
PET in GIT Malignancies - The Egyptian Society of Nuclear ...
Upload
independentCategory
view
1download
0
PII S0360-3016(00)00771-9
PHYSICS CONTRIBUTION
INTENSITY-MODULATED WHOLE PELVIC RADIATION THERAPY INPATIENTS WITH GYNECOLOGIC MALIGNANCIES
JOHN C. ROESKE, PH.D.,* ANTHONY LUJAN, PH.D.,* JACOB ROTMENSCH, M.D.,*†
STEVE E.WAGGONER, M.D.,† DIANE YAMADA , M.D.,† AND ARNO J. MUNDT, M.D.*
*Department of Radiation and Cellular Oncology, and†Department of Obstetrics and Gynecology, Section of Gynecologic Oncology,University of Chicago, Chicago, IL
Purpose: To evaluate the ability of intensity-modulated radiation therapy (IMRT) to reduce the volume of smallbowel irradiated in women with gynecologic malignancies receiving whole pelvic radiotherapy (WPRT).Methods and Materials: Ten women with cervical (5) or endometrial (5) cancer undergoing WPRT were selectedfor this analysis. A planning CT scan of each patient was obtained following administration of oral, i.v., and rectalcontrast. The clinical target volume (CTV) was defined as the proximal vagina, parametrial tissues, uterus (ifpresent), and regional lymph nodes. The CTV was expanded uniformly by 1 cm in all directions to produce aplanning target volume (PTV). The bladder, rectum, and small bowel were also delineated in each patient. Twoplans were created: a standard “4-field box” with apertures shaped to the PTV in each beam’s eye view and anIM-WPRT plan designed to conform to the PTV while minimizing the volume of normal tissues irradiated. Bothplans were normalized to deliver 45 Gy to the PTV. Isodose distributions and dose–volume histograms (DVH)were compared.Results: The IM-WPRT plan reduced the volume of small bowel irradiated in all 10 patients at doses above 30Gy. At the prescription dose, the average volume of small bowel irradiated was reduced by a factor of two (17.4vs. 33.8%,p 5 0.0005). In addition, the average volume of rectum and bladder irradiated at the prescription dosewas reduced by 23% in both cases (p 5 0.0002 andp 5 0.0005, respectively). The average PTV doses deliveredby the conventional and IM-WPRT plans were 47.8 Gy and 47.4 Gy, respectively. Corresponding maximumdoses were 50.0 Gy and 54.8 Gy, respectively. However, on average, only 3.2% of the PTV received greater than50.0 Gy in the IM-WPRT plans.Conclusion: Our results suggest that IM-WPRT is an effective means of reducing the volume of small bowelirradiated in women with gynecologic malignancies receiving WPRT. This approach potentially offers a methodfor reducing small bowel complications in patients with gynecologic malignancies. © 2000 Elsevier Science Inc.
Gynecology, Whole pelvic radiation therapy, Inverse planning, Intensity modulation.
INTRODUCTION
Whole pelvic radiation therapy (WPRT) is commonly used inthe treatment of many gynecologic malignancies, particularlycervical and endometrial carcinomas. In addition to the treat-ment of the primary site, WPRT is used to sterilize metastaticdisease in the pelvic lymph nodes. Treatment of these nodes,however, entails irradiation of a considerable volume of smallbowel. Unsurprisingly, small bowel sequelae are among themost important acute and chronic toxicities in these patients (1,2). Sequelae include small bowel obstruction, enteritis, anddiarrhea. However, more subtle problems including malab-
sorption of vitamin B12, bile acids and lactose have beenreported following small bowel irradiation (3–6).
The incidence and severity of small bowel sequelae inwomen undergoing WPRT can be reduced by a variety ofmeans. The benefits of multiple fields, high energy beams,customized blocking and low daily fraction sizes are wellknown (2). Various agents have also been proposed aspossible radioprotectors of the small bowel (7–13). Since itis a mobile structure, mechanical means have been used todisplace the small bowel from the pelvis during treatment(14–17). However, such methods are often cumbersome (onboth patients and staff) and may be difficult to reproduce.
Reprint requests to: Dr. John C. Roeske, Department of Radia-tion and Cellular Oncology, University of Chicago, MC 9006,5758 South Maryland Avenue, Chicago, IL 60637. E-mail:[email protected]
Presented at the 40th annual Meeting of the American Societyfor Therapeutic Radiology and Oncology, Phoenix, AZ (USA),October 25–29, 1998.Acknowledgment—The authors thank Jong Kung, Ph.D., for help-ful discussions associated with the early stages of this work.
The research reported in this publication is supported by a grantfrom the Illinois Department of Public Health. Its contents aresolely the responsibility of the authors and do not necessarilyreflect the official views of the Illinois Department of PublicHealth.
Accepted for publication 10 July 2000.
Int. J. Radiation Oncology Biol. Phys., Vol. 48, No. 5, pp. 1613–1621, 2000Copyright © 2000 Elsevier Science Inc.Printed in the USA. All rights reserved
0360-3016/00/$–see front matter
1613

Surgical approaches to hold the small bowel in the upperabdomen out of the treatment field include absorbablemeshes (18–21), tissue expanders (22–24), and omento-plasty (25). While feasible in patients undergoing surgery,such approaches are not applicable to women undergoingdefinitive or preoperative RT. Moreover, such approacheshave a small but finite risk of small bowel injury (23, 26).
An approach that has received little attention in thesepatients is intensity-modulated radiation therapy (IMRT).Unlike conventional approaches, IMRT utilizes treatmentbeams of varying intensity allowing the high-dose region tobe conformed to the shape of the target volume. IMRT hasbeen shown to be a promising approach in other diseasesites. In prostate cancer, it has been used to minimize thevolume of bladder and rectum irradiated (27). IMRT hasreduced the dose to the parotid glands in head and neckcancer patients undergoing RT (28). Promising results havealso been published in tumors of the lung, central nervoussystem, and breast (29–31). Given this background, wepostulated that IMRT may prove a useful tool in the treat-ment of patients undergoing WPRT. The purpose of thisstudy is to evaluate the ability of IMRT to reduce thevolume of small bowel irradiated in women with gyneco-logic malignancies undergoing WPRT.
