How to move beyond PONV: Redefining Regional Anesthesia Outcomes
46
Colin J.L. McCartney Colin J.L. McCartney MBChB FCARCSI FRCA FRCPC MBChB FCARCSI FRCA FRCPC Director of Regional Anesthesia Research Director of Regional Anesthesia Research Department of Anesthesia Department of Anesthesia Sunnybrook Health Sciences Centre Sunnybrook Health Sciences Centre Professor of Anesthesia Professor of Anesthesia University of Toronto University of Toronto How to Move Beyond How to Move Beyond PONV: PONV: Redefining Regional Anesthesia Redefining Regional Anesthesia Outcomes Outcomes
Transcript of How to move beyond PONV: Redefining Regional Anesthesia Outcomes

Colin J.L. McCartney Colin J.L. McCartney MBChB FCARCSI FRCA FRCPCMBChB FCARCSI FRCA FRCPCDirector of Regional Anesthesia ResearchDirector of Regional Anesthesia ResearchDepartment of AnesthesiaDepartment of AnesthesiaSunnybrook Health Sciences CentreSunnybrook Health Sciences CentreProfessor of Anesthesia Professor of Anesthesia University of TorontoUniversity of Toronto
How to Move Beyond How to Move Beyond PONV:PONV:
Redefining Regional Anesthesia Redefining Regional Anesthesia Outcomes Outcomes

Goals: Regional Goals: Regional AnesthesiaAnesthesia
What is important for patient, What is important for patient, providers and the systemproviders and the system
What methods have been used to What methods have been used to assess outcomes?assess outcomes?
What methods should we use to What methods should we use to assess outcomes?assess outcomes?
What do we need?What do we need?

Goals: Regional Goals: Regional AnesthesiaAnesthesia
What is important for patient, What is important for patient, providers and the systemproviders and the system
What methods have been used to What methods have been used to assess outcomes?assess outcomes?
What methods should we use to What methods should we use to assess outcomes?assess outcomes?
What do we need?What do we need?

What is important for What is important for the patient?the patient?


Will the surgery affect my ability to Will the surgery affect my ability to care for myself?care for myself?
Will I need physical therapy?Will I need physical therapy? How mobile will I be after surgery?How mobile will I be after surgery? When will I be able to walk normally When will I be able to walk normally again?again?


What is important for What is important for the provider?the provider?

What do surgeons want?What do surgeons want?

What do surgeons want?What do surgeons want?

External pressuresExternal pressures

Problems with current Problems with current metrics for success?metrics for success?
Do current metrics really measure Do current metrics really measure quality?quality?
Does early discharge really reflect Does early discharge really reflect good early care?good early care?
Does low readmission reflect better Does low readmission reflect better medium term care?medium term care?
What about functional outcomes? What about functional outcomes? Physician visits at 1 year? Early pain Physician visits at 1 year? Early pain control?control?
Does it matter?Does it matter?

Reality on the ground?Reality on the ground? Major factors inhibiting early Major factors inhibiting early rehabilitation: pain, nausea, rehabilitation: pain, nausea, dizzyness, motor blockdizzyness, motor block
Is early pain control after discharge Is early pain control after discharge a problem: probably yesa problem: probably yes
Does TJA reduce pain and improve Does TJA reduce pain and improve function: yesfunction: yes
Is chronic pain after TKA a problem: Is chronic pain after TKA a problem: probably yes for atleast 20% of probably yes for atleast 20% of patientspatients

Confessions of a Confessions of a frustrated frustrated
physiotherapist?physiotherapist? Factors impeding Factors impeding rehabilitation:rehabilitation:
– PainPain– NauseaNausea– DizzynessDizzyness– Motor blockMotor block

Is pain after discharge Is pain after discharge a problem?a problem?
Andersen LO et al 2009: 52% Andersen LO et al 2009: 52% moderate pain and 16% severe pain moderate pain and 16% severe pain one month post TKAone month post TKA
Chan EY et al 2013: 52% reported Chan EY et al 2013: 52% reported that worst pain was first two weeks that worst pain was first two weeks at homeat home
Bremner S et al 2012: Reluctance of Bremner S et al 2012: Reluctance of patients to take analgesics at homepatients to take analgesics at home

Is chronic pain after Is chronic pain after TKA a problem?TKA a problem?
300,000+ TKA in USA per year300,000+ TKA in USA per year >30% will have chronic pain at >30% will have chronic pain at 1 year after surgery1 year after surgery
We know little about associated We know little about associated factors, prevention, nature or factors, prevention, nature or how to manage this painhow to manage this pain
Beswick AD et al BMJ Open 2012, Puolakka PA et al EJA 2010

What does the literature What does the literature tell us?tell us?
Short term outcomes of importance Short term outcomes of importance undeniably support regional anesthesiaundeniably support regional anesthesia
Regional anesthesia does influence Regional anesthesia does influence major outcomesmajor outcomes
Medium and long term functional outcome Medium and long term functional outcome has not been well studied (or studied has not been well studied (or studied well)well)
LIA has been proven beneficial (in LIA has been proven beneficial (in short term and compared to placebo)short term and compared to placebo)
Better studies needed?!Better studies needed?!

