
Pro-apoptotic activity of α-bisabolol in preclinical models of primary human acute leukemia cells
Upload
independentCategory
view
1download
0
HLA-DR-, CD33+, CD56+, CD16- Myeloid/Natural Killer Cell Acute Leukemia: A Previously Unrecognized Form of Acute Leukemia Potentially
Misdiagnosed as French-American-British Acute Myeloid Leukemia"3
By Amy A. Scott, David R. Head, Kenneth J. Kopecky, Frederick R. Appelbaum, Karl S. Theil, Michael R. Grever, I-Ming Chen, Michael H. Whittaker, Barbara B. Griffith, Jonathan D. Licht, Samuel Waxman, Margaret M. Whalen,
Arthur D. Bankhurst, Lynn C. Richter, Thomas M. Grogan, and Cheryl L. Willrnan
We have identified and characterized a previously unrecog- nized form of acute leukemia that shares features of both myeloid and natural killer (NK) cells. From a consecutive series of 350 cases of adult de novo acute myeloid leukemia (AML), we identified 20 cases (6%) with a unique immuno- phenotype: CD33'. CD56'. CDlla', CD13'", CD15'". CD34', HLA-DR-, CD16-. Multicolor flow cytometric assays con- firmed the coexpression of myeloid (CD33, CD13, CD151 and NK cell-associated (CD561 antigens in each case, whereas reverse transcription polymerase chain reaction (RT-PCR) assays confirmed the identity of CD56 (neural cell adhesion molecule) in leukemic blasts. Although two cases expressed CD4, no case expressed CD2, CD3, or CD8 and no case showed clonal rearrangement of genes encoding the T-cell receptor (TCR /3, 7, S) . Leukemic blasts in the majority of cases shared unique morphologic features (deeply invagi- nated nuclear membranes, scant cytoplasm with fine azuro- philic granularity, and finely granular Sudan black B and my- eloperoxidase cytochemical reactivity) that were remarkably similar to those of acute promyelocytic leukemia (APL); par- ticularly the microgranular variant (FAB AML-M3v). How- ever, all 20 cases lacked the t(15;17) and 17 cases tested lacked the promyelocyticlretinoic acid receptor (Y (RARru)
CUTE MYELOID LEUKEMIA (AML) constitutes a heterogeneous group of leukemic disorders with di-
verse biologic and clinical features. Traditionally, AML has been classified by morphologic and cytochemical criteria,
A
From the University of New Mexico (UNM) School of Medicine, Departments of Pathology, Medicine, and the UNM Cancer Center, Center for Molecular and Cellular Diagnostics, Albuquerque, NM; The Southwest Oncology Group (SWOG) Leukemia Biology Pro- gram, San Antonio, T X ; St Jude Children's Research Hospital, De- partment of Pathology, Memphis, TN; Fred Hutchinson Cancer Re- search Center, Seattle, WA; The Ohio State University, Departments of Pathology and Medicine, Columbus, OH; The Mount Sinai Medi- cal Center, Departments of Medicine and Molecular Biology, New York, NY; The University of Arizona and the SWOG Lymphoma Biology Repository, Tucson, AZ.
Submitted October 6, 1993; accepted March 8, 1994. Supported by Department of Health and Human Services Grants
No. CA32102, CA32734 (both supporting the SWOG Leukemia and Lymphoma Biology Programs), and CA59936 (supporting S. W. and J.D.L.); A.A.S. is a recipient of a Clinical Oncology Fellowship Award from the American Cancer SocieQ (No. 93-138-1).
Presented in part at the 82nd annual meeting of the United States and Canadian Academy of Pathology in New Orleans, L A , March 16, 1993.
Address reprint requests to SWOG Operations Ofice, 14980 Omi- cron Dr, San Antonio, Ix 782453218,
The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked "advertisement" in accordance with 18 U.S.C. section 1734 solely to indicate this fact. 0 1994 by The American Society of Hematology. OOO6-4971/94/8401-0026$3.00/0
244
fusion transcript in RT-PCR assays; 12 cases had 46,XX or 46,XY karyotypes, whereas 2 cases had abnormalities of chromosome 17q: 1 with de1(17)(q25) and the other with t(11;17)(q23;q21) and the promyelocytic leukemia zinc finger/RARa fusion transcript. All cases tested (6/20), includ- ing the case with t(11;17), failed t o differentiate in vitro in response to all-trans retinoic acid (ATRA), suggesting that these cases may account for some APLs that have not shown a clinical response t o ATRA. Four of 6 cases tested showed functional NK cell-mediated cytotoxicity, suggesting a rela- tionship between these unique CD33'. CD56'. CD16- acute leukemias and normal CD56'. CD16- NK precursor cells. Us- ing a combination of panning and multiparameter flow cyto- metric sorting, we identified a normal CD56'. CD33'. CD16- counterpart cell at a frequency of 1% to 2% in the peripheral blood of healthy individuals. Our studies suggest that this form of acute leukemia may arise from transformation of a precursor cell common to both the myeloid and NK cell lineages; thus we propose the designation myeloid/NK acute leukemia. Recognition of this new leukemic entity will be important in distinguishing these ATRA-nonresponsive cases from ATRA-responsive true APL. 0 1994 by The American Society of Hematology.
formalized in the French-American-British (FAB) classifi- cation ~ y s t e m . " ~ However, more recent analyses of the im- munophenotypic, cytogenetic, molecular, and cellular fea- tures of AML blasts have identified unique biologic subsets of AML."'' Assessment of these biologic parameters is now allowing for more precise diagnosis, classification, and more accurate prognostication of AML patients; moreover, these biologic and genetic parameters are beginning to have a significant impact on therapeutic decision making.'"'
From a series of 350 consecutive adult de novo AML patients (initially identified by morphologic and cytochemi- cal criteria) who were candidates for Southwest Oncology Group (SWOG) treatment protocols, we identified 20 cases of a previously unrecognized form of acute leukemia. These 20 cases were distinguished by their lack of expression of HLA-DR and by their unusual coexpression of myeloid and natural killer (NK) cell-associated antigens. Although the morphologic features of these cases were inconsistently clas- sified by submitting SWOG institutions, the majority of cases were noted upon review to bear a striking morphologic and immunophenotypic resemblance to AML cases of the FAB- M3 subtype, particularly the microgranular variant (M3v). In this report, we fully characterize the morphologic, immu- nophenotypic, cytogenetic, molecular, and biologic features of this unique type of acute leukemia. Our finding that these leukemia cases show functional NK cell-type mediated cyto- toxicity and our identification of a normal myeloid/NK coun- terpart cell in the peripheral blood of healthy individuals suggest that this unique form of acute leukemia may arise from transformation of a precursor cell common to the my- eloid and NK cell lineages.
Blood, VOI 84, NO 1 (July 1). 1994: PP 244-255

MYELOID/NATURAL KILLER CELL ACUTE LEUKEMIA
MATERIALS AND METHODS
Sample acquisition and morphologic review. This study was based on specimens of bone marrow (BM) or peripheral blood (PB) submitted to the SWOG Reference Laboratory and Myeloid Reposi- tory at the UNM Cancer Center according to standard procedures of SWOG. Briefly, pretreatment specimens of BM andor PB are submitted to the Repository for patients who are candidates for SWOG AML treatment studies. Upon initial receipt, leukemic blasts are enriched on Ficoll-Hypaque gradients (Pharmacia, Piscataway, NJ) and the leukemic blast percentage is determined by analysis of Wright-stained cytospins. All cases are immediately analyzed for the expression of a panel of hematopoietic cell surface antigens using multicolor flow cytometry. Residual leukemic cells are cryo- preserved as sterile, viable cell suspensions at - 135°C; these cryo- preserved specimens were used for the additional biologic assays undertaken in this study.
Pretreatment Wright-stained BM aspirates and PB specimens as well as a panel of submitted or centrally performed cytochemical stains (Sudan black B [SBB], alpha napthyl butyrate esterase, my- eloperoxidase [MPO], and chloracetate esterase) were reviewed by members of the SWOG Leukemia Review Panel. Additional mor- phologic and cytochemical studies were also performed on air-dried aspirates and on thawed, previously cryopreserved cell suspensions and were reviewed by three of the authors (AS., D.H., C.W.) and Dr Kathy Foucar (University of New Mexico, Albuquerque, NM). All cases were classified using standard FAB criteria and were alter- natively classified as myeIoidNK acute leukemia if they had a dis- tinct set of reproducible morphologic and cytochemical features dif- ferent from those detailed in the current FAB classification system (see ResuIts).l4 Three cases reported in this study were ultimately not registered on a SWOG clinical trial (Table l ; Cases 12, 14, and 15); however, slides from each case were submitted by SWOG institutional pathologists and underwent an identical process of mor- phologic review.
Immunophenotypic/fiow cytometric analysis. The cell surface antigen profile of leukemic blasts in each case initially were deter- mined on fresh cells at the time of sample submission using standard two-color flow cytometric analysis with a panel of monoclonal anti- bodies (MoAbs) as previously de~cribed. '~"~ The mononuclear cell component after Ficoll-Hypaque gradient separation was washed, then incubated in staining media with directly-conjugated [either fluorescein isothiocyanate (FITC) or phycoerythrin (PE)] MoAbs for 30 minutes at 4°C [Leu19 (CD56), MY10 (CD34), LeuMl (CDlS), Leu1 la (CD16), Leu12 (CD19). Leu16 (CD20). Leu5b (CD2), CR1 (CD35), CDIla, LeuMS (CDllc), GpIIbflIIa (CD41). Leu 5b (CD2), Leu4 (CD3). and HLA-DR (all supplied by Becton Dickin- son, San Jose, CA); and MY9 (CD33), MY4 (CDwl4). and MY7 (CD13) (all supplied by Coulter, Inc, Hialeah, E)]. Background staining was determined using isotype controls (FITC- or PE-conju- gated IgGl and PE-conjugated IgG2). After washing, samples were analyzed immediately with a Becton Dickinson FACScan flow cy- tometer. Although the percent viability of both fresh and thawed, previously cryopreserved leukemic cell suspensions usually ex- ceeded 90%, dead cells were excluded from flow cytometric analysis with propidium iodide gating.I3 Flow cytometric data were analyzed with FACScan software (Becton Dickinson) and results expressed as units of mean channel fluorescence shift relative to background control levels; composite two-color dot plots and contour plots were generated using the Lyses I1 analysis system (Becton Dickinson).
