Immunostimulatory DNA Inhibits Transforming Growth Factor Expression and Airway Remodeling
11
Immunostimulatory DNA Inhibits Transforming Growth Factor- Expression and Airway Remodeling Jae Youn Cho, Marina Miller, Kwang Je Baek, Ji Won Han, Jyothi Nayar, Monica Rodriguez, Sook Young Lee, Kirsti McElwain, Shauna McElwain, Eyal Raz, and David H. Broide Department of Medicine, University of California San Diego School of Medicine, La Jolla, California Immunostimulatory sequences of DNA (ISS) inhibit eosinophilic air- way inflammation, Th2 responses, and airway hyperreactivity (AHR) in mouse models of acute ovalbumin (OVA)-induced airway inflam- mation. To determine whether ISS inhibits airway remodeling, we developed a mouse model of airway remodeling in which OVA- sensitized mice were repeatedly exposed to intranasal OVA adminis- tration for 1–6 mo. Mice chronically exposed to OVA developed sustained eosinophilic airway inflammation and sustained AHR to methacholine compared with control mice. In addition, the mice chronically exposed to OVA developed features of airway remodel- ing, including thickening of the peribronchial smooth muscle layer, peribronchial myofibroblast accumulation, expression of the profi- brotic growth factor transforming growth factor-, and subepithel- ial collagen deposition (assessed by quantitation of the area of peribronchial trichrome staining using image analysis, and immuno- staining with anti–collagen V antibodies). Administration of ISS systemically every other week significantly inhibited the develop- ment of AHR, eosinophilic inflammation, airway mucus production, and importantly, airway remodeling in mice chronically exposed to OVA for 3–6 mo. In addition, ISS significantly reduced bronchoal- veolar lavage and lung levels of the profibrotic cytokine trans- forming growth factor-. These studies demonstrate that ISS pre- vents not only Th2-mediated airway inflammation in response to acute allergen challenge, but also airway remodeling associated with chronic allergen challenge. As several Th2 cytokines (interleukin [IL]-4, IL-5, IL-9, IL-13) are considered to play an important role in the pathogenesis of asthma, therapeutic strategies based on globally inhibiting Th2 cells, or alternatively inhibiting individual Th2 cytokines, are currently being investigated as novel therapies in mouse models of asthma as well as in human clinical trials (1). The importance of individual Th2 cytokines to asthma is suggested from their individual ability to induce many of the inflammatory features noted in the airways of individuals with allergic asthma. For example, IL-4 is a switch factor for IgE synthesis, IL-5 an eosino- phil growth factor, IL-9 induces mucus secretion, and IL-13 induces airway hyperreactivity (1). One novel therapeutic strat- egy to inhibit Th2 responses in asthma is to use immunostimula- tory sequences (ISS) of DNA. Several studies have demonstrated that ISS are effective in inhibiting Th2 cytokine responses, eosin- ophilic airway inflammation, mucus production, and airway reac- tivity to methacholine in mouse models of acute asthma (2–10). (Received in original form February 28, 2003 and in revised form October 29, 2003) Address correspondence to: David H. Broide, M.B., Ch.B., University of California San Diego, Basic Science Building, Room 5090, 9500 Gilman Drive, La Jolla, CA 92093-0635. E-mail: [email protected] Abbreviations: airway hyperresponsiveness, AHR; bronchoalveolar lavage, BAL; enzyme-linked immunosorbent assay, ELISA; interferon, IFN; interleukin, IL; immunostimulatory sequences, ISS; mutated oligodeoxynucleotide, M-ODN; oli- godeoxynucleotide, ODN; ovalbumin, OVA; Periodic Acid Schiff, PAS; phos- phate-buffered saline, PBS; Respiratory Syncutial Virus, RSV; transforming growth factor, TGF. Am. J. Respir. Cell Mol. Biol. Vol. 30, pp. 651–661, 2004 Originally Published in Press as DOI: 10.1165/rcmb.2003-0066OC on November 14, 2003 Internet address: www.atsjournals.org ISS inhibits Th2 responses in mice when administered as preven- tive therapy before airway antigen challenge (2–6), or as therapy to reverse already established airway eosinophilic inflammation (7, 9, 10). ISS is effective in inhibiting Th2-mediated eosinophilic inflammation in the lung when administered either systemically or delivered directly to the mucosa of the airway (2). A single systemic dose of ISS inhibits Th2 responses to ovalbumin (OVA) inhalation challenge for at least 4 wk (6). The mechanism by which ISS inhibits Th2 responses and eosinophilic inflammation in mouse models of asthma is not completely understood. The effect of ISS on T lymphocytes is indirect, as these cells do not express toll receptor-9 (TLR-9), which bind and mediate ISS signaling (11). ISS activates cells of the innate immune system (mainly dendritic cells and macro- phages) to generate cytokines such as interferon (IFN)- and IL-12, which promote naive T lymphocytes to develop into Th1 cells (12). However, although it is evident that ISS both induces Th1 responses and inhibits Th2 responses in vivo, it is not clear that induction of the Th1 response is necessary for the inhibitory effect of ISS on Th2 responses. This is evident from studies demonstrating that adoptive transfer of antigen-specific Th1 cells aggravates antigen-induced Th2 responses in the airway (13), suggesting that induction of Th1 responses may not mediate the beneficial effect of ISS in vivo in mouse models of asthma. ISS may therefore have a broader range of anti-inflammatory effects than initially suggested from its initial description as a Th1 adjuvant. In addition to the inhibitory effect of ISS on allergen-induced airway inflammation and airway hyperreactivity, ISS also dem- onstrates antiviral and anti-inflammatory effects in a mouse model of Respiratory Syncytial Virus (RSV) induced airway inflammation, suggesting that it might also protect against viral triggers of asthma (14). ISS inhibits both RSV viral load, as well as airway inflammation and mucus expression in mice challenged intranasally with RSV (14). The mechanism of the inhibitory effect of ISS is likely to be mediated by induction of antiviral cytokines, including IFN-, IFN-, and IFN-, which inhibit RSV replication in vitro (14). Although these studies have demonstrated that ISS may have benefit as therapy in acute allergen- and acute viral-induced asthma, they do not address whether ISS can inhibit features of airway remodeling associated with more chronic asthma. Asthma represents chronic inflammation of the airways followed by re- pair. The end result of repeated cycles of inflammation and repair may be imperfect repair resulting in a structurally and functionally abnormal remodeling of the airways. The structural remodeling changes noted in asthmatic airway include subepi- thelial fibrosis, an increased smooth muscle mass, and an increase in mucous glands (15). Attempts to study the mechanism and significance of airway remodeling in asthma have been hindered in humans with asthma by the difficulties inherent in prospec- tively following sufficient numbers of individuals with asthma with chronic airway inflammation for sufficient time periods (? years, ? decades) to observe whether remodeling of the airways
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of Immunostimulatory DNA Inhibits Transforming Growth Factor Expression and Airway Remodeling

Immunostimulatory DNA Inhibits Transforming GrowthFactor-� Expression and Airway RemodelingJae Youn Cho, Marina Miller, Kwang Je Baek, Ji Won Han, Jyothi Nayar, Monica Rodriguez, Sook Young Lee, Kirsti McElwain,Shauna McElwain, Eyal Raz, and David H. Broide
Department of Medicine, University of California San Diego School of Medicine, La Jolla, California
Immunostimulatory sequences of DNA (ISS) inhibit eosinophilic air-way inflammation, Th2 responses, and airway hyperreactivity (AHR)in mouse models of acute ovalbumin (OVA)-induced airway inflam-mation. To determine whether ISS inhibits airway remodeling, wedeveloped a mouse model of airway remodeling in which OVA-sensitized mice were repeatedly exposed to intranasal OVA adminis-tration for 1–6 mo. Mice chronically exposed to OVA developedsustained eosinophilic airway inflammation and sustained AHR tomethacholine compared with control mice. In addition, the micechronically exposed to OVA developed features of airway remodel-ing, including thickening of the peribronchial smooth muscle layer,peribronchial myofibroblast accumulation, expression of the profi-brotic growth factor transforming growth factor-�, and subepithel-ial collagen deposition (assessed by quantitation of the area ofperibronchial trichrome staining using image analysis, and immuno-staining with anti–collagen V antibodies). Administration of ISSsystemically every other week significantly inhibited the develop-ment of AHR, eosinophilic inflammation, airway mucus production,and importantly, airway remodeling in mice chronically exposed toOVA for 3–6 mo. In addition, ISS significantly reduced bronchoal-veolar lavage and lung levels of the profibrotic cytokine trans-forming growth factor-�. These studies demonstrate that ISS pre-vents not only Th2-mediated airway inflammation in response toacute allergen challenge, but also airway remodeling associatedwith chronic allergen challenge.
As several Th2 cytokines (interleukin [IL]-4, IL-5, IL-9, IL-13)are considered to play an important role in the pathogenesis ofasthma, therapeutic strategies based on globally inhibiting Th2cells, or alternatively inhibiting individual Th2 cytokines, arecurrently being investigated as novel therapies in mouse modelsof asthma as well as in human clinical trials (1). The importanceof individual Th2 cytokines to asthma is suggested from theirindividual ability to induce many of the inflammatory featuresnoted in the airways of individuals with allergic asthma. Forexample, IL-4 is a switch factor for IgE synthesis, IL-5 an eosino-phil growth factor, IL-9 induces mucus secretion, and IL-13induces airway hyperreactivity (1). One novel therapeutic strat-egy to inhibit Th2 responses in asthma is to use immunostimula-tory sequences (ISS) of DNA. Several studies have demonstratedthat ISS are effective in inhibiting Th2 cytokine responses, eosin-ophilic airway inflammation, mucus production, and airway reac-tivity to methacholine in mouse models of acute asthma (2–10).
