
recurrent miscarriages and associated obstetric complications
Upload
independentCategory
view
3download
0
O
LtWJ
Onlc
S2i
RpS
C2
Ccspsmcc
FMGWDSaOHUC
R2
R
0©d
Research www.AJOG.org
3
BSTETRICS
aparoscopic cervico-isthmic cerclage: surgicalechnique and obstetric outcomesendy L. Whittle, MD, PhD; Sukhbir S. Singh, MD; Lisa Allen, MD; Louise Glaude, RN;
acqueline Thomas, MD; Rory Windrim, MD; Nicholas Leyland, MD
fctam
Cpo
K
BJECTIVE: The purpose of the study is to review the surgical tech-ique, complication rate and obstetric outcome associated with the
aparoscopic approach to the placement of the cervico-isthmicerclage.
TUDY DESIGN: A prospective cohort study was conducted from003-2008 and compared with previously reported cases of cervico-
sthmic cerclage by laparotomy and laparoscopy.
ESULTS: Thirty-one patients underwent cerclage placement duringregnancy and 34 patients were not pregnant at the time of the surgery.
009;201:364.e1-7.
ctuTanIatiasltntalwfpvcmpemmarotomy approach, it h
see Table of Contents
64.e1 American Journal of Obstetrics & Gynecology OCTOBER 2009
rom uterine vessel bleeding or impaired surgical visibility; 2 pregnan-ies were lost perioperatively. No other complications occurred. The fe-al salvage rate (n � 67 pregnancies) was 89% with a mean gestationalge of 35.8 � 2.9 weeks. Six pregnancies were lost in the second tri-ester due to the consequences of acute or subacute chorioamnionitis.
ONCLUSION: Our findings suggest that the cervico-isthmic cerclagelaced laparoscopically compares favorably with the traditional laparot-my approach.
ey words: abdominal cerclage, cervico-isthmic cerclage,
even cases were converted to laparotomy due to complications arising laparoscopy, laparotomyite this article as: Whittle WL, Singh SS, Allen L, et al. Laparoscopic cervicoisthmic cerclage: surgical technique and obstetric outcomes. Am J Obstet Gynecol
tbjtoltitpl
MAst(e0pobpctncnci
ervical incompetence occurs in0.5-1% of all pregnancies, has a re-
urrence risk of �30% and typically pre-ents in the second trimester as pelvicressure and cervical dilation in the ab-ence of uterine activity or ruptured
embranes.1 The etiology of cervical in-ompetence can be classified as (1) a me-hanical failure of the cervix to remain
rom the Division of Maternal-Fetaledicine, Department of Obstetrics andynaecology, Mount Sinai Hospital (Drshittle and Windrim and Ms Glaude); theepartment of Obstetrics and Gynaecology,
t. Joseph’s Health Care Centre (Drs Singhnd Leyland); and the Department ofbstetrics and Gynaecology, Mount Sinaiospital (Drs Allen and Thomas),niversity of Toronto, Toronto, ON,anada.
eceived Nov. 10, 2008; revised Feb. 25,009; accepted July 14, 2009.
eprints not available from the authors.
002-9378/free2009 Published by Mosby, Inc.
oi: 10.1016/j.ajog.2009.07.018
For Editors’ Commentary,
losed against the increasing uterine dis-ention pressure, or (2) a functional fail-re due to premature cervical ripening.1
he cervical cerclage through a vaginalpproach was introduced as a mecha-ism to reinforce the cervical integrity.n 1965, Benson and Durfee2 introducedn alternative to the vaginal approach—he placement of a cerclage at the cervicalsthmus: a noose-like suture positionedround the isthmus in the avascularpace above the cardinal and uterosacraligaments placed by laparotomy.3 Thisechnique was intended when the vagi-al approach was not feasible due to al-
ered cervical anatomy (ie, congenitalnomaly, scarring due to cone biopsy, oraceration at delivery); the indicationas extended by Novy4 to include a
ailed transvaginal cerclage in a previousregnancy. Cervico-isthmic cerclage re-iews quote a successful pregnancy out-ome rate from 76.5-100%; however, theorbidity associated with the surgical
rocedure is significant.5 In an era whenndoscopic surgery provides a mini-ally invasive alternative with docu-ented benefit over the traditional lap-
as been proposed t
hat the cervico-isthmic cerclage coulde completed laparoscopically.6 The ob-
ective of the present study is to reviewhe surgical technique, morbidity, andbstetric outcome associated with the
aparoscopic approach to placement ofhe cervico-isthmic cerclage. Our find-ngs will be compared with reports ofhe traditional cervico-isthmic cerclagelaced by laparotomy and more recently
aparoscopy.7-30
ATERIALS AND METHODSprospective observational cohort
tudy was conducted from January 2003o June 2008 at Mount Sinai HospitalToronto, Canada) with institutionalthics board approval (MSH REB no. 06-149-E). The indication for cerclagelacement was a presumptive diagnosisf mechanical cervical incompetenceased on the Novy criteria.4 Pregnantatients underwent pelvic ultrasound toonfirm viability, and were offered firstrimester aneuploidy screening or diag-ostic chorionic villi sampling prior toerclage placement. After surgery, preg-ant patients underwent routine cervi-al/vaginal swabs and urine culture. Allnfections were treated with routine an-