Cytogenetic analysis. Pretreatment BM andlor PB samples were prepared for cytogenetic analysis by direct andor short term (24 to 72 hour) unstimulated cultures at approved SWOG cytogenetics laboratories.15 A minimum of 20 G-banded metaphases were ana- lyzed in each case, and chromosomes were identified and clonal abnormalities classified according to the International System for
245
Table 1. Morphologic, Immunophenotypic, and Cytogenetic Characteristics of Myeloid/NK Precursor Cell Leukemia Cases
Case No. FAB* lmmunophenotype Kavotype
1 M7 HLA-DR-.CD34+.CD33+.CDl5+ CD13+,CD56+,CD16~,CDlla+
2 My/NK HLA-DR-,CD34',CD33',CDl5+
3 M1 HLA-DR~.CD34',CD33'.CDl5+
4 My/NK HLA-DR-,CD34+,CD33+,CDl5+
5 My/NK HLA-DR-,CD34-,CD33'
6 My/NK HLA-DR-,CD34-,CD33+
7 My/NK HLA-DR-,CD34-,CD33+
8 M2 HLA-DR-,CD34-,CD33'
9 My/NK HLA-DR-,CD34-,CD33'
10 M2 HLA-DR-,CD34-,CD33'
CD13+,CD56+,CDl6~,CDlla'
CD13+,CD56+,CD16~,CD1la'
CD13+,CD56+,CD16~,CDlla'
CD13+,CD56+,CD16-,CDlla'
CD13+.CD56+,CD16-,CDllai
CD13+,CD56+,CD16~,CDlla+
CD13',CD56+,CD16-,CDlla+
CD13'.CD56+,CD16~,CDlla+,CD4+
CD13',CD56+,CD16~,CDlla+,CD4+
11 My/NK HLA-DR-,CD34-,CD33'
12 M2 HLA-DR-,CD34-,CD33'
13 My/NK HLA-DR-,CD34-,CD33'
14 My/NK HLA-DR-,CD34-.CD33+
15 My/NK HLA-DR-,CD34-,CD33-
16 M2 HLA-DR-,CD34-,CD33+
CD13-,CD56',CD16-
CD13-,CD56'.CD16-
CD13-,CD56'.CD16-
CD13-,CD56+,CD16-
CD13',CD56+,CD16-
CD13+,CD56+,CD16-
17 My/NK HLA-DR-,CD34-,CD33-
18 My/NK HLA-DR-,CD34-,CD33-
19 M2 HLA-DR-,CD34+,CD33'
20 My/NK HLA-DR-,CD34-,CD33'
CD13+.CD56+,CD16-
CD13',CD56',CD16-
CD13'.CD56+,CD16-
CD56+,CD16-
47,XY.+8,1(16;21) (pll;q22)
46,XY
ND
46,XX
46,XY
46,XX
ND
46,XY
46,XX
45,XY,-ll,-14,-17,-22, +i(17q),+der(221t(717;22) (pll;pll)/44,idem, -2O,der(ll)t(l1;14) (p13;qlll
46,XY
46,XY
ND
46,XY
46,XX,de117(q25)
46,XX.t(11;17) (q23;qZl)
46,XX
46,XY
ND
47 XX,+8,de1(13) . . ,. ..
(q172q174)
with the background isotope control fluorescence intensity. Positivity is defined as greater than 20% of fluorescence intensity compared
same as previous clone; ND, not determined or unsuccessful. Abbreviations: My/NK. myeloid/natural killer cell morphologic features; idem,
that subtype is provided. Alternatively, if features were most consistent with the If morphologic features were consistent with a particular FAB subtype, then
myeloid/NK (My/NK) subtype, then that designation is provided.
Human Cytogenetic Nomenclature (ISCN) (1985) and ISCN ( 1991).16,'7 Representative original karyotypes were submitted for central review to the SWOG Cytogenetics Working Group (R. Ellen Magenis, Chair) and were rereviewed by one of us (K.T.).
Reverse-transcriptase polymerase chain reaction (RT-PCR) and oligonucleotide probe hybridization assays for CD56 neural cell adhesion molecule (NCAM). To detect CD56 NCAM transcripts in leukemic blasts, RT-PCR assays were performed on total RNA isolated from cases 8 and 15 (Table l ) , as previously described." The CD56+ myeloma cell line 8226Dox40 was used as a high-level positive control." RNA from a case of AML that was not a myeloid NK leukemia case and that exhibited 1% expression of CD56 by flow cytometric analysis was used as a negative control. Briefly, cDNA was synthesized from 1 pg of total cellular RNA in 20 pL of a solution containing 5 mmoVL MgClz, 50 mmoVL KCL, 10 mmoVL TRIS-HCL (pH 8.3). 20 U RNase inhibitor, 50 U reverse

246 SCOTT ET AL
transcriptase, 0.75 pmol/L of downstream primer, and 1 mmol/L of each deoxynucleotide triphosphate (dNTP). The samples were incubated in a thermal cycler (Perkin Elmer-Cetus, Norwalk, CT) at 42°C for 30 minutes and 99°C for S minutes, To amplify the cDNA, SS p L of a PCR master mix was added to each tube to yield a final concentration of 2 mmol/L MgCl?, 50 mmol/L KCI, and I O mmol/L TRIS-HCI (pH 8.3), along with one Ampliwax PCR Gem (Perkin Elmer-Cetus) to enable hot-start PCR. Tubes were heated to 70°C for 3 minutes and cooled to 15°C for 3 minutes. A final 25 pL volume of PCR mix that now included Amplitaq DNA polymer- ase (2.5 Ull00 pL) and the upstream primer (final concentration =
0.15 pmol/L). PCR was performed for 45 cycles as follows: 1 cycle at 95°C for 3 minutes, 60°C for 3 minutes, and 72°C for 3 minutes; 43 cycles at 45 seconds at 95”C, 1 minute at 60T, and 1 minute at 72°C; and finally, 1 cycle of 95°C for 45 seconds, 60°C for 1 minute and 72°C for 5 minutes. The NCAM primers yielding a 493-hp product were as follows: upstream primer, 5’-GCCCATCCTCAA- ATACAAAGC-3’ (NCAM residues 1,684 through I ,704), and downstream primer, S’-GGTCCTGAACACAAAATGAGC-3’ (NCAM residues 2,156 through 2,176). Ten microliters of the RT-PCR prod- uct was electrophoresed in agarose gels and standard Southern blot transfer was performed.” Nitrocellulose membranes were prehybrid- ized for 1 hour at 65°C in 5 mL of Rapid-Hyb buffer (Amersham, Arlington Heights, IL). Final hybridization was performed with a 525-bp PCR-synthesized NCAM DNA probe spanning the region initially amplified in the patient samples [S’ primer: NCAM residues 1,667 through 1,686 (S’-GAGGCCACAGGTGGGGTGCC-3’); 3’ primer: NCAM residues 2,175 through 2,194 (S’GGCTGTGGG- CTGGGCCGAGG-3‘)I. The probe was random primed (Boehr- inger-Mannheim Biochemicals, Indianapolis, IN) and the membrane was hybridized for I hour at 65°C. Stringency washes included one wash of IS minutes at room temperature in 0.1 X SSC, 0.1 o/o sodium dodecyl sulfate (SDS), followed by two 15-minute washes in 0.1 X SSC, 0.1% SDS at 65°C followed by autoradiography.
RT-PCR ussa.ys for promyelocytic (PML)/retinoic acid receptor cu (RARcu) mRNA transcripts. RNA was isolated from 17/20 myeloid/NK leukemia cases with residual cryopreserved cells (all cases except cases 6 ,9 , and 13; Table I ) and from 3 AML-M3 cases with a confirmed t(15;17).” The RT-PCR amplification method used was similar to that of Biondi et al.’” One microgram of total cellular RNA was incubated for I O minutes at 23°C IS minutes at 42°C and 5 minutes at 99°C in a total volume of 20 pL containing 2 pL of 10 X buffer ( 1 0 0 m m o l k TRIS pH 8.3, O S mol/L KCI, and 50 mmol/L MgCI?), 2 p L of IO mmol/L dNTPs, O S pL of 100 pmol/ p L random hexamers (Boehringer-Mannheim), 0.5 pL of RNAsin (20 U/0.5 pL) (Promega, Madison, WI), 2.0 p L of SO mmol/L dithio- threitol, 0.2.5 pL of Moloney murine leukemia virus (MMLV) re- verse transcriptase ( S O U0.25 pL) (GIBCO-BRL, Gaithersburg, MD), and 7.75 p,L of diethylprocarbonate-treated H20. Five microli- ters of this reaction was then used for nested RT-PCR assays using primer sequences to detect PML/RARa fusion mRNAs as previously described: M2R8 (M2 derived from PML exon S and R8 from RARa exon 3) to analyze breakpoint cluster regions (bcr) 1 and 2 and M4R8 (M4 derived from PML exon 3) to analyze bcr region 3.2‘).21 After amplification, 15 p L of the PCR reaction was fractionated and visualized in ethidium bromide-stained agarose gels. Amplification of 02-microglobulin mRNA, using S pL of the cDNA was performed as an internal control for RNA integrity and PCR reaction fidelity in each sample, using an annealing temperature of 5SOC.”
RT-PCR assays jiw the promyelocytic leukemia zinc j n g e r (PLZF)/RARa mRNA transcripts. RT-PCR was performed to de- tect the PLZF/RARa-fusion transcript arising from the t( l l ;17), as previously described.” Total RNA (4 pg) from each leukemic sam- ple was hybridized to a primer (5”TGGATGCTGCGGCGGAAG- AAGCCCTTGCAG-3’) complementary to the B region of the RARa gene and reverse transcribed by incubation with 200-U
MMLV reverse transcriptase (GIBCO-BRL) at 37°C for 45 minutes. One tenth of the cDNA product was then amplified by PCR using Taq polymerase (Promega) in 100-pL volume with a primer comple- mentary to the B region of the RARa (5”GGGCACTATCTC- TTCAG-3’ ) and a primer complementary to the B region of PLZF (5”CTGTCTCCATGGACTTC-3’ ), with two cycles at 98°C for 5 0 seconds, 47°C for 1.5 minutes, and 72°C for 2 minutes. 32 cycles at 98°C for 25 seconds, 47°C for l .S minutes, and 72°C for 2 minutes. and a final extension for 12 minutes at 72°C. Ten microliters of the PCR products were electrophoretically separated through a 1.44 agarose gel, transferred to nitrocellulose, prehybridized, and hybrid- ized overnight in 5 X salt sodium phosphate and ethylendiamine tetra-acetate (SSPE), 5 X Denhardt’s, 1 mg/mL salmon sperm DNA at 63°C with a radiolabeled oligonucleotide complementary to PLZF (S‘-TGGAGCAGCACAGGAAGCTGC-3’ ). located 3’ to the PLZF amplification primer. After washing, the filters were autoradio- graphed. A previously identified AML patient with t(1 1;17) and a PLZFRARa-fusion product was used as a positive control.”,”
In vitro differentiation studies with ATRA. Previously cryopre- served leukemic blasts from four patients (cases 1 I , 14, IS, and 16; Table 1) and from two AML-M3 patients with a confirmed t( 15;17) were thawed in 37°C defrosting medium [RPMI 1640; 20% fetal calf serum (FCS)], centrifuged at 1,100 rpm for 5 minutes and then resuspended in complete culture medium (RPMI 1640, 2 0 8 FCS, antibiotics). Cells were cultured with or without l PmolLATRA (Sigma Chemical Co. St Louis, MO) for 7 days as previously de- scribed.”~?’ Aliquots of cells removed at time 0 and days 2, 5. and 7 were analyzed by cytologic evaluation and differential count of Wright and SBB-stained cytospins. Maturation was defined by a gain in cytoplasmic volume, loss of cytoplasmic granularity after the promyelocytic stage, and nuclear segmentation.
