Hybrid SPECT-CT: An Additional Technique for Sentinel Node Detection of Patients with Invasive...
9
Bladder Cancer Hybrid SPECT-CT: An Additional Technique for Sentinel Node Detection of Patients with Invasive Bladder Cancer Amir Sherif a, * ,1 , Ulrike Garske b,1 , Manuel de La Torre c , Magnus Tho ¨rn d a Department of Urology, Uppsala University Hospital, Uppsala, Sweden b Department of Medical Sciences/Nuclear Medicine,Uppsala University Hospital, Uppsala, Sweden c Department of Pathology and Cytology, Uppsala University Hospital, Uppsala, Sweden d Department of Surgery, Karolinska Institute, South Stockholm General Hospital, Stockholm, Sweden european urology 50 (2006) 83–91 available at www.sciencedirect.com journal homepage: www.europeanurology.com Article info Article history: Accepted March 1, 2006 Published online ahead of print on March 20, 2006 Keywords: Bladder cancer Computed tomography Lymphoscintigraphy Sentinel node Abstract Objectives: To explore the feasibility of performing lymphoscintigraphy com- bined with computed tomography (CT) for preoperative detection of sentinel lymph nodes in patients with invasive bladder cancer. Materials: Six consecutive patients scheduled for radical cystectomy underwent lymphoscintigraphy after transurethral injection of Albures-technetium 99m in the detrusor muscle peritumourally both with planar imaging and with single- photon emission computed tomography/CT (SPECT/CT). CT for anatomic fusion was performed directly after the SPECT/CT and both investigations were combined to a fused image. Radical cystectomy started with extended lymphadenectomy and intraoperative detection of sentinel nodes with both Geiger probe and dye marker. The conventional planar lymphoscintigraphies and the fused SPECT/CT were compared with each other and with the outcome of intraoperative sentinel node detection and final histopathologic analyses. Results: The method allowed anatomically detailed preoperative visualisation of 21 sentinel nodes in five of the six patients, whereas planar pictures only visualised two sentinel nodes in two of six patients. Two patients had lymph node metastases and in the other four the nodes were negative. The combined method visualised all metastatic sentinel nodes, whereas planar lymphoscinti- graphy detected only one of six node metastases. Conclusions: The combination of lymphoscintigraphy with CT enhanced preo- perative anatomic localisation of sentinel nodes in bladder cancer and aided in the identification of sentinel nodes during surgery. The yield of detected sentinel nodes, both metastatic and nonmetastatic, was markedly increased using the combined method compared to conventional planar lymphoscintigraphy. # 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved. 1 Both authors contributed equally to this work. * Corresponding author. Department of Urology, Akademiska University Hospital, SE-751 85 Uppsala, Sweden. Fax: +46 18 50 79 07. E-mail address: [email protected] (A. Sherif). 0302-2838/$ – see back matter # 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2006.03.002
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Hybrid SPECT-CT: An Additional Technique for Sentinel Node Detection of Patients with Invasive...
Bladder Cancer
Hybrid SPECT-CT: An Additional Technique for Sentinel NodeDetection of Patients with Invasive Bladder Cancer
Amir Sherif a,*,1, Ulrike Garske b,1, Manuel de La Torre c, Magnus Thorn d
aDepartment of Urology, Uppsala University Hospital, Uppsala, SwedenbDepartment of Medical Sciences/Nuclear Medicine,Uppsala University Hospital, Uppsala, SwedencDepartment of Pathology and Cytology, Uppsala University Hospital, Uppsala, SwedendDepartment of Surgery, Karolinska Institute, South Stockholm General Hospital, Stockholm, Sweden
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 8 3 – 9 1
avai lab le at www.sciencedi rect .com
journa l homepage: www.europeanurology.com
Article info
Article history:Accepted March 1, 2006Published online ahead ofprint on March 20, 2006
Keywords:Bladder cancerComputed tomographyLymphoscintigraphySentinel node
Abstract
Objectives: To explore the feasibility of performing lymphoscintigraphy com-bined with computed tomography (CT) for preoperative detection of sentinellymph nodes in patients with invasive bladder cancer.Materials: Six consecutive patients scheduled for radical cystectomy underwentlymphoscintigraphy after transurethral injection of Albures-technetium 99m inthe detrusor muscle peritumourally both with planar imaging and with single-photon emission computed tomography/CT (SPECT/CT). CT for anatomic fusionwas performed directly after the SPECT/CT and both investigations were combinedtoa fused image. Radical cystectomy started with extended lymphadenectomy andintraoperative detection of sentinel nodes with both Geiger probe and dye marker.The conventional planar lymphoscintigraphies and the fused SPECT/CT werecompared with each other and with the outcome of intraoperative sentinel nodedetection and final histopathologic analyses.Results: The method allowed anatomically detailed preoperative visualisation of21 sentinel nodes in five of the six patients, whereas planar pictures onlyvisualised two sentinel nodes in two of six patients. Two patients had lymphnode metastases and in the other four the nodes were negative. The combinedmethod visualised all metastatic sentinel nodes, whereas planar lymphoscinti-graphy detected only one of six node metastases.Conclusions: The combination of lymphoscintigraphy with CT enhanced preo-perative anatomic localisation of sentinel nodes in bladder cancer and aided inthe identification of sentinel nodes during surgery. The yield of detected sentinelnodes, both metastatic and nonmetastatic, was markedly increased using thecombined method compared to conventional planar lymphoscintigraphy.# 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved.
1 Both authors contributed equally to this work.* Corresponding author. Department of Urology, Akademiska University Hospital, SE-751 85Uppsala, Sweden. Fax: +46 18 50 79 07.E-mail address: [email protected] (A. Sherif).
