
Immunomodulation of tissue-engineered transplants: in vivo bone generation from...
9
Abstract Subcutaneously implanted, in vitro engineered tissue is generally affected by the immune system of the host even in autogenous transplantation. The aim of this study was to investigate immunomodulation of subcuta- neously implanted tissue-engineered cartilage transplants by intramuscular methylprednisolone application. Trans- plants consisted of auricular rabbit chondrocytes, polylac- tide-polyglycolide co-polymer fleeces and species-specific fibrin or agarose. The transplants were subcutaneously implanted in the ridge. Thereafter, animals were separated into two groups, one with and one without methylpred- nisolone treatment. The specimens were histologically in- vestigated after 6 and 12 weeks. Fleece fiber degradation was complete after 12 weeks, and all transplants showed areas of calcification. The corticosteroid-treated group presented pronounced trabecular bone generation without fibrous tissue infiltration. The untreated group showed sporadic islets of calcification without coherent bone for- mation, and adjacent fibrous tissue had infiltrated the trans- plants. Native controls and corticoid-treated transplants did not exhibit bone generation or signs of fibrous tissue infiltration. This study found that immunomodulation by intramuscular methylprednisolone application protects tis- sue-engineered autogenous chondrocyte transplants from fibrous tissue infiltration and induces trabecular bone for- mation. Keywords Tissue engineering · Cartilage · Bone · Corticosteroids · Methylprednisolone · Tissue transplantation Introduction Clinical applications of tissue-engineered cartilage in the fields of otorhinolaryngology, craniofacial, orthopedic and head and neck surgery may include the restoration of trau- matic and tumorous lesions as well as the correction of congenital defects. In contrast to orthopaedic indications, clinical application in the fields of otorhinolaryngology and plastic reconstructive surgery is still not performed due to an unpredictable extent of resorption of the trans- plants by the activated host immune system after subcuta- neous implantation. Subcutaneously implanted tissue is generally affected by the immune system of the host even in autogenous models. Due to surgical trauma, tissue-en- gineered transplants are initially affected by the activation of a complex inflammation cascade leading to the inhibi- tion of chondrocyte redifferentiation and neomatrix for- mation [1]. Glucocorticoids lessen the effects of released mediators like histamine and serotonin and reduce capil- lary dilation with subsequent edema, leukocyte migration and fibrin deposition in and around the focus of inflam- mation. Inflammation-mediated factors are also reduced: elevated lipocortin decreases prostaglandin and throm- boxane secretion. The reduction of phospholipase A2 leads to a decrease in prostaglandins and leukotrienes. Under glucocorticoid treatment, fewer macrophages and neutrophils are evident in the inflammation. Gluco- corticoids are effective immunomodulators because of their antiphlogistic effect, the disruption of antigen presenting Andreas Haisch · Frank Wanjura · Cornelia Radke · Korinna Leder-Jöhrens · Andreas Gröger · Michaela Endres · Svea Klaering · Alexander Loch · Michael Sittinger Immunomodulation of tissue-engineered transplants: in vivo bone generation from methylprednisolone-stimulated chondrocytes Eur Arch Otorhinolaryngol (2004) 261 : 216–224 DOI 10.1007/s00405-003-0646-3 Received: 17 October 2002 / Accepted: 11 June 2003 / Published online: 25 July 2003 MISCELLANEOUS A. Haisch (✉) · F. Wanjura · A. Gröger Department of Otorhinolaryngology, Head and Neck Surgery, University Medical Center Benjamin Franklin, Free University of Berlin, Hindenburgdamm 30, 12200 Berlin, Germany Tel.: +49-30-84452440, Fax: +49-30-84454460, e-mail: [email protected] C. Radke Department of Pathology, Charité, Humboldt University of Berlin, Schumannstr. 20-21, 10098 Berlin, Germany K. Leder-Jöhrens Department of Pathology, University Medical Center Benjamin Franklin, Free University of Berlin, Hindenburgdamm 30, 12200 Berlin, Germany M. Endres · S. Klaering · A. Loch · M. Sittinger Interdisciplinary Tissue Engineering Laboratories, Department of Rheumatology, Charité, Humboldt University of Berlin, Tucholskystr. 2, 10115 Berlin, Germany © Springer-Verlag 2003
-
Upload
charite-de -
Category
Documents
-
view
2 -
download
0
Transcript of Immunomodulation of tissue-engineered transplants: in vivo bone generation from...

Abstract Subcutaneously implanted, in vitro engineeredtissue is generally affected by the immune system of thehost even in autogenous transplantation. The aim of thisstudy was to investigate immunomodulation of subcuta-neously implanted tissue-engineered cartilage transplantsby intramuscular methylprednisolone application. Trans-plants consisted of auricular rabbit chondrocytes, polylac-tide-polyglycolide co-polymer fleeces and species-specificfibrin or agarose. The transplants were subcutaneouslyimplanted in the ridge. Thereafter, animals were separatedinto two groups, one with and one without methylpred-nisolone treatment. The specimens were histologically in-vestigated after 6 and 12 weeks. Fleece fiber degradationwas complete after 12 weeks, and all transplants showedareas of calcification. The corticosteroid-treated grouppresented pronounced trabecular bone generation withoutfibrous tissue infiltration. The untreated group showedsporadic islets of calcification without coherent bone for-mation, and adjacent fibrous tissue had infiltrated the trans-plants. Native controls and corticoid-treated transplants
did not exhibit bone generation or signs of fibrous tissueinfiltration. This study found that immunomodulation byintramuscular methylprednisolone application protects tis-sue-engineered autogenous chondrocyte transplants fromfibrous tissue infiltration and induces trabecular bone for-mation.
