Investigating the decision-making needs of HIV-positive women in Africa using the Ottawa...
13
Investigating the decision-making needs of HIV-positive women in Africa using the Ottawa Decision-Support Framework: Knowledge gaps and opportunities for intervention Marion Doull a, * , Annette O’Connor b , M.J. Jacobsen b , Vivian Robinson a , Laura Cook c , Caroline Nyamai-Kisia d , Peter Tugwell a a Centre for Global Health, Institute of Population Health, University of Ottawa, Ottawa, Canada K1N 6N5 b University of Ottawa and Ottawa Health Research Institute, Ottawa, Canada c Arthritis Community Research and Evaluation Unit, Division of Outcomes and Population Health, Toronto Western Hospital Research Institute, Toronto, Canada d AfriAfya, Harnessing ICTs for Health, Nairobi, Kenya Received 22 February 2006; received in revised form 22 June 2006; accepted 29 June 2006 Abstract Objective: To examine HIV-positive women’s decision making in the context of pregnancy and HIV/AIDS and to explore interventions that may enhance and develop women’s decision-making capacity in the sub-Saharan African context. Methods: The Ottawa Decision-Support Framework was used to assemble evidence of women’s decision-making needs. Several electronic databases were searched and an Internet search of the World Wide Web was conducted to search grey literature sources. An evidence-based approach to assessing benefits, harms and current practices was employed. Results: Several gaps in our knowledge about women’s decision making in the context of pregnancy and HIV were identified. The availability of evidence varied for each decision; however, significant gaps included: evidence around testing for ones status, advanced directives for self and child, disclosure (specifically, the impact of), others perceptions of antiretroviral use and data on termination of pregnancies. Conclusion: Decision making as a concept was generally not addressed in the MTCT literature. Evidence regarding the perceptions of women and others regarding the various decisions was often not available and subsequently an important aspect of MTCT interventions neglected. Practice implications: Incorporating a multi-disciplinary decision-support framework may prove useful to promote women’s autonomy and involvement in MTCT-related decision making. # 2006 Elsevier Ireland Ltd. All rights reserved. Keywords: HIV/AIDS; Pregnancy; Decision making; Reproductive health 1. Introduction Research has consistently shown that maternal health and well-being are crucial to child health and survival in the developing world. However, this knowledge has not resulted in consistent and equitable treatment and care for HIV- positive women. HIV-positive pregnant women are often seen as mothers first rather than individuals in their own right. This paper will examine HIV-positive women’s decision making in the context of pregnancy and HIV/ AIDS and will explore interventions that may enhance and develop women’s decision-making capacity in this arena. It is believed that women themselves are an underused resource in their care and treatment and that decision- support interventions such as ‘health coaching’ may help to capitalize on women’s unique knowledge and skills. The Health Coach approach is a shared decision-making style of counselling based on the Ottawa Decision-Support www.elsevier.com/locate/pateducou Patient Education and Counseling 63 (2006) 279–291 * Corresponding author. Tel.: +1 613 562 5800x2509; fax: +1 613 562 5659. E-mail address: [email protected] (M. Doull). 0738-3991/$ – see front matter # 2006 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.pec.2006.06.020
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Investigating the decision-making needs of HIV-positive women in Africa using the Ottawa...

www.elsevier.com/locate/pateducou
Patient Education and Counseling 63 (2006) 279–291
Investigating the decision-making needs of HIV-positive women in
Africa using the Ottawa Decision-Support Framework:
Knowledge gaps and opportunities for intervention
Marion Doull a,*, Annette O’Connor b, M.J. Jacobsen b, Vivian Robinson a,Laura Cook c, Caroline Nyamai-Kisia d, Peter Tugwell a
a Centre for Global Health, Institute of Population Health, University of Ottawa, Ottawa, Canada K1N 6N5b University of Ottawa and Ottawa Health Research Institute, Ottawa, Canada
c Arthritis Community Research and Evaluation Unit, Division of Outcomes and Population Health,
Toronto Western Hospital Research Institute, Toronto, Canadad AfriAfya, Harnessing ICTs for Health, Nairobi, Kenya
Received 22 February 2006; received in revised form 22 June 2006; accepted 29 June 2006
Abstract
Objective: To examine HIV-positive women’s decision making in the context of pregnancy and HIV/AIDS and to explore interventions that
may enhance and develop women’s decision-making capacity in the sub-Saharan African context.
Methods: The Ottawa Decision-Support Framework was used to assemble evidence of women’s decision-making needs. Several electronic
databases were searched and an Internet search of the World Wide Web was conducted to search grey literature sources. An evidence-based
approach to assessing benefits, harms and current practices was employed.
Results: Several gaps in our knowledge about women’s decision making in the context of pregnancy and HIV were identified. The availability
of evidence varied for each decision; however, significant gaps included: evidence around testing for ones status, advanced directives for self
and child, disclosure (specifically, the impact of), others perceptions of antiretroviral use and data on termination of pregnancies.
Conclusion: Decision making as a concept was generally not addressed in the MTCT literature. Evidence regarding the perceptions of
women and others regarding the various decisions was often not available and subsequently an important aspect of MTCT interventions
neglected.
Practice implications: Incorporating a multi-disciplinary decision-support framework may prove useful to promote women’s autonomy and
involvement in MTCT-related decision making.
# 2006 Elsevier Ireland Ltd. All rights reserved.
Keywords: HIV/AIDS; Pregnancy; Decision making; Reproductive health
1. Introduction
Research has consistently shown that maternal health and
well-being are crucial to child health and survival in the
developing world. However, this knowledge has not resulted
in consistent and equitable treatment and care for HIV-
positive women. HIV-positive pregnant women are often
* Corresponding author. Tel.: +1 613 562 5800x2509;
fax: +1 613 562 5659.
E-mail address: [email protected] (M. Doull).
0738-3991/$ – see front matter # 2006 Elsevier Ireland Ltd. All rights reserved
doi:10.1016/j.pec.2006.06.020
seen as mothers first rather than individuals in their own
right. This paper will examine HIV-positive women’s
decision making in the context of pregnancy and HIV/
AIDS and will explore interventions that may enhance and
develop women’s decision-making capacity in this arena. It
is believed that women themselves are an underused
resource in their care and treatment and that decision-
support interventions such as ‘health coaching’ may help to
capitalize on women’s unique knowledge and skills.
The Health Coach approach is a shared decision-making
style of counselling based on the Ottawa Decision-Support
.

M. Doull et al. / Patient Education and Counseling 63 (2006) 279–291280
Table 2
Ottawa Decision-Support Framework: determinants of decisions
Perceptions of decision
Knowledge
Expectations
Values
Decisional conflict
Stage of decision making
Predisposition
Perceptions of others
Perceptions of others’ opinions and practices
Support
Pressures
Roles in decision making
Framework that is designed to support individuals in making
decisions that are consistent with personal values [1B]. Early
feasibility studies in Chile have shown that this type of
decision-making counselling was effective in empowering
disadvantaged women to more effectively manage their
health and that of their families [2B]. This approach blends
concepts from decision support and peer-based counselling
by training community members as ‘health coaches’ who are
from the same cultural background as their clients. The
health coach is trained to help individuals build decision-
making skills, clarify values and build skills in accessing
appropriate health care.
