
Prevalence and Treatment Patterns of Pelvic Health Disorders ...
57
® Prevalence and Treatment Patterns of Pelvic Health Disorders Among U.S. Women Submitted to: The National Women’s Health Resource Center Submitted by: The Lewin Group, Inc. June 2007
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Prevalence and Treatment Patterns of Pelvic Health Disorders ...

®
Prevalence and Treatment Patterns of Pelvic Health Disorders Among U.S. Women
Submitted to:
The National Women’s Health Resource Center
Submitted by:
The Lewin Group, Inc.
June 2007

Prevalence and Treatment Patterns of Pelvic Health Disorders
Among U.S. Women
Submitted to: The National Women’s Health Resource Center
Submitted by: The Lewin Group, Inc.
June 2007

Pelvic Health Disorders
Table of Contents
Introduction and Key Findings ....................................................................... 1-1
Key Findings ..................................................................................................... 1-2
Organization of the Report ................................................................................... 1-6
Menorrhagia .............................................................................................. 2-1
Background ...................................................................................................... 2-1
Prevalence ....................................................................................................... 2-1
Diagnosis and Treatment Gaps ............................................................................... 2-2
Treatment Options and Patterns of Care ................................................................... 2-3
Uterine Fibroids
Background ...................................................................................................... 3-1
Prevalence ....................................................................................................... 3-1
Diagnosis and Treatment Gaps ............................................................................... 3-3
Treatment Options and Patterns of Care ................................................................... 3-3
Stress Urinary Incontinence .......................................................................... 4-1
Background ...................................................................................................... 4-1
Prevalence ....................................................................................................... 4-1
Diagnosis and Treatment Gaps ............................................................................... 4-3
Treatment Options and Patterns of Care ................................................................... 4-4
Pelvic Organ Prolapse .................................................................................. 5-1
Background ...................................................................................................... 5-1
Prevalence ....................................................................................................... 5-2
Diagnosis and Treatment Gaps ............................................................................... 5-3
Treatment Options and Patterns of Care ................................................................... 5-4
Conclusion ................................................................................................ 6-1
Reference List ........................................................................................... 7-1
Appendix A: Glossary....................................................................................A-1
Appendix B: Methods....................................................................................B-1
i

Pelvic Health Disorders Introduction and Key Findings
Introduction and Key Findings
At some point in their lifetime, most women are likely to experience a pelvic health concern, ranging from minor inflammation to more complex problems such as menstrual and/or urinary irregularities. Such conditions can be traced to a variety of factors, including pregnancy and childbirth, genetic factors, obesity, medications and complications of surgical procedures.
As many of these risk factors also are highly correlated with age, it is critically important to examine how Baby Boomer women are affected by pelvic health disorders (PHDs). In fact, the onset of many PHDs is frequently between the ages of 40 and 60. Gaining a stronger understanding of the current prevalence and treatment patterns of PHDs for Baby Boomer women can help inform and educate policymakers and practitioners about the severity, frequency and diagnosis of these disorders, as well as appropriate treatment options.
This report, funded by the National Women’s Health Resource Center (NWHRC), examines four pelvic health disorders – menorrhagia, uterine fibroids, stress urinary incontinence (SUI) and pelvic organ prolapse (POP) – that commonly affect women and, in particular, Baby Boomer women born between 1946 and 1964.
The goal of this report is to address the following five primary questions for each of the respective pelvic health disorders:
1) What is the prevalence among women in the U.S., and how does prevalence differ by age and other demographic variables? How are Baby Boomer women affected?
2) How do these disorders affect women and, in particular, Baby Boomers in the U.S.? What is their overall impact on quality of life?
3) To what extent is the magnitude and severity of these disorders properly recognized and understood by public health practitioners, researchers and policymakers?
4) Does a treatment gap exist (the gap between the prevalence of the disorder and treatment)? Are there any barriers women face when attempting to access treatment for these disorders?
5) Do current treatment patterns reflect the most effective and appropriate standards of practice? Are clinical practice guidelines followed by physicians?
A detailed literature review and analysis of hospital discharge data was employed to address the aforementioned questions, however, not all questions could be answered fully, as there has been limited research on most of these topics and the available literature often was incomplete or outdated. Specifically, there have been few large-scale, representative studies and surveys on the incidence, prevalence and treatment patterns of each disorder, much less studies that look at the comorbidity of these often related disorders. Information also is limited on demographic patterns, including age and economic factors (for example, health insurance coverage) that may influence the onset of each disorder and access to care.
1-1

Pelvic Health Disorders Introduction and Key Findings
Key Findings
The following key findings emerged with respect to menorrhagia, uterine fibroids, stress urinary incontinence and pelvic organ prolapse, both from a review of the current literature and analysis of inpatient hospital discharge data.
1) At least one-third of all women in the United States will be treated for one or more pelvic health disorders by the age of 60—this will total at least 35 million of the 116 million women now 18 or older and 13 million of the 40 million Baby Boomers.
Exhibit 1: Prevalence of Pelvic Health Disorders
Among All Women and Baby Boomer Women
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Menorrhagia* Uterine Fibroids^ SUI POP
Baby Boomers+All Women Baby Boomers+Baby Boomers+All WomenAll Women
30%
40%
20-25%
35%
26-31%33%
N/A
40%
* Self-reported “excessive flow”. ^ Symptomatic. + Rate is for women aged 50-70 years. N/A: not available.
2) The Baby Boomer generation is currently in the phase of life with the highest rate of onset for pelvic health disorders. The incidence of SUI and POP is more common in women aged 40 to 60 years. In addition, the prevalence of menorrhagia increases with age, peaking just before menopause.
3) African American women are more likely to have uterine fibroids, while Caucasian women are more likely to be affected by stress urinary incontinence and pelvic organ prolapse. Epidemiological studies examining rates of hysterectomies among African American and Caucasian women have found that African American women are more likely to have fibroids and tend to be younger at the time of diagnosis and treatment.
1-2

Pelvic Health Disorders Introduction and Key Findings
4) Pelvic health disorders have a substantial impact on women’s health and their quality of life. These disorders often cause complications with sexual dysfunction, fertility and pregnancy, anemia, abdominal pain and pressure, low self-esteem and depression.
5) Women’s reluctance to consult their physician about symptoms associated with pelvic health disorders results in under- and/or misdiagnosis, further complicating the treatment and overall understanding of the impact of these disorders on U.S. women and Baby Boomers.
All four disorders are suspected to be under diagnosed among women in the U.S. due to: a) lack of understanding by women that certain symptoms may be abnormal (e.g., pelvic pain, heavy menses); and b) the embarrassing nature of the disorder (e.g., urinary leakage associated with SUI), making women reluctant to report symptoms.
Approximately 50 to 75 percent of women who likely have stress urinary incontinence fail to tell their health care providers about their symptoms and, therefore, are never properly diagnosed and treated.
Only 10 to 20 percent of women with pelvic organ prolapse seek medical care for the condition and many do not report their symptoms to physicians due to embarrassment or a general belief that the disorder is merely a normal part of the aging process.
6) Uterine fibroids and menorrhagia are the leading indications for hysterectomy in the United States. Nearly one-third of all hysterectomies are performed to treat uterine fibroids.
Approximately 600,000 hysterectomies are performed each year, and their use has remained relatively constant over the last two decades.
Exhibit 2: Annual Trends in Hysterectomies
1988-2005
0
100
200
300
400
500
600
700
1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
100,
000s
Source: Analysis of National Hospital Discharge Survey by The Lewin Group
1-3

Pelvic Health Disorders Introduction and Key Findings
In 2005, hysterectomies were more common among women between the ages of 40 and 49 relative to other age groups (this pattern has held true for several decades).
Exhibit 3: Annual Number and Rate of Hysterectomies, by Age
2005
0
50
100
150
200
250
300
0
20
40
60
80
100
120
0-19Years
20-29Years
30-39Years
40-49Years
50-59Years
70+Years
60-69Years
Num
ber
of H
yste
rect
omie
sRate of H
x/10,000W
omen/Year
Source: Analysis of National Hospital Discharge Survey by The Lewin Group.
7) More invasive forms of hysterectomy still are most commonly used to treat uterine fibroids and menorrhagia, despite the availability of less invasive surgical alternatives and medical treatments that don’t require hospitalization or extended recovery time. Recent technological advances have broadened the options available to patients, however, evidence suggests such advances have not been incorporated broadly into physician practice patterns.
The last decade has yielded significant improvements in minimally invasive techniques for the treatment of menorrhagia and uterine fibroids, including the use of laparoscopic and hysteroscopic procedures such as laparoscopic hysterectomy, myomectomy, endometrial ablation and uterine artery embolization. These approaches require smaller incisions, resulting in shorter inpatient stays or even outpatient surgical or in-office procedures, reduced pain and discomfort, fewer complications and faster recoveries that enable patients to return to routine activities in a shorter period of time.
Despite the availability of less invasive approaches, abdominal hysterectomy is still the most common form of surgical treatment in cases where uterine fibroids or menorrhagia is the primary diagnosis.
In 2005, 44 percent (256,300) of all hysterectomies performed were for women with a primary diagnosis of uterine fibroids or menorrhagia. Of these procedures, nearly 71
1-4

Pelvic Health Disorders Introduction and Key Findings
percent (181,627) were performed for Baby Boomer women with a primary or secondary diagnosis of uterine fibroids or menorrhagia.
Only approximately 15 percent of all hysterectomies for Baby Boomers, as well as women generally, were performed using the less invasive laparoscopic method.
8) Current patterns of care indicate that clinically recommended and effective treatments generally are employed for each disorder. However, some clinicians and researchers are concerned about the common use of hysterectomies for menorrhagia and uterine fibroids, as well as the rate of anterior repairs used to treat stress urinary incontinence.
Several studies have found that for approximately 15 percent of women diagnosed with menorrhagia, the actual cause of excessive bleeding is von Willebrand disease, a bleeding disorder that causes blood to not clot properly. Due to inaccurate diagnosis, women with von Willebrand disease may be receiving inappropriate treatments, such as hormonal therapies or surgical procedures (e.g., hysterectomies or endometrial ablation) that do not address the underlying cause of their symptoms.
In approximately 10 percent of surgical cases for SUI, anterior repairs are performed, despite numerous studies demonstrating that they are not as effective as alternative surgical procedures and have higher rates of complications.
Despite the high prevalence, and the impact on quality of life associated with pelvic health disorders, there has been limited epidemiological study of these conditions in the U.S., particularly with respect to how Baby Boomers are affected. The literature suggests that many patients, clinicians and policymakers may not have the information they need for adequate diagnosis or to make truly informed decisions about appropriate treatments. Given the prevalence of these conditions and their substantial impact on women’s lives, future research priorities should include:
Development of standard measures of the overall impact (e.g., quality of life and costs) and severity of pelvic health disorders on women and, in particular, Baby Boomer women.
Longitudinal studies to identify lifetime incidence, prevalence, patterns of care, risk factors and comorbidity between these related disorders.
Development and adoption of standard, clinically accepted definitions for each disorder that further clarify to what extent symptoms should be deemed problematic and, therefore, warrant treatment.
Methodologically rigorous studies of minimally invasive and medical treatments for pelvic health disorder to obtain long-term data on their effectiveness and impacts.
1-5

Pelvic Health Disorders Introduction and Key Findings
Organization of the Report
This report is organized into the following five sections and appendices:
Section I: Introduction and Key Findings, including an overview of the report and key findings for each pelvic health disorder
Section II: Prevalence and Treatment of Menorrhagia
Section III: Prevalence and Treatment of Uterine Fibroids
Section IV: Prevalence and Treatment of Stress Urinary Incontinence
Section V: Prevalence and Treatment of Pelvic Organ Prolapse
Section VI: Conclusion
Appendix A: Glossary
Appendix B: Methods
1-6

Pelvic Health Disorders Menorrhagia
Menorrhagia
Background
Menorrhagia is the most common type of abnormal uterine bleeding, characterized by heavy and prolonged menstrual bleeding. Clinically, menorrhagia is defined as blood loss of 80ml or more per menstrual cycle or menses lasting longer than seven days (menstrual flow that soaks through one or more sanitary pads or tampons every hour for several consecutive hours).1 There is a marked variation in a woman’s sensitivity to this degree of blood loss, with many women either over- or under-reporting their menstrual loss. One study found that 40 percent of women who met the clinical definition of menorrhagia considered their periods either “light” or “moderate”.2
Although menorrhagia is not a life-threatening condition, it can have a negative impact on a woman’s lifestyle and self-esteem. Some of the possible complications resulting from menorrhagia include iron deficiency, anemia and infertility.
Over onaffecte40s andas theyhormondescribthat arBoomer Babymenocohoof woexpe
In 20werewommenoBoom180,0
Some studies suggest that a specific cause for menorrhagia is identified in less than 50 percent of affected women.3 The most common causes of menorrhagia are hormonal imbalances and uterine fibroids. Other less common causes include polyps, ovarian cysts and endometrial or cervical cancer.1
The onset of the disorder can vary, however, teenagers often experience menorrhagia in the 12 to 18 months after their first menstrual period (menarche), while women in their 40s and 50s tend to experience menorrhagia when they approach menopause due to hormonal imbalances. Most women diagnosed with menorrhagia are over 30.1
Prevalence
Overall, using a broad definition of menorrhagia (self-reported excessive or heavy menses) the general consensus in the field is that approximately 30 percent of women experience menorrhagia in their lifetime. However, the most widely cited U.S. and international population-based studies and reviews have found that the prevalence of women who meet the clinica(blood loss of 80ml or more per menstrual cycle) is between 9 amillion women.2, 4-6
Baby Boomers particularly are affected by menorrhagia, as onewomen found that 39.5 percent of women aged 45 to 60 years rmenstrual periods.7 Using the stricter clinical definition of the percent of all women diagnosed with menorrhagia are older th
The Impact of Menorrhagia on Baby Boomers
e-third of all Baby Boomers are d by menorrhagia. Women in their 50s tend to experience the disorder approach menopause due to al imbalances. The following es other key aspects of the disorder e relevant particularly to the Baby generation: Boomers particularly are affected by rrhagia, as one study of an Italian
rt of women found that 39.5 percent men aged 45 to 60 years reported
riencing heavy menstrual periods. 05, over 250,000 hysterectomies performed in the United States for en with a primary diagnosis of rrhagia or uterine fibroids. For Babyers with the same diagnoses, 00 hysterectomies were perf
over
ormed.
l definition for menorrhagia nd 14 percent, or 6.8 to 10.6
study of an Italian cohort of eported experiencing heavy disorder, approximately 50 an 45 years of age.8
2-1

Pelvic Health Disorders Menorrhagia
Exhibit 4: Prevalence of Menorrhagia, All Women vs. Baby Boomer Women
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
All Women Baby Boomers
9.0-14.0%^8.8-12.6%+
30.0%*
40.0%+
80+ ml Flow per MonthHeavy Menses/Excessive Flow80+ ml Flow per MonthHeavy Menses/Excessive Flow
Sources: Oehler, 2003; Shaw, 2007; Marino, 2004; Hallberg, 1966; Cole, 1971; Dilley, 2002; Van Eijkeren, 1989. * n=108 million, based on 2000 U.S. Census data. ^ n=76 million women, aged 15 to 51 years, based on 2000 U.S. Census data. + n=39.5 million women, aged 40 to 60 years, based on 2000 U.S. Census data.
It is widely accepted that the prevalence of menorrhagia increases with age.9 However, it is difficult to obtain good estimates of menorrhagia, as most available data is based on individuals seeking care for the disorder rather than population-based studies.
Diagnosis and Treatment Gaps
Many researchers suspect that menorrhagia may be either under or misdiagnosed in the general population.5, 10 Women often do not to report symptoms of the disorder to their physician, because they either are unaware that heavy menses is a treatable condition or that they are embarrassed by the nature of the problem.11 Even if the excessive or heavy bleeding does not meet the clinical definition of menorrhagia, some studies have found that even blood flow between 61 to 80ml per month still may cause medical problems (e.g., anemia) that warrant treatment.2 Some studies also suggest that up to two-thirds of women presenting with menorrhagia do not get treatment, despite discussing their options with a physician.12, 13
Research also suggests that physicians may be overlooking the true cause of menorrhagia in some women, leading to the use of inappropriate treatment options or no treatment at all. Up to 2 million women in the United States may have an undiagnosed bleeding disorder, which occurs when the blood does not clot properly.14 One study of a clinical population found that 47 percent of women with menorrhagia had hemostatic abnormalities, including platelet
2-2

