allegations concerning the abuse or neglect of children in care
Upload
khangminh22Category
view
1download
0
Childhood trauma, abuse and neglect:
Truths and consequences
Bessel A van der Kolk MD
Medical director Trauma Center @ JRI
Professor of Psychiatry, Boston University School of Medicine
National Child Traumatic Stress Network
Trauma changes the brain

Imprint of trauma is in the areas of the brain devoted to survival
1. In response to threat people, like all animals, mobilize for automatic physical action.
How to restore focus and calm to the traumatized brain?
Community, touch, safety, belonging, taking effective action
Imagination is the key to survival
Imagination is absolutely critical to the quality of our lives.
Our imagination enables us to leave our routine everyday existence by
fantasizing about travel, food, sex, falling in love, or having the last
word— all the things that make life interesting. Imagination gives us the
opportunity to envision new possibilities— it is an essential launchpad
for making our hopes come true.
It fires our creativity, relieves our boredom, alleviates our pain, enhances
our pleasure, and enriches our most intimate relationships.
When people are compulsively and constantly pulled back into the past,
to the last time they felt intense involvement and deep emotions, they
suffer from a failure of imagination, a loss of the mental flexibility.
Without imagination there is no hope, no chance to envision a better
future, no place to go, no goal to reach
van der Kolk Body keeps the Score, 2014.
Freedman, Kaplan & Sadock’s
Comprehensive Textbook of Psychiatry, II. 1975
‘There is little agreement about the role of father-daughter incest
as a source of serious subsequent psychopathology.
The father-daughter liaison satisfies instinctual drives in a setting
where mutual alliance with an omnipotent adult condones the
transgression. .. The act offers an opportunity to test in reality an
infantile fantasy whose consequences are found to be gratifying
and pleasurable.
..….. such incestuous activity diminishes the subject’s chance of
psychosis and allows for a better adjustment to the external world.
…… the vast majority of them were none the worse for the
experience.
Incest in the United States: one out of 1.1 million women
Friedman & Kapla
How do you take a trauma history?
TRAUMATIC ANTECENDENTS QUESTIONNAIRE I
I. Demographics
- current household composition, occupation, etc.
- who do you rely on for practical help
- who do you rely on for emotional help
II. Current Health
III. Family of origin demographics
- who in your family was affectionate with you
- who recognized you as a special person
- was there anyone you felt safe with growing up?
IV. Childhood caretakers and separations
Herman and van der Kolk
V. Peer relationships and childhood strength
VI. Family Alcoholism
VII. Family discipline and conflict resolution
- who made the rules and enforced discipline at home
- description of family rules
- usual ways of disciplining children: scolding, withholding privileges, spanking, verbal abuse, hitting, hitting with objects
- usual way parents solved disagreements: never angry, talking, yelling, threatening to hit, breaking and throwing, hitting
VIII. Early sexual experiences
TRAUMATIC ANTECENDENTS QUESTIONNAIRE II

Childhood antecedents of self-destructive behavior
(van der Kolk, Perry & Herman, 1991)
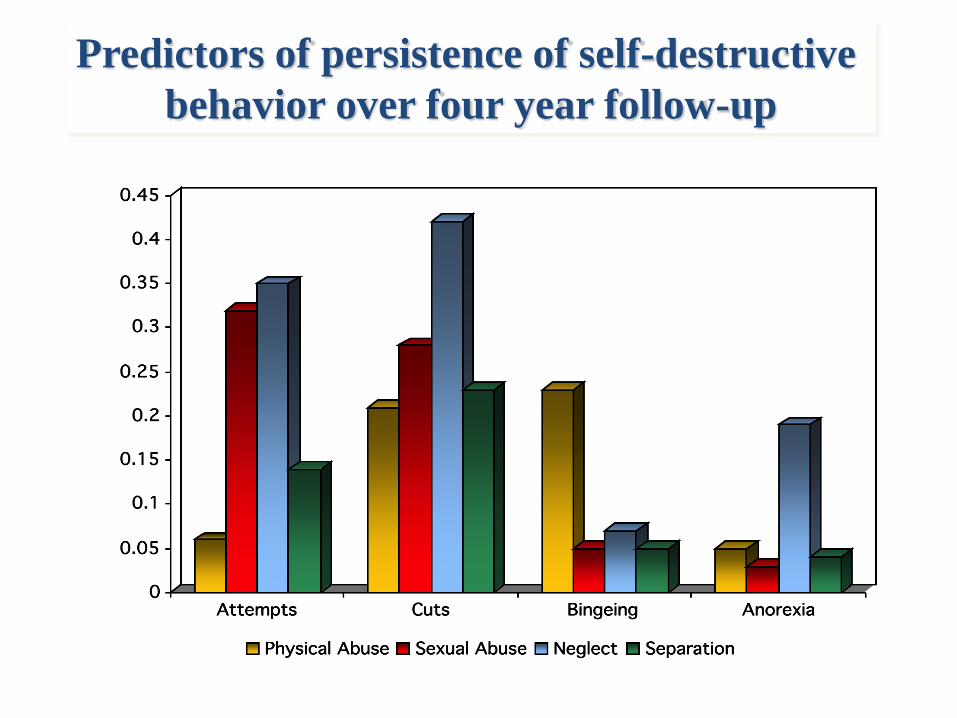
Predictors of persistence of self-destructive
behavior over four year follow-up

