Assessing risks, costs, and benefits of laparoscopic hernia repair.
17
Annu. Rev. Medicine 1998. 49:95–109 Copyright © 1998 by Annual Reviews Inc. All rights reserved ASSESSING RISKS, COSTS, AND BENEFITS OF LAPAROSCOPIC HERNIA REPAIR Muhammed Ashraf Memon, MBBS, DCH, FRCSI, FRCSEd, FRCSEng Laparoscopic Surgical Research Fellow, Department of Surgery, Creighton University School of Medicine, Omaha, Nebraska 68131; e-mail: [email protected] Robert J. Fitzgibbons, Jr., MD, FACS Professor and Chief, Division of General Surgery, Creighton University School of Medicine, Omaha, Nebraska 68131; e-mail [email protected] KEY WORDS: hernia, inguinal surgery; surgery, laparoscopic; laparoscopic economics; cost- benefit analysis; cost and cost analysis ABSTRACT Laparoscopic inguinal herniorrhaphy (LIHR) was introduced with the fol- lowing potential advantages: less postoperative discomfort and pain, re- duced recovery time that allows earlier return to full activity, easier repair of a recurrent hernia, the ability to treat bilateral hernias concurrently, the per- formance of a simultaneous diagnostic laparoscopy, ligation of the hernia sac at the highest possible site, improved cosmesis, and decreased incidence of recurrence. Potential disadvantages include complications, such as bowel, bladder, and vascular injuries; potential adhesive complications at sites where the peritoneum has been breached or prosthetic material has been placed; the apparent need, at least at the present, for a general anesthetic; and the increased cost because of expensive equipment needs. Most surgeons agree that LIHR has a role in the management of patients with a recurrent hernia after a conventional inguinal herniorrhaphy (CIHR), bilateral inguinal hernia, or a need for laparoscopy for another procedure, such as laparoscopic cholecystectomy. The routine use of LIHR for the unilateral, uncomplicated hernia is a more contentious issue. 0066-4219/98/0201-0095$08.00 95 Annu. Rev. Med. 1998.49:95-109. Downloaded from www.annualreviews.org by University of Queensland on 06/11/11. For personal use only.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Assessing risks, costs, and benefits of laparoscopic hernia repair.
Annu. Rev. Medicine 1998. 49:95–109Copyright © 1998 by Annual Reviews Inc. All rights reserved
ASSESSING RISKS, COSTS, AND
BENEFITS OF LAPAROSCOPIC
HERNIA REPAIR
Muhammed Ashraf Memon, MBBS, DCH, FRCSI, FRCSEd,
FRCSEng
Laparoscopic Surgical Research Fellow, Department of Surgery, Creighton University
School of Medicine, Omaha, Nebraska 68131; e-mail: [email protected]
Robert J. Fitzgibbons, Jr., MD, FACS
Professor and Chief, Division of General Surgery, Creighton University School of
Medicine, Omaha, Nebraska 68131; e-mail [email protected]
KEY WORDS: hernia, inguinal surgery; surgery, laparoscopic; laparoscopic economics; cost-
benefit analysis; cost and cost analysis
ABSTRACT
Laparoscopic inguinal herniorrhaphy (LIHR) was introduced with the fol-lowing potential advantages: less postoperative discomfort and pain, re-duced recovery time that allows earlier return to full activity, easier repair ofa recurrent hernia, the ability to treat bilateral hernias concurrently, the per-formance of a simultaneous diagnostic laparoscopy, ligation of the hernia sacat the highest possible site, improved cosmesis, and decreased incidence ofrecurrence. Potential disadvantages include complications, such as bowel,bladder, and vascular injuries; potential adhesive complications at siteswhere the peritoneum has been breached or prosthetic material has beenplaced; the apparent need, at least at the present, for a general anesthetic; andthe increased cost because of expensive equipment needs. Most surgeonsagree that LIHR has a role in the management of patients with a recurrenthernia after a conventional inguinal herniorrhaphy (CIHR), bilateral inguinalhernia, or a need for laparoscopy for another procedure, such as laparoscopiccholecystectomy. The routine use of LIHR for the unilateral, uncomplicatedhernia is a more contentious issue.
0066-4219/98/0201-0095$08.00
95
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.
INTRODUCTION
Groin hernia is one of the most common afflictions of adults, especially men(1). The earliest recordings of medical history include discussions about effec-tive means of treatment. Approximately 500,000 to 750,000 herniorrhaphiesare performed in the United States each year (2–6). It was the most commonsurgical operation performed by general surgeons in the United States in 1991according to data from the National Center for Health Statistics, Hyattsville,Maryland (7). There are large, direct costs for the surgical procedure and sig-nificant indirect costs because of time away from normal activities. The over-all cost to society for treatment of this condition would be even greater if theestimated 800,000 patients per annum in the United States who choose not tohave their inguinal hernias repaired had changed their minds (8).
Many different types of surgical procedures are currently used to repair an in-guinal hernia, and there is a lack of consensus among surgeons concerning the bestprocedure. The perfect method for inguinal herniorrhaphy has yet to be developed.It is not surprising, therefore, that numerous modifications of existing proce-dures have been described and that new procedures are regularly being developed.
BACKGROUND
Modern surgical thinking concerning inguinal herniorrhaphy has been domi-nated by the principles first set forth by Bassini, who in 1884 developed a tech-nique for inguinal herniorrhaphy that included high ligation of the sac and re-inforcement of the inguinal floor (9). His operation was associated with alower operative mortality, and the recurrent hernia rate was one fifth of thatwhich was commonly accepted at the time. Modifications of Bassini’s repairhave been described by McVay (10), Halsted (11), Shouldice, and others(12–15) in attempts to further reduce the recurrence rate and to avoid compli-cations. Impressively low recurrence rates have been achieved with thesevariations in the hands of experts. However, postoperative pain has generallybeen considered excessive by both surgeons and patients, presumably result-ing from the tension created by suturing together tissues that are not naturallyin apposition (16). In addition, chronic groin pain syndromes have plaguedthese procedures. A randomized, prospective trial published from Canada byCunningham et al disclosed an astonishing rate of long-term pain after thesekinds of repairs (63% at 1 year and 53% at 2 years with 10% being severe) (17).Finally, in general surgical practice outside of specialty centers using any ofthese conventional methods, the recurrence rate requiring re-operation re-mains approximately 10%, as evidenced by a population-based study per-formed by the Rand Corporation and by the high incidence of recurrent herniasat enrollment in most published series (Table 1 & 2).
96 MEMON & FITZGIBBONS JR.
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.