0302-2838/$ – see back matter # 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2006.03.002
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 8 3 – 9 184
1. Introduction
Detection of sentinel nodes as a tool for node staginghas been explored and implemented with clinicalsuccess in the surgical treatment of breast cancer [1]and malignant melanoma [2]. Recently, we per-formed sentinel node detection in patients withinvasive bladder cancer [3]. The dynamic detectionof sentinel nodes reveals not only the pathoana-tomic localisation of possible nodal metastases, incontrast to restricted lymphadenectomy, which isbased on assumptions of lymph drainage in healthyindividuals, but also provides a means to examineearly metastatic progression in aspects of clonalityand biomarker profiles [4]. The majority of patientsundergoing cystectomy and traditional restrictedlymphadenectomy have no lymph node metastasesaccording to histopathologic examination [5]. Asubstantial percentage of these patients still haverecurrences and die from disseminated disease. Theoverall 5-yr survival rate of only 50% in patientsundergoing cystectomy is postulated to be caused byundetected metastatic spread to unidentified nodes.It is possible that staging could be improved andresult in more accurate assessment of nodal status ifsentinel nodes could be identified and examined in amajority of patients with invasive urothelial bladdercancer. The concept of sentinel node detectionincludes detection of lymph nodes that are sug-gested to be primed in receiving metastatic depositsat one time or another. The individual sentinel nodestatus is thus considered to reflect the actualoccurrence of primed sentinel nodes at the momentof excision, with or without metastatic deposits. Onetechnical problem with the interpretation of planarlymphoscintigraphy in the conventional manner, asin our first study, is the difficulty in preoperativelyidentifying the precise anatomic localisation of thedetected node. In most cases the nodes can beidentified once intraoperative detection conse-quently is added to the examination, but still thecertainty of lymphoscintigraphic localisation ofnodes needs to be discussed and reassessed caseby case. The problems of limited detection on planarlymphoscintigraphy, with an underestimation ofactual number of sentinel nodes, has also beenhighlighted by other investigators [6]. In our firstpilot study, planar lymphoscintigraphy yielded asentinel node detection rate of 67% and twometastatic sentinel nodes of four, that is, 50%, werealso recorded.
The purpose of this trial was to use a techniquefor better anatomic localisation of sentinel nodesand also to improve detection rates. Therefore weexplored a newly described method in which single-
photon emission computed tomography (SPECT) wascombined with computed tomography (CT) foranatomic fusion (SPECT/CT). So far this techniquehas been successful in sentinel node detection ofmalignant melanoma in two published reports [7,8]and has been presented as a suitable method forsentinel node detection in prostatic carcinoma [9,10].In the study of Even-Sapir et al., in 9 of 21 patientswith a primary tumour located in the head and neckor trunk region, SPECT/CT fused images detectedsentinel nodes that were missed on planar images.Two of these were metastatic sentinel nodes [8]. In areport from Wagner et al., comparing planar lym-phoscintigraphy with SPECT/CT, 30 patients withsquamous cell carcinoma of the head and neck regionwere investigated. Forty-nine sentinel nodes weredetected by SPECT/CT and 38 nodes by planarlymphoscintigraphy. The investigators even con-cluded that SPECT/CT is more sensitive to tumor-adjacent sentinel nodes than detection by g-probe,due to the high activity at the injection site causingobscuring and difficult detection [11].
2. Patients and methods
2.1. Patients
The study included six consecutive patients with urothelial
bladder cancer admitted to the University Hospital of Uppsala
from October 2002 to January 2003 for cystectomy. The four
men and two women were aged 59–75 yr. All six tumours
originated from urothelial epithelium and were assessed as
muscle invasive, T2a-T2b in five patients and as T1G3 with
multiple carcinomas in situ (CIS) in one, according to the TNM
classification of 1997 (Union Internationale Contre le Cancer)
and histopathologically graded according to criteria of the
World Health Organization and the International Pathology
Consensus Committee (1988). Preoperative work-up with CT,
intravenous pyelogram, and plain chest radiography did not
show any local or distant metastases.
None of the patients had received neoadjuvant therapy.
The study was approved both by the regional ethical
committee and the regional radiation ethical committee. All
six patients gave their informed consent to participate.