Keywords Tissue engineering · Cartilage · Bone · Corticosteroids · Methylprednisolone · Tissue transplantation
Introduction
Clinical applications of tissue-engineered cartilage in thefields of otorhinolaryngology, craniofacial, orthopedic andhead and neck surgery may include the restoration of trau-matic and tumorous lesions as well as the correction ofcongenital defects. In contrast to orthopaedic indications,clinical application in the fields of otorhinolaryngologyand plastic reconstructive surgery is still not performeddue to an unpredictable extent of resorption of the trans-plants by the activated host immune system after subcuta-neous implantation. Subcutaneously implanted tissue isgenerally affected by the immune system of the host evenin autogenous models. Due to surgical trauma, tissue-en-gineered transplants are initially affected by the activationof a complex inflammation cascade leading to the inhibi-tion of chondrocyte redifferentiation and neomatrix for-mation [1]. Glucocorticoids lessen the effects of releasedmediators like histamine and serotonin and reduce capil-lary dilation with subsequent edema, leukocyte migrationand fibrin deposition in and around the focus of inflam-mation. Inflammation-mediated factors are also reduced:elevated lipocortin decreases prostaglandin and throm-boxane secretion. The reduction of phospholipase A2 leadsto a decrease in prostaglandins and leukotrienes.
Under glucocorticoid treatment, fewer macrophagesand neutrophils are evident in the inflammation. Gluco-corticoids are effective immunomodulators because of theirantiphlogistic effect, the disruption of antigen presenting
Andreas Haisch · Frank Wanjura · Cornelia Radke ·Korinna Leder-Jöhrens · Andreas Gröger ·Michaela Endres · Svea Klaering · Alexander Loch ·Michael Sittinger
Immunomodulation of tissue-engineered transplants: in vivo bone generation from methylprednisolone-stimulated chondrocytes
Eur Arch Otorhinolaryngol (2004) 261 : 216–224DOI 10.1007/s00405-003-0646-3
Received: 17 October 2002 / Accepted: 11 June 2003 / Published online: 25 July 2003
MISCELLANEOUS
A. Haisch (✉) · F. Wanjura · A. GrögerDepartment of Otorhinolaryngology, Head and Neck Surgery,University Medical Center Benjamin Franklin, Free University of Berlin, Hindenburgdamm 30, 12200 Berlin, GermanyTel.: +49-30-84452440, Fax: +49-30-84454460,e-mail: [email protected]
C. RadkeDepartment of Pathology, Charité, Humboldt University of Berlin, Schumannstr. 20-21, 10098 Berlin, Germany
K. Leder-JöhrensDepartment of Pathology, University Medical Center Benjamin Franklin, Free University of Berlin, Hindenburgdamm 30, 12200 Berlin, Germany
M. Endres · S. Klaering · A. Loch · M. SittingerInterdisciplinary Tissue Engineering Laboratories, Department of Rheumatology, Charité, Humboldt University of Berlin, Tucholskystr. 2, 10115 Berlin, Germany
© Springer-Verlag 2003

cells (APC) and the reduced expression of MHC mole-cules. In light of these facts, the presented study was de-signed to investigate the potential of corticosteroids forprolonging graft survival of tissue-engineered auricularchondrocytes by protecting the transplant from the host’sunspecific immune system and by stimulating chondro-cyte differentiation. Methylprednisolone is a commonly usedand relatively simple tool for immunomodulation withfewer side effects and a well-documented therapeutic im-pact.
Materials and methods
Native elastic auricular cartilage was taken from six New Zealandwhite rabbits. The animals were anesthetized with 0.3 ml of xy-
lazine-hydrochloride (Rhompun) and 0.5 ml of ketamine (Ketan-est)/kg BW. A piece of cartilage (1.5×1.5 cm) was separated from theperichondrium and the soft tissue by retroauricular incision. Theskin wound was sutured with vicryl 4–0. The cartilage was sent tothe lab, cleaned with ethanol (70%) and rinsed with PBS (Dul-becco Biochrom KG, Germany). It was then chopped into piecesof 0.09 cm2 and enzymatically digested for 24 h in Spinner flasks:RPMI medium (Dulbecco Biochrom KG, Germany) with collage-nase I and II and hyaluronidase (Boehringer, Germany). Cells werecounted in a Neubauer chamber. After two passages, the cells wereharvested for transplant formation.
Species-specific fibrin glue
Rabbit plasma (Kraeber, Germany) was cryoprecipitated to con-centrate fibrinogen. Thrombin was adsorbed out of the supernatantby sephadex A-50 (Sephadex, Germany) and eluted by a 2 M NaClbuffer. This elution was desalted by dialysis for 1 h in 0.01 molar
217
Table 1 Transplant formationand division into groups

trisodium citrate buffer and subsequently for 12 h in buffer with aphysiological salt concentration.
