The effect of Alaska's home visitation program for high-risk families on trends in abuse and neglect
17
Child Abuse & Neglect 32 (2008) 317–333 The effect of Alaska’s home visitation program for high-risk families on trends in abuse and neglect Bradford D. Gessner ∗ Alaska Division of Public Health, P.O. Box 240249, 3601 C Street Suite 576, Anchorage, AK 99524, USA Received 30 October 2006; received in revised form 25 July 2007; accepted 14 August 2007 Abstract Objectives: At 6 sites serving 21 communities, Alaska implemented Healthy Families Alaska, a home visitation program using paraprofessionals designed to decrease child abuse and neglect. The primary study objective was to compare changes over time in Child Protective Services outcomes by Healthy Families Alaska enrollment status. Methods: Enrollment status was linked to birth certificates for birth years 1996–2002 which in turn was linked to the Alaska Child Protective Services database for outcome years 1996–2004. All children were followed through the study databases until age 2 years. Results: There were 40,099 children born during 1996–2002 to residents of Healthy Families Alaska communities and 985 were enrolled in the program. Physical abuse referrals among enrolled children decreased from 73 to 42 per 1000 child-years of follow-up from 1996–1998 to 2000–2002 (p = .005); all of this decrease occurred among children who received 20 or more home visitations. This decrease may have been unrelated to program impact as a similar decrease in referral was seen among unenrolled high-risk children. Compared to unenrolled high-risk children, enrolled children had a modest decrease in the proportion with substantiated neglect but no difference in the proportion with neglect referral or physical abuse referral or substantiation. Conclusions: Little evidence exists that Alaska’s home visitation program had a measurable impact on child maltreatment outcomes. Practice implications: Within Alaskan communities that had a home visitation program targeting families at high risk for child abuse, changes in Child Protective Services outcomes among children less than 2 years of age were followed over time by program enrollment status. Enrollment was associated with a substantial decrease in physical abuse referrals, but a similar decrease was seen among unenrolled high-risk children. No improvement was seen in physical abuse substantiation. A greater number of home visitations was not associated with fewer abuse outcomes. This work supports most of the recent literature, which questions the field effectiveness of home visitation programs. In combination with other studies, the current work may lead decision-makers and funding agencies to re-examine ∗ Corresponding author. 0145-2134/$ – see front matter © 2008 Elsevier Ltd. All rights reserved. doi:10.1016/j.chiabu.2007.08.004
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of The effect of Alaska's home visitation program for high-risk families on trends in abuse and neglect

Child Abuse & Neglect 32 (2008) 317–333
The effect of Alaska’s home visitation program for high-riskfamilies on trends in abuse and neglect
Bradford D. Gessner ∗
Alaska Division of Public Health, P.O. Box 240249, 3601 C Street Suite 576, Anchorage, AK 99524, USA
Received 30 October 2006; received in revised form 25 July 2007; accepted 14 August 2007
Abstract
Objectives: At 6 sites serving 21 communities, Alaska implemented Healthy Families Alaska, a home visitationprogram using paraprofessionals designed to decrease child abuse and neglect. The primary study objective was tocompare changes over time in Child Protective Services outcomes by Healthy Families Alaska enrollment status.Methods: Enrollment status was linked to birth certificates for birth years 1996–2002 which in turn was linked tothe Alaska Child Protective Services database for outcome years 1996–2004. All children were followed throughthe study databases until age 2 years.Results: There were 40,099 children born during 1996–2002 to residents of Healthy Families Alaska communitiesand 985 were enrolled in the program. Physical abuse referrals among enrolled children decreased from 73 to 42per 1000 child-years of follow-up from 1996–1998 to 2000–2002 (p = .005); all of this decrease occurred amongchildren who received 20 or more home visitations. This decrease may have been unrelated to program impactas a similar decrease in referral was seen among unenrolled high-risk children. Compared to unenrolled high-riskchildren, enrolled children had a modest decrease in the proportion with substantiated neglect but no difference inthe proportion with neglect referral or physical abuse referral or substantiation.Conclusions: Little evidence exists that Alaska’s home visitation program had a measurable impact on childmaltreatment outcomes.Practice implications: Within Alaskan communities that had a home visitation program targeting families at highrisk for child abuse, changes in Child Protective Services outcomes among children less than 2 years of age werefollowed over time by program enrollment status. Enrollment was associated with a substantial decrease in physicalabuse referrals, but a similar decrease was seen among unenrolled high-risk children. No improvement was seen inphysical abuse substantiation. A greater number of home visitations was not associated with fewer abuse outcomes.This work supports most of the recent literature, which questions the field effectiveness of home visitation programs.In combination with other studies, the current work may lead decision-makers and funding agencies to re-examine
∗ Corresponding author.
0145-2134/$ – see front matter © 2008 Elsevier Ltd. All rights reserved.doi:10.1016/j.chiabu.2007.08.004

318 B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333
the usefulness of home visitation programs, particularly those using a methodology similar to that implemented inAlaska.© 2008 Elsevier Ltd. All rights reserved.
Keywords: Abuse; Alaska; Healthy Families America; Home visitation; Neglect; Physical abuse; Prevention
Introduction
During 1995, the State of Alaska implemented Healthy Families Alaska, a home visitation programdesigned to decrease child abuse and neglect and improve other child health outcomes. This decision wasbased on the Healthy Families America initiative promoted by the National Committee to Prevent ChildAbuse (now Prevent Child Abuse America), which in turn was based on initial promising results fromother sites (Olds, Henderson, Chamberlin, & Tatelbaum, 1986; Olds & Kitzman, 1990). After severalyears of implementation, the Alaska State legislature required an evaluation of the home visitationapproach and, from 2000 to 2004, a randomized trial of the Healthy Families Alaska program at six siteswas conducted. This study has now been completed and results reported (Duggan, Caldera, Rodriguez,Burrell, & Shea, 2004).
Since the initial promising results, several studies from other areas have found that home visitationprograms could decrease the risk of child abuse and neglect under some circumstances (Eckenrode et al.,2000; Olds et al., 1997), prompting the US Centers for Disease Control and Prevention to recommendthese programs for child abuse prevention (Centers for Disease Control and Prevention, 2003). However,similar to most studies, including those conducted more recently (Duggan, McFarlane, et al., 2004;Sweet & Appelbaum, 2004), no or minimal impact on child abuse was found in Alaska (Duggan,Caldera, et al., 2004).
The primary goal of Healthy Families Alaska was to decrease the occurrence of abuse and neglect am-ong high-risk families, and specifically that 95% of target children would have no substantiated child abuseor neglect. However, the randomized program evaluation found that Healthy Families Alaska “did not pre-vent child maltreatment, reduce malleable parent risks for maltreatment, or improve child health.” Sixteenpercent of enrolled children compared to 17% of unenrolled children experienced substantiated neglector abuse during the first 2 years of life, and both groups had similar rates of abuse when stratified by age.
Negative results could have occurred because of specific program implementation problems. Evenat the best performing sites, service delivery fell short of program standards. The highest site specificretention was 45% at 2 years and the highest visitation rate averaged once per 2 weeks versus a goal ofonce a week. Almost half of families had no individualized family support plan. Home visitors usuallydid not address the risk factors for child maltreatment that led to program enrollment, namely poor mentalhealth, domestic violence, and substance abuse. Finally, while in theory program delivery guidelines werecodified, substantial changes occurred in service delivery over time. A full description of the HealthyFamilies Alaska program, including its implementation and results of the randomized trial, is available athttp://hss.state.ak.us/ocs/Publications/JohnsHopkins HealthyFamilies.pdf (last accessed 10 April 2007).
In addition to implementation issues, program design and analysis issues may have unfairly biasedresults toward the null. All randomized home visitation evaluations conducted to date, including Alaska’s,have been by necessity nonblinded. Because of this, program staff may have delivered services to controlfamilies beyond those that they would have received in the absence of the study. This problem was

B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333 319
augmented in Alaska where the study was designed to provide enhanced community resources referralimmediately before randomization to children in both the intervention and control arms. Consequently, notrue control population existed. Additionally, Healthy Families Alaska may have decreased true episodesof child maltreatment but this effect could have been masked if home visitors identified and reportedadditional cases of maltreatment. Presumably, as home visitor competency increased over time, thiseffect should have diminished and rates of decline in maltreatment outcomes should have been higheramong enrolled than control families. However, the published analysis of Healthy Families Alaska didnot evaluate changes in maltreatment outcomes over time.
To address these latter methodological limitations, the current study was conducted to determine ifall children enrolled in Healthy Families Alaska throughout the state (including those in the interventionarm of the study) experienced a greater decrease in child abuse over time than that documented among alland high-risk unenrolled children living in Healthy Families Alaska communities (the majority of whomhad received no change in services during the evaluation period). By linking Healthy Families Alaskaenrollment status to Child Protective Services records and birth certificates, it became possible to useas controls the general population of children in the Healthy Families Alaska communities and childrenidentified as high-risk based on birth certificate characteristics. This approach thus reduced the potentialbias caused by provision of enhanced resources either before or after study enrollment to all childrenenrolled in Healthy Families Alaska.
Methods
Healthy Families Alaska background
Healthy Families Alaska began serving clients during 1995 in Juneau and the Central Kenai Peninsula(Kenai, Soldotna, Sterling, Clam Gulch, Cohoe, Funny River, Kasilof, Nikiski, Ninilchik, Salamatof, andRidgeway) followed in 1996 by Anchorage, Dillingham, Fairbanks, and the Matanuska-Susitna Borough(Palmer, Sutton, Wasilla, Willow, Talkeetna, and Houston). The program in Dillingham ceased at the endof 2003 while that serving the Central Kenai Peninsula ceased mid-2005. Anchorage had two programsthrough 2005, one serving primarily Alaska Natives and the other non-Natives. The program in Bethelwas not included because it ended during 2000.
All families at Healthy Families Alaska sites were screened. Enrollment in Healthy Families Alaskawas offered to families identified as at-risk for poor health and social outcomes based on a score of atleast 25 on the Kempe Family Stress Checklist. The Kempe Family Stress Checklist is intended to assessthe parents’ ability to care for their child and is endorsed by Healthy Families America as a screeningtool (http://www.healthyfamiliesamerica.org/network resources/training.shtml, last accessed 27 October2006). It contains 10 items and scoring includes a component based on the professional judgment of theadministrator. All programs employed paraprofessionals as family support workers and the Central KenaiPeninsula program also employed public health nurses.
Study hypothesis and design
The primary study hypothesis was that—among children less than 2 years of age—Healthy FamiliesAlaska enrollment would have a measurable impact on substantiated physical abuse rates when compared

320 B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333
to all unenrolled children and two groups of unenrolled high-risk children from the same communities.Secondary hypotheses were that Healthy Families Alaska would impact abuse and neglect referral ratesand neglect substantiation.
These hypotheses were tested by (a) comparing abuse rates over time among the four groups, (b) byevaluating whether increasing numbers of home visitations led to decreased abuse rates, that is, whethera dose-response existed, and (c) by comparing the proportion of children experiencing abuse and neglectoutcomes overall and over time among the four groups. Method (a) was based on the concept that ifHealthy Families Alaska was effective, the impact on abuse should increase over time as personnelbecame better trained and more efficient; additionally, as deficiencies were identified, Healthy FamiliesAlaska was modified substantially and usually in ways that were designed specifically to improve effectson abuse rates.
Existing Alaska Department of Health and Social Services databases were linked and evaluated,including birth certificates, Child Protective Services records, and Healthy Families Alaska enroll-ment files. The birth certificate file for births occurring during 1996–2002 was considered the masterfile. The birth certificate file contained information on child’s date of birth, birth weight, and gesta-tion; maternal residence, age, education, race, marital status, and prenatal substance use; and paternalage and education. Using name and date of birth, the Alaska Bureau of Vital Statistics linked thisfile to the Child Protective Services database for suspected abuse and neglect cases reported during1996–2004. The Child Protective Services database extended for two more years than the birth cer-tificate database to ensure that all children had until age 2 years to experience an abuse or neglectoutcome. Variables included from the Child Protective Services database included date of the report,type of report (physical abuse, sexual abuse, or neglect), and whether the report was substantiatedor not.
Healthy Families Alaska participants were not representative of all children born in Alaska, but—asnoted above—were selected based on a Kempe Family Stress Checklist score indicating a high riskfor child abuse. Families not enrolled in Healthy Families Alaska did not complete this check-list and thus a rigorously comparable high-risk control group was not available. As a rough proxy,analysis was conducted of maltreatment outcomes among two groups of high-risk children. High-risk group number 1 comprised children born both preterm (i.e., at less than 37 weeks gestation)and to women with <12 years of education (n = 529). High-risk group number 2 comprised chil-dren born to unmarried women who reported prenatal alcohol use (n = 499). All four risk factorswere identified on the birth certificate. The chosen risk factors have been reported previously toincrease the risk of child maltreatment in Alaska (Gessner, Moore, Hamilton, & Muth, 2004) and else-where (Hibbard, Desch, American Academy of Pediatrics Committee on Child Abuse and Neglect,& American Academy of Pediatrics Council on Children with Disabilities, 2007; Overpeck, Brenner,Trumble, Trifiletti, & Berendes, 1998; Winpisinger, Hopkins, Indian, & Hostetler, 1991). Risk factorpairings were chosen to provide an adequate sample size in each category and to identify rela-tively independent groups: of the 529 children in high-risk group 1, 35 (7%) were in high-riskgroup 2.
