
Surgical Techniques & Interpretation
45
11/10/2015 1 Surgical Techniques & Interpretation November 9, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll Only: 1-408-435 -7088 or Submit a question to the Event Producer via the Q&A Panel For international support numbers visit: http://support.webex.com/support/phone-numbers.ht Questions may be submitted anytime during the presentation. To submit questions: Type your questions in the text entry box Click the Send Button Please direct your questions to “All Panelists” in the drop down
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Surgical Techniques & Interpretation

11/10/2015
1
Surgical Techniques & Interpretation
November 9, 2015
If you experience technical difficulty during the presentation:
Contact WebEx Technical Support directly at:
US Toll Free: 1-866-779-3239Toll Only: 1-408-435 -7088
orSubmit a question to the Event Producer via the Q&A Panel
For international support numbers visit:http://support.webex.com/support/phone-numbers.ht
Questions may be submitted anytime during the presentation.
To submit questions:
Type your questions in the text entry box
Click the Send Button
Please direct your questions to “All Panelists” in the drop down

11/10/2015
2
Pancreatic Cancer: Surgical Techniques
Christopher L. Wolfgang, MD, PhD, FACS
Chief of Hepatobiliary and Pancreatic Surgery
Professor of Surgery, Pathology and Oncology
Paul K. Neumann Professor of Pancreatic Cancer Research

11/10/2015
3
How do we win the war?
Local Battle
Systemic Battle
Local Battle

11/10/2015
4
The Local Battle is Fought
with Surgery

11/10/2015
5
Systemic Battle

11/10/2015
6
The Systemic Battle is Fought
With Chemotherapy or
Biological Therapy
How do we determine what
therapy someone with
pancreatic cancer receives?

11/10/2015
7
Clinical StagingClinical StagingClinical StagingClinical Staging
Potentially ResectablePotentially ResectablePotentially ResectablePotentially Resectable
(20%)(20%)(20%)(20%)• Localized
• Borderline
(potentially curable)
Unresectable (80%)Unresectable (80%)Unresectable (80%)Unresectable (80%)
• Metastatic
• Locally Advanced
(unlikely to be cured)
1. Systemic Spread
2. Local Tumor Relationship
Determination of ResectabilityDetermination of ResectabilityDetermination of ResectabilityDetermination of Resectability
• Metastatic
– Liver
– Peritoneum
– Lung
– CT scan
– PET scan
– Laparoscopic
Exploration
• Local Tumor
Relationships
– Superior Mesenteric
Artery/Celiac Axis
– Portal Vein/Superior
Mesenteric Vein
– Adjacent Organs
– CT scan
– EUS
– Not Surgical Exploration

11/10/2015
8

11/10/2015
9
Resectable Unresectable
Management
• Stage I/II (resectable)
– Surgery
– Adjuvant or Neoadjuvant Therapy
• Stage III (locally advanced, unresectable
and borderline resectable)
– Chemoradiotherapy for locally advanced
– Neoadjuvant for borderline
• Stage IV
– Systemic therapy

