
Measuring heat distribution in bone during radiofrequency ...

1
LAPAROSCOPIC RADIOFREQUENCY ABLATION OF SMALL RENAL
TUMORS: LONG-TERM ONCOLOGIC OUTCOMES
Daniel Ramirez, Yun-Bo Ma, Selahattin Bedir, Jodi Antonelli, Jeffery Cadeddu, Jeffery
Gahan
Department of Urology
UT Southwestern Medical Center
Dallas, TX
ªCorresponding Author:
Jeffery Cadeddu, MD
UT Southwestern Department of Urology
Moss Bldg, 8th
Fl, Ste 112
5323 Harry Hines Blvd.
Dallas, TX 75390-9110
Phone (214) 648-0202
Fax (214) 648-8786
Running title: " Laparoscopic radiofrequency ablation of small renal tumors: Long-term
oncologic outcomes." Key Words: radiofrequency ablation, small renal masses, laparoscopic ablative techniques
Page 1 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
2
Abstract
Introduction: Unlike percutaneous radiofrequency ablation (RFA) of small renal tumors, there
is limited data assessing the long-term efficacy of laparoscopic RFA. Though the ablation
cannot be visualized as reliably as with cryoablation, laparoscopic RFA allows for improved
mobilization and placement of probes under direct vision. We reviewed our experience with
laparoscopic RFA to assess long-term oncologic outcomes.
Methods: We performed a retrospective study of all patients who had undergone laparoscopic
RFA for pT1a renal tumors from April 2000 to April 2010. Demographic, clinical and
radiologic data were assessed to determine indications and evidence for recurrence of disease.
Radiologic recurrence was defined as any new enhancement (> 10 Hounsfield units) after
absence of enhancement on initial negative 6-week computed tomography.
Results: Data was available for 79 patients who had 111 small renal masses treated over the 10
year period. The median tumor diameter was 2.2 cm and intraoperative biopsy identified renal
cell carcinoma in 77%. The median follow-up was 59 months with an estimated 5-year
recurrence-free survival of 93.3%. The overall rate of complications was 8.8% with a 3.8% rate
of major complications.
Conclusions: Long-term experience with laparoscopic RFA demonstrates that it is a safe and
effective option for the treatment of small renal tumors. Five year oncologic outcomes appear to
be comparable to extirpation.
Page 2 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.

3
Introduction
The widespread use of cross-sectional abdominal imaging over the last twenty years has
increased the diagnosis of incidentally detected, low-stage renal tumors, resulting in a change in
their management.1,2
This development has prompted urologists to investigate less invasive
strategies aimed at maintaining local tumor control while preserving renal function and
improving patient quality of life outcomes.3,4
Renal tumor ablation, when compared to
extirpative treatment, has been associated with a low rate of complications, less morbidity and
improved recuperation. Recently, it has become an increasingly acceptable approach in
management of small renal tumors as the number of institutions performing renal mass ablation
is increasing. . A percutaneous approach, compared to laparoscopic, has historically been the
preferred method for the management of small renal masses undergoing radiofrequency ablation
(RFA) due to its less invasive nature. However, in certain scenarios, critical structures such as
ureter or bowel may exist in close proximity to the renal tumor. In these instances, a
laparoscopic approach may be necessary in order to mobilize these structures away from the
renal tumor thereby allowing direct visualization and delivery of ablative treatment. Currently,
the experience and follow-up of patients who have undergone a laparoscopic approach in the
radiofrequency ablation literature is limited.5-8
We reviewed our experience with laparoscopic
RFA to assess oncologic outcomes, safety and efficacy and provide the longest follow up in the
literature to date.
Methods and Patients
Institutional review board approval was gained to retrospectively review all patients who
underwent laparoscopic RFA from April 2000 to April 2010 at a single institution. There were
Page 3 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
4
a total of 80 patient identified who underwent laparoscopic RFA over this time frame. 79
of those patients had available clinical data and were included in the study. All patients
presented with an enhancing renal tumor seen on cross-sectional imaging and each elected to
undergo laparoscopic RFA. Intraoperative incisional biopsies (5 mm cup forceps) were obtained
routinely after ablation.8 Biopsy was done after ablation as a prior study from our
institution demonstrates that histological architecture is maintained in the tissue after
radiofrequency ablation is performed.9 Tissue samples were examined with hematoxyline-
eosin staining, and in some cases immunohistochemical staining was performed to assist in the
diagnosis.
