ANESTHESIA - MBBS UNIVERSITY EXAMS
209
ANESTHESIA
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of ANESTHESIA - MBBS UNIVERSITY EXAMS
ANESTHESIA
I. ANESTHETIC EQUIPMENT & MONITORS
HISTORY OF ANESTHESIA
• Dioscorides – used the term anesthesia
• Oliver Wendell Holmes – 1846 – termed anaesthesiology
• William T. G. Morton (The father of modern anaesthesia) – October 16, 1846 (World Ether day)
demonstrated general anesthetic effects of ether.
• Carl Koller-1884- introduced cocaine as an ophthalmic anesthetic
• Niemann-1860- introduced cocaine as a local anesthetic
• Joseph Priestley – produced Nitrous oxide- 1772
• Horace Walls: demonstrated use of Nitrous oxide for tooth extraction-1844
• On December 21, 1846, Robert Liston performed first surgical operation under ether anesthesia
• W. E. Clarke in 1841 administered anesthesia for a dental extraction [not made widely noted]
• August Bier- 1898-first spinal anesthesia/ father of spinal anesthesia
• Simpson: first to use chloroform
• John Lundy first used IV anesthetic thiopentone -1934
• Ferdinand Cathelin – 1901 – caudal epidural anesthesia
• Fidel Pages – 1921 – Lumbar epidural anesthesia
• Alexander Wood-1855 – invented needle & syringe
• Harold Griffith- 1942 – used curare
• Lofgren-1943- introduced Lidocaine
• John Lundy & Ralph waters: coined 'balanced anesthesia'
• Ketamine: first used by Domino & Corsen
• Succinyl choline: synthesized by Bovet
• First Boyle's machine: Edmund Gaske Boyle in 1917
• First endotracheal intubation: Ivan Magill
• First nasal intubation: Stanlers Rowbothon
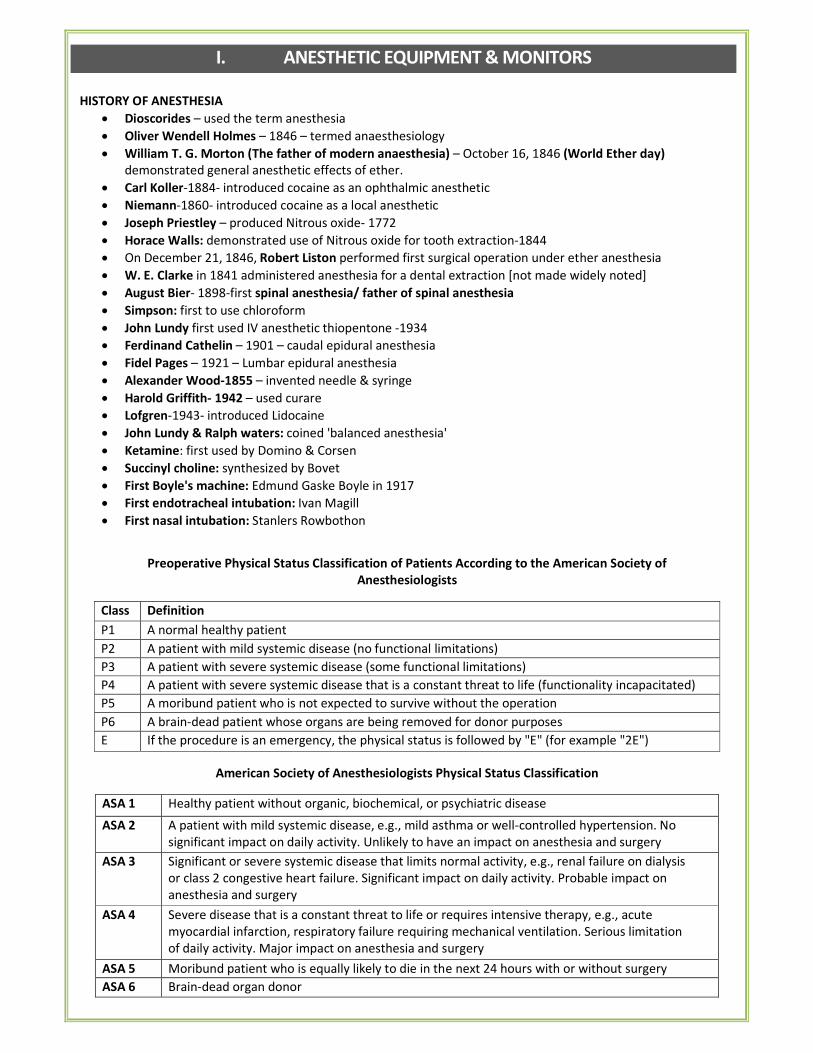
Preoperative Physical Status Classification of Patients According to the American Society of
Anesthesiologists
Class Definition
P1 A normal healthy patient
P2 A patient with mild systemic disease (no functional limitations)
P3 A patient with severe systemic disease (some functional limitations)
P4 A patient with severe systemic disease that is a constant threat to life (functionality incapacitated)
P5 A moribund patient who is not expected to survive without the operation
P6 A brain-dead patient whose organs are being removed for donor purposes
E If the procedure is an emergency, the physical status is followed by "E" (for example "2E")
American Society of Anesthesiologists Physical Status Classification
ASA 1 Healthy patient without organic, biochemical, or psychiatric disease
ASA 2 A patient with mild systemic disease, e.g., mild asthma or well-controlled hypertension. No
significant impact on daily activity. Unlikely to have an impact on anesthesia and surgery
ASA 3 Significant or severe systemic disease that limits normal activity, e.g., renal failure on dialysis
or class 2 congestive heart failure. Significant impact on daily activity. Probable impact on
anesthesia and surgery
ASA 4 Severe disease that is a constant threat to life or requires intensive therapy, e.g., acute
myocardial infarction, respiratory failure requiring mechanical ventilation. Serious limitation
of daily activity. Major impact on anesthesia and surgery
ASA 5 Moribund patient who is equally likely to die in the next 24 hours with or without surgery
ASA 6 Brain-dead organ donor
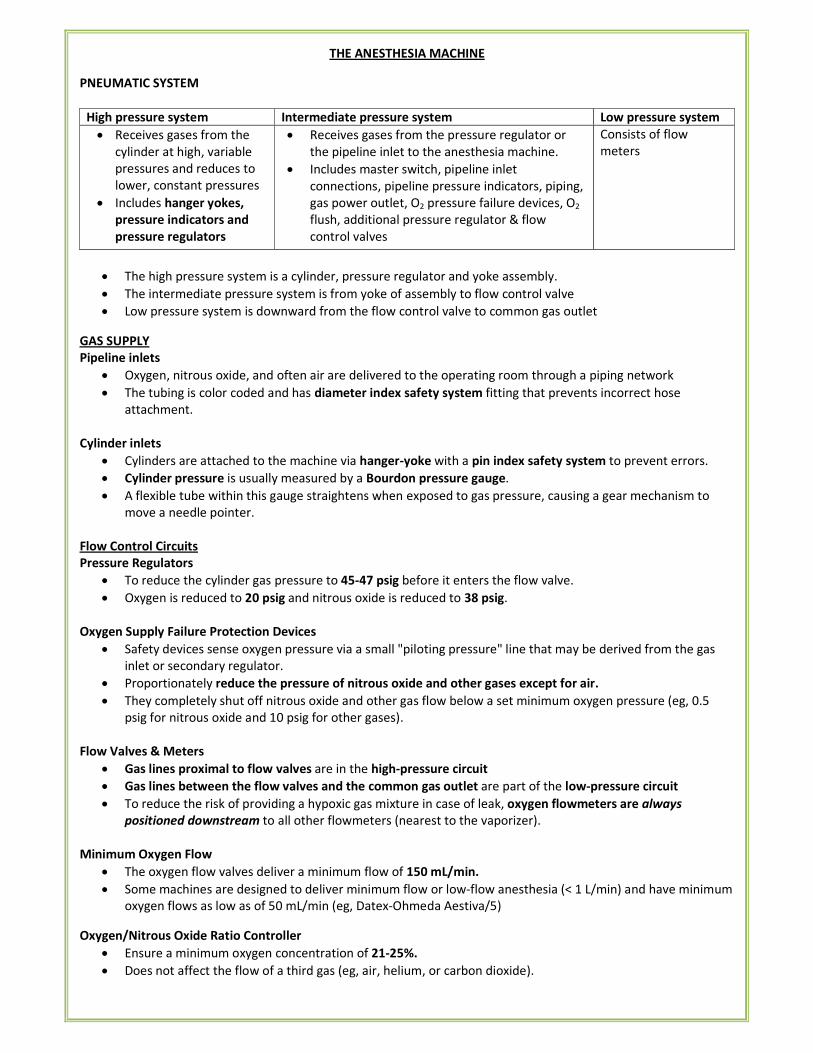
THE ANESTHESIA MACHINE
PNEUMATIC SYSTEM
High pressure system Intermediate pressure system Low pressure system
• Receives gases from the
cylinder at high, variable
pressures and reduces to
lower, constant pressures
• Includes hanger yokes,
pressure indicators and
pressure regulators
• Receives gases from the pressure regulator or
the pipeline inlet to the anesthesia machine.
• Includes master switch, pipeline inlet
connections, pipeline pressure indicators, piping,
gas power outlet, O2 pressure failure devices, O2
flush, additional pressure regulator & flow
control valves
Consists of flow
meters
• The high pressure system is a cylinder, pressure regulator and yoke assembly.
• The intermediate pressure system is from yoke of assembly to flow control valve
• Low pressure system is downward from the flow control valve to common gas outlet
GAS SUPPLY
Pipeline inlets
• Oxygen, nitrous oxide, and often air are delivered to the operating room through a piping network
• The tubing is color coded and has diameter index safety system fitting that prevents incorrect hose
attachment.
Cylinder inlets
• Cylinders are attached to the machine via hanger-yoke with a pin index safety system to prevent errors.
• Cylinder pressure is usually measured by a Bourdon pressure gauge.
• A flexible tube within this gauge straightens when exposed to gas pressure, causing a gear mechanism to
move a needle pointer.
Flow Control Circuits
Pressure Regulators
• To reduce the cylinder gas pressure to 45-47 psig before it enters the flow valve.
• Oxygen is reduced to 20 psig and nitrous oxide is reduced to 38 psig.
Oxygen Supply Failure Protection Devices
• Safety devices sense oxygen pressure via a small "piloting pressure" line that may be derived from the gas
inlet or secondary regulator.
• Proportionately reduce the pressure of nitrous oxide and other gases except for air.
• They completely shut off nitrous oxide and other gas flow below a set minimum oxygen pressure (eg, 0.5
psig for nitrous oxide and 10 psig for other gases).
Flow Valves & Meters
• Gas lines proximal to flow valves are in the high-pressure circuit
• Gas lines between the flow valves and the common gas outlet are part of the low-pressure circuit
• To reduce the risk of providing a hypoxic gas mixture in case of leak, oxygen flowmeters are always
positioned downstream to all other flowmeters (nearest to the vaporizer).
Minimum Oxygen Flow
• The oxygen flow valves deliver a minimum flow of 150 mL/min.
• Some machines are designed to deliver minimum flow or low-flow anesthesia (< 1 L/min) and have minimum
oxygen flows as low as of 50 mL/min (eg, Datex-Ohmeda Aestiva/5)
Oxygen/Nitrous Oxide Ratio Controller
• Ensure a minimum oxygen concentration of 21-25%.
• Does not affect the flow of a third gas (eg, air, helium, or carbon dioxide).
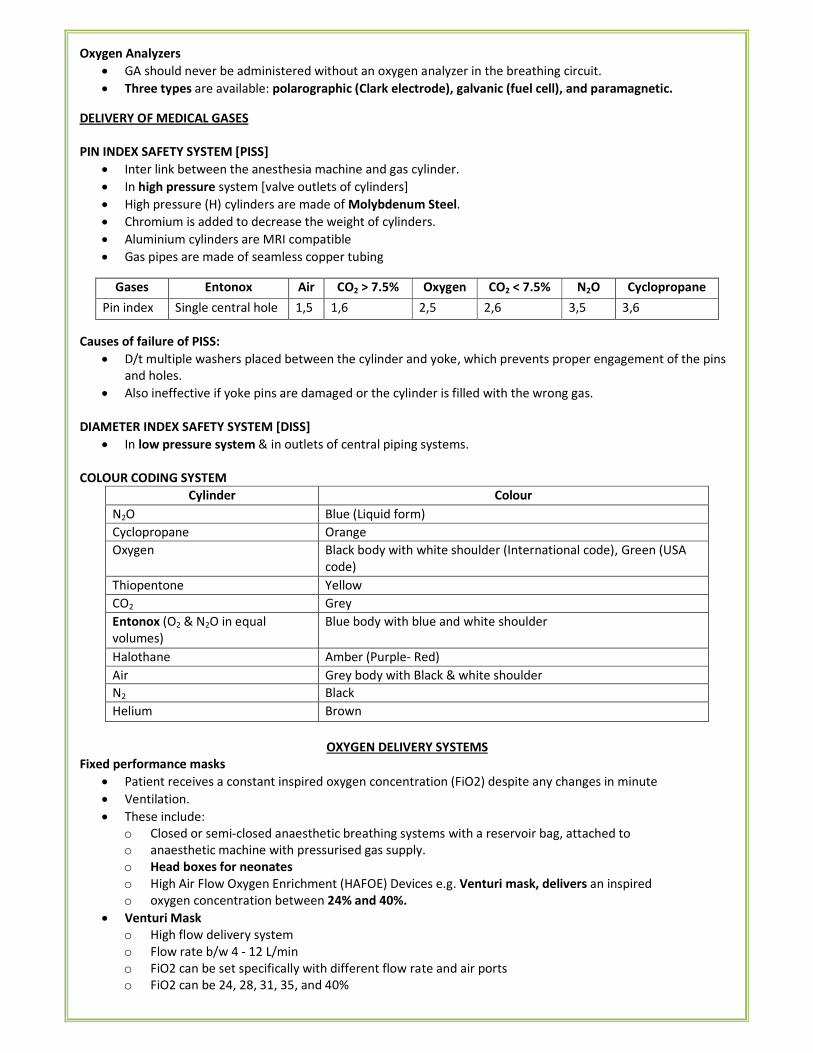
Oxygen Analyzers
• GA should never be administered without an oxygen analyzer in the breathing circuit.
• Three types are available: polarographic (Clark electrode), galvanic (fuel cell), and paramagnetic.
DELIVERY OF MEDICAL GASES
PIN INDEX SAFETY SYSTEM [PISS]
• Inter link between the anesthesia machine and gas cylinder.
• In high pressure system [valve outlets of cylinders]
• High pressure (H) cylinders are made of Molybdenum Steel.
• Chromium is added to decrease the weight of cylinders.
• Aluminium cylinders are MRI compatible
• Gas pipes are made of seamless copper tubing
Gases Entonox Air CO2 > 7.5% Oxygen CO2 < 7.5% N2O Cyclopropane
Pin index Single central hole 1,5 1,6 2,5 2,6 3,5 3,6
Causes of failure of PISS:
• D/t multiple washers placed between the cylinder and yoke, which prevents proper engagement of the pins
and holes.
• Also ineffective if yoke pins are damaged or the cylinder is filled with the wrong gas.
DIAMETER INDEX SAFETY SYSTEM [DISS]
• In low pressure system & in outlets of central piping systems.
COLOUR CODING SYSTEM
Cylinder Colour
N2O Blue (Liquid form)
Cyclopropane Orange
Oxygen Black body with white shoulder (International code), Green (USA
code)
Thiopentone Yellow
CO2 Grey
Entonox (O2 & N2O in equal
volumes)
Blue body with blue and white shoulder
Halothane Amber (Purple- Red)
Air Grey body with Black & white shoulder
N2 Black
Helium Brown
OXYGEN DELIVERY SYSTEMS
Fixed performance masks
• Patient receives a constant inspired oxygen concentration (FiO2) despite any changes in minute
• Ventilation.
• These include:
o Closed or semi-closed anaesthetic breathing systems with a reservoir bag, attached to
o anaesthetic machine with pressurised gas supply.
o Head boxes for neonates
o High Air Flow Oxygen Enrichment (HAFOE) Devices e.g. Venturi mask, delivers an inspired
o oxygen concentration between 24% and 40%.
• Venturi Mask
o High flow delivery system
o Flow rate b/w 4 - 12 L/min
o FiO2 can be set specifically with different flow rate and air ports
o FiO2 can be 24, 28, 31, 35, and 40%

o COPD patient that requires specific oxygen concentrations to administer high FiO2
but not
o too high such that the hypoxic drive to breath is blunted; titrate to keep saturation about 88%.
Variable performance masks/devices
• The oxygen concentration delivered depends on patient minute ventilation, peak inspiratory flow rate and
oxygen flow rate.
• Examples:
o Nasal Prongs:
� Low flow delivery system, > 6 L/min cause nasal mucosal drying
� Flow rate: 1 - 6 L/min
� FiO2 starts at 24% for 1L/min and increases 4% for each L/min up to 44% for 6 Lmin
� Well tolerated
� Use: minimal or no respiratory distress or oxygenation problem
o Nasal cannula:
� These do not increase dead space.
� Deliver 100% oxygen, but because the patient also breathes room air, the oxygen
� concentration ultimately delivered to the alveoli ranges from 24% to 44%.
� Inspiratory oxygen concentration depends on the flow rate
� No rebreathing occurs.
o Nasal catheters, 8FG
� Can be inserted into the nose as far as the pharynx
� A gas flow of 150m1/kg/min gives an inspired oxygen concentration of 50% in
� children less than 2 years
� No rebreathing occurs.
o Simple (Hudson) Face Mask (Rebreather)
� Have a small dead space.
� There is usually a small amount of rebreathing.
� Low flow delivery system
� Flow rate b/w 5 - 8 L/min
� FiO2: 5 - 6 is 40%, 6 - 7 is 50%, 7 - 8 is 60%
� Mask doesn't need tight seal
� Use: as per nasal prongs but require higher concentrations
BREATHING SYSTEMS
Insufflation
• Blowing of anesthetic gases across a patient's face.
• Avoids direct connection between a breathing circuit and a patient's airway.
• Valuable during pediatric inductions with inhalation anesthetics.
• There is no rebreathing of exhaled gases if the flow is high enough.
• Disadvantage: Ventilation cannot be controlled.
Open-Drop Anesthesia
• A highly volatile anesthetic—most commonly ether or halothane—is dripped onto a gauze-covered mask
(Schimmelbusch mask) applied to the patient's face.
• The vaporization lowers mask temperature, resulting in moisture condensation and a drop in anesthetic
vapor pressure
• May be used in locations or situations in which compressed medical gases are unavailable
Draw-Over Anesthesia
• In its most basic application, air is drawn through a low-resistance vaporizer as the patient inspires.
• Patients spontaneously breathing room air and a volatile, halogenated agent (nitrous oxide is never used
with draw-over devices) often manifest an oxygen saturation (Sp02) < 90%
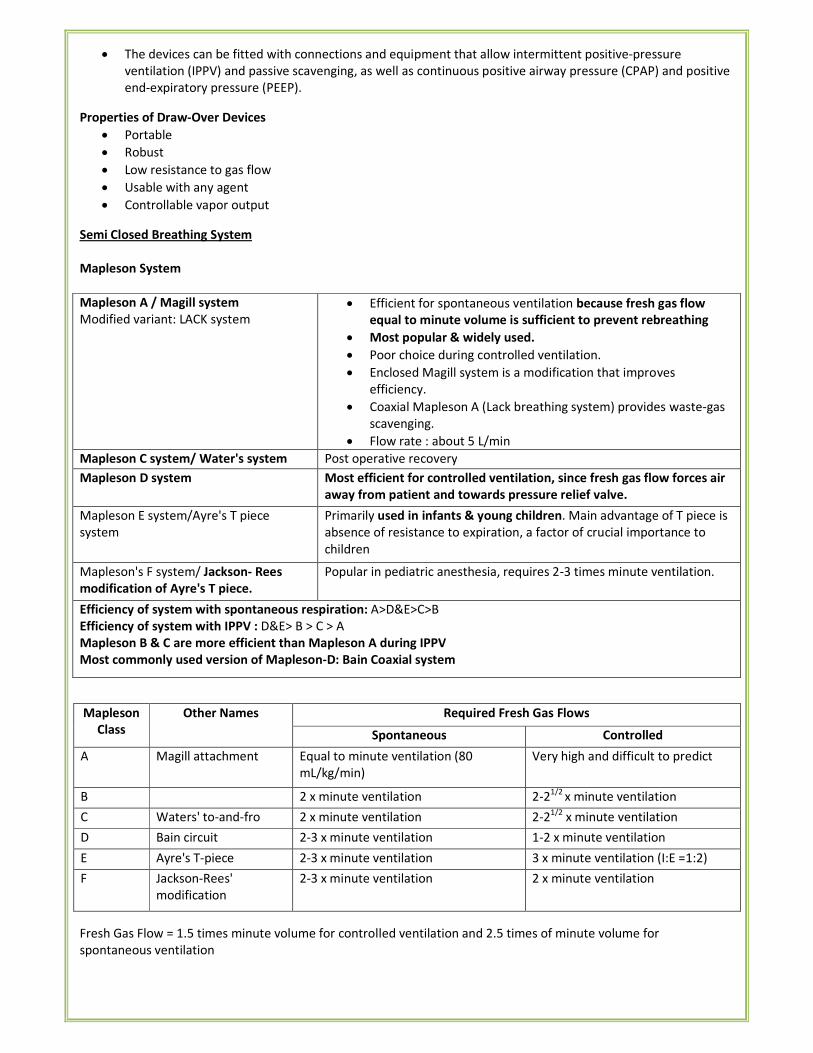
• The devices can be fitted with connections and equipment that allow intermittent positive-pressure
ventilation (IPPV) and passive scavenging, as well as continuous positive airway pressure (CPAP) and positive
end-expiratory pressure (PEEP).
Properties of Draw-Over Devices
• Portable
• Robust
• Low resistance to gas flow
• Usable with any agent
• Controllable vapor output
Semi Closed Breathing System
Mapleson System
Mapleson A / Magill system
Modified variant: LACK system
• Efficient for spontaneous ventilation because fresh gas flow
equal to minute volume is sufficient to prevent rebreathing
• Most popular & widely used.
• Poor choice during controlled ventilation.
• Enclosed Magill system is a modification that improves
efficiency.
• Coaxial Mapleson A (Lack breathing system) provides waste-gas
scavenging.
• Flow rate : about 5 L/min
Mapleson C system/ Water's system Post operative recovery
Mapleson D system Most efficient for controlled ventilation, since fresh gas flow forces air
away from patient and towards pressure relief valve.
Mapleson E system/Ayre's T piece
system
Primarily used in infants & young children. Main advantage of T piece is
absence of resistance to expiration, a factor of crucial importance to
children
Mapleson's F system/ Jackson- Rees
modification of Ayre's T piece.
Popular in pediatric anesthesia, requires 2-3 times minute ventilation.
Efficiency of system with spontaneous respiration: A>D&E>C>B
Efficiency of system with IPPV : D&E> B > C > A
Mapleson B & C are more efficient than Mapleson A during IPPV
Most commonly used version of Mapleson-D: Bain Coaxial system
Mapleson
Class
Other Names Required Fresh Gas Flows
Spontaneous Controlled
A Magill attachment Equal to minute ventilation (80
mL/kg/min)
Very high and difficult to predict
B 2 x minute ventilation 2-21/2
x minute ventilation
C Waters' to-and-fro 2 x minute ventilation 2-21/2
x minute ventilation
D Bain circuit 2-3 x minute ventilation 1-2 x minute ventilation
E Ayre's T-piece 2-3 x minute ventilation 3 x minute ventilation (I:E =1:2)
F Jackson-Rees'
modification
2-3 x minute ventilation 2 x minute ventilation
Fresh Gas Flow = 1.5 times minute volume for controlled ventilation and 2.5 times of minute volume for
spontaneous ventilation
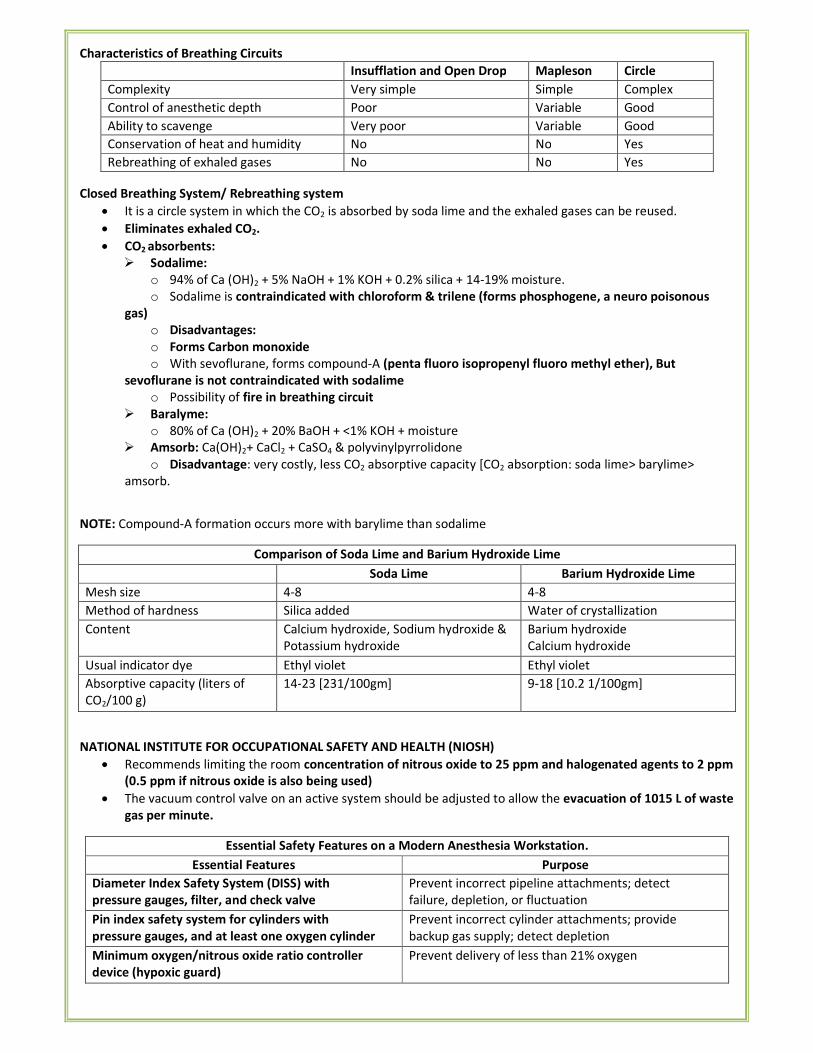
Characteristics of Breathing Circuits
Insufflation and Open Drop Mapleson Circle
Complexity Very simple Simple Complex
Control of anesthetic depth Poor Variable Good
Ability to scavenge Very poor Variable Good
Conservation of heat and humidity No No Yes
Rebreathing of exhaled gases No No Yes
Closed Breathing System/ Rebreathing system
• It is a circle system in which the CO2 is absorbed by soda lime and the exhaled gases can be reused.
• Eliminates exhaled CO2.
• CO2 absorbents:
� Sodalime:
o 94% of Ca (OH)2 + 5% NaOH + 1% KOH + 0.2% silica + 14-19% moisture.
o Sodalime is contraindicated with chloroform & trilene (forms phosphogene, a neuro poisonous
gas)
o Disadvantages:
o Forms Carbon monoxide
o With sevoflurane, forms compound-A (penta fluoro isopropenyl fluoro methyl ether), But
sevoflurane is not contraindicated with sodalime
o Possibility of fire in breathing circuit
� Baralyme:
o 80% of Ca (OH)2 + 20% BaOH + <1% KOH + moisture
� Amsorb: Ca(OH)2+ CaCl2 + CaSO4 & polyvinylpyrrolidone
o Disadvantage: very costly, less CO2 absorptive capacity [CO2 absorption: soda lime> barylime>
amsorb.
NOTE: Compound-A formation occurs more with barylime than sodalime
Comparison of Soda Lime and Barium Hydroxide Lime
Soda Lime Barium Hydroxide Lime
Mesh size 4-8 4-8
Method of hardness Silica added Water of crystallization
Content Calcium hydroxide, Sodium hydroxide &
Potassium hydroxide
Barium hydroxide
Calcium hydroxide
Usual indicator dye Ethyl violet Ethyl violet
Absorptive capacity (liters of
CO2/100 g)
14-23 [231/100gm] 9-18 [10.2 1/100gm]
NATIONAL INSTITUTE FOR OCCUPATIONAL SAFETY AND HEALTH (NIOSH)
• Recommends limiting the room concentration of nitrous oxide to 25 ppm and halogenated agents to 2 ppm
(0.5 ppm if nitrous oxide is also being used)
• The vacuum control valve on an active system should be adjusted to allow the evacuation of 1015 L of waste
gas per minute.
Essential Safety Features on a Modern Anesthesia Workstation.
Essential Features Purpose
Diameter Index Safety System (DISS) with
pressure gauges, filter, and check valve
Prevent incorrect pipeline attachments; detect
failure, depletion, or fluctuation
Pin index safety system for cylinders with
pressure gauges, and at least one oxygen cylinder
Prevent incorrect cylinder attachments; provide
backup gas supply; detect depletion
Minimum oxygen/nitrous oxide ratio controller
device (hypoxic guard)
Prevent delivery of less than 21% oxygen
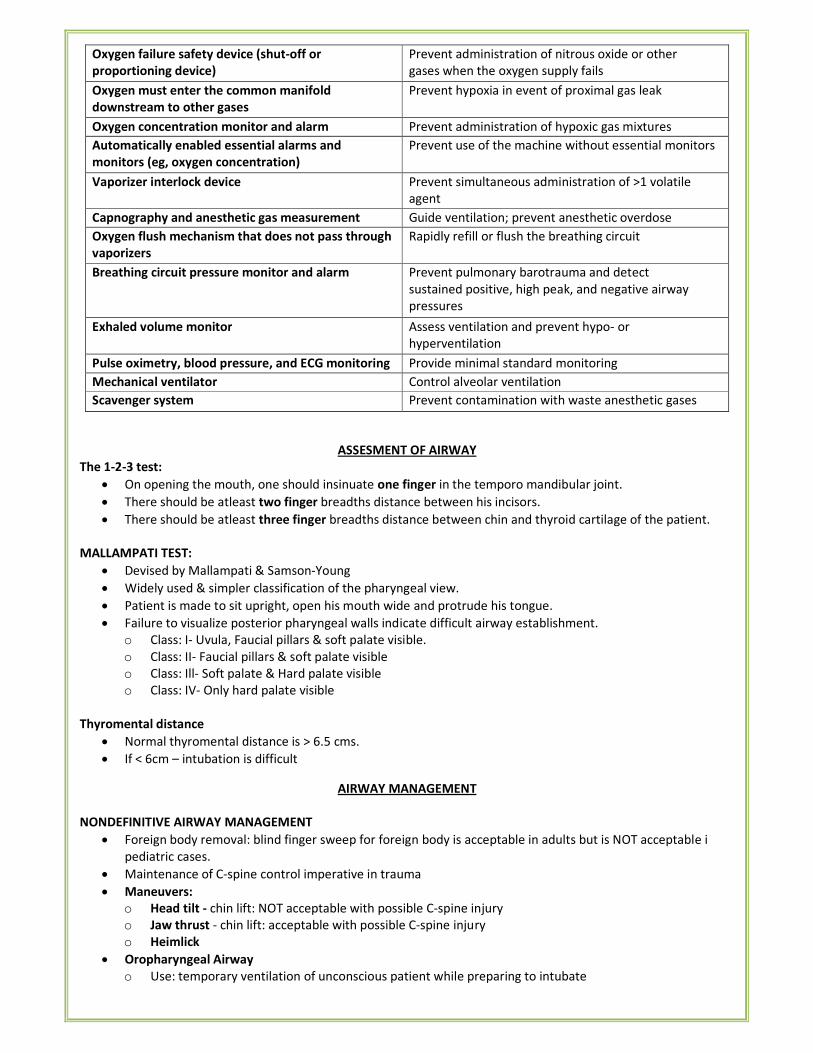
Oxygen failure safety device (shut-off or
proportioning device)
Prevent administration of nitrous oxide or other
gases when the oxygen supply fails
Oxygen must enter the common manifold
downstream to other gases
Prevent hypoxia in event of proximal gas leak
Oxygen concentration monitor and alarm Prevent administration of hypoxic gas mixtures
Automatically enabled essential alarms and
monitors (eg, oxygen concentration)
Prevent use of the machine without essential monitors
Vaporizer interlock device Prevent simultaneous administration of >1 volatile
agent
Capnography and anesthetic gas measurement Guide ventilation; prevent anesthetic overdose
Oxygen flush mechanism that does not pass through
vaporizers
Rapidly refill or flush the breathing circuit
Breathing circuit pressure monitor and alarm Prevent pulmonary barotrauma and detect
sustained positive, high peak, and negative airway
pressures
Exhaled volume monitor Assess ventilation and prevent hypo- or
hyperventilation
Pulse oximetry, blood pressure, and ECG monitoring Provide minimal standard monitoring
Mechanical ventilator Control alveolar ventilation
Scavenger system Prevent contamination with waste anesthetic gases
ASSESMENT OF AIRWAY
The 1-2-3 test:
• On opening the mouth, one should insinuate one finger in the temporo mandibular joint.
• There should be atleast two finger breadths distance between his incisors.
• There should be atleast three finger breadths distance between chin and thyroid cartilage of the patient.
MALLAMPATI TEST:
• Devised by Mallampati & Samson-Young
• Widely used & simpler classification of the pharyngeal view.
• Patient is made to sit upright, open his mouth wide and protrude his tongue.
• Failure to visualize posterior pharyngeal walls indicate difficult airway establishment.
o Class: I- Uvula, Faucial pillars & soft palate visible.
o Class: II- Faucial pillars & soft palate visible
o Class: Ill- Soft palate & Hard palate visible
o Class: IV- Only hard palate visible
Thyromental distance
• Normal thyromental distance is > 6.5 cms.
• If < 6cm – intubation is difficult
AIRWAY MANAGEMENT
NONDEFINITIVE AIRWAY MANAGEMENT
• Foreign body removal: blind finger sweep for foreign body is acceptable in adults but is NOT acceptable i
pediatric cases.
• Maintenance of C-spine control imperative in trauma
• Maneuvers:
o Head tilt - chin lift: NOT acceptable with possible C-spine injury
o Jaw thrust - chin lift: acceptable with possible C-spine injury
o Heimlick
• Oropharyngeal Airway
o Use: temporary ventilation of unconscious patient while preparing to intubate
o Not be tolerated by conscious patient b/c gag reflex and produces vomiting
o Proper size: corner of mouth to external auditory canal
• Nasopharyngeal Airway
o Use: temporary airway management in pt who would not tolerate an oropharyngeal airway or if it is
difficult to insert (trismus, mouth trauma, etc); less likely to induce vomiting
• Jet Insufflation (Needle Cricothroidotomy)
o Short term oxygenation until more definitive AW can be established
• Other
o Esophageal Obturator AW (EOA), Esophogastric Tube AW (EGTA), Pharygotracheal Lumen AW (PTLA),
Esophageal Tracheal Combitube, (ETC)
DEFINITIVE AIRWAY MANAGEMENT
• Endotracheal Intubation
o Indications:
� For supporting ventilation in patient with pathologic disease:
� Upper airway obstruction,
� Respiratory failure,
� Loss of consciousness
� For supporting ventilation during general anaesthesia (most common):
� Type of surgery:
� Operative site near the airway,
� Thoracic or abdominal surgery,
� Prone or lateral surgery,
� Long period of surgery
� Patient has risk of pulmonary aspiration
� Difficult mask ventilation
Tracheal Tube
• Used to deliver anesthetic gases directly into the trachea and allow the most control of ventilation and
oxygenation.
• Us are most commonly made from polyvinyl chloride.
• The shape and rigidity of TTs can be altered by inserting a stylet.
• Murphy tubes have a hole (the Murphy eye) to decrease the risk of occlusion should the distal tube opening
abut the carina or trachea.
• Uncuffed tubes are usually used in children to minimize the risk of pressure injury and postintubation croup.
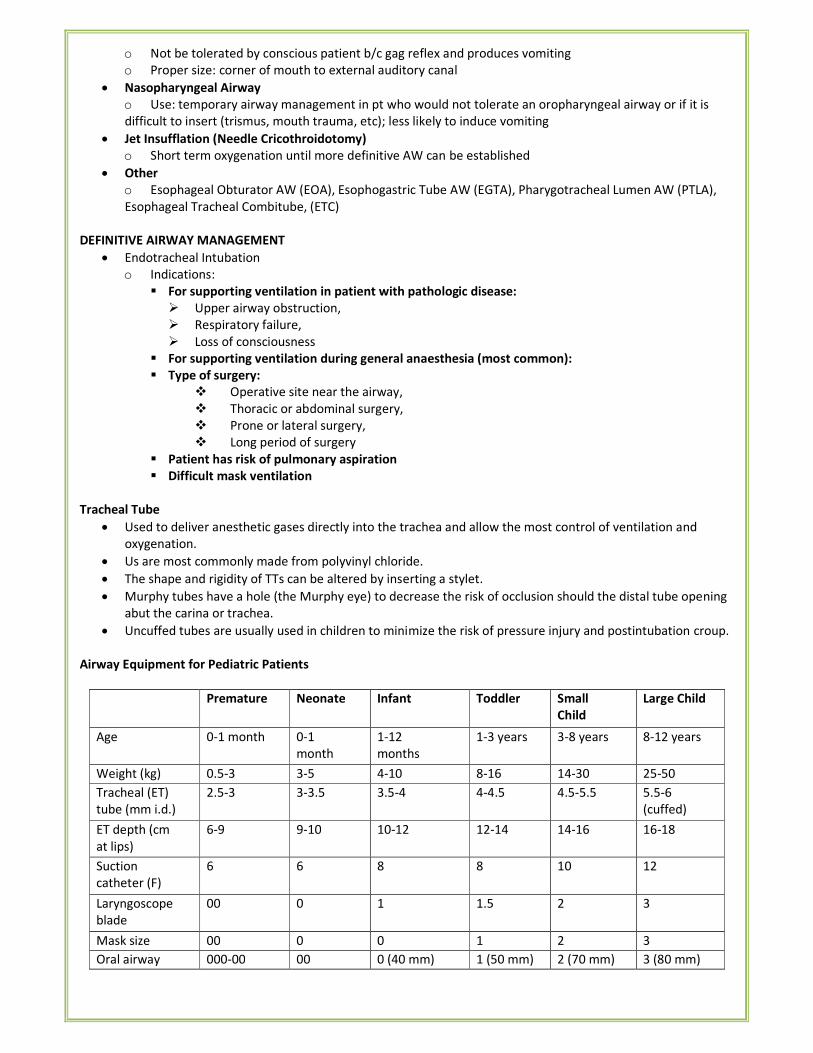
Airway Equipment for Pediatric Patients
Premature Neonate Infant Toddler Small
Child
Large Child
Age 0-1 month 0-1
month
1-12
months
1-3 years 3-8 years 8-12 years
Weight (kg) 0.5-3 3-5 4-10 8-16 14-30 25-50
Tracheal (ET)
tube (mm i.d.)
2.5-3 3-3.5 3.5-4 4-4.5 4.5-5.5 5.5-6
(cuffed)
ET depth (cm
at lips)
6-9 9-10 10-12 12-14 14-16 16-18
Suction
catheter (F)
6 6 8 8 10 12
Laryngoscope
blade
00 0 1 1.5 2 3
Mask size 00 0 0 1 2 3
Oral airway 000-00 00 0 (40 mm) 1 (50 mm) 2 (70 mm) 3 (80 mm)
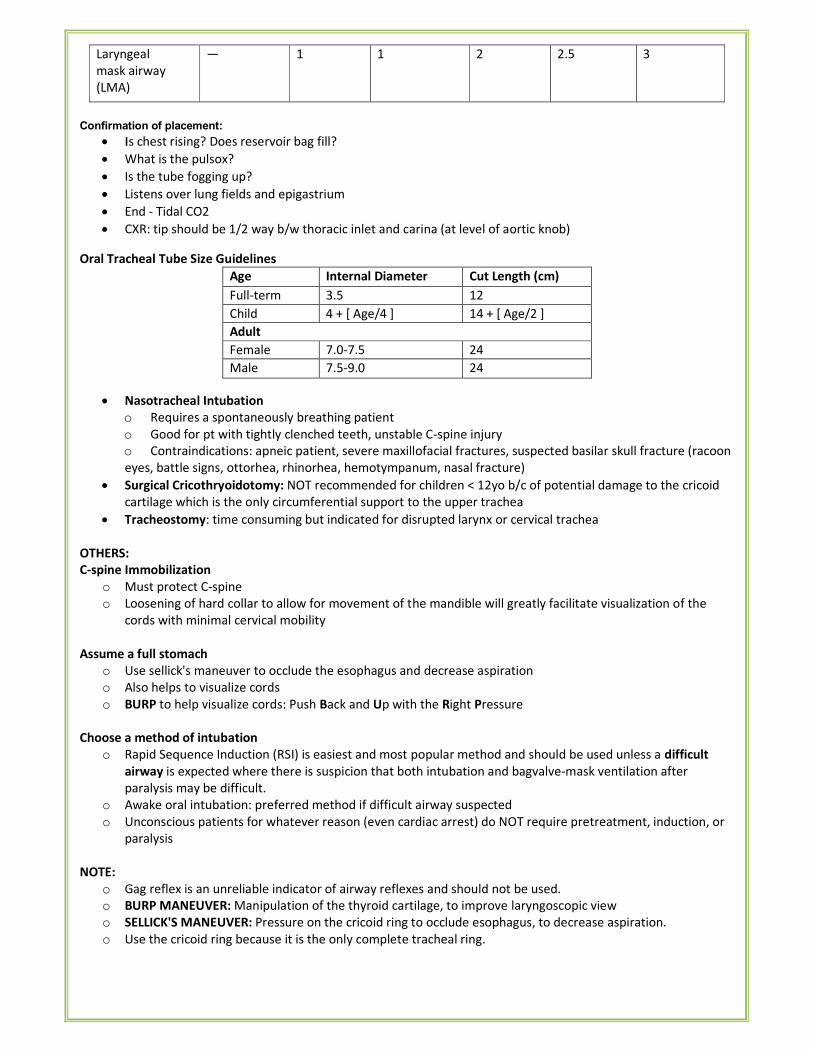
Laryngeal
mask airway
(LMA)
— 1 1 2 2.5 3
Confirmation of placement:
• IIs chest rising? Does reservoir bag fill?
• What is the pulsox?
• Is the tube fogging up?
• Listens over lung fields and epigastrium
• End - Tidal CO2
• CXR: tip should be 1/2 way b/w thoracic inlet and carina (at level of aortic knob)
Oral Tracheal Tube Size Guidelines
Age Internal Diameter
(mm)
Cut Length (cm)
Full-term
infant
3.5 12
Child 4 + [ Age/4 ] 14 + [ Age/2 ]
Adult
Female 7.0-7.5 24
Male 7.5-9.0 24
• Nasotracheal Intubation
o Requires a spontaneously breathing patient
o Good for pt with tightly clenched teeth, unstable C-spine injury
o Contraindications: apneic patient, severe maxillofacial fractures, suspected basilar skull fracture (racoon
eyes, battle signs, ottorhea, rhinorhea, hemotympanum, nasal fracture)
• Surgical Cricothryoidotomy: NOT recommended for children < 12yo b/c of potential damage to the cricoid
cartilage which is the only circumferential support to the upper trachea
• Tracheostomy: time consuming but indicated for disrupted larynx or cervical trachea
OTHERS:
C-spine Immobilization
o Must protect C-spine
o Loosening of hard collar to allow for movement of the mandible will greatly facilitate visualization of the
cords with minimal cervical mobility
Assume a full stomach
o Use sellick's maneuver to occlude the esophagus and decrease aspiration
o Also helps to visualize cords
o BURP to help visualize cords: Push Back and Up with the Right Pressure
Choose a method of intubation
o Rapid Sequence Induction (RSI) is easiest and most popular method and should be used unless a difficult
airway is expected where there is suspicion that both intubation and bagvalve-mask ventilation after
paralysis may be difficult.
o Awake oral intubation: preferred method if difficult airway suspected
o Unconscious patients for whatever reason (even cardiac arrest) do NOT require pretreatment, induction, or
paralysis
NOTE:
o Gag reflex is an unreliable indicator of airway reflexes and should not be used.
o BURP MANEUVER: Manipulation of the thyroid cartilage, to improve laryngoscopic view
o SELLICK'S MANEUVER: Pressure on the cricoid ring to occlude esophagus, to decrease aspiration.
o Use the cricoid ring because it is the only complete tracheal ring.
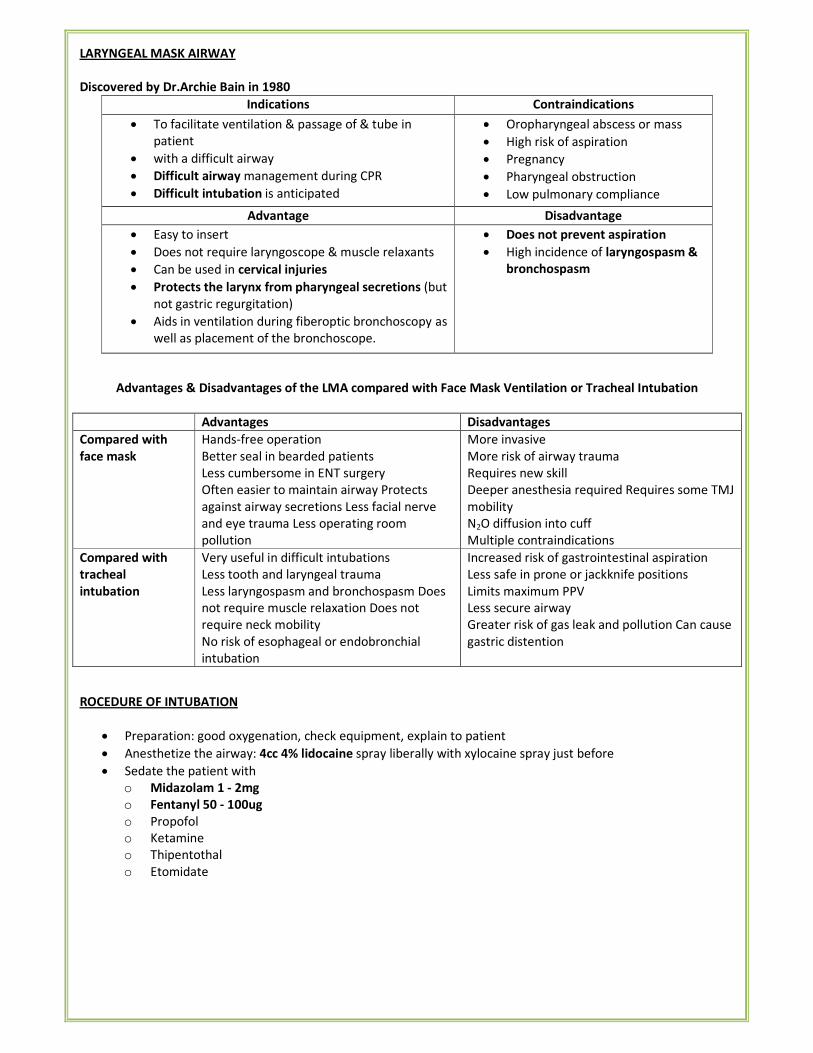
LARYNGEAL MASK AIRWAY
Discovered by Dr.Archie Bain in 1980
Indications Contraindications
• To facilitate ventilation & passage of & tube in
patient
• with a difficult airway
• Difficult airway management during CPR
• Difficult intubation is anticipated
• Oropharyngeal abscess or mass
• High risk of aspiration
• Pregnancy
• Pharyngeal obstruction
• Low pulmonary compliance
Advantage Disadvantage
• Easy to insert
• Does not require laryngoscope & muscle relaxants
• Can be used in cervical injuries
• Protects the larynx from pharyngeal secretions (but
not gastric regurgitation)
• Aids in ventilation during fiberoptic bronchoscopy as
well as placement of the bronchoscope.
• Does not prevent aspiration
• High incidence of laryngospasm &
bronchospasm
Advantages & Disadvantages of the LMA compared with Face Mask Ventilation or Tracheal Intubation
Advantages Disadvantages
Compared with
face mask
Hands-free operation
Better seal in bearded patients
Less cumbersome in ENT surgery
Often easier to maintain airway Protects
against airway secretions Less facial nerve
and eye trauma Less operating room
pollution
More invasive
More risk of airway trauma
Requires new skill
Deeper anesthesia required Requires some TMJ
mobility
N2O diffusion into cuff
Multiple contraindications
Compared with
tracheal
intubation
Very useful in difficult intubations
Less tooth and laryngeal trauma
Less laryngospasm and bronchospasm Does
not require muscle relaxation Does not
require neck mobility
No risk of esophageal or endobronchial
intubation
Increased risk of gastrointestinal aspiration
Less safe in prone or jackknife positions
Limits maximum PPV
Less secure airway
Greater risk of gas leak and pollution Can cause
gastric distention
ROCEDURE OF INTUBATION
• Preparation: good oxygenation, check equipment, explain to patient
• Anesthetize the airway: 4cc 4% lidocaine spray liberally with xylocaine spray just before
• Sedate the patient with
o Midazolam 1 - 2mg
o Fentanyl 50 - 100ug
o Propofol
o Ketamine
o Thipentothal
o Etomidate
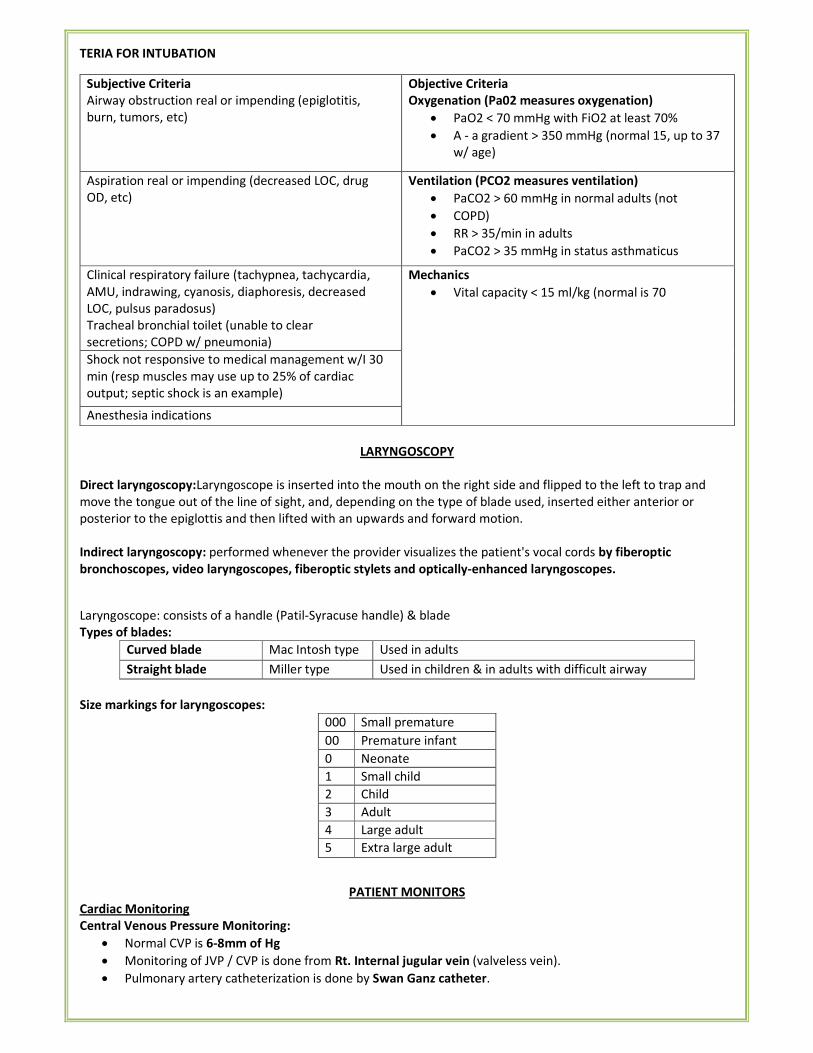
TERIA FOR INTUBATION
Subjective Criteria
Airway obstruction real or impending (epiglotitis,
burn, tumors, etc)
Objective Criteria
Oxygenation (Pa02 measures oxygenation)
• PaO2 < 70 mmHg with FiO2 at least 70%
• A - a gradient > 350 mmHg (normal 15, up to 37
w/ age)
Aspiration real or impending (decreased LOC, drug
OD, etc)
Ventilation (PCO2 measures ventilation)
• PaCO2 > 60 mmHg in normal adults (not
• COPD)
• RR > 35/min in adults
• PaCO2 > 35 mmHg in status asthmaticus
Clinical respiratory failure (tachypnea, tachycardia,
AMU, indrawing, cyanosis, diaphoresis, decreased
LOC, pulsus paradosus)
Tracheal bronchial toilet (unable to clear
secretions; COPD w/ pneumonia)
Mechanics
• Vital capacity < 15 ml/kg (normal is 70
Shock not responsive to medical management w/I 30
min (resp muscles may use up to 25% of cardiac
output; septic shock is an example)
Anesthesia indications
LARYNGOSCOPY
Direct laryngoscopy:Laryngoscope is inserted into the mouth on the right side and flipped to the left to trap and
move the tongue out of the line of sight, and, depending on the type of blade used, inserted either anterior or
posterior to the epiglottis and then lifted with an upwards and forward motion.
Indirect laryngoscopy: performed whenever the provider visualizes the patient's vocal cords by fiberoptic
bronchoscopes, video laryngoscopes, fiberoptic stylets and optically-enhanced laryngoscopes.
Laryngoscope: consists of a handle (Patil-Syracuse handle) & blade
Types of blades:
Curved blade Mac Intosh type Used in adults
Straight blade Miller type Used in children & in adults with difficult airway
Size markings for laryngoscopes:
000 Small premature
infant 00 Premature infant
0 Neonate
1 Small child
2 Child
3 Adult
4 Large adult
5 Extra large adult
PATIENT MONITORS
Cardiac Monitoring
Central Venous Pressure Monitoring:
• Normal CVP is 6-8mm of Hg
• Monitoring of JVP / CVP is done from Rt. Internal jugular vein (valveless vein).
• Pulmonary artery catheterization is done by Swan Ganz catheter.
• Swan Ganz catheter measures mixed venous pressure:
o Pressure in right atrium (0-8 mm of Hg)
o Pressure in right ventricle (15 – 25/0-8mm of Hg)
o Pressure in pulmonary artery (15-25/5-15 mm Hg)
o Pulmonary capillary wedge pressure (4 -12 mm Hg)
o Left atrium (4-12mm Hg).
• The best indicator for tissue perfusion or cardiac output is mixed venous O2 saturation.
• Best clinical guide for cardiac output is urinary output.
Transesophageal Echocardiography:
• Most sensitive for wall motion abnormalities and to detect ischemia and air embolism during intraoperative
period.
• For detecting arrhythmias in ECG lead II is preferred.
• For detecting ischemia in ECG lead V5 is preferred.
• Inferior wall MI shows abnormality in lead II,III and aVF.
BP Monitoring:
• For invasive BP monitoring, radial artery is most preferred.
• For radial artery cannulation, Allen's test should be performed to assess the patency of ulnar artery.
• Allen's Test:
o Hand circulation is stopped by occluding both radial and ulnar arteries.
o The pressure over ulnar artery is released while maintaining pressure on radial artery.
o Note the return of normal color of palm.
o If color returns to normal in < 7 sec, then radial artery cannulation can be done.
o If refill time is >15 sec then radial artery cannulation is contra-indicated.
o 7 – 14 sec is borderline.
Respiratory Monitoring
Pulse Oximeter:-
• It is used to detect hypoxia in intra – operative and post – operative period.
• Pulse oxymeter measures percentage saturation of oxygen.
• The normal O2 saturation is 98%
• Oximetry depends on the observation that oxygenated and reduced hemoglobin differ in their absorption of
red and infrared light (Lambert–Beer law)
• Oxyhemoglobin (HbO2) absorbs more infrared light (960 nm)
• Deoxyhemoglobin absorbs more red light (660 nm) and appears blue or cyanotic to the naked eye.
• Change in light absorption during arterial pulsations is the basis of oximetric determinations.
• Following factors lead to inaccurate reading in pulse oxymeter:
o Methemoglobin (shows 85% saturation always)
o Carboxy hemoglobin (shows 95% saturation always, over read d/t Hb CO)
o Fetal hemoglobin (at very high levels only)
o Cyanide poisoning (higher values)
o Anemia (lower values)
o Hemoglobin S
o Mal positioning of sensor
o Poor peripheral pulsation
o Skin pigmentation
o Dyes- methylene blue, indocyanine green
o Optical interference
o Electrical interference
o Nail polish & covering
• Severe Hyperbilirubinemia does not affect readings of pulseoximetry.
ETCO2 (capnography):
• The most commonly used type of capnograph plots Pco2 versus time.
• Capnography uses infrared light which is absorbed by CO2
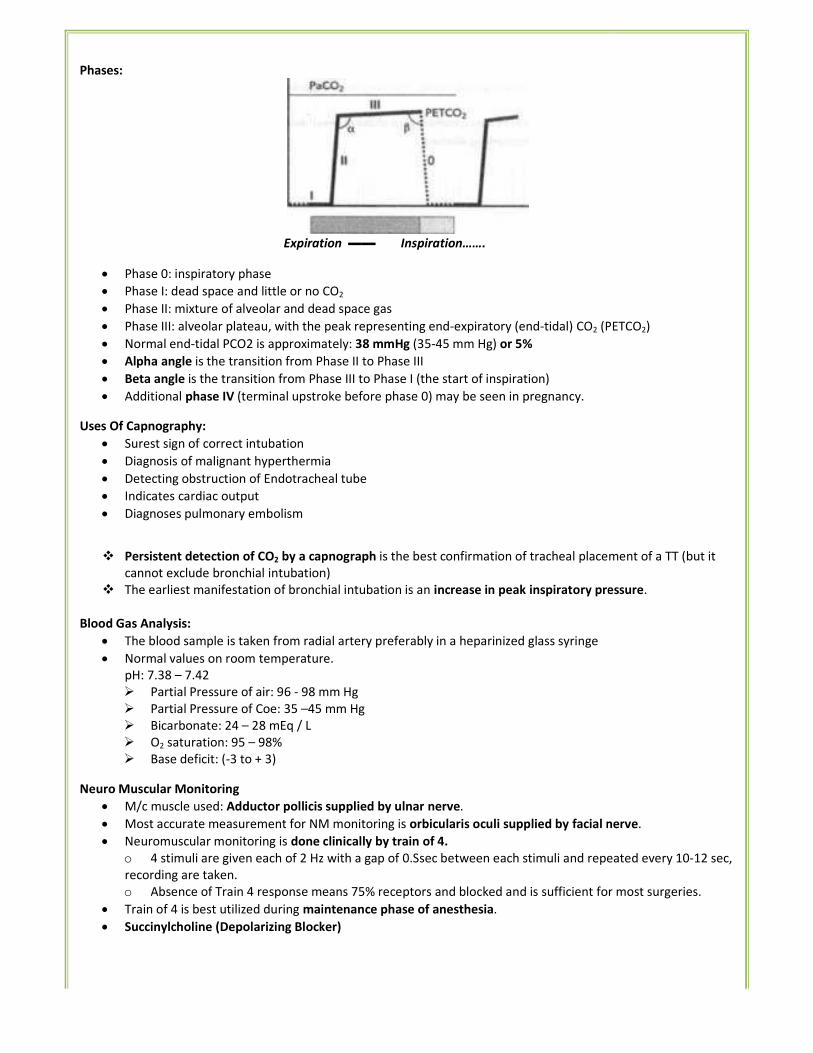
Phases:
Expiratio
• Phase 0: inspiratory phase
• Phase I: dead space and little or no C
• Phase II: mixture of alveolar and dead
• Phase III: alveolar plateau, with the p
• Normal end-tidal PCO2 is approximat
• Alpha angle is the transition from Ph
• Beta angle is the transition from Pha
• Additional phase IV (terminal upstrok
Uses Of Capnography:
• Surest sign of correct intubation
• Diagnosis of malignant hyperthermia
• Detecting obstruction of Endotrachea
• Indicates cardiac output
• Diagnoses pulmonary embolism
� Persistent detection of CO2 by a capn
cannot exclude bronchial intubation)
� The earliest manifestation of bronchi
Blood Gas Analysis:
• The blood sample is taken from radia
• Normal values on room temperature
pH: 7.38 – 7.42
� Partial Pressure of air: 96 - 98 m
� Partial Pressure of Coe: 35 –45 m
� Bicarbonate: 24 – 28 mEq / L
� O2 saturation: 95 – 98%
� Base deficit: (-3 to + 3)
Neuro Muscular Monitoring
• M/c muscle used: Adductor pollicis s
• Most accurate measurement for NM
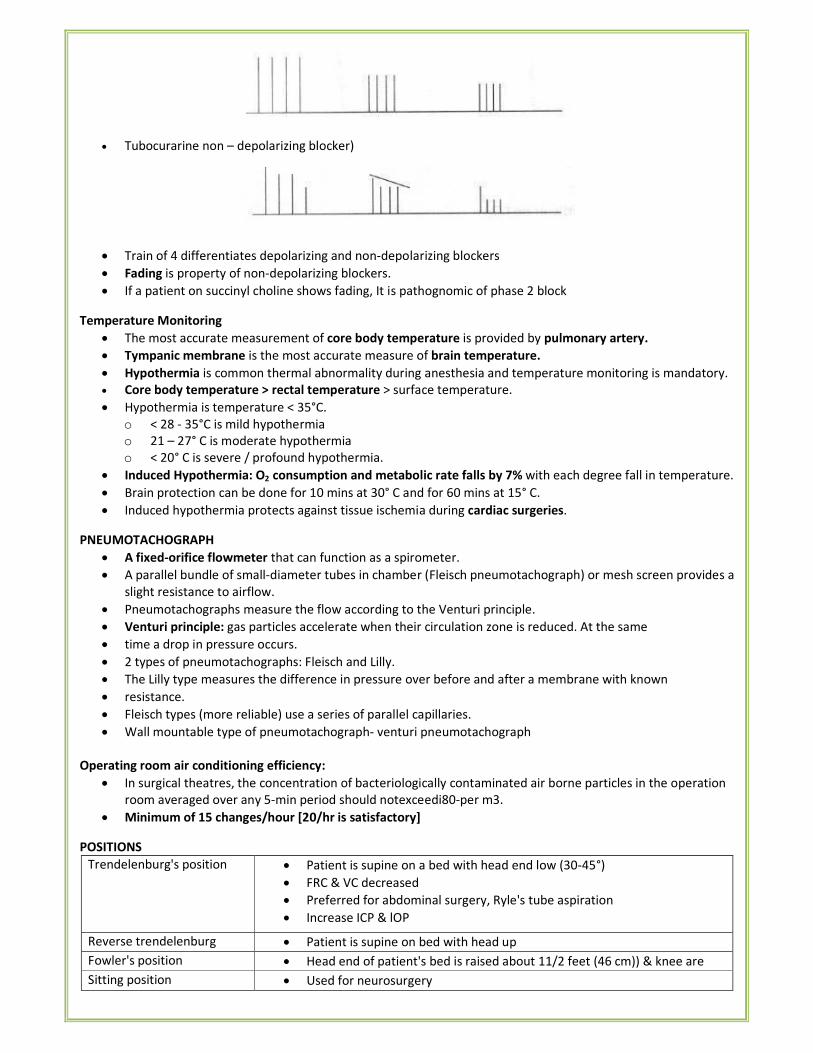
• Neuromuscular monitoring is done cl
o 4 stimuli are given each of 2 Hz w
recording are taken.
o Absence of Train 4 response me
• Train of 4 is best utilized during main
• Succinylcholine (Depolarizing Blocke
ration ▬▬ Inspiration…….
no CO2
dead space gas
he peak representing end-expiratory (end-tidal) CO2 (PE
imately: 38 mmHg (35-45 mm Hg) or 5%
Phase II to Phase III
Phase III to Phase I (the start of inspiration)
stroke before phase 0) may be seen in pregnancy.
rmia
cheal tube
capnograph is the best confirmation of tracheal placem
ion)
nchial intubation is an increase in peak inspiratory pres
adial artery preferably in a heparinized glass syringe
ture.
8 mm Hg
45 mm Hg
cis supplied by ulnar nerve.
NM monitoring is orbicularis oculi supplied by facial ne
ne clinically by train of 4.
Hz with a gap of 0.Ssec between each stimuli and repea
means 75% receptors and blocked and is sufficient for
aintenance phase of anesthesia.
ocker)
(PETCO2)
cement of a TT (but it
pressure.
al nerve.
epeated every 10-12 sec,
for most surgeries.
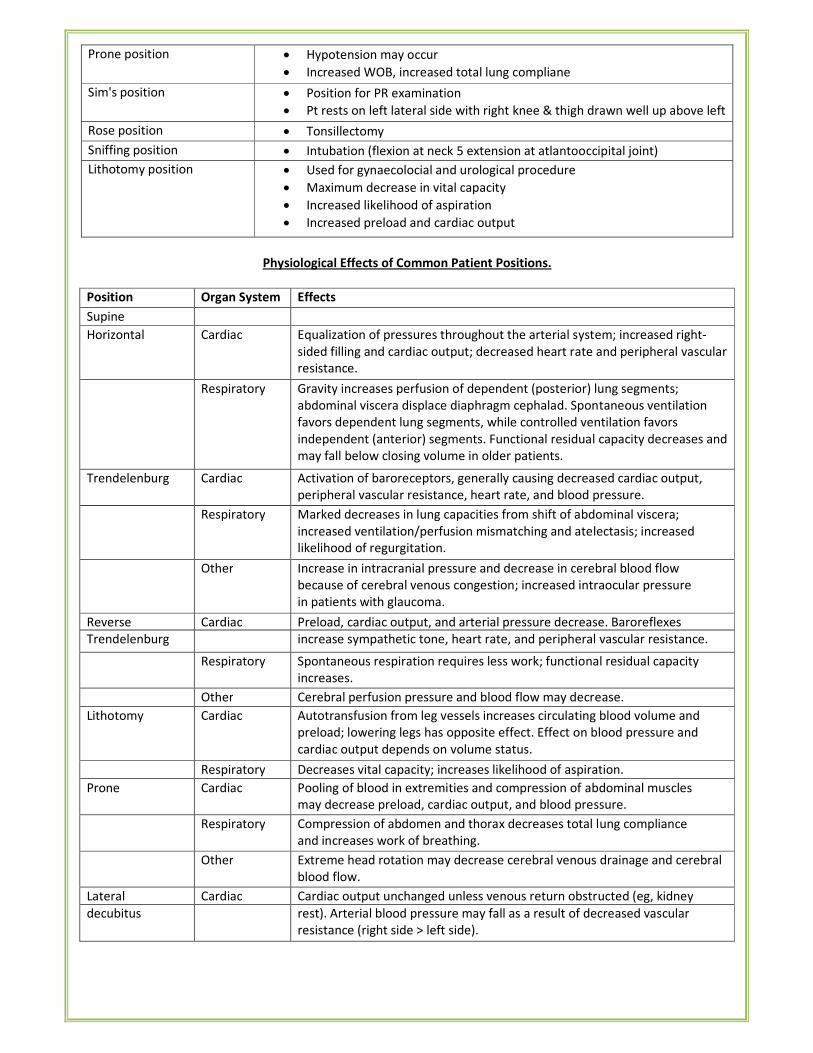
• Tubocurarine non – depolarizing blocker)
• Train of 4 differentiates depolarizing and non-depolarizing blockers
• Fading is property of non-depolarizing blockers.
• If a patient on succinyl choline shows fading, It is pathognomic of phase 2 block
Temperature Monitoring
• The most accurate measurement of core body temperature is provided by pulmonary artery.
• Tympanic membrane is the most accurate measure of brain temperature.
• Hypothermia is common thermal abnormality during anesthesia and temperature monitoring is mandatory.
• Core body temperature > rectal temperature > surface temperature.
• Hypothermia is temperature < 35°C.
o < 28 - 35°C is mild hypothermia
o 21 – 27° C is moderate hypothermia
o < 20° C is severe / profound hypothermia.
• Induced Hypothermia: O2 consumption and metabolic rate falls by 7% with each degree fall in temperature.
• Brain protection can be done for 10 mins at 30° C and for 60 mins at 15° C.
• Induced hypothermia protects against tissue ischemia during cardiac surgeries.
PNEUMOTACHOGRAPH
• A fixed-orifice flowmeter that can function as a spirometer.
• A parallel bundle of small-diameter tubes in chamber (Fleisch pneumotachograph) or mesh screen provides a
slight resistance to airflow.
• Pneumotachographs measure the flow according to the Venturi principle.
• Venturi principle: gas particles accelerate when their circulation zone is reduced. At the same
• time a drop in pressure occurs.
• 2 types of pneumotachographs: Fleisch and Lilly.
• The Lilly type measures the difference in pressure over before and after a membrane with known
• resistance.
• Fleisch types (more reliable) use a series of parallel capillaries.
• Wall mountable type of pneumotachograph- venturi pneumotachograph
Operating room air conditioning efficiency:
• In surgical theatres, the concentration of bacteriologically contaminated air borne particles in the operation
room averaged over any 5-min period should notexceedi80-per m3.
• Minimum of 15 changes/hour [20/hr is satisfactory]
POSITIONS
Trendelenburg's position • Patient is supine on a bed with head end low (30-45°)
• FRC & VC decreased
• Preferred for abdominal surgery, Ryle's tube aspiration
• Increase ICP & lOP
Reverse trendelenburg • Patient is supine on bed with head up
Fowler's position • Head end of patient's bed is raised about 11/2 feet (46 cm)) & knee are
elevated Sitting position • Used for neurosurgery
Prone position • Hypotension may occur
• Increased WOB, increased total lung compliane
Sim's position • Position for PR examination
• Pt rests on left lateral side with right knee & thigh drawn well up above left
Rose position • Tonsillectomy
Sniffing position • Intubation (flexion at neck 5 extension at atlantooccipital joint)
Lithotomy position • Used for gynaecolocial and urological procedure
• Maximum decrease in vital capacity
• Increased likelihood of aspiration
• Increased preload and cardiac output
Physiological Effects of Common Patient Positions.
Position Organ System Effects
Supine
Horizontal Cardiac Equalization of pressures throughout the arterial system; increased right-
sided filling and cardiac output; decreased heart rate and peripheral vascular
resistance.
Respiratory Gravity increases perfusion of dependent (posterior) lung segments;
abdominal viscera displace diaphragm cephalad. Spontaneous ventilation
favors dependent lung segments, while controlled ventilation favors
independent (anterior) segments. Functional residual capacity decreases and
may fall below closing volume in older patients.
Trendelenburg Cardiac Activation of baroreceptors, generally causing decreased cardiac output,
peripheral vascular resistance, heart rate, and blood pressure.
Respiratory Marked decreases in lung capacities from shift of abdominal viscera;
increased ventilation/perfusion mismatching and atelectasis; increased
likelihood of regurgitation.
Other Increase in intracranial pressure and decrease in cerebral blood flow
because of cerebral venous congestion; increased intraocular pressure
in patients with glaucoma.
Reverse Cardiac Preload, cardiac output, and arterial pressure decrease. Baroreflexes
Trendelenburg increase sympathetic tone, heart rate, and peripheral vascular resistance.
Respiratory Spontaneous respiration requires less work; functional residual capacity
increases.
Other Cerebral perfusion pressure and blood flow may decrease.
Lithotomy Cardiac Autotransfusion from leg vessels increases circulating blood volume and
preload; lowering legs has opposite effect. Effect on blood pressure and
cardiac output depends on volume status.
Respiratory Decreases vital capacity; increases likelihood of aspiration.
Prone Cardiac Pooling of blood in extremities and compression of abdominal muscles
may decrease preload, cardiac output, and blood pressure.
Respiratory Compression of abdomen and thorax decreases total lung compliance
and increases work of breathing.
Other Extreme head rotation may decrease cerebral venous drainage and cerebral
blood flow.
Lateral Cardiac Cardiac output unchanged unless venous return obstructed (eg, kidney
decubitus rest). Arterial blood pressure may fall as a result of decreased vascular
resistance (right side > left side).
Respiratory Decreased volume of dependent lung; increased perfusion of dependent
lung. Increased ventilation of dependent lung in awake patients (no V/Q
mismatch); decreased ventilation of dependent lung in anesthetized patients
V/Q mismatch). Further decreases in dependent lung ventilation with
paralysis and an open chest.
Sitting Cardiac Pooling blood in lower body decreases central blood volume. Cardiac
output and arterial blood pressure fall despite rise in heart rate and
systemic vascular resistance.
Respiratory Lung volumes and functional residual capacity increase; work of
breathing increases.
Other Cerebral blood flow decreases.
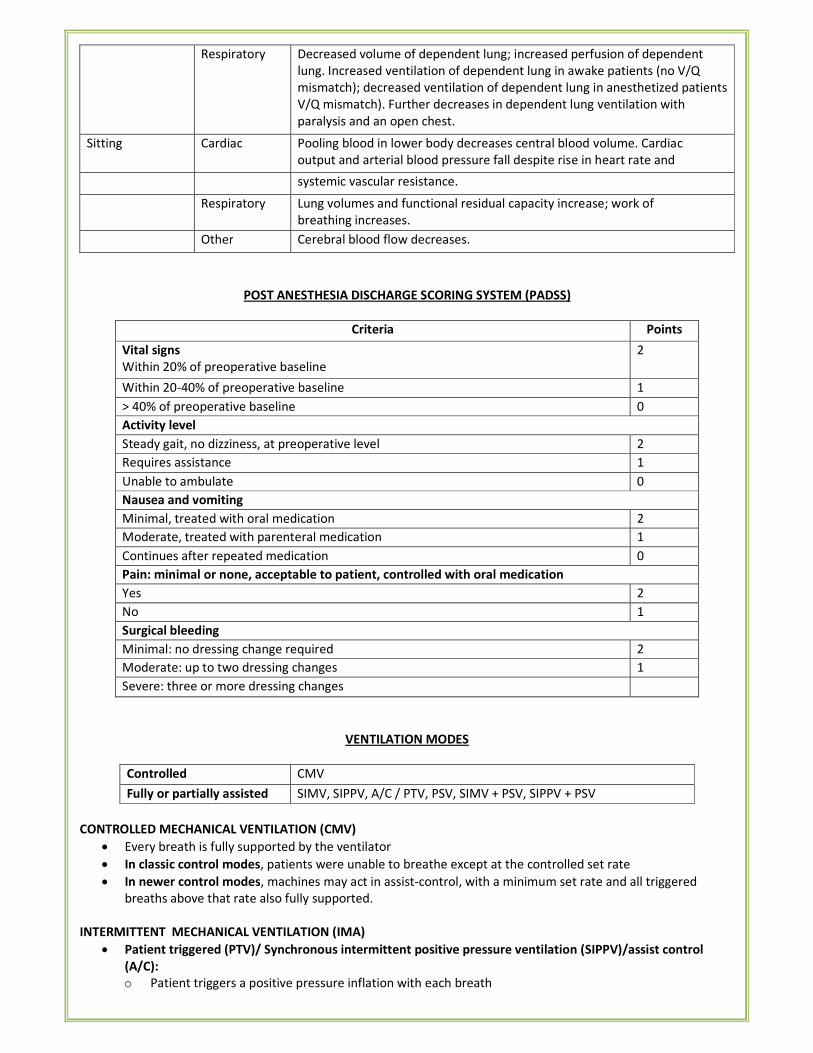
POST ANESTHESIA DISCHARGE SCORING SYSTEM (PADSS)
Criteria Points
Vital signs
Within 20% of preoperative baseline
2
Within 20-40% of preoperative baseline 1
> 40% of preoperative baseline 0
Activity level
Steady gait, no dizziness, at preoperative level 2
Requires assistance 1
Unable to ambulate 0
Nausea and vomiting
Minimal, treated with oral medication 2
Moderate, treated with parenteral medication 1
Continues after repeated medication 0
Pain: minimal or none, acceptable to patient, controlled with oral medication
Yes 2
No 1
Surgical bleeding
Minimal: no dressing change required 2
Moderate: up to two dressing changes 1
Severe: three or more dressing changes
VENTILATION MODES
Controlled CMV
Fully or partially assisted SIMV, SIPPV, A/C / PTV, PSV, SIMV + PSV, SIPPV + PSV
CONTROLLED MECHANICAL VENTILATION (CMV)
• Every breath is fully supported by the ventilator
• In classic control modes, patients were unable to breathe except at the controlled set rate
• In newer control modes, machines may act in assist-control, with a minimum set rate and all triggered
breaths above that rate also fully supported.
INTERMITTENT MECHANICAL VENTILATION (IMA)
• Patient triggered (PTV)/ Synchronous intermittent positive pressure ventilation (SIPPV)/assist control
(A/C):
o Patient triggers a positive pressure inflation with each breath
• Synchronized Intermittent Mandatory Ventilation (SIMV):
o Patient is able to trigger only a pre-set number of positive pressure inflations.
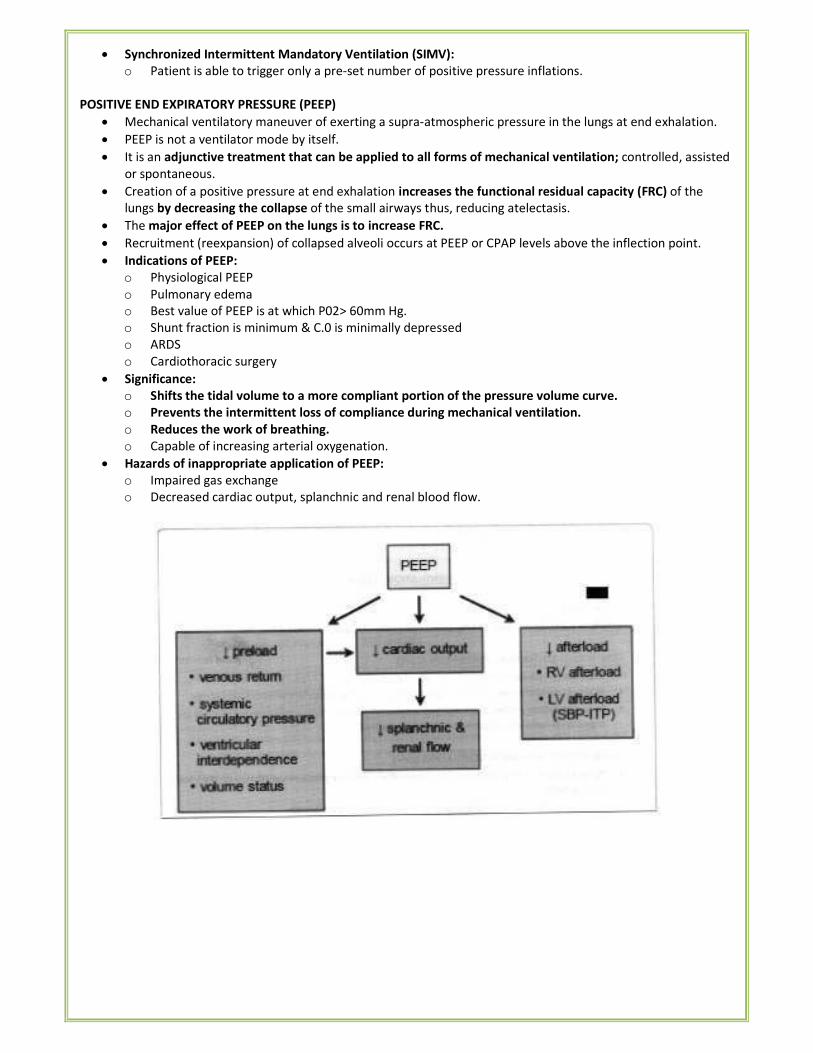
POSITIVE END EXPIRATORY PRESSURE (PEEP)
• Mechanical ventilatory maneuver of exerting a supra-atmospheric pressure in the lungs at end exhalation.
• PEEP is not a ventilator mode by itself.
• It is an adjunctive treatment that can be applied to all forms of mechanical ventilation; controlled, assisted
or spontaneous.
• Creation of a positive pressure at end exhalation increases the functional residual capacity (FRC) of the
lungs by decreasing the collapse of the small airways thus, reducing atelectasis.
• The major effect of PEEP on the lungs is to increase FRC.
• Recruitment (reexpansion) of collapsed alveoli occurs at PEEP or CPAP levels above the inflection point.
• Indications of PEEP:
o Physiological PEEP
o Pulmonary edema
o Best value of PEEP is at which P02> 60mm Hg.
o Shunt fraction is minimum & C.0 is minimally depressed
o ARDS
o Cardiothoracic surgery
• Significance:
o Shifts the tidal volume to a more compliant portion of the pressure volume curve.
o Prevents the intermittent loss of compliance during mechanical ventilation.
o Reduces the work of breathing.
o Capable of increasing arterial oxygenation.
• Hazards of inappropriate application of PEEP:
o Impaired gas exchange
o Decreased cardiac output, splanchnic and renal blood flow.
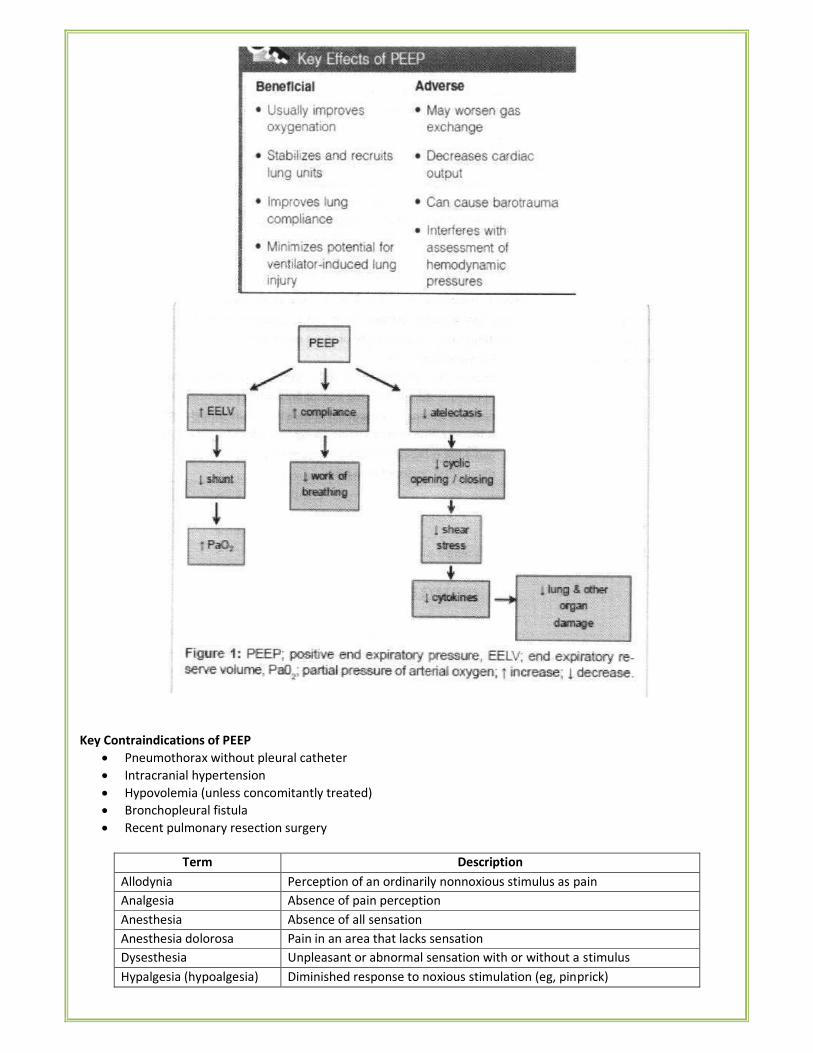
Key Contraindications of PEEP
• Pneumothorax without pleural catheter
• Intracranial hypertension
• Hypovolemia (unless concomitantly treated)
• Bronchopleural fistula
• Recent pulmonary resection surgery
Term Description
Allodynia Perception of an ordinarily nonnoxious stimulus as pain
Analgesia Absence of pain perception
Anesthesia Absence of all sensation
Anesthesia dolorosa Pain in an area that lacks sensation
Dysesthesia Unpleasant or abnormal sensation with or without a stimulus
Hypalgesia (hypoalgesia) Diminished response to noxious stimulation (eg, pinprick)
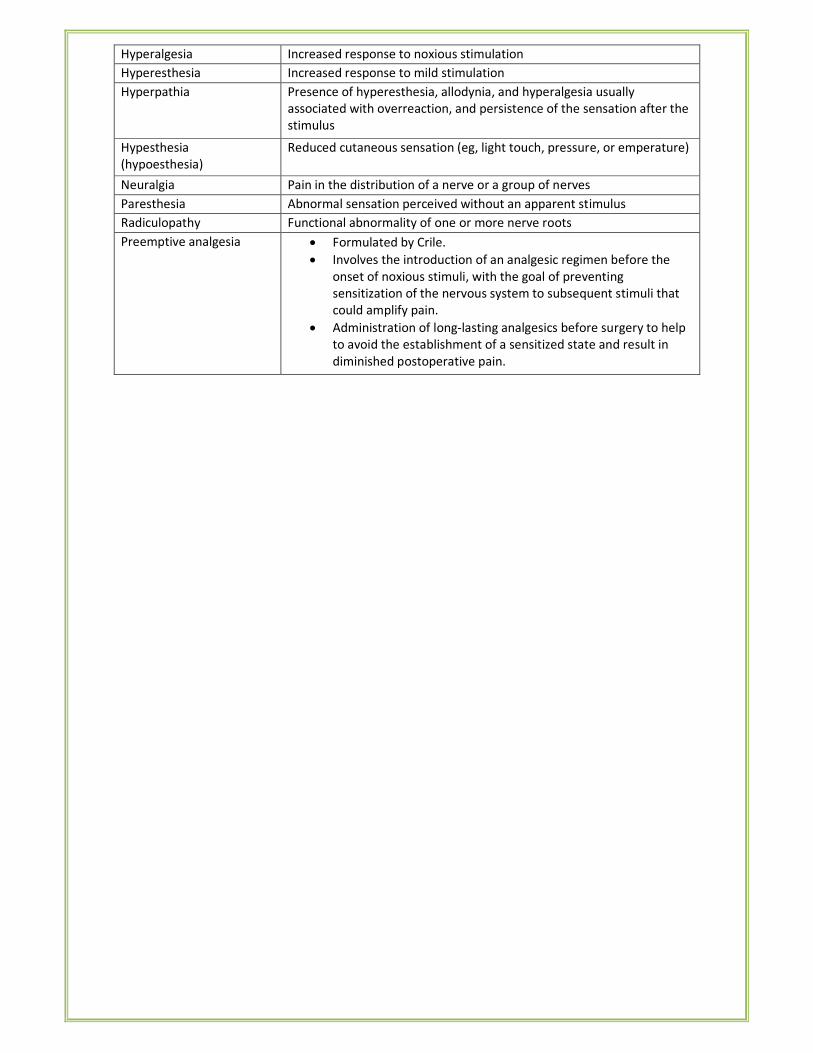
Hyperalgesia Increased response to noxious stimulation
Hyperesthesia Increased response to mild stimulation
Hyperpathia Presence of hyperesthesia, allodynia, and hyperalgesia usually
associated with overreaction, and persistence of the sensation after the
stimulus
Hypesthesia
(hypoesthesia)
Reduced cutaneous sensation (eg, light touch, pressure, or emperature)
Neuralgia Pain in the distribution of a nerve or a group of nerves
Paresthesia Abnormal sensation perceived without an apparent stimulus
Radiculopathy Functional abnormality of one or more nerve roots
Preemptive analgesia • Formulated by Crile.
• Involves the introduction of an analgesic regimen before the
onset of noxious stimuli, with the goal of preventing
sensitization of the nervous system to subsequent stimuli that
could amplify pain.
• Administration of long-lasting analgesics before surgery to help
to avoid the establishment of a sensitized state and result in
diminished postoperative pain.
II. CLINICAL PHARMACOLOGY OF ANESTHETIC DRUGS
STAGES OF ANESTHESIA (Guedel's staging based on ether)
• Stage I: Analgesia:
o Loss of pain sensation results from interference with sensory transmission in the Spinothalamic tract.
o The patient is conscious and conversational.
o Amnesia and a reduced awareness of pain occur as Stage II is approached.
• Stage II: Excitement:
o The patient experiences delirium and possibly violent, combative behavior.
o There is a rise and irregularity in blood pressure.
o The respiratory rate may increase.
o To avoid this stage of anesthesia, a short-acting barbiturate, such as thiopental, is given intravenously
before inhalation anesthesia is administered.
• Stage III: Surgical anesthesia:
o Regular respiration and relaxation of the skeletal muscles occur in this stage.
o Eye reflexes decrease progressively, until the eye movements cease and the pupil is fixed.
o Surgery may proceed during this stage.
• Stage IV: Medullary paralysis:
o Severe depression of the respiratory and vasomotor centers occurs during this stage.
o Death can rapidly ensue unless measures are taken to maintain circulation and respiration.
CLASSIFICATION OF GENERAL ANESTHETICS
Inhalational agents Intravenous agents
Gaseous Volatile Inducing agent Slower acting
Nitrous
oxide
Xenon
Alkanes:
Halothane
Ethers: Ether,
Enflurane,
Desflurane,
Isoflurane,
Sevoflurane
Propofol
Methohexitone
Thiopentone
Etomidate
Benzodiazepines
Dissociative anesthesia: Ketamine
Neurolept analgesia: Fentanyl +
Droperidol
INHALATION ANESTHETICS
IMPORTANT FACTS:
• IDEAL GAS Obeys Charles, Boyle's & Avogadro's law
• Charles's law: at constant pressure V a T.
• Boyle's law: at constant temperature V a 1/P.
• Unitary hypothesis: all inhalation agents share a common mechanism of action at the molecular level.
• Meyer—Overton rule: Anesthetic potency of inhalation agents correlates directly with their lipid solubility.
• General anesthesia typically reduces both VO2 and VCO2 by about 15%.
• The greatest reductions are in cerebral and cardiac O2 consumption.
• Three factors affect anesthetic uptake:
� Solubility in the blood
� Alveolar blood flow
� Difference in partial pressure between alveolar gas and venous blood.
MINIMAL ALVEOLAR CONCENTRATION
• MAC is alveolar concentration of an inhaled anesthetic that prevents movement in 50% of patients in
response to a standardized stimulus (eg:- surgical incision)
• MAC is a useful measure as it measures the potency of inhalational agents.
• 0.3 to 0.4 MAC is associated with awakening from anesthesia (MAC awake)
• There is 6% decrease in MAC per decade of age.
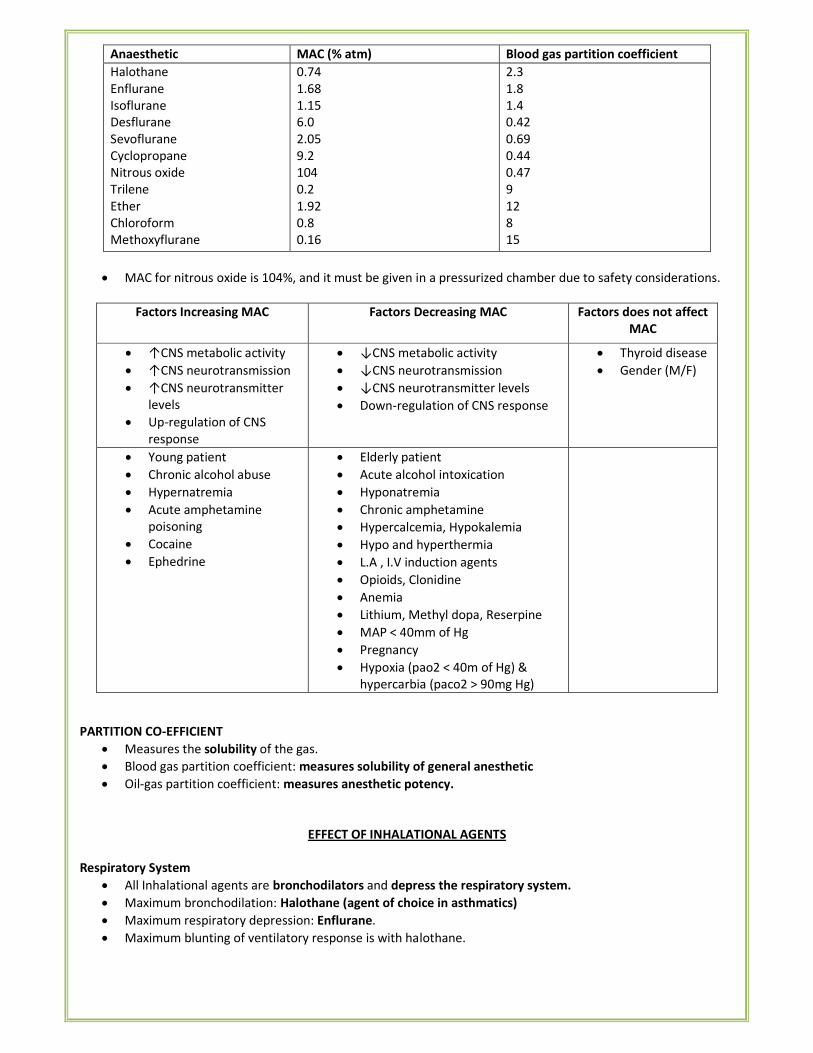
Anaesthetic MAC (% atm) Blood gas partition coefficient
Halothane
Enflurane
Isoflurane
Desflurane
Sevoflurane
Cyclopropane
Nitrous oxide
Trilene
Ether
Chloroform
Methoxyflurane
0.74
1.68
1.15
6.0
2.05
9.2
104
0.2
1.92
0.8
0.16
2.3
1.8
1.4
0.42
0.69
0.44
0.47
9
12
8
15
• MAC for nitrous oxide is 104%, and it must be given in a pressurized chamber due to safety considerations.
Factors Increasing MAC Factors Decreasing MAC Factors does not affect
MAC
• ↑CNS metabolic activity
• ↑CNS neurotransmission
• ↑CNS neurotransmitter
levels
• Up-regulation of CNS
response
• ↓CNS metabolic activity
• ↓CNS neurotransmission
• ↓CNS neurotransmitter levels
• Down-regulation of CNS response
• Thyroid disease
• Gender (M/F)
• Young patient
• Chronic alcohol abuse
• Hypernatremia
• Acute amphetamine
poisoning
• Cocaine
• Ephedrine
• Elderly patient
• Acute alcohol intoxication
• Hyponatremia
• Chronic amphetamine
• Hypercalcemia, Hypokalemia
• Hypo and hyperthermia
• L.A , I.V induction agents
• Opioids, Clonidine
• Anemia
• Lithium, Methyl dopa, Reserpine
• MAP < 40mm of Hg
• Pregnancy
• Hypoxia (pao2 < 40m of Hg) &
hypercarbia (paco2 > 90mg Hg)
PARTITION CO-EFFICIENT
• Measures the solubility of the gas.
• Blood gas partition coefficient: measures solubility of general anesthetic
• Oil-gas partition coefficient: measures anesthetic potency.
EFFECT OF INHALATIONAL AGENTS
Respiratory System
• All Inhalational agents are bronchodilators and depress the respiratory system.
• Maximum bronchodilation: Halothane (agent of choice in asthmatics)
• Maximum respiratory depression: Enflurane.
• Maximum blunting of ventilatory response is with halothane.
Cardiovascular System
• All inhalational agents decrease cardiac output except isoflurane and desflurane.
• Maximum decrease in C.O- halothane
• C.0 is best maintained by isoflurane because of reflex tachycardia.
• All inhalational agents are pulmonary vasodilators except N2O which is pulmonary vasoconstrictor
• All inhalational agents reduce mucociliary activity of airways except ether.
• Maximum inhibition of baroreceptor reflexes is with Halothane.
