The state of therapy modalities in clinic for biliary tract cancer
Upload
khangminh22Category
view
4download
0
Early Management of Operative Injuries of theExtrahepatic Biliary Tract
1. WILLIAM BROWDER, M.D.,* JAMES B. DOWLING, M.D.,t K. KRISTENE KOONTZ, M.D.,* and MARTIN S. LITWIN, M.D.§
Since 1980, the authors have managed 19 patients with opera-tive injuries to their biliary tracts. Eleven patients (58%) in-curred their injuries during cholecystectomies for acute chole-cystitis (average age-56 years); seven patients (37%) receivedtheir injuries during elective cholecystectomies (averageage-24 years); and in one patient (5%) the inqury occurredduring gastrectomy. In group I were eight patients in whominJuries were recognized and repaired intraoperatively duringtheir initial operations. Seven of these patients (88%) had pri-mary duct reanastomoses, and one patient had a choledocho-duodenostomy. All healed without further surgery, and nonelater had cholangitis develop. In group II were 11 patientsdiagnosed and reoperated later after surgery (mean time untildiagnosis, 12 days). Seven of these patients (64%) were man-aged with Roux-en-Y hepaticojejunostomies or choledochoje-junostomies. Four patients had cholangitis develop after sur-gery: two had demonstrable anastomic stenosis and two had nostenosis. Three of these four patients (75%) who had cholan-gitis develop did not have stents used in their repairs. Theoverall mortality rate in this series of 19 patients was 11%. Themajor risk factors for biliary tract injury were the presence ofacute cholecystitis and of anatomically small biliary ducts. Forthis latter reason, younger patients who had elective cholecys-tectomies were particularly at risk. In delayed repair, the useof internal stents appeared to be useful in preventing the laterdevelopment of stenosis and/or cholangitis; however, recurrentcholangitis developed in two patients who did not have demon-strable anastomotic stenoses.
OPE RATIVE INJURIES to the biliary tract are un-common and devastating problems. The inci-dence of such injuries ranges in from 0.2 to
0.9% of patients having cholecystectomies.' 2 Not infre-
Presented at the 98th Annual Meeting of The Southern SurgicalAssociation, Palm Beach, Florida, November 30-December 3, 1986.
* Associate Professor of Surgery and Physiology.t Clinical Associate Professor of Surgery.t Senior Surgical Resident.§ Robert and Viola Lobrano Professor of Surgery.Reprint requests: I. William Browder, M.D., Department ofSurgery,
Tulane University Medical Center, 1430 Tulane Avenue, New Or-leans, LA 70112.Submitted for publication: December 31, 1986.
From the Department of Surgery, Tulane University MedicalCenter, and the Mahorner Clinic, New Orleans, Louisiana
quently, a biliary tract injury leads to chronic biliarystricture with resulting jaundice, biliary cirrhosis, andhepatic failure if the stricture is not corrected surgically.Repairs of such strictures may require multiple opera-tions and lead to high morbidity and mortality rates,particularly in those patients in whom liver disease andportal hypertension eventually develop.
In several reports it has been noted that proper earlymanagement can markedly improve ultimate success inthese difficult patients.3'4 Because such early manage-ment may be critical in the outcome of these patients,we report our experience since 1980 with the initialmanagement ofpatients who had iatrogenic biliary tractinjuries.
Materials and Methods
Since 1980, we have been consulted to assist in themanagement of 19 patients with operative injuries totheir biliary tracts. Eight ofthese patients had their inju-ries diagnosed intraoperatively (group I), while 11 ofthepatients were referred up to 3 weeks after their initialbiliary tract surgeries, when their injuries had occurred(group II). Records of these 19 patients have been ana-lyzed, with particular attention paid to risk factors forthe mechanisms of their biliary tract injuries. Technicalaspects ofthe individual repairs and morbidity and mor-tality rates were also reviewed. Finally, all living patientswere contacted to ascertain any recurrent symptoms oroccurrence of biliary strictures.
Results
The group of 19 patients who had biliary tract injuriesconsisted of 12 females and seven males. Ages ranged
649

Ann. Surg, * June 1987
TABLE 1. Nineteen Biliary Tract Injuries
Time of Injury Recognition
Type of Intraoperative PostoperativeInjury (Group I) (Group II) Totals
Ligation 0 7 7Partial
transection 5 1 6Complete
transection 3 1 4Resection 0 2 2
from 17 to 82 years (mean age 46 years). The originalprocedures related to the biliary injuries were cholecys-tectomies for acute cholecystitis in 11 patients (meanage 56 years), cholecystectomies for chronic cholecys-titis in seven patients (mean age 24 years), and emer-
gency gastrectomy for bleeding duodenal ulcer in one
patient (age 82 years). Of the five patients who were
younger than 30 years of age, four were noted by theirprimary surgeons to have a common bile duct measur-
ing less than 5 mm in diameter. The original surgeon
was a resident in six cases and a board-certified surgeon
in 13 cases.The types of injuries encountered in the 19 patients
are listed in Table 1. The only type of injury noted
FIG. 1. Location of operative injuries to the biliary tract. In this studyof 19 patients, the site injured most frequently was at the cystic duct-common ductjunction (1 1 patients, 58%). Less common sites ofinjurywere to the common hepatic duct just before its bifurcation (3 patients,16%), to the common bile duct just above the duodenum (3 patients,16%), to the left hepatic duct (1 patient, 5%), and to an anomalous righthepatic duct coming off the cystic duct (1 patient, 5%).