ACE Study N=17,337
Emotional abuse 10.6
(Did a parent or other adult in the household . . .)
1) Often or very often swear at you, insult you, or put you down?
2) Sometimes, often, or very often act in a way that made you fear that you might be
physically hurt?
10.6
Physical 28.3
(Did a parent or other adult in the household . . .)
1) Often or very often push, grab, slap, or throw something at you?
2) Often or very often hit you so hard that you had marks or were injured?
28.3
Sexual 20.7
(Did an adult or person at least 5 years older ever . . .)
1) Touch or fondle you in a sexual way?
2) Have you touch their body in a sexual way?
3) Attempt oral, anal, or vaginal intercourse with you?
4) Actually have oral, anal, or vaginal intercourse with you?
20.7
Household dysfunction
Substance abuse 26.9
1) Live with anyone who was a problem drinker or alcoholic?
2) Live with anyone who used street drugs?
26.9
Mental illness 19.4
1) Was a household member depressed or mentally ill?
2) Did a household member attempt suicide?
19.4
Mother treated violently 12.7
(Was your mother (or stepmother)):
1) Sometimes, often, or very often pushed, grabbed,
slapped, or had something thrown at her?
2) Sometimes, often, or very often kicked, bitten, hit with a
fist, or hit with something hard?
12.7
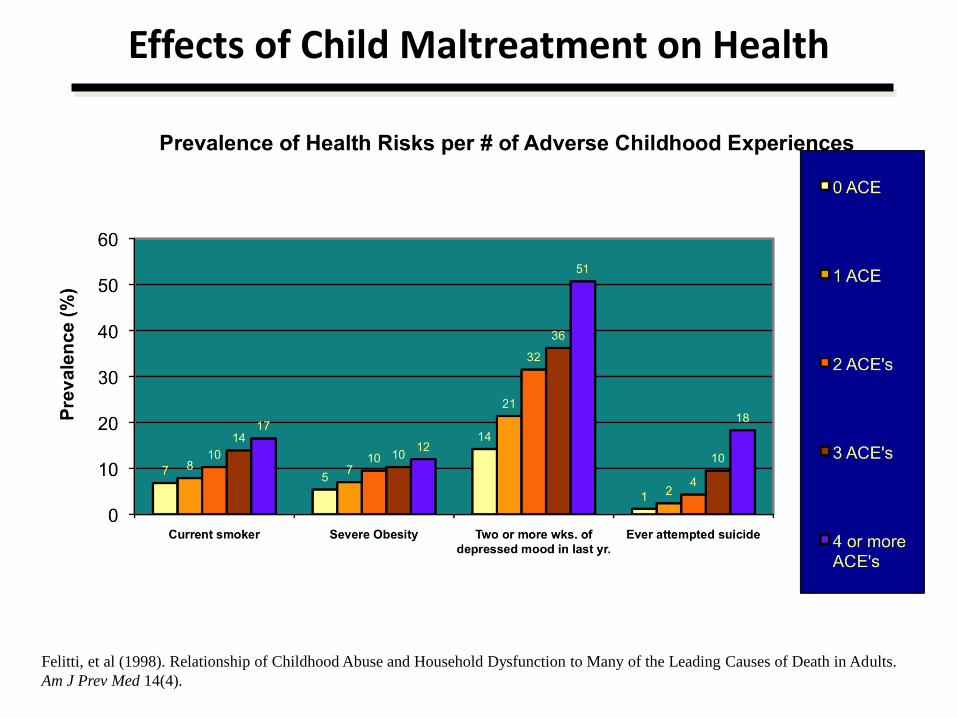
Felitti, et al (1998). Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults.
Am J Prev Med 14(4).
Effects of Child Maltreatment on Health
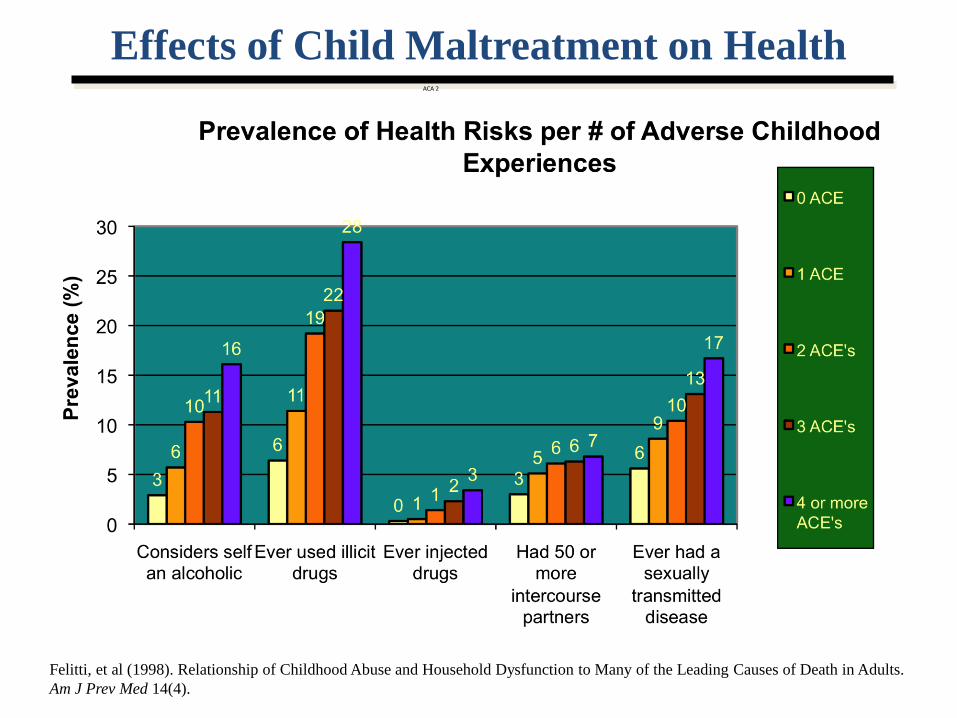
Felitti, et al (1998). Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults.
Am J Prev Med 14(4).
Effects of Child Maltreatment on Health ACA 2
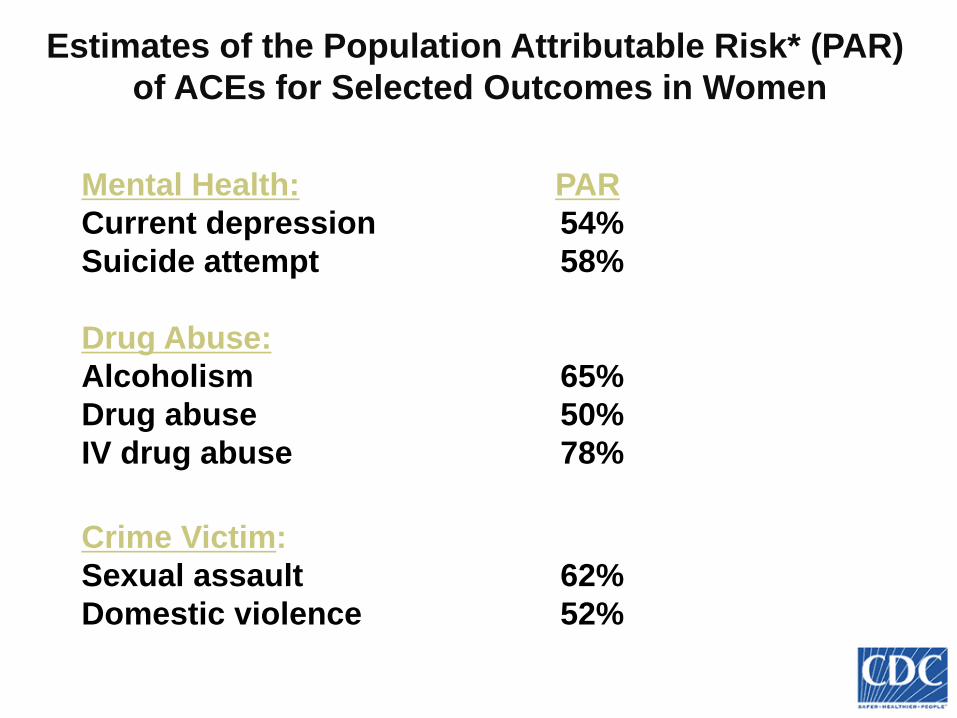
Estimates of the Population Attributable Risk* (PAR)
of ACEs for Selected Outcomes in Women
Mental Health: PAR
Current depression 54%
Suicide attempt 58%
Drug Abuse:
Alcoholism 65%
Drug abuse 50%
IV drug abuse 78% Crime Victim:
Sexual assault 62%
Domestic violence 52%
*Based upon the prevalence of one or more ACEs (62%) and the adjusted odds ratio >1 ACE.
I - Childhood Adversities
The ACE study demonstrated how pervasive trauma is, and that multiple systems are effected by early trauma,
abuse and deprivation
Scope of Childhood Trauma
• The U.S. Centers for Disease Control (CDC) estimates that 1 in 8 children between ages 2 and 17 is a victim of maltreatment.
• Developmental Victimization Study finds that 71% of U.S. children had at least one form of victimization
• Great Smokey Mountain Study finds that 67.8% of children were traumatized in some fashion by age 16 years
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
3,500,000
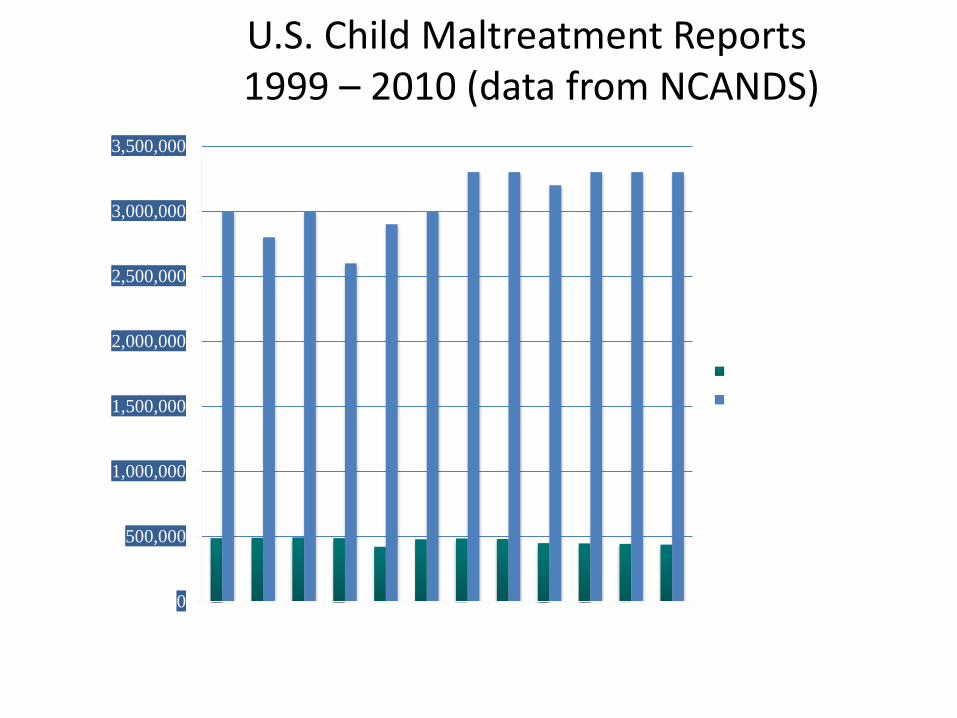
U.S. Child Maltreatment Reports 1999 – 2010 (data from NCANDS)
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
3,500,000
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Substantiated Cases
Estimated Referrals
DSM IV Field Trial for PTSD
Van der Kolk, Pelcovitz, Roth, 1994
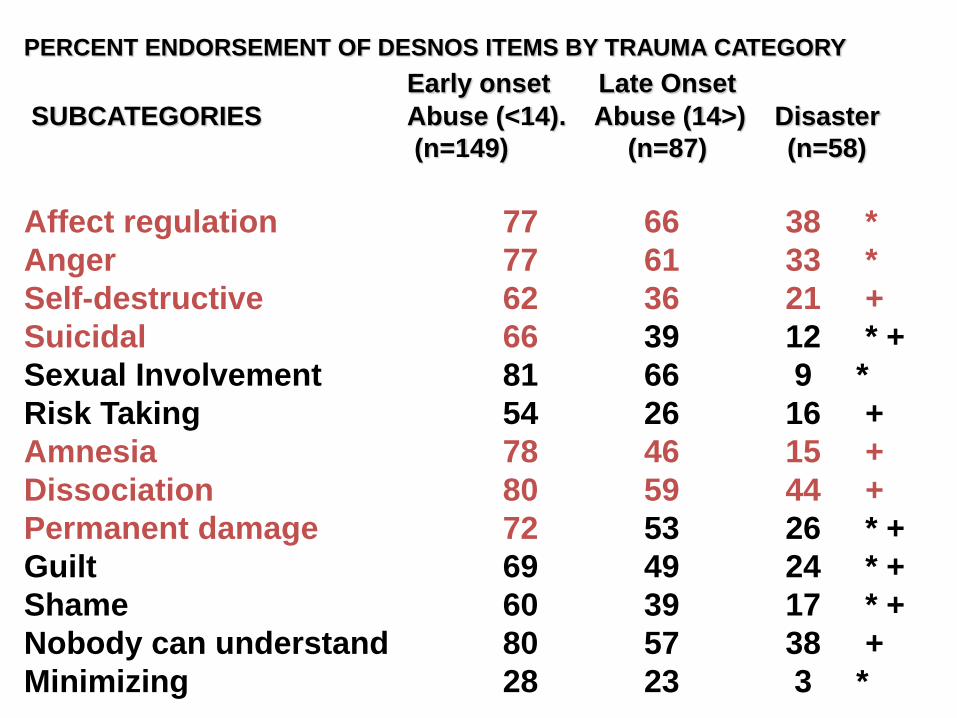
PERCENT ENDORSEMENT OF DESNOS ITEMS BY TRAUMA CATEGORY
Early onset Late Onset
SUBCATEGORIES Abuse (<14). Abuse (14>) Disaster
(n=149) (n=87) (n=58)
Affect regulation 77 66 38 *
Anger 77 61 33 *
Self-destructive 62 36 21 +
Suicidal 66 39 12 * +
Sexual Involvement 81 66 9 *
Risk Taking 54 26 16 +
Amnesia 78 46 15 +
Dissociation 80 59 44 +
Permanent damage 72 53 26 * +
Guilt 69 49 24 * +
Shame 60 39 17 * +
Nobody can understand 80 57 38 +
Minimizing 28 23 3 *
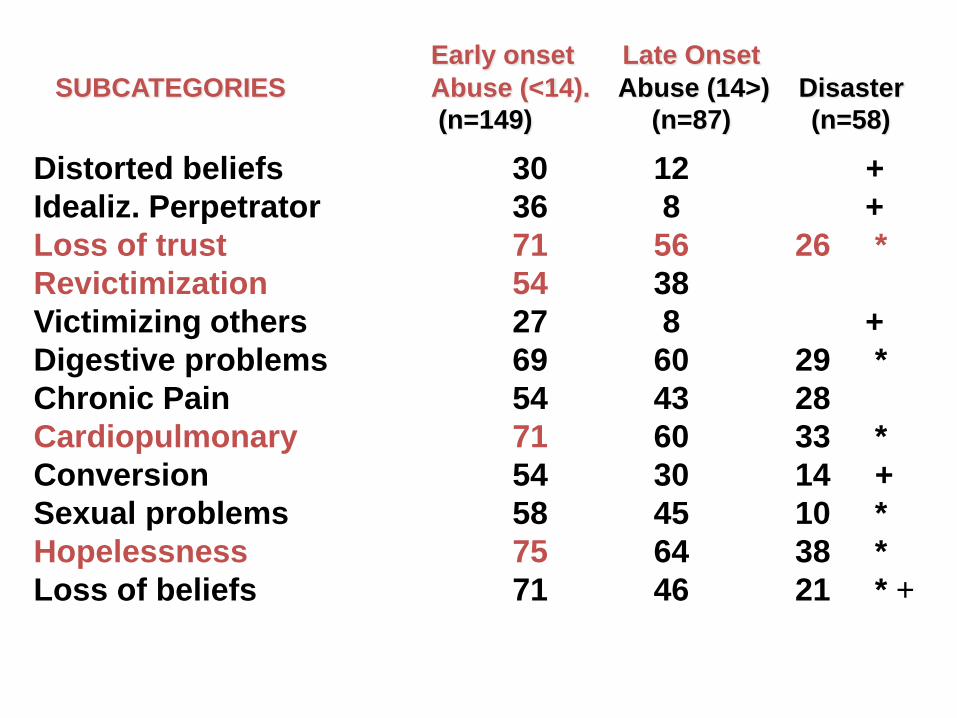
Distorted beliefs 30 12 +
Idealiz. Perpetrator 36 8 +
Loss of trust 71 56 26 *
Revictimization 54 38
Victimizing others 27 8 +
Digestive problems 69 60 29 *
Chronic Pain 54 43 28
Cardiopulmonary 71 60 33 *
Conversion 54 30 14 +
Sexual problems 58 45 10 *
Hopelessness 75 64 38 *
Loss of beliefs 71 46 21 * +
Early onset Late Onset
SUBCATEGORIES Abuse (<14). Abuse (14>) Disaster
(n=149) (n=87) (n=58)

Correlates of Disturbed Attachment vs. Unresolved
Trauma
Symptom Profile
Disturbed Attachment
(Secure vs. Not)
Unresolved
Trauma (Ut vs. not)
PTSD Severity
Affect Dysregulation
Capacity for NMR
Anger Expression
Chronic Suicidality and Self
Injury
Disturbances in Relation to Others
Perceptions of
Belonging/Support
Cumulative Revictimization
Somatization
---
.17*
Stovall-McClough & Cloitre (2006) JCCP

Correlates of Disturbed Attachment vs. Unresolved
Trauma
Symptom Profile
Disturbed Attachment
(Secure vs. Not)
Unresolved
Trauma (Ut vs.
not)
PTSD Severity
Affect Dysregulation
Capacity for NMR
Anger Expression
Chronic Suicidality and Self
Injury
Disturbances in Relation to
Others
Perceptions of
Belonging/Support
Cumulative Revictimization
Somatization
---
.24**
.22*
.19*
.29**
.26**
.23**
.17*
---
---
---
---
---
---
Child Maltreatment and Public Health
• Single most preventable cause of mental illness
• Single most preventable cause of drug and alcohol abuse in women
• Single most preventable cause of HIV high-risk behavior (IV drugs, promiscuity)
• Significant contributor to leading causes of death (heart disease, cancer, stroke, diabetes, suicide)
OhioCanDo4Kids.Org
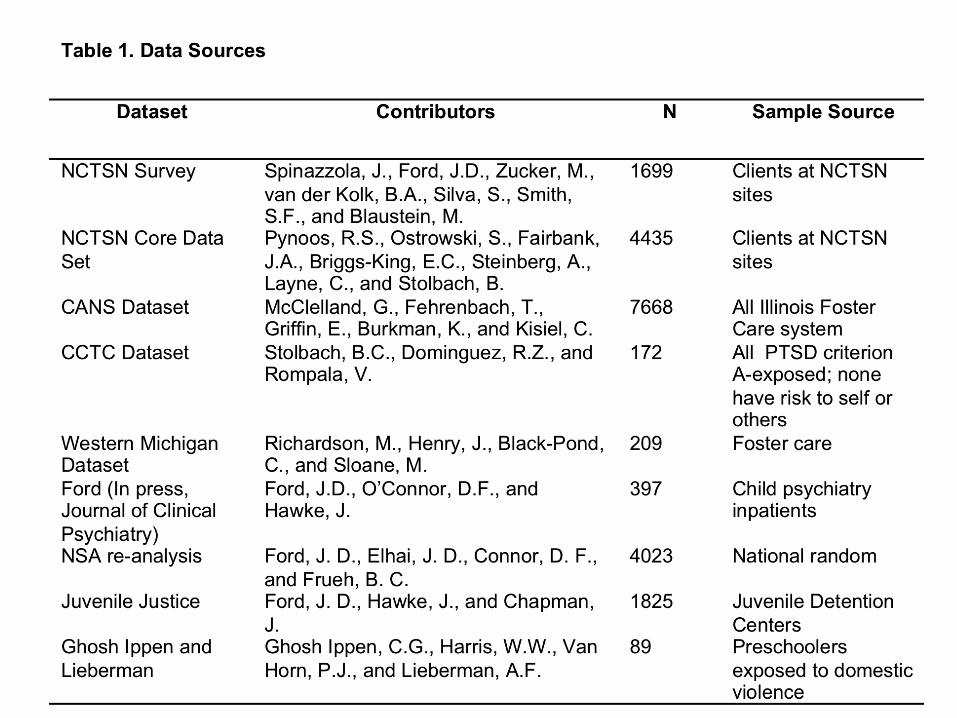
Complex Trauma in the National Child Traumatic Stress Network
Joseph Spinazzola, Ph.D., Julian Ford, Ph.D., Margaret Blaustein, Ph.D., Melissa Brymer, Psy.D., Laura Gardner,
BsPH, Susan Silva, Ph.D., Stephanie Smith, Ph.D. Bessel van der Kolk, M.D.,
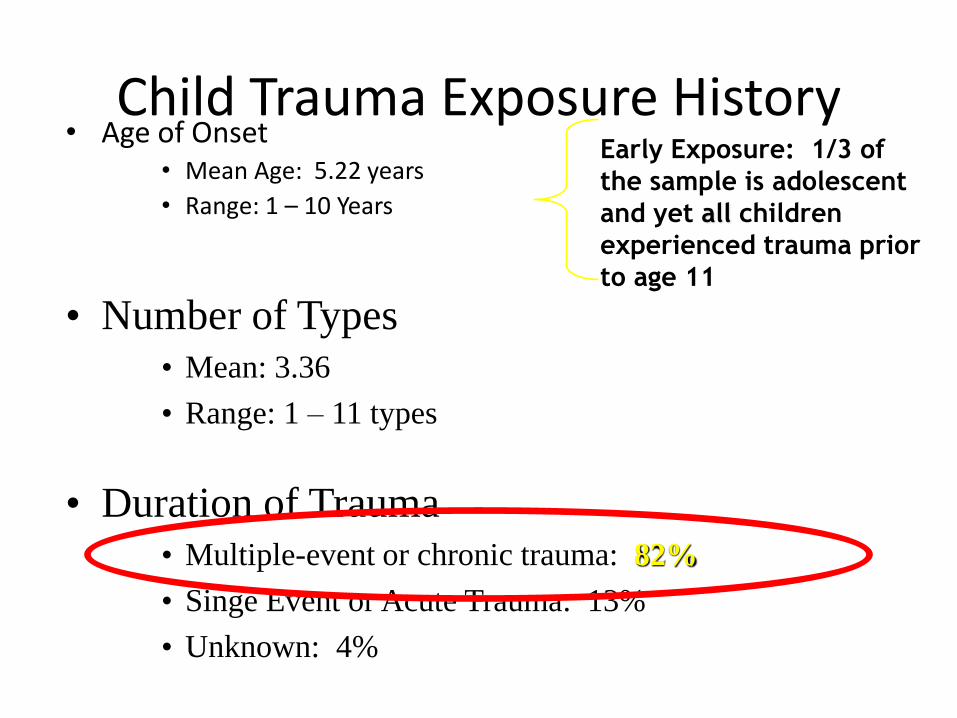
Child Trauma Exposure History • Age of Onset
• Mean Age: 5.22 years
• Range: 1 – 10 Years
Early Exposure: 1/3 of
the sample is adolescent
and yet all children
experienced trauma prior
to age 11
• Duration of Trauma • Multiple-event or chronic trauma: 82%
• Singe Event or Acute Trauma: 13%
• Unknown: 4%
• Number of Types • Mean: 3.36
• Range: 1 – 11 types