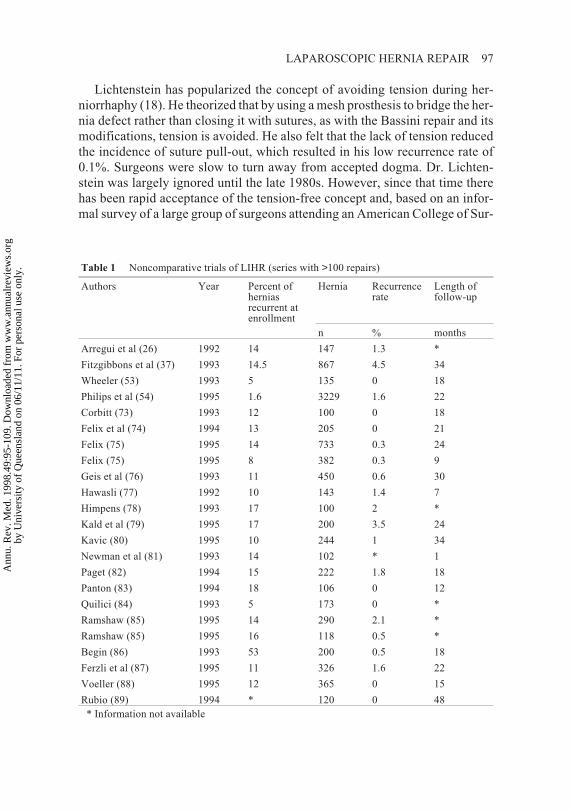
Lichtenstein has popularized the concept of avoiding tension during her-niorrhaphy (18). He theorized that by using a mesh prosthesis to bridge the her-nia defect rather than closing it with sutures, as with the Bassini repair and itsmodifications, tension is avoided. He also felt that the lack of tension reducedthe incidence of suture pull-out, which resulted in his low recurrence rate of0.1%. Surgeons were slow to turn away from accepted dogma. Dr. Lichten-stein was largely ignored until the late 1980s. However, since that time therehas been rapid acceptance of the tension-free concept and, based on an infor-mal survey of a large group of surgeons attending an American College of Sur-
LAPAROSCOPIC HERNIA REPAIR 97
Table 1 Noncomparative trials of LIHR (series with >100 repairs)
Authors Year Percent ofherniasrecurrent atenrollment
Hernia Recurrencerate
Length offollow-up
n % months
Arregui et al (26) 1992 14 147 1.3 *
Fitzgibbons et al (37) 1993 14.5 867 4.5 34
Wheeler (53) 1993 5 135 0 18
Philips et al (54) 1995 1.6 3229 1.6 22
Corbitt (73) 1993 12 100 0 18
Felix et al (74) 1994 13 205 0 21
Felix (75) 1995 14 733 0.3 24
Felix (75) 1995 8 382 0.3 9
Geis et al (76) 1993 11 450 0.6 30
Hawasli (77) 1992 10 143 1.4 7
Himpens (78) 1993 17 100 2 *
Kald et al (79) 1995 17 200 3.5 24
Kavic (80) 1995 10 244 1 34
Newman et al (81) 1993 14 102 * 1
Paget (82) 1994 15 222 1.8 18
Panton (83) 1994 18 106 0 12
Quilici (84) 1993 5 173 0 *
Ramshaw (85) 1995 14 290 2.1 *
Ramshaw (85) 1995 16 118 0.5 *
Begin (86) 1993 53 200 0.5 18
Ferzli et al (87) 1995 11 326 1.6 22
Voeller (88) 1995 12 365 0 15
Rubio (89) 1994 * 120 0 48
* Information not available
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.
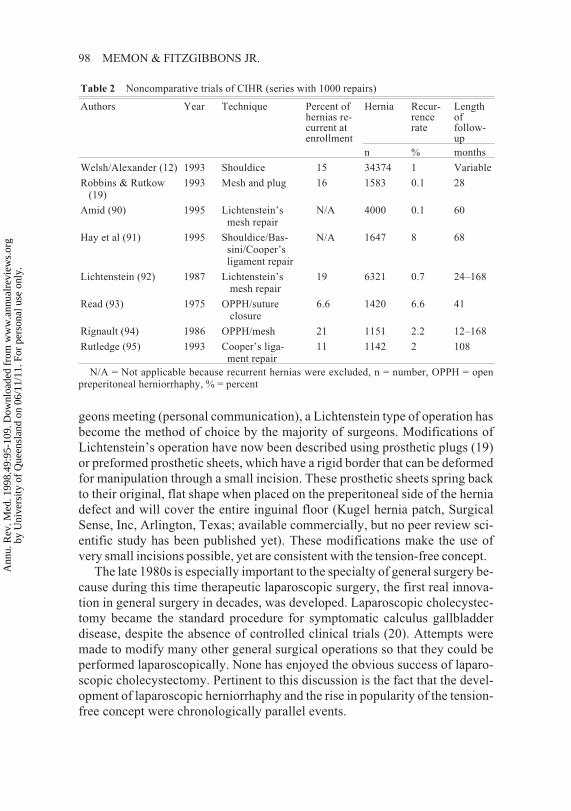
geons meeting (personal communication), a Lichtenstein type of operation hasbecome the method of choice by the majority of surgeons. Modifications ofLichtenstein’s operation have now been described using prosthetic plugs (19)or preformed prosthetic sheets, which have a rigid border that can be deformedfor manipulation through a small incision. These prosthetic sheets spring backto their original, flat shape when placed on the preperitoneal side of the herniadefect and will cover the entire inguinal floor (Kugel hernia patch, SurgicalSense, Inc, Arlington, Texas; available commercially, but no peer review sci-entific study has been published yet). These modifications make the use ofvery small incisions possible, yet are consistent with the tension-free concept.
The late 1980s is especially important to the specialty of general surgery be-cause during this time therapeutic laparoscopic surgery, the first real innova-tion in general surgery in decades, was developed. Laparoscopic cholecystec-tomy became the standard procedure for symptomatic calculus gallbladderdisease, despite the absence of controlled clinical trials (20). Attempts weremade to modify many other general surgical operations so that they could beperformed laparoscopically. None has enjoyed the obvious success of laparo-scopic cholecystectomy. Pertinent to this discussion is the fact that the devel-opment of laparoscopic herniorrhaphy and the rise in popularity of the tension-free concept were chronologically parallel events.
98 MEMON & FITZGIBBONS JR.
Table 2 Noncomparative trials of CIHR (series with 1000 repairs)
Authors Year Technique Percent ofhernias re-current atenrollment
Hernia Recur-rencerate
Lengthoffollow-up
n % months
Welsh/Alexander (12) 1993 Shouldice 15 34374 1 Variable
Robbins & Rutkow(19)
1993 Mesh and plug 16 1583 0.1 28
Amid (90) 1995 Lichtenstein’smesh repair
N/A 4000 0.1 60
Hay et al (91) 1995 Shouldice/Bas-sini/Cooper’sligament repair
N/A 1647 8 68
Lichtenstein (92) 1987 Lichtenstein’smesh repair
19 6321 0.7 24–168
Read (93) 1975 OPPH/sutureclosure
6.6 1420 6.6 41
Rignault (94) 1986 OPPH/mesh 21 1151 2.2 12–168
Rutledge (95) 1993 Cooper’s liga-ment repair
11 1142 2 108
N/A = Not applicable because recurrent hernias were excluded, n = number, OPPH = openpreperitoneal herniorrhaphy, % = percent
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.

