International Maritime Health Foundation - Via Medica Journals
98
International Maritime Health, 2020, Vol. 71, No. 4 2020, Vol. 71, No. 4 nr ISSN 1641–9251 www.intmarhealth.pl Official scientific forum of the: International Maritime Health Foundation Indexed/abstracted in: CrossRef, DOAJ, EBSCO, ESCI, FMJ, Google Scholar, Index Copernicus, Medical Journals Links, Medline, Ministry of Science and Higher Education, Polish Medical Bibliography, Scopus, SJR, Ulrich's Periodicals Directory, WorldCat
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of International Maritime Health Foundation - Via Medica Journals

Inte
rnatio
nal M
aritim
e H
ealth
, 2020, V
ol. 7
1, N
o. 4
MARITIME MEDICINE Original articles
Anish Arvind Hebbar, Nitin Mukesh
COVID-19 and seafarers’ rights to shore leave, repatriation and medical assistance: a pilot study ............................................................ 217
Getu Gamo Sagaro, Gopi Battineni, Nalini Chintalapudi, Marzio Di Canio, Francesco Amenta
Telemedical assistance at sea in the time of COVID-19 pandemic .......................................... 229
Farhad Azimi Yancheshmeh, S. Hossain Mousavizadegan, Amin Amini, Andrew P. Smith, Reza Kazemi
Poor sleep quality, long working hours and fatigue in coastal areas: a dangerous combination of silent risk factors for deck officers on oil tankers ...237
Alexis Maffert, Barbara Aupy
Optokinetic stimulation efficiency for sea sickness treatment ................................... 249
Review articles
Devran Yazır, Bekir Şahin, Tsz Leung Yip, Po-Hsing Tseng
Effects of COVID-19 on maritime industry: a review .................................................................. 253
Elisabeth Stoll, Klaus Püschel, Volker Harth, Marcus Oldenburg
Prevalence of alcohol consumption among seafarers and fishermen ....................................... 265
Marcus Oldenburg, Lukas Belz, Filip Barbarewicz, Volker Harth, Hans-Joachim Jensen
Work profile of maritime pilots in Germany ......... 275
Case report
Ajit C. Kulkarni
A case of neurocysticercosis with an unusual presentation on high seas .................................... 278
TRAVEL MEDICINEReview article
Krzysztof Korzeniewski
Extreme traveler .................................................... 281
VARIAOriginal article
Giulio Nittari, Graziano Pallotta, Ravjyot Singh Khuman, Francesco Amenta
TelePharmaSea: proposing a novel approach to automate, organize and simplify management of medical chest on board commercial vessels ............................... 291
LETTERS TO THE EDITOR
Ken Inoue, Nursultan Seksenbayev, Timur Moldagaliyev, Yoshihiro Noso, Nobuo Takeichi, Yoshiyuki Ohira, Zhannat Sarsembina, Nargul Ospanova, Noriyuki Kawano, Haruo Takeshita, Masaharu Hoshi
Adequate measures to prevent medical personnel from contracting COVID-19 should be promptly implemented: support from numerous agencies is needed ................................................................ 296
Ken Inoue, Nursultan Seksenbayev, Timur Moldagaliyev, Nobuo Takeichi, Yoshihiro Noso, Zhannat Sarsembina, Nargul Ospanova, Haruo Takeshita, Yoshiyuki Ohira, Noriyuki Kawano, Masaharu Hoshi
Changes in university classes as COVID-19 continues and new findings regarding future university instruction methods: from the perspective of Japan and Semey, Republic of Kazakhstan ........................................ 297
Manik Sharma
Design of brain-computer interface-based classification model for mining mental state of COVID-19 afflicted mariner’s ............................ 298
Dominique Jégaden, David Lucas
About the relationship between ship noise and the occurrence of arterial hypertension in seafarers .............................................................. 301
Richard Pougnet, Pol Bleunven, Brice Loddé, David Lucas, Jean-Dominique Dewitte, Laurence Pougnet
Sexually transmitted infection and seafarers: raising awareness on preventing prostitution? ..... 303
2020, Vol. 71, No. 4 nr ISSN 1641–9251
www.intmarhealth.pl
"International Maritime Health" is indexed at: CrossRef, DOAJ, EBSCO, ESCI, FMJ, Google Scholar, Index Copernicus, Medical Journals Links, Medline, Ministry of Science and Higher Education, Polish Medical Bibliography, Scopus, SJR, Ulrich's Periodicals Directory, WorldCat.
Official scientific forum of the:
InternationalMaritime
HealthFoundation
Indexed/abstracted in: CrossRef, DOAJ, EBSCO, ESCI, FMJ, Google Scholar, Index Copernicus,
Medical Journals Links, Medline, Ministry of Science and Higher Education, Polish Medical Bibliography, Scopus, SJR,
Ulrich's Periodicals Directory, WorldCat
CONTENTS

INTERNATIONAL MARITIME HEALTHFormer: Bulletin of the Institute of Maritime and Tropical Medicine in Gdynia, issued since 1949Owner: International Maritime Health FoundationThe international multidisciplinary journal devoted to research and practice in the field of: maritime medicine, travel and tropical medicine, hyperbaric and underwater medicine, sea-rescue, port hygienic and sanitary problems, maritime psychology.
Supported financially by:
Editor-in-ChiefMaria JeżewskaMedical University of Gdańsk, Institute of Maritime and Tropical Medicine, Gdynia, Poland(http://www.immt.gdynia.pl/) See our website for information on sending manuscript, aims, scope, instructions for authors (reviewers), editorial board members, guidelines for scientific demands etc.https://journals.viamedica.pl/international_maritime_healthwww.intmarhealth.plwww.imhf.pl
Publisher of the International Maritime HealthPublishing, Subscription and Advertising Office: VM Media sp. z o.o. VM Group sp.k.ul. Świętokrzyska 73, 80–280 Gdańsk, Poland, tel. (+48 58) 320 94 94, fax (+48 58) 320 94 60e-mail: [email protected], http://www.viamedica.pl
Subscription rates: Paper subscription, 4 issues incl. package and postage institutional — 120 euro. The above prices are inclusive of regular postage costs. Payment should be made to: VM Media sp. z o.o. VM Group sp.k., Grupa Via Medica, Bank BGŻ Paribas SA account number: 15 1600 1303 0004 1007 1035 9021; SWIFT: PPABPLPK. Single issues, subsriptions orders and requests for sample copies should be send to e-mail: [email protected]. Electronic orders option available at: https://journals.viamedica.pl/international_maritime_health
Advertising: for details on media opportunities within this journal please contact the advertising sales: VM Media sp. z o.o. VM Group sp.k., ul. Świętokrzyska 73, 80–280 Gdańsk, Poland, tel. (+48 58) 320 94 94, fax (+48 58) 320 94 60, e-mail: [email protected] Editors accept no responsibility for the advertisement contents.
"International Maritime Health" is edited by: International Maritime Health Foundation (IMHF) and Polish Society of Maritime, Tropical and Travel Medicine in Gdynia (PSMTTM).Address: 9B Powstania Styczniowego street, 81–519 Gdynia, Poland Secretary: Leszek Mayer MD, e-mail: [email protected]
All rights reserved, including translation into foreign languages. No part of this periodical, either text or illustration, may be used in any form whatsoever. It is particularly forbidden for any part of this material to be copied or translated into a mechanical or electronic language and also to be recorded in whatever form, stored in any kind of retrieval system or transmitted, whether in an electronic or mechanical form or with the aid of photocopying, mi-crofilm, recording, scanning or in any other form, without prior written permission of the publisher. The rights of the publisher and authors are protected by national copyright laws and by international conventions, and their violation will be punishable by penal sanctions.
Legal note: http://czasopisma.viamedica.pl/IMH/about/legalNote
"International Maritime Health" is indexed at: CrossRef, DOAJ (Directory of Open Access Journals), EBSCO, ESCI (Emerging Sources Citation Index), FMJ, Google Scholar, Index Copernicus, Medical Journals Links, Medline, Ministry of Science and Higher Education, Polish Medical Bibliography, Scopus, SJR, Ulrich's Periodicals Directory, WorldCat. Position in Index Copernicus ranking system is available at: www.indexcopernicus.com.
Copyright © 2020 Polish Society of Maritime Tropical and Travel MedicinePrinted in the Republic of PolandISSN: 1641–9251
Norwegian Centre for Maritime and Diving Medicine,
Bergen, Norway
Polish Society of Maritime, Tropical and Travel Medicine,
Gdynia, Poland
NORWEGIAN CENTRE FORMARITIME AND DIVING MEDICINE
HELSE BERGEN, Haukeland University
Hospital, Bergen, Norway
Norwegian Association of Maritime Medicine,
Bergen, Norway
INFORMATION FOR AUTHORSThe International Maritime Health will publish original papers on medical and health problems of seafarers, fishermen,
divers, dockers, shipyard workers and other maritime workers, as well as papers on tropical medicine, travel medicine, epidemiology, and other related topics.
Typical length of such a paper would be 2000–4000 words, not including tables, figures and references. Its construc-tion should follow the usual pattern: abstract (structured abstract of no more than 300 words); key words; introduction; participants; materials; methods; results; discussion; and conclusions/key messages.
Case Reports will also be accepted, particularly of work-related diseases and accidents among maritime workers.All papers will be peer-reviewed. The comments made by the reviewers will be sent to authors, and their criticism and
proposed amendments should be taken into consideration by authors submitting revised texts.Review articles on specific topics, exposures, preventive interventions, and on the national maritime health services will
also be considered for publication. Their length will be from 1000 to 4000 words, including tables, figures and references.Letters to the Editor discussing recently published articles, reporting research projects or informing about workshops
will be accepted; they should not exceed 500 words of text and 5 references.There also will be the section Chronicle, in which brief reports will be published on the international symposia and
national meetings on maritime medicine and health, on tropical parasitology and epidemiology, on travel medicine and other subjects related to the health of seafarers and other maritime workers. Information will also be given on training activities in this field, and on international collaborative projects related to the above subjects.
All articles should be submitted to IMH electronically online at www.intmarhealth.pl where detailed instruction regarding submission process will be provided.
Only English texts will be accepted.Manuscripts should be typed in double line spacing on numbered pages and conform to the usual requirements (Ref.:
International Committee on Medical Journals Editors. Uniform Requirements for Manuscripts Submitted to Biomedical Journals, JAMA, 1997; 277: 927–934).
Only manuscripts that have not been published previously, and are not under consideration by another publisher, will be accepted.
Full texts of oral presentations at meetings (with abstracts printed in the conference materials) can be considered.All authors must give written consent to publication of the text.Manuscripts should present original material, the writing should be clear, study methods appropriate, the conclusions
should be reasonable and supported by the data. Abbreviations, if used, should be explained.Drugs should be referred to by their approved names (not by trade names). Scientific measurements should be given
in SI units, except for blood pressure, which should be expressed in mm Hg.Authors should give their names, addresses, and affiliations for the time they did the work. A current address of one
author should be indicated for correspondence, including telephone and fax numbers, and e-mail address.All financial and material support for the reported research and work should be identified in the manuscript.
REFERENCESReferences should be numbered in the order in which they appear in the text. At the end of the article the full list of
references should give the names and initials of all authors (unless there are more than six authors, when only the first three should be given followed by: et al.).
The authors’ names are followed by the title of the article; the title of the journal abbreviated according to Medline; the year of publication, the volume number; and the first and last page numbers. Please note: References you should include DOI numbers of the cited papers (if applicable) – it will enable the references to be linked out directly to prop-er websites. (e.g. Redon J, Cifkova R, Laurent S et al. Mechanisms of hypertension in the cardiometabolic syndrome. J Hypertens. 2009; 27(3): 441–451, doi: 10.1097/HJH.0b013e32831e13e5.).
Reference to books should give the title, names of authors or of editors, publisher, place of publication, and the year.Information from yet unpublished articles, papers reported at meetings, or personal communications should be cited
only in the text, not in References.For full information for authors refer to the web page: www.intmarhealth.pl.

EDITORIAL BOARD: Hyperbaric and diving medicine Marit GrönningDepartment of Occupational Medicine, Haukeland University Hospital, Bergen, Norway e-mail: [email protected]
Telemedicine, maritime medicineAlf Magne Horneland NCMDM, Haukeland University Hospital, Bergen, Norway e-mail: [email protected]
Francesco AmentaCIRM Rome, University of Camerino, Italy e-mail: [email protected]
Epidemiology and occupational medicineOlaf Chresten JensenCentre of Maritime Health and Society, University of Southern Denmark, Esbjerg, Denmark e-mail: [email protected]
Jorgen Riis Jepsen Centre of Maritime Health and Society, University of Southern Denmark, Esbjerg, Denmark e-mail: [email protected]
Naval medicine, public healthJon Magnus HagaNCMDM, Haukeland University Hospital, Bergen, Norway e-mail: [email protected]
Epidemiology, travel and tropical medicineKrzysztof KorzeniewskiDepartment of Epidemiology and Tropical Medicine Military Institute of Medicine, Warsaw, Poland e-mail: [email protected]
Maritime and travel medicineNebojša Nikolić Faculty of Medicina, University of Rijeka, Croatia e-mail: [email protected]
Cardiology, maritime emergencies and accidentsMarcus Oldenburg Department of Maritime Medicine, Institute of Occupational and Maritime Medicine (ZfAM) University of Hamburg, Germany e-mail: [email protected]
Mental health and health promotion Vsevolod RozanovOdessa National Mechnikov University, Odessa, Ukraine e-mail: [email protected]
Psychology and safety at workAndy Smith Centre for Occupational and Health Psychology Cardiff University, United Kingdom e-mail: [email protected]
EDITOR-IN-CHIEF: Maria Jeżewska Medical University of Gdańsk, Institute of Maritime and Tropical Medicine, 9B Powstania Styczniowego street, 81–519 Gdynia, Poland, e-mail: [email protected], tel: (+48) 601 67 65 33, fax: (+48 58) 622 33 54
DEPUTY EDITOR-IN-CHIEF: Eilif DahlNCMDM, Haukeland University Hospital, Bergen, Norwaye-mail: [email protected]
Stephen E. Roberts School of Medicine Swansea University, United Kingdom e-mail: [email protected]
HONORARY EDITOR: Bogdan Jaremin e-mail: [email protected]
SECRETARY of the EDITORIAL BOARD:Leszek Mayer e-mail: [email protected]
PUBLISHER EDITOR:Joanna Niezgoda Via Medica, Gdańsk, Polande-mail: [email protected]
STATISTICAL EDITOR:Paweł Zagożdżon Department of Hygiene and Epidemiology Medical University of Gdańsk, Poland e-mail: [email protected]
LANGUAGE EDITORTim CarterNCMDM, Haukeland University Hospital, Bergen, Norway e-mail: [email protected]

EDITORIAL ADVISORY BOARD:Gregory Chan Chung Tsing National University of Singapore, Singapore e-mail: [email protected]
Ilona Denisenko IMHA, WISTA, Russian Federation e-mail: [email protected]
Jordi Desola CRIS-UTH, University of Barcelona, Spain e-mail: [email protected], [email protected]
Lucero Prisno Don Eliseo III University of Liverpool, UK e-mail: [email protected]
Karl Faesecke Hamburg Hyperbaric Center, Germany e-mail: [email protected]
Marta Grubman-Nowak IMTM, MUG, Gdynia, Poland e-mail: [email protected]
Christos Hadjichristodoulou University of Thessaly, Larissa, Greece e-mail: [email protected]
Henrik Lyngbeck Hansen CMHS University of Southern Denmark, Denmark e-mail: [email protected]
Suresh N. Idnani IMHA, ICSW, Goa, India e-mail: [email protected]
Dominique Jegaden FSMH, Brest University, France e-mail: [email protected]
Piotr Kajfasz Medical University of Warsaw, Poland e-mail: [email protected]
Jacek Kot IMTM MUG, Gdynia, Poland e-mail: [email protected]
Raymond Lucas George Washington, University Washington DC, USA e-mail: [email protected]
Alessandro Marroni DAN Europe, Italy/Malta e-mail: [email protected]
Bente Elisabeth Moen University of Bergen, Norway e-mail: [email protected]
Wacław Leszek Nahorski Medical University of Gdańsk, Poland e-mail: [email protected]
Ralph Nilsson Sahlgrenska University Goteborg, Sweden e-mail: [email protected]
Marcin RenkeMedical University of Gdańsk, Poland e-mail: [email protected]
Giovanna Ricci University of Camerino, Italy e-mail: [email protected]
Przemysław RutkowskiDepartment of Nephrology, Transplantology and Internal Diseases, MUG, Poland e-mail: [email protected]
Maria Luisa Sanchez K Line Clinic, Manila, Philippines e-mail: [email protected]
Bernd Fred Schepers German Maritime Health Association e-mail: [email protected]
Klaus Seidenstuecker Chairman German Maritime Health Association e-mail: [email protected]
Suzanne Louise StannardNCMDM, Haukeland University Hospital, Bergen, Norway e-mail: [email protected]
Robert Steffen ISPM, University of Zurich, Switzerland e-mail: [email protected]
Agnar Ström TvetenNCMDM, Radio Medico Norway e-mail: [email protected]
Einar Thorsen Department Occupational Medicine, Haukeland University Hospital, Bergen, Norway e-mail: [email protected]
Arne Johan Ulven NCMDM, Haukeland University Hospital, Bergen, Norway e-mail: [email protected]
Donald A. Velasco University of the Immaculate Conception, Davao City, Philippines e-mail: [email protected]
Karin Westlund Sahlgrenska University Hospital Got henburg, Sweden e-mail: [email protected]
Stephen Williams Institute of Cruise Ship Medicine, Miami Beach, USA e-mail: [email protected]

CONTENTS
MARITIME MEDICINE Original articles
Anish Arvind Hebbar, Nitin Mukesh
COVID-19 and seafarers’ rights to shore leave, repatriation and medical assistance: a pilot study ............................................................ 217
Getu Gamo Sagaro, Gopi Battineni, Nalini Chintalapudi, Marzio Di Canio, Francesco Amenta
Telemedical assistance at sea in the time of COVID-19 pandemic .......................................... 229
Farhad Azimi Yancheshmeh, S. Hossain Mousavizadegan, Amin Amini, Andrew P. Smith, Reza Kazemi
Poor sleep quality, long working hours and fatigue in coastal areas: a dangerous combination of silent risk factors for deck officers on oil tankers ...237
Alexis Maffert, Barbara Aupy
Optokinetic stimulation efficiency for sea sickness treatment ................................... 249
Review articles
Devran Yazır, Bekir Şahin, Tsz Leung Yip, Po-Hsing Tseng
Effects of COVID-19 on maritime industry: a review .................................................................. 253
Elisabeth Stoll, Klaus Püschel, Volker Harth, Marcus Oldenburg
Prevalence of alcohol consumption among seafarers and fishermen ....................................... 265
Marcus Oldenburg, Lukas Belz, Filip Barbarewicz, Volker Harth, Hans-Joachim Jensen
Work profile of maritime pilots in Germany ......... 275
Case report
Ajit C. Kulkarni
A case of neurocysticercosis with an unusual presentation on high seas .................................... 278
TRAVEL MEDICINEReview article
Krzysztof Korzeniewski
Extreme traveler .................................................... 281
VARIAOriginal article
Giulio Nittari, Graziano Pallotta, Ravjyot Singh Khuman, Francesco Amenta
TelePharmaSea: proposing a novel approach to automate, organize and simplify management of medical chest on board commercial vessels ............................... 291
LETTERS TO THE EDITOR
Ken Inoue, Nursultan Seksenbayev, Timur Moldagaliyev, Yoshihiro Noso, Nobuo Takeichi, Yoshiyuki Ohira, Zhannat Sarsembina, Nargul Ospanova, Noriyuki Kawano, Haruo Takeshita, Masaharu Hoshi
Adequate measures to prevent medical personnel from contracting COVID-19 should be promptly implemented: support from numerous agencies is needed ................................................................ 296
Ken Inoue, Nursultan Seksenbayev, Timur Moldagaliyev, Nobuo Takeichi, Yoshihiro Noso, Zhannat Sarsembina, Nargul Ospanova, Haruo Takeshita, Yoshiyuki Ohira, Noriyuki Kawano, Masaharu Hoshi
Changes in university classes as COVID-19 continues and new findings regarding future university instruction methods: from the perspective of Japan and Semey, Republic of Kazakhstan ........................................ 297
Manik Sharma
Design of brain-computer interface-based classification model for mining mental state of COVID-19 afflicted mariner’s ............................ 298
Dominique Jégaden, David Lucas
About the relationship between ship noise and the occurrence of arterial hypertension in seafarers .............................................................. 301
Richard Pougnet, Pol Bleunven, Brice Loddé, David Lucas, Jean-Dominique Dewitte, Laurence Pougnet
Sexually transmitted infection and seafarers: raising awareness on preventing prostitution? ..... 303


Dear Readers, Dear Writers,Dear IMH Friends,
The year 2020 is coming to an end.It has been a very difficult time for all of us.The COVID-19 pandemic has changed our professional and social lives. It has changed us and our families. It has affected our health. The pandemic has challenged many fields, particularly medicine and pharmaceuticals.On the eve of a new year, we celebrate many achievements of science and medicine.We trust that the vaccination will be delivered to all the people in the world very soon. However, we still wait for the effective remedy. This is the greatest challenge of all.And in this extraordinary reality I venture to wish you all a very healthy Christmas.A big thank you to all the Authors for bringing wonderful articles to IMH this year.We always await new interesting reports, especially now, about the fight against the pandemic on land and at sea.Let this Christmas be filled with warmth and peace.Let it be the time of reflection on our lives.Be patient; look after yourselves and your families. Avoid any unnecessary risk and keep the distance.
Stay healthy!Maria Jeżewska
IMH Editor-in-Chief


Anish Arvind Hebbar, Assistant Professor (Maritime Safety and Environmental Protection), World Maritime University, Fiskehamngatan 1, 201 24 Malmö, Sweden,
e-mail: [email protected]
COVID-19 and seafarers’ rights to shore leave, repatriation and medical assistance: a pilot study
Anish Arvind Hebbar , Nitin Mukesh
World Maritime University, Malmö, Sweden
ABSTRACTBackground: The well-being of the world’s 1.65 million seafarers is expected to be secured by the rights established under the Maritime Labour Convention (MLC), 2006 with active monitoring of its implementa-tion by the flag administrations through the International Maritime Organisation (IMO) and International Labour Organisation (ILO). However, the substantial gains achieved since entry into force of MLC in August 2013 appear to have been severely dented by the COVID-19 global pandemic. The aim of the study was to examine, on a pilot basis, the disruptions and challenges to the observance of seafarers’ rights to shore leave, repatriation and medical assistance as an immediate consequence of COVID-19. Materials and methods: The impact of COVID-19 on seafarers’ rights was examined in three dimensions — shore leave, repatriation and medical assistance. Questionnaires were administered online from June to August 2020 to 450 seafarers, top 10 ship-management companies, 35 shipping companies and ma-ritime administrations of top 5 seafarer supplying countries. The paper discusses the results of the survey.Results: The research revealed a previously unknown majority preference for shore leave, that diminished sharply during COVID-19. Impact on work-performance and well-being of seafarers was revealed with only a fifth of the seafarers having willingly agreed to an extension of contract. This study revealed incidence rates at 6 months into the pandemic of several parameters — delayed repatriations (21.44%) that includes crew with contract extensions (12.48%), crew with completed contract awaiting repatriation (8.96%) and crew that had exceeded 12-month continuous service (0.82%). Compensation, if provided, is meagre and was affecting ratings the most. Deprivation of medical assistance was also revealed. Conclusions: The well-being of seafarers would likely remain vulnerable to breaches, unless measures are put in place to safeguard the rights assured under MLC in the face of uncertainties caused by a pandemic such as COVID-19.
(Int Marit Health 2020; 71, 4: 217–228)
Key words: seafarer, well-being, rights, shore leave, repatriation, medical assistance, MLC, COVID-19
�
INTRODUCTIONDespite the Maritime Labour Convention (MLC), 2006 [1]
of the International Labour Organisation (ILO) setting out the seafarers’ rights along with their working and living conditions on board a ship, the outbreak of COVID-19 pandemic in March 2020 placed seafarers in a rather precarious situation. A sur-vey by the International Transport Workers’ Federation (ITF) in September 2020 showed that 73.3% of seafarers were worried about ‘being tired and fatigued’, while 60.1% said it was more likely than not that they or their crewmates would be ‘involved in an accident (…) due to tiredness or fatigue’ [2].
Anecdotal evidence of consequences to the well-being of the seafarers since the outbreak has been sporadic, yet unceasing. The incessant monthly cycle of 300,000 repatri-ations was abruptly halted by sweeping travel restrictions [3], with seafarers waiting to join a ship stranded ashore, and those on board resigned to their fate. With persisting lock-downs, shore leave was restricted as was also the access to medical assistance [4]. Suicides committed by seafarers such as the 39-year-old crewmember on the Regal Princess reflect the deep anxiety and depression caused by the pandemic [5]. The ITF, to which a majority of the world’s 1.65 million
www.intmarhealth.pl 217
Int Marit Health 2020; 71, 4: 217–228
10.5603/IMH.2020.0040 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
ORIG INAL ART ICLE

seafarers pledge allegiance, went to the extent of issuing a statement assuring assistance to seafarers to exercise their right to stop work, leave ship and return home [6]. The International Maritime Organisation (IMO) was joined by several United Nations organisations when it emphasised the contribution of international trade and supply chains to a sustainable socio-economic recovery during COVID-19 [7].
Seafaring features among the most dangerous occupa-tions in the world with at least three times more fatalities than the most dangerous occupation on land [8], and seri-ous depredations of seafarers’ rights appear to be almost the norm. Piracy and kidnapping for ransom are serious risks. Abandonment of seafarers has been recognised as a historic problem with no easy solution until amendments were incorporated in MLC [9]. Ill-treatment through unfair contracts, insufficient shore leave, and inability to contact families while at sea, etc. are, perhaps, endemic to shipping and increasingly prompting seafarers to move from ship to shore [10]. Criminalisation for marine pollution incidents [11] including the Wakashio spill in August 2020 [12], and subsequent neglect by employers [13] is a persisting con-cern for seafarers [12]. COVID-19 presents unprecedented challenges to the rights of seafarers over and above the persisting issues, and deserves comprehensive research as to its consequences to the seafarer’s well-being. This research attempts to fill an emergent gap in knowledge by exploring the impact of the COVID-19 pandemic on the seafarers’ rights to shore leave, repatriation and medical assistance and, consequently, their well-being.
PROVISION OF SEAFARERS’ RIGHTS IN INTERNATIONAL INSTRUMENTS
The rights of seafarers for shore leave, repatriation and medical assistance are well-defined in MLC 2006. It requires seafarers to be granted shore leave for the sake of their well-being and health. Repatriation shall be at no cost to the seafarer. The maximum period of service on board shall be less than 12 months. If the ship-owner can-not repatriate a seafarer then the competent authority of the flag will arrange repatriation or the state which they are citizen of or the state from which the seafarer is to be repatriated may arrange repatriation and its cost may be recovered from the ship-owner or from the flag state of the vessel. All member states have to ensure that all seafarers are covered for protecting their health and have sufficient medical care during their shipboard tenure, provided free of cost, and that a seafarer in need of urgent medical care is provided access to shore medical facilities [1].
The Seafarer Employment Agreement (SEA) governed by MLC [1], specifies a fixed tenure, but allows extension of con-tract by 1 or 2 months if repatriation cannot be affected due to operational exigencies, for example an inconvenient port.
The Seafarer Identity Document Convention (Revised), 2003 [14] facilitates access to ports, shore leave, transit, transfer and repatriation obviating any requirement to hold visa for these purposes. However, an authority can deny permission of shore leave based on national security, public safety, and public health.
International Maritime Organisation instruments encour-age cooperation and coordination among member states for implementing the procedure and conditions related to shore leave [15] and call for a balanced approach between port re-lated security and seafarers’ right of access to shore leave and social facilities ashore [16]. Furthermore, search and rescue services are required to perform co-ordination of provision of medical advice, initial medical assistance and evacuation [17].
The International Health Regulations (IHR), 2005 [18] are of relevance for repatriation of seafarers. IHR call upon states to respect the traveller whereas the lockdown initiat-ed by states restricts the rights of movement of seafarers [19]. Although national legislation usually decides on the conflicts of human and labour rights, IHR attempts to resolve the conflict by reminding that measures taken to protect public health should be less invasive on other rights.
There are differing views on the positive impact of MLC. In a pilot study on board Danish flagged vessels in 2018, Danish seafarers opined that MLC did not have any signifi-cant impact in their case since most standards were already in place and some were even inferior to those currently implemented. Rather, MLC added to an otherwise heavy burden of administrative tasks, paperwork and checklists [20]. State practice of providing protection to seafarers has been studied from flag, port and coastal state perspective [21], and vulnerability to abuse is higher when serving on board ships flagged in open registries [22]. The observation that, ‘the greatest difficulty faced by seafarers is the fact that their legal rights are often hard to discern, as are the jurisdictions in which these rights can be enforced’ appears to hold good despite the adoption of MLC as validated by case studies in Panama and the Philippines [23]. Therefore, although theoretically the rights of a seafarer are secured by MLC, in practice, those rights may be subverted by the maze of laws and policies regulating the shipping industry [24].
SHORE LEAVEShore leave for seafarers is a longstanding issue. As
far back as 1943, in “Aguilar v. Standard Oil Company”, the Supreme Court in the United States ruled that shore leave is, “an elemental necessity (…), not merely a personal diversion” and emphasised that, “no crew would be taken if it could never obtain it” [25]. Leisure outside of the ves-sel during a port call plays a vital role in the well-being of a seafarer and, while needs may vary between individuals, professional obligations could be an inhibiting factor [26].
Int Marit Health 2020; 71, 4: 217–228
www.intmarhealth.pl218

Implementation of post 9–11 security measures deprived seafarers of their customary right to shore leave exposing them to prejudicial and other negative treatment. In one ex-treme case, a seafarer spent a night in jail and was deported for stepping ashore to make a call from a public telephone only metres from his ship [27]. Giving due priority to wel-fare would require seafarers to be given due respect and transformed as the subjects of the shipping industry [28]. Studies attribute denial of shore leave to a social agenda for dealing with perceived risk, with attendant sociological impacts and technical consequences [29].
REPATRIATIONRepatriation has received scant attention in literature,
primarily in the context of medical assistance. Repatriation consequent to an injury or illness has been studied from the perspective of risk [30]. Long tenure on board enhances the risk of medical repatriation, and a study of Filipino seafarers investigated whether 200 days may be the upper limit [31].
MEDICAL ASSISTANCEThe seafarers’ right to medical assistance has been equat-
ed with the right to life which is a fundamental human right [32], but globalisation created the possibility of disposable worker protections, including seafarer health protection. Technological advancements yield benefits, and disadvantages. Tele Medical Assistance Service (TMAS) has improved access to healthcare for seafarers on board [33, 34] and reduced requirement of medical evacuations [35]. On the other hand, a case study of the United States revealed that neoliberal policies taken together with technology could create conditions that may for example, increase health inequity among seafarers [36]. Medical assistance to seafarers has been the focus of several case studies [37–40], but it draws little attention and receives limited public resources for provision of services [32]. More-over, identifying and addressing special health and welfare needs of women seafarers is a work in progress [41].
COVID-19 AND SEAFARERS’ WELL-BEINGCOVID-19 disrupted the entire scheme of repatriation.
While ITF attempted to study the matter, media reports captured diverse issues surrounding the repatriation of seafarers. Shipping community have had to go the extra mile to manage crew change since support from the flag states was less than desirable [42], although, crew change was marginally easier at places where flights were operational [43]. Within the community, ship-owners reportedly faced lack of cooperation from several charterers [44]. Mean-while, International Chamber of Shipping proposed that the industry cannot afford to lose the faith of government [45]. In this context, this research survey helps to bring forward the ground reality.
A few early studies in the early months of COVID-19 re-port the exposure of seafarers to work-related stress aggra-vated by the uncertainties of the pandemic. One study used indications drawn up by the Centro Internazionale Radio Medico (C.I.R.M.) [46]. A survey of 72 seafarers using the General Health Questionnaire (GHQ12) confirmed excess work-related stress in the pandemic situation although an earlier study of 350 seafarers with higher resilience, longer experience and greater support at work reported lower levels of stress at sea [47].
The aim of the study is to examine, on a pilot basis, the disruptions and challenges to the observance of seafarers’ rights to shore leave, repatriation and medical assistance as an immediate consequence of COVID-19.
This study is conducted in the backdrop of the concern about the underway United Nations human rights treaty body review process that commenced in April 2020 over the fact that the outcome of the review process may result in less robust state oversight and human rights compliance in the future [48].
The study attempts to shed greater light on the state of well-being of the world’s seafarers whose facilitation is vital to world trade. The possibilities for amelioration are linked to the expectations placed on the ongoing efforts at enhanced cooperation among all the relevant United Nations agencies — the International Maritime Organisation (IMO), International Labour Organisation (ILO), World Health Organization (WHO) and International Civil Aviation Organ-isation (ICAO) — maritime stakeholders and in particular shipping and ports, to collectively address the pandemic and minimise the risk for global trade and on human health [49].
MATERIALS AND METHODS The conceptual framework (Fig. 1) for the research was
based on the hypothesis that the COVID-19 pandemic di-rectly impacts the well-being of seafarers by impinging on their rights established under MLC. The research, therefore,
Figure 1. Conceptual framework for the research
www.intmarhealth.pl 219
Anish Arvind Hebbar, Nitin Mukesh, Impact of COVID-19 on seafarer’s wellbeing

adopted a questionnaire survey based on a purposive con-venience sampling to examine the impact of COVID-19 on seafarers’ rights in three dimensions — shore leave, repatri-ation and medical assistance. The questionnaire was admin-istered online, from June to August 2020. Besides 450 sea-farers, top 10 ship-management companies, 35 shipping companies and 33 maritime administrations including top 5 seafarer supplying nations were invited to participate in the survey owing to their role as providers of the rights.
Each group — seafarers, companies, administrations — received a separate set of survey questions. Whereas the seafarers’ questionnaire focused on their experienc-es in the three dimensions linked to their well-being, the company and administration received questions relating to their guidelines, response action and coordination with stakeholders. The questionnaires were approved by the Research and Ethics Committee of the univer-sity and the survey was based on informed consent of the participants.
Response was received from 288 seafarers, 18 ship-ping companies including 4 ship-management companies and 6 maritime administrations including top 2 seafarer supplying nations yielding an individual response rate of 64.0% and institutional response rate of 35.89%. 30% of the individuals were masters of vessels and 66.67% were serving on board at the time of responding to the question-naire. The 18 participating companies collectively manage 74,701 seafarers aboard 2,240 ships.
RESULTS AND DISCUSSION
DENIAL OF SHORE LEAVEFear of the COVID-19 pandemic was all pervasive, and
seafarers were not spared of the consequential lockdowns and movement restrictions. During the pandemic, 95% of the surveyed seafarers experienced denial of shore leave. Two-thirds could not even disembark from the gangway while less than a third managed to disembark, if only for reading draft. Apart from state imposed lockdowns, restric-tions were imposed by the terminal, port, shipowner, and company, including 80% of the surveyed companies. These restrictions which appear to have been imposed of own accord and, perhaps, without knowledge or directives of the flag administration are violative of MLC.
On the other hand, given the imminent risk, 75% sea-farers apparently accepted the restrictions and did not wish to avail shore leave during the pandemic. 62% suggested a strong probability of suffering an infection besides 32% who feared a moderate probability. The study revealed a previously unknown majority preference for shore leave at every port during normal times that diminished sharply during the COVID-19 pandemic, due to the imminent risk of
infection during shore leave. Figure 2 presents the survey results of denial of shore leave.
IMPACT OF SHORE LEAVE DENIALProlonged restriction on board without shore leave will
likely take toll, particularly on the mental state, work per-formance and health of the seafarer. The study explored all of these aspects. Two out of 5 seafarers felt unhappy, 3 out of 10 felt stressed, and 1 in 6 felt completely fa-tigued. Overall, other than the 7.7% hardy seafarers who believed that they were happy regardless of circumstances, an overwhelming 88% seafarers were visibly impacted by absence of shore leave. The possibility to choose only one option revealed the stronger among the feelings although a person could feel unhappy, stressed and fatigued at the same time, as revealed through comments by 4 partici-pants. The seafarers’ state of happiness was explored in a specific question, later.
Absence of shore leave impacted work performance and, perceivably, the health of seafarers, with only 1 in 6 participants indicating that performance was not affected against 4 in 5 seafarers who reported moderate effect due to denial of shore leave. Adverse effect on health was report-ed to be on a similar scale with 1 in 3 suggesting moderate effect against only 1 in 4 seafarers having felt no effect.
The impact of denial of shore leave (Fig. 3) is a significant finding of the study and confirms the concerns being raised in several quarters since the outbreak of the pandemic. Diminishing shore leave incredibly influences the well-being of those who frequently face long voyages without a break at any port. This is genuinely tragic. Shore leave is the priv-ilege of each seafarer and permitting them sufficient shore leave in the long run increments the general efficiency of work on board.
It appears that companies are mindful of the adverse impacts since majority (65%) provided additional enter-tainment facilities on board although some (25%) took no interest in the matter.
CONTRACT EXTENSION AS COLLATERALThe widely prevailing narrative on uncertainties of re-
patriation was reinforced by the survey with only 14.5% seafarers being repatriated timely after contract completion and contract extension emerging as a collateral impact (Fig. 4). One in 10 seafarers suffered 1 to 2 months delay, an equal proportion suffered three to 4 months delay, and some were repatriated as many as 4 months on contract completion. The bulk of contracts were extended due to COVID-19. A cause for concern is the fact that more than half of the seafarers on board during COVID-19 had their contract extended, half of which were against free will. 7.9% contracts were extended beyond 12 months.
Int Marit Health 2020; 71, 4: 217–228
www.intmarhealth.pl220

A B
C D
Figure 3. Impact of shore leave denial; A. Shore leave denial — overall impact; B. Seafarers’ happiness status during COVID-19; C. Shore leave denial — impact on work; D. Shore leave denial — impact on health
A B
C D
E F
Figure 2. Denial of shore leave; A. Grant of shore leave; B. Permission to disembark; C. Company policy on shore leave; D. Belief in COVID-19 risk on availing shore leave; E. Shore leave expectation in normal times; F. Shore leave expectation during COVID-19
www.intmarhealth.pl 221
Anish Arvind Hebbar, Nitin Mukesh, Impact of COVID-19 on seafarer’s wellbeing

A B
C D
E
Figure 4. Contract extension as collateral impact; A. Timeliness of repatriations during COVID-19; B. Stay on board exceeding 12 months; C. Status of contract extension due to COVID-19; D. Contract extension — willingness; E. Seafarers exceeded Seafarer Employment Agreement + 1 month clause by per cent of companies
The largescale contract extensions are despite MLC requiring that no seafarer be employed beyond 12 months. A seafarer has the right to repatriation once the contract terminates, or simply wants to terminate it for justified/compassionate reasons. Apparently, the company negotiated with the seafarers so as to acquire additional time to coordinate repatriation.
The company survey (Table 1) yielded further insights on contract extensions. The 18 surveyed companies, that among them managed 74,701 seafarers, reported 6,695 having completed contract and awaiting repatri-ation despite extending contract of another 9,324 crew of whom 615 had exceeded 12 months of continuous service, in violation of MLC standard A2.5, and the Col-
lective Bargaining Agreement. Almost all surveyed com-panies reported contract extensions (Table 1) and overall, 6 months into the pandemic, the incidence rate of delayed repatriations, contract extensions, crew with completed contract awaiting repatriation and crew that had exceed-ed 12-months continuous service was 21.44%, 12.48%, 8.96% and 0.82%, respectively. Seafarers who have ex-ceeded the +1-month clause of the contract may not be mentally prepared for further stay on board, which may reflect on work performance. Mental fatigue plays a major role in the condition of work.
Regardless, companies suggested satisfactory outcome for repatriations in contrast to the seafarers’ response, and the wider belief in the maritime fraternity. 80% companies
Int Marit Health 2020; 71, 4: 217–228
www.intmarhealth.pl222

Table 1. Consolidated company particulars
Company Number of ships managed by company
Number of seafarers managed by company
Number of crew with extended contract
Number of crew with completed contract
Number of crew exceeded 12-month service
A 150 5000 0 0 0
B 55 1500 6 22 2
C 300 12000 3600 30 0
D 102 5300 827 1300 37
E 19 450 50 175 0
F 1 6 6 0 0
G 22 650 80 110 0
H 9 200 27 37 0
I 515 11000 220 1038 65
J 8 300 59 78 0
K 122 3200 240 120 0
L 2 25 5 0 0
M 150 6000 1100 900 90
N 600 21000 2680 2308 0
O 12 1500 100 80 0
P 146 5650 238 420 421
Q 17 800 67 74 0
R 10 120 25 3 0
Total 2,240 74,701 9,324 6,695 615
Incidence rate (%)
12.48 8.96 0.82
Figure 5. Seafarers’ opinion on stakeholder efforts for their relief and repatriation
were required to provide additional budget for repatriations although most companies could not specify the exact in-crease in budget. One company, however, stated that there was no limit to the budget for repatriating crew.
RELIEF AND REPATRIATION EFFORTSThe perspectives of seafarers on the relief and repa-
triation efforts of stakeholders are quite revealing (Fig. 5). The company is expected to act appropriately to resolve the
www.intmarhealth.pl 223
Anish Arvind Hebbar, Nitin Mukesh, Impact of COVID-19 on seafarer’s wellbeing

A B
Figure 6. Vessel diversion for crew repatriations; A. Vessel diversion by companies for repatriation; B. Number of crew repatriated by vessel diversion
issue, which includes consulting the concerned authority on repatriation matters. However, opinion was split, and only 37% seafarers felt that the efforts by the company were non-existent, insufficient, or the company appeared to be helpless. As such, flag state is deemed to have a greater role in facilitating repatriation of seafarers under jurisdiction. The study indicated marginally better sentiments on part of the seafarers towards the flag administration as compared to the shipping companies. Overall, whereas 40% of par-ticipants were satisfied with flag state, company and trade union effort, more than 20% felt that efforts were lacking. Despite all endeavours, the fact remains that crew remain stranded and await relief and repatriation, and needless to mention, they remain under tremendous pressure.
VESSEL DIVERSIONMajority of companies reported vessel diversions for
crew change (Fig. 6) and accepted that it was a challenge to send crew home due to lockdown, and the remainder reporting nil diversion or no requirement of diversion, should be treated with caution. Contrary to media reports [44], a majority of companies agreed that owners and charterers were also supportive for diverting vessel for crew change, and that steps taken for repatriating seafarers are work-ing effectively. Baltic and International Maritime Council’s COVID-19 crew change clause in the time charter also re-portedly facilitates the deviation of vessel [50].
COMPENSATION FOR DELAYED REPATRIATIONAny incentive or bonus by the company for extended stay
on board is well deserved and a great morale booster for the seafarer. While 41% seafarers reported being compensated with a bonus or increment in basic or full wages, 32% were not compensated for their extended stay on board.
The company response mirrored that of the seafar-ers. 75% companies offered compensation in some form — increment in basic wages, bonus, prolonged service al-
lowances, etc. and also provided additional entertainment facility on board and periodically contacted the seafarer’s family (Fig. 7), which is truly heart-warming.
Not honouring the clause for compensating extension of scheduled tour length is a violation of SEA. Management recognition could motivate a seafarer to willingly continue on board whereas inadequate or no compensation (25% companies) and failing to ensure the welfare of seafarers could have adverse consequences for the crew, and thereby the safety of the ship and the environment.
MEDICAL ASSISTANCE AND COVID-19 READINESS
Limited availability of medical assistance appears to have been a collateral impact of COVID-19 to not only seafar-ers but also community at large. IMO too recognised the grav-ity of the problem and its consequences for seafarers [51]. While vessels are equipped to deal with COVID-19 to the extent possible, access to medical assistance ashore when calling at a port emerged as a major challenge. Most par-ticipants agreed that their vessel was adequately equipped to deal with COVID-19 prevention (Fig. 8) and as such, 47.8% of participants did not experience any sick seafarer on board. None experienced COVID-19 infection to any of their shipmates sailing with them. However, 15.4% of par-ticipants were of the view that seafarers were not provided with medical assistance ashore.
Medical evacuation coverage for COVID-19 infected sea-farers is a critical aspect of medical care to seafarers. Only half of the surveyed companies trusted the sufficiency of their policy for dealing with any COVID-19 infections, and 10% companies clearly admitted that it was not sufficient. With the exception of one case, none of the respondent companies had suffered any COVID-19 infection in their fleet although there were cases of other medical emer-gencies. Companies largely accepted (65%) that there was no additional insurance cover for COVID-19 except for P&I
Int Marit Health 2020; 71, 4: 217–228
www.intmarhealth.pl224

