-building and improve links between HIV prevention, reproductive health promotion and the prevention of sexual and gender-based violence.
• A culture should be developed among peacekeepers that encourages and enables them to act as agents of change for HIV prevention and human rights education in the wider community, enabling them to respond to heightened risks in humanitarian cri-ses, peacekeeping and post-conflict peacebuilding.
Prevention programmes among uniformed servicesHIV prevention among uniformed services personnel has concentrated on providing peer education. This has been supported – albeit unevenly – by service provision, including:

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–2010xvi
HIV testing, antiretroviral therapy, managing sexually transmitted infections and provid-ing condoms. Despite these efforts, high-risk behaviour among uniformed personnel is still widespread. There is still a paucity of strategic information about the effectiveness of HIV prevention programmes among uniformed services and what should constitute a minimum standard package of HIV-related activities and their scope.
For Member States and the United Nations
• Member States still need to implement effective long-term strategies for HIV educa-tion, prevention and treatment of their personnel, with special emphasis on preventing sexual violence against girls and women as an important part of their preparation for peacekeeping operations.
• “Know your HIV risk” should become part of all DPKO missions. As part of a con-solidated approach, standardized behavioural and HIV surveillance methods should be developed and people trained to use them. Knowledge of the effects of alcohol and substance use on HIV high-risk behaviour should be improved among uniformed ser-vice personnel and substance abuse programmes developed.
• The Medical Services Division, Medical Support Section DFS and DPKO databases should be strengthened to report on AIDS-related illnesses according to an agreed template and indicators. Capacity in monitoring and evaluation needs to be built at the mission level by appointing and training monitoring and evaluation officers. This would also support the evaluation of peacekeeping practices to be undertaken at the end of assignments and missions.
• Promote and scale up South–South cooperation (military–military, police–military and civil–military) using best practices on HIV prevention programmes.
AIDS and securityAlthough the AIDS, Security and Conflict Initiative (ASCI) has been able to quell some of the earlier fears about soaring rates of infection among soldiers and the risks posed by HIV to the potential collapse of states, it has also identified very specific implications for the operational capacity of armies and police: the role of sexual violence in increasing the risk of HIV transmission, how HIV affects local governance and community survival and the spe-cific HIV-related risks associated with post-conflict transitions. Epidemiological measures of impact – incidence and prevalence – have failed to capture these social and political impli-cations. More attention needs to be paid to how AIDS adversely affects the functioning of local and regional government as well as macro level impacts. Local and regional government structures are important – along with health and police services – in facilitating personal and local security. This evidence indicates (a) the importance of maintaining and expanding antiretroviral therapy; (b) the desirability of further detailed studies of the effects of HIV on local and regional government capacity in circumstances in which (i) the HIV prevalence exceeds 5% in the general population and (ii) budgetary and human resource constraints already compromise the capabilities of local and regional government.
Post-conflict transitions are both a period of heightened vulnerability to HIV trans-mission and a neglected element in AIDS policy and programming. Greater policy attention and service continuity is needed in post-conflict situations to respond to the complexities of context, increased population mobility, the demobilization of combatants, disruptions in the provision of humanitarian assistance to displaced people and refugees in camp settings and the overloading of health and social services in areas of population return. Disarmament, demobilization and reintegration programmes are an important and consistently overlooked focus for HIV prevention and response, especially among military and extended families and women and children associated with armed forces.

Executive Summary xvii
For Member States and the United Nations
• Further empirical research is required to better measure and more effectively respond to the relationships between AIDS, conflict and state fragility. Further studies are also needed on the relationship between HIV morbidity and mortality and the competence and capacity of local and regional authorities in Member States, and such studies need to be given priority when the HIV prevalence in the general population reaches or exceeds 5%.
• Major policy gaps in responding to AIDS and security should be addressed. There are currently substantial HIV policy and programmatic gaps and discontinuities during post-conflict transitions between emergency assistance and reconstruction and devel-opment efforts.
• Interventions related to AIDS should start in crisis settings as part of early recovery programmes, and disarmament, demobilization and reintegration should be the entry point for institutionalizing these policies and practices.
• The capacity of relevant agencies and partners to incorporate HIV interventions within disarmament, demobilization and reintegration programming should be strengthened through appropriate staffing, training and resource mobilization.
Police and other uniformed servicesHIV prevention efforts have neglected police and other law enforcement and uniformed ser-vices personnel, including customs, navy, immigration and corrections. The risks of HIV transmission, especially in epidemics concentrated among people who inject drugs and sex workers, are influenced by law enforcement practices and, in turn, by the drug trade and human trafficking and by the people who control sex work, including pimps, “protectors”, traffickers and long-term clients. Cross-border issues, including the trafficking of women, the drug trade and sexual exploitation and abuse at border-crossing points, are all related to the risks of HIV transmission. The previously underestimated role of some groups of law enforce-ment personnel as core group transmitters or maintaining populations warrants further explo-ration. Bilateral or multilateral exchange and cooperation is a prerequisite for addressing these questions, and borders should be a special focus for HIV efforts. The nexus between HIV/AIDS, the international trade in illicit drugs, related sex trafficking activities, drug use and the emergence of “narco states” in several parts of the world demands particular attention.
For Member States
• Laws to combat and criminalize discrimination and violence against populations at higher risk of HIV exposure should be enforced. To this end, law enforcement officers should be trained and enabled to defend human rights, especially when reaching out to women and populations at higher risk such as sex workers, men who have sex with men, people who inject drugs and migrants.
For Member States and the United Nations
• More focus on AIDS should be placed across borders and in relation to traffic and trade. Particular attention needs to be paid to the security concerns related to the nexus between policing, AIDS, the international trade in illicit drugs, related sex trafficking activities, drug use and violence against women

Overall recommendationA new agenda for United Nations Security Council Resolution 1308 is needed. It should consider the changed context and new evidence that has emerged since Resolution 1308 was adopted with a view to enhancing existing programmes to more effectively prevent HIV, ensure security and build peace.

Acknowledgement is made of the valuable input provided by:United Nations Department of Peacekeeping Operations field missions, UNAIDS regional support teams, the AIDS programmes of Member States, the EuropeanUnion, the United States Department of Defence HIV/AIDS Prevention Program, the United States President’s Emergency Plan for AIDS Relief, the Global Fund to Fight AIDS, Tuberculosis and Malaria, the regional military networks, the Global Task Force on HIV among Uniformed Services, Southern African Development Community, United Nations Action Against Sexual Violence in Conflict network, WHO, UNDP, UNFPA, UNICEF, UNODC, UN Women, UNITAID, the United Nations Office for the Coordination of Humanitarian Affairs and the range of individual researchers whose work is cited in this report, as well as the large number of individual respondents to requests for information on progress at the country, regional and global levels.
ACKNOWLEDGMENTS

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–2010xx

A decade of United Nations and Security Council involvement with the AIDS response
SECTION
ONE


3
A decade of United Nations and Security Council involvement with the AIDS response
This section outlines the history of the United Nations Security Council’s engagement with the AIDS response. The next section describes the global context within which United Nations Security Council Resolution 1308 was passed and developments in that context in the past decade.
United Nations Security Council Resolution 1308In 2000, United Nations Security Council Resolution 1308 (S/RES/1308) acknowledged the extent of the AIDS epidemic worldwide and especially the severity of the crisis in Africa and called for a wide range of action to address the implications of the HIV pandemic for international peace and security. The Resolution recognized that the AIDS epidemic is exacerbated by conditions of violence and instability, which increase the risk of exposure to the disease through large movements of people, widespread uncertainty over conditions and reduced access to health care. Concerned that an unchecked AIDS epidemic might pose a risk to stability and security, the Security Council set out a range of measures. It asked the Joint United Nations Programme on HIV/AIDS (UNAIDS), the United Nations Depart-ment of Peacekeeping Operations (DPKO) and Member States to respond to the effects of HIV on the health of peacekeeping and support personnel and develop long-term strategies for HIV prevention as an important part of Member States’ preparation for participation in peacekeeping operations. The Resolution called on the Secretary-General to take further steps to ensure that pre-deployment orientation and training on preventing HIV became a standard part of preparing peacekeepers for missions.
Declaration of Commitment on HIV/AIDSIn 2001 the United Nations General Assembly Special Session on HIV/AIDS adopted the Declaration of Commitment on HIV/AIDS, committing to take up the challenge of AIDS and mobilize a comprehensive response to the epidemic. Under the section on HIV/AIDS in conflict- and disaster-affected regions, paragraphs 77 and 78 specifically addressed the uniformed services.
• By 2003, have in place national strategies to address the spread of HIV among national uniformed services, where this is required, including armed forces and civil defence forces, and consider ways of using personnel from these services who are educated and trained in HIV/AIDS awareness and prevention to assist with HIV/AIDS awareness and prevention activities, including participation in emergency, humanitarian, disaster relief and rehabilitation assistance.
• By 2003, ensure the inclusion of HIV/AIDS awareness and training, including a gender component, into guidelines designed for use by defence personnel and other

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–20104
personnel involved in international peacekeeping operations, while also continuing with ongoing education and prevention efforts, including pre-deployment orienta-tion, for these personnel.
United Nations Security Council Resolution 1325The United Nations Security Council adopted Resolution 1325 on women, peace and secu-rity in October 2000. It recognized the impact of armed conflict on women and girls and called for effective institutional arrangements to guarantee their protection and full partici-pation in peace processes. In the context of the Security Council’s call for Member States to provide training guidelines and materials on the protection, rights and the particular needs of women related to HIV, Member States were also invited to incorporate HIV awareness training into their national training programmes for military and civilian police personnel in preparation for deployment.
United Nations Security Council Resolution 1820The United Nations Security Council adopted Resolution 1820 on Women, Peace and Secu-rity in June 2008. It urged troop- and police-contributing countries to take appropriate action to strengthen efforts to implement the policy of zero tolerance of sexual exploitation and abuse among United Nations peacekeeping forces as a way of reducing the risk of HIV transmission. It also called for including HIV prevention and response in and around United Nations–managed camps for refugees and internally displaced people, in all disarmament, demobi-lization and reintegration processes and in justice and security sector reform efforts assisted by the United Nations. The Security Council further encouraged support for appropriate regional and sub regional bodies to consider developing and implementing policies, activities, and advocacy to benefit women and girls affected by sexual violence in both armed conflict and in post-conflict situations. As one strategy to decrease post-conflict violence, the Security Council called for urgent efforts to scale up reintegration efforts for demobilized personnel.
United Nations Security Council Resolution 1888The Security Council’s recognition of the links between HIV gender relations and sexual and gender-based violence (Secretary-General of the United Nations, 2009) and peace and security (Security Council Resolution 1325) has created an unprecedented opportunity to align action for HIV prevention and against sexual violence and responses to both. The Security Council’s resolutions on gender, women and sexual violence (Resolutions 1888 and 1889) provide additional impetus for aligning and intensifying actions in these two areas.
The Security Council adopted Resolution 1888 in September 2009. It specifically man-dates peacekeeping missions to protect women and children from sexual violence during armed conflict and calls for this to be achieved through: technical support to troop- and police-contributing countries, including guidance for military, civilian and police personnel at risk from HIV in the pre-and post- deployment phases; induction and in-service training, par-ticularly among civilian superiors and military commanders; encouragement of commitment and political will among civilian and military leaders so as to prevent HIV; responsibility for HIV policy and practice within military command structures with lines of accountability and disciplinary and enforcement mechanisms to prevent sexual violence among the ranks as well as within local communities; and recognition of the role of the United Nations Peacebuild-ing Commission in addressing AIDS as a way to reduce instability in post-conflict situations.

A decade of United Nations and Security Council involvement with the AIDS response 5
United Nations Security Council Resolution 1889The United Nations Security Council adopted Resolution 1889 in 2009. It focused on gen-der, women and sexual violence and called for a wide range of measures to strengthen the participation of women at all stages of peace processes. It focused on the period after peace agreements have been reached. It specifically calls for greater physical security and better socioeconomic conditions, to be achieved through education, income-generating activities, access to basic services and any related resolutions to include provision for promotion of gen-der equality and the empowerment of women in post-conflict situations.
United Nations Security Council Resolution 1960In December 2010, the Security Council condemned the widespread and systematic use of sexual abuse against civilian populations in situations of armed conflict. It called for an end to all acts of sexual violence. In Resolution 1960, The Security Council asked parties to armed conflict to make commitments against the use of sexual violence and to investigate alleged abuses, which the Secretary-General was asked to monitor. The Security Council stated its intention when reviewing or adopting sanctions to designate criteria pertaining to acts of rape and other forms of sexual violence. The Security Council praised the work of gender advisers and looked forward to the appointment of women protection advisers in peacekeeping missions.
States were encouraged to use scenario-based training materials provided by the Secre-tary-General before the deployment of peacekeeping operations, with the Security Council pledging to pay attention to sexual violence in mandate renewals and authorizations. Fur-ther, states were asked to deploy more women as police and military personnel in peacekeep-ing operations. The Secretary-General was asked to strengthen the policy of zero tolerance of sexual exploitation and abuse by United Nations personnel and report regularly to the Council on progress in implementing the current resolution.
The changing global context of Resolution 1308
AIDS, health and securityThe belief that the AIDS epidemic might be a threat to global security became established for a number of confluent reasons. In December 1999, then United States Ambassador Rich-ard Holbrooke had seen the condition of children orphaned by AIDS in Lusaka, Zambia. Thereafter he urged the United Nations Security Council to seize the issue. Security Council Resolution 1308 of July 2000 was a direct result, stating that: “… the HIV/AIDS pandemic, if unchecked, may pose a risk to stability and security”. It was widely believed that the pan-demic could contribute to the breakdown of states in some of the most severely affected areas of the world and that the breakdown of already fragile states represents a threat to global and national security.
Such ideas were not new. In 1987, a study published by the Council on Foreign Rela-tions (Garrett, 2005) concluded that HIV would have a serious destabilizing effect on sub-Saharan Africa. It warned that, without intervention, much of the region could plummet into a period of civil war, unrest and downward economic spirals. In January 2000, a United States National Intelligence Council (2000a) report concluded: “In our view, the infectious disease burden will add to political instability and slow democratic development in sub-Saharan Africa, parts of Asia and the former Soviet Union, while also increasing political tensions in and among some developed countries.” More specifically, this report claimed

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–20106
that: “Infectious diseases also will affect national security and international peacekeeping efforts as militaries and military recruitment pools experience increased deaths and disabili-ties from infectious diseases. The greatest impact will be among hard-to-replace officers, non-commissioned officers and enlisted soldiers with specialized skills and among militaries with advanced weapons and weapons platforms of all kinds.” In 2000, the United States National Intelligence Council (2000b) reported: “In the absence of a major medical breakthrough, the relentless progression of AIDS and other diseases will decimate the economically productive adult population, sharply accentuate the continent’s youth bulge and generate a huge cohort of orphaned children. This condition will strain the ability of the extended family system to cope and will contribute to higher levels of dissatisfaction, crime and political volatility”. In the same report, the United States National Intelligence Council (2000b) predicted that, “AIDS and malaria alone will reduce gross domestic product (GDP) in several sub-Saharan African countries by 20% or more by 2010,” and at the micro-level, would have such a devas-tating impact on villages and families that HIV “will strain the ability of the extended fam-ily system to cope and will contribute to higher levels of dissatisfaction, crime and political volatility.” A further scenario (United States National Intelligence Council, 2002) identified a “second wave” of countries – China, India, the Russian Federation, Ethiopia and Nigeria – predicting a trajectory of generalized epidemics and potential socio-political crises that would pose a threat to global security. Given how the epidemic was then understood, such dire warnings seemed plausible. Nevertheless, things have changed; better knowledge is now available. The situation is more complex and more subtle but still requires urgent action.
Changes since 2000The success of the Global Fund to Fight AIDS, Tuberculosis and Malaria, United States President’s Emergency Plan for AIDS Relief and UNAIDS in taking forward the agenda of antiretroviral therapy has demonstrated the creative potential of the United Nations System working with national governments, multilateral and bilateral donors, the private sector, civil society, opinion leaders and international political and humanitarian figures. Today more than 5.2 million people living with HIV are receiving treatment. Increased access to treatment has markedly reduced HIV-related mortality, enabling people to lead healthy lives. It has reduced HIV transmission and therefore affected the trajectory of the epidemic. Nevertheless, universal access to HIV prevention, treatment, care and support remains an unrealized goal; only one third of the people who need antiretroviral therapy receive it. Social, cultural and economic position often determines access to HIV prevention, treat-ment, care and support. Universal access is closely linked to broader social, economic, politi-cal and cultural determinants of health and illness beyond HIV. Paramount among these is gender, which does not mean “women” but describes the biological and social, economic and cultural factors that shape relations between men and women and thus their HIV risk and access to prevention, treatment, care and support.
The relationships between HIV and national security are better understood
AIDS has so far not resulted in the sudden collapse of already fragile states. It is true that countries with lower income have major HIV epidemics, especially those with marked inequality. Nevertheless, no strong evidence indicates that the fragility of states alone pro-duces worse epidemics (Iqbal & Zorn, 2010). AIDS has not caused the sudden collapse of social, economic and political order in individual countries or internationally, but this insight should not encourage complacency. The indicators conventionally used to measure the fragility of states do not necessarily measure the subtle and often long-term effects of an AIDS epidemic. Nor is sufficiently long-term information available to determine how such