Met Full Criteria for PTSD
73.5
24.5
0
10
20
30
40
50
60
70
80
90
100
NO
Yes
Perc
en
t
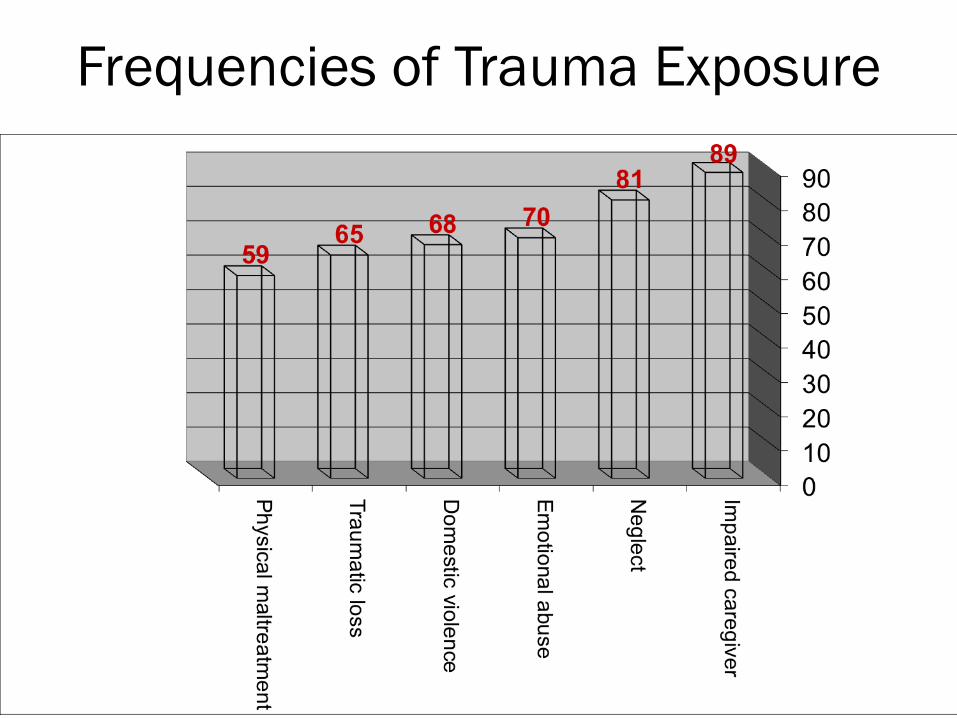
Frequencies of Trauma Exposure
COMPLEX POSTTRAUMATIC SEQUELAE

Complex Posttraumatic Sequelae:
Most Frequent Difficulties
61.5% 59.2% 57.9%53.1%
45.8%
0%
15%
30%
45%
60%
75%
Affect
Dys
regu
latio
n
Attent
ion/
Con
cent
ratio
n
Neg
ative
Self-I
mag
e
Impul
se C
ontro
l
Aggre
ssio
n/Risk-
taking
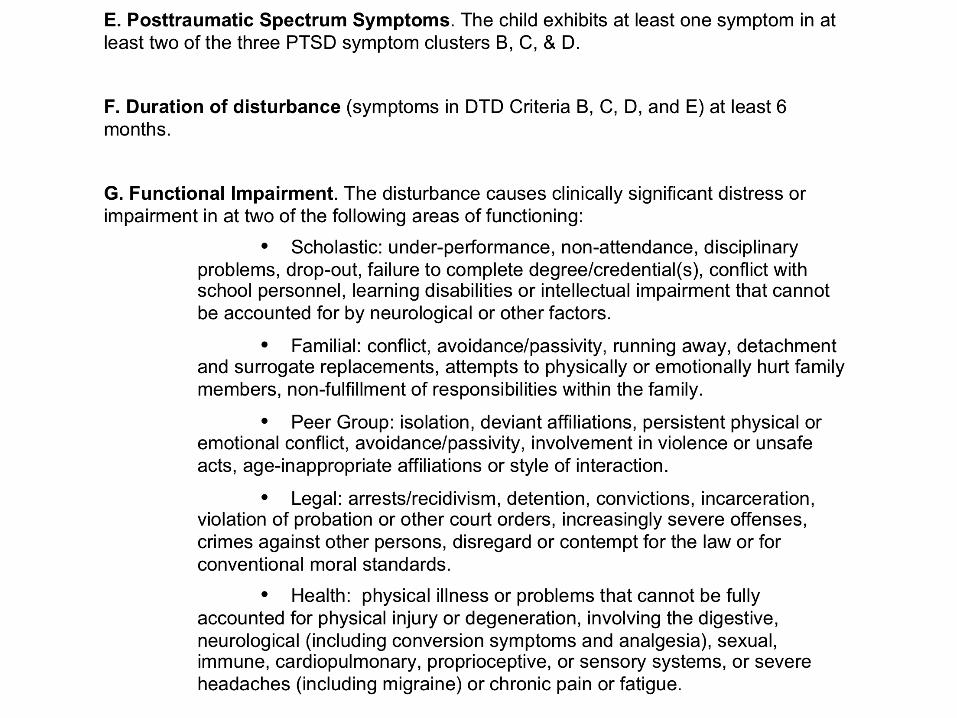
Proposal to include Developmental Trauma Disorder in the DSM 5
Joseph Spinazzola PhD Julian Ford PhD
Wendy D’Andrea PhD Bradley Stolbach PhD Dante Cicchetti PhD
Marylene Cloitre PhD Alicia Lieberman MD
Frank Putnam MD Glenn Saxe MD
Martin Teicher MD PhD Robert Pynoos PD
Bessel A. van der Kolk MD
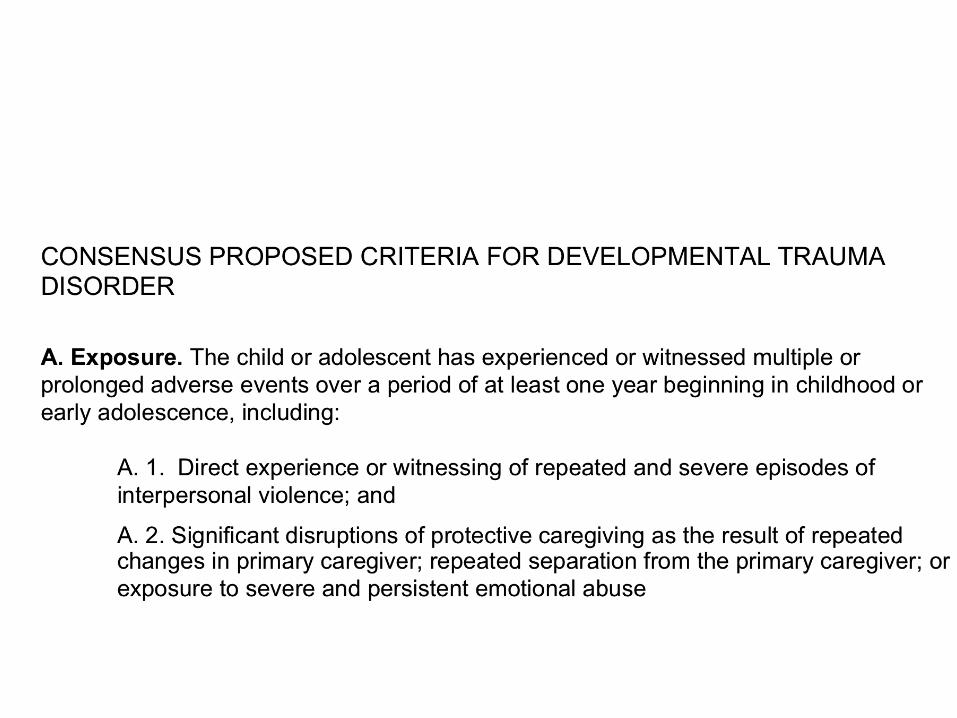
Developmental Trauma Disorder
Statement of Purpose
The goal of introducing the diagnosis of Developmental Trauma
Disorder is to capture the reality of the clinical presentations of children
and adolescents exposed to chronic interpersonal trauma and thereby
guide clinicians to develop and utilize effective interventions and for
researchers to study the neurobiology and transmission of chronic
interpersonal violence.
Children who have developed in the context of ongoing danger,
maltreatment, and inadequate caregiving systems are ill-served by the
current diagnostic system, as it frequently leads to no diagnosis, multiple
unrelated diagnoses, an emphasis on behavioral control without
recognition of interpersonal trauma and lack of safety in the etiology of
symptoms, and a lack of attention to ameliorating the developmental
disruptions that underlie the symptoms.

Othe past 25 years there has been a relatively independent and parallel emergence of
I. The field of Developmental Psychopathology (e.g. Maughan & Cicchetti, 2002;Sroufe,
2005, Putnam, Trickett,2008 Yehuda, & McFarlane, 1997), which has documented the
effects of interpersonal trauma and disruption of caregiving systems on the development
of affect regulation, attention, cognition, perception, and interpersonal relationships.
II. The other significant development has been the increasing documentation of the
effects of adverse early life experiences on brain development (e.g. De Bellis et al., 2002;
Teicher et al., 2003), neuroendocrinology (e.g.Hart, Gunnar, & Cicchetti, 1995;) and
immunology (e.g. Putnam et al., 1997; Wilson et al, 1999).

Developmental Trauma Disorder
Disorder of
1) Self-regulation
2) Focused attention
3) Focused collaborative engagement with self and others

The DSM V taskforce response
The consensus was that there is just too little evidence, at this time, to include DTD in the DSM-V
Minnesota Study of Risk & Adaptation
• 180 children and their families.
• Starting 3 months before the children were born and followed for 30 years into adulthood, measuring all major aspects of the child’s functioning and surrounding circumstances.
• extensive prenatal interviews and testing of parents,
• began collecting data on the infants at birth, beginning with nurses’ ratings in the newborn nursery and continuing with home assessments at 7 and 10 days.
• 11 additional direct assessments between 3 -30 months, and 4 more prior to school entry.
• Assessments were then made almost yearly until age 13, with follow-ups at ages 16, 17½, 19, 21, 23, 26, and 28.
Classification of 212 kids @ 2 months,
• 55% secure, • 22% avoidant, • 23% resistant.
• At 18 months, • 61% secure, • 22% avoidant, • 17% resistant
• Of the 189 dyads assessed at both time periods, 74% of
secure infants remained secure, 45% of avoidant infants remained avoidant, and 37% of the resistant infants remained stable (Egeland & Farber, 1984).
Disorganized attachment
• Humans flee from a source of threat and also, when threatened, to flee to the caregiver (who can protect or carry the infant to safety).
• If the caregiver is the source of threat, the infant is placed in an irresolvable paradox. It is not possible to flee toward and away from the same locus simultaneously.
• Contradictory behaviors, unfocused or anomalous behavior, a collapse in organized functioning, and other signs of behavioral conflict.
Minnesota Study of Risk & Adaptation
Attachment patterns persist
• These patterns become prototypes for subsequent regulation, even when apart from the caregiver.
• Anxious attachment: Patterns of regulation of the anxiously attached groups seriously compromise later functioning. Chronic vigilance, apprehension, and worry about needs being met take a toll.
• Avoidant attachment: Blunting one's feelings so as not to express needs, isolating oneself, feeling alienated from others, and failing to turn to them and stress, makes life very difficult, especially in the social arena
• Disorganized attachment: Being disorganized and disoriented cuts one off from vital experiences or originate inside and outside of the self.
Attentional problems • Both intrusive behavior at 6 months and overstimulation
(boundary violation) @ 42 months predicted activity and
attention problems in kindergarten, ( Jacobvitz &Sroufe, 1987)
• Both caregiver intrusiveness at 6 months and boundary violation
(overstimulation) at 42 months predicted attentional problems.
• Conduct problems. A very large number of studies have found an
association between parental neglect or harsh treatment and
later conduct problems (Elder, Nguyen and Caspi, 1985).
Socialization of violence
• Harsh, chaotic treatment leads to interpersonal alienation and anger
• lack of internalized empathy, and impulse control problems due to a early dysregulation,
• As a result, these children engage in disruptive, oppositional, and aggressive behaviors.
• Such behavior prompts further anger in, and harsh treatment from, parents and alienate teachers and peers, leading to further rejection all around.

