Plasma proteome changes in cardiovascular disease patients: novel isoforms of apolipoprotein A1
Upload
independentCategory
view
0download
0
at SciVerse ScienceDirect
The Breast 21 (2012) 165e170
Contents lists available
The Breast
journal homepage: www.elsevier .com/brst
Original article
Immunophenotyping analysis in invasive micropapillary carcinoma of the breast:Role of CD24 and CD44 isoforms expression
Sara Simonetti a,*, Luigi Terracciano b, Inti Zlobec b, Ergin Kilic b, Loredana Stasio a, Maria Quarto c,Guido Pettinato a, Luigi Insabato a,*
aDepartment of Functional and Biomorphological Science, University “Federico II”, Via S. Pansini 5, 80131 Naples, ItalybDepartment of Pathology, University of Basel, SwitzerlandcDepartment of Physic Sciences, University “Federico II”, Naples, Italy
a r t i c l e i n f o
Article history:Received 1 January 2011Received in revised form28 June 2011Accepted 2 September 2011
Keywords:Invasive micropapillary carcinoma of thebreastInverted polarityLymph-vascular invasion propensityCD24CD44 isoforms
Abbreviations: IMPC, invasive micropapillary carcarcinoma.* Corresponding authors. Tel.: þ39 0817463442; fa
E-mail addresses: [email protected] (S. Simo(L. Terracciano), [email protected] (I. Zlobec), kilicinwind.it (L. Stasio), [email protected] (M. Quar(G. Pettinato), [email protected] (L. Insabato).
0960-9776/$ e see front matter � 2011 Elsevier Ltd.doi:10.1016/j.breast.2011.09.004
a b s t r a c t
We analyzed immunohistochemically the expression of CD24 and spliced variants of CD44v5 and v9 ininvasive micropapillary carcinoma (IMPC) of the breast that is a rather aggressive tumor characterized byalteration of cells adhesion molecules, early lymph node metastases and poor prognosis. We analyzed 31high-grade IMPCs and compared their expression to 22 high grade (G3) invasive ductal carcinomas of thebreast (IDCs). We found a higher expression of CD24 in high-grade IMPCs with a peculiar inverted apicallocalization, compared to IDCs, showing a strong cytoplasmic staining; normal breast tissue resultedcompletely negative. IMPCs showed reduced expression of CD44v5 and CD44v9 compared with IDCs, butwithout a statistical significant difference. This study demonstrated that IMPC represents a distinct entityof breast carcinoma with high expression of CD24 with a typical inverted apical membrane pattern andreduction of CD44 isoforms v5 and v9, compared to IDCs. These features could explain the high lymph-vascular invasion propensity and higher metastatic capability of these tumors and could be a useful toolfor a future targeted therapy.
� 2011 Elsevier Ltd. All rights reserved.
Introduction
The mechanisms by which metastases develop are variable andrequire several steps including loss of contact with neighboringcells, penetration of vessel walls, adhesion at the new localizationand angiogenesis. These processes involve a series of proteins andadhesion molecules such as CD44, cadherins or selectins.1 CD44 isa family of transmembrane glycoproteins generated from a singlelarge gene that contains 10 exons producing 10 isoforms (v1-10)that are different in their extracellular domains as result of alter-native splicing. Hyaluronan is the main ligand of CD44 and thefunction of the standard form (CD44s) is to regulate the homing oflymphocytes.2,3 Some variant isoforms are overexpressed in humantumors and seem to be involved in the formation and development
cinoma; IDC, invasive ductal
x: þ39 0817463475.netti), [email protected]@uke.de (E. Kilic), elle.dt@to), [email protected]
All rights reserved.