Pelvic Health Disorders Menorrhagia
dysfunction, von Willebrand’s disease or coagulation factor deficiencies.3 According to the Centers for Disease Control and Prevention, separate studies conducted in Europe and the United States have shown that approximately 15 percent of women with menorrhagia may have von Willebrand disease (VWD), an inherited bleeding disorder.14
Treatment Options and Patterns of Care
The appropriate treatment for menorrhagia depends on the cause and severity of the bleeding, as well as the woman’s age and desire to have children. Treatment options typically include either medication or surgical treatment, including less invasive surgical procedures. Medical treatment is indicated when there is no obvious pelvic abnormality (e.g., uterine fibroids or polyps) and the woman wishes to retain her fertility. Effectiveness of medication treatments range but, in one study, it was only 15 percent and can have significant side effects.8, 15 Surgical treatment options range from less invasive procedures that remove the interior uterine lining to more invasive procedures that remove the uterus completely. Surgical procedures may be necessary to deal with pelvic abnormalities such as uterine fibroids, which often are associated with menorrhagia.16
Exhibit 5 describes the type of treatment options available for women with menorrhagia, including the degree of effectiveness and possible complications of each treatment.
Exhibit 5: Medical and Surgical Treatment Options for Menorrhagia
Option Effectiveness Potential Risks/Complications
Medical
Progestin Therapy Most frequently prescribed medicine for menorrhagia. Can reduce menstrual blood flow by 15%.1
Weight gain, headaches, edema and depression.
Oral Contraceptives Up to 60% effective at reducing menstrual blood flow.
Headaches, nausea, mood disturbance, breast tenderness and weight gain.17
Progestogens (to correct hormonal imbalance)
Norethisterone and medroxyprogresterone commonly are used. Up to 20% effective at reducing blood loss.
Similar to those associated with oral contraceptives.
Levonorgestrel-releasing Intrauterine System (a device implanted in the uterus for five years)
One study found reduced blood loss by 94%15, and that it was more effective than ablation.18
Intermenstrual bleeding, breast tenderness.
Danazol (a drug that suppresses the hormones that increase the endometrium)
Up to 100% effective at reducing menstrual blood loss.8
Developing male characteristics (e.g., facial hair, muscle mass).19
Nonsteroidal Anti-inflammatory Drugs
Can reduce menstrual blood flow by 25-35%.
Gastrointestinal problems.20
2-3

Pelvic Health Disorders Menorrhagia
Option Effectiveness Potential Risks/Complications
Surgical
Hysterectomy (surgical removal of the uterus via the abdomen or the vagina that can include using a laparoscope). Some hysterectomy methods that involve a laparoscope include laparoscopic supracervical hysterectomy (LSH) and laparoscopic-assisted vaginal hysterectomy.
100% effective at improving heavy menstrual bleeding.
Hysterectomy permanently impairs fertility. Longest recovery time associated with abdominal hysterectomy. There is a higher risk of infection following hysterectomy compared to ablation or resection procedures. More expensive than ablation or resection, and there is a longer operating and recovery period.
Endometrial or Uterine Ablation (removal of the endometrium or lining of the uterus); current UK guidelines for menorrhagia identify thermal balloon endometrial ablation and microwave endometrial ablation as the best treatment options in cases where surgical intervention is appropriate.21
Ablation procedures are less invasive and safer than hysterectomy and transcervical resection.22 According to research, 70-90% of patients reported successful reduction in menstrual bleeding following balloon ablation surgery.8 Some studies indicate the effects of microwave ablation are similar to hysterectomy (96% vs. 100%, respectively), but with the advantage of keeping the uterus intact.23
Additional surgery may be required. Short-term side effects include mild pain or discomfort resulting from surgery.
Transcervical Resection of the Endometrium (TCRE)
Achieves a nearly 86% success rate in reducing heavy menstrual flow. Reduced post-operative recovery time versus hysterectomy.
Resection has more complications than other procedures (i.e., ablation) that are equally effective.22 The primary risk is uterine perforation.13
Dilation & Curettage (D&C) (expanding the entrance of the uterus in order to scrape away the lining of the uterus and take tissue samples).
Effective at temporarily (2-6 months) stopping bleeding.24 Commonly used as a diagnostic technique to investigate the cause of heavy menstrual bleeding.
This procedure is now viewed as a temporary treatment with limited efficacy.17
The American College of Obstetricians and Gynecologists (ACOG) recommends that treatment for menorrhagia begin with the least invasive therapy.25 Exhibit 6 summarizes the 2000 ACOG recommendations for menorrhagia with respect to screening, treating and the overall management of the disorder.
Exhibit 6: Summary of ACOG Recommendations for Menorrhagia
Diagnosis/Screening Women with abnormal uterine bleeding should be screened for von Willebrand's disease, especially when bleeding otherwise is not easily explained or does not respond to medical therapy.
Treatment
The first treatment of choice for menorrhagia is medical therapy with oral contraceptives or cyclic progestins. Women for whom medical therapy is ineffective and who no longer desire future childbearing are candidates for endometrial ablation, which appears to be an efficient and cost-effective alternative treatment to hysterectomy.
2-4

Pelvic Health Disorders Menorrhagia
Despite guidelines recommending the initial use of medically less invasive surgical treatments, there is concern about the over use of hysterectomies to treat menorrhagia.10 Some research suggests that the majority of hysterectomies performed for menorrhagia are unnecessary, due to the fact that a large number of post-hysterectomy specimens show no abnormality, there is a non-trivial risk of complications, the high monetary cost and high disability during recuperation. 26
Hysterectomies still are commonly used to treat menorrhagia, especially for women who also have been diagnosed with uterine fibroids and who are in their later reproductive years.11, 12 In 2005, over 250,000 hysterectomies were performed in the United States for women with a primary diagnosis of menorrhagia or uterine fibroids. For Baby Boomers with the same diagnoses, over 180,000 hysterectomies were performed. Although the use of laparoscopic procedures for these diagnoses is increasing (from 23,615 procedures in 2000 to 39,473 in 2005), abdominal and vaginal hysterectomies still comprise nearly 85 percent of all hysterectomies performed for the treatment of menorrhagia and/or uterine fibroids.11, 27
Numerous surgical alternatives to hysterectomy have been developed for women that seek safe, effective and less invasive options.10, 28 Consistent with current ACOG guidelines, endometrial ablation increasingly is used to treat menorrhagia. According to one study, as of 2002, more than 100,000 women worldwide were treated with uterine balloon ablation (a form of endometrial ablation).11 In addition to providing a less invasive alternative, endometrial ablation is less costly, less traumatic than hysterectomy, causes less postoperative morbidity and is associated with a shorter recovery period.29-31 Studies comparing endometrial ablation to hysterectomy have found that both procedures are safe and effective.23, 32, 33 Endometrial ablation is performed as an outpatient procedure and can also be performed in an office setting.34, 35
However, endometrial ablation is not suitable for all types of menorrhagia, and women must have a benign cause for their menorrhagia and have no desire for future fertility before considering this option.12 In addition, treating women with endometrial ablation who have large fibroids on the uterus is associated with a higher incidence of complications.36 This underscores the need to carefully diagnose and rule out other disorders before selecting the appropriate treatment option for menorrhagia. In addition, a Cochrane review of published studies comparing endometrial ablation to hysterectomy found that endometrial ablation does not work for a fraction of patients, and they may require additional surgery to address the symptoms of menorrhagia.30
Endometrial resection is another treatment option that is less invasive than hysterectomy. One study found that resection complete relief of menorrhagia was achieved more often in women aged 45 years or older than in those aged 44 years or younger.37
Although ACOG guidelines recommend that women with abnormal uterine bleeding be screened for von Willebrand’s disease (VWD), a 2002 survey of gynecologists in Georgia indicates that only 4 percent of physicians consider the disease in the differential diagnosis of menorrhagia.5 The treatment of VWD as the underlying cause of menorrhagia requires a different course of treatment, including treatment with synthetic hormones called Desmopressin or with replacement therapy that are given by injection or nasal spray to increase the level of von Willebrand factor in the blood.38 Some concern exists that early recourse to surgical procedures to treat menorrhagia, such as hysterectomy, may not address the actual underlying cause.39
2-5
Pelvic Health Disorders Uterine Fibroids
Uterine Fibroids
Background
The Impact of Uterine Fibroids on Baby Boomers
Thirty-five percent of all Baby Boomers experience symptomatic uterine fibroids. Fibroids can be highly problematic for this generation, as the size of fibroids generally increase with age (until menopause) due to changes in hormonal levels during reproductive years. The following describes other key aspects of the disorder that are relevant particularly to the Baby Boomer generation: Approximately 70 percent of Caucasian women and 80 percent of African American women develop uterine fibroids by the age of 50 (average age of menopause is 51).
Most fibroids are diagnosed in women between the ages of 40 and 44 years.
Of the approximately 332,000 hysterectomies performed on Baby Boomer women in 2005, approximately 55 percent (181,627) were for a primary diagnosis of either uterine fibroids or menorrhagia.
Over seventy percent (2,700) of the uterine artery embolization procedures performed in 2005 were for Baby Boomers. The number of myomectomies dropped considerably for Baby Boomers between 2000 (11,000 p
Uterine fibroids (also called uterine leiomyomas or myomas) are smooth muscle tumors of the uterus and, generally, they are benign. Traditionally, fibroids are classified based on their location in relation to the uterine wall as either pedunculated, subserosal, intramural or submucosal. Pedunculated fibroids are attached to the uterus by a connective tissue stalk; they may be either intra-abdominal or in the uterine cavity. Subserosal fibroids lie just underneath the parietal peritoneum (outer layer) covering the uterus. Intramural fibroids are those where the bulk of the fibroid lies within the myometrium (middle of the uterine wall). Submucosal fibroids have all or a substantial part of their surface immediately beneath the endometrium (lining of the uterus). The location and size of the fibroid helps to determine appropriate treatment options.
The exact cause of fibroids is unknown, however, ovarian hormones are believed to play a key role in the etiology of uterine fibroids.40 Fibroids tend to develop after puberty and regress after menopause. Heredity, race and obesity also are known risk factors. Uterine fibroids often are diagnosed based on the physical appearance of an enlarged uterus on pelvic examination.41 Ultrasonography or magnetic resonance imaging also are used to confirm the diagnosis.41
The major symptoms associated with fibroids include heavy menstrual bleeding (menorrhagia), pelvic pressure and pain and infertility.41 Fibroids also may increase the risk of preterm labor and delivery and the risk for cesarean delivery.42
Whether symptomatic or asymptomatic, since uterine fibroids are associated with other serious health conditions (e.g., heavy menstrual bleeding), failing to properly diagnose and treat the disorder may result in other medical conditions (e.g., anemia).2
rocedures) and 2005 (6,000 procedures). Prevalence
Uterine fibroids are the most common benign tumors found in premenopausal women.43 Approximately 70 percent of Caucasian women and 80 percent of African American women develop fibroids by the age of 50.44 For many of these women, they may not be aware that they have fibroids, as they often are asymptomatic.44 As a result, much of the literature for uterine fibroids is based on samples of clinical cases and women who undergo treatment.
3-1

Pelvic Health Disorders Uterine Fibroids
Fibroids are symptomatic in approximately 20 to 25 percent of all reproductive age women (aged 30 to 60 years).7, 45 In one population-based study, approximately 35 percent of women aged 45 to 60 years had symptomatic uterine fibroids.7
The prevalence and the size of uterine fibroids increase with age (until menopause), due to changes in hormonal levels during women’s reproductive years. Approximately 35 percent of women in their 30s and 40s have either symptomatic or asymptomatic uterine fibroids.44 Most fibroids are diagnosed in women between the ages of 40 and 44 years.46 African American women are more likely than Caucasian women to have symptomatic fibroids and are diagnosed earlier in life, while Asian and Hispanic women have rates similar to Caucasian women.41, 46
Exhibit 7: Prevalence of Uterine Fibroids
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
All Women* Baby Boomers^
20-25%
35%
Source: Lewin Group analysis of the U.S. Census Bureau data, 2004. Prevalence estimates based on the following sources: Day Baird, 2002; Marino 2004; Buttram 1981. * Includes women aged 30 to 60 years. ^Includes women aged 45 to 60.
For many women with fibroids, their symptoms are reduced or relieved at the time of menopause as their hormone levels decline. However, some studies have found that women taking hormone replacement therapy (HRT) to alleviate symptoms of menopause are at increased risk of developing symptomatic uterine fibroids.41 One study of postmenopausal women found HRT does increase uterine size in the first two years of use, however, the increased size appears to decline in the third year of HRT treatment.47
3-2

Pelvic Health Disorders Uterine Fibroids
Diagnosis and Treatment Gaps
Current research available on uterine fibroids does not address how many women who have fibroids (either symptomatic or asymptomatic) seek treatment for the condition. What is known is that many other conditions have symptoms that mimic uterine fibroids (e.g., menorrhagia, pelvic pain and pressure, pregnancy complications) and that, consequently, a large majority of women with fibroids may not report any symptoms related to the disorder to their physicians because they may mistake them for these disorders.42
For women with asymptomatic fibroids, there is no evidence to suggest that failure to treat with medical or surgical therapy will result in harmful outcomes. In addition, women with symptomatic fibroids may not require treatment if a woman is close to menopausal age, making it more likely that the symptoms will decline naturally.48 However, leaving the condition untreated (whether medically or surgically) may have serious health consequences, as some of the symptoms associated with fibroids (e.g., heavy menstrual bleeding) may lead to other medical conditions (e.g., anemia, infertility) if left untreated.2
Treatment Options and Patterns of Care
There are a variety of effective treatments for uterine fibroids. While hysterectomy has been a leading option for many years, technological advances have broadened the options available to patients and medical practitioners. Selection of the type of treatment is determined by the size and location of the fibroid, symptoms of the disorder and the age and reproductive desires of the woman.41 Fibroids that do not cause symptoms, that are small or that occur in a woman nearing menopause often do not require treatment.41
Fibroids may be treated medically or with surgery (including the use of minimally invasive procedures). Hysterectomy is a common and highly effective surgical treatment option that removes the uterus along with the fibroids, and the peak incidence for hysterectomies due to fibroids occurs around age 45.43 The procedure can be performed abdominally or through laparoscopically assisted vaginal procedures. Myomectomy is another surgical treatment option that removes the fibroid(s) while preserving the uterus.
Uterine artery embolization (UAE) is a newer, minimally invasive form of treatment that reduces blood supply to fibroids, resulting in a decrease in size. Endometrial ablation can be used for some fibroids on the inner wall of the uterus. MRI guided focused ultrasound surgery is the newest minimally invasive treatment option, but little is known about its effectiveness. Medical treatments for uterine fibroids do not tend to be effective, long-term solutions.49
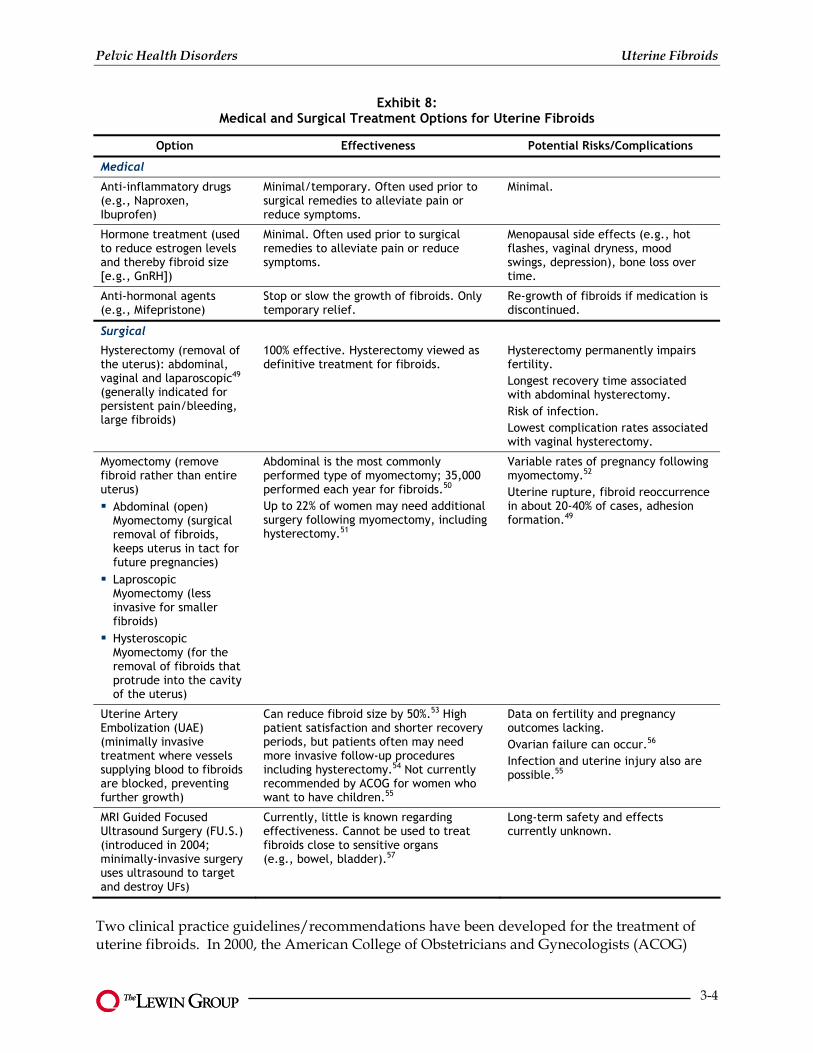
Exhibit 8 describes the various treatment options, their effectiveness and potential complications.
3-3
Pelvic Health Disorders Uterine Fibroids
Exhibit 8: Medical and Surgical Treatment Options for Uterine Fibroids
Option Effectiveness Potential Risks/Complications
Medical
Anti-inflammatory drugs (e.g., Naproxen, Ibuprofen)
Minimal/temporary. Often used prior to surgical remedies to alleviate pain or reduce symptoms.
Minimal.
Hormone treatment (used to reduce estrogen levels and thereby fibroid size [e.g., GnRH])
Minimal. Often used prior to surgical remedies to alleviate pain or reduce symptoms.
Menopausal side effects (e.g., hot flashes, vaginal dryness, mood swings, depression), bone loss over time.
Anti-hormonal agents (e.g., Mifepristone)
Stop or slow the growth of fibroids. Only temporary relief.
Re-growth of fibroids if medication is discontinued.
Surgical
Hysterectomy (removal of the uterus): abdominal, vaginal and laparoscopic49 (generally indicated for persistent pain/bleeding, large fibroids)
100% effective. Hysterectomy viewed as definitive treatment for fibroids.
Hysterectomy permanently impairs fertility. Longest recovery time associated with abdominal hysterectomy. Risk of infection. Lowest complication rates associated with vaginal hysterectomy.
Myomectomy (remove fibroid rather than entire uterus)
Abdominal (open) Myomectomy (surgical removal of fibroids, keeps uterus in tact for future pregnancies) Laproscopic Myomectomy (less invasive for smaller fibroids) Hysteroscopic Myomectomy (for the removal of fibroids that protrude into the cavity of the uterus)
Abdominal is the most commonly performed type of myomectomy; 35,000 performed each year for fibroids.50 Up to 22% of women may need additional surgery following myomectomy, including hysterectomy.51
Variable rates of pregnancy following myomectomy.52 Uterine rupture, fibroid reoccurrence in about 20-40% of cases, adhesion formation.49
Uterine Artery Embolization (UAE) (minimally invasive treatment where vessels supplying blood to fibroids are blocked, preventing further growth)
Can reduce fibroid size by 50%.53 High patient satisfaction and shorter recovery periods, but patients often may need more invasive follow-up procedures including hysterectomy.54 Not currently recommended by ACOG for women who want to have children.55
Data on fertility and pregnancy outcomes lacking. Ovarian failure can occur.56 Infection and uterine injury also are possible.55
MRI Guided Focused Ultrasound Surgery (FU.S.) (introduced in 2004; minimally-invasive surgery uses ultrasound to target and destroy UFs)
Currently, little is known regarding effectiveness. Cannot be used to treat fibroids close to sensitive organs (e.g., bowel, bladder).57
Long-term safety and effects currently unknown.
Two clinical practice guidelines/recommendations have been developed for the treatment of uterine fibroids. In 2000, the American College of Obstetricians and Gynecologists (ACOG)
3-4