ibiotic therapy; if the test of cure indi-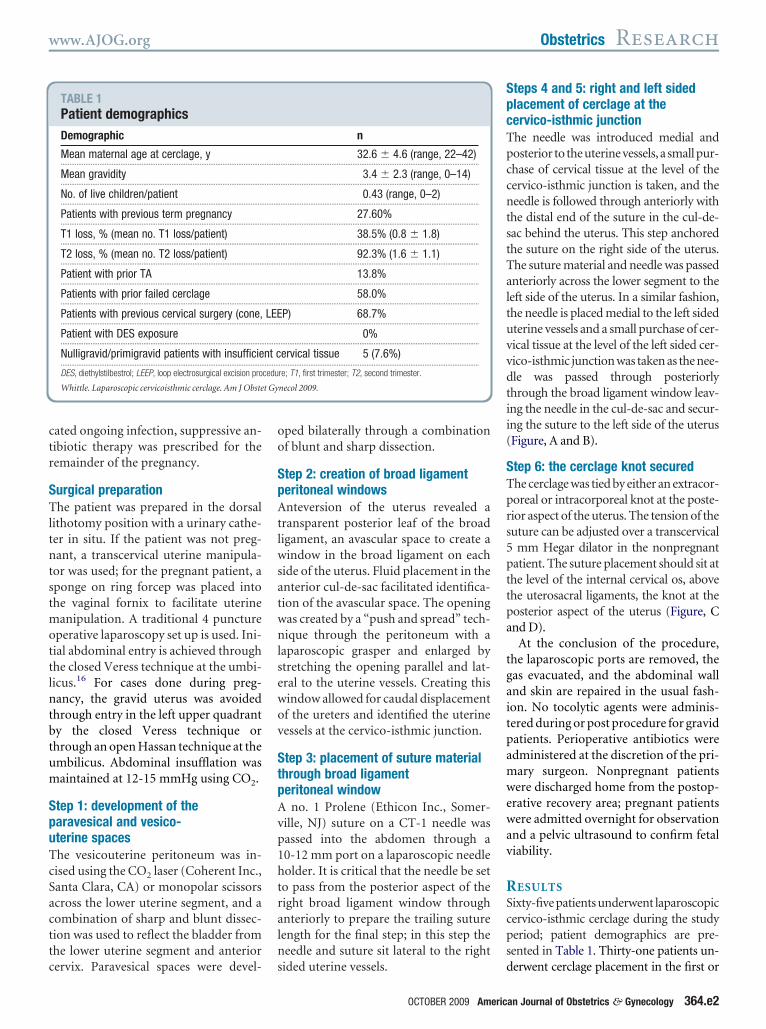
ctr
STltntstmottlntbtum
SpuTcSacttc
oo
SpAtlwsatwnlsewov
StpAvp1htraln
SpcTpccntstTaltuvvdtii(
STprs5pttpa
tgaitpamwewav
RScps
t Gy
www.AJOG.org Obstetrics Research
ated ongoing infection, suppressive an-ibiotic therapy was prescribed for theemainder of the pregnancy.
urgical preparationhe patient was prepared in the dorsal
ithotomy position with a urinary cathe-er in situ. If the patient was not preg-ant, a transcervical uterine manipula-
or was used; for the pregnant patient, aponge on ring forcep was placed intohe vaginal fornix to facilitate uterine
anipulation. A traditional 4 punctureperative laparoscopy set up is used. Ini-ial abdominal entry is achieved throughhe closed Veress technique at the umbi-icus.16 For cases done during preg-ancy, the gravid uterus was avoided
hrough entry in the left upper quadranty the closed Veress technique orhrough an open Hassan technique at thembilicus. Abdominal insufflation wasaintained at 12-15 mmHg using CO2.
tep 1: development of thearavesical and vesico-terine spaceshe vesicouterine peritoneum was in-ised using the CO2 laser (Coherent Inc.,anta Clara, CA) or monopolar scissorscross the lower uterine segment, and aombination of sharp and blunt dissec-ion was used to reflect the bladder fromhe lower uterine segment and anterior
TABLE 1Patient demographicsDemographic
Mean maternal age at cerclage, y...................................................................................................................
Mean gravidity...................................................................................................................
No. of live children/patient...................................................................................................................
Patients with previous term pregnancy...................................................................................................................
T1 loss, % (mean no. T1 loss/patient)...................................................................................................................
T2 loss, % (mean no. T2 loss/patient)...................................................................................................................
Patient with prior TA...................................................................................................................
Patients with prior failed cerclage...................................................................................................................
Patients with previous cervical surgery (cone,...................................................................................................................
Patient with DES exposure...................................................................................................................
Nulligravid/primigravid patients with insufficie...................................................................................................................
DES, diethylstilbestrol; LEEP, loop electrosurgical excision pro
Whittle. Laparoscopic cervicoisthmic cerclage. Am J Obste
ervix. Paravesical spaces were devel- s
ped bilaterally through a combinationf blunt and sharp dissection.
tep 2: creation of broad ligamenteritoneal windowsnteversion of the uterus revealed a
ransparent posterior leaf of the broadigament, an avascular space to create aindow in the broad ligament on each
ide of the uterus. Fluid placement in thenterior cul-de-sac facilitated identifica-ion of the avascular space. The openingas created by a “push and spread” tech-ique through the peritoneum with a
aparoscopic grasper and enlarged bytretching the opening parallel and lat-ral to the uterine vessels. Creating thisindow allowed for caudal displacementf the ureters and identified the uterineessels at the cervico-isthmic junction.
tep 3: placement of suture materialhrough broad ligamenteritoneal window
no. 1 Prolene (Ethicon Inc., Somer-ille, NJ) suture on a CT-1 needle wasassed into the abdomen through a0-12 mm port on a laparoscopic needleolder. It is critical that the needle be seto pass from the posterior aspect of theight broad ligament window throughnteriorly to prepare the trailing sutureength for the final step; in this step theeedle and suture sit lateral to the right
n
32.6 � 4.6 (range, 22–42)..................................................................................................................
3.4 � 2.3 (range, 0–14)..................................................................................................................