11/10/2015
10
Multidisciplinary Care: Especially Important for
Pancreatic Cancer
Biopsy Proven or Suspected Pancreatic Cancer
Staging Work-up: Genetics, Family Hx, Functional Status
Imaging: 3-D CT scan, MRI, Functional Imaging
Labs: CBC, Liver function, Ca 19-9
Borderline Resectable Unresectable
SurgeryNeoadj CRT
Metastatic or Unresectable
Chemotherapy CRT Chemo SBRT
or
3X10
Surgery
(IORT?)
ADJ Tx
Resectable
Pancreatic MDC: Case Review
Review Images
CT/PET/MRI/
EUS
Discuss Case
and reach
consensus
Review
Pathology
See patients and
discuss options
Present Cases
using outline
Enroll in trials/studies
Dictate note and cc to
referring physicians
• Oncology
• Radiation
Oncology
• Surgery
• Pathology
• Diagnostic
Imaging
• Pain Medicine
11/10/2015
11
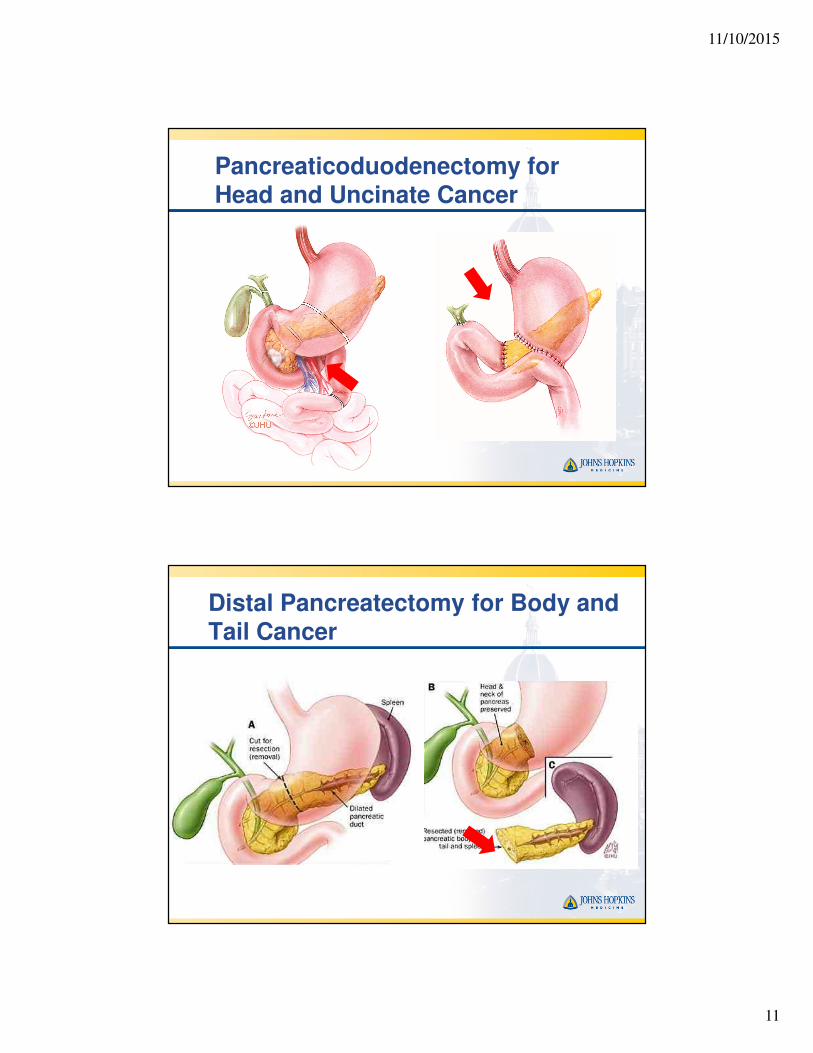
Pancreaticoduodenectomy for Head and Uncinate Cancer
Distal Pancreatectomy for Body and Tail Cancer

11/10/2015
12
Atlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and Hepato----PancreatoPancreatoPancreatoPancreato----Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)
Atlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and Hepato----PancreatoPancreatoPancreatoPancreato----Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)

11/10/2015
13
Atlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and Hepato----PancreatoPancreatoPancreatoPancreato----Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)
Atlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and Hepato----PancreatoPancreatoPancreatoPancreato----Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)

11/10/2015
14
Atlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and Hepato----PancreatoPancreatoPancreatoPancreato----Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)
Atlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and HepatoAtlas of Upper Gastrointestinal and Hepato----PancreatoPancreatoPancreatoPancreato----Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)Biliary Surgery (Douglas Evans)

11/10/2015
15
Surgical Margins

11/10/2015
16
Minimally Invasive Whipple
Operation
(Robotic or Laparoscopic)

11/10/2015
17
Vessel Involvement
(Stage III)

11/10/2015
18
Resection determined by vessel
involvement
AHPBA/SSO/SSAT/NCCN
Resectable BorderlineLocally
Advanced
SMV/PV No contactAbut, encase or
occludeNot
reconstructable
SMA/Hepatic No contact Abut Encase
CHA No contactAbut or short-
segment encaseLong-segment
encase
Celiac Trunk No contact No contact Any contact
BorderlineLocally
advancedResectable
Sandone 5A

11/10/2015
19

11/10/2015
20

11/10/2015
21
Locally Advanced and
Unresectable
Sandone 2

11/10/2015
22
Sandone 6
MLC 406 US Rev B
How Electroporation Works

11/10/2015
23
NanoKnife® System
SMVSMASMV
SMA

11/10/2015
24
Preoperative CT
2/06

11/10/2015
25
Pancreatic Cancer is Almost
Always a Systemic Disease at
the Time of Diagnosis