• All inhalational agents reduce BP except cyclopropane.
• Isoflurane is the agent of choice for controlled hypotension.
• Isoflurane is agent of choice for cardiac patients because of maintenance of C.O and minimum response on
baroreceptor reflexes.
• Maximum inhibition of myocardial contractility - Halothane.
• Halothane sensitizes the heart to arrhythmogenic action of adrenaline
• Halothane is contraindicated in patients with Pheochromocytoma
Central Nervous System
• All inhalational agents increase intracranial tension.
• Maximum increase in intracranial tension is with enflurane.
• Minimum increase in ICT is isoflurane and Desflurane < 6%
• Inhalational agent of choice for neurosurgeries is Isoflurane.
Kidneys
• Nephrotoxicity is d/t fluoride content.
• Anesthetics are fluorinated to make them non-inflammatory.
• Maximum fluoride content is seen in methoxyflurane (maximum nephrotoxicity)
• Methoxyflurane produces vasopressin resistance, polyuric renal failure
Others
• N2O can cause bone marrow suppression, Vitamin B12 deficiency and megaloblastic anemia
• All inhalational agents relaxes the uterus.
• Maximum uterine relaxation - halothane and thus halothane is agent of choice for internal version and
manual removal of placenta.
• Hyperglycemia is produced by ether, cyclopropane and desflurane.
• All inhalational agents increase intra ocular pressure
• All inhalational agents are good skeletal muscle relaxants except N2O.
• Maximim skeletal muscle relaxation is by ether
• Ether and cyclopropane are highly inflammable. Cautery should not be used with these agents.
• All inhalational agents undergo metabolism by oxidation.
• Halothane is metabolized by reduction and oxidation.
Extent of metaholism of inhalational anesthetics
• Methoxyflurane > 70% (maximum metabolism)
• Halothane > 40%
• Enflurane 8%
• Sevoflurane 2-5%
• Isoflurane < 2%
• Desflurane < 0.05% (least metabolism)
• N2O does not undergo any metabolism
PHARMACOLOGY OF INDIVIDUAL AGENTS
NITROUS OXIDE (laughing gas)
• Has second gas effect during induction & diffusion hypoxia after discontinuation of anesthesia in recovery
phase.
• As N2O is used in high concentration (70-80%) it leads to entry of N2O in blood at a rate higher than minute
(1 lit/min) volume.
• N2O has low blood solubility. So it rapidly diffuse into alveoli & dilutes the alveolar air-Partial Pressure of O2
in alveoli is reduced i.e. diffusion hypoxia
• Diffusion hypoxia is prevented by administering 100% oxygen for 5-10 min after discontinuing N2O
• Poynting effect: Entonox (50% O2 & 50% N2O) & mixture of gases (O2 & N2O) keeps them in gaseous form.
• If another potent anesthetic eg. Halothane is added, it also will be delivered to the blood at a rate higher
than minute volume & the induction will be faster.
• N2O is a good analgesic but weak anaesthetic and poor muscle relaxant. Hence it is not a complete
anaesthetic.
• N2O has blood gas coefficient of 0.47 and has fast induction
• It has MAC value of 104; Hence Potency is low
• N2O is used as a carrier gas given in a mixture of 33% O2 and 66% N2O
• Contraindications for N2O :
o Middle ear surgeries and tympanoplasty
o Laparoscopic surgeries, Eye surgeries
o Acute intestinal obstruction and volvulus
o Microlaryngeal surgeries
o Pneumothorax, pneumoperitonium
o Pneumoencephalos.
• It should be avoided in patients with pulmonary hypertension
• Adverse effects: bone marrow depression (agranulocytosis, megaloblastic anemia) and even neurological
deficiencies (peripheral neuropathies and pernicious anemia).
ENTONOX
• 50-50 mixture of N2O & O2
• Cylinder is blue coloured with white shoulder
• Uses - analgesia for wound dressing, chest physiotherapy, removal of chest drains labour analgesia, & dental
surgery
• It is good analgesic (d/to N2O)
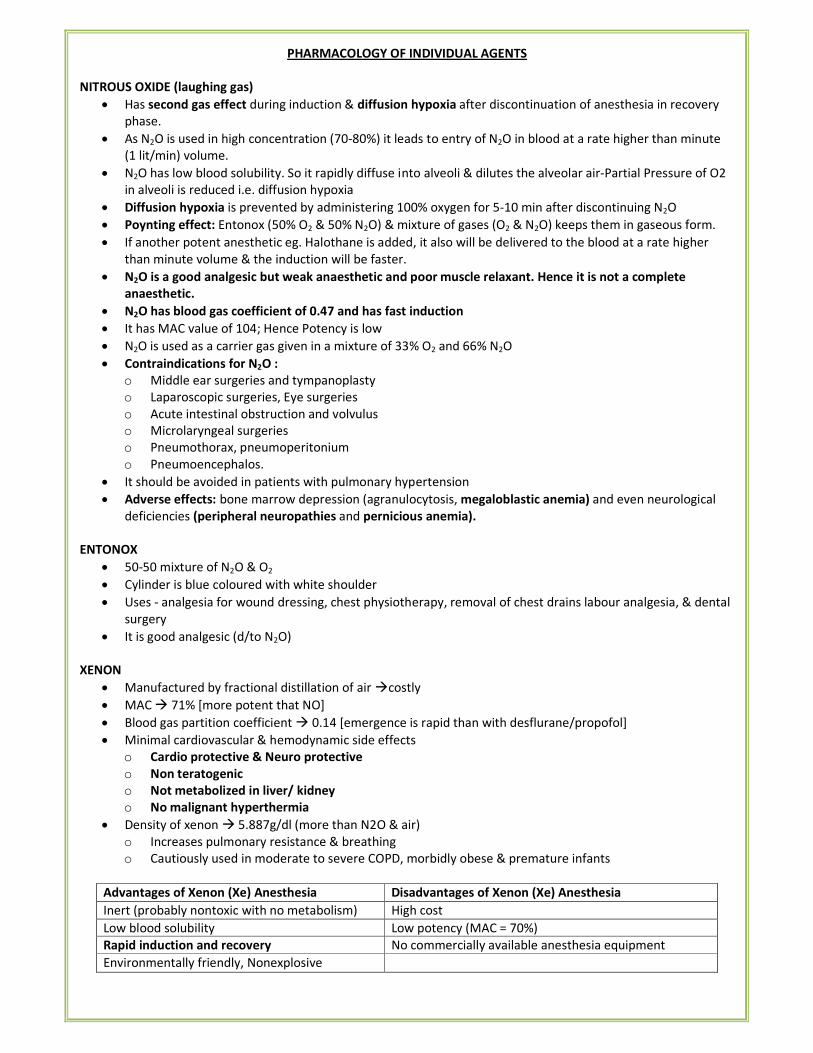
XENON
• Manufactured by fractional distillation of air �costly
• MAC � 71% [more potent that NO]
• Blood gas partition coefficient � 0.14 [emergence is rapid than with desflurane/propofol]
• Minimal cardiovascular & hemodynamic side effects
o Cardio protective & Neuro protective
o Non teratogenic
o Not metabolized in liver/ kidney
o No malignant hyperthermia
• Density of xenon � 5.887g/dl (more than N2O & air)
o Increases pulmonary resistance & breathing
o Cautiously used in moderate to severe COPD, morbidly obese & premature infants
Advantages of Xenon (Xe) Anesthesia Disadvantages of Xenon (Xe) Anesthesia
Inert (probably nontoxic with no metabolism) High cost
Low blood solubility Low potency (MAC = 70%)
Rapid induction and recovery No commercially available anesthesia equipment
Environmentally friendly, Nonexplosive
HALOTHANE (2, bromo, 2 chloro, 1, 1, 1 trifluoroethane)
• Least expensive & least pungent.
• Potent anesthetic, no analgesia.
• Dissolve rubber and corrodes metals.
• Drager Narko test is done for halothane.
• Contains 0.01% thymol for stability.
• Decomposed by light but is stable in amber coloured bottles.
• 15-20% is metabolized.
• May persist in the liver upto 12 days & not given in same patient within 3 months (potent hepato toxic).
• Relaxes skeletal and uterine muscle & blood vessels.
• Not hepatotoxic in children and combined with its pleasant odor, suitable in children for inhalation
induction.
• Causes 5’H’
o Malignant Hyperthermia,
o Hepatitis (centrilobular necrosis) extremely rare (1 per 35,000 cases)
o Hypotension
o Hypercapnia
o Heart rate decreases (myocardial depression)
• Decreases 10P, but ICT is increased
• Shivering & tremors common (H-shakes) in early post-operative period
• Myocardial depression of halothane is exacerbated by β-blockers and calcium channel-
• blocking agents.
• The combination of halothane and aminophylline � serious ventricular arrhythmias.
Contraindications for halothane:
• Pregnancy because it increases the risk of post -partum hemorrhage
• Liver dysfunction & Previous use within 3 months: due to halothane hepatitis
• Hypovolemia & severe cardiac disease (aortic stenosis); due to negative ionotropic effect
• Pheochromocytoma & exogenous catecholamines administration as it sensitize heart to catecholamines.
� Best uterine relaxant is Halothane followed by ether.
� Best muscle relaxant is ether followed by halothane.
FLURANES
• Enflurane
� Contraindicated in epilepsy
� Increases cerebral blood flow, secretion of CSF, resistance to CSF flow & intra cranial pressure
� High voltage high frequency EEG changes can progress to spike & wave pattern that culminates in frank
tonic clonic seizures.
� This epileptiform activity is exacerbated by high anesthetic concentrations & hypocapnia, so
hyperventilation is not recommended to attenuate Enflurane induced intracranial hypertension.
• Isoflurane
� AOC in neurosurgery
� Causes coronary steal syndrome
� Least effect on myocardial contractility [most cardio stable volatile agent]
• Enflurane & Halothane: myocardial depressants
• Desflurane: transient sympathetic activation, broken down to carbon monoxide by dry barium hydroxide
���� carbon monoxide poisoning.
• Sevoflurane
� Sweet odour
� Metabolized to HFIP [Hexa flour !so propyl]
� Induction agent of choice in children
• Halothane and isoflurane: sensitizes the heart to circulating catecholamines (adr/NA)
• Seizures are seen in enflurane & desflurane (lesser extent)
HEPATOTOXICITY OF ANESTHETIC AGENTS:
• Depends on
o Gender (Female> male)
o Age (middle age adults)
o Obesity
o Enzyme induction
o Prior anesthetic exposure
o Genetics
• Hepatotoxicity of inhalational agents is due to TFA [Tri flour acetyl] metabolite.
• Therefore, hepatotoxicity is proportional to the percentage of metabolism.
• % metabolism: halothane (20%) > Sevoflurane (2-5%)> Enflurane (2-4%)> Isoflurane (0.2%)>desflurane
(0.02%)
• But sevoflurane does not cause hepatotoxicity because its metabolite is HFIP (not TFA)
NEPHROTOXICITY OF ANESTHETIC AGENTS:
• Methoxyflurane:
o Most potent inhalation agent, but its high solubility and low vapor pressure limited its rate of induction
and emergence
o Highly nephrotoxic (high fluoride content)
o Causes polyuric (High output), vasopressin-resistant renal failure
o Tendency of oxalate stone formation
• Prolonged use of Enflurane: Leads to significant fluoride production and nephrotoxicity.
• Though sevoflurane produces fluoride, nephrotoxicity is rare in usual therapeutic doses
• Halothane, Isoflurane Desflurane: fluoride production is negligible, Can be used in Renal failure.
• Halothane & Isoflurane decreases renal blood flow, GRF & urinary output but Desflurane do not.
TRICHLOROETHYLENE (TRILENE)
• It is potent nerve poison.
• Vth & VII th CN are most commonly involved
• Produces analgesia in distribution of 5th
cranial nerve & relieves trigeminal neuralgia.
• It is not used in closed circuit (Soda lime ) because toxic product may be formed
• At 125°C or in presence of O2 as by cautery it decomposes into phosgene (COCl2) & Hcl
• Does not depress myocardium & respiration (like N2O)
• Not inflammable.
• Disadvantage : Sensitizes heart to adrenaline (Occasional dysrhythmia)
• Highly potent analgesic because MAC is low 17% (MAC α�
�������)
• Used for labour analgesia
ETHER
• Ether has slow induction with slow recovery and is very unpleasant.
• Induces laryngeal spasm and makes induction even slower.
• Stimulates salivary and bronchial secretions. So atropine pre medication is required.
• Highly inflammable and explosive, it should not be used when diathermy is needed in the airway
• Muscle relaxants need no to be used as ether itself produce excellent relaxation.
• Ether liberates catecholamines and tends to maintain blood pressure.
• No sensitization of myocardium to circulating catecholamines.
• It is a complete anaesthetic nearer to ideal anaesthetic.
• Ether does not affect the mucociliary action and is good bronchodilator.
• Ether has good anaesthetic, good analgesic, good skeletal muscle relaxant.
• Ether does not cause depression of myocardium but instead causes tachycardia and hypertension.
• Ether has highest instance of nausea and vomiting among inhalational agents.
• Ether causes hyperglycemia and is contraindicated in diabetes
• Guedel's 4 stages of anaesthesia were based on ether.
• Ether is safe in unskilled professionals and is very economical.
Preservatives
• Halothane: 0.01% thymol
• Ketamine: Benzethonium chloride
• Thiopentone: Anhydrous sodium carbonate (6%) & nitrogen gas
• Ether: propyl galate/ hydroquinone/ diphenylamine
NONVOLATILE ANESTHETIC AGENTS
PROPOFOL
Cardiovascular Neurologic Metabolic
• Depresses entricular
systolic function
• Vasodilatation results
from calcium channel
blockade.
• In patients undergoing
coronary artery bypass
surgery, it decreases
mean arterial blood
pressure, stroke volume
and increases heart rate
• Reduce neuronal
damage by
depressing cerebral
metabolism.
• Decreases cerebral
oxygen
consumption,
cerebral blood flow
and cerebral glucose
use
• The emulsion used as the vehicle for propofol
contains soybean oil and egg lecithin and
supports bacterial growth; iatrogenic
contamination leading to septic shock.
• Currently available preparations contain EDTA,
metabisulfite, or benzyl alcohol as a
bacteriostatic agent.
• Because EDTA chelates trace metals,
particularly zinc, serum zinc levels should be
measured daily during continuous infusions
• Hyperlipidemia may occur in infants and small
children
• Water-soluble phosphorylated prodrug: fospropofol [hydrolyzed by endothelial cell surface alkaline
phosphatases]
• Hypnotic agent associated with pleasant emergence and little hangover.
• 1% xylocaine is also given along with it to reduce pain on injection.
• Preferred agent for sedation and hypnosis and in particular for patients with altered level of consciousness.
• Anesthetic of Choice
o Malignant hyperpyrexia
o Day care surgery
o Total IV anesthesia (used along with alfentanil)
• Has anti-oxidant, anti- emetic, anti convulsant, bronchodilator & anti pruritic property.
• The rapid recovery of neurologic status makes it a good sedative in ICU patients.
• Diprivan (1% formulation): contains 10% soya oil, 1.25% egg phophatide & 2.25 %glycerol.
PROPOFOL INFUSION SYNDROME-PRIS:
• Occurs if given at the rate of 4mg/kg/hour or more for 48hrs or longer.
• Lethal disorder as it interferes with mitochondrial oxidation.
• Features:
o Acute refractory bradycardia leading to asystole
o Metabolic acidosis
o Rhabdomyolysis
o Hyperlipidemia
o Enlarged/fatty liver
o Cardiomyopathy with acute cardiac failure, skeletal myopathy
THIOPENTONE
• Ultra short acting barbiturate used for induction.
• The duration of action of highly lipid-soluble barbiturates (thiopental, thiamylal, and
methohexital) is determined by redistribution, not metabolism or elimination.
• Although thiopental is highly protein bound (80%), its great lipid solubility and high nonionized fraction
(60%) account for maximal brain uptake within 30 s.
Actions:
CNS:
• Cerebro protective
• Decreases cerebral blood flow & intra cranial tension.
• Decreases cerebral O2 consumption & increases the perfusion pressure.
• Anti-analgesic (can produce hyperalgesia by reducing the threshold of pain)
• It has anticonvulsant / anti-epileptic property
Eye:
• Pupils first dilate & then constrict.
• Decrease in IOT
• Loss of eye lash reflex- sign of adequate induction
Musculo - skeletal system: Tremors, twitching, respiratory excitation including cough, hiccup
Respiratory system: Transient apnea, respiratory depression [double apnea], upper airway obstruction
Larynx: Laryngospasm & hiccups
Other Features:
• It is not a muscle relaxant.
• Has anti-thyroid properties because it has thiourilene structure.
• Ringer lactate should not be used for reconstitution as it gets precipitated with it.
• IV agent of choice for cerebral protection.
• It crosses BBB and Placental barrier
Complications:
• Induces ALA synthetase ���� acute intermittent porphyria.
• Perivenous and IM injections cause tissue necrosis and ulcerations due to high alkalinity
• Intra-arterial injections lead to arterial spasm which is prevented by using 2.5% solution, injecting very
slowly and in incremental doses.
• Thiopentone should be avoided in asthmatics, hypotension, and shock, patients on Beta blockers,
hypokalemia, heart blocks, valvular stenosis and dystrophia myotonia.
METHOHEXITONE
• Ultra short acting barbiturate. More potent than thiopentone.
• Induces seizures and is the agent of choice for electroconvulsive therapy
ETOMIDATE
• Used to induce anesthesia.
• Hypnotic agent but lacks analgesic activity.
• Water solubility is poor, so etomidate is formulated in a propylene glycol solution.
• Induction is rapid, and the drug is short-acting.
• Only used for patients with coronary artery disease or CVS dysfunction, such as shock.
• Etomidate is hydrolyzed in the liver, no effect on the heart and circulation.
• Adverse effect: decrease in plasma cortisol and aldosterone levels due to inhibition of 11-α-ahydroxylase.
KETAMINE
• A short-acting, non barbiturate anesthetic
• Structural analogue of phencyclidine
• N-methyl-D-aspartate receptor (NMDA) a subtype of the glutamate receptor antagonist.
• Causes profound analgesia, dissociative anesthesia and catatonia
• Anesthesia of choice in shock.
• It is associated with emergence psychoto mimetic side effects "DISSOCIATIVE ANESTHESIA" (delirium,
illusions, hallucination) it is less common in children and pretreatment with lorazepam (drug of choice)
• Only IV anesthetic agent with both anesthetic and analgesic activity
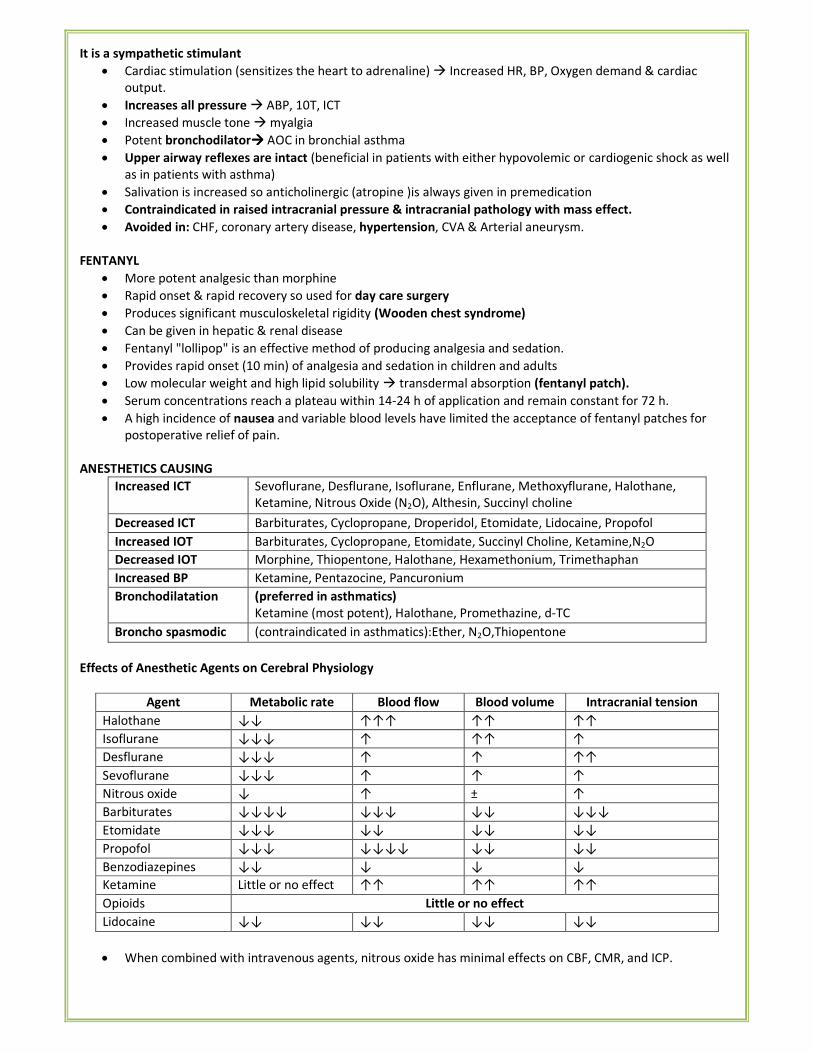
It is a sympathetic stimulant
• Cardiac stimulation (sensitizes the heart to adrenaline) � Increased HR, BP, Oxygen demand & cardiac
output.
• Increases all pressure � ABP, 10T, ICT
• Increased muscle tone � myalgia
• Potent bronchodilator���� AOC in bronchial asthma
• Upper airway reflexes are intact (beneficial in patients with either hypovolemic or cardiogenic shock as well
as in patients with asthma)
• Salivation is increased so anticholinergic (atropine )is always given in premedication
• Contraindicated in raised intracranial pressure & intracranial pathology with mass effect.
• Avoided in: CHF, coronary artery disease, hypertension, CVA & Arterial aneurysm.
FENTANYL
• More potent analgesic than morphine
• Rapid onset & rapid recovery so used for day care surgery
• Produces significant musculoskeletal rigidity (Wooden chest syndrome)
• Can be given in hepatic & renal disease
• Fentanyl "lollipop" is an effective method of producing analgesia and sedation.
• Provides rapid onset (10 min) of analgesia and sedation in children and adults
• Low molecular weight and high lipid solubility � transdermal absorption (fentanyl patch).
• Serum concentrations reach a plateau within 14-24 h of application and remain constant for 72 h.
• A high incidence of nausea and variable blood levels have limited the acceptance of fentanyl patches for
postoperative relief of pain.
ANESTHETICS CAUSING
Increased ICT Sevoflurane, Desflurane, Isoflurane, Enflurane, Methoxyflurane, Halothane,
Ketamine, Nitrous Oxide (N2O), Althesin, Succinyl choline
Decreased ICT Barbiturates, Cyclopropane, Droperidol, Etomidate, Lidocaine, Propofol
Increased IOT Barbiturates, Cyclopropane, Etomidate, Succinyl Choline, Ketamine,N2O
Decreased IOT Morphine, Thiopentone, Halothane, Hexamethonium, Trimethaphan
Increased BP Ketamine, Pentazocine, Pancuronium
Bronchodilatation (preferred in asthmatics)
Ketamine (most potent), Halothane, Promethazine, d-TC
Broncho spasmodic (contraindicated in asthmatics):Ether, N2O,Thiopentone
Effects of Anesthetic Agents on Cerebral Physiology
Agent Metabolic rate Blood flow Blood volume Intracranial tension
Halothane ↓↓ ↑↑↑ ↑↑ ↑↑
Isoflurane ↓↓↓ ↑ ↑↑ ↑
Desflurane ↓↓↓ ↑ ↑ ↑↑
Sevoflurane ↓↓↓ ↑ ↑ ↑
Nitrous oxide ↓ ↑ ± ↑
Barbiturates ↓↓↓↓ ↓↓↓ ↓↓ ↓↓↓
Etomidate ↓↓↓ ↓↓ ↓↓ ↓↓
Propofol ↓↓↓ ↓↓↓↓ ↓↓ ↓↓
Benzodiazepines ↓↓ ↓ ↓ ↓
Ketamine Little or no effect ↑↑ ↑↑ ↑↑
Opioids Little or no effect
Lidocaine ↓↓ ↓↓ ↓↓ ↓↓
• When combined with intravenous agents, nitrous oxide has minimal effects on CBF, CMR, and ICP.
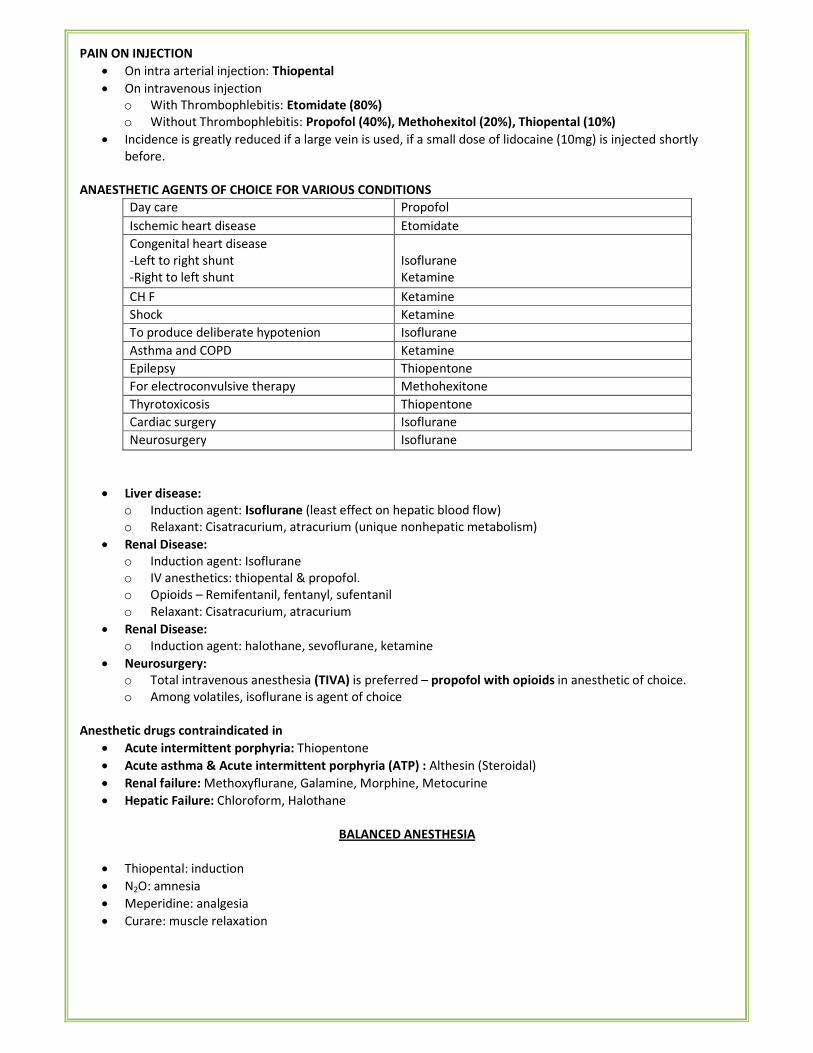
PAIN ON INJECTION
• On intra arterial injection: Thiopental
• On intravenous injection
o With Thrombophlebitis: Etomidate (80%)
o Without Thrombophlebitis: Propofol (40%), Methohexitol (20%), Thiopental (10%)
• Incidence is greatly reduced if a large vein is used, if a small dose of lidocaine (10mg) is injected shortly
before.
ANAESTHETIC AGENTS OF CHOICE FOR VARIOUS CONDITIONS
Day care Propofol
Ischemic heart disease Etomidate
Congenital heart disease
-Left to right shunt
-Right to left shunt
Isoflurane
Ketamine
CH F Ketamine
Shock Ketamine
To produce deliberate hypotenion Isoflurane
Asthma and COPD Ketamine
Epilepsy Thiopentone
For electroconvulsive therapy Methohexitone
Thyrotoxicosis Thiopentone
Cardiac surgery Isoflurane
Neurosurgery Isoflurane
• Liver disease:
o Induction agent: Isoflurane (least effect on hepatic blood flow)
o Relaxant: Cisatracurium, atracurium (unique nonhepatic metabolism)
• Renal Disease:
o Induction agent: Isoflurane
o IV anesthetics: thiopental & propofol.
o Opioids – Remifentanil, fentanyl, sufentanil
o Relaxant: Cisatracurium, atracurium
• Renal Disease:
o Induction agent: halothane, sevoflurane, ketamine
• Neurosurgery:
o Total intravenous anesthesia (TIVA) is preferred – propofol with opioids in anesthetic of choice.
o Among volatiles, isoflurane is agent of choice
Anesthetic drugs contraindicated in
• Acute intermittent porphyria: Thiopentone
• Acute asthma & Acute intermittent porphyria (ATP) : Althesin (Steroidal)
• Renal failure: Methoxyflurane, Galamine, Morphine, Metocurine
• Hepatic Failure: Chloroform, Halothane
BALANCED ANESTHESIA
• Thiopental: induction
• N2O: amnesia
• Meperidine: analgesia
• Curare: muscle relaxation
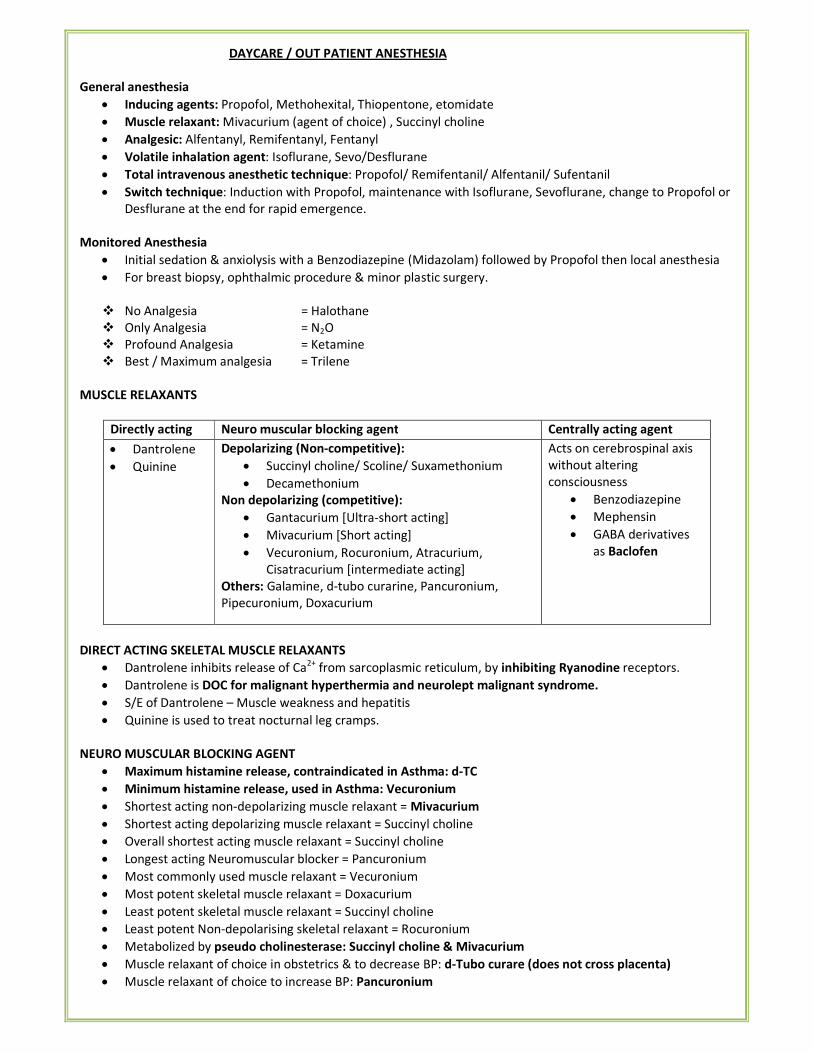
DAYCARE / OUT PATIENT ANESTHESIA
General anesthesia
• Inducing agents: Propofol, Methohexital, Thiopentone, etomidate
• Muscle relaxant: Mivacurium (agent of choice) , Succinyl choline
• Analgesic: Alfentanyl, Remifentanyl, Fentanyl
• Volatile inhalation agent: Isoflurane, Sevo/Desflurane
• Total intravenous anesthetic technique: Propofol/ Remifentanil/ Alfentanil/ Sufentanil
• Switch technique: Induction with Propofol, maintenance with Isoflurane, Sevoflurane, change to Propofol or
Desflurane at the end for rapid emergence.
Monitored Anesthesia
• Initial sedation & anxiolysis with a Benzodiazepine (Midazolam) followed by Propofol then local anesthesia
• For breast biopsy, ophthalmic procedure & minor plastic surgery.
� No Analgesia = Halothane
� Only Analgesia = N2O
� Profound Analgesia = Ketamine
� Best / Maximum analgesia = Trilene
MUSCLE RELAXANTS
Directly acting Neuro muscular blocking agent Centrally acting agent
• Dantrolene
• Quinine
Depolarizing (Non-competitive):
• Succinyl choline/ Scoline/ Suxamethonium
• Decamethonium
Non depolarizing (competitive):
• Gantacurium [Ultra-short acting]
• Mivacurium [Short acting]
• Vecuronium, Rocuronium, Atracurium,
Cisatracurium [intermediate acting]
Others: Galamine, d-tubo curarine, Pancuronium,
Pipecuronium, Doxacurium
Acts on cerebrospinal axis
without altering
consciousness
• Benzodiazepine
• Mephensin
• GABA derivatives
as Baclofen
DIRECT ACTING SKELETAL MUSCLE RELAXANTS
• Dantrolene inhibits release of Ca2+
from sarcoplasmic reticulum, by inhibiting Ryanodine receptors.
• Dantrolene is DOC for malignant hyperthermia and neurolept malignant syndrome.
• S/E of Dantrolene – Muscle weakness and hepatitis
• Quinine is used to treat nocturnal leg cramps.
NEURO MUSCULAR BLOCKING AGENT
• Maximum histamine release, contraindicated in Asthma: d-TC
• Minimum histamine release, used in Asthma: Vecuronium
• Shortest acting non-depolarizing muscle relaxant = Mivacurium
• Shortest acting depolarizing muscle relaxant = Succinyl choline
• Overall shortest acting muscle relaxant = Succinyl choline
• Longest acting Neuromuscular blocker = Pancuronium
• Most commonly used muscle relaxant = Vecuronium
• Most potent skeletal muscle relaxant = Doxacurium
• Least potent skeletal muscle relaxant = Succinyl choline
• Least potent Non-depolarising skeletal relaxant = Rocuronium
• Metabolized by pseudo cholinesterase: Succinyl choline & Mivacurium
• Muscle relaxant of choice in obstetrics & to decrease BP: d-Tubo curare (does not cross placenta)
• Muscle relaxant of choice to increase BP: Pancuronium
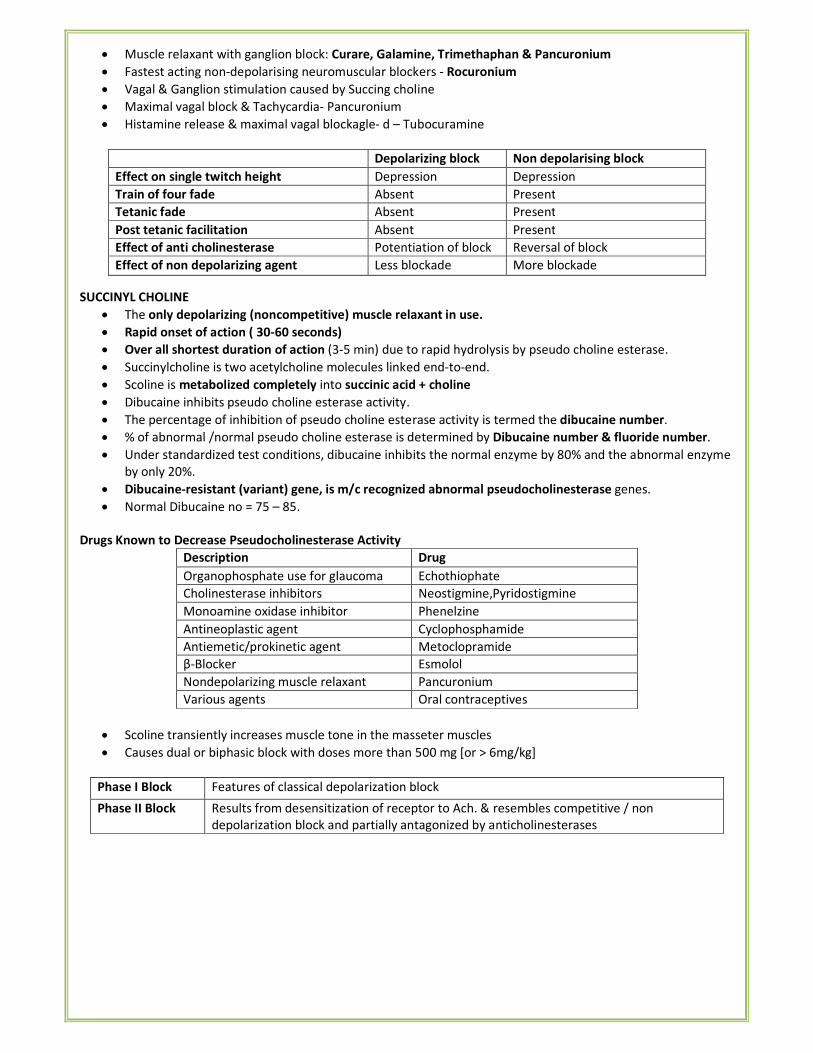
• Muscle relaxant with ganglion block: Curare, Galamine, Trimethaphan & Pancuronium
• Fastest acting non-depolarising neuromuscular blockers - Rocuronium
• Vagal & Ganglion stimulation caused by Succing choline
• Maximal vagal block & Tachycardia- Pancuronium
• Histamine release & maximal vagal blockagle- d – Tubocuramine
Depolarizing block Non depolarising block
Effect on single twitch height Depression Depression
Train of four fade Absent Present
Tetanic fade Absent Present
Post tetanic facilitation Absent Present
Effect of anti cholinesterase Potentiation of block Reversal of block
Effect of non depolarizing agent Less blockade More blockade
SUCCINYL CHOLINE
• The only depolarizing (noncompetitive) muscle relaxant in use.
• Rapid onset of action ( 30-60 seconds)
• Over all shortest duration of action (3-5 min) due to rapid hydrolysis by pseudo choline esterase.
• Succinylcholine is two acetylcholine molecules linked end-to-end.
• Scoline is metabolized completely into succinic acid + choline
• Dibucaine inhibits pseudo choline esterase activity.
• The percentage of inhibition of pseudo choline esterase activity is termed the dibucaine number.
• % of abnormal /normal pseudo choline esterase is determined by Dibucaine number & fluoride number.
• Under standardized test conditions, dibucaine inhibits the normal enzyme by 80% and the abnormal enzyme
by only 20%.
• Dibucaine-resistant (variant) gene, is m/c recognized abnormal pseudocholinesterase genes.
• Normal Dibucaine no = 75 – 85.
Drugs Known to Decrease Pseudocholinesterase Activity
Description Drug
Organophosphate use for glaucoma Echothiophate
Cholinesterase inhibitors Neostigmine,Pyridostigmine
Monoamine oxidase inhibitor Phenelzine
Antineoplastic agent Cyclophosphamide
Antiemetic/prokinetic agent Metoclopramide
β-Blocker Esmolol
Nondepolarizing muscle relaxant Pancuronium
Various agents Oral contraceptives
• Scoline transiently increases muscle tone in the masseter muscles
• Causes dual or biphasic block with doses more than 500 mg [or > 6mg/kg]
Phase I Block Features of classical depolarization block
Phase II Block Results from desensitization of receptor to Ach. & resembles competitive / non
depolarization block and partially antagonized by anticholinesterases
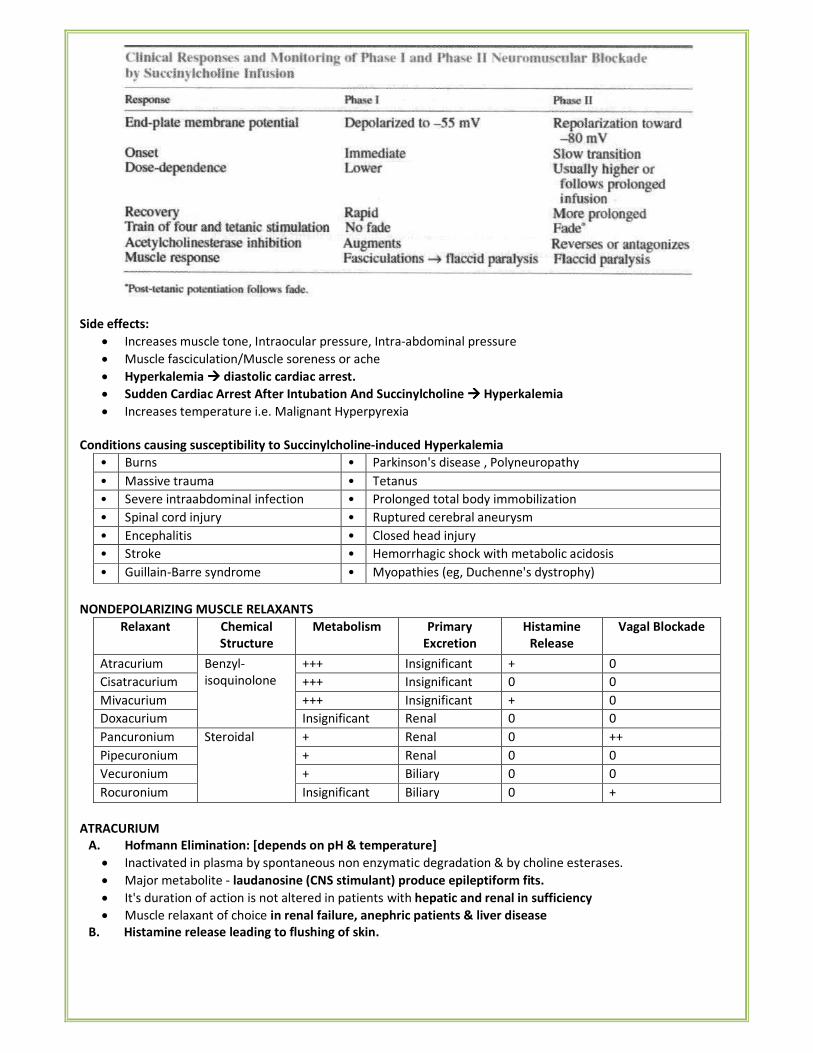
Side effects:
• Increases muscle tone, Intraocular pressure, Intra-abdominal pressure
• Muscle fasciculation/Muscle soreness or ache
• Hyperkalemia ���� diastolic cardiac arrest.
• Sudden Cardiac Arrest After Intubation And Succinylcholine ���� Hyperkalemia
• Increases temperature i.e. Malignant Hyperpyrexia
Conditions causing susceptibility to Succinylcholine-induced Hyperkalemia
• Burns • Parkinson's disease , Polyneuropathy
• Massive trauma • Tetanus
• Severe intraabdominal infection • Prolonged total body immobilization
• Spinal cord injury • Ruptured cerebral aneurysm
• Encephalitis • Closed head injury
• Stroke • Hemorrhagic shock with metabolic acidosis
• Guillain-Barre syndrome • Myopathies (eg, Duchenne's dystrophy)
NONDEPOLARIZING MUSCLE RELAXANTS
Relaxant Chemical
Structure
Metabolism Primary
Excretion
Histamine
Release
Vagal Blockade
Atracurium Benzyl-
isoquinolone
+++ Insignificant + 0
Cisatracurium +++ Insignificant 0 0
Mivacurium +++ Insignificant + 0
Doxacurium Insignificant Renal 0 0
Pancuronium Steroidal + Renal 0 ++
Pipecuronium + Renal 0 0
Vecuronium + Biliary 0 0
Rocuronium Insignificant Biliary 0 +
ATRACURIUM
A. Hofmann Elimination: [depends on pH & temperature]
• Inactivated in plasma by spontaneous non enzymatic degradation & by choline esterases.
• Major metabolite - laudanosine (CNS stimulant) produce epileptiform fits.
• It's duration of action is not altered in patients with hepatic and renal in sufficiency
• Muscle relaxant of choice in renal failure, anephric patients & liver disease
B. Histamine release leading to flushing of skin.
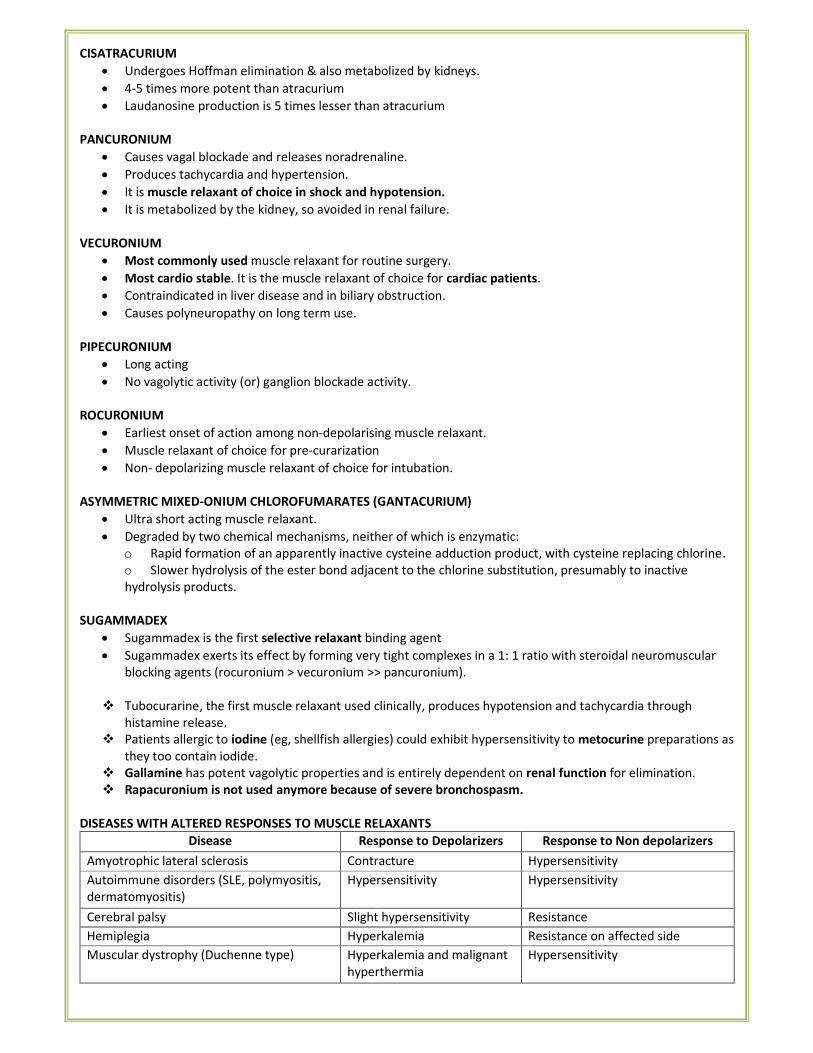
CISATRACURIUM
• Undergoes Hoffman elimination & also metabolized by kidneys.
• 4-5 times more potent than atracurium
• Laudanosine production is 5 times lesser than atracurium
PANCURONIUM
• Causes vagal blockade and releases noradrenaline.
• Produces tachycardia and hypertension.
• It is muscle relaxant of choice in shock and hypotension.
• It is metabolized by the kidney, so avoided in renal failure.
VECURONIUM
• Most commonly used muscle relaxant for routine surgery.
• Most cardio stable. It is the muscle relaxant of choice for cardiac patients.
• Contraindicated in liver disease and in biliary obstruction.
• Causes polyneuropathy on long term use.
PIPECURONIUM
• Long acting
• No vagolytic activity (or) ganglion blockade activity.
ROCURONIUM
• Earliest onset of action among non-depolarising muscle relaxant.
• Muscle relaxant of choice for pre-curarization
• Non- depolarizing muscle relaxant of choice for intubation.
ASYMMETRIC MIXED-ONIUM CHLOROFUMARATES (GANTACURIUM)
• Ultra short acting muscle relaxant.
• Degraded by two chemical mechanisms, neither of which is enzymatic:
o Rapid formation of an apparently inactive cysteine adduction product, with cysteine replacing chlorine.
o Slower hydrolysis of the ester bond adjacent to the chlorine substitution, presumably to inactive
hydrolysis products.
SUGAMMADEX
• Sugammadex is the first selective relaxant binding agent
• Sugammadex exerts its effect by forming very tight complexes in a 1: 1 ratio with steroidal neuromuscular
blocking agents (rocuronium > vecuronium >> pancuronium).
� Tubocurarine, the first muscle relaxant used clinically, produces hypotension and tachycardia through
histamine release.
� Patients allergic to iodine (eg, shellfish allergies) could exhibit hypersensitivity to metocurine preparations as
they too contain iodide.
� Gallamine has potent vagolytic properties and is entirely dependent on renal function for elimination.
� Rapacuronium is not used anymore because of severe bronchospasm.
DISEASES WITH ALTERED RESPONSES TO MUSCLE RELAXANTS
Disease Response to Depolarizers Response to Non depolarizers
Amyotrophic lateral sclerosis Contracture Hypersensitivity
Autoimmune disorders (SLE, polymyositis,
dermatomyositis)
Hypersensitivity Hypersensitivity
Cerebral palsy Slight hypersensitivity Resistance
Hemiplegia Hyperkalemia Resistance on affected side
Muscular dystrophy (Duchenne type) Hyperkalemia and malignant
hyperthermia
Hypersensitivity
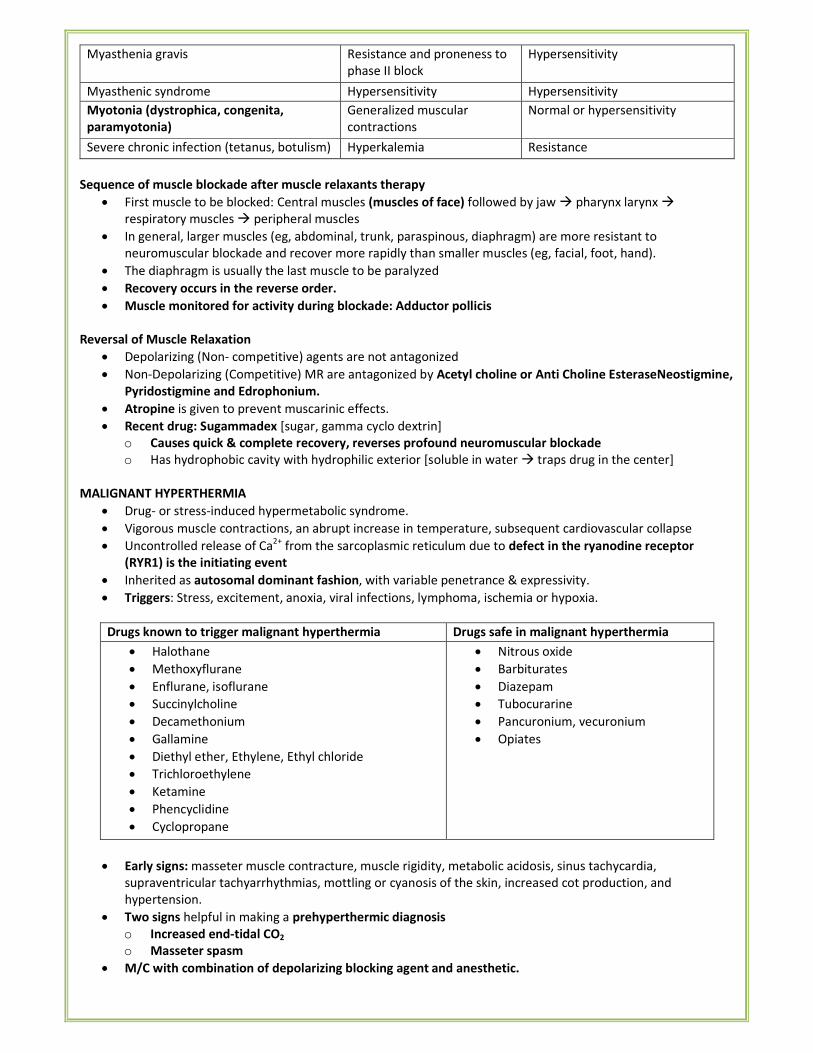
Myasthenia gravis Resistance and proneness to
phase II block
Hypersensitivity
Myasthenic syndrome Hypersensitivity Hypersensitivity
Myotonia (dystrophica, congenita,
paramyotonia)
Generalized muscular
contractions
Normal or hypersensitivity
Severe chronic infection (tetanus, botulism) Hyperkalemia Resistance
Sequence of muscle blockade after muscle relaxants therapy
• First muscle to be blocked: Central muscles (muscles of face) followed by jaw � pharynx larynx �
respiratory muscles � peripheral muscles
• In general, larger muscles (eg, abdominal, trunk, paraspinous, diaphragm) are more resistant to
neuromuscular blockade and recover more rapidly than smaller muscles (eg, facial, foot, hand).
• The diaphragm is usually the last muscle to be paralyzed
• Recovery occurs in the reverse order.
• Muscle monitored for activity during blockade: Adductor pollicis
Reversal of Muscle Relaxation
• Depolarizing (Non- competitive) agents are not antagonized
• Non-Depolarizing (Competitive) MR are antagonized by Acetyl choline or Anti Choline EsteraseNeostigmine,
Pyridostigmine and Edrophonium.
• Atropine is given to prevent muscarinic effects.
• Recent drug: Sugammadex [sugar, gamma cyclo dextrin]
o Causes quick & complete recovery, reverses profound neuromuscular blockade
o Has hydrophobic cavity with hydrophilic exterior [soluble in water � traps drug in the center]
MALIGNANT HYPERTHERMIA
• Drug- or stress-induced hypermetabolic syndrome.
• Vigorous muscle contractions, an abrupt increase in temperature, subsequent cardiovascular collapse
• Uncontrolled release of Ca2+
from the sarcoplasmic reticulum due to defect in the ryanodine receptor
(RYR1) is the initiating event
• Inherited as autosomal dominant fashion, with variable penetrance & expressivity.
• Triggers: Stress, excitement, anoxia, viral infections, lymphoma, ischemia or hypoxia.
Drugs known to trigger malignant hyperthermia Drugs safe in malignant hyperthermia
• Halothane
• Methoxyflurane
• Enflurane, isoflurane
• Succinylcholine
• Decamethonium
• Gallamine
• Diethyl ether, Ethylene, Ethyl chloride
• Trichloroethylene
• Ketamine
• Phencyclidine
• Cyclopropane
• Nitrous oxide
• Barbiturates
• Diazepam
• Tubocurarine
• Pancuronium, vecuronium
• Opiates
• Early signs: masseter muscle contracture, muscle rigidity, metabolic acidosis, sinus tachycardia,
supraventricular tachyarrhythmias, mottling or cyanosis of the skin, increased cot production, and
hypertension.
• Two signs helpful in making a prehyperthermic diagnosis
o Increased end-tidal CO2
o Masseter spasm
• M/C with combination of depolarizing blocking agent and anesthetic.
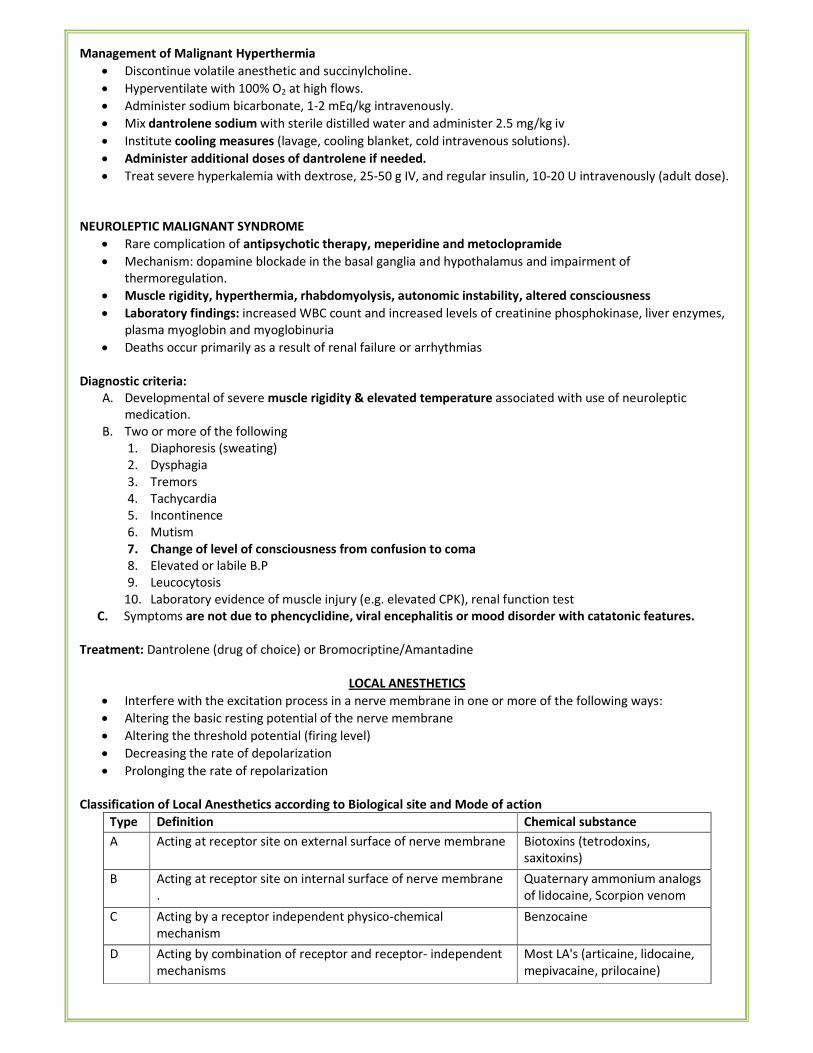
Management of Malignant Hyperthermia
• Discontinue volatile anesthetic and succinylcholine.
• Hyperventilate with 100% O2 at high flows.
• Administer sodium bicarbonate, 1-2 mEq/kg intravenously.
• Mix dantrolene sodium with sterile distilled water and administer 2.5 mg/kg iv
• Institute cooling measures (lavage, cooling blanket, cold intravenous solutions).
• Administer additional doses of dantrolene if needed.
• Treat severe hyperkalemia with dextrose, 25-50 g IV, and regular insulin, 10-20 U intravenously (adult dose).
NEUROLEPTIC MALIGNANT SYNDROME
• Rare complication of antipsychotic therapy, meperidine and metoclopramide
• Mechanism: dopamine blockade in the basal ganglia and hypothalamus and impairment of
thermoregulation.
• Muscle rigidity, hyperthermia, rhabdomyolysis, autonomic instability, altered consciousness
• Laboratory findings: increased WBC count and increased levels of creatinine phosphokinase, liver enzymes,
plasma myoglobin and myoglobinuria
• Deaths occur primarily as a result of renal failure or arrhythmias
Diagnostic criteria:
A. Developmental of severe muscle rigidity & elevated temperature associated with use of neuroleptic
medication.
B. Two or more of the following
1. Diaphoresis (sweating)
2. Dysphagia
3. Tremors
4. Tachycardia
5. Incontinence
6. Mutism
7. Change of level of consciousness from confusion to coma
8. Elevated or labile B.P
9. Leucocytosis
10. Laboratory evidence of muscle injury (e.g. elevated CPK), renal function test
C. Symptoms are not due to phencyclidine, viral encephalitis or mood disorder with catatonic features.
Treatment: Dantrolene (drug of choice) or Bromocriptine/Amantadine
LOCAL ANESTHETICS
• Interfere with the excitation process in a nerve membrane in one or more of the following ways:
• Altering the basic resting potential of the nerve membrane
• Altering the threshold potential (firing level)
• Decreasing the rate of depolarization
• Prolonging the rate of repolarization
Classification of Local Anesthetics according to Biological site and Mode of action
Type Definition Chemical substance
A Acting at receptor site on external surface of nerve membrane Biotoxins (tetrodoxins,
saxitoxins)
B Acting at receptor site on internal surface of nerve membrane
.
Quaternary ammonium analogs
of lidocaine, Scorpion venom
C Acting by a receptor independent physico-chemical
mechanism
Benzocaine
D Acting by combination of receptor and receptor- independent
mechanisms
Most LA's (articaine, lidocaine,
mepivacaine, prilocaine)
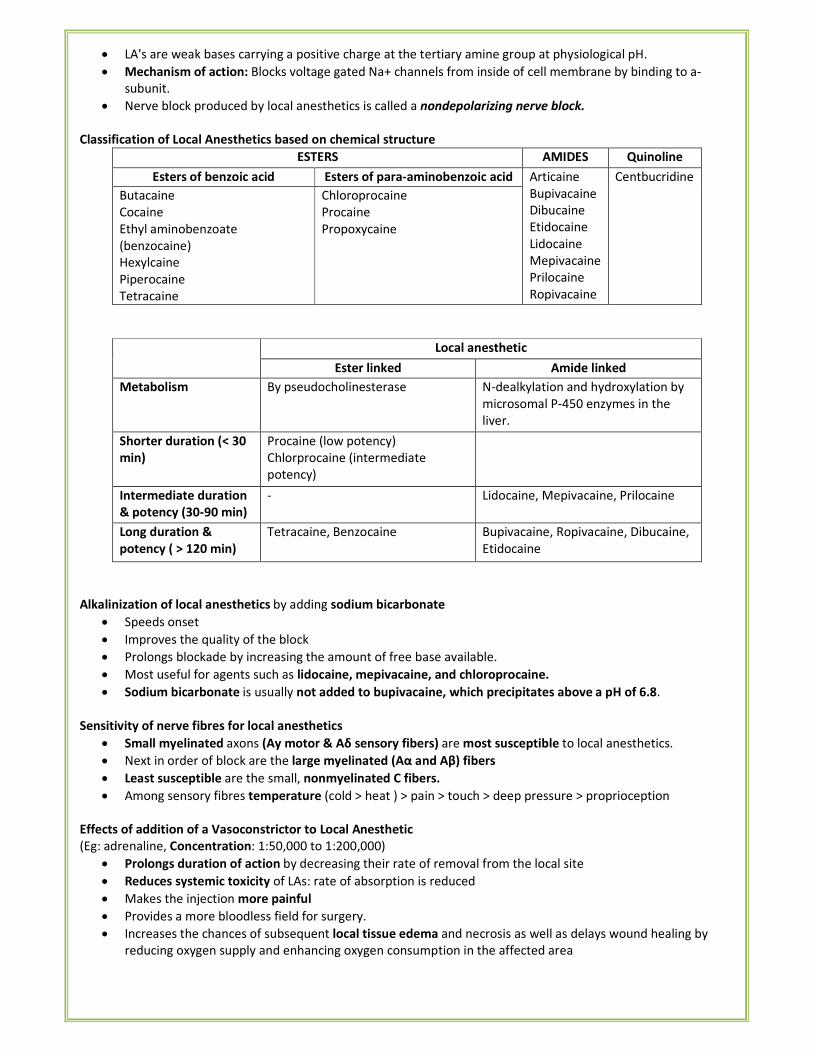
• LA's are weak bases carrying a positive charge at the tertiary amine group at physiological pH.
• Mechanism of action: Blocks voltage gated Na+ channels from inside of cell membrane by binding to a-
subunit.
• Nerve block produced by local anesthetics is called a nondepolarizing nerve block.
Classification of Local Anesthetics based on chemical structure
ESTERS AMIDES Quinoline
Esters of benzoic acid Esters of para-aminobenzoic acid Articaine
Bupivacaine
Dibucaine
Etidocaine
Lidocaine
Mepivacaine
Prilocaine
Ropivacaine
Centbucridine
Butacaine
Cocaine
Ethyl aminobenzoate
(benzocaine)
Hexylcaine
Piperocaine
Tetracaine
Chloroprocaine
Procaine
Propoxycaine
Local anesthetic
Ester linked Amide linked
Metabolism By pseudocholinesterase N-dealkylation and hydroxylation by
microsomal P-450 enzymes in the
liver.
Shorter duration (< 30
min)
Procaine (low potency)
Chlorprocaine (intermediate
potency)
Intermediate duration
& potency (30-90 min)
- Lidocaine, Mepivacaine, Prilocaine
Long duration &
potency ( > 120 min)
Tetracaine, Benzocaine Bupivacaine, Ropivacaine, Dibucaine,
Etidocaine
Alkalinization of local anesthetics by adding sodium bicarbonate
• Speeds onset
• Improves the quality of the block
• Prolongs blockade by increasing the amount of free base available.
• Most useful for agents such as lidocaine, mepivacaine, and chloroprocaine.
• Sodium bicarbonate is usually not added to bupivacaine, which precipitates above a pH of 6.8.
Sensitivity of nerve fibres for local anesthetics
• Small myelinated axons (Ay motor & Aδ sensory fibers) are most susceptible to local anesthetics.
• Next in order of block are the large myelinated (Aα and Aβ) fibers
• Least susceptible are the small, nonmyelinated C fibers.
• Among sensory fibres temperature (cold > heat ) > pain > touch > deep pressure > proprioception
Effects of addition of a Vasoconstrictor to Local Anesthetic
(Eg: adrenaline, Concentration: 1:50,000 to 1:200,000)
• Prolongs duration of action by decreasing their rate of removal from the local site
• Reduces systemic toxicity of LAs: rate of absorption is reduced
• Makes the injection more painful
• Provides a more bloodless field for surgery.
• Increases the chances of subsequent local tissue edema and necrosis as well as delays wound healing by
reducing oxygen supply and enhancing oxygen consumption in the affected area
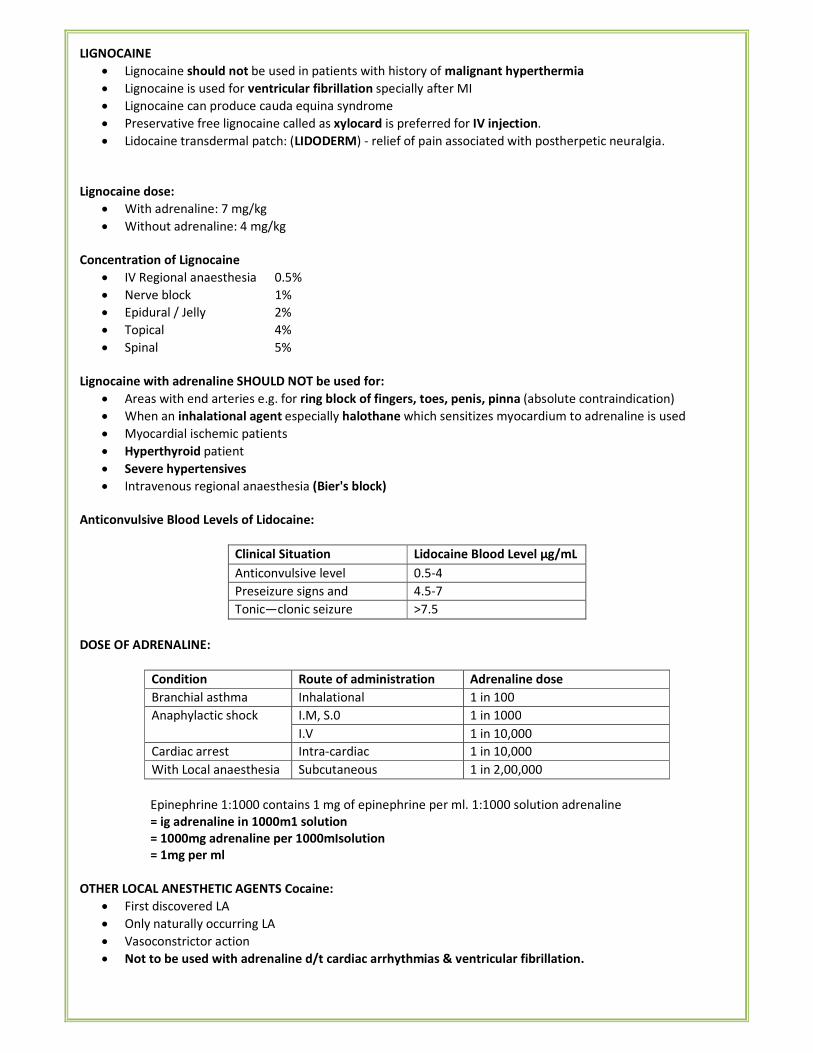
LIGNOCAINE
• Lignocaine should not be used in patients with history of malignant hyperthermia
• Lignocaine is used for ventricular fibrillation specially after MI
• Lignocaine can produce cauda equina syndrome
• Preservative free lignocaine called as xylocard is preferred for IV injection.
• Lidocaine transdermal patch: (LIDODERM) - relief of pain associated with postherpetic neuralgia.
Lignocaine dose:
• With adrenaline: 7 mg/kg
• Without adrenaline: 4 mg/kg
Concentration of Lignocaine
• IV Regional anaesthesia 0.5%
• Nerve block 1%
• Epidural / Jelly 2%
• Topical 4%
• Spinal 5%
Lignocaine with adrenaline SHOULD NOT be used for:
• Areas with end arteries e.g. for ring block of fingers, toes, penis, pinna (absolute contraindication)
• When an inhalational agent especially halothane which sensitizes myocardium to adrenaline is used
• Myocardial ischemic patients
• Hyperthyroid patient
• Severe hypertensives
• Intravenous regional anaesthesia (Bier's block)
Anticonvulsive Blood Levels of Lidocaine:
Clinical Situation Lidocaine Blood Level μg/mL
Anticonvulsive level 0.5-4
Preseizure signs and
symptoms
4.5-7
Tonic—clonic seizure >7.5
DOSE OF ADRENALINE:
Condition Route of administration Adrenaline dose
Branchial asthma Inhalational 1 in 100
Anaphylactic shock I.M, S.0 1 in 1000
I.V 1 in 10,000
Cardiac arrest Intra-cardiac 1 in 10,000
With Local anaesthesia Subcutaneous 1 in 2,00,000
Epinephrine 1:1000 contains 1 mg of epinephrine per ml. 1:1000 solution adrenaline
= ig adrenaline in 1000m1 solution
= 1000mg adrenaline per 1000mIsolution
= 1mg per ml
OTHER LOCAL ANESTHETIC AGENTS Cocaine:
• First discovered LA
• Only naturally occurring LA
• Vasoconstrictor action
• Not to be used with adrenaline d/t cardiac arrhythmias & ventricular fibrillation.
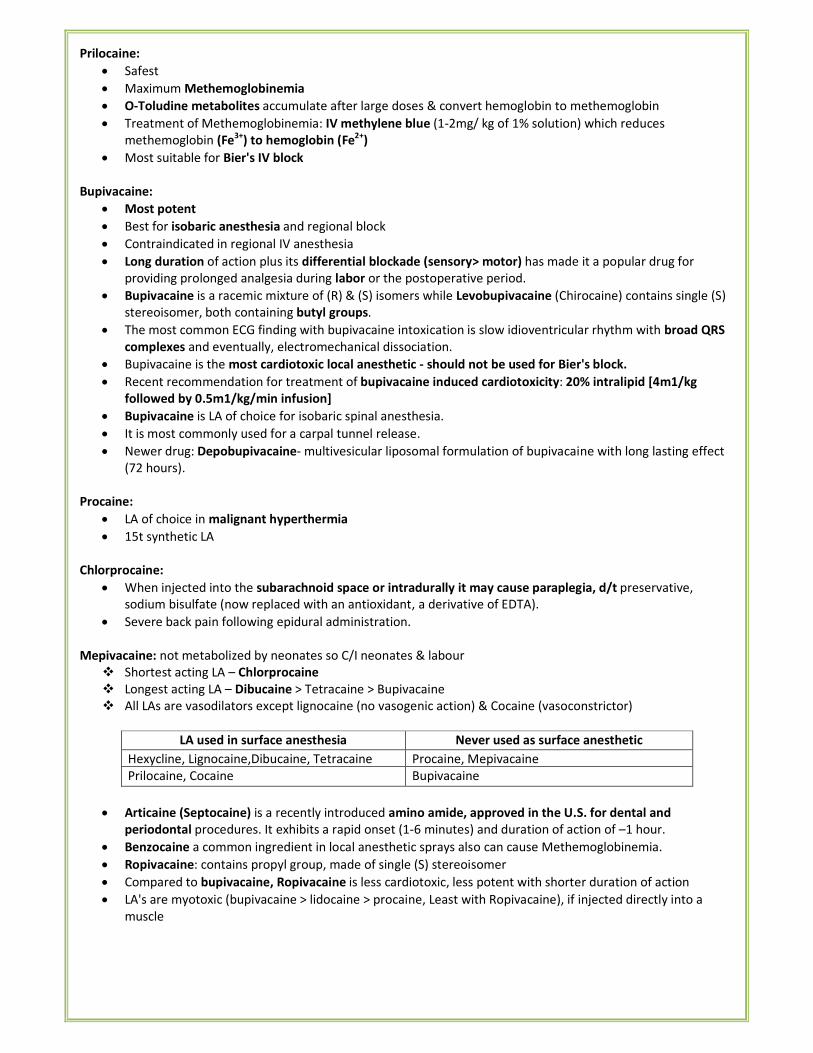
Prilocaine:
• Safest
• Maximum Methemoglobinemia
• O-Toludine metabolites accumulate after large doses & convert hemoglobin to methemoglobin
• Treatment of Methemoglobinemia: IV methylene blue (1-2mg/ kg of 1% solution) which reduces
methemoglobin (Fe3+) to hemoglobin (Fe2+)
• Most suitable for Bier's IV block
Bupivacaine:
• Most potent
• Best for isobaric anesthesia and regional block
• Contraindicated in regional IV anesthesia
• Long duration of action plus its differential blockade (sensory> motor) has made it a popular drug for
providing prolonged analgesia during labor or the postoperative period.
• Bupivacaine is a racemic mixture of (R) & (S) isomers while Levobupivacaine (Chirocaine) contains single (S)
stereoisomer, both containing butyl groups.
• The most common ECG finding with bupivacaine intoxication is slow idioventricular rhythm with broad QRS
complexes and eventually, electromechanical dissociation.
• Bupivacaine is the most cardiotoxic local anesthetic - should not be used for Bier's block.
• Recent recommendation for treatment of bupivacaine induced cardiotoxicity: 20% intralipid [4m1/kg
followed by 0.5m1/kg/min infusion]
• Bupivacaine is LA of choice for isobaric spinal anesthesia.
• It is most commonly used for a carpal tunnel release.
• Newer drug: Depobupivacaine- multivesicular liposomal formulation of bupivacaine with long lasting effect
(72 hours).
Procaine:
• LA of choice in malignant hyperthermia
• 15t synthetic LA
Chlorprocaine:
• When injected into the subarachnoid space or intradurally it may cause paraplegia, d/t preservative,
sodium bisulfate (now replaced with an antioxidant, a derivative of EDTA).
• Severe back pain following epidural administration.
Mepivacaine: not metabolized by neonates so C/I neonates & labour
� Shortest acting LA – Chlorprocaine
� Longest acting LA – Dibucaine > Tetracaine > Bupivacaine
� All LAs are vasodilators except lignocaine (no vasogenic action) & Cocaine (vasoconstrictor)
LA used in surface anesthesia Never used as surface anesthetic
Hexycline, Lignocaine,Dibucaine, Tetracaine Procaine, Mepivacaine
Prilocaine, Cocaine Bupivacaine
• Articaine (Septocaine) is a recently introduced amino amide, approved in the U.S. for dental and
periodontal procedures. It exhibits a rapid onset (1-6 minutes) and duration of action of –1 hour.
• Benzocaine a common ingredient in local anesthetic sprays also can cause Methemoglobinemia.
• Ropivacaine: contains propyl group, made of single (S) stereoisomer
• Compared to bupivacaine, Ropivacaine is less cardiotoxic, less potent with shorter duration of action
• LA's are myotoxic (bupivacaine > lidocaine > procaine, Least with Ropivacaine), if injected directly into a
muscle
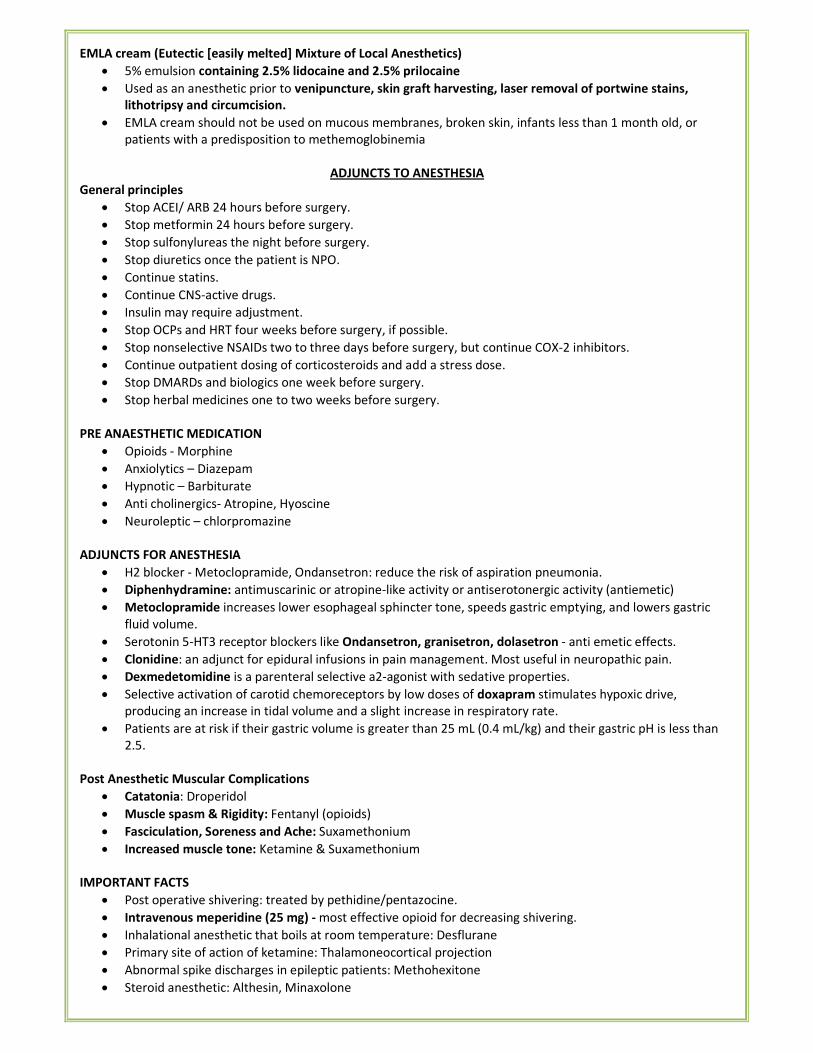
EMLA cream (Eutectic [easily melted] Mixture of Local Anesthetics)
• 5% emulsion containing 2.5% lidocaine and 2.5% prilocaine
• Used as an anesthetic prior to venipuncture, skin graft harvesting, laser removal of portwine stains,
lithotripsy and circumcision.
• EMLA cream should not be used on mucous membranes, broken skin, infants less than 1 month old, or
patients with a predisposition to methemoglobinemia
ADJUNCTS TO ANESTHESIA
General principles
• Stop ACEI/ ARB 24 hours before surgery.
• Stop metformin 24 hours before surgery.
• Stop sulfonylureas the night before surgery.
• Stop diuretics once the patient is NPO.
• Continue statins.
• Continue CNS-active drugs.
• Insulin may require adjustment.
• Stop OCPs and HRT four weeks before surgery, if possible.
• Stop nonselective NSAIDs two to three days before surgery, but continue COX-2 inhibitors.
• Continue outpatient dosing of corticosteroids and add a stress dose.
• Stop DMARDs and biologics one week before surgery.
• Stop herbal medicines one to two weeks before surgery.
PRE ANAESTHETIC MEDICATION
• Opioids - Morphine
• Anxiolytics – Diazepam
• Hypnotic – Barbiturate
• Anti cholinergics- Atropine, Hyoscine
• Neuroleptic – chlorpromazine
ADJUNCTS FOR ANESTHESIA
• H2 blocker - Metoclopramide, Ondansetron: reduce the risk of aspiration pneumonia.
• Diphenhydramine: antimuscarinic or atropine-like activity or antiserotonergic activity (antiemetic)
• Metoclopramide increases lower esophageal sphincter tone, speeds gastric emptying, and lowers gastric
fluid volume.
• Serotonin 5-HT3 receptor blockers like Ondansetron, granisetron, dolasetron - anti emetic effects.
• Clonidine: an adjunct for epidural infusions in pain management. Most useful in neuropathic pain.
• Dexmedetomidine is a parenteral selective a2-agonist with sedative properties.
• Selective activation of carotid chemoreceptors by low doses of doxapram stimulates hypoxic drive,
producing an increase in tidal volume and a slight increase in respiratory rate.
• Patients are at risk if their gastric volume is greater than 25 mL (0.4 mL/kg) and their gastric pH is less than
2.5.
Post Anesthetic Muscular Complications
• Catatonia: Droperidol
• Muscle spasm & Rigidity: Fentanyl (opioids)
• Fasciculation, Soreness and Ache: Suxamethonium
• Increased muscle tone: Ketamine & Suxamethonium
IMPORTANT FACTS
• Post operative shivering: treated by pethidine/pentazocine.
• Intravenous meperidine (25 mg) - most effective opioid for decreasing shivering.
• Inhalational anesthetic that boils at room temperature: Desflurane
• Primary site of action of ketamine: Thalamoneocortical projection
• Abnormal spike discharges in epileptic patients: Methohexitone
• Steroid anesthetic: Althesin, Minaxolone
• Heid brink meter indicates: flow rate of gases
• Armoured ET tube: used in neurosurgery
• Aspiration of gastric contents: Mendelson's syndrome
• First reflex to appear during recovery from anesthesia: swallowing
• 5 % CO2 is used for creating pneumoperitoneum during laparoscopy
• A mixture of 80% helium and 20% O2 is used for tracheal obstruction.
• M/C complication in pediatric anesthesia: laryngospasm.
• M/C complication in adult patients under GA: Dysarhythmias & Hypotension
• Neurolept analgesia: Fentanyl + Droperidol
• Neurolept anesthesia: Fentanyl + Droperidol + 65% N2O + 35% O2
III. REGIONAL ANESTHESIA & PAIN MANAGEMENT
Baricity of Anesthetic Agents
• Higher the dosage or site of injection, the higher the level of anesthesia obtained.
• Migration of the drug in CSF depc.t.ius on its specific gravity relative to CSF (baricity).
• A hyperbaric solution is denser (heavier) than CSF, whereas a hypobaric solution is less dense (lighter) than
CSF.
• Solutions can be made hyperbaric by adding glucose or hypobaric by adding sterile water.
• In head-down position, a hyperbaric solution spreads cephalad and a hypobaric anesthetic solution moves
caudad; and vice-versa in head-up position
• Anesthetic agents are mixed with CSF (at least 1:1) to make their solutions isobaric.
• Hyperbaric bupivacaine and tetracaine are most commonly used agents for spinal anesthesia.
• Both are relatively slow in onset (5-10 min) and have a prolonged duration (90-120 min).
• Hyperbaric spinal anesthesia is more commonly used than the hypobaric or isobaric techniques.
• The level of anesthesia is dependent on the patient's position during and immediately following the
injection.
• In the sitting position, "saddle block" can be achieved by keeping the patient sitting for 3-5 min following
injection so that only the lower lumbar nerves and sacral nerves are blocked.
INTRAVENOUS REGIONAL ANESTHESIA (BIER'S BLOCK)
• It consists of injection of LA in a vein of a tourniquet occluded limb.
• 0.5% Lidocaine is most commonly used in drug
• Mainly used for upper limb orthopedic procedures as it is most difficult to obstruct blood supply of lower
limb.
SPINAL ANESTHESIA
• The principal site of action for neuraxial blockade is the nerve root.
• Neuraxial anesthesia does not block the vagus nerve.
• The drug is injected in subarachnoid space (piamater and arachnoid membrane)
• Injection below L1 in adults and L3 in children avoids trauma to the spinal cord.
• Quincke needle is a cutting needle with end injection.
• Blunt tip (pencil-point) needles decrease the incidence of postdural puncture headache.
• Heavily myelinated, small preganglionic sympathetic fibers and pain fibers are blocked first.
• Motor fibers are blocked last.
• The level of motor block is two to four dermatomes lower than the level of sensory anesthe
• Sequence of blockade autonomic � sensory � motor
Confirmation of spinal needle: feel of two "pops".
• The first is penetration of the ligamentum flavum
• The second is penetration of the dura-arachnoid membrane.
Factors Affecting the Level of Spinal Anesthesia
Most important factors Other factors
• Baricity of anesthetic solution
• Position of the patient during &
• Immediately after injection
• Drug dosage
• Site of injection
• Age, Patient height, Pregnancy
• Cerebrospinal fluid
• Curvature of the spine
• Drug volume
• Intra -abdominal pressure
• Needle direction
• MOA- Local anesthetic acts on spinal nerves and dorsal ganglia
• Unconsciousness, apnea, and hypotension resulting from high levels of spinal anesthesia are referred to as a
"high spinal" or "total spinal."
• Complications of SAB:
o Hypotension –M/c complication of SAB. Preventive measures are head low position to increase venous
return, fluid preloading with RL, prophylactic vasopressor, oxygen supplementation
o Bradycardia –M/c arrhythmia
o Apnea
o Cardiac arrest
o Anaphylaxis
o Nausea & Vomiting
o 6th
cranial nerve is M/c nerve involved due to longest intracranial course.
o Transient neurological symptoms (TNS), also called as transient radicular irritation
o Post Dural puncture Headache (PDPH)
Post Dural Puncture Headache (PDPH)
• Presents 12-24hrs after spinal block
• Usually occipital but can also be frontal
• Increases on sitting & relieved on lying down
• Lasts for 7-10 days but may be for 3 weeks
• Cause – Due to CSF leakage through dural rent
• Treatment:
o Small size needle
o Adequate hydration
o Prone or supine position
o Analgesic
o Oral or I/V caffeine
o Autologous epidural blood patch (most effective): stop further leakage of CSF by either mass effect or
coagulation
Factors that may increase the incidence of Post–spinal Puncture Headache
Age Younger more frequent
Gender Females > males
Needle size Larger > smaller
Needle bevel Less when the needle bevel is placed in the long axis of the neuraxis
Pregnancy More when pregnant
Dural punctures (no.) More with multiple punctures
Factors not increasing the incidence of Post–spinal Puncture Headache
Continuous spinals
Timing of ambulation
Contraindications to spinal anaesthesia
Absolute Relative
• Raised intracranial pressure
• Patient refusal
• Shock: Hypotension and hypovolemia
• Infants and children- control of level is difficult.
• Bleeding disorders
• Patient's on anticoagulants
• Infection of the local site and
• Septicemias
• Vertebral abnormalities (kyphosis, lordosis, etc.)
• Aortic and mitral stenosis
• MI
• Heart block
• Spinal deformities
• Psychiatric and CNS disorders
Agents used in Spinal Anesthesia
• Bupivacaine: 0.5% in 8.25% dextrose, 0.5% plain
• Lidocaine: 2% plain, 5% in 7.5% dextrose
• Procaine: 10% plain, 2.5% in water
• Tetracaine: 0.5% in water, 0.5% in D5W
Parameter Spinal Anesthesia Epidural Anesthesia
Level performed Lumbar Any Level
Cost Cheaper Expensive
Onset of Effect 2- 3 minutes 15 – 20 minutes
Duration of Effect Lesser Prolonged
Quality of block Total Patchy
Post spinal head ache Present Absent
Epidural hematoma Less common More common
Total spinal Rare High chances
Intravascular injection Rare High chances
Drug toxicity Less common More common
Catheter complication Absent Present
EPIDURAL BLOCK
• Drug is injected in the epidural space between the ligamentum flavum and the duramater.
• The standard (Tuohy needle, directional needle) epidural needle has a blunt bevel with a gentle curve of 15-
30° at the tip.
• Straight needles without a curved tip (Crawford needles): higher incidence of dural puncture but facilitate
passage of an epidural catheter.
• Methods to locate epidural space (negative pressure test)
− Hanging drop technique
− Loss of resistance (preferred)
− Macintosh extradural space indicator
• Indications for Epidural Anesthesia:
o Mainly used for controlling post – operative pain & Chronic cancer pain
o Painless labor
o Can be used for all surgeries done by spinal anesthesia
• Advantages of epidural anaesthesia
o Less hypotension
o No postspinal headache
o Level of block can be extended
o Any duration of surgery can be performed
CAUDAL BLOCK (EPIDURAL SACRAL BLOCK)
• Sacral epidural anesthesia is referred to as a caudal block.
• Drug penetrates the sacrococcygeal ligament covering the sacral hiatus that is created by the unfused S4
and S5 laminae.
• Also employed for labor and postoperative analgesia.
• Mainly used in children for perineal and genitourinary surgery.
• Within the sacral canal, the anesthesia bathes the S2–S4 spinal nerve roots, including the pain fibers from
the uterine cervix and superior vagina, and the afferent fibers from the pudendal nerve.
• The entire birth canal, pelvic floor, and majority of the perineum are anesthetized
• Lower limbs are not usually affected.
• The pain fibers from the uterine body (superior to the pelvic pain line) ascend to the inferior thoracic-
superior lumbar levels; these and the fibers superior to them are not affected by the anesthetic, so the
mother is aware of her uterine contractions.
• With epidural anesthesia, no " spinal headache" occurs because the vertebral epidural space is not
continuous with the cranial extradural (epidural) space
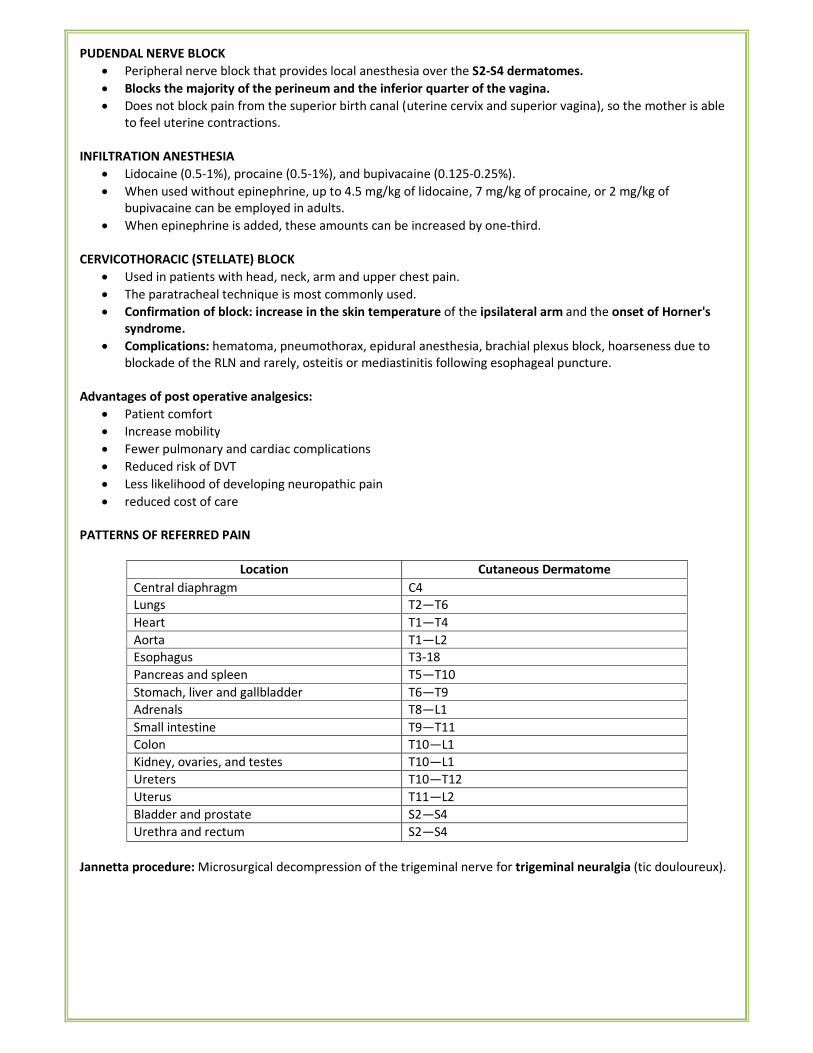
PUDENDAL NERVE BLOCK
• Peripheral nerve block that provides local anesthesia over the S2-S4 dermatomes.
• Blocks the majority of the perineum and the inferior quarter of the vagina.
• Does not block pain from the superior birth canal (uterine cervix and superior vagina), so the mother is able
to feel uterine contractions.
INFILTRATION ANESTHESIA
• Lidocaine (0.5-1%), procaine (0.5-1%), and bupivacaine (0.125-0.25%).
• When used without epinephrine, up to 4.5 mg/kg of lidocaine, 7 mg/kg of procaine, or 2 mg/kg of
bupivacaine can be employed in adults.
• When epinephrine is added, these amounts can be increased by one-third.
CERVICOTHORACIC (STELLATE) BLOCK
• Used in patients with head, neck, arm and upper chest pain.
• The paratracheal technique is most commonly used.
• Confirmation of block: increase in the skin temperature of the ipsilateral arm and the onset of Horner's
syndrome.
• Complications: hematoma, pneumothorax, epidural anesthesia, brachial plexus block, hoarseness due to
blockade of the RLN and rarely, osteitis or mediastinitis following esophageal puncture.
Advantages of post operative analgesics:
• Patient comfort
• Increase mobility
• Fewer pulmonary and cardiac complications
• Reduced risk of DVT
• Less likelihood of developing neuropathic pain
• reduced cost of care
PATTERNS OF REFERRED PAIN
Location Cutaneous Dermatome
Central diaphragm C4
Lungs T2—T6
Heart T1—T4
Aorta T1—L2
Esophagus T3-18
Pancreas and spleen T5—T10
Stomach, liver and gallbladder T6—T9
Adrenals T8—L1
Small intestine T9—T11
Colon T10—L1
Kidney, ovaries, and testes T10—L1
Ureters T10—T12
Uterus T11—L2
Bladder and prostate S2—S4
Urethra and rectum S2—S4
Jannetta procedure: Microsurgical decompression of the trigeminal nerve for trigeminal neuralgia (tic douloureux).
