
Increasing intrathecal lymphocytosis and immunoglobulin G production in neurologically asymptomatic...
14
Journal of Neuroimmunology, 19 (1988) 291 - 304 Elsevier JNI 00634 291 Increasing intrathecal lymphocytosis and immunoglobulin G production in neurologically asymptomatic HIV-1 infection Mats A. Andersson 1, Tomas B. Bergstr/Sm 3, Christian Blomstrand ~, Svante H. Hermodsson 3, Charles HS.kansson 2 and Gun-Britt E. L~Swhagen 2 Department of I Neurology. 2 Dermatology and ~ Virology, Unit,ersity of Gothenburg, Sahlgren's Hospital. Gothenburg~ Sweden (Received 6 April 1988) (Accepted 18 April 1988) Key words: Human immunodeficiencyvirus; Immunology; Cytology, CSF; Protein, CSF: IgG Summary Cerebrospinal fluid from 34 human immunodeficiency virus (HIV-1) seropositive patients, only four of whom had HIV-related neurological symptoms, was examined by cytology, protein quantification, isoelectric focusing and specific serological tests. CSF lymphocytosis and evidence of intrathecal lgG production, found in 21 and 20 respectively of the 34 patients, correlated significantly with the duration of the infection. Increasing IgG index was found in two patients with repeated CSF examinations during > 7 years. Intrathecal HIV antibodies were detected on Western blot in 32/34 patients. HIV antigen test positive in 5/34 sera was negative in all 34 CSF samples. Intrathecal B cell activation seems to increase during the early HIV infection. Introduction Human immunodeficiency virus (HIV-1) has the ability not only to create an immunodeficiency state by infecting and destroying T helper lymphocytes but also Address for correspondence: Mats Andersson, Department of Neurology, Sahlgren's Hospital, S-413 45 Gothenburg, Sweden. 0165-5728/88/$03.50 (O 1988 Elsevier Science Publishers B.V. (Biomedical Division)
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Increasing intrathecal lymphocytosis and immunoglobulin G production in neurologically asymptomatic...

Journal of Neuroimmunology, 19 (1988) 291 - 304 Elsevier
JNI 00634
291
Increasing intrathecal lymphocytosis and immunoglobulin G production
in neurologically asymptomatic HIV-1 infection
Mats A. Andersson 1, Tomas B. Bergstr/Sm 3, Christian Blomstrand ~, Svante H. Hermodsson 3, Charles HS.kansson 2
and Gun-Britt E. L~Swhagen 2 Department of I Neurology. 2 Dermatology and ~ Virology, Unit,ersity of Gothenburg, Sahlgren's Hospital.
Gothenburg~ Sweden
(Received 6 April 1988) (Accepted 18 April 1988)
Key words: Human immunodeficiency virus; Immunology; Cytology, CSF; Protein, CSF: IgG
Summary
Cerebrospinal fluid from 34 human immunodeficiency virus (HIV-1) seropositive patients, only four of whom had HIV-related neurological symptoms, was examined by cytology, protein quantification, isoelectric focusing and specific serological tests. CSF lymphocytosis and evidence of intrathecal lgG production, found in 21 and 20 respectively of the 34 patients, correlated significantly with the duration of the infection. Increasing IgG index was found in two patients with repeated CSF examinations during > 7 years. Intrathecal HIV antibodies were detected on Western blot in 32/34 patients. HIV antigen test positive in 5 /34 sera was negative in all 34 CSF samples. Intrathecal B cell activation seems to increase during the early HIV infection.
Introduction
Human immunodeficiency virus (HIV-1) has the ability not only to create an immunodeficiency state by infecting and destroying T helper lymphocytes but also
Address for correspondence: Mats Andersson, Department of Neurology, Sahlgren's Hospital, S-413 45 Gothenburg, Sweden.
0165-5728/88/$03.50 (O 1988 Elsevier Science Publishers B.V. (Biomedical Division)
292
the ability to infect the central nervous system (CNS). HIV has been isolated from cerebrospinal fluid (CSF) and brain tissue in patients with acquired immuno- deficiency syndrome (AIDS) and AIDS-related complex (ARC) (Ho et al., 1985; Levy et al., 1985), and HIV genome has been detected by hybridization technique in brain tissue from AIDS patients (Shaw et al., 1985). Furthermore, chimpanzees have been HIV infected by inoculation of brain tissue from AIDS patients (Gajdusek et al., 1985). Increased intrathecal lgG production and pleocytosis have been reported in patients with AIDS and ARC (Resnick et al., 1985; Elovaara et al., 1987). The majority of these patients had neurological symptoms and were examined at a late stage of the disease, but a few asymptomatic HIV-seropositive patients were also reported to have increased intrathecal IgG production. Goudsmit et al. (1986b) reported CSF findings from ten HIV-seropositive men who also had syphilis. The aim of the present study was to examine the CSF and especially the lgG production in a larger population of patients with HIV infection at an early neurologically asymptomatic stage. Opportunistic and other infections would then be less likely to interfere with the results. We also wanted to correlate the findings to the duration of the infection, in order to get a temporal profile of the intrathecai IgG response.