Pelvic Health Disorders Uterine Fibroids
issued guidelines that focused on medical and surgical alternatives in the management of uterine fibroids, including medications, hysterectomy and other operative procedures. In 2004, the Society of Interventional Radiology (SIR) issued recommendations on the use of uterine artery embolization (UAE). Exhibit 9 summarizes both ACOG’s and SIR’s recommendations for the treatment of uterine fibroids.
Exhibit 9: Summary of ACOG and SIR Recommendations for Uterine Fibroids
The American College of Obstetricians & Gynecologists (ACOG) Level A (consistent with scientific evidence)
In women with symptomatic leiomyomas, hysterectomy provides a definitive cure. In women with symptomatic leiomyomas, abdominal myomectomy is a safe and effective option for women who wish to retain their uterus. If this option is selected, women should be counseled preoperatively about the relatively high risk of reoperation. Use of gonadotropin-releasing hormone (GnRH) agonists preoperatively is beneficial, especially when improvement of hematologic status and uterine shrinkage are important goals. Benefits of the use of GnRH agonists should be weighed against their cost side effects for individual patients. The use of vasopressin at the time of myomectomy appears to limit blood loss.
The American College of Obstetricians & Gynecologists (ACOG) Level C (based primarily on consensus and expert opinion)
Laparoscopic myomectomy appears to be a safe and effective option for women with a small number of moderately sized uterine leiomyomas who do not desire future fertility. Further studies are necessary to evaluate the safety of this procedure for women planning pregnancy. Hysteroscopic myomectomy is an effective option for controlling menorrhagia in women with submucosal leiomyomas. Although endometrial ablation appears to be an effective option in controlling menorrhagia in women without leiomyomas, further studies are needed in women who have clinically significant leiomyomas. Because leiomyomas may be a factor in infertility for some patients, the issues are complex, and myomectomy should not be performed without first completing a comprehensive fertility evaluation. Although postmenopausal women with leiomyomas may have more bleeding problems and some increase in leiomyoma size while taking hormone replacement therapy, there appears to be no reason to withhold this treatment option from women who desire or need such therapy.
The Society of Interventional Radiology
Uterine artery embolization should be offered only to patients with symptomatic uterine fibroids. In addition, every patient who undergoes UAE should have a complete gynecological examination within 12 months before the procedure to confirm the diagnosis of UF and exclude other significant pathology.
Although ACOG identified hysterectomies as a “definitive” treatment for symptomatic uterine fibroids, concern remains about the high use of the procedure given the availability of medical as well as less invasive surgical treatment options.58, 59 In 2005, 256,300 hysterectomies were performed for women diagnosed with a primary diagnosis of either uterine fibroids or menorrhagia. Although the use of hysterectomy has declined approximately 10 percent since 2000, over 77 percent of these procedures performed in 2005 were abdominal, the most invasive form of hysterectomy.27
Hysterectomy also is commonly used to treat Baby Boomers with primary diagnosis of either uterine fibroids or menorrhagia. Of the approximately 332,000 hysterectomies performed on Baby Boomer women in 2005, approximately 55 percent (181,627) were for a primary diagnosis
3-5

Pelvic Health Disorders Uterine Fibroids
of either uterine fibroids or menorrhagia. Of these procedures, less than 15 percent were performed laproscopically.27
Exhibit 10: Total Number of Discharges for Hysterectomy
Baby Boomer Women with a Primary Diagnosis of Menorrhagia or Uterine Fibroids 2000-2005
0
20
40
60
80
100
120
140
160
180
200
220
240
2000 2001 2002 2003 2004 2005
100,
000s
Abdominal HysterectomiesLaparoscopic HysterectomiesTotal HysterectomiesVaginal HysterectomiesAbdominal HysterectomiesLaparoscopic HysterectomiesTotal HysterectomiesVaginal Hysterectomies
234,969
31,292
135,084148,083
163,601
179,355193,318
159,715
215,378
240,931
217,021
199,764
181,627
18,831
32,76019,144
26,55121,807
28,887
18,035
36,668
18,230
36,110
18,760
Note: Abdominal hysterectomies includes the categories of total abdominal, subtotal abdominal and radical abdominal. Vaginal hysterectomies include the categories of vaginal and radical vaginal. Laparoscopic hysterectomies includes the categories of laparoscopically assisted vaginal and laparoscopic service. Source: Lewin analysis of National Hospital Discharge Survey data, 2000-2005.
Although the use of uterine artery embolization (UAE) to treat uterine fibroids remains small compared to hysterectomy, the procedure is more common in treating symptomatic uterine fibroids. An estimated 13,000-14,000 UAE procedures (inpatient and outpatient) are performed annually in the U.S..60 In addition, inpatient UAE procedures for women with a primary diagnosis of uterine fibroids increased 40 percent between 2000 and 2005, from 2,700 to 3,800 respectively. Baby Boomers accounted for over 70 percent (2,700 cases) of the UAE procedures performed in 2005.27
Studies comparing UAE to hysterectomy have found that both procedures are safe and effective.61 In addition, a recent systematic review of the literature comparing UAE to hysterectomy found that UAE has a shorter hospital stay and a quicker return to routine activities.62 Some studies also have concluded that UAE is more cost-effective than hysterectomy.63
Still, current research also indicates the need for further studies on the safety and overall effectiveness of UAE. Some studies have documented that complications, such as ovarian failure, can occur in a small percentage of patients after UAE56 and that the potential need for subsequent surgery (resorting to hysterectomy after less invasive treatments have been
3-6

Pelvic Health Disorders Uterine Fibroids
attempted) may be greater than is the case with abdominal hysterectomy.64 ACOG recommends that women who wish to retain their fertility be fully informed of the lack of evidence regarding the effect of UAE on fertility and pregnancy outcomes before they decide to undergo the procedure.65
Despite ACOG’s guideline indicating that myomectomy is a safe and effective alternative for women with uterine fibroids who want to retain their uterus, the number of procedures performed in recent years has increased only slightly. In 2000, approximately 21,000 inpatient myomectomy procedures were performed, compared to 23,000 in 2005. The number of myomectomies dropped considerably for Baby Boomers between 2000 (11,000 procedures) versus 2005 (6,000 procedures). Relatively infrequent use of the procedure may be due to the risk of recurring fibroids or the increased use of less invasive procedures. One study found that 27 percent of the women who had a myomectomy had recurring fibroids within 10 years.66 Studies comparing UAE to myomectomy report that women undergoing UAE returned to work sooner, spent half as many days in the hospital and didn’t need general anesthesia.67 However, no noticeable difference was observed between the procedures in terms of improving the symptoms of uterine fibroids.67
The treatment of African American women with uterine fibroids differs compared to the types of treatment received by Caucasian women. The time from diagnosis of uterine fibroids to hysterectomy is longer for African Americans than for Caucasians, however African American women tend to undergo hysterectomy at a younger age than Caucasian women due to their earlier age at diagnosis.46 In addition, studies suggest that African American women are more likely to have in-hospital complications from surgical therapy, which can be attributed at least, in part, to having larger and more numerous fibroids than Caucasian women.68
Patterns also differ with respect to treating pregnant women. Some evidence suggests that the presence of uterine fibroids is associated with pregnancy complications. A population-based study in Washington found that pregnant women with fibroids were more likely to experience pregnancy complications (e.g., pain, first trimester bleeding, premature rupture of membranes and abruption) than women without fibroids.69 Studies also have found that pregnant women with fibroids are more likely to have labor and delivery complications (e.g., breech position, cesarean delivery) than pregnant women without fibroids.69 As a result, pregnant women with uterine fibroids are more likely to undergo laparotomy than are pregnant women without fibroids.70
3-7

Pelvic Health Disorders Stress Urinary Incontinence
Stress Urinary Incontinence
Background
Stress urinary incontinence (SUI), the most common form of urinary incontinence, involves the involuntary leakage of urine upon effort or exertion, such as sneezing or coughing. 71 The two basic underlying causes of SUI are weakening of pelvic muscles that support the bladder and urethra (urethral hypermobility) or abnormalities in the urethral sphincter (intrinsic sphincter deficiency, ISD). These two conditions also may coexist.
Symptoms include the accidental leakage of urine during physical activities such as sneezing, coughing, laughing, lifting or exercising. Other physical symptoms include vaginal discharge, vulvar irritation, pain during intercourse and unpleasant odors. Women with slight incontinence generally have a few drops of leakage a few times each month, whereas women with severe incontinence experience large amounts of leakage at least once every week. 72 Therefore, SUI is viewed commonly as an embarrassing and bothersome medical condition which can have a significant impact on a woman’s quality of life. The condition may result in social isolation, loss of self-esteem, increased expenses, emotional distress, sexual dysfunction and depression.73
SUI may coexist with urge incontinence. Urge incontinence, also known as overactive bladder, is characterized by a sudden uncontrollable urge to urinate. The presence of both SUI and urge incontinence in a patient is known as mixed incontinence and affects an estimated 30 percent of women with SUI. 74, 75
Common risk factors for SUI in women include pregnancy and childbirth, previous pelvic or vaginal surgery, high-impact physical activity, menopausal status and anatomic or neurologic abnormalities and advancing age. Smoking and chronic conditions such as respiratory ailments, obesity, constipation and chronic coughing also predispose women to SUI. 76
An essential aspect of managing SUI is an accurate diagnosis of the cause(s). The selection of a treatment option, especially surgical, will vary based on the presence of either urethral hypermobility, ISD or both.77 Treatment options also must be assessed based on the severity of the symptoms, patient preference, potential child-bearing and overall health and medical history of the patient. Basic evaluation of women with symptoms of SUI involves a careful review of medical history and physical examination. A comprehensive assessment may include urodynamic testing, post-void residual (PVR), urinary stress test and cystoscopy.78
Behavioral interventions, such as pelvic floor muscle exercises and lifestyle changes, usually are the first line of therapy recommended to patients, especially for mild to moderate SUI. Although available to patients in Europe, currently, there are no medications approved for the treatment of SUI in the U.S..78 Generally, surgical interventions are used for moderate to severe SUI, but only after non-surgical treatments have been proven ineffective.78, 79
Prevalence
Stress urinary incontinence is a common condition affecting women of all ages—particularly those who have had a vaginal delivery—with a higher prevalence in women between the ages of 40 and 60 years. Based on data from two national cross-sectional studies conducted in the U.S., SUI has a significant impact on Baby Boomer women, with an estimated 13.5 million
4-1

Pelvic Health Disorders Stress Urinary Incontinence
women (33 percent) suffering from the disorder.73, 80,a Overall, SUI has a negative impact on nearly 30 percent of all women over the age of 18 in the U.S. (31 million), with prevalence estimates ranging between 26 to 31 percent.73, 80,b
The Impact of Stress Urinary Incontinence on Baby Boomers
One-third of all Baby Boomers (13.5 million women) are affected by stress urinary incontinence. The following describes other key aspects of the disorder that are particularly relevant to the Baby Boomer generation: The prevalence of severe SUI (large amounts of leakage at least once a week) increases with age. Approximately 29 percent of women aged 25 to 44 years experience severe symptoms of SUI, compared to 33 percent of women aged 45 to 60 years and 86 percent of women aged 60 years and older.
Women who seek treatment for SUI are generally over the age of 60 due to the increasing severity of their symptoms.
However, prevalence rates for SUI cited in the literature differ as a result of variation in survey methods, definitions of incontinence and study populations. This is further complicated by the fact that the majority of research is concentrated on the prevalence of overall urinary incontinence, with only a limited number of studies that are specific to SUI. For example, the EPINCONT survey, a well-known study conducted in Norway in the late 1990s, found prevalence for stress and mixed UI to be as low as 12 and 21 percent, respectively. Similarly, a meta-analysis of 48 epidemiologic studies between 1954 and 1998 determined prevalence rates of 17 and 27 percent for stress and mixed urinary incontinence. While a more specific definition of SUI is needed in the field in order to provide accurate prevalence estimates, there is agreement among research that SUI is the most common form of urinary incontinence and a growing problem among women.
Exhibit 11: Prevalence of Stress Urinary Incontinence
All Women and Baby Boomer Women
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
All Women(n=108M)
Baby Boomers*(n=39.6M)
26-31%
50%
33%
30.1M13.1M
Source: Muller, 2005; Fultz 2003. *Includes women aged 45 to 64.
4-2
a Based on average of SUI prevalence among women aged 40-60 years cited in the studies and 2000 Census Data. b Based on average of overall SUI prevalence cited in the studies and 2000 Census Data.

