Antibiotic Prophylaxis in Gastric, Biliary and Colonic Surgery
8
Antibiotic Prophylaxis in Gastric, Biliary and Colonic Surgery H. HARLAN STONE, M.D., C. ANN HOOPER, B.S., B.A., LAURA D. KOLB, B.S., CAROL E. GEHEBER, B.S., E. JANELLE DAWKINS, B.S. Antibiotic prophylaxis for surgery has appeared indicated when- ever likelihood of infection is great or consequences of such are catastrophic. For better clarification, a prospective, randomized, double-blind study was run on 400 patients undergoing elective gastric, biliary, and colonic operations. There were four treat- ment categories, with antibiotic being instituted 12 hours pre- operatively, just prior to operation, after operation, or not at all. During operation, samples of blood, viscera, muscle, and fat were taken for determination of antibiotic concentration. Both aerobic and anaerobic cultures were also taken of any viscus entered, peritoneal cavity, and incision. Similar cultures were run on all postoperative infections. Results demonstrated that the incidence of wound infection could be reduced significantly by the preopera- tive administration of antibiotic in operations on the stomach (22% to 4%), on the biliary tract (11% to 2%), and large bowel (16% to 6%). Less impressive results were obtained for peritoneal sepsis. Initiation of antibiotic postoperatively gave an almost identical infection rate as if antibiotic had not been given (15% and 16%, respectively). TrHE VALUE as well as dangers of prophylactic anti- biotics has been hotly debated for the past three decades. Lack of concrete data, as might be derived from either rigidly controlled laboratory studies or prospective randomized clinical trials, has by no means limited these arguments. Only the animal experiments of Burke4 and relatively sophisticated clinical trials by Polk,10, Ledger,7 and a few others have given any true insight as to the benefits of such a program.1 3'4'8 9 All other supportive re- ports have primarily been emotional claims, based upon either poorly or totally uncontrolled scientific evidence. There are, in addition, other advantages that might be gained through the administration of prophylactic anti- biotics. Hospital beds possibly could be conserved through a shortened average patient stay. Hospital costs From the Joseph B. Whitehead Department of Surgery, Emory University School of Medicine, 69 Butler St., S.E., Atlanta, Georgia 30303 could then likewise be reduced if less hospital days were consumed and if reoperation for some complicating in- fection were not as frequently required; while antibiotic use might even be decreased if fewer postoperative infections developed and, especially, if the duration of antibiotic prophylaxis was cut to a bare minimum. Nevertheless, potential harm resulting from routine antibiotic therapy cannot be ignored. Drug toxicity, allergic reactions, and in particular the evolution of resistant bacterial strains certainly appear to be potential if not actual significant threats. Clinical Trial To evaluate these several aspects of prophylactic anti- biotic therapy as well as to confirm the already reported benefits of its application, a prospective randomized and double-blinded study was carried out on the surgical wards of Grady Memorial Hospital. After 20 months (the trial period ending February 29, 1976), 400 consecutive patients admitted for elective operations on the stomach, biliary tract, and/or colon had been enrolled in the study. The only exceptions to inclusion into the study were antibiotic therapy with parenteral or orally absorbable agents during the 10 days immediately preceding opera- tion, conditions present that already demanded antibiotic prophylaxis (i.e., heart valve disease), known allergy to a cephalosporin, and an age of less than two years. Pa- tients undergoing colon surgery, however, did receive 1 gm of oral neomycin every 4 to 6 hours for two days prior to operation as well as 500 mg of erythromycin 443 Presented at the Annual Meeting of the American Surgical Associa- tion, New Orleans, Louisiana, April 7-9, 1976. Supported in part by a grant from Eli Lilly and Company.
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Antibiotic Prophylaxis in Gastric, Biliary and Colonic Surgery
Antibiotic Prophylaxis in Gastric, Biliary and Colonic Surgery
H. HARLAN STONE, M.D., C. ANN HOOPER, B.S., B.A., LAURA D. KOLB, B.S., CAROL E. GEHEBER, B.S.,E. JANELLE DAWKINS, B.S.
Antibiotic prophylaxis for surgery has appeared indicated when-ever likelihood of infection is great or consequences of such arecatastrophic. For better clarification, a prospective, randomized,double-blind study was run on 400 patients undergoing electivegastric, biliary, and colonic operations. There were four treat-ment categories, with antibiotic being instituted 12 hours pre-operatively, just prior to operation, after operation, or not at all.During operation, samples of blood, viscera, muscle, and fat weretaken for determination of antibiotic concentration. Both aerobicand anaerobic cultures were also taken of any viscus entered,peritoneal cavity, and incision. Similar cultures were run on allpostoperative infections. Results demonstrated that the incidenceof wound infection could be reduced significantly by the preopera-tive administration of antibiotic in operations on the stomach (22%to 4%), on the biliary tract (11% to 2%), and large bowel (16% to6%). Less impressive results were obtained for peritoneal sepsis.Initiation of antibiotic postoperatively gave an almost identicalinfection rate as if antibiotic had not been given (15% and 16%,respectively).
TrHE VALUE as well as dangers of prophylactic anti-biotics has been hotly debated for the past three
decades. Lack of concrete data, as might be derived fromeither rigidly controlled laboratory studies or prospectiverandomized clinical trials, has by no means limited thesearguments. Only the animal experiments of Burke4 andrelatively sophisticated clinical trials by Polk,10, Ledger,7and a few others have given any true insight as to thebenefits of such a program.1 3'4'8 9 All other supportive re-ports have primarily been emotional claims, based uponeither poorly or totally uncontrolled scientific evidence.There are, in addition, other advantages that might be
gained through the administration of prophylactic anti-biotics. Hospital beds possibly could be conservedthrough a shortened average patient stay. Hospital costs
From the Joseph B. Whitehead Department of Surgery,Emory University School of Medicine,
69 Butler St., S.E., Atlanta, Georgia 30303
could then likewise be reduced if less hospital days wereconsumed and if reoperation for some complicating in-fection were not as frequently required; while antibioticuse might even be decreased if fewer postoperativeinfections developed and, especially, if the duration ofantibiotic prophylaxis was cut to a bare minimum.
