
Catheter Ablation Versus Antiarrhythmic Drug Therapy for ...

Radiofrequency Catheter Ablation ofSupraventricular Tachycardia SubstratesAfter Mustard and Senning Operationsfor d-Transposition of the Great ArteriesRonald J. Kanter, MD, FACC,* John Papagiannis, MD,§ Michael P. Carboni, MD,*Ross M. Ungerleider, MD, FACC,† William E. Sanders, MD, FACC,\ J. Marcus Wharton, MD, FACC‡Durham and Chapel Hill, North Carolina, and Athens, Greece
OBJECTIVES The purpose of this study was to determine the efficacy and risks of radiofrequency ablationof various forms of supraventricular tachycardia after Mustard and Senning operations ford-transposition of the great arteries.
BACKGROUND In this patient group, the reported success rate of catheter ablation of intraatrial reentrytachycardia is about 70% with a negligible complication rate. There are no reports of the useof radiofrequency ablation to treat other types of supraventricular tachycardia.
METHODS Standard diagnostic criteria were used to determine supraventricular tachycardia type.Appropriate sites for attempted ablation included 1) intraatrial reentry tachycardia: presenceof concealed entrainment with a postpacing interval similar to tachycardia cycle length; 2)focal atrial tachycardia: a P-A interval #220 ms; and 3) typical variety of atrioventricular(AV) node reentry tachycardia: combined electrographic and radiographic features.
RESULTS Nine Mustard and two Senning patients underwent 13 studies to successfully ablate allsupraventricular tachycardia substrates in eight (73%) patients. Eight of eleven (73%) patientshaving intraatrial reentry tachycardia, 3/3 having typical AV node reentry tachycardia, and2/2 having focal atrial reentry tachycardia were successfully ablated. Among five patientshaving intraatrial reentry tachycardia (IART) and not having ventriculoatrial (V-A) conduc-tion, two suffered high-grade AV block when ablation of the systemic venous portion of themedial tricuspid valve/inferior vena cava isthmus was attempted.
CONCLUSIONS Radiofrequency catheter ablation can be effectively and safely performed for certain supraven-tricular tachycardia types in addition to intraatrial reentry. A novel catheter course is requiredfor slow pathway modification. High-grade AV block is a potential risk of lesions placed inthe systemic venous medial isthmus. (J Am Coll Cardiol 2000;35:428–41) © 2000 by theAmerican College of Cardiology
The Mustard and Senning operations were developed assurgical treatments for transposition of the great arteries.These operations fell into disfavor in part owing to a highincidence of arrhythmias at long-term follow-up. Intraatrialrentry tachycardia (IART) has been reported to occur in 2%to 10% of Mustard and Senning patients at 4 to 10 years’follow-up (1–5). Sudden cardiac death has been reported tooccur late after these operations in 3% to 15% of patients(1,2,6,7), and a rapid ventricular response to paroxysmalatrial tachycardias has been thought to be the cause of death
in many instances. Such morbidity and mortality hasprompted an aggressive treatment philosophy. Older ther-apies have been far from perfect; antiarrhythmic drugs arefraught with proarrhythmic and noncardiac complicationsand with incomplete efficacy; antitachycardia pacing is onlyeffective for slower tachycardias and may accelerate them tomore dangerous, faster ones; and bradycardia pacing isadjunctive therapy, at best (8).
Based upon the high efficacy of radiofrequency catheterablation to treat adults with typical atrial flutter (9,10),several investigators have reported a favorable early experiencein Mustard and Senning patients having IART (11–14). Theseresearchers utilized principles of concealed entrainmentmapping (11–13), identification of nonconducting anatomicbarriers (11,14) and presence of split potentials (13) toablate IART circuits successfully in 70% to 80% of patients(11–13).
From the Departments of *Pediatrics, †Surgery, and ‡Internal Medicine, DukeUniversity School of Medicine, Durham, North Carolina; the §Department ofPediatric Cardiology, Onassis Cardiac Surgery Center, Athens, Greece; and the\Department of Internal Medicine, University of North Carolina at Chapel HillSchool of Medicine, Chapel Hill, North Carolina.
Manuscript received November 17, 1998; revised manuscript received September 3,1999, accepted October 18, 1999.
Journal of the American College of Cardiology Vol. 35, No. 2, 2000© 2000 by the American College of Cardiology ISSN 0735-1097/00/$20.00Published by Elsevier Science Inc. PII S0735-1097(99)00557-4

Although these reports only described experience withIART, other supraventricular tachycardias may occur inpatients with transposition. This report presents a singleinstitution’s experience with radiofrequency catheter abla-tion for various supraventricular tachycardias in patientswho had undergone Mustard or Senning operations.
METHODS
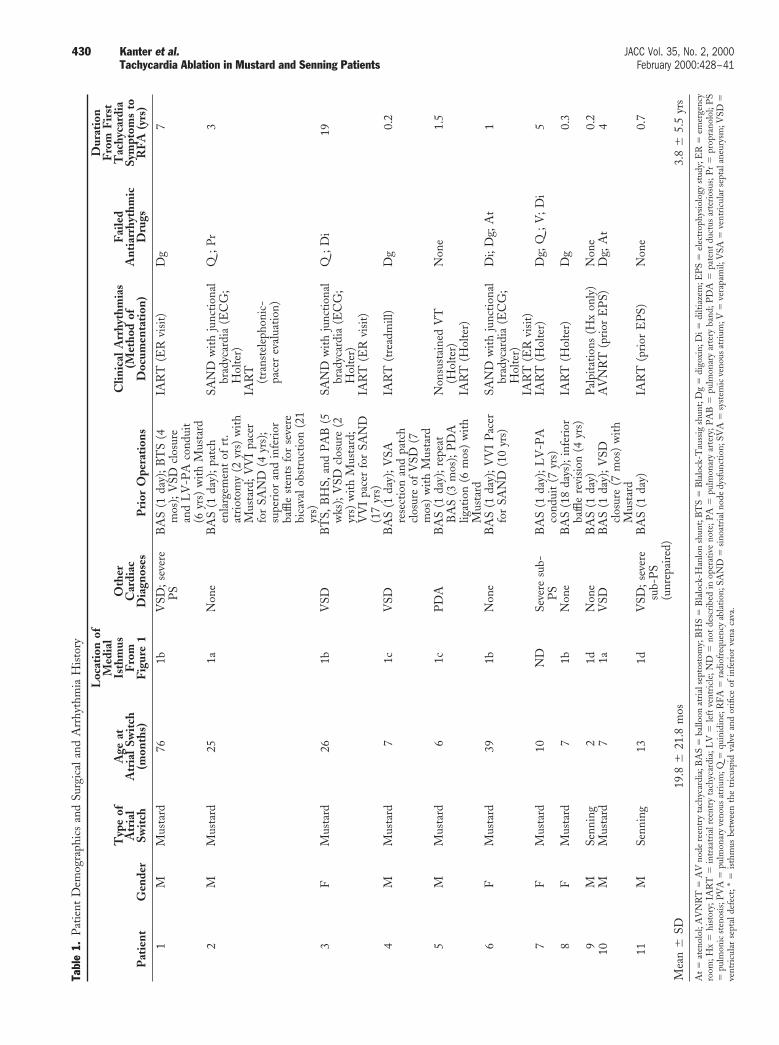
Patient selection. All patients referred to Duke UniversityMedical Center from January 1994 to March 1998 forelectrophysiologic study and radiofrequency catheter abla-tion following Mustard or Senning operations were in-cluded (n 5 10). An eleventh patient (patient 10) under-went his procedure at the University of North CarolinaMemorial Hospital, where the first author (R.J.K.) partici-pated. Patient demographic, surgical, and clinical arrhyth-mia data appear in Table 1. Supraventricular tachycardiahad been documented in all patients, except patient 9, inwhom the history suggested the diagnosis. Informed con-sent was obtained using a protocol approved by the DukeUniversity Institutional Review Board for the first sevenpatients. A standard consent for electrophysiologic studyand catheter ablation was obtained from the last fourpatients.