A B
Figure 8. Medical assistance to seafarers and COVID-19 readiness; A. Vessel readiness for COVID-19 — seafarers’ perceptions; B. Access to medical assistance ashore during COVID-19
A B
C D
Figure 7. Compensation for delayed repatriation; A. Compensation for extended stay — seafarer poll; B. Compensation for extended stay — company poll; C. Company contact with seafarer family — frequency; D. Whether additional entertainment facilities provided on board — company poll
Figure 9. Seafarers’ awareness of instruments related to their rights
www.intmarhealth.pl 225
Anish Arvind Hebbar, Nitin Mukesh, Impact of COVID-19 on seafarer’s wellbeing

cover. A majority (57.9%) of owners, charterers, ship-man-agement would accept a deviation for medical care for a COVID-19 infected crew, 15.5% categorically rejected the possibility of a deviation. As discussed before, regardless of the refusal by a small fraction of industry, denial of medical care to a seafarer is not acceptable under MLC, or Collective Bargaining Agreement.
SEAFARERS’ AWARENESS OF REGULATIONSThe study suggests that only about 70% of participants
had full awareness of the international regulations pertain-ing to shore leave, repatriation and medical assistance, while a quarter of the respondents indicated some aware-ness of the provisions (Fig. 9). Member states especially seafarer providing nations, companies, seafarer unions and other relevant stakeholders should take note of the fact that around 5% of seafarers are not aware at all of their rights and, therefore, more vulnerable to deprivation.
CONCLUSIONSShore leave is key to mental well-being and requires
utmost facilitation. Crew change merits standardised inter-national protocols supported by designation of seafarers as key worker. Binding seafarers into contracts without their will is a serious human rights violation calling for more stringent legal safeguards and diligent monitoring by flag states. Well-being of seafarers remains vulnera-ble to breaches, unless seafarers are apprised of their rights through a formal Standards of Training, Certifica-tion and Watchkeeping for Seafarers training module and measures devised to safeguard the rights assured under MLC. The experiences gained and lessons learned from the COVID-19 pandemic should be drivers for improving resilience in meeting extraordinary situations in the future.
ACKNOWLEDGEMENTSSeafarers, companies and maritime administration re-
spondents are thanked for their kind participation. Shan-tanu Hebbar’s assistance with data summarisation and visualisation is gratefully acknowledged.
REFERENCES1. International Labour Organisation, (ILO). Maritime Labour Conven-
tion, (MLC), 2006. UNTS volume-2952-I-51299.2. International Transport Workers’ Federation (ITF). COVID corner-cut-
ting will lead to deaths, ‘environmental catastrophe’ – new shipping report. https://www.itfseafarers.org/en/news/covid-corner-cuttin-g-will-lead-deaths-environmental-catastrophe-new-shipping-report (2020, 20 September).
3. International Maritime Organization (IMO). Joint statement. IMO--UNCTAD – Call for collaborative action in support of keeping ships moving, ports open and cross-border trade flowing during the COVID-19 pandemic. Circular letter no.4204/add.21. https://wwwcdn.imo.org/localresources/en/MediaCentre/HotTopics/Do-
cuments/COVID%20CL%204204%20adds/Circular%20Letter%20No.4204-Add.21%20-%20Joint%20Statement%20Imo-Unctad%20-%20Call%20For%20Action%20Keeping%20Ships%20Moving.pdf (2020, June 8).
4. International Maritime Organization (IMO). Coronavirus (CO-VID-19) – Preliminary list of recommendations for Governments and relevant national authorities on the facilitation of maritime trade during the COVID-19 pandemic. Circular LetterNo.4204/Add.6. https://wwwcdn.imo.org/localresources/en/MediaCentre/HotTopics/Documents/Circular%20Letter%20No.4204Add.6%20%20Coronavirus%20Covid-19%20Preliminary%20List%20Of%20Recommendations.pdf (2020, March 27).
5. Greenfield P, McCormick E. Hunger strikes and deaths as mental health crisis grips stranded cruise ships. The Guardian. https://www.theguardian.com/environment/2020/may/14/deaths-and--hunger-strikes-point-to-mental-health-crisis-on-stranded-cruise-ships (2020, May 14).
6. International Transport Workers’ Federation (ITF). Enough is enough. https://www.itfseafarers.org/en/news/eno-ugh-enough-worlds-seafarers-wi l l -now-exercise-r ight - le -ave-ships-amid-covid-19-failures#:~:text=Covid%2D19%20failu-res-,Enough%20is%20enough%3A%20World’s%20seafarers%20will%20now%20exercise%20right%20to,ships%20amid%20Covid%2D19%20failures&text=The%20International%20Trans-port%20Workers’%20Federation,leave%20ships%2C%20and%20return%20home (2020, 15 June).
7. International Maritime Organization (IMO), United Nations Conferen-ce on Trade and Development (UNCTAD). Joint statement in support of keeping ships moving, ports open and cross-border trade flowing during the COVID-19 pandemic. https://unctad.org/meetings/en/Sessional Documents/osg_2020-06-08_stat01_en.pdf (2020, June 8).
8. Li KX, Ng JM. International maritime conventions: Seafarers’ safety and human rights. J. Mar. L. & Com. 2002; 33: 381.
9. International Labour Organisation (ILO). 2014. Amendments (2014) to the Maritime Labour Convention, 2006. 2014. http://www.ilo.org/wcmsp5/groups/public/---ed_norm/---relconf/documents/meetingdocument/wcms_248905.pdf (2014, June 11).
10. Caesar DL, Cahoon SC, Fei J. Understanding and managing the complexity of retention issues for 21st century seafarers in the global shipping industry. 2014 International Association of Maritime Economists Conference (IAME 2014) 2014 (pp. 1-20).
11. Kirby SM. The continuing criminalization of seafarers: Where to go from here? In: Chircop A, Letalik N, McDorman TL & Rolston SJ, editors. The regulation of international shipping: International and comparative perspectives: Essays in honour of Edgar Gold. Marti-nusNijhoff, Leiden, Netherlands 2012: 443–464.
12. Lloyd’s List, 2020. Wakashio master arrested in Mauritius. 2020, August 18. https://lloydslist.maritimeintelligence.informa.com/LL1133565/Wakashio-master-arrested-in-Mauritius (November 10, 2020).
13. Couper A. Perceptions and attitudes of seafarers towards mariti-me regulations: An historical perspective. In: Chircop A, Letalik N, McDorman TL & Rolston SJ, editors. The regulation of international shipping: International and comparative perspectives: Essays in honour of Edgar Gold. MartinusNijhoff, Leiden, Netherlands 2012: 429–442.
14. International Labour Office. Seafarer Identity Documents Convention (Revised) 2003: ILO Convention No. 185. ISBN 978-92-2-118339-6.
15. International Maritime Organization (IMO). Facilitating shore leave and access to ships, removing unnecessary restrictions imposed by
Int Marit Health 2020; 71, 4: 217–228
www.intmarhealth.pl226

divergences in implementation of the ISPS Code. FAL.3/Circ.201. https://wwwcdn.imo.org/localresources/en/OurWork/Facilitation/FAL%20related%20nonmandatory%20documents/FAL.3-Circ.201.pdf (2010, September 27).
16. International Maritime Organization (IMO). Reminder in connection with shore leave and access to ships. MSC.1/Circ.1342. https://wwwcdn.imo.org/localresources/en/OurWork/Security/Docu-ments/MSC.1%20Circ.1342.pdf (2010, May 27).
17. International Maritime Organization (IMO). Medical Assistance at sea. MSC/Circ.960. https://wwwcdn.imo.org/localresources/en/OurWork/Safety/Documents/MSC.1-Circ.960%20-%20Medical%20Assistance%20At%20Sea.PDF (2000, June 20).
18. World Health Organization (WHO). International health regulations (2005). UNTS v2509 (p.79) 2005.
19. von Tigerstrom BJ, Halabi SF, Wilson KR, et al. COVID-19 travel re-strictions and the International Health Regulations, 2005. BMJ Glob Health. 2020; 5(5): e002629, doi: 10.1136/bmjgh-2020-002629, indexed in Pubmed: 32424016.
20. Fotteler ML, Jensen OC, Andrioti D. Seafarers’ views on the impact of the Maritime Labour Convention 2006 on their living and working conditions: results from a pilot study. Int Marit Health. 2018; 69(4): 257–263, doi: 10.5603/IMH.2018.0041, indexed in Pubmed: 30589065.
21. Piniella FS, Francisca JB. The protection of Seafarers: State Practice and the emerging new International regime. State Practice and International Law Journal. 2015; 2: 43–67.
22. Kabai M. The maritime labour convention and open registries: hand in glove or chalk and cheese. Int J Marine Coastal Law. 2015; 30(1): 189–198, doi: 10.1163/15718085-12341341.
23. Aguda OO. Maritime labour convention 2006: implications for seafarers after a decade. Nnamdi Azikiwe University Journal of International Law and Jurisprudence. 2017; 8(2): 125–134.
24. Guillot-Wright S. The changing economic structure of the maritime industry and its adverse effects on seafarers’ health care rights. Int Marit Health. 2017; 68(2): 77–82, doi: 10.5603/IMH.2017.0015, indexed in Pubmed: 28660609.
25. Mcconnell ML. The ILO’s Seafarers’ Identity Documents Convention (Revised), 2003 (n° 185) after more than a decade: Ahead of its time or case of good intentions gone wrong? In: Chaumette, P coordinator. Seafarers: An international labour market in perspective, University of Nantes. Gomylex, Bilbao, Spain 2016: 285–334.
26. Oldenburg M, Jensen HJ. Maritime welfare facilities - utilization and relevance for the compensation of shipboard stress. J Occup Med Toxicol. 2019; 14: 11, doi: 10.1186/s12995-019-0231-3, indexed in Pubmed: 31043998.
27. Balbaa A. Protecting seafarer’s rights – The need to review the imple-mentation of the ISPS code. In: Association of Maritime Universities (IAMU) 6th Conference, 2005, October.
28. Graham C. Maritime security and seafarers’ welfare: Towards har-monization. WMU Journal of Maritime Affairs. 2009; 8(1): 71–87, doi: 10.1007/bf03195154.
29. Manuel M. Potential sociological impacts of unfair treatment of seafarers. Maritime Policy & Management. 2011; 38(1): 39–49, doi: 10.1080/03088839.2010.533714.
30. Lefkowitz RY, Slade MD, Redlich CA. Risk factors for merchant se-afarer repatriation due to injury or illness at sea. Int Marit Health. 2015; 66(2): 61–66, doi: 10.5603/IMH.2015.0016, indexed in Pubmed: 26119673.
31. Abaya A, Rivera J, Roldan S, et al. Does long-term length of stay on board affect the repatriation rates of seafarers? Int Marit Health. 2018; 69(3): 157–162, doi: 10.5603/imh.2018.0025.
32. Zhang P, Shan D, Zhao M, et al. Navigating seafarer’s right to life across the shipping industry. Marine Policy. 2019; 99: 80–86, doi: 10.1016/j.marpol.2018.10.002.
33. Nittari G, Pirillo I, Amenta F, et al. The right to medical assistance for seafarers. Ethical and practical consequences of the introduction of telemedicine to improve healthcare on board ships. Marine Policy. 2019; 106: 103525, doi: 10.1016/j.marpol.2019.103525.
34. Lee A, Sikka N, O’Connell F, et al. Telepsychiatric assessment of a mariner expressing suicidal ideation. Int Marit Health. 2015; 66(1): 49–51, doi: 10.5603/IMH.2015.0012, indexed in Pubmed: 25792168.
35. Westlund K, Attvall S, Nilsson R, et al. Telemedical Maritime As-sistance Service (TMAS) to Swedish merchant and passengers ships 1997-2012. Int Marit Health. 2016; 67(1): 24–30, doi: 10.5603/IMH.2016.0006, indexed in Pubmed: 27029926.
36. Guillot-Wright S. The changing economic structure of the maritime industry and its adverse effects on seafarers’ health care rights. Int Marit Health. 2017; 68(2): 77–82, doi: 10.5603/IMH.2017.0015, indexed in Pubmed: 28660609.
37. Holt TE, Tveten A, Dahl E. Medical emergencies on large passenger ships without doctors: the Oslo-Kiel-Oslo ferry experience. Int Marit Health. 2017; 68(3): 153–158, doi: 10.5603/IMH.2017.0027, indexed in Pubmed: 28952660.
38. Kulkarni AC. Medical evacuation on high seas. Int Marit Health. 2019; 70(4): 216–219, doi: 10.5603/IMH.2019.0034, indexed in Pubmed: 31891174.
39. Dahl E. Sick leave aboard: a one-year descriptive study among crew on a passenger ship. Int Marit Health. 2005; 56(1-4): 5–16, indexed in Pubmed: 16532581.
40. Nittari G, Arcese A, Battineni G, et al. Design and evolution of the Seafarer’s Health Passport for supporting (tele)-medical assistance to seafarers. Int Marit Health. 2019; 70(3): 151–157, doi: 10.5603/IMH.2019.0024, indexed in Pubmed: 31617938.
41. Stannard S, Vaughan C, Swift O, et al. Women seafarers’ health and welfare survey. Int Marit Health. 2015; 66(3): 123–138, doi: 10.5603/IMH.2015.0027, indexed in Pubmed: 26394312.
42. Gemma P. Seafarer crisis is a challenge for the whole marine sector. Lloyd’s List. 2020, August 4 (https://lloydslist.maritimeintelligence.informa.com/LL1133377/Seafarer-crisis-is-a-challenge-for-the-who-le-marine-sector).
43. Walia I. Pacific basin chief urges governments to allow crew changes. Lloyd’s List. 2020, August 6 (https://lloydslist.maritimeintelligence.informa.com/LL1133416/Pacific-Basin-chief-urges-governments--to-allow-crew-changes).
44. Nigel L. Charterers lambasted for indifference to crews’ plight. Lloyd’s List, 2020. https://lloydslist.maritimeintelligence.informa.com/LL1133427/Charterers-lambasted-for-indifference-to-crews-plight (2020, August 6).
45. Blenkey N. 2020. ICS: Failures to follow protocols threaten crew change progress. https://www.marinelog.com/shipping/ics-failures--to-follow-protocols-threaten-crew-change-progress/ (2020, July 24).
46. Sossai P, Uguccioni S, Mela GS, et al. Coronavirus variant COVID-19 pandemic: a report to seafarers. Int Marit Health. 2020; 71(3): 191–194, doi: 10.5603/IMH.2020.0034, indexed in Pubmed: 33001431.
47. Pesel G, Canals ML, Sandrin M, et al. Wellbeing of a selection of seafarers in Eastern Adriatic Sea during the COVID-19 pandemic 2020. Int Marit Health. 2020; 71(3): 184–190, doi: 10.5603/IMH.2020.0033, indexed in Pubmed: 33001430.
48. Sarkin J. The 2020 United Nations human rights treaty body review process: prioritising resources, independence and the
www.intmarhealth.pl 227
Anish Arvind Hebbar, Nitin Mukesh, Impact of COVID-19 on seafarer’s wellbeing

domestic state reporting process over rationalising and stre-amlining treaty bodies. Int J Human Rights. 2020: 1–27, doi: 10.1080/13642987.2020.1822337.
49. Doumbia-Henry C. Shipping and COVID-19: protecting seafarers as frontline workers. WMU J Marit Affairs. 2020; 19(3): 279–293, doi: 10.1007/s13437-020-00217-9.
50. Baltic and International Maritime Council. (2020). COVID crew change clause for Time Charter Parties. https://www.bimco.org/contracts-and-clauses/bimco-clauses/current/
covid-19-crew-change-clause-for-time-charter-parties-2020 (2020, September 16).
51. International Maritime Organisation (IMO). Coronavirus (COVID-19) Recommendations for port and coastal states on the prompt disembarkation of seafarers for medical care ashore during the COVID-19 pandemic. Circular letter no 4204/Add.23. 2020, Au-gust 3 (https://wwwcdn.imo.org/localresources/en/MediaCentre/HotTopics/Documents/COVIDCL4204adds/CircularLetterNo.4204-Add.26-Coronavirus(Covid-19)-GuidanceOnCruiseEU.pdf).
Int Marit Health 2020; 71, 4: 217–228
www.intmarhealth.pl228

Getu Gamo Sagaro, PhD, Telemedicine and Telepharmacy Centre, School of Medicinal and Health Products Sciences, University of Camerino, Via Madonna Delle Carceri 9,
62032 Camerino MC, Italy, e-mail: [email protected]
Telemedical assistance at sea in the time of COVID-19 pandemic
Getu Gamo Sagaro1 , Gopi Battineni1 , Nalini Chintalapudi1 , Marzio Di Canio2 , Francesco Amenta1, 2
1Telemedicine and Telepharmacy Centre, School of Medicinal and Health Products Sciences, University of Camerino, Italy 2Research Department, International Radio Medical Centre (C.I.R.M.), Rome, Italy
ABSTRACTBackground: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the aetiological factor of COVID-19 infection, poses problems in providing medical assistance at sea. Ships are in an isolated environment, and most of the merchant ships do not carry medical personnel or medical supplies. Tele-medicine offers a real possibility to provide reasonable quality medical assistance to seagoing vessels. The fact that ships may touch ports in affected areas, the difficulties for seafarers to be assisted ashore due to quarantine measures and the crews’ lack of turnover make medical assistance at sea difficult. This study has compared maritime telemedical assistance data before and during the COVID-19 pandemic to propose prevention measures.Materials and methods: The study was based on the data from medical records of Centro Internazionale Radio Medico (C.I.R.M.) database of seafarers assisted from January 1 to June 30, in the years 2017–2020. The data were collected separately for each year. Age, sex, rank, and pathologies affecting the assisted seafarers were considered. Common signs of COVID-19 infection such as fever, cough, sore throat, short-ness of breath, and other respiratory symptoms were analysed. Results: From January 1, 2017, to December 31, 2019, C.I.R.M. assisted 15,888 patients on board ships. During the first 6 months of the years under evaluation, C.I.R.M. assisted 2,419 patients in 2017, 2,444 patients in 2018, 2,694 patients in 2019, and 3,924 in 2020. The number of assisted cases almost doubled in the first 6 months (from January to June) of 2020 compared to the same period of the previous years. Gastrointestinal disorders, injuries/traumas, and dermatological pathologies were the first, second, and third most often reported causes of illness on board over the 4-year study period. A higher number of seafarers with fever, cough, sore throat, and shortness of breath were assisted during the COVID-19 pandemic than before the coronavirus outbreak. Medical requests for fever increased significantly during the COVID-19 pandemic compared to the same period from 2017 to 2019.Conclusions: The requests for medical advice for fever, sore throat, and shortness of breath were significantly more common during the coronavirus epidemic. Close follow-up, regular health education on preventing coronavirus transmission, personal protective equipment, adequate environmental hygiene, and applying other standard precautions could help minimise the risk factors for the spread of COVID-19.
(Int Marit Health 2020; 71, 4: 229–236)
Key words: COVID-19 pandemic, seafarers, medical advice, infection
�
INTRODUCTIONCoronavirus is the member of a large family of viruses
causing several pathologies affecting the pulmonary system ranging from the common cold to severe respiratory syn-dromes such as the Middle East respiratory syndrome (MERS)
and the severe acute respiratory syndrome (SARS) [1]. SARS- -CoV-2, which is also called novel coronavirus, originated from Wuhan City in China [2]. Globally, until May 31, 2020, 5,934,936 cases were registered with 367,166 deaths [3]. Despite the apparent reduction in the number of COVID-19 cas-
www.intmarhealth.pl 229
Int Marit Health 2020; 71, 4: 229–236
10.5603/IMH.2020.0041 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
ORIG INAL ART ICLE

es, the fact that there is no medication or vaccine for this deadly and highly transmissible virus makes this medical emergency still a serious issue worldwide.
It is far more challenging and difficult to treat the COVID-19 on board a ship than ashore. Ships at sea are an example of isolated communities, and the fact that the majority of cargo ships do not carry doctors or adequately trained paramedics makes the possibilities of intervention more difficult. The shipping sector carries 90% of global trade and is the main artery of international supply chains. It was reported that in April 2020, the volume of global mer-chandise trade was decreased by approximately 13%, and there are estimates of a 25% reduction in shipping, with a forecast of 10% annual fall of maritime traffic in 2020 [4].
The situation on the cruise ship Diamond Princess is a perfect illustration of the difficulties in providing medical assistance on board a ship during the COVID-19 outbreak. The Diamond Princess is a British registered cruise ship that arrived offshore of Yokohama port on the evening of February 3 (Monday), 2020 and on that day the quarantine began [5]. There were 2,666 passengers and 1,045 crew members on board of the ship (a total of more than 3,700), and even though the ship had medical facilities on board and was assisted by the Japanese Health authorities, the quarantine lasted until February 20, and 619 of 3,700 pas-sengers and crew members (17%) were tested positive [6]. Despite the discussions about the effectiveness of public health countermeasures taken on that occasion, the situa-tion demonstrates how problematic it is to manage epidemic situations on board a ship [6].
The COVID-19 pandemic represents a serious problem for seafarers. From an organisation’s point of view, seafarers have to face considerable problems joining and leaving their ships in ports (each month, around 100,000 seafarers are involved in crew changes). The prohibition, or at least delays in being allowed to return home, the extension of tours of duty with the consequent fatigue caused by an increased workload, isolation, and social pressures for seafarers due to forced separation from their families, all increases dis-tress among seafarers. The pandemic also has a direct influence on the health condition of seafarers. There are quarantine restrictions for international seafarers on being able to go ashore for medical treatment or access port-based welfare services as well as restrictions on the delivery to ships of essential medical supplies, in cases where ships are refused entry into ports [4].
The problem of providing medical care on board ships not carrying a doctor has always been a significant chal-lenge. Since the first license of a radio medical service for seafarers issued by the State of New York (the USA) on November 18, 1920, several radio medical services have been operational, starting with radio signals and Morse
code, evolving through telephones to full-blown telemed-icine solutions [7]. In addition to all the challenges facing telemedicine for users and providers on land, several are to be met at sea. Technological limitations and organisational challenges are abundant, but we also have significant med-ical challenges [8]. At present, telemedicine offers the best possibility to provide medical assistance to ships without a doctor on board, although obviously it has its downfalls [7].
In view of both health and organisational problems experienced by seafarers due to the diffusion of COVID-19, e.g. closure of ports, etc., we have decided to analyse the impact of the pandemic on telemedical advice requests to the Centro Internazionale Radio Medico (C.I.R.M.). C.I.R.M. is the Italian Telemedical Maritime Assistance Service (TMAS) [9], and with more than 100,000 patients assisted on board ships, it represents the TMAS with the largest experience of medical assistance at sea in the world.
The present study has analysed the C.I.R.M. medical assistance data generated in the period from January 1, 2017 to December 31, 2019 used as a reference, and subsequently the data of medical assistance from January 1, 2020 to June 30, 2020. The starting date of January 1, 2020 was chosen since, on December 31, 2019, the World Health Organization (WHO) China Country Office was in-formed of cases of pneumonia of unknown aetiology in Wuhan City, Hubei Province of China.
MATERIALS AND METHODSThis retrospective study has analysed the C.I.R.M. data of
seafarers assisted from January 1 to June 30 during the years 2017–2020. The data were collected separately for each year. Age, sex, rank, and pathologies reported by the assisted seafarers were considered. Common signs of COVID-19 infec-tion such as fever, cough, sore throat, shortness of breath, and other respiratory symptoms were also analysed.
Medical conditions reported by seafarers were classified according to the International Statistical Classification of Dis-eases and Related Health Problems 10th Revision [10]. The data were analysed by descriptive statistics, including mean, median, and standard deviation for continuous variables. The c2 or Fisher tests were used for assessing the significance of dif-ferences between patients reporting the signs of COVID-19 be-fore and during the COVID-19 pandemic. A two-tailed p-value less than 0.05 was considered statistically significant, and the Stata software (Version 15) was used for data analysis.
RESULTS
ANALYSIS OF C.I.R.M. MEDICAL ASSISTANCE DATA 2017–2020
In total, from January 1, 2017 to December 31, 2019, C.I.R.M. assisted 15,888 patients on board ships. As shown
Int Marit Health 2020; 71, 4: 229–236
www.intmarhealth.pl230
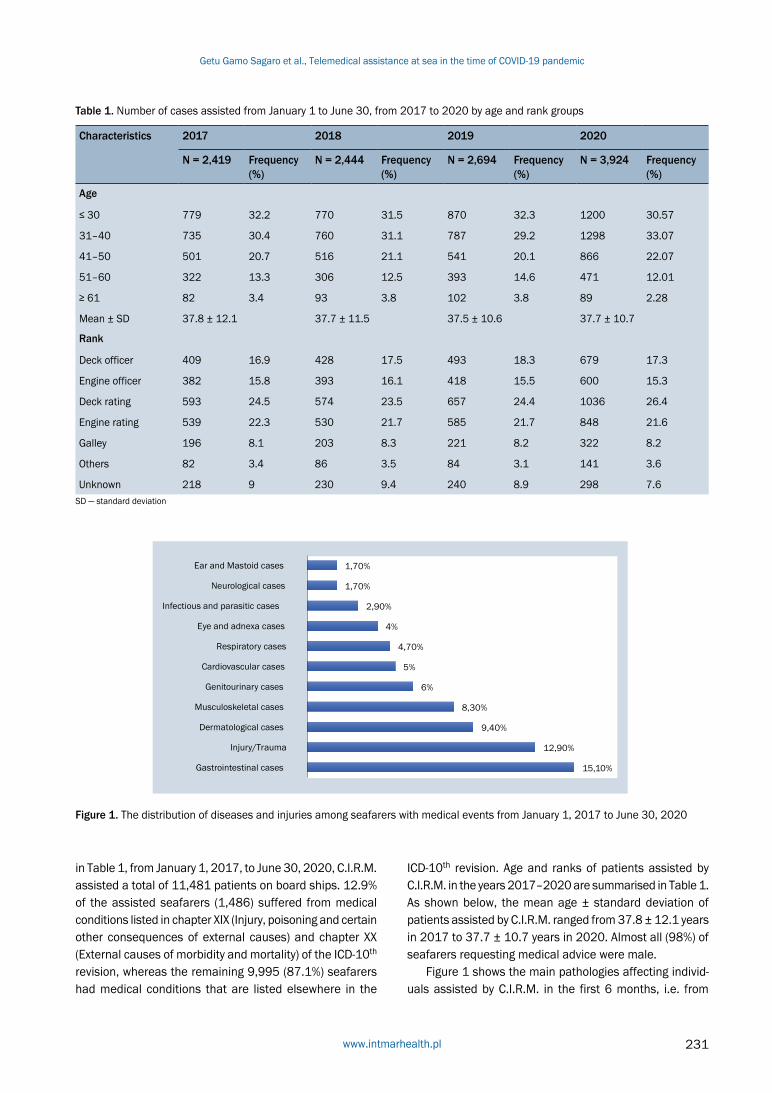
Table 1. Number of cases assisted from January 1 to June 30, from 2017 to 2020 by age and rank groups
Characteristics 2017 2018 2019 2020
N = 2,419 Frequency (%)
N = 2,444 Frequency (%)
N = 2,694 Frequency (%)
N = 3,924 Frequency (%)
Age
≤ 30 779 32.2 770 31.5 870 32.3 1200 30.57
31–40 735 30.4 760 31.1 787 29.2 1298 33.07
41–50 501 20.7 516 21.1 541 20.1 866 22.07
51–60 322 13.3 306 12.5 393 14.6 471 12.01
≥ 61 82 3.4 93 3.8 102 3.8 89 2.28
Mean ± SD 37.8 ± 12.1 37.7 ± 11.5 37.5 ± 10.6 37.7 ± 10.7
Rank
Deck officer 409 16.9 428 17.5 493 18.3 679 17.3
Engine officer 382 15.8 393 16.1 418 15.5 600 15.3
Deck rating 593 24.5 574 23.5 657 24.4 1036 26.4
Engine rating 539 22.3 530 21.7 585 21.7 848 21.6
Galley 196 8.1 203 8.3 221 8.2 322 8.2
Others 82 3.4 86 3.5 84 3.1 141 3.6
Unknown 218 9 230 9.4 240 8.9 298 7.6SD — standard deviation
Figure 1. The distribution of diseases and injuries among seafarers with medical events from January 1, 2017 to June 30, 2020
in Table 1, from January 1, 2017, to June 30, 2020, C.I.R.M. assisted a total of 11,481 patients on board ships. 12.9% of the assisted seafarers (1,486) suffered from medical conditions listed in chapter XIX (Injury, poisoning and certain other consequences of external causes) and chapter XX (External causes of morbidity and mortality) of the ICD-10th revision, whereas the remaining 9,995 (87.1%) seafarers had medical conditions that are listed elsewhere in the
ICD-10th revision. Age and ranks of patients assisted by C.I.R.M. in the years 2017–2020 are summarised in Table 1. As shown below, the mean age ± standard deviation of patients assisted by C.I.R.M. ranged from 37.8 ± 12.1 years in 2017 to 37.7 ± 10.7 years in 2020. Almost all (98%) of seafarers requesting medical advice were male.
Figure 1 shows the main pathologies affecting individ-uals assisted by C.I.R.M. in the first 6 months, i.e. from
www.intmarhealth.pl 231
Getu Gamo Sagaro et al., Telemedical assistance at sea in the time of COVID-19 pandemic
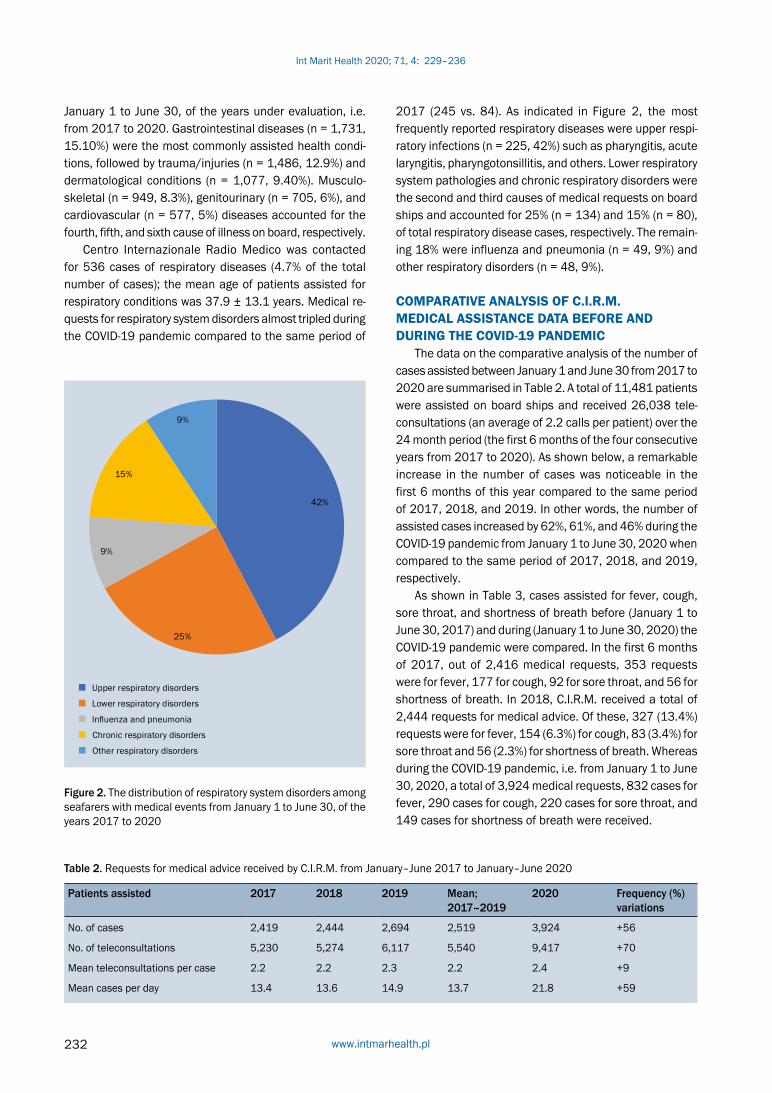
Figure 2. The distribution of respiratory system disorders among seafarers with medical events from January 1 to June 30, of the years 2017 to 2020
January 1 to June 30, of the years under evaluation, i.e. from 2017 to 2020. Gastrointestinal diseases (n = 1,731, 15.10%) were the most commonly assisted health condi-tions, followed by trauma/injuries (n = 1,486, 12.9%) and dermatological conditions (n = 1,077, 9.40%). Musculo-skeletal (n = 949, 8.3%), genitourinary (n = 705, 6%), and cardiovascular (n = 577, 5%) diseases accounted for the fourth, fifth, and sixth cause of illness on board, respectively.
Centro Internazionale Radio Medico was contacted for 536 cases of respiratory diseases (4.7% of the total number of cases); the mean age of patients assisted for respiratory conditions was 37.9 ± 13.1 years. Medical re-quests for respiratory system disorders almost tripled during the COVID-19 pandemic compared to the same period of
Table 2. Requests for medical advice received by C.I.R.M. from January–June 2017 to January–June 2020
Patients assisted 2017 2018 2019 Mean; 2017–2019
2020 Frequency (%) variations
No. of cases 2,419 2,444 2,694 2,519 3,924 +56
No. of teleconsultations 5,230 5,274 6,117 5,540 9,417 +70
Mean teleconsultations per case 2.2 2.2 2.3 2.2 2.4 +9
Mean cases per day 13.4 13.6 14.9 13.7 21.8 +59
2017 (245 vs. 84). As indicated in Figure 2, the most frequently reported respiratory diseases were upper respi-ratory infections (n = 225, 42%) such as pharyngitis, acute laryngitis, pharyngotonsillitis, and others. Lower respiratory system pathologies and chronic respiratory disorders were the second and third causes of medical requests on board ships and accounted for 25% (n = 134) and 15% (n = 80), of total respiratory disease cases, respectively. The remain-ing 18% were influenza and pneumonia (n = 49, 9%) and other respiratory disorders (n = 48, 9%).
COMPARATIVE ANALYSIS OF C.I.R.M. MEDICAL ASSISTANCE DATA BEFORE AND DURING THE COVID-19 PANDEMIC
The data on the comparative analysis of the number of cases assisted between January 1 and June 30 from 2017 to 2020 are summarised in Table 2. A total of 11,481 patients were assisted on board ships and received 26,038 tele-consultations (an average of 2.2 calls per patient) over the 24 month period (the first 6 months of the four consecutive years from 2017 to 2020). As shown below, a remarkable increase in the number of cases was noticeable in the first 6 months of this year compared to the same period of 2017, 2018, and 2019. In other words, the number of assisted cases increased by 62%, 61%, and 46% during the COVID-19 pandemic from January 1 to June 30, 2020 when compared to the same period of 2017, 2018, and 2019, respectively.
As shown in Table 3, cases assisted for fever, cough, sore throat, and shortness of breath before (January 1 to June 30, 2017) and during (January 1 to June 30, 2020) the COVID-19 pandemic were compared. In the first 6 months of 2017, out of 2,416 medical requests, 353 requests were for fever, 177 for cough, 92 for sore throat, and 56 for shortness of breath. In 2018, C.I.R.M. received a total of 2,444 requests for medical advice. Of these, 327 (13.4%) requests were for fever, 154 (6.3%) for cough, 83 (3.4%) for sore throat and 56 (2.3%) for shortness of breath. Whereas during the COVID-19 pandemic, i.e. from January 1 to June 30, 2020, a total of 3,924 medical requests, 832 cases for fever, 290 cases for cough, 220 cases for sore throat, and 149 cases for shortness of breath were received.
Int Marit Health 2020; 71, 4: 229–236
www.intmarhealth.pl232

Table 3. Number of cases assisted at sea for common COVID-19 signs and symptoms during the first 6 months of 2017 to 2020
Symptom 2017 2018 2019 2020
N = 2,419 Frequency (%)
N = 2,444 Frequency (%)
N = 2,694 Frequency (%)
N = 3,924 Frequency (%)
Fever*, #, ^ 353 14.6 327 13.4 466 17.3 832 21.2
Cough^ 177 7.3 154 6.3 140 5.2 290 7.4
Sore throat*, #, ^ 92 3.8 83 3.4 119 4.4 220 5.6
Shortness of breath*, #, ^ 56 2.3 56 2.3 35 1.3 149 3.8
*P < 0.05 for comparison of fever, cough, sore throat, and shortness of breath 2020 vs. 2017#P < 0.05 for comparison of fever, cough, sore throat, and shortness of breath 2020 vs. 2018^P < 0.05 for comparison of fever, cough, sore throat, and shortness of breath 2020 vs. 2019
Table 4. Requests for medical advice received by C.I.R.M. from January 1 to June 30, from 2017 to 2020 per month.
Month Patients assisted Frequency (%) variations*
Mean patients per day
2017 2018 2019 Mean 2020 2017 2018 2019 2020
January 414 404 478 432 506 +17 13.4 13.0 15.4 16.3
February 342 354 411 369 456 +24 12.2 12.6 14.6 16.2
March 401 404 437 414 651 +57 12.9 13.0 14.1 21
April 395 395 438 409 716 +75.06 13.2 13.2 14.6 23.8
May 414 422 475 437 834 +90.85 13.4 13.6 15.3 26.9
June 453 465 455 457 761 +66.52 15.1 15.5 15.1 25.4
*Frequency variations from the mean value (2017–2019) and 2020
Medical requests for fever during the first 6 months of the COVID-19 pandemic had doubled compared to the first half of 2017. From January 1 to June 30, 2020, C.I.R.M. received nearly 3 times more medical requests for fever than during the same period of 2018 and nearly 2 times more requests than in the same period of 2019. The differ-ence in the number of medical requests for fever during the COVID-19 pandemic was statistically significant compared to the same period of 2017 [c2 (1) = 29.55, p < 0.0005], 2018 [c2 (1) = 43.12, p < 0.0005] and 2019 [c2 (1) = 10.25, p = 0.001]. Medical requests for cough were more common in the first 6 months of this year compared to the same period from 2017 to 2019. The increase in the number of teleconsultations for cough between the year 2020 and 2019 was found to be statistically significant [c2 (1) = 10.82, p = 0.001]. There were nearly 3 times more medical re-quests for sore throat during the COVID-19 outbreak than during the first 6 months of 2017 and 2018 and nearly twice as many as in the same period of 2019. The increase in the frequency of medical requests for sore throat in the first 6 months of the COVID-19 pandemic was statistical-ly significant in comparison to the same period of 2017 [c2 (1) = 9.10, p = 0.002], 2018 [c2 (1) = 14.37, p = 0.0002] and 2019 [c2 (1) = 3.98, p = 0.04].
Requests for medical assistance due to shortness of breath were approximately 4 times more frequent during
the first 6 months of this year compared to the same pe-riod of 2019 [c2 (1) = 34.15, p < 0.0005]. Differences for this medical problem were almost 3 times significantly higher than in the same period of 2017 [c2 (1) = 9.43, p = 0.002] and 2018 [c2 (1) = 9.84, p = 0.002].
Table 4 presents the number of medical requests from January 1 to June 30, 2017 to 2020 on a monthly and av-erage daily basis. As shown in this table, from May 2017 to May 2020, the number of assisted cases was doubled (it increased from 19% to 39%). In comparison to the same period of 2019, the highest increase was observed between March and May 2020 (Table 4).
Depending on the intensity of the symptoms, dedicated software assigned a triage tag to the first request for med-ical advice from a ship. The triage system aims to prioritise incoming medical requests and identify those who cannot wait to be consulted. A triage system is essential for sorting and classifying patients, determining their needs, and estab-lishing treatment priorities. During outbreaks of infectious diseases, like COVID-19, it is used to separate patients likely to be infected with the pathogen of concern from those with other medical conditions. The system employed by C.I.R.M. uses four colour coded triage tags (white, green, yellow, and red) to classify the intensity of self-reported symptoms in those on board ships. Accordingly, the white tag indicates a mild case; the green tag indicates a moderate case;
www.intmarhealth.pl 233
Getu Gamo Sagaro et al., Telemedical assistance at sea in the time of COVID-19 pandemic

the yellow tag indicates an urgent case, and the red tag indicates a severe case. As shown in Table 5, most of the C.I.R.M. assisted cases were coded with white or green tags. For example, 73.5% (611) of fever cases reported in the first 6 months of this year were classified as moderate cases (Table 5).
DISCUSSIONThere were a total of 11,481 requests for assistance to
C.I.R.M. due to occupational injuries and illnesses over the 24 month period (in the first 6 months of 2017 until 2020). In terms of the types of pathologies requiring medical advice, gastrointestinal disorders and trauma/injuries were among the most commonly reported medical conditions occurring on board during the study period and were responsible for 15.10% and 12.90% of all requests, respectively. The findings reported in this study concerning injuries are in line with the Polish TMAS report [11]. A previous research study conducted by C.I.R.M. has shown that digestive system dis-orders were the most commonly reported causes of illness on board during the periods: 1952–1961, 1962–1971, and 1972–1981. After the 1980s, these pathologies held the second place [12]. The present study has reported that gastrointestinal cases were the number one cause of pa-thologies on board during the study period. These findings are consistent with those reported by the Swedish TMAS [13]. A higher prevalence of gastrointestinal conditions could be attributed to various factors, such as ingesting
contaminated food or water, and contact with contaminated environment. Dermatological and musculoskeletal cases were the third and fourth most common reason for seeking help from C.I.R.M doctors during the study period.
In this study, our attention was focused on the cases assisted in the first 6 months of the COVID-19 pandemic (Jan-uary–June 2020). Considering the fact that on board cargo ships asking for telemedical advice a definite COVID-19 diag-nosis cannot be made, we have investigated the occurrence of common signs of the coronavirus infection, including fever, cough, sore throat, and shortness of breath. Accord-ingly, a higher number of cases assisted on board during COVID-19 pandemic (3,924 cases) than during the same months of the year before the outbreak (2,694 cases) was noticeable. In the first 6 months of this year, a higher number of seafarers with fever, cough, sore throat, and shortness of breath asked for telemedical advice compared to the years from 2017 to 2019. This could indicate a possible occur-rence of some COVID-19-like pathologies on board ships but might as well be a sign of fear among seafarers and/or ship passengers of having developed the COVID-19 infection.
A study conducted on the Diamond Princess cruise ship reported that approximately 3,700 passengers and crew mem-bers were quarantined on February 3, 2020, in the port of Yo-kohama, Japan. By the end of the quarantine, nearly 700 coro-navirus cases had been confirmed by laboratory test [14]. The same study revealed that the first verified COVID-19 case in a crew member occurred in food service workers [14].
Table 5. The intensity of patients’ symptoms helped during the first 6 months from January 1 to June 30, 2017–2020
Year Triage tag Common symptoms of COVID-19 pandemic
Fever Cough Sore throat Shortness of breath
2017 White 104 (29.5%) 47 (28.3%) 44 (47.8%) 3 (5.6%)
Green 212 (60%) 109 (65.7%) 46 (50%) 23 (42.6%)
Yellow 33 (9.4%) 10 (6%) 2 (2.2%) 27 (50%)
Red 4 (1.1%) 0 (0%) 0 (0%) 1 (1.9%)
2018 White 62 (19%) 29 (20.4%) 21 (26.6%) 1 (2.2%)
Green 236 (72.8%) 106 (74.7%) 54 (68.4%) 26 (57.8%)
Yellow 23 (7%) 7 (4.9%) 4 (5%) 16 (35.6%)
Red 3 (0.93%) 0 (0%) 0 (0%) 2 (4.4%)
2019 White 86 (18.5%) 31 (22%) 18 (17.6%) 2 (4.4%)
Green 331 (71%) 80 (57%) 73 (71.6%) 18 (40%)
Yellow 47 (10%) 28 (20%) 10 (9.8%) 22 (48.9%)
Red 2 (0.43%) 1 (0.71%) 1 (0.98%) 3 (6.7%)
2020 White 163 (19.6%) 40 (13.8%) 50 (22.7%) 9 (6%)
Green 611 (73.5%) 222 (76.6%) 158 (71.8%) 94 (63%)
Yellow 53 (6.4%) 27 (9.3%) 11 (5%) 40 (26.8%)
Red 4 (0.48%) 1 (0.35%) 1 (0.46%) 6 (13.3%)
Int Marit Health 2020; 71, 4: 229–236
www.intmarhealth.pl234

As already mentioned a higher number of requests for assistance to the TMAS services in the time of COVID-19 pan-demic may indicate a growing number of COVID-19 infec-tions among seafarers, but on the other hand, it might also be a sign of panic and conviction that fever and shortness of breath are inevitably a sign of COVID-19 infection. Al-though shortness of breath and fever are the very common symptoms of a coronavirus infection, it is difficult to make a definite diagnosis from ashore unless quick diagnostic tests are available on board. There are at least several other pulmonary pathologies, including asthma, chronic obstructive pulmonary disorders and community-acquired pneumonia, which can cause shortness of breath, fever, cough, and dyspnoea.
In this particular situation, it is essential to take early warning symptoms if one of the crew members is sick. In this time of local and global distress, people on board ships who develop emergency warning signs for coronavirus should get medical attention as soon as possible. It is impossible to carry highly sensitive diagnostic systems for COVID-19 on board due to the costs involved and the difficulties in han-dling these systems by non-experts, e.g. ship officers. Based on our own experience, the availability of a pulse oximeter on board has allowed us to manage several doubtful cas-es. With an approach consisting of starting oxygen therapy in patients showing relevant respiratory symptoms and blood oxygen level below 92%, we could effectively manage all cases of pulmonary pathologies reported to C.I.R.M. without losing any of the patients.
Centro Internazionale Radio Medico statistics show that cardiovascular and respiratory system conditions are the sixth and seventh most common causes of illness on board (Fig. 1). Several recent studies related to coronavirus infec-tion have reported that people with underlying illnesses, par-ticularly chronic illnesses such as cardiovascular disease, respiratory problems, and adults over 65 years of age, are at an increased risk of a severe course of the COVID-19 pan-demic once infected [15, 16]. Therefore, a crew member with underlying health conditions like hypertension, dia-betes, chronic obstructive pulmonary diseases, or cardio-vascular disease should receive more medical attention. Potential risk areas on board should be identified, adequate health education must be provided to crew members and passengers, and environmental sanitation should be car-ried out correctly. Similarly, a study conducted on board a cruise vessel reported that the crew dining area was the primary area of congregation for the crew, and 15 out of 20, confirmed cases in crew members occurred in food service workers [14]. Hence, dining areas and the crew member living places, especially the galley, should be sanitised on a regular basis to prevent transmission. Moreover, all crew members should maintain standard recommendations to
prevent the spread of COVID-19 infection on board. These include covering the mouth and nose when coughing and sneezing, proper handwashing, cooking meat and eggs thoroughly, avoiding close contact with any crew member who shows symptoms of a respiratory disease.
Seafaring is one of the most hazardous occupations as far as personal health and occupational safety are con-cerned. Additionally, ships are one of the most crowded environments, where apart from injuries/traumas, seafarers are continuously exposed to infectious agents such as those transmissible by direct contact or droplets [17]. To prevent this novel and deadly pandemic (COVID-19 infection), any crew member who has had close contact with a confirmed case should quarantine and monitor his/her symptoms. For any early warning signs like fever, cough, shortness of breath, sore throat, and dyspnoea, the contact of a TMAS for proper treatment of the case is strongly recommended.
CONCLUSIONSDuring the COVID-19 pandemic, telemedical advice on
board was required for a higher number of seafarers. Fever, sore throat, and dyspnoea were the primary reasons for the more frequent requests for maritime telemedical advice, which were remarkably increased during the coronavirus outbreak. Close follow-up, regular health education on pre-venting coronavirus, using personal protective equipment, and adequate environmental hygiene could help minimise the potential risk factors for the COVID-19 transmission. Standard precautions such as frequent handwashing, cov-ering the mouth and nose when coughing and sneezing, avoiding close contact with any crew member showing early warning symptoms should be applied by all crew members regardless of suspected or confirmed cases.
ACKNOWLEDGEMENTS This work was supported by a grant No. 1508 from the
ITF Seafarers’ Trust, London, United Kingdom.
CONFLICT OF INTEREST The authors declare that they have no conflicts of in-
terest.
REFERENCES1. de Wit E, van Doremalen N, Falzarano D, et al. SARS and MERS:
recent insights into emerging coronaviruses. Nat Rev Microbiol.
2016; 14(8): 523–534, doi: 10.1038/nrmicro.2016.81, indexed
in Pubmed: 27344959.
2. Mizumoto K, Chowell G. Transmission potential of the novel
coronavirus (COVID-19) onboard the diamond Princess Cruises
Ship, 2020. Infect Dis Model. 2020; 5: 264–270, doi: 10.1016/j.
idm.2020.02.003, indexed in Pubmed: 32190785.
3. Glass C, Cash J, Mullen J. Coronavirus Disease (COVID-19). Family
Practice Guidelines. 2020, doi: 10.1891/9780826153425.0016b.
www.intmarhealth.pl 235
Getu Gamo Sagaro et al., Telemedical assistance at sea in the time of COVID-19 pandemic

4. ILO. ILO Sectoral Brief: COVID-19 and maritime shipping and fishing, 2020; No. March, pp. 1–8.
5. Takeuchi I. COVID-19 first stage in Japan - how we treat ‘Diamond Princess Cruise Ship’ with 3700 passengers? Acute Med Surg. 2020; 7(1): e506, doi: 10.1002/ams2.506, indexed in Pubmed: 32313661.
6. Rocklöv J, Sjödin H, Wilder-Smith A. COVID-19 outbreak on the Dia-mond Princess cruise ship: estimating the epidemic potential and effectiveness of public health countermeasures. J Travel Med. 2020; 27(3), doi: 10.1093/jtm/taaa030, indexed in Pubmed: 32109273.
7. Sagaro GG, Amenta F. Past, present, and future perspectives of telemedical assistance at sea: a systematic review. Int Marit Health. 2020; 71(2): 97–104, doi: 10.5603/IMH.2020.0018, indexed in Pubmed: 32604452.
8. Amenta DTF, Tveito A., TELEMEDICINE AT SEA: COMMUNICATIO-NAL CHALLENGES, ISfTeH e-Journal, 2007; pp. 219–222 [Online]. https://www.isfteh.org/media/med_e_tel_2007.
9. Mahdi SS, Amenta F. Eighty years of CIRM. A journey of commitment and dedication in providing maritime medical assistance. Int Marit Health. 2016; 67(4): 187–195, doi: 10.5603/IMH.2016.0036, indexed in Pubmed: 28009394.
10. WHO. International statistical classification of diseases and related health problems:10th revision. 2016; vol. 1, no. Fifth edition 2016 [On-line]. www.who.int/about/licensing/copyright_form/en/index.html.
11. Szafran-Dobrowolska J, Renke M, Wołyniec W. Telemedical Maritime Assistance Service at the University Center of Maritime and Tropi-
cal Medicine in Gdynia. The analysis of 6 years of activity. Med Pr. 2020; 71(2): 121–125, doi: 10.13075/mp.5893.00897, indexed in Pubmed: 31929519.
12. Amenta F, Dauri A, Rizzo N. Organization and activities of the Inter-national Radio Medical Centre (CIRM). J Telemed Telecare. 1996; 2(3): 125–131, doi: 10.1258/1357633961929907, indexed in Pubmed: 9375045.
13. Westlund K, Attvall S, Nilsson R, et al. Telemedical Maritime As-sistance Service (TMAS) to Swedish merchant and passengers ships 1997-2012. Int Marit Health. 2016; 67(1): 24–30, doi: 10.5603/IMH.2016.0006, indexed in Pubmed: 27029926.
14. Kakimoto K, Kamiya H, Yamagishi T, et al. Initial Investigation of Transmission of COVID-19 Among Crew Members During Quaranti-ne of a Cruise Ship — Yokohama , Japan , February 2020, 69, 11, 312–313.
15. Guo Y, et al. The origin , transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak – an update on the status. 2020: 1–10.
16. CDC. People Who Are at Higher Risk for Severe Illness | CDC. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-at-higher-risk.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fspecific-groups%2Fpe-ople-at-higher-risk.html (accessed Apr. 09, 2020).
17. Rashid H, Haworth E, Shafi S, et al. Pandemic influenza: mass gatherings and mass infection. Lancet Infectious Diseases. 2008; 8(9): 526–527, doi: 10.1016/s1473-3099(08)70186-5.
Int Marit Health 2020; 71, 4: 229–236
www.intmarhealth.pl236