I n vitro cytotoxicify ussuys. The cytotoxicity of previously cryo- preserved leukemic cell suspensions from six myeloid/NK leukemia cases with residual cells (cases 3, I O [a posttreatment relapse speci- men was analyzed as pretreatment cells were not available], 12, 14, IS, and 19, Table I ) was tested in a ”Chromium (Cr) release func- tional assay.” An NK leukemia cell line (IMC-I; recently developed in our laboratory) and an AML-M3 sample with a confirmed t( I 5 ; 17) were used as controls.2x Target cells included the NK cell-susceptible K562 (human erythroleukemia) line. Target cells were incubated with ”Cr (New England Biolabs, Boston, MA) in I mL of bovine calf serum (BCS) ( S O pCi/l X IO” cells) for 2 hours at 37°C in air/ CO2 (19: l ) . The cells were then washed three times with complete medium (RPMI 1640, 10% BCS, and 50 U of PenicillidmL, 5 0 pg/ mL of Streptomycin, and 50 pg/mL Gentamicin (Sigma). Cryopre- served leukemic cells (effector cells) were defrosted in warm de- frosting medium, centrifuged at l , l00 rpm for 5 minutes, and then resuspended in complete media. Effector cells were added ( 5 X I O 5 cells/100 pL for a 50: I ratio) to the wells of round-bottom microtiter plates (Costar, Cambridge, MA), and were diluted at ratios of 25: I (2.5 X 1O5/10O pL), 12.5:l (1.25 X 10’/100 pL). 6.25:l (6.25 X
10‘/100pL),and3.12:1 (3.12X lO‘/lOOpL).Forassayswhere 12:l was the highest effector:target ratio used, effectors at 1.2 X IO’ cells/100 pL were added to the wells and the appropriate dilutions were made. Each ratio was tested in triplicate. Targets were added ( l X 10‘ cells/100 pL) to each well, and the plate was centrifuged at 501: for 3 minutes and incubated for 4 hours at 37°C (air/COz. l9:l). Effector and target cell mixtures were assayed before incuba- tion with recombinant interleukin-2 (IL-2) (Chiron Corp, Emoryville, CA) to obtain a baseline at day 0. Cells were also assayed after effector cells were precultured for 48 hours with 1,000 UlmL IL-2 and complete media (5% CO2, 37°C). After incubation and removal of the IL-2, the supernatant was collected using a harvesting press (Skatron, Sterling, VA) and counted for radioactivity for 1 minute in a gamma counter. Specific lysis (%) was determined as follows: 100 X [(test cpm - spontaneous cpm)/(maximum cpm - spontane-

MYELOID/NATURAL KILLER CELL ACUTE LEUKEMIA
ous cpm)], with maximum release determined by adding 100 pL of target cells to wells containing 100 pL of 10% Triton X-100.27
Isolation of a nonleukemic CD33+, CD.56+, C D 1 6 normal coun- terpart cell. NK cells were isolated from PB buffy coats of four healthy blood donors, with a pooled average cell count of 4.7 X 109/L, as previously des~ribed.~~-~ ' Mononuclear cells were collected by Ficoll-Hypaque centrifugation at 1,360 rpm (400g) for 25 to 30 minutes resuspended in 2 mL of RPMI, and layered on top of an equal amount of FCS and centrifuged again at 800 rpm for 5 minutes to remove platelets. The cell pellet was resuspended in complete medium (RPMI 1640, 20% FCS), plated on plastic petri dishes and incubated overnight at 37°C in a CO2 incubator to remove adherent monocytes. The nonadherent cell fraction was washed and T lym- phocytes were removed by incubation with mouse anti-CD3 anti- body, followed by rosetting with sheep red blood cells coated with rabbit-antimouse IgG. A second Ficoll-Hypaque centrifugation was performed to remove rosetted T cells and the nonrosetted cell layer was harvested. This NK cell-enriched population was then directly labeled for three-color flow cytometric analysis; cells were stained with purified CD56 antibody (Becton Dickinson), washed, and then labeled with biotinylated goat-antimouse IgG F(ab);. After a blocking step with goat serum, the cells were labeled with FITC- conjugated CD33 (Coulter) and PE-conjugated CD16 (Becton Dick- inson). After washing with Hanks' Balanced Salt Solution (HBSS), the cells were labeled with streptavidin PE-conjugated Texas Red (RED613) (Life Technologies, Becton Dickinson, San Jose, CA) and then washed and resuspended in HBSS. Cells were initially sorted using forward-angle light-scatter and side-scatter parameters on a Coulter 753 Cell Sorter to select for a small to medium-sized, nongranular population; cells stained with mouse isotype control antibodies were used as a negative control to establish gating param- eters. Additional gating was performed on CD56+ and CD33' cells to obtain CD16' and C D 1 6 populations for cytospin morphologic and cytochemical evaluation.
Clinical and outcome data. Clinical data for patients registered on treatment studies SWOG 8600 or 9031 were obtained from SWOG central data base and were subjected to standard SWOG
2 41
procedures for reporting and quality control. Seventeen of these patients were registered on SWOG AML frontline studies (11 on SWOG 8600, 3 on SWOG 9031, and 2 on SWOG 9034); three patients were not ultimately registered on any SWOG treatment study (cases 12, 14, and 15, Table 1). Data for patients registered on study SWOG 9034, an intergroup study coordinated by Eastern Cooperative Oncology Group (ECOG), were obtained from the ECOG central data base. Data for patients who were not registered on SWOG treatment studies (cases 12, 14, and 15, Table 1) were obtained from the hematologist-oncologist responsible for the pa- tient's care. Overall survival was measured from the day of registra- tion on SWOG treatment study (or the start date of induction therapy for non-SWOG patients) until death from any cause. Relapse-free survival (RFS) was measured from the onset of complete response until relapse or death from any cause, with observation censored at the date of last contact for living patients with no report of relapse. Median durations of survival and R F S were obtained from distribu- tions estimated by the method of Kaplan and Meier.3' The BM differential data listed in Table 2 is based on the local institutional pathology.
RESULTS
Flow cytometric immunophenotypic studies. Pretreat- ment BM and PB specimens from patients who were candi- dates for frontline AML treatment studies SWOG 8600, 903 1, and 9034 were reviewed for possible inclusion in this study. Specimens from 350 consecutive patients were exam- ined and flow cytometric analysis of hematopoietic cell sur- face antigen expression showed 20 cases (6%) with a unique immunophenotypic profile. These 20 cases were character- ized by a lack of expression of HLA-DR and by the coex- pression of various myeloid (CD33, CD13, CD15) and NK cell-associated (CD56) surface antigens; the detailed immu- nophenotypic profile in each case is provided in Table 1. Like AML cases of the FAB M3 subtype, all cases consis-
Table 2. MyeloidlNK Precursor Cell Acute Leukemia Cases: Pretreatment Clinical Characteristics and Therapeutic Response
WBC BM BM Case No. Age/Sex (XIOs/L) (% blasts) (96 prornyelocytes)
Extramedullary Bleeding Response to Survival Disease Diathesis Induction TX (dl
1 52/M 4.7 71 4 None, CNS Unk None CR 282 2 681M 33.8 98 <l None None ED 23 3 35lF 155.1 98 0 None None CR 486+ 4 43/F 6.2 92 0 None, CNS Unk None CR 754+ 5 18tM 16.2 >95 0 None None CR 1,309
7 43lM 78.7 90 0 H. S Mild CR 1,620+ 8 64lM 53.9 96 1 None None NASS 19 9 72lF 88.6 91 <l None Mild NR 61 +
10 41iM 1 .o 81 1 None Mild NR 68 11 281M 86.1 ND ND H, Ing None CR 1,798+ 12 66/M 13.9 88 7 None Mild CR 1,085+ 13 44lF 91.7 99 0 Ax, Ing None NASS 14
1.990+ 48tM 328.0 >95 0 None None NR 45
15 48lF 212.1 99 0 None Mild CR 901 16 351F 45.2 47 10 None Moderate NR 350 17 48iF 71.3 98 0 ANOS Mild CR 18 601M 98.2 82 Unk None Mild CR 19 48lF 89.0 79 0 cx Mild ED 5
6 62lF 218.0 93 0 None None CR 133
28+ 146+
20 57tF 8.2 90 Unk None None NR 81
Abbreviations: Extramedullary disease: Ax, axillary lymphadenopathy; Cx, cervical lymphadenopathy; Ing, inguinal lymphadenopathy; ANOS, adenopathy Site unspecified; S, splenomegaly; H, hepatomegaly; CNS, central nervous system. Response to induction therapy (Tx): CR. complete remission; ED, early death; NASS, not adequately assessed; NR, no response; ND, not done; Unk, unknown.