Anatomic descriptions. All operative reports were re-viewed by a pediatric cardiac surgeon (R.M.U.) with atten-tion to the locations of all incisions and the ultimatelocation of the coronary sinus with respect to the inferiorsuture line of the atrial baffle. Specific handling of thecoronary sinus was described for 10 of the 11 patients (Fig.1). If the baffle suture line kept the coronary sinus ostium inthe systemic venous atrium, the medial isthmus between thetricuspid valve annulus and inferior vena cava was necessar-ily bisected, perhaps with the majority on the systemicvenous side (Fig. 1c). Superiorly, this suture line alwaysdeviates from the tricuspid annulus to avoid the atrioven-tricular (AV) node. Hence, at least part of the medialisthmus would remain on the pulmonary venous side. If thecoronary sinus was incised or other efforts made to redirectthe ostium into the systemic venous atrium surgically, it wasconcluded that the great majority of the isthmus remainedin the pulmonary venous atrium (Fig. 1b). Likewise, if theostium was kept in the pulmonary venous atrium, themedial isthmus remained there as well (Fig. 1a).
The isthmus between the tricuspid valve annulus and theinferior vena cava orifice was arbitrarily divided into medial,
mid, and lateral portions. If the tricuspid annulus were theface of a clock in a left anterior oblique projection, theanterior aspect of the medial isthmus would range from 4:00to 5:00 o’clock, the mid isthmus from 5:00 to 7:00 o’clock,and the lateral isthmus from 7:00 to 8:00 o’clock, with eachportion extending as a wedge posteriorly to the inferior venacava orifice. The relationship of the isthmus subdivisions tothe eustachian ridge was not considered, because the oper-ative reports never mentioned this structure.
Definitions of tachycardia types. Tachycardia types weredetermined by a combination of surface electrocardio-graphic features and intracardiac electrophysiologic charac-teristics.
Intraatrial reentry tachycardia was paroxysmal in onset andtermination and had a regular nonsinus P-wave morphol-ogy. It was inducible by atrial programmed stimulation oratrial burst pacing and had periods of second-degree AVblock with a constant atrial cycle length. The mechanism ofmacroreentry was supported by demonstration of manifestentrainment.
Focal atrial tachycardia (FAT) was different from IART inits surface electrocardiographic appearance and intracardiacelectrogram features. The P waves were discrete, with a clearisoelectric inter-P-wave interval in all leads. Split andfractionated electrograms were not present in regions ofearliest atrial activation, including successful ablation sites.Unlike IART, manifest entrainment could not be demon-strated.
Typical variety of AV node reentry tachycardia was diag-nosed when a regular, narrow-complex tachycardia could beinduced by atrial or ventricular programmed stimulation inassociation with a 1:1 AV relationship, a ventriculoatrial(V-A) interval #70 ms, and concentric atrial activation.Because a His bundle recording could not be consistentlyobtained, standard maneuvers to dissociate ventricular oratrial electrograms from the tachycardia circuit were notpossible. Additional findings supporting the diagnosis in-cluded 1) initiation of tachycardia during atrial extrastimu-lus testing following an AV interval increase of $50 msduring a decrease in atrial prematurity of 10 ms; 2) theobservation that a single atrial extrastimulus initiates tachy-cardia following a double ventricular response; or 3) theability of adenosine to terminate tachycardia following anatrial electrogram.
Technique of electrophysiologic study. Antiarrhythmicmedications were discontinued at least four half-lives beforeeach study. Intravenous propofol was used as a generalanesthetic agent (15), except in Patients 2 and 6, who werestudied under conscious sedation. Hemodynamic measure-ments were obtained in all patients, except Patients 6 and10, in whom echocardiographic evaluation was performed.Diagnostic electrode catheters with close spacing (2 to10 mm) were placed in the left ventricle, systemic venousatrium, and the inferior portion of the systemic venousremnant of the atrial septum in the region of the coronary
Abbreviations and AcronymsAV 5 atrioventricularFAT 5 focal atrial tachycardiaIART 5 intraatrial reentry tachycardiaV-A 5 ventriculoatrial
429JACC Vol. 35, No. 2, 2000 Kanter et al.February 2000:428–41 Tachycardia Ablation in Mustard and Senning Patients
Tabl
e1.
Pat
ient
Dem
ogra
phic
san
dSu
rgic
alan
dA
rrhy
thm
iaH
isto
ry
Pat
ient
Gen
der
Typ
eof
Atr
ial
Swit
ch
Age
atA
tria
lSw
itch
(mon
ths)
Loc
atio
nof
Med
ial
Isth
mus
Fro
mF
igur
e1
Oth
erC
ardi
acD
iagn
oses
Pri
orO
pera
tion
s
Clin
ical
Arr
hyth
mia
s(M
etho
dof
Doc
umen
tati
on)
Fai
led
Ant
iarr
hyth
mic
Dru
gs
Dur
atio
nF
rom
Fir
stT
achy
card
iaSy
mpt
oms
toR
FA
(yrs
)
1M
Mus
tard
761b
VSD
;sev
ere
PS
BA
S(1
day)
;BT
S(4
mos
);V
SDcl
osur
ean
dL
V-P
Aco
ndui
t(6
yrs)
with
Mus
tard
IAR
T(E
Rvi
sit)
Dg
7
2M
Mus
tard
251a
Non
eB
AS
(1da
y);p
atch
enla
rgem
ent
ofrt
.at
riot
omy
(2yr
s)w
ithM
usta
rd;V
VI
pace
rfo
rSA
ND
(4yr
s);
supe
rior
and
infe
rior
baffl
est
ents
for
seve
rebi
cava
lobs
truc
tion
(21
yrs)
SAN
Dw
ithju
nctio
nal
brad
ycar
dia
(EC
G;
Hol
ter)
IAR
T(t
rans
tele
phon
ic-
pace
rev
alua
tion)
Q;P
r3
3F
Mus
tard
261b
VSD
BT
S,B
HS,
and
PA
B(5
wks
);V
SDcl
osur
e(2
yrs)
with
Mus
tard
;V
VI
pace
rfo
rSA
ND
(17
yrs)
SAN
Dw
ithju
nctio
nal
brad
ycar
dia
(EC
G;
Hol
ter)
IAR
T(E
Rvi
sit)
Q;D
i19
4M
Mus
tard
71c
VSD
BA
S(1
day)
;VSA
rese
ctio
nan
dpa
tch
clos
ure
ofV
SD(7
mos
)w
ithM
usta
rd
IAR
T(t
read
mill
)D
g0.
2
5M
Mus
tard
61c
PD
AB
AS
(1da
y);r
epea
tB
AS
(3m
os);
PD
Alig
atio
n(6
mos
)w
ithM
usta
rd
Non
sust
aine
dV
T(H
olte
r)IA
RT
(Hol
ter)
Non
e1.
5
6F
Mus
tard
391b
Non
eB
AS
(1da
y);V
VI
Pac
erfo
rSA
ND
(10
yrs)
SAN
Dw
ithju
nctio
nal
brad
ycar
dia
(EC
G;
Hol
ter)
IAR
T(E
Rvi
sit)
Di;
Dg;
At
1
7F
Mus
tard
10N
DSe
vere
sub-
PS
BA
S(1
day)
;LV
-PA
cond
uit
(7yr
s)IA
RT
(Hol
ter)
Dg;
Q;V
;Di
5
8F
Mus
tard
71b
Non
eB
AS
(18
days
);in
feri
orba
ffle
revi
sion
(4yr
s)IA
RT
(Hol
ter)
Dg
0.3
9M
Senn
ing
21d
Non
eB
AS
(1da
y)P
alpi
tatio
ns(H
xon
ly)
Non
e0.