Nevertheless, potential harm resulting from routineantibiotic therapy cannot be ignored. Drug toxicity,allergic reactions, and in particular the evolution ofresistant bacterial strains certainly appear to be potentialif not actual significant threats.
Clinical Trial
To evaluate these several aspects of prophylactic anti-biotic therapy as well as to confirm the already reportedbenefits of its application, a prospective randomized anddouble-blinded study was carried out on the surgicalwards of Grady Memorial Hospital. After 20 months (thetrial period ending February 29, 1976), 400 consecutivepatients admitted for elective operations on the stomach,biliary tract, and/or colon had been enrolled in the study.The only exceptions to inclusion into the study were
antibiotic therapy with parenteral or orally absorbableagents during the 10 days immediately preceding opera-tion, conditions present that already demanded antibioticprophylaxis (i.e., heart valve disease), known allergy toa cephalosporin, and an age of less than two years. Pa-tients undergoing colon surgery, however, did receive 1gm of oral neomycin every 4 to 6 hours for two daysprior to operation as well as 500 mg of erythromycin
443
Presented at the Annual Meeting of the American Surgical Associa-tion, New Orleans, Louisiana, April 7-9, 1976.
Supported in part by a grant from Eli Lilly and Company.

STONE AND OTHERS
base every 6 hours for 24 hours preoperatively. Routineattempts were made to preclude any consideration ofantibiotic prophylaxis with respect to decision foroperation, procedure performed, and general postoper-ative care.
Antibiotic Administration
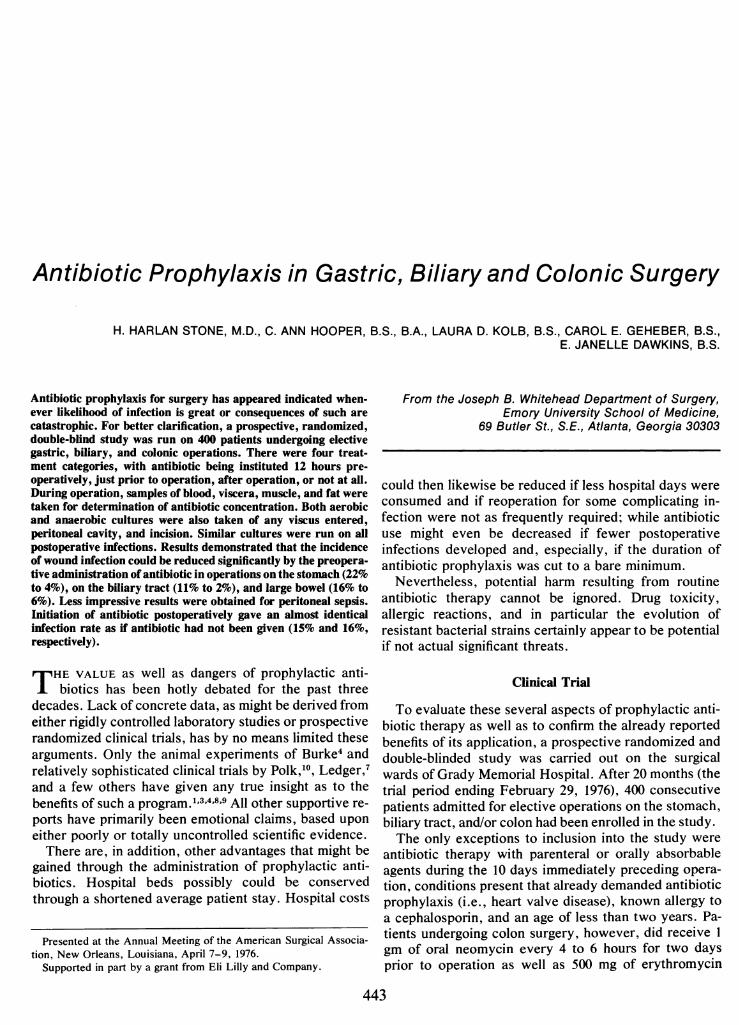
Each patient was given an intramuscular injection ofeither antibiotic (I gm of tefazolin) or placebo (equiv-alent volume of diluent) on the evening before opera-tion, on call to the operating room and on that sameevening after return to either the ward or the intensivecare unit, on the morning of the day following surgery,and again during the evening of the first postoperativeday (Fig. 1). Scaled down doses were used for children,with weight being the prime determinant. The solutionsfor injection had previously been assembled in patientnumber packets, so that there were five vials in each packand each vial was coded as to time when it should begiven. Details in randomization were unknown to all con-cerned with patient care, although the master key wasreadily available in the event that a possible drug orinfectious complication demanded that the code bebroken.Drug dosage had been set up so that equal numbers
of patients had their prophylactic antibiotic initiatedapproximately 12 hours preoperatively, one hour prior tooperation, or within an hour following completion of theoperation (Fig. 1). Twenty-five per cent of the patientsreceived no antibiotic at all. When given, cefazolin wasadministered in three consecutive injections for a totaldose of 3 gms over a period of approximately 24 hours.No other antimicrobial was given thereafter, that is,unless an established infection could be documentedor the patient's clinical course became highly suggestiveof a developing septic complication.
Sampling During Operation
At surgery, 9 specific specimens were taken. An at-tempt was generally made to obtain all samples withina few minutes of each other. Once the abdomen had beenopened, both peripheral as well as portal venous bloodwere drawn for determination of antibiotic blood levels.Likewise, liquid contents ofthe organ ofoperation (gastricjuice, bile, and/or colon contents) were obtained forsimilar analyses of antibiotic concentration. A modifiedwell-diffusion technique was used for these studies.13
Biop§ies of viscera resected as well as abdominal wallmuscle and subcutaneous fat were also taken. Thesespecimens were immediately frozen and then sent at inter-vals to the Lilly Research Laboratories for determina-tion of antibiotic tissue concentration.