of metastases.4e6 Increased expression of CD44v5 is frequentlyassociated with cancer progression, lymph nodes metastasis andshort relapse-free survival in gastrointestinal tumors.7,8 On theother hand, the abnormal expression of CD44v9 has been associ-ated with invasion ability of tumoral cells and metastasis.9
In breast cancer expression of CD44 isoforms seems to play animportant role for the development of lymph node metastasis andtumor progression. Bankfalvi et al. analyzed the expression ofCD44s and its variants in benign and malignant breast lesions,finding a significant increase in malignant and premalignantlesions compared to normal breast tissue. In invasive ductal carci-noma (IDC), they observed loss of CD44v3 and v6, and an increaseof CD44v4 and v5; in invasive lobular carcinoma loss of CD44v4 andv6, and gain of CD44s, v5 and v9. CD44v3, v5 and v6 are associatedwith a decreased disease-free survival but fails to be independentprognosticators.10 Nevertheless some studies have analyzed therole of CD44v9 in estrogen receptor-positive breast tumors,however without a significant correlation with the prognosis.Whereas negativity for CD44v9 seems to be an independent factorfor predicting the recurrence of node-negative breast cancer.11
Recently, attention has shifted to CD24 because of its importantrole in the development of cancer metastases12 and as a marker of

Table 1Clinicopathological features of high grade IMPCs compared with high grade IDCs.
IMPCs IDCs P value
AgeMean 58 57 0.137Range 29e82 32e78
No of Cases (%)Grade1 0 (0) 0 (0)2 0 (0) 0 (0)3 31 (100) 22 (100)
StagePT1 12 (39) 7 (32) 0.830pT2 14 (45) 10 (45)pT3 2 (6) 3 (14)pT4 3 (10) 2 (9)
Lymph nodespN0 2 (7) 16 (27) <0.05pN1 14 (45) 10 (27)pN2 13 (41) 3 (32)pN3 2 (7) 3 (14)
IHC characteristicsERþ 9 (29) 17 (77) <0.05PRþ 8 (26) 17 (77) <0.05HER2þ 27 (87) 5 (14) <0.05
IMPCs ¼ Invasive micropapillary carcinomas. IDCs ¼ Invasive ductal carcinoma.IHC ¼ Immunohistochemistry; ERþ ¼ Immunopositivity for estrogen receptor.PRþ¼ Immunopositivity for progesterone receptor. HER2þ¼ immunoreactivity forHER2 oncoprotein.
S. Simonetti et al. / The Breast 21 (2012) 165e170166
malignancy in several tumor types. In fact, protein overexpressionhas been associatedwith high grade or invasive neoplasms, positivenodal status, and shorter patient disease-free survival in colon,ovary, kidney, prostate, lung, and other tumors.13,14 CD24 is anadhesion mucin-like molecule indentified as an alternative ligandof P-selectin, a receptor present in activated platelets and endo-thelial cells whose expression could increase the ability of cancercells to metastasize.12 Although CD24 seems to influence lymphoidand hematopoietic cell maturation and to be involved in theregulation of cell proliferation and interaction12,13, its functionremains unclear. In breast cancer, CD24 is abundantly expressed,increasing with the histological grade of the tumor. Differentexpression has also been observed in breast carcinomas (cyto-plasmic pattern) versus benign breast tumors (apical pattern).Therefore, CD24 is considered a marker of tumor progression andpoor prognosis.15e17 Recently, Li et al. observed a great proportion
Fig. 1. Histologic features of IMPC of the breast (A). Unlike IDC (B), this tumor is characterizfibrous stroma.
of tumor cells expressing CD24 in an uncommon variant of ductalcarcinoma of the breast, invasive micropapillary carcinoma (IMPC),associated with lymph node invasion.18
IMPCs of the breast are rare (0.7e3% of all invasive breastcarcinomas), and aggressive subtypes of IDC, described for the firsttime by Siariaunkgul et al.19 and best characterized by Luna-Moréet al.20,21 and Middleton et al.22 Morphologically IMPCs showa peculiar architecture characterized by pseudopapillary structurescomposed of cell clusters with inverted polarity and floating inempty spaces, lined by delicate strands of fibrous stroma.19e23
Invasive micropapillary pattern has been described in tumors ofseveral organs, such as ovary, salivary gland, colon, bladder andlung24e27 and clinically is nearly always associated with poorprognosis and high incidence of lymph node metastases.23,28,29
Although many studies have tried to explain the peculiar featuresof these tumors, analyzing adhesion molecules markers or severalmolecular characteristics,23,25,27,28,30 the bases of their biologicbehavior remain unclear and several efforts have to be made tobetter understand this rare variant of carcinoma.