210
MM
usta
rd7
1aV
SDB
AS
(1da
y);V
SDcl
osur
e(7
mos
)w
ithM
usta
rd
AV
NR
T(p
rior
EP
S)D
g;A
t4
11M
Senn
ing
131d
VSD
;sev
ere
sub-
PS
(unr
epai
red)
BA
S(1
day)
IAR
T(p
rior
EP
S)N
one
0.7
Mea
n6
SD19
.86
21.8
mos
3.8
65.
5yr
s
At5
aten
olol
;AV
NR
T5
AV
node
reen
try
tach
ycar
dia;
BA
S5
ballo
onat
rial
sept
osto
my;
BH
S5
Bla
lock
-Han
lon
shun
t;B
TS
5B
lalo
ck-T
auss
igsh
unt;
Dg
5di
goxi
n;D
i5di
ltiaz
em;E
PS
5el
ectr
ophy
siol
ogy
stud
y;E
R5
emer
genc
yro
om;H
x5
hist
ory;
IAR
T5
intr
aatr
ialr
eent
ryta
chyc
ardi
a;L
V5
left
vent
ricl
e;N
D5
not
desc
ribe
din
oper
ativ
eno
te;P
A5
pulm
onar
yar
tery
;PA
B5
pulm
onar
yar
tery
band
;PD
A5
pate
ntdu
ctus
arte
rios
us;P
r5
prop
rano
lol;
PS
5pu
lmon
icst
enos
is;P
VA
5pu
lmon
ary
veno
usat
rium
;Q5
quin
idin
e;R
FA5
radi
ofre
quen
cyab
latio
n;SA
ND
5si
noat
rial
node
dysf
unct
ion;
SVA
5sy
stem
icve
nous
atri
um;V
5ve
rapa
mil;
VSA
5ve
ntri
cula
rsep
tala
neur
ysm
;VSD
5ve
ntri
cula
rse
ptal
defe
ct;*
5is
thm
usbe
twee
nth
etr
icus
pid
valv
ean
dor
ifice
ofin
feri
orve
naca
va.
430 Kanter et al. JACC Vol. 35, No. 2, 2000Tachycardia Ablation in Mustard and Senning Patients February 2000:428–41

sinus ostium. A His bundle recording was only obtainedduring ablation for AV node reentry tachycardia. A fourthdiagnostic catheter, consisting of 5 to 10 bipoles, was placedwithin the systemic venous atrium from the inferior to thesuperior vena cava. In the Mustard patients, signals from theinferior-most bipoles recorded signals from the medialisthmus or right side of the inferior remnant of the atrialseptum, the middle bipoles from the posterior wall of thenative left atrium, and the superior-most bipoles from theright side of the superior remnant of the atrial septum (Fig.2). In the two Senning patients, this catheter mapped theposterior length of the systemic venous tube—inferiorly,from the right side of the atrial septal remnant (due tosurgical septectomy) adjacent to the IVC; then along the
atrial septal flap; and superiorly, to the right side of the atrialseptal remnant adjacent to the superior vena cava (Fig. 2).Patient 11 required transhepatic venous access, becausethere was bilateral iliofemoral venous thrombosis. Eachpatient was heparinized and the activated clotting timemaintained at 250 to 300 s.
Standard pacing maneuvers were performed at baselineand under the influence of isoproterenol at 0.03 to 0.07mg/kg/min. A 4-mm tip ablation catheter (EP Technol-ogies, Sunnyvale, California; or Cordis-Webster, Bald-win Park, California) was then used for mapping pur-poses. Surface lead gains were increased to permitidentification of the P-wave onset, and atria were mappedduring tachycardia for presystolic activity and for splitpotentials. When 1:1 or 2:1 AV conduction was present,adenosine was used to identify P-wave onset. Regions inwhich there was electrical activity preceding P-waveonset were paced at cycle lengths 20 to 40 ms shorter thanthe atrial tachycardia cycle length to determine thepresence of concealed entrainment.
Selection of sites for radiofrequency ablation. IART. Anisthmus of atrial tissue was selected for creation of linearlesions based upon electrophysiologic characteristics andknowledge of the adjacent lines of conduction block, bothnatural and surgical. The presence of atrial presystolicactivity was felt to be necessary, and was accompanied bysplit potentials if the site was adjacent to a suture line.Entrainment with concealed fusion proved that a site wascritical to the IART circuit, if the atrial activation sequencewas identical to that of tachycardia and if the postpacinginterval was #30 ms longer than the IART cycle length(13). Natural barriers to conduction included the superiorand inferior vena cava orifices and the tricuspid and mitralvalve annuli. In Mustard patients, the baffle suture line andthe right atriotomy were also potential lines of conductionblock (Fig. 2). In Senning patients, the surgical anatomy ismore complex, and there were several potential surgical linesof conduction block: 1) the suture line where the atrial septalflap forms a roof over the pulmonary veins; 2) the edge ofthe atrial septal remnant; 3) the suture line where the rightatrial freewall attaches to the atrial septal remnant to formthe roof over the systemic venous tube (Fig. 2, bottom:A–C); and 4) the suture line where the rightward mostsection of the pulmonary venous atrium is attached to theremaining right atrial freewall (Fig. 2, bottom: D–F).
FAT. Foci of earliest atrial activation were sought. Basedupon published data from patients having atrial ectopictachycardia (16), sites activated at least 20 ms prior to theP-wave onset were considered starting points for detailedmapping.
In cases of IART and FAT, radiofrequency ablation wasconsidered successful if energy delivery during the tachycar-dia terminated the tachycardia, and if it could not be
Figure 1. Diagrams of the pulmonary venous atrium followingMustard (a– c) and Senning (d) operations as viewed from a rightanterior oblique projection. They illustrate the variations of surgi-cal handling of the coronary sinus and medial isthmus between theinferior vena cava orifice and the tricuspid valve. (a) Inferior atrialbaffle suture line is placed posterior to the coronary sinus ostium,keeping it and nearly all of the medial isthmus on the pulmonaryvenous side (Patients 2, 10). (b) Suture line is in approximately thesame location as in (a), but the ostium is surgically redirectedposteriorly into the systemic venous atrium (Patients 1, 3, 6, 8). (c)Suture line is placed anterior to the coronary sinus ostium, keepingit and a large portion of the medial isthmus on the systemic venousside (Patients 4, 5). (d) Right atrial freewall edge (arrows), whichserves as a roof over the systemic venous tube, is sutured posteriorto the coronary sinus ostium, similar in location to (a) (Patients 9,11). AVN 5 compact AV node; CSO 5 coronary sinus ostium;TV 5 septal leaflet of tricuspid valve; cross-hatched area 5medial isthmus; shaded area 5 region of “slow” inputs into AVnode; stippled area 5 region of “fast” inputs into AV node.
431JACC Vol. 35, No. 2, 2000 Kanter et al.February 2000:428–41 Tachycardia Ablation in Mustard and Senning Patients

reinduced for at least 60 min, at baseline and under theinfluence of isoproterenol.
ATRIOVENTRICULAR NODE REENTRY TACHYCARDIA. Ra-diofrequency modification of the slow inputs to the AVnode was attempted using established principles publishedfrom patients having normal hearts (17,18). Access to thetricuspid annulus was possible only using an arterial cathe-ter, which was retroflexed across the tricuspid valve into thepulmonary venous atrium. The catheter was pulled back androtated clockwise until there was a dominant ventricularsignal. Subtle flexion or extension was performed until a His
bundle electrogram was obtained (Fig. 3, left). The catheterwas further extended inferiorly until this electrogram disap-peared (Fig. 3, right). Radiofrequency energy was deliveredat this site during sinus rhythm. Accelerated junctionalrhythm was considered a sensitive indicator of the appro-priateness of the ablation site, and inability to reinduce AVnode reentry tachycardia after 60 min was considered aspecific indicator of successful ablation.