11/10/2015
26
1980s (N=65) 1990s (N=512) 2000s (N=1115)
months 12 24 36 48 60 12 24 36 48 60 12 24 36 48 60
# at risk 42 23 16 12 10 355 189 139 108 96 740 414 232 162 110
Survival Of Pancreatic Cancer By Decade

11/10/2015
27
Personalized Approach
To Treatment
PalB2
• Partner and Localizer of BRCA2
• 3% of familial pancreatic cancer (also a
cause of familial breast cancer)
• Familial predisposition genes can be
discovered by sequencing all known
genes in a single patient!!
S. Jones, et al. Science 2009
EP Slater, et al. Clin Genet. 2010
11/10/2015
28
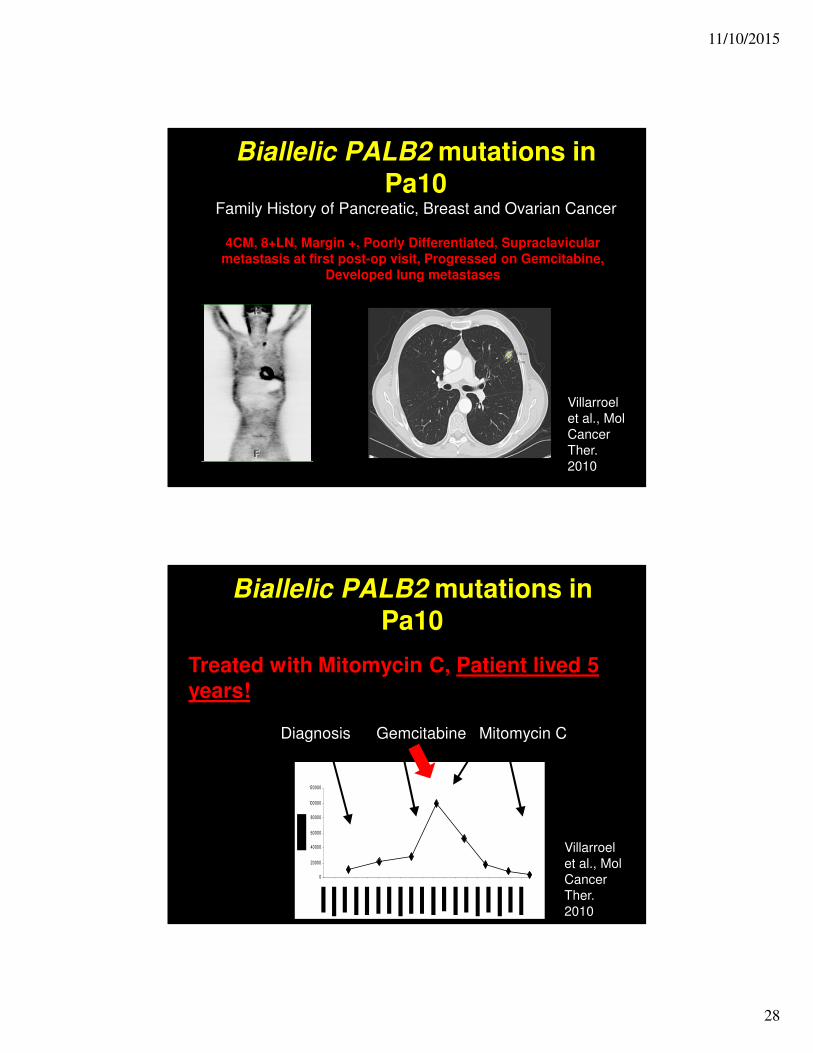
Biallelic PALB2 mutations in Pa10
Family History of Pancreatic, Breast and Ovarian Cancer
4CM, 8+LN, Margin +, Poorly Differentiated, Supraclavicular
metastasis at first post-op visit, Progressed on Gemcitabine,
Developed lung metastases
Villarroel
et al., Mol
Cancer
Ther.
2010
Biallelic PALB2 mutations in Pa10
Treated with Mitomycin C, Patient lived 5
years!
0
20000
40000
60000
80000
100000
120000
GemcitabineDiagnosis Mitomycin C
Villarroel
et al., Mol
Cancer
Ther.
2010

