
Impact of experience with a retrograde-viewing device on adenoma detection rates and withdrawal...
9
ORIGINAL ARTICLE: Clinical Endoscopy Impact of experience with a retrograde-viewing device on adenoma detection rates and withdrawal times during colonoscopy: the Third Eye Retroscope study group Daniel C. DeMarco, MD, Elizabeth Odstrcil, MD, Luis F. Lara, MD, David Bass, MD, Chase Herdman, MD, Timothy Kinney, MD, Kapil Gupta, MD, Leon Wolf, MD, Thomas Dewar, MD, Thomas M. Deas, MD, Manoj K. Mehta, MD, M. Badar Anwer, MD, Randall Pellish, MD, J. Kent Hamilton, MD, Daniel Polter, MD, K. Gautham Reddy, MD, Ira Hanan, MD Dallas, North Richland Hills, Fort Worth, Texas, Minneapolis, Minnesota, Evanston, Chicago, Illinios, Celebration, Florida, Worcester, Massachusetts, USA Background: Colonoscopy has been adopted as the preferred method to screen for colorectal neoplasia in the United States. However, lesions can be missed because of numerous factors, including location on the proximal aspect of folds or flexures, where they may be difficult to detect with the forward-viewing colonoscope. The Third Eye Retroscope (TER) is a disposable device that is passed through the instrument channel of a standard colonoscope to provide a retrograde view that complements the forward view of the colonoscope during withdrawal. Objective: To evaluate whether experience with the TER affects polyp detection rates and procedure times in experienced endoscopists who had not previously used the equipment. Design, Setting, Patients: This was an open-label, prospective, multicenter study at 9 U.S. sites, involving 298 patients presenting for colonoscopy, evaluating the use of the TER in combination with a standard colonoscope. Interventions: After cecal intubation, the TER was inserted through the instrument channel of the colonoscope. During withdrawal, the forward and retrograde video images were observed simultaneously on a wide-screen monitor. Main Outcome Measurements: Primary outcome measures were the number and size of adenomas and all polyps detected with the standard colonoscope and with the colonoscope combined with the TER. Secondary outcome measures were withdrawal phase time and total procedure time. Each endoscopist examined 20 subjects, divided into quartiles according to the order of their procedures, and results were compared among quartiles. Results: Overall, 182 polyps were detected with the colonoscope and 27 additional polyps with the TER, a 14.8% increase (P .001). A total of 100 adenomas were detected with the colonoscope and 16 more with the TER, a 16.0% increase (P .001). For procedures performed after each endoscopist had completed 15 procedures while using the TER, the mean additional detection rates with the TER were 17.0% for all polyps (P .001) and 25.0% for adenomas (P .001). For lesions 6 mm or larger, the overall additional detection rates with the TER for all polyps and for adenomas were 23.2% and 24.3%, respectively. For lesions 10 mm or larger, the overall additional detection rates with the TER for all polyps and for adenomas were 22.6% and 19.0%, respectively. The mean withdrawal times in the first and fourth quartiles were 10.6 and 9.2 minutes, respectively (P .044). Limitations: There was no randomization or separate control group. The endoscopists judged whether each lesion could have been detected with the colonscope alone by using their standard technique. Conclusions: Polyp detection rates improved significantly with the TER, especially after 15 procedures, when the mean additional detection rate for adenomas was 25.0%. Additional detection rates with the TER for medium-size and large adenomas were greater than for smaller lesions. These results suggest that, compared with a colonoscope alone, a retrograde-viewing device can increase detection rates for clinically significant adenomas without detriment to procedure time or procedure complications. (Clinical trial registration number: NCT00969124.) ( Gastrointest Endosc 2010;71:542-50.) 542 GASTROINTESTINAL ENDOSCOPY Volume 71, No. 3 : 2010 www.giejournal.org
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Impact of experience with a retrograde-viewing device on adenoma detection rates and withdrawal...
5
ORIGINAL ARTICLE: Clinical Endoscopy
Impact of experience with a retrograde-viewing device on adenomadetection rates and withdrawal times during colonoscopy:the Third Eye Retroscope study group
Daniel C. DeMarco, MD, Elizabeth Odstrcil, MD, Luis F. Lara, MD, David Bass, MD, Chase Herdman, MD,Timothy Kinney, MD, Kapil Gupta, MD, Leon Wolf, MD, Thomas Dewar, MD, Thomas M. Deas, MD,Manoj K. Mehta, MD, M. Badar Anwer, MD, Randall Pellish, MD, J. Kent Hamilton, MD, Daniel Polter, MD,K. Gautham Reddy, MD, Ira Hanan, MD
Dallas, North Richland Hills, Fort Worth, Texas, Minneapolis, Minnesota, Evanston, Chicago, Illinios, Celebration,Florida, Worcester, Massachusetts, USA
Background: Colonoscopy has been adopted as the preferred method to screen for colorectal neoplasia in theUnited States. However, lesions can be missed because of numerous factors, including location on the proximalaspect of folds or flexures, where they may be difficult to detect with the forward-viewing colonoscope. TheThird Eye Retroscope (TER) is a disposable device that is passed through the instrument channel of a standardcolonoscope to provide a retrograde view that complements the forward view of the colonoscope duringwithdrawal.
Objective: To evaluate whether experience with the TER affects polyp detection rates and procedure times inexperienced endoscopists who had not previously used the equipment.
Design, Setting, Patients: This was an open-label, prospective, multicenter study at 9 U.S. sites, involving 298patients presenting for colonoscopy, evaluating the use of the TER in combination with a standard colonoscope.
Interventions: After cecal intubation, the TER was inserted through the instrument channel of the colonoscope.During withdrawal, the forward and retrograde video images were observed simultaneously on a wide-screenmonitor.
Main Outcome Measurements: Primary outcome measures were the number and size of adenomas and allpolyps detected with the standard colonoscope and with the colonoscope combined with the TER. Secondaryoutcome measures were withdrawal phase time and total procedure time. Each endoscopist examined 20subjects, divided into quartiles according to the order of their procedures, and results were compared amongquartiles.