Statistical analysis. Descriptive data are presented as themean 6 SD, or, when appropriate, with 95% confidenceintervals (CI). The Fisher exact test was used to analyze dataon a nominal scale. Data obtained on a continuous scale
Figure 2. Diagrams of surgical anatomy with suture lines and of typical electrode catheter placement in Mustard and Senning patients.All important structures posterior to the level of the tricuspid valve are shown. The pulmonary venous atrium and the systemic venous baffle(cutaway) are illustrated in the Mustard diagram. The circle representing the coronary sinus ostium (CS os) is broken to emphasize itsinconstant relationship with the adjacent portion of the baffle’s suture line. In the Senning diagram, only the systemic venous atrium andthe anterior atrial septal remnant portion of the pulmonary venous atrium are shown. See text for details. LA 5 left atrial catheter; LAA 5left atrial appendage; LV 5 left ventricular catheter; MV 5 direction of mitral valve location; RAA 5 right atrial appendage.
432 Kanter et al. JACC Vol. 35, No. 2, 2000Tachycardia Ablation in Mustard and Senning Patients February 2000:428–41

were analyzed using the Student t test. A p value ,0.05 wasconsidered statistically significant.
RESULTS
Patient characteristics. Eleven patients, ranging in agefrom 11 to 29 years, underwent 13 electrophysiologicprocedures 10 to 27 years following their atrial switchoperation (Tables 1 and 2). They had been symptomatic fortwo months to 19 years. Two patients had experiencedsyncope, two patients had symptomatic sustained IARTrequiring cardioversion, five patients had symptomatic non-
sustained palpitations, and two patients had asymptomaticIART on Holter monitoring.
The patients had undergone Mustard or Senning opera-tions ranging from 2 to 76 months of age (Table 1). Basedupon the operative notes, the medial portion of the isthmusof tissue between the tricuspid valve and inferior vena cavalorifice was almost exclusively left in the pulmonary venousatrium in eight patients (Fig. 1a,b,d) and was bisectedbetween systemic and pulmonary venous atria in two pa-tients (Fig. 1c). In patient 7 the operative note did notprovide sufficient detail to determine this information. Sixpatients had coexisting structural cardiac defects, which are
Figure 3. Posteroanterior (PA) and lateral (Lat) radiographs and electrograms during mapping for and ablation of the typical variety ofAV node reentry tachycardia in Patient 9. (Bottom Left) The ablation catheter (Abl) was first used to identify the region of the His bundleusing the retrograde aortic approach. (Bottom Right) The successful ablation site (Abl) of the “slow” inputs to the AV node. Radiographson the left are lower magnification than those on the right. Baff 5 systemic venous baffle multipole catheter. Bipole 4 is most superior andbipole 7 most inferior; HLA 5 high anatomic left atrial catheter; LV 5 left ventricular catheter; PSRA 5 posteroseptal right atrialcatheter. The electrograms are from the most proximal bipole. See text for details.
433JACC Vol. 35, No. 2, 2000 Kanter et al.February 2000:428–41 Tachycardia Ablation in Mustard and Senning Patients

Tabl
e2.
Car
diac
Cat
hete
riza
tion
and
Ele
ctro
phys
iolo
gySt
udy
Res
ults
Pat
ient
Age
atSt
udy
(yrs
)H
emod
ynam
icA
bnor
mal
itie
sB
asel
ine
Rhy
thm
AV
BC
L(m
s)V
AB
CL
(ms)
Tac
hyca
rdia
sIn
duce
dC
ycle
Len
gth
(ms)
116
Com
plet
eSV
Cob
stru
ctio
n;sm
all
VSD
;mild
LV
OT
O(2
0m
mH
g)
Nor
mal
sinu
s42
036
0(is
o)IA
RT
280
223
Mild
bica
valo
bstr
uctio
n(3
–4m
mH
g)V
VIR
pace
d29
0N
oco
nduc
tion
IAR
T25
5
329
Non
eV
VIR
pace
d40
0N
oco
nduc
tion
IAR
T24
54
11M
ildL
VO
TO
(32
mm
Hg)
;R
Vdy
sfun
ctio
n(R
VE
DP
512
)
Nor
mal
sinu
s34
0N
oco
nduc
tion
IAR
T22
0
515
Non
eN
orm
alsi
nus
440
No
cond
uctio
nIA
RT
250
629
Hem
odyn
amic
stud
yno
tpe
rfor
med
VV
IRpa
ced
430
No
cond
uctio
nFA
T(is
o)32
0IA
RT
#1(is
o)21
5IA
RT
#230
029
Hem
odyn
amic
stud
yno
tpe
rfor
med
VV
IRpa
ced
280
390
IAR
T#2
310
716
Mild
LV
OT
O(3
0m
mH
g)N
orm
alsi
nus
300
No
cond
uctio
nFA
T(is
o)40
5
18M
ildL
VO
TO
(30
mm
Hg)
Nor
mal
sinu
s44
0N
oco
nduc
tion
IAR
T24
0
817
Non
eN
orm
alsi
nus
410
620
(300
with
iso)
IAR
T23
5T
ypic
alA
VN
RT
330
911
Mild
supe
rior
baffl
eob
stru
ctio
n(2
mm
Hg)
Junc
tiona
lat
55be
ats/
min
260
690
IAR
T24
5
Typ
ical
AV
NR
T31
0
1021
Hem
odyn
amic
stud
yno
tpe
rfor
med
Junc
tiona
lat
60be
ats/
min
400
500
Typ
ical
AV
NR
T52
0IA
RT
(iso)
250
1113
Unr
estr
ictiv
eV
SD;
arte
rial
O2
satu
ratio
n—91
%;
seve
reL
VO
TO
(80
mm
Hg)
Nor
mal
sinu
s33
067
0IA
RT
#123
0
IAR
T#2
(iso)
200
Mea
n6
SD19
.06
6.6
yrs
365
ms
(95%
CI
532
8–40
2)IA
RT
524
4m
s(9
5%C
I5
229–
257)
FAT
536
5m
s(9
5%C
I5
280–
446)
AV
NR
T5
387
ms
(95%
CI
525
6–51
8)
AV
BC
L5
atri
oven
tric
ular
bloc
kcy
cle
leng
th;A
VN
RT
5A
Vno
dere
entr
yta
chyc
ardi
a;FA
T5
foca
latr
ialt
achy
card
ia;I
AR
T5
intr
aatr
ialr
eent
ryta
chyc
ardi
a;is
o5
isop
rote
reno
l;L
VO
TO
5le
ftve
ntri
cula
rou
tflow
trac
tobs
truc
tion;
RV
ED
P5
righ
tve
ntri
cula
ren
d-di
asto
licpr
essu
re;S
VC
5su
peri
orve
naca
va;V
AB
CL
5ve
ntri
culo
atri
albl
ock
cycl
ele
ngth
;VSD
5ve
ntri
cula
rse
ptal
defe
ct.
434 Kanter et al. JACC Vol. 35, No. 2, 2000Tachycardia Ablation in Mustard and Senning Patients February 2000:428–41

listed in Table 2. Three patients had undergone rate-adaptive, single chamber, ventricular pacing for “sick sinussyndrome,” and none had undergone implantation of anatrial pacing lead.
Electrophysiologic study and radiofrequency ablation.Baseline hemodynamic and electrophysiologic data appearin Table 2. Antegrade AV conduction was present anddecremental in every case. Because a stable His bundlerecording was not obtained in every patient, the anatomiclocation of AV and V-A block was not always available.Ventriculoatrial conduction was present in six of the eightpatients in whom the medial isthmus was known to bemostly on the pulmonary venous side, but was absent in thetwo patients in whom the native coronary sinus ostium wasleft on the systemic venous side (p 5 NS). Atrioventricularnode reentry tachycardia was not inducible in any patientlacking V-A conduction. It was inducible in three patientshaving V-A conduction (50%) (p 5 NS).