(Received in original form February 28, 2003 and in revised form October 29, 2003)
Address correspondence to: David H. Broide, M.B., Ch.B., University of CaliforniaSan Diego, Basic Science Building, Room 5090, 9500 Gilman Drive, La Jolla, CA92093-0635. E-mail: [email protected]
Abbreviations: airway hyperresponsiveness, AHR; bronchoalveolar lavage, BAL;enzyme-linked immunosorbent assay, ELISA; interferon, IFN; interleukin, IL;immunostimulatory sequences, ISS; mutated oligodeoxynucleotide, M-ODN; oli-godeoxynucleotide, ODN; ovalbumin, OVA; Periodic Acid Schiff, PAS; phos-phate-buffered saline, PBS; Respiratory Syncutial Virus, RSV; transforming growthfactor, TGF.
Am. J. Respir. Cell Mol. Biol. Vol. 30, pp. 651–661, 2004Originally Published in Press as DOI: 10.1165/rcmb.2003-0066OC on November 14, 2003Internet address: www.atsjournals.org
ISS inhibits Th2 responses in mice when administered as preven-tive therapy before airway antigen challenge (2–6), or as therapyto reverse already established airway eosinophilic inflammation(7, 9, 10). ISS is effective in inhibiting Th2-mediated eosinophilicinflammation in the lung when administered either systemicallyor delivered directly to the mucosa of the airway (2). A singlesystemic dose of ISS inhibits Th2 responses to ovalbumin (OVA)inhalation challenge for at least 4 wk (6).
The mechanism by which ISS inhibits Th2 responses andeosinophilic inflammation in mouse models of asthma is notcompletely understood. The effect of ISS on T lymphocytes isindirect, as these cells do not express toll receptor-9 (TLR-9),which bind and mediate ISS signaling (11). ISS activates cellsof the innate immune system (mainly dendritic cells and macro-phages) to generate cytokines such as interferon (IFN)-� andIL-12, which promote naive T lymphocytes to develop into Th1cells (12). However, although it is evident that ISS both inducesTh1 responses and inhibits Th2 responses in vivo, it is not clearthat induction of the Th1 response is necessary for the inhibitoryeffect of ISS on Th2 responses. This is evident from studiesdemonstrating that adoptive transfer of antigen-specific Th1 cellsaggravates antigen-induced Th2 responses in the airway (13),suggesting that induction of Th1 responses may not mediate thebeneficial effect of ISS in vivo in mouse models of asthma. ISSmay therefore have a broader range of anti-inflammatory effectsthan initially suggested from its initial description as a Th1 adjuvant.
In addition to the inhibitory effect of ISS on allergen-inducedairway inflammation and airway hyperreactivity, ISS also dem-onstrates antiviral and anti-inflammatory effects in a mousemodel of Respiratory Syncytial Virus (RSV) induced airwayinflammation, suggesting that it might also protect against viraltriggers of asthma (14). ISS inhibits both RSV viral load, as wellas airway inflammation and mucus expression in mice challengedintranasally with RSV (14). The mechanism of the inhibitoryeffect of ISS is likely to be mediated by induction of antiviralcytokines, including IFN-�, IFN-�, and IFN-�, which inhibitRSV replication in vitro (14).
Although these studies have demonstrated that ISS may havebenefit as therapy in acute allergen- and acute viral-inducedasthma, they do not address whether ISS can inhibit features ofairway remodeling associated with more chronic asthma. Asthmarepresents chronic inflammation of the airways followed by re-pair. The end result of repeated cycles of inflammation andrepair may be imperfect repair resulting in a structurally andfunctionally abnormal remodeling of the airways. The structuralremodeling changes noted in asthmatic airway include subepi-thelial fibrosis, an increased smooth muscle mass, and an increasein mucous glands (15). Attempts to study the mechanism andsignificance of airway remodeling in asthma have been hinderedin humans with asthma by the difficulties inherent in prospec-tively following sufficient numbers of individuals with asthmawith chronic airway inflammation for sufficient time periods (?years, ? decades) to observe whether remodeling of the airways

652 AMERICAN JOURNAL OF RESPIRATORY CELL AND MOLECULAR BIOLOGY VOL. 30 2004
occurs. In addition, most individuals with asthma are on anti-inflammatory therapy, which may prevent remodeling of theairways. Mouse models of asthma have provided important in-sight into the mechanism of acute allergen-induced airway in-flammation and airway hyperreactivity (AHR), but have beenconsidered unsuitable for the study of airway remodeling asrecurrent nebulized antigen challenge induces tolerance insteadof chronic airway inflammation (which is considered to precedeairway remodeling). Our laboratory and others (16) have suc-cessfully developed a method of allergen administration thatinduces chronic eosinophilic inflammation and airway remodel-ing in mice for at least 6 mo. Associated with the developmentof chronic eosinophilic inflammation, these mice repetitivelychallenged with allergen develop sustained AHR, increased col-lagen synthesis, and increased expression of the lung epithelialmucus gene Muc-5ac. In this study we investigated the abilityof ISS to inhibit features of airway remodeling associated withrepetitive antigen challenge in OVA-sensitized mice.
Materials and Methods
Induction of Chronic Pulmonary Eosinophilic Inflammation
Female BALB/c mice (16 mice/group; Jackson Laboratory, Bar Harbor,ME) were used when they reached 8–10 wk of age. Mice were immu-nized subcutaneously on Days 0, 7, 14, and 21 with 25 �g of OVA(grade V; Sigma, St. Louis, MO) adsorbed to 1 mg of alum (Aldrich)in 200 �l normal saline. Intranasal OVA challenges (20 ng/50 �l inphosphate-buffered saline [PBS]) were administered on Days 27, 29,and 31 under isoflurane (Vedco, Inc., St Joseph, MO) anesthesia. Intra-nasal OVA challenges were then repeated twice a week for 1, 3, or6 mo (see Figure 1 for protocol). Age- and sex-matched control micewere sensitized but not challenged with OVA during the 1-, 3-, or6-mo study. Mice were killed 24 h after the final OVA challenge andbronchoalveolar lavage (BAL) fluid (BALF) and lungs were analyzed.In selected experiments mice were killed on Day 32 24 h after comple-tion of the acute OVA challenge protocol. All animal experimentalprotocols were approved by the University of California, San DiegoAnimal Subjects Committees.
Therapeutic Intervention with ISS
Different groups of mice (16 mice/group) were administered intraperi-toneal endotoxin-free (� 1 ng/mg DNA) phosphorothioate ISS-ODN(5�-TGACTGTGAACGTTCGAGATGA-3�) (100 �g in 100 �l of ster-ile, endotoxin-free PBS; Trilink, San Diego, CA), mutated oligodeoxy-nucleotide (M-ODN) (5�-TGACTGTGAAGGTTGGAGATGA-3�)which lacks the CpG motif present in ISS, or diluent control starting1 d before the first intranasal OVA challenge on Day 27, and thencontinuing every other week 1 d before intranasal challenges for 1, 3,or 6 mo. In selected experiments, in mice challenged repetitively withOVA for 3 mo, we ended the experiment either in the week in whichmice had received ISS, or in the week that they had not received ISS.Previous studies in our laboratory have demonstrated that ISS, but not
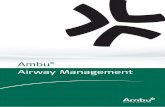
Figure 1. Mouse OVA experimental protocol. Mice were immunizedsubcutaneously on Days 0, 7, 14, and 21 with OVA. Intranasal OVAchallenges were administered on Days 27, 29, and 31, and then repeatedtwice a week for 1, 3, or 6 mo. Age- and sex-matched control mice weresensitized but not challenged with OVA during the 1-, 3-, or 6-mo study.Mice were killed 24 h after the final OVA challenge, and BALF and lungswere analyzed. ISS or diluent control was administered intraperitoneallystarting 1 d before the first intranasal OVA challenge on Day 26, andthen continued every other week 1 d before intranasal challenges for 1,3, or 6 mo.
M-ODN, inhibits OVA-induced eosinophilic inflammation and AHRwhen administered 1 d before OVA challenge (2), and that this inhibi-tory effect lasts at least 4 wk (6).
Determination of Airway Responsiveness to MCh In Vivo
We measured airway responsiveness to MCh using noninvasive as wellas invasive methods.
Noninvasive measurement of airway responsiveness. Airway respon-siveness was assessed 24 h after the final OVA challenge (after 1, 3, or6 mo of repetitive OVA challenges), using a single-chamber whole bodyplethysmograph obtained from Buxco (Troy, NY), as previously de-scribed in this laboratory (2). The enhanced pause (Penh) correlatesclosely with pulmonary resistance measured by conventional two-cham-ber plethysmography in ventilated mice as measured in our (9) and otherlaboratories (17). In the plethysmograph, mice were exposed for 3 minto nebulized PBS and subsequently to increasing concentrations of nebu-lized MCh (Sigma, St. Louis, MO) in PBS using an Aerosonic ultrasonicnebulizer (DeVilbiss, Somerset, PA). After each nebulization, recordingswere taken for 3 min. The Penh values measured during each 3-minsequence were averaged and are expressed for each MCh concentrationas the percentage of baseline Penh values following PBS exposure (2).
Measurements of airway responsiveness in intubated and ventilatedmice. In selected experiments airway resistance was measured with anin-line pressure transducer and software program (Scireq, Montreal,PQ, Canada) in intubated and ventilated mice connected to a rodentventilator as previously described in this laboratory (9). Airway resis-tance measurements were taken at baseline, after nebulized PBS, andafter each increasing concentration of nebulized MCh (9).