Farhad Azimi Yancheshmeh, Amirkabir University of Technology, Tehran, Iran, tel/fax: +98-9398473283, e-mail: [email protected]
Poor sleep quality, long working hours and fatigue in coastal areas: a dangerous combination of silent
risk factors for deck officers on oil tankers
Farhad Azimi Yancheshmeh1 , S. Hossain Mousavizadegan1, Amin Amini1 , Andrew P. Smith2 , Reza Kazemi3
1Amirkabir University of Technology, Tehran, Iran 2Cardiff University, Cardiff, United Kingdom
3Shiraz University of Medical Science, Shiraz, Iran
ABSTRACT Background: The high number of marine incidents in port and coastal areas due to the tired deck officers’ erroneous actions are one of the major challenges of marine transportation. Approaching, berthing, and cargo handling (ABC) are the most stressful and exhausting operations of the ship in these areas, which are carried out consecutively and uninterruptedly.Materials and methods: This study examined Psychomotor Vigilance Task (PVT) performance, Arrow Flan-ker Task performance and the Pittsburgh Sleep Quality Index (PSQI) of 70 deck officers of ocean-going oil tankers with 4on–8off shifts at the end of the first shift of cargo-handling operations. In this case, they had worked more than 14 hours continuously. Also, their level of sleepiness was assessed using the Karolinska Sleepiness Scale (KSS) at the beginning, middle, and end of their first shift of handling operation. Results: The results were analysed according to the duration at sea and deck officers rank. PSQI, KSS, PVT mean reaction times and lapses, and also Flanker’s variables were higher among the chief and second officers who were present on board between 0–30 days. The state of officers who were present on board between 31 to 60 days was better than the officers with 0–30 and 61–90 days’ duration at sea. In addition, the results show that sleep quality during tour of duty affects cognitive performance and sleepiness of officers during cargo handling operations. Conclusions: The paper concludes by discussing possible solutions for reducing fatigue and human error among seafarers.
(Int Marit Health 2020; 71, 4: 237–248)
Key words: deck officers, fatigue, cognitive performance, sleepiness, sleep quality, approaching, berthing, cargo handling operation, oil tankers
�
INTRODUCTIONMaritime transportation experts have made consider-
able attempts to reduce marine accidents that mostly occur in coastal areas and ports [1], but the statistics show that there has not been a considerable reduction in the num-ber of these accidents and incidents [2–4]. Approaching port, berthing, and cargo handling (ABC) are three of the most important ship operations in the coastal water of the destination port and many accidents have occurred during
these operations. The statistics suggest that almost 78% [5] and 70% [6] of maritime casualties are happening during these operations and a substantial number of them were due to the human erroneous actions especially made by the deck officers [7].
The navigation officers of ocean going oil tankers are divided into two groups of day work and shift work in the long duration of the tour of duty. The day work officer is the ship’s captain who has the highest age and maritime
www.intmarhealth.pl 237
Int Marit Health 2020; 71, 4: 237–248
10.5603/IMH.2020.0042 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
ORIG INAL ART ICLE

experience among the navigation officers, and whose work shift is from 8.00–17.00. Moreover, the shift work officers are further divided into three groups of first officers with the work shifts (04:00 to 08:00 and 16:00 to 20:00), second officers with the work shifts (00:00 to 04:00 and 12:00 to 16:00) and third officers with the work shifts (08:00 to 12:00 and 20:00 to 24:00), where the first officers have the highest age and maritime experience among these three groups, and the second and third officers take the next places, respectively. The total work shifts of these officers form a fixed work/rest cycle [8].
Many studies have shown that one of the main problems of shift workers is their working at night and sleeping during the day which results in circadian misalignment, consider-able level of fatigue, decreased cognitive performance at night, and also leads to sleepiness during both day and night shifts [9–11]. This is a problem even for deck officers who have been involved for a long time in shift working because studies show that the endogenous rhythms of less than 3% of people, who continually work night shifts, can completely adapt to the night work shifts [11, 12]. In addition, deck officers spend a lot of time in a restricted and confined environment and face some problems due to the nature of marine occupations, including sleeping in a moving and noisy environment that is constantly influenced by the vi-brations of the engine room [13–15]. As a result, sleeping is continuously disturbed and restricted; restorative sleep is hindered [14, 16]. Some other outcomes resulting from the above-mentioned situation are a chronic reduction of sleep quality [17, 18], fatigue and development of sleep disorders like obstructive sleep apnoea and insomnia [19, 20].
Various definitions of fatigue have been proposed and cover a state resulting from factors such as insufficient sleep, extended wakefulness, and work/rest requirements out of sync with circadian rhythms, which possibly cause decrements in vigilance and cognitive performance [17, 21, 22]. Sleep quality is one of the influential factors in fatigue and perfor-mance [23–25] and it refers to how well individuals sleep and can include quantitative aspects of sleep like sleep latency, sleep hours, and depth of sleep [26]. Many studies have shown that one of the most important factors that affects nav-igation officers’ performance during ship operation like cargo handling is fatigue and sleepiness [9, 27], and several marine disasters involving e.g. the Exxon Valdez, ferry MS Herald of Free Enterprise, Jambo, and Shen Neng ships were because of the tiredness of deck officers happening in coastal areas and narrow straits with heavy traffic load [28–30].
Several weeks after the start of the tour of duty and passing through seas and canals, vessels usually reach coastal and approach areas in order to perform cargo han-dling operation [27]. Navigation officers, who are suffering from the above mentioned problems, start conducting ship
operations in these areas. In the operations in coastal areas and ports, deck officers face more restrictions and difficulties than in open seas because of heavy traffic load and congested waters [27]. Generally, the procedure, which is followed to increase the safety as well as the efficiency of the approaching operations, is as follows: the officers of the previous shift participate in the first 2 hours of the present shift while the watch-keeping officers of the next shift take part in the last 2 hours of the current shift. As a result, the rest hours decrease while the workload of officers increases [27]. Immediately as the approaching operation finishes and the vessel approaches the berth, the berthing operation begins. The berthing operation normally takes about 4 to 5 hours for oil tankers; and to conduct this operation, the first and second officers are present on the forward and aft stations of the ship along with the teams of seamen. Another team including the master, pilot, third officer, and wheelman manage the operation from the bridge. As the berthing opera-tion completes, cargo handling operations start immediately. This operation is really stressful and mainly calculation-driven and requires high accuracy and precision. There are many different important issues, including vessel stability, envi-ronmental protection, and application of port regulations, that have to be taken into account constantly [27]. In this phase, many inspectors and auditors inspect the ship multi-ple times, thereby disrupting the working and resting hours of the officers. It is also worth noting that all of these steps have to be taken as quickly as possible because any loss of time can cause significant financial penalties. This issue is one of the most important reasons for fatigue and stress of deck officers during ABC operations [27, 31].
The above mentioned situations put deck officers in a lot of stressful situations for a long time, that is, 15–16 hours, with minimum rest time, and long working hours which could be considered as an important risk factor for fatigue and sleepiness [27, 32]. They must also perform several cog-nitive activities like arithmetic and calculation-driven tasks simultaneously while they are bombarded by a large volume of internal and external stimuli. Under such circumstances, considering the limited capacity of the human brain, the high load of mental activities exceeds the operators’ mental capacity and causes mental fatigue [19, 33]. Figure 1 pres-ents an infographic of the problems faced by the navigation officers from the beginning of the tour of duty up until the beginning of the cargo handling operation.
Long working hours and high workload could greatly affect the performance of navigation officers during the sen-sitive cargo handling operation which is dependent on their cognitive abilities, by increasing their fatigue and sleepiness [34]. For example, Guo et al. [35] showed that mental fatigue causes reduced response inhibition in drivers and Boksem et al. [36] has shown that fatigue can cause a sustained
Int Marit Health 2020; 71, 4: 237–248
www.intmarhealth.pl238
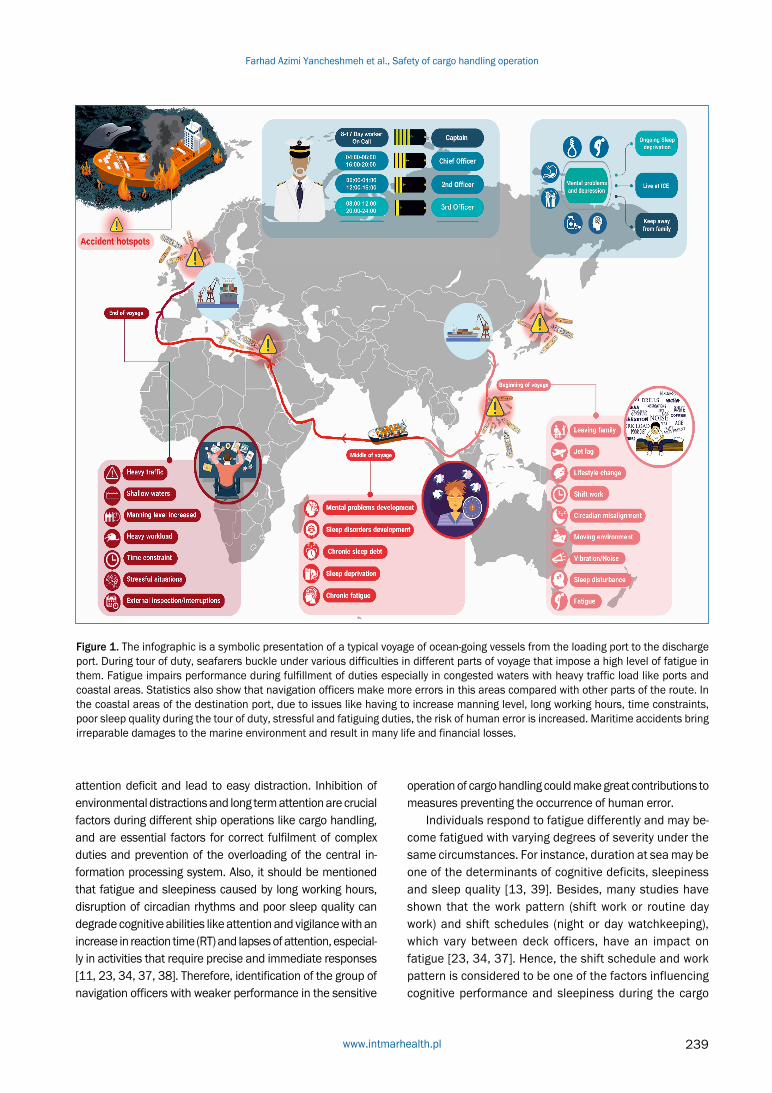
Figure 1. The infographic is a symbolic presentation of a typical voyage of ocean-going vessels from the loading port to the discharge port. During tour of duty, seafarers buckle under various difficulties in different parts of voyage that impose a high level of fatigue in them. Fatigue impairs performance during fulfillment of duties especially in congested waters with heavy traffic load like ports and coastal areas. Statistics also show that navigation officers make more errors in this areas compared with other parts of the route. In the coastal areas of the destination port, due to issues like having to increase manning level, long working hours, time constraints, poor sleep quality during the tour of duty, stressful and fatiguing duties, the risk of human error is increased. Maritime accidents bring irreparable damages to the marine environment and result in many life and financial losses.
attention deficit and lead to easy distraction. Inhibition of environmental distractions and long term attention are crucial factors during different ship operations like cargo handling, and are essential factors for correct fulfilment of complex duties and prevention of the overloading of the central in-formation processing system. Also, it should be mentioned that fatigue and sleepiness caused by long working hours, disruption of circadian rhythms and poor sleep quality can degrade cognitive abilities like attention and vigilance with an increase in reaction time (RT) and lapses of attention, especial-ly in activities that require precise and immediate responses [11, 23, 34, 37, 38]. Therefore, identification of the group of navigation officers with weaker performance in the sensitive
operation of cargo handling could make great contributions to measures preventing the occurrence of human error.
Individuals respond to fatigue differently and may be-come fatigued with varying degrees of severity under the same circumstances. For instance, duration at sea may be one of the determinants of cognitive deficits, sleepiness and sleep quality [13, 39]. Besides, many studies have shown that the work pattern (shift work or routine day work) and shift schedules (night or day watchkeeping), which vary between deck officers, have an impact on fatigue [23, 34, 37]. Hence, the shift schedule and work pattern is considered to be one of the factors influencing cognitive performance and sleepiness during the cargo
www.intmarhealth.pl 239
Farhad Azimi Yancheshmeh et al., Safety of cargo handling operation
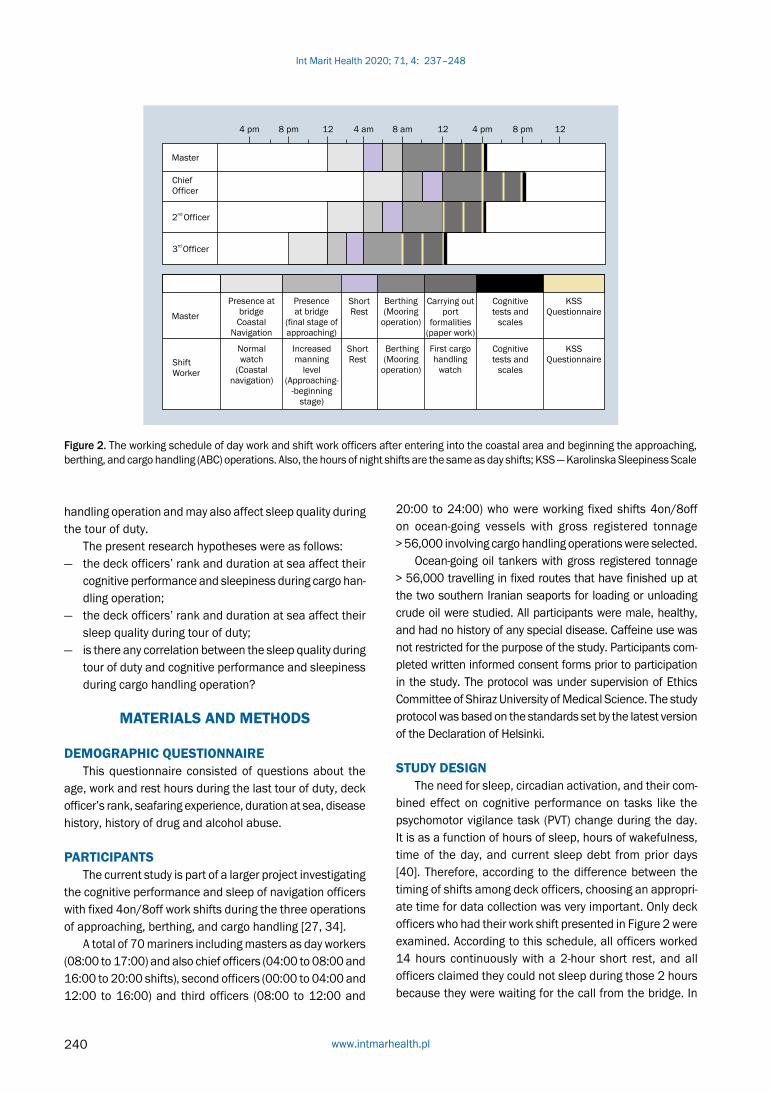
Figure 2. The working schedule of day work and shift work officers after entering into the coastal area and beginning the approaching, berthing, and cargo handling (ABC) operations. Also, the hours of night shifts are the same as day shifts; KSS — Karolinska Sleepiness Scale
handling operation and may also affect sleep quality during the tour of duty.
The present research hypotheses were as follows: — the deck officers’ rank and duration at sea affect their
cognitive performance and sleepiness during cargo han-dling operation;
— the deck officers’ rank and duration at sea affect their sleep quality during tour of duty;
— is there any correlation between the sleep quality during tour of duty and cognitive performance and sleepiness during cargo handling operation?
MATERIALS AND METHODS
DEMOGRAPHIC QUESTIONNAIREThis questionnaire consisted of questions about the
age, work and rest hours during the last tour of duty, deck officer’s rank, seafaring experience, duration at sea, disease history, history of drug and alcohol abuse.
PARTICIPANTSThe current study is part of a larger project investigating
the cognitive performance and sleep of navigation officers with fixed 4on/8off work shifts during the three operations of approaching, berthing, and cargo handling [27, 34].
A total of 70 mariners including masters as day workers (08:00 to 17:00) and also chief officers (04:00 to 08:00 and 16:00 to 20:00 shifts), second officers (00:00 to 04:00 and 12:00 to 16:00) and third officers (08:00 to 12:00 and
20:00 to 24:00) who were working fixed shifts 4on/8off on ocean-going vessels with gross registered tonnage > 56,000 involving cargo handling operations were selected.
Ocean-going oil tankers with gross registered tonnage > 56,000 travelling in fixed routes that have finished up at the two southern Iranian seaports for loading or unloading crude oil were studied. All participants were male, healthy, and had no history of any special disease. Caffeine use was not restricted for the purpose of the study. Participants com-pleted written informed consent forms prior to participation in the study. The protocol was under supervision of Ethics Committee of Shiraz University of Medical Science. The study protocol was based on the standards set by the latest version of the Declaration of Helsinki.
STUDY DESIGN The need for sleep, circadian activation, and their com-
bined effect on cognitive performance on tasks like the psychomotor vigilance task (PVT) change during the day. It is as a function of hours of sleep, hours of wakefulness, time of the day, and current sleep debt from prior days [40]. Therefore, according to the difference between the timing of shifts among deck officers, choosing an appropri-ate time for data collection was very important. Only deck officers who had their work shift presented in Figure 2 were examined. According to this schedule, all officers worked 14 hours continuously with a 2-hour short rest, and all officers claimed they could not sleep during those 2 hours because they were waiting for the call from the bridge. In
Int Marit Health 2020; 71, 4: 237–248
www.intmarhealth.pl240

fact, ABC procedures were aligned at a specific time of day for all participants of the same rank, but consistently differed between ranks. Also, 16-hour wakefulness was an appropriate time for cognitive performance assessment [38]; hence, the data collection time was chosen at the end of the first cargo handling shift. Also, as they were awake for at least 10 hours, the effect of sleep inertia was not an issue.
Due to the times of sunrise and sunset in that port and the seasons of collecting data, the time window from 8am to 8pm was considered as day, and therefore it can be said that all the operators’ data were gathered during the day shifts. During the evaluation of cognitive performance, participants were in a closed and quiet room without any noise or visual disturbance. This room was located away from bridge and cargo control room, and all participants were supervised by an experimenter.
COGNITIVE PERFORMANCE ASSESSMENTS Psychomotor Vigilance Task (PVT). The psychomotor
vigilance is a neurobehavioral assessment test that was per-formed to evaluate sustained attention between different groups of deck officers. This test has high ecological validity and reliability and many studies have shown its sensitivity to fatigue, sleepiness, and circadian misalignment [10, 40, 41]. First, each participant was piloted to get familiar with the procedure so they were instructed to use their dominant finger to show the quickest reaction to a simple visual stim-ulus (a red light display). Each PVT administration lasted 10 min with a random inter-stimulus interval of 2–10 s.
Arrow Flanker Task. The Flanker task assesses the indi-vidual’s inhibitory control of attention or selective attention capacity by taking into account the relevant stimulus while ignoring the irrelevant stimuli [42, 43]. The Flanker task requires participants to respond quickly (inter-trial interval = 1200 ms) via a forced-choice keypress to central target arrows (< or >) flanked by either congruent (<<<<<.>>>>>) or incongruent (<<><<.>><>>) arrows. Each trial started with the presentation of a central fixation cross “+”, which lasted for 1000 ms and the arrow appeared 200 ms later after the fixation cross disappeared. They were instructed that the arrows would appear rapidly, so they must react quickly to perform the task; however, it was emphasized that speed and accuracy were equally important. The whole test was 10 min with 300 trials with congruent and incongruent trials being presented randomly with equal probabilities.
KAROLINSKA SLEEPINESS SCALE (KSS) In the present study, the KSS was used to measure the
subjective level of sleepiness at a particular time during the day [44, 45]. Previous research studies have evaluated the validity and reliability of the KSS through other subjective indicators of sleepiness such as electroencephalograph-
ic, behavioural variables, etc. [44, 45]. The instrument is scored on a nine-point scale indicating 1 (very alert), 3 (alert), 5 (neither alert and nor sleepy), 7 (sleepy), and 9 (very sleepy and trying to stay awake).
SLEEP QUALITY ASSESSMENTThe Pittsburgh Sleep Quality Index (PSQI) was selected
to examine subjective sleep quality [26]. This 19-item ques-tionnaire was developed to analyse the sleep quality of the respondents over the last month. The PSQI consists of self-rat-ed questions and differentiates “poor” from “good” sleep by measuring seven domains: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep dis-turbances, use of sleep medication, and daytime dysfunction over the last month. Each element was scored from 0 to 3 and then summed into a global PSQI-score. Scores exceeding five indicate low sleep quality [26]. The PSQI has previously been validated with satisfactory validity and reliability [46].
DATA ANALYSISIBM_SPSS_Statistics 23 (2014) was used to perform
statistical analyses. In the PVT, RT was measured as the time between the onset of the red circle and the first key-press. Based on previous research on PVT [47], the following outcome measures of PVT performance were included: 1) mean RT, 2) number of lapses, defined as RT > 500 ms (errors of omission). In the Flanker task, response time was measured as the time between the onset of the arrow and the first keypress. Response accuracy and number of errors were calculated as the percentage of correct responses. The difference between RT in congruent and incongruent trials was defined as Dif-RT and the difference between the per-centage of correct responses in congruent and incongruent was defined as Dif-error. These variables measure the in-hibitory control of attention by participants.
The Kolmogorov–Smirnov tests and also investigation of kurtosis and skewness of different variables revealed that all data were normally distributed. Analyses results were carried out in SPSS using the ANOVA test to compare sleep quality scores between different groups, and a MANO-VA to compare PVT and Flanker scores between different groups. A Tukey’s test, an independent sample T-test, and a Spearman’s correlation test were used for specific com-parisons. The significance level for each test was p = 0.05.
RESULTSNumber, mean age, mean seafaring experience, and
ranges are presented in Table 1. In order to analyse the re-sults, the participants were divided into four groups from the deck officers’ rank perspective and into three groups from the duration at sea perspective (0–30 days, 31–60 days, 61–90 days).
www.intmarhealth.pl 241
Farhad Azimi Yancheshmeh et al., Safety of cargo handling operation
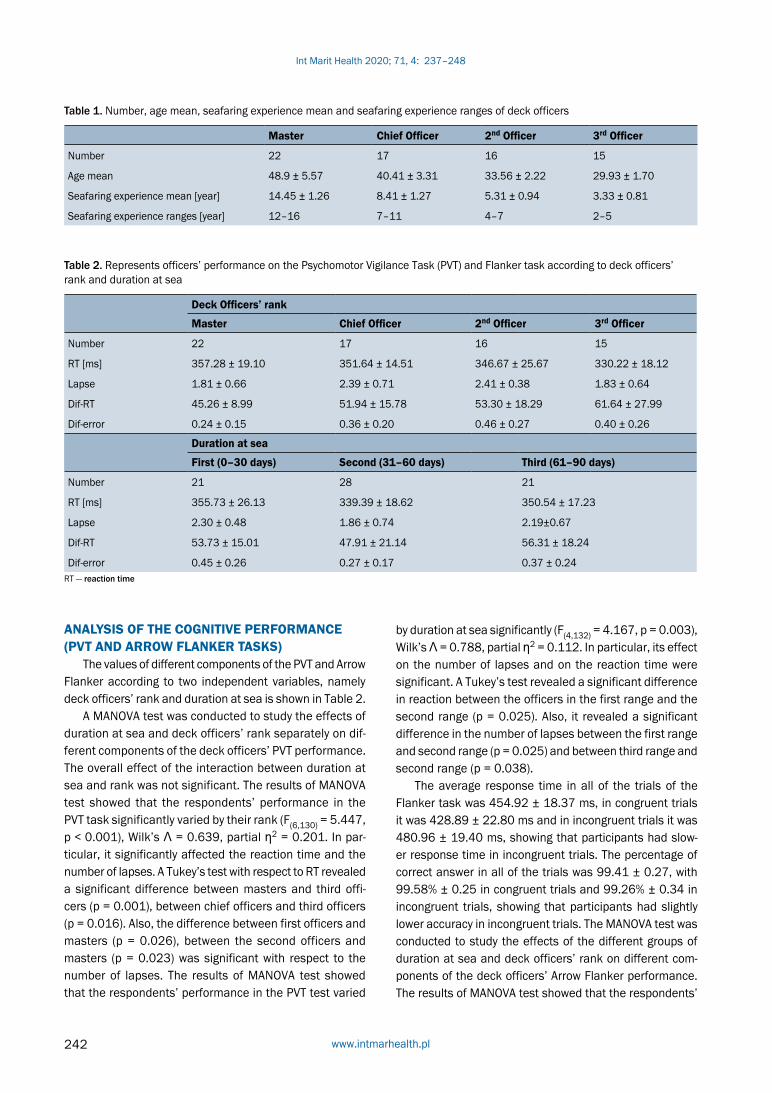
Table 1. Number, age mean, seafaring experience mean and seafaring experience ranges of deck officers
Master Chief Officer 2nd Officer 3rd Officer
Number 22 17 16 15
Age mean 48.9 ± 5.57 40.41 ± 3.31 33.56 ± 2.22 29.93 ± 1.70
Seafaring experience mean [year] 14.45 ± 1.26 8.41 ± 1.27 5.31 ± 0.94 3.33 ± 0.81
Seafaring experience ranges [year] 12–16 7–11 4–7 2–5
Table 2. Represents officers’ performance on the Psychomotor Vigilance Task (PVT) and Flanker task according to deck officers’ rank and duration at sea
Deck Officers’ rank
Master Chief Officer 2nd Officer 3rd Officer
Number 22 17 16 15
RT [ms] 357.28 ± 19.10 351.64 ± 14.51 346.67 ± 25.67 330.22 ± 18.12
Lapse 1.81 ± 0.66 2.39 ± 0.71 2.41 ± 0.38 1.83 ± 0.64
Dif-RT 45.26 ± 8.99 51.94 ± 15.78 53.30 ± 18.29 61.64 ± 27.99
Dif-error 0.24 ± 0.15 0.36 ± 0.20 0.46 ± 0.27 0.40 ± 0.26
Duration at sea
First (0–30 days) Second (31–60 days) Third (61–90 days)
Number 21 28 21
RT [ms] 355.73 ± 26.13 339.39 ± 18.62 350.54 ± 17.23
Lapse 2.30 ± 0.48 1.86 ± 0.74 2.19±0.67
Dif-RT 53.73 ± 15.01 47.91 ± 21.14 56.31 ± 18.24
Dif-error 0.45 ± 0.26 0.27 ± 0.17 0.37 ± 0.24RT — reaction time
ANALYSIS OF THE COGNITIVE PERFORMANCE (PVT AND ARROW FLANKER TASKS)
The values of different components of the PVT and Arrow Flanker according to two independent variables, namely deck officers’ rank and duration at sea is shown in Table 2.
A MANOVA test was conducted to study the effects of duration at sea and deck officers’ rank separately on dif-ferent components of the deck officers’ PVT performance. The overall effect of the interaction between duration at sea and rank was not significant. The results of MANOVA test showed that the respondents’ performance in the PVT task significantly varied by their rank (F(6,130) = 5.447, p < 0.001), Wilk’s Ʌ = 0.639, partial ƞ2 = 0.201. In par-ticular, it significantly affected the reaction time and the number of lapses. A Tukey’s test with respect to RT revealed a significant difference between masters and third offi-cers (p = 0.001), between chief officers and third officers (p = 0.016). Also, the difference between first officers and masters (p = 0.026), between the second officers and masters (p = 0.023) was significant with respect to the number of lapses. The results of MANOVA test showed that the respondents’ performance in the PVT test varied
by duration at sea significantly (F(4,132) = 4.167, p = 0.003), Wilk’s Ʌ = 0.788, partial ƞ2 = 0.112. In particular, its effect on the number of lapses and on the reaction time were significant. A Tukey’s test revealed a significant difference in reaction between the officers in the first range and the second range (p = 0.025). Also, it revealed a significant difference in the number of lapses between the first range and second range (p = 0.025) and between third range and second range (p = 0.038).
The average response time in all of the trials of the Flanker task was 454.92 ± 18.37 ms, in congruent trials it was 428.89 ± 22.80 ms and in incongruent trials it was 480.96 ± 19.40 ms, showing that participants had slow-er response time in incongruent trials. The percentage of correct answer in all of the trials was 99.41 ± 0.27, with 99.58% ± 0.25 in congruent trials and 99.26% ± 0.34 in incongruent trials, showing that participants had slightly lower accuracy in incongruent trials. The MANOVA test was conducted to study the effects of the different groups of duration at sea and deck officers’ rank on different com-ponents of the deck officers’ Arrow Flanker performance. The results of MANOVA test showed that the respondents’
Int Marit Health 2020; 71, 4: 237–248
www.intmarhealth.pl242

Table 3. Sleepiness comparison between the day shifts and night shifts for each group of the officers and the comparison between the sleepiness processes during each shift
Deck Officers’ rank
P-value3rd Officer2nd OfficerChief OfficerMaster
0.0034.20 ± 0.865.18 ± 0.915.17 ± 0.884.54 ± 0.85KSS1
0.0384.60 ± 0.735.43 ± 1.035.35 ± 0.704.81 ± 1.18KSS2
0.1305 ± 1.255.56 ± 1.205.88 ± 0.855.22 ± 1.15KSS3
Duration at sea
P-valueThird rangeSecond rangeFirst range
0.0044.85 ± 0.794.35 ± 0.915.23 ± 0.94KSS1
0.0175 ± 0.834.71 ± 0.935.52 ± 1.07KSS2
0.4555.38 ± 1.075.25 ± 1.105.66 ± 1.27KSS3KSS — Karolinska Sleepiness Scale
Table 4. Sleep quality according to the different ranges of duration at sea. The worst sleep quality was observed respectively in the officers who are in the first range (i.e., respondents who spent between 0 to 30 days) and the third range (i.e., respondents who spent between 61 to 90 days)
Deck Officers’ rank
P-value3rd Officer2nd OfficerChief OfficerMaster
0.0186.13 ± 1.307.31 ± 1.357.23 ± 1.146.63 ± 0.90PSQI
Duration at sea
P-valueThird rangeSecond rangeFirst range
0.0077.09 ± 1.226.28 ± 0.977.28 ± 1.30PSQIPSQI — Pittsburgh Sleep Quality Index
performance in this task significantly varied by their rank (F(6,130) = 2.624, p = 0.020), Wilk’s Ʌ = 0.796, partial ƞ2 = 0.108. In particular, rank significantly affected Dif-error. A Tukey’s test with respect to Dif-error revealed significant difference between second officers and masters (p = 0.018). The results of MANOVA test, showed that the respondents’ performance in the Arrow Flanker task significantly varied with duration at sea (F(4,132) = 3.424, p = 0.011), Wilk’s Ʌ = 0.821, partial ƞ2 = 0.094. In particular, its effect on the number of Dif-error was significant. A Tukey’s test revealed a significant difference in Dif-error between the officers in the first range and the second range (p = 0.024).
KSS ANALYSISThe average of KSS1, KSS2, and KSS3 values for dif-
ferent ranks among the officers, and the different ranges of duration at sea, are presented in Table 3. The one-way between subject ANOVA results showed that the KSS1 and KSS2 were significantly different for the different ranks of deck officers. The post-hoc Tukey test also demonstrated that the KSS1 scores were significantly higher among the first and second officers, compared to the third officers (p = 0.014, p = 0.013, respectively). Moreover, the one-way between subject ANOVA results also showed that KSS1, and
KSS2 were significantly different for the different ranges of duration at sea. Additionally, the post-hoc Tukey test also re-vealed that the KSS1 scores were significantly higher among the officers present in the first range, than the officers in the second range (p = 0.03). Furthermore, the results of this test for the KSS2 scores, show that the officers in the first range have significantly higher scores compared to the officers in the second range (p = 0.012).
PSQI ANALYSISThe mean sleep quality score of the participants over
the last month was 6.82 ± 1.22 and this indicated that their mean scores were significantly higher than standard score which is 5 (p < 0.001) that represents poor sleep quality. Ac-cording to the results, 89% of the respondents had low sleep quality. The mean sleep quality for the different deck offi-cers’ rank is presented Table 4. In the following data analy-sis, a one-way ANOVA was carried out to study the difference between the mean sleep quality scores of different groups of deck officers’ rank, revealing a significant difference be-tween the sleep quality of the deck officers. A Tukey’s test revealed a significant difference between the first officer and third officers (p = 0.045) and also between the second officers and third officers (p = 0.031).
www.intmarhealth.pl 243
Farhad Azimi Yancheshmeh et al., Safety of cargo handling operation

officers and first officers had the highest sleepiness and weak-est sleep quality and cognitive performance with regards most variables, and subsequently they experienced more fatigue.
During the tour of duty, the first and second officers have workshifts from 4am to 8am and 24 to 4 am, respective-ly. Performing the workshifts against the circadian rhythm and in times when the highest pressure for sleeping sup-press the human body, results in the weakening of the cog-nitive performance and acute fatigue in the short term, and in chronic fatigue and sleep deprivation in the long term [9, 10, 23, 34]. Moreover, sleeping during the day weakens the sleep quality of these officers to a great extent, and would not be sufficiently restorative, which is another reason for their fatigue [16, 48]. When combined with long working hours and the heavy workload of the ABC operations, these problems could be one of the main factors in impairing their perfor-mance during sensitive operations such as cargo handling.
Interestingly, although ship masters are usually day workers, their sleep quality is low presumably due to the significant work stress, excessive workload, and need for emergency preparedness [19, 49]. Captains suffer from a disturbed working and rest regime (unfixed working hours, even during the rest waiting for a call to taking place). Numerous captains, for instance, stated that sometimes they have to wake up several times during the night and be present on the bridge after receiving a call from an officer on the bridge to handle the situation [49]. The results of the current study agree with previous results regarding the worse performance of captains in the cognitive tests [50]. Factors such as the variety of inspections at port, time con-straints, and receiving numerous e-mails from the shipping company, cargo owners, and ship charterers impose an additional workload on captains [27]. Captains have the greatest seafaring experience and highest age among the deck officers, and increasing age reduces sleep quality and affects fatigue [17, 51]. Also, with an increase in seafaring experience and the increased responsibilities carried out by the officers on ships, their occupational stress and fatigue rises [13]. However, Hystad and Ed [13] stated that older and more experienced mariners are more capable of dealing with the circumstances. Further research is required to give a better understanding of the effect of age and working experience on cognitive performance.
The results obtained regarding duration at sea and sleep quality of the participants also suggest that the par-ticipants in the first range, i.e. 0–30 days, had the lowest sleep quality. This finding is in line with previous studies [7, 15], which reflected the difficulty and complexity of the process of adaptation of mariners to different and unique ship conditions on the first days of joining a ship and also some problems like jet lag. Surprisingly, it is stated that two-third of mariners directly start their work shifts without
Table 5. Represents Pearson correlation test. The results show that sleep quality affects their Psychomotor Vigilance Task (PVT) performance as indexed by reaction time (RT) and lapse and also sleepiness of participants
Variables Correlation P-value
PVT
RT-pre 0.386** 0.001
RT-post 0.361* 0.002
Lapse-pre 0.223 0.064
Lapse-post 0.215 0.074
Arrow Flanker
Dif-RT(pre) 0.027 0.824
Dif-RT(post) 0.094 0.437
Dif-error(pre) 0.329* 0.005
Dif-error(post) 0.505** 0.000
Karolinska Sleepiness Scale (KSS)
KSS1 0.365* 0.002
KSS2 0.332* 0.005
KSS3 0.385** 0.001
*p < 0.05; **p < 0.001
A one-way ANOVA was also carried out to study the dif-ference between the mean sleep quality scores of different groups of duration at sea, revealing a significant difference between the sleep quality of the deck officers. A Tukey’s test revealed that the officers in the first range had significantly lower sleep quality than the officers in the second range (p = 0.011) and also that the officers in the third range had significantly lower sleep quality than the officers in the second range (p = 0.046).
Results of the Pearson’s correlation in Table 5 showed a positive and significant correlation between sleep quality of officers during tour of duty and their cognitive perfor-mance and sleepiness during cargo handling operation.
DISSCUSION AND CONCLUSIONS The fatigue and sleepiness caused by poor sleep quality,
high workload and long working hours are the most critical factors that impair the performance of navigation officers during cargo handling operations. The comparison of the participants’ performance on the PVT and their KSS ratings in the present study with similar research conducted in simulator like HORIZON shows more fatigue in the real situ-ation. The results of the present study show that the officers with 4–8 shifts have more fatigue than the officers with 6–6 shifts in simulator-based studies like HORIZON [28].
The analysis of the results of the PVT, Flanker tasks, KSS and also PSQI based on deck officer’s rank revealed that second
Int Marit Health 2020; 71, 4: 237–248
www.intmarhealth.pl244

taking rest at the end of a flight after reaching the port where the ship is moored [52] which can cause more problems for night shift workers. It is worth noting that the alteration of the circadian rhythm, the stress of being separated from their families and changes in their sleeping environment not only lead to sleep deprivation but also causes problems such as insomnia, dysthymia and depression [53]. Now, imagine officers who are night shift workers, have joined the ship recently, and have to perform their duty on ABC operations. What a dangerous combination of risk factors this is for them! According to the PSQI, sleep disorders such as feeling warm or cold, coughing, snoring, having nightmares, waking up at midnight, and using sleeping pills were more prevalent among officers, who worked for 0 to 30 days on ships. Although individuals adapt more to the conditions of a tour of duty over the time, the other stressful factors and fatigue resulting from living and working at sea, including sleep debt, chronic sleep loss, and psychological problems resulting from living in the isolated and confined environment increase [51]. This could be the reason for poor sleep quality of officers in the third range (61 to 90 days).
The analysis of the participants’ performance in the KSS, PVT and Flanker based on duration at sea suggest that the participants in the first range, i.e., 0 to 30 days, who suffered lower sleep quality, showed more sleepiness, higher reaction time and number lapses and also had poorer inhibitory control of attention than the other ranges. These findings are in accor-dance with the results reported about the increased fatigue and subsequently decrements in sustained attention due to reduced quality and duration of sleep [51, 54]. However, par-ticipants who spent 61 to 90 days at sea showed more sleep-iness and weaker sleep quality and cognitive performance than the participants in the second range. Chronic exposure to stressors and fatiguing factors, and also the clear relationship between fatigue severity and duration of exposure to fatigue, means that duration at sea negatively affects their cognitive performance, sleepiness and sleep quality. This finding is similar to the findings reported regarding supply vessels [13].
The results of the Flanker task indicate significant differ-ences between some variables and the officers who worked the night shift in the latest tour of duty and stayed between 0 and 30 days or 61 to 90 days on the ship, had poorer inhibitory control of attention and made more mistakes in the Flanker task. These findings are in accordance with the results listed in studies [55] suggesting that individuals working the night shifts committed more errors than day workers. In addition to fatigue and sleep quality, depres-sion is another factor that affects the executive functions of the respondents [56]. However, given the mild to severe depression of mariners [14], it could be stated that depres-sion affects their response inhibition ability, which calls for further research.
The sleepiness resulting from low sleep quality com-bined with acute fatigue caused by stressful operations in the port, approaching, and coastal areas can create task deviation and heighten the risk of operational errors by navigation officers by reducing their cognitive abilities [57]. Despite the presence of work and rest hours regulations stipulated in the Maritime Labour Convention (MLC2006) as well as Standards of Training, Certification, and Watch-keeping (STCW), it seems that for commercial reasons, deck officers have to sometimes ignore these regulations [27]. Therefore, it is highly recommended that a new and specific framework is developed, involving a short rest break or nap for deck officers, especially those that joined the ship recently, and have a night shift in the last tour of duty and also have excessive workload in their duties after cargo handling operations. Azimi Yancheshmeh et al. [27, 34] also show that the existence of rest time between the berthing and cargo handling operations can have a significant effect on reducing the sleepiness and improving the cognitive performance of these officers during their first workshift in cargo handling operation.
Recently, the Oil Companies International Marine Forum (OCIMF) and the International Association of Independent Tanker Owners (INTERTANKO) released an article about the necessity of behavioural competency assessment. They believe that in order to reduce incidents, marine industries’ primary focus should be placed on training and assessing non-technical skills (soft skills) like team working, communication, situation awareness, decision making, result focus, and leadership which have been named competency domains. It is highly recommended by them to perform these assessments during critical ship operations like ABC [58]. It is worth noting that all of these competency domains are affected by fatigue directly and indirectly, especially during ABC. For example, fatigue can degrade situation awareness or decision making abilities through cognitive performance degradation. Sometimes, seafarers technically know how to perform their duties and also desire to act in that way but have made errors during performance of a task due to fatigue. On the one hand, OCIMF and INTERTANKO suggest that officers with greater experience and higher rank should have more soft skills due to the nature of their responsibilities. However, the present study showed that this group of officers had lower sleep quality and became more fatigued. Hence, it is deemed necessary for the assessor to focus on the level of seafarer fatigue while performing behavioural assessments in order to achieve more precise results.
Moreover, it seems there is a lack of a device similar to alcohol test devices to immediately measure the level of sleepiness in highly regulated industries. Such a device would enable the masters or port state control inspectors
www.intmarhealth.pl 245
Farhad Azimi Yancheshmeh et al., Safety of cargo handling operation

to assess the capacity of the deck officers for the accom-plishment of their tasks in their work shifts. Furthermore, it should be noted that much research demonstrates that insomnia is one of the main consequences of chronic sleep restriction and chronic sleep debt which is prevalent among seafarers [19, 59]. Using sleeping pills can be useful but this method has side effects like headache, dizziness, memory problems, and sleepiness. Non-pharmacological solutions such as a relaxation technique are one of the best methods for resolving sleep problems.
It is worth mentioning that cost-effectiveness is still one of the priorities for ship and cargo owners and maritime transportations companies due to the culture dominating maritime transportation. For example, deck officers may ar-rive at a destination with fatigue and poor sleep quality due to long tour of duty and then be involved in the tiresome and complicated approaching and berthing operations. Before handling cargo operations, such individuals need a reason-able amount of time to recover from work-related fatigue. However, the stakeholders, shipping companies, and cargo owners are not interested in the increased duration of stay of vessels in wharves due to the dire financial consequences or add a cargo officer to help the officers during cargo han-dling operation. This priority may increase the likelihood of a commitment to errors by the navigation officers.
LIMITATIONS OF THE STUDYShip’s type, cargo, and the crew nationality all contribute
to the degree of fatigue experienced by the ship crew [19]. However, in the present study, only ocean-going vessels were studied. Another limitation of the present study was its cross-sectional structure. Hence, any decisive conclusion needs to be drawn from further longitudinal research [60]. The seafarers were also assured that their participation in this study was not going to have any adverse occupational effect on them. Unfortunately, in the marine community, the inappropriate culture and fear of dismissal by the ship-owners or shipping companies causes problems. Hence, workers tried to hide many of their problems and hardships while answering the surveys [31]. In addition to the above-mentioned issues, there are other limitations associated with this field study such as time restrictions on presence on board. Similarly, the authors had to use subjective sleep quality which in comparison of objective sleep quality has lower precision.
It should be noted that in order to evaluate the sleep quality among those individuals who had worked offshore for less than a month, they were asked to answer questions proportionate to the length of time they were at sea.
Another limitation of this study is the low number of participants. Finally, it should be noted that the most im-portant information about fatigue comes from on-board field
studies. While time-consuming and personnel intensive, it is these studies that best allow a realistic assessment of the working and living conditions likely to produce high levels of fatigue and which therefore are needed in greater numbers.
DATA AVAILABILITYThe datasets generated during and/or analysed during
the current study are available from the corresponding authors on reasonable request.
CONFLICT OF INTERESTThe authors declare no competing interests.
REFERENCES1. Ugurlu O, Yildirim U, Yuksekyildiz E. Marine accident analysis with
GIS. J Shipp Ocean Eng. 2013; 3(1-2): 21.2. Akyuz E, Celik M. Utilisation of cognitive map in modelling human
error in marine accident analysis and prevention. Saf Scie. 2014; 70: 19–28, doi: 10.1016/j.ssci.2014.05.004.
3. Hu S, Zhang J. Risk assessment of marine traffic safety at coastal water area. Procedia Engineering. 2012; 45: 31–37, doi: 10.1016/j.proeng.2012.08.116.
4. Knudsen O, Hassler B. IMO legislation and its implementation: Accident risk, vessel deficiencies and national administrative practices. Marine Policy. 2011; 35(2): 201–207, doi: 10.1016/j.marpol.2010.09.006.
5. Kim I, Lee Hh, Lee D. Development of a new tool for objective risk assessment and comparative analysis at coastal waters. J Int Marit Saf Environ Aff Shipp. 2019; 2(2): 58–66, doi: 10.1080/25725084.2018.1562511.
6. European Maritime Safety Agency (EMSA), Annual overview of marine casualties and incidents. 2017.
7. Rutenfranz J. Work at sea: a study of sleep, and of circadian rhythms in physiological and psychological functions, in watchkeepers on merchant vessels. Int Arch Occup Environ Health. 1988; 60(6): 331–339.
8. Short MA, Agostini A, Lushington K, et al. A systematic review of the sleep, sleepiness, and performance implications of limited wake shift work schedules. Scand J Work Environ Health. 2015; 41(5): 425–440, doi: 10.5271/sjweh.3509, indexed in Pubmed: 26103467.
9. Duffy JF, Zitting KM, Czeisler CA. The case for addressing ope-rator fatigue. Rev Hum Factors Ergon. 2015; 10(1): 29–78, doi: 10.1177/1557234X15573949, indexed in Pubmed: 26056516.
10. Van Dongen HPA, Dinges DF. Sleep, circadian rhythms, and psy-chomotor vigilance. Clin Sports Med. 2005; 24(2): 237–49, vii, doi: 10.1016/j.csm.2004.12.007, indexed in Pubmed: 15892921.
11. Chellappa SL, Morris CJ, Scheer FA. Effects of circadian misalign-ment on cognition in chronic shift workers. Sci Rep. 2019; 9(1): 699, doi: 10.1038/s41598-018-36762-w, indexed in Pubmed: 30679522.
12. Folkard S. Do permanent night workers show circadian adjustment? A review based on the endogenous melatonin rhythm. Chronobiol Int. 2008; 25(2): 215–224, doi: 10.1080/07420520802106835, indexed in Pubmed: 18533325.
13. Hystad SW, Eid J. Sleep and fatigue among seafarers: the role of environmental stressors, duration at sea and psychological capital. Saf Health Work. 2016; 7(4): 363–371, doi: 10.1016/j.shaw.2016.05.006, indexed in Pubmed: 27924241.
Int Marit Health 2020; 71, 4: 237–248
www.intmarhealth.pl246

14. Carotenuto A. Psychological stress in seafarers: a review. Int Marit Health. 2012; 63(4): 188–194.
15. Wadsworth EJK, Allen PH, Wellens BT, et al. Patterns of fatigue among seafarers during a tour of duty. Am J Ind Med. 2006; 49(10): 836–844, doi: 10.1002/ajim.20381, indexed in Pubmed: 16948149.
16. Allen P, Wardsworth E, Smith A. Seafarers’ fatigue: a review of the recent literature. Int Marit Health. 2008; 59(1-4): 81–92.
17. International Maritime Organization (IMO), Guidelines on fatigue 2019.
18. Tamura Y, Kawada T, Sasazawa Y. Effect of ship noise on sleep. J Sound Vib. 1997; 205(4): 417–425, doi: 10.1006/jsvi.1997.1007.
19. Jepsen JR, Zhao Z, van Leeuwen WMA. Seafarer fatigue: a review of risk factors, consequences for seafarers’ health and safety and options for mitigation. Int Marit Health. 2015; 66(2): 106–117, doi: 10.5603/IMH.2015.0024, indexed in Pubmed: 26119681.
20. Strauch B. Investigating fatigue in marine accident investigations. Procedia Manuf. 2015; 3: 3115–3122, doi: 10.1016/j.prom-fg.2015.07.859.
21. Gawron VJ, French J, Funke D. An overview of fatigue. In: P.A. Han-cock, P. Desmond (Eds.) Stress, workload and fatigue. Lawrence Elbaum, 2020 NY.
22. Phillips R. A review of definitions of fatigue – And a step towards a whole definition. Trans Res Part F Traffic Psychol Behav. 2015; 29: 48–56, doi: 10.1016/j.trf.2015.01.003.
23. Kazemi R, Haidarimoghadam R, Motamedzadeh M, et al. Effects of shift work on cognitive performance, sleep quality, and sleepiness among petrochemical control room operators. J Circadian Rhythms. 2016; 14: 1, doi: 10.5334/jcr.134, indexed in Pubmed: 27103934.
24. Benitez A, Gunstad J. Poor sleep quality diminishes cognitive functioning independent of depression and anxiety in healthy young adults. Clin Neuropsychol. 2012; 26(2): 214–223, doi: 10.1080/13854046.2012.658439, indexed in Pubmed: 22335237.
25. Wadsworth EJK, Allen PH, McNamara RL, et al. Fatigue and health in a seafaring population. Occup Med (Lond). 2008; 58(3): 198–204, doi: 10.1093/occmed/kqn008, indexed in Pubmed: 18310605.
26. Buysse D, Reynolds C, Monk T, et al. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989; 28(2): 193–213, doi: 10.1016/0165-1781(89)90047-4.
27. Azimi Yancheshmeh F et al., Challenges contributing to navigation officers’ fatigue during approaching, berthing and cargo handling operations: a safety culture perspective (pre-submission). 2020.
28. HORIZON, Project Horizon-a wake-up call. 2012, Research Report.29. National Transportation Safety Board (NTSB), Marine Accident
Report: Grounding of the US Tankship Exxon Valdez: on Bligh Reef, Prince William Sound, Near Valdez, Alaska, March 24, 1989. 1990: The Board. 1989.
30. Sheen, J., MV Herald of Free Enterprise. Published by: Department of Transport, London, Hr. Majesty’s Stationary Office, Report of Court No. 8074, Formal Investigation, 1987.
31. Rajapakse A, Emad G, Lützhöft M, et al. A study on time constraints and task deviations at sea leading to accidents – a cultural-histo-rical perspective. Marit Policy Manag. 2019; 46(4): 436–452, doi: 10.1080/03088839.2019.1574407.
32. Uğurlu Ö. A case study related to the improvement of working and rest hours of oil tanker deck officers. Marit Policy Manag. 2015; 43(4): 524–539, doi: 10.1080/03088839.2015.1040476.
33. Kato Y, Endo H, Kizuka T. Mental fatigue and impaired response processes: event-related brain potentials in a Go/NoGo task. Int
J Psychophysiol. 2009; 72(2): 204–211, doi: 10.1016/j.ijpsy-cho.2008.12.008, indexed in Pubmed: 19135100.
34. Azimi Yancheshmeh F et al. Investigating the effect of shift schedules on the sleep quality, cognitive performance and sleepiness of oil tankers’ deck officers at the first cargo handling operation shift. (pre-submission). 2020.
35. Guo Z, Chen R, Liu X, et al. The impairing effects of mental fatigue on response inhibition: An ERP study. PLoS One. 2018; 13(6): e0198206, doi: 10.1371/journal.pone.0198206, indexed in Pubmed: 29856827.
36. Boksem MAS, Meijman TF, Lorist MM. Effects of mental fatigue on attention: an ERP study. Brain Res Cogn Brain Res. 2005; 25(1): 107–116, doi: 10.1016/j.cogbrainres.2005.04.011, indexed in Pubmed: 15913965.
37. Kazemi R, Motamedzade M, Golmohammadi R, et al. Field study of effects of night shifts on cognitive performance, salivary melatonin, and sleep. Saf Health Work. 2018; 9(2): 203–209, doi: 10.1016/j.shaw.2017.07.007, indexed in Pubmed: 29928535.
38. Van Dongen HPA, Maislin G, Mullington JM, et al. The cumulative cost of additional wakefulness: dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation. Sleep. 2003; 26(2): 117–126, doi: 10.1093/sleep/26.2.117, indexed in Pubmed: 12683469.
39. Carter T. Working at sea and psychosocial health problems Report of an International Maritime Health Association Workshop. Travel Med Infect Dis. 2005; 3(2): 61–65, doi: 10.1016/j.tmaid.2004.09.005, indexed in Pubmed: 17292007.
40. Dinges D, Powell J. Microcomputer analyses of performance on a portable, simple visual RT task during sustained operations. Behav Res Methods Instrum Comput. 1985; 17(6): 652–655, doi: 10.3758/bf03200977.
41. Lim J, Dinges DF. A meta-analysis of the impact of short-term sleep deprivation on cognitive variables. Psychol Bull. 2010; 136(3): 375––389, doi: 10.1037/a0018883, indexed in Pubmed: 20438143.
42. Diamond A. Executive Functions. Ann Rev Psychol. 2013; 64(1): 135–168, doi: 10.1146/annurev-psych-113011-143750.
43. Eriksen B, Eriksen C. Effects of noise letters upon the identification of a target letter in a nonsearch task. Percept Psychophys. 1974; 16(1): 143–149, doi: 10.3758/bf03203267.
44. Kaida K. Validation of the Karolinska sleepiness scale against performance and EEG variables. Clin Neurophysiol. 2006; 117(7): 1574–1581.
45. Gillberg M, Kecklund G, Akerstedt T. Relations between performance and subjective ratings of sleepiness during a night awake. Sleep. 1994; 17(3): 236–241, doi: 10.1093/sleep/17.3.236, indexed in Pubmed: 7939123.
46. Sohn SIl, Kim DoH, Lee MiY, et al. The reliability and validity of the Korean version of the Pittsburgh Sleep Quality Index. Sleep Breath. 2012; 16(3): 803–812, doi: 10.1007/s11325-011-0579-9, indexed in Pubmed: 21901299.
47. Basner M, Dinges DF. Maximizing sensitivity of the psycho-motor vigilance test (PVT) to sleep loss. Sleep. 2011; 34(5): 581–591, doi: 10.1093/sleep/34.5.581, indexed in Pubmed: 21532951.
48. Allen P, Wardsworth E, Smith A. The prevention and management of seafarers’ fatigue: a review. Int Marit Health. 2007; 58(1-4): 167–177.
49. Phillips R. Sleep, watchkeeping and accidents: a content analysis of incident at sea reports. Trans Res Part F Traffic Psychol Behav. 2000; 3(4): 229–240, doi: 10.1016/s1369-8478(01)00007-9.
www.intmarhealth.pl 247
Farhad Azimi Yancheshmeh et al., Safety of cargo handling operation

