Epidermal growth factor-related peptides and their receptors in human malignancies
Upload
independentCategory
view
2download
0
J Cutan Pathol 2012: 39: 971–976doi: 10.1111/j.1600-0560.2012.01978.xJohn Wiley & Sons. Printed in Singapore
Copyright © 2012 John Wiley & Sons A/S
Journal ofCutaneous Pathology
Leukemia cutis in association withcutaneous epidermal malignancies
Background: Epidermal malignancies developing in association withhematolymphoid malignancies are exceptional. Only one prior case ofmyeloid leukemia cutis with a cutaneous epidermal malignancy hasbeen reported.Methods: We report two cases; one occurred in association withsquamous cell carcinoma (SCC) and another with basal cell carcinoma(BCC).Results: Both patients were 83-year-old males without establishedhistories of systemic hematopoietic disorders; one presented with anerythematous papule on the right upper back and the other with anodule on the left wrist. One biopsy revealed nodular BCC with anassociated perivascular myeloid leukemic infiltrate showingimmunohistochemical positivity for CD43 and CD45. The other biopsyshowed SCC associated with a leukemic infiltrate in sheets with myeloidblasts, eosinophilic myelocytes and maturing myeloid precursors. Themyeloid cells showed immunohistochemical expression of CD43,CD68, CD33, CD117 and myeloperoxidase. Both patients hadmyeloblasts on peripheral blood smear. One patient declined furthertreatment and died of disease 5 weeks after the initial biopsy. The otherpatient underwent chemotherapy and is alive after 6 months.Conclusion: Although most inflammatory infiltrates associated withcutaneous epidermal malignancies are reactive, careful examination isnecessary to exclude systemic hematopoietic disease, especially inelderly patients.
Keywords: basal cell carcinoma, collision tumors, leukemia cutis,squamous cell carcinoma
Ra S, Su A, Ellison D, Koperski J, Bonilla M, Robbins B. Leukemiacutis in association with cutaneous epidermal malignancies.J Cutan Pathol 2012; 39: 971–976. © 2012 John Wiley & Sons A/S.
Seong Ra1,2, Albert Su2,Doug Ellison1, JudithKoperski3, Maria Bonilla4 andBruce Robbins1
1San Diego Pathologists Medical Group, SanDiego, CA, USA,2Department of Pathology, UCLA MedicalCenter, Los Angeles, CA, USA,3Dermatologists Medical Group Encinitas,San Diego, CA, USA, and4Torrey Pines Dermatology, San Diego, CA,USA
Seong Ra, MD,San Diego Pathologists Medical Group, Inc.,7592 Metropolitan Drive, Suite 405/406,San Diego, CA 92108, USATel: +1 619 297 4900Fax: +1 619 297 5460e-mail: [email protected]
Accepted for publication May 28, 2012
Epidermal malignancies in association with hema-tolymphoid malignancies are exceptional. Mostof these cases involve chronic lymphocyticleukemia/small lymphocytic lymphoma accom-panying a cutaneous epidermal malignancy.1– 3
Epidermal proliferations/carcinomas have also beenreported accompanying CD30-positive lymphopro-liferative disorders and T-cell lymphomas.4– 7 Onlyone prior case of myeloid leukemia cutis in associationwith a cutaneous epidermal malignancy [basal cellcarcinoma (BCC)] has been reported.8 We review the
clinicopathologic features of two cases: one with squa-mous cell carcinoma (SCC) and another with BCC.
Materials and methodsBoth cases were retrieved from the surgical pathologyfiles of San Diego Pathologists Medical Group, Inc.Clinical and follow-up information were obtainedfrom the referring physicians. The surgical specimenswere fixed in 10% buffered formalin and representa-tive sections were routinely processed and embedded
971
Ra et al.