Lung Eosinophil Counts
The killed mice had their tracheas surgically exposed and cannulatedwith 27-gauge silicon tubing attached to a 23-gauge needle on a 1-mltuberculin syringe. Following instillation of 800 �l of sterile salinethrough the trachea into the lung, BALF was withdrawn and cytospun(3 min at 500 rpm) onto microscope slides. Eosinophil counts wereperformed as previously described (2).
Quantification of Airway Remodeling
Lungs in the different groups of mice were equivalently inflated withan intratracheal injection of a similar volume of 4% paraformaldehydesolution (Sigma) to preserve the pulmonary architecture. The inflatedlungs were embedded in paraffin, stained with either hematoxylin andeosin, Periodic Acid Schiff (PAS), Trichrome stain, or processed forimmunohistochemistry. The analyses were performed by investigatorsblinded to the treatment groups.
Peribronchial trichrome staining. The area of peribronchial tri-chrome staining in paraffin-embedded lung was outlined and quantifiedusing a light microscope (Leica DMLS; Leica Microsystems Inc., DePew, NY) attached to an image analysis system (Image-Pro Plus; MediaCybernetics, Silver Spring, MD). Results are expressed as the areaof trichrome staining per micron length of basement membrane ofbronchioles 150–200 �m of internal diameter. At least 10 bronchioleswere counted in each slide.
Lung immunohistochemical staining (�-smooth muscle actin, collagen).Six-micron-thick sections of lung from each paraffin block were deparaf-finized with xylene and hydrated in ethanol and PBS pH 7.4. Endoge-nous peroxidase activity was quenched by incubating lung sectionswith 0.3% hydrogen peroxide in anhydrous methanol for 5 min. Afterwashing with PBS, the lung sections were incubated with 1% goatserum for 10 min to block nonspecific antibody binding.
For immunohistochemical detection of �-smooth muscle actin, thelung sections were incubated overnight at 4�C with either a primarymonoclonal Ab directed against �-smooth muscle actin (Sigma), oras a negative control mouse serum instead of the primary antibody.Immunoreactivity was detected by sequential incubations of lung sec-tions with a biotinylated secondary antibody, followed by peroxidasereagent and AEC chromogen (3-amino-9-ethylcarbazole). The lungsections were briefly incubated with hematoxylin counterstain for 30 s,and then mounted with aqueous mounting media. Similar methods wereused for incubation of anti-collagen primary antibodies (anti-collagensubtypes I, III, V; Polyscience, Warrington, PA) for immunohistochemi-cal detection of collagen. Mouse collagen subtypes were detected using

Cho, Miller, Baek, et al.: ISS DNA Inhibits Airway Remodeling 653
a biotinylated secondary antibody, followed by peroxidase reagent andDAB (3,3�-diaminobenzidine) chromogen (Vector, Burlingame, CA).
The area of immunostaining (�-smooth muscle actin or collagen)in each paraffin embedded lung was outlined and quantified using alight microscope attached to an image analysis system. Results areexpressed as the area of immunostaining per micron length of basementmembrane of bronchioles 150–200 �m of internal diameter. At least10 bronchioles were counted in each slide.
Peribronchial airway smooth muscle thickness. The thickness of theairway smooth muscle layer was measured using an image analysissystem. Lungs that had been fixed in 3% gluteraldehyde and 1% osmiumtetroxide were stained with Basic Fuchsin-Toluidine Blue, which al-lowed the best visualization of the peribronchial smooth muscle layer.The thickness of the peribronchial smooth muscle layer (the transversediameter) was measured from the innermost aspect to the outermostaspect of the circumferential smooth muscle layer. The smooth musclelayer thickness in at least 10 bronchioles of similar size (150–200 �m)were counted on each slide.
Quantitation of airway mucus expression. To quantitate the level ofmucus expression in the airway, the number of PAS-positive and PAS-negative epithelial cells in individual bronchioles were counted as pre-viously described in this laboratory (14). At least 10 bronchioles werecounted in each slide. Results are expressed as the % of PAS-positivecells/bronchiole, which is calculated from the number of PAS-positiveepithelial cells per bronchus divided by the total number of epithelialcells of each bronchiole.
Measurement of BAL and Lung Cytokines Associated with AirwayRemodeling (TGF-�1, IL-13) and Lung Cytokines Associatedwith Th1 versus Th2 Responses (IFN-�, IL-5)
The concentrations of TGF-�1 and IL-13 in BAL fluid were assayedby enzyme-linked immunosorbent assay (ELISA) according to the man-ufacturer’s instructions (R&D Systems, Minneapolis, MN). Before theTGF-�1 assay, the BAL samples were treated with 2.5 N acetic acid toactivate any latent TGF-�1 to immunoreactive TGF-�1 (18). Acidifiedsamples were neutralized by 2.7 N NaOH. The TGF-�1 and IL-13ELISA assays each have a sensitivity of 61 pg/ml.
The concentrations of TGF-�1 and IL-13, as well as IFN- � andIL-5, were also assayed in lung tissue by ELISA. Lungs homogenizedin lysis buffer (0.5% Triton X-100, 150 mM NaCl, 15 mM Tris, 1 mMCaCl2, 1 mM MgCl2) were centrifuged at 10,000 � g for 20 min. Afterthe lung supernatant was passaged through a 0.8 �m-pore-size filter,the lung supernatant was assayed for cytokines and protein content. Thelung supernatant protein content was assayed using a Micro BCATMprotein assay reagent kit (Pierce, Rockford, IL) which has a sensitivityof 0.5 �g/ml. Levels of cytokines in lung supernatants were measuredby ELISA and results are expressed as pg cytokine/mg protein.
Statistical Analysis
Results in the different groups of mice were compared by ANOVAusing the nonparametric Kruskal-Wallis test followed by post-testingusing Dunn’s multiple comparison of means. All results are presentedas mean SEM. A statistical software package (Graph Pad Prism, SanDiego, CA) was used for the analysis. P values of � 0.05 were consideredstatistically significant.
Results
Effect of ISS on Airway Responsiveness
Mice sensitized to OVA and challenged with repetitive intrana-sal administration of OVA developed sustained increases inairway responsiveness to MCh compared with control OVA-sensitized mice not repetitively challenged with OVA (Figure2A). The increase in airway responsiveness was evident at allthe time points studied, e.g., 1 mo (P 0.05 versus control),3 mo (P 0.05 versus control), or 6 mo (P 0.05 versus control)(Figure 2A). Systemic administration of ISS significantly reducedairway responsiveness to MCh in mice repetitively challengedwith OVA compared with untreated mice repetitively challenged
with OVA at 1 mo (P 0.05), 3 mo (P 0.05), and 6 mo (P 0.05) (Figure 2A).
We also measured airway responsiveness to MCh in intubatedand ventilated mice. Mice challenged repetitively with OVAfor 3 mo developed significant increases in airway resistancein response to MCh challenge as compared with non–OVA-challenged control mice (P 0.01) (Figure 2B). ISS significantlyreduced airway resistance to MCh in OVA-challenged mice (P 0.05), whereas M-ODN did not have any effect on inhibitingOVA-induced increases in airway resistance to MCh (P ns)(Figure 2B).
Effect of ISS on BAL Eosinophils
The absolute number of BAL eosinophils in mice sensitized toOVA and repetitively challenged with OVA was significantlygreater than in control non–OVA-challenged mice at 1 mo(45.9 5.55 � 103 versus 0.3 0.1 � 103 BAL eosinophils) (P 0.0001), 3 mo (34.9 5.8 � 103 versus 0.10 0.03 � 103 BALeosinophils) (P 0.0001), and 6 mo (8.9 2.3 � 103 versus0.1 0.1 � 103 BAL eosinophils) (P 0.0001) (Figure 3A).Although the number of BAL eosinophils in mice repetitivelychallenged with OVA were still significantly increased at 6 mocompared with control non–OVA-challenged mice (8.9 � 103
versus 0.1 � 103 BAL eosinophils), the number of BAL eosino-phils in mice repetitively challenged with OVA was lower at6 mo (8.9 � 103 BAL eosinophils) compared with mice repeti-tively challenged with OVA at 1 mo (45.9 � 103 BAL eosino-phils) and 3 mo (34.9 � 103 BAL eosinophils).
Systemic administration of ISS before initiation of repetitiveOVA challenges significantly reduced the absolute number ofBAL eosinophils compared with untreated mice challenged re-petitively with OVA at 1 mo (16.87 4.58 � 103 versus 45.9 5.55 � 103 BAL eosinophils) (P 0.001) and 3 mo (13.3 3.9 �103 versus 34.9 5.8 � 103 BAL eosinophils) (P 0.001),whereas the reduction at 6 mo did not reach statistical signifi-cance (4.1 0.7 � 103 versus 8.9 2.3 � 103 BAL eosinophils)(P 0.15) (Figure 3A).
Systemic administration of an M-ODN to mice repetitivelychallenged with OVA for 3 mo did not inhibit BAL eosinophiliacompared with untreated mice challenged repetitively with OVA(P ns) (Figure 3B).
Effect of ISS on BAL Mononuclear Cells
The absolute number of BAL mononuclear cells in mice sensi-tized to OVA and repetitively challenged with OVA was signifi-cantly greater than in control non–OVA-challenged mice at1 mo (25.4 4.3 � 103 versus 4.5 1.3 � 103 BAL mononuclearcells) (P 0.01), 3 mo (29.1 7.0 � 103 versus 2.9 0.6 � 103
BAL mononuclear cells) (P 0.01), and 6 mo (51.2 8.6 �103 versus 4.2 1.0 � 103 BAL mononuclear cells) (P 0.01)(Figure 3C).
