Positioning for Anesthesia and Surgery
21
24 cr LU U Positioning for Anesthesia and Surgery Celeste G. Villanueva Positioning the patient for a surgical procedure provides the surgeon with the maximum acceptable access to the operative field. Two equally important objectives of pa- tient positioning are to allow access to the patient for the safe administration of anesthesia and to ensure the opti- mal physiologic function of all body systems. Proper po- sitioning clearly contributes to the success of a surgical procedure and is an important factor in anesthesia- related morbidity and mortality. Patient positioning is potentially an issue in two sit- uations: when inadequate surgical posture compromises good exposure, thereby prolonging and possibly compli- cating surgery, or when the patient's position is so opti- ma! in terms of exposure that the patient's physiologic limits are exceeded. The responsibility of adapting a po- sition dictated by the operative procedure without com- promising the patient falls primarily to the anesthetist. A position-related anesthetic misadventure was doc- umented as early as 1849 when an intraoperative death that was possibly attributable to a posture change. John Griffith, a 31-year-old U.S. seaman, received a chloroform anesthetic via an open mask technique in the sitting po- s ition. Soon after anesthetization, the patient was placed in the lateral position for a hemorrhoidectomy. The doc- umented record of events indicates that directly after the Posture change occurred, Mr. Griffith ceased to breathe a nd was pulseless. History also records that all efforts to ^store the patient were ineffective (Little, I960). Alterations in the body's physiology caused by posi- l <oning patients for surgical procedures were the focus of study as early as 1933 (Button). The subsequent thirty years witnessed the publication of several landmark stud- ies that correlated physiologic changes, particularly those involving the circulatory and respiratory systems, with varying surgical positions (Courington & Little, 1968; Henschel, Wyant, Dobkin, & Henschel, 1957; Slocum, Hoeflich, &Allen, 1947). Since the 1960s Martin and his associates (Martin, 1997a, 1997b, 1997c; Martin & Warner, 1997) have con- tributed significantly to the body of knowledge pertain- ing to this basic, but often ignored, aspect of clinical practice. Their work has raised the level of understand- ing of positioning issues beyond anecdotal folklore to statistical assessments of huge patient databases. These types of studies are particularly timely in an era of pa- tient risk management, performance improvement by care givers, and outcome analysis of anesthetic care. Taking a different historical perspective of patient positioning, the continual evolution of new and innova- tive surgical techniques highly depends on the possibil- ity of placing patients in extreme or nonanatomic posi- tions that challenge the physiologic limits of the patient. Because of a greater understanding in the field of anes- thesiology of the physiological consequences and man- agement of patients in these "unusual" positions, patients can safely undergo newer procedures and surgical tech- niques can continue to evolve. This chapter discusses the basic principles of safe positioning, conveys the importance of proper posi- tioning from a medicolegal perspective, presents an overview of the alterations in body physiology caused by 543
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Positioning for Anesthesia and Surgery

24 crLU
U
Positioning for Anesthesiaand SurgeryCeleste G. Villanueva
Positioning the patient for a surgical procedure providesthe surgeon with the maximum acceptable access to theoperative field. Two equally important objectives of pa-tient positioning are to allow access to the patient for thesafe administration of anesthesia and to ensure the opti-mal physiologic function of all body systems. Proper po-sitioning clearly contributes to the success of a surgicalprocedure and is an important factor in anesthesia-related morbidity and mortality.
Patient positioning is potentially an issue in two sit-uations: when inadequate surgical posture compromisesgood exposure, thereby prolonging and possibly compli-cating surgery, or when the patient's position is so opti-ma! in terms of exposure that the patient's physiologiclimits are exceeded. The responsibility of adapting a po-sition dictated by the operative procedure without com-promising the patient falls primarily to the anesthetist.
A position-related anesthetic misadventure was doc-umented as early as 1849 when an intraoperative deaththat was possibly attributable to a posture change. JohnGriffith, a 31-year-old U.S. seaman, received a chloroformanesthetic via an open mask technique in the sitting po-sition. Soon after anesthetization, the patient was placedin the lateral position for a hemorrhoidectomy. The doc-umented record of events indicates that directly after thePosture change occurred, Mr. Griffith ceased to breatheand was pulseless. History also records that all efforts to^store the patient were ineffective (Little, I960).
Alterations in the body's physiology caused by posi-l<oning patients for surgical procedures were the focus
of study as early as 1933 (Button). The subsequent thirtyyears witnessed the publication of several landmark stud-ies that correlated physiologic changes, particularlythose involving the circulatory and respiratory systems,with varying surgical positions (Courington & Little,1968; Henschel, Wyant, Dobkin, & Henschel, 1957;Slocum, Hoeflich, & Allen, 1947).
Since the 1960s Martin and his associates (Martin,1997a, 1997b, 1997c; Martin & Warner, 1997) have con-tributed significantly to the body of knowledge pertain-ing to this basic, but often ignored, aspect of clinicalpractice. Their work has raised the level of understand-ing of positioning issues beyond anecdotal folklore tostatistical assessments of huge patient databases. Thesetypes of studies are particularly timely in an era of pa-tient risk management, performance improvement bycare givers, and outcome analysis of anesthetic care.
Taking a different historical perspective of patientpositioning, the continual evolution of new and innova-tive surgical techniques highly depends on the possibil-ity of placing patients in extreme or nonanatomic posi-tions that challenge the physiologic limits of the patient.Because of a greater understanding in the field of anes-thesiology of the physiological consequences and man-agement of patients in these "unusual" positions, patientscan safely undergo newer procedures and surgical tech-niques can continue to evolve.
This chapter discusses the basic principles of safepositioning, conveys the importance of proper posi-tioning from a medicolegal perspective, presents anoverview of the alterations in body physiology caused by
543

544 PART V Perioperative Management, Techniques, and Applications
posture changes in general with emphasis on the circu-latory, respiratory, and peripheral nervous systems, andpresents common surgical positions along with the mostimportant anesthetic implications entailed by each.
> PRINCIPLES OF SAFE POSITIONING
Basic Elements of Safe PositioningThe essential elements of safe patient positioning paral-lel what most practitioners consider basic componentsof the principles and practice of anesthesia: a strong the-oretical knowledge base, forethought and organization,attention to detail, a collaborative effort, proper equip-ment, and vigilance.
An adequate fund of knowledge for proper posi-tioning involves an understanding of the changes in bodyphysiology, particularly in cardiopulmonary dynamics,that occur when a patient is placed in the various surgi-cal postures. A. solid grasp of the practical aspects ofaccomplishing certain positions also is necessary. Per-haps most critical is an awareness of the sometimes direconsequences of improperly positioning a patient. Last,an empathic awareness by the clinician of the discomfortassociated with various surgical positions is extremelyhelpful. In many training programs, novice anesthetistsare placed in each of the common postures to allowthem to experience how difficult it can be to attain acomfortable and safe position without compromisingoperative exposure.
Forethought and organization refer to the carefulplanning of position changes by each member of the in-traoperative team. This implies an adequate understand-ing of the logistics of the particular surgical procedure,the specific requirements of the operating surgeon, andthe medical condition of the patient. Of critical impor-tance, especially when attempting a complex positionchange, is the pharmacologic strategy developed by theanesthetist. A combination of agents, as well as the titra-tion of their dosages and levels, is chosen based on theprimary goal of circulatory and pulmonary stability.Proper planning also includes the development of a strat-egy for keeping intact the intravenous and monitor-ing lines, airway maintenance device, and all other de-vices attached to the patient during rotational positionchanges.
Safe positioning requires meticulous attention todetail. Moreover, attentiveness to detail is possible onlywhen sufficient time is available and when involved per-sonnel are focused on the procedure at hand. A commonpitfall for many anesthesia students is to allow them-selves to be rushed unprepared into a complex position-ing sequence by an impatient surgical or anesthesia staff.It also is extremely important that all members of the po-
sitioning team be satisfied with every detail of the finalposture of the patient prior to sterile preparation anadraping of the surgical field. Any uneasiness that remainsabout aspects of the position or physiological status <>fthe patient (as it relates to positioning) is greatly majyij.fled after the surgical incision is made when access tothe patient to correct a problem is difficult or impossiblewithout a major disruption of the procedure (Colvin1987).
The importance of a collaborative effort by the p<).sitioning team—surgeons, anesthetists, nurses and tech-nicians—cannot be overemphasized. Clear and continu-ous communication between members is the hallmark ofa successful and efficient team. The question of who isultimately responsible for properly positioning a patientfor surgery can be hotly debated in legal circles, but themost correct and comprehensive answer is that all mem-bers of the team share this responsibility. Specific rolesmay vary between institutions and surgical practices.However, a reasonable generalization is that the anes-thetist determines when the patient is physiologicallyprepared for a posture change and the actual pace andtiming of the positioning maneuvers. The anesthetisttakes direct physical responsibility for maintaining thestability of the head and neck and protecting the eyesand ears from trauma and the patency of the airway dur-ing all position changes.
The availability and functionality of the propeiequipment necessary to achieve and maintain theproper position should be established prior to anes-thetizing the patient and initiating a positioning process.In large, busy operating room suites this often representsthe biggest challenge.
Vigilance is especially critical to avoid complica-tions from positioning. Adequate anesthesia for surgicalpain also implies that pain due to an uncomfortable po-sition or a position that exceeds the patient's usualanatomic or physiologic limits is eliminated. In addition,the signs and symptoms of many position-related prob-lems are not manifest on a monitor. Frequent visual in-spection and palpation of the patient's body parts thaiare at risk are usually the best monitors for proper posi-tioning.
Preanesthetic Evaluation
A preanesthetic positioning assessment focuses on thepatient, the surgical procedure, and the positioningteam. Identifying risk factors for positioning complica-tions is the major objective of the preanesthetic assess-ment. An evaluation of the patient's cardiopulmoiuryreserve is critical, as the subsequent discussions of <-'ir-culatory and respiratory alterations will make evidentAdditional risk factors focus on the potential t(!
position-related neuropathies. A study identified factors
Chapter 24 Positioning for Anesthesia and Surgery 545
that were strongly predictive for the development of mo-tor neuropathy in lower extremities (Warner, Warner, &
^Martin, 1994).These results can certainly be extrapolatedto include risk for developing neuropathies in areasother than the lower extremities. The factors identifiedinclude a low body mass index (less than or equal to 20),increasing age, a history of smoking within 1 month of asurgical procedure, and preexisting diabetes or vasculardisease.
Identifying and documenting preanesthetic muscu-loskeletal limitations and preexisting neurologic deficitsor neuropathies are part of a thorough patient evalua-tion. The practice of incorporating a "dry run" of the spe-cific surgical posture is a prudent undertaking, especiallyin situations where preoperative neuropathies exist. Inthis process, the awake patient places himself in the de-sired surgical position, communicating to the team thetolerable limits of his extremity and joint movements,and directing the placement of padding in potentialproblem areas.
Specific knowledge of the surgical procedure itselfalso is part of a preanesthetic evaluation. The best sourceof information in this matter is the primary surgeon in-volved in the case. Clarifying the exact purpose of thesurgery (biopsy versus excision, partial versus total re-section of an organ, diagnostic procedure prior to a ther-apeutic maneuver) is a perfectly reasonable request in anera when options concerning virtually every aspect of aprocedure are numerous. Other useful bits of informa-tion are the likelihood of an intraoperative positionchange (or in some cases even a change in the operatingtable) and the anticipated duration of a case, as the dura-tion of time spent in a particular extreme position hasbeen found to correlate directly with the developmentof nerve damage (Warner, Warner, & Martin, 1994).