Similar interventions, under the banners of ‘expert
patients’ and ‘self-management programs’ have been
successful in improving patient outcomes in most developed
countries [3B,4G,5G]. However, with the exception of a
recently published paper [6B], the idea of HIV-positive
women’s involvement in treatment and care models for the
prevention of MTCT and future self-care activities have not
been explored.
Antenatal care is often the entry point for women into the
health care system. In many countries, it is also the first time
a woman will undergo, or be offered, HIV testing if she has
not sought out testing previously. Therefore, pregnancy can
open a Pandora’s box of health issues for women,
particularly when HIV/AIDS is a concern. Should a woman
test positive for HIV during pregnancy she is faced with a
cascade of complex and sensitive decisions (Table 1). These
decisions depend on context and resources available, and
women often lack the information, support and resources to
make informed choices.
This cascade of decisions requires women to act as
autonomous decision makers in settings where women often
traditionally follow the advice of health care workers or
family members [7B]. Complicating this issue is the fact that
there may unclear evidence about the choice options and
outcomes and decisions may be highly dependent on values.
These factors increase the importance of a context specific
evidence-based decision-making framework for health care
workers or trained lay workers to use to coach women
through the decisions. Furthermore, the importance of
actively involving HIV-positive women in the decision-
making process, either as lay coaches/counsellors or
Table 1
Potential decision cascade (dependent on context and setting)
1. To test for HIV status?
2. To disclose status (and to whom)?
3. What type of HIV treatment (e.g. take antiretrovirals (ARVs)
to prevent transmission to child (PMTCT))?
4. To continue with pregnancy?
5. What method of delivery (e.g. caesarean, vaginal)?
6. Who to help with delivery (e.g. midwife, traditional birth
attendant, general practitioner)?
7. Where to deliver (home or hospital)?
8. To breast-feed or not?
9. How to take care of self and child in the future (advanced directives)?
patients, is highlighted by the complexity of pregnancy
and HIV-related decision making.
The Ottawa Decision-Support Framework provides a
framework to promote high-quality decisions, defined as
informed and consistent with individual values [8B]. The
decision-support approach depends on the amount and
quality of information about the likely harms and benefits of
options. Effective care decisions are those in which the
benefits are large compared to the harms, or best-practices
(e.g. testing for HIV status). Preference-sensitive decisions
are those that are dependent on patient values (e.g.
disclosure of HIV status to partners or family) and unknown
effectiveness decisions are those in which the evidence of
benefits and harms is inconclusive or varied. According to
the Ottawa Decision-Support Framework (ODSF) decision
making is also dependent on several interrelated factors or
determinants (Table 2). Furthermore, the ODSF asserts that
decision-support tools such as health coaching and
evidence-based decision aids are integral to the decision-
making process [9B].
This review maps nine decisions that pregnant women
face according to the Ottawa Decision-Support Framework
and looks specifically at the African context. We highlight
the evidence about alternatives, current decision-making
practices, and gaps. We then focus on perceptions of
pregnant women and perceptions of others to explain the
gaps. Throughout the paper, we highlight areas in which the
implementation of a decision-support intervention, such as
the use of decision aids and health coaching, may assist
Resources to make decision
Personal
Previous experience
Self-confidence
Motivation
Skill in decision making
External
Support (information, advice, emotional, instrumental, financial,
professional help) from social networks and agencies
Characteristics
Client: age, sex, marital status, education, occupation, culture, locale,
medical diagnosis and duration, health status
Practitioner: age, sex, education, specialty, culture,
practice locale, experience, counselling style

M. Doull et al. / Patient Education and Counseling 63 (2006) 279–291 281
women to make evidence-based decisions in the context of
MTCT and narrow the evidence-practice gap.
2. Methods
We searched the following electronic databases for
evidence about decision making by HIV-positive women and
MTCT interventions: The Cochrane Library, MEDLINE,
EMBASE, CINAHL, PubMED, AIDSLINE, PsycINFO,
Sociofile and SPECTR (Social, Psychological, Educational
and Criminological Trials Register). We also used Google to
search websites of the World Health Organization,
UNAIDS, UNICEF, The Centre for Disease Control/USAID
(United States) and other sites. The searches included both
textwords and MESH headings for knowledge, attitudes,
practices, needs and decision-making skills of women with
HIV.
We used elements of the Ottawa Decision-Support
Framework (ODSF) to identify evidence around the
cascade of nine decisions; barriers and facilitators to
making those decisions; decision determinants; efficacy of
interventions to support decision making. Citations in the
search strategy were screened for relevant articles based on
each decision. Studies were included if they provided
evidence regarding interventions for a decision or if they
provided information on any of the above listed decision
determinants. Efforts were made to include as many
studies as possible for each decision within the space
limitations. In order to develop a complete picture of the
evidence, we used data from both Africa and other
countries; we recognize that this may affect the reliability
of our conclusions. Non-governmental (NGO) reports and
project specific reports (white papers) were found using
the web search and were used fill evidence gaps in the
peer-reviewed scientific literature. Considering that in
some regions NGOs and United Nations affiliates are the
main providers of HIV/AIDS treatment, care and support
these ‘white papers’ are an essential and often unmatched
form of evidence.
Evidence from quantitative studies is graded to indicate
the strength of the study design and confidence in results.
We used the hierarchy of evidence and grading system
developed by the Ottawa Methods Group for clinical
practice guidelines and decision aids [10B]. Evidence is
ranked as platinum [P]: a systematic review with at least
two RCTs; gold [G]: one RCT with minimum sample size
of 50; silver [S]: systematic review or RCT that does not
meet criteria for platinum or gold; bronze [B]: evidence
from at least one case series without controls or evidence
from expert opinion [10B]. While not HIV-specific, the
methods developed by the Ottawa Methods Group were
used here as they are straight forward, user friendly and are
applicable across subject areas. This grading method was
used in order to give the reader an indication of the strength
of evidence for each decision; it was not used to screen
articles for inclusion; however, where platinum evidence
was available it was reported first (i.e. systematic reviews)
in an effort to provide a complete, yet brief picture.
Qualitative evidence [Q] was used to gather contextual
information. The qualitative evidence was not graded as the
use of grading systems and quality checklists for qualitative
studies is highly contested and their use may not accurately
reflect the quality of a paper in the ‘quantitative’ sense
[11B,12B].
3. Results
The results are structured according to the cascade of
decisions. Evidence on benefits and harms for all of the
decision interventions are summarized in Table 3. For
intervention effectiveness (benefits and harms) platinum
level evidence was used first if available [10B]. The
availability of evidence for each decision varied significantly
and thus general conclusions cannot be drawn. A summary
of decision-support intervention strategies to address each
decision can be found in Table 4.
3.1. To test for HIV status?
UNAIDS estimates that 9 out of 10 HIV-positive people
do not know their serostatus.
3.1.1. Benefits and harms
Voluntary counselling and testing (VCT) is considered
‘best practice’ and ‘effective care’ decision because of gold-
level evidence showing significant reduction in risk
behaviours with uncommon adverse effects [13G]. In an
RCT of 3000 women, negative life events, such as
estrangement from peers, employer discrimination and
family neglect were uncommon (1–4% overall) [14G] with
the exception of break-up of a sexual relationship. There
were no statistically significant differences between groups,
but rates of physical abuse (18% versus 5%) and break-up of
marriage (15% versus 3%) were higher with VCT.