0.43 (range, 0–2)..................................................................................................................
27.60%..................................................................................................................
38.5% (0.8 � 1.8)..................................................................................................................
92.3% (1.6 � 1.1)..................................................................................................................
13.8%..................................................................................................................
58.0%..................................................................................................................
P) 68.7%..................................................................................................................
0%..................................................................................................................
ervical tissue 5 (7.6%)..................................................................................................................
re; T1, first trimester; T2, second trimester.
necol 2009.
ided uterine vessels. d
OCTOBER 2009 Americ
teps 4 and 5: right and left sidedlacement of cerclage at theervico-isthmic junctionhe needle was introduced medial andosterior to theuterinevessels, a smallpur-hase of cervical tissue at the level of theervico-isthmic junction is taken, and theeedle is followed through anteriorly with
he distal end of the suture in the cul-de-ac behind the uterus. This step anchoredhe suture on the right side of the uterus.he suture material and needle was passednteriorly across the lower segment to theeft side of the uterus. In a similar fashion,he needle is placed medial to the left sidedterine vessels and a small purchase of cer-ical tissue at the level of the left sided cer-ico-isthmic junction was taken as the nee-le was passed through posteriorlyhrough the broad ligament window leav-ng the needle in the cul-de-sac and secur-ng the suture to the left side of the uterusFigure, A and B).
tep 6: the cerclage knot securedhe cerclage was tied by either an extracor-oreal or intracorporeal knot at the poste-ior aspect of the uterus. The tension of theuture can be adjusted over a transcervical
mm Hegar dilator in the nonpregnantatient. The suture placement should sit athe level of the internal cervical os, abovehe uterosacral ligaments, the knot at theosterior aspect of the uterus (Figure, Cnd D).
At the conclusion of the procedure,he laparoscopic ports are removed, theas evacuated, and the abdominal wallnd skin are repaired in the usual fash-on. No tocolytic agents were adminis-ered during or post procedure for gravidatients. Perioperative antibiotics weredministered at the discretion of the pri-ary surgeon. Nonpregnant patientsere discharged home from the postop-
rative recovery area; pregnant patientsere admitted overnight for observation
nd a pelvic ultrasound to confirm fetaliability.
ESULTSixty-five patients underwent laparoscopicervico-isthmic cerclage during the studyeriod; patient demographics are pre-ented in Table 1. Thirty-one patients un-
.........
.........
.........
.........
.........
.........
.........
.........
LEE.........
.........
nt c.........
cedu
erwent cerclage placement in the first or
an Journal of Obstetrics & Gynecology 364.e2
satvc(2
tecdggc
cwsecmlmttthi
incptiinwtacpdcd1eg2tTccwtpfrc1c
t3(phwid
et G
Research Obstetrics www.AJOG.org
3
econd trimester (�16 weeks’ gestation)nd 34 patients were not pregnant at theime of the surgery. Seven cases were con-erted to laparotomy due to either compli-ations arising from uterine vessel bleedingn � 5) or impaired surgical visibility (n �) due to morbid obesity; 6 of these pa-
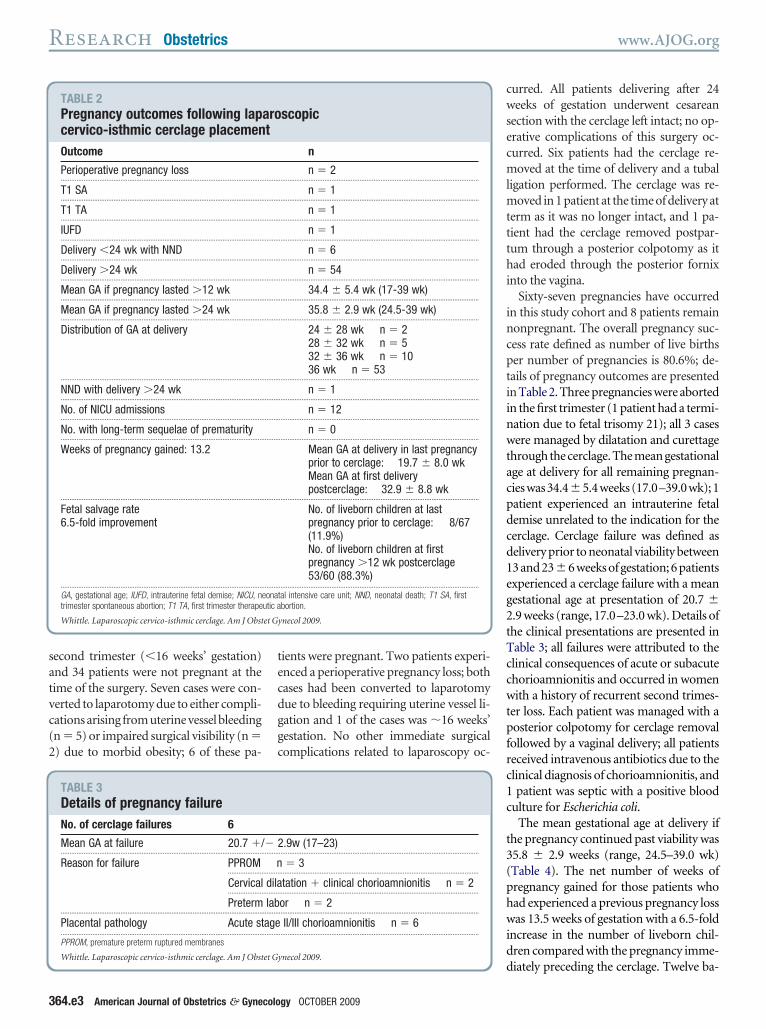
TABLE 2Pregnancy outcomes following lapcervico-isthmic cerclage placemenOutcome
Perioperative pregnancy loss...................................................................................................................
