Influence of bispectral index monitoring on decision making during cardiac anesthesia
8
Original contribution Influence of bispectral index monitoring on decision making during cardiac anesthesia George Vretzakis MD (Assistant Professor) a , Eleni Ferdi MD (Anesthesiologist) a , Helena Argiriadou MD (Anesthesiologist) a , Basilios Papaziogas (Lecturer) b, * , Dimitrios Mikroulis MD (Cardiac Surgeon) c , Miltiadis Lazarides MD (Cardiac Surgeon) c , George Bitzikas MD (Cardiac Surgeon) c , George Bougioukas MD c a Department of Cardiac Anesthesia, University Hospital of Alexandroupolis, 68100 Alexandroupolis, Greece b 2nd Surgical Clinic, Aristotle University of Thessaloniki, 54635 Thessaloniki, Greece c Clinic of Cardiac and Thoracic Surgery, Democritus University of Thrace, 68100 Alexandroupolis, Greece Received 5 January 2004; accepted 1 December 2004 Abstract Study Objective: To assess bispectral index (BIS) monitoring on decision making during cardiac surgery with cardiopulmonary bypass (CPB) by measuring the number of preset standardized comments with and without knowing the BIS value and by classifying the interventions following the BIS data. Design: Prospective, randomized study. Setting: University Hospital. Patients: One hundred twenty-one patients scheduled for elective cardiac surgery (89 coronary patients, 24 valve replacement patients, and 8 valve replacement and coronary surgery). Interventions: Patients were divided into 3 groups. An observing anesthesiologist recorded on a special form (bparallelQ anesthesia record) data from the devices of the workstation and the BIS monitor. Conditions in which BIS monitoring was subjectively considered that might have been useful in anesthetic decision making were recorded as bevents.Q In group A (36 patients), the responsible anesthesiologist had continuous access to BIS information. In group B (44 patients), intraoperative anesthetic management was bblindedQ to BIS values, whereas in group C (41 patients), the anesthesiologist observing the BIS monitor was free to inform the attending anesthesiologist about the BIS score. The number of events was considered as negatively reflecting the quality of the clinical course of a patient. The reduction of events was considered as improvement in decision making. All patients received the same anesthetic regimen (propofol + remifentanil). Monitoring was equal in all cases. Mild hypothermic CPB was applied in 73 patients. Statistical analysis used 1-way analysis of variance, Student 2-tailed t test, and v 2 analysis. Main Results: Patient demographic data, underlying pathology, operation performed, hypothermia application, times of anesthesia, duration of operation, and CPB were similar in the 3 groups. In group B, the BIS value was considered by the observer as useful to know in 220 events (5.00 F 1.58 per patient). In group C, the BIS value was considered by the observer as useful to know in 143 events 0952-8180/$ – see front matter D 2005 Elsevier Inc. All rights reserved. doi:10.1016/j.jclinane.2004.12.018 T Corresponding author. 551 33 Thessaloniki, Greece. Tel.: +30 2310 992562; fax: +30 2310 992563. Keywords: Bispectral index monitoring; Cardiac anesthesia; Decision support; Hypothermia Journal of Clinical Anesthesia (2005) 17, 509–516
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Influence of bispectral index monitoring on decision making during cardiac anesthesia

Original contribution
Influence of bispectral index monitoring on decisionmaking during cardiac anesthesia
George Vretzakis MD (Assistant Professor)a, Eleni Ferdi MD (Anesthesiologist)a,Helena Argiriadou MD (Anesthesiologist)a, Basilios Papaziogas (Lecturer)b,*,Dimitrios Mikroulis MD (Cardiac Surgeon)c, Miltiadis Lazarides MD (Cardiac Surgeon)c,George Bitzikas MD (Cardiac Surgeon)c, George Bougioukas MDc
aDepartment of Cardiac Anesthesia, University Hospital of Alexandroupolis, 68100 Alexandroupolis, Greeceb2nd Surgical Clinic, Aristotle University of Thessaloniki, 54635 Thessaloniki, GreececClinic of Cardiac and Thoracic Surgery, Democritus University of Thrace, 68100 Alexandroupolis, Greece
Received 5 January 2004; accepted 1 December 2004
0952-8180/$ – see front matter D 2005
doi:10.1016/j.jclinane.2004.12.018
T Corresponding author. 551 33 The
Keywords:Bispectral index
monitoring;
Cardiac anesthesia;
Decision support;
Hypothermia
AbstractStudy Objective: To assess bispectral index (BIS) monitoring on decision making during cardiac
surgery with cardiopulmonary bypass (CPB) by measuring the number of preset standardized comments
with and without knowing the BIS value and by classifying the interventions following the BIS data.
Design: Prospective, randomized study.
Setting: University Hospital.
Patients: One hundred twenty-one patients scheduled for elective cardiac surgery (89 coronary patients,24 valve replacement patients, and 8 valve replacement and coronary surgery).
Interventions: Patients were divided into 3 groups. An observing anesthesiologist recorded on a specialform (bparallelQ anesthesia record) data from the devices of the workstation and the BIS monitor.