Results: Overall, 182 polyps were detected with the colonoscope and 27 additional polyps with the TER, a 14.8%increase (P � .001). A total of 100 adenomas were detected with the colonoscope and 16 more with the TER, a16.0% increase (P � .001). For procedures performed after each endoscopist had completed 15 procedures whileusing the TER, the mean additional detection rates with the TER were 17.0% for all polyps (P � .001) and 25.0%for adenomas (P � .001). For lesions 6 mm or larger, the overall additional detection rates with the TER for allpolyps and for adenomas were 23.2% and 24.3%, respectively. For lesions 10 mm or larger, the overall additionaldetection rates with the TER for all polyps and for adenomas were 22.6% and 19.0%, respectively. The meanwithdrawal times in the first and fourth quartiles were 10.6 and 9.2 minutes, respectively (P � .044).
Limitations: There was no randomization or separate control group. The endoscopists judged whether eachlesion could have been detected with the colonscope alone by using their standard technique.
Conclusions: Polyp detection rates improved significantly with the TER, especially after 15 procedures, whenthe mean additional detection rate for adenomas was 25.0%. Additional detection rates with the TER formedium-size and large adenomas were greater than for smaller lesions. These results suggest that, comparedwith a colonoscope alone, a retrograde-viewing device can increase detection rates for clinically significantadenomas without detriment to procedure time or procedure complications. (Clinical trial registrationnumber: NCT00969124.) (Gastrointest Endosc 2010;71:542-50.)
42 GASTROINTESTINAL ENDOSCOPY Volume 71, No. 3 : 2010 www.giejournal.org

dtr
dactcpwv
if
B
Sicvc
iicfls
A
Drcp
C0d
R
CJTTMNHWI
RDD
ID
DeMarco et al Impact of experience with a retrograde-viewing device on adenoma detection rates during colonoscopy
w
Colorectal cancer is the second leading cause of cancereath in the United States.1 Current strategies for reducinghe toll from colorectal cancer focus on early detection andemoval of potential precancerous lesions.
Colonoscopy is currently regarded as the criterion stan-ard for the detection of polyps and cancers in the colonnd is the preferred method of screening for colorectalancer in the United States.2-6 However, evidence showshat polyps and other lesions can be missed duringolonoscopy,7-16 at least in part because of location on theroximal aspect of flexures, rectal valves, or haustral folds,here they can be difficult to see with the forward-iewing colonoscope.13
Therefore, detection rates might be enhanced by anncreased ability to visualize areas behind flexures andolds.
ACKGROUND
The Third Eye Retroscope (TER) (Avantis Medicalystems, Inc, Sunnyvale, Calif) is a disposable auxiliarymaging device that is inserted through the instrumenthannel of a standard colonoscope to provide a retrogradeiew of the colon during the withdrawal phase of aolonoscopy.17-19
After the colonoscope has been advanced to the cecumn the usual manner, the TER is inserted through thenstrument channel. As it emerges from the distal tip of theolonoscope, the TER automatically bends 180 degrees toorm a J shape (Fig. 1) so that its sensor and integratedight source are directed back toward the tip of the colono-cope. The device is then withdrawn together with the
bbreviation: TER, Third Eye Retroscope.
ISCLOSURE: The following author disclosed a financial relationshipelevant to this publication: D.C. DeMarco: Consultant for Spirus Medi-al. All other authors disclosed no financial relationships relevant to thisublication.
opyright © 2010 by the American Society for Gastrointestinal Endoscopy.016-5107/$36.00oi:10.1016/j.gie.2009.12.021
eceived September 4, 2009. Accepted December 4, 2009.
urrent affiliations: Baylor University Medical Center (D.C.D, E.O., L.F.L.,.K.H., D.P.), Dallas, Texas, North Hills Hospital (D.B.), North Richland Hills,exas, S.W. Fort Worth Endoscopy Center (C.H. T.D., T.M.D.), Fort Worth,exas, Hennepin County Medical Center (T.K., K.G.), Minneapolis,innesota, University of Texas Southwestern (L.W.), Dallas, Texas,orthShore University HealthSystem (M.K.M.), Evanston, Illinois, Floridaospital (M.B.A.), Celebration, Florida, University of Massachusetts (R.P.),orcester, Massachusetts, University of Chicago (K.G.R., I.H.), Chicago,
llinois.
eprint requests: Daniel C. DeMarco, MD, Baylor University Medical Center,igestive Health Associates of Texas, 712 North Washington, Suite 200,allas, TX 75246.
f you would like to chat with an author of this article, you may contact Dr.
eMarco at [email protected].ww.giejournal.org V
colonoscope, thus providing a continuous retrograde viewto complement the forward view of the colonoscope.
Previous studies showed that the TER can increasedetection rates for adenomas and other polyps.18,19 Pre-liminary data also suggested that experience with the TERincreases polyp detection rates and procedure efficiency.This study was designed to evaluate whether there is alearning curve for the TER in terms of both efficacy forpolyp detection and procedure time.
METHODS
Fifteen experienced endoscopists at 9 U.S. sites partic-ipated in an open-label, prospective study to determinepolyp detection rates and procedure time while perform-ing colonoscopy by using a standard colonoscope (CF-Q160AL, CF-Q180AL, or CF-H180AL; Olympus America,Inc, Center Valley, Pa) with the addition of the TER, aretrograde-viewing auxiliary imaging device, during thewithdrawal phase. The participating endoscopists had noprevious experience with the TER other than a trainingsession with an anatomical model.
Subjects were invited to participate in the study if theywere undergoing colonoscopy for colorectal neoplasiascreening, for polyp surveillance, or for diagnostic workup(including anemia, abdominal pain, abnormal imaging)and if they were able to understand and provide writtenconsent for the procedure.
Exclusion criteria included history of colon resection,known inflammatory bowel disease, polyposis syndrome,radiation therapy to abdomen or pelvis, suspicion ofchronic stricture potentially precluding complete colonos-copy, presence of diverticulitis or toxic megacolon, andconcurrent enrollment in another clinical investigation.
The study was approved by the institutional reviewboard of each participating institution, and all patients
Capsule Summary
What is already known on this topic
● In screening for colorectal neoplasia, the standardforward-viewing colonoscope may not detect lesions onthe proximal aspect of folds or flexures.
What this study adds to our knowledge
● In a prospective, multicenter study, detection of polypsincreased 14.8% and detection of adenomas increased16% with the addition of a retrograde-viewing devicecompared with the standard colonoscope alone.