Patients and methods
Since August 1986 all HIV-seropositive patients attending the Department of Dermatology, Sahlgren's Hospital have been offered a neurological examination including lumbar puncture. Hitherto 34 consecutive patients have been examined and included in this study. Three of the patients were female (Nos. 23, 30 and 33), two were heterosexual (Nos. 25 and 27) and 29 homosexual men (ages 19-69 years; mean 36 years). Fifteen of the 34 patients fulfilled the criteria for lymphadenopathy syndrome (LAS), as defined by Centers for Disease Control (CDC). In one patient (No. 3), complaining of remarkable fatigue, a low-grade malignant lymphoma of T cell origin was diagnosed in a lymph node from the axilla 3 months before entrance into the study. There were no signs of extranodal involvement. The other patients had no HIV-related clinical symptoms such as weight loss, fever, diarrhoea, signifi- cant fatigue or night sweats.
Chest X-rays performed in 28 patients were normal. Routine laboratory tests were normal except in patient No. 13 who had a sedimentation rate of 50 mm. A history of treated syphilitic infection was given by nine patients. Three patients (Nos. 1, 15 and 28) had episodes of anal herpes during the last year. The diagnosis of patient No. 15 has later been revised to AIDS because of severe persistent anal herpes. At the time of lumbar puncture the patient was treated with acyclovir and free of symptoms. Two patients (Nos. 8 and 23) had herpes zoster 1 and 6 months before the lumbar puncture. The duration of the HIV infection could be determined in 23 patients. In 12 cases the examination of stored sera gave the time for seroconversion. In the remaining the duration was estimated from data in the history. This included results of contact tracing which was performed together with a specialized health worker.

293
The patients were separated into three groups according to the duration of their infection: less than 1 year, 1-3 years, and more than 3 years. In 11 patients it was not possible to estimate the duration of the infection.
All patients were neurologically examined by the same neurologist (M.A.). A lumbar puncture was performed under standardized conditions in the morning with the patient in a recumbent position. 20 ml of CSF was collected in standardized portions, and 10 ml of blood was drawn at the same time. CSF and serum samples were stored at - 70 o C.
The total number of lymphocytes in peripheral blood with surface antigen CD4 (helper T cells), CD8 (cytotoxic/suppressor T ceils) and C D 4 / C D 8 ratios were determined using monoclonal antibodies (Ortho, U.S.A.).
CSF cells were routinely counted in a Fuchs-Rosenthai chamber. Pleocytosis was defined as > 5 leukocytes//xi. Cytological preparations were done in a cytocentri- fuge and the cells were stained with May-Griinwald-Giemsa solution.
The protein concentration of the CSF was determined according to Lowry et al. (1951) as modified by Lous et al. (1956). Albumin (alb) and immunoglobulin G (IgG) were measured with electroimmunodiffusion ad modum Laurell (1966). Blood-brain barrier damage was estimated using the CSF alb (mg/ l ) / s e rum alb (g/ l ) ratio. Reference values: < 6 for patients 15-44 years, < 7 for patients 45-54 years.
Intrathecal immunoglobulin production was calculated by two different for- mulas: the IgG index according to Tibbling et al. (1977), reference value _< 0.70, and Tourtellotte's formula for IgG production (TourteUotte et al., 1985), reference value _< 3 mg/day.
Isoelectric focusing of unconcentrated CSF and serum diluted 1/200 was per- formed as previously described (Wikkels6 et al., 1984). Intrathecal immunoglobulin production was considered to be present when one or more bands in the gamma region was found exclusively in the CSF or was stronger in CSF than in serum. Bands that could be caused by naturally occurring CSF enriched proteins like gamma trace, beta trace and a band at isoelectric point (pI ) 7.4 (Wikkels6 et al., 1983) were excluded. In doubtful cases the IgG nature of the bands was confirmed with a direct immunofixation technique using antibodies to human IgG, specific for gamma chains (Dakopatts, Denmark).
Screening for opportunistic viral infections was performed by inoculation of CSF on green monkey kidney cells, human fibroblasts and A549 cells. The cell lines were cultured for 2-6 weeks after inoculation. Peripheral blood leukocytes were cocul- tured with human fibroblasts for 24 h and then removed by washing. The human fibroblasts were screened for cytopathogenic effect once weekly during 6 weeks.
CSF and serum samples were analysed for IgG antibodies against cytomega- lovirus (CMV), herpes simplex virus (HSV) type 1 and 2, varicella zoster virus (VZV), morbilli virus and Toxoplasma gondii using enzyme-linked immunosorbent assay (ELISA). Serum samples were also tested for IgM antibodies against CMV and HSV with ELISA. IgM antibodies against Toxoplasma gondii and Epstein-Barr virus (EBV) and IgG antibodies against Borrelia were analysed by immunofluores- cence. Sera were also tested for IgG antibodies against hepatitis B core and surface

294
antigen and for presence of hepatitis B surface antigen (HBsAg). Serum samples were screened for syphilis with the Wasserman test (WR) and Venereal Disease Research Laboratory (VDRL) test. Both CSF samples and sera were analysed by the Treponema pallidum haemagglutination assay (TPHA) test.
Antibodies against HIV were detected using both a direct (Behring, F.R.G.) and a competitive ELISA (Wellcome, U.K.). Positive samples were further analysed by Western blot (WB) using commercially available HIV strips (Du Pont, Switzerland). The strips were washed with Tris-buffered saline (TBS) and 0.3% Tween for 30 min at 37°C. After preincubation with TBS containing 3% bovine serum albumin and 4% fetal calf serum, serum samples (dilution 1/200) and CSF samples (dilution 1/10) were added. After incubation overnight at room temperature, the strips were washed and incubated with rabbit anti-human lgG conjugated to horseradish peroxidase and developed after washing (Towbin et al., 1979).