METHODS AND MATERIALS
Patient populationTen consecutive women with cervical (5) or endometrial
(5) carcinoma undergoing WPRT were prospectively se-lected. The cervical cancer patients had Stage IB–IIB dis-ease and were receiving WPRT before intracavitary brachy-therapy. The endometrial cancer patients had Stage IC–IIBdisease and were treated postoperatively. The prescribedWPRT dose in all patients was 45 Gy in 1.8-Gy dailyfractions.
SimulationTo minimize setup variability, a custom immobilization
device (Alpha Cradle, Smithers Medical Product, Inc.,North Canton, OH) was fabricated with each patient in thesupine position. A computed tomography (CT) scan of eachpatient in the treatment position was then obtained using ourdepartmental scanner (PQ5000, Marconi Medical Systems,Cleveland, OH). The scan parameters consisted of a largefield-of-view pelvic protocol with a 4-mm slice thickness/table index. The CT scans were obtained from the L2vertebral body to 5-cm below the ischial tuberosities with anaverage of 80 images per patient. Oral, i.v., and rectalcontrast were administered to all patients before the CTscan.
Target definitionFollowing the ICRU 50 recommendations (32), a clinical
target volume (CTV) was contoured on individual axial CTslices in all patients. The CTV included the upper one-halfof the vagina and parametrial tissues. In women with an
intact uterus, the entire uterus was included. Contrast-en-hanced vessels plus a 2-cm margin were used to define thecommon, external, and internal iliac nodal regions to thelevel of the L4–5 interspace. The presacral region wasincluded to the bottom of the S3 vertebral body to ensurecoverage of the presacral lymph nodes and attachment ofthe uterosacral ligament. A volume-rendered image of theCTV for a typical patient is shown in Fig. 1. The CTV wasexpanded uniformly by 1 cm in all directions to produce aplanning target volume (PTV). This margin is traditionallyused in conventional WPRT and was applied to IM-WPRTfor comparison purposes.
The rectum and bladder were also contoured for eachpatient. The rectum was defined from the level of the sacralpromontory to the ischial tuberosities. The peritoneal cavity(excluding the rectum and bladder) from the level of L4–5was used to define the small bowel region (SBR). Theindividual loops of small bowel were not separately con-toured.
Conventional treatment planningConventional WPRT plans were generated using our
three-dimensional treatment-planning system (PLanUNC)(33). The isocenter was placed at the geometric center of thePTV. A 4-field “box” plan was designed using 18-MVphotons with apertures shaped to the PTV in each beam’s-eye-view. The fields consisted of anterior, posterior, right,and left lateral beam directions. Field sizes were adjusted toensure coverage of the PTV with a 1-cm margin in alldirections to account for beam penumbra. Weights of theindividual fields were optimized to maximize dose unifor-mity in the PTV, and wedges were used as needed. All planswere normalized to cover 98% of the PTV with 45 Gy. The2% underdose represents those voxels at the periphery. This
Fig. 1. Volume rendering of the clinical target volume for a typicalpatient.
1614 I. J. Radiation Oncology● Biology ● Physics Volume 48, Number 5, 2000
normalization provided conformal coverage while minimiz-ing dose nonuniformity within the target. Dose–volumehistograms (DVHs) were calculated for the PTV, SBR,rectum, and bladder.
IMRT planningIMRT plans were generated using a commercial inverse
treatment-planning system (CORVUS, Version 3.0, NO-MOS Corporation, Sewickley, PA). Briefly, this planningsystem produces optimal intensity-modulation profiles us-ing a simulated annealing algorithm. The prescription doseis defined by the user along with all dose–volume con-straints of the PTV and normal tissues. To select the optimalnumber of fields and beam energy, plans for a test patientwere generated using 4–11 equally spaced, coplanar, 6- and18-MV photon beams. Dose constraints were set to mini-mize the volume of normal tissue receiving the prescriptiondose without compromising PTV coverage. Plans werecompared in terms of isodose distributions as well as normaltissue and PTV DVHs (data not shown). This analysisdemonstrated that increasing the beam number was associ-ated with better dose conformation to the PTV. However, nosignificant improvement was evident with the use of morethan nine beams. These results are consistent with theoret-ical studies showing that more than 7–9 fields does notsignificantly improve dose conformation (34, 35). In addi-tion, we noted slightly better PTV dose conformation using6-MV photons.
Based the above analysis, a 9-field, 6-MV, coplanar,IMRT plan was generated for each patient using an identicalset of dose–volume constraints. Fields were equally spacedat 40° intervals consisting of the following gantry angles: 0,40, 80, 120, 160, 200, 240, 280, and 320°. As in conven-tional planning, all plans were normalized to cover 98% ofthe PTV with the prescription dose. DVHs were calculatedfor PTV, SBR, rectum, and bladder.
ComparisonAverage and maximum doses of the PTV were calculated
for the conventional and IM-WPRT plans and compared.The percent volume of the normal tissues (SBR, rectum, andbladder) was obtained at six dose levels (10, 20, 30, 40, 45,and 50 Gy) from the individual DVHs. At each level, thepercent volume for both the conventional and IM-WPRTplans was averaged. These average values were then com-pared using Student’st test.