Pelvic Health Disorders Stress Urinary Incontinence
Prevalence estimates differ according to symptom severity. Approximately half of women with SUI (53 percent ) have slight incontinence, while 17 percent have severe incontinence.81 The prevalence of severe SUI also increases with age, with 29 percent, 33 percent and 86 percent of women aged 25 to 44 years, 45 to 60 years and 60 years and older experiencing severe symptoms of SUI, respectively. 81, 82
An estimated three-quarters of women with SUI report symptoms to be bothersome, while more than one-quarter report moderate to extremely bothersome symptoms.73, 81 Of women with more bothersome symptoms, 54 percent believe their symptoms have a moderate to extreme impact on physical activities, 43 percent perceived a similar impact on confidence, 39 percent on daily activities and 37 percent on social activities.73 As a result, one study reported that nearly 60 percent of women experiencing symptoms of SUI underwent some change in their lifestyle, another trend that increases with age.80
Prevalence of SUI also varies based on race. Caucasian women are 2.8 times more likely to have weekly stress incontinence than African American women. Research has suggested that the higher prevalence among Caucasian women may be due to anatomic differences, such as shorter urethra and weaker pelvic floor muscles.83 Other risk factors that have an impact on prevalence include childbirth and previous pelvic surgery. Prevalence of SUI is significantly greater in women who have had vaginal deliveries, and it increases with each additional birth. In addition, women who have undergone previous pelvic surgery, especially hysterectomy, are at a 40 percent increased risk of developing SUI.76
Diagnosis and Treatment Gaps
Despite the fact that nearly one in every four women in the U.S. has SUI, the condition is both under diagnosed and underreported among all women.80, 84, 85 A study published in 2005 found that only 47 percent of women with SUI had ever consulted a physician about their symptoms.80 Studies also indicate that, while increasing symptom severity and duration are factors associated with treatment seeking, less than half of all women with the highest severity of SUI inquire about urinary incontinence treatment options.73 Studies examining overall urinary incontinence have reported that only an estimated 30 percent of all women tell their medical providers about their symptoms, with a lower consultation rate for SUI patients compared with other types of urinary incontinence.84-88 Therefore, overall, approximately 50 to 75 percent of women with stress urinary incontinence fail to tell their medical providers about their problems and get medical evaluation and treatment.73, 80, 84-89
Treatment seekers for urinary incontinence most often are women over the age of 60 with significantly worse urinary symptoms. In addition, positive attitudes toward health care contribute to the likelihood of women talking to their medical providers about SUI symptoms. For example, those who discuss the condition with physicians are more likely to schedule physician visits for routine physicals or preventive care and seek out medical information.84, 85 Those who do not seek treatment typically are younger and are less likely to view their symptoms as bothersome.
The embarrassment of talking about incontinence also prevents many women from discussing their symptoms with physicians. 84, 85 Overall, research indicates that SUI is widely misunderstood by all women. An unpublished online survey conducted across four U.S. cities in 2007 found that at least half of surveyed women were not aware of SUI and that, on average,
4-3
Pelvic Health Disorders Stress Urinary Incontinence
only 20 percent of those aware of the disorder had learned about it from their physician.90 These statistics are consistent with another study reporting that nearly 54 percent of all women and 34 percent of those failing to seek treatment view incontinence as a normal part of the aging process.
Physicians, thus, are encouraged to be proactive in asking and informing their patients about SUI symptoms.73 Researchers also recommend educating physicians and the general public about factors associated with treatment seeking and available treatment options, in order to increase the proportion of women seeking and receiving timely care.73, 84, 85, 91
Treatment Options and Patterns of Care
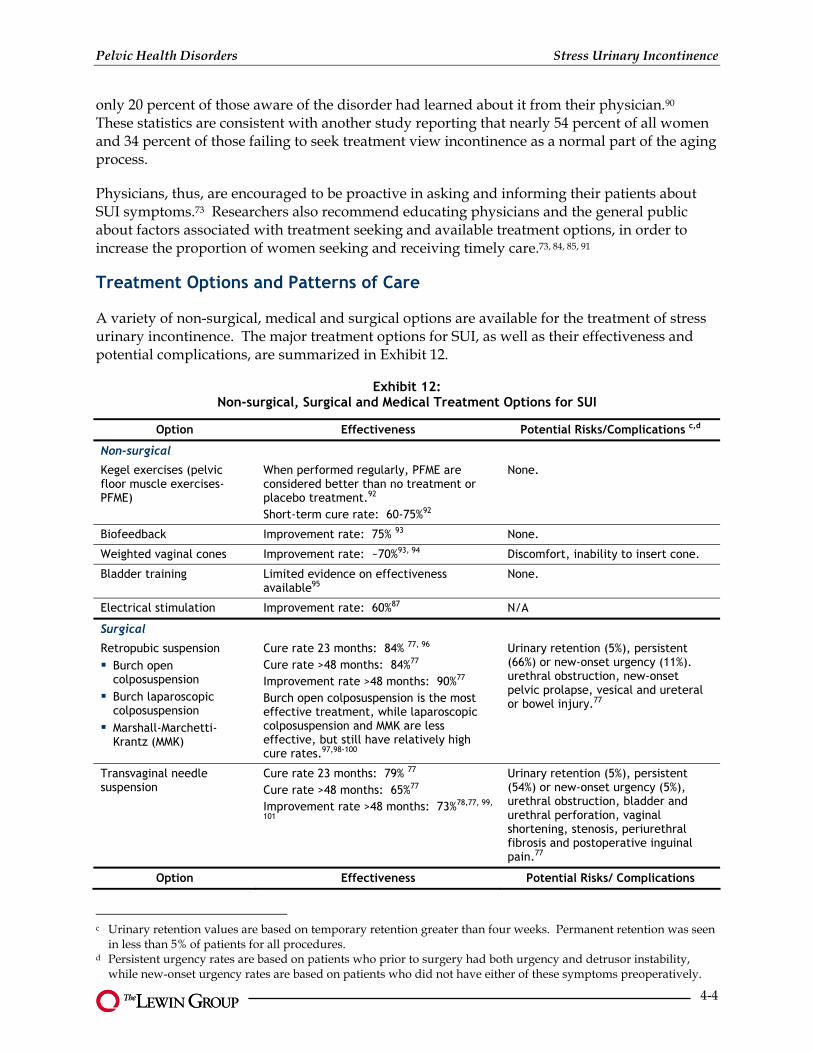
A variety of non-surgical, medical and surgical options are available for the treatment of stress urinary incontinence. The major treatment options for SUI, as well as their effectiveness and potential complications, are summarized in Exhibit 12.
Exhibit 12: Non-surgical, Surgical and Medical Treatment Options for SUI
Option Effectiveness Potential Risks/Complications c,d
Non-surgical
Kegel exercises (pelvic floor muscle exercises-PFME)
When performed regularly, PFME are considered better than no treatment or placebo treatment.92 Short-term cure rate: 60-75%92
None.
Biofeedback Improvement rate: 75% 93 None.
Weighted vaginal cones Improvement rate: ~70%93, 94 Discomfort, inability to insert cone.
Bladder training Limited evidence on effectiveness available95
None.
Electrical stimulation Improvement rate: 60%87 N/A
Surgical
Retropubic suspension
Burch open colposuspension Burch laparoscopic colposuspension Marshall-Marchetti-Krantz (MMK)
Cure rate 23 months: 84% 77, 96 Cure rate >48 months: 84%77 Improvement rate >48 months: 90%77 Burch open colposuspension is the most effective treatment, while laparoscopic colposuspension and MMK are less effective, but still have relatively high cure rates.97,98-100
Urinary retention (5%), persistent (66%) or new-onset urgency (11%). urethral obstruction, new-onset pelvic prolapse, vesical and ureteral or bowel injury.77
Transvaginal needle suspension
Cure rate 23 months: 79% 77 Cure rate >48 months: 65%77 Improvement rate >48 months: 73%78,77, 99,
101
Urinary retention (5%), persistent (54%) or new-onset urgency (5%), urethral obstruction, bladder and urethral perforation, vaginal shortening, stenosis, periurethral fibrosis and postoperative inguinal pain.77
Option Effectiveness Potential Risks/ Complications
c Urinary retention values are based on temporary retention greater than four weeks. Permanent retention was seen
in less than 5% of patients for all procedures. d Persistent urgency rates are based on patients who prior to surgery had both urgency and detrusor instability,
while new-onset urgency rates are based on patients who did not have either of these symptoms preoperatively.
4-4
Pelvic Health Disorders Stress Urinary Incontinence
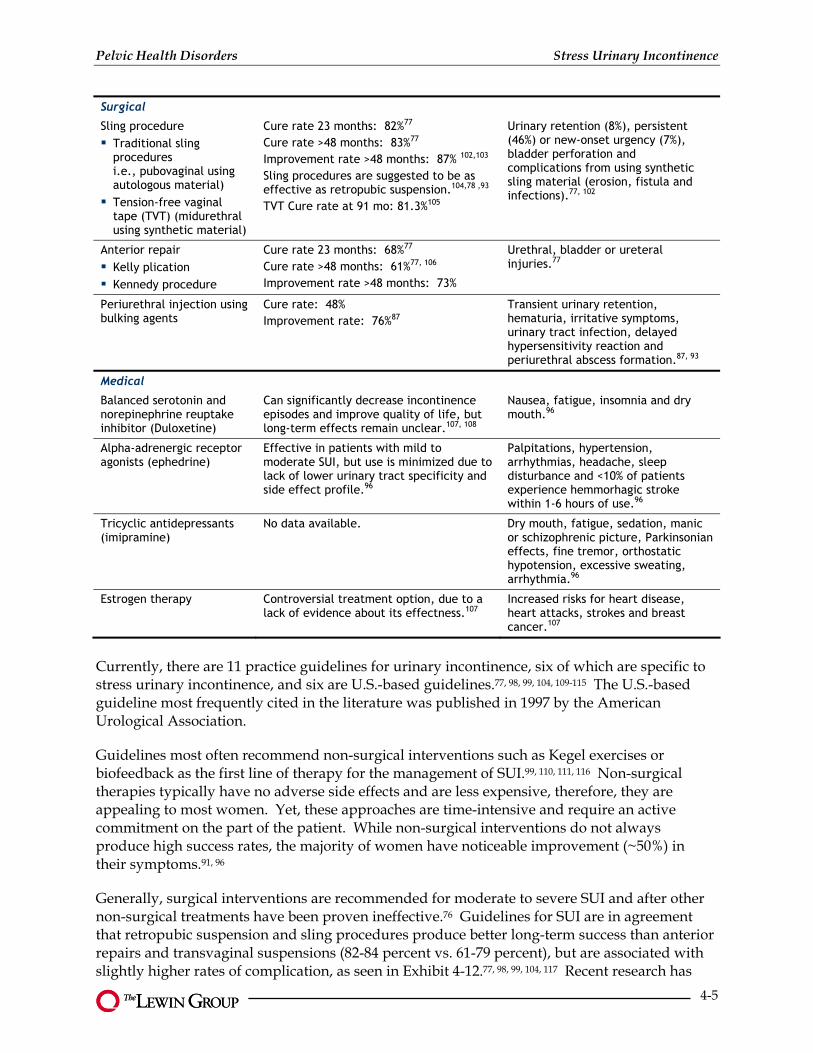
Surgical
Sling procedure
Traditional sling procedures i.e., pubovaginal using autologous material) Tension-free vaginal tape (TVT) (midurethral using synthetic material)
Cure rate 23 months: 82%77 Cure rate >48 months: 83%77 Improvement rate >48 months: 87% 102,103 Sling procedures are suggested to be as effective as retropubic suspension.104,78 ,93 TVT Cure rate at 91 mo: 81.3%105
Urinary retention (8%), persistent (46%) or new-onset urgency (7%), bladder perforation and complications from using synthetic sling material (erosion, fistula and infections).77, 102
Anterior repair Kelly plication Kennedy procedure
Cure rate 23 months: 68%77 Cure rate >48 months: 61%77, 106 Improvement rate >48 months: 73%
Urethral, bladder or ureteral injuries.77
Periurethral injection using bulking agents
Cure rate: 48% Improvement rate: 76%87
Transient urinary retention, hematuria, irritative symptoms, urinary tract infection, delayed hypersensitivity reaction and periurethral abscess formation.87, 93
Medical
Balanced serotonin and norepinephrine reuptake inhibitor (Duloxetine)
Can significantly decrease incontinence episodes and improve quality of life, but long-term effects remain unclear.107, 108
Nausea, fatigue, insomnia and dry mouth.96
Alpha-adrenergic receptor agonists (ephedrine)
Effective in patients with mild to moderate SUI, but use is minimized due to lack of lower urinary tract specificity and side effect profile.96
Palpitations, hypertension, arrhythmias, headache, sleep disturbance and <10% of patients experience hemmorhagic stroke within 1-6 hours of use.96
Tricyclic antidepressants (imipramine)
No data available. Dry mouth, fatigue, sedation, manic or schizophrenic picture, Parkinsonian effects, fine tremor, orthostatic hypotension, excessive sweating, arrhythmia.96
Estrogen therapy Controversial treatment option, due to a lack of evidence about its effectness.107
Increased risks for heart disease, heart attacks, strokes and breast cancer.107
Currently, there are 11 practice guidelines for urinary incontinence, six of which are specific to stress urinary incontinence, and six are U.S.-based guidelines.77, 98, 99, 104, 109-115 The U.S.-based guideline most frequently cited in the literature was published in 1997 by the American Urological Association.
Guidelines most often recommend non-surgical interventions such as Kegel exercises or biofeedback as the first line of therapy for the management of SUI.99, 110, 111, 116 Non-surgical therapies typically have no adverse side effects and are less expensive, therefore, they are appealing to most women. Yet, these approaches are time-intensive and require an active commitment on the part of the patient. While non-surgical interventions do not always produce high success rates, the majority of women have noticeable improvement (~50%) in their symptoms.91, 96
Generally, surgical interventions are recommended for moderate to severe SUI and after other non-surgical treatments have been proven ineffective.76 Guidelines for SUI are in agreement that retropubic suspension and sling procedures produce better long-term success than anterior repairs and transvaginal suspensions (82-84 percent vs. 61-79 percent), but are associated with slightly higher rates of complication, as seen in Exhibit 4-12.77, 98, 99, 104, 117 Recent research has
4-5

Pelvic Health Disorders Stress Urinary Incontinence
compared the Burch colposuspension, a commonly performed retropubic suspension, with the pubovaginal sling procedure using autologous rectus fascia. The study indicates that the autologous fascial sling resulted in a higher success rates over a 24-month period for the treatment of SUI, but with greater morbidity.118 The study also notes that there has been a recent transition in clinical practice from the use of fascial sling and Burch procedures to the newer midurethral synthetic sling procedures, such as the tension-free vaginal tape.118, 119 However, researchers agree that more well-designed randomized trials are needed to compare the efficacy of midurethral synthetic slings with pubovaginal fascial slings or Burch procedures. Nevertheless, both sling procedures and retropubic suspensions are proven to be the most effective surgical treatments for SUI. 77, 106, 118, 120, 121
Other surgical procedures or devices, such as periurethral injection or the artificial urinary sphincter, are noted in the guidelines as alternatives for the management of intrinsic sphincter deficiency (ISD), however, they have low success rates and a high likelihood of complications. Artificial urinary sphincters also are not commonly recommended for women. Currently, there are no medications recommended or approved in the United States for the treatment of SUI.122,123
Recent research on treatment patterns in SUI patients is unavailable.124 However, patterns of care for SUI based on claims and hospital discharge data, as well as physician survey results, from 1995 through 2000 seem to be consistent with current guidelines. Women with minimal or moderate SUI symptoms typically elect conservative therapy options such as biofeedback, while retropubic suspension and sling procedures are the most common surgical treatments.125-128
Of the small fraction of women who do seek treatment for SUI, the percentage of women choosing surgery is increasing.91, 125, 129, 130 One study found that an estimated 30 percent of women with SUI underwent at least one SUI-related procedure between 1995 and 2000. 125, e In addition, traditionally, SUI surgery has been followed by hospitalization and a period of recovery.130, 131 However, hospitalizations for SUI surgeries declined between 1996 and 2005. This trend may reflect the increased utilization of ambulatory surgical procedures for SUI and is further supported by evidence that newer procedures, such as collagen implants and TVT, which can be completed in less than one hour, without a significant incision and with fewer complications and faster recovery times, are becoming increasingly prevalent. 27, 131,120, 132
While retropubic suspension and sling procedures are referenced as the most common surgical procedures for SUI, data indicates that anterior repairs still are being used despite substantial evidence indicating that that this procedure has poor short- and long-term efficacy compared to other procedures for SUI.77, 133 There was a notable decline between 1995 and 2000 in anterior repairs and other less effective procedures such as transvaginal needle suspensions. However, these two approaches individually still comprise about 10 percent of all surgeries conducted in SUI patients.125 While a more detailed analysis is needed, it has been hypothesized that continued use may be attributed to physician and patient preference for less invasive surgery. At the same time, it also may reveal the need for better education of physicians regarding the outcomes of different procedures for SUI or the need for additional training in more effective SUI operations.79, 125, 129, 134
e As mentioned above, other research has shown that an estimated 50-70% of women do not seek treatment for SUI.
Thus, this figure may overrepresent the use of surgery among the total population of stress incontinent women.125
4-6
Pelvic Health Disorders Stress Urinary Incontinence
Patterns of care indicate that most surgical procedures have less than a 10 percent risk of temporary postoperative urinary retention and generally less than 5 percent risk of permanent urinary retention, with a somewhat higher risk among women who underwent sling procedures.77, 125 While there is no statistically significant difference among surgical procedures in regard to persistent or new-onset postoperative urgency, generally, there is a slightly higher likelihood of these conditions following retropubic suspensions and sling procedures. 77 A study examining health care utilization among women with SUI also noted that only an estimated 14 percent of all SUI surgical patients file a UI-related claim more than six months after their surgery. 125
Treatment patterns also vary by race and geographic location. Caucasian women have an overall surgery rate that is nearly five times greater than African American women. In addition, the rate of surgery is significantly higher in the South compared to other regions of the U.S.. 125,
129
4-7