A decade of United Nations and Security Council involvement with the AIDS response 7
a long-wave event plays out over the longer term (Seeley, 2011; Seeley et al., 2010). Research in South Africa (Chirambo & Steyn, 2009) shows that, although the AIDS epidemic has not resulted in sudden economic and political change, unusual levels of mortality and mor-bidity among local government officials and councillors may adversely affect the operation of local and ultimately national politics, albeit ameliorated by the increased availability of antiretroviral therapy.
The evidence from recent studies (AIDS, Security and Conflict Initiative, 2011) is striking: the effects of HIV on governance are all at the margin, nowhere more significantly than in the effects of sexual violence on girls and women, with consequences for their future employment, parenting and ultimately the wider social fabric and thus national as well as personal security. These effects are most pronounced at the local level and depend on the intersection of other factors, including poverty, emigration of skilled labour, and governance crises, which are not related to HIV.
The pre-conflict, conflict and post-conflict continuum
Resolution 1308 called on the Secretary-General to take further steps to ensure that pre-deployment orientation and training on preventing HIV would become a standard part of preparing peacekeepers for missions. It also called on UNAIDS to continue to strengthen cooperation with interested Member States. The result was the development of a Coopera-tion Framework Agreement between UNAIDS and DPKO, signed in January 2001. This provides the basis for joint activities by UNAIDS and DPKO. In 2005, the activities of HIV units in DPKO were expanded to follow up the recommendations of a 2005 Presi-dential Statement of the United Nations Security Council and of the 2001 United Nations General Assembly Special Session on HIV/AIDS. In 2005, UNAIDS and DPKO reported on progress in the five years since Resolution 1308 was adopted. Attention was given to the potential for uniformed services to provide leadership in championing HIV prevention and to the engagement of defence and interior ministries in addressing HIV transmission risk among uniformed services and mitigating potential effects on force capability (UNAIDS, 2005a). UNAIDS outlined two challenges: the need to increase access by peacekeepers to voluntary counselling and testing for HIV and the need to ensure that programmes are con-sistently implemented. DPKO called for increased command responsibility for HIV preven-tion within military forces and for reducing high-risk HIV behaviour among peacekeeping personnel. DPKO noted that HIV testing and counselling remained a controversial and divisive issue. The peacekeepers surveyed generally had high HIV awareness, but only a few had received training from within their battalions or detachments, showing that the cover-age of HIV training before deployment was still low (DPKO, 2005).
Armed conflict and the absence of armed conflict are best seen as a continuum, a fluid and unpredictable risk environment. Such risk environments typically exhibit multiple ten-sions and switches between stability and stasis, insecurity and volatility. Conflict can some-times be a protective factor against HIV when low-prevalence populations are less mobile and isolated and have increased access to humanitarian support and HIV prevention ser-vices, care and treatment. However, in other circumstances, factors such as mixing between high- and low-prevalence populations during migration, return and reintegration processes, limited access to health services and increased sexual violence and exploitation contribute to increased risk. Sexual violence is often used as a weapon of war. Because of unrest, break-down of social relations and social norms as a result of conflict, post-conflict transitions are also risk environments in which behaviour such as sexual violence can increase. In such cir-cumstances, the processes of disarmament, demobilization and reintegration of armed forces can be used as an entry point for HIV prevention. Further, the task of engaging with HIV is not finished when the conflict has ended: soldiers, their families and survivors of violence all face continuing disruption and the social and psychosocial challenges familiar in post-

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–20108
conflict populations. Trauma of conflict endures for many years, adversely affects people’s physical and mental functioning and may cause them to do things that make them more sus-ceptible to acquiring HIV infection. For these reasons, long-term civil society intervention is necessary for combatants, their families and for the general population in post-conflict areas.
Better understanding of the situation in uniformed services
In 2000, the number of people estimated to be living with HIV had passed 28 million, with an estimated 3.1 million people newly infected and at least 1.8 million AIDS-related deaths that year, bringing the total number of deaths to more than 20 million. Of the 28 million people living with HIV at that time, more than 20 million were concentrated in sub-Saharan Africa. This was the region of the world in which most United Nations peacekeepers were deployed, and much of the concern about HIV and peacekeeping centred on the assump-tion that personnel coming from areas with a high HIV prevalence might constitute an important source of HIV transmission to local populations. For peacekeepers from countries with a low HIV prevalence and deployed in countries with far higher rates of HIV, concern centred on new exposure risks. Indeed, in 2000, many peacekeepers were serving in areas in which the HIV prevalence was up to six times higher than in their countries of origin (United States National Intelligence Council, 2000). At the time, it was also widely believed that peacekeepers were especially at risk for HIV transmission because of their relative youth, long periods of separation from family and sexual partners, the culture of aggressive mas-culinity in military units, substance abuse (especially alcohol) and relatively high disposable income that could lead to situations of sexual violence, exploitation and transactional sex for women in the communities. There was concern that soldiers’ rates of sexually transmitted infections, including HIV, were two to five times higher than the general population, with even greater ratios in times of conflict (UNAIDS, 1998). These concerns led to warnings about the dissolution of command structures, loss of experienced officers and potential for accelerated spread of infection throughout the general population and peacekeeping person-nel. A small but growing body of evidence suggests that these assumptions about the recip-rocal and mutually reinforcing aspects of HIV and insecurity should now be re-examined (Barnett & Prins, 2006). In addition, it is recognized that the HIV prevalence within the uniformed services is related to age, rank, time in service, the maturity of the epidemic, the repertoires of violence, military sexual trauma and the policies and activities of the com-mand. AIDS can threaten the operational capability of armies, primarily at the tactical level, to maintain combat effectiveness, unit cohesion, morale and discipline and human resource quality. Once again, the processes are unlikely to be sudden and more likely to be subtle: the impact of HIV on an army depends on other factors, such as military budget allocations, educational and development levels in the country and whether the army is primarily an infantry army or a mechanized force dependent on specialists.
Better understanding of the social determinants of health and well-being
Recent evidence (Commission on Social Determinants of Health, 2008) demonstrates that health and well-being are not primarily a matter of health care and health services: they are associated with factors outside the health care sphere. Above all, they are associated with security in the widest sense of human security as well as national security: they are associ-ated with the conditions in which people may flourish and realize their individual and joint potential (Sen, 1999). The conditions for human security include protection against poverty and protection from sexual violence. Thus, conditions of work, security from economic, gen-der or ideological exploitation, good governance, educational opportunity and many other factors affect health outcomes. Social, economic and cultural inequality and insecurity, lack of hope for the future (Barnett & Weston, 2008) and absence of control over one’s destiny

A decade of United Nations and Security Council involvement with the AIDS response 9
affect people’s health status and health outcomes. There is a direct line between the condi-tions for human security and those for national security.
One condition for long-term security is the construction and financial support of sys-tems of global public goods. Evidence from 15 years of experience building novel international institutions to fight AIDS and other infectious diseases shows what can be done. UNAIDS, the Global Fund to Fight AIDS, Tuberculosis and Malaria and UNITAID are examples of novel ways of mobilizing resources for public health initiatives in resource-constrained set-tings. Such visionary initiatives are part of what the United Nations System envisaged in the 1990s when it established the global public goods agenda, arguing (Kaul et al., 1999): “We should be … willing to pay for global goods that serve our common interests, be they shared systems of environmental controls, the destruction of nuclear weapons, the control of trans-mittable diseases such as malaria and HIV, the prevention of ethnic conflicts or the reduc-tion of refugee flows. And we should be prepared to finance such goods through innovative mechanisms based on the principles of reciprocity and collective responsibility …”
It is no accident that new institutions – UNAIDS, the Global Fund and UNITAID – have been constructed in the face of two pandemic diseases, HIV and tuberculosis (TB), and another endemic disease, malaria. National boundaries can offer no protection against such threats; success will only be possible though concerted global action using the instruments of global public goods spanning public, business, civil society and multilateral sectors. Such public goods and their institutional mechanisms can play an important part in protecting individual, national and international security in an ever more densely interrelated world.
This reportFollowing the first progress report (UNAIDS, 2005b), a Security Council Presidential State-ment asked DPKO and UNAIDS to provide regular briefings on progress “as a measure to strengthen commitment and accountability at the highest levels to sustained monitoring and evaluation of HIV programmes” and, in doing so, to help to maintain the momentum created by Resolution 1308.
This progress report documents progress since 2005 on the following four actions iden-tified in Resolution 1308:
• to document the potential damaging impact of HIV and AIDS on the health of inter-national peacekeeping personnel and uniformed services;
• for the United Nations to provide training for peacekeeping personnel on issues related to preventing HIV and to continue further development of pre-deployment orienta-tion and training for all peacekeeping personnel;
• for Member States, as an important part of their preparation to participate in peace-keeping operations, to develop effective long-term strategies for HIV and AIDS educa-tion and treatment of their uniformed service personnel; and
• to encourage interested Member States to increase international cooperation among their relevant national bodies and thus to assist in creation and execution of policies for HIV and AIDS prevention, voluntary and confidential testing and counselling and treatment for personnel to be deployed in international peacekeeping operations.

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201010
UN P
hoto
/Mar
ie F
rech
on

HIV and Uniformed Services
SECTION
TWO


HIV and Uniformed Services
International peacekeepers
New mix of troop-contributing countriesSince Resolution 1308 was adopted, a growing number of unstable political situations have required a significantly increased deployment of peacekeepers around the world. In 2000 the number of peacekeepers worldwide was 37,000, but by 2011, there were 98,837 international peacekeepers comprising troops (82,196), police (14,377) and military experts on mission (2264) with the surge in peacekeeping. A total of 10,209 civilians are also participating in peace operations. United Nations peacekeeping missions comprise troops and police from 115 countries. The number of missions has increased to 15 (see map).
The growing need for peacekeeping operations has been matched by a growing num-ber of countries contributing troops and police. In 2000, the top main troop-contributing countries in terms of numbers of personnel were Nigeria, Bangladesh, India, Ghana, Jordan, Australia, Ukraine, Kenya, Pakistan and Poland, but by 2011, the top ten were Pakistan, Bangladesh, India, Nigeria, Egypt, Nepal, Jordan, Rwanda, Ghana and Uruguay.
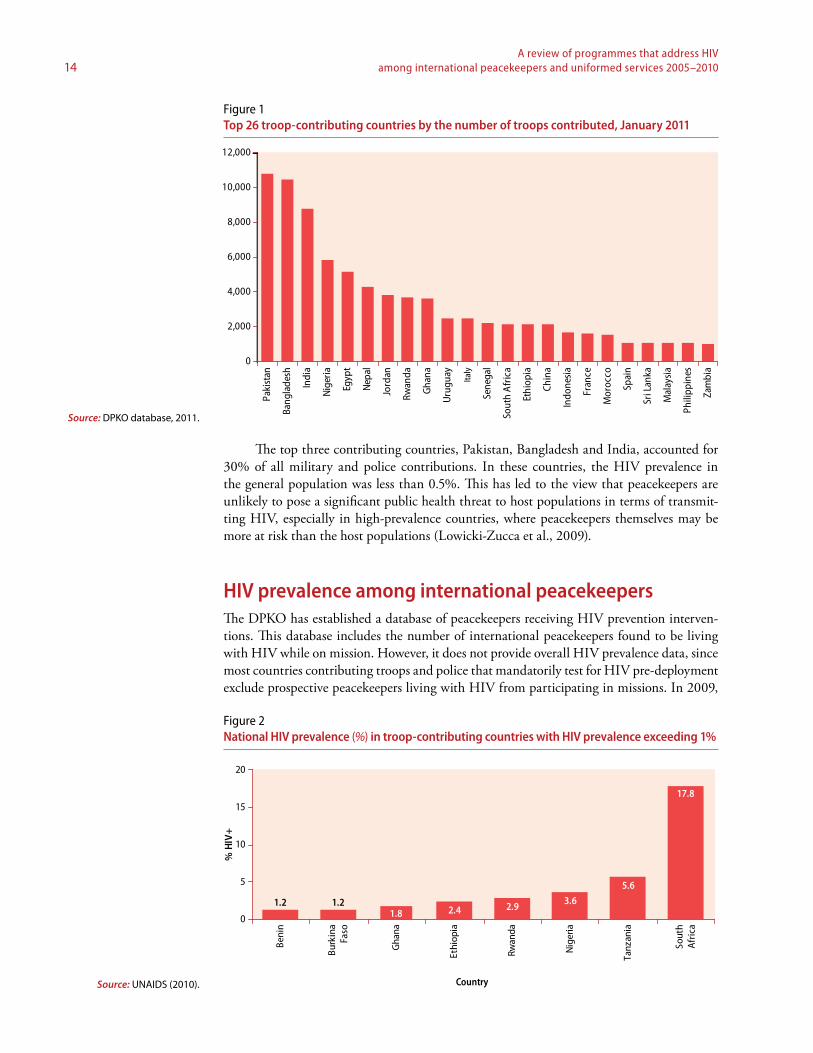
In 2011, 49 countries contributed less than 100 personnel and 26 countries contrib-uted more than 1000 (Fig. 1). Among these 26 countries, only 8 have HIV prevalence higher than 1% in the general population.
* political mission
UNFICYPCyprus
UNDOFSyria
UNTSOMiddle East
UNIFILLebanon
UNMOGIPIndia and Pakistan
MINURSOWestern Sahara
UNMIKKosovo
UNAMIDDarfur, Sudan
UNAMA*Afghanistan
UNMITTimor-Leste
UNMISSudan
MONUSCODem. Rep. of the Congo
UNOCICôte d'Ivoire
UNMILLiberia
MINUSTAHHaiti
Map No. 4259 Rev. 12(E) UNITED NATIONSJanuary 2011
Department of Field SupportCartographic Section
MISSIONS ADMINISTERED BY THE DEPARTMENT OF PEACEKEEPING OPERATIONS
MapCurrent DPKO missions
A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201014
The top three contributing countries, Pakistan, Bangladesh and India, accounted for 30% of all military and police contributions. In these countries, the HIV prevalence in the general population was less than 0.5%. This has led to the view that peacekeepers are unlikely to pose a significant public health threat to host populations in terms of transmit-ting HIV, especially in high-prevalence countries, where peacekeepers themselves may be more at risk than the host populations (Lowicki-Zucca et al., 2009).
HIV prevalence among international peacekeepersThe DPKO has established a database of peacekeepers receiving HIV prevention interven-tions. This database includes the number of international peacekeepers found to be living with HIV while on mission. However, it does not provide overall HIV prevalence data, since most countries contributing troops and police that mandatorily test for HIV pre-deployment exclude prospective peacekeepers living with HIV from participating in missions. In 2009,
0
2,000
4,000
6,000
8,000
10,000
12,000
Paki
stan
Bang
lade
sh
Indi
a
Nig
eria
Egyp
t
Nep
al
Jord
an
Rwan
da
Gha
na
Uru
guay
Italy
Sene
gal
Sout
h A
fric
a
Ethi
opia
Chin
a
Indo
nesi
a
Fran
ce
Mor
occo
Spai
n
Sri L
anka
Mal
aysi
a
Phili
ppin
es
Zam
bia
Figure 1Top 26 troop-contributing countries by the number of troops contributed, January 2011
Source: DPKO database, 2011.
Figure 2National HIV prevalence (%) in troop-contributing countries with HIV prevalence exceeding 1%
Source: UNAIDS (2010).
1.2 1.21.8 2.4 2.9 3.6
5.6
17.8
0
5
10
15
20
Beni
n
Burk
ina
Faso
Gha
na
Ethi
opia
Rwan
da
Nig
eria
Tanz
ania
Sout
hA
fric
a
Country
% H
IV+

How HIV affects security 15
10,409 peacekeepers requested voluntary counselling and testing in DPKO mission: of these. The percentage of international uniformed personnel reported to be living with HIV varied between missions and was in the range of 1.0% to 2.4%.
HIV status and HIV-related repatriationsA 2007 survey of 48,116 peacekeeping personnel in three missions (MINUSTAH, MONUC and UNMIL) found that, from August 2001 to June 2007, 25 peacekeepers from the three missions had died from AIDS-related causes (24 UNMIL and 1 MONUC), and 105 had been repatriated for HIV-related reasons (100 UNMIL and 5 MONUC). Of these repatria-tions, more than half came from one troop-contributing country, and most were from two troop-contributing countries that did not practice pre-deployment HIV testing (Likimani, 2007a, b) (Fig. 3).The institution of mandatory pre-deployment HIV testing and the non-deployment of per-sonnel living with HIV from certain countries could account for more recent reductions in HIV-related repatriations. For example, troop-contributing country B introduced pre-deployment testing in September 2006, whereas troop-contributing country A started in early 2006 and now only deploys HIV-negative soldiers. The 2007 report indicates that some military forces take the approach that, since peacekeeping is voluntary, soldiers presenting for pre-deployment medical examinations have by default “volunteered” for HIV testing, while others received mandatory HIV testing. Reports from the field in mid-2007 indi-cate that HIV testing conducted by national military forces very rarely includes counselling (Likimani, 2007a, b).
More comprehensive data from DPKO-DFS shows the profile of peacekeeping person-nel living with AIDS who were repatriated, evacuated or died in service due to HIV-related causes during the period 2005 to the end of 2009. Of 110 staff affected, only 3 were women and most were military personnel (49%) (Fig. 4). Mortality has sharply declined since 2005. Earlier diagnosis of HIV, changing attitudes towards personnel living with HIV, absence of AIDS symptoms and early repatriation are the main causes of this decline. Troop-con-tributing countries raise the cost of repatriation and evacuation as an issue. Many countries have initiated mandatory pre-deployment HIV testing to reduce the possibility of soldiers living with HIV being deployed and subsequently requiring repatriation. However, as shown
Figure 3Number of HIV-related repatriation by troop-contributing country (TCC), October 2003 to June 2007
Source: DPKO database, 2010.0
60
20
30
40
50
60
2003 2004 2005 2006 2007 Total
TCC ATCC BTCC DTCC EOthers

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201016
below, other countries such as South Africa and Zambia encourage troops living with HIV to be deployed as long as they are fit for service, with troop-contributing countries prepared to cover any treatment and associated costs while personnel are on active service.
The adequacy of medical reporting has been questioned as to whether it is complete in terms of both content and timing (Likimani, 2007a), and it remains unclear whether and to what extent current reporting provides clear information on the cause of death. In particular, it is not clear whether the primary cause of death is correctly attributed to AIDS or whether other co infections such as malaria, meningitis or TB are recorded as the cause of death.
HIV prevalence among uniformed services
Military personnelObtaining information about the HIV prevalence among national military personnel remains difficult. By the end of 2008, the United States Department of Defence HIV/AIDS Prevention Program found that half the 18 national military forces with which they worked were collecting data on HIV prevalence. In some countries, the most recent data were for 2001. Recent United States Department of Defence HIV/AIDS Prevention Program data on the prevalence of HIV infection in 33 national military forces show that this information was publicly available in less than half (42%) of them. Surveys are planned or underway in 22 countries, which should help provide a more complete picture of the HIV epidemic among military populations by the end of 2011 (United States Department of Defence HIV/AIDS Prevention Program, 2011). Available data from selected countries (Table 1) indicate that the HIV prevalence varied from a low of 0.6% among recruits in Vietnam to 10.1% for recruits in Equatorial Guinea. However, countries with known severe HIV epidemics, such as South Africa, do not appear in the table. In two countries with more than one study, time-series data were available, but data were derived from convenience samples and were not necessarily representative of the entire military. In the most severely affected countries in southern Africa, the HIV prevalence among uniformed services personnel is recognized to be slightly more than that of the general male population, between 15% and 30%. The HIV prevalence within the uniformed services is related to a range of factors and increases with age, time in service, the maturity of the epidemic, the repertoires of violence and the policies and activities of the command (AIDS, Security and Conflict Initiative, 2009).
Figure 4Number of HIV-related repatriation, evacuation and mortality cases by personnel group, 2005 to the end of 2009 (n = 110)
Source: DPKO database, 2010. 0
2
4
6
8
10
12
14
16
2005 2006 2007 2008 2009
UNPOLMilitary
Military ObserverInternational
National

How HIV affects security 17
In 2008, data for 21 African military forces showed that the HIV prevalence was ele-vated compared with the general population. They also showed that recent conflict slightly increases the HIV prevalence among men in the military compared with the civilian popu-lation (Ba et al. 2008). Data reliability remains a serious concern. A study of five Central American countries shows fairly low official HIV prevalence figures and argues that serious underreporting is occurring at the national level (Kruijt & Balconi, 2008). Moreover, with-out systematic HIV testing, reliable figures for the military and police are absent. Cases are revealed only when individuals living with HIV choose to disclose their serostatus (Kruijt & Balconi, 2008). Data are almost totally lacking on HIV among demobilized soldiers and their partners and similarly among soldiers who have served in peacekeeping missions after they return to their country (AIDS, Security and Conflict Initiative, 2009).
Although the United States Department of Defence HIV/AIDS Prevention Program has been providing considerable support to national military forces to improve their HIV-related data, military personnel are increasingly aware of the need to “know their epidemic”. For example, the Botswana Defence Forces have argued for more accurate data on HIV prevalence not only to understand the magnitude of the problem but also to be able to iden-tify which units are most severely affected and to identify the drivers of the epidemic within the military (Tiroyamodimo, 2010). Military personnel from Uganda have echoed this view on the grounds that HIV prevalence data cannot and should not be extrapolated from gen-eral population data and assumptions about the military “soldiering lifestyle” and that, even within the same forces, sexual behaviour differs significantly (Kusasira, 2010).
In India, data were available for three branches of the uniformed services (army, navy and air force); the HIV prevalence declined among uniformed service personnel from 2005 to 2009. The HIV prevalence varied from about 0.03% to 0.3% in 2009, depending on the sec-tor of the uniformed services (unpublished country presentation, 2010). Another example of good practice comes from Thailand, where the HIV prevalence among men 21 years old who where conscripted into the army by lottery was 2.9% in 1993 but 10% in the Northern Prov-ince. Following a sustained and intensive HIV prevention programme and including inter-ventions for the military within the national AIDS policy, the HIV prevalence was halved by 2000 and was further reduced to 0.5% at the end of 2009; Fig. 5 shows the trends from 1989 to 2009 at the national level and the contrasting situation, much less favourable, in Myanmar.
Figure 5HIV prevalence among military recruits in Myanmar and Thailand, 1989–2009
Source: National AIDS pro-grammes, 2010.
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5 ThailandMyanmar
1989
1991
1993
1995
1997
1999
2001
2003
2005
2007
2009

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201018
Table 1Knowledge about HIV prevalence in various military forces
Country
HIV prevalence in general population
(%) 2009HIV prevalence in military forces (%) Comments
Angola 2.0 3–11 2003 study provided prevalence range
Bahamas 3.1 NA A study of knowledge, attitudes and practices funded by the United States Department of Defence HIV/AIDS Prevention Program was to be conducted in 2010
Belize ... NA Study underway
Benin 1.2 2.2 The military conducted a seroprevalence study in 2005
Brazil 0.6 0.63 Country presentation 2009
Botswana 24.8 NA Study underway
Cameroon 5.3 11.3 According to a prevalence study in 2005
Chad 3.4 9.3 (2009)5.3 (2003)
According to a prevalence study in 2003 and a new prevalence study from one location in 2009
Côte d’Ivoire 3.4 4.7 TRaC (tracking) survey with PSI around behaviour conducted in 2008
Democratic Republic of the Congo
... 5.73.8
Survey 2000Survey 2007
Djibouti 2.5 1.2 The military conducted a 2006 seroprevalence study – not validated by their national AIDS programme
Dominican Republic 0.9 NA Study was to be conducted in 2010
Ecuador 0.4 1.25 Country presentation
Equatorial Guinea 5.0 10.1 2008 survey conducted and limited to certain sites
Ethiopia ... 7.2 urban recruits3.8 rural recruits
Abebe et al. (2003)
Gabon 5.2 4.3 Seroprevalence study done in May 2007
Ghana 1.8 NA Incidence estimated
Guatemala 0.8 0.7 According to a 2003 seroprevalence study
Guinea 1.3 6.6 Rate is according to a 2001 national study – the report was not seen
Honduras 0.8 NA Study was planned for 2010/2011
Jamaica 1.7 NA Study in planning phase
Lesotho 23.6 NA Study underway
Mozambique 11.5 NA Study underway
Paraguay 0.3 Military 0.4Police 0.8
2009 country presentation
Peru 0.4 Army 0.6Marines 0.5Air Force 0.1National Police 0.2
2009 country presentation
Congo (Brazzaville) 3.4 2.6 (2007)4.3 (2003)
Seroprevalence study done in April 2007 and prevalence rates released by Ministry of Defence
Rwanda 2.9 NA Study underway
Senegal 0.9 0.7 Study done in 2006 by military and national AIDS secretariat
Sierra Leone 1.6 3.3 Armed Forces conducted a seroprevalence study in 2007
Sudan – Sudan People’s Liberation Army
1.1 NA Study underway
Swaziland 25.9 NA Study underway
Trinidad and Tobago 1.5 NA Study about to begin
Gambia 2.0 NA Study to begin in 2010
Uganda 6.5 NA Study underway
Viet Nam 0.4 0.6% Estimated among recruits
Zambia 13.5 NA 2004 study conducted
Sources: United States Department of Defence HIV/AIDS Prevention Program (2011) and UNAIDS (2011).

How HIV affects security 19
In conclusion, there is mixed evidence on whether peacekeepers and military and police pose a public health threat as a population group, with a higher risk of transmitting HIV to the host community or to the general population in the home countries. Comparing the HIV prevalence in the military and police with the prevalence among similar age groups in the general population of their countries shows some evidence that they have similar or higher rates.
National law enforcement officersPolice forces and law enforcement officers play a critical role in enforcing the rule of law and the internal peace and security of a nation. However, the impact of AIDS on the police and their role in the response to AIDS are much-neglected areas of research; there is a dearth of data on HIV prevalence among law enforcement officers. Some evidence from Cambodia, India, Kenya and Malawi suggests that the HIV prevalence among these forces may not only be high but perhaps several times higher than that of the general population. More needs to be known about how HIV affects the police and their work in the wider community.

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201020
UN P
hoto
/Stu
art P
rice

Section three 21
Progress in implementation: preventing HIV infection among peacekeeping personnel
SECTION
THREE


Progress in implementation: preventing HIV infection among peacekeeping personnel
New policy environment on HIV counselling and testingOn 1 December 2007, the DPKO-DFS HIV Policy Directive was issued on the roles, responsibilities and functions of HIV units in United Nations DPKO peacekeeping opera-tions (DPKO, 2007). HIV units have two key roles: to provide awareness and prevention programmes to mission personnel: to integrate AIDS into mission mandates. The Policy Directive describes the key principles underlying the work of DPKO in relation to HIV: respect for human rights and non-discrimination; gender sensitivity; partnerships; and effi-ciency. In 2009, DPKO and DFS reiterated the organizational policy on safeguarding the personal health information of United Nations personnel; they reminded all missions that all personal information on individual health status must be marked as “strictly confidential”, and access to this information is limited to key clinical, technical and administrative staff (DPKO code cable to field missions, 2009: Maintaining confidentiality of personal health information). A third role is needed, which is outreach to support the host country civil soci-ety capacity-building in HIV. This is attributed to the high demand experienced with respec-tive host countries and the limitations experienced with funds and programmes in meeting such demands on the ground. Eritrea was a documented example of combined efforts of the national army and DPKO responding to AIDS together (UNAIDS, 2003).
DPKO HIV units are responsible for conducting four types of training: (1) HIV induc-tion training (mandatory for all personnel within six weeks of deployment) and refresher training for contingents deployed for longer than six months; (2) peer education training of personnel to establish a cadre of peer educators among the troop contingents and formed police units; (3) training counsellors in voluntary, confidential counselling and testing (vol-untary, confidential counselling and testing) for HIV; and (4) training of change agents for HIV integration into disarmament, demobilization and reintegration programmes. Mission HIV units are responsible for providing voluntary, confidential counselling and testing ser-vices based on an opt-in model, male and female condoms and post-exposure prophylaxis kits as well as guidance on universal precautions.
An HIV testing policy for uniformed peacekeepers was developed in 2004 and is being revised. It is based on the WHO-recommended shift towards provider-initiated testing and counselling and the fact that many countries contributing troops and police routinely test all troops and personnel for HIV before deployment on international missions. The existing testing policy is explicit that the sole criterion for deploying and retaining a peacekeeper is “fitness to perform peacekeeping duties during the term of deployment ... the HIV status of an individual is not in itself considered an indication of fitness for deployment in a peacekeeping mission.” South Africa and Zambia have recently revisited the non-engagement of personnel

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201024
living with HIV in active service, as is the norm in many African countries, with a view to basing involvement in peacekeeping on fitness for service and not on HIV status (see below).
Pre-deployment guidelines have a list of chronic medical conditions, including clinical AIDS, that preclude individuals from being deployed to international peacekeeping mis-sions. Following a survey conducted in 2007 (DPKO 2008a, b), it was recommended that provider-initiated testing and counselling for HIV be considered for pre-deployment medi-cal examinations, since the current guidelines use clinical symptoms for diagnosing AIDS, a method that has limited sensitivity and may miss a substantial number of staff members living with HIV (Likimani, 2007a). This recommendation was followed up by a position statement on HIV testing issued by the United Nations Medical Directors (2008). It rec-ommends that the 2004 United Nations policy on HIV testing be amended to encourage voluntary confidential medical interventions and provider-initiated testing and counselling (including history-taking, diagnostic testing and subsequent management) as a regular part of occupational health-oriented patient contact.
DPKO’s policy on voluntary confidential counselling and testing often differs from those of national military forces. For instance, the 2007 MINUSTAH knowledge, attitude and practice survey reported high rates of pre-deployment HIV testing: 95% of peacekeep-ers in Haiti had been HIV tested as part of pre-deployment screening. Of these, almost half were not offered or given any counselling with the HIV test. A further 11% were voluntarily counselled and tested for HIV in MINUSTAH (Tomczyk, 2007; Tomczyk et al., 2007). Atul Khare, Assistant Secretary-General, DPKO, visited the mission HIV unit on World AIDS Day in 2008 and agreed to be voluntarily tested for HIV. Finn Reske-Nielsen, Deputy Special Representative for the Secretary-General in UNMIT, was tested in 2009, and the United Nations Police Commissioner and two Deputy Commissioners at UNMIT came forward for testing in 2010. In UNMIS, during commemoration of World AIDS Day in 2010, the Minister of Health, the Chair of the South Sudan AIDS Commission and the Chief of Staff of the Sudan People’s Liberation Army led in HIV testing. Such visible and proactive attitudes among senior leadership are important steps to reducing stigma and dis-crimination and normalizing HIV testing.
Despite the new policy directive, fear of inadequate confidentiality can be a reason for not seeking testing and counselling. This indicates that the presence of a policy does not necessarily translate into good practice. At the 2007 and 2008 annual HIV workshops, HIV advisers and focal points agreed to advocate for implementing minimum standards for HIV services across all missions, an activity that is still ongoing. There was a need to update, harmonize and integrate DPKO standards in conducting voluntary and confidential coun-selling and testing across missions. In 2009, DPKO headquarters convened two regional meetings to train two batches of 25 field mission staff members from 18 DPKO and United Nations peace missions in Nairobi and 15 in Kathmandu.
International non-civilian peacekeepers are not considered United Nations employees – their contracts are with their national military force from which they have been seconded to the United Nations. National military forces are therefore responsible for updating their policies in accordance with international good practice. While on mission, DPKO HIV units provide training in awareness and prevention and voluntary counselling and testing for peacekeepers but cannot provide access to treatment care and support services. The national government is responsible for this in accordance with national protocols.
The programmes, which are implemented by mission HIV units and focal points, have core components: i) conducting awareness and prevention training, ii) providing voluntary counselling and testing, iii) training change agents for HIV mainstreaming in the disarma-ment, demobilization and reintegration process, iv) making condoms available to all per-sonnel, v) peer education training and vi) training of HIV counsellors. Messages delivered centre on the “ABC” approach: Abstinence and being faithful to one faithful partner are

Section three 25
promoted as primary preventive means, and consistent condom use is encouraged to ensure safer sex. In UNAMID, both male and female condom types are available and accessible to peacekeepers at strategic locations within the mission.
In 2000, only four HIV advisers were available to United Nations peacekeeping mis-sions. This had increased to 10 HIV advisers by 2005 (plus support from United Nations Volunteers and professionals from host countries) and focal points in smaller missions. Because of an increased number of missions and expanded scope, HIV programming for international peacekeepers has since been strengthened. As of the end of 2009, there were 9 Chief of HIV officers/policy advisers stationed in bigger missions plus 78 support staff and 12 focal points working in 11 smaller missions. Chief HIV officers/ policy advisers and focal points are an integral part of every United Nations peacekeeping mission, and pre-deployment HIV training has become standardized in all countries. Cosponsors such as UNFPA are taking an active role in pre-deployment training for police and military (such as in Bangladesh, Nepal and Paki-stan, while in 2005, UNMIS sensitized over 300 military observers during centralized pre-deployment in Kenya), are working with HIV advisers in peacekeeping missions to strengthen their HIV programmes (such as Côte d’Ivoire, the Democratic Republic of the Congo, Leba-non and Sudan/Darfur) and are providing joint support to disarmament, demobilization and reintegration programmes to support successful demobilization and reintegration of ex-com-batants in Côte d’Ivoire, the Democratic Republic of the Congo, Liberia, Nepal and Sudan.
Increased HIV awareness and prevention trainingPeacekeeper HIV induction training increased almost seven-fold between 2005 (the time of the last report to the United Nations Security Council) and the end of 2010. During the same period, the number of peacekeepers in field missions increased from 69,838 to nearly 100,000. In 2005, 11% had received HIV induction training. This had increased to 55% by the end of December 2010 (Fig. 6).In 2008, in conjunction with Integrated Training Services, the DPKO HIV induction and awareness training module was revised for inclusion in the compulsory United Nations Stan-
Figure 6Total number of UN peacekeepers receiving HIV induction training by category and year, 2004–2010
Source: DPKO database, 2011.0
10000
20000
30000
40000
50000
60000
2004 2005 2006 2007 2008 2009 2010
MilitaryPoliceCivilianTotal
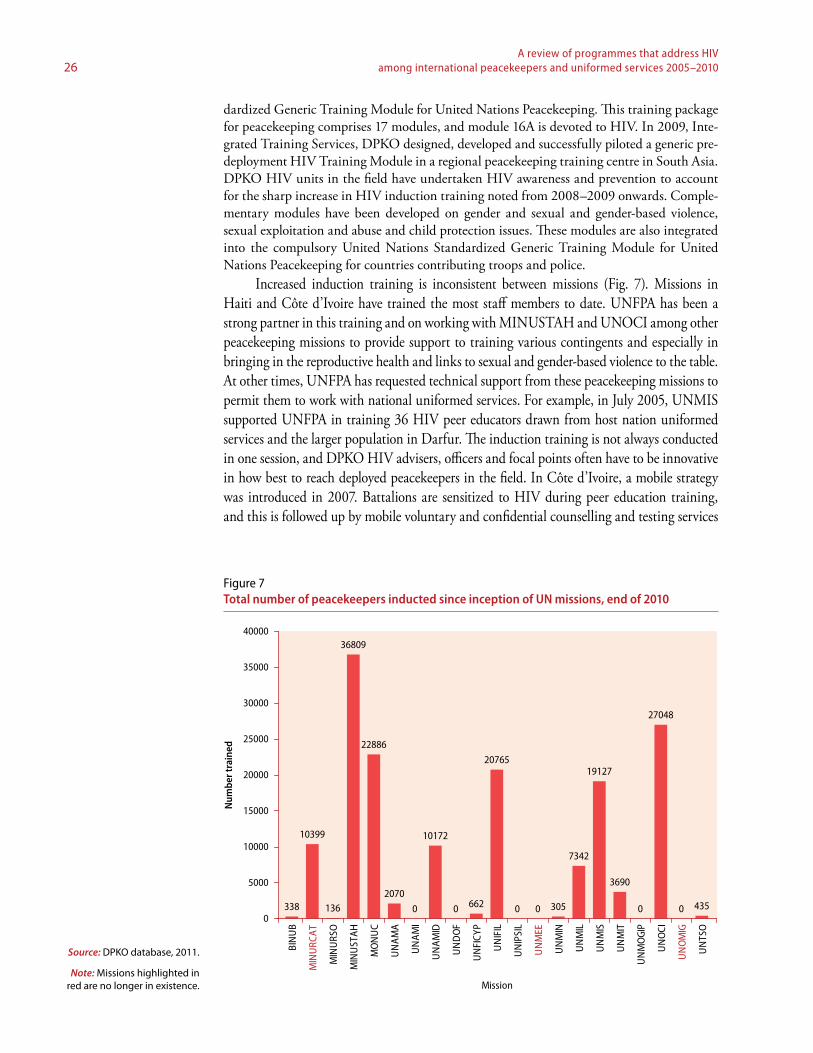
A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201026
dardized Generic Training Module for United Nations Peacekeeping. This training package for peacekeeping comprises 17 modules, and module 16A is devoted to HIV. In 2009, Inte-grated Training Services, DPKO designed, developed and successfully piloted a generic pre-deployment HIV Training Module in a regional peacekeeping training centre in South Asia. DPKO HIV units in the field have undertaken HIV awareness and prevention to account for the sharp increase in HIV induction training noted from 2008–2009 onwards. Comple-mentary modules have been developed on gender and sexual and gender-based violence, sexual exploitation and abuse and child protection issues. These modules are also integrated into the compulsory United Nations Standardized Generic Training Module for United Nations Peacekeeping for countries contributing troops and police.
Increased induction training is inconsistent between missions (Fig. 7). Missions in Haiti and Côte d’Ivoire have trained the most staff members to date. UNFPA has been a strong partner in this training and on working with MINUSTAH and UNOCI among other peacekeeping missions to provide support to training various contingents and especially in bringing in the reproductive health and links to sexual and gender-based violence to the table. At other times, UNFPA has requested technical support from these peacekeeping missions to permit them to work with national uniformed services. For example, in July 2005, UNMIS supported UNFPA in training 36 HIV peer educators drawn from host nation uniformed services and the larger population in Darfur. The induction training is not always conducted in one session, and DPKO HIV advisers, officers and focal points often have to be innovative in how best to reach deployed peacekeepers in the field. In Côte d’Ivoire, a mobile strategy was introduced in 2007. Battalions are sensitized to HIV during peer education training, and this is followed up by mobile voluntary and confidential counselling and testing services
Figure 7Total number of peacekeepers inducted since inception of UN missions, end of 2010
Source: DPKO database, 2011.
Note: Missions highlighted in red are no longer in existence.
338
10399
136
36809
22886
2070
0
10172
0 662
20765
0 0 305
7342
19127
3690
0
27048
0 4350
5000
10000
15000
20000
25000
30000
35000
40000
BIN
UB
MIN
URC
AT
MIN
URS
O
MIN
UST
AH
MO
NU
C
UN
AM
A
UN
AM
I
UN
AM
ID
UN
DO
F
UN
FICY
P
UN
IFIL
UN
IPSI
L
UN
MEE
UN
MIN
UN
MIL
UN
MIS
UN
MIT
UN
MO
GIP
UN
OCI
UN
OM
IG
UN
TSO
Mission
Num
ber t
rain
ed

