Imaging of Genitourinary Trauma
10
1514 AJR:192, June 2009 tients with blunt and penetrating renal trau- ma [1, 3]; the liver and the spleen are the most common intraabdominal organs to be injured with blunt trauma [8]. Patients who present with either gross hematuria or shock are apt to have nongenitourinary intraab- dominal injury in 24% and 65% of cases, re- spectively [9], attesting to the severity of the trauma. In this article, we discuss the role of imag- ing in the management of patients with geni- tourinary trauma. Adrenal Trauma Incidence and Significance Trauma to the adrenal glands is unusual because of their relatively well-protected po- sition deep in the retroperitoneum, so injury to these organs occurs in the setting of mas- sive trauma [10, 11]. The incidence of adre- nal injury in patients with blunt trauma is reported to be 0.15–4% in different series [10–13]. Rana et al. [11] reported traumatic adrenal hemorrhage in 5% of patients with an injury severity score (ISS) greater than 40 compared with a 0.4% incidence in pa- tients with an ISS of 0–19, whereas Stawicki et al. [10] reported that mean ISS scores were more than two times higher in patients with adrenal injury than in those without. Patients with adrenal gland trauma have a higher mor- tality rate than do trauma patients without Imaging of Genitourinary Trauma Parvati Ramchandani 1 Philip Michael Buckler Ramchandani P, Buckler PM 1 Both authors: Department of Radiology, University of Pennsylvania Medical Center, 3400 Spruce St., Philadelphia, PA 19104. Address correspondence to P. Ramchandani ([email protected]). Genitourinary Imaging • Review AJR 2009; 192:1514–1523 0361–803X/09/1926–1514 © American Roentgen Ray Society W ide-impact blunt abdominal trauma is responsible for most closed injuries of the genitouri- nary organs, with motor vehicle crashes being the most common cause in the Western hemisphere [1, 2]. The incidence of penetrating trauma is also increasing, which is seen particularly in inner city trauma cen- ters, and is becoming a major cause of renal injury [3, 4]. A European registry of road traffic crash victims compiled between 1996 and 2001 recorded trauma to the genitouri- nary system in 0.46% of cases (199 of 43,056 cases) [2]. Motor vehicle crashes were most frequently associated with renal and bladder injuries (43% and 16% of cases, respective- ly), whereas accidents involving two-wheeled motorized vehicles were associated with in- jury to the male external genital organs in 64% of cases, with testicular injury account- ing for two thirds of cases, and renal injury in 28% of cases [2]. Other series have report- ed renal trauma in 1.2% of 500,000 patients hospitalized for trauma in the United States [5], and a 3% incidence of renal and testicu- lar trauma in 14,763 children evaluated in a U. S. emergency department [6]. In victims of penetrating trauma, renal injury may be seen in 3–5.7% of cases [3, 7]. Associated multiorgan injury is common with both blunt and penetrating renal trauma and may be seen in many as 80–95% of pa- Keywords: blunt trauma, genital trauma, genitourinary trauma, kidney, penetrating trauma, scrotum, testicle, ureter DOI:10.2214/AJR.09.2470 Received January 30, 2009; accepted without revision January 30, 2009. FOCUS ON: OBJECTIVE. Blunt and penetrating abdominal trauma can cause significant injury to the genitourinary organs, and radiologic imaging plays a critical role both in diagnosing these in- juries and in determining the management. In this article, we describe and illustrate the spec- trum of injuries that can occur in the genitourinary system in order to facilitate accurate and rapid recognition of the significant injuries. CONCLUSION. Imaging plays a crucial role in the evaluation of the genitourinary tract in a patient who has suffered either blunt or penetrating trauma because multiorgan injury is common in such patients. Contrast-enhanced CT is the primary imaging technique used to evaluate the upper and lower urinary tract for trauma. Cystography and urethrography re- main useful techniques in the initial evaluation and follow-up of trauma to the urinary blad- der and urethra. Ramchandani and Buckler Genitourinary Trauma Genitourinary Imaging Review Downloaded from www.ajronline.org by 114.79.28.198 on 09/11/14 from IP address 114.79.28.198. Copyright ARRS. For personal use only; all rights reserved
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Imaging of Genitourinary Trauma

1514 AJR:192, June 2009
tients with blunt and penetrating renal trau-ma [1, 3]; the liver and the spleen are the most common intraabdominal organs to be injured with blunt trauma [8]. Patients who present with either gross hematuria or shock are apt to have nongenitourinary intraab-dominal injury in 24% and 65% of cases, re-spectively [9], attesting to the severity of the trauma.
In this article, we discuss the role of imag-ing in the management of patients with geni-tourinary trauma.
Adrenal TraumaIncidence and Significance
Trauma to the adrenal glands is unusual because of their relatively well-protected po-sition deep in the retroperitoneum, so injury to these organs occurs in the setting of mas-sive trauma [10, 11]. The incidence of adre-nal injury in patients with blunt trauma is reported to be 0.15–4% in different series [10–13]. Rana et al. [11] reported traumatic adrenal hemorrhage in 5% of patients with an injury severity score (ISS) greater than 40 compared with a 0.4% incidence in pa-tients with an ISS of 0–19, whereas Stawicki et al. [10] reported that mean ISS scores were more than two times higher in patients with adrenal injury than in those without. Patients with adrenal gland trauma have a higher mor-tality rate than do trauma patients without
Imaging of Genitourinary Trauma
Parvati Ramchandani1
Philip Michael Buckler
Ramchandani P, Buckler PM
1Both authors: Department of Radiology, University of Pennsylvania Medical Center, 3400 Spruce St., Philadelphia, PA 19104. Address correspondence to P. Ramchandani ([email protected]).
Genitour inar y Imaging • Review
AJR 2009; 192:1514–1523
0361–803X/09/1926–1514
© American Roentgen Ray Society
Wide-impact blunt abdominal trauma is responsible for most closed injuries of the genitouri-nary organs, with motor vehicle
crashes being the most common cause in the Western hemisphere [1, 2]. The incidence of penetrating trauma is also increasing, which is seen particularly in inner city trauma cen-ters, and is becoming a major cause of renal injury [3, 4]. A European registry of road traffic crash victims compiled between 1996 and 2001 recorded trauma to the genitouri-nary system in 0.46% of cases (199 of 43,056 cases) [2]. Motor vehicle crashes were most frequently associated with renal and bladder injuries (43% and 16% of cases, respective-ly), whereas accidents involving two-wheeled motorized vehicles were associated with in-jury to the male external genital organs in 64% of cases, with testicular injury account-ing for two thirds of cases, and renal injury in 28% of cases [2]. Other series have report-ed renal trauma in 1.2% of 500,000 patients hospitalized for trauma in the United States [5], and a 3% incidence of renal and testicu-lar trauma in 14,763 children evaluated in a U. S. emergency department [6]. In victims of penetrating trauma, renal injury may be seen in 3–5.7% of cases [3, 7].
Associated multiorgan injury is common with both blunt and penetrating renal trauma and may be seen in many as 80–95% of pa-
Keywords: blunt trauma, genital trauma, genitourinary trauma, kidney, penetrating trauma, scrotum, testicle, ureter
DOI:10.2214/AJR.09.2470
Received January 30, 2009; accepted without revision January 30, 2009.
FOCU
S O
N:
OBJECTIVE. Blunt and penetrating abdominal trauma can cause significant injury to the genitourinary organs, and radiologic imaging plays a critical role both in diagnosing these in-juries and in determining the management. In this article, we describe and illustrate the spec-trum of injuries that can occur in the genitourinary system in order to facilitate accurate and rapid recognition of the significant injuries.
