
HYPONATREMIA AND THE SYNDROME - NCBI
9
[systematic review * examen critique systematique I HYPONATREMIA AND THE SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE ASSOCIATED WITH THE USE OF SELECTIVE SEROTONIN REUPTAKE INHIBITORS: A REVIEW OF SPONTANEOUS REPORTS Barbara A. Liu,* MD, FRCPC; Nicole Mittmann,*t MSc; Sandra R. Knowles,* BScPhm; Neil H. Shear,*t MD, FRCPC . _ | l__l l .I l l - Objective: To review reported cases of hyponatremia and the syndrome of inappropriate secretion of an- tidiuretic hormone (SIADH) associated with the use of selective serotonin reuptake inhibitors (SSRls). Data sources: A search of MEDLINE for reports of hyponatremia and SIADH associated with the use of fluoxetine, fluvoxamine, paroxetine or sertraline published between January 1980 and May 1995. Un- published reports of cases were requested from the pharmaceutical industry, the Ontario Medical Asso- ciation, the Health Protection Branch of Health Canada, the US Food and Drug Administration and the World Health Organization. Data selection and extraction: Spontaneous reports from postmarketing surveillance. Data synthesis: A total of 736 cases of hypernatremia and SIADH associated with SSRI use were reported. Fluoxetine was involved in 554 (75.3%) of the cases, paroxetine in 91 (12.4%), sertraline in 86 (11.7%) and fluvoxamine in 11 (1.5%). Reports of 30 cases were published. The remaining 706 cases were re- ported to monitoring bodies and the pharmaceutical industry. According to information in the pub- lished reports, the median time to onset of hyponatremia was 13 days (range 3 to 120 days). Most (83%) of the published cases involved patients 65 years of age or more, as compared with 74% of the unpublished cases. Conclusion: Elderly people may be at increased risk for hyponatremia associated with SSRI use. Physi- cians caring for elderly patients should be aware of this potentially serious but reversible adverse effect. Further research is required to determine the incidence of this adverse effect, the relative risk of hy- ponatremia and SIADH in different age groups and the risk associated with different SSRI drugs. Objectif: Examiner des cas signales d'hyponatremie et de syndrome d'antidiurese inappropriee lies 'a l'uti- lisation d'inhibiteurs specifiques du recaptage de la serotonine. Sources de donnees: Recherche dans MEDLINE de comptes rendus d'hyponatremie et de syndrome d'antidiurese inappropriee lies 'a l'utilisation de fluoxetine, de fluvoxamine, de paroxetine ou de sertra- line, publies entre janvier 1980 et mai 1995. On a demande des comptes rendus de cas non publies a l'industrie pharmaceutique, 'a l'Association medicale de l'Ontario, 'a la Direction generale de la protec- tion de la sante de Sante Canada, a la Food and Drug Administration des ltats-Unis et 'a l'Organisation mondiale de la sante. Selection et extraction des donnees Rapports spontanes issus des activites de pharmacovigilance. Synthese des donnees On a signale au total 736 cas d'hypernatremie et de syndrome d'antidiurese inap- propriee lies a l'utilisation d'inhibiteurs specifiques du recaptage de la serotonine. La fluoxetine etait im- pliquee dans 554 (75,3 %) des cas, la paroxetine dans 91 (12,4 %), la sertraline dans 86 (11,7 %), et la fluvoxamine dans 11 (1,5 %). Des comptes rendus ont ete publies sur 30 cas. Les 706 cas restants ont et signales aux organismes de surveillance et 'a l'industrie pharmaceutique. Selon les renseignements From *the Division of Clinical Pharmacology, Sunnybrook Health Science Centre, University of Toronto, and tthe Department of Pharmacology, University of Toronto, Toronto, Ont. This article was presented in part at the International Conference on Pharmacoepidemiology, Aug. 27-30, 1995, Montreal, Que. Reprint requests to: Dr. Neil H. Shear, Division of Clinical Pharmacology, Sunnybrook Health Science Centre, Rm. E240, 2075 BayviewAve., North York ON M4N 3M5 0 1996 Canadian Medical Association (text and abstractresume) CAN MED ASSOC J * SEPT. 1, 1996; 155 (5) 519 <- For prescribing information see page 596
-
Upload
khangminh22 -
Category
Documents
-
view
6 -
download
0
Transcript of HYPONATREMIA AND THE SYNDROME - NCBI

[systematic review * examen critique systematique I
HYPONATREMIA AND THE SYNDROMEOF INAPPROPRIATE SECRETION OF ANTIDIURETIC
HORMONE ASSOCIATED WITH THE USE OF SELECTIVESEROTONIN REUPTAKE INHIBITORS:A REVIEW OF SPONTANEOUS REPORTS
Barbara A. Liu,* MD, FRCPC; Nicole Mittmann,*t MSc; Sandra R. Knowles,* BScPhm; Neil H. Shear,*t MD, FRCPC
._| l _ _ l l .I l l -
Objective: To review reported cases of hyponatremia and the syndrome of inappropriate secretion of an-tidiuretic hormone (SIADH) associated with the use of selective serotonin reuptake inhibitors (SSRls).