● After each endoscopist had completed 15 procedureswith the device, detection rates for polyps and adenomasincreased to 17% and 25%, respectively.
signed an informed consent. Between January and June
olume 71, No. 3 : 2010 GASTROINTESTINAL ENDOSCOPY 543

2d
maoPppttw
tdpfmc
cmfvocTwatwss
diwc
Fstc
Impact of experience with a retrograde-viewing device on adenoma detection rates during colonoscopy DeMarco et al
5
009, subjects were enrolled in sequence until each en-oscopist had completed 20 procedures.
Because the TER reduces suction capacity approxi-ately 50% when it is in the channel, endoscopists were
dvised to lavage and suction any residual stool and poolsf fluid during colonoscope insertion. The Ottawa Bowelreparation Quality Scale20 was used to grade the bowelreparation. If bowel preparation was deemed to be ofoor quality and if the endoscopist was unable to cleansehe bowel adequately to perform a high-quality examina-ion, the patient was excluded from the study and the TERas not used.During each procedure, the colonoscope was advanced
o the cecum in the usual manner and its position wasocumented with photographs of the ileocecal valve, ap-endiceal orifice, or terminal ileum. Polyps that wereound during colonoscope insertion were immediately re-oved and counted as having been found with the
olonoscope.After water irrigation of the instrument channel of the
olonoscope, the TER was inserted through the channel,uch as one would insert a polypectomy snare or biopsy
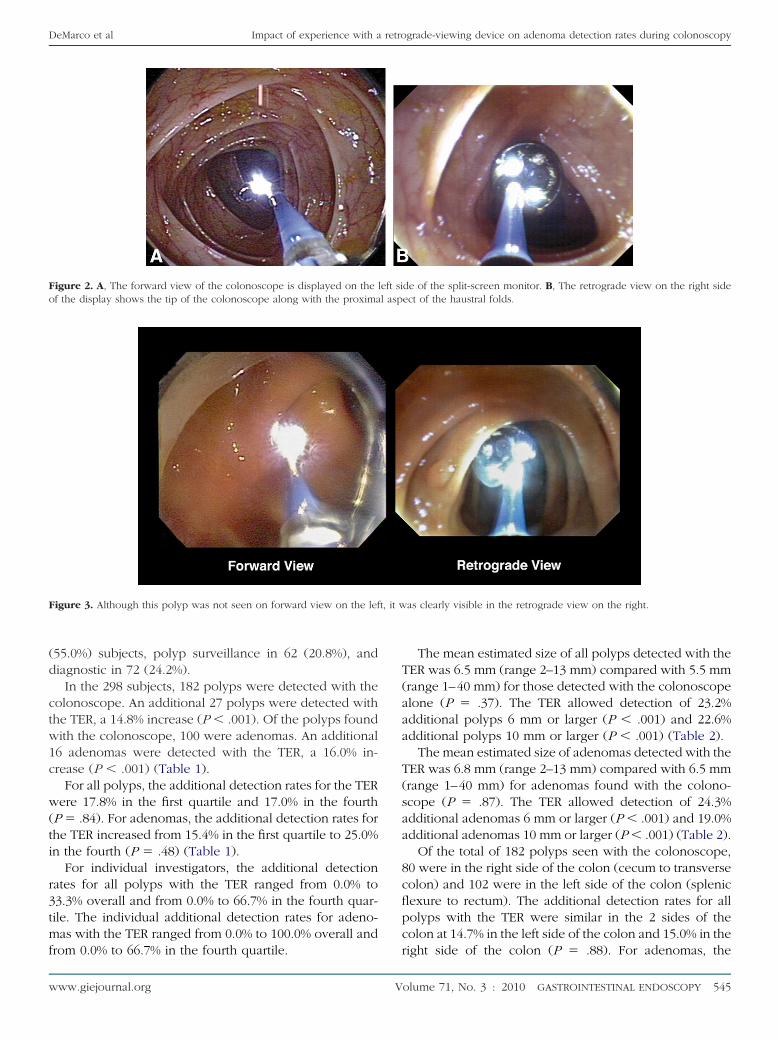
orceps. During withdrawal, the forward and retrogradeideo images were observed simultaneously side by siden a wide-screen monitor (Fig. 2). When necessary, theolonoscope water jet was used to clean the lens of theER. When a polyp was seen, the endoscopist indicatedhether it could have been seen with the colonoscopelone by using a routine degree of deflection of the tip ofhe colonoscope or whether it was found only because itas detected with the TER (Fig. 3). When a polyp was
een both with the colonoscope and the TER, the colono-cope was credited with finding it.
For each polyp, the endoscopist indicated its size, itsistance from the anal verge, and the segment of the colonn which it was found. When a polyp was seen duringithdrawal, the TER was removed while maintaining the
igure 1. After insertion through the instrument channel, the TER as-umes a J shape so that its sensor and light source are directed backoward the tip of the colonoscope, providing a retrograde view toomplement the forward view of the colonoscope.
olonoscope in place. The polyp was then removed by
44 GASTROINTESTINAL ENDOSCOPY Volume 71, No. 3 : 2010
using the tip of the colonoscope or the instrument (snareor biopsy forceps). Because each polyp was removed atthe time that it was found, there was no possibility that alesion could be counted twice.
Total procedure time started with colonoscope inser-tion and ended when the colonoscope was withdrawnpast the anal verge. Withdrawal time began when theendoscopist began to withdraw the colonoscope and TERtogether through the colon and ended when both werewithdrawn through the anal verge. Any pauses forpolypectomies, biopsies, or extensive bowel cleansingwere subtracted so that the withdrawal time would repre-sent the time that was devoted to examining the colonmucosa. A research assistant was present during the pro-cedure to record findings and procedure times as directedby the endoscopist.
Primary outcome measures were the number and sizeof the polyps detected with the colonoscope, and thenumber and size of the additional polyps that were foundonly because they were first detected with the TER. Sec-ondary outcome measures were the withdrawal phasetime and total procedure time.
Statistical analysisThe 20 subjects who were enrolled by each endoscopist
were divided into quartiles, ie, the first 5 constituted thefirst quartile, the second 5 the second quartile, and so on.The learning curve was evaluated by comparing resultsamong quartiles. The exact binomial test was used todetermine the significance of the increased detection ratesby using the TER.