24% SCOTT ET AL
Fig 1. Two-color contour plots derived from three-color flow cyto- metric analysis of gated blasts from a representative case of myeloid/ NK acute leukemia with PE, FITC, and Texas Red (TR)-conjugated antibodies. (A) Coexpression of CD33-PE (Y-axis) and CD56-TR IX- axis). (B) Expression of CD33-PE (Y-axis) and lack of expression of HU-DR-TR (X-axis). (C) Expression of CD33-PE (Y-axis) and lack of expression of CD16-FITC (X-axis). (D) Expression of CD56-TR (X-axis) and lack of expression of CD16-FITC (Y-axis).
tently lacked expression of HLA-DR. an antigen that is pref- erentially expressed by myeloblasts and lost during matura- tion to the promyelocytic Although two cases were positive for CD4, this antigen is not T-cell lineage specific and may frequently be expressed on AML blasts and on a subset of PB monocytes.5.x The absence of T-cell lineage commitment was further confirmed by the lack of expression of the T-cell lineage-associated antigens CD2, CD3, and CD8 and by a lack of clonal rearrangement of genes encod- ing the T-cell receptor (TCRP, y , 61, and 62; data not shown). All cases were characterized by the expression of the myeloid-associated antigens CD33, CD13, and/or CD1 5; the hematopoietic stem and progenitor cell antigen CD34 was expressed at low antigen density in 6/20 cases (Table l ) . All cases expressed CD56 (a variantly spliced form of the NCAM)"3"4 at high antigen density and did not express CD16 (the immunoglobulin Fcy receptor). The CD1 la adhe- sion molecule required for NK cell-mediated cytotoxic- ity,'5.36 was also expressed at high antigen density in all cases in which it was assessed (Table I , Cases I through 10). Coexpression of CD56 and myeloid-associated antigens (CD33, CD13, and CD15) was confirmed in each case by two- and three-color flow cytometric studies (Fig 1).
RT-PCR and oligonucleotide probe hybridization assays for CD56 (NCAM). To confirm that CD56, and not a cross- reactive epitope, was expressed in the myeloid/NK acute leukemia cases, RT-PCR assays were performed to detect CD56 (NCAM) mRNA transcripts in leukemic blasts. A major 493-bp CD56 (NCAM) PCR product was identified in each of two cases tested (Cases 8 and 15; Table 1) (Fig
2A). The analysis also included the CD56' myeloma cell line 8226/Dox40 used as a high-level positive control and an AML case with very low CD56 expression ( 1 % by flow cytometry) as a negative control. The identity of this 493- bp product has been previously confirmed by DNA sequenc- ing.Ix Hybridization of the RT-PCR products with an NCAM DNA probe confirmed the specificity of the RT-PCR prod- ucts (Fig 2B).
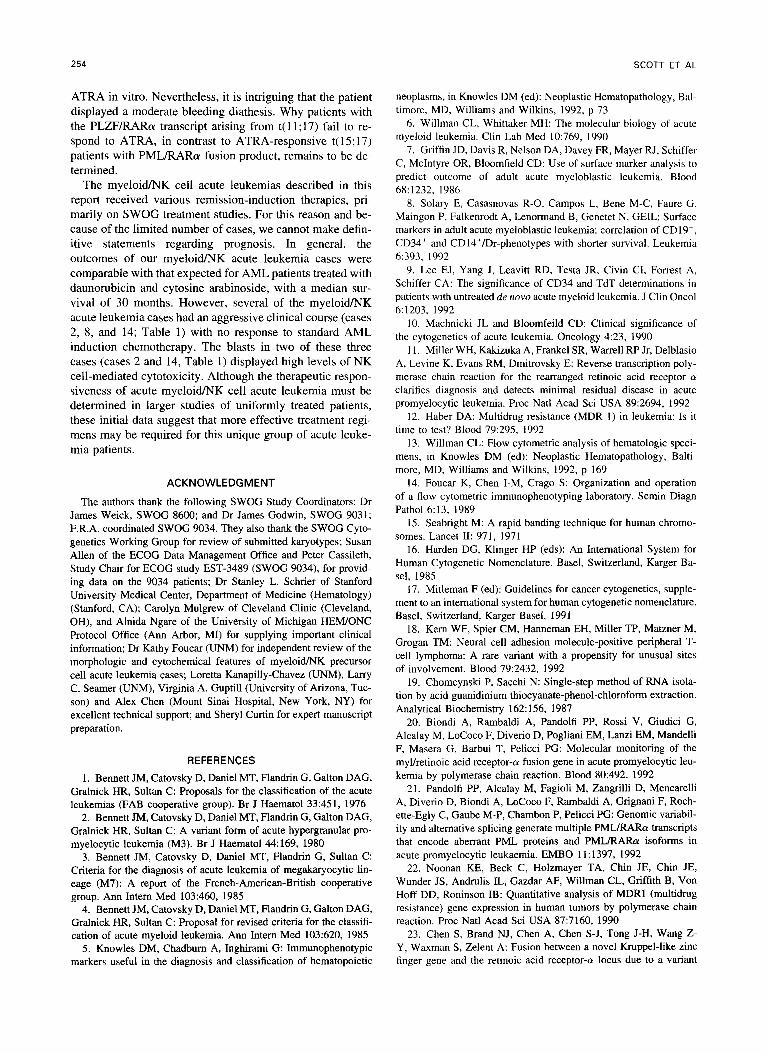
Review of morphologic and cwdlernical features. The referring institutional FAB diagnoses were as follows for the 20 cases: 1 MO/L2, 10 M I , 5 M2, 2 M3, and 2 M4. Upon rereview of BM aspirates and PB smears in each case by the SWOG Leukemia Review Panel, the majority of the cases ( 1 3/20) were noted to have distinct, yet similar mor- phologic and cytochemical features (which we have chosen to designate myeloid/NK acute leukemia; Table l ) . These features included strikingly invaginated nuclear membranes, scant to moderate cytoplasm with fine to moderately coarse azurophilic granules, and weak to moderate finely granular SBB and/or MP0 cytochemical reactivity (Fig 3, A and C). Although these features were highly reminiscent of AML- M3, particularly the microgranular variant (AML-M3v) (Fig 3B), distinct differences were apparent. Whereas occasional myeloid/NK blasts had conspicuous cytoplasmic granules, they were not as prominent as typical AML-M3 blasts; more- over, the pattern of weak or moderate finely granular SBB or MP0 positivity was distinct from the intense and dense SBB and MP0 staining of AML-M3 and M3v (Fig 3D). Rare myeloid/NK blasts contained Auer rods; bundles of Auer rods (faggot cells) characteristic of FAB M3 were not present. All cases were characterized by a high marrow-blast percentage (median blast cell percentage, 92%; range of 47% to 99%); however, in contrast to cases of AML-M3, in- creased numbers of marrow promyelocytes were not seen (Table 2). Increased numbers of cells with large granular
S 1 2 3 4 S 1 2 3 4
a493 bp
Fig 2. (A) Ethidium-stained gel of NCAM RT-PCR products. DNA size markers (in bp) are shown in lane S. A major 493-bp NCAM RT- PCR product is detected in the CD56' 822WDOX40 cell line used as a positive control (lane 1) while an AML sample lacking CD56 (<l% by flow cytometry) essentially lacks this product (lane 41. Two CD56' myeloid/NK cell acute leukemia cases in lane 2 (Case 8; Table 1) and lane 3 (Case 15; Table 1) show the major 493-bp NCAM RT-PCR product. (B) Autoradiograph of the gel in A hybridized with an NCAM- specific DNA probe. Hybridization confirms the specificity of the NCAM RT-PCR products; lanes as identified in Fig 2A.
MYELOID/NATURAL KILLER CELL ACUTE LEUKEMIA
Fig 3. Morphologic and cytochemical features of myeloidlNK acute leukemias in comparison to AML- M3v blasts. (A) Wright-stained myeloidlNK leukemic blasts; note deeply invaginated nuclear membranes and fine azurophilic granularity of cytoplasm. Origi- nal magnification x 1,OOO. (B) Wright-stained AML- Mhr; note similarities to A. Original magnification x 1,OOO. (C) SBB-stained myeloid/NK leukemic blasts; note finely granular staining pattern. (D) SBB-stained AML-Mhr blasts; note intense and dense staining pattern.
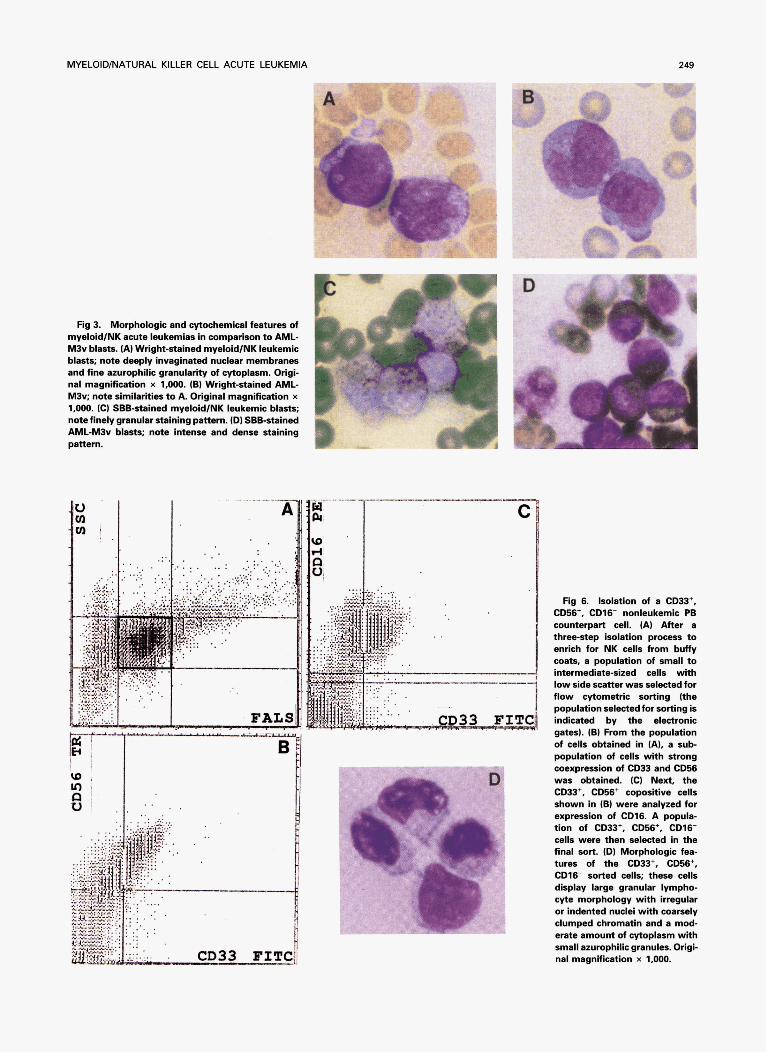
Rg 6. Isolation of a CD33+, C m + , CD16- nonleukemic PB counterpart cell. (A) After a three-step isolation process to enrich for NK cells from buffy coats, a population of small to intermediate-sized cells with low side scatter was selected for flow cytometric sorting (the population selected for sorting is indicated by the electronic gates). (B) From the population of cells obtained in (A), a sub- population of cells with strong coexpression of CD33 and CD56 was obtained. (C) Next, the CD33+, C m + copositive cells shown in (B) were analyzed for expression of CD16. A popula- tion of CD33+, CD=+, CD16- cells were then selected in the final sort. (D) Morphologic fea- tures of the CD33+, CD56+, CD16- sorted cells; these cells display large granular lympho- cyte morphology with irregular or indented nuclei with coarsely clumped chromatin and a mod- erate amount of cytoplasm with small azurophilic granules. Origi- nal magnification x 1,OOO.