Polyelectrolyte membrane
Capsule preparation was performed using two polyionic reactioncomponents. Sodium cellulose sulfate (NaCs: MW: 711KD) servedas the polyanion and polydiallyl dimethyl ammonium chloride(PDADMAC) as the polycation. The heterogenic NaCs solutionwas used to build the capsule core and the PDADMAC solution asa precipitation bath supplying the second reaction component forPEC formation at the capsule surface. Before encapsulation wasperformed, 2.5% NaCs was sterilized by heat and 4% PDADMACwith a molecular weight of 35 KD by filtration. The encapsulationprocess was initiated by dipping the cartilage into the highly vis-cous NaCs solution until it was entirely covered by a thin layer ofNaCs. For precipitation and capsule formation, the cartilage wasstored in the PDADMAC solution for 120 min. Under these reac-tion conditions, a membrane was formed with a cut-off of 20 KD.The encapsulated cartilage was then directly implanted subcuta-neously in the ridge of the rabbits [2].
Agarose
Two percent low-melting point agarose (Sigma, Germany) in PBS(Dulbecco, Germany) was used.
Transplant formation
We employed 1.0×1.0×0.2 cm [3] pieces of polymer constructs(PGA/PLA scaffold, Ethicon) to fill with chondrocyte suspension.A cell suspension (25×106 chondrocytes/ml) of HAM’s F12 me-dium (Dulbecco Biochrom KG, Germany) with proline, glutamine,penicillin/streptomycin, HEPES, ascorbic acid and rabbit serumwas produced and mixed with allogeneic fibrin at a ratio of 3:1(“fibrin-TX,” 4/rabbit).
Four additional “fibrin-TX” per rabbit were encapsulated by apolyelectrolyte membrane (“capsule-TX”). Another four trans-plants consisted of agarose (Sephadex, Germany) and cell suspen-sion (25×106 chondrocytes/ml) of HAM’s F12 medium at a ratio of3:1 (“agarose-TX”). Two pieces of native cartilage served as thecontrol. One rabbit was killed; the “transplants” served as in vitrocontrols.
The 70 transplants mentioned above were implanted in theback of five rabbits: four fibrin-TX, four capsule-TX, four agarose-TX and two native controls per rabbit (Table 1).
Experimental design
The animals were divided into two groups: (1) the group treatedwith and (2) without methylprednisolone. Group 1 received a dailyintramuscular injection of methylprednisolone for 3 weeks (1 mg/kgbw, including dose reduction at the end, Table 2).
Surgery in rabbits
Animals were anesthetized and subcutaneous pockets (four para-median lines: three with one of each four TX, one with two nativecontrols) were prepared in their backs. The rabbits were killed byan intravenous injection of potassium after 6 (two rabbits) and 12weeks (three rabbits). Specimens were explanted for histologicalexamination. Perioperative single-shot antibiotics (Tardomyocel,Bayer, Germany) were given to all animals.
Group 1 received i.m. methylprednisolone (Urbason 16, Hoechst,Germany) according to the regimen in Table 2. To gradually raisethe dose systemically, we surrounded the transplant of group 1 withtriamcinolone acetonide (Lederlon, Lederle, Germany). Group 2was left untreated.
All animal experiments were carried out according to the poli-cies and principles established by the Animal Welfare Act, theNIH Guide for care and use of laboratory animals and the NationalAnimal Welfare Guidelines. The experiments were approved bythe local legal representative (Landesamt für Arbeitsschutz, Ge-sundheitsschutz und technische Sicherheit, Berlin; registration no.092/99).
Histologic investigation
Longitudinal microsections were prepared for hematoxylin-eosinstaining.
Results
Six weeks in vivo
Macroscopically, the explanted specimens were white toyellowish in color and had a fibroelastic solid consistency.The specimens from the methylprednisolone-treated groupdid not change size from the time of implantation: 1 cm×1 cm×0.2 cm (see Figs. 1, 2). The specimens of the un-treated group were hardly visible and could not be clearlydistinguished from the surrounding connective tissue.
After 6 weeks in vivo all of the tissue-engineered trans-plants in both groups showed areas of osteoblasts and os-teocytes in addition to regions with cartilage-like mor-phology and fleece fiber remnants. In the untreated group,invading granulocytes and macrophages, representing anunspecific immune reaction, were seen inside and at themargins of the transplant.
While marked trabecular bone formation and hemopoi-etic bone marrow with erythroblasts and megacaryocyticswere found in the corticosteroid-treated group, an unspe-cific immune reaction was not evident (Figs. 3, 4, 5).