Differences in withdrawal times, total procedure times,and the size of polyps detected with the colonoscope andwith the TER were evaluated by using analysis of variance.Differences in polyp detection between the left and rightside of the colon were determined by using the Fisherexact test. For statistical purposes, the numbers of polypswere analyzed independently of whether a patient hadmore than 1 polyp detected. No corrections were made forthe multiplicity of tests performed.
RESULTS
Of the 328 subjects who were enrolled, 30 (9.1%) werewithdrawn per protocol for inadequate bowel preparation(n � 15), inability to reach the cecum (n � 9), previouslyunrecognized diseases in which use of the TER was con-sidered by the endoscopists to be a potential risk factor(colitis, polyposis, severe diverticulosis; n � 3), technicalerror (incorrect cap placed on the colonoscope; n � 1),and protocol violation (n � 2).
Of the 298 subjects who completed the study, 144(48.3%) were men and 154 (51.7%) were women, and theirmean age was 56.8 years (standard deviation 11.3; range
22-90 years). The indications were screening in 164www.giejournal.org
(d
ctw1c
w(ti
r3tmf
Fo l asp
F t, it w
DeMarco et al Impact of experience with a retrograde-viewing device on adenoma detection rates during colonoscopy
w
55.0%) subjects, polyp surveillance in 62 (20.8%), andiagnostic in 72 (24.2%).
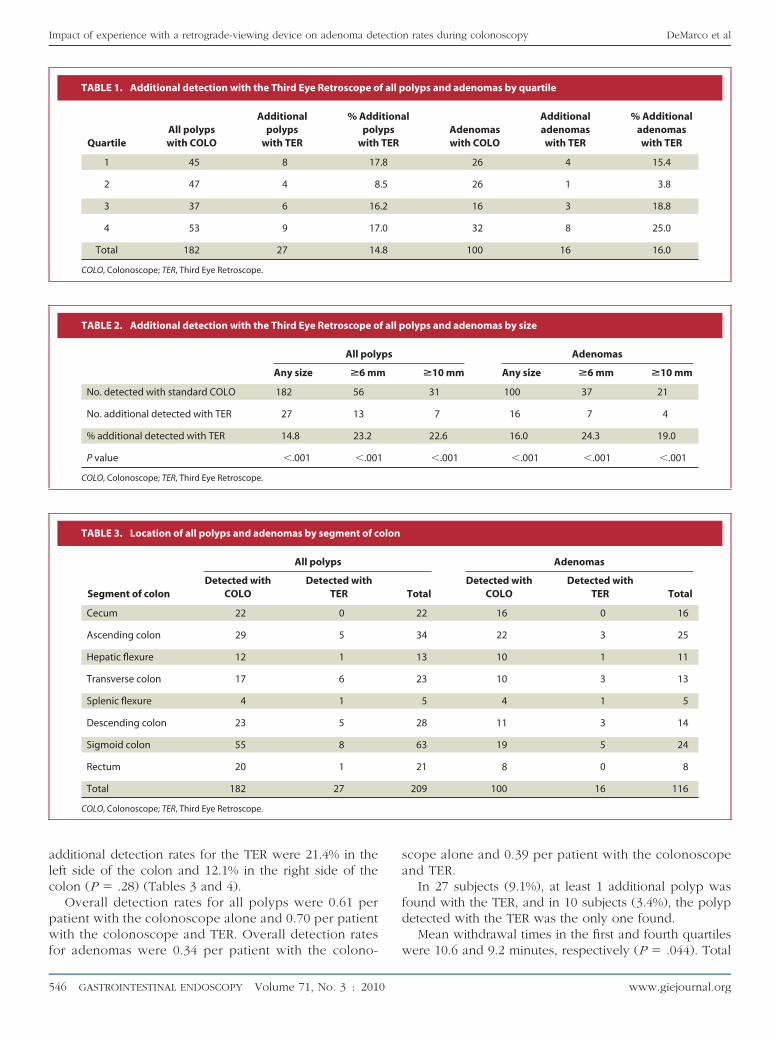
In the 298 subjects, 182 polyps were detected with theolonoscope. An additional 27 polyps were detected withhe TER, a 14.8% increase (P � .001). Of the polyps foundith the colonoscope, 100 were adenomas. An additional6 adenomas were detected with the TER, a 16.0% in-rease (P � .001) (Table 1).
For all polyps, the additional detection rates for the TERere 17.8% in the first quartile and 17.0% in the fourth
P � .84). For adenomas, the additional detection rates forhe TER increased from 15.4% in the first quartile to 25.0%n the fourth (P � .48) (Table 1).
For individual investigators, the additional detectionates for all polyps with the TER ranged from 0.0% to3.3% overall and from 0.0% to 66.7% in the fourth quar-ile. The individual additional detection rates for adeno-as with the TER ranged from 0.0% to 100.0% overall and
igure 2. A, The forward view of the colonoscope is displayed on thef the display shows the tip of the colonoscope along with the proxima
igure 3. Although this polyp was not seen on forward view on the lef
rom 0.0% to 66.7% in the fourth quartile.
ww.giejournal.org V
The mean estimated size of all polyps detected with theTER was 6.5 mm (range 2–13 mm) compared with 5.5 mm(range 1–40 mm) for those detected with the colonoscopealone (P � .37). The TER allowed detection of 23.2%additional polyps 6 mm or larger (P � .001) and 22.6%additional polyps 10 mm or larger (P � .001) (Table 2).
The mean estimated size of adenomas detected with theTER was 6.8 mm (range 2–13 mm) compared with 6.5 mm(range 1–40 mm) for adenomas found with the colono-scope (P � .87). The TER allowed detection of 24.3%additional adenomas 6 mm or larger (P � .001) and 19.0%additional adenomas 10 mm or larger (P � .001) (Table 2).