Conditions in which BIS monitoring was subjectively considered that might have been useful in
anesthetic decision making were recorded as bevents.Q In group A (36 patients), the responsible
anesthesiologist had continuous access to BIS information. In group B (44 patients), intraoperative
anesthetic management was bblindedQ to BIS values, whereas in group C (41 patients), the
anesthesiologist observing the BIS monitor was free to inform the attending anesthesiologist about
the BIS score. The number of events was considered as negatively reflecting the quality of the clinical
course of a patient. The reduction of events was considered as improvement in decision making. All
patients received the same anesthetic regimen (propofol + remifentanil). Monitoring was equal in all
cases. Mild hypothermic CPB was applied in 73 patients. Statistical analysis used 1-way analysis of
variance, Student 2-tailed t test, and v2 analysis.
Main Results: Patient demographic data, underlying pathology, operation performed, hypothermia
application, times of anesthesia, duration of operation, and CPB were similar in the 3 groups. In group
B, the BIS value was considered by the observer as useful to know in 220 events (5.00 F 1.58 per
patient). In group C, the BIS value was considered by the observer as useful to know in 143 events
Journal of Clinical Anesthesia (2005) 17, 509–516
Elsevier Inc. All rights reserved.
ssaloniki, Greece. Tel.: +30 2310 992562; fax: +30 2310 992563.

G. Vretzakis et al.510
(3.49 F 1.31 per patient, P b 0.001) and, at the same time, the attending anesthesiologist was informed
about BIS. In 112 (78.3%) cases, measures were taken. Titration of anesthetic drugs was done in
79 (70.5%) patients, whereas titration of vasoactive drugs was done in 9 (8.0%) patients, titration of both
in 13 (11.6%) patients, and other diagnostic or corrective actions in 11 (9.8%) patients. Distributions of
BIS values did not differ statistically (39.19 F 10.32, 37.38 F 10.21, and 38.29 F 10.01 in group A,
group B, and group C, respectively). bZenithQ and bnadirQ BIS values after induction also did not differ
statistically. Awakening and extubation times were similar in both groups.
Conclusions: Subjectivity, although reduced as much as possible, can play a confining role in the
value of our results. The usefulness of BIS monitoring is shown by the fact that BIS data resulted in
corrective measures. Attending anesthesiologist’s actions, based on BIS information, reduced the events
in group C.
D 2005 Elsevier Inc. All rights reserved.
1. Introduction
The bispectral index (BIS) offers a simple method for
continuous brain status monitoring throughout the admin-
istration of anesthetic or sedative drugs. Bispectral index
monitoring is considered a reliable tool in assessing the
level of consciousness. It is currently accepted that
induction and maintenance of anesthesia are associated with
a decrease in BIS value, and that increasing concentrations
of either volatile or intravenous anesthetics further decrease
the BIS value. This measurement of the hypnotic effect
proved to be accurate and reliable in nearly all patients and
clinical settings. The use of BIS monitoring has grown
rapidly in the care of patients, as it is safe and inexpensive
and it does not require special training.
During cardiac surgery, one of the aims of anesthetic
management is to achieve a level of adequacy that
eliminates the stress response, without unjustifiably pro-
longing the postoperative mechanical support of breathing.
In these operations, the result of anesthetic drugs may be
affected by various factors. Acute and significant fluctua-
tions in plasma drug concentration as a result of priming,
alterations in the rate of diuresis or in the concentration of
binding proteins, modification of the function of organs
contributing to drug metabolism, and temperature fluctua-
tions are some of the factors that may alter drug kinetics or
affect the pharmacodynamic action of anesthetic or sedative
administration. Furthermore, the relation between the
hypnotic and analgesic depth and the usual clinical criteria
of their estimation is unclear because of the administration
of various drugs such as catecholamines and b-blockers,among others, and because of the manipulations in the
central circulation. All of the above, combined with the
problem of bawarenessQ and the benefits of early extubation,
justify the application of BIS monitoring in assessing the
patient’s hypnotic state. Nevertheless, its utility during
cardiac operations and its role on decision making are
unclear. This study aimed to determine whether BIS
monitoring enhances decision making as measured by
standardized comments and interventions following the
knowledge of BIS value.
2. Materials and methods
2.1. Patient data, anesthesia, and operation
After receiving protocol approval by the Ethical Com-
mittee of the University Hospital of Alexandroupolis/
Greece, we initially enrolled into the study 130 patients
who were scheduled for elective cardiac operations. Those
patients undergoing boff-pumpQ techniques and those with
significantly compromised left ventricular function in the
preoperative evaluation were excluded from the study. In all
patients, ejection fraction (EF) was greater than 45% (mean
EF, 49.5% F 4.6%) as measured by preoperative angioven-
triculography. Patients scheduled for a combined caro-
tid endarterectomy procedure were also excluded from
the study.
Premedication consisted of diazepam 10 mg given orally
1 hour before admission to the operating room (OR). On
arrival in the OR, patients were connected to standard
monitoring (Solar 8000, Marquette Medical Systems,
Milwaukee, Wis) and a peripheral intravenous catheter
and a radial intra-arterial catheter were placed. Intraoper-
ative electrocardioscopy consisted of 5-lead, ST-segment
analysis. Anesthetic induction was achieved with a slow,
single-dose administration of midazolam (1-3 mg) plus
fentanyl (100-250 lg) plus etomidate (0.2 mg/kg) and
neuromuscular blockade with pancuronium (0.12 mg/kg).
