Continuous 500,000Year Climate Record from Vein Calcite in Devils Hole, Nevada
Upload
independentCategory
view
2download
0
This article was published in an Elsevier journal. The attached copyis furnished to the author for non-commercial research and
education use, including for instruction at the author’s institution,sharing with colleagues and providing to institution administration.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Vein graft anastomoses with magnets*,**
Christoph Heitmann a, Farah N. Khan a, Detlev Erdmann a,Kevin C. Olbrich a, A. Adam Sharkawy b, Bruce Klitzman a,*
a Kenan Plastic Surgery Research Laboratories and Biomedical Engineering, Duke University Medical Center,Circuit Dr, Research Park 4, Box 3906, Durham NC 27710, USAb Ventrica, Inc., 5055 Brandin Ct, Fremont, CA 94538,USA
Received 3 March 2006; accepted 4 October 2006
KEYWORDSReconstructivesurgery;Sutureless;Dog
Summary Background: Performing vascular anastomoses requires complete circumferentialaccess and is time-consuming and technically challenging. The purpose of our study was to as-sess a sutureless magnetic device for anastomosing vein grafts.Methods and results: Oval magnets with a lumen were placed in six male foxhounds. The fem-oral artery was ligated and an 8 cm length of femoral vein was harvested and reversed. Aftera 4 mm venotomy or arteriotomy, one magnet was inserted into each vessel lumen and a secondmagnet was placed outside the vessel but aligned directly over the intraluminal magnet, form-ing a magnetic port in each vessel. The graft and target vessels were then allowed to self-alignand seal, creating a side-to-side anastomosis. Patency was confirmed with duplex Doppler ul-trasound scans after 6 and 13 weeks and during explantation after 14 weeks. At that time, thecontralateral femoral vein was harvested and an acute graft was created as a control. Macro-scopically there was no sign of stenoses or aneurysms. After explant, saline was perfusedthrough all grafts and the hydrodynamic resistance was quantified. There was no significantdifference in resistance between the acute and 14-week grafts indicating stenosis. Microscopicexamination of 14-week anastomoses showed that all blood-contacting surfaces were well-endothelialised.Conclusions: The magnetic vascular coupler allowed sutureless anastomoses between bloodarteries and veins. This device might prove useful for anastomosis of large and small vessels,as well as for anastomosis or approximation of non-vascular structures such as peripheralnerves, fallopian tubes or ureters.ª 2007 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
* Ventrica was acquired by Medtronic, Inc., which now controls the rights to this technology.** Some data were presented at the Plastic Surgery Research Council in Las Vegas, April, 2003 and some at the Second World Society ofReconstructive Microsurgery, Heidelberg, Germany, June 2003, where it received the ‘Best Basic Science’ paper award.
* Corresponding author. Tel.: þ1 919 684 3929.E-mail address: [email protected] (B. Klitzman).
1748-6815/$-seefrontmatterª2007BritishAssociationofPlastic,ReconstructiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.doi:10.1016/j.bjps.2006.10.017
Journal of Plastic, Reconstructive & Aesthetic Surgery (2007) 60, 1296e1301
Author's personal copy
Through the development and refinement of microsurgicalinstruments, sutures, needles, and optical magnification,the vascular anastomosis as envisioned 100 years ago hasbecome a surgical reality.1e3 Yet there continue to bedrawbacks in performing sutured vascular anastomoses forreconstructive surgery since the procedure demands exten-sive training if high patency rates are to be achieved.4 Con-sequently, the search for new methods that result in fasterand easier vascular anastomoses have included microclips,a pre-armed device, and ring couplers.5e8
Using a magnetic vascular positioning device, we as-sessed sutureless vascular anastomoses. The basis for thisassessment is our group’s recent report on the feasibility ofperforming an arteriovenous fistula using magnets.9 Themodel presented has a limited number of surgical applica-tions. Thus this report depicts a more clinically relevantmodel, namely vein grafts for plastic and reconstructivesurgeons. This model creates a vein graft that is function-ally two end-to-end anastomoses. Additionally, the veingraft model differs substantially from the fistula in its lowerblood flow, greater risk of occlusion, and the presence ofboth proximal and distal anastomoses The two specific con-cerns during the investigation of this model were that: (1)the direct contact between the blood and the magnetmay cause thrombosis, particularly with lower blood flowthan the fistula model, and (2) the foreign body responsemay cause unacceptable intimal or adventitial hyperplasialeading to a narrowing of the anastomoses. Other groupshave demonstrated the use of identical magnets for per-forming anastomoses in coronary vessels. Thus, the purposeof this study was to assess the feasibility of using the mag-nets for anastomoses in a reconstructive surgical model ofa vein graft.