Assessing the preparedness of the intraoperative po-sitioning team may seem too basic a concept to includein this discussion. However, a single experience with theanxiety produced when an inexperienced or inattentiveteam member fails to support the patient's limb or is un-able to attach a critical stabilizing device is enough toconvince most anesthetists that all team membersshould be ready prior to embarking on major positionchanges.
Postanesthetic Evaluation
The postanesthetic aspect of positioning principles isbased on the importance of prompt recognition of com-plications to institute diagnostic procedures, consulta-tions, and therapeutic measures. Major assessment pointsinclude hemodynamic stability, new-onset of sensory ormotor neuropathies not explained by the anesthetic tech-nique used, sustained or unexplained pain, and swelling,lacerations, or hematomas in a nonoperative site.
Evaluation of the Operating Table
There is a wide range of operating tables, ranging frombasic, manually operated models to sophisticated, elec-tronically controlled varieties. Specific tables are fre-quently used for certain surgical subspecialties andrequire a complete training session to be operated prop-erly.
For the anesthetist in the early stages of training thebest practice is to include a preoperative check of thesurgical table as part of the daily setup routine. It is par-ticularly important to determine the center of gravity ofthe table established for each procedure. Most operatingrooms use tables whose tops move in relation to the sta-bilizing, fixed pedestal. Although this feature vastly im-proves access for radiologic equipment (fluoroscopeswith C-shaped camera arms) underneath the table sur-face, an obese patient placed too far from the table's cen-ter of gravity may cause the entire unit to fall. In addition,a preoperative check of the table should include gainingfamiliarity with the specific workings of the table's con-trol panel and ensuring the functionality of all of its mov-ing parts. Realizing that a table is not functioning or thatone is unable to manipulate the table because of lack ofknowledge during the surgical procedure when the pa-tient is already fully anesthetized predisposes to compli-cations.
Armboards that are routinely attached to the surgi-cal table and the padding used for various aspects of po-sitioning often are viewed as mundane elements of posi-tioning. However, their proper use is essential to avoidcomplications and provide quality care. The sectionsthat discuss specific positions address proper placementof these items.
Another practice that will help ensure patient andprovider safety is clearly to announce operating table po-sition changes prior to instituting the change to allow allmembers of the surgical staff to protect the patient andthemselves from the harmful consequences of movingtable components.
> MEDICOLEGAL ASPECTSOF POSITIONING
A major source of professional liability in anestheticpractice continues to be patient injuries caused by re-lated positioning-problems, most notably peripheral neu-ropathies. A retrospective study of a large closed claimsdatabase was undertaken to determine the frequency ofnerve damage in the overall incidence of anesthesia-related injury (Kroll, Caplan, Posner, Ward, & Cheney.1990). Fifteen percent of 1541 claims reviewed involvednerve injury directly related to anesthesia. Interestingly,the standard of care had been met in these nerve-related
546 PART V Perioperative Management, Techniques, and Applications
injury claims significantly more often than in claims notinvolving nerve injury, a finding that the authors of thestudy partly attribute to the unclear mechanism of themost common type of nerve injury (ie, ulnar neuropathy,which is discussed in a subsequent section of this chap-ter.)
In 1994 the major insurer of nurse anesthetists inthe United States reported that nerve-related and arm- orshoulder-related events were the ninth and tenth, re-spectively, most common allegations made againstCRNAs insured by their company during the 5 yearsprior to the report (St. Paul Medical Services, 1994). Al-though more recent data indicate that this statistic maynot repeat itself in the subsequent 5 years (St. Paul Med-ical Services, 1997), it is clear that perioperative nerve-related injuries, correctly assumed to be most often relatedto positioning issues, should be of major concern to allanesthesia clinicians.
It has been clearly established (Stoelting, 1993) thatanesthesia-related neuropathies can easily occur despitethe use of "textbook" positioning. A clear message to theanesthetist in training certainly is to heed the basic prin-ciples and proper methods of positioning about to bediscussed in the rest of the chapter and the lessons gen-erated by innumerable malpractice cases involving posi-tioning in anesthesia and surgery: Develop the habit ofclearly and consistently documenting the measurestaken to protect the patient adequately.
*> THE PHYSIOLOGY OFPOSTURE CHANGE
Prior to discussing the various surgical positions, itseems logical to examine the normal physiologic state ofhealthy, awake humans in the two positions in which wespend the majority of our lives, erect and supine. Morespecifically, what is relevant to the anesthetist is an un-derstanding of the physiologic adaptations involved inchanging from an erect to a supine position, as the ma-jority of surgical procedures are done in some variationof the basic supine position. This discussion of physio-logic adaptations focuses on the cardiovascular and pul-monary systems.
K CARDIOVASCULAR SYSTEM
The posture change from erect to supine in an awake,healthy individual is accompanied by a series of com-pensatory autonomic reflexes that provide circulatoryhomeostasis. The specific reflexes involved in maintain-ing a stable blood pressure and adequate tissue perfusionare the "low-pressure" reflexes, the arterial baroreceptorreflex, and the Bainbridge reflex.
The low-pressure receptors (also referred to a.mechanoreceptors or cardiopulmonary receptors) ar*located in the great veins, the atria and the ventriclesThey are components of a negative feedback system- anincrease in intravascular volume stimulates the recep.tors to generate an increase in vagal activity via themedullary vasomotor center, resulting in a reflex inhibi-tion of sympathetic outflow (O'Brien & Ebert, 199~)Conversely, a decrease in blood volume will cause sym-pathetic excitation. This physiologic response is distinctfrom, but works in concert with, the arterial barorecep-tor reflex.
The arterial baroreceptor reflex originates in thepressure-sensitive receptors of the carotid sinus and aor-tic arch. These receptors send afferent impulses throughthe glossopharyngeal and vagus nerves to the medullaryvasomotor center, which relays efferent sympathetic andparasympathetic outflow. Increased arterial blood pres-sure sensed by the baroreceptors ultimately results in in-creased vagal tone as well as diminished sympathetic ac-tivity, which leads to decreased heart rate and myocardialcontractility.
The Bainbridge reflex involves an adjustment ofheart rate in response to atrial volume; its baroreceptorsare located in the right atrium and great veins. Changingfrom an erect to the supine position increases venous re-turn because of gravitational changes. This increasedatrial volume stimulates an increase in heart rate thatserves to prevent blood from pooling in the veins, atria,and pulmonary system and to promote more effectiveleft ventricular filling.
The cumulative effect of these aforementioned au-tonomic reflexes when activated by a postural changefrom upright to supine has been determined in two stud-ies (Korner. 1971; Ward, Danzinger, & Bonica, 1966).There is a decrease in mean arterial pressure (systolicblood pressure is unchanged, diastolic pressure de-creased), heart rate, and peripheral vascular resistancewith a simultaneous increase in cardiac output andstroke volume (primarily due to the increased venous re-turn).
The vigor of the protective cardiovascular reflexesjust described is impaired by disease, injury, and ;inevthesia. Postural changes that normally cause little or nochange in blood pressure and tissue perfusion will causea significant fall in both blood pressure and perfusion inthe anesthetized patient (Biddle & Caunady, 1990). Thisis especially true if the patient is repositioned in the im-mediate postinduction period. Clearly, an anesthetized in-dividual with impaired cardiovascular reserve will beeven less tolerant of the circulatory changes that accom-pany position changes.
The pharmacologic agents most commonly utilizedin general anesthesia are volatile agents, barbiturates,benzodiazepines, which all depress the sympathetic re-

Chapter 24 Positioning for Anesthesia and Surgery 547
to position changes.The cifcuiatbi-y effect of this^pressed response is a tendency for blood to pool in pe-ripheral, dependent veins, decreasing venous return andcardiac output, with resultant hypotension. These sym-patholytic effects of anesthetic drugs are dose related;the clinical corollary to this principle is to avoid dosagesof drugs that will cause deep or even moderate levels ofanesthesia prior to major position changes. Drugs withjjjgher degrees of myocardial depression should, ofcourse, be avoided until after the positioning process iscomplete.
Maintaining a minimal level of general anesthesiaprior to a position change to prevent circulatory depres-sion entails the risk of patient movement and thereforeinjury during positioning. If the anesthesia-induced de-pression of muscle tone is insufficient, muscle rigidityalso can occur. The use of muscle relaxants prior to po-sitioning is a common practice used to prevent either ofthe aforementioned events. However, this technique isnot without its drawbacks. A relaxed and unprotectedhead and neck, joint, or limb is at higher risk for injury ifit is inadequately controlled during positioning.
It also is not uncommon for a minimally anes-thetized patient to become hypertensive during positionmaneuvering secondary to tracheal and joint stimulation.If an elevated blood pressure places the patient at in-creased cardiovascular risk, therapeutic measures shouldbe anticipated and implemented prior to completing theposture change: increased doses of analgesics, titration ofan antihypertensive agent that is appropriate for the pa-tient, or judicious increases in the concentration of an in-halation agent.
Additional measures to prevent hypotension relatedto posture changes that should be instituted prior to po-sitioning are (1) administration of a bolus of intravenousfluid to increase the intravascular volume; (2) applicationof compression (active or passive) devices to the lowerextremities to minimize venous pooling; (3) institution ofposition changes gradually and carefully, allowing the de-pressed circulatory system slowly to adapt to posturalchanges. This is especially critical at the termination ofsurgery when intravascular volume shifts can adverselyinfluence circulatory homeostasis.
Epidural and subarachnoid anesthetics result in asympathetic blockade; hence, depending on the levelof the blockade, avoiding hypotension with posturechanges can be a challenge. The choice of local anes-thetic (type, baricity, dose) as well as the timing and tech-nique to achieve an anesthetic level (incremental dosingvia a catheter versus a single dose) relative to the posi-tion change may be helpful to prevent a severe hypoten-sive episode. Judicious use of intravenous fluids and va-sopressors, the mainstay of treatment for hypotensionsecondary to the sympatholysis of regional anesthetics, isparticularly effective in these situations.
Respiratory SystemA study has quantified the gravitational forces in thesupine position on upper airway anatomy. In an awakeindividual the change from an erect to a supine positionresults in an increase in soft palate thickness and area, adecrease in the vertical length of the airway, and a 29%decrease in the oropharyngeal area (Pae, Lowe, & Sasaki.1994). Clinically, this may have major implications for air-way assessment and management. The following discus-sion on the effects of posture change on respiratoryphysiology is divided in terms of ventilation, perfusion.with some mention of specific lung volumes.
In normal respiration the lung expands in an infe-rior-superior direction as the diaphragm moves. Di-aphragmatic movement in the supine position accountsfor 66% of quiet ventilation; therefore, any limitationcaused by a surgical position on the movement of this'important respiratory muscle contributes heavily to anydeleterious effect. In an awake, spontaneously breathingindividual in the supine position, the abdominal contentslimit excursion and force the diaphragm cephalad, re-ducing functional residual capacity (FRC) by approxi-mately 800 mL (Lumb & Nunn, 1991).Total lung capacity(TLQ also is decreased. Froese and Bryan (1974) demon-strated that in a supine, anesthetized, spontaneouslybreathing state the diaphragm is placed further cepha-lad, and in an anesthetized, paralyzed state the diaphragmis pushed further still. Little (I960) noted that all of thecommon surgical positions do in fact restrict diaphrag-matic movement.