To clarify the high incidence of lymph node metastases andaggressive clinical behavior in IMPCs, we analyzed immunohisto-chemical expression of CD24 and CD44 variants in these tumors,comparing to high grade IDCs and normal breast tissue.
Materials and methods
Patients
In a previous study we analyzed morphologically and immu-nohistochemically 62 cases of IMPCs of the breast of differenttumoral grades, from the files of the Department of Pathology,University of Naples Federico II, Italy.23 Of these cases we identified31 cases of high-grade IMPCs and added 22 cases of high gradeIDCs. A total of 53 high grade breast tumors (31 IMPCs and 22 IDCs)were selected for this study. The diagnosis of all the cases, lymph-vascular invasion and lymph node metastasis were evaluated in4 mm sections, stained with H/E, by two independent pathologists(LI and SS), according to the criteria of the literature.19e23 Forlymph-vascular invasion in doubt cases an immunohistochemicalstaining with CD31 was done. The slides were graded according theNottingham modification of the Bloom-Richardson method.31 Themicropapillary pattern was exclusive or prevalent (>50%) in 18tumors (58%) and partial (<50%) in 13 (42%). Normal breast tissuepresent in the sections of 26 cases (18 IMPCs and 8 IDCs) was also
ed by pseudopapillary structures floating in empty spaces lined by delicate strands of

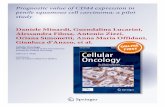
Fig. 2. Immunohistochemical staining for CD24 IMPCs and IDCs of the breast. A) In IMPCs CD24 showed a characteristic inverted apical localization in the neoplastic cells.B) Immunohistochemical staining for CD24 in IDCs showing a strong cytoplasmic staining. C) In normal breast tissue CD24 expression resulted negative.
S. Simonetti et al. / The Breast 21 (2012) 165e170 167
evaluated for immunohistochemical analysis. Clinicopathologicalfinding of both populations are showed in Table 1. Microscopicfeatures of IMPCs and IDCs are showed in Fig. 1.
Immunohistochemistry
Immunohistochemical staining was performed on 4-mm thicksections from formalin fixed, paraffin embedded tissues. Thefollowing antibodies were used: mouse monoclonal antibodyagainst CD24 (clone SN3b Neomarkers, Thermo Scientific, CA, USA),at a dilution of 1:200, CD44v5 (clone VFF-8, Novocastra Laborato-ries, Newcastle, UK) at a dilution of 1:800, and CD44v9 (clone VVF-10, Novocastra Laboratories) at a dilution of 1:400. The sampleswere deparaffinized with xylene and rehydrated in a series ofethanols. Endogenous peroxidase was blocked at room tempera-ture by 3% hydrogen peroxide for 15 min. Antigen retrieval wasperformed in 0.01 M citrate buffer (pH 6.0) in a microwave for20 min. The slides were incubated with the antibodies against
Fig. 3. Immunohistochemical expression of CD44v5 in IMPCs (A) and IDCs (B) of the breascytoplasmic membrane toward the matrix border. In IDCs we observed expression of CD44
CD24, CD44v5, and CD44v9, treated with the streptavidin-biotin-peroxidase complex method (DAKO, Glostrup Denmark) with dia-minobenzidine as a chromogen and counterstained with hema-toxylin. Human tonsil tissue was included as positive control.Omission of primary antibody and substitution with phosphate-buffered saline were used as negative control. Accordingly to theliterature, no detectable CD24 immunoreactivity in any part of thetumor was considering as negative; a range between a weak butunequivocal staining in both cytoplasm and/or membrane of tumorcells to strong expression was defined as positive. Apical or cyto-plasmic staining pattern for CD24was also evaluated.15e17 For CD44variants (v5 and v9) immunopositivity was established as found inthe literature. The following score was used: 0, negative staining; 1,weak expression in <5% of the membrane of tumor cells; 2,moderate or strong expression in 5e75% of the membrane of tumorcells; 3, strong expression in >75% of the membrane of tumor cells.A score of 0 or 1 was considered as negative, and a score of 2 or 3was considered positive.10
t. Arrows show the reduction or loss of immunohistochemical staining in the part ofv5 protein in all the perimeter of the membrane (B).