CONCLUSION. Imaging plays a crucial role in the evaluation of the genitourinary tract in a patient who has suffered either blunt or penetrating trauma because multiorgan injury is common in such patients. Contrast-enhanced CT is the primary imaging technique used to evaluate the upper and lower urinary tract for trauma. Cystography and urethrography re-main useful techniques in the initial evaluation and follow-up of trauma to the urinary blad-der and urethra.
Ramchandani and BucklerGenitourinary Trauma
Genitourinary ImagingReview
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.198
on
09/1
1/14
fro
m I
P ad
dres
s 11
4.79
.28.
198.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:192, June 2009 1515
Genitourinary Trauma
adrenal injury, attesting to the severity of the trauma. In the series by Stawicki et al., patients with adrenal injury had a five times higher mortality rate than those without ad-renal injury, and Rana et al. reported a 10% mortality rate with adrenal injury compared with 4% without. It follows that multiorgan injury is common in these patients, although isolated adrenal injury may be seen in 2–6% of cases [11–15].
Imaging FeaturesTraumatic adrenal injuries tend to affect
the right adrenal gland disproportionately, with only the right adrenal gland being af-fected in more than 70% of cases [10–15] (Fig. 1A). Isolated left adrenal injury is less common, and bilateral adrenal injury is the least common, occurring in fewer than 1% of cases. It is speculated that the right adrenal gland is more vulnerable to injury for sev-eral reasons: Its confined position allows di-rect compression of the right adrenal gland between the liver and the spine, and the di-rect entry of the short right adrenal vein into the inferior vena cava (IVC) contributes to an acute rise in intraadrenal venous pressure during the abdominal compression associat-ed with blunt trauma [16].
The typical appearance of a traumatic ad-renal injury is an expansile, hyperattenuat-ing, round or oval hematoma with a mean diameter of 2.8 cm and mean attenuation of 52–54 HU [11, 13] (Fig. 1A). Other findings seen are irregularity or obliteration of the gland by hemorrhage, periadrenal fat strand-ing, and mild to moderate enlargement of the gland due to edema or contusion. Active adrenal hemorrhage may be seen. Mild en-largement of the adrenal gland may be a har-
binger of a delayed adrenal hematoma [17]. On follow-up CT examinations, hematomas should decrease in size or resolve [11] (Figs. 1A and 1B). Adrenal masses that remain un-changed over several weeks may represent a disorder other than trauma—most often an adenoma—and should be further evaluated as deemed clinically appropriate [11]. Con-versely, it is important to recognize that an adrenal abnormality in the absence of a his-tory of significant trauma is unlikely to rep-resent a traumatic adrenal injury [11, 13]. Bilateral adrenal hemorrhage, particular-ly in the setting of minimal trauma, should prompt a search for an underlying coagula-tion abnormality. A preexisting adrenal dis-order can predispose the adrenal gland to in-jury and hemorrhage with relatively minor trauma [18].
Sonography is a particularly useful tech-nique to evaluate children who have sus-tained trauma. The adrenal gland may be enlarged and may show hypoechoic areas of hemorrhage [19] (Fig. 1C).
Unilateral adrenal injury is of little clin-ical significance, with therapeutic interven-tions required only for the associated injuries that commonly accompany adrenal trauma. Bilateral adrenal injury may rarely cause en-docrine abnormalities such as adrenal insuf-ficiency or posttraumatic pheochromocyto-ma-like syndrome [20, 21].
Renal TraumaRole of Imaging
The primary role of imaging in renal trau-ma is to accurately assess the severity and extent of injury, evaluate the injured kidney for underlying disorders, evaluate the anato-my and function of the opposite kidney, and
assess for other associated injuries. Contrast-enhanced MDCT is the imaging technique of choice to evaluate the entire urinary tract, including the renal vasculature, renal paren-chyma, and the collecting system [4, 22, 23]. The role of IV urography (IVU) is currently relegated to situations in which CT may not be available, or as a one-shot study in the op-erating room, where a film is obtained 10–15 minutes after contrast injection to grossly as-sess symmetry of excretion and to look for contrast extravasation that would indicate in-jury to the collecting system [24]. The low sensitivity of IVU for detecting or character-izing injuries limits its usefulness in the rou-tine evaluation of a trauma patient [25].
Grading InjuriesThe severity of renal injuries is graded
from 1 to 5 (least to most severe) accord-ing to a classification system developed by the Organ Injury Scaling Committee of the American Association for the Surgery of Trauma (AAST) and is called the organ in-jury scale (OIS) [26–28]. The grading sys-tem was primarily devised as a clinical re-search tool for 32 different organs and organ systems, including the different parts of the urinary tract, to ensure accurate and repro-ducible classification of injury severity. The grading system for renal injuries is yet to be modified to better integrate abnormalities seen only on imaging, such as arterial con-trast extravasation and quantification of he-matoma size [27].
Renal injuries are graded as follows [26–28]: Grade 1 injuries are characterized by
A
Fig. 1—Traumatic adrenal hematoma. A, 52-year-old man after motorcycle collision. Unenhanced CT scan reveals high-density right adrenal mass (arrow) suspected to be hematoma.B, Follow-up contrast-enhanced CT scan obtained approximately 10 weeks later in same patient as in A shows resolution of right adrenal hematoma.C, 12-year-old boy after motor vehicle collision who has right adrenal hemorrhage. Sagittal sonogram shows right adrenal gland to be enlarged and predominantly hypoechoic, consistent with acute hemorrhage.
CBDow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.198
on
09/1
1/14
fro
m I
P ad
dres
s 11
4.79
.28.
198.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
1516 AJR:192, June 2009
Ramchandani and Buckler
renal contusion without a parenchymal lac-eration, and a nonexpanding subcapsular he-matoma. Grade 2 injuries show superficial cortical lacerations that are < 1 cm deep (and thus do not involve the collecting system) and a nonexpanding perinephric hematoma. Grade 3 injuries have deeper lacerations, > 1 cm deep, that do not extend into the collect-ing system, and nonexpanding perinephric hematoma. Grade 4 injuries show lacera-tions that extend into the collecting system and injury to the main and segmental renal vessels. Grade 5 injuries show shattering of the kidney and dispersion of the avulsed por-tions, avulsion, laceration or thrombosis of the main renal vessels, hilar injury, and ure-teropelvic junction (UPJ) avulsion.
Most renal injuries are minor; contusions account for 64–81% of all renal injuries [5, 28] (Fig. 2A). In a multicenter study of 6,231
patients with renal trauma, Wessels et al. [5] found contusions or hematomas in 64.4% of patients, lacerations in 26.3% (Fig. 3), paren-chymal disruption in 5.3%, and vascular in-juries in 4% of cases (Figs. 2–6). Penetrating trauma resulted in more severe renal injuries than did blunt trauma, with a higher propor-tion of lacerations, parenchymal disruption, and vascular injury [5].
Imaging FindingsIndications for imaging—The degree of
hematuria that should lead to radiologic eval-uation of the urinary tract in a victim of blunt trauma is controversial because there is no absolute correlation between the presence or degree of hematuria and the amount of re-nal injury that is present [29]. Consensus re-view of experts indicates that hemodynami-cally stable adults with blunt trauma should
undergo radiographic evaluation if they have gross hematuria or microhematuria and a systolic blood pressure < 90 mm Hg [27]; 12.5% of such patients have a major renal in-jury [30]. Adult patients with blunt trauma who have microhematuria and systolic blood pressure > 90 mm Hg have only a 0.2% inci-dence of major renal injury [30] and do not require imaging evaluation. Additional pa-tients in whom imaging evaluation should be considered even in the absence of hematuria are those with vertical deceleration injuries (falls), those who were in high-speed motor vehicle collisions, and those with multiple associated injuries [27, 30, 31]. Radiologic evaluation of all patients suffering penetrat-ing injury is recommended because there is poor correlation between hematuria and se-verity of injury [30].