Resilience • “Resilient” children had an early positive foundation that supported their
recovery
• Masten (2001) “ordinary magic.” Children with histories of early positive care and early histories of competence are significantly less likely to evince problem behavior in the face of stress than those with unsupportive histories
• “If self-esteem and trust are established early, children are more resilient in the face of environmental stress. They may show poor adaptation during an overwhelming crisis, but when the crisis has passed and the environment is again positive, they may respond more quickly.” (Sroufe, 1978, p. 56).
• Changes in family stress; changes in parents’ characteristics, such as depression; and changes in parenting practices all are associated with changes in child behavior
Minnesota Study of Risk & Adaptation
• By being told repeatedly that something does not hurt and that big boys do not cry children learn to not recognize such feelings.
• A girl repeatedly told by her mother that father died in a car accident, when the child found him hanging, can lead her not to access the memory of the witnessed death and to have no place to put the attendant feelings.
• In addition, of course this child would and emotional abandonment by mother to death off the father in her experienced losses.
Denial -- Sroufe, 2005
Karlen Lyon-Ruth’s Harvard Family Pathways longitudinal study
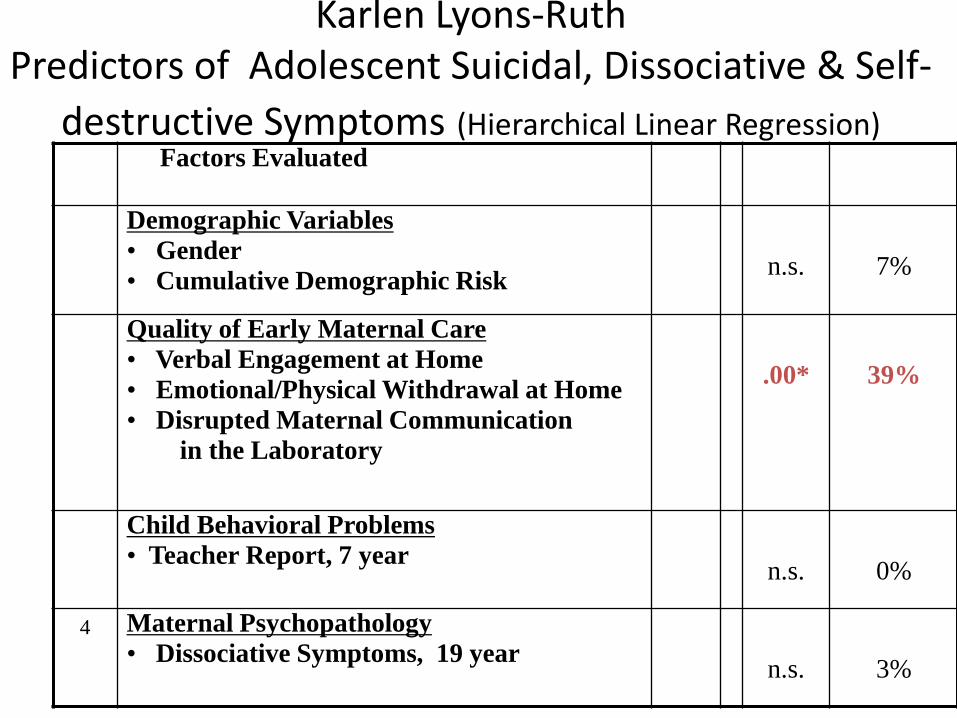
Karlen Lyons-Ruth Predictors of Adolescent Suicidal, Dissociative & Self-
destructive Symptoms (Hierarchical Linear Regression) Step Factors Evaluated ∆ F p Variance
Explained
1 Demographic Variables
• Gender
• Cumulative Demographic Risk
1.34
n.s.
7%
2 Quality of Early Maternal Care
• Verbal Engagement at Home
• Emotional/Physical Withdrawal at Home
• Disrupted Maternal Communication
in the Laboratory
8.30
.00*
39%
3 Child Behavioral Problems
• Teacher Report, 7 year
.01
n.s.
0%
4 Maternal Psychopathology
• Dissociative Symptoms, 19 year
1.71
n.s.
3%

Dissociation
Dissociation is manifested in feeling lost, overwhelmed, abandoned, torn, disconnected from the world, unloved, empty, helpless, trapped, or weighed down. Lyons Ruth found that lack of emotional responsiveness at home at 12 months of age strongly predicted these symptoms in young adults.
Frank W. Putnam MD