Systemic administration of ISS before initiation of repetitiveOVA challenges did not significantly change the absolute num-ber of BAL mononuclear cells compared with untreated micechallenged repetitively with OVA at 1 mo (P ns), 3 mo (P ns), or 6 mo (P ns) (Figure 3C).
ISS Reduces Peribronchial Fibrosis
We performed initial experiments to determine whether there aredifferences in peribronchial trichrome staining in mice followingacute versus chronic OVA exposure. Acute OVA challenge inOVA-sensitized mice did not induce increased peribronchial tri-chrome staining (acute OVA versus no-OVA) (P ns), whereas3 mo of repetitive OVA challenges did induce significant in-creases in peribronchial trichrome staining (chronic OVA versusno-OVA) (P 0.004) (Figure 4A).

654 AMERICAN JOURNAL OF RESPIRATORY CELL AND MOLECULAR BIOLOGY VOL. 30 2004
Figure 2. ISS inhibits airway reactivity to MCh in mice repetitively challenged with OVA. (A ) Noninvasive pulmonary function tests. Mice repetitivelychallenged with OVA for 1 mo (P 0.05, OVA versus control), 3 mo (P 0.05, OVA versus control), or 6 mo (P 0.05, OVA versus control)developed increased airway responsiveness to MCh 48 mg/ml compared with control non–OVA-challenged mice as assessed by measurement ofPenh. Systemic administration of ISS to mice repetitively challenged with OVA significantly reduced airway responsiveness to MCh 48 mg/ml comparedwith untreated mice repetitively challenged with OVA for 1 mo (P 0.05 versus ISS � OVA versus OVA), 3 mo (P 0.05 versus ISS � OVA versusOVA), or 6 mo (P 0.05 versus ISS � OVA versus OVA). Triangles, OVA; inverted triangles, OVA � ISS; circles, no OVA. (B ) Measurementsof airway resistance in intubated and ventilated mice. Mice challenged repetitively with OVA for 3 mo developed significant increases in airwayresistance in response to MCh challenge as compared with non–OVA-challenged control mice (P 0.01, MCh 48 mg/ml). ISS significantly reducedairway resistance to MCh in OVA-challenged mice (P 0.05, MCh 48 mg/ml), whereas M-ODN did not have any effect on inhibiting OVA-inducedincreases in airway resistance to MCh. Circles, M-ODN � OVA; triangles, OVA; inverted triangles, ISS � OVA; squares, no OVA.
We used two image analysis methods to quantitate peribron-chial fibrosis, namely the area of peribronchial trichrome stain-ing, and the area of peribronchial immunostaining with anti–collagen V Ab (expressed as the stained area in �m2/�mcircumference of bronchiole). The area of peribronchial trichromestain in mice which were repetitively challenged with OVA wassignificantly greater than in control non–OVA-challenged mice at3 mo (0.60 0.08 versus 0.26 0.03 �m2/�m circumference ofbronchiole) (P 0.004), and 6 mo (0.79 0.09 versus 0.36 0.04�m2/�m circumference of bronchiole) (P 0.0001), whereas theincrease at 1 mo did not reach statistical significance (0.58 0.04versus 0.32 0.04 �m2/�m circumference of bronchiole) (P 0.12) (Figures 4B and 4C).
Systemic administration of ISS to mice repetitively challengedwith OVA significantly reduced the area of trichrome stainingcompared with untreated mice repetitively challenged with OVAat 3 mo (0.27 0.03 versus 0.60 0.08 �m2/�m circumferenceof bronchiole) (P 0.0003), and 6 mo (0.40 0.02 versus0.79 0.09 �m2/�m circumference of bronchiole) (P 0.0001)(Figures 4B and 4C). Pretreatment with ISS did not significantlyinhibit levels of trichrome staining at 1 mo in mice repetitivelychallenged with OVA compared with untreated mice repetitivelychallenged with OVA (0.58 0.04 versus 0.55 0.06 �m2/�mcircumference of bronchiole) (P ns) (Figure 4C).
The area of peribronchial trichrome staining noted in micerepetitively challenged with OVA and pretreated with ISS for3 mo was reduced to levels of background peribronchial tri-chrome staining noted in non–OVA-challenged control mice
(0.27 0.04 versus 0.27 0.03 �m2/�m circumference of bron-chiole) (Figure 4C). Similar beneficial effects of ISS on reducingperibronchial trichrome staining to levels of non–OVA-chal-lenged mice were also noted in mice treated with ISS for 6mo (0.40 0.02 versus 0.36 0.04 �m2/�m circumference ofbronchiole) (Figure 4C).
To determine whether the timing of the administration ofISS (ISS was administered every 2 wk) in relation to the finalOVA challenge influences its effect on the extent of peribron-chial trichrome staining, we evaluated the extent of peribronchialtrichrome staining in mice challenged repetitively with OVA for3 mo, ending the experiment either in the week mice had receivedISS, or in the week that they had not received ISS. Systemicadministration of ISS every other week significantly reduced thelevels of peribronchial trichrome staining in mice challengedrepetitively with OVA for 3 mo, when ISS was administeredeither in the same week as the final OVA challenge (P 0.001,OVA� ISS versus OVA), or when ISS was administered 2 wkbefore the final OVA challenge (P 0.003, OVA� ISS/offversus OVA) (Figure 4D).
To investigate whether ISS directly affected peribronchialtrichrome staining in the absence of allergen challenge, we ad-ministered ISS every other week without OVA challenge tomice for 3 mo. ISS did not significantly influence peribronchialtrichrome staining compared with non–OVA-challenged, non–ISS-treated control mice (Figure 4E).
Systemic administration of an M-ODN to mice repetitivelychallenged with OVA for 3 mo did not reduce peribronchial

Cho, Miller, Baek, et al.: ISS DNA Inhibits Airway Remodeling 655
Figure 3. Effect of ISS on BAL cells. (A ) Inhibition of BAL eosinophilia by ISS. Mice repetitively challenged with OVA for 1 mo (P 0.0001,OVA versus no OVA), 3 mo (P 0.0001, OVA versus no OVA), or 6 mo (P 0.0001, OVA versus no OVA) had increased numbers of BALeosinophils compared with control non–OVA-challenged mice. Systemic administration of ISS in mice repetitively challenged with OVA significantlyreduced levels of BAL eosinophils, compared with untreated mice repetitively challenged with OVA for 1 mo (P 0.001, ISS � OVA versusOVA) and 3 mo (P 0.001, ISS � OVA versus OVA), whereas the reduction at 6 mo did not reach statistical significance (P 0.15, ISS � OVAversus OVA). Open bars, no OVA; filled bars, OVA; diagonally striped bars, OVA � ISS. (B ) Effect of M-ODN on BAL eosinophilia. Micerepetitively challenged with OVA for 3 mo had increased numbers of BAL eosinophils compared with control non–OVA-challenged mice (P
0.001, OVA versus no OVA). Systemic administration of ISS in mice repetitively challenged with OVA significantly reduced levels of BAL eosinophils,compared with untreated mice repetitively challenged with OVA for 3 mo (P 0.01, OVA � ISS versus OVA). Systemic administration of anM-ODN to mice repetitively challenged with OVA for 3 mo did not inhibit BAL eosinophila compared with mice challenged repetitively withOVA (P ns, OVA � M-ODN versus OVA). (C ) Effect of ISS on BAL mononuclear cells. Mice repetitively challenged with OVA for 1 mo(P 0.01, OVA versus no OVA), 3 mo (P 0.01, OVA versus no OVA), or 6 mo (P 0.01, OVA versus no OVA) had increased numbers ofBAL mononuclear cells compared with control non–OVA-challenged mice. Systemic administration of ISS before initiation of repetitive OVAchallenges did not significantly change the absolute number of BAL mononuclear cells compared with untreated mice challenged repetitively withOVA at 1 mo, 3 mo, or 6 mo. Open bars, no OVA; filled bars, OVA; diagonally striped bars, OVA � ISS.
trichrome staining compared with mice challenged repetitivelywith OVA (Figure 4F).
Effect of ISS on Peribronchial Collagen Immunostaining
Pilot immunostaining studies of remodeled airways with anti–collagen I, III, and V Abs demonstrated that anti-collagen stain-ing with the anti–collagen V Ab was reproducibly detected,whereas staining with anti–collagen I and III Abs was morevariable in the lungs of mice repetitively challenged with OVA.Therefore we quantitated only anti–collagen V immunostaining.The area of peribronchial collagen V immunostaining in mice whichwere repetitively challenged with OVA was significantly greaterthan in control non–OVA-challenged mice at 3 mo (0.32 0.02versus 0.15 0.02 �m2/�m circumference of bronchiole) (P 0.0001) (Figure 4G). Systemic administration of ISS to mice repeti-tively challenged with OVA significantly reduced the area of colla-gen V immunostaining compared with untreated mice repetitivelychallenged with OVA at 3 mo (0.17 0.02 versus 0.32 0.02�m2/�m circumference of bronchiole) (P 0.0001) (Figure 4G).
Effect of ISS on Peribronchial Smooth Muscle Layer Thickness
The thickness of the peribronchial smooth muscle layer (mea-sured in �m) in mice repetitively challenged with OVA wassignificantly greater than in control non–OVA-challenged miceat 1 mo (13.6 0.4 versus 5.3 0.5 �m) (P 0.0001), 3 mo(14.3 0.7 versus 8.9 0.6 �m) (P 0.0001), and 6 mo (15.0 0.4 versus 8.3 0.4 �m) (P 0.0001) (Figure 5A).