3.1.2. Current practice
At United Nations MTCT pilot sites, 64–83% of women
consent to have an HIV test after counselling [15B]. Testing
acceptability among women is greater after pre-test
individual or group counselling, with test acceptance
ranging from 89 to 93% [16S].
3.1.3. Mother’s perception of decision
Reported reasons for test refusal in African antenatal care
settings include the prohibitive cost of tests, fear of AIDS,
concerns about confidentiality of test results, partner’s
reactions, belief that the benefits of knowing does not
outweigh the risks of subsequent disclosure; lack of medical
care for HIV-positive persons negates advantages of
knowing [17B,18Q]. Confidentiality concerns are not only

M. Doull et al. / Patient Education and Counseling 63 (2006) 279–291282
Table 3
Summary of MTCT decisions and evidence of efficacy of intervention options
Decision Type of decision Evidence of efficacy of interventions
Benefits Harms
Voluntary counselling
and testing (VCT)
Preference sensitive Known HIV status: implications
for risk reduction [13G]a
Unknown HIV statusc
Negative life events
uncommon (1–4% overall)
[14G]a
Disclosure of status Preference sensitive Health benefits, risk reduction,
care and support [23G,24S,20Q]a
Stigma and discrimination
[23G]b
Condom use is higher when both
individuals in a relationship disclose
their serostatus and when the male
partner is seronegative [20Q]a
Blame, anger, violence
[20Q,32B]b
Treatment Effective care ARV zidovudine reduced the risk of
MTCT significantly in comparison
to a placebo (RR 0.54,95% CI,
0.42–0.69) [33P]a
Long-term effects of
ARV use unknownc
Zidovudine reduces risk of infant
death within first year of life
(OR 0.57, 95%CI, 0.38–0.85) and
risk of maternal death (OR 0.32,
95%CI, 0.16–0.66) [33P]a
Increase in transmission
of drug resistant strains
of HIV [40B]b
ARV Nevirapine when compared
with Zidovudine showed significant
risk reduction of MTCT (0R 0.51,
95%CI, 0.33–0.79) [33P]a
Pregnancy termination Preference sensitive Removes risk of HIV transmission
to childa
Risks to physical and mental
health particularly in areas
where abortion practices are
illegal or unsafeb
Delivery method,
assistance and location
Effective care/
preference sensitive
Method: caesarean section effective
in reducing the risk of MTCT,
transmission is reduced from
10/100 to less than 9/100 [48P]a
Method: caesarean
section without resources
and trained staff can lead
to injury or deathb
Infant feeding Preference sensitive/
unknown effectiveness
Cumulative probability at 2 years
of HIV infection was 36.7% (CI,
29.4–44.0%) in breast-feeding
group vs. 20.5% (CI, 14.0–27.0%)
in formula-feeding group (1 RCT,
n = 401) [55G]c
Breast-feeding protects
maternal and child
health [61B]a
Options: breast-feeding
or formula-feeding
Exclusive breast-feeding reduces
transmission of HIV by 61% as
compared to mixed feeding [57S]c
Risk of HIV transmission
from breast milk 16.2%
compared to
formula-feeding [55G]c
Formula-feeding risk of
water-borne diseases
and malnutrition [61B]b
Advanced directives Preference sensitive Succession planning prevents
institutionalization of childrena
Stigma and discriminationb
Disclosure to children can strengthen
family bonds & promote precautionary
behaviours among children [68S]a
Evidence grades: B, bronze; S, silver; G, gold; P, platinum; Q, qualitative.a Scientific evidence of benefit.b Scientific evidence of harm.c Unclear whether benefits outweigh harms, conflicting evidence.

M. Doull et al. / Patient Education and Counseling 63 (2006) 279–291 283
Table 4
Decision-support intervention summary and MTCT decisions
Types of decisions
and links with MTCT
Common approaches
and interventions
Delivery strategies
and resources
Evaluation and
outcome measures
Effective care (benefits
large compared to harms)
Assess perceptions
of decision
Health coaching services
(in person, group,
telephone call centre)
Improved knowledge
Testing for status Assess decision-making needs
(resources, available support)
Online decision-support
tools (Ottawa Guide)
to capture process of
decision support
Positive attitudes
ARV treatment Provide decision support Library of decision aids
and interventions
Self-confidence/skills in
behaviour change
Facilitate progress in decision
making and implementation
Training programs
for coaches (professional
schools, high schools)
Satisfaction with process
Preference sensitive
(dependent on patient values)
Facilitate transfer of learning
to future decisions
Clear values and realistic
expectations
Disclosure Inform Increased uptake of health
interventions
Continuing with pregnancy Clarify values Continuance of chosen option
Advanced directives Improved health outcomes
and quality of life
Safety
Unknown effectiveness
(insufficient data to judge)
Reduced distress/regret
Method/location/
assistance with deliverya
Breast-feeding vs. formula-feedinga
a Some decisions are deemed to have insufficient evidence given the context. For example, we know that caesareans work in ideal settings but if this is not a
reality whether the risks outweigh the benefits is inconclusive.
about results of the test (i.e. that someone at the clinic will
divulge results) but also that the testing process is not
confidential (i.e. waiting in line at the clinic) [18Q]. Reasons
for supporting routine HIV screening of pregnant women
include protection of the unborn baby, initiation of early
treatment if positive, and protection of other patients and
health care workers [19Q].
3.1.4. Perceptions of others
Community members and fear of disclosure play a role in
deciding whether to accept and return for test results where
results are not immediately available after testing [20Q]. A
significant barrier to VCT in some settings is the attitudes
and beliefs of health care providers who often push for
testing regardless of the personal consequences to the
woman [21Q].
3.1.5. Opportunities for decision support
Test acceptance increases with counselling but other
factors such as health care worker beliefs and individual
values still dictate individual decision making. A structured
decision aid used with counselling would systematically
take women through each stage of the decision highlighting
pros and cons of options, values clarification and often
includes stories or vignettes about what others would do in
their situation, addressing many of the barriers to testing
outlined above [22B].
3.2. To disclose (and to whom)?
There is limited evidence of the impact of disclosure of
HIV status in Africa.
3.2.1. Benefits and harms
Disclosure of HIV status is associated with beneficial
health effects including increased support from health care
providers and risk reduction by the individual
[20Q,23G,24S]. Harms include the possibility of stigmati-
zation and discrimination [14G,25Q]. However, commu-
nity-based services may be able to mitigate these negative
reactions [26Q].
3.2.2. Current practice
Test outcomes significantly affect disclosure patterns—
52% of those testing HIV positive disclosed their status
versus 79% who tested negative [23G]. Some women did not
disclose their HIV status to health care workers to avoid
discrimination (4/59) and about one-quarter reported
receiving substandard care because of their status or being
scolded by nurses for becoming pregnant [25B]. Only 32%
of women in Burkina Faso informed their partners of their
HIV status [27B], while in Tanzania 22% of women did
[28G]. In Rwanda, 85% of HIV-positive women stated that
they had informed their partners of testing but only 51%
intended to inform them of the results [29S]. Private

M. Doull et al. / Patient Education and Counseling 63 (2006) 279–291284
disclosure (to close family or friends) does occur but public
disclosure is very rare [18Q].
3.2.3. Mother’s perception of decision
Reasons for non-disclosure were similar across studies
and included fear of social stigma, divorce, accusations of
infidelity, family conflict, forced eviction from home,
rejection and abandonment [27B,28G,29S,30S].