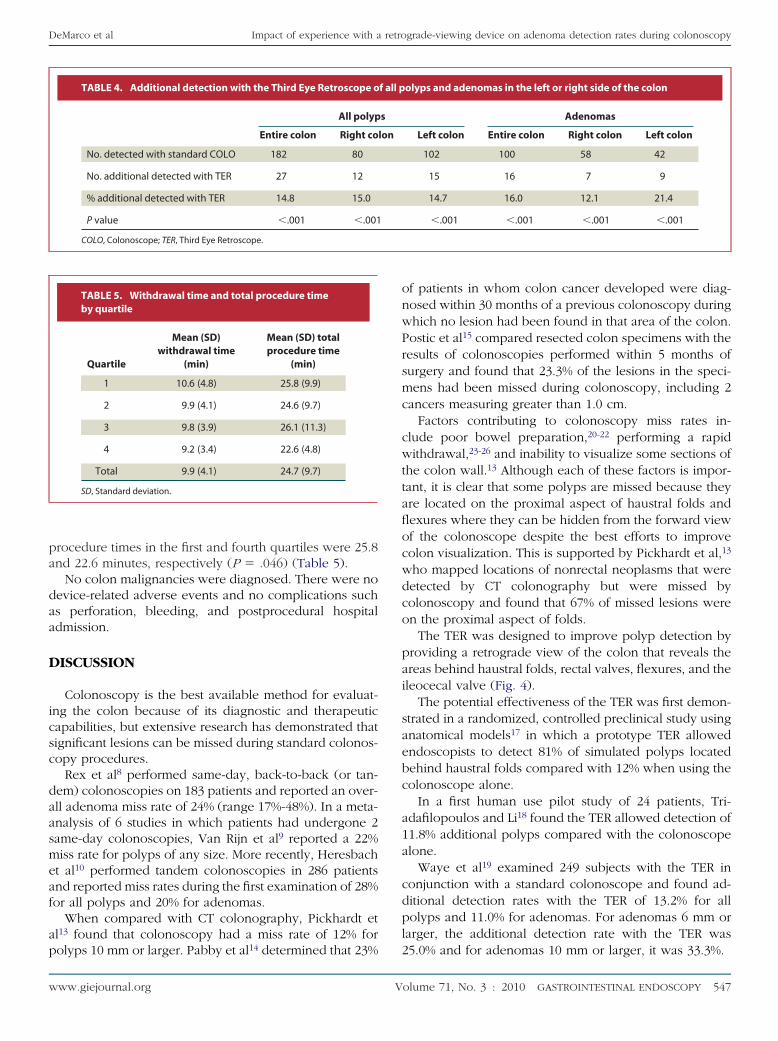
Of the total of 182 polyps seen with the colonoscope,80 were in the right side of the colon (cecum to transversecolon) and 102 were in the left side of the colon (splenicflexure to rectum). The additional detection rates for allpolyps with the TER were similar in the 2 sides of thecolon at 14.7% in the left side of the colon and 15.0% in the
de of the split-screen monitor. B, The retrograde view on the right sideect of the haustral folds.
as clearly visible in the retrograde view on the right.
left si
right side of the colon (P � .88). For adenomas, the
olume 71, No. 3 : 2010 GASTROINTESTINAL ENDOSCOPY 545
alc
pwf
Impact of experience with a retrograde-viewing device on adenoma detection rates during colonoscopy DeMarco et al
5
dditional detection rates for the TER were 21.4% in theeft side of the colon and 12.1% in the right side of theolon (P � .28) (Tables 3 and 4).
Overall detection rates for all polyps were 0.61 peratient with the colonoscope alone and 0.70 per patientith the colonoscope and TER. Overall detection rates
TABLE 1. Additional detection with the Third Eye Retroscope o
QuartileAll polypswith COLO
Additionalpolyps
with TER
% Addpol
with
1 45 8 17
2 47 4 8
3 37 6 16
4 53 9 17
Total 182 27 14
COLO, Colonoscope; TER, Third Eye Retroscope.
TABLE 2. Additional detection with the Third Eye Retroscope o
All poly
Any size >6 mm
No. detected with standard COLO 182 56
No. additional detected with TER 27 13
% additional detected with TER 14.8 23.2
P value �.001 �.001
COLO, Colonoscope; TER, Third Eye Retroscope.
TABLE 3. Location of all polyps and adenomas by segment of c
Segment of colon
All polyps
Detected withCOLO
Detected withTER
Cecum 22 0
Ascending colon 29 5
Hepatic flexure 12 1
Transverse colon 17 6
Splenic flexure 4 1
Descending colon 23 5
Sigmoid colon 55 8
Rectum 20 1
Total 182 27
COLO, Colonoscope; TER, Third Eye Retroscope.
or adenomas were 0.34 per patient with the colono-
46 GASTROINTESTINAL ENDOSCOPY Volume 71, No. 3 : 2010
scope alone and 0.39 per patient with the colonoscopeand TER.
In 27 subjects (9.1%), at least 1 additional polyp wasfound with the TER, and in 10 subjects (3.4%), the polypdetected with the TER was the only one found.
Mean withdrawal times in the first and fourth quartiles
olyps and adenomas by quartile
lAdenomaswith COLO
Additionaladenomaswith TER
% Additionaladenomaswith TER
26 4 15.4
26 1 3.8
16 3 18.8
32 8 25.0
100 16 16.0
olyps and adenomas by size
Adenomas
>10 mm Any size >6 mm >10 mm
31 100 37 21
7 16 7 4
22.6 16.0 24.3 19.0
�.001 �.001 �.001 �.001
Adenomas
TotalDetected with
COLODetected with
TER Total
22 16 0 16
34 22 3 25
13 10 1 11
23 10 3 13
5 4 1 5
28 11 3 14
63 19 5 24
21 8 0 8
209 100 16 116
f all p
itionaypsTER
.8
.5
.2
.0
.8
f all p
ps
olon
were 10.6 and 9.2 minutes, respectively (P � .044). Total
www.giejournal.org
pa
daa
D
icsc
daasmeaf
ap
DeMarco et al Impact of experience with a retrograde-viewing device on adenoma detection rates during colonoscopy
w
rocedure times in the first and fourth quartiles were 25.8nd 22.6 minutes, respectively (P � .046) (Table 5).
No colon malignancies were diagnosed. There were noevice-related adverse events and no complications suchs perforation, bleeding, and postprocedural hospitaldmission.
ISCUSSION
Colonoscopy is the best available method for evaluat-ng the colon because of its diagnostic and therapeuticapabilities, but extensive research has demonstrated thatignificant lesions can be missed during standard colonos-opy procedures.