during surgery (group I) was partial or complete tran-section of the bile duct. In contrast, the injury recog-nized most frequently later in the period after surgery(group II) was ligation of the common bile duct.The locations of the various injuries to the biliary
tract are varied (Fig. 1). By far most injuries (58%) oc-curred at the cystic duct-common duct junction (11patients). Another patient received an injury to ananomalous right hepatic duct that joined the cystic ductjust before its junction with the common duct.
In the 11 patients in group II, cholangiography duringsurgery was not used effectively. In six of these patients,cholangiography was not performed during surgery be-cause of the intense inflammation associated with theiracute cholecystitis and the surgeons' desire to avoid un-necessary delay. In three other patients, cholangiogra-phy was not performed during surgery because the sur-geon suspected nothing abnormal. In the remaining twopatients, cholangiography was performed during sur-gery; however, one received an injury after the x-ray wasdone and in the other patient the cholangiogram takenduring surgery was incorrectly interpreted.The repair of biliary tract injuries in patients in group
I was accomplished by primary reanastomosis in sevenpatients (Table 2). These seven patients included fivewho had partial transections and two who had completetransections of their biliary tracts. The additional pa-tient had choledochoduodenostomy because the biliarytract injury was in close juxtaposition to the duodenum.The average length oftime required for recognition of
the biliary tract injuries after surgery in patients in groupII was 12 days (range: 5 to 21 days). The average biliru-bin of these patients at the time of diagnosis was 7.0 mgpercent (range: 3 mg/dl to 17 mg/dl). Cholangitis didnot occur before surgery in any of these patients. Diag-nostic workup to confirm the presence of biliary tractinjuries in patients in group II included endoscopic ret-rograde cholangiopancreatography (ERCP) in six pa-tients and percutaneous transhepatic cholangiography(PTC) in five patients; two of these 11 patients had bothERCP and PTC.The 11 patients in group II had a variety of reparative
procedures (Table 2). All were performed within 3 weeksof their original operations. The procedure most fre-quently performed in patients in this group (64%) wasRoux-en-Y hepaticojejunostomy or choledochojejunos-tomy; this was performed in seven patients who hadinjuries of either the common hepatic or the commonbile duct. In three other patients who had injuries oftheir common bile ducts, choledochoduodenostomieswere done. In one patient, a partial transection of thecommon duct at the cystic duct-common bile ductjunction occurred, and a primary anastomosis was per-formed.
650 BROWDER AND OTHERS

BILIARY TRACT INJURIES 651TABLE 2. Techniques ofRepair and Use ofStents in Biliary Tract Injuries
No. ofPatients Type of Repair Use of Stent Result
Group I: Intraoperative diagnosisPartial transection 5 Reanastomosis 3-T-tube Excellent
2-none I -bile fistula*Complete transection 3 Reanastomosis (2) 2-T-tube I-bile fistula*
Choledochoduodenostomy (1) 1-T-tube Excellent
Group II: Postoperative diagnosisLigation 7 Choledochoduodenostomy (3) 1-catheter Excellent
2-none 1-cholangitisRoux-en-Y hepaticojejunostomy (3) 2-catheter I-cholangitis
1-none ExcellentRoux-en-Y choledochojejunostomy 1-none 1 -cholangitis
(1)Resection 2 Roux-en-Y hepaticojejunostomy 2-none 1 cholangitisComplete transection 1 Roux-en-Y choledochojejunostomy I-T-tube ExcellentPartial transection 1 Reanastomosis i-T-tube Excellent
* Both healed without reoperation and with no residual stricture.