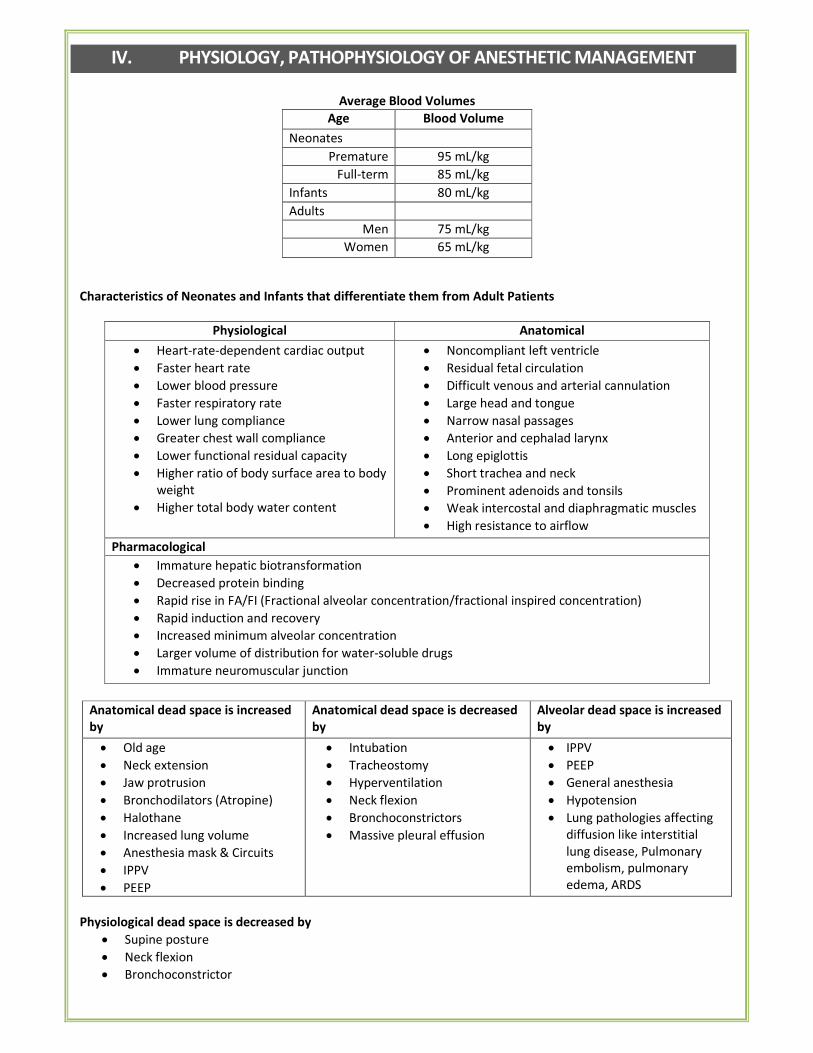
IV. PHYSIOLOGY, PATHOPHYSIOLOGY OF ANESTHETIC MANAGEMENT
Average Blood Volumes
Age Blood Volume
Neonates
Premature 95 mL/kg
Full-term 85 mL/kg
Infants 80 mL/kg
Adults
Men 75 mL/kg
Women 65 mL/kg
Characteristics of Neonates and Infants that differentiate them from Adult Patients
Physiological Anatomical
• Heart-rate-dependent cardiac output
• Faster heart rate
• Lower blood pressure
• Faster respiratory rate
• Lower lung compliance
• Greater chest wall compliance
• Lower functional residual capacity
• Higher ratio of body surface area to body
weight
• Higher total body water content
• Noncompliant left ventricle
• Residual fetal circulation
• Difficult venous and arterial cannulation
• Large head and tongue
• Narrow nasal passages
• Anterior and cephalad larynx
• Long epiglottis
• Short trachea and neck
• Prominent adenoids and tonsils
• Weak intercostal and diaphragmatic muscles
• High resistance to airflow
Pharmacological
• Immature hepatic biotransformation
• Decreased protein binding
• Rapid rise in FA/FI (Fractional alveolar concentration/fractional inspired concentration)
• Rapid induction and recovery
• Increased minimum alveolar concentration
• Larger volume of distribution for water-soluble drugs
• Immature neuromuscular junction
Anatomical dead space is increased
by
Anatomical dead space is decreased
by
Alveolar dead space is increased
by
• Old age
• Neck extension
• Jaw protrusion
• Bronchodilators (Atropine)
• Halothane
• Increased lung volume
• Anesthesia mask & Circuits
• IPPV
• PEEP
• Intubation
• Tracheostomy
• Hyperventilation
• Neck flexion
• Bronchoconstrictors
• Massive pleural effusion
• IPPV
• PEEP
• General anesthesia
• Hypotension
• Lung pathologies affecting
diffusion like interstitial
lung disease, Pulmonary
embolism, pulmonary
edema, ARDS
Physiological dead space is decreased by
• Supine posture
• Neck flexion
• Bronchoconstrictor
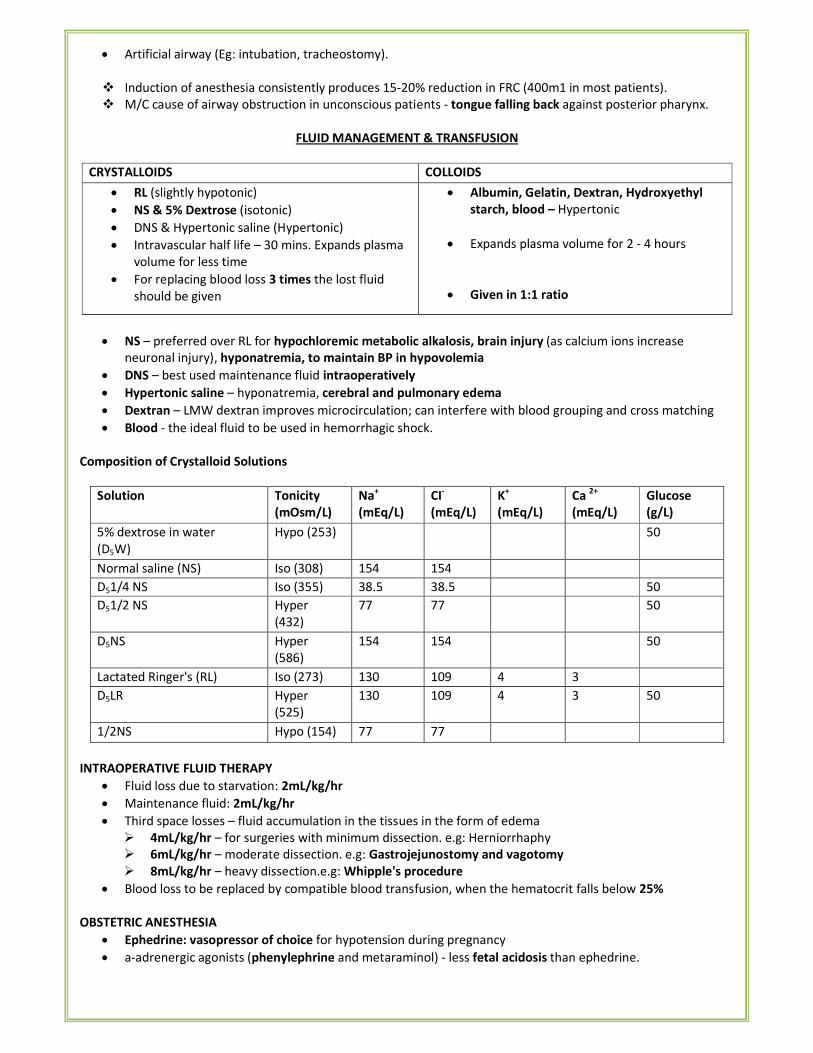
• Artificial airway (Eg: intubation, tracheostomy).
� Induction of anesthesia consistently produces 15-20% reduction in FRC (400m1 in most patients).
� M/C cause of airway obstruction in unconscious patients - tongue falling back against posterior pharynx.
FLUID MANAGEMENT & TRANSFUSION
CRYSTALLOIDS COLLOIDS
• RL (slightly hypotonic)
• NS & 5% Dextrose (isotonic)
• DNS & Hypertonic saline (Hypertonic)
• Intravascular half life – 30 mins. Expands plasma
volume for less time
• For replacing blood loss 3 times the lost fluid
should be given
• Albumin, Gelatin, Dextran, Hydroxyethyl
starch, blood – Hypertonic
• Expands plasma volume for 2 - 4 hours
• Given in 1:1 ratio
• NS – preferred over RL for hypochloremic metabolic alkalosis, brain injury (as calcium ions increase
neuronal injury), hyponatremia, to maintain BP in hypovolemia
• DNS – best used maintenance fluid intraoperatively
• Hypertonic saline – hyponatremia, cerebral and pulmonary edema
• Dextran – LMW dextran improves microcirculation; can interfere with blood grouping and cross matching
• Blood - the ideal fluid to be used in hemorrhagic shock.
Composition of Crystalloid Solutions
Solution Tonicity
(mOsm/L)
Na+
(mEq/L)
CI-
(mEq/L)
K+
(mEq/L)
Ca 2+
(mEq/L)
Glucose
(g/L)
5% dextrose in water
(D5W)
Hypo (253) 50
Normal saline (NS) Iso (308) 154 154
D51/4 NS Iso (355) 38.5 38.5 50
D51/2 NS Hyper
(432)
77 77 50
D5NS Hyper
(586)
154 154 50
Lactated Ringer's (RL) Iso (273) 130 109 4 3
D5LR Hyper
(525)
130 109 4 3 50
1/2NS Hypo (154) 77 77
INTRAOPERATIVE FLUID THERAPY
• Fluid loss due to starvation: 2mL/kg/hr
• Maintenance fluid: 2mL/kg/hr
• Third space losses – fluid accumulation in the tissues in the form of edema
� 4mL/kg/hr – for surgeries with minimum dissection. e.g: Herniorrhaphy
� 6mL/kg/hr – moderate dissection. e.g: Gastrojejunostomy and vagotomy
� 8mL/kg/hr – heavy dissection.e.g: Whipple's procedure
• Blood loss to be replaced by compatible blood transfusion, when the hematocrit falls below 25%
OBSTETRIC ANESTHESIA
• Ephedrine: vasopressor of choice for hypotension during pregnancy
• a-adrenergic agonists (phenylephrine and metaraminol) - less fetal acidosis than ephedrine.
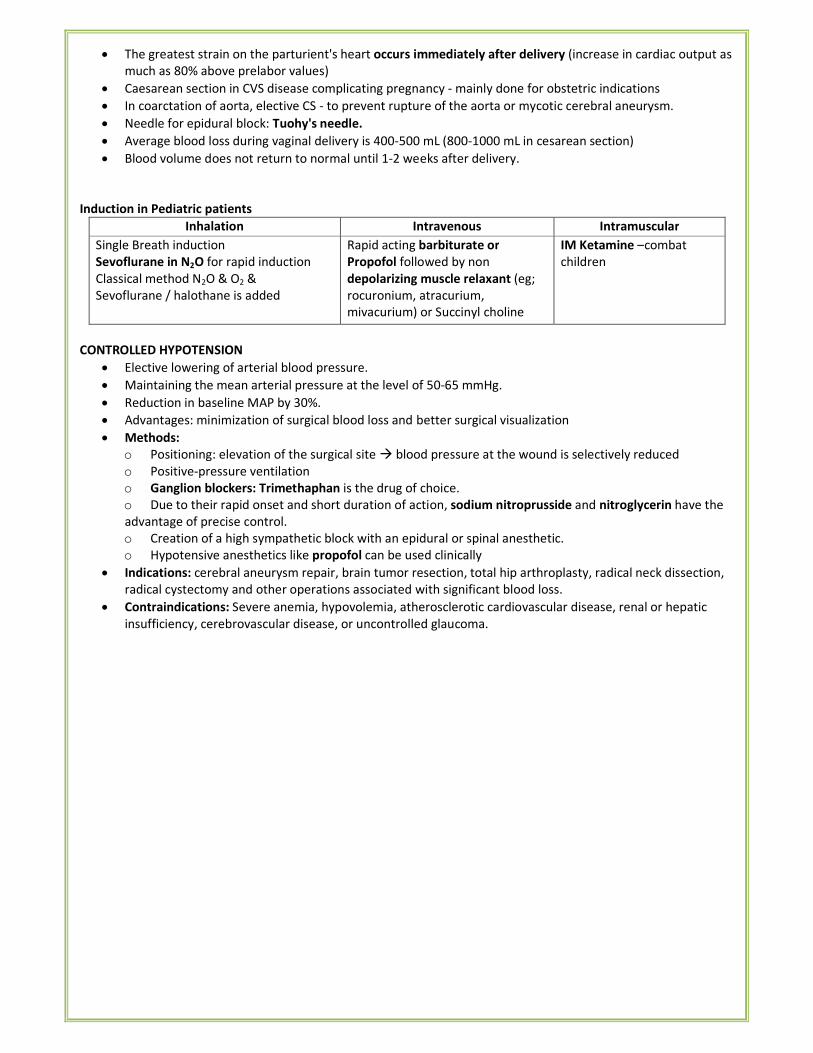
• The greatest strain on the parturient's heart occurs immediately after delivery (increase in cardiac output as
much as 80% above prelabor values)
• Caesarean section in CVS disease complicating pregnancy - mainly done for obstetric indications
• In coarctation of aorta, elective CS - to prevent rupture of the aorta or mycotic cerebral aneurysm.
• Needle for epidural block: Tuohy's needle.
• Average blood loss during vaginal delivery is 400-500 mL (800-1000 mL in cesarean section)
• Blood volume does not return to normal until 1-2 weeks after delivery.
Induction in Pediatric patients
Inhalation Intravenous Intramuscular
Single Breath induction
Sevoflurane in N2O for rapid induction
Classical method N2O & O2 &
Sevoflurane / halothane is added
Rapid acting barbiturate or
Propofol followed by non
depolarizing muscle relaxant (eg;
rocuronium, atracurium,
mivacurium) or Succinyl choline
IM Ketamine –combat
children
CONTROLLED HYPOTENSION
• Elective lowering of arterial blood pressure.
• Maintaining the mean arterial pressure at the level of 50-65 mmHg.
• Reduction in baseline MAP by 30%.
• Advantages: minimization of surgical blood loss and better surgical visualization
• Methods:
o Positioning: elevation of the surgical site � blood pressure at the wound is selectively reduced
o Positive-pressure ventilation
o Ganglion blockers: Trimethaphan is the drug of choice.
o Due to their rapid onset and short duration of action, sodium nitroprusside and nitroglycerin have the
advantage of precise control.
o Creation of a high sympathetic block with an epidural or spinal anesthetic.
o Hypotensive anesthetics like propofol can be used clinically
• Indications: cerebral aneurysm repair, brain tumor resection, total hip arthroplasty, radical neck dissection,
radical cystectomy and other operations associated with significant blood loss.
• Contraindications: Severe anemia, hypovolemia, atherosclerotic cardiovascular disease, renal or hepatic
insufficiency, cerebrovascular disease, or uncontrolled glaucoma.
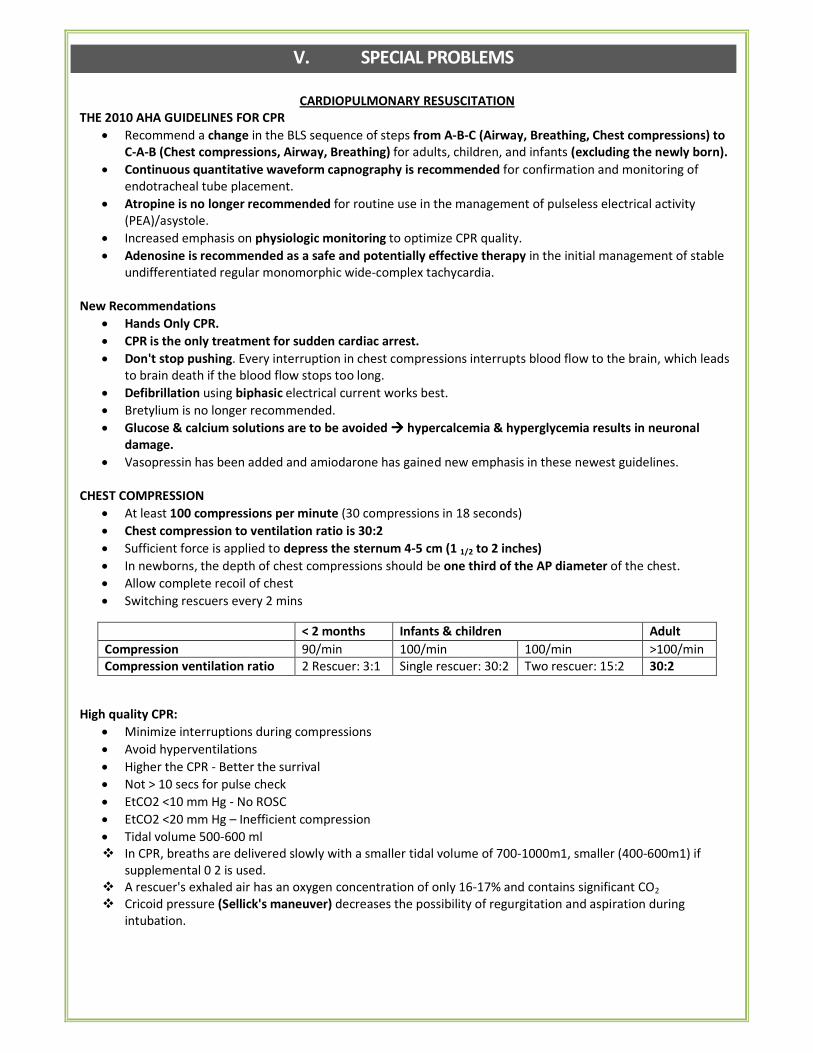
V. SPECIAL PROBLEMS
CARDIOPULMONARY RESUSCITATION
THE 2010 AHA GUIDELINES FOR CPR
• Recommend a change in the BLS sequence of steps from A-B-C (Airway, Breathing, Chest compressions) to
C-A-B (Chest compressions, Airway, Breathing) for adults, children, and infants (excluding the newly born).
• Continuous quantitative waveform capnography is recommended for confirmation and monitoring of
endotracheal tube placement.
• Atropine is no longer recommended for routine use in the management of pulseless electrical activity
(PEA)/asystole.
• Increased emphasis on physiologic monitoring to optimize CPR quality.
• Adenosine is recommended as a safe and potentially effective therapy in the initial management of stable
undifferentiated regular monomorphic wide-complex tachycardia.
New Recommendations
• Hands Only CPR.
• CPR is the only treatment for sudden cardiac arrest.
• Don't stop pushing. Every interruption in chest compressions interrupts blood flow to the brain, which leads
to brain death if the blood flow stops too long.
• Defibrillation using biphasic electrical current works best.
• Bretylium is no longer recommended.
• Glucose & calcium solutions are to be avoided ���� hypercalcemia & hyperglycemia results in neuronal
damage.
• Vasopressin has been added and amiodarone has gained new emphasis in these newest guidelines.
CHEST COMPRESSION
• At least 100 compressions per minute (30 compressions in 18 seconds)
• Chest compression to ventilation ratio is 30:2
• Sufficient force is applied to depress the sternum 4-5 cm (1 1/2 to 2 inches)
• In newborns, the depth of chest compressions should be one third of the AP diameter of the chest.
• Allow complete recoil of chest
• Switching rescuers every 2 mins
< 2 months Infants & children Adult
Compression 90/min 100/min 100/min >100/min
Compression ventilation ratio 2 Rescuer: 3:1 Single rescuer: 30:2 Two rescuer: 15:2 30:2
High quality CPR:
• Minimize interruptions during compressions
• Avoid hyperventilations
• Higher the CPR - Better the surrival
• Not > 10 secs for pulse check
• EtCO2 <10 mm Hg - No ROSC
• EtCO2 <20 mm Hg – Inefficient compression
• Tidal volume 500-600 ml
� In CPR, breaths are delivered slowly with a smaller tidal volume of 700-1000m1, smaller (400-600m1) if
supplemental 0 2 is used.
� A rescuer's exhaled air has an oxygen concentration of only 16-17% and contains significant CO2
� Cricoid pressure (Sellick's maneuver) decreases the possibility of regurgitation and aspiration during
intubation.
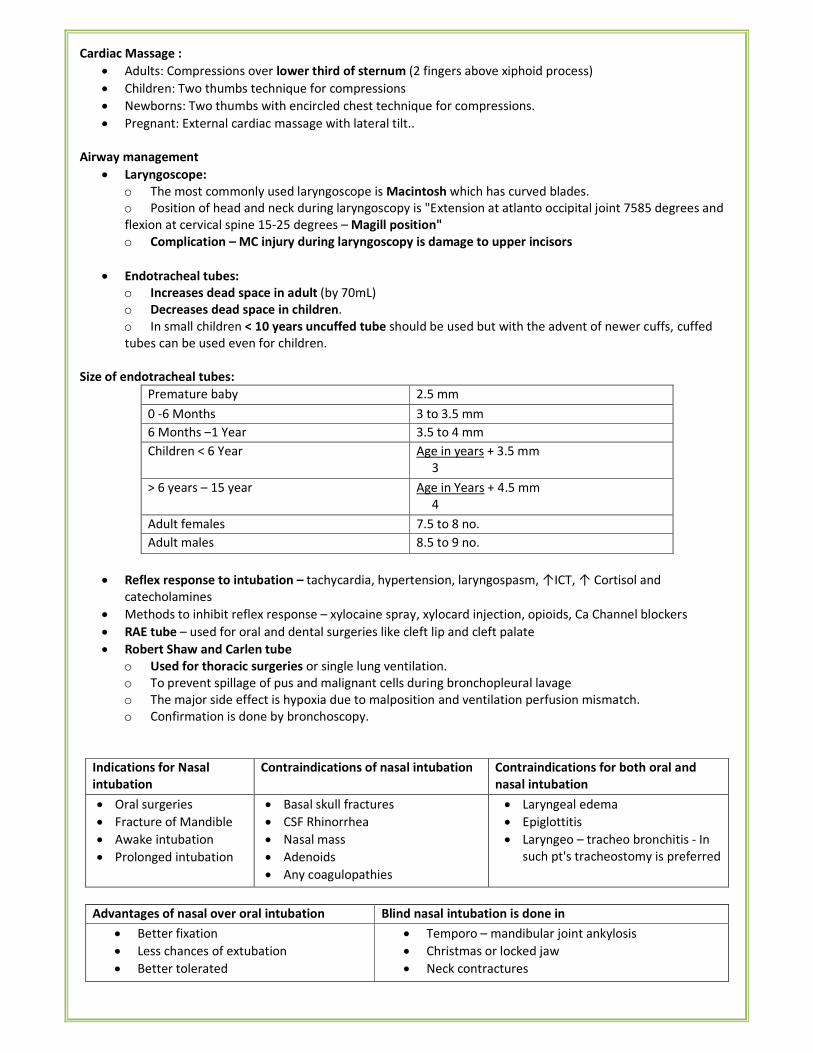
Cardiac Massage :
• Adults: Compressions over lower third of sternum (2 fingers above xiphoid process)
• Children: Two thumbs technique for compressions
• Newborns: Two thumbs with encircled chest technique for compressions.
• Pregnant: External cardiac massage with lateral tilt..
Airway management
• Laryngoscope:
o The most commonly used laryngoscope is Macintosh which has curved blades.
o Position of head and neck during laryngoscopy is "Extension at atlanto occipital joint 7585 degrees and
flexion at cervical spine 15-25 degrees – Magill position"
o Complication – MC injury during laryngoscopy is damage to upper incisors
• Endotracheal tubes:
o Increases dead space in adult (by 70mL)
o Decreases dead space in children.
o In small children < 10 years uncuffed tube should be used but with the advent of newer cuffs, cuffed
tubes can be used even for children.
Size of endotracheal tubes:
Premature baby 2.5 mm
0 -6 Months 3 to 3.5 mm
6 Months –1 Year 3.5 to 4 mm
Children < 6 Year Age in years + 3.5 mm
3
> 6 years – 15 year Age in Years + 4.5 mm
4
Adult females 7.5 to 8 no.
Adult males 8.5 to 9 no.
• Reflex response to intubation – tachycardia, hypertension, laryngospasm, ↑ICT, ↑ Cortisol and
catecholamines
• Methods to inhibit reflex response – xylocaine spray, xylocard injection, opioids, Ca Channel blockers
• RAE tube – used for oral and dental surgeries like cleft lip and cleft palate
• Robert Shaw and Carlen tube
o Used for thoracic surgeries or single lung ventilation.
o To prevent spillage of pus and malignant cells during bronchopleural lavage
o The major side effect is hypoxia due to malposition and ventilation perfusion mismatch.
o Confirmation is done by bronchoscopy.
Indications for Nasal
intubation
Contraindications of nasal intubation Contraindications for both oral and
nasal intubation
• Oral surgeries
• Fracture of Mandible
• Awake intubation
• Prolonged intubation
• Basal skull fractures
• CSF Rhinorrhea
• Nasal mass
• Adenoids
• Any coagulopathies
• Laryngeal edema
• Epiglottitis
• Laryngeo – tracheo bronchitis - In
such pt's tracheostomy is preferred
Advantages of nasal over oral intubation Blind nasal intubation is done in
• Better fixation
• Less chances of extubation
• Better tolerated
• Temporo – mandibular joint ankylosis
• Christmas or locked jaw
• Neck contractures
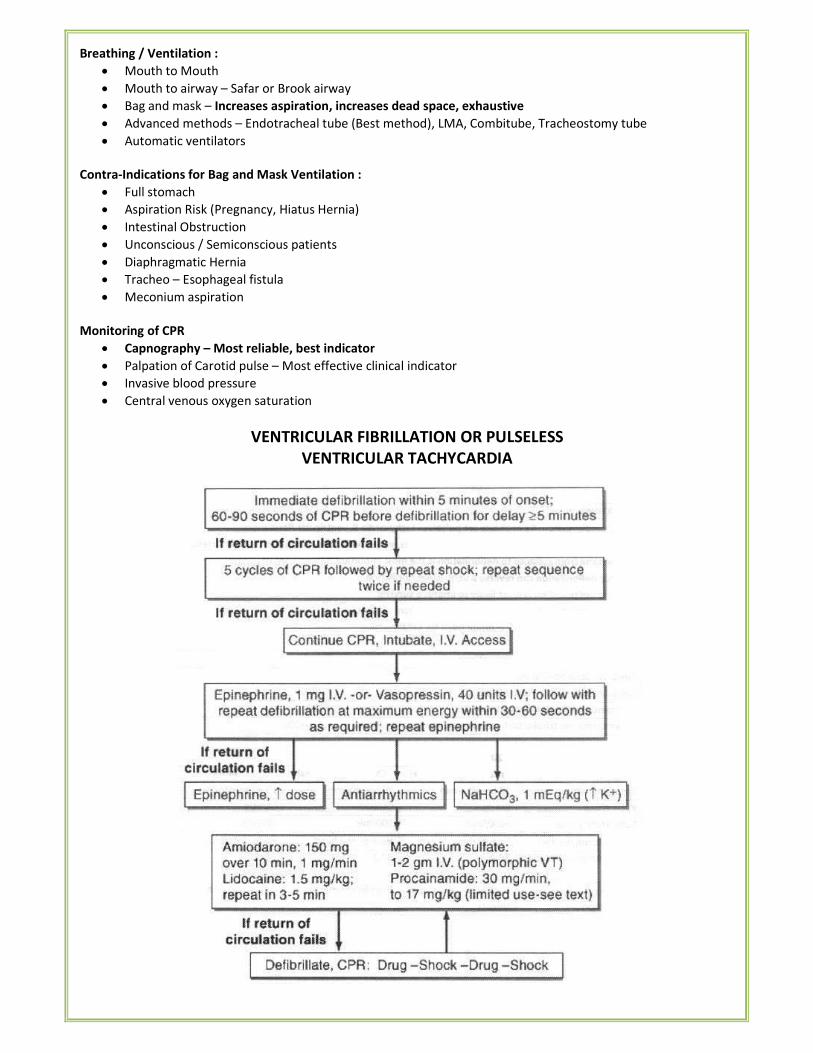
Breathing / Ventilation :
• Mouth to Mouth
• Mouth to airway – Safar or Brook airway
• Bag and mask – Increases aspiration, increases dead space, exhaustive
• Advanced methods – Endotracheal tube (Best method), LMA, Combitube, Tracheostomy tube
• Automatic ventilators
Contra-Indications for Bag and Mask Ventilation :
• Full stomach
• Aspiration Risk (Pregnancy, Hiatus Hernia)
• Intestinal Obstruction
• Unconscious / Semiconscious patients
• Diaphragmatic Hernia
• Tracheo – Esophageal fistula
• Meconium aspiration
Monitoring of CPR
• Capnography – Most reliable, best indicator
• Palpation of Carotid pulse – Most effective clinical indicator
• Invasive blood pressure
• Central venous oxygen saturation
VENTRICULAR FIBRILLATION OR PULSELESS
VENTRICULAR TACHYCARDIA
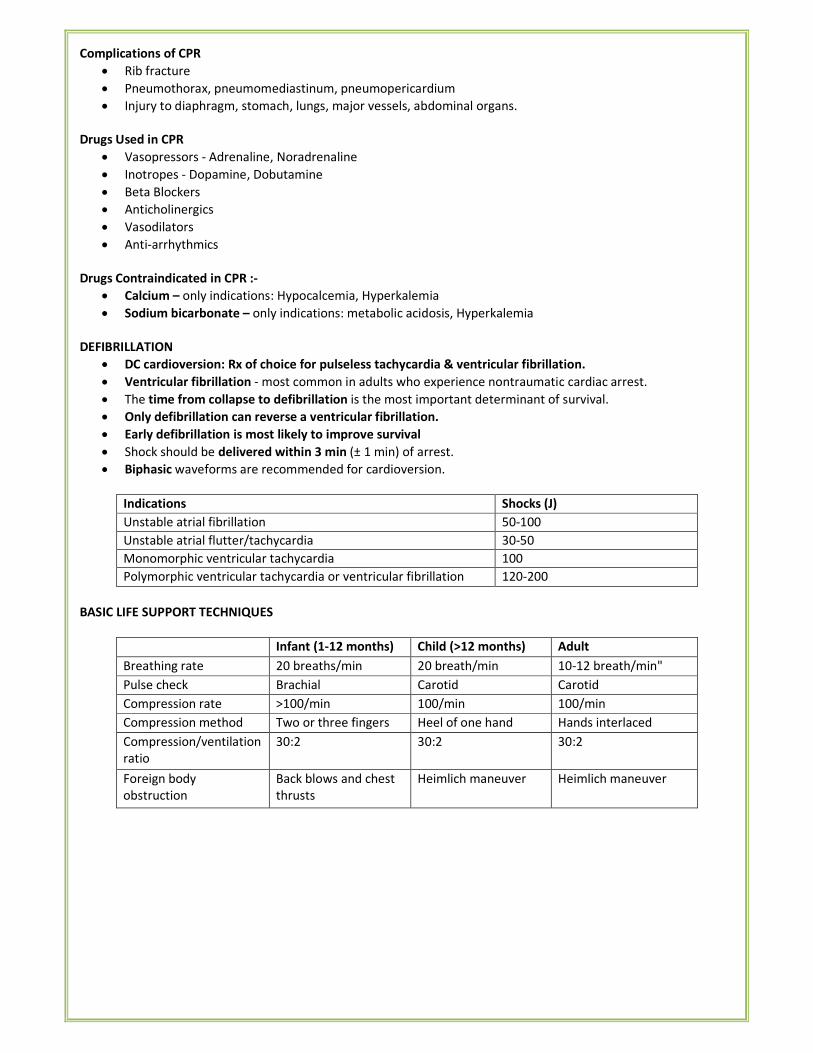
Complications of CPR
• Rib fracture
• Pneumothorax, pneumomediastinum, pneumopericardium
• Injury to diaphragm, stomach, lungs, major vessels, abdominal organs.
Drugs Used in CPR
• Vasopressors - Adrenaline, Noradrenaline
• Inotropes - Dopamine, Dobutamine
• Beta Blockers
• Anticholinergics
• Vasodilators
• Anti-arrhythmics
Drugs Contraindicated in CPR :-
• Calcium – only indications: Hypocalcemia, Hyperkalemia
• Sodium bicarbonate – only indications: metabolic acidosis, Hyperkalemia
DEFIBRILLATION
• DC cardioversion: Rx of choice for pulseless tachycardia & ventricular fibrillation.
• Ventricular fibrillation - most common in adults who experience nontraumatic cardiac arrest.
• The time from collapse to defibrillation is the most important determinant of survival.
• Only defibrillation can reverse a ventricular fibrillation.
• Early defibrillation is most likely to improve survival
• Shock should be delivered within 3 min (± 1 min) of arrest.
• Biphasic waveforms are recommended for cardioversion.
Indications Shocks (J)
Unstable atrial fibrillation 50-100
Unstable atrial flutter/tachycardia 30-50
Monomorphic ventricular tachycardia 100
Polymorphic ventricular tachycardia or ventricular fibrillation 120-200
BASIC LIFE SUPPORT TECHNIQUES
Infant (1-12 months) Child (>12 months) Adult
Breathing rate 20 breaths/min 20 breath/min 10-12 breath/min"
Pulse check Brachial Carotid Carotid
Compression rate >100/min 100/min 100/min
Compression method Two or three fingers Heel of one hand Hands interlaced
Compression/ventilation
ratio
30:2 30:2 30:2
Foreign body
obstruction
Back blows and chest
thrusts
Heimlich maneuver Heimlich maneuver
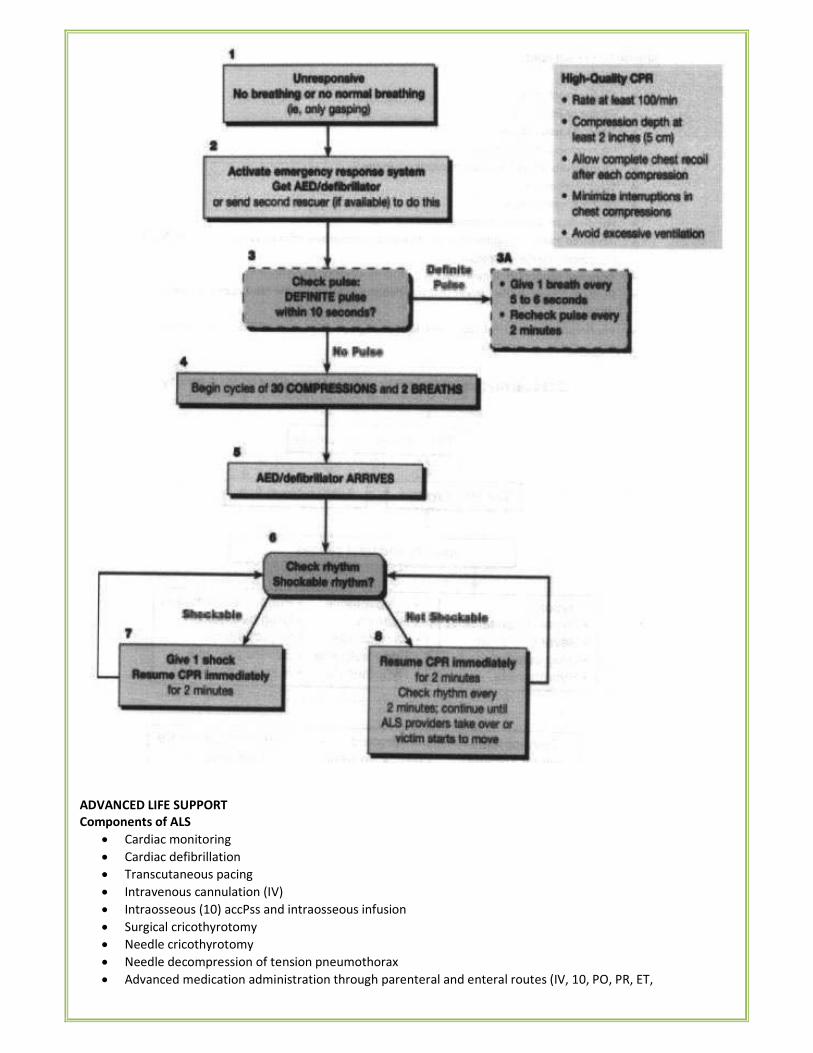
ADVANCED LIFE SUPPORT
Components of ALS
• Cardiac monitoring
• Cardiac defibrillation
• Transcutaneous pacing
• Intravenous cannulation (IV)
• Intraosseous (10) accPss and intraosseous infusion
• Surgical cricothyrotomy
• Needle cricothyrotomy
• Needle decompression of tension pneumothorax
• Advanced medication administration through parenteral and enteral routes (IV, 10, PO, PR, ET,
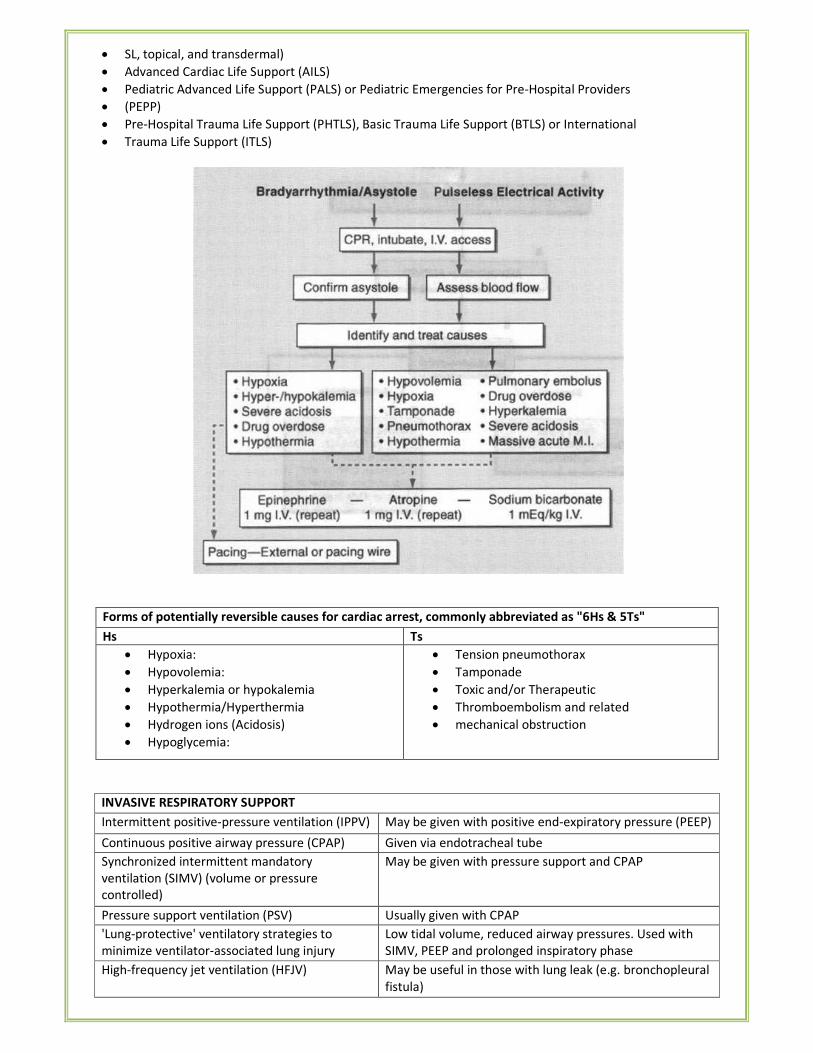
• SL, topical, and transdermal)
• Advanced Cardiac Life Support (AILS)
• Pediatric Advanced Life Support (PALS) or Pediatric Emergencies for Pre-Hospital Providers
• (PEPP)
• Pre-Hospital Trauma Life Support (PHTLS), Basic Trauma Life Support (BTLS) or International
• Trauma Life Support (ITLS)
Forms of potentially reversible causes for cardiac arrest, commonly abbreviated as "6Hs & 5Ts"
Hs Ts
• Hypoxia:
• Hypovolemia:
• Hyperkalemia or hypokalemia
• Hypothermia/Hyperthermia
• Hydrogen ions (Acidosis)
• Hypoglycemia:
• Tension pneumothorax
• Tamponade
• Toxic and/or Therapeutic
• Thromboembolism and related
• mechanical obstruction
INVASIVE RESPIRATORY SUPPORT
Intermittent positive-pressure ventilation (IPPV) May be given with positive end-expiratory pressure (PEEP)
Continuous positive airway pressure (CPAP) Given via endotracheal tube
Synchronized intermittent mandatory
ventilation (SIMV) (volume or pressure
controlled)
May be given with pressure support and CPAP
Pressure support ventilation (PSV) Usually given with CPAP
'Lung-protective' ventilatory strategies to
minimize ventilator-associated lung injury
Low tidal volume, reduced airway pressures. Used with
SIMV, PEEP and prolonged inspiratory phase
High-frequency jet ventilation (HFJV) May be useful in those with lung leak (e.g. bronchopleural
fistula)
Extracorporeal techniques May be useful in severe acute respiratory failure
NON-INVASIVE RESPIRATORY SUPPORT
Continuous positive airway pressure (CPAP) Inspiratory and expiratory pressures the same
Non-invasive positive support ventilation ± CPAP
Bilevel positive airway pressure (BiPAP) Inspiratory and expiratory pressures set separately
WEANING METHODS:
• The most useful weaning parameters are
o Arterial blood gas tensions
o Respiratory rate
o Rapid shallow breathing index (RSBI).
• The most common techniques to wean a patient from the ventilator include
o SIMV
o Pressure support
o Periods of spontaneous breathing alone on a T- Piece or on low levels of CPAP.
o Noninvasive positive-pressure ventilation
• The traditional method is to allow the patient to breathe entirely spontaneously for a short time, following
which respiratory support is reinstituted.
MANAGEMENT OF PRE EXISTING DRUG THERAPIES DURING ANAESTHESIA
Oral Hypoglycemic Drugs Omit morning dose in case of minor surgery
For major surgeries: shift to Insulin 48 hrs before surgery
OCP's Stop 4 weeks before to decrease thromboembolism
Oral Anti-coagulants Stop 4 days ahead of surgery & shift to LMW heparins. Heparin should
be stopped one day before surgery.
In case of emergency Vit K is given if at least 6 hrs are available.
If the surgery is to be performed immediately fresh frozen plasma is to
be given.
Unfractionated heparin stop 6 hrs before surgery
LMWH stop 12 hrs before surgery
Anti hypertensive drugs Should be continued. For ACE inhibitors and ARBS's morning dose is
withheld
Anti Anginal Drugs Antithyroid
Drugs, Anti Epileptic Drugs
Levodopa Anticholinesterases
Should be continued and even morning dose is given.
Antiplatelet Drugs Clopidogrel- stop 1 week before surgery. In emergency platelet
transfusion should be given prior to surgery.
Aspirin can be continued on the day of surgery.
Lithium Should be stopped 48 -72 Hrs before.
Smoking Should be ideally stopped 6-8 weeks before (complete ciliary recovery )
Antitubercular Drugs Should be continued with monitoring of liver function test
Aminoglycosides Has neuromuscular blocking activity so it is shift to another antibiotic
48 hrs prior to surgery
Fasting guidelines before surgical procedures
Adults Children
• Clear fluids – 2 hours
• Semisolids – 4 hours
• Solid foods – 6hours
• Clear fluids – 2 hours
• Breast milk – 4 hours
• Formula milk, solid foods – 6 hours
Indications for Central Venous Catheterization
Pulmonary artery catheterization (with coagulopathy) External jugular vein
Hemodialysis
Plasmapheresis
Preoperative preparation
Fluid management of ARDS (CVP monitoring)
Internal jugular vein
Pulmonary artery catheterization [with pulmonary compromise or high-level
positive end-expiratory pressure (PEEP)]
Emergency transvenous pacemaker
Right internal
jugular vein
Total parenteral nutrition (TPN)
Hypovolemia, inability to perform peripheral catheterization
General purpose venous access, vasoactive agents, caustic medications, radiologic
procedures
Subclavian vein
Cardiopulmonary arrest
Hypovolemia, inability to perform peripheral catheterization
Emergency airway management
Inability to lie supine
Central venous oxygen satuation monitoring
Femoral vein
*****END*****
DERMATOLOGY
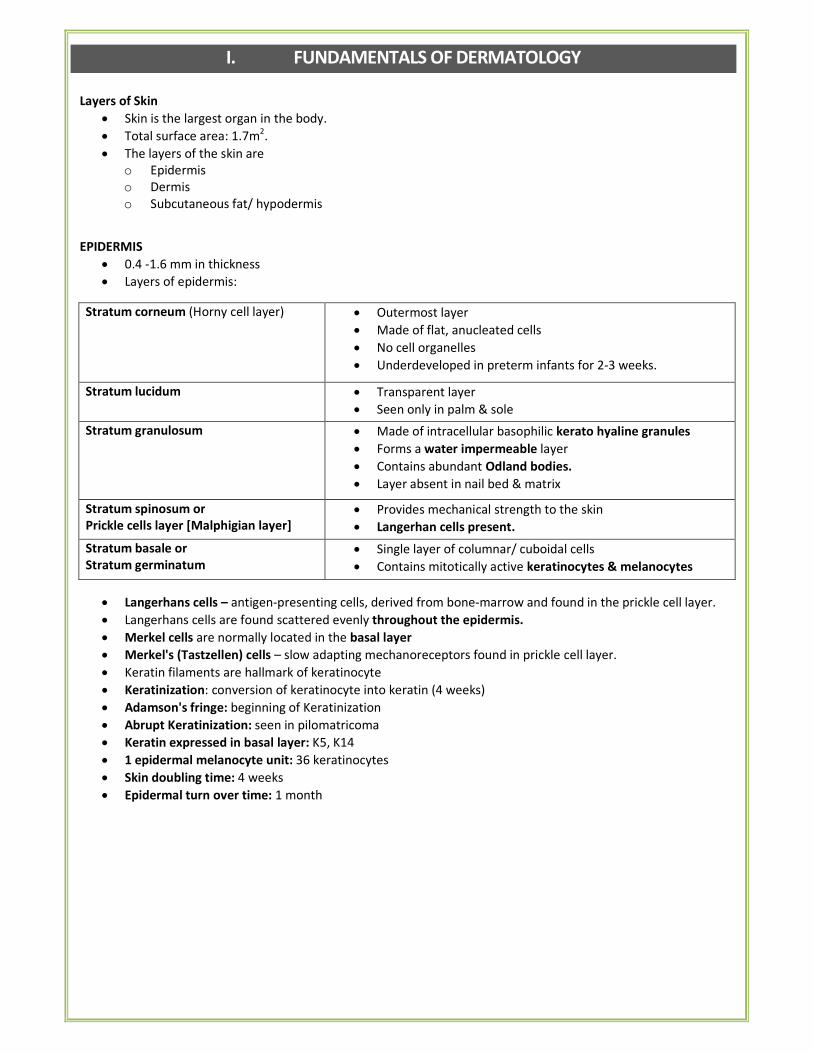
I. FUNDAMENTALS OF DERMATOLOGY
Layers of Skin
• Skin is the largest organ in the body.
• Total surface area: 1.7m2.
• The layers of the skin are
o Epidermis
o Dermis
o Subcutaneous fat/ hypodermis
EPIDERMIS
• 0.4 -1.6 mm in thickness
• Layers of epidermis:
Stratum corneum (Horny cell layer) • Outermost layer
• Made of flat, anucleated cells
• No cell organelles
• Underdeveloped in preterm infants for 2-3 weeks.
Stratum lucidum • Transparent layer
• Seen only in palm & sole
Stratum granulosum • Made of intracellular basophilic kerato hyaline granules
• Forms a water impermeable layer
• Contains abundant Odland bodies.
• Layer absent in nail bed & matrix
Stratum spinosum or
Prickle cells layer [Malphigian layer]
• Provides mechanical strength to the skin
• Langerhan cells present.
Stratum basale or
Stratum germinatum
• Single layer of columnar/ cuboidal cells
• Contains mitotically active keratinocytes & melanocytes
• Langerhans cells – antigen-presenting cells, derived from bone-marrow and found in the prickle cell layer.
• Langerhans cells are found scattered evenly throughout the epidermis.
• Merkel cells are normally located in the basal layer
• Merkel's (Tastzellen) cells – slow adapting mechanoreceptors found in prickle cell layer.
• Keratin filaments are hallmark of keratinocyte
• Keratinization: conversion of keratinocyte into keratin (4 weeks)
• Adamson's fringe: beginning of Keratinization
• Abrupt Keratinization: seen in pilomatricoma
• Keratin expressed in basal layer: K5, K14
• 1 epidermal melanocyte unit: 36 keratinocytes
• Skin doubling time: 4 weeks
• Epidermal turn over time: 1 month
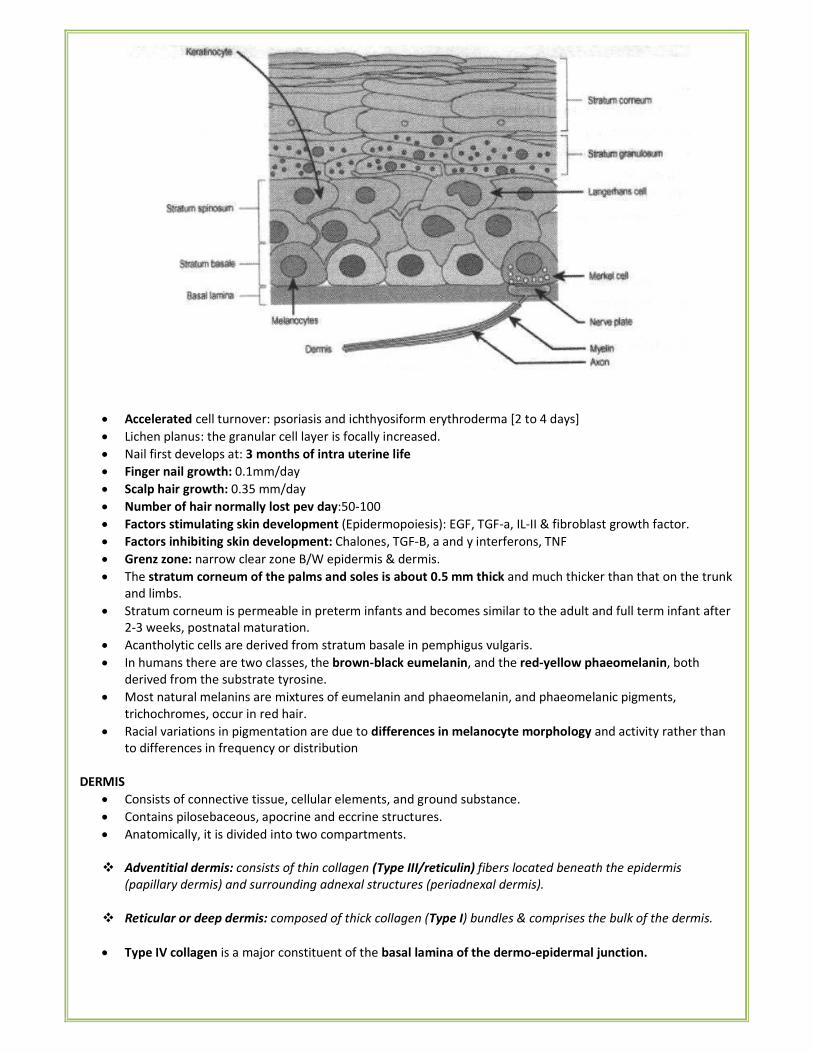
• Accelerated cell turnover: psoriasis and ichthyosiform erythroderma [2 to 4 days]
• Lichen planus: the granular cell layer is focally increased.
• Nail first develops at: 3 months of intra uterine life
• Finger nail growth: 0.1mm/day
• Scalp hair growth: 0.35 mm/day
• Number of hair normally lost pev day:50-100
• Factors stimulating skin development (Epidermopoiesis): EGF, TGF-a, IL-II & fibroblast growth factor.
• Factors inhibiting skin development: Chalones, TGF-B, a and y interferons, TNF
• Grenz zone: narrow clear zone B/W epidermis & dermis.
• The stratum corneum of the palms and soles is about 0.5 mm thick and much thicker than that on the trunk
and limbs.
• Stratum corneum is permeable in preterm infants and becomes similar to the adult and full term infant after
2-3 weeks, postnatal maturation.
• Acantholytic cells are derived from stratum basale in pemphigus vulgaris.
• In humans there are two classes, the brown-black eumelanin, and the red-yellow phaeomelanin, both
derived from the substrate tyrosine.
• Most natural melanins are mixtures of eumelanin and phaeomelanin, and phaeomelanic pigments,
trichochromes, occur in red hair.
• Racial variations in pigmentation are due to differences in melanocyte morphology and activity rather than
to differences in frequency or distribution
DERMIS
• Consists of connective tissue, cellular elements, and ground substance.
• Contains pilosebaceous, apocrine and eccrine structures.
• Anatomically, it is divided into two compartments.
� Adventitial dermis: consists of thin collagen (Type III/reticulin) fibers located beneath the epidermis
(papillary dermis) and surrounding adnexal structures (periadnexal dermis).
� Reticular or deep dermis: composed of thick collagen (Type I) bundles & comprises the bulk of the dermis.
• Type IV collagen is a major constituent of the basal lamina of the dermo-epidermal junction.
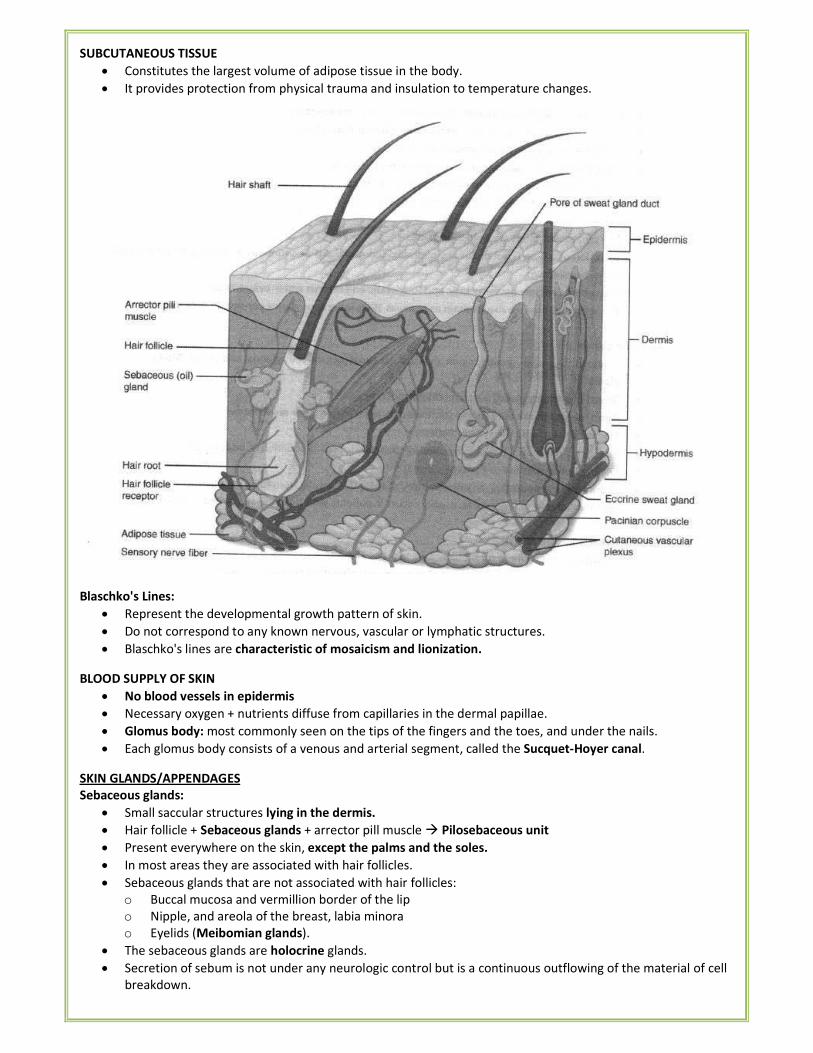
SUBCUTANEOUS TISSUE
• Constitutes the largest volume of adipose tissue in the body.
• It provides protection from physical trauma and insulation to temperature changes.
Blaschko's Lines:
• Represent the developmental growth pattern of skin.
• Do not correspond to any known nervous, vascular or lymphatic structures.
• Blaschko's lines are characteristic of mosaicism and lionization.
BLOOD SUPPLY OF SKIN
• No blood vessels in epidermis
• Necessary oxygen + nutrients diffuse from capillaries in the dermal papillae.
• Glomus body: most commonly seen on the tips of the fingers and the toes, and under the nails.
• Each glomus body consists of a venous and arterial segment, called the Sucquet-Hoyer canal.
SKIN GLANDS/APPENDAGES
Sebaceous glands:
• Small saccular structures lying in the dermis.
• Hair follicle + Sebaceous glands + arrector pill muscle � Pilosebaceous unit
• Present everywhere on the skin, except the palms and the soles.
• In most areas they are associated with hair follicles.
• Sebaceous glands that are not associated with hair follicles:
o Buccal mucosa and vermillion border of the lip
o Nipple, and areola of the breast, labia minora
o Eyelids (Meibomian glands).
• The sebaceous glands are holocrine glands.
• Secretion of sebum is not under any neurologic control but is a continuous outflowing of the material of cell
breakdown.
• The sebum is mildly bacteriostatic and fungistatic and retards water evaporation.
• The scalp and the face may contain as many as 1000 sebaceous glands per square centimetre
Apocrine glands:
• Found in the axillae, genital region, external ear canal (ceruminous glands) and eyelid (Moll's glands).
• Breast (mammary gland) is also modified apocrine gland.
• Apocrine glands are adrenergic; stimulated by epinephrine > nor epinephrine
• Do not develop until the time of puberty.
• The secretions may act as pheromones (responsible for the production of body odor).
• Obstruction results in Fox Fordyce's disease
• Hidradenitis suppurativa, an inflammatory process that results from follicular obstruction and
retention of follicular products, usually occurs in patients with the acne-seborrhea complex.
Eccrine sweat (merocrine) glands:
• Distributed everywhere on the skin surface
• Most numerous on sole of foot (620/cm2) and least abundant on the back (64/cm9
• Glands first appear on volar surface of hands & feet in 3.5 month old fetus
• Develop as a downgrowth from the primitive epidermis.
• The eccrine sweat glands and the vasculature of the skin maintain stable internal body temperature.
• Their prime stimulus is heat and their activity is under the control of hypothalamus.
• Both adrenergic and cholinergic fibers innervate the glands.
• Blockage of the eccrine ducts results in miliaria (prickly heat).
• If eccrine glands are congenitally absent, as in anhidrotic ectodermal dysplasia, a life-threatening
hyperpyrexia may develop.
Fox Fordyce's Spot (Disease)
• Fordyce spots are visible sebaceous glands without hair follicles.
• Extremely common, benign condition.
• Tiny white / yellowish focally grouped papules in buccal mucosa and vermilion border of lips, scrotum, shaft
of penis and labia
• No treatment is indicated other than reassurance.
Epidermal Stem Cells
• Three main locations of epidermal stem cells in the adult skin
o Bulge region of the hair follicle
o Interfollicular epidermis (IFE)
o Sebaceous gland
� Stem cells of small blood vessels: Pericytes
� Skin stem cells occur in the basal layer of the epidermis and at the base of hair follicles.
TERMINOLOGIES
• Acantholysis: loss of cohesion between epidermal cells, seen in all types of pemphigus.
• Acanthosis: increased thickness of the prickle cell layer due to stimulation of basal layer.
• Dyskeratosis: premature keratinization of epidermal cells.
• Foam cells: lipid-laden macrophages containing dead lepra bacilli.
• Hydropic degeneration of basal cells: vacuolization of basal cells seen in LE, dermatomyositis, early lichen
planus.
• Hyperkeratosis: Increased thickening of stratum corneum.
• Parakeratosis: presence of immature nucleated cells in stratum corneum.
• Spongiosis: accumulation of fluid between epidermal cells, seen in acute eczema.
Skin Lesions
Flat lesions:
• Macule: < 2 cm, colored. Examples: white (vitiligo), brown (café au lait spot), purple (petechia).
• Patch: > 2 cm, colored.
• Purpura: Extravasation of RBCs in the skin, blanches on pressure.
• Telangiectasia: Permanent dilatation of superficial vessels.
Elevated lesions:
• Papule: < 1 cm, solid. Examples: acne, warts, small lesions of psoriasis.
• Nodule: 1-5 cm, solid. Examples: tumors, granuloma annulare
• Tumor: > 5 cm, solid.
• Plaque: > 1 cm, flat topped. Example: psoriasis.
• Vesicle: < 1 cm, fluid-filled. Example: blisters of herpes simplex.
• Bullae: > 1 cm, fluid-filled. Example: bullous impetigo.
• Pustule: Vesicle filled with leukocytes. Examples: acne, folticulitis.
• Wheal: circumscribed, flat-topped, firm elevation of skin resulting from tense edema of the papillary dermis.
Example: urticaria
Secondary changes
Scales Dry, thin plates of keratinized epidermal cells (stratum corneum) Example: psoriasis,
Lichenification Induration of skin with exaggerated skin lines and a shiny surface resulting from chronic
rubbing of the skin. Example: atopic dermatitis.
Impetiginization Bacterial infection resulting in exudation and golden-yellow crusting
Erosion and
oozing
A moist, circumscribed, slightly depressed area representing a blister base with the roof of
the blister removed. Examples: burns, impetigo. Most oral blisters present as erosions.
Crusts Dried exudate of plasma on the surface of the skin following acute dermatitis. Examples:
impetigo, contact dermatitis.
Fissures A linear split in the skin extending through the epidermis into the dermis. Example: angular
cheilitis.
Scars A flat, raised, or depressed area of fibrotic replacement of dermis or subcutaneous tissue.
Atrophy Depression of the skin surface caused by thinning of one or more layers of skin.
Example: lichen sclerosis.
Configuration of lesions
Annular
(circular)
Annular nodules represent granuloma annulare; annular scaly papules are more apt to be
caused by dermatophyte infections.
Linear (straight
lines)
Linear papules represent lichen striatus; linear vesicles, incontinentia pigmenti; linear
papules with burrows, scabies.
Grouped Grouped vesicles occur in herpes simplex or zoster.
INTRA-EPIDERMAL BLISTERS:
Granular layer Spinous layer Supra basal layer Basal Layer
Friction blister
Pemphigus foliaceous
Sub corneal pustular
dermatosis
Staphylococcal skin scald
syndrome / Bullous impetigo
Eczematous
dermatitis
Herpes virus infection
Familial benign
pemphigus
Pemphigus vulgaris
Darier's disease
Lupus erythematosus
Lichen planus
Epidermolysis bullosa simplex
BLISTERS AT DERMAL EPIDERMAL JUNCTIONS:
Junctional (at the lamina lucida) Dermolytic (Below basal lamina)
Bullous Pemphigoid
Erythema multiforme
Junctional Epidermolysis bullosa
Epidermolysis bullosa dystrophicans
Epidermolysis bullosa acquisita
Porphyria cutanea tarda
Dermatitis herpetitiformis
DIAGNOSTIC TECHNIQUES
Disease Diagnosed by
Atopic Dermatitis
Contact Dermatitis
Donovanosis (GI)
Chancroid
Clinical evaluation
Patch Test
Microscopy (Donovan bodies/Safety pin appearance)
Gram staining(gram negative rods/ school of fish / rails road appearance
• Grattage test: Psoriasis
• Pethergy test: Behcet's syndrome
• Patch test: Contact dermatitis
• Dermatoscopy (Epiluminescence microscopy, dermoscopy): method of observing superficial layers of skin
using 10-100 X magnification under oil immersion.
Tzanck Smear
• Most commonly used in the diagnosis of herpes virus infection – shows multinucleated giant cells.
• Also used in pemphigus – shows acantholysis.
SKIN BIOPSY
There are four principal techniques for performing skin biopsies:
• Surgical excision with suturing:
o Good cosmetic result
o Entire lesion is removed.
o Disadvantage: most time consuming of the three techniques, removal of the sutures.
• Punch biopsy:
o Inadequate for evaluation of vesiculobullous diseases
o Should be deep enough to include subcutaneous fat if used for diagnosis of panniculitis or
o tumors in a subcutaneous location.
o Pigmented lesions should not be punched unless they can be completely excised.
• Excision with scissors:
o Useful for certain types of elevated lesions and in areas in which the cosmetic result is not too
important.
o Advantage of this procedure is the speed and the simplicity with which it can be done.
• Shave biopsy:
o Can be performed superficially or deeply.
o Hemostasis can be accomplished by pressure, light electrosurgery, Monsel solution, or aluminium
chloride solution.
o Not recommended for excision of melanocytic lesions or other potentially malignant tumor where
margin assessment is required.
WOOD'S LAMP
It is a source of ultra violet light (mainly long wave UV-A, at a wavelength of 360nm), from which virtually all variable
rays have been excluded by filter (made of nickel oxide i.e. Ni02 and Si). It is used in:
• Fungal infections like:
o Tinea capitis = yellow green fluorescence.
o Pityriasis versicolor = golden yellow / apple green
• Bacterial infections like:
o Erythrasma & Acne = Coral red / pink
o Pseudomonas pyocyanea = yellow-green
• Pigmentary disorder
o Vitiligo = total white
o Ash-leaf macules in tuberous sclerosis = blue white
• Urine examination in Porphyria (red / pink urine)
• Squamous cell carcinoma of skin = red fluorescence
Type of collagen Location
I Bone
II Cartilage, vitreous tumour, Intervertebral disc
III Extensive - skin, lung, hollow organ (vascular system)
IV Basement membrane, Eye lens
VII Anchoring fibrils at Dermo-epidermal junction
VIII Endothelium
X Hypertrophic cartilage
XVII Skin, hemidesmosomes
XVIII Liver, kidney
XIX Rhabdomyasarcoma cells
Distributions of Glycosaminoglycans (GAGS):
Hyaluronic acid Synovial fluid, Vitreous humour, Loose connective tissue
Chondroitin sulphate Cartilage, bone, cornea
Keratan sulphate-I Cornea
Keratan sulphate-II Loose connective tissue
Heparin Mast cells
Heparan sulfate Skin, Fibroblasts
Dermatan sulphate Wide distribution
PANNICULUS ADIPOSUS
• The panniculus adiposus is the fatty layer of the subcutaneous tissues, superficial to a deeper vestigial layer
of muscle, the panniculus carnosus.
• It includes structures that are considered fascia by some sources but not by others.
• Eg: Fascia of Camper, superficial cervical fascia.
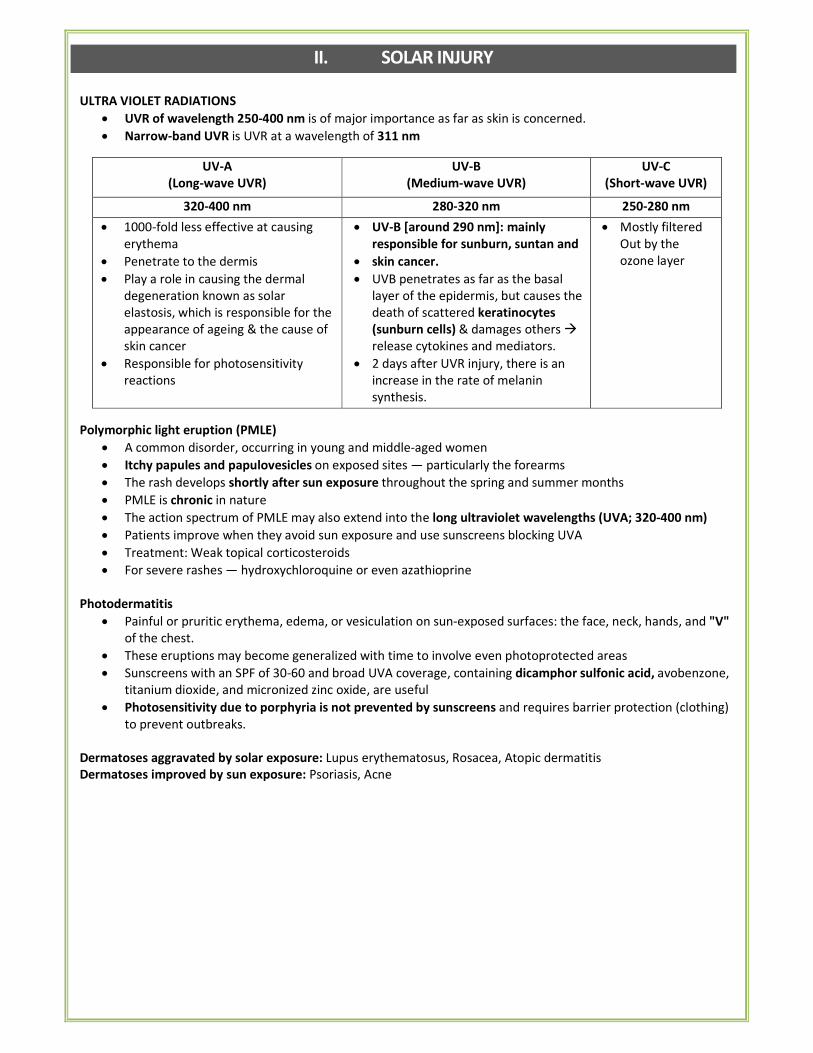
II. SOLAR INJURY
ULTRA VIOLET RADIATIONS
• UVR of wavelength 250-400 nm is of major importance as far as skin is concerned.
• Narrow-band UVR is UVR at a wavelength of 311 nm
UV-A
(Long-wave UVR)
UV-B
(Medium-wave UVR)
UV-C
(Short-wave UVR)
320-400 nm 280-320 nm 250-280 nm
• 1000-fold less effective at causing
erythema
• Penetrate to the dermis
• Play a role in causing the dermal
degeneration known as solar
elastosis, which is responsible for the
appearance of ageing & the cause of
skin cancer
• Responsible for photosensitivity
reactions
• UV-B [around 290 nm]: mainly
responsible for sunburn, suntan and
• skin cancer.
• UVB penetrates as far as the basal
layer of the epidermis, but causes the
death of scattered keratinocytes
(sunburn cells) & damages others �
release cytokines and mediators.
• 2 days after UVR injury, there is an
increase in the rate of melanin
synthesis.
• Mostly filtered
Out by the
ozone layer
Polymorphic light eruption (PMLE)
• A common disorder, occurring in young and middle-aged women
• Itchy papules and papulovesicles on exposed sites — particularly the forearms
• The rash develops shortly after sun exposure throughout the spring and summer months
• PMLE is chronic in nature
• The action spectrum of PMLE may also extend into the long ultraviolet wavelengths (UVA; 320-400 nm)
• Patients improve when they avoid sun exposure and use sunscreens blocking UVA
• Treatment: Weak topical corticosteroids
• For severe rashes — hydroxychloroquine or even azathioprine
Photodermatitis
• Painful or pruritic erythema, edema, or vesiculation on sun-exposed surfaces: the face, neck, hands, and "V"
of the chest.
• These eruptions may become generalized with time to involve even photoprotected areas
• Sunscreens with an SPF of 30-60 and broad UVA coverage, containing dicamphor sulfonic acid, avobenzone,
titanium dioxide, and micronized zinc oxide, are useful
• Photosensitivity due to porphyria is not prevented by sunscreens and requires barrier protection (clothing)
to prevent outbreaks.
Dermatoses aggravated by solar exposure: Lupus erythematosus, Rosacea, Atopic dermatitis
Dermatoses improved by sun exposure: Psoriasis, Acne
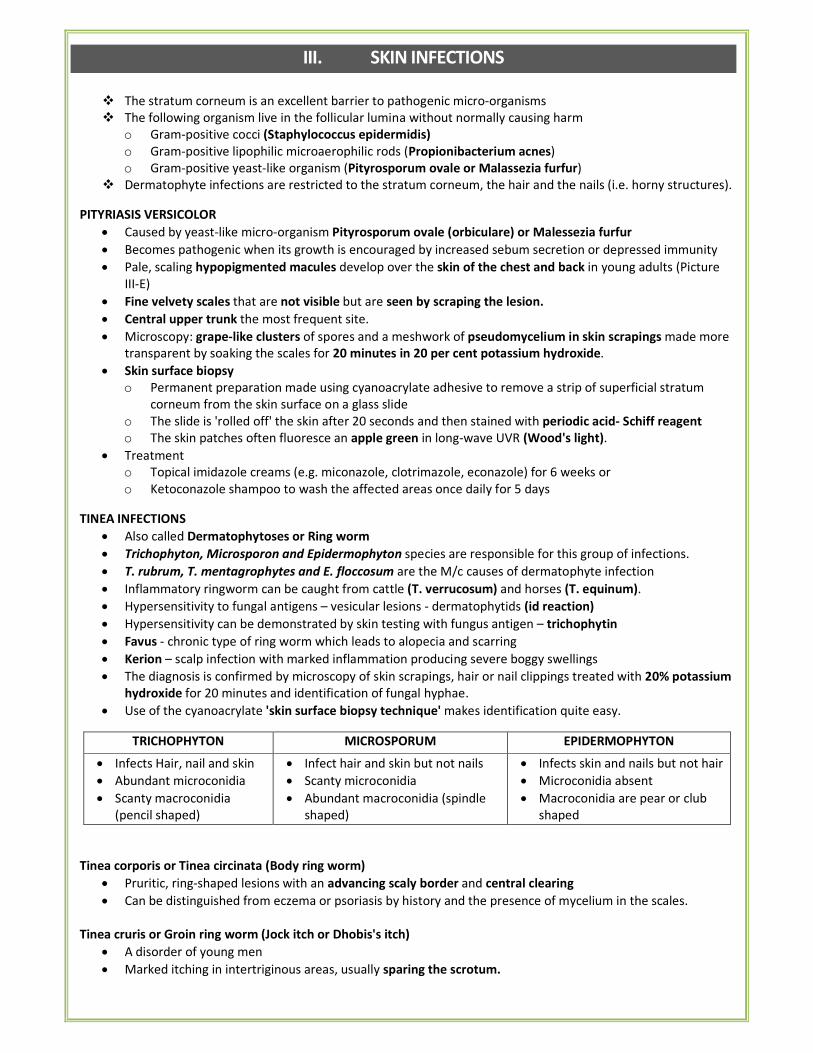
III. SKIN INFECTIONS
� The stratum corneum is an excellent barrier to pathogenic micro-organisms
� The following organism live in the follicular lumina without normally causing harm
o Gram-positive cocci (Staphylococcus epidermidis)
o Gram-positive lipophilic microaerophilic rods (Propionibacterium acnes)
o Gram-positive yeast-like organism (Pityrosporum ovale or Malassezia furfur)
� Dermatophyte infections are restricted to the stratum corneum, the hair and the nails (i.e. horny structures).
PITYRIASIS VERSICOLOR
• Caused by yeast-like micro-organism Pityrosporum ovale (orbiculare) or Malessezia furfur
• Becomes pathogenic when its growth is encouraged by increased sebum secretion or depressed immunity
• Pale, scaling hypopigmented macules develop over the skin of the chest and back in young adults (Picture
III-E)
• Fine velvety scales that are not visible but are seen by scraping the lesion.
• Central upper trunk the most frequent site.
• Microscopy: grape-like clusters of spores and a meshwork of pseudomycelium in skin scrapings made more
transparent by soaking the scales for 20 minutes in 20 per cent potassium hydroxide.
• Skin surface biopsy
o Permanent preparation made using cyanoacrylate adhesive to remove a strip of superficial stratum
corneum from the skin surface on a glass slide
o The slide is 'rolled off' the skin after 20 seconds and then stained with periodic acid- Schiff reagent
o The skin patches often fluoresce an apple green in long-wave UVR (Wood's light).
• Treatment
o Topical imidazole creams (e.g. miconazole, clotrimazole, econazole) for 6 weeks or
o Ketoconazole shampoo to wash the affected areas once daily for 5 days
TINEA INFECTIONS
• Also called Dermatophytoses or Ring worm
• Trichophyton, Microsporon and Epidermophyton species are responsible for this group of infections.
• T. rubrum, T. mentagrophytes and E. floccosum are the M/c causes of dermatophyte infection
• Inflammatory ringworm can be caught from cattle (T. verrucosum) and horses (T. equinum).
• Hypersensitivity to fungal antigens – vesicular lesions - dermatophytids (id reaction)
• Hypersensitivity can be demonstrated by skin testing with fungus antigen – trichophytin
• Favus - chronic type of ring worm which leads to alopecia and scarring
• Kerion – scalp infection with marked inflammation producing severe boggy swellings
• The diagnosis is confirmed by microscopy of skin scrapings, hair or nail clippings treated with 20% potassium
hydroxide for 20 minutes and identification of fungal hyphae.
• Use of the cyanoacrylate 'skin surface biopsy technique' makes identification quite easy.
TRICHOPHYTON MICROSPORUM EPIDERMOPHYTON
• Infects Hair, nail and skin
• Abundant microconidia
• Scanty macroconidia
(pencil shaped)
• Infect hair and skin but not nails
• Scanty microconidia
• Abundant macroconidia (spindle
shaped)
• Infects skin and nails but not hair
• Microconidia absent
• Macroconidia are pear or club
shaped
Tinea corporis or Tinea circinata (Body ring worm)
• Pruritic, ring-shaped lesions with an advancing scaly border and central clearing
• Can be distinguished from eczema or psoriasis by history and the presence of mycelium in the scales.
Tinea cruris or Groin ring worm (Jock itch or Dhobis's itch)
• A disorder of young men
• Marked itching in intertriginous areas, usually sparing the scrotum.
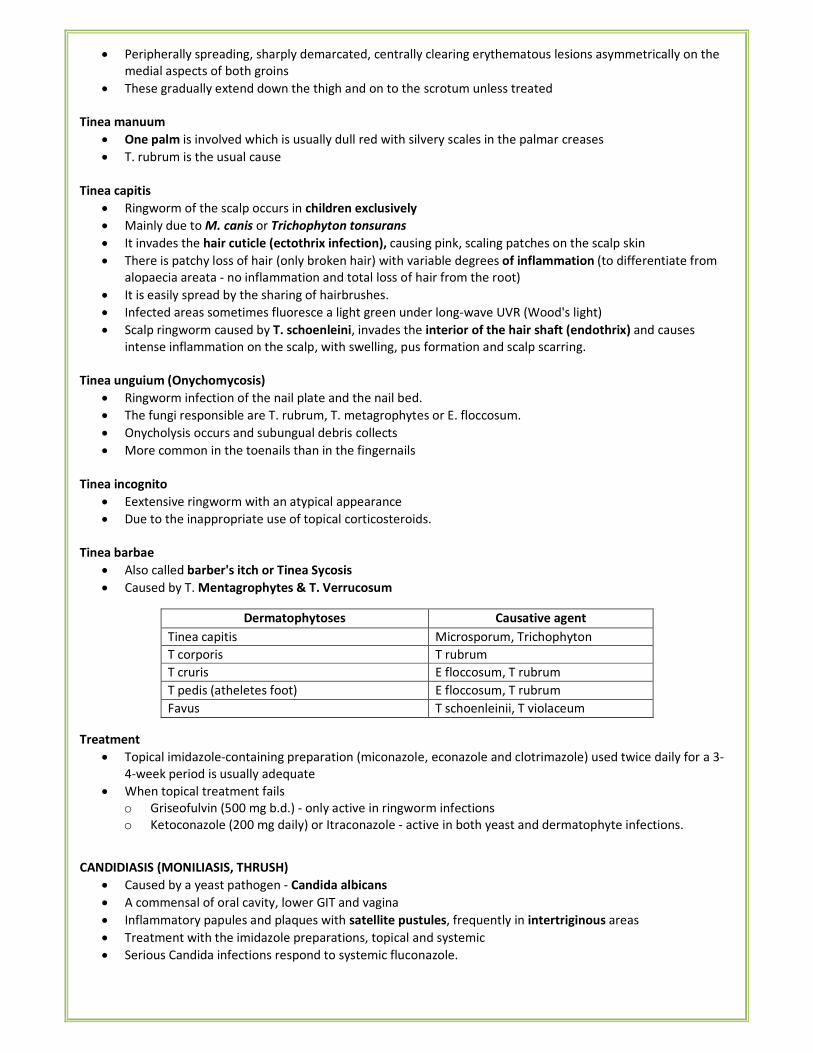
• Peripherally spreading, sharply demarcated, centrally clearing erythematous lesions asymmetrically on the
medial aspects of both groins
• These gradually extend down the thigh and on to the scrotum unless treated
Tinea manuum
• One palm is involved which is usually dull red with silvery scales in the palmar creases
• T. rubrum is the usual cause
Tinea capitis
• Ringworm of the scalp occurs in children exclusively
• Mainly due to M. canis or Trichophyton tonsurans
• It invades the hair cuticle (ectothrix infection), causing pink, scaling patches on the scalp skin
• There is patchy loss of hair (only broken hair) with variable degrees of inflammation (to differentiate from
alopaecia areata - no inflammation and total loss of hair from the root)
• It is easily spread by the sharing of hairbrushes.
• Infected areas sometimes fluoresce a light green under long-wave UVR (Wood's light)
• Scalp ringworm caused by T. schoenleini, invades the interior of the hair shaft (endothrix) and causes
intense inflammation on the scalp, with swelling, pus formation and scalp scarring.
Tinea unguium (Onychomycosis)
• Ringworm infection of the nail plate and the nail bed.
• The fungi responsible are T. rubrum, T. metagrophytes or E. floccosum.
• Onycholysis occurs and subungual debris collects
• More common in the toenails than in the fingernails
Tinea incognito
• Eextensive ringworm with an atypical appearance
• Due to the inappropriate use of topical corticosteroids.
Tinea barbae
• Also called barber's itch or Tinea Sycosis
• Caused by T. Mentagrophytes & T. Verrucosum
Dermatophytoses Causative agent
Tinea capitis Microsporum, Trichophyton
T corporis T rubrum
T cruris E floccosum, T rubrum
T pedis (atheletes foot) E floccosum, T rubrum
Favus T schoenleinii, T violaceum
Treatment
• Topical imidazole-containing preparation (miconazole, econazole and clotrimazole) used twice daily for a 3-
4-week period is usually adequate
• When topical treatment fails
o Griseofulvin (500 mg b.d.) - only active in ringworm infections
o Ketoconazole (200 mg daily) or Itraconazole - active in both yeast and dermatophyte infections.
CANDIDIASIS (MONILIASIS, THRUSH)
• Caused by a yeast pathogen - Candida albicans
• A commensal of oral cavity, lower GIT and vagina
• Inflammatory papules and plaques with satellite pustules, frequently in intertriginous areas
• Treatment with the imidazole preparations, topical and systemic
• Serious Candida infections respond to systemic fluconazole.
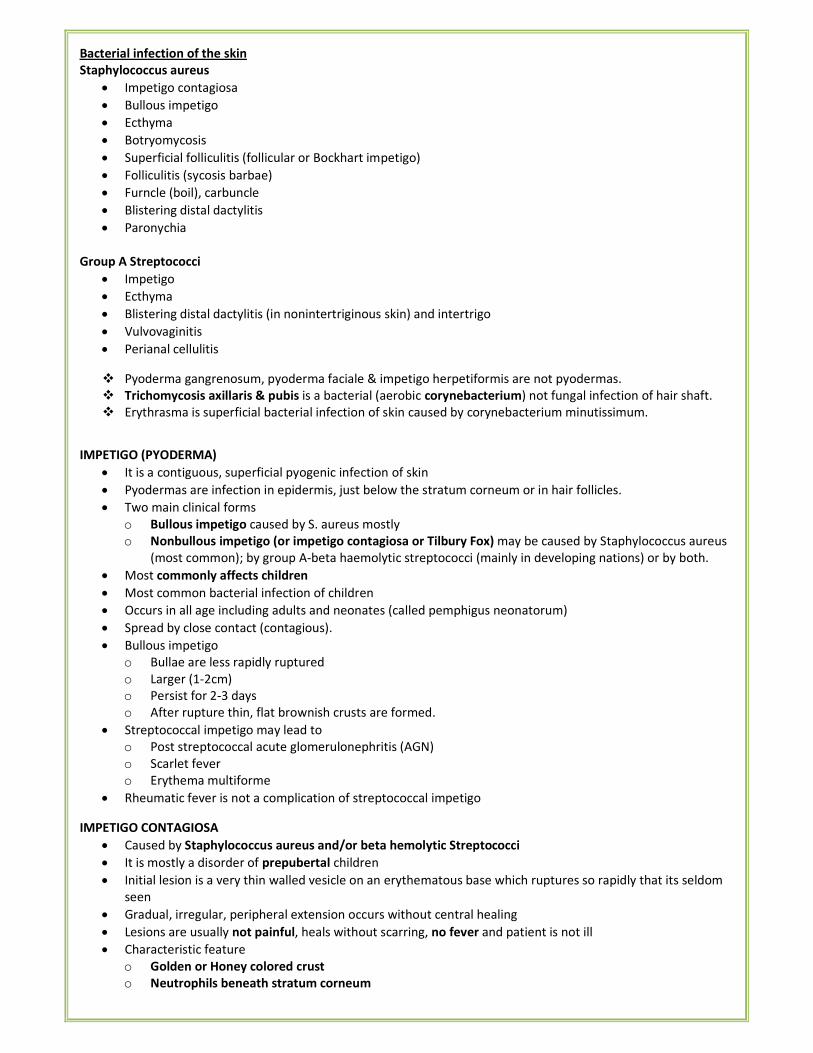
Bacterial infection of the skin
Staphylococcus aureus
• Impetigo contagiosa
• Bullous impetigo
• Ecthyma
• Botryomycosis
• Superficial folliculitis (follicular or Bockhart impetigo)
• Folliculitis (sycosis barbae)
• Furncle (boil), carbuncle
• Blistering distal dactylitis
• Paronychia
Group A Streptococci
• Impetigo
• Ecthyma
• Blistering distal dactylitis (in nonintertriginous skin) and intertrigo
• Vulvovaginitis
• Perianal cellulitis
� Pyoderma gangrenosum, pyoderma faciale & impetigo herpetiformis are not pyodermas.
� Trichomycosis axillaris & pubis is a bacterial (aerobic corynebacterium) not fungal infection of hair shaft.
� Erythrasma is superficial bacterial infection of skin caused by corynebacterium minutissimum.
IMPETIGO (PYODERMA)
• It is a contiguous, superficial pyogenic infection of skin
• Pyodermas are infection in epidermis, just below the stratum corneum or in hair follicles.
• Two main clinical forms
o Bullous impetigo caused by S. aureus mostly
o Nonbullous impetigo (or impetigo contagiosa or Tilbury Fox) may be caused by Staphylococcus aureus
(most common); by group A-beta haemolytic streptococci (mainly in developing nations) or by both.
• Most commonly affects children
• Most common bacterial infection of children
• Occurs in all age including adults and neonates (called pemphigus neonatorum)
• Spread by close contact (contagious).
• Bullous impetigo
o Bullae are less rapidly ruptured
o Larger (1-2cm)
o Persist for 2-3 days
o After rupture thin, flat brownish crusts are formed.
• Streptococcal impetigo may lead to
o Post streptococcal acute glomerulonephritis (AGN)
o Scarlet fever
o Erythema multiforme
• Rheumatic fever is not a complication of streptococcal impetigo
IMPETIGO CONTAGIOSA
• Caused by Staphylococcus aureus and/or beta hemolytic Streptococci
• It is mostly a disorder of prepubertal children
• Initial lesion is a very thin walled vesicle on an erythematous base which ruptures so rapidly that its seldom
seen
• Gradual, irregular, peripheral extension occurs without central healing
• Lesions are usually not painful, heals without scarring, no fever and patient is not ill
• Characteristic feature
o Golden or Honey colored crust
o Neutrophils beneath stratum corneum
• Face around nose and mouth) and limbs are most commonly affected
Erysipelas
• Caused by the beta-haemolytic Streptococcus
• Sudden onset of a well-marginated, painful and swollen erythematous area, on the face or lower limbs.
• The inflammation may be very intense and the area may become haemorrhagic and even blister.
• There is usually an accompanying pyrexia and malaise.
Pyoderma faciale
• Also called rosacea fulminas or rosacea conglobate
• Occurs mainly in adult women (in 20s)
• Sudden, severe eruption of confluent papules, nodules, pustules, cystic swellings which may be
interconnected by draining sinuses usually confined to face, involving checks, chin, nose, & forehead
• Comedones are usually absent or inconspicuous, as are other features of acne vulgaris or rosacea
• Some cases may develop during pregnancy or medication (interferon alpha-2B & ribavirin therapy for
hepatitis C)
TOXIC EPIDERMAL NECROLYSIS/ STAPHYLOCOCCAL SCALDED SKIN SYNDROME (SSSS)
Also called LyeII syndrome
• Caused by ET (Exfoliative / Erythematogenic toxin) producing Staph. aureus (phage group II)
• Most common site of infection is extracutaneous
• Wide spread erythematous blisterous eruption with striking desquamation of large areas of skin (Nikolsky
sign positive) as seen in scald or burn.
• Mucosa is not involved.
• Initial findings are redness & tenderness of central face, neck, truck & interiginous zone followed by short
lived flaccid bullae & slough or exfoliation or peeling of superficial epidermis.
• Treated by IV antibiotics
CUTANEOUS TUBERCULOSIS
Lupus Vulgaris
• Slowly progressive, granulomatous plaque on the skin
• It slowly increases in size, over one, two or three decades.
• Blanching with a glass microscope slide (diascopy) will reveal grey-green foci (apple jelly nodules)
Tuberculosis Verrucosa Cutis (Warty Tuberculosis)
• Seen on the backs of the hands, knees, elbows and buttocks whenever abrasive contact with the earth and
tubercle bacilli has been made.
• Thickened, warty plaques are present - sometimes misdiagnosed as viral warts
Different types of cutaneous TB
• Lupus vulgaris (Apple-jelly nodules)
• Lupus miliaris disseminate faciei
• Lichen scrofulosoeum
• Scrofuloderma (skin T.B. secondary to underlying structure)
• Tuberculosis cutis orificalis (TB. of orifices - oral, anal, urogenital)
• Papulo necrotic tuberculids
• Erythema nodosum
• Erythema induratum
• Acne agmination
Other Mycobacterial Infections
Swimming pool granuloma
• Caused by Mycobacterium marinum
• Causes plaques, abscesses and erosions on the elbows and knees in particular.
• The condition responds to minocycline or a trimethoprimsulphamethoxazole combination.
Buruli ulcer
• Mycobacterium ulcerans is responsible for this disorder
• Surgical removal is currently the best treatment.
SARCOIDOSIS
• Bluish chilblain-likeswellings of the fingers, nose and ears (lupus pernio) – infiltrated by typical sarcoid tissue
• Erythema nodosum – not infiltrated by typical sarcoid tissue
• Histologically of the typical Sarcoid lesion: 'naked' tubercle, which contains foci of macrophages and giant
cells without many surrounding lymphocytes.
LYME DISEASE
• Caused by the Borrelia burgdorfii
• Early stages - erythema chronicum migrans
• Late stages - skin atrophy (acrodermatitis chronica atrophicans), or fibrosis
Viral infection of the skin
HERPES SIMPLEX
• Type I is responsible for the common herpetic infection of the face and oropharynx
• Type II herpes simplex infects the genitalia
• 20 % suffer from recurrent 'cold sores', precipitated by minor pyrexial disorders or sun exposure.
• Commonly, the lesions occur around the mouth or on the lip.
• Genital herpes affects the glans penis and the shaft of the penis.
• In women, the vulval region or labia minora is usually involved
HERPES ZOSTER (SHINGLES)
• Mostly affects those past the age of 50 years
• Also affects immunosuppressed individuals
• Due to the reactivation of a latent virus in a posterior root ganglion of a spinal nerve
• Starts with paraesthesiae or pain in the distribution of one or more dermatomes (Picture III-F)
• Dermatome frequently affected - thoracic
• Involvement of one of the branches of the trigeminal ganglion, with lesions in the distribution of the
maxillary, mandibular or ophthalmic sensory nerves, is common
• Lesions are confined to the skin innervated by the dorsal primary root (s) infected
VIRAL WARTS
• Caused by a member of the human papillomavirus family
• Epidermodysplasia vericuformis
o Congenital condition
o Plane warts spread extensively on the arms, face, trunk and limbs
o Some lesions can transform to squamous cell carcinoma
• Verruca vulgaris (Picture III-G)
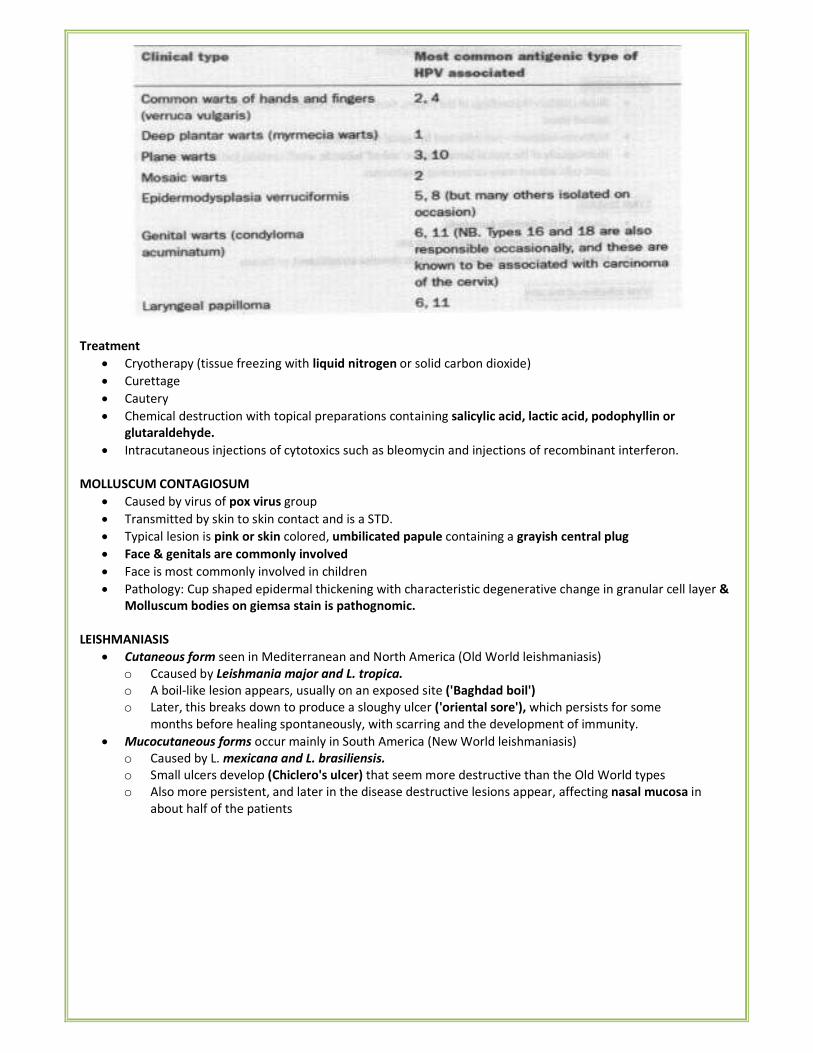
Treatment
• Cryotherapy (tissue freezing with liquid nitrogen or solid carbon dioxide)
• Curettage
• Cautery
• Chemical destruction with topical preparations containing salicylic acid, lactic acid, podophyllin or
glutaraldehyde.
• Intracutaneous injections of cytotoxics such as bleomycin and injections of recombinant interferon.
MOLLUSCUM CONTAGIOSUM
• Caused by virus of pox virus group
• Transmitted by skin to skin contact and is a STD.
• Typical lesion is pink or skin colored, umbilicated papule containing a grayish central plug
• Face & genitals are commonly involved
• Face is most commonly involved in children
• Pathology: Cup shaped epidermal thickening with characteristic degenerative change in granular cell layer &
Molluscum bodies on giemsa stain is pathognomic.
LEISHMANIASIS
• Cutaneous form seen in Mediterranean and North America (Old World leishmaniasis)
o Ccaused by Leishmania major and L. tropica.
o A boil-like lesion appears, usually on an exposed site ('Baghdad boil')
o Later, this breaks down to produce a sloughy ulcer ('oriental sore'), which persists for some
months before healing spontaneously, with scarring and the development of immunity.
• Mucocutaneous forms occur mainly in South America (New World leishmaniasis)
o Caused by L. mexicana and L. brasiliensis.
o Small ulcers develop (Chiclero's ulcer) that seem more destructive than the Old World types
o Also more persistent, and later in the disease destructive lesions appear, affecting nasal mucosa in
about half of the patients
IV. SKIN INFESTATIONS
ECTOPARASITES
Phthirus pubis Pubic lice infestation
Pediculus humanus Pediculosis
Sarcoptes scabiei Scabies
SCABIES
Epidemiology:
• Infestation caused by Acarus hominis/Sarcoptes scabie.
• Incubation period is 2-4 weeks.
• Itching worse at night is most common symptom.
• Family history of similar itchy eruptions in close contact
• On an average, an adult has 12 mites and an infant 20 mites.
Primary lesions:
• Serpentine (S-shaped) burrows traversed by parasite in stratum corneum (pathognomic lesion)
• Most common sites involved: Inter digital space, Anterior wrist, Ulnar border of hand
• An imaginary circle intersecting the main sites of involvement—axillae, elbow flexures, wrists and
• hands and groins - 'circle of Hebra'.
• In infants and elderly: Scalp, Face, Neck, Palms & Soles, Penis also involved
• Papules & papulo-vesicles: due to hypersensitivity to the mite.
• Fine pin head size follicular papules
Secondary lesions:
• Pustules due to 2° infection is one of commonest form of presentation.
• Eczematized crusted lesion, in infants & children are predominant lesions.
• Nodular lesions are seen on scrotum (most common), groin, and anterior axillary fold (Nodular scabies).
Types:
• Crusted or Norwegian scabies
o Most severe form
o The average number of mites in these cases is 2 million
o Seen in immuno compromised, mentally ill patients, GVDH, leprosy, leukemia
o Psoriatiform or warty lesions accompanied by nail hyperkeratosis
o No burrows
o Minimal itching
o Highly contagious
o Ivermectin is the treatment of choice
• Scabies incognetio - wrongly treated with steroids.