Pelvic Health Disorders Pelvic Organ Prolapse
Pelvic Organ Prolapse
Background
Pelvic organ prolapse (POP) refers to the downward descent of female pelvic organs, resulting in protrusion into or out of the vaginal canal. Prolapse is classified according to the site of prolapse and the organ involved:
Upper vaginal prolapse: uterus (uterine prolapse) or vagina (vaginal vault prolapse)
Anterior vaginal wall prolapse: bladder (cystocele) or urethra (urethrocele)
Posterior vaginal wall prolapse: rectum (rectocele) or bowel (enterocele)
The cause of prolapse is multifactorial, although vaginal delivery, increasing body mass index and advancing age are the most consistent risk factors cited in the literature. Other factors such as previous prolapse surgery or hysterectomy, chronic straining, pregnancy, family history and connective tissue disorders also may predispose some women to weakened and stretched pelvic muscles and tissues, resulting in prolapse. 135-137
With only 10 to 20 percent of women experiencing noticeable symptoms, prolapse often can be asymptomatic and only diagnosed following clinical examination.138, 139 POP rarely results in severe morbidity or mortality, but symptoms of the condition can have a significant impact on a woman’s daily activities and quality of life. Women experiencing symptoms of prolapse are likely to report a feeling of pelvic fullness or pressure and a sensation of a vaginal bulge or protrusion. Other common symptoms include urinary problems such as incontinence, dyspareunia (painful intercourse), pain or bleeding from the vagina, lower back pain and difficulty with bowel movements; however, these symptoms are not uniquely specific to POP.140
Women experiencing symptoms suggestive of prolapse should seek medical care and undergo a pelvic examination. The severity of prolapse is classified in clinical practice using the Pelvic Organ Prolapse Quantification (POP-Q) system (stages 0-4) or the Baden-Walker system (grades 0 to 4) as seen in Exhibit 13. 141
Exhibit 13: Summary of POP-Q and Baden-Walker POP Classification Systems
Pelvic Organ Prolapse Quantification System Baden–Walker System
Stage 0: No prolapse. Stage I: The most distal portion of the prolapse is more than 1 cm above the level of the hymen. Stage II: The most distal portion of the prolapse is between 1 cm above and 1 cm below the hymen. Stage III: The most distal portion of the prolapse is more than 1 cm below the hymen but protrudes no further than 2 cm less than the total vaginal length. Stage IV: Eversion of the total lower genital tract is essentially complete.
Grade 0: Normal position for each respective site. Grade 1: Descent halfway to the hymen. Grade 2: Descent to the hymen. Grade 3: Descent halfway past the hymen. Grade 4: Maximum possible descent for each site.
5-1

Pelvic Health Disorders Pelvic Organ Prolapse
The Impact of Pelvic Organ Prolapse on Baby Boomers
Forty percent of women aged 40 to 79 are affected by pelvic organ prolapse. Other key aspects of the disorder affecting Baby Boomers include: Large scale studies consistently report a higher prevalence of POP among women aged 50 years and older, with a peak among those aged 60 to 69 years.
The risk of prolapse increases nearly 20 percent with each additional vaginal delivery up to five births.
The most common indication for hysterectomy in women aged 55 years and older in the US is prolapse. The number of other prolapse surgeries performed in women aged 50 years and older also is increasing, with a peak incidence in individuals between the ages of 60 and 69 years.
It is estimated that the demand for prolapse surgery likely will increase by nearly 45 percent in the next 30 years as Baby Boomers age.
Treatment options for symptomatic women include non-surgical interventions such as pelvic floor muscle exercises or lifestyle modifications, pessary use and surgery. Surgical strategies for prolapse are classified either as reconstructive or obliterative. Reconstructive techniques can be performed using either an abdominal or vaginal approach. Obliterative techniques are performed less often and result in the loss of vaginal sexual function.135, 137
Pelvic organ prolapse is a major health concern affecting a significant percentage of women throughout the United States. Since the prevalence of the disorder increases with age, there is growing concern that the changing demographics of the U.S. population will lead to even more women affected by POP.
Prevalence
Despite the fact that POP is a common disorder among women, there is a lack of epidemiological studies assessing its prevalence.135 In addition, there is no clear consensus among studies on a specific definition regarding the level of prolapse that represents disorder or is considered clinically significant to warrant treatment.135, 141 However, in the Women’s Health Initiative, a cross-sectional analysis of 27,342 women, 40 percent of women aged 50 to 79 years were found to have some form of POP, with most women experiencing cystocele, rectocele and uterine prolapse, respectively.142 In a multicenter study of 1,004 women between the ages of 18 and 83 seen for routine gynecologic care, 24 percent were identified as having no prolapse, 38 percent with stage I, 35 percent with stage II, 2 percent with stage III and no women exhibited stage IV prolapse.143 Therefore, some loss of utero-vaginal support occurs in most adult women.135
Although POP affects women of all ages, overall prevalence increases with age.143 Large scale studies consistently find a higher prevalence of POP among women aged 50 years and older, with a peak among those aged 60 to 69 years.144, 145 Various obstetric factors also are related to the risk of prolapse, such as vaginal delivery. A study conducted among Swedish women between the ages of 20 to 59 revealed that nearly half of all parous women have some form of prolapse, which may or may not be symptomatic.145 Some research also suggests that having a caesarean section instead of a vaginal delivery may decrease a woman’s risk of having prolapse.146 Finally, increasing body mass index also contributes to the risk of developing POP.142,143, 147
With the aging of the Baby Boomer population, demand for services to treat POP are predicted to increase at twice the rate of growth of women between the ages of 30 and 89.148, 149
5-2

Pelvic Health Disorders Pelvic Organ Prolapse
Exhibit 14: Prevalence of Pelvic Organ Prolapse
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
All Women(n=108M)
Baby Boomers*(n=39.6M)
N/A
85%
40%
15.8M
Source: Hendrix, 2002; Swift, 2005. N/A denotes not available. * Includes women aged 45 to 64.
Diagnosis and Treatment Gaps
It is estimated that only 10 to 20 percent of women with POP seek medical care.150, 151 Failure to seek care may be attributed to a lack of awareness and education about POP, according to findings from a recent, nationwide online survey of women aged 21 years and older. The unpublished study reported that 4 out of 5 women have never heard about POP. In addition, of the small fraction of women who are aware of the disorder, only 1 in 7 (14 percent) learn about the condition from their physician. 152
Many women suffering from the disorder tend to underreport their condition, due to embarrassment about discussing the problem with a health provider as well as the belief that POP is a normal part of the aging process.139 Research also indicates that the low number of women seeking treatment is largely a result of the difficulty in self-diagnosing the disorder. Despite its high prevalence, most women with POP are not clinically affected because they have “mild” symptoms.145 For this reason, POP commonly is diagnosed only after physical examination in asymptomatic women.153
Women are more likely to seek treatment when symptoms are more severe and have a significant impact on daily activities and/or quality of life. In addition, women seeking treatment for advanced POP tend to have poorer body image and quality of life, relative to women seen for routine gynecologic care with normal vaginal support. However, further research is needed in order to assess the relative importance of body image in a woman’s decision to seek treatment.154
5-3

Pelvic Health Disorders Pelvic Organ Prolapse
Treatment Options and Patterns of Care
There are numerous non-surgical and surgical therapies available for treating POP in symptomatic women. For asymptomatic patients or women whose symptoms are not sufficiently bothersome to justify active intervention, observation is typically the best option.
For symptomatic women with mild symptoms of any form of POP, the most common non-surgical treatment option is the use of a pessary. On the contrary, surgical treatment options vary based on the type and severity of prolapse. The choice of treatment depends on a variety of factors, including which organs are involved, the severity of the symptoms and what other medical conditions are present. The major surgical options for treatment of POP, as well as their effectiveness and potential complications, are noted in Exhibit 15.
Exhibit 15: Surgical Treatment Options for POP
Option Effectiveness Potential Risks/Complications
Reconstructive Techniques
Upper Vaginal Prolapse155
Hysterectomy Often done alongside other procedures for upper vaginal prolapse, such as sacral colpoplexy. 156 Hysterectomy + sacrospinous ligament fixation success rate: 72%156
Increased risk of developing other types of prolapse, particularly vaginal vault prolapse. Results in increased risk of postoperative mesh erosion into the vagina when done with other procedures.157, 158
Abdominal sacral colpopexy, open or laparoscopic (with or without mesh)
Success rate: 78–100% 135, 136, 155, 156, 159 Abdominal sacral coloplexy (using synthetic mesh) is proven to have lower recurrent prolapse but a longer operating time, greater morbidity and higher cost than vaginal sacrospinous ligament suspension.135, 159 Laparoscopic approach is as successful as the open technique, yet has slightly longer operating time. 135, 160, 161
Intra-abdominal adhesions, small bowel obstruction, hemorrhage, urinary incontinence, mesh erosion, fecal incontinence, pelvic pain.
Vaginal sacrospinous ligament suspension or fixation
Sacrospinous ligament suspension success rate: 65-90%156
Hemorrhage, damage to the pudendal and sciatic nerves, severe pain in legs, buttocks, genitals and pelvic area.
Iliocococcygeus ligament fixation
Subjective success rate: 91% Objective success rate: 53%162
Postoperative cystocele, hemorrhage, dyspareunia and nerve entrapment.
High uterosacral ligament suspension (vaginal)
Success rate: 87-92%135, 156 Uretal injury, small bowel injury, suture erosion.
Mayo culdoplasty Subjective success rate: 82%156
5-4

Pelvic Health Disorders Pelvic Organ Prolapse
Option Effectiveness Potential Risks/Complications
Reconstructive Techniques
Anterior Vaginal Prolapse
Anterior colporrhaphy (with or without mesh/graft material)
Success rate: 80-100% (case series); 40-60% (randomized trials)135, 156, 163 Mesh may be used to help support vaginal wall and keep prolapsed organs in place, especially in women who have recurrent prolapse.
Dyspareunia, incontinence, mesh erosion.
Paravaginal repair (vaginal or abdominal)
Abdominal success rate: 75-97% Vaginal success rate: 67-100%135, 164, 165
Severe pain, uretal injury and vaginal abscesses.
Posterior Vaginal Prolapse
Posterior coloporrhaphy (with midline plication of the subepithelial tissue or levator ani)
With midline fascial plication Objective success rate at 24 months: 79% Subjective success rate at 24 months: 89% 135, 166-168
Exceptionally high rates of dyspareunia in posterior coloporrhaphy with plication of the levator ani.
Site-specific repairs Success rate: 80-100%135 Site-specific repair is associated with
higher anatomic recurrence rates and similar rates of dyspareunia and bowel symptoms than standard posterior colporrhaphy.169
Greater chance of recurrent prolapse within one year in site-specific repair (33%), than in traditional midline plication (14%).141, 169
ObliterativeTechniques
Colpocleisis Success rate: 90-100% Shortened operative time, decreased perioperative morbidity and a very low prolapse recurrence risk. 135
Loss of ability to engage in vaginal intercourse.
The quality of evidence pertaining to various surgical procedures for POP is limited.170 In addition, the array of available treatment options for POP reflects the lack of agreement in the field as to the optimal treatment.155 However, in February 2007, the American College of Obstetricians and Gynecologists (ACOG) published clinical management guidelines for POP that review and provide recommendations on current treatment options.141 In addition, the International Continence Society (ICS) has published research recommendations on surgical treatment options based on extensive review of POP literature.156
ACOG highlights the importance of conducting a thorough assessment of the nature and severity of a POP patient’s symptoms, as well as the extent of prolapse. The guidelines conclude, based on evidence, that the only symptom specific to prolapse is the feeling of a vaginal bulge or protrusion (Grade A evidence). ACOG also suggests that women with asymptomatic or mildly symptomatic prolapse may forego treatment until symptoms warrant concern. ACOG recommends that pessaries should be considered first for treatment of POP in symptomatic patients prior to the use of surgical interventions (Grade B evidence). Other non-surgical therapies including symptom-directed therapy, such as lifestyle interventions or pelvic floor muscle exercises, may be suggested despite the lack of evidence-based data supporting their use.
5-5

Pelvic Health Disorders Pelvic Organ Prolapse
More severe prolapse should be treated with surgical interventions. A summary of the recommendations published by ACOG and ICS is provided in Exhibit 16.
Exhibit 16: Summary of ACOG and ICS Treatment Recommendations
Upper Vaginal Prolapse
Abdominal sacral colpopexy has less apical failure and less postoperative dyspareunia and stress incontinence compared to vaginal sacrospinous ligament fixation, but also is associated with more complications. (Grade B, ACOG; Grade A, ICS). Abdominal surgery also is noted as having increased short-term morbidity. (Grade A, ICS). Uterosacral ligament suspension also is commonly suggested for upper vaginal prolapse, however sacrospinous ligament or iliococcygeus fascia fixation are recommended for use when the uterosacral ligaments are not easily accessible or are unable to offer sufficient support (Grade B, ACOG; Level III, ICS). While hysterectomy alone traditionally has been the most common surgical approach for upper vaginal prolapse, it does not always address the underlying cause of uterine or vaginal vault prolapse. Therefore, other procedures for upper vaginal prolapse should be performed after remote or concomitant hysterectomy to address the problem (ACOG and ICS).
Women Who Want to Avoid Hysterectomy
May elect either uterosacral or sacrospinous ligament fixation by the vaginal approach or sacral hysteropexy or colpopexy by the abdominal approach (ACOG). Hysteropexy should not be performed using the ventral abdominal wall for support, due to the greater chance for recurrent prolapse, particularly enterocele (Grade B, ACOG). Round ligament suspension also is stated to be ineffective in treating uterine or vaginal vault prolapse (Grade B, ACOG).
Anterior Vaginal Prolapse May be treated either with anterior coloporrhaphy or paravaginal repair, which can be performed vaginally or retropubically by open or laparascopic techniques (ACOG and ICS).
Posterior Vaginal Prolapse
Levator plication increases the risk of sexual and defecatory dysfunction and, therefore, should have limited use for treatment of POP (Grade B, ICS). Transvaginal posterior repair is recommended over the transanal approach, due to lower recurrence rates of posterior prolapse and less complications141,
156 (Grade B, ACOG).
Women Who Are at Increased Risk of Complications from Surgical Procedures
For women who are at high risk for complications with reconstructive procedures and who no longer desire vaginal intercourse, colpocleisis can be offered (Grade C, ACOG, ICS).
Currently Available Graft Materials
Cadaveric fascia should not be used as a graft material for abdominal sacral colpopexy, because of a substantially higher risk of recurrent prolapse than with synthetic mesh (Grade A, ACOG).
Stress Incontinent Women
Stress incontinent women with positive stress test results (prolapse reduced) are at higher risk for developing postoperative stress incontinence after prolapse repair alone compared with women with negative stress test results (prolapse reduced) (Grade A, ACOG). For stress incontinent women planning abdominal sacral colpopexy, regardless of the results of the preoperative stress testing, the addition of the Burch procedure substantially reduced the likelihood of postoperative stress incontinence without increasing urgency symptoms or obstructed voiding (Grade A, ACOG).
5-6