2.2. Preoperative sentinel node detection
Lymphoscintigraphy was performed after injection of Albures-
technetium 99m (Scanflex, Nycomed Amersham, Milan, Italy)
in the detrusor muscle peritumourally. One surgeon (A.S.) was
the principal investigator in all six patients. A 3.7F, 35-cm long
Williams cystoscopy needle (Cook Urological, Spencer, IN)
directed by an Albarran bridge was used. A total of 50–60 MBq
was injected into each patient; the dose was divided into four
equal parts as described previously [3].The patients were
transferred to the Department of Nuclear Medicine 2–3 h after
injection. First, planar scintigraphy of the pelvis in anterior,
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 8 3 – 9 1 85
posterior, and lateral views was performed. We defined a
sentinel node detected at planar lymphoscintigraphy as a
delineated spot with increased radioactivity clearly separated
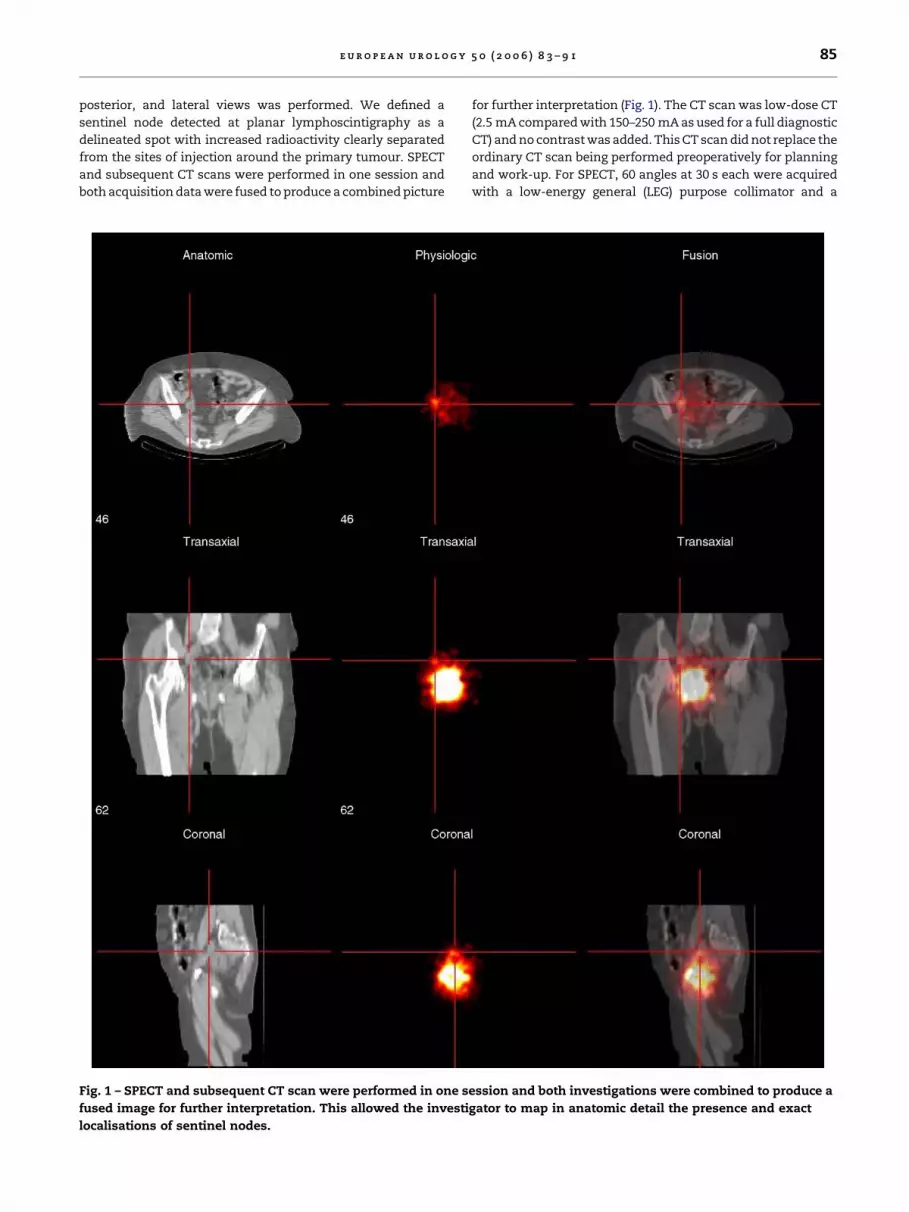
from the sites of injection around the primary tumour. SPECT
and subsequent CT scans were performed in one session and
both acquisition data were fused to produce a combined picture
Fig. 1 – SPECT and subsequent CT scan were performed in one s
fused image for further interpretation. This allowed the investi
localisations of sentinel nodes.
for further interpretation (Fig. 1). The CT scan was low-dose CT
(2.5 mA compared with 150–250 mA as used for a full diagnostic
CT) and no contrast was added. This CT scan did not replace the
ordinary CT scan being performed preoperatively for planning
and work-up. For SPECT, 60 angles at 30 s each were acquired
with a low-energy general (LEG) purpose collimator and a
ession and both investigations were combined to produce a
gator to map in anatomic detail the presence and exact
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 8 3 – 9 186
ye
rker
Intr
ao
pg-
dete
ctio
np
Tst
age
pN
sta
ge
To
tal
no
.h
arv
est
ed
no
des
To
tal
no
.d
ete
cted
sen
tin
el
no
des
Fa
lse-
neg
ati
ve
sen
tin
el
no
des
es)
10
pT
2b
pN
022
2–
01
pT
3b
pN
020
6–
06
pT
3a
pN
018
6–
12
pT
ap
N+
94
–
02
pT
3b
pN
+6
3–
00
pT
cis
pN
024
0–
ogra
ph
y/c
om
pu
ted
tom
ogra
ph
y;
intr
ao
p.:
intr
ao
pera
tiv
e.
128 � 128 matrix. The examination was performed with
anatomic enhancement on a g-camera Millennium VG5 with
Hawkeye (General Electric); attenuation correction using the CT
attenuation map and reconstruction of the raw data were
carried out on an Entegra workstation (General Electric). One
investigator (U.G.) was the sole interpreter of the lymphoscinti-
graphies and the combined pictures of hybrid SPECT/CT.
2.3. Intraoperative sentinel node detection
Prior to major surgery the patient was initially in the lithotomy
position and a second cystoscopy was performed. A total of
1 ml Patent blue (Bleu Patente V; Guerbet Laboratory, Issy les
Moulineaux, France), divided into four equal portions, was
injected peritumourally, with the intent to spot the same
positions as previously done with radioactive tracer. If >24 h
had elapsed since the latter, renewed injections of Albures-
technetium 99m were performed as described above. Intrao-
peratively we performed both detections with the help of a
handheld g-probe and visual detection of possibly blue-
colored nodes.
2.4. Surgery
One surgeon (A.S.) was the main surgeon in all six laparo-
tomies. All six patients underwent cystectomy with lympha-
denectomy and received urinary diversions accordingly.
Lymphadenectomies were mainly carried out after the
cystectomy or cystoprostatectomy, before formation of the
urinary outlet. Lymphadenectomy included all sentinel nodes
by the different described modalities and nonsentinel lymph
nodes in obturator regions and along iliac vessels with the
intent to include nodes up to the aortic bifurcation bilaterally.