A B C
D E F
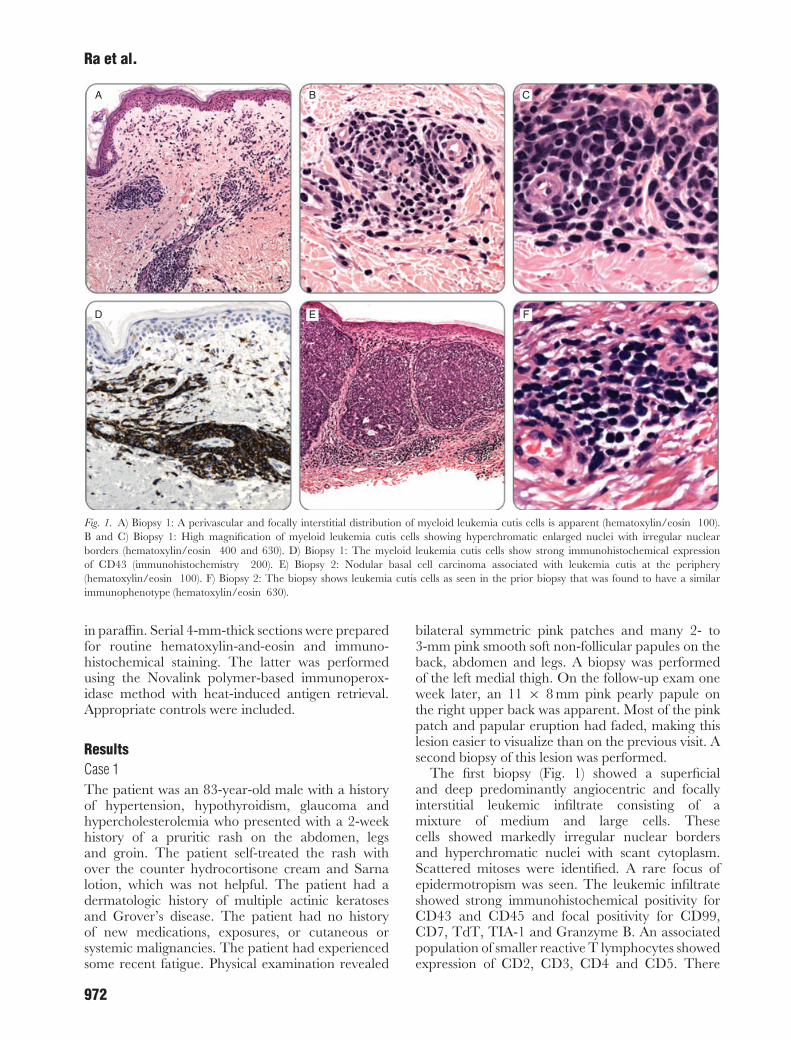
Fig. 1. A) Biopsy 1: A perivascular and focally interstitial distribution of myeloid leukemia cutis cells is apparent (hematoxylin/eosin 100).B and C) Biopsy 1: High magnification of myeloid leukemia cutis cells showing hyperchromatic enlarged nuclei with irregular nuclearborders (hematoxylin/eosin 400 and 630). D) Biopsy 1: The myeloid leukemia cutis cells show strong immunohistochemical expressionof CD43 (immunohistochemistry 200). E) Biopsy 2: Nodular basal cell carcinoma associated with leukemia cutis at the periphery(hematoxylin/eosin 100). F) Biopsy 2: The biopsy shows leukemia cutis cells as seen in the prior biopsy that was found to have a similarimmunophenotype (hematoxylin/eosin 630).
in paraffin. Serial 4-mm-thick sections were preparedfor routine hematoxylin-and-eosin and immuno-histochemical staining. The latter was performedusing the Novalink polymer-based immunoperox-idase method with heat-induced antigen retrieval.Appropriate controls were included.
ResultsCase 1The patient was an 83-year-old male with a historyof hypertension, hypothyroidism, glaucoma andhypercholesterolemia who presented with a 2-weekhistory of a pruritic rash on the abdomen, legsand groin. The patient self-treated the rash withover the counter hydrocortisone cream and Sarnalotion, which was not helpful. The patient had adermatologic history of multiple actinic keratosesand Grover’s disease. The patient had no historyof new medications, exposures, or cutaneous orsystemic malignancies. The patient had experiencedsome recent fatigue. Physical examination revealed
bilateral symmetric pink patches and many 2- to3-mm pink smooth soft non-follicular papules on theback, abdomen and legs. A biopsy was performedof the left medial thigh. On the follow-up exam oneweek later, an 11 × 8 mm pink pearly papule onthe right upper back was apparent. Most of the pinkpatch and papular eruption had faded, making thislesion easier to visualize than on the previous visit. Asecond biopsy of this lesion was performed.