Imaging abnormalities—Renal contusions are seen as areas of ill-defined decreased en-hancement (Fig. 2A), whereas areas of seg-mental infarction due to laceration, thrombo-sis, or dissection of segmental arteries appear as sharply demarcated linear or wedge-shaped nonenhancing areas (Fig. 2B). Lacer-ations appear as irregular or linear parenchy-mal defects that may contain clot (Fig. 3A). In a shattered kidney, foci of active arterial extravasation should be distinguished from islands of viable renal parenchyma that are still enhancing (Fig. 3B). Subcapsular hema-tomas are seen as round or elliptical high-at-tenuation (40–70 HU) collections of clotted blood [22, 23].
When a renal laceration is detected on CT, a 10-minute delayed scan should be obtained to assess the collecting system and evaluate for urinary extravasation (Figs. 4A–4C and 5). Delayed images are also helpful for char-acterizing the nature of a perinephric fluid collection and for distinguishing a hematoma from a urinoma [32] (Fig. 5). UPJ injuries are discussed later with other ureteral injuries.
Segmental arterial injuries may cause areas of segmental infarction, pseudoaneurysms, or arteriovenous fistulae. Global infarction can be due to renal artery thrombosis related to intimal dissection from a deceleration inju-ry, or to renal artery avulsion, in which case a perinephric hematoma should be present (Fig. 6A). Venous injuries with blunt trauma are rare and usually occur in association with arterial pedicle injuries and severe parenchy-mal injuries, although isolated renal venous injury without arterial or parenchymal injury has been reported with trauma sustained dur-ing martial arts [33] (Fig. 6B).
A
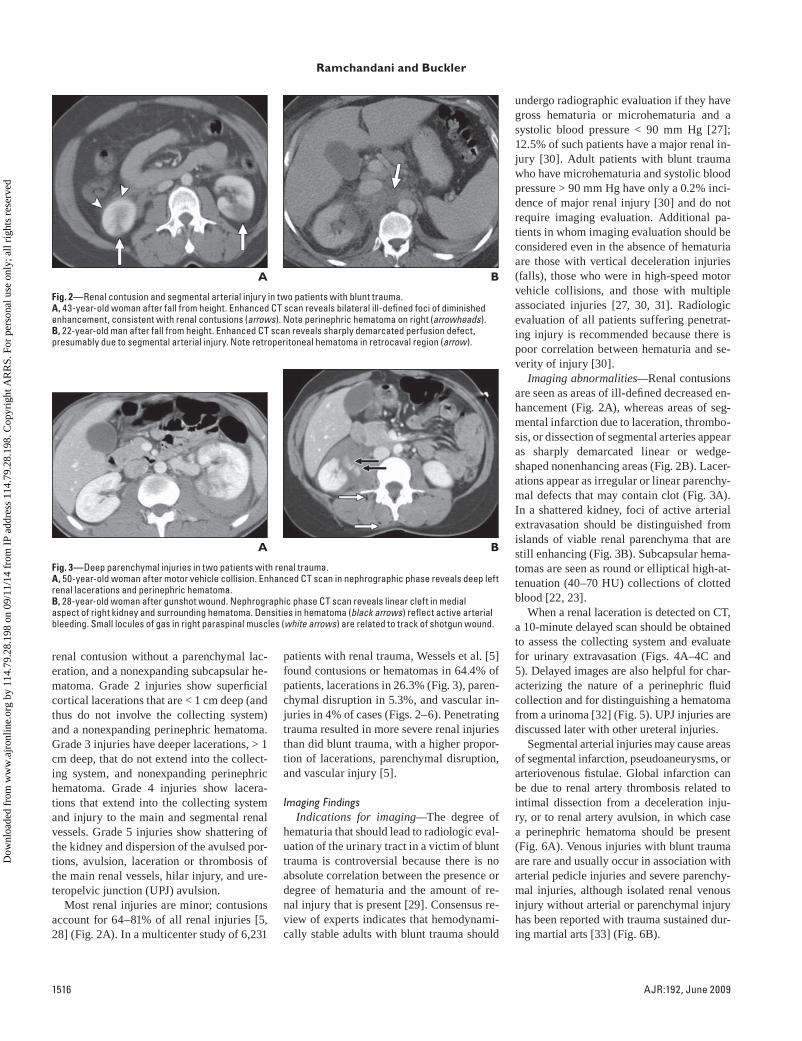
Fig. 2—Renal contusion and segmental arterial injury in two patients with blunt trauma.A, 43-year-old woman after fall from height. Enhanced CT scan reveals bilateral ill-defined foci of diminished enhancement, consistent with renal contusions (arrows). Note perinephric hematoma on right (arrowheads).B, 22-year-old man after fall from height. Enhanced CT scan reveals sharply demarcated perfusion defect, presumably due to segmental arterial injury. Note retroperitoneal hematoma in retrocaval region (arrow).
B
A
Fig. 3—Deep parenchymal injuries in two patients with renal trauma.A, 50-year-old woman after motor vehicle collision. Enhanced CT scan in nephrographic phase reveals deep left renal lacerations and perinephric hematoma.B, 28-year-old woman after gunshot wound. Nephrographic phase CT scan reveals linear cleft in medial aspect of right kidney and surrounding hematoma. Densities in hematoma (black arrows) reflect active arterial bleeding. Small locules of gas in right paraspinal muscles (white arrows) are related to track of shotgun wound.
B
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.198
on
09/1
1/14
fro
m I
P ad
dres
s 11
4.79
.28.
198.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:192, June 2009 1517
Genitourinary Trauma
Underlying renal parenchymal abnorma-lities can predispose the kidney to injury. These abnormalities include cysts, tumors, chronic hydronephrosis, and congenital anom-alies such as a horseshoe kidney, ectop ic kid-ney, congenital UPJ obstruction, and poly-cystic kidneys [25, 34] (Fig. 7). Trauma in abnormal kidneys tends to be confined to the kidneys, to occur with relatively minor trau-ma, and to result in macrohematuria more frequently. Children, particularly those with congenital anomalies, have been considered to be at greater risk for renal trauma, but in a small published series [6] congenital anoma-lies were not found to increase the incidence of renal injuries.
ManagementNonoperative management is the accepted
standard of care for minor injuries. No fol-low-up imaging is recommended for grades 1 and 2 injuries (minor renal injuries). Pa-tients with grade 3 lacerations who are hemo-dynamically stable and show no devitalized fragments also require no follow-up imag-ing [27]. Delayed or secondary hemorrhage may occur from 2 to 38 days later in patients with deep lacerations, particularly those due to stab wounds, likely because of pseudoan-eurysm or formation of an arteriovenous fis-tula [35, 36]. These can usually be well man-aged with standard angiographic techniques. Grade 4 lacerations require follow-up CT at 36–72 hours to monitor extravasation from the collecting system. Because urine extrava-sation resolves spontaneously in 80–90% of cases, expectant management is the appro-priate therapy for most such patients [37]. If
A
Fig. 4—Collecting system injury in 18-year-old man with blunt abdominal trauma shown on delayed excretory phase imaging.A, Nephrographic phase CT scan shows severely lacerated right kidney and large surrounding fluid collection of hematoma and urinoma.B, Excretory phase of CT urogram shows extravasation of urine from right kidney (arrows).C, Sagittal multiplanar reformation of same study as in B shows numerous lacerations (arrows) in right kidney as well as extravasated urine (arrowheads).
CB
A
Fig. 5—45-year-old woman with perinephric fluid who was involved in motor vehicle collision.A, CT scan in early excretory phase shows right renal lacerations and perinephric fluid.B, Late excretory phase image shows that perinephric fluid is combination of hematoma and extravasated urine.