Finally, both aerobic and anaerobic cultures were taken
of the contents of the organ subjected to operation,the peritoneal cavity, and the subcutaneous portion of theincision at the time of closure. Sensitivity testing wassubsequently run on all aerobic isolates to the 30 mcgdisc of cefazolin.2
FollowupPostoperatively, all patients were carefully followed for
evidences of infection developing within the abdomenand/or surgical incision. In addition, complicating infec-tions in other areas were specifically noted. Appropriateaerobic and anaerobic cultures were taken from all sitesof known as well as even suspected sepsis. Aerobicbacterial isolates were also tested for sensitivity to theprophylactic antibiotic, i.e., cefazolin, at a 30 mcg discsize.2Complications of drug therapy, other postoperative
problems, total as well as postoperative hospital stay,all details related to indications for surgery, type ofoperation, general status of the patient, and, finally,eventual outcome were faithfully recorded. These itemswere later used to confirm the purity of the randomiza-tion process plus the identification of any significantinfluence, other than the prophylactic antibiotic, on theincidence of subsequent infection.
Results
At the completion of the clinical trial, there were 100patients for analysis in each treatment category. Gastricsurgery had been performed on 96, a biliary tractprocedure on 131, and colon surgery on 190-therebygiving a total of 417 operations. The extra 17 were ac-counted for by the fact that these patients had had asurgical procedure carried out in two, rather thanjust one,area of study.Ages ranged from 2 to 86 years, with an average of 47.6.
There were 179 males and 221 females; 312 were Negro,while 88 were Caucasian. No significant difference couldbe found between the four assigned treatment groupswith respect to type of operation, indication for surgery,age, sex, or race.There were four postoperative deaths, three of which
occurring in patients who had had two procedures doneat the one operation. Otherwise, no major difference wasapparent between the several therapy categories.
Antibiotic Distribution
Concentrations of cefazolin were not significantlydifferent when portal was compared to peripheral venousblood (Table 1). The average value was 13.7 mcg/ml.
Administration of cefazolin 8 to 12 hours prior tooperation gave approximately 40% higher tissue levels
444 Ann. Surg. o October 1976
ANTIBIOTIC PROPHYLAXIS
FIG. 1. Times of antibioticadministration. Placebo in-jections are indicated by an
"O"; cefazolin was givenat times marked by an "X."
than if the antibiotic had been started a mere hour pre-
operatively (Table 1). Concentrations of cefazolin in sub-cutaneous fat were less than half that of the blood when-ever antibiotic therapy had been instituted only an hourbefore hand. In fact, antibiotic concentrations in fat and inbowel wall were consistently below values discovered inother tissues. Stomach and gallbladder had biologicallymeasurable concentrations of cefazolin in their walls thateven surpassed concomitant blood levels, yet such may
well have been due to the additive bacteriocidal effectof acid and bile, respectively.
Analyses of bile and gastric juice for cefazolinconcentrations were undoubtedly spurious because oftheir already known antimicrobial actions (Table 1).Similarly, the preoperative administration of oral neo-
mycin and erythromycin base may well have accountedfor the apparent presence of study antibiotic in coloncontents, irrespective as to whether cefazolin had beenadministered preoperatively or not.
Incidence of Infection
The reduction in incidence of intraperitoneal sepsiswas relatively significant (P = 0.05) whenever prophy-
Table 1. Distribution of Chefazolin at Operation:Antibiotic Administered Preoperatively
Antibiotic BegunPreoperatively
8-12 Hours 1 Hour
Peripheral venous blood mcg/ml 14.1 13.5Portal venous blood mcg/ml 13.8 13.4Abdominal muscle mcg/gm 14.0 9.3Subcutaneous fat mcg/gm 9.8 6.3Gastric secretions mcg/ml 14.3 11.2Bile mcg/ml 22.5 21.4Colon contents mcg/ml 22.3 20.4Stomach wall mcg/gm 15.9 12.9
Gall bladder wall mcg/gm 21.3 14.9Colon wall mcg/gm 11.0 9.8
lactic antibiotic had been started preoperatively (Table 2).Results were much more impressive with procedures on
the colon than for operations on the stomach and biliarytract. However, no real difference could be discernedbetween the two groups receiving preoperative cefazolin,that is, between those patients having such therapyinstituted 8 to 12 hours prior to operation and thosewhose antibiotic was not begun until just an hour beforesurgery. By contrast, the incidence of peritoneal sepsiswas essentially the same as if no antibiotic had beengiven whenever cefazolin administration had been put offuntil after operation.
Differences in wound infection rate were much more
dramatic than were those for intraperitoneal sepsis (Table3). Overall, there was an almost four-fold greater inci-dence of infection within the incision when antibioticwas withheld than when such had been given preopera-
tively. Initiating cefazolin therapy after operation gave
approximately the same results as if the parenteral anti-biotic had been completely withheld. All of thesefigures were highly significant (P = .01). As with intra-peritoneal infection, results obtained in the two preoper-ative treatment groups were almost identical.