11/10/2015
29
Summary• There are 2 battles to fight to win the war on
pancreatic cancer
– Systemic and Local
• The treatment for pancreatic cancer is based on the
stage
• Surgery plays an important role in localized disease
• Whipple Operation – pancreatic head lesions
• Distal Pancreatectomy and Splenectomy for body
and tail lesions
• Most surgical failures are systemic
– Chemotherapy is used to combat this problem

11/10/2015
30
Interpretation
Martha Bishop Pitman, MD
Director of Cytology
Massachusetts General Hospital
Associate Professor of Pathology
Harvard Medical School
Patient Care Team
Microscope Clipart by ben : Science Cliparts #17424- ClipartSE
www.freepik.com

11/10/2015
31
Pathologist
• A medical doctor specialist in pathology;
specifically, a physician who interprets and
diagnoses the changes caused by disease in
tissues and body fluids.
Pancreatic Mass
– Abdominal/back pain
– Jaundice
– Dark urine/light stool
– Fatigue
– Fullness after eating
– Weight loss
– New onset or worsening
diabetes
– Solid mass
– Anywhere in the pancreas, most
common in the pancreatic head
(pancreas surrounded by the
duodenum)
– Irregular borders
Symptoms Radiological Imaging
HeadHeadHeadHead BodyBodyBodyBody TailTailTailTail
PancreasPancreasPancreasPancreas
No symptoms
– Radiological imaging for
another reason

11/10/2015
32
Diagnosis
Clinical diagnosis
(radiologist, gastroenterologist and surgeon)
– Symptoms
– Radiological imaging
– History of past illness
– History of family illness
– Physical examination
Diagnosis
Pathological Diagnosis
(Pathologist)
– Blood tests (clinical pathology)
– Tissue tests (anatomic pathology)
• Examination of cells (cytology) or tissue (histology)
under the microscope

11/10/2015
33
Normal Pancreas
Histology for Pathologists, S. Mills. LWW
HEAD BODY TAIL
Normal Pancreas Histology
•Exocrine Pancreas (enzymes)
•Acinar cells
•Ductal cells
•Endocrine Pancreas (hormones, e.g. insulin)
•Islet cells
11/10/2015
34
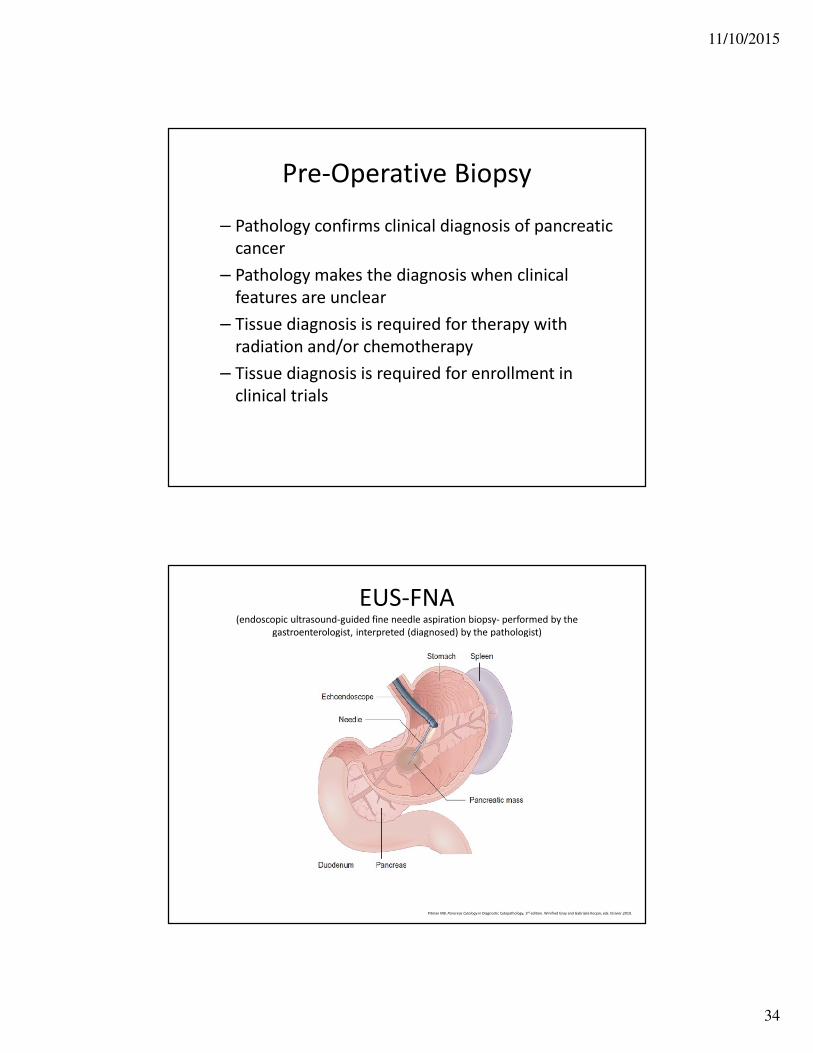
Pre-Operative Biopsy
– Pathology confirms clinical diagnosis of pancreatic
cancer
– Pathology makes the diagnosis when clinical
features are unclear
– Tissue diagnosis is required for therapy with
radiation and/or chemotherapy
– Tissue diagnosis is required for enrollment in
clinical trials
EUS-FNA(endoscopic ultrasound-guided fine needle aspiration biopsy- performed by the
gastroenterologist, interpreted (diagnosed) by the pathologist)
Pitman MB. Pancreas Cytology in Diagnostic Cytopathology, 3rd edition. Winifred Gray and Gabrijela Kocjan, eds. Elsivier.2010.