Table 2Immunohistochemical results for CD24 and CD44 isoforms staining in IMPCs of thebreast compared with IDCs and NTs.
IHC Results IMPCs IDCs NTs P value
N. of Cases (%)
CD24 þ Cytoplasm 4 (13) 12 (55) 0 (0) <0.05
CD24 þ Apical 27 (87) 6 (27) 0 (0) <0.05CD44v5þ 14 (45) 14 (63) 8 (31) 0.075
S. Simonetti et al. / The Breast 21 (2012) 165e170168
Statistical analysis
The correlation between CD24, CD44v5 and CD44v9 proteinexpression and clinicopathological features of IMPCs, IDCs andnormal tissues, were evaluated using the Chi-square test. The tStudent test was used for continuous variable. The P values �0.05denote statistical significance. Statistical analysis was performedusing Stata software (Stata Corp., College Station, Tex., USA).
CD44v9þ 23 (74) 18 (81) 17 (65) 0.435
IMPCs ¼ Invasive micropapillary carcinoma of the breast. IDCs ¼ Invasive ductalcarcinoma. NTs ¼ Normal breast tissues.
Results
In IMPCswe found expression of CD24 in 27/31 (87%) cases, witha characteristic apical localization (Fig. 2A); moreover 4 tumors(13%) simultaneously presented a cytoplasmic staining. Strikingly,we observed an inverted apical staining of CD24 in IMPCs, as shownin Fig. 2A. Membrane expression for CD44v5 and CD44v9 wasfound in 14/31 (45%) (Fig. 3A) and in 23/31 (74%) cases (Fig. 4A),respectively. Interestingly, we observed in IMPCs an incompletestaining of the cytoplasmic membrane with a lack of expression ofthe protein of both variables of CD44 in the part of cytoplasmicmembrane toward the matrix border (Fig. 3A and Fig. 4A arrows).IDCs showed expression of CD24 in 12/22 (54%) cases with strongcytoplasmic staining (Fig. 2B). We observed a significantly statis-tical difference in the apical and cytoplasmic expression of CD24 inIDCs and IMPCs (p < 0.001), with a predominance of cytoplasmiclocalization in IDCs and apical expression in IMPCs. We foundmembrane expression of CD44v5 in 14/22 (63%) IDCs (Fig. 3B) andpositivity for CD44v9was observed in 18/22 (81%) cases (Fig. 4B). Innormal breast tissue CD24 expression was not found (Fig. 2C)immunopositivity for CD44v5 and CD44v9 was observed in 8/26(31%) and in 17/26 (65%) cases, respectively (Table 2).
We have not found association between CD24, CD44v5 and v9expression and clinical and pathological risk factors such as tumorsize, HER2/neu positivity or estrogen and progesterone receptorexpression (data not shown). A trend of statistical significance wasobserved between CD24 staining and the number of metastaticlymph nodes in both subtypes of carcinomas (p ¼ 0.061). Whereaswe have not found association between CD44v5 and v9 expressionand lymph node metastasis (p ¼ 0.165 and p ¼ 0.618 respectively),as shown in Table 3. Separately, IMPCs with lymph node invasionshowed positivity for CD24 in 26/29 (90%) cases, for CD44v5 in 13/29 (45%) cases and for CD44v9 in 22/29 (76%) cases, whereas IDCswith lymph node invasion expressed CD24 in 12/16 (75%) of thecases, CD44v5 in 11/16 (69%) of the cases and for CD44v9 in 13/16(81%) of the cases. There is not statistical significant differencesamong CD24, CD44v5 and CD44v9 expression and lymph nodemetastasis, comparing IMPCs and IDCs (Table 3).
