
IL10 -1082, IL10 -819 and IL10 -592 polymorphisms are associated with chronic periodontitis in a...
28
1 Atanasovska-Stojanovska A, Trajkov D, Popovska M, Spiroski M. IL10 -1082, IL10 -819 and IL10 -592 polymorphisms are associated with chronic periodontitis in a Macedonian population. Hum Immunol. 2012 Jul;73(7):753- 8. Epub 2012 Apr 23. PubMed PMID: 22537751. IL10 -1082, IL10 -819 and IL10 -592 polymorphisms are associated with chronic periodontitis in a Macedonian population Aneta Atanasovska-Stojanovska 1 , Dejan Trajkov 2 , Mirjana Popovska 1 , Mirko Spiroski 2 * 1 Dental Clinical Center, Department of Oral Pathology and Periodontology, Faculty of Stomatology, University "Ss. Cyril and Methodius", Skopje, Republic of Macedonia; 2 Institute of Immunobiology and Human Genetics, Faculty of Medicine, University "Ss. Cyril and Methodius", Skopje, Republic of Macedonia Running title: IL10 gene polymorphisms and chronic periodontitis *Corresponding Author: Mirko Spiroski, MD, PhD. Institute of Immunobiology and Human Genetics, Faculty of Medicine, University "Ss. Cyril and Methodius", 1109 Skopje, PO Box 60, Republic of Macedonia. Tel.: +389-2-3110556. Fax: +389-2-3110558. URL: http://www.iibhg.ukim.edu.mk . E-mail: [email protected] Conflict of interest and source of funding statement
Transcript of IL10 -1082, IL10 -819 and IL10 -592 polymorphisms are associated with chronic periodontitis in a...

1
Atanasovska-Stojanovska A, Trajkov D, Popovska M, Spiroski M. IL10 -1082,
IL10 -819 and IL10 -592 polymorphisms are associated with chronic
periodontitis in a Macedonian population. Hum Immunol. 2012 Jul;73(7):753-
8. Epub 2012 Apr 23. PubMed PMID: 22537751.
IL10 -1082, IL10 -819 and IL10 -592 polymorphisms are associated with
chronic periodontitis in a Macedonian population
Aneta Atanasovska-Stojanovska1, Dejan Trajkov2, Mirjana Popovska1, Mirko
Spiroski2*
1Dental Clinical Center, Department of Oral Pathology and Periodontology,
Faculty of Stomatology, University "Ss. Cyril and Methodius", Skopje, Republic of
Macedonia; 2Institute of Immunobiology and Human Genetics, Faculty of
Medicine, University "Ss. Cyril and Methodius", Skopje, Republic of Macedonia
Running title: IL10 gene polymorphisms and chronic periodontitis
*Corresponding Author:
Mirko Spiroski, MD, PhD. Institute of Immunobiology and Human Genetics, Faculty of Medicine, University "Ss. Cyril and Methodius", 1109 Skopje, PO Box 60, Republic of Macedonia. Tel.: +389-2-3110556. Fax: +389-2-3110558. URL: http://www.iibhg.ukim.edu.mk. E-mail: [email protected]
Conflict of interest and source of funding statement

2
This research is part of the project “Molecular analysis of cytokine gene
polymorphisms in the Republic of Macedonia” supported by the Ministry of
Education and Science from Republic of Macedonia (Project No. 13-874/3-05).
We declare we have no conflict of interest.

3
Abstract
Genetic polymorphisms in the interleukin 10 (IL10) gene have been
reported to influence the host response to microbial challenge by altering levels
of cytokine expression. We analyzed nucleotide polymorphisms in the promoter
region of the IL10 gene and its relation with periodontal disease in a Macedonian
population. The study population consisted of 111 unrelated subjects with chronic
periodontitis and 299 healthy controls. DNA was isolated and IL10 genotyping
performed by PCR-SSP (Heidelberg kit) for the alleles and genotypes of IL10 -
1082, IL10 -819 and IL10 -592. Frequencies of IL10 haplotypes and the
haplotype zygotes were also examined. Comparisons between groups were
tested using the Pearson's p-value. After Bonferroni adjustment, significant
associations were detected between subjects with chronic periodontitis and IL10
genotypes (IL10 -1082/A:G was negative or protective and IL10 -1082/G:G was
positive or susceptible). Cytokine polymorphism on the IL10 gene appears to be
associated with susceptibility to chronic periodontitis in Macedonians.
Key words: chronic periodontitis; IL10 gene; gene polymorphism; genetics.

4
1. Introduction
Chronic periodontitis like many other common diseases (e.g.,
cardiovascular diseases, diabetes, Crohn’s disease) is considered to be a
complex multifactorial disease.. These diseases are of relative late of onset (i.e.,
postjuvenile or adult onset) and are relatively common. The phenotype of the
complex diseases is determined by both genetic and the environmental factors
that affect the individual. Although pathogenic bacteria and various other
environmental factors (e.g., smoking and stress) [1] are involved in pathogenesis
of chronic periodontitis, also genetic factors are evidenced in the aetiology of
chronic periodontitis [2, 3].
There are a large number of scientific papers searching for the role of
genes and their variants (polymorphisms) in host responses in chronic
periodontitis, and in the progression of the disease [4-12]. The genetic
polymorphisms may in some situations cause a change in the protein or its
expression possibly resulting in alterations in innate and adaptive immunity and
may thus be deterministic in disease outcome [11]. Genetic polymorphisms may
also be protective for a disease [12].
Interleukine-10 (IL-10) is considered an antiinflammatory cytokine,
downregulating the proinflammatory immune response of the monocytes and
macrophages. IL-4 and IL-10 display additive effects and induce a strong
increase in the number of viable cells. Moreover, IL-10 induces activated B cells
to secrete large amounts of IgG, IgA, and IgM, and the combination of IL-10 and
IL-4 results in the secretion of the four immunoglobulin isotypes. Thus, IL-10 may