11/10/2015
35
EUS-FNA
The National Pancreas Foundation
Pre-Operative Pathology(Cytology)
Diagnosis: Pancreatic Ductal adenocarcinoma
https://therestlesslegsblog.wordpress.com/2010/04/

11/10/2015
36
Pre-Operative Diagnosis
Benign Malignant
Pre-Operative Diagnosis
Ductal Adenocarcinoma Neuroendocrine Tumor
11/10/2015
37
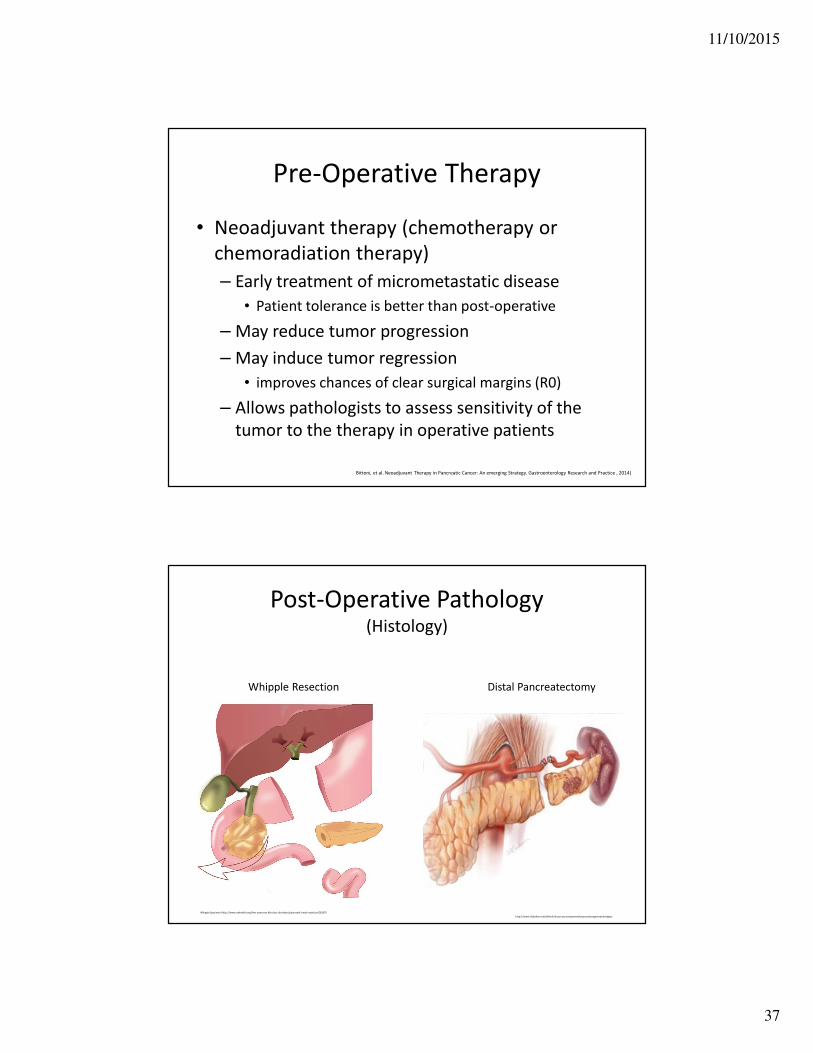
Pre-Operative Therapy
• Neoadjuvant therapy (chemotherapy or
chemoradiation therapy)
– Early treatment of micrometastatic disease
• Patient tolerance is better than post-operative
– May reduce tumor progression
– May induce tumor regression
• improves chances of clear surgical margins (R0)
– Allows pathologists to assess sensitivity of the
tumor to the therapy in operative patients
Bittoni, et al. Neoadjuvant Therapy in Pancreatic Cancer: An emerging Strategy. Gastroenterology Research and Practice , 2014)
Post-Operative Pathology(Histology)
Whipple Specimen (http://www.uwhealth.org/liver-pancreas-bile-duct-disorders/pancreatic-head-resection/26267)
http://www.slideshare.net/drferzli/trocar-port-placementforproceduregeneralstrategies
Whipple Resection Distal Pancreatectomy