Data sources: A search of MEDLINE for reports of hyponatremia and SIADH associated with the use offluoxetine, fluvoxamine, paroxetine or sertraline published between January 1980 and May 1995. Un-published reports of cases were requested from the pharmaceutical industry, the Ontario Medical Asso-ciation, the Health Protection Branch of Health Canada, the US Food and Drug Administration andthe World Health Organization.
Data selection and extraction: Spontaneous reports from postmarketing surveillance.Data synthesis: A total of 736 cases of hypernatremia and SIADH associated with SSRI use were reported.
Fluoxetine was involved in 554 (75.3%) of the cases, paroxetine in 91 (12.4%), sertraline in 86 (11.7%)and fluvoxamine in 11 (1.5%). Reports of 30 cases were published. The remaining 706 cases were re-ported to monitoring bodies and the pharmaceutical industry. According to information in the pub-lished reports, the median time to onset of hyponatremia was 13 days (range 3 to 120 days). Most(83%) of the published cases involved patients 65 years of age or more, as compared with 74% of theunpublished cases.
Conclusion: Elderly people may be at increased risk for hyponatremia associated with SSRI use. Physi-cians caring for elderly patients should be aware of this potentially serious but reversible adverse effect.Further research is required to determine the incidence of this adverse effect, the relative risk of hy-ponatremia and SIADH in different age groups and the risk associated with different SSRI drugs.
Objectif: Examiner des cas signales d'hyponatremie et de syndrome d'antidiurese inappropriee lies 'a l'uti-lisation d'inhibiteurs specifiques du recaptage de la serotonine.
Sources de donnees: Recherche dans MEDLINE de comptes rendus d'hyponatremie et de syndromed'antidiurese inappropriee lies 'a l'utilisation de fluoxetine, de fluvoxamine, de paroxetine ou de sertra-line, publies entre janvier 1980 et mai 1995. On a demande des comptes rendus de cas non publies al'industrie pharmaceutique, 'a l'Association medicale de l'Ontario, 'a la Direction generale de la protec-tion de la sante de Sante Canada, a la Food and Drug Administration des ltats-Unis et 'a l'Organisationmondiale de la sante.
Selection et extraction des donnees Rapports spontanes issus des activites de pharmacovigilance.Synthese des donnees On a signale au total 736 cas d'hypernatremie et de syndrome d'antidiurese inap-
propriee lies a l'utilisation d'inhibiteurs specifiques du recaptage de la serotonine. La fluoxetine etait im-pliquee dans 554 (75,3 %) des cas, la paroxetine dans 91 (12,4 %), la sertraline dans 86 (11,7 %), et lafluvoxamine dans 11 (1,5 %). Des comptes rendus ont ete publies sur 30 cas. Les 706 cas restants ontet signales aux organismes de surveillance et 'a l'industrie pharmaceutique. Selon les renseignements
From *the Division of Clinical Pharmacology, Sunnybrook Health Science Centre, University of Toronto, and tthe Department of Pharmacology, University of Toronto, Toronto, Ont.
This article was presented in part at the International Conference on Pharmacoepidemiology, Aug. 27-30, 1995, Montreal, Que.
Reprint requests to: Dr. Neil H. Shear, Division of Clinical Pharmacology, Sunnybrook Health Science Centre, Rm. E240, 2075 BayviewAve., North York ON M4N 3M5
0 1996 Canadian Medical Association (text and abstractresume)
CAN MED ASSOC J * SEPT. 1, 1996; 155 (5) 519<- For prescribing information see page 596

contenus dans les rapports publies, la periode moyenne d'apparition de l'hyponatremie s'est etablie a13 jours (fourchette de 3 'a 120 jours). La plupart (83 %) des cas publies mettaient en cause des pa-tients de 65 ans ou plus, comparativement a 74 % des cas non publies.
Conclusion Les personnes agees peuvent risquer davantage d'etre atteintes d'hyponatremie liee 'a l'utilisa-tion d!inhibiteurs specifiques du recaptage de la serotonine. Les medecins qui traitent des patients agesdevraient etre conscients de cet effet indesirable qui pourrait etre grave, mais qui est reversible. Desrecherches plus poussees s'imposent pour determiner l'incidence de cet effet indesirable, le risque re-latif d'hyponatr6mie et de syndrome d'antidiurese inappropriee dans des groupes deage diffents et lerisque lie aux differents inhibiteurs specifiques du recaptage de la serotonine.
The use of selective serotonin reuptake inhibitors(SSRIs) in elderly people has been associated with
reports of hyponatremia, some of which are compatiblewith the syndrome of inappropriate secretion of antidi-uretic hormone (SIADH). Internists and primary carephysicians are most often responsible for managing el-derly patients when they present with electrolyte distur-bances, yet few physicians are aware of this potentiallyfatal but reversible adverse effect. Most published re-ports on this topic have appeared in the psychiatric liter-ature.
Patients with hyponatremia may be asymptomatic orpresent with nausea, anorexia, muscle cramps, weakness,fatigue, confusion and disorientation. Severe hypona-tremia may result in serious neurologic sequelae such ascoma and seizures, and death. Both the magnitude andrate of development of hyponatremia are important de-terminants of the severity of clinical symptoms.'