T1 SA...................................................................................................................
T1 TA...................................................................................................................
IUFD...................................................................................................................
Delivery �24 wk with NND...................................................................................................................
Delivery �24 wk...................................................................................................................
Mean GA if pregnancy lasted �12 wk...................................................................................................................
Mean GA if pregnancy lasted �24 wk...................................................................................................................
Distribution of GA at delivery
...................................................................................................................
NND with delivery �24 wk...................................................................................................................
No. of NICU admissions...................................................................................................................
No. with long-term sequelae of prematurity...................................................................................................................
Weeks of pregnancy gained: 13.2
...................................................................................................................
Fetal salvage rate6.5-fold improvement
...................................................................................................................
GA, gestational age; IUFD, intrauterine fetal demise; NICU, ntrimester spontaneous abortion; T1 TA, first trimester therape
Whittle. Laparoscopic cervico-isthmic cerclage. Am J Obst
TABLE 3Details of pregnancy failureNo. of cerclage failures 6
Mean GA at failure 20.7 �/...................................................................................................................
Reason for failure PPROM....................
Cervical....................
Preterm...................................................................................................................
Placental pathology Acute st...................................................................................................................
PPROM, premature preterm ruptured membranes
Whittle. Laparoscopic cervico-isthmic cerclage. Am J Obstet G
64.e3 American Journal of Obstetrics & Gynecolo
ients were pregnant. Two patients experi-nced a perioperative pregnancy loss; bothases had been converted to laparotomyue to bleeding requiring uterine vessel li-ation and 1 of the cases was �16 weeks’estation. No other immediate surgicalomplications related to laparoscopy oc-
scopic
n
n � 2..................................................................................................................
n � 1..................................................................................................................
n � 1..................................................................................................................
n � 1..................................................................................................................
n � 6..................................................................................................................
n � 54..................................................................................................................
34.4 � 5.4 wk (17-39 wk)..................................................................................................................
35.8 � 2.9 wk (24.5-39 wk)..................................................................................................................
24 � 28 wk n � 228 � 32 wk n � 532 � 36 wk n � 1036 wk n � 53
..................................................................................................................
n � 1..................................................................................................................
n � 12..................................................................................................................
n � 0..................................................................................................................
Mean GA at delivery in last pregnancyprior to cerclage: 19.7 � 8.0 wkMean GA at first deliverypostcerclage: 32.9 � 8.8 wk
..................................................................................................................
No. of liveborn children at lastpregnancy prior to cerclage: 8/67(11.9%)No. of liveborn children at firstpregnancy �12 wk postcerclage53/60 (88.3%)
..................................................................................................................
tal intensive care unit; NND, neonatal death; T1 SA, firstbortion.
ynecol 2009.
.9w (17–23)..................................................................................................................
� 3.................................................................................................................
tation � clinical chorioamnionitis n � 2.................................................................................................................
or n � 2..................................................................................................................
II/III chorioamnionitis n � 6..................................................................................................................
dynecol 2009.
gy OCTOBER 2009
urred. All patients delivering after 24eeks of gestation underwent cesarean
ection with the cerclage left intact; no op-rative complications of this surgery oc-urred. Six patients had the cerclage re-oved at the time of delivery and a tubal
igation performed. The cerclage was re-oved in 1 patient at the time of delivery at
erm as it was no longer intact, and 1 pa-ient had the cerclage removed postpar-um through a posterior colpotomy as itad eroded through the posterior fornix
nto the vagina.Sixty-seven pregnancies have occurred
n this study cohort and 8 patients remainonpregnant. The overall pregnancy suc-ess rate defined as number of live birthser number of pregnancies is 80.6%; de-ails of pregnancy outcomes are presentedn Table 2. Three pregnancies were abortedn the first trimester (1 patient had a termi-ation due to fetal trisomy 21); all 3 casesere managed by dilatation and curettage
hrough the cerclage. The mean gestationalge at delivery for all remaining pregnan-ieswas34.4�5.4weeks(17.0–39.0wk);1atient experienced an intrauterine fetalemise unrelated to the indication for theerclage. Cerclage failure was defined aselivery prior to neonatal viability between3 and 23�6 weeks of gestation; 6 patientsxperienced a cerclage failure with a meanestational age at presentation of 20.7 �.9 weeks (range, 17.0–23.0 wk). Details ofhe clinical presentations are presented inable 3; all failures were attributed to thelinical consequences of acute or subacutehorioamnionitis and occurred in womenith a history of recurrent second trimes-
er loss. Each patient was managed with aosterior colpotomy for cerclage removal
ollowed by a vaginal delivery; all patientseceived intravenous antibiotics due to thelinical diagnosis of chorioamnionitis, andpatient was septic with a positive blood
ulture for Escherichia coli.The mean gestational age at delivery if
he pregnancy continued past viability was5.8 � 2.9 weeks (range, 24.5–39.0 wk)Table 4). The net number of weeks ofregnancy gained for those patients whoad experienced a previous pregnancy lossas 13.5 weeks of gestation with a 6.5-fold
ncrease in the number of liveborn chil-ren compared with the pregnancy imme-
arot
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
eonautic a
� 2.........
n.........
dila.........
lab.........
age.........
iately preceding the cerclage. Twelve ba-

bittpts3tmdgo
mamdctbpt
oclef
CCnl
wtnbtidishpaoucpeshssnmcwpht
STav
pvo5psfpoctlpcaciimabvibgaopdlosccmpitttwesrptreawsafs
et G
www.AJOG.org Obstetrics Research
ies were admitted to the neonatalntensive care unit, 1 baby died due to ex-reme prematurity, and no other long-erm sequelae of prematurity were re-orted. Nine patients have had a seconderm (�37 weeks) pregnancy with theame cerclage in situ, and 1 patient has had
term pregnancies. Two patients had awin gestation at the time of cerclage place-
ent in the first trimester; both patientselivered healthy children after 34 weeks ofestation with no long-term complicationsf preterm birth.Overall, the timing of cerclage place-ent did not influence the gestational age
t delivery but cerclage failure did occurore often when the cerclage was placed
uring that pregnancy (Table 4). The indi-ation for cerclage did not affect the gesta-ional age at delivery, but in the small num-er of patients for whom the cerclage waslaced due to insufficient cervical tissuehere was no cerclage failure (Table 4).
