
Local Immunoglobulin E in the Nasal Mucosa: Clinical Implications

Recurrence of Immunoglobulin A Nephropathy With Immunoglobulin A Antineutrophil Cytoplasmic Antibodies
Following Renal Transplantation
Stephane d. Martin, MD, Marie A.P. Audrain, MD, Thierry Baranger, MD, Anne Moreau, MD, Jacques Dantal, MD, Angelo Testa, MD, and Vincent L.M. Esnault, PhD
• We previously reported the presence of immunoglobulin A (IgA) antineutrophil cytoplasmic antibodies (ANCAs) in patients presenting IgA nephropathy (IgAN), particularly when associated with Henoch-Sch6nlein purpura. Most of the patients exhibited IgA ANCAs directed at an unknown 50-kd neutrophil protein but no IgG ANCAs. A subgroup of patients presented IgG as well as IgA ANCAs, suggesting an overlap syndrome between Henoch- Sch6nlein purpura and microscopic polyangiitis. We aimed at confirming the correlation of IgA ANCA titer with disease activity in a patient presenting IgAN relapse following kidney transplantation. The ANCAs were searched for by isotype- and antigen-specific enzyme-linked immunosorbent assay. Specificity was confirmed by antigen- specific enzyme-linked immunosorbent assay and Western blot analysis. At the onset of the disease in 1989, the patient presented with ANCAs of IgA and IgG class with specificity for myeloperoxidase and no rheumatoid factor. End-stage renal failure developed 1 year afterward. In 1991, he received a cadaveric renal allograft, and 9 months later developed acute nephrotic syndrome with rapidly progressive renal failure and recurrence of IgAN on the kidney transplant. An increase in IgA but not IgG ANCAs was found on clinical relapse after kidney transplantation. We conclude that rare patients may present an overlap syndrome between IgG ANCA-positive systemic vasculitis and IgAN, characterized by the presence of IgG and IgA anti-myeloperoxidase antibodies. © 1997 by the National Kidney Foundation, Inc.
INDEX WORDS: Antineutrophil cytoplasmic antibodies; Henoch-Sch6nlein purpura; immunoglobulin A; immuno- globulin A nephropathy; myeloperoxidase; transplantation.
T HE COURSE of primary IgA nephropathy (IgAN) is not always benign, as progression
to renal failure occurs in one third of cases. ~ Patients may even present with rapidly progres- sive glomerulonephritis and extensive epithelial crescent formation. 2 Immunoglobulin A ne- phropathy recurs in the kidney transplant in ap- proximately 50% of cases, often with little clini- cal effects) Immunoglobulin A antineutrophil cytoplasmic antibodies (ANCAs) have been re- ported in severe IgAN when associated with Henoch-SchOnlein purpura (HSP) 4-6 and IgA ANCA titer correlated with disease activity. 4 We report a case of crescentic IgAN recurrence after renal transplantation following an increase in IgA ANCA titer.
PATIENTS AND METHODS
uria (4 g/d) and microhematuria. Rheumatoid factor and anti- nuclear antibodies were absent, and complement levels of C3 and C4 fractions were normal. Renal biopsy was performed 1 week after presentation. Histologic examination revealed proliferative glomerulonephritis, with 50% extracapillary crescents, moderate focal tubular atrophy, minor interstitial cellular infiltration, and no significant arterial lesions (Fig 1A). Immunoftuorescence microscopy disclosed bright gran- ular IgA and C3 deposits within mesangial areas, as well as IgG and fibrin in crescents (Fig 1B). Final diagnosis was IgAN. In spite of a short steroid course, renal function deteri- orated progressively and hemodialysis was started in Septem- ber 1990.
