
The Role of Inflammation in Retinal Neurodegeneration and ...
Upload
independentCategory
view
4download
0
216 | MARCH 2002 | VOLUME 3 www.nature.com/reviews/neuro
R E V I E W S
The central nervous system (CNS) mounts an organized INNATE IMMUNE RESPONSE during systemic bac-terial/viral infection. This inflammatory response is characterized by the expression of various immuno-logical proteins in the CIRCUMVENTRICULAR ORGANS
(CVOs) and other structures devoid of blood–brainbarrier (BBB). The response extends progressively toaffect microglia across the brain parenchyma and maylead to the onset of an ADAPTIVE IMMUNE RESPONSE.Molecules of both the innate and adaptive immuneresponses are induced in a wide diversity of neurologi-cal disorders, including Alzheimer’s disease,Parkinson’s disease, Huntington’s disease, multiplesclerosis and amyotrophic lateral sclerosis (ALS). Therecent discovery of this immune response in the brainrevives the idea that immunological challenges mightbe aetiological factors in sporadic cases of neuro-degeneration, and indicates that primary causes of suchdegeneration could originate outside the CNS. Indeed,the mechanisms that underlie 90% of ALS cases,sporadic Parkinson’s disease and Alzheimer’s diseaseremain elusive, and bacterial/viral infections have beenproposed as a primary cause. Furthermore, peripheralantibodies generated by damaged peripheral tissues inneurological conditions that include STIFF-MAN SYNDROME
and RASSMUSSEN ENCEPHALITIS can induce neuronal deathby targeting specific antigens.
Progress in the use of anti-inflammatory therapiesand immunization in animal models of neurodegener-ative disorders points to the importance of the immuneresponse in neurodegeneration. Whereas regulation ofthe innate immune response could be decisive in thedevelopment of both sporadic and familial forms ofneurological disorders, molecules of the innate immuneresponse can also trigger the production of neuro-trophic factors, and promote repair and remyelinationin response to injury, trauma and toxin-induceddemyelination. Here, we review the mechanisms thatunderlie the dichotomous role of the inflammatoryresponse of the brain, a response that can, on the onehand, protect neurons and, on the other, be a directcause of degeneration.
Innate immunityHost organisms detect the presence of infection by recog-nizing specific elements produced by microorganisms1.These elements — the so-called PATHOGEN-ASSOCIATED
MOLECULAR PATTERNS (PAMPs) — are recognized by spe-cific cells of the immune system as inducers of innateresponses to bacterial infection. The reaction to endo-toxin lipopolysaccharide (LPS), an important com-ponent of the outer membranes of GRAM-NEGATIVE
BACTERIA, is the best-characterized example of innaterecognition that leads to a robust inflammatory
INNATE IMMUNITY: THE MISSINGLINK IN NEUROPROTECTION ANDNEURODEGENERATION?Minh Dang Nguyen*, Jean-Pierre Julien* and Serge Rivest‡
Innate immunity was previously thought to be a nonspecific immunological programme that wasengaged by peripheral organs to maintain homeostasis after stress and injury. Emergingevidence indicates that this highly organized response also takes place in the central nervoussystem. Through the recognition of neuronal fingerprints, the long-term induction of the innateimmune response and its transition to an adaptive form might be central to the pathophysiologyand aetiology of neurodegenerative disorders. Paradoxically, this response also protects neuronsby favouring remyelination and trophic support afforded by glial cells.
INNATE IMMUNITY
The early response of a host toinfection. One of its mainfeatures is the pro-inflammatoryresponse induced by antigen-presenting cells —macrophages, dendritic cellsand, in the brain, microglialcells. This response is followedby an adaptive response that ismediated by the clonal selectionof lymphocytes, which leads tolong-term immune protection.
*Centre for Research inNeurosciences, McGillUniversity, The MontréalGeneral Hospital ResearchInstitute, Montréal, Québec,H3G 1A4, Canada.‡Laboratory of MolecularEndocrinology, CHULResearch Center and Laval University,2705 Boulevard Laurier,Sainte-Foy, Québec,G1V 4G2, Canada.Correspondence to S.R.e-mail: [email protected]: 10.1038/nrn752
NATURE REVIEWS | NEUROSCIENCE VOLUME 3 | MARCH 2002 | 217
R E V I E W S
CIRCUMVENTRICULAR ORGANS
Brain regions that have a richvascular plexus with aspecialized arrangement of theblood vessels. The junctionsbetween the capillary endothelialcells are not tight in the bloodvessels of these regions, allowingthe diffusion of large molecules.These organs include theorganum vasculosum of thelamina terminalis, thesubfornical organ, the medianeminence and the areapostrema. Although notincluded as circumventricularorgans, the choroid plexus andleptomeninges are also highlyvascularized and are rapidlyactivated by circulatingpathogens.
multiple leucine-rich repeats, whereas TLR cytoplasmicdomains are similar to the cytoplasmic portion of theinterleukin 1 (IL-1) receptor (IL-1R), commonly knownas Toll/IL-1R homologous regions (TIR domains)1,3,4.Distinct TLRs have been proposed as key molecules in theselective recognition of the main PAMPs that are pro-duced by either Gram-negative or Gram-positive bacteria(FIG. 1). The observations that mutations of the mouse Lpslocus abolish the response to LPS, and that this locusencodes TLR4, provided the first evidence that this partic-ular receptor might be involved in the innate immuneresponse to Gram-negative bacteria5,6. By contrast, TLR2-deficient mice show a normal inflammatory responseto LPS7, but macrophages from these animals are lessresponsive to Gram-positive bacterial cell walls andpeptidoglycan7. These results are evidence of TLR selec-tivity in PAMP recognition, although other TLRs canrecognize the same components of both Gram-negativeand Gram-positive bacteria (see below).
response by phagocytic cells2. Peptidoglycan and lipotei-choic acid from GRAM-POSITIVE BACTERIA are other PAMPsthat have the ability to activate the NUCLEAR FACTOR κB
(NFκB) signalling pathways and the production ofCYTOKINES. The secretion of cytokines by circulatingmonocytes/neutrophils and tissue macrophages inresponse to PAMPs requires a cascade of signallingevents, the details of which have been clarified in recentyears. In particular, the involvement of TOLL-LIKE RECEPTORS
(TLRs) has received significant attention.The Toll protein was first discovered as an essential
molecule for the establishment of the dorsoventral axis inthe Drosophila embryo. TLRs are mammalian homo-logues of this protein, which are expressed at the surfaceof a specific group of immune cells known as the ANTIGEN-
PRESENTING CELLS (APCs). These cells are rapidly activatedby pathogens that bind to specific TLRs. Members of theTLR family share characteristic extracellular and cyto-plasmic domains3. Their extracellular domains include
TNF
TNF
TNFR1
PP
P UbUb
Ub
Ub
ATP
Degraded IκB
2Pi
2ADP2ATP
RIP
LPS (Gram–)dsRNA
Nucleus
Cytoplasm
IRAK
Ubiquitin-conjugating
enzymes
NIK
NIK
IκB-α
Target genes
LTA, PGN (Gram+)
Flagellin Bacterial DNA
NIK
NIK
NIK
NIK
P
TRADD
IL-1R
TRAF6
TRAF2
IL-1
ACP1
IL-1
MyD88
TLR2 TLR6TLRX
IRAKMyD88
TRAF6
IRAKIRAK
TRAF6
IκB
TRAF6
TLR3CD14
TLR4TLR5MyD88 MyD88
IRAKTRAF6
MyD88TLR9
IRAKTRAF6
MyD88
p65p50
IκB
p65p50
IκB
p65
p65
p50
p50p65p50
γ β αIKAP
Proteasome
p65 p50
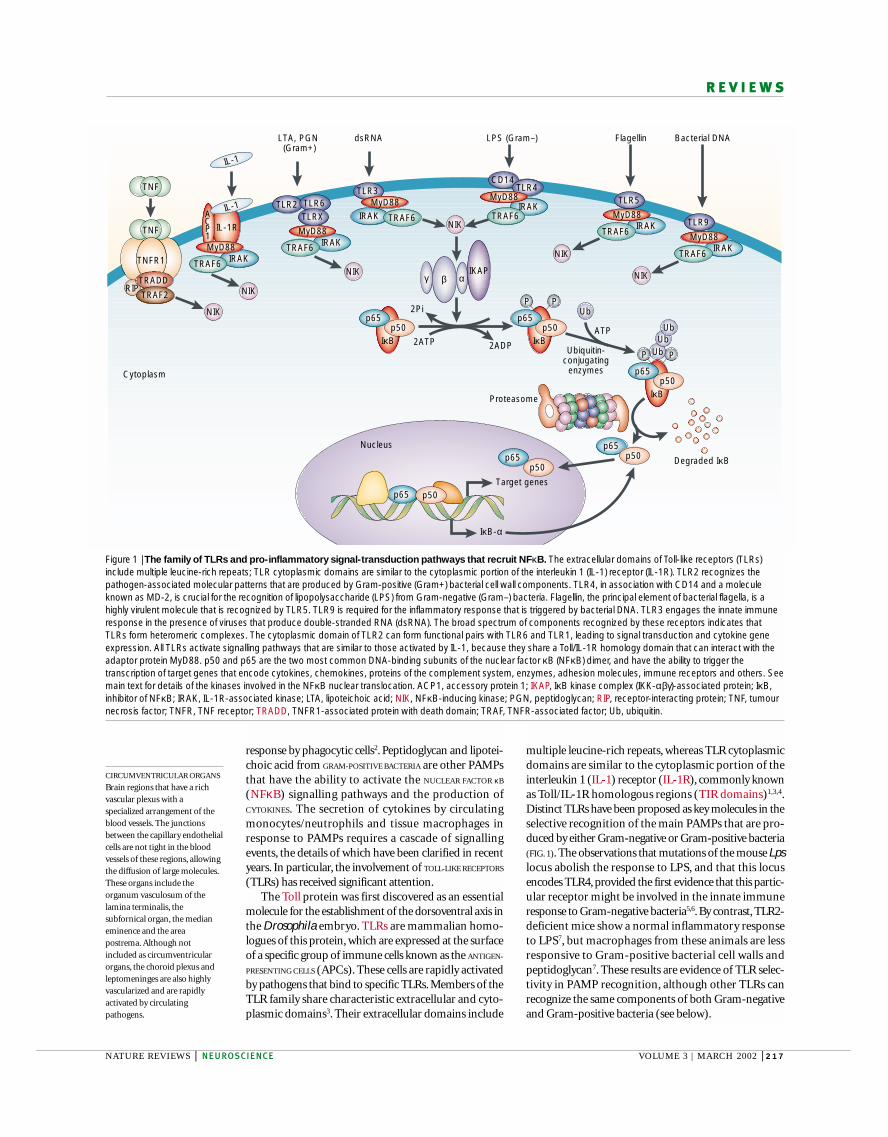
Figure 1 | The family of TLRs and pro-inflammatory signal-transduction pathways that recruit NFκB. The extracellular domains of Toll-like receptors (TLRs)include multiple leucine-rich repeats; TLR cytoplasmic domains are similar to the cytoplasmic portion of the interleukin 1 (IL-1) receptor (IL-1R). TLR2 recognizes thepathogen-associated molecular patterns that are produced by Gram-positive (Gram+) bacterial cell wall components. TLR4, in association with CD14 and a moleculeknown as MD-2, is crucial for the recognition of lipopolysaccharide (LPS) from Gram-negative (Gram–) bacteria. Flagellin, the principal element of bacterial flagella, is ahighly virulent molecule that is recognized by TLR5. TLR9 is required for the inflammatory response that is triggered by bacterial DNA. TLR3 engages the innate immuneresponse in the presence of viruses that produce double-stranded RNA (dsRNA). The broad spectrum of components recognized by these receptors indicates thatTLRs form heteromeric complexes. The cytoplasmic domain of TLR2 can form functional pairs with TLR6 and TLR1, leading to signal transduction and cytokine geneexpression. All TLRs activate signalling pathways that are similar to those activated by IL-1, because they share a Toll/IL-1R homology domain that can interact with theadaptor protein MyD88. p50 and p65 are the two most common DNA-binding subunits of the nuclear factor κB (NFκB) dimer, and have the ability to trigger thetranscription of target genes that encode cytokines, chemokines, proteins of the complement system, enzymes, adhesion molecules, immune receptors and others. Seemain text for details of the kinases involved in the NFκB nuclear translocation. ACP1, accessory protein 1; IKAP, IκB kinase complex (IKK-αβγ)-associated protein; IκB,inhibitor of NFκB; IRAK, IL-1R-associated kinase; LTA, lipoteichoic acid; NIK, NFκB-inducing kinase; PGN, peptidoglycan; RIP, receptor-interacting protein; TNF, tumournecrosis factor; TNFR, TNF receptor; TRADD, TNFR1-associated protein with death domain; TRAF, TNFR-associated factor; Ub, ubiquitin.