After tracheal intubation, all patients were placed on
mechanical ventilation (Julian, Dr7eger, Lqbeck, Germany)
that was targeted to slight hypocapnia (33 mm Hg b Paco2
b37 mm Hg), based on repeated arterial blood gas sampling.
Inspiratory fraction of oxygen in air was between 0.5 and
1.0. For the anesthesia maintenance, patients received a
propofol infusion targeted to a 3-lg/mL plasma concentra-
tion, facilitated by a pump (Fresenius, Vial, Brezins,
France). Infusion rates were manually calculated to ensure
a stable concentration during the next 30 minutes, that is, the
time necessary for further anesthetic and surgical preparation.
A continuous infusion of remifentanil (c20 lg/kg per hour)was also administered as a means of providing analgesia.
The attending anesthesiologist was free to change those
rates during the procedure. The insertion of a triple-lumen

Decision-support by bispectral index during cardiac anesthesia 511
central venous catheter and a pulmonary artery catheter
(Oximetry TD catheter, Edwards Lifesciences, Germany)
was followed by the esophageal placement of a multiplane
echocardiographic probe (Toshiba Medical Systems, Tokyo,
Japan). During field preparation, echocardiographic exami-
nation was performed and the probe was positioned in the
stomach, displaying the two cavities by short axis. All
patients were operated on while on cardiopulmonary bypass
(CPB) and with cardioplegic arrest. Mild hypothermia
(c338C) was applied in 79 (60.7%) patients. In the
remainder of the patients, body temperature was allowed to
decrease naturally. In the period near the completion of the
main surgical procedure, before aortic unclamping and
during the rest of CPB, active rewarming aided by the
heart-lung machine was applied in all patients.
2.2. BIS monitoring, patient groups, and datacollection
Before anesthetic induction and after skin preparation,
the BIS sensor was placed and connected to the monitor
(BIS/XP, Aspect Medical systems, Natick, Mass). We
accepted a BIS value of less than 40 as indicating, with
high probability, that a patient is unconscious. Patients were
randomly allocated to 1 of 3 groups. In group A, the
responsible anesthesiologist had continuous access to BIS
values. In group B and group C, the BIS monitor was
located in a remote position from the bworkstationQ and BIS
values were thus unavailable. An observer anesthesiologist
noted BIS values and collected data from the monitoring
devices and infusion pumps on a special form (a bparallelQanesthesia record). For every case, participating anesthesi-
ologists were appointed randomly from a population of
three. All had at least 1 year of experience in everyday BIS
monitoring. During the anesthetic procedure and in relation
to the BIS value, the observer had the option of writing
down standardized comments as follows:
1. Expected BIS value (ie, from 45 to 35 with the plus
administration of a single dose of 50 mg of propofol
or from 35 to 30 with the initiation of hypothermic
perfusion or from 35 to 40 during rewarming);
2. Expected tendency but unexpected deviation in BIS
value (ie, very low values, less than 20 during the
insertion of the pulmonary artery catheter or rising
with rewarming or falling after the sternotomy
closure but gaps greater than 10 compared with the
previous value);
3. Unexpected BIS value. This option was for values
difficult to interpret for the period of the operation in
relation to the administrated dose of hypnotics (ie, a
value of 50 during left internal mammary artery
preparation, when in usual circumstances this period
is characterized by stability). Abrupt changes in
BIS values, not fitting to the data from the avail-
able monitoring, were included here (ie, from 35 to
45 with the use of an external pacemaker or with other
external interference without artifact recognition);
4. The BIS value would be useful. This option was for
situations where the patient and the BIS trending
were more or less stable but the absolute value
would be useful for the titration of drugs (ie, BIS in
a very low [near 20] or high [near 50] level). It was
also for problematic conditions where the knowl-
edge of patient’s hypnotic state would result in an
integrated or more comprehensive approach (ie,
BIS stable and expected in a patient with compro-
mised hemodynamics);
5. BIS value mandatory to know (ie, BIS values
increasing above 50 for more than 5 minutes or
BIS value above 60 in any case).
This categorization came after analyzing and discussing a
number of pilot cases. It became clear that additional
categorization for more objective clarification of clinical
situations would result in an extended, difficult protocol.
The standardized comments had qualitative character and
numbering was done for ease of data collection and
processing. The observer was free to record a standardized
comment whether it was subjectively estimated that the BIS
value toward the clinical conditions was similar as above.
The participating anesthesiologists considered this catego-
rization adequate for the description and judgment of
clinical events.
In group B, anesthetic support was concluded without
any information about the BIS value (bblindQ to BIS). In
group C, the observer recording a standardized comment
was free to inform the attending anesthesiologist only about
the BIS readings (BIS value, SQI percentage, EMG
percentage). At this moment, the attending anesthesiologist
could also ask to see the electroencephalogram waveform
while BIS trending was covered. The attending anesthesi-
ologist had to evaluate this information and act at his or her
own judgment. Taking into consideration the BIS data and
evaluating its clinical significance (useless, expected,
relationship to the drugs administered or to the condition
of the patient or to the phase of the procedure, unexpected,
useful, etc), the attending anesthesiologist decided whether,
and how, to intervene. However, BIS monitoring is unable
to predict future changes. For this reason, BIS values above
50 for more than 5 minutes (for two bsamplesQ conse-
quently), although until 60 indicating low probability of
explicit recall, were considered a transition from the deep
hypnotic state and the patient was recorded as a standard-
ized comment of 5. In this case (BIS value mandatory to
know), as a protocol obligation to our Ethical Committee,
the anesthesia provider was immediately informed and the
patient was removed to a subgroup (B1 and C1), irrespec-
tive of his or her original group allocation. For patients in
group B, study blindness to BIS had to be violated.