Table 5 presents the outcome of previ-usly published retrospective cohorts ofervico-isthmic cerclage placed by bothaparotomy and laparoscopy with an op-rative complication rates of 0-25% andetal survival rates between 60-100%.
OMMENTervical incompetence, defined as preg-ancy loss following painless cervical di-
TABLE 4Effect of timing and indication for cIndication for cervico-isthmic cerclage
..........................................................................................................
Previous T2 loss �/� cone biopsy..........................................................................................................
Previous failed vaginal cerclage �/� con..........................................................................................................
Nulliparous with prior cone biopsy
...................................................................................................................
Timing of cerclage: mean GA at delivery forpregnancies �12 w
..........................................................................................................
Cerclage placed in pregnancy..........................................................................................................
Cerclage placed nonpregnant...................................................................................................................
Pregnancy failures (perioperative loss, IUFD, d�24 w, NND)
..........................................................................................................
Cerclage placed in pregnancy..........................................................................................................
Cerclage placed nonpregnant...................................................................................................................
IUFD, intrauterine fetal demise; NND, neonatal death.
Whittle. Laparoscopic cervico-isthmic cerclage. Am J Obst
atation, has been traditionally treated s
ith a cerclage placed in the vaginal por-ion of the cervix in the subsequent preg-ancy.1 This therapeutic intervention isased on the assumption that the struc-ural integrity of the cervical tissue hasnsufficient strength to act as a barrier toelivery against the increasing intrauter-
ne pressure of the growing gestationalac.1 When this vaginal cerclage fails toold the cervix closed or cannot belaced due to insufficient cervical tissue,n alternative approach is the placementf a cerclage at the cervico-isthmus of theterus. Conventionally, this type of cer-lage is placed in the first trimester ofregnancy through a laparotomy; how-ver, with the advent of minimally inva-ive surgery, placement by laparoscopyas been described in case reports anderies (Table 5).7-30 The purpose of thistudy was to describe the surgical tech-ique for the laparoscopic cervico-isth-ic cerclage, its associated obstetric out-
omes, and compare these outcomesith the traditional laparotomy ap-roach using previously reported co-orts that describe both rates of opera-ive complications and fetal survival.
urgical considerationshe advantages of a minimally invasivepproach are well established; we pro-ide evidence that this approach confers
clage on pregnancy outcome
..................................................................................................................
31.2 �/� 7.8 w (17–38 w)..................................................................................................................
opsy 34.1 �/� 5.3 w (20–38 w)..................................................................................................................
1 delivery at 34 w.......................................................................
3 delivery at �37 w..................................................................................................................
..................................................................................................................
32.9 �/� 8.8 w..................................................................................................................
34.5 �/� 4.9 w..................................................................................................................
ery
..................................................................................................................
n � 7..................................................................................................................
n � 2..................................................................................................................
ynecol 2009.
imilar if not a slightly improved rate of e
OCTOBER 2009 Americ
erioperative complications as the cer-ico-isthmic cerclage placed by laparot-my (10% vs 0-25%, respectively; Table). The main complication of either ap-roach was excessive blood loss—in oureries no patient required a blood trans-usion. The second most common com-lication was the conversion to laparot-my due to surgical visibility—such aomplication should be considered inhe context that 58 women were spared aaparotomy by having the cerclagelaced laparoscopically. Since the cer-lage is placed similar to a “noose” in therea of the cervical isthmus, a potentialomplication is compression of the uter-ne vessels leading to compromised uter-ne blood flow and subsequent fetal de-
ise; our perioperative losses could bettributed to uterine vessel compressionut may also be in part due to specificessel ligation to arrest excessive bleed-ng. The reported perioperative loss ratey us and others did not occur with anyreater incidence using the laparoscopicpproach and likely is a risk of this typef cerclage regardless of the surgical ap-roach. As the uterine size increases itoes become a technically more chal-
enging procedure; although we reportednly 2 cases of cerclage placement in theecond trimester, 1 was complicated byonversion and fetal loss. In addition, theonversion to laparotomy did occurore frequently when the patient was
regnant. Placement of this cerclage us-ng a vaginal approach with tissue dissec-ion similar to that of a vaginal hysterec-omy has recently been described; thisechnique may be advantageous foromen who present in the late first or
arly second trimester.31 A #1 Proleneuture was chosen in this study with theationale based on ease of handling forlacement and removal compared withhe traditional 5 mm Mersilene tape; thisationale is similarly supported by Rustt al32 in the choice of suture material forvaginal cerclage. The successful resultse present support the use of this type of
uture material in regard to its integritynd strength. Concerning the techniqueor knot tying, since the Roeder knottrength has been determined to be
er
.........
.........
e bi.........
.........
.........
.........
.........
eliv
.........
.........