Psychobiological Effects of Sexual Abuse: 20 Years Later
Frank W. Putnam, MD Professor of Pediatrics and Psychiatry
Cincinnati Children’s Hospital Medical Center
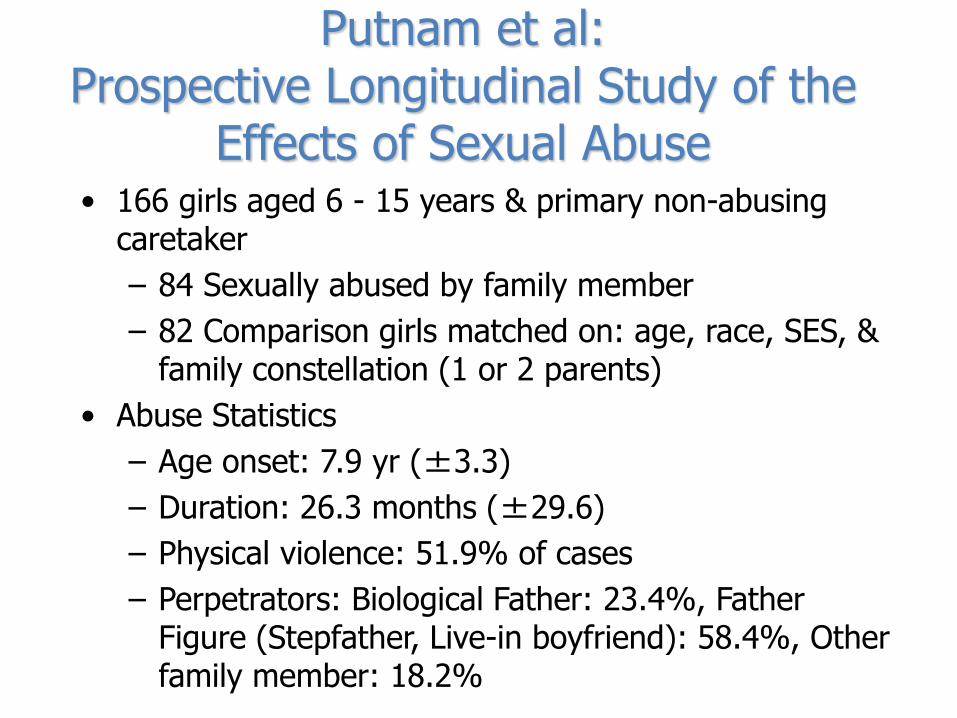
Putnam et al: Prospective Longitudinal Study of the
Effects of Sexual Abuse • 166 girls aged 6 - 15 years & primary non-abusing
caretaker
– 84 Sexually abused by family member
– 82 Comparison girls matched on: age, race, SES, & family constellation (1 or 2 parents)
• Abuse Statistics
– Age onset: 7.9 yr (±3.3)
– Duration: 26.3 months (±29.6)
– Physical violence: 51.9% of cases
– Perpetrators: Biological Father: 23.4%, Father Figure (Stepfather, Live-in boyfriend): 58.4%, Other family member: 18.2%
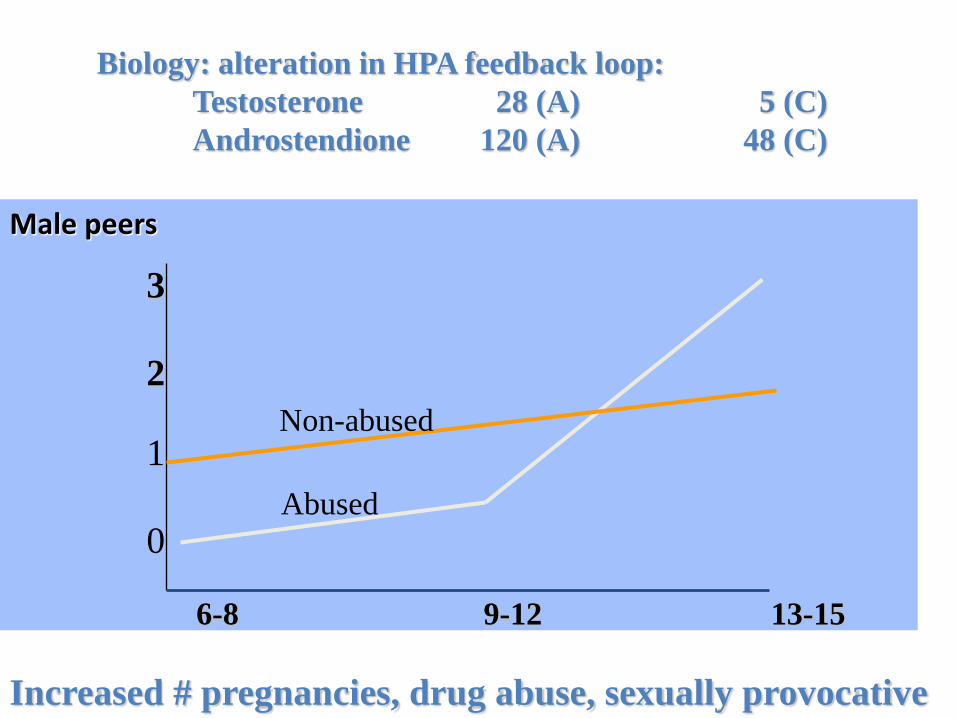
Male peers
Putnam Peer graph
6-8 9-12 13-15
3
2
1
0
Biology: alteration in HPA feedback loop:
Testosterone 28 (A) 5 (C)
Androstendione 120 (A) 48 (C)
Increased # pregnancies, drug abuse, sexually provocative
Non-abused
Abused
Roth S, Newman E, Pelcovitz D, van der Kolk BA, Mandel FS: Complex PTSD in victims exposed to sexual and physical abuse: results from the DSM-IV Field Trial for Posttraumatic Stress Disorder. J Trauma Stress 1997; 10:539-555
van der Kolk BA, Pelcovitz D, Roth S, Mandel FS, McFarlane A, Herman JL: Dissociation, somatization, and affect dysregulation: the complexity of adaptation to trauma. Am J Psychiatry 1996; 153):83-93 Pelcovitz D, van der Kolk BA, Roth S, Mandel F, Kaplan S, Resick P: Development of a criteria set and a structured interview for disorders of extreme stress (SIDES). J Trauma Stress 1997; 10:3-16 Ogata SN, Silk KR, Goodrich S, Lohr NE, Westen D, Hill EM: Childhood sexual and physical abuse in adult patients with borderline personality disorder. Am J Psychiatry 1990; 147:1008-1013
M C. Zanarini, F R. Frankenburg, E D. Dubo, A E. Sickel, A Trikha, A Levin, V Reynolds; Axis I Comorbidity of Borderline Personality Disorder. American Journal of Psychiatry. 1998 Dec;155(12):1733-1739. Shearer SL, Peters CP, Quaytman MS, Ogden RL: Frequency and correlates of childhood sexual and physical abuse histories in adult female borderline inpatients. Am J Psychiatry 1990; 147:214–216 Westen D, Ludolph P, Misle B, Ruffins S, Block J: Physical and sexual abuse in adolescent girls with borderline personality disorder. Am J Orthopsychiatry 1990; 60:55–66 Zanarini MC, Williams AA, Lewis RE, Reich RB, Vera SC, Marino MF, Levin A, Yong L, Frankenburg FR: Reported pathological childhood experiences associated with the development of borderline personality disorder. Am J Psychiatry 1997; 154:1101–1106
Most
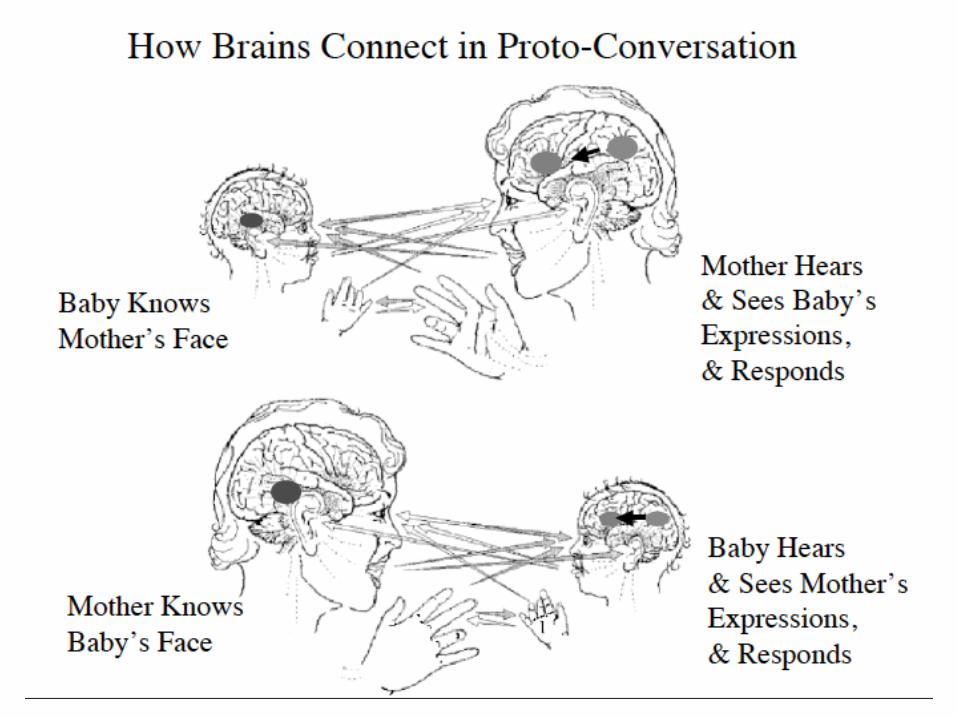
Mind and brain grow in the context of attachment.
We are living rhythm machines
What cannot be communicated to
the (m)other cannot be
communicated to the self.
Bowlby (1991)
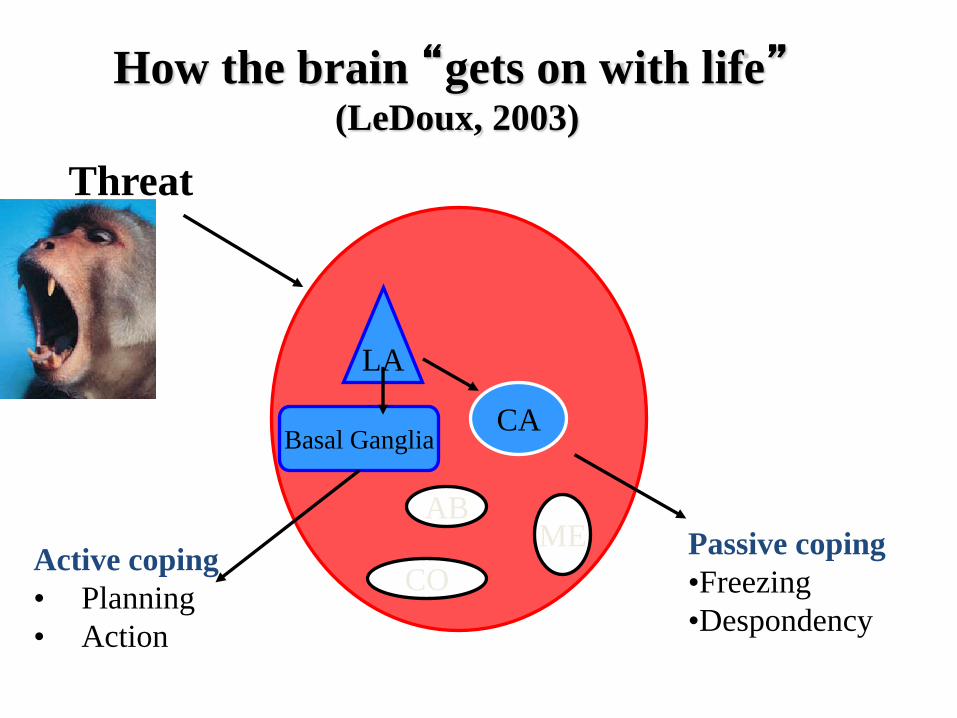
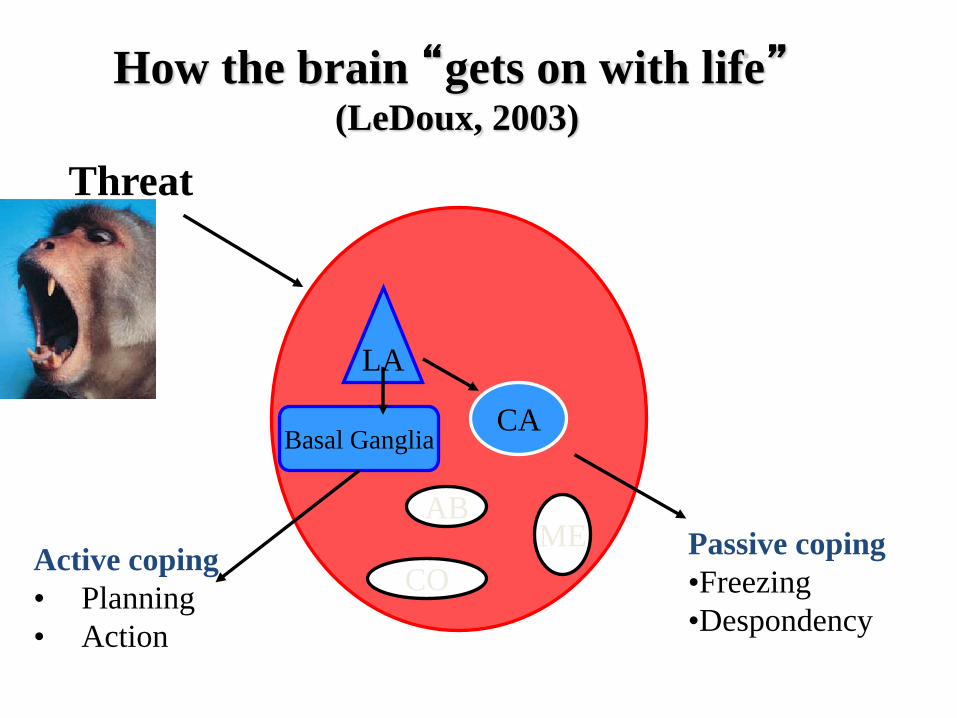
How the brain “gets on with life” (LeDoux, 2003)
Threat
LA
CA Basal Ganglia
AB ME
CO Passive coping
•Freezing
•Despondency
Active coping
• Planning
• Action
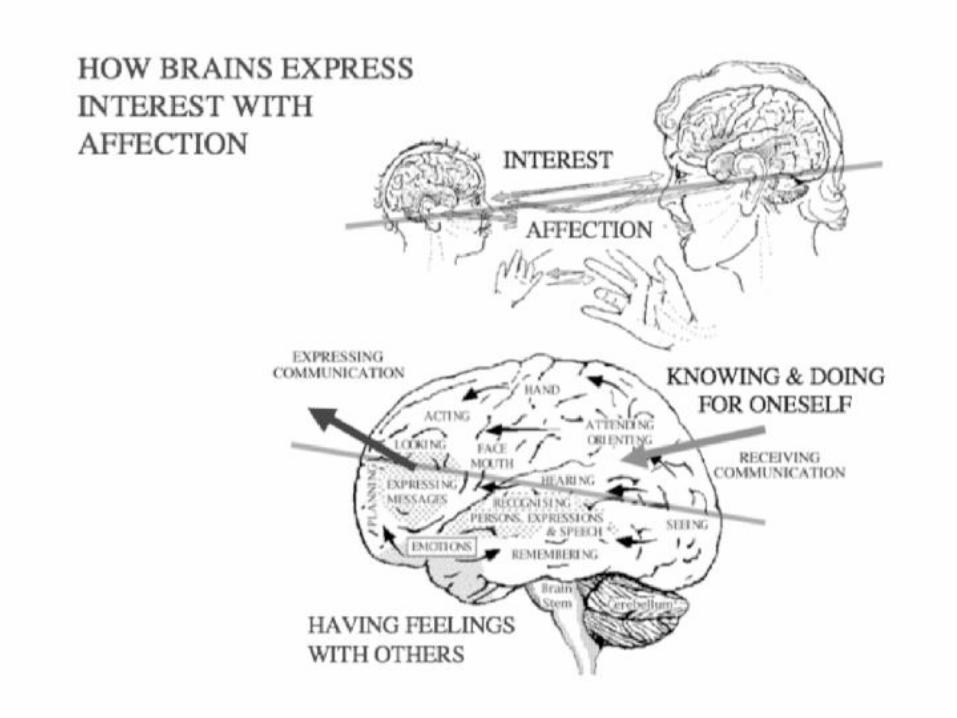
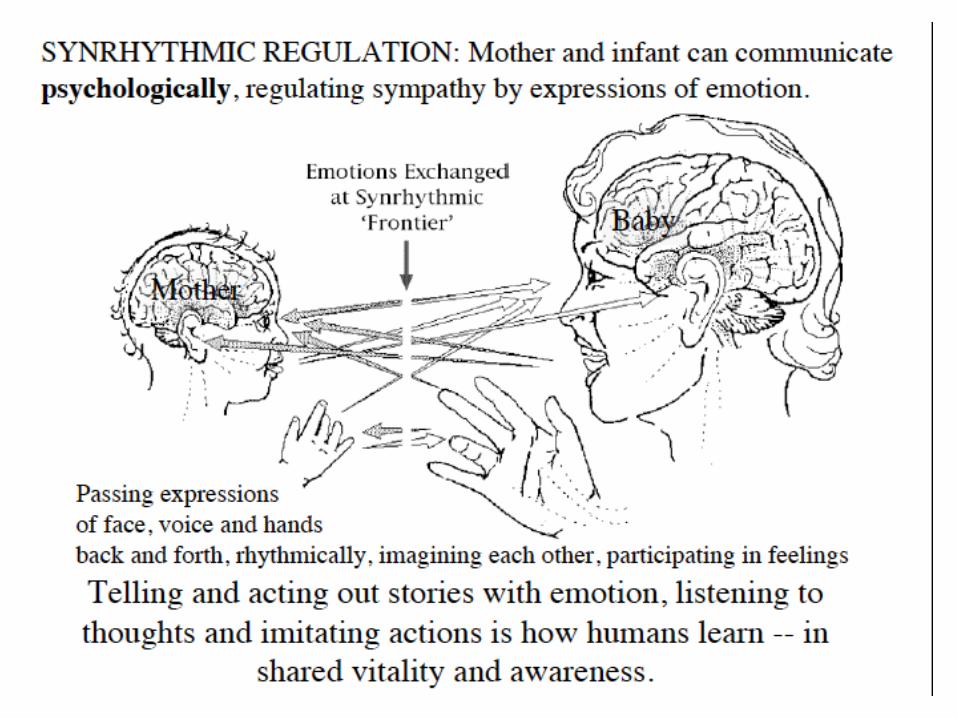
Brain and mind are programmed to playfully engage with others to communicate intentions, experiences and feelings.
Sharing and synchrony is fundamental for development of mind and brain.
That is what we have brains for.
Lack of synchrony, sharing and attunement has devastating consequences.
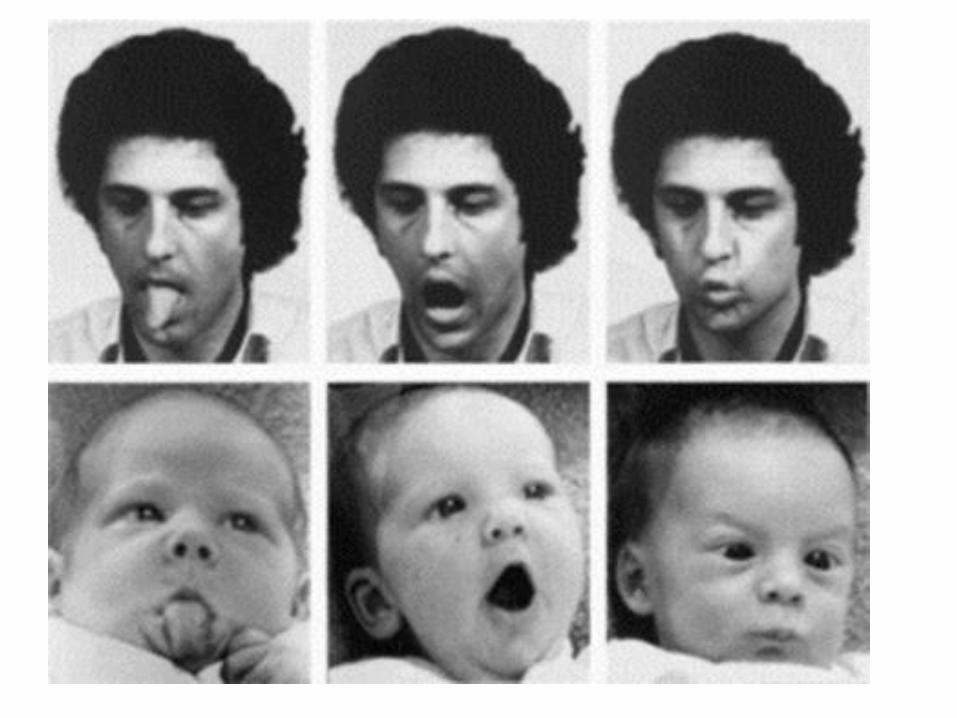
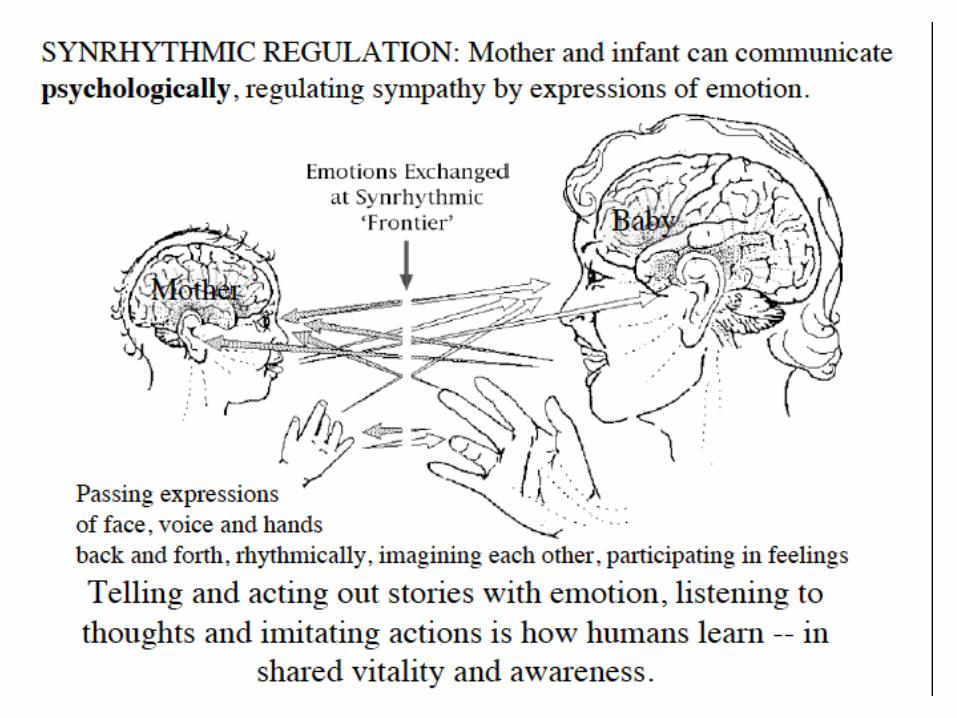
Rhythms & synchrony
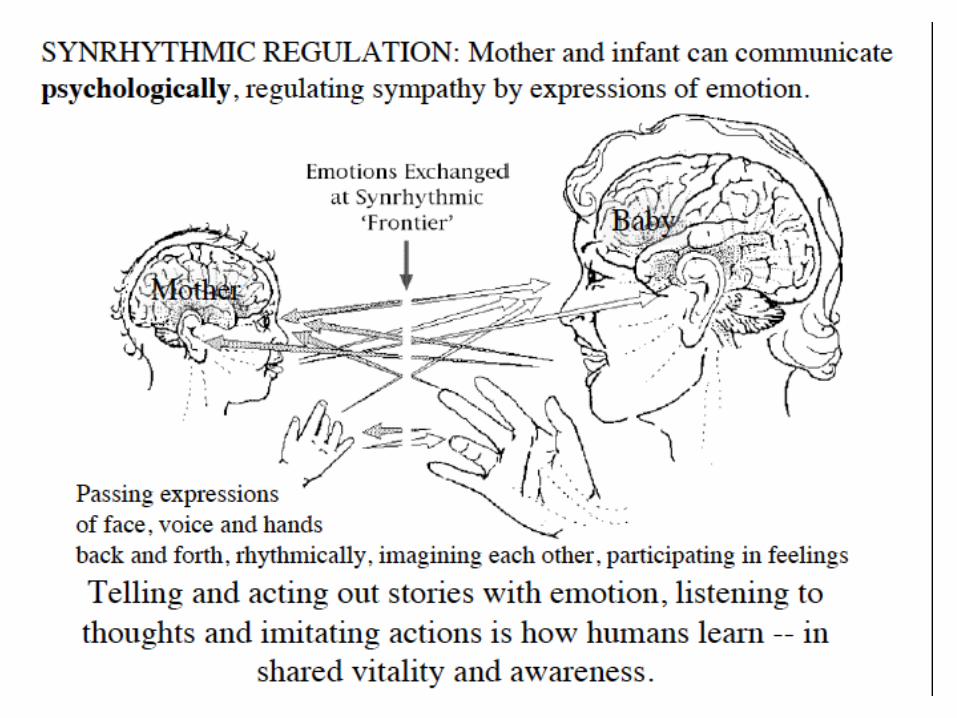
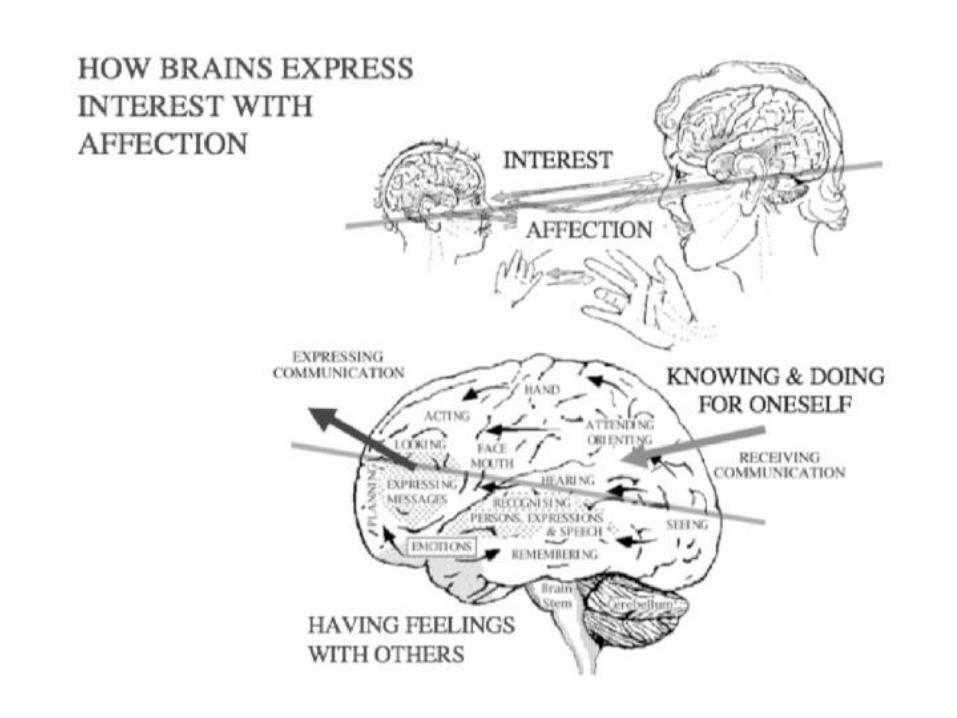
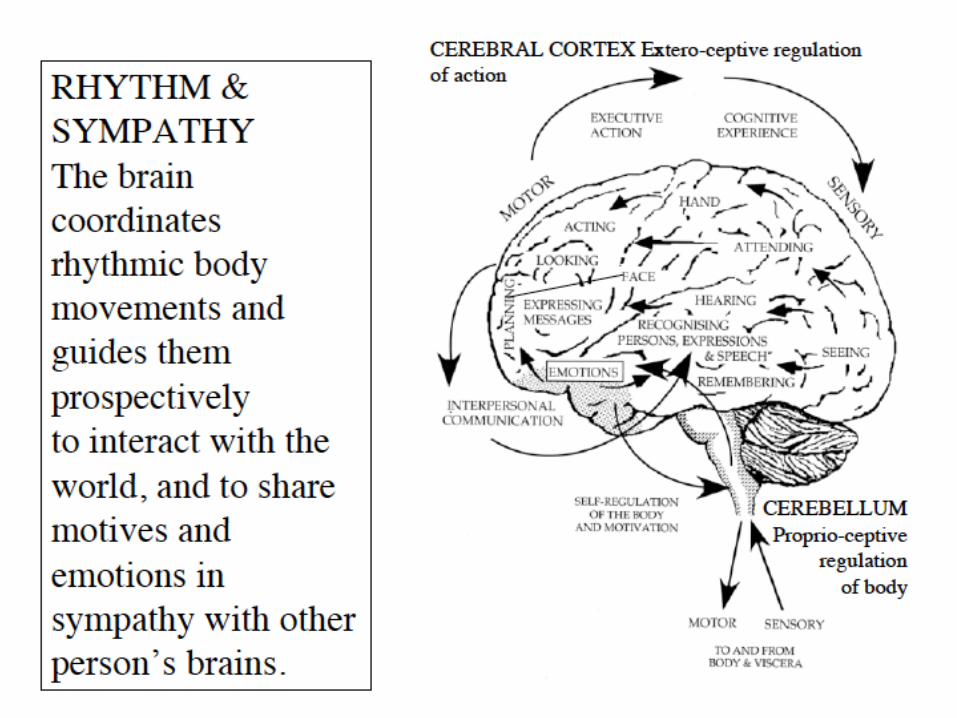
• States of mind are expressed as body movements, facial expressions and gestures that communicate in rhythms physical synchrony.
• This sharing is the foundation of mental health, therapy and all learning and education.
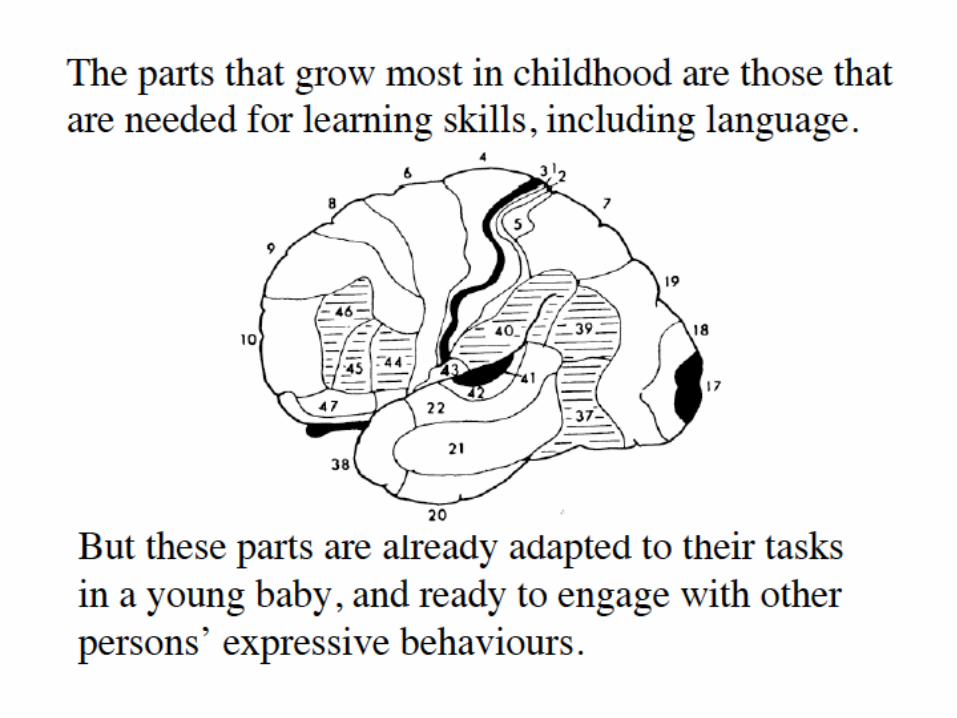
II Trauma & Brain Development