RESULTS
Example caseConventional and IM-WPRT treatment plans for an ex-
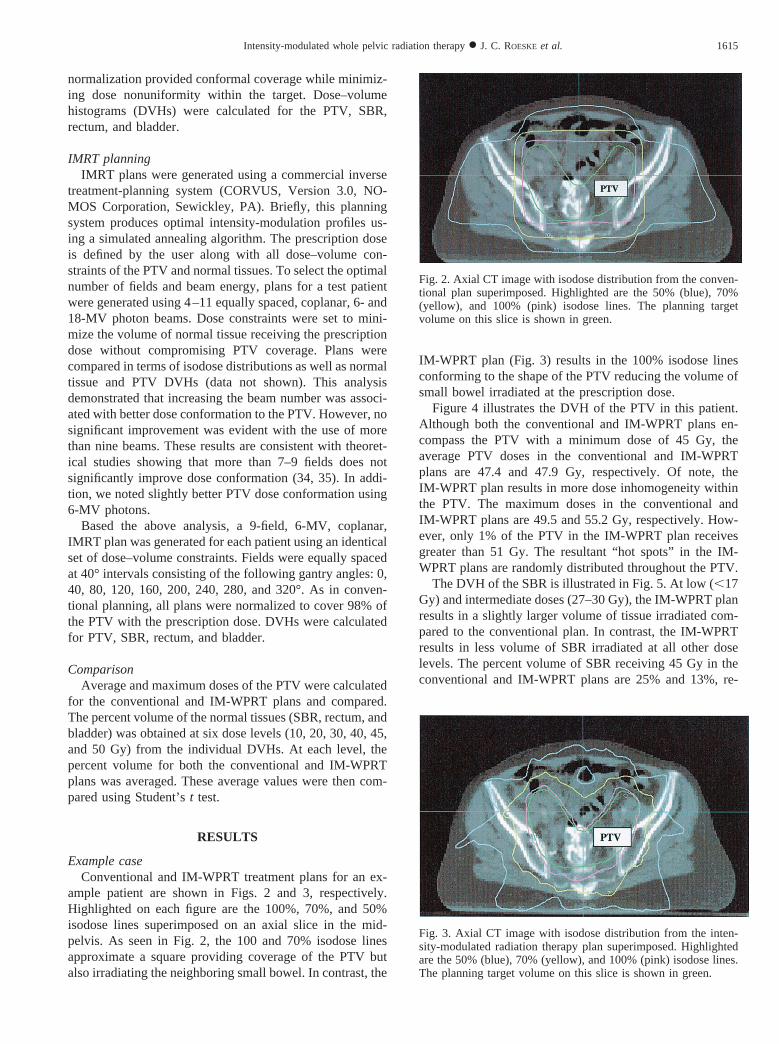
ample patient are shown in Figs. 2 and 3, respectively.Highlighted on each figure are the 100%, 70%, and 50%isodose lines superimposed on an axial slice in the mid-pelvis. As seen in Fig. 2, the 100 and 70% isodose linesapproximate a square providing coverage of the PTV butalso irradiating the neighboring small bowel. In contrast, the
IM-WPRT plan (Fig. 3) results in the 100% isodose linesconforming to the shape of the PTV reducing the volume ofsmall bowel irradiated at the prescription dose.
Figure 4 illustrates the DVH of the PTV in this patient.Although both the conventional and IM-WPRT plans en-compass the PTV with a minimum dose of 45 Gy, theaverage PTV doses in the conventional and IM-WPRTplans are 47.4 and 47.9 Gy, respectively. Of note, theIM-WPRT plan results in more dose inhomogeneity withinthe PTV. The maximum doses in the conventional andIM-WPRT plans are 49.5 and 55.2 Gy, respectively. How-ever, only 1% of the PTV in the IM-WPRT plan receivesgreater than 51 Gy. The resultant “hot spots” in the IM-WPRT plans are randomly distributed throughout the PTV.
The DVH of the SBR is illustrated in Fig. 5. At low (,17Gy) and intermediate doses (27–30 Gy), the IM-WPRT planresults in a slightly larger volume of tissue irradiated com-pared to the conventional plan. In contrast, the IM-WPRTresults in less volume of SBR irradiated at all other doselevels. The percent volume of SBR receiving 45 Gy in theconventional and IM-WPRT plans are 25% and 13%, re-
Fig. 2. Axial CT image with isodose distribution from the conven-tional plan superimposed. Highlighted are the 50% (blue), 70%(yellow), and 100% (pink) isodose lines. The planning targetvolume on this slice is shown in green.
Fig. 3. Axial CT image with isodose distribution from the inten-sity-modulated radiation therapy plan superimposed. Highlightedare the 50% (blue), 70% (yellow), and 100% (pink) isodose lines.The planning target volume on this slice is shown in green.
1615Intensity-modulated whole pelvic radiation therapy● J. C. ROESKE et al.
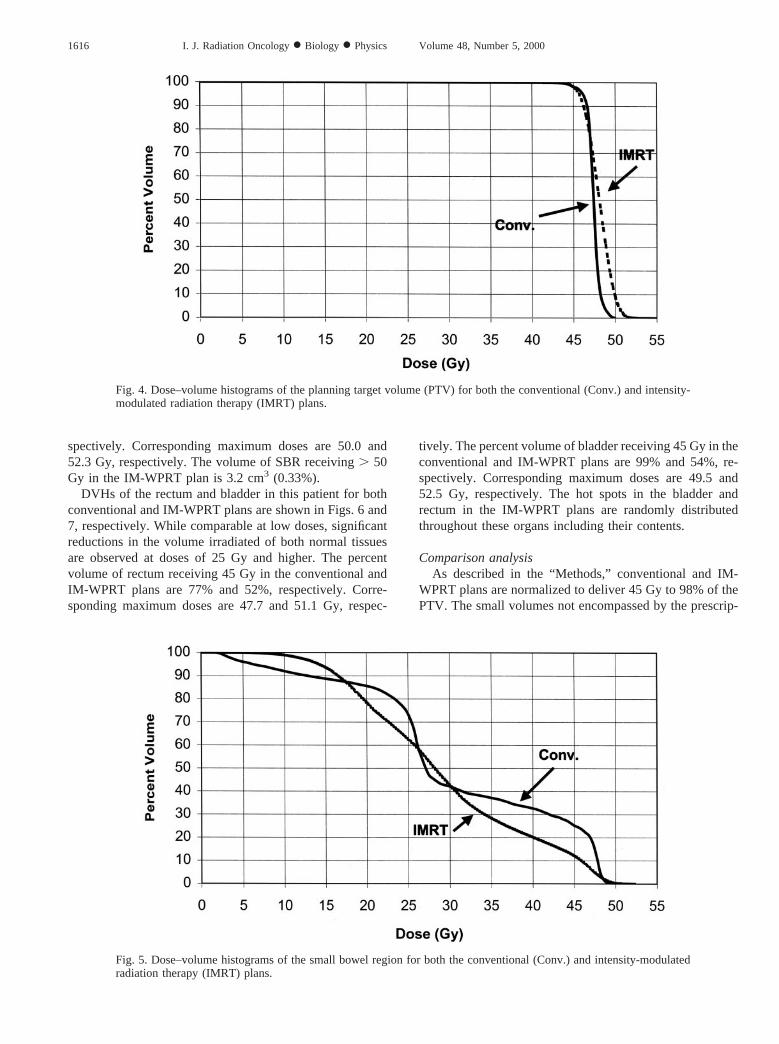
spectively. Corresponding maximum doses are 50.0 and52.3 Gy, respectively. The volume of SBR receiving. 50Gy in the IM-WPRT plan is 3.2 cm3 (0.33%).
