
Impact on Stroke Subtype Diagnosis of Early Diffusion-Weighted Magnetic Resonance Imaging and...
10
Lance J. Lee, Chelsea S. Kidwell, Jeffry Alger, Sidney Starkman and Jeffrey L. Saver Imaging and Magnetic Resonance Angiography Impact on Stroke Subtype Diagnosis of Early Diffusion-Weighted Magnetic Resonance Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2000 American Heart Association, Inc. All rights reserved. is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Stroke doi: 10.1161/01.STR.31.5.1081 2000;31:1081-1089 Stroke. http://stroke.ahajournals.org/content/31/5/1081 World Wide Web at: The online version of this article, along with updated information and services, is located on the http://stroke.ahajournals.org//subscriptions/ is online at: Stroke Information about subscribing to Subscriptions: http://www.lww.com/reprints Information about reprints can be found online at: Reprints: document. Permissions and Rights Question and Answer process is available in the Request Permissions in the middle column of the Web page under Services. Further information about this Once the online version of the published article for which permission is being requested is located, click can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Stroke in Requests for permissions to reproduce figures, tables, or portions of articles originally published Permissions: by guest on November 21, 2014 http://stroke.ahajournals.org/ Downloaded from by guest on November 21, 2014 http://stroke.ahajournals.org/ Downloaded from
Transcript of Impact on Stroke Subtype Diagnosis of Early Diffusion-Weighted Magnetic Resonance Imaging and...

Lance J. Lee, Chelsea S. Kidwell, Jeffry Alger, Sidney Starkman and Jeffrey L. SaverImaging and Magnetic Resonance Angiography
Impact on Stroke Subtype Diagnosis of Early Diffusion-Weighted Magnetic Resonance
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2000 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.31.5.1081
2000;31:1081-1089Stroke.
http://stroke.ahajournals.org/content/31/5/1081World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on November 21, 2014http://stroke.ahajournals.org/Downloaded from by guest on November 21, 2014http://stroke.ahajournals.org/Downloaded from

Impact on Stroke Subtype Diagnosis of EarlyDiffusion-Weighted Magnetic Resonance Imaging and
Magnetic Resonance AngiographyLance J. Lee, MD; Chelsea S. Kidwell, MD; Jeffry Alger, PhD;
Sidney Starkman, MD; Jeffrey L. Saver, MD
Background and Purpose—The purpose of the present study was to assess the diagnostic usefulness of earlydiffusion-weighted MRI (DWI) and MR angiography (MRA) in patients with ischemic stroke. Past approaches to strokediagnosis required a series of diagnostic tests over several days of hospitalization. New magnetic resonancemethodologies that include DWI and MRA may allow more rapid characterization of stroke pathophysiology. However,no previous study has assessed the impact on formal stroke subtype diagnosis of early imaging with DWI/MRA.
Methods—We analyzed 46 consecutive patients with acute ischemic stroke who underwent DWI/MRA within 24 hours ofadmission. Initial diagnoses were rendered with use of the 2 most widely used formal stroke subtype classificationschemes, the TOAST and the Oxfordshire methods, which were applied to patients after CT/conventional MRI butbefore DWI/MRA. Modified TOAST and Oxfordshire diagnoses were then rendered based on the results of day 1 DWI,MRA, and DWI plus MRA. Final TOAST/Oxfordshire diagnoses at discharge were taken as the gold standard.
Results—Compared with final diagnoses, pre-MRI TOAST diagnoses matched final diagnoses in 48%, improving to 83%after DWI alone, 56% after MRA alone, and 94% after DWI plus MRA. For the TOAST diagnostic subtypes oflarge-vessel atherothromboembolism and small-vessel disease, pre-MRI diagnoses matched final diagnoses in 56% and35% of patients, respectively, improving to 89% and 100% after DWI/MRA. Pre-MRI Oxfordshire diagnoses matchedfinal diagnoses in 67% of patients, improving to 100% after DWI.
Conclusions—The use of DWI/MRA within 24 hours of hospitalization substantially improves the accuracy of thediagnosis of early ischemic stroke subtype. When initial management and clinical trial eligibility decisions areinfluenced by stroke subtype, day 1 multimodal MRI is advantageous as a guide to therapy.(Stroke.2000;31:1081-1089.)
