The Neural Basis of Anosognosia for Spatial Neglect After Stroke
11
The Neural Basis of Anosognosia for Spatial Neglect After Stroke Simone Vossel, PhD; Peter H. Weiss, MD; Philipp Eschenbeck, PhD; Jochen Saliger; Hans Karbe, MD; Gereon R. Fink, MD Background and Purpose—The present study investigated the lesion anatomy of anosognosia for visuospatial neglect resulting from right hemispheric stroke. Methods—In 63 patients, self-ratings of performance in paper-and-pencil tests were contrasted with external performance ratings. Lesion analysis was conducted on patient subgroups with different degrees of anosognosia but comparable visuospatial impairment. Results—Independent of the severity of visuospatial neglect per se, damage to the right angular and superior temporal gyrus was associated with higher levels of anosognosia. Conclusions—Using a novel assessment of anosognosia for spatial neglect, the present study relates stroke-induced self-awareness deficits to inferior parietal and superior temporal brain damage. (Stroke. 2012;43:1954-1956.) Key Words: lesion analysis neglect self-awareness D espite the severe impact of stroke-induced impairments on daily life, some patients remain unaware of their deficits, that is, show anosognosia. 1 Previous studies demon- strated that the majority of patients with reduced self-awareness for hemiplegia/hemiparesis have right hemispheric brain dam- age. 2,3 No study has yet focused on the lesion anatomy of self-awareness deficits for visuospatial neglect, although these are even more prevalent than for hemiplegia. 4 The present study investigated anosognosia for spatial neglect and its neuroanato- my in patients with different degrees of impaired self-awareness but comparable visuospatial impairment. Patients and Methods Sixty-three patients with unilateral right hemispheric stroke (22 females) and 18 healthy control subjects (7 females) gave written informed consent. Lesions were confirmed by CT or MRI. The study had been approved by the local ethics committee. Participants performed 6 paper-and-pencil tests from the Behavioral Inattention Test 5 (star and line cancellation, line bisection, figure copying, clock drawing, text reading). Subse- quent to each subtest, the patients rated their performance on a 5-point scale (ranging from 1, severe difficulties to 5, no difficulties). An equivalent rating was performed by one of the investigators (P.E.) to evaluate the patient’s difficulties during task performance. This external rating was moreover used to relate the patients’ performance to that of healthy control subjects (patients performing 3 SDs below the mean of control subjects were regarded to have substantial visuospatial deficits; Table 1). Interrater agreement with 2 additional raters (evaluating the performance of 39 patients who gave their consent to video recordings) and correlations with objective performance measures (line bisection deviation and cancellation laterality quotients) were determined to ensure the reliability and validity of the external ratings. To quantify the degree of unawareness for visuospatial neglect, the following index was calculated: Table 1. Descriptive Data (MeanSD) Age, y Time Poststroke Total Score External Rating Total Score Self-Rating Anosognosia Index Healthy elderly control subjects (n18) 51.76.4 ... 29.30.96 28.91.8 0.010.04 Patients performing within 3 SDs from control subjects (n34) 55.114.9 111.0274.1 28.11.4 28.02.0 0.000.04 Patients performing 3 SDs below control subjects (n22)* 64.010.3 112.7191.1 20.04.9 25.52.7 0.380.5 *Note that only patients with matching pair member (ie, included in the lesion analyses) are listed. Received March 12, 2012; final revision received April 5, 2012; accepted April 6, 2012. From the Cognitive Neuroscience, Institute of Neuroscience & Medicine (INM-3; S.V., P.H.W., P.E., G.R.F.), Research Centre Ju ¨lich, Ju ¨lich, Germany; the Department of Neurology (P.H.W., G.R.F.), University Hospital Cologne, Cologne, Germany; Hochschule fu ¨r Gesundheit (P.E.), University of Applied Sciences, Bochum, Germany; and the Neurological Rehabilitation Centre Godesho ¨he (J.S., H.K.), Bonn, Germany. The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA.112. 657288/-/DC1. Correspondence to Simone Vossel, PhD, Institute of Neuroscience and Medicine (INM-3), Research Centre Ju ¨lich, Leo-Brandt-Str 5, 52425 Ju ¨lich, Germany. E-mail [email protected] © 2012 American Heart Association, Inc. Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.112.657288 1954 by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of The Neural Basis of Anosognosia for Spatial Neglect After Stroke

The Neural Basis of Anosognosia for Spatial NeglectAfter Stroke
Simone Vossel, PhD; Peter H. Weiss, MD; Philipp Eschenbeck, PhD; Jochen Saliger;Hans Karbe, MD; Gereon R. Fink, MD
Background and Purpose—The present study investigated the lesion anatomy of anosognosia for visuospatial neglectresulting from right hemispheric stroke.