DVHs of the rectum and bladder in this patient for bothconventional and IM-WPRT plans are shown in Figs. 6 and7, respectively. While comparable at low doses, significantreductions in the volume irradiated of both normal tissuesare observed at doses of 25 Gy and higher. The percentvolume of rectum receiving 45 Gy in the conventional andIM-WPRT plans are 77% and 52%, respectively. Corre-sponding maximum doses are 47.7 and 51.1 Gy, respec-
tively. The percent volume of bladder receiving 45 Gy in theconventional and IM-WPRT plans are 99% and 54%, re-spectively. Corresponding maximum doses are 49.5 and52.5 Gy, respectively. The hot spots in the bladder andrectum in the IM-WPRT plans are randomly distributedthroughout these organs including their contents.
Comparison analysisAs described in the “Methods,” conventional and IM-
WPRT plans are normalized to deliver 45 Gy to 98% of thePTV. The small volumes not encompassed by the prescrip-
Fig. 4. Dose–volume histograms of the planning target volume (PTV) for both the conventional (Conv.) and intensity-modulated radiation therapy (IMRT) plans.
Fig. 5. Dose–volume histograms of the small bowel region for both the conventional (Conv.) and intensity-modulatedradiation therapy (IMRT) plans.
1616 I. J. Radiation Oncology● Biology ● Physics Volume 48, Number 5, 2000

tion isodose are located at the periphery of the PTV in bothplans. The average PTV doses delivered by the conventionaland IM-WPRT plans are 47.86 0.5 Gy and 47.46 0.4 Gy,respectively. Corresponding maximum doses are 50.06 1.5Gy and 54.86 1.7 Gy, respectively. However, on average,only 3.2% of the PTV receives greater than 50.0 Gy in theIM-WPRT plan.
Table 1 summarizes the comparison of conventional andIM-WPRT plans of the SBR volume irradiated in these 10patients. At the 10-Gy level, a larger volume of the SBR is
included in the IM-WPRT plan. However, the IM-WPRTplan results in significant reductions in the SBR volumeirradiated at the 20, 40, and 45 Gy levels. At the 30-Gylevel, there is no significant difference in the SBR volumeirradiated. Moreover, the percent SBR volume irradiated atthe prescription dose (45 Gy) is reduced by nearly a factorof two in the IM-WPRT plan (17.4 vs. 33.8%,p 5 0.0005).The comparison of the SBR volumes irradiated at the 45-Gylevel in each of the 10 patients is illustrated graphically inFig. 8. Of note, a reduction in the volume of SBR irradiated
Fig. 6. Dose–volume histograms of the rectum for both the conventional (Conv.) and intensity-modulated radiationtherapy (IMRT) plans.
Fig. 7. Dose–volume histograms of the bladder for both the conventional (Conv.) and intensity-modulated radiationtherapy (IMRT) plans.
1617Intensity-modulated whole pelvic radiation therapy● J. C. ROESKE et al.
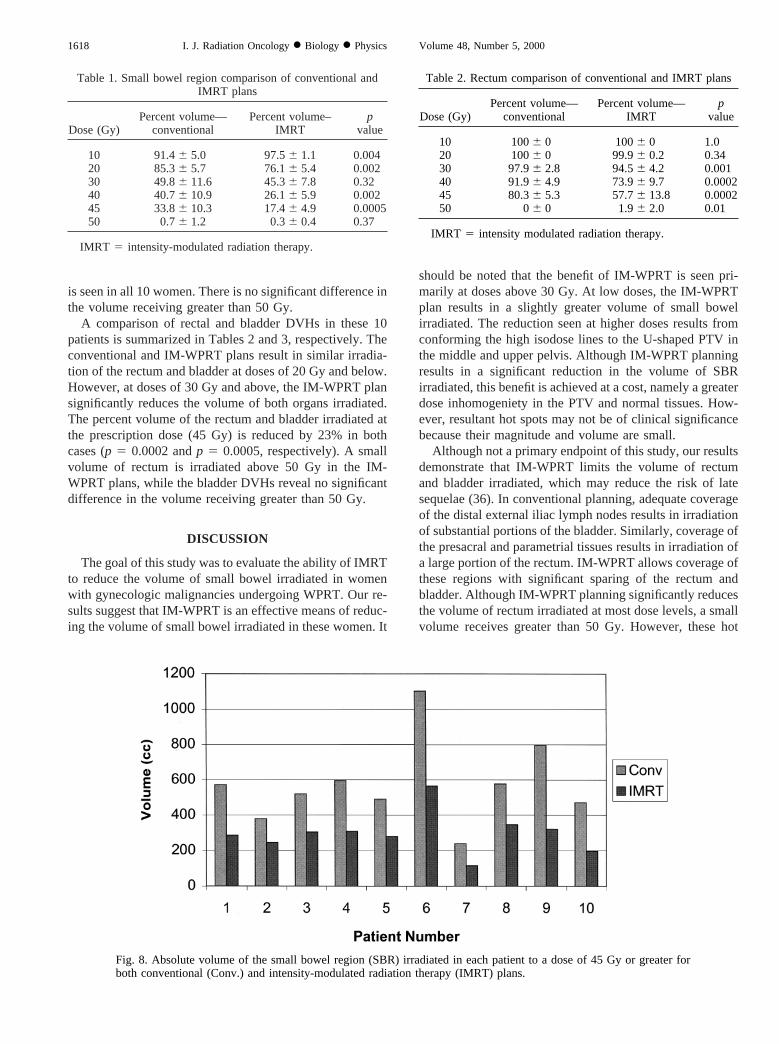
is seen in all 10 women. There is no significant difference inthe volume receiving greater than 50 Gy.