LAPAROSCOPIC INGUINAL HERNIORRHAPHY
Laparoscopic inguinal hernia repair (LIHR) was developed with the followingpotential advantages in mind: less postoperative discomfort and pain, reducedrecovery time that allows earlier return to full activity, easier repair of a recur-rent hernia because the repair is performed in tissue that has not been previ-ously dissected, the ability to treat bilateral hernias concurrently, the perform-ance of a simultaneous diagnostic laparoscopy, the highest possible ligation ofthe hernia sac, and improved cosmesis (21–25). In addition, it was theorizedthat LIHR might have a lower recurrence rate than conventional inguinal her-niorrhaphy (CIHR) because of the mechanical advantage gained by placing theprosthesis in the preperitoneal space and the tension-free nature of the repair(26, 27).
These potential advantages of laparoscopic herniorrhaphy must be inter-
preted in the light of the possible disadvantages of a laparoscopic approach.
These include complications related to the laparoscopy such as bowel perfo-
ration or major vascular injury, potential adhesive complications at sites
where the peritoneum has been breached or prosthetic material has been
placed, the apparent need, at least at the present time, for a general anesthetic,
and increased cost because of the expensive equipment needs (28). The con-
ventional operation can be performed under local anesthesia on an outpa-
tient basis, with minimal risk of intra-abdominal injury, and the cost is less
(29–31).The LIHRs performed earlier on in surgeons’ learning curves were plagued
by two serious flaws. The first was an unacceptably high recurrence rate that
approached 20% (32, 33), due to the nonscientific repair method of simply fill-
ing the defect with large plugs or sheets of prosthetic material, while failing to
address the weakened inguinal floor. This problem was soon identified, and
surgeons started routinely using a large, flat prosthesis to support the entire in-
guinal floor. This modification has tremendously improved the recurrence rate
in contemporary series. Table 1 is a summary of recently published non-
comparative, mainly single-center series of laparoscopic hernia repairs. The
recurrence rates are essentially the same as those reported with the conven-
tional method for studies of the same design (Table 2).The second flaw was an unacceptably high incidence of neuralgia (34–37).
This problem was also rapidly solved as surgeons became familiar with the
posterior abdominal wall anatomy as seen from the laparoscopic prospective.
Surgeons learned to avoid stapling in critical areas where nerves traverse. Only
now that such technical problems have been solved and the operation has been
standardized can the true benefits be assessed.
LAPAROSCOPIC HERNIA REPAIR 99
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.

BENEFITS OF LAPAROSCOPIC INGUINALHERNIORRAHPHY
Conventional (open) hernia repair methods such as Bassini, McVay, Stoppa,or Shouldice suffer from one major disadvantage, i.e. a slow and painful recov-ery process. This is attributed to a number of factors that include a large skinincision, injury to various nerves, entrapment of nerves by postoperative scarformation or by suture, and presence of tissue tension. It is now believed thatthe presence of tissue tension in a hernia repair plays a significant role in bothshort- and long-term pain and recurrence (38). The postoperative recoveryprocess, therefore, is generally better with a tensionless herniorrhaphy, such asLichtenstein (39). LIHR was envisioned to allow for the best of both worlds byavoiding a large groin incision and subsequent scarring and by placing theprosthesis in a tension-free manner. This would be most beneficial in patientswith recurrent hernia after a failed CIHR or with bilateral or other complicatedhernias.
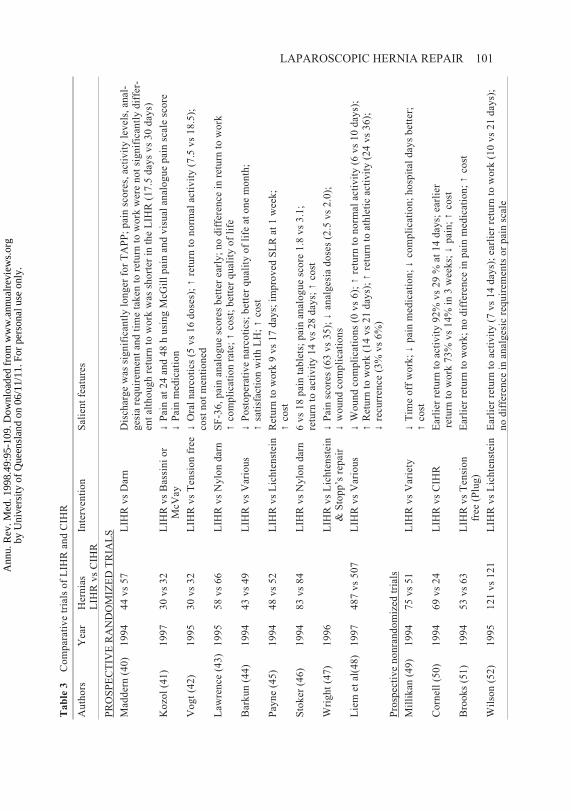
In Table 3, 13 trials [9 randomized prospective (40–48) and 4 non-randomized (49–52) trials] comparing laparoscopic and conventional herniarepair have been summarized. All of the comparative trials except one (40)have shown a statistically significant benefit for LIHR patients over both ten-sion and tension-free CIHRs in one or more of the parameters studied. A re-cently published prospective randomized trial (48) that enrolled 997 patientsclearly showed that LIHR patients had significantly less postoperative pain, asmeasured by a visual analogue pain scale, returned to normal work and athleticactivities much faster, and had a significantly lower recurrence rate at the endof two years. In addition, the incidence of wound abscesses was significantlyless in the LIHR group.
THE RISKS ASSOCIATED WITH LAPAROSCOPICHERNIORRHAPHY
The overall complication rate with LIHR is slightly lower than in conventionalrepairs (28), but the difference is not great. Some of the complications associ-ated with LIHR have been more severe and life threatening than those seen inCIHR and include bladder and bowel perforation (42, 53), bowel obstructionor herniation at trocar sites (54–57), major vascular injury (58), and colovesi-cal fistula (59). Table 4 summarizes possible complications of laparoscopicherniorrhaphy by separating them into three groups: (a) those related to thelaparoscopy; (b) those related to the patient, i.e. general complications; and (c)those related to the herniorrhaphy. Except for complications unique to lapa-roscopy, the incidence of other complications is similar for both procedures.
100 MEMON & FITZGIBBONS JR.
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.