The first biopsy (Fig. 1) showed a superficialand deep predominantly angiocentric and focallyinterstitial leukemic infiltrate consisting of amixture of medium and large cells. Thesecells showed markedly irregular nuclear bordersand hyperchromatic nuclei with scant cytoplasm.Scattered mitoses were identified. A rare focus ofepidermotropism was seen. The leukemic infiltrateshowed strong immunohistochemical positivity forCD43 and CD45 and focal positivity for CD99,CD7, TdT, TIA-1 and Granzyme B. An associatedpopulation of smaller reactive T lymphocytes showedexpression of CD2, CD3, CD4 and CD5. There
972

Leukemia cutis associated with BCC and SCC
A B C
D E F
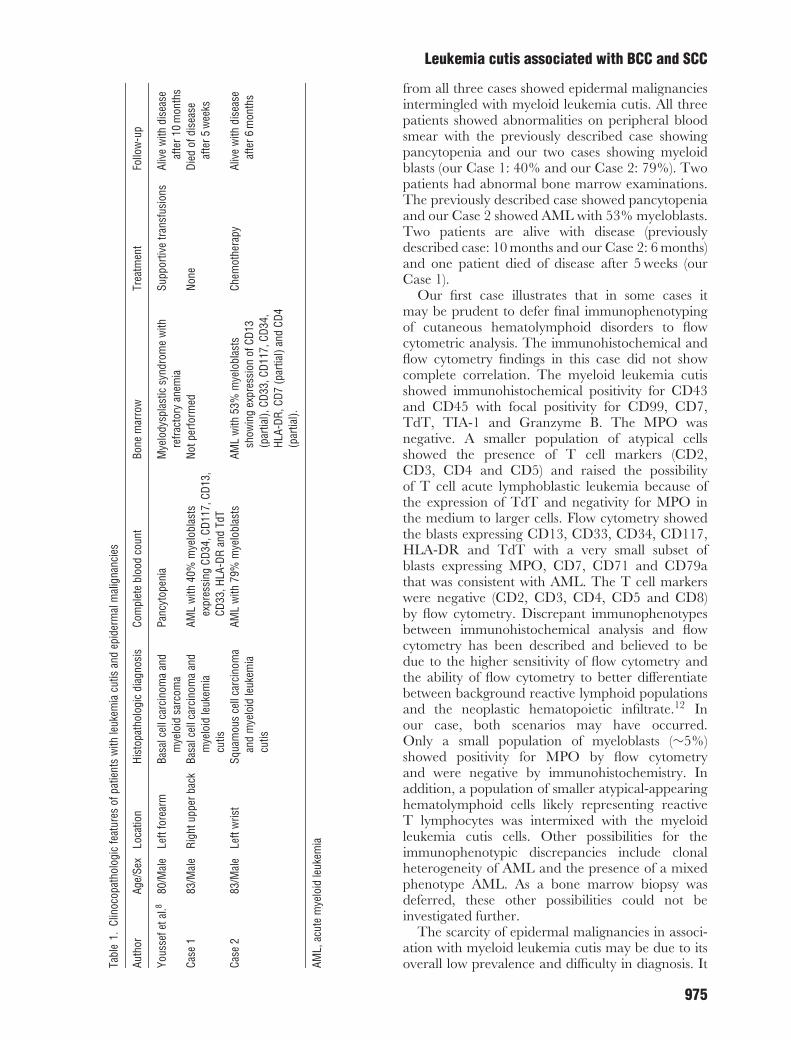
Fig. 2. A and B) Infiltrating keratinizing nests of squamous cell carcinoma in association with sheets of myeloid leukemia cutis cells(hematoxylin/eosin 50 and 100). C) Sheets of leukemia cutis cells (hematoxylin/eosin 200). D) The myeloid leukemia cutis cells show strongimmunohistochemical expression of myeloperoxidase (immunohistochemistry 200). E) High magnification of an invasive nest of squamous cellcarcinoma surrounded by sheets of myeloid leukemia cutis cells (hematoxylin/eosin 400). F) High magnification shows myeloid leukemia cutiscells with myeloblasts showing enlarged vesicular nuclei with irregular nuclear membranes and prominent nucleoli. Eosinophilic myelocytesand maturing myeloid precursors are also noted (hematoxylin/eosin 630).