Table 2. Peritoneal Infection
Antibiotic BegunAreaof 8-12 hr I hr 1-4 hr Never
Operation Preop Preop Postop Given Totals
Gastric 22 27 24 23 96
Infected 1 1 1 2 5Incidence 5% 4% 4% 9%o 5%
Biliary 29 31 33 38 131Infected 1 0 1 1 3Incidence 3% - 3% 3% 2%
Colonic 54 47 46 43 190
Infected 1 1 3 3 8
Incidence 2% 2% 7% 7% 4%Totals 100 100 100 100 400
Infected 2 2 5 6 15
Incidence 2% 2% 5% 5% 4%
445
PRE-OP DAY OF POST-OPGROUP DAY 1 OPERATION DAY AGROU l|AM PM-t AM |PM ||AM |PE
I x x x 0 0
Ii 0 X X X 0
III 0 0 X X X
IV 0 0 0 0 0
Vol. 184oNo. 4
Ann. Surg. EOctober 1976
Table 3. Wound Infection
Antibiotic BegunAreaof 8-12 hr I hr 1-4 hr Never
Operation Preop Preop Postop Given Totals
Gastric 22 27 24 23 96Infected 1 1 4 5 11Incidence 5% 4% 17% 22% 11%
Biliary 29 31 33 38 131Infected 1 0 3 4 8Incidence 3% 9% 11% 6%
Colonic 54 47 46 43 190Infected 3 3 7 7 20Incidence 6% 6% 15% 16%c 11%
Totals 100 100 100 100 400Infected 4 3 14 15 36Incidence 4% 3% 14% 15% 9%
Bacterial Contamination
Exactly half of the patients had positive cultures of thewound and/or peritoneum at the time of operation; and,of these, 35 or 17.5% had Staphylococcus aureus as oneof the bacterial contaminants (Table 4). Preoperativeantibiotic prophylaxis gave a wound infection rate of only7% in those patients with culture proven contamination;while postoperative cefazolin administration or no anti-biotic treatment at all produced infection rates of 24%and 29%, respectively, for the same degree of bacterialcontamination. The incidence of wound infection due toStaphylococcus aureus was similarly affected in bothtreatment groups by the action of preoperative prophy-lactic therapy.A striking contrast to this increased incidence of in-
fection was the exceedingly rare development of inci-
Table 4. Bacterial Contamination and Wound Infection
Operative Culture of Woundand Peritoneum
Antibiotic Positive Positive NegativeBegun Culture Staph. Culture
Preoperative 96 13 104Infected 7 1 0Incidence 7% 8% 0%
Postoperative 55 10 45Infected 13 3 1Incidence 24% 30%W 2%
Never given 49 12 51Infected 14 3 1Incidence 29% 25% 2%
sional sepsis when all intraoperative wound as well as
peritoneal cultures had been negative (Table 4).Although the majority of bacterial isolates recovered
from organs of operation could be classified as gram-
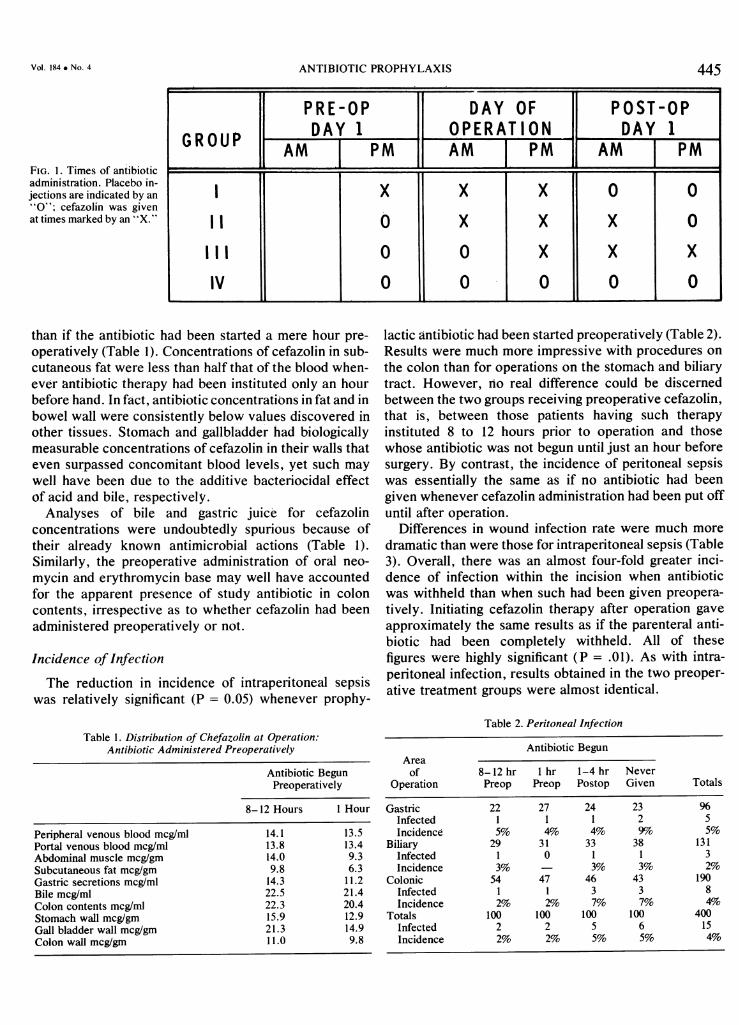
negative rods, such species were even more predominantin operations on the colon (Table 5). In addition,anaerobes and Enterococcus were also plentiful in thecolonic flora. Antimicrobial sensitivity of the 790aerobic isolates obtained at operation was 74.8% to the 30mcg cefazolin disc. On the other hand, the actual andnot just potential contaminants (i.e., isolates from thewound and/or peritoneum alone) had a much greatersusceptibility to cefazolin (91.2%) (Fig. 2). Aerobicbacteria cultured from all complicating wound andperitoneal infections, however, had sensitivities thataveraged only 39% (Table 5 and Fig. 2).The total number of bacteria contaminating the wound
also appeared to influence the likelihood of subsequent
TABLE 5. Bacterial Sensitivities to Cefazolin: Testing to 30 mcg Antibiotic Disc.
Gastric Isolates Biliary Isolates Colon Isolates Total Initial Infection Isolates
Per cent Per Cent Per Cent Per Cent Per CentSpecies Isolated Number Sensitive Number Sensitive Number Sensitive Number Sensitive Number Sensitive
E. coli 49 47 31 30 159 137 239 90%G 18 61%E. species 4 2 2 2 8 6 14 71% - -Klebsiella-Enterobacter 6 5 2 2 16 15 24 92% 8 38%Klebsiella species 32 31 13 12 58 54 103 94% 8 75%Proteus mirablis 13 12 3 3 17 16 33 94% 4 50%cProteus species 8 1 2 0 38 10 48 23% 12 68%Pseudomonas 6 0 0 21 0 27 O% 7 0%Other G-neg rods 13 13 8 4 7 6 28 82% 10 10%Staph aureus 24 24 36 34 33 32 93 97% 11 64%oB. Streptococcus 3 3 1 1 2 2 6 10%-Enterococcus 43 22 18 4 205 54 266 30%o 22 9WMisc. aerobes 4 4 0 5 3 9 78%-Bacteroides 23 * 6 * 52 * 81 * 2 *Eubacteria 13 * 4 * 32 * 49 * I *Pepto & Peptostrepto 17 * 3 * 16 * 36 * 1 *Clostridia 10 * 5 * 21 * 36 * *Misc. anaerobes 79 * 27 * 69 * 175 * 18 *C. albicans 3 * 0 * 6 * 9 * 0 *
* Sensitivities not run.