Treatment
• Drug of choice : 5% Permethrin (1st
) BHC (2nd
).
• Oral drug (Only): Ivermectin.
• Other drugs : Benzyl benzoate 25%, Crotamiton 10%, Malathion, Monosulfiram.
• Drug safe in pregnancy & infants < 2 months: precipitated sulfur 5-10%.
• Scabicides should be applied to the whole body (below jaw line in adults) to all members of family whether
symptomatic or not.
PEDICULOSIS
• Macula cerulea (bluish stain on the skin d/t louse bite) is a typical lesion of Pediculosis
P. Capitis
• Transmitted by Head louse
• Involves scalp � mobile dandruff
• Common in girls with long hairs
• The diagnosis is made by seeing the lice in the scalp or more often, nits glued to the hair shaft
P. Corporis (Vagabond's disease.)
• Transmitted by Body louse
• The body louse transmits
o Epidemic typhus
o Trench fever
o Relapsing fever
• The diagnos s is positively established by finding the lice or nits in the seams of clothing
• Treatmeot: disinfection of clothes with 10% DDT or 1% BHC + Pediculocide drug application
Pthirus Pubis (Pubic louse):
• Is a STD, can also infest body, axillary, and eyelash hairs
• In children the common areas of involvement are the eyebrows and eyelashes (pediculosis palpebrum)
• Diagnosis is made on seeing black speck like bodies attached to the root of hair at an angle—t.,e crab lice
V. IMMUNE MEDIATED SKIN DISORDERS
URTICARIA (nettlerash, 'weals' and 'hives')
• Urticaria is a vascular reaction pattern characterised by transient, erythematous, oedematous papules or
plaques (wheals) of varying sizes and shapes which are usually pruritic.
• Angioedema is the same process but involves the deep dermis, subcutaneous and submucosal tissues
• Urticaria — dermal edema
• Angioedema — subcutaneous, submucosal edema
• Result of histamine release from mast cells in the skin.
• Type I hypersensitivity mediated by histamine.
• Lesions are itchy, red papules and plaques of variable size that arise suddenly, often within a few minutes
THE 'PHYSICAL' URTICARIAS
Cold urticaria
• Occur after exposure to the cold.
• The reaction can be elicited by an ice block.
• There is a familial form.
Pressure urticaria
• Lesions develop some time (up to several hours) after pressure on the skin
• For example from belts or other tight clothing, or from the rungs of a ladder.
Dermographism
• Many patients with urticaria mark easily when their skin is rubbed firmly, for example with a key.
• This is an exaggerated 'triple response' and is quite troublesome to some patients
Solar urticaria
• Urticaria spots develop on exposed skin a few minutes after exposure to the sun.
• It is a skin sign of one systemic disease— erythropoietic protoporphyria
Cholinergic Urticaria
• Irritating, small urticaria spots develop after exercise, hot baths, emotions
• Occurs after stimuli that evoke sweating from the post-ganglionic cholinergically enervated sweat glands.
DRUG-INDUCED URTICARIA
• Penicillin
• NSAIDs
• Sulphonamides
• Aspirin
Urticaria lesions are seen in patients with
• Mastocytosis (urticaria pigmentosa)
• Hypo- or hyperthyroidism
• Systemic-onset juvenile idiopathic arthritis (Still's disease)
ERYTHEMA MULTIFORME (EM)
• EM minor: an acute, self-limiting, usually mild, often recurrent inflammatory syndrome characterised by
symmetrically distributed erythematous papular, urticaria and typical iris/target shaped lesions (Picture:V-
A)
o Cause: Herpes simplex virus – most common cause of recurrent EM
• EM major: more severe variant with extensive mucous membrane involvement and constitutional symptoms
o Cause: HSV, Mycoplasma, Drugs (sulfonamides, phenytoin, barbiturates, aminopenicillins, non-
nucleoside reverse transcriptase inhibitors, and carbamazepine)
o Hemorrhagic crusts of lips
• The term "erythema multiforme major" has been replaced by three terms
o Stevens-Johnson syndrome (SJS), with < 10% BSA skin loss
o Toxic epidermal necrolysis (TEN) when there is > 30% BSA skin loss
o SJS/TEN overlap for cases with between 10% and 30% BSA denudation.
• Skin biopsy is diagnostic.
• Direct immunofluorescence studies are negative
ERYTHEMA NODOSUM
• Painful crops of nodules develop in response to antigenic stimuli mostly in shins & forearms.
• Women are predominantly affected by a ratio of 10:1 over men
Causes of erythema nodosum
• Tuberculosis – most common
• Sarcoidosis
• Leprosy (lepromatous type LL & BL)
• Brucellosis
• Streptococcal infection
• Ulcerative colitis & Crohn's disease
• Oral contraceptives
LUPUS ERYTHEMATOSUS
• Skin involvement is the 2nd
most common clinical manifestation after joint inflammation and is found in up to
70% of patients
• The two most common forms of chronic cutaneous lupus erythematosus (CCLE) are
o Chronic scarring (discoid) lesions (DLE)
o Erythematous non-scarring red plaques (Subacute cutaneous LE) (SCLE).
• Discoid LE (DLE) or Chronic cutaneous LE
• The lesions are most commonly found on face and neck
• Permanent hair loss (scarring alopecia) and loss of pigmentation are common sequelae of discoid lesions.
• There is atrophy, telangiectasia, depigmentation, and follicular plugging by scales
• When the scale is removed, its underside shows small excrescences that correlate with the openings of hair
follicles (carpet tacking or thumbtack like)
• The disorder may be aggravated or initiated by exposure to the sun.
• Histology: epidermal degenerative changes are more marked, with scattered cytoid body formation and
patchy epidermal atrophy and thickening
Treatment
• Sun avoidance and use of sunscreens
• Individual lesions sometimes respond to potent topical corticosteroid
• For unresponsive lesions - hydroxychloroquine (200-400 mg per day) is often helpful.
SYSTEMIC SCLEROSIS
Progressive systemic sclerosis
• The disease is mostly seen in young women
• Gradual thickening and stiffening of the skin of the hands and face
• This causes a characteristic beak-like facial appearance, with narrowing of the mouth
• There are pigmentary changes over the face and neck in the form of hyperpigmentation and depigmentation
(pepper-salt pigmentation) (Picture V-B)
• Telangiectatic macules appear over the face and deposits of calcium develop in the skin.
• Fingers: sclerodactyly or sausage shaped fingers with taut skin over the fingers and thimble pitted scars over
fingertips
• Raynaud's phenomenon is almost a constant feature
• CRST syndrome (Calcinosis cutis, Raynaud phenomenon, Sclerodactyly, and Telangiectasia)
• When there is also dysphagia due to Esophageal involvement - CREST syndrome
Morphoea or Localized Scleroderma.
• Linear scleroderma - involvement of the face and/or forehead manifesting as Parry-Romberg syndrome and
'en coup de sabre (depressed sclerotic groove over the frontal/frontoparietal region of the scalp)
• Anti-topoisomerase II antibodies have been detected in 76% of patients with localised scleroderma and in
85% of cases of generalised morphea
• These antibodies, in contrast to antitopoisomearsel/scl-70 antibodies have been found in 14% of the patients
with systemic scleroderma.
DERMATOMYOSITIS
• An idiopathic inflammatory myopathy of striated muscles along with characteristic cutaneous findings
• Linked to human leucocyte antigen (HLA) DR3, DRS, DR7
• The pathognomonic cutaneous features
o Heliotrope rash (periorbital confluent macular mauve or violaceous erythema)
o Gottron's papules (papules having violaceous hue overlying the dorsolateral aspect of interphalangeal
or metacorpophalangeal joints)
• Other cutaneous features are
o Malar erythema
o Poikiloderma (variegated telangiectasia along with atrophy and hyperpigmentation)
o Periungual and cuticular changes (cuticular hypertrophy with haemorrhagic infarcts)
o Mechanics hands (fingertip erythema and scaling).
o Calcinosis cutis - firm yellow or flesh coloured nodules extruding calcium through the skin
IMMUNE MEDIATED BULLOUS DISORDERS:
Intra-epidermal bullae Sub-epidermal bullae
• Pemphigus vulgaris
• Pemphigus vegetans
• Pemphigus foliaceous
• Pemphigus erythematosus
• Drug induced pemphigus
• Paraneoplastic pemphigus
• Bullous pemphigoid
• Cicatricial pemphigoid
• Dermatitis herpetiformis
• Linear IgA buloous dermatosis
• Pemphigoid gestationis
• Epidermolysis bullosa aquisita
Clinical Histology Immunopathology Auto antigens
Pemphigus
foliaceous
Crusts and shallow
erosions on scalp,
central face, upper
chest and back
Acantholytic blister
formed in
superficial
layer of epidermis;
Cell surface deposits
of IgG on
keratinocytes
(epidermis)
Desmogleins (Dsg1)
Pemphigus
vulgaris
Picture: V-C
Flaccid blisters,
Painless,
MC site: buccal
mucosa
Nikolsky sign: + ve
Acantholytic blister
formed in supra
basal layer of
epidermis
Cells surface
deposits
of IgG on
keratinocytes
(epidermis)
Dsg 3 (+ Dsg 1 in
patient with skin
involvement)
Bullous
Pemphigoid
Picture: V-D
(Senile
Large tense blisters,
Painless
MC site: extremities
Nikolsky sign: - ye
Blister formed in
sub epidermal
region; eosinophil-
rich infiltrate
Linear band of IgG
and C3 across the
basement embrane
zone (BMZ)
Proteins in basal
keratinocytes
Bullous Pemphigoid
AntiGen. Two
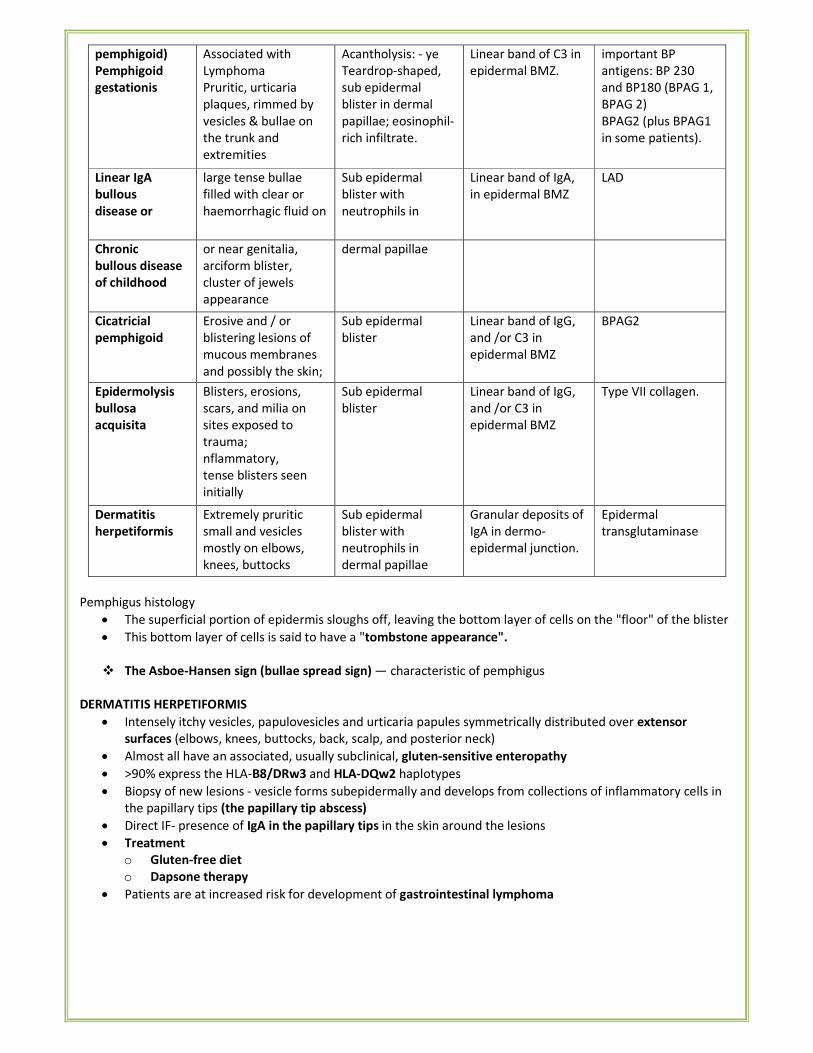
pemphigoid)
Pemphigoid
gestationis
Associated with
Lymphoma
Pruritic, urticaria
plaques, rimmed by
vesicles & bullae on
the trunk and
extremities
Acantholysis: - ye
Teardrop-shaped,
sub epidermal
blister in dermal
papillae; eosinophil-
rich infiltrate.
Linear band of C3 in
epidermal BMZ.
important BP
antigens: BP 230
and BP180 (BPAG 1,
BPAG 2)
BPAG2 (plus BPAG1
in some patients).
Linear IgA
bullous
disease or
large tense bullae
filled with clear or
haemorrhagic fluid on
Sub epidermal
blister with
neutrophils in
Linear band of IgA,
in epidermal BMZ
LAD
Chronic
bullous disease
of childhood
or near genitalia,
arciform blister,
cluster of jewels
appearance
dermal papillae
Cicatricial
pemphigoid
Erosive and / or
blistering lesions of
mucous membranes
and possibly the skin;
Sub epidermal
blister
Linear band of IgG,
and /or C3 in
epidermal BMZ
BPAG2
Epidermolysis
bullosa
acquisita
Blisters, erosions,
scars, and milia on
sites exposed to
trauma;
nflammatory,
tense blisters seen
initially
Sub epidermal
blister
Linear band of IgG,
and /or C3 in
epidermal BMZ
Type VII collagen.
Dermatitis
herpetiformis
Extremely pruritic
small and vesicles
mostly on elbows,
knees, buttocks
Sub epidermal
blister with
neutrophils in
dermal papillae
Granular deposits of
IgA in dermo-
epidermal junction.
Epidermal
transglutaminase
Pemphigus histology
• The superficial portion of epidermis sloughs off, leaving the bottom layer of cells on the "floor" of the blister
• This bottom layer of cells is said to have a "tombstone appearance".
� The Asboe-Hansen sign (bullae spread sign) — characteristic of pemphigus
DERMATITIS HERPETIFORMIS
• Intensely itchy vesicles, papulovesicles and urticaria papules symmetrically distributed over extensor
surfaces (elbows, knees, buttocks, back, scalp, and posterior neck)
• Almost all have an associated, usually subclinical, gluten-sensitive enteropathy
• >90% express the HLA-B8/DRw3 and HLA-DQw2 haplotypes
• Biopsy of new lesions - vesicle forms subepidermally and develops from collections of inflammatory cells in
the papillary tips (the papillary tip abscess)
• Direct IF- presence of IgA in the papillary tips in the skin around the lesions
• Treatment
o Gluten-free diet
o Dapsone therapy
• Patients are at increased risk for development of gastrointestinal lymphoma
MASTOCYTOSIS (URTICARIA PIGMENTOSA)
• Systemic mastocytosis is defined by a clonal expansion of mast cells that in most instances is indolent and
nonneoplastic
• Cutaneous mastocytosis (CM)
o Urticaria pigmentosa (UP)/maculopapularcutaneous mastocytosis (MPCM)
o Variants: plaque form, nodular form; telangiectasia macularis eruptiva perstans (TMEP); diffuse
cutaneous mastocytosis (DCM)
o Solitary mastocytoma of skin
• The cutaneous lesions of urticaria pigmentosa are reddish-brown macules or papules that respond to
trauma with urtication and erythema (Darier's sign).
• Urticaria pigmentosa is the most common manifestation of mastocytosis, both in adults & children.
Diseases with numerous telangiectasias
• cirrhosis of the liver,
• Osler-Weber-Rendu disease, which also has mucous membrane involvement,
• lupus erythematosus
• scleroderma,
• dermatomyositis,
• cutaneous polyarteritis,
• metastatic carcinoid syndrome,
• ataxia telangiectasia,
• angiokeratoma corporis diffusum,
• telangiectasia macularis eruptiva perstans, and
• rosacea.
• overlying basal cell cancers
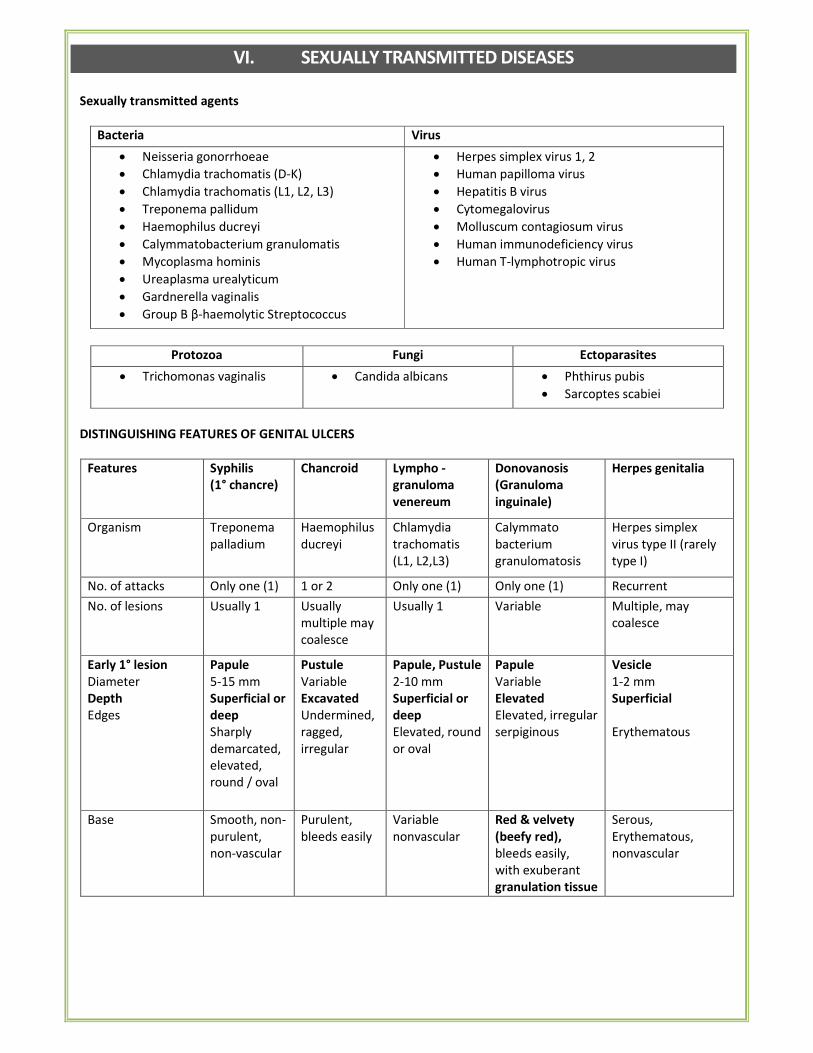
VI. SEXUALLY TRANSMITTED DISEASES
Sexually transmitted agents
Bacteria Virus
• Neisseria gonorrhoeae
• Chlamydia trachomatis (D-K)
• Chlamydia trachomatis (L1, L2, L3)
• Treponema pallidum
• Haemophilus ducreyi
• Calymmatobacterium granulomatis
• Mycoplasma hominis
• Ureaplasma urealyticum
• Gardnerella vaginalis
• Group B β-haemolytic Streptococcus
• Herpes simplex virus 1, 2
• Human papilloma virus
• Hepatitis B virus
• Cytomegalovirus
• Molluscum contagiosum virus
• Human immunodeficiency virus
• Human T-lymphotropic virus
Protozoa Fungi Ectoparasites
• Trichomonas vaginalis • Candida albicans • Phthirus pubis
• Sarcoptes scabiei
DISTINGUISHING FEATURES OF GENITAL ULCERS
Features Syphilis
(1° chancre)
Chancroid Lympho -
granuloma
venereum
Donovanosis
(Granuloma
inguinale)
Herpes genitalia
Organism Treponema
palladium
Haemophilus
ducreyi
Chlamydia
trachomatis
(L1, L2,L3)
Calymmato
bacterium
granulomatosis
Herpes simplex
virus type II (rarely
type I)
No. of attacks Only one (1) 1 or 2 Only one (1) Only one (1) Recurrent
No. of lesions Usually 1 Usually
multiple may
coalesce
Usually 1 Variable Multiple, may
coalesce
Early 1° lesion
Diameter
Depth
Edges
Papule
5-15 mm
Superficial or
deep
Sharply
demarcated,
elevated,
round / oval
Pustule
Variable
Excavated
Undermined,
ragged,
irregular
Papule, Pustule
2-10 mm
Superficial or
deep
Elevated, round
or oval
Papule
Variable
Elevated
Elevated, irregular
serpiginous
Vesicle
1-2 mm
Superficial
Erythematous
Base Smooth, non-
purulent,
non-vascular
Purulent,
bleeds easily
Variable
nonvascular
Red & velvety
(beefy red),
bleeds easily,
with exuberant
granulation tissue
Serous,
Erythematous,
nonvascular
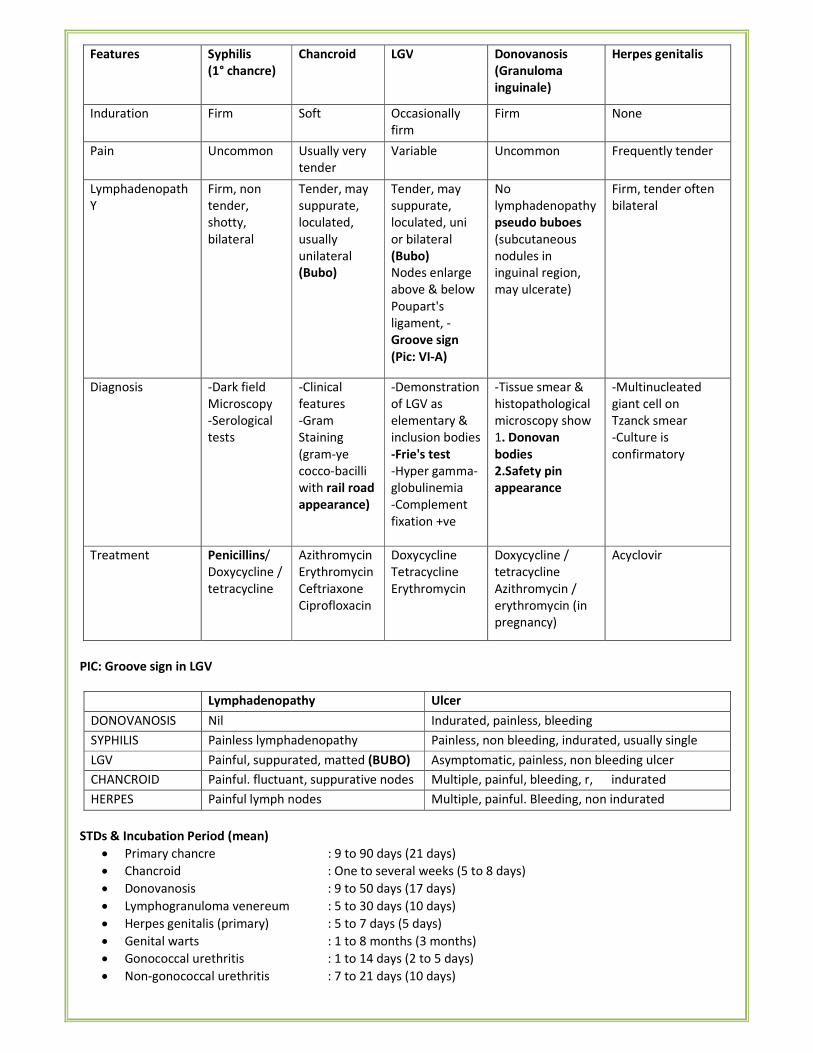
Features Syphilis
(1° chancre)
Chancroid LGV Donovanosis
(Granuloma
inguinale)
Herpes genitalis
Induration Firm Soft Occasionally
firm
Firm None
Pain Uncommon Usually very
tender
Variable Uncommon Frequently tender
Lymphadenopath
Y
Firm, non
tender,
shotty,
bilateral
Tender, may
suppurate,
loculated,
usually
unilateral
(Bubo)
Tender, may
suppurate,
loculated, uni
or bilateral
(Bubo)
Nodes enlarge
above & below
Poupart's
ligament, -
Groove sign
(Pic: VI-A)
No
lymphadenopathy
pseudo buboes
(subcutaneous
nodules in
inguinal region,
may ulcerate)
Firm, tender often
bilateral
Diagnosis -Dark field
Microscopy
-Serological
tests
-Clinical
features
-Gram
Staining
(gram-ye
cocco-bacilli
with rail road
appearance)
-Demonstration
of LGV as
elementary &
inclusion bodies
-Frie's test
-Hyper gamma-
globulinemia
-Complement
fixation +ve
-Tissue smear &
histopathological
microscopy show
1. Donovan
bodies
2.Safety pin
appearance
-Multinucleated
giant cell on
Tzanck smear
-Culture is
confirmatory
Treatment Penicillins/
Doxycycline /
tetracycline
Azithromycin
Erythromycin
Ceftriaxone
Ciprofloxacin
Doxycycline
Tetracycline
Erythromycin
Doxycycline /
tetracycline
Azithromycin /
erythromycin (in
pregnancy)
Acyclovir
PIC: Groove sign in LGV
Lymphadenopathy Ulcer
DONOVANOSIS Nil Indurated, painless, bleeding
SYPHILIS Painless lymphadenopathy Painless, non bleeding, indurated, usually single
LGV Painful, suppurated, matted (BUBO) Asymptomatic, painless, non bleeding ulcer
CHANCROID Painful. fluctuant, suppurative nodes Multiple, painful, bleeding, r, indurated
HERPES Painful lymph nodes Multiple, painful. Bleeding, non indurated
STDs & Incubation Period (mean)
• Primary chancre : 9 to 90 days (21 days)
• Chancroid : One to several weeks (5 to 8 days)
• Donovanosis : 9 to 50 days (17 days)
• Lymphogranuloma venereum : 5 to 30 days (10 days)
• Herpes genitalis (primary) : 5 to 7 days (5 days)
• Genital warts : 1 to 8 months (3 months)
• Gonococcal urethritis : 1 to 14 days (2 to 5 days)
• Non-gonococcal urethritis : 7 to 21 days (10 days)
� Esthiomine: vaginal & rectal strictures & elephantiasis of the vulva. (Seen in LGV)
� Lipschutz ulceration: Non veneral ulcer of the vulva or lower vagina. (Ulcus Vulvae acutum) seen in Behcet's
disease. Similar to aphthous ulcers
MANAGEMENT OF STD's
CHANCROID:
• Based on history: sexual exposure with infected person, short incubation period & morphology.
• Confirmed by demonstration of organisms from smears taken from bubo.
• Smears are stained with gram's or Pappenheim's stain.
• Ito-Reenstierna intradermal test: becomes positive 1 or 2 weeks after appearance of sore & persists positive
for life.
• Injection of 0.1ml of suspension of killed organism & inferred as positive if a nodule of > 5mm appears after
24 hours.
• Treatment: erythromycin & Ceftriaxone.
LGV:
• History of occurrence of herpetiform lesions on the genitals, few days after intercourse, followed by painful
unilateral, multilocular inguinal bubo.
• Culture, Frei's intrademal test, complement fixation test can be done.
• Tetracyclines are the DOC.
GRANULOMA INGUINALE:
• Confirmed by demonstration of Donovan bodies in the tissue smears & also by HPE.
• Giemsa stain.
• Few large cells containing cystic spaces, often with nuclei pushed to one side & darkly staining (cells of
Greenblatt) are conspicuous.
• Rx: streptomycin, tetracyclines & cotrimoxazole.
REACTIVE ARTHRITIS (REITER'S SYNDROME)
• 50 – 80% are HLA B27 positive
• Oligoarthritis, conjunctivitis, urethritis, and mouth ulcers most common features
• Most cases of reactive arthritis develop within 1-4 weeks after either a gastrointestinal infection (with
Shigella, Salmonella, Yersinia, Campylobacter) or a sexually transmitted infection (with Chlamydia
trachomatis or Ureaplasma urealyticum)
• Psoriasiform skin lesions develop on the soles and toes
• These are often severe, persistent, aggressive and pustular (keratoderma blenorrhagica)
• Inflamed, red, scaling patches may also develop on the glans penis (circinate balanitis)
VII. ECZEMA AND DERMATITIS
Types of eczema
Endogenous eczema Exogenous eczema
• Atopic dermatitis
• Seborrhoeic dermatitis
• Nummular eczema
• Pompholyx (Dyshidrotic eczema)
• Asteatotic eczema
• Stasis dermatitis
• Juvenile plantar dermatitis
• Lichen simplex chronicus
• Irritant contact dermatitis
• Allergic contact dermatitis
• Photodermatitis
• Infectious eczematoid dermatitis
ATOPIC DERMATITIS
• Synonyms: Neurodermatitis, Besnier's prurigo, Infantile eczema
• Positive family history of allergic rhinitis, asthma or eczema
• Pruritis is the most common symptom
• Course marked by exacerbations and remissions
• Clinical course lasting longer than 6 weeks
• Lichenification of skin
• Infantile pattern: involves face, neck, extensor surfaces and groin.
• Childhood and adolescent pattern: involves flexural skin, particularly in the antecubital fossa and popliteal
fossa.
• Cutaneous stigmata of AD
o Perioral pallor
o Extra fold of skin beneath the lower eyelid (Dennie-Morgan folds)
o Increased palmar skin markings
o Increased incidence of cutaneous infections, particularly Staphylococcus aureus
• Diagnosis: clinically - dry skin, severe itching, flexural lichenification, hand eczema, nipple eczerr and eyelid
eczema in adults, history of atopy in the family/patient, and raised IgE serum levels.
CONTACT DERMATITIS
Irritant contact dermatitis
• Synonyms: Occupational dermatitis, Housewive's eczema
• Materials may injure by direct toxic action (irritants)
• Due to contact with irritants like detergents, acids, alkaline chemicals, oils, organic solvents etc
• Housewife's eczema, diaper dermatitis and industrial dermatitis are examples of cumulative irritant contact
dermatitis.
• Most common site affected is hand.
• Most common cause of contact dermatitis in Indian women – detergent.
Allergic contact dermatitis
• May induce immunological reaction of delayed hypersensitivity type (allergens) – Allergic contact dermatitis
• Most common metal causing contact dermatitis is nickel.
• Most common cause of air-borne contact dermatitis– parthenium.
• Barloque dermatitis due to cosmetics.
• Diagnosis: Patch test.
o Skin hypersensitivity test (delayed type).
o Readings are made after 48 hours.
Differences Between Irritant and Allergic Contact Dermatitis
Irritant CD Allergic CD
Symptoms Acute Stinging, smarting ���� itching Itching ���� pain
Chronic Itching/pain Itching/pain
Lesions Acute Erythema ���� vesicle ���� erosion ����
crust ���� scaling
Erythema ���� papules ���� vesicles ���� erosions
���� crust ���� scaling
Chronic Papules, plaques, fissures, scaling,
crusts
Papules, plaques, scaling, crusts
Margination
and site
Acute Sharp, strictly confined to site of
exposure
Sharp, confined to site of exposure but
spreading in the periphery; usually tiny
papules; may become generalized
Chronic III-defined III-defined, spreads
Evolution Acute Rapid (few hours after exposure) Not so rapid (12 to 72 h after exposure)
Chronic Months to years of repeated
exposure
Months or longer; exacerbation after every
reexposure
Causative
agents
Dependent on concentration of
agent and state of skin barrier;
occurs only above threshold level
Relatively independent of amount applied,
usually very low concentrations sufficient
but depends on degree of sensitization
Incidence May occur in practically everyone Occurs only in the sensitized
Hand Eczema
• Caused by chronic exposure to water and detergent.
• Dryness and cracking of the skin of hands with variable erythema and edema
• Diagnosis: Scratch test with latex extract.
Nummular (Discoid) Eczema
• Characterized by circular or oval 'coin-like' lesion.
• Most common sites are – trunk and extensor surfaces of extremities (pretibial skin and dorsum of hands)
• Most commonly affects men in middle age group.
Asteatotic Eczema
• Also called the 'Winter-itch' or Xerotic eczema or Eczema craquelee
• Seen in elderly people in dry season.
• Characterized by fine cracks in the areas of dry skin over the anterior surface of legs.
Venous eczema (Gravitational eczema or Stasis Dermatitis)
• Due to venous incompetence and chronic edema.
• Site – over the medial aspect of the ankle.
Seborrheic Dermatitis
• Most common in infants and very young. Most common location is the scalp.
• Greasy scales overlying erythematous patches or plaques
• Scaling of the external auditory canal is common
• In the first week of life, it typically occurs in the scalp ("cradle cap"), face, or groin
• In adults, it is seen in patients with Parkinson's disease, CVA and HIV infection
• Leser-Trelat sign: Sudden eruption of multiple seborrheic keratosis lesions in associated internal malignancy
Lichen Simplex Chronicus (Circumscribed neuro dermatitis)
• End stage of various eczematous disorders
• Lichenification (thickening) of skin due to chronic scratching and rubbing.
• Most common sites – nuchal region, dorsum of feet and ankles
Pompholyx (Dyshidrotic Eczema)
• Affects young adults
• Characterised by sudden crops of highly pruritic, deep-seated sago-like vesicles on the palms, sides of fingers
and/or soles
PELLAGRA
• Deficiency disease caused by lack of niacin (nicotinic acid), occurs chiefly in countries where corn (maize), a
poor source of tryptophan is basic food stuff.
• Its clinical presentations is "3-D"
� Dementia
� Diarrhea
� Dermatitis
o Most characteristic manifestation
o Occurs in form of pigmented, scaly, sharply demarcated & frequently changing cracked skin on parts
exposed to sunlight
o Various types on location
� Pellagrous glove [lesion on hand]
� Pellagrous boot [lesion on boot]
� Casal necklace [lesion around neck]
� Deficiency of vitamin A leads to follicular hyperkeratosis and roughening of the skin (phrynoderma).
ACRODERMATITIS ENTEROPATHICA
• Autosomal recessive
• Inherited form of zinc deficiency
• Result of a mutation in a zinc transport protein - decreased ability to absorb zinc from dietary sources
• Triad of
o Acral dermatitis (face, hands, feet, anogenital area)
o Alopecia
o Diarrhea
• Requires lifelong zinc supplementation
• 1-3 mg/kg of zinc gluconate or sulfate is administered orally each day
� Acrodermatitis chronica atrophicans: skin atrophy in Lyme's disease
� Acrodermatitis continua/ Acrodermatitis pustulosa: form of pustular psoriasis
EXFOLIATIVE DERMATITIS (EXFOLIATIVE ERYTHRODERMA)
• Generalized redness and scaling of the skin of >30% BSA.
• A preexisting dermatosis is the cause of exfoliative dermatitis in two-thirds of cases, including
� Psoriasis
� Atopic dermatitis
� Contact dermatitis
� Pityriasis rubra pilaris
� Seborrheic dermatitis.
• Reactions to topical or systemic drugs account 20-40% of cases
• Cancer (lymphoma, solid tumors and, most commonly, cutaneous T cell lymphoma) for 10-20%.
VIII. PAPULOSQUAMOUS DISORDERS
PSORIASIS
• Typical lesions are erythematous (red), raised, scaly, well demarcated plaques
• Characteristically presents with silvery mica scales.
• Sites: extensor aspect of trunk & limbs preferentially
• Due to increased cell turn over resulting in marked epidermal skin thickening (acanthosis)
• 50% have positive family history
• Associated with HLA-Cw6 (most common)
• Deletion of 2 late cornified envelope (LCE) genes, LCE3C and LCE3B, is a common genetic factor for
susceptibility to psoriasis
• Obesity is another factor associated with psoriasis. Weight loss results in significant improvement
Triggering factors
• Trauma (Koebner phenomenon)
• Season (worsens in winter)
• Emotional stress
• Upper respiratory tract infections
• Drugs like beta-blockers, lithium and chloroquine
• Withdrawal of systemic steroids can lead to precipitation of pustular psoriasis.
Variants
Plaque type
• Most common type
• Slow, indolent course
• The most commonly involved areas: elbows, knees and scalp
Inverse psoriasis
• Affects the intertriginous regions including the axilla, groin, submammary region, and navel
• May be moist and without scale due to their locations
Guttate psoriasis (eruptive psoriasis)
• Most common in children and young adults
• It develops acutely in individuals without psoriasis or in those with chronic plaque psoriasis
• Patients present with many small erythematous, scaling papules, frequently after upper respiratory tract
infection with β-hemolytic streptococci
Pustular psoriasis
• Generalized eruption of sterile pustules
• Fever
• Intense erythema
• Local irritants, pregnancy, medications, infections, and systemic glucocorticoid withdrawal can precipitate
this form of psoriasis
• Types
� Palmo plantar
� Acrodermatitis continua
� Pustular bacterids
� Generalized pustular (Von Zumbusch disease)
Psoriatic arthritis (PsA)
Occurs in 5 – 10% of patients with psoriasis. There are five subtypes
• Symmetric: resembles rheumatoid arthritis, but is usually milder
• Asymmetric: can involve any joint; present as sausage digits (Pencil in cup or Opera glass deformity)
• Distal interphalangeal predominant (DIP): the classic form
• Spondylitis
• Arthritis mutilans: severe and deforming, affects primarily the small joints of the hands and feet.
� Scalp psoriasis: Pityriasis amaintaceae
� Rupoid psoriasis: classically present in Reiter's syndrome (HLA-B 27)
Koebner's / Isomorphic phenomenon
• Psoriasis appears at the site of minor injury such as scratch or graze.
• Koebner phenomenon is also seen in
� Lichen planus
� Vitiligo
� Toxic Epidermal Necrolysis
� Molluscum contagiosum
� Kaposi sarcoma
� Necrobiosis lipoidica
� Discoid lupus erythematosus.
• Appears usually 7 to 14 days after injury (i.e. trauma or surgery).
• It is an all or none phenomenon (i.e. if psoriasis occurs at one site of injury it does so means will occur at all
sites of injury)
� Reverse Koebner phenomenon (reaction) is clearing of existing psoriasis lesions following injury. It also
obeys an all or none rule, and Koebner and reverse Koebner reactions are mutually exclusive.
� Pseudo – isomorphic phenomenon is due to autoinoculation & is seen in infections like
� Plane warts
� Molluscum contagiosum
• Auspitz sign -a characteristic finding of psoriasis in which removal of scales leads to pinpoint bleeding
• Removal of scales reveals a glistening red membrane of Berkeley
• Grattage Test — on scratching scales appear
• Wornoff Ring — White halo around lesion
• Candle grease sign
• In nails
� Onycholysis (separation of nail plate from nail bed)
� Thimble-pitting of nail plate
• Not seen in psoriasis
� Alopecia
� Mucosal involvement
� CNS involvement
• Histological features
� Elongation of rete-ridges
� Parakeratosis
� Hypogranulosis
� Munro's micro abscesses in the horny layer
� Spongiform pustules of Kogoj
• The psoriatic epidermis shows rapid transition of epidermal cells in as fast as 2 days as compared to 13 days
in normal epidermis
• Itching may or may not present
Key diagnostic points for psoriasis
� Erythematous scaly plaques
� Well-defined border
� Scales dry loose and micaceous
� Koebner phenomenon seen
� Auspitz sign positive
� Regular, circular pits on nail plates
� Involvement of DIP joints of fingers and toes
� Histopathological: Spongiform pustules of Kogoj
Treatment
• Treatment of choice: PUVA therapy
• DOC for psoriatic arthropathy: Methotrexate
• Tar preparations, Vit-D3 analogs like calcipotriol, Anthralin etc... can be used locally
• DOC in AIDS with psoriasis & pustular psoriasis: Synthetic retinoid — acitretin
• Biological agents used in the treatment of psoriasis
� Alefacept (anti-CD2)
� Etarnacept, Adalimumab, Infliximab (anti-TNFα)
Differential diagnosis of round, red, scaling patches
Disease Features
Psoriasis Well-defined, thickened, scaly plaques, usually multiple
Discoid eczema Moderately well-defined edge; slightly scaly, pink patches, limited in number
Ringworm Annular with central clearing; microscopy and culture of scales will reveal fungal mycelium
Bowen's disease Often slightly irregular in shape; edge is well defined; biopsy is decisive
PHOTO CHEMOTHERAPY (PUVA)
• Photosensitizing drug Psoralen + UV-A (300-400nm)
• The UV-A is supplied by special fluorescent lamps housed in cabinets or special frames over beds
• The main psoralen used is 8-methoxy psoralen
• Psoralen is given orally 2 hours before exposure & the dose 0.6 mg/kg
• Decrease DNA synthesis in psoriasis & increase melanin synthesis in Vitiligo
• UV-light therapy is contraindicated in patients receiving cyclosporine
Uses Side effects
• Psoriasis
• Vitiligo
• Cutaneous T Cell Lymphoma (Mycosis fungoides)
• Pityriasis lichenoides chronica
• Atopic dermatitis
• Pompholyx
• Long term (Major):
� Skin cancer
� Cataract
� Photo (premature) aging
• Minor (Short term): Nausea, Burning, Pruritis,
Xeroderma
LICHEN PLANUS
• Affects the skin, scalp, nails, and mucous membranes
• The primary cutaneous lesions are pruritic, polygonal, flat-topped, violaceous papules.
• Close examination of the surface of these papules reveals a network of gray lines (Wickham's striae)
• The skin lesions but have a predilection for the wrists, shins, lower back, and genitalia
• Buccal mucosa is particularly involved
Variants
• Hypertrophic lichen planus- commonest variant, thickened, mauvish papules or nodules of irregular shape
with a warty or scaling surface.
• Annular lichen planus: ring-type configuration, on the male genitalia and lower abdomen.
• Lichen nitidus: is a rare variant, numerous tiny, pink, flat-topped papules develop.
• Bullous lichen planus: blistering occurs on some lesions.
• Lichen plano-pilaris: predominantly involves the hair follicles. Affected sites lose their terminal hair and
develop horny spines. Involvement of scalp results in scarring alopecia
Clinical presentation of Lichen planus
Lesions Characteristic features Histology
• Plain (flat) topped
• Polygonal
• Purple (violaceous)
• Pruritic
• Papule
• Pterygium (thinning) of
nails
• Pigmentation on healing
• Wickham's stria
• Lace-like pattern due to
involvement of buccal and
vaginal mucosa
• Koebner's phenomenon
• Scarring alopecia
• Band-like infiltration of lymphocytes
in the upper dermis
• Formation of saw tooth profile &
cytoid (civatte) body.
• Epidermal thinkening
• Subepidermal lichenoid band
• Max Joseph histological cleft
� Associated with: Squamous cell carcinoma, Hepatitis — C
� Treatment: topical steroids are the mainstay of treatment
PITYRIASIS ROSEA
• The exact aetiology of PR is not known though HHV-6 and 7 have been implicated.
• First manifestation is an annular lesions of 2-6 cm diameter (the herald patch)
• The centers of the lesions have a crinkled or "cigarette paper" appearance
• Followed by smaller annular or papular lesions, predominantly on the trunk along the cleavage lines.
• The eruption has a characteristic 'bathing suit' distribution (trunk and proximal parts of limbs)
• Lesions on the back are parallel to ribs giving 'Christmas tree' appearance or 'hanging curtain sign'
• PR shares many clinical features with the eruption of secondary syphilis, but palm and sole lesions are
extremely rare in PR and common in secondary syphilis.
• Course — usually self-limiting.
PITYRIASIS RUBRA PILARIS
• Reddish orange scaly plaques
• Palmoplantar keratoderma
• Keratotic follicular papules
• Disease begins on the face and scalp, with pinkness and scaling
• The histological appearance: distinctive accentuation of the dermal papillae and the undulations of the
dermoepidermal junction are much less marked than in psoriasis.
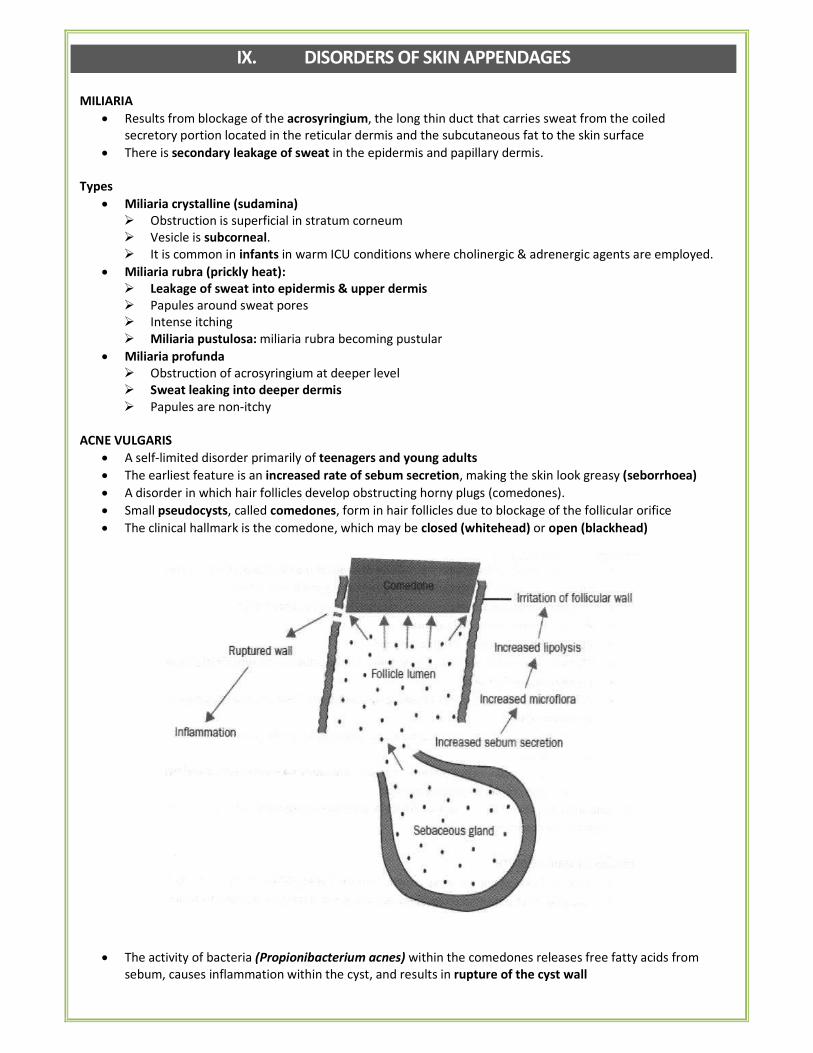
IX. DISORDERS OF SKIN APPENDAGES
MILIARIA
• Results from blockage of the acrosyringium, the long thin duct that carries sweat from the coiled
secretory portion located in the reticular dermis and the subcutaneous fat to the skin surface
• There is secondary leakage of sweat in the epidermis and papillary dermis.
Types
• Miliaria crystalline (sudamina)
� Obstruction is superficial in stratum corneum
� Vesicle is subcorneal.
� It is common in infants in warm ICU conditions where cholinergic & adrenergic agents are employed.
• Miliaria rubra (prickly heat):
� Leakage of sweat into epidermis & upper dermis
� Papules around sweat pores
� Intense itching
� Miliaria pustulosa: miliaria rubra becoming pustular
• Miliaria profunda
� Obstruction of acrosyringium at deeper level
� Sweat leaking into deeper dermis
� Papules are non-itchy
ACNE VULGARIS
• A self-limited disorder primarily of teenagers and young adults
• The earliest feature is an increased rate of sebum secretion, making the skin look greasy (seborrhoea)
• A disorder in which hair follicles develop obstructing horny plugs (comedones).
• Small pseudocysts, called comedones, form in hair follicles due to blockage of the follicular orifice
• The clinical hallmark is the comedone, which may be closed (whitehead) or open (blackhead)
• The activity of bacteria (Propionibacterium acnes) within the comedones releases free fatty acids from
sebum, causes inflammation within the cyst, and results in rupture of the cyst wall
• The first lesions, usually comedones, develop on the forehead (pre-adolescent acne)
• At its peak, acne covers the entire face (adolescent acne)
• In mature adults (25 years plus) it settles on the jaw area and the adjacent neck (adult acne).
• The scars formed after healing are often quite irregular and tend to form 'bridges'
• Even the smaller inflamed papules can cause scars - pock-like or triangular indentations (ice-pick scars).
• Acne fulminans
� Lesions quite suddenly become very inflamed
� Affected individual is unwell and develops fever and arthralgia.
• Treatment:
� Oral tetracycline or erythromycin.
� Topical — retinoic acid (for nodulocystic acne), benzoyl peroxide, salicylic acid.
� Sebum production is decreased by sebotrophic agents (directly) and antiandrogens (indirectly)
o Tretinoin (all trans retinoic acid)-1st generation (1G)
o Isotretinoin (13-cis isomer of tretinoin)-2G
o Adapalene — 3G
o Tazarotene — 4th
generation
ROSACEA (ACNE ROSACEA)
• Common chronic inflammatory acneiform disorder of the facial pilosebaceous units, coupled with an
increased reactivity of capillaries leading to flushing and telangiectasia.
• It is seen almost exclusively in adults, rarely affecting patients <30 years.
• Rosacea is more common in women
• But those most severely affected are men
• Characterized by the presence of erythema, telangiectases, and superficial pustules
• Comedones are not seen
• Predisposing factors: History of flushing associated with heat, emotional stimuli, alcohol, hot drinks or spicy
foods.
• Site: typically involves the central face. This does not affect the trunk.
• Complications
� Nose – connective tissue overgrowth (Rhinophyma – sebaceous gland hypertrophy)
� Eye – keratitis, uveitis, chalazion.
� Chloracne- extremely severe form of industrial acne due to exposure to complex chlorinated naphthalenic
compounds and dioxin.
PHASES OF HAIR GROWTH
• Anagen: Phase of normal active growth, lasts for 3 years, 90% of hairs are in this phase
• Catagen: Brief transition phase (between anagen and telogen) during which hair growth stops, lasts for 3
weeks
• Telogen: Resting phase, lasts for 3 months
• Exogen: Hair shedding phase (relationship between hair shaft and base of telogen follicle)
• Duration and rate of growth of anagen phase determine the ultimate length of hair in that area.
• Eyebrows, eyelashes, and axillary pubic hair: anagen phase is short; telogen phase prolonged.
• Scalp, beard: relatively long anagen phase.
• Terminal scalp hair follicles: 100,000 at birth; genetically determined to produce long, thick pigmented hairs.
• Vellus hairs: present over most of the body; genetically predestined to produce hairs that are short, fine,
non-pigmented.
HAIR LOSS (ALOPECIA)
• Shedding of hair is termed effluvium or defluvium
PATTERN ALOPECIA or MALE ALOPECIA or ANDROGENIC ALOPECIA
• Most common type
• Autosomal dominant
• Progressive form of alopecia
• Mostly seen in men
• The earliest changes occur at the anterior portions of the calvarium on either side of the "widow's peak" and
on the crown (vertex).
• Loss of hair starts in both temporal regions.
Treatment:
• Chemical castration with anti-androgen-prostagen combination in women by cyproterone acetate &
ethinylestranol – Dianette.
• Anti hypertensive (Vasodilator) – Minoxidil & Tretinoin
• 5-alpha-reductase inhibitor – Finasteride.
ALOPECIA AREATA
• Autoimmune disorder of hair follicles causing loss of hair in sharply defined areas of skin
• Results from arrest of hair follicles in late anagen phase.
• 10-20% patients give a family history
• Polygenic inheritance
• HLA DR4, DR5, DQ3 are associated with severe alopecia
• HLA DQ3 and DR11 – associated with alopecia totalis & universalis
• 'Exclamation mark' hairs at the margin of the lesions.
• Non scarring & non patterned alopecia
• Particularly common between the ages of 15 and 30 years.
• Alopecia totalis is total or almost total loss of scalp hair.
• Alopecia universalis is loss of all body hair.
o Sites of Predilection: Scalp, eyebrows, eyelashes, pubic hair, beard.
o Nails: Fine pitting ("hammered brass") of dorsal nail plate, mottled lunula, trachyonychia (rough nails),
onychomadesis (separation of nail from matrix).
• Ophiasis is alopecia along scalp margin. (band-like hair loss in the occipital and temporal scalp),
• Sisaipho (predilection for parietal scalp mimicking androgenetic alopaecia),
• Classical feature is sparing of gray/white hairs.
• Positively associated with autoimmune disorders
• Alopecia Aerata + Vitiligo + Uveitis Vogt Koyanagi syndrome
• Dense 'bee swarm'-like cluster of lymphocytes can be seen around the follicles in biopsies.
• Treatment: Potent topical steroids or systemic steroids, PUVA, dithranol, allergic sensitization with
diphencyprone and topical minoxidil
TELOGEN EFFLUVIUM
• Transitory increase in the number of hairs in the telogen (resting) phase of the hair growth cycle.
• This may occur spontaneously, may appear at the termination of pregnancy, may be precipitated by crash
dieting, high fever, stress from surgery or shock, malnutrition, or hormonal contraceptives.
• Telogen effluvium usually has a latent period of 2-4 months
• The prognosis is generally good
ALOPECIA MUCINOSA
• Non scarring alopecia
• Mucin deposition in hair follicles & sebaceous glands causing epithelial reticular degeneration
• MC site: face & scalp
SCARRING/CICATRICAL ALOPECIA
• Due to inflammatory process like discoid lupus erythematosus and lichen planus
• Result in permanent loss of hair in the affected area.
• Most common congenital cicatrial alopecia is aplasia cute's congenita (i.e. focal absence of epidermis with
or with or with out other layers).
• Pseudopelade - small, rounded patches of scarring alopecia without any inflammation.
DISORDERS OF NAILS
Koilonychia (Spoon nail)
The nail is concave with raised edges
Iron deficiency anemia
Lichem planus
Hypothyroidism
Racquet Nail
Width of nail bed & nail plate is greater than their length
Premature obliteration of epiphyseal line
Anonychia
Absence of all or part of one or several nails
Lichen panus
With tong. bone anomalies
Beau's Line
Poor nutrition to matrix 1/t a defective band of nail
formation resulting in transverse groove of thin nail
plate.
Any severe systemic illness
Onychomadesis : Separation of nail from matrix
Longitudinal ridges with beaded and/or Fir tree
appearance
Median canaliform dystrophy of Heller
Trachyonychia (Rough sand paper nail) 20 nail dystrophy (alopecia areata)
External chemical treatment
Leuconychia : White discolouration of nail Nail matrix dysfunction
Apparent leuconychia
White appearance d/t changes in underlying tissue
Tery's nail, half & half nail
Muehrck's paired narrow white band
Onychogryphosis (Ram's horn or Oyster – Nail)
Nail is severly distorted, thickened, opaque, brownish,
sparaled & with out attachment to nail bed
Pressure from foot wear in elderly
Hook Nail Lack of support from short bony phalynx
Pterygium Dorsal pterygium in lichen planus
Ventral pterygium in scleroderma with Raynaud's
phenomenon, causalgia of median nerve,
formaldehyde containing nail cosmetics.
Onycholysis : Detachment of nail plate from its bed
starting at its distal &/or lateral attachment
Psoriasis
Reiter's syndrome
Onychorrhexis : Splitting & roughness of nail plate Lichen planus
Onychoptosis defluvium (Alopecia unguim)
Component of alopecia
Alopecia areata
Koenen's Periungal Fibroma Tuberous sclerosis (50% cases)
Mee's Line Arsenic Poisoning.
Pitting Deep & irregular pits: psoriasis, atopic dermatitis
Superficial & geometric pits in alopecia areata.
Melanonychia
Presence of melanin in nail plate presenting as single /
multiple longitudinal brown — black band.
-Single band: nail matric nevus or melanoma
(deserve biopsy), trauma (usually in 4/5th toe nail)
-Multiple band: dark race, pregnancy, inflmatory
nail disorder, Lauiger — Huntziker syndrome (with
pigmented macules on lip & genitals), AIDS,
Addison syndrome
Muehrck's lines Hypoalbuminemia
Brown nail Arsenic poisoning
Addison's disease
Blue nail Wilson's disease
X. GENODERMATOSES & DISORDERS OF KERATINIZATION
Genodermatoses: diseases which are transmitted genetically from parents to children.
NEUROFIBROMATOSIS (VON RECKLINGHAUSEN'S DISEASE)
• Autosomal dominant
• Plexiform neurofibroma - soft, doughy, subcutaneous swelling having a bag of worm feeling and run along
nerves
• Multiple, brownish macules (Café au lait macules)
• Tiny specks of brownish macules in the axilla (axillary freckling)
TUBEROUS SCLEROSIS (SYN. BOURNEVILLES DISEASE)
• Two third cases – sporadic, others - Autosomal dominant,
• Multiple, brown, soft, grouped papules present in the perinasal area and cheeks in a butterfly distribution
These are called facial angiofibromas (misnamed as adenoma sebaceum)
• Ungual or subungual fibromas, (Koenen's tumours) are small fleshy tumours that grow around and under
the toenails or fingernails
• Hypomelanotic macules ('ash leaf spots') are white or light coloured patches on skin (only visible sign of
tuberous sclerosis at birth)
• Shagreen patches are areas of thick leathery skin which is dimpled like an orange peel and is usually found
on the lower back or nape of the neck
• Café au lait macules can be seen
ICTHYOSIS
• Characterised by the accumulation of 'fish-like' scales due to abnormal epidermal cell kinetics
• Autosomal dominant Icthyosis
� Icthyosis vulgaris – most common type
� X-linked icthyosis (seen in boys only)
• Autosomal recessive Icthyosis – more severe than the dominant form
� Lamellar icthyosis
� Icthyosiform erythroderma
Icthyosis vulgaris
• Begins in the first year of life
• Dry, scaly skin over the extensor aspects of the arms and legs
• The scales are larger over the lower extremities
• Mild keratoderma or (thickening of the skin over the palms and soles)
• The dryness becomes worse during winters and improves in summers and humid weather
• Histologically, the only abnormality detectable is a much diminished granular cell layer.
X-linked ichthyosis
• Deficiency of steroid sulphatase
• The scales are dirty brown in colour and affect both the extensor and flexural surfaces of the extremities
with prominent involvement of the neck and trunk
• These male children are often the products of postmature pregnancies and difficult labours.
• Associated disorders: cryptorchidism, ectropion
� Acquired icthyosis: The most important cause underlying malignant disease – particularly lymphoma –such
as Hodgkin's disease
� Tylosis: Marked thickening of palmar and plantar skin due to localized abnormality of keratinization.
XERODERMA PIGMENTOSUM
• An autosomal recessive disorder of DNA repair
• The most common defect - nucleotide excision repair (NER) enzymes are mutated.
• History - the child cries on exposure to light
• Skin turns erythematous on exposure to sun
• Development of freckles and lentiginosis on the exposed area of the body, such as the extensor aspect of
arms, face and the neck are early signs
• Later by adulthood squamous cell carcinoma, basal cell carcinoma, and malignant melanoma may form
EPIDERMOLYSIS BULLOSA
• An inherited defect in the keratin formation
• Characterised by the formation of multiple blisters on gentle rubbing or on minimal skin trauma especially
over the trauma prone areas of the body
• There may be blisters in the pharynx, larynx, eyes and the genital mucosa.
• There may be contractures and mitten like deformities of hands in the severe variants
• Pyloric stenosis and squamous cell carcinoma are other complications
PALMOPLANTAR KERATODERMA
• Inherited defects due to mutations in the enzymes involved in the synthesis of keratin
• Skin over palms and soles becomes hard, thick, dry and hyperkeratotic
REFSUM'S SYNDROME (HEREDOPATHIA ATACTICA NEURITIS FORMIS)
• Autosomal recessive,
• Accumulation of phytanic acid in all the tissues
• Cerebellar ataxia, polyneuritis, retinitis pigmentosa, nerve deafness, generalized ichthyosiform scaling.
DARIER'S DISEASE (KERATOSIS FOLLICULITIS)
• Inherited as an autosomal dominant disorder, but also occurs sporadically.
• Appearance of groups of brownish, horny papules over the central trunk, shoulders, face and elsewhere
• Oral cavity shows: Cobble stone appearance
• V shaped nicking of nails seen
• Presence of tiny pits on the palms
• There is a curious loss of cohesion between keratinocytes above the basal layer
XI. PEDIATRIC DERMATOLOGY
NEONATAL DERMATOLOGY
Transient Neonatal Pustular Melanosis
• Onset at birth
• Common in darkly pigmented infants
• Smear of sterile pustule shows numerous neutrophils
• Histology: subcorneal pustules with neutrophils
Erythema Toxicum Neonatorum
• Onset typically 24 – 48 h after birth
• Occurs in half of all full-term infants
• Presents with blotchy erythematous macules, papules, pustules, and wheals
• Smear of sterile vesicle/pustule shows eosinophils
• Histology: subcorneal pustules with eosinophils, associated with pilosebaceous unit
Neonatal Cephalic Pustulosis (Neonatal Acne)
• Onset typically within first 30 days
• Malassezia spp. implicated in pathogenesis
• Presents with erythematous follicular comedones, papules, and pustules on face
• Histology: follicular pustules with neutrophils
Sclerema Neonatorum
• Onset usually within first week of life
• Form of panniculitis in severely ill, premature infants; often fatal
• Presents with diffuse woody hardening of skin
• Spares genitalia, palms, and soles
• Histology: needle-shaped clefts with necrotic adipocytes with little surrounding inflammation
Seborrheic Dermatitis
• Onset typically 1 week after birth; lasts several months, mostly resolves by 1 year of age
• Presents with ill-defined erythematous patches with waxy scale over scalp ("cradle cap"), ± axillae and groin
Aplasia Cutis Congenita (ACC)
• Onset before birth
• Localized defect in epidermis, dermis and/or fat
• Typically along midline
• Presents with erosion, ulceration, scar, or membranous defect (ovoid lesion covered by an epithelial
membrane)
• Hair collar sign: ring of dark long hair encircling lesion; ± marker of underlying neural tube defect
Cutis Marmorata Telangiectatica Congenita (CMTC)
• Onset at birth
• Typically improves with age
• Presents with blanching reticulated vascular pattern on trunk/extremities with segmental distribution
• Associated anomalies in 1/2 of patients (varicosities, nevus flammeus, macrocephaly, ulceration, hypoplasia,
and/or hypertrophy of soft tissue and bone)
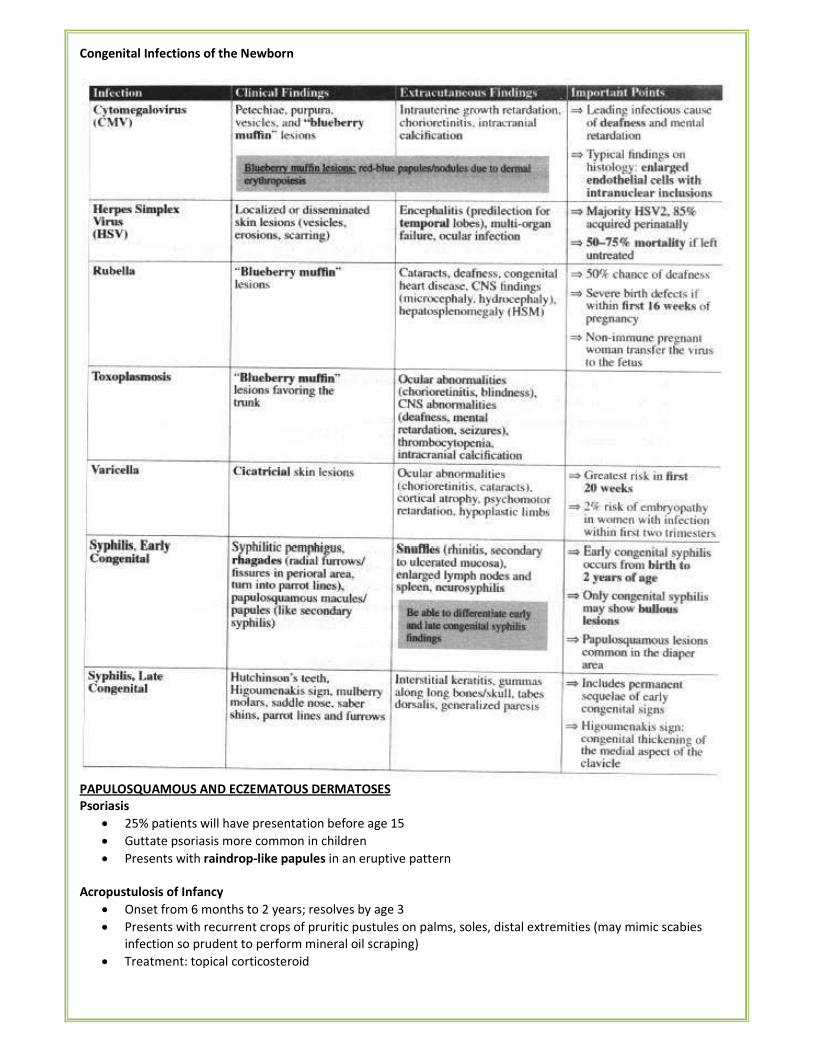
Congenital Infections of the Newborn
PAPULOSQUAMOUS AND ECZEMATOUS DERMATOSES
Psoriasis
• 25% patients will have presentation before age 15
• Guttate psoriasis more common in children
• Presents with raindrop-like papules in an eruptive pattern
Acropustulosis of Infancy
• Onset from 6 months to 2 years; resolves by age 3
• Presents with recurrent crops of pruritic pustules on palms, soles, distal extremities (may mimic scabies
infection so prudent to perform mineral oil scraping)
• Treatment: topical corticosteroid
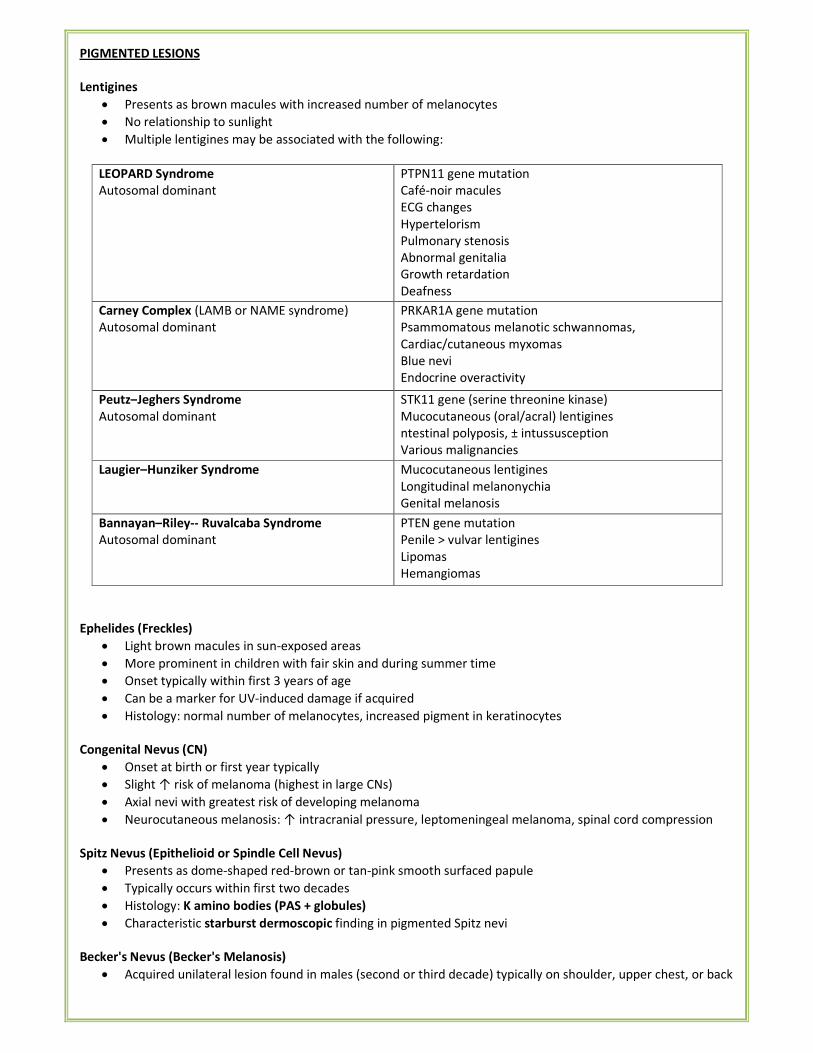
PIGMENTED LESIONS
Lentigines
• Presents as brown macules with increased number of melanocytes
• No relationship to sunlight
• Multiple lentigines may be associated with the following:
LEOPARD Syndrome
Autosomal dominant
PTPN11 gene mutation
Café-noir macules
ECG changes
Hypertelorism
Pulmonary stenosis
Abnormal genitalia
Growth retardation
Deafness
Carney Complex (LAMB or NAME syndrome)
Autosomal dominant
PRKAR1A gene mutation
Psammomatous melanotic schwannomas,
Cardiac/cutaneous myxomas
Blue nevi
Endocrine overactivity
Peutz–Jeghers Syndrome
Autosomal dominant
STK11 gene (serine threonine kinase)
Mucocutaneous (oral/acral) lentigines
ntestinal polyposis, ± intussusception
Various malignancies
Laugier–Hunziker Syndrome Mucocutaneous lentigines
Longitudinal melanonychia
Genital melanosis
Bannayan–Riley-- Ruvalcaba Syndrome
Autosomal dominant
PTEN gene mutation
Penile > vulvar lentigines
Lipomas
Hemangiomas
Ephelides (Freckles)
• Light brown macules in sun-exposed areas
• More prominent in children with fair skin and during summer time
• Onset typically within first 3 years of age
• Can be a marker for UV-induced damage if acquired
• Histology: normal number of melanocytes, increased pigment in keratinocytes
Congenital Nevus (CN)
• Onset at birth or first year typically
• Slight ↑ risk of melanoma (highest in large CNs)
• Axial nevi with greatest risk of developing melanoma
• Neurocutaneous melanosis: ↑ intracranial pressure, leptomeningeal melanoma, spinal cord compression
Spitz Nevus (Epithelioid or Spindle Cell Nevus)
• Presents as dome-shaped red-brown or tan-pink smooth surfaced papule
• Typically occurs within first two decades
• Histology: K amino bodies (PAS + globules)
• Characteristic starburst dermoscopic finding in pigmented Spitz nevi
Becker's Nevus (Becker's Melanosis)
• Acquired unilateral lesion found in males (second or third decade) typically on shoulder, upper chest, or back
• Hyperpigmented hypertrichotic patch or plaque associated with underlying smooth muscle hamartoma
(arrector pili)
• Histology: ↑ melanin in epidermis, often smooth muscle hamartoma present in dermis
Blue Nevus
• Congenital or acquired (typically early childhood)
• Multiple blue nevi associated with Carney complex (LAMB/NAME syndrome)
• Histology: normal epidermis, many elongated dendritic melanocytes within dermis, large amounts of
melanin often seen within melanocytes
Nevus of Ota (Nevus Fuscoceruleus Ophthalmomaxillaris, Oculodermal Melanocytosis, Congenital melanosis bulbi)
• Onset either near birth or during puberty
• Mostly in women
• Caused by the entrapment of melanocytes in the upper third of the dermis
• Presents as unilateral (90%), blue-gray hyperpigmented macules in the face (forehead, temple, malar area,
or periorbital skin)
• Typically involving ophthalmic and maxillary branches of trigeminal nerve
• Most common extracutaneous sites: sclera (increased risk of glaucoma)
• Malignant melanoma develops very rarely
• Mongolian spot - a birthmark caused by entrapment of melanocytes in the dermis but is located in the
lumbosacral region.
Nevus of Ito (Nevus Fuscoceruleus Acromiodeltoideus)
• Similar presentation to nevus of Ota
• Usually unilateral
• Typically occurs in shoulder region (supraclavicular, scapular, and deltoid)
Hori's Nevus (Acquired Nevus of Ota-like Macules)
• Onset in late adolescence
• Bilateral nevus of Ota-like macules of the zygomatic region
• May be misdiagnosed as melasma
Nevus achromicus (Nevus depigmentosus)
• An uncommon birthmark characterised by a well-defined pale patch.
• Often, smaller hypopigmented macules arise around the edges, resembling a splash of paint
• Achromic naevus is not completely white (differentiates from vitilligo)
• Achromic naevi are usually solitary (in contrast to tuberous sclerosis, where multiple pale patches occur and
are called ash-leaf spots)
• Most commonly seen on the upper chest, but may also arise on the limbs
Congenital Dermal Melanocytosis (Mongolian Spot)
• Common in infants with pigmented skin
• Presents with blue-gray macules or patches typically over lumbosacral skin or buttocks
TELANGIECTASIAS
Spider Angioma (Spider Nevus)
• Common acquired lesion seen in children and adults
• Comprised of central arteriole with radiating thin walled vessels
• Temporary obliteration seen with compression
• Multiple lesions associated with liver disease, pregnancy, and estrogen therapy
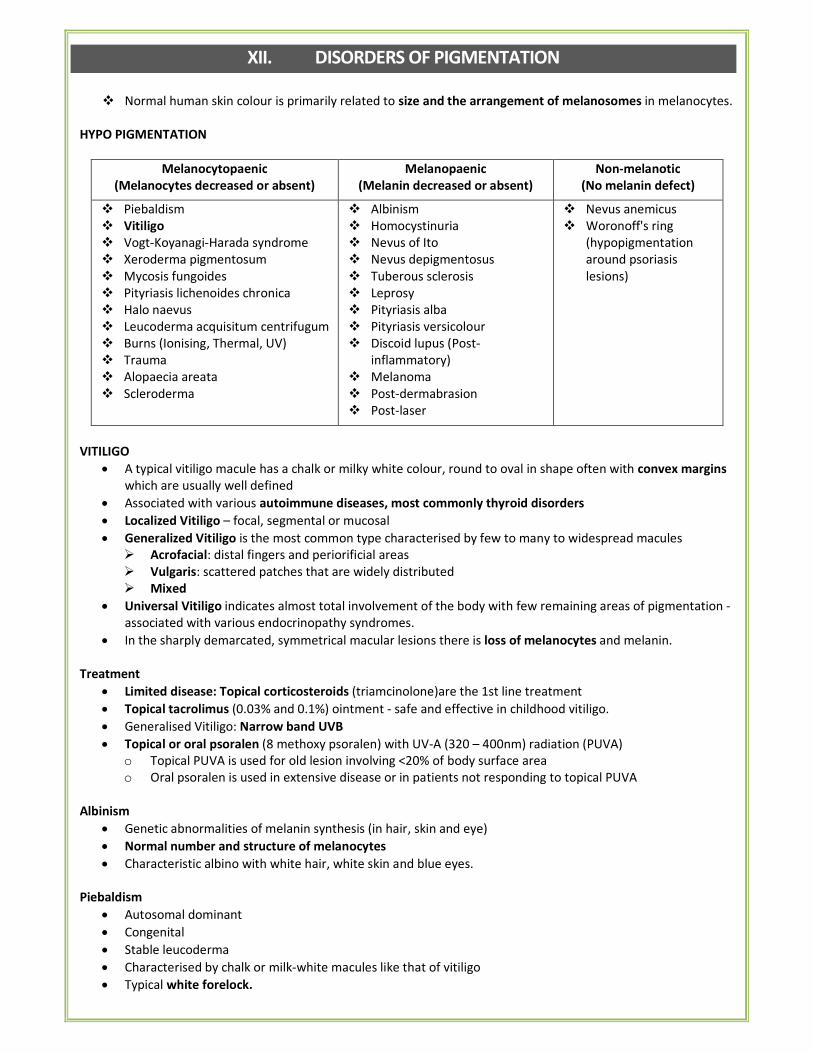
XII. DISORDERS OF PIGMENTATION
� Normal human skin colour is primarily related to size and the arrangement of melanosomes in melanocytes.
HYPO PIGMENTATION
Melanocytopaenic
(Melanocytes decreased or absent)
Melanopaenic
(Melanin decreased or absent)
Non-melanotic
(No melanin defect)
� Piebaldism
� Vitiligo
� Vogt-Koyanagi-Harada syndrome
� Xeroderma pigmentosum
� Mycosis fungoides
� Pityriasis lichenoides chronica
� Halo naevus
� Leucoderma acquisitum centrifugum
� Burns (Ionising, Thermal, UV)
� Trauma
� Alopaecia areata
� Scleroderma
� Albinism
� Homocystinuria
� Nevus of Ito
� Nevus depigmentosus
� Tuberous sclerosis
� Leprosy
� Pityriasis alba
� Pityriasis versicolour
� Discoid lupus (Post-
inflammatory)
� Melanoma
� Post-dermabrasion
� Post-laser
� Nevus anemicus
� Woronoff's ring
(hypopigmentation
around psoriasis
lesions)
VITILIGO
• A typical vitiligo macule has a chalk or milky white colour, round to oval in shape often with convex margins
which are usually well defined
• Associated with various autoimmune diseases, most commonly thyroid disorders
• Localized Vitiligo – focal, segmental or mucosal
• Generalized Vitiligo is the most common type characterised by few to many to widespread macules
� Acrofacial: distal fingers and periorificial areas
� Vulgaris: scattered patches that are widely distributed
� Mixed
• Universal Vitiligo indicates almost total involvement of the body with few remaining areas of pigmentation -
associated with various endocrinopathy syndromes.
• In the sharply demarcated, symmetrical macular lesions there is loss of melanocytes and melanin.
Treatment
• Limited disease: Topical corticosteroids (triamcinolone)are the 1st line treatment
• Topical tacrolimus (0.03% and 0.1%) ointment - safe and effective in childhood vitiligo.
• Generalised Vitiligo: Narrow band UVB
• Topical or oral psoralen (8 methoxy psoralen) with UV-A (320 – 400nm) radiation (PUVA)
o Topical PUVA is used for old lesion involving <20% of body surface area
o Oral psoralen is used in extensive disease or in patients not responding to topical PUVA
Albinism
• Genetic abnormalities of melanin synthesis (in hair, skin and eye)
• Normal number and structure of melanocytes
• Characteristic albino with white hair, white skin and blue eyes.
Piebaldism
• Autosomal dominant
• Congenital
• Stable leucoderma
• Characterised by chalk or milk-white macules like that of vitiligo
• Typical white forelock.
White patch of skin: differential diagnosis (Mnemonic: "Vitiligo PATCH")
• Vitiligo
• Pityriasis alba/ Post-inflammatory hypopigmentation
• Age related hypopigmentation
• Tinea versicolor/ Tuberous sclerosis (ash-leaf macule)
• Congenital birthmark
• Hansen's (leprosy)
HYPERPIGMENTATION
Melanocytotic
(increase in number of melanocytes)
Melanotic
(increase in melanin)
• Lentigines
• Peutz-Jegher syndrome
• PUVA therapy
• Lentigo, solar, UV (radiation tanning)
• Café-au-lait macules
• Freckles
• Naevus spilus
• Hemochromatosis
• Melasma
• Exogenous ACTH
• Chronic pruritis
• Post inflammatory
• Melanoma,
• Mastocytosis
• Acanthosis nigricans
MELASMA
• Dark areas appear symmetrically across the cheeks, around the eyes and over the forehead, giving a mask-
like appearance
• It is much more common in women
• Seen more often in people with dark skin
• The majority of cases appear related to pregnancy or oral contraceptives
• High expression of α-MSH in the lesional keratinocytes plays an important role in the melanisation of skin
• Topical hydroquinone (2% to 4%) with retinoids and or steroids is the usual treatment
XIII. SKIN IN SYSTEMIC DISEASES & MISCELLANEOUS
PARANEOPLASTIC SIGNS OF INTERNAL MALIGNANCY
• Acanthosis nigricans - Brown-back velvety plaques over neck and flexures
• Acute febrile neutrophilic dermatosis - Tender, red plaques over limbs and face in a middle-aged lady
• (Sweet's syndrome)
• Acquired Ichthyosis - Dry fish-like skin most commonly in Hodgkin's lymphoma
• Clubbing - Severe grades of clubbing with lung carcinoma
• Dermatomyositis - 10% cases have associated with internal malignancy
• Erythema gyratum repens - Concentric rings of erythema and scaling over trunk (Ca bronchus)
• Hypertrophic osteoarthropathy - Subperiosteal new bone formation
• Migratory thrombophlebitis – Pancreatic cancer
• Myeloma-associated amyloidosis - Skin nodules and purpura
Associated with endocrine neoplasm
• Necrolytic migratory Erythema – Glucagonoma
• Necrobiosis lipoidica diabeticorum – Diabetes mellitus
• Addisonian pigmentation - Adrenal corticotropin hormone (ACTH) secreting neoplasms
• Carcinoid tumours - Flushing of face and upper trunk
ACANTHOSIS NIGRICANS
• It is a velvety hyperpigmentation, thickening & increased rugosity of skin
• Primarily involves flexures – axilla & groin.
• Thickened areas bear skin tags & seborrheic warts
• In majority of patients, it is associated with obesity (pseudo acanthosis nigricans) and insulin resistance
• The skin changes are reversible on weight reduction.
• It can reflect internal malignancy – most commonly gastrointestinal malignancy
• Also seen in: Endocrine diseases like Cushings syndrome, Acromegaiy, Poiycystic ovarian disease, insulin
resistant DM
• HAIR- AN syndrome: in women, the triad of
� Hyperandrogenism
� Insulin-resistance
� Acanthosis nigricans
NECROBIOSIS LIPOIDICA DIABETICORUM
• A disorder of collagen degeneration with a granulomatous response, thickening of blood vessel walls, and
fat deposition
• The main complication of the disease is ulceration, usually occurring after trauma
• Strongly associated with diabetes mellitus
• Usually present with shiny, asymptomatic patches that slowly enlarge over months to years
• The patient's main complaint is the unsightly cosmetic appearance of the lesions.
• Most cases of necrobiosis lipoidica occur on the pretibial area
ERYTHEMA MARGINATUM
• Major criteria for diagnosis of rheumatic fever
• Extremely rare in Indians
• Erythematous pink rashes with a clear center and round or serpiginous margin.
• Not raised above the skin
• They are brought on by application of heat
• Most commonly seen on the trunk and proximal parts of extremities, but never on face.
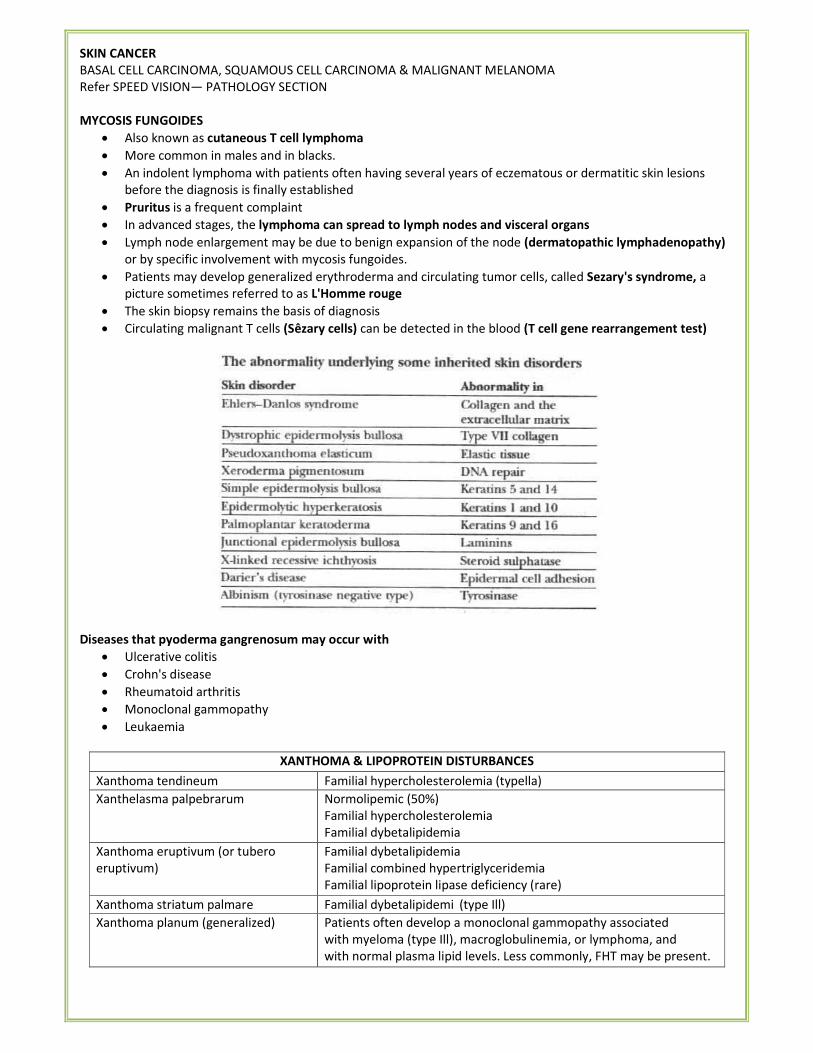
SKIN CANCER
BASAL CELL CARCINOMA, SQUAMOUS CELL CARCINOMA & MALIGNANT MELANOMA
Refer SPEED VISION— PATHOLOGY SECTION
MYCOSIS FUNGOIDES
• Also known as cutaneous T cell lymphoma
• More common in males and in blacks.
• An indolent lymphoma with patients often having several years of eczematous or dermatitic skin lesions
before the diagnosis is finally established
• Pruritus is a frequent complaint
• In advanced stages, the lymphoma can spread to lymph nodes and visceral organs
• Lymph node enlargement may be due to benign expansion of the node (dermatopathic lymphadenopathy)
or by specific involvement with mycosis fungoides.
• Patients may develop generalized erythroderma and circulating tumor cells, called Sezary's syndrome, a
picture sometimes referred to as L'Homme rouge
• The skin biopsy remains the basis of diagnosis
• Circulating malignant T cells (Sêzary cells) can be detected in the blood (T cell gene rearrangement test)
Diseases that pyoderma gangrenosum may occur with
• Ulcerative colitis
• Crohn's disease
• Rheumatoid arthritis
• Monoclonal gammopathy
• Leukaemia
XANTHOMA & LIPOPROTEIN DISTURBANCES
Xanthoma tendineum Familial hypercholesterolemia (typella)
Xanthelasma palpebrarum Normolipemic (50%)
Familial hypercholesterolemia
Familial dybetalipidemia
Xanthoma eruptivum (or tubero
eruptivum)
Familial dybetalipidemia
Familial combined hypertriglyceridemia
Familial lipoprotein lipase deficiency (rare)
Xanthoma striatum palmare Familial dybetalipidemi (type Ill)
Xanthoma planum (generalized) Patients often develop a monoclonal gammopathy associated
with myeloma (type Ill), macroglobulinemia, or lymphoma, and
with normal plasma lipid levels. Less commonly, FHT may be present.
CONDITION CAUSE
Necrotizing fasciitis
Erysipelas
Strep. Pyogenes
Ecthyma Pseudomonas
Erythrasma Corynebacterium minuttissmus
Erythema migrans Borrelia burgdorferi
Erythema Ab Igne Repetitive exposure to infrared rays
Erythema annulare centifugum Hypersensitivity [gyrate erythema]
Erythema gyratum repens Associated with malignancy [M/C: lung, esophagus, breast]
Erythema dyschromicum perstans Ashy dermatosis, idiopathic
Erythema chronicum migrans Cutaneous manifestation of stage I Lyme disease
Erythema elevatum diutinum Localized fibrosing small vessel vasculitis
Erythema induratum of Bazin Tuberculosis
Erythema infectiosum Parvovirus B 19
Lesion Found in
Erythema pernio (chill blain) Cold
Lupus pernio & Epitheloid granuloma Sarcoidosis
Lupus profundus SLE
Lupus Vulgaris Cutaneous TB
Phrynoderma Vit-A deficiency
Essential fatty acid deficiency
Sauroderma/Crocodile skin Icthyosis Vulgaris
Weldt sores Desert areas
Black hairy tongue Broad spectrum antibiotics
Oral Hairy Leukoplakia AIDS (not candidiasis)
Rain drop pigmentation Chronic Arsenic Poisoning
Pyoderma Gangrenosa Ulcerative Colitis
Slapped Cheek appearance Erythema infectiosum
Honey Crust Impetigo
Angioid Streak Pseudoxanthoma Elasticum
Axillary freckling & Lisch nodule (Iris hamartoma) Neurofibromatosis
Cradle cap appearance Seborrheic Dermatitis (Pityriasis capitis)
Coyenne pepper stippling (d/t hemosiderin) Plasma cell balenitis of Zoom
NIKOLSKY SIGN: Positive in
• Pemphigus Vulgaris / foliaceous & Epidermolysis bullosa congenita
• Staphylococcal Skin Scald Syndrome (SSSS) & Toxic Epidermal Necrolysis (TEN)
• Stevens Johnson Syndrome
• Leukemia
• Herpes
� The Asboe-Hansen sign ("indirect Nikolsky sign" or "Nikolsky II sign") refers to the extension of a blister to
adjacent unblistered skin when pressure is put on the top of the bulla
SIGNS IN DERMATOLOGY
• Antenna sign – Keratosis Pilaris
• Asboe Hansen sign (Bulla spread sign) – Pemphigus
• Auspitz sign – Psoriasis
• Button hole sign – Neurofibromatosis.
• Birbeck's granules: Langhan cell histiocytosis
• Chandelier's sign - Gonorrhea in women
• Candle sign & last cuticle sign: Psoriasis
• Carpet tack's sign – DLE
• Cerebriform tongue sign – Pemphigus vegetans
• Coup'd'ongue sign –Tinea versicolor
• Crowe's sign – Axillary freckling in Neurofibromatosis
• Comby sign: Measles
• Russell's sign: Bulimia Nervosa
• Premalatha Sign: Pemphigus Vulgaris
• Deckchair sign: Papulo erythrodema
• Dimple sign (Fitzpatrick sign ) – Dermato fibro sarcoma protuberans, differentiates dermatofibroma
• from malignant melanoma
• Dubois sign – Short little finger in congenital syphilis
• Dory flap sign: Primary chancre
• Flag sign – Kwashiorkor
• Forscheimer sign – Enanthema on soft palate in Rubella
• Groove sign of Greenblat – LGV
• Head light sign – Perinasal and periorbital pallor in Atopic dermatitis
• Hertoghe's sign – Loss of lateral third of eyebrow in Atopic dermatitis
• Higouminaki's sign – Congenital syphilis; thickened sternal portion of clavicle.
• Leopard sign: Onchocerciasis
• Milian's ear sign – Erysipelas can spread into the pinna (being cuticular infection), whereas cellulitis cannot
spread to the pinna due to close adhesion of skin to cartilage of ear (without any areolar tissue.)
• Oil drop sign – Discoloration of nail bed in Psoriasis.
• Ollendorf sign – Papule is very tender to touch in secondary syphilis
• Osler's sign – Alkaptonuria
• Pillow sign – Netherton's syndrome; hair shaft defect patient sees hair on pillow on getting up in the morning
• Trichrome sign – Vitiligo
• Romana's sign -T.Cruzi; Chaga's disease
• Shawl sing – Erythema over the upper back and shoulders in dermatomyositis
• Wrist sign , Thumb sign or Steinberg's thumb – Marfan syndrome
IMPORTANT PEARLS:
• Area of skin: 1.7m2, constitutes 4kg of body weight in adult man.
• Spongiform pustule of Kogoj: accumulation of neutrophils in Malphigian layer.
• Tzanck cell: keratinocyte.
• Clue cells: vaginal epithelial cells
• Fordyce spots: ectopic sebaceous glands
• Target lesions: Erythema multiforme
• Binkley's spots: Diabetic dermatopathy
• Muehrcke's nail: seen in chronic hypoalbuminemia
• Circle of Hebra: seen in scabies
• Ritter's disease: caused by Staph. aureus
• Lichen nitidus: claw clutching a ball appearance
• Anatomist's wart: Tuberculosis verrucosa cutis/Warty TB
• Remote reverse Koebner phenomenon: Vitiligo
• Dermographism: Urticaria
• White dermographism: Atopy
• Myrmecia warts: Plantar warts
• Dermatomyositis: Helitrope rash/ Gottron sign/ Gottron papule
• Most common form of oral candidiasis: acute pseudo membranous
• M/c dermatophyte producing favus: T. schoenleinii
• M/c photodermatoses: Polymorphic Light Eruptions (PLE)
• M/c form of cutaneous TB: Lupus Vulgaris
• M/c manifestation of gonococcal infection in males: Anterior urethritis
• M/c manifestation of acute gonococcal infection in females: endocervicitis
• M/c cause of vaginal discharge in India: Bacterial vaginosis
• M/c cosmetic allergen: fragrances > hair dye
• M/c site of trophic ulcer: ball of great toe
• M/c teeth affected in leprosy: upper incisors
• Black Piedra/ Trichomycosis nodularis: Piedraia hortae.
• White piedra: Trichosporon ovoides
• Copper penny bodies: Chromomycosis
• Endothrix dermatophytosis in India is due to: T. Violaceum
• Profeta's law: fetus maybe born normal but may develop signs of early congenital syphilis during first few
weeks/months
• Colle's law: syphilitic infant may not infect its own mother but is capable of infecting others.
• Truck driver's disease: Hydradenitis suppurative of perianal region in males
• Kligman's formula/ Triluma cream: 5% hydroxyquinone, 0.1% dexamethasone, 0.1% Tretinoin (For
Chloasma)
• Thinning of nails : involves nail matrix
• Dilapidated brick walls: Hailey-Hailey disease
• Syringoma: Tadpole like appearance
• Miescher's granuloma: Erythema nodosum
• Cork screw hair: Scurvy
• Selenium deficiency: Pseudoalbinism
• Louis bar syndrome: Ataxia telangiectasia
• Pseudo-Hutchinson's sign: Bowen's disease
• Hutchinson's sign: Melanoma in nail matrix
• Keratosis follicularis squamosa: lotus leaves on water appearance
• Jigsaw puzzle appearance: cylindroma
• Trimethylamine: fish odour syndrome
• Urbach Wiethe disease: lipoid proteinosis
• Mauserung phenomenon: icthyosis bullosa of Siemens
• Basal cell carcinoma: Bazex syndrome
• Erythema induratum affecting legs of young women: Bazin's disease
• Mouse ear appearance: X- ray feature of psoriatic arthritis
• Least affected in Atopic dermatitis: Mid chest
• Pharyngeal dysmotility: seen in polymyositis
• Green nail syndrome with fruity odor: Pseudomonas aeruginosa
• Haverhill fever/ erythema arthriticum: Streptobacillus moniliformis
• Jungle sore: cutaneous diphtheria
• Woody fibrosis: actinomycosis
• Mickey mouse ears: Cockayne syndrome
• Subcutaneous fat necrosis: Carcinoma pancreas
• Cigarette paper scars: Ehler Danlos Syndrome
• Hot tub follicles: Pseudomonas aeruginosa
• Slavic leprosy: Rhinoscleroma
• Pretibial fever: leptospirosis
• Alkaptonuria: sweat that stains
• Pseudo-Cushing's disease: chronic alcoholism
• Angel's kiss: Nevus flammeus
• Bath itch: Polycythemia rubra vera
• Nostalgia parasthetica: itch in interscapular region
• Effective drug for pruritus due to polycythemia rubra vera: Aspirin
• Mediator of pruritus in Hodgkin's Lymphoma: Leukopeptidase
• Syphilitic gumma: involves left atrium & septum
• Secondary syphilis never involves: bone
• Photopatch testing: patch testing + UV irradiation [to document photoallergy]
• Worm eaten skull: Gummatous osteoperiosteitis of skull bones in syphilis
• Earliest feature of congenital syphilis: nasal discharge
• Pseudo paralysis of parrot in congenital syphilis: due to osteochondritis.
• Olympian brow: Supra orbital thickening in syphilis
• Wooly headedness: adverse effect of Dapsone
• Blaschko's lines: system of lines along which many linear nevus & dermatoses arrange themselves.
• Weber Christian panniculitis: seen in pancreatic disorders
• Shell nail: seen in bronchiectasis
• Foshay test: 48-hour intradermal test that, if positive, indicates tularemia.
• The intradermal reaction (sporotriquin test) - confirm the diagnosis for sporotrichosis.
• Berloque dermatitis: increased pigmentation due to cosmetics
• Treatment of choice for pruritis due to Uremia: UV light
• Acantholytic cells can be seen in bedside Tzanck test
• Pigmented purpuric dermatoses: shows recent pinpoint cayenne pepper—colored hemorrhages associated
with older hemorrhages and hemosiderin deposition.