Ta
ble
1–
Pa
tien
tch
ara
cteri
stic
sa
nd
resu
lts
of
sen
tin
el
no
de
dete
ctio
n
Pa
tien
tn
o.
Age, y
Sex
Cli
nic
al
sta
ge
Pla
na
rly
mp
ho
scin
t.S
PE
CT
/CT
Dm
a
(No
.o
fd
ete
cted
no
d
164
MT
21
2
272
MT
20
6
374
MT
20
6
475
FT
20
4
573
FT
21
3
659
MT
1G
3,
CIS
00
Ly
mp
ho
scin
t:ly
mp
ho
scin
tigra
ph
y;
SP
EC
T/C
T:
sin
gle
-ph
oto
nem
issi
on
com
pu
ter
tom
3. Results
3.1. Lymph node yield
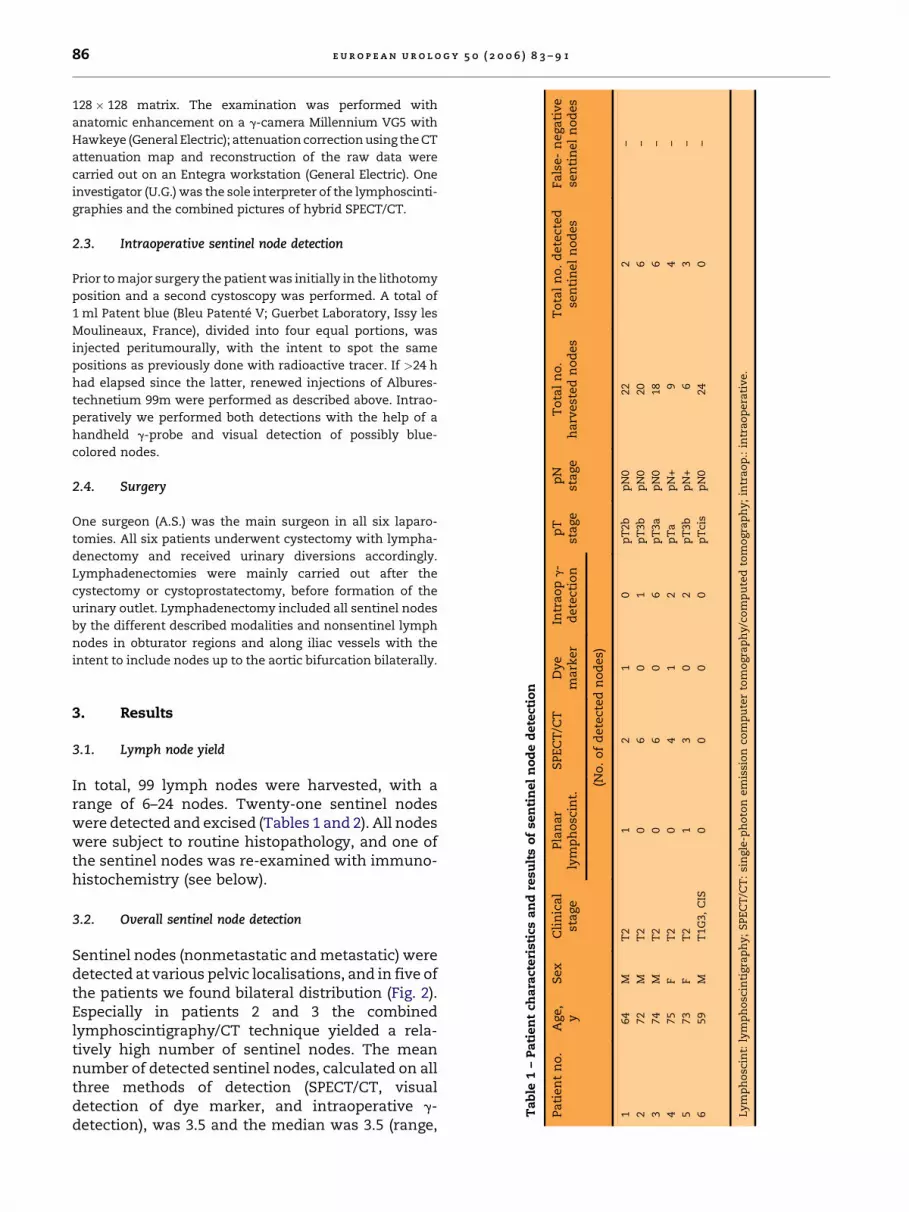
In total, 99 lymph nodes were harvested, with arange of 6–24 nodes. Twenty-one sentinel nodeswere detected and excised (Tables 1 and 2). All nodeswere subject to routine histopathology, and one ofthe sentinel nodes was re-examined with immuno-histochemistry (see below).