was no significant immunohistochemical expressionof CD20, PAX-5, CD79a, CD8, CD30, CD68,CD163, myeloperoxidase (MPO), CD33, CD56,Alk-1, CD117 and CD10. The Ki-67 proliferationindex was ∼10%.
The second biopsy (Fig. 1) showed an epidermal-based proliferation of basal cells with prominentperipheral palisading and associated mucinousstroma. Large nodules of neoplastic basal cells withoccasional cystic change were seen within the dermis.Prominent intratumoral apoptoses and rare mitoseswere identified. Solar elastosis of the dermis wasnoted. An associated angiocentric leukemic infiltratecharacterized by medium to large sized cells withirregular nuclear borders, open chromatin andscant cytoplasm was seen at the periphery. Raremitoses were identified. No epidermotropism wasseen. Immunohistochemical stains showed a similarimmunophenotype as the prior biopsy.
Due to the initial biopsy findings, the patient wasreferred to an oncologist who initiated a systemicwork up. A peripheral blood smear showed acute
myelogenous leukemia (AML) with 40% myeloblaststhat showed expression of CD34, CD117, CD13,CD33, HLA-DR and TdT on flow cytometry. Avery small subset of blasts (∼5%) were positive forMPO, CD7, CD71 and CD79a. The patient declinedfurther treatment and died of disease 5 weeks fromthe time of the initial biopsy.
Case 2The patient was an 83-year-old male who presentedwith a 1.2 cm enlarging pruritic nodule of theleft wrist. He had reported a possible arthropodbite at the site approximately 1 month before.The patient did not have prior history ofmalignancy. A biopsy was performed (Fig. 2) thatrevealed SCC surrounded by sheets of a leukemicinfiltrate. The SCC was characterized by varyingsized infiltrating nests of neoplastic keratinocyteswithin the dermis. Some of the nests showedprominent keratinization and invaded to a depthof at least 3 mm. The neoplastic keratinocytes
973

Ra et al.
showed variation in size and shape of nucleiwith some displaying prominent nucleoli. Scatteredmitoses were seen. Solar elastosis was noted. Theleukemic infiltrate consisted of immature largemyeloid precursors showing prominent nucleoliwith vesicular chromatin and granular cytoplasm.Occasional eosinophilic myelocytes were identified.Focal maturing myeloid precursors were seen.Scattered mitoses were noted. The leukemic cellsshowed immunohistochemical expression of CD43,MPO, CD33, CD117 and CD34 (weak, focal). Therewas no immunohistochemical expression for CD3and CD20.
Due to the biopsy findings, the patient was referredto an oncologist who initiated a systemic work up.A peripheral blood smear showed 79% myeloblasts.A bone marrow biopsy showed 53% myeloblastsshowing flow cytometric expression of CD13 (partial),CD33, CD117, CD34, HLA-DR, CD7 (partial) andCD4 (partial). Only limited follow up information isavailable; however, the patient was alive 6 monthsafter the biopsy and had undergone at least tworounds of chemotherapy.
DiscussionWe herein describe the clinicopathologic features oftwo cases of myeloid leukemia cutis in associationwith epidermal malignancies. The presence of thesemalignancies within a single biopsy may be achance occurrence and represent a collision tumor.Alternatively, a relationship exists between the twomalignancies where one component induces/drivesthe proliferation of the other. These two possibilitiesare explored.
Cutaneous collision tumors show the presenceof more than one neoplasm in a single cutaneousspecimen and are scarce with one of the largeststudies documenting 69 cases out of over 40,000 cases(<0.2%).9 Collision tumors are thought to occur bychance occurrence and typically involve commoncutaneous lesions. The most common lesions foundby Boyd et al.9 were nevus and seborrheic keratosis,BCC and nevus, BCC and seborrheic keratosis, andactinic keratosis and nevus.