218
Table 2 Intramuscular im-munomodulation of rabbits(treated group)
Day Mg methyl-prednisolone per b.w. (kg)
1 1.002 1.003 1.004 1.005 0.756 0.757 0.758 0.759 0.50
10 0.5011 0.5012 0.5013 0.2514 0.2515 0.2516 0.2517 0.1018 0.1019 0.1020 0.10
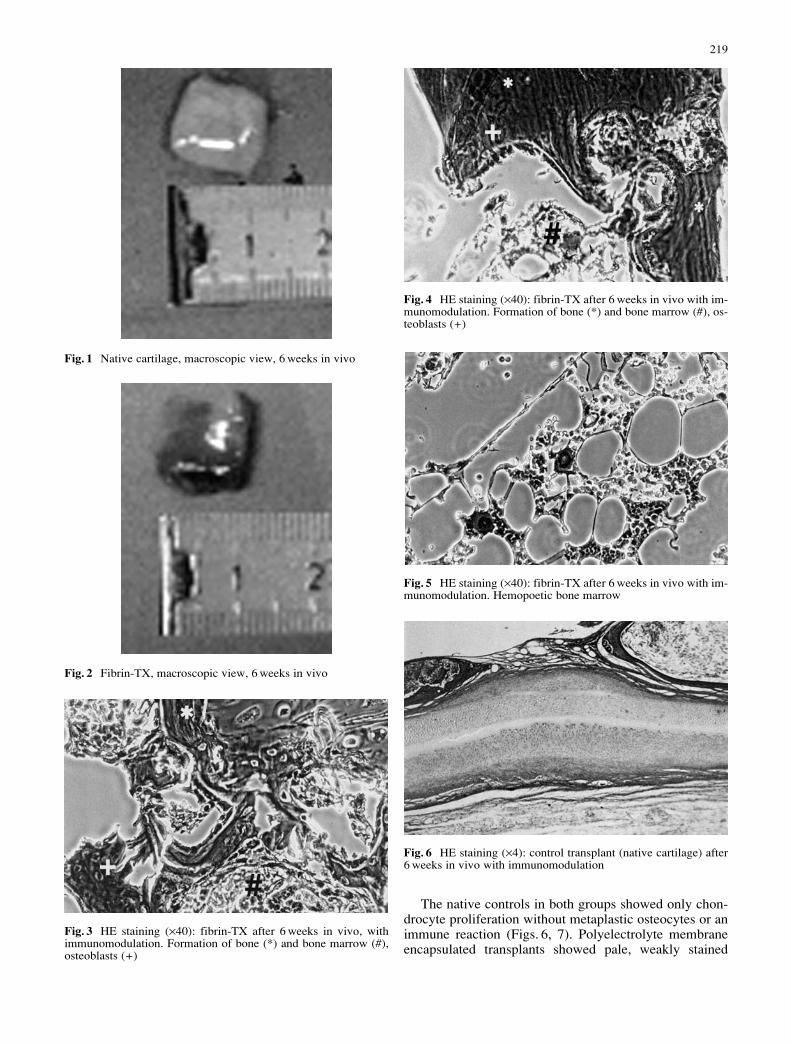
The native controls in both groups showed only chon-drocyte proliferation without metaplastic osteocytes or animmune reaction (Figs. 6, 7). Polyelectrolyte membraneencapsulated transplants showed pale, weakly stained
219
Fig. 1 Native cartilage, macroscopic view, 6 weeks in vivo
Fig. 2 Fibrin-TX, macroscopic view, 6 weeks in vivo
Fig. 3 HE staining (×40): fibrin-TX after 6 weeks in vivo, withimmunomodulation. Formation of bone (*) and bone marrow (#),osteoblasts (+)
Fig. 4 HE staining (×40): fibrin-TX after 6 weeks in vivo with im-munomodulation. Formation of bone (*) and bone marrow (#), os-teoblasts (+)
Fig. 5 HE staining (×40): fibrin-TX after 6 weeks in vivo with im-munomodulation. Hemopoetic bone marrow
Fig. 6 HE staining (×4): control transplant (native cartilage) after6 weeks in vivo with immunomodulation
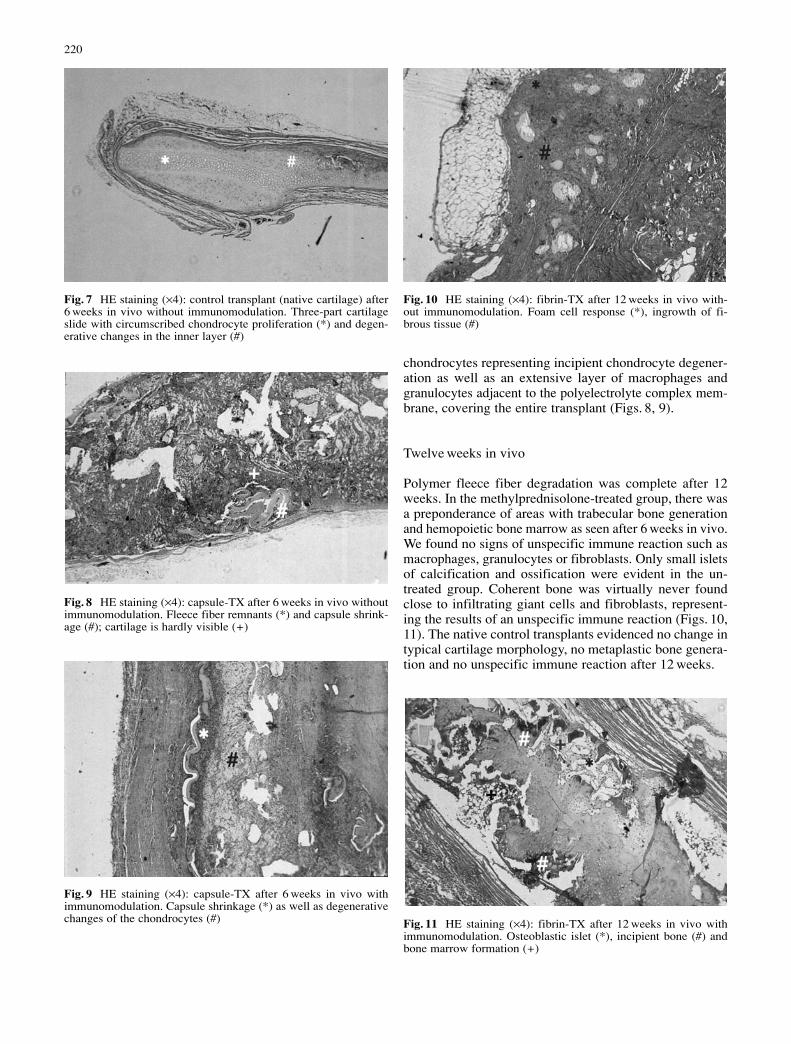
chondrocytes representing incipient chondrocyte degener-ation as well as an extensive layer of macrophages andgranulocytes adjacent to the polyelectrolyte complex mem-brane, covering the entire transplant (Figs. 8, 9).