446 STONE AND OTHERS

ANTIBIOTIC PROPHYLAXIS
C')zcog~u)E0
(02-o00z0=L) 2
0
0.0
1%1*1
100
Pm-operativ Post-0pative Never GivenTIME OF BEGINNING ANTIBIOIlC
FIG. 2. Antibiotic sensitivities of the bacterial isolates. Bacterialsusceptibility to 30 mcg discs of cefazolin is charted according totime of initiating antibiotic therapy. Shaded bars represent results ob-tained from taking initial isolates, while the clear bars reflect sensitivitiesof bacteria cultured from subsequent wound and/or peritonealinfections.
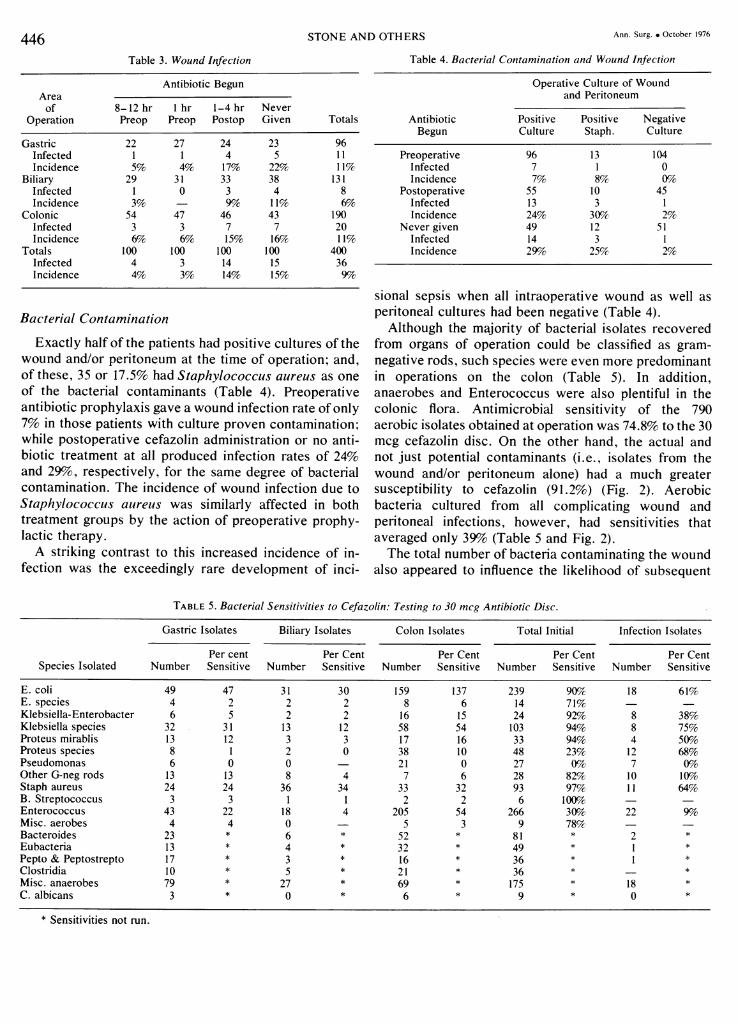
infection (Fig. 3). This was especially true in patientsnot given preoperative antibiotic or in whom cefazolinadministration was delayed until the patient had reachedthe recovery room. Nevertheless, antibiotic therapy in
80
FIG. 3. Relationship of thenumber of bacterial speciescontaminating the incisionat the time of wound clos-ure and incidence of sub-sequent wound infection.
06O
60
z
Z 400
IL0
0Z 20b
PREIOPECEFA2
no way altered the infection rate when the contaminat-ing bacteria were already resistant to the antimicrobialagent given, i.e., cefazolin.
This relationship of number of bacterial species toincidence of complicating infection was dramatically re-flected in the culture data as well as the disease processfor which gastric operations were done (Table 6). Hyper-acidity was associated with a relatively sterile stomachlumen and accordingly resulted in only a single postopera-tive infection. Such contrasted strikingly to the 30%oaverage infection rate when surgery was performed forgastric cancer or a benign gastric ulcer.
Cause ofInfection
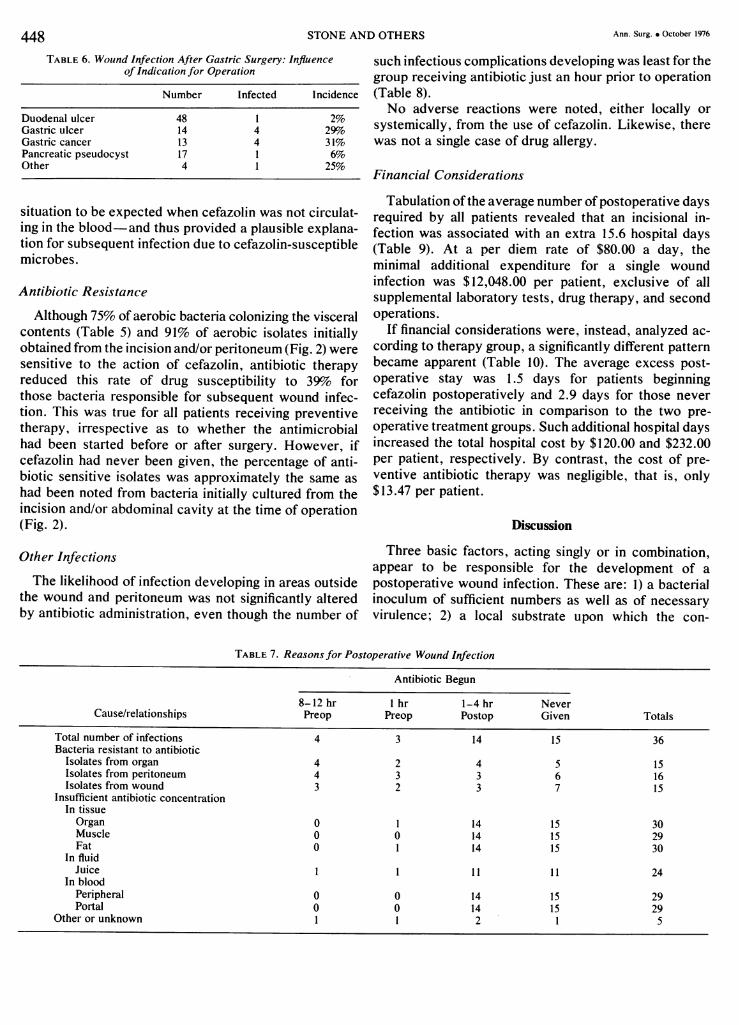
All seven of the wound infections occurring in pa-tients who received preoperative antibiotic could be ex-plained, at least on theoretical grounds, by a wound and/orperitoneal contamination by cefazolin-resistant bacteria(Table 7). One of the patients, in addition, had an anti-biotic concentration in his subcutaneous fat which mightwell be deemed insufficient for the control of an inoculumcontaining otherwise susceptible pathogens.