In our entire study of 19 patients, an early morbidityrate occurred in three patients (morbidity rate 16%). Intwo patients in group I, transient bile fistulae developedafter reanastomosis of their biliary tract injuries at thetime of cholecystectomies for acute cholecystitis. Bothhealed spontaneously, and neither has had a stricturedevelop during a 1-year follow-up period. An additionalpatient in group II had a fecal fistula develop when thetransverse colon was injured at the time of Roux-en-Yhepaticojejunostomy. One year later, it was necessary toperform a transverse colectomy; the patient has nosymptoms 2 years later.The decision to use a stent as well as the type of stent
used varied for each of the 19 patients. In a total of 11patients (58%), the repairs were stented (Table 2). Theaverage duration of stenting was 9 weeks (range: 1rtionth to 1 year).The mean follow-up time in our study is 2.5 years
(range: 3 months to 6 years). During this period, fourpatients (31%) have had episodes of cholangitis. All ofthese patients were in group II, and in three of these fourpatients the repairs were not stented. In group II, one offive patients (20%) whose repairs were stented and threeof six patients (50%) whose repairs were not stented hadcholangitis develop.A brief analysis of the patients in whom cholangitis
developed is also of interest. One patient in whom acholedochoduodenostomy was performed has had epi-sodes of chills, fever, and mild bilirubin elevation ashigh as 3.0 mg/dl every 12-15 months. Other liverfunction studies have been normal, and no obstructioncan be demonstrated at the site of the choledochoduo-denostomy. Two other patients who had Roux-en-Y he-paticojejunostomies have had episodes of cholangitis.One of these patients was found to have an anastomotic
stricture and had revision of the anstomosis 8 monthsafter surgery; this patient has had no further symptomsof cholangitis. The other patient has recurrent episodesof cholangitis approximately once each year. Extensiveworkup has revealed no obstruction at the hepaticoje-junostomy, and there is no reflux of barium up the je-junal Roux-en-Y loop. This patient's cholangitis re-sponds rapidly to antibiotics taken orally, and he has notbeen operated on again. The fourth patient had a Roux-en-Y choledochojejunostomy, and now has recurrentepisodes of cholangitis that occur approximately 8-12months apart. Workup has revealed partial obstructionat the choledochojejunostomy, but the patient refusesreoperation at this time.There have been two deaths in our study of 19 pa-
tients (mortality rate 11%). An 82-year-old woman whohad emergency gastrectomy for a bleeding duodenalulcer had an injury to the common duct that requiredcholedochoduodenostomy. Her course after surgery wasmarked by recurrent bouts of abdominal sepsis andrenal failure, and she died 1 month later. A second pa-tient died 18 months after cholecystectomy for acutecholecystitis. The common bile duct was transected andrepaired, but the patient later died after development ofmultiple bowel fistulae and intra-abdominal abscesses.
Discussion
In our experience with biliary tract injuries, youngand middle-aged patients seemed to be at higher riskthan older patients for occurrence of operative injuries.The mean age of our patients was 46 years, very similarto that reported by others.5 6 This finding may be relatedto the higher incidence of cholecystitis in patients ofthese ages. A proposed risk factor in the occurrence of
Vol. 205 * No. 6
BROWDER AND OTHERS
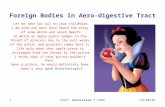
FIG. 2. Operative injuries to the biliary tract. The presence of a smallcommon duct is an important contributory factor in the occurrence ofthese injuries. In this patient, the common duct had been severedduring emergency cholecystectomy for acute cholecystitis. Five daysafter his cholecystectomy, jaundice developed and he was operated onagain. At that time it was found that the common duct had beensevered, and a small segment of it had been removed. Because the endsappeared to come together easily, a primary repair had been donearound a #8 French T-tube inserted through the anastomotic line intothis small duct. When a stent is inserted through an anastomotic line,circumferential duct repair cannot be accomplished. For this reason,the anastomosis is inherently weaker, this is especially true when a
portion ofthe duct has been removed and there is tension on the sutureline. Under such conditions the suture line will ultimately retract, anda stricture will form. The sequence of events in this typical patient isfurther illustrated in Figures 3, 4, and 5.
biliary tract injuries in such patients is the presence ofinflammatory changes in the area ofthe portal triad thatobscure normal anatomic features. In our study, 11 pa-tients (58%) had acute cholecystitis at the time of theircholecystectomies. The relatively high frequency of oc-currence of common hepatic and right and left hepaticduct injuries in our study (11 patients-58%) might beexplained by difficulties in dissecting in the area of thehepatic hilum in the presence of acute inflammatorychanges. Others have also noted the increased incidenceof acute cholecystitis in patients who have operative in-juries to the biliary tree.8
An additional finding in our study was that, in 80% ofthe patients younger than 30 years of age, the biliaryduct anatomy was noted by the operating surgeon to beunusually small, estimated to be less than 5 mm in di-ameter. The average age ofour patients who had electivecholecystectomy for chronic cholecystitis was 24 years.
Because the biliary ducts in young people are usuallysmall, this finding supports the concept that small ductanatomy, as frequently noted in the younger patient,may also be an important contributing factor in theoccurrence of biliary tract injures (Fig. 2).
Inexperience of the operating surgeon has also beenproposed as a factor in the cause of these injuries; how-ever, there is controversy in the surgical literature re-
garding this issue. Adren-Sandberg et al., in a report of65 operative biliary tract injuries, noted that, even
though most of the surgeons in his study were still intraining, 80% of them had performed 25-100 cholecys-tectomies.5 Other reports have noted that about half ofthe biliary tract injuries occurred when established andexperienced surgeons were operating.6'9 In this presentreport, 13 (68%) of the injuries occurred when a board-certified surgeon was operating. While experience is ofimportance, of course, on the basis of this report, andthose in the literature, it appears that there may be fac-tors involved in this injury of greater importance thanrelative inexperience of the operating surgeon.