250 SCOTT ET AL
lymphocyte (LGL) morphology associated with the NK cell lineage were seen in the BM aspirates and PB smears of some cases (data not shown); whether these cells were de- rived from the leukemic clone or represented residual normal NK cells is not known. Whereas seven of the remaining cases (cases 1 ,3 ,8 , IO, 12, 16, and 19; Table 1) had morpho- logic and cytochemical similarities to cases designated as myeloid/NK acute leukemia, the overall features were equally consistent with an M1, M2, or M7 designation in the FAB classification system and these cases are designated in this fashion (Table l).
Pretreatment clinical characteristics and therapeutic re- sponse. Detailed pretreatment clinical characteristics and therapeutic responses are provided in Table 2. Median age at time of treatment was 48 years (range, 18 to 72 years) with an equal sex distribution (10 women, 10 men). The majority of patients presented with high white blood cell counts at presentation with a median of 75.0 X 109/L (range of 1.0 X 109/L to 328.0 X lo9& Table 2). The median PB lymphocyte count was 3,8OO/pL (range, 400 to 15,3OO/pL); 9/18 cases had counts greater than 4,00O/pL (data not shown). Extramedullary disease, including hepatospleno- megaly and lymphadenopathy, was noted in only 5 patients; among 18 patients in whom central nervous system (CNS) involvement was assessed, none displayed evidence of CNS involvement at presentation or relapse. In contrast to AML- M3 patients, less than half of the myeloid/NK leukemia pa- tients had a bleeding diathesis at presentation. Eight cases (Table 2) had a mild bleeding diathesis consisting of pete- chial and/or mucosal hemorrhage, whereas 2 patients dis- played disseminated intravascular coagulopathy; 1 displayed a mild bleeding diathesis (case 12, Table 2) and 1 a moderate diathesis (case 16, Table 2).
Thirteen patients were treated with standard-dose cytosine arabinoside and daunorubicin (8 on SWOG 8600, 3 on SWOG 903 1, and 2 off protocol) and three with standard- dose cytosine arabinoside plus idarubicin (2 on SWOG 9034 and 1 off protocol). The other four patients received high- dose cytosine arabinoside and daunorubicin on SWOG 8600 (2 with 2.0/g/M2/d X 6 days and 2 with 3.0/g/M2/d X 6 days). Eleven patients achieved complete remission (CR). In five of these cases, relapse occurred after 90 days, 98 days, 15 months, 16 months, or 27 months; the other six patients remain alive without report of relapse at 28 days, 112 days, 16 months, 24 months, 42 months, and 59 months after achieving CR. Eleven patients have died and the other nine remain alive at between 28 days and 65 months (median 16 months). The estimated median survival is 30 months.
Cytogenetic review. Pretreatment cytogenetic studies were available for 16/20 cases and 12 of these cases had no detectable cytogenetic abnormality (Table 1). A balanced reciprocal t( 15;17)(q22;ql1-21) is a characteristic feature of acute promyelocytic leukemia (APL; A M L - M ~ M ~ v ) and is detectable in 50% to 70% of APL cases by standard karyo- typic analy~is.~’ However, despite the morphologic and im- munophenotypic similarities between our cases and AML- M3v, no case contained a t(15;17) on routine cytogenetic analysis (Table I) . Two cases had karyotypic abnormalities involving chromosome 17q (Table 1): case 16 with t(11;17)(q23;q21) and case 15 with de1(17)(q25). Case 1,
with morphologic features most consistent with FAB AML- M7 was characterized by a 47,XY,+8,t(16;21)(pl l;q22), whereas case 10 contained a t ( l l ; l4)(pl3;ql l ) (Table l ) .
RT-PCR screerxfor the PML-RARa fusion transcript. Be- cause of the morphologic and immunophenotypic similarities of our cases to A M L - M ~ v and because of the preponderance of 46,XY or 46,XX karyotypes, we were concerned that the t( 15; 17) might have been missed in routine cytogenetic analysis. Therefore, we used RT-PCR assays to screen RNA isolated from 17 of 20 cases with residual cells (all cases except 9, 13, and 19; Table 1) for the PML/RARa chimeric transcript which arises from the t( 15;17). All RNA samples from myeloid/NK cases and from three APL cases with con- firmed t( 15; 17) used as controls contained amplifiable 02- microglobulin transcripts (Fig 4A). In contrast to APL/FAB- M3 cases (Fig 4, B and C, lanes 12 through 14), all 17 of the myeloid/NK leukemia cases analyzed lacked the PML/ RARa fusion mRNA (Fig 4, B and C, lanes 2 through 1 1; data on remaining cases not shown), confirming that myeloid/NK acute leukemia cases are genetically and molec- ularly distinct from APL/AML-M3.
RT-PCR screen ,for the PLZFiRARa fusion transcript. The AML-associated t( 1 1 ; 17)(q23;q2 1.1) has recently been cloned and characterized.*’ Like cases of true APL with a t( 15; 17), the t( 1 1 ; 17) involves the RARa gene in the same intron on chromosome 17q21; but in contrast to APL, the t( 11;17) results in a fusion of RARa with a novel gene designated PLZF on chromosome 1 1q23.23 As one of our cases had a cytogenetically detectable t( 1 1 ; 17)(q2 1 ;q23) (case 16; Table l) , we wanted to test for the presence of the PLZF/RARa fusion transcript in this case, and to determine whether any of the other cases (particularly those with 46,XX or 46,XY karyotypes) contained a PLZF/RARa fusion mRNA. RT-PCR for the PLZFIRARa fusion mRNA, as shown in Fig 4D, detected a 319-bp PLZF/RARa product in our case with a t( 1 1;17) (Fig 4D, lane 12) as well as in a positive control sample. However, none of the eleven other myeloid/NK acute leukemia cases tested expressed this fu- sion product (Fig 4D). Thus, although the t( 11;17)(q23;q21) appears to be associated with the myeloid/NK leukemia cell phenotype, other genetic abnormalities, yet to be defined, must be present in the majority of the myeloid/NK acute leukemia cases.
Response of cases to ATRA-Induced differentiation. A hallmark of APL with t(15;17) and the PMLIRARa fusion transcript is an induction of differentiation in vitro and in vivo in response to ATRA.”-4’ The in vitro responsiveness of AML cases with t( 1 1;17) to ATRA has not been previously determined. Because of the morphologic and immunopheno- typic similarity of our cases to APL and the inclusion of one case with a t( 1 1;17)(q23;q21) involving the RARa gene in our series, we sought to determine the responsiveness of myeloid/NK acute leukemia cases to ATRA in vitro. Resid- ual cryopreserved cells from six patients (Cases 3, 11, 14, 15, 16, and 19; Table l), all of whom had Ficoll-Hypaque- enriched cryopreserved blast cell percentages exceeding 90%, and two control cases of APL/AML-M3 were cultured in vitro in medium with or without ATRA. Morphologic differentiation was assessed at time 0 and on days 2,5, and 7 postculture. ATRA-induced granulocytic differentiation was

MYELOID/NATURAL KILLER CELL ACUTE LEUKEMIA 251
A
B
C
D
1 2 3 4 5 6 7 8 9 1 0 1 1 1 2 1 3 14
4 324 bp
1 2 3 4 5 6 7 8 9 l0 11 12 1 3 W 1-1
4319bp
Fig 4. RT-PCR assays for PML/RARa and PLZFlRARa fusion transcripts. In A through C (all ethidium-stained gels of RT-PCR products), the samples in each lane are identical: lane 1 (blank control); lane 2 (HL60 cells used as a negative controll; lanes 3 through 11 (myeloid/NK leukemia samples); lanes 12 and 13 (APL/AML-M3 samples with a PML/RARa-fusion mRNA involving the bcr 1); lane 14 IAPL/AML-M3 sample with a PML/RARa fusion involving the bcr 3 PML reg i~n) .~" ' (A) 104-bp RT-PCR product of PZ-microglobulin mRNA, amplified as an internal control in each case. (B and C). Nested RT-PCR for the PMLIRARa fusion with the M2-RS primers (B), which detect a 326-bp PCR product arising from the PML bcr 1, and M4-R8 primers (C), which detect a 324-bp PCR product arising from the PML bcr3); see Materials and Methods. Compared with APL/AML-M3 controls, all myeloid/NK leukemia cases lack the PMLlRARa fusion. (D) RT-PCR analysis with primers to detect the PUFIRARa-fusion mRNA. Lanes 1 through 11 Imyeloid/NK leukemia cases); lane 12 (myeloid/NK leukemia case 16 with t(11;17)); lanes 13 and 14 (APL/AML-M3 controls); lane 15 ([+l, AML control case with t(ll;171); and lane 16 (1-1, blank control). Lanes 12 and 15 show a 319- bp PLZF/RARa-fusion product.