Subgroups were created for further analysis of these
patients. In group A, the attending anesthesiologist had
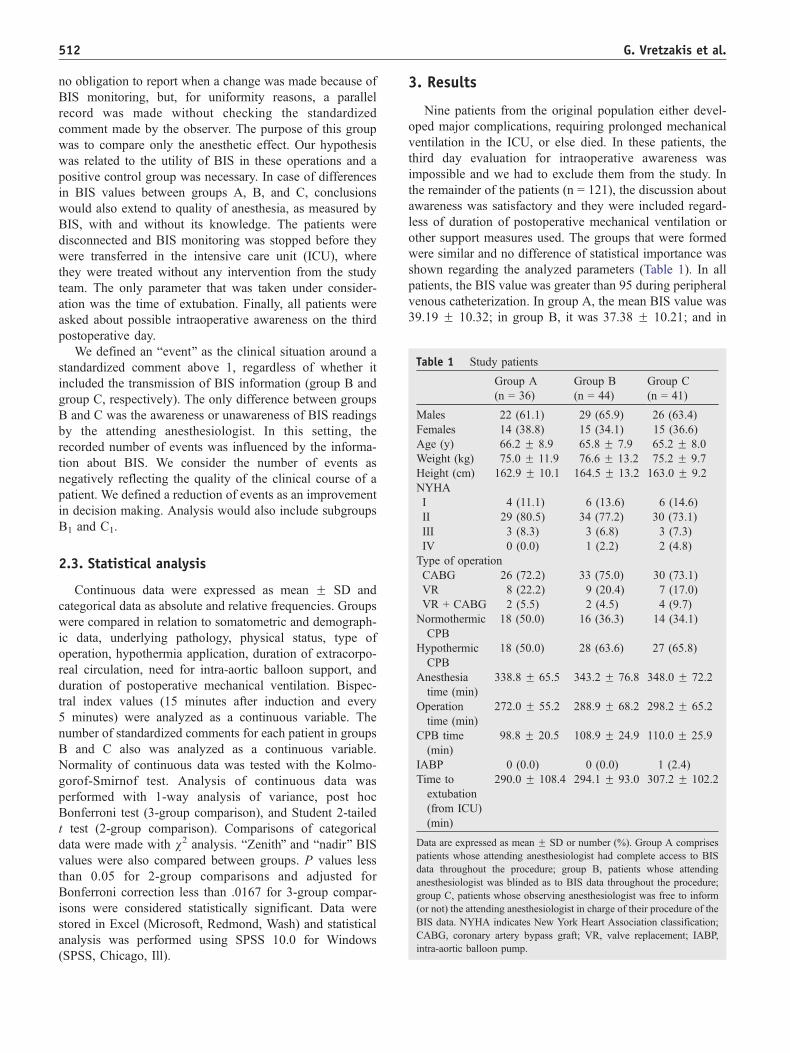
Table 1 Study patients
Group A
(n = 36)
Group B
(n = 44)
Group C
(n = 41)
Males 22 (61.1) 29 (65.9) 26 (63.4)
Females 14 (38.8) 15 (34.1) 15 (36.6)
Age (y) 66.2 F 8.9 65.8 F 7.9 65.2 F 8.0
Weight (kg) 75.0 F 11.9 76.6 F 13.2 75.2 F 9.7
Height (cm) 162.9 F 10.1 164.5 F 13.2 163.0 F 9.2
NYHA
I 4 (11.1) 6 (13.6) 6 (14.6)
II 29 (80.5) 34 (77.2) 30 (73.1)
III 3 (8.3) 3 (6.8) 3 (7.3)
IV 0 (0.0) 1 (2.2) 2 (4.8)
Type of operation
CABG 26 (72.2) 33 (75.0) 30 (73.1)
VR 8 (22.2) 9 (20.4) 7 (17.0)
VR + CABG 2 (5.5) 2 (4.5) 4 (9.7)
Normothermic
CPB
18 (50.0) 16 (36.3) 14 (34.1)
Hypothermic
CPB
18 (50.0) 28 (63.6) 27 (65.8)
Anesthesia
time (min)
338.8 F 65.5 343.2 F 76.8 348.0 F 72.2
Operation
time (min)
272.0 F 55.2 288.9 F 68.2 298.2 F 65.2
CPB time
(min)
98.8 F 20.5 108.9 F 24.9 110.0 F 25.9
IABP 0 (0.0) 0 (0.0) 1 (2.4)
Time to
extubation
(from ICU)
(min)
290.0 F 108.4 294.1 F 93.0 307.2 F 102.2
Data are expressed as mean F SD or number (%). Group A comprises
patients whose attending anesthesiologist had complete access to BIS
data throughout the procedure; group B, patients whose attending
anesthesiologist was blinded as to BIS data throughout the procedure;
group C, patients whose observing anesthesiologist was free to inform
(or not) the attending anesthesiologist in charge of their procedure of the
BIS data. NYHA indicates New York Heart Association classification;
CABG, coronary artery bypass graft; VR, valve replacement; IABP,
intra-aortic balloon pump.
