An Alerting System Improves Adherence to Follow-up Recommendations From Colonoscopy Examinations
11
CLINICAL—ALIMENTARY TRACT An Alerting System Improves Adherence to Follow-up Recommendations From Colonoscopy Examinations DANIEL A. LEFFLER,* NAAMA NEEMAN, ‡ JAMES M. RABB,* JACOB Y. SHIN, ‡ BRUCE E. LANDON, § KUMAR PALLAV,* Z. MYRON FALCHUK,* and MARK D. ARONSON ‡ *Department of Gastroenterology, ‡ Department of Medicine, Beth Israel Deaconess Medical Center, Boston, Massachusetts; § Department of Health Care Policy, Harvard Medical School, Boston, Massachusetts This article has an accompanying continuing medical education activity on page e13. Learning Objective: Upon completion of this CME module successful learners will be able to explain issues in follow-up colonoscopy adherence and identify potential solutions to improve follow up and reduce risk. See related article, Hjelkrem M et al, on page 326 in CGH; see editorial on page 1129. BACKGROUND & AIMS: Systems are available to en- sure that results of tests are communicated to patients. However, lack of adherence to recommended follow-up evaluation increases risk for adverse health outcomes and medical or legal issues. We tested the effective- ness of a novel follow-up system for patients due for surveillance colonoscopy examinations. METHODS: Electronic medical records from colonoscopies per- formed 5 years prior were reviewed to identify individ- uals due for a repeat surveillance colonoscopy exami- nation. Patients were assigned to groups that received the standard of care or a newly developed follow-up system that included a letter to the primary care pro- vider, 2 letters to the patient, and a telephone call to patients who had not yet scheduled an examination by the procedure due date. The primary end point was the percentage of patients who scheduled or completed the colonoscopy examination within 6 months of the due date. Secondary end points included detection rate for adenomas, sex- and ethnicity-specific follow-up rates, and patient satisfaction. RESULTS: Of 2609 patient records reviewed, 830 (31.8%) were found to be due for a surveillance colonoscopy examination in the study period. At the conclusion of the study, 241 (44.7%) patients in the intervention arm had procedures sched- uled or completed, compared with 66 (22.6%) in the control group (P .0001). The follow-up system ap- peared particularly effective among non-white pa- tients; patients reported general satisfaction with the reminder program. CONCLUSIONS: A simple pro- tocol of letters and a telephone call to patients who are due for colonoscopy examinations significantly improved adherence to endoscopic follow-up rec- ommendations. This work provides justification for the creation of reminder systems to improve patient adherence to medical recommendations. Keywords: Quality Improvement; Screening; Colon Cancer Surveillance; Efficacy. D ata from randomized controlled trials and observa- tional studies show that colonoscopy is associated with a reduction in both colorectal cancer incidence and mortality. 1,2 Colorectal cancer arises from a series of sequential genetic mutations that result first in adeno- matous polyps, which then progress on to the develop- ment of cancer. As the only screening method that di- rectly visualizes the entire colon, colonoscopy has become a preferred method of colorectal cancer screening in the United States. 3 Although evidence-based guidelines for colon cancer screening and surveillance exist, 4 there are significant issues with patient adherence to recommendations re- garding colonoscopy. Many studies document barriers to initial colonoscopy, 5–11 but even after the initial colono- scopy is performed, appropriate follow-up testing often is neglected with potentially serious consequences. Limited data suggest that between 15% and 30% of patients, including those with a history of polyps, do not adhere to surveillance colonoscopy recommendations, although these studies were in selected groups and likely were not representative of a typical colonoscopy surveillance pop- Abbreviations used in this paper: BIDMC, Beth Israel Deaconess Medical Center; EMR, electronic medical record; PCP, primary care physician. © 2011 by the AGA Institute 0016-5085/$36.00 doi:10.1053/j.gastro.2011.01.003 CLINICAL– ALIMENTARY TRACT GASTROENTEROLOGY 2011;140:1166 –1173
-
Upload
hms-harvard -
Category
Documents
-
view
1 -
download
0
Transcript of An Alerting System Improves Adherence to Follow-up Recommendations From Colonoscopy Examinations
H
CLIN
ICA
L–A
LIMEN
TARY
TRA
CT
GASTROENTEROLOGY 2011;140:1166–1173
CLINICAL—ALIMENTARY TRACT
An Alerting System Improves Adherence to Follow-up RecommendationsFrom Colonoscopy Examinations
DANIEL A. LEFFLER,* NAAMA NEEMAN,‡ JAMES M. RABB,* JACOB Y. SHIN,‡ BRUCE E. LANDON,§ KUMAR PALLAV,*Z. MYRON FALCHUK,* and MARK D. ARONSON‡
*Department of Gastroenterology, ‡Department of Medicine, Beth Israel Deaconess Medical Center, Boston, Massachusetts; §Department of Health Care Policy,arvard Medical School, Boston, Massachusetts
This article has an accompanying continuing medical education activity on page e13. Learning Objective: Uponcompletion of this CME module successful learners will be able to explain issues in follow-up colonoscopy adherence
and identify potential solutions to improve follow up and reduce risk.wmsmmrbi
See related article, Hjelkrem M et al, on page326 in CGH; see editorial on page 1129.
BACKGROUND & AIMS: Systems are available to en-sure that results of tests are communicated to patients.However, lack of adherence to recommended follow-upevaluation increases risk for adverse health outcomesand medical or legal issues. We tested the effective-ness of a novel follow-up system for patients due forsurveillance colonoscopy examinations. METHODS:Electronic medical records from colonoscopies per-formed 5 years prior were reviewed to identify individ-uals due for a repeat surveillance colonoscopy exami-nation. Patients were assigned to groups that receivedthe standard of care or a newly developed follow-upsystem that included a letter to the primary care pro-vider, 2 letters to the patient, and a telephone call topatients who had not yet scheduled an examination bythe procedure due date. The primary end point was thepercentage of patients who scheduled or completed thecolonoscopy examination within 6 months of the duedate. Secondary end points included detection rate foradenomas, sex- and ethnicity-specific follow-up rates,and patient satisfaction. RESULTS: Of 2609 patientrecords reviewed, 830 (31.8%) were found to be due fora surveillance colonoscopy examination in the studyperiod. At the conclusion of the study, 241 (44.7%)patients in the intervention arm had procedures sched-uled or completed, compared with 66 (22.6%) in thecontrol group (P � .0001). The follow-up system ap-peared particularly effective among non-white pa-tients; patients reported general satisfaction with thereminder program. CONCLUSIONS: A simple pro-tocol of letters and a telephone call to patients who
are due for colonoscopy examinations significantlyimproved adherence to endoscopic follow-up rec-ommendations. This work provides justificationfor the creation of reminder systems to improvepatient adherence to medical recommendations.
Keywords: Quality Improvement; Screening; Colon CancerSurveillance; Efficacy.
Data from randomized controlled trials and observa-tional studies show that colonoscopy is associated
ith a reduction in both colorectal cancer incidence andortality.1,2 Colorectal cancer arises from a series of
equential genetic mutations that result first in adeno-atous polyps, which then progress on to the develop-ent of cancer. As the only screening method that di-
ectly visualizes the entire colon, colonoscopy hasecome a preferred method of colorectal cancer screening
n the United States.3
Although evidence-based guidelines for colon cancerscreening and surveillance exist,4 there are significantissues with patient adherence to recommendations re-garding colonoscopy. Many studies document barriers toinitial colonoscopy,5–11 but even after the initial colono-scopy is performed, appropriate follow-up testing often isneglected with potentially serious consequences. Limiteddata suggest that between 15% and 30% of patients,including those with a history of polyps, do not adhere tosurveillance colonoscopy recommendations, althoughthese studies were in selected groups and likely were notrepresentative of a typical colonoscopy surveillance pop-
Abbreviations used in this paper: BIDMC, Beth Israel DeaconessMedical Center; EMR, electronic medical record; PCP, primary carephysician.