218 | MARCH 2002 | VOLUME 3 www.nature.com/reviews/neuro
R E V I E W S
ADAPTIVE IMMUNITY
Also known as acquiredimmunity, it describes theresponse of antigen-specificlymphocytes to antigen and thedevelopment of immunologicalmemory. It is mediated by theclonal selection of lymphocytes.
STIFF-MAN SYNDROME
A neuromuscular disorder thatis characterized by progressiverigidity and a hyperactive startlereflex that results in thecontraction of muscles, causingviolent spasms.
RASMUSSEN ENCEPHALITIS
A childhood disease that ischaracterized by seizures,hemiparesis, inflammation andmental deterioration.
PATHOGEN-ASSOCIATED
MOLECULAR PATTERNS
Specific elements that areproduced by microorganismsand can induce innate immuneresponses. These elements arerecognized by specific receptorsthat are expressed at the surfaceof macrophages, dendritic cellsand microglia.
GRAM-NEGATIVE BACTERIA
Bacteria that do not retain abasic blue dye during the Gram-stain procedure. Their cell wallsare thin, consisting of a layer oflipopolysaccharide outside apeptidoglycan layer.
activation of NFκB by many stimuli, although onlyIKK-β is essential for activating NFκB in response tocytokines and PAMPs. Indeed, IKK-β is the target ofupstream signals generated by pro-inflammatory stim-uli that give rise to phosphorylation of the inhibitor ofNFκB (IκB) at Ser32/36 and proteasomal degradationafter polyubiquitination13,14. This event frees NFκB, andallows its nuclear translocation and the subsequent acti-vation of target genes (FIG. 1). Recruitment of theMyD88/IRAK/TRAF6 complex can also activate mito-gen-activated protein kinase (MAPK) kinases (MKKs);in particular, the JUN kinase pathway that leads to acti-vation of the activator protein 1 (AP-1) transcriptionfactor. A well-known consequence of the nuclear trans-location of AP-1 and NFκB is the transcriptional activa-tion of numerous pro-inflammatory genes, whichencode cytokines, CHEMOKINES, proteins of the COMPLEMENT
SYSTEM, enzymes (such as cyclooxygenase 2 and theinducible form of nitric oxide synthase), adhesion mole-cules and immune receptors. All of these molecules areinvolved in engaging and controlling the innate immuneresponse, which is essential for pathogen elimination,and in orchestrating the transition to an adaptiveimmune response (BOX 1).
Innate immune response in the CNSFor a long time, the brain was considered to be a privi-leged organ from an immunological point of view,owing to its inability to mount an immune responseand process antigens. Although this is partly true, theCNS shows a well-organized innate immune reactionin response to systemic bacterial infection and cerebralinjury. The CD14 and TLR4 receptors are constitutivelyexpressed in the CVOs15,16. Circulating LPS also causesa rapid increase in CD14 in these brain regions, and adelayed response takes place in cells located at theboundaries of the CVOs and in microglia across the brain parenchyma. A similar expression pattern wasrecently found for the gene that encodes TLR2 in thebrains of mice after a single systemic injection of LPS17.The signal was first detected in regions devoid of BBB(FIG. 2). A second wave of TLR2 expression was detectedin the surrounding parenchymal cells, which alsoexpressed the microglial marker Iba1. The rapid induc-tion of IκB and the upregulation of MyD88 indicatethat LPS-induced TLR2 transcription is dependent onthe NFκB pathway17.
The activation of parenchymal microglia duringendotoxaemia is associated with a robust induction ofgenes that encode cytokines, chemokines and proteinsof the complement system18–23. This phenomenon issurprising, because access of circulating endotoxins tocerebral tissue is limited by the BBB. However, thereare structures that are devoid of BBB that seem to actas immune sentinels for the brain. These include theorganum vasculosum of the lamina terminalis, subfor-nical organ, median eminence, area postrema, CHOROID
PLEXUS and LEPTOMENINGES. The basal expression of CD14and TLR4 is likely to be central to the pro-inflamma-tory signal-transduction events that originate in theseregions during the innate immune response. Indeed,
Eight further members of the TLR family have beencharacterized so far. Flagellin, the principal element ofbacterial flagella, is a highly virulent molecule that is rec-ognized by the TLR5 receptor8, whereas TLR9 isrequired for the inflammatory response that is triggeredby bacterial DNA9. TLRs also trigger an innate immuneresponse to viruses that produce double-stranded RNA.For example, TLR3-deficient mice show reducedresponses to the synthetic double-stranded-RNA ana-logue polyinosine-polycytidylic acid10. In addition,TLRs can form multimeric complexes to increase thespectrum of molecules that they recognize. So, dimer-ization of the cytoplasmic domain of TLR2 does notinduce cytokine production in macrophages, whereassimilar dimerization of the TLR4 cytoplasmic domain isassociated with pro-inflammatory signalling11. Also, thecytoplasmic domain of TLR2 can form functional pairswith TLR6 and TLR1, leading to signal transductionand cytokine expression11. So, whereas the TLR4homodimer is responsible for triggering NFκB inresponse to cell wall components of Gram-negative bac-teria, a more complex combinatorial repertoire isneeded to discriminate between PAMPs found innature.
Because of the presence of the TIR domain, TLRsactivate signalling pathways that are similar to thoseengaged by IL-1. The TIR domain can interact withMyD88 (FIG. 1). This adaptor protein has an amino-terminal DEATH DOMAIN that associates with the IL-1R-associated kinase (IRAK), a serine kinase that activatesanother adaptor molecule — tumour necrosis factor(TNF) receptor (TNFR)-associated factor 6 (TRAF6).Recruitment of TRAF6 leads to activation of the proteinkinase IKK (IκB kinase), which is composed of two catalytic subunits (IKK-α and IKK-β) and one regula-tory subunit (IKK-γ/NEMO)12. IKK-γis required for the
Box 1 | Transition from innate to adaptive immune response
Although long considered as nonspecific, the innate immune reaction might be crucial inthe transmission of appropriate information to the immune cells that are involved inacquired immunity. Macrophages and DENDRITIC CELLS express as many as ten differentToll-like receptors (TLRs), which recognize specific components of bacteria and viruses3.The identification of these receptors provided evidence that pathogen-associatedmolecular patterns (PAMPs) recognize specific endogenous receptors that are expressedon the surface of antigen-presenting cells. Cytokines that act on the macrophage itself areproduced minutes after TLR activation, whereas those that mediate the transition frominnate to adaptive immune response appear after a few hours. Binding of PAMPs to theirrespective TLRs leads to the release of interleukin 12 (IL-12), a cytokine that is involved inthe transition from innate to adaptive immunity. Indeed, macrophage-derived IL-12stimulates the differentiation of a subset of T lymphocytes (CD4+) into T
H1 helper cells,
which produce interferon-γ(IFN-γ). TH
1 cells are believed to be crucial to thepathogenesis of multiple sclerosis, especially during the demyelinating episodes. Helper T lymphocytes can also differentiate into T
H2 cells, but this phenomenon requires IL-4
production from antigen-activated T cells, and the contribution of the innate immuneresponse in this process remains unclear. The balance between T
H1 (pro-inflammatory)
and TH
2 (anti-inflammatory) cytokines in the brain might have a profound impact onneuronal elements. Although the link between the innate immune reaction and acquiredimmunity has been better clarified in recent years, there are many questions aboutwhether defects in this fine interplay are direct causes of autoimmune diseases indifferent organs and in the central nervous system.

NATURE REVIEWS | NEUROSCIENCE VOLUME 3 | MARCH 2002 | 219
R E V I E W S
GRAM-POSITIVE BACTERIA
Bacteria that retain a basic bluedye during the Gram-stainprocedure. Their cell wall isthicker than that of Gram-negative bacteria, containingmore peptidoglycan.
NUCLEAR FACTOR κB
A family of transcription factorsthat are important for pro-inflammatory and anti-apoptoticresponses.
CYTOKINES
In general terms, cytokines areproteins made by cells that affectthe behaviour of other cells.They are produced mainly by theimmune system.
TOLL-LIKE RECEPTORS
A large family of receptors thatare expressed at the surface ofleukocytes and microglial cells.They are responsible forengaging the innate immunesystem in response to pathogens.
ANTIGEN-PRESENTING CELLS
Specialized cells that presentspecific antigens to T cells.Macrophages and dendritic cellsare the main antigen-presentingcells; in the CNS, the antigen-presenting cells are the microglia.
DEATH DOMAIN
A protein–protein interactiondomain found in many proteinsthat are involved in signallingand apoptosis.
CHEMOKINES
Small, secreted proteins thatstimulate the motile behaviourof leukocytes.
COMPLEMENT SYSTEM
A set of plasma proteins thatattack extracellular pathogens.The pathogen becomes coatedwith complement proteins thatfacilitate pathogen removal byphagocytes.