In addition to diaphragmatic movement, thorax ex-pansion plays a major role in normal ventilation. Me-chanical interference with chest movement that limitslung expansion perhaps is the single most important ef-fect of posture on respiration (little, I960). The follow-ing figures are extracted from Little's data. The percent-ages represent the degree to which the vital capacity(VC) decreased in healthy, awake subjects from a sittingposition into the indicated common surgical positions.These percentages may be decreased further in the anes-thetized individual:
Supine 9.5%Reverse Trendelenburg 9%Prone 10%Lateral 10%Jackknife 12.5%Gallbladder 13.5%Kidney 14.5%Trendelenburg 14.5%Lithotomy 18%
The concept of regional variations in ventilation (V)and perfusion (Q) should be familiar to a student of anes-thesiology. The reader is encouraged to review these

548 PART V Perioperative Management, Techniques, and Applications
concepts in the classic textbooks and schematics of West(1995) when analyzing the effect of various positionchanges on respiration on an awake, spontaneouslybreathing individual. A simplistic view of regional per-fusion is that blood flow essentially follows gravitationalforces. The lower or dependent lung area will, generallyspeaking, be better perfused than the upper or nonde-pendent lung areas. A similarly simplistic view of regionalvariations in ventilation is that ventilation decreases withdistance up the lung. Stated differently, alveoli in lower,dependent lung areas have a smaller initial volume and alarger change in volume than those in the upper, nonde-pendent lung areas. Hence, ventilation is greater in thedependent lung areas. Interestingly, radiologic evidenceindicates that ventilation always is greater in the depen-dent portion of the lungs regardless of the surgical pos-ture (Jenkins, 1968).
After summarily reviewing the changes in cardiores-piratory physiology involved in changing from the erectto the supine position in an awake individual and dis-cussed how anesthesia disrupts the body's instinctual re-flexes and mechanisms, the following statement shouldbe noted. Changes related to positioning in cardiorespi-ratory dynamics in anesthetized patients are very diffi-cult for the clinician to predict because an individual'sresponse depends on a variety of factors, some of whichare in a dynamic state themselves. These factors includethe body habitus, the anesthetic drug levels at any giventime, the patient's circulating volume, and whether ven-tilation is spontaneous or controlled.
Gastrointestinal System
In the supine position, esophageal sphincter tone in-creases (Babka, Hager, & Castell, 1973). This is a helpfulnatural counteraction to increased esophageal reflux ten-dencies in the supine state. The reflux is due to in-creased intragastric pressure. Not surprisingly, gastricemptying time also is significantly longer in the supineposition (Hulme-Moir, Donnan, & McAlister, 1973). Thesephysiologic findings provide strong rationales for rapid-sequence induction protocols.
Obesity constitutes one of the gravest hazards inanesthesia. Excess weight markedly restricts the di-aphragm, with a reduction in the tidal volume (VT ) andfunctional residual capacity (FRC). Extreme obesity,therefore, exaggerates all of the deleterious effects ofsurgical posture and accelerates the clinical manifesta-tions of respiratory insufficiency (Courington & Little,1968). Further implications of obesity will be discussedin subsequent sections on the specific surgical postures.
Muscular System
A combination of general anesthesia and muscle relax-ants produces complete muscle relaxation, as does sub-
arachnoid anesthesia. This profound muscle relaxationcauses the legs to lie flat on the operating table and un.duly stretches ligaments and muscles of the lower spinc
This stretch is responsible for most cases of backache inthe postoperative period. Soft padding should be placedunder the legs and back to prevent this discomfort.
The other important factor affecting the likelihoodof backache is the duration of surgery. In cases lasting ito 60 minutes, 18% of the patients developed postopera-tive backache, whereas in those procedures lasting 181to 240 minutes, 34% developed backache (Hicks & Koer-bacher, 1992). The long-term effect of this finding is un-clear.
* PERIPHERAL NERVE INJURIESASSOCIATED WITH POSITIONING
Mechanisms of Injury
Peripheral neuropathies continue to persist as the mostcommon, serious perioperative complications related topositioning. As such, a multitude of studies have beendone, many of them attempting to elucidate the precisemechanism of a specific nerve group's injury. In truth,the etiologic factors in perioperative peripheral nerve le-sions are complex and interrelated; they include preex-isting medical conditions, the effects of anesthesia, in ad-dition to intraoperative and postoperative positioning.
From a physiologic point of view, the most likelycauses of nerve injury are section (intentional or inad-vertent), compression, traction, and ischemia; the latterthree are the ones most likely related to positioning.Compression injuries are the result of externally appliedmechanical forces, a category that includes tourniquetcompression, crush injuries, tumors, hematomas, edema,and increased intrafascicular pressure. Nerves that passimmediately adjacent to a hard structure (eg, the radialnerve as it courses around the humeral shaft) are partic-ularly prone to this type of injury. Traction or stretchinginjuries can certainly be the result of positioning. Trac-tion decreases the cross-sectional area of a nerve, raisesthe pressure in the nerve, and compresses the nerve $blood supply; this can lead to permanent damage andnecrosis. Ischemic injuries occur when a peripheralnerve's blood supply is compressed or actually severed(as in femoral artery penetration or damage during can-nulation).
A special mention should be made here concerningpneumatic arterial tourniquets in relation to peripheralnerve injuries as tourniquets are used extensively in the
operating room; in some institutions, proper placementand monitoring of the tourniquet are considered thepurview of the anesthesia team. The high pressure gen-crated by tourniquets causes both compression •in"ischemic-type injuries to peripheral nerves. The
Chapter 24 Positioning for Anesthesia and Surgery 549
Of injury depends on both the quantity and duration ofpressure; injury is related more to duration than to quan-tity (Nakata & Stocking, 1997). It is customary to limitthe tourniquet time to approximately 1 hour in the up-per limb and 2 hours for the lower limb. If these time lim-itations are exceeded before the surgical procedureends, temporary decompression of the tourniquetshould be strongly considered to allow normal nerveconduction to be reestablished before reinflating thetourniquet.
The patient under general anesthesia is at higherrisk of injury to peripheral nerves for two major reasons:(1) muscle tone is lost; and (2) the patient's perceptivesense of impending nerve damage (paresthesias, pain, orboth) is absent.
The intent of this chapter is not to provide a de-tailed discussion of this important aspect of positioning,so the reader is referred to the works of Dylewsky andMcAlpine (1997), Dawson and Krarup (1989), and Brittand Gordon (1964) for excellent reviews.
Brachial Ptexus
The brachial plexus is by far the nerve group most vul-nerable to damage from improper positioning. A 1988study by Cooper, Jenkins, Bready, and Rockwood citedthe overall incidence of this injury at 0.02%. Interestingly,this statistic was very similar to one generated by a simi-lar study published 15 years earlier (Parks, 1973).
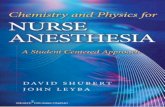
Stretching is the chief cause of damage to thebrachial plexus. Many intraoperative maneuvers can pro-duce stretching, but perhaps the most common are ab-duction and dorsal extension of the arm on an armboardat an angle of more than 60 degrees to the operatingtable. When the arm is extended to a maximum of 90 de-grees and the hand is forcibly pronated, the brachialplexus is stretched across the humeral-clavicular joint,leading to injury (Figs. 24-1 and 24-2).
Suspension of the arm from the ether screen in anysurgical position (most commonly occurs in the lateraldecubitus) that produces an upper arm abductiongreater than 90 degrees with the forearm pronatedshould be avoided (Fig. 24-3). The clinical picture in pa-tients who have had a stretch injury to the brachialplexus usually is a relatively painless motor deficit com-monly affecting the upper roots (C5-7). Surgical explo-ration is not indicated for this injury. The majority of pa-tients recover within 3 months, although protracted andincomplete recoveries have been reported (Dawson &Krerup, 1989).
A brachial plexus injury distinctly related to the ster-nal retraction used in open-heart surgery has been stud-ied by several investigators (Hanson et al., 1983; Leder-man et al., 1982). According to the results of thesestudies, pain from the nerve lesion is a prominent fea-ture, and recovery is long.
Figure 24-1. Nerve damage occurs when the brachiaf plexus isstretched when the arm is abducted, extended, and-'externallyrotated and the head is deviated to the opposite side... (CourtesyDepartment of Art as Applied to Medicine, Faculty of,,Medicine,University of Toronto.)
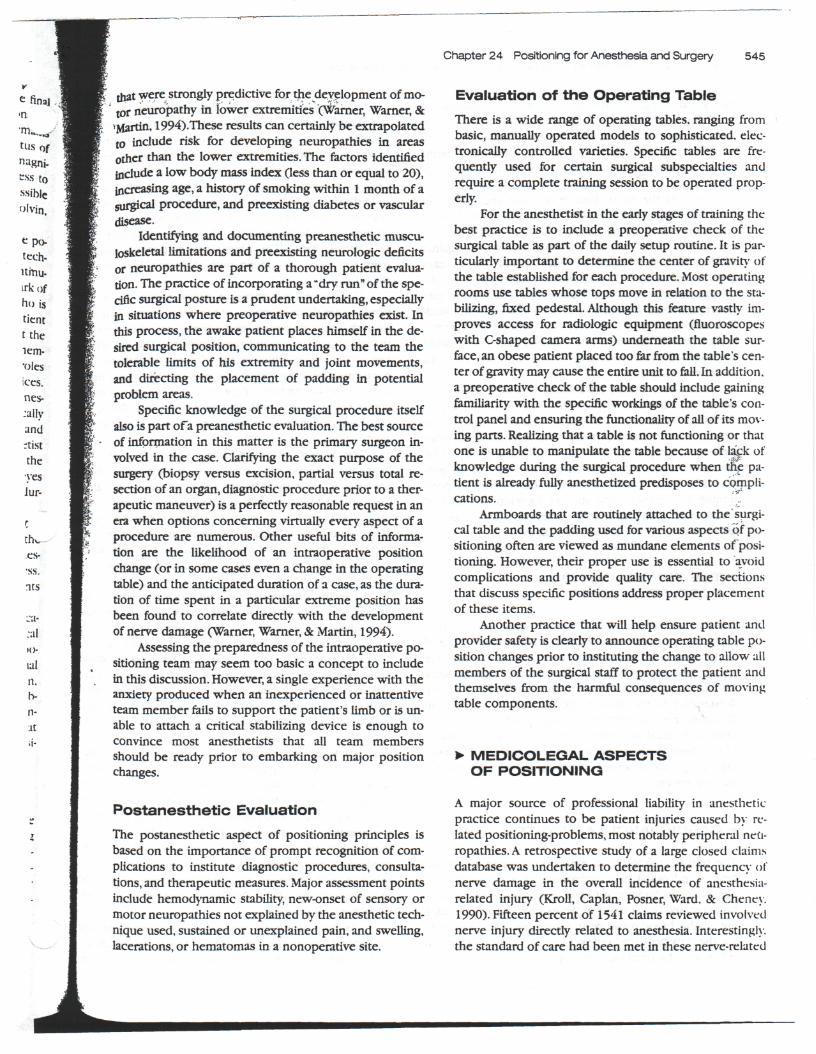
Figure 24-2. Damaging stretching of the brachial plexus around thetendon of pectoralis minor when the shoulder girdle falls back withthe arm abducted, extended, and externally rated. (CourtesyDepartment of Art as Applied to Medicine, Faculty of Medicine.University of Toronto.)

550 PART V Perioperative Management, Techniques, and Applications
Figure 24-3. Stretching of the brachial plexus around the clavicleand tendon of pectoralis minor by fixation of the abducted arm to theframe of an ether scree'n is to be avoided. (Courtesy Department ofArt as Applied to Medicine, Faculty of Medicine, University ofToronto.)