50. Umut T, Tavacioglu L, Bolat P. Age and experience based neuroco-gnitive performance of seafarers. Eng Sci. 2017 ; 12(3): 168–177, doi: 10.12739/NWSA.2017.12.3.1A0385.
51. Sąlyga J, Kušleikaitė M. Factors influencing psychoemotional strain and fatigue, and relationship of these factors with health complaints at sea among Lithuanian seafarers. Medicina. 2012; 47(12): 99, doi: 10.3390/medicina47120099.
52. Cardiff University. Cardiff University Seafarers Fatigue Film. 2012. https://www.youtube.com/watch?v=ua-ppReV684.
53. Baron KG, Reid KJ. Circadian misalignment and health. Int Rev Psychia-try. 2014; 26(2): 139–154, doi: 10.3109/09540261.2014.911149, indexed in Pubmed: 24892891.
54. Krueger G. Sustained work, fatigue, sleep loss and performance: A review of the issues. Work & Stress. 1989; 3(2): 129–141, doi: 10.1080/02678378908256939.
55. Finn P. The effects of shift work on the lives of employees. Monthly Lab Rev. 1981; 104: 31.
56. Dillon DG, Wiecki T, Pechtel P, et al. A computational analysis of flanker interference in depression. Psychol Med. 2015; 45(11): 2333–2344, doi: 10.1017/S0033291715000276, indexed in Pubmed: 25727375.
57. Ansiau D, Wild P, Niezborala M, et al. Effects of working conditions and sleep of the previous day on cognitive performance. Appl Ergon. 2008; 39(1): 99–106, doi: 10.1016/j.apergo.2007.01.004, indexed in Pubmed: 17434440.
58. OCIMF and INTERTANKO, Behavioural competency assessment and verification for vessel operators. 2018.
59. Akerstedt T. Shift work and disturbed sleep/wakefulness. Occup Med (Lond). 2003; 53(2): 89–94, doi: 10.1093/occmed/kqg046, indexed in Pubmed: 12637592.
60. Zapf D, Dormann C, Frese M. Longitudinal studies in organizational stress research: A review of the literature with reference to metho-dological issues. J Occup Health Psychol. 1996; 1(2): 145–169, doi: 10.1037/1076-8998.1.2.145.
Int Marit Health 2020; 71, 4: 237–248
www.intmarhealth.pl248

Dr. Alexis Maffert, Head and Neck Surgery Department, HIA Clermont Tonnerre, rue du colonel Fonferrier, 29200 Brest, France, e-mail: [email protected]
Optokinetic stimulation efficiency for sea sickness treatment
Alexis Maffert , Barbara Aupy
Head and Neck Surgery Department, HIA Clermont Tonnerre, Brest, France
ABSTRACT Background: Sea sickness is the type of motion sickness induced by maritime transport. Its prevention through optokinetic exercises is efficient. The object of this study is to evaluate the efficiency experienced by the patients as well as the impact on other motion sicknesses. Materials and methods: One hundred and forty-one patients underwent optokinetic treatment methods between 2006 and 2014. The following parameters were studied and scored on a numeric scale: sea sickness, intensity of vomiting and ability to hold position and duties on board. Results: Study parameters significantly improved by optokinetic reeducation method. Sea sickness was reduced by a factor of 2. Study settings were also stable over years. Other motion sicknesses were also improved with this optokinetic stimulation. Conclusions: Treating sea sickness by optokinetic stimulation reeducation gives good results parti-cularly improving its related clinical manifestations, therefore allowing seamen to properly hold their functions on board. Its efficiency lasts in time and seems promising for the management of other motion sicknesses.
(Int Marit Health 2020; 71, 4: 249–252)
Key words: sea sickness, motion sickness, optokinetic stimulation, sensory conflict
�
INTRODUCTIONMotion sicknesses are the set of neurovegetative mani-
festations presented by an individual subjected to passive movements induced by any means of transportation. Sea sickness is the maritime induced motion sickness. Amari-nage corresponds to the period of a few days necessary for the organism to adapt to the marine environment; beyond 2 days of physiological adaptation, one speaks of seasick-ness. A third of the population is sensitive to seasickness, another third will be sensitive in rough conditions and the last third during extreme conditions [1].
Balance comes as the result of central integration of multiple pieces of information from the vestibulum, the peripheral retina and from proprioceptive sensors. During movement, potential conflict arising from these different sources is the origin of motion sickness.
At sea, accelerations are intricate, unpredictable, related to the boat movement in the swell [2]. These moves have
a mainly vertical component [3] with hyper and mostly hypo gravity phenomena, all the more disturbing as they occur at low frequency (< 0.3 Hz).
Several medicinal solutions, such as antihistamines or anticholinergics, have been proposed with moderate effi-ciency but many side effects [4] sometimes making them unsuitable for professionals (alertness disorders).
An optokinetic stimulation reeducation technique is performed in our service and obtains good results [5]. It aims at creating sensory conflict in order to provoke and optimise the organism’s adaptation.
Trendel et al. [5] showed the method’s efficiency in 2010. This method also works better than placebo [6]. Re-education takes place after clinical examination and vestibular explorations in order to check the good running of inner ears and exclude patients with underlying pathologies. Reeducation consists in 10 sessions of optokinetic stimulation to which pro-prioceptive perturbations and cervical movements are added.
www.intmarhealth.pl 249
Int Marit Health 2020; 71, 4: 249–252
10.5603/IMH.2020.0043 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
ORIG INAL ART ICLE

We were interested in what the patient felt in terms of seasickness, vomiting and ability to hold his function on board so as to assess the method’s efficiency.
MATERIALS AND METHODSThis was a retrospective study concerning patients
enrolled in the service from January 2006 to December 2014 with at least 1 year follow-up to the end of the reed-ucation. To be included, a patient had to have attended at least 8 sessions of reeducation, to accept to participate, to be of age, without underlying pathology that could disturb the response to the reeducation and to be consulting for seasickness and not for other motion sickness.
Patients were asked to answer a series of questions so that they could evaluate on a numeric scale the intensity of their sea sickness, their vomiting and their ability to work on board before and after reeducation.
We analysed the patients’ data (age, sex, number of days at sea since reeducation and time since reeducation) as well as parameters such as seasickness intensity, vomiting intensity and inability to work on board.
Data were analysed with software R® version 3.2.4, with a risk threshold alpha = 0.05.
RESULTS
POPULATIONOne hundred and forty-one patients were included in
the study according to de defined criteria. Among these patients, 60 were professionals (military or not).
Median age was 45 years old (from 22 to 73 years old). There was a majority of men (61%) with a sex ratio at 1.56. The average number of days at sea since reeducation
was 88.62 days with a 95% confidence interval (955 CI) of 69.15–107.29 and average time since reeducation was 3.65 years with 95% CI of 3.33–3.97 (from 1 to 9 years, me-dian is 3 years). There was no difference between genders for age (p = 0.4544), number of days at sea (p = 0.1967) and time since reeducation (p = 0.2038).
PARAMETERS ANALYSISThe perceived intensity of seasickness significantly
improved from 7.92 to 4.28 with p < 0.0001 (Table 1). This improvement was also observed according to gender. Observed differences between genders before and after reeducation were not significantly different from general population of the study (p = 0.2787 and p = 0.8458).
Vomiting intensity and working on board inability were also significantly improved (p < 0.0001 and p < 0.0001) with a score from 6.68 to 2.89 for vomiting and from 7.2 to 3.81 for inability. For each sex the improvement was signifi-cant for these two parameters (p < 0.0001 and p < 0.0001). There was no difference between sexes before and after reeducation (p = 0.6982 and p = 0.5609 for vomiting and p = 0.2796 and p = 0.2994 for inability).
These parameters were analysed in function of elapsed time since reeducation. There was no significant difference in terms of age (Kruskal-Wallis test, p = 0.5827) and num-ber of days at sea (p = 0.3377). There was no significant difference between groups for sea sickness intensity before and after reeducation (Kruskal-Wallis test, p = 0.3332 and p = 0.3046). The same applies to vomiting (before, p = 0.9978 and after, p = 0.3529) and to working on board inability (before, p = 0.2187 and after, p = 0.7147).
Whatever elapsed time since reeducation, there was a significant improvement of sea sickness intensity per-
Table 1. Results before and after reeducation
Before reeducation After reeducation P
Seasickness intensity
Total 7.92 [7.60–8.23] 4.28 [3.82–4.73] < 0.0001
Male 7.78 [7.36–8.20] 4.31 [3.75–4.87] < 0.0001
Female 8.13 [7.65–8.61] 4.22 [3.43–5.00] < 0.0001
Vomiting intensity
Total 6.68 [6.25–7.12] 2.89 [2.44–3.33] < 0.0001
Male 6.75 [6.22–7.28] 2.99 [2.44–3.54] < 0.0001
Female 6.57 [5.80–7.34] 2.72 [1.94–3.49] < 0.0001
Working on board inability
Total 7.20 [6.81–7.59] 3.81 [3.32–4.29] < 0.0001
Male 7.03 [6.53–7.53] 3.60 [3.02–4.19] < 0.0001
Female 7.47 [6.82–8.12] 4.14 [3,28–5.01] < 0.0001Data are shown as mean and 95% confidence interval
Int Marit Health 2020; 71, 4: 249–252
www.intmarhealth.pl250

ceived by patients (Table 2). Other parameters (vomiting and working ability) were also improved except for the 1-year elapsed group (p = 0.0742 for vomiting intensity and p = 0.2276 for working on board inability).
OTHER MOTION SICKNESSESFifty-one (including 27 female) individuals out of the
141 patients studied reported feeling an improvement for at least 1 type of motion sickness. Car sickness was incrim-inated by 48 (94%) patients then air sickness (51%) and train sickness (49%) (Table 3).
In this patient group, the mean age was 44.37 years old, 95% CI 40.85–47.89 with a median at 46 years old. There was no difference in age between this group and our study population (p = 0.9095), nor between sexes (p = 0.6878 for men and p = 0.5964 for women). These patients had fewer days at sea than the total study popula-tion with 58.71 days with 95% CI 37.26–80.16 (p = 0.042) and the elapsed time since reeducation was not different from the study population with an average of 3.63 years and 95% CI 3.15–4.11 (p = 0.9305).
Among these patients who showed improvement in another motion sickness, the proportion of women is sig-nificantly higher (c2 test, p = 0.0207)
For each kind of motion sickness, the reported improve-ment was very significant (p < 0.0001). This improvement was also found for each gender. For males, the improve-ment was significant with p < 0.0001 for car sickness, p = 0.0032 for airsickness and p = 0.0043 for train sickness. For females, the improvement was also significant with p < 0.0001 for car sickness, p = 0.0094 for airsickness and p = 0.0007 for train.
DISCUSSIONThe choice of quantifying motion sickness scores on
a numeric scale has been justified by the subjectivity inher-ent to the Graybiel and Miller’s scale [7] and the need for an easy to use evaluation method. Sea sickness presents itself with a variety of symptoms but vomiting dominates the situation and is the only easily apprehendable sign. Furthermore, even for leisure activities, seafarers have to play a part on board and the assessment of the ability to be effective on board often unfortunately takes a second place in medical approach when it is a main complaint.
This latest element needs to be noticed. The purpose that any practitioner should be aiming is the ability of the patient to ensure his function on board even though few symptoms of seasickness are still remaining. That is why even improving clinical is not good enough to evaluate the success of seasickness treatment and the reason we tried to appreciate the ability to be effective on board.
Visual stimulation alone produces symptoms of motion sickness [5]. This is also true in driving simulators or virtual reality [8]. Optokinetic stimulation relies on vestibulo-visual conflict and allows sensitisation of the vestibulum from visual stimulation [5, 8, 9].
We had an older population than Trendel’s (44.1 vs. 32.8 years old); which can be explained by the larger share of military people in Trendel’s study [5]. In our study, 61% were men, which is similar to Trendel’s 58.7%.
The end of the studied period has been defined by an evolution in our seasickness treatment management. Over the most recent years, the cognitive part of the seasickness has been included and the patients were initiated to the op-
Table 2. Significance of observed improvement function of elapsed time since reeducation
Elapsed time since reeducation [years]
1 2 3 4 5 ≥ 6
Number (male) 10 (8) 34 (21) 37 (23) 24 (16) 11 (5) 25 (13)
Difference of seasickness intensity before and after reeducation
p = 0.0271 p < 0.0001 p < 0.0001 p <0.0001 p = 0.0105 p = 0.0004
Difference of vomiting intensity before and after reeducation
p = 0.0742 p < 0.0001 p < 0.0001 p = 0.0001 p = 0.041 p < 0.0001
Difference of working on board ability before and after reeducation
p = 0.2276 p < 0.0001 p < 0.0001 p < 0.0001 p = 0.0237 p < 0.0001
Table 3. Improvement in other motion sickness
N (proportion) Discomfort before Discomfort after P
Car sickness 48 (94%) 5.78 [5.01–6.56] 2.32 [1.67–2.97] < 0.0001
Air sickness 26 (51%) 4.68 [3.57–5.79] 1.80 [1.08–2.52] < 0.0001
Train sickness 25 (49%) 4.65 [3.54–5.77] 1.19 [0.58–1.80] < 0.0001
Data are shown as number (%) or mean and 95% confidence interval
www.intmarhealth.pl 251
Alexis Maffert, Barbara Aupy, Optokinetic stimulation efficiency for sea sickness treatment

timisation of the potential techniques [10]. Some sessions of reeducation were also replaced by virtual reality exercises in standing positions. More recently, new seasickness meth-ods of management in our department use virtual reality in a sitting position associated to vertical movements thanks to a mobile deck since 2016.
A period of at least 1 year was required in the study conditions in order to evaluate benefits over time and rely on a sufficiently large number of days at sea to attest the meaningfulness of the results. With 88 days at sea on aver-age, the seamen in the study have regularly been confronted to sea sickness. Because of the length of the reeducation method (10 sessions of optokinetic stimulation), priority should be given to patients whose exposure is frequent and for long periods.
One of the interests of this study was to be able to appreciate the stability of the benefits or the effectiveness of this method of sea sickness reeducation. We found an average of 3.65 years since reeducation but the analysis in subgroups according to the delay since reeducation showed a stability over time of the effectiveness of this method.
In the literature, there is a female predominance for seasickness (sex ratio 1.7/1) with a faster symptom ap-pearance and more intense clinical manifestations [11–13]. We did not find any difference between genders in terms of intensity of manifestations for seasickness. Bos et al. [14] also contested this otherwise usually admitted difference. However, in the population showing improvement in other motion sicknesses, we also had a female predominance (p = 0.0207), that corresponds to that of the literature [11, 12].
The proportion of people reporting an improvement in other motion sickness was higher than we might have initially thought (nearly one third of the patients followed for seasickness). Carsickness is the most described and im-proved motion sickness. Other motion sicknesses improved whereas only seasickness was targeted. This illustrates the similarities of the triggering mechanisms and their inter-actions in the onset of clinical manifestations. It would be necessary to set up a dedicated prospective study protocol to evaluate this improvement.
CONCLUSIONSAlthough longer (10 sessions) but with no risk and no
side effects, sea sickness reeducation by optokinetic stim-ulation, progressively sensitised by the addition of head movement and disturbance of plantar somatosensory infor-mation, provides satisfactory results on vomiting intensity and seasickness intensity for people suffering from it.
This method provides long-term benefits over sever-al years.
Nevertheless, the reduction or even cessation of vom-iting does not eliminate the feeling of seasickness but it
allows keeping a position on board and thus ensuring the operational capacity of seafarers. So the evaluation of the efficiency of seasickness treatment should take care of the ability of to perform their duties on board and not only the clinical results and symptoms reduction.
The optokinetic stimulation method seems to have a very interesting impact on motion sicknesses other than maritime conditions, which phenomenon should be studied with dedicated prospective protocols.
CONFLICT OF INTEREST The authors declare that they have no conflict of interest.
REFERENCES1. Sherman CR. Motion sickness: review of causes and pre-
ventive strategies. J Travel Med. 2002; 9(5): 251–256, doi : 10.2310/7060.2002.24145, indexed in Pubmed: 12962599.
2. Bles W, Bos JE, de Graaf B, et al. Motion sickness: only one provoca-tive conflict? Brain Res Bull. 1998; 47(5): 481–487, doi: 10.1016/s0361-9230(98)00115-4, indexed in Pubmed: 10052578.
3. Khalid H, Turan O, Bos J, et al. Application of the subjective vertical–horizontal-conflict physiological motion sickness model to the field trials of contemporary vessels. Ocean Engineering. 2011; 38(1): 22–33, doi: 10.1016/j.oceaneng.2010.09.008.
4. Bonne L, Loaec E, Aupy B, et al. Cinétose. EMC - Oto-rhino-laryngol-ogie. 2017; 12(1): 1–5.
5. Trendel D, Haus-Cheymol R, Erauso T, et al. Optokinetic stimulation rehabilitation in preventing seasickness. Eur Ann Otorhinolar-yngol Head Neck Dis. 2010; 127(4): 125–129, doi: 10.1016/j.anorl.2010.07.006, indexed in Pubmed: 20860921.
6. Ressiot E, Dolz M, Bonne L, et al. Prospective study on the efficacy of optokinetic training in the treatment of seasickness. Eur Ann Otorhinolaryngol Head Neck Dis. 2013; 130(5): 263–268, doi: 10.1016/j.anorl.2012.03.009, indexed in Pubmed: 23562228.
7. Graybiel A, Wood CD, Miller EF, et al. Diagnostic criteria for grading the severity of acute motion sickness. Aerosp Med. 1968; 39(5): 453–455, indexed in Pubmed: 5648730.
8. Bos JE, Bles W. Motion sickness induced by optokinetic drums. Aviat Space Environ Med. 2004; 75(2): 172–174, indexed in Pubmed: 14960055.
9. Rine RM, Schubert MC, Balkany TJ. Visual-vestibular habituation and balance training for motion sickness. Phys Ther. 1999; 79(10): 949–957, indexed in Pubmed: 10498971.
10. Perreaut P. ‘Comprendre et Pratiquer les Techniques d’Optimisation du Potentiel’ 2014 Inter Editions.
11. Golding JF, Kadzere P, Gresty MA. Motion sickness susceptibility fluctuates through the menstrual cycle. Aviat Space Environ Med. 2005; 76(10): 970–973, indexed in Pubmed: 16235881.
12. Matchock RL, Levine ME, Gianaros PJ, et al. Susceptibility to nausea and motion sickness as a function of the menstrual cycle. Womens Health Issues. 2008; 18(4): 328–335, doi: 10.1016/j.whi.2008.01.006, indexed in Pubmed: 18485739.
13. Flanagan MB, May JG, Dobie TG. Sex differences in tolerance to visually-induced motion sickness. Aviat Space Environ Med. 2005; 76(7): 642–646, indexed in Pubmed: 16018346.
14. Bos JE, Damala D, Lewis C, et al. Susceptibility to seasickness. Ergonom-ics. 2007; 50(6): 890–901, doi: 10.1080/00140130701245512, indexed in Pubmed: 17457748.
Int Marit Health 2020; 71, 4: 249–252
www.intmarhealth.pl252

Dr. Devran Yazır, Surmene Faculty of Marine Sciences, Karadeniz Technical University, 61530 Surmene/Trabzon, Turkey, tel/fax: 04623778073, e-mail: [email protected]
Effects of COVID-19 on maritime industry: a review
Devran Yazır1 , Bekir Şahin1 , Tsz Leung Yip2 , Po-Hsing Tseng3
1Surmene Faculty of Maritime Sciences, Karadeniz Technical University, Trabzon, Turkey 2Department of Logistics and Maritime Studies, the Hong Kong Polytechnic University, Hong Kong
3Department of Shipping and Transportation Management, National Taiwan Ocean University, Taiwan
ABSTRACTCOVID-19 is a global disease that has quickly shaken the world economy since the beginning of 2020 and consequently has significantly affected the shipping industries development (including shipping operators, port operators, government authorities, shippers, seafarers, passengers, supply chain operators, etc.). Currently, the clinical management of COVID-19 remains unclear. In order to understand the newest chal-lenges and figure out potential solutions for the maritime industries post COVID-19, this paper selected four shipping industries (including dry bulk, tanker, container, and cruiser sector) and reviewed these industries’ newest development. The research findings can strengthen the awareness of COVID-19 and reduce opera-tional risk and further improve business performance for the maritime related industries and authorities.
(Int Marit Health 2020; 71, 4: 253–264)
Key words: COVID-19, coronavirus, shipping industry, tanker, cruise
�
INTRODUCTIONWith the reference to the warning of the World Health
Organization (WHO) against various pneumonia cases that were detected in Wuhan city on December 31, 2019 in China. The information regarding an outbreak risk began to spread rapidly in the world. Chinese authorities announced on January 7, 2020, they have identified a new type of virus related to viruses like SARS and MERS. This new virus was temporarily called ‘2019-nCoV’. On 11 February 2020, WHO announced that COVID-19 was the official name for the disease induced by the new coronavirus [1]. COVID-19 has resulted in the deaths of hundreds of thousands of people worldwide since December 2019 [2].
It has also contributed to significant declines in econom-ic development and had major impacts on several national economies. In some countries, since measures have been taken to safeguard public health, industrial production and energy usage have been decreased by up to 30% in only a few weeks [3]. Most of the food supply chains were harmed or threatened by the outbreak of COVID-19.
Lack of intermediate goods from China due to COVID-19 caused many companies to suffer. Commodity
prices dropped; especially crude oil saw the lowest prices in history. People’s travel opportunities have been restricted, the transportation and carrying sector has been adversely affected. As a result, almost all countries shrank in the first quarter of 2020. This situation naturally caused economists to make some predictions for the rest of 2020 according to pessimistic and optimistic scenarios. According to these scenarios, even if the global economy improves in the sec-ond half, 2020 will not be very good both in terms of the global economy and global transportation. This situation can be seen from the growth expectations of the International Monetary Fund (IMF) [4].
The container industries have faced many new chal-lenges in recent year, such as trade regulation (e.g. US-Chi-na trade war), shipping fleet deployment, green shipping and green port issues (e.g. sulphur content in fuels). The emergence of COVID-19 has brought new challenges for shipping operation and management. For example, security check of port can result in extra waiting time for berthing operations, inland seaport transshipment operation, hin-terland transportation management, etc. The change of trade volume affects the freight and charter rates in the
www.intmarhealth.pl 253
Int Marit Health 2020; 71, 4: 253–264
10.5603/IMH.2020.0044 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
REV IEW ART ICLE

container shipping market and shipping operators must think how to figure out resilience strategies to reduce the potential operation loss and make this market back on a growth track.
During the early of the year 2020, many cruise ships have berthed at ports empty of passengers due to the influ-ence of COVID-19. The spread of viral pandemics has made this industry face serious challenges since it has involved public health and life safety problems. Past studies have mainly focused on specific case (e.g. Diamond Princess Cruise Ship) [5, 6] and explored treatment process. The insight studies of analysing market response strategies for COVID-19 outbreak period in the cruise industries are still limited. These contents will be further analysed and help cruise industries pass COVID-19 storm and develop new market opportunities.
This paper provides a comprehensive literature review to criticise the effects of COVID-19 on shipping industry. As COVID-19 is new to academia and the world and has yet to be researched, we tried to combine all related sources such as academic papers, magazines and corporate web-sites. It is believed that this study will contribute to fighting COVID-19 in shipping industry by increasing the awareness and taking measures and pre-cautions.
DRY BULK SHIPPINGIt can be stated that with the global pandemic of
COVID-19, the agricultural sector’s versatility has been tested. The global downfall in the demand of hotels and restaurants, caused agricultural commodities prices to drop by 20% [7]. Countries around the world have taken sever-al preventive actions to manage the exponentially rising spread. Nonetheless, aside from the restaurant and hotel services, most of the agriculture and food supply chains were considered in much better condition than the general economy during the pandemic [8].
Unquestionably, that is because people continue to con-sume, and particularly, stock up on dry food based on their stay at home. However, the food industry has been chal-lenged by panic-stricken people who stockpile excessively [9]. This has led to increased concerns about food shortages in sterilized milk, pasta, rice, and canned foods. This high demand for food products also hindered the delivery of online purchase food. Dry food and detergent sales have been exploded online, and while companies struggled with excessive demands, orders were delivered late or never arrived at all [10].
To put it another way, concerns about food shortage mean that the vulnerable population that cannot afford to stockpile food would not be able to find food. The result was the implementation of new restrictions to provide food to those who need it most of time [11].
Besides the aforementioned information, the poor coun-tries and their food shortages have become more preva-lent rapidly with the global epidemic [12, 13]. Accordingly, governments have taken various measures to protect the integrity of food supply chains. Therefore, besides compro-mising human health, it can be said that pandemics have posed major economic and sociocultural hazards [14, 15].
Even though the agriculture sector’s economic risks are deemed lower during the pandemic, if agricultural supply chains continue to crumble, employees are more likely to suffer because of employment gaps or an increase in the working hours. The reason for this can be stated as agriculture is the main industry that provides for 37% of total employment opportunities, and most of the paid agri-cultural workers are working seasonally and without social security [16].
Agricultural products are transported by land route, railway, and seaway. Dry bulk is transported to ports by land and rail, and between ports by seaway [8]. Throughout the pandemic, every dry bulk trade mechanism was influ-enced significantly by COVID-19 outbreak-related interven-tions. Since governments limited transport connections with other countries according to the physical distance rules, this situation particularly affected the trade performed via international maritime transportation [17].
As maritime shipping constitutes approximately 90% of global goods trade, disrupted port facilities prevent the distri-bution of imported food. International Maritime Organisation (IMO) has therefore consistently stressed the significance of not inconveniencing the maritime trade [1]. It has also high-lighted the necessity of taking certain health measures for this. After the disclosure of the pandemic, cargo ships with bulk ocean freight have been equipped with crews isolated from residents on the mainland due to the fear of transmit-ting COVID-19 on board. Since the marine containers could not make new loading during their return to Asian countries that are frequently importing, empty container problems arose [18]. Therefore, due to the pandemic, spending extra time and money turned into a necessity for a new loading. For example, a health screening was required for the crew, so the landing was prohibited. Harbours were in a state of deadlock due to the shortage of workers and failing to carry cargo quickly; thus, refrigerated warehouses have become unusable for fresh food [19]. These delays caused perishable goods to spoil in a short-time and increased food waste. Also, the suspension of containers during the quarantine period caused serious economic problems in maritime trade.
As seen in Figure 1, the Baltic Exchange Dry Index start-ed to fall in October 2019 and continued to downward momentum by reaching more than 80% fall in February 2020. After that date, certain rises were observed and lev-els in November 2019 were almost achieved in July 2020.
Int Marit Health 2020; 71, 4: 253–264
www.intmarhealth.pl254

The coronavirus (COVID-19) outbreak increased food safety risks in Asia and the Pacific. Since the increased health risks have led to travel restrictions, disruptions in domestic and international food supply chains have reduced food availability and accessibility [20]. In addition to interna-tional transportation and logistics limitations, interruptions experienced in food supply chains also stem from the travel restrictions and employee sicknesses observed during the planting and harvesting period [20]. Employment gaps and income losses also put people at risk of starvation and malnutrition. Besides, the international lockdown of borders and export restrictions limited import-dependent countries’ access to certain food products [20].
Following the announcement of COVID-19 as a pan-demic, food prices in India, which is among the countries where dry food is produced most in Asia, have increased considerably since transport services have been suspended and fresh materials were not accessible [21]. This situation has damaged the harvest of wheat in Northern India, while volunteer students were sought for the harvest of grapes in Pune. Owing to the fear of contamination, onion harvesting was hindered at Maharashtra due to the fleeing of drivers and personnel. Food processing operations have ceased notwithstanding the high demand for processed foods such as instant noodles and biscuits. Giant food companies like Nestle and PepsiCo were unable to boost production since all workers returned to their villages. Afterward, flour and
Figure 1. Baltic Exchange Dry Index Monthly Open Values [23]
grain imports decreased significantly due to export bans on wheat in Uzbekistan. Owing to disruptions in the global supply chain and distribution networks generated by the pandemic, Indonesia has limited its import capacity. The transport of dry food was restricted in the People’s Repub-lic of China, and the delivery of agricultural products was interrupted due to labour shortages [22].
Furthermore, it was found that the demand for food is decreasing due to certain factors. According to Michael Bourke [12], COVID-19 would possibly reduce the supply of both fresh and dried products traded as follows:
— greatly decreased change-ability of the population and possible interruption of transport/supply chains;
— spoilage in fresh food marketing and, accordingly, in-creases in fresh food prices;
— interruption of supply of foreign food chains, such as products dependent on rice and flour;
— disruptions in the supply of food chains based on sugar, eggs, poultry, pork products, and canned tuna fish;
— closing of many shops because of lack in supply or civil disorder;
— loss of income by many people in both the formal and grey economy, and thereby, a decrease in purchasing power of food that affects rural and urban people.The combination of trade-policy shocks and
COVID-19 seems to have triggered a major storm. A single incident may not be sufficient to prompt the rethinking of
www.intmarhealth.pl 255
Devran Yazır et al., Effects of COVID-19 on maritime industry: a review

global value chains; however, the two can be merged. The US-China trade battle, the current restrictions on the export of medicinal and agricultural goods, has created uncertainty regarding the future of free trade [24]. Ergo, global value chains linked to dry grain and sea transport have been assumed to be reshaped after the pandemic.
Scientists warn us that extreme weather conditions caused by climate change and infectious diseases will trig-ger new outbreaks [25]. In case of a determined action against climate changes and epidemics have not been taken, resonant shocks in the global economic system would have become widespread. Countries would need to diversify their supplier sources to prevent problems affecting a spe-cific supplier or geographical region. For instance, numerous Eastern European and Eastern and Southern Mediterranean countries have a competitive advantage over goods export-ed by China [26]. Countries firstly will need to increase their development efforts regarding export by maritime transport and dry food investment to seize the opportunity to enter global value chains or intensify their share.
TANKER AND LNG SHIPPING
TANKER SHIPPING MARKET IN TURMOILOpinions and concerns about the problems that
COVID-19 will cause in the maritime sector were conveyed to the European Union by the European Community Ship-owners Association (ECSA) and the European Transport Workers’ Federation (ETF). In the letter, it is stated that the measures to restrict the movement of people to minimise the risk of infection in many countries are understandable, but these measures also have serious consequences on the movement of seafarers. Also, the closure of the ports is stated as a related effect. Moreover, it is emphasized that workers on both the sea and the land experience various problems that require urgent intervention. It was said in the letter to be very important for the ships to approach the port when necessary and for the personnel to join and leave their ships with as few obstacles as possible. Also, this situation was getting harder with the restrictions in the ports and the reductions of the flights. The shipping industry, therefore, called on the operator and owner to continue operating the ship. It also said crew members have the flexibility to enable them to leave the ship and return to their homes. It also requests that the crew members are exempted from nation-al travel prohibitions so that they can join their ships and maintain the operability of their supply lines. It was reported that seafarers should be treated differently when they return to their countries, and just like healthcare professionals and security forces, seafarers are key employees. So, it was stated that governments should pay special attention to seafarers in this way [27].
Seafarers who are not allowed to leave the ship due to travel restrictions may be forced to stay on the ship longer than usual. Besides, educational institutions such as the Training Support Command (TSC) San Diego were closed to limit the spread of the virus. Due to concerns that certificate periods may expire as a result of seafarers failing to receive the necessary training to extend their certificates, the United Kingdom Maritime and Coast Guard Agency (MCA) advises on seafarers’ training as the COVID-19 outbreak continues. In this context, the maritime sector called on the Flag and the Port States to extend the validity period of the certificates for at least 3 months and demands that regional Port State control regimes around the world act for this situation [27].
In the January–February period of tanker transportation, China’s daily oil shipment fell by almost 0.4 billion tons from January 10 to February 18, from an average of 3.5 billion DWT. However, with the fall of oil prices, oil shipment in-creased again. In the period until the first week of April, both crude oil imports and iron ore imports increased by 2% compared to the same period of 2019 [4].
After a bad 4.5–5 months in terms of many segments of maritime transport (excluding tanker transport), the pan-demic is controlled, and then the pandemic can be finished at the end of May and if the second outbreak does not ap-pear, the remaining 8 months may be better. In the following times, a higher trend may be a maritime sector in 2021 by all segments. But the remedy for this improvement may be the cause of a new debt crisis in 2022–2023 [4].
According to the data of BIMCO, the COVID-19 pan-demic influenced all over the world, causing delays or cancellations of contracts in the shipbuilding industry and postponement of new building deliveries. Shipbuilding contract activities fell by 55%. Ship deliveries decreased by 16.7% in the first quarter of this year compared to the same period last year. Both parts of the tanker shipping industries saw deliveries reduced by half compared to the first quarter of 2019; 49% and 43%, respectively for crude oil and product tankers. While 5.7 million DWT crude oil tankers were delivered in the first quarter of the year, 4 million DWT of them came from the delivery of 13 Very Large Crude Carrier (VLCC) [28].
Petroleum exporting countries have found a storage formula to take advantage of this period after oil prices, which have experienced a historic decline. Refineries, which fill their tanks with cheap oil to the brim, searched for more rental tankers. While the rental prices of tanker ships are rising, the value of companies is rising rapidly. The corona-virus epidemic, the giant sector of centuries changed the balances in oil [27].
Stopping travel due to epidemic disease and interruption of hundreds of businesses has reduced oil consumption from 100 million barrels to 30 million barrels. This led to
Int Marit Health 2020; 71, 4: 253–264
www.intmarhealth.pl256

a rapid decline in oil prices. The price of Brent oil, which was traded at $66 a year earlier, fell below $20 a barrel. Oil importing countries closely follow the oil market to benefit from the low price in oil [27].
While storage companies are looking for tankers to transport oil from all around, sector agents say that it is difficult to find a rental tank for a while. Maritime companies’ officials state that the rents of tanker ships have lined with the increase in demand. In international markets, the share values of tanker companies started to increase rapidly [27].
Long Range 2 (LR2) product tankers (80,000–119,999 DWT) daily earnings were $165,000, whereas before 2001 it was around $80,000. Aframax (750,000 DWT) crude oil tanker earns almost the same money daily as VLCC crude oil tanker, which takes more than 2 times crude oil. The daily income of Long Range 1 (LR1) product tankers (55,000–79,999 DWT) is $110,000 and the previous gain is around $65,000. Medi-um-range (MR) product tankers (25,000–54,999 DWT) dai-ly earnings are around $75,000, and Handysize (10,000– –24,999 DWT) daily earnings are around $90,000 [29].
As almost all land refineries are full, so, product tankers are used as storehouses. Therefore, as the demand for product tankers has increased, the profit of these tankers has increased more than ever [29].
Due to the tightness in large tonnage VLCC and Suezmax tanker ships, very few loadings and unloading ports serve such ships in the open sea [29].
Although MRs, Handysize, and LRs type tanker ships do cargo loading and unloading in different hemispheres, they have been left in the discharge port for a long time and caused the ships to be used as warehouses [29]. Crude oil tankers are used as warehouses due to the decrease in crude oil prices and the increase in prices in the future, because of the buy-to-sell strategy [29]. COVID-19 caused a lack of demand all over the world. Therefore, the depreci-ation in the crude oil market prices is expected to continue for a while. And crude oil ships are used as warehouses for a long time and the freight prices of these ships are expected to increase due to excess demand [29].
The maritime and tanker sector is in a vicious circle due to the epidemic. It is said by the authorized people that there is a big decline in the industry in the world and we are still in the middle of this decline. It is also estimated that this situation will continue for a while [30].
According to the report of Diamond S maritime compa-ny, the first quarter of 2020’s ship rental net income was 45 million dollars and it was seen that it decreased 1 million dollars compared to the first quarter of the previous year [30]. Oil supply to ships has decreased due to the confusion in the oil market, although this has a positive effect on ship charter rates. However, long waiting times for vessels negatively affect shipowners [30].
Fifty-four per cent of the Suezmax crude oil tankers op-erating at the Diamond S shipping company were rented in the first quarter of 2020 with the spot. In the second quarter of the year, the daily rents of this type of ship increased to $48700 and remained below expectations [30].
In January and February 2020, Suezmax tankers were rented at a low rental price. While these ships were expected to evacuate in March and April, they had to wait idly during these months due to logistics restrictions, oil refineries being closed, and refineries being full.
The shipowners suffered losses during this period as the demurrage paid by the hirer was less than the daily rent on empty waiting days [30].
Eighty per cent of Diamond S maritime company ships are operated as spot and 20% as time charters. Due to the pandemic in the world, spot market ship rents are expected to decrease in the future. For this reason, it is estimated that time charter ship rentals will gradually increase in the tanker market [30].
In the process of the epidemic, tanker shares cause financial damage to its investors in a short time. In the long term, the coronavirus epidemic should pass in a short time for the shares to profit their investors. This stagnation will continue from 2020 through 2021 when tankers are used as warehouses due to the epidemic. Also, whenever the world economy returns to normal, the recession will end. It is estimated that the markets will stop decreasing in the first quarter of 2021 [31].
The International Energy Agency (IEA) explains that quantity, time graph, and estimates for the use of oil as a floating tank in tankers are interpreted in Figures 2, 3 and 4 [31].
According to Webber Research and Advisory data, VLCC ship daily rents in 2020 are estimated to be $85,000, and VLCC ship daily rents will be $65,000 in 2021 [31].
According to the analyses, the usage, daily earnings, and estimated earnings ratios of VLCC ships are as indicated in the chart [31]. According to the 2019 annual report, Liquefied Natural Gas (LNG) demand is 12.5% around the world. This corresponds to 359 million tons. Due to LNG’s low carbon emission, its demand is expected to double by 2040. In 2019, Bangladesh, India, and Pakistan recorded the highest growth in demand (19%) from Asian countries, besides China’s 14% supply growth. Although the LNG tank-er market is stagnant in a short time due to coronavirus, it is estimated that the market will grow gradually since the demand will increase after 2020 [32].
THE EFFECT OF COVID-19 DISEASE ON THE MARITIME SECTOR AND FUTURE FORECASTS
COVID-19 significantly affected the maritime industry. Damage to the maritime industry, which has an important
www.intmarhealth.pl 257
Devran Yazır et al., Effects of COVID-19 on maritime industry: a review

Figure 2. Floating storage scenarios [33]
Figure 3. VLCC utilisation and earnings estimate forecast [33]
share in the conduct of trade activities in the world, will indicate the effect of this negativity in a short time. Unfor-tunately, developing countries like us will get their share from this negatively. It seems that there is still no definitive solution for COVID-19 and countries are still spending on their capital. Now, even if we haven’t felt the effect of this so far, it is clear that this situation will lead to an economic crisis soon.
As is known, the incubation period of this virus is 14 days. Therefore, the first thing that comes to mind in
the maritime sector will be an important question “whether the ships coming to the ports will be kept for 14 days to be able to take free practice”. Especially, the arrival of the ships coming to/going from places where the ports of calling such as China, Italy, Spain, USA, etc. show the effect of Corona (taking into account the death cases) during this period will cause the maritime trade. Large accumulation, delays, and commercial losses will arise from this situation. In addition, inspections will become more frequent on ships and new checklists will be created.
Int Marit Health 2020; 71, 4: 253–264
www.intmarhealth.pl258

Figure 4. Global container throughput and container trade [35]
It has been also seen in the guide published by the Turkish shipowners’ association; the pre-survey inspection intervals for Turkish Flagged ships in Port Directorates have been extended. Besides, Port State Inspection applications to foreign-flagged ships have been suspended, and man-datory surveys and certificates have been extended. These show that there will be some breaks in these lines and their repair time will have an effect over time. Suspension of personnel certification procedures will lead to accumulation and confusion in the next stage.
At the same time, it will be more difficult for ship crews to go out in the usual ports. When the outgoing personnel come back to the ship, they will be quarantined for a while and will create extra work burden such as take someone’s temperature by the relevant officers.
How healthy the replenishment to be made to the ships will become controversial. Besides, garbage from ships will be questioned. From now on, it will be discussed that there is also a warehouse for the garbage received from ships and the disposal of the garbage in this warehouse. New stan-dards and classifications will emerge in the garbage system.
Restrictions and regulations will come for the crew to leave the ship. Currently, the changes seem to be postponed in many countries. The Maritime Labour Convention (MLC) will be revised. Countries that will consider the incubation period of COVID-19 will also emerge in crew changes and it will be considered that the ship has not visited any port in the last 14 days. However, for those leaving the ship, there will also be a follow-up period and whether the crew leaving the ship experience any symptoms.
Cruise ships and maritime tourism will also suffer great-ly from this situation. Sectors such as these will be given
more care and attention because the rich people’s life is very valuable. This sector may suffer for a long time if the necessary measures are not taken.
“Electronic solutions” will enter our lives in a short time to make communication and transactions with the ship crew faster. E-signature will increase. Besides, if internet access can be provided anywhere in the world, which is the project of Elon Musk, human-ship control will be provided with camera systems. Over time, a great advance will be taken to accelerate the transition to a fully artificial intelligence ship control. Moreover, investment in transportation systems such as “hyperloop one” will be further increased and these studies will be given new momentum. This means that in the future time, it may leave some of the loads on maritime transport to a new system in a faster process than expected.
CONTAINER SHIPPING: SUCCESSFUL TURNAROUND
During the COVID-19, the freight and charter rates in the container shipping segment dropped by 4.76%. In 2019, about 5.99% of the fleet was out of service (compared with 2.86% in 2018). Ivanov estimated about 9% of container ship-ping fleet became idle due to COVID-19 [34]. In the meantime, prices (rates) have recovered, but they are still well below their record levels just before COVID-19. Although the next few years will see additional capacity introduced into the market — and especially in the very large container ship segment — demand is likely to grow faster than supply on average. The problem of overcapacity will therefore be mitigated. In 2021, charter rates could drop by significant double-digit percentage.
The medium-term outlook for the sector is intact. World seaborne container trade is likely to expand by an average of
www.intmarhealth.pl 259
Devran Yazır et al., Effects of COVID-19 on maritime industry: a review

7.44% in 2021. Container shipping is thus the fastest grow-ing mode of transport. The drivers remain the increasing international division of labour and productivity gains within the sector. All the same, container shipping increasingly finds itself faced with political and economic challenges and risks. These include stricter environmental regulation, capacity bottlenecks at ports, rising fuel prices and protec-tionist tendencies.
2020 SEES GLOBAL CONTAINER THROUGHPUT SINK FOR THE FIRST TIME
The US-China Trade War of 2018/2019 hit the global container shipping business hard. World seaborne container trade fell for the first time in the annals of the sector in 2020, contracting by –8.47%, according to Shipping Intelligence Network [35]. Prices (freight and charter rates) fell by 4.76%. At its height some 5.99% of the fleet (based on capacity in TEU) was laid up, which means that in 2019 about 300 ships had been taken out of service. International shipping lines suffered losses. The reasons for these losses are obvious: the global pandemic was marked by a slump in trading activities and investment. This had a knock-on effect on container shipping since the fortunes of the sector are very closely correlated with global trade developments.
From a regional standpoint it was the China ports that were particularly hard hit by the US-China Trade War and COVID-19. In 2019 container throughput increased by 4.4% at China ports and by 2.3% worldwide. The biggest decline of around 6% was posted by the West Coast of United States ports (Long Beach, Los Angeles, Seattle-Tacoma) that are small by international standards. Of the world’s 220 biggest ports, China suffered the decline at 5.7% [36]. The significant drop of China external trade was one major reason. Asian ports were less affected by the COVID-19, as the pandemic environment there was much less serious than in Europe and the United States. In both the Asia (excluding China) the de-crease in container throughput in 2020 was about 5.6% [36].
CONTAINER SHIPPING ENJOYS MULTIPLE ADVANTAGES
Before the slump in container throughput in 2019, the container sector posted very high growth rates. Between 2003 and 2018, for instance, global container throughput rose by an annual average rate of more than 35%. The dis-crepancy between the 2020 figure and the prior long-term performance highlights the scale of the COVID-19.
The reasons for the historically very high growth in con-tainer shipping include the increasing international division of labour and the growing liberalisation of world trade (e.g. China’s WTO accession in 2001). Furthermore, the share of goods that are ideal for shipping via container (semis and finished products) has risen steadily over the last few years,
and advances in container technology allow more and more goods to be transported via container (e.g. containers for refrigerated goods or liquids). In addition, container ships possess specific advantages over traditional general car-go freighters: shorter loading and unloading times reduce turnaround times in the port, which cuts costs. Also, the options for onward conveyance via other modes of transport are better with containers than with general cargo. Ever bigger and faster ships have enabled constant productivity gains, although the increase in capacity over recent years has cranked up the price pressure in the sector. Extensive investment in port infrastructure has been and remains essential for fast growth. Especially in Asia a very large number of container terminals have been expanded or built from scratch in the last few years.
CONTAINER SHIPPING CELEBRATES AN IMPRESSIVE COMEBACK
Global container shipping has managed a complete turn-around following the COVID-19. Global container through-put probably rose from approximately –8.47% in 2020 to +7.44% in 2021 [35]. The key factor in this recovery was the stock-building by the industrial sector and the swift economic recovery in many countries that was often driven by external trade. Particularly the upturn in Asia helped to get container shipping back on a growth track. The world’s leading exporter, China, will boost its shipments. Other Asian economies, too, will bolster the sector. Overall, container throughput in Asia probably increased in 2021, where-as North America and Western Europe are likely to have achieved only below average growth.
ASIA SETTING THE PACEThe focus of the global container shipping sector has
been steadily shifting outwards from China in any case over recent years. Some 70% of global container throughput is handled by ports in Asia. In 2019, nine out of the ten biggest container ports in the world were in Asia (namely, Shanghai, Singapore, Ningbo-Zhoushan, Shenzhen Guang-zhou, Busan, Hong Kong, Qingdao, and Tianjin). In the year 2004, the figure was 6 (namely, Hong Kong, Singapore, Shanghai, Shenzhen, Busan, and Kaohsiung). China was the dominant force in this respect, being home to 6 of the current top 10 ports. Looking at container trade by shipping route reveals that at least one port in Asia is involved in around 50% of all movements. This illustrates that global container shipping not only benefits from the manufacturing in Asia of consumer goods for Western Europe or the United States, but that in addition the trade links and the interna-tional division of labour between Asian countries have also increased significantly. There are individual ports that are highly specialised in the pure transshipment of containers,
Int Marit Health 2020; 71, 4: 253–264
www.intmarhealth.pl260

thus operating primarily as hubs for global and regional container shipping and handling relatively little local traffic. Overall, besides China there are smaller developing coun-tries and emerging markets (e.g. Malaysia, Vietnam, India) that are also continually investing in their port capacities.
OUTLOOK INTACT — LIMITING FACTORS IN VIEWAs previously mentioned, the short-term outlook for con-
tainer shipping remains bright with annual growth in contain-er throughput expected to average 7.44% in 2021. Going forward, momentum will continue to be generated by the established stalwarts: the continuing increase in the inter-national division of labour, rising incomes and consumption opportunities in many emerging markets and the thereby initiated trade flows are the most important drivers on the demand side. Rising incomes in important emerging markets — above all in China — may also enable the sector to mitigate the problem of unequal flows and thus reduce the share of empty container journeys; this would result in considerable cost savings. To date, on routes from China to Europe and the United States the share of laden containers is higher than on the return leg.
On the supply side productivity improvements suggest that container shipping will continue to post high growth rates. These include larger ships (and growing transship-ment shares) as well as more efficient loading and unloading systems at the terminals. In addition, the containerization level will increase worldwide; however, the containerisation level at many ports is already high, which makes a further increase virtually impossible. Slow steaming cancels out some of the productivity gains, unless high freight rates make faster speeds more economically lucrative.
Despite this generally rosy outlook the container shipping sector faces many challenges that may limit its growth potential:
— Maritime shipping is becoming the focus of national and international climate and environmental policy. Discus-sion is currently underway about a variety of measures that could mitigate the negative ecological impact of ship-ping (e.g. CO2 and pollutant emissions). These include emissions trading, efficiency standards or reducing the sulphur content in fuels. In the end, the shipping lines face higher costs because they will have to invest in their fleets in order to comply with the new standards. In addition, the sector’s competitiveness relative to oth-er modes of transport is declining. In terms of energy consumption per transported tonne, though, maritime shipping remains the most efficient mode of transport.
— Capacity bottlenecks at the ports (e.g. terminals, inland seaport traffic) can result in waiting times for contain-er ships as could often be observed, for instance, on the east coast of the emerging Asian countries before
the COVID-19. Insufficient shipping depths also act as a brake on the sector’s growth. The growing importance of very large container ships makes a deepening of the waterways/shipping lanes necessary at many ports (e.g. in India, Vietnam). The expansion of the port infrastruc-ture required by the transport industry often flounders because of financial limitations or political resistance.
— During the global recession after the COVID-19, pro-tectionist ideas will experience a renaissance in many countries. The danger that the liberalization of global trade becomes mired permanently is at least no lower now than before the COVID-19.
— The rising number of pirate attacks in several mari-time regions (recently off West Africa, IMB report 2020) means higher costs for ship owners, for instance for insurance or for modifying their ships (e.g. installing shelters for the crews) [37].
— Many seafarers have suffered the COVID-19. The availabil-ity of qualified nautical personnel is a medium to long-term challenge for the sector; personnel costs are set to rise.All in all, the container trade sector’s growth prospects
are subject to political challenges (US-China Trade War) and health challenges (COVID-19). Ultimately, however, global container shipping will remain the fastest growing mode of transport over the medium-term [38].
CRUISE SECTORThe cruise has become a popular international transporta-
tion mode with comfortable environment (e.g. entertainment services, restaurant, hotel, etc.) in recent years [39]. Gener-ally, one cruise can carry about 3,000 passengers at least in one trip (3–10 days or longer). It is argued that passengers easily contact each other through engaging social activities in the nearly close space during the trip. It is well known that coronavirus disease has brought significant risk in the cruise and the space characteristic of cruise has increased expan-sion speed of COVID-19 and brought potential risk of public health in the cruise related industries [6, 40–43].
Based on the report of Centres for Disease Control and Prevention (US), it is suggested that people with a high risk of serious illness should defer travel on cruise. Since year 2020, cruise has brought negative image for the public due to the effect of COVID-19 and consequently affected the operation strategies for the cruise companies and related industries (e.g. terminal operators). Basically, cruise com-panies will reduce revenue (e.g. ship tickets, passengers’ expenditure during onboard and onshore trips, terminal charging, etc.) affect the stock price of cruise industries when COVID-19 has continuously existed. Also, related industries (e.g. port authorities, travel agencies, tour bus companies, etc.) must adjust their service contents and operational strategies in order to reduce potential costs.
www.intmarhealth.pl 261
Devran Yazır et al., Effects of COVID-19 on maritime industry: a review