3.2.4. Perceptions of others
Community members may assume the HIV-positive
status of women if their husbands died of an AIDS-related
illness [31Q]. A study in Burkina Faso found that informed
partners reacted with indifference (72%) or had an
encouraging attitude (24%) and no cases of domestic
violence were reported [27B]. In Rwanda, 62% of women
reported a positive reaction from their partners, 17%
reported blame or anger, and 21% reported fear, disbelief
or shock [20Q]. A study in Burkina Faso revealed that 18%
of HIV-positive women disclosed to their husbands and the
only reason women refused to disclose was fear of domestic
violence [32B]. In this study, impact of disclosure on
relations with primary male partners was limited: 2/54
women separated from their husbands after disclosure; but
most remained together and practiced more abstinence and
condom use [32B].
3.2.5. Opportunities for decision support
Decision support is effective in helping individuals to
clarify their values and also to obtain realistic expecta-
tions of the decision outcomes [22B]. This aspect of
decision support may be particularly useful given the
evidence above that many women fear adverse outcomes
of disclosure but less report experiencing adverse
outcomes.
3.3. What type of treatment (i.e. antiretrovirals)?
The evidence below is only for antiretrovirals (ARVs)
administered in labour or during pregnancy to prevent
MTCT. In the developing world, the combination ARV
regimen for treatment of HIV for both the mother and child,
if infected, has been unfortunately rarely available, primarily
due to prohibitive cost. Recently, efforts have been initiated
to expand access to ARV treatment.
3.3.1. Benefits and harms
A Cochrane systematic review demonstrated that both
short-course zidovudine and single-dose nevirapine are
effective for reducing MTCT [33P]. Short-course zido-
vudine reduced the relative risk of MTCT by 54% versus
placebo; an absolute reduction of 12 out of 100 children
compared to 24 children infected without treatment [33P].
Zidovudine also reduced the risk of both infant and
maternal death [33P]. A single dose of Nevirapine at the
onset of labour reduced MTCT by half (OR 0.51)
compared to intra and postpartum doses of Zidov-
udine [33P]. Short-course combination therapies of
zidovudine and lamivudine (3TC) were also effective in
reducing the risk of MTCT when administered during the
antenatal and intrapartum period or during the intrapartum
and postpartum period, when compared with a placebo
[33P].
Evidence about long-term effects of ARV use for the
prevention of MTCT is lacking. There is evidence of
nevirapine resistance both among women and children,
which could lead to limited future treatment options
[34S,35G]. A 2-year study of 2414 uninfected children
exposed to ARV demonstrated increased early anaemia, but
no other adverse effects [36B]. Potential side-effects of
zidovudine for the mother include headache, gastrointestinal
intolerance and bone marrow toxicity (anaemia), all of
which subside with use [37B]. No major adverse effects for
the newborn have been reported, although long-term follow-
up of children exposed to zidovudine in utero are still needed
[37B].
3.3.2. Current practice
Administration of ARV treatment varies widely
according to setting. In studies where an ARV dose
was planned directly before labour, 40% of women did not
reach the clinic to give birth [38G]. Evaluation of the
United Nations MTCT pilot projects found that 40–60%
of women who test positive at clinic sites received ARVs
[15B]. Reasons why women often do not receive the full
course of ARVs vary but may include timing of arrival at
health facility, delivery at home, lack of disclosure to
labour ward staff, partner opposition, concerns about
taking drugs during pregnancy, and incomplete adherence
[15B,39B].
3.3.3. Mother’s perceptions
Factors that influence women’s decisions about ARV
treatment include: perceptions of, relationships with and
trust in, health care providers, beliefs about ARVs including
efficacy, side-effects and perceptions of peers and family
(particularly mothers) and other HIV-positive women [40Q].
Pregnant HIV-positive women were concerned they would
be denied other health services if they refused ARV
treatment [40Q].
3.3.4. Perceptions of others
Social factors may affect the administration of intra-
partum doses. One study found that women were reluctant to
receive ARVs in the delivery room when family members
were present for fear of disclosing their status [41G].
3.3.5. Opportunities for decision support
ARV treatment is considered an effective care decision
(benefits are large compared to harms) and in this case,
the role of a health coach is mainly to inform. Key
outcomes of decision support in this case would be

M. Doull et al. / Patient Education and Counseling 63 (2006) 279–291 285
reduced decisional conflict and improved knowledge, both
of which have been shown to significantly improve via the
use of decision aids [42P]. Decision aids have also been
shown in some cases to increase the uptake of health
interventions but this has not been tested with ARV-
related decisions [42P].
3.4. To continue with pregnancy?
Pregnancy termination in response to an HIV-positive
diagnosis is an unlikely choice in Africa, due to moral,
social, cultural, legal and economic reasons.
3.4.1. Benefits and harms
Pregnancy termination removes the risk of HIV
transmission to the child. For an HIV-infected woman, it
also eliminates the personal, emotional, social and financial
burden of caring for a child. Potential harms include risk of
death and other medical complications due to unsafe
abortion procedures, loss of future financial security, loss of
family, and risk of poor emotional and mental health. Over
4 million unsafe abortions occur each year in Africa.
However, this figure does not distinguish between HIV-
positive and HIV-negative women [43B].
3.4.2. Current practice
Access to safe legal abortion is severely restricted in
Africa, with the exception of some countries such as South
Africa.
3.4.3. Mother’s perceptions
Factors influencing reproductive decision making
include personal health, desire for children, religious
beliefs, beliefs about abortion, knowing children born to
HIV-infected women who were HIV negative, knowledge
and beliefs about HIV, previous childbearing experience,
attitudes of families, partners and health care providers,
access to health care, ethnicity, socioeconomic status,
concerns about child and child’s future, drug use behaviours
and being in an abusive relationship [44B,45S,46Q]. A
survey of 209 HIV-positive women in Zimbabwe found that
nearly two-thirds would have had an abortion if it was
available, primarily because the pregnancy was unplanned
or unwanted [25B].
3.4.4. Opportunities for decision support
Whether to continue with one’s pregnancy is a
preference-sensitive decision, one that is highly dependent
on values. This decision is also highly dependent on
context and thus may not be a choice in some settings. A
health coach’s role in this case would be to work through
the decision help women clarify their values by describing
the physical, social and emotional consequences of the
options, describe how others have decided and asking
women to explicitly rank those benefits/harms they most
value [47B]. Explicit values clarification helps to improve
agreement between values and the actual choice made
[47B].
3.5. Method, location and assistance with delivery
How and where a woman gives birth is an extremely
context specific decision. In many settings women may not
have the choice or resources to make a decision regarding
the method, location or type of person providing assistance
during the delivery.
3.5.1. Benefits and harms of caesarean
A Cochrane systematic review found that caesarean
section delivery is very effective in preventing MTCT.
Without caesarean, 10 out of 100 children were infected,
with caesarean, 9 fewer were infected out of 100 [48P]. In
many African settings, there is little choice in who provides
care, and there is a lack of evidence of birth outcomes with
different health care providers (e.g. midwife, traditional
birth attendant (TBA), general practitioner).
3.5.2. Current practice
A study in rural Malawi revealed that 95% of women
(HIV-positive and negative) deliver vaginally [49B]. Women
may not seek or be able to seek delivery from trained
individuals [49B,50B,51B]. For example, in Malawi,
approximately 36% of deliveries were assisted by an
untrained individual, 35% by a TBA, 26% by a medical
professional and 3% delivered alone [49B]. In most African
hospitals, HIV is not considered an indication for caesarean
due to limited resources and trained individuals.