LAPAROSCOPIC HERNIA REPAIR 101T
ab
le3
Co
mp
arat
ive
tria
lso
fL
IHR
and
CIH
R
Au
tho
rsY
ear
Her
nia
sL
IHR
vs
CIH
RIn
terv
enti
on
Sal
ien
tfe
atu
res
PR
OS
PE
CT
IVE
RA
ND
OM
IZE
DT
RIA
LS
Mad
der
n(4
0)
19
94
44
vs
57
LIH
Rv
sD
arn
Dis
char
ge
was
sig
nif
ican
tly
lon
ger
for
TA
PP
;p
ain
sco
res,
acti
vit
yle
vel
s,an
al-
ges
iare
qu
irem
ent
and
tim
eta
ken
tore
turn
tow
ork
wer
en
ot
sig
nif
ican
tly
dif
fer-
ent
alth
ou
gh
retu
rnto
wo
rkw
assh
ort
erin
the
LIH
R(1
7.5
day
sv
s3
0d
ays)
Ko
zol
(41
)1
99
73
0v
s3
2L
IHR
vs
Bas
sin
io
rM
cVay
↓P
ain
at2
4an
d4
8h
usi
ng
McG
ill
pai
nan
dv
isu
alan
alo
gu
ep
ain
scal
esc
ore
↓P
ain
med
icat
ion
Vo
gt
(42
)1
99
53
0v
s3
2L
IHR
vs
Ten
sio
nfr
ee↓
Ora
ln
arco
tics
(5v
s1
6d
ose
s);↑
retu
rnto
no
rmal
acti
vit
y(7
.5v
s1
8.5
);co
stn
ot
men
tio
ned
Law
ren
ce(4
3)
19
95
58
vs
66
LIH
Rv
sN
ylo
nd
arn
SF
-36
,p
ain
anal
og
ue
sco
res
bet
ter
earl
y;
no
dif
fere
nce
inre
turn
tow
ork
↑co
mp
lica
tio
nra
te;↑
cost
;b
ette
rq
ual
ity
of
life
Bar
ku
n(4
4)
19
94
43
vs
49
LIH
Rv
sV
ario
us
↓P
ost
op
erat
ive
nar
coti
cs;
bet
ter
qu
alit
yo
fli
feat
on
em
on
th;
↑sa
tisf
acti
on
wit
hL
H;↑
cost
Pay
ne
(45
)1
99
44
8v
s5
2L
IHR
vs
Lic
hte
nst
ein
Ret
urn
tow
ork
9v
s1
7d
ays;
imp
rov
edS
LR
at1
wee
k;
↑co
st
Sto
ker
(46
)1
99
48
3v
s8
4L
IHR
vs
Ny
lon
dar
n6
vs
18
pai
nta
ble
ts;
pai
nan
alo
gu
esc
ore
1.8
vs
3.1
;re
turn
toac
tiv
ity
14
vs
28
day
s;↑
cost
Wri
gh
t(4
7)
19
96
LIH
Rv
sL
ich
ten
stei
n&
Sto
pp
’sre
pai
r↓
Pai
nsc
ore
s(6
3v
s3
5);
↓an
alg
esia
do
ses
(2.5
vs
2.0
);↓
wo
un
dco
mp
lica
tio
ns
Lie
met
al(4
8)
19
97
48
7v
s5
07
LIH
Rv
sV
ario
us
↓W
ou
nd
com
pli
cati
on
s(0
vs
6);
↑re
turn
ton
orm
alac
tiv
ity
(6v
s1
0d
ays)
;↑
Ret
urn
tow
ork
(14
vs
21
day
s);↑
retu
rnto
ath
leti
cac
tiv
ity
(24
vs
36
);↓
recu
rren
ce(3
%v
s6
%)
Pro
spec
tiv
en
on
ran
do
miz
edtr
ials
Mil
lik
an(4
9)
19
94
75
vs
51
LIH
Rv
sV
arie
ty↓
Tim
eo
ffw
ork
;↓
pai
nm
edic
atio
n;↓
com
pli
cati
on
;h
osp
ital
day
sb
ette
r;↑
cost
Co
rnel
l(5
0)
19
94
69
vs
24
LIH
Rv
sC
IHR
Ear
lier
retu
rnto
acti
vit
y9
2%
vs
29
%at
14
day
s;ea
rlie
rre
turn
tow
ork
73
%v
s1
4%
in3
wee
ks;
↓p
ain
;↑
cost
Bro
ok
s(5
1)
19
94
53
vs
63
LIH
Rv
sT
ensi
on
free
(Plu
g)
Ear
lier
retu
rnto
wo
rk;
no
dif
fere
nce
inp
ain
med
icat
ion
;↑
cost
Wil
son
(52
)1
99
51
21
vs
12
1L
IHR
vs
Lic
hte
nst
ein
Ear
lier
retu
rnto
acti
vit
y(7
vs
14
day
s);
earl
ier
retu
rnto
wo
rk(1
0v
s2
1d
ays)
;n
od
iffe
ren
cein
anal
ges
icre
qu
irem
ents
or
pai
nsc
ale
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.

Complications related to the patient are minimized with CIHR when the opera-tion is performed under local anesthesia, although many patients find this ap-proach unacceptable. To summarize, the potential for severe, life-threateningcomplications is greater with LIHR than CIHR, although the overall incidenceof complications between the two procedures is similar (28). The question be-comes, “Does the benefit of LIHR justify the increased risk of severe compli-cations?”
COST CONSIDERATIONS
If one includes the factors of surgical procedure and time away from normaldaily activities, the estimated cost of repairing 500,000 to 700,000 inguinalhernias per annum is approximately $3 billion (2, 4, 5, 7, 8, 60). It has been es-timated that herniorrhaphies cause the loss of 10 million working days eachyear , at a cost that has not been precisely defined but is obviously significant.Failure of the primary hernia repair (i.e. recurrence) requiring re-operation fur-ther increases the management costs of this routine procedure.
Cost-Benefit and Cost-Effective Analysis
Cost-benefit and cost-effective analyses measure and compare the vital gainsand losses associated with different methods of patient management. Doubilet etal (61) described four important measurements for any event that is introducedinto clinical practice to improve costeffectiveness. These include (a) cost sav-ings; (b) effectiveness in improving health care; (c) cost savings, with an equalor better health outcome; and (d) additional benefit worth the additional cost.
102 MEMON & FITZGIBBONS JR.
Table 4 Complications (37)
Related to laparoscopy Related to the patient Related to the herniorrhaphy
I. BleedingA. Abdominal wallB. Intra-abdominalC. Retroperitoneal
II. Visceral injuryA. Bowel perforationB. Bladder perforation
III. Bowel obstructionA. Trocar or peritoneal clo-
sure site herniaB. Adhesions
IV. Diaphragmatic dysfunc-tion
V. Wound infectionVI. Hypercapnia
I. UrinaryII. IleusIII. Aspiration pneumoniaIV. Cardiovascular and
Respiratory insufficiencyV. Nausea and vomiting
I. NeurologicalII. Cord & testicularIII. HydroceleIV. Wound infectionV. Prosthetic infectionVI. SeromaVII. Retroperitoneal hema-
tomaForeign body reaction to
mesh
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.

COST SAVINGS According to Stahlgren (62), there are four ways to achieve cost
savings when treating an adult patient with an inguinal hernia: (a) avoid unneces-
sary operations; (b) perform outpatient or ambulatory surgery; (c) reduce the
cost of the operation and hospitalization; and (d) minimize the incidence of re-
currence and wound infection by using appropriate surgical techniques with
known results.
