
Transmission of solitary pulse in dissipative nonlinear transmission lines
Upload
independentCategory
view
3download
0
ARTICLE IN PRESS
www.elsevier.com/locate/braindev
Brain & Development xxx (2008) xxx–xxx
Original article
Primary soliter and multiple intracranial cyst hydatid disease:Report of five cases
Huseyin Per a,*, Sefer Kumandas� a, Hakan Gumus� a, Ali Kurtsoy b
a Department of Pediatric Neurology, Medical Faculty, Erciyes University, 38039 Kayseri, Turkeyb Department of Neurosurgery, Medical Faculty, Erciyes University, 38039 Kayseri, Turkey
Received 17 November 2007; received in revised form 22 March 2008; accepted 30 March 2008
Abstract
Echinococcosis is a parasitic disease caused by infestation of various body tissues by the encysted larvae of Echinococcosis gran-
ulosa, the tapeworm. The disease because of the inefficiency of environmental health and protective care and dealing with animals isprevalent in South America, Africa, Australia, the Mediterranean countries and the Middle East. Cerebral hydatid cysts are rare andcomprise only 0.5–3% of all reported hydatid cysts. Brain involvement is seen rare and primary form is very rare. We report fivecases of primary hydatid disease of the brain. In three cases (60%), brain involvement was solitary, while two cases (40%) had pri-mary multiple intracranial hydatid cysts. This study confirms that hydatid disease is a difficult health problem in Turkey.� 2008 Elsevier B.V. All rights reserved.
Keywords: Intracranial; Cyst hydatid; Primary; Multiple
1. Introduction
Cerebral hydatid cysts are rare and comprise only0.5–3% of all reported hydatid cysts. Cerebral hydatidcyst is considered a childhood disease, and estimated50–75% of cases involving the central nervous systemoccurring in the paediatric age group [1–4]. Cerebralhydatid cysts are usually solitary and unilocular or mul-tilocular although multiple cysts have been reported.Multiple cerebral hydatid cysts usually occur as a resultof surgical or traumatic rupture, but spontaneous rup-ture also is possible [5–13].
We reported five cases of primary hydatid disease ofbrain. In three cases (60%), brain involvement was soli-tary, while two cases (40%) had multiple intracranialhydatid cysts. The surgical and medical treatmentsapplied to five patients were observed for 1–17 years
0387-7604/$ - see front matter � 2008 Elsevier B.V. All rights reserved.
doi:10.1016/j.braindev.2008.03.009
* Corresponding author. Tel.: +90 (352) 2405005; fax: +90 (352)4375825.
E-mail address: [email protected] (H. Per).
Please cite this article in press as: Per H et al., Primary soliter and mdoi:10.1016/j.braindev.2008.03.009
and the results and the complications of the five caseswere presented.
2. Materials and methods
The retrospective study was carried out at the Pediat-ric Neurology and Neurosurgery Department of ErciyesUniversity, Kayseri, in Turkey. This study included fivepatients who were treated for primary intracranial hyda-tid cysts. They were four male and one female patients.Their ages were between 11 and 16, with an average ageof 14. Three patients were evaluated with MRI and twopatients were evaluated with CT of brain. Cerebral MRimaging, at field strength of 1.5 T, was performed onpatients. Present clinical symptoms and signs werereviewed. All lesions were surgically removed. Allpatients underwent a chest X-ray, echocardiographyand abdominal ultrasound to reveal any hydatid diseasein the lung, heart , and/or liver. The post operative com-plications were documented and the outcome of thepatients was evaluated.