CD14
The first lipopolysaccharidereceptor to be characterized. Itexists two forms: membraneCD14 (mCD14) and solubleCD14 (sCD14). mCD14 ispresent at the surface of myeloidcells and acts as aglycosylphosphatidylinositol(GPI)-anchored membraneglycoprotein, whereas sCD14lacks the GPI anchor, but canbind LPS to activate cells that aredevoid of mCD14, such asendothelial cells.
itself acts as an autocrine and paracrine factor toupregulate the LPS receptor. The binding of TNF to itstype 1 receptor — TNFR1 (p55) — leads to the activa-tion and translocation of NFκB into the nucleus, anevent that modulates CD14 expression. TNF-α caninduce a transient increase in plasma CD14 levels,which is accompanied by increased CD14 mRNA in lung, liver and kidney24. Pre-treatment of mice with anti-TNF-α antibodies significantly preventsLPS-induced CD14 transcription25.
TNF can also induce its own production by auto-crine stimulation, which is followed by the synthesis of
the TLR4/CD14-positive cells of the CVOs mightselectively recognize cell wall components of Gram-negative bacteria to allow LPS signalling and rapidtranscription of pro-inflammatory cytokines duringendotoxaemia, first within these organs and lateracross the brain parenchyma. Interestingly, systemicinjection of the bacterial endotoxin causes expressionof CD14 messenger RNA in the brain in a pattern thatis closely related to the induction of TNF-α, with bothrapid and delayed responses15,20. Although a large bodyof evidence indicates that CD14 is necessary for LPS totrigger cytokine transcription, it is possible that TNF-α
Veh
LPS 6 h
ME
3VLHA
SFO
ChpAmygdala
6 h 1.5 h
12 h 12 h 3 h
24 h 24 h 24 h
LPS
LPS
Figure 2 | Response wave of TLR2-expressing cells across the mouse brain to bacterial endotoxin LPS. After a singlesystemic injection of lipopolysaccharide (LPS), induction of Toll-like receptor 2 (TLR2) starts in the circumventricular organs,choroid plexus (Chp), leptomeninges and blood vessels. Six hours after injection, a localized hybridization signal is detected in themedian eminence (ME)/arcuate nucleus (left column), and at the edge of the fimbria, stria terminalis and optic tract (middlecolumn). The choroid plexus and subfornical organ (SFO) already show a strong signal 3 h after the injection (right column). Lateron, the message spreads over these structures, reaching deeper parenchymal regions 24 h after the challenge (bottom panels).Magnification, x10. 3V, third ventricle; LHA, lateral hypothalamic area; Veh, vehicle injection. Adapted with permission from REF. 17
© 2001 International Society for Neurochemistry.

220 | MARCH 2002 | VOLUME 3 www.nature.com/reviews/neuro
R E V I E W S
CHOROID PLEXUS
A site of production ofcerebrospinal fluid in the adultbrain. It is formed by theinvagination of ependymal cellsinto the ventricles, whichbecome richly vascularized.
DENDRITIC CELLS
Also known as interdigitatingreticular cells because of theirbranched morphology, dendriticcells are the most potentstimulators of T-cell responses.
LEPTOMENINGES
The pia mater and the arachnoidconsidered together.
TNF-αTumour necrosis factor-α.A cytokine produced bymacrophages that has multiplefunctions in the immuneresponse.
Dual nature of innate immunity in the CNSThe roles of TLR2, TLR4 and CD14 in the CNS areunknown. The constitutive expression of CD14 in theCVOs and its upregulation in the brain parenchymaafter LPS injection indicate a potential role for thismolecule in protecting nerve cells against LPS particles.The macrophages and microglia in the CVOs arestrategically positioned to respond rapidly to circulat-ing endotoxin or bacteria, whereas parenchymalmicroglia serve as the phagocytic population of cells inthe brain in case of invasion. The BBB is altered duringsevere endotoxaemia and neurodegeneration. Thisalteration might allow the diffusion of molecules thatnormally have no access to the parenchymal elements.Although activation of microglial cells could rapidlyeliminate this foreign material, sustained activity ofthese cells might have detrimental effects and be associ-ated with neurodegenerative disorders. In this regard,robust and rapid transcriptional activation of TLR2and CD14 takes place in the brains of mice with EXPERI-
MENTAL AUTOIMMUNE ENCEPHALOMYELITIS (EAE), an experi-mental model of multiple sclerosis26. This observationis in agreement with the fact that this demyelinatingdisease has a well-known immune aetiology, beingassociated with the chronic induction of inflammatorymolecules. However, a similar induction of TLR2 wasfound after stab injury, viral meningitis and, surpris-ingly, in transgenic mice that overexpress a mutantform of superoxide dismutase 1 that is found in ALS(REF. 27, and S.R. and colleagues, unpublished observa-tions). So, proteins of the innate immune system can beinduced not only by PAMPs, but also by brain injuryand during some neurodegenerative disorders. Whathappens first remains unknown, and the role of thisinnate immune response in the brain has yet to beunravelled. It is possible that, in addition to its well-known role as a sensor of PAMPs and as an OPSONIZATION
factor of LPS particles, CD14 might also have a role inpriming and sustaining the activity of microglial cellswithin the brain parenchyma. This could contribute toan exaggerated immune response and be potentiallydetrimental for neurons.
LPS-induced pro-inflammatory signal-transductionpathways are generally not associated with neurodegen-eration, although a few studies have provided evidenceof LPS-induced neurotoxicity28,29. Such discrepanciescould be explained by the use of different techniques toassay neurodegeneration and/or by differences in theregions under scrutiny. So, injection of bacterial endo-toxin in the hippocampus, cortex or substantia nigra ofadult rats produced neurodegeneration only in the sub-stantia nigra29. The authors of this study suggested thatthe differential susceptibility to LPS might be attribut-able to differences in the number of microglial cells ineach region, and might reflect the levels of inflamma-tion-related factors produced by these cells29. Moreover,it is possible that specific populations of neurons aremore susceptible to inflammatory molecules than oth-ers and that, despite their role in eliminating pathogensfrom the CNS, microglia and their secreted products areharmful to some neurons.
other pro-inflammatory cytokines, such as IL-1β andIL-6. In the brain, TNF seems to activate parenchymalmicroglia in a paracrine manner during endotox-aemia. Indeed, central injection of rat TNF-α causes arobust expression of the genes that encode IκB-α ,TNF-α and CD14 within microglial cells across thebrain parenchyma20. Systemic injection with endo-toxin LPS causes a similar microglial activation that isprevented by inhibiting the activity of TNF-α in theCNS20. We suggest that circulating LPS might bind itstransmembrane receptors on macrophages andmicroglia of the CVOs, stimulating NFκB signallingand triggering TNF-α transcription. This cytokinecould, in turn, activate NFκB signalling and gene tran-scription in adjacent microglial cells (FIG. 3). So, cen-trally produced TNF-α is probably essential for theactivation of parenchymal microglial cells duringsevere endotoxaemia. These events might be central tothe orchestration of coordinated inflammatoryresponses that activate the resident phagocytic cells of the brain.
LBP
LPSLPSLBP
Autocrine effect
Changes ingene
expression
CVO-residentmacrophages
microglia
Parenchymalmicroglia
Paracrine effect
CD14TLR4
TRADD/TRAF2/RIP
TNFR1
MEKK3
IRAK/TRAF6MyD88
TNF-α
NFκBNFκB
Blood vessel
TRADD/TRAF2/RIP
MEKK3
Figure 3 | Autocrine and paracrine roles of TNF-α in the synthesis of CD14 in microglialcells during endotoxaemia. Cell wall components of Gram-negative bacteria might berecognized by TLR4/CD14-positive cells of the circumventricular organs (CVOs), allowing LPSsignalling and rapid transcription of pro-inflammatory cytokines, first within these organs andlater across the brain parenchyma. We suggest that circulating LPS targets its receptors inCVO macrophages and microglia, stimulating the NFκB signalling pathway and triggering TNF-α transcription. The cytokine might in turn bind its cognate receptor (TNFR1) and lead tothe formation of the TRADD/TRAF2/RIP complex, which could activate NFκB signalling inadjacent microglia. Such events probably contribute to transcriptional activation of CD14, TNF-α and TLR2 in the brains of endotoxin-treated animals. Expression levels of genes that are constitutively expressed in the CVOs increase in response to circulating LPS, whereasexpression of TLR4 is decreased. This downregulation of the endotoxin receptor is central tothe control of LPS tolerance. LBP, LPS-binding protein; LPS, lipopolysaccharide; MEKK3,mitogen-activated protein kinase kinase kinase 3; NFκB, nuclear factor κB; RIP, receptor-interacting protein; TLR, Toll-like receptor; TNF-α, tumour necrosis factor-α; TRADD, TNFR1-associated protein with death domain; TRAF2, TNFR-associated factor 2.

NATURE REVIEWS | NEUROSCIENCE VOLUME 3 | MARCH 2002 | 221
R E V I E W S
EXPERIMENTAL AUTOIMMUNE
ENCEPHALOMYELITIS
A rodent model of multiplesclerosis that is characterized byepisodes of spasticity andtremor.
OPSONIZATION
The alteration of the surface of apathogen so that it can beingested by a phagocyte.
HELPER T CELLS
At least two distinct subsets ofactivated CD4+ T lymphocyteshave been described. T
H1 cells
produce IFN-γ, lymphotoxinand TNF-α, and support cell-mediated immunity. T
H2 cells
produce IL-4, IL-5 and IL-13,support humoural immunity,and downregulate T
H1
responses.
FAS
A transmembrane protein thatmediates apoptosis and might beinvolved in the negative selectionof autoreactive T cells in thethymus.
cytokine promotes IGF1 receptor resistance in neuronsand inhibits IGF1-receptor-mediated phosphorylationof the docking molecule insulin receptor substrate 2and activation of the downstream survival enzymephosphatidylinositol 3-kinase37. Despite this evidence,there are conflicting results on the role of TNF in eitherexacerbating or attenuating brain damage in differentpathological situations. In an elegant study, Arnett et al.38 used mice that lack TNF-α and its associatedreceptors to study demyelination and remyelination.Lack of TNF-α led to a significant delay in remyelina-tion, which was associated with a reduction in the poolof proliferating oligodendrocyte progenitors and areduction in the number of mature oligodendrocytes.TNFR2, but not TNFR1, mediated this reparative roleof TNF, indicating that the dual role of this cytokine indemyelination and remyelination depends partly oncytokine receptor type38.
But the role of TNF and other cytokines in myelina-tion and demyelination could be more complex. HELPER
T CELLS also produce TNF, together with interferon-γ(IFN-γ), and migrate in the CNS of EAE animals.Although it is not known how this phenomenon takesplace, a subset of helper T cells — activated T
H1 cells —
and their secreted cytokines are believed to have a signif-icant involvement in the aetiology of multiple sclerosisand demyelination. It is therefore possible that TNF andIFN-γact synergistically to damage neurons and othercells of the CNS. Moreover, transgenic mice that expressIFN-γ in the hippocampus show an enhancedmicroglial reactivity to lesion-induced neuronal injury,indicating that IFN-γmight act as an amplifier of theresponse39. Treatment with IFN-γfailed to alter cell sur-vival or expression of myelin basic protein in culturedhuman oligodendrocytes, but these cells are more sus-ceptible to FAS-mediated apoptosis, an effect that is augmented by TNF40. On the other hand, acute admin-istration of TNF into the cerebral tissue is not generallyassociated with demyelination, despite the robust andtransient inflammatory reaction that occurs across thebrain parenchyma20. We therefore propose that recep-tors and cytokines that are involved in the innateimmune response (such as TNF) are beneficial to cere-bral tissue and crucial in protecting against pathogensand toxin-induced demyelination. By contrast, mol-ecules of the adaptive immune system, especially thoseproduced by the T
H1 subset of helper T cells (such as
IFN-γ) might promote demyelination.