Regarding past research cases about cruise issues, in Taiwan, the one Diamond Princess Cruise Ship with high COVID-19 risk passengers docked at Keelung Port on 31 Jan-uary 2020 [5]. In Japan, the authorities have faced a similar problem when Diamond Princess Cruise Ship (carrying ap-proximately 3,700 passengers and crew) docked at Yoko-hama Port from 20 January to 9 February 2020 [44–46].
In the United States, there were 28.4 million for-eign-born workers in 2019 [47]. And these workers might come from hospitality workers who have contacted infected COVID-19 patients and potential people. In the United States, it is estimated that approximately 200 cruise passengers cases of COVID-19 were confirmed from multiple cruise ship voyages and this number has accounted for about 17% of total reported United States cases during February 3 — March 13, 2020 [48]. Sönmez et al. [49] also found that COVID-19 has resulted in mental and physical pressure on the health and safety of immigrant hospitality workers. Es-timates of the reproduction number (R0) for COVID-19 are crucial to understanding the health risk on board. Based on the Diamond Princess cruise ship where an outbreak occurred on a cruise ship, it is estimated that the value of reproductive number R0 ranges from 2.28 [50] to 14.8 [51].
In order to make sure the health and safety of cruise passengers and crew and avoid the expansion of COVID-19, four suggestions are provided below [41, 52–54].
First, the government authorities (e.g. public health au-thorities and hospitals) should enhance maritime medicine techniques, treatment, and health care for already infected people and implemented effective strategies to track poten-tially infected passengers and understand theirs’ contract history [e.g. (1) using big data to track the health status of all cruise passengers with potential contact; (2) using mobile sensor data for identifying the possible contacts; (3) Health Insurance Claims data should be strictly implemented for all cruise passengers and crew; (4) conducting preboarding screening for any potential risk people and material]. Sec-ond, the cruise ships must be equipped with suitable on-board medical facilities and qualified (available) profession-als (e.g. ship’s medical staff) around the clock 24/7 in order to provide initial medical care for (potentially) ill passengers and avoid disease transmission. Safety education training works for all crews and well information announcements for the passengers through public address systems should be strengthened in order to effectively respond to any emergen-cy clinical situations. Third, cruise companies should rethink their product strategies and attract potential customers through cooperation and brand management when such a global epidemic has been controlled and cruise industries have started to recover in the future. Finally, cruise com-panies and government authorities should strengthen risk management abilities through effective regulation rules in
order to prevent any potential or new threat (such as the sudden global emergence of COVID-19 illness) in the future. Also, resilience building is important for cruise stakeholders (e.g. cruise companies, port operators, supply chain opera-tors, insurance companies, etc.) to maintain current profit or reduce potential loss in an uncertain market environment.
CONCLUSIONSThe maritime industries are critical in the global econo-
my and social well-being. This review has provided a timely and relevant study to understanding the four major sectors in maritime industries with practical insights. It has con-ducted a systematic and concise overview of contemporary issues of maritime operations and management. It attempts to conclude with a useful discussion of challenges and disruptions that are being faced by the maritime industries.
The COVID-19 has already brought significant impacts on maritime industries since early 2020. Based on the literature, this paper has overviewed recent industries de-velopment trends, new challenges and potential solutions regarding dry bulk, tanker, container and cruise sectors. Two research findings are summarised below.
First, the operators (e.g. shipowners, exporters, importers, terminal operators, shipping carriers, etc.) of these indus-tries have faced operational losses and inconvenience due to health and safety consideration. For example, seafarers or passengers who entered or departed from international ports must be detected and received mandatory investigation and/or strictly quarantined for 14 days due to incubation of vi-rus. These restrictions and regulations have inevitably affected the freight rates, charter rates, revenues and earnings as well as the utilisation of facilities and human resources. In particu-lar, the cruise industries have faced huge losses since the cab-ins, nearly closed space, might increase the risk of COVID-19 infection. Second, it is believed that effective Port State In-spections based on IMO conventions and big data applica-tions could reduce potential operation risk in the era post the COVID-19 and provide successful turnaround opportunities.
ACKNOWLEDGEMENTSThis research has been partially supported by the Ministry of
Science and Technology, Taiwan (MOST109-2410-H-019-027) and The Hong Kong Polytechnic University (G-UAFE).
We also would like to thank Prof. Dr. Ahmet Soylu for his su-pervision, and the Norwegian University of Science and Technol-ogy (NTNU) for hosting Dr. Bekir Sahin to conduct his research.
REFERENCES1. International Maritime Organization (IMO). (2020). Circular Letter
No.4204/Add.1. http://www.imo.org/en/MediaCentre/HotTopics/Documents/CL.4204-Add.1%20English.pdf (Retrieved September 20, 2020).
Int Marit Health 2020; 71, 4: 253–264
www.intmarhealth.pl262

2. Worldmeter (2020). Reported cases and deaths by country, terri-tory or conveyance. https://www.worldometers.info/coronavirus/ (Retrieved September 30, 2020).
3. McKibbin WJ, Fernando R. The Global Macroeconomic Impacts of COVID-19: Seven Scenarios. 2020. CAMA Working Paper No. 19/2020.
4. Sismanyazıcı H. (2020). Koronavirus dünya ekonomisini sallıyor. 7deniz Dergisi. 44, 18-22. https://issuu.com/7denizdergisi/docs/7_deni_z_44_e_dergi_ (Retrieved May 25, 2020).
5. Chen CM, Jyan HW, Chien SC, et al. Containing COVID-19 Among 627,386 Persons in Contact With the Diamond Princess Cruise Ship Passengers Who Disembarked in Taiwan: Big Data Analytics. J Med Internet Res. 2020; 22(5): e19540, doi: 10.2196/19540, indexed in Pubmed: 32353827.
6. Dahl E. Coronavirus (Covid-19) outbreak on the cruise ship Dia-mond Princess. Int Marit Health. 2020; 71(1): 5–8, doi: 10.5603/MH.2020.0003, indexed in Pubmed: 32212140.
7. Bhosale J. (2020). Prices of agricultural commodities drop 20% post COVID-19 outbreak. https://economictimes.indiatimes.com/news/economy/agriculture/prices-of-agricultural-commodi-ties-drop-20-post-covid-19outbreak/articleshow/74705537.cms (Retrieved September 30, 2020).
8. Gray R. Agriculture, transportation, and the COVID‐19 crisis. Canadian Journal of Agricultural Economics/Revue canadienne d’agroeconomie. 2020; 68(2): 239–243, doi: 10.1111/cjag.12235.
9. The Guardian (2020). MPs in plea to government over UK’s COVID-19 stockpiling, World news, The Guardian. https://www.theguardian.com/world/2020/mar/21/mps-plea-government-uk-covid-19-stock-piling-coronavirus/ (Retrieved September 21, 2020).
10. BBC News (2020). Online shopping website Ocado suspends ser-vice. https://www.bbc.com/news/business-51941987/ (Retrieved September 22, 2020).
11. BBC News (2020). Stockpiling ‘will hit vulnerable’, food bank warns. https://www.bbc.com/news/uk-england-beds-bucks-herts51856592 (Retrieved September 22, 2020).
12. Michael Bourke MK. (2020). Potential response to COVID-19 in PNG: support for food production. https://devpolicy.org/potential-re-sponse-to-covid-19-in-pngsupport-for-food-production-20200421-1 (Retrieved September 26, 2020).
13. Tantau M. (2020). Is Indonesia Facing a Looming Food Crisis? The Diplomat. 5 May. https://thediplomat.com/2020/05/is-indone-sia-facing-a-looming-food-crisis/ (Retrieved September 22, 2020).
14. CDC COVID-19 Response Team. Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19) - United States, February 12-March 16, 2020. MMWR Morb Mortal Wkly Rep. 2020; 69(12): 343–346, doi: 10.15585/mmwr.mm6912e2, indexed in Pubmed: 32214079.
15. Nicola M, Alsafi Z, Sohrabi C, et al. The socio-economic implica-tions of the coronavirus pandemic (COVID-19): A review. Int J Surg. 2020; 78: 185–193, doi: 10.1016/j.ijsu.2020.04.018, indexed in Pubmed: 32305533.
16. Hurst P, Termine P, Karl M. Agricultural workers and their contribu-tion to sustainable agriculture and rural development. FAO-ILO-IUF. ILO, Geneva 2005.
17. Arifin MD. (2020). Impacts of Coronavirus COVID-19 on the Global Shipping and Maritime Industry in Indonesia and How to Overcome the Coronavirus Outbreak Based on WHO and IMO recommenda-tions, Project: Coronavirus COVID-19. https://doi.org/10.31224/osf.io/6wy5c (Retrieved September 20, 2020).
18. Shih W (2020). COVID-19 and global supply chains: Watch out for bullwhip effects. Forbes. https://www.forbes.com/sites/wil-lyshih/2020/02/21/covid-19-and-global-supply-chains-watch-out-
for-bullwhip-effects/?sh=87e70d971951 (Retrieved September 27, 2020).
19. North (2020). COVID-19: Coronavirus Outbreak – Impact on Shipping *Update*, 15 April. https://www.nepia.com/ industry-news/corona-virus-outbreak-impact-on-shipping/ (Retrieved September 24, 2020).
20. Kim K., Kim S., Park C.-Y. Food Security in Asia and the Pacific amid the COVID-19 Pandemic, ADB Briefs 2020, No. 139.
21. Food and Agriculture Organization (FAO). (2020). Local food systems and COVID-19; A glimpse on India’s responses. http://www.fao.org/in-action/food-for-cities-programme/news/detail/en/c/1272232/ (Retrieved September 23, 2020).
22. Shulang Fei JN. (2020). Local food systems and COVID-19: A look into China’s responses. http://www.fao.org/in-action/food-for-cities-programme/news/detail/en/c/1270350/ (Retrieved September 23, 2020).
23. Economics T. (2020). Baltic Exchange Dry Index. https://tradingeco-nomics.com/commodity/baltic (Retrieved September 23, 2020).
24. Javorcik B. 8-Global supply chains will not be the same in the post-COVID-19 world. COVID-19 and Trade Policy: Why Turning Inward Won’t Work. CEPR Press, 2020, p. 111.
25. Warning S. (2020). Coronavirus pandemic. https://www.scien-tistswarning.org/2020/06/04/coronavirus-pandemic/ (Retrieved October 01, 2020).
26. For Reconstruction, E. B., Development (2020). COVID-19: from shock to recovery. Regional economic prospects April 2020.
27. 7deniz (2020). STK’lardan AB’ye mektup, 7deniz Dergisi, 44, 74-75. https://issuu.com/7denizdergisi/docs/7_deni_z_44_e_dergi_ (Retrieved September 25, 2020).
28. 7deniz (2020). BIMCO: Gemi inşa siparişleri düşüyor, 7deniz Dergisi, 44, 52. https://issuu.com/7denizdergisi/docs/7_deni_z_44_e_dergi_ (Retrieved September 25, 2020).
29. Miller G. (2020). Tanker craziness continues as product carriers hit record high. Clarkson’s platou securities. https://www.freightwaves.com/news/tanker-craziness-continues-as-product-carriers-hit-re-cord-high (Retrieved September 26, 2020).
30. Miller G. (2020). Tanker veteran warns on rates: The storm is coming. https://www.freightwaves.com/news/tanker-veteran-warns-on-rates-the-storm-is-coming (Retrieved September 26, 2020).
31. Miller G. (2020). Tanker stocks surge as global oil market collapses. https://www.freightwaves.com/news/tanker-stocks-surge-as-global-oil-market-collapses (Retrieved September 26, 2020).
32. Miller G. (2020). Today’s Pickup: Shell expects to see LNG demand double by 2040. https://www.freightwaves.com/news/todays-pickup-shell-expects-to-see-lng-demand-double-by-2040 (Retrieved September 26, 2020).
33. Webber Research & Advisory (2020). Tanker stocks could emerge as COVID-19 relapse hedge. https://www.freightwaves.com/news/tanker-stocks-could-emerge-as-covid-19-relapse-hedge (Retrieved September 20, 2020).
34. Ivanov D. Predicting the impacts of epidemic outbreaks on global supply chains: A simulation-based analysis on the coronavirus out-break (COVID-19/SARS-CoV-2) case. Transp Res E Logist Transp Rev. 2020; 136: 101922, doi: 10.1016/j.tre.2020.101922, indexed in Pubmed: 32288597.
35. Shipping Intelligence Network (2020). Shipping intelligence network. https://sin.clarksons.net/ (Retrieved September 20, 2020).
36. Drewry (2020). Drewry. https://www.drewry.co.uk/ (Retrieved September 21, 2020).
37. Wong MC, Yip TL. Maritime piracy: an analysis of attacks and violence. Int J Shipp Transp Log. 2012; 4(4): 306, doi: 10.1504/ijstl.2012.049315.
www.intmarhealth.pl 263
Devran Yazır et al., Effects of COVID-19 on maritime industry: a review

38. Wong MC, Yip TL. Influence of transportation infrastructure on the relationship between institutions and economic performance. Marit Business Rev. 2019; 4(4): 395–412, doi: 10.1108/mabr-09-2019-0038.
39. Kang J. Identifying antecedents and consequences of well-being: The case of cruise passengers. Tourism Management Perspectives. 2020; 33: 100609, doi: 10.1016/j.tmp.2019.100609.
40. Cruise Lines International Association (2020). CLIA announces voluntary suspension in US cruise operations. Washington, DC. Cruise Line International Association. https://cruising.org/en/News-and-Research/Press-Room/2020/August/CLIA-Announc-es-Third-Voluntary-Suspension-of-US-Cruise-Operations (Retrieved September 19, 2020).
41. Mizumoto K, Chowell G. Transmission potential of the novel coronavirus (COVID-19) onboard the diamond Princess Cruises Ship, 2020. Infect Dis Model. 2020; 5: 264–270, doi: 10.1016/j.idm.2020.02.003, indexed in Pubmed: 32190785.
42. World Health Organization (WHO) (2020). Situation report-141 coronavirus disease 2019 (COVID-19) 9 June 2020. Geneva. WHO. https://www.who.int/emergencies/diseases/novel-corona-virus-2019/situation-reports/ (Retrieved September 29, 2020).
43. Zhu Na, Zhang D, Wang W, et al. China Novel Coronavirus Investi-gating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med. 2020; 382(8): 727–733, doi: 10.1056/NEJMoa2001017, indexed in Pubmed: 31978945.
44. Ministry of Health, Labour and Welfare (2020). The first case of novel coronavirus infection in Japan, Tokyo. Ministry of Health, Labour and Welfare. https://www.mhlw.go.jp/stf/newpage_08906.html (Retrieved September 29, 2020).
45. National Institute of Infectious Diseases (NIID). (2020). Manual of laboratory diagnosis of novel coronavirus. Japan, Tokyo. NIID. https://www.niid.go.jp/niid/ja/labo-manual.html#class0 (Retrieved September 23, 2020).
46. Yamagishi T, Kamiya H, Kakimoto K, et al. Descriptive study of COVID-19 outbreak among passengers and crew on Diamond Prin-cess cruise ship, Yokohama Port, Japan, 20 January to 9 February 2020. Euro Surveill. 2020; 25(23), doi: 10.2807/1560-7917.ES.2020.25.23.2000272, indexed in Pubmed: 32553062.
47. BLS (2020). The employment situation — March 2020. Bureau of Labor Statistics, US Department of Labor. https://www.bls.gov/news.release/archives/empsit_04032020.htm (Retrieved September 27, 2020).
48. CDC (2020). Coronavirus disease 2019 (COVID-19): Cases in US Atlanta, GA: US Department of Health and Human Services, United States Centers for Disease Control and Prevention (CDC). https://www.cdc.gov/coronavirus/2019-ncov/cases-in-us.html (Retrieved September 28, 2020).
49. Sönmez S, Apostolopoulos Y, Lemke MK, et al. Understanding the effects of COVID-19 on the health and safety of immigrant hospitality workers in the United States. Tour Manag Perspect. 2020; 35: 100717, doi: 10.1016/j.tmp.2020.100717, indexed in Pubmed: 32834958.
50. Zhang S, Diao M, Yu W, et al. Estimation of the reproductive number of novel coronavirus (COVID-19) and the probable outbreak size on the Diamond Princess cruise ship: A data-driven analysis. Int J Infect Dis. 2020; 93: 201–204, doi: 10.1016/j.ijid.2020.02.033, indexed in Pubmed: 32097725.
51. Rocklöv J, Sjödin H, Wilder-Smith A. COVID-19 outbreak on the Diamond Princess cruise ship: estimating the epidemic potential and effectiveness of public health countermeasures. J Travel Med. 2020; 27(3), doi: 10.1093/jtm/taaa030, indexed in Pubmed: 32109273.
52. Geldsetzer P. Knowledge and Perceptions of COVID-19 Among the General Public in the United States and the United King-dom: A Cross-sectional Online Survey. Ann Intern Med. 2020; 173(2): 157–160, doi: 10.7326/M20-0912, indexed in Pubmed: 32196071.
53. Kakimoto K, Kamiya H, Yamagishi T, et al. Initial Investigation of Transmission of COVID-19 Among Crew Members During Quarantine of a Cruise Ship - Yokohama, Japan, February 2020. MMWR Morb Mortal Wkly Rep. 2020; 69(11): 312–313, doi: 10.15585/mmwr.mm6911e2, indexed in Pubmed: 32191689.
54. Subramanian S. (2020). The Ordeal of the Diamond Princess Crew. The Diplomat 22 February. https://thediplomat.com/2020/02/the-ordeal-of-the-diamond-princess-crew/ (Retrieved September 22, 2020).
Int Marit Health 2020; 71, 4: 253–264
www.intmarhealth.pl264

Dr. Marcus Oldenburg, Institute for Occupational and Maritime Medicine, University Medical Centre Hamburg-Eppendorf (UKE), Seewartenstrasse 10, 20459 Hamburg,
Germany, tel: +49 40 428 374 308, fax: +49 40 427 311 393, e-mail: [email protected]
Prevalence of alcohol consumption among seafarers and fishermen
Elisabeth Stoll1, Klaus Püschel2, Volker Harth1 , Marcus Oldenburg1
1Institute for Occupational and Maritime Medicine Hamburg (ZfAM), University Medical Centre Hamburg-Eppendorf (UKE), Hamburg, Germany
2Department of Legal Medicine, University Medical Centre Hamburg-Eppendorf, Hamburg, Germany
ABSTRACTBackground: Over the decades, several published studies showing the relevance of alcohol use among seafarers/fishermen have highlighted the dangers of alcohol consumption during working time. The present study aims to provide an up-to-date overview of the prevalence of alcohol consumption among seafarers/fishermen. It also points out their consumption behaviour, depending on socio-demographic and job-related factors.Materials and methods: To detect relevant studies for this systematic review, the electronic database PubMed was searched. All identified studies published between January 2014 and September 2019 were included using the subsequent terms: (alcohol OR ethanol) AND (seafarer OR fishermen OR ship crew OR merchant ship).Results: According to the applied search string, 18 studies were identified. Thirteen of them were selected for this review. The results of the studies about alcohol consumption among seafarers and fishermen showed a wide range of prevalence, from 11.5% to 89.5% (median 53.0%). Concerning seafarers no stratified data were available for further analyses. Among fishermen alcohol consumption has decreased over the period examined (56.9% [2010–2014] vs. 42.3% [2015–2018]). The evaluation of socio-demographic factors showed alcohol consumption was less prevalent in fishermen > 60 years (15.0%). Furthermore, a higher prevalence of alcohol intake was found in those with a lower education (63.9%). In respect of job-related data, 61.0% of the alcohol consuming fishermen reported they had been involved in an accident due to alcohol consumption.Conclusions: The consumption of alcohol among fishermen has declined over time. Compared with the land-based European population, seafarers and fishermen show a lower prevalence of alcohol use, at least during their stay on board. Due to the limited data available — especially concerning seafarers — further studies on the prevalence of alcohol consumption among shipboard crews are recommended. In particular, these should provide more data on alcohol consumption related to socio-demographic and job-related factors.
(Int Marit Health 2020; 71, 4: 265–274)
Key words: seafarer, fishermen, alcohol, drugs, dependence
�
INTRODUCTIONAccording to the World Health Organization (WHO) Global
Status Report 2018 [1] on current drinkers, more than half of the population in America, Europe and the West Pacific aged ≥ 15 consumed alcohol. The highest total alcohol consumption of 9.8 litres per capita per year was observed among Europeans [1]. In 2016, about 3 million people
worldwide died from hazardous alcohol intake. There are more deaths related to alcohol than to tuberculosis (TBC), human immunodeficiency virus/acquired immune deficien-cy syndrome (HIV/AIDS) or diabetes [1].
Over the decades, some studies have been published showing the prevalence of alcohol use among seafarers. One of the most extensive reviews on this topic, performed by
www.intmarhealth.pl 265
Int Marit Health 2020; 71, 4: 265–274
10.5603/IMH.2020.0045 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
REV IEW ART ICLE
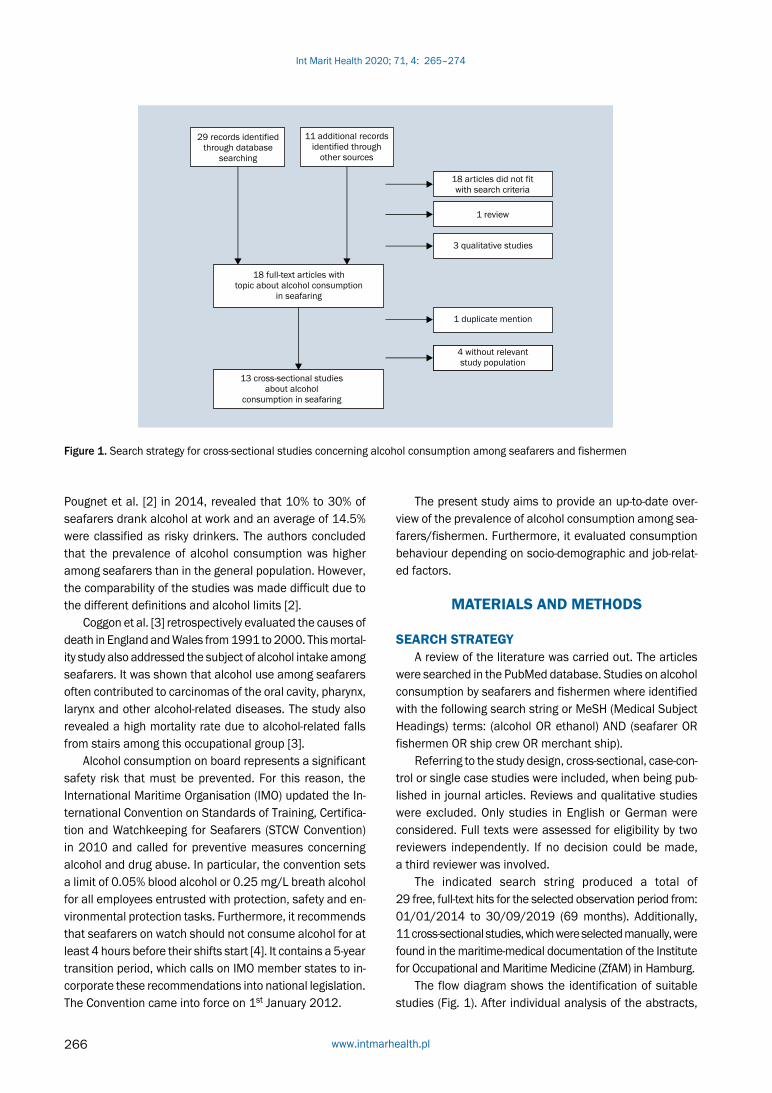
Pougnet et al. [2] in 2014, revealed that 10% to 30% of seafarers drank alcohol at work and an average of 14.5% were classified as risky drinkers. The authors concluded that the prevalence of alcohol consumption was higher among seafarers than in the general population. However, the comparability of the studies was made difficult due to the different definitions and alcohol limits [2].
Coggon et al. [3] retrospectively evaluated the causes of death in England and Wales from 1991 to 2000. This mortal-ity study also addressed the subject of alcohol intake among seafarers. It was shown that alcohol use among seafarers often contributed to carcinomas of the oral cavity, pharynx, larynx and other alcohol-related diseases. The study also revealed a high mortality rate due to alcohol-related falls from stairs among this occupational group [3].
Alcohol consumption on board represents a significant safety risk that must be prevented. For this reason, the International Maritime Organisation (IMO) updated the In-ternational Convention on Standards of Training, Certifica-tion and Watchkeeping for Seafarers (STCW Convention) in 2010 and called for preventive measures concerning alcohol and drug abuse. In particular, the convention sets a limit of 0.05% blood alcohol or 0.25 mg/L breath alcohol for all employees entrusted with protection, safety and en-vironmental protection tasks. Furthermore, it recommends that seafarers on watch should not consume alcohol for at least 4 hours before their shifts start [4]. It contains a 5-year transition period, which calls on IMO member states to in-corporate these recommendations into national legislation. The Convention came into force on 1st January 2012.
The present study aims to provide an up-to-date over-view of the prevalence of alcohol consumption among sea-farers/fishermen. Furthermore, it evaluated consumption behaviour depending on socio-demographic and job-relat-ed factors.
MATERIALS AND METHODS
SEARCH STRATEGYA review of the literature was carried out. The articles
were searched in the PubMed database. Studies on alcohol consumption by seafarers and fishermen where identified with the following search string or MeSH (Medical Subject Headings) terms: (alcohol OR ethanol) AND (seafarer OR fishermen OR ship crew OR merchant ship).
Referring to the study design, cross-sectional, case-con-trol or single case studies were included, when being pub-lished in journal articles. Reviews and qualitative studies were excluded. Only studies in English or German were considered. Full texts were assessed for eligibility by two reviewers independently. If no decision could be made, a third reviewer was involved.
The indicated search string produced a total of 29 free, full-text hits for the selected observation period from: 01/01/2014 to 30/09/2019 (69 months). Additionally, 11 cross-sectional studies, which were selected manually, were found in the maritime-medical documentation of the Institute for Occupational and Maritime Medicine (ZfAM) in Hamburg.
The flow diagram shows the identification of suitable studies (Fig. 1). After individual analysis of the abstracts,
Figure 1. Search strategy for cross-sectional studies concerning alcohol consumption among seafarers and fishermen
Int Marit Health 2020; 71, 4: 265–274
www.intmarhealth.pl266

18 articles did not fit with the search criteria. Furthermore, one review about this topic was excluded. Three more stud-ies were precluded because of their qualitative study design.
In total, 18 cross-sectional studies were identified and the full text of all these articles has been reviewed. Four studies were excluded as they did not rely on seafarers, fishermen or crews of merchant ships. Another one was precluded because of duplicate mention.
All identified cross-sectional studies were analysed in respect of the examined study population, the definition of alcohol, the prevalence of alcohol consumption among sea-farers/fishermen and their alcohol consumption depending on socio-demographic and job-related factors.
AUDITTwo of the examined articles [5, 6] used Alcohol Use
Disorder Identification Test (AUDIT) as a standardized questionnaire survey. AUDIT serves to identify persons with hazardous and harmful patterns of alcohol consumption. It was first published in 1989 by the WHO [7]. The ques-tionnaire also provides a framework for interventions to help hazardous and harmful drinkers to reduce or stop drinking and thus to avoid the harmful consequences of their alcohol intake. Addiction to alcohol and specific con-sequences of harmful alcohol consumption can also be identified with the help of AUDIT, which is consistent with the ICD-10 definitions of alcohol dependence and harmful alcohol use. The survey consists of 10 questions, with the following themes: recent alcohol consumption, dependence symptoms and alcohol-related problems [7]. Five possible answers, with a rating score from 0 to 4, are given for each of these 10 questions. The maximum score is 40. If the to-tal score exceeds 8 points, hazardous and harmful alcohol consumption as well as possible alcohol dependency are proposed as results. In some studies with a greater range of subjects with alcohol-related problems, the following limits for specific measures are recommended:
— results between 8 and 15 points are suitable for simple advice focusing on reducing hazardous alcohol con-sumption;
— values between 16 and 19 indicate short consultation and continuous monitoring;
— AUDIT values of 20 or more clearly justify further diag-nostic evaluation of alcohol dependence.
AUDIT-CAnother study [8] used, inter alia, AUDIT-consumption
questions (AUDIT-C) to assess the health risks of alcohol consumption. AUDIT-C is a modified short version of the AUDIT questionnaire survey and was designed to identify hazardous and harmful alcohol intake in primary care [9]. AUDIT-C contains the first three questions of AUDIT. Five
possible answers with a rating score from 0 to 4 are given for each question. The maximum score is 12. The test is con-sidered as positive if the score exceeds the following values:
— ≥ 5 for men; — ≥ 4 for women.
The resulting suspicion of harmful and dangerous al-cohol consumption or even alcohol dependence should be confirmed by an additional AUDIT [9].
RESULTS
CHARACTERISTICS AND METHODS OF SELECTED ARTICLES
The study populations of the selected articles were investigated between 2010 and 2018. The populations ranged from 136 to 2,060 participants (median 835). The average age of the participants ranged from 36.1 years to 53 years (median 40 years). Four of the 13 studies were conducted in Morocco, 2 studies in India, 1 study each was investigated in France, Croatia, Greece, Denmark, the Seychelles and the Philippines and 1 study was carried out anonymously. Eight of the 13 studies were conducted among fishermen [5, 6, 8, 10–14] and 5 among seafarers [15–19].
Three [5, 6, 11] of the 13 studies investigated the con-sumption of alcohol among seafarers and fishermen as the main question (Table 1). Ten studies focused on a different question and surveyed alcohol consumption only as an accompanying parameter or risk factor.
Six of the 13 identified studies did not define the mean-ing of alcohol consumption (Table 1) [10–13, 17, 18]. Based on AUDIT, 2 studies defined alcohol intake among users [5, 6]. Fort et al. [8] used AUDIT-C to show the possible dependence on alcohol, and they used an alcohol consump-tion profile to show consumers with excessive (67.7%) and without excessive (21.8%) profiles [8]. The other 4 studies applied individual questionnaires with various and het-erogeneous definitions of alcohol consumption (Table 1) [14–16, 19]. Slišković and Penezić [15], for example, re-quested the amount (standard drink unit/typical day) and frequency of alcohol intake.
PREVALENCE OF ALCOHOL CONSUMPTION The prevalence of alcohol consumption among sea-
men showed a wide range from 11.5% to 89.5% (median 53.0%) [5, 6, 8, 10–17], with differences in respect of the occupational group; fishermen ranged from 35.4% to 89.5% (median 47.7%) vs. seafarers from 11.5% to 79.4% (median 58.5%). With an overall prevalence of alcohol consumption among seafarers of only 11.5%, the study by Mahdi et al. [18] was significantly different from other studies.
www.intmarhealth.pl 267
Elisabeth Stoll et al., Alcohol consumption among seafarers and fishermen

Table 1. Characteristics and methods of selected articles
Author (year)
Aim of the study Population Year of inve-stigation
Methods Definition of alcohol
Laraqui et al. (2017)
To determine the preva-lence of the use and misuse of addictive substances in fisher-men
1,219 male fisher-men of Morocco
2014 AUDIT Alcohol consumption is quantified by the number of standard drinks containing a fixed amount of 10 g of pure alcohol per day (toxic habits) [drink of 10 cL table wine at 12° = drink of 25 cL of beer at 5° = drink of 3 cL of whisky at 40° = drink of 7 cL of aperitif at 18°]. Among drinkers AUDIT was used. A score ≥ 8 is considered to indicate hazardo-us or harmful alcohol use. The authors also assumed a misuse (dependence) if the AUDIT score exceeded ≥ 8
Kumar et al. (2018)
To assess:(a) harmful alcohol use and dependence on alcohol(b) socio-demographic factors associated with harmful alcohol use and probable dependence among alcohol users
304 fishermen of South India
02/2015 AUDIT An AUDIT score ≥ 8 was considered as “harm-ful use of alcohol”. An AUDIT score ≥ 20 was considered as “probable dependence on al-cohol”. The questionnaire focused on alcohol use within the past 1 year
Fort et al. (2016)
To evaluate the use of cannabis and cocaine among fishermen
1,024 French fishermen (1,009 males; 15 females)
02/2012– 03/2013
AUDIT-C and alco-hol con-sumption profile
AUDIT-C: an addiction to alcohol is possible for a score ≥ 5 for men and ≥ 4 for women. Alco-hol consumption profile: (a) non-consumers: those who never drink, (b) consumers without excessive alcohol risk: those who never drink ≤ 6 glasses on a single occasion AND ≤ 14 drinks/week for woman, ≤ 21drinks/week for men (c) consumers with an excessive alcohol risk: one of the two following conditions have to be met: drinking ≥ 15 glasses/week for women, ≥ 22 glasses/week for men OR ≥ 6 glasses on one occasion more frequently than once a month
Slišković and Penezić (2016)
To compare the preva-lence of various lifesty-le factors during stay on board ship and on shore
530 Croatian seafarers
2014 Individual question-naire
Alcohol consumption was measured with ques - tions about frequency and quantity. Quantity was measured as standard drink unit/typical day. The standard drink unit was defined as 1 beer (330 mL), 1 glass of wine (140 mL) or 1 measure of a spirit (40 mL)
Laraqui et al. (2018)
To assess the stress in fishermen by analysing its relationship with sociodemographic and professional characte-ristics and evaluating work stressors
828 fishermen of Northern Morocco
01–04/2018 Individual question-naire
Alcohol consumption was not defined
Rane et al. (2016)
To assess the preva-lence of tobacco and alcohol consumption among fishermen
825 fishermen from Udupi Taluk (India)
01–06/2015 Individual question-naire
Alcohol consumption was not defined
Anzil et al. (2016)
To assess the prevalen-ce of deleterious habits and oral mucosal le-sions among fishermen
362 fishermen of Mahe, Seychelles (266 males; 96 female)
Interview by a trained interviewer
Alcohol consumption was not defined
Gregorio et al. (2016)
To determine the know-ledge, attitudes and practices related to car-diovascular diseases of Filipino seafarers
136 male Filipino seafarers
02–03/2010 Individual question-naire
The consumption of alcohol was surveyed in relation to the past 4 weeks and the number of times in which the respondents drank alco-hol during the specified period
Æ
Int Marit Health 2020; 71, 4: 265–274
www.intmarhealth.pl268

Author (year)
Aim of the study Population Year of inve-stigation
Methods Definition of alcohol
Laraqui et al. (2017)
To investigate the potential fishermen’s psychological functio-ning which induces risk taking behaviours
1,413 traditional fishermen 1,049 administrative staff on land of Northern Morocco
2016 Individual question-naire
Alcohol consumption was not defined
Laraqui et al. (2017)
To assess the know-ledge, attitudes and practices of seafarers in relation to sexually transmitted infections
1,376 male sailors of Northern Morocco
2014 Individual question-naire
Alcohol consumption was not defined
Mahdi et al. (2016)
To assess the habits and problems of dental hygiene of seafarers as well as their attitudes
2,060 seafarers who asked Centro Internazionale Radio Medico for medical advice
01.07.2014– 31.10.2014
Individual question-naire
Alcohol consumption was not defined
Tu and Jap-sen (2016)
To address the preva-lence of hypertension among Danish seafa-rers and discuss poten-tial risk factors for hy-pertension in maritime settings
629 Danish seafarers
10/2011– 06/2012
Individual question-naire
Alcohol consumption was defined as beverages per week at home: (a) 1–7 beverages, (b) 8–14 beverages, (c) > 15 beverages
Frantzeskou et al. (2016)
To examine the health status and the health risk factors present in Greek fishery workers by exploring their wor-king environment
161 Greek fisher-men
08/2013– 11/2013
Individual question-naire
The daily alcohol consumption was divided into (a) ≥ 300 mL/day and (b) ≥ 500 mL/day
AUDIT — Alcohol Use Disorder Identification Test; AUDIT-C — AUDIT-consumption questions
Table 1. cont. Characteristics and methods of selected articles
The prevalence of alcohol consumption among fish-ermen showed a median of 56.9% in the investigation period from 2010 to 2014 and a median of 42.3% between 2015 and 2018. Concerning seafarers, no stratified data were available for further analyses.
Based on AUDIT, Kumar et al. [5] revealed a prevalence of harmful alcohol use of 60.8% among fishermen of South India. In this study, the prevalence of dependence was 9.9% [5] compared to Laraqui et al. [6], who also used AUDIT and reported a prevalence of dependence of 19.0% among fishermen of Morocco. Fort et al. [8] showed that 33.9% of French fishermen had a positive AUDIT-C and 67.7% an excessive alcohol consumption profile. Other studies, for example Slišković and Penezić [15], showed a significantly higher prevalence of alcohol consumption among Croatian seafarers at home (93.0%) than on board (55.5%). Tu and Jepsen [19] also showed a high prevalence of alcohol intake among Danish seafarers at home (71.9%).
ALCOHOL CONSUMPTION DEPENDING ON SOCIO--DEMOGRAPHIC CHARACTERISTICS
Only three of the examined studies provided data on the alcohol use in relation to the seafarers’ age. The study
by Laraqui et al. [6] revealed that fishermen younger than 40 years more often had (64.9%) toxic alcohol consumption. Furthermore, 64.2% of these subjects were regarded to be alcohol-dependent [6]. Kumar et al. [5] revealed a high prev-alence of alcohol consumption among fishermen in the age groups 19–39 (44.8%) and 40–59 (49.0%), but to a less extent in older fishermen (> 60 years; 15.0%) [5]. Rane et al. [11] observed a high alcohol use, in particular, in fishermen aged 29–38 years (35.9%) compared to younger and old-er fishermen.
Only 3 studies gave information about alcohol con-sumption in relation to the educational level of the sea-farers. All the studies demonstrated that subjects with secondary or high school education were characterised by a lower alcohol intake, compared to those seafarers with a primary educational level [5, 6, 11]. This result was also evident among the seafarers defined as de-pendent [6].
The greatest co-dependency among seafarers examined by four studies was found in the combination of alcohol and tobacco (6.1%, 11.8%, 22.9%, 80.9%) [6, 11, 12, 18]. The combined use of other substances such as alcohol and cannabis was rather low at 3.8% (Table 2) [6].
www.intmarhealth.pl 269
Elisabeth Stoll et al., Alcohol consumption among seafarers and fishermen

Table 2. Prevalence of alcohol consumption depending on socio-demographic factors
Author (y) Prevalence of alcohol consumption Co-dependence Educational level Prevalence of alcohol consumption in relation to age [y]
Laraqui et al. (2017)
The prevalence of toxic alcohol was 36.5% (445/1,219). In relation to all examined parti-cipants the misuse (dependence) was 19.0% (232/445). Among consumers, the prevalence of misuse (dependence) was 52% (232/445)
Toxic habit:T + A = 6.1%A + C = 3.8%T + C + A = 4.5%T + A + OPS = 3.4%C + A + OPS = 0.6%T + A + C + OPS = 1.9%
Toxic habits: Illiterate 13.4% Primary 52.4% Secondary 34.2% Superior 0.0% Misuse/dependence: Illiterate 18.5% Primary 47.4% Secondary 34.4% Superior 0.0%
Toxic habits: < 40 y — 64.9% ≥ 40 y — 35.1% Misuse/depen-dence: < 40 y — 64.2% ≥ 40 y — 35.8%
Kumar et al. (2018)
79% (241/304) of fishermen reported alcohol consumption in the past 1 year. In relation to the participants the prevalence of harmful use was 60.8% (185/304) and of probable dependence 9.9% (30/304). Among consumers, the preva-lence of harmful use was 76.8% (185/241) and probable alcohol dependence 12.4% (30/241)
Participants reported alcohol consumption in the past 1 year: Illiterate 17.8% Primary and middle school 46.1%High school and above 36.1%
Participants repor-ted alcohol con-sumption in the past 1 year: 19–39 y — 44.8% 40–59 y — 49.0% ≥ 60 y — 15.0%
Fort et al. (2016)
89.5% (917/1,024) of fishermen reported alcohol consumption. 33.9% (350/1,024) were positive according to AUDIT-C. Alcohol con-sumption profile: (a) 10.5% (107/1,024); (b) 21.8% (208/1,024); (c) 67.7% (709/1024)
Slišković and Penezić (2016)
55.5% (294/530) of seafarers reported alcohol consumption on board compared to 93.0% (492/530) at home. Weekly and daily alcohol use on board was less frequent than at home (18.0% vs. 42.0%). Alcohol quantity shows gre-ater prevalence of zero consumption of alcohol in a typical day on board (58.3%) than in the home situation (24.2%)
Laraqui et al. (2018)
35.4% (293/828) of fishermen reported alco-hol consumption
Rane et al. (2016)
45.6% (376/825) of fishermen reported alco-hol consumption
22.9% had a habit of using tobacco and alcohol
Illiterate 31.9%Literate but no formal education 5.3% Primary 43.9%Secondary 19.4%
19–28 y — 13.6% 29–38 y — 35.9% 39–48 y — 25.5% ≥ 49 y — 25.0%
Anzil et al. (2016)
48.8% (177/362) of fishermen reported alco-hol consumption
11.8% smoked tobacco and consumed alcohol 13.2% chewed tobacco and consumed alcohol 11.4% had all the three habits
Gregorio et al. (2016)
79.4% (108/136) of fishermen reported alco-hol consumption within the past 4 weeks
Laraqui et al. (2017)
38.9% (550/1,413) of fishermen reported alco-hol consumption
Laraqui et al. (2017)
58.3% (802/1,376) of seaman reported alco-hol consumption
Mahdi et al. (2016)
11.5% (236/2,060) of seafarers reported alco-hol consumption on a regular basis
80.9% of alcohol consu-mers also smoked
Tu and Jap-sen (2016)
71.9% (452/629) of seafarers reported weekly alcohol consumption at home [(a) 38.6%, (b) 18.3%, (c) 14.9%)]. Seafarers who consumed > 15 alcoholic beverages a week had the highest prevalence of hypertension (55.3%)
Frantzeskou et al. (2016)
53% of fishermen reported daily alcohol consumption [(a) 34.0%, (b) 19%)]
A — alcohol; C — cannabis; OPS — others psychotropic substances; T — tobacco; y — years
Int Marit Health 2020; 71, 4: 265–274
www.intmarhealth.pl270

PREVALENCE OF ALCOHOL CONSUMPTION DEPENDING ON JOB-RELATED CHARACTERISTICS
Concerning the perceived stress level on board, Laraqui et al. [10] described a higher prevalence of alco-hol consumption in the self-reported stress group than in the non-self-reported stress group (41.9% vs. 27.2%; p < 0.001). Sliškivić and Penezić [15] showed no correlation between stress on board and drinking behaviour, regardless of whether the seafarer stayed at sea (r = –0.02), or ashore (r = –0.08). Furthermore, Rane et al. [11] observed no statis-tically significant correlation between alcohol consumption and stress among fishermen (p = 0.19).
Only 2 studies examined the association of alcohol consumption and the length of employment, and they pro-vided contradicting findings. Laraqui et al. [6] found a high consumption among fishermen with 5 to 15 years of em-ployment at sea (50.1%) in comparison to those with more than 15 years of employment (38.4%) [6]. In contrast, Kumar et al. [5] observed alcohol consumption less frequently among fishermen with 0–10 years of employment (14.0%) compared to those with longer job experience (more than 40.0%) [5].
Laraqui et al. [6] showed that working more than 8 hours per day was associated with alcohol consumption among 79.3% of fishermen with a toxic habit. Furthermore, Kumar et al. [5] described that the majority (62.7%) of the alcohol consuming fishermen spent 6 to 24 hours at sea. In addi-tion, the latter study revealed that 61.0% of the fishermen reported that they had been involved in an accident due to alcohol consumption (Table 3) [5].
DISCUSSIONThe present review focussed on studies about alcohol
prevalence among seafarers and fishermen and their al-cohol consumption, depending on socio-demographic and job-related factors, in the period from January 2014 to September 2019. As a limitation of this review, the results of the included studies are only comparable to a limited extent due to their different or missing definitions of al-cohol intake. Thus, general conclusions should be viewed critically. Furthermore, most of the studies focussed on different topics in seafaring and alcohol consumption was only an incidental aspect, for example as a risk factor for cardiovascular diseases or in the context of oral hygiene.
There was a wide range from 11.5% to 89.0% in the prevalence of alcohol consumption among the seafaring populations examined. This result was confirmed by a se-parate analysis of the prevalence of alcohol consumption by fishermen (35.4% to 89.5%) and seafarers (11.5% to 79.4%). A difference became apparent when comparing the median of fishermen and seafarers (47.7% vs. 58.5%). However, since the data were based on self-reporting data,
it can be assumed that the use of alcohol at sea was high-er than published due to social desirability [15]. In 2014, 76.1% of people in the European Union aged 15 years and older stated they had consumed alcohol in the previous 24 months [20]. Compared to the included studies, 9 out of 13 publications revealed lower consumption levels. If the range of results is listed by date of investigation, a decrease in alcohol use among fisherman can be observed over time (median before and after 2014: 56.9% vs. 42.3%). This could be the consequence of greater public awareness about alcohol-related illnesses or due to the introduction of legal regulations such as the STCW Convention [4].
The prevalence of alcohol consumption from 2015 to 2018 is solely based on data collection conducted among fishermen. Due to missing current data there is a need for further investigations also among seafarers to be able to make more precise statements for this occupational group.
The significantly lowest alcohol prevalence among sea-farers, at 11.5%, was shown by Mahdi et al. [18]. Firstly, a reason for this outcome could be an underreporting due to the different aim of this study, which dealt with dental hygiene and oral health status among seafarers and raised alcohol consumption only as an accompanying factor. Sec-ondly, the data collection took place in the context of emer-gency care carried out by the Centro Internationale Radio Medico. It is likely that the seafarers were hesitant in this situation to speak openly about the subject of alcohol use.
In the German general population, 16% of the sub-jects aged 18–64 stated a risky alcohol consumption in 2015 [21]. Compared to this, a 4-fold higher finding of harmful (60.8%) [5]/risky (67.7/%) [8] alcohol consumption was reported among fishermen. Therefore, an elevated risk for this occupational group concerning risky consumption can be possible. This can probably be explained by the fact that alcohol intake in traditional fishing is partly not subject to regulation [5] or by the especially high work-related stress level on fishing vessels due to heavy vessel movements, hard physical work and economic pressure. However, due to the lack of data, this result should be viewed with caution and makes further investigations in this context necessary.
This review showed an increased alcohol consumption in middle age, which, however, decreased with rising age. This can be explained by the healthy worker effect and the adaptation of the older employees to the stressful working conditions on board.
According to Pougnet et al. [2] and the present review, the greatest co-dependence in shipboard crews was found in the simultaneous consumption of alcohol and tobacco. To a minor extent, this may be explained by the observed finding of Rane et al. [11] that most fishermen believed in an increase in labour productivity through alcohol and tobacco consumption. According to the latter study, other
www.intmarhealth.pl 271
Elisabeth Stoll et al., Alcohol consumption among seafarers and fishermen