An attempt to evaluate intrathecal production of HIV IgG antibodies was made by incubating the HIV strips with CSF samples diluted to 1/10 and the correspond- ing serum samples diluted to equal IgG concentrations. The band patterns were then compared visually.
HIV-1 antigen was detected in serum and CSF samples using a commercially available enzyme immunoassay (Abbot Laboratories, F,R.G.).
Pitman's non-parametric permutation test (Bradley, 1968), and multiple linear regression analysis were used to analyse correlations between different variables in the material.
Results
No patients had symptoms indicating meningitis. Only four patients suffered from moderate tension headache, which is not more than expected in view of the psychological stress connected with the HIV disease.
Four patients (Nos. 2, 21, 30 and 34) had symptoms where a relation to the HIV infection could not be excluded. Patient No. 2 had an episode with unilateral optic neuritis. Patient No. 21 had several episodes with brain stem dysfunction lasting only minutes each time. Patient No. 30 had symptoms clinically indistinguishable from transient ischaemic attacks, three attacks of visual field defects and one with vertigo. Patient No. 34 had a slight intention tremor in one leg, without any other signs of cerebellar damage.
All patients had serum antibodies against HIV by both the direct and the competitive ELISA as well as by WB. Thirty-three of 34 patients had CSF IgG antibodies against HIV detected by at least one of the ELISA tests. Thirty-two of 34 patients were considered CSF HIV IgG antibody positive in WB when the criteria for positivity were presence of at least two bands (antibodies against both core and envelope). The two remaining patients, Nos. 16 and 21, had only one detectable band (gpl60 and p24, respectively).
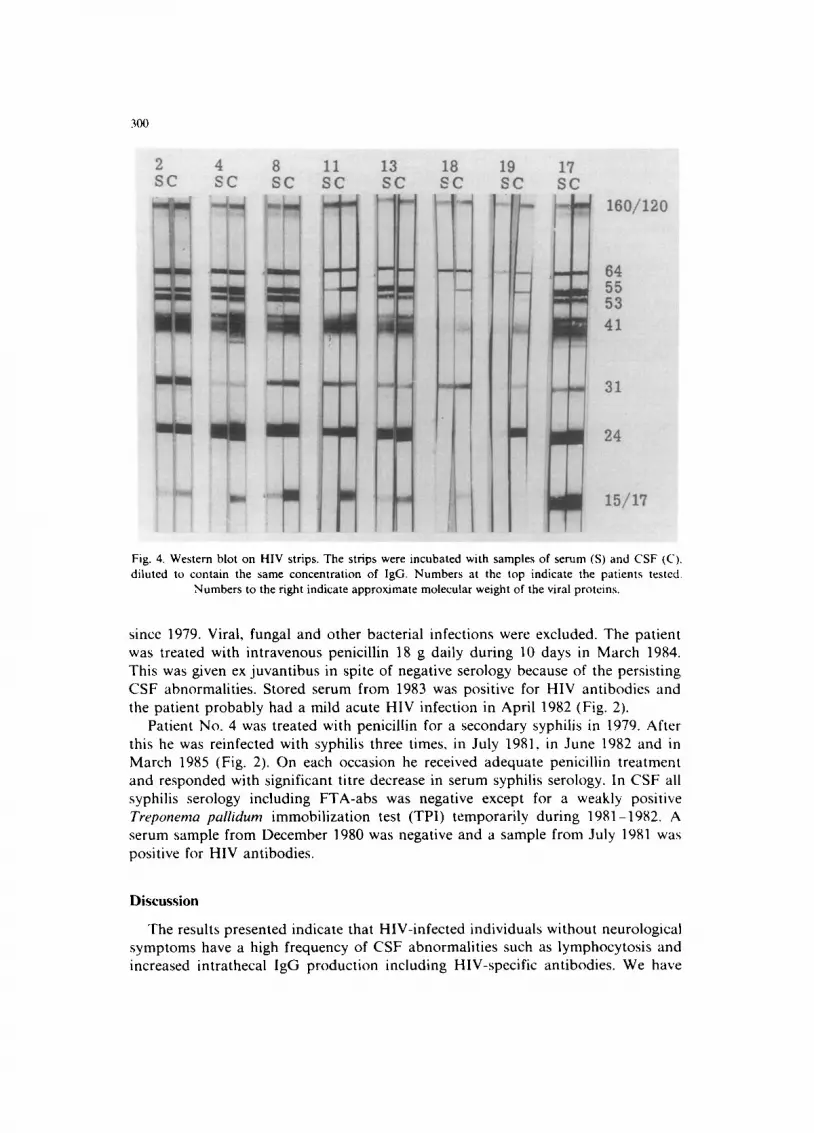
When CSF and corresponding serum samples from each patient were diluted to contain equal concentrations of IgG, the WB pattern indicated intrathecai produc-

295
tion of HIV antibodies in ten patients. CSF from the patients (Nos. 2, 4, 8, 11, 13, 18, 19, 28, 29 and 32) displayed stronger reactions than serum to at least two viral proteins (Fig. 4). Patient No. 19 with shorter infection duration, No. 28 with unknown duration and No. 29 differed from the others by showing a strong reactivity in CSF against p24 but none against p15. In the other seven patients, however, the p15 band was stronger with CSF than with serum. In patients No. 2, 4, 11, 18, 19 and 32 stronger CSF reactivity was also noted against p55. A relative increase in the reaction to one of the bands, which was noted in four patients (Nos. 3, 6, 12 and 15), should probably also be taken as a sign of intrathecal production.