Key Words: angiography, magnetic resonancen magnetic resonance imaging, diffusion-weightedn stroke classification
The diagnosis of ischemic stroke subtype in the first fewhours after hospital arrival has traditionally been per-
formed through educated guesswork. Deductions regardingneuroanatomic localization, involved vascular territory, andetiologic vascular mechanism are reached on the basis ofclues in the clinical history and the pattern of deficits onphysical examination. The contribution of imaging has gen-erally been confined to the exclusion of primary intracerebralhemorrhage with a negative early CT scan. This conventionalapproach has substantial accuracy limitations, even whenformal stroke subtype classification criteria are used. Forexample, the TOAST trialists reported that initial subtype
diagnoses matched final diagnoses in only 62% of cases.1
Other investigators have also found accuracy in the range of50% to 70%.2–5
Newer MRI techniques may assist early stroke subtypediagnosis. Diffusion-weighted MRI (DWI) can render ische-mic fields visible within minutes of ischemia onset in animalmodels, and clinical studies have demonstrated the efficacy ofDWI in humans in early visualization of the site and extent ofischemia.6–15 However, the impact of DWI findings on earlyischemic stroke subtype diagnosis has not been systemati-cally investigated. Magnetic resonance angiography (MRA)allows rapid characterization of the cervical and cephalic
Received December 6, 1999; final revision received February 21, 1999; accepted February 21, 2000.From the University of California Los Angeles Stroke Center (L.J.L., C.S.K., J.A., S.S., J.L.S.) and the Departments of Neurology (L.J.L., C.S.K., S.S.,
J.L.S.), Radiology (J.A.), and Emergency Medicine (S.S.), University of California Los Angeles Medical Center.This work was presented in preliminary form at the 50th meeting of the American Academy of Neurology, Minneapolis, Minn, April 1998.Correspondence to Jeffrey L. Saver, MD, UCLA, Reed Neurologic Research Center, 710 Westwood Plaza, Los Angeles, CA 90095. E-mail
[email protected] supplemental figure delineating a formal algorithm to render the baseline TOAST diagnosis (based on clinical examination and CT scan) has been
filed with the National Auxiliary Publications Service (NAPS) and is available for a nominal fee by writing to ASIS/NAPS, c/o Microfiche Publications,Burrows Systems, 248 Hempstead Turnpike, West Hempstead, NY 11552-2664 (516-481-2300).
© 2000 American Heart Association, Inc.
Stroke is available at http://www.strokeaha.org
1081 by guest on November 21, 2014http://stroke.ahajournals.org/Downloaded from

large vessels. MRA detects and grades cervical internalcarotid stenosis with an accuracy of 85% to 96% comparedwith digital subtraction angiography.16–21 With the use ofMRA, stenoses and occlusions of intracranial vessels areidentified with 80% to 100% sensitivity and specificitycompared with catheter angiography.22–25 However, studiesof MRA have generally been performed days after strokeoccurrence rather than in the acute setting. In addition, priorinvestigations have generally focused on MRA/angiographycorrelations and have not systematically investigated theimpact of MRA on stroke subtype diagnosis.
Together, DWI and cervical and cephalic MRA have thepotential to identify the site of brain ischemia and the site oflarge-vessel disease within the first hours after stroke onset
and hospital admission, providing detailed pathophysiologi-cal information that may improve the accuracy of strokesubtype diagnoses rendered in the acute phase. We thereforeassessed the diagnostic usefulness of combined DWI andMRA obtained within 24 hours of admission in acute ische-mic stroke through the use of the 2 most widely used formalmethods for stroke subtype classification: the TOAST andOxfordshire classification criteria.
Subjects and MethodsThe University of California Los Angeles Stroke Center StrokePatient Registry was reviewed to identify all ischemic stroke patientswho underwent intracranial MRA, extracranial MRA, and DWIimaging within 24 hours of admission between January 1, 1997, andMarch 31, 1998.
Figure 1. Algorithm to render modified TOAST stroke subtype diagnosis, with MRA and DWI findings and clinical history and physicalexamination incorporated.
TABLE 1. Final Stroke Subtype Diagnosis and Initial (Before MRA/DWI) TOASTStroke Subtype Diagnosis
InitialDiagnosis(BeforeMRA/DWI)
Final Discharge Diagnosis
LargeVessel Cardioembolic
SmallVessel Others
UnknownCause
No. of InitialTOAST Diagnoses
Large vessel 5 0 1 0 0 6
Cardioembolic 0 2 0 0 0 2
Small vessel 1 0 8 0 2 11
Others 0 0 0 1 0 1
Unknowncause
3 3 14 0 6 26
Total 9 5 23 1 8 46
1082 Stroke May 2000
by guest on November 21, 2014http://stroke.ahajournals.org/Downloaded from

Ischemic stroke subtype diagnoses were rendered retrospectivelyat 5 possible time points: (1) immediately before DWI/MRA imaging(based on history, physical examination, and CT or conventionalMRI studies), (2) immediately after DWI imaging (without MRAdata), (3) immediately after MRA imaging (without DWI data), (4)immediately after combined DWI/MRA, and (5) at hospital dis-charge (final diagnosis).
MRI was performed with a 1.5-T Siemens Vision MR systemequipped with echo planar imaging data acquisition capabilitydesigned to obtain rapid diffusion images. Diffusion imaging wasperformed with a slice thickness of 7 mm with no interslice gap and2 levels of diffusion sensitization (b50, 1000 s/mm2). The higherlevel of diffusion sensitization was replicated in each of the 3orthogonal, principal gradient directions (read, slice select, phaseencode [X,Y, Z] planes), and DWI images were formed from theaverage of these. Extracranial MRA was performed with settingsof TR 25, TE 9, flip angle 35°, images interpolated to 3.0-mmslice thickness, matrix 1923256, field of view 19, and superiorsaturation band. Intracranial MRA was performed with settings ofTR 35, TE 7.2, flip angle 20°, images interpolated to 1.5-mm slicethickness, matrix 2003512, field of view 20, and superiorsaturation band. MRA images were processed with a maximumintensity projection, 3-dimensional time-of-flight technique. CTscans were obtained with 2 General Electric high-speed scannerswith 5-mm slice thickness.