Patients who never received preventative antibioticor whose antimicrobial therapy was begun in the post-operative phase had infection rates, specifically due tocefazolin-resistant bacteria, that were almost identicalto what had been noted for the preoperative treatmentgroups (Table 7). However, none of the tissues of thelate or not-treated patients contained antibiotic-a
.pATIV/E I CEFAZOLIN NEVER ORZOLIN POST-OPERATIVELY
/
o--o Cefozwin ms=stant
Ir . sC,nI I I I I, I I II 2 3 4 5 5+ 1 2 3
NUMBER OF BACTERIAL SPECIES ISOLATED(from incision at time of closu)
4 5 5+
447Vol. 184 a No. 4
Ann. Surg. v October 1976
TABLE 6. Wound Infection After Gastric Surgery: Influenceof Indication for Operation
Number Infected Incidence
Duodenal ulcer 48 1 2%Gastric ulcer 14 4 29%oGastric cancer 13 4 31%Pancreatic pseudocyst 17 1 6%Other 4 1 25%
situation to be expected when cefazolin was not circulat-ing in the blood-and thus provided a plausible explana-tion for subsequent infection due to cefazolin-susceptiblemicrobes.
Antibiotic Resistance
Although 75% of aerobic bacteria colonizing the visceralcontents (Table 5) and 91% of aerobic isolates initiallyobtained from the incision and/or peritoneum (Fig. 2) weresensitive to the action of cefazolin, antibiotic therapyreduced this rate of drug susceptibility to 39o forthose bacteria responsible for subsequent wound infec-tion. This was true for all patients receiving preventivetherapy, irrespective as to whether the antimicrobialhad been started before or after surgery. However, ifcefazolin had never been given, the percentage of anti-biotic sensitive isolates was approximately the same ashad been noted from bacteria initially cultured from theincision and/or abdominal cavity at the time of operation(Fig. 2).
Other Infections
The likelihood of infection developing in areas outsidethe wound and peritoneum was not significantly alteredby antibiotic administration, even though the number of
such infectious complications developing was least for thegroup receiving antibiotic just an hour prior to operation(Table 8).No adverse reactions were noted, either locally or
systemically, from the use of cefazolin. Likewise, therewas not a single case of drug allergy.
Financial Considerations
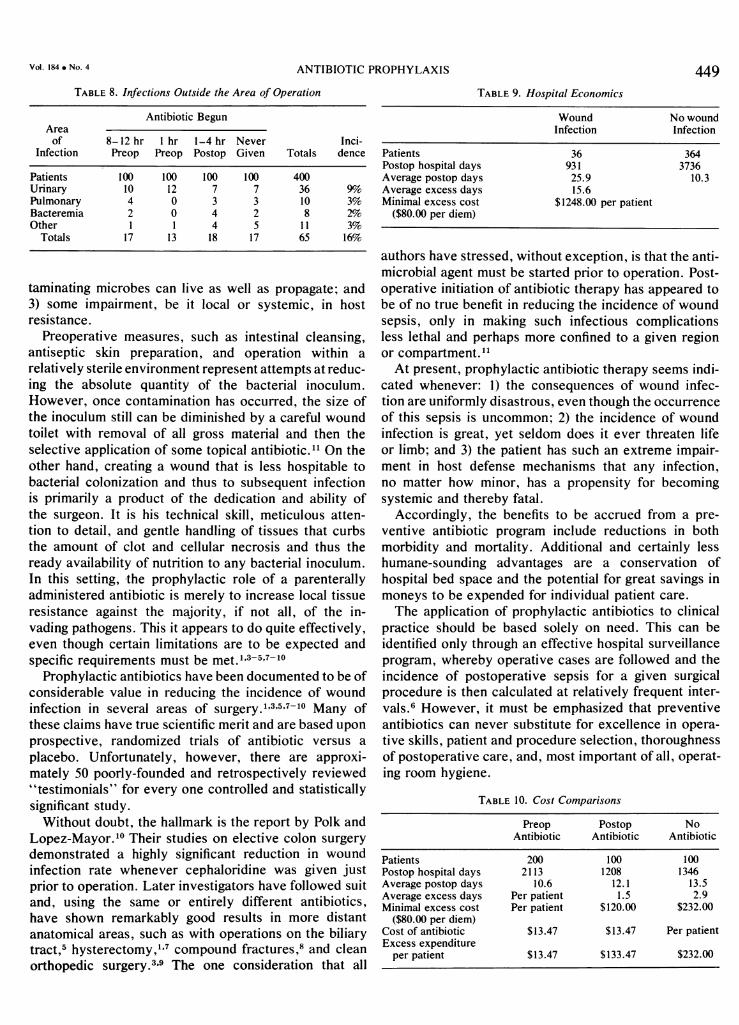
Tabulation of the average number of postoperative daysrequired by all patients revealed that an incisional in-fection was associated with an extra 15.6 hospital days(Table 9). At a per diem rate of $80.00 a day, theminimal additional expenditure for a single woundinfection was $12,048.00 per patient, exclusive of allsupplemental laboratory tests, drug therapy, and secondoperations.