Methods
Animal protocol
This protocol was approved by the Institutional Animal Careand Use Committee of Duke University. Six male foxhounds(approximately 25 kg) received 325 mg clopidogrel and325 mg aspirin at least two days preoperatively. Then theanimals received daily 75 mg of clopidogrel and 325 mg ofaspirin until the day of operation. On the day of surgery,no antiplatelet medications were received by the animaluntil postoperative recovery. For the surgery, they had anantecubital vein cannulated and were intubated and anaes-thetised with 1.5e2.5% isoflurane in oxygen. With the ani-mal in a supine position, the right groin and medial thighwere shaved, prepped with povidone/iodine, and drapedwith sterile towels. Aseptic surgical technique was used.Lactated Ringer’s solution (400e500 ml) was administeredintraoperatively. The common femoral artery (approxi-mately 4 mm initial external diameter) and vein (approxi-mately 6 mm diameter) were exposed through a 10 cmlongitudinal incision and isolated using loupe magnification.
The femoral artery was occluded temporarily withatraumatic clamps, with proximal and distal clamps sepa-rated by approximately 7 cm. One longitudinal arteriotomy(4 mm long) was performed approximately 6 mm distal tothe proximal clamp and one 6 mm proximal to the distal
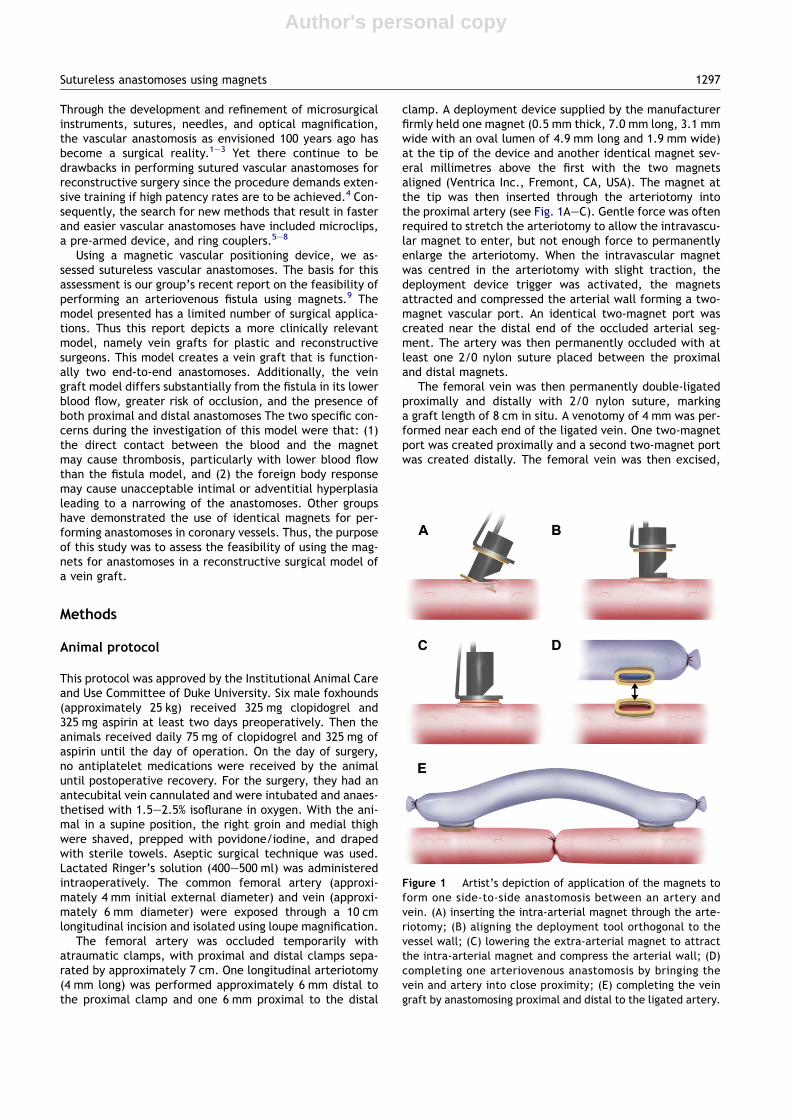
clamp. A deployment device supplied by the manufacturerfirmly held one magnet (0.5 mm thick, 7.0 mm long, 3.1 mmwide with an oval lumen of 4.9 mm long and 1.9 mm wide)at the tip of the device and another identical magnet sev-eral millimetres above the first with the two magnetsaligned (Ventrica Inc., Fremont, CA, USA). The magnet atthe tip was then inserted through the arteriotomy intothe proximal artery (see Fig. 1AeC). Gentle force was oftenrequired to stretch the arteriotomy to allow the intravascu-lar magnet to enter, but not enough force to permanentlyenlarge the arteriotomy. When the intravascular magnetwas centred in the arteriotomy with slight traction, thedeployment device trigger was activated, the magnetsattracted and compressed the arterial wall forming a two-magnet vascular port. An identical two-magnet port wascreated near the distal end of the occluded arterial seg-ment. The artery was then permanently occluded with atleast one 2/0 nylon suture placed between the proximaland distal magnets.