All patients were treated with a Model 1500X Rita 250 watt radiofrequency generator
with Starburst XL probes (AngioDynamics, Latham, NY) as previously described. 8 Briefly,
probes were inserted percutaneously under laparoscopic guidance after exposure of the renal
tumor. Laparoscopic ultrasound was used to confirm proper probe deployment. The probe tines
were deployed 5-10 mm beyond the diameter of the lesion, and ablation was performed in two,
size-determined cycles to a target temperature of 105 degrees Celsius. A contrast-enhance
computed tomography (CT) scan was obtained 6 weeks post-operatively to confirm complete
ablation of the target lesion. Radiologic surveillance consisted of contrast-enhanced axial
imaging at 6 months, 12 months and at least annually thereafter. Pretreatment and follow up
serum creatinine and glomerular filtration rate (GFR) were obtained and recorded, as were
comorbidities, ASA score, age and post-operative pathology results.
Incomplete ablation was defined as residual enhancement of the target lesion at 6 weeks
of follow up. Recurrence was defined as an increase in tumor size or enhancement (> 10 HU) in
the vicinity if the treated tumor.
Page 4 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.

5
Descriptive analysis was performed to characterize the patient population. Paired t test
was employed for evaluation of the changes in creatinine and eGFR after treatment. Estimated