Fig. 4. Membrane expression of CD44v9 in IMPCs (A). Immunohistochemical staining for CDCD44v9 in the apical membrane of IMPCs cells.
Discussion
Invasive micropapillary component has been described inseveral type of carcinomas and associated with poor prognosis andlymph nodes invasion.24e27 Due to its low frequency, it is not clearlyknown which kind of molecular alterations are related to itsmorphologic and clinical behavior and many studies are necessaryto thoroughly analyze these entities. IMPC is a rare subtype ofductal carcinoma of the breast with an unusual and distinctivehistologic pattern, and with peculiar molecular features.19e23,30
IMPC occurs in about 0.7e3% of all breast cancers and it ischaracterized by a high histologic grade, pseudopapillary structureswith alteration of adhesion molecules, high propensity forlymphatic dissemination and an aggressive biological behav-ior.19e21 Recently it has been observed that IMPCs have a prevalenceof CD44s(þ)/CD24(�/low) tumor cells and a proportion of CD24(þ)tumor cells higher than IDCs, showing a tumor-initiating pheno-type and associationwith lymph nodemetastasis.18 In our series weobserved similar features of IMPCs compared with IDCs, andconsidering CD44v5 and CD44v9 separately, we have not founddifferences in the expression of these isoforms to identify the“stem-cell phenotype” (data not shown).
Although various biological markers have been studied in thesetumors and it seems that this subtype of breast cancer is a distinctentity even at the molecular level,20,23,28e30 their origin is stillunclear.
In previous studies we described, in 62 cases of IMPCs of thebreast, morphologic and immunophenotypic features of prognosticimportance such as DNA ploidy, cell proliferation index, proto-oncogene expression of Her2/neu and p53, expression of metas-tases suppressor genes, and hormonal receptor immunoreactivity,to explain the aggressive behavior of these tumors.23
A unique feature of this breast carcinoma subtype is that theneoplastic cells are organized in clusters with reversed polarity,
44v9 showed a strong membrane staining in IDCs (B). Arrows show loss or reduction of

Table 3CD24 and CD44 isoforms expression in IMPCs and IDCs patients with lymph node metastasis.
Type of tumor Number oflymph node
CD24 CD44v5 CD44v9
Total, n Positive (%) p-value Total, n Positive (%) p-value Total, n Positive (%) p-value
IMPCs þ IDCs 1e3 19 68 0.061 19 63 0.165 19 84 0.6184e9 17 88 17 35 17 719þ 9 44 9 67 9 78
IDCs 1e3 6 67 0.837 6 67 0.953 6 67 0.3134e9 4 50 4 75 4 759þ 6 67 6 67 6 100
IMPCs 1e3 13 85 0.168 13 62 0.104 13 92 0.0744e9 13 100 13 23 13 699þ 3 67 3 67 3 33
IMPCs ¼ Invasive micropapillary carcinomas of the breast. IDCs ¼ invasive ductal carcinomas.