Innate immunity and neurodegenerationThe activation of microglia and astrocytes, which isindicative of inflammation, occurs in the CNS of patientswith Alzheimer’s, Parkinson’s and Huntington’s diseases,multiple sclerosis and ALS41–43. The serum and cere-brospinal fluid of these patients show elevated levels ofmolecules of the innate immune system, such as IL-6, IL-1β and TNF-α41–43. IL-1β and TNF-α are secreted byactivated parenchymal microglia and can be potentinducers of cell death in models of neurodegeneration,which can be alleviated by anti-inflammatory drugs andneutralizing antibodies41,44–47.Although this effect depends
A detrimental effect of this sort might be observedwhen the cerebral tissue is exposed to very high concen-trations of LPS and other PAMPs; for example, in casesof bacterial meningitis in children. It is interesting tonote that immature brains are more susceptible to theinflammatory response: LPS administration to 7-day-oldrats markedly sensitizes the brain to injury and inducescerebral infarction in response to short periods ofhypoxia/ischaemia that cause little or no injury bythemselves30. Although the expression of both CD14and TLR4 was altered in these brains, there was nodirect evidence of a contribution of these receptors inhypoxia/ischaemia-induced cerebral injury.
Although the innate immune response might have adetrimental effect in the nervous system, it is clear that italso has a beneficial role. Pro-inflammatory cytokinesare produced as early as 15 minutes after acute traumato the CNS31. This form of traumatic injury is typicallyaccompanied by the migration of inflammatory cellsinto the damaged tissue. However, it takes several hoursfor this phenomenon to take place, and parenchymalelements of the brain produce molecules of the innateimmune response at early time points. Indeed, we haveprovided anatomical evidence that cytokine transcriptsappear in microglia 3 and 12 hours after corticallesions31. Activated microglia have also been observedwithin and adjacent to the primary traumatic injury sitewithin one hour, whereas infiltration of mononuclearcells became prominent only 48 hours after injury32,33.The temporal profile of neurotrophic factor inductionthat follows the endogenous production of pro-inflam-matory cytokines after injury points to a potential roleof the inflammatory response in mediating neuro-trophic responses. TNF and IL-1 are two of the maincytokines that are detected within parenchymalmicroglia along the lesion site31, and a role for IL-1β inthe induction of nerve growth factor expression byastrocytes has been reported34,35. Microglial-derived IL-1is also required for the astrocytic production of ciliaryneurotrophic factor (CNTF)31 and insulin-like growthfactor 1 (IGF1)36, both of which promote repair of theinjured CNS. Remyelination is impaired in mice thatlack IL-1β, and there is also a profound delay in the differ-entiation of oligodendrocyte progenitors36. This indicatesthat early production of IL-1β by parenchymal micro-glial cells might be essential for triggering the release ofneurotrophic factors by astrocytes and facilitating thematuration of precursor cells (FIG. 4).
Although TNF and IL-1 have numerous overlap-ping activities in the immune system, TNF does notseem to be required for the release of neurotrophic fac-tors, at least not for that of CNTF. The production ofCNTF is totally abolished in IL-1β-deficient mice,although TNF expression remains comparable to thatof wild-type animals after CNS injury 31. Whereas IL-1might be crucial in increasing the production of neuro-trophic factors by astrocytes, TNF might act on microgliain an autocrine and paracrine manner (FIGS 3 and 4).Paradoxically, TNF-induced microglial activity mightbe detrimental to the brain by promoting apoptosis ofoligodendrocytes and preventing remyelination. This

222 | MARCH 2002 | VOLUME 3 www.nature.com/reviews/neuro
R E V I E W S
CASPASES
Cysteine proteases involved inapoptosis, which cleave atspecific aspartate residues.
PROSTAGLANDINS
Biologically active metabolites ofarachidonic acid and otherlipids. Prostaglandins have manyfunctions; for example, they areinvolved in vasodilation,bronchodilation, inflammatoryreactions and the regulation ofcell proliferation. They are alsoinvolved in the control ofendocrine functions.
CYCLIN-DEPENDENT KINASES
Enzymes that phosphorylateproteins that are involved inDNA synthesis and mitosis.They require a cyclin partner foractivity and substrate specificity.
BCL PROTEINS
Molecules that are associatedwith B-cell leukaemia andlymphoma. Bcl2 is amitochondrial protein of theinner membrane that can blockapoptosis.
immunity in neurodegeneration raises questions aboutthe fundamental capability of the CNS to control exces-sive inflammation and to drive adequately the innateimmune response for neuroprotection.
Common stressors (such as oxidative damage, mito-chondrial dysfunction and excitotoxicity) and down-stream effector molecules (such as CYCLIN-DEPENDENT
KINASES, caspases, BCL2 FAMILY MEMBERS and nitric oxide) areinvolved in the death of selective neuronal populationsin animal models of ALS, and in Alzheimer’s, Parkinson’sand Huntington’s diseases43,49,50. It is unlikely that theseare the sole factors that dictate the specificity of neuro-degeneration or that trigger the inflammation process.
on the model and the cellular environment, IL-1β hasthe ability to activate CASPASES, whereas, in addition toactivating caspases (such as IL-1), TNF-α also inhibitsthe IGF1-dependent survival of neurons37,47. In additionto the secretion of cytokines, microglial cells producetoxic molecules such as nitric oxide and PROSTAGLANDINS,which might further contribute to the degenerative cas-cade41–43. By acting as APCs and controlling the transitionto the adaptive immune response, microglial cells aremediators of the innate response in the CNS42,48 (BOX 1).However, it remains unclear whether the innate mecha-nisms in the CNS are fine-tuned to handle chronicimmune challenges. The long-term induction of innate
IL-1R1
TNFR2
NTs(e.g. NGF, CNTF)
?
TNFR1
Remyelination
Neurogenesis
Neuron
Astrocyte
Pathogens (PAMPs)Injury/traumaStressors
MEKK3 NFκB
Microglialcell
TNF-α
Stem cellprogenitor
MyD88 NTs
NFκB
++
TLRs
TNFR1
MyD88
NFκB
Microglialcell
TNF-αIL-1β
IL-1β
TNF-α
TRADDRIP
TRAF2MEKK3
TRADDRIP
TRAF2
Figure 4 | Potential beneficial roles of pro-inflammatory cytokines during the innate immune reaction. Pathogens(including bacteria and viruses), injury and stressors stimulate Toll-like receptors (TLRs) that are expressed at the surface of microglialcells, the antigen-presenting cells of the central nervous system (CNS). This allows the recruitment of adaptor proteins and activationof the pro-inflammatory signal-transduction pathways that ultimately trigger cytokine transcription. Tumour necrosis factor-α (TNF-α)and interleukin 1β (IL-1β) are the two main cytokines involved in the early innate immune response. Once released, these cytokinesact on different cell types in the CNS. TNF-α acts as an autocrine and paracrine factor through its type 1 receptor (TNFR1) to activatethe microglia further, whereas IL-1β binds to its type 1 receptor (IL-1R1) in astrocytes, leading to the production of neurotrophins(NTs), such as nerve growth factor (NGF) and ciliary neurotrophic factor (CNTF). These NTs might act on progenitors to favourremyelination after mechanical or toxin-induced injury. TNF-α could also bind to TNFR2 at the surface of specific progenitors topromote their differentiation into mature and functional oligodendrocytes. MEKK3, mitogen-activated protein kinase kinase kinase 3;NFκB, nuclear factor κB; PAMPs, pathogen-associated molecular patterns; RIP, receptor-interacting protein; TRADD, TNFR1-associated protein with death domain; TRAF, TNFR-associated factor.

NATURE REVIEWS | NEUROSCIENCE VOLUME 3 | MARCH 2002 | 223
R E V I E W S
MAJOR HISTOCOMPATIBILITY
COMPLEX
There are two classes of MHCmolecules. MHC class Imolecules are found on thesurface of most cells and presentproteins that are generated in thecytosol to T lymphocytes. MHCclass II molecules are expressedonly at the surface of activatedantigen-presenting cells, andthey present peptides that havebeen degraded in cellular vesiclesto T cells.
FINGERPRINT
A distinct set of proteinsexpressed by a given populationof neurons, which mightaccount for the specializedbiochemical properties of theseneurons, and make themvulnerable to an immunechallenge by acting as antigens.
PARANEOPLASTIC
NEUROLOGICAL DISEASES
A set of neurodegenerativedisorders that arise in thecontext of cancer and arebelieved to be mediated by theimmune system. Patientsharbour autoantibodies that aretargeted to specific tumour andneuronal antigens (onconeuralantigens).
ALTERNATIVE SPLICING
During splicing, introns areexcised from RNA aftertranscription and the cut endsare rejoined to form acontinuous message. Alternativesplicing allows the production ofdifferent messages from thesame DNA molecule.
GEPHYRIN
A cytosolic protein that clustersglycine and GABA
Areceptors at
synapses.
AMPHIPHYSIN
A molecule located at thepresynaptic terminal thatinteracts with several proteinsthat are important in thesynaptic-vesicle cycle.
been proposed that peripheral antibodies recognize theneuronal antigen and disrupt its normal function, lead-ing to cell death. NOVA1 (neuro-oncological ventralantigen 1), the POMA antigen, a protein expressed exclu-sively in neurons of the ventral horn and hindbrain,binds the pre-mRNAs of the glycine receptor α2 andGABA
A(γ-aminobutyric acid type A) receptor γ2 sub-
units, and regulates their ALTERNATIVE SPLICING62–64. POMAantibodies disrupt the binding of NOVA1 to these pre-mRNAs62,63. Mice that are null for Nova1 show abnormalsplicing of the glycine α2 receptor subunit, developmotor defects and neurological features of POMA, andundergo neuronal apoptotic death in ventral, but notdorsal, spinal cord and brainstem65.
In the case of ALS, the administration of immuno-globulin G (IgG) that is isolated from patients inducestoxicity in motor neurons of mice and in a hybrid cellline of motor neurons by disrupting calcium homeo-stasis60,66–68. Mice injected intraperitoneally with IgGfrom ALS patients also recruit activated microglial cellsin the ventral horn of spinal cord, emphasizing the closerelationship between peripheral challenge, microglialactivation and selective neuronal degeneration69.