A comparison of rectal and bladder DVHs in these 10patients is summarized in Tables 2 and 3, respectively. Theconventional and IM-WPRT plans result in similar irradia-tion of the rectum and bladder at doses of 20 Gy and below.However, at doses of 30 Gy and above, the IM-WPRT plansignificantly reduces the volume of both organs irradiated.The percent volume of the rectum and bladder irradiated atthe prescription dose (45 Gy) is reduced by 23% in bothcases (p 5 0.0002 andp 5 0.0005, respectively). A smallvolume of rectum is irradiated above 50 Gy in the IM-WPRT plans, while the bladder DVHs reveal no significantdifference in the volume receiving greater than 50 Gy.
DISCUSSION
The goal of this study was to evaluate the ability of IMRTto reduce the volume of small bowel irradiated in womenwith gynecologic malignancies undergoing WPRT. Our re-sults suggest that IM-WPRT is an effective means of reduc-ing the volume of small bowel irradiated in these women. It
should be noted that the benefit of IM-WPRT is seen pri-marily at doses above 30 Gy. At low doses, the IM-WPRTplan results in a slightly greater volume of small bowelirradiated. The reduction seen at higher doses results fromconforming the high isodose lines to the U-shaped PTV inthe middle and upper pelvis. Although IM-WPRT planningresults in a significant reduction in the volume of SBRirradiated, this benefit is achieved at a cost, namely a greaterdose inhomogeniety in the PTV and normal tissues. How-ever, resultant hot spots may not be of clinical significancebecause their magnitude and volume are small.
Although not a primary endpoint of this study, our resultsdemonstrate that IM-WPRT limits the volume of rectumand bladder irradiated, which may reduce the risk of latesequelae (36). In conventional planning, adequate coverageof the distal external iliac lymph nodes results in irradiationof substantial portions of the bladder. Similarly, coverage ofthe presacral and parametrial tissues results in irradiation ofa large portion of the rectum. IM-WPRT allows coverage ofthese regions with significant sparing of the rectum andbladder. Although IM-WPRT planning significantly reducesthe volume of rectum irradiated at most dose levels, a smallvolume receives greater than 50 Gy. However, these hot
Table 1. Small bowel region comparison of conventional andIMRT plans
Dose (Gy)Percent volume—
conventionalPercent volume–
IMRTp
value
10 91.46 5.0 97.56 1.1 0.00420 85.36 5.7 76.16 5.4 0.00230 49.86 11.6 45.36 7.8 0.3240 40.76 10.9 26.16 5.9 0.00245 33.86 10.3 17.46 4.9 0.000550 0.76 1.2 0.36 0.4 0.37
IMRT 5 intensity-modulated radiation therapy.
Fig. 8. Absolute volume of the small bowel region (SBR) irradiated in each patient to a dose of 45 Gy or greater forboth conventional (Conv.) and intensity-modulated radiation therapy (IMRT) plans.
Table 2. Rectum comparison of conventional and IMRT plans
Dose (Gy)Percent volume—
conventionalPercent volume—
IMRTp
value
10 1006 0 1006 0 1.020 1006 0 99.96 0.2 0.3430 97.96 2.8 94.56 4.2 0.00140 91.96 4.9 73.96 9.7 0.000245 80.36 5.3 57.76 13.8 0.000250 06 0 1.96 2.0 0.01
IMRT 5 intensity modulated radiation therapy.
1618 I. J. Radiation Oncology● Biology ● Physics Volume 48, Number 5, 2000

spots are randomly distributed throughout the rectal vol-ume. Thus, many are within the lumen of the rectum and notalong its surface. Moreover, these hot spots are small andnot concentrated within the portion of rectum that wouldreceive high doses from subsequent intracavitary brachy-therapy.
The concept of conformally shaping the dose distributionto the pelvic lymph nodes to reduce the volume of normaltissue irradiated was first discussed in the 1970s (37). Re-searchers at the Harvard Joint Center for Radiation Therapyproposed a technique known as computer-controlled radia-tion therapy. Briefly, this technique required a patient to betranslated longitudinally during the course of treatmentwhile the dose rate, gantry angle, and collimator jaws werevaried. This resulted in a conformal dose distribution to thepelvic and para-aortic lymph node regions. However, giventhe available technology at that time, this approach was notclinically implemented. Today, modern computer-con-trolled linear accelerators equipped with dynamic multileafcollimators, along with commercial inverse planning soft-ware make the implementation and delivery of conformalnodal irradiation possible. Recently, investigators at Wash-ington University have presented data evaluating the use ofIMRT planning in the treatment of locally advanced cervi-cal cancer with extended field RT. Similar to our results,significant reductions in the volume of small bowel, rectumand bladder irradiated at the prescription dose wereachieved (38).