B
A
Fig. 6—Traumatic renal arterial and venous injury in two patients.A, 23-year-old man with vascular pedicle injury after motorcycle collision. Nephrographic phase CT scan shows near total absence of enhancement in left kidney. Left renal artery (arrow) terminates abruptly. There was also left perinephric hematoma as well as hemoperitoneum from associated splenic injury (not shown).B, 52-year-old man after blunt trauma during karate practice resulting in traumatic left renal vein thrombosis. Contrast-enhanced CT scan shows large filling defect (white arrows) in left renal vein. Also note relatively delayed enhancement of left kidney, which is still in corticomedullary phase, compared with right kidney, which already shows some contrast excretion into collecting system (black arrow). Left kidney is enlarged, and perinephric fluid and stranding are present.
B
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.198
on
09/1
1/14
fro
m I
P ad
dres
s 11
4.79
.28.
198.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

1518 AJR:192, June 2009
Ramchandani and Buckler
urine leaks persist, retrograde or antegrade stenting may help to promote resolution of the extravasation and avoid surgery [25]. Urino-mas that form as a complication of urine ex-travasation can also be successfully managed by percutaneous drainage [25]. Angiography is used largely to treat complications detected on CT, such as suspected renal artery throm-bosis or segmental arterial injury, in patients in whom stenting or embolization is feasible [38]. Surgical management is considered in patients with renal pedicle injury or a severe-ly damaged and shattered kidney [27].
Sequelae of Renal TraumaMinor renal injuries (grades 1 and 2) heal
completely and leave no residual change in the kidney on follow-up CT [39]. Higher-grade injuries can cause permanent scars in the affected kidney [39, 40]. Most (64%) grade 3 and all grades 4 and 5 injuries re-sult in permanent parenchymal scarring of the kidneys.
Ureteral TraumaCauses
Ureteral injuries from external trauma are unusual but when they occur are usually re-lated to penetrating trauma, primarily gun-shot wounds [41, 42]. As with all cases of penetrating trauma, multiple associated in-traabdominal organ injuries are often pres-ent [42]. Missile paths that are in proximity to the ureter can also cause significant tissue damage and may have a delayed presentation. Blunt trauma usually affects the UPJ and is related to rapid deceleration injury [41].
Iatrogenic ureteral injuries can occur dur-ing gynecologic, obstetric, urologic, colorec-
tal, general, or vascular surgery [43]; gyne-cologic surgery accounts for more than half of all iatrogenic injuries [41]. The pelvic ure-ters are the most commonly affected, and preoperative imaging or ureteral stenting to facilitate intraoperative ureteral identifica-tion appear not to be helpful in preventing injury [41]. Patients may present with flank or abdominal pain, elevated serum blood urea nitrogen and creatinine levels, vaginal urinary leakage, fever, or other nonspecific symptoms. If the injury is recognized intra-operatively, the ureter can be repaired im-mediately. Unfortunately, the diagnosis of an iatrogenic ureteral injury can be delayed for several weeks until the patient becomes symptomatic.
Hematuria is an unreliable indicator of ureteral trauma and may be absent in many patients [41, 42].
Imaging FeaturesThe AAST-OIS grades of ureteral injuries
are as follows: grade 1, ureteral contusion; grade 2, less than 50% partial transection; grade 3, more than 50% partial transection; grade 4, complete transection; and grade 5, complete transection and extensive devascu-larization [44]. To our knowledge, no studies have compared imaging findings with opera-tive findings to determine whether the grades of ureteral trauma can be recognized on ra-diographic imaging.
Preoperative imaging may not be per-formed in patients with penetrating trau-ma because these patients are often rapidly transferred to the operating room for explo-ration [42]. One-shot preoperative or intra-operative IVU may show contrast extravasa-tion, but it is often not performed because of poor diagnostic performance and the delays inherent in performing the examination in an unstable patient [24, 41, 42]. In the delayed setting, complete IVU or contrast-enhanced CT with imaging in the delayed phase may show contrast extravasation from the ure-ter or partial or complete ureteral obstruc-tion in patients with ureteral injury. CT may also show urinary ascites or urinoma; a high index of suspicion should be maintained in postoperative patients with intraabdominal fluid collections to accurately assess the uri-nary tract for urine leaks and to characterize any fluid collections (Fig . 8).
In patients with blunt trauma and sus-pected UPJ injury, CT with excretory phase imaging is a reliable tool for evaluation. Features that suggest UPJ injury include pre-
dominantly medial perirenal contrast ex-travasation in the absence of renal paren-chymal injury [45]. If the UPJ is lacerated, contrast material will be present in the distal ureter; and with transection, the distal ure-ter will not be opacified. In equivocal cases, retrograde pyelography can be helpful in dis-tinguishing partial laceration from complete transection [41]. The distinction is important because lacerations are managed with a ure-teral stent, whereas transections require sur-gical repair.
Urinary Bladder TraumaClassification
Bladder injuries are classified by the AAST-OIS scale into five grades [44]; grade 1, which includes contusion, intramural he-matoma, and partial thickness laceration; grade 2, extraperitoneal wall lacerations < 2 cm; grade 3, extraperitoneal lacerations > 2 cm and intraperitoneal lacerations < 2 cm; grade 4, intraperitoneal lacerations > 2 cm; and grade 5, intraperitoneal or extraperito-neal lacerations that extend into the bladder neck or trigone. A second classification sys-tem endorsed by a consensus panel of the So-ciete Internationale D’Urologie [46] classifies bladder injury into four types, which do not take into account the length or extent of the bladder wall laceration: type 1 is bladder con-tusion; type 2, intraperitoneal rupture; type 3, extraperitoneal rupture; and type 4, combined injury. Radiologic imaging is better suited to conform to the latter classification and is di-rected toward determining whether there is a full-thickness tear of the bladder as judged by contrast extravasation on CT cystography or
Fig. 7—42-year-old woman with bleeding from left renal angiomyolipoma after motor vehicle collision. Contrast-enhanced CT scan shows large exophytic mass containing fat (white arrow) and multiple foci of contrast extravasation (black arrows). Note surrounding hematoma and anterior displacement of kidney.
Fig. 8—Right ureteral injury as a complication of hysterectomy in 51-year-old woman. Delayed axial image from CT urography shows jet of contrast material (arrow) extending from injured right ureter. Large amount of urinomatous ascites is present, with some layering of contrast material present dependently in pelvis.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.198
on
09/1
1/14
fro
m I
P ad
dres
s 11
4.79
.28.
198.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:192, June 2009 1519
Genitourinary Trauma
conventional cystography monitored by radi-ography or fluoroscopy.
CausesThe most frequent causes of bladder trauma
are motor vehicle crashes (in which both seat belt compression of the bladder and ejection injuries may be responsible), falls, crush in-juries, and blows to the lower abdomen [46]. Sixty percent to 90% (mean, 80%) of patients with bladder injuries due to blunt trauma have associated pelvic fractures [46], and approxi-mately 30% of patients with pelvic fractures will have some bladder injury, including blad-der contusion [47]. Twenty-five percent of in-traperitoneal bladder ruptures occur in patients without a pelvic fracture [48]. Simultaneous ruptures of the bladder and prostatomembra-neous urethra can occur in 10–29% of males undergoing trauma [49].