Avoid unnecessary operations Surgeons routinely recommend elective in-guinal herniorrhaphy at the time of diagnosis for two reasons: fear of hernia ac-cident, i.e. obstruction and /or strangulation, and progression of the hernia withtime, making repair more difficult (63). In fact, the natural history of a groinhernia is not known. At the present time, there is no predictor of which herniawill become strangulated or when strangulation might occur. Since inguinalherniorrhaphy is currently performed routinely on diagnosis, there are no re-cent data documenting the incidence of hernia accident in adults.
An analysis of hernia management without operation was performed by
Neuhauser (64) that combined unpublished data from Cali, Colombia, in the
1970s with data from a study published in 1896, which described 10,000 pa-
tients enrolled in Berger’s truss clinic in Paris. The author found the annual
risk of a hernia accident for all ages to be 0.00291–0.0037. The incidence of
strangulation in patients 65 years of age was estimated to be 0.00291/year, or
0.044 during the remaining 15 years of life expectancy (64). Based on this an-
nual risk of a hernia accident and considering the life expectancy and operative
mortality rates for an uncomplicated herniorrhaphy in the Medicare population
from 1971, Neuhauser showed that elective operation has a greater loss of life
for a 65-year-old, although the absolute difference was negligible. Therefore,
in an older population, simple observation or truss may well be justified. Even
a truss, which costs between $80–100, including fitting, may not be necessary.
A recent report (65) revealed a truss to be uncomfortable and of no benefit in
controlling the hernia in the majority (69%) of patients. It was further sug-
gested that a truss may increase the incidence of complications and may make
eventual hernia repair more difficult. If hernia repair can be avoided altogether
in a significant number of patients, the impact on overall cost would be more
substantial than the difference between CIHR and LIHR.
Performing outpatient or ambulatory surgery Outpatient inguinal hernior-rhaphy can be performed for approximately half the cost of an inpatient proce-dure (66, 67). It is estimated that if one half of these procedures were per-formed in the outpatient setting, there would be a savings of approximately$200 million yearly in the United States. As Schultz (68) pointed out, promot-
LAPAROSCOPIC HERNIA REPAIR 103
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.

ing LIHR in more cost-efficient surroundings, such as an office surgical suite,could readily improve its acceptance by health-care insurers.
Reduce costs of the operation and hospitalization Most surgeons assumethat the laparoscopic procedure is more expensive because of the use of dispos-able items. Indeed, Schultz (68) showed the higher cost of LIHRs was secon-dary to the increased direct costs, which include supplies, equipment, and op-erating room charges. However, he concluded that this higher cost is offset bythe indirect savings in the health-care experience caused by the patient’s pre-dictable prompt return to unrestricted employment and resumption of produc-tivity. Schurz et al (69) also emphasized the use of cost-conscious techniques(i.e. avoidance of disposable equipment) as the key factor in offsetting highercost. Nevertheless, the authors conceded that despite all these measures, thecosts and charges of LIHR will never be as low as CIHR.
On the other hand, Lenker et al and others (70, 71) recently showed that
with the use of a strict cost-control protocol that eliminated all disposable
items except the hernia prosthesis and substituted epidural for general anesthe-
sia, the average cost for a herniorrhaphy could be made equal for LIHR and
CIHR. In fact, the authors showed that bilateral hernias actually could be re-
paired at a lesser cost laparoscopically than with a CIHR. It will be interesting
to see if the same results can be achieved when similar cost-control practices
are applied to both groups.
Minimize recurrence and complications There are a number of factors thatadversely affect patient outcome in inguinal herniorrhaphy, including (a) typeof hernia repair; (b) size of hernia; (c) surgical technique; (d) hemostasis; (e)avoidance of excessive tissue tension; and (f) comorbid conditions, such asrespiratory or cardiovascular diseases or obesity. These factors have beenshown to affect the incidence of recurrence and complications, both of whichcan magnify cost through such factors as prolonged hospital stay, prolongedcourse of antibiotics, reoperation, increased incidence of pain and disability,lost productivity, repeated follow-up outpatient visits, and the need for a sec-ond intervention (72).
Perioperative efforts to control these factors are extremely important. For ex-
ample, the incidence of wound infection following CIHR is estimated to be ap-
proximately 2% (100,000). Reducing this number even slightly would also lead
to significant savings because of the number of herniorrhaphies performed per
annum. A recent randomized, controlled prospective study found that the inci-
dence of wound infection with LIHR was significantly less than with CIHR
(48). Because LIHR is a very new procedure, it is reasonable to assume that
further modifications of the procedure will result in further decrease in the in-
104 MEMON & FITZGIBBONS JR.
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.

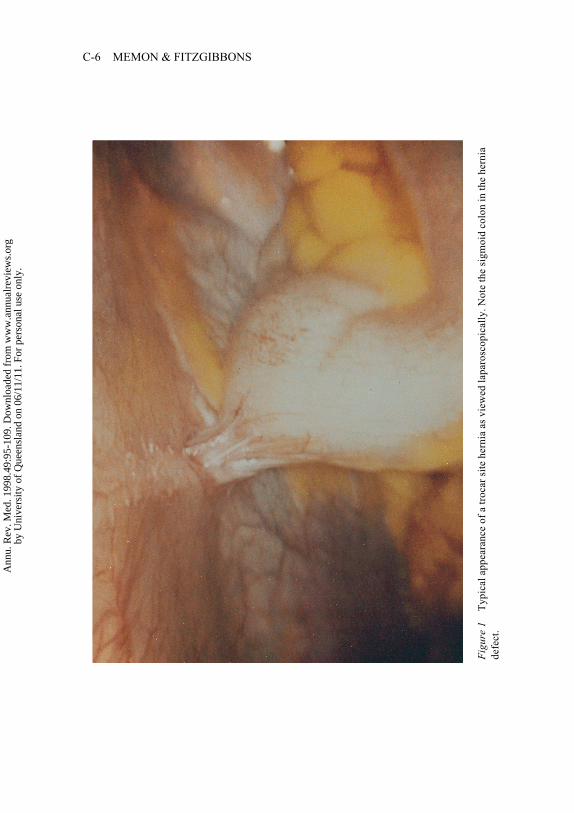
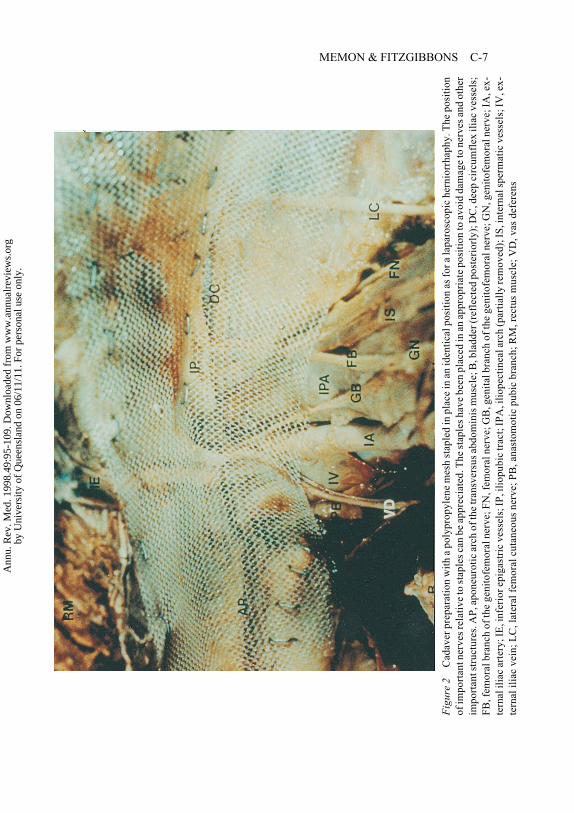
cidence of complications. Indeed, the two complications of trocar site hernia-tion (Figure 1; see color section, p. C-6) and neuralgia (Figure 2, p. C-7) wereidentified early and now have been virtually eliminated by closing all trocarsites and not stapling in inappropriate areas.