5
play an important role in the amplification of humoral responses. [13]. Auto-
antibodies may also play a role in chronic periodontitis [14–16]. IL-10 is produced
by monocytes, macrophages, and T cells and plays a role in the regulation of
proinflammatory cytokines such as IL-1 and TNF-α.
The gene encoding for IL-10 is mapped on chromosome 1q31-q32, in a cluster
with closely related interleukin genes, including IL-19, IL-20, and IL-24. Several
promoter polymorphisms have been described in the IL10 gene: -1087 (-1082), -
819 (-824), -627, -592 (-597), and -590. The IL10 -1082, -819, and -592
polymorphisms show strong linkage disequilibrium and form two common
haplotypes. The G to A nucleotide polymorphism occurs within a putative Ets
transcription factor–binding site. The C to T nucleotide polymorphism lies within a
putative positive regulatory region, and the C to A polymorphism lies within a
putative STAT 3 binding site and a negative regulatory region [17]. Initial in vitro
work on peripheral blood mononuclear cell (PBMC) cultures has suggested that
the GCC/GCC genotype is associated with higher IL-10 production than other
genotypes [18, 19]. IL-10 has a protective role towards periodontal tissue
destruction, inhibiting both matrix metalloproteinases (MMP) and receptor
activator for nuclear factor-κB (RANK) systems [20, 21].
The aim of this study was to analyze three single-nucleotide
polymorphisms (SNPs) (-1082, -819, -590) in the promoter region of IL10 gene
(on location 1q31-q32) and its relation with periodontal disease in a Macedonian
population.

6
2. Material and Methods
Healthy subjects were recruited from the patient pool at the Clinic for Oral
Diseases and Periodontology, University Clinical Centre of Stomatology, Skopje,
Macedonia [22-26]. All subjects were at least 20 years of age, had at least 20
teeth present, were from Macedonian ethnic background to the third generation,
and were unrelated residents from different geographical regions of the Republic
of Macedonia.
The chronic periodontitis group consisted of 111 subjects previously
diagnosed with moderate or severe chronic periodontal disease. Diagnosis
chronic (adult) periodontitis (CP), was established clinically and by x-ray
verification, in accordance to criteria of American Academy of Periodontal
Disease (AAP, 1999) [27, 28] presence of chronic gingivorrhagia, bleeding on
probing, clinical attachment loss (CAL), and horizontal or vertical loss of alveolar
bone. Degree of clinical attachment loss, in all patients was defined with
confirmed periodontal probe. For each tooth, maximal CAL (distance between
the cement-enamel junction and the bottom of the pocket) were derived by
measuring six sites around each tooth and recording the maximum values.
Patients were selected if they showed attachment loss in ≥ 30% of the teeth, with
a minimum CAL of 4 mm. Degree of gingival inflammation was fortified pursuant
to Loe-Silness’ index [29]. 0 – normal gingival (pale pink color, with hard and
paltry granular consistency); 1 – mild inflammation (marginal gingiva is mildly red,
with small oedema and does not bleed on mild provocation); 2 – modest
inflammation (gingiva with red color, with emphasized oedema on the free

7
gingival, there is bleeding on mild pressure with plug); 3 – strong inflammation
(gingiva with clearly red color, with lot of oedemas, with tendency for
spontaneous bleedings).The measures were evaluated on bucal, lingual, mesial
and distal side of each tooth, of each quadrant. Bleeding on probing BOP was
graded 1, if it occurred within 30 sec. If not it was graded 0. Excluding criteria
were: 1) diseases of oral soft and hard tissues in oral cavity, excluding caries and
periodontitis; 2) presence of orthodontic apparatuses (prosthesis) in mouth; 3)
usage of systemic antibiotics in period of three months before engagement in this
study; 4) pregnancy and lactation; 5) diabetes; 6) appliance of immune-
suppressive therapy; 7) history of any general disease which violates functions of
immune system; and 8) current or former smokers.
The healthy control group consisted of 299 subjects displaying no sites
with a probing depth >3 mm, no clinical attachment loss > 2 mm, gingival index of
1, and BOP 6.8 ± 6.4%. The study was approved by the Committee of the
Ministry of Education and Science from the Republic of Macedonia, as well as
the Ethical Committee of the Medical Faculty in Skopje [23] and was part of the
Cytokine Polymorphisms and Expression, 15th International Histocompatibility
and Immunogenetics Workshop (IHIWS).
2.1 Testing Polymorphism on IL10 gene
Genomic DNA was isolated by the phenol-chloroform [30] method from
peripheral leukocytes and samples stored in the Macedonian bank for human
DNA as previously described [31]. IL10 gene polymorphisms were determined