.........
quivalent to the intracorporeal knot,
an Journal of Obstetrics & Gynecology 364.e4

tmwcfcelp
OI8lp
acpcbccsiab(
tdtneomdainsP
et G
Research Obstetrics www.AJOG.org
3
he posterior location of our knot place-ent favors the Roeder knot especiallyith the bulky pregnant uterus.33 We
onclude that the laparoscopic approachor the placement of the cervico-isthmicerclage confers a similar rate of periop-rative complications as the traditionalaparotomy and is best completed non-regnant or early in the first trimester.
bstetric considerationsn our series, the fetal survival rate was0.6%; however, taking into account that 3osses were in the first trimester and that 1
TABLE 5Cumulative results of cervico-isthmcerclage placed by laparoscopy inCerclage placed by laparotomy:study and year
Benson and Durfee 1965...................................................................................................................
Watkins 1972...................................................................................................................
Mahran 1978...................................................................................................................
Olsen and Tobiassen 1982...................................................................................................................
Novy 1982...................................................................................................................
Wallenberg and Lotgering 1987...................................................................................................................
Herron and Parer 1988...................................................................................................................
Van Dongen et al 1991...................................................................................................................
Novy 1991...................................................................................................................
Cammarano et al 1995...................................................................................................................
Anthony et al 1997...................................................................................................................
Craig and Fliegner 1997...................................................................................................................
Turnquest et al 1999...................................................................................................................
Davis et al 2000...................................................................................................................
Lotgering et al 2006...................................................................................................................
Debbs et al 2007...................................................................................................................
Scibetta et al 1998...................................................................................................................
Lesser et al 1998...................................................................................................................
Mingione et al 2003...................................................................................................................
Cho et al 2003...................................................................................................................
Gallot et al 2003...................................................................................................................
Ghomi et al 2006...................................................................................................................
Aboujaoude et al 2007...................................................................................................................
Agdi et al 2008...................................................................................................................
Reid et al 2008...................................................................................................................
Current study...................................................................................................................a Intraoperative complications include: cystotomy, bleeding �
Whittle. Laparoscopic cervico-isthmic cerclage. Am J Obst
atient suffered an intrauterine demise not o
64.e5 American Journal of Obstetrics & Gynecolo
ttributable to the cerclage, the true cer-lage success rate should be defined by theregnancies lost at the time of surgery (2ases) and the number of live, take homeabies (58 cases) after the first trimester isompleted. By this definition, the rate oferclage success was 89%, making the ob-tetric outcome after laparoscopic cervico-sthmic cerclage comparable to that of thebdominal approach and to that reportedy others using a laparoscopic approachTable 5).
Based on the failures that occurred in
cerclage placed during pregnancy bth pregnant and nonpregnant patientient Pregnancy
no.Intraoperrate, %
13 Not repor.........................................................................................................................
2 Not repor.........................................................................................................................
10 0.........................................................................................................................
17 Not repor.........................................................................................................................
22 Not repor.........................................................................................................................
16 0.........................................................................................................................
13 Not repor.........................................................................................................................
16 14.2.........................................................................................................................
21 0.........................................................................................................................
29 21.7.........................................................................................................................
15 7.6.........................................................................................................................
5 25.........................................................................................................................
12 0.........................................................................................................................
40 0.........................................................................................................................
101 5.........................................................................................................................
75 4.........................................................................................................................
1 0.........................................................................................................................
1 0.........................................................................................................................
12 9.........................................................................................................................
19 0.........................................................................................................................
2 0.........................................................................................................................
1 0.........................................................................................................................
1 0.........................................................................................................................
1 0.........................................................................................................................
0 0.........................................................................................................................
67 10.7.........................................................................................................................
, bleeding requiring transfusion, perioperative pregnancy loss, ru
ynecol 2009.
ur series, what has become apparent is s
gy OCTOBER 2009
hat cervical incompetence is a complexisease that cannot be treated solely withhe placement of a cerclage—either vagi-ally or at the cervico-isthmus; multipletiologies lead to a common final pathwayf undesired cervical dilatation and efface-ent. Cervical incompetence should be
escribed in 2 main categories: mechanicalnd functional. Mechanical incompetencemplies that the cervical components doot have the strength to maintain thetructure of the cervix through gestation.1
ostulated risk factors include: cervical
aparotomy and cervico-isthmic
e complicationa Fetal survivalrate, %
82..................................................................................................................
100..................................................................................................................
70..................................................................................................................
88..................................................................................................................
95..................................................................................................................
94..................................................................................................................
85..................................................................................................................
96..................................................................................................................
90..................................................................................................................
93..................................................................................................................
87..................................................................................................................
60..................................................................................................................
83..................................................................................................................
97..................................................................................................................
93.5..................................................................................................................
96..................................................................................................................
100..................................................................................................................
100..................................................................................................................
83..................................................................................................................
95..................................................................................................................
100..................................................................................................................
100..................................................................................................................
Not reported..................................................................................................................
100..................................................................................................................
100..................................................................................................................
80..................................................................................................................
d fetal membranes.
ic y lbo sPatno.
ativ
10 ted......... .........
2 ted......... .........
10......... .........
17 ted......... .........
16 ted......... .........
13......... .........
8 ted......... .........
14......... .........
20......... .........
23......... .........
13......... .........
4......... .........
11......... .........
40......... .........
101......... .........
75......... .........
1......... .........
1......... .........
11......... .........
20......... .........
3......... .........
1......... .........
1......... .........
1......... .........
2......... .........
65......... .........
500c pture
tructural anomalies due to in utero dieth-

ycvttisedctg
ww
athptparnpirfu
tlflccwpfhwSflrc
ApotSW
www.AJOG.org Obstetrics Research
lstilbestrol exposure, overdilatation of theervix during pregnancy termination, cer-ical trauma from conization or loop elec-rosurgical excision procedures, congeni-al mullerian anomalies, obstetric traumancluding cervical lacerations, prolongedecond stage of labor, precipitous deliv-ry.1 Each risk factor describes a type ofamage to the anatomic elements of theervix and should be the defining indica-ion(s) for the cervico-isthmic cerclage re-ardless of the surgical approach.