Rex et al8 performed same-day, back-to-back (or tan-em) colonoscopies on 183 patients and reported an over-ll adenoma miss rate of 24% (range 17%-48%). In a meta-nalysis of 6 studies in which patients had undergone 2ame-day colonoscopies, Van Rijn et al9 reported a 22%iss rate for polyps of any size. More recently, Heresbach
t al10 performed tandem colonoscopies in 286 patientsnd reported miss rates during the first examination of 28%or all polyps and 20% for adenomas.
When compared with CT colonography, Pickhardt etl13 found that colonoscopy had a miss rate of 12% for
TABLE 4. Additional detection with the Third Eye Retroscope o
All polyp
Entire colon Right co
No. detected with standard COLO 182 80
No. additional detected with TER 27 12
% additional detected with TER 14.8 15.0
P value �.001 �.001
COLO, Colonoscope; TER, Third Eye Retroscope.
TABLE 5. Withdrawal time and total procedure timeby quartile
Quartile
Mean (SD)withdrawal time
(min)
Mean (SD) totalprocedure time
(min)
1 10.6 (4.8) 25.8 (9.9)
2 9.9 (4.1) 24.6 (9.7)
3 9.8 (3.9) 26.1 (11.3)
4 9.2 (3.4) 22.6 (4.8)
Total 9.9 (4.1) 24.7 (9.7)
SD, Standard deviation.
olyps 10 mm or larger. Pabby et al14 determined that 23%
ww.giejournal.org V
of patients in whom colon cancer developed were diag-nosed within 30 months of a previous colonoscopy duringwhich no lesion had been found in that area of the colon.Postic et al15 compared resected colon specimens with theresults of colonoscopies performed within 5 months ofsurgery and found that 23.3% of the lesions in the speci-mens had been missed during colonoscopy, including 2cancers measuring greater than 1.0 cm.
Factors contributing to colonoscopy miss rates in-clude poor bowel preparation,20-22 performing a rapidwithdrawal,23-26 and inability to visualize some sections ofthe colon wall.13 Although each of these factors is impor-tant, it is clear that some polyps are missed because theyare located on the proximal aspect of haustral folds andflexures where they can be hidden from the forward viewof the colonoscope despite the best efforts to improvecolon visualization. This is supported by Pickhardt et al,13
who mapped locations of nonrectal neoplasms that weredetected by CT colonography but were missed bycolonoscopy and found that 67% of missed lesions wereon the proximal aspect of folds.
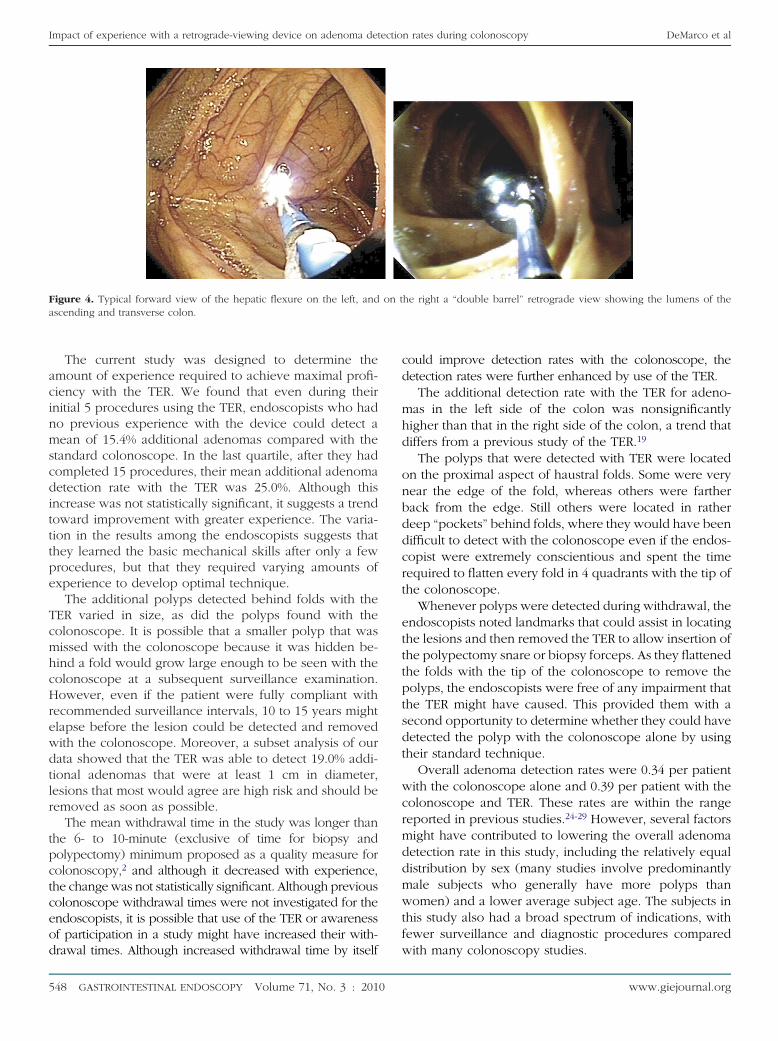
The TER was designed to improve polyp detection byproviding a retrograde view of the colon that reveals theareas behind haustral folds, rectal valves, flexures, and theileocecal valve (Fig. 4).
The potential effectiveness of the TER was first demon-strated in a randomized, controlled preclinical study usinganatomical models17 in which a prototype TER allowedendoscopists to detect 81% of simulated polyps locatedbehind haustral folds compared with 12% when using thecolonoscope alone.
In a first human use pilot study of 24 patients, Tri-adafilopoulos and Li18 found the TER allowed detection of11.8% additional polyps compared with the colonoscopealone.