ultiple intracranial cyst hydatid disease: ..., Brain Dev (2008),

2 H. Per et al. / Brain & Development xxx (2008) xxx–xxx
ARTICLE IN PRESS
3. Patient reports
3.1. Patient 1
A 15-year-old boy was admitted to our Neurosur-gery Department with 2-month history of severeheadache and intellectual deterioration. Ten daysprior to admission he developed progressive dyspha-sia. Neurological examination revealed bilateral papil-ledema, expressive dysphasia, and obdundation. CTshowed four spherical, well-defined cystic lesionsoccupying the left supratentorial hemisphere. Ofthese, three were located in the frontoparietal region,and one measuring 1 cm in diameter, in the occipitalregion. Laboratory studies were normal and therewas no evidence of hydatid disease elsewhere. Thecysts were extirpated without rupture. The postopera-tive course was uneventful. The patient’s neurologiccondition markedly improved and he was free ofsymptoms when discharged on the 15th day afteradmission. Seven months later, a new CT performedbecause of dysphasia, revealed a large recurrent cystin the sylvian cistern. The cysts were removed intactusing the same operative technique [13]. Pathologicalexamination confirmed that the surgical specimenswere hydatid cysts with scoleces. The patient wasadmitted 2 years later after the second operation.The liver cyst hydatid was detected. The patient dieddue to anaphylactic shock in operation.
3.2. Patient 2
A previously healthy 15-year–old boy was admittedto our Pediatric Neurology Department complainingof severe headache, faintness, diplopia and thrice vomit-ing everyday. His complaints started 10 days ago. Onadmission, he had signs of raised intracranial pressure:papilledema edema, silence left hemiparesia and positiveleft Babinski sign. A computed-tomography scan andMRI images showed a cystic lesion in the right temporo-parietal region. X-ray of chest and ultrasonography ofthe abdomen were normal. The cyst was delivered with-out rupture. Pathological examination confirmed thatthe surgical specimens were hydatid cysts with scoleces.Medical therapy of the patient was ordered with 200 mgof albendazole three times a day throughout 3 months.The postoperative course was uneventful, and thepatient showed a marked recovery in his neurologicalstatus.
3.3. Patient 3
A 14-year old girl of rural origin was admitted to thehospital because of severe headache, nausea, vomitingand seizure. Her complaints started 4 weeks ago. Onphysical examination, the patient appeared tired but
Please cite this article in press as: Per H et al., Primary soliter and mdoi:10.1016/j.braindev.2008.03.009
not acutely ill. The results of the physical examinationwere normal. A computed tomography scan showed acystic lesion in the right posterior parietal region andwas not seen midline shift and edema. X-ray of her chestand ultrasonography of her abdomen were normal. Thecyst was extirpated without rupture. Pathological exam-ination confirmed that the surgical specimens werehydatid cysts with scoleces. Medical therapy of thepatient was ordered with 200 mg of albendazole threetimes a day during three months. The postoperativecourse was uneventful, and the patient showed a markedrecovery in her neurological status. But; her hydatid cystrecurred in the same region 1 year later. The cyst wasremoved without rupture.
3.4. Patient 4
A previously healthy 16-year-old boy complaining ofsevere headache, intermittent vomiting for 2 monthsand impaired vision was admitted to the Pediatric Neu-rology Department. On examination, he had signs ofraised intracranial pressure: right papilledema andimpaired vision. Magnetic resonance imaging showeda cystic lesion in the right parietal region (Fig. 1A–C). The cyst extirpated was uncomplicated (Fig. 1D).Pathological examination confirmed that the surgicalspecimens were hydatid cysts with scoleces. The post-operative course was uneventful, and the patientshowed a marked recovery in his neurological status.Medical therapy of the patient was ordered with200 mg of albendazole three times a day throughout3 months.