Systemic administration of ISS significantly reduced the peri-bronchial smooth muscle layer thickness in mice repetitivelychallenged with OVA compared with untreated mice repetitivelychallenged with OVA at 1 mo (7.5 0.8 versus 13.6 0.4 �m)(P 0.0001), 3 mo (9.8 0.5 versus 14.3 0.7 �m) (P 0.0001), and 6 mo (11.5 0.3 versus 15.0 0.4 �m) (P 0.0001)(Figure 5A).
Effect of ISS on the Area of Peribronchial Myofibroblast �-SmoothMuscle Actin Immunostaining
The area of peribronchial myofibroblast �-smooth muscle actinimmunostaining was quantified by image analysis and expressedas the stained area in �m2/�m circumference of a bronchiole.Acute OVA challenge in OVA-sensitized mice did not induceincreased peribronchial �-smooth muscle actin immuonostaining(acute OVA versus no-OVA) (P ns), whereas 3 mo of repeti-tive OVA challenges did induce significant increases in peri-bronchial �-smooth muscle actin immunostaining (chronic OVAversus no-OVA) (P 0.0001) (Figure 5B). The area of peribron-chial �-smooth muscle actin immunostaining in mice repetitivelychallenged with OVA was significantly greater than in controlnon–OVA-challenged mice at 1 mo (0.88 0.06 versus 0.60 0.09 �m2/�m circumference of bronchiole) (P 0.004), 3 mo(0.97 0.06 versus 0.49 0.02 �m2/�m circumference of bron-chiole) (P 0.0001), and 6 mo (0.94 0.07 versus 0.48 0.03�m2/�m circumference of bronchiole) (P 0.0001) (Figures 5Cand 5D).
Systemic administration of ISS before repetitive OVA chal-lenges significantly reduced the area of �-smooth muscle actinimmunostaining compared with untreated mice challenged re-petitively with OVA at 3 mo (0.80 0.11 versus 0.97 0.06�m2/�m circumference of bronchiole) (P 0.0001), and 6 mo(0.72 0.05 versus 0.94 0.06 �m2/�m circumference of bron-chiole) (P 0.001) (Figures 5C and 5D). Pretreatment with ISSfor 1 mo did not significantly inhibit the area of �-smooth muscleactin immunostaining in mice repetitively challenged with OVA,compared with untreated mice repetitively challenged with OVAat 1 mo (P ns).
Effect of ISS on BALF TGF-�1 and IL-13 Levels
As both TGF-�1 and IL-13 are able to induce peribronchial fibro-sis (19), we measured levels of these cytokines in BALF and lung

656 AMERICAN JOURNAL OF RESPIRATORY CELL AND MOLECULAR BIOLOGY VOL. 30 2004
tissue. Levels of BAL TGF-�1 were significantly increased inmice exposed to repetitive OVA challenge compared with controlnon–OVA-challenged mice at 1 mo (300 17 versus 135 5pg/ml TGF-�1) (P 0.03), 3 mo (356 28 versus 156 37pg/ml TGF-�1) (P 0.03), and 6 mo (369 74 versus 146 8 pg/ml TGF-�1) (P 0.03) (Figure 6A). ISS significantly re-duced levels of BAL TGF-�1 in mice exposed to repetitive OVAchallenge compared with untreated mice challenged repetitivelywith OVA at 3 mo (356 28 versus 241 19 pg/ml TGF-�1)(P 0.05), and at 6 mo (369 74 versus 269 37 pg/ml TGF-�1)(P 0.05), but not at 1 mo (Figure 6A).
Similarly, levels of lung TGF-�1 were significantly increasedin mice exposed to repetitive OVA challenge for 3 mo comparedwith control non–OVA-challenged mice (1,946 261 versus664 75 pg TGF-�1/mg lung protein) (P 0.02) (Figure 6B).
ISS significantly reduced levels of lung TGF-�1 in mice exposedto repetitive OVA challenge compared with untreated mice chal-lenged repetitively with OVA (939 171 versus 1,946 261pg TGF-�1/mg lung protein) (P 0.05) (Figure 6B).
Levels of BAL IL-13 were significantly increased in miceexposed to repetitive OVA challenge compared with control non–OVA-challenged mice at 1 mo (3,768 245 versus 1,850 112pg/ml IL-13) (P 0.05), 3 mo (4,189 731 versus 1,597 590pg/ml IL-13) (P 0.05), and 6 mo (3,341 212 versus 1,910
125 pg/ml IL-13) (P 0.05) (Figure 6C). ISS significantly reducedlevels of BAL IL-13 in mice exposed to repetitive OVA challengeat 1 mo (3,768 245 versus 2,798 100 pg/ml IL-13) (OVA versusOVA�ISS) (P 0.05) (Figure 6C). Although ISS also reduced

Cho, Miller, Baek, et al.: ISS DNA Inhibits Airway Remodeling 657
Figure 4. ISS reduces peribronchial fibrosis. (A ) Peribronchial fibrosis: effect of acute versus chronic OVA challenges. Acute OVA challenge inOVA-sensitized mice did not induce increased peribronchial trichrome staining (acute OVA versus no-OVA) (P ns), whereas 3 mo of repetitiveOVA challenges did induce significant increases in peribronchial trichrome staining (chronic OVA versus no-OVA) (P 0.004). (B ) Peribronchialtrichrome staining. Control bronchi derived from mice not challenged with OVA (panel A) exhibited minimal peribronchial trichrome staining (bluecolor). In contrast repetitive OVA challenge for 3 months induced circumferential peribronchial trichrome staining (panel B), which was significantlyinhibited by ISS therapy (panel C). (C ) Effect of ISS on area of peribronchial trichrome staining. Mice repetitively challenged with OVA for 3months (P 0.004, OVA versus no OVA), or 6 mo (P 0.0001, OVA versus no OVA), but not 1 mo (P ns, OVA versus no OVA), developedincreased peribronchial trichrome staining compared with control non–OVA-challenged mice. Systemic administration of ISS significantly reducedlevels of peribronchial trichrome staining in mice challenged repetitively with OVA, compared with untreated mice challenged repetitively withOVA for 3 mo (P 0.0003, versus ISS � OVA versus OVA) or 6 mo (P 0.0001, ISS � OVA versus OVA). Open bars, no OVA; filled bars,OVA; diagonally striped bars, OVA � ISS. (D ) Effect of timing of administration of ISS and final OVA challenge on peribronchial trichromestaining. Mice repetitively challenged with OVA for 3 mo had increased peribronchial trichrome staining compared with control non–OVA-challengedmice (P 0.004, OVA versus no OVA). Systemic administration of ISS every other week significantly reduced the levels of peribronchial trichromestaining in mice challenged repetitively with OVA for 3 mo, when ISS was administered either in the same week as the final OVA challenge (P
0.001, OVA� ISS versus OVA), or when ISS was administered 2 wk before the final OVA challenge (P 0.003, OVA�ISS/off versus OVA). (E )Effect of the administration of ISS in the absence of OVA challenge on peribronchial trichrome staining. To investigate whether ISS directly affectedperibronchial trichrome staining in the absence of allergen challenge, we administered ISS every other week without OVA challenge to mice for3 mo. ISS did not significantly influence peribronchial trichrome staining compared with control non–OVA-challenged mice that were not treatedwith ISS. In contrast, systemic administration of ISS significantly reduced the levels of peribronchial trichrome staining in mice challenged repeti-tively with OVA for 3 mo (P 0.01, OVA�ISS versus OVA). (F ) Effect of M-ODN on peribronchial trichrome staining. Mice repetitivelychallenged with OVA for 3 mo had increased levels of peribronchial trichrome staining compared with control non–OVA-challenged mice (P
0.001, OVA versus no OVA). Systemic administration of ISS to mice repetitively challenged with OVA significantly reduced levels of peribronchialtrichrome staining compared with untreated mice repetitively challenged with OVA for 3 mo (P 0.01, OVA � ISS versus OVA). Systemic admin-istration of an M-ODN to mice repetitively challenged with OVA for 3 mo did not inhibit peribronchial trichrome staining compared with untreatedmice challenged repetitively with OVA (P ns, OVA � M-ODN versus OVA). (G ) Collagen V immunostaining. Mice repetitively challengedwith OVA for 3 mo developed increased peribronchial collagen V immunostaining compared with control non–OVA-challenged mice (P 0.0001,OVA versus no OVA). Systemic administration of ISS significantly reduced levels of peribronchial collagen V immunostaining in mice challengedrepetitively with OVA, compared with untreated mice challenged repetitively with OVA for 3 mo (P 0.0001, ISS � OVA versus OVA).�
levels of BAL IL-13 in mice exposed to repetitive OVA chal-lenge at 3 mo and 6 mo compared with untreated mice challengedrepetitively with OVA, this reduction was not statistically sig-nificant (Figure 6C). ISS did not significantly reduce levels oflung IL-13 in mice exposed to repetitive OVA challenge com-pared with untreated mice challenged repetitively with OVA(data not shown).
Effect of ISS on Lung IL-5 and IFN-� Levels
Systemic administration of ISS to mice repetitively challengedwith OVA for 3 mo significantly inhibited levels of lung IL-5(511 115, versus 310 57 pg IL-5/mg lung protein) (OVAversus OVA � ISS) (P 0.05). As anticipated repetitive OVAchallenge for 3 mo induced a Th2 response (e.g., IL-5), but didnot induce the Th1 cytokine IFN-� (� 9 pg IFN-�/mg lungprotein). Interestingly, repetitive administration of ISS for 3 moin OVA-challenged mice was associated with inhibition of Th2responses, but not induction of Th1 responses in the lung (� 9pg IFN-�/mg lung protein).
