Comorbid physical health conditions and anxiety disorders: a population-based exploration of...
9
Psychiatric–Medical Comorbidity The Psychiatric–Medical Comorbidity section will focus on the prevalence and impact of psychiatric disorders in patients with chronic medical illness as well as the prevalence and impact of medical disorders in patients with chronic psychiatric illness. Comorbid physical health conditions and anxiety disorders: a population-based exploration of prevalence and health outcomes among older adults Renée El-Gabalawy, M.A. a, ⁎ , Corey S. Mackenzie, Ph.D. a , Shahin Shooshtari, Ph.D. b,d , Jitender Sareen, M.D. a,c,d a Department of Psychology, University of Manitoba, Winnipeg, MB Canada R3E 3N4 b Department of Family Social Sciences, University of Manitoba, Winnipeg, MB Canada R3E 3N4 c Department of Psychiatry, University of Manitoba, Winnipeg, MB Canada R3E 3N4 d Department of Community Health Sciences, University of Manitoba, Winnipeg, MB Canada R3E 3N4 Received 24 April 2011; accepted 15 July 2011 Abstract Objective: The primary objectives of this study were to examine the likelihood of anxiety disorders among respondents with common physical health conditions and to explore the associations between this comorbidity and older adults' perceived mental and physical health. Method: The sample consisted of older adults from the Canadian Community Health Survey 1.2 (n=12,792). Trained lay interviewers assessed psychiatric disorders based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, criteria. Physical health conditions were based on self-reported diagnoses by health professionals. Multiple logistic regressions examined whether suffering from a physical health condition increased the odds of any assessed anxiety disorder (panic, agoraphobia, social phobia and posttraumatic stress disorder). Multiple linear regressions examined associations between self-rated health and comorbid physical health conditions and anxiety. Results: After adjusting for confounding variables, the presence of chronically painful conditions (i.e., arthritis, back pain and migraine) and of other commonly occurring diseases (i.e., allergies, cataracts and gastrointestinal, lung and heart disease) were positively associated with anxiety. The comorbidity of anxiety with allergies, cataracts, arthritis and lung disease resulted in poorer self-rated physical and/or mental health after adjusting for confounding variables. Conclusion: Health problems in older adults are associated with increased odds of anxiety, and this comorbidity is associated with poorer self-reported health than medical problems or anxiety alone. These findings have important clinical implications for health professionals. © 2011 Elsevier Inc. All rights reserved. Keywords: Anxiety; Medical conditions; Comorbidity; Older adults; Epidemiology Recently, there has been an expanding body of literature investigating the relationship between physical health conditions and mental disorders. Existing research has focused primarily on mood disorders and, to a lesser extent, anxiety disorders in conjunction with physical health conditions in the general adult population [1–5]. However, it is unclear which physical health conditions are more likely to co-occur with anxiety and what the outcomes of this comorbidity are in older adults, who are more likely to experience physical health conditions and have a high rate of anxiety disorders [6] that can persist for years [7]. Clarifying these issues is imperative because both anxiety and various physical health conditions significantly affect the quality of life of large and rapidly growing numbers of North American older adults [8]. The current research aims to examine the Available online at www.sciencedirect.com General Hospital Psychiatry 33 (2011) 556 – 564 ⁎ Corresponding author. E-mail address: [email protected] (R. El-Gabalawy). 0163-8343/$ – see front matter © 2011 Elsevier Inc. All rights reserved. doi:10.1016/j.genhosppsych.2011.07.005
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Comorbid physical health conditions and anxiety disorders: a population-based exploration of...
Available online at www.sciencedirect.com
General Hospital Psychiatry 33 (2011) 556–564
Psychiatric–Medical ComorbidityThe Psychiatric–Medical Comorbidity section will focus on the prevalence and impact of psychiatric disorders in patients with chronic medical illness as well
as the prevalence and impact of medical disorders in patients with chronic psychiatric illness.
Comorbid physical health conditions and anxiety disorders:a population-based exploration of prevalence and
health outcomes among older adultsRenée El-Gabalawy, M.A.a,⁎, Corey S. Mackenzie, Ph.D.a,Shahin Shooshtari, Ph.D.b,d, Jitender Sareen, M.D.a,c,d
aDepartment of Psychology, University of Manitoba, Winnipeg, MB Canada R3E 3N4bDepartment of Family Social Sciences, University of Manitoba, Winnipeg, MB Canada R3E 3N4
cDepartment of Psychiatry, University of Manitoba, Winnipeg, MB Canada R3E 3N4dDepartment of Community Health Sciences, University of Manitoba, Winnipeg, MB Canada R3E 3N4
Received 24 April 2011; accepted 15 July 2011
Abstract
Objective: The primary objectives of this study were to examine the likelihood of anxiety disorders among respondents with commonphysical health conditions and to explore the associations between this comorbidity and older adults' perceived mental and physical health.Method: The sample consisted of older adults from the Canadian Community Health Survey 1.2 (n=12,792). Trained lay interviewersassessed psychiatric disorders based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, criteria. Physicalhealth conditions were based on self-reported diagnoses by health professionals. Multiple logistic regressions examined whethersuffering from a physical health condition increased the odds of any assessed anxiety disorder (panic, agoraphobia, social phobia andposttraumatic stress disorder). Multiple linear regressions examined associations between self-rated health and comorbid physical healthconditions and anxiety.Results: After adjusting for confounding variables, the presence of chronically painful conditions (i.e., arthritis, back pain and migraine) andof other commonly occurring diseases (i.e., allergies, cataracts and gastrointestinal, lung and heart disease) were positively associated withanxiety. The comorbidity of anxiety with allergies, cataracts, arthritis and lung disease resulted in poorer self-rated physical and/or mentalhealth after adjusting for confounding variables.Conclusion: Health problems in older adults are associated with increased odds of anxiety, and this comorbidity is associated with poorerself-reported health than medical problems or anxiety alone. These findings have important clinical implications for health professionals.© 2011 Elsevier Inc. All rights reserved.
Keywords: Anxiety; Medical conditions; Comorbidity; Older adults; Epidemiology
Recently, there has been an expanding body of literatureinvestigating the relationship between physical healthconditions and mental disorders. Existing research hasfocused primarily on mood disorders and, to a lesser extent,anxiety disorders in conjunction with physical healthconditions in the general adult population [1–5]. However,
⁎ Corresponding author.E-mail address: [email protected] (R. El-Gabalawy).
0163-8343/$ – see front matter © 2011 Elsevier Inc. All rights reserved.doi:10.1016/j.genhosppsych.2011.07.005
it is unclear which physical health conditions are more likelyto co-occur with anxiety and what the outcomes of thiscomorbidity are in older adults, who are more likely toexperience physical health conditions and have a high rate ofanxiety disorders [6] that can persist for years [7]. Clarifyingthese issues is imperative because both anxiety and variousphysical health conditions significantly affect the quality oflife of large and rapidly growing numbers of North Americanolder adults [8]. The current research aims to examine the

557R. El-Gabalawy et al. / General Hospital Psychiatry 33 (2011) 556–564
comorbidity of anxiety and a broad range of physical healthconditions, and explore whether this relationship is associ-ated with poorer self-reported physical and mental healththan either condition alone.