The femoral vein was then permanently double-ligatedproximally and distally with 2/0 nylon suture, markinga graft length of 8 cm in situ. A venotomy of 4 mm was per-formed near each end of the ligated vein. One two-magnetport was created proximally and a second two-magnet portwas created distally. The femoral vein was then excised,
Figure 1 Artist’s depiction of application of the magnets toform one side-to-side anastomosis between an artery andvein. (A) inserting the intra-arterial magnet through the arte-riotomy; (B) aligning the deployment tool orthogonal to thevessel wall; (C) lowering the extra-arterial magnet to attractthe intra-arterial magnet and compress the arterial wall; (D)completing one arteriovenous anastomosis by bringing thevein and artery into close proximity; (E) completing the veingraft by anastomosing proximal and distal to the ligated artery.
Sutureless anastomoses using magnets 1297

Author's personal copy
reversed and brought into proximity of the femoral arteryto allow self-alignment of the magnetic ports, completingboth of the anastomoses (Fig. 2).
Finally, the arterial vessel clamps were released torestore blood flow to the limb through the bypass graft.The wounds were closed using 3/0 absorbable suture forthe muscle and subcutaneous layers and 3/0 nylon suturefor the cutaneous layer.
Postoperatively, the animals were allowed unrestrictedactivity in individual runs and again received 75 mg clopi-dogrel and 325 mg aspirin daily. One animal had a seromaand was placed on prophylactic antibiotic for seven daysuntil the seroma resolved.
The patency of each graft was assessed after 6 weeksand 13 weeks using a colour duplex Doppler scanner (Philips5500, 7 MegaHertz linear probe). Video waveform record-ings were made of each graft.
Explant
After 14 weeks, animals were again anaesthetised usingisoflurane. All grafts were surgically exposed and cannu-lated proximally and then rinsed with Ringer’s solution. Atthe same time, the initial operative procedure was re-peated on the contralateral hind limb of three dogs. Allgrafts (acute and 14 week) were then gently flushed withsaline and harvested.
Resistance measurement
The resistance measurements of all grafts were performedusing a roller pump (Masterflex, Cole-Parmer InstrumentCo., Chicago, IL, USA) to drive saline at 90 ml/min throughpolyethylene tubing (PE240; inner diameter 1.67 mm). Apressure transducer (Fiber Optic Sensor Technologies,Inc., Ann Arbor, MI, USA) was connected via a stopcock tothe inflow tubing and measured the pressure with no graftat 90 ml/min. The femoral artery was then cannulatedproximally with the PE240 tubing and the saline exitedthrough the distal artery. The exiting stream did not raise
more than approxiamately 1 cm above the vessel endwhen turned upright, indicating a pressure of less than1 mmHg in the vein.
The hydrodynamic resistance of the entire graft wascalculated by dividing the inflow pressure by the flow rate.Then, the vein wall opposite the proximal anastomosis waswidely resected to allow saline to exit immediately afterpassing through the proximal anastomosis. Therefore, thepressure readings divided by the flow rate, reflected theresistance of only the proximal anastomosis. The vein wallopposite the distal anastomosis was then resected and thePE240 tubing was inserted into the distal artery. Thepressure readings were repeated using retrograde flow tothen estimate distal anastomotic resistance.