*****END*****
PSYCHIATRY
I. HISTORY OF PSYCHIATRY
PIONEERS IN THE FIELD OF PSYCHIATRY
• Emil Kraepelin: Divided major mental illness into Dementia precox and Manic depressive insanity
• Sigmund Freud:
o Founder of Psychoanalysis
o Dream interpretation
o Theory of infantile sexuality
o Structural and topographical model of mind
o Theory of instincts
o Ego defence mechanisms
o Id, ego and superego
o Stages of psychosexual development
• Eugen Blueler: Gave 4 A's of schizophrenia. (Autism, Affective flattening, Ambivalence, loosening of
Association)
• Leo Kanner defined autism
• Skinner – operant conditioning
• Pavlov- classical conditioning
• John F cade - Lithium
• Reserpine – First drug used in treating psychosis
• Ugo Cerletti and Lucio Bini - ECT
• Egas Moniz and Almenda Lima – Psychosurgery (prefrontal leucotomy)
• Emil Durkeim – Sociology theory of suicide
• Thomas Sydenham – Hysteria
• Adolf Meyer: founder of psychobiology
• John Broadus Watson: founder of behaviorism
• Philippe Pinel: abandoned forceful restraints, proposed morale & humane Rx of the mentally ill.
• Paolo Zacchia – first forensic psychiatrist
• Johann Weyer – Father of modern psychiatry
Personality Coined the term
Eugen Bleuler Schizophrenia
James Braid Hypnosis
Reil Johan Christian Psychiatry
Eward Hecker Hebephrenia
Emil Kraeplin Dementia precox
Sigmund Freud Free association
Oedipus complex, Electra complex
Penis envy, Psychoanalysis
Ego defence mechanism
Pleasure principle, Reality principle
Alfred Adler Inferiority complex
II. FUNDAMENTALS IN PSYCHIATRY
Diagnosis and Classification in Psychiatry
The Five Axes of DSM-IV-TR
• AXIS I: Clinical Psychiatric Diagnosis
• AXIS II: Personality Disorder and Mental Retardation
• AXIS III: General Medical Conditions
• AXIS IV: Psychosocial and Environment Problems
• AXIS V: Global Assessment of functioning: Current and in past one year (Rated on a scale)
Normal experiences
• Hypnagogic hallucinations (Abnormal perception at the time of falling asleep)
• Hypnopompic hallucinations (Abnormal perception at the time of waking up)
• Near death experiences (complex hallucinatory phenomenon in people who perceive death to be imminent)
• Pseudo hallucinations
• Ideas of reference
• Panoramic memory
THINKING PROCESSES
• Abstract thinking: thinker can conceptualize or generalize, understanding that each concept can have
multiple meanings.
• Concrete thinking: thinking is limited to what's in front of the face, and the here and now.
Freud's Primary and Secondary thinking processes:
Primary Process:
• Drive-dominated, prelogical, preverbal, imaginative thinking
• Consists of those mental processes which are directly related to functions of the primitive life forces
associated with the Id
• The Id has no contact with reality and works on the Pleasure Principle.
• Primary Process is characteristic of unconscious mental activity; marked by unorganized, non-logical
thinking and by the tendency to seek immediate discharge and gratification of instinctual urges.
• When Primary Process plays a significant role in a person's thinking he is incapable of being inner-directed.
Secondary Process:
• Reality oriented, goal-directed, logically ordered, rational, concrete and/or abstract conceptual thinking
• Consists of those mental processes which are directly related to learned and acquired functions of the Ego
• Characteristic of conscious and preconscious mental activity; marked by logical thinking and by the
tendency to delay gratification by regulation of the discharge of instinctual demands.
TERMINOLOGIES IN PSYCHIATRY
• Apraxia: Inability to perform skilled motor movements in the presence of normal comprehension, muscle
strength and coordination
• Aphasia: Loss or impairment of linguistic ability as a result of brain damage
• Agnosia: Deficits in self-experience (anosognosia – denial of illness)
• Anhedonia: Lack of interest in pleasurable activities (depression)
• Catastrophic reaction: Sudden agitation, anger when demented persons or persons with head injury are
asked to perform tasks beyond their capacity
• Compulsion: An act performed repeatedly to reduce anxiety in response to obsessive thought
• Confabulation: falsification of memory in clear consciousness (Korsakoff's psychosis)
o Due to hypothalamic-diencephalic lesions
o Does not occur in bilateral hippocampal lesions (insight also preserved)
o Two types:
1. Momentary - brief in content and has to be provoked; can be traced to a time-dislocated true
memory
2. Fantastic - sustained; spontaneous and elaborate with grandiose, far-fetched content
• Coprolalia: Forced vocalization of obscene words or phrases (Tourette's syndrome)
• Deja vu: Familiarity of unfamiliar situation
• Jamais vu: Unfamiliarity of the familiar situation (temporal lobe epilepsy/schizophrenia)
• Echolalia: Repetition of phrases or sentences (schizophrenia/Mental retardation/learning
disability/dementia/head injury/Tourette's syndrome)
• Echopraxia: Repetition of acts done by examiner
• Perseveration: Persisting with same reply beyond point of relevance (Organic brain lesions) "where do you
live?", "London", "How old are you", "London"...
• Palilalia – perseverated word is repeated with increasing frequency
• Logoclonia – perseveration of the last syllable of the last word
• Neologism: New word formation (schizophrenia)
• Palimpsest: Also called as alcoholic black out
• Stereotypy: Repetitive and bizarre movement, non- goal directed (schizophrenia, autism)
• Verbal stereotypy - repetition of a word or phrase (Stock word) which has no immediate relevance to the
context.
• Abreaction: A process by which repressed material, particularly painful experience or a conflict is brought
back to consciousness.
• Alexithymia: Inability to describe or being aware of one's emotions.
• Mood is the pervasive feeling tone which is sustained (lasts for some length of time) and colours the total
experience of the person.
• Affect is the outward objective expression of the immediate, cross-sectional experience of emotion at a
given time.
Neurotransmitters & Associated Disorders
• OCD: decrease in serotonin.
• Alzheimer's disease: decrease in Ach & Nor-adrenaline.
• Schizophrenia: increased serotonin, nor adrenaline & dopamine.
• Depression: decreased serotonin, nor adrenaline & dopamine.
Features Psychosis Neurosis
Judgment
Insight
Personality
Contact with reality
Lacking or impaired Present
Delusions/ Hallucinations Common Usually not present
Examples 1. Schizophrenia
2. Delusional disorder
3. Mood disorder
� Mania
� Depression
� Bipolar disorder
1. Phobia
2. Dissociative disorder
3. Conversion / somatoform disorder
4. OCD (Obsession Compulsive Disorder)
5. Anxiety: Generalized anxiety & Panic
disorder
DISORDERS OF PERCEPTION
• Hallucination
• Illusion
• Derealization
• Depersonalization
Hallucination
• Perceptions which arise in the absence of any external stimulus.
• Characteristics:
o Unwilled - not subject to conscious manipulation
o Has the same qualities of a real perception, i.e. Vivid, solid
o Perceived as being located in the external world occurs in five sensory modalities (auditory, visual,
olfactory, gustatory, tactile)
• Auditory hallucination — commonest type in psychiatric disorders
• Visual hallucination - Suspect organic etiology/ withdrawal states)
o Unformed hallucinations - flashing or steady spots, colored lines and shapes
o Formed hallucinations - vivid objects, flowers, animals and persons
o Visual hallucinations of temporal lobe are usually complex, formed hallucinations
o Unformed hallucinations are common with disorders of the occipital lobe
• Olfactory hallucination- Temporal lobe epilepsy
• Tactile hallucination - Cocaine/alcohol abusers
• Gustatory hallucination - schizophrenia/temporal lobe epilepsy/ Lithium/disuifiram users
• Hypnagogic hallucinations (Abnormal perception at the time of falling asleep)
• Hypnopompic hallucinations (Abnormal perception at the time of waking up)
• Extracampine hallucinations: hallucinations outside the field of sensory perception (eg: outside visual
field).
HALLUCINATIONS PSEUDOHALLUCINATIONS
Bright vivid perception just like reality The lack of vividness (e.g., impossible to distinguish
male and female voices)
Patient gets it with natural way of perception (with
eyes, ears etc.) from the real perpetual space (extra-
projection)
Patient got it with other perception (internal vision
or hearing) from out of perpetual space (e.g., intra-
projection)
Confidence in the fact that other people have the
same perceptions
Ideas of distant influence organized especially for
the patient
Excitement or attempts to act with the false objects.
More frequent in the evening and night
Indifferent behavior or passive defence (e.g.,
attempts to shield with metal net or screen)
Typical delirium and other organic disorders Typical for paranoid schizophrenia
Charles Bonnet Syndrome (CBS)
• A disorder in which patients with normal cognition experience consistent or periodic complex (formed) visual
hallucinations
• Have no evidence of dementia, drug abuse, neurological or psychiatric abnormalities
Illusion three types
• A type of false perception in which the perception of a real world object is combined with internal imagery
to produce a false internal perception
• Affect illusion: Misperception + heightened emotion (e.g., while walking across a lonely park at night, briefly
seeing a tree moving in the wind as an attacker)
• Completion illusion: it depends on inattention such as misreading words in newspapers
• Pareidolic illusion: These are meaningful perceptions produced when experiencing a poorly defined stimulus
(seeing faces in fire or clouds)
Depersonalization-Derealisation syndrome
• Depersonalization - alteration in the perception of self, so that feeling of one's own reality is temporarily
changed or lost
• The person affected is not delusionally convinced about the change, and instead describes it to have
occurred, as-f
• Derealisation – alteration in the perception of the external world, so that feeling of reality of external world
s temporarily changed or lost
• Both are 'as – if' phenomenon
• Insight is present
• Episodes occur in the presence of a clear sensorium
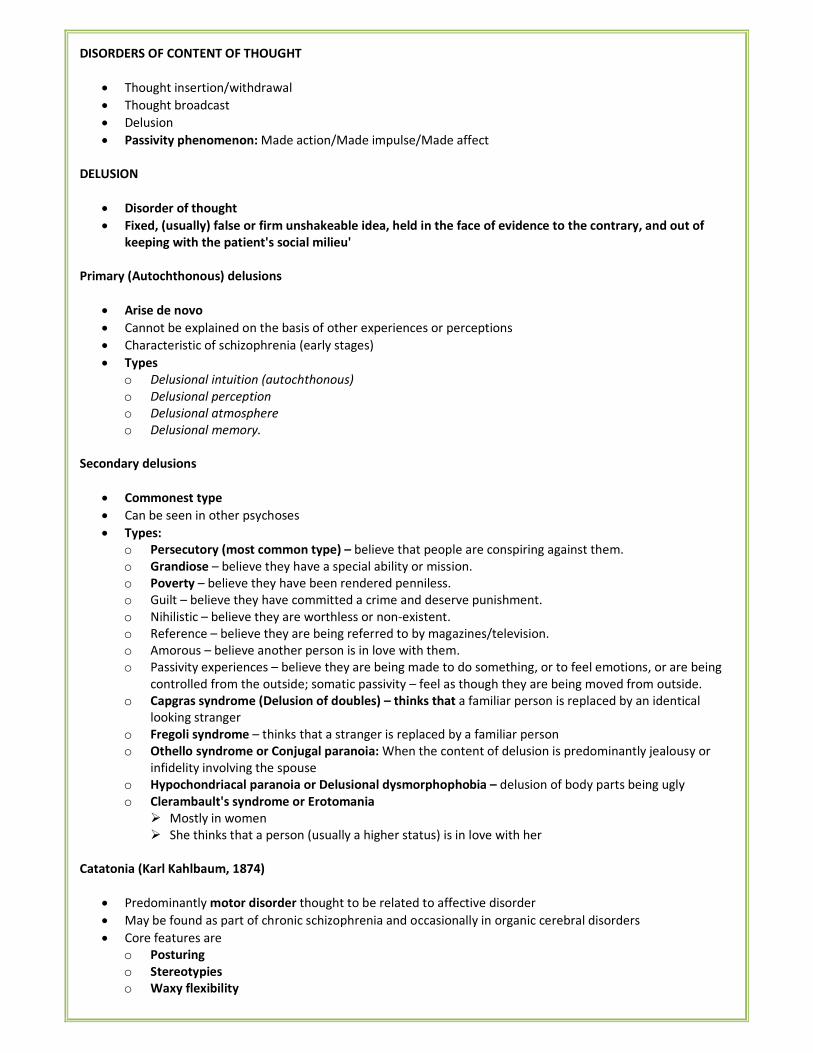
DISORDERS OF CONTENT OF THOUGHT
• Thought insertion/withdrawal
• Thought broadcast
• Delusion
• Passivity phenomenon: Made action/Made impulse/Made affect
DELUSION
• Disorder of thought
• Fixed, (usually) false or firm unshakeable idea, held in the face of evidence to the contrary, and out of
keeping with the patient's social milieu'
Primary (Autochthonous) delusions
• Arise de novo
• Cannot be explained on the basis of other experiences or perceptions
• Characteristic of schizophrenia (early stages)
• Types
o Delusional intuition (autochthonous)
o Delusional perception
o Delusional atmosphere
o Delusional memory.
Secondary delusions
• Commonest type
• Can be seen in other psychoses
• Types:
o Persecutory (most common type) – believe that people are conspiring against them.
o Grandiose – believe they have a special ability or mission.
o Poverty – believe they have been rendered penniless.
o Guilt – believe they have committed a crime and deserve punishment.
o Nihilistic – believe they are worthless or non-existent.
o Reference – believe they are being referred to by magazines/television.
o Amorous – believe another person is in love with them.
o Passivity experiences – believe they are being made to do something, or to feel emotions, or are being
controlled from the outside; somatic passivity – feel as though they are being moved from outside.
o Capgras syndrome (Delusion of doubles) – thinks that a familiar person is replaced by an identical
looking stranger
o Fregoli syndrome – thinks that a stranger is replaced by a familiar person
o Othello syndrome or Conjugal paranoia: When the content of delusion is predominantly jealousy or
infidelity involving the spouse
o Hypochondriacal paranoia or Delusional dysmorphophobia – delusion of body parts being ugly
o Clerambault's syndrome or Erotomania
� Mostly in women
� She thinks that a person (usually a higher status) is in love with her
Catatonia (Karl Kahlbaum, 1874)
• Predominantly motor disorder thought to be related to affective disorder
• May be found as part of chronic schizophrenia and occasionally in organic cerebral disorders
• Core features are
o Posturing
o Stereotypies
o Waxy flexibility
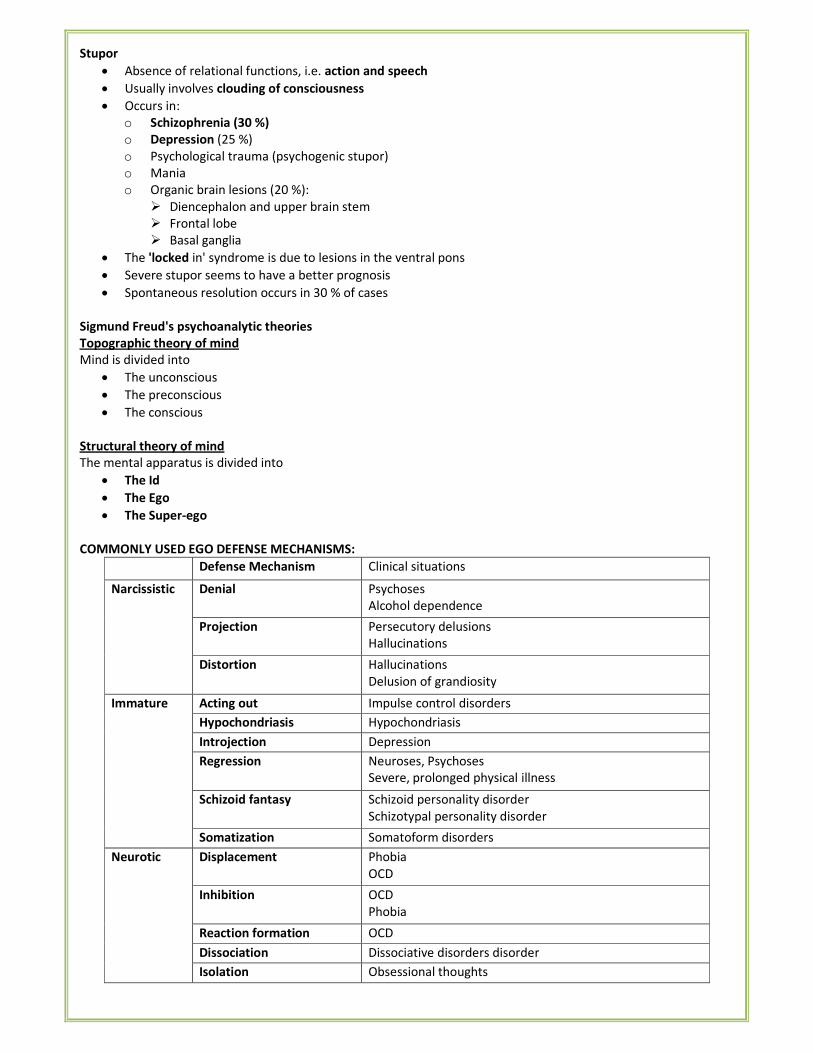
Stupor
• Absence of relational functions, i.e. action and speech
• Usually involves clouding of consciousness
• Occurs in:
o Schizophrenia (30 %)
o Depression (25 %)
o Psychological trauma (psychogenic stupor)
o Mania
o Organic brain lesions (20 %):
� Diencephalon and upper brain stem
� Frontal lobe
� Basal ganglia
• The 'locked in' syndrome is due to lesions in the ventral pons
• Severe stupor seems to have a better prognosis
• Spontaneous resolution occurs in 30 % of cases
Sigmund Freud's psychoanalytic theories
Topographic theory of mind
Mind is divided into
• The unconscious
• The preconscious
• The conscious
Structural theory of mind
The mental apparatus is divided into
• The Id
• The Ego
• The Super-ego
COMMONLY USED EGO DEFENSE MECHANISMS:
Defense Mechanism Clinical situations
Narcissistic Denial Psychoses
Alcohol dependence
Projection Persecutory delusions
Hallucinations
Distortion Hallucinations
Delusion of grandiosity
Immature Acting out Impulse control disorders
Hypochondriasis Hypochondriasis
Introjection Depression
Regression Neuroses, Psychoses
Severe, prolonged physical illness
Schizoid fantasy Schizoid personality disorder
Schizotypal personality disorder
Somatization Somatoform disorders
Neurotic Displacement Phobia
OCD
Inhibition OCD
Phobia
Reaction formation OCD
Dissociation Dissociative disorders disorder
Isolation Obsessional thoughts
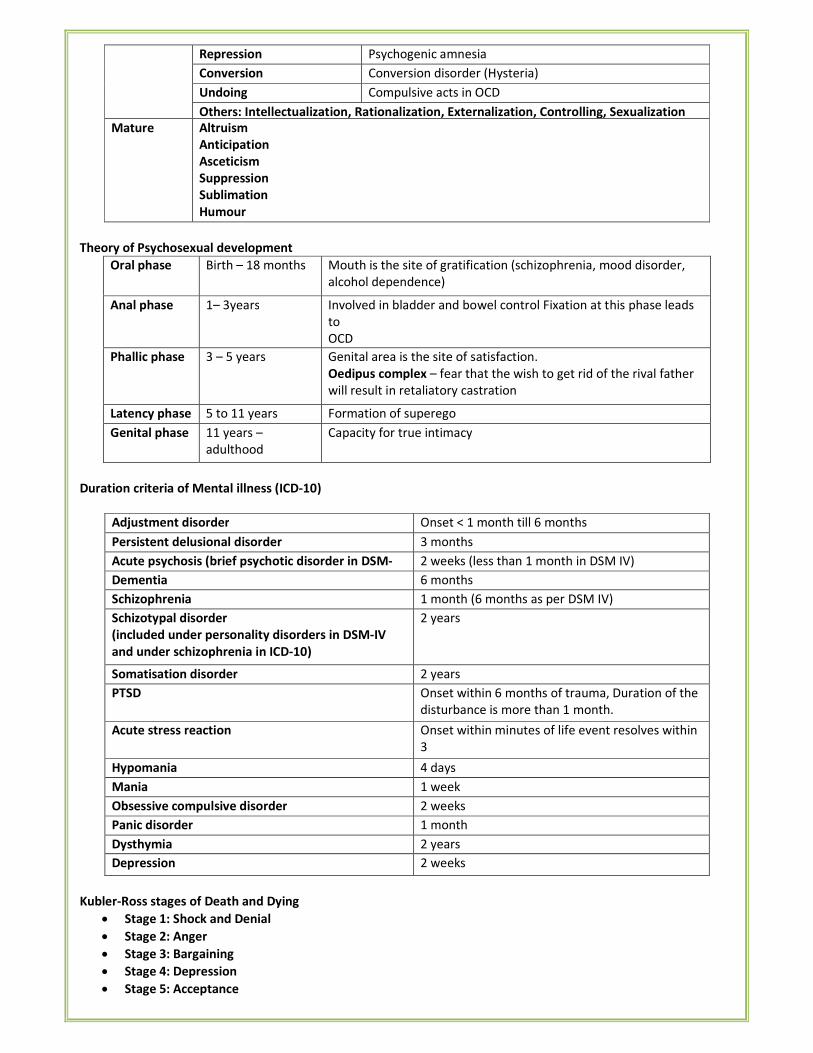
Repression Psychogenic amnesia
Conversion Conversion disorder (Hysteria)
Undoing Compulsive acts in OCD
Others: Intellectualization, Rationalization, Externalization, Controlling, Sexualization
Mature Altruism
Anticipation
Asceticism
Suppression
Sublimation
Humour
Theory of Psychosexual development
Oral phase Birth – 18 months Mouth is the site of gratification (schizophrenia, mood disorder,
alcohol dependence)
Anal phase 1– 3years Involved in bladder and bowel control Fixation at this phase leads
to
OCD
Phallic phase 3 – 5 years Genital area is the site of satisfaction.
Oedipus complex – fear that the wish to get rid of the rival father
will result in retaliatory castration
Latency phase 5 to 11 years Formation of superego
Genital phase 11 years –
adulthood
Capacity for true intimacy
Duration criteria of Mental illness (ICD-10)
Adjustment disorder Onset < 1 month till 6 months
Persistent delusional disorder 3 months
Acute psychosis (brief psychotic disorder in DSM-
IV)
2 weeks (less than 1 month in DSM IV)
Dementia 6 months
Schizophrenia 1 month (6 months as per DSM IV)
Schizotypal disorder
(included under personality disorders in DSM-IV
and under schizophrenia in ICD-10)
2 years
Somatisation disorder 2 years
PTSD Onset within 6 months of trauma, Duration of the
disturbance is more than 1 month.
Acute stress reaction Onset within minutes of life event resolves within
3
days Hypomania 4 days
Mania 1 week
Obsessive compulsive disorder 2 weeks
Panic disorder 1 month
Dysthymia 2 years
Depression 2 weeks
Kubler-Ross stages of Death and Dying
• Stage 1: Shock and Denial
• Stage 2: Anger
• Stage 3: Bargaining
• Stage 4: Depression
• Stage 5: Acceptance
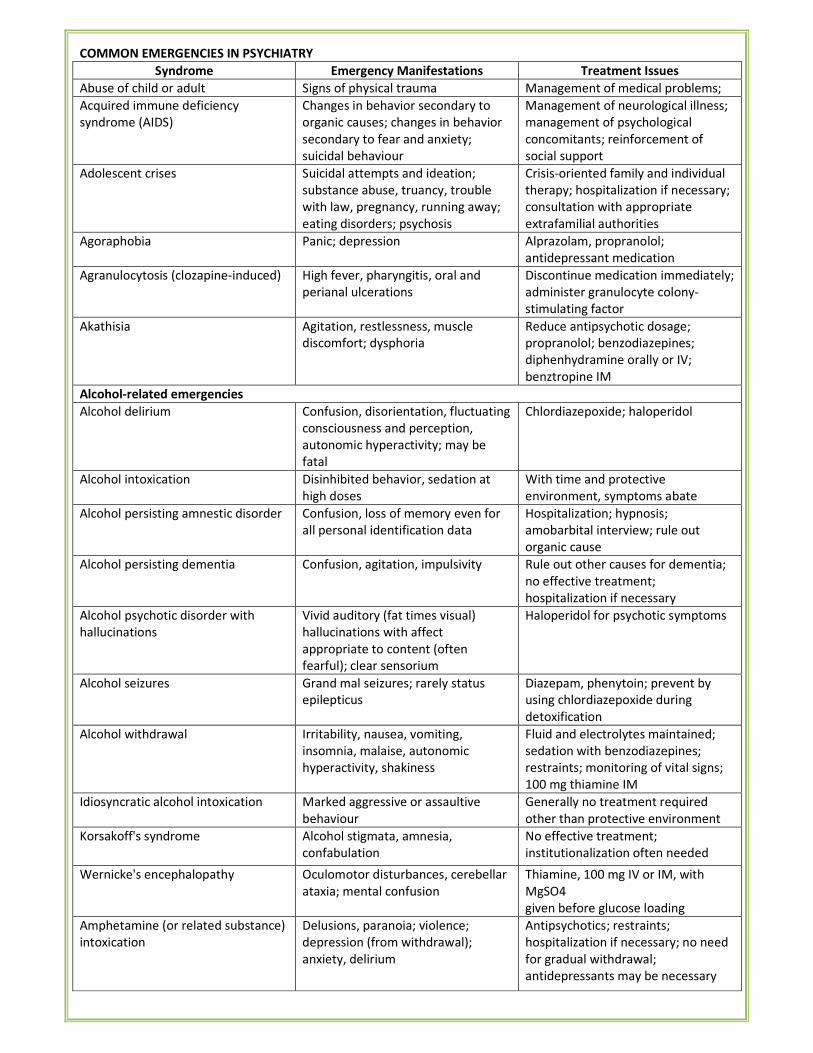
COMMON EMERGENCIES IN PSYCHIATRY
Syndrome Emergency Manifestations Treatment Issues
Abuse of child or adult Signs of physical trauma Management of medical problems;
Acquired immune deficiency
syndrome (AIDS)
Changes in behavior secondary to
organic causes; changes in behavior
secondary to fear and anxiety;
suicidal behaviour
Management of neurological illness;
management of psychological
concomitants; reinforcement of
social support
Adolescent crises Suicidal attempts and ideation;
substance abuse, truancy, trouble
with law, pregnancy, running away;
eating disorders; psychosis
Crisis-oriented family and individual
therapy; hospitalization if necessary;
consultation with appropriate
extrafamilial authorities
Agoraphobia Panic; depression Alprazolam, propranolol;
antidepressant medication
Agranulocytosis (clozapine-induced) High fever, pharyngitis, oral and
perianal ulcerations
Discontinue medication immediately;
administer granulocyte colony-
stimulating factor
Akathisia Agitation, restlessness, muscle
discomfort; dysphoria
Reduce antipsychotic dosage;
propranolol; benzodiazepines;
diphenhydramine orally or IV;
benztropine IM
Alcohol-related emergencies
Alcohol delirium Confusion, disorientation, fluctuating
consciousness and perception,
autonomic hyperactivity; may be
fatal
Chlordiazepoxide; haloperidol
Alcohol intoxication Disinhibited behavior, sedation at
high doses
With time and protective
environment, symptoms abate
Alcohol persisting amnestic disorder Confusion, loss of memory even for
all personal identification data
Hospitalization; hypnosis;
amobarbital interview; rule out
organic cause
Alcohol persisting dementia Confusion, agitation, impulsivity Rule out other causes for dementia;
no effective treatment;
hospitalization if necessary
Alcohol psychotic disorder with
hallucinations
Vivid auditory (fat times visual)
hallucinations with affect
appropriate to content (often
fearful); clear sensorium
Haloperidol for psychotic symptoms
Alcohol seizures Grand mal seizures; rarely status
epilepticus
Diazepam, phenytoin; prevent by
using chlordiazepoxide during
detoxification
Alcohol withdrawal Irritability, nausea, vomiting,
insomnia, malaise, autonomic
hyperactivity, shakiness
Fluid and electrolytes maintained;
sedation with benzodiazepines;
restraints; monitoring of vital signs;
100 mg thiamine IM
Idiosyncratic alcohol intoxication Marked aggressive or assaultive
behaviour
Generally no treatment required
other than protective environment
Korsakoff's syndrome Alcohol stigmata, amnesia,
confabulation
No effective treatment;
institutionalization often needed
Wernicke's encephalopathy Oculomotor disturbances, cerebellar
ataxia; mental confusion
Thiamine, 100 mg IV or IM, with
MgSO4
given before glucose loading
Amphetamine (or related substance)
intoxication
Delusions, paranoia; violence;
depression (from withdrawal);
anxiety, delirium
Antipsychotics; restraints;
hospitalization if necessary; no need
for gradual withdrawal;
antidepressants may be necessary
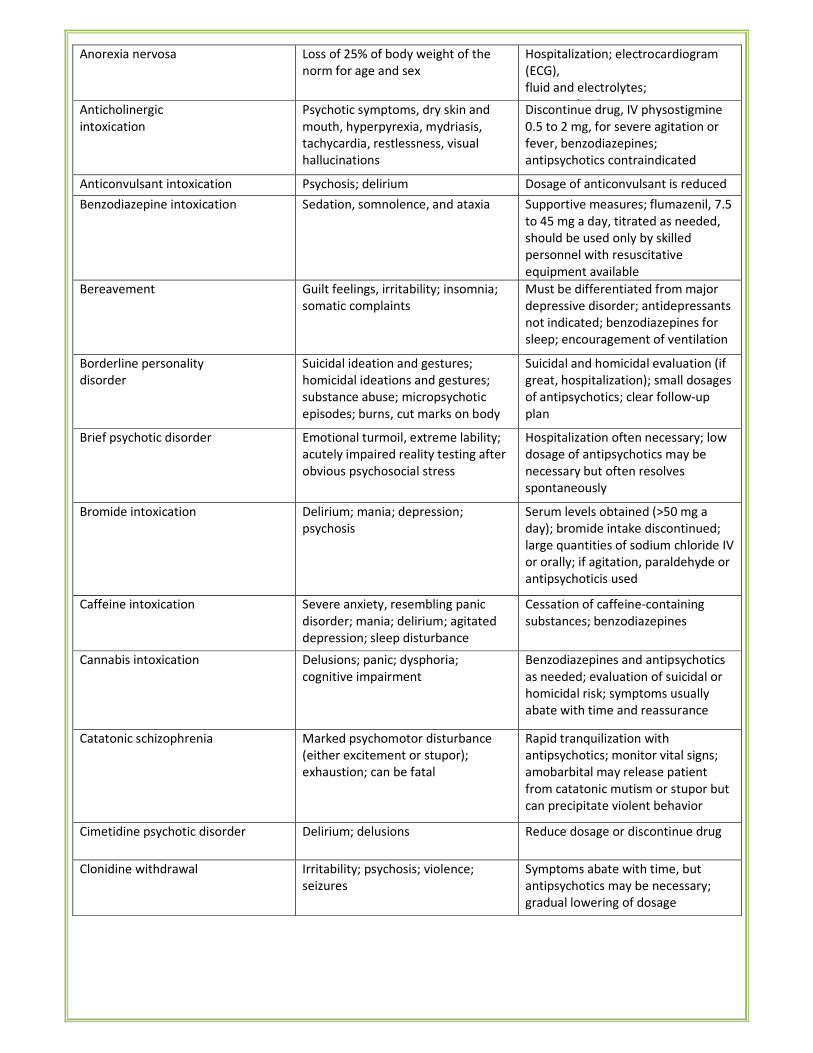
Anorexia nervosa Loss of 25% of body weight of the
norm for age and sex
Hospitalization; electrocardiogram
(ECG),
fluid and electrolytes;
neuroendocrine Anticholinergic
intoxication
Psychotic symptoms, dry skin and
mouth, hyperpyrexia, mydriasis,
tachycardia, restlessness, visual
hallucinations
Discontinue drug, IV physostigmine
0.5 to 2 mg, for severe agitation or
fever, benzodiazepines;
antipsychotics contraindicated
Anticonvulsant intoxication Psychosis; delirium Dosage of anticonvulsant is reduced
Benzodiazepine intoxication Sedation, somnolence, and ataxia Supportive measures; flumazenil, 7.5
to 45 mg a day, titrated as needed,
should be used only by skilled
personnel with resuscitative
equipment available
Bereavement Guilt feelings, irritability; insomnia;
somatic complaints
Must be differentiated from major
depressive disorder; antidepressants
not indicated; benzodiazepines for
sleep; encouragement of ventilation
Borderline personality
disorder
Suicidal ideation and gestures;
homicidal ideations and gestures;
substance abuse; micropsychotic
episodes; burns, cut marks on body
Suicidal and homicidal evaluation (if
great, hospitalization); small dosages
of antipsychotics; clear follow-up
plan
Brief psychotic disorder Emotional turmoil, extreme lability;
acutely impaired reality testing after
obvious psychosocial stress
Hospitalization often necessary; low
dosage of antipsychotics may be
necessary but often resolves
spontaneously
Bromide intoxication Delirium; mania; depression;
psychosis
Serum levels obtained (>50 mg a
day); bromide intake discontinued;
large quantities of sodium chloride IV
or orally; if agitation, paraldehyde or
antipsychoticis used
Caffeine intoxication Severe anxiety, resembling panic
disorder; mania; delirium; agitated
depression; sleep disturbance
Cessation of caffeine-containing
substances; benzodiazepines
Cannabis intoxication
Delusions; panic; dysphoria;
cognitive impairment
Benzodiazepines and antipsychotics
as needed; evaluation of suicidal or
homicidal risk; symptoms usually
abate with time and reassurance
Catatonic schizophrenia Marked psychomotor disturbance
(either excitement or stupor);
exhaustion; can be fatal
Rapid tranquilization with
antipsychotics; monitor vital signs;
amobarbital may release patient
from catatonic mutism or stupor but
can precipitate violent behavior
Cimetidine psychotic disorder Delirium; delusions Reduce dosage or discontinue drug
Clonidine withdrawal Irritability; psychosis; violence;
seizures
Symptoms abate with time, but
antipsychotics may be necessary;
gradual lowering of dosage
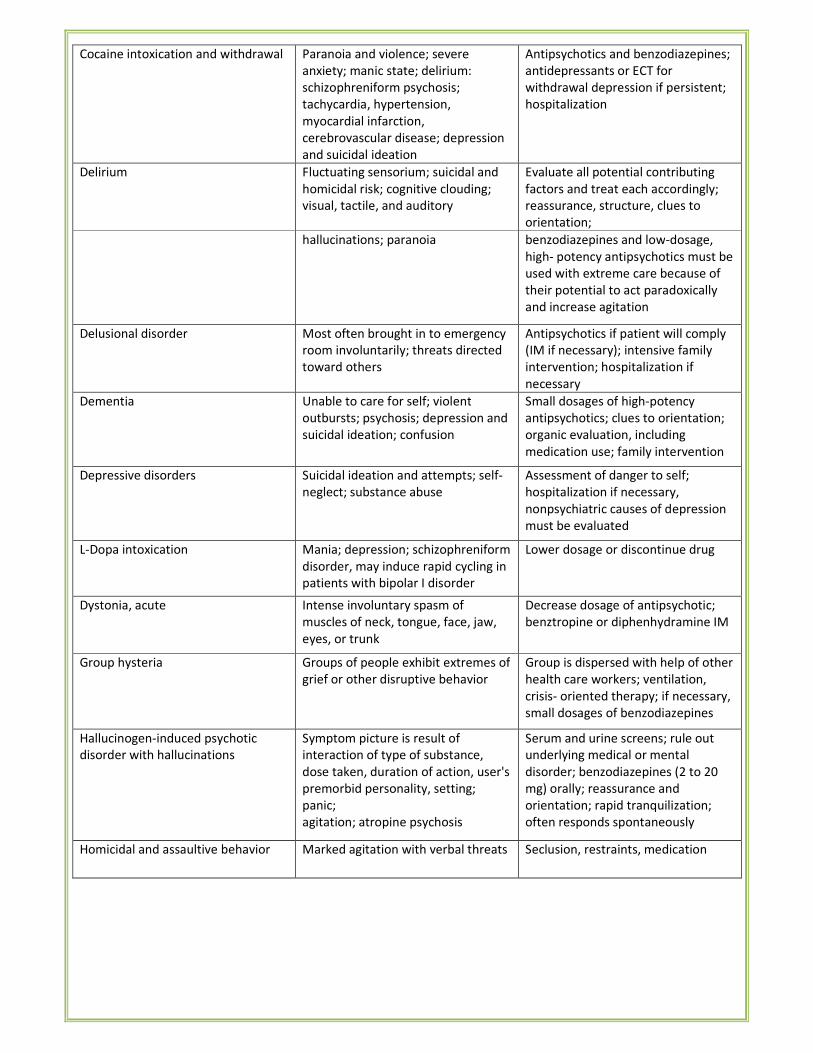
Cocaine intoxication and withdrawal Paranoia and violence; severe
anxiety; manic state; delirium:
schizophreniform psychosis;
tachycardia, hypertension,
myocardial infarction,
cerebrovascular disease; depression
and suicidal ideation
Antipsychotics and benzodiazepines;
antidepressants or ECT for
withdrawal depression if persistent;
hospitalization
Delirium Fluctuating sensorium; suicidal and
homicidal risk; cognitive clouding;
visual, tactile, and auditory
Evaluate all potential contributing
factors and treat each accordingly;
reassurance, structure, clues to
orientation;
hallucinations; paranoia benzodiazepines and low-dosage,
high- potency antipsychotics must be
used with extreme care because of
their potential to act paradoxically
and increase agitation
Delusional disorder Most often brought in to emergency
room involuntarily; threats directed
toward others
Antipsychotics if patient will comply
(IM if necessary); intensive family
intervention; hospitalization if
necessary
Dementia Unable to care for self; violent
outbursts; psychosis; depression and
suicidal ideation; confusion
Small dosages of high-potency
antipsychotics; clues to orientation;
organic evaluation, including
medication use; family intervention
Depressive disorders Suicidal ideation and attempts; self-
neglect; substance abuse
Assessment of danger to self;
hospitalization if necessary,
nonpsychiatric causes of depression
must be evaluated
L-Dopa intoxication Mania; depression; schizophreniform
disorder, may induce rapid cycling in
patients with bipolar I disorder
Lower dosage or discontinue drug
Dystonia, acute Intense involuntary spasm of
muscles of neck, tongue, face, jaw,
eyes, or trunk
Decrease dosage of antipsychotic;
benztropine or diphenhydramine IM
Group hysteria Groups of people exhibit extremes of
grief or other disruptive behavior
Group is dispersed with help of other
health care workers; ventilation,
crisis- oriented therapy; if necessary,
small dosages of benzodiazepines
Hallucinogen-induced psychotic
disorder with hallucinations
Symptom picture is result of
interaction of type of substance,
dose taken, duration of action, user's
premorbid personality, setting;
panic;
agitation; atropine psychosis
Serum and urine screens; rule out
underlying medical or mental
disorder; benzodiazepines (2 to 20
mg) orally; reassurance and
orientation; rapid tranquilization;
often responds spontaneously
Homicidal and assaultive behavior Marked agitation with verbal threats Seclusion, restraints, medication
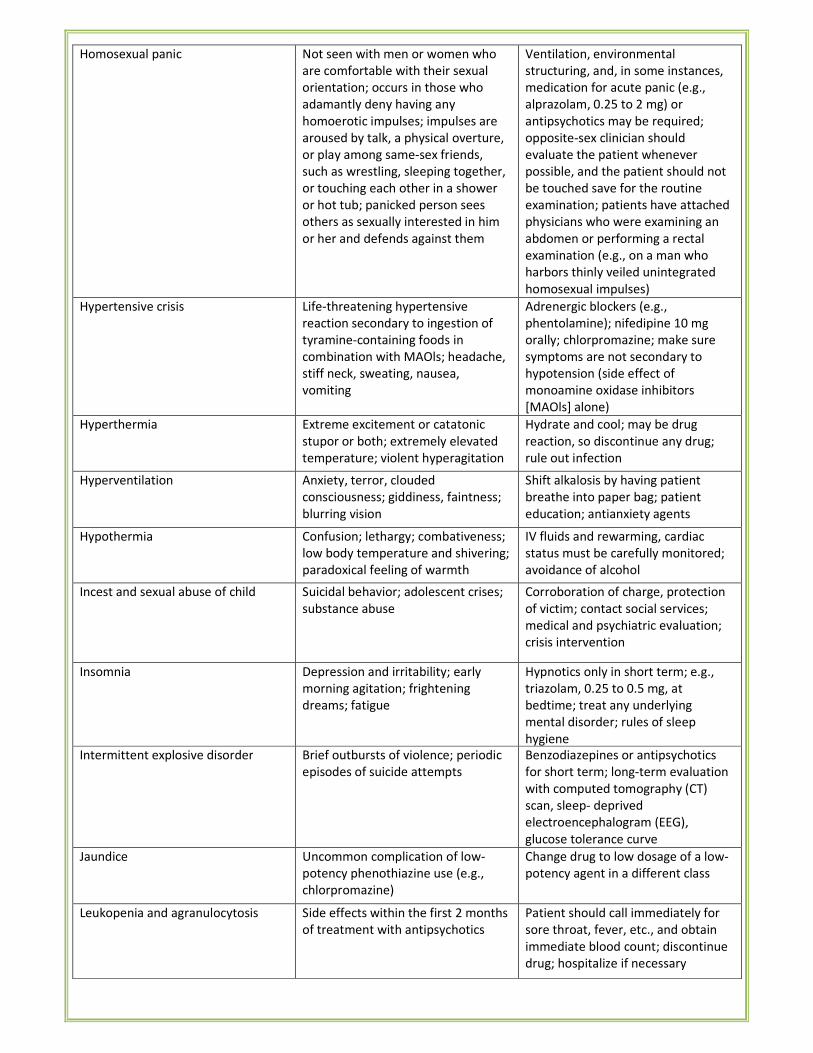
Homosexual panic Not seen with men or women who
are comfortable with their sexual
orientation; occurs in those who
adamantly deny having any
homoerotic impulses; impulses are
aroused by talk, a physical overture,
or play among same-sex friends,
such as wrestling, sleeping together,
or touching each other in a shower
or hot tub; panicked person sees
others as sexually interested in him
or her and defends against them
Ventilation, environmental
structuring, and, in some instances,
medication for acute panic (e.g.,
alprazolam, 0.25 to 2 mg) or
antipsychotics may be required;
opposite-sex clinician should
evaluate the patient whenever
possible, and the patient should not
be touched save for the routine
examination; patients have attached
physicians who were examining an
abdomen or performing a rectal
examination (e.g., on a man who
harbors thinly veiled unintegrated
homosexual impulses)
Hypertensive crisis Life-threatening hypertensive
reaction secondary to ingestion of
tyramine-containing foods in
combination with MAOls; headache,
stiff neck, sweating, nausea,
vomiting
Adrenergic blockers (e.g.,
phentolamine); nifedipine 10 mg
orally; chlorpromazine; make sure
symptoms are not secondary to
hypotension (side effect of
monoamine oxidase inhibitors
[MAOls] alone)
Hyperthermia Extreme excitement or catatonic
stupor or both; extremely elevated
temperature; violent hyperagitation
Hydrate and cool; may be drug
reaction, so discontinue any drug;
rule out infection
Hyperventilation Anxiety, terror, clouded
consciousness; giddiness, faintness;
blurring vision
Shift alkalosis by having patient
breathe into paper bag; patient
education; antianxiety agents
Hypothermia Confusion; lethargy; combativeness;
low body temperature and shivering;
paradoxical feeling of warmth
IV fluids and rewarming, cardiac
status must be carefully monitored;
avoidance of alcohol
Incest and sexual abuse of child Suicidal behavior; adolescent crises;
substance abuse
Corroboration of charge, protection
of victim; contact social services;
medical and psychiatric evaluation;
crisis intervention
Insomnia Depression and irritability; early
morning agitation; frightening
dreams; fatigue
Hypnotics only in short term; e.g.,
triazolam, 0.25 to 0.5 mg, at
bedtime; treat any underlying
mental disorder; rules of sleep
hygiene
Intermittent explosive disorder Brief outbursts of violence; periodic
episodes of suicide attempts
Benzodiazepines or antipsychotics
for short term; long-term evaluation
with computed tomography (CT)
scan, sleep- deprived
electroencephalogram (EEG),
glucose tolerance curve
Jaundice Uncommon complication of low-
potency phenothiazine use (e.g.,
chlorpromazine)
Change drug to low dosage of a low-
potency agent in a different class
Leukopenia and agranulocytosis Side effects within the first 2 months
of treatment with antipsychotics
Patient should call immediately for
sore throat, fever, etc., and obtain
immediate blood count; discontinue
drug; hospitalize if necessary
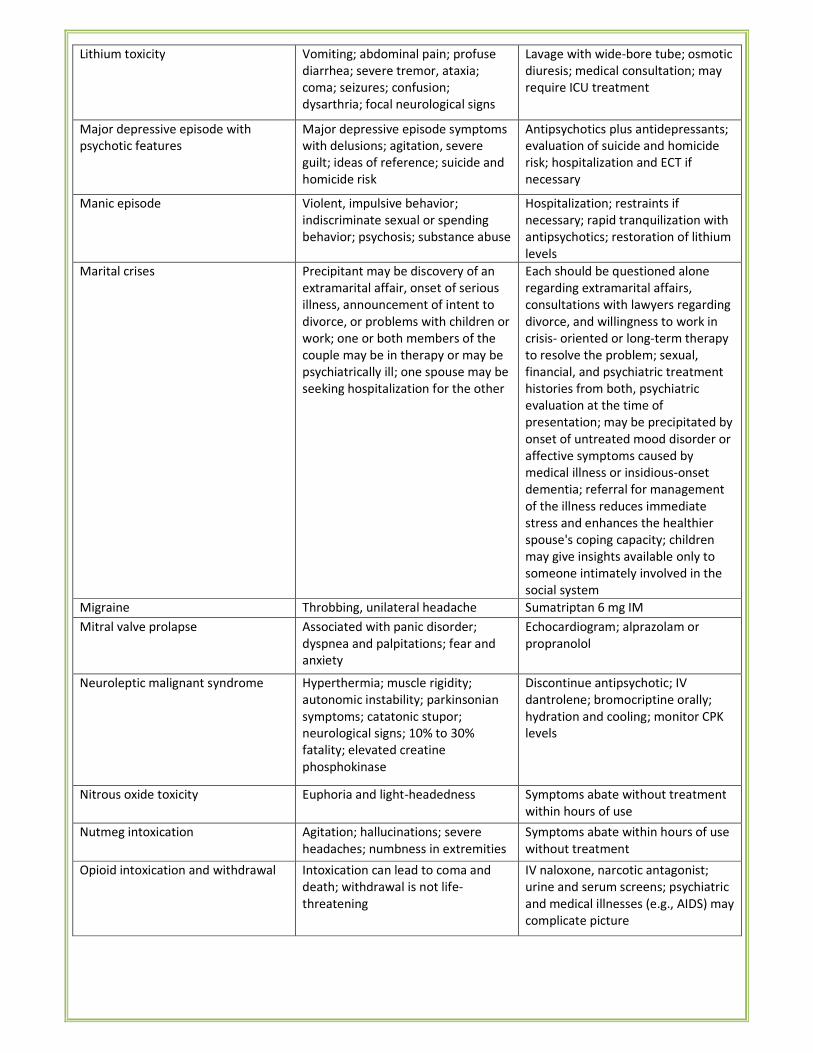
Lithium toxicity Vomiting; abdominal pain; profuse
diarrhea; severe tremor, ataxia;
coma; seizures; confusion;
dysarthria; focal neurological signs
Lavage with wide-bore tube; osmotic
diuresis; medical consultation; may
require ICU treatment
Major depressive episode with
psychotic features
Major depressive episode symptoms
with delusions; agitation, severe
guilt; ideas of reference; suicide and
homicide risk
Antipsychotics plus antidepressants;
evaluation of suicide and homicide
risk; hospitalization and ECT if
necessary
Manic episode Violent, impulsive behavior;
indiscriminate sexual or spending
behavior; psychosis; substance abuse
Hospitalization; restraints if
necessary; rapid tranquilization with
antipsychotics; restoration of lithium
levels
Marital crises Precipitant may be discovery of an
extramarital affair, onset of serious
illness, announcement of intent to
divorce, or problems with children or
work; one or both members of the
couple may be in therapy or may be
psychiatrically ill; one spouse may be
seeking hospitalization for the other
Each should be questioned alone
regarding extramarital affairs,
consultations with lawyers regarding
divorce, and willingness to work in
crisis- oriented or long-term therapy
to resolve the problem; sexual,
financial, and psychiatric treatment
histories from both, psychiatric
evaluation at the time of
presentation; may be precipitated by
onset of untreated mood disorder or
affective symptoms caused by
medical illness or insidious-onset
dementia; referral for management
of the illness reduces immediate
stress and enhances the healthier
spouse's coping capacity; children
may give insights available only to
someone intimately involved in the
social system
Migraine Throbbing, unilateral headache Sumatriptan 6 mg IM
Mitral valve prolapse Associated with panic disorder;
dyspnea and palpitations; fear and
anxiety
Echocardiogram; alprazolam or
propranolol
Neuroleptic malignant syndrome Hyperthermia; muscle rigidity;
autonomic instability; parkinsonian
symptoms; catatonic stupor;
neurological signs; 10% to 30%
fatality; elevated creatine
phosphokinase
Discontinue antipsychotic; IV
dantrolene; bromocriptine orally;
hydration and cooling; monitor CPK
levels
Nitrous oxide toxicity Euphoria and light-headedness Symptoms abate without treatment
within hours of use
Nutmeg intoxication Agitation; hallucinations; severe
headaches; numbness in extremities
Symptoms abate within hours of use
without treatment
Opioid intoxication and withdrawal Intoxication can lead to coma and
death; withdrawal is not life-
threatening
IV naloxone, narcotic antagonist;
urine and serum screens; psychiatric
and medical illnesses (e.g., AIDS) may
complicate picture
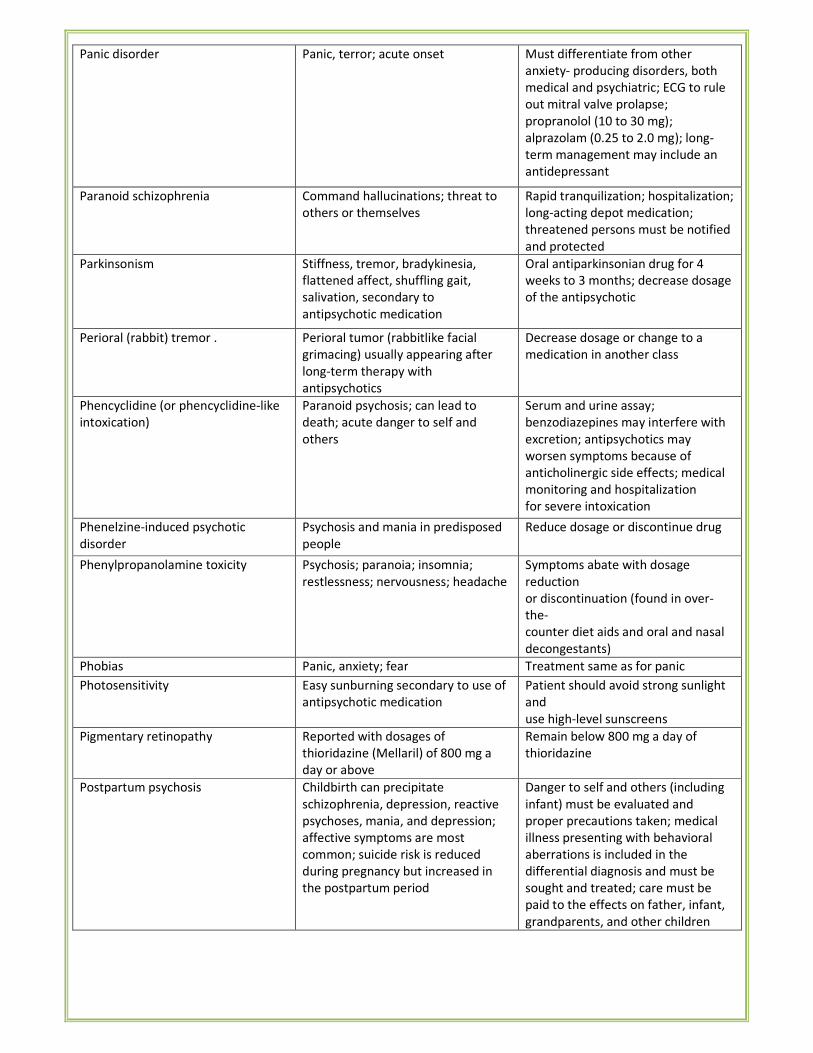
Panic disorder Panic, terror; acute onset Must differentiate from other
anxiety- producing disorders, both
medical and psychiatric; ECG to rule
out mitral valve prolapse;
propranolol (10 to 30 mg);
alprazolam (0.25 to 2.0 mg); long-
term management may include an
antidepressant
Paranoid schizophrenia Command hallucinations; threat to
others or themselves
Rapid tranquilization; hospitalization;
long-acting depot medication;
threatened persons must be notified
and protected
Parkinsonism Stiffness, tremor, bradykinesia,
flattened affect, shuffling gait,
salivation, secondary to
antipsychotic medication
Oral antiparkinsonian drug for 4
weeks to 3 months; decrease dosage
of the antipsychotic
Perioral (rabbit) tremor . Perioral tumor (rabbitlike facial
grimacing) usually appearing after
long-term therapy with
antipsychotics
Decrease dosage or change to a
medication in another class
Phencyclidine (or phencyclidine-like
intoxication)
Paranoid psychosis; can lead to
death; acute danger to self and
others
Serum and urine assay;
benzodiazepines may interfere with
excretion; antipsychotics may
worsen symptoms because of
anticholinergic side effects; medical
monitoring and hospitalization
for severe intoxication
Phenelzine-induced psychotic
disorder
Psychosis and mania in predisposed
people
Reduce dosage or discontinue drug
Phenylpropanolamine toxicity Psychosis; paranoia; insomnia;
restlessness; nervousness; headache
Symptoms abate with dosage
reduction
or discontinuation (found in over-
the-
counter diet aids and oral and nasal
decongestants)
Phobias Panic, anxiety; fear Treatment same as for panic
disorder Photosensitivity Easy sunburning secondary to use of
antipsychotic medication
Patient should avoid strong sunlight
and
use high-level sunscreens
Pigmentary retinopathy Reported with dosages of
thioridazine (Mellaril) of 800 mg a
day or above
Remain below 800 mg a day of
thioridazine
Postpartum psychosis Childbirth can precipitate
schizophrenia, depression, reactive
psychoses, mania, and depression;
affective symptoms are most
common; suicide risk is reduced
during pregnancy but increased in
the postpartum period
Danger to self and others (including
infant) must be evaluated and
proper precautions taken; medical
illness presenting with behavioral
aberrations is included in the
differential diagnosis and must be
sought and treated; care must be
paid to the effects on father, infant,
grandparents, and other children
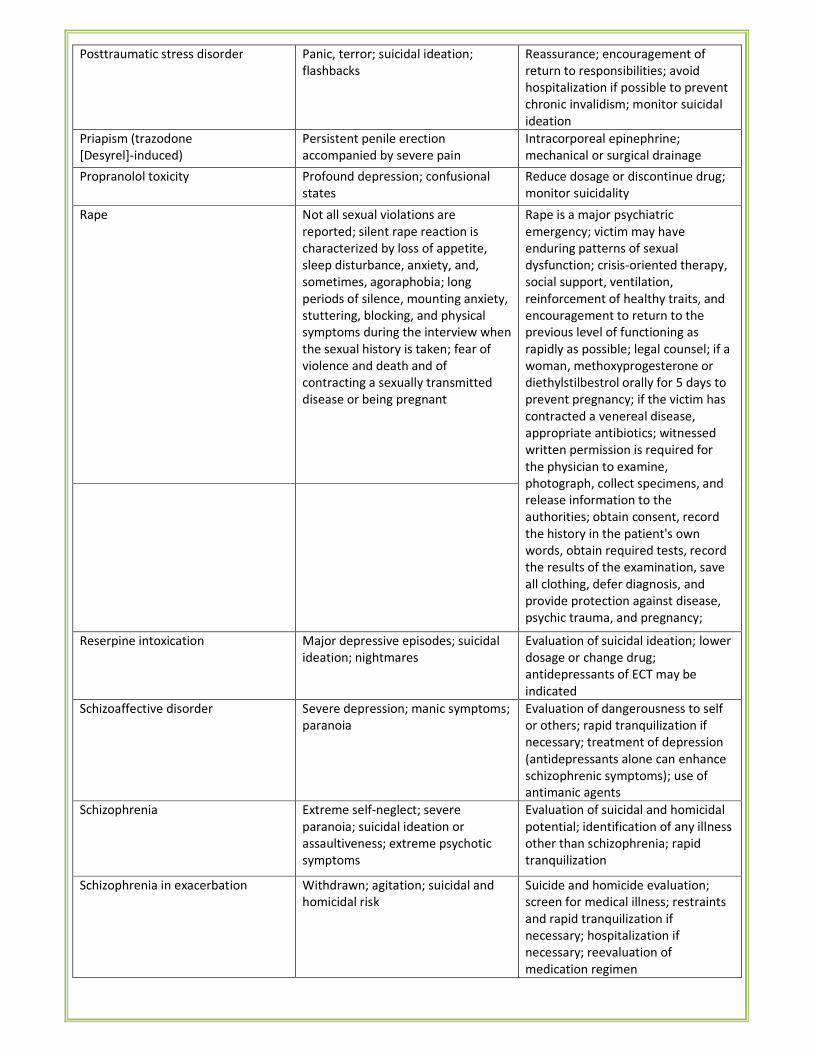
Posttraumatic stress disorder Panic, terror; suicidal ideation;
flashbacks
Reassurance; encouragement of
return to responsibilities; avoid
hospitalization if possible to prevent
chronic invalidism; monitor suicidal
ideation
Priapism (trazodone
[Desyrel]-induced)
Persistent penile erection
accompanied by severe pain
Intracorporeal epinephrine;
mechanical or surgical drainage
Propranolol toxicity Profound depression; confusional
states
Reduce dosage or discontinue drug;
monitor suicidality
Rape Not all sexual violations are
reported; silent rape reaction is
characterized by loss of appetite,
sleep disturbance, anxiety, and,
sometimes, agoraphobia; long
periods of silence, mounting anxiety,
stuttering, blocking, and physical
symptoms during the interview when
the sexual history is taken; fear of
violence and death and of
contracting a sexually transmitted
disease or being pregnant
Rape is a major psychiatric
emergency; victim may have
enduring patterns of sexual
dysfunction; crisis-oriented therapy,
social support, ventilation,
reinforcement of healthy traits, and
encouragement to return to the
previous level of functioning as
rapidly as possible; legal counsel; if a
woman, methoxyprogesterone or
diethylstilbestrol orally for 5 days to
prevent pregnancy; if the victim has
contracted a venereal disease,
appropriate antibiotics; witnessed
written permission is required for
the physician to examine,
photograph, collect specimens, and
release information to the
authorities; obtain consent, record
the history in the patient's own
words, obtain required tests, record
the results of the examination, save
all clothing, defer diagnosis, and
provide protection against disease,
psychic trauma, and pregnancy;
Reserpine intoxication Major depressive episodes; suicidal
ideation; nightmares
Evaluation of suicidal ideation; lower
dosage or change drug;
antidepressants of ECT may be
indicated
Schizoaffective disorder Severe depression; manic symptoms;
paranoia
Evaluation of dangerousness to self
or others; rapid tranquilization if
necessary; treatment of depression
(antidepressants alone can enhance
schizophrenic symptoms); use of
antimanic agents
Schizophrenia Extreme self-neglect; severe
paranoia; suicidal ideation or
assaultiveness; extreme psychotic
symptoms
Evaluation of suicidal and homicidal
potential; identification of any illness
other than schizophrenia; rapid
tranquilization
Schizophrenia in exacerbation Withdrawn; agitation; suicidal and
homicidal risk
Suicide and homicide evaluation;
screen for medical illness; restraints
and rapid tranquilization if
necessary; hospitalization if
necessary; reevaluation of
medication regimen
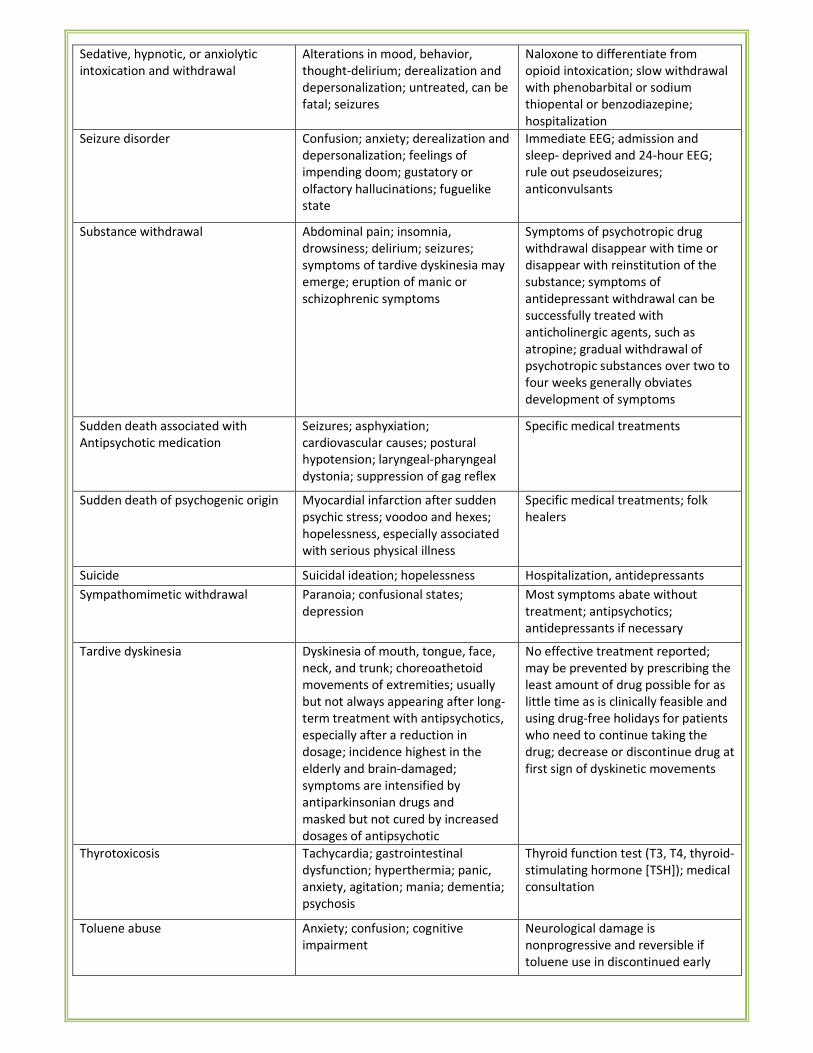
Sedative, hypnotic, or anxiolytic
intoxication and withdrawal
Alterations in mood, behavior,
thought-delirium; derealization and
depersonalization; untreated, can be
fatal; seizures
Naloxone to differentiate from
opioid intoxication; slow withdrawal
with phenobarbital or sodium
thiopental or benzodiazepine;
hospitalization
Seizure disorder Confusion; anxiety; derealization and
depersonalization; feelings of
impending doom; gustatory or
olfactory hallucinations; fuguelike
state
Immediate EEG; admission and
sleep- deprived and 24-hour EEG;
rule out pseudoseizures;
anticonvulsants
Substance withdrawal Abdominal pain; insomnia,
drowsiness; delirium; seizures;
symptoms of tardive dyskinesia may
emerge; eruption of manic or
schizophrenic symptoms
Symptoms of psychotropic drug
withdrawal disappear with time or
disappear with reinstitution of the
substance; symptoms of
antidepressant withdrawal can be
successfully treated with
anticholinergic agents, such as
atropine; gradual withdrawal of
psychotropic substances over two to
four weeks generally obviates
development of symptoms
Sudden death associated with
Antipsychotic medication
Seizures; asphyxiation;
cardiovascular causes; postural
hypotension; laryngeal-pharyngeal
dystonia; suppression of gag reflex
Specific medical treatments
Sudden death of psychogenic origin Myocardial infarction after sudden
psychic stress; voodoo and hexes;
hopelessness, especially associated
with serious physical illness
Specific medical treatments; folk
healers
Suicide Suicidal ideation; hopelessness Hospitalization, antidepressants
Sympathomimetic withdrawal Paranoia; confusional states;
depression
Most symptoms abate without
treatment; antipsychotics;
antidepressants if necessary
Tardive dyskinesia Dyskinesia of mouth, tongue, face,
neck, and trunk; choreoathetoid
movements of extremities; usually
but not always appearing after long-
term treatment with antipsychotics,
especially after a reduction in
dosage; incidence highest in the
elderly and brain-damaged;
symptoms are intensified by
antiparkinsonian drugs and
masked but not cured by increased
dosages of antipsychotic
No effective treatment reported;
may be prevented by prescribing the
least amount of drug possible for as
little time as is clinically feasible and
using drug-free holidays for patients
who need to continue taking the
drug; decrease or discontinue drug at
first sign of dyskinetic movements
Thyrotoxicosis Tachycardia; gastrointestinal
dysfunction; hyperthermia; panic,
anxiety, agitation; mania; dementia;
psychosis
Thyroid function test (T3, T4, thyroid-
stimulating hormone [TSH]); medical
consultation
Toluene abuse Anxiety; confusion; cognitive
impairment
Neurological damage is
nonprogressive and reversible if
toluene use in discontinued early
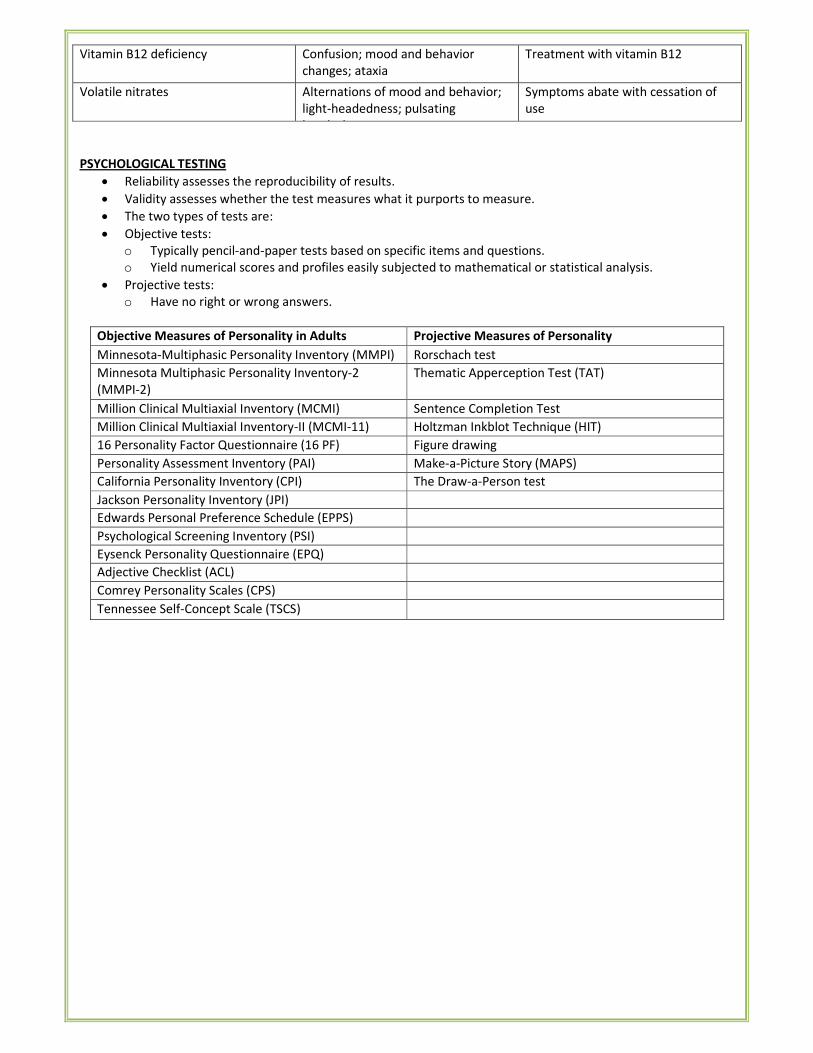
Vitamin B12 deficiency Confusion; mood and behavior
changes; ataxia
Treatment with vitamin B12
Volatile nitrates Alternations of mood and behavior;
light-headedness; pulsating
headache
Symptoms abate with cessation of
use
PSYCHOLOGICAL TESTING
• Reliability assesses the reproducibility of results.
• Validity assesses whether the test measures what it purports to measure.
• The two types of tests are:
• Objective tests:
o Typically pencil-and-paper tests based on specific items and questions.
o Yield numerical scores and profiles easily subjected to mathematical or statistical analysis.
• Projective tests:
o Have no right or wrong answers.
Objective Measures of Personality in Adults Projective Measures of Personality
Minnesota-Multiphasic Personality Inventory (MMPI) Rorschach test
Minnesota Multiphasic Personality Inventory-2
(MMPI-2)
Thematic Apperception Test (TAT)
Million Clinical Multiaxial Inventory (MCMI) Sentence Completion Test
Million Clinical Multiaxial Inventory-II (MCMI-11) Holtzman Inkblot Technique (HIT)
16 Personality Factor Questionnaire (16 PF) Figure drawing
Personality Assessment Inventory (PAI) Make-a-Picture Story (MAPS)
California Personality Inventory (CPI) The Draw-a-Person test
Jackson Personality Inventory (JPI)
Edwards Personal Preference Schedule (EPPS)
Psychological Screening Inventory (PSI)
Eysenck Personality Questionnaire (EPQ)
Adjective Checklist (ACL)
Comrey Personality Scales (CPS)
Tennessee Self-Concept Scale (TSCS)
III. DELIRIUM AND DEMENTIA
DELIRIUM
• Most common organic mental disorder seen in clinical practice
Etiology:
• Seen in approximately 10 to 30 % of medically ill patients who are hospitalized
• The incidence is higher in postoperative patients
• Predisposing factors
� Preexisting brain damage (e.g., dementia, cerebrovascular disease, tumor)
� History of delirium
� Alcohol or drug dependence & withdrawal
� Generalized or focal cerebral lesion
� Chronic medical illness
� Surgical procedure and postoperative period
� Treatment with psychotropic medicines
� Present or past history of head injury
� Diabetes, Cancer
� Sensory impairment (e.g., blindness)
� Male gender
Diagnostic Criteria for Delirium, Not Induced by Alcohol and Other Psychoactive Substances
A. There is clouding of consciousness, i.e., reduced clarity of awareness of the environment, with reduced
ability to focus, sustain, or shift attention.
B. Disturbance of cognition is manifest by both:
1. impairment of immediate recall and recent memory, with relatively intact remote memory;
2. disorientation in time, place, or person.
C. At least one of the following psychomotor disturbances is present:
1. rapid, unpredictable shifts from hypoactivity to hyperactivity;
2. increased reaction time;
3. increased or decreased flow of speech;
4. enhanced startle reaction.
D. There is disturbance of sleep or of the sleep-wake cycle, manifest by at least one of the following:
1. insomnia, which in severe cases may involve total sleep loss, with or without daytime drowsiness, or
reversal of the sleep-wake cycle;
2. nocturnal worsening of symptoms;
3. disturbing dreams and nightmares, which may continue as hallucinations or illusions after awakening.
E. Symptoms have rapid onset and show fluctuations over the course of the day.
F. There is objective evidence from history, physical and neurological examination, or laboratory tests of an
underlying cerebral or systemic disease (other than psychoactive substance-related) that can be presumed
to be responsible for the clinical manifestations in Criteria A to D.
Comments
• Emotional disturbances such as depression, anxiety or fear, irritability, euphoria, apathy, or wondering
perplexity, disturbances of perception (illusions or hallucinations, often visual), and transient delusions are
typical but are not specific indications for the diagnosis. A fourth character may be used to indicate whether
or not the delirium is superimposed on dementia
o Delirium, not superimposed on dementia
o Delirium, superimposed on dementia
o Other delirium
o Delirium, unspecified
Clinical Features:
• Sudden onset with fluctuating course
• Cognitive impairment
• Clouding of consciousness — decreased awareness of surroundings and decreased ability to respond to
environmental stimuli
• Disorientation (mostly in time)
• Perceptual disturbances - Illusions, hallucinations
• Delirium may first present with daytime drowsiness and night time insomnia (sun downing)
• Motor symptoms: asterixis, incoordination, carphologia or floccillation (picking movements at cover-sheets
and clothes), Multifocal myoclonus
• When a psychiatric illness causes symptoms of delirium, patients are said to have a pseudodelirium
• Delirium can occur in older patients wearing eye patches after cataract surgery (black-patch delirium)
Treatment
• Primary goal: treat the underlying cause.
• Commonly used drug: haloperidol.
DEMENTIA
• Impairment of intellectual functions
• Impairment of memory (predominantly of recent memory, especially in early stages),
• Deterioration of personality with lack of personal care.
• Impairment of judgment and impulse control
• Impairment of abstract thinking.
• No impairment of consciousness
Additional features:
• Emotional lability (marked variation in emotional expression)
• Catastrophic reaction (when confronted with an assignment which is beyond the residual intellectual
capacity, patient may go into a sudden rage).
• Thought abnormalities, e.g. perseveration, delusions.
• Urinary and faecal incontinence may develop in later stages.
• Disorientation in time; disorientation in place and person may also develop in later stages.
• Neurological signs may or may not be present, depending on the underlying cause.
Dementia Pseudodementia (Depression)
Patient rarely complains of cognitive
impairment
Patient usually always complains about memory
impairment Patient often emphasizes achievements Patient often emphasizes disability
Patients often appears unconcerned Patient very often communicates distress
Usually labile affect Severe depression on examination
Patient makes errors on cognitive examination Do not know' answers are more frequent
Impairment of recent memory Rarely impaired
Confabulation may be present Confabulation very rare
Consistently poor performance on similar tests Marked variability in performance on similar tests
History of depression less common Past history of manic and/ or depression episodes
Features Cortical Dementia Subcortical Dementia
Site of lesion Cortex (frontal and temporo parieto-
occipital association areas, hippocampus)
Subcortical grey matter (thalamus, basal
ganglia, and rostral brain stem)
Examples Alzheimer's disease, Pick's disease Huntington' chorea, Parkinson's disease,
Progressive supranuclear palsy, Wilson's
disease
Severity Severe Mild to moderate
Motor system Usually normal Dysarthria, flexed/extended posture, tremors,
dystonic, chorea, ataxia, rigidity
Other features Simple delusions; depression uncommon;
severe aphasia, amnesia, agnosia,
apraxia, acalculia, slowed cognitive speed
(bradyphrenia)
Complex delusions; depression common;
rarely mania
Memory deficit
(Short-term)
Recall helped very little by cues Recall partially helped by cues and recognition
tasks
Reversible causes of dementia:
• Hypothyroidism
• Infections
• B1 B12 deficiency
• Wilsons disease
• NPH
Feature Dementia Delirium
Onset Slow Rapid
Duration Months to years Hours to weeks
Consciousness Normal Clouded
Orientation Normal until late stages Disturbed
Memory Immediate retention and recall
normal
Recent memory disturbed
Impaired remote memory in late
stages
Impaired recent and immediate memory
Attention and
concentration
Usually normal Disturbed
Comprehension Impaired only in late stages Impaired
Speech Word-finding difficulty Incoherent (slow or rapid)
Sleep-wake cycle Normal Frequent disruption (e.g., day & night
reversal)
Thoughts Impoverished Disorganized
Awareness Unchanged Reduced
ALZHEIMER'S DISEASE
• Most common cause of dementia (> 50%)
NINCDS-ARDRA CRITERIA used for diagnosis
• Presence of dementia
• Deficits in at least two areas of cognition
• Progressive deterioration
• No clouding of consciousness
• Age between 40 and 90
• Absence of systemic disorders
• Neurofibrillary tangles
• Beta amyloid plaques
• Apolipoprotein E4
Clinical features:
• Delayed recall is the best overall discriminator for early Alzheimer's disease
• Early dementia is probable with a MMSE score of 24-27
• CT- cortical atrophy over parietal and temporal lobes
• MRI- atrophy of grey matter (hippocampus, amygdala, medial temporal lobe)
Multi — infarct Dementia
• Second most common cause of dementia (10-15%)
• Some studies indicate that multi-infarct dementia is probably far more common in India.
• It is also one of the important treatable causes of dementia.
• Characterized by :
o An abrupt onset
o Acute exacerbations (due to repeated infarctions),
o Stepwise clinical deterioration (step-ladder pattern),
o Fluctuating course,
o Presence of hypertension (most commonly) or any other significant cardiovascular disease, and
o History of previous stroke or transient ischemic attacks (TIAs).
• Focal neurological signs are frequently present.
• Insight into the illness is usually present in the early part of the course.
• Emotional lability is common.
• EEG - focal area of slowing
• CT scan or MRI - multiple infarcts
AIDS Dementia Complex
• Seen in about 50-70% of patients suffering from AIDS
• Triad of cognitive, behavioral and motoric deficits of subcortical dementia type.
• Cranial CT scan can show cortical atrophy 1-4 months before the onset of clinical dementia
Lewy Body Dementia
• Second most common cause of the degenerative dementias
• Typically, the clinical features include:
o Fluctuating cognitive impairment over weeks or months
o Lucid intervals can be present in between fluctuations.
o Recurrent and detailed visual hallucinations.
o Spontaneous extrapyramidal symptoms such as rigidity and tremors.
o Neuroleptic sensitivity syndrome - marked sensitivity typical doses of antipsychotic drugs (resulting in
severe extrapyramidal side-effects with use of antipsychotics).
� Antipsychotics (Haloperidol and Risperidone) use to treat disruptive behavior in dementia has decreased
markedly due to possible association with increased mortality
� Antipsychotics should be avoided if Lewy body dementia is suspected
ORGANIC HALLUCINOSIS
• Presence of persistent or recurrent hallucinations due to an underlying organic cause.
• Usually visual (most common) or auditory in nature.
Etiology
• Drugs: Hallucinogens (LSD, psilocybin, mescaline), cocaine, cannabis, phencyclidine etc.
• Alcohol: In alcoholic hallucinosis, auditory hallucinations are usually more common.
• Sensory deprivation.
• 'Release' hallucinations due to sensory pathway disease, e.g. bilateral cataracts, otosclerosis, optic neuritis.
• Brain stem lesions (peduncular hallucinosis).
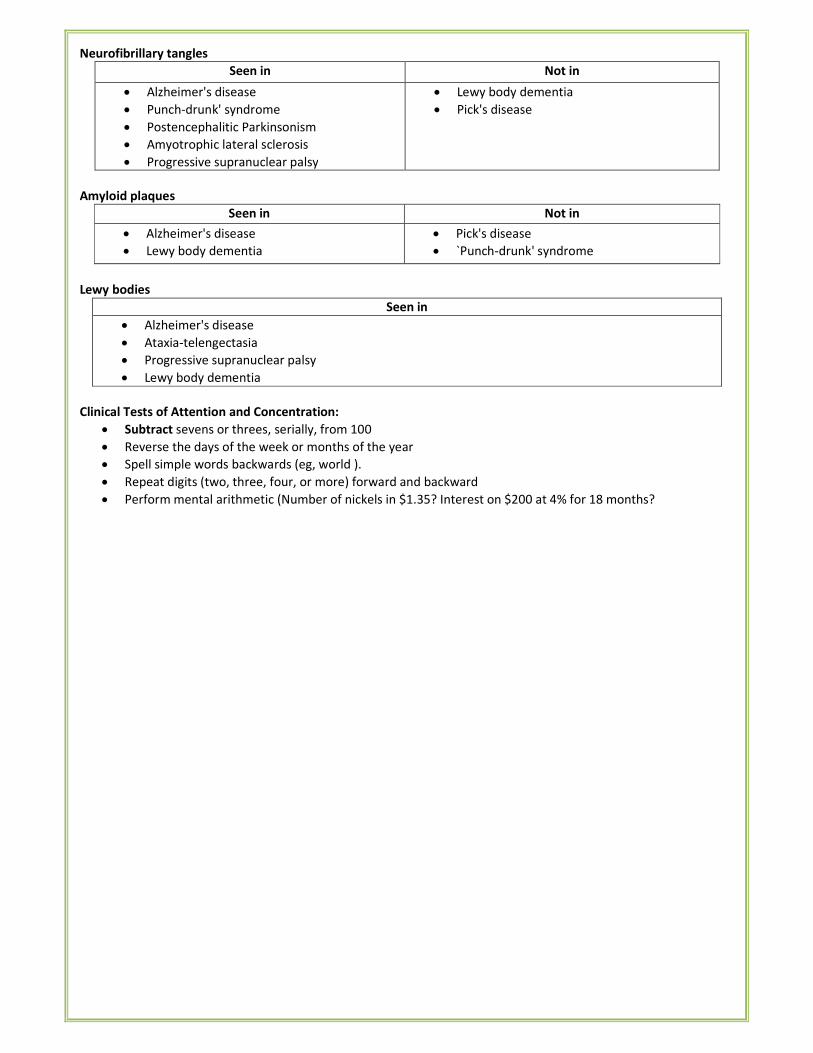
Neurofibrillary tangles
Seen in Not in
• Alzheimer's disease
• Punch-drunk' syndrome
• Postencephalitic Parkinsonism
• Amyotrophic lateral sclerosis
• Progressive supranuclear palsy
• Lewy body dementia
• Pick's disease
Amyloid plaques
Seen in Not in
• Alzheimer's disease
• Lewy body dementia
• Pick's disease
• `Punch-drunk' syndrome
Lewy bodies
Seen in
• Alzheimer's disease
• Ataxia-telengectasia
• Progressive supranuclear palsy
• Lewy body dementia
Clinical Tests of Attention and Concentration:
• Subtract sevens or threes, serially, from 100
• Reverse the days of the week or months of the year
• Spell simple words backwards (eg, world ).
• Repeat digits (two, three, four, or more) forward and backward
• Perform mental arithmetic (Number of nickels in $1.35? Interest on $200 at 4% for 18 months?
IV. PSYCHOACTIVE SUBSTANCE ABUSE
Complications of alcoholism
DELIRIUM TREMENS
• Most severe alcohol withdrawal syndrome
• It occurs usually within 2-4 days of complete or significant abstinence from heavy alcohol drinking
• The course is short, with recovery occurring within 3-7 days.
• This is an acute organic brain syndrome (delirium) with characteristic features of:
o Clouding of consciousness
o Disorientation in time and place.
o Poor attention span and distractibility.
o Visual (also auditory) hallucinations and illusions, which are often vivid and very frightening.
o Marked autonomic disturbance - tachycardia, fever, hypertension, sweating, mydriasis
o Psychomotor agitation and ataxia.
o Insomnia, with a reversal of sleep-wake pattern.
o Dehydration with electrolyte imbalance.
• It is extremely important not to administer 5% dextrose in delirium tremens without thiamine
Alcoholic seizures ('rum fits')
• Generalized tonic clonic seizures
• Usually occurs 12-48 hours after a heavy bout of drinking
• Often these patients have been drinking alcohol in large amounts on a regular basis for many years.
• Multiple seizures (2-6 at one time) are more common than single seizures.
• In 30% of the cases, delirium tremens follows.
Alcoholic hallucinosis
• Presence of hallucinations (usually auditory) during partial or complete abstinence
• They occur during clear consciousness
WERNICKE'S ENCEPHALOPATHY
• An acute reaction to a severe deficiency of thiamine
• Commonest cause - chronic alcohol use.
• Ophthalmoplegia with bilateral external rectus paralysis
• Higher mental function disturbance: disorientation, confusion, recent memory disturbances, poor attention
span and distractibility
• Apathy and ataxia.
• Neuronal degeneration and haemorrhage are seen in thalamus, hypothalamus, mammillary bodies and
midbrain.
• Completely reversible with treatment
Korsakoff's psychosis
• Often follows Wernicke's encephalopathy; and referred to as Wernicke-Korsakoff syndrome.
• Gross memory disturbances, with confabulation
• 20 percent of patients with Korsakoff's syndrome recover
• Insight is often impaired.
• Neuropathological lesions are symmetrical and paraventricular, involving the mammillary bodies, the
thalamus, the hypothalamus, the midbrain, the pons, the medulla, the fornix, and the cerebellum.
Marchiafava — Bignami disease
• Disorientation, epilepsy, ataxia, dysarthria, hallucinations, spastic limb paralysis, and deterioration of
personality and intellectual functioning
• There is a widespread demyelination of corpus callosum, optic tracts and cerebellar peduncles.
� Legal limit for driving in India: 30 mg/100 ml (Section 185 of the Motor Vehicle Act, 1988)
Screening test for alcoholism:
• MAST (Michigan Alcoholism Screening Test)
• CAGE questionnaire test
CAGE Questionnaire
• Ever had to Cut down the amount of alcohol
• Been Annoyed by people's criticism of alcoholism
• Felt Guilty of drinking.
• Need of an Eye opener.
Withdrawal syndrome: Drugs of 1st choice — Chlordiazepoxide (diazepam 2nd)
Treatment of Alcohol Dependence
• Behaviour therapy
• Psychotherapy
• Group therapy
• Deterrent agents
� The deterrent agents are also known as alcohol sensitizing drugs.
� Disulfiram (tetraethyl thiuram disulfide) — most commonly used
� Other deterrent agents: Citrated calcium carbimide (CCC), Metronidazole. animal charcoal, a fungus
(coprinus atramentarius), sulfonylureas and certain cephalsoporins
• Anti — craving agents
� Acamprosate - interacts with NMDA receptor — mediated glutamatergic neurotransmission in the
various brain regions and reduces Ca++ fluxes through voltage — operated channels.
� Naltrexone - probably interferes with alcohol — induced reinforcement by blocking opioid receptors
� SSRIs (such as fluoxetine)
OPIUM ABUSE
• Opium use has increased markedly all over the world in the past few decades
• India is surrounded both sides by the infamous routes of illicit transport – Golden triangle (BurmaThailand-
Laos) and Golden Crescent (Iran-Afghanistan-Pakistan)
• Heroin (Di-acetyl-morphine) can be smoked or chased (chasing the dragon)
• Tolerance to heroin occurs very rapidly
Withdrawal syndrome
• Occurs typically within 12-24 hours
• Lacrimation, rhinorrhea, pupillary dilation. sweating, diarrhea, yawning, tachycardia, insomnia, raised
body temperature, muscle cramps, piloerection
Treatment
• Overdose: Naloxone
• Withdrawal: Methadone (1st choice), Clonidine (2' choice); others: LAAM, buprenorphine
• Maintenance: Methadone
Nicotine withdrawal
• Anxiety, restlessness, poor concentration, decreased sleep, increased appetite, exacerbation of psychiatric
symptoms
• Drugs used in smoking cessation: Bupropion (amfebutamone), Varenicline
Substance Characteristic feature
Cocaine Magnus symptom (cocaine bugs/tactile hallucinations)
Cannabis Run amok, Amotivation syndrome, Flash backs, Hemp insanity,
Alcohol Mc-Evan's sign, Morbid jealousy
LSD Bad trips, Flash backs
Amphetamine Paranoid hallucinatory syndrome (like paranoid schizophrenia)
Phencyclidine (angel dust) Dissociative anesthesia
� LSD: No withdrawal syndrome
� Cannabis: No physical dependence; mild to marked psychological dependence
� Cocaine: Mild physical dependence; severe psychological dependence
� Amok is an episode of acute violent behavior for which the person claims amnesia. Seen in cannabis abuse.
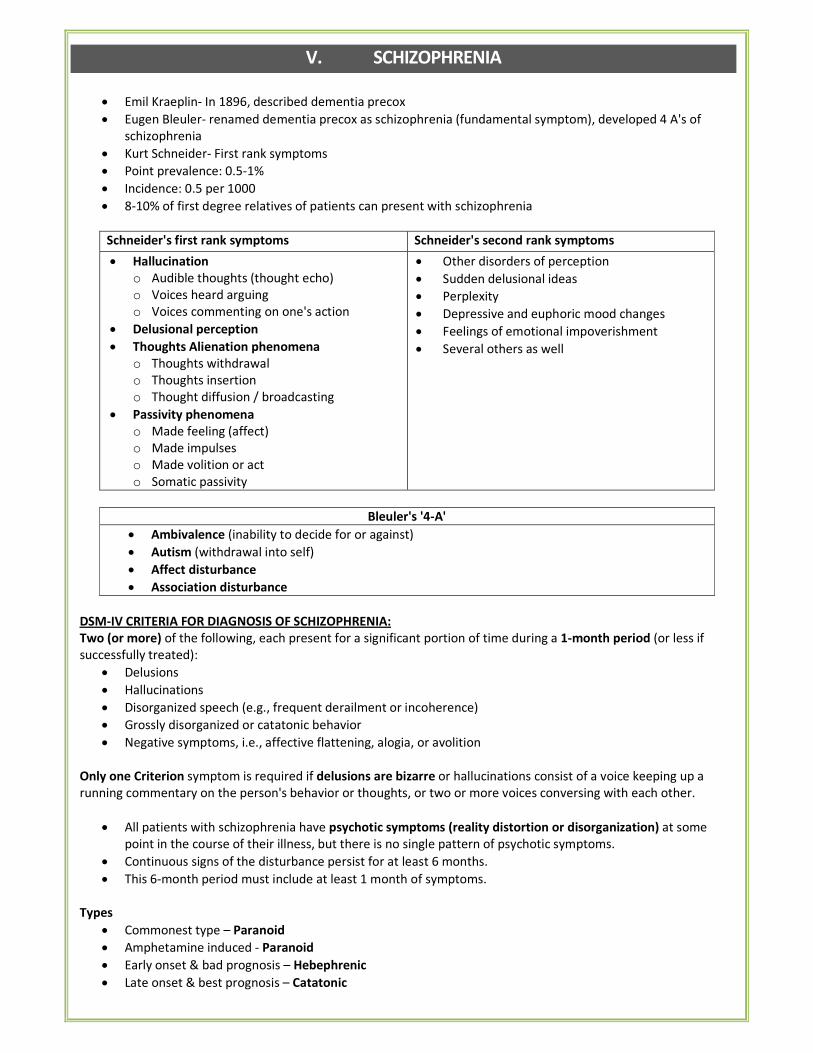
V. SCHIZOPHRENIA
• Emil Kraeplin- In 1896, described dementia precox
• Eugen Bleuler- renamed dementia precox as schizophrenia (fundamental symptom), developed 4 A's of
schizophrenia
• Kurt Schneider- First rank symptoms
• Point prevalence: 0.5-1%
• Incidence: 0.5 per 1000
• 8-10% of first degree relatives of patients can present with schizophrenia
Schneider's first rank symptoms Schneider's second rank symptoms
• Hallucination
o Audible thoughts (thought echo)
o Voices heard arguing
o Voices commenting on one's action
• Delusional perception
• Thoughts Alienation phenomena
o Thoughts withdrawal
o Thoughts insertion
o Thought diffusion / broadcasting
• Passivity phenomena
o Made feeling (affect)
o Made impulses
o Made volition or act
o Somatic passivity
• Other disorders of perception
• Sudden delusional ideas
• Perplexity
• Depressive and euphoric mood changes
• Feelings of emotional impoverishment
• Several others as well
Bleuler's '4-A'
• Ambivalence (inability to decide for or against)
• Autism (withdrawal into self)
• Affect disturbance
• Association disturbance
DSM-IV CRITERIA FOR DIAGNOSIS OF SCHIZOPHRENIA:
Two (or more) of the following, each present for a significant portion of time during a 1-month period (or less if
successfully treated):
• Delusions
• Hallucinations
• Disorganized speech (e.g., frequent derailment or incoherence)
• Grossly disorganized or catatonic behavior
• Negative symptoms, i.e., affective flattening, alogia, or avolition
Only one Criterion symptom is required if delusions are bizarre or hallucinations consist of a voice keeping up a
running commentary on the person's behavior or thoughts, or two or more voices conversing with each other.
• All patients with schizophrenia have psychotic symptoms (reality distortion or disorganization) at some
point in the course of their illness, but there is no single pattern of psychotic symptoms.
• Continuous signs of the disturbance persist for at least 6 months.
• This 6-month period must include at least 1 month of symptoms.
Types
• Commonest type – Paranoid
• Amphetamine induced - Paranoid
• Early onset & bad prognosis – Hebephrenic
• Late onset & best prognosis – Catatonic
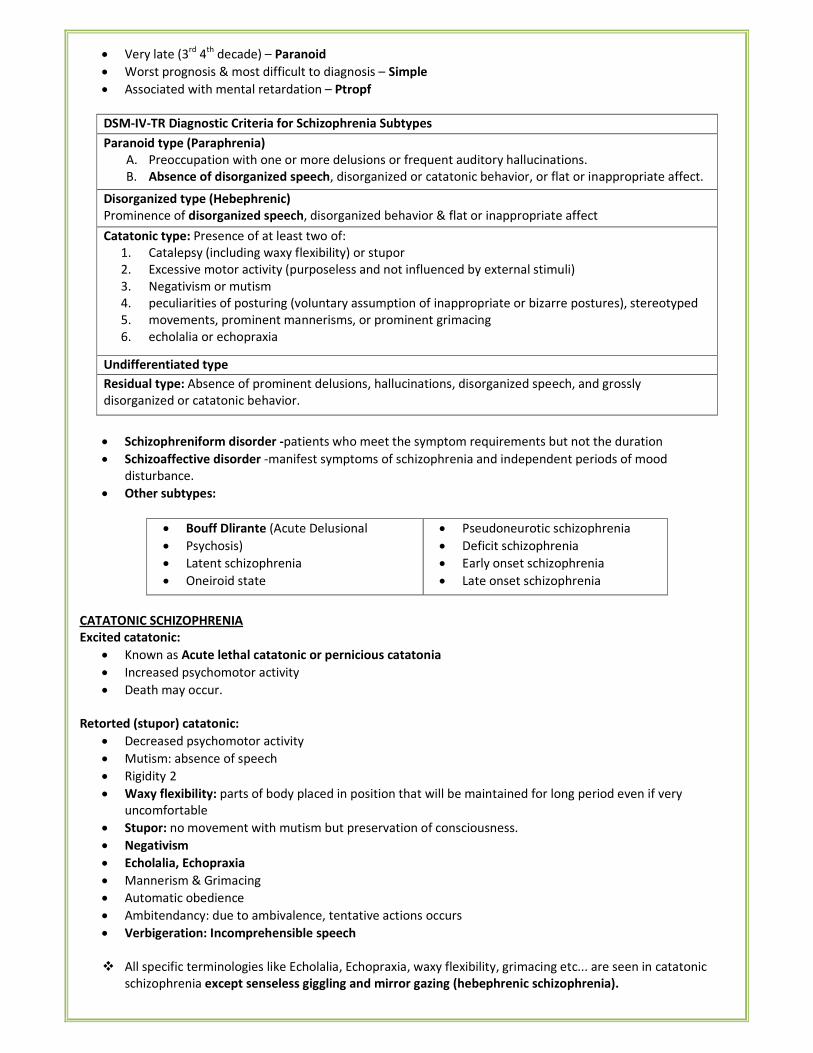
• Very late (3rd
4th
decade) – Paranoid
• Worst prognosis & most difficult to diagnosis – Simple
• Associated with mental retardation – Ptropf
DSM-IV-TR Diagnostic Criteria for Schizophrenia Subtypes
Paranoid type (Paraphrenia)
A. Preoccupation with one or more delusions or frequent auditory hallucinations.
B. Absence of disorganized speech, disorganized or catatonic behavior, or flat or inappropriate affect.
Disorganized type (Hebephrenic)
Prominence of disorganized speech, disorganized behavior & flat or inappropriate affect
Catatonic type: Presence of at least two of:
1. Catalepsy (including waxy flexibility) or stupor
2. Excessive motor activity (purposeless and not influenced by external stimuli)
3. Negativism or mutism
4. peculiarities of posturing (voluntary assumption of inappropriate or bizarre postures), stereotyped
5. movements, prominent mannerisms, or prominent grimacing
6. echolalia or echopraxia
Undifferentiated type
Residual type: Absence of prominent delusions, hallucinations, disorganized speech, and grossly
disorganized or catatonic behavior.