Ulnar Nerve
Perioperative lesions of the ulnar nerve are well recog-nized as a complication of surgery and anesthesia, andthey often are the focus of litigation. The ulnar nerve isespecially vulnerable to injury because it passes posteri-orly under the medial epicondyle of the elbow. At the el-bow, both the ulnar nerve and the ulnar collateral arterypass superficially through the cubital tunnel as theycourse from the arm to the forearm. Clinical manifesta-tions of ulnar nerve damage include a "clawlike" hand,impaired adduction or abduction of the medial four dig-its, and a sensory deficit in the ulnar nerve distribution.
Wadsworth (1974) describes the cubital tunnel ex-ternal compression syndrome, which is often cited as anexplanation for the unexpected appearance of postoper-ative ulnar nerve palsy. Based on this perspective, ulnarnerve damage is a complication that can theoretically beprevented by proper arm positioning. If the arm is re-stricted to the patient's side, pronation (palms down) ofthe forearm prevents excess compression on the cubitaltunnel. When the arm is abducted on a padded arm-board, there is some disagreement regarding what con-stitutes proper position of the forearm, pronation orsupination (palms up). Many practitioners believe thatforearm pronation promotes cubital tunnel contact with
flat and/or hard surfaces (ie, the metal frame of the op.crating table), resulting in a more vulnerable ulnar nerveHowever, forearm supination frees the cubital tunnelfrom compression, but may cause stretching of thebrachial plexus and potential injury.
Compression of the ulnar nerve also may resultwhen the elbow is allowed to sag slightly over the sideof the side of the operating table or when the arms arefolded across the abdomen or chest (Fig. 24-4).
With the forearm in either the pronated orsupinated position, the cubital tunnel is best protectedwhen sufficient padding is placed around the elbow andwhen the forearm is judiciously positioned. Some prac-titioners choose to alternate (when possible) the an-esthetized patient's arm between the pronated andsupinated position.
It is important for clinicians to recognize that theexact mechanism of ulnar nerve palsy has not been elu-cidated, that in fact multiple mechanisms can contributeto the problem. This situation prompts Stocking (1993)to pose the question of whether ulnar nerve palsy is apreventable complication at all. Alvine and Schurrer(1987) propose that a preexisting subclinical ulnar neu-ropathy may be worsened by the effects of a surgicalprocedure. The large retrospective study of Warner.Warner, and Martin (1994) indicates that being male iy.extremes of body habitus, and prolonged hospitalizationare risk factors strongly associated (despite proper posi-tioning) with perioperative ulnar neuropathy. The clini-cal lessons implied by these studies is that a history ofpreanesthetic ulnar neuropathies should be elicited fromthe patient and documented, all positioning precautionsshould indeed be taken to prevent a perioperative ulnurneuropathy from developing. Preventive measuresshould be carefully documented.
Figure 24-4. Ulnar nerve injury is caused by compression betweenthe medial epicondyle of the humerus and the edge of the operatingtable. Inset: Anomalous position of ulnar nerve. (Courtesy Depart-ment of Art as Applied to Medicine, Faculty of Medicine, Universityof Toronto.)

Chapter 24 Positioning for Anesthesia and Surgery 551
Radial NerveWhen the arm is compressed between the body and thevertical bar of the ether screen or any other table attach-ment (eg, Bookwalter retractor) there is danger of dam-age to the radial nerve if the nerve is pinched betweenthe screen and spiral groove of the humerus (Fig. 24-5).Clinically, radial nerve injury is manifested by wrist dropand the inability to extend the metacarpophalangealjoints due to paralysis of the extensor muscles in theforearm.
peroneal and Saphenous NervesThe most frequently damaged nerves of the lower ex-tremities are the common peroneal and its distalbranches and the saphenous (Warner, Martin, Schroeder,Offord, & Chute, 1994). The common peroneal nerve isinjured in the lithotomy position when the legs areplaced in stirrups. This posture causes the flbular neck torest against the vertical bar of the lithotomy stirrup, thuscompressing the nerve (Fig. 24-6).
Common peroneal neuropathies are manifested byfoot drop, loss of dorsal extension of the toes, an inabil-ity to evert the foot, and sensory loss in the dorsal areaof the foot. The major preventive measure is to place softpadding between the leg and the stirrup.
Saphenous nerve damage occurs in the lithotomyposition when the legs are suspended lateral to the ver-
CORRECTFigure 24-6. Common peroneal nerve compression betweenlithotomy stirrup and neck of fibula. This may be avoided by padding(see inset). (Courtesy Department of Art as Applied to Medicine,Faculty of Medicine, University of Toronto.)
Figure 24-5. Damaging compression of the radial nerve betweenthe humerus and an ether screen. (Courtesy Department of Art asApplied to Medicine, Faculty of Medicine, University of Toronto.)
CORRECTFigure 24-7. Saphenous nerve compressed between lithotomystirrup and tibia. (Courtesy Department of Art as Applied toMedicine, Faculty of Medicine, University of Toronto.)
552 PART V Perioperative Management, Techniques, and Applications
tical brace of the stirrup, potentially causing compres-sion between the stirrup and the tibia (Fig. 24-7), orwhen excessive pressure on the medial aspect of the calfor tibial condyle is placed by the "knee crutch" stirrup.
Paresthesias along the medial and anteromedial as-pects of the calf are the major symptoms of saphenousnerve lesions. Prevention also is accomplished by usingsoft padding between the legs and stirrup apparatus.
»> BASIC POSITIONS USED INANESTHESIA AND SURGERY
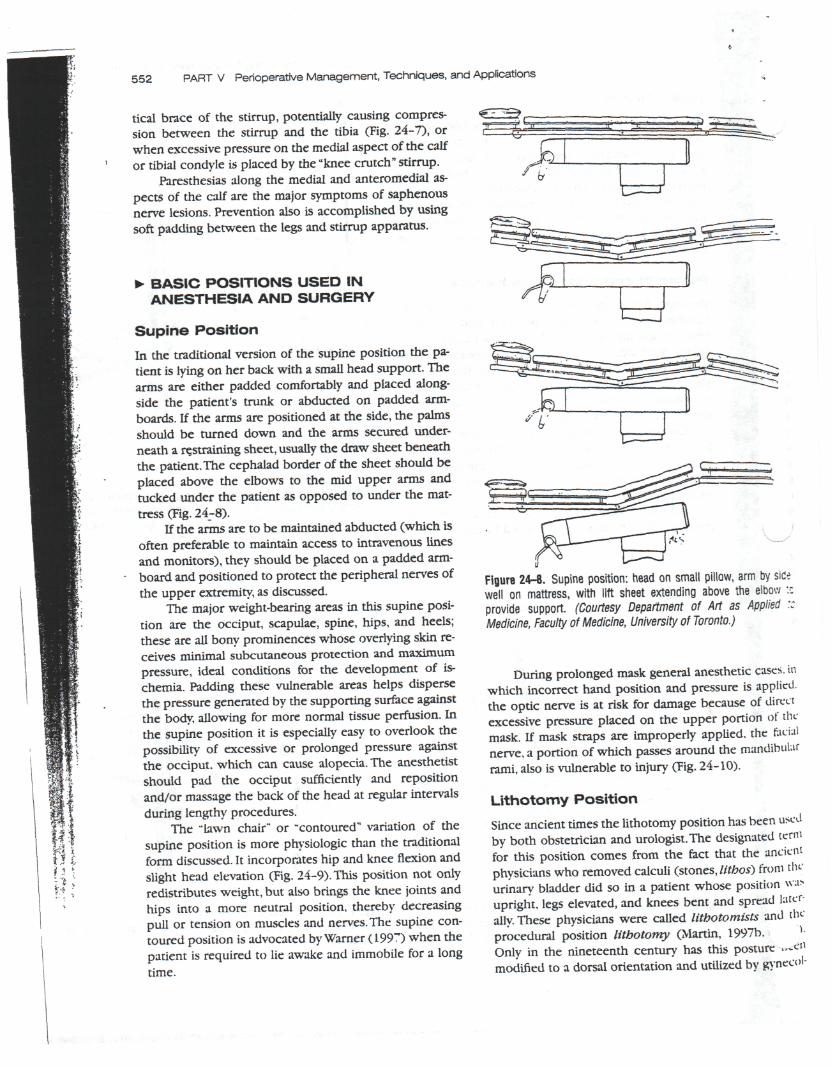
Supine PositionIn the traditional version of the supine position the pa-tient is lying on her back with a small head support. Thearms are either padded comfortably and placed along-side the patient's trunk or abducted on padded arm-boards. If the arms are positioned at the side, the palmsshould be turned down and the arms secured under-neath a restraining sheet, usually the draw sheet beneaththe patient. The cephalad border of the sheet should beplaced above the elbows to the mid upper arms andtucked under the patient as opposed to under the mat-tress (Fig. 24-8).
If the arms are to be maintained abducted (which isoften preferable to maintain access to intravenous linesand monitors), they should be placed on a padded arm-board and positioned to protect the peripheral nerves ofthe upper extremity, as discussed.
The major weight-bearing areas in this supine posi-tion are the occiput, scapulae, spine, hips, and heels;these are all bony prominences whose overlying skin re-ceives minimal subcutaneous protection and maximumpressure, ideal conditions for the development of is-chemia. Padding these vulnerable areas helps dispersethe pressure generated by the supporting surface againstthe body, allowing for more normal tissue perfusion. Inthe supine position it is especially easy to overlook thepossibility of excessive or prolonged pressure againstthe occiput, which can cause alopecia. The anesthetistshould pad the occiput sufficiently and repositionand/or massage the back of the head at regular intervalsduring lengthy procedures.
The "lawn chair" or "contoured" variation of thesupine position is more physiologic than the traditionalform discussed. It incorporates hip and knee flexion andslight head elevation (Fig. 24-9). This position not onlyredistributes weight, but also brings the knee joints andhips into a more neutral position, thereby decreasingpull or tension on muscles and nerves. The supine con-toured position is advocated by Warner (199") when thepatient is required to lie awake and immobile for a longtime.
Figure 24-8. Supine position: head on small pillow, arm by sidewell on mattress, with lift sheet extending above the elbow •.provide support. (Courtesy Department of Art as Applied :Medicine, Faculty ol Medicine, University of Toronto.)
During prolonged mask general anesthetic cases, inwhich incorrect hand position and pressure is applied,the optic nerve is at risk for damage because of directexcessive pressure placed on the upper portion of themask. If mask straps are improperly applied, the facialnerve, a portion of which passes around the mandibularrami, also is vulnerable to injury (Fig. 24-10).
Lithotomy PositionSince ancient times the lithotomy position has been usedby both obstetrician and urologist. The designated termfor this position comes from the fact that the ancientphysicians who removed calculi (stones, lithos) from tin-urinary bladder did so in a patient whose position va>upright, legs elevated, and knees bent and spread later-ally. These physicians were called lithotomists and tin-procedural position lithotomy (Martin, 1997b.Only in the nineteenth century has this posture —enmodified to a dorsal orientation and utilized by gynecol-

Chapter 24 Positioning for Anesthesia and Surgery 553
Figure 24-9. Supine position: Establishing the "lawn chair"position with hip and knee flexion and a pillow for the head. (FromMartin [1997]. Reprinted with permission.)
ogists; it may have been the most convenient arrange-ment by which to visualize the reproductive tract of thefemale and conduct a bimanual examination.