Almost half of our patients (46%) had their injuriesdiscovered during surgery. In another study, 85% of in-juries were recognized during surgery,5 but most reportsin the literature indicated recognition rates during sur-
gery of 12-22%.`-9In these 19 patients, the most frequent injury (37%)
was ligation of the common bile duct and the mostcommon site of injury (58%) was the cystic duct-com-mon bile duct junction. In Glenn's extensive report of100 biliary tract injuries, he also noted that the cysticduct-common bile ductjunction was the most commonsite of injury.'0 Presumably, tension on a short cysticduct tents the common bile duct upward, allowing thecystic duct ligature to be secured around the displacedcommon bile duct. Careful attention to the junction ofthe cystic duct with the common bile duct should aid inprevention of this injury by this particular mechanism.Additionally, in our study one injury occurred to an
anomalous right hepatic duct as itjoined the cystic duct.Others have also reported injury to this anomalousduct.8 Awareness of possible anatomic variants in thisarea will help to prevent this particular injury.Our data on the use of cholangiography during sur-
gery is also of interest. In the 11 patients in group IIwhose injuries were not diagnosed during their originaloperations, only two patients had cholangiograms per-formed during surgery. In one ofthese studies the x-rays
652 Ann. Surg. * June 1987
BILIARY TRACT INJURIES
I-
were misinterpreted as showing no injury, and in theother the injury occurred after the study was performed.Collins and Gorey noted that cholangiograms duringsurgery had been performed during the initial operationin only 21% of their patients who had biliary tract inju-ries." When the surgeon encounters an anatomic abnor-mality or considers the possibility ofbile duct injury, it isimperative that a cholangiogram be performed duringsurgery and that the cholangiogram be correctly inter-preted.5 Maneuvers during surgery after completion ofthe cholangiogram should also be kept to a minimumunless bleeding or other difficulties demand continuedactivity.
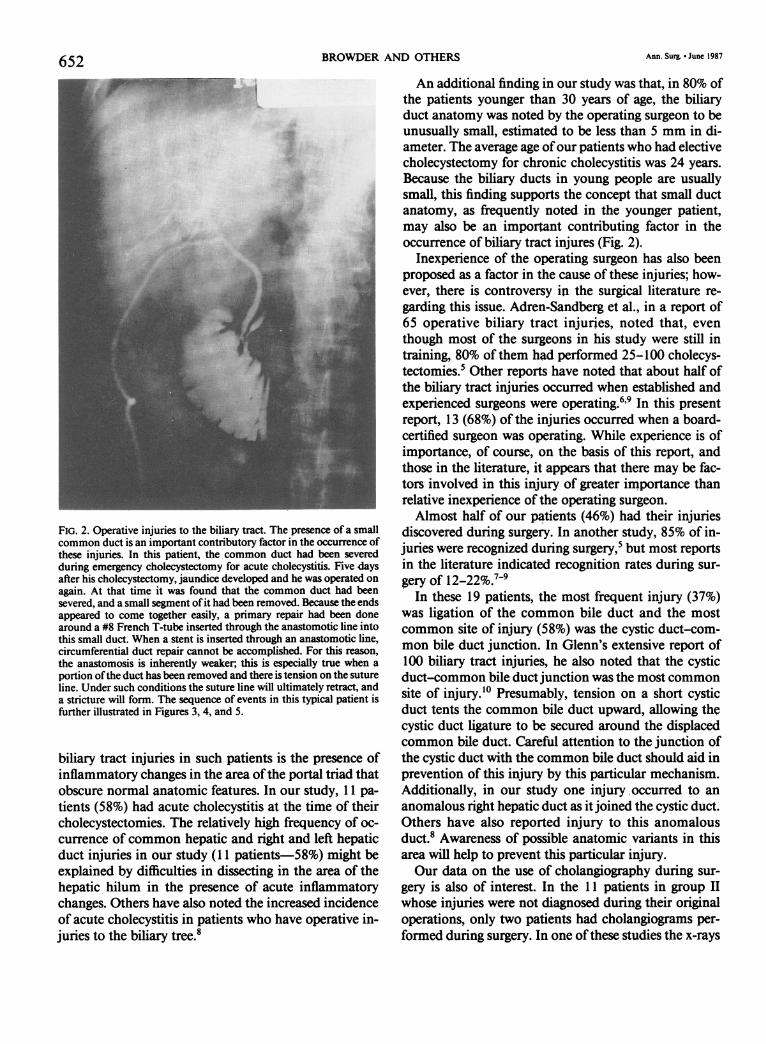
FIGS. 3A-C. The simultaneous use of both ERCP and PTC allows aclear definition of the extent of the duct damage. In this patient A.ERCP clearly identified a common bile duct obstruction, and B. PTCdemonstrated the location of the proximal end of the obstruction. C.The combined simultaneous use ofboth ERCP (1) and PTC (2) furtherdemonstrated the extent of the intervening stricture (3) that hadformed.
In our patients in group I, early recognition of thebiliary tract injuries clearly and beneficially influencedtheir ultimate outcome. Seven of the eight injuries rec-
ognized during surgery were repaired by primary rean-astomosis. Even though two ofthese patients had biliaryfistulae develop, both healed spontaneously withoutreoperation. Furthermore, during an average follow-upperiod of 2.5 years, a biliary stricture had not occurredin any of these patients. To date, our results are some-what better in this regard than those reported by An-dran-Sandberg et al.12 In their patients, 32% of thosewho had primary reanastomoses required reoperation,usually because of chronic biliary fistulae, and another
653Vol. 205 * No. 6

654 BROWDER AND OTHERS
-= -----In most (64%) of the patients in group II who had_ ._ ..........reoperation for their biliary tract injuries, Roux-en-Y
hepaticojejunostomy or choledochojejunostomy wasperformed, depending upon the location of the injury.Several investigators have cautioned against primaryreanastomosis in this setting, because such an approachseems to have resulted in an inordinately high incidenceof strictures.8" Duct stricture is particularly apt to occurwhen a portion of duct has been resected and there is
........tension on the suture line. Under such circumstances itis to be expected that the suture line will retract andhealing by scar contracture will occur (Fig. 4). Sutureline contracture may also occur at the anastomosis inthe absence of tension unless a large and patulous anas-tomotic opening is created and maintained. Insertion ofa stent through the suture line prevents circumferentialsuturing from being accomplished and forms an inher-ently weaker and inadequately small anastomosis. Forthese reasons, stents should be inserted into the ductthrough an opening separate from the anastomotic line,either in another portion ofthe duct or through the wall
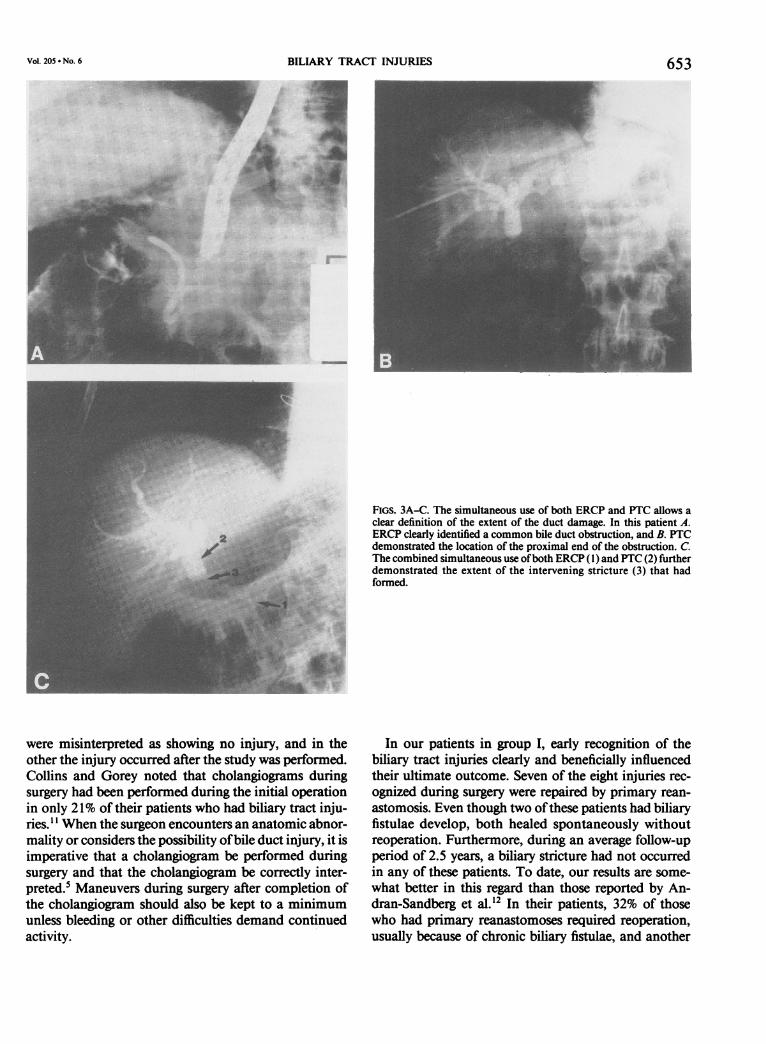
FIG. 4. Operative injuries to the biliary tract. As shown in Figure 1, a eithe in oer poto of the ductordthrughateswalT-tube had been inserted into the duct through the primary anasto- of the visceral loop to which the duct had been anasto-mosis. In this cholangiogram taken 5 weeks after reanastomosis, re- mosed (Fig. 5).traction of both ends of the duct at the suture line is clearly evident.The stricture noted in Figure 3C progressively formed after removal ofthis T-tube.
37% of their patients later had strictures develop thatrequired reoperation.12 Warren et al. noted that biliarystrictures almost always occur within 3 years of the in-jury.'3 The average follow-up period in our study of 2.5years should be long enough to assure our success rate insuch patients. It may be of significance that the most(63%) ofthese injuries that were repaired primarily werepartial transections in which a portion of the common
.30
duct remained intact. Belzer's and Dunphy's classic ani-mal experiments demonstrated that such injuries areassociated with a decreased incidence of biliary stric-ture.'4
Patients in group II who had the diagnoses of biliarytract injuries made after their initial biliary tract opera-tions all had jaundice develop. All diagnoses were madewithin 3 weeks of the injuries, and there were no epi-sodes of cholangitis seen before their repairs. Theworkup of such patients is straightforward, with effortsbeing directed primarily toward radiographic visualiza-tion of their biliary tracts. Early in our experience em-phasis was placed upon ERCP (Fig. 3A). As PTC hasbecome increasingly available, it has become quite ap-becomeainrentthatthisicng aile,whith hisualesb e quit am. FIG. 5. Operative injuries to the biliary tract. An hepaticojejunostomyparent that this technique, which visualizes the proximal was done. A T-tube was inserted through the wall of the Roux loop,point of obstruction, is more valuable to the surgeon and a long arm was used to stent the anastomosis. Six days later, the(Fig. 3B). The combined use ofPTC and ERCP is also of T-tube was clamped and the patient was discharged from the hospital.
great use, paacularly when either* as eginent ofduct has The T-tube was removed 3 months later. Two years later the patient'sgreat use, particularly when either a segment Of duct has liver function test results have returned to normal, and he has nobeen resected or a stricture has occurred (Fig. 3C). symptoms.
Ann. Surg. * June 1987

BILIARY TRACT INJURIES 655The overall morbidity rate in the management of the
injuries in our study was 37%. Others have reportedmorbidity rates ranging from 22 to 32% in this verydifficult group of patients.7'8 The most serious morbidproblem in our patients has been that of recurrent cho-langitis; this has occurred in four patients, all of whomwere in group II. In two ofthese patients an anastomoticstenosis was demonstrated by PTC; one had surgicalrevision with relief of symptoms, whereas the other hasrefused surgical intervention. In two other patients noanastomotic stenoses have been demonstrated by PTC,and there was no reflux up their Roux-en-Y loops. Bis-muth et al. also described five patients with recurrentepisodes of cholangitis after Roux-en-Y hepaticojejun-ostomy in whom there was neither obstruction at theiranastomoses nor reflux of barium up their Roux-en-Yloops.'5 Based upon these experiences and those of Bis-muth et al., we are forced to conclude that cholangitismay occur after Roux-en-Y choledochoenterostomywithout an apparent anatomic cause.A critical question investigated in this study is the role
of internal stents in preventing subsequent biliary stric-tures. Once a biliary stricture occurs, ultimate mortalityrates range from 9 to 27% and usually result from hepa-tic failure.3"0 Whether or not internal stenting decreasesstricture formation is controversial. Several investigatorsfeel strongly that stents are beneficial and that the longera stent is in place, the better the result."3 Others havecontended that the necessity for long-term stents (6months to 1 year) exists only when there is marked fi-brosis in the area at the time ofreoperation.6'9 Our use ofstents in this study varied, with 11 of 19 (58%) patientshaving some type of internal stenting. Stenting in thepatients whose injuries were recognized and repairedduring surgery during their initial operations (group I)appeared to have little influence on their subsequentdevelopment of cholangitis, because none of these pa-tients had this complication develop. Even though thisexperience with a somewhat limited follow-up period(mean 2.5 years) does not clearly demonstrate the effi-cacy and need for use of stents in patients whose injuriesare discovered during surgery, we recommend at leastshort-term stenting (6-8 weeks) in such patients. Theprimary utility of stents in this group of patients is fordiversion of bile to allow healing of the repair and toprovide a means for subsequent radiographic examina-tion.
Stenting may have been ofgreater importance when itwas used for biliary tract injuries managed by reopera-tion (group II). It seems significant that three ofthe fourpatients in group II who later had cholangitis did nothave internal stenting at the time of their reparativeoperations. As a result ofthis experience, it is our recom-mendation that biliary tract injuries recognized later
and repaired during a secondary operation, when fi-brosis and inflammation are more marked, should haveinternal stenting for a period of 3-6 months. Eventhough the need for stents is not clear-cut, we believethat this approach will aid in ensuring healing with anadequate bile duct lumen.The overall mortality rate in our study of patients
managed within 3 weeks of their biliary tract injurieswas 11% (two patients); abdominal sepsis and organ fail-ure were the causes of death. This mortality rate is simi-lar to that in other reports that have noted an earlymortality rate ranging from 3 to 18% in this group ofseriously ill patients.`~
Conclusions
Factors associated with high rsk for biliary tract in-jury include acute cholecystitis and anatomically smallbiliary ducts, as are usually found in younger patients.The most common site of iatrogenic injury to the extra-hepatic biliary system is at the cystic duct-common bileduct junction. Failure to perform cholangiography dur-ing surgery may contribute to failure to diagnose biliarytract injuries during surgery. Injuries recognized duringsurgery can be repaired primarily with acceptable re-sults, but injuries diagnosed after surgery should be re-paired with Roux-en-Y choledochoenterostomies orwith the use of anastomic stents. Recurrent cholangitismay be related to the omission of stent usage and mayoccur in patients after surgery, even in the absence ofanastomotic stenoses.
References
1. Smith EB. latrogenic injuries to extrahepatic ducts and associatedvessels: a 25 year analysis. J Natl Med Assoc 1982; 74:735-738.
2. Hermann RE. A plea for a safer technique of cholecystectomy.Surgery 1976; 79:609-611.
3. Blumgart LH, Kelley CJ, Benjamin IS. Benign bile duct stricturefollowing cholecystectomy: critical factors in management. Br JSurg 1984; 71:836-843.
4. Warren KW, Mountain JC, Midell Al. Management of stricturesof the biliary tract. Surg Clin North Am 1971; 51:711-731.
5. Andren-Sandberg A, Alinder G, Bengmark S. Accidental lesionsof the common bile duct at cholecystectomy. Pre- and periop-erative factors of importance. Ann Surg 1985; 201:328-332.
6. Riggs T, Foshag L, Vargish T, Zimmerman B. Biliary tract injuriesfollowing routine cholecystectomy. Am Surg 1986; 52:312-314.
7. Hillis TM, Westbrook KC, Caldwell FT, Read R. Surgical injuryofthe common bile duct. Am J Surg 1977; 134:712-716.
8. Castrini G, Pappalardo G. Iatrogenic strictures of the bile ducts:our experience with 66 cases. World J Surg 1981; 5:753-758.
9. Kune G. Bile duct injury during cholecystectomy: causes, preven-tion and surgical repair in 1979. Aust NZ J Surg 1979; 49:35-40.
10. Glenn F. Iatrogenic injuries to the biliary ductal system. SGO1978; 146:430-434.
11. Coffins PG, Gorey TF. Iatrogenic biliary stricture: presentationand management. Br J Surg 1984; 71:980-982.
Vol. 205 * No. 6

656 BROWDER AND OTHERS Ann. Surg. * June 1987
12. Andren-Sandberg A, Johansson S, Bengmark S. Accidental lesionsof the common bile duct at cholecystectomy. II. Results oftreatment. Ann Surg 1985; 201:452-455.
13. Warren K, Poulantzas J, Kune G. Use of Y-tube splint in therepair of biliary strictures. SGO 1966; 122:785-790.
14. Belzer FO, Watts JM, Ross HB, Dunphy JE. Auto-reconstructionof the common bile duct after venous patch graft. Ann Surg1965; 162:346-355.
15. Bismuth H, Franco D, Corlette M, Hepp J. Longterm results ofRoux-en-Y hepaticojejunostomy. SGO 1978; 146:161-167.
DISCUSSION
DR. G. RAINEY WILLIAMS (Oklahoma City, Oklahoma): This beau-tiful presentation certainly adds to our knowledge ofhow to manage ahistorically difficult group of patients.The central question, of course, is why did these injuries occur, and
then the corollary, how they can be prevented. The authors did notaddress this because I suspect they do not know why the injuriesoccurred. I have diligently pursued this in a sizable series of patientsand conclude that it should be part of our surgical litany that nocholecystectomy is routine.
I believe one of the valuable aspects of this paper is the demonstra-tion that primary repair of a ductal injury recognized at the time islikely to be successful. Many ofus have believed this for some time, butit is hard to find data, and although these may not prove it, they aresupportive.
I agree that the most important diagnostic maneuver is the percu-taneous transhepatic cholangiography, and in these days of cost con-tainment we should go straight to that procedure. If it is successful, andit should be in about 95% ofattempts, it is no additional trouble to passa catheter into the biliary system and leave it. This catheter can do fourthings. First, it can decompress the biliary system. We agree with Pittand associates that this is not particularly valuable. The second thing isthat if the catheter is stiff enough, you can sometimes feel it, therebyminimizing the dissection. If you cannot feel it, you can inject dyethrough it and take a picture on the operating table. Either of thesemaneuvers may save significant operative time. Finally, if there is atube in place and you decide to use a stent, it is easy to attach the stentto the end of the catheter and withdraw it, thereby putting a transhe-patic stent in place.
Finally, without going into it in depth, I disagree with the authorsabout the use of stents. We rarely use them and have had a very lowincidence of postoperative cholangitis.