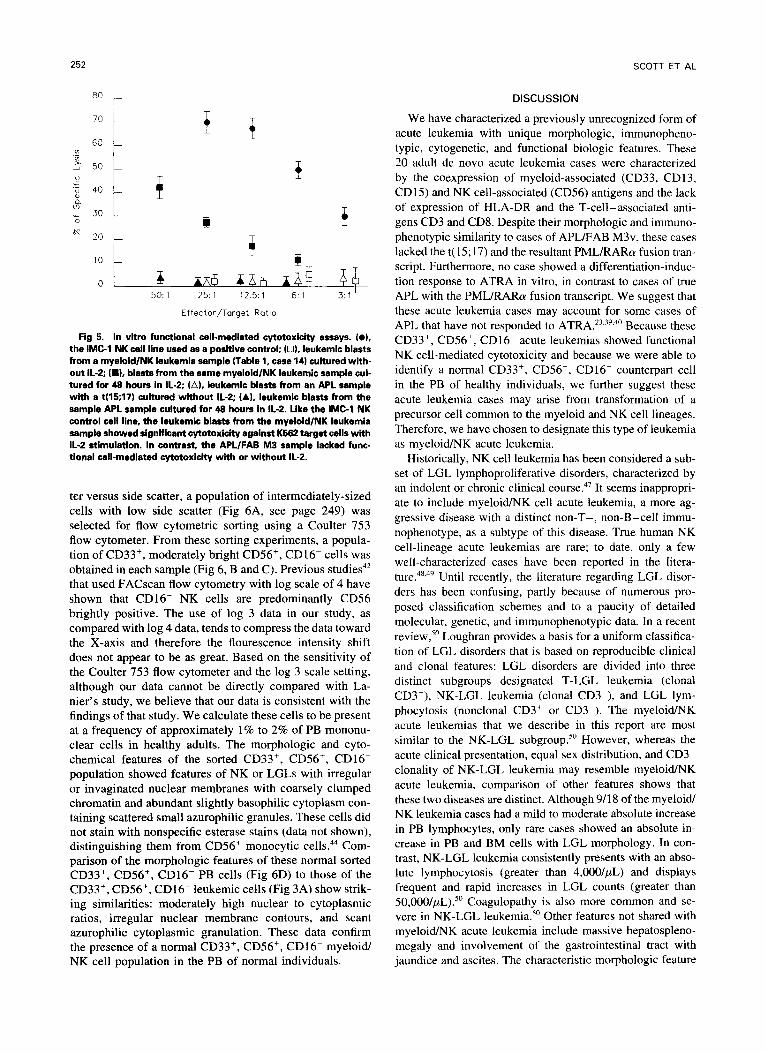
observed in none of the six myeloid/NK acute leukemia or increased cytotoxicity compared with freshly isolated PB cases, including case 16 (Table I ) with a t(l1;17) (data not NK cells'* (Fig 5). NK cell-mediated cytotoxicity was also shown). In contrast, both control APL/AML-M3 cases analyzed in two cases of APL with a confirmed t( l5;17) (Fig showed myelocytic differentiation with decreased blast per- 5). Four cases (cases 3, IO, 14, and 19; Table 1) displayed centages at days 5 and 7 (data not shown). These results significant cytotoxic activity with IL-2, as compared with further support the distinct biologic nature of myeloid/NK the positive NK leukemia control cell line (Fig 5; showing acute leukemia and confirm the nonresponsiveness of these the data from case 14). In contrast, both cases of APL/FAB cases to ATRA in vitro. M3 lacked cytotoxic activity (Fig 5). This demonstration of
Assessment of N K cell-mediated functional cytotoxicity. functional cell-mediated cytotoxicity in the leukemic cells Because the myeloid/NK acute leukemia cases coexpressed further supports a relationship between myeloid/NK acute the CD56 and CD1 la antigens essential for functional NK leukemias and cells derived from the NK lineage. cell-mediated cytotoxicity in addition to sharing the CD56', Isolation of a CD33', CD%', C D 1 6 nonleukemic coun- CD16- phenotype of NK precursor cells, we sought to deter- terpart cell. Although our myeloid/NK acute leukemia mine whether these leukemic cases displayed functional NK cases expressed the CD56', CD16- phenotype of NK pre- cell-mediated cytotoxicity.""" Cytotoxicity was assessed in cursor cells, they also coexpressed the myeloid-associated a standard "Cr release functional assay using the NK cell- antigen CD33. As previous studies characterizing CD56+, susceptible line K562 as a target cell (Fig 5). Leukemic CD16- NK precursor cells have not included an analysis of blasts from six cases [cases 3, I O (results obtained with myeloid antigens such as CD33,42-4h we sought to determine relapse material), 12, 14, 15, and 19; (Table l ) ] were added whether the coexpression of CD33 in our cases reflected an as effector cells; in each case selected for analysis, the leuke- aberrant leukemic phenotype or whether a CD33', CD56', mic blast cell percentage in the enriched cryopreserved cell CD16- rnyeloid/NK cell was present in normal BM and suspensions exceeded 90% and no cells with LGL morphol- PB. Using PB buffy coats from four healthy donors, a three- ogy were evident in the preassay or postassay samples. The step isolation process was performed to enrich for NK cells. levels of cytotoxicity in these leukemic samples were com- Cells obtained by these methods were labeled with CD33, pared with those of a positive control cell line, the IL-2- CD56, and CD16 antibodies and sorted using multiparame- dependent IMC-I NK leukemia cell line that displays equal ter flow cytometry. From plots of forward-angle light scat-
252
ao r
SCOTT ET AL
DISCUSSION
We have characterized a previously unrecognized form of acute leukemia with unique morphologic, immunopheno- typic, cytogenetic, and functional biologic features. These 20 adult de novo acute leukemia cases were characterized by the coexpression of myeloid-associated (CD33, CD13, CD 15) and NK cell-associated (CD56) antigens and the lack of expression of HLA-DR and the T-cell-associated anti- gens CD3 and CD8. Despite their morphologic and immuno- phenotypic similarity to cases of APL/FAB M3v, these cases lacked the t( 15; 17) and the resultant PML/RARa fusion tran- script. Furthermore, no case showed a differentiation-induc- tion response to ATRA in vitro, in contrast to cases of true APL with the PML/RARa fusion transcript. We suggest that these acute leukemia cases may account for some cases of APL that have not responded to ATRA.23.3y~40 Because these CD33+, CD56+, CD16- acute leukemias showed functional NK cell-mediated cytotoxicity and because we were able to identify a normal CD33+, CD56+, CD16- counterpart cell in the PB of healthy individuals, we further suggest these acute leukemia cases may arise from transformation of a precursor cell common to the myeloid and NK cell lineages. Therefore, we have chosen to designate this type of leukemia as myeloid/NK acute leukemia.
Historically, NK cell leukemia has been considered a sub- set of LGL lymphoproliferative disorders, characterized by an indolent or chronic clinical co~rse .~ ' It seems inappropri- ate to include myeloid/NK cell acute leukemia, a more ag- gressive disease with a distinct non-T-, non-B-cell immu- nophenotype, as a subtype of this disease. True human NK cell-lineage acute leukemias are rare; to date, only a few well-characterized cases have been reported in the litera- t~re.".~' Until recently, the literature regarding LGL disor- ders has been confusing, partly because of numerous pro- posed classification schemes and to a paucity of detailed molecular, genetic, and immunophenotypic data. In a recent review,'" Loughran provides a basis for a uniform classifica- tion of LGL disorders that is based on reproducible clinical and clonal features: LGL disorders are divided into three distinct subgroups designated T-LGL leukemia (clonal CD3+), NK-LGL leukemia (clonal CD3-), and LGL lym- phocytosis (nonclonal CD3' or CD3-). The myeloid/NK acute leukemias that we describe in this report are most similar to the NK-LGL subgroup." However, whereas the acute clinical presentation, equal sex distribution, and CD3- clonality of NK-LGL leukemia may resemble myeloid/NK acute leukemia, comparison of other features shows that these two diseases are distinct. Although 9/18 of the myeloid NK leukemia cases had a mild to moderate absolute increase in PB lymphocytes, only rare cases showed an absolute in- crease in PB and BM cells with LGL morphology. In con- trast, NK-LGL leukemia consistently presents with an abso- lute lymphocytosis (greater than 4,0OO/pL) and displays frequent and rapid increases in LGL counts (greater than 50,000/pL).50 Coagulopathy is also more common and se- vere in NK-LGL le~kemia.~" Other features not shared with myeloid/NK acute leukemia include massive hepatospleno- megaly and involvement of the gastrointestinal tract with jaundice and ascites. The characteristic morphologic feature
V .- L
'6 40
Ln ," 30 I 20
T 7 i
I r
T
& I
l i
50: 1 25: 1 12.5: 1 6.1 3: l i
Effector/Target Ratio
Fig 5. In vitro functional cell-mediated cytotoxicity assays. (01, the IMC-l NK cell line used as a positive control; (0). leukemic blasts from a myeloid/NK leukemia sample (Table 1, case 14) cultured with- out IL-2; ( W , blasts from the same myeloid/NK leukemic sample cul- tured for 48 hours in IL-2; (A), leukemic blasts from an APL sample with a t(15;17) cultured without IL-2; (AI, leukemic blasts from the sample APL sample cultured for 48 hours in IL-2. Like the IMC-l NK control cell line, the leukemic blasts from the myeloid/NK leukemia sample showed significant cytotoxicity against K562 target cells with 11-2 stimulation. In contrast, the APLlFAB M3 sample lacked func- tional call-mediated cytotoxicity with or without IL-2.
ter versus side scatter, a population of intermediately-sized cells with low side scatter (Fig 6A, see page 249) was selected for flow cytometric sorting using a Coulter 753 flow cytometer. From these sorting experiments, a popula- tion of CD33+, moderately bright CD56+, CD16- cells was obtained in each sample (Fig 6, B and C). Previous studies4* that used FACscan flow cytometry with log scale of 4 have shown that CD16- NK cells are predominantly CD56 brightly positive. The use of log 3 data in our study, as compared with log 4 data, tends to compress the data toward the X-axis and therefore the flourescence intensity shift does not appear to be as great. Based on the sensitivity of the Coulter 753 flow cytometer and the log 3 scale setting, although our data cannot be directly compared with La- nier's study, we believe that our data is consistent with the findings of that study. We calculate these cells to be present at a frequency of approximately 1% to 2% of PB mononu- clear cells in healthy adults. The morphologic and cyto- chemical features of the sorted CD33+, CD56+, CD16- population showed features of NK or LGLs with irregular or invaginated nuclear membranes with coarsely clumped chromatin and abundant slightly basophilic cytoplasm con- taining scattered small azurophilic granules. These cells did not stain with nonspecific esterase stains (data not shown), distinguishing them from CD56+ monocytic cellsu Com- parison of the morphologic features of these normal sorted CD33+, CD56+, CD16- PB cells (Fig 6D) to those of the CD33+, CD56+, CD16- leukemic cells (Fig 3A) show strik- ing similarities: moderately high nuclear to cytoplasmic ratios, irregular nuclear membrane contours, and scant azurophilic cytoplasmic granulation. These data confirm the presence of a normal CD33', CD56+, CD16- myeloid NK cell population in the PB of normal individuals.