The HIV-1 antigen test was positive in sera from all three women and the two heterosexual men (Nos. 25 and 27), but negative in all 29 homosexual men. The CSF samples from all the 34 patients were negative in the antigen test.
Screening for other infections All CSF and peripheral blood samples gave negative results after attempts to
isolate virus. No evidence of intrathecal antibody production, seroconversion or significant titre rise between sequential sera was found against CMV, HSV-1, HSV-2, VZV, morbilli or Toxoplasma gondii in any of the patients. No serum IgM antibodies against HSV, CMV or Toxoplasma gondii were detected. Twenty-two patients had IgG serum antibodies to hepatitis B virus, one of them after vaccina- tion though, and two patients were HBsAg positive.
Nine patients had a positive TPHA titre in serum. All of them had a history of treated syphilis. Patient No. 4 had had four and patient No. 7 two syphilitic infections. Seven patients (Nos. 7, 9, 11, 12, 16, 22 and 26) treated more than 2 years before the lumbar puncture were all seronegative in WR a n d / o r VDRL. Two patients (Nos. 4 and 6) treated during 1985 were still seropositive in WR and VDRL but with significant decrease of the titre. All but two patients were TPHA negative in CSF. Patient Nos. 6 and 22 had a low TPHA titre (1 /20 and 1/40 respectively) in CSF compared to 1/1280 in both sera, The fluorescent treponemal antibody absorption test (FTA-abs) was negative in CSF of these two patients.
All patients but one were negative for Borrelia antibodies in serum. Patient No. 6 with positive WR and VDRL in serum also had a slightly raised Borrelia titre probably reflecting cross-reactivity with Treponema pallidum (Stiernstedt et al., 1985).
CSF cellular reaction Twenty-one of the 34 patients had an increased number of mononuclear cells in
CSF (Table 1). Twenty-six patients including those with pleocytosis had pathologi- cal cytology with activated small and medium-sized lympht~cytes and plasma cells. Two additional patients showed slight activation of monocytes without pleocytosis. Six patients had normal cytology. No po!ymorphonuclear cells or phagocytes were found in any of the patients.
Protein determinations A raised CSF/serum albumin ratio indicating a blood-brain barrier damage was
found in six of 34 patients. Four of these had a duration of HIV infection of more

296
T A B L E 1
L A B O R A T O R Y F I N D I N G S IN 34 P A T I E N T S W I T H HIV I N F E C T I O N
Dura t ion Pat ient C D 4 ~ CSF Cyto logy C S F / S IgG IgG IEF g No. mono d alb index " synth, t (No. bands) h
< 1 year 14 0.40 3
G r o u p I 16 S ,i 0.80 3
19 0.49 3
Mean 3
1 - 3 years 1 0.89 3 G r o u p II 6 S 0.90 10
7 S 0.73 1 10 LAS b 0.81 1
15 0.06 2
18 0.87 3
21 0.38 8
23 LAS 0.23 6
Mean 4
< 3 years 3 LAS 0.28 21 G r o u p I11 4 S 0.44 6
11 LAS, S 0.39 9
12 LAS. S 0.43 26
13 0.58 28 17 LAS 0.50 14
20 I,AS 0.30 4 22 LAS, S 0.37 19
27 0.23 1
29 0.81 9 30 LAS 0.49 4
33 0.21 8
Mean 15
U n k n o w n 2 0.47 53 G r o u p IV 5 0.60 20
8 LAS 0.67 14
9 LAS, S 0.50 13 24 0.47 3
25 I,AS 0.31 8 26 LAS, S 0.42 11 28 I.AS 0.93 1
31 0.62 6
32 0.41 26 34 LAS 0.61 13
Mean 25
R ' 4.5 0.70 2 I k 6.2 0.61 2 N i 1.6 0.53 - 4
4.6 0.61 0
I 3.4 0.78 3
I 3.8 0.91 7 N 4.9 0.67 2
N 5.9 0.58 0
N 2.6 0.92 4
I 3.1 0.88 6
I 6.0 0.88 21
I 1.9 0.68 - 4
4.2 0.80 6
9.2 0.90 42
3.5 1.01 10
5.2 0.98 25
6.4 1.26 54 8.6 1.35 81
16.8 1.27 158 R 5.3 0.55 - 2
I 5.6 0.81 13 N 3.3 (I.54 - 3
i 3.6 0.86 5 1 5.7 0.64 5
I 5.7 0.75 8
7.9 1.05 52
6.5 1.63 66 3.7 (I.82 4
3.0 1.53 25 3.1 0.64 - 2 4.2 0.37 - 7
5.3 0.49 - 5
5.5 0.75 5
N 5.1 0.52 - 2 I 4.6 0.64 1 I 7.1 1 .25 35
I 4.1 0.99 14
4.1 1.16 23
I (2) N N
1 (2) I (2) N
N I (7) I (7) ! (5) N
+ B "' (11) (5)
(6)
(171 (14)
+ B (7)
N I (7) N I (7) l (1) 1 (4)
I (9) I (4) I (15 ) N N
N N
N I (4) 1 (151 I (8)
" S = pa t ien ts wi th his tory of t reated syphil is ; b I,AS = l y m p h a d e n o p a t h y syndrome: " C D 4 = helper-T
lymphocy tes in per iphera l blood; d CSF m o n o = n u m b e r of mononuc l ea r c e l l s / # l in ce rebrosp ina l fluid; ~" IgG index = (CSF I g G / s e r u m I g G ) / ( C S F a l b / s e r u m alb); r IgG synthes is = in t ra theca l IgG synthes is in m g / 1 0 0 ml accord ing to Tour te l lo t te ' s formula; g IEF = isoelectr ic focusing; h No. bands = n u m b e r of CSF enr iched IgG bands ; ' R = unspecif ic cell react ion; k I = pa t te rn suggest ing immuno log ica l ac t iva- t ion; t N = normal pa t te rn ; m B = bar r ie r d a m a g e pat tern .