Bladder contusion is related to mucosal in-jury from trauma. No abnormalities are de-tectable on imaging studies [50]. Intraperito-neal rupture occurs when there is a blow to or compression of the lower abdomen in a pa-tient with a distended urinary bladder, caus-ing a sudden rise in the intraluminal pres-sure of the bladder and rupture of the dome, which is the weakest portion of the bladder. The dome of the distended bladder is cov-ered by peritoneum, so an injury at this site causes intraperitoneal extravasation. Intra-
peritoneal injury accounts for approximately one third of bladder injuries. Extraperitoneal ruptures account for approximately 60% of major bladder injuries and are usually asso-ciated with pelvic fractures, although the ex-act mechanism of injury remains the subject of debate. The bladder injury may be relat-ed either to direct laceration by sharp bony spicules of pelvic fractures or to a contra-coup mechanism caused by ligamentous in-jury and associated bladder tears. Extraperi-toneal ruptures are further classified into two groups, simple and complex, by Sandler et al. [50]. In simple extraperitoneal rupture, con-trast extravasation is confined to the pelvic extraperitoneal space; whereas in complex extraperitoneal rupture, extravasated con-trast material can disperse widely into the anterior abdominal wall, the penis, the scro-tum, and the perineum as a result of disrup-tion of the fascial planes of the pelvis by the injury. Complex injuries may result in con-fusion during image interpretation, causing confined extraperitoneal injuries to be mis-interpreted as combined extraperitoneal and intraperitoneal injuries or to be mistaken for the presence of a coexisting urethral injury [50, 51].
The presence of both intraperitoneal and extraperitoneal bladder injuries is known as a combined bladder injury and occurs in ap-proximately 5% of major bladder injuries.
ImagingIndications for imaging—Gross hematu-
ria with pelvic fracture is an absolute indica-tion for evaluation of the bladder in a patient with trauma [51, 52] because such patients have a high likelihood of injury. Morey et al. [52] reported that of their 53 patients with bladder injury, all had hematuria, and 85% had pelvic fractures. In the series by Quagli-ano et al. [51], 32% of patients with pelvic fracture and gross hematuria were found to have bladder injury. Gross hematuria with-out pelvic fracture, microhematuria with pel-vic fracture, and isolated microhematuria are considered relative indications for evaluation of the bladder, with imaging recommended in patients with clinical symptoms such as suprapubic pain or voiding difficulties [52].
Both CT cystography and conventional cystography are similar in their sensitivity and specificity for detecting and character-izing bladder injury [51, 53].
Conventional cystography—The identifi-cation of contrast material outside the con-fines of the urinary bladder confirms the diagnosis of bladder rupture. With extraperi-toneal leaks, the contrast agent remains con-fined to the pelvis (Fig. 9); with intraperitone-al leaks, contrast material may outline bowel loops and extend into the paracolic gutters and diffusely into the peritoneal cavity (Fig. 10A). In a patient with blood at the urethral
A
Fig. 9—34-year-old man with extraperitoneal bladder rupture after motor vehicle collision. Extraluminal bladder contrast is not seen when there is passive filling of bladder with excreted IV contrast material but is visualized well when bladder is actively distended on CT cystogram.A, Delayed axial image from contrast-enhanced CT of pelvis shows excreted contrast material (and Foley catheter balloon) in bladder as well as small amount of surrounding fluid (arrows), but no extraluminal contrast material is detected. Note that bladder appears quite distended.B–D, CT cystograms show extraperitoneal rupture and large amount of contrast material in prevesical space and extending into superficial soft tissues.
CB D
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.198
on
09/1
1/14
fro
m I
P ad
dres
s 11
4.79
.28.
198.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

1520 AJR:192, June 2009
Ramchandani and Buckler
meatus, there is a high likelihood of urethral injury, and retrograde urethrography should be performed before bladder catheterization [54]. The bladder should be distended until a detrusor contraction is obtained in order to avoid a false-negative study.
Cystography has an accuracy rate of 85–100% for detecting bladder injury [50–52]. Cystography should ideally be performed with fluoroscopic guidance. The minimal se-quence of films for cystography is prelimi-nary radiography of the pelvis, a film of the maximally filled bladder, and a postdrainage film to detect extraluminal contrast leak from a posterior wall injury that may be obscured on the filled film. Because these patients of-ten have associated pelvic fractures, oblique views may not be feasible. Bladder injury may be identified only on the postdrainage film in approximately 10% of cases [48].
CT cystography—Active distention of the urinary bladder with contrast material is es-sential for a high-quality CT cystogram that is reliable in excluding a bladder leak [50–55]. It is important to recognize that passive distention of the bladder, using excreted con-trast material only, during a routine abdom-inopelvic CT study cannot be relied on to diagnose bladder rupture, even with clamp-ing of a urethral catheter [50, 55, 56], even if the bladder appears to be distended (Fig. 9). CT performed with excreted contrast ma-terial only may show intraperitoneal or ex-traperitoneal fluid but cannot differentiate urine from ascites. A minimum of 300–350 mL of diluted contrast media should be in-stilled into the bladder followed by axial CT imaging of the pelvis [56]. Multiplanar ref-ormation (MPR) may be helpful to better de-lineate the site of the bladder rupture; Chan et al. [53] found that additional sagittal and coronal MPR images were particularly use-ful in showing perforations at the dome of the bladder. A postvoid or postdrainage film is unnecessary and redundant in CT cystog-raphy [53].
Quagliano et al. [51] reported sensitivity and specificity of 95% and 100%, respective-ly, for both CT cystography and convention-al cystography. Other authors have reported similar high sensitivity and specificity for CT cystography [53, 57].
Quagliano et al. [51] distended the blad-der with diluted contrast material before per-forming routine abdominopelvic CT and re-ported satisfactory results. Other authors have reported performing CT cystography on a second imaging series after initial rou-
tine diagnostic CT of the abdomen and pelvis [57]. The absence of pelvic ascites is report-ed to be quite helpful in excluding bladder rupture [58].
In extraperitoneal injuries, contrast mate-rial may be confined to the pelvis (a molar-tooth appearance may be seen to the pattern of contrast extravasation) or may extend be-yond the perivesical space with a complex extraperitoneal injury (Fig. 10B). Intraperito-neal injuries outline bowel loops and diffuse through the mesenteric folds (Fig. 10A).
Urethral TraumaClassification
Male urethral trauma was originally clas-sified by Colapinto and McCallum [59] on the basis of the appearance of the urethra on retrograde urethrography. This classification was subsequently modified and expanded to better predict continence [60]. Male urethral injuries are primarily of two types, depend-ing on the cause of the trauma. They may be associated with a fracture of the anterior pelvic arch and affect about 5% of men who sustain a pelvic fracture. These injuries usu-ally involve the membranous urethra and are due to shearing and rupturing of the pubo-prostatic ligaments. A hematoma forms in the retropubic and perivesical spaces [48]; identification of this hematoma on CT scans is an important clue to the presence of a ure-thral injury.
The second main type of injury results from a straddle injury, which directly in-jures the bulbous urethra. The frequency of anterior urethral injuries is one third that
of posterior urethral injuries [61]. A direct blow to the perineum compresses the ure-thra and corpus spongiosum between the ex-ternal hard object and the inferior aspect of the symphysis pubis. In most cases, no pelvic fracture occurs. Straddle injuries can cause either partial or complete rupture of the bul-bous urethra [48] (Fig. 11A).
Posterior urethral injuries associated with a pelvic fracture are classified into five types [48, 59, 60]: type I, posterior urethra stretched but intact; type II, urethra disrupted at the membranoprostatic junction above the uro-genital diaphragm (Fig. 11B); type III, mem-branous urethra disrupted, with extension to the proximal bulbous urethra or disruption of the urogenital diaphragm (most common); type IV, bladder neck injury with extension into the urethra; type IVa, injury of the base of the bladder and periurethral extravasation simulating a true type IV urethral injury; and type V, partial or complete pure anterior ure-thral injury. A European consensus commit-tee [61] endorsed the Goldman classification [60] but recommended simplification; they suggested that assessment be aimed at de-termining whether the injury is a partial or complete disruption of the anterior or poste-rior urethra, and whether posterior urethral injuries are complicated by extension to the bladder neck or rectum [61].