The presence of collision tumors involving thepresence of leukemia cutis is exceptional withmost of the described cases involving chroniclymphocytic leukemia/small lymphocytic lymphomain association with BCC and SCC.1– 3 The presenceof a collision tumor composed of these entitiesseems logical as chronic lymphocytic leukemia/smalllymphocytic lymphoma is the most commonleukemia/lymphoma in adults in western nations10
and BCC and SCC are the most frequent types ofnon-melanoma skin cancers.11 Patients with chronic
lymphocytic leukemia/small lymphocytic lymphomaare reported to have an eight fold increased riskfor developing non-melanoma skin cancers probablysecondary to antecedent immune dysfunction.3 Mostpatients are typically known to have a priordiagnosis; however, in some cases, the diagnosis isunknown.1
Epidermal proliferations/carcinomas have alsobeen described in association with CD30-positivelymphoproliferative disorders and some cutaneousT-cell lymphomas.5– 7 Rather than occurring bychance, some believe that the hematolymphoidmalignancy is driving the proliferation of the epider-mal component. One purported epithelial inductionmechanism includes the production of local factorsby the hematolymphoid component including epi-dermal growth factor, transforming growth factor,fibroblast growth factor and platelet-derived growthfactor.5– 7 Also, the production of certain cytokineshas been hypothesized to inhibit apoptotic home-ostatic mechanisms within keratinocytes throughinhibiting the binding of CD95 with its ligand.5
Alternatively, the cutaneous epidermal malignancymay attract the hematolymphoid malignancy. Inchronic lymphocytic leukemia/small lymphocyticlymphoma, it has been thought that the epidermalmalignancy can express specific tumor antigens thatcan draw neoplastic lymphocytes. Another explana-tion is that the neoplastic lymphocytes may be partof a generalized immune response to the epidermalmalignancy.3
Both of our cases show the presence of more thanone neoplasm within a single cutaneous specimenand would arguably qualify as cutaneous ‘collisiontumors’. However, true collision tumors are thoughtto occur by chance. If a possible link exists betweenthe two malignancies, then some believe that thesewould not qualify as true collision tumors. Also, inCase 1, the patient had a high burden of myeloidleukemia cutis that may have been present inreaction to any skin lesions or in normal appearingskin. The myeloid leukemia cutis would have beenmore of an ‘innocent bystander’ if this was the case.However, without additional biopsies this conceptcannot be proven.
There has only been one previously describedcase of myeloid leukemia cutis in association withnon-melanoma skin cancer. Youssef et al.8 describeda BCC in conjunction with myeloid leukemia cutis.No cases of SCC with myeloid leukemia cutishave been previously described. The previouslydescribed case shares many similarities to our twocases (Table 1). All three patients were elderly malesranging in age from 80 to 83 yrs. and were relativelyhealthy at the time of presentation. No patient had aprior history of a hematologic malignancy. Pathology
974
Leukemia cutis associated with BCC and SCC
Tabl
e1.
Clin
ocop
atho
logi
cfe
atur
esof
patie
nts
with
leuk
emia
cutis
and
epid
erm
alm
alig
nanc
ies
Auth
orAg
e/Se
xLo
catio
nHi
stop
atho
logi
cdi
agno
sis
Com
plet
ebl
ood
coun
tBo
nem
arro
wTr
eatm
ent
Follo
w-u
p
Yous
sefe
tal.8
80/M
ale
Left
fore
arm
Basa
lcel
lcar
cino
ma
and
mye
loid
sarc
oma
Panc
ytop
enia
Mye
lody
spla
stic
synd
rom
ew
ithre
fract
ory
anem
iaSu
ppor
tive
trans
fusi
ons
Aliv
ew
ithdi
seas
eaf
ter1
0m
onth
sCa
se1
83/M
ale
Righ
tupp
erba
ckBa
salc
ellc
arci
nom
aan
dm
yelo
idle
ukem
iacu
tis
AML
with
40%
mye
lobl
asts
expr
essi
ngCD
34,C
D117
,CD1
3,CD
33,H
LA-D
Ran
dTd
T
Notp
erfo
rmed
None
Died
ofdi
seas
eaf
ter5
wee
ks
Case
283
/Mal
eLe
ftw
rist
Squa
mou
sce
llca
rcin
oma
and
mye
loid
leuk
emia
cutis
AML
with
79%
mye
lobl
asts
AML
with
53%
mye
lobl
asts
show
ing
expr
essi
onof
CD13
(par
tial),
CD33
,CD1
17,C
D34,
HLA-
DR,C
D7(p
artia
l)an
dCD
4(p
artia
l).