G. Vretzakis et al.512
no obligation to report when a change was made because of
BIS monitoring, but, for uniformity reasons, a parallel
record was made without checking the standardized
comment made by the observer. The purpose of this group
was to compare only the anesthetic effect. Our hypothesis
was related to the utility of BIS in these operations and a
positive control group was necessary. In case of differences
in BIS values between groups A, B, and C, conclusions
would also extend to quality of anesthesia, as measured by
BIS, with and without its knowledge. The patients were
disconnected and BIS monitoring was stopped before they
were transferred in the intensive care unit (ICU), where
they were treated without any intervention from the study
team. The only parameter that was taken under consider-
ation was the time of extubation. Finally, all patients were
asked about possible intraoperative awareness on the third
postoperative day.
We defined an bevent Q as the clinical situation around a
standardized comment above 1, regardless of whether it
included the transmission of BIS information (group B and
group C, respectively). The only difference between groups
B and C was the awareness or unawareness of BIS readings
by the attending anesthesiologist. In this setting, the
recorded number of events was influenced by the informa-
tion about BIS. We consider the number of events as
negatively reflecting the quality of the clinical course of a
patient. We defined a reduction of events as an improvement
in decision making. Analysis would also include subgroups
B1 and C1.
2.3. Statistical analysis
Continuous data were expressed as mean F SD and
categorical data as absolute and relative frequencies. Groups
were compared in relation to somatometric and demograph-
ic data, underlying pathology, physical status, type of
operation, hypothermia application, duration of extracorpo-
real circulation, need for intra-aortic balloon support, and
duration of postoperative mechanical ventilation. Bispec-
tral index values (15 minutes after induction and every
5 minutes) were analyzed as a continuous variable. The
number of standardized comments for each patient in groups
B and C also was analyzed as a continuous variable.
Normality of continuous data was tested with the Kolmo-
gorof-Smirnof test. Analysis of continuous data was
performed with 1-way analysis of variance, post hoc
Bonferroni test (3-group comparison), and Student 2-tailed
t test (2-group comparison). Comparisons of categorical
data were made with v2 analysis. bZenithQ and bnadir Q BISvalues were also compared between groups. P values less
than 0.05 for 2-group comparisons and adjusted for
Bonferroni correction less than .0167 for 3-group compar-
isons were considered statistically significant. Data were
stored in Excel (Microsoft, Redmond, Wash) and statistical
analysis was performed using SPSS 10.0 for Windows
(SPSS, Chicago, Ill).
3. Results
Nine patients from the original population either devel-
oped major complications, requiring prolonged mechanical
ventilation in the ICU, or else died. In these patients, the
third day evaluation for intraoperative awareness was
impossible and we had to exclude them from the study. In
the remainder of the patients (n = 121), the discussion about
awareness was satisfactory and they were included regard-
less of duration of postoperative mechanical ventilation or
other support measures used. The groups that were formed
were similar and no difference of statistical importance was
shown regarding the analyzed parameters (Table 1). In all
patients, the BIS value was greater than 95 during peripheral
venous catheterization. In group A, the mean BIS value was
39.19 F 10.32; in group B, it was 37.38 F 10.21; and in

Decision-support by bispectral index during cardiac anesthesia 513
group C, it was 38.29 F 10.01, without any difference of
statistical importance between groups (Table 2). No patient
was moved from group B or group C to the B1 or C1
subgroups. In other words, the observer anesthesiologist
never noted a standardized comment of 5. Distribution of
the zenith BIS values did not differ statistically, and there
was no difference in the nadir BIS values.
Our results are shown in Table 2. The difference between
those patients who were operated on during active hypo-
thermia and those who were operated on during normother-
mia is shown. In addition, 4 distinct periods of the procedure
for each subgroup (hypothermic, normothermic) are dis-
played. In all groups, in patients who were operated on
under hypothermia, the BIS values of each period (pre-
sternotomy, pre-CPB, etc) differed statistically (P b 0.01).
In group A patients who were operated on without active
hypothermia, pre-sternotomy values (44.58 F 10.33) were
statistically different from pre-CPB values (39.21 F 9.16,
P b 0.001). Similar statistical differences were noted in
groups B and C. In the same subgroup of patients from
group A, the BIS values did not differ statistically between
the CPB and the rewarming to the end of operation periods,
as was also noted for similar patients in groups B and C.
In group A, in the period from sternotomy to institution of
CPB, BIS values were 38.08 F 8.20 and 39.21 F 9.16 (ns)
with respect to whether hypothermia was to be applied. In
the next operative period, from institution of CPB to the
beginning of rewarming, BIS values were 33.91 F 6.66 and
37.22F 8.98 (P b 0.001), respectively. In group B and with
respect to the above-mentioned periods, BIS values were
Table 2 Results
Group A (n = 36)
BIS valuea 39.19 F 10.32
Zenith BISa 52.08 F 12.22
Nadir BISa 26.73 F 2.82
Standardized comments N1 none
Standardized comment N1 per pt none
Propofol administration (mL/kg per hour) 0.470 F 0.053b
Remifentanil (ml/kg per hour) 0.190 F 0.021
CBP temp (hypothermic pts) (8C) 33.82 F 0.563
CBP temp (normothermic pts) (8C) 5.15 F 0.427
BIS values
Hypothermic pts (n = 18)
Pre-sternotomy perioda 43.90 F 11.82
Pre-bypass period 38.08 F 8.20
CPB 33.91 F 6.66
Rewarming–end of operation 37.54 F 8.02
Normothermic pts (n = 18)
Pre-sternotomy perioda 44.58 F 10.33
Pre-bypass period 39.21 F 9.16
CPB 37.22 F 8.98
Rewarming–end of operation 39.07 F 9.81a Values not including the awake patient until 15 minutes after induction.b Denotes statistical difference (3-group comparison).