GFR was calculated using the abbreviated MDRD equation. The Kaplan-Meier method was
used to determine estimated 5-year overall and recurrence free survival.
Results
Patient demographic data is listed in Table 1. Our patient population had a mean age of
63.8 years and a mean ASA score of 2.6. A total of 111 tumors in 79 patients were treated with
laparoscopic RFA. The mean size of the treated renal mass was 2.2 cm with a range of 0.9-4.2
cm. Six patients had solitary kidneys and 15 patients were diagnosed with pre-treatment
chronic kidney disease.
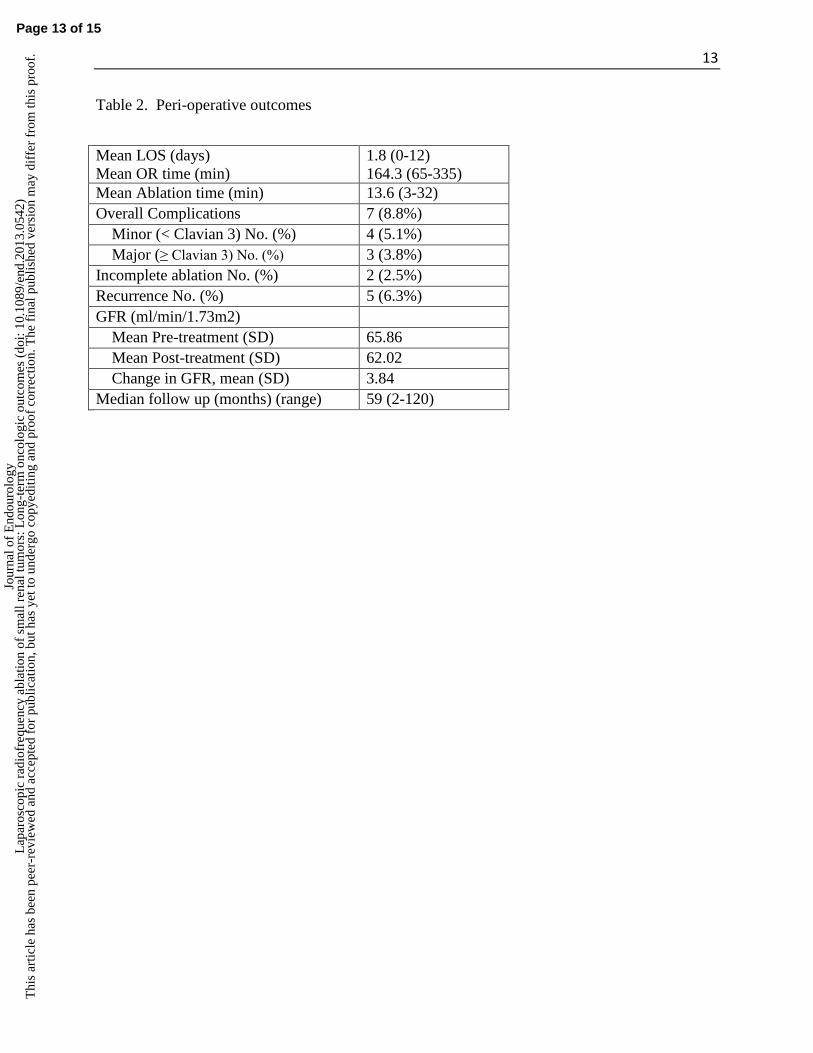
Table 2 lists perioperative outcomes. Mean OR time was 164 minutes (range 65-335
minutes) with a mean estimated blood loss (EBL) of 29 mL (range 0-400 mL). Mean length of
stay (LOS) was 1.8 days (range of 0-12 days). One patient required a 12-day hospitalization due
to a persistent ileus and ultimately was found to have renal pelvis obstruction. The overall rate
of complications was 8.8% (n = 7). Four (5.1%) of these complications were minor (Clavien
grade 1-2). Three (3.8%) complications were major (Clavien grade 3b) with 2 patients requiring
repeat surgery for obstruction of the collecting system at the ureteropelvic junction, 1 patient
requiring conversion to laparoscopic nephrectomy and 1 patient requiring stent placement for