The majority of research investigating comorbid mentaland physical health problems has focused on mood disordersin the general adult population. For example, the relationshipbetween mood disorders and physical health conditions suchas arthritis, asthma and diabetes, and the negative effect ofthese co-occurring conditions on quality of life have beenwell-established [1,2]. There has also been a growing bodyof research examining the relationship between anxietydisorders and physical health conditions in the general adultpopulation. Population-based research, including the WorldMental Health Survey initiative, focused on adults across thelife span has also found significant associations betweenanxiety disorders and physical health conditions [9,10], withthe combination of the two resulting in greater clinicalseverity after controlling for confounding variables such associodemographics and other mental disorders [3–5,11,12].Preliminary research suggests that anxiety may be morelikely than depression to co-occur with physical healthconditions, and this co-occurrence may result in greater roleimpairment [13]. However, it is unclear whether these resultsgeneralize to older adults who typically suffer from a greaternumber of physical health problems.
Prevalence rates of anxiety disorders in older adults areestimated to be between 3.2% and 14.2% [14], and researchwith clinical samples suggests that a significant proportion ofolder adults with anxiety disorders are at increased risk ofmedical conditions and disability [15,16]. For example, areview by Palmer and colleagues [17] indicated thathyperthyroidism, diabetes, heart disease, chronic obstructivepulmonary disease and gastrointestinal disease are associatedwith increased prevalence of anxiety in clinical samples.Furthermore, a dose–response relationship appears to exist,where older adults suffering from a greater number of somatic[18] and pain [19,20] conditions are at greater risk of anxiety. Itis not clear, however, whether this research with clinicalsamples generalizes to the general population. Moreover,research with clinical samples has not tended to adjust forphysical and mental health comorbidity in order to determinethe independent relationships of various physical healthconditions with anxiety. Preliminary population-based re-search has found that psychiatric and physical comorbidityamong older adults is particularly common; however, specificphysical health conditions and the effects of this comorbidityhave not yet been investigated among this population [10].
The current study addressed this gap in knowledge usinga nationally representative sample of older adults. The aimsof this study were threefold. First, we extended prior clinicaland community research by examining whether a number ofhighly prevalent physical health conditions increase the oddsof suffering from a co-occurring anxiety disorder in olderadults after controlling for sociodemographic variables andmood and substance use disorders. Second, we attempted to
replicate prior clinical research suggesting a dose–responserelationship whereby the risk of suffering from a co-occurring anxiety disorder increases linearly with increasingnumbers of physical health problems. Third, we examinedwhether suffering from comorbid physical health conditionsand any anxiety disorder was associated with poorer self-rated physical and mental health after controlling forsociodemographic variables, other mental disorders andother physical health conditions.
1. Methods
We analyzed data from the Canadian Community HealthSurvey Cycle 1.2–Mental Health and Well-Being (CCHS1.2) Master File maintained at the Statistics Canada ResearchData Centre in Winnipeg, Manitoba, Canada. The CCHS 1.2was conducted in 2002, has a 77% response rate and includes36,984 representative Canadians aged 15 years or olderliving in private dwellings in the 10 provinces [21]. Eligiblerespondents were chosen using a multistage, stratified clusterdesign. The survey excluded military personnel and in-dividuals living in institutions or on Indian Reserves. Inaddition, respondents whose cognitive, mental or physicalhealth prevented them from responding were excluded fromthe survey. Most (86%) of the interviews were conducted inperson using a computer-assisted application; the rest wereconducted by telephone. The method of sample selection forhousehold interviews and the description of the CCHS 1.2field procedures appear elsewhere [21]. As is the case inprevious research [22,23], our analyses were restricted toparticipants 55 years of age or older (n=12,792) to enhancestatistical power and because the traditional age cutoff of 65years is increasingly irrelevant as individuals often retiresignificantly earlier than age 65 years or long after it [24].
1.1. Study measures
1.1.1. Sociodemographic variablesSociodemographic variables in this study included sex,
age, marital status, education and income. We assessed agecontinuously and categorized both marital status (married/common law, widowed, separated/divorced and nevermarried) and level of education (less than secondary school,secondary school graduate/no postsecondary education,some postsecondary education and postsecondary degree/diploma). We categorized income into four quartiles (lowerincome, lower middle, upper middle and high income).
1.1.2. Anxiety disorders and other psychiatric disordersLay interviewers from the community who were
extensively trained and included people with a wide rangeof language competencies assessed past-year anxietydisorders and other psychiatric disorders using a modifiedversion of the World Mental-Health Composite InternationalDiagnostic Interview (CIDI) based on Diagnostic andStatistical Manual of Mental Disorders, Fourth Edition,

558 R. El-Gabalawy et al. / General Hospital Psychiatry 33 (2011) 556–564
criteria. One or more screening questions identified coresymptoms, and individuals were screened into appropriatediagnostic modules of the survey. We generated diagnosticvariables reflecting any mood disorder (i.e., major depres-sion, mania), any substance use disorder (i.e., alcoholdependence, drug dependence) and any anxiety disorder(i.e., panic disorder, agoraphobia, social phobia) as beingpresent or absent in the past 12 months. We used past-yeardiagnoses because lifetime diagnoses are particularlyinaccurate in older adult samples [25]. In addition, thesurvey assessed past-year posttraumatic stress disorder(PTSD) in the chronic conditions section. Respondentsindicated whether they had been diagnosed with PTSD by ahealth professional. Thus, we maintained past-year consis-tency by including those who endorsed this question in the“any anxiety disorder” category. Good concordance has beendemonstrated between lay-person-administered CIDI diag-noses and clinician-administered structured clinical inter-view diagnoses [26].
able 1ample characteristics
ariable Weighted prevalence 95% CI
exMale 46.8 46.06–47.60Female 53.2 52.40–53.94ducationLess than secondary 39.7 38.42–40.96Secondary degree 16.7 15.71–17.65Some postsecondary 5.6 5.06–6.27Postsecondary degree/diploma 38.0 36.76–39.31arital statusMarried/common law 68.3 67.22–69.29Widowed 18.3 17.52–19.17Separated/divorced 8.2 7.62–8.78Single 5.2 4.64–5.86ast-year household income1st (lowest) quartile 12.4 11.65–13.262nd (second lowest) quartile 28.6 27.33–29.813rd (second highest) quartile 36.0 34.72–37.214th (highest) quartile 23.1 21.89–24.28ny anxiety disorder total 7.7 7.11–8.41hysical health conditionsAllergies 28.6 27.49–29.67Cataracts 13.9 13.12–14.78Hypertension 35.2 34.01–36.39Heart disease 15.6 14.78–16.50Arthritis or rheumatism 39.4 38.19–40.64Back pain 26.1 25.05–27.26Migraine 6.8 6.17–7.42Gastrointestinal disease 9.2 8.41–10.09Lung disease 12.0 11.20–12.78Cancer 5.0 4.33–5.67Underweight 2.8 2.37–3.21Obesity 19.0 17.98–19.96Diabetes 11.5 10.68–12.27Thyroid disease 10.2 9.51–10.84
1.1.3. Physical health conditionsThe CCHS 1.2 assessed the presence or absence of 23
common physical health conditions. We excluded a numberof these conditions because of their low prevalence (e.g.,epilepsy) among the study population and because of unclearor ambiguous clinical diagnostic criteria (e.g., chronicfatigue). We grouped together conditions that met ourinclusion criteria if they had similar clinical presentations, ifthey had been grouped together in prior research [27] or ifthey behaved similarly in the regression analyses. Weassessed the following outcomes: (a) allergies (i.e., food orother), (b) cataracts, (c) hypertension, (d) heart disease, (e)arthritis or rheumatism, (f) back pain, (g) migraine, (h)gastrointestinal disease (i.e., bowel disease, or stomach orintestinal ulcers), (i) lung disease (i.e., asthma, bronchitis,emphysema or chronic obstructive pulmonary disease), (j)thyroid disease, (k) diabetes, (l) cancer and (m) obesity/underweight. With the exception of obesity/underweight,physical health conditions were based on self-reports of“long-term conditions which are expected to last or havealready lasted 6 months or more and that have beendiagnosed by a health professional.” Research has foundacceptable to good concordance between self-reportedphysical health conditions and diagnoses by medicalprofessionals [28]. We assessed obesity and underweightby calculating body mass index (BMI) scores for eachrespondent. A BMI greater than 30 was indicative of beingoverweight, and a BMI less than 19 was indicative of beingunderweight. We calculated BMI by dividing body weight(in pounds) by height² (in inches) multiplied by 703, which isin accordance with previous studies [29].