If financial considerations were, instead, analyzed ac-
cording to therapy group, a significantly different patternbecame apparent (Table 10). The average excess post-operative stay was 1.5 days for patients beginningcefazolin postoperatively and 2.9 days for those neverreceiving the antibiotic in comparison to the two pre-operative treatment groups. Such additional hospital daysincreased the total hospital cost by $120.00 and $232.00per patient, respectively. By contrast, the cost of pre-ventive antibiotic therapy was negligible, that is, only$13.47 per patient.
Discussion
Three basic factors, acting singly or in combination,appear to be responsible for the development of apostoperative wound infection. These are: 1) a bacterialinoculum of sufficient numbers as well as of necessaryvirulence; 2) a local substrate upon which the con-
TABLE 7. Reasons for Postoperative Wound Infection
Antibiotic Begun
8-12 hr I hr 1-4 hr NeverCause/relationships Preop Preop Postop Given Totals
Total number of infections 4 3 14 15 36Bacteria resistant to antibiotic
Isolates from organ 4 2 4 5 15Isolates from peritoneum 4 3 3 6 16Isolates from wound 3 2 3 7 15
Insufficient antibiotic concentrationIn tissueOrgan 0 1 14 15 30Muscle 0 0 14 15 29Fat 0 1 14 15 30
In fluidJuice 1 1 11 11 24
In bloodPeripheral 0 0 14 15 29Portal 0 0 14 15 29
Other or unknown 1 1 2 1 5
448 STONE AND OTHERS
ANTIBIOTIC PROPHYLAXIS
TABLE 8. Infections Outside the Area of Operation
Antibiotic BegunAreaof 8-12 hr 1 hr 1-4 hr Never Inci-
Infection Preop Preop Postop Given Totals dence
Patients 100 100 100 100 400Urinary 10 12 7 7 36 9%OPulmonary 4 0 3 3 10 3%Bacteremia 2 0 4 2 8 2%Other I 1 4 5 11 3%
Totals 17 13 18 17 65 16%O
taminating microbes can live as well as propagate; and3) some impairment, be it local or systemic, in hostresistance.
Preoperative measures, such as intestinal cleansing,antiseptic skin preparation, and operation within a
relatively sterile environment represent attempts at reduc-ing the absolute quantity of the bacterial inoculum.However, once contamination has occurred, the size ofthe inoculum still can be diminished by a careful woundtoilet with removal of all gross material and then theselective application of some topical antibiotic."1 On theother hand, creating a wound that is less hospitable tobacterial colonization and thus to subsequent infectionis primarily a product of the dedication and ability ofthe surgeon. It is his technical skill, meticulous atten-tion to detail, and gentle handling of tissues that curbsthe amount of clot and cellular necrosis and thus theready availability of nutrition to any bacterial inoculum.In this setting, the prophylactic role of a parenterallyadministered antibiotic is merely to increase local tissueresistance against the majority, if not all, of the in-vading pathogens. This it appears to do quite effectively,even though certain limitations are to be expected andspecific requirements must be met. 1'3-5'7-10
Prophylactic antibiotics have been documented to be ofconsiderable value in reducing the incidence of woundinfection in several areas of surgery.13'57-10 Many ofthese claims have true scientific merit and are based uponprospective, randomized trials of antibiotic versus a
placebo. Unfortunately, however, there are approxi-mately 50 poorly-founded and retrospectively reviewed"testimonials" for every one controlled and statisticallysignificant study.Without doubt, the hallmark is the report by Polk and
Lopez-Mayor.10 Their studies on elective colon surgerydemonstrated a highly significant reduction in woundinfection rate whenever cephaloridine was given justprior to operation. Later investigators have followed suitand, using the same or entirely different antibiotics,have shown remarkably good results in more distantanatomical areas, such as with operations on the biliarytract,5 hysterectomy,1'7 compound fractures,8 and cleanorthopedic surgery.3'9 The one consideration that all
449TABLE 9. Hospital Economics
Wound No woundInfection Infection
Patients 36 364Postop hospital days 931 3736Average postop days 25.9 10.3Average excess days 15.6Minimal excess cost $1248.00 per patient
($80.00 per diem)
authors have stressed, without exception, is that the anti-microbial agent must be started prior to operation. Post-operative initiation of antibiotic therapy has appeared tobe of no true benefit in reducing the incidence of woundsepsis, only in making such infectious complicationsless lethal and perhaps more confined to a given regionor compartment.11At present, prophylactic antibiotic therapy seems indi-
cated whenever: 1) the consequences of wound infec-tion are uniformly disastrous, even though the occurrenceof this sepsis is uncommon; 2) the incidence of woundinfection is great, yet seldom does it ever threaten lifeor limb; and 3) the patient has such an extreme impair-ment in host defense mechanisms that any infection,no matter how minor, has a propensity for becomingsystemic and thereby fatal.
Accordingly, the benefits to be accrued from a pre-ventive antibiotic program include reductions in bothmorbidity and mortality. Additional and certainly lesshumane-sounding advantages are a conservation ofhospital bed space and the potential for great savings inmoneys to be expended for individual patient care.The application of prophylactic antibiotics to clinical
practice should be based solely on need. This can beidentified only through an effective hospital surveillanceprogram, whereby operative cases are followed and theincidence of postoperative sepsis for a given surgicalprocedure is then calculated at relatively frequent inter-vals.6 However, it must be emphasized that preventiveantibiotics can never substitute for excellence in opera-tive skills, patient and procedure selection, thoroughnessof postoperative care, and, most important of all, operat-ing room hygiene.