The primary untoward effect of the lithotomy posi-tion on an anesthetized patient's circulatory system ismanifested at the termination of the procedure as the pa-
Figure 24-10. Motor root of facial nerve injured by traction on theangle of the mandible. (Courtesy Department tf Art as Applied toMedicine, Faculty of Medicine, University of Toronto.)
tient is taken out of the lithotomy position. This maneu-ver may be accompanied by a dangerous lowering of theblood pressure, caused by too rapid a filling of the dilatedperipheral vascular bed of the previously elevated ex-tremities. The degree of hypotension is directly propor-tional to the amount of impairment of the vasoregulatorymechanisms of the upper and lower extremities, whichin turn is predicated by the patient's cardiovascular re-serve, the anesthetic level, duration of time spent in litho-tomy, and the intravascular volume (Batillo & Hendler,1993). Fortunately, the degree of hypotension also highlydepends on the speed with which the lower extremity islowered. The circulatory insult can be minimized oreven eradicated by slowly, steadily lowering the legs andlightening the anesthetic level and restorating the in-travascular volume beforehand.
A study by Little (I960) reveals that the vital capac-ity in the lithotomy position in awake, spontaneouslybreathing humans is reduced by 18%. However, Henschelet al., (1957) and Jones and Jacoby (1955) had estab-lished that tidal volume (VT) provides a better reflectionof the respiratory condition of the anesthetized patient.Their data indicated that the lithotomy position caused a3% decrease in VT, that an additional 10 degrees of head-down tilt caused a 14% decrease, and that a 20-degreehead-down tilt caused a 15% decrease in VT. It also is wellrecognized that in lithotomy there is a correlation be-tween the degree of thigh flexion on the abdomen andVT decreases (Walsh, 1994). A tenet of pulmonary func-tion in patients under anesthesia is that ventilatory re-strictions caused by the anesthetic state itself increaseprogressively during the course of the operation; if an al-ready decreasing VT is further reduced by a certain pos-ture (eg, lithotomy plus head-down tilt), the potential forgeneral fatigue of the respiratory muscles becomesgreater as time spent in the posture increases. From aclinical point of view, in the vast majority of patients ma-jor respiratory limitations produced by the lithotomy po-sition can be corrected using an endotracheal tube andassisted or controlled ventilation.
Extremity-supporting devices attached to the frameof the operating table are needed to place the patient inthe lithotomy position. The three most common config-urations for these leg holders are the "candy cane pole"(Fig. 24-6), the "knee crutch," and the "knee crutch withan adjustable knee and foot support" (Fig. 24-1,1).
The candy cane pole should be used for relativelyshort procedures because the apparatus design (freeswinging cloth slings for the feet) allows the lower ex-tremities to move. The legs are thus easily displaced fromtheir proper position either by operative team memberswho inadvertently push against the patient or the stir-rups or by the patient (who may or may not be anes-thetized). As described in the section relating to periph-eral nerve injuries, the common peroneal and saphenous

f!a554 PART V Perioperative Management, Techniques, and Applications
Figure 24-11. Lithotomy position: Note placement of legs intostirrups and buttocks on table. (From Martin [1997]. Reprinted withpermission.)
nerves are at risk when the lithotomy position is estab-lished with the candy cane poles.
The advantage of the knee crutch with the leg andfoot support is that it evenly distributes the weight of thelower extremity. Its proper use depends on team mem-bers who have the knowledge and take the time to ad-just the hip, knee, and foot supports according to the pa-tient's anatomy. The obturator, saphenous, and femoralnerves are all at risk when this particular leg holder isused because the weight of the legs within the supportcan cause compression of the aforementioned nerves.Compression syndromes have been well established aspotential complications of several variations of the litho-tomy position. Martin (1992), in an extensive review ar-ticle, delineates some clear guidelines for anesthetists toemploy to avoid this complication, including maintainingblood pressure at normal ranges for the patient as hy-potension and loss of driving blood flow in elevated ex-tremities facilitates the muscle compression and is-chemic process.
There are several basic steps to place the patient inthe lithotomy position. First, it is imperative that theequipment chosen be appropriate to the patient'slength, body habitus, and range of both hip and kneejoints. Second, if both extremities are to be placed inholders, both legs must be flexed and extended simulta-neously to prevent a torsion injury to relaxed musclesand ligaments or joint and spinal injury, including hip dis-articulation. Backache is not an uncommon postopera-tive complaint following lithotomy. Third, symmetrical
placement of both legs must be established in the hold,ers, again to prevent rotational spine or joint injury. Theanesthetist with a clear vantage point at the head of th*surgical table often is consulted to determine whetherthe patient is symmetrically placed. Finally, the -takedown" maneuver of the lithotomy position entails a coordinated, smooth, slow lowering of the legs.
There are several options for proper arm placementin the lithotomy position: Both arms on padded boards-one arm on a board, the other placed across the chest: orboth arms on the chest. The anesthetist must adhere 10the precautions previously discussed when placing thearms on armboards. When positioning the arm or armson the chest, care must be taken to ensure that the el-bow does not rest on the metal edge of the operatingtable. Not only does this place pressure on the ulnarnerve, but also it inadvertently incorporates the patientinto the electrocautery grounding site. The arm shouldnot be acutely flexed across the chest. An angle of morethan 100 degrees at the elbow can compromise the ar-terial supply to the lower arm and hand. Finally, placingthe arm at the patient's side is discouraged. The fingersmay potentially extend beyond the table break, becomeentrapped between the two table sections and, as thelower piece is raised when the surgical procedure i<completed, result in damage to or even amputation ofone or more fingers.
Head-Down TiltInterestingly in 1956 Inglis and Brooke stated "From thestandpoint of the anesthesiologist, placing a patient in Jhead-down position has real problems and few assets."Yet in current anesthesia practice, despite the fact thatmost anesthesia providers continue to hold the sameopinion as Inglis did in the late 1950s, the head-down tiltis used daily, frequently with the lithotomy position anda pneumoperitoneum, as required for laparoscopicsurgery. The use of head-down tilt still presents reulproblems and a host of challenges to the anesthetist, pri-marily because of a variety of cardiovascular and respira-tory insults.
The following represents a simplistic summary otthe cardiovascular response of a healthy, normovoleniic.anesthetized patient to minimal head-down tilt (MHI)T).the term currently used to describe a tilt ranging from10 to 20 degrees. The central blood volume is incrr.istrdsignificantly (from 500 to 1000 mL).The rapid rise of hy-drostatic pressure is sensed by the arterial barorecep-tors, which stimulates the expected reflex vasodihuationand decreased stroke volume, resulting in decreased cudiac output and reduced perfusion of vital organs. Thc
brain is especially vulnerable to decreased perfusion be-cause a head-down tilt also increases cerebral venouspressure, compromising cerebral perfusion pressure-

Chapter 24 Positioning for Anesthesia and Surgery 555
tilt in patients with known or suspected in-athology is absolutely contraindicated,
The vast majority of patients have an adequate car-diopulmonary reserve, and the physiologic challenge ofdie head-down tilt is met with normal compensatory re-sponses. Assuming proper anesthetic management, pa-tients tolerate the position well. In contrast, anesthetizedpatients with diminished cardiopulmonary reserveclearly do not tolerate a MHDT, as evidenced by rightventricular dilation, decreased right ventricular ejectionfraction, and impaired oxygenation (Reich, Konstadt,Raissi, Hubbard, & Thys, 1989). Steep head-down tilt(SHDT), or approximately 30 to 45 degrees of tilt, has thepotential to increase central blood volume and pul-monary blood flow enough to cause acute cardiac failurein normal individuals, hence the risk for failure in alreadycompromised patients is quite significant. Furthermore,when returning to the horizontal position, the patientwith decreased cardiovascular reserve will be very muchat risk for a severe hypotensive episode. Limiting or elim-inating SHDT in these patients is the best preventive
. measure for such untoward cardiac events. If one mustbe placed in MHDT, a slow, controlled shift of position,along with repetitive checks of the blood pressure facili-tate the ability of compromised vasculature to adjust to anewly enlarged circulatory capacitance.
The potential for MHDT or SHDT to mask intraoper-ative blood loss has very important implications for theclinician. Unsuspected or underestimated hypovolemiawill manifest as sudden hypotension when the patient isreturned to the supine and horizontal position. Accuratefluid deficit calculation and appropriate and timely re-placement are the key elements to avoiding this situation.
An allusion was made earlier to the frequent use ofthe head-down tilt during laparoscopic surgery. Duringrecent years, advances in instrumentation and surgicaltechnique have resulted in much more extensive, pro-longed laparoscopic procedures, especially in the fieldsof gynecology and general surgery. These intraabdominalprocedures require the establishment of a pneumoperi-toneum. In addition, MHDT, SHDT, and various degrees oflithotomy are positions that the anesthetist commonlyanticipates as part of the procedure. The cumulative ef-fects of these factors on the patient's cardiopulmonarysystem represent the bulk of the anesthetic challenge. A1989 study (Johannsen, Andersen, & Juhl) of healthywomen undergoing elective diagnostic laparoscopiesdocuments decreased stroke and cardiac indices (an av-erage decrease of 42% for each index during periods ofmaximum hemodynamic stress) that were directly cor-related to abdominal insufflation and head-down tilt. De-spite these significant numerical changes, patients withhealthy cardiac function tolerate such hemodynamicstresses, in part because anesthesia clinicians adhere tobasic principles of safe positioning.
A recent study by Harris, Ballantyne, Luther, and Per-rino (1996) of elderly patients with significant coexistingcardiopulmonary disease undergoing elective laparo-scopic colectomies investigated cardiovascular perfor-mance with special emphasis on the response to SHDT.The magnitude of the adverse hemodynamic responsesof these patients to the routine maneuvers of the proce-dure prompted the authors to recommend the use ofpulmonary artery catheterization and/or transesopha-geal echocardiography in this setting. Most practitionerswould agree that the prudent approach in this settingwould be to establish clear benefits of proceeding witha laparoscopic approach (entailing obligatory placementin some degree of head-down tilt) over the risk of theprocedure.
The respiratory effects of the head-down tilt are theresult of the abdominal contents being pushed upagainst the diaphragm, the respiratory muscle that doesmost of the work of breathing under anesthesia. Theworkload of the diaphragm is greatly increased. In addi-tion to lung ventilation it must lift the viscera, predispos-ing the patient to atelectasis. Pulmonary compliance, VT,and FRC also are diminished, resulting in increased workof breathing and varying degrees of ventilation-perfu-sion mismatch. Gravitational forces cause an increasedpulmonary blood volume, contributing to the aforemen-tioned decrease in pulmonary compliance.
The anticipated placement of an anesthetized pa-tient in MHDT or SHDT obligates the anesthetist to insertan endotracheal tube and to use positive-pressure, con-trolled, mechanical ventilation. Judicious manipulation ofventilatory settings enables the delivery of adequate ven-tilation and oxygenation. The position of the endotra-cheal (ET ) tube while the patient is in a head-down tiltmust be monitored carefully. A tube previously wellpositioned in the trachea can enter the right mainstembronchus after the patient is tilted head down as the ab-dominal and thoracic contents are pushed cephalad. TheET tube position should be checked after each positionalmodification, however minor, and periodically through-out the period in which the patient is in a head-downorientation.
Laparoscopic procedures require MHDT or SHDTand a pneumoperitoneum introduces an additional chal-lenge to the anesthetist: an increased CO2 load due to thecontinuous insufflation of gas must be excreted via ven-tilation to avoid hypercapnia and acidosis. According toHirvonen, Nuutinen, and Kauko (1995), it seems moreefficient to handle the increased ventilation require-ment by increasing VT and keeping the respiratory- fre-quency low.