3.5. Patient 5
A previously healthy 11-year-old boy complaining ofheadache, vomiting, diplopia for about 10 days wasadmitted to our Pediatric Neurology Department. Thereview of the family history disclosed no abnormalities.On examination, he had signs of raised intracranial pres-sure: with bilaterally sixth nerve palsy. Funduscopicexamination revealed papilledema. Routine blood anal-yses were within normal limits. A magnetic resonanceimaging showed cystic lesions (60 mm–20 mm–30 mmin diameter) but without rim enhancement or perifocaledema (Fig. 2A and B). Extensive screen for anothercyst elsewhere in the body revealed negative results.Chest radiography, echocardiography, ultrasonographyof the abdomen was normal. The operative approachwas planned with neuronavigation (BrainLab Vectorvision2, Munich, Germany). A large parietooccipitalcraniotomy was performed and firstly a large cyst weredelivered by using Dowling technique [1] (Fig. 2C),and then other cysts were delivered similarly (Fig. 2D).Pathological examination confirmed that the surgicalspecimens were hydatid cysts with scoleces. The postop-
ultiple intracranial cyst hydatid disease: ..., Brain Dev (2008),

Fig. 1. T2-weighted axial (A), T1-weighted sagittal (B) and T2-weighted coronal (C) images are showing the gigantic right parietal hydatid cyst. (D)The removed cyst is seen after the operation.
H. Per et al. / Brain & Development xxx (2008) xxx–xxx 3
ARTICLE IN PRESS
erative course was uneventful, and the patient showed amarked recovery in his neurological status.
4. Results
The ages of our cases were between 11 and 16 andfour of the patients were male (80%) and one was female(20%). On admission, one of the patients had seizureand all of them had a headache accompanied by vomit-ing. Primary single and multiple hydatid cysts weredetermined in our five cases. Primer hydatid cysts wereonly seen on cerebral hemispheres in three patients(right parietal, right temporoparietal and right posteriorparietal). Two cases had primary multiple intracranialinvolvement. Six cysts were located in the right cerebralhemisphere, while four cysts were located in the left one.
All patients were operated. Total removals of thecysts without rupture were achieved in all patients.Albendazole which is a broad-spectrum oral antihelmin-tic was given to all patients for 3 months. CT scan andMRI were applied to all cases during the preoperativeperiod. After the surgical intervention complex partialepilepsy, hemiparesis, strabismus developed in the cases
Please cite this article in press as: Per H et al., Primary soliter and mdoi:10.1016/j.braindev.2008.03.009
were improved successively. Between the 1st and 17thyear of follow-up period, no sequel has been found inany patients, except one whose seizures continued.Recurrence was seen in only two patients. One patientdied (Table 1).