The growing human brain needs to become part of an integrated society of brains, a world that itself is a self-regulating or sustaining organism – a Sociosphere.
After birth the growth of the body and brain transforms activity into experience and experience into action.
The brain seeks experience and is changed by it.
Martin Teicher MD PhD
Martin Teicher MD PhD
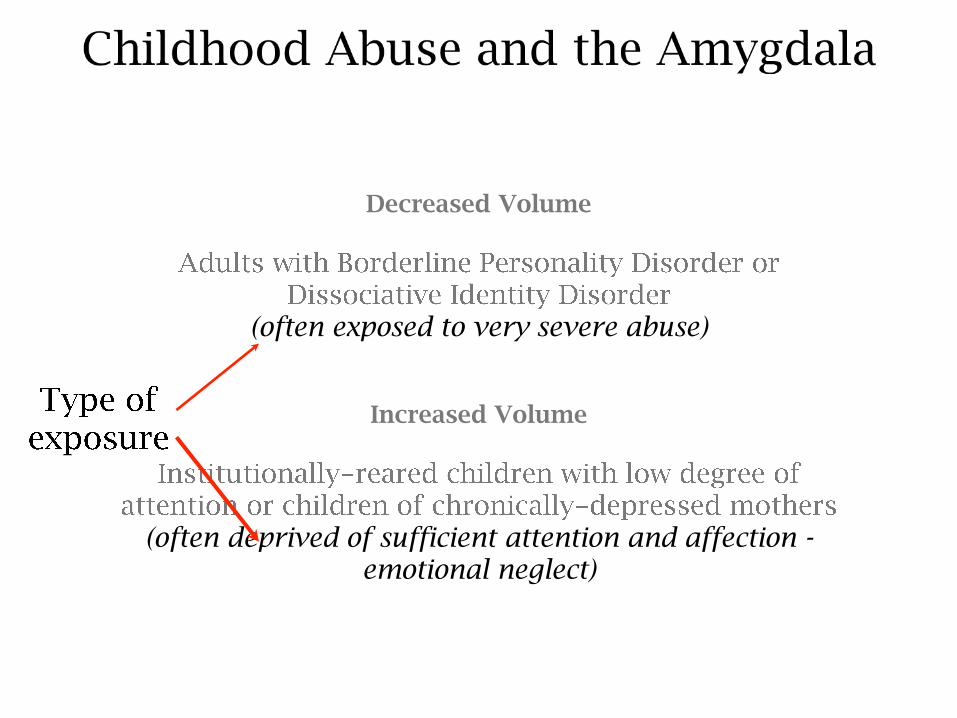
Decreased Volume
(often exposed to very severe abuse)
Increased Volume
(often deprived of sufficient attention and affection - emotional neglect)
Martin Teicher MD PhD