Twelve weeks in vivo
Polymer fleece fiber degradation was complete after 12weeks. In the methylprednisolone-treated group, there wasa preponderance of areas with trabecular bone generationand hemopoietic bone marrow as seen after 6 weeks in vivo.We found no signs of unspecific immune reaction such asmacrophages, granulocytes or fibroblasts. Only small isletsof calcification and ossification were evident in the un-treated group. Coherent bone was virtually never foundclose to infiltrating giant cells and fibroblasts, represent-ing the results of an unspecific immune reaction (Figs. 10,11). The native control transplants evidenced no change intypical cartilage morphology, no metaplastic bone genera-tion and no unspecific immune reaction after 12 weeks.
220
Fig. 7 HE staining (×4): control transplant (native cartilage) after6 weeks in vivo without immunomodulation. Three-part cartilageslide with circumscribed chondrocyte proliferation (*) and degen-erative changes in the inner layer (#)
Fig. 10 HE staining (×4): fibrin-TX after 12 weeks in vivo with-out immunomodulation. Foam cell response (*), ingrowth of fi-brous tissue (#)
Fig. 11 HE staining (×4): fibrin-TX after 12 weeks in vivo withimmunomodulation. Osteoblastic islet (*), incipient bone (#) andbone marrow formation (+)
Fig. 8 HE staining (×4): capsule-TX after 6 weeks in vivo withoutimmunomodulation. Fleece fiber remnants (*) and capsule shrink-age (#); cartilage is hardly visible (+)
Fig. 9 HE staining (×4): capsule-TX after 6 weeks in vivo withimmunomodulation. Capsule shrinkage (*) as well as degenerativechanges of the chondrocytes (#)
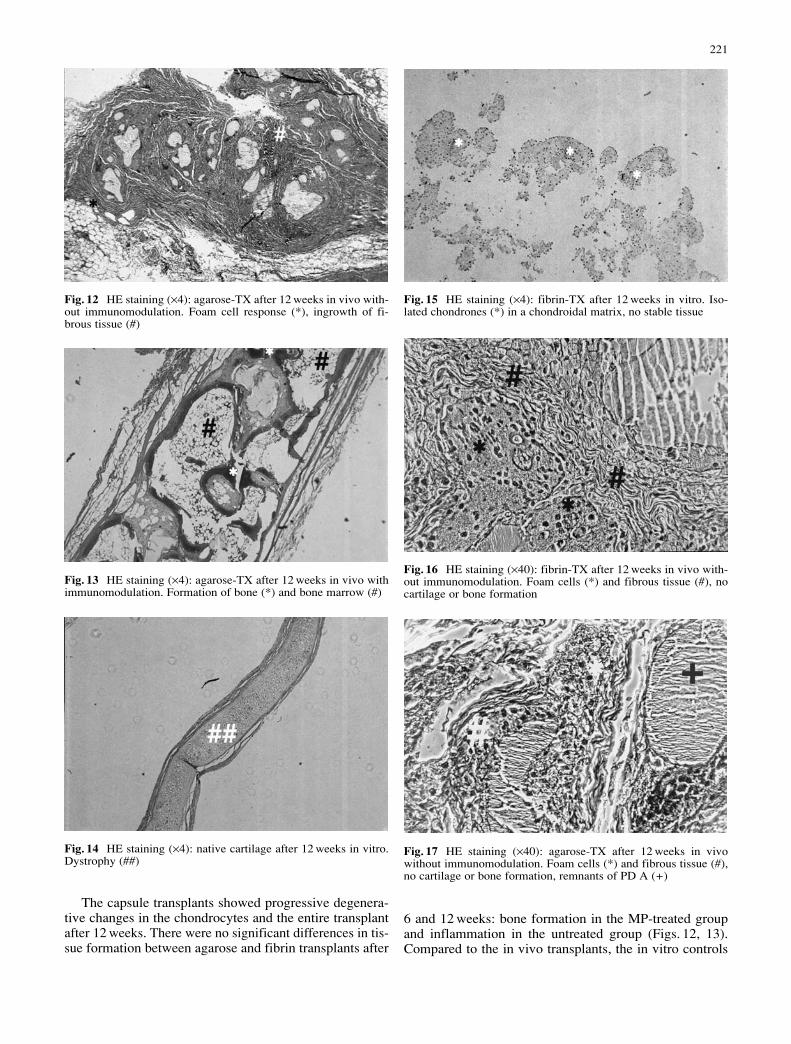
The capsule transplants showed progressive degenera-tive changes in the chondrocytes and the entire transplantafter 12 weeks. There were no significant differences in tis-sue formation between agarose and fibrin transplants after
6 and 12 weeks: bone formation in the MP-treated groupand inflammation in the untreated group (Figs. 12, 13).Compared to the in vivo transplants, the in vitro controls
221
Fig. 12 HE staining (×4): agarose-TX after 12 weeks in vivo with-out immunomodulation. Foam cell response (*), ingrowth of fi-brous tissue (#)
Fig. 16 HE staining (×40): fibrin-TX after 12 weeks in vivo with-out immunomodulation. Foam cells (*) and fibrous tissue (#), nocartilage or bone formation
Fig. 17 HE staining (×40): agarose-TX after 12 weeks in vivowithout immunomodulation. Foam cells (*) and fibrous tissue (#),no cartilage or bone formation, remnants of PD A (+)
Fig. 15 HE staining (×4): fibrin-TX after 12 weeks in vitro. Iso-lated chondrones (*) in a chondroidal matrix, no stable tissue
Fig. 13 HE staining (×4): agarose-TX after 12 weeks in vivo withimmunomodulation. Formation of bone (*) and bone marrow (#)
Fig. 14 HE staining (×4): native cartilage after 12 weeks in vitro.Dystrophy (##)

showed only slight cartilage formation (Figs. 14, 15). Theviolent immune reactions in transplants that had not un-dergone immunomodulation are exemplified by a fibrinand an agarose transplant in Figs. 16, 17.