The caveats discussed in the previous sections onpreventing peripheral neuropathies secondary to posi-tioning certainly apply to this position. An additionalpotential etiology of brachial plexus injury in the head-
556 PART V Perioperative Management, Techniques, and Applications
down tilt occurs when shoulder braces, attached to thesurgical table, are used to prevent the patient from slid-ing in a cephalad direction. If shoulder braces are used,they should be placed laterally so that their pressure ison the area of the acromioclavicular articulation and notdirectly on either the clavicle or the root of the neck. Awide variety of options for securing the patient safely tothe table in this position are explained comprehensivelyin Martin (1997a, pp. 95-124).
Lateral Decubitus Position
Lateral decubitus often is referred to as the standard tho-racotomy position because it affords optimal exposureand access to thoracic structures. In addition to thoracicprocedures, this position is utilized for cardiac, thoraco-vascular, and gastroesophageal surgeries. The flexed vari-ation of the lateral decubitus is most commonly used inurologic procedures (nephrectomies); still other slightvariations allow this position to be used in neurosur-gical (craniotomies, laminectomies) and orthopedic (hiparthroplasties) procedures.
Utilizing the correct terminology when describingthis position is helpful in protecting the patient and thecare team from-instituting a surgical intervention on theincorrect side of the patient. Lateral, lateral decubitus,and lateral recumbent are synonymous; the term gener-ally used is lateral decubitus. Right lateral decubitusrefers to a position in which the patient is lying on theright side and is appropriate for surgical procedures inwhich the left side is uppermost and vice versa.
An anesthetized patient in virtually all of the lateralpositions exhibits a decrease in arterial pressure; the low-est pressures have been observed in the right lateral de-cubitus and the right lateral flexed decubitus variations.Cardiac output tends to remain stable in all of the lateralpositions (Eggers, DeGroot, Tanner, & Leonard, 1963).The position-related blood pressure changes are attribut-able in most cases to a reduced systemic vascular resis-tance as opposed to decreased venous return. However,in the extreme flexed lateral position with the lower ex-tremities markedly dependent, impaired venous returncauses the decrease in arterial pressure.
Although most clinical studies have documentedthat cardiovascular compromise due to the lateral posi-tions per se is uncommon, cardiovascular collapse dur-ing lateral positioning still is possible in the anesthetizedpatient. In addition, the lateral decubitus position causesa shift of the mediastinum toward the downside and ro-tates the heart on its axis, relative "anatomical" changesthat can interfere with venous return and cardiac output.
The mechanical interference with thorax expansioncaused by the lateral decubitus position in an anes-thetized patient is manifested by a 10% to 14% decreasein tidal volume (Henschel et al., 1957), irrespective of a
regional or general anesthetic. The effects of the ladecubitus position on the respiratory system aretionally discussed in terms of ventilation/perfiisj()n
(V/Q) ratios or mismatch. As a clinician, one is inter-ested in V/Q ratios that are generated in the four scenar-ios listed in the next paragraph. To understand thechanges in ventilation, remember that it is the mechanicalefficiency of contraction of either the upper lung hemidi.aphragm or the lower lung hemidiaphragm that eon-fers preferential ventilation. In anesthetized states, thehemidiaphragm of the lower lung becomes mechanicalhless efficient and contracts less, and therefore ventilationis decreased.
• Scenario 1. In an awake, spontaneously breath-ing patient Q is greater in the lower lung becauseof gravitational flow while preferential V occimin the lower lung, resulting in minimal V/Q mis-match.
« Scenario 2. In an anesthetized, spontaneouslybreathing patient with a closed chest Q is greaterin the lower lung and V is greater in the upperlung, resulting in V/Q mismatch in both lungs.
• Scenario 3. In an anesthetized, paralyzed patieniwith a closed chest Q is greater in the lower lung.and, because paralysis and positive pressure ven-tilation further decrease the mechanicalciency of the lower hemidiaphragm, V is ev*,..-greater in the upper lung, resulting in increasedV/Q mismatch.
• Scenario 4. In an anesthetized, paralyzed patientwith an open chest Q is greater in the lower lung.and, because the upper lung is no longer re-stricted by the chest wall, it becomes even morecompliant, greatly increasing ventilation, result-ing in a further increase in V/Q mismatch.
From a practical point of view, any degree of" Y/omismatch predisposes the patient to hypoxia: under-standing when and why a patient is at higher risk for tin-undesireable state provides the rationale by which theanesthetist will choose ventilatory parameters, whetheror not paralysis is advantageous, as well as the percentage of oxygen to deliver. As it is not within the scopeof this chapter, this discussion does not take into accountthe various techniques by which differential ventilationof either lung can be accomplished. The reader is re-ferred to the works of Cohen (1995).
In the basic lateral decubitus position the patient i*turned 90 degrees to the horizontal surface of the tahlfand stabilized. Flexing the lower leg at the hip and kneewhile keeping the upper leg straight enhances stabilityadditional stabilizing devices include broad strips ofelastic adhesive tape, velcro-type bands, or quick-re,belts. All of these devices should be placed acro^the hips just below the iliac crest and across the show'

Chapter 24 Positioning for Anesthesia and Surgery 557
der and secured to the undersides of the operating tabletp ensure stability. Another alternative device to stabilizethe patient is the bean bag (Vacu-Pac) that is shaped us-ing a vacuum and placed beneath the patient as amolded support. Once the pelvics and thorax have beenstabilized, the bony prominences of the lower extremi-ties should be padded.
Proper placement of the arms in the basic positionis important to adding stability, as well as protecting theupper extremity peripheral nerve groups. The downsidearm usually is flexed and tucked under the pillow thatsupports the head. A small chest pad must be placedunder the downside thorax just caudad to, but not in, theaxilla; the purpose of this pad is to relieve pressure fromthe head of the downside humerus and to avoid com-pression of the brachial plexus. A covered, 1-L intra-venous fluid bag frequently is used as a chest pad. Thisaccessory is very commonly referred to as the axillaryroll, a misnomer, that often is improperly positioned byuninformed individuals. During the final position check,the anesthetist must verify proper placement of thechest pad.
The upper arm usually is placed according to surgi-cal needs. For nonthoracic procedures, there are severalsafe options: the arm can rest in an extended position ontop of several pillows placed on an armboard positioned90 degrees to the table, or the arm can be flexed at theelbow and extended to varying degrees and supportedon a pillow that lies adjacent to the patient's face. Otheroptions for upper-arm support in an elevated positionare a double-deck ("airplane") armboard (Fig. 24-12),Mayo stand, or suspension from the ether screen. Theuse of the last three items often are discouraged becausethey greatly increase the susceptibility of upper-armstretch or compression. With any of these options, bodyalignment must be maintained, brachial plexus stretchmust be avoided, and adequate perfusion of both armsand hands must be ensured via pulse palpation, capillaryrefill check, or a pulse oximeter probe.
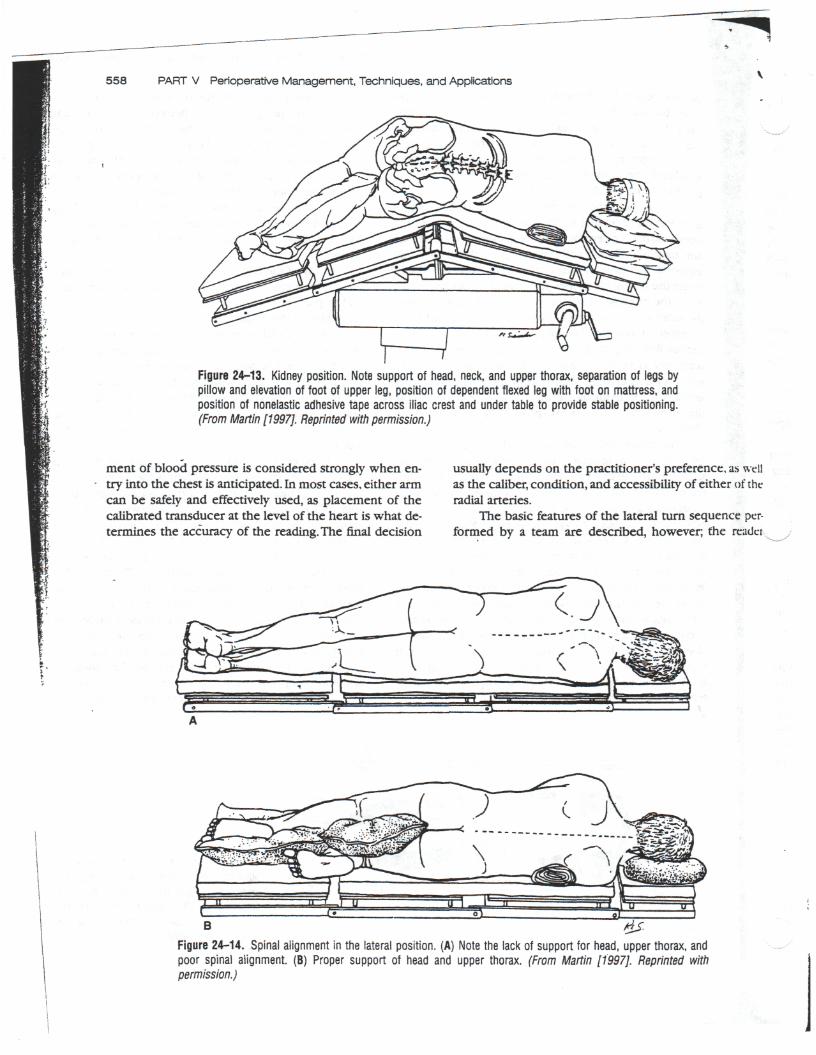
The flexed lateral decubitus (kidney) position is es-tablished by using the break between the upper andlower sections of the table. This break must be at thelevel of the iliac crest (Fig. 24-13). The "flex" in the tablecauses the lateral muscles to be stretched. The table canbe placed in a head-up tilt, making the operative site par-allel to the floor. The lower leg usually is slightly flexed,the upper leg remains extended, and a pillow or paddingis placed between the two. Care must be taken not to al-low the legs to overhang or touch the table's metalframe.
In any of the lateral decubitus positions, proper cer-vical spine alignment with head and neck support is cru-cial to prevent neck injury or brachial plexus injury viastretching of the upside neck (Fig. 24-14). The downsideeye, ear, and facial nerve must be protected from exces-sive pressure or rough surfaces. Ocular damage to thedownside eye is a particularly devastating complicationconsidering it is highly preventable. Corneal abrasionsare the result of careless eyelid protection, and retinalartery thrombosis (which can cause permanent blind-ness) is caused by excessive pressure on the down-side eye.
Placement of a blood pressure-measuring device inthe lateral decubitus position often is the focus of a pre-operative planning session. If a noninvasive blood pres-sure (NIBP) cuff is to be used, the following principlesshould be recognized: (1) there is approximately a32-mm Hg discrepancy in blood pressure between thetwo arms in the lateral position (the upper arm will in-dicate the lower of the two numbers); (2) the NIBP i.smore likely to be underestimated (relative to the truepressure of the heart or the brain) when the cuff isplaced in the upper arm; some practitioners prefer thisto minimize the risk of unrecognized hypotension,which may be more problematic than unrecognized hy-pertension; (3) placing the NIBP cuff on the downsidearm may compress the axillary artery (Lawson & Meyer,1997). Using an intraarterial catheter for direct measure-
••• \\ Figure 24-12. Lateral position. Note theplacement of support, flexion of lower leg,extension of upper leg, separation by pillow.placement of IV catheter, grounding pad.blood pressure cuff, and strap across iliaccrest. (From Martin [1997]. Reprinted withpermission.)