Chem
othe
rapy
Aliv
ew
ithdi
seas
eaf
ter6
mon
ths
AML,
acut
em
yelo
idle
ukem
ia
from all three cases showed epidermal malignanciesintermingled with myeloid leukemia cutis. All threepatients showed abnormalities on peripheral bloodsmear with the previously described case showingpancytopenia and our two cases showing myeloidblasts (our Case 1: 40% and our Case 2: 79%). Twopatients had abnormal bone marrow examinations.The previously described case showed pancytopeniaand our Case 2 showed AML with 53% myeloblasts.Two patients are alive with disease (previouslydescribed case: 10 months and our Case 2: 6 months)and one patient died of disease after 5 weeks (ourCase 1).
Our first case illustrates that in some cases itmay be prudent to defer final immunophenotypingof cutaneous hematolymphoid disorders to flowcytometric analysis. The immunohistochemical andflow cytometry findings in this case did not showcomplete correlation. The myeloid leukemia cutisshowed immunohistochemical positivity for CD43and CD45 with focal positivity for CD99, CD7,TdT, TIA-1 and Granzyme B. The MPO wasnegative. A smaller population of atypical cellsshowed the presence of T cell markers (CD2,CD3, CD4 and CD5) and raised the possibilityof T cell acute lymphoblastic leukemia because ofthe expression of TdT and negativity for MPO inthe medium to larger cells. Flow cytometry showedthe blasts expressing CD13, CD33, CD34, CD117,HLA-DR and TdT with a very small subset ofblasts expressing MPO, CD7, CD71 and CD79athat was consistent with AML. The T cell markerswere negative (CD2, CD3, CD4, CD5 and CD8)by flow cytometry. Discrepant immunophenotypesbetween immunohistochemical analysis and flowcytometry has been described and believed to bedue to the higher sensitivity of flow cytometry andthe ability of flow cytometry to better differentiatebetween background reactive lymphoid populationsand the neoplastic hematopoietic infiltrate.12 Inour case, both scenarios may have occurred.Only a small population of myeloblasts (∼5%)showed positivity for MPO by flow cytometryand were negative by immunohistochemistry. Inaddition, a population of smaller atypical-appearinghematolymphoid cells likely representing reactiveT lymphocytes was intermixed with the myeloidleukemia cutis cells. Other possibilities for theimmunophenotypic discrepancies include clonalheterogeneity of AML and the presence of a mixedphenotype AML. As a bone marrow biopsy wasdeferred, these other possibilities could not beinvestigated further.
The scarcity of epidermal malignancies in associ-ation with myeloid leukemia cutis may be due to itsoverall low prevalence and difficulty in diagnosis. It
975

Ra et al.
is estimated that about 13,000 cases AML will bediagnosed this year in the United States and that9000 people will die from it.10 Skin involvementonly occurs in less than 3% of patients with knownmyeloid malignancies with most patients having aknown or concurrent diagnosis.13 It is in the esti-mated 8% of cases of myeloid leukemia cutis that hadno known disease that can be especially challenging toidentify.14 In the face of an obvious epidermal lesion,the presence of subtle leukemia cutis can be easilyoverlooked. In addition, the diagnosis of myeloidleukemia cutis can be difficult upon due to its varietyof histopathologic patterns. The myeloid infiltratecommonly shows a diffuse, nodular, or nodular anddiffuse architecture; however, less common patternsthat have been described include single filing ofmyeloid cells, a granuloma annulare-like pattern, aperivascular pattern and a solitary dermal nodule.14
The examination of the infiltrate associatedwith any epidermal malignancy is important. Inaddition to potentially diagnosing patients with apreviously unknown hematologic malignancy, thediagnosis of myeloid leukemia cutis may haveclinical implications. One study has shown thatpatients with AML and leukemia cutis have aremarkable propensity to relapse in extramedullarysites following marrow transplantation.15 Anotherstudy showed that these patients may be candidatesfor intensified treatment such as allogeneic bonemarrow or autologous stem cell transplantation infirst complete remission.13
AcknowledgementsThis paper was presented in part at The American Society ofDermatopathology meeting in Seattle Washington, October 2011.