3.5.3. Location of delivery
Location of delivery is a major reason why women do not
undergo caesarean sections when needed [49B,50B,52Q].
For example, in rural Malawi, 71% of women deliver at
home or at a TBA facility, 17% at a health center and 11% in
a hospital [49B].
3.5.4. Perceptions of others
Research from Zimbabwe reports that most women who
gave birth while HIV positive were treated well by health
care providers at formal health care facilities; however, 25%
(n = 209) felt that they did not receive proper care because of
their HIV status [25B].
3.5.5. Opportunities for decision support
The provision of decision support via evidence-based
decision aids would be difficult in this case because there is a
lack of context specific data on outcomes. In order to assist
decision-making health coaches need to be able to provide
evidence-based information on the pros and cons of decision
options [22B]. More research is needed to determine the
comparability of outcomes (i.e. post-caesarean section) by
place of delivery (rural, urban) and by method of assistance
(physician, nurse, TBA).

M. Doull et al. / Patient Education and Counseling 63 (2006) 279–291286
3.6. To breast-feed or not?
The decision to breast-feed or formula-feed is highly
preference-sensitive (dependent on values), and also
depends on several health system, individual and environ-
mental factors.
3.6.1. Benefits and harms of exclusive formula-feeding
and exclusive breast-feeding
Breast-feeding protects the child against childhood
diseases, malnutrition and water-borne diseases and has
beneficial health effects for mothers including reduction in
breast cancer, ovarian cancer, and lactational amenorrhea
that promotes greater birth spacing [53B,54B]. However,
breast-feeding has been shown to result in 16.2% higher
post-natal transmission of HIV than formula-feeding in a
large RCT in Africa [55G,56G]. Over 75% of the HIV
transmission occurred in the first 6 months of breast-feeding.
However, breast-feeding is superior to mixed feeding
(breast-feeding mixed with other liquids, solids and
formula). Exclusive breast-feeding reduced post-natal
transmission of HIV by 61% compared to mixed feeding
and this protective effect was still significant 18 months
post-delivery [57S]. Mixed feeding (breast-feeding mixed
with other liquids, solids or formulas) is more harmful than
exclusive formula-feeding, resulting in a four-fold increase
in post-natal transmission of HIVand a three-fold increase in
HIV transmission plus death [57S].
The increased risk of transmission with mixed feeding
may be due to reduced immune benefits from the minimal
breast milk that infants ingest as well as introduction of other
foods to an immature system which may cause damage to
the mucosal linings of the gut allowing the virus easier
passage [58S,59B]. However, the evidence on reasons for
this increased risk is not conclusive.
Breast-feeding may result in higher maternal mortality
for women with HIV, but results are conflicting. For
example, one study found 11% mortality with breast-feeding
versus 4% with formula-feeding [56G] an another study
found no difference in maternal mortality (0.5% versus 2%
mortality, for breast-feeding and formula-feeding, respec-
tively) [60B]. Formula-feeding may be harmful in resource
poor settings where safe water and adequate formula may
not be available.
3.6.2. Current practice
The WHO and UNAIDS now recommend that for HIV-
positive women, breast-feeding should be avoided when
safe, acceptable, feasible and sustainable alternate feeding
sources are available [61B]. If these conditions cannot be
met, exclusive breast-feeding is recommended and should be
discontinued as soon as possible given local and personal
circumstances [61B].
Despite these recommendations, common practice is
mixed feeding. Many women in Africa choose to breast-feed
despite counselling recommending otherwise because of the
prohibitive cost of alternatives, fear of disclosing HIV status,
and awareness of risks of not breast-feeding for their child
given their setting [7B,62S]. Rates of breast-feeding
recorded in several antiretroviral RCTs range from 53 to
97% of women for a median time of 7 weeks to 19 months
[38G,63G,64G].
3.6.3. Mother’s perceptions
Women have a misconception that breast milk alone is
not enough for healthy child development and there are
cultural taboos about colostrum and early milk production in
some settings [7B]. Formula-feeding alone is also not
considered healthy [7B].
3.6.4. Perceptions of others
In many settings, breast-feeding is linked to social and
cultural norms and expectations. Women report that they
may be abused, ridiculed or interpreted as selfish or
promiscuous; that partners refused money to buy formula;
and that their family would disapprove [7B,65Q].
Some health care workers are unsupportive of formula-
feeding. A study in South Africa found that nurses insisted
women breast-feed after delivery, regardless of personal
choice, and they did not counsel women about potential risks
of breast-feeding if HIV positive [65B]. Research from
Tanzania found that counsellors often received contradictory
information about breast-feeding and transferred this
uncertainty to their clients [21Q].
Research in Zambia and Kenya found that counsellors
there provide appropriate information but fail to account for
women’s social and economic circumstances when making
feeding recommendations [62S].
3.6.5. Opportunities for decision support
A decision-support strategy may assist in realigning
expectations regarding infant feeding options and clarifying
evidence and misinformation. However, this decision
illustrates the vital importance of context specific deci-
sion-support tools that account for cultural beliefs and social
circumstances. For example, the best evidence may point to
formula-feeding as the option with the most ‘pros’ but this
may not be the case in places where access to clean water is
not guaranteed. Furthermore, the role of decision support is
to assist people in making the choice that is most consistent
with their values, which will vary significantly by setting.
3.7. Advanced directives for self and child
There is little evidence about these practices.
3.7.1. Benefits and harms
Formal succession planning including identification of a
primary caregiver is well accepted by children (over two-
thirds in one study) [66S,67B]. Planned succession prevents
institutionalization of children. Children raised in institu-
tions reach lower levels of education and lack social and

M. Doull et al. / Patient Education and Counseling 63 (2006) 279–291 287
cultural skills [68B]. Making arrangements for future care
involves testing and disclosure of status to children and
relatives (see decision #2). Disclosure can strengthen family
bonds and can promote HIV/AIDS precautionary behaviours
among children [69S].
3.7.2. Current practice
Less than half of women in Uganda disclose their HIV
status to their children [66S]. Also, in Uganda, 53% of
parents had appointed a guardian for their children but 53%
had not disclosed their status [69S]. The rights of orphaned
children to familial inheritance is a significant concern
among HIV-positive parents; however, only 10% of parents
had a written will [66S].
Prevention of unintended pregnancies among HIV-
positive women is a key WHO strategy, yet a review
suggests that MTCT and family planning programs are not
well integrated [17B,70B]. Research from Zimbabwe
revealed a shift in contraception use after a HIV-positive
diagnosis [25B]. Zambian data reveal that at six months
postpartum, contraception use was similar for HIV-positive
and negative women, with the exception of condom use
occurring more often by HIV-positive women [71B].
However, many HIV-positive women with regular partners
reported using no family planning methods [71B].
3.7.3. Mothers perceptions
Family planning is a key aspect of self-care for HIV-
positive women. Desire for children varies considerably
amongst HIV-positive women and is often dependent on the
number of children they already have, whether they are in a
new relationship, desires of their partners and/or their
previous experiences with child birth (i.e. miscarriages, still
births) [25B]. Despite knowledge that pregnancy could
seriously harm their health, many thought the benefits
outweighed the risks [25B].