Section three 27
where they are stationed. This approach has made it possible to scale up access to voluntary, confidential counselling and testing. In UNAMID, towards the end of 2009, 4 HIV units have been established resulting in wider coverage of the peacekeepers; Darfur has an area similar to that of France and has 30,000 UNAMID peacekeepers covered by only 23 HIV unit staffers. In Haiti, MINUSTAH has two voluntary, confidential counselling and test-ing centres as well as a mobile team that is deployed regularly to the regions to provide HIV counselling and testing to contingents and staff members who wish to be tested. UNMIS uses the initiative of mobile voluntary, confidential counselling and testing services to cover all mission sectors.
Increased number of peer educatorsThe number of peacekeepers trained as peer educators increased by 50% from 2005 to the end of 2008 (Fig. 8). However, the numbers trained decreased in 2009 because of training budget cuts and the lack of availability of peacekeepers from operational duties but increased again in 2010, except for national uniformed services. In UNAMID, a few peer education training courses were conducted in 2009 with the support of UNFPA.
Questions have been raised about the sustainability of training peer educators. As mili-tary contingents rotate every 6–9 months, their continuation as peer educators on return and the probability of re-deployment for United Nations peacekeeping is not predictable. Some missions have trained a few national uniformed services personnel as peer educators so that they can train other national staff and local community members. Another possibility is to focus more on training civilians who have longer stays in the mission, versus the military and police personnel, whose rotation varies from 3 to 12 months.
The quality and coverage of HIV interventions varies considerably between missions depending on mission mandates, geography, size and deployment of peacekeepers. Although they all carry out HIV induction programmes, there were marked differences in peer educa-tion training, post-exposure prophylaxis procurement and availability and voluntary, confi-
Figure 8Number of peacekeepers trained as peer educators, 2004–2010
Source: DPKO database, 2011.0
200
400
600
800
1000
1200
1400
1600
1800
2004 2005 2006 2007 2008 2009 2010
Int'l Uniformed ServiceNat'l Uniformed ServiceCivilianTotal

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201028
dential counselling and testing across all missions. According to an earlier DPKO monitoring and evaluation assessment, voluntary, confidential counselling and testing was the “least uni-formly available service across all missions”. Among missions that offer voluntary, confidential counselling and testing, there was a range of services from referral to the medical unit to providing static, mobile or combined static-mobile voluntary, confidential counselling and testing services to remote areas of deployment. Voluntary, confidential counselling and test-ing provision was the top request for support from HIV field staff (DPKO database, 2009).
Progress in distributing condomsMaking condoms available constitutes one element in DPKO’s comprehensive HIV preven-tion strategy, which is implemented in conjunction with clear rules on appropriate behav-iour and stringent measures against sexual exploitation and abuse. The number of condoms distributed to peacekeepers has risen dramatically (31 times), from about 210,400 in 2005 to 6,527,000 in 2009 (Fig. 9). Compared with the number of peacekeepers in the post, this represents an increase from an average of 3 condoms per peacekeeper in 2005 to 66.5 con-doms per peacekeeper in 2009. Although this is a dramatic increase, the number of condoms available may still not meet the sexual health needs of peacekeepers.
Making condoms available is one component of the DPKO strategy for HIV preven-tion, which is implemented in conjunction with clear rules on appropriate behaviour and stringent measures against sexual exploitation and abuse. There is no contradiction between making condoms available in peacekeeping missions and the United Nations policy of zero tolerance towards sexual exploitation and abuse. DPKO has made it clear that all condom dispensers in missions must be marked with a text that explicitly reminds personnel of the prohibition against sexual exploitation and abuse. More information is needed on sexual behaviour so that behaviour change interventions can be appropriately targeted and male
Box 2Involvement of command structure
In Lebanon, the active engagement and involvement of UNIFIL mission top management and leadership has lead to increased emphasis on HIV prevention interventions. Mission managers have been key advocates in promoting HIV programmes. For example, in 2009 the Office of the Force Commander took the lead in organizing the World AIDS Day event, which increased the profile of the event and attention on HIV prevention. Following an HIV orientation session, the commander of one of the European contingents decided to be tested for HIV, and this encouraged many of the troops in the contingent to come forward for voluntary testing.
Source: DPKO database, 2010.
Box 1Training national staff as peer leaders
In Haiti, MINUSTAH trained peer leaders after initial HIV awareness raising. Peer leaders were selected from the military, civilians (national and international) and United Nations Police. Following training, many peer leaders became active in training their peers through formal and informal sessions. The most active peer leaders were subsequently nominated as HIV focal points (total 25 in 2008) within their respective community or constituency. They provide support to the regional HIV response in accordance with the National AIDS Strategic Plan.
Source: DPKO database, 2010.

Section three 29
and female condom requirements can be more accurately estimated and the condoms and lubricants targeted to those who need them.
Improvement in HIV-related servicesThe number of staff requesting voluntary, confidential counselling and testing while
on mission increased from 1830 in 2005 to more than 14,000 by the end of 2010 (Fig. 10). In the context of the number of peacekeepers in post, the update of voluntary, confidential counselling and testing increased from less than 3% of the staff in 2005 to more than 15%
Figure 9Total number of condoms distributed to peacekeepers in all missions, 2004–2010
Source: DPKO database, 2011.0
1000
2000
3000
4000
5000
6000
7000
2004 2005 2006 2007 2008 2009 2010
Thou
sand
s
Figure 10Number of UN peacekeepers and civilians seeking HIV counselling and testing, 2005–2010
Source: DPKO database, 2011.
0
2000
4000
6000
8000
10000
12000
14000
2005 2006 2007 2008 2009 2010Year
No.
of V
CCT
adm
inis
tere
d
Military
Police
Civilian

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201030
in 2010. The number of sites at which voluntary, confidential counselling and testing was conducted increased from 2 in 2005 to 13 in 2009.
The services related to HIV and voluntary counselling and testing and the quality of these services offered diverge widely from mission to mission. Although all missions with HIV programming carry out basic HIV sensitization, there were differences in the availabil-ity of other mandated services (peer education training, post-exposure prophylaxis coverage and voluntary counselling and testing services across missions). In the 2007 Annual HIV Workshop in Brindisi, Italy, the HIV advisers and focal points agreed to advocate for pro-moting and implementing minimal standards in HIV service provision across all missions. The Southern African Development Community has now endorsed this.
As with other HIV prevention interventions, the provision and uptake of voluntary, confidential counselling and testing services among peacekeeping personnel varies consider-ably. Missions that have adopted mobile combined with mobile-static counselling and test-ing services have been more successful in increasing access to services. In UNOCI (Côte d’Ivoire), a strong partnership developed between the HIV unit and medical units. Medical units provide a private space for voluntary, confidential counselling and testing counselling and send laboratory technicians for mobile HIV testing in remote locations where peace-keepers are deployed. Emphasis on mobile testing and an increase in the number of trained counsellors has led to increased in uptake of voluntary, confidential counselling and testing services from 6% in 2005 to 29% at the end of 2009.
As noted above in Lebanon, the involvement of the command structure increased voluntary HIV testing in one contingent. In Timor-Leste, voluntary, confidential counsel-ling and testing campaigns have been conducted with the involvement and strong support from UNMIT senior leadership in conjunction with government, the Gender Affairs Unit and Human Rights Unit of UNMIT and other stakeholders. The uptake of voluntary, con-fidential counselling and testing services among United Nations military and civilian peace-keepers, both national and international, has increased since 2008, but this has not been so marked among United Nations Police. Implementation of the UN Cares strategy on HIV has been reported to be an important part of mission response to peacekeepers living with HIV in Haiti and Timor-Leste.
Many troop-contributing countries have a national mandatory HIV testing policy for their uniformed personnel, and this is used both before and after deployment in DPKO peacekeeping operations. However, DPKO is not normally informed of the overall results. This has hampered DPKO’s response and ability to evaluate HIV testing and counselling intervention programmes (Tomczyk et al., 2007).
Data are not routinely available on the availability and use of post-exposure prophy-laxis at missions. Some reports from the field tell of stock-outs of post-exposure prophylaxis; similarly, missions such as UNMIT in Timor-Leste describe the post-exposure prophylaxis custodian system as an example of good practice. In Darfur, the involvement of UNAMID police advisers has been critical in increasing access to post-exposure prophylaxis for both peacekeeping personnel and civilian populations in need (DPKO database, 2010).
HIV and behaviour changeMonitoring and evaluation systems are slowly developing but are hampered by the lack of tradition of assessing the outcome of activities. A survey of HIV knowledge, attitudes and practices was conducted on a sample of 849 United Nations peacekeepers from 11 coun-tries and one United Nations force (Argentina, Bolivia, Brazil, Chile, Ecuador, Guatemala, Peru, Philippines, Nigeria, Senegal, Uruguay and UNPOL) based in Haiti (MINUSTAH) in May 2007. The total peacekeeping staff at the mission was 8810, and they came from 42 countries. Thus, the sample was about 10% of the total troops deployed. The response rate was 78%, and the sample comprised 19% commissioned officers, 54% non-commissioned

Section three 31
officers and 27% troops, with an age range of 26.6 to 42.2 years. Of the respondents, 76% reported this was their first United Nations mission, and the average number of months they had been deployed was 5.3 months. Of the sample, 99% had heard of HIV, 89% received training before deployment and 65% received training in MINUSTAH. Despite this high level of exposure to training about HIV, misconceptions about HIV transmission were common, but their knowledge of HIV transmission and prevention was high and var-ied by country from 47% to 68%. Fifty-nine per cent did not have an HIV awareness card (Tomczyk et al., 2007). Less than 3% of respondents reported having sex while on mission (most of these reported sex with a regular partner). However, 29% had sex while on leave or compulsory time off. Of these, 43% did not use a condom with their last partner while on leave. In Darfur, Sudan, half the peacekeepers using condoms reported that condoms were very difficult or difficult to access (DPKO database, 2007). Other surveys of knowledge, attitudes and practices conducted among peacekeepers in Liberia in 2004 and in Haiti in 2007 reported findings about inconsistent condom use (Table 2).
No data are available on the effectiveness of the various behaviour change interven-tions used. In Haiti, the percentage of personnel who reported being trained about HIV issues before deployment ranged from 61% to 96%, and the percentage who had received training in MINUSTAH ranged from 2% to 99%. Training levels did not correlate with knowledge levels, and this is significant: it underlines the importance of quality control and continual reinforcement of key messages. Data are insufficient to measure change over time following HIV prevention programmes. Although military HIV prevention programmes have undoubtedly improved, much more remains to be done to improve them and to reduce the number of people newly infected (United States Department of Defence HIV/AIDS Prevention Program, 2009).
UNMIL (2004) MINUSTAH (2007)
Men among total troops (%) 99 99
Total troops (n) 15 880 8 810
Sample (n) 667 849
Married or long-term partners (%) 88 79
Age (years), mean 34.5 34.7
Education (%)
Secondary education 60 46.2
Higher education 36 35.5
Deployment (months) >6 5.3
HIV training (%)
Pre-deployment 56–100 65–89
In-mission awareness 88 65 (military)83 (United Nations Police)
HIV knowledge (2 of 3 modes of transmission) 83 4.7–56 (military)64 (United Nations Police)
HIV attitudes and behaviour
Perceived HIV risk (%)
None 51 42
Low 37 43
High 10 11.4
Sexual history: had sex in mission (%) 21 6.529.2 (during compensatory time off)
Condom use Inconsistent Inconsistent
Table 2Comparison of KAPB surveys among peacekeepers in UNMIL, Liberia (2004) and MINUSTAH, Haiti (2007)
Source: DPKO database, 2005, 2007.

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201032
Support for local communitiesIn collaboration with United Nations theme groups, Chief HIV officers/policy advisors also seek to mainstream AIDS into mission mandates (such as the training of local police in Haiti and the training of the local community, regular police, prison wardens and prison-ers in Sudan) and undertake outreach to local communities (such as collaboration with the Society for Women and AIDS in Africa in Sierra Leone). In Eritrea, peacekeepers organized joint peer education training on HIV with the national army. Overall, outreach education among uniformed services personnel and communities has reached several million men and women directly or indirectly. UNFPA has also supported prevention work with host communities living and working near uniformed services and the families of uniformed personnel. In the Latin America region, there is civil–military cooperation between the health ministries and the uniformed services with a long history of sharing and coordinat-ing resources, many of them under formal agreements and alliances. Some examples of this partnership and coordination are Bolivia’s Health Sentry Soldier Programme, includ-ing HIV prevention for civilian populations; the support of Brazil’s Army to the National AIDS Programme in the western Brazilian Amazon providing HIV testing, treatment and care to the entire civil population (70% indigenous); the prevention, treatment and care programme of the Committee for the Prevention and Control of HIV/AIDS in the Armed Forces and National Police of Peru (COPRECOS Peru), which corresponds to 2% of the total national response; and the Dominican Armed Forces, which assist 6–10% of the civil-ian population in their military health services and support the HIV national monitoring and evaluation system.
Mainstreaming HIV into disarmament, demobilization and reintegration and security sector reformUnited Nations mechanisms involved in disarmament, demobilization and reintegra-tion integrate HIV prevention, treatment, care and support into their normative proto-cols. These protocols are now operational in several countries (including Colombia, Côte d’Ivoire, Indonesia, Nepal and Sudan). The Integrated Disarmament, Demobilization and Reintegration Standards are based on two decades of disarmament, demobilization and reintegration experience on five continents. The standards cover 24 areas of disarmament, demobilization and reintegration, including HIV and AIDS, and were launched in 2006. The standards link disarmament, demobilization and reintegration initiatives related to HIV to national and local AIDS control programmes and strategies.
One important activity has been to put in place coordination efforts to ensure that deployment prevention programmes are aligned with pre-deployment training in coun-
Box 3HIV counselling and testing among military personnel and their families in Mozambique
HIV counselling and testing among military personnel was launched in 2004. By the end of 2009, eight static military HIV counselling and testing facilities had been opened, and 10,000 military personnel and their sexual partners and families had been tested for HIV. Community counselling and testing provided in residential areas adjacent to barracks and in neighbouring military units have helped to reach soldiers’ partners and families. The promotion and provision of services is coordinated with clinical treatment companions and the involvement of trained military and civil counsellors and health care providers.
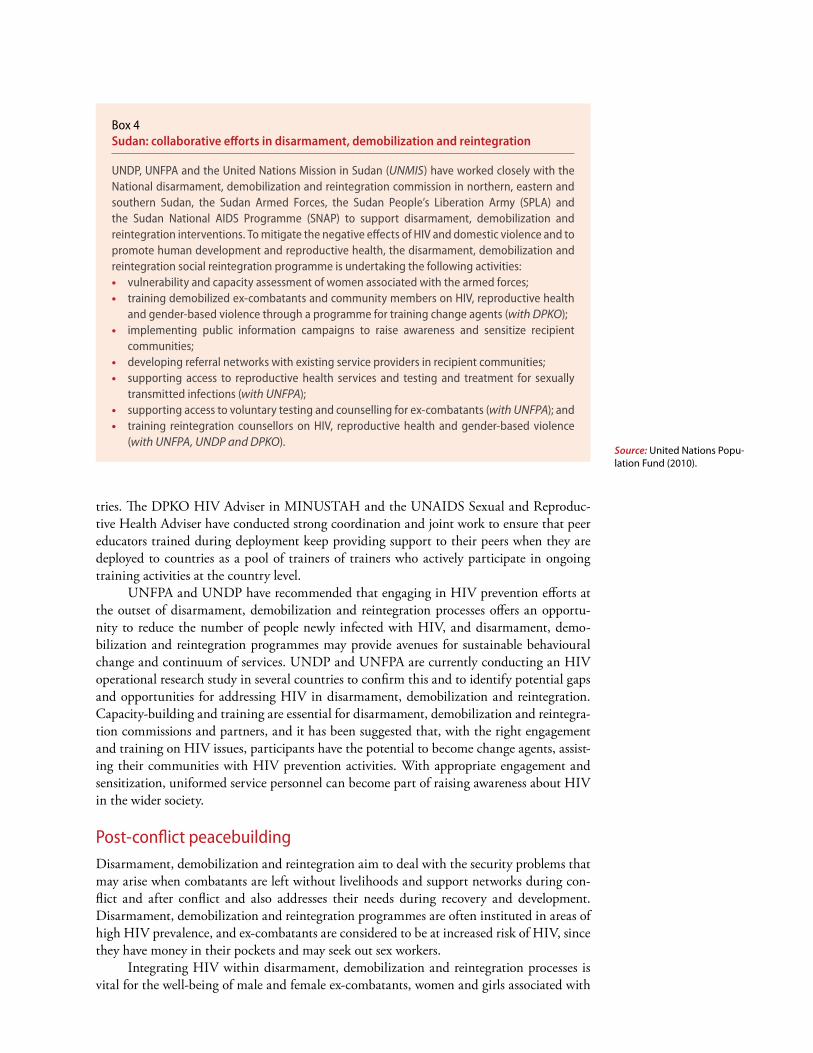
tries. The DPKO HIV Adviser in MINUSTAH and the UNAIDS Sexual and Reproduc-tive Health Adviser have conducted strong coordination and joint work to ensure that peer educators trained during deployment keep providing support to their peers when they are deployed to countries as a pool of trainers of trainers who actively participate in ongoing training activities at the country level.
UNFPA and UNDP have recommended that engaging in HIV prevention efforts at the outset of disarmament, demobilization and reintegration processes offers an opportu-nity to reduce the number of people newly infected with HIV, and disarmament, demo-bilization and reintegration programmes may provide avenues for sustainable behavioural change and continuum of services. UNDP and UNFPA are currently conducting an HIV operational research study in several countries to confirm this and to identify potential gaps and opportunities for addressing HIV in disarmament, demobilization and reintegration. Capacity-building and training are essential for disarmament, demobilization and reintegra-tion commissions and partners, and it has been suggested that, with the right engagement and training on HIV issues, participants have the potential to become change agents, assist-ing their communities with HIV prevention activities. With appropriate engagement and sensitization, uniformed service personnel can become part of raising awareness about HIV in the wider society.
Post-conflict peacebuildingDisarmament, demobilization and reintegration aim to deal with the security problems that may arise when combatants are left without livelihoods and support networks during con-flict and after conflict and also addresses their needs during recovery and development. Disarmament, demobilization and reintegration programmes are often instituted in areas of high HIV prevalence, and ex-combatants are considered to be at increased risk of HIV, since they have money in their pockets and may seek out sex workers.
Integrating HIV within disarmament, demobilization and reintegration processes is vital for the well-being of male and female ex-combatants, women and girls associated with
Box 4Sudan: collaborative efforts in disarmament, demobilization and reintegration
UNDP, UNFPA and the United Nations Mission in Sudan (UNMIS) have worked closely with the National disarmament, demobilization and reintegration commission in northern, eastern and southern Sudan, the Sudan Armed Forces, the Sudan People’s Liberation Army (SPLA) and the Sudan National AIDS Programme (SNAP) to support disarmament, demobilization and reintegration interventions. To mitigate the negative effects of HIV and domestic violence and to promote human development and reproductive health, the disarmament, demobilization and reintegration social reintegration programme is undertaking the following activities:• vulnerability and capacity assessment of women associated with the armed forces;• training demobilized ex-combatants and community members on HIV, reproductive health
and gender-based violence through a programme for training change agents (with DPKO);• implementing public information campaigns to raise awareness and sensitize recipient
communities;• developing referral networks with existing service providers in recipient communities;• supporting access to reproductive health services and testing and treatment for sexually
transmitted infections (with UNFPA);• supporting access to voluntary testing and counselling for ex-combatants (with UNFPA); and• training reintegration counsellors on HIV, reproductive health and gender-based violence
(with UNFPA, UNDP and DPKO).Source: United Nations Popu-lation Fund (2010).