11/10/2015
38
Tissue Processing
http://amida13.isi.uu.nl/?q=node/2
Pathological Diagnosis and Staging
• Tumor type
• Tumor size
• Tumor extent
• Surgical margins
• Lymph node involvement
• Distant spread (metastasis)

11/10/2015
39
Pathological Diagnosis: Tumor Type
• Ductal Adenocarcinoma (~90%)
AFIP Atlas of Tumor Pathology; 4th Series Fascicle 6
Pathological Diagnosis: Tumor Type
• Neuroendocrine Tumors (~10%)
AFIP Atlas of Tumor Pathology; 4th Series Fascicle 6

11/10/2015
40
Pathological Diagnosis: Tumor Type
• Rare other types
– Solid-pseudopapillary neoplasm
– Acinar cell carcinoma
– Pancreatoblastoma
– Lymphoma
– Sarcoma
AFIP Atlas of Tumor Pathology; 4th Series Fascicle 6
Solid-pseudopapillary neoplasm
Fine needle aspiration biopsy
Pathological Diagnosis: Tumor Size
Pea, cherry, walnut, and kiwi show tumor sizes.
www.pancreaticcancer.net.au

11/10/2015
41
Pathological Diagnosis
• Careful evaluation of
the surgical specimen
– Visual inspection of
tissue may not equate to
tumor under the
microscope
– Tumor and fibrosis are
both firm tissues
– Malignant glands can
extend beyond what is
seen as firm white tissueDuctal adenocarcinomaAFIP Atlas of Tumor Pathology; 4th Series Fascicle 6
Pathological Diagnosis: Tumor Extent
and Surgical Margins
http://www.rcpa.edu.au/Library/Practising-Pathology/Macroscopic-Cut-Up/Specimen/Gastrointestinal/Pancreas/Pancreas-resection
Cancer invasion of a nerve
Cancer invasion of a small vessel
Ductal adenocarcinomaAFIP Atlas of Tumor Pathology; 4th Series Fascicle 6
Cancers 2010, 2(4), 2001-2010

11/10/2015
42
Pathological Diagnosis: Lymph Node
involvement
http://medcell.med.yale.edu
Pathological Diagnosis: Metastasis
• Requires biopsy of distant tissue site and
diagnosis of cancer consistent with origin in
the pancreas: most common
– Liver
– Lung
– Adrenal glands
– Skin
Fine needle aspiration biopsy

11/10/2015
43
Pathological Staging:TNM Classification System
pT1 pT2
pT4N1
pT3
http://www.cancerresearchuk.org
American Joint Committee on Cancer(AJCC, 7th edition)

11/10/2015
44
Pathology Report
• Tumor Type– Ductal adenocarcinoma
– Neuroendocrine tumor
– Other
• Tumor Grade– Low grade or high grade
• Tumor extent
• High-risk histological findings– Invasion of the blood
vessels, lymphatic system, nerves
• Tumor Stage
Patient Care Team
Microscope Clipart by ben : Science Cliparts #17424- ClipartSE
www.freepik.com

11/10/2015
45
Thank you
Thank you for your participation.
If you have questions, please contact Patient Central at
(877) 272-6226 or e-mail [email protected].
www.pancan.org or wagehope.org




















