Implication of soluble and membrane HLA class I and serum IL10 in liver graft acceptance
10
Implication of Soluble and Membrane HLA Class I and Serum IL-10 in Liver Graft Acceptance Alfredo Minguela, Alberto Torı ´o, Luis Marı ´n, Manuel Muro, Luisa M. Villar, Julian Dı ´az, Pablo Ramı ´rez, Pascual Parrilla, Ana M. Garcı ´a-Alonso, and Marı ´a R. A ´ lvarez-Lo ´ pez ABSTRACT: Membrane HLA class-I expression (mHLA-I), soluble HLA class-I antigens (sHLA-I) and interleukin (IL)-10 are different factors implicated in the special acceptance of liver allograft. In this study, pre- and post-operative levels of mHLA-I in peripheral blood lym- phocytes (PBL) and serum sHLA-I were analyzed in 86 liver transplants, immunosuppressed with Cyclosporine-A, methylprednisolone and azathioprine, and classified into acute-rejection (AR, n 5 28) and non-acute-rejection (NAR, n 5 58) groups. Serum IL-10 was studied in 47 recipients (AR-group, n 5 16 and NAR-group, n 5 31). Pre-transplant values of mHLA-I and sHLA-I showed a bimodal distribution (high/low) in NAR-recipients, but in AR-patients were mainly included in the low expres- sion/secretion zone (mHLA-I, p , 0.02 and sHLA-I, p , 0.05). Consequently, average pre-transplant mHLA-I (868 6 109 versus 998 6 123, p , 0.05) and sHLA-I (1.3 6 0.4 versus 2.02 6 0.7 mg/ml, p , 0.01) was lower in the AR- than in the NAR-group. After transplant both parameters decreased in the NAR-group, but increased in AR-recipients previous to and on rejection diagnosis day. Additionally, serum IL-10 levels were significantly higher (p , 0.01) in the NAR than in the AR-group during the first 24 h post-transplant. In conclusion, low pre-trans- plant mHLA-I and sHLA-I levels pre-dispose liver recip- ients to acute rejection, whereas early post-transplant increases of serum IL-10 appear to be related to a good liver allograft acceptance. Human Immunology 60, 500 –509 (1999). © American Society for Histocompat- ibility and Immunogenetics, 1999. Published by Elsevier Science Inc. KEYWORDS: soluble HLA class I; HLA class I expres- sion; IL-10; liver transplant tolerance; acute rejection ABBREVIATIONS AR acute rejection BD Becton Dickinson CsA cyclosporine-A CTL cytotoxic T lymphocytes ELISA enzyme-linked immunosorbent assay FITC fluorescein isothiocyanate IFN-g interferon-g IL interleukin mAb monoclonal antibodies MFI mean fluorescence intensity mHLA-I membrane HLA class-I NAR non-acute-rejection OLT orthotopic liver transplant PBL peripheral blood lymphocytes sHLA-I soluble HLA class-I TcR T cell receptor INTRODUCTION Both cellular and humoral immunologic mechanisms are involved in the spontaneous tolerance observed in liver transplant [1–3], among them the functional inactiva- tion of donor-reactive cells and the blockage of donor specific cytotoxic T lymphocytes (CTL) [4, 5]. Some studies have found that the liver is the major producer of soluble HLA class-I (sHLA-I) molecules. These mole- cules appear to be important natural immunoregulatory factors in vivo capable of inducing donor specific toler- ance [6] by inhibiting recipient cytotoxic response [2]. In addition, after liver transplant a systemic release of interleukin (IL)-10 by Kuppfer cells [7] or hepatocytes [8], might also contribute to reducing the immunogenic From the Section of Immunology (A.M., A.T., L.M., M.M., J.D., A.M.G-A., M.R.A-L.) and Surgical Service (P.R., P.P.), University Hospital Virgen-Arrixaca, Murcia, Spain; and the Immunology Service, Hospital Ramo ´n-Cajal, Madrid, Spain (L.M.V.). Address reprint requests to: M. R. A ´ lvarez-Lo ´pez, Seccio ´n de Inmunolo- gı´a, Hospital U. Virgen de la Arrixaca, El Palmar, 30120-Murcia, Spain; Tel: 134-968-369692; Fax: 134-968-369678. E-Mail: [email protected]. Received October 27, 1998; revised December 12, 1998; accepted January 4, 1999. Human Immunology 60, 500 –509 (1999) 0198-8859/99/$–see front matter © American Society for Histocompatibility and Immunogenetics, 1999 Published by Elsevier Science Inc. PII S0198-8859(99)00016-6
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Implication of soluble and membrane HLA class I and serum IL10 in liver graft acceptance

Implication of Soluble and Membrane HLAClass I and Serum IL-10 in LiverGraft AcceptanceAlfredo Minguela, Alberto Torıo, Luis Marın,Manuel Muro, Luisa M. Villar, Julian Dıaz,Pablo Ramırez, Pascual Parrilla,Ana M. Garcıa-Alonso, and Marıa R. Alvarez-Lopez
ABSTRACT: Membrane HLA class-I expression(mHLA-I), soluble HLA class-I antigens (sHLA-I) andinterleukin (IL)-10 are different factors implicated in thespecial acceptance of liver allograft. In this study, pre- andpost-operative levels of mHLA-I in peripheral blood lym-phocytes (PBL) and serum sHLA-I were analyzed in 86liver transplants, immunosuppressed with Cyclosporine-A,methylprednisolone and azathioprine, and classified intoacute-rejection (AR, n 5 28) and non-acute-rejection(NAR, n 5 58) groups. Serum IL-10 was studied in 47recipients (AR-group, n 5 16 and NAR-group, n 5 31).
Pre-transplant values of mHLA-I and sHLA-I showed abimodal distribution (high/low) in NAR-recipients, butin AR-patients were mainly included in the low expres-sion/secretion zone (mHLA-I, p , 0.02 and sHLA-I, p ,0.05). Consequently, average pre-transplant mHLA-I(868 6 109 versus 998 6 123, p , 0.05) and sHLA-I
(1.3 6 0.4 versus 2.02 6 0.7 mg/ml, p , 0.01) was lowerin the AR- than in the NAR-group. After transplant bothparameters decreased in the NAR-group, but increased inAR-recipients previous to and on rejection diagnosis day.Additionally, serum IL-10 levels were significantly higher(p , 0.01) in the NAR than in the AR-group during thefirst 24 h post-transplant. In conclusion, low pre-trans-plant mHLA-I and sHLA-I levels pre-dispose liver recip-ients to acute rejection, whereas early post-transplantincreases of serum IL-10 appear to be related to a goodliver allograft acceptance. Human Immunology 60,500–509 (1999). © American Society for Histocompat-ibility and Immunogenetics, 1999. Published by ElsevierScience Inc.