Outcomes
Healthy Families Alaska received funding primarily based on its promise to prevent child abuse andneglect. Based on this, five outcomes were evaluated: any Child Protective Services referral, referral for

B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333 321
neglect, referral for abuse, referral for substantiated neglect, and referral for substantiated abuse. Abuseepisodes occurring prenatally—usually due to maternal substance use—were not included. Sexual abusewas not evaluated because this outcome was rare during the first 2 years of life.
Analysis
The study employed a retrospective cohort design. The unit of analysis was the outcome and rates werecalculated as outcomes per 1000 child-years of follow-up. All children born in the study communitieswere assumed to have been followed from birth to the second birthday since data were not available forchildren who died or left these communities before age 2 years. Rates were also calculated for the numberof children experiencing a particular outcome per 1000 child-years of follow-up. This was done becauseof concern that a few children experiencing a large number of referrals might lead to misinterpretation ofprogram impact.
This was a program effectiveness evaluation, that is, it measured how well the home visitation programworked when implemented in the general population rather than in a primarily experimental setting(Clemens, Brenner, Rao, Tafari, & Lowe, 1996). Consequently, children were compared based on HealthyFamilies Alaska enrollment regardless of whether or not any home visits actually occurred (of the 985enrolled children, 90 received no home visits). As discussed above, additional analyses were conductedto evaluate the effect of number of visits on outcomes.
Children could experience different maltreatment outcomes. Each outcome category included allepisodes of that outcome (e.g., substantiated physical abuse) regardless of whether the child experiencedan outcome in a different category (e.g., neglect referral).
Ethical review
The current manuscript presents a program evaluation that used existing public health databases housedwithin the Alaska Department of Health and Social Services. No additional information from subjectswas obtained and no subjects were contacted. As an evaluation of a public health program using internaldatabases by a legally empowered governmental authority for the development of public health recommen-dations, no institutional review board approval was sought or obtained. Following the decision to publishresults, approval was obtained from the University of Alaska, Anchorage Institutional Review Board. TheAlaska Department of Health and Social Services has a commitment to patient confidentiality includ-ing formal confidentiality procedures and training, password-encrypted data files, password-protectedcomputer log-on, and a firewall specific to Section of Epidemiology server where final data files werehoused.
Results
Background
There were 40,099 children born during 1996–2002 to residents of Healthy Families Alaska commu-nities; 23,929 (60%) children were born to Anchorage residents. During the 9-year period of follow-upfor abuse and neglect outcomes and among all 40,099 children, 3909 (9.7%) were referred to Child
322 B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333
Protective Services during the first 2 years of life with a total of 7138 referrals (range, 1–15 per child);2839 (7.1%) were referred for neglect (total referrals, 4589; range, 1–11 per child) and 1356 (3.4%) hadsubstantiated neglect (total outcomes, 1856; range, 1–8 per child); 902 (2.2%) were referred for physicalabuse (total referrals, 1042; range, 1–5 per child) and 336 (.8%) experienced substantiated physical abuse(total outcomes, 357; range, 1–3 per child).
Within the study communities, 985 (2.5%) infants were enrolled in Healthy Families Alaska. Comparedto all unenrolled infants within these communities, enrolled infants were more likely to be born pretermor low birth weight, to be born to a mother who used tobacco or alcohol prenatally, and to be born toyoung, less educated, and unmarried parents (Table 1). Enrolled children were similar to both groupsof unenrolled high-risk children. Among enrolled children, no change over time was noted for trends indemographic characteristics available from the birth certificates (such as maternal and paternal age andeducation, infant birth weight and gestation, parental marital status, and maternal prenatal substance use)(data not shown).
Evaluation of abuse and neglect events
Children enrolled in Healthy Families Alaska experienced a greater mean number of Child ProtectiveServices outcomes per child than unenrolled children (Table 2), an expected outcome given that childrenwere enrolled based on their high risk for abuse and neglect. However, enrolled children experiencedno difference in abuse or neglect outcomes when compared to either group of unenrolled high-riskchildren. Among enrolled children, referral to Child Protective Services over time varied from 338(during 1998–2000) to 376 (during 1996–1998) per 1000 child-years of follow-up with no statisti-cally significant change over time. Among all unenrolled children, referral rates varied from 75 (during1996–1998) to 88 (during 1999–2001) per 1000 child-years of follow-up. Among unenrolled childrenborn preterm and to less educated women, referral rates varied from 306 (during 1996–1998) to 405(during 2000–2002) per 1000 child-years of follow-up while among unenrolled children born to unmar-ried women who reported prenatal alcohol use, rates varied from 258 (during 1999–2001) to 308 (during1996–1998).
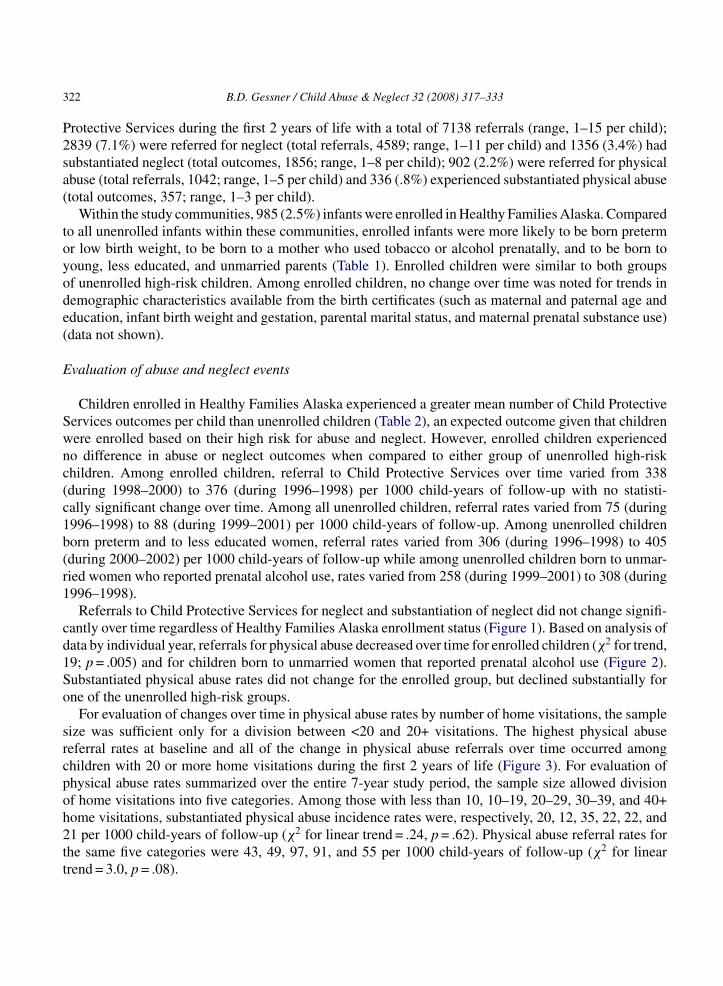
Referrals to Child Protective Services for neglect and substantiation of neglect did not change signifi-cantly over time regardless of Healthy Families Alaska enrollment status (Figure 1). Based on analysis ofdata by individual year, referrals for physical abuse decreased over time for enrolled children (χ2 for trend,19; p = .005) and for children born to unmarried women that reported prenatal alcohol use (Figure 2).Substantiated physical abuse rates did not change for the enrolled group, but declined substantially forone of the unenrolled high-risk groups.