In August 1991, patient CJ received a cadaveric kidney graft. Immunosuppressive treatment consisted of antithymo- cyte globulin for 18 days, followed by cyclosporin in associa- tion with azathioprine and prednisone. Four weeks after trans- plantation, serum creatinine level was 1.41 mg/dL, with neither proteinuria nor hematuria. In May 1992, the patient exhibited nephrotic syndrome, microscopic hematuria, and increased serum creatinine level (2.26 mg/dL), but no extrare-
Patient CJ
In June 1989, a 68-year-old man was admitted to our unit because of weakness, weight loss, hypertension, and renal failure. He had no history of hypertension, purpuric rash, or joint pain. There was no family history of renal disease and he had not taken any nephrotoxic drugs. At admission, arterial blood pressure was 150/100 mm Hg, and an extensive physi- cal examination, including the ears, nose, throat, and lungs, was normal. Laboratory tests showed elevated serum creati- nine (7.5 mg/dL) and C-reacfive protein (116 rag/L). Hemo- globin was 11.2 gtdL. Total IgG serum level was increased, whereas IgA and IgM serum levels were both decreased. There was no hypoalbuminemia. Urinalysis revealed protein-
From the Nephrology and Transplantation Department, the Immunology Department, and the Anatomopathology De- partment, Nantes University Hospital, France.
Received April 18, 1996; accepted in revised form August 27, 1986.
Supported in part by the Fondation pour la Recherche Mddicale and the Ddlggation d la Recherche Clinique of Nantes University Hospital.
Address reprint requests to Vincent L.M. Esnault, PhD, Service de Ndphrologie-lmmunologie Clinique, HOtel Dieu, 44035 Nantes, France.
© 1997 by the National Kidney Foundation, Inc. 0272-6386/97/2901-001753.00/0
American Journal of Kidney Diseases, Vol 29, No 1 (January), 1997: pp 125-131 125

126 MARTIN ET AL
Fig 1. (A) Light microscopy. Section of the native kidney showing glomerulonephritis with segmental and focal fibrinoid deposits and a cellular crescent. (B) Immunofluorescence microscopy. Section of the native kidney showing mesangial and parietal IgA deposits.

IGA ANCA AND RENAL TRANSPLANTATION 127
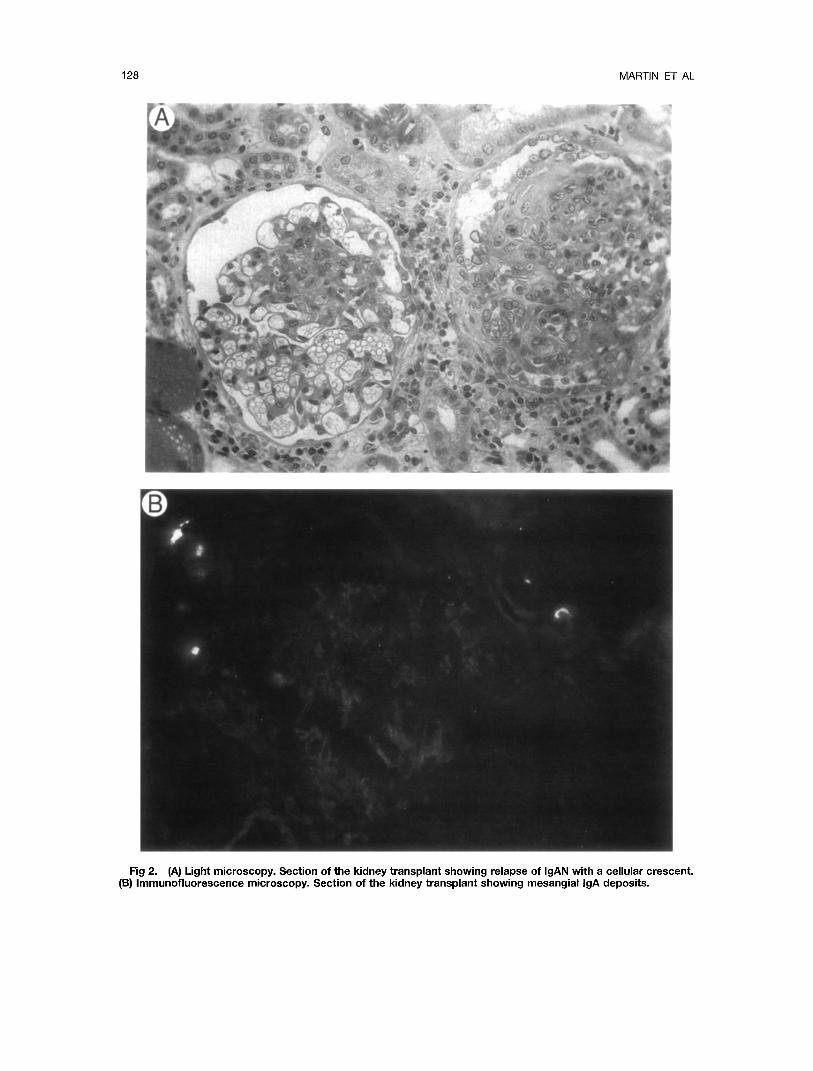
nal symptoms. Allograft biopsy showed recurrence of IgAN with 50% crescents and no signs of acute cellular rejection (Fig 2A). Immunofluorescence microscopy matched the ini- tial native kidney biopsy with IgA and C3, as well as with little IgG and fibrin deposits (Fig 2B) and no superimposed features of transplant glomerulopathy or cellular rejection. Intravenous methylprednisone treatment was given (5 mg/kg the first 2 days, 4 mg/kg the third day, 3 mg/kg the fourth day, and 2 mg/kg the fifth day), but proteinuria remained stable and renal function declined progressively. Hemodialy- sis was begun in September 1993.