Discussion
Many studies have focused on cartilage transplantation,cartilage engineering and the repair of connective tissuedefects in recent years. Biodegradable scaffolds have beenexamined for tissue engineering constructs [3, 4], andmethods have been developed to facilitate cultivation forlong-term experiments [5]. Autogenous cartilage trans-plants have been carried out in several animal models [6].Animal experiments were the first steps on the way toclinical application: The use of bovine chondrocytes forneocartilage formation in nude mice [7] showed that tis-sue-engineered cartilage can be maintained on preshapedbiodegradable scaffolds [8] and biomechanical propertiesare dependent on the number of seeded cells [9].
Tissue engineering required the development of encap-sulation techniques [10]. Fibrin monomers were success-fully used to encapsulate isolated chondrocytes [11]. More-over, alginate was discovered to be a good material for en-capsulation of tissue-engineered transplants [12]. Usingsmall cartilage implants encapsulated with polyelectrolytecomplex membranes, Haisch and Groeger found that graftinfiltration by cells of the unspecific immune system waslower than in the unencapsulated controls [2].
The most interesting issue is the mechanism of bonegeneration. Physiologically, bone formation occurs whennewly developed cartilage is infiltrated by blood vesselsand replaced by bone, i.e., endochondral ossification. Ac-tive bone marrow results during bone generation by circu-lating hemopoetic cells settling in the appropriate histo-logical structure. The literature contains references to ap-positional bone formation lining cartilage [13]. Direct dif-ferentiation of mesenchymal cells to osteoblasts as inskull, clavicle and mandible bones is called intramembra-nous ossification. Current techniques in bone engineeringhave focused on osteocytes and periosteal cells [14]. Osteo-cytes from limb allografts developed into bone after trans-plantation [15], and bone formation from tissue-engineeredperiosteum-derived cells healed bone defects in rats [16].However, surgery is painful and may involve severe peri-operative complications like osteomyelitis. Easily accessi-ble tissue like auricular chondrocytes would be ideal foravoiding this painful and difficult procedure. Auricularcartilage is harvested by an established surgical methodwith an easy access and minimal risk of surgical compli-cations. But how could these cells be stimulated to differ-entiate to osteoblasts? Expression of the differentiationfactor “Cbfa1” enables mesenchymal cells to differentiateto chondrocytes or osteoblasts. Cbfa1 seems to be an im-portant factor in osteoblast differentiation [17]. In addi-tion, BMP-7-transfected chondrocytes differentiate to bone[18]. However, there is an easier way to stimulate thechondrocytes using the corticosteroid as a growth hor-
mone [19]. There have already been many studies on car-tilage engineering: Interest developed in bone morpho-genetic proteins (BMPs) 10 years ago [20, 21], and inter-face problems between bone and cartilage in joint defectshave been a subject of investigation in tissue engineeringsince the early 1990s [22].
In this study, methylprednisolone induces bone forma-tion in in vivo engineered chondrocyte polymer fleece hy-drogel. Chondrocyte dedifferentiation was observed, andcalcifications were seen in the untreated group 2. Some ofthese calcifications are due to necrosis, resulting from un-specific inflammation. The strong bone formation in thetransplants of the treated group can only be explained bythe interaction of methylprednisolone with (1) the acidicmilieu of the degrading scaffold fibers, (2) the ectopic im-plantation of auricular chondrocytes into the ridge and (3)the rabbit animal model by itself. The findings describedconcerning graft survival indicating reduced unspecificimmune reaction and the need for immunomodulation con-tradict investigations by Dorfman et al., who successfullygenerated autologous myoblasts without requiring im-munomodulation for redifferentiation [23].