Histology
Following the resistance measurement all specimens wereimmersed in 10% buffered formalin. For histologic evalua-tion of the anastomoses, the magnets were removed usingan operating microscope for microdissection in such a wayas to disturb the anastomosis as little as possible, partic-ularly the luminal wall. Then, the specimens were embed-ded in paraffin and 5-mm-thick sections were stained withhematoxylin-eosin. For evaluation of the vessel wall thick-ness, cross sections were obtained as follows: (1) proximalartery proximal to the magnets, (2) proximal vein adjacentto the magnets, (3) distal vein adjacent to the magnets,and (4) distal artery distal to the magnets. In the vesselcross sections, the total thickness of the vessel wall wasmeasured at the 0�, 90�, 180� and 270� positions.
Statistics
All data are expressed as means� standard error. Differ-ences between groups were compared using a Student’st-test with a P value of 0.05 or less required for statisticalsignificance.
Results
All six dogs survived the placement of the magnets. Due topretreatment with anti-platelet medication, introperativehomeostasis required more aggressive cautery and vesselligation than usual. Deployment of the magnets was rapidand easy. When the arterial clamps were released, the veindistended considerably (to two to three times normaldiameter) and turbulence could be clearly observedthrough the thin venous wall. One animal developeda seroma that was treated conservatively with antibioticsuntil it resolved. Some animals were ambulating withinhours of recovery, while all animals appeared to havenormal gait after the first several days of recovery andthroughout the study.
All grafts were patented by colour duplex Dopplerscanning at 6 and 13 weeks postoperatively and underdirect observation on the day of sacrifice. At explant,fibrosis made explantation somewhat difficult. The wall ofthe vein graft thickened to completely encompass themagnets and the wall of the cul-de-sac ligated end
Figure 2 Intraoperative photograph of the vein graft afterfinishing both proximal (left) and distal (right) anastomoses.
1298 C. Heitmann et al.

Author's personal copy
retracted so that it appeared as an end-to-side anastomo-sis. The magnets were not visible from the abluminal side,but were clearly visible through the vessel wall whenobserved from the luminal side. There appeared to becomplete endothelialisation of the magnet surface inter-facing with the blood (Fig. 3A, B). There was no apparentinflammatory reaction in the tissue adjacent to the graftand there was no evidence of aneurysm or pseudoaneurysmformation.
Hydrodynamic resistance was not significantly differentbetween the acute and 14 week grafts (Fig. 4), althoughcautious interpretation is warranted since the sample sizewas not large. Individual anastomosis resistance averaged0.119 mmHg min/ml at the proximal end and 0.158 mmHgmin/ml at the distal end of the 14 week grafts and0.114 mmHg min/ml at the proximal and 0.120 mmHg min/ml at the distal ends of the acute grafts. The whole grafthad resistances of 0.216 mmHg min/ml after 14 weeks and0.158 mmHg min/ml acutely.
Histological examination of the anastomoses revealeda continuity of the endothelium, from the arterial vessel
wall through the anastomotic port to the venous vesselwall. The magnets represented only about one-fifth of thevessel wall thickness and were fully integrated into thevessel wall. The tissue was acellular (Fig. 5AeD), whilethere was no sign of compression necrosis and vessel walldegradation at the site of the original vessel walls, thus sug-gesting some pressure effects. There were only a few in-flammatory cells observed, but no evidence of a profoundforeign body reaction, such as foreign body giant cells, orof an ongoing aggressive inflammatory response, such asneutrophils or monocytes.
The medial venous wall of chronic grafts (0.12 mm) wassignificantly thicker than the acute grafts (0.023 mm;Fig. 6). There were no other significant differences inwall thickness between acute and 14 week grafts. The prox-imal and distal vein wall thicknesses were not significantlydifferent. The 14-week arterial wall thicknesses were0.29 mm (proximal) and 0.22 mm (distal). The acute proxi-mal and distal arterial wall thicknesses were both 0.30 mm.
Discussion
Suture and non-suture techniques of vascular anastomoseshave been previously described. Suture methods wereintroduced one Century ago by Abbe (1894), Payr (1900)and Carrel (1902).10e12 However, before Jacobsen andSuarez introduced the operative microscope, these methodswere not widely used.3 The microscope enhanced the out-come of hand-sewn anastomoses performed with suturesattached to needles.10 Today, vascular, cardiothoracic,neurological, orthopaedic, otolaryngology, and plastic andreconstructive surgeons perform vascular anastomoses.