An important issue in the planning of IM-WPRT isproper target delineation. Target delineation is not a trivialprocess in these patients and requires considerable knowl-edge of pelvic anatomy and patterns of disease failure.Because the lymph nodes at risk are not directly visualized,contrast-enhanced vessels must be used to define lymphnodal regions. We used generous 2-cm margins around thepelvic vessels to ensure coverage of these regions. It ispossible, however, that smaller margins may be adequate,which would further reduce the dose to the neighboringsmall bowel. In women with intact uteri, we elected toinclude the entire uterus in the PTV. However, irradiation ofthe entire uterus may not be necessary in early stage cervicalcancer patients without evidence of endometrial extension.
Accurate setup and immobilization are also paramount toachieving a favorable outcome in patients treated usingIMRT. Typically, WPRT patient setup is accomplished
using external markers tattooed onto the skin at simulation.At the time of treatment, patients are aligned using thesemarkers and a precision laser system. Studies have shownthis method results in both systematic and random errors(39–43). Mocket al.measured patient setup errors using anelectronic portal imaging device (EPID) in 25 women un-dergoing treatment for gynecologic malignancies. System-atic errors in setup were 1.5 mm, 2.9 mm, and 3.0 mm in theleft–right (LR), anterior–posterior (AP), and superior–infe-rior (SI) directions, respectively. Random setup errors wereobserved with a standard deviation ranging from 3.5 to 4.8mm (40). Rudatet al. observed random and systematicerrors in patient setup ranging from 2.5 to 3.9 mm (39).Cruetzberget al. examined setup errors in the LR and APdirections for patients aligned using a laser system only.Their results indicated that systematic errors ranged from3.0 to 3.3 mm, while random errors ranged from 2.3 to 3.1mm (43). Several authors have proposed various methods toreduce the magnitude and frequency of these errors. Luchkaet al. found that use of daily online portal imaging reducedthe frequency of large errors (.10 mm) from 10% to 2%(42). Rattrayet al. evaluated a new pelvic stabilizationdevice (the pelvic cradle) which appears promising in re-ducing setup uncertainties. The use of this device resulted ina reduction of the mean deviation from 3.8 mm to 2.0 mmin the LR direction and from 3.9 mm to 2.5 mm in the SIdirection (44). Investigation and understanding of setupuncertainties can potentially lead to a smaller CTV-to-PTVmargin that may, in turn, result in further reduction in thevolume of normal tissues irradiated. Margin design optimi-zation for IM-WPRT is the subject of ongoing research atour center.
Another important issue is organ motion within the pel-vis. Most organ motion studies in patients with pelvic ma-lignancies have focused on prostate cancer. Serial imaginghas demonstrated significant variations in the volumes ofthe rectum and bladder during a course treatment (45–47).Our own work has demonstrated that the rectal and bladdervolumes varied by as much as6 30% from the initialplanning CT scan (45). Few studies exist regarding organmotion in the female pelvis because many of the normaltissues are almost uniformly irradiated by the large WPRTfields. Thus, until now, organ motion has not been animportant issue. Gerstneret al.showed that bladder volumewas correlated with the volume of small bowel in thetreatment field. Patients with smaller bladder volumestended to have a larger volume of small bowel in the field(48). Buchaliet al. examined the effect of a full vs. emptybladder at the time of simulation. Their results indicated thatvariations in bladder filling caused significant motion of theuterus with median displacements of 7 mm and 4 mm in theSI and AP directions, respectively (49). Given the steepdose gradients present in the IM-WPRT plans, this type ofmotion could potentially result in underdosing portions ofthe CTV, or overdosing surrounding normal tissues. Thus,protocols designed to limit variations in organ motion mustbe developed in order for IM-WPRT to be successful.
Table 3. Bladder comparison of conventional and IMRT plans
Dose (Gy)Percent volume—
conventionalPercent volume—
IMRTp
value
10 1006 0 1006 0 1.020 1006 0 99.96 0.3 0.3430 1006 0 96.56 2.3 0.0540 99.86 0.4 86.16 7.2 0.000145 99.36 1.3 76.66 11.7 0.000550 5.36 9.0 2.56 2.6 0.37
IMRT 5 intensity modulated radiation therapy.
1619Intensity-modulated whole pelvic radiation therapy● J. C. ROESKE et al.

IM-WPRT has a number of potential applications. Asdemonstrated here, this approach allows the delivery ofconventional doses with less irradiation of normal tissues.IM-WPRT may also provide the ability to safely deliverhigher than conventional doses in select patients providedthat the resultant hot spots are small, not excessive inmagnitude, and not located in critical structures. This is anappealing approach in node positive cervical cancer patientsgiven their high rate of pelvic failure following surgery andadjuvant RT (50). We are currently evaluating the use ofIMRT planning as a means of delivering high central dosesin women with cervical cancer unable to undergo brachy-therapy. A central boost delivered with IMRT in conjunc-tion with conventional WPRT is currently being exploredby Kavanaghet al. (51). Finally, IM-WPRT may also beapplicable to other disease sites that routinely receive WPRTincluding bladder, anal, prostate and rectal cancers (52).
Several questions remain to be answered. First, it isunclear whether IM-WPRT is feasible in a busy clinic.Treatment planning and delivery are more time consumingthan the conventional 4-field box approach. We are cur-rently conducting a feasibility study of IM-WPRT inwomen with endometrial and cervical cancer. With experi-ence, it is our feeling that the time required for treatmentplanning and delivery will be considerably shortened. Weare also attempting to further optimize the treatment planand immobilization in these patients. We are incorporatinga video-assisted positioning system for our patients that hasbeen beneficial in other treatment sites (53). Finally, themost important question is whether dosimetric improve-ments seen here will translate to reduced treatment sequelae.Patients are being followed closely to answer this question.Only with adequate patient numbers and follow-up can thetrue benefit of IM-WPRT be assessed.