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201034
armed groups and their recipient communities. The disarmament, demobilization and rein-tegration process provides an opportunity to reach out to vulnerable groups and contributes to effective recovery and provides an opportunity to create links with national actors to address the needs of vulnerable groups over the long term. Disarmament, demobilization and reintegration programmes have been a consistently overlooked focus for HIV prevention and response, including their nearly exclusionary approach towards military families and women and children associated with armed forces and groups. Successful interventions in Côte d’Ivoire, Liberia, Nepal, Niger, Sierra Leone and Sudan (including Darfur) and have shown that dedicated staff capacity within a coordinated national disarmament, demobiliza-tion and reintegration response greatly improves the successful integration of HIV concerns.


UN P
hoto
/Mar
tine
Perr
et

Progress in implementation: preventing HIV among uniformed services personnel
SECTION
FOUR


Progress in implementation: preventing HIV among uniformed services personnel
Including HIV prevention for uniformed services in national AIDS strategiesUNAIDS reviewed national AIDS strategies in early 2010. Information collected from 62 countries showed that 38 strategies referred to the military, 39 to uniformed services in general, 19 to the police or law enforcement officers, 18 to prison staff and two to HIV pre-vention among demobilized soldiers. Some strategies mentioned security service personnel; individual country strategies also mentioned child soldiers, peacekeepers and drug treatment staff. However, a simple mention of uniformed services in these plans does not necessar-ily mean that any implementation occurred. Some countries do not have fully developed national AIDS policies but use national strategic frameworks to provide the action frame-work. These plans identify the military as the most vulnerable group but do not make provi-sion for intervention with priorities.
Progress reports on the implementation of the Declaration of Commitment on HIV/AIDS (UNAIDS, 2011) show trends over time from 2005 to 2009 (Fig. 11). For the years 2005, 2007 and 2009, 122, 147 and 182 countries reported, respectively. In 2009, nearly
Figure 11Percentage of countries reporting progress in HIV prevention, treatment and care programmes among uniformed services, 2005, 2007 and 2009 (percent)
Source: UNAIDS (2011).
0
10
20
30
40
50
60
70
80
90
Stra
tegy
BCC
Cond
om
prov
isio
n
Test
ing
&
Coun
selli
ng
STI S
ervi
ces
Trea
tmen
t
Care
&
Supp
ort
200520072009

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201040
80% of the reporting countries had a national strategy or an action framework for address-ing HIV issues among their national uniformed services, and 65% reported that antiret-roviral therapy services were implemented beyond the pilot stage. Progress in HIV testing and counselling services was spectacular, from 13% to 74%. In 2009, in about one third of countries, HIV testing was mandatory for military recruitment.
National AIDS strategic plans appear to more frequently include uniformed services in Latin America and the Caribbean. Of the 18 countries in this region, 12 included uniformed services in their plans and an additional 3 referred to activities conducted with the police. In most countries, uniformed personnel have been recognized as a population of interest, and interventions addressing them are considered a major opportunity for promoting behav-ioural change, especially for reducing stigma and discrimination against the populations at higher risk of HIV exposure. Uniformed services are often country partners that sit in decision-making forums such as country coordinating mechanisms, national AIDS councils and human rights national observatories and participate in decision-making processes and policy development as well as monitoring and evaluation mechanisms such as the national reports following up the United Nations General Assembly Special Session on HIV/AIDS.
Increased HIV preventionThe lesson learned from Latin America and the Caribbean is that an effective national AIDS response should involve sectors other than health, such as social, economic, legal and cultural sectors. A discrete uniformed service response is not the most effective way to address the problem. Moreover, the uniformed services have a fundamental role to play in the national AIDS response through military logistics and technical personnel as well as assisting civilian populations during situations of humanitarian relief (UNAIDS Regional Support Team for Latin America, 2010). The inclusion of HIV prevention and an AIDS response in national strategic plans in Latin America and the Caribbean has led to a comprehensive response, with all countries including human rights and gender equality as a core component of activi-ties and having surveys of knowledge, attitudes and behaviour in place to monitor changes in sexual and HIV risk behaviour (Table 3).
Before a regional meeting of military personnel held in Botswana in 2009, an assess-ment was conducted on HIV and AIDS interventions for the military in 11 countries of the South African Development Community. The results of the assessment indicate that all the military forces that responded to the survey were conducting HIV prevention programmes. However, coverage of interventions for military personnel varied widely, as did the topics and approaches. Only half the national forces surveyed had written HIV policies and, of these, 71% of the policies include HIV testing. Many different behaviour change methods are used in the South African Development Community region, with peer education being most common. Training was much less frequent on more recently introduced topics such as male circumcision and gender-based violence (United States Department of Defence HIV/AIDS Prevention Programme, 2009).
Alignment of military HIV policies with national programmesUNAIDS reviewed the HIV testing policies of 15 major troop-contributing countries and found that all subscribe to voluntary, confidential counselling and testing in principle but most apply pre-recruitment screening. Only Ethiopia, France and Jordan do not apply pre- or post-deployment testing. Policies are being reviewed in Senegal and South Africa. Most troop-contributing countries do not deploy personnel identified as living with HIV and repatriate any personnel found to be living with HIV while on mission (Kenny, 2009). Troop-contributing countries may explore the possibility of referrals by the health services to the national AIDS programmes to obtain antiretroviral therapy regimens not provided in

Progress in implementation: preventing HIV among uniformed services personnel 41
United Nations missions. On the other hand, in selected situations, the civilian peacekeepers can be reimbursed for their antiretroviral therapy and other health care expenses through their health insurance.
Additional information from 64 countries found that 35 of 52 countries have official or draft policies on pre-recruitment HIV testing, and 39 of 49 countries conduct either or both pre- and post-deployment HIV testing. A few countries allow recruits known to be living with HIV into the military, and 11 of 34 countries deploy troops known to be living with HIV as peacekeepers (Kenny, 2009). Research also shows that elements of AIDS policy and programming in the military are poorly aligned with national or civilian policies. A particular harmonization challenge is providing counselling, care and treatment for those who are discharged from the army after having tested HIV-positive (AIDS, Security and Conflict Initiative, 2009).
Military hospitals usually offer soldiers living with HIV free care and treatment, and they often stand a better chance of accessing antiretroviral therapy than does the general population. The support of the United States President’s Emergency Plan for AIDS Relief has facilitated considerable expansion of antiretroviral therapy and care of opportunistic infections. The South African Defence Force, for example, partnered with the United States National Institute of Health to provide antiretroviral therapy to soldiers living with HIV and their dependants in early 2004 – before the life-prolonging medicines became available in the public health system. Managing AIDS treatment is more problematic when soldiers are in the field. Only Botswana and South Africa supply their troops living with HIV with antiretroviral therapy during deployment. In some other militaries, soldiers who test HIV positive before foreign deployment are reassigned. Soldiers weakened by AIDS-related ill-nesses and unfit to perform their duties are usually encouraged to retire. Retired personnel usually continue receiving free health care.
Country
HIV included in academic curricula?
HIV peer educator network?
Human rights and gender
equality addressed?
Access to voluntary
counselling and testing?
Survey of knowledge, attitudes and
practices to monitor progress?
Belize Yes No Yes Yes Yes
Bolivia No Yes Yes Yes Yes
Brazil Yes Yes Yes Yes Yes
Colombia (armed forces) Yes Yes Yes Yes Yes
Colombia (police) Yes Yes Yes Yes Yes
Costa Rica Yes Yes Yes Yes Yes
Dominican Republic Yes Yes Yes Yes Yes
El Salvador Yes No Yes Yes Yes
Haiti No No Yes Yes Yes
Honduras Yes Yes Yes Yes Yes
Mexico Yes Yes Yes Yes Yes
Nicaragua (armed forces) Yes Yes Yes Yes Yes
Nicaragua (police) Yes Yes Yes Yes Yes
Panama Yes No Yes Yes Yes
Peru Yes Yes Yes Yes Yes
Uruguay Yes Yes Yes Yes Yes
Venezuela (Bolivarian Republic of)
Not observed Yes Yes Not observed Yes
Table 3Main achievements of country projects in Latin America and the Caribbean
Source: UNAIDS Regional Sup-port Team for Latin America (2010).

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201042
Following national policies, with the support of United States President’s Emergency Plan for AIDS Relief, male circumcision campaigns and efforts are underway in the militar-ies of Botswana, Ethiopia, Lesotho, Mozambique, Namibia, Nigeria, Rwanda, Swaziland, Uganda, United Republic of Tanzania and Zambia. The military setting is conducive to pro-viding the infrastructure for service delivery and follow-up. It also provides the opportunity to address additional prevention and men’s health issues. In addition, civilians use military health care sites and can benefit from their services. In Rwanda, the offer of male circumci-sion has begun in the military, and training and capacity-building of health workers from Army health services has started (WHO and UNAIDS, 2009).
UNAIDS found that 9 of 44 countries allow recruits known to be living with HIV into the military, and 11 of 34 countries deploy troops known to be living with HIV as peacekeepers (Kenny, 2009). Soldiers living with HIV have been publicizing the important role they can play in developing and implementing HIV programmes to reduce stigma and improve the well-being of soldiers living with HIV and their families (United States Depart-ment of Defence HIV/AIDS Prevention Programme, 2009).
HIV and behavioural changeInformation on 25,453 uniformed service personnel (24,402 men and 1,049 women) from 11 countries in the Latin America and the Caribbean region was gathered from knowledge, attitude and practice surveys. Seven countries are contributing countries to peacekeeping operations, especially Brazil and Uruguay, with more than 2000 troops. Most of the data were collected in 2005–2006, and the most recent study was in the Dominican Republic in 2009. The prevalence of knowing how to prevent HIV varied from 50% in El Salvador to 97% in Uruguay. It is striking that consistent condom use did not exceed 50% in any coun-try even though high-risk HIV behaviour was widely reported (figure 12). In the Dominican Republic, 47% of uniformed service personnel engaging in high-risk HIV behaviour did not use a condom if they had consumed alcohol. The level of discrimination attitudes is very high in the surveyed countries in the Caribbean region compared with the other countries in South America (Fig. 11). In 2009, high-risk sexual behaviour was studied among military personnel in the Dominican Republic who were stationed at border-crossing zones from Haiti into the Dominican Republic. A stratified systematic random sampling strategy was used, and questionnaires were verbally administered to 498 military personnel. The results of this study showed a high prevalence of high-risk sexual behaviour. In the past 12 months, 94% of respondents had had sex. Forty-one per cent reported sex with a casual partner; 19% reported sex with a sex worker (Anastario et al., 2010).
In Brazil, conscripts with low educational levels had a significantly higher HIV preva-lence (0.16%) than those who had completed high school (0.06%). A confirmed history of syphilis and a report of previous sexually transmitted infection were important predic-tors of HIV infection. Data from Costa Rica show that 3.3% of male respondents had had forced sex with another individual and 1.9% had used their position of authority to this end. Among female respondents, 10% reported having had sex against their will while deployed (UNAIDS Regional Support Team for Latin America, 2010). High rates of homophobia were reported among uniformed service personnel in the Latin American and Caribbean region (UNAIDS Regional Support Team for Latin America, 2010). Data from Latin Amer-ica show that, although uniformed personnel in countries have a high level of knowledge on HIV prevention and transmission, much still needs to be done regarding behaviour change related to condom use and stigma and discrimination.
In Senegal, the Senegalese Armed Forces conducted a behavioural and HIV prevalence survey of 747 male military personnel in seven sites in 2006 and compared the results with those from a 2002 survey of 1114 military staff (Dieng, 2008). The HIV prevalence was

Progress in implementation: preventing HIV among uniformed services personnel 43
0.7% and the syphilis prevalence 1.2% in the armed forces in 2006 (biological data were not obtained in 2002): those 40–49 years old had the highest HIV prevalence, 2%. The rate among married men was 3% versus 0.3% in single men. These findings are consistent with other surveys showing that the HIV prevalence is related to age and length of service (AIDS, Security and Conflict Initiative, 2009). None of the officers tested for HIV was found to be living with HIV: the HIV prevalence was highest among troops and military staff deployed overseas. The study found a high level of awareness of HIV (99%). Information was obtained mainly from the media but also from colleagues (39%) and conferences and group discus-sions (69%). Correct information about HIV had increased between 2002 and 2006, with a decrease in the number of military personnel who thought that HIV could be transmitted by mosquitoes (from 43% in 2002 to 26% in 2006) and an increase from 62% in 2002 to 90% in 2006 of those who knew that people living with HIV may appear to be healthy. However, increases were noted in high-risk sexual behaviour, with a decrease in the age of first sexual intercourse, an increase in casual sexual relations from 14% in 2002 to 22% in 2006 and an increase in sexual relations with sex workers from 4% in 2002 to 7% in 2006. However, consistent use of condoms with sex workers was reported to be high: 90% in 2002 and 92% in 2006 (Dieng, 2008).
Bing et al. (2008) reported an increase in HIV risk perception and condom use among personnel in Angola’s military and found a significant increase in the use of condoms during vaginal sex three months after education on HIV prevention. A survey conducted among 3141 Nigerian military personnel reported only 39% condom use despite 95% awareness about HIV risks and 86% familiarity with the symptoms of sexually transmitted infections (Kershaw, 2008). A study by the International Centre for Ethnic Studies (2008) found that, although three quarters of Sri Lankan soldiers surveyed were aware that condoms helped prevent HIV, the actual use in practice was much lower as reported for recent contacts – both heterosexual and homosexual.
One of the advantages national military forces have in implementing HIV prevention programmes compared with international peacekeeping forces is the length of time that
Figure 12KABP survey results by country: selected countries in South America and the Caribbean, 2005, 2007 and 2009
Source: UNAIDS Regional Sup-port Team for Latin America (2010).
0
20
40
60
80
100
120
Boliv
ia
Bras
il
Colo
mbi
a
Cost
a Ri
ca
Dom
inic
anRe
publ
ic
El S
alva
dor
Hai
ti
Hon
dura
s
Peru
Urug
uay
Vene
zual
a
% good knowledge of HIV transmission modes
% demonstrating stigma and discrimination
% good knowledge of HIV prevention
% stating consistentcondom use
A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201044
personnel are in post and their availability for training. There are very few published evalua-tions of the effectiveness of HIV prevention programmes in national military forces, but the findings from one demonstrate the need for intensive and sustained training for behaviour change to be adopted. One study compared two samples of 568 military personnel in 12 sites in Angola (Bing et al., 2008). One group received 4.5 days of intensive HIV preven-tion training and 0.5 days of training in malaria prevention. The control group received the reverse amounts of training. The training was followed up by monthly booster sessions and knowledge and behaviour was measured at baseline and at three and six months. The group receiving the intensive HIV prevention training had greater condom use and less unpro-tected anal sex at three months and reduced unprotected vaginal sex and fewer partners at both three and six months. This was coupled with greater HIV knowledge and perceived HIV vulnerability than the control group at three and six months. The authors argue that, even in resource-limited post-conflict countries, the military can provide effective HIV pre-vention education for personnel, including among their female partners, which can con-tribute to soldiers becoming agents for change and providing HIV prevention in the wider community (Bing et al., 2008).
The limited number of published studies of evaluated HIV and AIDS interventions in the military mainly results from financial constraints but also from weak monitoring and evaluation capacity. Where resources are available, funders may not request outcome assess-ments or governments may be wary that the results will generate criticism of inadequate prevention programmes. In some countries, assessments are conducted but they are not published, as they are considered to contain classified information that could compromise national security (Cornman, 2010).
Increased funding for HIV interventions for national uniformed servicesSince 2006, countries have had increased capacity and funding for HIV programming among militaries as part of national HIV strategic plans and national budgets. Of 62 coun-tries reviewed, more than 40 had policies for military forces, police and other uniformed per-sonnel as part of their national HIV strategic plans. The United States President’s Emergency Plan for AIDS Relief, which supports 71 countries, is an example of increased donor support for HIV programming among military and police forces. United States programme fund-ing for military-to-military assistance with HIV activities shows a fivefold increase over the past decade. The prevention efforts of the United States Department of Defence HIV/AIDS Prevention Programme support peer education, HIV prevention programmes for people liv-ing with HIV and male circumcision. In Latin America, the resource mobilization efforts carried out by uniformed personnel to ensure the sustainability of interventions were con-ducted at the regional and country levels with donors (such as the United States Agency for International Development, GIZ, the United Kingdom Department of International Devel-opment and multilaterals) interested in supporting this strategy. This reflects the national authorities’ interest in keeping it in the national HIV agenda. It also became an integral part of the UNAIDS country and regional work plans, United Nations joint programmes and Programme Acceleration Funds proposals.
The Global Fund to Fight AIDS, Tuberculosis and Malaria for the first time awarded US$ 58.8 million for a regional project submitted by the Committee for the Prevention and Control of HIV/AIDS in the Armed Forces and National Police of Latin America and the Caribbean (LAC COPRECOS) for uniformed services in 15 countries of Latin America and the Caribbean region. The approval of this proposal has opened a new dimension for financ-ing for regional networks of uniformed services working with HIV. The project, entitled AVANZADA, seeks to address identified gaps in HIV response efforts among uniformed service personnel and to establish sustainable programmes and services.

Progress in implementation: preventing HIV among uniformed services personnel 45
An example of innovative funding is the EU-UNDP-UNFPA Joint Programme HIV and Sexually Transmitted Infection Prevention among Uniformed Services in Ukraine with financial support from the EU. Established in 2005, the Programme was aimed at prevent-ing HIV and other health risks, such as drug abuse and sexually transmitted infections, and forming commitment for healthy lifestyles and safe behaviour among the uniformed services in Ukraine. The overall programme budget was €2.5 million. The World Bank has also contributed important funding for uniformed services through its Multi-Country HIV/AIDS Program for Africa.
Other uniformed servicesThe role of other uniformed services such as law enforcement and prison staff in HIV pre-vention and protecting vulnerable groups is still undeveloped. Some best practices have emerged, but the coverage of HIV prevention and services among police and other personnel is still low. A network of police called the Law Enforcement and Harm Reduction Network (LEAHRN) has been created in Asia. They are also building a wider approach to the inter-section of law enforcement and public health, and have a research partnership looking at harm reduction impact on police policy and practice in Cambodia, the Lao People’s Demo-cratic Republic and Viet Nam.
The first global workshop on HIV and police took place in 2007. It identified specific vulnerability in these forces and the potential role of police and law enforcement agencies in overall national responses and recommended that specifically tailored interventions be identified and implemented. UNAIDS and UNODC jointly reviewed police practices with most vulnerable populations affected by HIV and HIV intervention programming for their own staff. It is envisaged that this will feed into global guidance for building police capacity to create an enabling environment for national HIV responses. In Latin America, UNODC has been implementing, with the support of the UNAIDS Cosponsors Regional Group, a regional HIV project in more than 10 countries, and a regional observatory on HIV and prisons has been established.
In 2009, representatives of police from countries in Asia and the Pacific established the Asia and Pacific Regional Network on Police and AIDS. This defined a regional strategy as to how police can contribute to creating an enabling environment for AIDS programming among populations at higher risk.
Some best practices have also emerged in Asia. In India, for example, DISHA Jana Kalyan Kendra is an NGO that was founded in 1995 with the active collaboration of the Asansol Police. It serves a population of about 1500 sex workers and their clients. The Super-intendent of Police and the Additional Superintendent have played a very active role since the beginning, and the involvement of police is regarded as a major factor in the success of DISHA. As a result of their involvement, the police have changed their attitudes towards the sex workers and are more sympathetic towards them. The sex workers, as they go about their work as peer educators and counsellors, feel protected by the police and receive considerable support from them (UNAIDS India, 2010).
Box 4Armed forces and law enforcement agencies – Ukraine regional meeting
A consultation on uniformed services held in Ukraine in 2007 drew 86 participants from 24 countries and included UNFPA staff, national partners and other key partners working with the uniformed services, including United Nations agencies, regional networks, international and local NGOs and the United States Department of Defense.
Source: UNFPA (2008).

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201046
UNODC has provided support to Tihar prison in India, one of the largest in Asia. Tihar has trained prison and paramedical staff in HIV and injecting drug use awareness and developed an appraisal system to assess the performance of workers and inviting feed-back from them on HIV prevention activities. In UNAMID, the HIV and AIDS Unit has teamed up with the Prisons Advisory Unit under the Rule of Law Section to provide train-ing, including HIV awareness for the prison officers all over Darfur.
The role of uniformed services in natural disasters can be critical, as shown recently in Haiti and Pakistan. Engaging the uniformed services in HIV and gender-based violence pre-vention efforts during natural disasters should be an important new role. In 2010, COPRE-COS LAC supported the Dominican Republic in implementing a contingency plan for HIV and emergencies in the border region between Haiti and the Dominican Republic and played a key role in coordinating national HIV and emergency actors.
Sexual violenceSexual violence against girls is increasingly being recognized as having dire public health effects and long-term effects on security. Biological transfer of HIV is more likely when sex is accompanied by violence, and sexual relations characterized by violence are statistically more likely to lead to infection (WHO and Global Coalition on Women and AIDS, 2004; Sexual Violence Research Initiative, 2007). In non-conflict settings, sexually transmitted infections are among the most common health problems following sexual assault (Adlington & Burnett, 2004). Factors that may increase HIV transmission during forced sex include the higher likelihood of genital injury and trauma and the higher prevalence of HIV and sexu-ally transmitted infections observed among perpetrators. Genital injury influences the risk of HIV transmission (Adlington & Burnett, 2004). Evidence also indicates that children and older women are more susceptible to genital injury following rape due to size and mucosal characteristics that are specific to the less-developed reproductive tracts of younger girls and women and the more fragile reproductive tract lining among older women (Sommers et al., 2006; WHO and Global Coalition on Women and AIDS, 2004). Thus, girls who experience sexual violence have an increased biological risk of contracting HIV and other sexually trans-mitted infections. Evidence also suggests that sexual violence alters the life path of many girls, leading them down a road of depression, substance abuse and high-risk behaviour. In sub-Saharan Africa, girls are 2–4.5 times more likely to acquire HIV infection than boys, and women constitute about 60% of those living with HIV.
The effects of violence against girls and women in non-conflict situations extend far beyond poor health outcomes. Sexual violence is a powerful reason why girls miss out on educational opportunities. This lack of access to education reduces a girl’s potential for a bet-ter life and damages her prospects of earning a sustainable income, perpetuating the cycle of vulnerability and undermining economic growth. Over the long term, this harm to young women adversely affects their capabilities as parents and citizens, thus contributing funda-mentally to undermining social cohesion and the welfare of future generations.
Work with the police to address sex work and violence has started in several countries. In Sierra Leone, UNFPA, in collaboration with the National AIDS Secretariat and the Sierra Leone Police, has launched the Sierra Leone Police AIDS Policy, which aims at reducing the rate at which police officers acquire HIV infection. Several countries have implemented cooperation between police, sex workers and NGOs to sensitize the police to the harass-ment and violence experienced by street-based sex workers. The violence or harassment can originate from either clients or the police or both. Sex workers associated with the police document human rights violations in Kenya and in cooperation with representatives of the judicial system (penalization) in South Africa. Special training for the police is organized in Nepal, Peru and Kyrgyzstan. Cooperation with the police is often critical for sex workers’

associations because the decriminalization of the sex work industry in some states, such as in India and Pakistan, does not necessarily or automatically reduce harassment and/or sexual violence by the police and/or religious authorities. In 2007, the Global Consultation on the Police and HIV/AIDS identified the roles of police and law enforcement agencies in overall HIV national responses. UNAIDS and UNODC jointly reviewed police practices in col-laboration with the populations at higher risk of HIV exposure to coordinate global guid-ance for building police capacity in creating a more positive environment for the national HIV responses.
Box 5HIV, human rights and gender training
Côte d’Ivoire has the highest prevalence of HIV infection in western Africa – an estimated 3.4% in the general adult population. An innovative partnership between UNDP, UNFPA, UNAIDS and UNOCI has provided joint training for uniformed personnel on HIV, human rights, gender equality and technical support on HIV and disarmament, demobilization and reintegration. This initiative offers an opportunity to reduce the number of people newly infected with HIV, especially since more than 3000 ex-combatants have returned to their families and communities of origin. It also destigmatizes HIV, addresses discrimination and facilitates care and protection for people living with HIV in the armed forces.
Source: United Nations Development Programme (2010).

UN P
hoto
/Mar
tine
Perr
et

Increased partnerships and regional networks
SECTION
FIVE

Increased partnerships and regional networks
Partnerships
Global Task Force on HIV among Uniformed ServicesSince 2001, the UNAIDS Office on AIDS, Security and Humanitarian Response, together with the United States Department of Defence, has been chairing an international Task Force for strengthening and coordinating implementation of AIDS strategies among uni-formed services worldwide. In addition, as result of continued advocacy, leading regional security bodies have increasingly acknowledged the need to mainstream AIDS in their oper-ations. The UNAIDS Office on AIDS, Security and Humanitarian Response has worked closely with the Commonwealth of Independent States and the African Union and its Peace and Security Council and has formalized partnerships with COPRECOS LAC and the Pacific Islands Chief of Police Forum.
Global Task Force on HIV among Uniformed ServicesThe Global Task Force on HIV among Uniformed Services is an informal coalition of United Nations agencies, national military forces, international donors and organizations, leading think tanks and academic centres and international NGOs working together to promote global collaboration and partnership on AIDS and security and to meet the expanding need of HIV/AIDS programmes for uniformed services globally.
The development of tools to assist uniformed services in integrating HIV prevention, testing, treatment and care standards into their structures has been a priority for the Task Force. As a result, the Task Force has developed a range of resources for guidance, program-ming and information purposes, and for use within uniformed services.
International Committee on Military MedicineThe main aims of the International Committee on Military Medicine are to maintain rela-tions between the various military medical services of its Member States in order to pro-mote medico-military scientific activities and to participate in developing medical activities during humanitarian operations. For the International Committee on Military Medicine, preventing HIV infection among uniformed personnel is a priority. This involves discussing information, sharing lessons learned from the field and reciprocal representation in meetings with other organizations. AIDS remains one of the major public health concerns for health services supporting uniformed personnel. On 14 September 2009, the Deputy Executive Director of UNAIDS and the Secretary-General of the International Committee on Mili-tary Medicine signed a memorandum of understanding to facilitate cooperation between the two organizations in such areas as advocacy, sharing information and technical support.

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201052
International Centre for Technical CooperationThe International Centre for Technical Cooperation is a partnership between the Govern-ment of Brazil and UNAIDS and was created in 2004 to strengthen South–South technical cooperation in responding to AIDS. COPRECOS LAC is an accredited International Centre for Technical Cooperation training institute and has conducted two regional training courses for 52 police and military officers: the first one on capacity-building of uniformed service personnel in managing HIV and sexually transmitted infections (2006). The second course in 2007 focused on building capacity in monitoring and evaluating HIV programmes.
International Military HIV/AIDS ConferenceThe International Military HIV/AIDS Conference in Arusha, United Republic of Tanzania in 2010 brought together representatives from 60 military forces, including nearly 40 from Africa, to share information and work together in developing a joint strategy for combating the pandemic.
Regional networksRegional networks of military personnel were created: to advocate for HIV programmes among military forces in regions and their integration into national strategic plans and responses; to foster intra- and interregional collaboration and the exchange of best prac-tices and lessons learned; to set minimum standards and develop regional policies on HIV programming among military forces and to standardize interventions and training as far as possible; and to mobilize resources at both the country and regional levels.
African initiativesThe Inter Africa Group human security programme seeks to develop human security con-cepts relevant to the Horn of Africa region and to broaden participation with the Afri-can Union, the Intergovernmental Authority on Development, comprising six countries in eastern Africa, and the New Partnership for Africa’s Development. This is being achieved through a combination of research and analysis, advocacy, consultation and capacity-build-ing. The human security programme naturally includes activities on preventing HIV within the military.
The African Union plays an important role in peace and security in Africa. The launch of UNAMID, deployed in Darfur, marked an important step in linking African and inter-national efforts in securing and consolidating peace in Africa. It has also underlined the need for greater support in the areas of equipment, maintenance and other logistical issues. The G8 is supporting peacekeeping operation training centres in Africa, such as the Kofi Annan International Peace Training Centre and the École du Maintien de La Paix in Bamako, Mali. Plans are being developed for long-term, sustainable and flexible funding mechanisms for African-led peacekeeping efforts so that African partners can tackle existing and new chal-lenges at the pre- and post-conflict stage (G8, 2008).
In the East African Community, Article 118 of the Treaty for the Establishment of the East African Community calls for Partner States to cooperate in health activities and undertake joint activities to prevent and control communicable diseases and epidemics such as HIV that might endanger the health and welfare of people in the Community. The East African Community Developmental Strategy recognizes that HIV adversely affects national security and seriously threatens regional sustainable development and the East African Com-munity integration agenda. To address this, the Council of Ministers has directed that HIV be mainstreamed into regional peace and security sectors by convening regional advocacy, sensitization and health awareness meeting, seminars, and workshops for East African Com-

Increased partnerships and regional networks 53
munity military, police, paramilitary and institutions through East African Community Defence Liaison Officers. The East African Community Regional Armed Forces HIV/AIDS Prevention Seminar, a regional seminar held in 2010, examined progress made to date and drew attention to the use of alcohol and drugs by armed forces personnel and the role of these substances in HIV transmission, the need for workplace HIV polices to be implemented and for more comprehensive and integrated sexual and reproductive health services (including HIV and sexually transmitted infections) to be provided within functioning health systems (East African Community, 2010).
Southern Africa
South African Development Community Military Health Services Committee on HIV and AIDSThe South African Development Community Business Plan for 2004–2009 mentioned work with uniformed services, and its strategic framework for 2009–2015 recognizes the importance of the South African Development Community in relation to human security and HIV. “… It is essential that security operations take fully into account matters relating to HIV prevention, relating to the security services, and in relation to populations affected by insecurity, such as displaced people and refugees.” In 2009, the South African Develop-ment Community developed regional minimum standards for harmonized programming for control and management of HIV and AIDS, malaria and tuberculosis among military forces. In March, 2009, the Botswana Defence Force and United States Department of Defence HIV/AIDS Prevention Programme co-hosted the 2009 Military HIV Prevention Conference: Militaries Leading Prevention Efforts to Fight HIV.
Initial consultations on the creation of a regional network on HIV and the military occurred at the 15th International Conference on AIDS and Sexually Transmitted Infec-tions in Africa in Dakar, Senegal in December 2008. A satellite session entitled Integration of HIV into Humanitarian Response – Challenges and Lessons Learned included topics such as: AIDS among uniformed services, mobilizing military leaders against AIDS in the region, South African Development Community regional initiatives on AIDS and military forces, HIV programmes for the military forces in Senegal, HIV and disarmament, demo-bilization and reintegration in the peacekeeping mission in Côte d’Ivoire and HIV pro-grammes for the police in Sierra Leone.
The HIV Regional Network of Military Forces in West and Central Africa was offi-cially launched in July 2009. It provides technical support to strengthen national AIDS programming and encourages its members to share their respective experiences and practices and to standardize procedures.
Box 6Minimum standards relevant to HIV and AIDS in the military
Fitness for duty rather than HIV serostatus must be the guiding principle for medical discharges.During military service, there should be routine comprehensive health assessments including HIV testing, always accompanied by pre- and post-test counselling.Deployment should be subject to a health assessment and be based on individual health status.Deployment of military people living with HIV should be based on WHO criteria and not solely on a HIV-positive test result.The physician caring for the military person living with HIV should make the final decision on deployment based on medical status, duration and type of deployment and health services available in the mission area. Source: South African Devel-
opment Community (2009).