Short term items of Short term items of importance and importance and
correlation with factors correlation with factors impeding rehabilitation:impeding rehabilitation:PainPainNauseaNauseaDizzynessDizzynessMotor blockMotor block Rudan et al J Arthroplasty

Regional anesthesia and multimodal Regional anesthesia and multimodal analgesia reduces pain and nauseaanalgesia reduces pain and nausea
Richman JL et al 2005

Regional anesthesia and Regional anesthesia and multimodal analgesia multimodal analgesia
reduces pain and nauseareduces pain and nausea
Cepeda et al 2005

Does regional anesthesia Does regional anesthesia impact mortality?impact mortality?

Rodgers A et al BMJ 2000
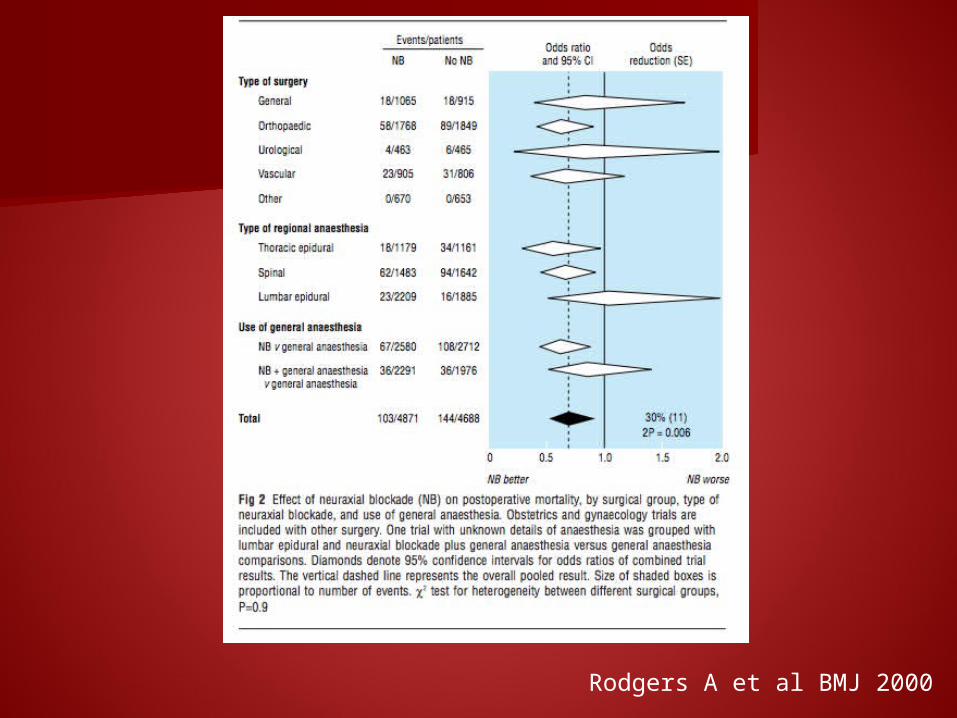
Rodgers A et al BMJ 2000

400 hospitals between 2006-10400 hospitals between 2006-10 Data from primary hip/knee Data from primary hip/knee arthroplastyarthroplasty
Subgrouped by anesthetic techniqueSubgrouped by anesthetic technique 30 day morbidity and mortality data30 day morbidity and mortality data
Anesthesiology 2013

382,000 patients382,000 patients 25% neuraxial25% neuraxial Neuraxial associated with less Neuraxial associated with less mortality, length of stay, in-mortality, length of stay, in-patient morbiditypatient morbidity
Anesthesiology 2013


Does regional anesthesia Does regional anesthesia impact short and longer-impact short and longer-
term function?term function?

Data from Brian’s studyData from Brian’s study
RCDB 50 patients undergoing TKARCDB 50 patients undergoing TKA cFNB or placebocFNB or placebo Multimodal analgesiaMultimodal analgesia Time to achieve three distinct Time to achieve three distinct discharge criteriadischarge criteria