Mean (S.E.) 95% CI
ge 67.1 (0.10) 66.87–67.24ental health status 3.9 (0.01) 3.86–3.91hysical health status 3.3 (0.01) 3.26–3.31
1.1.4. Perceived physical and mental health statusParticipants rated their (a) physical health and (b) mental
health on a scale from 1 (poor) to 5 (excellent).
1.2. Analytic strategy
We used weighted frequencies to derive estimates of theprevalence of the variables used in the analyses among thetotal older adult sample. We also calculated weightedprevalence rates of “any anxiety disorder” among eachphysical health condition group using χ2 analyses.
To address the first study objective, we examined whethersuffering from specific physical health conditions affectedthe odds of suffering from co-occurring any anxiety disorder(i.e., panic disorder, agoraphobia, social phobia and/orPTSD) using logistic regressions. We could not investigateanxiety disorders individually due to a lack of statisticalpower. In addressing the second study objective, weexplored whether suffering from multiple physical healthconditions (i.e., 1, 2, 3 or ≥4) was associated with co-occurring any anxiety disorder using logistic regressionmodeling. Multivariate statistical models in both sets of
TS
V
S
E
M
P
AP
AMP
559R. El-Gabalawy et al. / General Hospital Psychiatry 33 (2011) 556–564
analyses were adjusted for (a) sociodemographics and (b)mood and substance use disorders. To address the third studyobjective, we first compared differences in self-reportedmental health between individuals with physical healthproblems alone to individuals with physical health problemscomorbid with “any anxiety disorder.” Specifically, weexamined whether anxiety plus the physical health conditionof interest vs. the physical health condition alone wasassociated with poorer physical health (i.e., physical healthburden resulting from the comorbid anxiety disorder). In thesecond set of physical health analyses, the reference groupwas changed to physical health conditions comorbid with“any anxiety disorder” to examine how individuals with “anyanxiety disorder” alone compare to this group with regard toself-reported physical health (dependent variable). Specifi-cally, we examined whether anxiety plus the physical healthcondition of interest vs. anxiety alone is associated withpoorer mental health (i.e., mental health burden resultingfrom the comorbid physical health condition). We ranbivariate unadjusted models comparing mean health out-come scores as well as models adjusting for (a) socio-demographics and mood and substance use disorders and (b)sociodemographics, mood and substance use disorders, andall other physical health conditions excluding the conditionof interest. We carried out this final set of analyses byspecifying the calculation of least square covariate correctedmeans within SUDAAN's [30] linear regression module,which is mathematically equivalent to analysis of covari-ance. All analyses employed appropriate weights for theCCHS 1.2 to ensure that the data were representative of thegeneral population aged 55+ years. We used the boot-strapped weights provided by Statistics Canada and the
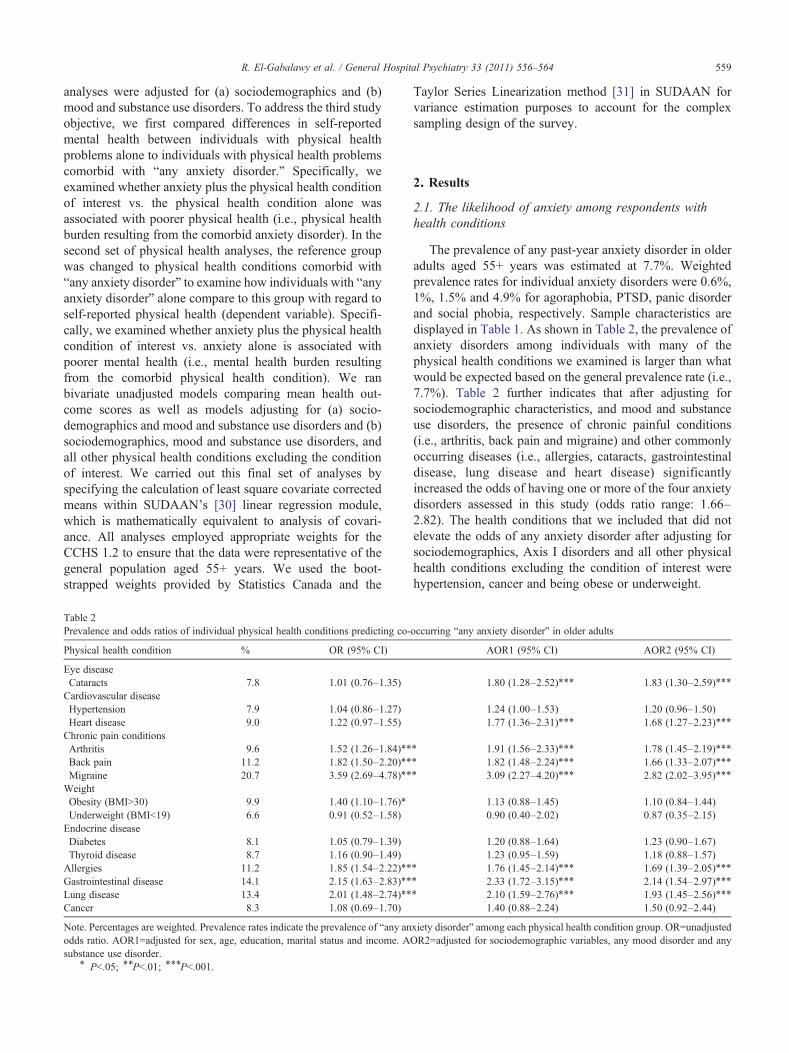
Table 2Prevalence and odds ratios of individual physical health conditions predicting co-
Physical health condition % OR (95% CI)
Eye diseaseCataracts 7.8 1.01 (0.76–1.35)Cardiovascular diseaseHypertension 7.9 1.04 (0.86–1.27)Heart disease 9.0 1.22 (0.97–1.55)Chronic pain conditionsArthritis 9.6 1.52 (1.26–1.84)⁎⁎
Back pain 11.2 1.82 (1.50–2.20)⁎⁎
Migraine 20.7 3.59 (2.69–4.78)⁎⁎
WeightObesity (BMIN30) 9.9 1.40 (1.10–1.76)⁎
Underweight (BMIb19) 6.6 0.91 (0.52–1.58)Endocrine diseaseDiabetes 8.1 1.05 (0.79–1.39)Thyroid disease 8.7 1.16 (0.90–1.49)Allergies 11.2 1.85 (1.54–2.22)⁎⁎
Gastrointestinal disease 14.1 2.15 (1.63–2.83)⁎⁎
Lung disease 13.4 2.01 (1.48–2.74)⁎⁎
Cancer 8.3 1.08 (0.69–1.70)
Note. Percentages are weighted. Prevalence rates indicate the prevalence of “any anodds ratio. AOR1=adjusted for sex, age, education, marital status and income. Asubstance use disorder.