Given that each of the cerclage failurese reported in our series occurred in
FIGURE
, Laparoscopic intraabdominal view of the placerepare the trailing suture length for the final stepf the placement of the suture through both perithe suture placement in the sit at the level of thechematic representation of cervico-isthmic cerchittle. Laparoscopic cervicoisthmic cerclage. Am J Obstet G
omen who presented with symptoms o
nd signs consistent with chorioamnioni-is, we propose that these patients mayave an underlying pathology resulting inrematurity that is not solely attributableo mechanical cervical failure. A similarroposal has been suggested by Drakely etl,34 who reported a 5% dual pathologyate in women with second trimester preg-ancy loss. Functional incompetence is theremature triggering of the cervical ripen-
ng process that occurs at term; postulatedisk factors include subacute or acute in-ection of the genitourinary tract and/orterine cavity, abnormal placental devel-
D
nt of the suture to pass from the posterior aspecthis step the needle and suture sit lateral to the ual broad ligament windows in preparation for theernal cervical os, above the uterosacral ligamente placement (blue) medial to the uterine vesselsol 2009.
pment, suspension of the antiinflamma- p
OCTOBER 2009 Americ
ory effects of progesterone, and pretermabor.1 Each risk factor describes a proin-ammatory environment that promoteservical ripening for which a cervical cer-lage will not suspend. The patients forhom the cerclage failed in this presentregnancy each presented with a clear in-
ectious/inflammatory process and eachad experienced a previous pregnancy lossith a similar presentation. Himes andimhan35 have reported that placental in-ammatory lesions including acute cho-ioamnionitis are associated with a signifi-ant risk of recurrent spontaneous
the broad ligament window through anteriorly toe vessels. B, Laparoscopic intraabdominal view
ot tying. C, Laparoscopic intraabdominal view ofhe knot at the posterior aspect of the uterus. D,d above the uterosacral ligaments.
me t of; in terinone knint s, tlag an
ynec
reterm birth. Furthermore, Edmondson
an Journal of Obstetrics & Gynecology 364.e6

elttipipirvrbctomcspparihccutcsdplao
csdoalrn
R1tm2vo13b1
4ctn5Sdn6sc7LcZ8aB9Acs21dpt11nwnq1ScJ1Plc21aO1vnM1Mts1i11cO1mc62dc
2cp2d12cd12lfn2PimG2im12ccM2RceA2ec23dcwc33mp23Bsgdn3Pt13Mp3pG3Rcw
Research Obstetrics www.AJOG.org
3
t al36 reported that chronic endometritiseading to chronic deciduitis plays a role inhe etiology of preterm labor and prema-ure ruptured membranes. Detailed exam-nation of the past obstetric history andlacental pathology(ies) is imperative to
dentify risk factors for pregnancy loss, inarticular a history of recurrent infectious/
nflammatory preterm birth, that are notelated to the structural integrity of the cer-ix. In such cases, counseling in regard toealistic expectations of the cerclage muste undertaken and potential role forhronic antibiotic and/or progesteroneherapy must be explored. However, eachf the patients who failed the cervico-isth-ic cerclage had a previous failed vaginal
erclage, which can cause damage to thetructural integrity of the cervix, com-ounding the risk for pregnancy loss by su-erimposing risk for mechanical failure onbackground of inflammatory/infectious
isk factors for premature cervical ripen-ng. As such, we recommend a compre-ensive evaluation of all women prior toervico-isthmic cerclage placement in-luding: radiographic evaluation of theterine cavity, thrombophilia screen, de-
ailed evaluation of obstetric history espe-ially placenta pathology, cervico-vaginalwabs, and endometrial biopsy if any evi-ence of inflammatory lesions within therevious placental pathology. Patient se-
ection remains the greatest challenge tond predictor of cerclage success regardlessf the location of its placement.In summary, our data indicated that the
ervico-isthmic cerclage placed laparo-copically compares favorably with the tra-itional laparotomy approach in regard toperative technique, risk of complications,nd obstetric outcome; in the carefully se-ected patient this cerclage may provide aeasonable alternative to achieve preg-ancy success. f
EFERENCES. Shennan A, Jones B. The cervix and prema-urity: aetiology, prediction and prevention. Se-in Fetal Neonatal Med 2004;9:471-9.. Benson RC, Durfee RB. Transabdominal cer-ico uterine during pregnancy for the treatmentf cervical incompetency. Obstet Gynecol965;25:145-55.. McDonald IA. Suture of the cervix for inevita-le miscarriage. J Obstet Gynaecol Br Emp
957;64:346-50. 164.e7 American Journal of Obstetrics & Gynecolo
. Novy MJ. Transabdominal cervicoisthmicerclage for the management of repetitive abor-ion and premature delivery. Am J Obstet Gy-ecol 1982;1:44-54.. Lotgering FK, Gaugler-Senden IP, LotgeringF, Wallenburg HC. Outcome after transab-ominal cervicoisthmic cerclage. Obstet Gy-ecol 2006;107:779-84.. Scibetta JJ, Sanko SR, Phipps WR. Laparo-copic transabdominal cervicoisthmic cer-lage. Fertil Steril 1998;69:161-3.. Reid GD, Wills HJ, Shukla A, Hammill P.aparoscopic transabdominal cervico-isthmicerclage: a minimally invasive approach. Aust NJ Obstet Gynaecol 2008;48:185-8.