Pelvic Health Disorders Pelvic Organ Prolapse
While current research on treatment patterns in POP patients is scarce, usually pessaries are the first line of therapy and the only non-surgical device used by 86 percent of gynecologists and 98 percent of urogynecologists, consistent with ACOG guidelines.135, 148 Also, in agreement with guidelines, colpoclesis is performed only in women who are willing to forego the possibility of vaginal intercourse and, thus, is the least common prolapse surgery.141, 156 Epidemiologic evidence demonstrates that most POP surgery in the United States is performed vaginally rather than abdominally.135, 149, 156, 171, 172 Current guidelines suggest that the abdominal route may be more effective and durable in correcting anatomy and preserving lower urinary tract function, however, there is a trade-off between effectiveness and higher chance of complications.
Trends through 1997 indicate that, by age 80, nearly one in every 10 women will have undergone surgery for pelvic organ prolapse or urinary incontinence.149 Approximately 200,000 inpatient procedures are performed annually for prolapse in the United States.141, 171 Yet, surgically managed patients comprise only a small percentage of symptomatic patients, since many either opt for conservative treatments or fail to seek medical care. 149
Consistent with the general prevalence of POP, the rate of surgery increases with age. The most common indication for hysterectomy in women aged 55 years and older in the U.S. is prolapse.141, 173 Also, the number of other prolapse surgeries performed in women aged 50 years and older is increasing, with a peak incidence in individuals between the ages of 60 and 69.171 Estimates indicate that demand for prolapse surgery likely will increase by nearly 45 percent in the next 30 years.171
Based on hospital discharge data through 1997, the most common prolapse procedures among women aged 50 years and older are cystocele and rectocele repairs. In addition, reoperation is required in an estimated 29 percent of all cases, suggesting a potentially high rate of surgical failure.149 However, the high incidence of reoperation also suggests to some clinicians and researchers that previous prolapse surgery may predispose an individual to the development of prolapse in another region.149
Finally, treatment patterns vary by race and geographic location. Caucasian women are three times more likely to undergo POP surgery compared to African American or Hispanic women. Also, surgeries for POP are more predominant in the South and Midwest, rather than in Eastern parts of the U.S..171, 172
5-7

Pelvic Health Disorders Conclusion
Conclusion
Approximately one-third of all women in the United States are affected by one or more pelvic health disorders by the age of 60, including menorrhagia, uterine fibroids, stress urinary incontinence and pelvic organ prolapse. These conditions are common, affecting women of all ages, however, the highest rate of onset for pelvic health disorders tends to be for women born between 1946 and 1964, the Baby Boomer generation. Such conditions can be traced to a variety of factors, including pregnancy and childbirth, genetic factors, obesity, medications and complications of surgical procedures.
This report, funded by the National Women’s Health Resource Center (NWHRC), examines five key questions with respect to the prevalence and treatment of menorrhagia, uterine fibroids, stress urinary incontinence (SUI) and pelvic organ prolapse (POP):
1) What is the prevalence among women in the U.S. and how does prevalence differ by age and other demographic variables? How are Baby Boomer women affected?
2) How do these disorders affect women and, in particular, Baby Boomers in the U.S.? What is their overall impact on quality of life?
3) To what extent is the magnitude and severity of these disorders properly recognized and understood by public health practitioners, researchers and policymakers?
4) Does a treatment gap exist (the gap between the prevalence of the disorder and treatment)? Are there any barriers women face when attempting to access treatment for these disorders?
5) Do current treatment patterns reflect the most effective and appropriate standards of practice? Are clinical practice guidelines followed by physicians?
Although the literature suggests that a significant number of women and, in particular, Baby Boomer women, are affected by these disorders, to date, there has been limited epidemiological study of these conditions in the U.S.. Additional key findings from this report include:
Pelvic health disorders have a substantial impact on women’s health and their quality of life, often resulting in complications with fertility and pregnancy, anemia, abdominal pain and pressure, low self-esteem, sexual dysfunction and depression.
Women’s reluctance to consult their physician about symptoms associated with pelvic health disorders results in under- and/or misdiagnosis, further complicating the treatment and overall understanding of the impact of these disorders on U.S. women and Baby Boomers.
Approximately 600,000 hysterectomies are performed each year in the United States, nearly one-third of which are performed to treat patients diagnosed with uterine fibroids and/or menorrhagia.
Despite the availability of less invasive approaches, abdominal hysterectomy is still the most common form of surgical treatment in cases where uterine fibroids or menorrhagia is the primary diagnosis. In 2005, 44 percent of all hysterectomies performed were for women
6-1
Pelvic Health Disorders Conclusion
with a primary diagnosis of uterine fibroids or menorrhagia. Of these procedures, nearly 71 percent were performed for Baby Boomer women with a primary or secondary diagnosis of uterine fibroids or menorrhagia.
The available literature indicates that clinically recommended and effective treatments generally are employed for pelvic health disorders, however, concern remains about the common use of hysterectomies to treat menorrhagia and uterine fibroids, as well as the rate of anterior repairs used to treat stress urinary incontinence.
Given the prevalence of these conditions and their substantial impact on women’s lives, future research priorities should include:
Development of standard measures of the overall impact (e.g., quality of life and costs) and severity of pelvic health disorders on women and, in particular, Baby Boomer women.
Longitudinal studies to identify lifetime incidence, prevalence, patterns of care, risk factors and comorbidity between these related disorders.
Development and adoption of standard, clinically accepted definitions for each disorder that further clarify to what extent symptoms should be deemed problematic and, therefore, warrant treatment.
Methodologically rigorous studies of minimally invasive and medical treatments for pelvic health disorder to obtain long-term data on their effectiveness and impacts.
6-2

Pelvic Health Disorders Reference List
Reference List
1. Shaw J. Menorrhagia. http://www.emedicine.com/med/topic1449.htm . Accessed on May 2, 2007 @ eMedicine.com
2. Hallberg L, Hogdahl AM, Nilsson L, Rybo G. Menstrual blood loss--a population study. Variation at different ages and attempts to define normality. Acta Obstet Gynecol Scand 1966;45(3):320-351.
3. Philipp CS, Faiz A, Dowling N, et al. Age and the prevalence of bleeding disorders in women with menorrhagia. Obstet Gynecol 2005;105(1):61-66.
4. Cole SK, Billewicz WZ, Thomson AM. Sources of variation in menstrual blood loss. J Obstet Gynaecol Br Commonw 1971;78(10):933-939.
5. Dilley A, Drews C, Lally C, Austin H, Barnhart E, Evatt B. A survey of gynecologists concerning menorrhagia: perceptions of bleeding disorders as a possible cause. J Womens Health Gend Based Med 2002;11(1):39-44.
6. Van Eijkeren MA, Christiaens GC, Sixma JJ, Haspels AA. Menorrhagia: a review. Obstet Gynecol Surv 1989;44(6):421-429.
7. Marino JL, Eskenazi B, Warner M, et al. Uterine leiomyoma and menstrual cycle characteristics in a population-based cohort study. Hum Reprod 2004;19(10):2350-2355.
8. Barrow C. Balloon endometrial ablation as a safe alternative to hysterectomy. AORN J 1999;70(1):80, 83-80, 90.
9. Van Voorhis BJ. Genitourinary symptoms in the menopausal transition. Am J Med 2005;118 Suppl 12B:47-53.
10. Oehler MK, Rees MC. Menorrhagia: an update. Acta Obstet Gynecol Scand 2003;82(5):405-422.
11. Warren M. The need for proper diagnosis and treatment of menorrhagia. Menopause Management . 2002. 2007.
12. Abbott JA, Garry R. The surgical management of menorrhagia. Hum Reprod Update 2002;8(1):68-78.
13. Shaw RW, Brickley MR, Evans L, Edwards MJ. Perceptions of women on the impact of menorrhagia on their health using multi-attribute utility assessment. Br J Obstet Gynaecol 1998;105(11):1155-1159.
14. Centers for Disease Control & Prevention, Department of Health & Human Services. Health Matters for Women Newsletter. Centers for Disease Control & Prevention . 2002. 2007.
7-1

Pelvic Health Disorders Reference List
15. Marjoribanks J, Lethaby A, Farquhar C. Surgery versus medical therapy for heavy menstrual bleeding. Cochrane Database Syst Rev 2006;(2):CD003855.
16. Lumsden MA, Wallace EM. Clinical presentation of uterine fibroids. Baillieres Clin Obstet Gynaecol 1998;12(2):177-195.
17. Fernandez H, Capella S, Audibert F. Uterine thermal balloon therapy under local anaesthesia for the treatment of menorrhagia: a pilot study. Hum Reprod 1997;12(11):2511-2514.
18. Busfield RA, Farquhar CM, Sowter MC, et al. A randomised trial comparing the levonorgestrel intrauterine system and thermal balloon ablation for heavy menstrual bleeding. BJOG 2006;113(3):257-263.
19. Beaumont H, Augood C, Duckitt K, Lethaby A. Danazol for heavy menstrual bleeding (Review). [1]. 2007. The Cochrane Collaboration.
20. Lethaby A, Augood C, Duckitt K. Nonsteroidal anti-inflammatory drugs for heavy menstrual bleeding. Cochrane Database Syst Rev 2002;(1):CD000400.
21. National Institute for Clinical Excellence. Fluid-filled thermal balloon and microwave endometrial ablation techniques for heavy menstrual bleeding. 2004. London (UK), National Institute for Clinical Excellence.
22. Bongers MY, Mol BW, Dijkhuizen FP, Brolmann HA. Is balloon ablation as effective as endometrial electroresection in the treatment of menorrhagia? J Laparoendosc Adv Surg Tech A 2000;10(2):85-92.
23. Lin H. Comparison between microwave endometrial ablation and total hysterectomy. Chin Med J (Engl ) 2006;119(14):1195-1197.
24. Dilation and Curettage. eMedicineHealth . 2007.
25. ACOG Committee on Practice Bulletins -- Gynecology. ACOG Practice Bulletin: management of anovulatory bleeding. Intl J Gynaecol Obstet 2001;72(3):263-271.
26. League DD. Endometrial ablation as an alternative to hysterectomy. AORN J 2003;77(2):322-338.
27. The Lewin Group Analysis of 1996-2005 Hospital Discharge Data. 2007.
28. Istre O, Qvigstad E. Current treatment options for abnormal uterine bleeding: an evidence-based approach. Best Pract Res Clin Obstet Gynaecol 2007.
29. Dwyer N, Hutton J, Stirrat GM. Randomised controlled trial comparing endometrial resection with abdominal hysterectomy for the surgical treatment of menorrhagia. Br J Obstet Gynaecol 1993;100(3):237-243.
7-2

Pelvic Health Disorders Reference List
30. Lethaby A, Shepperd S, Cooke I, Farquhar C. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding. Cochrane Database Syst Rev 2000;(2):CD000329.
31. Garside R, Stein K, Wyatt K, Round A, Pitt M. A cost-utility analysis of microwave and thermal balloon endometrial ablation techniques for the treatment of heavy menstrual bleeding. BJOG 2004;111(10):1103-1114.
32. Aberdeen Endometrial Ablation Trials Group. A randomised trial of endometrial ablation versus hysterectomy for the treatment of dysfunctional uterine bleeding: outcome at four years. Br J Obstet Gynaecol 1999;106(4):360-366.
33. Furst SN, Philipsen T, Joergensen JC. Ten-year follow-up of endometrial ablation. Acta Obstet Gynecol Scand 2007;86(3):334-338.
34. Andersson S, Mints M. Thermal balloon ablation for the treatment of menorrhagia in an outpatient setting. Acta Obstet Gynecol Scand 2007;86(4):480-483.
35. Clark TJ, Gupta JK. Outpatient thermal balloon ablation of the endometrium. Fertil Steril 2004;82(5):1395-1401.
36. Robson S, Devine B. Two cases of leiomyoma necrosis after thermal balloon endometrial ablation. J Minim Invasive Gynecol 2007;14(2):250-252.
37. Seidman DS, Bitman G, Mashiach S, Hart S, Goldenberg M. The effect of increasing age on the outcome of hysteroscopic endometrial resection for management of dysfunctional uterine bleeding. J Am Assoc Gynecol Laparosc 2000;7(1):115-119.
38. National Heart Lung and Blood Institute. von Willebrand's Disease. National Heart Lung and Blood Institute . 2007. 5-16-2007.
39. Dilley A, Drews C, Miller C, et al. von Willebrand disease and other inherited bleeding disorders in women with diagnosed menorrhagia. Obstet Gynecol 2001;97(4):630-636.
40. Andersen J. Growth factors and cytokines in uterine leiomyomas. Semin Reprod Endocrinol 1996;14(3):269-282.
41. Stewart EA. Uterine fibroids. Lancet 2001;357(9252):293-298.
42. Payson M, Leppert P, Segars J. Epidemiology of myomas. Obstet Gynecol Clin North Am 2006;33(1):1-11.
43. Farquhar CM, Naoom S, Steiner CA. The impact of endometrial ablation on hysterectomy rates in women with benign uterine conditions in the United States. Int J Technol Assess Health Care 2002;18(3):625-634.
44. Day Baird D, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol 2003;188(1):100-107.
7-3

Pelvic Health Disorders Reference List
45. Buttram VC, Jr. Uterine leiomyomata--aetiology, symptomatology and management. Prog Clin Biol Res 1986;225:275-296.
46. Marshall LM, Spiegelman D, Barbieri RL, et al. Variation in the incidence of uterine leiomyoma among premenopausal women by age and race. Obstet Gynecol 1997;90(6):967-973.
47. Yang CH, Lee JN, Hsu SC, Kuo CH, Tsai EM. Effect of hormone replacement therapy on uterine fibroids in postmenopausal women--a 3-year study. Maturitas 2002;43(1):35-39.
48. Cramer SF, Marchetti C, Freedman J, Padela A. Relationship of myoma cell size and menopausal status in small uterine leiomyomas. Arch Pathol Lab Med 2000;124(10):1448-1453.
49. Gupta JK HM LMA. Uterine artery embolization for symptomatic uterine fibroids. (Protocol). Cochrane Database Syst Rev 2005;(1).
50. National Center for Health Statistics. Ambulatory procedures in the United States. 1998. Hyattsville, Maryland, Public health Service.
51. Reed SD, Newton KM, Thompson LB, McCrummen BA, Warolin AK. The incidence of repeat uterine surgery following myomectomy. J Womens Health (Larchmt) 2006;15(9):1046-1052.
52. Poncelet C, Benifla JL, Madelenat P. [Myoma and infertility]. J Gynecol Obstet Biol Reprod (Paris) 1999;28(7):761-767.
53. Lumsden MA. Embolization versus myomectomy versus hysterectomy: which is best, when? Hum Reprod 2002;17(2):253-259.
54. David M, Ebert AD. Treatment of uterine fibroids by embolization--advantages, disadvantages, and pitfalls. Eur J Obstet Gynecol Reprod Biol 2005;123(2):131-138.
55. American College of Obstetricians & Gynecologists. Uterine Fibroids. 2007. Education Pamphlet AP074.
56. Olive DL, Lindheim SR, Pritts EA. Non-surgical management of leiomyoma: impact on fertility. Curr Opin Obstet Gynecol 2004;16(3):239-243.
57. Womenshealth.gov, U.S.Department of Health and Human Services. The National Women's Health Information Center. 2007.
58. Bernstein S, Fiske M, McGlynn E, Gifford D. A review of the literature on indications, effectiveness, and risks. Santa Monica, CA: RAND 1997;Publication MR-592 / 2-AHCPR.
59. Broder M, Kanouse D, Bernstein S. Assessing symptoms before hysterectomy: Is the medical record accurate? American Journal of Obstetrics & Gynecology 2001;185(1):97-102.
7-4

Pelvic Health Disorders Reference List
60. The Society of Interventional Radiology. Uterine fibroids symptoms and diagnosis. The Society of Interventional Radiology . 2007.
61. Spies J, Niedzwiecki G, Goodwin S, et al. Training standards for physicians performing uterine artery embolization for leiomyomata. Consensus statement developed by the Task Force on Uterine Artery Embolization and the Standards Division of the Society of Interventional Radiology--August 2000. J Vasc Interv Radiol 2003;14(9 Pt 2):S369-S371.
62. Gupta JK, Sinha AS, Lumsden MA, Hickey M. Uterine artery embolization for symptomatic uterine fibroids. Cochrane Database Syst Rev 2006;(1):CD005073.
63. Beinfeld MT, Bosch JL, Isaacson KB, Gazelle GS. Cost-effectiveness of uterine artery embolization and hysterectomy for uterine fibroids. Radiology 2004;230(1):207-213.
64. Marshburn PB, Matthews ML, Hurst BS. Uterine artery embolization as a treatment option for uterine myomas. Obstet Gynecol Clin North Am 2006;33(1):125-144.
65. ACOG Committee Opinion. Uterine artery embolization. Obstet Gynecol 2004;103(2):403-404.
66. Candiani GB, Fedele L, Parazzini F, Villa L. Risk of recurrence after myomectomy. Br J Obstet Gynaecol 1991;98(4):385-389.
67. Goodwin SC, Bradley LD, Lipman JC, et al. Uterine artery embolization versus myomectomy: a multicenter comparative study. Fertil Steril 2006;85(1):14-21.
68. Kjerulff KH, Guzinski GM, Langenberg PW, Stolley PD, Moye NE, Kazandjian VA. Hysterectomy and race. Obstet Gynecol 1993;82(5):757-764.
69. Coronado GD, Marshall LM, Schwartz SM. Complications in pregnancy, labor, and delivery with uterine leiomyomas: a population-based study. Obstet Gynecol 2000;95(5):764-769.
70. Burton CA, Grimes DA, March CM. Surgical management of leiomyomata during pregnancy. Obstet Gynecol 1989;74(5):707-709.
71. Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn 2002;21(2):167-178.
72. Sandvik H, Hunskaar S, Seim A, Hermstad R, Vanvik A, Bratt H. Validation of a severity index in female urinary incontinence and its implementation in an epidemiological survey. J Epidemiol Community Health 1993;47(6):497-499.
73. Fultz NH, Burgio K, Diokno AC, Kinchen KS, Obenchain R, Bump RC. Burden of stress urinary incontinence for community-dwelling women. Am J Obstet Gynecol 2003;189(5):1275-1282.
7-5