Martin Teicher MD PhD
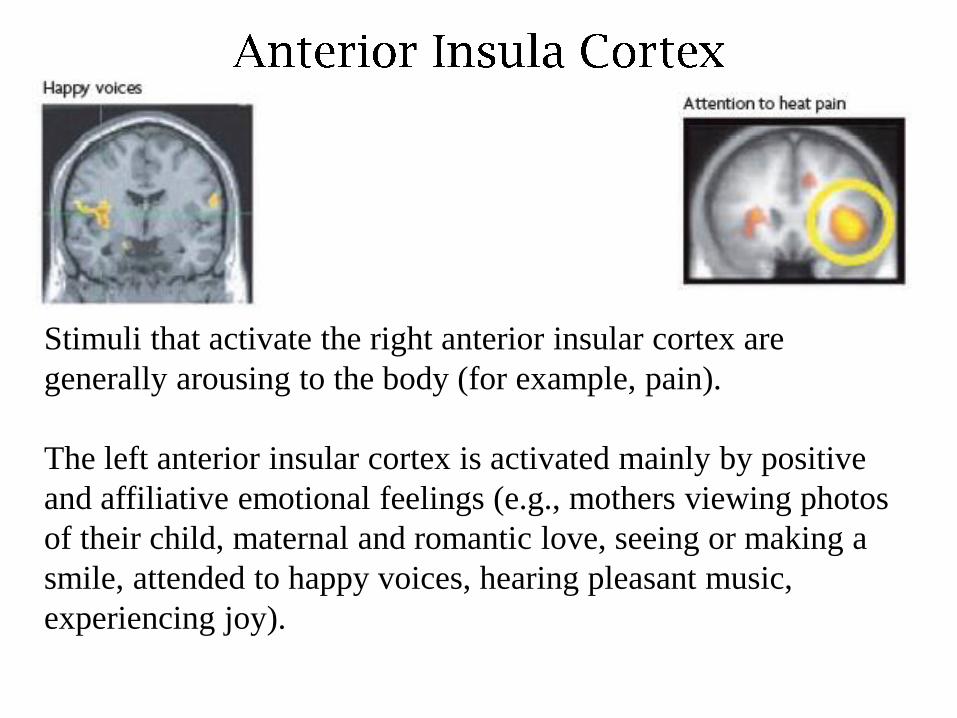
Stimuli that activate the right anterior insular cortex are
generally arousing to the body (for example, pain).
The left anterior insular cortex is activated mainly by positive
and affiliative emotional feelings (e.g., mothers viewing photos
of their child, maternal and romantic love, seeing or making a
smile, attended to happy voices, hearing pleasant music,
experiencing joy).
Trauma and the body
Sensorimotor Psychotherapy
Alignment Cartoon
Sensormotor Psychotherapy Institute
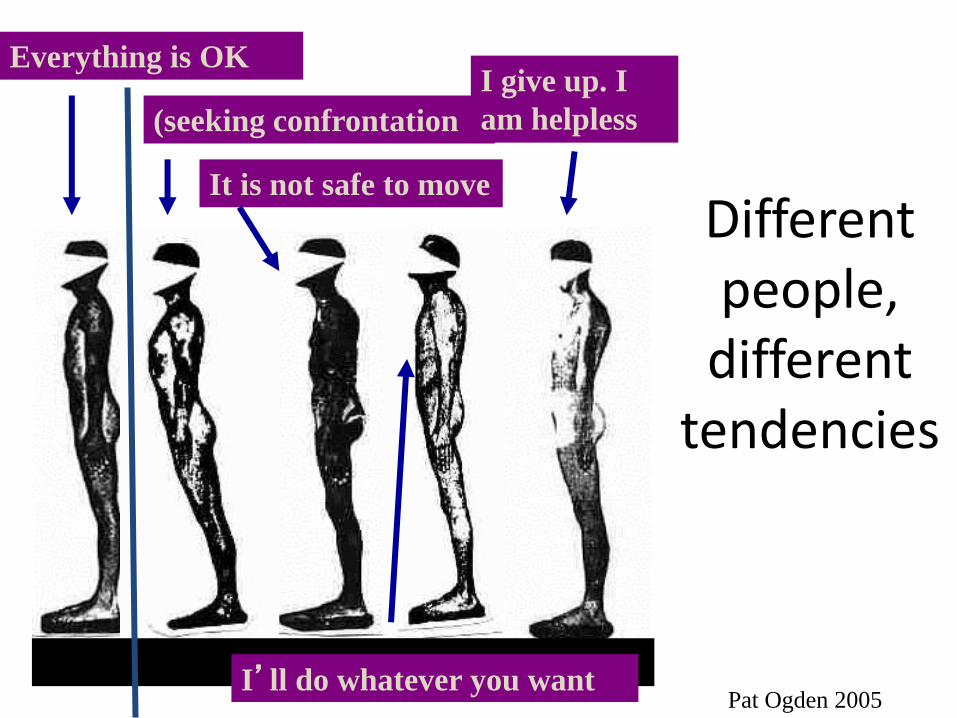
Different people,
different tendencies
Everything is OK
(seeking confrontation
It is not safe to move
I’ll do whatever you want
I give up. I
am helpless
Pat Ogden 2005
ARC Model (Blaustein & Kinniburgh)
• The child and adults in their environment and focuses on four key areas:
– Building safe Attachments
– Enhancing Self Regulatory Capacities
– Increase Competence in Multiple Domains
– Trauma processing
ARC Model: Kinniburgh, Henderson &
Cook (2003)

Overcoming trauma
1. Effective action
How the brain “gets on with life” (LeDoux, 2003)
Threat
LA
CA Basal Ganglia
AB ME
CO Passive coping
•Freezing
•Despondency
Active coping
• Planning
• Action

2. Trauma Processing
EMDR

Overcoming trauma
4. Accessing the emotional brain- knowing one’s self
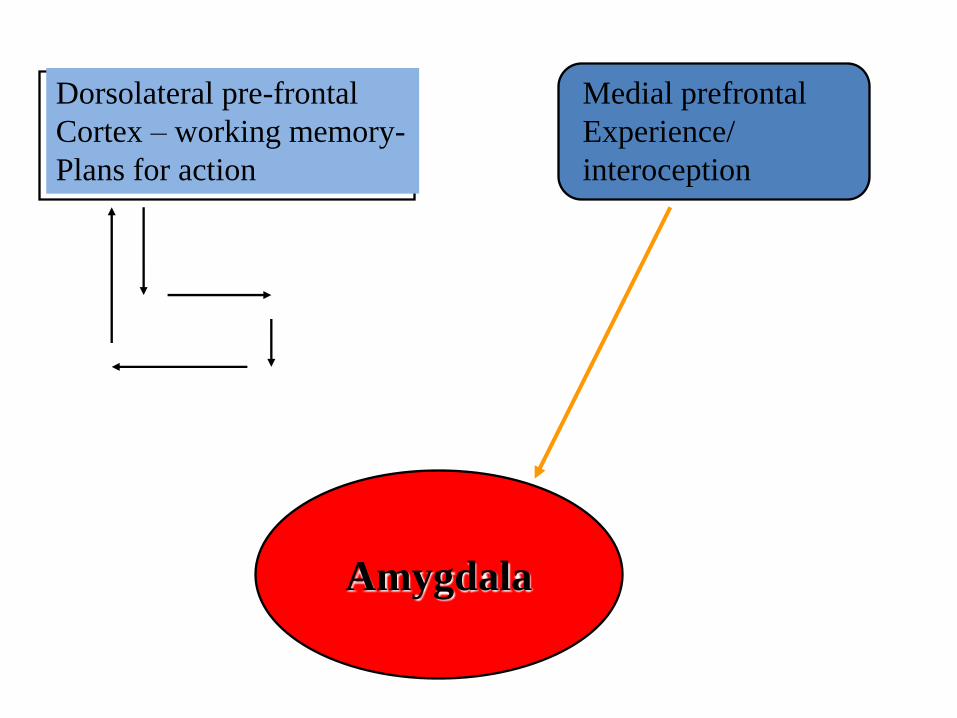
Amygdala
Dorsolateral pre-frontal
Cortex – working memory-
Plans for action
Medial prefrontal
Experience/
interoception
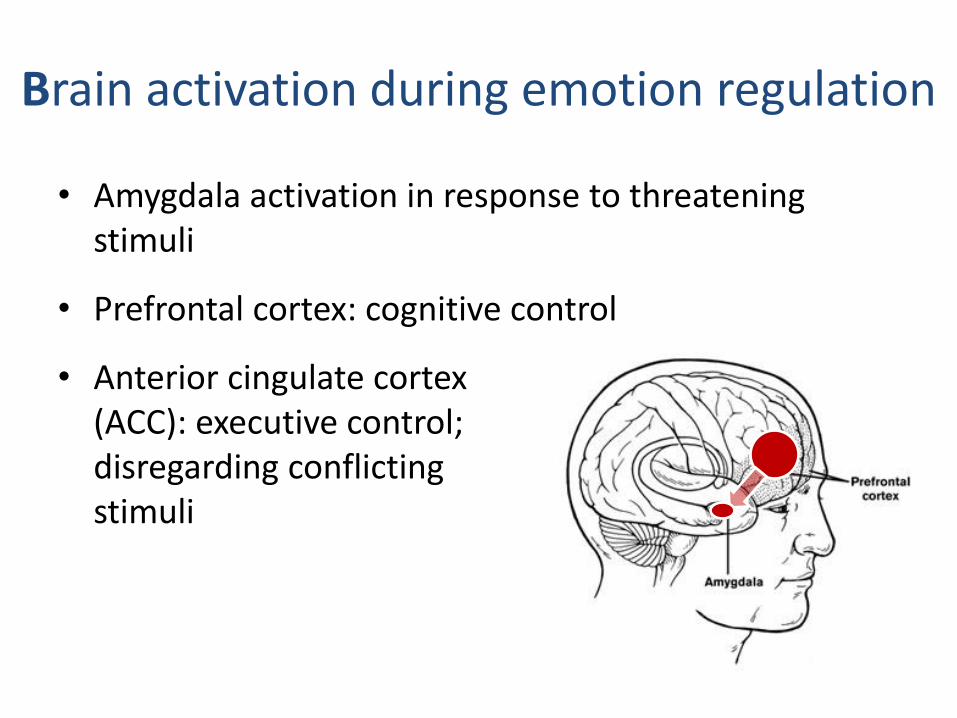
• Amygdala activation in response to threatening stimuli
• Prefrontal cortex: cognitive control
• Anterior cingulate cortex (ACC): executive control; disregarding conflicting stimuli
Brain activation during emotion regulation

Overcoming trauma: self-regulation
Heart Rate Variability (HRV)
1. Improving Heart Rate Variability
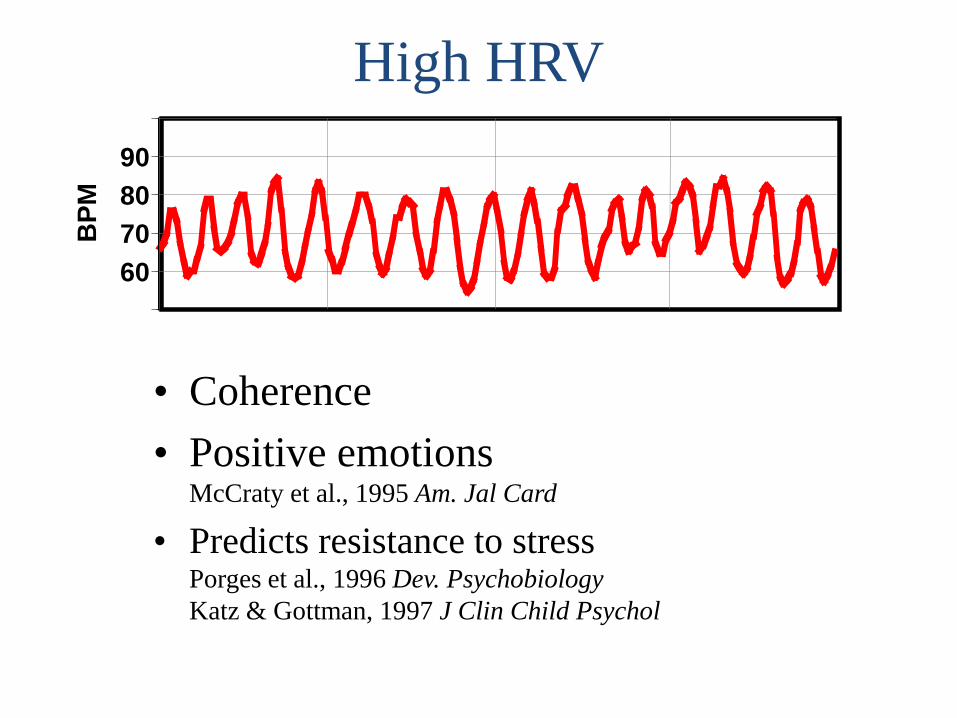
High HRV
60
70
80
90
BP
M
• Coherence
• Positive emotions McCraty et al., 1995 Am. Jal Card
• Predicts resistance to stress Porges et al., 1996 Dev. Psychobiology
Katz & Gottman, 1997 J Clin Child Psychol
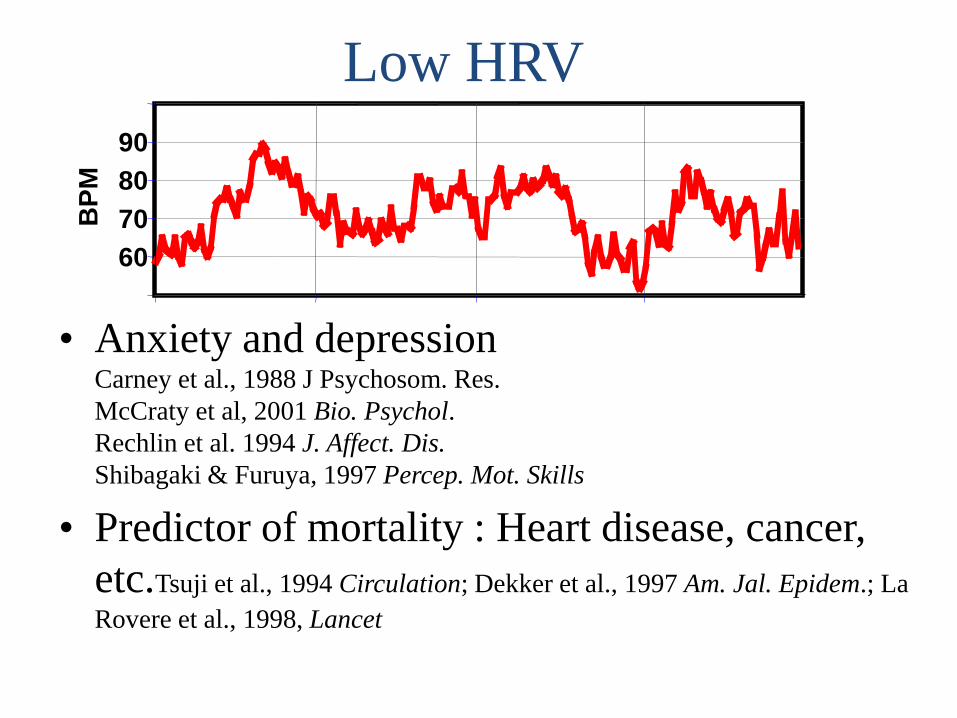
Low HRV
60
70
80
90
BP
M
• Anxiety and depression Carney et al., 1988 J Psychosom. Res.
McCraty et al, 2001 Bio. Psychol.
Rechlin et al. 1994 J. Affect. Dis.
Shibagaki & Furuya, 1997 Percep. Mot. Skills
• Predictor of mortality : Heart disease, cancer,
etc.Tsuji et al., 1994 Circulation; Dekker et al., 1997 Am. Jal. Epidem.; La
Rovere et al., 1998, Lancet
Improving self reguation
2. Yoga