urinary fistula. The mean tumor size of the patients with grade 3b complications was 3.2 cm.
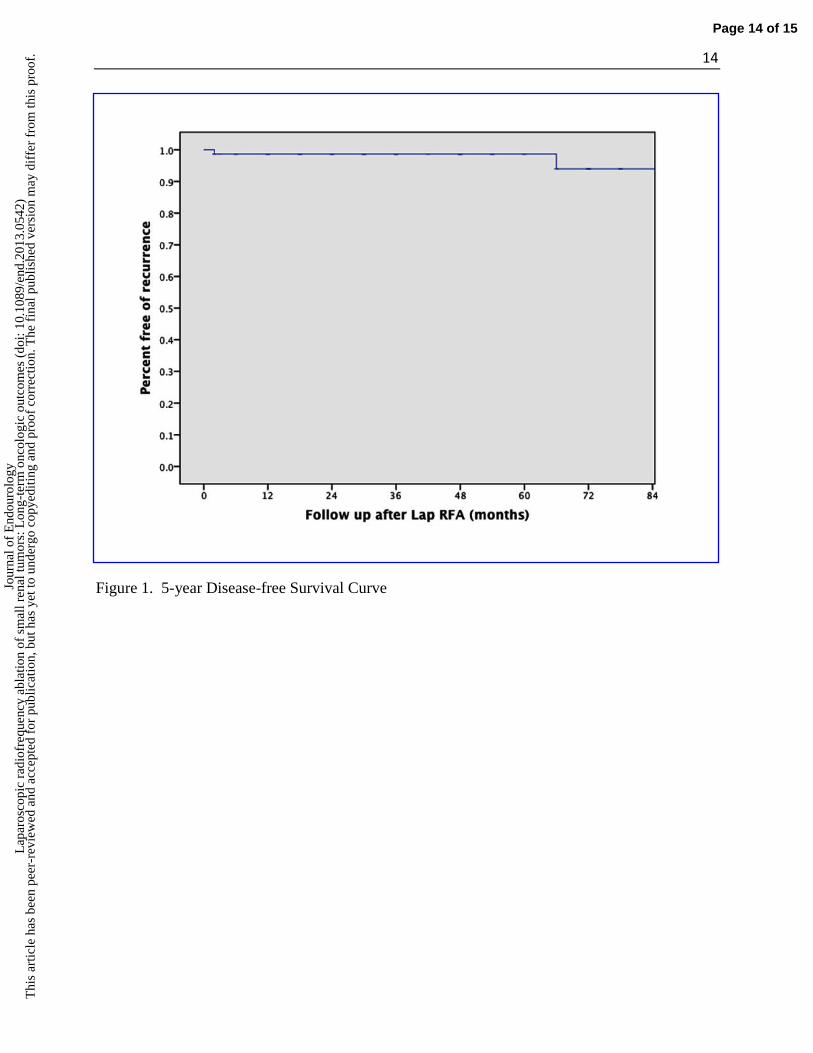
The median follow up was 59 months. Two patients (2.5%) had incomplete ablation of
their lesions on follow up CT at 6 weeks and both patients were treated successfully with salvage
percutaneous ablation. Estimated 5 year recurrence-free survival was 93.3% with only 3 patients
Page 5 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
6
having recurrence of disease. The 2 patients with persistent enhancing lesions on follow up
imaging at 6 weeks were included in the recurrence-free survival calculation (Figure 1A). Of the
5 patients who had recurrence or persistent disease, the mean tumor size was 2.1 cm and the
mean and median time to recurrence were 55.5 months and 39 months, respectively. The 5-year
recurrence-free survival among the patients with biopsy proven RCC was 92%. Both 5-year
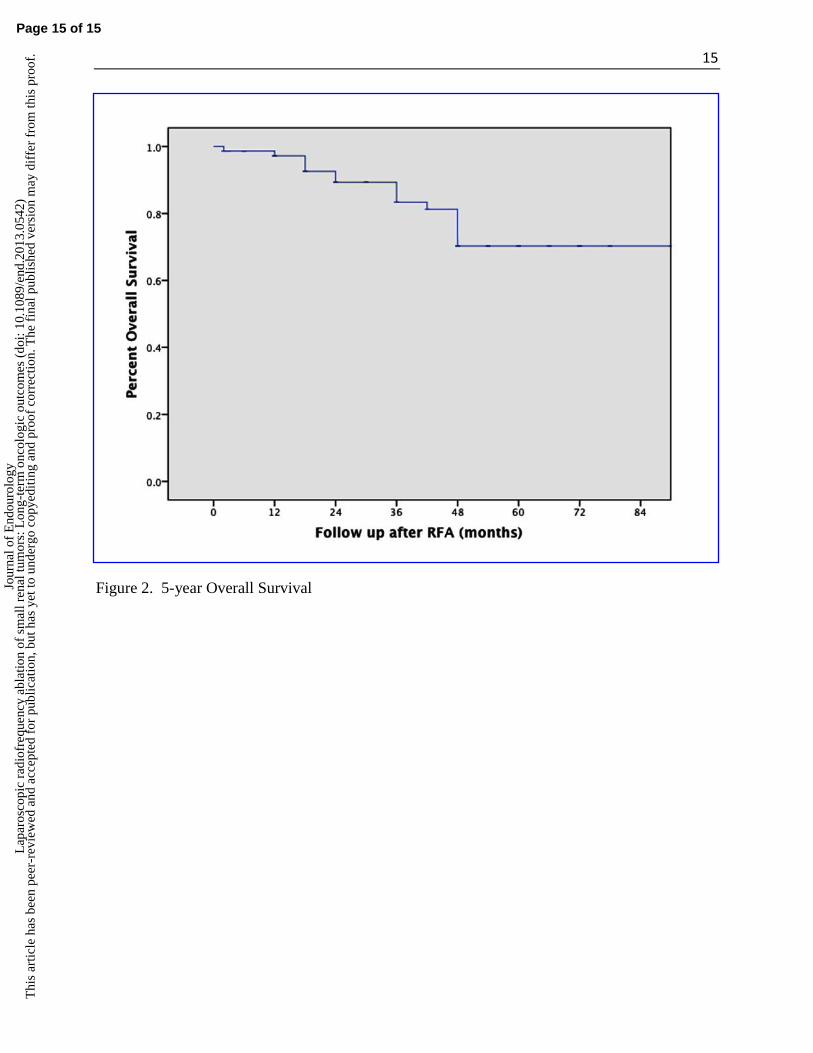
cancer-specific survival and metastatic-free survival were 100% in our cohort. Estimated 5-year
overall survival for our cohort of patients was 72% (Figure 1B). GFR data was collected during
pre-treatment evaluation and repeated at 12 months. Mean pre-treatment GFR was 65.9
ml/min/1.73m2 and 12 month mean post-treatment GFR was 62.0 ml/min/1.73m2 representing a
decrease in GFR of 5.8% over 12 months, though this change was not statistically significant.