3.2. Overall sentinel node detection
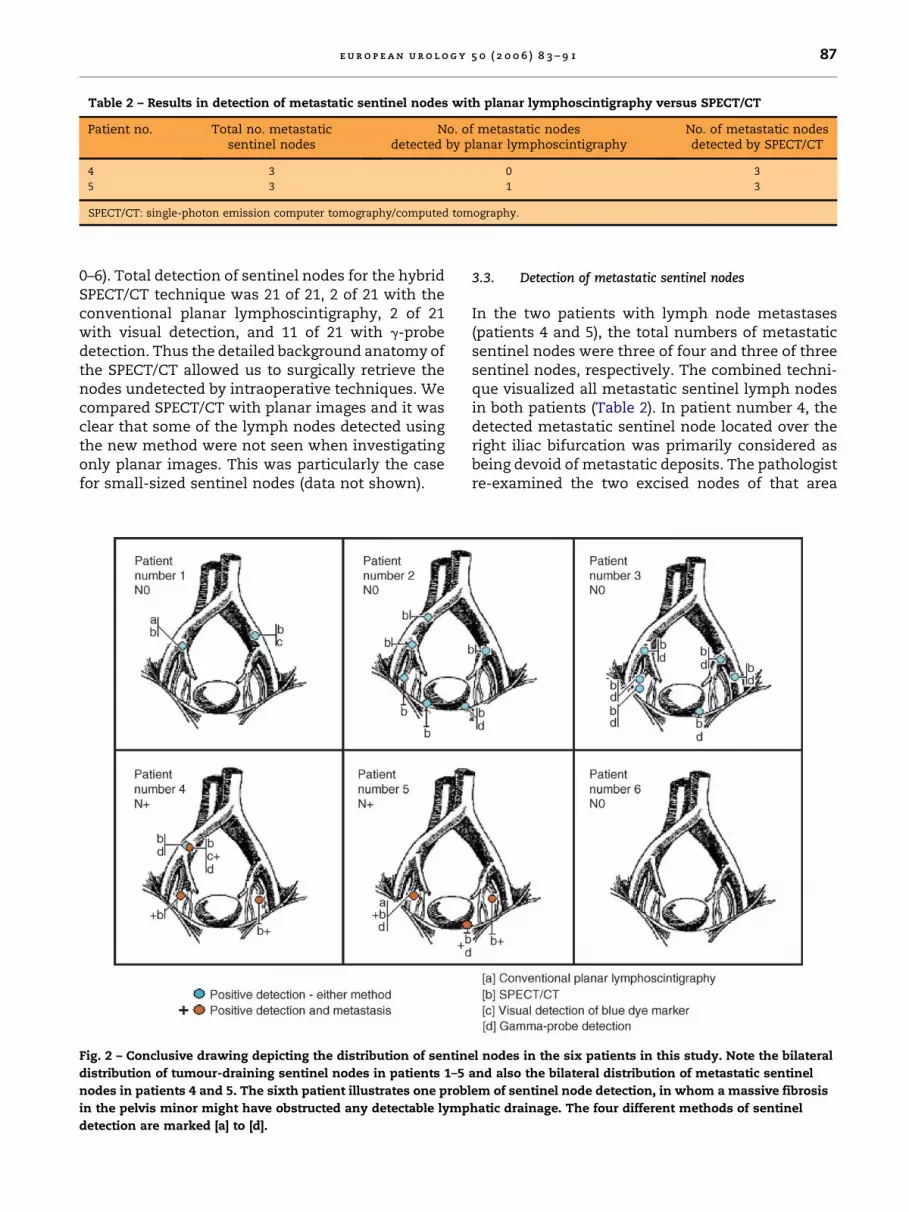
Sentinel nodes (nonmetastatic and metastatic) weredetected at various pelvic localisations, and in five ofthe patients we found bilateral distribution (Fig. 2).Especially in patients 2 and 3 the combinedlymphoscintigraphy/CT technique yielded a rela-tively high number of sentinel nodes. The meannumber of detected sentinel nodes, calculated on allthree methods of detection (SPECT/CT, visualdetection of dye marker, and intraoperative g-detection), was 3.5 and the median was 3.5 (range,
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 8 3 – 9 1 87
Table 2 – Results in detection of metastatic sentinel nodes with planar lymphoscintigraphy versus SPECT/CT
Patient no. Total no. metastaticsentinel nodes
No. of metastatic nodesdetected by planar lymphoscintigraphy
No. of metastatic nodesdetected by SPECT/CT
4 3 0 3
5 3 1 3
SPECT/CT: single-photon emission computer tomography/computed tomography.
0–6). Total detection of sentinel nodes for the hybridSPECT/CT technique was 21 of 21, 2 of 21 with theconventional planar lymphoscintigraphy, 2 of 21with visual detection, and 11 of 21 with g-probedetection. Thus the detailed background anatomy ofthe SPECT/CT allowed us to surgically retrieve thenodes undetected by intraoperative techniques. Wecompared SPECT/CT with planar images and it wasclear that some of the lymph nodes detected usingthe new method were not seen when investigatingonly planar images. This was particularly the casefor small-sized sentinel nodes (data not shown).
Fig. 2 – Conclusive drawing depicting the distribution of sentin
distribution of tumour-draining sentinel nodes in patients 1–5
nodes in patients 4 and 5. The sixth patient illustrates one probl
in the pelvis minor might have obstructed any detectable lymp
detection are marked [a] to [d].