References1. Padgett JK, Parlette HL 3rd, English JC 3rd.
A diagnosis of chronic lymphocytic leukemiaprompted by cutaneous lymphocytic infiltratespresent in mohs micrographic surgery frozensections. Dermatol Surg 2003; 29: 769.
2. Smoller BR, Warnke RA. Cutaneous infil-trate of chronic lymphocytic leukemia andrelationship to primary cutaneous epithelialneoplasms. J Cutan Pathol 1998; 25: 160.
3. Wilson ML, Elston DM, Tyler WB, MarksVJ, Ferringer T. Dense lymphocytic infiltratesassociated with non-melanoma skin cancer inpatients with chronic lymphocytic leukemia.Dermatol Online J 2010; 16: 4.
4. Cespedes YP, Rockley PF, Flores F, Ruiz P,Kaiser MR, Elgart GW. Is there aspecial relationship between CD30-positivelymphoproliferative disorders and epidermalproliferation? J Cutan Pathol 2000; 27: 271.
5. Lin JH, Lee JY. Primary cutaneousCD30 anaplastic large cell lymphoma withkeratoacanthoma-like pseudocarcinomatoushyperplasia and marked eosinophilia and neu-trophilia. J Cutan Pathol 2004; 31: 458.
6. Scarisbrick JJ, Calonje E, Orchard G, ChildFJ, Russell-Jones R. Pseudocarcinomatouschange in lymphomatoid papulosis andprimary cutaneous CD30+ lymphoma: aclinicopathologic and immunohistochemicalstudy of 6 patients. J Am Acad Dermatol2001; 44: 239.
7. Yanagi T, Shimizu T, Kodama K, Nemoto-Hasebe I, Kasai M, Shimizu H. CD30-positiveprimary cutaneous anaplastic large-cell lym-phoma and definite squamous cell carcinoma.Clin Exp Dermatol 2009; 34: e293.
8. Youssef AH, Zanetto U, Kaur MR, ChanSY. Granulocytic sarcoma (leukaemia cutis)in association with basal cell carcinoma. Br JDermatol 2006; 154: 201.
9. Boyd AS, Rapini RP. Cutaneous collisiontumors. An analysis of 69 cases and reviewof the literature. Am J Dermatopathol 1994;16: 253.
10. Howlader N, Noone AM, Krapcho M, et al.SEER Cancer Statistics Review, 1975–2008,National Cancer Institute. Bethesda, MD,http://seer.cancer.gov/csr/1975_2008/,based on November 2010 SEER data
submission, posted to the SEER web site,2011.
11. Alam M, Ratner D. Cutaneous squamous cellcarcinoma. N Eng J Med 2001; 344: 975.
12. Kelemen K, White CR, Gatter K, Braziel RM,Fan G. Immunophenotypic correlationbetween skin biopsy and peripheral blood find-ings in mycosis fungoides. Am J Clin Pathol2010; 134: 739.
13. Agis H, Weltermann A, Fonatsch C, et al.A comparative study on demographic,hematological, and cytogenetic findings andprognosis in acute myeloid leukemia with andwithout leukemia cutis. Ann Hematol 2002;81: 90.
14. Benet C, Gomez A, Aguilar C, Delattre C,et al. Histologic and immunohistologiccharacterization of skin localization of myeloiddisorders: a study of 173 cases. Am J ClinPathol 2011; 135: 278.
15. Michel G, Boulad F, Small TN, et al.Risk of extramedullary relapse followingallogeneic bone marrow transplantation foracute myelogenous leukemia with leukemiacutis. Bone Marrow Transplant 1997; 20: 107.
976
Copyright © 2022 FDOKUMEN