REFERENCES
1. Perez CA, Breaux S, Bedwinek JM,et al. Radiation therapyalone in the treatment of carcinoma of the uterine cervix: II.Analysis of complications.Cancer1984;54:235–246.
2. Corn BW, Lanciano RM, Greven KM,et al. Impact of im-proved irradiation technique, age, and lymph node samplingon the severe complication rate of surgically staged endome-trial cancer patients: a multivariate analysis.J Clin Oncol1994;12:510–515.
3. Beer WH, Fan A, Halsted CH. Clinical and nutritional impli-cations of radiation enteritis.Am J Clin Nutr1985;41:85–91.
4. Snijders-Keiholz A, Griffioen G,et al. Vitamin B12 malab-sorption after irradiation for gynaecological tumours.Antican-cer Res1993;13(5C):1877–1881.
5. Yeoh E, Horowitz M, Russo A,et al.A retrospective study ofthe effects of pelvic irradiation for carcinoma of the cervix ongastrointestinal function.Int J Radiat Oncol Biol Phys1993;26:229–237.
6. Thomson AB, Cheeseman CI, Walker K. Late effects ofabdominal radiation on intestinal uptake of nutrients.RadiatRes1986;107:344–353.
7. Beyzadeoglu M, Balkan M, Demiriz M,et al.Protective effectof vitamin A on acute radiation injury in the small intestine.Radiat Med1997;15:1–5.
8. Felemovicius I, Bonsack ME, Baptista ML,et al. Intestinalradioprotection by vitmain E (alpha-tocopherol).Ann Surg1995;222:504–508.
9. Travis EL, Thames HD Jr, Tucker SL,et al. Protection ofmouse jejunal crypt cells by WR-2721 after small doses ofradiation.Int J Radiat Oncol Biol Phys1986;12:807–814.
10. Felemovicius I, Bonsack ME, Griffin RJ,et al. Radioprotec-tion of the rat intestinal mucosa by tirilazad.Int J RadiatOncol Biol Phys1998;73:219–223.
11. Delaney JP, Bonsack ME, Felemovicius I. Misoprostol in theintestinal lumen protects against radiation injury of the mu-cosa of the small bowel.Radiat Res1994;137:405–409.
12. Rose PG, Halter SA, Su CM. The effect of indomethacin onacute radiation induced gastrointestinal injury: A morphologicstudy.J Surg Oncol1992;49:231–238.
13. Henriksson R, Franzen L, Littbrand B. Effects of sucralfate onacute and late bowel discomfort following radiotherapy ofpelvic cancer.J Clin Oncol1992;10:969–975.
14. Fu YT, Lam LC, Tze JM. Measurement of irradiated smallbowel volume in pelvic irradiation and the effect of a belly-board.Clin Oncol (R Coll Radiol)1995;7:188–192.
15. Gallagher MJ, Brereton HD, Rostock RA,et al.A prospectivestudy of treatment techniques to minimize the volume ofpelvic small bowel with reduction of acute and late effectsassociated with pelvic irradiation.Int J Radiat Oncol BiolPhys1986;12:1565–1573.
16. Das IJ, Lanciano RM, Movsas B,et al. Efficacy of a bellyboard device with CT-simulation in reducing small bowelvolume within pelvic irradiation fields.Int J Radiat Oncol BiolPhys1997;39:67–76.
17. Shanahan TG, Mehta MP, Bertelrud KL,et al. Minimizationof small bowel volume within treatment fields utilizing cus-tomized “belly boards.”Int J Radiat Oncol Biol Phys.1990;19:469–476.
18. Rodier JF, Janser JC, Rodier D,et al. Prevention of radiationenteritis by an absorbable polygolycolic acid mesh sling. A60-case multicentric study.Cancer1991;68:2545–2549.
19. Devereux DF, Kavanah MT, Feldman MI,et al. Small bowelexclusion from the pelvis by a polyglycolic acid mesh sling.J Surg Oncol1984;26:107–112.
20. Soper JT, Clarke-Pearson DL, Creasman WT. Absorbablesynthetic mesh (910-plyglactin) intestinal sling to reduce ra-diation-induced small bowel injury in patients with pelvicmalignancies.Gynecol Oncol1988;29:283–289.
21. Van Kasteren YM, Burger CW, Meijer OW,et al.Efficacy ofa synthetic mesh sling in keeping the small bowel in the upperabdomen to prevent radiation enteropathy in gynecologic ma-lignancies.Eur J Obstet Gynecol Reprod Biol1993;50:211–218.
22. Coucke PA, Cuttat JF, Mirimanoff RO. Small bowel protec-tion with “STEP.” Silastic tissue expander prosthesis.Strahl-enther Onkol1992;168:226–229.
23. Hoffman JP, Lanciano R, Carp NZ,et al. Morbidity afterintraperitoneal insertion of saline-filled tissue expanders forsmall bowel exclusion from radiotherapy treatment fields: aprospective four year experience with 34 patients.Ann Surg1994;60:473–482.
24. Armstrong JG, Harrison LB, Dattoli M,et al. The use of aprosthetic tissue expander to displace bowel from a brachy-therapy implant site.Int J Radiat Oncol Biol Phys1990;19:1521–1523.
25. Logmans A, van Lent M, van Geel AN,et al. The pedicledomentoplasty, a simple and effective surgical technique toacquire a safe pelvic radiation field: Theoretical and practicalaspects.Radiother Oncol1994;33:269–271.
1620 I. J. Radiation Oncology● Biology ● Physics Volume 48, Number 5, 2000

26. Sloan DA. Complete small bowel obstruction in the earlypostoperative period complicating surgical sling procedure.Am Surg1994;60:282–286.
27. Reinstein LE, Wang XH, Burman CM,et al. A feasibilitystudy of inverse treatment planning for cancer of the prostate.Int J Radiat Oncol Biol Phys1998;40:207–214.
28. Verellen D, Linthout N, van den Berge D,et al. Initial expe-rience with intensity-modulated conformal radiation therapyfor the treatment of the head and neck region.Int J RadiatOncol Biol Phys1997;39:99–114.