⁎ Pb.05; ⁎⁎Pb.01; ⁎⁎⁎Pb.001.
Taylor Series Linearization method [31] in SUDAAN forvariance estimation purposes to account for the complexsampling design of the survey.
2. Results
2.1. The likelihood of anxiety among respondents withhealth conditions
The prevalence of any past-year anxiety disorder in olderadults aged 55+ years was estimated at 7.7%. Weightedprevalence rates for individual anxiety disorders were 0.6%,1%, 1.5% and 4.9% for agoraphobia, PTSD, panic disorderand social phobia, respectively. Sample characteristics aredisplayed in Table 1. As shown in Table 2, the prevalence ofanxiety disorders among individuals with many of thephysical health conditions we examined is larger than whatwould be expected based on the general prevalence rate (i.e.,7.7%). Table 2 further indicates that after adjusting forsociodemographic characteristics, and mood and substanceuse disorders, the presence of chronic painful conditions(i.e., arthritis, back pain and migraine) and other commonlyoccurring diseases (i.e., allergies, cataracts, gastrointestinaldisease, lung disease and heart disease) significantlyincreased the odds of having one or more of the four anxietydisorders assessed in this study (odds ratio range: 1.66–2.82). The health conditions that we included that did notelevate the odds of any anxiety disorder after adjusting forsociodemographics, Axis I disorders and all other physicalhealth conditions excluding the condition of interest werehypertension, cancer and being obese or underweight.
occurring “any anxiety disorder” in older adults
AOR1 (95% CI) AOR2 (95% CI)
1.80 (1.28–2.52)⁎⁎⁎ 1.83 (1.30–2.59)⁎⁎⁎
1.24 (1.00–1.53) 1.20 (0.96–1.50)1.77 (1.36–2.31)⁎⁎⁎ 1.68 (1.27–2.23)⁎⁎⁎
⁎ 1.91 (1.56–2.33)⁎⁎⁎ 1.78 (1.45–2.19)⁎⁎⁎⁎ 1.82 (1.48–2.24)⁎⁎⁎ 1.66 (1.33–2.07)⁎⁎⁎⁎ 3.09 (2.27–4.20)⁎⁎⁎ 2.82 (2.02–3.95)⁎⁎⁎
1.13 (0.88–1.45) 1.10 (0.84–1.44)0.90 (0.40–2.02) 0.87 (0.35–2.15)
1.20 (0.88–1.64) 1.23 (0.90–1.67)1.23 (0.95–1.59) 1.18 (0.88–1.57)
⁎ 1.76 (1.45–2.14)⁎⁎⁎ 1.69 (1.39–2.05)⁎⁎⁎⁎ 2.33 (1.72–3.15)⁎⁎⁎ 2.14 (1.54–2.97)⁎⁎⁎⁎ 2.10 (1.59–2.76)⁎⁎⁎ 1.93 (1.45–2.56)⁎⁎⁎
1.40 (0.88–2.24) 1.50 (0.92–2.44)
xiety disorder” among each physical health condition group. OR=unadjustedOR2=adjusted for sociodemographic variables, any mood disorder and any

Table 3Logistic regressions predicting co-occurring “any anxiety disorder” among older adults with one or more physical health conditions
Number of physicalhealth conditions
Any anxiety disorderodds ratio (95% CI)
AOR1 AOR2
1 0.79 (0.54–1.16) 1.24 (0.80–1.94) 1.18 (0.74–1.87)2 1.75 (1.20–2.55)⁎⁎ 3.22 (2.13–4.86)⁎⁎⁎ 2.94 (1.92–4.48)⁎⁎⁎
3 2.01 (1.40–2.89)⁎⁎⁎ 3.44 (2.31–5.11)⁎⁎⁎ 2.86 (1.93–4.24)⁎⁎⁎
≥4 3.08 (2.22–4.28)⁎⁎⁎ 5.77 (3.95–8.43)⁎⁎⁎ 5.21 (3.55–7.66)⁎⁎⁎
Note. AOR1=adjusted for sex, age, education, marital status and income. AOR2=adjusted for sociodemographic variables, any mood disorder and any substanceuse disorder.
⁎Pb.05; ⁎⁎Pb.01; ⁎⁎⁎Pb.001.
560 R. El-Gabalawy et al. / General Hospital Psychiatry 33 (2011) 556–564
The logistic regressions in Table 3 demonstrate that as thenumber of physical health conditions increases, so do theodds of having any comorbid anxiety disorder even afteradjusting for sociodemographics and Axis I mental disorders.This relationship, however, was statistically significant onlyfor individuals with two or more physical health problems.
2.2. Physical and mental health associated with comorbidity
In order to explore the association of comorbid any anxietydisorder and health problems on perceived health, we firstexplored whether suffering from any anxiety disorder inaddition to the physical health condition of interest conferredpoorer self-rated physical health compared to the physicalhealth condition alone (i.e., anxiety+physical health conditionvs. physical health condition of interest alone predicting self-perceived physical health). As shown in Table 4, in theunadjusted model, all physical health conditions andcomorbid anxiety were associated with poorer physical healthratings than the physical health condition alone. Moreover,after adjusting for sociodemographics and mental disorders,all physical health conditions, with the exception of migraineand gastrointestinal disease, in conjunction with anxiety wereassociated with poorer self-rated physical health. However,after additionally adjusting for other physical health condi-tions excluding the condition of interest, only allergies,cataracts, lung disease and arthritis had significant indepen-
Table 4Self-reported physical health among older adults with physical health conditions a
Physical healthcondition
Model 1 (mean physical health score, S.E.) Model 2 (mea
Conditionalone
Condition+anxiety
Wald F Conditionalone
Cataracts 3.01 (0.03) 2.56 (0.12) 12.99⁎⁎⁎ 3.04 (0.04)Heart disease 2.91 (0.03) 2.58 (0.11) 8.92⁎⁎ 2.62 (0.03)Arthritis 2.98 (0.02) 2.58 (0.07) 33.04⁎⁎⁎ 2.98 (0.02)Back pain 2.97 (0.03) 2.65 (0.08) 13.66⁎⁎⁎ 2.98 (0.03)Migraine 3.04 (0.07) 2.60 (0.16) 6.17⁎ 3.07 (0.07)Allergies 3.13 (0.03) 2.64 (0.07) 41.82⁎⁎⁎ 3.14 (0.03)Gastrointestinal
disease2.49 (0.06) 1.99 (0.17) 8.12⁎⁎⁎ 2.50 (0.06)
Lung disease 2.75 (0.04) 2.43 (0.11) 7.43⁎⁎ 2.75 (0.04)
Note. Model 1=unadjusted. Model 2=adjusted for sociodemographic variables, asociodemographic variables, Axis I mental disorder and comorbid physical healtindicative of poorer self-rated physical health.