Methods—In 63 patients, self-ratings of performance in paper-and-pencil tests were contrasted with external performanceratings. Lesion analysis was conducted on patient subgroups with different degrees of anosognosia but comparablevisuospatial impairment.
Results—Independent of the severity of visuospatial neglect per se, damage to the right angular and superior temporalgyrus was associated with higher levels of anosognosia.
Conclusions—Using a novel assessment of anosognosia for spatial neglect, the present study relates stroke-inducedself-awareness deficits to inferior parietal and superior temporal brain damage. (Stroke. 2012;43:1954-1956.)
Key Words: lesion analysis � neglect � self-awareness
Despite the severe impact of stroke-induced impairmentson daily life, some patients remain unaware of their
deficits, that is, show anosognosia.1 Previous studies demon-strated that the majority of patients with reduced self-awarenessfor hemiplegia/hemiparesis have right hemispheric brain dam-age.2,3 No study has yet focused on the lesion anatomy ofself-awareness deficits for visuospatial neglect, although theseare even more prevalent than for hemiplegia.4 The present studyinvestigated anosognosia for spatial neglect and its neuroanato-my in patients with different degrees of impaired self-awarenessbut comparable visuospatial impairment.
Patients and MethodsSixty-three patients with unilateral right hemispheric stroke (22females) and 18 healthy control subjects (7 females) gave writteninformed consent. Lesions were confirmed by CT or MRI. The studyhad been approved by the local ethics committee.
Participants performed 6 paper-and-pencil tests from theBehavioral Inattention Test5 (star and line cancellation, linebisection, figure copying, clock drawing, text reading). Subse-quent to each subtest, the patients rated their performance on a5-point scale (ranging from 1, severe difficulties to 5, nodifficulties). An equivalent rating was performed by one of theinvestigators (P.E.) to evaluate the patient’s difficulties duringtask performance. This external rating was moreover used torelate the patients’ performance to that of healthy control subjects(patients performing �3 SDs below the mean of control subjectswere regarded to have substantial visuospatial deficits; Table 1).Interrater agreement with 2 additional raters (evaluating theperformance of 39 patients who gave their consent to videorecordings) and correlations with objective performance measures(line bisection deviation and cancellation laterality quotients)were determined to ensure the reliability and validity of theexternal ratings.
To quantify the degree of unawareness for visuospatial neglect,the following index was calculated:
Table 1. Descriptive Data (Mean�SD)
Age, yTime
PoststrokeTotal Score
External RatingTotal ScoreSelf-Rating
AnosognosiaIndex
Healthy elderly control subjects (n�18) 51.7�6.4 . . . 29.3�0.96 28.9�1.8 0.01�0.04
Patients performing within 3 SDs fromcontrol subjects (n�34)
55.1�14.9 111.0�274.1 28.1�1.4 28.0�2.0 0.00�0.04
Patients performing �3 SDs belowcontrol subjects (n�22)*
64.0�10.3 112.7�191.1 20.0�4.9 25.5�2.7 �0.38�0.5
*Note that only patients with matching pair member (ie, included in the lesion analyses) are listed.
Received March 12, 2012; final revision received April 5, 2012; accepted April 6, 2012.From the Cognitive Neuroscience, Institute of Neuroscience & Medicine (INM-3; S.V., P.H.W., P.E., G.R.F.), Research Centre Julich, Julich,
Germany; the Department of Neurology (P.H.W., G.R.F.), University Hospital Cologne, Cologne, Germany; Hochschule fur Gesundheit (P.E.),University of Applied Sciences, Bochum, Germany; and the Neurological Rehabilitation Centre Godeshohe (J.S., H.K.), Bonn, Germany.
The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA.112.657288/-/DC1.
Correspondence to Simone Vossel, PhD, Institute of Neuroscience and Medicine (INM-3), Research Centre Julich, Leo-Brandt-Str 5, 52425 Julich,Germany. E-mail [email protected]
© 2012 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.112.657288
1954 by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from

anosognosia index�� external rating�� self-rating
� external rating
To evaluate the validity of this new measure, the anosognosia indexwas correlated with the Awareness Questionnaire6 (n�62).
Lesions were mapped on a template brain with 5-mm axial slicedistance using MRIcroN. Due to the high correlation betweenanosognosia and the severity of visuospatial neglect (see the online-only Data Supplement), lesion analyses were confined to specific
patient subgroups. For patients showing visuospatial deficits, patientpairs with identical external rating were identified. Subsequently,each pair member was allocated to 1 of 2 groups based on his or herself-rating. Patients without matching pair members (n�5) or withidentical scores (n�2) had to be discarded from these analyses. Thisprocedure yielded 2 groups of 11 patients each with identicalexternally evaluated performance but different degrees of anosogno-sia. Importantly, all other measures of visuospatial neglect did notdiffer significantly between both groups (Table 2). Lesions werecompared with a voxelwise Liebermeister test7 using a permutationthreshold of P�0.05.
ResultsCorrelation analyses between the demographic and neuropsy-chological variables revealed that anosognosia was moresevere with increasing age (see the online-only Data Supple-ment). Moreover, the degree of anosognosia significantlycorrelated with the performance in the 2 cancellation tasks,ipsilesional line bisection errors and with the external ratingscore.
Lesion analysis was based on matched patient subgroupswith identical test performance but different degrees ofanosognosia (Table 2).
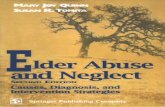
The Figure depicts the statistical test on the lesion locationsof the 2 subgroups. In the group with more severe anosog-nosia, a significantly higher number of patients had lesionsaffecting the right angular gyrus and the superior temporalgyrus when compared with the group with lower anosognosia(but comparable visuospatial impairment).
Table 2. Descriptive and Neuropsychological Data (Mean�SD)of the 2 Matched Patient Groups
LowerAnosognosia
HigherAnosognosia P*
No. 11 11 . . .
Age, y 60.3�9.4 67.7�10.1 0.091
Days poststroke 104.3�192 121.2�200 0.837
LQ line cancellation �0.26�0.4 �0.23�0.4 0.571
LQ star cancellation �0.30�0.5 �0.32�0.4 0.941
Mean bisection error 1.44�3.2 2.1�2.0 0.540
Total score external rating(maximum 30)
20�5 20�5
Matching criteria
Total score self-rating(maximum 30)
23.6�2.3 27.4�1.6
Anosognosia index �0.28�0.5 �0.47�0.5
LQ indicates laterality quotient.*Paired t test (matched patient pairs).
Figure. Results of the lesion analyses. LpermutFWE indicates critical test score for significance after multiple comparison correction.
Vossel et al Anosognosia for Spatial Neglect After Stroke 1955
by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from

To illustrate the lesion locations related to the presence ofvisuospatial neglect irrespective of anosognosia in thesepatients per se, the lesions of these patients were contrastedwith those of the remaining patients with normal perfor-mance. This analysis revealed that regions within a dorsalfrontoparietal network and underlying white matter, togetherwith inferior parietal brain areas (Figure), were more fre-quently damaged in patients with severely impaired visuospa-tial functions.
Lesion volume was significantly higher in patients withstrong spatial neglect than in the remaining patients(t[54]�4.4; P�0.001), whereas no significant lesion volumedifference was observed between the matched higher andlower anosognosia groups (t[10]��1.3; P�0.226).
The total rating score of all 3 raters revealed high interrateragreement (mean Pearson correlation coefficient r�0.973; all3 coefficients �0.96; P�0.001) and was highly correlatedwith the laterality quotients and line bisection errors (see theonline-only Data Supplement). The anosognosia index sig-nificantly correlated with the Awareness Questionnaire(r��0.46; P�0.001).
DiscussionBy contrasting subjective with objective performance ratingsin visuospatial paper-and-pencil tests, the present study in-vestigated anosognosia for spatial neglect and its neuralanatomy. Independent of the severity of the visuospatialdeficit per se, damage to the right inferior parietal andsuperior temporal cortex was associated with higher anosog-nosia, whereas anosognosia was not related to lesion size.The new anosognosia test showed good reliability andvalidity.
Anosognosia was strongly associated with different mea-sures of visuospatial neglect. Moreover, as previously re-ported,8 anosognosia was more severe with higher age.Hence, age might constitute an important factor for thedevelopment of anosognosia. Interestingly, unawareness forhemiplegia has also been critically related to visuospatialdeficits.9 Note, however, that anosognosia for hemiplegia hasalmost exclusively been studied in patients with visuospatialimpairment.10,11 Although contrasting lesions of patients withspatial neglect with and without anosognosia for hemiplegiacontrols for the presence of a visuospatial impairment, theseverity of the visuospatial impairments may still differbetween groups. For this reason, a matching procedure wasused in the current study to control for the severity of thevisuospatial deficits. This analysis revealed that lesions af-fecting the right angular and right superior temporal gyruswere more prevalent in the group with more severe anosog-nosia. This finding is in line with theoretical models ofimpaired self-awareness for attentional deficits.12 Moreover,our results parallel findings from Berti et al10 in the domain ofhemiplegia, because they also suggest function-specific neu-ral correlates of self-awareness.
Patients with parietal lesions fail to integrate informationabout performance outcome into future task execution plans,that is, they do not benefit from error feedback in subsequenttrials of a task.13 Along these lines, anosognosia for spatialneglect may be caused by a deficient performance monitoringin relation to discrepancies between intended and actualachievements. Further support for this notion comes fromstudies in the motor system, which show that the parietalcortex is crucially involved in the conscious detection ofdiscrepancies between intended actions and perceived move-ment consequences.14
AcknowledgmentsWe thank all our patients and are grateful to our colleagues from theResearch Centre Julich and the University Hospital Cologne as wellas the Max-Planck Institute for Neurological Research Cologne forproviding the opportunity to acquire MRI scans.
Sources of FundingS.V. is supported by the Deutsche Forschungsgemeinschaft (Vo1733/1-1).
DisclosuresNone.
References1. Prigatano GP. The Study of Anosognosia. New York, NY: Oxford Uni-
versity Press; 2010.2. Orfei MD, Robinson RG, Prigatano GP, Starkstein S, Ruesch N, Bria P,
et al. Anosognosia for hemiplegia after stroke is a multifaceted phe-nomenon: a systematic review of the literature. Brain. 2007;130:3075–3090.
3. Pia L, Neppi-Modona M, Ricci R, Berti A. The anatomy of anosognosiafor hemiplegia: a meta-analysis. Cortex. 2004;40:367–377.
4. Azouvi P, Samuel C, Louis-Dreyfus A, Bernati T, Bartolomeo P, BeisJM, et al. Sensitivity of clinical and behavioural tests of spatial neglectafter right hemisphere stroke. J Neurol Neurosurg Psychiatry. 2002;73:160–166.
5. Wilson BA, Cockburn J, Halligan P. Behavioural Inattention Test (BIT).Titchfield, Hampshire, UK: Thames Valley Test Company; 1987.
6. Sherer M, Bergloff P, Boake C, High W, Levin E. The AwarenessQuestionnaire: factor structure and internal consistency. Brain Inj. 1998;12:63–68.
7. Rorden C, Karnath H-O, Bonilha L. Improving lesion-symptom mapping.J Cogn Neurosci. 2007;19:1081–1088.
8. Appelros P, Karlsson GM, Hennerdal S. Anosognosia versus unilateralneglect. Coexistence and their relations to age, stroke severity, lesion siteand cognition. Eur J Neurol. 2007;14:54–59.
9. Vocat R, Staub F, Stroppini T, Vuilleumier P. Anosognosia for hemi-plegia: a clinical–anatomical prospective study. Brain. 2010;133:3578–3597.
10. Berti A, Bottini G, Gandola M, Pia L, Smania N, Stracciari A, et al.Shared cortical anatomy for motor awareness and motor control. Science.2005;309:488–491.
11. Karnath H-O, Baier B, Nagele T. Awareness of the functioning of one’sown limbs mediated by the insular cortex? J Neurosci. 2005;25:7134–7138.
12. Prigatano GP. Principles of Neuropsychological Rehabilitation. NewYork, NY: Oxford University Press; 1999.
13. Seki K, Ishiai S, Koyama Y, Sato S. Unassociated responses to tworelated task demands: a negative factor for improvement of unilateralspatial neglect. Neuropsychologia. 1999;37:75–82.
14. Desmurget M, Sirigu A. A parietal–premotor network for movementintention and motor awareness. Trends Cogn Sci. 2009;13:411–419.
1956 Stroke July 2012
by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from

FinkSimone Vossel, Peter H. Weiss, Philipp Eschenbeck, Jochen Saliger, Hans Karbe and Gereon R.
The Neural Basis of Anosognosia for Spatial Neglect After Stroke
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2012 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STROKEAHA.112.657288
2012;43:1954-1956; originally published online May 24, 2012;Stroke.
http://stroke.ahajournals.org/content/43/7/1954World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2016/04/07/STROKEAHA.112.657288.DC3.html http://stroke.ahajournals.org/content/suppl/2013/10/02/STROKEAHA.112.657288.DC2.html http://stroke.ahajournals.org/content/suppl/2012/06/13/STROKEAHA.112.657288.DC1.html
Data Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from

SUPPLEMENTAL MATERIAL
The neural basis of anosognosia for spatial neglect after stroke

Supplementary methods
Five-point scale for the self-rating of performance by the patients:
1) I have insuperable difficulties and I am not able to solve the task. I am not able tocorrect my errors.
2) I have severe difficulties and can only insufficiently solve the task. I make manyerrors and I am hardly able to correct these.
3) I have moderate difficulties but I can solve the task sufficiently. I make many errorsbut I am able to correct on average every second error.
4) I have mild difficulties but I can solve the task well. I make few errors and I am ableto correct most of these.
5) I do not have any difficulties in solving the task. I do not make any errors.

Supplementary tables
Table S1. Intercorrelations between demographic and neuropsychological variables,and the anosognosia index.
*p<.05; **p<.0014 (corresponding to Bonferroni-correction for 35 tests). Note that negative
LQ values indicate fewer hits in contralesional (left) as compared to ipsilesional (right) space.
Positive values in the line bisection test indicate ipsilesional (rightward) bisection errors.
Negative values in the awareness index reflect better self- than external ratings. The
Landmark-M test1 was additionally completed by the patients to differentiate between
perceptual-attentional and motor-intentional aspects of visuospatial functioning. This test was
not used for the assessment of anosognosia.
1. Bisiach E, Ricci R, Lualdi M, Colombo MR. Perceptual and response bias in unilateral
neglect: two modified versions of the Milner landmark task. Brain Cogn. 1998; 37:369-386.
age - -.20 -.17 .23 .24 .07 -.38* -.27*
days post-stroke -.05 -.05 .01 -.01 -.12 .03 .03
LQ line cancellation .66** -.63** -.49** -.13 .70** .73**
LQ star cancellation -.79** -.64** -.29* .77** .77**
mean bisection error .77** .31* -.74** -.75**
Landmark-Mperceptual bias
.02 -.63** -.52**
Landmark-M responsebias
-.25 -.21
total score externalrating
.86**
anosognosia index

Stroke 日本語版 Vol. 7, No. 322
図 病変解析の結果。LpermutFWE:多重比較補正後の有意性の限界テストスコア。
健康な対照より成績が 3SD超下の患者:病態失認 重度対軽度(n=2×11,視空間欠損の重症度について一致させた)
上側頭回 角回0
0
MNI-Z-17 -7 3 13 23 28 33 38 43 53 63 73 83
1 2 3 4
0.9 1.8 2.7
健康な対照より成績が 3SD超下の患者(n=22)対残りの患者(n=34)
permutFWE
permutFWE
脳卒中後に見られる空間無視に対する病態失認の神経基盤The Neural Basis of Anosognosia for Spatial Neglect After Stroke
Simone Vossel, PhD1; Peter H. Weiss, MD1,2; Philipp Eschenbeck, PhD1,3; Jochen Saliger4;Hans Karbe, MD4; Gereon R. Fink, MD1,2
1 Cognitive Neuroscience, Institute of Neuroscience & Medicine (INM-3), Research Centre Jülich, Jülich,Germany; 2 Department of Neurology, University Hospital Cologne, Cologne, Germany; 3 Hochschule für Gesundheit, University of Applied Sciences, Bochum, Germany; and 4 Neurological Rehabilitation Centre Godeshöhe, Bonn, Germany.
Abstract
背景および目的:本研究では,右大脳半球の脳卒中に起因する視空間無視の病態失認における病変の解剖学的構造を調べた。方法:63 例の患者を対象に,筆記テストの成績の自己評価を外部の成績評価と対比させた。病態失認の程度は異なるが視空間能障害は同等な患者サブグループについて病変
解析を行った。結果:視空間無視自体の重症度とは関係なく,右角回および上側頭回の損傷がより重度の病態失認と関連していた。結論:本研究では,空間無視の病態失認の新たな評価により,脳卒中により誘発された自己認識の欠如は下頭頂部および上側頭部の脳損傷と関連している。
Stroke 2012; 43: 1954-1956

66
3(27)’2012 ЭКСПЕРИМЕНТАЛЬНО-ТЕОРИТИЧЕСКИЕ ВОПРОСЫ
Нейрональные основы анозогнозии при пространственном игнорировании после инсульта
Источник. S. Vossel, P.H. Weiss, P. Eschenbeck, J. Saliger, H. Karbe, G.R. Fink. The neural basis of anosognosia for spatial neglect after stroke. Stroke 2012;43:6:1954–1956.
Дополнительная информация доступна on-line по адресу: http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA.112.657288/-/DC1 Cognitive Neuroscience, Institute of Neuroscience & Medicine, Research Centre Jülich, Jülich, Germany; the Department of Neurology, University Hospital Cologne, Cologne, Germany; Hochschule für Gesundheit, University of Applied Sciences, Bochum, Germany; and the Neurological Rehabilitation Centre Godeshöhe, Bonn, Germany.
Предпосылки и цель исследования. В исследовании изучали анатомию поражения головного мозга при анозогнозии со зрительно-про-странсвенным игнорированием, развившимся после инсульта в правом полушарии головного мозга. Методы. У 63 пациентов результаты самооценки письменных тестов сравнивали с объективной оценкой тестов. Провели анализ поражения головного мозга у пациентов с различной степенью анозогнозии, но сопоставимыми зрительно-пространственными нарушениями. Результаты. Независимо от тяжести зрительно-пространственного игнорирования как такового, повреждение правой угловой и верхней височной извилин было ассоцииро-вано с более выраженной анозогнозией. Выводы. С помощью нового метода оценки анозогнозии при пространственном игнорировании, в настоящем исследовании удалось установить, что дефицит самосознания после инсульта связан с локализацией поражения в нижней теменной и верхней височной извилинах головного мозга.
Ключевые слова: анализ очага поражения (lesion analysis), игнорирование (neglect), самооценка (self-awareness)
Несмотря на выраженное влияние последствий инсульта на повседневную жизнь, некоторые паци-енты не признают наличие у них дефекта, т. е. у них развивается анозогнозия [1]. В ранее проведенных исследованиях показали, что у большинства пациентов со сниженной самооценкой в отношении наличия у них гемиплегии/гемипареза, поражения локализова-лись в правом полушарии головного мозга [2, 3]. Ни в одном исследовании до сих пор не изучали локали-зацию поражения, обусловливающего развитие дефи-цита самоосознания при зрительно-пространственном игнорировании, хотя эти нарушения более распростра-нены, чем гемиплегия [4]. В настоящем исследовании изучали анозогнозию при пространственном игнори-ровании и ее нейроанатомический субстрат у пациен-тов с различной степенью нарушения самоосознания, но сопоставимыми зрительно-пространственными нарушениями.
■ ПАЦИЕНТЫ И МЕТОДЫ
Шестьдесят три пациента с односторонним инсуль-том в правом полушарии головного мозга (из них 22 женщины) и 18 здоровых лиц контрольной группы (из них 7 женщин) подписали письменное инфор-мированное согласие на участие в исследовании. Наличие поражения вещества головного мозга под-тверждали при проведении компьютерной томографии (КТ) или магнитно-резонансной томографии (МРТ). Исследование было одобрено локальным этическим комитетом.
Участники выполнили 6 письменных тестов из Behavioral Inattention Test [5] (вычеркивание звездо-
чек и линий, деление линий пополам, копирование фигур, рисование часов, чтение текста). Затем пациен-ты самостоятельно оценивали результаты каждого суб-теста по 5-балльной шкале (1 балл — серьезные затруд-нения, 5 баллов — отсутствие трудностей). Один из исследователей проводил аналогичную оценку резуль-татов тестов для выявления ошибок пациентов во время выполнения заданий. Эту фактическую оценку впоследствии использовали для изучения соотноше-ния между результатами тестирования пациентов и лиц контрольной группы (критерием наличия выражен-ного зрительно-пространственного дефицита считали обнаружение снижения показателей тестов пациентов на 3 стандартных отклонения по отношению к показа-телям лиц контрольной группы, таблица 1). Для обес-печения надежности и достоверности фактической оценки результатов изучили межэкспертную согласо-ванность с 2 экспертами (оценка результатов 39 паци-ентов, давших согласие на видеозапись тестирования), а также рассчитали корреляцию с объективными кри-териями оценки (отклонения в делении линии попо-лам и коэффициент латерализации вычеркивания).
Для количественной оценки степени неосведомлен-ности о наличии зрительно-пространственного игно-рирования рассчитали следующий индекс:
Индекс анозогнозии = Σ фактическая оценка – Σ самоценка Σ фактическая оценка
Для оценки достоверности этого нового показате-ля определили корреляцию индекса анозогнозии с результатами анкетирования с помощью опросника Awareness Questionnaire (n=62) [6].
Локализацию поражения вещества головного мозга размечали на модели с интервалом между аксиаль-ными срезами 5 мм с помощью программного обес-печения MRIcroN. Из-за высокой корреляции между
© American Heart Association, Inc., 2012 Адрес для корреспонденции: Simone Vossel, PhD, Institute of Neuroscience and Medicine (INM-3), Research Centre Jülich, Leo-Brandt-Str 5, 52425 Jülich, Germany. E-mail: [email protected]

67
3(27)’2012
анозогнозией и тяжестью зрительно-пространствен-ного игнорирования (см. дополнительные данные on-line), анализ поражений был ограничен определенны-ми подгруппами пациентов. Для пациентов со зри-тельно-пространственным дефектом выявляли пары пациентов с одинаковыми показателями фактической оценки результатов тестирования. Впоследствии каж-дого пациента в паре распределяли в одну из 2 групп в зависимости от его (ее) самооценки. Пациентов без соответствующей пары (n=5) или с идентичными результатами оценки (n=2) исключили из анализа. В результате этой процедуры получили 2 группы по 11 пациентов в каждой с одинаковыми оценками резуль-татов тестов, но разной степенью анозогнозии. Важно отметить, что существенного различия по всем другим характеристикам зрительно-пространственного игно-рирования между пациентами обеих групп не было (таблица 2). Поражения сравнивали путем проведения теста voxelwise Liebermeister test [7] с помощью порого-вого значения р<0,05.
■ РЕЗУЛЬТАТЫ
По результатам корреляционного анализа демо- графических и нейропсихологических показателей выявили наличие прямой зависимости тяжести ано-зогнозии от возраста (см. дополнительные данные on-line). Кроме того, степень анозогнозии достоверно коррелировала с результатами 2 заданий на вычерки-вание, ошибками в делении линий пополам на стороне поражения и фактической оценкой результатов.
Анализ поражений был основан на сравнении под-групп пациентов с одинаковыми результатами тести-
рования, но с разной степенью анозогнозии (табли-ца 2).
На рисунке (см. цв. вклейку) изображен статистичес-кий тест по локализации поражений в 2 подгруппах. В группе с тяжелой анозогнозией у значительно боль-шего числа пациентов очаги поражения локализова-лись в правой угловой извилине и верхней височной извилине, по сравнению с группой с менее выражен-ной анозогнозией (но сопоставимыми зрительно-про-странственными нарушениями).
Для иллюстрации локализации поражений, связан-ных с наличием зрительно-пространственного игно-рирования, независимо от анозогнозии как таковой, сравнивали локализацию поражений у этих пациентов с локализацией у пациентов, показавших нормальные результаты тестирования. По результатам проведен-ного анализа выявили, что у пациентов с тяжелыми нарушениями зрительно-пространственного гнозиса чаще были повреждены области в пределах дорзальной лобно-теменной зоны и белого вещества, а также в нижних теменных областях головного мозга (см. рису-нок на цв. вклейке).
Объем поражения был значительно выше у пациен-тов с выраженным пространственным игнорировани-ем, чем у остальных (t [54]=4,4; р<0,001), в то время как достоверных различий в объеме поражения между соответствующими группами с тяжелой и менее выра-женной анозогнозией не было (t [10] =–1,3; р=0,226).
Результирующий показатель оценок всех трех экс-пертов охарактеризовался высокой межэкспертной согласованностью (средний коэффициент корреляции Пирсона r=0,973; все 3 коэффициента >0,96; р<0,001) и был тесно связан с выявленной латерализацией
Таблица 1. Описательные данные (среднее±СО)
Группа Возраст, годыВремя от начала
инсульта, дниОбщая фактическая оценка результатов
Общая самооценка результатов
Индекс анозогнозии
Здоровые пожилые участники контрольной группы (n=18)
51,7±6,4 … 29,3±0,96 28,9±1,8 0,01±0,04
Пациенты с результатами в пределах 3 СО относительно результатов контрольной группы (n=34)
55,1±14,9 111,0±274,1 28,1±1,4 28,0±2,0 0,00±0,04
Пациенты с результатом на 3 СО ниже результатов контрольной группы (n=22)*
64,0±10,3 112,7±191,1 20,0±4,9 25,5±2,7 -0,38±0,5
Примечание. Важно отметить, что указаны данные только пациентов, для которых была соответствующая пара (т. е. только те, чьи данные вошли в анализ поражений)
Таблица 2. Описательные и нейропсихологические данные (среднее±СО) 2 сформированных групп пациентов
Характеристика группы Умеренная анозогнозия Тяжелая анозогнозия р*
Число пациентов, n 11 11 . . .
Возраст, годы 60,3±9,4 67,7±10,1 0,091
Число дней от начала инсульта 104,3±192 121,2±200 0,837
LQ в тесте вычеркивания линий -0,26±0,4 -0,23±0,4 0,571
LQ в тесте вычеркивания звездочек -0,30±0,5 -0,32±0,4 0,941
Средняя ошибка деления пополам, баллы 1,44±3,2 2,1±2,0 0,540
Общая фактическая оценка результатов тестирования (максимум 30 баллов), баллы 20±5 20±5
Критерий подбора соответствия
Общая субъективная оценка результатов (максимум 30 баллов), баллы 23,6±2,3 27,4±1,6
Индекс анозогнозии -0,28±0,5 -0,47±0,5
Примечание. LQ — коэффициент латерализации. * — Парный t-тест (сформированные пары пациентов)

68
3(27)’2012 ЭКСПЕРИМЕНТАЛЬНО-ТЕОРИТИЧЕСКИЕ ВОПРОСЫ
и наличием ошибок в делении линии пополам (см. дополнительные данные on-line). Индекс анозогнозии достоверно коррелировал с результатами заполнения опросника Awareness Questionnaire (r= 0,46; р<0,001).
■ ОБСУЖДЕНИЕ
В настоящем исследовании путем сравнения субъ-ективных и объективных оценок письменных тестов изучали анозогнозию при пространственном игно-рировании и ее анатомический субстрат. Независимо от тяжести зрительно-пространственного дефицита как такового, повреждения правой нижней теменной и верхней височной областей головного мозга были ассоциированы с более тяжелой анозогнозией, в то время как степень анозогнозии не была ассоциирована с размером очага поражения. Новый тест на наличие анозогнозии продемонстрировал хорошую надежность и достоверность.