Discussion
Within the realm of tissue ablation, different techniques have been implemented to target
renal tumors. In the cryoablation literature, a laparoscopic approach has been preferred over a
percutaneous approach. This may be because the expanding “ice ball” is easily visualized on
ultrasound, allowing for the identification of an adequate ablation margin. For RFA, this
relationship is reversed with more studies reporting a percutaneous technique as compared to a
laparoscopic one. The reasons for this are not clear; although the relative difficulty of RFA
probe placement with ultrasound guidance and the lack of a clearly defined ablation zone may be
contributing factors. Despite these drawbacks, a laparoscopic approach may be preferred for
RFA in certain situations where the proximity of critical structures to the renal tumor is of
concern. Laparoscopic RFA allows for the mobilization of the ureter, bowel and other
structures away from the ablation zone and theoretically ensures their safety. For this reason,
complications of in-situ ablation of small renal tumors have been relatively low.10-13
Within our
series, the overall complication rate was 8.8% with only 3.8% of patients suffering major
Page 6 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
7
complications (≥ Clavien grade 3). In contrast to the cryoablation literature, hemorrhage was not
an observed complication; however, 2 of the 3 major complications were related to injury to the
ureter or collecting system. The patients who suffered ureteropelvic junction obstruction
had tumors that were more anteriorly and medially located. These complications occurred
early in our series and as our experience progressed, patients with more medially located
tumors or tumors close to the collecting system were ultimately excluded from undergoing
laparoscopic RFA. The surgical complications encountered in our series were felt to be due
to direct use of the RFA probe and location of the tumor, not directly due to laparoscopic
dissection techniques.
Previous studies have reported similar complication rates. In 2004, Johnson et al
described a series of 139 cryoablations and 133 RF ablations and found an overall complication
rate of 11%, with 1.8% classified as major events.13
A meta-analysis by Novick et al reported a
4.9% incidence of major complications after cryoablation and a 6.0% rate of major
complications after RFA.14
While this and other data suggests that complication rates between
cryoablation and RFA appear similar, it has been widely reported that the risk of major urologic
complications is lower with ablative techniques when compared to either open or laparoscopic
partial nephrectomy.
As for oncologic outcomes of laparoscopic RFA, a recent series by Ji et al
demonstrated local tumor control in 98.1%. 6 Within our series, oncologic outcomes where
comparable with an estimated 5-year recurrence free survival of 93.3% and a 5-year metastatic
free survival of 100%. In comparison to percutaneous series, there appear to be no difference in
oncologic outcome measures.8 While the vast majority of RFA studies demonstrate favorable
oncologic outcomes, follow-up is limited and this is a common criticism of ablation therapy
Page 7 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
8
Thus the importance of this study which provides 5-year follow-up data (median 59 months)
demonstrating lasting efficacy for laparoscopic RFA.
Oncologic outcomes of RFA are often compared to extirpative therapy, with a somewhat
increased rate of local recurrence seen in RFA series. However, distant recurrence remains an
uncommon event using either technique with multiple studies confirming this result. Levinson et
al published one of the first long-term RFA reviews which demonstrated a 90.3% recurrence-free
survival and a 100% disease-specific survival 10
. Although recent data suggests that residual
tumor after local treatment may predispose patients to distant recurrence, this was not seen in our
series as no patients developed metastatic disease15
. This may be in part the result of
aggressively treating all patients with residual tumor (enhancement at 6 weeks) with immediate
re-ablation. Joniau et al showed that the success rate for RFA could be improved with repeated
ablations increasing from 86.9% after a single treatment to 93.8% after 2 or more treatments. 11
This ability to perform RFA in succession is an additional advantage of ablative therapies.