⁎Pb.05; ⁎⁎Pb.01; ⁎⁎⁎Pb.001.
dent effects, in combination with anxiety, on perceivedphysical health. These results indicate that, in many cases,anxiety in addition to a physical health condition increases thelikelihood of poorer physical health ratings. However, theseresults suggest that these poor physical health ratings may belargely driven by medical comorbidity as indicated by thesmaller number of significant associations in model 3.
Table 5 shows the results of our analyses exploringwhether suffering from a physical health condition inaddition to any anxiety disorder conferred poorer self-reported mental health compared to suffering from anxietyalone (i.e., anxiety+physical health condition vs. anxietyalone predicting self-perceived mental health). In contrast tothe physical health outcomes, fewer physical healthconditions with co-occurring any anxiety disorder weresignificantly associated with poorer self-reported mentalhealth. Specifically, in the unadjusted model, all physicalhealth conditions and comorbid anxiety, with the exceptionof cataracts and migraine, were associated with poorer self-reported mental health than anxiety alone. Additionally, onlyallergies, gastrointestinal disease, lung disease and cataractswere significant in the model adjusting for sociodemo-graphics and mental disorders. When additionally control-ling for comorbid physical health conditions, only comorbidany anxiety disorder and lung disease were significantlyassociated with poorer self-reported mental health.
lone vs. physical health conditions and comorbid “any anxiety disorder”
n physical health score, S.E.) Model 3 (mean physical health score, S.E.)
Condition+anxiety
Wald F Conditionalone
Condition+anxiety
Wald F
2.54 (0.13) 12.50⁎⁎⁎ 3.03 (0.03) 2.69 (0.12) 6.58⁎
2.38 (0.11) 4.13⁎ 2.62 (0.03) 2.42 (0.11) 2.812.70 (0.06) 16.72⁎⁎⁎ 2.97 (0.02) 2.81 (0.06) 5.13⁎
2.75 (0.08) 7.35⁎⁎ 2.97 (0.03) 2.83 (0.07) 3.122.76 (0.15) 3.44 3.04 (0.06) 2.86 (0.14) 1.312.68 (0.07) 38.23⁎⁎⁎ 3.12 (0.03) 2.84 (0.07) 14.92⁎⁎⁎
2.12 (0.18) 3.86 2.49 (0.06) 2.19 (0.17) 2.72
2.46 (0.10) 7.31⁎⁎ 2.75 (0.04) 2.50 (0.11) 4.21⁎
ny mood disorder and any substance use disorder. Model 3=adjusted forh conditions. Reference=physical health condition alone. Lower scores are

Table 5Self-reported mental health among older adults with “any anxiety disorder” alone vs. “any anxiety disorder” and comorbid physical health conditions
Physical healthcondition
Model 1 (mean mental health score, S.E.) Model 2 (mean mental health score, S.E.) Model 3 (mean mental health score, S.E.)
Anxiety alone Condition+anxiety Wald F Anxiety alone Condition+anxiety Wald F Anxiety alone Condition+anxiety Wald F
Cataracts 3.29 (0.06) 3.15 (0.12) 1.18 3.32 (0.05) 3.03 (0.14) 3.86⁎ 3.31 (0.05) 3.08 (0.13) 2.79Heart disease 3.31 (0.06) 3.08 (0.10) 4.23⁎ 3.31 (0.06) 3.13 (0.10) 2.59 3.31 (0.05) 3.15 (0.10) 1.76Arthritis 3.39 (0.08) 3.14 (0.07) 5.89⁎ 3.33 (0.07) 3.22 (0.07) 1.27 3.29 (0.07) 3.26 (0.07) 0.07Back pain 3.36 (0.07) 3.13 (0.08) 4.42⁎ 3.33 (0.06) 3.19 (0.08) 1.65 3.30 (0.06) 3.24 (0.08) 0.38Migraine 3.28 (0.05) 3.22 (0.15) 0.13 3.25 (0.05) 3.38 (0.13) 0.86 3.24 (0.05) 3.45 (0.13) 2.25Allergies 3.38 (0.07) 3.11 (0.08) 6.86⁎⁎ 3.38 (0.07) 3.12 (0.07) 6.95⁎⁎ 3.36 (0.07) 3.17 (0.07) 3.26Gastrointestinaldisease
3.29 (0.05) 2.84 (0.19) 5.05⁎ 3.29 (0.05) 2.93 (0.17) 4.48⁎ 3.29 (0.05) 2.95 (0.18) 3.34
Lung disease 3.34 (0.06) 2.98 (0.11) 9.86⁎⁎ 3.33 (0.06) 3.05 (0.09) 7.61⁎⁎ 3.33 (0.05) 3.08 (0.09) 5.06⁎
Note. Model 1=unadjusted. Model 2=adjusted for sex, age, education, marital status, income, any mood disorder and any substance use disorder. Model3=adjusted for sociodemographic variables, Axis I mental disorder and comorbid physical health conditions. Reference=anxiety alone. Lower scores areindicative of poorer self-rated mental health.
⁎Pb.05; ⁎⁎Pb.01; ⁎⁎⁎Pb.001.
561R. El-Gabalawy et al. / General Hospital Psychiatry 33 (2011) 556–564
3. Discussion
To the best of our knowledge, this is the first study to utilizea nationally representative sample of older adults to examinethe prevalence and health outcomes of comorbid anxietydisorders and physical health conditions. Two key findingsemerged from this investigation. First, our data provide strongsupport for higher rates of anxiety disorders among older adultswho experience a variety of physical health conditions.Importantly, these relationships remained significant afteradjusting for sociodemographics and mood and substance usedisorders. Furthermore, our data indicated that as the number ofphysical health conditions increased, so did the odds ofsuffering from a comorbid anxiety disorder. Second, comorbidany anxiety disorder and physical health problems had strongereffects on self-rated physical health than on self-rated mentalhealth. However, for bothmental and physical health outcomes,many of the health conditions that resulted in poorer healthratings when combined with anxiety no longer had uniqueeffects once we adjusted for other physical health conditions.
With respect to our first key finding, we found that anumber of chronic painful conditions and other commonlyoccurring diseases in older adults elevated the odds ofsuffering from a comorbid anxiety disorder, even after takinginto account several possible confounding factors. Conversely,anxiety disorders were not more common among older adultswith hypertension, with cancer and who were obese/underweight. These findings are consistent with prior clinicalresearch with older adults validating a link between cardio-vascular problems and anxiety [32–34], respiratory/lungdisease and anxiety [35,36], and gastrointestinal disease andanxiety [37]. Our results were also partially consistent with theone community-based examination of anxiety and medicalconditions among older Dutch individuals. Both that study andours found that joint disease, heart disease and lung diseasewere significantly associatedwith anxiety, whereas cancerwasnot. In contrast, only our study found a relationship betweenanxiety and gastrointestinal disease [18]. However, it isnoteworthy that these medical conditions were categorized
differently, and thus, comparisons should be interpretedcautiously. The inconsistent results may be due to the factthat the Dutch study had a smaller sample size ormay be due toregional or cultural differences between the two samples.