3.7.4. Opportunities for decision support
Presently, advanced directives for both mother and family
are a neglected aspect of MTCT-related programming.
Integrating decision-support interventions into the con-
tinuum of MTCT-related decisions offers an opportunity to
encourage families to consider advance planning more
systemically.
4. Discussion and conclusion
4.1. Discussion
We have identified several gaps in our knowledge about
women’s decision making in the context of pregnancy and
HIV as well as an urgent need for interventions to promote
women’s autonomy and involvement in decision making for
their health. Research has shown clinically important
benefits of nevirapine, highly active antiretroviral therapy
(HAART) and the entire complement of MTCT-prevention
interventions. MTCT programs could prevent 50% of infant
HIV infections; combination ARV treatment as advocated in
the MTCT Plus Initiative could prevent over 90% of infant
HIV infections [72B]. However, implementing these
strategies with demonstrated effectiveness has been proble-
matic. This review addresses an important aspect of
intervention implementation—patient decision making in
the context of pregnancy and HIV/AIDS. The perspective of
HIV-positive women is missing in the HIV/AIDS literature,
particularly their views on decision-making and the difficult
choices they face when pregnant. ‘Expert-patients’, those
who are actively involved in their medical decision-making
and are equipped with the tools to make such decisions are
on the rise in most developed countries around the world.
Exploration of these topics in the context of HIV/AIDS in
the developing world has not been examined. Maternal to
child transmission of the HIV virus is preventable if a series
of clinical, social and personal decisions are made and most
importantly, if resources are made available to facilitate
these decisions.
4.2. Conclusion
Decision making as a concept was generally not
addressed in the MTCT literature. Evidence about the
perceptions of women and others regarding the decisions
was often not available and subsequently an important
aspect of MTCT interventions neglected. Essentially, the
context within which health care workers must advise
women, and women must act on their advice, is ignored.
This review has also outlined areas where decision-support
activities may be beneficial to improve self-care practices
and appropriate utilization of resources. Incorporating a
multi-disciplinary decision-support framework may prove
useful in this context to empower women to become
effective health decision-makers.
4.3. Practice implications
One key strategy to improving uptake and implementa-
tion of MTCT and MTCT Plus programs is improved
counselling strategies [39B,73B]. The implementation of the
Thai national program for the prevention of MTCT
highlights counselling strategies as central and in need of
ongoing attention and improvement [73B]. Moreover, a
report on the implementation of MTCT prevention programs
at 18 sites in South Africa calls for increased training of ‘lay’
counsellors as a key ingredient for program success [67B].
Counsellors provide the first point of access to information
and resources for women considering HIV testing and are
essential post-testing, whether one’s result is positive or
negative. Counselling strategies need to incorporate broader
issues that go beyond making decisions about HIV testing to
include empowerment, ongoing psychological and emo-
tional support and access to resources.

M. Doull et al. / Patient Education and Counseling 63 (2006) 279–291288
We have illustrated here the potential role that a Health
Coach approach—one that advocates shared counselling and
employs lay or peer counsellors can play in the care and
treatment of HIV-positive women. Health coaching makes a
unique contribution as it is distinct from traditional
counselling because coaches build their clients’ skills in
decision making, which can be used in the future, whereas
counsellors may encourage dependency if they do not build
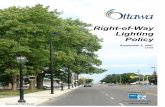
skills. Furthermore, coaches are trained to be neutral and
Fig. 1. Example data summary form for the Ottawa De
provide evidence and support versus advice, which is
emphasized in traditional counselling. An example of a
decision-support worksheet used by a health coach reveals
this personalization (see Fig. 1).
Health coaching supports women to make their own
choices that are consistent with their values and beliefs.
This process also has the supplementary benefit of
improving decision-making ability for subsequent deci-
sion making, a skill that may be essential given the
cision-Support Guide: Health Coach Worksheet.

M. Doull et al. / Patient Education and Counseling 63 (2006) 279–291 289
cascade of decisions involved in MTCT (see Table 4 for a
summary of MTCT decisions and decision-support
intervention approaches). Finally, health coaches tailor
decision support to the specific circumstances of each
client with the intention of improving the relevance of the
options, which is of particular importance to women in
resource poor settings.
The Health Coach Program is an attempt to intervene in
fairly complex clinical decisions at a level that is grounded
in individual experience and context. Therefore, the Health
Coach Program may be effective in improving decision-
making in contexts where this is not a traditional practice.
As illustrated in this review, the role of HIV-positive women
as decision makers invested in their own health and well-
being is not well addressed in the MTCT intervention
literature. Further research examining the impact of
involving HIV-positive women as decision makers is
needed and may provide important insights into MTCT
intervention efforts.
Acknowledgements
The authors would like to acknowledge the contributions
of Dr. Wafaa El-Sadr and Tanya Doherty for their insightful
and informative comments on this paper.
Funding: Marion Doull is funded by the Institute of
Gender and Health, Canadian Institutes for Health Research
Doctoral Scholarship Award. Annette O’Connor is funded
by the Canada Research Chair in Health Care Consumer
Decision Support and Peter Tugwell by the Canada Research
Chair on Health Equity.
References
[1] O’Connor AM, Tait V, Stacey D, Legare F. Communicating the
benefits and harms of estrogen–progestin hormone therapy with
decision aids. Medscape Women Health E-J 2003;8.
[2] Lange I, Campos MS, Urrutia M, Jaimovich S, Campos C, Penazola B.
Decision making needs of low income Chilean women. In: Proceed-
ings of the Sixth Annual Canadian Conference on International
Health; 1999.
[3] Glasgow RE, Orleans CT, Wagner EH, Curry SJ, Solberg LI. Does the
chronic care model serve also as a template for improving prevention?
Milbank Q 2001;79:579–612.
[4] Lorig KR, Sobel DS, Stewart AL, Brown BW, Bandura A, Ritter P,
Gonzalez VM, Laurent DD, Holman HR. Evidence suggesting that a
chronic disease self-management program can improve health status
while reducing hospitalization. Med Care 1999;37:5–14.
[5] Lorig KR, Ritter P, Stewart AL, Sobel DS, Brown BW, Bandura A,
Gonzalez VM, Laurent DD, Holman HR. Chronic disease self-man-
agement program 2-year health status and health care utilization
outcomes. Med Care 2001;39:1217–23.
[6] Kober K, Van Damme. Expert patients and AIDS care Antwerp:
Department of Public Health Institute of Tropical Medicine; 2006.
[7] Bassett MT. Psychosocial and community perspectives on alternatives
to breastfeeding. Ann NY Acad Sci 2000;918:128–35.
[8] O’Connor AM, Drake E, Fiset V, Graham I, Laupacis A, Tugwell P.
The Ottawa patient decision aids. Eff Clin Pract 1999;2:163.
[9] O’Connor AM, Jacobsen MJ, Stacey D. An evidence-based approach
to managing women’s decisional conflict. J Obstet Gynecol Neonatal
Nurs 2002;31:570.
[10] Tugwell P, Tugwell P, Shea B, Boers M, Brooks P, Simon L, Strand V,
Wells G, editors. Evidence-based rheumatology. London: Brit Med J
Books; 2004.
[11] Barbour R. Checklists for improving rigour in qualitative research: a
case of the tail wagging the dog. Br Med J 2001;322:1115.
[12] Dixon-Woods M, Shaw RL, Agarwal S, Smith JA. The problem of
appraising qualitative research. Qual Saf Health Care 2004;13:223.