558 PART V Perioperative Management, Techniques, and Applications
Figure 24-13. Kidney position. Note support of head, neck, and upper thorax, separation of legs bypillow and elevation of foot of upper leg, position of dependent flexed leg with foot on mattress, andposition of nonelastic adhesive tape across iliac crest and under table to provide stable positioning.(From Martin [1997]. Reprinted with permission.)
ment of blood pressure is considered strongly when en-try into the chest is anticipated. In most cases, either armcan be safely and effectively used, as placement of thecalibrated transducer at the level of the heart is what de-termines the accuracy of the reading. The final decision
usually depends on the practitioner's preference, us wellas the caliber, condition, and accessibility of either of theradial arteries.
The basic features of the lateral turn sequence per-formed by a team are described, however; the reudei
BFigure 24-14. Spinal alignment in the lateral position. (A) Note the lack of support for head, upper thorax, andpoor spinal alignment. (B) Proper support of head and upper thorax. (From Martin [1997]. Reprinted withpermission.)

Chapter 24 Positioning for Anesthesia and Surgery 559
should note that the many fine details or variations ofthis sequence are best gained by demonstration and ex-perience as well as studying a more in-depth referencetext (Lawson & Meyer, 1997).The patient must be turnedas a unit, and body alignment must be maintained at alltimes. A minimum of three people are required: a coor-dinator (the anesthetist) who supports and turns the headand neck and maintains the airway; one individual as-signed to turn and support the shoulders and thorax; andone individual designated to turn and support the hipsand legs. It is highly desirable to have a fourth team mem-ber to place the chest pad under the downside thorax, asthe head, neck, shoulder, and thorax are slightly elevatedand to place the appropriate padding while the patientis being secured to the table.
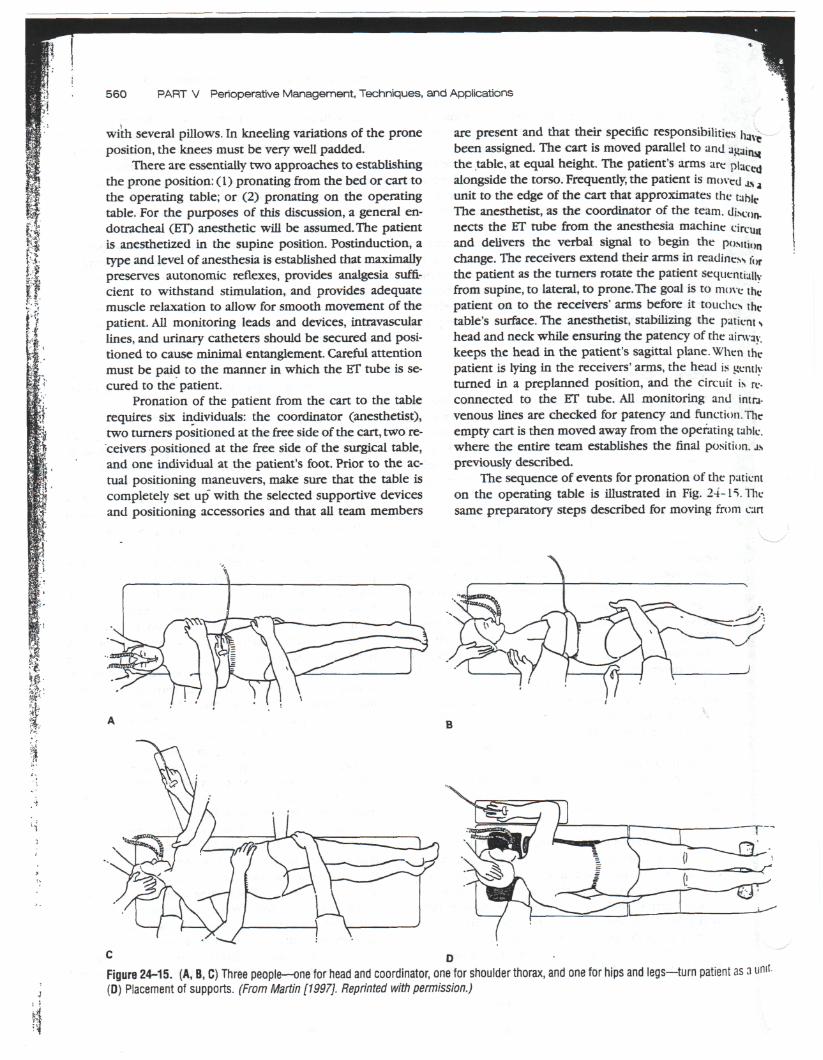
Prone Position
The prone position also is referred to as the ventral de-cubitus, or face-down, position. It is the most awkwardfor patients of all ages and sizes. There are numerousvariations of this position: the Georgia,cation of the Georgia, the Overhold,Brown, to name a few. In addition, sevibles designed specifically for variatioiposture carry the designer's name.
In a healthy anesthetized individu;diovascular problems are unusual in thdespite the usual depression of thesatorv autonomic reflexes. However, if
he Smith modifi-and the Sellor-ral operating ta-is of the prone
1, significant car-prone position,
lormal compen-he inferior vena
i
cava (IVC) and the femoral veins are compressed, venousreturn can be severely compromised and cause a de-crease in cardiac filling and hypotension. A compressedJVC forces venous return to occur through vessels thathave lesser flow capabilities, often the venous plexus ofthe vertebral column (Walsh, 1994). Decreased strokevolume and cardiac index have been Demonstrated inanesthetized prone patients (Backofen & Schauble,1985). Generally speaking, if IVC and flmoral vein com-pression are avoided, the untoward cardiovascular sideeffects of the prone position will be minimized.
If the patient's head is positioned below the level ofthe heart, venous pressure increases, causing increases inthe carotid vasculature, increased intracranial pressure,venous congestion of the head and neck, and ocularedema. Improper positioning causes compression of thechest and abdomen and the work of breathing is greatlyincreased. Furthermore, mechanical ventilation may beassociated with increased airway pressures and largertidal volumes, potentiating the risk for pulmonary baro-trauma (Martin. We, pp. 155-196). The study by Pelosiet al. (1995) demonstrates that, if the position is accom-plished properly, ensuring free abdominal and chestmovement, lung and chest wall mechanics are not signif-icantly altered, and lung volumes (VT and FRC) are
markedly improved, as is oxygenation.The same group ofinvestigators (Pelosi et al., 1996) demonstrated a similarfinding in obese (BMI greater than 30 kg/m2) patients.
An essential feature of the classic, horizontal proneposition is the ventral support device, either a chest rollor frame. The cephalad end of the support deviceshould be placed just below the clavicles and shouldextend just to the iliac crest. Free excursion of the an-terior thorax and the abdominal wall must be possiblewhen the patient is pronated on the device. Placing thefemale breasts can be challenging, especially if they arelarge and pendulous. The question posed by the posi-tioning team is whether to displace the breasts (relativeto the ventral supportive device) medially or laterally.Although Martin (1997c, pp. 155-196) generally recom-mends a medial displacement, it is prudent to individu-alize this particular decision according to the patient'sanatomy. The male genitalia should not be compressedor rotated.
The arms can be either extended above the head orplaced alongside the torso. If the former option is cho-sen, the arms must be placed on well-padded armboards,which are positioned parallel to the table. The armsshould be minimally abducted and the upper arm ex-tended and the elbow flexed. The upper arm should besupported to the same elevation as the thorax to preventpull and stretch on the brachial plexus. Padding shouldbe placed so that there is no pressure on the axilla or theelbow. The presence of effective radial pulses should bepalpated regularly. The option of placing the arms along-side the torso should be exercised in patients withknown or suspected thoracic outlet syndrome (TOS).such as those with a history of inability to raise theirhands above their head normally without experiencingnumbness, tingling, or pain. Arms placed alongside thetorso for any reason should have a restraining sheet thatis snug enough to secure the arms, without compromis-ing circulation. The usual vulnerable areas should bepadded, and adequate radial pulses established.
Head and neck positioning must be approachedwith an extreme degree of care, followed by frequentchecking for the development of untoward effects, espe-cially in the downside eye, ear, facial structures,and nose.Injury* to these structures can easily occur from pro-tracted pressure from the weight of the head against thetable surface. If there are no special headrests, the headshould be supported and padded, turned slightly to oneside, avoiding neck torsion. Extreme head or neck rota-tion may compress both the vertebral and carotid arter-ies and their branches. Managing a severely arthritic orunstable cervical spine represents a special challengeand should be extensively discussed with the entire po-sitioning team prior to instituting a position change.
Padding should be placed under the iliac crests andknees, and the dorsum of the feet should be supported
560 PART V Perioperative Management, Techniques, and Applications
1
iII
Jr
with several pillows. In kneeling variations of the proneposition, the knees must be very well padded.
There are essentially two approaches to establishingthe prone position: (1) pronating from the bed or cart tothe operating table; or (2) pronating on the operatingtable. For the purposes of this discussion, a general en-dotracheal (ET) anesthetic will be assumed. The patientis anesthetized in the supine position. Postinduction, atype and level of anesthesia is established that maximallypreserves autonomic reflexes, provides analgesia suffi-cient to withstand stimulation, and provides adequatemuscle relaxation to allow for smooth movement of thepatient. All monitoring leads and devices, intravascularlines, and urinary catheters should be secured and posi-tioned to cause minimal entanglement. Careful attentionmust be paid to the manner in which the ET tube is se-cured to the patient.
Pronation of the patient from the cart to the tablerequires six individuals: the coordinator (anesthetist),two turners positioned at the free side of the cart, two re-ceivers positioned at the free side of the surgical table,and one individual at the patient's foot. Prior to the ac-tual positioning maneuvers, make sure that the table iscompletely set up" with the selected supportive devicesand positioning accessories and that all team members
are present and that their specific responsibilities hav
been assigned. The cart is moved parallel to and againwthe table, at equal height. The patient's arms are placedalongside the torso. Frequently, the patient is moved a.s iunit to the edge of the cart that approximates the tableThe anesthetist, as the coordinator of the team. di.x.()n.nects the ET tube from the anesthesia machine circuuand delivers the verbal signal to begin the p()Mti,m
change. The receivers extend their arms in readiness f()r
the patient as the turners rotate the patient sequentiallyfrom supine, to lateral, to prone.The goal is to move thepatient on to the receivers' arms before it touches thetable's surface. The anesthetist, stabilizing the patient shead and neck while ensuring the patency of the airway,keeps the head in the patient's sagittal plane. When thepatient is lying in the receivers' arms, the head is gentlyturned in a preplanned position, and the circuit i* re-connected to the ET tube. All monitoring and intra-venous lines are checked for patency and function.Theempty cart is then moved away from the operating table.where the entire team establishes the final position. a.spreviously described.
The sequence of events for pronation of the patienton the operating table is illustrated in Fig. 24-15. Thesame preparatory steps described for moving from can
Figure 24-15. (A, B, C) Three people—one for head and coordinator, one for shoulder thorax, and one for hips and legs—turn patient as a unit-(D) Placement of supports. (From Martin [1997]. Reprinted with permission.)

Chapter 24 Positioning for Anesthesia and Surgery 561
to table are followed. The team, coordinated by the anes-thetist, moves the patient in the supine position towardthe turners' side of the table. Almost immediately, thepatient is turned to the lateral position briefly, thenpronated, after which the team members establish the fi-nal, proper posture.
Head-Elevated PositionThe classic, high-sitting position is used in neurosurgeryfor occipital craniotomies and cervical laminectomies.The lower-sitting positions, more commonly called the"beach chair" or "barber chair" are used in head, neck,and shoulder surgeries.