MYELOID/NATURAL KILLER CELL ACUTE LEUKEMIA 253
of NK-LGL leukemia is the presence of increased PB and BM cells with LGL morphology with or without coarse cyto- plasmic granules, rather than the unique blast cell features of myeloid/NK acute leukemia. The immunophenotype of NK-LGL leukemia (CD3-, CD56+, CD25-, CD16+, and CD579 is also distinctly different from myeloid/NK acute leukemia. Although expression of stem cell, myeloid-associ- ated, and adhesion molecules have not yet been thoroughly studied in NK-LGL leukemia, the HLA-DR+/CD56+ NK- LGL leukemia cases reported by I m a m ~ r a ~ ~ were CD13- and CD33-negative, supporting our theory that NK-LGL leuke- mia and myeloid/NK acute leukemia are separate and distinct diseases. In contrast to myeloid/NK acute leukemia, many clonal NK-LGL cases have been reported to have simple or complex abnormalities of chromosome 5.50*5' Finally, in contrast to the majority of our myeloid/NK acute leukemia cases, most NK-LGL leukemia patients have had rapidly progressive clinical courses and have died within several months of presentation despite aggressive treatment. Thus, although the myeloidrNK acute leukemias that we present in this report and cases of NK-LGL leukemia have some shared features and both may be related to the NK cell lineage, distinct biologic and clinical differences are appar- ent.
All myeloid/NK acute leukemia cases expressed the CD56 antigen at high density. CD56 is an isoform of the well- characterized NCAM that mediates celVcell adhesive inter- a c t i o n ~ . ~ ~ . ~ ~ . ~ CD56+, CD16+ NK cells express a variantly spliced form of CD56 that mediates NK cell-target Expression of CD56, in addition to the CD1 l a adhesion molecule also expressed on myeloid/NK acute leukemia cases, is required for NK cell-mediated cytotoxic effector function.36.44 In addition to the characteristic expression of CD56 on normal NK cells, CD56 is also expressed on a subset of CD3+ cytotoxic T cells, and a subset of PB mono- cyte~.~~.'"' In hematopoietic neoplasms, CD56 has also been detected on clinically aggressive T-cell lymphomas, plasma cell myelomas, and de novo AMLs with t(8;21), t(8;16), and other monocytic leukemia-associated cytogenetic abnor- m a l i t i e ~ . ' ~ * ~ ~ - ~ ~ The forms of CD56 expressed by various he- matopoietic neoplasms are highly variable as a result of both alternative splicing and differential glyc~sylation'~; these al- ternative isoforms may account in part for the different bio- logic behaviors of CD56' neoplasms.
Expression of CD16 is not uniform in cells of NK lineage and is not necessary for NK cell function. In contrast to initial reports of diminished cytotoxicity of CD56', CD16- NK cells, subsequent studies have shown that CD56+, CD16- NK cells may have increased cy to toxi~i ty .4* .~~~~~ Thus, the lack of expression of CD16 in our cases does not preclude NK cell lineage and the cytotoxicity shown by our CD33+, CD56+, CD16-, CDlla+ cases is not unexpected. Although the majority of PB NK cells coexpress CD56 and CD16, a CD56+, CD16- NK cell population has been identi- fied at frequency of less than 2% in normal PB.43,46 It has been suggested that CD56+ NK cells that are CD16- or CDi6'" are NK cell precursors because these CD56+, CD16- cells comprise the majority of NK cells found in the BM and splenic pools.44,46 Natural killer cells with a similar phe- notype have also been generated from primitive CD34',
HLA-DR- progenitors in long-term BM cultures supple- mented with IL-2.45 Unfortunately, the coexpression of my- eloid-associated antigens has not been examined in most NK cell studies; thus, we cannot determine whether the CD56', CD16- NK precursor cells identified in those studies corre- spond to or are distinct from the CD33+, CD56+, CD16- leukemic cells that we have identified in this report. As NK cells are known to be BM-derived, we speculate that the normal CD33+, CD56+, CD16- cells that we have identified may be a precursor population common to the myeloid and NK cell lineage.45 It will be interesting to determine the growth factor dependence of these cells in future studies, and whether the CD33 antigen is lost upon culture of these cells with IL-2 that may promote further differentiation into the NK lineage. Finally, we speculate that the CD33+, CD56+, CD16- acute leukemias that we have identified may represent leukemic transformation of this normal CD33+, CD56+, CD16- normal counterpart cell.
Despite morphologic and immunophenotypic similarities, myeloid/NK acute leukemia cases lacked the t( 15;17) and failed to show a differentiation-induction response to ATRA in vitro. Distinguishing these myeloid/NK acute leukemias from cases of true APL will be important for clinical studies of ATRA. De Rossi et a13* have proposed that immuno- phenotypiclflow cytometric analysis could be used to make a precise diagnosis of APL; the diagnostic profile proposed was CD33+, CD13+, CD9+ (a B-cell and granulocytic marker), HLA-DR-, and CD7-. Unfortunately, the immuno- phenotypic studies presented in this report show that this profile would not distinguish cases of true APL from myeloid/NK cell acute leukemia cases. Our studies suggest that myeloid/NK cell acute leukemias could be distinguished from cases of true APL by inclusion of the CD56 and CD16 antigens in the proposed diagnostic panel. However, this immunophenotypic approach may still not allow precise di- agnosis; in a review of the immunophenotypic data of 50 SWOG APL/AML-M3 cases [(with a confirmed t(15;17)], we identified two APL cases with expression of CD56 at high antigen density (data not shown). Thus, we propose that all acute leukemia cases with morphologic features similar to APL be initially analyzed by flow cytometric immunopheno- typing using a panel that includes the HLA-DR, CD34, CD33, CD15, CD16, CD56, and CDlla antigens, and by careful morphologic examination with rigid adherence to criteria for A M L - M ~ N ~ V . Diagnostic confirmation of APL versus myeloid/NK acute leukemia should include RT-PCR studies to assess the presence or absence of the PMWRARa fusion transcript. With the morphologic and immunopheno- typic similarity of myeloidlNK acute leukemia cases to APL, it is of interest that one of our myeloid/NK acute leukemia cases was associated with a t( 1 1 ; 17)(q23;q2 1) that results in fusion of the RARa and PLZF genes.23 PLZF has some homology with the zinc finger gene MZFl and is a putative transcription factor preferentially expressed by myeloid cells.23 Although the t(11;17) was initially cloned from a case of APL, our myeloid/NK acute leukemia patient with t( l 1 ; 17) did not have features of APL.23-24 Morphologically, this patient was classified as M2 by FAB criteria and had 10% promyelocytes in the BM. The patient did not respond to chemotherapy, nor did the patient's cells respond to
254 SCOTT ET AL
ATRA in vitro. Nevertheless, it is intriguing that the patient displayed a moderate bleeding diathesis. Why patients with the PLZFmARa transcript arising from t(l1;17) fail to re- spond to ATRA, in contrast to ATRA-responsive t(15;17) patients with PMLmARa fusion product, remains to be de- termined.
The myeloid/NK cell acute leukemias described in this report received various remission-induction therapies, pri- marily on SWOG treatment studies. For this reason and be- cause of the limited number of cases, we cannot make defin- itive statements regarding prognosis. In general, the outcomes of our myeloid/NK acute leukemia cases were comparable with that expected for AML patients treated with daunorubicin and cytosine arabinoside, with a median sur- vival of 30 months. However, several of the myeloid/NK acute leukemia cases had an aggressive clinical course (cases 2, 8, and 14; Table 1) with no response to standard AML induction chemotherapy. The blasts in two of these three cases (cases 2 and 14, Table 1) displayed high levels of NK cell-mediated cytotoxicity. Although the therapeutic respon- siveness of acute myeloid/NK cell acute leukemia must be determined in larger studies of uniformly treated patients, these initial data suggest that more effective treatment regi- mens may be required for this unique group of acute leuke- mia patients.
ACKNOWLEDGMENT
The authors thank the following SWOG Study Coordinators: Dr James Weick, SWOG 8600; and Dr James Godwin, SWOG 9031: F.R.A. coordinated SWOG 9034. They also thank the SWOG Cyto- genetics Working Group for review of submitted karyotypes; Susan Allen of the ECOG Data Management Office and Peter Cassileth, Study Chair for ECOG study EST-3489 (SWOG 9034), for provid- ing data on the 9034 patients: Dr Stanley L. Schrier of Stanford University Medical Center, Department of Medicine (Hematology) (Stanford, CA); Carolyn Mulgrew of Cleveland Clinic (Cleveland, OH), and Alnida Ngare of the University of Michigan HEWONC Protocol Office (Ann Arbor, MI) for supplying important clinical information: Dr Kathy Foucar (UNM) for independent review of the morphologic and cytochemical features of myeloid/NK precursor cell acute leukemia cases: Loretta Kanapilly-Chavez (UNM), Larry C. Seamer (UNM), Virginia A. Guptill (University of Arizona, Tuc- son) and Alex Chen (Mount Sinai Hospital, New York, NY) for excellent technical support: and Sheryl Curtin for expert manuscript preparation.