[13] Voluntary HIV-1 counselling and testing efficacy group. Efficacy of
voluntary HIV-1 counselling and testing in individuals and couples in
Kenya, Tanzania, and Trinidad: a randomised trial. Lancet 2000;356:
103–12.
[14] Gregorich S, Grinstead O, Hogan M, Balmer D, Sangiwa G, Furlonge
C, Coates T. Being tested for HIV does not increase the incidence of
negative life events in three developing countries: results from the
voluntary HIV counselling and testing study. In: Proceedings of the
12th World AIDS Conference; 1998 [Abstract no. 24328].
[15] Rutenberg N, Baek C, Kalibala S, Rosen J. Evaluation of United
Nations supported pilot projects for the prevention of mother-to-child
transmission of HIV New York: UNICEF; 2003.
[16] Cartoux M, Sombie I, Van de Perre P, Meda N, Tiendrebeogo S, Dabis
F. Evaluation of 2 techniques of HIV pre-test counselling for pregnant
women in West Africa DITRAME study group. Int J STD AIDS
1999;10:199–201.
[17] Preble E, Huber D, Piwoz E. Family planning and the prevention of
mother-to-child transmission of HIV: technical and programmatic
issues. Advance Africa 2003; available at: www.advanceafrica.org.
[18] Nyblade L, Pande R, Mathur S, Macquarrie K, Kidd R, Banteyerga H,
Kidanu A, Kilonzo G, Mbwambo J, Bond V, Disentangling HIV. AIDS
stigma in Ethiopia Tanzania and Zambia Washington: International
Centre for Research on Women (ICRW); 2003.
[19] Orji EO, Sotiloye D, Fawole AO, Huyinbo KI. Attitude of Abeokuta
pregnant women to routine human immunodeficiency virus screening.
Niger J Med 2001;10:173–6.
[20] Keogh P. The social impact of HIV infection on women in Kigali
Rwanda: a prospective study. Soc Sci Med 1994;38:1047–53.
[21] de Paoli M, Manongi R, Klepp K. Counselor’s perspectives on
antenatal HIV testing and infant feeding dilemmas facing women
with HIV in Northern Tanzania. Reprod Health Matters 2002;10:
144–56.
[22] O’Connor AM. Using patient decision aids to promote evidence-based
decision making. Evid Based Med 2001;6:100.
[23] Grinstead OA, Gregorich SE, Choi KH, Coates T. Positive and
negative life events after counselling and testing: the voluntary
HIV-1 counselling and testing efficacy study. AIDS 2001;15:1045–52.
[24] Coates T, Sangiwa G, Balmer D, Gregorich S, Kamenga C. Voluntary
counselling and testing (VCT) reduces risk behavior in developing
countries: results from the voluntary counselling and testing study. In:
Proceedings of the 12th World AIDS Conference; 1998 [Abstract no.
133/33269].
[25] Feldman R, Maposhere C. Safer sex and reproductive choice: findings
from ’positive women: voices and choices’ in Zimbabwe. Reprod
Health Matters 2003;11:162–73.
[26] Kaleeba N, Kalibala S, Kaseje M, Ssebbanja P, Anderson S, Van Praag
E, Tembo G, Katabira E. Participatory evaluation of counselling,
medical and social services of the AIDS Support Organization (TASO)
in Uganda. AIDS Care 1997;9:13–26.
[27] Issiaka S, Cartoux. Living with HIV: women’s experience in Burkina
Faso West Africa. AIDS Care 2001;13:123–8.
[28] Kilewo C, Massawe A, Lyamuya E, Semali I, Kalokola F, Urassa E,
Giattas M, Temu F, Karlsson K, Mhalu F, Biberfeld G. HIV counsel-
ling and testing of pregnant women in sub-Saharan Africa: experi-
ences from a study on prevention of mother-to-child HIV-1
transmission in Dar es Salaam Tanzania. J Acquir Immune Defic
Syndr 2001;28:458–62.

M. Doull et al. / Patient Education and Counseling 63 (2006) 279–291290
[29] Ladner J, Leroy V, Msellati P, Nyiraziraje M, De Clercq A, Van de
Perre P, Dabis F. A cohort study of factors associated with failure to
return for HIV post-test counselling in pregnant women: Kigali
Rwanda. AIDS 1996;10:69–75.
[30] Heyward WL, Batter VL, Malulu M, Mbuyi N, Mbu L, St. Louis M,
Kamenga M, Ryder R. Impact of HIV counselling and testing among
child-bearing women in Kinshasa Zaire. AIDS 1993;7:1633–7.
[31] Paxton S. The paradox of public HIV disclosure. AIDS Care
2002;14:559–67.
[32] Nebie Y, Meda N, Leroy V, Mendelbrot L, Yaro S, Sombie I,
Cartoux M, Tiendrebeogo S, Dao B, Ouangre A, Nacro B, Fao P,
Ky-Zerbo O, Van de Perre P, Dabis F. Sexual and reproductive life
of women informed of their HIV seropositivity: a prospective
cohort study in Burkina Faso. J Acquir Immune Defic Syndr
2001;28:367–72.
[33] Brocklehurst P, Volmink J. Antiretrovirals for reducing the risk of
mother-to-child transmission of HIV infection. Cochrane Database
Syst Rev )2002;(2).
[34] Jourdain G, Ngo-Giang-Huong N, Le Cœur S, Bowonwaranuwong C,
Kantipong P, Leechanachai P, Ariyadej S, Leenasirimakul P, Hammer
S, Lallemant M. Intrapartum exposure to nevirapine and subsequent
maternal responses to nevirapine-based antiretroviral therapy. N Engl
J Med 2005;351:229–40.
[35] Gray G, Urban M, Chersich M, Bolton C, van Niekerk R, Violari A,
Stevens W, McIntyre J. A randomized trial of two postexposure
prophylaxis regimens to reduce mother-to-child transmission in
infants of untreated mothers. AIDS 2005;19:1289–97.
[36] European Collaborative Study. Exposure to antiretroviral therapy in
utero or early life: the health of uninfected children born to HIV-
infected women. J Acquir Immune Defic Syndr 2003;32:380–7.
[37] World Health Organization. Safety and tolerability of zidovudine.
Department of Reproductive Health and Research, World Health
Organization. WHO/HIS/2000.01. 2001; available at: http://
www.who.int/reproductive-health/docs/zidovudine.html, accessed
November 28, 2005.
[38] Dabis F, Msellati P, Meda N, Weiffens-Ekra C, You B, Manigart O,
Leroy V, Simonon A, Cartoux M, Combe P, Ouange A, Ramon R, Ky-
Zerbo O, Montcho C, Salamon R, Rouzioux C, Van de Perre P,
Mandelbrot L. 6-Month efficacy, tolerance, and acceptability of a
short regimen of oral zidovudine to reduce vertical transmission of
HIV in breastfed children in Cote d’Ivoire and Burkina Faso: a double-
blind placebo-controlled multicentre trial. Lancet 1999;353:
786–92.
[39] McCoy D, Besser M, Visser R, Doherty T. Interim findings on the
national PMTCT pilot sites: lessons and recommendations South
Africa: Health Systems Trust; 2002.
[40] Misener TR, Sowell RL. HIV-infected women’s decisions to take
antiretrovirals. West J Nurs Res 1998;20:431–47.