For evaluation of changes over time in physical abuse rates by number of home visitations, the samplesize was sufficient only for a division between <20 and 20+ visitations. The highest physical abusereferral rates at baseline and all of the change in physical abuse referrals over time occurred amongchildren with 20 or more home visitations during the first 2 years of life (Figure 3). For evaluation ofphysical abuse rates summarized over the entire 7-year study period, the sample size allowed divisionof home visitations into five categories. Among those with less than 10, 10–19, 20–29, 30–39, and 40+home visitations, substantiated physical abuse incidence rates were, respectively, 20, 12, 35, 22, 22, and21 per 1000 child-years of follow-up (χ2 for linear trend = .24, p = .62). Physical abuse referral rates forthe same five categories were 43, 49, 97, 91, and 55 per 1000 child-years of follow-up (χ2 for lineartrend = 3.0, p = .08).

B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333 323
Table 1Birth characteristics of children residing in communities with a Healthy Families Alaska program, among children enrolled inHealthy Families Alaska, all unenrolled children in study communities, unenrolled high-risk children 1 (born at <37 weeks ges-tation and to women with <12 years education) and unenrolled high-risk children 2 (born to unmarried mothers with documentedprenatal alcohol use); Alaska, birth years 1996–2002
Birth characteristic Enrolled Not enrolled Not enrolled, high-risk 1 Not enrolled, high-risk 2
Maternal education (years)<12 363 (39%) 4,914 (13%) 529 (100%) 146 (31%)12 427 (45%) 15,126 (40%) 0 223 (47%)>12 153 (16%) 17,974 (47%) 0 103 (22%)
Paternal education (years)<12 127 (20%) 2,632 (7.9%) 110 (33%) 40 (17%)12 376 (59%) 14,319 (43%) 177 (53%) 113 (49%)>12 133 (21%) 16,514 (49%) 49 (15%) 78 (34%)
Maternal age (years)<20 338 (34%) 4,232 (11%) 184 (35%) 51 (10%)20–29 500 (51%) 10,786 (53%) 248 (47%) 267 (54%)30+ 146 (15%) 14,083 (36%) 97 (18%) 181 (36%)
Paternal age (years)<20 138 (16%) 1,603 (4.3%) 76 (16%) 15 (4%)20–29 476 (55%) 16,548 45%) 222 (48%) 150 (36%)30+ 259 (30%) 18,800 (51%) 165 (36%) 254 (61%)
Birth weight (g)400–1499 5 (.5%) 416 (1.1%) 69 (13%) 13 (3%)1500–2499 64 (6.5%) 1,983 (5.1%) 233 (45%) 58 (12%)2500–5499 911 (93%) 36,598 (94%) 221 (42%) 422 (86%)
Gestation (weeks)23–31 8 (.8%) 458 (1.2%) 84 (16%) 16 (3%)32–36 99 (10%) 2,798 (7.2%) 442 (84%) 61 (12%)37–43 872 (89%) 35,571 (92%) 0 417 (84%)
Parents marriedYes 296 (30%) 26,421 (68%) 176 (33%) 0No 687 (70%) 12,634 (32%) 353 (67%) 499 (100%)
Maternal prenatal alcohol useYes 44 (4.5%) 1,088 (2.8%) 42 (8.1%) 499 (100%)No 935 (96%) 37,616 (97%) 478 (92%) 0
Maternal prenatal tobacco useYes 399 (41%) 6,674 (17%) 231 (44%) 338 (68%)No 586 (59%) 32,135 (83%) 293 (56%) 158 (32%)
Evaluation of children referred for abuse and neglect
For the entire 7-year birth cohort, compared to all unenrolled children, children enrolled in HealthyFamilies Alaska were approximately four times more likely to receive a Child Protective Services referraland to experience substantiated neglect and abuse (Table 3). Compared to the two unenrolled high-risk

324 B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333
Table 2Mean number of Child Protective Services outcomes per child during the first 2 years of life among children enrolled inHealthy Families Alaska compared to all unenrolled children in study communities, unenrolled high-risk children 1 (born at <37weeks gestation and to women with <12 years education) and unenrolled high-risk children 2 (born to unmarried mothers withdocumented prenatal alcohol use); Alaska, birth years 1996–2002
Child Protective Services outcome Mean number of outcomes
HFA enrolled Not enrolled(p-value*)
High-risk 1(p-value*)
High-risk 2(p-value*)
Any referral .75 .16 (<.001) .73 (.83) .62 (.07)Neglect referral .44 .11 (<.001) .52 (.14) .45 (.84)Substantiated neglect .18 .043 (<.001) .22 (.25) .24 (.10)Abuse referral .12 .024 (<.001) .10 (.43) .08 (.12)Substantiated abuse .042 .0081 (<.001) .051 (.44) .044 (.84)
*p-Values refer to comparison of this group to HFA-enrolled children.
Figure 1. Rates of neglect referrals (a) and substantiated neglect (b) during the first 2 years of life, among Healthy FamiliesAlaska enrolled children (n = 985), all unenrolled children (n = 39,570), unenrolled children born preterm and to mothers with<12 years of education (n = 529), and unenrolled children born to unmarried women with documented prenatal alcohol use(n = 499); Alaska, birth years 1996–2002.
B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333 325
Figure 2. Rates of physical abuse referrals (a) and substantiated physical abuse (b) during the first 2 of life, among HealthyFamilies Alaska enrolled children (n = 985), all unenrolled children (n = 39,570), unenrolled children born preterm and to motherswith <12 years of education (n = 529), and unenrolled children born to unmarried women with documented prenatal alcohol use(n = 499); Alaska, birth years 1996–2002.
Figure 3. Rates of referral for and substantiation of physical abuse during the first 2 years of life by Child Protective Servicesamong children enrolled in Healthy Families Alaska (HFA), by number of HFA home visits; Alaska, birth years 1996–2002.