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201054
Latin America and the CaribbeanCOPRECOS LAC. In a historical decision foreseeing the security implications of the HIV epidemic, in 1992 COPRECOS was created at the national level in Peru; and in 1995, COPRECOS LAC was created to better respond to the HIV needs of the uniformed person-nel in countries and when deployed to United Nations missions. In 2005, the Latin Ameri-can Chapter of the International Committee on Military Medicine recognized COPRECOS LAC as its official technical HIV and AIDS advisory group in fulfilment of the Resolution on the Commitment to Fight against the HIV Epidemic signed by 113 countries during the Fourth World Congress on Military Medicine held in Washington, DC, in 2004. COPRE-COS LAC has now 22 country members, and has been very active in promoting universal access to prevention, treatment, care and support. As part of its resource mobilization strat-egy, COPRECOS LAC submitted a proposal to the Global Fund to Fight AIDS, Tubercu-losis and Malaria, which was approved in funding Round 9 (2009). The proposal seeks to address identified gaps in HIV response efforts among uniformed services in countries in Latin America and the Caribbean, establishing the sustainability of programmes and ser-vices. The beneficiary countries are Argentina, Plurinational State of Bolivia, Brazil, Colom-bia, Dominican Republic, Ecuador, El Salvador, Guatemala, Haiti, Honduras, Nicaragua, Panama, Paraguay, Peru and Uruguay. The expected outcomes of this regional project are: developing a formal educational programme for police and armed forces training institutes with a gender and human rights approach; reducing stigma and discrimination against pop-ulations at higher risk of HIV exposure; promoting the HIV awareness and strong leadership of high-ranking officials; generating strategic information (second-generation surveillance); institutionally strengthening COPRECOS LAC countries; and promoting male and female condom programmes and voluntary counselling and testing services. Gender has been an important issue COPRECOS LAC has addressed since its inception. Policies and regula-tions related to gender bias, discrimination, harassment and violence in the military and police vary greatly between countries. Each COPRECOS LAC country has had to address the issue of gender with regard to the training, placement, combat and operations, leadership and health care related to women recruits and officers. As such, one of the primary reasons for establishing COPRECOS LAC was to address the effects of HIV on women, especially their reproductive and sexual health as members of the uniformed services, family members or members of the local communities.
Asia and Pacific Regional Network on Police and AIDSIn Asia and the Pacific, where the HIV epidemic is concentrated among well-defined groups of populations at higher risk, the most appropriate regional networks of uniformed ser-vice personnel have involved the police. Law enforcement officers are often in contact with people who inject drugs, men who have sex with men and sex workers, and they can either hamper or support national AIDS programmes depending on how they carry out their law enforcement duties. In 2009, representatives of police from countries of the region estab-lished the Asia and Pacific Regional Network on Police and AIDS. This Network is in the process of defining a regional strategy on how police can create an enabling environment for AIDS programming among populations at higher risk. In 2009, the Secretariat of the Pacific Islands Chiefs of Police conducted the first-ever behavioural research project for police by police. The research is designed to ask questions about the participants’ knowledge, attitudes and behaviour on the following key themes: policing, alcohol, drugs, human rights, HIV and their personal relationships. More than 900 men and women police officers have been involved in the research to date.


A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201056
UN P
hoto
/Mar
co D
orm
ino

Conclusion and recommendations
SECTION
SIX


Conclusion and recommendations
The United Nations, Member States and partners are making good progress in implement-ing United Nations Security Council Resolution 1308 at the international, regional and national levels. During the past five years, UNAIDS, DPKO and partners have succeeded in moving the response to Resolution 1308 from a project approach to a programme approach, integrating HIV interventions within the uniformed services into the national response in countries. However, due to the changing landscape of security threats, the nature of conflicts and the evolving evidence on the relationship between AIDS and security, the premise, the context, the evidence and the response to Resolution 1308 now need to be re-examined in the light of new priorities in the Security Council and the response to AIDS needs to be refocused among uniformed services, to better promote human security and to contribute to building peace.
Findings and recommendationsPeacekeeping, peacebuilding and command-centred approachesThe prevalence of HIV infection among peacekeeping personnel tends to reflect the preva-lence among young men of similar age groups in their countries of origin. The HIV preva-lence in national uniformed services (including national police services) is similar to that of the general population, with some exceptions in countries in sub-Saharan Africa – but not, as was postulated in 2000, 2–5 times higher than in comparable civilian populations. The inci-dence of HIV infection tends to rise with increasing duration of deployment in a duty area. This underlines the need to intensify HIV prevention while personnel are deployed.
Some of the HIV prevention successes in military forces have been achieved through approaches that place responsibility for HIV policy and practice within the army command rather than on the health services alone. Research during the past five years indicates that command-centred approaches to HIV prevention are likely to be more effective in reduc-ing HIV risk among rank and file than solely relying upon education and training based on individual behavioural or medical approaches. A command-centred approach requires systematic assessment of HIV within an institution and the design and adoption of policies that address prevention, treatment, care and support for uniformed services personnel and their families. An essential element of the command-centred approach is the development of lines of accountability and enforcement of mechanisms to prevent sexual violence within military institutions. Also critical is to ensure that the needs of women living with HIV who experienced rape or other sexual violence committed by members of national, regional and multinational forces, be they civilian, police or military, are addressed comprehensively. The Military Institutional Audit and Force Capabilities Framework assessment, as outlined by Cranfield University for the AIDS, Security and Conflict Initiative, includes tools that can support this approach.
Integrating HIV prevention and response into the design and command of AIDS policies in international peace support operations, (which must address issues of pre- and post-deployment testing, including people living with HIV in the forces), should be aligned
A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201060
with the operational demands of the mission and the capacity of troop-contributing coun-tries. In all situations, testing should be accompanied by counselling and treatment refer-ral. Building on the operational tools of a command-centred approach to HIV prevention, DPKO and UNAIDS should consider developing a third tool specific to peace support missions: an HIV security risk assessment to be carried out as part of establishing a peace support mission, performed before deployment or on arrival at the mission area. The DPKO would be responsible for this, but it would be coordinated among actual or poten-tial troop-contributing countries. This tool would map findings from the Force Capabili-ties Framework and Military Institutional Audit tools in the particular operational mandate and locality. The mission would undertake measures to ensure the continuity of AIDS pro-grammes through troop rotations, for example, making sure that best practices are sustained.
For Member States and the United Nations
• Move to military command responsibility for HIV policy development and implemen-tation. This requires developing clear lines of accountability and enforcement mecha-nisms. Accountability for addressing sexual violence should be placed on command structures but also on peer co-responsibility through peer education programmes about sexual violence and human rights.
• The notion of zero tolerance for sexual abuse, both within peace support missions and between peacekeepers and the host population, should be coupled to the agendas of structural prevention and the command-centred approach. Zero tolerance should not be a pretext for a command to halt prevention measures, such as condom distribution, based on a policy of exclusive abstinence.
• The practices of national, regional and United Nations peace support missions should be aligned. The ultimate goal is a universal standard of HIV prevention, treatment, care and support across all troop/police-contributing countries, in accordance with universal access goals. An interim objective is sufficient alignment of policy and prac-tice to enable a common treatment protocol among the different contingents compris-ing a peace support operation. This requires involving commanders and also touches on the issue of mandatory testing. Member States should review their HIV testing and counselling policies to ensure confidentiality and referral to a continuum of care for personnel found to be living with HIV. Members of national uniformed services living with HIV should be deployed based on their fitness to perform duties, with competent medical authorities determining and documenting this fitness.
• The synergy between peacekeeping and peacebuilding should be addressed. There should be increased dialogue amongst partners and institutions with complementary mandates in this area – the United Nations Security Council, the United Nations Peacebuilding Commission, the African Union Peace and Security Council and other regional mechanisms – to address the heightened risks of HIV during post-conflict peacebuilding and to ensure the continuity of HIV prevention during post-conflict transitions, including disarmament, demobilization and reintegration.
Resolution 1308: contributing to United Nations efforts on peacebuilding and preventing violence against womenInsufficient progress has been achieved to ensure that implementing Resolution 1308 is also contributing to United Nations efforts on peacebuilding and preventing violence against women. In accordance with Security Council Resolutions 1325, 1820, 1888 and 1960, there is now an opportunity to scale up and focus these efforts. These efforts need to be aware of the Security Council’s framing of sexual violence as a core civilian protection concern. This view is reflected in successive Security Council resolutions: 1820 (2008), 1888 (2009) and

Conclusion and recommendations 61
1960 (2010). These are historic resolutions: they recognize the relationship between prevent-ing and addressing wartime sexual violence and ensuring sustainable peace and security.
Although there is a better understanding of the conflict and post-conflict continuum as a period of heightened risk for sexual violence and acquiring HIV infection, there is a variance in the findings of the limited research on links between sexual violence and HIV. The AIDS, Security and Conflict Initiative research indicates three central explanations for the dissonance of findings about the reciprocal links between sexual violence and HIV: (1) the underestimation of physiological susceptibility and social risk factors in epidemiological and behavioural models of transmission risk; (2) the absence of reliable baseline and compara-tive data for the incidence and prevalence of both HIV and sexual violence before, during and after conflicts take place; and (3) the lack of agreement on definitions of sexual violence as measurement indicators. Nevertheless the combined effects of sexual violence against girls and women and increased risk of HIV transmission have profound implications for individual and possibly national security.
Recognition must be given to violence, and especially sexual violence, as a physiological and social factor in the risk of HIV transmission and in HIV, humanitarian, public health and security policies. The role of force or coercion should be made explicit in data linking HIV with social and behavioural factors. The prevention of sexual violence and prevention of HIV must be more closely aligned, and preventing sexual violence should be central to AIDS policies and strategies in conflict-affected environments.
Although HIV prevention is often a first-line response to sexual violence by treating sexually transmitted infections, providing post-exposure prophylaxis and other measures, the prevention of sexual violence is rarely considered an entry point for HIV prevention in the context of security and humanitarian responses, including through disarmament, demo-bilization and reintegration programmes and reconstruction and early recovery programmes.
UNAIDS is working as part of United Nations Action against Sexual Violence in Con-flict and being supported by the United States National Institute of Health in convening a scientific research planning meeting to support advancing UNAIDS’ priority commitment to stop violence against women and girls and to align global, regional and national strategies for preventing sexual violence and AIDS. This expert group meeting of leading virologists, epidemiologists, mathematical modellers, social scientists and public health specialists will be convened with the aim of identifying new approaches for assessing the role of sexual violence in HIV risk transmission. The course of this debate, and its conclusions, will have significant implications for the global HIV response, security sector reforms and humanitarian action and should be considered a priority for future work on addressing conflict-related sexual violence and HIV.
For Member States and the United Nations
• HIV prevention strategies should be aligned with preventing and responding to sexual violence against women and girls (and sometimes, boys and men) in conflict.
• Measures and training for preventing sexual violence should be scaled up and inte-grated into policing and law enforcement practices – especially in relation to stig-matized and criminalized activities and populations at higher risk of HIV exposure. Much more work needs to be done as part of policing and law enforcement practices to address the nexus between sexual violence, trafficking of women and girls, trafficking of drugs and the heightened risk of HIV.
• The prevention of sexual violence should be considered an entry point for HIV preven-tion in the context of security and humanitarian responses, including through disar-mament, demobilization and reintegration programmes and reconstruction and early recovery programmes.

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201062
• Uniformed personnel and others should be trained to understand clearly the implica-tions and effects of sexual violence on victims and perpetrators alike.
For the United Nations
• The prevention of conflict-related violence should be better integrated into disarma-ment, demobilization and reintegration programmes. In so doing, care should be accorded to the specific needs of female combatants and girls and women associated with armed forces, including their reproductive health needs.
• Partnerships should be renewed between DPKO and other United Nations and non–United Nations partners to facilitate capacity-building and improve links between HIV prevention, reproductive health promotion and the prevention of sexual and gender-based violence.
• A culture should be developed among peacekeepers that encourages and enables them to act as agents of change for HIV prevention and human rights education in the wider community, enabling them to respond to heightened risks in humanitarian cri-ses, peacekeeping and post-conflict peacebuilding.
Prevention programmes among uniformed servicesHIV prevention among uniformed services personnel has concentrated on providing peer education. This has been supported – albeit unevenly – by service provision, including: HIV testing, antiretroviral therapy, managing sexually transmitted infections and provid-ing condoms. Despite these efforts, high-risk behaviour among uniformed personnel is still widespread. There is still a paucity of strategic information about the effectiveness of HIV prevention programmes among uniformed services and what should constitute a minimum standard package of HIV-related activities and their scope.
For Member States and the United Nations
• Member States still need to implement effective long-term strategies for HIV educa-tion, prevention and treatment of their personnel, with special emphasis on preventing sexual violence against girls and women as an important part of their preparation for peacekeeping operations.
• “Know your HIV risk” should become part of all DPKO missions. As part of a con-solidated approach, standardized behavioural and HIV surveillance methods should be developed and people trained to use them. Knowledge of the effects of alcohol and substance use on HIV high-risk behaviour should be improved among uniformed ser-vice personnel and substance abuse programmes developed.
• The Medical Services Division, Medical Support Section DFS and DPKO databases should be strengthened to report on AIDS-related illnesses according to an agreed template and indicators. Capacity in monitoring and evaluation needs to be built at the mission level by appointing and training monitoring and evaluation officers. This would also support the evaluation of peacekeeping practices to be undertaken at the end of assignments and missions.
• Promote and scale up South–South cooperation (military–military, police–military and civil–military) using best practices on HIV prevention programmes.
AIDS and securityAlthough the AIDS, Security and Conflict Initiative (ASCI) has been able to quell some of the earlier fears about soaring rates of infection among soldiers and the risks posed by HIV to the potential collapse of states, it has also identified very specific implications for the

Conclusion and recommendations 63
operational capacity of armies and police: the role of sexual violence in increasing the risk of HIV transmission, how HIV affects local governance and community survival and the spe-cific HIV-related risks associated with post-conflict transitions. Epidemiological measures of impact – incidence and prevalence – have failed to capture these social and political impli-cations. More attention needs to be paid to how AIDS adversely affects the functioning of local and regional government as well as macro level impacts. Local and regional government structures are important – along with health and police services – in facilitating personal and local security. This evidence indicates (a) the importance of maintaining and expanding antiretroviral therapy; (b) the desirability of further detailed studies of the effects of HIV on local and regional government capacity in circumstances in which (i) the HIV prevalence exceeds 5% in the general population and (ii) budgetary and human resource constraints already compromise the capabilities of local and regional government.
Post-conflict transitions are both a period of heightened vulnerability to HIV trans-mission and a neglected element in AIDS policy and programming. Greater policy attention and service continuity is needed in post-conflict situations to respond to the complexities of context, increased population mobility, the demobilization of combatants, disruptions in the provision of humanitarian assistance to displaced people and refugees in camp settings and the overloading of health and social services in areas of population return. Disarmament, demobilization and reintegration programmes are an important and consistently overlooked focus for HIV prevention and response, especially among military and extended families and women and children associated with armed forces.
For Member States and the United Nations
• Further empirical research is required to better measure and more effectively respond to the relationships between AIDS, conflict and state fragility. Further studies are also needed on the relationship between HIV morbidity and mortality and the competence and capacity of local and regional authorities in Member States, and such studies need to be given priority when the HIV prevalence in the general population reaches or exceeds 5%.
• Major policy gaps in responding to AIDS and security should be addressed. There are currently substantial HIV policy and programmatic gaps and discontinuities during post-conflict transitions between emergency assistance and reconstruction and devel-opment efforts.
• Interventions related to AIDS should start in crisis settings as part of early recovery programmes, and disarmament, demobilization and reintegration should be the entry point for institutionalizing these policies and practices.
• The capacity of relevant agencies and partners to incorporate HIV interventions within disarmament, demobilization and reintegration programming should be strengthened through appropriate staffing, training and resource mobilization.
Police and other uniformed servicesHIV prevention efforts have neglected police and other law enforcement and uniformed ser-vices personnel, including customs, navy, immigration and corrections. The risks of HIV transmission, especially in epidemics concentrated among people who inject drugs and sex workers, are influenced by law enforcement practices and, in turn, by the drug trade and human trafficking and by the people who control sex work, including pimps, “protectors”, traffickers and long-term clients. Cross-border issues, including the trafficking of women, the drug trade and sexual exploitation and abuse at border-crossing points, are all related to the risks of HIV transmission. The previously underestimated role of some groups of law enforce-ment personnel as core group transmitters or maintaining populations warrants further explo-

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201064
ration. Bilateral or multilateral exchange and cooperation is a prerequisite for addressing these questions, and borders should be a special focus for HIV efforts. The nexus between HIV/AIDS, the international trade in illicit drugs, related sex trafficking activities, drug use and the emergence of “narco states” in several parts of the world demands particular attention.
For Member States
• Laws to combat and criminalize discrimination and violence against populations at higher risk of HIV exposure should be enforced. To this end, law enforcement officers should be trained and enabled to defend human rights, especially when reaching out to women and populations at higher risk such as sex workers, men who have sex with men, people who inject drugs and migrants.
For Member States and the United Nations
• More focus on AIDS should be placed across borders and in relation to traffic and trade. Particular attention needs to be paid to the security concerns related to the nexus between policing, AIDS, the international trade in illicit drugs, related sex trafficking activities, drug use and violence against women
Overall recommendationA new agenda for United Nations Security Council Resolution 1308 is needed. It should consider the changed context and new evidence that has emerged since Resolution 1308 was adopted with a view to enhancing existing programmes to more effectively prevent HIV, ensure security and build peace.