S. Simonetti et al. / The Breast 21 (2012) 165e170 169
probably due to modifications in cell adhesion molecules. Inprevious studies some of these molecules such as MUC1, E-cad-herin or standard CD44 isoform have been analyzed and theirmembrane expression has been found altered, indicating inversionof cell polarization.22,23,28,32 The role of CD44 and its isoforms in thedevelopment of IMPCs remains unclear. A significant loss orreduction of standard CD44 isoform immunoreactivity was foundby Gong et al. in 23 IMPCs of the breast associated with a strongexpression of E-cadherin in cases with high incidence of lymph-vascular permeation and lymph node dissemination.32
Our results showed a high expression of CD44 variants v5 and v9in IDCs (63% and 81% of the cases, respectively), as described inliterature,10 and high level in IMPCs of both isoforms, althoughwitha lower percentage of positive cases (Table 2).Moreover in IMPCsweobserved a characteristic incomplete staining of the cytoplasmicmembrane with a lack of expression of the protein of both variablesof CD44 in the part of cytoplasmic membrane toward the matrixborder (Figs. 3A and 4A arrows). Strikingly we described thisparticular immunohistochemical feature observed for Her2 and E-cadherin expressions in our previous study.23 Even in the paperpublished by Gong et al. E-cadherin shows the lack of signal in thesame location of our series, however they did not comment it.32 Thepartial expression of these proteins seems to be a unique feature ofIMPCs. Therefore we might suppose that in these tumors adhesionmolecules lose their bindingwith the surrounding stroma, probablydue to specific capability of IMPCs cells to modify the stroma viaparacrine interactions and lead to loss of myoepithelial cells. Thishypothesis may explain the formation of empty spaces inwhich cellclusters float, their propensity for lymphatic invasion and thedevelopment of early metastases. Numerous evidences havedemonstrated that there is a strong correlation between cancer cellsand tumor microenvironment, which actively contributes to tumorinitiation, progression and metastases.33 In breast carcinomas,myoepithelial cells seem to play an import role of interactionbetween the luminal epithelial cells and the surrounding stroma,bringing important regulatory signals for the maintenance ofnormal breast structure and polarity of epithelial cells.34
An important factor related to the development of lymph nodemetastases, high grade or invasive neoplasms and reduction ofpatient survival in several tumors is the cell adhesion moleculeCD24. This marker has been found significantly overexpressed inseveral malignancies and plays an important role in the develop-ment of metastasis and poor prognosis.12,14,17,35 It has beenobserved that the loss of CD24 function in tumoral cells in vitro andin vivo reduced cell proliferation and microvessel density andincreased apoptosis, suggesting the CD24 knockdown as a potentialanti-tumoral therapeutic approach.35,36 In our series we describeda higher expression of CD24 in IMPCs comparing to IDCs (87% and54% respectively), with a peculiar apical localization in IMPCs, andnegativity in normal breast tissue (Table 2).
Conclusion
This study helps to confirm that IMPCs should be considereda histologic and molecular distinct subtype of invasive breastcarcinoma. These tumors showed high expression of CD24 with aninverted apical membrane pattern, compared with IDCs andexpression of the adhesion molecules CD44 isoforms v5 and v9with an incomplete staining of the membrane toward the extra-cellular matrix. These features might explain the loss of epithelialcellsestroma interaction and its propensity for lymphatic invasion.Moreover the increased expression of CD24 might be a useful toolfor a future targeted therapy.
Authors’ contributions
SS, IL, LT and GP participated in the design of the study and itswriting. IZ, LK, and LS carried out the immunohistochemical assays.MQ realized the statistical tests. SS, IL, LT and GP have madesubstantial contributions to analysis and interpretation of data. Allauthors read and approved the final manuscript.
Conflict of interest statementThe authors declare that they have no competing financial
interests.
References
1. Achen MG, Stacker SA. Molecular control of lymphatic metastasis. Ann N Y AcadSci 2008;1131:225e34.
2. Rudzki Z, Jothy S. CD44 and the adhesion of neoplastic cells. Mol Pathol1997;50:57e71.
3. Sneath RJ, Mangham DC. The normal structure and function of CD44 and itsrole in neoplasia. Mol Pathol 1998;51:191e200.
4. Katsura M, Furumoto H, Nishimura M, Kamada M, Aono T. Overexpression ofCD44 variants 6 and 7 in human endometrial cancer. Gynecol Oncol1998;71:185e9.