Sera Collection
Five sera of patient CJ were stored at -80°C at different stages of the disease: at onset of IgAN in 1989, during hemo- dialysis in 1990, before kidney transplantation in 1991, during IgAN relapse in 1992, and at the beginning of hemodialysis in 1993.
Controls included 20 IgG anti-myeloperoxidase (MPO)- positive patients, 11 IgAN patients, and 12 normal blood donors, as well as a pool of 50 normal blood donor sera.
Immunoglobulin G Antineutrophil Cytoplasmic Antibody Tests
Indirect immunofluorescence was performed as described] Sera containing perinuclear ANCAs were also tested for anti- nuclear activity on HEp2 cells (Immunoconcept; Sacramento, CA).
Immunoglobulin G anti-MPO antibodies were searched for by an enzyme-linked immunosorbent assay (ELISA) using the reference commercial purified preparation (Calbiochem, La Jolla, CA) diluted 0.5 #g/mL in borate-buffered saline. Briefly, after coating MPO, nonspecific binding sites were blocked and sera were incubated at a 1:50 dilution as de- scribed, s The detection system was an alkaline phosphatase- conjugated goat anti-human IgG polyclonal reagent (Sigma A3150) diluted 1:1,000 before addition of the substrate (Sigma 104; St Louis, MO).
For these ANCA tests, results were expressed as the per- centage of binding of a 100% positive serum using linear regression analysis.
ImmunoglobuIin A Antineutrophil Cytoplasmic Antibody Tests
Indirect imrnunofluorescence was derived from the IgG ANCA indirect immunofluorescence assay by changing the detection system using an FITC-conjugated goat anti-human specific IgA polyclonal reagent (F204, Dako; Copenhagen, Denmark). Immunoglobulin A anti-MPO was derived from the IgG ANCA ELISA assay by changing the detection sys- tem using an alkaline phosphatase-conjugated goat anti-hu- man IgA polyclonal reagent (Sigma, A9669).
Anti-proteinase 3 antibodies were searched for by an ELISA according to Rasmussen et al, 9 as well as by a com- mercially available ELISA kit (IBL, Hamburg, Germany) ac- cording to the manufacturer's instructions. Anti-elastase ac- tivity was searched for by ELISA using elastase (Calbiochem, 324681) diluted to 1 mg/mL in phosphate-buffered saline, t° In both assays the detection system was changed for detection of IgA ANCAs as above.
in these assays, serum dilution was determined for each sample from total IgA levels to obtain a final IgA concentra- tion of 100 mg/L for both patient and control sera. Positivity was defined as an absorbance greater than 2 SD above the mean value of a panel of normal blood donor sera.
Immunoglobulin A Rheumatoid Factor Enzyme- Linked Immunosorbent Assay
Immunoglobulin A anti-IgG rheumatoid factor were searched for according to the method of Sinico et alJ j
Inhibition Studies
The specificity of IgA ANCA binding in the anti-MPO ELISA was confirmed by inhibition studies. Binding inhibi- tion was searched for following preincubation of test sera (diluted 1:20) with MPO (Sigma; diluted in phosphate-buf- fered saline containing 1% bovine serum albumin and 01% Tween 20, with concentrations ranging from 20 to 0.019 #g/ mL) in glass tubes for 1 hour at 37°C. Results were expressed as the percentage of inhibition of test serum binding calcu- lated according to the following formula: %inhibition = (S - S/MPO)/S, where S represents the binding of test serum and S/MPO represents binding of the test serum after preincu- bation with MPO.
Western Blot Studies .for ImmunoglobuIin A Antineutrophil Cytoplasmic Antibodies
Western blot analysis was done according to LaemmliJ 2 sodium dodecylsulfate-polyacrylamide gel electrophoresis (SDS-PAGE) was performed with purified unboiled MPO (1 ~g/lane) in nonreducing buffer. Immunoglobulin G anti- MPO and anti-lactoferrin monoclonals (diluted 1:4 in Tris- buffered saline containing 1% Tween 20 and 2% dried skimmed milk [TBSTM]) as well as IgA ANCA-positive and control sera (100 #g/mL IgA final concentration in TBSTM) were incubated with nitrocellulose strips for 2 hours at room temperature. After washing, binding was detected using a mouse anti-human IgA monoclonal re- agent (Chaffi; Clonatec, Paris, France) diluted 1:250 fol- lowed by an alkaline phosphatase-conjugated polyclonal goat IgG anti-mouse IgG (Bioatlantic, Nantes, France) di- luted 1:2,000 in TBSTM.
RESULTS
Immunoglobulin G Antineutrophil Cytoplasmic Antibody Tests
Al l p a t i e n t C J se ra w e r e p o s i t i v e in I g G ind i -
r ec t i m m u n o f l u o r e s c e n c e , w i t h p e r i n u c l e a r s t a in -
ing a n d w i t h o u t a n t i n u c l e a r a n t i b o d y . Al l f ive
se ra e x h i b i t e d I g G A N C A a n t i - M P O ac t iv i ty ,
w i t h b i n d i n g d e c r e a s i n g r e g u l a r l y f r o m 5 0 % to
2 0 % (pos i t i v i ty o v e r 15%) (Fig 3A) .
Immunoglobulin A Antineutrophil Cytoplasmic Antibody Tests
I n d i r e c t i m m u n o f l u o r e s c e n c e s tud ies u s i n g pa -
t i en t C J se ra s h o w e d a typ i ca l A N C A s t a i n i n g
128 MARTIN ET AL
Fig 2. (A) Light microscopy. Section of the kidney transplant showing relapse of IgAN with a cellular crescent. (B) Immunofluorescence microscopy. Section of the kidney transplant showing mesangial IgA deposits.

IGA ANCA AND RENAL TRANSPLANTATION 129
60
50
~ 4 0 ¢ - , m
"o e -
, N
3 0
0
2 0
10
A I / I ~ i
.
0 I I I I O') O g 04 03 60 O'~ O'~ O'1 13') O) 13') ~ O'1
',r- ',P- ~ 'v'-
>,,,
I- "o
¢j ,m
K O
1,2
1
0,8
0,6
0,4
0 , 2
0 I I I I 0 ",- 0,I CO
Fig 3. (A) Immunoglobulin G anti-MPO ELISA (Cal- biochem) showing high activity at onset in 1989 and decreasing activity during the course of the disease. (B) Immunoglobulin A anti-MPO ELISA (Calbiochem) showing high activity at onset in 1989 and during re- lapse of IgAN after kidney transplantation in 1992; weak IgA ANCA anti-MPO activity is noted at end- stage renal failure in 1989 and during hemodialysis in 1990.
with anti-IgA reagents with mainly membrane fluorescence as previously described. 4 All patient CJ sera exhibited IgA ANCA anti-MPO activity, with strong positivity at the onset of the disease and during relapse after kidney transplantation, In contrast, IgA ANCA activity was weak during hemodialysis and before kidney transplantation
(Fig 3B). No reactivity was found to proteinase 3 and elastase. Immunoglobulin A anti-IgG rheu- matoid factor activity was not detectable.