Because of the dearth of literature examining associationsbetween anxiety and physical health conditions in olderadults, it is difficult to make other direct comparisons toprevious studies. However, in comparison to research withthe general adult population, our results were also partiallyconsistent with a population-based study that used physicianassessments of medical conditions in a German sample [5].Similarly, that study found that the presence of an anxietydisorder was significantly associated with several physicalhealth conditions (except diabetes) and that the strongestassociation was with migraine headaches. Conversely, theirstudy found no relationship with cardiac disease [5]. Onceagain, this may be due to differences in categorizations ofphysical health conditions or differences in the samples.
Although our data cannot speak as to why some physicalhealth conditions were linked to anxiety whereas others werenot, it is worth noting that the physical health conditions thatwere associated with anxiety in this study have the capacity tobe severe and debilitating. For example, arthritis, back painand migraine are often associated with severe chronic pain andimpairment [38,39]. In contrast, with the exception of cancer,hypertension and obesity/underweight often are not associatedwith severe and distressing symptoms, which may reduce thelikelihood of their associations with anxiety. Alternatively, the“any anxiety disorder” group may have not captured distinctrelationships between different types of anxiety disorders andanxiety disorders that were not included in the survey. Priorresearch has found that these relationships do exist [10]. Forexample, PTSD has been found to be significantly associatedto obesity in the general adult population [10]. Similarly, interms of cancer, prior population-based research has found thatadults 55 to 75 years of agewith this disease (but not those overthe age of 75 years) have an increased risk of suffering fromagoraphobia, a decreased risk of suffering from social phobiaand no relationship with panic [40]. It is also possible that the

562 R. El-Gabalawy et al. / General Hospital Psychiatry 33 (2011) 556–564
link between cancer and anxiety is relatively weak in olderadults due to survivor effects, where only older adults with lesssevere forms of cancer are still alive and included in the survey.
Results of the current study further suggest that sufferingfrom a greater number of physical health conditions isassociated, in a linear fashion, with increased odds ofsuffering from comorbid anxiety even after controlling forsociodemographics and Axis I mental disorders. In fact, theodds ratio for greater than four conditions was very large,which implies a strong association. This finding builds onprevious research with both younger and older adults findinga dose–response relationship between physical healthproblems and both anxiety [18,41,42] and depression [43].There is also reason to believe that this dose–responserelationship may result in poorer health outcomes for olderindividuals, even though our data do not address thisspecifically. In indirect support, we found that severalphysical health conditions and comorbid anxiety predictedpoorer self-rated health, but that when we controlled formedical comorbidity, many of these associations lostsignificance. The fact that having multiple physical healthconditions increases the likelihood of having an anxietydisorder, and that their comorbidity often reduces self-ratedhealth, is especially relevant for older adults given that healthproblems are increasingly common with increasing age.
The second key finding from this study is that older adultssuffering from co-occurring anxiety and several physicalhealth conditions reported poorer self-rated health thanindividuals who suffered from either physical healthproblems or anxiety alone. When controlling for bothpsychiatric and medical comorbidity, co-occurring anxietyand allergies, lung disease, cataracts and arthritis predictedpoorer self-rated physical health. It is possible that olderadults who suffer from anxiety may experience psychoso-matic reactions which exacerbate physical discomfort fromtheir existing medical condition(s). In support of this notion,older adults who suffer from anxiety frequently reportsomatic complaints [44]. Furthermore, the lower threshold ofpain hypothesis [45] suggests that prolonged physiologicalarousal from stress resulting from both anxiety and pain canimpair body systems, particularly the cardiovascular andmetabolic systems, the brain and the immune system [46],and therefore potentially exacerbate pain.
In contrast to the relatively robust combined effects ofanxiety and physical health conditions on self-reportedphysical health, comorbid anxiety and health conditionshad fewer effects on self-reported mental health. In fact, aftercontrolling for sociodemographic factors and both psychiat-ric and medical comorbidity, only lung disease and co-occurring anxiety negatively affected perceived mentalhealth. This finding is supported by prior research suggestingthat psychiatric conditions such as anxiety contribute to theetiology, course and clinical expression of lung disease[47,48]. In fact, anxiety is considered among the mostfrequently reported predictors of poor quality of life in lungdisease sufferers [49]. Thus, prior research suggests that there
may be a particularly strong psychological component to lungdisease that can result in poorer mental health. Takentogether, these self-reported health results have importantimplications for older adults. First and most importantly,prior research has shown that self-reported physical andmental health predicts functional decline and mortality[50,51], disability [52], greater morbidity [53], greater healthcare use [54] and slower recovery from illness [55] in bothyounger and older adults. Finally, this suggests that in thosewith a comorbid anxiety disorder and physical healthcondition, the anxiety may be influencing older adults'perceptions of their physical health and perhaps alsoexacerbating pain. Therefore, appropriate treatment ofanxiety in comorbid relationships may reduce levels of painand may impact functioning. Moreover, this suggests thatphysical health conditions, when comorbid with anxiety, maybe influencing older adults' health status, which may lead togreater psychological burden.
Although our cross-sectional data do not allow us toexamine possible causal pathways or mechanisms behind thesubstantial degree of co-occurrence between physical healthconditions and anxiety, we can speculate on what they mightbe. First, a direct relationship may exist between physicalhealth conditions and anxiety. For example, emotionalarousal associated with uncertain outcomes in relation tophysical health conditions may elicit anxiety in older adults.This is supported by Clark's cognitive model which suggeststhat catastrophic misinterpretation of bodily sensations canexacerbate arousal and lead to anxiety [49,56]. Individualswho have been diagnosed with serious allergies, forexample, often live with constant vigilance and fear ofserious adverse reactions [57]. Conversely, anxiety mayincrease susceptibility to physical health conditions ifprolonged physiological arousal results in the deteriorationof neural, bone and muscle tissue [45]. Second, symptoms ofanxiety and physical health conditions may mutuallymaintain one another [58]. For example, anxiety may reducethe capacity to deal effectively with physical health problemsby, for example, decreasing adherence to treatment, whichmay in turn exacerbate symptomatology associated with thephysical health condition [59]. Mutual maintenance ofanxiety and physical health conditions may be alsounderstood in the context of anxiety sensitivity, which mayexacerbate pain in those with anxiety [45]. In addition, priorresearch has found that anxiety sensitivity is elevated inindividuals with comorbid anxiety and musculoskeletal pain,and may play a role in maintaining symptoms of both anxietyand the physical health condition [45]. Third, a number ofother potential mediators, such as personality, environmentaland biological characteristics, may explain the associationbetween anxiety and physical health conditions. Longitudi-nal research is needed to explore possible causal relation-ships between anxiety and physical health problems amongthis population.
The results of the current study must be considered inlight of several limitations. First, physical health diagnoses

563R. El-Gabalawy et al. / General Hospital Psychiatry 33 (2011) 556–564
and the assessment of PTSD were based on self-reports.Although individuals reported whether they were diagnosedby a health professional, this does not eliminate a possiblereporting bias. However, prior research has found anacceptable concordance between self-reports and medicalrecords of physical health diagnoses [13,28]. Second, theCCHS 1.2 assessed a limited number of anxiety disorders, sowe were not able to explore associations between physicalhealth problems and obsessive–compulsive disorder orgeneralized anxiety disorder. Thus, the prevalence of “anyanxiety disorder” is likely considerably underestimated. Thisis particularly important for generalized anxiety disorder,which is one of the most prevalent anxiety disorders amongolder adults [6,60]. In fact, prior clinical research has foundthat generalized anxiety disorder is significantly associatedwith diabetes and gastrointestinal conditions in older adults[37]. Future epidemiological research should aim to examinethe relationship of generalized anxiety disorder and medicalconditions in the elderly. Third, the CCHS 1.2 only surveyedcommunity-dwelling individuals, so the results cannot begeneralized to institutionalized older adults. Given thatinstitutionalized older adults tend to be less healthy thancommunity-dwelling individuals, it is possible that ourresults would be more pronounced in that population.