5. Kunishi M, Kayada Y, Yoshiga K. Down-regulated expression of CD44 variant 6in oral squamous cell carcinomas and its relationship to regional lymph nodemetastasis. Int J Oral Maxillofac Surg 1997;26:280e3.
6. Lee LN, Kuo SH, Lee YC, Chang YL, Chang HC, Jan IS, et al. CD44 splicing patternis associated with disease progression in pulmonary adenocarcinoma. J FormosMed Assoc 2005;104:541e8.
7. Li DM, Li SS, Zhang YH, Zhang HJ, Gao DL, Wang YX. Expression of humanchorionic gonadotropin, CD44v6 and CD44v4/5 in esophageal squamous cellcarcinoma. World J Gastroenterol 2005;11:7401e4.
8. Vizoso FJ, Fernández JC, Corte MD, Bongera M, Gava R, Allende MT, et al.Expression and clinical significance of CD44V5 and CD44V6 in resectablecolorectal cancer. J Cancer Res Clin Oncol 2004;130:679e86.
9. Sato S, Miyauchi M, Kato M, Kitajima S, Kitagawa S, Hiraoka M, et al. Upre-gulated CD44v9 expression inhibits the invasion of oral squamous cell carci-noma cells. Pathobiology 2004;71:171e5.
10. Bànkfalvi A, Terpe HJ, Breukelmann D, Bier B, Rempe D, Pschadka G, et al. Gainsand losses of CD44 expression during breast carcinogenesis and tumourprogression. Histopathology 1998;33:107e16.
11. Umemura S, Komaki K, Noguchi S, Shiba E, Toi M, Kimijima II, et al. Prognosticfactors for node-negative breast cancers: results of a study program by theJapanese breast cancer society. Breast Cancer 1998;5:243e9.

S. Simonetti et al. / The Breast 21 (2012) 165e170170
12. Kristiansen G, Sammar M, Altevogt P. Tumour biological aspects of CD24,a mucin-like adhesion molecule. J Mol Histol 2004;35:255e62.
13. Baumann P, Cremers N, Kroese F, Orend G, Chiquet-Ehrismann R, Uede T, et al.CD24 expression causes the acquisition of multiple cellular properties associ-ated with tumor growth and metastasis. Cancer Res 2005;65:10783e93.
14. Lim SC, Oh SH. The role of CD24 in various human epithelial neoplasias. PatholRes Pract 2005;201:479e86.
15. Bircan S, Kapucuoglu N, Baspinar S, Inan G, Candir O. CD24 expressionin ductal carcinoma in situ and invasive ductal carcinoma of breast:an immunohistochemistry-based pilot study. Pathol Res Pract 2006;202:569e76.
16. Fogel M, Friederichs J, Zeller Y, Husar M, Smirnov A, Roitman L, et al. CD24 isa marker for human breast carcinoma. Cancer Lett 1999;143:87e94.
17. Kristiansen G, Winzer KJ, Mayordomo E, Bellach J, Schlüns K, Denkert C, et al.CD24 expression is a new prognostic marker in breast cancer. Clin Cancer Res2003;9:4906e13.
18. Li W, Liu F, Lei T, Xu X, Liu B, Cui L, et al. The clinicopathological significance ofCD44(þ)/CD24(-/low) and CD24(þ) tumor cells in invasive micropapillarycarcinoma of the breast. Pathol Res Pract 2010;206:828e34.
19. Siriaunkgul S, Tavassoli FA. Invasive micropapillary carcinoma of the breast.Mod Pathol 1993;6:660e2.
20. Luna-More S, de los Santos F, Breton JJ, Canadas MA. Estrogen and proges-terone receptors, c-erbB-2, p53, and Bcl-2 in thirty-three invasive micro-papillary breast carcinomas. Pathol Res Pract 1996;192:27e32.