Waye et al19 examined 249 subjects with the TER inconjunction with a standard colonoscope and found ad-ditional detection rates with the TER of 13.2% for allpolyps and 11.0% for adenomas. For adenomas 6 mm orlarger, the additional detection rate with the TER was
olyps and adenomas in the left or right side of the colon
Adenomas
Left colon Entire colon Right colon Left colon
102 100 58 42
15 16 7 9
14.7 16.0 12.1 21.4
�.001 �.001 �.001 �.001
f all p
s
lon
25.0% and for adenomas 10 mm or larger, it was 33.3%.
olume 71, No. 3 : 2010 GASTROINTESTINAL ENDOSCOPY 547
acinmscditttpe
TcmhcHrewdtlr
tpctceod
Fa
Impact of experience with a retrograde-viewing device on adenoma detection rates during colonoscopy DeMarco et al
5
The current study was designed to determine themount of experience required to achieve maximal profi-iency with the TER. We found that even during theirnitial 5 procedures using the TER, endoscopists who hado previous experience with the device could detect aean of 15.4% additional adenomas compared with the
tandard colonoscope. In the last quartile, after they hadompleted 15 procedures, their mean additional adenomaetection rate with the TER was 25.0%. Although thisncrease was not statistically significant, it suggests a trendoward improvement with greater experience. The varia-ion in the results among the endoscopists suggests thathey learned the basic mechanical skills after only a fewrocedures, but that they required varying amounts ofxperience to develop optimal technique.
The additional polyps detected behind folds with theER varied in size, as did the polyps found with theolonoscope. It is possible that a smaller polyp that wasissed with the colonoscope because it was hidden be-ind a fold would grow large enough to be seen with theolonoscope at a subsequent surveillance examination.owever, even if the patient were fully compliant with
ecommended surveillance intervals, 10 to 15 years mightlapse before the lesion could be detected and removedith the colonoscope. Moreover, a subset analysis of ourata showed that the TER was able to detect 19.0% addi-ional adenomas that were at least 1 cm in diameter,esions that most would agree are high risk and should beemoved as soon as possible.
The mean withdrawal time in the study was longer thanhe 6- to 10-minute (exclusive of time for biopsy andolypectomy) minimum proposed as a quality measure forolonoscopy,2 and although it decreased with experience,he change was not statistically significant. Although previousolonoscope withdrawal times were not investigated for thendoscopists, it is possible that use of the TER or awarenessf participation in a study might have increased their with-
igure 4. Typical forward view of the hepatic flexure on the left, andscending and transverse colon.
rawal times. Although increased withdrawal time by itself
48 GASTROINTESTINAL ENDOSCOPY Volume 71, No. 3 : 2010
could improve detection rates with the colonoscope, thedetection rates were further enhanced by use of the TER.
The additional detection rate with the TER for adeno-mas in the left side of the colon was nonsignificantlyhigher than that in the right side of the colon, a trend thatdiffers from a previous study of the TER.19
The polyps that were detected with TER were locatedon the proximal aspect of haustral folds. Some were verynear the edge of the fold, whereas others were fartherback from the edge. Still others were located in ratherdeep “pockets” behind folds, where they would have beendifficult to detect with the colonoscope even if the endos-copist were extremely conscientious and spent the timerequired to flatten every fold in 4 quadrants with the tip ofthe colonoscope.
Whenever polyps were detected during withdrawal, theendoscopists noted landmarks that could assist in locatingthe lesions and then removed the TER to allow insertion ofthe polypectomy snare or biopsy forceps. As they flattenedthe folds with the tip of the colonoscope to remove thepolyps, the endoscopists were free of any impairment thatthe TER might have caused. This provided them with asecond opportunity to determine whether they could havedetected the polyp with the colonoscope alone by usingtheir standard technique.
Overall adenoma detection rates were 0.34 per patientwith the colonoscope alone and 0.39 per patient with thecolonoscope and TER. These rates are within the rangereported in previous studies.24-29 However, several factorsmight have contributed to lowering the overall adenomadetection rate in this study, including the relatively equaldistribution by sex (many studies involve predominantlymale subjects who generally have more polyps thanwomen) and a lower average subject age. The subjects inthis study also had a broad spectrum of indications, withfewer surveillance and diagnostic procedures compared
he right a “double barrel” retrograde view showing the lumens of the
on twith many colonoscopy studies.
www.giejournal.org

tDwcHdccpaw
bcosteewAam
C
dfiwt1Aalp
cdd
R
DeMarco et al Impact of experience with a retrograde-viewing device on adenoma detection rates during colonoscopy
w
Limitations of the study included the lack of randomiza-ion or blinding and the lack of a separate control group.eterminations regarding adequacy of bowel cleansing andhether each polyp could have been detected with the
olonoscope alone involved a judgment by the endoscopist.owever, to prevent an unfair advantage for the TER, polypetection was biased toward the colonoscope. Increasedleansing during intubation likely enhanced detection by theolonoscope before the TER was inserted, and the endosco-ists were instructed to remove such lesions immediately. Ifpolyp was found with both the colonoscope and TER, itas counted as detection with the colonoscope.Especially before they gained experience in observing
oth sides of the split-screen video display, some endos-opists might have focused more on the novel TER imagen the right side of the screen, resulting in failure to detectome lesions in the colonoscope view on the left side ofhe screen. However, such an effect would be expected toxaggerate the additional detection rate for TER in thearlier quartiles more so than in the later quartiles, and thatould be counter to the trend shown in the study results.lso, observation of multiple views has not adverselyffected endoscopy efficacy in other gastroenterologicalodalities such as capsule endoscopy.30
ONCLUSIONS
Experienced endoscopists new to the TER were able toetect a mean of 15.4% additional adenomas during theirrst 5 procedures. After completing at least 15 proceduresith the device, their mean additional detection rates with
he TER compared with the colonoscope alone were7.0% for all polyps and 25.0% for adenomas of all sizes.dditional detection rates with the TER for medium-sizend large adenomas were greater than those for smalleresions. Procedure times did not vary significantly as morerocedures were performed.These results suggest that, compared with routine
olonoscopy, a retrograde-viewing device can increaseetection rates for clinically significant adenomas withoutetriment to procedure time or procedure complications.
EFERENCES
1. Jemal A, Siegel R, Ward E, et al. Cancer Statistics, 2009. Ca Cancer J Clin2009;59:225-49.
2. Rex DK, Bond JH, Winawer S, et al. Quality in the technical performanceof colonoscopy and the continuous quality improvement process forcolonoscopy: recommendations of the U.S. Multi-Society Task Force onColorectal Cancer. Am J Gastroenterol 2002;97:1296-308.
3. U.S. Preventive Services Task Force. Screening for colorectal cancer: U.S.Preventive Services Task Force recommendation statement. Ann InternMed 2008;149:627-37.