Effect of ISS on Airway Mucus Expression
The percentage of airway epithelium which stained positive withPAS in mice repetitively challenged with OVA was significantlygreater than in control non–OVA-challenged mice at 1 mo(13.1 1.6 versus 0.1 0.01%) (P 0.0001), 3 mo (22.1 2.8versus 0.1 0.01%) (P 0.0001), and 6 mo (22.9 3.4 versus0.2 0.2%) (P 0.0005) (Figures 7A and 7B).
Systemic administration of ISS in mice repetitively challengedwith OVA significantly reduced the percentage of airway epithe-lium staining positively with PAS compared with untreated micerepetitively challenged with OVA at 1 mo (5.1 0.9, versus13.1 1.6%) (P 0.0005), 3 mo (7.4 1.3 versus 22.1 2.8%)(P 0.0003), and 6 mo (8.4 1.2 versus 22.9 3.4%) (P 0.02) (Figure 7B).
Systemic administration of an M-ODN to mice repetitivelychallenged with OVA for 3 mo did not reduce the percentageof airway epithelium staining positively with PAS compared withuntreated mice challenged repetitively with OVA (Figure 7C).
Discussion
In this study we demonstrate that repetitive airway allergen chal-lenge in mice induces many of the features of airway remodelingnoted in human asthma and that ISS significantly inhibits airwayremodeling. Mice exposed to repetitive OVA challenge developsustained airway hyperreactivity to MCh for up to 6 mo. Thisairway hyperreactivity is not only associated with Th2 cytokineexpression, eosinophilic inflammation, and mucus expression,but also with features of airway remodeling including increasedthickness of the peribronchial smooth muscle layer, peribron-chial myofibroblast accumulation, increased levels of lungTGF-�1, and peribronchial fibrosis. In contrast, acute OVA chal-lenge did not induce the airway remodeling changes detectedwith repetitive OVA challenge. The time course studies demon-strate that the majority of airway remodeling in this model occursduring the first month of chronic allergen challenge. While manyof the effects of ISS on airway remodeling are apparent at the1-mo time point, some effects of ISS are only apparent at the3-mo time point (Figure 4C, trichrome stain, and Figure 5D,�-smooth muscle actin immunostain, which are reduced by ISS at3 mo, but not at 1 mo). Repeated systemic dosing with ISS every2 wk results in sustained inhibition of airway hyperreactivity toMCh for at least 6 mo. In addition ISS administration signifi-cantly inhibits features of airway remodeling including mucusproduction, peribronchial myofibroblast accumulation, levels ofthe profibrotic cytokine TGF-�1, peribronchial fibrosis, and re-ducing the thickness of the peribronchial smooth muscle layer.

658 AMERICAN JOURNAL OF RESPIRATORY CELL AND MOLECULAR BIOLOGY VOL. 30 2004
Figure 5. ISS inhibits thickness of peribronchial smooth muscle layer and myofibroblasts. (A) Peribronchial smooth muscle layer thickness. Micerepetitively challenged with OVA for 1 mo (P 0.0001, OVA versus no OVA), 3 mo (P 0.0001, OVA versus no OVA), or 6 mo (P 0.0001,OVA versus no OVA), developed increased thickness of the peribronchial smooth muscle layer compared with control non–OVA-challenged mice.Systemic administration of ISS significantly reduced the peribronchial smooth muscle layer thickness in mice challenged repetitively with OVA, comparedwith untreated mice challenged repetitively with OVA for 1 mo (P 0.0001, versus ISS � OVA versus OVA), 3 mo (P 0.0001, versus ISS � OVAversus OVA), or 6 mo (P 0.0001, ISS � OVA versus OVA). Open bars, no OVA; filled bars, OVA; diagonally striped bars, OVA � ISS. (B)Peribronchial �-smooth muscle actin immunostaining: effect of acute versus chronic OVA challenges. Acute OVA challenge in OVA-sensitized micedid not induce increased peribronchial �-smooth muscle actin immuonostaining (acute OVA versus no-OVA) (P ns), whereas 3 mo of repetitiveOVA challenges did induce significant increases in peribronchial �-smooth muscle actin immunostaining (chronic OVA versus no-OVA) (P 0.0001).(C) Peribronchial myofibroblast immunostaining. Control bronchi derived from mice not challenged with OVA (panel a) exhibited peribronchialmyofibroblast immunostaining (red color). Repetitive OVA challenge for 3 mo induced an increase in the area of myofibroblast immunostaining (panelb), which was significantly inhibited by ISS therapy (panel c). (D) ISS reduces peribronchial myofibroblast immunostaining. Mice repetitively challengedwith OVA for 1 mo (P 0.004, OVA versus no OVA), 3 mo (P 0.0001, OVA versus no OVA), or 6 mo (P 0.0001, OVA versus noOVA), developed an increase in the area of peribronchial myofibroblast immunostaining compared with control non–OVA-challenged mice. Systemicadministration of ISS significantly reduced the area of peribronchial myofibroblast immunostaining in mice challenged repetitively with OVA, comparedwith untreated mice challenged repetitively with OVA for 3 mo (P 0.001, ISS � OVA versus OVA) or 6 mo (P 0.0001, ISS � OVA versusOVA), but not for 1 mo (P ns, ISS � OVA versus OVA). Open bars, no OVA; filled bars, OVA; diagonally striped bars, OVA � ISS.
This study shares similarities and differences with a recentstudy which demonstrated that CpG inhibited airway remodelingin a mouse model of asthma (20). Previous studies demonstratedthat pretreatment with CpG inhibited lung eosinophilic inflam-mation, airway hyperreactivity to methacholine, peribronchialtrichrome staining, and mucus expression in mice challengedwith antigen for 6 wk (20). This study extended these observa-tions by demonstrating that ISS inhibited an additional key com-ponent of the remodeled airway wall, namely peribronchial
smooth muscle layer thickness. As smooth muscle plays a keyrole in airway hyperreactivity in asthma, the ability of ISS toreduce the thickness of the airway smooth muscle layer may bean important mechanism by which ISS inhibits airway hyper-reactivity. In addition, we have made the novel observationsthat ISS inhibits accumulation of myofibroblasts, peribronchialcollagen V deposition, ongoing Th2 cytokine responses, anddemonstrated that repeated dosing with ISS could inhibit airwayremodeling and airway hyperresponsiveness for up to 6 mo.

Cho, Miller, Baek, et al.: ISS DNA Inhibits Airway Remodeling 659
Figure 6. ISS reduces levels of TGF-�1 in BAL fluid and lung. (A ) BAL TGF-�1. Mice repetitively challenged with OVA for 1 mo (P 0.03,OVA versus no OVA), 3 mo (P 0.03, OVA versus no OVA), or 6 mo (P 0.03, OVA versus no OVA) had increased levels of BAL TGF-�1compared with control non–OVA-challenged mice. Systemic administration of ISS significantly reduced levels of BAL TGF-�1 in mice challengedrepetitively with OVA, compared with untreated mice challenged repetitively with OVA for 3 mo (P 0.05, ISS � OVA versus OVA) or 6 mo(P 0.05, ISS � OVA versus OVA), but not for 1 mo. Open bars, no OVA; filled bars, OVA; diagonally striped bars, OVA � ISS. (B ) LungTGF-�1. Mice repetitively challenged with OVA for 3 mo had increased levels of lung TGF-�1 compared with control non–OVA-challenged mice(P 0.03, OVA versus no OVA). Systemic administration of ISS significantly reduced levels of lung TGF-�1 in mice challenged repetitively withOVA, compared with untreated mice challenged repetitively with OVA for 3 mo (P 0.05, versus ISS � OVA versus OVA). (C ) BAL IL-13.Mice repetitively challenged with OVA for 1 mo (P 0.05, OVA versus no OVA), 3 mo (P 0.05, OVA versus no OVA), or 6 mo (P 0.05,OVA versus no OVA), had increased levels of BAL IL-13 compared with control non–OVA-challenged mice. Systemic administration of ISSsignificantly reduced levels of BAL IL-13 in mice challenged repetitively with OVA for 1 mo (P 0.05, ISS � OVA versus OVA). Although ISSreduced levels of BAL IL-13 in mice challenged repetitively with OVA for 3 or 6 mo, this was not statistically significant (P ns, ISS � OVAversus OVA). Open bars, no OVA; filled bars, OVA; diagonally striped bars, OVA � ISS.
Finally, our study is the first to demonstrate that ISS inhibitsTGF-�1 expression in both BALF and lung of the remodeledairway, and suggests that ISS mediated inhibition of lung TGF-�1expression is an important mechanism by which ISS inhibitsairway remodeling.
In humans, the basement membrane of airway epithelium iscomprised of two layers, the basal lamina (referred to as thetrue basement membrane and of normal thickness in asthma)and the lamina reticularis, which is thickened in asthma (15).The thickened lamina reticularis is comprised of collagen typeI, III, V, and fibronectin which are likely produced by myofi-broblasts (15). In addition to trichrome staining, we have usedan anti–collagen V Ab in this study to demonstrate increasedperibronchial collagen deposition in mice which develop airwayremodeling in response to repetitive allergen challenge. Thedegree of thickening of the basement membrane in asthma hasbeen correlated with the severity of asthma in some but not allstudies (15). Differences in the results of these studies is probablydue to study design, and the fact that for ethical reasons, it willnever be possible to design the ideal experimental study in hu-man asthma in which anti-inflammatory therapy is withheld insubjects with mild, moderate, and severe asthma for sufficientperiods of time (? years) to determine whether severity of asthmacorrelates with features of airway remodeling.