21. Luna-More S, Gonzalez B, Acedo C, Rodrigo I, Luna C. Invasive micropapillarycarcinoma of the breast. A new special type of invasive mammary carcinoma.Pathol Res Pract 1994;190:668e74.
22. Middleton LP, Tressera F, Sobel ME, Bryant BR, Alburquerque A, Grases P, et al.Infiltrating micropapillary carcinoma of the breast. Mod Pathol1999;12:499e504.
23. Pettinato G, Manivel CJ, Panico L, Sparano L, Petrella G. Invasive micropapillarycarcinoma of the breast: clinicopathologic study of 62 cases of a poorlyrecognized variant with highly aggressive behavior. Am J Clin Pathol2004;121:857e66.
24. Compérat E, Roupret M, Yaxley J, Reynolds J, Varinot J, Ouzaïd I, et al. Micro-papillary urothelial carcinoma of the urinary bladder: a clinicopathologicalanalysis of 72 cases. Pathology 2010;42:650e4.
25. De Oliveira Duarte Achcar R, Nikiforova MN, Yousem SA. Micropapillary lungadenocarcinoma: EGFR, K-ras, and BRAF mutational profile. Am J Clin Pathol2009;131:694e700.
26. Nagao T, Gaffey TA, Visscher DW, Kay PA, Minato H, Serizawa H, et al. Invasivemicropapillary salivary duct carcinoma: a distinct histologic variant with bio-logic significance. Am J Surg Pathol 2004;28:319e26.
27. Verdú M, Román R, Calvo M, Rodón N, García B, González M, et al. Clinico-pathological and molecular characterization of colorectal micropapillarycarcinoma. Mod Pathol 2011;24:729e38.
28. Li YS, Kaneko M, Sakamoto DG, Takeshima Y, Inai K. The reversed apical patternof MUC1 expression is characteristics of invasive micropapillary carcinoma ofthe breast. Breast Cancer 2006;13:58e63.
29. Zekioglu O, Erhan Y, Ciris M, Bayramoglu H, Ozdemir N. Invasive micropapillarycarcinoma of the breast: high incidence of lymph node metastasis withextranodal extension and its immunohistochemical profile compared withinvasive ductal carcinoma. Histopathology 2004;44:18e23.
30. Marchiò C, Iravani M, Natrajan R, Lambros MB, Savage K, Tamber N, et al.Genomic and immunophenotypical characterization of pure micropapillarycarcinomas of the breast. J Pathol 2008;215:398e410.
31. Robbins P, Pinder S, de Klerk N, Dawkins H, Harvey J, Sterrett G, et al. Histo-logical grading of breast carcinomas: a study of interobserver agreement. HumPathol 1995;26:873e9.
32. Gong Y, Sun X, Huo L, Wiley EL, Rao MS. Expression of cell adhesion molecules,CD44s and E-cadherin, and microvessel density in invasive micropapillarycarcinoma of the breast. Histopathology 2005;46:24e30.
33. De Wever O, Demetter P, Mareel M, Bracke M. Stromal myofibroblasts aredrivers of invasive cancer growth. Int J Cancer 2008;123:2229e38.
34. Gudjonsson T, Adriance MC, Sternlicht MD, Petersen OW, Bissell MJ. Myoepi-thelial cells: their origin and function in breast morphogenesis and neoplasia.J Mammary Gland Biol Neoplasia 2005;10:261e72.
35. Kristiansen G, Denkert C, Schluns K, Dahl E, Pilarsky C, Hauptmann S. CD24 isexpressed in ovarian cancer and is a new independent prognostic marker ofpatient survival. Am J Pathol 2002;161:1215e21.
36. Smith SC, Oxford G, Wu Z, Nitz MD, Conaway M, Frierson HF, et al. Themetastasis-associated gene CD24 is regulated by Ral GTPase and is a mediatorof cell proliferation and survival in human cancer. Cancer Res2006;66:1917e22.
Copyright © 2022 FDOKUMEN