326B
.D.G
essner/C
hildA
buse&
Neglect32
(2008)317–333
Table 3The number of children experiencing Child Protective Services outcomes during the first 2 years of life, comparing children enrolled in Healthy Families Alaskato all unenrolled children in study communities, unenrolled high-risk children 1 (born at <37 weeks gestation and to women with <12 years education) andunenrolled high-risk children 2 (born to unmarried mothers with documented prenatal alcohol use); Alaska, birth years 1996–2002
Risk group Any referral Referral for neglect Substantiated neglect Referral for abuse Substantiated abuse
Enrolled (n = 985) 332 (34%) 249 (25%) 125 (13%) 89 (9.0%) 37 (3.8%)
Not enrolled (n = 39,144) 3577 (9.1%) 2590 (6.6%) 1231 (3.1%) 813 (2.1%) 299 (.8%)
Risk ratio (95% CI)a 3.7 (3.4, 4.0) 3.8 (3.4, 4.3) 4.0 (3.4, 4.8) 4.3 (3.5, 5.4) 4.9 (3.5, 6.9)
Not enrolled, high-risk 1 (n = 529) 191 (36%) 146 (27%) 80 (15%) 47 (8.9%) 25 (4.7%)
Risk ratio (95% CI)a .93 (.81, 1.1) .92 (.77, 1.1) .84 (.65, 1.1) 1.0 (.73, 1.4) .80 (.48, 1.3)
Not enrolled, high-risk 2 (n = 499) 171 (34%) 133 (27%) 91 (18%) 41 (8.2%) 22 (4.4%)
Risk ratio (95% CI)a .98 (.85, 1.1) .95 (.79, 1.1) .70 (.54, .89) 1.1 (.77, 1.6) .85 (.51, 1.4)
a CI = confidence interval. Risk ratio and CI refer to comparison of HFA-enrolled children to this group

B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333 327
groups, enrolled children had a modestly decreased risk of having one or more referrals for substantiatedneglect but no difference in other outcomes.
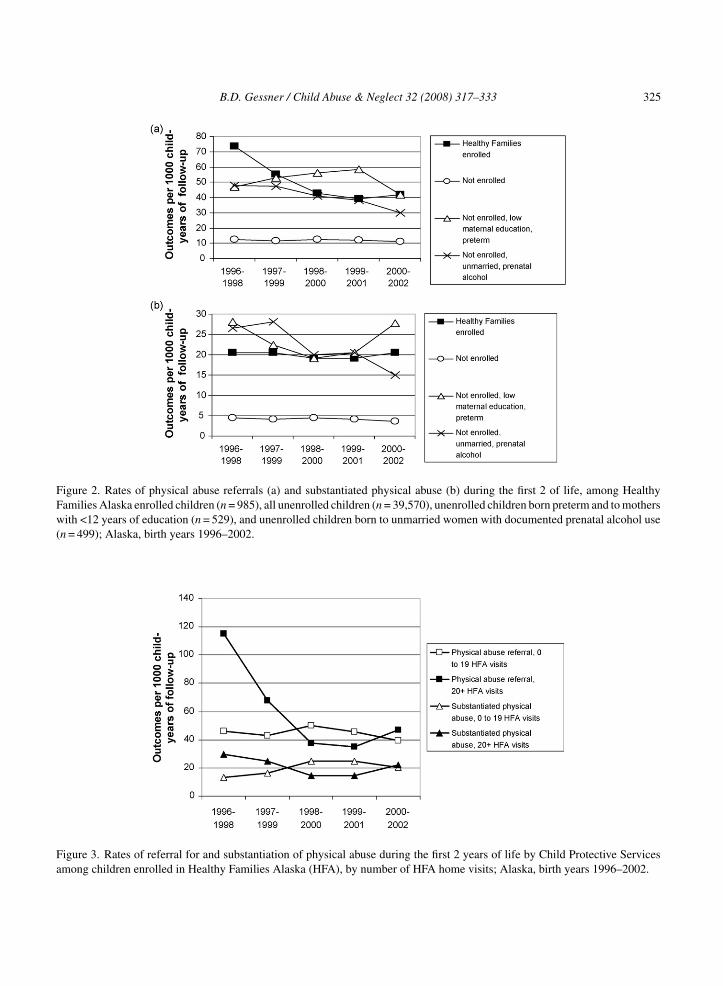
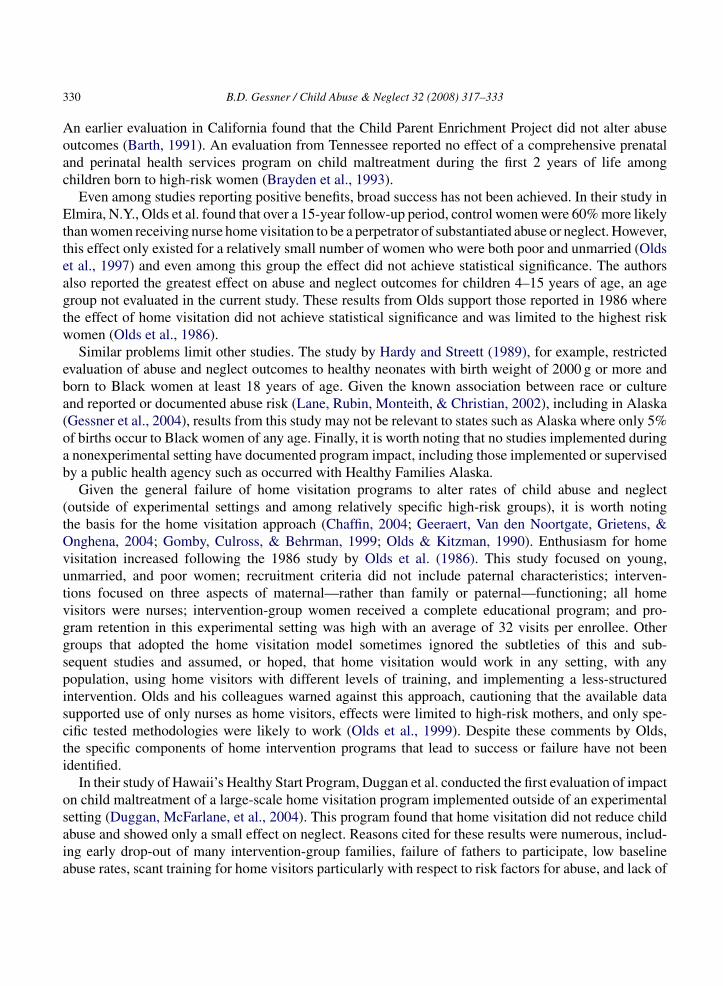
Compared to the two unenrolled high-risk groups, Healthy Families Alaska-enrolled children hada lower rate of experiencing abuse and neglect outcomes during the first month of life (Figure 4).Thereafter rates were similar among all three groups or higher among enrolled children such thatby age 2 years, the final proportions that had experienced an abuse or neglect outcome were nearlyidentical.