Independent of any surgical Specialty, the standard forthe performance of vascular and microvascular anastomo-ses is manual suturing, even though it continues to posesome technical challenges.4 Thus, these risks provoke a de-sire to improve technique segue advances such as minimallyinvasive procedures.11,12 For this reason, many surgical spe-cialties have attempted to develop non-suture vascularanastomoses.13e16 Some of them include mechanicaldevices, which use the methods of stapling, clipping andcoupling. Recently, tissue bonding with glueing or laser weld-ing has been introduced. Even though other devices exist, thesurgical community has not embraced any method as beingclearly better than manual suturing. Ring couplers, biocom-patible glues and lasers are a few examples of anastomotic
Figure 3 (A, B) Macro photographs of the 14 week explantedanastomosis showing the gold-coloured magnets. The shinymottled appearance is typical of endothelial coverage. (A)View from the lumen of the vein looking through the anastomo-sis to the artery. Note some ingrowth of tissue from the ‘toe’and ‘heel’, but far less from the sides of the magnets. (B)Oblique view showing the stack of four magnets that compriseeach anastomosis.
Figure 4 Hydrodynamic resistances after acute or chronicimplantation for proximal anastomoses alone, distal anastomo-ses alone, and the whole graft.
Sutureless anastomoses using magnets 1299

Author's personal copy
techniques that the surgical community has not yetembraced over manual suturing.5,17e21 Ring couplers havegained limited acceptance in clinical applications due totheir requirements of a specific size match between graftand target vessels, a relatively long, free segment of vesselfor eversion, and a somewhat exclusive suitability for end-
to-end anastomoses In addition, biocompatible glues areemployed widely in medicine, yet they are not widely ac-cepted for vascular anastomoses.21,22 Lastly, laser weldinghas been used to assist vascular anastomoses with goodpatency, but pseudoaneurysm formation and anastomoticrupture has limited its clinical acceptance.4,17e20,23
One procedure, not mentioned above, is a techniquethat Obora first presented: the use of magnets for anasto-moses in dogs and rats in 1978.24 A very different designusing magnets is presented here for performing suturelessanastomoses. With this design, there is no need for broadsurgical exposure of the vessels, freeing of the surroundingtissues or eversion of the vessel walls. Once the arterial andvenous ports are firmly in place, artery and vein are broughtin proximity and the side-to-side vascular anastomosis iscompleted through self-alignment of the magnets. In a re-cent report from our group, the feasibility of using thesemagnets to create an AeV fistula was demonstrated ina high-flow model.9
The follow up at 14 weeks in our study did not revealanastomotic stenoses or aneurysms. Although there wassome reduction in the long axis diameter of the lumen ofthe magnets (heel-to-toe; see Fig. 3), the short axis was rel-atively unaffected. As expected, this slight long-axis
Figure 5 Micrographs of the anastomoses, stained with hematoxylin & eosin. (A) M1 to M4 indicates the locations of the fourmagnet struts. Note that the magnets are fully incorporated into the remodelled vessel wall (1.25� objective). (B) Higher magni-fication view of the M1 magnet that had been initially placed inside the femoral vein and has now become fully endothelialisedwithin 14 weeks (4� objective). (C) Endothelium covering the luminal side of the magnet (10� objective). (D) Acellular tissuein between magnets with no apparent necrosis (10� objective).
Figure 6 Comparison of total vessel wall thickness of chronic(solid bars) and acute (open bars) arteries and vein grafts.
1300 C. Heitmann et al.

Author's personal copy
narrowing did not increase the resistance measurably be-tween the acute and 14 week explants. Microscopically,all intraluminal magnets were endothelialised and onlya small inflammatory or foreign body reaction was ob-served. We were concerned that the dramatic turbulencethat was grossly observed at the anastomoses would tendto activate platelets and increase thromobosis. Althoughno thrombotic occlusion was observed in this study, therecould still have been some platelet activation that couldhave encouraged cell proliferation and structural changesnear the anastomoses or led to microemboli impinging onthe microvessels downstream.
In summary, the simplicity of the magnet technique andits high patency rate encourages further studies in vesselsof different sizes, locations and blood flows. The magnet-based anastomotic device may have substantial benefit inminimally invasive surgery, such as vascular surgery, traumasurgery and reconstructive surgery.