The number of myofibroblasts in the subepithelium are in-creased in asthma and their numbers correlate with the thicknessof the basement membrane (15). Myofibroblasts are a majorsource of collagenous and noncollagenous extracellular matrixmolecules. In humans with asthma, allergen inhalation increasesthe number of myofibroblasts (21). The myofibroblast may con-tribute to airway remodeling by release of extracellular matrixcomponents (fibronectin, laminin, elastin) and cytokines. Myo-fibroblast supernatants enhance eosinophil survival in vitro (22).Myofibroblasts can be detected by immunostaining lung sectionswith an anti–�-smooth muscle antibody (15). The number ofperibronchial myofibroblasts increased in mice following chronicallergen administration suggesting that the increased numbersof myofibroblasts could be contributing to the deposition ofcollagen in the peribronchial region.
This study also demonstrated a significant increase in BALFand lung levels of the profibrotic cytokine TGF-�1. TGF-�1
stimulates fibroblasts to produce extracellular matrix proteins(collagen, fibronectin), decreases the production of enzymes thatdegrade the extracellular matrix (collagenase), and increases theproduction of proteins that inhibit enzymes that degrade theextracellular matrix (tissue inhibitor of metalloprotease, orTIMP) (23). The net effect is to increase the production ofextracellular matrix proteins. In subjects with asthma, increasedlevels of TGF-�1 have been reported in BAL and biopsy speci-mens (24, 25). TGF-�1 expression correlates with the degreeof subepithelial fibrosis, and levels of TGF-�1 are significantlyincreased in patients with severe asthma who have prominentairway eosinophilic inflammation (24, 25). However, not all stud-ies show an increase in TGF-�1 in asthma (26). In the lung TGF-�can be generated by multiple cell types (TGF-�1, macrophages,eosinophils, epithelium, endothelium, connective tissue cells,hematpoetic cells; TGF-�2, epithelial, neuronal cells; TGF-�3,mesenchymal cells) (23).
IL-13 is postulated to be a key mediator of tissue fibrosiscaused by Th2 lymphocytes. IL-13 is a potent stimulator of fi-broblast proliferation and collagen production in vitro (19, 27).In vivo studies in a parasite model of liver fibrosis demonstratethat an IL-13 inhibitor blocks the development of hepatic fibrosisduring this Th2-dominated inflammatory response (27). Simi-larly, recent in vivo studies with transgenic mice which overex-press IL-13 in airway epithelium demonstrate that the fibrogeniceffects of IL-13 are mediated by TGF-�1 (19). In vivo in theseepithelial targeted IL-13 transgenic mice, IL-13 selectively stimu-lated TGF-�1 (but not TGF-�2 or TGF-�3) production by mac-rophages in particular with lesser amounts of TGF-�1 beingproduced by epithelium and eosinophils (19). As IL-13–inducedlung fibrosis is significantly reduced by treatment with a TGF-�1antagonist (19), these studies suggest that the peribronchial fi-brogenic effects of IL-13 are mediated to a great extent bythis TGF-�1 pathway. In this study we have demonstrated thatperibronchial fibrosis is associated with increased levels of bothIL-13 and TGF-�1 suggesting that the IL-13/TGF-�1/peribronchialfibrosis pathway may be operative in this chronic allergen-inducedmodel of airway remodeling. We have also demonstrated thatISS significantly reduces peribronchial fibrosis as well as levels ofTGF-�1 with lesser inhibitory effects on levels of IL-13 suggestingthat ISS may be reducing TGF-� levels and peribronchial fibrosis

660 AMERICAN JOURNAL OF RESPIRATORY CELL AND MOLECULAR BIOLOGY VOL. 30 2004
Figure 7. ISS reduces airway mucus. (A ) PAS staining. Control bronchi derived from mice not challenged with OVA (panel a) exhibited minimalepithelial PAS staining (red color). In contrast repetitive OVA challenge for 3 mo induced circumferential epithelial PAS staining (panel b), whichwas significantly inhibited by ISS (panel c). (B ) ISS inhibits PAS staining of airway epithelium. Mice repetitively challenged with OVA for 1 mo(P 0.0001, OVA versus no OVA), 3 mo (P 0.0001, OVA versus no OVA), or 6 mo (P 0.0005, OVA versus no OVA), had increased PASstaining of airway epithelium compared with control non–OVA-challenged mice. Systemic administration of ISS significantly reduced the PASstaining of airway epithelium in mice challenged repetitively with OVA, compared with untreated mice challenged repetitively with OVA for 1 mo(P 0.0005, ISS � OVA versus OVA), 3 mo (P 0.0003, ISS � OVA versus OVA), or 6 mo (P 0.02, ISS � OVA versus OVA). Open bars,no OVA; filled bars, OVA; diagonally striped bars, OVA � ISS. (C ) Effect of M-ODN on peribronchial trichrome staining. Mice repetitivelychallenged with OVA for 3 mo developed increased levels of PAS staining of airway epithelium compared with control non–OVA-challenged mice(P 0.0001, OVA versus no OVA). Systemic administration of ISS in mice repetitively challenged with OVA significantly reduced levels of PASstaining of airway epithelium compared with untreated mice repetitively challenged with OVA for 3 mo (P 0.01, OVA � ISS versus OVA).Systemic administration of an M-ODN to mice repetitively challenged with OVA for 3 mo did not inhibit levels of PAS staining of airway epitheliumcompared with mice challenged repetitively with OVA (P ns, OVA � M-ODN versus OVA).
by mechanisms other than reducing levels of the Th2 cytokineIL-13. Although this study has demonstrated that ISS both inhib-its the expression of TGF-� as well as inhibits airway remodeling,further studies are needed to determine whether this is an associ-ation or a cause-and-effect relationship.
Mucus hypersecretion and mucus plugging of the airways arecharacteristic features of human asthma (28). Acute allergenchallenge in mouse models of asthma induces Muc-5ac mRNAand protein expression, as well as goblet cell metaplasia in mu-rine airways (29). Adoptive transfer of Th2 cells induces airwaymucus expression (30). When overexpressed in vivo, each Th2cytokine (IL-4, IL-9, IL-13) induces goblet cell metaplasia in themurine lung (31). However, only IL-9 directly induces epithelialgoblet cell metaplasia and human MUC5 gene expression (32).Neither IL-4 nor IL-13 directly induce Muc 5ac gene expressionwhen administered to epithelial cells in vitro (31). Thus, it isassumed that the actions of IL-4 and IL-13 are upstream of IL-9and act via indirect effects on as yet unknown cells or pathways(31). The mechanism by which ISS inhibits Muc 5ac mRNA andmucus expression in our chronic model of airway remodeling islikely due to the ability of ISS to inhibit Th2-derived cytokines
known to be important in stimulating mouse airway mucus pro-duction, including IL-4 (31) and IL-9 (33).
Airway smooth muscle hyperplasia is an important compo-nent of the structural changes that constitute airway remodeling(15). Indeed, airway smooth muscle cells obtained by airwaybiopsy from subjects with asthma grow in vitro at twice the rateof airway smooth muscle cells derived from control subjectswithout asthma (34). Because exaggerated airway narrowing inresponse to a variety of stimuli is a characteristic feature ofasthma, airway smooth muscle hyperplasia may play an impor-tant role in this exaggerated airway response. Extracellular ma-trix proteins such as collagen, fibronectin, and laminin can affectthe growth and expression of contractile proteins in airwaysmooth muscle cells. For example, airway smooth muscle cellscultured on collagen produce a proliferative rather than a con-tractile phenotype (35). This study demonstrates that repetitiveallergen challenge in mice induces an increased thickness ofthe peribronchial smooth muscle layer. Further studies are inprogress to determine the levels of expression of extracellularmatrix components and smooth muscle mitogens, which could

Cho, Miller, Baek, et al.: ISS DNA Inhibits Airway Remodeling 661
contribute to the increased airway smooth muscle thickness andthe mechanism by which ISS might inhibit this process.
In summary, this study demonstrates that repetitive allergenchallenge induces sustained AHR for up to 6 mo in a mousemodel of asthma. The sustained AHR is associated with in-creased levels of the profibrotic cytokine TGF-�1 and airwayremodeling. As ISS inhibits expression in the lung of severalkey Th2 cytokines including IL-4 (3), IL-5 (2), and IL-9 (33),ISS has the potential to inhibit many of the cytokine pathwaysimportant to the pathogenesis of asthma. Interestingly, repetitiveadministration of ISS for 3 mo in OVA-challenged mice wasassociated with inhibition of Th2 responses, but not inductionof Th1 responses in the lung. This suggests that inhibition ofTh2 responses rather than induction of Th1 responses may bea more important therapeutic mechanism of action of ISS inmouse models of airway inflammation and AHR. In mouse mod-els, ISS is as effective as corticosteroids in preventing acuteallergen-induced airway eosinophilic inflammation and AHR(2), and reversing established acute allergen induced airway eo-sinophilic inflammation and AHR (9). This study demonstratesthat ISS can also prevent sustained AHR and airway remodelingin response to chronic allergen challenge. Further studies inhumans will help to determine whether using ISS in the preven-tion and/or treatment of asthma will be safe and effective.
Acknowledgments: This study was supported by NIH grants AI 33977 and AI38425 (to D.B.) and NIH grant AI 40682 (to E.R.).
References
1. Barnes, P. J. Cytokine modulators for allergic diseases. 2001. Curr. Opin.Allergy Clin. Immunol. 1:555–560.
2. Broide, D., J. Schwarze, H. Tighe, T. Gifford, M. D. Nguyen, S. Malek, J. V.Uden, E. Martin-Orozco, E. W. Gelfand, and E. Raz. 1998. Immunostimula-tory DNA sequences inhibit IL-5, eosinophilic inflammation, and airwayhyperresponsiveness in mice. J. Immunol. 161:7054–7062.