• Schizophreniform disorder -patients who meet the symptom requirements but not the duration
• Schizoaffective disorder -manifest symptoms of schizophrenia and independent periods of mood
disturbance.
• Other subtypes:
• Bouff Dlirante (Acute Delusional
• Psychosis)
• Latent schizophrenia
• Oneiroid state
• Pseudoneurotic schizophrenia
• Deficit schizophrenia
• Early onset schizophrenia
• Late onset schizophrenia
CATATONIC SCHIZOPHRENIA
Excited catatonic:
• Known as Acute lethal catatonic or pernicious catatonia
• Increased psychomotor activity
• Death may occur.
Retorted (stupor) catatonic:
• Decreased psychomotor activity
• Mutism: absence of speech
• Rigidity 2
• Waxy flexibility: parts of body placed in position that will be maintained for long period even if very
uncomfortable
• Stupor: no movement with mutism but preservation of consciousness.
• Negativism
• Echolalia, Echopraxia
• Mannerism & Grimacing
• Automatic obedience
• Ambitendancy: due to ambivalence, tentative actions occurs
• Verbigeration: Incomprehensible speech
� All specific terminologies like Echolalia, Echopraxia, waxy flexibility, grimacing etc... are seen in catatonic
schizophrenia except senseless giggling and mirror gazing (hebephrenic schizophrenia).
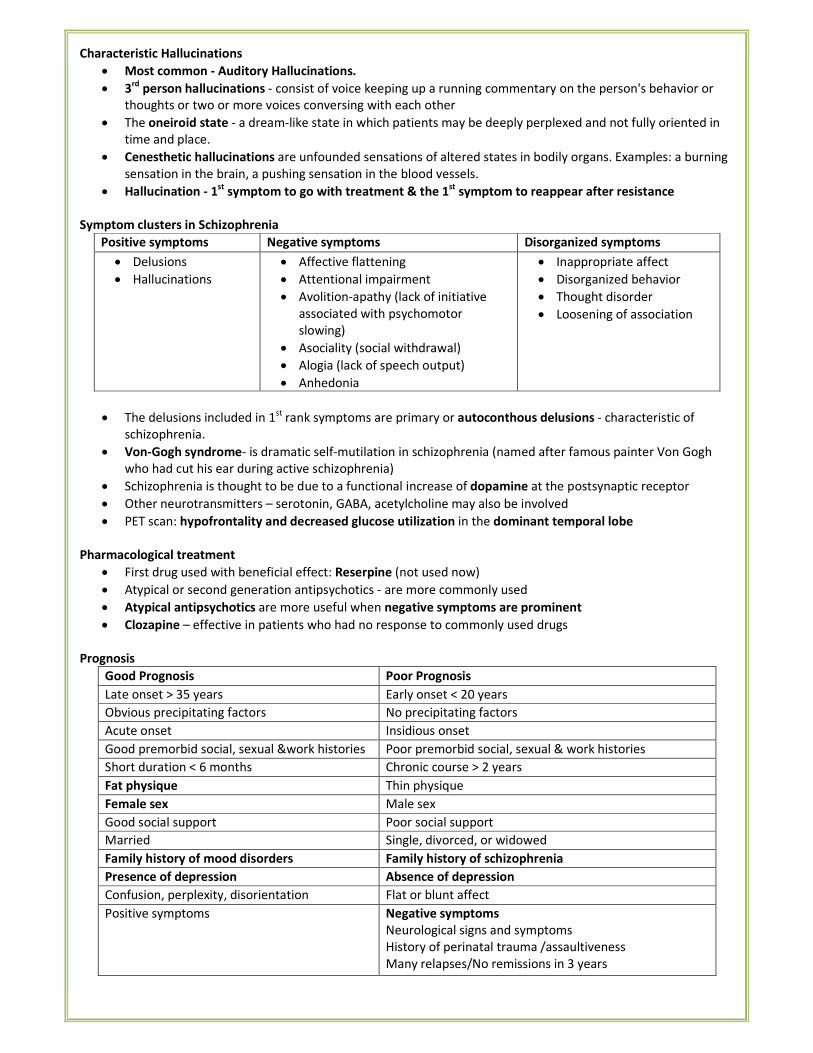
Characteristic Hallucinations
• Most common - Auditory Hallucinations.
• 3rd
person hallucinations - consist of voice keeping up a running commentary on the person's behavior or
thoughts or two or more voices conversing with each other
• The oneiroid state - a dream-like state in which patients may be deeply perplexed and not fully oriented in
time and place.
• Cenesthetic hallucinations are unfounded sensations of altered states in bodily organs. Examples: a burning
sensation in the brain, a pushing sensation in the blood vessels.
• Hallucination - 1st
symptom to go with treatment & the 1st
symptom to reappear after resistance
Symptom clusters in Schizophrenia
Positive symptoms Negative symptoms Disorganized symptoms
• Delusions
• Hallucinations
• Affective flattening
• Attentional impairment
• Avolition-apathy (lack of initiative
associated with psychomotor
slowing)
• Asociality (social withdrawal)
• Alogia (lack of speech output)
• Anhedonia
• Inappropriate affect
• Disorganized behavior
• Thought disorder
• Loosening of association
• The delusions included in 1st rank symptoms are primary or autoconthous delusions - characteristic of
schizophrenia.
• Von-Gogh syndrome- is dramatic self-mutilation in schizophrenia (named after famous painter Von Gogh
who had cut his ear during active schizophrenia)
• Schizophrenia is thought to be due to a functional increase of dopamine at the postsynaptic receptor
• Other neurotransmitters – serotonin, GABA, acetylcholine may also be involved
• PET scan: hypofrontality and decreased glucose utilization in the dominant temporal lobe
Pharmacological treatment
• First drug used with beneficial effect: Reserpine (not used now)
• Atypical or second generation antipsychotics - are more commonly used
• Atypical antipsychotics are more useful when negative symptoms are prominent
• Clozapine – effective in patients who had no response to commonly used drugs
Prognosis
Good Prognosis Poor Prognosis
Late onset > 35 years Early onset < 20 years
Obvious precipitating factors No precipitating factors
Acute onset Insidious onset
Good premorbid social, sexual &work histories Poor premorbid social, sexual & work histories
Short duration < 6 months Chronic course > 2 years
Fat physique Thin physique
Female sex Male sex
Good social support Poor social support
Married Single, divorced, or widowed
Family history of mood disorders Family history of schizophrenia
Presence of depression Absence of depression
Confusion, perplexity, disorientation Flat or blunt affect
Positive symptoms Negative symptoms
Neurological signs and symptoms
History of perinatal trauma /assaultiveness
Many relapses/No remissions in 3 years
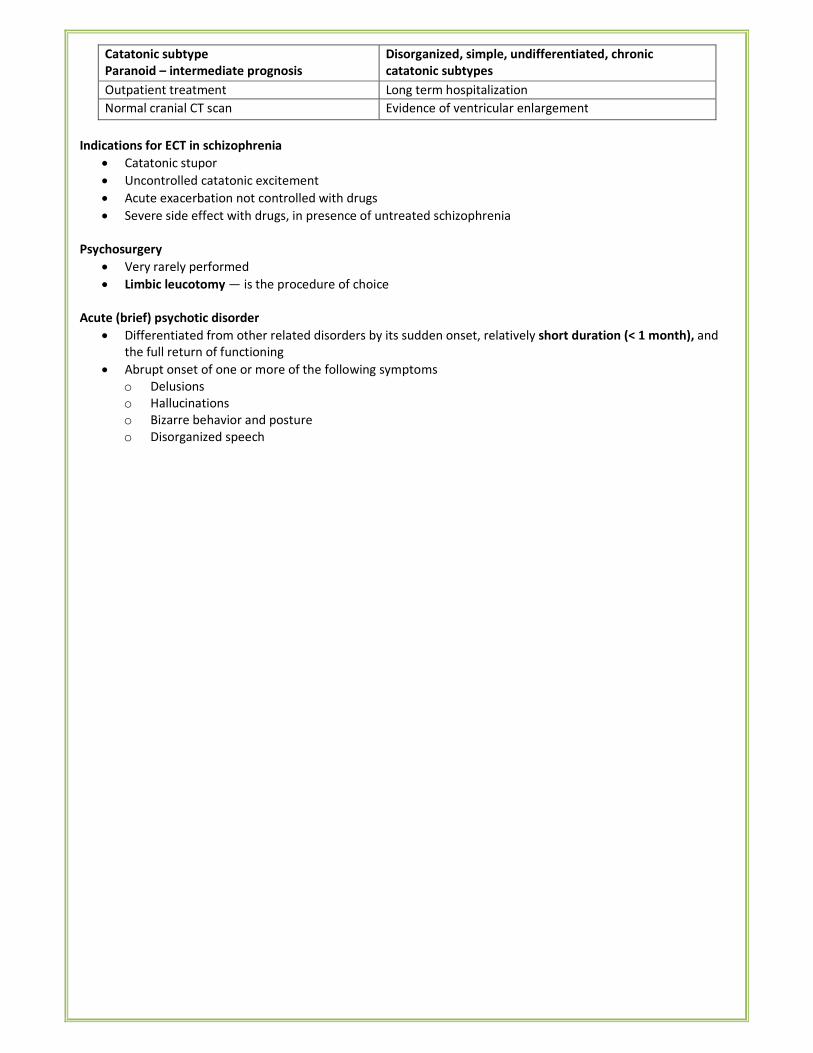
Catatonic subtype
Paranoid – intermediate prognosis
Disorganized, simple, undifferentiated, chronic
catatonic subtypes
Outpatient treatment Long term hospitalization
Normal cranial CT scan Evidence of ventricular enlargement
Indications for ECT in schizophrenia
• Catatonic stupor
• Uncontrolled catatonic excitement
• Acute exacerbation not controlled with drugs
• Severe side effect with drugs, in presence of untreated schizophrenia
Psychosurgery
• Very rarely performed
• Limbic leucotomy — is the procedure of choice
Acute (brief) psychotic disorder
• Differentiated from other related disorders by its sudden onset, relatively short duration (< 1 month), and
the full return of functioning
• Abrupt onset of one or more of the following symptoms
o Delusions
o Hallucinations
o Bizarre behavior and posture
o Disorganized speech
VI. ANXIETY & STRESS RELATED DISORDERS
TYPES OF ANXIETY DISORDERS (DSM-IV-TR)
• Panic disorder with or without agoraphobia
• Agoraphobia with or without panic disorder
• Specific phobia
• Social phobia
• Obsessive-compulsive disorder (OCD)
• Posttraumatic stress disorder (PTSD)
• Acute stress disorder
• Generalized anxiety disorder
Anxiety
• It is the most common psychiatric symptom
• Physical symptoms
o Motor: tremors, muscle twitching
o Autonomic and visceral: sweating, palpitation, tachycardia, flushes, hyperventilation, dry mouth,
dizziness, diarrhea, mydriasis
• Psychological symptoms
o Cognitive: poor concentration, hyperarousal, vigilance or scanning, negative automatic thoughts
o Perceptual: derealisation, depersonalization
o Affective: fearfulness, irritability, inability to relax, fear of impending
o Others: insomnia, increased sensitivity to noise, exaggerated startle response
DIFFERENTIAL DIAGNOSIS OF ANXIETY:
Medical Illnesses Substance Use/Abuse Psychiatric Disorders
Cardiac Endocrinologic Prescription or over-the-
counter drug use
• Adjustment
disorders
• Affective disorder
• Dissociative
disorders
• Personality
disorders
• Somatoform
disorders
• Schizophrenia
(and other
psychotic
disorders)
• Angina
• Arrhythmias
• Congestive failure
• Infarction
• Mitral valve
prolapse
• Paroxysmal atrial
tachycardia
• Hyperthyroidism
• Cushing's disease
• Hyperparathyroidism
• Hypoglycemia
• Premenstrual
• syndrome
• Antidepressants
• Fenfluramine/phentermine
• Psychostimulants (eg,
methylphenidate,
amphetamine)
• Steroids
• Sympathomimetics
Neoplastic Neurologic Substance abuse
• Carcinoid
• Insulinoma
• Pheocromocytoma
• Huntington's disease
• Meniere's disease
• Migraine
• Multiple sclerosis
• Seizure disorder
• Transient ischemic
attack
• Vertigo
• Wilson's disease
• Alcohol/sedative
withdrawal
• Caffeine
• Hallucinogen
• Stimulant abuse (eg,
cocaine)
Pulmonary Other
• Asthma
• Embolism
• Obstruction
• Obstructive
• pulmonary
disease
• Porphyria
• Uremia
PANIC DISORDER
Panic attacks
• Occur in panic disorder, specific phobia, social phobia and PTSD
• Unexpected panic attacks occur at any time and are not associated with identifiable situational stimulus
• A discrete period of intense fear or discomfort in which four (or more) of the following symptoms develop
abruptly and reached a peak within 10 minutes.
o Palpitations, pounding heart, or accelerated heart rate
o Sweating
o Trembling or shaking
o Sensations of shortness of breath or smothering
o Feeling of choking
o Chest pain or discomfort
o Nausea or abdominal distress-
o Feeling dizzy, unsteady, lightheaded, or faint
o Derealization or depersonalization
o Fear of losing control or going crazy
o Fear of dying
o Paresthesias (numbness or tingling)
o Chills or hot flashes
Panic disorder
• Recurrent panic attacks
• Extreme fear and sense of impending death and doom
• Patients usually cannot name the source of their fear
• Generally lasts 20-30 minutes
• Depression and depersonalization may be seen
• Mental status examination: rumination, difficulty speaking, impaired memory
• Between attacks they have anticipatory anxiety about another attack
PHOBIA
• Insight is present.
• Agoraphobia
o Fear of open places, crowded places or any place from where there is no escape to safe place
o Most common & most disabling type
o More common in women
o Only one or two persons are relied upon - phobia companions.
• Social phobia – irrational fear of activities or social interaction
o Shy-Bladder: fear of urinating in public lavatory
o Erythro phobia: Fear of blushing.
• Simple (specific) phobia – irrational fear of objects or situations
o Claustro phobia- Fear of closed spaces
o Acrophobia – fear of high places.
o Algophobia – fear of pain
o Arachnophobia- fear of spiders
o Xeno phobia –fear of strangers
o Zoophobia – fear of animals
o Sito phobia - fear of eating
o Thanatophobia – fear of death
o Cynophobia: fear of dogs
o Mysophobia: fear of dirt & germs
o Pyrophobia: fear of fire
o Ailurophobia: fear of cats
Behavior therapy for phobia
• Flooding
• Systematic desensitization
• Exposure and response prevention
• Relaxation techniques
OBSESSIVE COMPULSIVE DISORDER
• Prevalence in the world 2-3%
Obsessions Compulsions
• An idea, impulse or image which intrudes into
the conscious awareness repeatedly
• It is recognized as one's own idea, but perceived
as ego-alien (foreign to one's personality)
• It is recognized as irrational and absurd (insight
present)
• Patient tries to resist but is unable to
• Failure to resist leads to marked distress
• A form of behaviour which usually follows
obsessions
• It is aimed at preventing or neutralizing the distress
or fear arising out of obsession
• The behaviour is not realistic and is either irrational
or excessive
• Insight is present
• The behaviour is performed with a sense of
subjective compulsion (urge or impulse to act)
Delusion is differentiated from obsession by
• The thought is not recognized as ego-alien
• The thought is not recognized as irrational
• The thought is never resisted
Clinical Manifestations
• Washers
o Most common type
o Obsession is of contamination with dirt, germs
o Compulsion — washing hands or body repeatedly, many times a day
o Spreads on to washing clothes, bathroom, bedroom, personal articles etc
• In all cases obsessive-compulsive activities take up >1 hour per day
• Depression is very commonly associated with OCD
• The disorder usually has a waxing and waning course
Psychodynamic theory of Freud
• Explains OCD by a defensive regression to anal-sadistic phase of development
• New defences are needed as reaction formation is not enough
• Isolation of affect � Obsessive thoughts
• Undoing � Compulsive acts
• Displacement � Phobias
Treatment of choice:
• First: Behavior therapy - Exposure & response prevention
• Second: Systematic desensitization
Medical treatment:
• Fluoxetine (Drug of choice) & other SSRI
• Fluvoxamine: Specific anti-obsession actions.
• Clomipramine (this TCA is most selective for serotonin reuptake) (Drug of IInd
choice)
POST —TRAUMATIC STRESS DISORDER (PTSD)
• Arises as a delayed/protracted response to an exceptionally stressful or catastrophic life event or situation
(e.g. war, rape, torture, serious accident)
• Recurrent and intrusive recollections of the stressful event either in flashbacks (image, thoughts or
perceptions) and/or in dreams
• Avoidance of the events or situations that arouse recollections of the stressful event
• Numbing of general responsiveness
• Amnesia for some aspects of the event
• Anhedonia (inability to experience pleasure)
• Hyperarousal
DSM-IV-TR definitions
• Acute stress disorder: symptoms appear within 4 weeks of the event and remits within 2 days to 4 weeks
• PTSD: occurs after 4 weeks of a stressful event and duration of symptoms > 1 month
• Delayed onset PTSD: occurs after 6 months
• Acute PTSD - duration of symptoms < 3 months; chronic PTSD: duration - > 3 months
Treatment
• SSRIs
• MAO inhibitors
• Benzodiazepines
• Behavior therapy, cognitive therapy
VII. MOOD DISORDERS
MOOD DISORDERS
• Manic episode
• Depressive episode
• Bipolar mood disorder
• Recurrent depressive disorder
• Persistent mood disorder
MANIC EPISODE Symptoms should last for atleast 1 week for diagnosis
• Elevated, Expansive or Irritable mood:
o Euphoria: mild elevation of mood, seen in hypomania [STAGE-1]
o Elation: moderate elevation of mood, seen in mania (STAGE-2]
o Exaltation: severe elevation of mood, seen in severe mania [STAGE-3]
o Ecstasy: very severe elevation of mood, seen in delirious/ stuporous mania [STAGE-4]
• Psychomotor activity
o Increased
o Rarely - manic stupor
• Speech and though
o Flight of ideas
o Prolixity
o Mood congruent psychotic features
o hallucinations
• Goal directed activity
• Reduced sleep
Treatment:
• Atypical antipsychotics (Risperidone, olanzapine, quetiapine, haloperidol)
• Mood stabilizers (Sodium valproate, Carbamazepine, Benzodiazepines, Lithium, Lamotrigine)
DEPRESSION Diagnostic Criteria
A. At least 2 weeks of duration
B. > 5 features should be present most of the day
• Depressant mood
• Loss of interest/pleasure (Absence of pleasure in normally pleasurable environment: Anhedonia) (Among
these two, one is essential for the diagnosis), plus
• Decrease or increase in appetite or significant weight loss/ gain
• Decrease / increase psychomotor activity (psychomotor retardation or agitation)
• Decrease / increase sleep (Insomnia/ hypersomnia)
• Fatigue
• Feeling of worthlessness or guilt
• Decreased concentration
• Recurrent thoughts of death.
Depressive ideation/Cognition:
• Sadness of mood (depression) is usually associated with pessimism, which can result in
o Hopelessness
o Helplessness
o Worthlessness
• Difficulty in thinking, concentration, indecisiveness
• Nihilistic delusions (e.g: world is coming to an end)
Somatic syndrome (Melancholia) in depression
• Significant decrease in appetite or weight
• Early morning awakening (atleast 2 hours early than the usual time)
• Diurnal variation (depression worst in the morning)
• Pervasive loss of interest and loss of reactivity to pleasurable stimuli
• Psychomotor agitation or retardation
Other features
• Pseudo-dementia
• Otto veraguth fold
• Depression is seen in - Myxedema, AIDS, Cancer, post MI, surgery & post-partum
• Depression is most common in middle age females
Theories
• Cognitive theory: Postulated by Aaron Beck consists of the following triad
o About self - Negative self-precept
o About the environment - Tendency to experience the world as hostile and demanding
o About the future — the expectation of suffering and failure
• Learned helplessness theory
Sleep studies
• Decreased REM latency (the time between falling asleep and the first REM period is decreased)
• Increased duration of the first REM period
• Delayed sleep onset
SUICIDE
• Suicide is intentional self-destruction.
• The term parasuicide refers to suicidal attempts or gestures.
• Patients suffering from severe depression with suicidal intent or attempt have a marked decrease in the
serotonergic function
• Official suicide rate in India in 2008 — 10.8 per 100000 population per year
• Most common mode of committing suicide — ingestion of poison (35%) hanging (32%)
• The psychiatric disorder with greatest risk of suicide in both sexes — Mood disorder
• Widely accepted theory for suicide:
o Sociological factors: Durkheim's Theory:
� Egoistic suicide applies to those who are not strongly integrated into any social group
� Altruistic suicide applies to those susceptible to suicide stemming from their excessive integration
into a group, with suicide being the outgrowth of the integration., for example, a soldier who
sacrifices his life in battle.
� Anomic suicide applies to persons whose integration into society is disturbed so that they cannot
follow customary norms of behavior.
o Psychological Factors: Freud's Theory/ Menninger's Theory
Evaluation of Suicide Risk
Variable High Risk Low Risk
Demographic and Social Profile
Age Over 45 years Below 45 years
Sex Male Female
Marital status Divorced or widowed Married
Employment Unemployed Employed
Interpersonal relationship Conflictual Stable
Family background Chaotic or conflictual Stable
Health
Physical Chronic illness Good health
Hypochondriac Feels healthy
Excessive substance intake Low substance use
Mental Severe depression Mild depression
Psychosis Neurosis
Severe personality disorder Normal personality
Substance abuse Social drinker
Hopelessness Optimism
Suicidal activity
Suicidal ideation Frequent, intense, prolonged Infrequent, low intensity, transient
Suicide attempt Multiple attempts First attempt
Planned Impulsive
Rescue unlikely Rescue inevitable
Unambiguous wish to die Primary wish for change
Communication internalized (self-
blame)
Communication externalized (anger)
Method lethal and available Method of low lethality or not readily
available Resources
Personal Poor achievement Good achievement
Poor insight Insightful
Affect unavailable/ poorly
controlled
Affect available and appropriately controlled
Social Poor rapport Good rapport
Socially isolated Socially integrated
Unresponsive family Concerned family
Risk Factors
• Age> 40 years
• Male sex
• Staying single
• Previous suicidal attempts
• Suicidal pre occupation (e.g. a written suicidal note)
• Depression
• Alcohol/ drug dependence
• Severe/ painful physical illness
• Recent serious loss or major stressful event
• Social isolation
• High degree of impulsivity
Risk factors for suicide in depression
• Early stages of depression
• Recovering from depression
• With mood disorder, personality disorder, psychosis, hypochondriac
• Child with conduct disorder or substance abuse
• 45 years male, unemployed, single, separated, divorced, widowed, recently bereaved, chronically ill
• Positive family history
Treatment
• Tricyclic anti-depressants: imipramine, amitriptyline
• SSRIs: fluoxetine, sertraline, citaprolam
• SNRIs: venlafaxine, duloxetine
Neurotransmitters
• Mania: increased norepinephrine at the synaptic cleft
• Depression: decreased norepinephrine and/or 5-HT
BIPOLAR MOOD DISORDER
• Previous called as Manic depressive psychosis (MDP)
• Unpredictable swings in mood from mania to depression at different times
• In the intervening period, patient may be normal
o Bipolar-1: episodes of severe mania and depression.
o Bipolar-2: episodes of hypomania and severe depression
• Rapid cyclers: > 4 episodes per year; mostly women
• Ultra-rapid cycling: episodes of mania and depression alternate very rapidly (in hours or days)
Good prognostic factors Poor prognostic factors
• Acute or abrupt onset
• Typical clinical features
• Severe depression
• Well-adjusted premorbid
personality
• Good response to treatment
• Comorbid medical disorder, personality disorder or
alcohol dependence
• Double depression (acute depressive episode
superimposed on chronic depression or dysthymia)
• Catastrophic stress or chronic ongoing stress
• Unfavorable early environment
• Marked Hypochondriacal features
• Mood incongruent psychotic features
• Poor drug compliance
Other forms of depression
� Atypical depression – a term that has been applied to a variety of presentations, but particularly to patients
who present with mild to moderate depression, some mood reactivity, reverse diurnal variation in mood (i.e.
worse in the evening), overeating, hypersomnia and fatigue.
� Dysthymia – depressive symptoms which are insufficient to meet the criteria for a clinical depression. The
patient's symptoms are present for 2 or more years. Can be associated with other psychiatric conditions
such as borderline personality disorder. Sufferers often go on to develop more serious mood disorder.
� Cyclothymic disorder – chronic mood fluctuations over at least 2 years with episodes of elation and of
depression insufficient to meet the criteria for a hypomanic depressive episode.
� Masked depression – a state in which depressed mood is not particularly prominent, but other features of
depressive disorder are present, e.g. sleep disturbance, diurnal mood variation, depressive cognitions.
� Mild depressive disorders – milder forms of the symptoms of depression, with less disruption to social
functioning. These are likely to be accompanied by prominent anxiety, phobic or obsessional symptoms.
� Recurrent brief depressive disorder – lasts for <2 weeks, usually around 2-3 days. Occurs around once per
month, with complete recovery between episodes. The actual symptoms collectively may fulfil the criteria
for mild, moderate or severe depression, but the difference is in the duration of the episode.
� SAD – a temporal relationship between the season of the year and the onset of depression. The depression
starts in autumn/winter and resolves in spring/ summer. There may be symptoms of depression and
additional atypical biological features such as carbohydrate craving, fatigue and hypersomnia.
Note:
� Dysthymia – if the symptoms consist of persistent mild depression
� Cyclothymia –frequent mood swings of mild depression and mild elation.
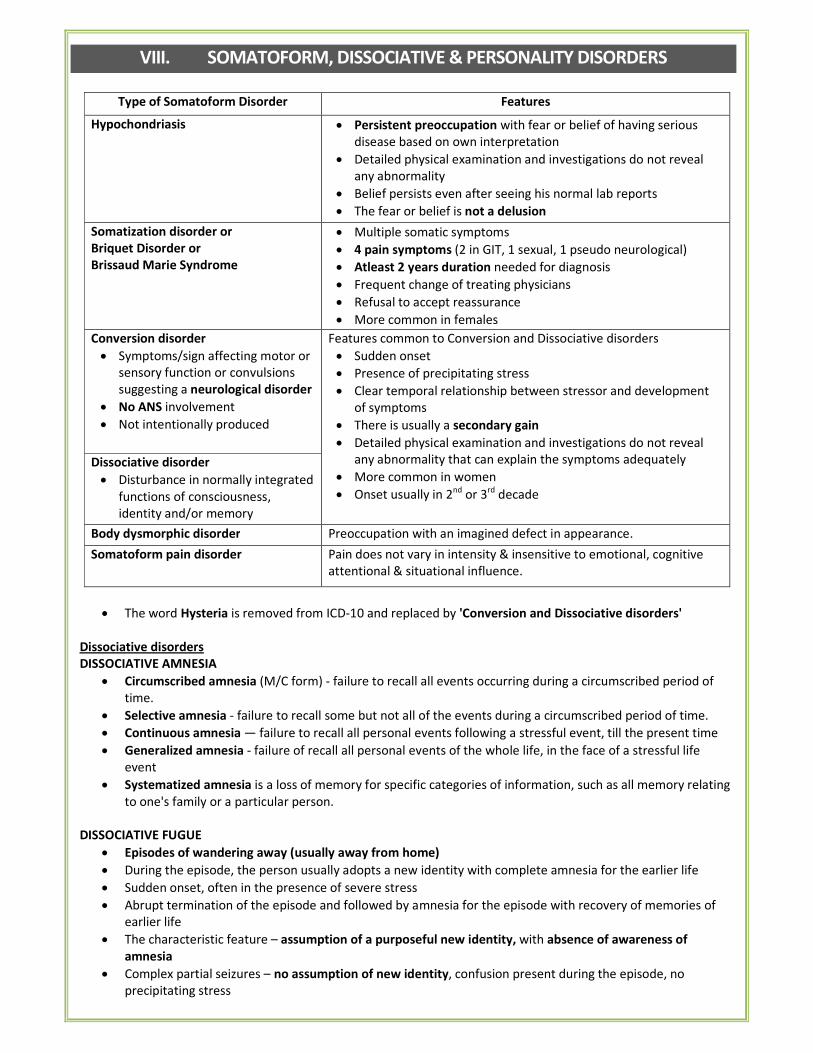
VIII. SOMATOFORM, DISSOCIATIVE & PERSONALITY DISORDERS
Type of Somatoform Disorder Features
Hypochondriasis • Persistent preoccupation with fear or belief of having serious
disease based on own interpretation
• Detailed physical examination and investigations do not reveal
any abnormality
• Belief persists even after seeing his normal lab reports
• The fear or belief is not a delusion
Somatization disorder or
Briquet Disorder or
Brissaud Marie Syndrome
• Multiple somatic symptoms
• 4 pain symptoms (2 in GIT, 1 sexual, 1 pseudo neurological)
• Atleast 2 years duration needed for diagnosis
• Frequent change of treating physicians
• Refusal to accept reassurance
• More common in females
Conversion disorder
• Symptoms/sign affecting motor or
sensory function or convulsions
suggesting a neurological disorder
• No ANS involvement
• Not intentionally produced
Features common to Conversion and Dissociative disorders
• Sudden onset
• Presence of precipitating stress
• Clear temporal relationship between stressor and development
of symptoms
• There is usually a secondary gain
• Detailed physical examination and investigations do not reveal
any abnormality that can explain the symptoms adequately
• More common in women
• Onset usually in 2nd or 3rd decade
Dissociative disorder
• Disturbance in normally integrated
functions of consciousness,
identity and/or memory
Body dysmorphic disorder Preoccupation with an imagined defect in appearance.
Somatoform pain disorder Pain does not vary in intensity & insensitive to emotional, cognitive
attentional & situational influence.
• The word Hysteria is removed from ICD-10 and replaced by 'Conversion and Dissociative disorders'
Dissociative disorders
DISSOCIATIVE AMNESIA
• Circumscribed amnesia (M/C form) - failure to recall all events occurring during a circumscribed period of
time.
• Selective amnesia - failure to recall some but not all of the events during a circumscribed period of time.
• Continuous amnesia — failure to recall all personal events following a stressful event, till the present time
• Generalized amnesia - failure of recall all personal events of the whole life, in the face of a stressful life
event
• Systematized amnesia is a loss of memory for specific categories of information, such as all memory relating
to one's family or a particular person.
DISSOCIATIVE FUGUE
• Episodes of wandering away (usually away from home)
• During the episode, the person usually adopts a new identity with complete amnesia for the earlier life
• Sudden onset, often in the presence of severe stress
• Abrupt termination of the episode and followed by amnesia for the episode with recovery of memories of
earlier life
• The characteristic feature – assumption of a purposeful new identity, with absence of awareness of
amnesia
• Complex partial seizures – no assumption of new identity, confusion present during the episode, no
precipitating stress
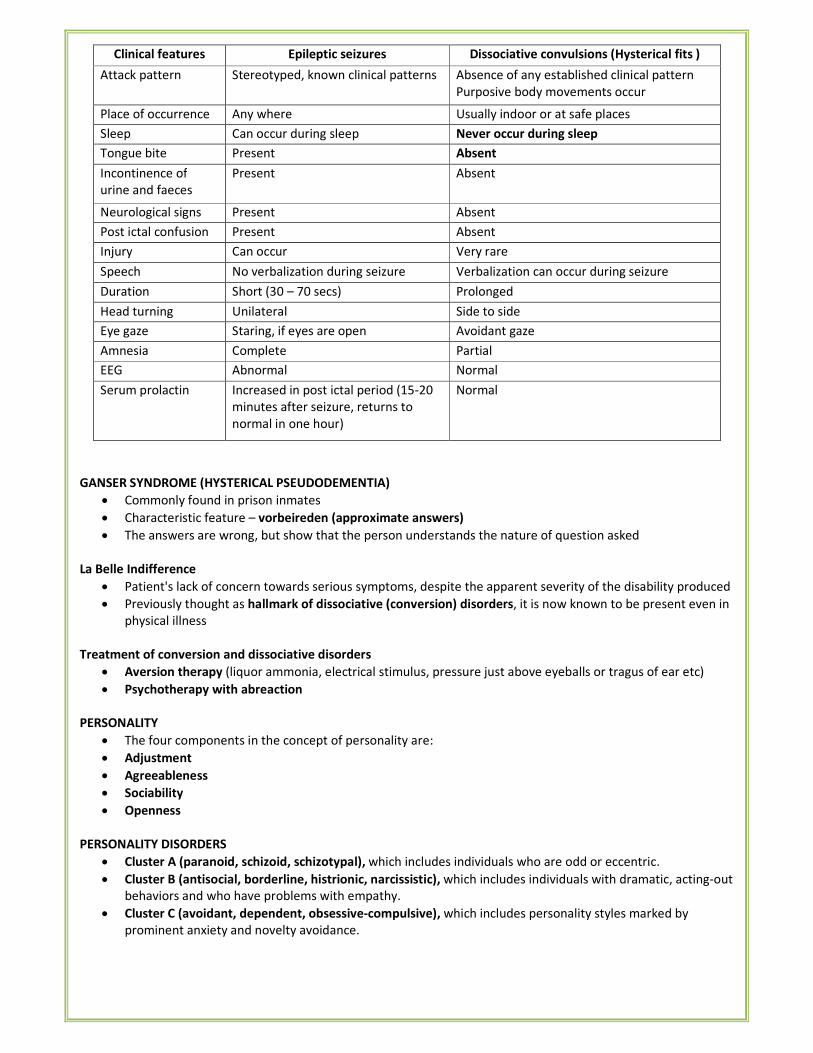
Clinical features Epileptic seizures Dissociative convulsions (Hysterical fits )
Attack pattern Stereotyped, known clinical patterns Absence of any established clinical pattern
Purposive body movements occur
Place of occurrence Any where Usually indoor or at safe places
Sleep Can occur during sleep Never occur during sleep
Tongue bite Present Absent
Incontinence of
urine and faeces
Present Absent
Neurological signs Present Absent
Post ictal confusion Present Absent
Injury Can occur Very rare
Speech No verbalization during seizure Verbalization can occur during seizure
Duration Short (30 – 70 secs) Prolonged
Head turning Unilateral Side to side
Eye gaze Staring, if eyes are open Avoidant gaze
Amnesia Complete Partial
EEG Abnormal Normal
Serum prolactin Increased in post ictal period (15-20
minutes after seizure, returns to
normal in one hour)
Normal
GANSER SYNDROME (HYSTERICAL PSEUDODEMENTIA)
• Commonly found in prison inmates
• Characteristic feature – vorbeireden (approximate answers)
• The answers are wrong, but show that the person understands the nature of question asked
La Belle Indifference
• Patient's lack of concern towards serious symptoms, despite the apparent severity of the disability produced
• Previously thought as hallmark of dissociative (conversion) disorders, it is now known to be present even in
physical illness
Treatment of conversion and dissociative disorders
• Aversion therapy (liquor ammonia, electrical stimulus, pressure just above eyeballs or tragus of ear etc)
• Psychotherapy with abreaction
PERSONALITY
• The four components in the concept of personality are:
• Adjustment
• Agreeableness
• Sociability
• Openness
PERSONALITY DISORDERS
• Cluster A (paranoid, schizoid, schizotypal), which includes individuals who are odd or eccentric.
• Cluster B (antisocial, borderline, histrionic, narcissistic), which includes individuals with dramatic, acting-out
behaviors and who have problems with empathy.
• Cluster C (avoidant, dependent, obsessive-compulsive), which includes personality styles marked by
prominent anxiety and novelty avoidance.
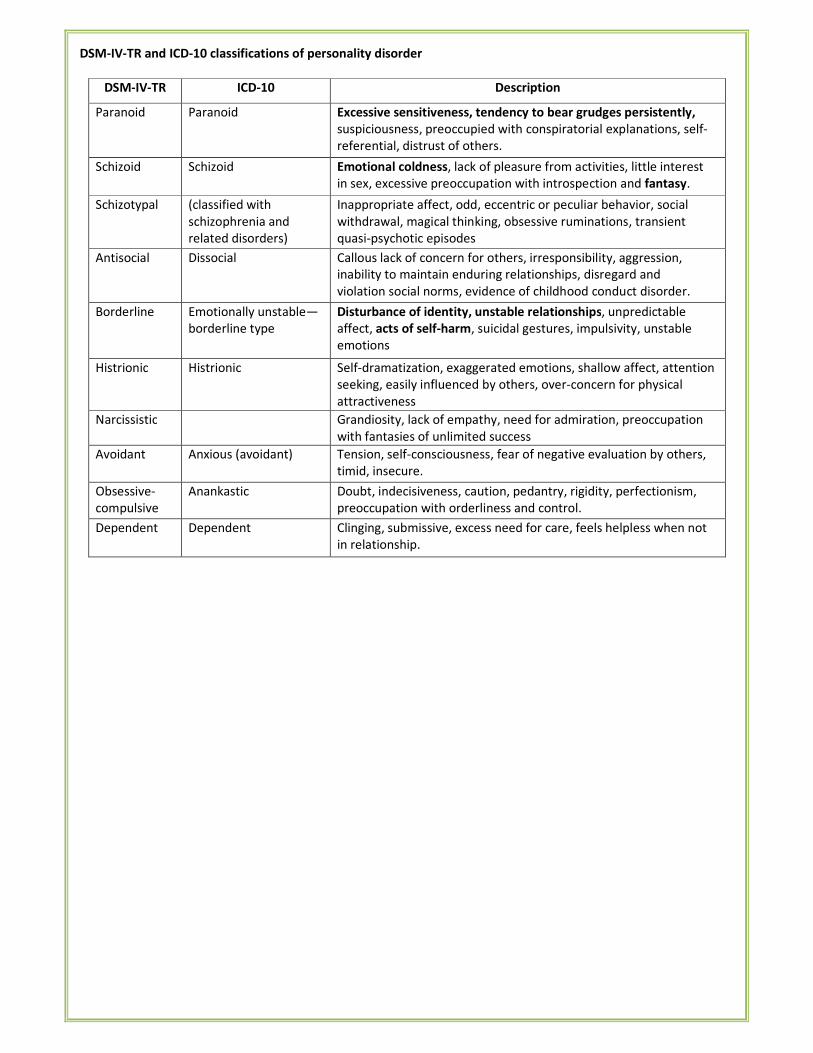
DSM-IV-TR and ICD-10 classifications of personality disorder
DSM-IV-TR ICD-10 Description
Paranoid Paranoid Excessive sensitiveness, tendency to bear grudges persistently,
suspiciousness, preoccupied with conspiratorial explanations, self-
referential, distrust of others.
Schizoid Schizoid Emotional coldness, lack of pleasure from activities, little interest
in sex, excessive preoccupation with introspection and fantasy.
Schizotypal (classified with
schizophrenia and
related disorders)
Inappropriate affect, odd, eccentric or peculiar behavior, social
withdrawal, magical thinking, obsessive ruminations, transient
quasi-psychotic episodes
Antisocial Dissocial Callous lack of concern for others, irresponsibility, aggression,
inability to maintain enduring relationships, disregard and
violation social norms, evidence of childhood conduct disorder.
Borderline Emotionally unstable—
borderline type
Disturbance of identity, unstable relationships, unpredictable
affect, acts of self-harm, suicidal gestures, impulsivity, unstable
emotions
Histrionic Histrionic Self-dramatization, exaggerated emotions, shallow affect, attention
seeking, easily influenced by others, over-concern for physical
attractiveness
Narcissistic Grandiosity, lack of empathy, need for admiration, preoccupation
with fantasies of unlimited success
Avoidant Anxious (avoidant) Tension, self-consciousness, fear of negative evaluation by others,
timid, insecure.
Obsessive-
compulsive
Anankastic Doubt, indecisiveness, caution, pedantry, rigidity, perfectionism,
preoccupation with orderliness and control.
Dependent Dependent Clinging, submissive, excess need for care, feels helpless when not
in relationship.
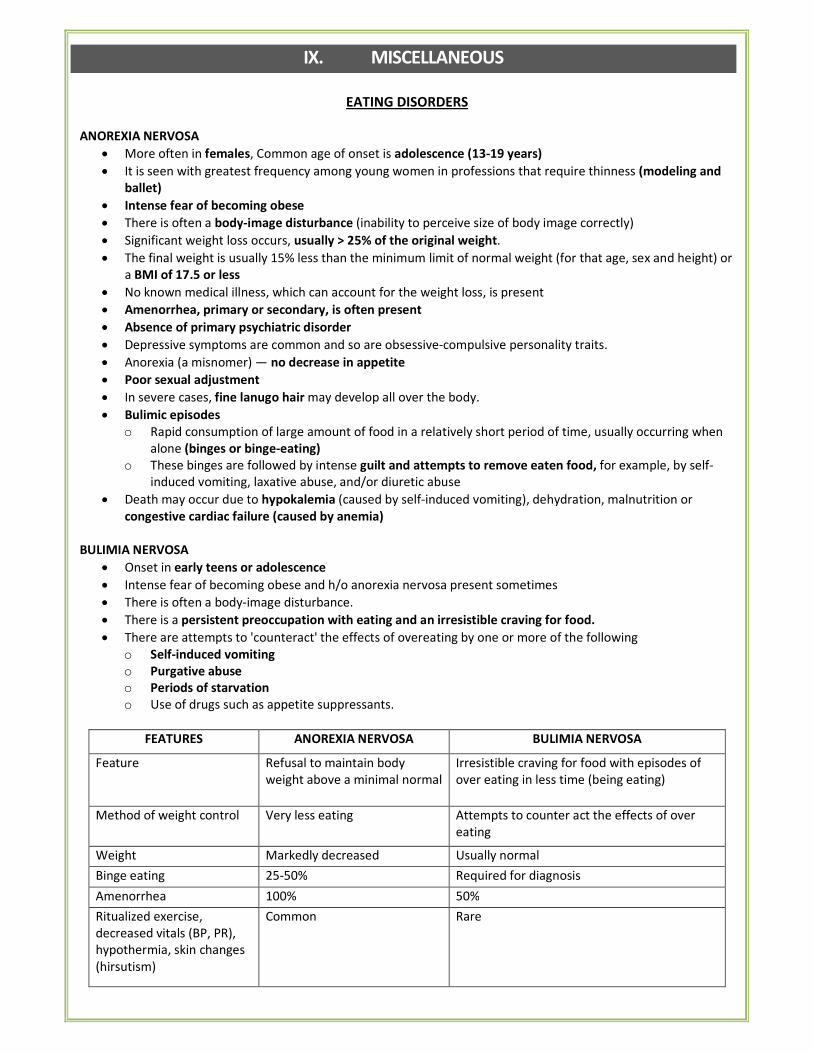
IX. MISCELLANEOUS
EATING DISORDERS
ANOREXIA NERVOSA
• More often in females, Common age of onset is adolescence (13-19 years)
• It is seen with greatest frequency among young women in professions that require thinness (modeling and
ballet)
• Intense fear of becoming obese
• There is often a body-image disturbance (inability to perceive size of body image correctly)
• Significant weight loss occurs, usually > 25% of the original weight.
• The final weight is usually 15% less than the minimum limit of normal weight (for that age, sex and height) or
a BMI of 17.5 or less
• No known medical illness, which can account for the weight loss, is present
• Amenorrhea, primary or secondary, is often present
• Absence of primary psychiatric disorder
• Depressive symptoms are common and so are obsessive-compulsive personality traits.
• Anorexia (a misnomer) — no decrease in appetite
• Poor sexual adjustment
• In severe cases, fine lanugo hair may develop all over the body.
• Bulimic episodes
o Rapid consumption of large amount of food in a relatively short period of time, usually occurring when
alone (binges or binge-eating)
o These binges are followed by intense guilt and attempts to remove eaten food, for example, by self-
induced vomiting, laxative abuse, and/or diuretic abuse
• Death may occur due to hypokalemia (caused by self-induced vomiting), dehydration, malnutrition or
congestive cardiac failure (caused by anemia)
BULIMIA NERVOSA
• Onset in early teens or adolescence
• Intense fear of becoming obese and h/o anorexia nervosa present sometimes
• There is often a body-image disturbance.
• There is a persistent preoccupation with eating and an irresistible craving for food.
• There are attempts to 'counteract' the effects of overeating by one or more of the following
o Self-induced vomiting
o Purgative abuse
o Periods of starvation
o Use of drugs such as appetite suppressants.
FEATURES ANOREXIA NERVOSA BULIMIA NERVOSA
Feature Refusal to maintain body
weight above a minimal normal
Irresistible craving for food with episodes of
over eating in less time (being eating)
Method of weight control Very less eating Attempts to counter act the effects of over
eating
Weight Markedly decreased Usually normal
Binge eating 25-50% Required for diagnosis
Amenorrhea 100% 50%
Ritualized exercise,
decreased vitals (BP, PR),
hypothermia, skin changes
(hirsutism)
Common Rare
Patient believes that their
body as a whole, or some part
of their body, is too fat.
-Dental caries are frequent
-Antisocial behavior &drug abuse is common
-Prognosis is worse
CULTURE BOUND SYNDROMES
• Dhat syndrome � fear of losing semen
• Amok � sudden, unprovoked episode of rage
• Koro � strong belief that his penis is shrinking
• Wihtigo (windigo) � belief that he has been transformed to a cannibal.
• Pibloktoq � Arctic Hysteria� Eskimos, extreme excitement of as long as 30 minutes' duration and
frequently followed by convulsive seizures and coma lasting as long as 12 hours
• Suchi-bai ���� purity mania
• Hwa-Byung / Wool-Hwa-Byung: Korean folk syndrome [anger syndrome] and is attributed to the
suppression of anger.
• Latah: hypersensitivity to sudden fright, often with echopraxia, echolalia, command obedience, and
dissociative or trance-like behavior.
• Locura: severe form of chronic psychosis [inherited vulnerability, the effect of multiple life difficulties, or a
combination of both factors]
• Mal de ojo: evil eye
• Ideas of nerves/Nervios: general state of vulnerability to stressful life experiences and to a syndrome
brought on by difficult life circumstances.
FACTITIOUS DISORDER (MUNCHAUSEN SYNDROME)
• Also known as hospital addiction, hospital hoboes, professional patients
• Simulate or fake diseases for the sole purpose of obtaining medical attention.
• No other recognized motive.
• Pseudologia fantastica - distort their clinical histories, lab reports and even facts about their lives
• Drug abuse is common
• They have superficial knowledge of medical terms
• Evidence of earlier treatment, usually surgical procedures, is often found in the form of multiple scars (e.g:
grid iron abdomen)
• They often tell lies and leave the hospital against medical advise
SLEEP
Two phases:
1. D-Sleep (desynchronized or dreaming sleep) OR REM-sleep (rapid eye movement sleep), active sleep or
paradoxical sleep.
2. S-Sleep (synchronized sleep), or NREM – sleep (non-REM sleep), quiet sleep, or orthodox sleep. S-sleep or
NREM-sleep is further divided into four stages, 1 to 4.
The EEG recording
• During the awake state shows alpha waves of 8-12 cycles/sec. frequency
• The onset of sleep is characterized by a disappearance of the alpha – activity.
• NREM –sleep
o Stage 1: first and the lightest stage of sleep, absence of alpha-waves, and low voltage, predominantly
theta activity.
o Stage 2: characterized by two typical EEG changes:
� Sleep spindles: Regular spindle shaped waves of 13-15 cycles/sec. frequency, lasting 0.5-2.0
seconds, with a characteristic waxing and waning amplitude.
� K-complexes: High voltage spikes present intermittently.
o Stage 3: appearance of high voltage, 751.1V, 6-waves of 0.5-3.0 cycles/sec.
o Stage 4: predominant δ-activity
The important time periods of the various sleep stages
• In an 8 hour sleep, usually 6-61/2
hours are spent in NREM –sleep & 11/2
– 2 hours in REM-sleep.
• Out of 6-6112 hours NREM-sleep period, only about 70-80 minutes are spent in Stage 4 sleep.
• The maximum Stage 4 sleep occurs in the first one-third of the night
• In the later part, the REM-sleep follows the Stage 3 NREM –sleep directly.
• REM-sleep occurs maximally in the last one-third of the night.
• REM-sleep occurs regularly after every 90-100 mins, with progressive lengthening of each REM period.
• The first REM period typically lasts for less than 10 minutes.
• Usually, there are 4-5 REM periods in the whole night of sleep.
• The usual sleep duration in newborn children is 16-18 hours/day, with nearly 8-10 hours spent in the REM-
sleep.
DISORDERS OF SLEEP
Nightmares
• Almost always occur during REM sleep and usually after a long REM period late in the night.
• The awakening may occur during any part of the sleep period, but typically during the second half.
Sleep terror: Arousal in the first third of the night during deep NREM (stages III and IV) sleep.
Kleine Levin syndrome
• Recurrent periods of prolonged sleep (from which patients may be aroused) with intervening periods of
normal sleep and alert waking
PARASOMNIAS
• Sleep walking and sleep terrors
• Common in preschool (3-6years) children
Characteristic Sleep walking Sleep terrors Night mares Nocturnal seizures
Timing during sleep First third First third Last third Variable, often during
sleep-wake transition
Stage of sleep Slow wave Slow wave REM Non REM > SWS
Arousal threshold High High Low High
Day time sleepiness None None Yes Probable '
Recall of event None None Frequent, vivid None
Incidence Common Rare Very common Rare
Family history Common Common None Variable
GENDER IDENTITY DISORDERS
• Common feature is a strong, persistent preference for living as a person of the other sex.
• Discontent with one's designated birth sex and a desire to have the body of the other sex, and to be
regarded socially as a person of the other sex.
• Gender identity disorder in adults ���� transsexualism.
• Cross-dressing is commonly known as transvestism, and the cross-dresser as a transvestite.
IMPULSE CONTROL DISORDERS
Kleptomania (pathological stealing)
• Failure to resist the impulse to steal useless objects that have little monetary value.
• Usually women
• No apparent motive
• Usually there is a feeling of tension before the act and sense of relief afterwards
• Differential diagnosis: Shoplifting (actions are usually well-planned and motivated by need or monetary
gain)
Pyromania (pathological fire-setting)
• Deliberate and purposeful fire setting on two or more occasions
• No apparent motive
• 90% are male.
� Pathological Gambling : Two or more gambling episodes per year which have not profitable outcome
� Trichotillomania: Recurrent pulling out of one's hair resulting in noticeable hair loss
� Dipsomania – irresistible urge to drink alcohol at regular intervals
� Mutilomania – irresistible urge to mutilate animals
• De Clerambult's syndrome: Erotic delusions
• Alice in Wonderland syndrome: Disturbance of one's view of self.
• Couvade syndrome: experiencing the symptoms of pregnancy in males
• Kanner's syndrome is autism with a normal ICI.
Asperger's syndrome, or schizoid personality of childhood, may be a mild form of autism and comprises eccentric
isolated behavior with circumscribed interests and stilted speech:
X. TREATMENT MODALITIES
ANTIPSYCHOTIC DRUGS
TYPICAL (Neuroleptics, D2 blockers) ATYPICAL
Phenothiazines Thioxanthines Butyrophenones Miscellaneous Clozapine , Olanzapine
Quetiapine,
Risperidone
Ziprasidone,
Iloperidone,
Lurasidone,
Aripiprazole,
Asenapine
Chlorpromazine
Thioridazine
Trifluoperazine
Fluphenazine
Flupenthixol
Thiothixene
Haloperidol
Droperidol
Penfluridol
Pimozide
Loxapine
• Longest acting: Fluphenazine (2-4 weeks), Penfluridol (1 week).
• Longest half- life: Aripiprazole (75 hours)
• Shortest half-life: Quetiapine (6 hours)
• Least potent: Chlorpromazine
• With antidepressant action: Flupenthixol.
• More emetic potential: Clozapine/ Olanzapine/ Risperidone/ Molindone
Actions
Extra pyramidal symptoms Sedation Hypotension Anti emetic
Maximum: Haloperidol
Least: Thioridazine
Almost nil: Clozapine,
Risperidone
Maximum: Chlorpromazine,
Triflupromazine,
Thioridazine, Clozapine &
Quetiapine
Maximum:
Thioridazine,
Clozapine &
Risperidone
Triflupromazine,
Trifluoperazine
Fluphenazine,
Haloperidol
• All anti psychotics are potent antiemetics except Thioridazine & atypical drugs.
• Low potency drugs possess significant α blocking (maximum with chlorpromazine) and anticholinergic
(maximum with thioridazine) properties.
• D2 receptors blockage in hypothalamus & pituitary � increase prolactin release � galactorrhoea &
amenorrhea.
• Aripiprazole: acts as a partial agonist at 5-HT1A and D2 receptors and antagonist at 5-HT2A receptors. It is
also known as dopamine- serotonin stabilizer.
• Ziprasidone: D2 +5-FIT2A/2c + H1-α 1 blocker
• Thioridazine: interferes with ejaculation, can cause cardiac arrhythmias and retinal damage.
• Asenapine: used sublingually for schizophrenia & acute mania.
• Amisulpiride: congener of sulpiride (typical antipsychotic) is categorized with the atypical antipsychotics
because it produces few extrapyramidal side effects and improves many negative symptoms of
schizophrenia as well. However, it retains high affinity for D2 (and D3) receptors and has low-affinity for 5-
HT2 receptors.
Clozapine:
• Most potent with least extrapyramidal S.E. & least antiemetic property
• Has weak D2 blocking action
• Reserve drug for resistant schizophrenia
• Most important side effect is agranulocytosis.
SIDE EFFECTS
• Extra pyramidal symptoms are due to D2 blockade in limbic system.
• Perioral movements [Rabbit syndrome]
� Within 7 days of starting or rapidly raising the dose of drugs — Neuroleptic induced dystonia
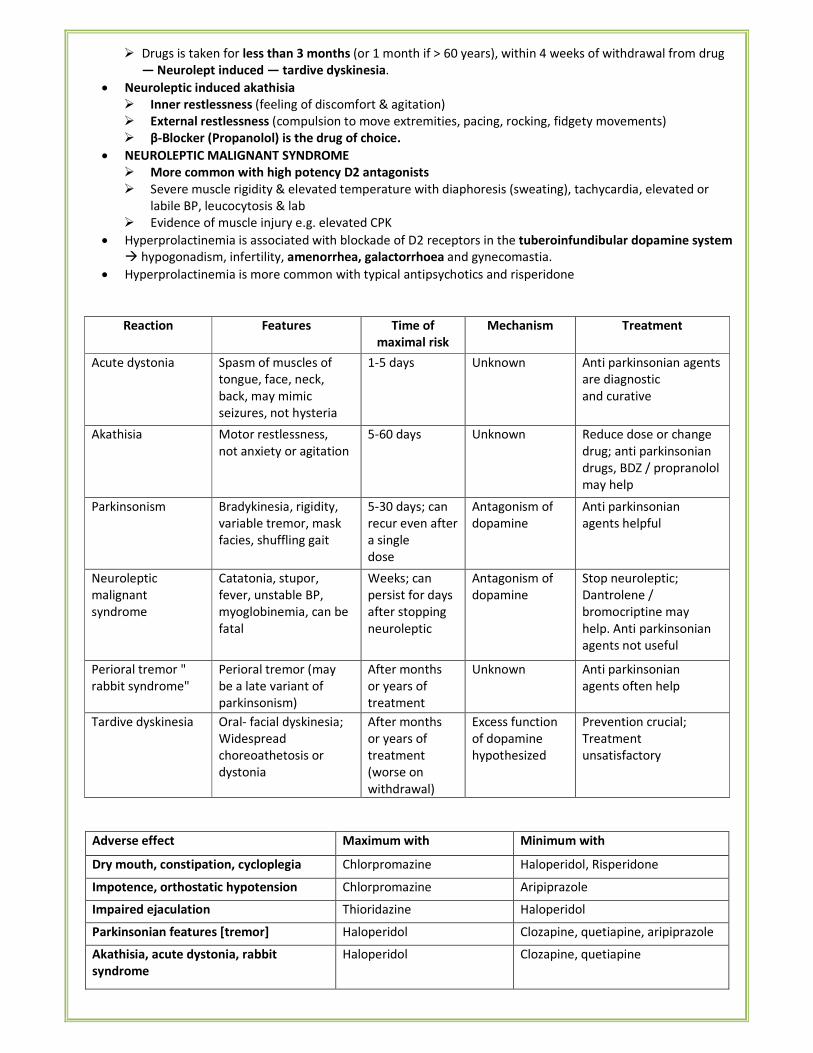
� Drugs is taken for less than 3 months (or 1 month if > 60 years), within 4 weeks of withdrawal from drug
— Neurolept induced — tardive dyskinesia.
• Neuroleptic induced akathisia
� Inner restlessness (feeling of discomfort & agitation)
� External restlessness (compulsion to move extremities, pacing, rocking, fidgety movements)
� β-Blocker (Propanolol) is the drug of choice.
• NEUROLEPTIC MALIGNANT SYNDROME
� More common with high potency D2 antagonists
� Severe muscle rigidity & elevated temperature with diaphoresis (sweating), tachycardia, elevated or
labile BP, leucocytosis & lab
� Evidence of muscle injury e.g. elevated CPK
• Hyperprolactinemia is associated with blockade of D2 receptors in the tuberoinfundibular dopamine system
� hypogonadism, infertility, amenorrhea, galactorrhoea and gynecomastia.
• Hyperprolactinemia is more common with typical antipsychotics and risperidone
Reaction Features Time of
maximal risk
Mechanism Treatment
Acute dystonia Spasm of muscles of
tongue, face, neck,
back, may mimic
seizures, not hysteria
1-5 days Unknown Anti parkinsonian agents
are diagnostic
and curative
Akathisia Motor restlessness,
not anxiety or agitation
5-60 days Unknown Reduce dose or change
drug; anti parkinsonian
drugs, BDZ / propranolol
may help
Parkinsonism Bradykinesia, rigidity,
variable tremor, mask
facies, shuffling gait
5-30 days; can
recur even after
a single
dose
Antagonism of
dopamine
Anti parkinsonian
agents helpful
Neuroleptic
malignant
syndrome
Catatonia, stupor,
fever, unstable BP,
myoglobinemia, can be
fatal
Weeks; can
persist for days
after stopping
neuroleptic
Antagonism of
dopamine
Stop neuroleptic;
Dantrolene /
bromocriptine may
help. Anti parkinsonian
agents not useful
Perioral tremor "
rabbit syndrome"
Perioral tremor (may
be a late variant of
parkinsonism)
After months
or years of
treatment
Unknown Anti parkinsonian
agents often help
Tardive dyskinesia Oral- facial dyskinesia;
Widespread
choreoathetosis or
dystonia
After months
or years of
treatment
(worse on
withdrawal)
Excess function
of dopamine
hypothesized
Prevention crucial;
Treatment
unsatisfactory
Adverse effect Maximum with Minimum with
Dry mouth, constipation, cycloplegia Chlorpromazine Haloperidol, Risperidone
Impotence, orthostatic hypotension Chlorpromazine Aripiprazole
Impaired ejaculation Thioridazine Haloperidol
Parkinsonian features [tremor] Haloperidol Clozapine, quetiapine, aripiprazole
Akathisia, acute dystonia, rabbit
syndrome
Haloperidol Clozapine, quetiapine
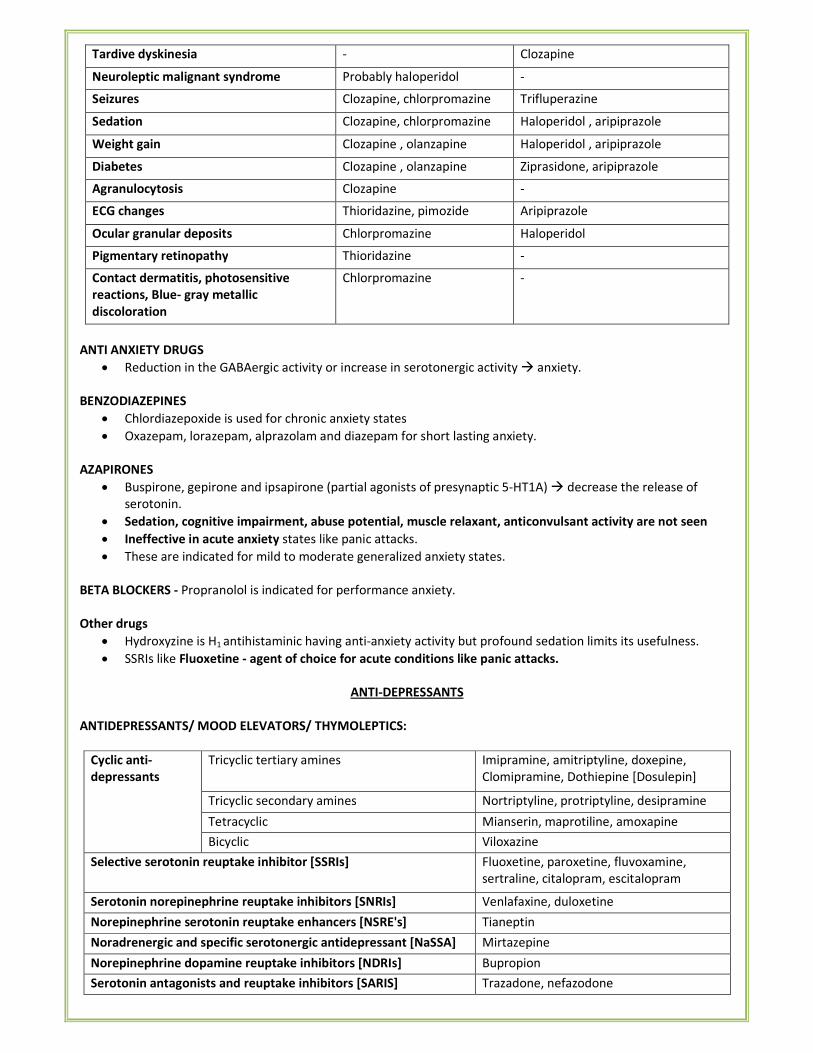
Tardive dyskinesia - Clozapine
Neuroleptic malignant syndrome Probably haloperidol -
Seizures Clozapine, chlorpromazine Trifluperazine
Sedation Clozapine, chlorpromazine Haloperidol , aripiprazole
Weight gain Clozapine , olanzapine Haloperidol , aripiprazole
Diabetes Clozapine , olanzapine Ziprasidone, aripiprazole
Agranulocytosis Clozapine -
ECG changes Thioridazine, pimozide Aripiprazole
Ocular granular deposits Chlorpromazine Haloperidol
Pigmentary retinopathy Thioridazine -
Contact dermatitis, photosensitive
reactions, Blue- gray metallic
discoloration
Chlorpromazine -
ANTI ANXIETY DRUGS
• Reduction in the GABAergic activity or increase in serotonergic activity � anxiety.
BENZODIAZEPINES
• Chlordiazepoxide is used for chronic anxiety states
• Oxazepam, lorazepam, alprazolam and diazepam for short lasting anxiety.
AZAPIRONES
• Buspirone, gepirone and ipsapirone (partial agonists of presynaptic 5-HT1A) � decrease the release of
serotonin.
• Sedation, cognitive impairment, abuse potential, muscle relaxant, anticonvulsant activity are not seen
• Ineffective in acute anxiety states like panic attacks.
• These are indicated for mild to moderate generalized anxiety states.
BETA BLOCKERS - Propranolol is indicated for performance anxiety.
Other drugs
• Hydroxyzine is H1 antihistaminic having anti-anxiety activity but profound sedation limits its usefulness.
• SSRIs like Fluoxetine - agent of choice for acute conditions like panic attacks.
ANTI-DEPRESSANTS
ANTIDEPRESSANTS/ MOOD ELEVATORS/ THYMOLEPTICS:
Cyclic anti-
depressants
Tricyclic tertiary amines Imipramine, amitriptyline, doxepine,
Clomipramine, Dothiepine [Dosulepin]
Tricyclic secondary amines Nortriptyline, protriptyline, desipramine
Tetracyclic Mianserin, maprotiline, amoxapine
Bicyclic Viloxazine
Selective serotonin reuptake inhibitor [SSRIs] Fluoxetine, paroxetine, fluvoxamine,
sertraline, citalopram, escitalopram
Serotonin norepinephrine reuptake inhibitors [SNRIs] Venlafaxine, duloxetine
Norepinephrine serotonin reuptake enhancers [NSRE's] Tianeptin
Noradrenergic and specific serotonergic antidepressant [NaSSA] Mirtazepine
Norepinephrine dopamine reuptake inhibitors [NDRIs] Bupropion
Serotonin antagonists and reuptake inhibitors [SARIS] Trazadone, nefazodone
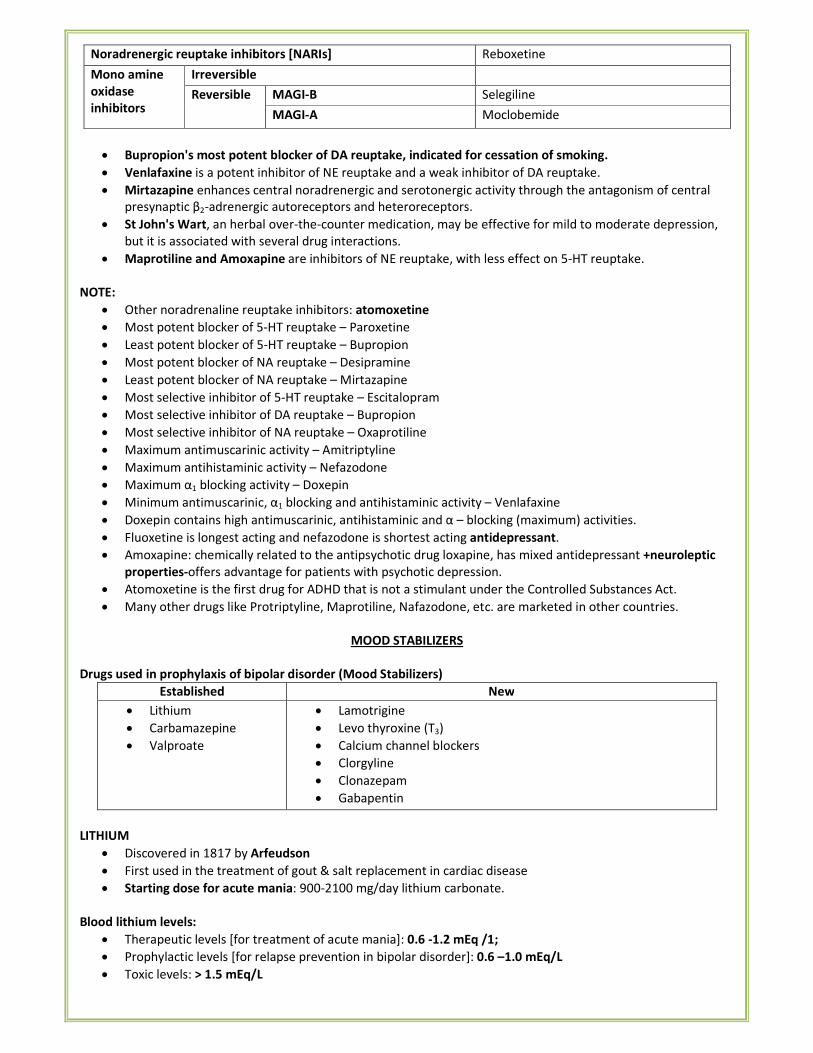
Noradrenergic reuptake inhibitors [NARIs] Reboxetine
Mono amine
oxidase
inhibitors
Irreversible
Reversible MAGI-B Selegiline
MAGI-A Moclobemide
• Bupropion's most potent blocker of DA reuptake, indicated for cessation of smoking.
• Venlafaxine is a potent inhibitor of NE reuptake and a weak inhibitor of DA reuptake.
• Mirtazapine enhances central noradrenergic and serotonergic activity through the antagonism of central
presynaptic β2-adrenergic autoreceptors and heteroreceptors.
• St John's Wart, an herbal over-the-counter medication, may be effective for mild to moderate depression,
but it is associated with several drug interactions.
• Maprotiline and Amoxapine are inhibitors of NE reuptake, with less effect on 5-HT reuptake.
NOTE:
• Other noradrenaline reuptake inhibitors: atomoxetine
• Most potent blocker of 5-HT reuptake – Paroxetine
• Least potent blocker of 5-HT reuptake – Bupropion
• Most potent blocker of NA reuptake – Desipramine
• Least potent blocker of NA reuptake – Mirtazapine
• Most selective inhibitor of 5-HT reuptake – Escitalopram
• Most selective inhibitor of DA reuptake – Bupropion
• Most selective inhibitor of NA reuptake – Oxaprotiline
• Maximum antimuscarinic activity – Amitriptyline
• Maximum antihistaminic activity – Nefazodone
• Maximum α1 blocking activity – Doxepin
• Minimum antimuscarinic, α1 blocking and antihistaminic activity – Venlafaxine
• Doxepin contains high antimuscarinic, antihistaminic and α – blocking (maximum) activities.
• Fluoxetine is longest acting and nefazodone is shortest acting antidepressant.
• Amoxapine: chemically related to the antipsychotic drug loxapine, has mixed antidepressant +neuroleptic
properties-offers advantage for patients with psychotic depression.
• Atomoxetine is the first drug for ADHD that is not a stimulant under the Controlled Substances Act.
• Many other drugs like Protriptyline, Maprotiline, Nafazodone, etc. are marketed in other countries.
MOOD STABILIZERS
Drugs used in prophylaxis of bipolar disorder (Mood Stabilizers)
Established New
• Lithium
• Carbamazepine
• Valproate
• Lamotrigine
• Levo thyroxine (T3)
• Calcium channel blockers
• Clorgyline
• Clonazepam
• Gabapentin
LITHIUM
• Discovered in 1817 by Arfeudson
• First used in the treatment of gout & salt replacement in cardiac disease
• Starting dose for acute mania: 900-2100 mg/day lithium carbonate.
Blood lithium levels:
• Therapeutic levels [for treatment of acute mania]: 0.6 -1.2 mEq /1;
• Prophylactic levels [for relapse prevention in bipolar disorder]: 0.6 –1.0 mEq/L
• Toxic levels: > 1.5 mEq/L
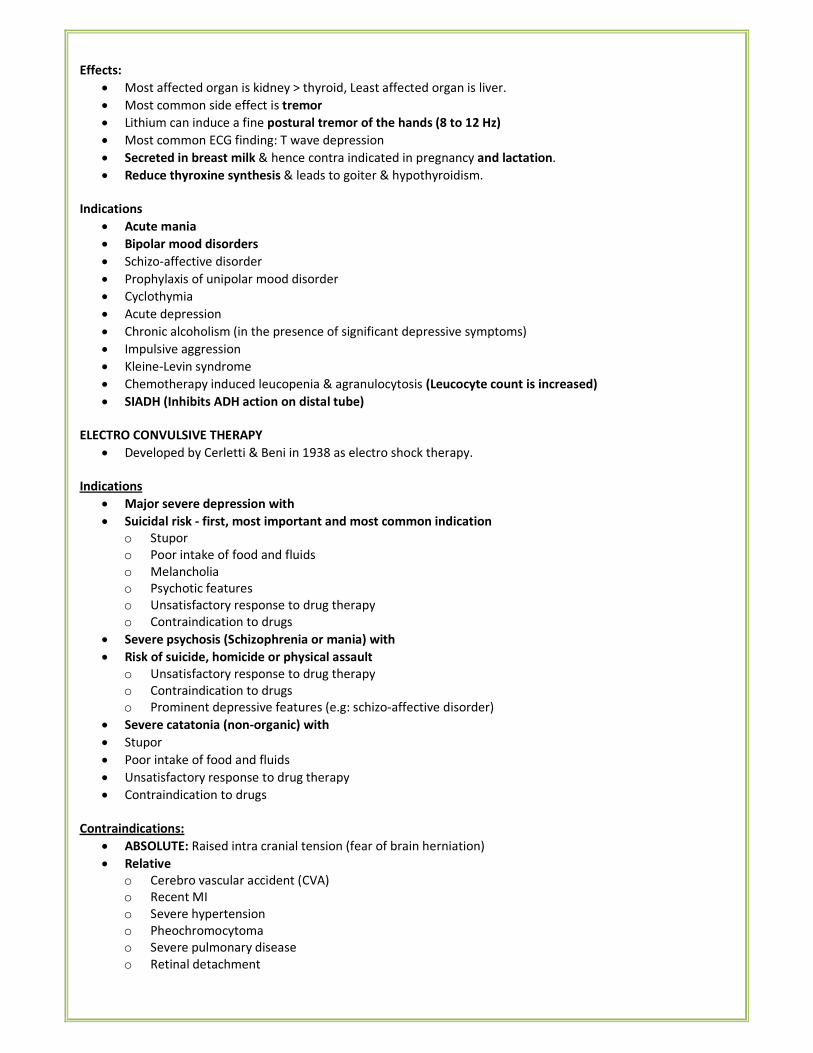
Effects:
• Most affected organ is kidney > thyroid, Least affected organ is liver.
• Most common side effect is tremor
• Lithium can induce a fine postural tremor of the hands (8 to 12 Hz)
• Most common ECG finding: T wave depression
• Secreted in breast milk & hence contra indicated in pregnancy and lactation.
• Reduce thyroxine synthesis & leads to goiter & hypothyroidism.
Indications
• Acute mania
• Bipolar mood disorders
• Schizo-affective disorder
• Prophylaxis of unipolar mood disorder
• Cyclothymia
• Acute depression
• Chronic alcoholism (in the presence of significant depressive symptoms)
• Impulsive aggression
• Kleine-Levin syndrome
• Chemotherapy induced leucopenia & agranulocytosis (Leucocyte count is increased)
• SIADH (Inhibits ADH action on distal tube)
ELECTRO CONVULSIVE THERAPY
• Developed by Cerletti & Beni in 1938 as electro shock therapy.
Indications
• Major severe depression with
• Suicidal risk - first, most important and most common indication
o Stupor
o Poor intake of food and fluids
o Melancholia
o Psychotic features
o Unsatisfactory response to drug therapy
o Contraindication to drugs
• Severe psychosis (Schizophrenia or mania) with
• Risk of suicide, homicide or physical assault
o Unsatisfactory response to drug therapy
o Contraindication to drugs
o Prominent depressive features (e.g: schizo-affective disorder)
• Severe catatonia (non-organic) with
• Stupor
• Poor intake of food and fluids
• Unsatisfactory response to drug therapy
• Contraindication to drugs
Contraindications:
• ABSOLUTE: Raised intra cranial tension (fear of brain herniation)
• Relative
o Cerebro vascular accident (CVA)
o Recent MI
o Severe hypertension
o Pheochromocytoma
o Severe pulmonary disease
o Retinal detachment
Types:
• Direct ECT (unmodified): ECT is given without muscle relaxants and anesthesia. Direct ECT causes decreased
intra ocular tension.
• Modified ECT: given with drug induced muscle relaxation and anesthesia.
Complications:
• ECT- Direct: Most common side effect is fracture T4T8 spine
• Modified —ECT: Most common is retrograde amnesia (ante grade amnesia is also found)
Light & melatonin therapy
• Based on the concept that humans are subject to circadian rhythms that affect physiological processes in
predictable ways
• By varying light exposure, circadian rhythms can be altered
• The concentration of melatonin in blood is highest at night and lowest or absent during the daylight
• Artificial bright light therapy is a proved method to treat depressive disorder with seasonal pattern which is
seen in winter months when daylight hours are reduced
BEHAVIOR THERAPY
Type Based on Used in
Systemic
desensitization
Reciprocal inhibition Phobias (treatment of choice)
OCD (treatment of choice)
Psycho-sexual dysfunctions
Aversion therapy Pairing of pleasant stimulus with an
unpleasant responses e.g. Pairing alcohol with
electric shock
Drug abuse
Sexual deviations
Flooding Direct exposure to phobia but escape not
possible
Phobias
Operant conditioning
for increasing a
behavior
Positive reinforcement
Negative reinforcement
Modeling
For augmenting an adaptive
behavior
Operant conditioning
for decreasing a
behavior
Time out
Punishment
Satiation(negative practice procedure)
For demoting maladaptive
behavior
Other physical treatments for Depression
Light therapy (phototherapy):
• For the treatment of "seasonal affective disorder" (SAD) by Rosenthal
• Effects of phototherapy may be independent of melatonin and produce a "phase advance" in circadian
rhythms (hence treatment may be best given first thing in the morning).
• Usually administered by use of a light box.
• Optimal intensity of light appears to be 10,000 lux.
• Ideal treatment duration is for 30 minutes (at 10,000 lux) a day.
• Although treatment response is generally noticeable within five days.
• For patients with seasonal depressive symptoms, maintenance therapy is recommended throughout the
winter months
Vagus nerve stimulation (VNS) therapy:
• Approved for severe, recurrent unipolar and bipolar depression in July 2005.
• Left cervical vagus nerve stimulation is accomplished through leads attached to a pulse generator implanted
in the left chest area.
• Response rates of 40-46% have been shown for treatment-resistant depressive disorder after 10 weeks to 9
months, with a remission rate of 29% at one year, suggesting that the effectiveness of VNS may have a slow
trajectory.
• VNS may be combined with essentially all existing treatments for depressive disorders.
• It has been safely used with antidepressants (including MAOIs) and can be temporarily shut off to allow for
ECT and restarted immediately post-ECT.
*****END*****
RADIODIAGNOSIS
&
RADIOTHERAPY
I. IMAGING TECHNIQUES
X- RAYS
• Are electromagnetic radiation
• Have penetrating power less than gamma rays but more than alpha and beta rays
• Can pass through human body, Cannot be absorbed completely
• Produced by Coolidge tube when fast moving stream of electrons produced by a cathode(Tungsten
filament) strikes the anode(tungsten/ molybdenum containing copper plate)
• X-rays are most scattered by H+ ions.
• Causes ionization in 3 ways: Photoelectric effect, Compton effect & Pair production
• Contrast can be increased by increasing the current (mA)
• Penetration can be increased by increasing the voltage (mV)
• Machine is kept at 6 feet distance form photographic plate to prevent magnification.
• Optimum distance of target film: 90-100cm
• Best chest X ray is done at: 120-150 kilovolt peak.
• Gunson method: X- ray of soft tissues of neck
• Cyclotron produces Gamma rays
ULTRASOUND (USG)
• Based on piezoelectric effect of crystals made up of lead zirconate titanate.
• Ian Donald - father of obstetric ultrasound. Also invented the B-mode scanner.
• Dr. John Wild and John Reid: invented an A-mode scanner for the detection of ovarian cancer.
• John Wild ("father of medical ultrasound") first used ultrasound to assess the thickness of bowel tissue.
• Contains waves with frequencies>20,000 Hz.
• In medical USG frequencies commonly used are 2-10 MHz
• Frequencies used:
• Trans abdominal ultrasound: 3-5 MHz,
o Trans-vaginal: 5-7.5MHz,
o Breast: 15 MHz,
o Gut wall: 7.5-20 MHz
o Vessels: 20 MHz
• Types of image display
o A –Mode � one dimensional picture, used only in eye scan
o B- Mode- � two dimensional picture, commonly used
o Real time scan � gives moving picture
o M-Mode � motion display (e.g. in ECHO)
• USG causes delirious effect on small micro-organisms by acoustic cavitation.
• Investigation of choice for obstetric conditions
DOPPLER
• Based on Doppler Effect (change in the perceived frequency of sound emitted by a moving source measures
blood flow). It provides both audio and video signals.
• Types: Continuous waves & Pulsed waves
• In Doppler imaging colour displays direction of blood flow. It is
Red --- when direction of flow is towards the transducer.
Blue --- if flow is away from transducer.
CT- scan or CAT scan
• Invented by God Frey Hounsfield in 1963, awarded Nobel Prize.
• Basic principle of CT is linear attenuation of x-rays.
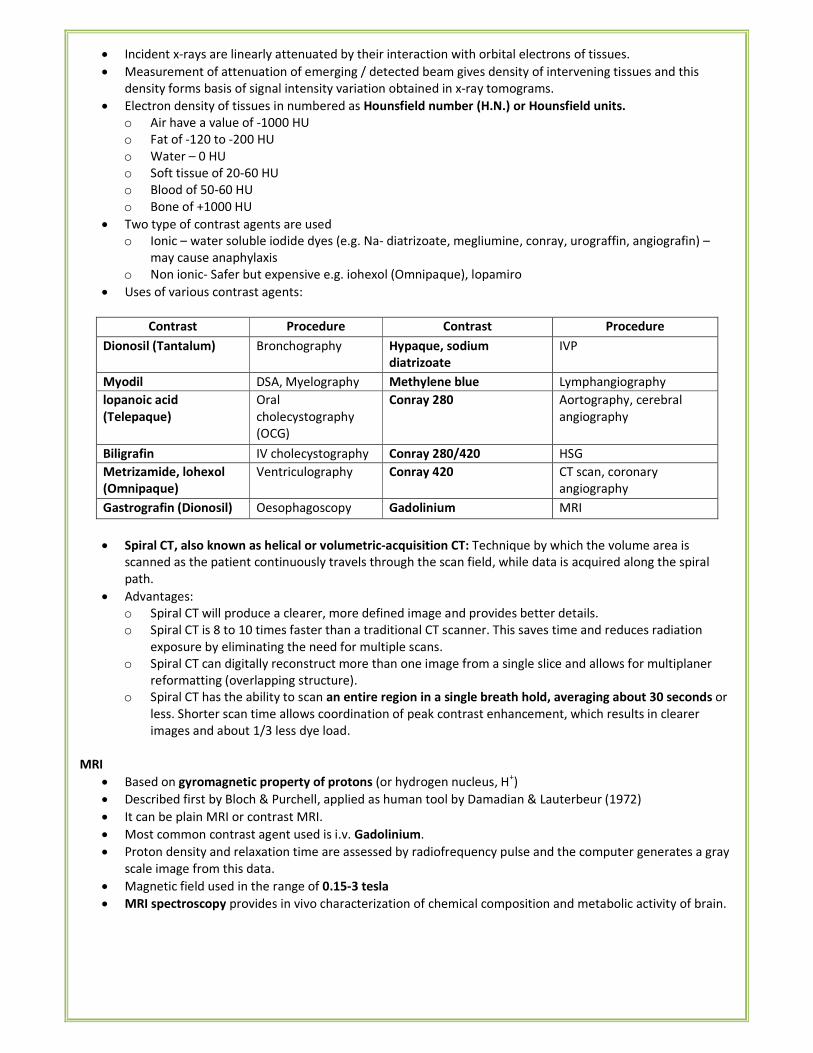
• Incident x-rays are linearly attenuated by their interaction with orbital electrons of tissues.
• Measurement of attenuation of emerging / detected beam gives density of intervening tissues and this
density forms basis of signal intensity variation obtained in x-ray tomograms.
• Electron density of tissues in numbered as Hounsfield number (H.N.) or Hounsfield units.
o Air have a value of -1000 HU
o Fat of -120 to -200 HU
o Water – 0 HU
o Soft tissue of 20-60 HU
o Blood of 50-60 HU
o Bone of +1000 HU
• Two type of contrast agents are used
o Ionic – water soluble iodide dyes (e.g. Na- diatrizoate, megliumine, conray, urograffin, angiografin) –
may cause anaphylaxis
o Non ionic- Safer but expensive e.g. iohexol (Omnipaque), lopamiro
• Uses of various contrast agents:
Contrast Procedure Contrast Procedure
Dionosil (Tantalum) Bronchography Hypaque, sodium
diatrizoate
IVP
Myodil DSA, Myelography Methylene blue Lymphangiography
lopanoic acid
(Telepaque)
Oral
cholecystography
(OCG)
Conray 280 Aortography, cerebral
angiography
Biligrafin IV cholecystography Conray 280/420 HSG
Metrizamide, lohexol
(Omnipaque)
Ventriculography Conray 420 CT scan, coronary
angiography
Gastrografin (Dionosil) Oesophagoscopy Gadolinium MRI
• Spiral CT, also known as helical or volumetric-acquisition CT: Technique by which the volume area is
scanned as the patient continuously travels through the scan field, while data is acquired along the spiral
path.
• Advantages:
o Spiral CT will produce a clearer, more defined image and provides better details.
o Spiral CT is 8 to 10 times faster than a traditional CT scanner. This saves time and reduces radiation
exposure by eliminating the need for multiple scans.
o Spiral CT can digitally reconstruct more than one image from a single slice and allows for multiplaner
reformatting (overlapping structure).
o Spiral CT has the ability to scan an entire region in a single breath hold, averaging about 30 seconds or
less. Shorter scan time allows coordination of peak contrast enhancement, which results in clearer
images and about 1/3 less dye load.
MRI
• Based on gyromagnetic property of protons (or hydrogen nucleus, H+)
• Described first by Bloch & Purchell, applied as human tool by Damadian & Lauterbeur (1972)
• It can be plain MRI or contrast MRI.
• Most common contrast agent used is i.v. Gadolinium.
• Proton density and relaxation time are assessed by radiofrequency pulse and the computer generates a gray
scale image from this data.
• Magnetic field used in the range of 0.15-3 tesla
• MRI spectroscopy provides in vivo characterization of chemical composition and metabolic activity of brain.
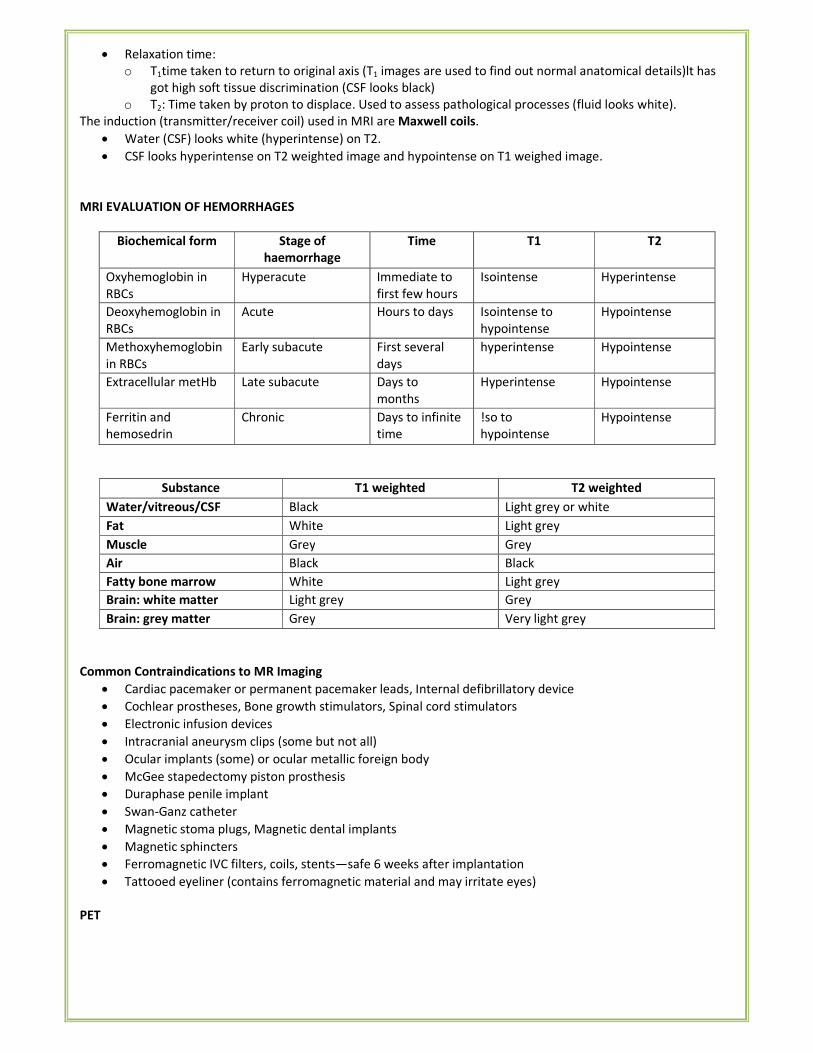
• Relaxation time:
o T1time taken to return to original axis (T1 images are used to find out normal anatomical details)lt has
got high soft tissue discrimination (CSF looks black)
o T2: Time taken by proton to displace. Used to assess pathological processes (fluid looks white).
The induction (transmitter/receiver coil) used in MRI are Maxwell coils.
• Water (CSF) looks white (hyperintense) on T2.
• CSF looks hyperintense on T2 weighted image and hypointense on T1 weighed image.
MRI EVALUATION OF HEMORRHAGES
Biochemical form Stage of
haemorrhage
Time T1 T2
Oxyhemoglobin in
RBCs
Hyperacute Immediate to
first few hours
Isointense Hyperintense
Deoxyhemoglobin in
RBCs
Acute Hours to days Isointense to
hypointense
Hypointense
Methoxyhemoglobin
in RBCs
Early subacute First several
days
hyperintense Hypointense
Extracellular metHb Late subacute Days to
months
Hyperintense Hypointense
Ferritin and
hemosedrin
Chronic Days to infinite
time
!so to
hypointense
Hypointense
Substance T1 weighted T2 weighted
Water/vitreous/CSF Black Light grey or white
Fat White Light grey
Muscle Grey Grey
Air Black Black
Fatty bone marrow White Light grey
Brain: white matter Light grey Grey
Brain: grey matter Grey Very light grey
Common Contraindications to MR Imaging
• Cardiac pacemaker or permanent pacemaker leads, Internal defibrillatory device
• Cochlear prostheses, Bone growth stimulators, Spinal cord stimulators
• Electronic infusion devices
• Intracranial aneurysm clips (some but not all)
• Ocular implants (some) or ocular metallic foreign body
• McGee stapedectomy piston prosthesis
• Duraphase penile implant
• Swan-Ganz catheter
• Magnetic stoma plugs, Magnetic dental implants
• Magnetic sphincters
• Ferromagnetic IVC filters, coils, stents—safe 6 weeks after implantation
• Tattooed eyeliner (contains ferromagnetic material and may irritate eyes)
PET
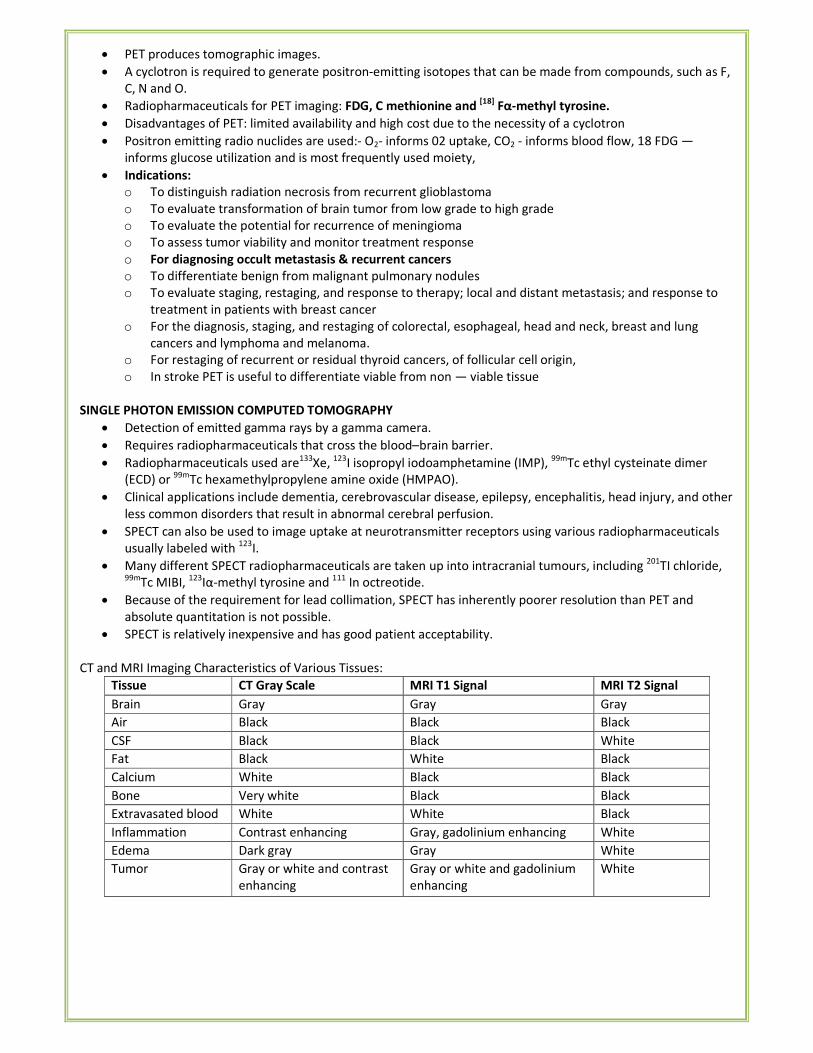
• PET produces tomographic images.
• A cyclotron is required to generate positron-emitting isotopes that can be made from compounds, such as F,
C, N and O.
• Radiopharmaceuticals for PET imaging: FDG, C methionine and [18]
Fα-methyl tyrosine.
• Disadvantages of PET: limited availability and high cost due to the necessity of a cyclotron
• Positron emitting radio nuclides are used:- O2- informs 02 uptake, CO2 - informs blood flow, 18 FDG —
informs glucose utilization and is most frequently used moiety,
• Indications:
o To distinguish radiation necrosis from recurrent glioblastoma
o To evaluate transformation of brain tumor from low grade to high grade
o To evaluate the potential for recurrence of meningioma
o To assess tumor viability and monitor treatment response
o For diagnosing occult metastasis & recurrent cancers
o To differentiate benign from malignant pulmonary nodules
o To evaluate staging, restaging, and response to therapy; local and distant metastasis; and response to
treatment in patients with breast cancer
o For the diagnosis, staging, and restaging of colorectal, esophageal, head and neck, breast and lung
cancers and lymphoma and melanoma.
o For restaging of recurrent or residual thyroid cancers, of follicular cell origin,
o In stroke PET is useful to differentiate viable from non — viable tissue
SINGLE PHOTON EMISSION COMPUTED TOMOGRAPHY
• Detection of emitted gamma rays by a gamma camera.
• Requires radiopharmaceuticals that cross the blood–brain barrier.
• Radiopharmaceuticals used are133
Xe, 123
I isopropyl iodoamphetamine (IMP), 99m
Tc ethyl cysteinate dimer
(ECD) or 99m
Tc hexamethylpropylene amine oxide (HMPAO).
• Clinical applications include dementia, cerebrovascular disease, epilepsy, encephalitis, head injury, and other
less common disorders that result in abnormal cerebral perfusion.
• SPECT can also be used to image uptake at neurotransmitter receptors using various radiopharmaceuticals
usually labeled with 123
I.
• Many different SPECT radiopharmaceuticals are taken up into intracranial tumours, including 201
TI chloride, 99m
Tc MIBI, 123
Iα-methyl tyrosine and 111
In octreotide.
• Because of the requirement for lead collimation, SPECT has inherently poorer resolution than PET and
absolute quantitation is not possible.
• SPECT is relatively inexpensive and has good patient acceptability.