© 2011 by the AGA Institute0016-5085/$36.00
doi:10.1053/j.gastro.2011.01.003

r
CLI
NIC
AL–
ALI
MEN
TARY
TRA
CT
April 2011 ALERTING SYSTEM 1167
ulation.12,13 Many practices and institutions currentlyhave systems in place to ensure and document that re-sults of tests, such as pathology findings after a polypec-tomy, are communicated to patients. Few institutions orpractices, however, have implemented systems to moni-tor and improve compliance with suggested follow-uptests. Reasons for the current lack of systems to improveadherence with endoscopic follow-up evaluation includethe length of time between procedures, controversy overoptimal follow-up periods, and uncertainty regardingspecialist vs primary care physician responsibility.
Regardless of cause, the lack of system-wide strategiesfor ensuring recommended follow-up evaluation afterprocedures carries with it many important clinical rami-fications. Most importantly, patient care is compromisedwhen delayed or missed procedures lead to the develop-ment of more advanced disease, as occurs when advancedlesions are found. In addition, there is an increased riskof litigation when there is no reminder system in place toinform patients of the need for repeat studies, and nodocumentation that patients have received adequate no-tification of the need for follow-up testing. Data from alarge malpractice carrier show that “missed diagnosis” ofcolorectal cancer is the second most common type ofcancer cited in malpractice claims, and that many ofthese claims were related to the lack of adequate fol-low-up evaluation and documentation systems.14 Al-though all follow-up medical tests are subject to variableadherence rates, colonoscopy presents particular diffi-culty for both patients and providers because of variabil-ity in the recommended follow-up interval and longlength of time between examinations.
To address the earlier-mentioned barriers for effectiveendoscopic follow-up evaluation, we developed, imple-mented, and tested a comprehensive follow-up manage-ment system for incorporation into the electronic medicalrecord (EMR) of a major gastroenterology referral centerthat performs approximately 10,000 screening colonosco-pies per year. This article describes the specifications of thefollow-up system created and the results of a randomizedcontrolled trial of the effectiveness of this system.
Materials and MethodsDevelopment of Principles for an AutomatedFollow-up Reminder SystemInterviews and meetings with primary care and
gastroenterology physicians suggested overlapping butnot identical requirements for a colonoscopy follow-upmanagement system that included the following 7 prin-ciples: (1) both the specialist and primary care physician(PCP) should be able to place and alter the colonoscopyreferral; (2) PCPs should be notified when the follow-upprocedure is due, and before the patient is contacted sothat, when appropriate, the order can be modified orcanceled; (3) for efficiency, patients first should be con-
tacted by letters, with telephone contact reserved fornecessary cases; (4) PCPs should be notified if a patientfails to keep recommended follow-up testing despite thereminders; (5) specialists should be able to choose on acase-by-case basis to be notified if the patient does notschedule/keep a follow-up appointment (eg, for fol-low-up evaluation of high-risk patients); (6) the remindersystem should be patient-dependent rather than provid-er-dependent so that the system will remain functionalregardless of whether the initial or ordering physician isstill involved in caring for the patient; and (7) the re-minder system should be integrated into the EMR in amanner that minimizes change to physician workflow.
Design of the Automated Follow-up ReminderSystemIn accordance with the 7 core principles listed
earlier, we developed a system algorithm wherein order-ing prompts are linked to the online pathology reports,to encourage specialists to order or modify follow-uprecommendations as necessary based on the pathologyresults. Links to current guidelines also are embedded inthe ordering system.
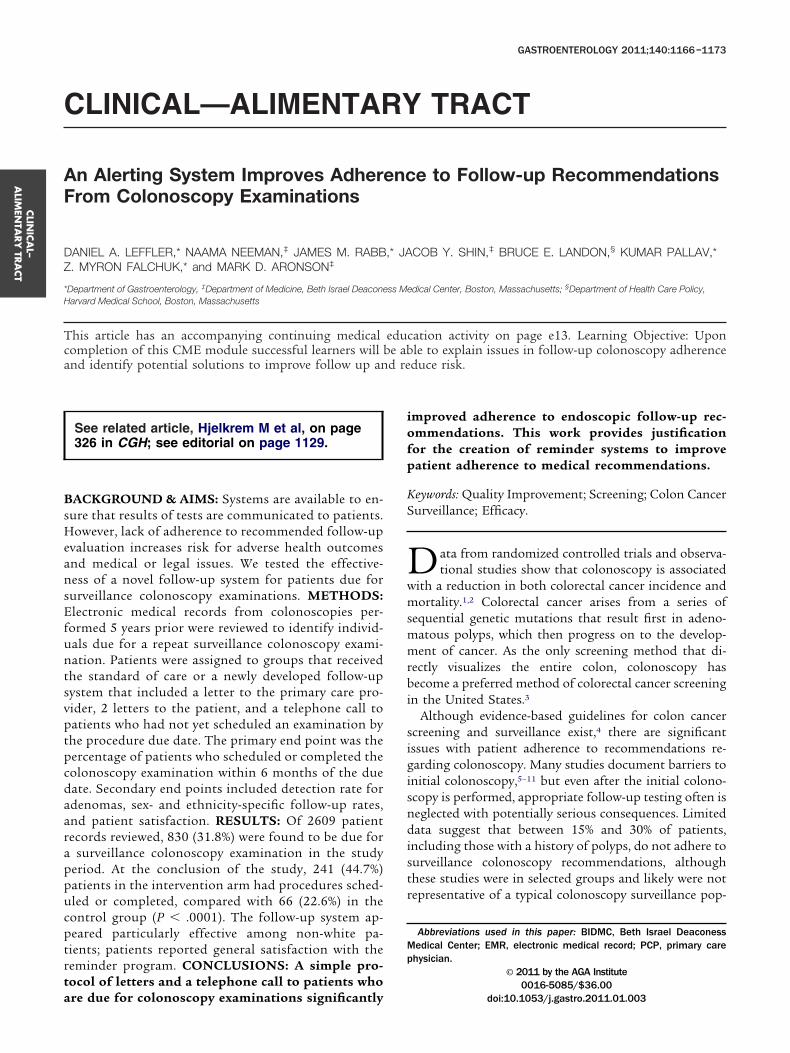
The system is initiated when a provider orders a fol-low-up test, indication, and a time interval until due. Theorder can be made or modified immediately after theprocedure, when the pathology report is received, or at anoffice visit. In addition, should guidelines change, proce-dures can be recalled by indication and the follow-upinterval can be altered as necessary. The system then liesdormant until 4 months before the due date for theprocedure. At that time the EMR of the patient is queriedfor a scheduled or completed procedure within 6 monthsof the due date. If none is found, a notification is sent tothe patient’s PCP that the patient is due for colonoscopyin the coming months, so that he/she can modify orcancel the order if necessary. If the PCP does not modifythe order, 3 months before the procedure due date thepatient is sent a standard reminder letter (Appendix 1).One month before the procedure due date, if no proce-dure has been scheduled or completed the patient is sentan identical reminder letter. Finally, if the due date passeswith no procedure scheduled or completed, and no cor-respondence from the patient, the system alerts admin-istrative staff to call the patient (Figure 1 shows a graphicepresentation of the follow-up algorithm).
Testing of the Automated Follow-up ReminderSystemThe follow-up reminder system is designed to be
forward looking (ie, the system is activated at the time ofthe index procedure. To assess system effectiveness in apractical time period, we evaluated records of all patientswho had undergone a colonoscopy at the institution 5years previously (from August 1, 2004, to February 28,2005). In this population, we looked for those who weredue for a 5-year follow-up study (from August 1, 2009, to
February 28, 2010) based on the endoscopist’s recom-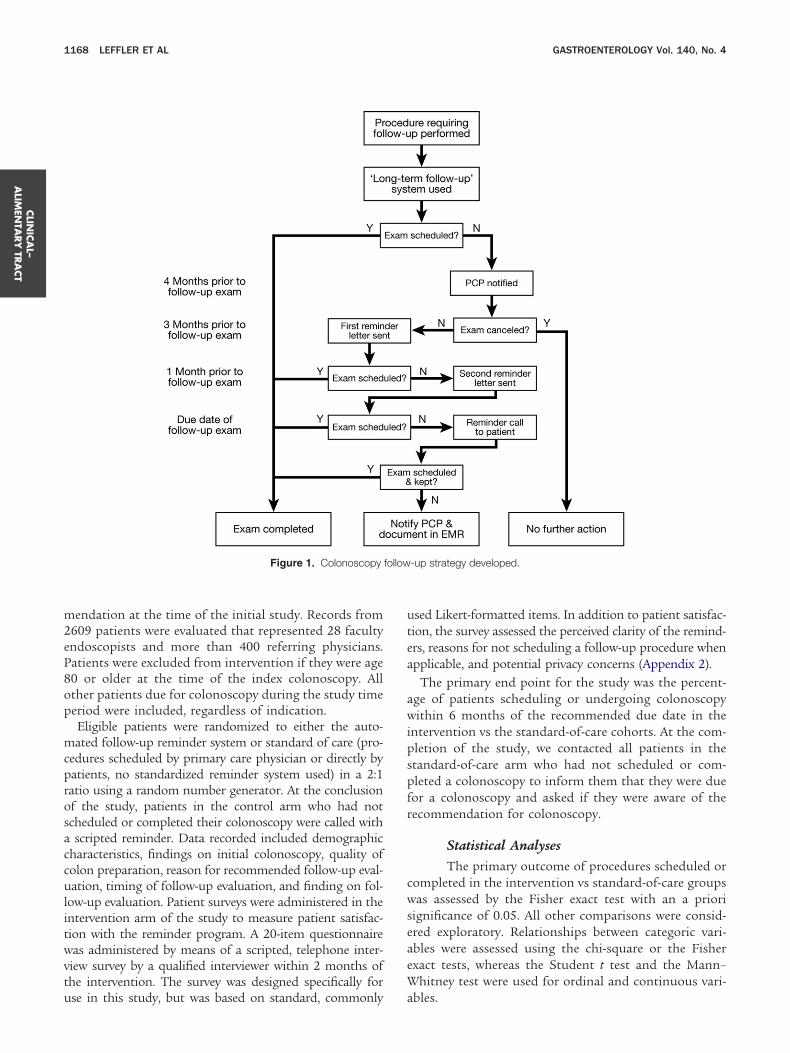
follow
CLIN
ICA
L–A
LIMEN
TARY
TRA
CT
1168 LEFFLER ET AL GASTROENTEROLOGY Vol. 140, No. 4
mendation at the time of the initial study. Records from2609 patients were evaluated that represented 28 facultyendoscopists and more than 400 referring physicians.Patients were excluded from intervention if they were age80 or older at the time of the index colonoscopy. Allother patients due for colonoscopy during the study timeperiod were included, regardless of indication.
Eligible patients were randomized to either the auto-mated follow-up reminder system or standard of care (pro-cedures scheduled by primary care physician or directly bypatients, no standardized reminder system used) in a 2:1ratio using a random number generator. At the conclusionof the study, patients in the control arm who had notscheduled or completed their colonoscopy were called witha scripted reminder. Data recorded included demographiccharacteristics, findings on initial colonoscopy, quality ofcolon preparation, reason for recommended follow-up eval-uation, timing of follow-up evaluation, and finding on fol-low-up evaluation. Patient surveys were administered in theintervention arm of the study to measure patient satisfac-tion with the reminder program. A 20-item questionnairewas administered by means of a scripted, telephone inter-view survey by a qualified interviewer within 2 months ofthe intervention. The survey was designed specifically for
Figure 1. Colonoscopy
use in this study, but was based on standard, commonly
used Likert-formatted items. In addition to patient satisfac-tion, the survey assessed the perceived clarity of the remind-ers, reasons for not scheduling a follow-up procedure whenapplicable, and potential privacy concerns (Appendix 2).
The primary end point for the study was the percent-age of patients scheduling or undergoing colonoscopywithin 6 months of the recommended due date in theintervention vs the standard-of-care cohorts. At the com-pletion of the study, we contacted all patients in thestandard-of-care arm who had not scheduled or com-pleted a colonoscopy to inform them that they were duefor a colonoscopy and asked if they were aware of therecommendation for colonoscopy.
Statistical AnalysesThe primary outcome of procedures scheduled or
completed in the intervention vs standard-of-care groupswas assessed by the Fisher exact test with an a priorisignificance of 0.05. All other comparisons were consid-ered exploratory. Relationships between categoric vari-ables were assessed using the chi-square or the Fisherexact tests, whereas the Student t test and the Mann–Whitney test were used for ordinal and continuous vari-
-up strategy developed.
ables.
out o
CLI
NIC
AL–
ALI
MEN
TARY
TRA
CT
April 2011 ALERTING SYSTEM 1169
Data were entered into a secure database (Access,Microsoft Office; Microsoft Corp, Redmond, WA) andreviewed for errors before analysis. Statistical analysiswas completed using SPSS for Windows (release 17.0,2008; SPSS, Inc, Chicago, IL). This project was ap-proved by the Beth Israel Deaconess Medical CenterInvestigational Review Board Protocol #2008-P-000426and funded by Controlled Risk Insurance Company(CRICO)-Risk Management Foundation (Cambridge,MA). The funder played no part in the design orconduct of the trial. This study is registered underclinicaltrials.gov number NCT01172080.
ResultsOf 2609 patients identified from August 1,
2004, to February 28, 2005, there were 830 (31.8%)eligible for randomization. The most common reasonsfor lack of eligibility were that patients were not yetdue for follow-up evaluation (32.5%) or had intervalcolonoscopies performed early for diagnostic purposes
Figure 2. Flow chart of study and major outcomes. *Majority owingprocedure, 13 (2.4%) were not able to be contacted, 13 (2.4%) moved
(18.7%) (Figure 2).
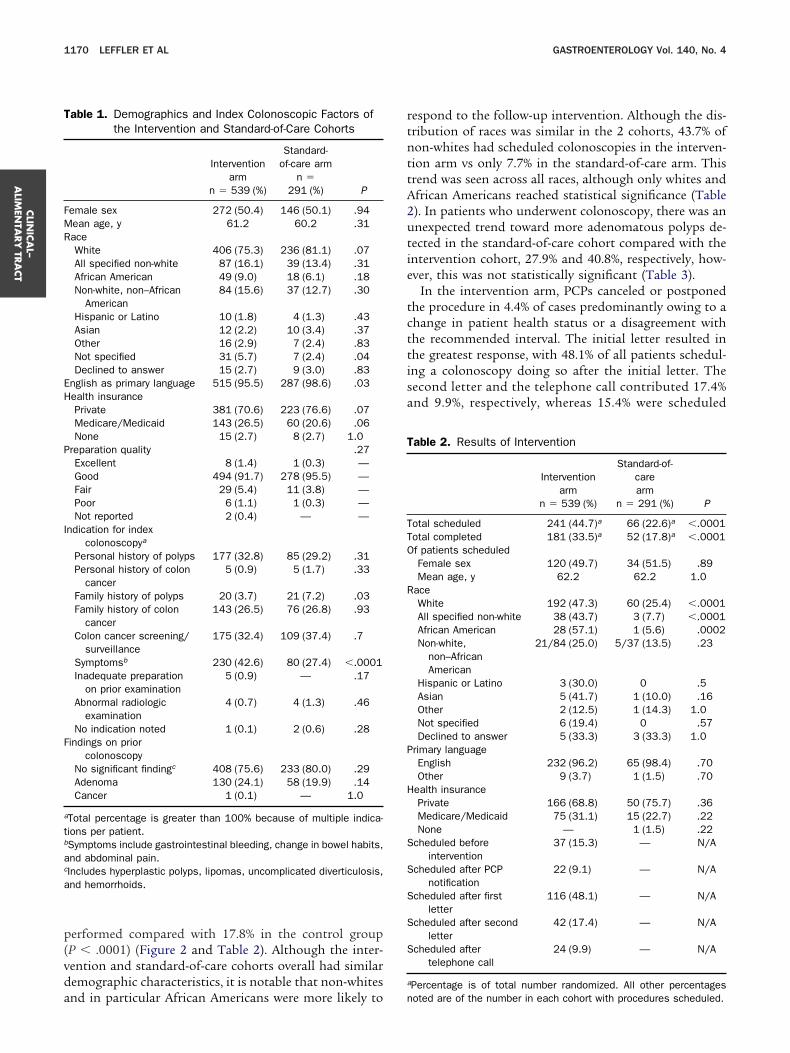
Of the 830 patients, 539 were randomized to the in-tervention arm and the remaining 291 were followed upwithout intervention. Demographics and index colono-scopic factors were similar in the intervention and con-trol cohorts with the exception of a slight predominanceof non-English speakers and unspecified race in theintervention arm (Table 1). The quality of colonoscopypreparations in the index procedures was similar in thecontrol and intervention arms. In the interventionarm, fewer patients had their initial procedures per-formed for a family history of polyps and more wereowing to the presence of symptoms (P � .03 and�.0001, respectively). Findings, and specifically ade-noma detection rates, at the index colonoscopy weresimilar in the 2 groups. Mean age and sex also weresimilar between the study groups (Table 1).
At the completion of the study, 44.7% of patientsrandomized to the intervention arm had proceduresscheduled compared with 22.6% in the control group(P � .0001). Similarly, at the completion of the study
vanced malignancy. **Of those not scheduled: 244 (45.2%) deferredf system, 3 (0.6%) reported comorbidity, and 1 (0.2%) was deceased.
to ad
33.5% of patients in the intervention arm had procedures
a
TO
CLIN
ICA
L–A
LIMEN
TARY
TRA
CT
1170 LEFFLER ET AL GASTROENTEROLOGY Vol. 140, No. 4
performed compared with 17.8% in the control group(P � .0001) (Figure 2 and Table 2). Although the inter-vention and standard-of-care cohorts overall had similardemographic characteristics, it is notable that non-whites
Table 1. Demographics and Index Colonoscopic Factors ofthe Intervention and Standard-of-Care Cohorts
Interventionarm
n � 539 (%)
Standard-of-care arm
n �291 (%) P
Female sex 272 (50.4) 146 (50.1) .94Mean age, y 61.2 60.2 .31Race
White 406 (75.3) 236 (81.1) .07All specified non-white 87 (16.1) 39 (13.4) .31African American 49 (9.0) 18 (6.1) .18Non-white, non–African
American84 (15.6) 37 (12.7) .30
Hispanic or Latino 10 (1.8) 4 (1.3) .43Asian 12 (2.2) 10 (3.4) .37Other 16 (2.9) 7 (2.4) .83Not specified 31 (5.7) 7 (2.4) .04Declined to answer 15 (2.7) 9 (3.0) .83
English as primary language 515 (95.5) 287 (98.6) .03Health insurance
Private 381 (70.6) 223 (76.6) .07Medicare/Medicaid 143 (26.5) 60 (20.6) .06None 15 (2.7) 8 (2.7) 1.0
Preparation quality .27Excellent 8 (1.4) 1 (0.3) —Good 494 (91.7) 278 (95.5) —Fair 29 (5.4) 11 (3.8) —Poor 6 (1.1) 1 (0.3) —Not reported 2 (0.4) — —
Indication for indexcolonoscopya
Personal history of polyps 177 (32.8) 85 (29.2) .31Personal history of colon
cancer5 (0.9) 5 (1.7) .33
Family history of polyps 20 (3.7) 21 (7.2) .03Family history of colon
cancer143 (26.5) 76 (26.8) .93
Colon cancer screening/surveillance
175 (32.4) 109 (37.4) .7
Symptomsb 230 (42.6) 80 (27.4) �.0001Inadequate preparation
on prior examination5 (0.9) — .17
Abnormal radiologicexamination
4 (0.7) 4 (1.3) .46
No indication noted 1 (0.1) 2 (0.6) .28Findings on prior
colonoscopyNo significant findingc 408 (75.6) 233 (80.0) .29Adenoma 130 (24.1) 58 (19.9) .14Cancer 1 (0.1) — 1.0
aTotal percentage is greater than 100% because of multiple indica-tions per patient.bSymptoms include gastrointestinal bleeding, change in bowel habits,and abdominal pain.cIncludes hyperplastic polyps, lipomas, uncomplicated diverticulosis,nd hemorrhoids.
and in particular African Americans were more likely to
respond to the follow-up intervention. Although the dis-tribution of races was similar in the 2 cohorts, 43.7% ofnon-whites had scheduled colonoscopies in the interven-tion arm vs only 7.7% in the standard-of-care arm. Thistrend was seen across all races, although only whites andAfrican Americans reached statistical significance (Table2). In patients who underwent colonoscopy, there was anunexpected trend toward more adenomatous polyps de-tected in the standard-of-care cohort compared with theintervention cohort, 27.9% and 40.8%, respectively, how-ever, this was not statistically significant (Table 3).
In the intervention arm, PCPs canceled or postponedthe procedure in 4.4% of cases predominantly owing to achange in patient health status or a disagreement withthe recommended interval. The initial letter resulted inthe greatest response, with 48.1% of all patients schedul-ing a colonoscopy doing so after the initial letter. Thesecond letter and the telephone call contributed 17.4%and 9.9%, respectively, whereas 15.4% were scheduled
Table 2. Results of Intervention
Interventionarm
n � 539 (%)
Standard-of-carearm
n � 291 (%) P
Total scheduled 241 (44.7)a 66 (22.6)a �.0001otal completed 181 (33.5)a 52 (17.8)a �.0001f patients scheduledFemale sex 120 (49.7) 34 (51.5) .89Mean age, y 62.2 62.2 1.0
RaceWhite 192 (47.3) 60 (25.4) �.0001All specified non-white 38 (43.7) 3 (7.7) �.0001African American 28 (57.1) 1 (5.6) .0002Non-white,
non–AfricanAmerican
21/84 (25.0) 5/37 (13.5) .23
Hispanic or Latino 3 (30.0) 0 .5Asian 5 (41.7) 1 (10.0) .16Other 2 (12.5) 1 (14.3) 1.0Not specified 6 (19.4) 0 .57Declined to answer 5 (33.3) 3 (33.3) 1.0
Primary languageEnglish 232 (96.2) 65 (98.4) .70Other 9 (3.7) 1 (1.5) .70
Health insurancePrivate 166 (68.8) 50 (75.7) .36Medicare/Medicaid 75 (31.1) 15 (22.7) .22None — 1 (1.5) .22
Scheduled beforeintervention
37 (15.3) — N/A
Scheduled after PCPnotification
22 (9.1) — N/A
Scheduled after firstletter
116 (48.1) — N/A
Scheduled after secondletter
42 (17.4) — N/A
Scheduled aftertelephone call
24 (9.9) — N/A
aPercentage is of total number randomized. All other percentages
noted are of the number in each cohort with procedures scheduled.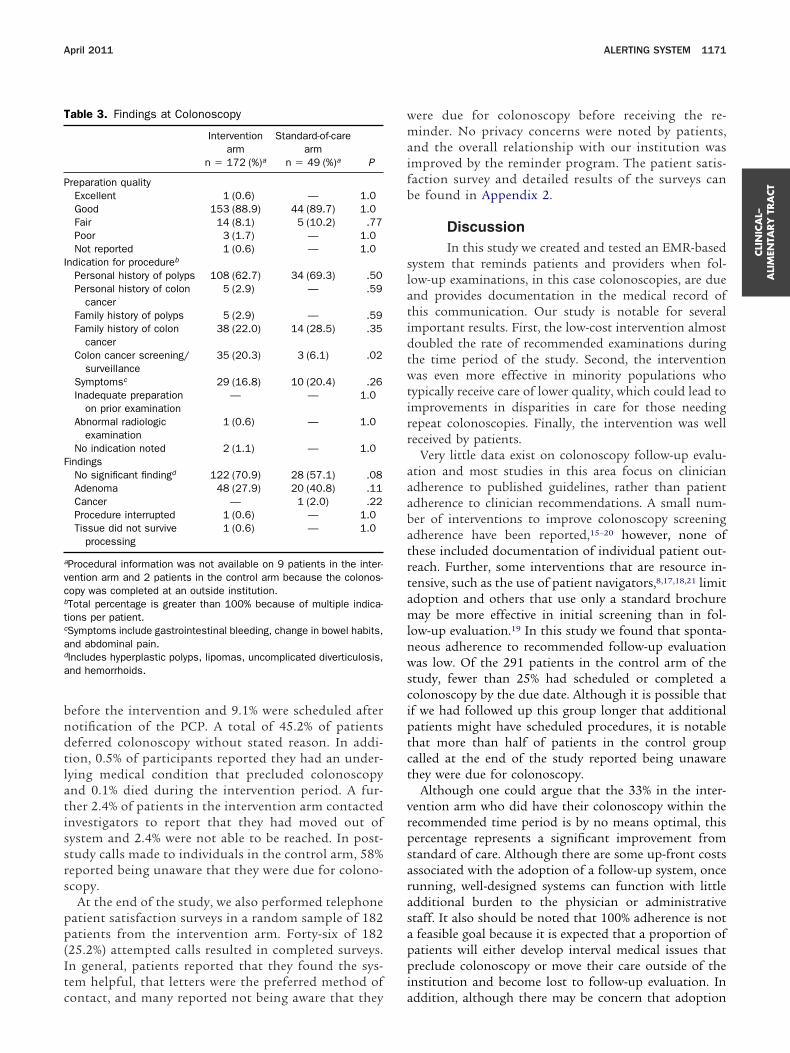
trt
P
I
vc
a
CLI
NIC
AL–
ALI
MEN
TARY
TRA
CT
April 2011 ALERTING SYSTEM 1171
before the intervention and 9.1% were scheduled afternotification of the PCP. A total of 45.2% of patientsdeferred colonoscopy without stated reason. In addi-tion, 0.5% of participants reported they had an under-lying medical condition that precluded colonoscopyand 0.1% died during the intervention period. A fur-ther 2.4% of patients in the intervention arm contactedinvestigators to report that they had moved out ofsystem and 2.4% were not able to be reached. In post-study calls made to individuals in the control arm, 58%reported being unaware that they were due for colono-scopy.
At the end of the study, we also performed telephonepatient satisfaction surveys in a random sample of 182patients from the intervention arm. Forty-six of 182(25.2%) attempted calls resulted in completed surveys.In general, patients reported that they found the sys-tem helpful, that letters were the preferred method of
Table 3. Findings at Colonoscopy
Interventionarm
n � 172 (%)a
Standard-of-carearm
n � 49 (%)a P
reparation qualityExcellent 1 (0.6) — 1.0Good 153 (88.9) 44 (89.7) 1.0Fair 14 (8.1) 5 (10.2) .77Poor 3 (1.7) — 1.0Not reported 1 (0.6) — 1.0
ndication for procedureb
Personal history of polyps 108 (62.7) 34 (69.3) .50Personal history of colon
cancer5 (2.9) — .59
Family history of polyps 5 (2.9) — .59Family history of colon
cancer38 (22.0) 14 (28.5) .35
Colon cancer screening/surveillance
35 (20.3) 3 (6.1) .02
Symptomsc 29 (16.8) 10 (20.4) .26Inadequate preparation
on prior examination— — 1.0
Abnormal radiologicexamination
1 (0.6) — 1.0
No indication noted 2 (1.1) — 1.0Findings
No significant findingd 122 (70.9) 28 (57.1) .08Adenoma 48 (27.9) 20 (40.8) .11Cancer — 1 (2.0) .22Procedure interrupted 1 (0.6) — 1.0Tissue did not survive
processing1 (0.6) — 1.0
aProcedural information was not available on 9 patients in the inter-ention arm and 2 patients in the control arm because the colonos-opy was completed at an outside institution.
bTotal percentage is greater than 100% because of multiple indica-tions per patient.cSymptoms include gastrointestinal bleeding, change in bowel habits,nd abdominal pain.
dIncludes hyperplastic polyps, lipomas, uncomplicated diverticulosis,and hemorrhoids.
contact, and many reported not being aware that they
were due for colonoscopy before receiving the re-minder. No privacy concerns were noted by patients,and the overall relationship with our institution wasimproved by the reminder program. The patient satis-faction survey and detailed results of the surveys canbe found in Appendix 2.
DiscussionIn this study we created and tested an EMR-based
system that reminds patients and providers when fol-low-up examinations, in this case colonoscopies, are dueand provides documentation in the medical record ofthis communication. Our study is notable for severalimportant results. First, the low-cost intervention almostdoubled the rate of recommended examinations duringthe time period of the study. Second, the interventionwas even more effective in minority populations whotypically receive care of lower quality, which could lead toimprovements in disparities in care for those needingrepeat colonoscopies. Finally, the intervention was wellreceived by patients.
Very little data exist on colonoscopy follow-up evalu-ation and most studies in this area focus on clinicianadherence to published guidelines, rather than patientadherence to clinician recommendations. A small num-ber of interventions to improve colonoscopy screeningadherence have been reported,15–20 however, none ofhese included documentation of individual patient out-each. Further, some interventions that are resource in-ensive, such as the use of patient navigators,8,17,18,21 limit
adoption and others that use only a standard brochuremay be more effective in initial screening than in fol-low-up evaluation.19 In this study we found that sponta-neous adherence to recommended follow-up evaluationwas low. Of the 291 patients in the control arm of thestudy, fewer than 25% had scheduled or completed acolonoscopy by the due date. Although it is possible thatif we had followed up this group longer that additionalpatients might have scheduled procedures, it is notablethat more than half of patients in the control groupcalled at the end of the study reported being unawarethey were due for colonoscopy.
Although one could argue that the 33% in the inter-vention arm who did have their colonoscopy within therecommended time period is by no means optimal, thispercentage represents a significant improvement fromstandard of care. Although there are some up-front costsassociated with the adoption of a follow-up system, oncerunning, well-designed systems can function with littleadditional burden to the physician or administrativestaff. It also should be noted that 100% adherence is nota feasible goal because it is expected that a proportion ofpatients will either develop interval medical issues thatpreclude colonoscopy or move their care outside of theinstitution and become lost to follow-up evaluation. In
addition, although there may be concern that adoption
si
onmcmsmepa
mtitPco
ifwocs.cpiTimdtowpscftc
sapcwsbrwrtwtgrcims
CLIN
ICA
L–A
LIMEN
TARY
TRA
CT
1172 LEFFLER ET AL GASTROENTEROLOGY Vol. 140, No. 4
of a follow-up system could increase malpractice riskthrough system failures both technical and human (in-correct addresses, order entry error), detailed discussionwith the risk management group that covers our centerand all affiliated groups suggested that these potentialrisks were substantially less than the risks associated withcurrent practice. Further studies will be necessary todetermine whether the documentation provided by thissystem will be sufficient to reduce the burden of malprac-tice claims related to inadequate follow-up evaluation.
Some practices may be reluctant to devote the re-sources necessary for the described workflow, however,despite potentially significant up-front costs, once initi-ated, the cost of maintaining a follow-up reminder sys-tem such as this is quite low and may even be revenue-generating. Further, if follow-up systems were to becomestandard in new EMR systems, cost would be negligibleand benefits would be persistent. It also is notable thatthe majority of effort was spent on the telephone recall,which was required for only about half of the interven-tion group. Although we believe that telephone calls areimportant, this step added only approximately 10% to theoverall scheduled procedures, and even without this stepthe difference in follow-up evaluation between thegroups remained highly significant (40.3% vs 22.6%; P �.0001).
In recent years there has been significant concern re-garding overuse of surveillance colonoscopy.22–24 It isnotable that 30.8% of patients studied were found to haveadenomatous polyps, a percentage similar to that seen inthe previous studies of surveillance colonoscopy,25 andeven the expected polyp detection rate at first screeningcolonoscopy.26,27 The high rate of adenoma detectionsuggests that recommendations for follow-up evaluationwere, in general, appropriate. We also would argue thatthe particular indications and time recommended forfollow-up evaluation in this cohort are tangential to theintervention tested. The follow-up system devised gener-alizes well across multiple different test indications andthe potential to improve adherence rates is clear. Further,the intervention was particularly effective in minoritypopulations, which traditionally have lower screeningand surveillance rates.28 This finding suggests that use ofimilar solutions can reduce the disparities seen in med-cal care across the US medical system.
Although our data provide strong support for the utilityf patient-centered reminder systems, we do recognize aumber of limitations. First, we focused on patients recom-ended for 5-year follow-up evaluation, whereas colonos-
opy may be recommended at nearly any interval from 6onths to 10 years. We chose this interval for the current
tudy, but we designed our prospective system to accom-odate any possible follow-up interval. Five-year follow-up
valuation was chosen to provide homogeneity to the studyopulation at a commonly recommended interval. Second,
lthough patients were randomized, PCPs were not, andost PCPs would have had patients in both the interven-ion and control arms. The reminders provided for thentervention cohort may have increased the PCPs awarenesso this matter in general, and hence increased reminders byCPs to patients in the control arm of recommendedolonoscopies. Such spillover, however, would have biasedur results to the null.
In addition, despite randomization, more individualsn the study cohort had the index colonoscopy performedor symptoms than in the control group. To investigatehether this factor could have significantly confoundedur results, we assessed for a correlation between priorolonoscopy for symptoms and scheduling of a follow-uptudy. In the control group there was no association (P �128), however, in the study group there was a significantorrelation (P � .003), with individuals having had theast colonoscopy performed for symptoms being signif-
cantly less likely to schedule a follow-up colonoscopy.he reason for this is unclear, but we speculate that
ndividuals who present for colonoscopy with symptomsay, on the whole, be less likely to have another proce-
ure when they are asymptomatic. Regardless of reason,his suggests that if the cohorts had been well matchedn reason for index colonoscopy, our finding likelyould have been more robust. We also recognize that theatient satisfaction survey was only completed in a smallubsample of the study population, and although nooncerns were elicited in this group, results may not beully representative. Finally, we acknowledge that, al-hough successful, this study was conducted at a singleenter and results may not be generalizable.
In summary, our automated, patient-dependent colono-copy follow-up reminder system significantly improveddherence with recommended surveillance colonoscopy andatient satisfaction. Although this study focused only onolonoscopy, it is expected that this approach would beidely applicable across different procedures and medical
pecialties. Overall, this study is congruent with the growingody of evidence that EMR systems can improve care andeduce error.29 At this stage it is unclear how EMR systemsill develop and how the general population’s growing
eliance on electronic means of communication will alterhe way patients and clinicians interact. Regardless ofhether information is transmitted on paper, in e-mails,
exts, or other media, we anticipate that the need for inte-rated systems to assist in prompting patients to obtainecommended care will increase. As electronic medical re-ord systems are adopted and refined, protocols for notify-ng and documenting communication regarding recom-
ended follow-up screening and diagnostic procedureshould be strongly considered.
Supplementary Material
Note: To access the supplementary material
accompanying this article, visit the online version of
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
CLI
NIC
AL–
ALI
MEN
TARY
TRA
CT
April 2011 ALERTING SYSTEM 1173
Gastroenterology at www.gastrojournal.org, and at doi:10.1053/j.gastro.2011.01.003.
References
1. Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectalcancer by colonoscopic polypectomy. The National Polyp StudyWorkgroup. N Engl J Med 1993;329:1977–1981.
2. Citarda F, Tomaselli G, Capocaccia R, et al. Efficacy in standardclinical practice of colonoscopic polypectomy in reducing colorec-tal cancer incidence. Gut 2001;48:812–815.
3. Screening for colorectal cancer: U.S. Preventive Services TaskForce recommendation statement. Ann Intern Med 2008;149:627–637.
4. Winawer S, Fletcher R, Rex D, et al. Colorectal cancer screeningand surveillance: clinical guidelines and rationale—updatebased on new evidence. Gastroenterology 2003;124:544–560.
5. Pignone MP, Lewis CL. Using quality improvement techniques toincrease colon cancer screening. Am J Med 2009;122:419–420.
6. Lloyd SC, Harvey NR, Hebert JR, et al. Racial disparities in coloncancer. Primary care endoscopy as a tool to increase screeningrates among minority patients. Cancer 2007;109:378–385.
7. Bajracharya SM. An assessment of the perceived barriers andstrategies to promoting early detection of colorectal cancer: apractitioners’ perspective. Int Q Community Health Educ 2006;26:23–44.
8. Nash D, Azeez S, Vlahov D, et al. Evaluation of an intervention toincrease screening colonoscopy in an urban public hospital set-ting. J Urban Health 2006;83:231–243.
9. Zimmerman RK, Tabbarah M, Trauth J, et al. Predictors of lowerendoscopy use among patients at three inner-city neighborhoodhealth centers. J Urban Health 2006;83:221–230.
0. Klabunde CN, Schenck AP, Davis WW. Barriers to colorectalcancer screening among Medicare consumers. Am J Prev Med2006;30:313–319.
1. Denberg TD, Melhado TV, Coombes JM, et al. Predictors ofnonadherence to screening colonoscopy. J Gen Intern Med 2005;20:989–995.
2. Colquhoun P, Chen HC, Kim JI, et al. High compliance ratesobserved for follow-up colonoscopy post polypectomy are achiev-able outside of clinical trials: efficacy of polypectomy is notreduced by low compliance for follow up. Colorectal Dis 2004;6:158–161.
3. Siddiqui AA, Patel A, Huerta S. Determinants of compliance withcolonoscopy in patients with adenomatous colon polyps in aveteran population. Aliment Pharmacol Ther 2006;24:1623–1630.
4. CRICO Risk Managment Foundation. Colorectal Cancer ScreeningAlgorithm. Available: http://www.rmf.harvard.edu/high-risk-areas/diagnosis/algorithms/colorectal-cancer-screening-algorithm.aspx. Date accessed: 3/17/2010.
5. Braun KL, Fong M, Kaanoi ME, et al. Testing a culturally appro-priate, theory-based intervention to improve colorectal cancerscreening among Native Hawaiians. Prev Med 2005;40:619–627.
6. Myers RE, Turner B, Weinberg D, et al. Impact of a physician-oriented intervention on follow-up in colorectal cancer screening.Prev Med 2004;38:375–381.
7. Lebwohl B, Neugut AI, Stavsky E, et al. Effect of a patient navi-gator program on the volume and quality of colonoscopy. J Clin
Gastroenterol October 2010. [Epub ahead of print].8. Christie J, Itzkowitz S, Lihau-Nkanza I, et al. A randomized con-trolled trial using patient navigation to increase colonoscopyscreening among low-income minorities. J Natl Med Assoc 2008;100:278–284.
9. Denberg TD, Coombes JM, Byers TE, et al. Effect of a mailedbrochure on appointment-keeping for screening colonoscopy: arandomized trial. Ann Intern Med 2006;145:895–900.
0. Khankari K, Eder M, Osborn CY, et al. Improving colorectal cancerscreening among the medically underserved: a pilot study withina federally qualified health center. J Gen Intern Med 2007;22:1410–1414.
1. Jandorf L, Gutierrez Y, Lopez J, et al. Use of a patient navigatorto increase colorectal cancer screening in an urban neighborhoodhealth clinic. J Urban Health 2005;82:216–224.
2. Lieberman DA, Holub J, Eisen G, et al. Utilization of colonoscopyin the United States: results from a national consortium. Gastro-intest Endosc 2005;62:875–883.
3. Schoen RE, Pinsky PF, Weissfeld JL, et al. Utilization of surveil-lance colonoscopy in community practice. Gastroenterology2010;138:73–81.
4. Laiyemo AO, Pinsky PF, Marcus PM, et al. Utilization and yield ofsurveillance colonoscopy in the continued follow-up study of thepolyp prevention trial. Clin Gastroenterol Hepatol 2009;7:562–567; quiz, 497.
5. Schoen RE. Surveillance after positive and negative colonoscopyexaminations: issues, yields, and use. Am J Gastroenterol 2003;98:1237–1246.
6. Barclay RL, Vicari JJ, Doughty AS, et al. Colonoscopic withdrawaltimes and adenoma detection during screening colonoscopy.N Engl J Med 2006;355:2533–2541.
7. Adler A, Pohl H, Papanikolaou IS, et al. A prospective randomisedstudy on narrow-band imaging versus conventional colonoscopyfor adenoma detection: does narrow-band imaging induce a learn-ing effect? Gut 2008;57:59–64.
8. Fenton JJ, Tancredi DJ, Green P, et al. Persistent racial and ethnicdisparities in up-to-date colorectal cancer testing in medicareenrollees. J Am Geriatr Soc 2009;57:412–418.
9. Schiff GD, Bates DW. Can electronic clinical documentation helpprevent diagnostic errors? N Engl J Med 2010;362:1066–1069.
Received November 22, 2010. Accepted January 10, 2011.
Reprint requestsAddress requests for reprints to: Daniel Leffler, MD, Department
of Gastroenterology, Beth Israel Deaconess Medical Center, 330Brookline Avenue, Boston, Massachusetts 02215. e-mail:[email protected]; fax: (617) 667-8144.
AcknowledgmentsThe authors greatly appreciate the assistance of Eileen Joyce and
Sara O’Conner in the Division of Gastroenterology, Beth IsraelDeaconess Medical Center, and Kenneth Sands, MD, Department ofMedicine, Beth Israel Deaconess Medical Center.
Clinical Trials Registration: clinicaltrials.gov #NCT01172080.
Conflicts of interestThe authors disclose no conflicts.
FundingSupported by Controlled Risk Insurance Company (CRICO)-Risk
Management Foundation. The study sponsor had no role in study
design, data collection, analysis, or interpretation.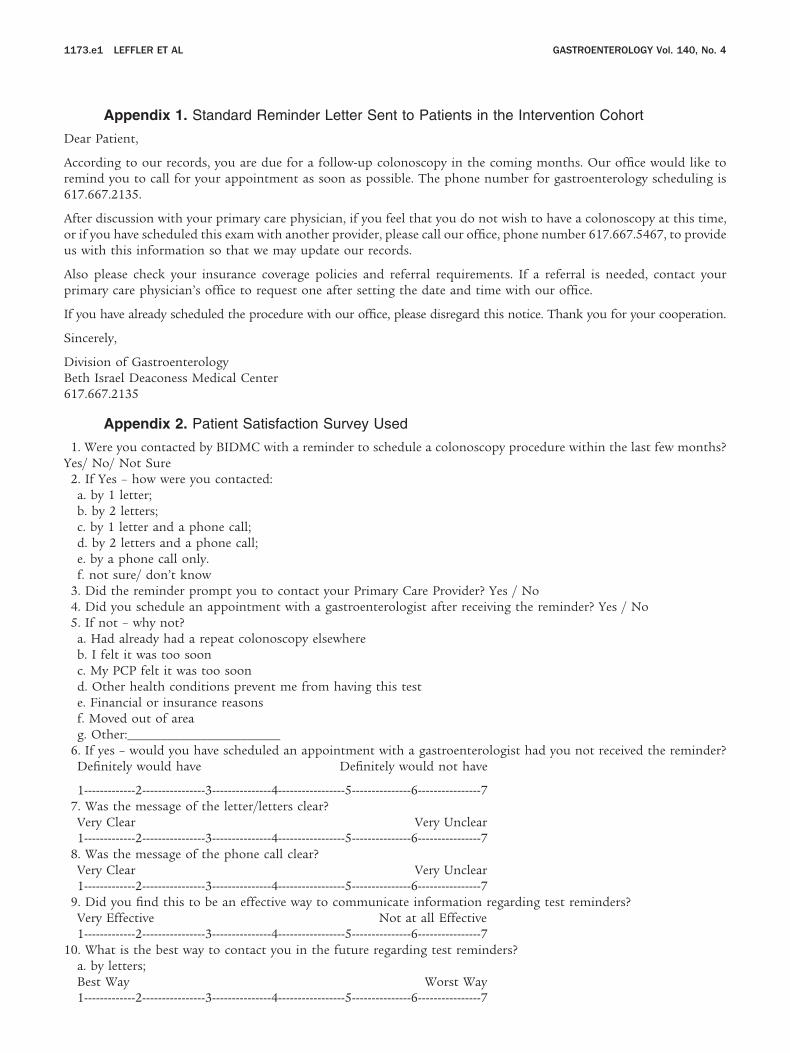
1173.e1 LEFFLER ET AL GASTROENTEROLOGY Vol. 140, No. 4
Appendix 1. Standard Reminder Letter Sent to Patients in the Intervention Cohort
Dear Patient,
According to our records, you are due for a follow-up colonoscopy in the coming months. Our office would like toremind you to call for your appointment as soon as possible. The phone number for gastroenterology scheduling is617.667.2135.
After discussion with your primary care physician, if you feel that you do not wish to have a colonoscopy at this time,or if you have scheduled this exam with another provider, please call our office, phone number 617.667.5467, to provideus with this information so that we may update our records.
Also please check your insurance coverage policies and referral requirements. If a referral is needed, contact yourprimary care physician’s office to request one after setting the date and time with our office.
If you have already scheduled the procedure with our office, please disregard this notice. Thank you for your cooperation.
Sincerely,
Division of GastroenterologyBeth Israel Deaconess Medical Center617.667.2135
Appendix 2. Patient Satisfaction Survey Used
1. Were you contacted by BIDMC with a reminder to schedule a colonoscopy procedure within the last few months?Yes/ No/ Not Sure
2. If Yes – how were you contacted:a. by 1 letter;b. by 2 letters;c. by 1 letter and a phone call;d. by 2 letters and a phone call;e. by a phone call only.f. not sure/ don’t know
3. Did the reminder prompt you to contact your Primary Care Provider? Yes / No4. Did you schedule an appointment with a gastroenterologist after receiving the reminder? Yes / No5. If not – why not?
a. Had already had a repeat colonoscopy elsewhereb. I felt it was too soonc. My PCP felt it was too soond. Other health conditions prevent me from having this teste. Financial or insurance reasonsf. Moved out of areag. Other:_______________________
6. If yes – would you have scheduled an appointment with a gastroenterologist had you not received the reminder?Definitely would have Definitely would not have
1-------------2----------------3---------------4-----------------5---------------6----------------77. Was the message of the letter/letters clear?
Very Clear Very Unclear1-------------2----------------3---------------4-----------------5---------------6----------------7
8. Was the message of the phone call clear?Very Clear Very Unclear1-------------2----------------3---------------4-----------------5---------------6----------------7
9. Did you find this to be an effective way to communicate information regarding test reminders?Very Effective Not at all Effective1-------------2----------------3---------------4-----------------5---------------6----------------7
10. What is the best way to contact you in the future regarding test reminders?a. by letters;Best Way Worst Way
1-------------2----------------3---------------4-----------------5---------------6----------------7
1
1
1
1
April 2011 ALERTING SYSTEM 1173.e2
b. by phone;Best Way Worst Way1-------------2----------------3---------------4-----------------5---------------6----------------7c. by e-mail;Best Way Worst Way1-------------2----------------3---------------4-----------------5---------------6----------------7d. by text messaging;Best Way Worst Way1-------------2----------------3---------------4-----------------5---------------6----------------7e. other ____________Best Way Worst Way1-------------2----------------3---------------4-----------------5---------------6----------------7
11. Would you like to receive reminders regarding colonoscopies and other tests in the future?Definitely Definitely not1-------------2----------------3---------------4-----------------5---------------6----------------7
2. Did getting this reminder raise any privacy concerns regarding your health information?Definitely Definitely not1-------------2----------------3---------------4-----------------5---------------6----------------7
3. How did getting a reminder to schedule a colonoscopy affect your relationship with BIDMC?Much Better Relationship Much Worse Relationship1-------------2----------------3---------------4-----------------5---------------6----------------7
14. Is English your primary language? Yes / No15. What is the highest grade in school or year of college that you completed?
___ 0. No formal schooling, or did not complete first grade___ 1. 1st grade___ 2. 2nd grade___ 3. 3rd grade___ 4. 4th grade___ 5. 5th grade___ 6. 6th grade___ 7. 7th grade___ 8. 8th grade___ 9. 9th grade___ 10. 10th grade___ 11. 11th grade___ 12. 12th grade___ 13. 1 year of college___ 14. 2 years of college or an Associate’s degree___ 15. 3 years of college___ 16. 4 years of college or a Bachelor’s degree___ 17. 1 or 2 years of graduate school or a Master’s degree___ 18. 3 years or more of graduate school or a Doctoral degree, Law degree___ 19. Trade, vocational, or technical school___ 20. GED
16. Are you of Spanish/Hispanic/Latino ethnicity? □ YES □ NO7. What do you consider to be your racial background? (check all that apply)
□ White□ Black or African American□ American Indian or Alaskan Native□ Asian□ Native Hawaiian or Pacific Islander□ Other
8. Which of the following best describes your current employment status? (read all options)□ Employed for wages□ Self-employed
□ Homemaker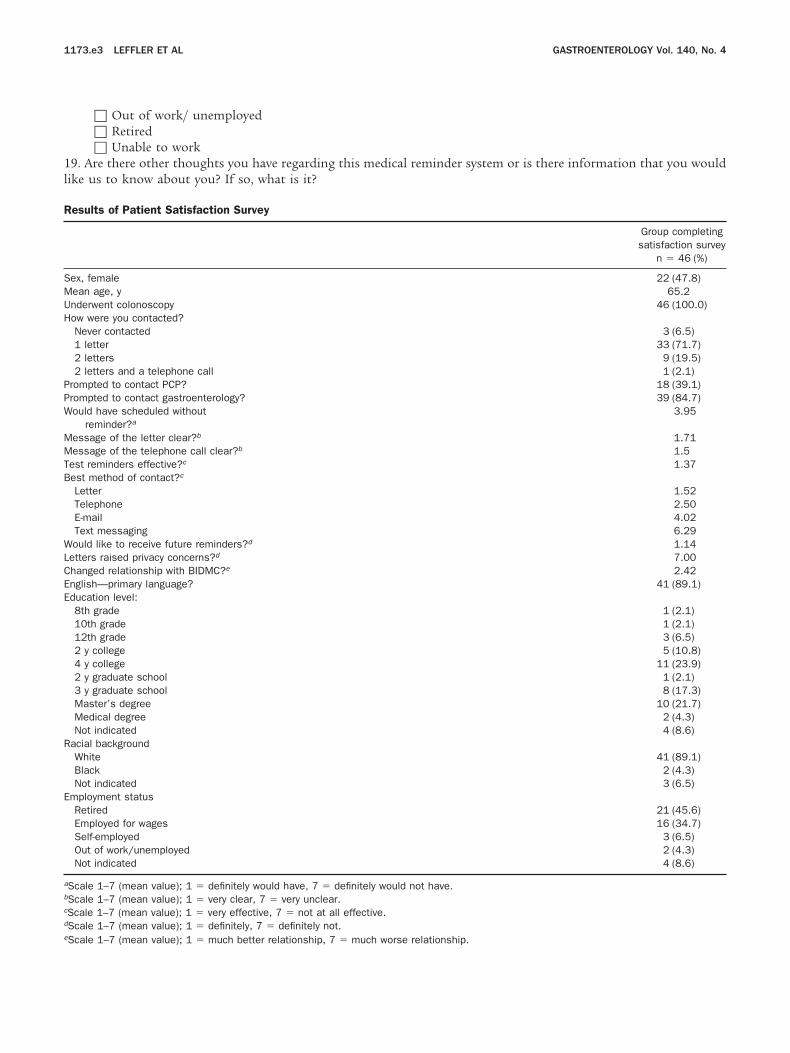
1l
SMUH
PPW
1173.e3 LEFFLER ET AL GASTROENTEROLOGY Vol. 140, No. 4
□ Out of work/ unemployed□ Retired□ Unable to work
9. Are there other thoughts you have regarding this medical reminder system or is there information that you wouldike us to know about you? If so, what is it?
Results of Patient Satisfaction Survey
Group completingsatisfaction survey
n � 46 (%)
ex, female 22 (47.8)ean age, y 65.2nderwent colonoscopy 46 (100.0)ow were you contacted?Never contacted 3 (6.5)1 letter 33 (71.7)2 letters 9 (19.5)2 letters and a telephone call 1 (2.1)
rompted to contact PCP? 18 (39.1)rompted to contact gastroenterology? 39 (84.7)ould have scheduled without
reminder?a3.95
Message of the letter clear?b 1.71Message of the telephone call clear?b 1.5Test reminders effective?c 1.37Best method of contact?c
Letter 1.52Telephone 2.50E-mail 4.02Text messaging 6.29
Would like to receive future reminders?d 1.14Letters raised privacy concerns?d 7.00Changed relationship with BIDMC?e 2.42English—primary language? 41 (89.1)Education level:
8th grade 1 (2.1)10th grade 1 (2.1)12th grade 3 (6.5)2 y college 5 (10.8)4 y college 11 (23.9)2 y graduate school 1 (2.1)3 y graduate school 8 (17.3)Master’s degree 10 (21.7)Medical degree 2 (4.3)Not indicated 4 (8.6)
Racial backgroundWhite 41 (89.1)Black 2 (4.3)Not indicated 3 (6.5)
Employment statusRetired 21 (45.6)Employed for wages 16 (34.7)Self-employed 3 (6.5)Out of work/unemployed 2 (4.3)Not indicated 4 (8.6)
aScale 1–7 (mean value); 1 � definitely would have, 7 � definitely would not have.bScale 1–7 (mean value); 1 � very clear, 7 � very unclear.cScale 1–7 (mean value); 1 � very effective, 7 � not at all effective.dScale 1–7 (mean value); 1 � definitely, 7 � definitely not.
eScale 1–7 (mean value); 1 � much better relationship, 7 � much worse relationship.