8
using the PCR-SSP (Heidelberg kit, Cytokine genotyping Tray, Invitrogen,
GmbH, Karlsruhe, Germany) at the Institute for Immunobiology and Human
Genetics at the Faculty of Medicine in Skopje [25, 32]. Briefly, the PCR-SSP
typing Heidelberg kit consists of PCR primer mixes aliquotted in 96 well PCR
trays. Master mix, which was supplied along with the reagents and consisted of
MgCl2, buffer, dNTP's, and glycerol was mixed with 1.2 - 3.0 μg DNA and 20 U
Taq polymerase and dispensed in the wells. The amplified products were
separated by 2% agarose gel electrophoresis, stained with 0.5 μg/mL ethidium
bromide and visualized by ultraviolet exposure. For IL10 gene with multiple
polymorphisms per gene [IL10 -1082 (rs1800896), IL10 -819 (rs1800871) and
IL10 -592 (rs1800872)] the Heidelberg PCR-SSP kit was able to detect true
haplotypes.
2.1. Statistical analysis
The population genetics analysis package, PyPop, developed by the
Biostatistics Core for the Workshop [33-35] was used for analysis of the IL10
data for this report. Allele frequencies and expected Hardy Weinberg proportions
(HWP) for each IL10 allele were determined [36]. The exact test for genotype
frequency deviation from HWP was calculated using the Arlequin implementation
accessed via PyPop [37]. Those alleles that did not fit HWP were evaluated to
determine whether there was an excess of homozygotes or heterozygotes, or if
any particular genotypes were significantly different from expected frequencies
by the chi square test. The Ewens-Watterson homozygozity test of neutrality

9
(EWN) (38) with Slatkin's exact p-values (SEPV) [39, 40] was used to indicate
any deviations from the hypothesis of neutral selection for each locus. Pearson's
p-values, crude Odds Ratio (OR) and Wald’s 95% confidence interval (CI) were
calculated for associations' analysis between IL10 (alleles, genotypes,
haplotypes, and diplotypes) and periodontal disease with Simple Interactive
Statistical Analysis (SISA) free statistical calculator
(http://www.quantitativeskills.com/sisa/statistics/twoby2.htm) with Bonferroni
corrected p-value [41]. P less than 0.05 were taken as significant.
3. Results
The clinical and demographic data of our Macedonian study populations
are shown in Table 1. As predicted, the values of the clinical parameters GI,
CAL, and BOP were higher in the chronic periodontitis group than in healthy
controls.
<<Table 1 near here>>
Observed versus expected cytokine genotypes for each IL10
polymorphism, Hardy Weinberg proportion (HWP), and Guo and Thompson
Hardy Weinberg Output (GTHWO) in healthy subjects and subjects with
periodontal disease is given in the Table 2. Observed frequencies of IL10 -1082
genotypes in the healthy population were significantly different from the
expectations (HWP P<0.001, GTHWO P<0.001). In subjects with periodontal

10
disease IL10 genotypes were in equilibrium with HWP and Guo and Thompson
Hardy Weinberg Output (GTHWO) was not significant (P> 0.05) (Table 2).
<<Table 2 near here>>
DNA from our 111 chronic periodontitis and 299 healthy controls were
analyzed for polymorphisms in the promoter (-1082, -819, -592) region of the
IL10 gene. Our results indicate non significant differences in the distribution of
alleles between the two groups at the IL10 -1082, IL10 -819, and IL10 -592 gene
polymorphism (Table 3).
Homozygosity for the A allele at position IL10 -1082 was seen in 30.6% of
subjects with chronic periodontitis compared to 23.4% of healthy subjects while
13.5% of chronic periodontitis subjects were homozygous for the G allele
compared to 5.7% of healthy subjects (Table 3). The distribution of the IL10 -
1082/A:G and IL10 -1082/G:G genotypes between groups was significantly
different after Bonferroni adjustment (P<0.004, OR=0.519, 95% CI=0.331-0.814
and P<0.009, OR=2.592, 95% CI=1.247-5.389, respectively). At the -819
position, 57.7% of chronic periodontitis subjects were homozygous for the C
allele compared to 51.8% of healthy subjects. Homozygosity for the C allele at
position -590 was noted in 55.9% of chronic periodontitis compared to 51.5% of
healthy subjects, but these differences failed to reach significance (P=0.294 and
0.433, respectively). Homozygous T allele at position -819 and A allele at
position -590 were noted in 3.6% of chronic periodontitis while 6.4% of healthy
subjects were homozygous for the T allele and 9.4% for the A allele, respectively.