The TOAST classification method has 5 stroke subtype categories:(1) large-vessel atherothromboembolic, (2) cardioembolic, (3) small-vessel, (4) stroke of other determined etiology, and (5) stroke of
undetermined etiology.26 The Oxfordshire classification methodcontains 4 subtypes based on anatomic distribution of infarcts andcorresponding clinical symptoms: (1) lacunar infarcts, (2) totalanterior circulation infarcts, (3) partial anterior infarcts, and (4) pos-terior circulation infarcts.27 Pre-DWI/MRA diagnoses and finaldiagnoses were rendered according to the standard TOAST andOxfordshire methods.26,27 For the DWI and post-MRA TOASTdiagnoses, we created modified TOAST classification criteria thatincorporate MRA alone, DWI alone, and MRA1DWI. For thepost-DWI Oxfordshire diagnoses, we created modified Oxfordshireclassification criteria that incorporate DWI.
The modified TOAST classification differs from the original in thefollowing ways: (1) vascular imaging by MRA was permitted toinfluence diagnosis in the same manner as carotid duplex, (2) DWIimaging of infarct size, location, and topography was permitted toinfluence diagnosis in the same manner as CT or conventional MRIof infarct size, location, and topography, and (3) if there was aconflict between history/physical examination findings and imagingfindings, imaging findings were accepted as decisive (eg, a patientwith a nonclassic lacunar clinical syndrome but a small, deep infarcton DWI and no large-vessel stenosis on MRA was classified ashaving a small-vessel stroke). To make application of the complexTOAST diagnostic method more uniform, we created formal algo-rithmic decision trees to guide diagnostic assignment (Figure 1 andsupplemental figure1). The modified Oxfordshire classification dif-fers from the original in 2 ways: (1) it incorporates DWI or otherparenchymal imaging findings, and (2) if there was a conflictbetween history/physical examination findings and imaging findings,
Figure 2. Impact of early imaging ondiagnosis. Each column represents thepercent of cases (n546) matching finalTOAST subtype diagnosis before andafter MRA, DWI, and combinedMRA/DWI.
TABLE 2. Final Stroke Subtype Diagnosis and TOAST Stroke Subtype DiagnosisAfter MRA/DWI
Initial Diagnosis(AfterMRA/DWI)
Final Discharge Diagnosis
LargeVessel Cardioembolic
SmallVessel Others
UnknownCause
No. of TOASTDiagnoses After
MRA/DWI
Large vessel 8 0 0 0 0 8
Cardioembolic 0 4 0 0 0 4
Small vessel 0 0 23 0 1 24
Others 0 0 0 1 0 1
Unknown cause 1 1 0 0 7 9
Total 9 5 23 1 8 46
Lee et al Impact of Early DWI and MRA on Stroke Subtyping 1083
by guest on November 21, 2014http://stroke.ahajournals.org/Downloaded from

imaging findings were accepted as decisive (eg, a patient with anonclassic lacunar clinical syndrome but a small, deep infarct onDWI was classified as “lacunar infarct-LACI”).
To guide early diagnoses, in addition to CT and conventionalMRI, results were available for all patients from chart medicalhistories and physical examinations, ECGs, chest radiographs, andcardiac enzyme, complete blood cell count, prothrombin time/INR,
partial thromboplastin time, electrolyte, glucose, blood urea nitro-gen, creatinine, and erythrocyte sedimentation rate tests. Finaldiagnoses at discharge also incorporated information from thesubsequent clinical course and additional diagnostic tests, includingVDRL, cholesterol panel, and transthoracic echocardiography for allpatients and transesophageal echocardiography, transcranial Dopp-ler, carotid duplex ultrasound, cerebral angiogram, cerebrospinal
Figure 3. Comparison chart of TOAST stroke subtype diagnoses based on history/examination with CT of head (if not, conventionalMR with T1-, T2-weighted images) findings before MRA/DWI, after MRA alone, after DWI alone, after MRA1DWI, and final diagnosisafter all the work-ups are completed.
1084 Stroke May 2000
by guest on November 21, 2014http://stroke.ahajournals.org/Downloaded from

fluid study, and specialized laboratory (hematologic/serologic/histo-logic) testing in selected patients.
TOAST and Oxfordshire algorithmic diagnoses were rendered by1 neurological reviewer (LL). In cases in which this reviewer judgedthat application of the TOAST and Oxfordshire algorithms was notimmediately straightforward, a second neurological reviewer (JLS)also performed a diagnostic analysis. Any discrepancies between the2 reviewers were settled by consensus discussion. Second reviewswere conducted in'25% of cases. Interrater agreement was.95%.
Diagnosis-related conventional MRI, DWI, and MRA scan infor-mation was obtained in the following manner. Official interpreta-tions by attending neuroradiologists were consulted by the neurolog-ical reviewers, and classification-relevant findings were abstracted.The neurological reviewers also personally examined each patient’sMRI films. There were no instances of disagreement between theformal neuroradiologic reading and the neurological reviewers’ scananalyses. In exceptional instances, the formal neuroradiologic reportdid not address all scan information potentially relevant to strokesubtype classification. In these cases, scan findings were based onthe neurological reviewers’ supplemental interpretation of the scan.
In abstracting information for stroke subtype classification, thereviewers followed a strategy of reviewing data in the order itbecame chronologically available during the hospital course, remain-ing blinded to data acquired later in the hospitalization beforerendering diagnoses at initial time points. In rare instances when datawere filed in charts out of chronological order, reviewers did becomeaware of later acquired data before rendering early diagnoses, butthey explicitly avoided incorporating such later data in following thediagnostic algorithms.
For statistical analysis, pre-DWI/MRA, post-DWI, post-MRA,and post-DWI/MRA diagnoses were cross-tabulated with final diag-noses. Final diagnoses were taken as a gold standard.
ResultsA total of 46 patients (22 men and 24 women) who underwentDWI/MRA within 24 hours of admission of stroke onset wereidentified. Of these, 39 underwent CT scanning before MRI,whereas 7 proceeded directly to MRI. Thirty-eight patients
presented with stroke to the emergency department (ED),whereas 8 patients developed stroke in the hospital.
Of the 38 patients presenting to the ED, 33 patientsunderwent CT scanning of the head. The average time fromED arrival to CT scan was a median of 1.25 hours and a meanof 2.00 hours (range 0.5 to 13 hours). The average time fromED arrival to MRI for the 38 patients was a median of 4.3hours and a mean of 7.7 hours (range 1 to 23 hours). For theentire cohort, the average time from stroke onset to CT was amedian of 10.0 hours and a mean of 21.9 hours (range 0.5 to180 hours). The average time from stroke onset to MRI wasa median of 19.0 hours and a mean of 32.3 hours (range 2 to190.5 hours).
The acute ischemic lesion was visualized in 6 of 39 (15%)patients on CT, 33 of 45 (73%) patients on T2-weighted MRI,and 45 of 46 (98%) on DWI. Multiple acute lesions on DWI(suggesting embolism) were seen in 6 patients (13%). Amongthe 46 patients studied, intracranial MRA visualized stenosesor occlusions in vessels relevant to the areas of ischemia in 7patients (15%), and extracranial MRA visualized relevantstenoses or occlusions in 3 patients (7%).
Data regarding the impact of DWI and MRA imaging ondiagnostic accuracy with the use of TOAST methods are shownin Tables 1 and 2 and Figure 2. Figure 3 illustrates the impact ofserial diagnostic testing in each of the patients in the cohort.Overall, the percent of cases matching final classification im-proved from 48% before DWI or MRA imaging to 56% with theaddition of MRA alone, 83% with the addition of DWI alone,and 94% with the addition of combined DWI and MRA. In thelarge-vessel atherothromboembolic category, pre-MRI diag-noses matched final diagnoses in 56% of patients and improvedto 89% with the addition of MRA alone, 56% with the addition
TABLE 3. Final Oxfordshire Stroke Subtype Diagnosis and Initial OxfordshireDiagnosis (Before MRA/DWI)
Initial OxfordshireDiagnosis(Before DWI)
Final Oxfordshire Diagnosis
TotalAnterior
PartialAnterior Lacunar Posterior
No. of Initial OxfordshireDiagnoses (Before DWI)
Total anterior 3 1 0 0 4
Partial anterior 0 9 5 2 16
Lacunar 0 3 15 1 19
Posterior 0 0 3 4 7
Total 3 13 23 7 46
TABLE 4. Final Oxfordshire Stroke Subtype Diagnosis and Initial OxfordshireDiagnosis (After MRA/DWI)
Initial OxfordshireDiagnosis(After DWI)
Final Oxfordshire Diagnosis
TotalAnterior
PartialAnterior Lacunar Posterior
No. of Initial OxfordshireDiagnoses After DWI
Total anterior 3 0 0 0 3
Partial anterior 0 14 0 0 14
Lacunar 0 0 23 0 23
Posterior 0 0 0 6 6
Total 3 14 23 6 46
Lee et al Impact of Early DWI and MRA on Stroke Subtyping 1085
by guest on November 21, 2014http://stroke.ahajournals.org/Downloaded from
of DWI alone, and 89% with the addition of combined DWI andMRA. In the small-vessel lacunar category, pre-MRI diagnosesmatched final diagnoses in 35% of patients, improving to 35%with the addition of MRA alone, 96% with the addition of DWIalone, and 100% with the addition of combined DWI andMRA. In the cardioembolic category, pre-MRI diagnosesmatched final diagnoses in 40% of cases, changing to 40%with the addition of MRA alone, 80% with the addition of
DWI, and 80% with the addition of combined DWI andMRA.
Data regarding the impact of imaging on Oxfordshireclassification are shown in Tables 3 and 4. The overallpercent of cases classified correctly improved from 67%before DWI to 100% after DWI.
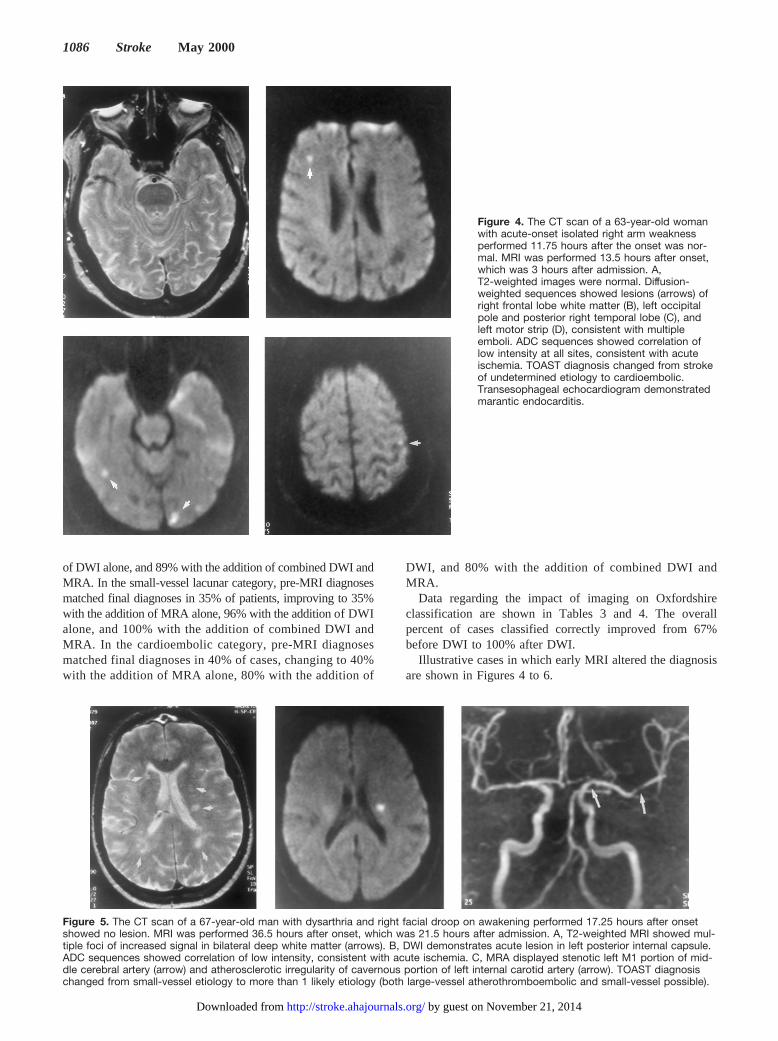
Illustrative cases in which early MRI altered the diagnosisare shown in Figures 4 to 6.
Figure 4. The CT scan of a 63-year-old womanwith acute-onset isolated right arm weaknessperformed 11.75 hours after the onset was nor-mal. MRI was performed 13.5 hours after onset,which was 3 hours after admission. A,T2-weighted images were normal. Diffusion-weighted sequences showed lesions (arrows) ofright frontal lobe white matter (B), left occipitalpole and posterior right temporal lobe (C), andleft motor strip (D), consistent with multipleemboli. ADC sequences showed correlation oflow intensity at all sites, consistent with acuteischemia. TOAST diagnosis changed from strokeof undetermined etiology to cardioembolic.Transesophageal echocardiogram demonstratedmarantic endocarditis.
Figure 5. The CT scan of a 67-year-old man with dysarthria and right facial droop on awakening performed 17.25 hours after onsetshowed no lesion. MRI was performed 36.5 hours after onset, which was 21.5 hours after admission. A, T2-weighted MRI showed mul-tiple foci of increased signal in bilateral deep white matter (arrows). B, DWI demonstrates acute lesion in left posterior internal capsule.ADC sequences showed correlation of low intensity, consistent with acute ischemia. C, MRA displayed stenotic left M1 portion of mid-dle cerebral artery (arrow) and atherosclerotic irregularity of cavernous portion of left internal carotid artery (arrow). TOAST diagnosischanged from small-vessel etiology to more than 1 likely etiology (both large-vessel atherothromboembolic and small-vessel possible).
1086 Stroke May 2000
by guest on November 21, 2014http://stroke.ahajournals.org/Downloaded from

DiscussionEarly classification of ischemic stroke subtype is of substan-tial practical clinical value.28,29 Classification aids earlyprognostication, identifying patients at increased risk of earlyneurological worsening, early recurrent stroke, medical com-plications, need for discharge to a long-term care facility, andlong-term death and disability.30,31 Long-term secondaryprevention therapies differ significantly among ischemicstroke subtypes. For example, surgical endarterectomy ispursued for large-vessel carotid atherothrombotic disease,anticoagulation is pursued for atrial fibrillation and othercauses of cardioembolism, and antiplatelet therapy is pursuedfor lacunar stroke. Earlier subtype diagnosis allows earlierplanning for institution of the appropriate long-term therapyand earlier hospital discharge.
In addition, many clinicians tailor acute stroke treatmentstrategies to stroke subtype. Large-scale clinical trials havenot yet demonstrated differential treatment effects amongsubtypes, but this in part may reflect imprecise entry strokesubtype diagnosis. Accurate early stroke subtype diagnosiswill likely be critical for the conduct of clinical trials ofemerging neurointerventional recanalization therapies.32 Tri-als of intra-arterial thrombolysis,33 acute cerebral angio-plasty,34 and other endovascular reperfusion techniques re-quire rapid, accurate identification of patients with largevessel occlusions.
Our data demonstrate that early, multimodal DWI/MRAsubstantially improves the accuracy of stroke subtype diag-nosis. Marked improvements in matching final diagnosiswere noted for both of the formal subtyping methods inwidespread use: the TOAST and the Oxfordshire classifica-tion systems.
With the TOAST method, early DWI/MRA substantiallyimproved the classification accuracy of early diagnoses oflarge-vessel atherothromboembolic and small-vessel (lacu-nar) subtypes. A tendency toward improved accuracy fordiagnosis of cardioembolic stroke was also noted, but con-clusions were limited by small patient numbers. Cardioem-bolic strokes were likely underrepresented in our cohort dueto an inherent limitation of MRI-dependent diagnosis strate-
gies. Acute MRI studies cannot be obtained in a subset ofpatients with cardiac sources of embolism, including patientswith cardiac pacemakers and patients who are hemodynam-ically unstable due to acute myocardial infarction or cardiacdysrhythmia.
It is noteworthy that the accuracy of stroke subtypediagnoses rendered after large-vessel imaging by MRA wassubstantially further improved by the addition of DWI deter-mination of ischemic insult topography. This observationsuggests limitations to acute diagnostic strategies that relyonly on standard CT plus vessel imaging with ultrasound(carotid duplex and transcranial), CT angiography, or MRA.DWI of infarct topography further assisted subtype diagnosisin several ways, including (1) in distinguishing when classiclacunar syndromes were indeed due to small, deep infarcts,1.5 cm in diameter versus due to larger territorial infarcts;(2) in conversely determining when nonclassic lacunar clin-ical syndromes were due to small, deep infarcts rather than tolarger insults; (3) in indicating multiple acute lesions in morethan 1 vascular territory in patients with only 1 symptomaticlesion, which is consistent with cardioembolism; and (4) indetermining the acute, symptomatic lesion from among sev-eral chronic deep and cortical lesions.
An important limitation of the present study is that the goldstandard, final diagnoses were not reached completely inde-pendent of the diagnostic test being evaluated. For thisreason, we have not expressed our detailed results in terms ofsensitivity, specificity, positive predictive value, and negativepredictive value; it would not be entirely statistically sound todo so. However, because it has been conventional to providethese measures in similar studies,1 for comparison purposesonly we note what our data would have yielded for the 2 mostcommon diagnostic categories. In the large-vessel athero-thromboembolic category, sensitivity and positive predictivevalues of initial TOAST diagnosis would have been 56% and83%, improving to 89% and 100% with the addition of MRAalone, 56% and 100% with the addition of DWI alone, and89% and 100% with the addition of combined MRA andDWI. In the small-vessel category, sensitivity and positivepredictive values of initial TOAST diagnoses would have
Figure 6. The CT scan of a 94-year-old man with several prior transientischemic attacks and strokes who pre-sented with slurred speech and gaitdifficulty performed 9.75 hours afteronset showed no lesion. MRI was per-formed 11.5 hours after onset, whichwas 3.5 hours after admission. A,T2-weighted sequences showed multi-ple, bilateral pontine, and cerebralwhite matter hyperintensities. B, DWIrevealed a single focus of increasedsignal in left pons. ADC sequencesshowed correlation of low intensity,consistent with acute ischemia. MRAshowed no large-vessel abnormality.TOAST diagnosis changed from strokeof undetermined etiology to small ves-sel. In addition, DWI distinguished thesingle site of active new ischemia frommultiple potentially relevant foci of T2abnormality.
Lee et al Impact of Early DWI and MRA on Stroke Subtyping 1087
by guest on November 21, 2014http://stroke.ahajournals.org/Downloaded from

been 35% and 73%, improving to 35% and 80% with theaddition of MRA alone, 96% and 92% with the addition ofDWI alone, and 100% and 96% with the addition of com-bined MRA and DWI. It is important to note that our datalikely underestimate the usefulness of DWI and MRA imag-ing in stroke subtype diagnosis. Our quantitative analysescapture only the impact of imaging with DWI and MRA onchanges in stroke subtype diagnosis and not the impact instrengthening the likelihood of initially correct subtype as-signments. For example, in the large-vessel atherothrombo-embolic category, DWI findings often increased the likeli-hood of a large-vessel mechanism by demonstrating infarcttopography compatible with large-vessel disease. Such afinding helps to move a diagnosis from “possible large-vesselatherothromboembolic” to “probable large-vessel athero-thromboembolic.” Similarly, MRA often strengthened thelikelihood of small-vessel disease by excluding a large-vesselstenosis or occlusion, making the diagnosis of small-vessellacunar even more probable.
Several groups have explored in an informal manner theaspects of the impact of early DWI and MRA imaging on theearly diagnosis of large-vessel syndrome35,36 or lacunar syn-dromes,37,38 but none have previously examined their effectacross all ischemic stroke subtypes or used formal diagnosticclassification algorithms. Our findings add to the growingliterature on the usefulness of DWI, MRA, and combinedDWI/MRA in the evaluation of acute ischemic stroke.7,39 Tothe usefulness of acute DWI volume in the prediction ofeventual functional outcome6,40,41and the usefulness of DWIin the differentiation of acute lesions from several chroniclesions,7,42 we may now add effectiveness in improvement ofthe accuracy of early stroke subtype diagnosis. In addition,we believe this study represents the first demonstration andquantitative assessment of the usefulness of combined cervi-cal and cephalic MRA in the diagnosis of stroke subtype.
In conclusion, imaging with DWI and MRA within 24hours of hospitalization substantially improves the accuracyof early ischemic stroke subtype diagnosis. When initialmanagement decisions and clinical trial eligibility are influ-enced by stroke subtype, day 1 multimodal MRI methodologywould be advantageous as a guide to therapy and to clinicaltrial enrollment. In addition, early multimodal MRI allowsthe rapid initiation of planning for long-term secondary strokeprevention therapy differentiated by stroke subtype.
AcknowledgmentsThis work was supported in part by National Institutes of Healthgrant K24-NS-02092-01. We thank David Schriger, MD, for expertstatistical assistance.
References1. Madden KP, Karanjia PN, Adams HP, Clarke WR, for the TOAST
Investigators. Accuracy of initial stroke subtype diagnosis in the TOASTstudy.Neurology. 1995;45:1975–1979.
2. Bogousslavsky J, Regli F, Besson G, Melo TP, Nater B. Early clinicaldiagnosis of stroke subtype.Cerebrovasc Dis. 1993;3:39–44.
3. Von Arbin M, Britton M, de Faire U, Helmers C, Miah K, Murray V.Accuracy of bedside diagnosis in stroke.Stroke. 1981;12:288–293.
4. Humphrey RD, Harrison MJ. How often can an embolic stroke bediagnosed clinically? A clinicopathological correlation.Postgrad Med J.1985;61:1039–1042.
5. Gross CR, Shinar D, Mohr JP, Hier DB, Caplan LR, Price TR, Wolf PA,Kase CS, Fishman IG, Calingo S, et al. Interobserver agreement in thediagnosis of stroke type.Arch Neurol. 1986;43:893–898.
6. Warach S, Dashe JF, Edelman RR. Clinical outcome in ischemic strokepredicted by early diffusion-weighted and perfusion magnetic resonanceimaging: a preliminary analysis.J Cereb Blood Flow Metab1996;16:53–59.
7. Lutsep HL, Albers GW, DeCrespigny A, Kamat GN, Marks MP, MoseleyME. Clinical utility of diffusion-weighted magnetic resonance imaging inthe assessment of ischemic stroke.Ann Neurol. 1997;41:574–580.
8. Baird AE, Benfield A, Gottfried Schlaug G, Siewerr B, Lovblad K-O,Edelman RR, Warach S. Enlargement of human cerebral ischemic lesionvolumes measured by diffusion-weighted magnetic resonance imaging.Ann Neurol. 1997;41:581–589.
9. Belliveau JW, Rosen BR, Kantor HL, Rzedzian RR, Kennedy DN,McKinstry RC, Vevea JM, Cohen MS, Pykett IL, Brady TJ. Functionalcerebral imaging by susceptibility-contrast NMR.Magn Reson Med.1990;14:538–546.
10. Busza AL, Allen KL, King MD, van Bruggen N, Williams SR, GadianDG. Diffusion-weighted imaging studies of cerebral ischemia in gerbils:potential relevance to energy failure.Stroke. 1992;23:1602–1612.
11. Minematsu K, Fisher M, Li L, Davis MA, Knapp AG, Cotter RE,McBurney RN, Sotak CH. Effects of novel NMDA antagonist on exper-imental stroke rapidly and quantitatively assessed by diffusion-weightedMRI. Neurology. 1993;43:397–403.
12. Minematsu K, Fisher M, Li L, Sotak CH. Diffusion and perfusionmagnetic resonance imaging studies to evaluate a noncompetitiveN-methyl-D-aspartate antagonist and reperfusion in experimental stroke inrats.Stroke. 1993;24:2074–2081.
13. Moseley ME, Cohen Y, Kucharczyk J, Mintorovitch J, Asgari HS,Wendland MF, Tsuruda J, Norman D. Diffusion-weighted MR imaging ofanisotropic water diffusion in cat central nervous system.Radiology.1990;176:439–445.
14. Moseley ME, Kucharczyk J, Mintorovitch J, Cohen Y, Kurhanewicz J,Derugin N, Asgari H, Norman D. Diffusion-weighted MR imaging ofacute stroke: correlation with T2-weighted and magnetic susceptibility-enhanced MR imaging in cats.Am J Neuroradiol. 1990;11:423–429.
15. Moseley ME, Cohen Y, Mintorovitch J, Chileuitt L, Shimizu H,Kucharczyk J, Wendland MF, Weinstein PR. Early detection of regionalcerebral ischemia in cats: comparison of diffusion- and T2-weighted MRIand spectroscopy.Magn Reson Med. 1990;14:330–346.
16. Liberopoulos K, Kaponis A, Kokkinis K, Pagratis N, Nicolakopoulou Z,Douskou M, Stringaris K, Clonaris C, Balas P. Comparative study ofmagnetic resonance angiography, digital subtraction angiography, duplexultrasound examination with surgical and histological findings of athero-sclerotic carotid bifurcation disease.Int Angiol. 1996;15:131–137.
17. Chiesa R, Melissano, G, Castellano R, Triulzi F, Anzalnoe N, Veglia F,Scotti G, Grossi A. Three dimensional time-of-flight magnetic resonanceangiography in carotid artery surgery: a comparison with digital sub-traction angiography.Eur J Vasc Surg. 1993;7:171–176.
18. Magarelli N, Scarabino T, Simeone AL, Florio F, Carriero A, Salvolini U,Bonomo L. Carotid stenosis: a comparison between MR and spiral CTangiography.Neuroradiology. 1998;40:367–373.
19. Remonda L, Heid O, Schroth G. Carotid artery stenosis, occlusion, andpseudo-occlusion: first-pass, gadolinium-enhanced, three-dimensionalMR angiography–preliminary study.Invest Radiol. 1998;33:560–572.
20. Willig DS, Turski PA, Frayne R, Graves VB, Korosec FR, Swan JS,Mistretta CA, Grist TM. Contrast-enhanced 3D MR DSA of the carotidartery bifurcation: preliminary study of comparison with unenhanced 2Dand 3D time-of-flight MR angiography.Radiology. 1998;208:447–451.
21. Jackson MR, Chang AS, Robles HA, Gillespie DL, Olsen SB, Kaiser WJ,Goff JM, O’Donnell SD, Rich NM. Determination of 60% or greatercarotid stenosis: a prospective comparison of magnetic resonanceangiography and duplex ultrasound with conventional angiography.AnnVasc Surg. 1998;12:236–243.
22. Johnson BA, Heiserman JE, Drayer BP, Keller PJ. Intracranial MRangiography: its role in the integrated approach to brain infarction.Am JNeuroradiol. 1994;15:901–908.
23. Dagirmanjian A, Ross JS, Obuchowski N, Lewin JS, Tkach JA, RuggieriPM, Masaryk TJ. High resolution, magnetization transfer saturation,variable flip angle, time-of-flight MRA in the detection of intracranialvascular stenoses.J Comput Assisted Tomogr. 1995;19:700–706.
1088 Stroke May 2000
by guest on November 21, 2014http://stroke.ahajournals.org/Downloaded from

24. Korogi Y, Takahashi M, Nakagawa T, Mabuchi N, Watabe T, ShiokawaY, Shiga H, O’Uchi T, Miki H, Horikawa Y, Fujiwara S, Furuse M.Intracranial vascular stenosis and occlusion: MR angiographic findings.Am J Neuroradiol. 1997;18:135–143.
25. Qureshi AI, Isa A, Cinnamon J, Fountain J, Ottenlips JR, Braimah J,Frankel MR. Magnetic resonance angiography in patients with braininfarction.J Neuroimaging. 1998;8:65–70.
26. Adams HP, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL,Marsh EE, the TOAST Investigators. Classification of subtype of acuteischemic stroke: definitions for use in a multicenter clinical trial.Stroke.1993;24:35–41.
27. Bamford J, Sandercock P, Dennis M, Burn J, Warlow C. Classificationand natural history of clinically identifiable subtypes of cerebralinfarction.Lancet. 1991;337:1521–1526.
28. Hennerici M, Schwartz A. Acute stroke subtypes—is there a need forreclassification?Cerebrovasc Dis. 1998;8(suppl 2):17–22.
29. Castillo V, Bogousslavsky J. Early classification of stroke.CerebrovascDis. 1997;7(suppl 3):5–11.
30. Pinto AN, Melo TP, Lourenco ME, Leandro MJ, Brazio A, Carvallho L,Franco AS, Ferro JM. Can a clinical classification of stroke predictcomplication and treatments during hospitalization?Cerebrovasc Dis.1998;8:204–209.
31. Rundek T, Elkind MS, Chen X, Boden-Albala B, Paik MC, Sacco R.Increased early stroke recurrence among patients with extracranial andintracranial atherosclerosis.Neurology. 1998;50:A75.
32. Caplan LR, Mohr JP, Kistler JP, Koroshetz W. Should thrombolytictherapy be the first line treatment for acute ischemic stroke? Thrombol-ysis—not a panacea for ischemic stroke.N Engl J Med. 1997;337:1309–1310.
33. Furlan A, Higashida R, Wechsler L, Gent M, Rowley H, Kase C, PessinM, Ahuja A, Callahan F, Clark WM, Silver F, Rivera F. Intra-arterialprourokinase for acute ischemic stroke: the PROACT II study: a ran-
domized controlled trial: Prolyse in Acute Cerebral Thromboembolism.JAMA. 1999;282:2003–2011.
34. Gomez CR, Wadlington VR, Terry JB, Vitek JJ, Roubin GS, Yadav SS.Neuroendovascular rescue: primary angioplasty for the management ofacute brain ischemia. Ann Neurol. 1998;44:468A.
35. Allder SJ, Moody AR, Martel AL, Morgan PS, Delay GS, Gladman JR,Fentem P, Lennox GG. Limitations of clinical diagnosis in acute stroke.Lancet. 1999;354:1523.
36. Sunshine JL, Tarr TW, Lanzieri CF, Landis DM, Selman WR, Lewin JS.Hyperacute stroke: ultrafast MR imaging to triage patients prior totherapy.Radiology. 1999;212:325–332.
37. Schonewille WJ, Tuhrim S, Singer MB, Atlas SW. Diffusion-weightedMRI in acute lacunar syndromes.Stroke. 1999;30:2066–2069.
38. Noguchi K, Nagayoshi T, Watanabe N, Kanazawa T, Toyoshima S,Morijiri M, Shojaku H, Shimizu M, Seto H. Diffusion-weighted echo-planar MRI of lacunar infarcts.Neuroradiology. 1998;40:448–451.
39. Rordorf G, Koroshetz WJ, Copen WA, Cramer SC, Schaefer PW, BudzikRF Jr, Schwamm LH, Buonanno F, Sorensen AG, Gonzalez G. Regionalischemia and ischemic injury in patients with acute middle cerebral arterystroke as defined by early diffusion-weighted and perfusion-weightedMRI. Stroke. 1998;29:939–943.
40. Barber PA, Darby DG, Desmond PM, Yang, Q, Gerraty RP, Jolley D,Donnan GA, Tress BM, Davis SM. Prediction of stroke outcome withechoplanar perfusion- and diffusion-weighted MRI.Neurology. 1998;51:418–426.
41. van Everdingen KJ, van der Grond J, Kappelle LJ, Ramos LM, Mali WP.Diffusion-weighted magnetic resonance imaging in acute stroke.Stroke.1998;29:1783–1790.
42. Singer MB, Chong J, Lu D, Schonewille WJ, Tuhrim S, Atlas SW.Diffusion-weighted MRI in acute subcortical infarction.Stroke. 1998;29:133–136.
Lee et al Impact of Early DWI and MRA on Stroke Subtyping 1089
by guest on November 21, 2014http://stroke.ahajournals.org/Downloaded from




