Discussion
Program effectiveness
Healthy Families Alaska screening criteria successfully identified families at high risk of experiencingchild abuse or neglect. Rates among enrolled children were approximately fourfold higher than among thecontrol population. The screening criteria utilized, however, were no more successful at identifying high-risk children than risk factors easily identifiable from the birth certificate. Moreover, having identifiedhigh-risk families, the current evaluation found little evidence that home visitation as implemented throughHealthy Families Alaska reduced rates of abuse and neglect.
The most promising finding among enrolled children was a 42% decrease in physical abuse refer-ral rates over time. This occurred despite no change among study communities in overall referralrates or among high-risk infants, the likelihood that children enrolled in Healthy Families Alaskareceived more scrutiny for potential abuse than other children, and no change in evaluated demo-graphic risk factors over time. The decrease in referral rates from 73 to 42 per 1000 child-yearsequates to approximately 61 prevented physical abuse referrals among the 985 children enrolled inHealthy Families Alaska. Nevertheless, the importance of this positive finding is tempered by thesimilar 38% decrease in physical abuse referral rates (from 48 to 30 per 1000 child-years) amongunenrolled children born to unmarried women who reported prenatal alcohol use. Consequently, it ispossible that the decrease in abuse referrals among enrolled children did not result from the HealthyFamilies Alaska program but rather from unmeasured events occurring in the study communities as awhole.
No change occurred in the rates of substantiated physical abuse among children enrolled in HealthyFamilies Alaska. It is conceivable that Healthy Families Alaska achieved a substantial reduction in abuserates immediately and then maintained this effect at a constant level over time. This seems unlikely forseveral reasons. As previously documented (Duggan, Caldera, et al., 2004), the Healthy Families Alaskaprogram underwent numerous changes over time as deficiencies were identified, many that were intendedto have an impact specifically on child maltreatment. If Healthy Families Alaska interventions wereeffective it seems unlikely that program staff would have made no improvements in service delivery. Thenumber of home visitations families received did not predict substantiated physical abuse rates, either forthe study as a whole or over time. Lastly, rates of substantiated physical abuse among enrolled childrenwere not substantially different from those among the evaluated unenrolled high-risk comparison groups.It is particularly striking that in comparison to enrolled children, unenrolled children born to unmarriedwomen with documented prenatal alcohol use had a higher initial rate of substantiated abuse but due toa 44% decline over the study period finished with a lower rate.
328 B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333
B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333 329
Compared to the two unenrolled high-risk groups, enrolled children had a modestly lower occurrenceof all abuse and neglect outcomes during the first month of life. Referrals during the first month of lifewere particularly high among children born to unmarried women with birth certificate documentation ofprenatal alcohol use. This finding may indicate a positive benefit of Healthy Families Alaska. However,after the first month of life, the proportion of children referred over time progressed at the same rateamong all three groups or was higher among enrolled children. By age 2 years, the final proportion ofchildren that had experienced abuse or neglect was similar among the three groups for all outcomes exceptsubstantiated neglect. Thus, if home visitation had a positive effect early in a child’s life, for examplethrough intensive efforts prenatally and during early infancy, this effect was short-lived.
In summary, the study results provide little indication that Healthy Families Alaska enrollment had asubstantial positive impact on child maltreatment. Nevertheless, several caveats bear mentioning. The sam-ple size may have been too small to document minor decreases in abuse and neglect rates. As others havenoted, it is particularly difficult to document impact among a population where abuse rates are relativelylow (Duggan, McFarlane, et al., 2004). Home visitors may have become more knowledgeable over timeabout identifying and referring abuse episodes that would lead to a finding of substantiation. This theory issupported by the finding that abuse referral rates were highest among children receiving the highest num-ber of home visitations and that all of the decrease over time in abuse referral rates occurred in this group.Additionally, Healthy Families Alaska may have had a true beneficial effect on abuse, but concentratedmainly on less severe episodes that did not meet the legal requirements for substantiation. This hypoth-esis is consistent with results from Figure 3, demonstrating a decline in physical abuse referrals, but notsubstantiated episodes, with increased home visitations. As discussed above, though, high-risk childrenwho did not receive the Healthy Families Alaska intervention also experienced declines in abuse referrals,suggesting that the decline among enrolled children may not have been the result of program impact.
Comparison to the literature
Some previous studies of home intervention programs have reported substantial reductions in childmaltreatment. For example, Olds et al. reported that among unmarried teenage parents, maltreatmentreports occurred among 19% of control families and 4% of treatment families during the first 2 years of achild’s life (Olds et al., 1986). Another study reported that women enrolled in home visitation programswere identified as perpetrators of abuse at about half the rate of other women over a 15-year period (Oldset al., 1997). A third trial using paraprofessional home visitors documented the occurrence of ChildProtective Services reports from 10% of control and 2% of intervention families (Hardy & Streett, 1989).
Other studies, however, have reported no effect of home visitation on child maltreatment. Forexample, the Hawaii Healthy Start Program did not prevent either self-reported or documented childabuse (Duggan, McFarlane, et al., 2004). A recent evaluation from California found that the HealthyStart model did not reduce the prevalence of mothers who were physically abusive over the first yearof a child’s life, although an enhanced model did lead to a reported benefit (Bugental et al., 2002).
Figure 4. Rates of neglect referral (a), neglect substantiation (b), physical abuse referral (c), and physical abuse substantiation(d) during the first 2 years of life among Healthy Families Alaska enrolled children, all unenrolled children, unenrolled childrenborn preterm and to mothers with <12 years of education, and unenrolled children born to unmarried women with prenatalalcohol use documented on the birth certificate; Alaska, birth years 1996–2002.
330 B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333
An earlier evaluation in California found that the Child Parent Enrichment Project did not alter abuseoutcomes (Barth, 1991). An evaluation from Tennessee reported no effect of a comprehensive prenataland perinatal health services program on child maltreatment during the first 2 years of life amongchildren born to high-risk women (Brayden et al., 1993).
Even among studies reporting positive benefits, broad success has not been achieved. In their study inElmira, N.Y., Olds et al. found that over a 15-year follow-up period, control women were 60% more likelythan women receiving nurse home visitation to be a perpetrator of substantiated abuse or neglect. However,this effect only existed for a relatively small number of women who were both poor and unmarried (Oldset al., 1997) and even among this group the effect did not achieve statistical significance. The authorsalso reported the greatest effect on abuse and neglect outcomes for children 4–15 years of age, an agegroup not evaluated in the current study. These results from Olds support those reported in 1986 wherethe effect of home visitation did not achieve statistical significance and was limited to the highest riskwomen (Olds et al., 1986).