CT and MRI Imaging Characteristics of Various Tissues:
Tissue CT Gray Scale MRI T1 Signal MRI T2 Signal
Brain Gray Gray Gray
Air Black Black Black
CSF Black Black White
Fat Black White Black
Calcium White Black Black
Bone Very white Black Black
Extravasated blood White White Black
Inflammation Contrast enhancing Gray, gadolinium enhancing White
Edema Dark gray Gray White
Tumor Gray or white and contrast
enhancing
Gray or white and gadolinium
enhancing
White
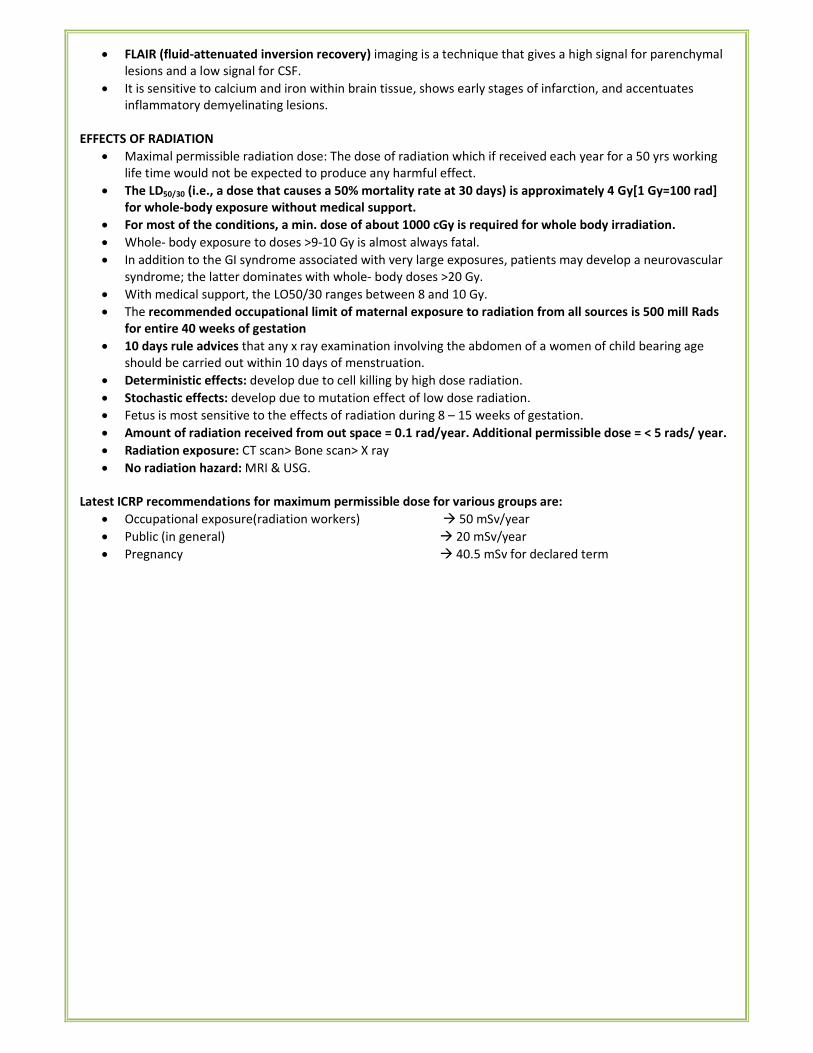
• FLAIR (fluid-attenuated inversion recovery) imaging is a technique that gives a high signal for parenchymal
lesions and a low signal for CSF.
• It is sensitive to calcium and iron within brain tissue, shows early stages of infarction, and accentuates
inflammatory demyelinating lesions.
EFFECTS OF RADIATION
• Maximal permissible radiation dose: The dose of radiation which if received each year for a 50 yrs working
life time would not be expected to produce any harmful effect.
• The LD50/30 (i.e., a dose that causes a 50% mortality rate at 30 days) is approximately 4 Gy[1 Gy=100 rad]
for whole-body exposure without medical support.
• For most of the conditions, a min. dose of about 1000 cGy is required for whole body irradiation.
• Whole- body exposure to doses >9-10 Gy is almost always fatal.
• In addition to the GI syndrome associated with very large exposures, patients may develop a neurovascular
syndrome; the latter dominates with whole- body doses >20 Gy.
• With medical support, the LO50/30 ranges between 8 and 10 Gy.
• The recommended occupational limit of maternal exposure to radiation from all sources is 500 mill Rads
for entire 40 weeks of gestation
• 10 days rule advices that any x ray examination involving the abdomen of a women of child bearing age
should be carried out within 10 days of menstruation.
• Deterministic effects: develop due to cell killing by high dose radiation.
• Stochastic effects: develop due to mutation effect of low dose radiation.
• Fetus is most sensitive to the effects of radiation during 8 – 15 weeks of gestation.
• Amount of radiation received from out space = 0.1 rad/year. Additional permissible dose = < 5 rads/ year.
• Radiation exposure: CT scan> Bone scan> X ray
• No radiation hazard: MRI & USG.
Latest ICRP recommendations for maximum permissible dose for various groups are:
• Occupational exposure(radiation workers) � 50 mSv/year
• Public (in general) � 20 mSv/year
• Pregnancy � 40.5 mSv for declared term
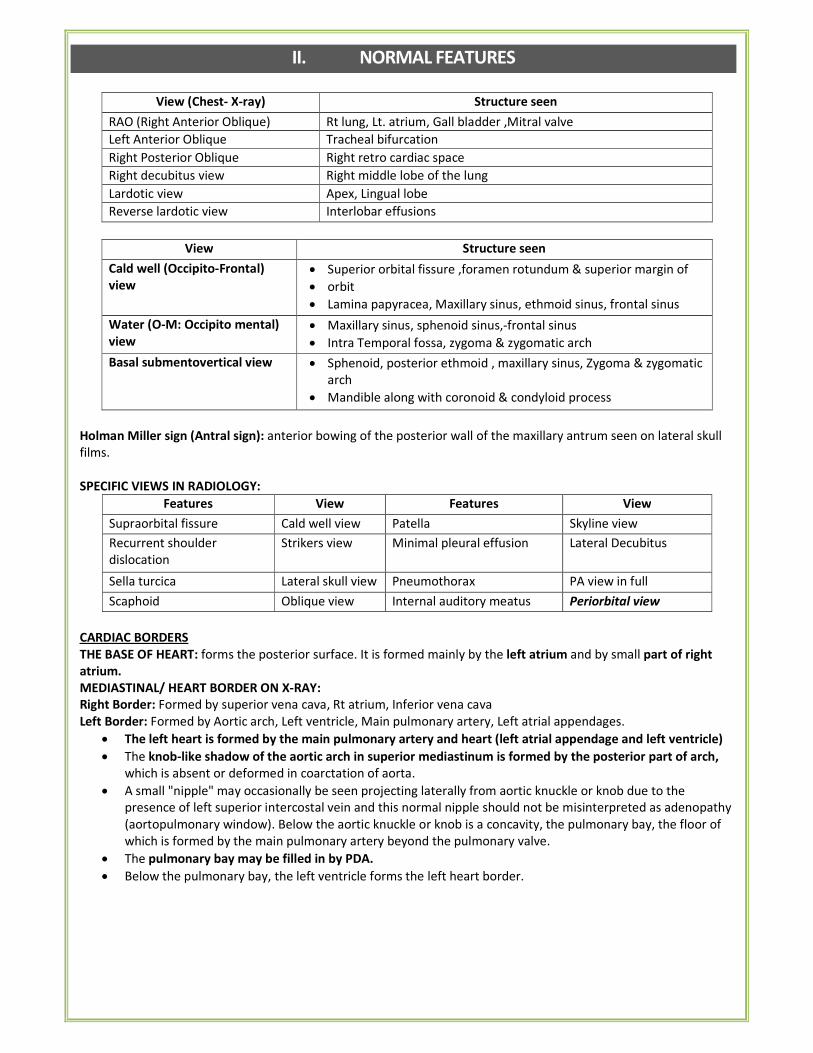
II. NORMAL FEATURES
View (Chest- X-ray) Structure seen
RAO (Right Anterior Oblique) Rt lung, Lt. atrium, Gall bladder ,Mitral valve
Left Anterior Oblique Tracheal bifurcation
Right Posterior Oblique Right retro cardiac space
Right decubitus view Right middle lobe of the lung
Lardotic view Apex, Lingual lobe
Reverse lardotic view Interlobar effusions
View Structure seen
Cald well (Occipito-Frontal)
view
• Superior orbital fissure ,foramen rotundum & superior margin of
• orbit
• Lamina papyracea, Maxillary sinus, ethmoid sinus, frontal sinus
Water (O-M: Occipito mental)
view
• Maxillary sinus, sphenoid sinus,-frontal sinus
• Intra Temporal fossa, zygoma & zygomatic arch
Basal submentovertical view • Sphenoid, posterior ethmoid , maxillary sinus, Zygoma & zygomatic
arch
• Mandible along with coronoid & condyloid process
Holman Miller sign (Antral sign): anterior bowing of the posterior wall of the maxillary antrum seen on lateral skull
films.
SPECIFIC VIEWS IN RADIOLOGY:
Features View Features View
Supraorbital fissure Cald well view Patella Skyline view
Recurrent shoulder
dislocation
Strikers view Minimal pleural effusion Lateral Decubitus
Sella turcica Lateral skull view Pneumothorax PA view in full
expiration Scaphoid Oblique view Internal auditory meatus Periorbital view
CARDIAC BORDERS
THE BASE OF HEART: forms the posterior surface. It is formed mainly by the left atrium and by small part of right
atrium.
MEDIASTINAL/ HEART BORDER ON X-RAY:
Right Border: Formed by superior vena cava, Rt atrium, Inferior vena cava
Left Border: Formed by Aortic arch, Left ventricle, Main pulmonary artery, Left atrial appendages.
• The left heart is formed by the main pulmonary artery and heart (left atrial appendage and left ventricle)
• The knob-like shadow of the aortic arch in superior mediastinum is formed by the posterior part of arch,
which is absent or deformed in coarctation of aorta.
• A small "nipple" may occasionally be seen projecting laterally from aortic knuckle or knob due to the
presence of left superior intercostal vein and this normal nipple should not be misinterpreted as adenopathy
(aortopulmonary window). Below the aortic knuckle or knob is a concavity, the pulmonary bay, the floor of
which is formed by the main pulmonary artery beyond the pulmonary valve.
• The pulmonary bay may be filled in by PDA.
• Below the pulmonary bay, the left ventricle forms the left heart border.
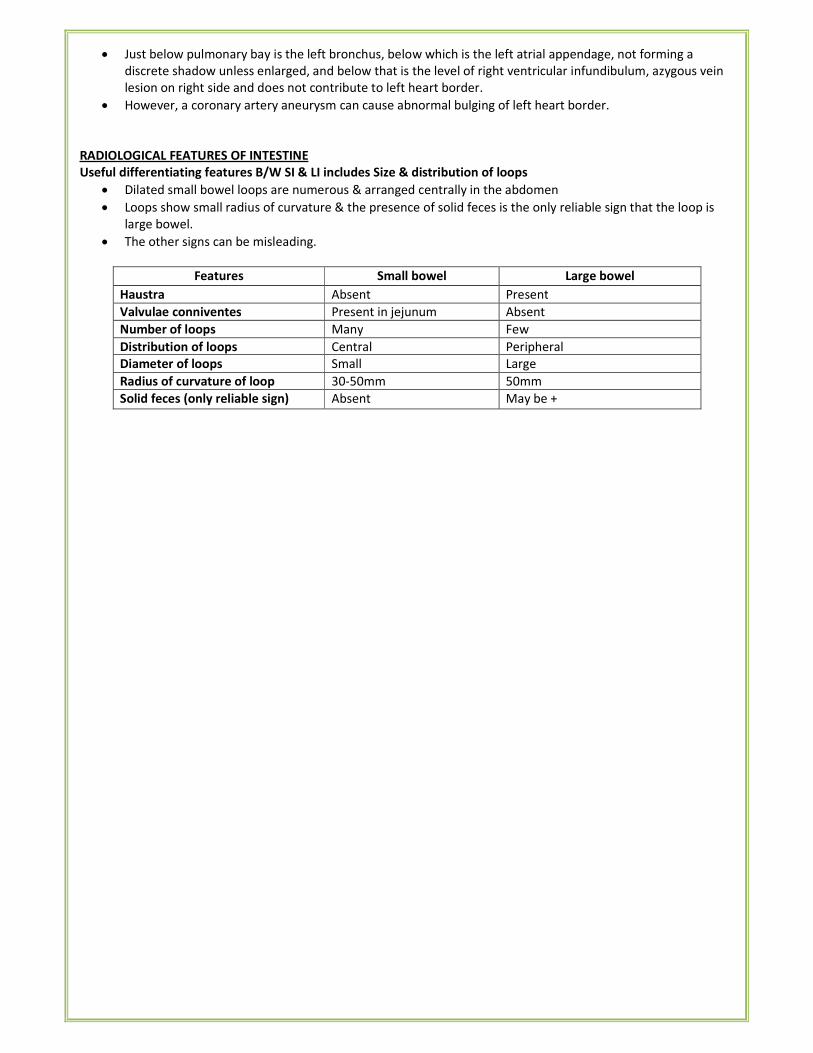
• Just below pulmonary bay is the left bronchus, below which is the left atrial appendage, not forming a
discrete shadow unless enlarged, and below that is the level of right ventricular infundibulum, azygous vein
lesion on right side and does not contribute to left heart border.
• However, a coronary artery aneurysm can cause abnormal bulging of left heart border.
RADIOLOGICAL FEATURES OF INTESTINE
Useful differentiating features B/W SI & LI includes Size & distribution of loops
• Dilated small bowel loops are numerous & arranged centrally in the abdomen
• Loops show small radius of curvature & the presence of solid feces is the only reliable sign that the loop is
large bowel.
• The other signs can be misleading.
Features Small bowel Large bowel
Haustra Absent Present
Valvulae conniventes Present in jejunum Absent
Number of loops Many Few
Distribution of loops Central Peripheral
Diameter of loops Small Large
Radius of curvature of loop 30-50mm 50mm
Solid feces (only reliable sign) Absent May be +
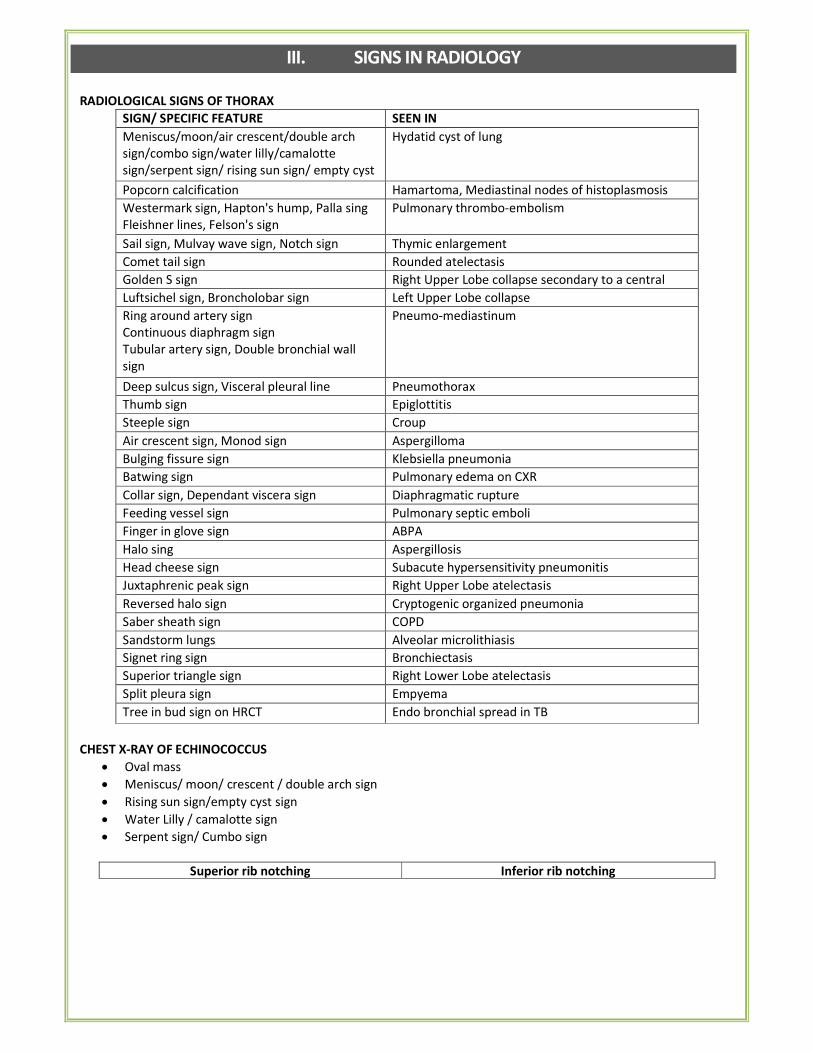
III. SIGNS IN RADIOLOGY
RADIOLOGICAL SIGNS OF THORAX
SIGN/ SPECIFIC FEATURE SEEN IN
Meniscus/moon/air crescent/double arch
sign/combo sign/water lilly/camalotte
sign/serpent sign/ rising sun sign/ empty cyst
sign
Hydatid cyst of lung
Popcorn calcification Hamartoma, Mediastinal nodes of histoplasmosis
Westermark sign, Hapton's hump, Palla sing
Fleishner lines, Felson's sign
Pulmonary thrombo-embolism
Sail sign, Mulvay wave sign, Notch sign Thymic enlargement
Comet tail sign Rounded atelectasis
Golden S sign Right Upper Lobe collapse secondary to a central
mass Luftsichel sign, Broncholobar sign Left Upper Lobe collapse
Ring around artery sign
Continuous diaphragm sign
Tubular artery sign, Double bronchial wall
sign
V sign of Naclerio, Spinnaker sail sign
Pneumo-mediastinum
Deep sulcus sign, Visceral pleural line Pneumothorax
Thumb sign Epiglottitis
Steeple sign Croup
Air crescent sign, Monod sign Aspergilloma
Bulging fissure sign Klebsiella pneumonia
Batwing sign Pulmonary edema on CXR
Collar sign, Dependant viscera sign Diaphragmatic rupture
Feeding vessel sign Pulmonary septic emboli
Finger in glove sign ABPA
Halo sing Aspergillosis
Head cheese sign Subacute hypersensitivity pneumonitis
Juxtaphrenic peak sign Right Upper Lobe atelectasis
Reversed halo sign Cryptogenic organized pneumonia
Saber sheath sign COPD
Sandstorm lungs Alveolar microlithiasis
Signet ring sign Bronchiectasis
Superior triangle sign Right Lower Lobe atelectasis
Split pleura sign Empyema
Tree in bud sign on HRCT Endo bronchial spread in TB
CHEST X-RAY OF ECHINOCOCCUS
• Oval mass
• Meniscus/ moon/ crescent / double arch sign
• Rising sun sign/empty cyst sign
• Water Lilly / camalotte sign
• Serpent sign/ Cumbo sign
Superior rib notching Inferior rib notching
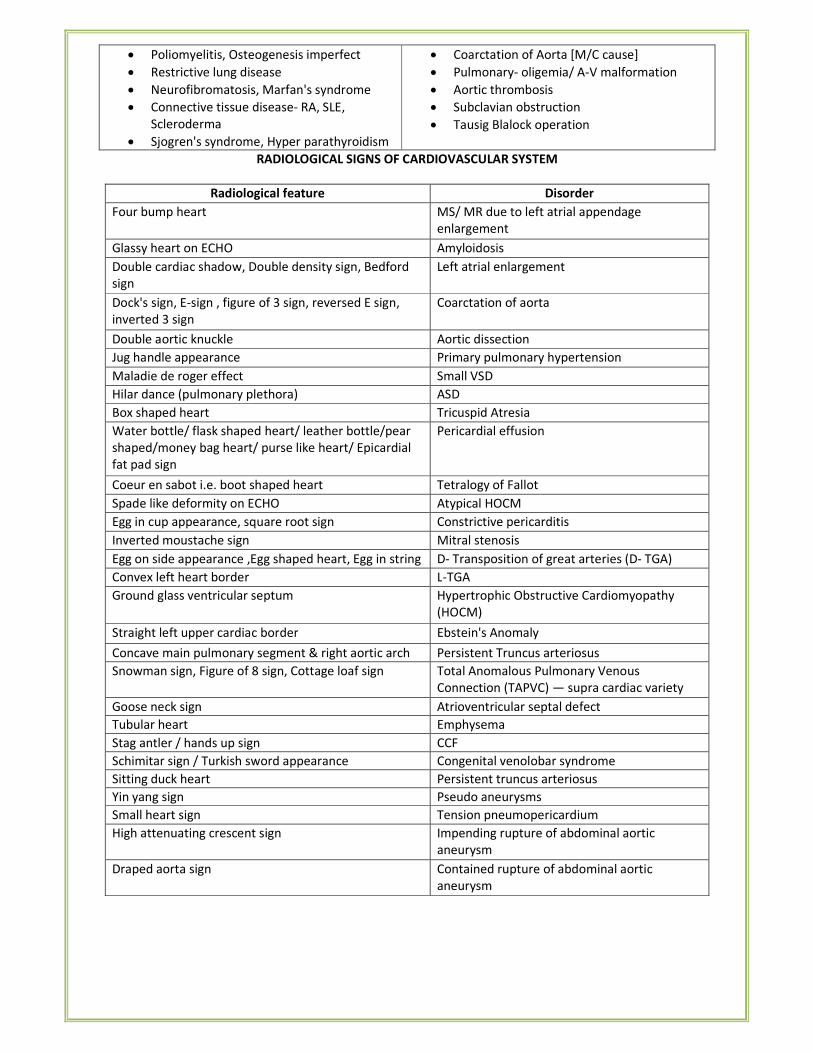
• Poliomyelitis, Osteogenesis imperfect
• Restrictive lung disease
• Neurofibromatosis, Marfan's syndrome
• Connective tissue disease- RA, SLE,
Scleroderma
• Sjogren's syndrome, Hyper parathyroidism
• Coarctation of Aorta [M/C cause]
• Pulmonary- oligemia/ A-V malformation
• Aortic thrombosis
• Subclavian obstruction
• Tausig Blalock operation
RADIOLOGICAL SIGNS OF CARDIOVASCULAR SYSTEM
Radiological feature Disorder
Four bump heart MS/ MR due to left atrial appendage
enlargement
Glassy heart on ECHO Amyloidosis
Double cardiac shadow, Double density sign, Bedford
sign
Left atrial enlargement
Dock's sign, E-sign , figure of 3 sign, reversed E sign,
inverted 3 sign
Coarctation of aorta
Double aortic knuckle Aortic dissection
Jug handle appearance Primary pulmonary hypertension
Maladie de roger effect Small VSD
Hilar dance (pulmonary plethora) ASD
Box shaped heart Tricuspid Atresia
Water bottle/ flask shaped heart/ leather bottle/pear
shaped/money bag heart/ purse like heart/ Epicardial
fat pad sign
Pericardial effusion
Coeur en sabot i.e. boot shaped heart Tetralogy of Fallot
Spade like deformity on ECHO Atypical HOCM
Egg in cup appearance, square root sign Constrictive pericarditis
Inverted moustache sign Mitral stenosis
Egg on side appearance ,Egg shaped heart, Egg in string D- Transposition of great arteries (D- TGA)
Convex left heart border L-TGA
Ground glass ventricular septum Hypertrophic Obstructive Cardiomyopathy
(HOCM)
Straight left upper cardiac border Ebstein's Anomaly
Concave main pulmonary segment & right aortic arch Persistent Truncus arteriosus
Snowman sign, Figure of 8 sign, Cottage loaf sign Total Anomalous Pulmonary Venous
Connection (TAPVC) — supra cardiac variety
Goose neck sign Atrioventricular septal defect
Tubular heart Emphysema
Stag antler / hands up sign CCF
Schimitar sign / Turkish sword appearance Congenital venolobar syndrome
Sitting duck heart Persistent truncus arteriosus
Yin yang sign Pseudo aneurysms
Small heart sign Tension pneumopericardium
High attenuating crescent sign Impending rupture of abdominal aortic
aneurysm
Draped aorta sign Contained rupture of abdominal aortic
aneurysm
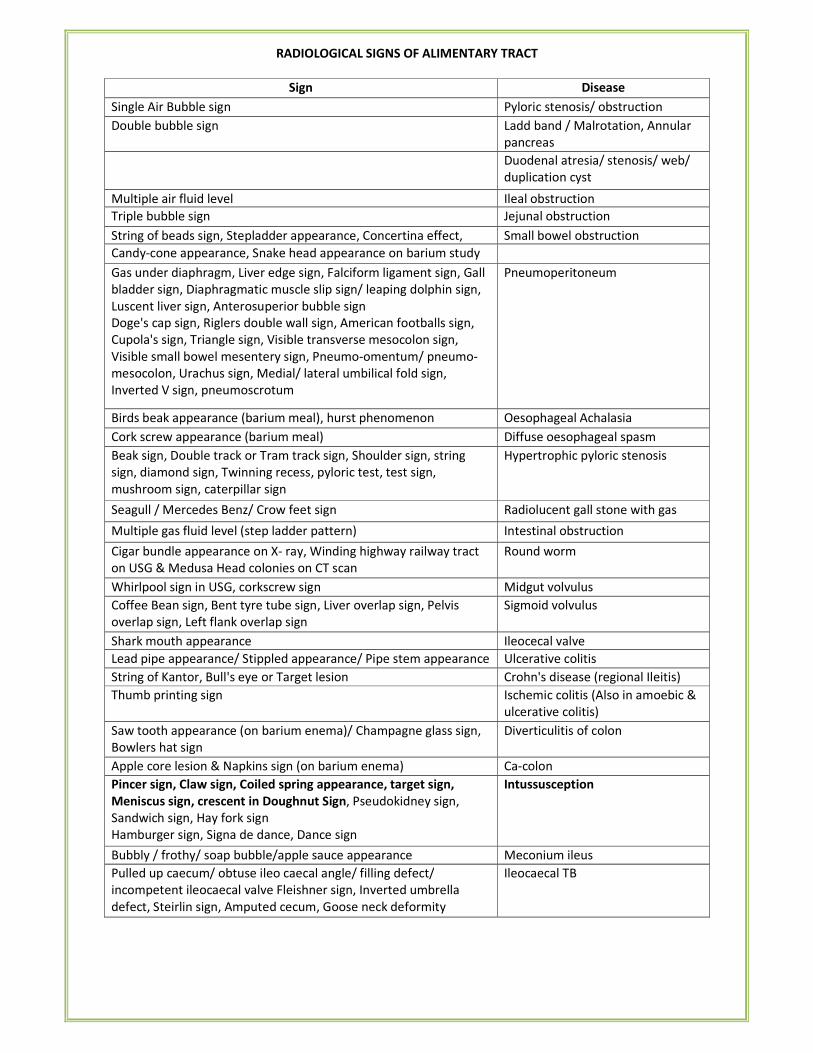
RADIOLOGICAL SIGNS OF ALIMENTARY TRACT
Sign Disease
Single Air Bubble sign Pyloric stenosis/ obstruction
Double bubble sign Ladd band / Malrotation, Annular
pancreas
Duodenal atresia/ stenosis/ web/
duplication cyst
Multiple air fluid level Ileal obstruction
Triple bubble sign Jejunal obstruction
String of beads sign, Stepladder appearance, Concertina effect, Small bowel obstruction
Candy-cone appearance, Snake head appearance on barium study
Gas under diaphragm, Liver edge sign, Falciform ligament sign, Gall
bladder sign, Diaphragmatic muscle slip sign/ leaping dolphin sign,
Luscent liver sign, Anterosuperior bubble sign
Doge's cap sign, Riglers double wall sign, American footballs sign,
Cupola's sign, Triangle sign, Visible transverse mesocolon sign,
Visible small bowel mesentery sign, Pneumo-omentum/ pneumo-
mesocolon, Urachus sign, Medial/ lateral umbilical fold sign,
Inverted V sign, pneumoscrotum
Pneumoperitoneum
Birds beak appearance (barium meal), hurst phenomenon Oesophageal Achalasia
Cork screw appearance (barium meal) Diffuse oesophageal spasm
Beak sign, Double track or Tram track sign, Shoulder sign, string
sign, diamond sign, Twinning recess, pyloric test, test sign,
mushroom sign, caterpillar sign
Hypertrophic pyloric stenosis
Seagull / Mercedes Benz/ Crow feet sign Radiolucent gall stone with gas
Multiple gas fluid level (step ladder pattern) Intestinal obstruction
Cigar bundle appearance on X- ray, Winding highway railway tract
on USG & Medusa Head colonies on CT scan
Round worm
Whirlpool sign in USG, corkscrew sign Midgut volvulus
Coffee Bean sign, Bent tyre tube sign, Liver overlap sign, Pelvis
overlap sign, Left flank overlap sign
Sigmoid volvulus
Shark mouth appearance Ileocecal valve
Lead pipe appearance/ Stippled appearance/ Pipe stem appearance Ulcerative colitis
String of Kantor, Bull's eye or Target lesion Crohn's disease (regional Ileitis)
Thumb printing sign Ischemic colitis (Also in amoebic &
ulcerative colitis)
Saw tooth appearance (on barium enema)/ Champagne glass sign,
Bowlers hat sign
Diverticulitis of colon
Apple core lesion & Napkins sign (on barium enema) Ca-colon
Pincer sign, Claw sign, Coiled spring appearance, target sign,
Meniscus sign, crescent in Doughnut Sign, Pseudokidney sign,
Sandwich sign, Hay fork sign
Hamburger sign, Signa de dance, Dance sign
Intussusception
Bubbly / frothy/ soap bubble/apple sauce appearance Meconium ileus
Pulled up caecum/ obtuse ileo caecal angle/ filling defect/
incompetent ileocaecal valve Fleishner sign, Inverted umbrella
defect, Steirlin sign, Amputed cecum, Goose neck deformity
Ileocaecal TB
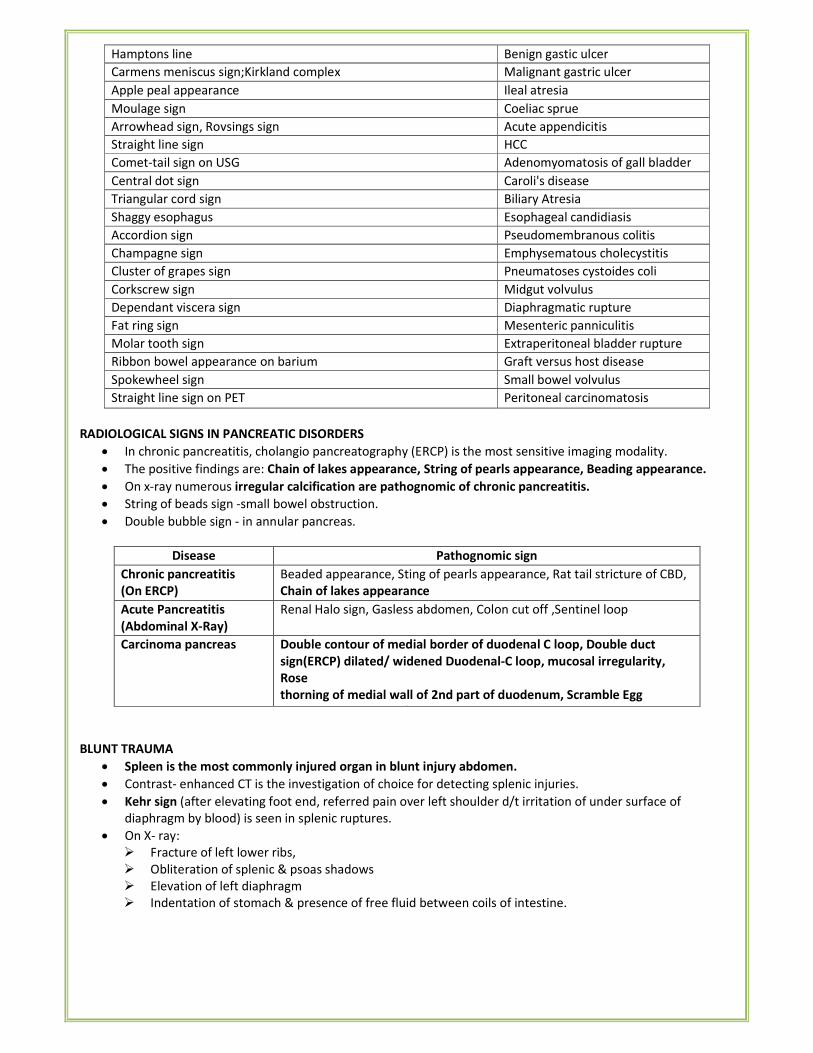
Hamptons line Benign gastic ulcer
Carmens meniscus sign;Kirkland complex Malignant gastric ulcer
Apple peal appearance Ileal atresia
Moulage sign Coeliac sprue
Arrowhead sign, Rovsings sign Acute appendicitis
Straight line sign HCC
Comet-tail sign on USG Adenomyomatosis of gall bladder
Central dot sign Caroli's disease
Triangular cord sign Biliary Atresia
Shaggy esophagus Esophageal candidiasis
Accordion sign Pseudomembranous colitis
Champagne sign Emphysematous cholecystitis
Cluster of grapes sign Pneumatoses cystoides coli
Corkscrew sign Midgut volvulus
Dependant viscera sign Diaphragmatic rupture
Fat ring sign Mesenteric panniculitis
Molar tooth sign Extraperitoneal bladder rupture
Ribbon bowel appearance on barium Graft versus host disease
Spokewheel sign Small bowel volvulus
Straight line sign on PET Peritoneal carcinomatosis
RADIOLOGICAL SIGNS IN PANCREATIC DISORDERS
• In chronic pancreatitis, cholangio pancreatography (ERCP) is the most sensitive imaging modality.
• The positive findings are: Chain of lakes appearance, String of pearls appearance, Beading appearance.
• On x-ray numerous irregular calcification are pathognomic of chronic pancreatitis.
• String of beads sign -small bowel obstruction.
• Double bubble sign - in annular pancreas.
Disease Pathognomic sign
Chronic pancreatitis
(On ERCP)
Beaded appearance, Sting of pearls appearance, Rat tail stricture of CBD,
Chain of lakes appearance
Acute Pancreatitis
(Abdominal X-Ray)
Renal Halo sign, Gasless abdomen, Colon cut off ,Sentinel loop
Carcinoma pancreas Double contour of medial border of duodenal C loop, Double duct
sign(ERCP) dilated/ widened Duodenal-C loop, mucosal irregularity,
Rose
thorning of medial wall of 2nd part of duodenum, Scramble Egg
appearance, Inverted/ Reverse-3 sign of frost berg
BLUNT TRAUMA
• Spleen is the most commonly injured organ in blunt injury abdomen.
• Contrast- enhanced CT is the investigation of choice for detecting splenic injuries.
• Kehr sign (after elevating foot end, referred pain over left shoulder d/t irritation of under surface of
diaphragm by blood) is seen in splenic ruptures.
• On X- ray:
� Fracture of left lower ribs,
� Obliteration of splenic & psoas shadows
� Elevation of left diaphragm
� Indentation of stomach & presence of free fluid between coils of intestine.
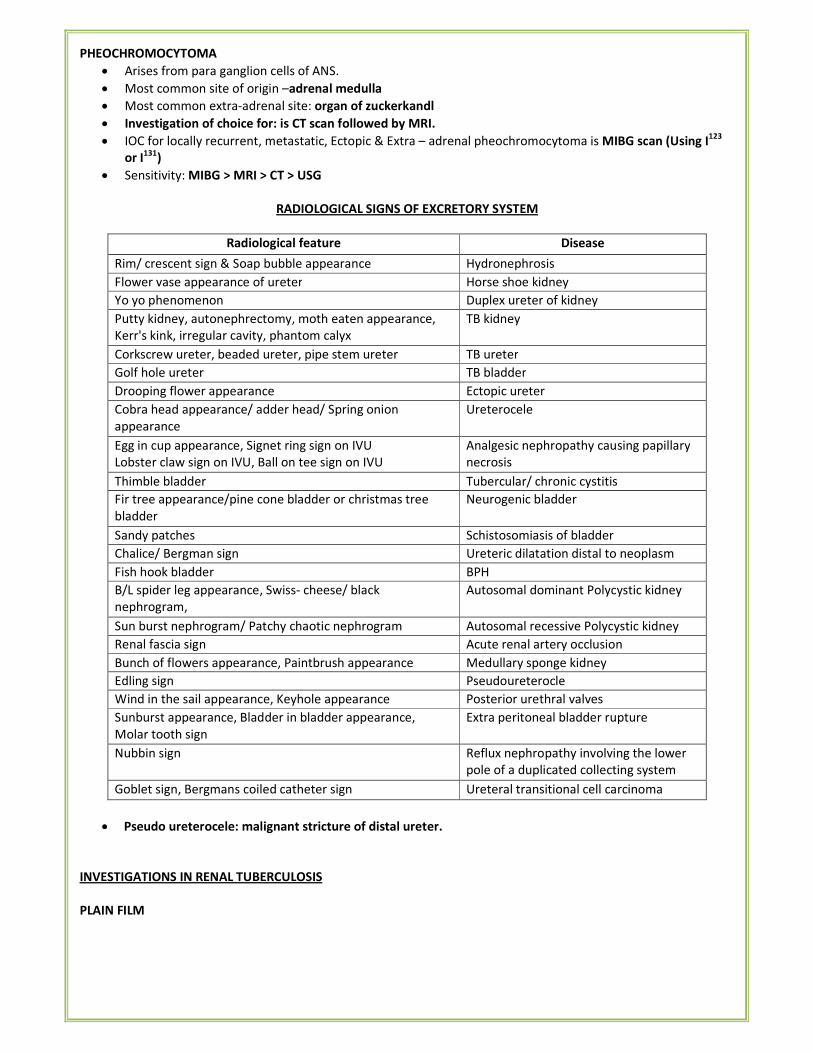
PHEOCHROMOCYTOMA
• Arises from para ganglion cells of ANS.
• Most common site of origin –adrenal medulla
• Most common extra-adrenal site: organ of zuckerkandl
• Investigation of choice for: is CT scan followed by MRI.
• IOC for locally recurrent, metastatic, Ectopic & Extra – adrenal pheochromocytoma is MIBG scan (Using I123
or I131)
• Sensitivity: MIBG > MRI > CT > USG
RADIOLOGICAL SIGNS OF EXCRETORY SYSTEM
Radiological feature Disease
Rim/ crescent sign & Soap bubble appearance Hydronephrosis
Flower vase appearance of ureter Horse shoe kidney
Yo yo phenomenon Duplex ureter of kidney
Putty kidney, autonephrectomy, moth eaten appearance,
Kerr's kink, irregular cavity, phantom calyx
TB kidney
Corkscrew ureter, beaded ureter, pipe stem ureter TB ureter
Golf hole ureter TB bladder
Drooping flower appearance Ectopic ureter
Cobra head appearance/ adder head/ Spring onion
appearance
Ureterocele
Egg in cup appearance, Signet ring sign on IVU
Lobster claw sign on IVU, Ball on tee sign on IVU
Analgesic nephropathy causing papillary
necrosis
Thimble bladder Tubercular/ chronic cystitis
Fir tree appearance/pine cone bladder or christmas tree
bladder
Neurogenic bladder
Sandy patches Schistosomiasis of bladder
Chalice/ Bergman sign Ureteric dilatation distal to neoplasm
Fish hook bladder BPH
B/L spider leg appearance, Swiss- cheese/ black
nephrogram,
Autosomal dominant Polycystic kidney
Sun burst nephrogram/ Patchy chaotic nephrogram Autosomal recessive Polycystic kidney
Renal fascia sign Acute renal artery occlusion
Bunch of flowers appearance, Paintbrush appearance Medullary sponge kidney
Edling sign Pseudoureterocle
Wind in the sail appearance, Keyhole appearance Posterior urethral valves
Sunburst appearance, Bladder in bladder appearance,
Molar tooth sign
Extra peritoneal bladder rupture
Nubbin sign Reflux nephropathy involving the lower
pole of a duplicated collecting system
Goblet sign, Bergmans coiled catheter sign Ureteral transitional cell carcinoma
• Pseudo ureterocele: malignant stricture of distal ureter.
INVESTIGATIONS IN RENAL TUBERCULOSIS
PLAIN FILM
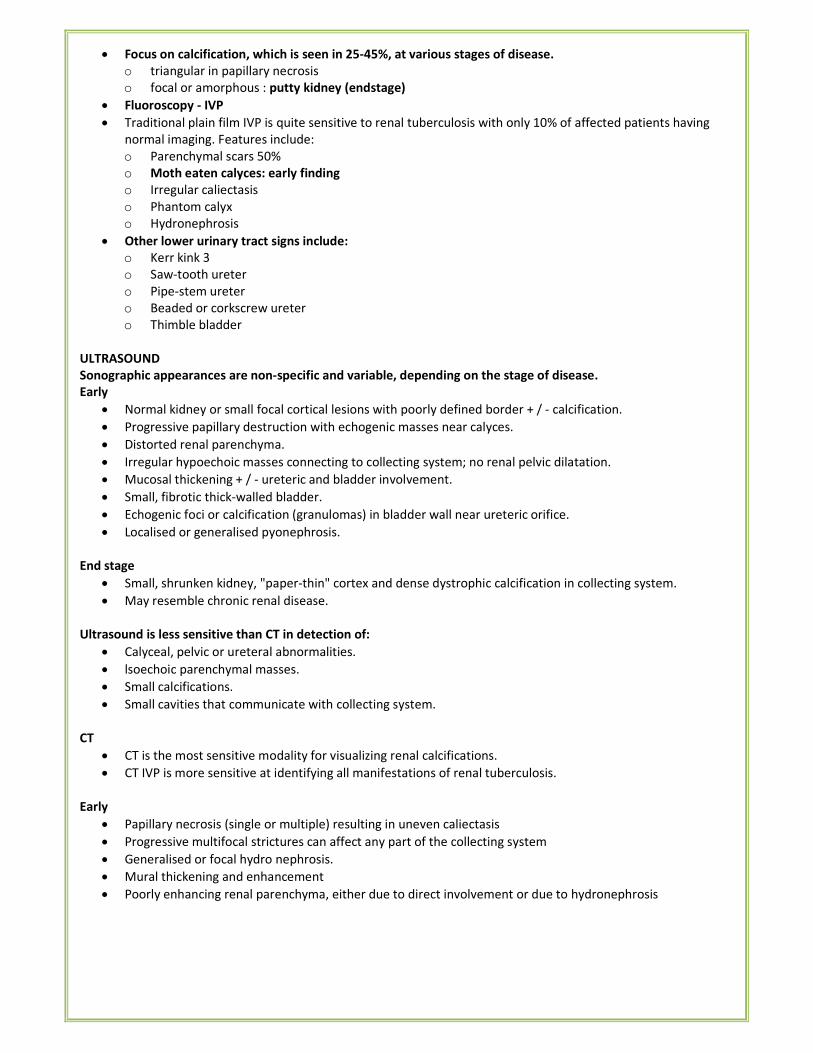
• Focus on calcification, which is seen in 25-45%, at various stages of disease.
o triangular in papillary necrosis
o focal or amorphous : putty kidney (endstage)
• Fluoroscopy - IVP
• Traditional plain film IVP is quite sensitive to renal tuberculosis with only 10% of affected patients having
normal imaging. Features include:
o Parenchymal scars 50%
o Moth eaten calyces: early finding
o Irregular caliectasis
o Phantom calyx
o Hydronephrosis
• Other lower urinary tract signs include:
o Kerr kink 3
o Saw-tooth ureter
o Pipe-stem ureter
o Beaded or corkscrew ureter
o Thimble bladder
ULTRASOUND
Sonographic appearances are non-specific and variable, depending on the stage of disease.
Early
• Normal kidney or small focal cortical lesions with poorly defined border + / - calcification.
• Progressive papillary destruction with echogenic masses near calyces.
• Distorted renal parenchyma.
• Irregular hypoechoic masses connecting to collecting system; no renal pelvic dilatation.
• Mucosal thickening + / - ureteric and bladder involvement.
• Small, fibrotic thick-walled bladder.
• Echogenic foci or calcification (granulomas) in bladder wall near ureteric orifice.
• Localised or generalised pyonephrosis.
End stage
• Small, shrunken kidney, "paper-thin" cortex and dense dystrophic calcification in collecting system.
• May resemble chronic renal disease.
Ultrasound is less sensitive than CT in detection of:
• Calyceal, pelvic or ureteral abnormalities.
• lsoechoic parenchymal masses.
• Small calcifications.
• Small cavities that communicate with collecting system.
CT
• CT is the most sensitive modality for visualizing renal calcifications.
• CT IVP is more sensitive at identifying all manifestations of renal tuberculosis.
Early
• Papillary necrosis (single or multiple) resulting in uneven caliectasis
• Progressive multifocal strictures can affect any part of the collecting system
• Generalised or focal hydro nephrosis.
• Mural thickening and enhancement
• Poorly enhancing renal parenchyma, either due to direct involvement or due to hydronephrosis
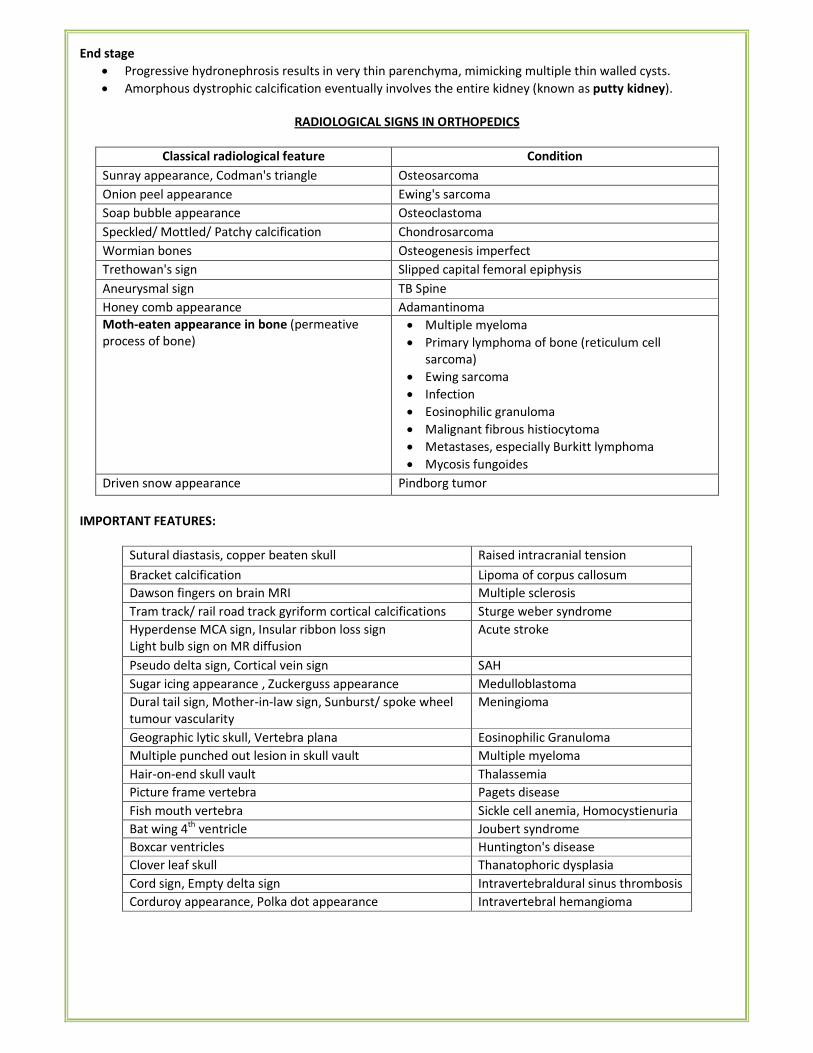
End stage
• Progressive hydronephrosis results in very thin parenchyma, mimicking multiple thin walled cysts.
• Amorphous dystrophic calcification eventually involves the entire kidney (known as putty kidney).
RADIOLOGICAL SIGNS IN ORTHOPEDICS
Classical radiological feature Condition
Sunray appearance, Codman's triangle Osteosarcoma
Onion peel appearance Ewing's sarcoma
Soap bubble appearance Osteoclastoma
Speckled/ Mottled/ Patchy calcification Chondrosarcoma
Wormian bones Osteogenesis imperfect
Trethowan's sign Slipped capital femoral epiphysis
Aneurysmal sign TB Spine
Honey comb appearance Adamantinoma
Moth-eaten appearance in bone (permeative
process of bone)
• Multiple myeloma
• Primary lymphoma of bone (reticulum cell
sarcoma)
• Ewing sarcoma
• Infection
• Eosinophilic granuloma
• Malignant fibrous histiocytoma
• Metastases, especially Burkitt lymphoma
• Mycosis fungoides
Driven snow appearance Pindborg tumor
IMPORTANT FEATURES:
Sutural diastasis, copper beaten skull Raised intracranial tension
Bracket calcification Lipoma of corpus callosum
Dawson fingers on brain MRI Multiple sclerosis
Tram track/ rail road track gyriform cortical calcifications Sturge weber syndrome
Hyperdense MCA sign, Insular ribbon loss sign
Light bulb sign on MR diffusion
Acute stroke
Pseudo delta sign, Cortical vein sign SAH
Sugar icing appearance , Zuckerguss appearance Medulloblastoma
Dural tail sign, Mother-in-law sign, Sunburst/ spoke wheel
tumour vascularity
Meningioma
Geographic lytic skull, Vertebra plana Eosinophilic Granuloma
Multiple punched out lesion in skull vault Multiple myeloma
Hair-on-end skull vault Thalassemia
Picture frame vertebra Pagets disease
Fish mouth vertebra Sickle cell anemia, Homocystienuria
Bat wing 4th
ventricle Joubert syndrome
Boxcar ventricles Huntington's disease
Clover leaf skull Thanatophoric dysplasia
Cord sign, Empty delta sign Intravertebraldural sinus thrombosis
Corduroy appearance, Polka dot appearance Intravertebral hemangioma
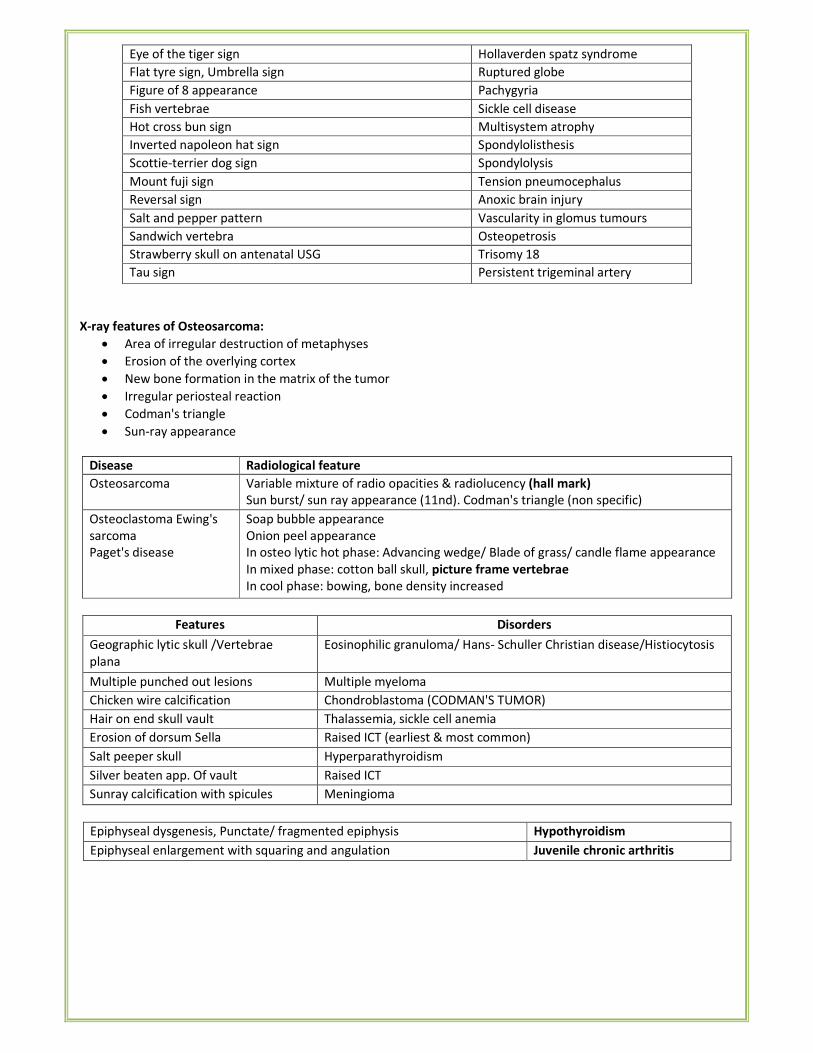
Eye of the tiger sign Hollaverden spatz syndrome
Flat tyre sign, Umbrella sign Ruptured globe
Figure of 8 appearance Pachygyria
Fish vertebrae Sickle cell disease
Hot cross bun sign Multisystem atrophy
Inverted napoleon hat sign Spondylolisthesis
Scottie-terrier dog sign Spondylolysis
Mount fuji sign Tension pneumocephalus
Reversal sign Anoxic brain injury
Salt and pepper pattern Vascularity in glomus tumours
Sandwich vertebra Osteopetrosis
Strawberry skull on antenatal USG Trisomy 18
Tau sign Persistent trigeminal artery
X-ray features of Osteosarcoma:
• Area of irregular destruction of metaphyses
• Erosion of the overlying cortex
• New bone formation in the matrix of the tumor
• Irregular periosteal reaction
• Codman's triangle
• Sun-ray appearance
Disease
Radiological feature
Osteosarcoma Variable mixture of radio opacities & radiolucency (hall mark)
Sun burst/ sun ray appearance (11nd). Codman's triangle (non specific)
Osteoclastoma Ewing's
sarcoma
Paget's disease
Soap bubble appearance
Onion peel appearance
In osteo lytic hot phase: Advancing wedge/ Blade of grass/ candle flame appearance
In mixed phase: cotton ball skull, picture frame vertebrae
In cool phase: bowing, bone density increased
Features Disorders
Geographic lytic skull /Vertebrae
plana
Eosinophilic granuloma/ Hans- Schuller Christian disease/Histiocytosis
Multiple punched out lesions Multiple myeloma
Chicken wire calcification Chondroblastoma (CODMAN'S TUMOR)
Hair on end skull vault Thalassemia, sickle cell anemia
Erosion of dorsum Sella Raised ICT (earliest & most common)
Salt peeper skull Hyperparathyroidism
Silver beaten app. Of vault Raised ICT
Sunray calcification with spicules Meningioma
Epiphyseal dysgenesis, Punctate/ fragmented epiphysis Hypothyroidism
Epiphyseal enlargement with squaring and angulation Juvenile chronic arthritis
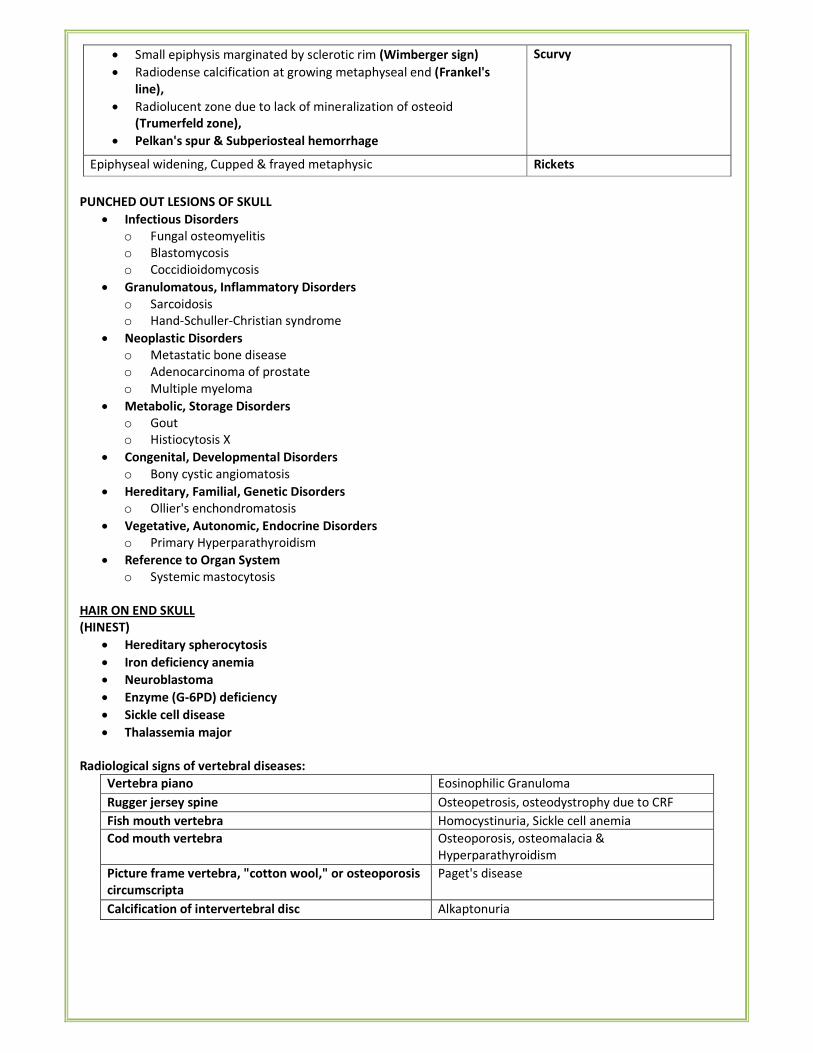
• Small epiphysis marginated by sclerotic rim (Wimberger sign)
• Radiodense calcification at growing metaphyseal end (Frankel's
line),
• Radiolucent zone due to lack of mineralization of osteoid
(Trumerfeld zone),
• Pelkan's spur & Subperiosteal hemorrhage
Scurvy
Epiphyseal widening, Cupped & frayed metaphysic Rickets
PUNCHED OUT LESIONS OF SKULL
• Infectious Disorders
o Fungal osteomyelitis
o Blastomycosis
o Coccidioidomycosis
• Granulomatous, Inflammatory Disorders
o Sarcoidosis
o Hand-Schuller-Christian syndrome
• Neoplastic Disorders
o Metastatic bone disease
o Adenocarcinoma of prostate
o Multiple myeloma
• Metabolic, Storage Disorders
o Gout
o Histiocytosis X
• Congenital, Developmental Disorders
o Bony cystic angiomatosis
• Hereditary, Familial, Genetic Disorders
o Ollier's enchondromatosis
• Vegetative, Autonomic, Endocrine Disorders
o Primary Hyperparathyroidism
• Reference to Organ System
o Systemic mastocytosis
HAIR ON END SKULL
(HINEST)
• Hereditary spherocytosis
• Iron deficiency anemia
• Neuroblastoma
• Enzyme (G-6PD) deficiency
• Sickle cell disease
• Thalassemia major
Radiological signs of vertebral diseases:
Vertebra piano Eosinophilic Granuloma
Rugger jersey spine Osteopetrosis, osteodystrophy due to CRF
Fish mouth vertebra Homocystinuria, Sickle cell anemia
Cod mouth vertebra Osteoporosis, osteomalacia &
Hyperparathyroidism
Picture frame vertebra, "cotton wool," or osteoporosis
circumscripta
Paget's disease
Calcification of intervertebral disc Alkaptonuria
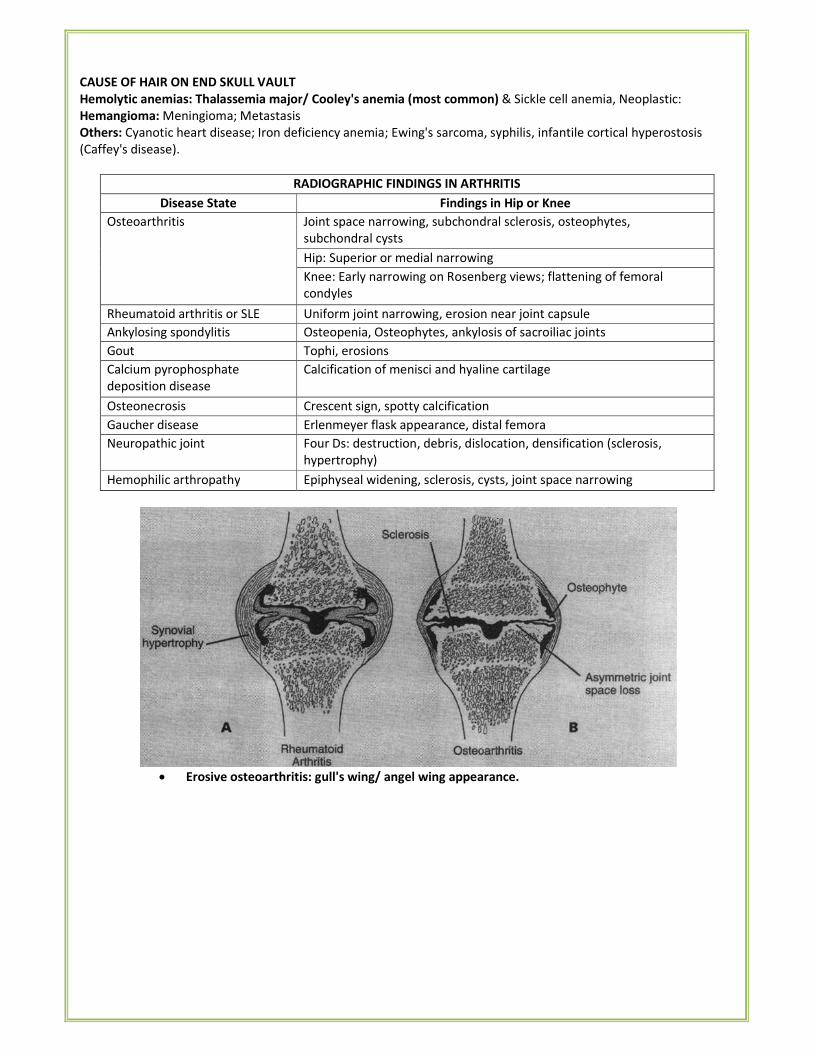
CAUSE OF HAIR ON END SKULL VAULT
Hemolytic anemias: Thalassemia major/ Cooley's anemia (most common) & Sickle cell anemia, Neoplastic:
Hemangioma: Meningioma; Metastasis
Others: Cyanotic heart disease; Iron deficiency anemia; Ewing's sarcoma, syphilis, infantile cortical hyperostosis
(Caffey's disease).
RADIOGRAPHIC FINDINGS IN ARTHRITIS
Disease State Findings in Hip or Knee
Osteoarthritis Joint space narrowing, subchondral sclerosis, osteophytes,
subchondral cysts
Hip: Superior or medial narrowing
Knee: Early narrowing on Rosenberg views; flattening of femoral
condyles
Rheumatoid arthritis or SLE Uniform joint narrowing, erosion near joint capsule
Ankylosing spondylitis Osteopenia, Osteophytes, ankylosis of sacroiliac joints
Gout Tophi, erosions
Calcium pyrophosphate
deposition disease
Calcification of menisci and hyaline cartilage
Osteonecrosis Crescent sign, spotty calcification
Gaucher disease Erlenmeyer flask appearance, distal femora
Neuropathic joint Four Ds: destruction, debris, dislocation, densification (sclerosis,
hypertrophy)
Hemophilic arthropathy Epiphyseal widening, sclerosis, cysts, joint space narrowing
• Erosive osteoarthritis: gull's wing/ angel wing appearance.
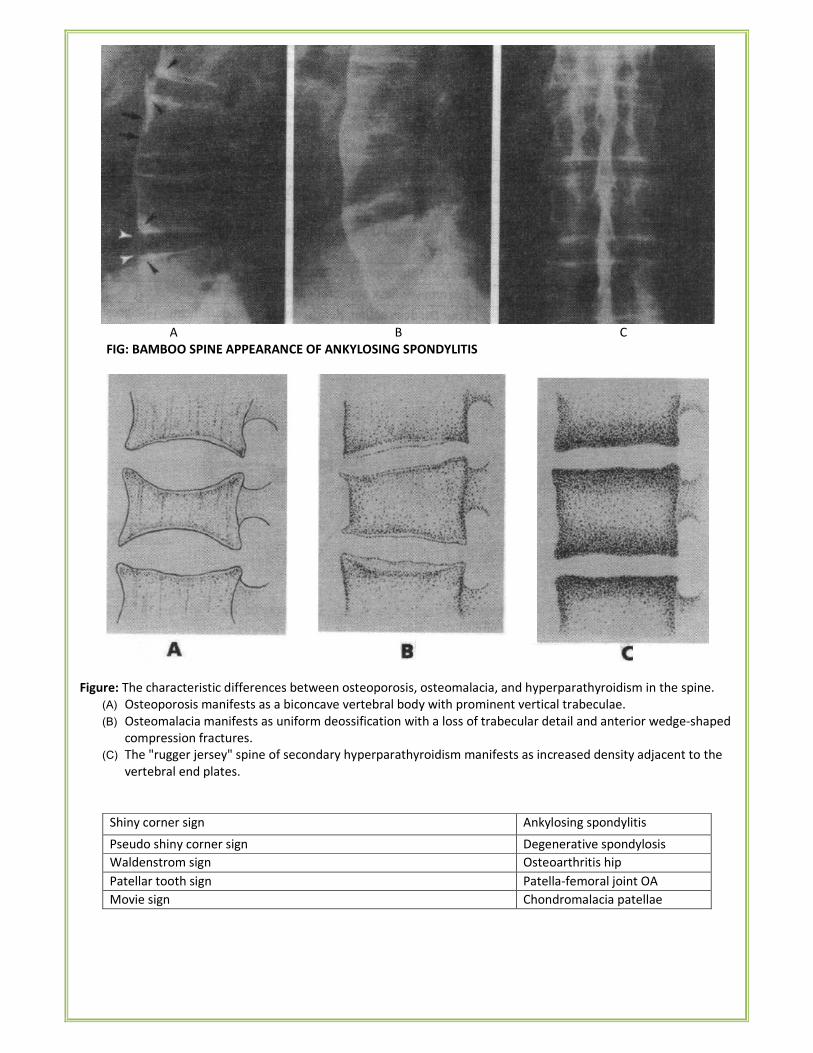
A B C
FIG: BAMBOO SPINE APPEARANCE OF ANKYLOSING SPONDYLITIS
Figure: The characteristic differences between osteoporosis, osteomalacia, and hyperparathyroidism in the spine.
(A) Osteoporosis manifests as a biconcave vertebral body with prominent vertical trabeculae.
(B) Osteomalacia manifests as uniform deossification with a loss of trabecular detail and anterior wedge-shaped
compression fractures.
(C) The "rugger jersey" spine of secondary hyperparathyroidism manifests as increased density adjacent to the
vertebral end plates.
Shiny corner sign Ankylosing spondylitis
Pseudo shiny corner sign Degenerative spondylosis
Waldenstrom sign Osteoarthritis hip
Patellar tooth sign Patella-femoral joint OA
Movie sign Chondromalacia patellae
Licked candy stick appearance, Jigsaw vertebra
Tumbling building block spine
Atrophic neuropathic arthritis
Migrating mouse sign
Apple core deformity of hip
Synovio-chondro-metaplasia
Cocktail sausage digit, spindle digit, ivory phalanx, Pencil in cup/
pestle and mortar/ mushroom and stem/ balancing pagoda/ cup in
saucer appearance, opera glass hand, whittling effect, mouse ears
sign
Psoriatic arthropathy
Bone in bone appearance, Sandwich vertebra, Rugger-jersey spine
Erlenmeyer flask deformity
Osteopetrosis
Flowing candlewax appearance Melorrhosteosis
Hot cross bun skull Cliedo-cranial dysplasia
Paired posterior iliac horns nail patella syndrome
Elephant ears, Mickey mouse ears, Clinodactyly Downs syndrome
Bare orbit, Empty orbit sign Neurofibromatosis-1
Hook shaped vertebral bodies, Cut corner sign MPS l/ hurler syndrome
Central beaking of vertebrae, Ape like pelvis MPS IV/ morquio syndrome
Gull wing sign Erosive OA
Steinberg sign Marfan syndrome
Pelkan spur/ Pencil thin cortex/ Corner sign of Parke
Trummerfield zone of rarefaction/ White line of Frankel/ Wimberger
sign
Scurvy
Looser zone/ lines, Milkmans fracture, Osteoid seams
Increment fracture, Umbau zones
Osteomalacia
Rugger jersey spine/ Brown tumours/ Pepper pot skull/ Subperiosteal
resorption of phalanges
Hyperparathyroidism
Cotton wool appearance, Candle flame/ blade of grass lysis
Picture frame vertebra
Pagets disease
Penumbra sign Brodies abscess
Inverted napoleon hat sign, Gendarme's cap sign
Bowline of Brailsford, Broken collar/ neck of scotty dog, Scottish
terrier sign
Spondylolisthesis
Button sequestrum, Floating teeth sign, Hole with hole appearance Histiocytosis-X
Swan neck deformity, Boutonniere deformity, Hitch hiker thumb
Hammer toes
RA
Trident hand, Tomb stone iliac bone, Cheuron sign Achondroplasia
Intervertebral disc calcification Alkaptonuria
Pear shaped vertebra Spondylo-epiphyseal dysplasia
congenita Hump shaped vertebra, Heaped up vertebra Spondylo-epiphyseal dysplasia
tarda Inferiorly beaked vertebra MPS l/ hurler syndrome
Centrally beaked vertebra MPS IV/ hunter syndrome
Biconcave lens vertebra Osteogenesis imperfecta
Spool shaped vertebra Pyknodysostosis
Bullet nose vertebra Achondroplasia
Vertebra with central anterior tongues Pseudochondroplasia
H shaped vertebra Thanatophoric dwarfism
FEATURES OF BRAIN HEMATOMA ON CT SCAN
Extradural Subdural Subarachnoid: (SAH)
• Biconvex (Lens
shaped/
lenticular)
• Hyper dense
in acute cases.
• Hypo dense in
Chronic cases
• Crescent
(Concavo-
Convex)
• Hyper dense
(<2 weeks)
• Isodense (2-4
wks)
• Hypo dense (> 4
wks)
• Non- contrast CT is investigation of choice for diagnosing
the hematoma.
• Four vessels (both carotids & both vertebra's) Digital
subtraction angiography (DSA) is the investigation of
choice for determining etiology.
• The hallmark of SAH is blood in CSF detected by lumbar
puncture.
• Lysis of blood in CSF causes Xanthochromia which is peak
at 48 hours.
• Most common intracranial lesion after head injury is subdural hematoma.
• Most common cause of SAH is head trauma.
• Investigation of choice for SAH is Non- contrast CT
• M.C. cause of spontaneous SAH is ruptured saccular aneurysm.
Diffuse axonal injury (DAI)
• It is caused by shearing of the white matter, often at the gray-white junction.
• May be due to the differing tissue density or fixation between two structures in differing response to
rotation, acceleration, and deceleration.
• Detection is often associated with changes in the lobar white matter, brainstem, and corpus callosum with
ovoid or elongated regions of decreased density.
• Patients usually present with severe impairment of consciousness from the moment of impact.
• MRI (FLAIR or T2 weighted) - most useful in defining the extent of axonal shearing and non-hemorrhagic
injury.
• CT results -often negative, but acute areas of petechial hemorrhage & cerebral edema have been seen in
early stages.
IMPORTANT SIGNS IN RADIOLOGY
• Puff of smoke sign: Moyamoya disease
• Polka dot sign: vertebral hemangioma
• Dripping candle wax sign: melorheostosis
• Accordion sign: pseudomembranous colitis
• Air crescent sign: aspergilloma
• Angelwing sign: pulmonary edema [bat wing sign]
• Air bronchogram sign: pneumonia
• Anteater's nose sign: tarsal coalition
• Apple core appearance: Ca Colon
• Blade of grass sign [Flame sign]: Paget's disease
• Bevelled edge appearance: eosinophilic granuloma
• Bowler hat sign, Mexican hat sign: colonic polyp
• Black pleura sign: alveolar microlithiasis
• Bird of prey sign: sigmoid volvulus
• Bone within bone appearance: osteopetrosis
• Breast within breast appearance: hamartoma of breast
• Bear paw sign: xanthogranulomatous Pyelonephritis
• Pelvic brim sign: Paget's disease
• Bite sign, crescent sign: avascular necrosis of femur
• Bulging fissure sign: Klebsiella pneumonia
• Banana sign/ lemon sign: neural tube defect
• Carman meniscus sign: Ca stomach
• Cotton wool appearance: Paget disease
• Cobra head appearance: Ureterocele
• Coblestone appearance: Crohn's disease
• C sign: tarsal coalition
• Coffee bean sign: sigmoid volvulus
• Colon cut off sign: acute pancreatitis
• Comb sign: Crohn's disease
• Comet tail sign: round atelectasis
• Comet sign: pelvic phlebolith
• Continuous diaphragm sign: pneumomediastinum
• Corduroy sign: vertebral hemangioma
• Corkscrew oesophagus: diffuse esophageal spasm
• Crazy paving sign: pulmonary alveolar proteinosis
• Champagne glass pelvis: Achondroplasia
• Celary stalk sign: rubella, osteopathia striata, anterior cruciate ligament degeneration
• Corkscrew sign: midgut volvulus
• Cottage loaf sign: diaphragmatic rupture
• Codfish vertebra: sickle cell disease
• Jerry Thomas sign: scapho lunate dislocation
• Dense MCA sign: hyperacute stroke(CT sign)
• Double bubble sign: duodenal atresia, annular pancreas
• Double density sign: enlarged left atrium (mitral stenosis)
• Doughnut sign: testicular torsion(nuclear scan)
• Draping aorta sign: leaking abdominal aortic aneurysm
• Deep sulcus sign: pneumothorax
• Double duct sign: periampullary, pancreatic Ca
• Erlenmeyer flask deformity: Gaucher's disease, thalassemia, osteopetrosis, pyle's disease
• Fat pad sign: pericardial effusion
• Foot ball/ falciform ligament sign: Pneumoperitoneum (infant)
• Fallen lung sign: fracture bronchus
• Fishhook ureter: BPH
• Flat waist sign: left lower lobe collapse
• Gloved finger sign: allergic bronchopulmonary aspergillosis
• Gull wing sign: erosive osteoarthritis
• Goose neck sign: endocardial cushion defect
• Hampton line: benign gastric ulcer
• Hampton hump: pulmonary infarction
• Honda sign: sacral insufficiency fracture
• Hide bound appearance: scleroderma
• Hair on end appearance: hemolytic anemia
• Hot nose sign: brain death
• Holly leaf appearance: asbestosis
• Hot cross bun sign: multi system atrophy-C
• Half moon/ light bulb sign: posterior shoulder dislocation
• Head cheese sign: hypersensitivity pneumonitis
• Ivory vertebra: osteoblastic vertebral metastasis
• Insular ribbon sign: acute cerebral infarct
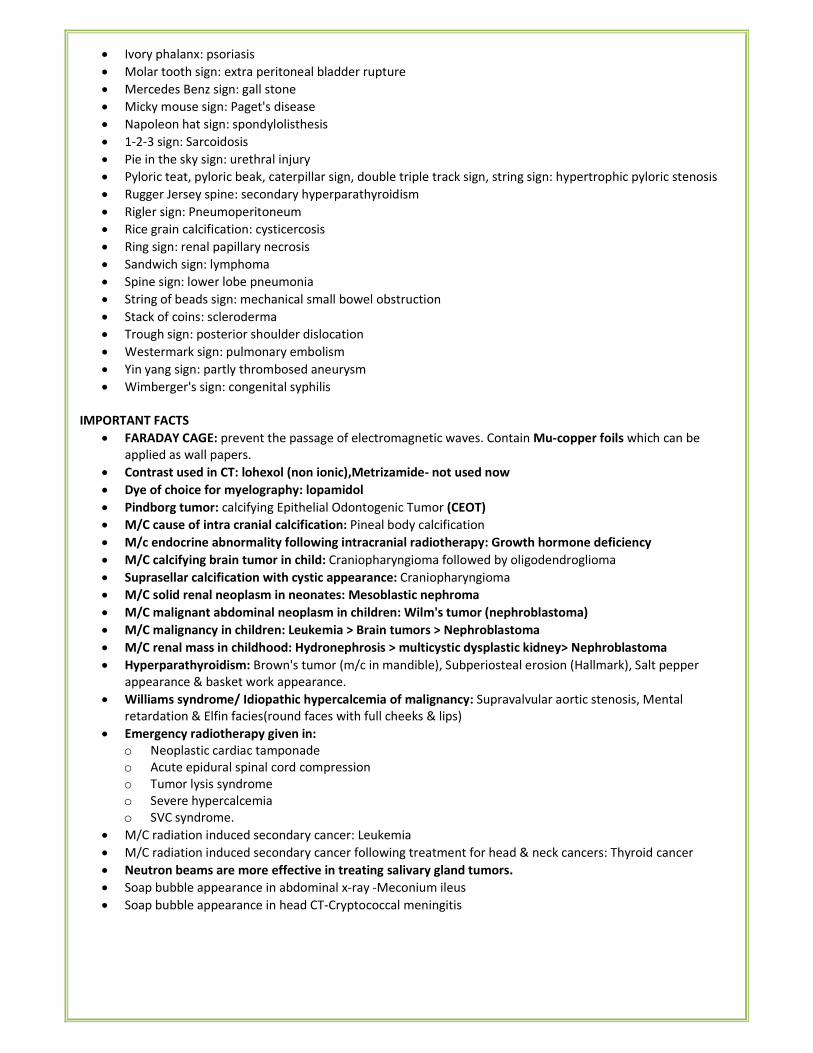
• Ivory phalanx: psoriasis
• Molar tooth sign: extra peritoneal bladder rupture
• Mercedes Benz sign: gall stone
• Micky mouse sign: Paget's disease
• Napoleon hat sign: spondylolisthesis
• 1-2-3 sign: Sarcoidosis
• Pie in the sky sign: urethral injury
• Pyloric teat, pyloric beak, caterpillar sign, double triple track sign, string sign: hypertrophic pyloric stenosis
• Rugger Jersey spine: secondary hyperparathyroidism
• Rigler sign: Pneumoperitoneum
• Rice grain calcification: cysticercosis
• Ring sign: renal papillary necrosis
• Sandwich sign: lymphoma
• Spine sign: lower lobe pneumonia
• String of beads sign: mechanical small bowel obstruction
• Stack of coins: scleroderma
• Trough sign: posterior shoulder dislocation
• Westermark sign: pulmonary embolism
• Yin yang sign: partly thrombosed aneurysm
• Wimberger's sign: congenital syphilis
IMPORTANT FACTS
• FARADAY CAGE: prevent the passage of electromagnetic waves. Contain Mu-copper foils which can be
applied as wall papers.
• Contrast used in CT: lohexol (non ionic),Metrizamide- not used now
• Dye of choice for myelography: lopamidol
• Pindborg tumor: calcifying Epithelial Odontogenic Tumor (CEOT)
• M/C cause of intra cranial calcification: Pineal body calcification
• M/c endocrine abnormality following intracranial radiotherapy: Growth hormone deficiency
• M/C calcifying brain tumor in child: Craniopharyngioma followed by oligodendroglioma
• Suprasellar calcification with cystic appearance: Craniopharyngioma
• M/C solid renal neoplasm in neonates: Mesoblastic nephroma
• M/C malignant abdominal neoplasm in children: Wilm's tumor (nephroblastoma)
• M/C malignancy in children: Leukemia > Brain tumors > Nephroblastoma
• M/C renal mass in childhood: Hydronephrosis > multicystic dysplastic kidney> Nephroblastoma
• Hyperparathyroidism: Brown's tumor (m/c in mandible), Subperiosteal erosion (Hallmark), Salt pepper
appearance & basket work appearance.
• Williams syndrome/ Idiopathic hypercalcemia of malignancy: Supravalvular aortic stenosis, Mental
retardation & Elfin facies(round faces with full cheeks & lips)
• Emergency radiotherapy given in:
o Neoplastic cardiac tamponade
o Acute epidural spinal cord compression
o Tumor lysis syndrome
o Severe hypercalcemia
o SVC syndrome.
• M/C radiation induced secondary cancer: Leukemia
• M/C radiation induced secondary cancer following treatment for head & neck cancers: Thyroid cancer
• Neutron beams are more effective in treating salivary gland tumors.
• Soap bubble appearance in abdominal x-ray -Meconium ileus
• Soap bubble appearance in head CT-Cryptococcal meningitis
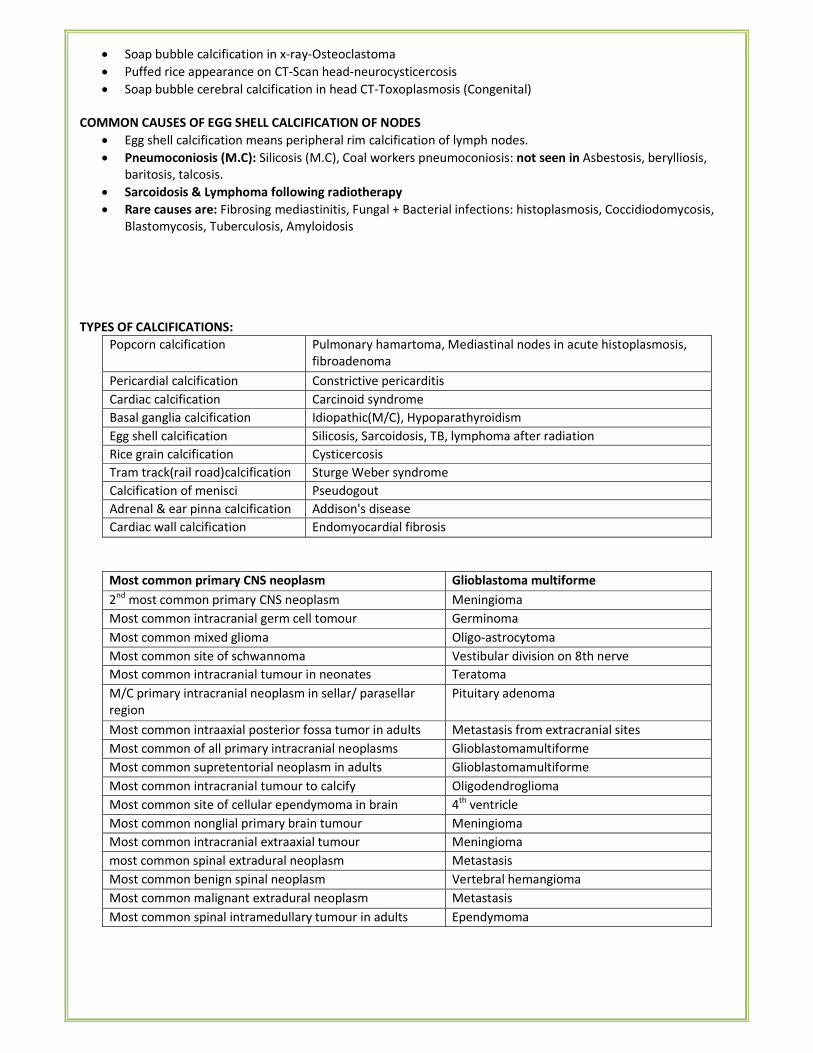
• Soap bubble calcification in x-ray-Osteoclastoma
• Puffed rice appearance on CT-Scan head-neurocysticercosis
• Soap bubble cerebral calcification in head CT-Toxoplasmosis (Congenital)
COMMON CAUSES OF EGG SHELL CALCIFICATION OF NODES
• Egg shell calcification means peripheral rim calcification of lymph nodes.
• Pneumoconiosis (M.C): Silicosis (M.C), Coal workers pneumoconiosis: not seen in Asbestosis, berylliosis,
baritosis, talcosis.
• Sarcoidosis & Lymphoma following radiotherapy
• Rare causes are: Fibrosing mediastinitis, Fungal + Bacterial infections: histoplasmosis, Coccidiodomycosis,
Blastomycosis, Tuberculosis, Amyloidosis
TYPES OF CALCIFICATIONS:
Popcorn calcification Pulmonary hamartoma, Mediastinal nodes in acute histoplasmosis,
fibroadenoma
Pericardial calcification Constrictive pericarditis
Cardiac calcification Carcinoid syndrome
Basal ganglia calcification Idiopathic(M/C), Hypoparathyroidism
Egg shell calcification Silicosis, Sarcoidosis, TB, lymphoma after radiation
Rice grain calcification Cysticercosis
Tram track(rail road)calcification Sturge Weber syndrome
Calcification of menisci Pseudogout
Adrenal & ear pinna calcification Addison's disease
Cardiac wall calcification Endomyocardial fibrosis
Most common primary CNS neoplasm Glioblastoma multiforme
2nd
most common primary CNS neoplasm Meningioma
Most common intracranial germ cell tomour Germinoma
Most common mixed glioma Oligo-astrocytoma
Most common site of schwannoma Vestibular division on 8th nerve
Most common intracranial tumour in neonates Teratoma
M/C primary intracranial neoplasm in sellar/ parasellar
region
Pituitary adenoma
Most common intraaxial posterior fossa tumor in adults Metastasis from extracranial sites
Most common of all primary intracranial neoplasms Glioblastomamultiforme
Most common supretentorial neoplasm in adults Glioblastomamultiforme
Most common intracranial tumour to calcify Oligodendroglioma
Most common site of cellular ependymoma in brain 4th
ventricle
Most common nonglial primary brain tumour Meningioma
Most common intracranial extraaxial tumour Meningioma
most common spinal extradural neoplasm Metastasis
Most common benign spinal neoplasm Vertebral hemangioma
Most common malignant extradural neoplasm Metastasis
Most common spinal intramedullary tumour in adults Ependymoma
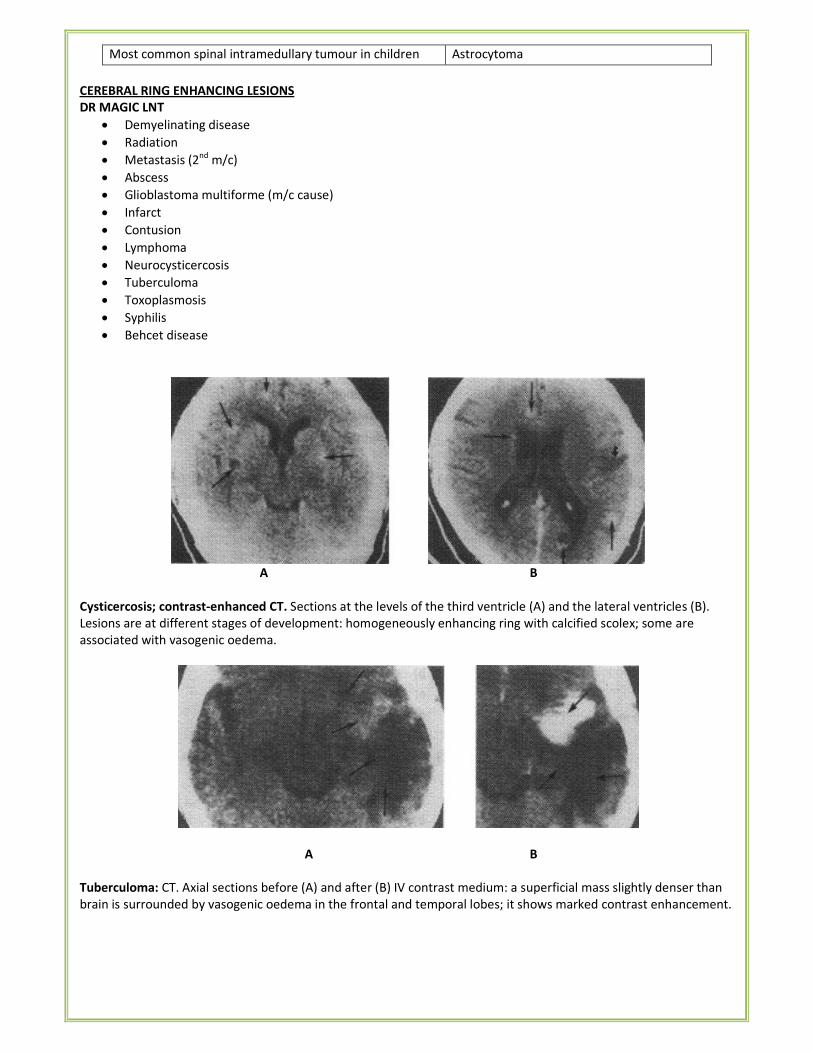
Most common spinal intramedullary tumour in children Astrocytoma
CEREBRAL RING ENHANCING LESIONS
DR MAGIC LNT
• Demyelinating disease
• Radiation
• Metastasis (2nd
m/c)
• Abscess
• Glioblastoma multiforme (m/c cause)
• Infarct
• Contusion
• Lymphoma
• Neurocysticercosis
• Tuberculoma
• Toxoplasmosis
• Syphilis
• Behcet disease
A B
Cysticercosis; contrast-enhanced CT. Sections at the levels of the third ventricle (A) and the lateral ventricles (B).
Lesions are at different stages of development: homogeneously enhancing ring with calcified scolex; some are
associated with vasogenic oedema.
A B
Tuberculoma: CT. Axial sections before (A) and after (B) IV contrast medium: a superficial mass slightly denser than
brain is surrounded by vasogenic oedema in the frontal and temporal lobes; it shows marked contrast enhancement.
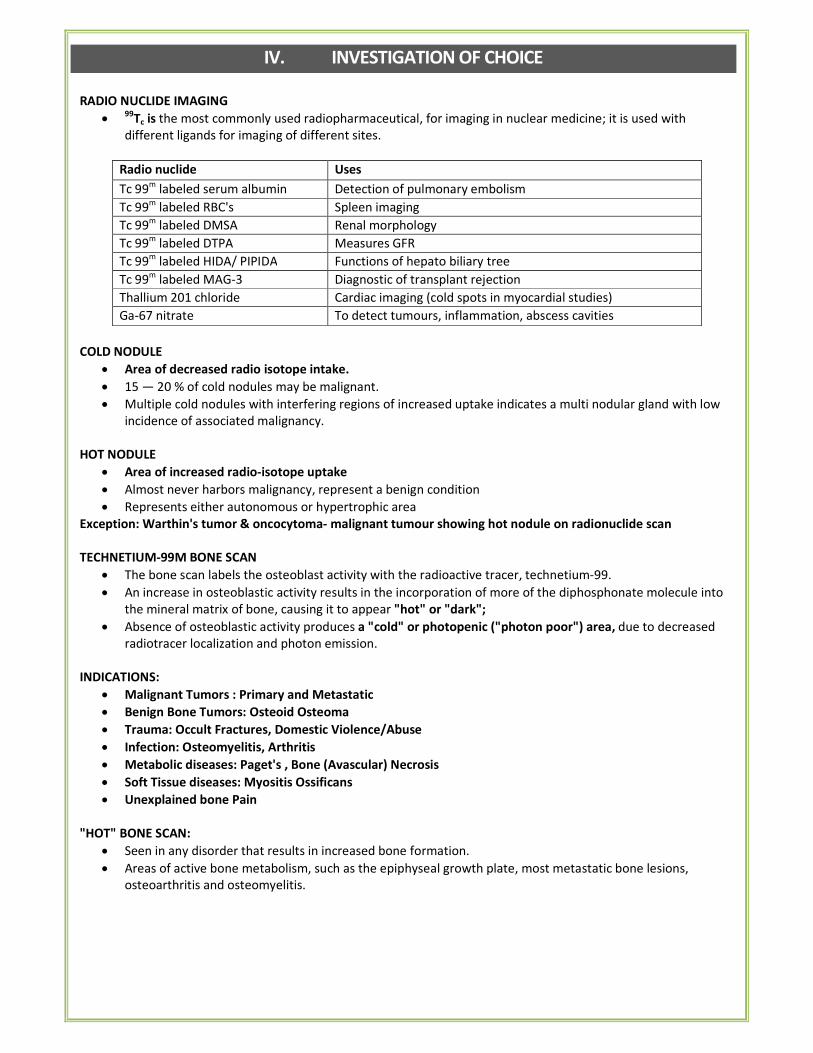
IV. INVESTIGATION OF CHOICE
RADIO NUCLIDE IMAGING
• 99Tc is the most commonly used radiopharmaceutical, for imaging in nuclear medicine; it is used with
different ligands for imaging of different sites.
Radio nuclide Uses
Tc 99m
labeled serum albumin Detection of pulmonary embolism
Tc 99m
labeled RBC's Spleen imaging
Tc 99m
labeled DMSA Renal morphology
Tc 99m
labeled DTPA Measures GFR
Tc 99m
labeled HIDA/ PIPIDA Functions of hepato biliary tree
Tc 99m
labeled MAG-3 Diagnostic of transplant rejection
Thallium 201 chloride Cardiac imaging (cold spots in myocardial studies)
Ga-67 nitrate To detect tumours, inflammation, abscess cavities
COLD NODULE
• Area of decreased radio isotope intake.
• 15 — 20 % of cold nodules may be malignant.
• Multiple cold nodules with interfering regions of increased uptake indicates a multi nodular gland with low
incidence of associated malignancy.
HOT NODULE
• Area of increased radio-isotope uptake
• Almost never harbors malignancy, represent a benign condition
• Represents either autonomous or hypertrophic area
Exception: Warthin's tumor & oncocytoma- malignant tumour showing hot nodule on radionuclide scan
TECHNETIUM-99M BONE SCAN
• The bone scan labels the osteoblast activity with the radioactive tracer, technetium-99.
• An increase in osteoblastic activity results in the incorporation of more of the diphosphonate molecule into
the mineral matrix of bone, causing it to appear "hot" or "dark";
• Absence of osteoblastic activity produces a "cold" or photopenic ("photon poor") area, due to decreased
radiotracer localization and photon emission.
INDICATIONS:
• Malignant Tumors : Primary and Metastatic
• Benign Bone Tumors: Osteoid Osteoma
• Trauma: Occult Fractures, Domestic Violence/Abuse
• Infection: Osteomyelitis, Arthritis
• Metabolic diseases: Paget's , Bone (Avascular) Necrosis
• Soft Tissue diseases: Myositis Ossificans
• Unexplained bone Pain
"HOT" BONE SCAN:
• Seen in any disorder that results in increased bone formation.
• Areas of active bone metabolism, such as the epiphyseal growth plate, most metastatic bone lesions,
osteoarthritis and osteomyelitis.
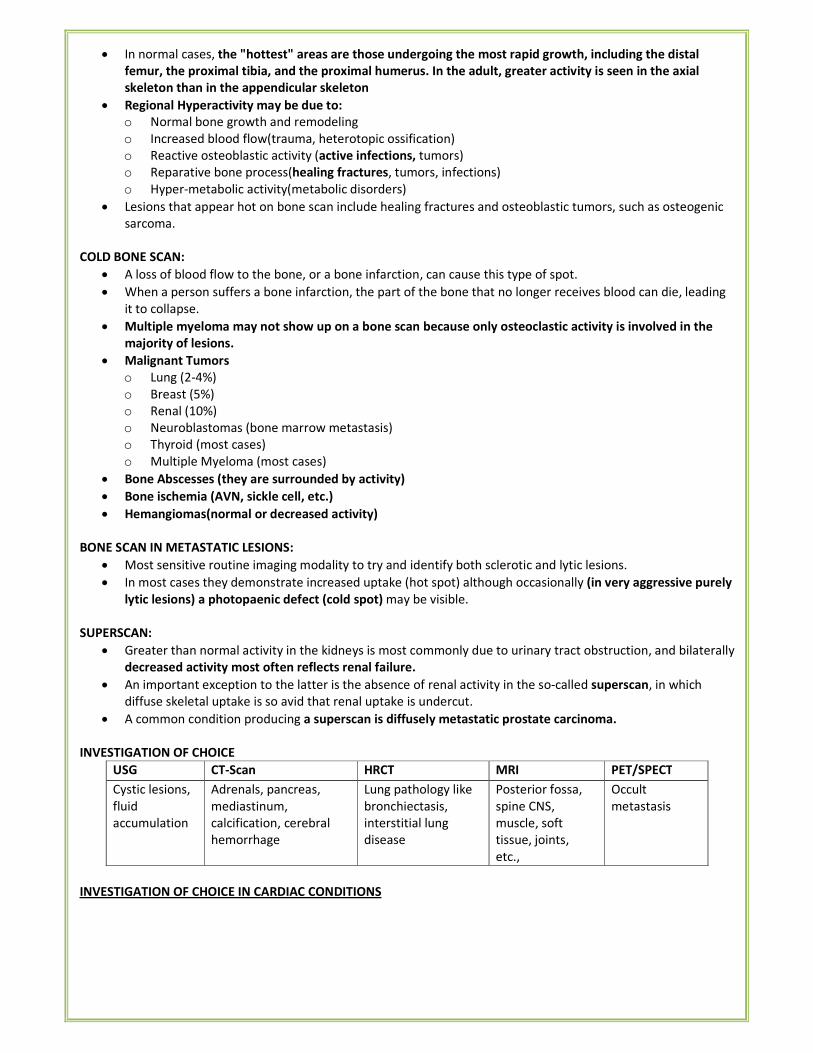
• In normal cases, the "hottest" areas are those undergoing the most rapid growth, including the distal
femur, the proximal tibia, and the proximal humerus. In the adult, greater activity is seen in the axial
skeleton than in the appendicular skeleton
• Regional Hyperactivity may be due to:
o Normal bone growth and remodeling
o Increased blood flow(trauma, heterotopic ossification)
o Reactive osteoblastic activity (active infections, tumors)
o Reparative bone process(healing fractures, tumors, infections)
o Hyper-metabolic activity(metabolic disorders)
• Lesions that appear hot on bone scan include healing fractures and osteoblastic tumors, such as osteogenic
sarcoma.