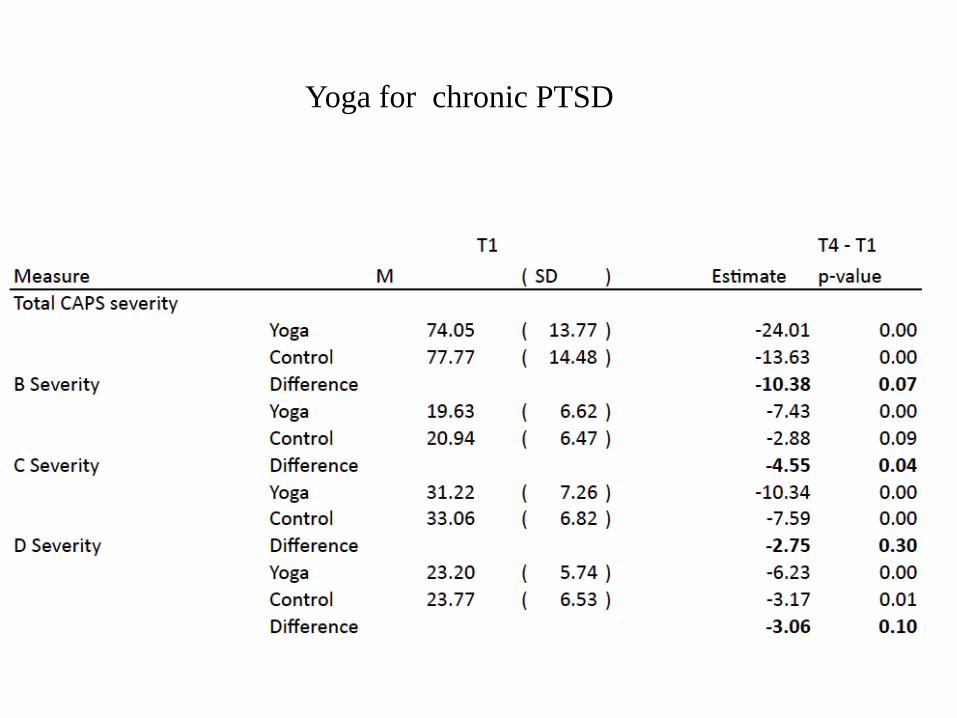
Yoga for chronic PTSD
Neurofeedback
Helping the brain to be connected to itself
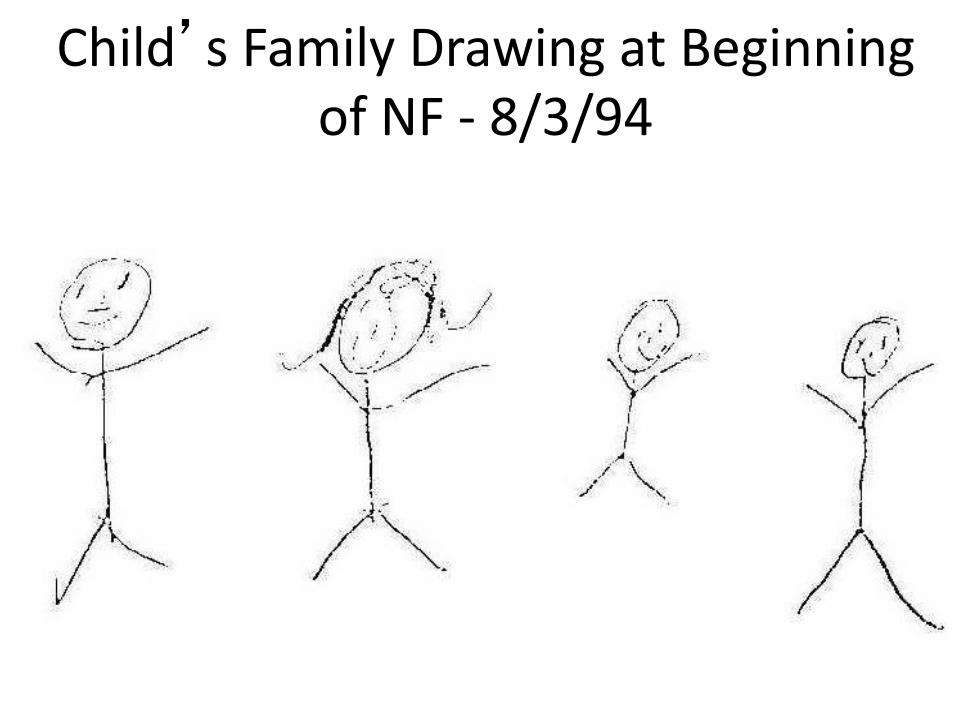
Child’s Family Drawing at Beginning of NF - 8/3/94
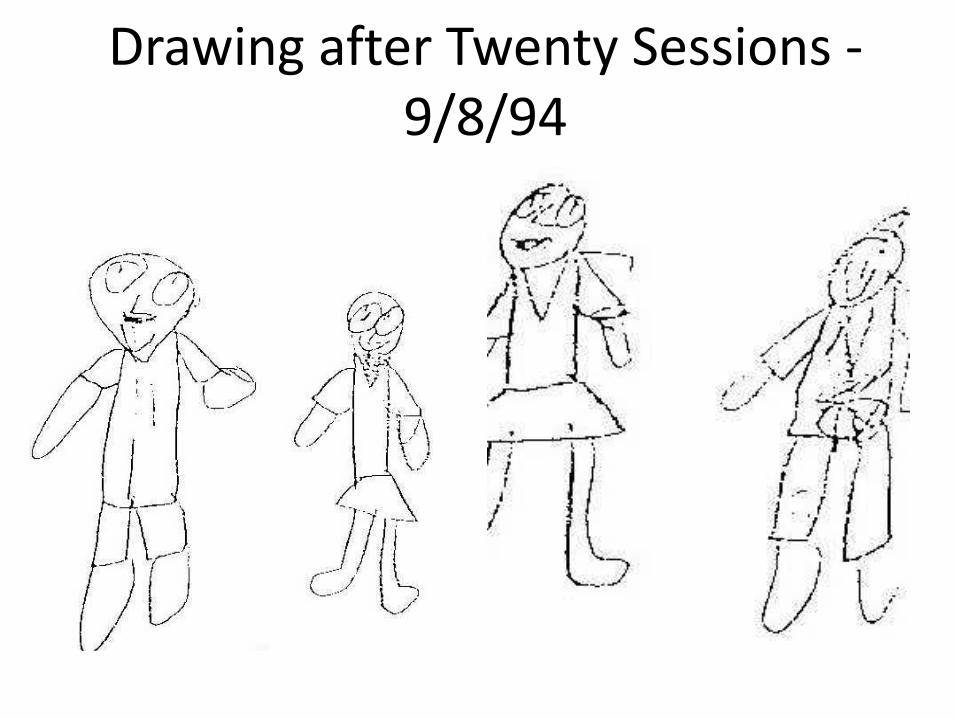
Drawing after Twenty Sessions - 9/8/94
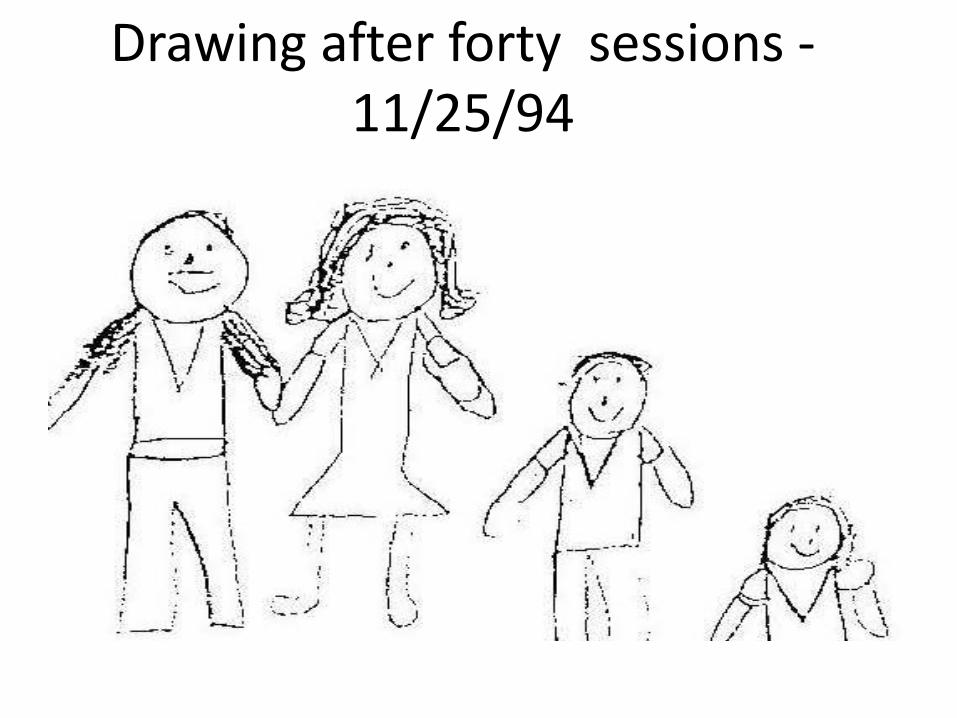
Drawing after forty sessions -11/25/94
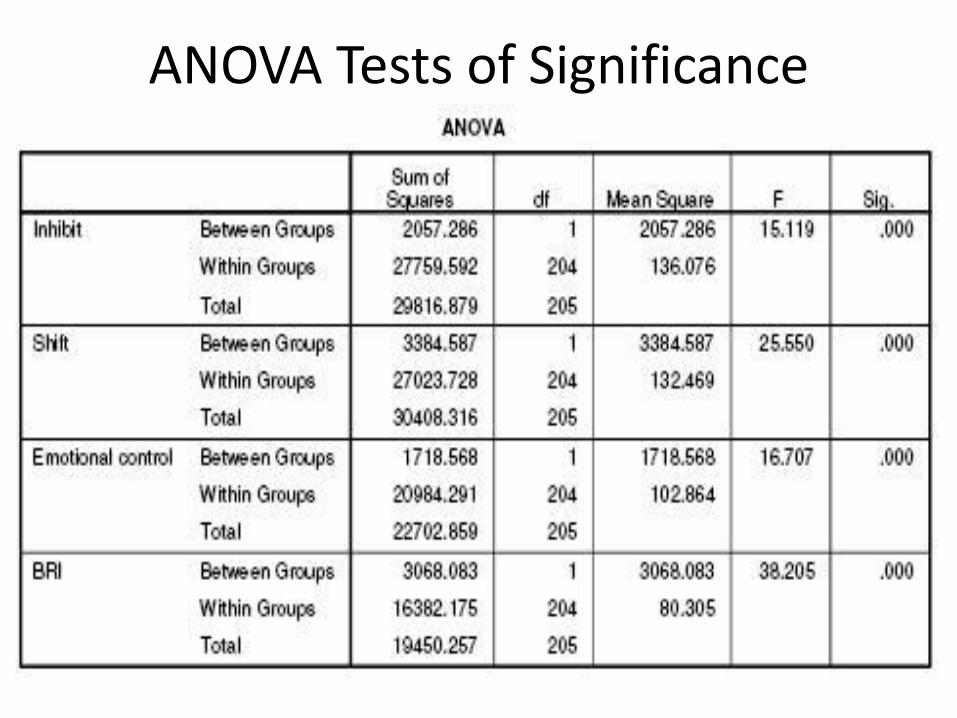
ANOVA Tests of Significance
Every once in a while, a book comes along that fundamentally changes the way we look at the world. Bessel Van der Kolk has written such a book. Having read THE BODY KEEPS THE SCORE, it will be impossible for us any longer to deny the profound extent of trauma and its impact on our lives. The arc of Van der Kolk’s story is vast and comprehensive—but he is such a skillful storyteller that he keeps us riveted to the page. I could not put this book down. It is, simply put, a great work.
•Stephen Cope, Founder and Director, Kripalu Institute for Extraordinary Living, author of Yoga and the Quest for the True Self“
In this inspirational work which seamlessly weaves keen clinical observation, neuroscience, historical analysis, the arts, and personal narrative, The book is full of wisdom, humanity, compassion and scientific insight, gleaned from a lifetime of clinical service, research and scholarship in the field of traumatic stress. A must read for mental health and other health care professionals, trauma survivors, their loved ones, and those who seek clinical, social, or political solutions to the cycle of trauma and violence in our society.”
•--Rachel Yehuda, PhD, Professor of Psychiatry and Neuroscience, Director of the Traumatic Stress Studies Division at the Mount Sinai School of Medicine New York NY.

For more information
Trauma Center Research Office
http://www.traumacenter.org
Copyright © 2022 FDOKUMEN