Similar problems limit other studies. The study by Hardy and Streett (1989), for example, restrictedevaluation of abuse and neglect outcomes to healthy neonates with birth weight of 2000 g or more andborn to Black women at least 18 years of age. Given the known association between race or cultureand reported or documented abuse risk (Lane, Rubin, Monteith, & Christian, 2002), including in Alaska(Gessner et al., 2004), results from this study may not be relevant to states such as Alaska where only 5%of births occur to Black women of any age. Finally, it is worth noting that no studies implemented duringa nonexperimental setting have documented program impact, including those implemented or supervisedby a public health agency such as occurred with Healthy Families Alaska.
Given the general failure of home visitation programs to alter rates of child abuse and neglect(outside of experimental settings and among relatively specific high-risk groups), it is worth notingthe basis for the home visitation approach (Chaffin, 2004; Geeraert, Van den Noortgate, Grietens, &Onghena, 2004; Gomby, Culross, & Behrman, 1999; Olds & Kitzman, 1990). Enthusiasm for homevisitation increased following the 1986 study by Olds et al. (1986). This study focused on young,unmarried, and poor women; recruitment criteria did not include paternal characteristics; interven-tions focused on three aspects of maternal—rather than family or paternal—functioning; all homevisitors were nurses; intervention-group women received a complete educational program; and pro-gram retention in this experimental setting was high with an average of 32 visits per enrollee. Othergroups that adopted the home visitation model sometimes ignored the subtleties of this and sub-sequent studies and assumed, or hoped, that home visitation would work in any setting, with anypopulation, using home visitors with different levels of training, and implementing a less-structuredintervention. Olds and his colleagues warned against this approach, cautioning that the available datasupported use of only nurses as home visitors, effects were limited to high-risk mothers, and only spe-cific tested methodologies were likely to work (Olds et al., 1999). Despite these comments by Olds,the specific components of home intervention programs that lead to success or failure have not beenidentified.
In their study of Hawaii’s Healthy Start Program, Duggan et al. conducted the first evaluation of impacton child maltreatment of a large-scale home visitation program implemented outside of an experimentalsetting (Duggan, McFarlane, et al., 2004). This program found that home visitation did not reduce childabuse and showed only a small effect on neglect. Reasons cited for these results were numerous, includ-ing early drop-out of many intervention-group families, failure of fathers to participate, low baselineabuse rates, scant training for home visitors particularly with respect to risk factors for abuse, and lack of

B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333 331
tested protocols and referral mechanisms. The authors recognized, though, that all of these explanationsamounted to untested hypotheses since no population-based home visitation model for child maltreat-ment prevention had been verified experimentally, and thus no gold standard for comparison existed.The authors concluded with a call for additional research before investing more resources in the homevisitation model. In an accompanying editorial, Chaffin supported the authors’ conclusions (Chaffin,2004).
The published report of the initial Healthy Families Alaska evaluation also supported these conclusions(Duggan, Caldera, et al., 2004). Like Hawaii, Healthy Families Alaska did not have a codified trainingor intervention component that specifically addressed determinants of abuse. Where written guidelinesexisted, evaluation showed that services actually delivered to enrolled families did not adhere to theseguidelines. Less than 60% of families were enrolled greater than 12 months. Even among those familiesthat had the highest level of intervention, less than one-third had interventions that addressed domesticviolence, substance use, or mental health (i.e., the major parental determinants of child abuse and neglect),possibly because home visitors felt ill-equipped to intervene in these areas. Similarly, approximately halfof families had no individualized family support plan. In practice Healthy Families Alaska screenedand primarily targeted mothers; however, data from Alaska has identified the biological father as themost common perpetrator of severe physical abuse in infants (Gessner et al., 2004). Lastly, the familyfocus of Healthy Families Alaska emphasized developing support plans in collaboration with the targetfamilies rather than specifically addressing important but sensitive risk factors for abuse even when thesewere identified. Again, no successful nonexperimental model for using home visitation to prevent childmaltreatment exists. Thus, it cannot be stated with certainty which if any of the above limitations ofHealthy Families Alaska affected program effectiveness.
Limitations
The current study had substantial limitations other than those previously noted. While control pop-ulations were evaluated, the study was not randomized. The study examined abuse reported to ChildProtective Services. The willingness of people to refer children to Child Protective Services may beinfluenced by characteristics such as poverty, race, and age and may not necessarily reflect the actualoccurrence of physical abuse. Changes in maltreatment rates over time documented by Child ProtectiveServices agencies may not reflect changes in the occurrence of maltreatment. For example, abuse referralor substantiation rates may change because of administrative changes in child welfare regulations, bud-getary changes, staff retention, degree and timing of staff education, political commitment, and publicawareness. These changes were not known to have occurred but if they did, they should have affected bothenrolled and unenrolled children. Because of this issue, the reader should be wary of drawing conclusionssolely from year-to-year changes in rates or case counts among enrolled children. Instead, the strengthof the study derives from comparing changes over time among enrolled children to changes among thethree comparison groups.
Implications for future work
Because so few approaches to child abuse prevention have been identified, it would be instructive to seeif the home visitation model in Alaska might achieve greater success if it were substantially revised. Thiswould include using trained professionals implementing specific interventions that address the critical

332 B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333
child abuse risk factors as well as implementation of previously successful cognitive approaches (Bugentalet al., 2002). For example, Duggan et al. have emphasized the importance of poor mental health, substanceuse, and domestic violence as contributing factors for child maltreatment (Duggan, Caldera, et al., 2004;Duggan, McFarlane, et al., 2004). A focused intervention could be developed to identify the contributionof these factors to child maltreatment by having home visitors address these outcomes at every visitregardless of the family’s agenda, connecting families to community resources specific to these riskfactors and documenting follow-up, and providing appropriate training to home visitors or, preferably,using mental health workers, domestic violence counselors, and drug abuse counselors as home visitors.
The hypothesis that retention of the home visitation model with substantial changes would improveprogram impact is untested: no empiric data exist supporting or refuting the idea that a more structuredapproach with better trained home visitors would result in a program that reduced child abuse. Thus, themost critical current need is for rigorous evaluations that can identify the components of successful homeintervention programs. Child maltreatment prevention advocates also must entertain the possibility thatmany and possibly most instances of child abuse occur in a complex setting that is not modifiable in partor entirely through parental participation in voluntary programs such as Healthy Families Alaska. Thisemphasizes the obligation of prevention advocates to include child welfare agencies as critical partnerswhen designing intervention programs.