COLD BONE SCAN:
• A loss of blood flow to the bone, or a bone infarction, can cause this type of spot.
• When a person suffers a bone infarction, the part of the bone that no longer receives blood can die, leading
it to collapse.
• Multiple myeloma may not show up on a bone scan because only osteoclastic activity is involved in the
majority of lesions.
• Malignant Tumors
o Lung (2-4%)
o Breast (5%)
o Renal (10%)
o Neuroblastomas (bone marrow metastasis)
o Thyroid (most cases)
o Multiple Myeloma (most cases)
• Bone Abscesses (they are surrounded by activity)
• Bone ischemia (AVN, sickle cell, etc.)
• Hemangiomas(normal or decreased activity)
BONE SCAN IN METASTATIC LESIONS:
• Most sensitive routine imaging modality to try and identify both sclerotic and lytic lesions.
• In most cases they demonstrate increased uptake (hot spot) although occasionally (in very aggressive purely
lytic lesions) a photopaenic defect (cold spot) may be visible.
SUPERSCAN:
• Greater than normal activity in the kidneys is most commonly due to urinary tract obstruction, and bilaterally
decreased activity most often reflects renal failure.
• An important exception to the latter is the absence of renal activity in the so-called superscan, in which
diffuse skeletal uptake is so avid that renal uptake is undercut.
• A common condition producing a superscan is diffusely metastatic prostate carcinoma.
INVESTIGATION OF CHOICE
USG CT-Scan HRCT MRI PET/SPECT
Cystic lesions,
fluid
accumulation
Adrenals, pancreas,
mediastinum,
calcification, cerebral
hemorrhage
Lung pathology like
bronchiectasis,
interstitial lung
disease
Posterior fossa,
spine CNS,
muscle, soft
tissue, joints,
etc.,
Occult
metastasis
INVESTIGATION OF CHOICE IN CARDIAC CONDITIONS
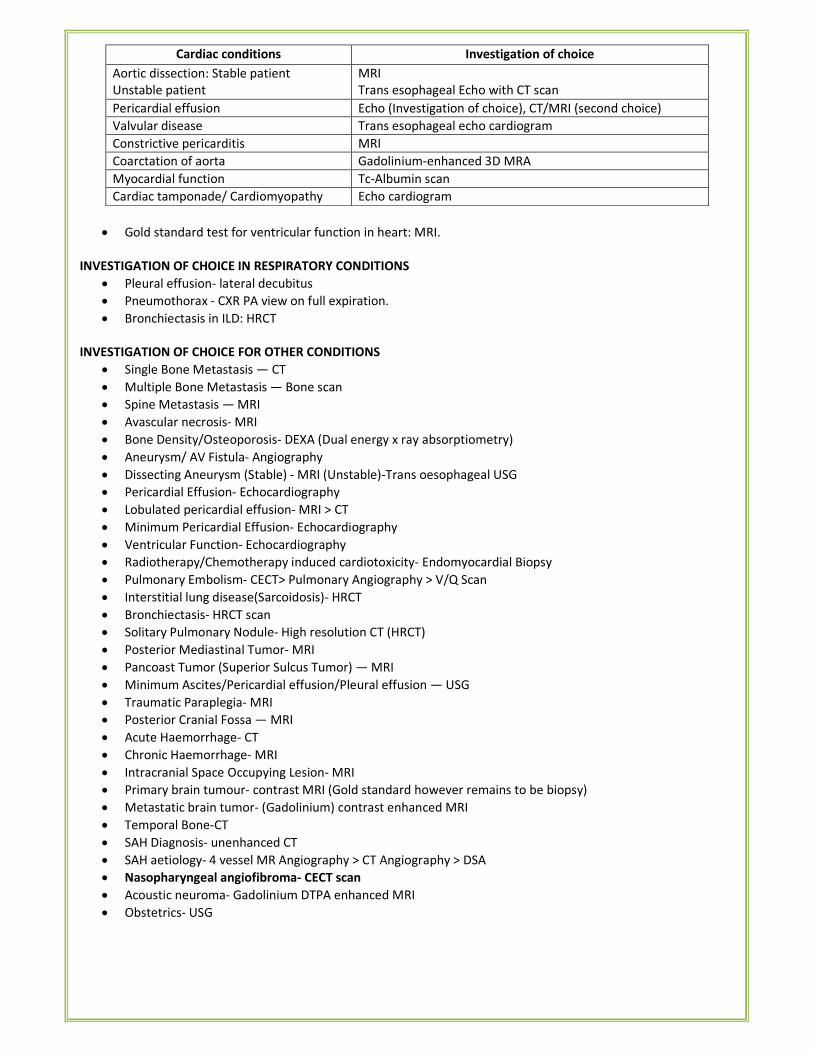
Cardiac conditions Investigation of choice
Aortic dissection: Stable patient
Unstable patient
MRI
Trans esophageal Echo with CT scan
Pericardial effusion Echo (Investigation of choice), CT/MRI (second choice)
Valvular disease Trans esophageal echo cardiogram
Constrictive pericarditis MRI
Coarctation of aorta Gadolinium-enhanced 3D MRA
Myocardial function Tc-Albumin scan
Cardiac tamponade/ Cardiomyopathy Echo cardiogram
• Gold standard test for ventricular function in heart: MRI.
INVESTIGATION OF CHOICE IN RESPIRATORY CONDITIONS
• Pleural effusion- lateral decubitus
• Pneumothorax - CXR PA view on full expiration.
• Bronchiectasis in ILD: HRCT
INVESTIGATION OF CHOICE FOR OTHER CONDITIONS
• Single Bone Metastasis — CT
• Multiple Bone Metastasis — Bone scan
• Spine Metastasis — MRI
• Avascular necrosis- MRI
• Bone Density/Osteoporosis- DEXA (Dual energy x ray absorptiometry)
• Aneurysm/ AV Fistula- Angiography
• Dissecting Aneurysm (Stable) - MRI (Unstable)-Trans oesophageal USG
• Pericardial Effusion- Echocardiography
• Lobulated pericardial effusion- MRI > CT
• Minimum Pericardial Effusion- Echocardiography
• Ventricular Function- Echocardiography
• Radiotherapy/Chemotherapy induced cardiotoxicity- Endomyocardial Biopsy
• Pulmonary Embolism- CECT> Pulmonary Angiography > V/Q Scan
• Interstitial lung disease(Sarcoidosis)- HRCT
• Bronchiectasis- HRCT scan
• Solitary Pulmonary Nodule- High resolution CT (HRCT)
• Posterior Mediastinal Tumor- MRI
• Pancoast Tumor (Superior Sulcus Tumor) — MRI
• Minimum Ascites/Pericardial effusion/Pleural effusion — USG
• Traumatic Paraplegia- MRI
• Posterior Cranial Fossa — MRI
• Acute Haemorrhage- CT
• Chronic Haemorrhage- MRI
• Intracranial Space Occupying Lesion- MRI
• Primary brain tumour- contrast MRI (Gold standard however remains to be biopsy)
• Metastatic brain tumor- (Gadolinium) contrast enhanced MRI
• Temporal Bone-CT
• SAH Diagnosis- unenhanced CT
• SAH aetiology- 4 vessel MR Angiography > CT Angiography > DSA
• Nasopharyngeal angiofibroma- CECT scan
• Acoustic neuroma- Gadolinium DTPA enhanced MRI
• Obstetrics- USG
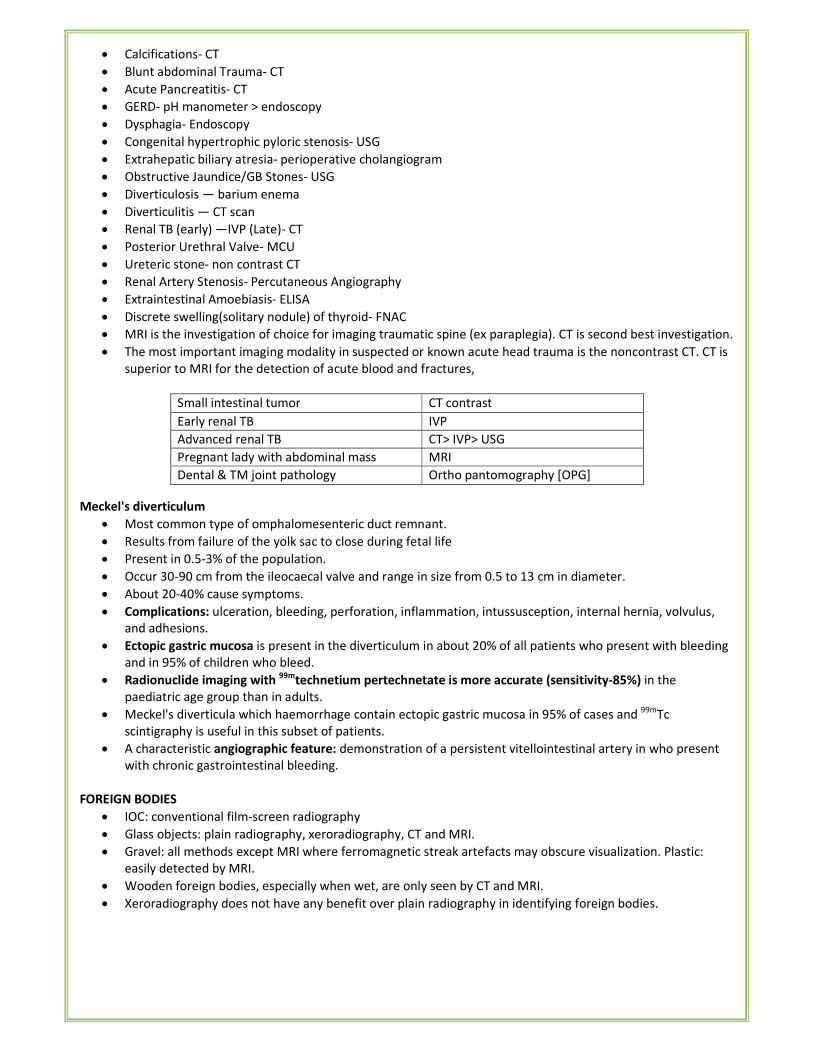
• Calcifications- CT
• Blunt abdominal Trauma- CT
• Acute Pancreatitis- CT
• GERD- pH manometer > endoscopy
• Dysphagia- Endoscopy
• Congenital hypertrophic pyloric stenosis- USG
• Extrahepatic biliary atresia- perioperative cholangiogram
• Obstructive Jaundice/GB Stones- USG
• Diverticulosis — barium enema
• Diverticulitis — CT scan
• Renal TB (early) —IVP (Late)- CT
• Posterior Urethral Valve- MCU
• Ureteric stone- non contrast CT
• Renal Artery Stenosis- Percutaneous Angiography
• Extraintestinal Amoebiasis- ELISA
• Discrete swelling(solitary nodule) of thyroid- FNAC
• MRI is the investigation of choice for imaging traumatic spine (ex paraplegia). CT is second best investigation.
• The most important imaging modality in suspected or known acute head trauma is the noncontrast CT. CT is
superior to MRI for the detection of acute blood and fractures,
Small intestinal tumor CT contrast
Early renal TB IVP
Advanced renal TB CT> IVP> USG
Pregnant lady with abdominal mass MRI
Dental & TM joint pathology Ortho pantomography [OPG]
Meckel's diverticulum
• Most common type of omphalomesenteric duct remnant.
• Results from failure of the yolk sac to close during fetal life
• Present in 0.5-3% of the population.
• Occur 30-90 cm from the ileocaecal valve and range in size from 0.5 to 13 cm in diameter.
• About 20-40% cause symptoms.
• Complications: ulceration, bleeding, perforation, inflammation, intussusception, internal hernia, volvulus,
and adhesions.
• Ectopic gastric mucosa is present in the diverticulum in about 20% of all patients who present with bleeding
and in 95% of children who bleed.
• Radionuclide imaging with 99mtechnetium pertechnetate is more accurate (sensitivity-85%) in the
paediatric age group than in adults.
• Meckel's diverticula which haemorrhage contain ectopic gastric mucosa in 95% of cases and 99m
Tc
scintigraphy is useful in this subset of patients.
• A characteristic angiographic feature: demonstration of a persistent vitellointestinal artery in who present
with chronic gastrointestinal bleeding.
FOREIGN BODIES
• IOC: conventional film-screen radiography
• Glass objects: plain radiography, xeroradiography, CT and MRI.
• Gravel: all methods except MRI where ferromagnetic streak artefacts may obscure visualization. Plastic:
easily detected by MRI.
• Wooden foreign bodies, especially when wet, are only seen by CT and MRI.
• Xeroradiography does not have any benefit over plain radiography in identifying foreign bodies.
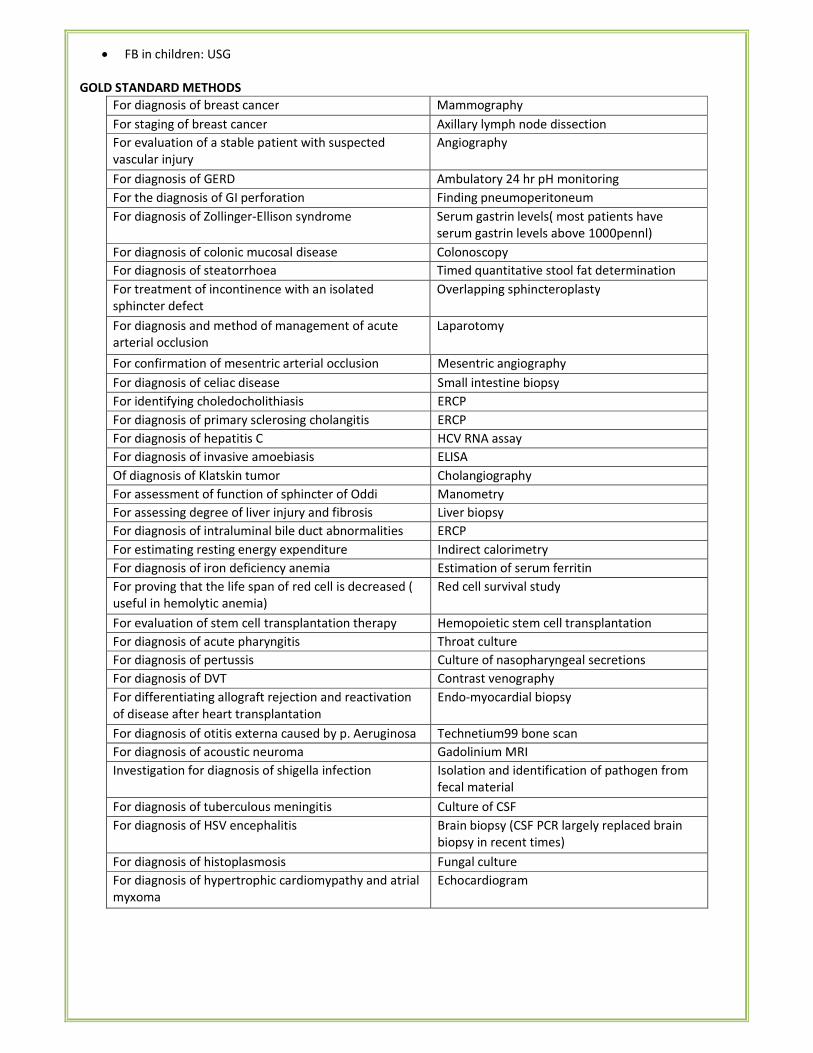
• FB in children: USG
GOLD STANDARD METHODS
For diagnosis of breast cancer Mammography
For staging of breast cancer Axillary lymph node dissection
For evaluation of a stable patient with suspected
vascular injury
Angiography
For diagnosis of GERD Ambulatory 24 hr pH monitoring
For the diagnosis of GI perforation Finding pneumoperitoneum
For diagnosis of Zollinger-Ellison syndrome Serum gastrin levels( most patients have
serum gastrin levels above 1000pennl)
For diagnosis of colonic mucosal disease Colonoscopy
For diagnosis of steatorrhoea Timed quantitative stool fat determination
For treatment of incontinence with an isolated
sphincter defect
Overlapping sphincteroplasty
For diagnosis and method of management of acute
arterial occlusion
Laparotomy
For confirmation of mesentric arterial occlusion Mesentric angiography
For diagnosis of celiac disease Small intestine biopsy
For identifying choledocholithiasis ERCP
For diagnosis of primary sclerosing cholangitis ERCP
For diagnosis of hepatitis C HCV RNA assay
For diagnosis of invasive amoebiasis ELISA
Of diagnosis of Klatskin tumor Cholangiography
For assessment of function of sphincter of Oddi Manometry
For assessing degree of liver injury and fibrosis Liver biopsy
For diagnosis of intraluminal bile duct abnormalities ERCP
For estimating resting energy expenditure Indirect calorimetry
For diagnosis of iron deficiency anemia Estimation of serum ferritin
For proving that the life span of red cell is decreased (
useful in hemolytic anemia)
Red cell survival study
For evaluation of stem cell transplantation therapy Hemopoietic stem cell transplantation
For diagnosis of acute pharyngitis Throat culture
For diagnosis of pertussis Culture of nasopharyngeal secretions
For diagnosis of DVT Contrast venography
For differentiating allograft rejection and reactivation
of disease after heart transplantation
Endo-myocardial biopsy
For diagnosis of otitis externa caused by p. Aeruginosa Technetium99 bone scan
For diagnosis of acoustic neuroma Gadolinium MRI
Investigation for diagnosis of shigella infection Isolation and identification of pathogen from
fecal material
For diagnosis of tuberculous meningitis Culture of CSF
For diagnosis of HSV encephalitis Brain biopsy (CSF PCR largely replaced brain
biopsy in recent times)
For diagnosis of histoplasmosis Fungal culture
For diagnosis of hypertrophic cardiomypathy and atrial
myxoma
Echocardiogram
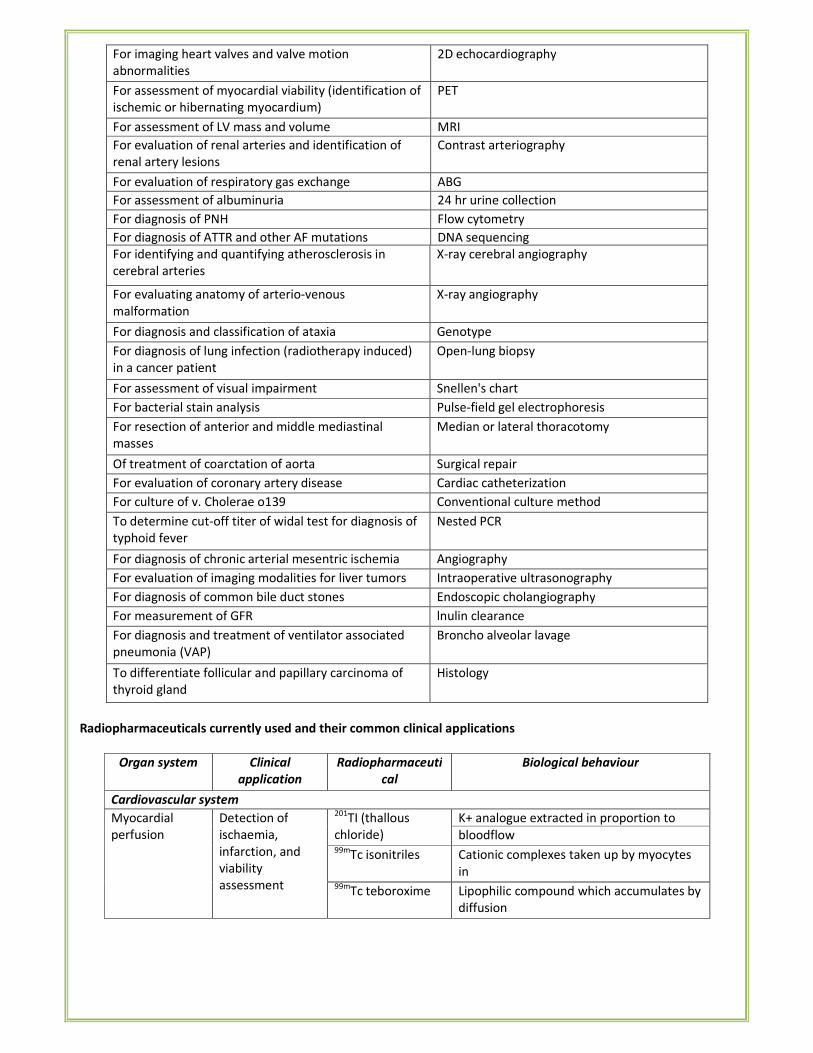
For imaging heart valves and valve motion
abnormalities
2D echocardiography
For assessment of myocardial viability (identification of
ischemic or hibernating myocardium)
PET
For assessment of LV mass and volume MRI
For evaluation of renal arteries and identification of
renal artery lesions
Contrast arteriography
For evaluation of respiratory gas exchange ABG
For assessment of albuminuria 24 hr urine collection
For diagnosis of PNH Flow cytometry
For diagnosis of ATTR and other AF mutations DNA sequencing
For identifying and quantifying atherosclerosis in
cerebral arteries
X-ray cerebral angiography
For evaluating anatomy of arterio-venous
malformation
X-ray angiography
For diagnosis and classification of ataxia Genotype
For diagnosis of lung infection (radiotherapy induced)
in a cancer patient
Open-lung biopsy
For assessment of visual impairment Snellen's chart
For bacterial stain analysis Pulse-field gel electrophoresis
For resection of anterior and middle mediastinal
masses
Median or lateral thoracotomy
Of treatment of coarctation of aorta Surgical repair
For evaluation of coronary artery disease Cardiac catheterization
For culture of v. Cholerae o139 Conventional culture method
To determine cut-off titer of widal test for diagnosis of
typhoid fever
Nested PCR
For diagnosis of chronic arterial mesentric ischemia Angiography
For evaluation of imaging modalities for liver tumors Intraoperative ultrasonography
For diagnosis of common bile duct stones Endoscopic cholangiography
For measurement of GFR lnulin clearance
For diagnosis and treatment of ventilator associated
pneumonia (VAP)
Broncho alveolar lavage
To differentiate follicular and papillary carcinoma of
thyroid gland
Histology
Radiopharmaceuticals currently used and their common clinical applications
Organ system Clinical
application
Radiopharmaceuti
cal
Biological behaviour
Cardiovascular system
Myocardial
perfusion
Detection of
ischaemia,
infarction, and
viability
assessment
201TI (thallous
chloride)
K+ analogue extracted in proportion to
bloodflow 99m
Tc isonitriles Cationic complexes taken up by myocytes
in
proportion to blood flow 99mTc teboroxime Lipophilic compound which accumulates by
diffusion
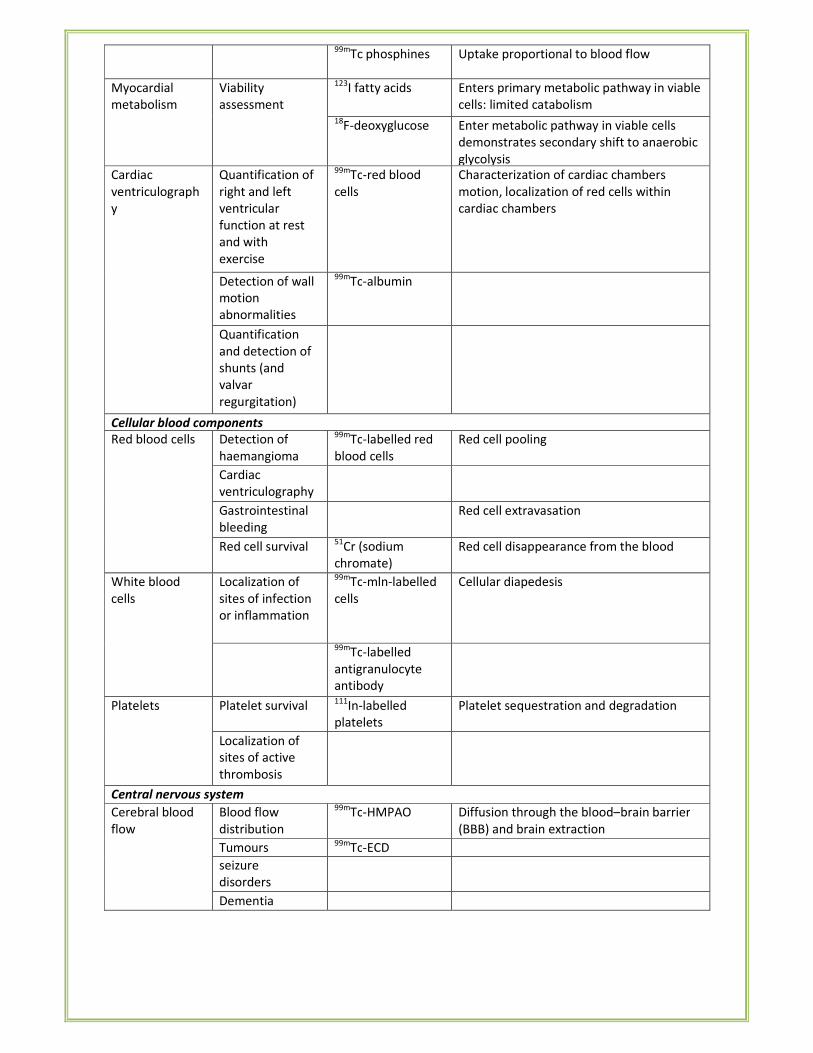
99mTc phosphines Uptake proportional to blood flow
Myocardial
metabolism
Viability
assessment
123I fatty acids Enters primary metabolic pathway in viable
cells: limited catabolism 18
F-deoxyglucose Enter metabolic pathway in viable cells
demonstrates secondary shift to anaerobic
glycolysis
Cardiac
ventriculograph
y
Quantification of
right and left
ventricular
function at rest
and with
exercise
99mTc-red blood
cells
Characterization of cardiac chambers
motion, localization of red cells within
cardiac chambers
Detection of wall
motion
abnormalities
99mTc-albumin
Quantification
and detection of
shunts (and
valvar
regurgitation)
Cellular blood components
Red blood cells Detection of
haemangioma
99mTc-labelled red
blood cells
Red cell pooling
Cardiac
ventriculography
Gastrointestinal
bleeding
Red cell extravasation
Red cell survival 51
Cr (sodium
chromate)
Red cell disappearance from the blood
White blood
cells
Localization of
sites of infection
or inflammation
99mTc-mln-labelled
cells
Cellular diapedesis
99m
Tc-labelled
antigranulocyte
antibody
Platelets Platelet survival 111
In-labelled
platelets
Platelet sequestration and degradation
Localization of
sites of active
thrombosis
Central nervous system
Cerebral blood
flow
Blood flow
distribution
99mTc-HMPAO Diffusion through the blood–brain barrier
(BBB) and brain extraction
Tumours 99m
Tc-ECD
seizure
disorders
Dementia
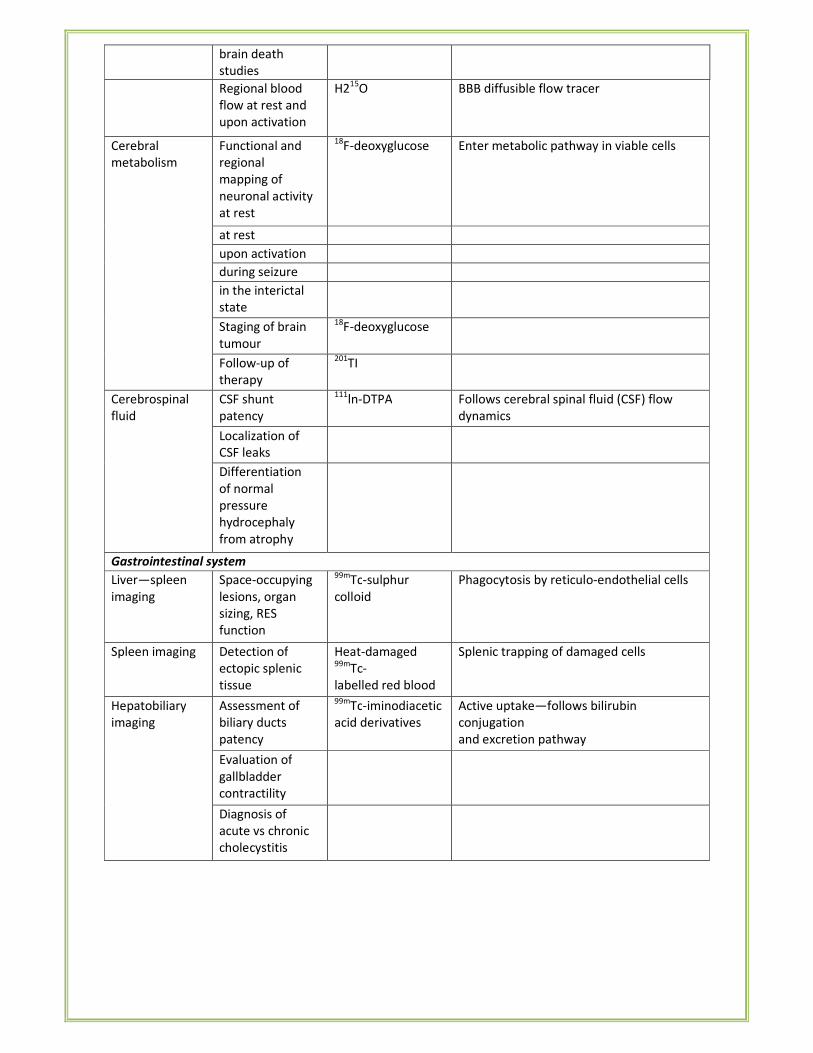
brain death
studies
Regional blood
flow at rest and
upon activation
H215
O BBB diffusible flow tracer
Cerebral
metabolism
Functional and
regional
mapping of
neuronal activity
at rest
18F-deoxyglucose Enter metabolic pathway in viable cells
at rest
upon activation
during seizure
in the interictal
state
Staging of brain
tumour
18F-deoxyglucose
Follow-up of
therapy
201TI
Cerebrospinal
fluid
CSF shunt
patency
111ln-DTPA Follows cerebral spinal fluid (CSF) flow
dynamics
Localization of
CSF leaks
Differentiation
of normal
pressure
hydrocephaly
from atrophy
Gastrointestinal system
Liver—spleen
imaging
Space-occupying
lesions, organ
sizing, RES
function
99mTc-sulphur
colloid
Phagocytosis by reticulo-endothelial cells
Spleen imaging Detection of
ectopic splenic
tissue
Heat-damaged 99m
Tc-
labelled red blood
cells
Splenic trapping of damaged cells
Hepatobiliary
imaging
Assessment of
biliary ducts
patency
99mTc-iminodiacetic
acid derivatives
Active uptake—follows bilirubin
conjugation
and excretion pathway
Evaluation of
gallbladder
contractility
Diagnosis of
acute vs chronic
cholecystitis
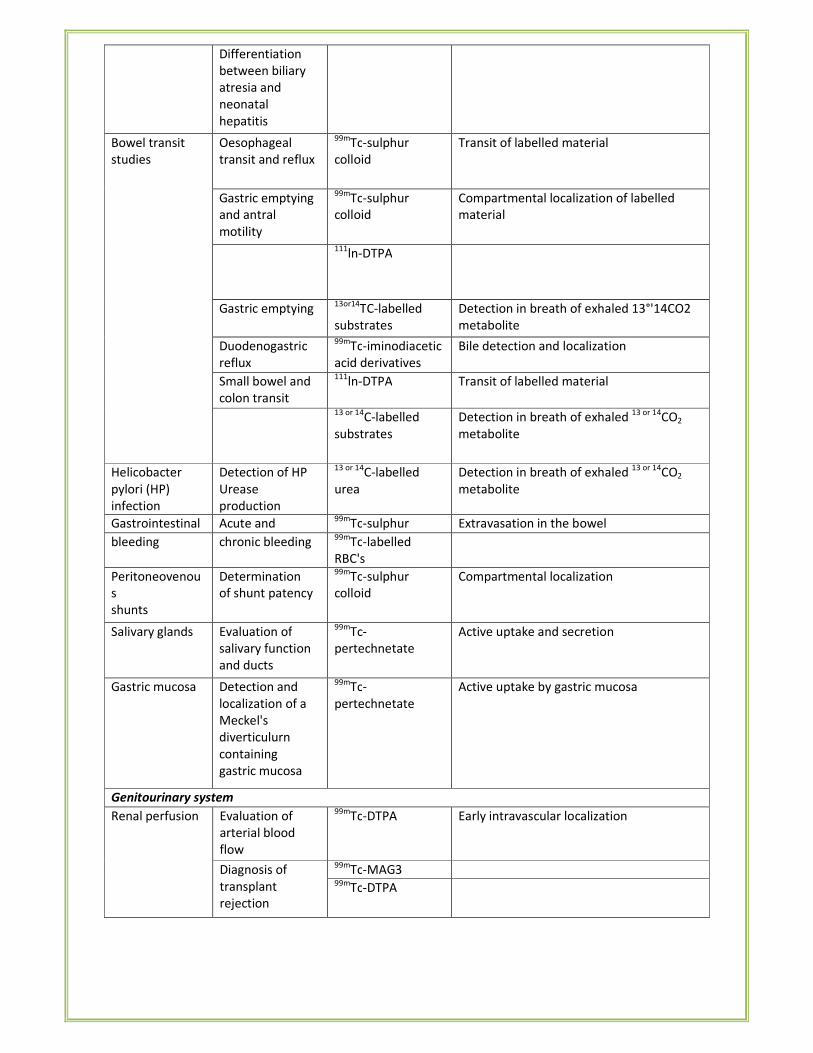
Differentiation
between biliary
atresia and
neonatal
hepatitis
Bowel transit
studies
Oesophageal
transit and reflux
99mTc-sulphur
colloid
Transit of labelled material
Gastric emptying
and antral
motility
99mTc-sulphur
colloid
Compartmental localization of labelled
material
111
ln-DTPA
Gastric emptying 13or14
TC-labelled
substrates
Detection in breath of exhaled 13°'14CO2
metabolite
Duodenogastric
reflux
99mTc-iminodiacetic
acid derivatives
Bile detection and localization
Small bowel and
colon transit
111ln-DTPA Transit of labelled material
13 or 14
C-labelled
substrates
Detection in breath of exhaled 13 or 14
CO2
metabolite
Helicobacter
pylori (HP)
infection
Detection of HP
Urease
production
13 or 14C-labelled
urea
Detection in breath of exhaled 13 or 14
CO2
metabolite
Gastrointestinal Acute and 99m
Tc-sulphur
colloid
Extravasation in the bowel
bleeding chronic bleeding 99m
Tc-labelled
RBC's
Peritoneovenou
s
shunts
Determination
of shunt patency
99mTc-sulphur
colloid
Compartmental localization
Salivary glands Evaluation of
salivary function
and ducts
patency
99mTc-
pertechnetate
Active uptake and secretion
Gastric mucosa Detection and
localization of a
Meckel's
diverticulurn
containing
gastric mucosa
99mTc-
pertechnetate
Active uptake by gastric mucosa
Genitourinary system
Renal perfusion Evaluation of
arterial blood
flow
99mTc-DTPA Early intravascular localization
Diagnosis of
transplant
rejection
99mTc-MAG3
99mTc-DTPA

Renal function GFR
measurement
51Cr-EDTA Clearance by glomerular filtration
Measurement of
effective renal
plasma flow;
tubular function
Tubular uptake
99mTc-MAG3
Renal
morphology
Detection of
renal infarct
99mTc-DMSA Retention in renal cortex
Global renal
morphology
Bladder Quantitation of
bladder residual
vesicoureteral
reflux
99mTc-DTPA Compartmental localization
Scrotum Differentiation
between acute
testicular torsion
99mTc-
pertechnetate
Early intravascular localization
Pulmonary system
Ventilation scan Evaluation of
regional
ventilation
133Xe gas Distributes in lungs in proportion to
regional
ventilation 81Kr
m gas
99mTc aerosols
Perfusion scan Detection of
pulmonary
emboli, right to
left shunts;
preoperative
and transplant
evaluation of
relative lung
perfusion
99mTc albumin
macroaggregates
Pulmonary capillary blockade
Parenchymal Interstitial lung 67
Ga Binds to transferrin in the intravascular
tissue disease staging
and therapeutic
evaluation
compartment,
Musculoskeletal
system
Detection of soft
tissue vs primary
bone disorders
during Phases I
and II of study
Detection of
benign, alignant,
and
infectious bone
lesions
99mTc-
polyphosphate
compounds
Intravascular and early soft tissue
distribution (Phase I and II)
Fixed to hydroxyapatite crystals (Phase Ill)
Thyroid-parathyroid
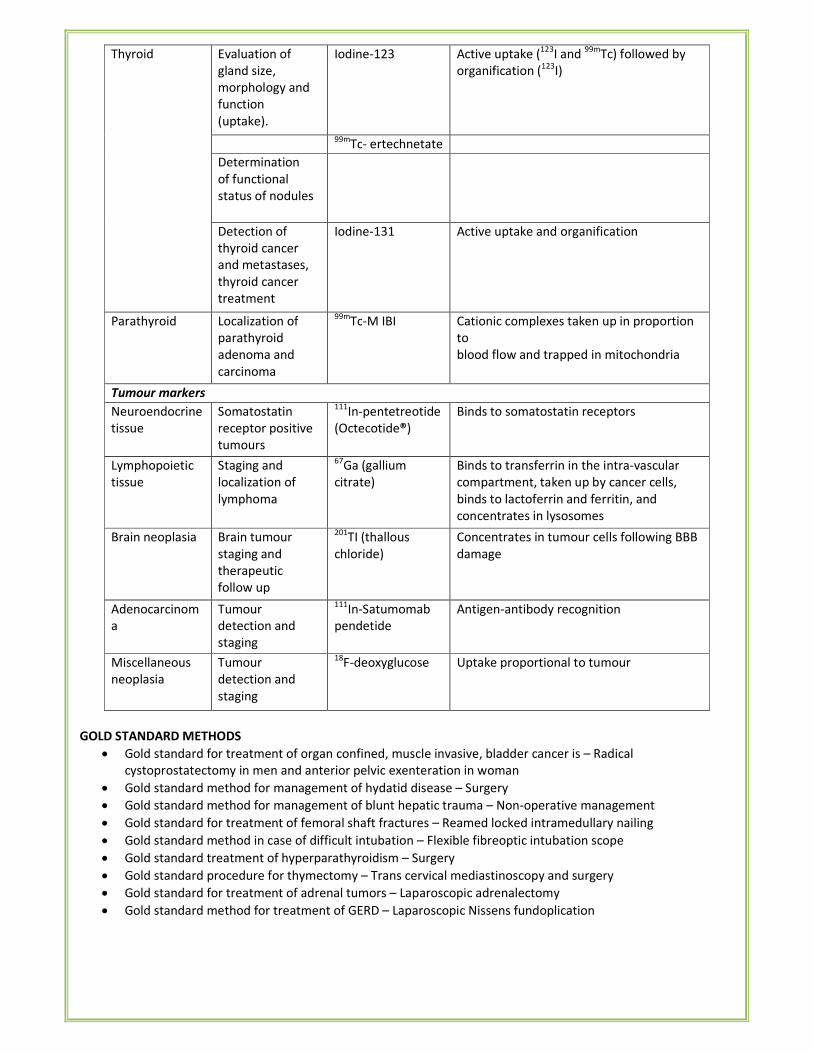
Thyroid Evaluation of
gland size,
morphology and
function
(uptake).
Iodine-123 Active uptake (123
I and 99m
Tc) followed by
organification (123
I)
99m
Tc- ertechnetate
Determination
of functional
status of nodules
Detection of
thyroid cancer
and metastases,
thyroid cancer
treatment
Iodine-131 Active uptake and organification
Parathyroid Localization of
parathyroid
adenoma and
carcinoma
99mTc-M IBI Cationic complexes taken up in proportion
to
blood flow and trapped in mitochondria
Tumour markers
Neuroendocrine
tissue
Somatostatin
receptor positive
tumours
111In-pentetreotide
(Octecotide®)
Binds to somatostatin receptors
Lymphopoietic
tissue
Staging and
localization of
lymphoma
67Ga (gallium
citrate)
Binds to transferrin in the intra-vascular
compartment, taken up by cancer cells,
binds to lactoferrin and ferritin, and
concentrates in lysosomes
Brain neoplasia Brain tumour
staging and
therapeutic
follow up
201TI (thallous
chloride)
Concentrates in tumour cells following BBB
damage
Adenocarcinom
a
Tumour
detection and
staging
111In-Satumomab
pendetide
Antigen-antibody recognition
Miscellaneous
neoplasia
Tumour
detection and
staging
18F-deoxyglucose Uptake proportional to tumour
GOLD STANDARD METHODS
• Gold standard for treatment of organ confined, muscle invasive, bladder cancer is – Radical
cystoprostatectomy in men and anterior pelvic exenteration in woman
• Gold standard method for management of hydatid disease – Surgery
• Gold standard method for management of blunt hepatic trauma – Non-operative management
• Gold standard for treatment of femoral shaft fractures – Reamed locked intramedullary nailing
• Gold standard method in case of difficult intubation – Flexible fibreoptic intubation scope
• Gold standard treatment of hyperparathyroidism – Surgery
• Gold standard procedure for thymectomy – Trans cervical mediastinoscopy and surgery
• Gold standard for treatment of adrenal tumors – Laparoscopic adrenalectomy
• Gold standard method for treatment of GERD – Laparoscopic Nissens fundoplication
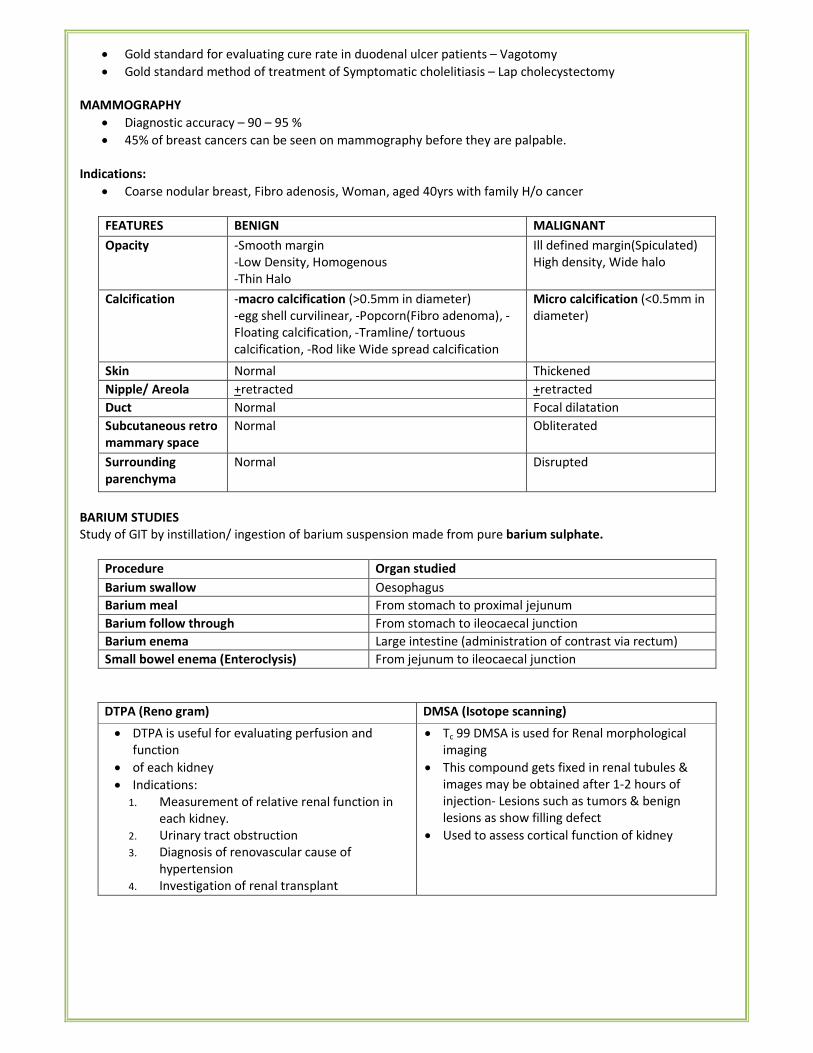
• Gold standard for evaluating cure rate in duodenal ulcer patients – Vagotomy
• Gold standard method of treatment of Symptomatic cholelitiasis – Lap cholecystectomy
MAMMOGRAPHY
• Diagnostic accuracy – 90 – 95 %
• 45% of breast cancers can be seen on mammography before they are palpable.
Indications:
• Coarse nodular breast, Fibro adenosis, Woman, aged 40yrs with family H/o cancer
FEATURES BENIGN MALIGNANT
Opacity -Smooth margin
-Low Density, Homogenous
-Thin Halo
Ill defined margin(Spiculated)
High density, Wide halo
Calcification -macro calcification (>0.5mm in diameter)
-egg shell curvilinear, -Popcorn(Fibro adenoma), -
Floating calcification, -Tramline/ tortuous
calcification, -Rod like Wide spread calcification
Micro calcification (<0.5mm in
diameter)
Skin Normal Thickened
Nipple/ Areola +retracted
_
+retracted
_ Duct Normal Focal dilatation
Subcutaneous retro
mammary space
Normal Obliterated
Surrounding
parenchyma
Normal Disrupted
BARIUM STUDIES
Study of GIT by instillation/ ingestion of barium suspension made from pure barium sulphate.
Procedure Organ studied
Barium swallow Oesophagus
Barium meal From stomach to proximal jejunum
Barium follow through From stomach to ileocaecal junction
Barium enema Large intestine (administration of contrast via rectum)
Small bowel enema (Enteroclysis) From jejunum to ileocaecal junction
DTPA (Reno gram) DMSA (Isotope scanning)
• DTPA is useful for evaluating perfusion and
function
• of each kidney
• Indications:
1. Measurement of relative renal function in
each kidney.
2. Urinary tract obstruction
3. Diagnosis of renovascular cause of
hypertension
4. Investigation of renal transplant
• Tc 99 DMSA is used for Renal morphological
imaging
• This compound gets fixed in renal tubules &
images may be obtained after 1-2 hours of
injection- Lesions such as tumors & benign
lesions as show filling defect
• Used to assess cortical function of kidney
• MCU is the most accurate method of demonstrating vesicoureteric reflux, and as this is important in children
with urinary tract infection and reflux nephropathy.
• The ascending urethrogram gives excellent anatomical information concerning the distal urethra as far as the
distal sphincter mechanism.
• Ultrasound and CT are the investigations of choice in the diagnosis and staging of renal tumours.
• Dynamic CT is more accurate than angiography in detecting a small neoplasm.
• Antegrade pyelography is an accurate method of demonstrating precisely the site of an obstruction to the
upper urinary tract.
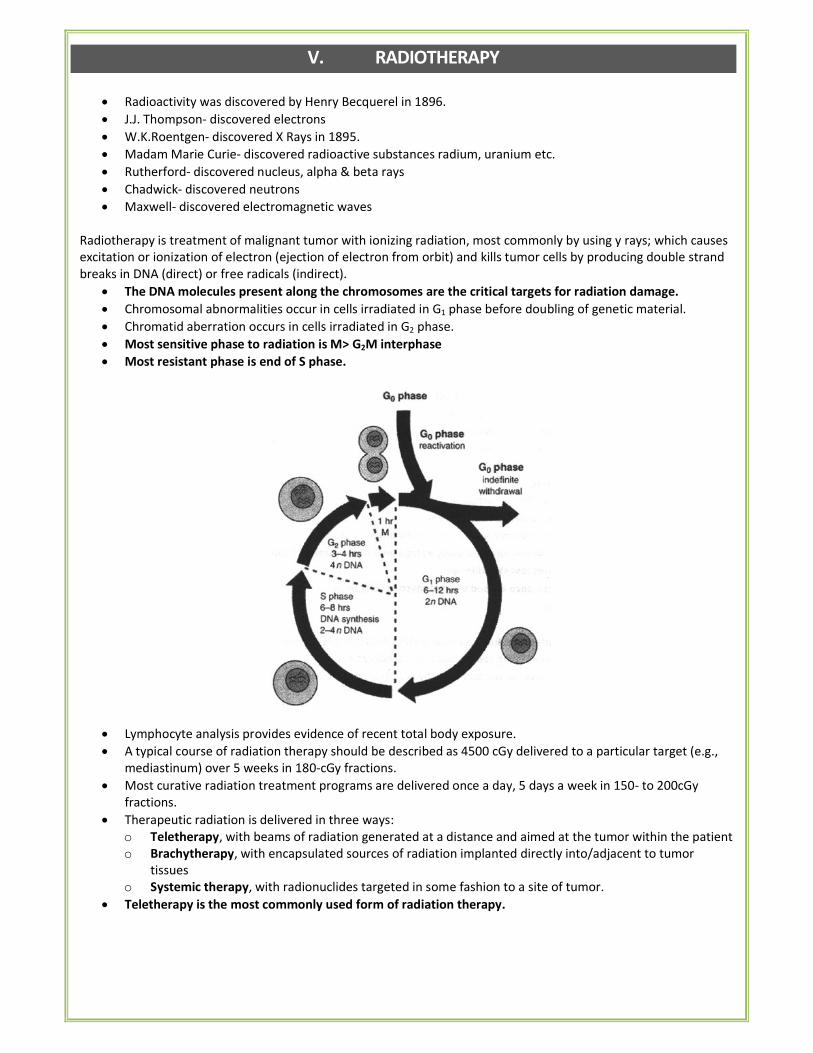
V. RADIOTHERAPY
• Radioactivity was discovered by Henry Becquerel in 1896.
• J.J. Thompson- discovered electrons
• W.K.Roentgen- discovered X Rays in 1895.
• Madam Marie Curie- discovered radioactive substances radium, uranium etc.
• Rutherford- discovered nucleus, alpha & beta rays
• Chadwick- discovered neutrons
• Maxwell- discovered electromagnetic waves
Radiotherapy is treatment of malignant tumor with ionizing radiation, most commonly by using y rays; which causes
excitation or ionization of electron (ejection of electron from orbit) and kills tumor cells by producing double strand
breaks in DNA (direct) or free radicals (indirect).
• The DNA molecules present along the chromosomes are the critical targets for radiation damage.
• Chromosomal abnormalities occur in cells irradiated in G1 phase before doubling of genetic material.
• Chromatid aberration occurs in cells irradiated in G2 phase.
• Most sensitive phase to radiation is M> G2M interphase
• Most resistant phase is end of S phase.
• Lymphocyte analysis provides evidence of recent total body exposure.
• A typical course of radiation therapy should be described as 4500 cGy delivered to a particular target (e.g.,
mediastinum) over 5 weeks in 180-cGy fractions.
• Most curative radiation treatment programs are delivered once a day, 5 days a week in 150- to 200cGy
fractions.
• Therapeutic radiation is delivered in three ways:
o Teletherapy, with beams of radiation generated at a distance and aimed at the tumor within the patient
o Brachytherapy, with encapsulated sources of radiation implanted directly into/adjacent to tumor
tissues
o Systemic therapy, with radionuclides targeted in some fashion to a site of tumor.
• Teletherapy is the most commonly used form of radiation therapy.
• X-rays and gamma rays are the forms of radiation most commonly used to treat cancer.
Radiation Content Penetrating
power
Ionizing
power
Damaging power Sources
α- Particle Helium nuclei
(i.e. 2 protons
& 2 neutrons
Poorest Maximum Most damaging Uranium,
Plutonium
β-Particle Either high
energy
electron or
antimatter
counterpart
positron
Greater than α -
particle (100)
Lesser than
α particle
< α particle Phosphorous-
32,strontium-
89,samarium-
132,1-131
X-Ray Low energy
photons
More than β-
particles
Lesser than
Β particle
<β Particle
Y-
Radiation
Very high
Energy
photons
More than X-
Rays 10000 i.e.,
Most penetrating
Minimum
ionizing
Least damaging Co-60, radium -
126.
Penetration power: y- ray > x ray > β particle > α particle
Ionizing & Damaging Power: α- particle> β-particle> x-ray > y ray
• Gamma rays are produced by decay of atomic nuclei in radioisotopes like cobalt & caesium.
• For deep seated tumors, X rays & Gamma rays are used, as high energy penetrating beam deliver a less
intense superficial dose & causes less skin damage.
• Electron beams have very low penetrance & used to treat mycosis fungoides.
• I-131: emits both beta & gamma rays.
• Californium: emits neutron.
• Heating of tungsten filament by battery produces electron beam which is targeted towards positive charged
tungsten or molybdenum containing copper block; this produces X-rays
• Linear accelerator and betatron are used to produce x-ray by accelerating electrons.
Neutrons
• Uncharged particulate radiation.
• Present in nuclear reactors and at high altitudes.
• Have highest penetrating power.
• Water and paraffin wax are effective in absorbing it.
• Predominant neutron emitter: californium.
BRACHYTHERAPY
• First proposed by Forssell in 1931.
• Delivered by two methods:
o Intra cavitatory therapy: Eg: Manchester system for Rx of Ca. cervix
o Interstitial implantation: Eg. HDR therapy for Ca. Bronchus & ca. Oesophagus.
• Radionuclides used in brachytherapy:
o Caesium 137, Cobalt 60, Iridium 192, Iodine 125, Radium 226, Radon 222, Strontium 90, Samarium 145,
Palladium 103, Gold 198, Yetrium 169.
• The characteristic features of Brachytherapy are:
o Maximum radiation effect can be obtained in diseased tissue.
o Minimum risk of to the normal tissue.
o It requires trained personnel & Invasive
o It is often used in brain tumours & cervical cancers.
UNITS OF RADIATION
Feature S.I. Unit Non S.I. Unit
Radioactivity Becquerel (Bq) Curie
Absorbed dose Gray (Gy) Rad
Dose equivalent Sievert (Sv) Rem
Exposure Coulombs/ kg Roentgen
ISOTOPES USED IN MEDICINE
Reactor Radioisotopes (half-life indicated in brackets):
• Molybdenum-99 (66 h): Used as the 'parent' in a generator to produce technetium-99m.
• Technetium-99m (6 h): Used in to image the skeleton and heart muscle in particular, but also for brain,
thyroid, lungs (perfusion and ventilation), liver, spleen, kidney (structure and filtration rate), gall bladder,
bone marrow, salivary and lacrimal glands, heart blood pool, infection and numerous specialized medical
studies.
• Uses of Technetium 99 tagged RBC's:
o Commonly indicated in Acute Lower Gastrointestinal Bleeding.
o Relatively sensitive & very specific imaging method for noninvasive diagnosis of liver hemangioma.
o Measurement of left ventricular ejection fraction. Assessment of regional wall motion (left and right
ventricles).
• Chromium-51 (28 d): Used to label RBC's and quantify gastro-intestinal protein loss.
• Cobalt-60 (10.5 months): Formerly used for external beam radiotherapy.
• Copper-64 (13 h): To study genetic diseases affecting copper metabolism. Eg: Wilson's and Menke's diseases.
• Dysprosium-165 (2 h): Used as an aggregated hydroxide for synovectomy treatment of arthritis.
• Erbium-169 (9.4 d): Use for relieving arthritis pain in synovial joints.
• Holmium-166 (26 h): Being developed for diagnosis and treatment of liver tumours.
• Iodine-125 (60 d): Used in brachytherapy (prostate and brain), to evaluate the filtration rate of kidneys and
to diagnose DVT in the leg. It is also used in radioimmuno-assays to show the presence of hormones in tiny
quantities.
• Iodine-131 (8 d): Used in treating thyroid cancer, imaging the thyroid; in diagnosis of abnormal liver
function, renal (kidney) blood flow and urinary tract obstruction. A strong gamma emitter, but used for beta
therapy.
• Iridium-192 (74 d): Supplied in wire form for use as an internal radiotherapy source for cancer treatment
• Iron-59 (46 d): Used in studies of iron metabolism in the spleen.
• Lutetium-177 (6.7 d): emits just enough gammas for imaging while the beta radiation does the therapy on
small (eg endocrine) tumours. Its half-life is long enough to allow sophisticated preparation for use.
• Palladium-103 (17 d): Used to make brachytherapy permanent implant seeds for early stage prostate cancer.
• Phosphorus-32 (14 d): Used in the treatment of polycythemia vera (excess red blood cells). Beta emitter.
• Potassium-42 (12 h): Used for the determination of exchangeable potassium in coronary blood flow.
• Rhenium-186 (3.8 d): Used for pain relief in bone cancer. Beta emitter with weak gamma for imaging.
• Rhenium-188 (17 h): Used to beta irradiate coronary arteries from an angioplasty balloon.
• Samarium-153 (47 h): Sm-153 is very effective in relieving the pain of secondary cancers lodged in
the bone, sold as Quadramet. Also very effective for prostate and breast cancer. Beta emitter.
• Selenium-75 (120 d): Used as seleno-methionine to study the production of digestive enzymes.
• Sodium-24 (15 h): For studies of electrolytes within the body.
• Strontium-89 (50 d): Very effective in reducing the pain of prostate & bone cancer. Beta emitter.
• Xenon-133 (5 d): Used for pulmonary (lung) ventilation studies.
• Ytterbium-169 (32 d): Used for cerebrospinal fluid studies in the brain.
• Ytterbium-177 (1.9 h): Progenitor of Lu-177.
• Yttrium-90 (64 h): for brachytherapy and as silicate colloid for relieving pain of arthritis. Pure beta emitter.
• Radioisotopes of caesium, gold and ruthenium are also used in brachytherapy.
Cyclotron Radioisotopes:
• Carbon-11, Nitrogen-13, Oxygen-15, Fluorine-18: positron emitters used in PET.
• F-18 in FDG in detection of cancers and the monitoring of progress in their treatment, using PET.
• Cobalt-57 (272 d): Used as a marker to estimate organ size and for in-vitro diagnostic kits.
• Gallium-67 (78 h): For tumour imaging & localization of inflammatory lesions (infections).
• Indium-111 (2.8 d): Used for specialist diagnostic studies, eg brain studies, infection and colon transit
studies.
• Iodine-123 (13 h): Used for diagnosis of thyroid function, a gamma emitter without the beta radiation of 1-
131.
• Krypton-81m (13 sec) from Rubidium-81 (4.6 h): Kr-81m gas can yield functional images of pulmonary
ventilation, e.g. in asthmatic patients, and for the early diagnosis of lung diseases and function.
• Rubidium-82 (65 h): Convenient PET agent in myocardial perfusion imaging.
• Strontium-92 (25 d): Used as the 'parent' in a generator to produce Rb-82.
• Thallium-201 (73 h): for diagnosis of coronary artery disease, other heart conditions such as heart muscle
death and for location of low-grade lymphomas.
T1/2 in hours T1/2 in days T1/2 in years
I132
-2.3 hours
Tc99
-6 hours
I123
-13 hours
I131
- 8 days; Gold- 2.7 days
Thallium-3.2 days; Radon-3.8 days
Xenon-5.2 days; P32
- 14 days
I125
- 60 days
Co60
- 5.2 years
Tritium- 12 years
St 90
- 28 years ; Cs132
- 30 years
Ra- 1622 years; U– 701 x 108 yrs
Co- 60 has the following features:
• Naturally occurring isotope
• Atomic. No. 27
• Atomic. Wt. 58.93
• Half- life 5.3 years
• Emits β and y- rays
• Used in both brachy & Teletherapy
Internal Contaminant Radionuclides: Properties and Treatment
Isotope
Name
Symbol Common
Usage
Radiation
Type, t%
Radiologic
t1/2
Biologic,
days
Exposure
Type
Focal
Accumulation
in Body
Treatment
Manganese Mn-56 Reactors,
research
laboratories
β, y, 2.6 h
5.7
External,
internal
Liver N/A
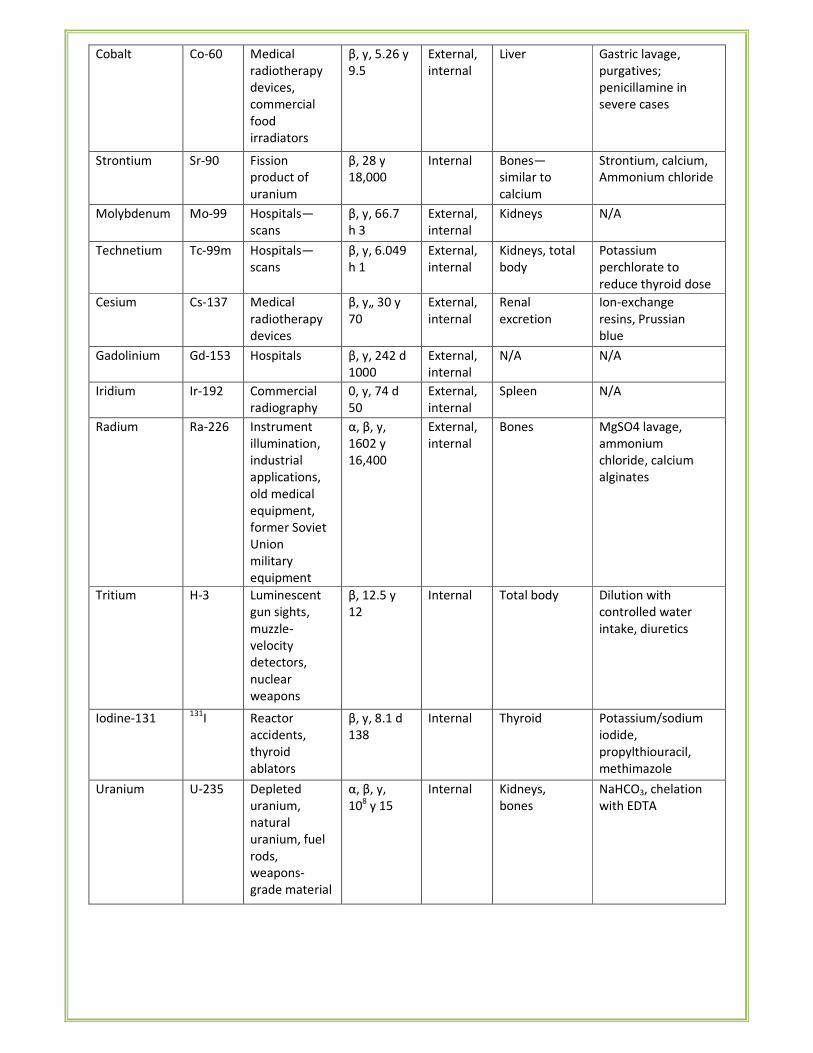
Cobalt Co-60 Medical
radiotherapy
devices,
commercial
food
irradiators
β, y, 5.26 y
9.5
External,
internal
Liver Gastric lavage,
purgatives;
penicillamine in
severe cases
Strontium Sr-90 Fission
product of
uranium
β, 28 y
18,000
Internal Bones—
similar to
calcium
Strontium, calcium,
Ammonium chloride
Molybdenum Mo-99 Hospitals—
scans
β, y, 66.7
h 3
External,
internal
Kidneys N/A
Technetium Tc-99m Hospitals—
scans
β, y, 6.049
h 1
External,
internal
Kidneys, total
body
Potassium
perchlorate to
reduce thyroid dose
Cesium Cs-137 Medical
radiotherapy
devices
β, y„ 30 y
70
External,
internal
Renal
excretion
Ion-exchange
resins, Prussian
blue
Gadolinium Gd-153 Hospitals β, y, 242 d
1000
External,
internal
N/A N/A
Iridium Ir-192 Commercial
radiography
0, y, 74 d
50
External,
internal
Spleen N/A
Radium Ra-226 Instrument
illumination,
industrial
applications,
old medical
equipment,
former Soviet
Union
military
equipment
α, β, y,
1602 y
16,400
External,
internal
Bones MgSO4 lavage,
ammonium
chloride, calcium
alginates
Tritium H-3 Luminescent
gun sights,
muzzle-
velocity
detectors,
nuclear
weapons
β, 12.5 y
12
Internal Total body Dilution with
controlled water
intake, diuretics
Iodine-131 131
I Reactor
accidents,
thyroid
ablators
β, y, 8.1 d
138
Internal Thyroid Potassium/sodium
iodide,
propylthiouracil,
methimazole
Uranium U-235 Depleted
uranium,
natural
uranium, fuel
rods,
weapons-
grade material
α, β, y,
108 y 15
Internal Kidneys,
bones
NaHCO3, chelation
with EDTA
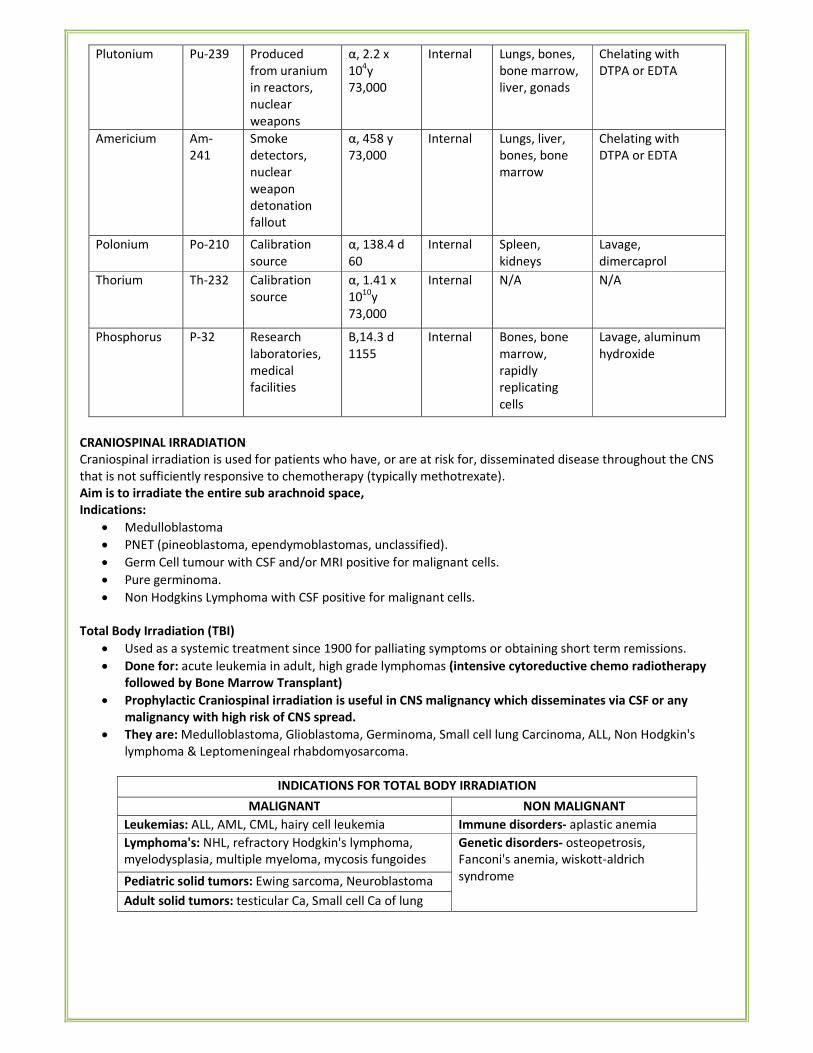
Plutonium Pu-239 Produced
from uranium
in reactors,
nuclear
weapons
α, 2.2 x
104y
73,000
Internal Lungs, bones,
bone marrow,
liver, gonads
Chelating with
DTPA or EDTA
Americium Am-
241
Smoke
detectors,
nuclear
weapon
detonation
fallout
α, 458 y
73,000
Internal Lungs, liver,
bones, bone
marrow
Chelating with
DTPA or EDTA
Polonium Po-210 Calibration
source
α, 138.4 d
60
Internal Spleen,
kidneys
Lavage,
dimercaprol
Thorium Th-232 Calibration
source
α, 1.41 x
1010
y
73,000
Internal N/A N/A
Phosphorus P-32 Research
laboratories,
medical
facilities
B,14.3 d
1155
Internal Bones, bone
marrow,
rapidly
replicating
cells
Lavage, aluminum
hydroxide
CRANIOSPINAL IRRADIATION
Craniospinal irradiation is used for patients who have, or are at risk for, disseminated disease throughout the CNS
that is not sufficiently responsive to chemotherapy (typically methotrexate).
Aim is to irradiate the entire sub arachnoid space,
Indications:
• Medulloblastoma
• PNET (pineoblastoma, ependymoblastomas, unclassified).
• Germ Cell tumour with CSF and/or MRI positive for malignant cells.
• Pure germinoma.
• Non Hodgkins Lymphoma with CSF positive for malignant cells.
Total Body Irradiation (TBI)
• Used as a systemic treatment since 1900 for palliating symptoms or obtaining short term remissions.
• Done for: acute leukemia in adult, high grade lymphomas (intensive cytoreductive chemo radiotherapy
followed by Bone Marrow Transplant)
• Prophylactic Craniospinal irradiation is useful in CNS malignancy which disseminates via CSF or any
malignancy with high risk of CNS spread.
• They are: Medulloblastoma, Glioblastoma, Germinoma, Small cell lung Carcinoma, ALL, Non Hodgkin's
lymphoma & Leptomeningeal rhabdomyosarcoma.
INDICATIONS FOR TOTAL BODY IRRADIATION
MALIGNANT NON MALIGNANT
Leukemias: ALL, AML, CML, hairy cell leukemia Immune disorders- aplastic anemia
Lymphoma's: NHL, refractory Hodgkin's lymphoma,
myelodysplasia, multiple myeloma, mycosis fungoides
Genetic disorders- osteopetrosis,
Fanconi's anemia, wiskott-aldrich
syndrome Pediatric solid tumors: Ewing sarcoma, Neuroblastoma
Adult solid tumors: testicular Ca, Small cell Ca of lung
• The standard treatment for brain metastases has been whole-brain radiotherapy (WBRT) usually
administered to a total dose of 3000 cGy in 10 fractions.
• This affords rapid palliation; approximately 80% of patients improve with glucocorticoids and radiation
therapy.
STEREOTACTIC RADIOSURGERY (SRS)
• Introduced by Lekshell in 1951.
• Treats brain disorders with a precise delivery of a single, high dose of radiation in a one-day session.
• Ideally confined to a lesion of 3-5cm size.
• Stereotactic radiosurgery (SRS) delivered through a variety of techniques including the gamma knife, linear
accelerator, proton beam and CyberKnife can deliver highly focused doses of RT, in a single fraction.
• Focused radiation beams are delivered to a specific area of the brain.
• It does not remove the tumor or lesion, but it distorts the DNA of the tumor cells.
• The cells then lose their ability to reproduce and retain fluids.
• Most of the beams used today are 4MV or 6MV beams.
• The three basic forms of stereotactic radiosurgery are:
o Particle beam (proton)
o Cobalt-60 based (photon), most well-known machine is the Gamma Knife.
o Linear accelerator based (linac)
Indications
• Arteriovenous Malformations
• Acoustic
• Neuromas
• Meningiomas
• Pineal and Pituitary Tumors
• Glial Tumors and Astrocytomas
• Low grade tumors
• Metastatic Brain Tumors
• Trigeminal Neuralgia
• Essential Tremor
• Parkinson's Tremor/Rigidity
• Current research areas include epilepsy,
headaches and neuro-psycho conditions.
INTENSITY MODULATED RADIATION THERAPY (IMRT)
• High precision radiotherapy by computer controlled X-ray accelerator to deliver precise radiation doses to a
malignant tumor or specific areas within the tumor.
• IMRT used in treatment of tumours of:
o Breast, Thyroid, lung, Prostate & Gynecological cancers
o Head & neck cancers
o Liver & brain cancers
o Lymphoma, sarcoma
INTRA OPERATIVE RADIOTHERAPY
• Applied with ortho voltage X —ray
• Specialized radiation technique for treating deeply located cancers with large single dose, avoiding damage
to the normal tissues.
• Intra operative electron beam followed by photons via X- rays & Gamma rays is the recent regimen.
• Used in pancreatic, gastric & rectal cancers; head & neck cancers, genitor urinary & gynecological cancers,
retroperitoneal sarcomas.
FAST NEUTRON RADIOTHERAPY (FNRT)
• Uses neutrons of megaelectron volts (MeV) energy.
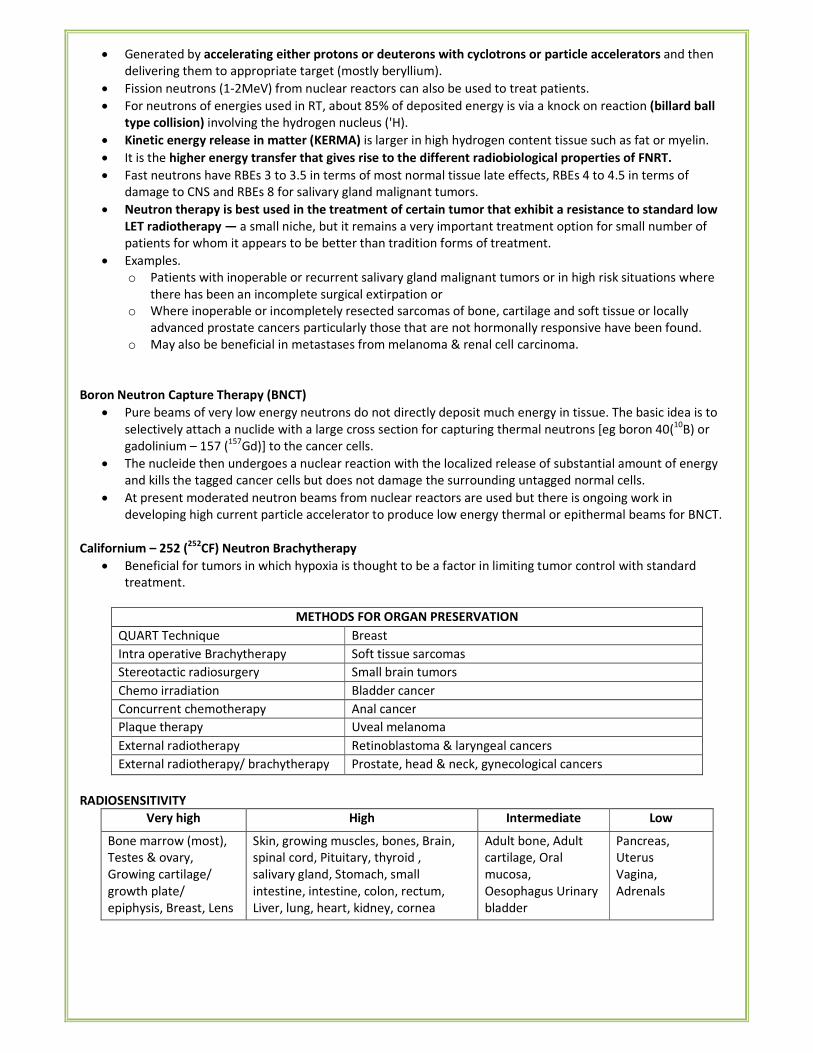
• Generated by accelerating either protons or deuterons with cyclotrons or particle accelerators and then
delivering them to appropriate target (mostly beryllium).
• Fission neutrons (1-2MeV) from nuclear reactors can also be used to treat patients.
• For neutrons of energies used in RT, about 85% of deposited energy is via a knock on reaction (billard ball
type collision) involving the hydrogen nucleus ('H).
• Kinetic energy release in matter (KERMA) is larger in high hydrogen content tissue such as fat or myelin.
• It is the higher energy transfer that gives rise to the different radiobiological properties of FNRT.
• Fast neutrons have RBEs 3 to 3.5 in terms of most normal tissue late effects, RBEs 4 to 4.5 in terms of
damage to CNS and RBEs 8 for salivary gland malignant tumors.
• Neutron therapy is best used in the treatment of certain tumor that exhibit a resistance to standard low
LET radiotherapy — a small niche, but it remains a very important treatment option for small number of
patients for whom it appears to be better than tradition forms of treatment.
• Examples.
o Patients with inoperable or recurrent salivary gland malignant tumors or in high risk situations where
there has been an incomplete surgical extirpation or
o Where inoperable or incompletely resected sarcomas of bone, cartilage and soft tissue or locally
advanced prostate cancers particularly those that are not hormonally responsive have been found.
o May also be beneficial in metastases from melanoma & renal cell carcinoma.
Boron Neutron Capture Therapy (BNCT)
• Pure beams of very low energy neutrons do not directly deposit much energy in tissue. The basic idea is to
selectively attach a nuclide with a large cross section for capturing thermal neutrons [eg boron 40(10
B) or
gadolinium – 157 (157
Gd)] to the cancer cells.
• The nucleide then undergoes a nuclear reaction with the localized release of substantial amount of energy
and kills the tagged cancer cells but does not damage the surrounding untagged normal cells.
• At present moderated neutron beams from nuclear reactors are used but there is ongoing work in
developing high current particle accelerator to produce low energy thermal or epithermal beams for BNCT.
Californium – 252 (252
CF) Neutron Brachytherapy
• Beneficial for tumors in which hypoxia is thought to be a factor in limiting tumor control with standard
treatment.
METHODS FOR ORGAN PRESERVATION
QUART Technique Breast
Intra operative Brachytherapy Soft tissue sarcomas
Stereotactic radiosurgery Small brain tumors
Chemo irradiation Bladder cancer
Concurrent chemotherapy Anal cancer
Plaque therapy Uveal melanoma
External radiotherapy Retinoblastoma & laryngeal cancers
External radiotherapy/ brachytherapy Prostate, head & neck, gynecological cancers
RADIOSENSITIVITY
Very high High Intermediate Low
Bone marrow (most),
Testes & ovary,
Growing cartilage/
growth plate/
epiphysis, Breast, Lens
Skin, growing muscles, bones, Brain,
spinal cord, Pituitary, thyroid ,
salivary gland, Stomach, small
intestine, intestine, colon, rectum,
Liver, lung, heart, kidney, cornea
Adult bone, Adult
cartilage, Oral
mucosa,
Oesophagus Urinary
bladder
Pancreas,
Uterus
Vagina,
Adrenals
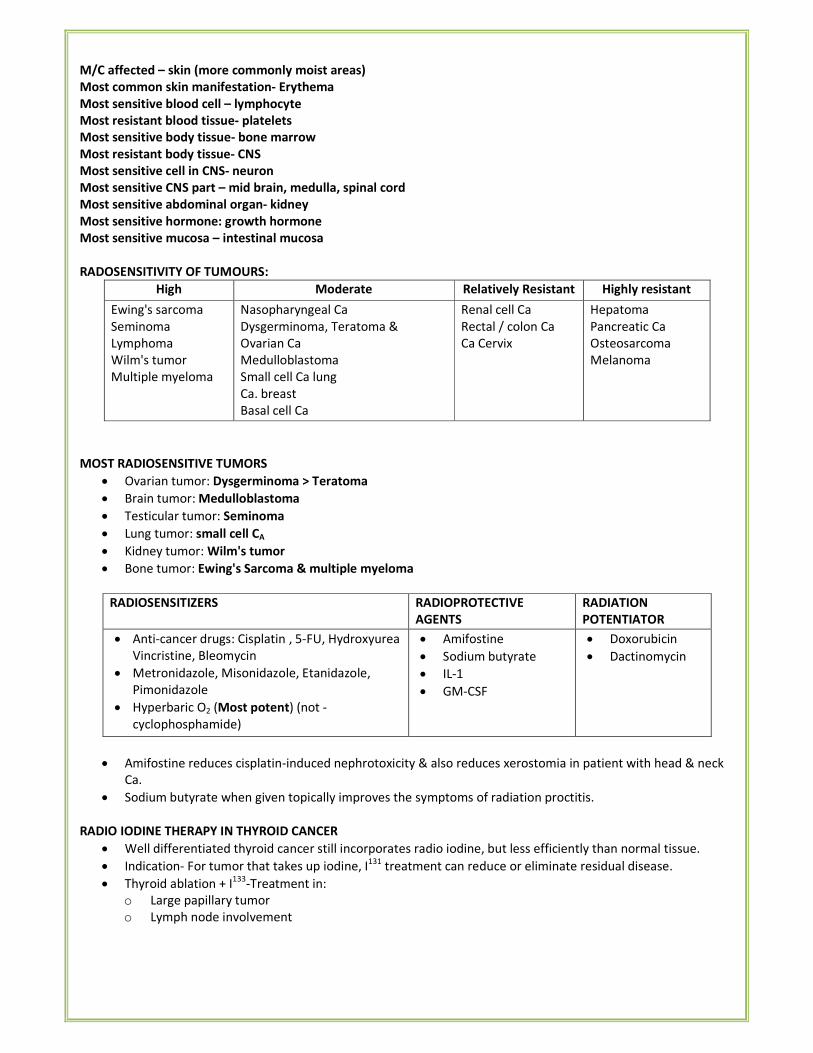
M/C affected – skin (more commonly moist areas)
Most common skin manifestation- Erythema
Most sensitive blood cell – lymphocyte
Most resistant blood tissue- platelets
Most sensitive body tissue- bone marrow
Most resistant body tissue- CNS
Most sensitive cell in CNS- neuron
Most sensitive CNS part – mid brain, medulla, spinal cord
Most sensitive abdominal organ- kidney
Most sensitive hormone: growth hormone
Most sensitive mucosa – intestinal mucosa
RADOSENSITIVITY OF TUMOURS:
High Moderate Relatively Resistant Highly resistant
Ewing's sarcoma
Seminoma
Lymphoma
Wilm's tumor
Multiple myeloma
Nasopharyngeal Ca
Dysgerminoma, Teratoma &
Ovarian Ca
Medulloblastoma
Small cell Ca lung
Ca. breast
Basal cell Ca
Renal cell Ca
Rectal / colon Ca
Ca Cervix
Hepatoma
Pancreatic Ca
Osteosarcoma
Melanoma
MOST RADIOSENSITIVE TUMORS
• Ovarian tumor: Dysgerminoma > Teratoma
• Brain tumor: Medulloblastoma
• Testicular tumor: Seminoma
• Lung tumor: small cell CA
• Kidney tumor: Wilm's tumor
• Bone tumor: Ewing's Sarcoma & multiple myeloma
RADIOSENSITIZERS RADIOPROTECTIVE
AGENTS
RADIATION
POTENTIATOR
• Anti-cancer drugs: Cisplatin , 5-FU, Hydroxyurea
Vincristine, Bleomycin
• Metronidazole, Misonidazole, Etanidazole,
Pimonidazole
• Hyperbaric O2 (Most potent) (not -
cyclophosphamide)
• Amifostine
• Sodium butyrate
• IL-1
• GM-CSF
• Doxorubicin
• Dactinomycin
• Amifostine reduces cisplatin-induced nephrotoxicity & also reduces xerostomia in patient with head & neck
Ca.
• Sodium butyrate when given topically improves the symptoms of radiation proctitis.
RADIO IODINE THERAPY IN THYROID CANCER
• Well differentiated thyroid cancer still incorporates radio iodine, but less efficiently than normal tissue.
• Indication- For tumor that takes up iodine, I131
treatment can reduce or eliminate residual disease.
• Thyroid ablation + I133
-Treatment in:
o Large papillary tumor
o Lymph node involvement
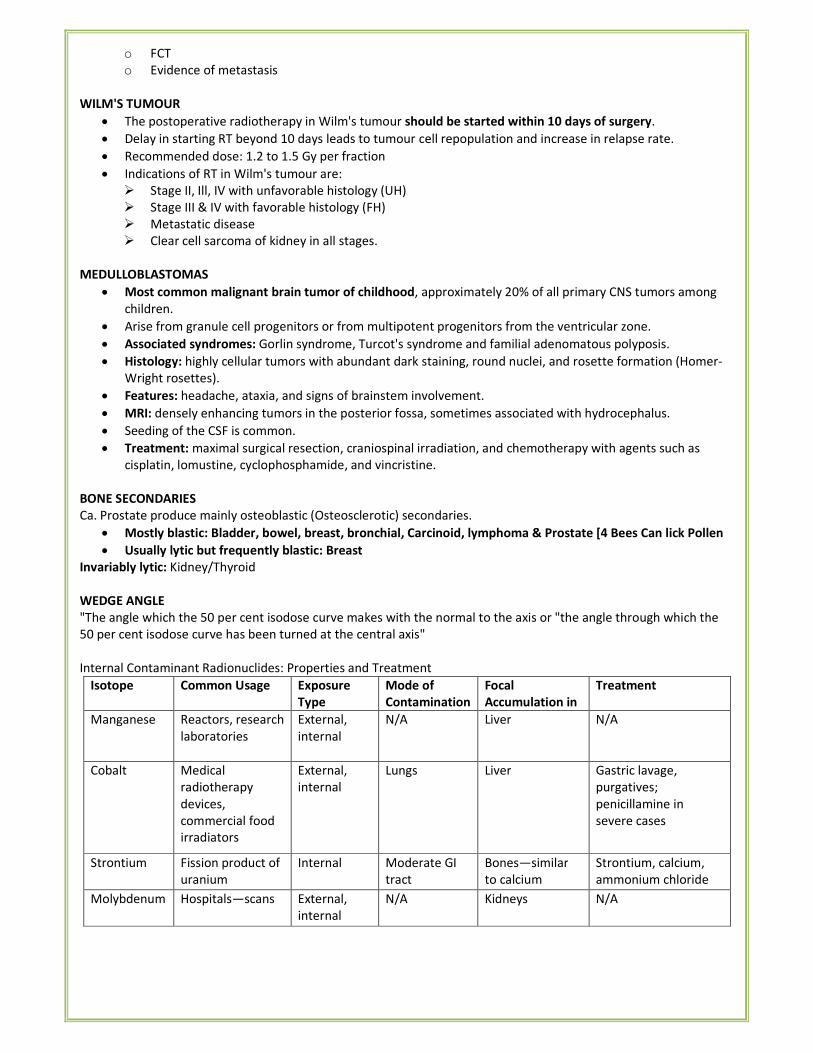
o FCT
o Evidence of metastasis
WILM'S TUMOUR
• The postoperative radiotherapy in Wilm's tumour should be started within 10 days of surgery.
• Delay in starting RT beyond 10 days leads to tumour cell repopulation and increase in relapse rate.
• Recommended dose: 1.2 to 1.5 Gy per fraction
• Indications of RT in Wilm's tumour are:
� Stage II, Ill, IV with unfavorable histology (UH)
� Stage III & IV with favorable histology (FH)
� Metastatic disease
� Clear cell sarcoma of kidney in all stages.
MEDULLOBLASTOMAS
• Most common malignant brain tumor of childhood, approximately 20% of all primary CNS tumors among
children.
• Arise from granule cell progenitors or from multipotent progenitors from the ventricular zone.
• Associated syndromes: Gorlin syndrome, Turcot's syndrome and familial adenomatous polyposis.
• Histology: highly cellular tumors with abundant dark staining, round nuclei, and rosette formation (Homer-
Wright rosettes).
• Features: headache, ataxia, and signs of brainstem involvement.
• MRI: densely enhancing tumors in the posterior fossa, sometimes associated with hydrocephalus.
• Seeding of the CSF is common.
• Treatment: maximal surgical resection, craniospinal irradiation, and chemotherapy with agents such as
cisplatin, lomustine, cyclophosphamide, and vincristine.
BONE SECONDARIES
Ca. Prostate produce mainly osteoblastic (Osteosclerotic) secondaries.
• Mostly blastic: Bladder, bowel, breast, bronchial, Carcinoid, lymphoma & Prostate [4 Bees Can lick Pollen
• Usually lytic but frequently blastic: Breast
Invariably lytic: Kidney/Thyroid
WEDGE ANGLE
"The angle which the 50 per cent isodose curve makes with the normal to the axis or "the angle through which the
50 per cent isodose curve has been turned at the central axis"
Internal Contaminant Radionuclides: Properties and Treatment
Isotope Common Usage Exposure
Type
Mode of
Contamination
Focal
Accumulation in
Treatment
Manganese Reactors, research
laboratories
External,
internal
N/A Liver N/A
Cobalt Medical
radiotherapy
devices,
commercial food
irradiators
External,
internal
Lungs Liver Gastric lavage,
purgatives;
penicillamine in
severe cases
Strontium Fission product of
uranium
Internal Moderate GI
tract
Bones—similar
to calcium
Strontium, calcium,
ammonium chloride
Molybdenum Hospitals—scans External,
internal
N/A Kidneys N/A
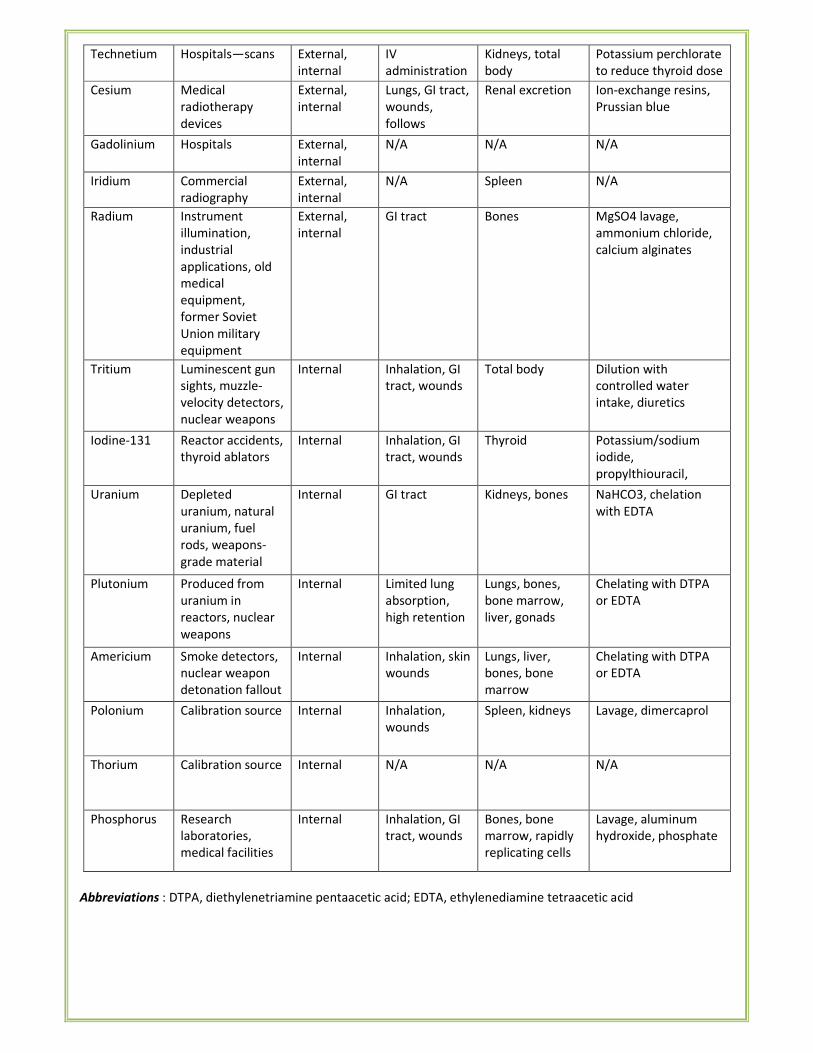
Technetium Hospitals—scans External,
internal
IV
administration
Kidneys, total
body
Potassium perchlorate
to reduce thyroid dose
Cesium Medical
radiotherapy
devices
External,
internal
Lungs, GI tract,
wounds,
follows
potassium
Renal excretion Ion-exchange resins,
Prussian blue
Gadolinium Hospitals External,
internal
N/A N/A N/A
Iridium Commercial
radiography
External,
internal
N/A Spleen N/A
Radium Instrument
illumination,
industrial
applications, old
medical
equipment,
former Soviet
Union military
equipment
External,
internal
GI tract Bones MgSO4 lavage,
ammonium chloride,
calcium alginates
Tritium Luminescent gun
sights, muzzle-
velocity detectors,
nuclear weapons
Internal Inhalation, GI
tract, wounds
Total body Dilution with
controlled water
intake, diuretics
Iodine-131 Reactor accidents,
thyroid ablators
Internal Inhalation, GI
tract, wounds
Thyroid Potassium/sodium
iodide,
propylthiouracil,
methimazole Uranium Depleted
uranium, natural
uranium, fuel
rods, weapons-
grade material
Internal GI tract Kidneys, bones NaHCO3, chelation
with EDTA
Plutonium Produced from
uranium in
reactors, nuclear
weapons
Internal Limited lung
absorption,
high retention
Lungs, bones,
bone marrow,
liver, gonads
Chelating with DTPA
or EDTA
Americium Smoke detectors,
nuclear weapon
detonation fallout
Internal Inhalation, skin
wounds
Lungs, liver,
bones, bone
marrow
Chelating with DTPA
or EDTA
Polonium Calibration source Internal Inhalation,
wounds
Spleen, kidneys Lavage, dimercaprol
Thorium Calibration source Internal N/A N/A N/A
Phosphorus Research
laboratories,
medical facilities
Internal Inhalation, GI
tract, wounds
Bones, bone
marrow, rapidly
replicating cells
Lavage, aluminum
hydroxide, phosphate
Abbreviations : DTPA, diethylenetriamine pentaacetic acid; EDTA, ethylenediamine tetraacetic acid
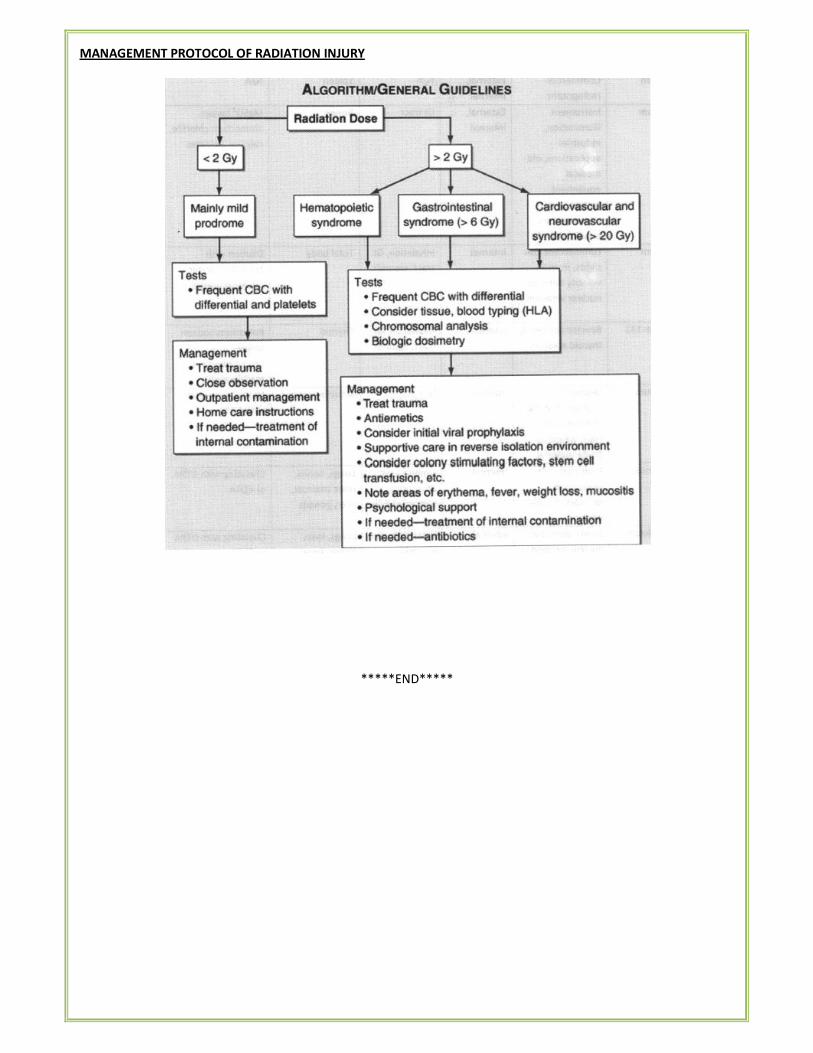
MANAGEMENT PROTOCOL OF RADIATION INJURY
*****END*****