EFFECTIVENESS IN IMPROVING HEALTH CARE According to Doubilet et al(61), the term effectiveness means a strategy that is most sensitive to produc-ing desired results without consideration of its monetary value. When applyingthis term to LIHR, its effectiveness can be measured in terms of: (a) its abilityto repair bilateral hernias concurrently without additional incisions; (b) theperformance of a simultaneous diagnostic laparoscopy; (c) better patient out-come; and (d) a low recurrence rate compared to CIHR (48). The ability to re-pair recurrent hernias with a low recurrence rate has to be considered the mosteffective application of the laparoscopic repair.
COST SAVING, WITH EQUAL OR BETTER HEALTH OUTCOME A procedure thatcosts less but does not increase morbidity or mortality will have the universalblessing of both the medical and business communities. A day case CIHR un-der local anesthesia is quite cost effective. However, the patient’s recovery isslower, and some patients find local anesthesia with sedation unacceptable. Nolarge-scale prospective comparative trials combining cost and outcomes be-tween LIHR and CIHR are currently available.
COST BENEFITS WITH ADDITIONAL COST This term implies health outcomeassociated with monetary implications. A given strategy is more cost effectivethan another if it is (a) less costly and at least as effective; (b) more effectiveand more costly, its additional benefit being worth its additional cost; or (c)less effective and less costly, the added benefit of the rival strategy not beingworth its cost (61). The proponents of LIHR argue that the procedure falls un-der (b); i.e. although more costly, the superior patient outcome is worth theadded cost. Indeed all of the comparative trials except one (40) in Table 3 haveshown a statistically significant advantage for LIHR patients over both tensionand tension-free CIHR in one or more of the parameters studied (these includedecreased analgesia requirement in the immediate postoperative period,and/or earlier return to normal activity, and/or improvement in the overallquality of life as measured by validated instruments, and/or a decreased recur-rence rate).
CONCLUSIONS
LIHR is a new and evolving procedure that has the potential to significantlydecrease the pain and recurrence rate associated with this common operation,
LAPAROSCOPIC HERNIA REPAIR 105
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.
especially when compared to tension-related CIHRs. Widespread use oftension-free repairs outside of specialty centers is a recent phenomenon, and itis possible that these repairs might be as minimally invasive as LIHRs whileavoiding potential complications associated with laparoscopy. The best indi-cations now for LIHR are: (a) recurrent hernia after a CIHR, because the op-eration is performed in normal, nonscarred tissue; (b) bilateral hernias, sinceboth sides can easily be repaired using the same small laparoscopy incisions;and (c) the presence of an inguinal hernia in a patient who requires a lapa-roscopy for another procedure, such as a laparoscopic cholecystectomy (as-suming the gram stain of the bile is negative). A more contentious issue is theuse of LIHR for the uncomplicated, unilateral hernia. Large randomized, pro-spective trials will be needed to determine whether the added risks and costsare worth the benefits.
Visit the Annual Reviews home page at http://www.AnnualReviews.org.
106 MEMON & FITZGIBBONS JR.
Literature Cited
1. Shackelford RT. 1955. Hernia of the gas-trointestinal tract. In Surgery of the Ali-mentary Tract, ed. RT Shackelford, pp.2155–441. Philadelphia: Saunders. 2575pp.
2. Nyhus LM, Bombeck CT, Klein MS.1991. Hernias. In Textbook of Surgery,ed. DC Sabiston Jr., 1134–48. Philadel-phia: Saunders. 2208 pp.
3. Rutkow IM, Robbins AW. 1995. Groinhernia. In Current Surgical Therapy, ed.JL Cameron, 481–86. St. Louis: Mosby.1118 pp.
4. Berliner SD. 1984. An approach to groinhernia. Surg. Clin. North Am. 64:197–213
5. Deysine M, Grimson RC, Soroff HS.1991. Inguinal herniorrhaphy. Reducedmorbidity by service standardization.Arch. Surg. 126:628–30
6. Nyhus LM, Klein MS, Rogers FB. 1991.Inguinal hernia. Curr. Probl. Surg. 28:401–50
7. Rutkow IM, Robbins AW. 1993. Demo-graphic, classificatory, and socioeco-nomic aspects of hernia repair in theUnited States. Surg. Clin. North Am. 73:413–26
8. Gaster J. 1970. Hernia: One day repair.New York: Hafner. 179 pp.
9. Bassini E. 1887. Nuovo metodo sulla curadadicale dell’ ernia inguinale. Arch. Soc.Ital. Chir. 4:380
10. McVay CB. 1948. Inguinal and femoralhernioplasty. Anatomic repair. Arch.Surg. 57:524–30
11. Halsted WS. 1893. The radical cure of in-guinal hernia in the male. Bull. JohnsHopkins Hosp. 4:17
12. Welsh DR, Alexander MA. 1993. TheShouldice repair. Surg. Clin. North Am.73:451–69
13. Shearburn EW, Myers RN. 1969.Shouldice repair for inguinal hernia. Sur-gery 66:450–59
14. Mansberger JA, Rogers DA, JenningsWD, et al. 1992. A comparison of a newtwo-layer anatomic repair to the tradi-tional Shouldice herniorrhaphy. Am.Surg. 58:211–12
15. Read RC, McLeod PC, Jr. 1981. Influ-ence of a relaxing incision on suture ten-sion in Bassini's and McVay's repairs.Arch. Surg. 116:440–45
16. Meakins JL, Barkun JS. 1997. Old andnew ways to repair inguinal hernias. N.Engl. J Med. 336:1596–97
17. Cunningham J, Temple WJ, Mitchell P, etal. 1996. Cooperative hernia study. Painin the postrepair patient. Ann. Surg. 224:598–602
18. Lichtenstein IL, Shulman AG, Amid PK,et al. 1989. The tension-free hernioplasty[see comments]. Am. J Surg. 157:188–93
19. Robbins AW, Rutkow IM. 1993. The
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.