3.3. Detection of metastatic sentinel nodes
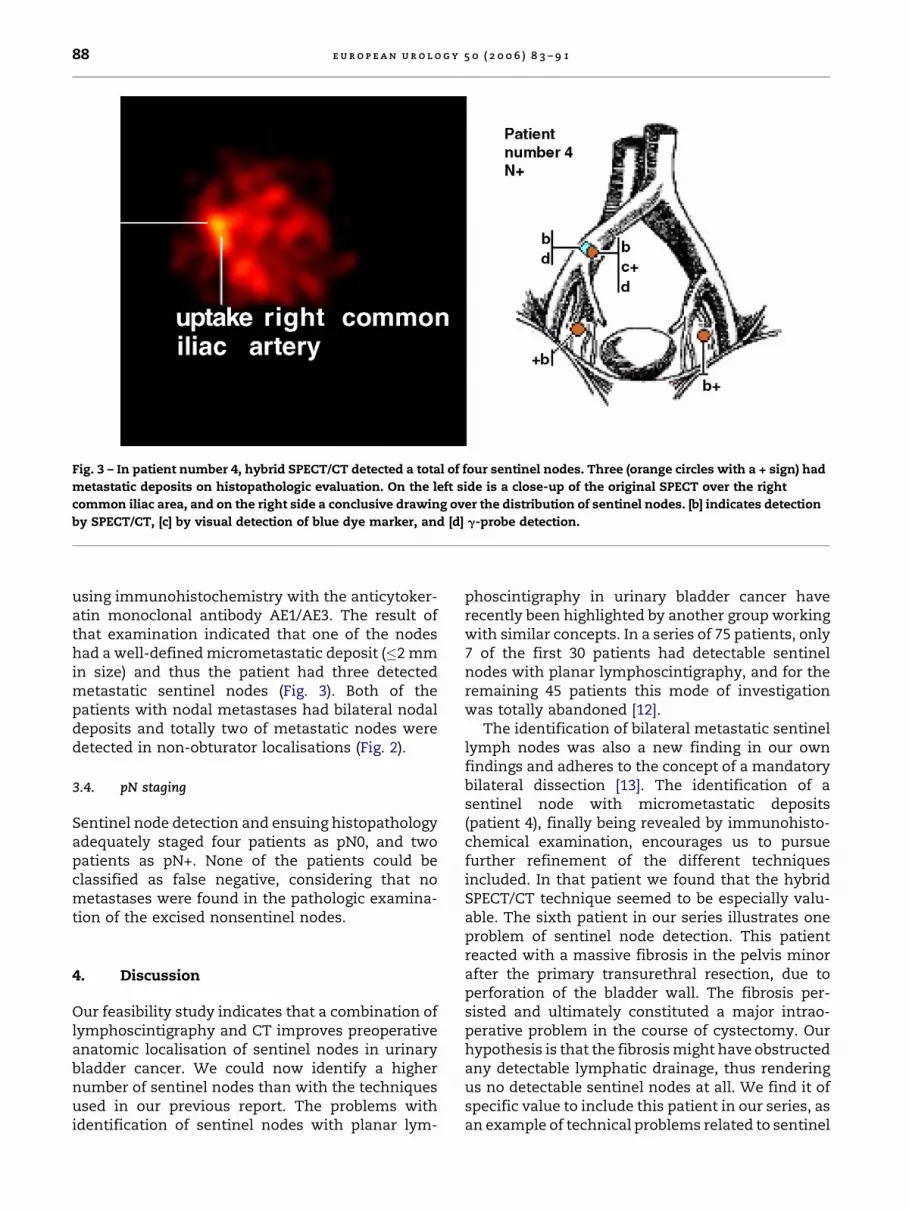
In the two patients with lymph node metastases(patients 4 and 5), the total numbers of metastaticsentinel nodes were three of four and three of threesentinel nodes, respectively. The combined techni-que visualized all metastatic sentinel lymph nodesin both patients (Table 2). In patient number 4, thedetected metastatic sentinel node located over theright iliac bifurcation was primarily considered asbeing devoid of metastatic deposits. The pathologistre-examined the two excised nodes of that area
el nodes in the six patients in this study. Note the bilateral
and also the bilateral distribution of metastatic sentinel
em of sentinel node detection, in whom a massive fibrosis
hatic drainage. The four different methods of sentinel
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 8 3 – 9 188
Fig. 3 – In patient number 4, hybrid SPECT/CT detected a total of four sentinel nodes. Three (orange circles with a + sign) had
metastatic deposits on histopathologic evaluation. On the left side is a close-up of the original SPECT over the right
common iliac area, and on the right side a conclusive drawing over the distribution of sentinel nodes. [b] indicates detection
by SPECT/CT, [c] by visual detection of blue dye marker, and [d] g-probe detection.
using immunohistochemistry with the anticytoker-atin monoclonal antibody AE1/AE3. The result ofthat examination indicated that one of the nodeshad a well-defined micrometastatic deposit (�2 mmin size) and thus the patient had three detectedmetastatic sentinel nodes (Fig. 3). Both of thepatients with nodal metastases had bilateral nodaldeposits and totally two of metastatic nodes weredetected in non-obturator localisations (Fig. 2).
3.4. pN staging
Sentinel node detection and ensuing histopathologyadequately staged four patients as pN0, and twopatients as pN+. None of the patients could beclassified as false negative, considering that nometastases were found in the pathologic examina-tion of the excised nonsentinel nodes.
4. Discussion
Our feasibility study indicates that a combination oflymphoscintigraphy and CT improves preoperativeanatomic localisation of sentinel nodes in urinarybladder cancer. We could now identify a highernumber of sentinel nodes than with the techniquesused in our previous report. The problems withidentification of sentinel nodes with planar lym-
phoscintigraphy in urinary bladder cancer haverecently been highlighted by another group workingwith similar concepts. In a series of 75 patients, only7 of the first 30 patients had detectable sentinelnodes with planar lymphoscintigraphy, and for theremaining 45 patients this mode of investigationwas totally abandoned [12].
The identification of bilateral metastatic sentinellymph nodes was also a new finding in our ownfindings and adheres to the concept of a mandatorybilateral dissection [13]. The identification of asentinel node with micrometastatic deposits(patient 4), finally being revealed by immunohisto-chemical examination, encourages us to pursuefurther refinement of the different techniquesincluded. In that patient we found that the hybridSPECT/CT technique seemed to be especially valu-able. The sixth patient in our series illustrates oneproblem of sentinel node detection. This patientreacted with a massive fibrosis in the pelvis minorafter the primary transurethral resection, due toperforation of the bladder wall. The fibrosis per-sisted and ultimately constituted a major intrao-perative problem in the course of cystectomy. Ourhypothesis is that the fibrosis might have obstructedany detectable lymphatic drainage, thus renderingus no detectable sentinel nodes at all. We find it ofspecific value to include this patient in our series, asan example of technical problems related to sentinel
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 8 3 – 9 1 89
node detection patients with in urinary bladdercancer.