TABLE 10. Cost Comparisons
Preop Postop NoAntibiotic Antibiotic Antibiotic
Patients 200 100 100Postop hospital days 2113 1208 1346Average postop days 10.6 12.1 13.5Average excess days Per patient 1.5 2.9Minimal excess cost Per patient $120.00 $232.00
($80.00 per diem)Cost of antibiotic $13.47 $13.47 Per patientExcess expenditure
per patient $13.47 $133.47 $232.00
VOl. 184 . NO. 4

450 STONE AND OTHERS Ann. Surg. * October 1976
Once the need for prophylactic antibiotic has beenjustified because of a proven significant incidence ofwound infection after surgery in a certain area or opera-tion for a specific patient condition, the responsiblebacteria must then be tabulated as a part of the samesurveillance procedure.6 From such data, plus informa-tion available from both the literature as well as thehospital laboratory on antimicrobial sensitivities of theseresponsible pathogens, several antibiotics can be intelli-gently evaluated for possible use in a preventiveprogram. Prime considerations are: 1) a reported as wellas the individual hospital experience confirming specificantibiotic effectiveness against the anticipated path-ogens; 2) lack of toxicity and rare allergic reactions;3) a tissue distribution that will permit the antimicrobialagent to reach those body areas with a known predilec-tion for postoperative infection and in concentrationsknown to be effective; 4) an established time/dose/routerelationship that will assure antibiotic tissue levels atthe time of anticipated contamination4; 5) elimination ofall antimicrobial agents which presently serve (or haveno immediately available substitute) as first choice anti-biotics for the more usual postoperative infections, suchas those of the wound or peritoneum; and 6) expectedcost of preventive drug therapy for each individualantibiotic under consideration.From such information, a practical selection as to
specific antibiotic for a given operation can then be made.In the future, cephalosporins will probably be the singlegroup of drugs most commonly employed, although re-quirements will indeed vary from hospital to hospital be-cause of entirely different infectious problems to be over-come. Thus, considerable variation in the exact prophy-lactic antibiotic program should be expected and evenencouraged. Nevertheless, it is extremely important thatpreventive treatment not be abused. Otherwise, surgicalskills will deteriorate; and antibiotic-resistant microbesmay then become even more dominant in the standardhospital flora than they now are.12
Conclusions
Antibiotic prophylaxis against sepsis following electivesurgery has appeared indicated whenever likelihood ofinfection is great or consequences of such, though rare,are catastrophic. For better clarification, the value of pre-ventive antimicrobials was assessed in a prospective,randomized, double-blind study of 400 patients under-going elective gastric, biliary, and colonic operations.There were four treatment categories, with antibiotic
(cefazolin) being instituted: 1) 12 hours preoperatively;2) just prior to operation; 3) just after operation; or 4)never. The placebo could be distinguished only bybreaking the numbered code. During operation, samplesofperipheral and portal venous blood, visceral secretions,
organ resected, abdominal muscle and subcutaneous fatwere taken for determination of antibiotic concentra-tion. Both aerobic and anaerobic cultures were alsotaken of any hollow viscus entered, peritoneal cavity,and abdominal incision at closure. Similar cultures wererun on all postoperative infections.
Results demonstrated that the incidence of wound in-fection could be cut significantly by timely administrationof prophylactic antibiotic in operations on the stomach(22% to 4%), on the biliary tract (11% to 2%) and largebowel (16% to 6%), all with P values of .01. Lessimpressive results, though almost as significant (P = 0.05),were obtained for peritoneal sepsis. However, for pro-phylaxis to be successful, the antibiotic had not onlyto be effective against anticipated bacterial con-taminants, but present in the circulating blood and, moreespecially, in local tissues at the time of contamina-tion. Indeed, initiation of antibiotic postoperatively gavealmost the same wound infection rate as if antibiotichad not been given at all (15% and 16%, respectively).
Evolution of antibiotic resistant bacterial strains andgreater hospital economy in beds and money were addi-tional important considerations.
References
1. Allen, J. L., Rampone, J. F., and Wheeless, C. R.: Use of aProphylactic Antibiotic in Elective Major Gynologic Opera-tions. Obstet. Gynecol., 39:218, 1972.
2. Bauer, A. W., Kirby, W. M. M., Sherris, J. C., and Turk, M.:Antibiotic Susceptibility Testing by a Standardized Single DiscMethod. Am. J. Clin. Pathol., 45:493, 1966.
3. Boyd, R. J., Burke, J. F., and Colton, T.: A Double-BlindClinical Trial of Prophylactic Antibiotics in Hip Fractures. J.Bone Joint Surg., 55-A:1251, 1973.
4. Burke, J. F.: The Effective Period of Preventive AntibioticAction in Experimental Incisions and Dermal Lesions. Surgery,50:161, 1961.
5. Chetlin, S. H., and Elliott, D. W.: Preoperative Antibiotics inBiliary Surgery. Arch. Surg., 107:319, 1973.
6. Cruse, P. J. E., and Foord, R.: A Five-Year ProspectiveStudy of 23,649 Surgical Wounds. Arch Surg., 107:206, 1973.
7. Ledger, W. J., Sweet, R. L., and Headington, J. T.: ProphylacticCephaloridine in the Prevention of Postoperative Pelvic Infec-tions in Premenopausal Women Undergoing Vaginal Hyster-ectomy. Am. J. Obstet. Gynecol., 115:766, 1973.
8. Patzakis, M. J., Harvey, J. P. and Ivler, D.: The Role of Anti-biotics in the Management of Open Fractures. J. Bone JointSurg., 56-A:532, 1974.
9. Pavel, A., Smith, R. L., Ballard, A., and Larsen, I. J.: ProphylacticAntibiotics in Clean Orthopaedic Surgery. J. Bone Joint Surg.,56-A: 777, 1974.
10. Polk, H. C., Jr., and Lopez-Mayor, J. F.: Postoperative WoundInfection: A Prospective Study of Determinant Factors andPrevention. Surgery, 66:97, 1969.
11. Stone, H. H., and Hester, T. R., Jr.: Incisional and PeritonealInfection After Emergency Celiotomy. Ann. Surg., 177:669,1973.
12. Stone, H. H., and Kolb, L. D.: The Evolution and Spread ofGentamicin-Resistant Pseudomonads. J. Trauma, 11:586, 1971.
13. Winters, R. E., Litwack, K. D., and Hewitt, W. L.: Relation Be-tween Dose and Levels of Gentamicin in Blood. J. Infect. Dis.,124; Supplement: 590, 1971.