35.04 F 7.68 and 37.11 F 8.04 (ns) and 32.47 F 5.78
and 36.09 F 8.67 (P b 0.001). In group C, BIS values were
35.92 F 6.90 and 37.88 F 7.72 (ns) and 33.04 F 5.00 and
37.01 F 7.94 (P b 0.001) in the hypothermic and
normothermic CPB patients, respectively. In the period from
rewarming to the end of the operation, BIS values were
increased significantly for the hypothermic CPB patients
regardless of their group allocation. Finally, as is shown
bhorizontallyQ in Table 2, comparisons of the 3 group
distributions revealed no differences in statistical importance.
In group B, a standardized comment above 1 was noted
in 220 cases (5.00 F 1.58 per patient). In group C, the
observer rated the BIS value qualitatively above 1 (stan-
dardized comment N1) in 143 cases (3.49 F 1.36 per
patient, P b 0.001) and so informed the attending anesthe-
siologist. In 112 (78.3%) of these events in group C, the
attending anesthesiologist proceeded to take corrective
measures. In 79 (70.5%) events, these measures involved
titration of anesthetics; in 9 (8.0%) events, they involved
titration of vasoactive drugs; and in 13 (11.6%) events, titra-
tion of both. Finally, in 11 (9.8%) cases, the attending
anesthesiologist took other diagnostic or corrective actions
or measures. In these cases, actions first written in the
parallel record, when the attending anesthesiologist became
aware of the BIS value of the event, were the following:
1. additional sampling for blood gas analysis (3);
2. zeroing of the pressure signals (3);
3. pump transfer to the heart-lung machine (valve ope-
ration with double venous cannulation) (2);
Group B (n = 44) Group C (n = 41) P
37.38 F 10.21 38.29 F 10.01 ns
53.72 F 12.04 49.82 F 11.90 ns
24.30 F 2.92 25.02 F 2.68 ns
220 143
5.00 F 1.58 3.49 F 1.36 b0.001
0.518 F 0.058 0.512 F 0.056 b0.0167
0.200 F 0.024 0.194 F 0.022 ns
33.74 F 0.478 33.76 F 0.502 ns
35.16 F 0.432 35.16 F 0.587 ns
(n = 28) (n = 27)
42.02 F 11.36 42.38 F 11.11 ns
35.04 F 7.68 35.92 F 6.90 ns
32.47 F 5.78 33.04 F 5.00 ns
36.86 F 7.87 37.49 F 7.11 ns
(n = 16) (n = 14)
42.96 F 12.08 44.09 F 13.62 ns
37.11 F 8.04 37.88 F 7.72 ns
36.09 F 8.67 37.01 F 7.94 ns
38.82 F 8.92 40.66 F 8.61 ns

G. Vretzakis et al.514
4. control and change of the anesthetic administration
line (2);
5. titration of ventilation (1).
These were or were not followed by other actions.
The consumption of propofol, normalized to the patient’s
weight and to duration of the duration, was statistically less
in group A (0.470 F 0.053 mL/kg per hour) than in groups
B or C (0.518 F 0.058 and 0.512 F 0.056 in mL/kg per
hour, respectively; ns). The normalized consumption of
remifentanil showed insignificant differences between the
3 groups (Table 2). Postoperatively, no intergroup differ-
ences were found with respect to time of extubation in the
ICU. Finally, no patient in any group experienced awareness
during anesthesia.
4. Discussion
Bispectral index monitoring has been reported to be
superior in evaluating anesthetic depth compared with other
clinical signs. In noncardiac anesthesia, BIS monitoring
helps to avoid underdosage or overdosage and their
consequences as light anesthesia or unjustified prolongation
of awakening. Furthermore, the usefulness of BIS as an
objective tool for the evaluation of needs and the analysis of
costs has also been documented [1-5]. However, none of
these studies has actually investigated its utility in decision
making. In cardiac anesthesia, some of the advantages of
BIS monitoring are minimized because the intraoperative
anesthetic drug support is usually based on the administra-
tion of large amounts of opioids [6,7]. Although its utility in
the titration of anesthetics or its accuracy is not altered with
the use of high doses of opioids, its ability to facilitate rapid
recovery and spontaneous ventilation is lost. Furthermore,
in these operations, the immediate weaning of ventilatory
support is impossible in most of the cases. Some inves-
tigators therefore wonder about the usefulness of BIS
monitoring in cardiac operations. Our study was designed
to clarify the contribution of intraoperative BIS monitoring
to decision making in the course of cardiac operations under
extracorporeal circulation and hypothermia.
To clarify our hypothesis, the study design excluded
patients undergoing off-pump techniques or patients who
would likely not be available for a third day of evaluation.