DR. JAMES D. HARDY (Jackson, Mississippi): I did not come pre-pared to discuss the paper, but there are two things I would like to drawattention to.
First, I want to add to the emphasis that has already been placed onavoiding permanent suture material inside the duct. Dr. Litwin hasindicted silk. Several years ago we treated a man with a gunshot woundof the liver whose bleeding had been controlled at his communityhospital, and he then was sent to us at University Hospital. Little ofthehepatic hilum was left. The stumps of the right and left hepatic ductswere found at a distance from each other, and a Roux-Y loop wasplaced using absorbable suture material for the internal sutures. Thepatient did well for several years. Later, a stricture developed, and oneofmy associates re-operated on the patient in my absence, but he usedProlene* sutures. Then, 2 or 3 years later the patient required stillanother exploration. Virtually every Prolene suture was surrounded bya hard berry-like calculus.My second point, though, and I believe it is even more important
than the first, is that when a patient who has had a bile duct stricturerepaired becomes jaundiced (the jaundice usually having been pre-ceded by a rising serum alkaline phosphatase level), recurrence ofstricture must be given first diagnostic consideration. The authors re-port that one or two of their patients had jaundice without a stricture.Perhaps in closing they would say more about these particular pa-tients? Biliary cirrhosis could have become a factor.
DR. ROBB H. RUTLEDGE (Fort Worth, Texas): Dr. Litwin's presen-tation shows us that the results of repair of an injured bile duct are
better if the problem is recognized and the repair done at the originaloperation. Forty per cent of his patients had repair primarily and faredbetter than the 60% who had repair secondarily. Forty per cent of theinjuries were a partial transection. He used both primary reanasto-moses and bypass procedures.
(Slide) Another method that occasionally will be helpful is a patchrepair. A patch can be used for a noncircumferential bile duct defect orfor a reanastomosis where only the back wall comes together withouttension.
(Slide) Depending on the circumstances, several patch materialsmay be available. Dr. Sandblom has reported on the successful use ofagallbladder patch. (Slide) Dr. Bengtsson has reported on a vascularizedjejunal patch. Both of these methods would have primary mucosalhealing.Other methods ofpatch repair (duodenal orjejunal onlay, prosthetic
material, or saphenous vein) all heal by ingrowth of columnar biliaryepithelium with the patch acting as a scaffold during the time of theautorepair. Although autologous material is preferred, Dr. Myers hashad a longstanding success with a patient with a knitted Teflone patch.
(Slide) A saphenous vein patch is especially appealing here. It can betailored to fit any bile duct defect. Belzer and Dunphy have shown thatthe vein patch shrinks, disappears, and cannot later be identified. It isessential to stent the vein patch for 2-4 months until the ingrowth ofbiliary epithelium is complete.
(Slide) In 1977, I used a vein patch to repair this noncircumferentialbiliary defect during a left hapatectomy. I left the T tube in about 3-4months. This worked well for about 4.5 years until the patient's deathof metastatic disease.
Dr. Litwin's report emphasized that biliary surgery must be donecarefully. If the bile duct is injured, immediate repair gives betterresults. Depending on the injury and tissues available, the surgeon hasa choice of several methods of repair.
DR. HERSCHEL A. GRAvES, JR. (Nashville, Tennessee): Dr. Litwin isto be congratulated for his impressive series of common bile ductinjuries and repair. I would like to present to you two contrasting casesthat have instructed me and may give you food for thought. It may be alittle bit at variance within the ongoing advice.Four years ago, a 25-year-old woman was referred to me 17 days
after her common duct had been unknowingly ligated during an elec-tive cholecystectomy and common duct exploration for stones. Heradmission bilirubin level was 30 mg/dL and she was afebrile and rela-tively asymptomatic. Her admission diagnosis was a retained commonbile duct stone. Her endoscopic retrograde cholangiopancreatographystudy, however, revealed blockage of the mid to upper common bileduct, and the transhepatic cholangiogram revealed the block to be justbelow the bifurcation ofthe right and left ducts. The diagnosis was nota retained stone but an iatrogenic common duct occlusion. The patientrefused additional surgery until after Christmas, 4 weeks hence, and adrainage catheter was left transhepatically. Even with this decompres-sion, she still had a large dilated ductal system that allowed a 2-cmanastomosis to a Roux-en-Y jejunal limb 1 month later, which in alllikelihood will never stricture.
In contrast, a 28-year-old woman was flown by helicopter from anoperating room 50 miles from Nashville immediately after a 1.5-cmplug had been resected from the common hepatic duct including thebifurcation. The ducts were small, the right and left branches measuredabout 3-4 mm each.On exploration, I considered ligating these small right and left ducts,
allowing them to dilate during the ensuing few weeks drawing on myexperience from a couple of years previously. However, such was notthe general recommendation from the surgical world and, as a repairwas technically feasible, the two hepatic ducts werejoined together side
Copyright © 2022 FDOKUMEN