[41] Wiktor SZ, Ekpini E, Karon JM. Short-course oral zidovudine for
prevention of mother-to-child transmission of HIV-1 in Abidjan Cote
d’Ivoire: a randomised trial. Lancet 1999;353:781–5.
[42] O’Connor AM, Stacey D, Rovner D, Holmes-Rovner M, Tetroe J,
Llewellyn-Thomas H, Entwistle V, Rostom A, Fiset V, Barry M, Jones
J. Decision aids for people facing health treatment or screening
decision (Cochrane Review). Cochrane Database Syst Rev )2003;(1).
[43] Ahman E, Shah I. Unsafe abortion: worldwide estimates for 2000.
Reprod Health Matters 2002;10:13–7.
[44] Selwyn PA, Carter RJ, Schoenbaum EE, Robertson VJ, Klein RS,
Rogers MF. Knowledge of HIV antibody status and decisions to
continue or terminate pregnancy among intravenous drug users. J
Am Med Assoc 1989;261:3567–71.
[45] Sunderland A, Minkoff HL, Handte J, Moroso G, Landesman S. The
impact of human immunodeficiency virus serostatus on reproductive
decisions of women. Obstet Gynecol 1992;79:1027–31.
[46] Richter DL, Sowell RL. Factors affecting reproductive decisions of
African American women living with HIV. Women Health 2002;36:
81–96.
[47] O’Connor AM, Llewellyn-Thomas HA, Flood AB. Modifying unwar-
ranted variation in health care: shared decision making using patient
decision aids. Health Aff 2004;63.
[48] Brocklehurst P. Interventions for reducing the risk of mother-to-child
transmission of HIV infection. Cochrane Database Syst Rev 2002;1.
[49] Kulmala T, Vaahtera M, Rannikko J, Ndekha M, Cullinan T, Salin ML,
Ashorn P. The relationship between antenatal risk characteristics,
place of delivery and adverse delivery outcome in rural Malawi. Acta
Obstet Gynecol Scand 2000;79:984–90.
[50] Saunders B. What’s it like to work in Zimbabwe. Pract Midwife
2002;5:36–9.
[51] Bulterys M, Glenn Fowler M, Shaffer N, Tih P, Greenberg A, Karita E,
Coovadia H, De Cock KM. Role of traditional birth attendants in
preventing perinatal transmission of HIV. Br Med J 2002;324:222–4.
[52] Amooti-Kaguna B, Nuwaha F. Factors influencing choice of delivery
sites in Rakai district of Uganda. Soc Sci Med 2000;50:203–13.
[53] Weinberg GA. The dilemma of postnatal mother-to-child transmission
of HIV: to breastfeed or not? Birth 2000;27:199–205.
[54] Coutsoudis A, Goga AE, Rollins N, Coovadia HM. The child health
group free formula milk for infants of HIV-infected women: blessing
or curse? Health Policy Plan 2002;17:154–60.
[55] Nduati R, John G, Mbori-Ngacha D, Richardson B, Overbaugh J,
Mwatha A, Ndinya-Achola J, Bwayo J, Onyango F, Hughes J, Kreiss J.
Effect of breastfeeding and formula feeding on transmission of HIV-1:
a randomized clinical trial. J Am Med Assoc 2000;283:1167–74.
[56] Nduati R, Richardson BA, John G, Mbori-Ngaccha D, Mwatha A,
Ndinya-Achola J, Bwayo J, Onyango FE, Kreiss J. Effect of breast-
feeding on mortality among HIV-1 infected women: a randomised
trial. Lancet 2001;357:1651–5.
[57] Iliff P, Piwoz E, Tavengwa N, Zunguza C, Marinda E, Nathoo K,
Moulton LH, Ward B. ZVITAMBO study group Humphrey J Early
exclusive breastfeeding reduces the risk of postnatal HIV-1 transmis-
sion and increases HIV-free survival. AIDS 2005;19:699–708.
[58] Coutsoudis A. Influence of infant feeding patterns on early mother-to-
child transmission of HIV-1 in Durban South Africa. Ann NYAcad Sci
2000;918:136–44.
[59] Willumsen J, Filteau S, Coutsoudis A, Newell M, Rollins N, Coovadia
H, Tomkins AM. Breastmilk RNA viral load in HIV-infected South
African women: effects of subclinical mastitis and infant feeding.
AIDS 2003;17:407–14.
[60] Coutsoudis A, Coovadia A, Pillay K, Kuhn L. Are HIV-infected
women who breastfeed at increased risk of mortality? AIDS
2001;15:653–5.
[61] UNICEF. HIV and infant feeding: a UNICEF fact sheet New York:
UNICEF; 2002.
[62] Coutsoudis A, Pillay K, Kuhn L, Spooner E, Tsai WY, Coovadia HM,
South African Vitamin study group. A method of feeding and trans-
mission of HIV-1 from mothers to children by 15 months of age:
prospective cohort study from Durban South Africa [comment]. AIDS
2001;15:379–87.
[63] Petra Study Team. Efficacy of three short-course regimens of zido-
vudine and lamivudine in preventing early and late transmission of
HIV-1 from mother to child in Tanzania, South Africa, and Uganda
(Petra study): a randomised, double-blind, placebo-controlled trial.
Lancet 2002;359:1178–86.
[64] Leroy V, Karon JM, Alioum A, Ekpini E, Ehounou R, Meda N,
Greenberg A, Msellati P, Hudgens M, Dabis F, Witkor S. Twenty-four
month efficacy of a maternal short-course zidovudine regimen to
prevent mother-to-child transmission of HIV-1 in West Africa. AIDS
2002;16:631–41.
[65] Seidel G, Sewpaul V, Dano B. Experiences of breastfeeding and
vulnerability among a group of HIV-positive women in Durban South
Africa. Health Policy Plan 2000;15:24–33.
[66] Gilborn LZ, Nyonyintono R, Kabumbuli R, Jagwe-Wadda G. Mak-
ing a difference for children affected by AIDS: baseline findings
from operations research in Uganda New York: Population Council;
2001.

M. Doull et al. / Patient Education and Counseling 63 (2006) 279–291 291
[67] UNAIDS. Investing in our future: psychosocial support for children
affected by HIV/AIDS: a case study of Zimbabwe and the United
Republic of Tanzania Geneva: UNAIDS; 2001.
[68] Phiri S, Webb D. In: Cornia AC, editor. The impact of HIV/AIDS on
orphans and programme and policy responses. Florence, Italy: AIDS,
Public Policy and Child Well-Being UNICEF; 2002.
[69] The Population Council. Succession planning in Uganda: early out-
reach for AIDS-affected children and their families Washington, DC:
Population Council/Horizons; 2003.
[70] Myer L, Rabkin M, Abrams E, Rosenfeld A, El-Sadr W. Focus on
women: linking HIV care and treatment with reproductive health
services in the MTCT-plus initiative. Reprod Health Matters
2005;13:136–46.
[71] Rutenberg N, et al. Family planning and PMTCT services: examining
interrelationships strengthening linkages Washington, DC: Population
Council; 2003.
[72] Global Health Council. MTCT Plus: spearheading HIV/AIDS pre-
vention and care for mothers and children. Global Health Council
2005.
[73] Kanshana S, Simonds RJ. National program for preventing mother-
child HIV transmission in Thailand: successful implementation and
lessons learned. AIDS 2002;16:953–9.