Ilfeld et al 2008

Buvanendran A et al A&A 2010
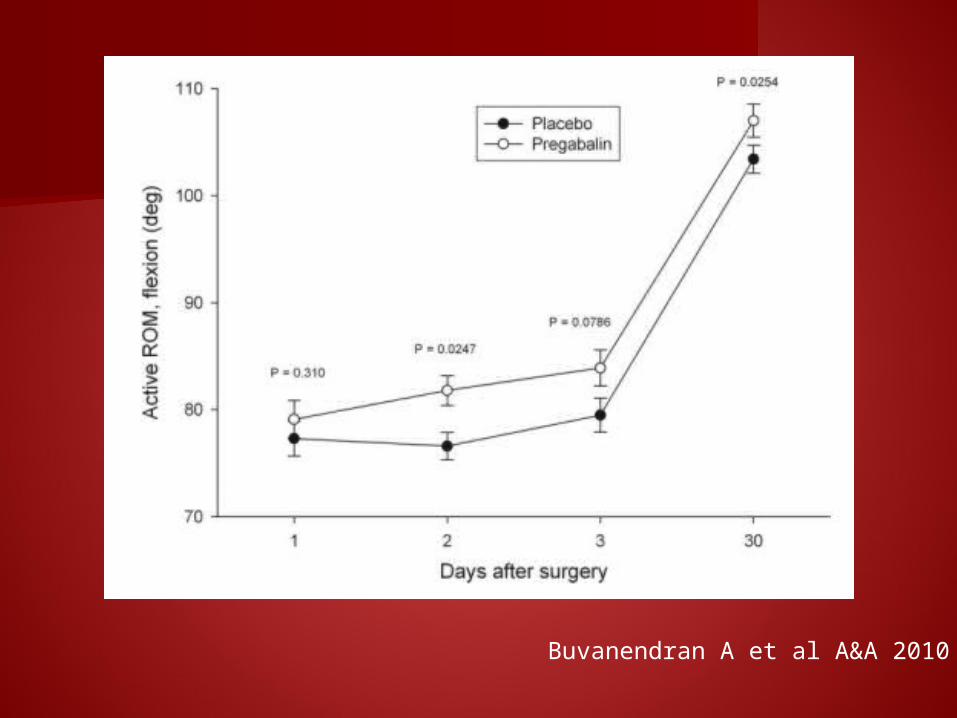
Buvanendran A et al A&A 2010

Measuring long-term Measuring long-term function?function?
What is important for patient, What is important for patient, providers and the systemproviders and the system
What methods have been used to What methods have been used to assess outcomes?assess outcomes?
What methods should we use to What methods should we use to assess outcomes?assess outcomes?
What do we need?What do we need?

What outcome measures What outcome measures should we be using and should we be using and
when?when?

Self-report measures: WOMAC, Knee Self-report measures: WOMAC, Knee Outcomes Severity Score (KOOS), Lower Outcomes Severity Score (KOOS), Lower Extremity Function Scale (LEFS)Extremity Function Scale (LEFS)
Physical performance outcomes: ROM, Physical performance outcomes: ROM, Quad strength, 6MWT, TUG, Stair time, Quad strength, 6MWT, TUG, Stair time, self-paced walk testself-paced walk test

Appropriate use of Appropriate use of functional outcomesfunctional outcomes
Combination of self-report (e.g. Combination of self-report (e.g. WOMAC) and physical performance WOMAC) and physical performance outcomes (e.g. 6MWT)outcomes (e.g. 6MWT)
Measures applied preoperatively and Measures applied preoperatively and at several time points in the at several time points in the postoperative periodpostoperative period
Use tests during period of maximal Use tests during period of maximal changechange
Aim: to demonstrate change in rate of Aim: to demonstrate change in rate of improvement or absolute changeimprovement or absolute change


Kennedy DM et al 2006

Buvanendran A et al A&A 2010

Timing of functional assessments:Timing of functional assessments:Early (<2wks): Knee flexion, Quad Early (<2wks): Knee flexion, Quad strength, TUGstrength, TUGIntermediate (6-12 wks): WOMAC, Intermediate (6-12 wks): WOMAC, LEFS, 6MWTLEFS, 6MWTLate (6-12 mths):as per Late (6-12 mths):as per intermediateintermediate

Where do we currently Where do we currently stand?stand?
Most studies assessing functional Most studies assessing functional outcome with RA have method outcome with RA have method limitationslimitations
Inadequate samples for functionInadequate samples for function Function not primary outcomeFunction not primary outcome Inappropriately used measuresInappropriately used measures
– Wrong measureWrong measure– Erroneous conclusionsErroneous conclusions– Single time pointSingle time point

Goals: Regional Goals: Regional AnesthesiaAnesthesia
What is important for patient, What is important for patient, providers and the systemproviders and the system
What methods have been used to What methods have been used to assess outcomes?assess outcomes?
What methods should we use to What methods should we use to assess outcomes?assess outcomes?
What do we need?What do we need?

What do we need?What do we need? Don’t lose focus on important outcomes Don’t lose focus on important outcomes for function: pain, nausea etcfor function: pain, nausea etc
Better studies examining function with Better studies examining function with adequate methodsadequate methods
Continue to advance practice and Continue to advance practice and improve quality and efficiency of careimprove quality and efficiency of care
Anesthesiologists need to be involved Anesthesiologists need to be involved in setting criteria and guidelines for in setting criteria and guidelines for perioperative careperioperative care



Summary:Summary: Both quality and efficiency are important Both quality and efficiency are important in patient carein patient care
Don’t sacrifice quality at expense of Don’t sacrifice quality at expense of efficiencyefficiency
Continue to focus on outcomes that matter Continue to focus on outcomes that matter to patients: function, postop painto patients: function, postop pain
Advocate for best practice at Advocate for best practice at governmental levelgovernmental level
We need better design for studies We need better design for studies examining functional outcomesexamining functional outcomes




![[Zukertort]The Colle Move by Move](https://static.fdokumen.com/doc/165x107/6333618d3108fad7760f05da/zukertortthe-colle-move-by-move.jpg)