Tabl
e 3.
Alc
ohol
con
sum
ptio
n de
pend
ing
on jo
b-re
late
d fa
ctor
s
Auth
or (y
ear)
Asso
ciat
ion
of a
lcoh
ol c
onsu
mpt
ion
w
ith s
tres
s lo
adDu
ratio
n of
em
ploy
-m
ent [
year
s =
y]Da
ily w
orki
ng [h
]Ti
me
spen
t in
sea
[h]
Freq
uenc
y go
ing
to
sea
Inju
ry b
ecau
se o
f al
coho
l drin
king
Lara
qui e
t al.
(201
7)
Toxi
c ha
bits
: <
5 y
— 1
1.5%
5–
15 y
— 5
0.1%
>
15 y
— 3
8.4%
M
isus
e/de
pend
ence
:<
5 y
— 9
.9%
5–
15 y
— 4
9.6%
>
15 y
— 4
0.5%
Toxi
c ha
bits
: ≤
8 h
— 2
0.7%
>
8 h
— 7
9.3%
Mis
use/
depe
nden
ce:
≤ 8
h —
14.
7%>
8 h
— 8
5.3%
Kum
ar e
t al.
(201
8)
Part
icip
ants
repo
rted
al
coho
l con
sum
ptio
n
in th
e pa
st 1
yea
r: 0–
10 —
14.
0%
11–2
0 —
41.
5%
≥ 21
— 4
3.6%
Pa
rtic
ipan
ts re
port
ed
alco
hol c
onsu
mpt
ion
in
the
past
1 y
ear:
0–5
h —
20.
3%
6–24
h —
62.
7%
≥ 25
h —
17.
0%
Part
icip
ants
repo
rted
al
coho
l con
sum
ptio
n
in th
e pa
st 1
yea
r: D
aily
78.
4%
Occ
asio
nally
21.
6%
Alco
hol c
onsu
mpt
ion
in th
e pa
st 1
yea
r: 61
.0%
Sliš
kovi
ć
and
Pene
zić
(2
016)
The
freq
uenc
y an
d qu
antit
y of
alc
ohol
co
nsum
ptio
n on
boa
rd a
nd a
t hom
e sh
owed
no
cor
rela
tion
with
str
ess
on b
oard
Lara
qui e
t al.
(201
8)Th
e pr
eval
ence
of a
lcoh
ol c
onsu
mpt
ion
w
as h
ighe
r in
the
grou
p of
par
ticip
ants
w
ith s
elf-r
epor
ted
stre
ss (4
1.9%
) tha
n in
the
gr
oup
with
non
-sel
f-rep
orte
d st
ress
(27.
2%)
Ran
e et
al.
(201
6)R
elat
ed to
eac
h fo
rm o
f alc
ohol
con
sum
ptio
n:
The
asso
ciat
ion
of s
tres
s an
d co
nsum
ptio
n
alco
hol w
as n
ot fo
und
to b
e st
atis
tical
ly
sign
ifica
nt c
ompa
red
to n
on-a
lcoh
olic
s
Int Marit Health 2020; 71, 4: 265–274
www.intmarhealth.pl272

fishermen further stated that they consumed alcohol and to-bacco to relieve themselves of the fatigue of overwork [11]. Although the consumption and possession of drugs is strictly forbidden on all ships, the intake of alcohol is permitted, with differences depending on the shipping company [15].
The investigation of alcohol consumption in connection with stress did not reveal a clear tendency, based on the results in two of 3 studies. Only Laraqui et al. [10] showed a significant association between alcohol consumption and stress. They claimed that fishermen compensate a decrease in alertness and an increase in fatigue through the con-sumption of substances such as alcohol. This consumption increases among fishermen with stress as compared to those without stress [10]. In contrast, Slišković and Penezić [15] found that stress on board was mainly related to a lack of sleep and an unhealthy diet, two factors that cannot be directly influenced by the seafarers [15]. These two con-flicting results and the limited data available make further investigations in this context necessary.
Alcohol intake in dependence of job-related factors was more difficult to assess due to the limited data available. Overall, there was an increase in consumption among fish-ermen who fished on a daily basis (78.4%) [5] and whose daily working time exceeded 8 hours (79.3%) [6]. Mental and physical isolation as well as coping with overtime and waiting time at sea are possible explanations for this [8]. Jégaden et al. [22] showed a higher tendency to get bored at sea according to the boredom scale results for ratings on board compared to those of officers and sedentary em-ployees. This boredom can be seen as the cause of all kinds of abuse [22].
This review revealed more studies on fishermen than on seafarers of merchant vessels in the search period in-dicated. Thus, the alcohol consumption in merchant sea-faring with a high proportion of Asian crew members can hardly be assessed; the cultural diversity of seafarers on board of merchant vessels influences the average alcohol consumption due to specific cultural habits, regulations, laws and religious beliefs [6]. Furthermore, the genetic vari-ance of the study participants should be considered within multiculturally manned vessels. Asians frequently show an atypical, inactive aldehyde dehydrogenase-2 (ALDH2) variant. Therefore, the consumption of alcohol leads to an increase in acetaldehyde concentration and subsequently to a “flush” syndrome. Consequently, alcohol consumption among Asians is rather low and abuse is rather rare.
CONCLUSIONSIn summary, among fishermen alcohol intake decreased
over the time period considered. In order to be able to make more accurate statements about the current prevalence of alcohol consumption among seafarers, further studies
are needed using a uniform definition of alcohol intake and harmful/hazardous and dependent alcohol consump-tion. AUDIT would be a suitable questionnaire to identify and define harmful/hazardous and dependent alcohol consumption. Further studies on alcohol intake and job related factors are recommended in order to increase the understanding of the prevalence and association of alcohol use on board.
CONFLICT OF INTERESTThere are no conflicts of interest.
REFERENCES1. World Health Organization. Global status report on alcohol
and health 2018. https://apps.who.int/iris/bitstream/han-dle/10665/274603/9789241565639-eng.pdf?ua=1 (Accessed August 2020).
2. Pougnet R, Pougnet L, Loddé B, et al. Consumption of addictive substances in mariners. Int Marit Health. 2014; 65(4): 199–204, doi: 10.5603/IMH.2014.0038, indexed in Pubmed: 25522703.
3. Coggon D, Harris EC, Brown T, et al. Occupation and mortality related to alcohol, drugs and sexual habits. Occup Med (Lond). 2010; 60(5): 348–353, doi: 10.1093/occmed/kqq040, indexed in Pubmed: 20407041.
4. STCW- A GUIDE FOR SEAFARER. 2010. https://www.mptusa.com%2Fpdf%2Fstcw_guide_english.pdf (Accessed August 2020).
5. Kumar AM, Ramaswamy G, Majella MG, et al. Alcohol, harmful use and dependence: Assessment using the WHO Alcohol Use Disorder Identification Test tool in a South Indian fishermen community. Ind Psychiatry J. 2018; 27(2): 259–263, doi: 10.4103/ipj.ipj_82_15, indexed in Pubmed: 31359981.
6. Laraqui O, Laraqui S, Manar N, et al. Prevalence of consumption of addictive substances amongst Moroccan fishermen. Int Marit He-alth. 2017; 68(1): 19–25, doi: 10.5603/IMH.2017.0004, indexed in Pubmed: 28357832.
7. Babor TF, Higgins-Biddle JC, Saunders JB, et al. AUDIT - The Alcohol Disorder Identification Test. 2019. https://www.who.int/publication-s-detail/audit-the-alcohol-use-disorders-identification-test-guideli-nes-for-use-in-primary-health-care (Accessed August 2020).
8. Fort E, Lassiège T, Bergeret A. Prevalence of cannabis and coca-ine consumption in French fishermen in South Atlantic region in 2012-2013 and its policy consequences. Int Marit Health. 2016; 67(2): 88–96, doi: 10.5603/IMH.2016.0018, indexed in Pubmed: 27364174.
9. Anderson P, Gual A, Colom J. Alcohol and primary healthcare: Clinical Guidelines on Identification and Brief Interventions. 2005. http://inebria.net/wp-content/uploads/2017/09/cg_1.pdf. (Accessed August 2020).
10. Laraqui O, Manar N, Laraqui S, et al. Occupational risk perception, stressors and stress of fishermen. Int Marit Health. 2018; 69(4): 233–242, doi: 10.5603/IMH.2018.0038, indexed in Pubmed: 30589062.
11. Rane PP, Narayanan P, Binu Vs, et al. Prevalence of Tobacco and Alcohol Consumption among Fishermen in Udupi Taluk’ Karnataka, India: a Cross-Sectional Study. Asian Pac J Cancer Prev. 2016; 17(4): 1733–1737, doi: 10.7314/apjcp.2016.17.4.1733, indexed in Pubmed: 27221846.
12. Anzil K, Mathews J, Sai AG, et al. Prevalence of deleterious oral habits and oral mucosal lesions among fishermen population of Mahe,
www.intmarhealth.pl 273
Elisabeth Stoll et al., Alcohol consumption among seafarers and fishermen

South India. J Contemp Dent Pract. 2016; 17(9): 745–749, doi: 10.5005/jp-journals-10024-1923, indexed in Pubmed: 27733718.
13. Laraqui O, Laraqui S, Manar N, et al. Risk-taking behaviours among fishermen in Morocco by the evaluation of “ordalique” functioning. Int Marit Health. 2017; 68(2): 83–89, doi: 10.5603/IMH.2017.0016, indexed in Pubmed: 28660610.
14. Frantzeskou E, Jensen OC, Linos A. Health status and occupational risk factors in Greek small fisheries workers. Int Marit Health. 2016; 67(3): 137–143, doi: 10.5603/IMH.2016.0026, indexed in Pubmed: 27681212.
15. Slišković A, Penezić Z. Lifestyle factors in Croatian seafarers as re-lating to health and stress on board. Work. 2017; 56(3): 371–380, doi: 10.3233/WOR-172501, indexed in Pubmed: 28339415.
16. Gregorio ER, Kobayashi J, Medina JR, et al. Knowledge, attitudes, and related practices of Filipino seafarers regarding cardiovascular diseases. Int Marit Health. 2016; 67(4): 214–222, doi: 10.5603/IMH.2016.0039, indexed in Pubmed: 28009390.
17. Laraqui S, Laraqui O, Manar N, et al. The assessment of seafarers’ knowledge, attitudes and practices related to
STI/HIV/AIDS in northern Morocco. Int Marit Health. 2017; 68(1): 26–30, doi: 10.5603/IMH.2017.0005, indexed in Pubmed: 28357833.
18. Mahdi SS, Sibilio F, Amenta F. Dental hygiene habits and oral he-alth status of seafarers. Int Marit Health. 2016; 67(1): 9–13, doi: 10.5603/IMH.2016.0003, indexed in Pubmed: 27029923.
19. Tu M, Jepsen JR. Hypertension among Danish seafarers. Int Marit Health. 2016; 67(4): 196–204, doi: 10.5603/IMH.2016.0037, indexed in Pubmed: 28009392.
20. Alcohol consumption statistics - Statistics Explained. 07.03.2020. https://ec.europa.eu/eurostat/statistics-explained/index.php/Alcohol_consumption_statistics (Accessed August 2020).
21. Lange C, Manz K, Rommel A, et al. Alkoholkonsum von Erwachsenen in Deutschland: Riskante Trinkmengen, Folgen und Maßnahmen: Robert Koch-Institut, Epidemiologie und Gesundheitsberichterstat-tung; 2016.
22. Jégaden D, Rio M, Lucas P, et al. L’étude de la disposition à l’ennui peut-elle être un outil pertinent dans la détermination de l’aptitude à l’embarquement. Medicina Maritima. 2013; 13: 26–38.
Int Marit Health 2020; 71, 4: 265–274
www.intmarhealth.pl274

Dr. Marcus Oldenburg, Institute for Occupational and Maritime Medicine, University Medical Centre Hamburg-Eppendorf (UKE), Seewartenstrasse 10, 20459 Hamburg,
Germany, tel: +49 40 428 374 308, fax: +49 40 427 311 393, e-mail: [email protected]
Work profile of maritime pilots in Germany
Marcus Oldenburg1 , Lukas Belz1 , Filip Barbarewicz1 , Volker Harth1 , Hans-Joachim Jensen1, 2
1Institute for Occupational and Maritime Medicine Hamburg (ZfAM), University Medical Centre Hamburg-Eppendorf (UKE), Germany 2Flensburg University of Applied Sciences, Germany
ABSTRACTLong and irregular shifts, unforeseeable operations and high responsibility are still prominent in the job of a pilot and pose high psycho-physical demands. Furthermore, there is a disturbed work-family balance. Working hours of pilots are highly variable and not bound by regulations due to irregularities of vessel traffic. The pilots have to work in a shifting rotation system. This paper demonstrates the stressors during their work routine and shows the usual working profile of a pilot during their service.
(Int Marit Health 2020; 71, 4: 275–277)
Key words: pilot, work profile, stressors
�
REVIEWIn the frame of globalisation and increasing trading
relations, international trade takes a key position in world economy. Almost 90% of modern global trade is depend-ing on sea transport. For this sector, seafarers, who are exposed to harsh conditions during ship operations, are essential [1–3]. Pilotage furthermore has a special role in the maritime industry [4].
During his service on the bridge, the pilot is officially only a consultant for the ship’s head of the watch. He knows local currents in relation to tides and current sea and weather conditions as well as depths and widths of the waterway. This knowledge is the foundation for important decisions for piloting to the port of destination. To know these regional factors, which can change spontaneously, for several ports is impossible for the ship’s master. The pilot’s expertise about his pilotage waters is necessary and cannot be re-placed by modern vessel traffic services and surveillance systems, radar, GPS or electronic chart systems.
CURRENT RELEVANCE OF PILOTS IN GERMANY
In the course of rising and internationally expanding trade, the size of vessels and their tonnage have increased continuously until today. Since the late nineties the maxi-mum twenty-foot equivalent unit (TEU) capacity of container ships has more than tripled resulting in bigger ships which are harder to operate in narrow channels (Table 1) [5].
With annual more than 100,000 vessel movements, the German Bight features one of the highest ship densities of the world. This amount of traffic, with the ongoing trend to larger vessels, enhances the risk of collisions and accidents with catastrophic impacts. Since 2015 there have been at least 112 maritime accidents in German waters each year [6].
In order to ensure traffic safety, there is an obligation to use pilot services for in and outgoing vessels. In Germany, the law of sea pilots (Seelotsgesetz) requests a permanent availability of pilots on 365 days at all times. This is surveyed strictly by regional supervisory authorities. For the river Elbe and the port of Hamburg there is a pilot acceptance obligation for all vessels, which are longer than 90 m overall and wider than 13 m and all tanker vessels. For a passage through the Kiel Canal any bigger ship passing the channel is obligated to take a channel pilot and a channel helmsman in order to avoid collisions.
Today, pilots in Germany are freelancers and execute the delegated pilotage services according to the law of sea pilots section 21 paragraph 1 SeeLG (1954) in self-adminis-tration. Pilots are therefore working in a self-employed and non-commercial environment, which is neither controlled by worker-protection laws nor the commercial inspectorate.
The usually unpredictable arrival of the ship, the trans-fer on board the ship and advising the captain during the passage through the specific waterway are general and typical features of the pilots’ job. Thus, according to the International Maritime Pilots Association (IMPA), the working
www.intmarhealth.pl 275
Int Marit Health 2020; 71, 4: 275–277
10.5603/IMH.2020.0046 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
REV IEW ART ICLE
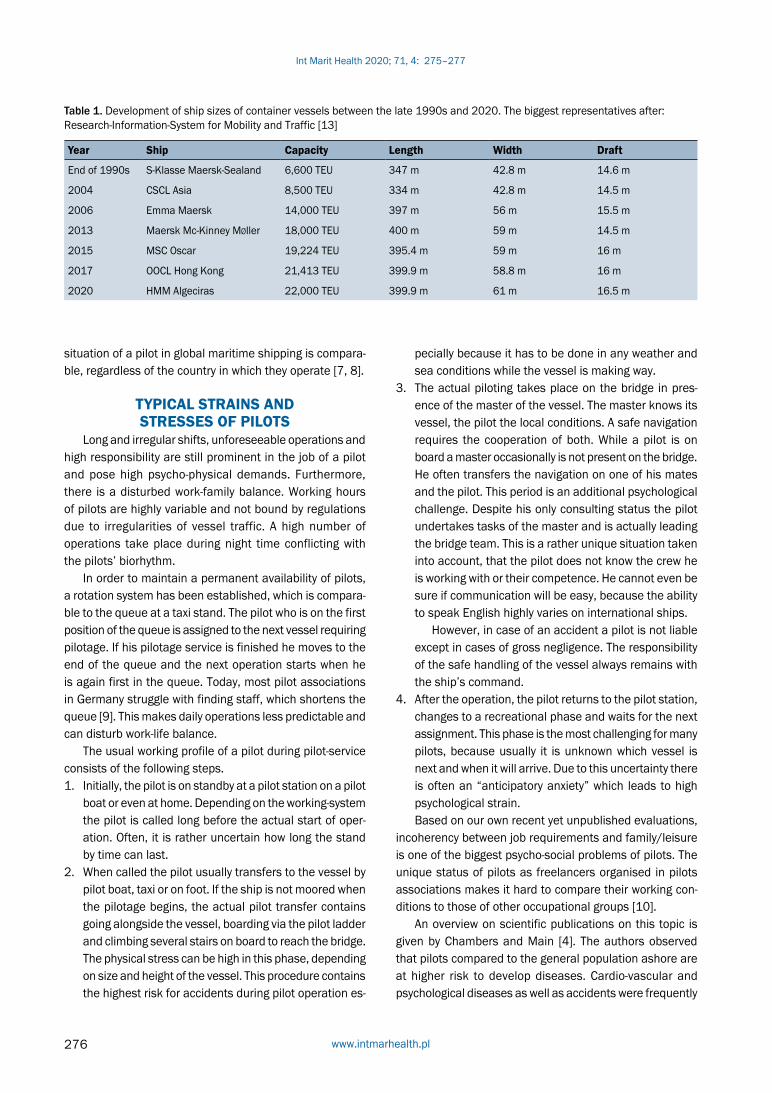
Table 1. Development of ship sizes of container vessels between the late 1990s and 2020. The biggest representatives after: Research-Information-System for Mobility and Traffic [13]
Year Ship Capacity Length Width Draft
End of 1990s S-Klasse Maersk-Sealand 6,600 TEU 347 m 42.8 m 14.6 m
2004 CSCL Asia 8,500 TEU 334 m 42.8 m 14.5 m
2006 Emma Maersk 14,000 TEU 397 m 56 m 15.5 m
2013 Maersk Mc-Kinney Møller 18,000 TEU 400 m 59 m 14.5 m
2015 MSC Oscar 19,224 TEU 395.4 m 59 m 16 m
2017 OOCL Hong Kong 21,413 TEU 399.9 m 58.8 m 16 m
2020 HMM Algeciras 22,000 TEU 399.9 m 61 m 16.5 m
situation of a pilot in global maritime shipping is compara-ble, regardless of the country in which they operate [7, 8].
TYPICAL STRAINS AND STRESSES OF PILOTS
Long and irregular shifts, unforeseeable operations and high responsibility are still prominent in the job of a pilot and pose high psycho-physical demands. Furthermore, there is a disturbed work-family balance. Working hours of pilots are highly variable and not bound by regulations due to irregularities of vessel traffic. A high number of operations take place during night time conflicting with the pilots’ biorhythm.
In order to maintain a permanent availability of pilots, a rotation system has been established, which is compara-ble to the queue at a taxi stand. The pilot who is on the first position of the queue is assigned to the next vessel requiring pilotage. If his pilotage service is finished he moves to the end of the queue and the next operation starts when he is again first in the queue. Today, most pilot associations in Germany struggle with finding staff, which shortens the queue [9]. This makes daily operations less predictable and can disturb work-life balance.
The usual working profile of a pilot during pilot-service consists of the following steps.1. Initially, the pilot is on standby at a pilot station on a pilot
boat or even at home. Depending on the working-system the pilot is called long before the actual start of oper-ation. Often, it is rather uncertain how long the stand by time can last.
2. When called the pilot usually transfers to the vessel by pilot boat, taxi or on foot. If the ship is not moored when the pilotage begins, the actual pilot transfer contains going alongside the vessel, boarding via the pilot ladder and climbing several stairs on board to reach the bridge. The physical stress can be high in this phase, depending on size and height of the vessel. This procedure contains the highest risk for accidents during pilot operation es-
pecially because it has to be done in any weather and sea conditions while the vessel is making way.
3. The actual piloting takes place on the bridge in pres-ence of the master of the vessel. The master knows its vessel, the pilot the local conditions. A safe navigation requires the cooperation of both. While a pilot is on board a master occasionally is not present on the bridge. He often transfers the navigation on one of his mates and the pilot. This period is an additional psychological challenge. Despite his only consulting status the pilot undertakes tasks of the master and is actually leading the bridge team. This is a rather unique situation taken into account, that the pilot does not know the crew he is working with or their competence. He cannot even be sure if communication will be easy, because the ability to speak English highly varies on international ships.
However, in case of an accident a pilot is not liable except in cases of gross negligence. The responsibility of the safe handling of the vessel always remains with the ship’s command.
4. After the operation, the pilot returns to the pilot station, changes to a recreational phase and waits for the next assignment. This phase is the most challenging for many pilots, because usually it is unknown which vessel is next and when it will arrive. Due to this uncertainty there is often an “anticipatory anxiety” which leads to high psychological strain.Based on our own recent yet unpublished evaluations,
incoherency between job requirements and family/leisure is one of the biggest psycho-social problems of pilots. The unique status of pilots as freelancers organised in pilots associations makes it hard to compare their working con-ditions to those of other occupational groups [10].
An overview on scientific publications on this topic is given by Chambers and Main [4]. The authors observed that pilots compared to the general population ashore are at higher risk to develop diseases. Cardio-vascular and psychological diseases as well as accidents were frequently
Int Marit Health 2020; 71, 4: 275–277
www.intmarhealth.pl276

found in 18 analysed studies. Specifically, on-call work periods that occur at irregular times with irregular pilotage are a major cause of poor sleep quality and quantity. These potential risks factors for fatigue can lead in the long-term to cognitive dysfunction and emotional disorders [11]. Ac-cording to Strauch [12], fatigue also poses a risk factor for accidents, although further studies are still needed to evaluate these relationships in more detail.
Furthermore, an unhealthy lifestyle is discussed as major risk factor among pilots. A former study revealed that this oc-cupational group compared to the general population is more likely to exhibit overweight, smoking, high lipid serum levels, lack of physical activity and unhealthy eating habits [13].
Closer analyses of this occupation show its impact on individual psycho-physical health and on concentration and performance levels of pilots. These influences are visible in sleeping disorders [14], cognitive disorders, limitation of vigilance [4] and more accidents [15]. In general, the health and wellbeing of pilots has been yet analysed insufficiently [16] and further research is necessary.
FUNDINGThis study was funded by the German Maritime Pilots’
Association, Hamburg, Germany.
CONFLICT OF INTERESTThere are no conflicts of interest.
REFERENCES1. Carotenuto A, Molino I, Fasanaro AM, et al. Psychological stress in
seafarers: a review. Int Marit Health. 2012; 63(4): 188–194, indexed in Pubmed: 24595974.
2. Nielsen MB, Bergheim K, Eid J. Relationships between work environ-ment factors and workers’ well-being in the maritime industry. Int Marit Health. 2013; 64(2): 80–88, indexed in Pubmed: 23788224.
3. Oldenburg M, Jensen HJ, Latza U, et al. The risk of coronary heart disease of seafarers on vessels sailing under a German flag. Int Marit Health. 2010; 62(3): 123–128, indexed in Pubmed: 21154298.
4. Chambers TP, Main LC. Symptoms of fatigue and coping strategies in maritime pilotage. Int Marit Health. 2015; 66(1): 43–48, doi: 10.5603/IMH.2015.0011, indexed in Pubmed: 25792167.
5. The Impact of Mega-Ships. International Transport Forum Policy Papers. Organisation for Economic Co-operation and Development, Paris. 2015, doi: 10.1787/5jlwvzcm3j9v-en.
6. Federal Bureau of Maritime Casualty Investigation. Jahresbericht 2019. 2020.
7. Marine Insight News Network. Maritime pilot and his duties. 2019. https://www.marineinsight.com/careers-2/maritime-pi-lot-and-his-duties/ (30.10.2020).
8. Andresen M, Domsch M, Cascorbi A. Working Unusual Hours and Its Relationship to Job Satisfaction: A Study of European Maritime Pilots. J Labor Res. 2007; 28(4): 714–734, doi: 10.1007/s12122-007-9010-5.
9. Runge W. Elblotsen haben Nachwuchssorgen 2019. https://www.welt.de/print/die_welt/hamburg/article198817903/Elblotsen-ha-ben-Nachwuchssorgen.html (24.08.2020).
10. Saarni H, Niemi L, Pentti J, et al. Is there need for change of health examinations for sea pilots? Bulletin of the Institute of Maritime and Tropical Medicine in Gdynia. 1992; 43(1-4): 25–34, indexed in Pubmed: 1345594.
11. Gregory K, Hobbs A, Parke B, et al. An evaluation of fatigue factors in maritime pilot work scheduling. Chronobiol Int. 2020 [Epub ahead of print]: 1–7, doi: 10.1080/07420528.2020.1817932, indexed in Pubmed: 32911999.
12. Strauch B. Investigating Fatigue in Marine Accident Investigations. Procedia Manufacturing. 2015; 3: 3115–3122, doi: 10.1016/j.promfg.2015.07.859.
13. Barbarewicz F, Jensen HJ, Harth V, et al. Psychophysical stress and strain of maritime pilots in Germany. A cross-sectional study. PLoS One. 2019; 14(8): e0221269, doi: 10.1371/journal.pone.0221269, indexed in Pubmed: 31415636.
14. Ferguson SA, Lamond N, Kandelaars K, et al. The impact of short, irregular sleep opportunities at sea on the alertness of marine pilots working extended hours. Chronobiol Int. 2008; 25(2): 399–411, doi: 10.1080/07420520802106819, indexed in Pubmed: 18484370.
15. Meere K, Van Da, Van Sp. Occupational injuries in Flemish pilots in Belgium. A questionnaire survey. Int Marit Health. 2005; 56(1-4): 67–77, indexed in Pubmed: 16532586.
16. Main LC, Chambers TP. Factors affecting maritime pilots’ health and well-being: a systematic review. Int Marit Health. 2015; 66(4): 220–232, doi: 10.5603/IMH.2015.0043, indexed in Pubmed: 26726893.
www.intmarhealth.pl 277
Marcus Oldenburg et al., Work profile of maritime pilots in Germany

Dr. Ajit C. Kulkarni, 3A Siddhi Vinayak Chambers, Opp. MIG Cricket Club, Bandra East, Mumbai 400051, India, tel: 2642 3428/2641 7143, cell: 98210 92233,
e-mail: [email protected]
A case of neurocysticercosis with an unusual presentation on high seas
Ajit C. Kulkarni
Medical Centre, Mumbai, India
ABSTRACTEvery seafarer undergoes a medical examination prior to joining a ship. Some disorders cannot be detected and they may appear while at sea. Diagnosing and managing them becomes extremely difficult for the Master being the caregiver on board. Large crude carriers often perform long voyages and due to their sheer size, do not enter any port. Helicopter evacuation of a sick or injured crew is the norm. They operate under strict chartering time lines which do not permit deviation from course. A case of hemiparesis on left side of body in a young hitherto healthy seafarer which was later diagnosed as a case of neurocysticercosis is described.
(Int Marit Health 2020; 71, 4: 278–280)
Key words: medical examination of seafarers, Radio Medical Advice, neurocysticercosis, seizure, Taenia solium
�
INTRODUCTIONSeafarers are required to undergo a medical examina-
tion prior to sailing to reduce risks to crew members and for the safe operations of the ship as well as to safeguard their personal health and safety at sea. Aim of the medical examination is to ensure that the seafarer is medically fit to perform his or her routine and emergency duties at sea and is not suffering from any medical condition likely to be aggravated by service at sea, to render him or her unfit for service or to endanger the health of other persons on board [1].
Master of the vessel is the caregiver on board and is required to have undergone a course in medical care as per the International Maritime Organisation (IMO) Standards of Training Certification and Watchkeeping (STCW) convention [2]. Due to advances in communication, he is able to seek medical advice by telephone, emails or video calls but han-dling any unusual medical condition is challenging and may also have a demoralizing effect on the crew.
CASE REPORTPreviously healthy 24 years old Indian 4th Engineer,
was sailing on a Hong Kong registered 320,051 DWT crude carrier for the past 10 weeks. Vessel was 333 m in length
(LOL) and had a speed of 13 knots per hour. The vessel had a mixed crew of Indian, Philippine and Indonesian nationals on board. The vessel was sailing in ballast to reach a loading port in Persian Gulf in 5 days.
The 4th Engineer woke up after a normal undisturbed sleep and realised that he had lost control in his left upper and lower limbs. He was dizzy and unsteady getting out of bed and walk to the rest room. He was unable to hold his toothbrush in his left hand to squeeze toothpaste on it. He called the Chief Engineer who in turn alerted the Master about the status of the 4th Engineer. After examining the patient, the Master called the author for Radio Medical Advice, being the medical Consultant to the Vessel Man-agement Company. There was no history of exertion, no syncope, speech was normal. No headache. No past history of any head injury. Other than weakness over the left side of the body and pain over left orbital area, the patient had no symptoms. He had voided urine in the morning without any difficulty. Pulse, respiration and blood pressure were within normal limits.
Master was advised steps in examining the central nervous system. Patient was fully conscious. Mental sta-tus examination with reference to attention, orientation and memory, both past and recent were normal. No signs
www.intmarhealth.pl
Int Marit Health 2020; 71, 4: 278–280
10.5603/IMH.2020.0047 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
CASE REPORT
278

of meningeal irritation. Examination of pupils and cranial nerves was normal. He needed to make special effort to carry out any activity with left upper and lower limbs. Power in left upper and lower limbs was found to be 4/5. Gait was unsteady. Romberg’s test with eyes closed was positive.
A provisional diagnosis of subarachnoid haemorrhage was made; however, there was no headache which normally accompanies such an episode. Patient was advised com-plete bed rest to be watched over by another crew member.
Operations manager was contacted by the Master and a three way conference call was held. Seriousness of the situation was conveyed and also that the seafarer needs to be evacuated ashore for hospitalisation and investigation was impressed upon. Vessel position was 12° 50 N and 73° 29 E, almost due west of Mangalore port on West coast of India. Well within the range of helicopter evacuation if the patient’s condition deteriorated. Patient’s condition was closely monitored every 8 hours. He remained dizzy, fully con-scious and had had cereal as meal. After 24 hours, patient’s condition remained unchanged. Small subarachnoid bleeds often resolve by itself and a decision was taken to sign off the patient in the loading port. Sailing along the West coast of India, the vessel remained within helicopter evacuation range from India and then Oman. The Agent in loading port was accordingly instructed that the crew member should be signed off and put on the first available flight to Mumbai, India. Over the next four days patient’s condition remained unchanged. Blood pressure, respiration was normal, blad-der and bowel control was normal. No headache. Patient was landed ashore in the Pilot boat, immigration formalities completed and he boarded a flight and arrived in Mumbai same day late evening. On arrival, he was taken to a hospital on a priority basis and on admission magnetic resonance imaging brain was carried out to diagnose the condition and plan line of treatment.
Magnetic resonance imaging study detected a solitary cystic lesion high up in right parietal lobe. The lesion was centrally hyperintense on both T2 W2 and inversion recovery magnetic resonance images with a hyper intense rim and surrounding vasogenic oedema. A small eccentric nodule was seen within the lesion. Post contrast image revealed peripheral enhancement. The findings were consistent with neurocysticercosis (NCC) (Fig. 1).
His liver function tests were normal. Fundus examination was normal. He was prescribed Tab Albendazole 400 mg twice daily for 8 days. Symptom exacerbation is common during the first week after antiparasitic treatment is ini-tiated. Use of steroids decreases this. Dexamethasone 0.1 mg/kg in three divided doses for 10 days was prescribed for the same to be tapered off [3]. As no active treatment was required, he was permitted to travel to his place of residence and consult a neurophysician for follow up.
DISCUSSIONSeizure is the most common symptom in a case of
NCC. To treat a seizure on board a vessel would not be an easy task. Midazolam (benzodiazepam) injection is the only medication recommended to be carried on board to treat seizure/epilepsy. It is to be administered intravenously, intramuscularly or intramucosal in the nostrils [4]. Presence of a seriously ill crew member on board demoralizes the rest of the crew extensively.
Neurocysticercosis is a parasitic disease caused by metacestodal stage of Taenia solium, and is one of the most common causes of epilepsy in man. The commonest manifestation of NCC in humans is acute symptomatic seizures. Seizures can be generalised, focal or rarely my-oclonus and acquired epileptic aphasia. It affects adults in their third or fourth decade of life [5].
Neurocysticercosis is one of the most important ne-glected tropical diseases in the third world countries. Cys-ticercosis is a serious public health problem especially in resource poor and developing countries including India. It is considered as a biological marker of social and economic development, it predominantly affects adults in their third or fourth decade of life [6].
Life cycle of Taenia solium comprises two natural hosts, man acts as definitive host harbouring the adult tape worm in the intestine passing the eggs in faeces. While pig is the intermediate host which ingests some of these eggs leading to development of cysticerci in internal organs like muscle and brain. Humans become infected by consuming pork contaminated with cysticerci. The scolex of adult worm is equipped with four lateral suckers and a rostellum is armed bearing 25–50 hooklets by which it attaches itself to the internal mucosa (Fig. 2).
Figure 1. Solitary cystic lesion in parietal lobe (all markings are deleted for confidentiality of identity of the patient)
www.intmarhealth.pl 279
Ajit C. Kulkarni, A case of neurocysticercosis with an unusual presentation on high seas

In the present case, the patient was a vegetarian and had never consumed pork. In India, in endemic areas, there is a large population that is vegetarian and do not consume pork. This significant number of vegetarians amongst NCC cases sug-gest other mode of transmission, e.g. contaminated salads [7].
Cysticercosis has been categorised as a potentially pre-ventable and eradicable disease. Tapeworm carriers are potential target for the control of cysticercosis. Emphasis should be on health education and mass administration of anthelminthics in endemic areas to remove tape worm carri-ers. Education of community based sanitation, building and usage of latrines and proper disposal of night soil coupled with healthy animal husbandry practices play a major role in control and eradication.
CONCLUSIONSLarge number of seafarers hail from South East Asia and
China where pork is consumed extensively. Screening every asymptomatic seafarer for NCC is not possible. Instead all reporting for pre-employment medical examination (PEME) could be administered tab Albendazole 400 mg as a sin-gle dose broad spectrum anthelmintic as a cost effective
measure. Food handlers should be additionally treated with anti-amoebic medication.
Patient remained prone to seizure and he may need anti-epileptic drugs and long convalescence. He would not be considered fit for sea service till 1 year after stoppage of anti-epileptic drugs. He was thus lost to follow up.
REFERENCES1. Guidelines on the Medical Examination of Seafarers. International
Labour Office Geneva, IMO. ISBN 978-92-2-127462-9.2. International Maritime Organization: Section A-VI/4, STCW Confe-
rence. 2/34, 3 August 2010.3. Garcia HH, Nash T, Brutto OD. Clinical symptoms, diagnosis, and
treatment of neurocysticercosis. Lancet Neurol. 2014; 13(12): 1202–1215, doi: 10.1016/s1474-4422(14)70094-8.
4. International Guide for Ships. 3rd Edition, World Health Organization. 2007. ISBN 978 924 154720. Page 118-121.
5. Malla BA. An overview of neurocysticercosis. J Pharmacognosy Phytochemistry. 2018; 7(6): 303–312.
6. Prasad KN, Prasad A, Verma A, et al. Human cysticercosis and Indian scenario: a review. J Biosci. 2008; 33(4): 571–582, doi: 10.1007/s12038-008-0075-y, indexed in Pubmed: 19208982.
7. Varma A, Gaur KJ. The clinical spectrum of neurocysticercosis in the Uttaranchal region. J Assoc Physicians India. 2002; 50: 1398–1400, indexed in Pubmed: 12583469.
Figure 2. Life cycle of Taenia solium
Int Marit Health 2020; 71, 4: 278–280
www.intmarhealth.pl280

Prof. Krzysztof Korzeniewski, MD, PhD, Military Institute of Medicine, Head of the Department of Epidemiology and Tropical Medicine, Szaserów St. 128, 04–141 Warsaw,
Poland; Medical University of Gdansk, Institute of Maritime and Tropical Medicine, Department of Occupational, Metabolic and Internal Diseases, Powstania Styczniowego St. 9B,
81–519 Gdynia, Poland, e-mail: [email protected]; [email protected]
Extreme traveler
Krzysztof Korzeniewski1, 2
1Department of Epidemiology and Tropical Medicine; Military Institute of Medicine, Warsaw, Poland 2Department of Occupational, Metabolic and Internal Diseases, Institute of Maritime and Tropical Medicine,
Medical University of Gdansk, Poland
ABSTRACTAlthough they may pose a serious health risk or may even turn out to be life-threatening, extreme sports, i.e. high-risk physical activities of varied difficulty, are growing in popularity among international travelers in recent years. Extreme sports encompass a wide range of activities such as scuba diving, rafting, surfing, bungee jumping and mountaineering. It is not unusual for travelers to engage in extreme sports far off the beaten path, in destinations where environmental conditions are difficult and specialist healthcare is not easily available. Therefore, before taking the decision to engage in any form of adventurous activity, travelers should be encouraged to take certain precautionary measures. The most important are: identifi-cation of potential health risk factors related to travel or the activity itself, physical conditioning and fitness training prior to travel (depending on the type of activity) and prophylaxis (a travel health kit, mandatory and recommended vaccinations, a pre-travel consultation to assess a person’s fitness to travel and identify any potential contraindications for certain types of adventure sports, a comprehensive travel insurance policy). The article focuses on popular extreme sports, common risk factors associated with extreme activities as well as the recommended prophylaxis and precautionary measures.
(Int Marit Health 2020; 71, 4: 281–290)
Key words: travelers, extreme sports, health hazards, prevention
�
INTRODUCTIONAlong with the increasing number of international tour-
ist arrivals, the number of travelers who are interested in adventurous activities is also increasing. According to sur-veys as much as 40% of travelers reported that they have engaged in extreme sports, such as scuba diving, rafting, surfing, bungee jumping or mountaineering during their travel [1, 2]. Extreme travel may be defined as participating in high-risk activities of varying degree of difficulty, usually in a remote destination where the environmental conditions are difficult and specialist healthcare is not readily accessi-ble. The most popular destinations are both in developing countries located in tropical or sub-tropical zone, as well as in the wilderness of developed regions in temperate climate. Extreme sports encompass a wide range of activities that can be divided into several different categories. The most popular water sports include scuba diving, surfing, wind-surfing and white-water rafting. As for the mountain sports,
the most popular are skiing, snowboarding and mountain-eering, while sky diving and paragliding are the top aerial activities. Other extreme sports such as bungee jumping or spelunking have also been gaining in popularity among trav-elers in recent years. When travelling abroad or engaging in extreme activities, travelers may encounter a wide range of health issues, either injuries or illnesses, which are normally treated or managed by specialists in travel or sports medi-cine. Therefore, it is necessary for health care professionals providing pre-travel advice to extreme travelers to have the basic knowledge on currently available prophylactic mea-sures as well as potential risk factors — both environmental and activity-related [3]. Although a vast majority of extreme travelers were found to be between 30 and 40 years old, extreme travel is also popular with older people. The two principle causes of mortality in travelers were found to be cardiovascular diseases (in the elderly) and injuries (in younger voyagers) [4]. It is well known that prolonged physi-
www.intmarhealth.pl 281
Int Marit Health 2020; 71, 4: 281–290
10.5603/IMH.2020.0048 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
REV IEW ART ICLE

cal activity and emotional stress associated with travel may unmask or exacerbate a cardiovascular disease; therefore, it is particularly important that older patients have a pre-travel consultation and undergo a comprehensive medical exam-ination before travel [5]. Myocardial infarctions normally occur within the first two days of travel [6]. Patients over the age of 50 with increased cardiovascular risk (e.g. obesity, arterial hypertension, and hypercholesterolemia) should at least have the electrocardiogram test performed before they travel. They should also be encouraged to have a specialist pre-travel consultation with a diabetologist (diabetes), en-docrinologist (thyroid disease) and a dentist (to treat any dental problems). Women are additionally recommended to have a gynecological consultation before travel. It is important that extreme travelers receive all mandatory and recommended vaccinations and pack a travel health kit containing all regularly taken medicines [7, 8]. Health care professionals offering pre-travel advice to extreme or adventurous travelers have an obligation to provide their patients with good medical advice on how to deal with any potential travel-related risk factors or medical conditions they may develop while travelling. The two principle health risk factors include long-term travel and journeying to remote destinations with harsh climate and poor sanitation. The highest single risk for extreme travelers is trauma. Most inju-ries which are reported in adventurous travelers result from the activity itself or travelling by local public transport. In the developing countries, most injuries seen in travelers result from traffic accidents [9]. The risk for a motor vehicle colli-sion is 6-fold higher when travelers are driving themselves, with an additional 2.5-fold higher risk if they need to drive on the opposite side of the road than in their home country [10, 11]. In order to reduce the risk of traffic accidents and accident-related injuries, travelers should avoid travelling at night and must never drive under the influence of alcohol or without their seatbelts fastened [9, 12].
TYPES OF EXTREME SPORTSTraditional, adventure activities have always been pop-
ular during journeys, but extreme sports are also becoming increasingly popular with both domestic and international travelers. Extreme sports are high-risk activities of varying difficulty (Table 1), which often require the use of profes-sional equipment. Adventurous activities are performed in hazardous environments (on land, in the air or in water) and are usually associated with a high degree of risk because they involve high speed (rafting, skiing) or are practiced in extreme environmental or weather conditions (scuba diving, mountaineering) [13, 14]. The typical mistake made by extreme travelers is the lack of preparation. Unfortunately, it is quite common that extreme travelers fail to purchase a comprehensive insurance policy covering for extreme sports injuries or forget to take a travel health kit with a supply of regularly taken prescription medications. They hardly ever seek pre-travel advice, although a consultation with an experienced health care professional might be very useful in assessing the health status of a traveler and identifying potential contraindications for certain types of adventure activities.
SCUBA DIVING A vast number of tour operators globally offer short
diving excursion as well as longer diving holidays. In coun-tries with a developed tourist industry (e.g. Thailand, Belize, Australia) it is necessary to hire a certified local instructor for anybody willing to go on a diving excursion; in the developing countries, however, the law may not be so strict. The two greatest risks for divers include drowning and decompres-sion sickness. The Diver’s Alert Network is an organization that offers substantial support in case of emergency. The organization can provide comprehensive diving insurance, their personnel can find the nearest functional hyperbaric chamber and assist with the hyperbaric treatment. Scuba
Table 1. Selected types of extreme sports, risks and preventive measures
Extreme sport Health risks Preventive measures
Scuba diving Decompression sickness, drowning, injuries (fauna and flora)
Decompression in a hyperbaric chamber or in water (if a hyperbaric chamber is unavailable)
Surfing Drowning, injuries Surfing with an experienced surfer/instructor
Rafting Drowning, injuries Using the services of certified operators
Bungee jumping Injuries Using the services of certified operators
Skiing, snowboarding, back country skiing
Injuries, avalanches Personal protective equipment, avalanche transceiver, CO2 scrubber
Mountaineering Acute mountains sickness, injuries, hypothermia, sunburns, frost bites
Experienced guides, supervised expedition with medi-cal support, avoiding rapid ascents, acclimatization
Spelunking Injuries, drowning, infectious diseases Experienced guides, avoiding the activity during rain, avoiding animal guano (bats), rabies vaccination
Int Marit Health 2020; 71, 4: 281–290
www.intmarhealth.pl282

diving far away from functional hyperbaric chambers re-quires alternative strategies for dealing with decompression sickness. One such strategy includes in-water recompres-sion, i.e. re-descending until symptoms subside and then slowly re-ascending with doubling one’s decompression time. This strategy, however, requires considerable expe-rience, sufficient air supply, good weather conditions and time [15]. A complete medical assessment of fitness to dive is a prerequisite for anyone planning to go scuba diving. Travelers willing to have a diving holiday, especially those who are planning to go diving for the first time, must be given a thorough medical examination on the basis of which an ex-perienced health care provider will be able to identify poten-tial risk factors and contraindications to dive. During such an examination, a physician will need to evaluate the condition of the diver’s respiratory and cardiovascular systems, their ears and paranasal sinuses as well as assess their mental health; it will also be necessary to collect information on the patient’s past medical history. Exposure to cold water, high ambient pressure and an increased volume of respiratory gases causes physiological and systemic changes which may unmask or aggravate certain pre-existing conditions [16, 17]. During a diving fitness health assessment, special attention should be given to patients with:
— respiratory illnesses — diving is contraindicated in pa-tients with asthma, bronchitis or pneumonia, patients who are susceptible to spontaneous pneumothorax, status post a thoracic surgery, airway obstruction or emphysema which can be seen on the chest X-ray; the above-listed conditions change the respiratory mechan-ics, in response to rapid changes in intrapulmonary pressures, a barotrauma may occur;
— illnesses of the ear and paranasal sinuses — diving is contraindicated in patients with chronic otitis media or sinusitis, marked stenosis of the auditory canal, perfo-rated tympanic membrane; the above-listed conditions will make it difficult or impossible to equalize pressure in the ear and in sinuses while diving; being under water with perforated eardrum may lead to irritation of the labyrinth and disorientation;
— illnesses which may disturb consciousness, e.g. epilep-sy or poorly controlled diabetes are a contraindication to diving;
— psychiatric illnesses and disorders — diving is contraindi-cated in patients with a psychosis, anxiety or personality disorders, intellectual disability, alcohol addiction or substance abuse;
— cardiovascular illnesses — diving is contraindicated in patients with poor exercise tolerance, a positive cardiac stress test and certain heart diseases (Table 2); the stress associated with diving increases blood pressure and can cause tachycardia, which in patients with cer-
tain cardiovascular diseases (e.g. arterial hypertension, coronary heart disease) may result in acute myocardi-al infarction and sudden death (12% of diving-related deaths are associated with cardiac events).Pregnancy is another absolute contraindication to diving.
Pregnant women should be discouraged from any diving-re-lated activity as it may result in developmental anomalies in the fetus (as a result of the effects of high partial pres-sure of oxygen). Women who have had a natural birth are not recommended to go scuba diving for at least 4 weeks after they have given birth; while women who have had a Cesarean section should not scuba dive for 8–12 weeks after delivery. Scuba diving is relatively contraindicated in people with class 3 obesity (body mass index > 40); obesity does not only decrease general physical fitness but it may also increase the risk of a decompression sickness due to a high content of total nitrogen in the body (nitrogen is more soluble in fat than in other tissues) [17–19].
People diving regularly should undergo a physical ex-amination at regular intervals. The World Recreational Scu-ba Training Council (www.wrstc.com) has introduced the physical examination guidelines for determining fitness or absolute contraindications to diving. The guidelines have also been approved by the Divers Alert Network (www.diveralertnetwork.org) and the Undersea and Hyperbar-ic Medicine Society (www.membership.uhms.org) [20]. A health care provider assessing a person’s fitness to dive will need to consider age and sex-related risk factors as well as the diver’s underlying conditions. Divers over the age of 50 should be informed of the fact that they have a lower level of fitness compared to younger people and that some underlying conditions and medications are con-sidered relative or absolute contraindications to diving. Aging is associated with a number of natural changes in the body. As the total muscle mass declines, the person’s general level of fitness is getting lower. Also, because their blood pressure increases, older people have a higher risk of developing a cardiovascular disease. Any person over the age of 50 who is willing to go diving should have their blood pressure controlled through regular exercise, limiting the amount of sodium in their diet and taking hypotension medications. They are also strongly recommended to have a pre-travel consultation with a cardiologist to assess the risk of myocardial ischemia. Aging is also associated with certain metabolic changes. A decrease in insulin secretion and progressing insulin resistance may lead to glucose intolerance and the development of senile diabetes. Older adults are more prone to asymptomatic hypoglycemia, which is considered a contraindication to diving. Due to a reduced production of thyroid hormones, the elderly will naturally have a higher sensitivity to environmental temperature, and will therefore be more susceptible to hypothermia or a heat
www.intmarhealth.pl 283
Krzysztof Korzeniewski, Extreme traveler