The original concept of sentinel node detectionwas based on the principle of one tumour-oneprimary sentinel node. However, the finding of morethan one sentinel node is often reported, as in a largebreast cancer multicentre study from 1998 (n = 443)where the mean number of sentinel nodes was2.6 � 2.2 [14]. The detection of second- and eventhird-echelon metastatic sentinel nodes adds moreconsiderations to the questions of defining theactual sentinel node [15]. At the time of presentationand detection, the presence of multiple detectablenodes, and also the presence of a number ofdetected metastatic sentinel nodes, is thus alsobeing displayed in this present study. The explana-tion might be found both in the individual biologictimetable of the actual tumour/patient, the timing ofdetection, and the possibility of larger tumourshaving different sections being drained into anato-mically different lymphatic routes. For example, in abiologically early setting, a patient might have onlyone single detectable sentinel node, with or withoutmetastatic deposits. Another patient, in a moreadvanced biologic setting, might have a number ofdetectable sentinel nodes, with a wide variation ofmetastatic spread or absence thereof. Simultaneoussentinel nodes might be considered to originatefrom different parts of a tumour with individual andseparate drainage routes being established withinthe same time frame. That could also serve as anexplanation for both crossover phenomena andbilateral distribution of nodal metastatic deposits.We consider all detected nodes as being so called‘‘hot nodes,’’ thus being detectable nodes by thedescribed methods. It should be pointed out that theterm ‘‘hot nodes’’ should be considered as includingboth first-echelon sentinel nodes (i.e., ‘‘true’’ senti-nel nodes) and second- and third-echelon drainingnodes. Until we have morphologic or biochemicalmarkers to differentiate between the position of thenodes in the draining system, we have made thechoice to designate all ‘‘hot nodes’’ as sentinelnodes. This is especially the case with the above-mentioned hypothetical argument of having differ-ent sections of the tumour being drained intodifferent subsets of draining areas. We wouldconsider it being suboptimal to just search for asingle draining node, especially because we knowthat usually more than one affected metastatic nodecan be found in many patients with nodal spreadand that distribution of metastatic nodes can befound in various localisations. In a recently pub-lished prospective trial from the Mansourah Center,bilateral nodal involvement was observed in 39% of
the patients with positive nodes [16]. Crossoverphenomena were reported in 7% of the patients inthe Swiss prospective investigation of 83 patientswith positive nodes undergoing cystectomy. Thisgroup also noted that of the 39 patients who had alateralized bladder tumour, 16 had nodes involvedon the contralateral side [17]. The insufficiency ofthe present TNM classification for describing andstratifying node-positive patients with urinarybladder cancer has recently been highlighted in areview discussing lymph node metastasis in thiscancer [18].
With this biologic background of advancedurinary bladder carcinomas, defining the firstsentinel node would mainly have an academicinterest, and the concept of one tumour-one nodecertainly also has to be challenged. To distinguishfirst-, second-, and third-echelon sentinel nodesfrom each other is another matter to be dealt with.In exceptionally clear cases, the suggested prepul-sion from one node to the second and so forth, canbe visualised intraoperatively in the initialmoments of traditional dynamic lymphoscintigra-phy. We do not propose that any general commonpattern of drainage can be discerned or establishedwith reference to tumour location and size [19]. Theconcept rather entails the possibility of multipleroutes of drainage, to one or more sentinel nodesor sentinel node regions. It has been suggestedthat an early nodal extension starts with theestablishment of specific routes for drainagethrough vascular endothelial growth factor (VEGF)C- and VEGF-D–induced tumor-specific lymphan-giogenesis [20,21], followed by independent meta-static progression taking place according to thespecific preconditions in every individual patient.This model might explain why we can detect anumber of unaffected but still established anddiscernable sentinel nodes in some patients. Inother patients one can assume that metastaticprogression occurs at a quicker pace, even thoughthe patient has only one or a few detectable sentinelnodes. In this present study we did not encounterany patients with false-negative sentinel nodes, bydefinition, undetected metastatic sentinel nodes.Still in a numerically larger study in which we areexploring the immunoresponse in sentinel nodes,we found a total of four false-negative nodes inthree patients [22]. We have also encountered thesame phenomena later on in a few more subsequentpatients being examined. The false-negative find-ings could either be explained by technical pro-blems related to the quality of tracer injection or bythe possibility described by other sentinel nodeinvestigators, where a completely tumour-engaged
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 8 3 – 9 190
metastatic sentinel node loses its ability to harbourtracer of any kind [23]. Our feasibility trial includes alow number of patients, and in future attempts wewould mainly aim to both increase the number ofinvestigated patients and also to have two separateinvestigators doing the preoperative imaging. Thiswould allow one investigator to interpret planarlymphoscintigraphy and independently haveanother investigator assess the SPECT/CT images.Ultimately the request for a more accuratestaging of nodal status is linked to our differentattempts to tailor treatment options for individualpatients. Another attempt to combine differentmodalities in the investigation of both nodal anddistant metastases in advanced bladder cancer is arecently published prospective trial on correlatingwhole-body fluorine-18 2-fluoro-2-dixoy-D-glu-cose-positron emission tomography (FDG-PET)and CT [24]. Attempts to further refine diagnosticaccuracy by combining these methods with sentinelnode detection seems to be the next temptingoption.
By refining the techniques that can be used fordetection of sentinel nodes, one might endeavour toincrease the amount of detected sentinel nodes,thus extending the options of further basic researchon the intrinsic factors governing routes of meta-static spread, presence or absence of metastaticnodes, molecular profiling of primary tumours,nonmetastatic and metastatic sentinel nodes,examination of immunologic interactions occurringin primary tumor and sentinel nodes [22], and,finally, also exploring mechanisms of lymphangio-genesis and metastatic tumor-homing.