11
Homozygosity for the T allele at position -819 and A allele at position -590 cannot
be statistically calculated because expected <5, χ2 test (Table 3).
<<Table 3 near here>>
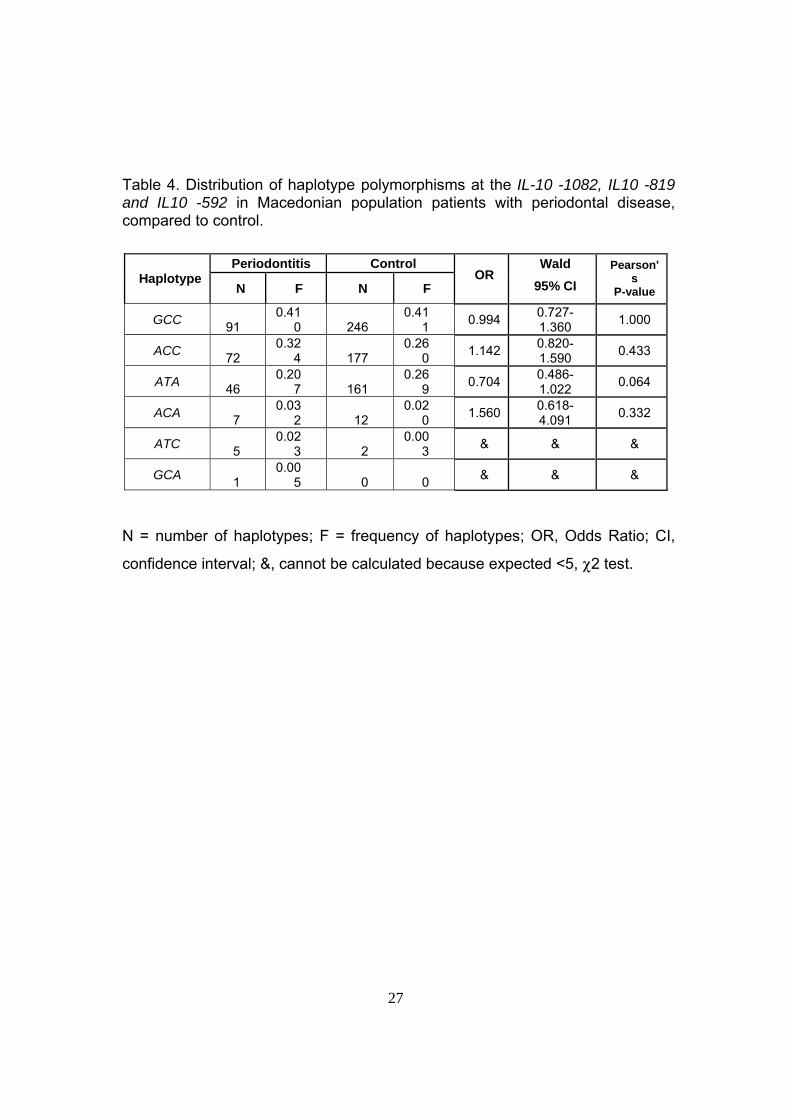
Six haplotypes were found in the chronic periodontitis group and in healthy
subjects with the highest frequency for IL10/GCC haplotype (0.410 in chronic
periodontitis and 0.411 in healthy subjects). Five haplotypes (IL10/ACC,
IL10/ATA, IL10/ACA, IL10/ATC, and IL10/GCA) were with lower frequency, but
differences between investigated groups were not significant (Table 4).
<<Table 4 near here>>
Table 5 shows the distribution of diplotypes (haplo-zygotes) between
groups. Of the 13 diplotypes identified in our study, three diplotypes were
significantly different between patients with chronic periodontitis and healthy
subjects (ACC:ATA, ATA:GCC, GCC:GCC), but failed to reach statistical
significance after Bonferroni adjustment. Three other diplotypes (ACC:ACC,
ACC:GCC, ATA:ATA) were statistically calculated, but differences failed to reach
significance. For seven haplotypes χ2 test was not calculated because the
expected frequencies were smaller than 5 (Table 5).
<<Table 5 near here>>
4. Discussion
In this paper we present the allelic, genotypic, and haplotypic
polymorphisms along the promoter region of the IL10 gene in a relatively

12
homogeneous population of Macedonian subjects with and without periodontal
disease.
In our study the distribution of the IL10 -1082/A:G and IL10 -1082/G:G
genotypes between groups was significantly different after Bonferroni
adjustment. Three diplotypes (ACC:ATA, ATA:GCC, GCC:GCC) were
significantly different between Macedonian patients with chronic periodontitis and
healthy subjects, but failed to reach statistical significance after Bonferroni
adjustment.
The smallest frequency of alleles, which is G allele for IL10 -1082 (-1087),
T allele for IL10 -819 (-824), and A allele for IL10 -590, is labelled with R (rare
allele) and the other allele is labelled with N (normal). The carriage rates of the
IL10 -1087 R allele (G allele) vary between 44% and 81% in Caucasians. The –
1082 (-1087) locus has not been associated with chronic periodontitis
susceptibility in most of Caucasian populations. However, the -1082 (-1087) N-
allele (A allele) was associated with chronic periodontitis in Swedish Caucasians
[42]. We present for the first time negative or protective association of IL10 -
1082/A:G with OR smaller than 1.0 (0.519) and positive or susceptible
association of IL10 -1082/G:G with OR higher than 1.0 (2.592) in Macedonian
Caucasians. However, there was no marked difference in -1082 IL10 genotype
frequencies between the controls and generalized aggressive periodontitis in
Iranian patients [43]. It was found that the proportion of IL-10+ cells in the
peripheral area of the periodontitis lesions was significantly larger in subjects with
the -1087 IL-10 GG genotype than in subjects with the AG or AA genotype [44],
13
which can be in agreement with our results. Recently, the mRNA expression of
Sp1 and IL-10 in patients with the GG genotype was four times higher than that
in patients with the AA genotype. Proportions of Sp1-positive cells overall and
Sp1-positive B cells were larger in patients with the GG genotype than in patients
with the AA genotype [45]. We can conclude from our and other published
results, that IL10 G allele at position -1082 play important role in the association
with chronic periodontitis.
The IL10 -819 polymorphism has been correlated with chronic
periodontitis in Brazilians but not in other populations [46]. Until now all three
studies on the IL10 -592 polymorphism have found a higher R-allele carriage rate
in chronic periodontitis patients [46–48]. The IL10 -592 R-allele carriage rates
varied in different populations between 68% and 75% in chronic periodontitis
patient and between 41% and 51% in controls.
One study on Japanese chronic periodontitis patients (N = 34) and
controls (N = 52) analyzed haplotypes consisting of the IL10 -1087, -819, and -
592 gene polymorphisms [49]. Only haplotype frequencies were reported and no
separate genotype frequencies were presented. No significant differences for the
carriage rates of the haplotypes of the IL10 gene were found between patients
and controls. Striking was the complete absence of the N-allele carriage at
position -1087 among the Japanese, in contrast to Caucasians, where the -1087
N-allele is the most occurring variant [42, 49].
The combination ATA/ATA, which is known as a 'low interleukin-10
producer', was found only in patients with aggressive periodontitis (15.6 vs. 0.0%,