. Agdi M, Tulandi T. Placement and removal ofbdominal cerclage by laparoscopy. Reprodiomed Online 2008;16:308-10.. Aboujaoude R, Maloof P, Alvarez M, Al Khan. A novel method for laparoscopic abdominalerclage utilizing minimally invasive hydrodis-ection: a case report. J Reprod Med007;52:428-30.0. Ghomi A, Rodgers B. Laparoscopic ab-ominal cerclage during pregnancy: a case re-ort and a review of the described operativeechniques. J Minim Invasive Gynecol 2006;3:337-41.1. Gallot D, Savary D, Laurichesse H, Bour-azeau JA, Amblard J, Lémery D. Experienceith three cases of laparoscopic transabdomi-al cervico-isthmic cerclage and two subse-uent pregnancies. BJOG 2003;110:696-700.2. Cho CH, Kim TH, Kwon SH, Kim JI, YoonD, Cha SD. Laparoscopic transabdominalervicoisthmic cerclage during pregnancy.Am Assoc Gynecol Laparosc 2003;10:363-6.3. Mingione MJ, Scibetta JJ, Sanko SR,hipps WR. Clinical outcomes following interval
aparoscopic transabdominal cervico-isthmicerclage placement: case series. Hum Reprod003;18:1716-9.4. Lesser KB, Childers JM, Surwit EA. Trans-bdominal cerclage: a laparoscopic approach.bstet Gynecol 1998;9:855-6.5. Leyland NA. Laparoscopic cervical cerclage—ideo presentation. American Association of Gy-ecologic Laparascopists 30th Annual Clinicaleeting; Miami, FL: 2002.6. BonjerHJ,HazebroekEJ,KazemierG,GiuffridaC, Meijer WS, Lange JF. Open versus closed es-
ablishment of pneumoperitoneum in laparoscopicurgery. Br J Surg 1997;84:599-602.7. Watkins RA. Transabdominal cervico-uter-
ne suture. Aust N Z J Obstet Gynaecol972;12:62-4.8. Mahran M. Transabdominal cervical cer-lage during pregnancy: a modified technique.bstet Gynecol 1978;52:502-6.9. Olsen S, Tobiassen T. Transabdominal isth-ic cerclage for the treatment of incompetent
ervix. Acta Obstet Gynecol Scand 1982;1:473-5.0. Wallenburg HC, Lotgering FK. Transab-ominal cerclage for closure of the incompetentervix. Eur J Obstet Gynecol Reprod Biol
987;25:121-9. Pgy OCTOBER 2009
1. Herron MA, Parer JT. Transabdominal cer-lage for fetal wastage due to cervical incom-etence. Obstet Gynecol 1988;71:865-8.2. Van Dongen PWJ, Nijhuis JG. Transab-ominal cerclage. Eur J Obstet Gynecol991;41:97-104.3. Novy MJ. Transabdominal cervicoisthmicerclage: a reappraisal 25 years after its intro-uction. Am J Obstet Gynecol 1991;164:635-41.4. Cammarano CL, Herron MA, Parer JT. Va-
idity of indications for transabdominal cerclageor cervical incompetence. Am J Obstet Gy-ecol 1995:172:1871-5.5. Anthony GS, Walker RG, Cameron AD,roce JL, Walker JJ, Calder AA. Transabdom-
nal cervico-isthmic cerclage in the manage-ent of cervical incompetence. Eur J Obstetynecol 1997;72:127-30.6. Craig S, Fliegner JRH. Treatment of cervical
ncompetence by transabdominal cervico-isth-ic cerclage. Aust NZ J Obstet Gynecol997;37:407-11.7. Turnquest MA, Britton KA, Brown HL. Out-ome of patients undergoing transabdominalerclage: a descriptive study. J Matern Fetaled 1999;8:225-7.8. Davis G, Berghella V, Talucci M, WapnerJ. Patients with a prior failed transvaginal cer-lage: a comparison of obstetric outcomes withither transabdominal or transvaginal cerclage.m J Obstet Gynecol 2000;183:836-9.9. Hole J, Tressler T, Martinez F. Elective andmergency transabdominal cervicoisthmic cer-lage for cervical incompetence. J Reprod Med003;48:596-600.0. Debbs RH, De La Vega GA, Pearson S, Seh-ev H, Marchiano D, Ludmir J. Transabdominalerclage after comprehensive evaluation ofomen with previous unsuccessful transvaginalerclage. Am J Obstet Gynecol 2007;197:17.e1-4.1. Katz M, Abrahams C. Transvaginal place-ent of cervicoisthmic cerclage: report onregnancy outcome. Am J Obstet Gynecol005;92:1989-92; discussion 1992-4.2. Rust OA, Atlas RO, Jones KJ, Benham BN,alducci J. A randomized trial of cerclage ver-us no cerclage among patients with ultrasono-raphically detected second-trimester pretermilatation of the internal os. Am J Obstet Gy-ecol 2000;183:830-5.3. Sharp HT, Dorsey JH, Chovan JD, HoltzM. A simple modification to add strength to
he Roeder knot. J Am Assoc Gynecol Laporsc996;3:305-7.4. Drakeley AJ, Quenby S, Farquharson RG.id-trimester loss—appraisal of a screeningrotocol. Hum Reprod 1998;13:1975-80.5. Himes KP, Simhan HN. Risk of recurrentreterm birth and placental pathology. Obstetynecol 2008;112:121-6.6. Edmondson N, Bocking A, Machin G, Rizek, Watson C, Keating S. The prevalence ofhronic deciduitis in cases of preterm laborithout clinical chorioamnionitis. Pediatr Dev
athol 2008;2:1.Copyright © 2022 FDOKUMEN




