One of the 20 IgG anti-MPO-positive controls also exhibited IgA anti-MPO activity. However, skin and kidney biopsies were not performed in this patient.
Inhibition Studies
The specificity of IgA anti-MPO positivity was tested in inhibition studies. Inhibition of binding was observed in ELISA after preincubation of the test sera in the liquid phase with purified MPO (Fig 4).
Myeloperoxidase Western Blot Studies
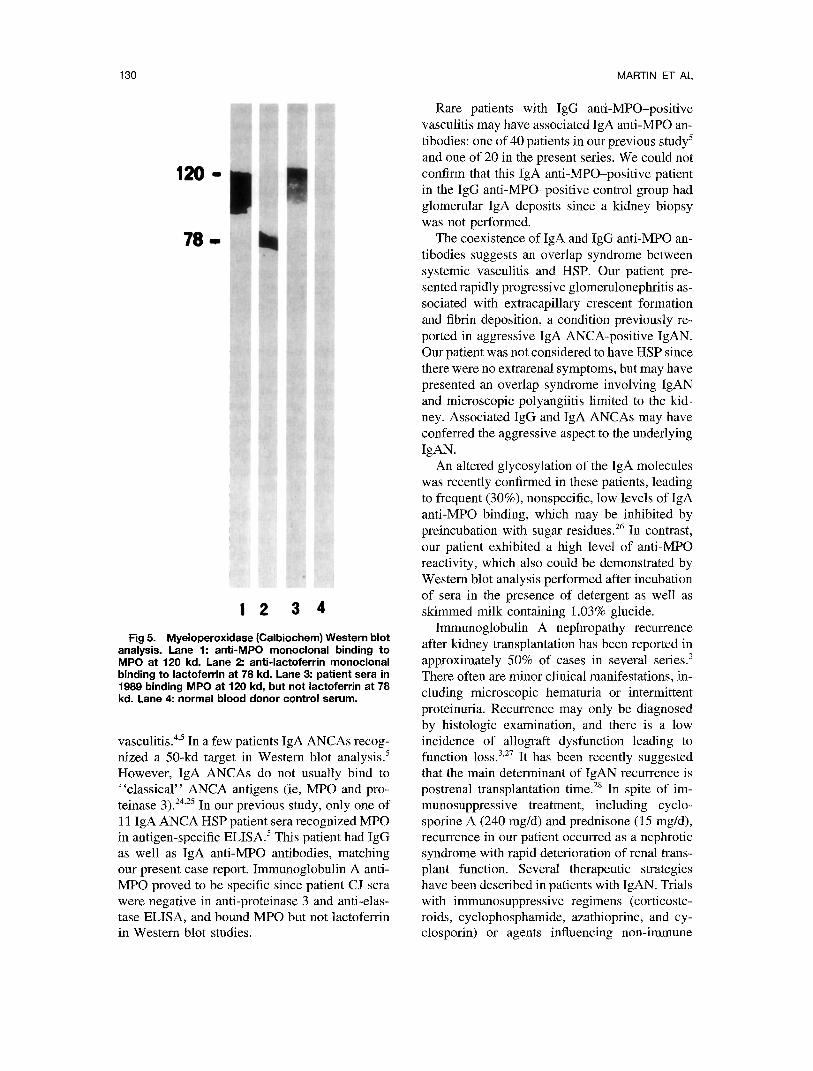
Anti-myeloperoxidase monoclonal (Fig 5, lane 1) exhibited binding at 120 kd, the size of the MPO tetramer, and anti-lactoferrin monoclonal (Fig 5, lane 2) at 78 kd, as previously described. ~3 Patient sera with IgA ANCA activity (Fig 5, lane 3) exhibited binding to MPO at 120 kd, but not to lactoferrin at 78 kd. Control sera (Fig 5, lane 4) exhibited no binding.