Table 2. Absolute and relative contraindications to recreational scuba diving [19]
System Absolute contraindications Relative contraindications
Pulmonary Spontaneous pneumothoraxCystic or cavitating lesionsActive asthma, exercise-, emotional-, or cold-induced bronchospasm
AsthmaObstructive and restrictive diseasesInterstitial diseasesIntrathoracic surgeryPulmonary exercise impairment
Ear, nose, throat Current tympanic membrane perforationTympanostomy tubes
Recurrent infections (e.g., otitis media, sinusitis)Eustachian tube dysfunction
Neurological History of seizures or epilepsyIntracranial tumorsHistory of transient ischemic attack or strokeSpinal cord injury with neurological deficitsSignificant motor deficits
Peripheral sensory nerve deficitsPrevious head injuryChronic illnesses (e.g., multiple sclerosis)Migraine
Endocrine and metabolic
Recently diagnosed diabetes or recent change in medication
DiabetesHormonal excess or deficiency
Behavioral or psychological
Psychosis or taking antipsychoticsHistory of panic disorderClaustrophobia or agoraphobia
History of substance abuse
Cardiovascular Ischemic heart diseaseIntracardiac shuntsValvular stenosisCongestive heart failureHypertrophic cardiomyopathyDysrhythmias requiring medicationHistory of immersion pulmonary edema
Previous ischemic heart disease or myocardial infarctionHypertension and antihypertensive medicationValvular regurgitationCardiovascular exercise impairment
Gastrointestinal Chronic or recurrent bowel obstructionAbdominal wall hernias Containing bowelSevere reflux disease
Peptic ulcerationInflammatory bowel disease
Other PregnancySignificant impairment of the senses (e.g., blindness)
Young agePrevious decompression illnessLow physical fitnessThird degree obesity (BMI > 40)
BMI — body mass index
stroke. Older adults are also more vulnerable to dehydration and suffer degenerative changes in the musculoskeletal system, which limit their physical fitness and mobility. Be-cause of the above mentioned age-related changes in the body, increased prevalence of underlying conditions and long-term pharmacotherapy or polypharmacy (defined as taking multiple medications daily, frequently associated with increased risk of adverse drug events or drug-drug interactions), the older travelers are strongly encouraged to have a consultation with a specialist and have all the necessary tests performed prior to making a decision to go scuba diving [17].
Although there are no formal age restrictions, the minimum age for recreational diving is considered to be 12 years, on condition that the child is physically and men-tally fit for diving (they have enough physical strength to carry scuba equipment and are emotionally mature) and has no contraindications to diving. Under the Polish law, diving and diving lessons are allowed in children over the age of
10 years old; but younger children have been reported to go scuba diving under the supervision of an expert instructor. However, most experts will agree that children should not be allowed to dive with their own scuba set using gas mix-tures or compressed air because they have a significantly higher risk of pulmonary barotraumas compared to adults (according to most diving medicine specialists young chil-dren and adolescents < 16 years old should only be allowed snorkeling). Those who support children’s diving assume that diving at a shallow depth is relatively safe. They are either unaware of the fact or they have forgotten that when a diver is breathing compressed air there is no such thing as a ‘safe depth’ because pulmonary barotraumas can occur even when a diver is ascending rapidly from the depth as low as 120 cm. Also, children are more at risk from ear barotraumas than most adults. This is because children are predisposed to middle ear infections, which in turn can lead to Eustachian tube dysfunction. Additionally, children under the age of 12 will generally find it more difficult to
Int Marit Health 2020; 71, 4: 281–290
www.intmarhealth.pl284

perform the Valsalva maneuver in order to equalize pres-sure in the middle ear (the Eustachian tube in children is shorter and at a more horizontal angle). Another important issue to consider is the fact that diving may affect bone development (micro bubbles entering the circulatory system may damage the epiphyseal plate of the long bones and inhibit their growth). To minimize the risk of a decompression sickness, children should not be allowed to descend deeper than 9 meters [17].
With respect to women divers, the only absolute con-traindication to diving is during pregnancy. Women who experience severe headaches or heavy bleeding during menstruation, which could affect their physical fitness, should be temporarily discouraged from diving [16]. Some researchers claim that oral contraceptives increase the risk of a decompression sickness, which might be associated with changes in blood coagulation. It has been estimated that women have a higher risk of developing a decompres-sion sickness because in general they have more body fat than men (an average of 25% in females vs. 14% in males) [17].
A large number of recreational divers need to take medications (e.g. to treat their underlying conditions or as chemoprophylaxis). Most drugs are not contraindicated in divers; there are some medications, however, which are absolutely or relatively contraindicated in divers. People who have just started a new drug regimen should report any side effects or adverse events that have occurred to their health care provider so that the medication can be changed before they go diving [21–23]. Table 3 shows the information on selected medications and their possible side effects or adverse events in divers.
According to the Divers Alert Network, cardiovascular diseases are the second most common cause of death in divers. Therefore, pre-travel assessment of fitness to dive is particularly important for patients with cardiovascular condi-tions [24]. Mild-to-moderate asthma with normal spirometry should not be considered an absolute contraindication to diving [25]. Diabetic patients can be considered fit to dive on condition that they receive a fixed-dose insulin therapy for at least 12 months or oral antidiabetic agents for at least 3 months before a dive; their level of HbA1c is ≤ 9.0%; they had no episodes of hyperglycemia or hypoglycemia within 12 months before diving [26]. Diving-related morbidity is not much different from morbidity rates associated with other sports. The incidence of decompression sickness has been estimated at 5–80 cases per 100,000 dives [27]. According to the American and European Divers Alert Network reports, the incidence of diving-related deaths has been estimated at 1/6000 dives per year. By contrast, the risk of jogging-relat-ed death is 1/7700 joggers per year [28]. Officially, drowning has been reported the major cause of diving associated
fatalities. In practice, however, the major areas of concern for specialists in diving medicine are issues associated with the use of breathing mixtures or hasty ascents as well as management of divers with underlying conditions which are contraindications to scuba diving [24, 28].
SURFINGSurfing is a type of activity which requires a good level of
physical fitness. Surfing-related injuries are quite common, especially in beginner surfers. In expert surfers they occur at a rate of 2.7–4.0 per 1000 surfing days. Most of the injuries occur while riding waves (higher waves are typically associated with a greater risk of an injury) but also while surfing over a coral reef rather than a sandy bottom [29]. It is less common for a surfer to sustain an injury while lying on the surfboard and paddling it, diving under or through a wave or getting into or out of water. Surfing-related injuries usually result from a collision with a surfboard, particularly its fins [30]. Injuries from sea creatures, like jellyfish, sea urchins and stingrays, are rare among surfers [31]. Most surfing-associated injuries affect the head, face, eyes, ears, extremities and trunk. The most common types of injuries are contused or lacerated wounds to the head, face or extremities (being the result of a collision with the seabed or the surfboard or contact with a coral reef, rocks or sea urchins) as well as fractures of the lower extremities, the skull, the face or cervical spine [29]. Head traumas resulting from a collision with the sea floor or the surfboard, can cause concussion, loss of consciousness and eventually drowning [31]. While an eye injury which has been a result of hitting the surfboard or its fins can cause eyeball rupture or orbital
Table 3. Selected medications and their possible adverse effects in divers [18]
Medications Note
Narcotic/analgesic Narcotic — contraindicated; NSAIDs — no contraindications
Cardiac Some hypotension medications can reduce exercise tolerance
Insulin Blood glucose concentration should be checked before each dive
Antidepressant Contraindicated
Anticonvulsant Contraindicated
Antimalarial Mefloquine — contraindicated; doxycycline, atovaquone/proguanil — no contraindica-tions
Sympathomimetics Pseudoephedrine can reduce the risk of pressure-related ear injury
Anti-motion sickness
Cause sedation, impair the activity of central nervous system
NSAIDs — non-steroidal anti-inflammatory drugs
www.intmarhealth.pl 285
Krzysztof Korzeniewski, Extreme traveler

fracture. The common extremity injuries include lacera-tions, sprains or fractures. Chest injuries with rib fractures usually result from a collision with a surfboard and spinal injuries are typically caused by hitting the seabed [32]. The back pain resulting from isometric hyperextension of the spine during paddling is the most common health problem among surfers [29]. Surfers not wearing neoprene wetsuits are recommended to use cream or lotion to protect their skin from sunburns and the effects of the wind and cold as well as wax their surfboard with special surfboard wax [29]. Swimming is the fundamental ability that every surfer should have; before learning to surf in water they should first have conditional and fitness training out of water. In order to avoid injuries surfers should be encouraged to wear wetsuits (which protect them from hypothermia, sunburn and skin abrasions), ear plugs (to protect their ears) and puncture-proof footwear which will reduce the risk of foot injuries. Rubber nose and fin guards will reduce the severity of injuries in case of a collision with the surfboard [29, 31]. The risk of an accident or an injury can be minimized by following the recommended surf safety rules (surfing with another person; avoiding areas packed with other surfers; being aware of the currents, local flora and fauna; know-ing the depth of the sea or the ocean; paying attention to warning signs) [29].
RAFTINGWhite water rafting is a type of extreme activity of riding
in a raft along a river with a strong current and rapids. The risks associated with white-water rafting can be classified into several different categories: injuries sustained from a collision with another person or hitting something inside or outside the raft; risks associated with freshwater expo-sure; overexertion and musculoskeletal overload associated with paddling; risks related with post-traumatic stress [33, 34]. Most injuries occur when a rafter is hit with a paddle or falls out of the raft, in such cases there is a high risk of drowning or sustaining a serious injury from smashing against the rocks [33, 35]. The injuries which are most commonly reported among rafters include: contused or lacerated wounds, sprains, fractures and contusions; mostly in the head or face (eyes, lips, nose, teeth) and knees [34, 36]. Injuries to the face are more common in women, while injuries to extremities are more frequent in men. Because on average women are physically weaker than men, they tend to sit in the middle or at the back of the raft. If the raft capsizes rafters who are sitting in the front section (usually men) collide with the people at the back, which can cause injuries in both [36]. The incidence of rafting-related injuries has been estimated at 26–44 per 100,000 people [34, 35]. Lack of adequate training (a typical training session before a rafting tour takes no more than 30 min) and poor fitness
of the participants pose additional risks for white water rafters, especially if rafting takes place in more dangerous settings and in rivers with very strong currents and rap-ids. Exposure to contaminated freshwater carries additional risk for rafters. There have been reports of outbreaks of infectious diseases among rafters, such as an outbreak of leptospirosis (in Costa Rica) [37], schistosomiasis (within the tributaries of the Nile in Uganda) [38] and of giardiasis [34]. If there is increased risk of exposure to contaminated fresh water and of developing leptospirosis during white water rafting, doxycycline in a single dose of 200 mg taken weekly is recommended as prophylaxis [37]. White water rafting operators have an obligation to provide each participant with personal protective equipment such as a helmet and a life jacket, while rafters are strongly recommended to do conditioning training before they go white water rafting [35].
BUNGEE JUMPINGThere is little data available on bungee jumping related
injuries. The only exception being the well documented cas-es of fatal accidents, mostly caused by the cord or harness failure, in which people fell to the ground and died because the landing spot had not been secured with a safety air cushion. The most common traumas include eye injuries associated with free falling and a rapid change of speed, in particular retinal, subconjunctival or vitreous hemorrhage. The lesions can be either unilateral or bilateral and may lead to vision impairment or seeing floaters [39]. Other, less common injuries include: traumatic carotid artery dissec-tion, pulmonary hemorrhage, subdural hemorrhage, a dis-located shoulder, peroneal nerve palsy [13, 40]. Prevention of injuries is primarily based on a medical examination and assessing a person’s fitness to bungee jump. Patients with vascular or ocular conditions are considered to have a high-er risk of a bungee jumping related injury [13].
SKIING, SNOWBOARDINGBoth skiing and snowboarding are considered quite
dangerous and can result in a wide range of sports injuries (affecting the head, lower and upper limbs, bones, joints). With regard to snowboarders, who represent approximately 30% of winter sports fans, injuries were found to be most common in beginners. Most skiing- and snowboarding-re-lated injuries are reported in men because they tend to ski faster and in a more risky manner compared to women [13]. In general, injury rates have been shown to be higher among beginner skiers and snowboarders because of their lack of skill and experience. Most skiing or snowboarding related injuries occur from falls on the slope or as a result of a collision with other skiers or snowboarders (the risk is 3-fold higher for skiers compared to snowboarders) [41, 42]. Skiers are much more likely to suffer sprains or injuries
Int Marit Health 2020; 71, 4: 281–290
www.intmarhealth.pl286

of the lower limbs, in particular anterior cruciate ligament injuries, compared to snowboarders. On the other hand, wrist and spine injuries are more common in snowboard-ers. Some authors have suggested that snowboarders have higher rates of head trauma and concussion as well as bone fractures in particular ankle fractures [43] in comparison to skiers [44]. Prevention of accidents and injuries is not only the matter of good technical training and physical prepa-ration, but also of high-quality safety gear. A good helmet can prevent a head injury while wrist guards are particularly useful for snowboarders [42]. Backcountry snow skiing is yet another type of extreme activity, which needs to be given special consideration. An important risk associated with backcountry skiing is the risk of avalanches, which is par-ticularly high during the winter months and that can never be fully eliminated, even if a traveler has all the necessary experience and is well prepared. Approximately 90% of av-alanches occur on slopes of between 30o and 45o, usually after a heavy snowfall, i.e. when the conditions for skiing seem to be perfect. Skiers are recommended to travel in groups and to have equipment which in case of emergency may save their life (an avalanche transceiver, a shovel, a CO2 scrubber) [45]. A study carried out by Radwin et al. [46] demonstrated that in most avalanche victims CO2 ne-crosis occurs much faster than hypoxia or hypothermia, which means that CO2 scrubbers offer the best chance of survival for avalanche victims.
MOUNTAINEERINGMountaineering at altitudes higher than 2500 meters
above sea level or quick ascent are associated with a num-ber of health risk factors, which include climbing-related injuries, hypoxia-induced illnesses and conditions which are attributable to the effects of cold or the sun [47]. The most common climbing-related illnesses are those associated with exposure to hypobaric and hypoxic conditions. The progression rate of the illness and the severity of symptoms will primarily depend on the elevation (at higher altitudes the atmospheric pressure decreases, and so does the oxygen content), time of exposure (hours, days, weeks), and the rate of ascent. The major risk factors for developing a high-alti-tude illness are associated with acclimatization, intensity of exercise, physical and mental condition of a climber and pre-existing illnesses. Acute mountain sickness (AMS) is the most common of the altitude-related illnesses in mountain climbers who have quickly changed elevation. A total of 10–20% of people who have climbed 1800–2400 meters in less than 24 hours develop the symptoms of AMS. A ma-jority of climbers who have climbed 3400–4300 meters suffer mild symptoms of AMS, while 12–18% may develop a severe form of AMS. The condition normally presents with headaches, dizziness, nausea and vomiting, loss of appetite,
sleep disorders and shortness of breath. The symptoms of AMS may affect those who have climbed from low to high altitude (e.g. from 500 m to 3000 m above sea level) within a short period of time, as well as those who, being at a high altitude, have climbed even higher. Thus, the cause of AMS is not high altitude itself, but rather making a quick ascent within a short period of time [47]. A total of 25–35% of passengers who have had a direct flight from lowland to highland destinations e.g. Lhasa in Tibet (3650 m above sea level) or La Paz in Bolivia (3800 m above sea level) develop symptoms of AMS [48]. AMS is best prevented by gradual acclimatization and discontinuation of further ascent if symptoms occur. The condition can be treated by descending to a lower altitude, administration of drugs and oxygen therapy (a portable hyperbaric chamber e.g. Gamow bag may be effective if it is available) [49]. According to study findings, acetazolamide has been most effective for prophylaxis and treatment of AMS; the drug accelerates ac-climatization through its diuretic effect, improves ventilation and sleep breathing patters. Acetazolamide does not mask the symptoms of AMS and can also be used for therapeutic purposes. The prophylactic dose in adults is 125–250 mg taken every 12 hours at least 24 hours before ascent, the therapy should continue for at least 48 hours after arrival at the highest altitude. Treatment doses of the drug are 250 mg taken every 12 hours; they should be continued for 24 hours after symptoms have subsided or after descent to a safer altitude [48]. High altitude pulmonary edema (HAPE) and high altitude cerebral edema (HACE) are the other two common conditions which are associated with hypobaric and hypoxic conditions. Unlike acute mountain sickness, HAPE and HACE may be life-threatening. The conditions are caused by decreased partial pressure of oxygen which leads to functional disorders, primarily of the central nervous system as well as the circulatory and respiratory systems. The progression rate of the illness and the severity of symptoms will mostly depend on the elevation itself, but also on a number of other factors such as age, physical and mental condition of a climber, hydration level, the use of medications as well as time of exposure to high altitude conditions and the rate of ascent [49]. HAPE is usually associated with hypoxia (resulting from pulmonary hypertension) and pulmonary edema (being the effect of increased vascular permeability). The estimated incidence of HAPE may range from 0.01% to even 15% in those rapidly climbing to very high altitudes and covering the distance of more than 2400 meters within a short period of time; other risk factors that increase the incidence of HAPE include genetic predisposition and past history of the condition [48]. Unlike AMS or HAPE, the incidence of HACE in climbers is much lower and is usually reported in climbers who have ascended to more than 3600 meters. In general, prolonged
www.intmarhealth.pl 287
Krzysztof Korzeniewski, Extreme traveler

exposure to hypoxic conditions increases permeability of cerebral vessels, thus, leading to edema. Other common medical problems that are reported in climbers include peripheral edema (usually affecting the lower or upper limbs or the face), retinal hemorrhage (usually asymptomatic), thromboembolism, immunosuppression and slow healing of wounds. Climbers are also at a higher risk of developing conditions associated with the exposure to cold (hypother-mia, frost bites, chilblains, trench foot, respiratory illnesses) or intense sunlight (sunburns, snow blindness) [47]. All climbers are strongly recommended to have a pre-travel consultation before they go mountaineering. A pre-travel consultation is a good opportunity to assess a person’s fitness to climb and identify any potential underlying con-ditions, this is extremely important because exposure to ex-treme environmental conditions may unmask or aggravate certain diseases. Climbers are also recommended to have a dentist appointment because exposure to hypoxic and hypobaric conditions can exacerbate inflammatory lesions of the pulp or periodontium. While travelers with pre-existing respiratory or cardiovascular diseases are encouraged to have a pre-travel consultation with their specialist. Severe chronic obstructive pulmonary disease, pulmonary hyper-tension presenting with clinical signs, decompensated heart failure and sickle-cell anemia are absolute contraindications to mountaineering [49].
SPELUNKINGRemote and technically difficult cave exploration has
been increasing in popularity among travelers in recent years. In principal, the major health risks include trauma and drowning in a flash flood, e.g. during a rainy season. In developing countries, quick evacuation may not be an option as the medical capabilities are limited. For their own safety, cave explorers are advised to inform local authorities of their plans, and organize the medical and evacuation support on their own. Spelunking is also associated with certain infectious risks, with histoplasmosis, a fungal infection caused Histoplasma capsulatum, being the most common cave-associated illness. The disease is transmitted through exposure to bird or bat guano, which is contaminated with infective spores [50, 51]. The biggest risk for spelunkers, however, is from rabies, a disease which is fatal for hu-mans. Cave-associated rabies is primarily transmitted from infected bats (bats account for 17% of all rabies cases in animals in the USA) [52]. Spelunkers need to be aware of the fact that rabies is not only transmitted through direct contact with an infected bat, but it can also spread indi-rectly, i.e. through exposure to the animal’s saliva, or even through aerosol transmission. This is possible with very large colonies of bats living in poorly ventilated caves with high humidity and temperature [53]. Rabies can be best
prevented through pre-exposure vaccination; in line with the proposed guidelines the rabies vaccine is “administered in 3 doses on days 0, 7 and 21 or 28; a complementary dose is administered 12 months after the primary course; booster doses are recommended every 5 years). In case of a direct contact with potentially rabid bats (being bit-ted or scratched), their feces or other secretions, it will be necessary to receive post-exposure vaccination. In patients who have received pre-exposure vaccination (in the last 5 years) post-exposure vaccination consists of 2 doses: the first on the day of exposure and the second 3 days after. In travelers who have not been immunized (their last vaccination was more than 5 years before, they have not completed the full vaccination course or have never received pre-exposure vaccination) post-exposure vaccination requires the administration of 5 doses of the rabies vaccine on days: 0 (the day of exposure), 3, 7, 14 and 28. Before administering the first dose of the vaccine, a non-immunized individual should also receive immunoglobulin RIG (HRIG: 20 IU/kg body mass or ERIG: 40 IU/kg body mass)” [12]. Another risk associated with spelunking is the risk of exposure to water contaminated with rodent or bat droppings or urine. Cave water tends to have a higher pH, which facilitates the growth of Leptospira, and may therefore be a potential source of leptospirosis. The best preventive measure against the disease is the adminis-tration of a single 200 mg dose of doxycycline weekly [54].
TRAVEL INSURANCE POLICYIf travelers are going to engage in any form of extreme
activities, they are strongly recommended to purchase a comprehensive travel insurance policy that would cover for the cost of treatment and assistance. The choice is nor-mally between the basic and extended insurance coverage, but extreme travelers need to be aware of the fact that most extreme activities are normally excluded from basic insur-ance plans. The typical travel insurance exclusions are [15]:
— scuba diving; — jet skiing; — animal or motor vehicle racing; — spelunking; — hang gliding, sky diving, parachuting, bungee jumping; — air sports, aviation (except as a passenger on a com-
mercial flight); — skiing and snowboarding, except for the purpose of rec-
reation (no insurance coverage in case of backcountry skiing/snowboarding or skiing/snowboarding against the advice of the local ski instructors of local authorities);
— mountaineering with the use of professional equipment (ropes) or above 4500 meters above sea level;
— any other sporting activity associated with an increased risk of injury.
Int Marit Health 2020; 71, 4: 281–290
www.intmarhealth.pl288

Extreme travelers are recommended to purchase a trav-el insurance policy covering for the costs of medical evacua-tion and repatriation and the costs of an emergency rescue operation which are not usually covered by the standard accident insurance policy. Their insurance policy should also cover for the costs of specialist treatment (e.g. treatment in a hyperbaric chamber for divers with decompression sick-ness), the costs of an emergency rescue operation at sea or in the mountains and include third party liability insurance (personal injury and property damage). The price of such comprehensive travel insurance will naturally depend on a variety of factors such as the nature of extreme sports (professionals vs. amateurs) or any underlying medical con-ditions an extreme traveler may have. Travelers need to bear in mind that their insurance company may refuse to pay the claim if damage or incident was associated with misuse of alcohol, drugs or other illegal substances [12].
REFERENCES1. Gundacker ND, Rolfe RJ, Rodriguez JM. Infections associated with
adventure travel: A systematic review. Travel Med Infect Dis. 2017; 16: 3–10, doi: 10.1016/j.tmaid.2017.03.010, indexed in Pubmed: 28351605.
2. Caine DJ. The epidemiology of injury in adventure and extreme sports. Med Sport Sci. 2012; 58: 1–16, doi: 10.1159/000338558, indexed in Pubmed: 22824836.
3. Goodyer L, Gibbs J. Medical supplies for travelers to deve-loping countries. J Travel Med. 2004; 11(4): 208–211, doi: 10.2310/7060.2004.19003, indexed in Pubmed: 15541222.
4. Jong EC. Approach to Travel Medicine and Contents of a Personal Travel Medicine Kit. In: Sanford CA, Pottinger PS, Jong EC (Eds). The Travel and Tropical Medicine Manual. 5th Edition. Marickville, Elsevier 2017.
5. Christenfeld N, Glynn LM, Phillips DP, et al. Exposure to New York City as a risk factor for heart attack mortality. Psychosom Med. 1999; 61(6): 740–743, doi: 10.1097/00006842-199911000-00003, indexed in Pubmed: 10593623.
6. Kop WJ, Vingerhoets Ad, Kruithof GJ, et al. Risk factors for myocardial infarction during vacation travel. Psychosom Med. 2003; 65(3): 396–401, doi: 10.1097/01.psy.0000046077.21273.ec, indexed in Pubmed: 12764212.
7. Wilder-Smith A, Khairullah NS, Song JH, et al. Travel health knowled-ge, attitudes and practices among Australasian travelers. J Travel Med. 2004; 11(1): 9–15, doi: 10.2310/7060.2004.13600, indexed in Pubmed: 14769281.
8. Cabada MM, Maldonado F, Mozo K, et al. Pre-travel preparation for Cusco, Peru: a comparison between European and North American travelers. J Travel Med. 2010; 17(6): 382–386, doi: 10.1111/j.1708-8305.2010.00461.x, indexed in Pubmed: 21050317.
9. Odero W, Garner P, Zwi A. Road traffic injuries in developing countries: a comprehensive review of epidemiological studies. Trop Med Int Health. 1997; 2(5): 445–460, indexed in Pubmed: 9217700.
10. Carey M, Aitken M. Motorbike Injuries in Bermuda: A Risk for To-urists. Annals of Emergency Medicine. 1996; 28(4): 424–429, doi: 10.1016/s0196-0644(96)70009-4.
11. Petridou E, Askitopoulou H, Vourvahakis D, et al. Epidemiology of road traffic accidents during pleasure travelling: the evidence from
the island of Crete. Accid Anal Prev. 1997; 29(5): 687–693, doi: 10.1016/s0001-4575(97)00038-9.
12. Korzeniewski K. Medycyna podróży. Kompendium [in Polish]. Wy-dawnictwo Lekarskie PZWL, Warszawa 2016.
13. Gomez AT, Rao A. Adventure and Extreme Sports. Med Clin North Am. 2016; 100(2): 371–391, doi: 10.1016/j.mcna.2015.09.009, indexed in Pubmed: 26900120.
14. Young CC. Extreme sports: injuries and medical coverage. Curr Sports Med Rep. 2002; 1(5): 306–311, doi: 10.1249/00149619-200210000-00009, indexed in Pubmed: 12831694.
15. Boulware DR. Travel medicine for the extreme traveler. Dis Mon. 2006; 52(8): 309–325, doi: 10.1016/j.disamonth.2006.08.004, indexed in Pubmed: 17101310.
16. Lynch JH, Bove AA. Diving medicine: a review of current evidence. J Am Board Fam Med. 2009; 22(4): 399–407, doi: 10.3122/jab-fm.2009.04.080099, indexed in Pubmed: 19587254.
17. Krzyżak J, Korzeniewski K. Medycyna dla nurkujących [in Polish]. Wydawnictwo 4Font 2020, Poznań 2020.
18. Marienau KJ, Arguin PM. Diving Medicine. In: Keystone JS, Freedman DO, Kozarsky PE, Connor BA, Nothdurft HD. [Eds]. Travel Medicine. Third Edition. Saunders, Philadelphia, PA 2013: 373–378.
19. Meintjes J. Diving Medicine. In: Keystone JS, Kozarsky PE, Connor BA, Northdurft HD, Mendelson M, Leder K. Travel Medicine. Fourth Edition. Elsevier Inc., USA 2019: 401–406.
20. Medical guidelines. Recreational Scuba Training Council. http://www.wrstc.com/downloads/10%20-%20Medical%20Guidelines.pdf (Accessed: 28 Sept 2017).
21. Harrison D, Lloyd-Smith R, Khazei A, et al. Controversies in the me-dical clearance of recreational scuba divers: updates on asthma, diabetes mellitus, coronary artery disease, and patent foramen ovale. Curr Sports Med Rep. 2005; 4(5): 275–281, doi: 10.1097/01.csmr.0000306222.19714.33, indexed in Pubmed: 16144586.
22. Dowse MS, Cridge C, Smerdon G. The use of drugs by UK recreational divers: prescribed and over-the-counter medications. Diving Hyperb Med. 2011; 41(1): 16–21, indexed in Pubmed: 21560980.
23. Leigh D. DAN discusses malaria and antimalarial drugs. Alert Diver, September 2020. http://www.diversalertnetwork.org/medical/articles/article.asp?articleid=80 (Accessed: 28 September 2017).
24. Denoble PJ, Caruso JL, Dear G. Common causes of open-circuit re-creational diving fatalities. Undersea Hyperb Med. 2008: 393–406, doi: 19175195.
25. Godden D, Currie G, Denison D, et al. British Thoracic Society guideli-nes on respiratory aspects of fitness for diving. Thorax. 2003; 58(1): 3–13, doi: 10.1136/thorax.58.1.3, indexed in Pubmed: 12511710.
26. Pollock NW, Uguccioni DM, Dear Gde L. [Eds]. Diabetes and recreatio-nal diving: guidelines for the future. Proceedings of the UHMS/DAN 2005 June 19 Workshop. Durham, NC: Divers, Alert Network 2005. Guidelines available at. http://www.diversalertnetwork.org/news/download/SummaryGuidelines.pdf (Accessed: 28 September 2017).
27. Bove AA, Moon RE. Patent foramen ovale – is it important to divers? In: Alert Diver, Sept/Oct 2004. http://diversalertnetwork.org/medical/articles/article.asp? articleid=70 (Accessed: 28 September 2017).
28. Vann RD, Lang MA. [Eds]. Recreational Diving Fatalities. Proceedings of the Dives Alert Network 2010 April 8-10 Workshop. Durham, NC. Available at:. http://d35gjurzz1vdcl. cloudfront.net/ftw-files/Fata-lities_Proceedings.pdf (Accessed: 28 September 2017).
29. Sunshine S. Surfing Injuries. Current Sports Medicine Reports. 2003; 2(3): 136–141, doi: 10.1249/00149619-200306000-00005, indexed in Pubmed: 12831652.
30. Nathanson A, Bird S, Dao L, et al. Competitive surfing injuries: a prospective study of surfing-related injuries among con-
www.intmarhealth.pl 289
Krzysztof Korzeniewski, Extreme traveler

test surfers. Am J Sports Med. 2007; 35(1): 113–117, doi: 10.1177/0363546506293702, indexed in Pubmed: 17021312.
31. Nathanson A, Haynes P, Galanis D. Surfing injuries. Am J Emerg Med. 2002; 20(3): 155–160, doi: 10.1053/ajem.2002.32650, indexed in Pubmed: 11992332.
32. Sano A, Yotsumoto T. Chest injuries related to surfing. Asian Cardiovasc Thorac Ann. 2015; 23(7): 839–841, doi: 10.1177/0218492315591103, indexed in Pubmed: 26071603.
33. Fiore DC, Houston JD. Injuries in whitewater kayaking. Br J Sports Med. 2001; 35(4): 235–241, doi: 10.1136/bjsm.35.4.235, indexed in Pubmed: 11477016.
34. Fiore D. Injuries Associated With Whitewater Rafting and Kayaking. Wilderness & Environmental Medicine. 2003; 14(4): 255–260, doi: 10.1580/1080-6032(2003)14[255:iawwra]2.0.co;2.
35. Wilson I, McDermott H, Munir F, et al. Injuries, ill-health and fata-lities in white water rafting and white water paddling. Sports Med. 2013; 43(1): 65–75, doi: 10.1007/s40279-012-0007-8, indexed in Pubmed: 23315757.
36. Whisman SA, Hollenhorst SJ. Injuries in commercial whitewater rafting. Clin J Sport Med. 1999; 9(1): 18–23, doi: 10.1097/00042752-199901000-00004, indexed in Pubmed: 10336047.
37. Centers for Disease Control and Prevention (CDC). Outbreak of leptospirosis among white-water rafters--Costa Rica, 1996. MMWR Morb Mortal Wkly Rep. 1997; 46(25): 577–579, indexed in Pub-med: 9214567.
38. Morgan OW, Brunette G, Kapella BK, et al. Schistosomiasis among recreational users of Upper Nile River, Uganda, 2007. Emerg In-fect Dis. 2010; 16(5): 866–868, doi: 10.3201/eid1605.091740, indexed in Pubmed: 20409387.
39. Jain AK, Gaynon M. Images in clinical medicine. Macular hemorrhage from bungee jumping. N Engl J Med. 2007; 357(3): e3, doi: 10.1056/NEJMicm064881, indexed in Pubmed: 17634454.
40. Manos D, Hamer O, Müller NL. Pulmonary hemorrhage resulting from bungee jumping. J Thorac Imaging. 2007; 22(4): 358–359, doi: 10.1097/RTI.0b013e31813fab8b, indexed in Pubmed: 18043394.
41. Wijdicks CA, Rosenbach BS, Flanagan TR, et al. Injuries in elite and recreational snowboarders. Br J Sports Med. 2014; 48(1): 11–17, doi: 10.1136/bjsports-2013-093019, indexed in Pubmed: 24282020.
42. Hume PA, Lorimer AV, Griffiths PC, et al. Recreational snow-sports injury risk factors and countermeasures: a meta-analysis review and Haddon matrix evaluation. Sports Med. 2015; 45(8): 1175–1190, doi: 10.1007/s40279-015-0334-7, indexed in Pubmed: 25946993.
43. Mahmood B, Duggal N. Lower extremity injuries in snowboarders. Am J Orthop (Belle Mead NJ). 2014; 43(11): 502–505, indexed in Pubmed: 25379746.
44. Stenroos A, Handolin L. Incidence of recreational alpine skiing and snowboarding injuries: six years experience in the largest ski resort in Finland. Scand J Surg. 2015; 104(2): 127–131, doi: 10.1177/1457496914532249, indexed in Pubmed: 24786173.
45. Radwin MI, Grissom CK. Technological advances in avalanche survival. Wilderness Environ Med. 2002; 13(2): 143–152, doi: 10.1580/1080-6032(2002)013[0143:taias]2.0.co;2, indexed in Pubmed: 12092969.
46. Radwin M, Grissom C, Scholand M, et al. Normal oxygenation and ventilation during snow burial by the exclusion of exhaled carbon dioxide. Wilderness & Environmental Medicine. 2001; 12(4): 256–262, doi: 10.1580/1080-6032(2001)012[0256:noavds]2.0.co;2.
47. Korzeniewski K. Health problems in high mountain conditions [in Polish]. Pol Merk Lek. 2008; 25(146): 161–165, indexed in Pub-med: 18942339.
48. Dietz TE, Hackett PH. High-Altitude Medicine. In: Keystone JS, Kozarsky PE, Connor BA, Northdurft HD, Mendelson M, Leder K. Travel Medicine. Fourth Edition. Elsevier Inc., USA 2019: 387–400.
49. Hartman-Ksycińska A, Kluz-Zawadzka J, Lewandowski B. High alti-tude illness. Przegl Epidemiol. 2016; 70(3): 490–499, indexed in Pubmed: 27888818.
50. Jülg B, Elias J, Zahn A, et al. Bat-associated histoplasmosis can be transmitted at entrances of bat caves and not only inside the caves. J Travel Med. 2008; 15(2): 133–136, doi: 10.1111/j.1708-8305.2008.00193.x, indexed in Pubmed: 18346250.
51. Norman FF, Martín-Dávila P, Fortún J, et al. Imported histoplasmo-sis: two distinct profiles in travelers and immigrants. J Travel Med. 2009; 16(4): 258–262, doi: 10.1111/j.1708-8305.2009.00311.x, indexed in Pubmed: 19674266.
52. Krebs JW, Noll HR, Rupprecht CE, et al. Rabies surveillance in the United States during 2001. J Am Vet Med Assoc. 2002; 221(12): 1690–1701, doi: 10.2460/javma.2002.221.1690, indexed in Pubmed: 12494966.
53. Messenger SL, Smith JS, Rupprecht CE. Emerging epidemiology of bat-associated cryptic cases of rabies in humans in the United Sta-tes. Clin Infect Dis. 2002; 35(6): 738–747, doi: 10.1086/342387, indexed in Pubmed: 12203172.
54. Mortimer R. Leptospirosis in a Caver Returned from Sarawak, Malay-sia. Wilderness & Environmental Medicine. 2005; 16(3): 129–131, doi: 10.1580/1080-6032(2005)16[129:liacrf]2.0.co;2.
Int Marit Health 2020; 71, 4: 281–290
www.intmarhealth.pl290
Dr. Graziano Pallotta, Scuola di Scienze del Farmaco e dei Prodotti della Salute, Università di Camerino, via Madonna delle Carceri 9, 62032 Camerino (MC) Italy,
e-mail: [email protected]
TelePharmaSea: proposing a novel approach to automate, organize and simplify management of medical chest on board commercial vessels
Giulio Nittari1 , Graziano Pallotta1 , Ravjyot Singh Khuman1 , Francesco Amenta1, 2
1Telemedicine and Telepharmacy Centre, School of Pharmacological Sciences and Health Products, University of Camerino, Italy 2Research Department, International Radio Medical Centre (C.I.R.M.), Rome, Italy
ABSTRACTBackground: The on-board pharmacy is the kit that allows the implementation healthcare on board ships, since it should contain everything that may be needed to guarantee proper and efficient health care interven-tions for seafarers. There are several problems that can lead to a difficult and non-optimal management of the on-board pharmacy. This work illustrates the “TelePharmaSea” software, specifically developed to optimise the management of the on-board pharmacy of commercial vessels without medical personnel. Materials and methods: We collected the Medical Scales of the various Flag States and brought them all into a standardised format which could be used. The Active Ingredients and Pharmaceutical form of each medicine is linked with the ATC Codes. Active Ingredients having similar effect are linked by ATC codes. Items that did not have an ATC code were given a unique system-generated code. Due to the proprietary nature of the software of which the database structure and functioning is unique, we cannot share the exact structure; however, the approach regarding the same has been highlighted.Results and Conclusions: The proposal of the TelePharmaSea software can be an effective tool capable of a significant improvement of the overall quality of medical and pharmacological assistance provided on ships without a doctor on board. The system can guarantee a better management of the on-board phar-macy’s inventory, and it may also reduce the risks of mistakes in drugs administration.
(Int Marit Health 2020; 71, 4: 291–295)
Key words: digital health, seafarers, health, safety, drug, monitoring
�
INTRODUCTION From the eighteenth to the nineteenth century, the phy-
sicians who embarked on board were carrying a cassette containing therapeutic prescriptions to be used in case of emergency [1].
Since the nineteenth century, many nations began to regulate hygiene matters aboard ships, and required the presence of a “medicine box” containing all the medicines used by sailors, with instructions for their use [2].
That is why, even today, all the medicines and all the medical supplies on board is called “ship medicine chest”. The types of activities performed on board a ship are entirely different from the ones performed onshore [3].
The situation is complicated by the fact that ships become both a workplace and a living environment for an extended period of time. Also, cargo ships do not carry qualified medical or paramedic personnel and sailors have a higher risk of accidents which may result in death or a serious injury [4].
One of the main problems arising from the early use of these chests was the diversity of content between different flag vessels. In this sense, the best solution to this problem is in international agreements, to be reviewed periodically to establish a scale of medicines, especially in relation to those which are the main health problems in which sailors are involved [5].
www.intmarhealth.pl 291
Int Marit Health 2020; 71, 4: 291–295
10.5603/IMH.2020.0049 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
ORIG INAL ART ICLE

The on-board pharmacy or “medical chest”, is a kit that allows the implementation of health care, providing thera-peutic interventions of first aid. It is therefore a vital asset, which must contain everything that might be needed to ensure proper and complete health care for sailors [6–8].
Nowadays, it is no longer a container enclosing medi-cines and medical devices, but rather a real pharmacy on board that has a wide range of health products. The man-ager of drug management is the master, or a designated officer, who also holds the responsibility of keeping the on-board pharmacy always stocked and efficient [9].
A large number of national and international regula-tions (World Health Organization [WHO], European Union) [10] makes it difficult for ship officers managing the ship’s pharmacy to perform their tasks.
Medicinal products are identified by the international non-proprietary name of the active principle and/or by their chemical or invented (branded) names [11]. This may make the identification of a medicinal product difficult, primarily if it is purchased abroad and the box and instructions are writ-ten in the language of the country where it is marketed [5].
Medicinal products considered restricted by some coun-tries are not restricted in the others. This could create confusion worsened by the fact that ship’s personnel do not usually have enough knowledge of pharmacology/pharmacy regulations to prepare a cabinet for restricted products before they stop in different countries [12, 13].
Another problem may occur as a result of a language barrier; if a given medicine has expired or has been used, it would be difficult to replace it with a local product, especially if it is labelled in a rare language [14].
Therefore, there is a simpler classification system of the medicinal compounds — the ATC (ATC: Anatomy, Therapeutic properties, Chemical, pharmacological properties) [5].
After carefully understanding the challenges, we decided to create an application that would have the potential to provide the solutions. Thus the idea of “TelePharmaSea” was developed.
The purpose of TelePharmaSea is to provide standard procedures for handling the on-board pharmacy and to au-tomatise some actions which are still carried out manually, offering unique opportunities to simplify the management of the ship’s pharmacy and consequently, to improve the quality of medical assistance on board ships.
MATERIALS AND METHODSWe collected the Medical Scales of the various Flag
States and brought them all into a standardised format which could be used. For the purpose of this exercise, we have only taken into consideration the scales pertaining to merchant vessels with no doctor on board.
The Active Ingredients and Pharmaceutical form of each medicine is linked with the ATC codes. The ATC/DDD system since its inception in 1996 has continued to expand and include most drugs promoted by WHO as the global standard for medicine classification and utilisation [15].
Active ingredients having similar effect are linked by ATC codes [16].
Items that did not have an ATC code were given a unique system-generated code.
The first step was to ensure that each item across the data had a Unique Code which would either be the ATC code or the Unique System-Generated Code and similar active ingredients documented.
Due to the proprietary nature of the software of which the database structure and functioning is unique, we cannot share the exact structure; however, the approach regarding the same has been highlighted (Fig. 1).
Figure 1. The figure shows the simplified relation of some of the various master tables; *defense against unauthorised access
Int Marit Health 2020; 71, 4: 291–295
www.intmarhealth.pl292

Thereafter a detailed database structure with several master tables was created to document the following: 1. Active Ingredient 2. ATC Code/Unique System Code 3. Pharmaceutical Forms 4. Similar Active Ingredients 5. Special Notes
Another master table was created to save Flag State de-tails:1. Flag State 2. Flag Icon 3. Country Associated
Corresponding tables were thereafter structured to link the Active Ingredients and the Flag States as well as record the additional information:1. Flag State 2. ATC Code/Unique System Code 3. Type of Vessel4. Minimum Quantity5. Special Notes
Data was meticulously added into the database by ap-proved and experienced pharmacist to ensure correct data transfer to the system. The data was further validated and screened by another pharmacist for the same purpose.
Each vessel is provided with a secure login for using the application for updating inventory, interacting with a quali-fied pharmacist as well as completing the requirements for the remote inspection and e-certification.
THE CHECKLIST FOR VESSELSA detailed medical checklist has been developed to
enhance the standards of sickbay management on board. The checklist was developed after detailed analysis on the factors leading to good practices and those requiring to be monitored routinely.
SECURITYAny system that involves issuing certificates or holds any
user information needs to have adequate security mecha-nisms to avoid misuse.
Methods used in the application are: — 2-step verification: The User is required to enter an OTP
which is sent to the registered ID for authorisation. This is mainly seen at the pharmacy side of the application;
— Fingerprint verification: For added security a fingerprint scan mechanism is used to grant access to authorised protocols of the application.
RESULTSA web-based platform with user access rights was devel-
oped as described above. A first step was to compare the different contents of the ship pharmacy as required by the
different Flag States. The platform has two intended users: (A) The vessel; (B) The pharmacist.
FEATURES — FLAG STATE COMPARISONS We were unable to find any previously published paper
that compared all the Flag State Medical Scales and attempt-ed to propose for a common standardised scale. This paper presents the solution whereby this can be easily achieved with the technological solution being put forth in this paper.
FEATURES — THE PHARMACISTThe pharmacist controls the information in the master
tables as well as completes the certification protocol of the system to generate an E-Certificate of conformity or non-conformity for the vessel (Table 1).
FEATURES — VESSELThe tasks required from the vessel side are summarised
in Table 2.
DISCUSSION
LIMITATIONSMost of the Flag State medical scales are in PDF format
with varying formats which posed a serious challenge in the initial data format standardisation. Sourcing the medical scales was a challenge and very few could be easily found on the website. Our collection of Flag State Medical Scales was based on information from only approved state sites for the Flag States, companies with vessels plying under the Flag State and data from Centro Internazionale Radio Medico (C.I.R.M.).
Mentioned flag stated and sources are the following: mentioned flag states and sources are the following: Austra-lia, Cyprus, C.I.R.M. Medical Scale, France, Gibraltar, Italy, Isle of Man, Liberia, Malta, Marshall Islands, Netherlands, Singapore, WHO [17–28].
STANDARDISED MEDICAL SCALEThe objective of this effort was to propose a viable solution
that can be further evaluated to automate, streamline and make easier the management of the medical chest and also provide a means that would allow for creating a standardised medical scale taking into consideration the various Flag States. There are limited studies that suggest the use of medicines with re-spect to medical scales to identify medicines and stocks that are no longer effective or used for care onshore. These can be replaced or delivering cost effective measures for the industry.
Therefore, we believe this easy to use system will lead the way to well-formatted medical scales that can easily be compared with various Flag States and thereafter champion the cause towards a standardized medical scale to benefit
www.intmarhealth.pl 293
Giulio Nittari et al., A novel approach for the management of medical chest onboard commercial vessels