Circulating antibodies produced by damaged periph-eral tissues could cross the BBB and target complexes ofantigens that are found exclusively in motor neurons. So,in Rasmussen encephalitis, peripheral antibodies aredirected against the AMPA (α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid) receptor subunitGluR3 and the synaptic protein Munc-18. These anti-bodies have been suggested to induce neuronal death byexcitotoxicity and altered synaptic activity, respec-tively59,70,71. In stiff-man syndrome, antibodies are directedagainst GEPHYRIN, glutamic acid decarboxylase (GAD) andAMPHIPHYSIN, indicating that the disorder might arisefrom disturbances in neurotransmission72–74 (TABLE 1).Moreover, stereotaxic injection of IgG from patientswith Alzheimer’s disease induces immune-mediated
Emerging evidence indicates that neurons are immuno-logically complex; for example, they express class I mol-ecules of the MAJOR HISTOCOMPATIBILITY COMPLEX (MHC)51–53.In the nervous system, these molecules mediate neuronalfunctions that are distinct from their usual roles inperipheral tissues53. However, it is possible that they alsoparticipate in the immune response by presenting anti-gens53,54. How might immunity in the CNS contribute toselective degeneration? It seems that different popula-tions of neurons express distinct sets of macromolecularprotein complexes, which account for their specializedbiochemical properties. These molecular FINGERPRINTS
(TABLE 1) might be involved in determining the specificfunctions of different neuronal populations, but theymight also make neurons prone to selective vulnerabilityby acting as antigens for peripheral antibodies55. Forexample, medium spiny neurons in the basal ganglia,which selectively express the protein DARPP-32, areselectively killed in Huntington’s disease.
A synergistic action of innate and adaptive immunityin selective neurodegeneration is particularly well illus-trated in a group of CNS disorders known as PARANEO-
PLASTIC NEUROLOGICAL DISEASES (PNDs)43,55,56. The serum ofpatients that suffer from these diseases commonly har-bours high titres of circulating cytokines and antibodiesthat cross-react in most cases with neuronal popu-lations43,55–57. Antibodies isolated from these patients areneurotoxic in vitro and in vivo58–61.
PNDs are characterized by the presence of tumoursoutside the CNS55. So, patients with paraneoplastic opso-clonus-myoclonus ataxia (POMA) show deficientinhibitory motor control of the eyes, limbs and trunk, aswell as gynaecological or small-cell lung cancer. Thehigh-titre peripheral antibodies of these patients staintheir systemic tumours, but also recognize neuronal anti-gens55. These antigens are termed ‘onconeural’ owing totheir cross-reactivity with tumour tissues, and are recog-nized by the immune system as foreign proteins. It has
Table 1 | Neuronal antigens in neurodegeneration and associated systemic challenges
Diseases Peripheral Neuronal Toxicity Referenceschallenges antigens
Paraneoplastic Cancers NOVA1 Aberrant RNA splicing of GABAA γ2 and 62–64neurological diseases glycine α2 receptor subunits
hu Deficient RNA binding 55
Cdr2 Cell-cycle signalling in neurons by 55disruption of Cdr2/c-Myc binding andc-Myc activity
mGluR1 Impaired cerebellar plasticity and motor 56learning
Amyotrophic lateral Lymphoma, virus? L-type Ca2+ Excitotoxicity; Ca2+-induced toxicity 60sclerosis channels
Rasmussen encephalitis Bacteria? GluR3 Excitotoxicity 70
Munc-18 Defective synaptic activity 71
Stiff-man syndrome ? Gephyrin Defects in neurotransmission 74
Diabetes mellitus GAD Defects in GABA synthesis; excitotoxicity 73
Cancer Amphiphysin Defects in presynaptic activity 72
Cdr2, cerebellar-degeneration-related protein 2; c-Myc, myelocytomatosis oncogene; GABA, γ-aminobutyric acid; GAD, glutamic acid decarboxylase; GluR3, ionotropic glutamate receptor 3; mGluR1, metabotropic glutamate receptor 1; NOVA1, neuro-oncologicalventral antigen 1.
224 | MARCH 2002 | VOLUME 3 www.nature.com/reviews/neuro
R E V I E W S
SUPPRESSOR T CELLS
Lymphocytes that can suppressthe activity of naive or effector T cells. They produce TGF-β,which inhibits T-cellproliferation.
CYTOTOXIC T CELLS
Lymphocytes that can kill othercells and are important in hostdefence against cytosolicpathogens. They are commonlyMHC class I CD8 cells.
CD4/CD8 RATIO
Most T lymphocytes express oneof two antigens — CD4 andCD8. CD4 is expressed by helperand inflammatory T cells and isa co-receptor for MHC class IImolecules. CD8 is expressed bycytotoxic T cells and is a co-receptor for MHC class Imolecules. An increasedCD4/CD8 ratio commonlyindicates heightened immunefunction, whereas a decreasedratio is indicative of prevalentdisease.
reaction42,75–78. Indeed, in ALS for example, increases inMHC II proteins and human leukocyte antigens in thecorticospinal tracts/anterior horns and elevation of theCD4/CD8 RATIO in serum have been reported, whereas B cells are conspicuously absent79–82.
On the basis of findings on the role of innate andadaptive immunity and BBB leakage, we propose a modelto explain the selective vulnerability of neurons thatoccurs in neurodegenerative disorders (FIG. 5).Accordingto this model, peripheral tissues express antigens that cor-respond to proteins found in macromolecular complexesof specific neuronal populations. These tissues undergoapoptosis and recruit at their site components of adaptiveimmunity.APCs recruited at the inflammatory site act asphagocytes, clearing up apoptotic debris, and present theantigen in association with the MHC I complex. Togetherwith co-stimulatory T cells, the APCs can activate anti-gen-specific CD8+ cells and CD4+ cells to help B cells toproduce antibodies. Some of these antibodies might crossthe BBB passively and bind to a neuronal antigen,
inflammatory injury to cholinergic neurons in the ratbasal forebrain, whereas injection of IgG from patientswith Parkinson’s disease causes selective damage toneurons of the substantia nigra58,61.
Although peripheral antibodies might disrupt thenormal role of these neuronal antigens, they are notsufficient to induce pathology. Indeed, reducing thetitre of antibodies in cases of PNDs does not slow downprogression of disease, and immunization of animalswith antibodies from patients with Rasmussenencephalitis or PNDs fails to induce pathology withfidelity55,56. It seems that toxicity of peripheral anti-bodies requires secretion of molecules of innate immu-nity in the CNS, increasing the permeability of the BBBand thereby favouring infiltration of components ofthe adaptive immune response in the brain. The find-ing of many diffusely scattered SUPPRESSOR/CYTOTOXIC
T CELLS mixed with macrophages in specific CNS tissues of patients with neurological disorders is indicative ofBBB leakage and the presence of an acquired immune
Intra-CNSchallenges
T-cellsT cells
∆VEGFPro-inflammatory cytokinesICAM1
Neuron
Dying neuron
6
7
Activated microglia
Systemic APC
Lymphoid organs
Increase neuronal MHC IChronic induction ofpro-inflammatory cytokines
Peripheral damage/dysfunction
Adaptiveimmunity
8
14
9
12
11
13
10
B cells5
4
3
2
1
Antigens
Antibodies
Blood BBB Brain
Basementmembrane
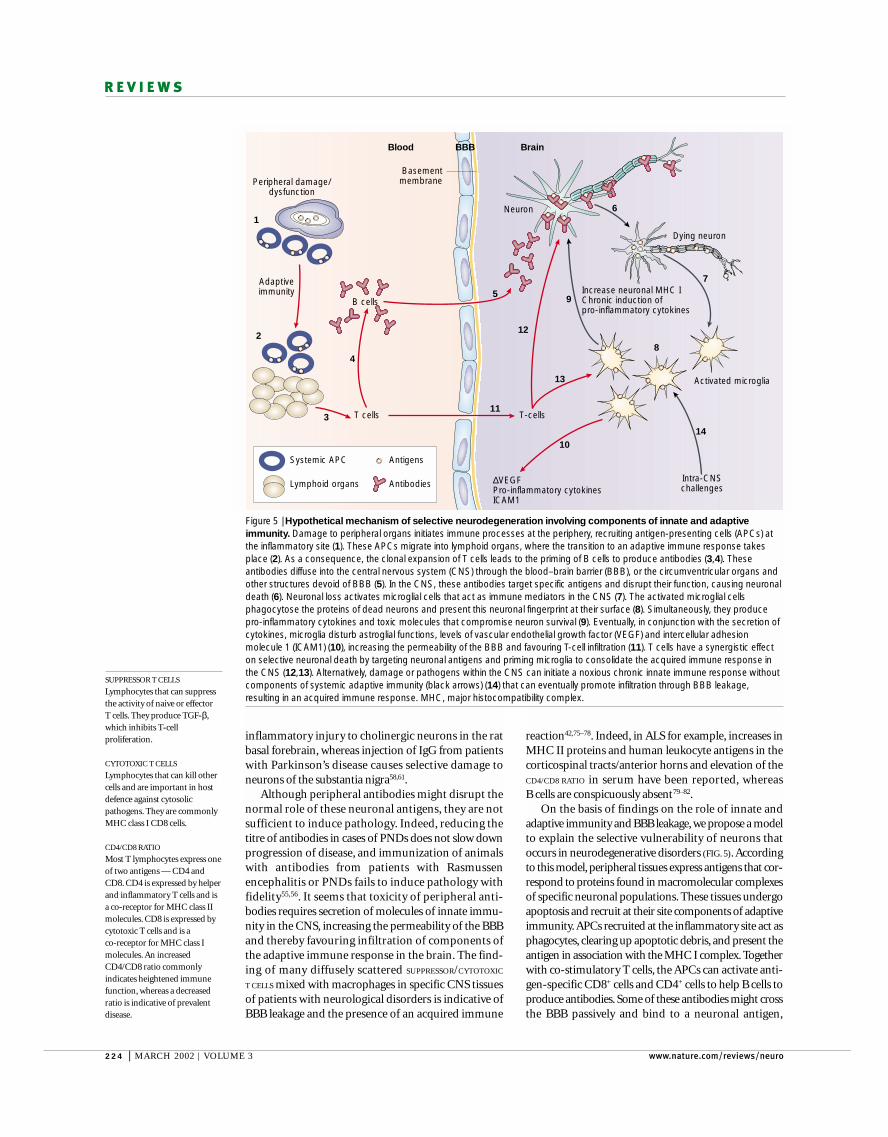
Figure 5 | Hypothetical mechanism of selective neurodegeneration involving components of innate and adaptiveimmunity. Damage to peripheral organs initiates immune processes at the periphery, recruiting antigen-presenting cells (APCs) atthe inflammatory site (1). These APCs migrate into lymphoid organs, where the transition to an adaptive immune response takesplace (2). As a consequence, the clonal expansion of T cells leads to the priming of B cells to produce antibodies (3,4). Theseantibodies diffuse into the central nervous system (CNS) through the blood–brain barrier (BBB), or the circumventricular organs andother structures devoid of BBB (5). In the CNS, these antibodies target specific antigens and disrupt their function, causing neuronaldeath (6). Neuronal loss activates microglial cells that act as immune mediators in the CNS (7). The activated microglial cellsphagocytose the proteins of dead neurons and present this neuronal fingerprint at their surface (8). Simultaneously, they producepro-inflammatory cytokines and toxic molecules that compromise neuron survival (9). Eventually, in conjunction with the secretion ofcytokines, microglia disturb astroglial functions, levels of vascular endothelial growth factor (VEGF) and intercellular adhesionmolecule 1 (ICAM1) (10), increasing the permeability of the BBB and favouring T-cell infiltration (11). T cells have a synergistic effecton selective neuronal death by targeting neuronal antigens and priming microglia to consolidate the acquired immune response inthe CNS (12,13). Alternatively, damage or pathogens within the CNS can initiate a noxious chronic innate immune response withoutcomponents of systemic adaptive immunity (black arrows) (14) that can eventually promote infiltration through BBB leakage,resulting in an acquired immune response. MHC, major histocompatibility complex.