ImagingWhen a patient with pelvic trauma pres-
ents with blood at the urethral meatus, or when urethral injury is suspected clinically, retrograde urethrography is essential before
A
Fig. 10—Intraperitoneal bladder injury and complex extraperitoneal bladder injury in two patients.A, 75-year-old woman with intraperitoneal bladder rupture after motor vehicle collision. CT cystogram shows defect in anterior bladder wall (arrow) as well as intraperitoneal contrast material outlining pelvic peritoneal reflections.B, 60-year-old woman after motor vehicle collision. Contrast extravasation from complex extraperitoneal rupture is extending high into pelvis in space of Retzius.
BDow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.198
on
09/1
1/14
fro
m I
P ad
dres
s 11
4.79
.28.
198.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
AJR:192, June 2009 1521
Genitourinary Trauma
attempting to catheterize the bladder [48, 60] to avoid traumatizing the urethra further and potentially converting a partial tear into a complete injury [48] (Fig. 11C). Retrograde urethrography is the diagnostic procedure of choice to evaluate patients with suspected urethral injury [48, 62, 63]. In patients with significant trauma, a suprapubic catheter may be placed for bladder drainage. However, it is not rare in modern trauma centers for a Foley catheter to be placed before retrograde ure-thrography so that fluid intake and output can be accurately monitored. CT may precede retrograde urethrography by hours or even days; it is therefore important to become fa-miliar with findings on CT that are reportedly seen with higher frequency in patients with posterior urethral injuries than in those with-out [64, 65]. These findings include obscura-tion of the urogenital diaphragmatic fat plane, hematoma of the ischiocavernosus and obturator internus muscles, obscuration of the prostatic contour, and obscuration of the bulbocavernosus muscle. Obscuration of the urogenital diaphragm fat plane was seen in 88% of patients with pelvic fracture and urethral injury versus only 3% of those with pelvic fracture but no urethral injury. Hema-toma of the ischiocavernosus muscle was seen in 88% of patients with urethral injury but in only 17% without urethral injury. Ob-scuration of the prostatic contour was seen in 59% with urethral injury but in only 7% without urethral injury. Obscuration of the bulbocavernosus muscle was seen in 47%
with urethral injury but in only 10% without urethral injury. Hematoma of the obturator internus muscle was seen in 53% with ure-thral injury but in only 13% without urethral injury (Fig. 11C).
Although MRI has no role in evaluating the urethra in the acute setting, it is useful in assessing posttraumatic pelvic anatomy, determining the position of the prostate and the amount of pelvic fibrosis, and estimating the length of the prostatomembraneous de-fect [62, 66].
Injuries to the female urethra are uncom-mon because of its short size and absence of firm attachment to the pubic bone. Female urethral injuries are often accompanied by vaginal and rectal injury [67].
Testicular TraumaThe testes can be injured with sporting ac-
tivities, which account for more than half of all cases of testicular injury [68]. Motor ve-hicle collisions are also an important cause, particularly two-wheeled motorized vehi-cles, when the testes are crushed between the bony pelvis and the fuel tank [2].
Imaging is useful in the triage of patients for surgical or nonsurgical management. Clinical examination may not be able to ac-curately determine the severity of injury be-cause the ecchymosis and the degree of he-matoma do not correlate accurately with the severity of testicular injury [69]. High-fre-quency sonography performed with a linear array transducer is the imaging technique
A
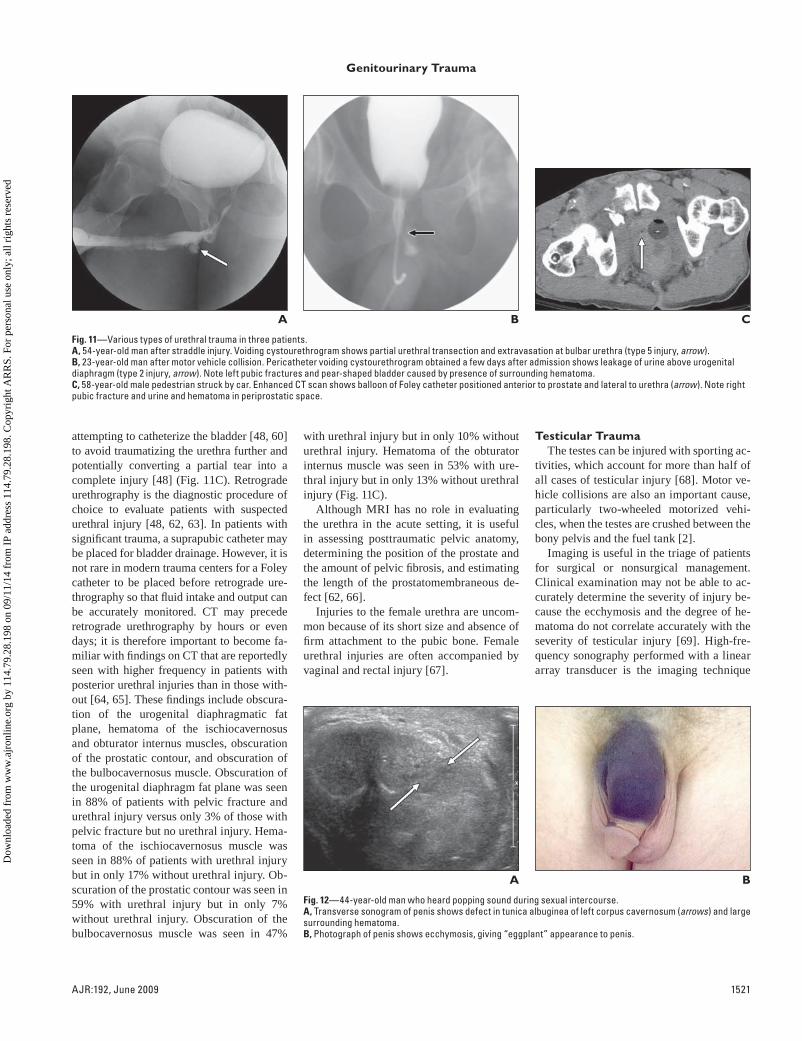
Fig. 11—Various types of urethral trauma in three patients.A, 54-year-old man after straddle injury. Voiding cystourethrogram shows partial urethral transection and extravasation at bulbar urethra (type 5 injury, arrow).B, 23-year-old man after motor vehicle collision. Pericatheter voiding cystourethrogram obtained a few days after admission shows leakage of urine above urogenital diaphragm (type 2 injury, arrow). Note left pubic fractures and pear-shaped bladder caused by presence of surrounding hematoma.C, 58-year-old male pedestrian struck by car. Enhanced CT scan shows balloon of Foley catheter positioned anterior to prostate and lateral to urethra (arrow). Note right pubic fracture and urine and hematoma in periprostatic space.
CB
A
Fig. 12—44-year-old man who heard popping sound during sexual intercourse.A, Transverse sonogram of penis shows defect in tunica albuginea of left corpus cavernosum (arrows) and large surrounding hematoma.B, Photograph of penis shows ecchymosis, giving “eggplant” appearance to penis.
B
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.198
on
09/1
1/14
fro
m I
P ad
dres
s 11
4.79
.28.
198.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

1522 AJR:192, June 2009
Ramchandani and Buckler
of choice; MRI is helpful in patients with equivocal findings.