DISCUSSION
The ANCAs were initially described to be of IgG class and used as markers of small vessel vasculitides, mainly Wegener's granulomatosis 14 and microscopic polyangiitis) Immunoglobulin M ANCAs also have been found in some pa- tients. 15 The main antigen targets for these auto- antibodies are proteinase 3,16'17 MPO, 18 and lacto- ferrin. 13 Immunoglobulin G ANCAs have been implicated In pathogenesis as titers show a corre- lation with disease activity and increase before clinical relapses.~9-21 The ANCAs can also induce neutrophil activation in vitro, z2'23 Immunoglobu- lin A ANCAs have been reported in IgAN and HSP, but rarely in IgG ANCA-positive systemic
=401 J I. • = _ . _ _ . - - = J "= j ' ~ 3O
2O
10 J "
~" O~ ~ I I I I I
o o o M P O c o n c e n t r a t i o n i n liquid phase ( m c g / m l )
Fig 4. Inhibition study of IgA anti-MPO activity after preincubation with MPO (Calbiochem) in liquid phase.
130 MARTIN ET AL
120 -
7 8 -
1 2 3 4
Fig 5. Myeloperoxidase (Calbiochem) Western blot analysis. Lane 1: anti-MPO monoclonal binding to MPO at 120 kd. Lane 2: anti-lactoferrin monoclonal binding to lactoferrin at 78 kd. Lane 3: patient sera in 1989 binding MPO at 120 kd, but not lactoferrin at 78 kd. Lane 4: normal blood donor control serum.
vasculitis. 4'5 In a few patients IgA ANCAs recog- nized a 50-kd target in Western blot analysis. 5 However, IgA ANCAs do not usually bind to "classical" ANCA antigens (ie, MPO and pro- teinase 3). 24,25 In our previous study, only one of 11 IgA ANCA HSP patient sera recognized MPO in antigen-specific ELISA. 5 This patient had IgG as well as IgA anti-MPO antibodies, matching our present case report. Immunoglobulin A anti- MPO proved to be specific since patient CJ sera were negative in anti-proteinase 3 and anti-elas- tase ELISA, and bound MPO but not lactoferrin in Western blot studies.
Rare patients with IgG anti-MPO-positive vasculitis may have associated IgA anti-MPO an- tibodies: one of 40 patients in our previous study 5 and one of 20 in the present series. We could not confirm that this IgA anti-MPO-positive patient in the IgG anti-MPO-positive control group had glomerular IgA deposits since a kidney biopsy was not performed.
The coexistence of IgA and IgG anti-MPO an- tibodies suggests an overlap syndrome between systemic vasculitis and HSP. Our patient pre- sented rapidly progressive glomerulonephritis as- sociated with extracapillary crescent formation and fibrin deposition, a condition previously re- ported in aggressive IgA ANCA-positive IgAN. Our patient was not considered to have HSP since there were no extrarenal symptoms, but may have presented an overlap syndrome involving lgAN and microscopic polyangiitis limited to the kid- ney. Associated IgG and IgA ANCAs may have conferred the aggressive aspect to the underlying IgAN.
An altered glycosylation of the IgA molecules was recently confirmed in these patients, leading to frequent (30%), nonspecific, low levels of IgA anti-MPO binding, which may be inhibited by preincubation with sugar residues. 26 In contrast, our patient exhibited a high level of anti-MPO reactivity, which also could be demonstrated by Western blot analysis performed after incubation of sera in the presence of detergent as well as skimmed milk containing 1.03% glucide.
Immunoglobulin A nephropathy recurrence after kidney transplantation has been reported in approximately 50% of cases in several series. 3 There often are minor clinical manifestations, in- cluding microscopic hematuria or intermittent proteinuria. Recurrence may only be diagnosed by histologic examination, and there is a low incidence of allograft dysfunction leading to func t ion loss. 3'27 It has been recently suggested that the main determinant of IgAN recurrence is postrenal transplantation time. 28 In spite of im- munosuppressive treatment, including cyclo- sporine A (240 rag/d) and prednisone (15 rag/d), recurrence in our patient occurred as a nephrotic syndrome with rapid deterioration of renal trans- plant function. Several therapeutic strategies have been described in patients with IgAN. Trials with immunosuppressive regimens (corticoste- roids, cyclophosphamide, azathioprine, and cy- closporin) or agents influencing non-imnmne

IGA ANCA AND RENAL TRANSPLANTATION 131
p a t h w a y s and con t r ibu t ing to g l o m e r u l a r in jury
(ant ip la te le t agents , u rok inase , e i c o s a p e n t o i c
acid) h a v e b e e n r epor t ed bu t s h o w conf l i c t ing results.a9
It m a y be c o n c l u d e d that I g A a n t i - M P O anti-
bod ie s o c c u r in a subgroup o f pat ients p resen t ing
s eve re I g A N and an ove r l ap s y n d r o m e i n v o l v i n g
I g A N and m i c r o s c o p i c po lyang i i t i s in w h i c h I g A
and I g G A N C A s coexis t . I m m u n o g l o b u l i n A
A N C A s but no t I g G a n t i - M P O titers cor re la ted
wi th d i sease act ivi ty . W e sugges t that this A N C A
ac t iv i ty c o n f e r r e d the a g g r e s s i v e aspec t o f this
I g A N . Fu r the r s tudies are n e e d e d to con f i rm the
p rognos t i c va lue o f I g A A N C A de tec t ion pr ior
to k i d n e y t ransp lan ta t ion in these rare pat ients .
REFERENCES
1. D'Amico G: The commonest glomernlonephritis in the world: IgA nephropathy. Q J Med 64:709-727, 1987
2. Diaz-Tejeiro R, Manuell F, Diez J, Esparza N, Errasta P, Purray A, Pardo J: Loss of renal graft due to recurrent IgA nephropathy with rapidly progressive course: An unusual clinical evolution. Nephron 54:341-343, 1990
3. Mathew TH: Recurrent disease after renal transplanta- tion. Transplant Rev 5:31-45 1991
4. Esnanlt VLM, Ronda N, Jayne DRW, Lockwood CM: Association of ANCA isotype and affinity with disease ex- pression. J Autoimmun 6:197-205, 1993
5. Ronda N, Esnault VLM, Layward L, Sepe V, Allen A, Feehally J, Lockwood CM: Anti-neutrophil cytoplasm anti- bodies (ANCA) of IgA isotype in adult Henoch-Sch6nlein purpura. Clin Exp Immunol 95:49-55, 1994
6. Van den Wall Bake AWL, Labatto S, Jonges L, Daha MR, Van Es LA: IgA antibodies directed against cytoplasmic antigens of polymorphonuclear leukocytes in patients with Henoch-SchSnl- ein purpura. Adv Exp Med Biol 216:1593-1598, 1987
7. Savage COS, Winearls CG, Jones S, Marshall PD, Lockwood CM: Prospective study of radioimmunoassay for antibodies against neutrophil cytoplasm in diagnosis of sys- temic vasculitis Lancet 1:1389-1393, 1987
8. Esnault VLM, Jayne DRW, Weetman AP, Lockwood CM: IgG subclass distribution and relative functional affinity of anti- myeloperoxidase antibodies in systemic vasculitis at presentation and during follow-up. Immunology 74:714-718, 1991
9. Rasmussen N, Sj61in C, Isaksson B, Bygren P, Wies- lander J: An ELISA for the detection of anti-neutrophil cyto- plasm antibodies (ANCA). J Intern Med 127:139-145, 1990
10. N~issberger L, Johansson A, Bjork S, Sjoholm AG, Stureelt G, Heubner A: Circulating anti-elastase in systemic lupus erythematosus. Lancet 1:509, 1989 (abstr)
11. Sinico RA, Fornasieri A, Maldifassi P, Colassanti G, D'Amico G: The clinical significance of IgA rheumatoid fac- tor in idiopathic IgA mesangial nephropathy (Berger's dis- ease). Clin Nephrol 30:182-186, 1988
12. Laemmli UK: Cleavage of structural proteins during the assembly of the head of bacteriophage T4. Nature 227:680-685, 1970
13. Esnault VLM, Short A, Audrain MAP, Sally JJ, Martin S J, Skehel M, Lockwood CM: Autoantibodies to lactoferrin
and histone in systemic vasculitis identified by antimyeloper- oxidase solid phase assays. Kidney Int 46:153-160, 1994
14. Van Der Woude FJ, Rasmussen N, Lobatto S, Wiik A, Van Es LA, Van der Giessen M, Van der Hem GK, The TH: Autoantibodies against neutrophils and monocytes; tool for diagnosis and marker of disease activity in Wegener's granulomatosis. Lancet 1:425-429, 1985
15. Esnault VLM, Soleimani B, Keogan M, Brownlee A, Jayne D, Lockwood CM: Association of IgM with IgG ANCA in patients presenting with pulmonary haemorrhage. Kidney Int 41:1304-1310, 1992
16. Ltidemann J, Utecht B, Gross WL: Anti-neutrophil cytoplasm antibodies in Wegener's granulomatosis recognize an elastinolytic enzyme. J Exp Med 171:357-362, 1990
17. Niles JL, McCluskey RT, Abroad MF, Arnouat MA: Wegener's granulomatosis autoantigen is a novel neutrophil serine proteinase. Blood 74:1988-1989, 1893
18. Falk R J, Jennette JC: Anti-neutrophil cytoplasmic auto- antibodies with specificity for myeloperoxidase in patients with systemic vasculitis and idiopathic necrotizing and crescentic glomemlonephritis. N Engl J Med 318:1651-1657, 1988
19. Nolle B, Specks U, Ludemann J, Rohrbach MS, De- remee RA, Gross WL: Anticytoplasmic autoantibodies: Their immunodiagnostic value in Wegener's granulomatosis. Ann Intern Med 111:28-40, 1989
20. Specks U, Wheatley CL, McDonald TJ, Rohrbach MS, Deremee RA: Anticytoplasmic autoantibodies in the diagno- sis and follow-up of Wegener's granulomatosis. Mayo Clin Proc 64:28-36, 1989
21. Cohen Tervaert JW, Huitema MG, Hene RJ, Sluiter WJ, The TH, Van der Hem GK, Kallemberg CGM: Preven- tion of relapses in Wegener's granulomatosis by treatment based on an antineutrophil cytoplasmic antibody titre. Lancet 336:709-711, 1990
22. Falk R, Terrel R, Charles L, Jennette J: Anti-neutrophil cytoplasmic autoantibodies induce neutrophils to degranulate and produce oxygen radicals in vitro. Proc Natl Acad Sci U S A 87:4115-4119, 1990
23. Keogan MT, Esnault VLM, Green A J, Lockwood CM, Brown DL: Activation of normal neutrophils by anti-neutrophil cytoplasm antibodies. Clin Exp Immunol 90:228-234, 1992
24. O'Donoghue DJ, Nusbaum P, Noel LH, Halbwachs- Mecartelli L, Lesavre PH: Antineutrophil cytoplasmic anti- bodies. Nephrol Dial Transplant 7:534-538, 1992
25. Sinico RA, Tadros M, Radice A, Pozzi C, Quarenghi M, Comotti C, Gregorini G, Castiglione A, Arrigo G, D'Am- ico G: Lack of IgA antineutrophil cytoplasmic antibodies in Henoch-Sch6nlein purpura and IgA nephropathy. Clin Immu- nol Immunopathol 73:19-26, 1994
26. Coppo R for the Italian Group of Renal Immunopa- thology: Serum IgA reacting with neutrophil cytoplasmic an- tigen (ANCA) in Henoch-Sch6nlein nephritis: Evidences of a non-immune binding based on carbohydrate interactions. EDTA Proceedings. Athens, Greece, 1995, p 16 (abstr)
27. Berger J, Noel LH, Nabarra B: Recurrence of mesan- gial IgA nephropathy after renal transplantation. Contrib Nephrol 40:290-295, 1984
28. Odum J, Peh CA, Clarkson AR, Bannister KM, Sey- mour AE, Gillis D, Thomas AC, Mathew TH, Woodroffe AJ: Recurrent mesangial IgA nephritis following renal trans- plantation. Nephrot Dial Transplant 9:309-312, 1994
29. Feehaly J: Strategies for the management of IgA ne- phropathy. Nephrol Dial Transplant 9:23-29, 1994 (suppl)
Copyright © 2022 FDOKUMEN



