KEYWORDS: soluble HLA class I; HLA class I expres-sion; IL-10; liver transplant tolerance; acute rejection
ABBREVIATIONSAR acute rejectionBD Becton DickinsonCsA cyclosporine-ACTL cytotoxic T lymphocytesELISA enzyme-linked immunosorbent assayFITC fluorescein isothiocyanateIFN-g interferon-gIL interleukin
mAb monoclonal antibodiesMFI mean fluorescence intensitymHLA-I membrane HLA class-INAR non-acute-rejectionOLT orthotopic liver transplantPBL peripheral blood lymphocytessHLA-I soluble HLA class-ITcR T cell receptor
INTRODUCTIONBoth cellular and humoral immunologic mechanisms areinvolved in the spontaneous tolerance observed in liver
transplant [1–3], among them the functional inactiva-tion of donor-reactive cells and the blockage of donorspecific cytotoxic T lymphocytes (CTL) [4, 5]. Somestudies have found that the liver is the major producer ofsoluble HLA class-I (sHLA-I) molecules. These mole-cules appear to be important natural immunoregulatoryfactors in vivo capable of inducing donor specific toler-ance [6] by inhibiting recipient cytotoxic response [2].In addition, after liver transplant a systemic release ofinterleukin (IL)-10 by Kuppfer cells [7] or hepatocytes[8], might also contribute to reducing the immunogenic
From the Section of Immunology (A.M., A.T., L.M., M.M., J.D.,A.M.G-A., M.R.A-L.) and Surgical Service (P.R., P.P.), UniversityHospital Virgen-Arrixaca, Murcia, Spain; and the Immunology Service,Hospital Ramon-Cajal, Madrid, Spain (L.M.V.).
Address reprint requests to: M. R. Alvarez-Lopez, Seccion de Inmunolo-gıa, Hospital U. Virgen de la Arrixaca, El Palmar, 30120-Murcia, Spain;Tel: 134-968-369692; Fax: 134-968-369678. E-Mail: [email protected].
Received October 27, 1998; revised December 12, 1998; accepted January4, 1999.
Human Immunology 60, 500–509 (1999)0198-8859/99/$–see front matter© American Society for Histocompatibility and Immunogenetics, 1999
Published by Elsevier Science Inc. PII S0198-8859(99)00016-6
potential of the liver graft. Despite these immunologicliver transplant characteristics, human liver recipientstreated with conventional immunosuppressive drugsgenerally do not become tolerant to grafts, because atleast 30% of recipients experience one or more histologicconfirmed acute rejection episodes that require addi-tional immunosuppression [9]. It has been reported thatthe acute rejection process induces a strong up-regulationof membrane HLA class-I (mHLA-I) both on hepatocytesand bile duct epithelia of the grafted liver [10–12] andalso that there is a considerable increase in serum sHLA-I[13]. Normal mHLA-I expression on peripheral bloodlymphocytes (PBL) seems to be important in the main-tenance of self-tolerance, since a reduced expression ofsuch molecules induce altered immunoresponse leadingto autoimmune diseases [14, 15].
The purpose of this study was to analyze the relation-ship between serum sHLA-I concentration, mHLA-I ex-pression on PBL and liver graft acceptance, as well as toevaluate the lymphocyte mHLA-I expression changesduring the rejection process, and the possible associationbetween IL-10 and sHLA-I levels with the liver-recipientalloresponse.
MATERIALS AND METHODSPatientsA total of 99 orthotopic liver transplants (OLT) per-formed over a period of 2 years, and 30 healthy volun-teers as a control group, were studied. After excludingpatients who died or lost the graft within the first monthafter transplant (n 511) and those showing the first acuterejection episode beyond the monitored period (n 5 2),the remaining 86 OLT-recipients, with different diag-
noses (Table 1), were divided into two groups: acute-rejection (AR-group, n 5 28) and non-acute-rejection(NAR-group, n 5 58). Immunosuppression consisted ofstandard triple-drug therapy with methylprednisolone,azathioprine and cyclosporine-A (CsA). Methylpred-nisolone (1g) was intravenously administered during theintra-operative period and then daily after transplant,with a gradual reduction from 200 to 20 mg/day bypost-operative day 7; Azathioprine at 1–2 mg/Kg/daywas also intravenously supplied until it was orally toler-ated, with a dose reduction when leukocyte counts fellbelow 5000 cells/ml; two intravenous doses of conven-tional-CsA at 2 mg/Kg/day or oral doses of 5–10 mg/Kg/day were given to maintain CsA blood levels between250–350 ng/ml. Additional individual regimens withbolus of 1g methylprednisolone were used in the case ofacute rejection episodes. Histologic diagnosis of acuterejection was based on the presence of at least two of thefollowing features: (1) mononuclear as well as mixedportal inflammation; (2) bile duct infiltration and dam-age; and (3) venous endothelitis of the portal tracts [1,16]. Doppler echography was carried out to excludehepatic ischemia due to hepatic artery or portal veinocclusion, and to establish an indication for liver biopsy.Informed consent was obtained from all recipients priorto experimental procedures.
Sample CollectionCytometric analysis was carried out on EDTA anticoag-ulated peripheral blood samples which were routinelycollected in the pre-operative (day 0) and post-operativeperiods: days 1 to 3, 4 to 6, 7 to 9, 10 to 13, 14 to 17,18 to 21, 22 to 25, and after day 25. Serum samples werealso collected pre-operative, 4, 12 and 24 h after trans-
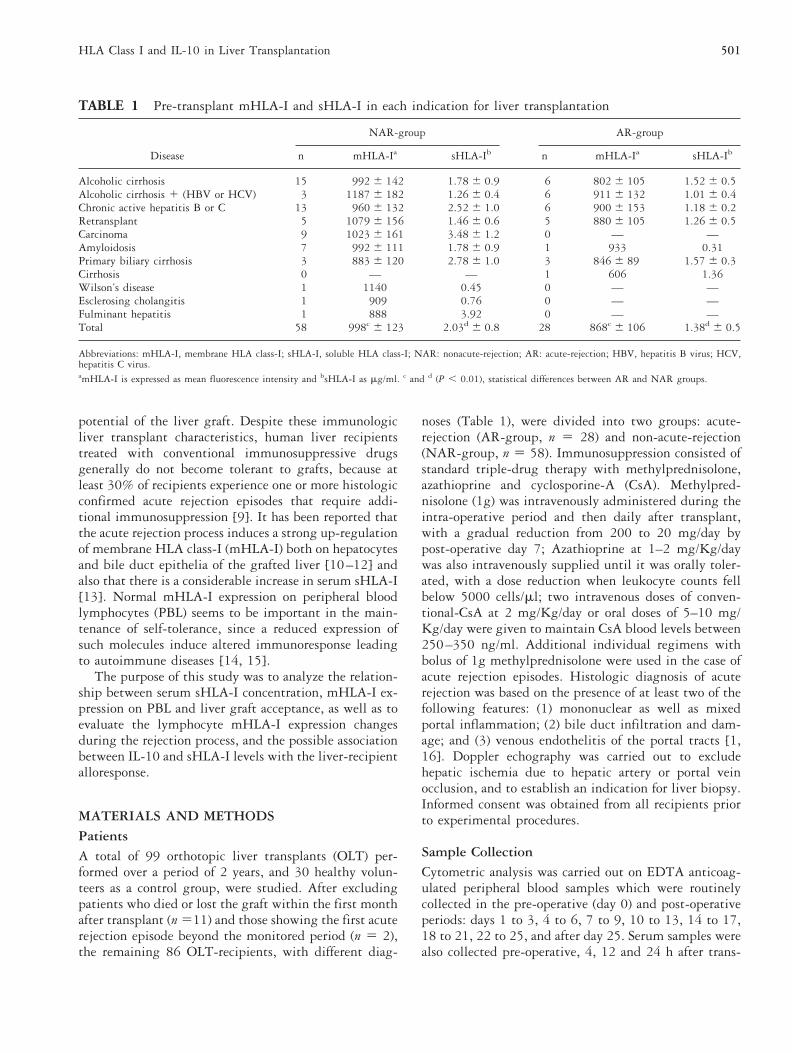
TABLE 1 Pre-transplant mHLA-I and sHLA-I in each indication for liver transplantation
Disease
NAR-group AR-group
n mHLA-Ia sHLA-Ib n mHLA-Ia sHLA-Ib
Alcoholic cirrhosis 15 992 6 142 1.78 6 0.9 6 802 6 105 1.52 6 0.5Alcoholic cirrhosis 1 (HBV or HCV) 3 1187 6 182 1.26 6 0.4 6 911 6 132 1.01 6 0.4Chronic active hepatitis B or C 13 960 6 132 2.52 6 1.0 6 900 6 153 1.18 6 0.2Retransplant 5 1079 6 156 1.46 6 0.6 5 880 6 105 1.26 6 0.5Carcinoma 9 1023 6 161 3.48 6 1.2 0 — —Amyloidosis 7 992 6 111 1.78 6 0.9 1 933 0.31Primary biliary cirrhosis 3 883 6 120 2.78 6 1.0 3 846 6 89 1.57 6 0.3Cirrhosis 0 — — 1 606 1.36Wilson’s disease 1 1140 0.45 0 — —Esclerosing cholangitis 1 909 0.76 0 — —Fulminant hepatitis 1 888 3.92 0 — —Total 58 998c 6 123 2.03d 6 0.8 28 868c 6 106 1.38d 6 0.5
Abbreviations: mHLA-I, membrane HLA class-I; sHLA-I, soluble HLA class-I; NAR: nonacute-rejection; AR: acute-rejection; HBV, hepatitis B virus; HCV,hepatitis C virus.amHLA-I is expressed as mean fluorescence intensity and bsHLA-I as mg/ml. c and d (P , 0.01), statistical differences between AR and NAR groups.
501HLA Class I and IL-10 in Liver Transplantation

plant and subsequently each day until day 15 and everythree days from day 15 to 30. Samples were always takenboth from overnight fasting patients and from healthyindividuals between 0700 and 0800. Serum sampleswere stored at 270°C until assay.
Flow Cytometry
After collection, peripheral blood cells were immediatelystained by a standard immunofluorescence method withdifferent monoclonal antibodies (mAb), acquiring 6 3103 lymphocytes in a FACScan flow cytometer (BectonDickinson -BD-, San Jose, CA), by setting up a lightscatter gate using an anti-CD45-PerCP/CD14-PE/HLA-I-FITC mAb combination. Mean Fluorescence Intensity(MFI) was used as a relative molecule-density measure-ment of HLA class-I, HLA class-II (HLA-DR) and T cellreceptor (TcR)-a/b on lymphocytes, monocytes andgranulocytes, and was calculated using PAINT-A-GATE-plus software (BD). Although the photoelectriccomponents of the FACScan flow cytometer were ad-justed daily, as previously described [16, 17], to avoidMFI variability caused by the instrument setting,mHLA-I/TcR-ab and mHLA-II/TcR-ab ratios werecalculated every day for each recipient, since the MFI ofTcR-ab on PBL was found to be practically invariableafter transplant.
Fluorescent mAbs, anti-CD45 (Hle-1, IgG1-PerCP,BD), anti-CD14 (Leu-M3, IgG2b-Phycoerythrin, BD),anti-HLA class-I (HLA-ABC, IgG2a-FICT, Serotec, Ox-ford, England), anti-HLA-DR (L243, IgG2a-FICT, BD),anti-CD3 (Leu4, IgG1-Phycoerythrin, BD), anti-TcR-ab (WT-31, IgG1-FICT, BD), at saturating con-centrations were used. Simultest IgG1-FITC/IgG2a-Phycoerythrin (BD) and IgG1-TRICOLOR (Caltag, SanFrancisco, CA) were also used as background fluorescencecontrol.
Quantification of Total Soluble HLA Class I
Total sHLA-I was measured by a sandwich ELISA in-volving the recognition of the b2-microglobulin-alphachain complex by W6/32 mAb [18] bound to the micro-ELISA well, and b2-microglobulin recognition by FG2/2-mAb [19] labelled with sulfo-NHS-biotin (Pierce,Rockford, USA) with minor modifications as describedpreviously [20]. After color development with streptavidin-peroxidase-conjugate (Boehringer-Mannhein, Mannhein,Germany) and 1,2-phenylendiamin (OPD, Merk, Ger-many) the concentration of sHLA-I was calculated bymeasuring absorbance at 492 nm. Optical density valueswere transformed into mg/ml using a standard curvemade with serial dilutions of a 0.8 mg/ml standardserum.
Quantification of Serum IL-10Serum IL-10 was measured in 47 recipients (AR, n 5 16and NAR, n 5 31) and in 30 healthy controls by asandwich ELISA following the manufacturer’s instruc-tions (Pharmingen, San Diego, CA), using recombinanthuman-IL-10 as reference-standard, JES3-9D7 as coatingmAb and biotinylated-JES3-12G8 as detection mAb. Ineach case, coating was performed overnight with 0.5mg/ml coating-mAb in bicarbonate buffer (0.1 MNaHCO3 pH 8.2) at 4°C; in order to block non-specificbinding, a 3% solution of BSA (Sigma, St. Louis, MO) inPBS was used at room temperature for 2 h. Afterwards,serial IL-10 standard dilution in 3% BSA-PBS and un-diluted serum samples were incubated overnight withconstant shaking at 4°C. A 45 min incubation withbiotinilated-mAb (0.5 mg/ml) in 3% BSA-PBS and asubsequent 30 min incubation with avidin-peroxidase(Sigma) were used for detection at 405 nm, using 2,29-Azino-bis(ethylbenzthiazoline-6-sulfonic-acid) substrate(ABTS, Sigma).
Statistical AnalysisData of mHLA-I and mHLA-II as well as serum sHLA-Iand IL-10 concentration were expressed as mean 6 SD.Additionally, these parameters were analyzed as post-transplant percentage changes calculated for each patientby contrasting them with their pre-transplant values,which were considered as 0% of change. Statistical anal-ysis was performed by a two-sample unpaired Student’st-test. Categorical data were analyzed using contingencytables and the chi-square test. Correlations were calcu-lated by Spearman regression analysis. Only P valuesbelow 0.05 were considered significant.
RESULTSPre-transplant Values of mHLA-I and sHLA-IAs shown in Fig. 1, the OLT-recipient mHLA-I andsHLA-I pre-transplant values were distributed in a bi-modal form; this fact allows us to distinguish patientswith high or low mHLA-I expression/sHLA-I secretionby setting a cut-off at 1000 MFI for mHLA and 1.4mg/ml for sHLA. Interestingly, this analysis demon-strated that most of the AR-recipients (22 out of 28,78.6%) were situated in the low mHLA-I expressiongroup (MFI , 1000), whereas NAR-patients were sim-ilarly distributed in both high and low expression groups(29 out of 58, 50%; p , 0.02). Moreover, 21 out of 28(75%) AR-recipients and 29 out of 58 (50%) NAR-recipients (p , 0.05) were included in the low sHLA-Isecretion group (sHLA-I,1.4 mg/ml). Consequently, av-erage pre-transplant values of mHLA-I and sHLA-I weresignificantly lower in the AR than in the NAR-group, afeature which was observed in all the indications for liver
502 A. Minguela et al.

transplantation (see Table 1). Nevertheless, it can beobserved that NAR-patients with chronic active hepati-tis B or C, carcinoma and primary biliary cirrhosisshowed the highest sHLA-I levels. In the control group,mHLA-I ranged from 600 to 1202 (9696153) andsHLA-I from 0.3 to 3.1mg/ml (1.3560.4 mg/ml). Pre-transplant mHLA-I was also analyzed in monocytes andgranulocytes, and in contrast to lymphocytes, no signif-icant difference between the AR and NAR groups wasfound (data not shown).
Post-transplant Evolution of mHLA-I, SHLA-I,and mHLA-IILymphocyte mHLA-I expression in the NAR-group wassignificantly down-regulated from days 1 to 6 post-transplant with respect to their pre-transplant values(p , 0.01). In the AR-group an initial significant down-regulation observed on days 1 to 3 (p , 0.05), was
compensated by a clear up-regulation from days 7 to 17post-transplant, reaching significant differences with re-spect to their own pre-transplant values (p , 0.01) aswell as to those exhibited by the NAR-group from days10 to 17 (p , 0.05; Fig. 2a). It is important to point outthat, in our study, all the acute rejection episodes tookplace between days 7 to 17 post-transplant. Figure 3shows lymphocyte mHLA-I histograms of one represen-tative patient from each of the AR and NAR groups.Additional studies of the mHLA-I expression on mono-cytes and granulocytes throughout the follow-up periodwere not able to demonstrate any significant differences,either with respect to their own pre-transplant values orbetween the values in the AR and NAR group (data notshown).
HLA class-II (HLA-DR) expression was down-regu-lated both on peripheral blood CD191 lymphocytes andmonocytes during the whole monitoring period, but thismolecule did not reveal significant differences when pa-tients from the AR and NAR groups were compared.
Soluble HLA class-I concentration experienced a deepfall both in the AR and NAR patients during the firstpost-transplant days; on the following monitored days,sHLA-I rose beyond their pre-transplant values but onlyin the AR-group and on days of maximum acute rejec-tion frequency (days 7 to 13, p , 0.01; Fig. 2a). Nev-ertheless, it is interesting that the absolute sHLA-I val-ues in the AR-group at no time surpassed those of the
FIGURE 1 Pre-transplant distribution of lymphocyte HLAclass-I (mHLA-I; A and B) and soluble HLA class-I (sHLA-I;C and D) values in liver recipients from the nonacute-rejection(NAR; o) and acute-rejection (AR; ■) groups. Mean Fluores-cence Intensity (MFI) was used to evaluate mHLA-I, whilesHLA was represented as mg/ml. Broken lines indicate cut-offvalues at 1000 MFI for mHLA and 1.4 mg/ml for sHLA. Abimodal distribution of both mHLA-I and sHLA-I values canbe observed in NAR-recipients, whereas AR-recipients aremainly included in the zone of low mHLA-I (MFI,1000; p ,0.02) and sHLA-I (sHLA-I,1.4mg/ml; p , 0.05).
503HLA Class I and IL-10 in Liver Transplantation
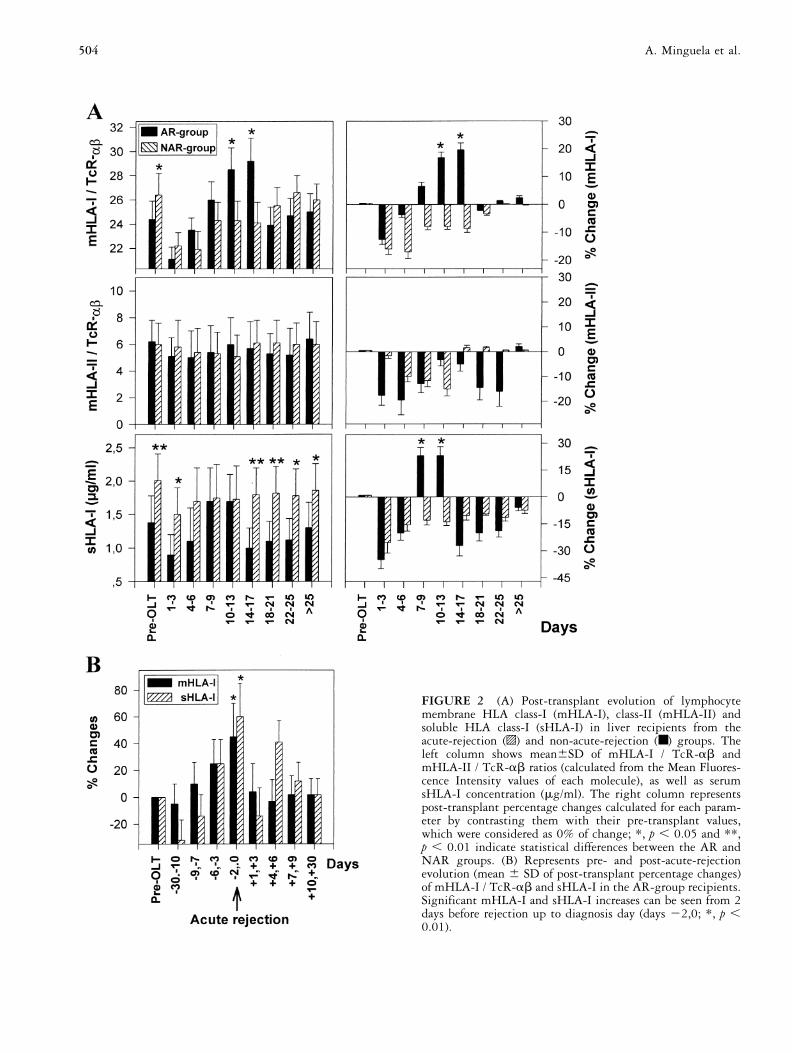
FIGURE 2 (A) Post-transplant evolution of lymphocytemembrane HLA class-I (mHLA-I), class-II (mHLA-II) andsoluble HLA class-I (sHLA-I) in liver recipients from theacute-rejection (o) and non-acute-rejection (■) groups. Theleft column shows mean6SD of mHLA-I / TcR-ab andmHLA-II / TcR-ab ratios (calculated from the Mean Fluores-cence Intensity values of each molecule), as well as serumsHLA-I concentration (mg/ml). The right column representspost-transplant percentage changes calculated for each param-eter by contrasting them with their pre-transplant values,which were considered as 0% of change; *, p , 0.05 and **,p , 0.01 indicate statistical differences between the AR andNAR groups. (B) Represents pre- and post-acute-rejectionevolution (mean 6 SD of post-transplant percentage changes)of mHLA-I / TcR-ab and sHLA-I in the AR-group recipients.Significant mHLA-I and sHLA-I increases can be seen from 2days before rejection up to diagnosis day (days 22,0; *, p ,0.01).
504 A. Minguela et al.

FIG
UR
E3
Lym
phoc
yte
HLA
clas
s-I
hist
ogra
ms
from
pre-
and
post
-tra
nspl
ant
peri
ods.
The
figu
rere
pres
ents
data
for
are
pres
enta
tive
reci
pien
tfr
omea
chof
the
AR
and
NA
Rgr
oups
.The
Mea
nFl
uore
scen
ceIn
tens
ity
6C
oeff
icie
ntof
Var
iati
on(M
FI6
CV
)is
show
nfo
rea
chda
y.O
nda
ys3
to10
,whi
chin
clud
eth
eda
yof
acut
ere
ject
ion
diag
nosi
s(d
ay8)
,an
mH
LA-I
up-r
egul
atio
nca
nbe
obse
rved
inth
eA
R-r
ecip
ient
,w
here
asth
ism
olec
ule
isdo
wn-
regu
late
din
the
NA
R-r
ecip
ient
.
505HLA Class I and IL-10 in Liver Transplantation

NAR-group. In addition, sHLA-I values positively cor-relate with the absolute number of PBL in the totalgroup of recipients as well as in the AR and NAR groups(p , 0.0001, in all cases).
Pre- and Post-acute Rejection Evolution ofmHLA-I and sHLA-ITo rule out data variability caused at the time of acuterejection appearance, we also studied mHLA-I andsHLA-I values in the AR-group recipients during pre-and post-rejection periods. In the Fig. 2b, it can beobserved that mHLA-I undergoes a gradual up-regula-tion from days 29 to 23 pre-rejection, reaching signif-icant increases only on the days of acute rejection diag-nosis (days 22 to 0, p , 0.01), and recovering theirpre-transplant values after anti-rejection therapy. How-ever, sHLA-I showed a significant decrease on days 230to 210 pre-rejection (p , 0.001), with a subsequentincrease that peaked on diagnosis day (p , 0.01). Al-though this augment was abrogated by anti-rejectiontherapy, following the first post-rejection days, sHLA-Iagain exceeded its pre-OLT values from days 14 to 19post-rejection.
Prognostic Value of mHLA-I andSHLA-I DeterminationsOn studying mHLA-I and sHLA-I evolution in eachrecipient during the monitoring period, it was observedthat 27 out of 28 (96.4%) AR-patients showed increasesof mHLA-I previous to and on days of acute rejection. Incontrast only 18 out of 58 (31%) NAR-recipients pre-sented mHLA-I increases in the follow-up period, al-though in these 18 patients other complications such asviral and bacterial infections, fever, graft dysfunction,cholestasis etc., which could possibly influence this in-crease, were frequently observed. On the other hand,clear increases in sHLA-I were found in 19 out of 28(67.8%) AR patients at the time of acute rejection, and,when the total follow-up period was analyzed, similarincreases were found in 13 out of 58 (22.4%) NAR-patients. Therefore, mHLA-I determination was moresensitive than the analysis of sHLA-I (96.4% versus67.8%) but also less specific (69% versus 77.6%). Nev-ertheless, taking the total number of recipients intoaccount, mHLA-I and sHLA-I variations throughout thefollow-up period were positively correlated (p , 0.004).
Serum IL-10 ConcentrationsIL-10 average values during the first 24 h post-transplantwere significantly different between the AR and NARgroups (p , 0.01). Both groups of recipients had similarpre-transplant values, which were no different to those ofcontrols (0.06 6 0.05 ng/ml). However, 4 h after trans-plant the NAR-group presented average values of
0.89 6 0.31 ng/ml, whereas the AR-group showed0.35 6 0.13 ng/ml (p , 0.01), a difference which stillremained 12 h (0.415 6 0.2 versus 0.22 6 0.1 ng/ml)and 24 h (0.21 6 0.18 versus 0.07 6 0.05 ng/ml) later.In contrast, on days of maximum acute rejection fre-quency, serum IL-10 concentrations from the AR-groupwere superior to those of the NAR-group, with signifi-cant differences on days 5 and 7 (p , 0.05; Fig. 4). It isimportant to notice that no differences were found in theearly post-transplant IL-10 levels when the initial recip-ient disease was considered.
DISCUSSIONThe data of this study show that in the NAR recipients,unlike in the AR patients, pre-transplant mHLA-I andsHLA-I values are distributed in a bimodal form (high/low), results which are in accordance with those de-scribed by McDonald et al. indicating that healthy in-dividuals can be divided into high and low sHLA-Isecretors [21]. Interestingly, this distribution was notobserved in patients suffering from rejection episodes(AR-group), who were included nearly homogeneouslyin the low expression/secretion group. This finding ap-pears to indicate that low mHLA-I expression or sHLA-Iconcentration are conditioning factors for acute rejection.At present, it is known that sHLA-I molecules [6, 22]and normal lymphocyte mHLA-I expression [14, 15] areinvolved in the maintenance of self-tolerance. Therefore,in liver transplant it is possible that individual differ-ences in sHLA-I secretion or abnormalities in the
FIGURE 4 Mean 6 SD of serum IL-10 (ng/ml) in theacute-rejection (AR) and non-acute-rejection (NAR) groups. *,p , 0.05 and **, p , 0.01 indicate statistical differencesbetween groups. Concentration of serum IL-10 in the controlgroup was 0.06 6 0.05 ng/ml.
506 A. Minguela et al.

mHLA-I expression of each recipient might conditionthe graft acceptance. Thus, it is interesting to note thatpatients with carcinoma showed the highest pre-trans-plant sHLA-I levels, which could have influenced theirlow acute rejection incidence. It is generally recognized:firstly, that peptides derived from polymorphic or con-served domains of the sHLA-I might inhibit the immuneresponse and CTL activity [6, 23, 24]; and secondly thatthe indirect presentation of sHLA-I by the recipientMHC, might trigger regulatory T cells that, in turn, willinduce anergy or suppression [25]. These observationssupport the possibility that sHLA-I behaves as an in vivonatural non-specific immunoregulatory factor whichblocks the allogeneic response, an effect that could be lessefficient in liver recipients with low sHLA-I levels.
It is important to note that irrespective of recipientclinic characteristics, or surgical and immunosuppressiverequirements, the observed pre-transplant sHLA-I dis-balance between groups was maintained at the end of thefollow-up period, even though it was transitorily offseton days of maximum acute rejection frequency (Fig. 2A).It should be emphasized that this feature is in agreementwith previous reports describing that the sHLA-I isconstant for long periods and not influenced by immu-nosuppressive therapies [26, 27]. Because of the fact thatinitial immunosuppression and post-transplant CsAblood levels were similar in all patients, their influenceon mHLA-I expression could also be excluded. It is truethat HLA class-I matching can condition the graft rejec-tion [28] and that sHLA-I secretion can be influenced bythe HLA phenotype of patients [29], but in any case, thecompatibility and phenotypic distribution were not ac-tually dissimilar in the study groups.
Different studies demonstrate that the liver is themajor source of sHLA-I [23, 30], and that in the rejec-tion process there occurs a strong mHLA-I up-regulationon hepatocytes and bile duct epithelia cells [10] whichdirectly favors donor sHLA-I shedding into circulation[13, 31, 32]. However, it cannot be excluded that thelymphocyte activation which takes place during the al-loresponse may contribute to the increase of total-sHLA-I as well [26, 32–35]. The last concept can besupported by the results presented here, which show alymphocyte mHLA-I up-regulation linked to acute re-jection, and a positive correlation of sHLA-I levels eitherwith the absolute number of PBL or mHLA-I values.
Despite the high correlation observed between rejec-tion and the increase of sHLA-I in previous studies [13,32], including our own, the analysis of total sHLA-I inliver recipients appears to be a non-specific parameter foracute rejection diagnosis. However, donor-derivedsHLA-I measurement might represent a more specifictest, useful in heart and liver transplant [26], but thisparameter is not always available [36]. From this stand-
point, our results demonstrate that cytometric analysis ofmHLA-I on recipient PBL represents a method of eval-uating acute rejection, with a degree of specificity similarto sHLA-I, but more sensitive and direct, with theadditional advantage of allowing the prediction of acuterejection as early as 2 days before the histologic diag-noses. Nevertheless, some patients without clinical rejec-tion evidence showed increases of mHLA-I or sHLA-I,although the existence of subclinical rejection processesshould not be disregarded [37].
On the other hand, it has been reported that IL-10 isa potent inhibitor of several processes involved in theallograft response, including MHC class-II and accessorymolecule expression [38], as well as the monocyte-de-pendent T cell proliferation [39, 40]. Alternatively,IL-10 induces in vitro MHC class-I down-regulation andrenders target cells insensitive to MHC class-I restrictedallospecific CTL-lysis [41, 42]. According to this mech-anism, the high serum IL-10 levels detected in the first24 h after liver graft, together with the mHLA-I down-regulation that happened in NAR-recipients (Fig. 2 and4), suggest that early in vivo IL-10 secretion could play arole in liver allograft acceptance. Experimental in vitro[43] and in vivo [44] assays have demonstrated that, theadministration of recombinant IL-10 efficiently preventsthe alloresponse when the cytokine is supplied at thebeginning of the allogeneic challenge, whereas main-tained treatments enhance the alloresponsiveness. In ad-dition, recipients with acute rejection showed serumIL-10 increases which coincided with the lymphoid ac-tivation induced in the rejection process, probably be-cause IL-10 was simultaneously secreted with other Tcell derived cytokines, particularly IL-4 and IFN-g [45,46]. All these facts together appear to indicate that IL-10interferes with an early T cell activation stage, whichfavors tolerance establishment, especially when short ini-tial treatments are used.
In conclusion, the data of this report demonstratefirstly that, not only a low serum sHLA-I concentration,but also a low pre-transplant HLA class-I expression onPBL, pre-dispose liver recipients to acute rejection, andsecondly, that high early post-operative IL-10 levels im-prove liver graft acceptance, providing a basis for con-sidering the potential therapeutic use of IL-10 in liver-graft tolerance induction. Nevertheless, further studiesare needed to confirm these results in other types ofgrafts and in more extensive series of liver transplants.
ACKNOWLEDGMENTS
This research was supported by grants from the Fondo deInvestigacion Sanitaria (F.I.S projects 94/0382 and 97/0397),Ministerio de Sanidad y Consumo and by “Caja Murcia”.Alfredo Minguela was fellow from F.I.S. (B.A.E. 96/5028).
507HLA Class I and IL-10 in Liver Transplantation

REFERENCES
1. Mor E, Solomon H, Gibbs JF, Holman MJ, GoldsteinRM, Husberg BS, Gonwa TA, Klintmalm GB: Acutecellular rejection following liver transplantation: clinicalpathologic features and effect on outcome. Semin LiverDis 12:28, 1992.
2. Kamada N: The liver as an immunosuppressive organ. InTilney NL, Strom TB, Paul LC (eds): Transplantationbiology: cellular and molecular aspects. Philadelphia: Lip-pincott-Raven, 1996.
3. Gonwa TA, Nery JR, Husberg BS, Klintmalm GB: Si-multaneous liver and renal transplantation in man. Trans-plantation 46:690, 1988.
4. Alters SE, Shizuru JA, Ackerman J, Grossman D, SeydelKB, Fathman CG: Anti-CD4 mediates clonal anergy dur-ing transplantation tolerance induction. J Exp Med 173:491, 1991.
5. Dallman MJ, Shiho O, Page TH, Wood KJ, Morris PJ:Peripheral tolerance to alloantigen results from alteredregulation of the interleukin-2 pathway. J Exp Med 173:79, 1991.
6. Krensky AM: T cells in autoimmunity and allograft re-jection. Kidney Internat 45:S50, 1994.
7. Le Moine O, Marchant A, Durand F, Ickx B, Pradier O,Belghiti J, Abramovicz D, Gelin M, Goldman M, DeviereJ: Systemic release of interleukin-10 during orthotopicliver transplant. Hepatology 20:889, 1994.
8. Alfrey EJ, Most D, Wang X, Lee LK, Holm B, KriegerNR, Sibley RK, Huie P, Dafoe DC: Interferon-gammaand interleukin-10 messenger RNA are up-regulated afterorthotopic liver transplantation in tolerant rats: evidencefor cytokine-mediated immune dysregulation. Surgery118:399, 1995.
9. Mirza DF, Gumson BK, Soonawalla Z, Pirenne J, MayerAD, Buckels JAC, McMaster P: Reduced acute rejectionafter liver transplantation with neoral-based triple immu-nosuppression. Lancet 349:701, 1997.
10. Nocera A, Pellicci R, Barocci S, Valente U, Cantarella S,Celada F, Callea F, Ceppa P, Leprini A: HLA antigensexpression and cellular infiltrate analysis in rejected andaccepted human liver allografts. Clin Transplant 5:23,1991.
11. Steinhoff G, Wonigeit K, Pichlmayer R: Analysis of se-quential changes in major histocompatibility complexexpression in human liver grafts after transplantation.Transplantation 45:394, 1988.
12. Rouger P, Gugenheim J, Gene P, et al.: Distribution ofthe MHC antigens after liver transplantation: relationshipwith biochemical and histological parameters. Clin ExpImmunol 80:404, 1990.
13. Puppo F, Pellice R, Brenci S, Nocera A, Morelli N,Dardano G, Bertocchi M, Antonucci A, Ghio M, Scud-eletti M, Barocci S, Valente U, Indiveri F: HLA class-I-soluble antigen serum levels in liver transplantation. A
predictor marker of acute rejection. Hum Immunol 40:166, 1994.
14. Faustman D, Li X, Lin HY, Fu Y, Eisenbarth G, AvruchM, Guo J: Linkage of faulty major histocompatibilitycomplex class-I to autoimmune diabetes. Science 254:1756, 1991.
15. Fu Y, Nathan DM, Li F, Li X, Faustman DL: Defectivemajor histocompatibility complex class-I expression onlymphoid cells in autoimmunity. J Clin Invest 91:2301,1993.
16. Garcıa-Alonso A M, Minguela A, Muro M, Ontanon J,Torıo A, Marın L, Lopez-Segura P, Miras M, Alvarez-Lopez MR: CD28 expression on peripheral blood T lym-phocytes after liver transplant: up-regulation in acuterejection. Hum Immunol 53:64, 1997.
17. Minguela A, Garcıa-Alonso AM, Marın L, Torıo A,Sanchez-Bueno F, Bermejo J, Parrilla P, Alvarez-LopezMR: Evidence of CD28 up-regulation on peripheral Tcells before liver transplant acute rejection. TransplantProc 29:499, 1997.
18. Barnstable CJ, Bodmer WF, Brown G, Galfre G, MilsteinC, Williams AF, Zeigler AZ: Production of monoclonalantibodies to group A erythrocytes, HLA and other hu-man cell surface antigens. Cell 14:9, 1978.
19. Bernabeu C, Morago G, Ortiz de Landazuru M, Carreira J,Sanchez-Madrid F: Anticuerpos momoclonales especıficospara antıgenos de histocompatibilidad y activacion deleucocitos humanos. Immunologia 5:83, 1986.
20. Ferreira A, Villar ML, Alvarez-Cermeno JC, Garcıa-Rod-rıguez MC, Fontan G, Goanzalez-Porque P: Quantifica-tion of soluble serum class-I antigens in healthy volunteersand AIDS patients. Clin Chem Acta 174:207, 1988.
21. McDonald JC, Gelder FB, Aultman DF, Landreneau MD,McMillan RW, Singh Y, Sorrells D, Liou WH: HLA inhuman serum-quantification of class-I by enzyme immu-noassay. Transplantation 53:445, 1992.
22. Buelow R, Burlinghan WJ, Clayberger C: Immunomodu-lation by soluble HLA class-I. Transplantation 59:649,1995.
23. Mathew JM, Shenoy S, Phelan D, Loweli J, Howard T,Mohanakumar T: Biochemical and immunological evalu-ation of donor-specific soluble HLA in the circulation ofliver transplant recipients. Transplantation 62:217, 1996.
24. Clayberger C, Lyu SC, Pouletty P, Kremsky AM: Peptidescorresponding to T cell receptor-HLA constant regionsinhibit class-I restricted immune responses. TransplantProc 25:477, 1993.
25. Grumet FC, Kirshnaswamy S, See-Tho K, Filvaroff E,Hiraki DD: Soluble form of an HLA-B7 class-I antigen(sHLA) specifically suppresses humoral alloimmunization.Hum Immunol 40:228, 1994.
26. Puppo F, Scudeletti M, Indiveri F, Ferrone S: Serum HLAclass-I antigens: markers and modulators of an immuneresponse? Immunol Today 16:124, 1995.
27. Drouet M, Petit B, Peyronnet P, Aussel L, Venot J,
508 A. Minguela et al.

Leroux-Robert C, Fauchet R: Soluble HLA class 1 anti-gens in kidney allograft recipients. Transplant Proc 27:1671, 1995.
28. Ontanon J, Muro M, Garcıa-Alonso AM, Minguela A,Torıo A, Bermejo J, Pons JA, Campos M, Alvarez-LopezMR: Effect of partial HLA-Class I match on acute rejec-tion in viral preinfected human liver allograft recipients.Transplantation 65:1047, 1998.
29. Adamashvili IM, Fraser PA, McDonald JC: Association ofserum concentrations of soluble class-I HLA with HLAallotypes. Transplantation 61:984, 1996.
30. Sumimoto R, Kamada N: Specific suppression of allograftrejection by soluble class-I antigen and complexes withmonoclonal antibody. Transplantation 50:678, 1990.
31. Hagihara M, Munkhbat B, Kanai N, Shimura T, KiuchiT, Inomata Y, Tanaka K, Yamamoto K, Tsuji K: Serumsoluble human leucocyte antigen class I in paediatric livertransplantation with live, related donors. Transpl Immu-nol 5:219, 1997.
32. Davies HFFS, Pollard SG, Calne RY: Soluble HLA anti-gens in the circulation of liver graft recipients. Transplan-tation 47:524, 1989.
33. Brieva JA, Villar LM, Leoro G, Alvarez-Cermeno JC,Roldan E, Gonzalez-Porque P: Soluble HLA class-I anti-gen secretion by normal lymphocytes: relationship withcell activation and effect of interferon-gamma. Clin ExpImmunol 82:390, 1990.
34. Villar LM, Roy G, Lazaro I, Alvarez-Cermeno JC, Gonza-lez M, Brieva JA, De la Sen ML, Leoro G, Bootello A,Gonzalez-Porque P: Detection of soluble class I molecules(non HLA-A or HLA-B) in serum, spleen membranes andlymphocytes in culture. Eur J Immunol 19:1835, 1989.
35. Aulitzky WE, Grosse-Wilde H, Westhoff U, Tilg H,Aulitzky W, Gastl G, Herold M, Habber C: Enhancedserum levels of soluble HLA class-I molecules are inducedby treatment with recombinant interferon-gamma (IFN-gamma). Clin Exp Immunol 86:236, 1991.
36. Koelman CA, Mulder A, Jutte NHPM, Vaessen LMB,Balk AHMM, Weimar W, Doxiadis IIN, Claas FHJ: Theapplication of human monoclonal antibodies for monitor-ing donor derived soluble HLA class I molecules in theserum of heart transplant recipients. Hum Immunol 59:106, 1998.
37. Klompmaker LJ, Gouw AS, Haagsma EB, Ten VergertEM, Verwer R, Slooff MJ: Selective treatment of earlyacute rejection after liver transplantation: effects on liver,infection rate, and outcome. Transpl Int 10:40, 1997.
38. Koppelman B, Neefjes JJ, de Vries JE, de Waal-MalefytR: Interleukin-10 down-regulates MHC class-II ab pep-tide complexes at the membrane of monocytes by affectingarrival and recycling. Immunity 7:861, 1997.
39. de Waal-Malefyt R, Haanen J, Spits S, Roncarlo MG,te-Velde A, Figfor C, Johnson K, Kastelin R, Yssel H, deVries JE: Interleukin 10 (IL-10) and viral IL-10 stronglyreduces antigen-specific human T cell proliferation bydiminishing the antigen presenting capacity of monocytesvia downregulation of class II MHC expression. J ExpMed 174:915, 1991.
40. Ding L, Linsley PS, Huang LY, Germain RN, ShevachEM: IL-10 inhibits macrophage costimulatory activity byselectively inhibiting the up-regulation of B-7 expression.J Immunol 151:1224, 1993.
41. Matsuda M, Salazar F, Peterson M, Masucci G, Hansson J,Pisa P, Zhang QJ, Masucci MG, Kiessling R: Interleukin10 pre-treatment protects target cells from tumor- andallo-specific cytotoxic T cells and downregulates HLAclass-I expression. J Exp Med 180:2371, 1994.
42. Rohrer JW, Coggin JH: CD8 T cell clones inhibit anti-tumor T cell function by secreting IL-10. J Immunol155:5719, 1995.
43. Peguet-Navarro J, Moulon C, Caux C, Dalbiez-GauthierC, Banchereau J, Schmitt D: Interleukin-10 inhibits theprimary allogenic T cell response to human epidermalLangerhans cells. Eur J Immunol 24:884, 1994.
44. Lowry RP, Konieczny B, Alexander D, Larsen C, PearsonT, Smith S, Narula S: Interleukin-10 eliminates anti-CD3monoclonal antibody-induced mortality and prolongheart allograft survival in inbred mice. Transplant Proc27:392, 1995.
45. Lang T, Krams SM, Martinez OM: Production of IL-4 andIL-10 does not lead to immune quiescence in vascularizedhuman organ grafts. Transplantation 62:776, 1996.
46. Schwarz M, Majdic O, Knapp W, Holter W: High-levelIL-10 production by monoclonal antibody-stimulated hu-man T cells. Immunology 86:364, 1995.
509HLA Class I and IL-10 in Liver Transplantation