LAPAROSCOPIC HERNIA REPAIR 107
mesh-plug hernioplasty. Surg. Clin.North Am. 73:501–12
20. Johnson A. 1997. Laparoscopic surgery.Lancet 349:631–35
21. Filipi CJ, Fitzgibbons RJ Jr, Salerno GM,et al. 1992. Laparoscopic herniorrhaphy.Surg. Clin. North Am. 72:1109–24
22. Fitzgibbons RJ Jr., Salerno GM, Filipi CJ,et al. 1994. A laparoscopic intraperitonealonlay mesh technique for the repair of anindirect inguinal hernia [see comments].Ann. Surg. 219:144–56
23. McKernan JB, Laws HL. 1993. Laparo-scopic repair of inguinal hernias using atotally extraperitoneal prosthetic ap-proach. Surg. Endosc. 7:26–28
24. Ger R, Mishrick A, Hurwitz J, et al. 1993.Management of groin hernias by lapa-roscopy. World J Surg. 17:46–50
25. Felix EL, Michas C. 1993. Double-buttress laparoscopic herniorrhaphy. J.Laparoendosc. Surg. 3:1–8
26. Arregui ME, Navarrete J, Davis CJ, et al.1993. Laparoscopic inguinal hernior-rhaphy. Techniques and controversies.Surg. Clin. North Am. 73:513–27
27. Spaw AT, Ennis BW, Spaw LP. 1991.Laparoscopic hernia repair: the anatomicbasis. J. Laparoendosc. Surg. 1:269–77
28. Memon MA, Rice D, Donohue JH. 1997.Laparoscopic herniorrhaphy. J. Am. Coll.Surg. 184:325–35
29. Lichtenstein IL, Shulman AG, Amid PK.1991. Laparoscopic hernioplasty. Arch.Surg. 126:1449
30. Barnes FE. 1993. Cost-effective herniarepair [letter, comment]. Arch. Surg. 128:600
31. Rutkow IM. 1992. Laparoscopic herniarepair. The socioeconomic tyranny of sur-gical technology [see comments]. Arch.Surg. 127:1271
32. Corbitt JD Jr. 1991. Laparoscopic her-niorrhaphy. Surg. Laparosc. Endosc. 1:23–25
33. Schultz L, Graber J, Pietrafitta J, et al.1990. Laser laparoscopic herniorraphy: aclinical trial preliminary results. J. Lapa-roendosc. Surg. 1:41–45
34. Broin EO, Horner C, Mealy K, et al. 1995.Meralgia paraesthetica following laparo-scopic inguinal hernia repair. An ana-tomical analysis. Surg. Endosc. 9:76–78
35. Seid AS, Amos E. 1994. Entrapment neu-ropathy in laparoscopic herniorrhaphy.Surg. Endosc. 8:1050–53
36. Kraus MA. 1993. Nerve injury duringlaparoscopic inguinal hernia repair. Surg.Laparosc. Endosc. 3:342–45
37. Fitzgibbons RJ, Jr, Camps J, Cornet DA,
et al. 1995. Laparoscopic inguinal her-niorrhaphy. Results of a multicenter trial[see comments]. Ann. Surg. 221:3–13
38. Rutkow IM. 1994. Open versus laparo-scopic groin herniorrhaphy: economic re-alities. In Inguinal Hernia: Advances orControversies? ed. ME Arregui, RF Na-gan, pp. 145–50. New York: RadcliffeMedical Press, Oxford. 517 pp.
39. Shulman AG, Amid PK, Lichtenstein IL.1994. Returning to work after hernior-rhaphy [editorial] [see comments]. Br.Med. J. 309:216–17
40. Maddern GJ, Rudkin G, Bessell JR, et al.1994. A comparison of laparoscopic andopen hernia repair as a day surgical proce-dure. Surg. Endosc. 8:1404–8
41. Kozol R, Lange PM, Kosir M, et al. 1997.A prospective, randomized study of openvs laparoscopic inguinal hernia repair: anassessment of postoperative pain. Arch.Surg. 132:292–95
42. Vogt DM, Curet MJ, Pitcher DE, et al.1995. Preliminary results of a prospec-tive, randomized trial of laparoscopic on-lay versus conventional inguinal hernior-rhaphy. Am. J. Surg. 169:84–89
43. Lawrence K, McWhinnie D, Goodwin A,et al. 1995. Randomised controlled trial oflaparoscopic versus open repair of ingui-nal hernia: early results. Brit. Med. J. 311:981–85
44. Barkun JS, Wexler MJ, Hinchey EJ, et al.1995. Laparoscopic versus open inguinalherniorrhaphy: preliminary results of arandomized controlled trial. Surgery 118:703–9
45. Payne JH Jr, Grininger LM, Izawa MT, etal. 1994. Laparoscopic or open inguinalherniorrhaphy? A randomized prospec-tive trial [see comments]. Arch. Surg.129:973–79
46. Stoker DL, Spiegelhalter DJ, Singh R, etal. 1994. Laparoscopic versus open ingui-nal hernia repair: randomised prospectivetrial [see comments]. Lancet 343:1243–-45
47. Wright DM, Kennedy A, Baxter JN, et al.1996. Early outcome after open versusextraperitoneal endoscopic tension-freehernioplasty: A randomized clinical trial.Surgery 119:552–57
48. Liem MSL, van der Graaf Y, van SteenselCJ, et al. 1997. Comparison of conven-tional anterior surgery and laparoscopicsurgery for inguinal hernia repair. N.Engl. J. Med. 336:1541–47
49. Millikan KW, Kosik ML, Doolas A.1994. A prospective comparison oftransabdominal preperitoneal laparo-
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.
108 MEMON & FITZGIBBONS JR.
scopic hernia repair versus traditionalopen hernia repair in a university setting.Surg. Laparosc. Endosc. 4:247–53
50. Cornell RB, Kerlakian GM. 1994. Earlycomplications and outcomes of the cur-rent technique of transperitoneal laparo-scopic herniorrhaphy and a comparison tothe traditional open approach. Am. J.Surg. 168:275–79
51. Brooks DC. 1994. A prospective com-parison of laparoscopic and tension-freeopen herniorrhaphy. Arch. Surg.129:361–66
52. Wilson MS, Deans GT, Brough WA.1995. Prospective trial comparingLichtenstein with laparoscopic tension-free mesh repair of inguinal hernia. Br. J.Surg. 82:274–77
53. Wheeler KH. 1993. Laparoscopic ingui-nal herniorrhaphy with mesh: an 18-month experience. J. Laparoendosc.Surg. 3:345–50
54. Phillips EH, Arregui M, Carroll BJ, et al.1995. Incidence of complications follow-ing laparoscopic hernioplasty. Surg. En-dosc. 9:16–21
55. Tsang S, Normand R, Karlin R. 1994.Small bowel obstruction: a morbid com-plication after laparoscopic hernior-rhaphy. Am. Surg. 60:332–34
56. Hendrickse CW, Evans DS. 1993. Intesti-nal obstruction following laparoscopic in-guinal hernia repair [see comments]. Br.J. Surg. 80:1432
57. Wegener ME, Chung D, Crans C. 1993.Small bowel obstruction secondary to in-carcerated Richter's hernia from laparo-scopic hernia repair. J. Laparoendosc.Surg. 3:173–76
58. Tetik C, Arregui ME. 1995. Prevention ofcomplications of open and laparoscopicrepair of groin hernias. In Principles ofLaparoscopic Surgery: Basic and Ad-vanced Techniques, ed. ME Arregui, RJFitzgibbons Jr, N Katkhouda, JB McKer-nan, H Rich, pp. 439–49. New York:Springer-Verlag. 852 pp.
59. Gray MR, Curtis JM, Elkington JS. 1994.Colovesical fistula after laparoscopic in-guinal hernia repair. Br. J. Surg. 81:1213–14
60. Haupt BJ. 1982. National Center forHealth Statistics, Utilization of Short-stayHospitals: Annual summary for theUnited States, 1980. Vital and Health Sta-tistics. Series 13, No.64:1–60
61. Doubilet P, Weinstein MC, McNeil BJ.1986. Use and misuse of the term “cost-effective” in medicine. N. Engl. J. Med.314:253–56
62. Stahlgren LH. 1997. Inguinal Hernia.Cost-Effective Surgical Management, ed.B Eiseman, L Stahlgren, pp. 217–19.Philadelphia: Saunders. 314 pp.
63. Williams JS, Hale HW. 1966. The advis-ability of inguinal herniorrhaphy in theelderly. Surg. Gynecol. Obstet. 122:100–4
64. Neuhauser D. 1977. Elective inguinalherniorrhaphy versus truss in the elderly.Costs, Risks, and Benefits of Surgery, ed.JP Bunker, BA Barnes, F Mosteller, pp.233–39. New York: Oxford Univ. 401 pp.
65. Law NW, Trapnell JE. 1992. Does a trussbenefit a patient with inguinal hernia? Br.Med. J. 304:1092
66. Rockwell E. 1982. Outpatient repair of in-guinal hernia. Am. J. Surg. 143:559–60
67. Russell IT, Devlin HB, Fell M, et al.1977. Day-case surgery for hernias andhaemorrhoids. A clinical, social, and eco-nomic evaluation. Lancet 1:844–47
68. Schultz LS. 1995. Laparoscopic vs ingui-nal hernia repairs. Outcomes and costs.Surg. Endosc. 9:1307–11
69. Schurz JW, Arregui ME, Hammond JC.1995. Open vs laparoscopic hernia repair.Analysis of costs, charges, and outcomes.Surg. Endosc. 9:1311–17
70. Lenker M, Hansen P, Kenyon T, et al.1997. Laparoscopic and open inguinalhernia repair costs can be made the same.Sages 1997 Final Program and AbstractsHandbook, 1:46 (Abstr.)
71. Heikkinen T, Haukipuro K, Leppala J, etal. 1997. Total costs of laparoscopic andLichtenstein inguinal hernia repairs: arandomized prospective study. Surg.Laparosc. Endosc. 7:1–5
72. Glassow F. 1964. Is postoperative woundinfection following simple inguinal her-niorrhaphy a predisposing cause of recur-rent hernia? Can. Med. Assoc. J. 91:870–-71
73. Corbitt JD Jr. 1993. Laparoscopic her-niorrhaphy. A preperitoneal tension-freeapproach. Surg. Endosc. 7:550–55
74. Felix EL, Michas CA, McKnight RL.1994. Laparoscopic herniorrhaphy.Transabdominal preperitoneal floor re-pair. Surg. Endosc. 8:100–3
75. Felix EL, Michas CA, Gonzalez MH, Jr.1995. Laparoscopic hernioplasty. TAPPvs TEP. Surg. Endosc. 9:984–89
76. Geis WP, Crafton WB, Novak MJ, et al.1993. Laparoscopic herniorrhaphy: re-sults and technical aspects in 450 con-secutive procedures. Surgery 114:765–72
77. Hawasli A. 1992. Laparoscopic inguinalherniorrhaphy: classification and 1 year
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.

LAPAROSCOPIC HERNIA REPAIR 109
experience. J. Laparoendosc. Surg. 2:137–43
78. Himpens JM. 1993. Laparoscopic ingui-nal hernioplasty. Repair with a conven-tional vs a new self-expandable mesh [seecomments]. Surg. Endosc. 7:315–18
79. Kald A, Smedh K, Anderberg B. 1995.Laparoscopic groin hernia repair: resultsof 200 consecutive herniorraphies. Br. J.Surg. 82:618–20
80. Kavic MS. 1995. Laparoscopic hernia re-pair. Three-year experience. Surg. En-dosc. 9:12–15
81. Newman L, 3d, Eubanks S, Mason E, etal. 1993. Is laparoscopic herniorrhaphy aneffective alternative to open hernia re-pair? J. Laparoendosc. Surg. 3:121–28
82. Paget GW. 1994. Laparoscopic inguinalherniorrhaphy. A personal audit of 222hernia repairs [see comments]. Med. J.Aust. 161:249–53
83. Panton ON, Panton RJ. 1994. Laparo-scopic hernia repair [see comments]. Am.J. Surg. 167:535–37
84. Quilici PJ, Greaney EM Jr, Quilici J, et al.1993. Laparoscopic inguinal hernia repairresults: 131 cases. Am. Surg. 59:824–30
85. Ramshaw BJ, Tucker JG, Mason EM, etal. 1995. A comparison of transabdominalpreperitoneal TAPP and total extraperito-neal approach TEPA laparoscopic her-niorrhaphies. Am. Surg. 61:279–83
86. Begin GF. 1993. Laparoscopic extraperi-toneal treatment of inguinal hernias in
adults. A series of 200 cases. Endosc.Surg. Allied. Technol. 1:204–6
87. Ferzli G, Kiel T. 1995. Evolving tech-niques in endoscopic extraperitoneal her-niorrhaphy. Surg. Endosc. 9:928–30
88. Voeller GR, Mangiante EC Jr, WilliamsC. 1995. Totally preperitoneal laparo-scopic inguinal herniorrhaphy using bal-loon dissection. Surg. Rounds 18:107–12
89. Rubio PA. 1994. Laparoscopic intraperi-toneal hernioplasty. Int. Surg. 79:293–95
90. Amid PK, Shulman AG, Lichtenstein IL.1995. The Lichtenstein open “tension-free” mesh repair of inguinal hernias.Surg. Today 25:619–25
91. Hay JM, Boudet MJ, Fingerhut A, et al.1995. Shouldice inguinal hernia repair inthe male adult: the gold standard? A mul-ticenter controlled trial in 1578 patients.Ann. Surg. 222:719–27
92. Lichtenstein IL. 1987. Herniorrhaphy. Apersonal experience with 6,321 cases.Am. J. Surg. 153:553–59
93. Read RC. 1975. Recurrence after preperi-toneal herniorrhaphy in the adult. Arch.Surg. 110:666–71
94. Rignault DP. 1986. Preperitoneal pros-thetic inguinal hernioplasty through aPfannenstiel approach. Surg. Gynecol.Obstet. 163:465–68
95. Rutledge RH. 1988. Cooper's ligament re-pair: a 25-year experience with a singletechnique for all groin hernias in adults.Surgery 103:1–10
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.
Ann
u. R
ev. M
ed. 1
998.
49:9
5-10
9. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Que
ensl
and
on 0
6/11
/11.
For
per
sona
l use
onl
y.