Methylprednisolone (MP) seems to be the best agentfor preventing unspecific immune reactions in the initialphase of wound healing following implantation-inducedtissue trauma. Immunosuppressives like cyclosporin are notnecessary because of the autogenous cells used for trans-plantation. This IL-2 inhibitor aims at specific T-cell-me-diated graft rejection. Our choice of MP was also supportedby the literature. In a rabbit ear model, composite graftsurvival was prolonged by perioperative and postopera-tive methylprednisolone treatment (30 mg/kg bw for 5 daysi.m.) and showed better results than a cyclooxygenase/lipooxygenase inhibitor [24]. MP (1.0 mg/kg bw) reducedcirculating Th-cells, while low-dose tacrolimus was prob-ably additive [25]. High-dose MP therapy may be compli-cated by side effects. A single high-dose (20 mg/kg bw)MP injection induced multifocal osteonecrosis in severalbones in a rabbit model [26]. Topical corticosteroids seemedto be the easiest way to increase the dose without causingcomplications. Topical steroids are now clinically used toprevent corneal graft rejection and are more suitable thancyclosporine [27], but a 3-week subcutaneous topical ap-plication is inconceivable.
Some aspects of the presented results disagree withpublished studies using MP for bone regeneration. Sup-pressive effects on bone growth were found for treatmentwith 1 mg/kg bw methylprednisolone in rabbit ulnar de-fects [28]. Long bone growth in rabbits decreased whenhydrocortisone was applied in daily doses of 4 mg/kg bwor 16 mg/kg bw [29]. Hydrocortisone treatment (2 mg/kgbw for 21 days) significantly depressed bone apposition inrabbits [30]. HOP levels as a marker for bone destructionand reduced bone formation were measured in hydrocorti-sone-treated (5 mg/kg) rabbits with radius fractures [31].
Corticosteroids are known to impair bone formation oreven induce osteonecrosis [32]. This property is also used todemonstrate adverse effects [33]. Thus, corticosteroids arenow clinically applied to inhibit ectopic bone formation [34].
222

Bilateral ossification of the earlobes has been describedin conjunction with addisonian crisis [35]. This could beexcluded as the cause of ossification here because none ofour rabbits showed signs of this disease.
Further investigations analyzing the pathways of corti-coid action in cartilage engineering are needed to clarifydifferences in the findings of this study and some of theabove-mentioned studies.
Conclusions
Autogenous transplant formation does not prevent unspe-cific immune reaction. Temporary systemic low-dose cor-ticosteroid application sufficiently suppresses the unspe-cific immune reaction for long-term graft survival and tis-sue differentiation in vivo. Furthermore, methylprednisolone(MP) stimulation of auricular chondrocytes allows tissueengineering of trabecular bone in the immunocompetentanimal after subcutaneous implantation. Thus, MP induceshypertrophy and transformation of chondrocytes into os-teocytes.
Acknowledgements The authors thank the DFG (German Re-search Foundation) for the grant Ha 2721-1-3.
References
1. Cao Y, Rodriguez A, Vacanti M, Ibarra C, Arevalo C, VacantiCA (1998) Comparative study of the use of poly, calcium algi-nate and pluronics in the engineering of autologous porcinecartilage. J Biomater Sci Polym Ed 9:475–487
2. Haisch A, Groger A, Radke C, Ebmeyer J, Sudhoff H, Gras-nick G, Jahnke V, Burmester GR, Sittinger M (2000) Macroen-capsulation of human cartilage implants: pilot study with poly-electrolyte complex membrane encapsulation. Biomaterials 21:1561–1566
3. Freed LE, Vunjak-Novakovic G, Biron RJ, Eagles DB, LesnoyDC, Barlow SK, Langer R (1994) Biodegradable polymer scaf-folds for tissue engineering. Biotechnology N Y 12:689–693
4. Sittinger M, Reitzel D, Dauner M, Hierlemann H, Hammer C,Kastenbauer E, Planck H, Burmester GR, Bujia J (1996) Re-sorbable polyesters in cartilage engineering: affinity and bio-compatibility of polymer fiber structures to chondrocytes. J Biomed Mater Res 33:57–63
5. Sittinger M, Schultz O, Keyszer G, Minuth WW, BurmesterGR (1997) Artificial tissues in perfusion culture. Artif Organs20:57–62
6. Desjardins MR, Hurtig MB, Palmer NC (1991) Heterotopictransfer of fresh and cryopreserved autogenous articular carti-lage in the horse. Vet Surg 20:434–445
7. Puelacher WC, Mooney D, Langer R, Upton J, Vacanti JP, Va-canti CA (1994) Design of nasoseptal cartilage replacementssynthesized from biodegradable polymers and chondrocytes.Biomaterials 15:774–778
8. Haisch A, Klaring S, Groger A, Gebert C, Sittinger M (2002)A tissue-engineering model for the manufacture of auricular-shaped cartilage implants. Eur Arch Otorhinolaryngol 259:316–321