References
1. Cobbett JR. Microvascular surgery. Surg Clin North Am 1967;47:521e42.
2. Smith JW. Microsurgery: review of the literature and discussionof microtechniques. Plast Reconstr Surg 1966;37:227e45.
3. Jacoboson HH, Miller DB, Suarez E. Microvascular surgery: a newhorizon in coronary artery surgery. Circulation 1960;22:767.
4. Werker PM, Kon M. Review of facilitated approaches to vascu-lar anastomosis surgery. Ann Thorac Surg 1997;63(Suppl. 6):S122e7.
5. Ahn CY, Shaw WW, Berns S, et al. Clinical experience with the3M microvascular coupling anastomotic device in 100 free-tissue transfers. Plast Reconstr Surg 1994;93:1481e4.
6. Heijmen RH, Hinchcliffe P, Borst C, et al. A novel one-shotanastomotic stapler prototype for coronary bypass graftingon the beating heart: feasibility in the pig. J Thorac CardiovascSurg 1999;117:117e25.
7. Kirsch WM, Zhu YH, Hardesty RA, et al. A new method for mi-crovascular anastomosis: report of experimental and clinicalresearch. Am Surg 1992;58:722e7.
8. Nataf P, Hinchcliffe P, Manzo S, et al. Facilitated vascularanastomoses: the one-shot device. Ann Thorac Surg 1998;66:1041e4.
9. Erdmann D, Sweis R, Heitmann C, et al. Side-to-side suturelessvascular anastomosis with magnets. J Vasc Surg 2004;40:505e11.
10. Abbe R. The surgery of the hand. NY Med J 1894;59:33e40.11. Carrel A. La technique operatoire des anastomoses vascularies
et la transplatation des visceres. Lyon Med 1902;89:859e63.12. Payr E. Beitrag zur Technik de Blugefass-und Nervennaht nebst
Mitteilungen uber die Verwendung eines resorbierbaren Metal-les in der Chirurgie. Arch Klin Chir 1900;62:67e93.
13. De Lorenzi F, van der Hulst RR, Boeckx WD. VCS auto suturestapled microvascular anastomoses in lower leg free flaps.Plast Reconstr Surg 2002;109:2023e30.
14. Solem JO, Boumzebra D, Al-Buraiki J, et al. Evaluation of a newdevice for quick sutureless coronary artery anastomosis in sur-viving sheep. Eur J Cardiothorac Surg 2000;17:312e8.
15. Zeebregts C, van den Dungen J, Buikema H, et al. Preservationof endothelial integrity and function in experimental vascularanastomosis with non-penetrating clips. Br J Surg 2001;88:1201e8.
16. Zegdi R, Lajos P, Ponzio O, et al. End-to-side anastomosisusing a new sutureless vascular prosthesis. Asaio J 2001;47:329e32.
17. McCarthy WJ, LoCicero J, Hartz RS, et al. Patency of laser-assisted anastomoses in small vessels: one-year follow-up.Surgery 1987;102:319e26.
18. Okada M, Shimizu K, Ikuta H, et al. An alternative method ofvascular anastomosis by laser: experimental and clinical study.Lasers Surg Med 1987;7:240e8.
19. Quigley MR, Bailes JE, Kwaan HC, et al. Aneurysm formationafter low power carbon dioxide laser-assisted vascular anasto-mosis. Neurosurgery 1986;18:292e9.
20. Dumanian GA, Dascombe W, Hong C, et al. A new photopoly-merizable blood vessel glue that seals human vessel anastomo-ses without augmenting thrombogenicity. Plast Reconstr Surg1995;95:901e7.
21. Nakayama K, Tamiya T, Yamamoto K, et al. A simple new appa-ratus for small vessel anastomosisi (free autograft of the sig-moid included). Surgery 1962;52:918e31.
22. Li YN, Wood MB. End-to-side-anastomosis in the dog using the3M precise microvascular anastomotic system: a comparativestudy. J Reconstr Microsurg 1991;7:345e50 [discussion 351e2].
23. Lerner R, Binur NS. Current status of surgical adhesives. J SurgRes 1990;48:165e81.
24. Obora Y, Tamaki N, Matsumoto S. Nonsuture microvascularanastomosis using magnet rings: preliminary report. SurgNeurol 1978;9:117e20.
Sutureless anastomoses using magnets 1301
Copyright © 2022 FDOKUMEN