The low preoperative EF is a persistent factor affecting the
time of extubation [8,9]. We also excluded patients
programmed for a combined carotid endarterectomy proce-
dure, as the relation of BIS readings to brain ischemia or
carotid clamping (ipsilateral or contralateral) is unclear. In
one report, BIS values were lower during hypoxia [10].
Currently, it seems that during episodes of brain hypoxia,
clinicians follow BIS values with a question mark. Finally,
we excluded 9 patients from the original population, as
they required prolonged mechanical ventilation in the ICU
or had a bad outcome; thus, a third day of evaluation for
intraoperative awareness was impossible. Nevertheless, the
intraoperative BIS values of the excluded subjects showed
no difference compared with all the others. Other character-
istics might affect their outcome, but this evaluation was
considered irrelevant to the hypothesis of our study.
In group B, anesthetic support was performed with no
access to BIS values. In 220 cases (5 times per patient),
checked as standardized comments, the observer considered
that BIS data would be useful, either because a particular act
had an insufficient result or it led to an unnecessarily greater
effect or because interpretation of the patient’s status was
incomplete and the measures taken were inadequate. Free
notes about the BIS value were plenty in the parallel
anesthesia record, concerning the changes in surgical
stimuli, the hemodilution, the alterations of temperature,
and the profound diuresis. In one case, malfunction of the
propofol pump was noticed by the observer before activa-
tion of the alarm.
In group C, the attending anesthesiologist was informed
about the BIS value in 143 cases (approximately 3.5 times
per patient). These cases were qualitatively similar to the
standardized comments in group B, they were checked in
the same way, and they were followed by similar free notes.
Information about BIS value resulted in fewer events. In
other words, the informed provider proceeded to actions that
reduced the number of incidents in which the BIS was
considered of value for management of the patient. The
value of BIS data is reflected in the fact that in most of the
cases (78.3%), measures were taken. Furthermore, this
positive value shows a decreased subjective dependence
by the observer on the standardized comments. The actions
of the attending anesthesiologist, after having the BIS data,
were grouped as per our results above. It seems that
knowledge of the adequacy or inadequacy of anesthesia
completes the hemodynamic image. In 15.3% of the total
events, the attending anesthesiologist addressed his actions
to the direction of hemodynamic handling, in spite of the
adequacy of the available monitoring. In many cases, the
decision to administer b-blockers and to increase or
decrease the inotropic and vasoactive drug administration
was made after taking into consideration the BIS value as
well. Finally, as it is reported, the attending anesthesiologist
proceeded to other diagnostic or corrective actions or
measures. In one case, during the pre-CPB period and after
a satisfactory control of the equipment, in a patient with a
heart rate (HR) of 100 beats per minute (bpm) and a blood
pressure (BP) of 145/88 mm Hg, hypoventilation was
proven when the attending anesthesiologist proceeded
to arterial blood gas analysis, as the BIS value was
47 (standardized comment = 4). It seemed that the BIS-
expressed adequacy of hypnosis turned his attention to other
causes of this hemodynamic picture. In another, a little
before sternotomy, the attending anesthesiologist only
confirmed the accuracy of transducers in a patient with an
HR of 62 bpm and BP of 75/52 mm Hg when the BIS value
was 18 (standardized comment = 2). It seemed that, waiting

Decision-support by bispectral index during cardiac anesthesia 515
for the sternotomy and knowing BIS, the responsible
anesthesiologist decided only to verify the BP level. The
attending anesthesiologist correctly re-zeroed the transducer
systems before transferring the patient to ICU, when in-
fusion of anesthetics was already lowered, HR was 65 bpm,
BIS values were 42 to 45 (standardized comment = 4), and
BP was falsely 178/100 mm Hg. He also proceeded to new
settings in the ventilatory mode in a patient who during left
internal mammary artery preparation was sweating, after
controlling the equipment and considering the BIS value of
45 (standardized comment = 4).
Patients from group A served somewhat as the control
group in this study. In many instances, the observer wrote,
as a free note in the parallel record, that anesthetic
management was targeted to some specific BIS score. At
most of the times, this was higher than what was displayed
on the BIS screen. That was common particularly during the
initiation of hypothermic CPB. Unfortunately, this obser-
vation cannot be further analyzed because of limitations in
our protocol. Although BIS values were highest in group A,
the anesthetic result, as measured by BIS, did not differ
between the 3 groups of patients. Furthermore, BIS values
could be considered low in all groups [11]. We believe that,
in our setting, these observations come from focusing
mainly on propofol’s plasma concentration [12]. Actually,
in group A, continuous BIS monitoring and lesser
uncertainty about adequacy of anesthesia allowed the
provider to significantly reduce propofol’s infusion rate. It
seems that, in the conditions of cardiac anesthesia, BIS
monitoring serves as a tool for significantly less adminis-
tration of anesthetics without increasing the frequency of
moving to clinically undesirable levels of anesthetic
inadequacy. Finally, the regimen that was used in our study
allowed low BIS values without the need for prolonged
postoperative mechanical ventilation, as has been seen
elsewhere [5]. Nevertheless, it could be suggested that
anesthesia guided to values closer to 50 would be more
appropriate for fast-tracking.