Наличие и выраженность анозогнозии были тесно связаны с различными показателями зрительно-про-странственного игнорирования. Кроме того, как сооб-щалось ранее [8], анозогнозия была более выраженной у лиц пожилого возраста. Таким образом, возраст можно считать важным фактором в развитии анозогно-зии. Интересно, что отрицание наличия гемиплегии также неразрывно связано со зрительно-пространс-твенным дефицитом [9]. Однако следует отметить, что анозогнозию при гемиплегии изучали преиму-щественно у пациентов со зрительно-пространствен-ными нарушениями [10, 11]. Несмотря на сравнение характера нарушений у пациентов с пространственным игнорированием с и без анозогнозии с лицами конт-рольной группы с гемиплегией по наличию зрительно-пространственных нарушений, их тяжесть у пациентов различных групп может различаться. По этой причи-
не в настоящем исследовании для контроля тяжести зрительно-пространственного дефицита использовали процедуру согласования. Этот анализ показал, что в группе с более тяжелой анозогнозией преобладали поражения правой угловой и правой верхней височ-ной извилин. Этот вывод согласуется с теоретически-ми моделями нарушения самооценки при дефиците внимания [12]. Кроме того, результаты исследования сопоставимы с выводами А. Berti и соавт. [10] отно-сительно гемиплегии, высказавших предположение о наличии функционально-специфических нейрональ-ных коррелят с самоосознанием.
Пациенты с поражением теменной доли не в состоя-нии интегрировать информацию о результате действия и планировать выполнение дальнейших заданий, т. е. они не извлекают пользу из ошибочной обратной связи в последующих попытках выполнения задания [13]. По этому принципу анозогнозия при пространс-твенном игнорировании может быть связана с недо-статочной оценкой результатов действий из-за рас-хождений между предполагаемыми и фактическими достижениями. Это предположение нашло поддержку в результатах исследований двигательной системы, демонстрирующих, что теменная кора играет решаю-щую роль в сознательном обнаружении расхождения между намеченными действиями и результатами вос-принимаемого движения [14].
■ БЛАГОДАРНОСТИ
Мы благодарим всех наших пациентов и признатель-ны нашим коллегам из Научно-исследовательского центра Юлиха и Университетской клиники Кельна, а также Института неврологических исследований Макса-Планка в Кельне за предоставленную возмож-ность провести МРТ исследование.
ЛИТЕРАТУРА
1. Prigatano G.P. The Study of Anosognosia. New York, NY: Oxford Uni-
versity Press; 2010.
2. Orfei M.D., Robinson R.G., Prigatano G.P., Starkstein S., Ruesch N.,
Bria P., et al. Anosognosia for hemiplegia after stroke is a multi-
faceted phe-nomenon: a systematic review of the literature. Brain.
2007;130:3075–3090.
3. Pia L., Neppi-Modona M., Ricci R., Berti A. The anatomy of
anosognosia for hemiplegia: a meta-analysis. Cortex. 2004;40:
367–377.
4. Azouvi P., Samuel C., Louis-Dreyfus A., Bernati T., Bartolomeo P.,
Beis J.M., et al. Sensitivity of clinical and behavioural tests of spatial
neglect after right hemisphere stroke. J Neurol Neurosurg Psychiatry.
2002;73:160–166.
5. Wilson B.A., Cockburn J., Halligan P. Behavioural Inattention Test
(BIT). Titchfield, Hampshire, UK: Thames Valley Test Company; 1987.
6. Sherer M., Bergloff P., Boake C., High W., Levin E. The Awareness
Questionnaire: factor structure and internal consistency. Brain Inj.
1998;12:63–68.
7. Rorden C., Karnath H.-O., Bonilha L. Improving lesion-symptom map-
ping. J Cogn Neurosci. 2007;19:1081–1088.
8. Appelros P., Karlsson G.M., Hennerdal S. Anosognosia versus unilat-
eral neglect. Coexistence and their relations to age, stroke severity,
lesion site and cognition. Eur J Neurol. 2007;14:54–59.
9. Vocat R., Staub F., Stroppini T., Vuilleumier P. Anosognosia for
hemi-plegia: a clinical–anatomical prospective study. Brain.
2010;133:3578–3597.
10. Berti A., Bottini G., Gandola M., Pia L., Smania N., Stracciari A.,
et al. Shared cortical anatomy for motor awareness and motor con-
trol. Science. 2005;309:488–491.
11. Karnath H.-O., Baier B., Nägele T. Awareness of the functioning
of one’s own limbs mediated by the insular cortex? J Neurosci.
2005;25:7134–7138.
12. Prigatano G.P. Principles of Neuropsychological Rehabilitation.
New York, NY: Oxford University Press; 1999.
13. Seki K., Ishiai S., Koyama Y., Sato S. Unassociated responses to
two related task demands: a negative factor for improvement of
unilateral spatial neglect. Neuropsychologia. 1999;37:75–82.
14. Desmurget M., Sirigu A. A parietal–premotor network for movement
intention and motor awareness. Trends Cogn Sci. 2009;13:
411–419.