Despite these limitations, the results of this study haveimportant implications for the detection and treatment of abroad range of physical health conditions and co-occurringanxiety. In particular, our results emphasize the need toscreen for anxiety disorders in physically unhealthy olderadults, particularly older adults suffering from multiplephysical health conditions. Screening for anxiety disorders ingeneral medical practices and specialty clinics is importantbecause of increased prevalence of anxiety across a varietyof health conditions, because comorbid anxiety and physicalhealth conditions often resulted in poorer physical healthand, in the case of lung disease, mental health, and becauseeffective treatments for anxiety disorders exist [61].Moreover, because of the possible reciprocal nature ofanxiety and physical health conditions, it is important forclinicians to effectively manage health problems in olderadults suffering from anxiety. Screening for comorbidanxiety and medical illness has the potential to enhance theprevention or early treatment of both conditions to improvethe quality of life of growing numbers of older adults.
Acknowledgments
Renée El-Gabalawy is supported by a Vanier CanadaGraduate Scholarship, Manitoba Graduate Scholarship,Research Data Centre Graduate Scholarship, and Universityof Manitoba Centre on Aging Fellowships. Corey S.Mackenzie is supported by a Manitoba Health ResearchCouncil Establishment Grant. Shahin Shooshtari is sup-ported by a Manitoba Research Data Centre Faculty Award.Jitender Sareen is supported by a Canadian Institutes ofHealth Research New Investigator Award (#152348) and the
Manitoba Health Research Council Chair Award. We wouldalso like to acknowledge Dr. Ian Clara at the ManitobaResearch Data Centre for his valuable input.
References
[1] Evans DL, Charney DS. Mood disorders and medical illness: a majorpublic health problem. Biol Psychiatry 2003;54(3):177–80.
[2] Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B.Depression, chronic diseases, and decrements in health: results fromthe World Health Surveys. Lancet 2007;370(9590):851–8.
[3] Katon W, Lin EH, Kroenke K. The association of depression andanxiety with medical symptom burden in patients with chronic medicalillness. Gen Hosp Psychiatry 2007;29(2):147–55.
[4] Sareen J, Cox BJ, Clara I, Asmundson GJ. The relationship betweenanxiety disorders and physical disorders in the U.S. NationalComorbidity Survey. Depress Anxiety 2005;21(4):193–202.
[5] Sareen J, Jacobi F, Cox BJ, Belik SL, Clara I, Stein MB. Disability andpoor quality of life associated with comorbid anxiety disorders andphysical conditions. Arch Intern Med 2006;166(19):2109–16.
[6] Beekman AT, Bremmer MA, Deeg DJ, et al. Anxiety disorders in laterlife: a report from the Longitudinal Aging Study Amsterdam. Int JGeriatr Psychiatry 1998;13(10):717–26.
[7] Schuurmans J, Comijs HC, Beekman AT, et al. The outcome of anxietydisorders in older people at 6-year follow-up: results from theLongitudinal Aging Study Amsterdam. Acta Psychiatr Scand2005;111(6):420–8.
[8] Alwahhabi F. Anxiety symptoms and generalized anxiety disorder inthe elderly: a review. Harv Rev Psychiatry 2003;11(4):180–93.
[9] Scott KM, Bruffaerts R, Tsang A, et al. Depression-anxiety relation-ships with chronic physical conditions: results from the World MentalHealth Surveys. J Affect Disord 2007;103(1–3):113–20.
[10] Scott KM, Von KM, Alonso J, et al. Age patterns in the prevalence ofDSM-IV depressive/anxiety disorders with and without physical co-morbidity. Psychol Med 2008;38(11):1659–69.
[11] Scott KM, Von KM, Alonso J, et al. Mental–physical co-morbidityand its relationship with disability: results from the World MentalHealth Surveys. Psychol Med 2009;39(1):33–43.
[12] McWilliams LA, Cox BJ, Enns MW. Mood and anxiety disordersassociated with chronic pain: an examination in a nationallyrepresentative sample. Pain 2003;106(1–2):127–33.
[13] Kessler RC, Ormel J, Demler O, Stang PE. Comorbid mental disordersaccount for the role impairment of commonly occurring chronicphysical disorders: results from the National Comorbidity Survey.J Occup Environ Med 2003;45(12):1257–66.
[14] Wolitzky-Taylor KB, Castriotta N, Lenze EJ, Stanley MA, CraskeMG. Anxiety disorders in older adults: a comprehensive review.Depress Anxiety 2010;27(2):190–211.
[15] Lenze EJ, Rogers JC, Martire LM, et al. The association of late-lifedepression and anxiety with physical disability: a review of theliterature and prospectus for future research. Am J Geriatr Psychiatry2001;9(2):113–35.
[16] Lu BY, Ahmed I. The mind–body conundrum: the somatopsychicperspective in geriatric depression. Am J Geriatr Psychiatry 2010;18(5):378–81.
[17] Palmer BW, Jeste DV, Sheikh JI. Anxiety disorders in the elderly:DSM-IV and other barriers to diagnosis and treatment. J Affect Disord1997;46(3):183–90.
[18] van Balkom AJ, Beekman AT, de BE, Deeg DJ, van DR, van TW.Comorbidity of the anxiety disorders in a community-based olderpopulation in the Netherlands. Acta Psychiatr Scand 2000;101(1):37–45.
[19] Richardson TM, Simning A, He H, Conwell Y. Anxiety and itscorrelates among older adults accessing aging services. Int J GeriatrPsychiatry 2010.

564 R. El-Gabalawy et al. / General Hospital Psychiatry 33 (2011) 556–564
[20] Smit F, Comijs H, Schoevers R, Cuijpers P, Deeg D, Beekman A.Target groups for the prevention of late-life anxiety. Br J Psychiatry2007;190:428–34.
[21] Gravel R, Beland Y. The Canadian Community Health Survey: mentalhealth and well-being. Can J Psychiatry 2005;50(10):573–9.
[22] Mackenzie CS, Scott T, Mather A, Sareen J. Older adults' help-seekingattitudes and treatment beliefs concerning mental health problems. AmJ Geriatr Psychiatry 2008;16(12):1010–9.
[23] Cairney J, Corna LM, Veldhuizen S, Herrmann N, Streiner DL.Comorbid depression and anxiety in later life: patterns of association,subjective well-being, and impairment. Am J Geriatr Psychiatry2008;16(3):201–8.
[24] Mackenzie CS, Pagura J, Sareen J. Correlates of perceived need for anduse of mental health services by older adults in the collaborativepsychiatric epidemiology surveys. Am J Geriatr Psychiatry 2010.
[25] Streiner DL, Patten SB, Anthony JC, Cairney J. Has 'lifetimeprevalence' reached the end of its life? An examination of the concept.Int J Methods Psychiatr Res 2009;18(4):221–8.