Imaging is directed toward determining whether testicular rupture is present. Sonog-raphy has a reported sensitivity of 100% and a specificity of 93.5% for the diagnosis of testicular rupture [70]. Heterogeneous echo-texture in the testis, testicular contour abnor-mality due to extrusion of the testes through a tunical defect, and disruption of the tunica albuginea are indicative of testicular rupture. Testicular fractures are surgically managed with débridement of extruded seminiferous tubules and closure of the tunical defect. The rate of testicular salvage is 90% if surgery is performed promptly. Testicular hematomas may also cause the echotexture to be hetero-geneous. The appearance of hematomas var-ies with their age, but they show no internal vascularity. Significant testicular hematomas should be monitored because they may be-come secondarily infected and necessitate orchiectomy. Other findings that may ac-company testicular trauma are a scrotal he-matocele, scrotal wall hematoma, and trau-matic epididymitis [68].
Penile FractureFracture of the penis occurs exclusively
with an erection, with aggressive vaginal in-tercourse being the most common cause. It is related to excessive bending of the erect penis and thrusting against the pubic sym-physis. The patient usually reports a crack-ing sound, immediate pain, and rapid detu-mescence. On physical examination, there is swelling and ecchymosis of the penile shaft, causing the so-called eggplant deformity (Fig. 12). A transverse tear occurs in the tu-nica albuginea, usually of one corporal cav-ernosal body, although both can be affected. If the clinical findings are equivocal, sonog-raphy or MRI [71–73] may help to show the defect in the tunica albuginea as well as the surrounding hematoma.
References 1. Baverstock R, Simons R, McLoughlin M. Severe
blunt renal trauma: a 7-year retrospective review
from a provincial trauma centre. Can J Urol 2001;
8:1372–1376
2. Paparel P, N’Diaye A, Laumon B, Caillot J-L,
Perrin P, Ruffion A. The epidemiology of trauma
of the genitourinary system after traffic accidents:
analysis of a register of over 43,000 victims. BJU
Int 2006; 97:338–341
3. Kansas BT, Eddy MJ, Mydlo JH, Uzzo RG. Inci-
dence and management of penetrating renal trau-
ma in patients with multiorgan injury: extended
experience at an inner city trauma center. J Urol
2004; 172:1355–1360
4. Smith J, Caldwell E, D’Amours S, Jalaludin B,
Sugrue M. Abdominal trauma: a disease in evolu-
tion. ANZ J Surg 2005; 75:790–794
5. Wessells H, Suh D, Porter JR, et al. Renal injury
and operative management in the United States:
results of a population-based study. J Trauma
2003; 54:423–430
6. McAleer IM, Kaplan GW, LoSasso BE. Congeni-
tal urinary tract anomalies in pediatric renal trau-
ma patients. J Urol 2002; 168:1808–1810
7. Shanmuganathan K, Mirvis SE, Chiu WC, Killeen
KL, Hogan GJF, Scalea TM. Penetrating torso
trauma: triple-contrast helical CT in peritoneal
violation and organ injury—a prospective study in
200 patients. Radiology 2004; 231:775–784
8. Yao DC, Jeffrey RB Jr, Mirvis SE, et al. Using
contrast-enhanced helical CT to visualize arterial
extravasation after blunt abdominal trauma: inci-
dence and organ distribution. AJR 2002; 178:17–
20
9. Knudson MM, McAninch JW, Gomez R, Lee P,
Stubbs HA. Hematuria as a predictor of abdominal
injury after blunt trauma. Am J Surg 1992; 164:
482–485
10. Stawicki SP, Hoey BA, Grossman MD, Anderson
HL III, Reed JF III. Adrenal gland trauma is as-
sociated with high injury severity and mortality.
Curr Surg 2003; 60:431–436
11. Rana AI, Kenney PJ, Lockhart ME, et al. Adrenal
gland hematomas in trauma patients. Radiology
2004; 230:669–675
12. Gabal-Shehab L, Alagiri M. Traumatic adrenal
injuries. J Urol 2005; 173:1330–1331
13. Sinelnikov AO, Abujudeh HH, Chan D, Novelline
RA. CT manifestations of adrenal trauma: experi-
ence with 73 cases. Emerg Radiol 2007; 13:313–
318
14. Pinto A, Scaglione M, Guidi G, Farina R, Acamp-
ora C, Romano L. Role of multidetector row com-
puted tomography in the assessment of adrenal
gland injuries. Eur J Radiol 2006; 59:355–358
15. Pinto A, Scaglione M, Pinto F, Gagliardi N, Ro-
mano L. Adrenal injuries: spectrum of CT find-
ings. Emerg Radiol 2003; 10:30–33
16. Sevitt S. Post-traumatic adrenal apoplexy. J Clin
Pathol 1955; 8:185–194
17. Oto A, Ozgen B, Akhan O, Besim A. Delayed
posttraumatic adrenal hematoma. Eur Radiol
2000; 10:903–905
18. Favorito LA, Lott FM, Cavalcante AG. Traumatic
rupture of adrenal pseudocyst leading to massive
hemorrhage in retroperitoneum. Int Braz J Urol
2004; 30:35–36
19. Capaccio E, Magnano GM, Valle M, Derchi LE.
Traumatic lesions of adrenal glands in paediat-
rics: about three cases. Radiol Med 2006; 111:
906–910
20. Francque SM, Schwagten VM, Ysebaert DK, Van
Marck EA, Beaucourt LA. Bilateral adrenal hae-
morrhage and acute adrenal insufficiency in a
blunt abdominal trauma: a case-report and litera-
ture review. Eur J Emerg Med 2004; 11:164–167
21. Schmidt J, Mohr VD, Metzger P, Zirngibl H. Post-
traumatic hypertension secondary to adrenal
hemorrhage mimicking pheochromocytoma: case
report. J Trauma 1999; 46:973–975
22. Park SJ, Kim JK, Kim KW, Cho KS. MDCT find-
ings of renal trauma. AJR 2006; 187:541–547
23. Kawashima A, Sandler CM, Corl FM, et al. Imag-
ing of renal trauma: a comprehensive review. Ra-
dioGraphics 2001; 21:557–574
24. Stevenson J, Battistella FD. The ‘one-shot’ intra-
venous pyelogram: is it indicated in unstable
trauma patients before celiotomy? J Trauma 1994;
36:828–833
25. Titton RL, Gervais DA, Boland GW, Mueller PR.
Renal trauma: radiologic evaluation and percuta-
neous treatment of nonvascular injuries. AJR
2002; 178:1507–1511
26. Moore EE, Shackford SR, Pachter HL, et al. Or-
gan injury scaling: spleen, liver, and kidney. J
Trauma 1989; 29:1664–1666
27. Santucci RA, Wessells H, Bartsch G, et al. Evalu-
ation and management of renal injuries: consen-
sus statement of the renal trauma subcommittee.
BJU Int 2004; 93:937–954
28. Santucci RA, McAninch JW, Safir M, Mario LA,
Susan MA, Segal MR. Validation of the Ameri-
can Association for the Surgery of Trauma Organ
Injury Severity Scale for the kidney. J Trauma
2001; 50:195–200
29. Sandler CM, Francis IR, Baumgarten DA, et al. Re-
nal trauma. In: ACR appropriateness criteria. Res-
ton, VA: American College of Radiology, 2007
30. Mee SL, McAninch JW, Robinson AL, Auerbach
PS, Carroll PR. Radiographic assessment of renal
trauma: a 10-year prospective study of patient se-
lection. J Urol 1989; 141:1095–1098
31. Brandes SB, McAninch JW. Urban free falls and
patterns of renal injury: a 20-year experience with
396 cases. J Trauma 1999; 47:643–649
32. Stuhlfaut JW, Lucey BC, Varghese JC, Soto JA.
Blunt abdominal trauma: utility of 5-minute de-
layed CT with a reduced radiation dose. Radiolo-
gy 2006; 238:473–479
33. Berkovich GY, Ramchandani P, Preate DL Jr,
Rovner ES, Shapiro MB, Banner MP. Renal vein
thrombosis after martial arts trauma. J Trauma
2001; 50:144–145
34. Schmidlin FR, Iselin CE, Naimi A, et al. The
higher injury risk of abnormal kidneys in blunt
renal trauma. Scand J Urol Nephrol 1998; 32:
388–392
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.198
on
09/1
1/14
fro
m I
P ad
dres
s 11
4.79
.28.