NATURE REVIEWS | NEUROSCIENCE VOLUME 3 | MARCH 2002 | 225
R E V I E W S
ISCHAEMIC PENUMBRA
A term that is generally used todefine ischaemic but still viablecerebral tissue that surrounds acore ischaemic zone.
HAEMORRHAGIC
TRANSFORMATION
Secondary bleeding that canoccur after an ischaemic episode.
PROGRESSIVE SUPRANUCLEAR
PALSY
A brain disorder that affects thecontrol of gait and balance. Themost obvious sign of the diseaseis an inability to direct the eyesproperly, reflecting lesions inbrainstem regions thatcoordinate eye movements.Patients often show alterationsof mood and behaviour,including depression, apathyand mild dementia.
In summary, the recognition of neuronal finger-prints might lead to the degeneration of specific neu-ronal populations in neurological disorders. The chronicstimulation of the innate immune response by microgliamight directly cause neuronal death. By producing pro-inflammatory molecules, this persistent response in theCNS might also promote site-specific leakage across theBBB, and the establishment of a noxious peripheraladaptive immune response by targeting neuronal anti-gens. Alternatively, a peripheral challenge might initiatesystemic inflammation, leading to selective neurodegen-eration. Although our understanding of the inflamma-tory mechanisms of neurodegeneration has improved, aknowledge of the peripheral sources that initiate CNSdegeneration is lacking.
Viral/bacterial aetiology in CNS degenerationAlthough best known for their detrimental effects onthe homeostasis of the whole organism, viral and bacte-rial infections can induce neuronal death and havetherefore been proposed as an aetiological factor in spo-radic cases of neurodegeneration. RNA and DNA frominfectious agents, and antibodies against viral proteinshave been found in the serum and CNS tissues ofpatients with neurological disorders. A role for viruses inthe pathogenesis of motor neuron disease is supportedby reports that phenotypes associated with ALS canoccur secondary to viral infections such as AIDS. In thiscase, the motor symptoms can be treated with antiviralagents89,90. Moreover, elevated titres of IgG againsthuman retroviral antigens, enterovirus RNA sequencesand human spuma retrovirus proteins have been foundin more than 50 patients with ALS91–95. The hypothesisof a viral aetiology in neurodegeneration is further sup-ported by findings that HIV can induce encephalitis anddementia, a syndrome that is found in Alzheimer’s dis-ease, frontotemporal dementia, ALS-parkinsonism/dementia complex of Guam and PROGRESSIVE SUPRANU-
CLEAR PALSY96. In addition, microbial and viral infectionsof genetically susceptible hosts have been proposed as aprimary cause of Rasmussen encephalitis97.
Other lines of evidence indicate that viruses and bac-teria might contribute to neurodegeneration. Humanfoamy virus proteins affect cerebellar granule cells in miceand produce an ataxic phenotype98, whereas experimen-tal pneumococcal meningitis in mice causes persistentspatial-learning deficits despite normal motor func-tions99. Mice infected with LP-BM5 murine leukaemiavirus generate antibodies that activate AMPA receptors100,supporting the idea that peripheral antibodies that arisefrom viral infection can induce neuronal death. Further-more, immunosuppressed mice that are genetically sus-ceptible to, and challenged with, lactate-dehydrogenase-elevating virus develop age-dependent poliomyelitis — aneuroparalytic disorder — and respiratory failure101.These animals show the important relationship betweengenetic factors, the immune response and infections inneurodegeneration. Together, these observations indicatethat viruses and bacteria, in conjunction with other envi-ronmental factors, such as trauma, chemical exposureand stress, might trigger selective neurodegeneration in
impairing its normal function. As a consequence, apop-tosis might occur in a subset of neurons. The apoptoticdebris would then be engulfed and presented to otherinvading T cells by parenchymal microglial cells.Microglia stimulate the production of molecules ofinnate immunity, such as cytokines, which increase thepermeability of the BBB and/or upregulate the neu-ronal MHC I complex. These events lead to the presen-tation of proteins specific to the degenerating neuronalpopulation, and might induce the selective killing ofthis population after T-cell infiltration. The initial chal-lenge will not necessarily come from the peripheraldamage. The stress could originate in the CNS andmight trigger a chronic innate immune response thateventually promotes infiltration and establishment ofacquired immunity in the CNS.
According to this model, the permeability of theBBB is crucial for the infiltration of both antibodies andlymphocytes. Perturbations in the stability of the BBBhave been reported in disease states such as Alzheimer’sdisease, stroke and HIV encephalitis42,83. The inductionof intercellular adhesion molecule 1 (ICAM1) by pro-inflammatory cytokines from the innate or the acquiredimmune reaction has a potent action on the permeabil-ity of the BBB, and β-amyloid deposits — one of themain agents involved in Alzheimer’s disease — causealterations in the BBB83,84. Another important factorthat controls the integrity of the BBB is vascularendothelial growth factor (VEGF)85. After a systemicchallenge, levels of VEGF are modulated to avoid theexacerbation of damage. The abnormal regulation ofVEGF levels might be a factor that predisposes the brainto uncontrolled inflammation. Indeed, administrationof recombinant human VEGF to rats 48 hours after an ischaemic episode increased angiogenesis in theISCHAEMIC PENUMBRA and significantly attenuated neuro-logical recovery 86. However, administration of VEGFone hour after the lesion significantly enhanced BBBleakage, HAEMORRHAGIC TRANSFORMATION and ischaemiclesions86. Chronic overexposure of normal brain toVEGF also increases the expression of ICAM1 andMHC complexes I and II, thereby favouring infiltra-tion87. The involvement of VEGF in immunity and neu-ronal survival is further supported by data showing thattargeted disruption of the hypoxia response element onthe VEGF gene in mice resulted in an inability to induceVEGF in hypoxic conditions. Mutant mice developedprofound progressive motor deficits between five andseven months of age, which were accompanied by theclassical hallmarks of ALS: accumulation of neuro-filament proteins in spinal cord and brainstem motorneurons, selective degeneration of motor axons, anddenervation-induced muscle atrophy 88. Remarkably, astrong astrocytosis, reminiscent of the intense inflam-mation and excitotoxicity that is found in ALS patients,occurred in the ventral horn of these mice88. AlthoughVEGF is not inflammatory by itself, it is possible thatthis factor modulates immune responses in the CNS bycontrolling the permeability of the BBB, allowing expo-sure of normally sequestered CNS antigens to peripheralimmune effector molecules.

226 | MARCH 2002 | VOLUME 3 www.nature.com/reviews/neuro
R E V I E W S
detrimental to the CNS, because it takes place rapidly inresponse to systemic and cerebral insults. The endoge-nous expression of CD14 and numerous TLRs mightengage pro-inflammatory signal-transduction pathwaysand the production of cytokines by microglia. One of thebeneficial consequences of such microglial reactivity isthe release of neurotrophic factors and other moleculesthat have important roles in brain homeostasis, neuro-protection and repair in the case of injury. Once engagedin severe infections, sustained microglial reactivity canoverproduce inflammatory molecules and alter the BBB,a mechanism that seems to be central to several neurode-generative disorders and demyelinating diseases. Asmicroglial cells are the APCs of the brain, they are proba-bly crucial for cell-specific immunity against neuronalelements.A better understanding of the innate immuneresponse in cerebral tissue could lead us to the funda-mental mechanisms that underlie the capability of thebrain to mount an inflammatory response that eitherprotects against or contributes to neuronal damage.
humans.Accordingly, a single infection would be able totrigger an innate immune response that can eventuallyprogress to a noxious adaptive immune response.
Concluding remarksThere is substantial evidence that molecules of theinnate immune reaction can be harmful to neurons andoligodendrocytes, whereas other observations indicatethat inflammation is actually beneficial to recovery. Thecellular source of the cytokines that are involved and thenature of their cognate receptors might help to explainthe discrepancies between studies. The chronic produc-tion of innate immune proteins and the presence of cellsof the adaptive immune system in the cerebral environ-ment could be essential features of neurodegeneration.However, this possibility has to be placed in a context ofcauses or consequences that involve many players,including genetic background, gender and environment.
The innate immune response that takes place in the CNS during systemic infection is unlikely to be
1. Anderson, K. V. Toll signaling pathways in the innate immuneresponse. Curr. Opin. Immunol. 12, 13–19 (2000).
2. Wright, S. D. Toll, a new piece in the puzzle of innateimmunity. J. Exp. Med. 189, 605–609 (1999).
3. Akira, S., Takeda, K. & Kaisho, T. Toll-like receptors: criticalproteins linking innate and acquired immunity. NatureImmunol. 2, 675–680 (2001).
4. Muzio, M., Polentarutti, N., Bosisio, D., Prahladan, M. K. &Mantovani, A. Toll-like receptors: a growing family of immune receptors that are differentially expressed andregulated by different leukocytes. J. Leukoc. Biol. 67,450–456 (2000).
5. Beutler, B. Tlr4: central component of the sole mammalianLPS sensor. Curr. Opin. Immunol. 12, 20–26 (2000).
6. Poltorak, A. et al. Defective LPS signaling in C3H/HeJ andC57BL/10ScCr mice: mutations in Tlr4 gene. Science 282,2085–2088 (1998).
7. Takeuchi, O. et al. Differential roles of TLR2 and TLR4 inrecognition of Gram-negative and Gram-positive bacterialcell wall components. Immunity 11, 443–451 (1999).The first demonstration that PAMPs found in naturetrigger innate immunity by selectively recognizing andactivating specific members of the TLR family.
8. Hayashi, F. et al. The innate immune response to bacterialflagellin is mediated by Toll-like receptor 5. Nature 410,1099–1103 (2001).
9. Hemmi, H. et al. A Toll-like receptor recognizes bacterialDNA. Nature 408, 740–745 (2000).
10. Alexopoulou, L., Holt, A. C., Medzhitov, R. & Flavell, R. A.Recognition of double-stranded RNA and activation of NF-κB by Toll-like receptor 3. Nature 413, 732–738 (2001).
11. Ozinsky, A. et al. The repertoire for pattern recognition ofpathogens by the innate immune system is defined bycooperation between Toll-like receptors. Proc. Natl Acad.Sci. USA 97, 13766–13771 (2000).The specific recognition of PAMPs depends on therepertoire of different TLRs, which can formheterodimers to allow pro-inflammatory signallingand gene transcription.
12. Chu, W. M. et al. JNK2 and IKKβ are required for activatingthe innate response to viral infection. Immunity 11, 721–731(1999).
13. Delhase, M., Hayakawa, M., Chen, Y. & Karin, M. Positiveand negative regulation of IκB kinase activity through IKKβsubunit phosphorylation. Science 284, 309–313 (1999).
14. Hu, Y. et al. Abnormal morphogenesis but intact IKKactivation in mice lacking the IKKα subunit of IκB kinase.Science 284, 316–320 (1999).
15. Lacroix, S., Feinstein, D. & Rivest, S. The bacterial endotoxinlipopolysaccharide has the ability to target the brain inupregulating its membrane CD14 receptor within specificcellular populations. Brain Pathol. 8, 625–640 (1998).
16. Laflamme, N. & Rivest, S. Toll-like receptor 4: the missinglink of the cerebral innate immune response triggered bycirculating Gram-negative bacterial cell wall components.FASEB J. 15, 155–163 (2001).
References 15 and 16 provide the first evidence that afine-tuned innate immune response takes place in theCNS after peripheral injection of LPS. This responseoriginates in the CVOs and progresses acrossmicroglial cells of the brain parenchyma.
17. Laflamme, N., Souci, G. & Rivest, S. Circulating cell wallcomponents derived from Gram-negative and not Gram-positive bacteria cause a profound transcriptional activationof the gene encoding toll-like receptor 2 in the CNS. J. Neurochem. 70, 648–657 (2001).
18. Brochu, S., Olivier, M. & Rivest, S. Neuronal activity andtranscription of proinflammatory cytokines, IκBα, and iNOSin the mouse brain during acute endotoxemia and chronicinfection with Trypanosoma brucei brucei. J. Neurosci. Res.57, 801–816 (1999).
19. Nadeau, S. & Rivest, S. Regulation of the gene encodingtumor necrosis factor α in the rat brain and pituitary inresponse to different models of systemic immune challenge.J. Neuropathol. Exp. Neurol. 58, 61–77 (1999).
20. Nadeau, S. & Rivest, S. Role of microglial-derived tumornecrosis factor in mediating CD14 transcription and NF-κBactivity in the brain during endotoxemia. J. Neurosci. 20,3456–3468 (2000).Reports a new mechanism of action for TNF-α in thepriming and crosstalk of parenchymal microglial cellsafter systemic injection of LPS.
21. Nadeau, S. & Rivest, S. The complement system is anintegrated part of the natural innate immune response in thebrain. FASEB J. 15, 1410–1412 (2001).
22. Quan, N., Whiteside, M. & Herkenham, M. Time course andlocalization patterns of interleukin-1β mRNA expression inthe brain and pituitary after peripheral administration oflipopolysaccharide. Neuroscience 83, 281–293 (1997).
23. Thibeault, I., Laflamme, N. & Rivest, S. Regulation of thegene encoding the monocyte chemoattractant protein 1(MCP-1) in the mouse and rat brain in response tocirculating LPS and proinflammatory cytokines. J. Comp.Neurol. 434, 461–477 (2001).
24. Fearns, C. & Loskutoff, D. J. Role of tumor necrosis factor αin induction of murine CD14 gene expression bylipopolysaccharide. Infect. Immun. 65, 4822–4831 (1997).
25. Fearns, C. & Ulevitch, R. J. Effect of recombinant interleukin-1β on murine CD14 gene expression in vivo.Shock 9, 157–163 (1998).
26. Zekki, H., Feinstein, D. L. & Rivest, S. The clinical course ofexperimental autoimmune encephalomyelitis is associatedwith a profound and sustained transcriptional activation ofthe genes encoding toll-like receptor 2 and CD14 in themouse CNS. Brain Pathol. (in the press).
27. Nguyen, M. D., Julien, J.-P. & Rivest, S. Induction ofproinflammatory molecules in mice with amyotrophic lateral sclerosis: no requirement for proapoptotic interleukin-1β in neurodegeneration. Ann. Neurol. 50,630–639 (2001).The first description of TLR2 induction in a model ofCNS degeneration. Indicates that innate immunity is
not only triggered by PAMPs, but might be a hallmarkof neurodegenerative disorders.
28. Castano, A., Herrera, A. J., Cano, J. & Machado, A.Lipopolysaccharide intranigral injection induces inflammatoryreaction and damage in nigrostriatal dopaminergic system.J. Neurochem. 70, 1584–1592 (1998).
29. Kim, W. G. et al. Regional difference in susceptibility tolipopolysaccharide-induced neurotoxicity in the rat brain:role of microglia. J. Neurosci. 20, 6309–6316 (2000).
30. Eklind, S. et al. Bacterial endotoxin sensitizes the immaturebrain to hypoxic-ischaemic injury. Eur. J. Neurosci. 13,1101–1106 (2001).
31. Herx, L. M., Rivest, S. & Yong, V. W. Central nervoussystem-initiated inflammation and neurotrophism in trauma:IL-1β is required for the production of ciliary neurotrophicfactor. J. Immunol. 165, 2232–2239 (2000).
32. Dusart, I. & Schwab, M. E. Secondary cell death and theinflammatory reaction after dorsal hemisection of the ratspinal cord. Eur. J. Neurosci. 6, 712–724 (1994).
33. Frank, M. & Wolburg, H. Cellular reactions at the lesion siteafter crushing of the rat optic nerve. Glia 16, 227–240 (1996).
34. Bandtlow, C. E. et al. Regional and cellular codistribution ofinterleukin-1β and nerve growth factor mRNA in the adult ratbrain. J. Cell Biol. 111, 1701–1711 (1990).
35. DeKosky, S. T. et al. Interleukin-1 receptor antagonistsuppresses neurotrophin response in injured rat brain. Ann. Neurol. 39, 123–127 (1996).
36. Mason, J. L., Suzuki, K., Chaplin, D. D. & Matsushima, G. K.Interleukin-1β promotes repair of the CNS. J. Neurosci. 21,7046–7052 (2001).
37. Venters, H. D. et al. A new mechanism ofneurodegeneration: a proinflammatory cytokine inhibitsreceptor signaling by a survival peptide. Proc. Natl Acad.Sci. USA 96, 9879–9884 (1999).
38. Arnett, H. A. et al. TNFα promotes proliferation ofoligodendrocyte progenitors and remyelination. NatureNeurosci. 4, 1116–1122 (2001).References 36 and 38 show a neuroprotective role of IL-1β and TNF-α by promoting remyelination in the CNS.
39. Jensen, M. B., Hegelund, I. V., Lomholt, N. D., Finsen, B. &Owens, T. IFNγenhances microglial reactions tohippocampal axonal degeneration. J. Neurosci. 20,3612–3621 (2000).
40. Pouly, S., Becher, B., Blain, M. & Antel, J. P. Interferon-γmodulates human oligodendrocyte susceptibility to Fas-mediated apoptosis. J. Neuropathol. Exp. Neurol.59, 280–286 (2000).
41. Pasinetti, G. M. Cyclooxygenase and inflammation inAlzheimer’s disease: experimental approaches and clinicalinterventions. J. Neurosci. Res. 54, 1–6 (1998).
42. Gonzalez-Scarano, F. & Baltuch, G. Microglia as mediatorsof inflammatory and degenerative diseases. Annu. Rev.Neurosci. 22, 219–240 (1999).
43. Julien, J.-P. Amyotrophic lateral sclerosis: unfolding thetoxicity of the misfolded. Cell 104, 581–591 (2001).

NATURE REVIEWS | NEUROSCIENCE VOLUME 3 | MARCH 2002 | 227
R E V I E W S
44. Stoll, G., Jung, S., Jander, S., van der Meide, P. & Hartung,H. P. Tumor necrosis factor-α in immune-mediateddemyelination and Wallerian degeneration of the ratperipheral nervous system. J. Neuroimmunol. 45, 175–182(1993).
45. Martin-Villalba, A. et al. Therapeutic neutralization of CD95-ligand and TNF attenuates brain damage in stroke. CellDeath Differ. 8, 679–686 (2001).
46. Robertson, J. et al. Apoptotic death of neurons exhibitingperipherin aggregates is mediated by the proinflammatorycytokine tumor necrosis factor-α. J. Cell Biol. 155, 217–226(2001).
47. Allan, S. M. & Rothwell, N. J. Cytokines and acuteneurodegeneration. Nature Rev. Neurosci. 2, 734–744(2001).
48. Hickey, W. F. & Kimura, H. Perivascular microglial cells of theCNS are bone marrow-derived and present antigen in vivo.Science 239, 290–292 (1988).Reports that perivascular microglia are bone-marrow-derived cells with features of macrophages, such asantigen processing and presentation. Indicates a fineinterplay between peripheral challenge and CNSmicroglia, as well as a potential role for bone-marrowtransplantation in replacing mutant and/or deficientmicroglia.
49. Mattson, M. P., Pedersen, W. A., Duan, W., Culmsee, C. &Camandola, S. Cellular and molecular mechanismsunderlying perturbed energy metabolism and neuronaldegeneration in Alzheimer’s and Parkinson’s diseases. Ann. NY Acad. Sci. 893, 154–175 (1999).
50. Albers, D. S. & Beal, M. F. Mitochondrial dysfunction andoxidative stress in aging and neurodegenerative disease. J. Neural Transm. 59, 133–154 (2000).
51. Neumann, H., Cavalie, A., Jenne, D. E. & Wekerle, H.Induction of MHC class I genes in neurons. Science 269,549–552 (1995).
52. Neumann, H., Schmidt, H., Cavalie, A., Jenne, D. &Wekerle, H. Major histocompatibility complex (MHC) class Igene expression in single neurons of the central nervoussystem: differential regulation by interferon (IFN)-γand tumor necrosis factor (TNF)-α. J. Exp. Med. 185, 305–316(1997).
53. Corriveau, R. A., Huh, G. S. & Shatz, C. J. Regulation ofclass I MHC gene expression in the developing and matureCNS by neural activity. Neuron 21, 505–520 (1998).Reports on MHC I expression and function indeveloping and mature CNS neurons. The MHC Iprobably participates in CNS immune function andmight have a role in neuronal signalling.
54. Darnell, R. B. Immunologic complexity in neurons. Neuron21, 947–950 (1998).
55. Musunuru, K. & Darnell, R. B. Paraneoplastic neurologicdisease antigens: RNA-binding proteins and signalingproteins in neuronal degeneration. Annu. Rev. Neurosci. 24,239–262 (2001).
56. Solimena, M. & De Camilli, P. Synaptic autoimmunity andthe Salk factor. Neuron 28, 309–310 (2000).
57. Whitney, K. D. & McNamara, J. O. Autoimmunity andneurological disease: antibody modulation of synaptictransmission. Annu. Rev. Neurosci. 22, 175–195 (1999).
58. Chen, S. et al. Experimental destruction of substantia nigrainitiated by Parkinson disease immunoglobulins. Arch. Neurol. 55, 1075–1080 (1998).
59. He, X. P. et al. Glutamate receptor GluR3 antibodies anddeath of cortical cells. Neuron 20, 153–163 (1998).
60. Engelhardt, J. I., Siklos, L., Komuves, L., Smith, R. G. &Appel, S. H. Antibodies to calcium channels from ALSpatients passively transferred to mice selectively increaseintracellular calcium and induce ultrastructural changes inmotoneurons. Synapse 20, 185–199 (1995).
61. Engelhardt, J. I. et al. Stereotaxic injection of IgG frompatients with Alzheimer disease initiates injury of cholinergicneurons of the basal forebrain. Arch. Neurol. 57, 681–686(2000).
62. Buckanovich, R. J. & Darnell, R. B. The neuronal RNAbinding protein Nova-1 recognizes specific RNA targets invitro and in vivo. Mol. Cell. Biol. 17, 3194–3201 (1997).
63. Buckanovich, R. J., Yang, Y. Y. & Darnell, R. B. Theonconeural antigen Nova-1 is a neuron-specific RNA-bindingprotein, the activity of which is inhibited by paraneoplasticantibodies. J. Neurosci. 16, 1114–1122 (1996).
64. Buckanovich, R. J., Posner, J. B. & Darnell, R. B. Nova, theparaneoplastic Ri antigen, is homologous to an RNA-binding protein and is specifically expressed in thedeveloping motor system. Neuron 11, 657–672 (1993).
65. Jensen, K. B. et al. Nova-1 regulates neuron-specificalternative splicing and is essential for neuronal viability.Neuron 25, 359–371 (2000).
66. Alexianu, M. E., Mohamed, A. H., Smith, R. G., Colom, L. V.& Appel, S. H. Apoptotic cell death of a hybrid motoneuroncell line induced by immunoglobulins from patients withamyotrophic lateral sclerosis. J. Neurochem. 63,2365–2368 (1994).
67. Engelhardt, J. I., Siklos, L. & Appel, S. H. Altered calciumhomeostasis and ultrastructure in motoneurons of micecaused by passively transferred anti-motoneuronal IgG. J. Neuropathol. Exp. Neurol. 56, 21–39 (1997).
68. Pullen, A. H. & Humphreys, P. Ultrastructural analysis ofspinal motoneurones from mice treated with IgG from ALSpatients, healthy individuals, or disease controls. J. Neurol.Sci. 180, 35–45 (2000).
69. Obal, I., Jakab, J. S., Siklos, L. & Engelhardt, J. I.Recruitment of activated microglia cells in the spinal cord ofmice by ALS IgG. Neuroreport 12, 2449–2452 (2001).
70. Rogers, S. W. et al. Autoantibodies to glutamate receptorGluR3 in Rasmussen’s encephalitis. Science 265, 648–651(1994).
71. Yang, R. et al. Autoimmunity to munc-18 in Rasmussen’sencephalitis. Neuron 28, 375–383 (2000).
72. De Camilli, P. et al. The synaptic vesicle-associated proteinamphiphysin is the 128-kD autoantigen of Stiff-Mansyndrome with breast cancer. J. Exp. Med. 178, 2219–2223(1993).
73. Li, L., Hagopian, W. A., Brashear, H. R., Daniels, T. &Lernmark, A. Identification of autoantibody epitopes ofglutamic acid decarboxylase in stiff-man syndrome patients.J. Immunol. 152, 930–934 (1994).
74. Butler, M. H. et al. Autoimmunity to gephyrin in Stiff-Mansyndrome. Neuron 26, 307–312 (2000).References 60, 64 and 70–74 report discoveries ofperipheral antibodies in different neurologicaldisorders. These antibodies recognize proteins thatare normally found in neurons, and trigger an adaptiveimmune response that leads to the disruption of theseneuronal proteins.
75. Li, Y. et al. Local-clonal expansion of infiltrating T lymphocytes in chronic encephalitis of Rasmussen. J. Immunol. 158, 1428–1437 (1997).
76. Albert, M. L. et al. Tumor-specific killer cells in paraneoplastic cerebellar degeneration. Nature Med. 4,1321–1324 (1998).
77. Whitney, K. D., Andrews, P. I. & McNamara, J. O.Immunoglobulin G and complement immunoreactivity in thecerebral cortex of patients with Rasmussen’s encephalitis.Neurology 53, 699–708 (1999).
78. Albert, M. L., Austin, L. M. & Darnell, R. B. Detection andtreatment of activated T cells in the cerebrospinal fluid ofpatients with paraneoplastic cerebellar degeneration. Ann. Neurol. 47, 9–17 (2000).
79. Provinciali, L. et al. Immunity assessment in the early stagesof amyotrophic lateral sclerosis: a study of virus antibodiesand lymphocyte subsets. Acta Neurol. Scand. 78, 449–454(1988).
80. Lampson, L. A., Kushner, P. D. & Sobel, R. A. Majorhistocompatibility complex antigen expression in theaffected tissues in amyotrophic lateral sclerosis. Ann. Neurol. 28, 365–372 (1990).
81. Troost, D., van den Oord, J. J. & Vianney de Jong, J. M.Immunohistochemical characterization of the inflammatoryinfiltrate in amyotrophic lateral sclerosis. Neuropathol. Appl.Neurobiol. 16, 401–410 (1990).
82. Panzara, M. A. et al. T cell receptor BV generearrangements in the spinal cords and cerebrospinal fluid ofpatients with amyotrophic lateral sclerosis. Neurobiol. Dis. 6,392–405 (1999).
83. Huber, J. D., Egleton, R. D. & Davis, T. P. Molecularphysiology and pathophysiology of tight junctions in theblood–brain barrier. Trends Neurosci. 24, 719–725 (2001).
84. Su, G. C., Arendash, G. W., Kalaria, R. N., Bjugstad, K. B. &Mullan, M. Intravascular infusions of soluble β-amyloidcompromise the blood–brain barrier, activate CNS glial cellsand induce peripheral hemorrhage. Brain Res. 818,105–117 (1999).
85. Dobrogowska, D. H., Lossinsky, A. S., Tarnawski, M. &Vorbrodt, A. W. Increased blood–brain barrier permeabilityand endothelial abnormalities induced by vascular endothelialgrowth factor. J. Neurocytol. 27, 163–173 (1998).
86. Zhang, Z. G. et al. VEGF enhances angiogenesis andpromotes blood–brain barrier leakage in the ischemic brain.J. Clin. Invest. 106, 829–838 (2000).
87. Proescholdt, M. A. et al. Vascular endothelial growth factor(VEGF) modulates vascular permeability and inflammation inrat brain. J. Neuropathol. Exp. Neurol. 58, 613–627 (1999).
88. Oosthuyse, B. et al. Deletion of the hypoxia-responseelement in the vascular endothelial growth factor promotercauses motor neuron degeneration. Nature Genet. 28,131–138 (2001).
89. MacGowan, D. J., Scelsa, S. N. & Waldron, M. An ALS-likesyndrome with new HIV infection and complete response toantiretroviral therapy. Neurology 57, 1094–1097 (2001).
90. Moulignier, A., Moulonguet, A., Pialoux, G. & Rozenbaum, W.Reversible ALS-like disorder in HIV infection. Neurology 57,995–1001 (2001).
91. Jubelt, B. Motor neuron diseases and viruses: poliovirus,retroviruses, and lymphomas. Curr. Opin. Neurol.Neurosurg. 5, 655–658 (1992).
92. Bartfeld, H. et al. Enteroviral-related antigen in circulatingimmune complexes of amyotrophic lateral sclerosis patients.Intervirology 30, 202–212 (1989).
93. Westarp, M. E. et al. Amyotrophic lateral sclerosis anenigmatic disease with B-cellular and anti-retroviral immuneresponses. Eur. J. Med. 2, 327–332 (1993).
94. Ferrante, P. et al. HTLV tax-rex DNA and antibodies inidiopathic amyotrophic lateral sclerosis. J. Neurol. Sci. 129,140–144 (1995).
95. Berger, M. M. et al. Detection and cellular localization ofenterovirus RNA sequences in spinal cord of patients withALS. Neurology 54, 20–25 (2000).
96. Price, R. W. AIDS dementia complex: a complex, slow virus‘model’ of acquired genetic neurodegenerative disease.Cold Spring Harb. Symp. Quant. Biol. 61, 759–770 (1996).
97. O’Meara, M. & Ouvrier, R. Viral encephalitis in children. Curr. Opin. Pediatr. 8, 11–15 (1996).
98. Lampe, J., Marino, S., Rethwilm, A. & Aguzzi, A.Degeneration of the cerebellar granule cell layer intransgenic mice expressing genes of human foamy virus.Neuropathol. Appl. Neurobiol. 24, 36–43 (1998).
99. Wellmer, A., Noeske, C., Gerber, J., Munzel, U. & Nau, R.Spatial memory and learning deficits after experimentalpneumococcal meningitis in mice. Neurosci. Lett. 296,137–140 (2000).
100. Koustova, E. et al. LP-BM5 virus-infected mice produceactivating autoantibodies to the AMPA receptor. J. Clin.Invest. 107, 737–744 (2001).
101. Schlenker, E. H., Jones, Q. A., Rowland, R. R., Steffen-Bien,M. & Cafruny, W. A. Age-dependent poliomyelitis in mice isassociated with respiratory failure and viral replication in thecentral nervous system and lung. J. Neurovirol. 7, 265–271(2001).
AcknowledgementsOur work is supported by the Canadian Institutes of HealthResearch (CIHR) and the Neuromuscular Research Partnership.M.D.N. is a recipient of a K. M. Hunter–CIHR Ph.D. Scholarship. J.-P.J. holds a CIHR Senior Investigator Award. S.R. is a CIHR Scientist and holds a Canadian Research Chair inNeuroimmunology. We thank G. Chabot, S. Nadeau and N. LaFlamme for assistance with the illustrations.
Online links
DATABASESThe following terms in this article are linked online to:FlyBase: http://flybase.bio.indiana.edu/TollLocusLink: http://www.ncbi.nlm.nih.gov/LocusLink/CD14 | GABAA receptor γ2 | GluR3 | glycine receptor α2 | Iba1 |IFN-γ | IKAP | IκB | IKK | IL-1 | IL-1R | IL-12 | IRAK | Munc-18 |MyD88 | NFκB | NIK | NOVA1 | RIP | TLRs | TNF-α | TNFR1 |TNFR2 | TRADD | TRAF2 | TRAF6OMIM: http://www.ncbi.nlm.nih.gov/Omim/ALS-parkinsonism/dementia complex of Guam | Alzheimer’sdisease | amyotrophic lateral sclerosis | frontotemporal dementia |Huntington’s disease | multiple sclerosis | Parkinson’s disease |stiff-man syndromePROSITE: http://www.expasy.ch/prosite/TIR domain
FURTHER INFORMATIONEncyclopedia of Life Sciences: http://www.els.net/antigen presentation to lymphocytes | blood–brain barrier |microglia | nervous and immune system interactions |neuroimmunologyAccess to this interactive links box is free online.
Copyright © 2022 FDOKUMEN




