Indeed, our success rates for ablation approaches 100% when success after re-ablation is
considered. In addition, overall survival is similar between patient undergoing RFA and
those undergoing active surveillance for small renal masses.16,17
One of the purported advantages of tumor ablation over extirpative treatment is renal
function preservation. A recent study from The Cleveland Clinic reviewed 427 patients who
underwent robotic-assisted laparoscopic partial nephrectomy with a mean tumor size of 3.0
cm. They found a mean decrease in eGFR of 8% at a median follow up less than 18
months.18
We found a decrease in mean eGFR of 5.8% at 1-year follow up. Thirty percent
(N=24) of patients in our study had CKD stage 3 or greater prior to treatment such that
distinguishing the proportion of renal function loss from RFA versus the natural history of their
Page 8 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.

9
pre-existing comorbidities was difficult. Nevertheless, there was no statistical loss in eGFR at 1
year. Multiple prospective reviews have shown a similar minimal effect of renal tumor RFA on
renal function.19,20
Several limitations of our study should be discussed. First, this was a retrospective study
making selection bias a concern, namely selecting for sicker, older patients as well as smaller
and anterior tumors. Also, the sample size is limited, however, when compared to previous
laparoscopic RFA series, the follow-up period is significantly improved. Another limitation of
this study is the analysis of renal function. Reporting renal function at one year may not truly
give insight as to the effect of nephron damage due to RFA; however, a longer follow-up would
allow competing risk factors to obfuscate the issue given a population with multiple co-
morbidities and preexisting CKD. Lastly, lack of contrast enhancement was used as a surrogate
for tumor destruction as opposed to ablation zone biopsy. Although this has been previously
debated, numerous studies support this as a suitable method for following patients after RFA.
Conclusion
Radiofrequency ablation through a laparoscopic approach is safe and effective in selected
patients. Long-term outcomes are excellent using this approach in terms of both local and distant
oncologic control and can be performed without a compromise to renal function.
Page 9 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.

10
References
1. Jayson M, Sanders H. Increased incidence of serendipitously discovered renal cell carcinoma. Urology. Feb 1998;51(2):203-205.
2. Volpe A, Panzarella T, Rendon RA, Haider MA, Kondylis FI, Jewett MA. The natural history of incidentally detected small renal masses. Cancer. Feb 15 2004;100(4):738-745.
3. Colombo JR, Jr., Kaouk JH. Minimally invasive management of renal cancer. Minerva Urol Nefrol. Jun 2007;59(2):159-165.
4. Pinto PA. Renal carcinoma: minimally invasive surgery of the small renal mass. Urol Oncol. May-Jun 2009;27(3):335-336.
5. Bensalah K, Zeltser I, Tuncel A, Cadeddu J, Lotan Y. Evaluation of costs and morbidity associated with laparoscopic radiofrequency ablation and laparoscopic partial nephrectomy for treating small renal tumours. BJU Int. Feb 2008;101(4):467-471.
6. Ji C, Li X, Zhang S, et al. Laparoscopic radiofrequency ablation of renal tumors: 32-month mean follow-up results of 106 patients. Urology. Apr 2011;77(4):798-802.
7. Lian H, Guo H, Zhang G, et al. Single-center comparison of complications in laparoscopic and percutaneous radiofrequency ablation with ultrasound guidance for renal tumors. Urology. Jul 2012;80(1):119-124.
8. Park S, Anderson JK, Matsumoto ED, Lotan Y, Josephs S, Cadeddu JA. Radiofrequency ablation of renal tumors: intermediate-term results. J Endo Urol. Aug 2006;20(8):569-573.
9. Margulis V, Matsumoto ED, Lindberg G, et al. Acute histologic effects of temperature-based radiofrequency ablation on renal tumor pathologic interpretation. Urology. Oct 2004;64(4):660-663.
10. Joniau S, Tailly T, Goeman L, Blyweert W, Gontero P, Joyce A. Kidney radiofrequency ablation for small renal tumors: oncologic efficacy. J Endo Urol. May 2010;24(5):721-728.
11. Levinson AW, Su LM, Agarwal D, et al. Long-term oncological and overall outcomes of percutaneous radio frequency ablation in high risk surgical patients with a solitary small renal mass. J Urol. Aug 2008;180(2):499-504; discussion 504.
12. Tracy CR, Raman JD, Donnally C, Trimmer CK, Cadeddu JA. Durable oncologic outcomes after radiofrequency ablation: experience from treating 243 small renal masses over 7.5 years. Cancer. Jul 1 2010;116(13):3135-3142.