Pelvic Health Disorders Reference List
74. Hampel C, Wienhold D, Benken N, Eggersmann C, Thuroff JW. Definition of overactive bladder and epidemiology of urinary incontinence. Urology 1997;50(6A Suppl):4-14.
75. Thom D. Variation in estimates of urinary incontinence prevalence in the community: effects of differences in definition, population characteristics, and study type. J Am Geriatr Soc 1998;46(4):473-480.
76. Luber KM. The definition, prevalence, and risk factors for stress urinary incontinence. Rev Urol 2004;6 Suppl 3:S3-S9.
77. American Urological Association. Female Stress Urinary Incontinence Clinical Guidelines report on the surgical management of female stress urinary incontinence. 1997.
78. Stress urinary incontinence: What matters? Temporal M, Newman D, Deutchman M, Kreder K, Minkin M, editors. FPEN Consensus Recommendation from an Expert Panel. Family Practice Education Network 5, 1-10. 2004.
79. Nygaard IE, Heit M. Stress urinary incontinence. Obstet Gynecol 2004;104(3):607-620.
80. Muller N. What Americans understand and how they are affected by bladder control problems: highlights of recent nationwide consumer research. Urol Nurs 2005;25(2):109-115.
81. Hannestad YS, Rortveit G, Sandvik H, Hunskaar S. A community-based epidemiological survey of female urinary incontinence: the Norwegian EPINCONT study. Epidemiology of Incontinence in the County of Nord-Trondelag. J Clin Epidemiol 2000;53(11):1150-1157.
82. Melville JL, Delaney K, Newton K, Katon W. Incontinence severity and major depression in incontinent women. Obstet Gynecol 2005;106(3):585-592.
83. Brown JS, Grady D, Ouslander JG, Herzog AR, Varner RE, Posner SF. Prevalence of urinary incontinence and associated risk factors in postmenopausal women. Heart & Estrogen/Progestin Replacement Study (HERS) Research Group. Obstet Gynecol 1999;94(1):66-70.
84. Hannestad YS, Rortveit G, Hunskaar S. Help-seeking and associated factors in female urinary incontinence. The Norwegian EPINCONT Study. Epidemiology of Incontinence in the County of Nord-Trondelag. Scand J Prim Health Care 2002;20(2):102-107.
85. Kinchen KS, Burgio K, Diokno AC, Fultz NH, Bump R, Obenchain R. Factors associated with women's decisions to seek treatment for urinary incontinence. J Womens Health (Larchmt ) 2003;12(7):687-698.
86. Dugan E, Roberts CP, Cohen SJ, et al. Why older community-dwelling adults do not discuss urinary incontinence with their primary care physicians. J Am Geriatr Soc 2001;49(4):462-465.
7-6

Pelvic Health Disorders Reference List
87. Smith PP, McCrery RJ, Appell RA. Current trends in the evaluation and management of female urinary incontinence. CMAJ 2006;175(10):1233-1240.
88. Burgio KL, Ives DG, Locher JL, Arena VC, Kuller LH. Treatment seeking for urinary incontinence in older adults. J Am Geriatr Soc 1994;42(2):208-212.
89. Seim A, Sandvik H, Hermstad R, Hunskaar S. Female urinary incontinence--consultation behaviour and patient experiences: an epidemiological survey in a Norwegian community. Fam Pract 1995;12(1):18-21.
90. Stress urinary incontinence web study. International Communications Research, January 2007.
91. Nygaard I, Thom DH. Urinary incontinence in women. In: Litwin M, Saigal CS, editors. Urologic Diseases of America. 2007 p. 157-192.
92. Hay-Smith EJ, Dumoulin C. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst Rev 2006;(1):CD005654.
93. Pesce F. Current management of stress urinary incontinence. BJU Int 2004;94 Suppl 1:8-13.
94. Herbison P, Plevnik S, Mantle J. Weighted vaginal cones for urinary incontinence. Cochrane Database Syst Rev 2002;(1):CD002114.
95. Wallace SA, Roe B, Williams K, Palmer M. Bladder training for urinary incontinence in adults. Cochrane Database Syst Rev 2004;(1):CD001308.
96. Smith AL, Moy ML. Modern management of women with stress urinary incontinence. Ostomy Wound Manage 2004;50(12):32-39.
97. Lapitan MC, Cody DJ, Grant AM. Open retropubic colposuspension for urinary incontinence in women. Cochrane Database Syst Rev 2005;(3):CD002912.
98. Royal College of Obstetricians and Gynaecologists. Guideline No. 35: Surgical treatment of urodynamic stress incontinence. 2003.
99. Bengston C, Kohli N, Loughlin K, Seligson J, Gharib S. Urinary incontinence: guide to diagnosis and management. 9. 2004. Brigham and Women's Hospital.
100. Dean NM, Ellis G, Wilson PD, Herbison GP. Laparoscopic colposuspension for urinary incontinence in women. Cochrane Database Syst Rev 2006;3:CD002239.
101. Glazener CM, Cooper K. Bladder neck needle suspension for urinary incontinence in women. Cochrane Database Syst Rev 2004;(2):CD003636.
102. Bullock TL, Ghoniem G, Klutke CG, Staskin DR. Advances in female stress urinary incontinence: mid-urethral slings. BJU Int 2006;98 Suppl 1:32-40.
7-7

Pelvic Health Disorders Reference List
103. Comiter CV. Surgery insight: management of failed sling surgery for female stress urinary incontinence. Nat Clin Pract Urol 2006;3(12):666-674.
104. Finnish Medical Society Duodecim. Urinary incontinence in women. 2005. Helinski, Finland, Duodecim Medical Publications Ltd.
105. Nilsson CG, Falconer C, Rezapour M. Seven-year follow-up of the tension-free vaginal tape procedure for treatment of urinary incontinence. Obstet Gynecol 2004;104(6):1259-1262.
106. Glazener CM, Cooper K. Anterior vaginal repair for urinary incontinence in women. Cochrane Database Syst Rev 2001;(1):CD001755.
107. Viktrup L, Bump RC. Pharmacological agents used for the treatment of stress urinary incontinence in women. Curr Med Res Opin 2003;19(6):485-490.
108. Mariappan P, Ballantyne Z, N'Dow JM, Alhasso AA. Serotonin and noradrenaline reuptake inhibitors (SNRI) for stress urinary incontinence in adults. Cochrane Database Syst Rev 2005;(3):CD004742.
109. Laycock J, Standley A, Crothers E, Naylor D, Frank M. Clinical guidelines for the physiotherapy management of females 16-65 with stress urinary incontinence. The Chartered Society of Physiotherapy. 2001.
110. Scottish Intercollegiate Guidelines Network (SNGI). Management of urinary incontinence in primary care. A national clinical guideline. 2004.
111. Dowling-Castronovo A. Urinary incontinence. Geriatric Nursing Protocols for Best Practice , 83-98. 2003.
112. Guideline: Recommendation for the management of stress and urge urinary incontinence in women. 2002. Austin, TX, University of Texas at Austin, School of Nursing.
113. Guideline: Nursing management of patients with urinary incontinence. 2003. Singapore Ministry of Health, Singapore.
114. Guideline: Promoting continence using prompted voiding. 2002. Toronto, Registered Nurses Association of Ontario (RNAO).
115. Continence for women. Evidence-based practice guideline. 2000. washington, DC, Association of Women's Health, Obstetric and Neonatal Nurses (AWHONN).
116. The Chartered Society of Physiotherapy. Clinical guidelines for the physiotherapy management of females 16-65 with stress urinary incontinence.
117. Robert M, Farrell SA, Easton WA, et al. Choice of surgery for stress incontinence. J Obstet Gynaecol Can 2005;27(10):964-980.
7-8

Pelvic Health Disorders Reference List
118. Albo ME, Richter HE, Brubaker L, et al. Burch Colposuspension versus Fascial Sling to Reduce Urinary Stress Incontinence. N Engl J Med 2007.
119. Paraiso MF. Laparoscopic Burch colposuspension and the tension-free vaginal tape procedure. Curr Opin Obstet Gynecol 2006;18(4):385-390.
120. Strohbehn K. Shades of Dry -- Curing Urinary Stress Incontinence. N Engl J Med 2007.
121. Weber AM, Walters MD. Burch procedure compared with sling for stress urinary incontinence: a decision analysis. Obstet Gynecol 2000;96(6):867-873.
122. Weiss BD. Selecting medications for the treatment of urinary incontinence. Am Fam Physician 2005;71(2):315-322.
123. Millard RJ, Moore K, Rencken R, Yalcin I, Bump RC. Duloxetine vs placebo in the treatment of stress urinary incontinence: a four-continent randomized clinical trial. BJU Int 2004;93(3):311-318.
124. Lightner DJ, Itano NM. Treatment options for women with stress urinary incontinence. Mayo Clin Proc 1999;74(11):1149-1156.
125. Kinchen KS, Long S, Orsini L, Crown W, Bump RC. Healthcare utilization among women who undergo surgery for stress urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct 2004;15(3):154-159.
126. Davila GW, Ghoniem GM, Kapoor DS, Contreras-Ortiz O. Pelvic floor dysfunction management practice patterns: a survey of members of the International Urogynecological Association. Int Urogynecol J Pelvic Floor Dysfunct 2002;13(5):319-325.
127. Kim HL, Gerber GS, Patel RV, Hollowell CM, Bales GT. Practice patterns in the treatment of female urinary incontinence: a postal and internet survey. Urology 2001;57(1):45-48.
128. O'Leary MP, Gee WF, Holtgrewe HL, et al. 1999 American Urological Association Gallup Survey: changes in physician practice patterns, treatment of incontinence and bladder cancer, and impact of managed care. J Urol 2000;164(4):1311-1316.
129. Waetjen LE, Subak LL, Shen H, et al. Stress urinary incontinence surgery in the United States. Obstet Gynecol 2003;101(4):671-676.
130. Boyles SH, Weber AM, Meyn L. Procedures for urinary incontinence in the United States, 1979-1997. Am J Obstet Gynecol 2003;189(1):70-75.
131. Boyles SH, Weber AM, Meyn L. Ambulatory procedures for urinary incontinence in the United States, 1994-1996. Am J Obstet Gynecol 2004;190(1):33-36.
132. National Institue of Diabetes and Digestive and Kidney Diseases. Urinary incontinence in women. 2007. 4-6-2007.
7-9

Pelvic Health Disorders Reference List
133. Black NA, Downs SH. The effectiveness of surgery for stress incontinence in women: a systematic review. Br J Urol 1996;78(4):497-510.
134. Korn AP, Learman LA. Operations for stress urinary incontinence in the United States, 1988-1992. Urology 1996;48(4):609-612.
135. Jelovsek JE, Maher C, Barber MD. Pelvic organ prolapse. Lancet 2007;369(9566):1027-1038.
136. Nygaard I, Bradley C, Brandt D. Pelvic organ prolapse in older women: prevalence and risk factors. Obstet Gynecol 2004;104(3):489-497.
137. Weber AM, Richter HE. Pelvic organ prolapse. Obstet Gynecol 2005;106(3):615-634.
138. Beck RP, McCormick S, Nordstrom L. A 25-year experience with 519 anterior colporrhaphy procedures. Obstet Gynecol 1991;78(6):1011-1018.
139. Shagam JY. Pelvic organ prolapse. Radiol Technol 2006;77(5):389-400.
140. Barber MD. Symptoms and outcome measures of pelvic organ prolapse. Clin Obstet Gynecol 2005;48(3):648-661.
141. ACOG Bulletin: No. 79: Clinical Management Guidelines: Pelvic Organ Prolapse. 2007.
142. Hendrix SL, Clark A, Nygaard I, Aragaki A, Barnabei V, McTiernan A. Pelvic organ prolapse in the Women's Health Initiative: gravity and gravidity. Am J Obstet Gynecol 2002;186(6):1160-1166.
143. Swift S, Woodman P, O'Boyle A, et al. Pelvic Organ Support Study (POSST): the distribution, clinical definition, and epidemiologic condition of pelvic organ support defects. Am J Obstet Gynecol 2005;192(3):795-806.
144. Swift SE. The distribution of pelvic organ support in a population of female subjects seen for routine gynecologic health care. Am J Obstet Gynecol 2000;183(2):277-285.
145. Samuelsson EC, Victor FT, Tibblin G, Svardsudd KF. Signs of genital prolapse in a Swedish population of women 20 to 59 years of age and possible related factors. Am J Obstet Gynecol 1999;180(2 Pt 1):299-305.
146. Lukacz ES, Lawrence JM, Contreras R, Nager CW, Luber KM. Parity, mode of delivery, and pelvic floor disorders. Obstet Gynecol 2006;107(6):1253-1260.
147. Moalli PA, Jones IS, Meyn LA, Zyczynski HM. Risk factors associated with pelvic floor disorders in women undergoing surgical repair. Obstet Gynecol 2003;101(5 Pt 1):869-874.
148. Trowbridge ER, Fenner DE. Conservative management of pelvic organ prolapse. Clin Obstet Gynecol 2005;48(3):668-681.
7-10

Pelvic Health Disorders Reference List
149. Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol 1997;89(4):501-506.
150. Thakar R, Stanton S. Management of genital prolapse. BMJ 2002;324(7348):1258-1262.
151. Beck RP. Pelvic relaxation prolapse. Principles and practice of clinical gynecology. New York: John Wiley; 1983 p. 677-685.
152. Prolapse awareness survey. International Communications Research, December 2006.
153. Drutz HP, Alarab M. Pelvic organ prolapse: demographics and future growth prospects. Int Urogynecol J Pelvic Floor Dysfunct 2006;17 Suppl 1:S6-S9.
154. Jelovsek JE, Barber MD. Women seeking treatment for advanced pelvic organ prolapse have decreased body image and quality of life. Am J Obstet Gynecol 2006;194(5):1455-1461.
155. Maher C, Baessler K, Glazener CM, Adams EJ, Hagen S. Surgical management of pelvic organ prolapse in women. Cochrane Database Syst Rev 2004;(4):CD004014.
156. Brubaker L, Bump R, Fynes M, Jacquetin B, Karram M, Kreder K, Maher C, Norton P. 3rd International Consultation on Continence: Chapter 21: Surgery for Pelvic Organ Prolapse. 2004.
157. Wu JM, Wells EC, Hundley AF, Connolly A, Williams KS, Visco AG. Mesh erosion in abdominal sacral colpopexy with and without concomitant hysterectomy. Am J Obstet Gynecol 2006;194(5):1418-1422.
158. Benson JT, Lucente V, McClellan E. Vaginal versus abdominal reconstructive surgery for the treatment of pelvic support defects: a prospective randomized study with long-term outcome evaluation. Am J Obstet Gynecol 1996;175(6):1418-1421.
159. Maher CF, Qatawneh AM, Dwyer PL, Carey MP, Cornish A, Schluter PJ. Abdominal sacral colpopexy or vaginal sacrospinous colpopexy for vaginal vault prolapse: a prospective randomized study. Am J Obstet Gynecol 2004;190(1):20-26.
160. Paraiso MF, Walters MD, Rackley RR, Melek S, Hugney C. Laparoscopic and abdominal sacral colpopexies: a comparative cohort study. Am J Obstet Gynecol 2005;192(5):1752-1758.
161. Rozet F, Mandron E, Arroyo C, et al. Laparoscopic sacral colpopexy approach for genito-urinary prolapse: experience with 363 cases. Eur Urol 2005;47(2):230-236.
162. Maher CF, Murray CJ, Carey MP, Dwyer PL, Ugoni AM. Iliococcygeus or sacrospinous fixation for vaginal vault prolapse. Obstet Gynecol 2001;98(1):40-44.
163. Weber AM, Walters MD, Piedmonte MR, Ballard LA. Anterior colporrhaphy: a randomized trial of three surgical techniques. Am J Obstet Gynecol 2001;185(6):1299-1304.
7-11