Table 1. Workflow of pharmacist’s activity
Add/edit item to master database
The pharmacist can add an item to the Master Tables. For this the pharmacist must mention the globally accepted ATC code or if not available ask the system to generate a Unique System Code
Add/edit flag state Flag State Medical Scales are not routinely updated. However, if there will be updates, the system permits the pharmacist to make changes which will automatically sync across and intimate the vessels and companies
Add/edit pharmaceutical forms
Over time medicines may be made available in multiple pharmaceutical forms or be available for different purposes. It is essential to mention the pharmaceutical form as the use and indications can vary. Should there be a need to update or add, the pharmacist is permitted to make the required change
Add/edit company and vessel
To be able to perform E-Inspection and E-Certifications it is important to link the system with the vessel/ /company. This allows for 2-wayflow of information required
Digital review of checklist from vessel
The checklist which was initially completed and shared using more conventional digital formats such as word or excel, now have a more secure and easier way of sending this information directly through the platform. No additional email and attachments would be required. The system which is secure can only be accessed by the authorized personnel
Digital review of inventory from vessel
The updated inventory of the vessel is synced periodically with the checklist which allows the pharmacist to easily review the quantities. The system provides automated alerts to the vessel and the pharmacist thereby allowing them to easily review the same
Assisted E-Certificate generation (2-step verification)
The automated system assists the pharmacist to quickly review the inventory based on required minimum quantities and the responses from the checklist to authorize the compliance certificate or alert the vessel of any incomplete measures
Assisted order form generation (2-step verification)
Order forms generally take the longest time and can be confusing with the correct pharmaceutical form; active ingredient, etc., should be mentioned for it to be correctly supplied to the vessel. Therefore, to mitigate the challenges, the system allows the pharmacist to auto generate an order form by automatically calculating the minimum quantities required. This saves time and prevents manual errors that could arise using the conventional forms of order forms
Table 2. Workflow of crew activity
Add new inventory (batch numbers)
The officer responsible for the medical chest on the vessel can easily update the inventory and manage stocks with different expiry dates. This allows for more accurate analysis of the medical chest and timely restocking alerts
Update inventory With the system being pre-setup as soon as the vessel logs in, the work of the officer responsible is reduced to ensuring the stock is routinely updated
Complete checklist Ideally it is recommended for the vessel to complete the checklist every quarter. This is also the frequency for the E-Certification. However, the officer responsible can run through the checklist at any time to document the medical management. These records are synced to the pharmacist
View certificate of compliance
Once the certificates are issued by the pharmacist, the officer responsible is able to view the same on the platform ensuring an automated digitalised archive of the records
the ship owners and management companies having fleets of various Flag States.
The C.I.R.M. medical scale has been developed using this system and by comparing the medical scales of the most commonly used Flag States. It also specifies the similar medicines which makes it essentially useful for a ship that needs to restock in a foreign port where the same active principle is not available.
E-COMPLIANCE FOR STOCKING AND DISPOSAL OF MEDICINES ON BOARD VESSELS
The system is complemented by service of TelePhar-maSea which includes access to skilled and experienced pharmacists. The connected framework allows for easy
compliance tracking, E-Inspections and guidelines for smart re-stocking and disposal of medicines on board. Continued efforts can lead a generally smart re-stocking effort for the industry bringing huge savings if correctly implemented [29].
CONCLUSIONSThe system developed holds specific database structure
and functioning to make it effective. The system can be used to assist Tele Medical Assistance Service (TMAS) centres as well as Tele-Pharmacists, shipping companies with the trends of consumptions of medicines which can be easily linked with the type of medical event. For data security and keeping in mind General Data Protection Regulation (GDPR), patient information will not be available; however,
Int Marit Health 2020; 71, 4: 291–295
www.intmarhealth.pl294

while providing medical assistance the tool can save con-siderable time for reviewing the medicines available based on the Flag State of the vessel. Later features could include where seafarer can track his/her consumption of medicines to be more aware of one’s health. The better inventory solution and classification guaranteed by TelePharmaSea may also reduce the risk of mistakes in the administration of medicines, with the potential of improving the handling of the ship’s pharmacy together with an overall enhancement of healthcare provided on board. The system can easily be expanded so as to have an impact on studying the effective-ness of medicines and general prescription patterns. This can lead to several insightful studies and a collaborative approach on highlighting the use of Medical Chest on board.
This paper proposed a solution derived from understand-ing and referencing the challenges that currently exist in achieving the same.
ACKNOWLEDGEMENTSThe support and the provision of data from C.I.R.M,
Rome, the Italian TMAS, and the Centre of Telepharmacy and Telemedicine of the University of Camerino (Italy) are gratefully acknowledged. We thank 3 Cube Services Pte. Ltd. (Private Limited company in Singapore) for their col-laboration to the study and for providing insights on the development of the TelePharmaSea software.
FUNDINGThis research received no specific grant from any funding
agency in the public, commercial, or not-for-profit sectors.
CONFLICT OF INTERESTThe authors declare that they have no competing in-
terests.
REFERENCES1. Goethe WHG, Watson EN, Jones DT. Handbook of Nautical Medicine.
Springer 1984.2. The Ship’s Medicine Chest and Medical Aid at Sea. U.S. Department
of Health and Human Services Public Health Service Office of the Surgeon General 2003 Edition.
3. Oldenburg M, Baur X, Schlaich C. Occupational Risks and Challenges of Seafaring. J Occup Health. 2010; 52(5): 249–256, doi: 10.1539/joh.k10004.
4. Nittari G, Peretti A, Sibilio F, et al. Development of software for handling ship’s pharmacy. Int Marit Health. 2016; 67(2): 72–78, doi: 10.5603/IMH.2016.0015, indexed in Pubmed: 27364171.
5. Tayebati SK, Nittari G, Mahdi SS, et al. Identification of World Health Organisation ship’s medicine chest contents by Anatomical Therapeutic Chemical (ATC) classification codes. Int Marit Health. 2017; 68(1): 39–45, doi: 10.5603/IMH.2017.0007, indexed in Pubmed: 28357835.
6. Wilson FE. International Medical Guide for Ships. Mil Med. 1968, doi: 10.1093/milmed/133.2.179a.
7. WHO. International Medical Guide for Ships: Including The Ship’s Medicine Chest. 2007.
8. McKay MP. Maritime health emergencies. Occup Med (Lond). 2007; 57(6): 453–455, doi: 10.1093/occmed/kqm053, indexed in Pubmed: 17652345.
9. Nittari G, Pirillo I, Amenta F, et al. The right to medical assistance for seafarers. Ethical and practical consequences of the introduction of telemedicine to improve healthcare on board ships. Marine Policy. 2019; 106: 103525, doi: 10.1016/j.marpol.2019.103525.
10. Amenta F, Dauri A, Rizzo N. Telemedicine and medical care to ships without a doctor on board. J Telemed Telecare. 1998; 4 Suppl 1: 44–45, doi: 10.1258/1357633981931407, indexed in Pubmed: 9640732.
11. Lenahan JL, McCarthy DM, Davis TC, et al. A drug by any other name: patients’ ability to identify medication regimens and its association with adherence and health outcomes. J Health Commun. 2013; 18 Suppl 1: 31–39, doi: 10.1080/10810730.2013.825671, indexed in Pubmed: 24093343.
12. Pécoul B, Chirac P, Trouiller P, et al. Access to essential drugs in poor countries: a lost battle? JAMA. 1999; 281(4): 361–367, doi: 10.1001/jama.281.4.361, indexed in Pubmed: 9929090.
13. Danzon PM, Furukawa MF. Prices and availability of pharmaceu-ticals: evidence from nine countries. Health Aff (Millwood). 2003; Suppl Web Exclusives: W3–W521, doi: 10.1377/hlthaff.w3.521, indexed in Pubmed: 15506157.
14. Nittari G, Pallotta G, Canio MDi, et al. Benzodiazepine prescriptions on merchant ships without a doctor on board: analysis from medical records of Centro Internazionale Radio Medico (CIRM). Int Marit He-alth. 2018; 69(1): 28–34, doi: 10.5603/IMH.2018.0005, indexed in Pubmed: 29611611.
15. Rønning MA. historical overview of the ATC/DDD methodology. WHO Drug Information. 2002.
16. Lim CM, Aryani Md Yusof F, Selvarajah S, et al. Use of ATC to descri-be duplicate medications in primary care prescriptions. Eur J Clin Pharmacol. 2011; 67(10): 1035–1044, doi: 10.1007/s00228-011-1025-4, indexed in Pubmed: 21499761.
17. Authority, A. G. A. M. S. Medical Carriage Requirements. 2016.18. Republic of Cyprus, Ministry of Communications and Works, Leme-
sos. Department of Merchant shipping, Lemesos. The Merchant Shipping (Minimum Requirements of Medical Treatment on Board Ships) Order of 2010 (P.I .233/2010).
19. Affaires Maritimes - France. Affaires Maritimes DIVISION 217 DISPO-SITIONS SANITAIRES. 1996.
20. Gibraltar Merchant Shipping (Medical Stores) Regulations 2000.21. Interministerial Decree 20, 1 October 2015 - Amendments to the
Schedule to the Decree of 25 May 1988 n. 279, which indicates medicines, the dressing objects and tools of which must be provided to national ships for merchant shipping, fishing and recreation.
22. Grace P. Department of Economic Development Isle of Man Ship Registry Consultation. 2015; 44: 1–19.
23. Wilson H. Constitution of the Republic of Liberia, 1847. Origins of West African Nationalism. 1969: 61–72, doi: 10.1007/978-1-349-15352-7_5.
24. Republic of Malta. Legal Notice 145 of 2013. Subsidiary Legislation 234.51. Maritime Labour Convention. 2013.
25. Freestone D, Schofield C. Republic of the Marshall Islands. Int J Mar Coastal Law. 2016; 31(4): 732–758, doi: 10.1163/15718085-12341413.
26. Waterstaat IV. Medical Supplies Seagoing Vessels. 2009.27. Merchant Shipping (Maritime Labour Convention) (Medicines And Me-
dical Equipment) Regulations 2014 — Singapore 2017; 91: 399–404.28. WHO. WHO Model List of Essential Medicines 20th List WHO Model
List of Essential Medicines (March 2017) Explanatory notes. World Heal. Organ. 2017.
29. United Nations. Review of Maritime Transport 2018. United Nations Publications, 2018.
www.intmarhealth.pl 295
Giulio Nittari et al., A novel approach for the management of medical chest onboard commercial vessels

Ken Inoue, MD, PhD, Research and Education Faculty, Medical Sciences Cluster, Health Service Centre, Kochi University, 2-5-1, Akebono-cho, Kochi-shi, Kochi 780-8520,
Japan, tel: +81-88-844-8158, fax: +81-88-844-8089, e-mail: [email protected]
Adequate measures to prevent medical personnel from contracting COVID-19
should be promptly implemented: support from numerous agencies is needed
Ken Inoue1 , Nursultan Seksenbayev2 , Timur Moldagaliyev2 , Yoshihiro Noso3 , Nobuo Takeichi4, 5 , Yoshiyuki Ohira6, 7 , Zhannat Sarsembina2 ,
Nargul Ospanova2 , Noriyuki Kawano5 , Haruo Takeshita8 , Masaharu Hoshi5
1Kochi University, Kochi, Japan 2Semey Medical University, Semey, Kazakhstan
3Hiroshima International University, Hiroshima, Japan 4Takeichi Clinic, Hiroshima, Japan
5Hiroshima University, Hiroshima, Japan 6International University of Health and Welfare, School of Medicine, Chiba, Japan
7Chiba University Hospital, Chiba, Japan 8Shimane University, Shimane, Japan
�
The importance of preventing medical personnel from contracting COVID-19 has been noted in Japan as else-where. Among the various medical personnel, nurses most often deal closely with patients. Caring for patients who have COVID-19 is a major risk for nurses, and the public needs to fully understand this fact.
The International Council of Nurses (ICN) reported that by mid-August 2020, 1,097 nurses in 44 countries had died from COVID-19 [Kochi Shimbun, 2020 September 16 evening: 2], and as that the description noted, it is likely that an even greater number of nurses’ deaths due to COVID-19 would have been identified if the reporting had been conducted in more countries. The ICN noted that an average of 10% of the medical personnel in 32 countries had contracted COVID-19 [Kochi Shimbun, 2020 September 16 evening: 2]. The ICN report also indicated that: (1) there is a lack of protective equipment for medical personnel working in long-term care facilities, (2) rumours that medical personnel are a source of infection can lead to discrimina-tion and violence, and (3) nurses are not being allowed to
move into rental housing [Kochi Shimbun, 2020 September 16 evening: 2].
Medical personnel are responding to COVID-19 despite the threat to their own lives. A common-sense approach and strong support are needed to address the three above-men-tioned issues. Responding to COVID-19 is also extremely mentally fatiguing for medical personnel. An extensive onsite follow-up is crucial to the mental healthcare of nurses and other medical staff who care for COVID-19 patients. Physical care for individual medical personnel should also be provided in the workplace. Assistance from the government (at various units’ levels) could facilitate a more robust care for nurses and other medical staff. Medical personnel are working in settings in which they are constantly dealing with the dangers and challenges of COVID-19, and they are under constant tension. Their mental and physical fatigue can intensify; if it worsens, it can lead to suicide. The government, workplac-es, and relevant agencies need to consider COVID-19 and its various impacts, and they need to work together when necessary to provide ongoing support to medical personnel.
www.intmarhealth.pl
Int Marit Health 2020; 71, 4: 296
10.5603/IMH.2020.0050 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
LETTER TO THE EDITOR
296

Ken Inoue, MD, PhD, Research and Education Faculty, Medical Sciences Cluster, Health Service Centre, Kochi University, 2-5-1, Akebono-cho, Kochi-shi, Kochi 780-8520,
Japan, tel: +81-88-844-8158, fax: +81-88-844-8089, e-mail: [email protected]
Changes in university classes as COVID-19 continues and new findings regarding future university
instruction methods: from the perspective of Japan and Semey, Republic of Kazakhstan
Ken Inoue1 , Nursultan Seksenbayev2 , Timur Moldagaliyev2 , Nobuo Takeichi3, 4 , Yoshihiro Noso5 , Zhannat Sarsembina2 , Nargul Ospanova2 , Haruo Takeshita6 ,
Yoshiyuki Ohira7, 8 , Noriyuki Kawano4 , Masaharu Hoshi4
1Kochi University, Kochi, Japan 2Semey Medical University, Semey, Kazakhstan
3Takeichi Clinic, Hiroshima, Japan 4Hiroshima University, Hiroshima, Japan
5Hiroshima International University, Hiroshima, Japan 6Shimane University, Shimane, Japan
7International University of Health and Welfare, School of Medicine, Chiba, Japan 8Chiba University Hospital, Chiba, Japan
�
As of September 17, 2020, there have been approx. 29.76 million cumulative cases of COVID-19 and approx. 940,000 deaths worldwide [1]. The respective numbers of COVID-19 cumulative cases and cumulative deaths in-clude the following data per country: USA, ~6.63 million and ~200,000; India, ~5.02 million and ~800,000; Brazil,
~4.42 million and ~130,000; Russia, ~1.08 million and
~20,000, and Peru, ~740,000 and ~30,000 [1].As of September 17, 2020, Japan has had ~80,000 cu-
mulative cases and ~1,500 cumulative deaths [2]. Kazakh-stan has had ~110,000 cumulative cases and ~1,600 cu-mulative deaths as of September 15, 2020 [3].
Concerned about the spread of COVID-19, the World Health Organization (WHO) declared the outbreak a Public Health Emergency of International Concern (PHEIC) at the end of January 2020. The number of COVID-19 cases contin-ued to increase worldwide, and on March 11, 2020 the WHO declared COVID-19 a pandemic. Lifestyles have changed in countries where COVID-19 is prevalent. Changes have also occurred in approaches to education.
At universities in both Japan and Semey, Republic of Kazakhstan (e.g., Semey Medical University), university classes were taught in-person prior to COVID-19. The first-term classes at universities, junior colleges, and technical colleges in Japan (the Japanese school year starts in April) have been ‘suspended (to be resumed at some later date)’ or converted to ‘online (remote classes)’ that are expected
to ‘continue online’ or ‘continue as a combination of online and in-person classes’. As one description has indicated, classes in the second term (starting in September or October) are scheduled to be ‘conducted both online and in person’ (80.1%) or ‘fully in-person’ (19.3%) [4].
Since the outbreak of COVID-19, Semey Medical Univer-sity has provided only online classes. Students have both positive and negative opinions regarding online classes. The continuation of COVID-19 is likely to affect students’ mental state. Online classes provide markedly fewer or zero chanc-es to attend school; this can lead to isolation and mental fatigue. A multi-faceted follow-up is needed for university students, to help them maintain a healthy mental state and enthusiasm for their education. Educational approaches are changing because of the situation related to COVID-19. Cur-rent educational approaches will be drawn upon and may be changed in this new global setting, but they must allow students to continue learning.
REFERENCES1. NHK. https://www3.nhk.or.jp/news/special/coronavirus/world-da-
ta/ (cited 2020 September 17).2. NHK. https://www3.nhk.or.jp/news/special/coronavirus/data-all/
(cited 2020 September 17).3. Ministry of Foreign Affairs of Japan. https://www.anzen.mofa.go.jp/
od/ryojiMailDetail.html?keyCd=98279 (cited 2020 September 17).4. Nihonkeizai Shimbun. https://www.nikkei.com/article/DGXMZO-
63845810V10C20A9CR8000 (cited 2020 October 1).
www.intmarhealth.pl 297
Int Marit Health 2020; 71, 4: 297
10.5603/IMH.2020.0051 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
LETTER TO THE EDITOR

Dr. Manik Sharma, Department of CSA, DAV University Jalandhar, 1544401 Jalandhar, India, e-mail: [email protected]
Design of brain-computer interface-based classification model for mining mental state
of COVID-19 afflicted mariner’s
Manik Sharma
Department of CSA, DAV University Jalandhar, India
�
The corona-virus (COVID-19) has tremendously crippled the whole world and eventually swayed the lifestyle, be-haviour, and cognitive health of the people [1]. To restrict the dissemination of COVID-19, most of the countries had imposed a partial or complete lockdown. However, nowa-days, most of the countries have started the unlocked-down phase. Most of the services have been restarted and the individuals are free to move as per the government adviso-ries and the precautionary measures.
The complete world trade business and the global econ-omy are significantly based upon the maritime industry and the seafarers. Shipping is recognised as a pillar of globalisa-tion and foreign exchange. More than 2 million seafarers are working across the globe and support to complete all the sea transactions [2]. Like other professionals, the extreme work-ing conditions, job responsibility, erratic schedule, chemi-cal hazards, salvage diving, asbestosis and psychosocial factors are inducing a high degree of stress (psychological disorders) among seafarers and mariners. Unfortunately, the effects of COVID-19 have also been seen on shipping and marine industry. The study has shown that during this pandemic (COVID-19) 50% (of the sample study) of the mariners did not feel safe and more than 50% employees were not satisfied with the precautionary measures taken to deal with this global epidemic [3]. All these concerns are devastating their mental as well as physical state. No doubt, the people have started their work; however, still, there is a great fear of having a COVID-19 infection.
The mental state of the individuals has been great-ly affected and consequently, most of the persons are suffering from different psychiatric and neuropsychiatric disorders. A single COVID-19 victim can create chaos in a ship. This chaos can trigger stress as well as other human psychological disorders among different persons travelling
through the ship. Therefore, to ensure the healthy state of the mariners, there is a need to examine the mental state (mind alertness) along with their body temperature (thermal checking). The mental state of the individuals can be easily accessed using electroencephalography (EEG) signals [4]. A brain-sense device can be used to capture the frequency of the brainwave signals and consequently, the mental state of a seafarer or mariner can be reflected. The key contribution of this research work is to present a framework (Fig. 1) for the diagnosis of the mental state of the mariners during the traumatic period of COVID-19.
The model is framed using an amalgamation of brain-com-puter interface (BCI) and soft computing techniques. BCI is an emerging research area in the domain of human-computer interaction. BCI is related to the communication of thoughts (originated in the brain) without using any muscular control [5]. In BCI systems, the brain activities are recorded in the form of the brainwaves and are transmitted to the computing machine for recording and pattern recognition. Some of the major applications of the BCI are prosthetic control (home appliances and wheelchair control), operator monitoring, forensics (lie detection, trust assessment), entertainment (mood assessment, thought control, response detection), healthcare (drowsiness detection, neuro-rehabilitation), and neuro-market [6]. In healthcare, BCI has been effectively employed in different areas ranging from prevention to re-habilitation. The effective outcomes of BCI in prevention (smoking, alcoholism), prognosis (neurological and psychi-atric disorders), and rehabilitation (brain, disability and psy-chiatric disorders) have also been witnessed [4]. Here, an artificial intelligent BCI has been proposed to generate and record the mental state (brain-waves) of the seafarers. The brain-sense devices are used for BCI. Some of the important characteristics of the brain-sense devices are [7]:
www.intmarhealth.pl
Int Marit Health 2020; 71, 4: 298–300
10.5603/IMH.2020.0052 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
LETTER TO THE EDITOR
298
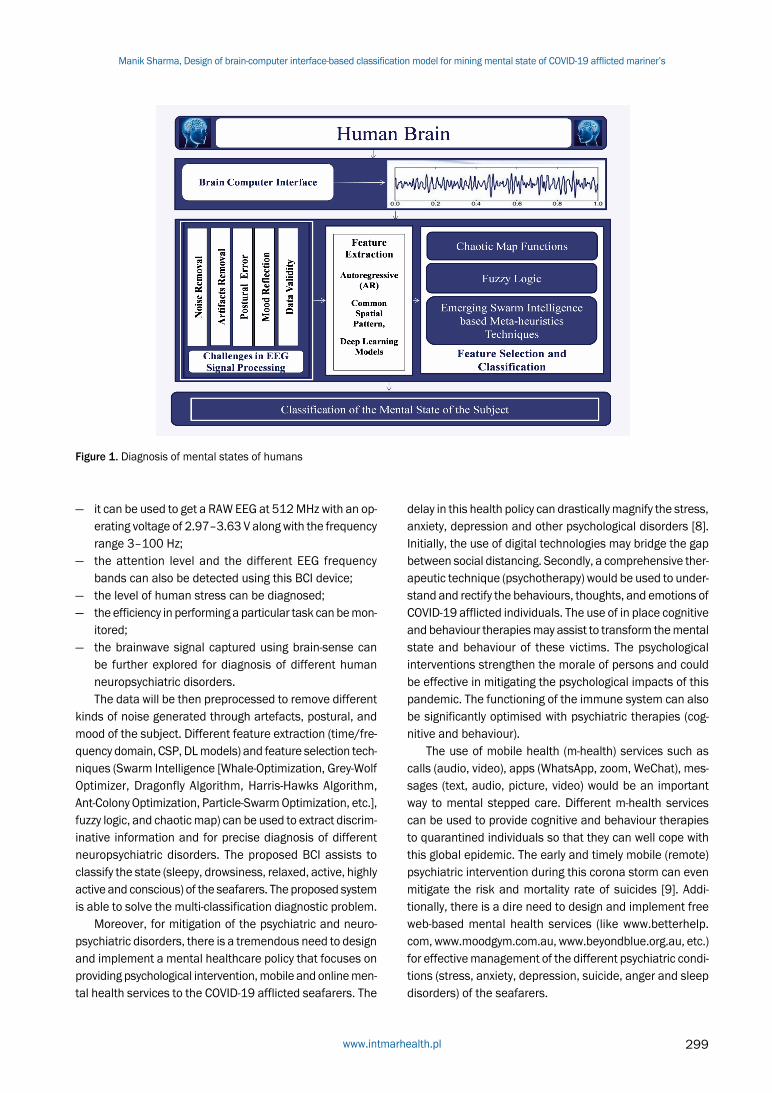
Figure 1. Diagnosis of mental states of humans
— it can be used to get a RAW EEG at 512 MHz with an op-erating voltage of 2.97–3.63 V along with the frequency range 3–100 Hz;
— the attention level and the different EEG frequency bands can also be detected using this BCI device;
— the level of human stress can be diagnosed; — the efficiency in performing a particular task can be mon-
itored; — the brainwave signal captured using brain-sense can
be further explored for diagnosis of different human neuropsychiatric disorders. The data will be then preprocessed to remove different
kinds of noise generated through artefacts, postural, and mood of the subject. Different feature extraction (time/fre-quency domain, CSP, DL models) and feature selection tech-niques (Swarm Intelligence [Whale-Optimization, Grey-Wolf Optimizer, Dragonfly Algorithm, Harris-Hawks Algorithm, Ant-Colony Optimization, Particle-Swarm Optimization, etc.], fuzzy logic, and chaotic map) can be used to extract discrim-inative information and for precise diagnosis of different neuropsychiatric disorders. The proposed BCI assists to classify the state (sleepy, drowsiness, relaxed, active, highly active and conscious) of the seafarers. The proposed system is able to solve the multi-classification diagnostic problem.
Moreover, for mitigation of the psychiatric and neuro-psychiatric disorders, there is a tremendous need to design and implement a mental healthcare policy that focuses on providing psychological intervention, mobile and online men-tal health services to the COVID-19 afflicted seafarers. The
delay in this health policy can drastically magnify the stress, anxiety, depression and other psychological disorders [8]. Initially, the use of digital technologies may bridge the gap between social distancing. Secondly, a comprehensive ther-apeutic technique (psychotherapy) would be used to under-stand and rectify the behaviours, thoughts, and emotions of COVID-19 afflicted individuals. The use of in place cognitive and behaviour therapies may assist to transform the mental state and behaviour of these victims. The psychological interventions strengthen the morale of persons and could be effective in mitigating the psychological impacts of this pandemic. The functioning of the immune system can also be significantly optimised with psychiatric therapies (cog-nitive and behaviour).
The use of mobile health (m-health) services such as calls (audio, video), apps (WhatsApp, zoom, WeChat), mes-sages (text, audio, picture, video) would be an important way to mental stepped care. Different m-health services can be used to provide cognitive and behaviour therapies to quarantined individuals so that they can well cope with this global epidemic. The early and timely mobile (remote) psychiatric intervention during this corona storm can even mitigate the risk and mortality rate of suicides [9]. Addi-tionally, there is a dire need to design and implement free web-based mental health services (like www.betterhelp.com, www.moodgym.com.au, www.beyondblue.org.au, etc.) for effective management of the different psychiatric condi-tions (stress, anxiety, depression, suicide, anger and sleep disorders) of the seafarers.
www.intmarhealth.pl 299
Manik Sharma, Design of brain-computer interface-based classification model for mining mental state of COVID-19 afflicted mariner’s

In light of the aforementioned findings, the proposed BCI based classification model will help mariner to diagnose their mental state so that if require the remote mental health services can be provided to alleviate the risk of any psychiatric and neuropsychiatric disorders.
REFERENCES1. Sharma S, Sharma M, Singh G. A chaotic and stressed environment
for 2019-nCoV suspected, infected and other people in India: Fear of mass destruction and causality. Asian J Psychiatr. 2020; 51: 102049, doi: 10.1016/j.ajp.2020.102049, indexed in Pubmed: 32278890.
2. Doumbia-Henry C. Shipping and COVID-19: protecting seafarers as frontline workers. WMU J Maritime Affairs. 2020; 19(3): 279–293, doi: 10.1007/s13437-020-00217-9.
3. Pesel G, Canals ML, Sandrin M, et al. Wellbeing of a selection of seafarers in Eastern Adriatic Sea during the COVID-19 pandemic 2020. Int Marit Health. 2020; 71(3): 184–190, doi: 10.5603/IMH.2020.0033, indexed in Pubmed: 33001430.
4. Lin CT, Chuang CH, Cao Z, et al. Forehead EEG in support of future feasible personal healthcare solutions: sleep management, heada-
che prevention, and depression treatment. IEEE Access. 2017; 5: 10612–10621, doi: 10.1109/access.2017.2675884.
5. Padfield N, Zabalza J, Zhao H, et al. EEG-Based Brain-Computer In-terfaces Using Motor-Imagery: Techniques and Challenges. Sensors (Basel). 2019; 19(6): 1423, doi: 10.3390/s19061423, indexed in Pubmed: 30909489.
6. Abdulkader S, Atia A, Mostafa MS. Brain computer interfacing: Ap-plications and challenges. Egyptian Info J. 2015; 16(2): 213–230, doi: 10.1016/j.eij.2015.06.002.
7. Avudaiammal R, Mystica K, Balaji A, et al. Brain Sense Controlled Wireless Robot: Interfacing Neurosky Brainsense to a Wheelchair Prototype. 2020 Third International Conference on Smart Sys-tems and Inventive Technology (ICSSIT). 2020, doi: 10.1109/icssit48917.2020.9214100.
8. Duan Li, Zhu G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry. 2020; 7(4): 300–302, doi: 10.1016/S2215-0366(20)30073-0, indexed in Pubmed: 32085840.
9. Reger MA, Stanley IH, Joiner TE. Suicide Mortality and Coronavirus Disease 2019-A Perfect Storm? JAMA Psychiatry. 2020 [Epub ahe-ad of print], doi: 10.1001/jamapsychiatry.2020.1060, indexed in Pubmed: 32275300.
Int Marit Health 2020; 71, 4: 298–300
www.intmarhealth.pl300

Dr. Dominique Jégaden, French Society for Maritime Medicine, Faculty of Medicine and Health Sciences, University of Western Brittany, Brest, France,
tel/fax: +33673018959, e-mail: [email protected]
About the relationship between ship noise and the occurrence of arterial hypertension in seafarers
Dominique Jégaden1 , David Lucas1, 2
1French Society for Maritime Medicine, Faculty of Medicine and Health Sciences, University of Western Brittany, Brest, France 2Centre for Professional and Environmental Pathologies, Morvan Teaching Hospital (CHRU), Brest, France
�
For more than 40 years, the relationship between noise exposure and the onset of high blood pressure is a contro-versial topic. The increased number of studies, reviews and meta-analyses on this subject highlights its relevance for public health. Indeed, noise is a ubiquitous stressor, and high blood pressure is a potentially life threatening disease.
A German team — Bolm-Audorff et al. [1] has just pub-lished in the ‘International Journal of Environmental Re-search and Public Health’, in August 2020, a new meta-anal-ysis on this subject (“Occupational noise and hypertension risk: A systematic review and meta-analysis”). They provide a clear evidence of relationship between exposure to in-dustrial noise above 85 dB (A) and the risk of high blood pressure (odds ratio: 1.72 [1.48–2.01]). Out of 4,583 pa-pers collected from international databases, they selected 180 eligible articles, and finally 23 articles were included in the meta-analysis. Surprisingly, one of the 23 selected papers is one of ours, published in 1986 in the French journal ‘Archives des Maladies Professionnelles’ [2]. In this study, we recruited 455 seafarers, all men aged from 40 to 55 years (164 engine room personnel and 291 deck crew). Toward the notch at 4000 Hz on audiometry, typical of hearing loss due to noise greater than 85 dB (A), we characterised impact of noise between these two seafarers’ subgroups. This notch was not found among deck crew [3]. We calculated a prevalence of confirmed hypertension of 18.90% (12.8–25%) and 11.68% (7.92–15.44%) among en-gine room personnel and deck crew, respectively (p < 0.05). No statistical relation between hearing loss’ level and hy-pertension was found. This risk was independent of other known risk factors of hypertension (obesity, alcoholism, hypertensive heredity). Moreover, we noticed in our results that the occurrence of hypertension was linked, on the one hand, to a high level of noise (> 85 dB [A]) and, on the other hand, to a long duration of exposure to noise
(greater than 20 years). Several other recent meta-analyses have also the same conclusion on a positive relationship between noise and hypertension [4–7]. Fu et al. [4] found a relative risk at 1.62 (1.40–1.88) and Skogstad et al. [5] at 1.68 (1.10–2.57), the same as ours.
The inclusion of our 40-year-old work in this recent me-ta-analysis, underlined some facts and questions:1. The maritime environment is unique. It could be consider
as an in vivo laboratory, allowing us to study the reac-tions of the human being exposed to physical constraints such as noise and vibrations, psychological constraints (stress, confinement, isolation, boredom), and still to infections in confined spaces, as we saw recently with the COVID-19 pandemic.
2. Few studies on arterial blood pressure and noise expo-sure were published in seafarers’ population. In their arti-cle on hypertension in Danish seamen, Tu and Jepsen [8] underlined this risk factor (“Measured noise levels are highest in the engine rooms, followed by the levels on deck. This may partly explain the high prevalence of hypertension for seafarers working in these two areas”.).
Oldenburg et al. [9, 10] noted that “particularly engine room officers and galley/operating staff are at a higher coronary risk”, without mentioning a possible relationship with noise.
3. It should suggest that technological advances on noise exposure prevention on board ships are signif-icant for 40 years (improvement of the insulation of living areas, automation of machines, soundproofed surveillance rooms, diesel-electric propulsion...) and therefore that seamen are today less exposed. Reduc-ing occupational noise exposure have effect on health status such as deafness or, as regards this letter, hypertension is expected. However, several recent studies corroborate that engine room workers are
www.intmarhealth.pl 301
Int Marit Health 2020; 71, 4: 301–302
10.5603/IMH.2020.0053 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
LETTER TO THE EDITOR
still exposed to harmful noise levels, above 85 dB (A), even today [11–13].
Turan et al. [14] consider that ships easily meet the International Maritime Organisation criteria, while peo-ple working on board such ships are still likely exposed to high noise levels [14]. The International Maritime Organisation noise code should therefore be updated in order to enforce lower noise levels on ships. The negative effects of noise exposure on human health are now well-known and many design solutions are now available to reduce noise levels.
4. We must also be careful on fishermen. Many of fishing vessels are still very noisy, and remember that this risk factor is added to many other risks of hypertension, such as obesity, sedentary lifestyle and alcoholism [15–17].
REFERENCES1. Bolm-Audorff U, Hegewald J, Pretzsch A, et al. Occupational noise
and hypertension risk: a systematic review and meta-analysis. Int J Environ Res Public Health. 2020; 17(17), doi: 10.3390/ijerph17176281, indexed in Pubmed: 32872306.
2. Jégaden D, Le Fluart C, Marie Y, et al. Contribution to the study noise-high blood pressure. Concerning 455 merchant sailors aged 40–55 years. (Contribution — l’étude de la relation bruit-hypertension artérielle. — propos de 455 marins de commerce âgés de 40 — 55 ans). Arch Mal Prof. 1986; 47: 15–20.
3. Jégaden D. Noise on board ships: its impact on the hearing function of merchant seamen (Bruit — bord des navires: son retentissement sur la fonction auditive des marins de commerce). Arch Mal Prof. 1984; 45(5): 345–349.
4. Fu W, Wang C, Zou Li, et al. Association between exposure to noise and risk of hypertension: a meta-analysis of observational epidemiological studies. J Hypertens. 2017; 35(12): 2358–2366, doi: 10.1097/HJH.0000000000001504, indexed in Pubmed: 28806352.
5. Skogstad M, Johannessen HA, Tynes T, et al. Occupational noise exposure and hearing: a systematic review. Int Arch Occup Environ Health. 2016; 89(3): 351–372, doi: 10.1007/s00420-015-1083-5, indexed in Pubmed: 26249711.
6. Yang Ye, Zhang E, Zhang J, et al. Relationship between occupational noise exposure and the risk factors of cardiovascular disease in China: a meta-analysis. Medicine (Baltimore). 2018; 97(30): e11720, doi: 10.1097/MD.0000000000011720, indexed in Pubmed: 30045338.
7. Pyko A, Lind T, Mitkovskaya N, et al. Transportation noise and incidence of hypertension. Int J Hyg Environ Health. 2018; 221(8): 1133–1141, doi: 10.1016/j.ijheh.2018.06.005, indexed in Pubmed: 30078646.
8. Tu M, Jepsen JR. Hypertension among Danish seafarers. Int Marit Health. 2016; 67(4): 196–204, doi: 10.5603/IMH.2016.0037, indexed in Pubmed: 28009392.
9. Oldenburg M, Jensen HJ, Latza U, et al. Coronary risks among sea-farers aboard German-flagged ships. Int Arch Occup Environ Health. 2008; 81(6): 735–741, doi: 10.1007/s00420-007-0261-5, indexed in Pubmed: 17909838.
10. Oldenburg M. Risk of cardiovascular diseases in seafarers. Int Marit Health. 2014; 65(2): 53–57, doi: 10.5603/IMH.2014.0012, indexed in Pubmed: 25231325.
11. Nikolic A, Nikolic E. Controlling risk due to noise on ferry boat. PROMET - Traffic&Transportation. 2013; 25(4): 387–394, doi: 10.7307/ptt.v25i4.305.
12. Borelli D., Schenone C. Seafarers’ woek exposure to tonal noise components. 23rd International Congress on Sound and Vibration, Athens (Greece), 10-14 Juy 2016.
13. Oldenburg M, Felten C, Hedtmann J, et al. Physical influences on seafarers are different during their voyage episodes of port stay, river passage and sea passage: A maritime field study. PLoS One. 2020; 15(4): e0231309, doi: 10.1371/journal.pone.0231309, indexed in Pubmed: 32267889.
14. Turan O, Helvacioglu IH, Insel M, et al. Crew noise exposure on board ships and comparative study of applicable stan-dards. Ships Offshore Structures. 2011; 6(4): 323–338, doi: 10.1080/17445302.2010.514716.
15. Zytoon M. Occupational noise exposure of fishermen aboard small and medium-scale fishing vessels. Int J Ind Ergon. 2013; 43(6): 487–494, doi: 10.1016/j.ergon.2012.08.001.
16. Levin J, Curry W, Shepherd S, et al. Hearing loss and noise exposure among commercial fishermen in the gulf coast. J Occupat Environ Med. 2016; 58(3): 306–313, doi: 10.1097/jom.0000000000000642.
17. Nguyen N. Noise exposure and its relationship with hypertension among fishermen in Thua Thien-Hue Province, Vietnam. J Integrat Com Health. 2020; 09(01): 3–16, doi: 10.24321/2319.9113.202001.
Int Marit Health 2020; 71, 4: 301–302
www.intmarhealth.pl302

Dr. Pougnet Richard, MD, PhD (Philosophy), LTh (Theology), Centre de Pathologies Professionnelles, CHRU Morvan, 2, av Foch, 29200 Brest, France,
e-mail: [email protected]
Sexually transmitted infection and seafarers: raising awareness on preventing prostitution?
Richard Pougnet1, 2, 3 , Pol Bleunven2, Brice Loddé1, 2, 4 , David Lucas1, 2, 4 , Jean-Dominique Dewitte1, 2, 3 , Laurence Pougnet1, 5
1Société Française de Médecine Maritime (SFMM), France 2Centre de Pathologies Professionnelles et Environnementales, CHRU Morvan, Brest, France
3Laboratoire d’Etudes et de Recherche en Sociologie (LABERS), EA 3149, Faculté des Lettres et Sciences Humaines, Victor Segalen, Université de Bretagne Occidentale, Brest, France
4Optimisation des Régulations Physiologiques (ORPHY), EA 4324, Université de Bretagne Occidentale, Brest, France 5Hôpital d’Instruction des Armées, Clermont-Tonnerre, Brest, France
�
According to a literature review studying sexually transmit-ted infections (STIs) amongst seafarers, 19.5% of seafarers have had an intercourse with a sex worker [1]. Reported rates range between 2.5% and 66.0% depending on the study. As high as these rates might seem, they resemble those of the general French male population, estimated at 15%.
The issue of STIs amongst seafarers is historically linked to prostitution. This became a noticeable matter of concern in the 19th century, when the health and efficiency of Brit-ish armed forces and navy soldiers was threatened by the spread of STIs, requiring political action to be taken. A se-ries of laws, known as the Contagious Diseases Acts, was introduced in an attempt to submit suspected prostitutes to undergo medical examinations, compelling them to be treated, if needed, in specialised STI hospitals [2].
This law sparked significant controversy, fuelled by a phi-losopher John Stuart Mill, who disapproved of this project [3]. He perceived the arrest and forced medical check-ups on suspected women as an infringement on personal freedom and an inequality between men and women. Moreover, he expressed his concerns about institutionalizing sex workers’ care, which could suggest that the authorities condoned prostitution by making it safer [4].
Nowadays, prostitution practices vary depending on the country. While some choose to enable it, others prohibit seeking a prostitute without penalising the sex workers themselves, and some countries outright ban and punish both sex workers and the clients.
Although the debate on prostitution issues goes be-yond the field of maritime medicine, maritime and military doctors should be aware of political, moral, philosophical and religious specificities that may vary from country to
country. This would enable them to give relevant advices to seafarers, regarding not only the risk of STIs itself, but also potential fine or jail penalties etc. These physicians should question their role in overall health promotion. Prevention of STIs could also be broadened on preventing prostitution itself. Sex workers are known to be a vulnerable population, threatened by insecurity, violence, drugs, infections, etc. Would it be unrealistic to expect these doctors to prevent seafarers from engaging with sex workers? Scientific litera-ture shows that interaction with sex workers is mainly linked to long distance journeys [1]. Promoting intellectual, leisure or spiritual activities could help in preventing this behaviour [5]. Investigating the reasons driving seafarers to seek intercourse with sex workers might also help in preventing these conducts. It is believed that peer pressure might have a role to play in that regard. Prevention must therefore be collective in order to change mentalities.
REFERENCES1. Pougnet R, Pougnet L, Dewitte JD, et al. Sexually transmitted
infections in seafarers: 2020’s perspectives based on a literature review from 2000-2020. Int Marit Health. 2020; 71(3): 166–173, doi: 10.5603/IMH.2020.0030, indexed in Pubmed: 33001427.
2. Nevins Birkbeck J, Ffolliott N. Contagious Diseases Acts. Br Med J. 1875; 743(1): 430–431.
3. Mill JS. Essays on Equality, Law, and Education. Robson JM (ed.), with an Introduction by S. Collini. Routledge & Kegan Paul - University of Toronto Press, London & Toronto 1984.
4. Guillin V. Biopolitique, utilitarisme et libéralisme. Archives de Philos-ophie. 2010; 73(4): 615, doi: 10.3917/aphi.734.0615.
5. Haglund KA, Fehring RJ. The association of religiosity, sexual edu-cation, and parental factors with risky sexual behaviors among ad-olescents and young adults. J Relig Health. 2010; 49(4): 460–472, doi: 10.1007/s10943-009-9267-5, indexed in Pubmed: 19565334.
www.intmarhealth.pl 303
Int Marit Health 2020; 71, 4: 303
10.5603/IMH.2020.0054 www.intmarhealth.pl
Copyright © 2020 PSMTTM ISSN 1641–9251
LETTER TO THE EDITOR


INTERNATIONAL MARITIME HEALTHFormer: Bulletin of the Institute of Maritime and Tropical Medicine in Gdynia, issued since 1949Owner: Polish Society of Maritime, Tropical and Travel MedicineThe international multidisciplinary journal devoted to research and practice in the field of: maritime medicine, travel and tropical medicine, hyperbaric and underwater medicine, sea-rescue, port hygienic and sanitary problems, maritime psychology.
Supported financially by:
Editor-in-ChiefMaria JeżewskaMedical University of Gdańsk, Institute of Maritime and Tropical Medicine, Gdynia, Poland(http://www.immt.gdynia.pl/) See our website for information on sending manuscript, aims, scope, instructions for authors (reviewers), editorial board members, guidelines for scientific demands etc.https://journals.viamedica.pl/international_maritime_healthwww.intmarhealth.pl
Publisher of the International Maritime HealthPublishing, Subscription and Advertising Office: VM Media sp. z o.o. VM Group sp.k.ul. Świętokrzyska 73, 80–280 Gdańsk, Poland, tel. (+48 58) 320 94 94, fax (+48 58) 320 94 60e-mail: [email protected], http://www.viamedica.pl
Subscription rates: Paper subscription, 4 issues incl. package and postage institutional — 120 euro. The above prices are inclusive of regular postage costs. Payment should be made to: VM Media sp. z o.o. VM Group sp.k., Grupa Via Medica, Bank BGŻ Paribas SA account number: 15 1600 1303 0004 1007 1035 9021; SWIFT: PPABPLPK. Single issues, subsriptions orders and requests for sample copies should be send to e-mail: [email protected]. Electronic orders option available at: https://journals.viamedica.pl/international_maritime_health
Advertising: for details on media opportunities within this journal please contact the advertising sales: VM Media sp. z o.o. VM Group sp.k., ul. Świętokrzyska 73, 80–280 Gdańsk, Poland, tel. (+48 58) 320 94 94, fax (+48 58) 320 94 60, e-mail: [email protected] Editors accept no responsibility for the advertisement contents.
"International Maritime Health" is edited by: Polish Society of Maritime, Tropical and Travel Medicine in Gdynia (PSMTTM).Address: 9B Powstania Styczniowego street, 81–519 Gdynia, Poland Secretary: Leszek Mayer MD, e-mail: [email protected]
All rights reserved, including translation into foreign languages. No part of this periodical, either text or illustration, may be used in any form whatsoever. It is particularly forbidden for any part of this material to be copied or translated into a mechanical or electronic language and also to be recorded in whatever form, stored in any kind of retrieval system or transmitted, whether in an electronic or mechanical form or with the aid of photocopying, mi-crofilm, recording, scanning or in any other form, without prior written permission of the publisher. The rights of the publisher and authors are protected by national copyright laws and by international conventions, and their violation will be punishable by penal sanctions.
Legal note: http://czasopisma.viamedica.pl/IMH/about/legalNote
"International Maritime Health" is indexed at: CrossRef, DOAJ (Directory of Open Access Journals), EBSCO, ESCI (Emerging Sources Citation Index), FMJ, Google Scholar, Index Copernicus, Medical Journals Links, Medline, Ministry of Science and Higher Education, Polish Medical Bibliography, Scopus, SJR, Ulrich's Periodicals Directory, WorldCat. Position in Index Copernicus ranking system is available at: www.indexcopernicus.com.
Copyright © 2020 Polish Society of Maritime Tropical and Travel MedicinePrinted in the Republic of PolandISSN: 1641–9251
International Maritime Health Association, Antwerp, Belgium
Norwegian Centre for Maritime and Diving Medicine,
Bergen, Norway
Polish Society of Maritime, Tropical and Travel Medicine,
Gdynia, Poland
NORWEGIAN CENTRE FORMARITIME AND DIVING MEDICINE
HELSE BERGEN, Haukeland University
Hospital, Bergen, Norway
Norwegian Association of Maritime Medicine,
Bergen, Norway
INFORMATION FOR AUTHORSThe International Maritime Health will publish original papers on medical and health problems of seafarers, fishermen,
divers, dockers, shipyard workers and other maritime workers, as well as papers on tropical medicine, travel medicine, epidemiology, and other related topics.
Typical length of such a paper would be 2000–4000 words, not including tables, figures and references. Its construc-tion should follow the usual pattern: abstract (structured abstract of no more than 300 words); key words; introduction; participants; materials; methods; results; discussion; and conclusions/key messages.
Case Reports will also be accepted, particularly of work-related diseases and accidents among maritime workers.All papers will be peer-reviewed. The comments made by the reviewers will be sent to authors, and their criticism and
proposed amendments should be taken into consideration by authors submitting revised texts.Review articles on specific topics, exposures, preventive interventions, and on the national maritime health services will
also be considered for publication. Their length will be from 1000 to 4000 words, including tables, figures and references.Letters to the Editor discussing recently published articles, reporting research projects or informing about workshops
will be accepted; they should not exceed 500 words of text and 5 references.There also will be the section Chronicle, in which brief reports will be published on the international symposia and
national meetings on maritime medicine and health, on tropical parasitology and epidemiology, on travel medicine and other subjects related to the health of seafarers and other maritime workers. Information will also be given on training activities in this field, and on international collaborative projects related to the above subjects.
All articles should be submitted to IMH electronically online at www.intmarhealth.pl where detailed instruction regarding submission process will be provided.
Only English texts will be accepted.Manuscripts should be typed in double line spacing on numbered pages and conform to the usual requirements (Ref.:
International Committee on Medical Journals Editors. Uniform Requirements for Manuscripts Submitted to Biomedical Journals, JAMA, 1997; 277: 927–934).
Only manuscripts that have not been published previously, and are not under consideration by another publisher, will be accepted.
Full texts of oral presentations at meetings (with abstracts printed in the conference materials) can be considered.All authors must give written consent to publication of the text.Manuscripts should present original material, the writing should be clear, study methods appropriate, the conclusions
should be reasonable and supported by the data. Abbreviations, if used, should be explained.Drugs should be referred to by their approved names (not by trade names). Scientific measurements should be given
in SI units, except for blood pressure, which should be expressed in mm Hg.Authors should give their names, addresses, and affiliations for the time they did the work. A current address of one
author should be indicated for correspondence, including telephone and fax numbers, and e-mail address.All financial and material support for the reported research and work should be identified in the manuscript.
REFERENCESReferences should be numbered in the order in which they appear in the text. At the end of the article the full list of
references should give the names and initials of all authors (unless there are more than six authors, when only the first three should be given followed by: et al.).
The authors’ names are followed by the title of the article; the title of the journal abbreviated according to Medline; the year of publication, the volume number; and the first and last page numbers. Please note: References you should include DOI numbers of the cited papers (if applicable) – it will enable the references to be linked out directly to prop-er websites. (e.g. Redon J, Cifkova R, Laurent S et al. Mechanisms of hypertension in the cardiometabolic syndrome. J Hypertens. 2009; 27(3): 441–451, doi: 10.1097/HJH.0b013e32831e13e5.).
Reference to books should give the title, names of authors or of editors, publisher, place of publication, and the year.Information from yet unpublished articles, papers reported at meetings, or personal communications should be cited
only in the text, not in References.For full information for authors refer to the web page: www.intmarhealth.pl.

Inte
rnatio
nal M
aritim
e H
ealth
, 2020, V
ol. 7
1, N
o. 4
MARITIME MEDICINE Original articles
Anish Arvind Hebbar, Nitin Mukesh
COVID-19 and seafarers’ rights to shore leave, repatriation and medical assistance: a pilot study ............................................................ 217
Getu Gamo Sagaro, Gopi Battineni, Nalini Chintalapudi, Marzio Di Canio, Francesco Amenta
Telemedical assistance at sea in the time of COVID-19 pandemic .......................................... 229
Farhad Azimi Yancheshmeh, S. Hossain Mousavizadegan, Amin Amini, Andrew P. Smith, Reza Kazemi
Poor sleep quality, long working hours and fatigue in coastal areas: a dangerous combination of silent risk factors for deck officers on oil tankers ...237
Alexis Maffert, Barbara Aupy
Optokinetic stimulation efficiency for sea sickness treatment ................................... 249
Review articles
Devran Yazır, Bekir Şahin, Tsz Leung Yip, Po-Hsing Tseng
Effects of COVID-19 on maritime industry: a review .................................................................. 253
Elisabeth Stoll, Klaus Püschel, Volker Harth, Marcus Oldenburg
Prevalence of alcohol consumption among seafarers and fishermen ....................................... 265
Marcus Oldenburg, Lukas Belz, Filip Barbarewicz, Volker Harth, Hans-Joachim Jensen
Work profile of maritime pilots in Germany ......... 275
Case report
Ajit C. Kulkarni
A case of neurocysticercosis with an unusual presentation on high seas .................................... 278
TRAVEL MEDICINEReview article
Krzysztof Korzeniewski
Extreme traveler .................................................... 281
VARIAOriginal article
Giulio Nittari, Graziano Pallotta, Ravjyot Singh Khuman, Francesco Amenta
TelePharmaSea: proposing a novel approach to automate, organize and simplify management of medical chest on board commercial vessels ............................... 291
LETTERS TO THE EDITOR
Ken Inoue, Nursultan Seksenbayev, Timur Moldagaliyev, Yoshihiro Noso, Nobuo Takeichi, Yoshiyuki Ohira, Zhannat Sarsembina, Nargul Ospanova, Noriyuki Kawano, Haruo Takeshita, Masaharu Hoshi
Adequate measures to prevent medical personnel from contracting COVID-19 should be promptly implemented: support from numerous agencies is needed ................................................................ 296
Ken Inoue, Nursultan Seksenbayev, Timur Moldagaliyev, Nobuo Takeichi, Yoshihiro Noso, Zhannat Sarsembina, Nargul Ospanova, Haruo Takeshita, Yoshiyuki Ohira, Noriyuki Kawano, Masaharu Hoshi
Changes in university classes as COVID-19 continues and new findings regarding future university instruction methods: from the perspective of Japan and Semey, Republic of Kazakhstan ........................................ 297
Manik Sharma
Design of brain-computer interface-based classification model for mining mental state of COVID-19 afflicted mariner’s ............................ 298
Dominique Jégaden, David Lucas
About the relationship between ship noise and the occurrence of arterial hypertension in seafarers .............................................................. 301
Richard Pougnet, Pol Bleunven, Brice Loddé, David Lucas, Jean-Dominique Dewitte, Laurence Pougnet
Sexually transmitted infection and seafarers: raising awareness on preventing prostitution? ..... 303
2020, Vol. 71, No. 4 nr ISSN 1641–9251
www.intmarhealth.pl
"International Maritime Health" is indexed at: CrossRef, DOAJ, EBSCO, ESCI, FMJ, Google Scholar, Index Copernicus, Medical Journals Links, Medline, Ministry of Science and Higher Education, Polish Medical Bibliography, Scopus, SJR, Ulrich's Periodicals Directory, WorldCat.
Official scientific forum of the:
InternationalMaritime
HealthAssociation
Indexed/abstracted in: CrossRef, DOAJ, EBSCO, ESCI, FMJ, Google Scholar, Index Copernicus,
Medical Journals Links, Medline, Ministry of Science and Higher Education, Polish Medical Bibliography, Scopus, SJR,
Ulrich's Periodicals Directory, WorldCat
CONTENTS