Hypothermia is known to cause increased sedation and
loss of consciousness. During cardiac operations, the effect
of hypothermia on BIS values has been extensively
evaluated [13-16], thus allowing decision making to be
based on BIS regardless of the temperature. In our patients,
the application of mild hypothermic CPB resulted in
decreased BIS values. The attending anesthesiologists had
adequate experience in everyday BIS monitoring and they
adjusted, blindly or not, the infusion rate of the anesthetic
drugs. We consider that this experience contributed to the
only small absolute decrease of BIS values during the
hypothermic CPB noted in our patients.
Observer subjectivity could play a limiting role in the
results noted in our study. We tried to reduce the subjective
character in our methods, although we accept that it is
always present to some extent in behavioral observations.
However, given the fact that information resulted in
measures and reduced events in group C and from the rest
of our findings as discussed above, the usefulness of BIS
monitoring during cardiac operations is evident. Actually,
our study directly shows the actions following the intermit-
tent knowledge of BIS value. In conclusion, our results
suggest that BIS data, as part of the intraoperative
assessment in cardiac operations, provide the clinician with
an ability to make more informed decisions about the dosing
and balance of anesthetic agents and other adjuvant
therapies such as analgesics and cardioactive agents.
Acknowledgments
The authors are indebted to several people for their
contribution to this work. We thank the statistician J
Tripsianis for helping us with the statistical analysis. We
also thank M Vergoulidou, D Kyriakidou, D Artemis, and D
Patridas, students of Medicine of the Democritus University
of Thrace, who worked willingly in the OR and ICU for the
collection and processing of the data.
References
[1] Glass PS, Bloom M, Kearse L, Rosow C, Sebel P, Manberg P.
Bispectral analysis measures sedation and memory effects of propofol,
midazolam, isoflurane and alfentanil in healthy volunteers. Anesthe-
siology 1997;86:836-47.
[2] Katoh T, Suzuki A, Ikeda K. Electroencephalographic derivatives as a
tool for predicting the depth of sedation and anesthesia induced by
sevoflurane. Anesthesiology 1998;88:642 -50.
[3] Struys M, Somers AA, Van Den Eynde N, et al. Cost reduction
analysis of propofol versus sevoflurane: maintenance of anaesthesia
for gynaecological surgery using the bispectral index. Eur J
Anaesthesiol 2002;19:727 -34.
[4] Yli-Hankala A, Vakkuri A, Annila P, Korttila K. EEG bispectral
index monitoring in sevoflurane or propofol anaesthesia: analysis of
direct costs and immediate recovery. Acta Anaesthesiol Scand 1999;
43:545-9.
[5] Lehmann A, Karzau J, Boldt J, Thaler E, Lang J, Isgro F. Bispectral
index-guided anesthesia in patients undergoing aortocoronary bypass
grafting. Anesth Analg 2003;96:336-43.
[6] Heck M, Kumle B, Boldt J, Lang J, Lehmann A, Saggau W.
Electroencephalogram bispectral index predicts hemodynamic and
arousal reactions during induction of anesthesia in patients undergoing
cardiac surgery. J Cardiothorac Vasc Anesth 2000;14:693-7.
[7] Driessen JJ, Harbers JB, van Egmond J, Booij LH. Evaluation of the
electroencephalographic bispectral index during fentanyl-midazolam
anaesthesia for cardiac surgery. Does it predict haemodynamic
responses during endotracheal intubation and sternotomy? Eur J
Anaesthesiol 1999;16:622 -7.
[8] Habib RH, Zacharias A, Engoren M. Determinants of prolonged
mechanical ventilation after coronary artery bypass grafting. Ann
Thorac Surg 1996;62:1164-71.
[9] Bezanson JL, Deaton C, Craver J, Jones E, Guyton RA, Weintraub
WS. Predictors and outcomes associated with early extubation in older
adults undergoing coronary artery bypass surgery. Am J Crit Care
2001;10:383-90.
[10] Okawa H, Hirota K, Sakai I, Tsubo T, Ishihara H, Matuki A. Early
detection of hypoxia with BIS monitoring during percutaneous
cardiopulmonary support. Masui 2001;50:429 -32.

G. Vretzakis et al.516
[11] Kelley SD, editor. Monitoring level of consciousness during anesthe-
sia and sedation. A clinician’s guide to the bispectral index. Natick
(Mass)7 Aspect Medical Systems Inc; 2003. p. 32- 47.
[12] White M, Kenny GN. Intravenous anaesthetic agents: delivery
systems. In: Nimmo WA, Rowbotham DJ, Smith G, editors.
Anaesthesia. 2nd ed. Oxford (UK)7 Blackwell Scientific Publications;
1994. p. 106 -8.
[13] Mathew JP, Weatherwax KJ, East CJ, White WD, Reves JG.
Bispectral analysis during cardiopulmonary bypass: the effect of
hypothermia on the hypnotic state. J Clin Anesth 2001;13:301-5.
[14] Hemmerling TM, Fortier JD. Falsely increased bispectral index
values in a series of patients undergoing cardiac surgery using
forced-air-warming therapy of the head. Anesth Analg 2002;95:
322-33.
[15] Doi M, Gajraj RJ, Mantzaridis H, Kenny GN. Effects of cardiopul-
monary bypass and hypothermia on electroencephalographic varia-
bles. Anaesthesia 1999;52:1048-55.
[16] Honan D, Doherty D, Frizelle H. A comparison of the effects of mild
versus moderate hypothermia during cardiopulmonary bypass on the
EEG bispectral index. Eur J Anaesthesiol 2002;19(S24):26.