14
p = 0.023) [50], but the Bonferroni adjustment was not applied. Without
Bonferroni correction, our results have shown significant association between
ACC:ATA, ATA:GCC, GCC:GCC diplotypes and patients with chronic
periodontitis. There was a significant (p approximately 0.02) main effect of IL10
haplotypes, with individuals having either the ATA/ACC or the ACC/ACC
genotype experiencing around 20% fewer probing depths of >or= 4 mm
compared to individuals with other genotypes, suggesting that the IL10 genotype
contributes to the progression of periodontal disease [51]. The IL10 gene
polymorphism at position -592C>A may be associated with a lower risk for
development of chronic periodontitis. The IL10 haplotype ATA is associated with
generalized aggressive periodontitis in a Taiwanese population [52].
Our study is subject to limitations. After Bonferroni correction of P-values,
we found smaller number of IL10 genotypes and diplotypes to be associated with
periodontal disease in Macedonians, but the inclusion of Bonferroni correction in
this report implies a higher likelihood of false negatives with subsequently less
significant associations with periodontal disease [41, 53]. Moreover, IL10 -1082
genotypes in healthy participants were not in HWP (P<0.001) and we should be
very careful about their associations with periodontal disease. Unfortunately, we
do not have any information about HWP in other published papers connected
with IL10 gene polymorphisms and associations with chronic periodontitis [42-52]
in order to compare connection of the results with HWP. The number of patients
in our study (111), as well as in other published papers [42-52], is very small. In
the association studies, there are possibilities that some positive results might be

15
spurious and some negative findings might be a consequence of low statistical
power. It could be due to their small sample size or methodological
shortcomings, such as the selection of an appropriate control group. It is
necessary to investigate IL10 gene polymorphisms in our population in well
defined subgroups of phenotypes with bigger number of participants in order to
have more precise conclusions for genetic background of development of chronic
periodontitis in Macedonians. Multicentric studies and/or meta-analysis of the
patients with chronic periodontitis and association with cytokine polymorphisms
should be very useful.
It can be concluded that, at least in Macedonian patients with chronic
periodontitis, some IL10 gene polymorphisms contribute to
susceptibility/protection to disease. Ethnic factors might play a role in the
variability of results in different populations. Therefore, additional studies are
needed to clarify this issue.
Acknowledgements
This research is part of the project “Molecular analysis of cytokine gene
polymorphisms in the Republic of Macedonia” supported by the Ministry of
Education and Science from Republic of Macedonia (Project No. 13-874/3-05).
The authors thank Elena Cvetkovska (Institute of Immunobiology and Human
Genetics, Faculty of Medicine, University “Ss Cyril and Methodius”, Skopje,
Republic of Macedonia) for isolation of genomic DNA and taking care of the
Macedonian Human DNA Bank (www.hdnamkd.org.mk).

16
References
[1] Borrell LN, Papapanou PN. Analytical epidemiology of chronic
periodontitis. J Clin Periodontol. 2005;32 Suppl 6:132-58.
[2] Michalowicz BS, Diehl SR, Gunsolley JC, Sparks BS, Brooks CN, Koertge
TE, Califano JV, Burmeister JA, Schenkein HA. Evidence of a substantial
genetic basis for risk of adult chronic periodontitis. J Periodontol.
2000;71(11):1699-707.
[3] Michalowicz BS, Aeppli D, Virag JG, Klump DG, Hinrichs JE, Segal NL,
Bouchard TJ Jr, Pihlstrom BL. Periodontal findings in adult twins. J
Periodontol. 1991;62(5):293-9.
[4] Loos BG, John RP, Laine ML. Identification of genetic risk factors for
chronic periodontitis and possible mechanisms of action. J Clin
Periodontol. 2005;32Suppl 6:159-79.
[5] Laine ML, Loos BG, Crielaard W. Gene polymorphisms in chronic
periodontitis. Int J Dent. 2010;2010:324719.
[6] Zhang J, Sun X, Xiao L, Xie C, Xuan D, Luo G. Gene polymorphisms and
chronic periodontitis. Periodontol 2000. 2011;56(1):102-24.
[7] Gera I, Vári M. [Genetic background of chronic periodontitis. Part II.
Genetic polymorphism in periodontal disease. A review of literature].
Fogorv Sz. 2009;102(4):131-40.

17
[8] Nikolopoulos GK, Dimou NL, Hamodrakas SJ, Bagos PG. Cytokine gene
polymorphisms in periodontal disease: a meta-analysis of 53 studies
including 4178 cases and 4590 controls. J Clin Periodontol.
2008;35(9):754-67.
[9] Takashiba S, Naruishi K. Gene polymorphisms in periodontal health and
disease. Periodontol 2000. 2006;40:94-106.
[10] Shapira L, Wilensky A, Kinane DF. Effect of genetic variability on the
inflammatory response to periodontal infection. J Clin Periodontol. 2005;32
Suppl 6:72-86.
[11] Kinane DF, Hart TC. Genes and gene polymorphisms associated with
periodontal disease. Crit Rev Oral Biol Med. 2003;14(6):430-49.
[12] Kornman KS, di Giovine FS. Genetic variations in cytokine expression: a
risk factor for severity of adult chronic periodontitis. Ann Periodontol.
1998;3(1):327-38.
[13] Rousset F, Garcia E, Defrance T, Péronne C, Vezzio N, Hsu DH,
Kastelein R, Moore KW, Banchereau J. Interleukin 10 is a potent growth
and differentiation factor for activated human B lymphocytes. Proc Natl
Acad Sci U S A. 1992;89(5):1890-3.
[14] Afar B, Engel D, Clark EA. Activated lymphocyte subsets in adult chronic
periodontitis. J Periodontal Res. 1992;27(2):126-33.