IART. This tachycardia was inducible in all patients, andtwo patients had two apparently different circuits. Theirmean cycle length was 244 6 13 ms (range: 200–280 ms).A tachycardia thought to represent a circuit reversal of apreviously identified circuit was counted as a single tachy-cardia. Radiofrequency energy was applied to the so-calledcritical zones of conduction as a series of stepwise connectedburns creating linear lesions. Focal lesions were neversuccessful for interrupting any IART. Overall, IART cir-cuits were successfully ablated in 8 of 11 (73%) patients(95% CI for failure rate: 2% to 52%).
Mustard patients. Among nine Mustard patients, 10apparently different IART circuits were identified. Theisthmus of tissue between the tricuspid valve and inferiorvena caval orifice was identified as a critical zone ofconduction for nine of these circuits, and the region be-tween the orifice of the superior vena cava and the supero-posterior remnant of the atrial septum was a critical zone forone circuit (Fig. 4). In all five patients in whom it wasattempted, concealed entrainment with a short postpacinginterval could be demonstrated on both systemic and pul-monary venous sides of the inferior baffle.
All IART circuits were successfully ablated in six (67%)patients (95% CI for failure rate: 2% to 64%). Of the ninecircuits involving the isthmus between the tricuspid valveand inferior vena caval orifice, only the medial isthmus couldbe negotiated from the systemic venous side due to thesurgical anatomy; the inferior/anterior portion of the bafflealways seemed to be very near the inferior vena caval orifice,leaving the entire mid- and lateral isthmus on the pulmo-nary venous side. Linear lesions were always attempted fromthe systemic venous side first, except in patient 2, due to thepresence of an intravascular stent. In the other eight, thisapproach was successful in one, abandoned in two becauseof increasing AV block, and unsuccessful in five. When thesystemic venous approach was unsuccessful, the retrograde,right ventricular approach to this region required prolapsing
the flexed catheter across the tricuspid valve into thepulmonary venous atrium. Interruption of IART was usu-ally only accomplished once the catheter tip was pulled backto the tricuspid valve annulus. In Patient 10, interruption ofthe IART circuit required that the linear lesion be extendedmore posteriorly to what was probably the right atriotomyscar. These pullbacks engaged the mid- or lateral isthmus,well away from the medial isthmus.
Senning patients. The two Senning patients had threeseemingly separate IART circuits (Fig. 4). In both patients,a critical zone of conduction was identified in the supero-posterior remnant of the atrial septum below the superiorvena caval orifice, but IART interruption did not occur untilthe linear lesions were continued inferiorly and posteriorlyto the uppermost suture line where the atrial septal flapforms the roof over the pulmonary veins (Fig. 4). Thecatheter could be felt to “hop” over the cut edge of the atrialseptal remnant to engage the more posterior structure. Inpatient 11, brief recurrences of this IART persisted untiladditional linear lesions were created posteriorly, from thesuperior-most portion of the native left atrium inferiorly tothis same suture line (Fig. 4, broken black rectangle). Thethird IART circuit had as a critical zone of conduction themid-isthmus, which had been entirely segregated from the
Figure 4. Locations of radiofrequency ablation attempts in Mus-tard and Senning patients. Illustrated are lesion locations forsupraventricular tachycardias successfully and unsuccessfully ab-lated. In patients whose tachycardias were successfully ablated,unsuccessful locations are not illustrated. In the Mustard diagram,the solid gray area represents the systemic venous atrium, and thestippled area, the isthmus between the tricuspid valve and inferiorvena cava. In the Senning diagram, the systemic venous atrium isopened, approximating the anatomy from Figure 2. The rightatrial freewall flap comprising the roof over the systemic venous(intercaval) atrium is also removed, revealing the entire atrial septalremnant. The portion remaining on the pulmonary venous atrial(PVA) side includes the tricuspid valve/inferior vena cava isthmus.See text for details. MV 5 mitral valve; SVA 5 systemic venousatrium; TV 5 tricuspid valve.
435JACC Vol. 35, No. 2, 2000 Kanter et al.February 2000:428–41 Tachycardia Ablation in Mustard and Senning Patients

systemic venous atrium by the inferior portion of thesuperoinferior suture line attaching the right atrial freewallonto the inferior remnant of the atrial septum, posterior tothe coronary sinus ostium (Fig. 4). Therefore, this couldonly be negotiated by using a retrograde arterial catheter andpulling back from this suture line to approximately “6o’clock” of the tricuspid valve annulus. Both patients hadsuccessful ablation of IART circuits.
FAT. There were two FATs, each in Mustard patients(Tables 2 and 3). Both were inducible with atrial pro-grammed stimulation. The cycle lengths of these tachycar-dias tended to be longer than those of the IARTs (363 6 60vs. 244 6 13 ms, p 5 0.2). The cycle length of the FATfrom patient 7 varied from 360 to 450 ms and was markedlyinfluenced by autonomic tone. It could also be terminatedby adenosine. Sites of earliest atrial activation were in thepulmonary venous atrium in one and the systemic venousatrium in the other. Both foci were immediately adjacent tosuture lines (Fig. 4) and were successfully ablated.
TYPICAL VARIETY OF AV NODE REENTRY TACHYCARDIA.
This tachycardia was inducible in two Mustard patients andone Senning patient, but prior to delivery of radiofrequencyenergy only in patient 10. The cycle lengths of thesetachycardias tended to be longer than those of the IARTs(387 6 116 vs. 244 6 13 ms, p 5 0.16). The V-A intervalsduring tachycardia were 27 to 65 ms.
These three patients were successfully treated by applyingradiofrequency energy along the tricuspid annulus below thelocation where a His bundle electrogram was observed(Figs. 3 and 4). Accelerated junctional rhythm was observedduring radiofrequency energy in each. The PR intervals andthe existence of V-A conduction were unaffected by theseablations.
Procedural issues and complications. These were lengthyprocedures, in part due to the inclusion of hemodynamicstudies. The total fluoroscopy times per patient (80 min;95% CI: 62–99 min) and procedure times (8.8 h; 95% CI:8.0 to 9.6 h) were longer than those reported from thePediatric Radiofrequency Registry (19).
Two patients suffered second- or third-degree AV blockduring delivery of radiofrequency energy from the systemicvenous side of the medial isthmus, and in one, it waspermanent. These were the only two patients in whom thecoronary sinus ostium was kept on the systemic venous sidewith no attempt at surgical redirection or incision of thecoronary sinus (p 5 0.02) (Fig. 1). These two patients weretwo of the five not having V-A conduction (p 5 NS).Among the eight patients whose medial isthmus was leftalmost exclusively on the pulmonary venous side, nonesuffered any degree of AV block (p 5 NS).
Follow-up. At 28 months’ mean follow-up (range: 4 to 54months), all 11 patients are alive (Table 4). Of those threewhose ablations were not thought to be successful, one hasa dual-chamber pacemaker for permanent second-degree
atrioventricular block, and the other two receive class Iantiarrhythmic drugs. All remain asymptomatic.
Among the eight patients whose ablations were thoughtto be successful, three receive digoxin, and one (Patient 10)atenolol. Digoxin had not been efficacious in those patientspreprocedure. Patient 10 suffered IART recurrences, begin-ning two months following his procedure, but he is nowcompletely controlled with atenolol. He had many recur-rences prior to the procedure while receiving atenolol.Patient 4 has episodes lasting ,3 s of a junctional tachy-cardia during exertion. All other patients remain asymptom-atic. In summary, seven of the eight patients (88%; 95% CIfor recurrence rate: 0% to 36%) whose procedures weresuccessful have had no supraventricular tachycardia recur-rences.