5. Conclusions
The combination of lymphoscintigraphy with CTenabled preoperative localisation of sentinel nodesin anatomic detail and facilitated detection duringoperation. Identification of more sentinel nodesthan expected might be due to timing of thescintigraphy; some identified nodes may thereforebe second- and third-echelon nodes. This additionaltechnique provides us with more information butshould be investigated further before any of theother methods of detection are excluded.
Acknowledgements
Dr Per Marits, MD, Department of Internal MedicineUppsala University Hospital, for providing us withdrawings.
References
[1] Schwartz GF. Clinical practice guidelines for the use of
axillary sentinel lymph node biopsy in carcinoma of the
breast: current update [review]. Breast J 2004;10:85–8.
[2] Reintgen D, Balch CM, Kirkwood J, et al. Recent advances
in the care of the patient with malignant melanoma. Ann
Surg 1997;225:1.
[3] Sherif A, De La Torre M, Malmstrom PU, Thorn M. Lym-
phatic mapping and detection of sentinel nodes in
patients with bladder cancer. J Urol 2001;166:812–5.
[4] Malmstrom PU, Ren ZP, Sherif A, de la Torre M, Wester K,
Thorn M. Early metastatic progression of bladder carci-
noma: molecular profile of primary tumor and sentinel
lymph node. J Urol 2002;168:2240–4.
[5] Bassi P, Ferrante GD, Piazza N, et al. Prognostic factors of
outcome after radical cystectomy for bladder cancer: a
retrospective study of a homogeneous patient cohort. J
Urol 1999;161:1494–7.
[6] Jansen L, Nieweg OE, Kapteijn AE, et al. Reliability of lym-
phoscintigraphy in indicatingthenumberofsentinelnodes
in melanoma patients. Ann Surg Oncol 2000;7:624–30.
[7] Kretschmer L, Altenvoerde G, Meller J, et al. Dynamic
lymphoscintigraphy and image fusion of SPECT and pel-
vic CT-scans allow mapping of aberrant pelvic sentinel
lymph nodes in malignant melanoma. Eur J Cancer
2003;39:175–83.
[8] Even-Sapir E, Lerman H, Lievshitz G, et al. Lymphoscinti-
graphy for sentinel node mapping using a hybrid SPECT/
CT system. J Nucl Med 2003;44:1413–20.
[9] Wurm TM, Eichhorn K, Corvin S, Anastidis AG, Bares R,
Stenzl A. Anatomic-functional image fusion allows
intraoperative sentinel node detection in prostate cancer
patients. American Urological Association, San Francisco.
J Urol 2004. p. 171, (abstract no. 854).
[10] Kizu H, Takayama T, Fukuda M, et al. Fusion of SPECT and
multidetector CT images for accurate localization of pel-
vic sentinel lymph nodes in prostate cancer patients. J
Nucl Med Technol 2005;33:78–82.
[11] Wagner A, Schicho K, Glaser C, et al. SPECT-CT for topo-
graphic mapping of sentinel lymph nodes prior to gamma
probe-guided biopsy in head and neck squamous cell
carcinoma. J Craniomaxillofac Surg 2004;32:343–9.
[12] Liedberg F, Chebil G, Thomas Davidsson T, Gudjonsson S,
Mansson W. Intraoperative sentinel node detection
improves nodal staging in invasive bladder cancer. J Urol
2006;175:84–9.
[13] Ghoneim MA, Abol-Enein H. Lymphadenectomy with
cystectomy: is it necessary and what is its extent? [review]
Eur Urol 2004;46:457–61.
[14] Krag D, Weaver D, Ashikaga T, et al. The sentinel node in
breast cancer—a multicenter validation study. N Engl J
Med 1998;339:941–6.
[15] Nieweg OE, Tanis PJ, Kroon BB. The definition of a sentinel
node. Ann Surg Oncol 2001;8:538–41.
[16] Abol-Enein H, El-Baz M, Abd El-Hameed MA, Abdel-Latif
M, Ghoneim MA. Lymph node involvement in patients
with bladder cancer treated with radical cystectomy: a
patho-anatomical study—a single center experience. J
Urol 2004;172:1818–21.
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 8 3 – 9 1 91
[17] Mills RD, Turner WH, Fleischmann A, Markwalder R,
Thalmann GN, Studer UE. Pelvic lymph node metastases
from bladder cancer: outcome in 83 patients after radical
cystectomy and pelvic lymphadenectomy. J Urol 2001;
166:19–23.
[18] Liedberg F, Mansson W. Lymph node metastasis in blad-
der cancer. Eur Urol 2006;49:13–21.
[19] Malmstrom PU, Sherif A, Thorn M. Re: extended radical
lymphadenectomy in patients with urothelial bladder
cancer: results of a prospective multicenter study. J Urol
2004;172:386, author reply p. 386.
[20] Jain RK, Padera TP. Development. Lymphatics make the
break. Science 2003;299:209–10.
[21] Alitalo K, Mohla S, Ruoslahti E. Lymphangiogenesis and
cancer: meeting report. Cancer Res 2004;64:9225–9.
[22] Marits P, Mona Karlsson M, Sherif A, Garske U, Thorn M,
Winqvist O. Detection of immune responses against urin-
ary bladder cancer in sentinel lymph nodes. Eur Urol
2006;49:59–70.
[23] Keshtgar MR, Ell PJ. Clinical role of sentinel-lymph-node
biopsy in breast cancer [review]. Lancet Oncol 2002;3:105–
10.
[24] Drieskens O, Oyen R, Van Poppel H, Vankan Y, Flamen P,
Mortelmans L. FDG-PET for preoperative staging of
bladder cancer. Eur J Nucl Med Mol Imaging 2005;32:
1412–7.