9. Duda GN, Haisch A, Endres M, Gebert C, Schroeder D, Hoff-mann JE, Sittinger M (2000) Mechanical quality of tissue engi-neered cartilage: results after 6 and 12 weeks in vivo. J BiomedMater Res 53:673–677
10. Sittinger M, Bujia J, Rotter N, Reitzel D, Minuth WW, Bur-mester GR (1996) Tissue engineering and autologous trans-plant formation: practical approaches with bioresorbable bio-materials and new cell culture techniques. Biomaterials 17:237–242
11. Sims CD, Butler PE, Cao YL, Casanova R, Randolph MA,Black A, Vacanti CA, Yaremchuk MJ (1998) Tissue engi-neered neocartilage using plasma derived polymer substratesand chondrocytes. Plast Reconstr Surg 101:1580–1585
12. Rowley JA, Madlambayan G. Mooney DJ (1999) Alginate hy-drogels as synthetic extracellular matrix materials. Biomateri-als 20:45–53
13. Isogai N, Landis W, Kim TH, Gerstenfeld LC, Upton J, Va-canti JP (1999) Formation of phalanges and small joints by tis-sue-engineering. J Bone Joint Surg Am 81:303–316
14. Breitbard AS (1998) Tissue engineered bone repair of calvarialdefects using cultured periosteal cells. Plast Reconstr Surg 101:567–576
15. Butler PE (1998) Cell transplantation from limb allografts.Plast Reconstr Surg 102:161–170
16. Puelacher WC (1996) Femoral shaft reconstruction using tis-sue-engineered growth of bone. Int J Oral Maxillofac Surg 25:223–228
17. Ducy P, Schinke T, Karsenty G (2000) The osteoblast: a so-phisticated fibroblast under central surveillance. Science 289:1501–1514
18. Ramoshebi LN, Ripamonti U (2000) Osteogenic protein-1, abone morphogenetic protein, induces angiogenesis in the chickchorioallantoic membrane and synergizes with basic fibroblastgrowth factor and transforming growth factor-beta1. Anat Rec259:97–107
19. Jaiswal N (1997) Osteogenic differentiation of purified, cul-ture-expanded human mesenchymal stem cells in vitro. J CellBiochem 64:295–312
20. Kaps C, Bramlage C, Smolian H, Haisch A, Ungethum U,Burmester GR, Sittinger M, Gross G, Haupl T (2002) Bonemorphogenetic proteins promote cartilage differentiation andprotect engineered artificial cartilage from fibroblast invasionand destruction. Arthritis Rheum 46:149–162
21. Viljanen VV, Lindholm TS (1993) Heterotopic osteoinductionin a rat membrane-isolated latissimus dorsi island flap. A pilotstudy. Ann Chir Gynaecol [Suppl] 207:55–62
22. Mow VC, Ratcliffe A, Rosenwasser MP, Buckwalter JA (1991)Experimental studies on repair of large osteochondral defects ata high weight bearing area of the knee joint: a tissue engineer-ing study. J Biomech Eng 113:198–207
23. Dorfman J, Duong M, Zibaitis A, Pelletier MP, Shum-Tim D,Li C, Chiu RC (1998) Myocardial tissue engineering with au-tologous myoblast implantation. J Thorac Cardiovasc Surg 116:744–751
24. Fann PC, Hartman DF, Goode RL (1993) Pharmacologic andsurgical enhancement of composite graft survival. Arch Oto-laryngol Head Neck Surg 119:313–319
25. Piekoszewski W, Chow FS, Jusko WJ (1994) Pharmacokineticand pharmacodynamic effects of coadministration of methyl-prednisolone and tacrolimus in rabbits. J Pharmacol Exp Ther269:103–109
26. Yamamoto T, Irisa T, Sugioka Y, Sueishi K (1997) Effects ofpulse methylprednisolone on bone and marrow tissues. Arthri-tis Rheum 40:2055–2064
27. Williams KA, Grutzmacher RD, Roussel TJ, Coster DJ (1985)A comparison of the effects of topical cyclosporine and topicalsteroid on rabbit corneal allograft rejection. Transplantation 39:242–244
28. Ho ML, Chang JK, Wang GJ (1995) Antinflammatory drug ef-fects on bone repair and remodeling in rabbits. Clin Orthop313:270–278
29. Moell C, Aronson AS, Selvik G (1988) Growth in rabbits dur-ing alternate-day cortisone injections: near normal growth ondays without cortisone. Acta Paediatr Scand 77:693–698
223

224
30. Tam CS, Cruickshank B, Swinson DR, Anderson W, LittleHA(1979) The response of bone apposition rate to some non-physiologic conditions. Metabolism 28:751–755
31. Lyritis G, Papadopoulou Z, Nikiforidis P, Batrinos M, VaronosD (1975) Effects of cortisone and an anabolic steroid uponplasma hydroxyproline during fracture healing in rabbits. ActaOrthop Scand 46:25–30
32. Orwin JF (1991) Use of the uncemented bipolar endoprosthesisfor the treatment of steroid-induced osteonecrosis of the hip inrenal transplantation patients. J Arthroplasty 6:1–9
33. Prisell PT (1997) Insulin-like growth factor I increases boneformation in old or corticosteroid trated rats. Acta Orthop Scand68:586–592
34. Brantus JF, Meunier PJ (1998) Effects of intravenous etidronateand oral corticosteroids in fibrodysplasia ossificans progres-siva. Clin Orthop 346:117–120
35. Rodriguez Rodriguez R, Ontanilla Lopez A, Rodriguez Ro-driguez C, Herrera Silva J, Echevarria Moreno M, MartinezDiestre MD (1991) Bilateral ossification of the earlobes. Ad-disonian crisis in the postoperative period. Rev Esp AnestesiolReanim 38:391–392




