5. Discussion
Cerebral hydatid cysts are rare and comprise only 2–3% of all reported hydatid cysts. It constitutes up to 3–4%of all intracranial space-occupying lesions [4,7,9,14–16].Cerebral hydatid cysts are usually solitary and unilocu-lar or multilocular although multiple cysts have beenreported [5–13]. Primary hydatid infection caused byembryos which escaped hepatic and pulmonary barriersis generally single and fertile. Cerebral hydatid cysts aremost often supratentorially localized in the distributionof the terminal branches of the middle cerebral artery,usually temporo-parieto-occipitally [9,7,18]. Multiplecerebral hydatid cysts are extremely rare and result fromspontaneous, traumatic or surgical rupture of a solitaryprimary cyst or as a consequence of a cyst rupture else-where and embolization of hydatids to the brain [6,13–
ultiple intracranial cyst hydatid disease: ..., Brain Dev (2008),
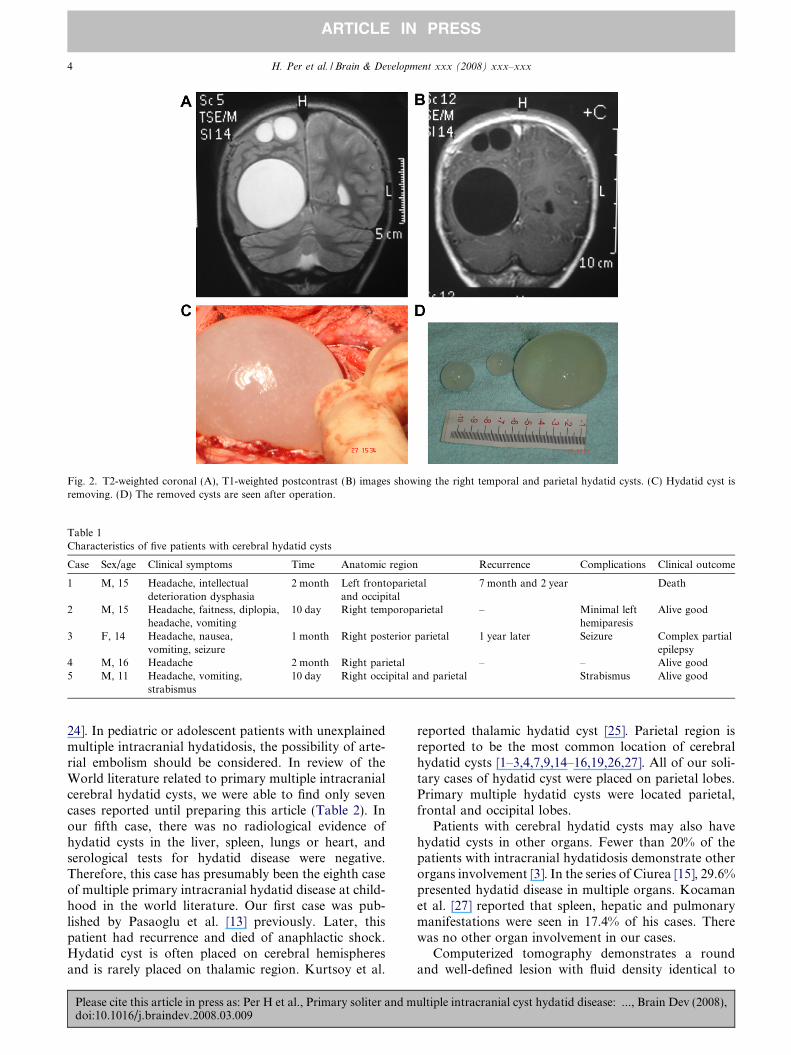
Fig. 2. T2-weighted coronal (A), T1-weighted postcontrast (B) images showing the right temporal and parietal hydatid cysts. (C) Hydatid cyst isremoving. (D) The removed cysts are seen after operation.
Table 1Characteristics of five patients with cerebral hydatid cysts
Case Sex/age Clinical symptoms Time Anatomic region Recurrence Complications Clinical outcome
1 M, 15 Headache, intellectualdeterioration dysphasia
2 month Left frontoparietaland occipital
7 month and 2 year Death
2 M, 15 Headache, faitness, diplopia,headache, vomiting
10 day Right temporoparietal – Minimal lefthemiparesis
Alive good
3 F, 14 Headache, nausea,vomiting, seizure
1 month Right posterior parietal 1 year later Seizure Complex partialepilepsy
4 M, 16 Headache 2 month Right parietal – – Alive good5 M, 11 Headache, vomiting,
strabismus10 day Right occipital and parietal Strabismus Alive good
4 H. Per et al. / Brain & Development xxx (2008) xxx–xxx
ARTICLE IN PRESS
24]. In pediatric or adolescent patients with unexplainedmultiple intracranial hydatidosis, the possibility of arte-rial embolism should be considered. In review of theWorld literature related to primary multiple intracranialcerebral hydatid cysts, we were able to find only sevencases reported until preparing this article (Table 2). Inour fifth case, there was no radiological evidence ofhydatid cysts in the liver, spleen, lungs or heart, andserological tests for hydatid disease were negative.Therefore, this case has presumably been the eighth caseof multiple primary intracranial hydatid disease at child-hood in the world literature. Our first case was pub-lished by Pasaoglu et al. [13] previously. Later, thispatient had recurrence and died of anaphlactic shock.Hydatid cyst is often placed on cerebral hemispheresand is rarely placed on thalamic region. Kurtsoy et al.