3. Kline, J. N., T. J. Waldschmidt, T. R. Businga, J. E. Lemish, J. V. Weinstock,P. S. Thorne, and A. M. Krieg. 1998. Modulation of airway inflammationby CpG oligodeoxynucleotides in a murine model of asthma. J. Immunol.160:2555–2559.
4. Sur, S., J. S. Wild, B. K. Choudhury, N. Sur, R. Alam, and D. M. Klinman.1999. Long term prevention of allergic lung inflammation in a mouse modelof asthma by CpG oligodeoxynucleotides. J. Immunol. 162:6284–6293.
5. Broide, D. H., G. Stachnick, D. Castaneda, J. Nayar, M. Miller, J. Cho, M.Rodriquez, M. Roman, and E. Raz. 2001. Immunostimulatory DNA medi-ates inhibition of eosinophilic inflammation and airway hyperreactivity in-dependent of natural killer cells in vivo. J. Allergy Clin. Immunol. 108:759–763.
6. Broide, D. H., G. Stachnick, D. Castaneda, J. Nayar, M. Miller, J. Y. Cho, M.Roman, J. Zubeldia, T. Hyashi, and E. Raz. 2001. Systemic administrationof immunostimulatory DNA sequences mediates reversible inhibition ofTh2 responses in a mouse model of asthma. J. Clin. Immunol. 21:175–182.
7. Serebrisky, D., A. A. Teper, C. K. Huang, S. Y. Lee, T. F. Zhang, B. H.Schofield, M. Kattan, H. A. Sampson, and X. M. Li. 2000. CpG oligodeoxy-nucleotides can reverse Th2-associated allergic airway responses and alterthe B7.1/B72 expression in a murine model of asthma. J. Immunol. 165:5906–5912.
8. Kline, J. N., A. M. Krieg, T. J. Waldschmidt, Z. K. Ballas, V. Jain, and T. R.Businga. 1999. CpG oligodeoxynucleotides do not require TH1 cytokinesto prevent eosinophilic airway inflammation in a murine model of asthma.J. Allergy Clin. Immunol. 104:1258–1264.
9. Ikeda, R. K., J. Nayar, J. Y. Cho, M. Miller, M. Rodriguez, E. Raz, and D.Broide. 2003. Resolution of airway inflammation following ova inhalation:comparison of ISS DNA and corticosteroids. Am. J. Respir. Cell Mol. Biol.28:655–663.
10. Kline, J. N., K. Kitagaki, T. R. Businga, and V. V. Jain. 2002. Treatment ofestablished asthma in a murine model using CpG oligodeoxynucleotides.Am. J. Physiol. Lung Cell. Mol. Physiol. 283:L170–L179.
11. Hemmi, H., O. Takeuchi, T. Kawai, T. Kaisho, S. Sato, H. Sanjo, M. Matsu-
moto, K. Hoshino, H. Wagner, K. Takeda, and S. Akira. 2000. A Toll-likereceptor recognizes bacterial DNA. Nature 408:740–745.
12. Horner, A. A., J. H. Van Uden, J. M. Zubeldia, D. Broide, and E. Raz.2001. DNA-based immunotherapeutics for the treatment of allergic disease.Immunol. Rev. 179:102–118.
13. Hansen, G., G. Berry, R. H. DeKruyff, and D. T. Umetsu. 1999. Allergen-specific Th1 cells fail to counterbalance Th2 cell-induced airway hyperreac-tivity but cause severe airway inflammation. J. Clin. Invest. 103:175–183.
14. Cho, J. Y., M. Miller, K. J. Baek, D. Castaneda, J. Nayar, M. Roman, E.Raz, and D. H. Broide. 2001. Immunostimulatory DNA sequences inhibitrespiratory syncytial viral load, airway inflammation, and mucus secretion.J. Allergy Clin. Immunol. 108:697–702.
15. Elias, J. A., Z. Zhu, G. Chupp, and R. J. Homer. 1999. Airway remodeling inasthma. J. Clin. Invest. 104:1001–1006.
16. Henderson, W. R., Jr., L. O. Tang, S. J. Chu, S. M. Tsao, G. K. Chiang, F.Jones, M. Jonas, C. Pae, H. Wang, and E. Y. Chi. 2002. A role for cysteinylleukotrienes in airway remodeling in a mouse asthma model. Am. J. Respir.Crit. Care Med. 165:108–116.
17. Hammelmann, E., J. Schwarze, K. Takeda, A. Oshiba, G. L. Larsen, C. G.Irvin, and E. W. Gelfand. 1997. Noninvasive measurement of airway respon-siveness in allergic mice using barometric plethysmography. Am. J. Respir.Crit. Care Med. 156:766–775.
18. Khalil, N. 1999. TGF-�: from latent to active. Microbes Infect. 1:1255–1263.19. Lee, C. G., R. J. Homer, Z. Zhu, S. Lanone, X. Wang, V. Koteliansky, J. M.
Shipley, P. Gotwals, P. Noble, Q. Chen, R. M. Senior, and J. A. Elias.2001. Interleukin-13 induces tissue fibrosis by selectively stimulating andactivating transforming growth factor beta(1). J. Exp. Med. 194:809–821.
20. Jain, V. V., K. Kitagaki, T. Businga, I. Hussain, C. George, P. O’Shaughnessy,and J. N. Kline. 2002. CpG-oligodeoxynucleotides inhibit airway remodelingin a murine model of chronic asthma. J. Allergy Clin. Immunol. 110:867–872.
21. Gizycki, M. J., E. Adelroth, A. V. Rogers, P. M. O’Byrne, and P. K. Jeffery.1997. Myofibroblast involvement in the allergen-induced late response inmild atopic asthma. Am. J. Respir. Cell Mol. Biol. 16:664–673.
22. Zhang, S., Q. Mohammed, A. Burbidge, C. M. Morland, and W. R. Roche.1996. Cell cultures from bronchial subepithelial myofibroblasts enhanceeosinophil survival in vitro. Eur. Respir. J. 9:1839–1846.
23. Blobe, G. C., W. P. Schiemann, and H. F. Lodish. 2000. Role of transforminggrowth factor beta in human disease. N. Engl. J. Med. 342:1350–1358.
24. Vignola, A. M., P. Chanez, G. Chiappara, A. Merendino, E. Pace, A. Rizzo,A. M. la Rocca, V. Bellia, G. Bonsignore, and J. Bousquet. 1997. Trans-forming growth factor-� expression in mucosal biopsies in asthma andchronic bronchitis. Am. J. Respir. Crit. Care Med. 156:591–599.
25. Redington, A. E., J. Madden, A. J. Frew, R. Djukanovic, W. R. Roche, S. T.Holgate, and P. H. Howarth. 1997. Transforming growth factor-�1 inasthma: measurement in bronchoalveolar lavage fluid. Am. J. Respir. Crit.Care Med. 156:642–647.
26. Hoshino, M., Y. Nakamura, and J. J. Sim. 1998. Expression of growth factorsand remodelling of the airway wall in bronchial asthma. Thorax 53:21–27.
27. Chiramonte, M. G., D. D. Donaldson, A. W. Cheever, and T. A. Wynn. 1999.An IL-13 inhibitor blocks the development of hepatic fibrosis during a T-helper type 2-dominated inflammatory response. J. Clin. Invest. 104:777–785.
28. Aikawa, T., S. Shimura, H. Sasaki, M. Ebina, and T. Takishima. 1992. Markedgoblet cell hyperplasia with mucus accumulation in the airways of patientswho died of severe acute asthma attack. Chest 101:916–921.
29. Alimann, M. Z., F. M. Piazza, D. M. Selby, N. Letwin, L. Huang, and M. C.Rose. 2000. Muc-5/5ac mucin, messenger RNA and protein expression aremarkers of goblet-cell metaplasia in murine airways. Am. J. Respir. CellMol. Biol. 22:253–260.
30. Cohn, L., R. J. Homer, A. Marinov, J. Rankin, and K. Bottomly. 1997. Inductionof airway mucus production by T helper 2 (Th2) cells: a critical role forinterleukin 4 in cell recruitment but not mucus production. J. Exp. Med.186:1737–1747.
31. Wills-Karp, M. 2000. Trophic slime, allergic slime. Am. J. Respir. Cell Mol.Biol. 22:637–639.
32. Longphre, M., D. Li, M. Gallup, E. Drori, C. L. Ordonez, T. Redman, S.Wenzel, D. E. Bice, J. V. Fahy, and C. Basbaum. 1999. Allergen-inducedIL-9 directly stimulates mucin transcription in respiratory epithelial cells.J. Clin. Invest. 104:1375–1382.
33. Ikeda, R. K., M. Miller, J. Nayar, L. Walker, J.-Y. Cho, K. McElwain, S.McElwain, E. Raz, and D. H. Broide. 2003. Accumulation of peribronchialmast cells in a mouse model of ovalbumin allergen induced chronic airwayinflammation: modulation by immunostimulatory DNA sequences. J. Im-munol. 171:4860–4867.
34. Johnson, P. R., M. Roth, M. Tamm, M. Hughes, Q. Ge, G. King, J. K. Burgess,and J. L. Black. 2001. Airway smooth muscle cell proliferation is increasedin asthma. Am. J. Respir. Crit. Care Med. 164:474–477.
35. Hirst, S. J., C. H. Twort, and T. H. Lee. 2000. Differential effects of extracellularmatrix proteins on human airway smooth muscle cell proliferation andphenotype. Am. J. Respir. Cell Mol. Biol. 23:335–344.