SIADH, the syndrome of inappropriate secretion ofantidiuretic hormone, occurs in association with reducedserum osmolality. This condition is characterized by hy-potonic hyponatremia (serum sodium level of less than130 mmol/L), inappropriately elevated urine osmolality(usually more than 200 mmol/kg) relative to plasmaosmolality, an elevated urine sodium level (typicallygreater than 20 mmol/L), expanded extracellular volume,and normal renal, adrenal and thyroid function.2 Thesyndrome may be caused by a number of disease pro-cesses (e.g., malignant neoplasms, nonmalignant pul-monary disease and central nervous system disorders)and medications. The list of medications known to causeSIADH includes several psychotropic agents. We be-lieve that SSRI antidepressants should be added to thatlist.We reviewed cases of SIADH and hyponatremia as-
sociated with SSRI use published in the literature as wellas unpublished reports collected from postmarketing sur-veillance. We examined trends in these reports in orderto identify the scope of the problem and possible riskfactors for these underrecognized adverse effects.
METHODS
We searched MEDLINE, using manual cross-referenc-ing, for reports of SSRI use and SIADH or hyponatremia
published between January 1980 and May 1995 usingthe following MeSH terms: "water-electrolyte imbal-ance," "hyponatremia," "inappropriate ADH syndrome"and "serotonin uptake inhibitors." In addition, we col-lected case reports from the manufacturers of the SSRIscurrently available in North America. We sent requestsfor information to the adverse drug monitoring pro-grams of the Ontario Medical Association (OMA), theHealth Protection Branch (HPB) of Health Canada, theUS Food and Drug Administration (FDA) and theWorld Health Organization (WHO). Duplicate reportswere identified on the basis of demographic details andcase descriptions. When overlap occurred, the reportswere attributed to the highest ranking source accordingto the following hierarchy: published literature; WHO;HPB, OMA or FDA; and the Canadian pharmaceuticalindustry.We did not attempt to assess causality or the criteria
used to diagnose hyponatremia or SIADH in the reportsreceived from independent monitoring bodies. In thepublished cases two of us (B.A.L. and S.R.K.) assessedcausality by consensus using a validated 10-item ratingsystem for adverse drug reactions.,
Published reports were analysed separately from un-published ones for trends, because the information inthe published reports was felt to be more detailed andmore reliable.
RESULTS
We found 736 cases of hyponatremia associated withSSRI use in the published literature and unpublished re-ports (Table 1). Reports from the FDA would have beenprovided at an estimated cost of US$1600 and thereforewere not requested for inclusion in our review. However,most of the reports sent to the WHO originated fromthe United States (84% [507/605]) and therefore werelikely part of the unreviewed FDA database.
PUBLISHED REPORTS
We found 30 cases in the literature (Table 2).4-22Twenty-five (83%) involved patients over 65 years ofage (range 47 to 92 years). The median time to onset ofhyponatremia was 13 days (range 3 to 120 days). In all
520 CAN MED ASSOC J * ler SEPT. 1996; 155 (5)

cases the patient's condition returned to normal 2 to 28days after discontinuation of the SSRI; in one case theSSRI was not withdrawn and fluid restriction was tem-porarily required to normalize the serum sodium level.The results of rechallenge were reported for five cases.An 83-year-old woman had recurrence of hyponatremiawithin 3 weeks after rechallenge with fluoxetine.'4 A 60-year-old man required ongoing fluid restriction to con-trol his serum sodium level after rechallenge with sertra-line.20 Jackson and associates'5 described a 77-year-oldwoman in whom hyponatremia compatible with SIADHdeveloped after treatment with fluoxetine; the elec-trolyte disturbance recurred within 4 days after switch-ing to sertraline. Two other patients were rechallenged
Table 1:. Summary of reports of hyponatremiaand syn:drome of inappropriate secret"ion ofantidiuret hormon (SIADH) assocatd wh-the use of selectve serotonin reu..ptakeinhibitors (SSRIs)
No. (and %)Variable of cases
CountryUnited States 523 (71.1)Australia and New Zealand 50 (6.8)United Kingdom 26 (3.5)Canada 26 (3.5)Europe 22 (3.0)South Africa 1 (0.1)Not specified 88 (12.0)SourceWorld Health Organization 605 (82.2)Health Protection Branch(Health Canada) or OntarioMedical Association 10 (1.4)Pharmaceutical industry 91 (12.4)Published literature 30 (4.1)
Age, yr<65 136 (18.5). 65 410 (55.7)Not specified 190 (25.8)SexMale 144 (19.6)Female 444 (60.3)Not specified 148 (20.1)SSRIFluoxetine 554* (75.3)Fluvoxamine 11 (1.5)Paroxetine 91* (12.4)Sertraline 86* (11.7)Total 736 (100.0)*In two cases the patient was exposed to both fluoxetine andparoxetine. and in four the patient was exposed to both fluoxe-tine and uertraiine.
with the implicated SSRI and were able to tolerate thedrug.e820
Challenge with another SSRI from the same class wasalso reported. In the case involving the 83-year-oldwoman reported by Druckenbrod and Mulsant'4 SIADHdeveloped 3 months after the start of fluoxetine therapy.Demeclocycline was required to control the hypona-tremia. The patient later received a trial of sertraline,which was discontinued because of diarrhea. There wasno mention of electrolyte disturbance, nor was the dura-tion of the sertraline therapy indicated. In the case in-volving the 77-year-old woman described by Jacksonand associates'5 the patient's sodium level returned tonormal after withdrawal of the fluoxetine. When she wassubsequently given sertraline, electrolyte disturbancecompatible with SIADH recurred.