29. Esik O, Bortfeld T, Bendl R,et al. Inverse radiotherapyplanning for a concave-convex PTV in cervical and uppermediastinal regions. Simulation of radiotherapy using an Al-derson-RANDO phantom.Strahlenther Onkol1997;174:193–200.
30. Meeks SL, Buatti JM, Bova FJ,et al. Potential clinical effi-cacy of intensity-modulated conformal therapy.Int J RadiatOncol Biol Phys1998;40:483–495.
31. Hong L, Hunt M, Chui C,et al. Intensity-modulated tangentialbeam irradiation of the intact breast.Int J Radiat Oncol BiolPhys1999;44:1155–1164.
32. International Commission on Radiation Units, and Measure-ments (ICRU). Report Number 50. Prescribing, recording andreporting photon beam therapy. Washington, DC: ICRU;1993.
33. Sailer SL, Chaney EL, Rosenman JG,et al. Treatment plan-ning at the University of North Carolina at Chapel Hill.SeminRadiat Oncol1992;2:267–273.
34. Bortfeld T, Schlegel W. Optimization of beam orientation inradiation therapy: some theoretical considerations.Phys MedBiol 1993;38:291–304.
35. Soderstrom S, Brahme A. Which is the most suitable numberof photon beam portals in coplanar radiation therapy?Int JRadiat Oncol Biol Phys1995;33:151–159.
36. Roeske JC, Mundt AJ, Halpern H,et al. Late rectal sequelaefollowing definitive radiation therapy for carcinoma of theuterine cervix: A dosimetric analysis.Int J Radiat Oncol BiolPhys1997;37:351–358.
37. Chin LM, Kijewski PK, Svensson GK,et al. A computer-controlled radiation therapy machine for pelvic and para-aorticnodal areas.Int J Radiat Oncol Biol Phys1981;7:61–70.
38. Portelance L, Chao C, Grigsby PW,et al. Intensity modulatedradiation therapy (IMRT) may reduce small bowel, rectum,and bladder complications in patients with cervical cancertreated to the pelvis and paraaortic area (Abstr.).Int J RadiatOncol Biol Phys1999;45(Suppl 1):211.
39. Rudat V, Flentje M, Oetzel D,et al. Influence of the position-ing error on 3D conformal dose distributions during fraction-ated radiotherapy.Radiother Oncol1994;33:56–63.
40. Mock U, Dieckman K, Wolff U,et al. Portal imaging baseddefinition of the planning target volume during pelvic irradi-ation for gynecological malignancies.Int J Radiat Oncol BiolPhys1999;45:227–232.
41. Huddart RA, Nahum A, Neal A,et al. Accuracy of pelvicradiotherapy: A prospective analysis of 90 patients in a ran-domised trial of blocked versus standard radiotherapy.Ra-diother Oncol1996;39:19–29.
42. Luchka K, Shalev S. Pelvic irradiation of the obese patient: Atreatment strategy involving megavoltage simulation and in-tratreatment setup corrections.Med Phys1996;23:1897–1902.
43. Creutzberg CL, Althoff VG, deHoog MD,et al. A qualitycontrol study of the accuracy of patient positioning in irradi-ation of pelvic fields.Int J Radiat Oncol Biol Phys1996;34:697–708.
44. Rattray G, Hopley S, Mason N,et al. Assessment of pelvicstabilization devices for improved field reproducibility.Aus-tralasian Radiol1998;42:118–125.
45. Roeske JC, Forman JD, Mesina CF,et al. Evaluation ofchanges in the size and location of the prostate, seminalvesicle, bladder, and rectum during a course of external beamradiation therapy.Int J Radiat Oncol Biol Phys1995;33:1321–1329.
46. Van Herk M, Bruce A, Kroes AP,et al. Quantification oforgan motion during conformal radiotherapy of the prostate bythree dimensional image registration.Int J Radiat Oncol BiolPhys1995;35:1311–1320.
47. Melian E, Mageras GS, Fuks Z,et al. Variation in prostateposition quantitation and implications for three-dimensionalconformal treatment planning.Int J Radiat Oncol Biol Phys1997;38:73–81.
48. Gerstner N, Wachter S, Knocke TH,et al. The benefit ofbeam’s eye view based 3D treatment planning for cervicalcancer.Radiother Oncol1999;51:71–78.
49. Buchali A, Koswig S, Dinges S, Rosenthal P, Salk J, LacknerG, Bohmer D, Schlenger L, Budach V. Impact of the fillingstatus of the bladder and rectum on their integral dose distri-bution and the movement of the uterus in the treatment plan-ning of gynaecological cancer.Radiother Oncol1999;52:29-34.
50. Stock RG, Chen AS, Flickinger JC,et al. Node-positive cer-vical cancer: impact of pelvic irradiation and patterns offailure. Int J Radiat Oncol Biol Phys1995;31:31–36.
51. Kavanagh BD, Wu Q, Arnfield M,et al. Whole pelvic inten-sity-modulated radiotherapy (IMRT) for cervix cancer using a“butterfly” isodose plan:in vivo dosimetric verification ofreduced rectal dose and clinical feasibility evaluation (Abstr.).Int J Radiat Oncol Biol Phys1999;45(Suppl. 1):412.
52. Robertson JM, Yan D, Girimonte PE,et al. The potentialbenefit of intensity modulated radiation therapy (IMRT) forrectal cancer (Abstr.).Int J Radiat Oncol Biol Phys1999;45(Suppl. 1):248–249.
53. Johnson LS, Milliken BD, Hadley SW,et al. Initial clinicalexperience with a video-based positioning system.Int J RadiatOncol Biol Phys1999;45:205–213.
1621Intensity-modulated whole pelvic radiation therapy● J. C. ROESKE et al.
Copyright © 2022 FDOKUMEN




















