When climate change couples social neglect: malaria dynamics in Panamá
Upload
independentCategory
view
1download
0
E M S / S P E C I A L C O N T R I B U T I O N
David Markenson, MDGeorge Foltin, MDMichael Tunik, MDArthur Cooper, MDHedda Matza-Haughton, MSW,
CSW Lenora Olson, MA Marsha Treiber, MPS
Published simultaneously inPediatric Emergency Care andPrehospital Emergency Care.
Authors’ affiliations are pro-vided at the end of this article.
[Markenson D, Foltin G, Tunik M, Cooper A, Matza-Haughton H, Olson L, Treiber M. Knowledge andattitude assessment and education of prehospital personnel in child abuse and neglect: report of aNational Blue Ribbon Panel. Ann Emerg Med. July 2002;40:89-101.]
I N T R O D U C T I O N
Violence against children, specifically in the area of child maltreatment, is a publichealth concern that has reached epidemic proportions. Prehospital providers, whooften witness scenes of child abuse and neglect, can fill an essential role in identifyingneglect and abuse in the home, at school, and in other locations.
In October 2001, a blue ribbon panel of national experts in emergency medical ser-vices (EMS), emergency medical services for children (EMSC), and child protectionservices (CPS) convened to discuss the prehospital provider’s role in identifying andreporting suspected child abuse and neglect. Significantly, this marked the first timenational experts from the worlds of child protection and EMSC met face-to-face toaddress this issue. With expertise in EMS education, pediatric emergency medicine,pediatric surgery, psychiatry and psychology, social work, legal practice, law enforce-ment, and fire and rescue services, the participants represented the entire continuumof care for at-risk children. When all available services are used and integrated, chil-dren are kept from falling through the cracks, and the highest quality of care possibleis provided for them.
Guided by research findings from a national survey conducted by the Center forPediatric Emergency Medicine (CPEM), the panel’s goals were to:
• Recommend content areas in child protection that will form the basis for futureeducational resources for prehospital providers
• Develop recommendations regarding advocacy and policy issues important toEMS and CPS
• Discuss plans for continued collaboration between the EMS and CPS worldsThis article presents a summary of their findings.
Knowledge and Attitude Assessment and
Education of Prehospital Personnel in Child
Abuse and Neglect: Report of a National Blue
Ribbon Panel
J U L Y 2 0 0 2 4 0 : 1 A N N A L S O F E M E R G E N C Y M E D I C I N E 8 9
47/1/125610doi:10.1067/mem.2002.125610

E M S A N D C H I L D A B U S EMarkenson et al
B A C K G R O U N D
In 2000, CPEM received federal funding from the EMSCProgram to launch a National Child Protection Educa-tion Project. To begin the project, CPEM established anadvisory board representing major national organiza-tions in EMS, EMSC, and child protection, as well as areview panel composed of individuals with expertise inthese areas. Working with the advisory board and re-view experts, the National EMSC Data Resource Center(NEDARC), and the National Registry of EmergencyMedical Technicians (NREMT), CPEM staff developeda questionnaire targeting EMTs and paramedics nation-wide. The survey instrument queried prehospitalproviders regarding (1) knowledge of signs and symp-toms associated with child abuse or neglect, (2) self effi-cacy and attitudes toward recognition and managementof child abuse or neglect, and (3) knowledge of identifi-cation, documentation, and reporting procedures forsuspected child abuse and neglect.
The questionnaire was pilot-tested and revised, andthen 10,000 copies were distributed to a representativecross-section of prehospital providers throughout theUnited States. Two mechanisms were used for distribu-tion: one was a sampling system previously developedfor the NREMT’s Longitudinal EMT Attributes andDemographic Study (LEADS) project, and the otherinvolved direct distribution to EMS offices in 15 statesand territories, where the surveys were subsequentlyadministered at regional training sites during certifica-tion courses and continuing medical education confer-ences. The overall return rate, independent of method,averaged 44%. The results were tabulated and ana-lyzed in collaboration with the NREMT and NEDARC.Following data analysis, the blue ribbon panel con-vened to review and discuss the results.
T H E C O N T I N U U M O F C A R E F O R T H E A B U S E DO R N E G L E C T E D C H I L D
Prehospital Phase
EMS providers are trained and either certified orlicensed. Levels are defined by the state and region andare based partially on the Department of Transporta-
9 0 A N N A L S O F E M E R G E N C Y M E D I C I N E 4 0 : 1 J U L Y 2 0 0 2
tion’s National Standard Curricula. In their originalforms, these curricula provided limited information onpediatric care and even less on child protection. In addi-tion to the time constraints in these curricula, a reviewof their outlines indicates that material focuses onrecognition of severe physical abuse, with little discus-sion of documentation and almost no discussion ofother manifestations of child maltreatment, interactionwith families, and issues of cultural diversity. Representa-tives from EMS and EMSC discussed the roles and re-sponsibilities of prehospital providers as well as train-ing for the different certification levels.
The Certified First Responder curriculum touchesonly briefly on pediatrics in a description of resuscita-tion techniques. No information on child abuse isgiven at this level. The EMT-basic program provides for6 hours of pediatric education, half of which is didacticmaterial. This level of training accounts for the educa-tion of the majority of EMS providers. Child abuse is arequired component of the didactic material withoutspecifying the exact time for this topic; traditionally,however, only 5 to 10 minutes is spent on this subject.The EMT-intermediate learns additional skills in adultcare together with a brief mention of pediatric airwayissues, but no additional information on child protec-tion issues is provided. The EMT-paramedic programprovides for expanded pediatric information andskills. Child abuse is a required component in this cur-riculum, but there is no set time for the didactic mate-rial and no opportunity for applied education using sce-narios or role-playing; typically, it is no more than 15 to20 minutes.
Each of these curricula includes practical compo-nents that could be applied to child abuse, such as thescene survey, during which EMS providers could gainvaluable information for CPS. However, the compo-nents are not taught within the framework of childabuse, so this opportunity is missed. Other topic areasthat could include child abuse information are patientassessment, mechanism of injury, focused history, doc-umentation, and communication with other health careprofessionals.
Because EMS providers are often called to the homeof the child, they can have an important role in identify-

E M S A N D C H I L D A B U S EMarkenson et al
medical or professional capacity, that the child theyobserve is an abused child. The definition of an abuseralso varies by state. It could be the parent or paramourof the parent, other relatives, other caregivers (eg, fos-ter parents, facility staff, and child care providers), orany other person with ongoing responsibility for thecare of a child.
Reporting is necessary so that further injury can beprevented and the safety of the child ensured. For anincident to be considered child maltreatment, the fol-lowing must be true.
• The alleged victim is younger than 18 years.• The alleged perpetrator has temporary or ongoing
responsibility for the child.• There is harm or substantial risk of harm to the child.• A specific incident or set of circumstances is evident
or manifest (as defined by individual state law).The first step in reporting suspected abuse and neglect
is to communicate with a hotline or another reportingmechanism.
The child protection worker who initially respondsto the complaint will determine whether the informa-tion meets the state’s criteria for abuse or neglect andwhether an investigation is warranted. If so, the ChildProtection Agency will initiate an investigation. Thisoften begins with interviews of the child, the caregiver,the alleged perpetrator, and, in some instances, the per-son who reported the information. The investigationwill determine whether there is sufficient evidence tosubstantiate a finding of abuse or neglect. Possible in-vestigative outcomes include “founded” or “indicated,”“unfounded” or “ruled out,” and “unsubstantiated.”
An outcome of “founded” or “indicated” means thatenough evidence is present to indicate that physicalabuse or neglect occurred. Depending on the circum-stances, the child may be allowed to remain in the homewhile various interventions are provided, such as homevisits by a social worker, counseling, parenting classes,or drug testing. Alternatively, if there is a high risk forfurther abuse or neglect, the child may be removed fromthe home. Planning must begin immediately, becausefederal law mandates that a permanent plan for a child’sliving arrangements be made within 18 months fromthe time the child enters the child welfare system.
ing and recording information that many medical andchild protection professionals do not have an opportu-nity to see.
It is imperative that prehospital providers and theirleadership, as well as child protection advocates, under-stand each other’s roles. For example, without an under-standing of the variety of child protection interventionspossible, prehospital providers who report their suspi-cions may see that the child was not removed from thehome and conclude that nothing came of their report.However, CPS professionals are encouraged to keepfamilies together when the child’s safety and well-beingis not compromised. CPS is a complex system; prehospi-tal personnel would benefit by understanding how it isdesigned to work and how cases move through it.
Child Protection Phase
The child protection phase begins after a prehospitalprovider has reported a suspicion of abuse or neglect.This phase encompasses interventions performed byhospital personnel and the local child protection agency.CPS professionals presented key issues in child protec-tion as they relate to EMS.
All states have laws, policies, and guidelines for childprotection, which are based on federal statutes. TheCPS agency in each state or region provides support ser-vices to families. CPS workers may remove childrenfrom unsafe homes; try to reunite children with theirparents or other primary caregivers when appropriate;and develop alternative permanency plans, includingadoption, when the latter is not possible. They also helpchildren develop independent living skills as they nearthe age of emancipation. Depending on local statutes,the family court may be involved alongside CPS.
Regional variations in child protection practices in-dicate that more uniform guidelines are needed. Forexample, states do not universally consider prehospitalpersonnel mandated reporters of suspected child abuseor neglect. Mandated reporters are generally defined asindividuals who, in the course of their employment,occupation, practice of their profession, or any capac-ity as required by state jurisdiction, come into contactwith children and report or cause a report to be madewhen they have reason to believe, on the basis of their
J U L Y 2 0 0 2 4 0 : 1 A N N A L S O F E M E R G E N C Y M E D I C I N E 9 1

E M S A N D C H I L D A B U S EMarkenson et al
A ruling of “unfounded” or “ruled out” means thatthere is insufficient evidence to indicate abuse or neglect.The case is closed unless additional information sup-ports a finding of abuse or neglect. Some states may electto enter a finding of “unsubstantiated.” This means thatthe court believes that abuse or neglect occurred, butevidence to support such a finding is lacking.
Multidisciplinary child protection teams in localhospitals and in some communities review all casesreported from their hospital or geographic areas. Theseteams often include a representative from CPS to helpfacilitate the flow of information, but the EMS commu-nity is rarely represented. This lack of representationhinders the efforts of EMS providers and child protec-tion workers to develop a mutual understanding of eachother’s roles; as a result, child protection workers oftenhave little knowledge of the information prehospitalproviders can furnish regarding the cases they examine.
Legal Issues Affecting the Continuum
A final presentation and discussion focused on legalissues of concern to EMS and CPS professionals.
Mandatory Reporting. All of the states and the Districtof Columbia have enacted a mandatory reporting statute.These statutes vary greatly from jurisdiction to jurisdic-tion, but all include a list of persons who qualify asmandated reporters. Typically, all persons who are em-ployed in occupations in which they deal with childrenor who come into contact with children are mandatoryreporters. This may include school personnel, doctors,medical examiners, daycare providers, social workers,mental health professionals, law enforcement officials,EMTs, and others in similar professions. Some jurisdic-tions even include photo developers who may discoverphotographs depicting pornographic images of under-age children. In approximately 18 states, anyone whosuspects child abuse or maltreatment is required toreport it, regardless of profession. It is vital for prehos-pital providers to be familiar with their jurisdiction’sdefinition of a mandated reporter.
Standard of Proof for Reporting. The standard to deter-mine whether a mandated reporter must notify authori-ties of suspected child abuse varies from state to state.Typically, a report is required whenever the reporter
9 2 A N N A L S O F E M E R G E N C Y M E D I C I N E 4 0 : 1 J U L Y 2 0 0 2
suspects or has reason to suspect child abuse or neglect.Suspicion can be based on physical observation, state-ments made by the child, statements overheard, or trans-fer of knowledge from another person.
Liability Issues. For a state to receive funding underthe Child Abuse Prevention and Treatment Act, it mustprovide immunity from prosecution to all good faithreports of suspected or known child abuse or neglect.Most states extend this immunity protection to includeall criminal and civil actions as well as all judicial pro-ceedings arising from the report.
In 45 jurisdictions and the District of Columbia,penalties are imposed if a mandated reporter fails tomake a report. Most states impose one of the followingstandards: “knowingly,” “knows or should have known,”or “willfully.” A minority of states imposes the standardof “intentionally or purposefully.” Penalties may in-clude forfeiture of license or certification, fines, orcriminal prosecution.
Confidentiality. To receive grant funding under theChild Abuse Prevention and Treatment Act, recordsmust be kept confidential to protect the identity of theparent or guardian. Mandatory reporters do not have alegal right to know the results of their report. They maybe entitled to information, however, if they have subse-quent involvement with the child.
R E S E A R C H F I N D I N G S
The research findings of the CPEM National ChildProtection Education Project were presented. Theassessment instrument previously described includeddemographic information; case scenarios; and ques-tions covering attitude, opinion, and knowledge ofchild abuse and neglect.
The responses showed the following trends: prehos-pital providers were more comfortable managing physi-cal abuse than neglect; they were uncomfortable man-aging sexual abuse and interacting with families ofabused and neglected children; and their confidence inthese areas tended to exceed their knowledge. Therewere significant knowledge gaps in the respondents’understanding of pediatric developmental stages andabilities, interaction with families, and the type of evi-

E M S A N D C H I L D A B U S EMarkenson et al
The panels made additional recommendations to:• Increase focus on similarities between EMS and
child protection roles• Develop educational materials in child protection
for EMS providers• Develop support systems for prehospital providers
who report child abuse and neglect• Ensure that mandated reporting laws are imple-
mented effectively• Emphasize that the EMS system encompasses pre-
hospital providers, hospital-based physicians, and hos-pital systems in a single continuum of care (ie, avoidcompartmentalizing prehospital care)
• Create opportunities for internships in which pre-hospital providers observe child protection workers,police officers, etc.
• Encourage increased focus on child abuse andneglect at state and national EMS conferences
• Encourage increased focus on the role of EMS inchild abuse and neglect at local and national child pro-tection conferences
• Communicate with national organizations to pro-mote the value of EMS in child protection investigations
T A S K G R O U P S A N D S P E C I F I CR E C O M M E N D A T I O N S
The Blue Ribbon Panel focused on the following majorissues in child protection to be considered a foundationfor the involvement of EMS in child protection. Theseissues will help in the development of educational re-sources and address policy, advocacy, and future actionsregarding EMS and child abuse and neglect. The issuesincluded:
• Definition of terms• Role of the prehospital provider• Challenges to the role of prehospital providers in
child protection• Legal and legislative issues for the prehospital
provider• Problems faced by prehospital providers• Prevention and identification of high-risk situations• Patient and family interaction• Recognition, assessment, and treatment
dence that is needed in order to report suspicions ofabuse or neglect. Prehospital providers perceived aneed for additional training in a multitude of areas; themost frequent requests involved cultural competency,interaction with families, and documentation.
Differences in overall trends were noted according tosex, type of provider, and years of service. The detailedresults have been submitted for publication.
G E N E R A L R E C O M M E N D A T I O N S
The panel participants defined several overall issues ofimportance for EMS and child protection and made thefollowing recommendations.
Mandated Reporters
In many states, EMS providers are not mandatedproviders, and in places where they are mandatedreporters, EMS providers, physicians, and child protec-tion workers may be unaware of this fact. Prehospitalproviders, as health care professionals responsible forthe care of children, should be considered mandatedreporters in all states and territories. Prehospitalproviders and child protection personnel should beeducated on this point.
Cross-disciplinary Cooperation
EMS providers and CPS experts, albeit knowledgeablein their own disciplines, do not possess comprehensiveknowledge of each other’s areas of expertise and function,and coordination and collaboration between EMS andCPS is virtually nonexistent. As such, further coopera-tion, coordination, and collaboration between EMS andCPS is needed.
Education
Prehospital providers should be better educated inthe following areas: their role in the child protectionsystem, assessment of children in different develop-mental stages, documentation, and reporting. Further-more, child protection workers and physicians shouldreceive training on the role of prehospital providers, theassessments they perform, and how they may identifyabuse and neglect.
J U L Y 2 0 0 2 4 0 : 1 A N N A L S O F E M E R G E N C Y M E D I C I N E 9 3

E M S A N D C H I L D A B U S EMarkenson et al
• Documentation and reporting procedures• Children with special health care needs • Cultural competency• General recommendations regarding policy, advo-
cacy, and future direction
Definition of Terms
Currently, there is no cross-disciplinary consensusregarding definitions of terms in the field of child abuseand neglect. During the meeting, the panel reviewedglossaries taken from EMS and child protection re-sources, identified differences in definitions, andselected key words and phrases to define in common(Table 1). Nationally recognized experts who havecompleted work in child protection and EMS will formdefinitions.
The basic vocabulary used by prehospital providersand child protection experts may differ, leading toinconsistency and confusion. For example, a prehospi-tal provider considers assessment to mean a physicalassessment conducted at the scene, whereas the childprotection professional considers it to mean a compre-hensive physical and psychosocial evaluation to deter-mine whether there are grounds for suspecting abuseand neglect. The EMS prehospital provider should usethe term suspected child abuse. Many do not know thatsuspicion is the only requirement for initial reporting;thereafter, local authorities will investigate to deter-mine whether definitive proof of child abuse or neglectexists. The definitions of suspected child abuse andneglect versus child abuse and neglect are key for pre-hospital providers in understanding their roles.
Role of the Emergency Medical Service Provider in ChildAbuse and Neglect
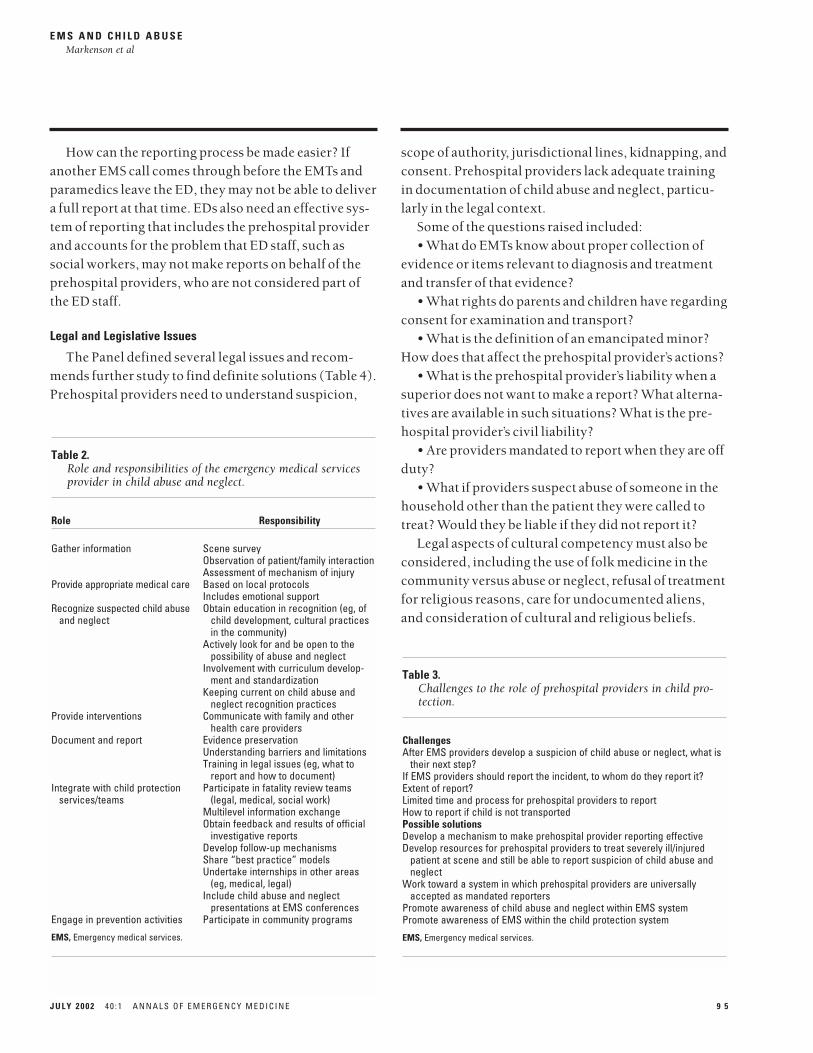
The prehospital provider’s role in child abuse andneglect was discussed, and associated responsibilitieswere outlined (Table 2).
It was discussed that the role of prehospital providersis to care for children, including providing emotionalsupport, and to adequately document their findings. Itwas recommended that prehospital providers be edu-cated in the areas of abuse and neglect, including recog-nition, treatment, documentation, and reporting.
9 4 A N N A L S O F E M E R G E N C Y M E D I C I N E 4 0 : 1 J U L Y 2 0 0 2
Recognition of child abuse depends partly on knowl-edge of child development stages; for example, in orderto decide whether a child is malnourished, the providermust be aware of what the normal weight should be forthe child. To assess whether a mechanism of injuryreported by the parent is plausible, the provider mustknow the average capabilities of a child that age (eg, “Isthis infant capable of rolling off a couch?”). Prehospitalproviders also require knowledge of cultural practicesand special needs children in the community. They needto understand proper reporting requirements and properobjective documentation methods that will hold up incourt, when necessary. Most importantly, they need toknow how to get their report to someone who has theauthority to activate the system on the child’s behalf.
Challenges to the Role of Prehospital Providers in ChildProtection
The panel discussed the challenges prehospitalproviders face in their role in child abuse and neglect(Table 3). For example, there is no universal conceptregarding where prehospital providers should delivertheir report. The assessment survey indicated that someproviders report suspicions to the emergency depart-ment physician; in most cases, a social worker subse-quently reports on behalf of the ED physician. However,professionals in CPS prefer to receive information “earlyand up front,” rather than second- or thirdhand. Shouldthe prehospital provider report directly to CPS?
Table 1.List of words and phrases to be defined.
MaltreatmentAbuseNeglect (eg, optimal care vs adequate care vs minimal care)Reasonable cause to believe/suspectSuspicionHigh-risk behaviorAssessment/history (physical vs psychosocial)Caretaker and caregiver (legal, local definitions)TreatmentDocumentationReportMandated reporterConsentSudden infant death syndrome (SIDS)
E M S A N D C H I L D A B U S EMarkenson et al
scope of authority, jurisdictional lines, kidnapping, andconsent. Prehospital providers lack adequate trainingin documentation of child abuse and neglect, particu-larly in the legal context.
Some of the questions raised included:• What do EMTs know about proper collection of
evidence or items relevant to diagnosis and treatmentand transfer of that evidence?
• What rights do parents and children have regardingconsent for examination and transport?
• What is the definition of an emancipated minor?How does that affect the prehospital provider’s actions?
• What is the prehospital provider’s liability when asuperior does not want to make a report? What alterna-tives are available in such situations? What is the pre-hospital provider’s civil liability?
• Are providers mandated to report when they are offduty?
• What if providers suspect abuse of someone in thehousehold other than the patient they were called totreat? Would they be liable if they did not report it?
Legal aspects of cultural competency must also beconsidered, including the use of folk medicine in thecommunity versus abuse or neglect, refusal of treatmentfor religious reasons, care for undocumented aliens,and consideration of cultural and religious beliefs.
How can the reporting process be made easier? Ifanother EMS call comes through before the EMTs andparamedics leave the ED, they may not be able to delivera full report at that time. EDs also need an effective sys-tem of reporting that includes the prehospital providerand accounts for the problem that ED staff, such associal workers, may not make reports on behalf of theprehospital providers, who are not considered part ofthe ED staff.
Legal and Legislative Issues
The Panel defined several legal issues and recom-mends further study to find definite solutions (Table 4).Prehospital providers need to understand suspicion,
J U L Y 2 0 0 2 4 0 : 1 A N N A L S O F E M E R G E N C Y M E D I C I N E 9 5
Table 2.Role and responsibilities of the emergency medical servicesprovider in child abuse and neglect.
Role Responsibility
Gather information Scene surveyObservation of patient/family interactionAssessment of mechanism of injury
Provide appropriate medical care Based on local protocolsIncludes emotional support
Recognize suspected child abuse Obtain education in recognition (eg, of and neglect child development, cultural practices
in the community)Actively look for and be open to the
possibility of abuse and neglectInvolvement with curriculum develop-
ment and standardizationKeeping current on child abuse and
neglect recognition practicesProvide interventions Communicate with family and other
health care providersDocument and report Evidence preservation
Understanding barriers and limitationsTraining in legal issues (eg, what to
report and how to document)Integrate with child protection Participate in fatality review teams
services/teams (legal, medical, social work)Multilevel information exchangeObtain feedback and results of official
investigative reportsDevelop follow-up mechanismsShare “best practice” modelsUndertake internships in other areas
(eg, medical, legal)Include child abuse and neglect
presentations at EMS conferencesEngage in prevention activities Participate in community programs
EMS, Emergency medical services.
Table 3.Challenges to the role of prehospital providers in child pro-tection.
ChallengesAfter EMS providers develop a suspicion of child abuse or neglect, what is
their next step?If EMS providers should report the incident, to whom do they report it?Extent of report?Limited time and process for prehospital providers to reportHow to report if child is not transportedPossible solutionsDevelop a mechanism to make prehospital provider reporting effectiveDevelop resources for prehospital providers to treat severely ill/injured
patient at scene and still be able to report suspicion of child abuse andneglect
Work toward a system in which prehospital providers are universallyaccepted as mandated reporters
Promote awareness of child abuse and neglect within EMS systemPromote awareness of EMS within the child protection system
EMS, Emergency medical services.

E M S A N D C H I L D A B U S EMarkenson et al
Problems Faced by Prehospital Providers
Although much of the discussion focused on keyissues related to the role of prehospital providers in childprotection, one discussion centered on specific possibleproblems faced by prehospital providers (Table 5).
Prehospital providers respond to a high volume ofadult calls but few calls involving children; of these,even fewer will involve child abuse and neglect. Pro-viders must be vigilant for signs of abuse or neglect dur-ing all pediatric calls, but they must also remember thatabused or neglected children may be present duringadult calls. Under the intense pressure of the acute careenvironment, providers perceive that they do not havetime to perform assessments beyond direct patient care.To address this dilemma, it is important to developgeneric guidelines that providers can follow at all scenes.These should include an assessment for possible childabuse and neglect during the scene survey any timechildren are present, with the goal of heighteningawareness of child abuse and neglect in any situation.This assessment need not interrupt patient care and
9 6 A N N A L S O F E M E R G E N C Y M E D I C I N E 4 0 : 1 J U L Y 2 0 0 2
may not require immediate documentation. It is suffi-cient for providers to mentally note elements that mayhelp in a later investigation, documenting these findingswhen the crisis is over.
There is some agreement that the essential role of theEMS provider includes identifying, recognizing, andreporting child abuse and neglect, but the manner inwhich this translates into practice, procedures, andguidelines varies among communities and EMS systems.The unclear role presents a problem for the provider inknowing his or her course of action. Some possible solu-tions are to encourage states to clarify language definingthe prehospital provider’s role as a mandated reporter ofchild abuse and neglect, and to decide whether providersare expected to report directly to the CPS agency or inte-grate reporting with other reporting mechanisms.
Problems are also caused by most prehospital pro-viders’ lack of familiarity with systems for reportingchild abuse and neglect in their state. Suggested solu-tions were to:
• Educate prehospital providers on state and localreporting requirements
• Establish protocols and systems to facilitate thereporting process for prehospital providers (eg, add acheck box to the run sheet of suspicions and who/wheredid/do they report [ED, physician, hotline])
Table 4.Legal and legislative issues for emergency medical servicesproviders.
Problems Possible Solutions
Differences in states regarding Recommendation to make every-who is a mandated reporter one a mandated reporter
Ambiguity in language Standardize languageAre EMS providers mandated Include clarification in law or
reporters when they are off duty? regulation as has been done forother mandated reporters
Contents of reports: how easy are Require documentation that reflects they to write? Are they formulated prehospital terminology and for EMS? available information
Multidisciplinary teams within CPS Provide for prehospital inclusion do not include EMS where these teams are mandated
Parental consent: what to do when Provide legal mechanism for parents want to accompany child transport of the possibly abused on transport or when parents refuse or neglected child without transport for their child parental consent
Legalities regarding cultural and Educate prehospital providers in religious attitudes toward medicine the legal issues regarding culturaland treatment and religious beliefs
Lack of training in legal aspects of Education in objective documenta-documentation tion, including noting child’s
emotions and objectively recordwhat is said
CPS, Child protection services; EMS, emergency medical services.
Table 5.Problems faced by prehospital providers.
Limited clinical exposure to child abuse/neglect because of the lowpercentage of pediatric calls
Limited opportunity for on-scene assessments beyond those essential todirect patient care
Lack of a clear, consistent role in reporting child abuse/neglect from stateto state and region to region
Lack of familiarity with mechanisms for reporting directly to the childprotection agency
Failure of child protection agency to include providers in the investigation/evaluation process
Child protection services have traditionally not been educated about theimportance of EMS in child maltreatment detection, evaluation, and, ifneeded, prosecution
Lack of inclusion in interdisciplinary teams dealing with child abuse andneglect (eg, child fatality reviews, child protection teams in hospitals)
Limited experience and education in recognizing subtle findings that, whenput together, might lead to the suspicion of child abuse and neglect
EMS, Emergency medical services.

E M S A N D C H I L D A B U S EMarkenson et al
Child protection professionals view risk as the po-tential for maltreatment or harm. Their assessment inthese cases focuses on whether the child is safe in thecurrent environment. Terms such as at risk or high riskdo not necessarily mean that maltreatment has occurred,but, rather, that the family requires interventions toprevent maltreatment from occurring. These situationsmay not yield reportable evidence of child abuse orneglect, yet a timely referral to social services may serveas a method of prevention. At-risk children could bene-fit if prehospital providers had the knowledge and skillsto identify these situations (Table 6).
It may be useful to place a check box on the patient carerecord so that providers could request a social work refer-ral when transporting an at-risk child to the hospital. Ifthe child is not transported, providers could give the fam-ily a brochure with referral information and telephonenumbers. This would give prehospital providers anopportunity to contribute to prevention efforts. Findingtime for prevention-related activities is a challenge forCPS professionals and prehospital providers alike.
Patient and Family Interaction
Prehospital providers receive limited training infamily and patient interaction, so they are not well
• Teach providers to document the scene with pho-tographs
• Educate providers about what should be includedwhen reporting
• Determine how reports should be coordinated andby whom
Recognizing child abuse often involves fitting to-gether many subtle clues. By themselves, these clues mayseem innocuous, but together they reveal a more suspi-cious picture. Prehospital providers have limited experi-ence recognizing the findings that create this picture, buttheir observations may be additive to other findings lead-ing to suspicion. A problem is that prehospital providersdo not often know that, even without reaching the levelof suspicion, documenting their findings may be helpfulto others involved in child protection.
Child protection workers generally do not contactthe prehospital provider during the investigation ofalleged child abuse or neglect. Providers have few inter-actions with CPS. In many cases, CPS professionals donot even know that they can contact prehospital pro-viders for information. As more prehospital providersobjectively document significant observations duringemergency calls, thereby conveying valuable informa-tion to investigative staff, the current gap between EMSand CPS will begin to close. Better linkages and com-munication between CPS and EMS will help to promotethis cooperation locally and nationally.
Currently, prehospital providers are not included ininterdisciplinary teams dealing with child abuse andneglect, such as child fatality reviews and child protec-tion teams in hospitals. EMS representation would giveprehospital providers an opportunity to hear about theoutcome of child abuse cases. Knowing that somethinghas been done to help the child will provide a strongincentive to report future findings.
High-risk Situations and Prevention
Prevention is a complex challenge for CPS profession-als and is even more so for the prehospital provider.Because of the low volume of pediatric calls, there is scantevidence to suggest whether EMS personnel can carry outprevention and identification of at-risk children, butpanel members agreed that it is within their purview.
J U L Y 2 0 0 2 4 0 : 1 A N N A L S O F E M E R G E N C Y M E D I C I N E 9 7
Table 6.Key knowledge points in identifying high-risk situations.
Criteria CPS uses to determine safety/lack of safety for child and definitionof safe/unsafe
Circumstances that indicate high riskWhen talking about safety in regard to child protection, refer to risk for
harm and risk for maltreatment.Determinants of accidental versus nonaccidental injuriesThreat-to-harm versus harm, at-risk versus high-riskNormal growth and developmentClinical presentations of child abuse (eg, findings that indicate accident vs
inflicted and common symptoms)Recognizing a hazardous environment (ie, not just a dirty or untidy home)Caregiver disabilities and characteristics that create a high-risk situation
(eg, mental and physical health, alcohol or other substance abuse)Criteria for rapid assessment for high-risk situationsDocumentation of observationsResources and referrals for at-risk families that do not need immediate CPSEffective ways to pass information and communicate concern to hospital
staff, referral agencies, or child protection workers
CPS, Child protection services.

E M S A N D C H I L D A B U S EMarkenson et al
equipped to cope with the volatile family situation thatmay accompany potential child abuse or neglect. CPEMresearch showed that EMTs and paramedics reportedthe least confidence in this area. Most respondents indi-cated a need for additional education in techniques forinterviewing and interacting with the family in such sit-uations. The Panel established key knowledge andskills issues in this area (Table 7).
Role-playing and scenarios are the best methods fortraining and educating providers in these techniques.Scripted questions may be helpful as well. Future tech-nology may bring additional tools to this arena, such asinteractive video presentations.
Recognition, Assessment, and Treatment
The results of CPEM’s survey demonstrated that pre-hospital providers need to broaden their view of assess-ment and open their eyes wider if they are to recognizepotential child abuse and neglect or children who are atrisk. The relative scarcity of pediatric calls contributesto this problem. Child protection professionals use abasic assessment framework, which assesses the ques-tions of who, what, where, when, and how, when inves-tigating a suspicion of child abuse; this could be readilyadapted for prehospital providers. Prehospital pro-viders should be reminded that they already acquiremost of this information when they perform the scene
9 8 A N N A L S O F E M E R G E N C Y M E D I C I N E 4 0 : 1 J U L Y 2 0 0 2
survey and determine the mechanism of injury. Becausemost prehospital providers have only been taught aboutsevere physical abuse and traumatic presentations intheir certification courses, it is clear that child abuseand neglect issues need to be incorporated into medicalpresentations (eg, apnea, lethargy, seizures) going fromthe general to the specific in child abuse and neglect.
Prehospital providers must be assured that they arenot expected to employ the specialized skills or fill therole of a social worker. Their role is not to fix the prob-lem at the scene, but, rather, to identify the problem andpass along the information. This is how they can actu-ally fix it.
Given that prehospital providers are afforded fewopportunities to practice their recognition, assessment,and treatment skills, the Panel agreed that frequenteducational opportunities are needed. Various teachingmethods were suggested; for example, experiencedproviders could act as mentors to help less seasonedproviders enhance their skills and knowledge.Additional questions about child abuse and neglectcould be added to examinations for the national registryand state certification. Helpful pocket resources thataddress child abuse and neglect could be developed.
The Panel suggested the following scenarios for role-playing to help with training in the areas of recognition,assessment, and treatment.
• What does one do when child abuse or neglect is sus-pected, and the family refuses treatment or transport?
• Can a child be transported without obvious medi-cal necessity?
• What does one do if abuse or neglect is suspected,but there is no medical need for transport?
• What does one do when the abused child is not thepatient for whom the ambulance was called?
Documentation and Reporting Procedures
The Panel agreed that the importance of proper docu-mentation cannot be overemphasized. Documentationreinforces memory, provides a vehicle for conveyinginformation to others, and increases the accuracy of testi-mony, if required. During every emergency call, prehos-pital providers should attune all of their senses to their
Table 7.Knowledge and skills in patient and family interaction.
General approachListenAskKeep in mind you don’t know! (ie, do not assume)
Cultural variationsDon’t make assumptions based on stereotypesBe realistically supportiveBe respectfulScripted questioning
Medically relevantForensically informed
Intervention strategies for the hostile patient and family (ie, unsafesituations that pose danger to the patient or provider)
How to spot red flagsDocumentation of interactions and statements; passing along information

E M S A N D C H I L D A B U S EMarkenson et al
help them assess children with special health care needsfor abuse and neglect (Table 9).
Cultural Competency
Prehospital providers require knowledge and skillsin cultural competency so that they can appropriatelyassess children from different cultural backgrounds forchild abuse and neglect (Table 10). Without this knowl-edge, provider bias may emerge, greatly affecting theaccuracy of the evaluation. To that end, EMS shouldinclude members of culturally diverse communities insuch areas as protocol development, multidisciplinaryteams, and general outreach. EMS participation in com-munity activities should be encouraged. EMS personnelneed resources that expand their knowledge of culturaldiversity within their communities. EMS agencies shouldbe encouraged to teach existing courses that includecultural competency training.
Advocacy and Future Meetings
The final portion of the meeting focused on futureneeds for advocacy and subsequent meetings (Table11). The Panel resolved that prevailing attitudes towardeducation in child abuse and neglect must be changedin order to advance the role of EMS in this arena. Itwould be helpful to produce a joint position paper onthis issue with EMS and CPS.
surroundings so that they can precisely describe theenvironment and, if appropriate, the mechanism ofinjury, even if there is no time to document them at thescene. It is imperative to use clear, objective language forall documentation and to avoid opinions and judgments.
All providers, regardless of whether they are mandatedreporters, must gain the requisite knowledge and skillsfor reporting (Table 8). Education efforts should coverthe definition of reporting, who is mandated to report, towhom the report is made, the mechanism for reporting,and reporting criteria, such as reasonable suspicion.
Children With Special Health Care Needs
The Panel agreed that knowledge about childrenwith special health care needs should be integrated withinformation on child abuse and neglect, because statis-tics have shown that these children are at high risk forabuse and neglect. Prehospital providers should bemade aware of this so that they can watch for signs ofchild maltreatment. Specific knowledge and skills can
J U L Y 2 0 0 2 4 0 : 1 A N N A L S O F E M E R G E N C Y M E D I C I N E 9 9
Table 8.Knowledge and skills for documentation.
Importance of proper documentation Methods for proper documentation, including phrasing and terminology Identify the mechanism of injury and child development issuesScene documentation, including environment and mechanism of injuryDocumentation checklist for efficiency, improved patient call reports, and
better identification of suspicious cases Details checklist (eg, accuracy, mechanism of injury; hygiene, prior medical
care, use of proper legal documentation)Awareness of inappropriate terminology Recording statements of bystanders
Table 9.Knowledge of children with special health care needs.
CSHCN are at high risk for child abuse and neglect Parents of CSHCN are at high risk for wrongful accusation of abuseInterviewing and interaction skills (use role-playing in training and
resource)Address CSHCN in case studies and scenarios for practice
CSHCN, Children with special health care needs.
Table 10.Cultural competency knowledge and skills for child abuseand neglect.
Child-specific cultural competency issues (most key points of curricula incultural competency are not specific to children but, rather, discussnormative cultural values and practices)
Knowledge of ethnic variations in the local neighborhoodIdentification of community leadersDifferentiating folk practices from child abuse and neglect for referral
purposesProvider practices and biasesPsychosocial issuesInterviewing techniques that account for cultural practices and normsInterviewing across language barriers (eg, identifying an appropriate
translator, such as a child or relative)Awareness of nonverbal cues by translator when another is translating for
patient

E M S A N D C H I L D A B U S EMarkenson et al
The Panel called for cross-disciplinary presentationsat EMS and child protection conferences so that eachdiscipline will understand the other’s role. EMS repre-sentatives should be included in hospital-based andother child protection interdisciplinary teams. In addi-tion, it was agreed that the EMSC National ResourceCenter would create, with the help of participants fromthe Blue Ribbon Panel, a fact sheet on EMS and childprotection for national distribution to the EMS world,promoting awareness of advocacy needs.
With regard to advocacy activities to improve exist-ing policy, most discussions focused on issues of man-dated reporting. Many states have statutes that makeprehospital providers mandated reporters but do notrequire mandated education. How can providers beexpected to report if they have no knowledge of thelaw? The Panel agreed that both education and report-ing must become mandatory. It was suggested that thereporting process be facilitated through a checklist orform that prehospital providers could incorporate intheir patient call record. It may be helpful to establishan outline for the form that could be used nationally,but each state will need to adapt this outline to its ownrequirements.
The Panel resolved to publish this summary of theconsensus conference simultaneously in EMS and childprotection journals, with the hope that it will help per-sonnel in EMS and CPS understand and remember theimportance of each other’s roles. Panel participants willfacilitate presentations on this topic at EMS and child
1 0 0 A N N A L S O F E M E R G E N C Y M E D I C I N E 4 0 : 1 J U L Y 2 0 0 2
protection meetings. The Panel suggested that educa-tional materials in EMS and child protection arenasincorporate cross-disciplinary information on eachprofession’s roles. Finally, the Panel recommended thatdata continue to be collected in the area of child protec-tion and EMS.
C O N C L U S I O N S
This conference provided an important first step inbridging the gap between the child protection and EMSworlds. The Blue Ribbon Panel recognized the impor-tance of the identification, recognition, documenta-tion, and reporting in child protection that prehospitalpersonnel can provide. Although prehospital providersare not mandated reporters in all states, it was felt thatthis should be advocated, and that providers must beeducated to fulfill this role.
Prehospital providers are in the unique position ofvisiting the home unannounced and seeing the actualmechanisms of injury. They may observe child protec-tion issues whether the child is the patient or a by-stander. Mechanisms should be established to helpproviders recognize situations that do not fit the criteriafor mandated reporting, so that they can help the fami-lies of at-risk children obtain social services that mayprotect these children from future harm.
Child protection experts must be educated as well, sothat they will better understand the prehospital provider’simportant role in identifying and reporting child mal-treatment. The continued cooperation of these two dis-ciplines is essential if we are to help children who sufferfrom maltreatment. Continued cooperation can be fos-tered through mutual understanding, increased pres-ence and participation at each other’s conferences, andpublication of research data from this field.
Medical Director, National Child Protection Education Project,Center for Pediatric Emergency Medicine, Director of PediatricCritical Care and Child Protection, Harlem Hospital Center, andAssistant Professor of Pediatrics, Columbia University College ofPhysicians and Surgeons, New York, NY (Markenson); Director,Center for Pediatric Emergency Medicine, Director of PediatricEmergency Medicine Program, Bellevue Hospital Center, andAssociate Professor of Pediatrics, New York University School of
Table 11.Recommendations for advocacy and collaboration.
Produce a joint position paper with EMS and child protection organizationsDeliver presentations on child abuse and neglect at EMS conferences Deliver presentations on EMS at child protection conferences Add EMS representatives to hospital-based and other child protection teamsCreate a fact sheet for national distribution to the EMS world Make education and reporting mandatory in all statesCreate a checklist or form that EMS can incorporate into its record and use
for reportingPublish meeting summary simultaneously in EMS and child protection journalsIncorporate cross-disciplinary material into EMS and CPS training to
delineate roles
CPS, Child protection services; EMS, emergency medical services.

E M S A N D C H I L D A B U S EMarkenson et al
A P P E N D I X .Blue Ribbon Panel participants, Center for PediatricEmergency Medicine staff, and local conference staff.
Blue Ribbon Panel Participants*
Beth L. Adams, RN, NREMT-P, National Association of Emergency MedicalServices Physicians
Seth Asser, MD, Cultural Competency ExpertEdward N. Bailey, MD, National Alliance of Children’s Trust and Prevention
FundsJane Ball, DrPH, RN, Emergency Medical Services for Children National
Resource CenterRintha Batson, EMT-P, National Association of Emergency Medical TechniciansKathleen Brown, MD, American College of Emergency PhysiciansCindy W. Christian, MD, Ambulatory Pediatric AssociationDavid Corwin, MD, American Academy of Child and Adolescent Psychiatry Cindy Doyle, RN, BSN, MA, Maternal and Child Health BureauDouglas S. Faust, PhD, American Psychological AssociationBruce E. Herman, MD, American Academy of PediatricsArthur Hesieh, MA, NREMT-P, National Association of Emergency Medical
Services EducatorsStephen Hise, National Association of State Emergency Medical Services
DirectorsSusan Hohenhaus, RN, CPEN, FNE, North Carolina Emergency Medical
Services for ChildrenMarilyn K. Johnson, RN, Emergency Nurses AssociationDan Kavanaugh, MSW, Maternal and Child Health BureauCarolyn Levitt, MD, National Children’s AllianceJeffrey T. Lindsey, MEd, EMT-P, International Association of Fire ChiefsStephen Ludwig, MD, American Academy of PediatricsJanet McCleery, RN, CPNP, National Association of Pediatric Nurse
PractitionersMargaret McHugh, MD, MPH, Child Protection and Development Center of
Bellevue HospitalDavid R. Miller, National Council of State Emergency Medical Services
Training Coordinators Thomas D. Morton, Child Welfare InstituteLenora Olson, MA, National EMSC Data Analysis Resource CenterNancy A. Peddle, PhD, Prevent Child Abuse AmericaDenice L. Reese, RN, CPNP, National Association of School NursesLaVoyce Reid, MSW, LCSW, National Association of Social Workers Murney Rinholm, Parent RepresentativeLaura Rogers, JD, National Center for Prosecution of Child AbusePaul Sowash, National Registry of Emergency Medical Technicians John Stuemky, MD, International Society for the Prevention of Child Abuse
and Neglect Chief Mary Ann Viverette, International Association of Chiefs of PoliceCenter for Pediatric Emergency Medicine StaffDavid Markenson, MD, EMT-P (Meeting Chair)Hedda Matza-Haughton, MSW, CSW (Meeting Co-Chair)Arthur Cooper, MD, MSLocal Conference Staff (National EMSC Resource Center)Shulamit Lewin, MHSYvonnada Cousins, BA Nikita Reed Donna M. Davidson, MPH Susan Eads Role, JD, MLS*Although these individuals were appointed to represent their organizations, and thecomments contained in this document represent the participants’ input, formalapproval of this summary was not obtained from the boards of these organizations.
Medicine, New York, NY (Foltin); Director of Research, PediatricEmergency Medicine Program, Bellevue Hospital Center, andAssistant Professor of Clinical Pediatrics, New York UniversitySchool of Medicine, New York, NY (Tunik); Director, PediatricSurgery and Pediatric Surgical Critical Care, Harlem HospitalCenter, and Associate Professor of Surgery, Columbia UniversityCollege of Physicians and Surgeons, New York, NY (Cooper);Project Coordinator, National Child Protection Project, Center forPediatric Emergency Medicine, New York, NY (Matza-Haughton);Associate Director of Programs, National Emergency MedicalServices for Children Data Analysis Resource Center, Inter-mountain Injury Control Research Center, and Assistant Professor,Department of Pediatrics, University of Utah, Salt Lake City, UT(Olson); Executive Director, Center for Pediatric EmergencyMedicine, and Assistant Research Scientist, New York UniversitySchool of Medicine, New York, NY (Treiber).
The research project members and staff attending this meetingwere supported by HRSA Grant No. 6 H34 MC 00077.
Address for reprints: David Markenson, MD, Director of PediatricCritical Care and Child Protection, Harlem Hospital Center, ColumbiaUniversity College of Physicians and Surgeons, 506 Lenox Avenue,MLK 17, New York, NY 10037; E-mail [email protected].
We thank the Emergency Medical Services for Children (EMSC)Program of the Maternal and Child Health Bureau (MCHB) of theDepartment of Health and Human Services for providing the finan-cial support for the meeting. We thank Cindy Doyle, RN, and DanKavanagh, MSW, of the MCHB EMSC Program, for their directionand assistance with this project and with the meeting; and JaneBall, PhD, Ken Allen, Yvonnada Cousins, and the staff of the EMSCNational Resource Center, who helped to coordinate the meeting.We express our appreciation to Lenora Olson, MA, and LawrenceCook, MStat, from the National Data Analysis Research Center; andWilliam Brown, NREMT-P, and Philip Dickison, NREMT-P, of theNational Registry of EMTs (NREMT) for help with data managementand analysis. The authors would also like to thank AndrewSkomorowsky, MFA, NREMT-P, from the Center for PediatricEmergency Medicine, whose help in the development and distribu-tion of the assessment tool and coordination of results dissemina-tion was invaluable.
Blue Ribbon Panel participants, Center for Pediatric EmergencyMedicine staff, and local conference staff are listed in theAppendix.
J U L Y 2 0 0 2 4 0 : 1 A N N A L S O F E M E R G E N C Y M E D I C I N E 1 0 1
Copyright © 2022 FDOKUMEN