There was no association found between the SSRIdose or the patient's age and the time of onset of hy-ponatremia in any of the published cases. Neither ofthese two variables correlated with the severity of thehyponatremic response. The SSRI dose was within thesuggested therapeutic dose range in all cases.
Concomitant illness or use of medications known tocause SIADH could be implicated in some of thecases. 610131-1820,21 Other reports ruled out the commoncauses of SIADH, such as pulmonary or cerebral pathol-ogy, and renal, thyroid or adrenal disease.5791"4 1922 Thepositive temporal association, the lack of alternativecauses and the reversal of hyponatremia after discontinu-ation of the SSRI offered good evidence of a causal rela-tionship. Using the adverse drug reaction rating scale toassess causality we found that 18 (60%) of the 30 reportswere possibly related to the SSRI, 9 (30%) were proba-bly related and 3 (10%) were definitely related.
UNPUBLISHED REPORTS
There were 706 reports of hyponatremia associatedwith SSRI use submitted to the OMA, the HPB, WHOand the pharmaceutical industry (Table 3). In 516 casesthe patient's age was reported: at least 384 (74.4%) ofthese involved patients over 65 years. According to in-formation from 266 cases, the median time to onset ofhyponatremia was 13 days (range 1 to 787 days). In al-most all (95.8% [346/361]) of the cases in which the re-sults of discontinuation of the drug were reported, thehyponatremia reversed after withdrawal of the SSRI.Challenge with the drug, attempted in 24 cases, resultedin recurrence of the hyponatremia in 16 cases (66.7%).Challenge with an alternative antidepressant from thesame SSRI class was reported in two cases in which hy-ponatremia had developed in 83-year-old women whilethey were taking fluoxetine. One woman was subse-quently treated with fluvoxamine, the other with paroxe-
CAN MED ASSOC J * SEPT. 1, 1996; 155 (5) 521

"0
F00
CuSLA,in
C
a
E
0
a
CaBi
522 CAN MED ASSOC J * le, SEPT. 1996; 155 (5)

-
ca > -o) 0o _
o)
_ E ' , E
V: z o n
EO2Ea
0
a)
Z CL
ci
a)
on(3)
a
( Ln
_n C
Z o E_
1-
a)
0
z
N
co)
cc
Z Z Z
O r- o
N 0
0 0 0 0
N N T
0
0
(N
LU LL L LL-
ao Cok.D C0 0 w
-oD
a)
C-
r-
a)
c0
ao
a4>0
0 a~
- (. '
CU aaC)
o
ot)
Lx0
0
C-)
E
a)a.2 0N a)Ca
--7S
'<)-0N0 Qa C tDX
-0 -
co
Ofccz
N0')CY)
CY)N
C-
--
0)
E0
oU
,\
I
Bo
a)
CL)
a-1
a)
I
E0
C-
C)
0
a)
Lac
o
=3
-o0)
c
CD-:r
-o
a)
X:
LI
._ _ a)
0 0 a a) 0
0o N
U U 0 .a >
N t
c
aD N
_
O~3 zCE
ut ZZ
LL LL
so r- r-
._
a
0)
0
0L
a)
m
IW-00
C)
a:-a
a)
3;
0
a
'-a
Oa)
o- aX)a1) 0
z
a)
z a oo
--2E
ECO a°
C:.t)<E E
In ,° F ECZ
x5: 75 0 u0
E) o--a E
a a) a> o
> )
>Ofa) -: C L0 O
a1)
a) -C~'- 'o:s a)
Q) _N.a)-:
Ca
c-
6
a
a)
E a)0-
XO
F--D
m
a)
S0
a)
-c'-C
. E
C
rcZ Z
COZ Z
O
N
CO 0 aCr) co) aO
OCo CY) -- ) co__ N Lo C0 0)
La N m m
NO 0 rCCr) D a' -
N N N N\N N
0 00 N anN -N \,- --I - _ -
0 0
Cr)t-C- r- It
a)c
V)
_,
CZ
1= a)
3;
0)
0
0 0
aD N-
o" C-\
m
a)
0
-j
a)
F-
CAN MED ASSOC J * SEPT. 1, 1996; 155 (5) 523
-o
0Eo c
a)
N.C
of cc ooZ Z Z N
ON C) 0
D ;T _ Ne
z z aIt
B)D
,Cz
ccOc
11
3;
Z
a'O-aQa
as
S a
at
ZUs
ODv
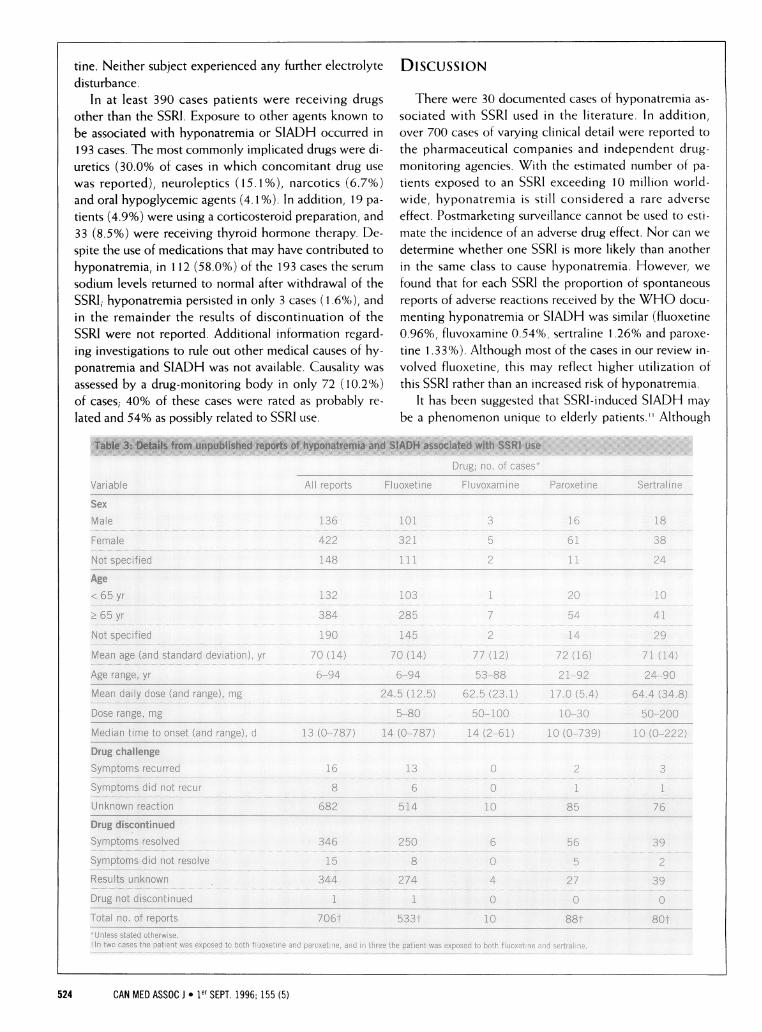
tine. Neither subject experienced any further electrolyte DISCUSSIONdisturbance.
In at least 390 cases patients were receiving drugs There were 30 documented cases of hyponatremia as-other than the SSRI. Exposure to other agents known to sociated with SSRI used in the literature. In addition,be associated with hyponatremia or SIADH occurred in over 700 cases of varying clinical detail were reported to193 cases. The most commonly implicated drugs were di- the pharmaceutical companies and independent drug-uretics (30.0% of cases in which concomitant drug use monitoring agencies. With the estimated number of pa-was reported), neuroleptics (15. 1 %), narcotics (6.7%) tients exposed to an SSRI exceeding 10 million world-and oral hypoglycemic agents (4.1%). In addition, 19 pa- wide, hyponatremia is still considered a rare adversetients (4.9%) were using a corticosteroid preparation, and effect. Postmarketing surveillance cannot be used to esti-33 (8.5%) were receiving thyroid hormone therapy. De- mate the incidence of an adverse drug effect. Nor can wespite the use of medications that may have contributed to determine whether one SSRI is more likely than anotherhyponatremia, in 112 (58.0%) of the 193 cases the serum in the same class to cause hyponatremia. However, wesodium levels returned to normal after withdrawal of the found that for each SSRI the proportion of spontaneousSSRI; hyponatremia persisted in only 3 cases (1 .6%), and reports of adverse reactions received by the WHO docu-in the remainder the results of discontinuation of the menting hyponatremia or SIADH was similar (fluoxetineSSRI were not reported. Additional information regard- 0.96%, fluvoxamine 0.54%, sertraline 1.26% and paroxe-ing investigations to rule out other medical causes of hy- tine 1.33%). Although most of the cases in our review in-ponatremia and SIADH was not available. Causality was volved fluoxetine, this may reflect higher utilization ofassessed by a drug-monitoring body in only 72 (10.2%) this SSRI rather than an increased risk of hyponatremia.of cases; 40% of these cases were rated as probably re- It has been suggested that SSRI-induced SIADH maylated and 54% as possibly related to SSRI use. be a phenomenon unique to elderly patients." Although
Table 3: Details from unpublished reports of hyponatremia and SIADH associated with SSRi 1:us.
524 CAN MED ASSOC J * ier SEPT. 1996; 155 (5)

the patients featured in the reports we reviewed ranged inage from 6 to 94 years, most were elderly. A number ofphysiologic changes in water homeostasis may predis-pose elderly people to hyponatremia from any cause. Inthis age group, the maximal diluting and concentratingcapacity of the kidney is impaired, 23 and ADH secretionmay be slightly increased.24 In addition, the ADH re-sponse to osmolar stimuli has been shown to be greaterin elderly people than in young control subjects.25 Thisincreased osmosensitivity may increase the risk forSIADH in elderly people. Alternatively, hyponatremiamay simply not be tolerated as well in elderly patientsand thus be more likely to require medical attention.
Sixty percent of the cases we reviewed involved fe-males and 20% males; in the remaining 20% sex was notspecified. In general, adverse drug reactions are reportedto occur more frequently in female patients.2S28 Severalfactors may contribute to an apparent sex-related differ-ence in the occurrence of hyponatremia and SSRI use.Female patients may have increased exposure to SSRIsbecause the incidence of depression is increased in thefemale population,29 or there may be sex-related bias inprescribing patterns. Patterns of health care utilizationhave been shown to differ between male and female pa-tient populations.303 This may affect not only drug ex-posures but also the detection, documentation and re-porting of adverse reactions.
Hyponatremia associated with SSRI use usually devel-ops soon after the start of drug therapy. The median timeto onset in the cases we reviewed was 13 days (based onreports from published and unpublished sources). Threequarters of the cases presented within 30 days after thestart of therapy. Routine monitoring of electrolyte levelsin elderly patients may be worth while, especially duringthe first 2 to 4 weeks of treatment. However, hypona-tremia may occur late in the course of SSRI therapy. Inour series, 29% of the patients presented more than 3months after SSRI therapy had been started.
Our assessment of causality in the published cases re-sulted in 40% being rated as either definitely or probablyrelated to SSRI use and the remaining cases being ratedas possibly related. Although we did not attempt to assesscausality in the unpublished cases, we found that reversalof hyponatremia after withdrawal of the SSRI occurred in58% of the 193 cases in which there was concomitant useof pharmaceutical agents known to cause SIADH. Chal-lenge with the implicated SSRI, attempted in 27 cases, re-sulted in the recurrence of hyponatremia in 18. Somecases of drug-induced SIADH have been reported to betransient.32 This may explain the lack of response to thechallenge seen in the other nine cases.
Hyponatremia is likely an effect common to this classof antidepressants. Considering the structural hetero-geneity of the four SSRIs reviewed, the adverse effect is
unlikely to be related to chemical structure. There arethree possible ways drugs can affect water homeostasis:they can increase ADH secretion centrally, potentiate theeffect of endogenous ADH at the renal medulla, and re-set the osmostat, thus lowering the threshold for ADHsecretion.ADH secretion from the posterior lobe of the pitu-
itary gland is thought to be affected by such nonosmolarfactors as angiotensin 11, noradrenaline, acetylcholineand endorphin levels.3334 Dopamine antagonists such ashaloperidol and domperidone have been shown in ani-mal models to facilitate ADH secretion3" and increasethirst by increasing angiotensin 11 levels.38 Noradrenalineinduces the release of ADH via a,-adrenergic receptors;stimulation of ac2-adrenergic and B-adrenergic receptorsmay, however, inhibit ADH release.9'40 Serotonin-medi-ated effects on 5-HT2 and 5-HT,c receptors have beenshown to induce release of ADH.442 Although the SSRIsare believed to be highly selective in their effect on sero-tonin reuptake, animal studies have shown that theSSRIs have some inhibitory effects on the reuptakeof dopamine and noradrenaline. However, the potencyof these effects varies greatly between the differentSSRIs.4344 The effect of various psychotropic drugs onneurotransmitters has been speculated to contribute toexcess ADH secretion; however, the exact mechanism ofSSRI-induced SIADH remains unknown.
Hyponatremia associated with SSRI use may be amanifestation of a drug interaction. SSRIs are known toinhibit a number of cytochrome P450 isoenzymes.45 Inseveral of the cases we reviewed, the patients were con-currently receiving a drug known to cause SIADH. Byinhibiting the metabolism of concomitant drugs such asneuroleptics, adverse effects on sodium metabolism maybe augmented.
There are several limitations one must consider whenevaluating reports from postmarketing surveillance. An in-cidence rate cannot be estimated, because the number ofpatients exposed is not available. Voluntary reporting mayunderrepresent the true incidence of adverse drug reac-tions. Reports may be biased because of perceived severityof the adverse effect, media bias or physician awareness ofa possible drug association. In addition, the quality of re-ports can vary greatly. In some reports, even the most ba-sic demographic information such as age and sex weremissing. Moreover, there may be overlap of reports be-tween the various sources. We identified 25 cases that hadbeen reported to more than one source. Duplication of re-ports may result in an overestimation of the event, an es-pecially important problem for rare adverse events.
The problem we encountered in attempting to accessinformation from the FDA has been reported previ-ously.Y1 Willingness of drug-monitoring bodies to shareinformation for medical practice and research in a timely
CAN MED ASSOC J * SEPT. 1, 1996; 155 (5) 525

fashion and without exorbitant service charges should beensured. In order for information regarding adverse drugreactions to be applied, accessibility, analysis and dis-semination of information are critical.
CONCLUSION
There is a large number of reports of SIADH and hy-ponatremia associated with SSRI use. This form of hy-ponatremia usually develops soon after the start of SSRItherapy, and the electrolyte disturbance in almost allcases reverses after withdrawal of the drug. There is noapparent relation with dose. Advanced age appears to bea risk factor for this adverse effect, as does the concomi-tant use of diuretics. Increased physician awareness ofthis potentially serious but treatable adverse effect isneeded. The use of SSRI antidepressants should be in-cluded in the differential diagnosis of drug-induced hy-ponatremia. Clinical deterioration should prompt anevaluation of electrolyte levels. Elderly patients shouldbe monitored closely in the first 4 weeks of SSRI therapyfor clinical signs suggestive of hyponatremia. Further re-search is required to evaluate the relation between age,sex and the risk of SSRI-induced hyponatremia. In addi-tion, the relative risk of hyponatremia associated witheach SSRI drug needs to be determined.
Since this review was completed, six additional cases of h)ypona-tremia and SIADH associated with SSRI use have appeared in theliterature.47-50 Five of the patients were women, and five were over65 years of age.
We thank the World Health Organization Collaborating Centre for In-ternational Drug Monitoring, the Adverse Drug Monitoring Division ofthe Health Protection Branch, Health Canada, and the Adverse DrugReaction Monitoring Program of the Ontario Medical Association. Theinformation obtained from each of these sources is not homogeneous, atleast with respect to the origin or likelihood that the pharmaceuticalproduct caused the adverse reaction. The opinions expressed in this arti-cle are those of the authors and do not represent the opinion of any ofthe aforementioned organizations.
Dr. Liu is supported by the Pfizer Fellowship from the Canadian Soci-ety for Clinical Pharmacology.
I. Bartter FC. The syndrome of inappropriate secretion of an-tidiuretic hormone (SIADH). Dis Mon 1973;20:3-46.
2. Bartter FC, Schwartz WB. The syndrome of inappropriatesecretion of antidiuretic hormone. Am J Med 1967;42:790-806.
3. Naranjo CA, Busto U, Sellers EM, et al. A method for esti-mating the probability of adverse drug reactions. Clin Phar-macol Ther 1981 i 30:239-45 .
4. Hwang AS, Magraw RM. Syndrome of inappropriate secre-tion of antidiuretic hormone due to fluoxetine [letter]. Am JPsychiatry 1989; 146:399.
5. Cohen BJ, Mahelsky M, Adler L. More cases of SIADH withfluoxetine [letter]. Amii J Psychiatry 1990; 147:948-9.
6. Gommans JH, Edwards RA. Fluoxetine and hyponatraemia[letter]. N Z Med J 1990; 103:106.
7. Marik PE, van Heerden W, Steenkamp V. Fluoxetine-induced syndrome of inappropriate antidiuretic hormoneexcretion [letter]. S Afr Med .J 1990;78:760- 1.
8. Staab JP, Yerkes SA, Cheney EM, Clayton AH. TransientSIADH associated with fluoxetine [letter]. Am J Psychiatry1990; 147:1569-70.
9. Vishwanath BM, Navalgund AA, Cusano W, NavalgundKA. Fluoxetine as a cause of SIADH [letter]. Am J Psychiatry1991 ; 148:542- 3.
10. Blacksten JV, Birt JA. Syndrome of inappropriate secretionof antidiuretic hormone secondary to fluoxetine. Ann Phar-macother 1993;27:723-4.
11. Kazal LA, Hall DL, Miller LG, Noel ML. Fluoxetine-in-duced SIADH: A geriatric occurrence? J Fam Pract 1993;36:341-3.
12. Ball CJ, Herzberg J. Hyponatraemia and selective serotoninreuptake inhibitors. Int J Geriatr Psychiatry 1994;9:819-22.
13. Pillans PI, Coulter DM. Fluoxetine and hyponatraemia - apotential hazard in the elderly. N Z Med J 1994; 107:85-6.
14. Druckenbrod R, Mulsant BH. Fluoxetine-induced syndromeof inappropriate antidiuretic hormone secretion: a geriatriccase report and a review of the literature. J Geriatr PsychiatryNeurol 1994;7:255-8.
15. Jackson C, Carson W, MarkowitzJ, MintzerJ. SIADH asso-ciated with fluoxetine and sertraline therapy [letter]. Am JPsychiatry 1995;152:809-8.
16. McHardy KC. Syndrome of inappropriate antidiuretic hor-mone secretion due to fluvoxamine therapy. Br J Clin Pharma-col 1993;47:62-3.
17. Goddard C, Paton C. Hyponatraemia associated withparoxetine [letter]. BMJ 1992;305: 1332.
18. Chua TP, Vong SK. Hyponatraemia associated with paroxe-tine [letter]. BMJ 1993;306:143.
19. Crews JR, Potts NLS, Schreiber J, Lipper S. Hyponatremiain a patient treated with sertraline [letter]. Am J Psychiatry1993l150:1564.
20. Doshi D, Borison R. Association of transient SIADH withsertraline [letter]. Am J Psychiatry 1994; 151:779-80.
21. Llorente MD, Gorelick M, Silverman MA. Sertraline as thecause of inappropriate antidiuretic hormone sercretion [let-ter]. J Clin Psychiatry 1994;j55:543-4.
526 CAN MED ASSOC J* ier SEPT. 1996; 155 (5)
22. Thornton SL, Resch DS. SIADH associated with sertralinetherapy [letter]. Am J Psycbiatry 1995;152:809.
23. Lindeman RD, Van Buren HC, Raisz LG. Osmolar concen-trating ability in healthy young men and hospitalized pa-tients without renal disease. N Engl J Med 1960;262: 1306-14.
24. Miller M. Fluid and electrolyte balance in the elderly. Geri-atrics 1987;42:65-76.
25. Helderman JH, Vestal RE, Rowe JW, Tobin JD, Andres R,Robertson GL. The response of arginine vasopressin to in-travenous ethanol and hypertonic saline in man: the impactof aging. J Gerontol 1978;33:39-47.
26. Seidl Lg, Thornton GF, Cluff LE. Epidemiological studies ofadverse drug reactions. Am J Public Health 1965;55: 1170-5.
27. Hurwitz N. Predisposing factors in adverse reactions todrugs. BMJ 1969;1:536-8.
28. Caranasos GH, Steart RB, Cluff LE. Drug-induced illnessleading to hospitalization. JAMA 1974;227:713-7.
29. Blazer D, Hughers DC, George LK. The epidemiology ofdepression in an elderly community population. Gerontologist1987;27:281-7.
30. Franks P, Clancy CM, Naumburg EH. Sex, access, and ex-cess. Ann Intern Med 1995; 123:548-50.
31. Verbrugge LM, Steiner RP. Physician treatment of men andwomen patients: Sex bias or appropriate care? Med Care1981; 19:609-32.
32. Weitzel WD, Shraberg D, Work J. Inappropriate ADH se-cretion: the role of drug re-challenge. Psycbosomatics 1980;21:771-9.
33. Ledingham JGG. Water and sodium homeostasis. In:Weatherall DJ, Ledingham JGG, Warrell DA, editors: Ox-ford Textbook of Medicine. vol 2. Oxford, England: Oxford Uni-versity Press, 1987:18-29
34. Spigset 0, Hedenmalm K. Hyponatraemia and the syn-drome of inappropriate antidiuretic hormone secretion(SIADH) induced by psychotropic drugs. Drug Safety1995; 12:209-25.
35. Cunningham ET Jr, Sawchenk PE. Reflex control of magno-cellular vasopressin and oxytocin secretion. Trends Neurosci1991;14:406-1 1.
36. Yamaguchi K, Hama H. Facilatory role of central dopaminein the osmotic release of vasopresin. Brain Res 1989;481:388-91.
37. Yamaguchi K, Hama H, Adachi C. Inhibitory role ofperiventricular dopaminergic mechanisms in hemorrhage-induced vasopressin secretion in conscious rats. Brain Res1990i513:335-8.
38. Verghese C, de Leon H, Simpson GM. Neuroendocrine fac-tors influencing polydipsia in psychiatric patients: an hy-pothesis. Neuropsychopbarmacology 1 993;9: 157-66.
39. Leibowitz SF, Jhanwar-Uniyal M, Dvorkin.B, et al. Distribu-tion of a-adrenergic and dopaminergic receptors in discretehypothalamic areas of rat. Brain Res 1982;233:97-1 14.
40. Leibowitz SF, Eidelman D, Suh JS, et al. Mapping study ofnoradrenergic stimulation of vasopressin release. Exp Neurol1990; l10:298-305.
41. Anderson IK, Martin GR, Ramage AG. Central administra-tion of 5-HT activates 5-HT1A receptors to cause sympa-thoexcitation and 5-HT2/5-HT1C receptors to release vaso-pressin in anaesthetized rats. Br J Pbarmacol 1992; 107:1020-8.
42. Brownfield MS, Greathouse H, Lorens SA, Armstrong H,Urban JH, Van de Kar LD. Neuropharmacological charac-terization of serotoninergic stimulation of vasopressin secre-tion in conscious rats. Neuroendocrinology 1988;47:277-83.
43. Grebb JB. Serotonin-specific reuptake inhibitors: introduc-tion and overview. In: Kaplan HI, Sadock BJ, editors. Com-prehensive Textbook of Psychiatry. vol 2. 6th ed. Baltimore:Williams and Wilkins, 1995:2054-6.
44. Bressler R, Katz MD. Drug therapy for geriatric depression.Drugs Aging 1993,3:195-219. A
45. Crewe JK, Lennard MS, Tucker GT, Woods FR, HaddockRE. The effect of selective serotonin re-uptake inhibitors oncytochrome P4502D6 (CYP2D6) activity in human liver mi-crosomes. Br J Clin Pharmacol 1992;347:262-5.
46. Vogt CL. Adverse drug reactions: getting information backfrom MEDWATCH [letter]. JAMA 1994;272:590.
47. Taylor IC, McConnell JG. Severe hyponatraemia associatedwith selective serotonin reuptake inhibitors. Scot Med J1995;40: 147-8.
48. Bluff DD, Oji N. SIADH in a patient receiving sertraline[letter]. Ann Intern Med 1995; 123:81 1.
49. Leung M, Remick R: Sertraline-associated hyponatremia[letter]. Can J Psychiatry 1 995;40:497-8..
50. Ayonrinde OT, Teutens SG, Sanfilippo FM. Paroxetine-induced SIADH [letter]. Med J Aust 1995;163:390.
CAN MED ASSOC J * SEPT. 1, 1996; 155 (5) 527




