18
[15] Berglundh T, Liljenberg B, Tarkowski A, Lindhe J. The presence of local
and circulating autoreactive B cells in patients with advanced chronic
periodontitis. J Clin Periodontol. 2002;29(4):281-6.
[16] Koutouzis T, Haber D, Shaddox L, Aukhil I, Wallet SM. Autoreactivity of
serum immunoglobulin to periodontal tissue components: a pilot study. J
Periodontol. 2009;80(4):625-33.
[17] Claudino M, Trombone AP, Cardoso CR, Ferreira SB Jr, Martins W Jr,
Assis GF, Santos CF, Trevilatto PC, Campanelli AP, Silva JS, Garlet GP.
The broad effects of the functional IL-10 promoter-592 polymorphism:
modulation of IL-10, TIMP-3, and OPG expression and their association
with periodontal disease outcome. J Leukoc Biol. 2008;84(6):1565-73.
[18] Crawley E, Kay R, Sillibourne J, Patel P, Hutchinson I, Woo P.
Polymorphic haplotypes of the interleukin-10 5' flanking region determine
variable interleukin-10 transcription and are associated with particular
phenotypes of juvenile rheumatoid arthritis. Arthritis Rheum.
1999;42(6):1101-8.
[19] Koss K, Satsangi J, Fanning GC, Welsh KI, Jewell DP. Cytokine (TNF
alpha, LT alpha and IL-10) polymorphisms in inflammatory bowel diseases
and normal controls: differential effects on production and allele
frequencies. Genes Immun. 2000;1(3):185-90.
[20] Garlet GP, Martins W Jr, Fonseca BA, Ferreira BR, Silva JS. Matrix
metalloproteinases, their physiological inhibitors and osteoclast factors are

19
differentially regulated by the cytokine profile in human periodontal
disease. J Clin Periodontol. 2004;31(8):671-9.
[21] Zhang X, Teng YT. Interleukin-10 inhibits gram-negative-microbe-specific
human receptor activator of NF-kappaB ligand-positive CD4+-Th1-cell-
associated alveolar bone loss in vivo. Infect Immun. 2006;74(8):4927-31.
[22] Atanasovska-Stojanovska A, Trajkov D, Nares S, Angelov N, Spiroski M.
IL4 gene polymorphisms and their relation to periodontal disease in a
Macedonian population. Hum Immunol. 2011;72(5):446-50.
[23] Atanasovska-Stojanovska A, Trajkov D, Popovska M, Spiroski M. Analysis
of Transforming Growth Factor-Beta1 Gene Polymorphisms in
Macedonian Patients with Chronic periodontitis. Maced J Med Sci. 2009;
2(1):30-35.
[24] Trajkov D, Arsov T, Petlichkovski A, Strezova A, Efinska-Mladenovska O,
Spiroski M. Cytokine gene polymorphisms in population of ethnic
Macedonians. Croat Med J 2005; 46: 685-692.
[25] Trajkov D, Atanasovska-Stojanovska A, Petlichkovski A, et al. (IL-1 gene
cluster polymorphisms in the Macedonian population. Mac J Med Sci
2008; 1: 21-28.
[26] Trajkov D., Arsov, T., Petlichkovski, A., et al. Distribution of the 22
cytokine gene polymorphisms in healthy Macedonian population.
Bratislavske Lekarske Listy 2009;110: 7-17.

20
[27] Armitage GC. Development of a classification system for periodontal
diseases and conditions. Ann Periodontol 1999;4(1):1-6.
[28] Burt B, Greenwell H, Fiorellini J, et al. Position paper: Epidemiology of
periodontal diseases. J Periodontol 2005; 76: 1406-1419.
[29] Loe H, Silness J. Periodontal disease in pregnancy. I. Prevalence and
severity. Acta Odontol Scand 1963; 21: 533-551.
[30] Towner P. Purification of DNA. In: Brown TA, ed. Essential molecular
biology, Oxford: Oxford University Press, 2005: 47-54.
[31] Spiroski M, Arsov T., Petlichkovski, A., et al. Case Study: Macedonian
Human DNA Bank (hDNAMKD) as a source for public health Genetics. In:
Georgieva L, Burazeri G, eds. Health determinants in the scope of new
public health. Sofia: Hans Jacobs Company, 2005: 33-44.
[32] Tseng LH, Chen PJ, Lin MT, et al. Simultaneous genotyping of single
nucleotide polymorphisms in the IL-1 gene complex by multiplex
polymerase chain reaction restriction fragment length polymorphism. J
Immunol Methods 2002; 267: 151-156.
[33] Lancaster A, Nelson MP, Meyer D, Thomson G, Single RM. PyPop: a
software framework for population genomics: analyzing large-scale multi-
locus genotype data. Pac Symp Biocomp 2003; 8: 514-525.
[34] Lancaster AK, Single RM, Solberg OD, Nelson MP, Thomson G. PyPop
update - a software pipeline for large-scale multilocus population
genomics. Tissue Antigens 2007;69 (Suppl 1): 192-197.