The circulatory changes in the classic sitting posi-tion are due to the profound effect of gravity. Pooling ofvenous blood in the dependent periphery is increasedby the vasodilatory and cardiac depressing effects of gen-eral anesthesia. The diminished venous return causes a12% to 20% decrease in stroke volume and cardiac index,with a compensatory increase in both the pulmonary
. and systemic vasculature. Most notable is a 15% decreasein the cerebral perfusion pressure (Milde, 1997). This isproblematic for patients with cerebrovascular disease,cervical spine changes, or longstanding hypertension.
Because of gravitational forces, respiratory mechan-ics and lung volumes are increased, as one would sur-mise. In fact, much less peak inspiratory pressure is re-quired to expand the alveoli of an individual in thesitting position than in the supine position, favoring thedevelopment of hyperventilation and excessive hypocar-bia. For neurosurgical patients or those with cerebrovas-cular disease, the resultant vasoconstrictive decrease incerebral blood flow could be disastrous. In the sitting po-sition, V/Q mismatch also can occur, as the upper-lungzones are far less perfused, yet more easily ventilated.
The risk of an air embolism in head-elevated posi-tions is well established. When a surgical field is locatedhigher than the level of the heart, a subatmospheric pres-sure differential is established, and air is more easily en-trained into open venous channels, with subsequent en-try into the central venous system. Current detectiontechniques are far more sensitive and can diagnose ve-nous air embolism before catastrophic cardiopulmonaryevents transgress. For an in-depth discussion of venousair embolism, the reader is referred to Young (1994). Fa-cial, tongue, and neck swelling can occur with the sittingposition because of malposition of the endotracheal tubeor oral airway, extreme neck flexion, or any conditionthat leads to decreased venous or lymphatic drainage.
The classic sitting position is shown in Fig. 24-16.Afull description and explanation of this highly special-ized position are beyond the scope of this chapter, andonly the basic elements of the posture are outlined. Thecervical, thoracic, and lumbar spine should be aligned.
Figure 24-16. Park bench position. Head in skeletal holder, legsflexed and at heart level, with support hose to thigh level. Access toanterior thoracic wall. (From Morgan, G. E., & Mikhail, M. S. [1996].Clinical anesthesiology [2nd erf., p.455]. Stamford, CT: Appleton &Lange. Adapted with permission.)
There are a wide variety of head-holding devices avail-able; the frame is usually attached to the back section ofthe table so the head can be lowered rapi'dly, if required.The legs are positioned at the level of the heart andslightly flexed at the knees. The footboard should bepadded and adjusted to prevent plantar flexion. Armsare crossed in the patient's lap with elbows flexed at 90degrees or less to give the anesthetist access to intravas-cular lines and monitors. Access to the anterior thoracicwall also is maintained for monitoring and maneuvers re-lated to a significant embolic event. Sufficient paddingshould be placed under the buttocks, knees, heels, and el-bows.
*• CASE STUDY
A 65-year-old female is scheduled for a left total hiparthroplasty. Her medical history is significant for hyper-tensive disease, well controlled with an ACE inhibitor. Shedenies any prior history of myocardial infarction, chestpain, or dyspnea on exertion; her exercise tolerance isdifficult to ascertain because of the osteoarthritic painshe has been experiencing in her left hip. However, sheused to tolerate moderate physical activity well. She hasa remote smoking history (stopped smoking 20 years

562 PART V Perioperative Management, Techniques, and Applications
ago) and denies any history of asthma, bronchitis, pneu-monia, or frequent urinary tract infections. Her medicalhistory is negative for diabetes, peripheral vascular dis-ease, or hepatic or neurologic disease. She denies anybleeding tendencies. Her osteoarthritis is symptomaticprimarily in her hip joint. However, she does have somepain and decreased dexterity in her hands. She has nor-mal range of motion and no pain in her cervical spine. Onphysical exam her heart sounds were normal and lungfields clear. Her airway was MP Class II, with normal TMdistance. Laboratory values are within normal limits. Herchest x-ray revealed normal heart size and essentiallyclear lung fields. Her EGG showed normal sinus rhythmwith nonspecific ST changes in the lateral leads. Sheweighs 65 kg, and her body mass index is 25. Thepatient will undergo a combination of epidural-general endotracheal anesthetic (ED-GETA) in the rightlateral decubitus position.
1. Why is an ED-GETA technique appropriate (in thelateral decubitus position) for this procedure in thispatient? -
A. regional anesthetic for total hip arthroplastiesis preferred by both surgeons and anesthetistsbecause of its clearly established benefits: de-creased blood loss, decreased risk of throm-boembolism, provision of postoperative analgesia,and avoidance of airway manipulation. How-ever, placing the patient in the lateral decubitusposition in an awake state often becomes veryuncomfortable after 1 to 2 hours because of pres-sure on the patient's downside. Arthritic diseasemay increase the potential for discomfort. Fur-thermore, although an ED block at the level of theT10 dermatome is sufficient to relieve surgicalpain, it is conceivable that a higher-level block maybe attained in the patient; higher levels may com-promise respiratory mechanics, especially in thelateral position. Therefore, the establishment ofGETA at the onset (with the patient's airway ac-cessible in the supine position) will obviate theneed for airway manipulation in the lateral positionand will prevent the patient from experiencing anydegree of discomfort during the procedure. Thisparticular patient appears to have a normal a'rwayand a reasonable degree of cardiopulmonary re-serve, making the benefits of GETA in this situationan acceptable risk. A caveat with the combinedED-GETA technique is that the potential for signif-icant hypotension is increased; general anesthe-sia usually is kept at the minimal possible level.
2. What special respiratory function concerns doesthe lateral decubitus position entail?
The decrease in the patient's respiratory mechan-ics already has been mentioned. The use of positivepressure ventilation (PPV) certainly compensatesfor the decrease in the lung volumes. In addition,
the anesthetized, paralyzed patient with a closerchest in the lateral position exhibits the potential fohypoxia due to V/Q mismatch. The lower (down,side) lung is underventilated and relatively overcer-
• fused. Simultaneously, the upper lung is oven/en ,̂lated (increased compliance) and underperfusec!Again, PPV delivered with an adequateoxygen tension helps prevent a hypoxic state.the patient is intubated, no muscle relaxants shcuabe necessary from a surgical point of view as r€
epidural anesthetic provides a motor block. Keec-ing the diaphragm unparaJyzed helps to decreasethe V/Q mismatch of the lateral position.
Because this patient does not appear to haveactive pulmonary disease, one may hope thatthere will be no perioperative respiratory proc-lems. However, total hip arthroplasties tend tcpromote large blood loss and overzealous fluid re-placement could manifest as pulmonary conges-tion. Judicious management of fluids and ventila-tory parameters will help prevent the occurrenceof problems.
3. What risk factors does this patient exhibit for pe-ripheral nerve injury? Which peripheral nerves areat risk for injury in the lateral decubitus positionand why? What preventive measures must ce
• taken for each nerve at risk?
With the exception of increasing age, this patientdoes not possess other risk factors identified fcrnerve injury. Her smoking history is noncontrbu-tory, and she does not have diabetes or peripheralvascular disease; her body mass index is weiwithin normal range. In this case the position ;tse:fimposes the greatest risk for nerve damage.
In the lateral decubitus position the brachelplexus is at especially high risk for both compres-sion and stretch injuries. Compression of thedownside arm's brachial plexus occurs if trelower shoulder and arm are allowed to reman di-rectly under the rib cage after assuming the lateralposition. Proper placement of a chest pad ia De-vice of sufficient bulk to support the chest wai.positioned just caudal to the axilla) is extreme!1/helpful in preventing this complication. The upsidearm's brachial plexus also is at risk for a stretch <"•jury if upper-arm abduction is greater than 90 de-grees or if cervical spine alignment is not proper:1,attained. Excessive dorsal extension and lateralflexion of the neck cause the angle between rl~ehead and shoulder tip to widen, resulting m 3stretched nerve bundle. Damage to the brachialplexus implies possible neurologic deficit tc thenerves distal to the axilla. In addition, the ulnar ancmedian nerves can be damaged by improper icareless management of the forearm of thedownside arm.
In the lateral decubitus position the common
j

Chapter 24 Positioning for Anesthesia and Surgery 563
peroneal nerve in the lower extremity \s at risk ofinjury because of inadequate padding betweenthe lateral aspect of the downside leg and the op-erating table surface.
Excessive pressure can damage the facialnerve and its branches. Another devastating, butpreventable, complication is retinal artery throm-bosis. The proper choice and placement of thehead support plus frequent monitoring of thedownside eye is the best preventive measure forthis complication.
4. Given the potential for hemodynamic instability(surgical blood loss in addition to position-relatedblood flow redistribution), where are blood pres-sure monitoring devices best placed?
The decision to use a direct blood pressure mea-surement via an intraarterial catheter (A-line) inaddition to a noninvasive blood pressure device(NIBP) will depend on the customary practiceof the • institution and practitioner preference.This particular patient does not exhibit significantexercis'e-limiting cardiac or pulmonary disease,.therefore the risk of an A-line placement might notbalance the benefits (beat-to-beat measure ofblood pressure, access for intraoperative labdraws) gained. However, the distinct possibilitiesfor hypotensive events due to the anesthetictechnique, the potential for blood loss, and thepossible use of methylmethacrylate cement toplace the prosthesis make a strong argument forplacing an A-line.
Irrespective of the monitoring options chosen,the following principles are helpful in placing themonitor. Discrepancies (5-20 mmHg) betweenthe readings of direct and indirect methods ofblood pressure measurement are common; thedirect A-line readings are invariably higher. Theo-retically, the accuracy of the A-line readingsshould not be influenced by the choice of arm inwhich the line is placed. It is the placement of thecalibrated transducer at the level of the heart thatconfers the veracity of the reading. Many practi-tioners prefer to use the radial artery of the down-side arm for cannulation because its placementon an armboard allows the volar surface of thewrist to be exposed and the arm is placed on astable, protected, and visible surface.
Many practitioners will place the NIBP cuff onthe upside arm to eliminate any inaccuracy that acompressed axillary artery may transfer to a cuffreading. There often is a discrepancy betweenthe NIBP readings in the upside versus the down-side arm. Blood pressure measurements in theupside arm often are too low, which decreasesthe risk of unrecognized hypotension, making itanother reason to place the cuff on the upsidearm. From a practical point of view, the upper armis the most accessible to monitor continually forproper cuff placement.
The clinical usefulness of a central venous linewith monitoring (CVP line) in this situation also isdebatable. The accuracy of a CVP reading in thelateral position is questionable because the usualexternal reference point for placement of thetransducer is difficult to define and utilize consis-tently. The monitoring of CVP trends may be ofbenefit in this position.
> SUMMARY
All of the common surgical positions are potentiallyharmful because of both the cardiopulmonary chal-lenges they present to an anesthetized patient and theperipheral nerve injuries they may cause. It is essentialfor the anesthetist to understand the physiologic basis ofthe hazards of positioning to protect the patient, whileoptimizing access to the operative site.
The ability to establish surgical positions in a safeand timely fashion entails both theoretical and practicalknowledge regarding each position, planning and orga-nizational skills, a consistent attention to detail, and theability to coordinate the activities of the personnel in-volved in positioning the patient. Acceptable patientoutcomes require continuous vigilance, with an eye forsome of the positioning complications that tend to occurin long surgical procedure.
Positioning the patient in some of the routine surgi-cal postures often becomes viewed as a mundane task.one in which a standard of care might easily be over-looked or omitted by any member of the positioningteam. The anesthetist should assume the role of theenforcer of the standards of quality care.