The results from Healthy Families Alaska in combination with those from Hawaii’s home visitationprogram also emphasize that results from small-scale trials in an experimental setting may not be appli-cable to other settings. Stated differently, program efficacy may not translate into program effectiveness,a concept previously described for large-scale introduction of vaccines (Clemens et al., 1996).
Summary
Children enrolled in Healthy Families Alaska had a fourfold greater risk of child abuse and neglectcompared to other children living in the same communities. However, maltreatment rates were similar tounenrolled high-risk groups identified through birth certificate characteristics, thus bringing into questionthe added value of the utilized screening criteria. Enrollment also was associated with a substantialdecrease in physical abuse referral, but this decrease was no greater than that seen among some unenrolledhigh-risk children. Enrolled children experienced no change over time in substantiated physical abuse orneglect rates, while one of the evaluated groups of unenrolled high-risk children experienced a decreasein physical abuse substantiation. Among enrolled children, the number of home visits did not predicta lower rate of substantiated physical abuse. Numerous problems with the design and implementationof Healthy Families Alaska may have led to lack of effectiveness. Given the absence of a successfulcomparison model, it is not clear which components of the program, if any, prevented achievement ofreductions in child maltreatment.
Acknowledgments
The author would like to acknowledge Debra Caldera for her assistance with implementation of HealthyFamilies Alaska and for providing critical review of the current manuscript. The author also would like toacknowledge Phillip Mitchell of the Alaska Bureau of Vital Statistics for preparing birth certificate dataand performing data linkage.

B.D. Gessner / Child Abuse & Neglect 32 (2008) 317–333 333
References
Barth, R. P. (1991). An experimental evaluation of in-home child abuse prevention services. Child Abuse & Neglect, 15, 363–375.Brayden, R. M., Altemeier, W. A., Dietrich, M. S., Tucker, D. D., Christensen, M. J., McLaughlin, F. J., & Sherrod, K. B. (1993).
A prospective study of secondary prevention of child maltreatment. Journal of Pediatrics, 122, 511–516.Bugental, D. B., Ellerson, P. C., Lin, E. K., Rainey, B., Kokotovic, A., & O’Hara, N. (2002). A cognitive approach to child abuse
prevention. Journal of Family Psychology, 16, 243–258.Chaffin, M. (2004). Is it time to rethink Health Start/Healthy Families? Child Abuse & Neglect, 28, 589–595.Centers for Disease Control and Prevention. (2003). First reports evaluating the effectiveness of strategies for preventing violence:
Early childhood home visitation and firearms laws: Findings from the Task Force on Community Preventive Services.Morbidity and Mortality Weekly Report, 52(RR-14), 1–9.
Clemens, J., Brenner, R., Rao, M., Tafari, N., & Lowe, C. (1996). Evaluating new vaccines for developing countries. Efficacy oreffectiveness? Journal of the American Medical Association, 275, 390–397.
Duggan, A., Caldera, D. L., Rodriguez, K., Burrell, L. D., & Shea, S. K. (2004a). Evaluation of the Healthy Families AlaskaProgram: Final report, July 29, 2004. Alaska Department of Health and Social Services. Available at: http://hss.state.ak.us/ocs/Publications/JohnsHopkins HealthyFamilies.pdf, last accessed April 10, 2007.
Duggan, A., McFarlane, E., Fuddy, L., Burrell, L., Higman, S. M., Windham, A., & Sia, C. (2004). Randomized trial of astatewide home visiting program: Impact in preventing child abuse and neglect. Child Abuse & Neglect, 28, 597–622.
Eckenrode, J., Ganzel, B., Henderson, C. R., Smith, E., Olds, D. L., Powers, J., Cole, R., Kitzman, H., & Sidora, K. (2000). Thelimiting effects of domestic violence. Journal of the American Medical Association, 284, 1385–1391.
Geeraert, L., Van den Noortgate, W., Grietens, H., & Onghena, P. (2004). The effects of early prevention programs for familieswith young children at risk for physical child abuse and neglect: A meta-analysis. Child Maltreatment, 9, 277–291.
Gessner, B. D., Moore, M., Hamilton, B., & Muth, P. T. (2004). The incidence of infant physical abuse in Alaska. Child Abuse& Neglect, 28, 9–23.
Gomby, D., Culross, P. L., & Behrman, R. E. (1999). Home visiting: Recent program evaluations—Analysis and recommenda-tions. The Future of Children, 9, 4–26.
Hardy, J. B., & Streett, R. (1989). Family support and parenting education in the home: An effective extension of clinic-basedpreventive health care services for poor children. Journal of Pediatrics, 115, 927–931.
Hibbard, R. A., Desch, L. W., & American Academy of Pediatrics Committee on Child Abuse and Neglect; American Academyof Pediatrics Council on Children with Disabilities. (2007). Maltreatment of children with disabilities. Pediatrics, 119,1018–1025.
Lane, W. G., Rubin, D. M., Monteith, R., & Christian, C. W. (2002). Racial differences in the evaluation of pediatric fracturesfor physical abuse. Journal of the American Medical Association, 288, 1603–1609.
Olds, D. L., Eckenrode, J., Henderson, C. R., Jr., Kitzman, H., Powers, J., Cole, R., Sidora, K., Morris, P., Pettitt, L. M., &Luckey, D. (1997). Long-term effects of home visitation on maternal life course and child abuse and neglect. Fifteen-yearfollow-up of a randomized trial. Journal of the American Medical Association, 278, 637–643.
Olds, D. L., Henderson, C. R., Chamberlin, R., & Tatelbaum, R. (1986). Preventing child abuse and neglect: A randomized trialof nurse home visitation. Pediatrics, 78, 65–78.
Olds, D. L., Henderson, C. R., Kitzman, H. J., Eckenrode, J. J., Cole, R. E., & Tatelbaum, R. C. (1999). Prenatal and infancyhome visitation by nurses: Recent findings. Future Child, 9, 44–65.
Olds, D. L., & Kitzman, H. (1990). Can home visitation improve the health of women and children at environmental risk?Pediatrics, 86, 108–116.
Overpeck, M. D., Brenner, R. A., Trumble, A. C., Trifiletti, L. B., & Berendes, H. W. (1998). Risk factors for infant homicidein the United States. New England Journal of Medicine, 339, 1211–1216.
Sweet, M. A., & Appelbaum, M. I. (2004). Is home visiting an effective strategy? A meta-analytic review of home visitingprograms for families with young children. Child Development, 75, 1435–1456.
Winpisinger, K. A., Hopkins, R. S., Indian, R. W., & Hostetler, J. R. (1991). Risk factors for childhood homicides in Ohio: Abirth certificate-based case-control study. American Journal of Public Health, 81, 1052–1054.