Please cite this article in press as: Per H et al., Primary soliter and mdoi:10.1016/j.braindev.2008.03.009
reported thalamic hydatid cyst [25]. Parietal region isreported to be the most common location of cerebralhydatid cysts [1–3,4,7,9,14–16,19,26,27]. All of our soli-tary cases of hydatid cyst were placed on parietal lobes.Primary multiple hydatid cysts were located parietal,frontal and occipital lobes.
Patients with cerebral hydatid cysts may also havehydatid cysts in other organs. Fewer than 20% of thepatients with intracranial hydatidosis demonstrate otherorgans involvement [3]. In the series of Ciurea [15], 29.6%presented hydatid disease in multiple organs. Kocamanet al. [27] reported that spleen, hepatic and pulmonarymanifestations were seen in 17.4% of his cases. Therewas no other organ involvement in our cases.
Computerized tomography demonstrates a roundand well-defined lesion with fluid density identical to
ultiple intracranial cyst hydatid disease: ..., Brain Dev (2008),

Table 2Primary multiple cerebral hydatid cysts published in the literature
Authors–Year Age, sex Localisation Treatment Outcome
Sharma et al. [24] 1982 9, F Five cysts in the right supratentorial region OP GoodPasaoglu et al. [13] 1989 15, M Four cysts left supratentorial region OP DeathIplikcioglu et al. [23] 1989 7, F Three cysts right frontal, two cysts left occipital, one cyst in the left frontal region OP GoodCataltepe et al. [22] 1991 8, M Two cysts in both parietooccipital regions OP GoodGupta et al. [20] 1991 18, M Multiple cysts in both cerebral and left Cerebellar hemispheres OP DeathNurchi et al. [21] 1992 9, ? Multiple cysts in the right parietal and occipital regions OP GoodOnal et al. [19] 2001 7, M Right frontal, left lateral ventricle OP Death
?, Details not reported.
H. Per et al. / Brain & Development xxx (2008) xxx–xxx 5
ARTICLE IN PRESS
cerebrospinal fluid, with or without septations or calcifi-cation. Compression of the midline structures and ven-tricles are seen in most of the cases. However edemaand contrast enhancement are usually absent inuntreated or uncomplicated cases. On MR, the signalintensity of the cyst is isointense with cerebrospinal fluidon all pulse sequences. Variable amounts of septa couldbe observed. Both CT and MRI demonstrate the cere-bral hydatid cysts adequately. MRI will be more widelyused for the diagnosis and surgical planning in cerebralhydatid disease. MRI scans show details that cannot beseen on CT scan. MRI demonstrates the hydatid cyst asa spherical thin-walled structure containing fluid withCSF imaging characters. The differential diagnosis ofintracranial hydatid cysts includes cystic lesions suchas porencephalic cyst, arachnoid cyst, cystic tumoursof the brain and pyogenic abscesses. In contrast to hyda-tid cysts, porencephalic cysts and arachnoid cysts arenot spherical in shape and are not surrounded entirelyby brain substance. Arachnoid cysts are extra-axialmasses that may deform adjacent brain. Porencephaliccysts result from insults to normal brain tissue and arelined by gliotic white matter that could easily be demon-strated with MR imaging [2,5,6,10,26]. In our cases, thetypical appearance of hydatid cyst was determined inCT and MRI.