21
[35] Single RM, Meyer D, Mack SJ, Lancaster A, Erlich HA, Thomson G. 14th
International HLA and Immunogenetics Workshop: report of progress in
methodology, data collection, and analyses. Tissue Antigens 2007; 69
(Suppl 1): 185-187.
[36] Guo SW, Thompson EA. Performing the exact test of Hardy Weinberg
proportion for multiple alleles. Biometrics 1992; 48: 361-372.
[37] Schneider S., Roessli, D., Excoffier, L. Arlequin version 2.000: a software
for population genetics data analysis. 2000; Geneva (Switzerland):
Genetics and Biometry Laboratory, University of Geneva.
[38] Watterson GA. The homozygozity test of neutrality. Genetics 1978; 88:
405-417.
[39] Slatkin M. An exact test for neutrality based on the Ewens sampling
distribution. Genet Res 1994; 64: 71-74.
[40] Slatkin M, Excoffier L. Testing for linkage disequilibrium in genotypic data
using the Expectation-Maximization algorithm. Heredity 1996; 76 (Pt 4):
377-383.
[41] Rice TK, Schork NJ, Rao DC. Methods for handling multiple testing. Adv
Genet 2008; 60: 293-308.
[42] Berglundh T, Donati M, Hahn-Zoric M, Hanson LA, Padyukov L.
Association of the -1087 IL 10 gene polymorphism with severe chronic
periodontitis in Swedish Caucasians. J Clin Periodontol. 2003;30(3):249-
54.

22
[43] Mellati E, Arab HR, Tavakkol-Afshari J, Ebadian AR, Radvar M. Analysis
of -1082 IL-10 gene polymorphism in Iranian patients with generalized
aggressive periodontitis. Med Sci Monit. 2007;13(11):CR510-514.
[44] Donati M, Liljenberg B, Padyukov L, Berglundh T. Local expression of
interleukin-10 and mCD14 in relation to the -1087 IL-10 and -159 CD14
gene polymorphisms in chronic periodontitis. J Periodontol.
2008;79(3):517-24.
[45] Larsson L, Thorbert-Mros S, Rymo L, Berglundh T. Interleukin-10
genotypes of the -1087 single nucleotide polymorphism influence sp1
expression in periodontitis lesions. J Periodontol. 2011;82(9):1376-82.
[46] Scarel-Caminaga RM, Trevilatto PC, Souza AP, Brito RB, Camargo LE,
Line SR. Interleukin 10 gene promoter polymorphisms are associated with
chronic periodontitis. J Clin Periodontol. 2004;31(6):443-8.
[47] Sumer AP, Kara N, Keles GC, Gunes S, Koprulu H, Bagci H. Association
of interleukin-10 gene polymorphisms with severe generalized chronic
periodontitis. J Periodontol. 2007;78(3):493-7.
[48] Claudino M, Trombone AP, Cardoso CR, Ferreira SB Jr, Martins W Jr,
Assis GF, Santos CF, Trevilatto PC, Campanelli AP, Silva JS, Garlet GP.
The broad effects of the functional IL-10 promoter-592 polymorphism:
modulation of IL-10, TIMP-3, and OPG expression and their association
with periodontal disease outcome. J Leukoc Biol. 2008;84(6):1565-73.

23
[49] Yamazaki K, Tabeta K, Nakajima T, Ohsawa Y, Ueki K, Itoh H, Yoshie H.
Interleukin-10 gene promoter polymorphism in Japanese patients with
adult and early-onset periodontitis. J Clin Periodontol. 2001;28(9):828-32.
[50] Reichert S, Machulla HK, Klapproth J, Zimmermann U, Reichert Y, Gläser
CH, Schaller HG, Stein J, Schulz S. The interleukin-10 promoter haplotype
ATA is a putative risk factor for aggressive periodontitis. J Periodontal
Res. 2008;43(1):40-7.
[51] Cullinan MP, Westerman B, Hamlet SM, Palmer JE, Faddy MJ, Seymour
GJ, Middleton PG, Taylor JJ. Progression of periodontal disease and
interleukin-10 gene polymorphism. J Periodontal Res. 2008;43(3):328-33.
[52] Hu KF, Huang KC, Ho YP, Lin YC, Ho KY, Wu YM, Yang YH, Tsai CC.
Interleukin-10 (-592 C/A) and interleukin-12B (+16974 A/C) gene
polymorphisms and the interleukin-10 ATA haplotype are associated with
periodontitis in a Taiwanese population. J Periodontal Res.
2009;44(3):378-85.
[53] Holm S. A simple sequentially rejective Bonferroni test procedure. Scand J
Statistics 1979; 6: 65-70.

24
Table 1. Demographic and periodontal findings of the Macedonian study
population.
Chronic periodontitis
(n = 111) Control group
(n = 299) P
Female (%) 41.90 54.60 NS Male (%) 58.10 46.40 NS Age, year (mean ± SD) 38.97 ± 10.12 35.20 ± 9.90 NS Loe-Silnes Index , GI (mean ± SD) 2.38 ± 0.67 0.5 ± 0 <0.001BOP, % (mean ± SD) 82.52 ± 8.14 6.8 ± 6.4 <0.001CAL (mean ± SD) 5.18 ± 0.716 1.8 ± 0.3 <0.001
SD, standard deviation; n, number of participants; NS, non significant; BOP, bleeding on probing; CAL, Clinical attachment loss.