DISCUSSION
Radiofrequency ablation of FAT and atrioventricularnode reentry tachycardia. The principal new informationin this report is a description of radiofrequency catheterablation of other supraventricular tachycardias in addition toIART following the Mustard and Senning operations. Sitesof focal atrial tachycardias on either systemic or pulmonaryvenous sides of the surgical baffles can be mapped andablated. These sites seemed to be immediately adjacent tobaffle suture lines. Criteria previously described for accuratelocalization of atrial ectopic tachycardia foci (16) were usefulin these two patients.
The typical variety of AV node reentry tachycardia wasinducible in three patients; however, in two it was only seenfollowing application of radiofrequency lesions to the me-dial isthmus for IART. These two cases could thereforehave been caused by alteration of conduction properties ofthe slow inputs to the AV node, and, hence, could beiatrogenic. Irrespective of the etiology, application of radio-frequency energy along the tricuspid valve on the pulmonaryvenous side, probably corresponding to M1 and M2 zones(20), resulted in accelerated junctional rhythm (21) andrendered the tachycardia as noninducible. Well-establishedcatheter ablation techniques (17,18,21) for the typical vari-ety of AV node reentry tachycardia, then, proved efficaciousin this patient group. The catheter course was similar to thatrequired for isthmus ablation from the pulmonary venousside. However, more clockwise torque was required torender the tip medial and against the anteroseptal tricuspidannulus. To avoid damage to the compact AV node, webelieve that it is critical to obtain a His bundle electrogramfirst. Flexion on the catheter may then be relaxed slightlyuntil the His bundle signal no longer is present and thereremain small atrial and large ventricular electrograms. Insummary, we found both electrographic and fluoroscopicinformation to be necessary for safe and successful manage-ment of the typical variety of AV node reentry tachycardia.
436 Kanter et al. JACC Vol. 35, No. 2, 2000Tachycardia Ablation in Mustard and Senning Patients February 2000:428–41

Tabl
e3.
Rad
iofr
eque
ncy
Abl
atio
nof
Supr
aven
tric
ular
Tac
hyca
rdia
san
dO
ther
Pro
cedu
ralI
ssue
s
Pat
ient
Dat
eof
Stud
yT
achy
card
ia
Cri
teri
afo
rL
ocat
ion
ofR
FE
nerg
yD
eliv
ery
Succ
essf
ul(y
es/n
o)M
ain
Site
ofSu
cces
sful
RF
AM
ain
Site
ofU
nsuc
cess
ful
RF
AN
o.of
RF
App
licat
ions
Flu
oros
copy
Tim
e(m
in)
Pro
cedu
reT
ime
(h)
Com
plic
atio
ns
11/
94IA
RT
CE
M;p
resy
stol
icpo
tent
ials
No
Med
iali
sthm
us(S
VA
linea
r;P
VA
foca
l)
2311
011
Upp
erbo
dyed
ema
(24
h)
28/
94IA
RT
CE
M;p
resy
stol
icpo
tent
ials
No
Mid
-an
dla
tera
lis
thm
us(P
VA
linea
ran
dfo
cal)
750
9.5
Non
e
33/
95IA
RT
CE
M;p
resy
stol
icpo
tent
ials
Yes
Med
iali
sthm
us(S
VA
linea
r)10
358.
5N
one
412
/95
IAR
TC
EM
;pre
syst
olic
pote
ntia
lsY
esM
id-i
sthm
us(P
VA
linea
r)M
edia
list
hmus
(SV
Alin
ear)
2065
9T
rans
ient
seco
nd-
degr
eeA
Vbl
ock
53/
96IA
RT
Pre
syst
olic
and
split
pote
ntia
lsN
oM
edia
list
hmus
(SV
Alin
ear)
340
8T
rans
ient
thir
d-de
gree
AV
bloc
k;pe
rman
ent
seco
nd-
degr
eeA
Vbl
ock
62/
96FA
TE
arlie
stat
rial
elec
trog
ram
(A-P
inte
rval
535
ms)
Yes
PV
A-l
eft
ofL
PV
s(f
ocal
)N
one
IAR
T#1
CE
M;p
resy
stol
icpo
tent
ials
Yes
SVC3
sept
alre
mna
nt(S
VA
linea
r)
2775
12
IAR
T#2
CE
M;p
resy
stol
icpo
tent
ials
Yes
Med
iali
sthm
us(S
VA
linea
r)4/
96IA
RT
#2C
EM
;pre
syst
olic
pote
ntia
lsY
esM
id-i
sthm
us(P
VA
linea
r)M
id-i
sthm
us(S
VA
linea
r)11
408
Non
e
74/
94FA
TE
arlie
stat
rial
elec
trog
ram
(A-P
inte
rval
561
ms)
Yes
Mid
-sep
tal
rem
nant
(SV
Afo
cal)
1775
10N
one
5/96
IAR
TC
EM
;pre
syst
olic
pote
ntia
lsY
esM
id-i
sthm
us(P
VA
linea
r)M
id-i
sthm
us(S
VA
linea
r)8
356.
5N
one
811
/96
IAR
TC
EM
;pre
syst
olic
pote
ntia
lsY
esM
id-i
sthm
us(P
VA
linea
r)M
edia
list
hmus
(SV
Alin
ear)
111
8N
one
Typ
ical
AV
NR
TA
nato
mic
loca
tion
of“s
low
inpu
ts”
toA
Vno
de;
acce
lera
ted
junc
tiona
lrh
ythm
Yes
Mid
-ist
hmus
TV
A(P
VA
foca
l)
20
(con
tinue
d)
{ }
}{
}{
}{
437JACC Vol. 35, No. 2, 2000 Kanter et al.February 2000:428–41 Tachycardia Ablation in Mustard and Senning Patients

Tabl
e3.
(con
tinue
d)
95/
97IA
RT
CE
M;p
resy
stol
icpo
tent
ials
Yes
SVC3
sutu
relin
eof
sept
alfla
p(S
VA
linea
r)
Mid
-ist
hmus
(PV
Alin
ear)
;med
ial
isth
mus
(SV
Alin
ear)
1788
7N
one
Typ
ical
AV
NR
TA
nato
mic
loca
tion
of“s
low
inpu
ts”
toA
Vno
de;
acce
lera
ted
junc
tiona
lrh
ythm
Yes
Mid
-sep
talT
VA
(PV
Afo
cal)
10
106/
97T
ypic
alA
VN
RT
Ana
tom
iclo
catio
nof
“slo
win
puts
”to
AV
node
;ac
cele
rate
dju
nctio
nal
rhyt
hm
Yes
Mid
-sep
talT
VA
(PV
Afo
cal)
710
28
Non
e
IAR
TC
EM
;pre
syst
olic
pote
ntia
lsY
esR
t.A
trio
tom
ysc
ar3
TV
A(P
VA
linea
r)
Med
iali
sthm
us(S
VA
linea
r)36
113/
98IA
RT
#1C
EM
;pre
syst
olic
pote
ntia
lsY
esL
ater
alis
thm
us(P
VA
linea
r)M
id-i
sthm
us(S
VA
linea
r)9
579
Non
e
IAR
T#2
CE
M;p
resy
stol
icpo
tent
ials
Yes
SVC
/sup
erio
rle
ftat
rium3
sutu
relin
eof
sept
alfla
p(S
VA
linea
r)
8
Mea
n6
SD21
/pt
(95%
CI:
14–2
8)80
min
/pt
(95%
CI:
62–9
9)8.
8h/
proc
edur
e(9
5%C
I:8.
0–9.