Pelvic Health Disorders Reference List
164. Mallipeddi PK, Steele AC, Kohli N, Karram MM. Anatomic and functional outcome of vaginal paravaginal repair in the correction of anterior vaginal wall prolapse. Int Urogynecol J Pelvic Floor Dysfunct 2001;12(2):83-88.
165. Young SB, Daman JJ, Bony LG. Vaginal paravaginal repair: one-year outcomes. Am J Obstet Gynecol 2001;185(6):1360-1366.
166. Kahn MA, Stanton SL. Posterior colporrhaphy: its effects on bowel and sexual function. Br J Obstet Gynaecol 1997;104(1):82-86.
167. Mellgren A, Anzen B, Nilsson BY, et al. Results of rectocele repair. A prospective study. Dis Colon Rectum 1995;38(1):7-13.
168. Maher CF, Qatawneh AM, Baessler K, Schluter PJ. Midline rectovaginal fascial plication for repair of rectocele and obstructed defecation. Obstet Gynecol 2004;104(4):685-689.
169. Abramov Y, Gandhi S, Goldberg RP, Botros SM, Kwon C, Sand PK. Site-specific rectocele repair compared with standard posterior colporrhaphy. Obstet Gynecol 2005;105(2):314-318.
170. Novara G, Artibani W. Surgery for pelvic organ prolapse: current status and future perspectives. Curr Opin Urol 2005;15(4):256-262.
171. Boyles SH, Weber AM, Meyn L. Procedures for pelvic organ prolapse in the United States, 1979-1997. Am J Obstet Gynecol 2003;188(1):108-115.
172. Brown JS, Waetjen LE, Subak LL, Thom DH, Van den ES, Vittinghoff E. Pelvic organ prolapse surgery in the United States, 1997. Am J Obstet Gynecol 2002;186(4):712-716.
173. Wilcox LS, Koonin LM, Pokras R, Strauss LT, Xia Z, Peterson HB. Hysterectomy in the United States, 1988-1990. Obstet Gynecol 1994;83(4):549-555.
7-12

Pelvic Health Disorders Appendix A: Glossary
Appendix A: Glossary
anemia – a low red blood cell count, caused by heavy menstrual bleeding or other blood loss; the most obvious symptom is fatigue.
anterior repair (coloporrhaphy) – the supportive tissue between the vagina and bladder is folded and stitched together so the bladder and urethra are in proper position.
artificial urinary sphincter – a mechanical device surgically implanted into the patient that consists of a cuff, placed around the bulbar urethra or bladder neck, a pressure-regulating balloon and a pump. The device is used to control opening and closing of the urethra manually and is not commonly recommended for women.
autologous – taken from an individual’s own tissues, cells or DNA.
Baby Boomers – women born between 1946 and 1964.
Baden Walker system – system of classifying the severity of prolapse and organized into grades 0 (normal position) to 4 (maximum possible descent). The grades are based on descent of organs in relation to the hymen.
benign – not cancerous.
biofeedback – a behavioral technique by which information about a normally unconscious physiologic process is presented to the patient and the clinician as a visual, auditory or tactile signal. The signal is derived from a measurable physiologic parameter which subsequently is used in an educational process to accomplish a specific therapeutic result. The signal is displayed in a quantitative way, and the patient is taught how to alter it and, thus, control the physiologic process.
bladder training – a behavioral technique that teaches the patient to resist or inhibit the urge to urinate and to urinate according to a schedule rather than urinating at the urge.
bleeding disorders – any disorder leading to bleeding or bruising.
Burch colposuspension – procedure done through an abdominal incision or through a laparoscope to support the bladder base by placing sutures in the vagina to attach it to a ligament on the pubic bone. Classified under retropubic suspension.
cervical cancer – cancer of the cervix (bottom portion of the uterus).
cesarean section – the surgical removal of an infant from the uterus from an incision in the abdomen when vaginal delivery is not possible.
colpocleisis – complete closure of the vagina while leaving channels at the side for drainage from the uterus (which is not removed). This procedure results in the loss of ability to have vaginal intercourse.
A-1

Pelvic Health Disorders Appendix A: Glossary
cystocele – occurs when the bladder prolapses, falling toward the vagina and creating a large bulge in the front vaginal wall.
cystometry – a test used to assess the function of the bladder by measuring the pressure/ volume relationship of the bladder. Cystometry is used to assess detrusor activity, sensation, capacity and compliance. There are different variations of the test depending on the problem being investigated but, regardless of the technique, cystometry involves insertion of a catheter into the bladder.
cytoscopy - inspection of the inside of the bladder.
detrusor instability – common cause of urge incontinence. Involuntary bladder contractions which occur despite one’s desire to postpone urination.
dysfunctional uterine bleeding – uterus bleeding unrelated to periods.
dysmenorrhea – painful periods.
electrical stimulation – the application of electric current to stimulate or inhibit the pelvic viscera or their nerve supply in order to induce a direct therapeutic response.
endometrial ablation – the removal of the endometrium (see below) using a variety of procedures including laser, microwave, electric current or heated fluid and freezing. This is a treatment for heavy menstrual bleeding that permanently stops menstruation and prevents future childbearing.
endometrial resection – a procedure to remove the lining of the uterus using a resectoscope (hysteroscope with a heated wire loop).
endometrial cancer – cancer of the endometrium (uterus lining).
endometrial hyperplasia – thickening of the endometrium (lining of the uterus).
endometriosis – misplaced uterus tissue causing scar tissue.
endometritis – inflammation of the endometrium (uterine lining).
enterocele – the weakening of the upper vaginal supports, resulting in the front and back walls of the vagina to separate and causing the intestines to push against the vaginal skin.
excessive menstrual bleeding – a period is heavy and associated with clots and flooding with excessive usage of sanitary pads.
fascia - specialized connective tissue layer which surrounds muscles, bones and joints.
GnRH – gonadotropin-releasing hormone, one of the hormones that regulates the female menstrual cycle.
A-2

Pelvic Health Disorders Appendix A: Glossary
GnRH agonists (gonadotropin-releasing hormone agonists) – a group of drugs which reduce a woman’s estrogen levels; these drugs are used to treat endometriosis and reduce the size of fibroids. These drugs prevent ovulation and cause an artificial menopause. They may cause symptoms similar to menopause and can cause bone mineral loss eventually leading to osteoporosis. For these reasons, GnRH agonists are most often a temporary treatment, relieving symptoms until other approaches can take effect.
hysterectomy – the removal of the uterus. During a simple hysterectomy only, the uterus and cervix are removed; during a total hysterectomy, the uterus and cervix are removed along with the ovaries and fallopian tubes. The more extensive procedure usually is used in cancer treatment. To treat fibroids and other pelvic health conditions, only a simple hysterectomy is usually required.
hysteroscopic resection – the removal of fibroids from the inner wall of the uterus with a fiberoptic device called a hysteroscope.
illiococcygeal ligament fixation – a vaginal procedure that attaches the top of the prolapsed vagina to pararectal supportive tissue.
infertility – the inability to have children; not being able to acheive pregnancy after one year of regular, unprotected sex or the inability to carry a pregnancy to a live birth.
intrinsic sphincter deficiency (ISD) – a cause of stress urinary incontinence in which the urethral sphincter is unable to contract and generate sufficient resistance in the bladder, especially during stress maneuvers.
Kelly or Kennedy plication - aimed at supporting and elevating the bladder neck and urethra to a high retropubic position. Kelly plication imbricates urethropelvic fascia and anterior vaginal wall to restore support to the floor of the urethra and bladder neck. The Kennedy procedure continues this plication to include the pubocervical fascia in order to restore support to the base of the bladder. These two procedures often are combined.
laparoscopy – this procedure uses a fibreoptic device called a laparoscope to examine the inside of the pelvic cavity. The laparoscope is inserted through a small incision in the abdomen.
laparotomy – traditional abdominal surgery.
leiomyomas – the medical term for fibroids.
levator ani – broad, thin muscle, situated on the side of the pelvis.
Marshall-Marchetti-Krantz (MMK) – surgical procedure that reinforces the bladder neck in order to prevent unintentional urine loss. Classified under retropubic suspension.
menarche – a woman’s first menstrual period.
A-3

Pelvic Health Disorders Appendix A: Glossary
menorrhagia – menstruation at regular cycle intervals but with excessive flow and duration. Clinically, it is defined as total blood loss exceeding 80 mL per cycle or menses lasting longer than 7 days.
menopause - the cessation of a woman’s menstrual periods.
menses – menstrual flow.
mixed urinary incontinence – the combination, in a patient, of urge urinary incontinence and stress urinary incontinence.
myomectomy – the surgical removal of a fibroid.
ovaries – female glands that produce eggs and the hormones estrogen and progesterone.
paravaginal repair (vaginal or abdominal approach) – support the vaginal wall by attaching it to the pelvic sidewall to fix a cystocele. A synthetic mesh or organic graft material made be placed to reinforce this repair.
parous – having given births to one or more viable children.
pelvic floor muscle exercises (PFME) – also known as Kegel’s exercises, they strengthen the support of the pelvic organs. They are useful in prolapse prevention, but once the symptoms of prolapse are severe, these exercises are of little benefit.
pelvic organ prolapse – the downward descent of female pelvic organs resulting in protrusion of the vagina, uterus or both.
Pelvic Organ Prolapse Quantification (POP-Q) system – system of classifying the severity of prolapse and organized into stages 0 (no prolapse) to 4 (severe prolapse). The stages are based on the maximal extent of prolapse relative to the hymen, in one or more compartments.
pessary – a device worn in the vagina like a diaphragm. Pessaries are used to support the vagina, bladder, rectum and uterus as necessary. They come in a variety of shapes and sizes and must be fitted by a doctor or nurse.
periurethral bulking injections – a surgical treatment for urethral sphincter insufficiency that involves injecting materials such as polytetrafluoroethylene (PTFE) or collagen into the periurethral area to increase urethral compression.
plication - fold, an angular or rounded shape made by folding.
posterior colporrhaphy – a vaginal procedure to reestablish the support between the vagina and rectum to fix a rectocele. A synthetic mesh or organic graft material made be placed to reinforce this repair.
post void residual measurement (PVR) – volume of urine remaining in the bladder immediately after urination.
A-4

Pelvic Health Disorders Appendix A: Glossary
progestogens – naturally-occuring hormones that shrink endometrial tissue; they are used as an endometriosis treatment but can have severe side effects.
prostaglandins – naturally-occuring hormones that cause the uterus to contract and are responsible for period cramps.
rectocele – this occurs when the end of the large bowel (rectum) loses support and falls into the back wall of the vagina, causing it to bulge.
reproductive age – from the first menstrual cycle until the onset of menopause; all the years a woman is able to conceive a child.
resection – the surgical removal of an organ or other structure.
retropubic suspension – utilize the strong components of the pelvic wall as anchoring tissue for sutures placed in the periurethral and perivesical tissues.
sacral colpopexy – a procedure (performed abdominally or laparoscopically) that attaches the top of the prolapsed vagina to the sacrum using either synthetic mesh or cadaveric material.
sacrospinous ligament suspension – a vaginal procedure that attaches the top of the prolapsed vagina to a ligament in the pelvis.
site-specific repairs - rebuild weakened endopelvic fascia, repair fascial tears and reattach prolapsed tissues to stronger sites.
sling procedures – surgical methods for treating urinary incontinence involving the placement of a sling, made either of tissue obtained from the person undergoing the sling procedure (autologous)or of tissue obtained from another source (synthetic or cadaver), under the urethrovesical junction and anchored to retropubic and/or abdominal structures.
stress urinary incontinence – a form of urinary incontinence characterized by the involuntary loss of urine upon effort or exertion, such as coughing, sneezing, laughing or physical exercise.
synthetic - substances produced by chemical or biochemical means; produced artificially, not natural.
tension-free vaginal tape (TVT) – newer sling procedure that uses a special type of midurethral mesh sling and typically is performed under local anesthesia on an outpatient basis.
transvaginal enterocele repair – closes the space between the vagina and rectum through a vaginal incision to prevent the small bowel from pushing the vagina out. This procedure also will resuspend the top of the vagina.
transvaginal needle suspension – sutures are threaded from the vagina to the anterior abdominal fascia and looped through the paraurethral tissue on each side of the bladder neck.
tumor – a mass of cells that may be benign or cancerous.
A-5
Pelvic Health Disorders Appendix A: Glossary
ultrasound –used to visualize soft body tissues by directing high frequency sound waves. The “echoes” produce an on-screen image. Thicker tissue appears lighter on the ultrasound screen. Ultrasound technology has been used for over 35 years and studies show it is safe.
uterus – the female organ that holds and sustains the fetus.
uterine artery embolization – a procedure that involves blocking the blood vessels that supply the tumor by injecting small particles into the arteries feeding the uterus.
uterine fibroids – benign nodules in the uterus wall.
urethral hypermobility – common cause of stress urinary incontinence. Involves the rotational descent of the proximal urethra and bladder neck into the vagina, associated with increases in abdominal pressure that occur with such activities as coughing.
urethrocele – bulging of the urethra into the lower one-third of the anterior vaginal wall.
urge incontinence – a form of urinary incontinence involving a strong, sudden need to urinate, followed by a bladder contraction, which results in leakage.
urinary incontinence – a condition in which a person is unable to hold urine and prevent its leakage.
urinary stress test - the patient is asked to stand with a full bladder and then cough.
urodynamic testing – evaluation of bladder and sphincteric function; also includes tests to measure pressure and urine flow.
uterine prolapse – involves weakening of a group of ligaments called the uterosacral ligaments at the top of the vagina. This causes the uterus to fall, which commonly causes both the front and back walls of the vagina to weaken as well.
uterosacral ligament suspension – suspends the top of the vagina to the uterosacral ligaments; can be performed vaginally or abdominally.
vaginal vault prolapse – the top of the vagina gradually falls toward the vaginal opening, causing the walls of the vagina to weaken. Eventually, the top of the vagina may protrude out of the body through the vaginal opening.
von Willebrand disease – a rare inherited blood coagulation disorder characterized by a deficiency or defect in plasma protein called the von Willebrand factor which leads to excessive bleeding problems.
Weighted vaginal cones – small weights that can be placed in your vagina to help you train your pelvic floor muscles. As the pelvic muscles become stronger, cones of increasing weight should be used.
A-6

Pelvic Health Disorders Appendix B: Methods
Appendix B: Methods
To answer questions on pelvic health disorder, a structured, detailed search strategy was employed to identify literature on both the prevalence and patterns of treatment for menorrhagia, uterine fibroids, stress urinary incontinence and pelvic organ prolapse. This search focused on obtaining English-language journal articles and reports pertaining to the four topical areas, as well as examining the available unpublished literature. Reference lists of key published literature also were reviewed to identify seminal or prominent literature in the field.
Several databases were used to search for literature, reports and clinical practice guidelines, including PubMed, the National Guidelines Clearinghouse and the Cochrane Collaboration. In addition, Google searches were performed to identify organizational websites containing information on each disorder (e.g., National Uterine Fibroids Foundation, Society of Interventional Radiology, National Association for Continence), as well as any non-peer reviewed literature and studies.
The following text and Medical Subject Headings (MeSH) search terms were used to conduct the literature review:
abnormal uterine bleeding baby boomer(s) endometrial ablation epidemiology endometrial ablation (thermal balloon ablation) endometrial or endometrial resection excessive menstrual bleeding extreme bleeding fibroids heavy menstrual bleeding hormonal contraceptives/oral contraceptive hysterectomy (including laparoscopic-assisted, vaginal and abdominal) hysteroscopic incidence
leiomyoma (including uterine leiomyomata) magnetic resolution imaging menorrhagia myomectomy pelvic organ prolapse/prolapse prevalence stress urinary incontinence treatment/treatment patterns urinary incontinence uterine fibroids uterine artery/fibroid embolization/UAE uterine fibroids women
Analysis of the National Hospital Discharge Survey also was conducted to identify treatment pattern trends for each disorder. Data were analyzed from 1996 to 2005 with respect to the types of procedures performed for all women and baby boomer women. For purposes of this analysis, Baby Boomer women were identified based on their age at time of discharge, including only women born between 1946 and 1964.
B-1

®
701
3
National Women’s Health Resource Center1750 K Street, NW Suite 350 Washington, DC 2006
1.877.986.9472
157 Broad StreetSuite 315 Red Bank, NJ 07
The Lewin Group, Inc. 130 Fairview Park Drive
Suite 800 Falls Church, VA 22042
703.269.5500




