[26] Haro JM, Arbabzadeh-Bouchez S, Brugha TS, et al. Concordance ofthe Composite International Diagnostic Interview Version 3.0 (CIDI3.0) with standardized clinical assessments in the WHOWorld MentalHealth surveys. Int J Methods Psychiatr Res 2006;15(4):167–80.
[27] Sareen J, Cox BJ, Stein MB, Afifi TO, Fleet C, Asmundson GJ.Physical and mental comorbidity, disability, and suicidal behaviorassociated with posttraumatic stress disorder in a large communitysample. Psychosom Med 2007;69(3):242–8.
[28] Kriegsman DM, Penninx BW, van Eijk JT, Boeke AJ, Deeg DJ. Self-reports and general practitioner information on the presence of chronicdiseases in community dwelling elderly. A study on the accuracy ofpatients' self-reports and on determinants of inaccuracy. J ClinEpidemiol 1996;49(12):1407–17.
[29] Mather AA, Cox BJ, Enns MW, Sareen J. Associations between bodyweight and personality disorders in a nationally representative sample.Psychosom Med 2008;70(9):1012–9.
[30] Shah BV, Barnswell BG, Bieler GS. SUDAAN user's manual: release9.0. Research Triangle Park, NC: Research Triangle Institute; 2004.
[31] Levy PS, Lemeshow S. Sampling of populations. New York: JohnWiley & Sons; 1999.
[32] Goldberg R, Morris P, Christian F, Badger J, Chabot S, Edlund M. Panicdisorder in cardiac outpatients. Psychosomatics 1990;31(2):168–73.
[33] Kubzansky LD, Koenen KC, Spiro III A, Vokonas PS, Sparrow D.Prospective study of posttraumatic stress disorder symptoms andcoronary heart disease in the Normative Aging Study. Arch GenPsychiatry 2007;64(1):109–16.
[34] Todaro JF, Shen BJ, Raffa SD, Tilkemeier PL, Niaura R. Prevalence ofanxiety disorders in men and women with established coronary heartdisease. J Cardiopulm Rehabil Prev 2007;27(2):86–91.
[35] Dowson C, Laing R, Barraclough R, et al. The use of the HospitalAnxiety and Depression Scale (HADS) in patients with chronicobstructive pulmonary disease: a pilot study. N Z Med J 2001;114(1141):447–9.
[36] Vogele C, von Leupoldt A. Mental disorders in chronic obstructivepulmonary disease (COPD). Respir Med 2008;102(5):764–73.
[37] Wetherell JL, Ayers CR, Nuevo R, Stein MB, Ramsdell J, PattersonTL. Medical conditions and depressive, anxiety, and somaticsymptoms in older adults with and without generalized anxietydisorder. Aging Ment Health 2010;14(6):764–8.
[38] Nicholl BI, Macfarlane GJ, Davies KA, Morriss R, Dickens C, McBethJ. Premorbid psychosocial factors are associated with poor health-related quality of life in subjects with new onset of chronic widespreadpain— results from the EPIFUND study. Pain 2009;141(1–2):119–26.
[39] Gureje O, Von KM, Simon GE, Gater R. Persistent pain and well-being: a World Health Organization study in primary care. JAMA1998;280(2):147–51.
[40] Rasic DT, Belik SL, Bolton JM, Chochinov HM, Sareen J. Cancer,mental disorders, suicidal ideation and attempts in a large communitysample. Psychooncology 2008;17(7):660–7.
[41] Russo J, Katon W, Sullivan M, Clark M, Buchwald D. Severity ofsomatization and its relationship to psychiatric disorders andpersonality. Psychosomatics 1994;35(6):546–56.
[42] Kubzansky LD, Kawachi I, Spiro III A, Weiss ST, Vokonas PS,Sparrow D. Is worrying bad for your heart? A prospective study ofworry and coronary heart disease in the Normative Aging Study.Circulation 1997;95(4):818–24.
[43] Stegmann ME, Ormel J, de GR, et al. Functional disability as anexplanation of the associations between chronic physical conditionsand 12-month major depressive episode. J Affect Disord 2010;124(1–2):38–44.
[44] Turnbull JM. Anxiety and physical illness in the elderly. J ClinPsychiatry 1989;50(Suppl):40–5.
[45] Asmundson GJ, Katz J. Understanding the co-occurrence of anxietydisorders and chronic pain: state-of-the-art. Depress Anxiety 2009;26(10):888–901.
[46] McEwen BS. Protective and damaging effects of stress mediators. NEngl J Med 1998 January 15;338(3):171–9.
[47] Mikkelsen RL, Middelboe T, Pisinger C, Stage KB. Anxiety anddepression in patients with chronic obstructive pulmonary disease(COPD). A review. Nord J Psychiatry 2004;58(1):65–70.
[48] Lehrer P, Feldman J, Giardino N, Song HS, Schmaling K.Psychological aspects of asthma. J Consult Clin Psychol 2002;70(3):691–711.
[49] Livermore N, Sharpe L, McKenzie D. Panic attacks and panic disorderin chronic obstructive pulmonary disease: a cognitive behavioralperspective. Respir Med 2010;104(9):1246–53.
[50] Idler EL, Benyamini Y. Self-rated health and mortality: a reviewof twenty-seven community studies. J Health Soc Behav 1997;38(1):21–37.
[51] Lee Y. The predictive value of self assessed general, physical, andmental health on functional decline and mortality in older adults.J Epidemiol Community Health 2000;54(2):123–9.
[52] Mansson NO, Rastam L. Self-rated health as a predictor of disabilitypension and death–a prospective study of middle-aged men. Scand JPublic Health 2001;29(2):151–8.
[53] Ferraro KF, Farmer MM,Wybraniec JA. Health trajectories: long-termdynamics among black and white adults. J Health Soc Behav 1997;38(1):38–54.
[54] Wolinsky FD, Culler SD, Callahan CM, Johnson RJ. Hospital resourceconsumption among older adults: a prospective analysis of episodes,length of stay, and charges over a seven-year period. J Gerontol1994;49(5):S240–52.
[55] Wilcox VL, Kasl SV, Idler EL. Self-rated health and physical disabilityin elderly survivors of a major medical event. J Gerontol B Psychol SciSoc Sci 1996;51(2):S96–104.
[56] Clark DM. A cognitive approach to panic. Behav Res Ther 1986;24(4):461–70.
[57] Jones SM, Scurlock AM. The impact of food allergy: the real qfearfactorq. Ann Allergy Asthma Immunol 2006;96(3):385–6.
[58] Sharp TJ, Harvey AG. Chronic pain and posttraumatic stress disorder:mutual maintenance? Clin Psychol Rev 2001;21(6):857–77.
[59] Katon WJ, Richardson L, Lozano P, McCauley E. The relationshipof asthma and anxiety disorders. Psychosom Med 2004;66(3):349–55.
[60] Mackenzie CS, Reynolds K, Chou KL, Pagura J, Sareen J. Prevalenceand correlates of generalized anxiety disorder in a national sample ofolder adults. Am J Geriatr Psychiatry 2011;19(4):305–15.
[61] Pinquart M, Duberstein PR. Treatment of anxiety disorders in olderadults: a meta-analytic comparison of behavioral and pharmacologicalinterventions. Am J Geriatr Psychiatry 2007;15(8):639–51.