6)
AV
NR
T5
atri
oven
tric
ular
noda
lree
ntry
tach
ycar
dia;
CE
M5
conc
eale
den
trai
nmen
tm
appi
ng;F
AT
5fo
cala
tria
ltac
hyca
rdia
;IA
RT
5in
traa
tria
lree
ntry
tach
ycar
dia;
LP
Vs
5le
ftpu
lmon
ary
vein
s;P
VA
5pu
lmon
ary
veno
usat
rium
;R
FA5
radi
ofre
quen
cyab
latio
n;SV
A5
syst
emic
veno
usat
rium
;SD
5st
anda
rdde
viat
ion;
SVC
5su
peri
orve
naca
va;T
VA
5tr
icus
pid
valv
ean
nulu
s.
438 Kanter et al. JACC Vol. 35, No. 2, 2000Tachycardia Ablation in Mustard and Senning Patients February 2000:428–41

Radiofrequency ablation of IART. Our overall acutesuccess rate for ablation of IART circuits (77% of circuits;73% of patients) compares favorably with that described inprevious reports (78% of circuits; 79% of patients) (11–13).Among Mustard patients having isthmus-dependent IART,Van Hare et al. (11) reported a relationship between thesurgically determined location of the coronary sinus ostiumand the location of successful radiofrequency ablation–pulmonary venous versus systemic venous side of the bafflesuture line. When the ostium was on the systemic venousside, ablation on the same side was required for successfulinterruption of IART, and vice versa (11). Our findings didnot agree with theirs.
Although the nomenclature in Table 1 is different fromthat used in the report by Van Hare et al., the “location ofthe medial isthmus” from Table 1 was similarly deducedfrom the description of the surgical handling of the coronarysinus. Whenever the coronary sinus was kept on thepulmonary venous side, or whenever it was surgically incisedto permit redirection into the systemic venous atrium, weconcluded that the medial isthmus was almost entirelypulmonary venous. Hence, a medial isthmus with bothsystemic and pulmonary venous components would corre-spond to a systemic venous coronary sinus in the Van Harestudy (11). With that explanation, in only three of fiveMustard patients in our series, in whom surgical proceduraldata were available, was the location of the coronary sinuspredictive of the site of successful ablation IART; in three offour patients in whom the coronary sinus was left on thepulmonary venous side, ablation was successful on that side,having first been unsuccessful on the systemic venous side.In the other patient (Patient 3), ablation was successful fromthe systemic venous side. Among the two patients in whom
the coronary sinus remained on the systemic venous side, inpatient 4 the ablation was successful from the pulmonaryvenous side, having failed from the systemic venous side.
There are several possible explanations for the discrep-ancy in these findings. The small numbers of patients inboth series make statistically based conclusions difficult.Second, with respect to the surgical handling of the coro-nary sinus, there may not be a fair comparison of patients inthe two experiences. For example, in several patients in ourseries, we concluded that the medial isthmus was kept onthe pulmonary venous side, when the coronary sinus ostiumwas surgically redirected to systemic venous atrium. If suchsurgical redirection was performed in the patients in theVan Hare series (11), then the expression “systemic venouscoronary sinus ostium” would not have equivalence. Third,because of our experience with AV block in two patientsduring application of radiofrequency energy to the systemicvenous side of the medial isthmus, we did not perform morethan two linear lesions in this region in any subsequentpatient before switching to the pulmonary venous approach.Hence, we became less aggressive.
Sites for delivery of radiofrequency ablation energy de-pended upon the tachycardia mechanism. For focal atrialtachycardia and AV node reentry tachycardia, the criteriaused are discussed above. For IART, various maneuverswere used: 1) identification of fractionated atrial electro-grams prior to the P-wave onset, preferably with splitpotentials, during tachycardia; 2) characterization of theanatomy based upon fluoroscopic location of the ablationcatheter during mapping; and 3) proof of participation ofthat region in the tachycardia circuit, using entrainmentwith concealed fusion. In agreement with previous reports(11–13), when concealed entrainment was accompanied by
Table 4. Current Patient Status at Last Follow-up
Patient
DurationSince Last RFA
(mos)
CurrentAntiarrhythmic
MedicationsCurrent
Rhythm Status
ClinicalTachycardiaRecurrences
1 54 Dg Normal sinus None2 47 Pr; Q AAICP paced None3 40 None VVIR paced None4 32 Dg Normal sinus None5 28 Diso DDD paced None6 27 None VVIR paced None7 26 Dg Normal sinus None8 20 None Normal sinus None9 14 Dg Junctional Brief palpitation
(,5 s runs,junctionaltachycardia)
10 13 At Junctional/sinus IART11 4 None Normal sinus None
Mean 6 SD 28 6 15 months(4–54 mos)
At 5 atenolol; Dg 5 digoxin; Diso 5 disopyramide; IART 5 intraatrial reentry tachycardia; Pr 5 propranolol; Q 5 quinidine;RFA 5 radiofrequency ablation.
439JACC Vol. 35, No. 2, 2000 Kanter et al.February 2000:428–41 Tachycardia Ablation in Mustard and Senning Patients

a postpacing interval #20 ms longer than the tachycardiacycle length, that location was considered to be a critical partof the tachycardia circuit. Knowledge of the anatomicboundaries of that portion of the circuit was then necessaryto permit successful radiofrequency ablation.
The observation in Mustard patients that entrainmentwith concealed fusion and a short postpacing interval couldbe demonstrated on both systemic and pulmonary venoussides of the lower atrial baffle suggested to us that the entireisthmus participates in the reentrant circuit and must betransected. As the baffle extends anteriorly, to encircle theinferior vena caval orifice, catheter manipulation suggestedthat no portion of the mid- or lateral isthmus remained onthe systemic venous side (Fig. 4). Except in patients inwhom a large portion of the medial isthmus remains on thesystemic venous side, the best opportunity for transectingthe entire isthmus is from the pulmonary venous side at thelevel of the mid- or lateral isthmus.
AV block during radiofrequency ablation. This is the firstreport of damage to AV conduction during radiofrequencyablation of the medial isthmus from the systemic venousside following the Mustard procedure. To understand howthis might have occurred, precise knowledge of the originalsurgical procedure is necessary. Essential components of theMustard operation include a subtotal atrial septectomyfollowed by placement of a complex baffle of pericardium orprosthetic material, described as “pant legs” in shape.Damage to anterior or “fast” inputs to the AV node mightbe expected by the septectomy, although there are nointraoperative mapping data that precisely address thisanatomic region. Electrocardiographic evidence for thiswould include first-degree AV block; however, prolongationof the PR interval is frequently seen after this procedure dueto severe intraatrial conduction delay (22). Confounding ourability to discriminate the anatomic level of PR intervalprolongation was an inability to obtain a reliable Hisrecording. Based upon our knowledge of AV node conduc-tion in the normal heart, we considered the presence ofintact V-A conduction as suggestive of at least adequatefunction of the “fast” inputs to the AV node.
With respect to posterior or “slow” inputs to the AVnode, conduction block to the entire posteroseptal regionhas been demonstrated during intraoperative mapping,when the coronary sinus was kept on the systemic venousside of the inferior baffle suture line (23). A portion of the“slow” inputs to the AV node are thought to exist in thisregion (Fig. 1). The two patients in our series suffering atleast transient second- or third-degree AV block wereamong the six in whom the coronary sinus ostium drainedinto the systemic venous side and the only two in whom ithad not been surgically redirected or incised. Therefore, thecombination of the original surgical technique plus ablationcatheter access to the medial isthmus from the systemicvenous side (Fig. 1c) may have caused “slow pathway”damage. If the absence of V-A conduction observed in these
two patients represents prior loss of “fast pathway” conduc-tion, then overall impairment of AV node conduction mightbe expected.