Cerebral hydatid cysts are benign, slowly growingcysts. The lesions may remain asymptomatic until theyare quite large. Headache and vomiting were the mostcommon presenting symptoms in this series, as in otherseries reported literature. Most common symptoms ofcentrally placed cases are headache, depending on sizeof cyst, and increasing intracranial pressure, vomitingand findings of extra pyramidal system sign. Evidenceof pyramidal tract dysfunction, appropriate to the loca-tion of the cyst, is noted in almost 90% of patients. Men-tal changes are noted in 25% of children, and seizureactivity in approximately 20%. Papiledema is usuallypresent in patients with intracranial hydatid cyst at thediagnosis. Other symptoms such as hemiparesis, sei-zures, visual field alteration and gait disorders may varywith the location of the cyst. It is reported that the mostcommon neurological damage is paralysis and very rarecomplications are partial and generalized seizure, sub-
Please cite this article in press as: Per H et al., Primary soliter and mdoi:10.1016/j.braindev.2008.03.009
dural effusion and ventricular dilatation in postoperativeperiod in hydatid cyst cases [1,3,4,7–9,12–16,19,20,27].In all cases related to cerebral hydatid cyst headacheand vomiting were determined.
Hydatid disease is generally a severe disease, withover 90% mortality in untreated patients. Intact deliveryof cerebral hydatid cysts should be the surgical aim in allcases. Such gigantic cysts are easily ruptured during theoperation and recurrence is the rule. Avoiding this risk,a cortical incision must be equal and appropriate to thecyst diameter. However, larger cortical incision maycause increasing morbidity. Stereotactic neuronaviga-tion system has proven to be a helpful tool for surgicaltreatment of different brain pathological condition. Thistechnology provides with continous interactive threedimensional images of formation location and surgicaltrajectory for the surgeon. It is useful in planning andguiding to surgery of intracranial mass lesions.Although primary cerebral cyst hydatid cases wereremoved without any rupture, there may be otherlesions which are likely to be out of central nervous sys-tem but not showed (as they are in cases of 1 and 3).Management of hydatid disease requires surgery andchemotherapy. Although albendazole is effective inhydatid disease, Hydatid cysts should be removed with-out rupture and all patients must receive albendazole atpre-and postoperative periods for 8 weeks [3,4,8,9,11–16,19–25,27]. In addition to surgical treatment, 10–15 mg/kg/day albendazole was regularly given during3 months in our cases. No side-effects related with alben-dazole was determined in our cases. In the series of Ersa-hin [7] including 19 children who underwent surgery forintracranial hydatid cysts recurrence was seen only in 2patients. Ciurea et al. [15], in a series of 27 children withcerebral hydatid cysts have 11 cases of recurrence(40.7%) due to cyst rupture at surgery. Only in two ofour case of hydatid cyst, recurrence was determined inthe follow-up.
Hydatid cyst is still a serious disease in Turkey.Proper treatment is absolutely necessary and thesepatients should be observed for a long time, regardingto recurrences and complications. And, we must givemore importance to environmental health and protec-tive health.
ultiple intracranial cyst hydatid disease: ..., Brain Dev (2008),

6 H. Per et al. / Brain & Development xxx (2008) xxx–xxx
ARTICLE IN PRESS
References
[1] Carrea R, Dowling Jr E, Guevara JA. Surgical treatment ofhydatid cysts of the central nervous system in pediatric age(Dowling’s technique). Childs Brain 1975;1:4–21.
[2] Cataltepe O, Colak A, Ozcan OE, Ozgen T. Intracranial hydatidcysts: experience with surgical treatment in 120 patients. Neuro-chirurgia 1992;35:108–11.
[3] Turgut M. Intracranial hydatidosis in Turkey: its clinical presen-tation, diagnostic studies surgical management, and outcome. Areview of 276 cases. Neurosurg Rev 2001;24:200–8.
[4] Dew HR. Primary cerebral hydatid disease. Aust N Z J Surg1995;24:161–71.
[5] Sahin-Akyar G. Computed tomography and magnetic resonanceimaging findings in cerebral hydatid disease. Radiography2002;8:251–8.
[6] Tuzun M, Altinors N, Arda IS, Hekimoglu B. Cerebral hydatidCT and MR findings. J Clin Imaging 2002;26:353–7.
[7] Ersahin Y, Mutluer S, Guzelbag E. Intracranial hydatid cysts inchildren. Neurosurgery 1993;33:219–25.
[8] Kaya U, Ozden B, Turker K, Tarcan B. Intracranial hydatidcysts. Study of 17 cases. J Neurosurg 1975;42:580–4.
[9] Krajewski R, Stelmasiak Z. Cerebral hydatid cyst in children.Child’s Nerv Syst 1991;7:154–5.
[10] Topal U, Parlak M, Kilic E, Sivri Z, Sadikoglu MY, Tuncel E. CTand MRI findings in cerebral hydatid disease. Eur Radiol1995;5:244–7.
[11] Popli MB, Khudale B. Primary multiple hydatid cysts of thebrain. Australas Radiol 1998;42:90–1.
[12] Yuceer N, Guven MB, Yilmaz H. Multiple hydatid cysts of thebrain: a case report and review of the literature. Neurosurg Rev1998;21:181–4.
[13] Pasaoglu A, Orhon C, Akdemir H. Multiple primary hydatidcysts of the brain. Turk J Pediatr 1989;31:57–61.
[14] Ayres CM, Dawey LM, German WJ. Cerebral hydatidosis.Clinical case report with review of pathogenesis. J Neurosurg1963;20:371–7.
Please cite this article in press as: Per H et al., Primary soliter and mdoi:10.1016/j.braindev.2008.03.009
[15] Ciurea AV, Vasilescu G, Nuteanu L, Carp N. Cerebral hydatidcyst in children. Experience of 27 cases. Child’s Nerv Syst1995;11:679–85.
[16] Ozek M. Complications of central nervous system hydatiddisease. Pediatr Neurosurg 1994;20:84–91.
[17] Mingde Q, Zheshang H. Echinococcosis of the central nervoussystem. Eur Neurol 1981;20:125–31.
[18] Turgut M, Benli K, Eryılmaz M. Secondary multiple intracranialhydatid cysts caused by intracerebral embolism of cardiacechinococcosis: an exceptional case of hydatidosis. J Neurosurg1997;86:714–8.
[19] Onal C, Unal F, Barlas O, Izgi N, Hepgul K, Turantan MI, et al.Long-term follow-up and results of thirty pediatric intracranialhydatid cysts: half a century of experience in the Department ofNeurosurgery of the School of Medicine at the University ofIstanbul (1952–2001). Pediatr Neurosurg 2001;35:72–81.
[20] Gupta S, Desai K, Goel A. Intracranial hydatid cyst: a reportof five cases and review of literature. Neurol India1999;47:214–7.
[21] Nurchi G, Floris F, Montaldo C, Mastio F, Peltz T, Coraddu M.Multiple cerebral hydatid disease: case report with magneticresonance imaging study. Neurosurgery 1992;30:436–8.
[22] Cataltepe O, Tahta K, Colak A, Erbengi A. Primary multiplecerebral hydatid cysts. Neurosurg Rev 1991;14:231–4.
[23] Iplikcioglu AC, Ozer AF, Benli K, Isik N, Erbengi A. Multiplecerebral hydatid cysts: report of two cases. Br J Neurosurg1989;3:217–9.
[24] Sharma A, Abraham J. Multiple giant hydatid cysts of the brain.Case report. J Neurosurg 1982;57:413–5.
[25] Kurtsoy A, Oktem S, Koc K, Akdemir H, Menku A. Successfulsurgical treatment of a thalamic hydatid cyst with contralateraltranscallosal approach. Pediatr Neurosurg 1999;31:96–9.
[26] El Shamam O, Amer T, Atta MA. Magnetic resonance imaging ofsimple and infected hydatid cysts of the brain. Magn ResonImaging 2001;19:965–74.
[27] Kocaman S, Ersahin Y, Mutluer S. Cerebral hydatid cysts inchildren. J Neurosci Nurs 1999;31:270–7.
ultiple intracranial cyst hydatid disease: ..., Brain Dev (2008),
Copyright © 2022 FDOKUMEN




