25
Table 2. Observed vs. expected cytokine genotypes for each IL10 -1082, IL10 -819 and IL10 -592 polymorphisms, Hardy Weinberg proportions (HWP), and Guo and Thompson Hardy Weinberg Output (GTHWO) in Macedonian population.
Polymorphism Genotype Observed number
Observed frequency
Expected number
p-value HWP p-value
GTHWO p-value
Control (n=299)
IL10 -1082 A:A A:G G:G
70 212 17
0.234 0.709 0.057
103.6 144.8
50.6
0.001* <0.001* <0.001*
<0.001* <0.001*
IL10 -819 C:C C:T T:T
155 125 19
0.518 0.418 0.064
158.2 118.6
22.2
0.798 0.555 0.495
0.348 0.391
IL10 -592 A:A A:C C:C
28 117 154
0.094 0.391 0.515
25.0 123.0 151.0
0.552 0.592 0.809
0.403 0.404
Periodontitis (n=111)
IL10 -1082 A:A A:G G:G
34 62 15
0.306 0.559 0.135
38.1 53.9 19.1
0.510 0.268 0.352
0.112 0.171
IL10 -819 C:C C:T T:T
64 43
4
0.577 0.387 0.036
65.9 39.3 5.9
0.819 0.553 0.443
0.319 0.428
IL10 -592 A:A A:C C:C
62 45
4
0.559 0.405 0.036
64.3 40.3 6.3
0.355 0.464 0.772
0.224 0.302

26
Table 3. Distribution of allele and genotype polymorphisms of the IL-10 -1082, IL10 -819 and IL10 -592 in Macedonian population patients with periodontal disease, compared to control.
Periodontitis Control Polymorphism
Allele or Genotype N F (%) N
F (%)
OR Wald
95% CI Pearson's
P-value
A 130 0.586 352 0.589IL10 -1082
G 92 0.414 246 0.4110.987
0.722-1.350
1.000
C 171 0.770 435 0.727IL10 -819
T 51 0.230 163 0.2731.256
0.876-1.802
0.214
A 53 0.239 173 0.289IL10 -590
C 169 0.761 425 0.7110.770
0.540-1.099
0.150
A:A 34 30.6 70 23.4 1.4440.890-2.344
0.135
A:G 62 55.9 212 70.9 0.5190.331-0.814
0.004* IL10 -1082
G:G 15 13.5 17 5.7 2.5921.247-5.389
0.009*
C:C 64 57.7 155 51.8 1.2650.815-1.963
0.294
C:T 43 38.7 125 41.8 0.8800.564-1.375
0.575 IL10 -819
T:T 4 3.6 19 6.4 & & &
A:A 4 3.6 28 9.4 & & &
A:C 45 40.5 117 39.1 1.0600.680-1.654
0.795 IL10 -590
C:C 62 55.9 154 51.5 1.1910.769-1.846
0.433
N = number of alleles or genotypes; F = frequency of alleles or genotypes; OR,
Odds Ratio; CI, confidence interval; *, statistically significant after Bonferroni
adjustment (p-value x number of alleles or genotypes) < 0.05; &, cannot be
calculated because expected <5, χ2 test.
27
Table 4. Distribution of haplotype polymorphisms at the IL-10 -1082, IL10 -819 and IL10 -592 in Macedonian population patients with periodontal disease, compared to control.
N = number of haplotypes; F = frequency of haplotypes; OR, Odds Ratio; CI,
confidence interval; &, cannot be calculated because expected <5, χ2 test.
Periodontitis Control Haplotype
N F N F OR
Wald
95% CI
Pearson's
P-value
GCC 91
0.410 246
0.411
0.994 0.727-1.360
1.000
ACC 72
0.324 177
0.260
1.142 0.820-1.590
0.433
ATA 46
0.207 161
0.269
0.704 0.486-1.022
0.064
ACA 7
0.032 12
0.020
1.560 0.618-4.091
0.332
ATC 5
0.023 2
0.003
& & &
GCA 1
0.005 0 0
& & &

28
Table 5. Percentage of diplotypes (haplo-zygotes) of polymorphisms of the IL10 -1082, IL10 -819 and IL10 -592 in Macedonian population patients with periodontal disease, compared to control.
Periodontitis Control Diplotype
N F (%) N F (%)
OR Wald
95% CI Pearson's
P-value
ACC:ACC 10 9.0 21 7.0 1.311 0.597-2.879 0.499 ACC:ATA 17 15.3 21 7.0 0.394 1.212-4.730 0.010 ACC:GCC 34 30.6 114 38.1 0.716 0.450-1.142 0.160 ATA:ATA 3 2.7 19 6.4 0.409 0.119-1.411 0.144 ATA:GCC 20 18.0 93 31.1 0.487 0.283-0.837 0.008 GCC:GCC 15 13.5 17 5.7 2.592 1.247-5.389 0.008 GCC:ACA 5 4.5 3 1.0 & & & ATC:GCC 2 1.8 2 0.7 & & & ACA:ATA 1 0.9 9 3.0 & & & ATC:ACC 1 0.9 0 0 & & & ATC:ATA 1 0.9 0 0 & & &
GCA:ATA 1 0.9 0 0 & & &
ATC:ACA 1 0.9 0 0 & & &
N = number of diplotypes; F = frequency of diplotypes; OR, Odds Ratio; CI,
confidence interval; &, cannot be calculated because expected <5, χ2 test.




