297
Cel ls/~l IgG index
30
26
20
15
10 •
5 ............................ ° .......
°
< 1 1 - 3 years
Albumin ratio
15
10
7 3
, , o
1 1 - 3 73 years
1.5
L
1.0 == n t
e o
0.5 • 00
Cells//JI
50
40
30
20
10
o . ,
1 1 - 3 ~ 3 years
N °
i# °
• i • ' '
t •
• Sole• • o•
o.s , .o llS 21o fgG index
Fig. 1. Correlation between duration of HIV-infection and number of CSF mononuclear cel ls/#l , intrathecal IgG production (IgG index), blood-brain barrier damage (CSF/serum albumin ratio), and correlation between number of CSF mononuclear cel ls /#l and IgG index (r = 0.70). Dotted lines show
upper normal limits.
than 3 years and two belonged to the group in which the duration could not be determined (Table 1).
IgG index was pathological in 20 of 34 patients, and 20 of 34 patients had a pathological IgG production according to the Tourtellotte formula. IgG index in relation to duration of infection is shown in Fig. 1.
Serum IgG was increased in 22 of the 34 patients (mean + SD = 18 __+ 5 g/I) and increasing in the groups with longer duration (0/3, 6 /8 and 10/12).
Is•electric focusing A pattern of CSF-enriched gamma region bands suggesting intrathecal IgG
production was present in 22 of 34 patients. With longer duration of HIV infection there was an increase in the frequency of abnormal IgG patterns and also in the
298
registered number of bands (Fig. 3). Two patients (Nos. 3 and 17) had a pattern indicating blood-brain barrier damage in combination with evidence of intrathecal lgG production. Twelve patients had a normal IEF pattern (Table 1).
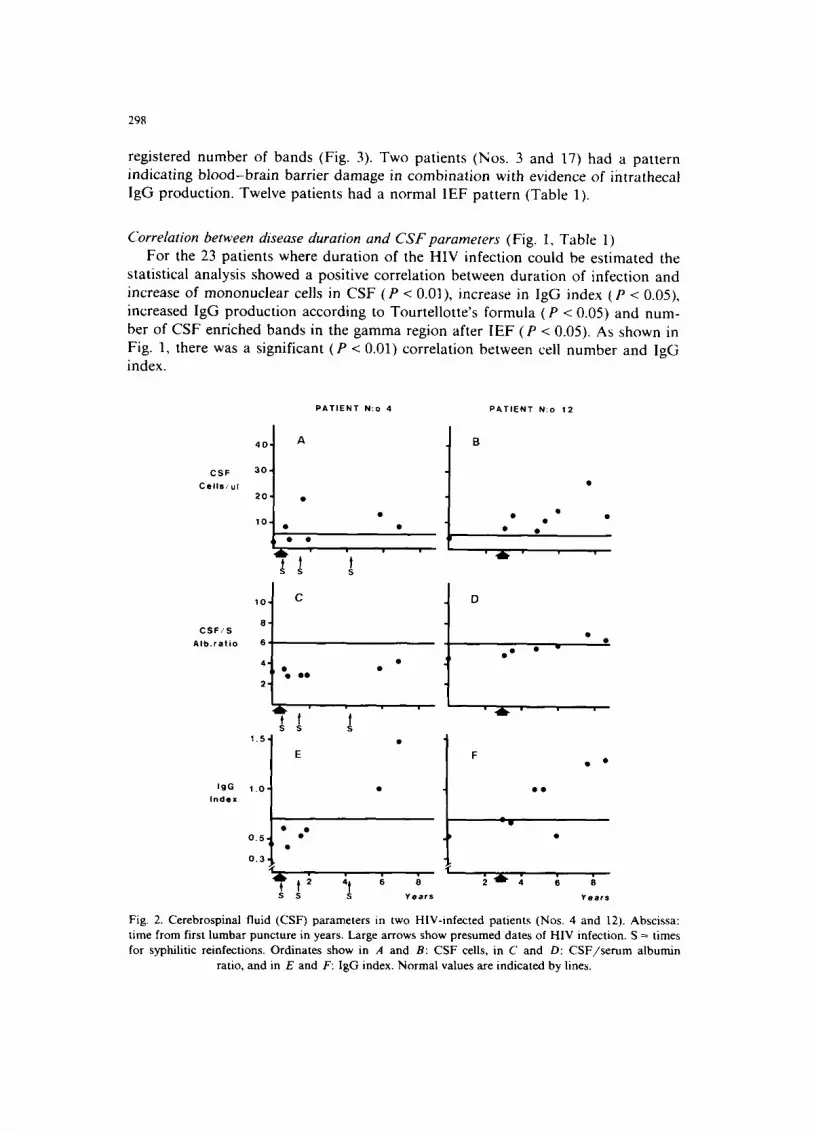
Correlation between disease duration and C S F parameters (Fig. 1, Table l) For the 23 patients where duration of the HIV infection could be estimated the
statistical analysis showed a positive correlation between duration of infection and increase of mononuclear cells in CSF (P < 0.01), increase in IgG index (P < 0.05), increased IgG production according to Tourtellotte's formula (P < 0.05) and num- ber of CSF enriched bands in the gamma region after IEF (P < 0.05), As shown in Fig. 1, there was a significant (P < 0.01) correlation between cell number and IgG index.
P A T I E N T N:o 4 P A T I E N T N:o 12
C S F
C e l l s / u l
4 0 -
3 0 -
2 0
1 0 • •
' i
C S F / S
A I b . r a t i o
I g G
i n d e x
1 0 .
8 '
6 .
4 -
2 .
4b-
1 . 5 .
1 . 0 -
0 . 5
0 , 3
C
OQ O • •
D
V
e
E
Iltl~
t :~ ;~ ~ ~ : ~ - ~, ~ S S Y e a r s Y e a r s
Fig. 2. Cerebrospinal fluid (CSF) parameters in two HIV-infected patients (Nos. 4 and 12). Abscissa: time from first lumbar puncture in years. Large arrows show presumed dates of HIV infection. S = times for syphilitic reinfections. Ordinates show in A and B: CSF cells, in C and D: C S F / s e r u m albumin
ratio, and in E and F: IgG index. Normal values are indicated by lines.

299
Two patients, Nos. 4 and 12, had several lumbar punctures during 7 and 8 years respectively because of t reatments and follow-up of syphilitic infections. Their data are shown in Fig. 2 and illustrate persisting pleocytosis and increase in lgG product ion with time.
Patient No. 12 was treated with penicillin in 1978 for a secondary syphilis. Since 1979 he has been W R and V D R L negative in serum and since 1982 also FTA-abs negative. WR, VDRL, FTA-abs and TPI have been repeatedly negative in CSF
t
q
I I
Fig. 3. lsoelectric focusing of serum and CSF in polyacrylamide gel. Samples from three patients (Nos. 16, 18 and 12) selected to represent different durations of HIV infection: < 1 year (left). 1--3 years
(middle) and > 3 years (right). Serum (left) and CSF proteins (right) in each pair.
300
2 SC
4 SC
8 SC
I I S C
13 S C
18 SC
Ill"
. ,
I I
19 S C
17 SC
eo/12o
84 55 53 41
31
24
l s / n
Fig. 4. Western blot on HIV strips. The strips were incubated with samples of serum (S) and CSF (C). diluted to contain the same concentration of IgG. Numbers at the top indicate the patients tested.
Numbers to the right indicate approximate molecular weight of the viral proteins.
since 1979. Viral, fungal and other bacterial infections were excluded. The patient was treated with intravenous penicillin 18 g daily during 10 days in March 1984. This was given ex juvantibus in spite of negative serology because of the persisting CSF abnormalities. Stored serum from 1983 was positive for HIV antibodies and the patient probably had a mild acute HIV infection in April 1982 (Fig. 2).
Patient No. 4 was treated with penicillin for a secondary syphilis in 1979. After this he was reinfected with syphilis three times, in July 1981, in June 1982 and in March 1985 (Fig. 2). On each occasion he received adequate penicillin treatment and responded with significant titre decrease in serum syphilis serology. In CSF all syphilis serology including FTA-abs was negative except for a weakly positive Treponema pallidum immobilization test (TPI) temporarily during 1981-1982. A serum sample from December 1980 was negative and a sample from July 1981 was positive for HIV antibodies.
Discussion
The results presented indicate that HIV-infected individuals without neurological symptoms have a high frequency of CSF abnormalities such as lymphocytosis and increased intrathecal lgG production including HIV-specific antibodies. We have
301
also found that the frequency of CSF abnormalities increased with the duration of infection.
CSF changes have been reported in primary HIV infection with neurological symptoms and in AIDS (Resnick et al,, 1985; Elovaara et al., 1987) while little is known about the asymptomatic stage in between. Our aim was to study CSF humoral immune reactions prospectively through this stage. Recruited mainly from a ward for health control, our patients probably represent the healthiest third of the individuals known to be HIV seropositive in the town of Gothenburg. Consistent with this assumption we found a low frequency of blood-brain barrier damage and absence of opportunistic infections. Similar data were reported for early asymptomatic cases in previous studies (Goudsmit et al., 1986b; Elovaara et al.. 1987), as well as failure to detect HIV antigen in CSF (Goudsmit et ai., 1986a).
The frequency of pathological pleocytosis and intrathecal IgG synthesis was similar in our and Goudsmit 's study, but Elovaara et al. (1987) found a lower incidence (3/18 and 6 /18) in their groups of patients with asymptomatic infection or LAS. The majority of the Finnish patients are reported to have a duration of HIV infection of less than 1 year, and although we are uncertain about the meaning of the expression 'confirmed duration' this might explain the differences. The frequency of pathological CSF findings in our groups varied from normal values in all patients with less than 1 year duration to almost 80% pathological in the group with more than 3 years duration.
When studying the total intrathecai IgG production, which is relevant for the comparison of the HIV infection with multiple sclerosis or other diseases of unknown aetiology, one has to consider the coexistence of other infections. There were no signs of opportunistic or other CNS infections that could interfere with the interpretation of our results. One could, however, speculate about the reactivation of earlier infections. Hepatitis B and syphilis were the only infections prevalent enough to be relevant. Syphilis but not hepatitis B is known to cause CSF pleocytosis and intrathecal IgG production. In a study from our laboratory on early syphilis intrathecal IgG production was found in ten and pleocytosis in 17 of 47 patients without neurological symptoms (LiSwhagen et al., 1983). The coexistence of HIV and syphilis infection is frequent as in all ten patients in the study of Goudsmit et al. (1986b). However, our patients with a history of syphilis were all adequately treated, seven patients more than 2 years, and two patients more than 1 year, before the study. All were FTA-abs negative in their CSF. When comparing the nine patients with a history of syphilis with the 25 patients without (Table 1) and when comparing the 22 patients with positive hepatitis B serology with the remaining patients, no significant difference was found in number of CSF cells or IgG index.
Four patients disclosed CNS symptoms that could possibly be caused by HIV. Optic neuropathy found in patient No. 2 has been described in a patient with AIDS and neurosyphilis but was thought to be caused by the syphilitic infection (Zaid- man, 1986), The episodic symptoms related by patient No. 21 show similarities to paroxysmal brain stem symptoms found in multiple sclerosis (MS) (Matthews, 1985). Since CSF IgG changes also are similar to MS, HIV infection should be excluded before a definite MS diagnosis is established.

302
Passive transfer of lgG antibodies from serum to CSF would result in identical WB antibody reactivity. Therefore, a stronger antibody reactivity in CSF than in serum samples as seen in ten patients was regarded as evidence of intrathecal production (Weber et al.. 1987). In addition the relative difference in band distribu- tion found in four patients might indicate intrathecal production. A complete correlation between patients having increased IgG index and patients having intrathecal HIV-specific antibody production was not found. This is in accordance with Resnick et al. (1985) who reported that only 0.2-2.8% of CSF IgG was specifically directed against HIV in patients with AIDS and ARC in their study.
All our patients with signs of intrathecal HIV-specific antibody production displayed increased IgG index except patients No. 19 and 28. These patients had a different antibody pattern with a prominent reaction against p24 and patient No. 19 differed from the others by shorter duration of infection. Goudsmit et al. (1986) described the same CSF WB pattern in a patient approximately half a year after seroconversion.
In the group with more than 3 years duration 9-10 of 12 patients showed pathological intrathecal IgG production in the quantitative and qualitative tests. This frequency is even higher than that reported for AIDS and ARC patients. Resnick et al. (1985) pointed out that two of their patients with neurological symptoms had a lower concentration of specific HTLV-III antibodies than two patients without neurological symptoms. Our results indicate that intrathecal B cell activation precedes stages with neurological symptoms.
There are several possible explanations for a polyclonal intrathecal activation of B cells in the HIV infection. Since it occurred in stages without immunodeficiency or opportunistic infections virus transformation by coinfection with EBV or CMV, suggested explanations in AIDS, are less likely. Polyclonal activation of B lympho- cytes by AIDS virus in vitro has been reported (Schnittman et al., 1986). Inter- ference with the function of regulatory lymphokines with defect down-regulation of B cells has been postulated. Recent reports that HIV-envelope protein has amino acid sequences homologous to regions of interleukin-2 (Weigent et al., 1986) and neuroleukin (Gurney, 1987) are interesting in this respect. Further studies are needed to show if this is relevant in vivo.
We conclude that intrathecal pleocytosis and polyclonal lgG production, increas- ing with time and occurring before neurological symptoms, seem to be prominent features in the natural history of HIV infection.
Acknowledgements
Gunilla Hallhagen, Ann Hult6n and Carina ,~strt~m are acknowledged for their enthusiastic work with the patients, and Marianne Andersson for skilful technical assistance.
This study was financially supported by the Gothenburg Society of Neurologi- cally Disabled, the G6teborg Medical Society and the Edith Jacobsson foundation.

303
References
Bradley, J.V. (1968) 4. Fisher's method of randomization. In: J.V. Bradley (Ed.), Distribution-free Statistical Tests, Prentice Hall, London, pp. 68-86.
Elovaara, 1., livanainen. M., Valle, S.-L.. Suni J., Tervo, T. and L~hdevirta. J. (1987) CSF protein and cellular profiles in various stages of HIV infection related to neurological manifestations. J. Neurol. Sci. 78, 331-342.
Gajdusek, D.C., Amyx, H.L., Gibbs, C.J., Asher, D.M., Rodgers-Johnson, P., Epstein, L.G., Sarin, P.S., Gallo, R.C., Maluish, A., Arthur, L.O., Montagnier, L. and Mildvan, D. (1985) Infection of chimpanzees by human T-lymphotropic retroviruses in brain and other tissues from AIDS patients. Lancet i, 55-56.
Goudsmit, J., De Wolf, F., Paul, D.A., Epstein, L.G., Lange, J.M., Krone, W.J., Speelman, H., Woltcrs, E.C., Van der N(×)rdaa, J., Oleske, J.M., Van der Helm, H.J. and Coutinho, R.A. (1986a) Expression of human immunodeficiency virus antigen (HIV-Ag) in serum and cerebrospinal fluid during acute and chronic infection. Lancet ii (26), 177-180.
Goudsmit. J., Wolters, E.C., Bakker, M., Smit, L., Van der Noordaa, J., Hische, E.A.I-t., Tutuarima, J.A. and Van der Helm, H.J. (1986b) Intrathecal synthesis of antibodies to HTLV-lll in patients without AIDS or AIDS related complex. Br. Med. J. 292, 1231-1234.
Gurney. M.E. (1987) Neuroleukin: basic biology and functional interaction with human immuno- deficiency virus. Immunol. Rev. 100, 203-223.
Ho, D.D.. Rota, T.R., Schooley, R.T., Kaplan, J.C., Allan, J.D., Groopman, J.E., Resnick, L., Felsen- stein, D., Andrews, C.A. and Hirsch, M.S. (1985) Isolation of HTLV-III from cerebrospinal fluid and neural tissues of patients with neurologic syndromes related to the acquired immunodeficiency syndrome. New Engl. J. Med. 313, 1493-1497.
Laurell, C.-B. (1966) Quantitative estimation of proteins by electrophoresis in agarose gel containing antibodies. Anal. Biochem. 15, 45-52.
Levy, J.A., Shimabukuro, J., Hollander, H., Mills, J. and Kaminsky, L. (1985) Isolation of AIDS-associ- ated retroviruses from cerebrospinal fluid and brain of patients with neurological symptoms. Lancet ii, 586-. 588.
Lous, P., Plum, C.M. and Schou, M. (1956) Kolorimetrisk bestemmelse af totalprotein og globulin i spinalvaske. Nord. Med. 55, 693-695.
L~Swhagen, G.-B., Andersson, M., Blomstrand, C. and Roupe, G. (1983) Central nervous system involvement in early syphilis. Part I. lntrathecal immunoglobulin production. Acta Derm.-Venereol. 63. 409-417.
Lowry, O.H., Rosebrough, N.J., Farr, A.L. and Randall, R.J. (1951) Protein measurement with the Folin phenol reagent. J. Biol. Chem. 193, 265-275.
Matthews, W.B. (1985) 5. Symptoms and signs. In: W.B. Matthews (Ed.), McAlpine's Multiple ,Sclerosis, Churchill Livingstone, New York, pp. 112-113.
Resnick, L., Di Marzo-Veronese, F., SchiJpbach, J., Tourtellotte, W.W., Ho, D.D., Miiller, F., Shapshak, P., Vogt, M., Groopman, J.E., Markham, P.D. and Gallo, R.C. (1985) Intra-blood-brain-barrier synthesis of HTLV-III specific lgG in patients with neurologic symptoms associated with AIDS or AIDS-related complex. New Engl. J. Med. 313, 1498-1504.
Schnittman, S.M., Lane, H.C., Higgins, S.E., Folks, T. and Fauci, A.S. (1986) Direct polyclonal activation of human B lymphocytes by the acquired immune deficiency syndrome virus. Science 233, 1084-1086.
Shaw, G.M., Harper, M.E., Hahn, B.H., Epstein, L.G., Gajdusek, D.C., Price. R.W., Navia, B.A., Petito, C.K., O'Hara, C.J., Groopman, J.E., Cho, E.-S., Oleske, J.M., Wong-Staal, F. and Gallo, R.C. (1985) HTLV-III infection in brains of children and adults with AIDS encephalopathy. Science 227, 177-182.
Stiernstedt, G.T., Granstr0m, M., Hederstedt, B. and Sk61denberg, B. (1985) Diagnosis of spirochetal meningitis by enzyme-linked immunosorbent assay and indirect immunofluorescence assay in serum and cerebrospinal fluid. J. Clin. Microbiol. 21, 1-7.
Tibbling, G., Link, H. and Ohman, S. (1977) Principles of albumin and IgG analyses in neurological disorders. 1. Establishment of reference values. Stand. J. Clin. Lab. Invest. 37, 385-390.
304
Tourtellotte, W.W., Potvin, A.R., Fleming, J.O., Murthy, K.N., l.evy, J., Syndulko, K. and Potvin, J.H. (1980) Multiple sclerosis: measurement and validation of central nervous system IgG synthesis rate. Neurology 30, 240-244.
Towbin, H., Staehelin, T. and Gordon. J. (1979) Electrophoretic transfer of proteins from polyacrylamide gels to nitrocellulose sheets: prcx:.edure and some applications. Proc. Natl. Acad. Sci. U.S.A. 76. 4350-4354.
Weber, Th., Btittner, W. and Felgenhauer, K. (1987) Evidence for different immune responses to HIV in CSF and serum? Klin. Wochenschr. 65, 259-263.
Wcigent. D.A., Hoeprich, P.D., Bost, K.L., Brunck, T.K., Rciher, W.E. and Blalock. J.E. (1986)The HTLV-III envelope protein contains a hexapeptide homologous to a region of interleukin-2 that binds to the interleukin-2 receptor. Biochem. Biophys. Res. Commun. 139, 367-374.
Wikkels6, C., Andersson, M., Von Essen, C., R~'~nnback, I,. and Blomstrand, C. (1983) Separation of cerebrospinal fluid-enriched proteins. J. Neurol. Sci. 60, 419-429.
Wikkels6, C., Andersson, M., Andersson, R. and BIomstrand, C. (1984) Isoelectric focusing followed by silver staining. A suitable method for routine investigation of cerebrospinal fluid proteins. Eur. Neurol. 23, 306-312.
Zaidman, G.W. (1986) Neurosyphilis and retrobulbar neuritis in a patient with AIDS. Ann. Ophthalmol. 18, 260-261.




