198.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
AJR:192, June 2009 1523
Genitourinary Trauma
35. Heyns CF, De Klerk DP, De Kock ML. Stab
wounds associated with hematuria: a review of 67
cases. J Urol 1983; 130:228–231
36. Lee DG, Lee SJ. Delayed hemorrhage from a
pseudoaneurysm after blunt renal trauma. Int J
Urol 2005; 12:909–911
37. Matthews LA, Smith EM, Spirnak JP. Nonopera-
tive treatment of major blunt renal lacerations
with urinary extravasation. J Urol 1997; 157:
2056–2058
38. Hagiwara A, Sakaki S, Goto H, et al. The role of
interventional radiology in the management of
blunt renal injury: a practical protocol. J Trauma
2001; 51:526–531
39. Dunfee BL, Lucey BC, Soto JA. Development of
renal scars on CT after abdominal trauma: does
grade of injury matter? AJR 2008; 190:1174–
1179
40. El-Sherbiny MT, Aboul-Ghar ME, Hafez AT,
Hammad AA, Bazeed MA. Late renal functional
and morphological evaluation after non-operative
treatment of high-grade renal injuries in children.
BJU Int 2004; 93:1053–1056
41. Brandes S, Coburn M, Armenakas N, McAninch
J. Diagnosis and management of ureteric injury:
an evidence-based analysis. BJU Int 2004; 94:
277–289
42. Best CD, Petrone P, Buscarini M, et al. Traumatic
ureteral injuries: a single institution experience
validating the American Association for the Sur-
gery of Trauma-Organ Injury Scale grading scale.
J Urol 2005; 173:1202–1205
43. Selzman AA, Spirnak JP. Iatrogenic ureteral inju-
ries: a 20-year experience in treating 165 injuries.
J Urol 1996; 155:878–881
44. Moore EE, Cogbill TH, Jurkovich GJ, et al. Organ
injury scaling. III: Chest wall, abdominal vascu-
lar, ureter, bladder, and urethra. J Trauma 1992;
33:337–339
45. Kawashima A, Sandler CM, Corriere JN, Rodgers
BM, Goldman SM. Ureteropelvic junction inju-
ries secondary to blunt abdominal trauma. Radi-
ology 1997; 205:487–492
46. Gomez RG, Ceballos L, Coburn M, et al. Consen-
sus statement on bladder injuries. BJU Int 2004;
94:27–32
47. Rehm CG, Mure AJ, O’Malley KF, Ross SE.
Blunt traumatic bladder rupture: the role of retro-
grade cystogram. Ann Emerg Med 1991; 20:845–
847
48. Sandler CM, Goldman SM, Kawashima A. Lower
urinary tract trauma. World J Urol 1998; 16:69–75
49. Cass AS. Diagnostic studies in bladder rupture:
indications and techniques. Urol Clin North Am
1989; 16:267–273
50. Sandler CM, Francis IR, Baumgarten DA, et al.
Suspected lower urinary tract trauma. In: ACR
appropriateness criteria. Reston, VA: American
College of Radiology, 2007
51. Quagliano PV, Delair SM, Malhotra AK. Diagno-
sis of blunt bladder injury: a prospective compara-
tive study of computed tomography cystography
and conventional retrograde cystography. J Trau-
ma 2006; 61:410–421
52. Morey AF, Iverson AJ, Swan A, et al. Bladder
rupture after blunt trauma: guidelines for diag-
nostic imaging. J Trauma 2001; 51:683–686
53. Chan DP, Abujudeh HH, Cushing GL Jr, Novel-
line RA. CT cystography with multiplanar refor-
mation for suspected bladder rupture: experience
in 234 cases. AJR 2006; 187:1296–1302
54. Schneider RE. Genitourinary trauma. Emerg Med
Clin North Am 1993; 11:137–145
55. Mee SL, McAninch JW, Federle MP. Computer-
ized tomography in bladder rupture: diagnostic
limitations. J Urol 1987; 137:207–209
56. Vaccaro JP, Brody JM. CT cystography in the
evaluation of major bladder trauma. RadioGraph-
ics 2000; 20:1373–1381
57. Peng MY, Parisky YR, Cornwell EE, Radin R,
Bragin S. CT cystography versus conventional
cystography in evaluation of bladder injury. AJR
1999; 173:1269–1272
58. Pao DM, Ellis JH, Cohan RH, Korobkin M. Util-
ity of routine trauma CT in the detection of blad-
der rupture. Acad Radiol 2000; 7:317–324
59. Colapinto V, McCallum RW. Injury to the male
posterior urethra in fractured pelvis: a new clas-
sification. J Urol 1977; 118:575–580
60. Goldman SM, Sandler CM, Corriere JN Jr,
McGuire EJ. Blunt urethral trauma: a unified,
anatomical mechanical classification. J Urol
1997; 157:85–89
61. Chapple C, Barbagli G, Jordan G, et al. Consensus
statement on urethral trauma. BJU Int 2004;
93:1195–1202
62. Kawashima A, Sandler CM, Wasserman NF, Le-
Roy AJ, King BF Jr, Goldman SM. Imaging of
urethral disease: a pictorial review. RadioGraph-
ics 2004; 24:S195–S216
63. Ingram MD, Watson SG, Skippage PL, Patel U.
Urethral injuries after pelvic trauma: evaluation
with urethrography. RadioGraphics 2004;
24[suppl 1]:S195–S216
64. Ali M, Safriel Y, Sclafani SJ, Schulze R. CT signs
of urethral injury. RadioGraphics 2003; 23:951–
963
65. Kenney PJ, Ali M, Safriel Y, Sclafani SJA,
Schulze R. Invited commentary. (authors’ re-
sponse) RadioGraphics 2003; 23:963–966
66. Narumi Y, Hricak H, Armenakas NA, Dixon CM,
McAninch JW. MR imaging of traumatic posteri-
or urethral injury. Radiology 1993; 188:439–443
67. Venn SN, Greenwell TJ, Mundy AR. Pelvic frac-
ture injuries of the female urethra. BJU Int 1999;
83:626–630
68. Bhatt S, Dogra VS. Role of US in testicular and scro-
tal trauma. RadioGraphics 2008; 28:1617–1629
69. Lupetin AR, King W 3rd, Rich PJ, Lederman RB.
The traumatized scrotum: ultrasound evaluation.
Radiology 1983; 148:203–207
70. Buckley JC, McAninch JW. Use of ultrasonogra-
phy for the diagnosis of testicular injuries in blunt
scrotal trauma. J Urol 2006; 175:175–178
71. Koga S, Santo Y, Arakaki Y, et al. Sonography in
fracture of the penis. Br J Urol 1993; 72:228–229
72. Choi MH, Kim B, Ryu JA, Lee SW, Lee KS. MR
imaging of acute penile fracture. RadioGraphics
2000; 20:1397–1405
73. Morey AF, Metro MJ, Carney KJ, Miller KS,
McAninch JW. Consensus on genitourinary trau-
ma: external genitalia. BJU Int 2004; 94:507–515
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.7
9.28
.198
on
09/1
1/14
fro
m I
P ad
dres
s 11
4.79
.28.
198.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved