Uncommon locations of hydatid cysts Pictorial review
15
Pictorial Review UNCOMMON LOCATIONS OF HYDATID CYSTS D. A. KıRES ¸ I, A. KARABACAKOG ˘ LU, K. O ¨ DEV and S. KARAKO ¨ SE Selcuk University Meram Medical Faculty, Department of Radiology, Konya, Turkey. Key words: Hydatid, unusual loca- lization, imaging. Correspondence: Demet Aydog ˘ du Kıres ¸ i, Department of Radiology, Selcuk University Meram Medical Faculty, 42080, Konya, Turkey. Fax þ90 332 3232641. E-mail: [email protected] Accepted for publication 1 August 2003. Abstract Hydatid disease is endemic in many parts of the world. It may develop in almost any part of the body. The location is mostly hepatic (75%) and pulmonary (15%), and only 10% occur in the rest of the body. In this article, the various imaging findings of hydatid cysts in unusual localizations are reviewed, based on our experience. Findings in brain, cavernous sinus, submandibular gland, thy- roid gland, heart, pleura, chest wall, retrocrural tissue, kidney, spleen, pancreas, peritoneal cavity and inguinal canal, breast, bone and soft tissue are discussed. Hydatid disease (HD) is prevalent and widespread in most sheep-raising countries in Asia, Australia, South America, Near East, and southern Europe. HD caused by Echinococcus granulosus (EG) is often manifested by a slowly growing cystic mass. Two classes of parasites are mainly involved: Cestoidea (flatworms, tapeworms) and Nematoda (roundworms). EG is a tapeworm and adult tapeworms live in the intestinal tract of infected dogs (6, 12, 22). Its eggs are excreted in the dog’s feces and swallowed by the intermediate hosts – sheep, cattle, goats, or humans. Humans may con- tract the infection either by direct contact with a dog or by ingestion of foods or fluids contaminated by the eggs. After ingestion, the eggs are freed from their coating and larvae penetrate the mucosa of the jejunum reaching through the venous and lymph- atic channels to every region of the body where they transform into small cysts. The cysts may be single or multiple, uni- or multiloculated, and thin or thick walled. A hydatid cyst has three layers. The outer layer is the pericyst, which is composed of a modi- fied host cell. The middle, or laminated, membrane is acellular. The inner layer, or endocyst, is produced by the parasite itself. More specific signs include calcification of the cyst wall, presence of daughter cysts, and membrane detachment. However, hydatid cysts with unusual localizations may cause serious problems in the differential diag- nosis. Radiological signs are usually non-specific, but serologic tests may help in the diagnosis (12). It may lodge in the liver, or pass to the lungs or other organs. It has been known to affect any organ in the body including brain, bone, spleen, kidney and pancreas. In this article, the various imaging findings of hydatid cysts with unusual localizations are reviewed, based on our experience. Acta Radiologica 44 (2003) 622–636 Copyright # Acta Radiologica 2003 Printed in Denmark . All rights reserved ACTA RADIOLOGICA ISSN 0284-1851 622
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Uncommon locations of hydatid cysts Pictorial review
Pictorial Review
UNCOMMON LOCATIONS OF HYDATID CYSTS
D. A. KıRESI, A. KARABACAKOGLU, K. ODEV and S. KARAKOSE
Selcuk University Meram Medical Faculty, Department of Radiology, Konya, Turkey.
Key words: Hydatid, unusual loca-lization, imaging.
Correspondence: Demet AydogduKıresi, Department of Radiology,Selcuk University Meram MedicalFaculty, 42080, Konya, Turkey.Fax þ90 332 3232641.E-mail: [email protected]
Accepted for publication 1 August 2003.
Abstract
Hydatid disease is endemic in many parts of the world. It may develop in almostany part of the body. The location is mostly hepatic (75%) and pulmonary(15%), and only 10% occur in the rest of the body. In this article, the variousimaging findings of hydatid cysts in unusual localizations are reviewed, based onour experience. Findings in brain, cavernous sinus, submandibular gland, thy-roid gland, heart, pleura, chest wall, retrocrural tissue, kidney, spleen, pancreas,peritoneal cavity and inguinal canal, breast, bone and soft tissue are discussed.
Hydatid disease (HD) is prevalent and widespreadin most sheep-raising countries in Asia, Australia,South America, Near East, and southern Europe.HD caused by Echinococcus granulosus (EG) isoften manifested by a slowly growing cystic mass.Two classes of parasites are mainly involved:Cestoidea (flatworms, tapeworms) and Nematoda(roundworms). EG is a tapeworm and adulttapeworms live in the intestinal tract of infecteddogs (6, 12, 22). Its eggs are excreted in the dog’sfeces and swallowed by the intermediate hosts –sheep, cattle, goats, or humans. Humans may con-tract the infection either by direct contact with adog or by ingestion of foods or fluids contaminatedby the eggs. After ingestion, the eggs are freed fromtheir coating and larvae penetrate the mucosa of thejejunum reaching through the venous and lymph-atic channels to every region of the body where theytransform into small cysts. The cysts may be single
or multiple, uni- or multiloculated, and thin or thickwalled. A hydatid cyst has three layers. The outerlayer is the pericyst, which is composed of a modi-fied host cell. The middle, or laminated, membraneis acellular. The inner layer, or endocyst, is producedby the parasite itself. More specific signs includecalcification of the cyst wall, presence of daughtercysts, and membrane detachment. However,hydatid cysts with unusual localizations maycause serious problems in the differential diag-nosis. Radiological signs are usually non-specific,but serologic tests may help in the diagnosis (12).It may lodge in the liver, or pass to the lungsor other organs. It has been known to affectany organ in the body including brain, bone,spleen, kidney and pancreas. In this article, thevarious imaging findings of hydatid cysts withunusual localizations are reviewed, based on ourexperience.
Acta Radiologica 44 (2003) 622–636 Copyright # Acta Radiologica 2003
Printed in Denmark . All rights reservedA C T A R A D I O L O G I C A
ISSN 0284-1851
622

Brain
Cerebral HD represents only 2% of all cerebralspace-occupying lesions even in the countrieswhere the disease is endemic. Cerebral hydatid dis-ease is most frequently supratentorial, involving themiddle cerebral arterial territory. Most commonly,cerebral HD shows signs and symptoms of raisedintracranial pressure, which include headache,vomiting, papil edema, or diminution of vision (16).Computed tomography (CT) and MR imaging
(MRI) show a large, well-defined, round or oval,non-enhanced cystic structure of cerebro-spinal fluiddensity or intensity. There is usually neither sur-rounding edema nor calcification, although there isconsiderable mass effect and there may be hydroce-phalus (Fig. 1) (10).Hydatid cysts should be differentiated from other
cystic lesions including arachnoid cysts, porence-phalic cysts, cystic tumors and abscesses. The ara-chnoid cyst is not round or surrounded by braintissue, as in the HD while porencepalic cysts usuallycommunicates with the ventricle. Cystic tumorsusually have a soft tissue component whichenhances after intravenous contrast, whereas anabscess usually shows enhancement and perifocaledema (12).
Parasellar Epidural
Intracranial extracerebral HD may occur in threeforms (4): (i) cranial: usually the bony spongiosa isthe first to be involved; (ii) cranial extradural: the
extradural space may be infected by embolization ofscolices or embryos via blood vessels, by extrusionof intracerebral cysts via healthy dura mater or byerosion of osseous hydatid into the extraduralspace; (iii) combined: there may be simultaneousintracerebral, extradural, and bony cysts. Of thethree forms, extradural HD forms an extremelyrare group. This is because the physiologic flow ofblood to the brain is mainly through the internalcarotid system, so the likelihood of the larvae trav-elling through the external carotid system is verylow (25). Moreover, the extradural vessels that maycarry the hexacanth embryo or scolices to the spacesare few and virtually non-existent. Because the loca-tion and the CT characteristics are so different fromthe other cysts, a preoperative diagnosis is difficultto make (13). An extradural location may beresponsible for the lobulated appearance on CT(Fig. 2) (7). An infected hydatid cyst with a well-defined capsule may have clearly demarcated bor-ders with or without rim enhancement.
Submandibular
Hydatid cysts in the maxillofacial region areextremely rare, with a prevalence of 2%. Thesecommonly appear as cystic lesions located in themandible, maxillary sinus, orbit, infratemporalfossa, pterygopalatine fossa, parapharyngealspace, tongue, parotid gland and submandibularsalivary gland (6, 22). The diagnosis of Echinococ-cus infestation is based on the history of the patient,
Fig. 1. Hydatid cyst of the brain in a 25-year-old woman with a headache, papiledema, and ataxia. Non-enhanced computed tomography (CT)shows a large, well-defined, unilocular cystic mass compressing the right lateral ventricle in the parietal lobe without perifocal edema.
UNCOMMON LOCATIONS OF HYDATID CYSTS
623
a
b
c
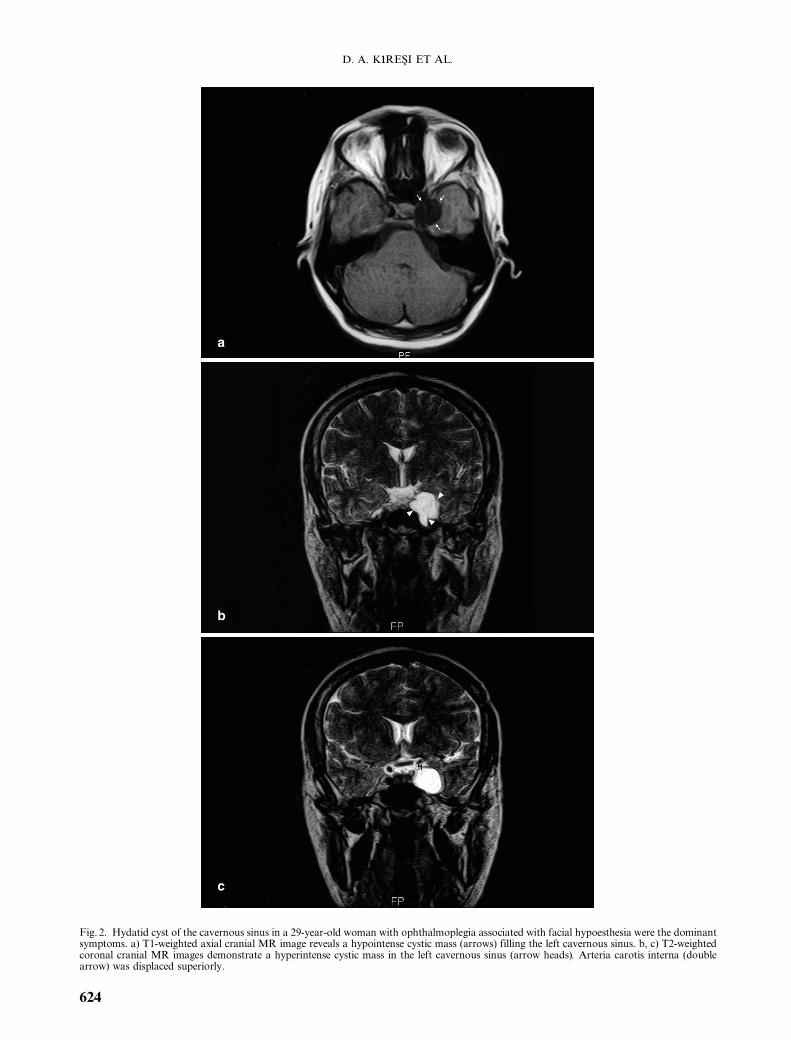
Fig. 2. Hydatid cyst of the cavernous sinus in a 29-year-old woman with ophthalmoplegia associated with facial hypoesthesia were the dominantsymptoms. a) T1-weighted axial cranial MR image reveals a hypointense cystic mass (arrows) filling the left cavernous sinus. b, c) T2-weightedcoronal cranial MR images demonstrate a hyperintense cystic mass in the left cavernous sinus (arrow heads). Arteria carotis interna (doublearrow) was displaced superiorly.
D. A. KıRESI ET AL.
624
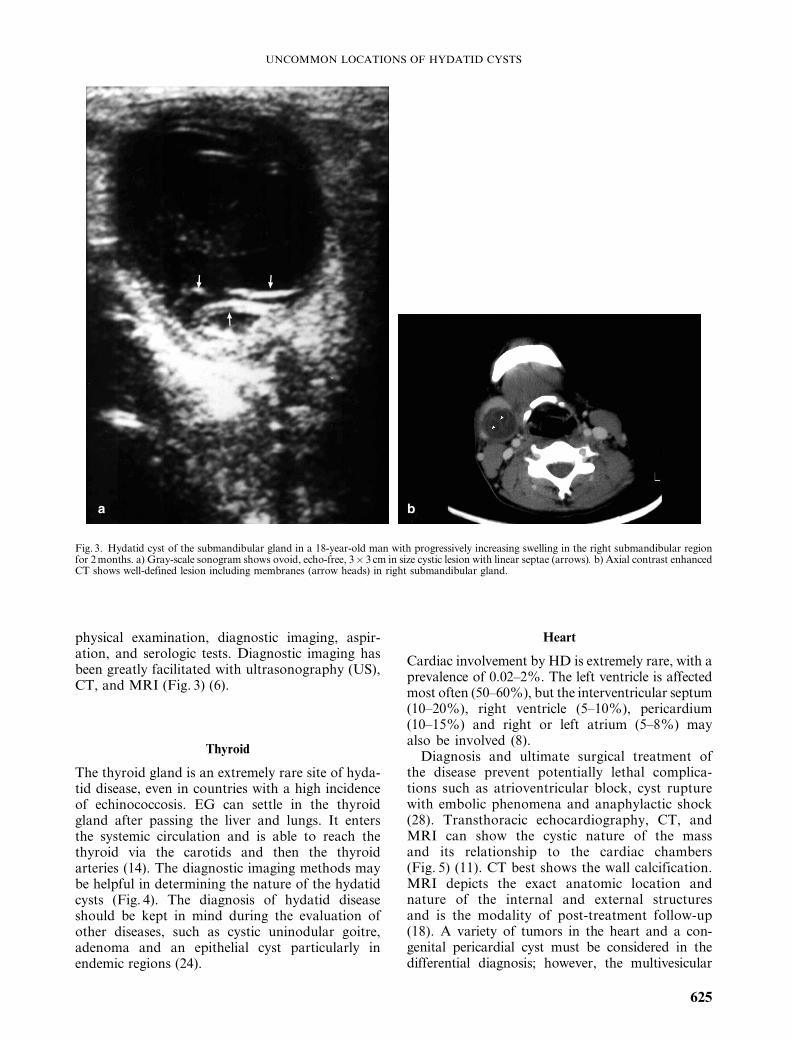
physical examination, diagnostic imaging, aspir-ation, and serologic tests. Diagnostic imaging hasbeen greatly facilitated with ultrasonography (US),CT, and MRI (Fig. 3) (6).
Thyroid
The thyroid gland is an extremely rare site of hyda-tid disease, even in countries with a high incidenceof echinococcosis. EG can settle in the thyroidgland after passing the liver and lungs. It entersthe systemic circulation and is able to reach thethyroid via the carotids and then the thyroidarteries (14). The diagnostic imaging methods maybe helpful in determining the nature of the hydatidcysts (Fig. 4). The diagnosis of hydatid diseaseshould be kept in mind during the evaluation ofother diseases, such as cystic uninodular goitre,adenoma and an epithelial cyst particularly inendemic regions (24).
Heart
Cardiac involvement by HD is extremely rare, with aprevalence of 0.02–2%. The left ventricle is affectedmost often (50–60%), but the interventricular septum(10–20%), right ventricle (5–10%), pericardium(10–15%) and right or left atrium (5–8%) mayalso be involved (8).Diagnosis and ultimate surgical treatment of
the disease prevent potentially lethal complica-tions such as atrioventricular block, cyst rupturewith embolic phenomena and anaphylactic shock(28). Transthoracic echocardiography, CT, andMRI can show the cystic nature of the massand its relationship to the cardiac chambers(Fig. 5) (11). CT best shows the wall calcification.MRI depicts the exact anatomic location andnature of the internal and external structuresand is the modality of post-treatment follow-up(18). A variety of tumors in the heart and a con-genital pericardial cyst must be considered in thedifferential diagnosis; however, the multivesicular
a b
Fig. 3. Hydatid cyst of the submandibular gland in a 18-year-old man with progressively increasing swelling in the right submandibular regionfor 2months. a) Gray-scale sonogram shows ovoid, echo-free, 3� 3 cm in size cystic lesion with linear septae (arrows). b) Axial contrast enhancedCT shows well-defined lesion including membranes (arrow heads) in right submandibular gland.
UNCOMMON LOCATIONS OF HYDATID CYSTS
625

a
b
c
Fig. 5. A cardiac hydatid cyst in a 20-year-old woman with chest pain. a) Transthoracic ultrasonography shows multivesicular (stars) appearanceof the cystic mass. b, c) Contrast-enhanced CT demonstrates cystic mass (arrow head) in the interventricular septum (arrows).
Fig. 4. Hydatid cyst of the thyroid gland in a 32-year-old woman. Contrast enhanced CT shows a well-defined, unilocular cystic mass includingmembranes (arrow head) in the left lobe of the thyroid gland.
D. A. KıRESI ET AL.
626
nature of the cystic mass can provide the truediagnosis.
Intrapleural and Chest Wall
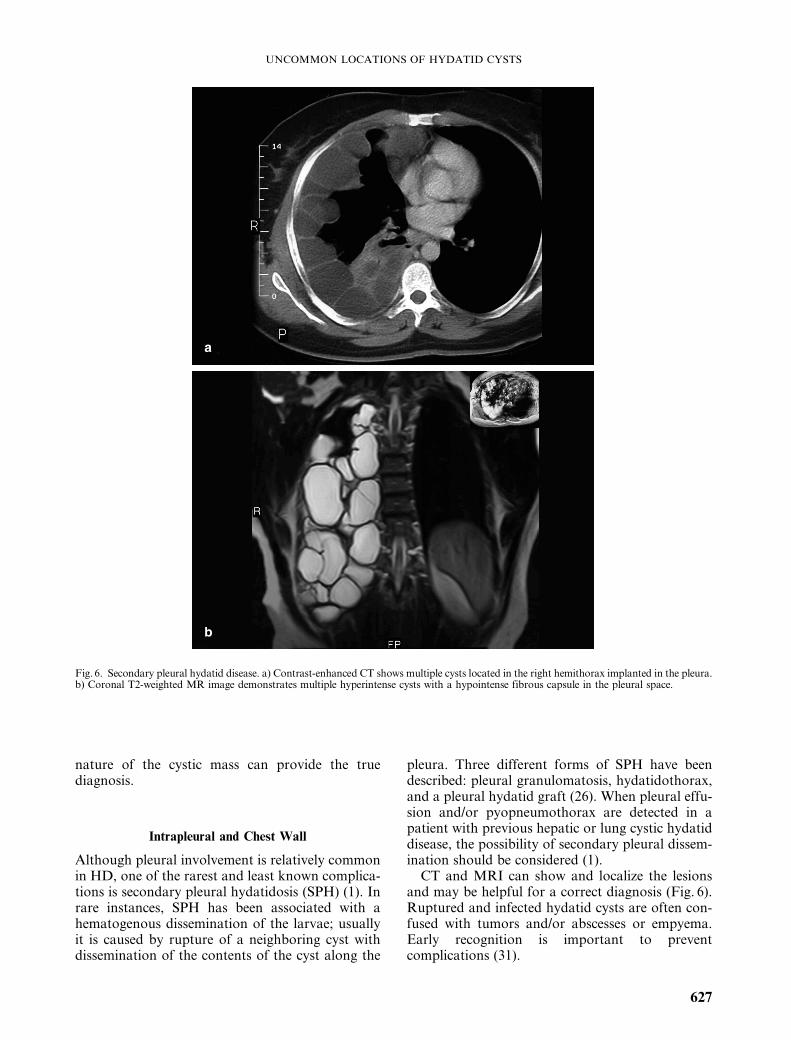
Although pleural involvement is relatively commonin HD, one of the rarest and least known complica-tions is secondary pleural hydatidosis (SPH) (1). Inrare instances, SPH has been associated with ahematogenous dissemination of the larvae; usuallyit is caused by rupture of a neighboring cyst withdissemination of the contents of the cyst along the
pleura. Three different forms of SPH have beendescribed: pleural granulomatosis, hydatidothorax,and a pleural hydatid graft (26). When pleural effu-sion and/or pyopneumothorax are detected in apatient with previous hepatic or lung cystic hydatiddisease, the possibility of secondary pleural dissem-ination should be considered (1).CT and MRI can show and localize the lesions
and may be helpful for a correct diagnosis (Fig. 6).Ruptured and infected hydatid cysts are often con-fused with tumors and/or abscesses or empyema.Early recognition is important to preventcomplications (31).
a
b
Fig. 6. Secondary pleural hydatid disease. a) Contrast-enhanced CT shows multiple cysts located in the right hemithorax implanted in the pleura.b) Coronal T2-weighted MR image demonstrates multiple hyperintense cysts with a hypointense fibrous capsule in the pleural space.
UNCOMMON LOCATIONS OF HYDATID CYSTS
627
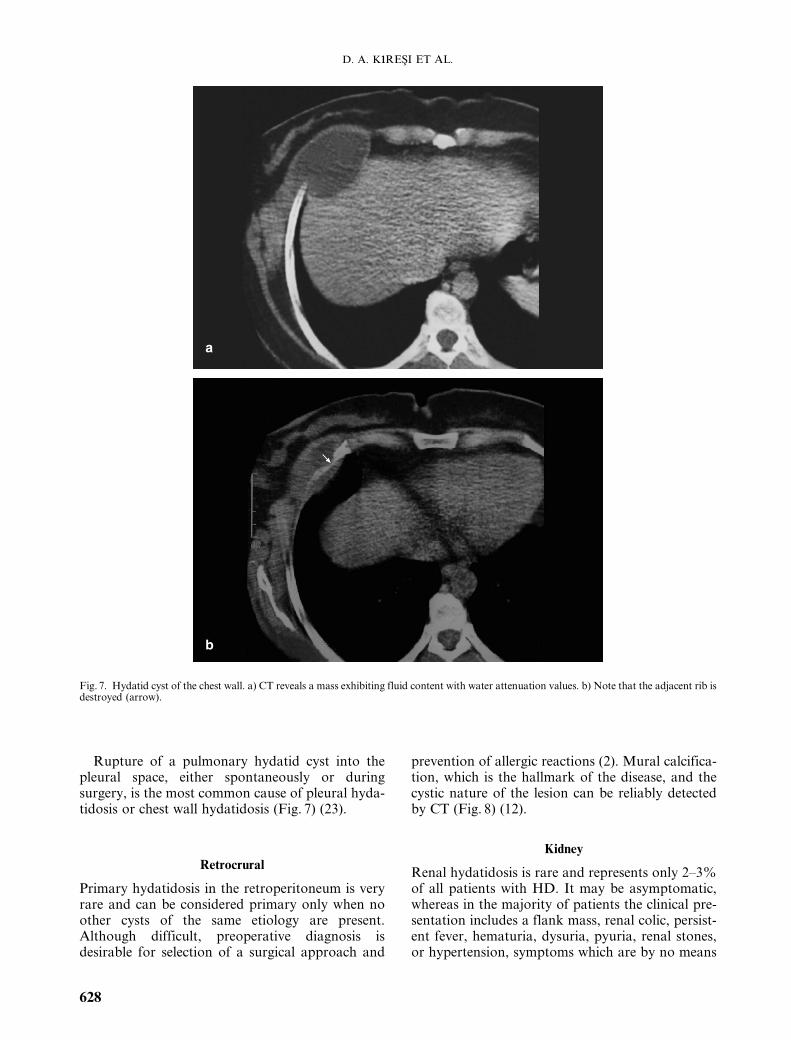
Rupture of a pulmonary hydatid cyst into thepleural space, either spontaneously or duringsurgery, is the most common cause of pleural hyda-tidosis or chest wall hydatidosis (Fig. 7) (23).
Retrocrural
Primary hydatidosis in the retroperitoneum is veryrare and can be considered primary only when noother cysts of the same etiology are present.Although difficult, preoperative diagnosis isdesirable for selection of a surgical approach and
prevention of allergic reactions (2). Mural calcifica-tion, which is the hallmark of the disease, and thecystic nature of the lesion can be reliably detectedby CT (Fig. 8) (12).
Kidney
Renal hydatidosis is rare and represents only 2–3%of all patients with HD. It may be asymptomatic,whereas in the majority of patients the clinical pre-sentation includes a flank mass, renal colic, persist-ent fever, hematuria, dysuria, pyuria, renal stones,or hypertension, symptoms which are by no means
b
a
Fig. 7. Hydatid cyst of the chest wall. a) CT reveals a mass exhibiting fluid content with water attenuation values. b) Note that the adjacent rib isdestroyed (arrow).
D. A. KıRESI ET AL.
628

a
b
c
Fig. 8. Retrocrural hydatid cyst in a 69-year-old woman. a) Contrast-enhanced CT demonstrates a hydatid cyst (star) in the retrocrural region.b, c) T2-weighted coronal MR images show a retrocrural cystic lesion with a hypointense fibrous capsula (black arrows) and an intrapleuralhydatid cyst in the same patient.
UNCOMMON LOCATIONS OF HYDATID CYSTS
629
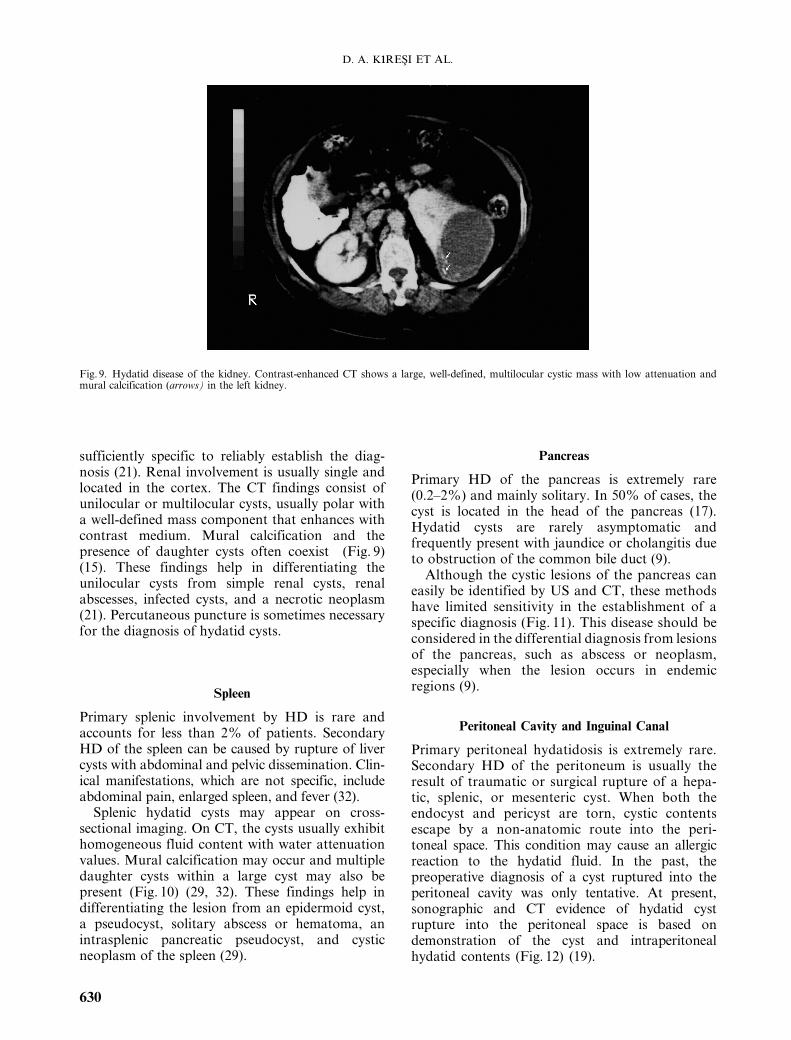
sufficiently specific to reliably establish the diag-nosis (21). Renal involvement is usually single andlocated in the cortex. The CT findings consist ofunilocular or multilocular cysts, usually polar witha well-defined mass component that enhances withcontrast medium. Mural calcification and thepresence of daughter cysts often coexist (Fig. 9)(15). These findings help in differentiating theunilocular cysts from simple renal cysts, renalabscesses, infected cysts, and a necrotic neoplasm(21). Percutaneous puncture is sometimes necessaryfor the diagnosis of hydatid cysts.
Spleen
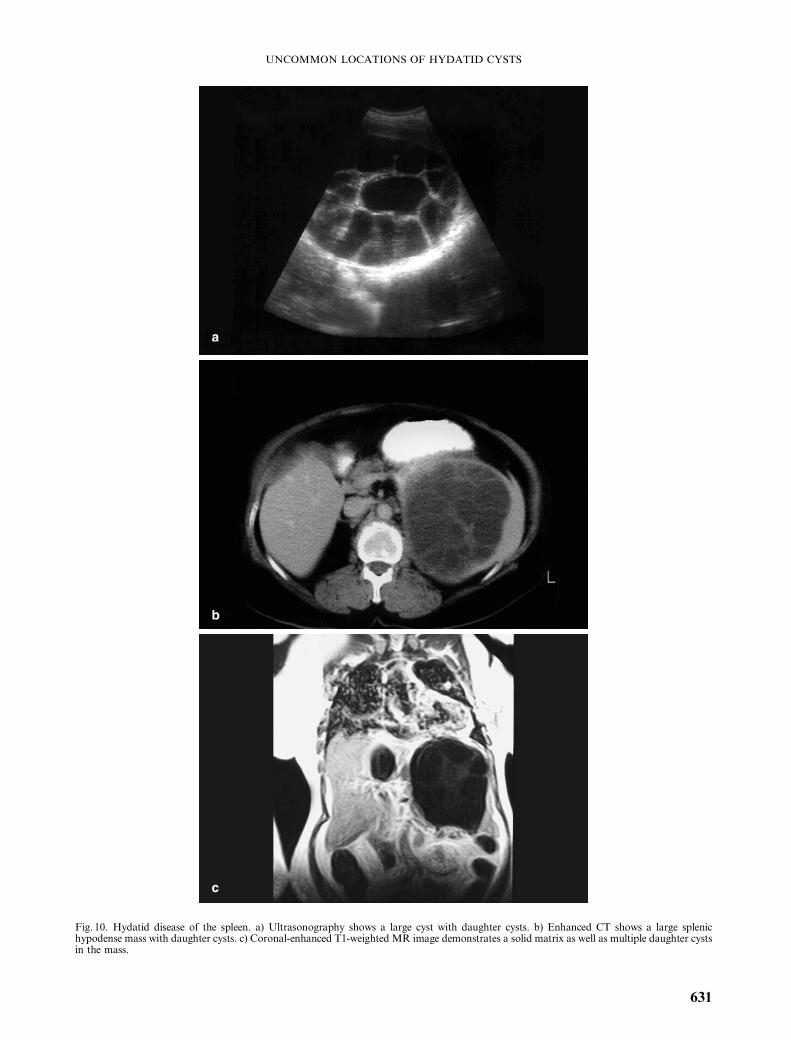
Primary splenic involvement by HD is rare andaccounts for less than 2% of patients. SecondaryHD of the spleen can be caused by rupture of livercysts with abdominal and pelvic dissemination. Clin-ical manifestations, which are not specific, includeabdominal pain, enlarged spleen, and fever (32).
Splenic hydatid cysts may appear on cross-sectional imaging. On CT, the cysts usually exhibithomogeneous fluid content with water attenuationvalues. Mural calcification may occur and multipledaughter cysts within a large cyst may also bepresent (Fig. 10) (29, 32). These findings help indifferentiating the lesion from an epidermoid cyst,a pseudocyst, solitary abscess or hematoma, anintrasplenic pancreatic pseudocyst, and cysticneoplasm of the spleen (29).
Pancreas
Primary HD of the pancreas is extremely rare(0.2–2%) and mainly solitary. In 50% of cases, thecyst is located in the head of the pancreas (17).Hydatid cysts are rarely asymptomatic andfrequently present with jaundice or cholangitis dueto obstruction of the common bile duct (9).
Although the cystic lesions of the pancreas caneasily be identified by US and CT, these methodshave limited sensitivity in the establishment of aspecific diagnosis (Fig. 11). This disease should beconsidered in the differential diagnosis from lesionsof the pancreas, such as abscess or neoplasm,especially when the lesion occurs in endemicregions (9).
Peritoneal Cavity and Inguinal Canal
Primary peritoneal hydatidosis is extremely rare.Secondary HD of the peritoneum is usually theresult of traumatic or surgical rupture of a hepa-tic, splenic, or mesenteric cyst. When both theendocyst and pericyst are torn, cystic contentsescape by a non-anatomic route into the peri-toneal space. This condition may cause an allergicreaction to the hydatid fluid. In the past, thepreoperative diagnosis of a cyst ruptured into theperitoneal cavity was only tentative. At present,sonographic and CT evidence of hydatid cystrupture into the peritoneal space is based ondemonstration of the cyst and intraperitonealhydatid contents (Fig. 12) (19).
Fig. 9. Hydatid disease of the kidney. Contrast-enhanced CT shows a large, well-defined, multilocular cystic mass with low attenuation andmural calcification (arrows) in the left kidney.
D. A. KıRESI ET AL.
630
a
b
c
Fig. 10. Hydatid disease of the spleen. a) Ultrasonography shows a large cyst with daughter cysts. b) Enhanced CT shows a large splenichypodense mass with daughter cysts. c) Coronal-enhanced T1-weighted MR image demonstrates a solid matrix as well as multiple daughter cystsin the mass.
UNCOMMON LOCATIONS OF HYDATID CYSTS
631

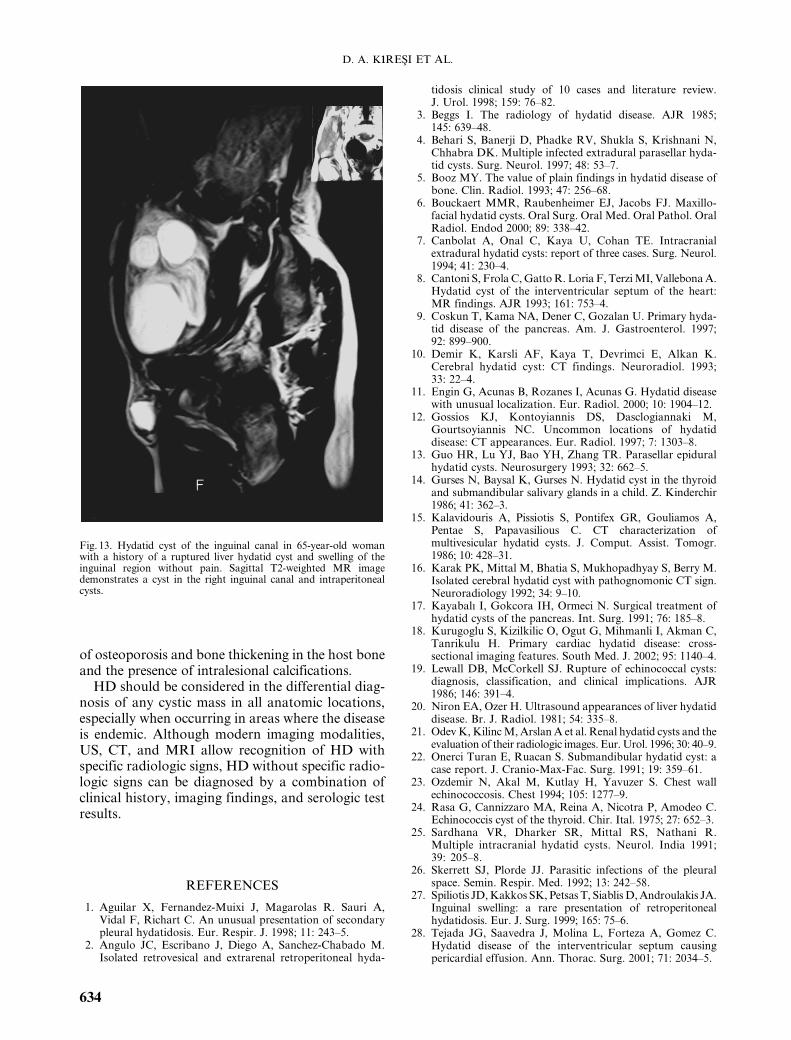
Inguinal cysts may cause inguinal pain andswelling mimicking an irreducible inguinal hernia;however, careful examination shows the intra-abdominal disease (27). The diagnosis is facilitatedby ultrasonography, CT and MRI as the examin-ations of choice in such cases (Fig. 13).
Breast
The breast is a rare location for a hydatid cyst; itaccounts for 0.2% of all occurrences. The ring-shaped structures inside the lesion are a reported
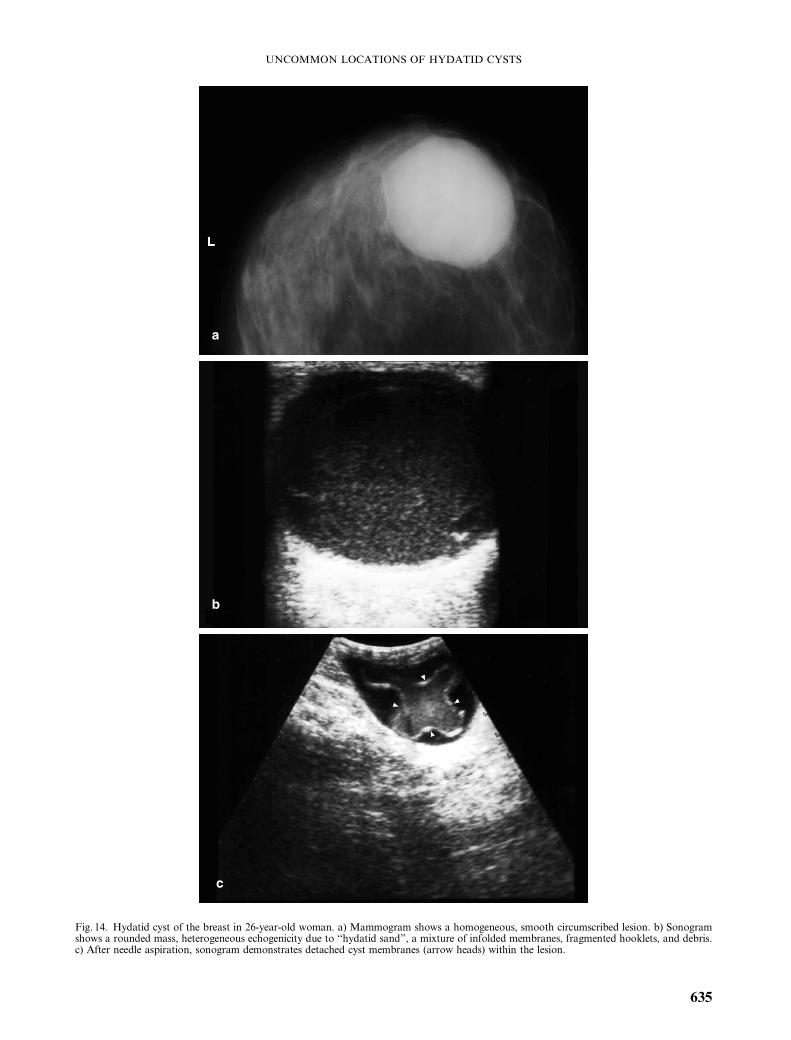
mammographic finding. When ring-shaped struc-tures are not present, the imaging features of ahydatid cyst are non-specific (30). The lesion isusually seen as a circumscribed mass. Hydatidsand, fluid-level in the mammary hydatid cystmay be seen by sonography (Fig. 14). The diag-nosis of a hydatid cyst of the breast based onresults of needle aspiration has previously beenreported, and no complication has beendescribed (20). The differential diagnosis includesa cyst, fibroadenoma, a phyllodes tumor, andcircumscribed carcinoma (30).
b
a
Fig. 11. Hydatid disease of the pancreas in a symptom-less patient. a) Ultrasonography shows a well-defined cystic lesion (star) without septae inthe body of the pancreas. b) Contrast-enhanced CT shows a well-defined mass with fluid contents showing water attenuation values in the bodyof the pancreas.
D. A. KıRESI ET AL.
632

Musculoskeletal System
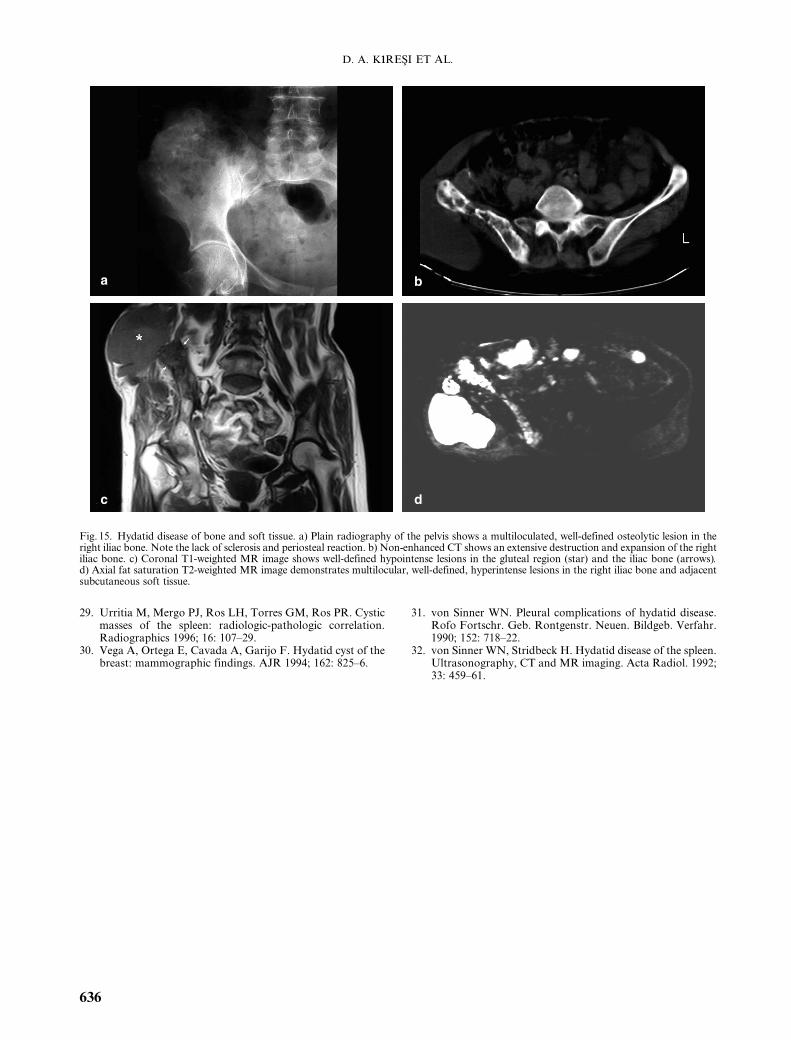
Skeletal involvement by primary HD is found inonly 0.5–4% of patients. HD in bones occursmostly in richly vascularized areas such as verte-brae, long-bone epiphyses, ilium, skull, ribs, andsoft tissue extension is frequent. Lesions in bonesmay present with pathological fractures showing noevidence of repair (12). In plain films, HD in boneproduces a well-defined, multiloculated, expansile,osteolytic lesion. Sclerosis and a periosteal reactionare uncommon (3). The CT appearances of bonelesions are similar to those demonstrated on plain
films. A well-defined, typically multiloculated,osteolytic lesion sometimes with coarse trabeculaeis usually seen, giving a honeycomb appearance,which is accompanied by expansion of the bone,thinning of its cortex, and extension into adjacentsoft tissue. CT and MRI are quite variable in therecognition of the extraosseous spread of the HDwithin the tissue (Fig. 15) (5). The differentialdiagnosis of a cystic soft tissue mass includes anabscess, chronic hematoma, a synovial cyst, and anecrotic malignant soft tissue tumor (11). Signsmeaningful for a differential diagnosis include lack
b
a
Fig. 12. Intraperitoneal hydatid cysts in a 47–year-old woman with a history of ruptured liver hydatid cysts. a) Contrast-enhanced CT shows athick-walled hydatid cyst with multiple daughter cysts. b) Sagittal T2-weighted MR image demonstrates an intraperitoneal cyst with multipledaughter cysts.
UNCOMMON LOCATIONS OF HYDATID CYSTS
633
of osteoporosis and bone thickening in the host boneand the presence of intralesional calcifications.
HD should be considered in the differential diag-nosis of any cystic mass in all anatomic locations,especially when occurring in areas where the diseaseis endemic. Although modern imaging modalities,US, CT, and MRI allow recognition of HD withspecific radiologic signs, HD without specific radio-logic signs can be diagnosed by a combination ofclinical history, imaging findings, and serologic testresults.
REFERENCES
1. Aguilar X, Fernandez-Muixi J, Magarolas R. Sauri A,Vidal F, Richart C. An unusual presentation of secondarypleural hydatidosis. Eur. Respir. J. 1998; 11: 243–5.
2. Angulo JC, Escribano J, Diego A, Sanchez-Chabado M.Isolated retrovesical and extrarenal retroperitoneal hyda-
tidosis clinical study of 10 cases and literature review.J. Urol. 1998; 159: 76–82.
3. Beggs I. The radiology of hydatid disease. AJR 1985;145: 639–48.
4. Behari S, Banerji D, Phadke RV, Shukla S, Krishnani N,Chhabra DK. Multiple infected extradural parasellar hyda-tid cysts. Surg. Neurol. 1997; 48: 53–7.
5. Booz MY. The value of plain findings in hydatid disease ofbone. Clin. Radiol. 1993; 47: 256–68.
6. Bouckaert MMR, Raubenheimer EJ, Jacobs FJ. Maxillo-facial hydatid cysts. Oral Surg. Oral Med. Oral Pathol. OralRadiol. Endod 2000; 89: 338–42.
7. Canbolat A, Onal C, Kaya U, Cohan TE. Intracranialextradural hydatid cysts: report of three cases. Surg. Neurol.1994; 41: 230–4.
8. Cantoni S, Frola C,GattoR. Loria F, TerziMI, VallebonaA.Hydatid cyst of the interventricular septum of the heart:MR findings. AJR 1993; 161: 753–4.
9. Coskun T, Kama NA, Dener C, Gozalan U. Primary hyda-tid disease of the pancreas. Am. J. Gastroenterol. 1997;92: 899–900.
10. Demir K, Karsli AF, Kaya T, Devrimci E, Alkan K.Cerebral hydatid cyst: CT findings. Neuroradiol. 1993;33: 22–4.
11. Engin G, Acunas B, Rozanes I, Acunas G. Hydatid diseasewith unusual localization. Eur. Radiol. 2000; 10: 1904–12.
12. Gossios KJ, Kontoyiannis DS, Dasclogiannaki M,Gourtsoyiannis NC. Uncommon locations of hydatiddisease: CT appearances. Eur. Radiol. 1997; 7: 1303–8.
13. Guo HR, Lu YJ, Bao YH, Zhang TR. Parasellar epiduralhydatid cysts. Neurosurgery 1993; 32: 662–5.
14. Gurses N, Baysal K, Gurses N. Hydatid cyst in the thyroidand submandibular salivary glands in a child. Z. Kinderchir1986; 41: 362–3.
15. Kalavidouris A, Pissiotis S, Pontifex GR, Gouliamos A,Pentae S, Papavasilious C. CT characterization ofmultivesicular hydatid cysts. J. Comput. Assist. Tomogr.1986; 10: 428–31.
16. Karak PK, Mittal M, Bhatia S, Mukhopadhyay S, Berry M.Isolated cerebral hydatid cyst with pathognomonic CT sign.Neuroradiology 1992; 34: 9–10.
17. Kayabalı I, Gokcora IH, Ormeci N. Surgical treatment ofhydatid cysts of the pancreas. Int. Surg. 1991; 76: 185–8.
18. Kurugoglu S, Kizilkilic O, Ogut G, Mihmanli I, Akman C,Tanrikulu H. Primary cardiac hydatid disease: cross-sectional imaging features. South Med. J. 2002; 95: 1140–4.
19. Lewall DB, McCorkell SJ. Rupture of echinococcal cysts:diagnosis, classification, and clinical implications. AJR1986; 146: 391–4.
20. Niron EA, Ozer H. Ultrasound appearances of liver hydatiddisease. Br. J. Radiol. 1981; 54: 335–8.
21. OdevK,KilincM,ArslanA et al. Renal hydatid cysts and theevaluation of their radiologic images. Eur. Urol. 1996; 30: 40–9.
22. Onerci Turan E, Ruacan S. Submandibular hydatid cyst: acase report. J. Cranio-Max-Fac. Surg. 1991; 19: 359–61.
23. Ozdemir N, Akal M, Kutlay H, Yavuzer S. Chest wallechinococcosis. Chest 1994; 105: 1277–9.
24. Rasa G, Cannizzaro MA, Reina A, Nicotra P, Amodeo C.Echinococcis cyst of the thyroid. Chir. Ital. 1975; 27: 652–3.
25. Sardhana VR, Dharker SR, Mittal RS, Nathani R.Multiple intracranial hydatid cysts. Neurol. India 1991;39: 205–8.
26. Skerrett SJ, Plorde JJ. Parasitic infections of the pleuralspace. Semin. Respir. Med. 1992; 13: 242–58.
27. Spiliotis JD,Kakkos SK, Petsas T, SiablisD,Androulakis JA.Inguinal swelling: a rare presentation of retroperitonealhydatidosis. Eur. J. Surg. 1999; 165: 75–6.
28. Tejada JG, Saavedra J, Molina L, Forteza A, Gomez C.Hydatid disease of the interventricular septum causingpericardial effusion. Ann. Thorac. Surg. 2001; 71: 2034–5.
Fig. 13. Hydatid cyst of the inguinal canal in 65-year-old womanwith a history of a ruptured liver hydatid cyst and swelling of theinguinal region without pain. Sagittal T2-weighted MR imagedemonstrates a cyst in the right inguinal canal and intraperitonealcysts.
D. A. KıRESI ET AL.
634
a
b
c
Fig. 14. Hydatid cyst of the breast in 26-year-old woman. a) Mammogram shows a homogeneous, smooth circumscribed lesion. b) Sonogramshows a rounded mass, heterogeneous echogenicity due to ‘‘hydatid sand’’, a mixture of infolded membranes, fragmented hooklets, and debris.c) After needle aspiration, sonogram demonstrates detached cyst membranes (arrow heads) within the lesion.
UNCOMMON LOCATIONS OF HYDATID CYSTS
635
29. Urritia M, Mergo PJ, Ros LH, Torres GM, Ros PR. Cysticmasses of the spleen: radiologic-pathologic correlation.Radiographics 1996; 16: 107–29.
30. Vega A, Ortega E, Cavada A, Garijo F. Hydatid cyst of thebreast: mammographic findings. AJR 1994; 162: 825–6.
31. von Sinner WN. Pleural complications of hydatid disease.Rofo Fortschr. Geb. Rontgenstr. Neuen. Bildgeb. Verfahr.1990; 152: 718–22.
32. von Sinner WN, Stridbeck H. Hydatid disease of the spleen.Ultrasonography, CT and MR imaging. Acta Radiol. 1992;33: 459–61.
a
c d
b
Fig. 15. Hydatid disease of bone and soft tissue. a) Plain radiography of the pelvis shows a multiloculated, well-defined osteolytic lesion in theright iliac bone. Note the lack of sclerosis and periosteal reaction. b) Non-enhanced CT shows an extensive destruction and expansion of the rightiliac bone. c) Coronal T1-weighted MR image shows well-defined hypointense lesions in the gluteal region (star) and the iliac bone (arrows).d) Axial fat saturation T2-weighted MR image demonstrates multilocular, well-defined, hyperintense lesions in the right iliac bone and adjacentsubcutaneous soft tissue.
D. A. KıRESI ET AL.
636