4. Rex DK, Johnson DA, Inadomi JM, et al. American College of Gastroen-terology guidelines for colorectal cancer screening 2008. Am J Gastro-
enterol 2009;104:739-50.ww.giejournal.org V
5. Levin B, Lieberman DA, Winawer SJ, et al. American Cancer Society Colo-rectal Cancer Advisory Group; US Multi-Society Task Force; AmericanCollege of Radiology Colon Cancer Committee. Screening and surveil-lance for the early detection of colorectal cancer and adenomatous pol-yps, 2008: a joint guideline from the American Cancer Society, the USMulti-Society Task Force on Colorectal Cancer, and the American Col-lege of Radiology. CA Cancer J Clin 2008;58:130-60.
6. Winawer SJ, Zauber AG, Rex DK, et al. Guidelines for colonoscopy sur-veillance after polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer and the American Cancer Soci-ety. Gastroenterology 2006;130:1872-85.
7. Hixson LJ, Fennerty MB, Sampliner RE, et al. Prospective blinded trial ofthe colonoscopic miss-rate of large colorectal polyps. Gastrointest En-dosc 1991;37:125-7.
8. Rex DK, Cutler CS, Mark DG, et al. Colonoscopic miss rates of adenomasdetermined by back-to-back colonoscopies. Gastroenterology 1997;112:24-8.
9. Van Rijn JC, Reitsma JB, Dekker E, et al. Polyp miss rate determined bytandem colonoscopy: a systemic review. Am J Gastroenterol 2006;101:343-50.
10. Heresbach D, Barrioz T, Ponchon T, et al. Miss rate for colorectal neoplas-tic polyps: a prospective multicenter study of back-to-back videocolonoscopies. Endoscopy 2008;40:284-90.
11. Soetikno RM, Kaltenbach T, Friedland S, et al. Prevalence of nonpolypoid(flat and depressed) colorectal neoplasms in asymptomatic and symp-tomatic adults. JAMA 2008;299:1027-35.
12. Van Gelder RE, Nio CY, Stoker J, et al. Computed tomographic colonog-raphy compared with colonoscopy in patients at increased risk for colo-rectal cancer. Gastroenterology 2004;127:41-8.
13. Pickhardt PJ, Nugent PA, Schindler WR, et al. Location of adenomasmissed by optical colonoscopy. Ann Intern Med 2004;141:352-9.
14. Pabby A, Schoen RE, Schatzkin A, et al. Analysis of colorectal canceroccurrence during surveillance colonoscopy in the dietary Polyp Pre-vention Trial. Gastrointest Endosc 2005;61:385-91.
15. Postic G, Lewin D, Wallace MB, et al. Colonoscopic miss rates deter-mined by direct comparison of colonoscopy with colon resection spec-imens. Am J Gastroenterol 2002;97:3182-5.
16. Bressler B, Paszat LF, Rabeneck L, et al. Colonoscopic miss rates for right-sided colon cancer: a population-based analysis. Gastroenterology2004;127:452-6.
17. Triadafilopoulos G, Watts HD, Van Dam J, et al. A novel retrograde-viewing auxiliary imaging device (Third Eye Retroscope) improves thedetection of simulated polyps in anatomic models of the colon. Gastro-intest Endosc 2007;65:139-44.
18. Triadafilopoulos G, Li J. A pilot study to assess the safety and efficacy ofthe Third Eye retrograde auxiliary imaging system during colonoscopy.Endoscopy 2008;40:478-82.
19. Waye JD, Russell IH, Fleischer DE, et al. A retrograde-viewing deviceimproves detection of adenomas in the colon: a prospective efficacyevaluation (with videos). Gastrointest Endosc 2010;71:551-6.
20. Rostom A, Jolicoeur E. Validation of a new scale for the assessment ofbowel preparation quality. Gastrointest Endosc 2004;59:482-6.
21. Harewood GC, Sharma VK, de Garmo P. Impact of colonoscopy prepa-ration quality on detection of suspected colonic neoplasia. GastrointestEndosc 2003;58:76-9.
22. Froehlich F, Wietlisbach V, Vader JP, et al. Impact of colonic cleansing onquality and diagnostic yield of colonoscopy: the European Panel of Ap-propriateness of Gastrointestinal Endoscopy European multicenterstudy. Gastrointest Endosc 2005;61:378-84.
23. Rex DK. Colonoscopic withdrawal technique is associated with ade-noma miss rates. Gastrointest Endosc 2000;51:33-6.
24. Barclay RL, Vicari JJ, Doughty AS, et al. Colonoscopic withdrawal timesand adenoma detection during screening colonoscopy. N Engl J Med2006;355:2533-41.
25. Sanchez W, Harewood GC, Petersen BT. Evaluation of polyp detection inrelation to procedure time of screening or surveillance colonoscopy.
Am J Gastroenterol 2004;99:1941-5.olume 71, No. 3 : 2010 GASTROINTESTINAL ENDOSCOPY 549

2
2
Impact of experience with a retrograde-viewing device on adenoma detection rates during colonoscopy DeMarco et al
5
6. Simmons DT, Harewood GC, Baron TH, et al. Impact of endoscopist with-drawal speed on polyp yield: implications for optimal colonoscopywithdrawal time. Aliment Pharmacol Ther 2006;24:965-71.
7. Schatzkin A, Lanza E, Corle D, et al. Lack of effect of a low-fat, high-fiberdiet on the recurrence of colorectal adenomas. N Engl J Med 2000;342:
1149-55.50 GASTROINTESTINAL ENDOSCOPY Volume 71, No. 3 : 2010
28. Lieberman DA, Weiss DG, Bond JH, et al. Use of colonoscopy to screen asymp-tomatic adults for colorectal cancer. N Engl J Med 2000;343:162-8.
29. Rex DK. Maximizing detection of adenomas and cancers duringcolonoscopy. Am J Gastroenterol 2006;101:2866-77.
30. Westerhof J, Koornstra JJ, Weersma RK. Can we reduce capsule endos-
copy reading times? Gastrointest Endosc 2009;69:497-502.GIE on Facebook
GIE now has a Facebook page. Fans will receive news, updates, and links toauthor interviews, podcasts, articles, and tables of contents. Search on Facebookfor “GIE: Gastrointestinal Endoscopy” and become a fan.
www.giejournal.org




