References
Abebe Y et al. (2003). HIV prevalence in 72,000 urban and rural male army recruits, Ethio-pia. AIDS, 17:1835–1840.
Adlington R, Burnett A (2004). Sexually transmitted infections as a consequence of rape. In: Peel M, ed. Rape as a method of torture. London, Medical Foundation for the Care of Victims of Torture:147–166.
AIDS, Security and Conflict Initiative (2009). HIV/AIDS, security and conflict: new reali-ties, new responses. New York, Social Science Research Council (SSRC) and the Neth-erlands Institute of International Relations, AIDS, Security and Conflict Initiative (http://asci.researchhub.ssrc.org, accessed 15 April 2011).
AIDS, Security and Conflict Initiative [web site] (2011). New York, AIDS, Security and Conflict Initiative (http://asci.researchhub.ssrc.org, accessed 15 April 2011).
Anastario MP, Tavarez MI, Chun H. Sexual risk behaviour among military personnel sta-tioned at border-crossing zones in the Dominican Republic. Revista Panamericana de Salud Pública/Pan American Journal of Public Health, 2010, 28:361–367.
Ba O et al. (2008). HIV/AIDS in African militaries: an ecological analysis. Medicine, Con-flict and Survival, 24:88–100.
Baliunas D et al. (/2010). Alcohol consumption and risk of incident human immunodefi-ciency virus infection: a meta-analysis. International Journal of Public Health, 55:159–166.
Barnett T, Dutta I (2008). HIV and state failure: is HIV a security risk? New York, AIDS, Security and Conflict Initiative.
Barnett T, Prins G (2006). HIV/AIDS and security: fact, fiction and evidence; a report to UNAIDS. International Affairs, 82:359–368.
Barnett T, Weston M (2008). Health, wealth, HIV and the economics hope. AIDS, 2(Suppl. 2):S27–S34.
Bing EG et al. (2008). Evaluation of a prevention intervention to reduce HIV risk among Angolan soldiers. AIDS Behaviour, 12:384–395.
Chirambo K, Steyn J (2009). AIDS and local government in South Africa. Pretoria, Institute for Democracy in South Africa.
Commission on Social Determinants of Health (2008). Closing the gap in a generation: health equity through action on the social determinants of health. Final report of the Commission on Social Determinants of Health. Geneva, World Health Organiza-tion (http://www.who.int/social_determinants/resources/gkn_lee_al.pdf, accessed 17 August 2010).
Cornman DC (2010). Behavioural HIV prevention interventions [slide presentation]. 2010 International Military HIV/AIDS Conference, Arusha, United Republic of Tanzania, 12–15 April 2010.
Dieng MK (2008). National survey on combined surveillance of STI and HIV/AIDS in the Senegalese Armed Forces [slide presentation]. 7th Annual Defence Institute for Medi-cal Operations HIV/AIDS Strategic Planning and Policy Course, San Antonio, Texas, December 2008.
DPKO (2005). Statement by Mr Jean-Marie Guehenno, Under Secretary General of the Department of Peacekeeping Operations on the implementation of Resolution 1308

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201066
(2000) on HIV/AIDS and international peacekeeping. New York, United Nations DPKO, 2005 (http://www.un.org/en/peacekeeping/articles/article180705.htm, accessed 15 April 2011).
DPKO (2010). Monthly summary of military and police contribution to United Nations operations. New York, United Nations (http://www.un.org/en/peacekeeping/contribu-tors/06-08.shtml).
East African Community (2010). East African Community Armed Forces Regional Work-shop on HIV and AIDS Prevention and Mainstreaming in the Peace and Security Sec-tors. Report of the Workshop held at the Serena Hotel, Kigali, Rwanda, 22–24 March 2010. Arusha, United Republic of Tanzania, EAC Secretariat.
G8 (2008). Progress report by the G8 Africa Personal Representatives (APRs) on imple-mentation of the Africa Action Plan. Tokyo, Group of 8 (G8) industrialized countries (http://www.mofa.go.jp/POLICY/economy/summit/2008/doc/pdf/0708_10_en.pdf, accessed 15 April 2011).
International Centre for Ethnic Studies (2009). A survey of HIV/AIDS awareness and risky sexual behaviour in a vulnerable population in Sri Lanka. New York, AIDS, Security and Conflict Initiative (ASCI Research Report No. 22).
Iqbal Z, Zorn C (2010). Violent conflict and the spread of HIV/AIDS in Africa. Journal of Politics, 72:149–162.
Kaul I, Grunberg I, Stern M, eds. (1999). Global public goods: international cooperation in the 21st century. New York, Oxford University Press.
Kenny L (2009). Towards universal access to integrated HIV prevention, treatment, care and support: militaries and other uniformed services [slide presentation]. 38th Interna-tional Congress on Military Medicine, Kuala Lumpur. Geneva, UNAIDS.
Kershaw RJ (2008). The impact of HIV/AIDS on the operational effectiveness of military forces. New York, AIDS, Security and Conflict Initiative (ASCI Research Report No. 4; http://asci.researchhub.rc.org/working-papers/Kershaw.pdf, accessed 15 April 2011).
Kruijt D, Balconi J (2008). HIV/AIDS and the Central American uniformed services. New York, AIDS, Security and Conflict Initiative (ASCI Research Report No. 3; http://asci.researchhub.ssrc.org/ hiv-aids-and-the-central-american-uniformed-services/attach-ment, accessed 15 April 2011).
Kusasira S (2010). The importance and implications of knowing the HIV epidemic in the military: the Uganda Peoples’ Defence Forces [slide presentation]. 2010 International Military HIV/AIDS Conference, Arusha, United Republic of Tanzania, 12–15 April 2010.
Likimani S (2007a). Medical and public health implications of HIV and AIDS in peace-keeping: field evaluation and analysis. Unpublished, DPKO.
Likimani S (2007b). Some implications of HIV at peacekeeping missions [slide presenta-tion]. DPKO Training Workshop on HIV/AIDS, Brindisi, Italy August 2007.
Lowicki-Zucca M, Karmin S, Dehne K-L (2009). HIV among peacekeepers and its likely impact on prevalence on host countries’ HIV epidemics. International Peacekeeping, 216:352–363.
Rawls J (1993). Political liberalism. New York, Columbia University Press.Sato A (2008). Is HIV/AIDS a threat to security in fragile states? New York, AIDS, Security
and Conflict Initiative, Social Science Research Council (ASCI Research Report No. 10).Secretary-General of the United Nations (2009). Women and peace and security: report of
the Secretary-General. New York, United Nations (S/2009/465).Garrett L (2005). HIV and national security: where are the links? New York, Council on
Foreign Relations.Seeley J (2011). The longitudinal impact of HIV/AIDS on agriculture and rural livelihoods
in Uganda: framing paper. Swindon, Economic and Social Research Council.

Conclusion and recommendations 67
Seeley J, Dercon S, Barnett T (2010). The effects of HIV/AIDS on rural communities in East Africa: a 20-year perspective. Tropical Medicine and International Health, 15:329–335.
Sen A (1999). Development as freedom. New York, Alfred A. Knopf.Sexual Violence Research Initiative (2007). Sexual violence and HIV. Pretoria, Sexual Vio-
lence Research Initiative.Shuper PA et al. (2009). Alcohol as a correlate of unprotected sexual behaviour among people
living with HIV/AIDS: review and meta-analysis. AIDS Behavior, 13:1021–1036.Sommers MS et al. (2006). The effects of age and ethnicity on physical injury from rape.
Journal of Obstetric, Gynecologic and Neonatal Nursing, 35:199–207.Tiroyamodimo O (2010). The importance and implications of knowing the HIV epidemic
in the military: Botswana Defence Force [slide presentation]. 2010 International Mili-tary HIV/AIDS Conference, Arusha, United Republic of Tanzania, 12–15 April 2010.
Tomczyk B (2007). Overview of HIV/AIDS knowledge, attitude and practice survey con-ducted among United Nations peacekeepers in Haiti [slide presentation]. New York, United Nations DPKO.
Tomczyk B et al. (2007). Results from a HIV/AIDS knowledge, attitude and practice survey conducted among United Nations peacekeepers in Haiti April to May 2007. New York, United Nations DPKO.
UNAIDS (1998). AIDS and the military: UNAIDS point of view. Geneva, UNAIDS (UNAIDS Best Practice Collection: Point of View; http://data.unaids.org/Publica-tions/IRC-pub05/militarypv_en.pdf, accessed 15 April 2011).
UNAIDS (2003). Fighting AIDS: HIV and AIDS prevention and care among armed forces and peacekeepers: the case of Eritrea. Geneva, UNAIDS (http://data.unaids.org/Pub-lications/IRC-pub05/armed_forces_eritrea_en.pdf, accessed 15 April 2011).
UNAIDS (2005a). Statement to the United Nations Security Council by Dr Peter Piot, UNAIDS Executive Director and Under Secretary-General of the United Nations, New York, 18 July 2005.
Geneva, UNAIDS (http://data.unaids.org/Media/Speeches02/sp_security_18july05_en.pdf, accessed 15 April 2011).
UNAIDS (2005b). On the front line: a review of policies and programmes to address HIV/AIDS among peacekeepers and uniformed services. Geneva, UNAIDS (http://data.unaids.org/UNA-docs&/report_shr_onfrontline_18july05_en.pdf, accessed 15 April 2011).
UNAIDS (2010). UNAIDS report on the global AIDS epidemic. Geneva, UNAIDS (http://www.unaids.org/globalreport/Global_report.htm, accessed 15 April 2011).
UNAIDS (2011). Monitoring country progress [web site]. Geneva, UNAIDS (http://www.unaids.org/en/dataanalysis/monitoringcountryprogress, accessed 15 April 2011).
UNAIDS India (2010). Changing attitudes, giving direction: a case study of DISHA Jana Kalyan Kendra, Asansol. Delhi, UNAIDS, 2010.
UNAIDS Regional Support Team for Latin America (2010). Regional report on HIV and security in Latin America and the Caribbean. Panama, UNAIDS Regional Support Team for Latin America.
United Nations Development Programme (2010). Bringing HIV related issues into humani-tarian instruments. New York, UNDP, 2010.
United Nations Medical Directors (2008). Position statement on HIV/AIDS. New York, United Nations Medical Directors, 2008.
United Nations Population Fund (2008). Working with the Uniformed Services Consulta-tion. Final report. Kyiv, Ukraine, 29 September–3 October 2008. New York, United Nations Population Fund.
United Nations Population Fund (2009a). Working with uniformed services to promote reproductive health and prevent HIV: UNFPA experience. Report. New York, UNFPA.

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201068
United Nations Population Fund (2009b). Working with uniformed services to promote reproductive health and prevent HIV: UNFPA experience. Fact sheet. New York, UNFPA.
United Nations Population Fund (2010). Unified Budget and Work plan broad activity implementation – biennial report (2008–2009). New York, UNFPA, 2010.
United Nations Security Council (2000). Resolution 1325. New York, United Nations. (http://www.un.org/events/res_1325e.pdf, accessed 15 April 2011).
United Nations Security Council (2008). Resolution 1820. New York, United Nations (http://daccess-dds-ny.un.org/doc/UNDOC/GEN/N08/391/44/PDF/N0839144.pdf?OpenElement, accessed 15 April 2011).
United Nations Security Council (2009a). Resolution 1888. New York, United Nations (http://www.un.org/News/Press/docs/2009/sc9753.doc.htm, accessed 15 April 2011).
United Nations Security Council (2009b). Resolution 1889. New York, United Nations, (http://www.un.org/News/Press/docs/2009/sc9759.doc.htm, accessed 15 April 2011).
United States Department of Defence HIV/AIDS Prevention Programme (2009). Military HIV Prevention Conference: Militaries Leading Prevention Efforts to Fight HIV/AIDS. Conference Report, Co-sponsored by: Department of Defence (DoD) HIV/AIDS Prevention Programme and Botswana Defence Force, Gaborone, Botswana, 2-5 March 2009.
United States Department of Defence HIV/AIDS Prevention Programme (2011). Depart-ment of Defence HIV/AIDS Prevention Programme (DHAPP) 2010 annual report. San Diego, CA, United States Department of Defence HIV/AIDS Prevention Pro-gramme.
United States National Intelligence Council (2000a). The global infectious disease threat and its implications for the United States. Washington, DC, United States National Intelligence Council (http://www.fas.org/irp/nic/infectious_diseases_paper.html, accessed 15 April 2011).
United States National Intelligence Council (2000b). Global trends 2015: a dialogue about the future with nongovernment experts. Washington, DC, United States National Intelligence Council.
United States National Intelligence Council (2002). The next wave of HIV/AIDS: Nigeria, Ethiopia, Russia, India, and China. Washington, DC, United States National Intelli-gence Council (http://www.dni.gov/nic/special_nextwaveHIV.html, accessed 15 April 2011).
Whiteside A, de Waal A, Gebre-Tensae (2006). AIDS, security and the military in Africa: a sober appraisal. African Affairs, 105(419):201–218.
WHO and Global Coalition on Women and AIDS (2004 ). Intimate partner violence and HIV/AIDS. Geneva, World Health Organization (http://www.who.int/hac/techguid-ance/pht/InfoBulletinIntimatePartnerViolenceFinal.pdf, accessed 15 April 2011).
WHO and UNAIDS (2009). Progress in male circumcision scale-up: country implemen-tation update. Geneva, World Health Organization (http://www.who.int/hiv/pub/malecircumcision/mc_update_2009.pdf, accessed 15 April 2011).
Bibliography
De Waal A (2010). HIV/AIDS and the challenges of security and conflict. Lancet, 375: 22–23.
DPKO (2004). HIV testing policy for uniformed peacekeepers. New York, United Nations DPKO.
DPKO (2007). Briefing note: reconciling the availability of condoms and the policy of zero-tol-erance in United Nations peacekeeping operations. New York, United Nations DPKO.
DPKO (2007). Provision of voluntary confidential counselling and testing in UN peace-keeping missions: survey of practice. New York, United Nations DPKO.
DPKO (2007). DPKO-DFS Policy Directive: the role and function of HIV/AIDS units in UN peacekeeping operations. New York, United Nations DPKO-DFS.
DPKO (2008). Basic pre-deployment training on HIV for UN peacekeepers. Module 16A of the United Nations Standardized Generic Training Module for Peacekeepers. Back-ground notes. New York, United Nations DPKO-DFS.
DPKO (2008). Basic pre-deployment training on HIV for UN peacekeepers [slide presenta-tion]. Module 16A of the United Nations Standardized Generic Training Module for Peacekeepers. New York, United Nations DPKO-DFS.
DPKO (2009). Maintaining confidentiality of personal health information: responsibility of key personnel in safeguarding private health information of United Nations personnel. New York, United Nations DPKO.
DPKO (2009). HIV voluntary confidential counselling and testing manual. New York, United Nations DPKO.
DPKO (2009). HIV voluntary confidential counselling and testing: Counselling Training Programme. Training report, Nairobi, Kenya, 24 to 29 May 2009. New York, United Nations DPKO.
DPKO (2009). HIV voluntary confidential counselling and testing: Counselling Training Programme. Training report, Kathmandu, Nepal, 8 to 14 November 2009. New York, United Nations DPKO.
DPKO (2010). Monthly summary of military and police contribution to United Nations operations. New York, United Nations DPKO (http://www.un.org/en/peacekeeping/contributors/documents/Yearly06.pdf, accessed 15 April 2011).
DPKO (2010). Gender statistics by mission. New York, United Nations DPKO (http://www.un.org/en/peacekeeping/contributors/gender/2009gender/dec09.pdf, accessed 15 April 2011).
DPKO (2010). HIV community of practice. New York, United Nations DPKO (http://www.peacekeepingbestpractices.unlb.org/PBPS/Pages/Public/search.aspx, accessed 15 April 2011).
European Centre for Disease Prevention and Control and WHO Regional Office for Europe (2009). HIV/AIDS surveillance in Europe 2008. Stockholm, European Centre for Disease Prevention and Control.
Felix JM (2010). Together in the defence of health: HIV counselling and testing campaign within the military in Mozambique [slide presentation]. 2010 International Military HIV/AIDS Conference, Arusha, United Republic of Tanzania, 12–15 April 2010.

A review of programmes that address HIV among international peacekeepers and uniformed services 2005–201070
Global Task Force on HIV among Uniformed Services (2007). Minutes of meeting 6–7 December 2007. Geneva, Global Task Force on HIV among Uniformed Services, 2007.
Musavengana T, Oxche T-R, Ndung’u I, eds. (2009). HIV and AIDS and the African mili-tary. Towards a common and comprehensive approach. Conference report. 11–13 March 2009, Jinja, Uganda. Pretoria, Institute for Security Studies.
Pearce H (2007). The police and HIV/AIDS: a literature review. New York, AIDS, Secu-rity and Conflict Initiative (ASCI Research Report No. 1, 2007; http://asci.research-hub.ssrc.org/the-police-and-hiv-aids-a-literature-review/attachment, accessed 15 April 2011).
Sayed O, Gutbi A (2010). Knowledge, attitude and practice survey on HIV. UNAMID Uniformed Peacekeepers in Darfur, Sudan.
Singh M (2010). Surveillance: HIV/AIDS scenario, Indian Armed Forces. 2010 Interna-tional Military HIV/AIDS Conference, Arusha, United Republic of Tanzania, 12–15 April 2010.
South African Development Community (2009). Regional minimum standards for har-monised control of HIV and AIDS, malaria and tuberculosis among SADC militaries. Gaborone, Botswana, Policy Development and Harmonisation, Directorate for Social and Human Development and Special Programmes, South African Development Community Secretariat.
South African Development Community (2009). Assessment report on status of HIV and AIDS, malaria and tuberculosis policies for the SADC militaries. Gaborone, Botswana, Policy Development and Harmonisation, Directorate for Social and Human Develop-ment and Special Programmes, South African Development Community Secretariat.
Tassie J-M. (2010). Second generation surveillance: overview [slide presentation]. Made on behalf of the UNAIDS/WHO Working Group on Global HIV/AIDS and STI Sur-veillance. 2010 International Military HIV/AIDS Conference, Arusha, United Repub-lic of Tanzania, 12–15 April 2010.
UNAIDS (2007). Safe, voluntary, informed male circumcision and comprehensive HIV prevention programming: guidance for decision-makers on human rights, ethical and legal considerations. Geneva, UNAIDS.
UNAIDS (2009). Joint action for results: UNAIDS outcome framework, 2009–2011. Geneva, UNAIDS (http://data.unaids.org/pub/Report/2010/jc1713_joint_action_en.pdf, accessed 15 April 2011).
UNAIDS (2010). UNAIDS Global report on the AIDS epidemic. Geneva, UNAIDS (http://www.unaids.org/globalreport).
United Nations (2001). Cooperation framework between the Joint United Nations Pro-gramme on HIV/AIDS (UNAIDS) and the United Nations Department of Peace-keeping Operations. New York, United Nations, 2001.
United Nations (2005). Statement by the President of the Security Council (S/PRST/2005/33). New York, United Nations, 2005.
United Nations (2010). The Millennium Development Goals report 2010. New York, United Nations, 2010.
United Nations Action against Sexual Violence in Conflict (2010). Women, peace and secu-rity: sexual violence in situations of armed conflict. Statement by the United Nations Special Representative of the Secretary General, Margot Wallström, to the United Nations Security Council Open Meeting, New York, 27 April 2010. New York, United Nations Action against Sexual Violence in Conflict.