13. Johnson DB, Solomon SB, Su LM, et al. Defining the complications of cryoablation and radio frequency ablation of small renal tumors: a multi-institutional review. J Urol. Sep 2004;172(3):874-877.
14. Novick RM, Mitzey AM, Brownfield MS, Elfarra AA. Differential localization of flavin-containing monooxygenase (FMO) isoforms 1, 3, and 4 in rat liver and kidney and evidence for expression of FMO4 in mouse, rat, and human liver and kidney microsomes. J Pharm Exp Therap. Jun 2009;329(3):1148-1155.
15. Yang B, Autorino R, Remer EM, et al. Probe ablation as salvage therapy for renal tumors in von Hippel-Lindau patients: the Cleveland Clinic experience with 3 years follow-up. Urol Oncol. Jul 2013;31(5):686-692.
16. Abou Youssif T, Kassouf W, Steinberg J, Aprikian AG, Laplante MP, Tanguay S. Active surveillance for selected patients with renal masses: updated results with long-term follow-up. Cancer. Sep 1 2007;110(5):1010-1014.
17. Mason RJ, Abdolell M, Trottier G, et al. Growth kinetics of renal masses: analysis of a prospective cohort of patients undergoing active surveillance. Eur Urol. May 2011;59(5):863-867.
18. Khalifeh A, Autorino R, Eyraud R, et al. Three-year Oncologic and Renal Functional Outcomes After Robot-assisted Partial Nephrectomy. Eur Urol. Nov 2013;64(5):744-750.
Page 10 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.

11
19. Raman JD, Thomas J, Lucas SM, et al. Radiofrequency ablation for T1a tumors in a solitary kidney: promising intermediate oncologic and renal function outcomes. Can J Urol. Apr 2008;15(2):3980-3985.
20. Shingleton WB, Sewell PE, Jr. Percutaneous renal cryoablation of renal tumors in patients with von Hippel-Lindau disease. J Urol. Mar 2002;167(3):1268-1270.
Page 11 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.

12
Table 1. Patient and Tumor characteristics
Patients No. 79
Total number of tumors 111
Single tumors 47
Multiple tumors 22
Bilateral tumors 10
Median Age (y) (range) 63.8 (18-35)
Mean ASA (SD) 2.6 (sd)
CKD ≥ 3 24
Mean Size (cm) (SD) 2.2 (sd)
Location No. (%)
Right 62 (55.9%)
Left 49 (44.1%)
Upper pole 26 (23.4%)
Mid pole 53 (47.7%)
Lower pole 32 (28.8%)
Anterior 55(49.5%)
Lateral 38 (34.2%)
Posterior 18 (16.2%)
Biopsy data No. (%)
RCC 61 (77.2%)
AML 6 (7.6%)
Oncocytoma 8 (10%)
Non-diagnostic 4 (5.1%)
Page 12 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
13
Table 2. Peri-operative outcomes
Mean LOS (days)
Mean OR time (min)
1.8 (0-12)
164.3 (65-335)
Mean Ablation time (min) 13.6 (3-32)
Overall Complications 7 (8.8%)
Minor (< Clavian 3) No. (%) 4 (5.1%)
Major (≥ Clavian 3) No. (%) 3 (3.8%)
Incomplete ablation No. (%) 2 (2.5%)
Recurrence No. (%) 5 (6.3%)
GFR (ml/min/1.73m2)
Mean Pre-treatment (SD) 65.86
Mean Post-treatment (SD) 62.02
Change in GFR, mean (SD) 3.84
Median follow up (months) (range) 59 (2-120)
Page 13 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
14
Figure 1. 5-year Disease-free Survival Curve
Page 14 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
15
Figure 2. 5-year Overall Survival
Page 15 of 15
Jour
nal o
f E
ndou
rolo
gyL
apar
osco
pic
radi
ofre
quen
cy a
blat
ion
of s
mal
l ren
al tu
mor
s: L
ong-
term
onc
olog
ic o
utco
mes
(do
i: 10
.108
9/en
d.20
13.0
542)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
Copyright © 2022 FDOKUMEN




