Study limitations. There are several limitations of thisstudy. Anatomic detail was inferred from the fluoroscopiclocation of catheters coupled with prior echocardiographicand angiographic information. Real-time transesophagealechocardiographic or intracardiac echographic (24) tech-niques would provide new and potentially more accurateinformation regarding anatomy and catheter contact. Map-ping IART in such complex structures may also benefitfrom new magnetic electroanatomic mapping techniquessuch as those described by Marchlinski et al. (25) and byDorostkar et al. (26). In our patients, no attempts weremade to demonstrate creation of bidirectional block toconduction, either during or following radiofrequency en-ergy delivery to IART circuits. This will require novelcatheter placement in future patients. The absence of areliable His bundle electrogram throughout all studiesprevented meaningful evaluation of AV node function. Thiswould have been most important in the two patientssuffering AV node damage. Follow-up longer than 28months will be necessary to determine the long-term effi-cacy of radiofrequency ablation for supraventricular tachy-cardias in these patients. In particular, it is hoped that therecurrence rate of IART will be as low as that seen in adultswith normal hearts and not as high as that seen in Fontanpatients. We speculate that the relatively normal atrial sizeand pressure in our patients—in distinction from thatobserved in Fontan patients—will predict this to be so.
Clinical implications. As the population of patients whohad undergone the Mustard or Senning operation ages,paroxysmal tachycardias remain their most significant clin-ical problem. The majority of these tachycardias are su-praventricular in origin, predominantly IART. Other thanatrial fibrillation, there appears to be no supraventriculartachycardia that should be considered exempt from candi-dacy for radiofrequency ablation following these operations.As in patients having normal cardiac anatomy and commonatrial flutter, risk of damage to the AV node should bediscussed with patients, as ablation of inputs to the AV nodemay occur.
AcknowledgmentsWe gratefully acknowledge Phyllis Bason for manuscriptpreparation and the Pediatric Catheterization Laboratoryand Electrophysiology Laboratory staffs for providing su-perb patient care. We also thank our referring physicianswho trusted us with the care of their patients.
Reprint requests and correspondence: Dr. Ronald J. Kanter,Duke University Medical Center, Box 3090, Durham, NC 27710.E-mail: [email protected].
440 Kanter et al. JACC Vol. 35, No. 2, 2000Tachycardia Ablation in Mustard and Senning Patients February 2000:428–41

REFERENCES
1. Hayes CJ, Gersony WM. Arrhythmias after the Mustard operation fortransposition of the great arteries: a long-term study. J Am CollCardiol 1986;7:133–7.
2. Gewillig M, Cullen S, Mertens B, et al. Risk factors for arrhythmiasand death after Mustard operation for simple transposition of the greatarteries. Circulation 1991;84:III187–92.
3. Garson A, Bink-Boelkens M, Hesslein PS, et al. Atrial flutter in theyoung: a collaborative study of 380 cases. J Am Coll Cardiol 1985;6:871–8.
4. Flinn CJ, Wolff GS, Campbell RM, et al. Natural history of supraven-tricular rhythms in 182 children following the Mustard operation.J Am Coll Cardiol 1983;1:613–8.
5. Gillette PC, El-Said GM, Siverajan N, et al. Electrophysiologicalabnormalities after Mustard’s operation for transposition of the greatarteries. Br Heart J 1974;36:186–91.
6. Ashraf MH, Cotroneo J, DiMarco D, Subramanian S. Fate oflong-term survivors of Mustard procedure (inflow repair) for simpleand complex transposition of the great arteries. Ann Thorac Surg1986;42:385–9.
7. Vetter VL, Tanner CS, Horowitz LN. Inducible atrial flutter after theMustard repair of complete transposition of the great arteries. Am JCardiol 1988;61:428–35.
8. Silka MJ, Manwill JR, Kron J, McAnulty DH. Bradycardia-mediatedtachyarrhythmias in congenital heart disease and responses to chronicpacing at physiologic rates. Am J Cardiol 1990;65:488–93.
9. Feld GK, Fleck P, Chen P-S, et al. Radiofrequency catheter ablationfor the treatment of human type I atrial flutter. Circulation 1992;86:1233–40.
10. Cosio FG, Lopez-Gil M, Goicolea A, et al. Radiofrequency ablationof the inferior vena cava-tricuspid valve isthmus in common atrialflutter. Am J Cardiol 1993;71:705–9.
11. Van Hare GF, Lesh MD, Ross BA, et al. Mapping and radiofrequencyablation of intraatrial reentrant tachycardia after the Senning orMustard procedures for transposition of the great arteries. Am JCardiol 1996;77:985–91.
12. Triedman JK, Saul JP, Weindling SN, Walsh EP. Radiofrequencyablation of intra-atrial reentrant tachycardia after surgical palliation ofcongenital heart disease. Circulation 1995;91:707–14.
13. Kalman JM, VanHare GF, Olgin JE, et al. Ablation of ‘incisional’reentrant atrial tachycardia complicating surgery for congenital heartdisease; use of entrainment to define critical isthmus of conduction.Circulation 1996;93:502–12.
14. Baker BM, Linsay BD, Bromberg BI, et al. Catheter ablation ofclinical intraatrial reentrant tachycardias resulting from previous atrialsurgery: localizing and transecting the critical isthmus. J Am CollCardiol 1996;28:411–7.
15. Lavoie J, Walsh EP, Burrows FA, et al. Effects of propofol orisoflurane anesthesia on cardiac conduction in children undergoingradiofrequency catheter ablation for tachydysrhythmias. Anesthesiol-ogy 1995;82:884–7.
16. Walsh EP, Saul JP, Hulse JE, et al. Transcatheter ablation of ectopicatrial tachycardia in young patients using radiofrequency current.Circulation 1992;86:1138–46.
17. Kay GN, Epstein AE, Dailey SM, Plumb VJ. Selective radiofrequencyablation of the slow pathway for the treatment of atrioventricular nodalreentrant tachycardia. Circulation 1992;85:1675–88.
18. Haissaguerre M, Gaita F, Fischer B, et al. Elimination of atrioven-tricular nodal reentrant tachycardia using discrete slow potentials toguide application of radiofrequency energy. Circulation 1992;85:2162–75.
19. Kugler JD, Danford DA, Deal BJ, et al. Radiofrequency catheterablation for tachyarrhythmias in children and adolescents. N EnglJ Med 1994;330:1481–7.
20. Keim S, Werner P, Jazayeri M, et al. Localization of the fast and slowpathways in atrioventricular nodal reentrant tachycardia by intraoper-ative ice mapping. Circulation 1992;86:919–24.
21. Jentzer JH, Goyal R, Williamson BD, et al. Analysis of junctionalectopy during radiofrequency ablation of the slow pathway in patientswith atrioventricular nodal reentrant tachycardia. Circulation 1994;90:2820–6.
22. Vetter VL, Tanner CS, Horowitz LN. Electrophysiologic conse-quences of the Mustard repair of d-transposition of the great arteries.J Am Coll Cardiol 1987;10:1265–73.
23. Wittig JH, deLeval MR, Stark J, Castaneda A. Intraoperative map-ping of atrial activation before, during, and after the Mustard opera-tion. J Thorac Cardiovasc Surg 1977;73:1–13.
24. Chu E, Fitzpatrick AP, Chin MC, et al. Radiofrequency catheterablation guided by intracardiac echocardiography. Circulation 1994;89:1301–5.
25. Marchlinski F, Callans D, Gottlieb C, et al. Magnetic electroanatomi-cal mapping for ablation of focal atrial tachycardias. Pacing ClinElectrophysiol 1998;21:1621–35.
26. Dorostkar PC, Cheng J, Scheinman MM. Electroanatomical mappingand ablation of the substrate supporting intraatrial reentrant tachycar-dia after palliation for complex congenital heart disease. Pacing ClinElectrophysiol 1998;21:1810–9.
441JACC Vol. 35, No. 2, 2000 Kanter et al.February 2000:428–41 Tachycardia Ablation in Mustard and Senning Patients
Copyright © 2022 FDOKUMEN




