REFERENCES
1. Bennett JM, Catovsky D, Daniel MT, Flandrin G, Galton DAG, Gralnick HR, Sultan C: Proposals for the classification of the acute leukemias (FAB cooperative group). Br J Haematol 33:451, 1976
2. Bennett JM, Catovsky D, Daniel MT, Flandrin G, Galton DAG, Gralnick HR, Sultan C: A variant form of acute hypergranular pro- myelocytic leukemia (M3). Br J Haematol 44: 169, 1980
3. Bennett JM, Catovsky D, Daniel MT, Flandrin G, Sultan C: Criteria for the diagnosis of acute leukemia of megakaryocytic lin- eage (M7): A report of the French-American-British cooperative group. Ann Intern Med 103:460, 1985
4. Bennett JM, Catovsky D, Daniel MT, Flandrin G, Galton DAG, Gralnick HR. Sultan C: Proposal for revised criteria for the classifi- cation of acute myeloid leukemia. Ann Intern Med 103:620, 1985
5 . Knowles DM, Chadburn A, Inghirami G: Immunophenotypic markers useful in the diagnosis and classification of hematopoietic
neoplasms, in Knowles DM (ed): Neoplastic Hematopathology, Bal- timore, MD, Williams and Wilkins, 1992, p 73
6. Willman CL, Whittaker MH: The molecular biology of acute myeloid leukemia. Clin Lab Med 10:769, 1990
7. Griffin JD, Davis R, Nelson DA, Davey FR, Mayer RJ, Schiffer C, McIntyre OR, Bloomfield CD: Use of surface marker analysis t o predict outcome of adult acute myeloblastic leukemia. Blood 68: 1232, 1986
8. Solary E, Casasnovas R-0, Campos L, Bene M-C, Faure G, Maingon P, Falkenrodt A, Lenormand B, Genetet N, GEIL: Surface markers in adult acute myeloblastic leukemia: correlation of CD19+, CD34' and CDlil+/Dr-phenotypes with shorter survival. Leukemia 6:393, 1992
9. Lee EJ, Yang J, Leavitt RD. Testa JR, Civin CI, Forrest A, Schiffer CA: The significance of CD34 and TdT determinations in patients with untreated de novo acute myeloid leukemia. J Clin Oncol 6:1203, 1992
10. Machnicki JL and Bloomfeild CD: Clinical significance of the cytogenetics of acute leukemia. Oncology 4:23, 1990
1 I . Miller WH, Kakizuka A, Frankel SR, Warrell RP Jr, Delblasio A, Levine K, Evans RM, Dmitrovsky E: Reverse transcription poly- merase chain reaction for the rearranged retinoic acid receptor a clarifies diagnosis and detects minimal residual disease in acute promyelocytic leukemia. Proc Natl Acad Sci USA 89:2694, 1992
12. Haber DA: Multidrug resistance (MDR 1) in leukemia: Is it time to test? Blood 79:295, 1992
13. Willman CL: Flow cytometric analysis of hematologic speci- mens, in Knowles DM (ed): Neoplastic Hematopathology, Balti- more, MD, Williams and Wilkins, 1992, p 169
14. Foucar K, Chen I-M, Crago S: Organization and operation of a flow cytometric immunophenotyping laboratory. Semin Diagn Pathol 6:13, 1989
15. Seabright M: A rapid banding technique for human chromo- somes. Lancet 11: 971, 1971
16. Harden DG, Klinger HP (eds): An International System for Human Cytogenetic Nomenclature. Basel, Switzerland, Karger Ba- sel, 1985
17. Mitleman F (ed): Guidelines for cancer cytogenetics, supple- ment to an international system for human cytogenetic nomenclature. Basel, Switzerland, Karger Basel, 1991
18. Kern WF, Spier CM, Hanneman EH, Miller TP, Matzner M, Grogan TM: Neural cell adhesion molecule-positive peripheral T- cell lymphoma: A rare variant with a propensity for unusual sites of involvement. Blood 79:2432, 1992
19. Chomcynski P, Sacchi N: Single-step method of RNA isola- tion by acid guanidinium thiocyanate-phenol-chloroform extraction. Analytical Biochemistry 162:156, 1987
20. Biondi A, Rambaldi A, Pandolfi PP, Rossi V, Giudici G, Alcalay M, LoCoco F, Diverio D, Pogliani EM, Lanzi EM, Mandelli F, Masera G, Barbui T, Pelicci PG: Molecular monitoring of the mylhetinoic acid receptor-@ fusion gene in acute promyelocytic leu- kemia by polymerase chain reaction. Blood 80:492, 1992
21. Pandolfi PP, Alcalay M, Fagioli M, Zangrilli D, Mencarelli A, Diverio D, Biondi A, LoCoco F, Rambaldi A, Grignani F, Roch- ette-Egly C, Gaube M-P, Chambon P, Pelicci PG: Genomic variabil- ity and alternative splicing generate multiple PML/RARa transcripts that encode aberrant PML proteins and PMLIRARa isoforms in acute promyelocytic leukaemia. EMBO 11: 1397, 1992
22. Noonan K E , Beck C, Holzmayer TA, Chin JE, Chin JE, Wunder JS, Andrulis IL, Gazdar AF, Willman CL, Griffith B, Von Hoff DD, Roninson IB: Quantitative analysis of MDRl (multidrug resistance) gene expression in human tumors by polymerase chain reaction. Proc Natl Acad Sci USA 87:7160, 1990
23. Chen S, Brand NJ, Chen A, Chen S-J, Tong J-H, Wang Z- Y, Waxman S, Zelent A: Fusion between a novel Kruppel-like zinc finger gene and the retinoic acid receptor-a locus due to a variant

MYELOIDNATURAL KILLER CELL ACUTE LEUKEMIA 255
t(l1;17) translocation associated with acute promyelocytic leukae- mia. EMBO 12:1161, 1993
24. Chen SX, Zelent A, Tong JH, Yu HQ, Wang ZY, Derre J, Berger R, Waxman S, Chen Z: Rearrangements of the retinoic acid receptor alpha and promyelocytic leukemia zinc finger genes re- sulting from t(l1;17)(q23;q21) in a patient with acute promyelocytic leukemia. J Clin Invest 91:2260, 1993
25. Breitman T, Collins SJ, Keene B: Terminal differentiation of human promyelocytic leukemic cells in primary culture in response to retinoic acid. Blood 57:1000, 1981
26. Breitman TR, Selonick SE, Collins SJ: Induction of differenti- ation of the human promyelocytic leukemia cell line (HL-60) by retinoic acid. Proc Natl Acad Sci USA 77:2936, 1980
27. Whalen MM, Roshi RN, Bankhurst AD: Effects of pertussis toxin treatment on human natural killer cell function. Immunology 76:402, 1992
28. Sever CE, Whalen M, Chen I-M, Doshi R, Bankhurst A, McConnell T, Willman CL: A new human natural killer leukemia cell line with a novel complex translocation: Functional and cytoge- netic characterization. Leukemia (in press)
29. Cosentino LM, Cathcart MK: A multi-step isolation scheme for obtaining CD16' human natural killer cells. J Immunol Methods 103:195, 1987
30. Ling N R , Bishop S, Jefferis R: Use of antibody-coated red cells for the sensitive detection of antigen and in rosette tests for cells bearing surface immunoglobulins. J Immunol Methods 15279, 1977
3 1. Kaplan EL, Meier P: Nonparametric estimation from incom- plete observations. J Amer Stat Assoc 53:457, 1958
32. De Rossi G , Avvisati G, Coluzzi S, Fenu S, LoCoco F, Lopez M, Nanni M, Pasqualetti D, Mandelli F: Immunological definition of acute promyelocytic leukemia (FAB M3): A study of 39 cases. Eur J Haematol 45:168, 1990
33. Lanier LL, Testi R, Bindl J, Phillips JH: Identity of Leu-l9 (CD56) leukocyte differentiation antigen and neural cell adhesion molecule. J Exp Med 169:2233, 1989
34. Nitta T, Yagita H, Sat0 K, Okumura K Involvement of CD56 ( N W - 1 k u - 19 Antigen) as an adhesion molecule in natural killer- target cell interaction. J Exp Med 170:1757, 1989
35. Ritz J, Schmidt RE, Michon J, Hercend T, Schlossman S F Characterization of functional surface structures on human natural killer cells. Adv Immunol 42:181, 1988
36. Amaout MA: Structure and function of the leukocyte adhe- sion molecules CDll/CD18. Blood 751037, 1990
37. Heim S, Mitelman F (eds): Acute nonlymphocytic leukemia, in Cancer Cytogenetics, New York, NY, Liss, 1987, p 65
38. Warrell RP Jr, Frankel SR, Miller WH Jr, Scheinbert DA, Itri LM, Hittelman WN, Vyas R, Andreeff M, Tafuri A, Jakubowski A, Gabrilove J, Gordon MS, Dmitrovsky E: Differentiation therapy of acute promyelocytic leukemia with tretinoin (ALL-Trans-Retinoic acid). N Engl J Med 324:1385, 1991
39. Chomienne C, Ballerini P, Balitrand N, Danie MT, Fenaux P, Castaigne S, Degos L: All-rrans retinoic acid in acute promyelocytic leukemias. 11. In vitro studies: Structure-function relationship. Blood 76:1710, 1990
40. Chen S-J, Zhu Y-J, Tong J-H, Dong S, Huang W, Chen Y, Xiang W-M, Zhang L, Li X-S, Qian G-Q, Wang Z-Y, Chen Z, Larsen C-J, Berger R: Rearrangements in the second intron of the
RAM gene are present in a large majority of patients with acute promyelocytic leukemia and are used as molecular marker for reti- noic acid-induced leukemic cell differentiation. Blood 78:2696, 1991
41. Castaigne S, Balitrand N, deThe H, Dejean A, Degos L, Cho- mienne C: A PMLdretinoic acid receptor a fusion transcript is con- stantly detected by RNA-based polymerase chain reaction in acute promyelocytic leukemia. Blood 79:3110, 1992
42. Lanier LL, Le AM, Civin CI, Loken MR, Phillips JH: The relationship of CD16 (Leu-l 1) and Leu-19 (NKH-l) antigen expres- sion on human peripheral blood NK cells and cytotoxic T lympho- cytes. J Immunol 136:4480, 1986
43. Nagler A, Lanier LL, Cwirla S, Phillips JH: Comparative studies of human FcRIII-positive and negative natural killer cells. J Immunol 143:3183, 1989
44. Robertson MJ, Ritz J: Biology and clinical relevance of hu- man natural killer cells. Blood 762421, 1990
45. Miller JS, Verfaillie C, McGlave P: The generation of human natural killer cells from CD34+/DR- primitive progenitors in long- term bone marrow culture. Blood 80:2182, 1992
46. Jacobs R, Stoll M, Stratmann G, Leo R, Link H, Schmidt RE: CD16- CD56' natural killer cells after bone marrow transplantation. Blood 79:3239, 1992
47. Pandolfi F, Loughran TP, Starkebaum G, Chisesi T, Barbui T, Chan WC, Brouet JC, DeRossi G, McKenna RW, Salsano F, Herrmann F, Vanoostveen .W, Schlimok G , Cafaro A, Zambello R, Garcia Rodriguez MC, Geisler CH, Pizzolo G, Steis RG, Brisbane JU, Kadin ME, Mantovovani A, Tagawa S, Fauci AS, Gastl G, Palutke M, Proctor SJ, Pross HF, Mancini P, Aiuti F, Semenzato: Clinical course and prognosis of the lymphoproliferative disease of granular lymphocytes. Cancer 65341, 1990
48. Sheridan W, Winton EF, Chan WC, Gordon DS, Vogler WR, Phillips C, Bongiovanni W, Waldmann TA: Leukemia of non-T lineage natural killer cells. Blood 72:1701, 1988
49. Imamura N, Kusunoki Y, Kawa-Ha K, Yumura K, Haha J, Oda K, Aba K, Dohy H, Inada T, Kajihara H, Kuramoto A: Aggres- sive natural killer cell IeukemiaAymphorna: Report of four cases and review of the literature. Br J Haematol 75:49, 1990
50. Loughran TP: Clonal diseases of large granular lymphocytes. Blood 82:1, 1993
51. Taniwaki M, Tagawa S, Nishigaki H, Horiike S, Misawa S, Shimazaki C, Maekawa T, Fujii H, Kitani T, Abe T : Chromosomal abnormalities define clonal proliferation in CD3- large granular lym- phocyte leukemia. Am J Hematol 33:32, 1990
52. Van Camp B, Durie BGM, Spier C, De Waele M, Van Riet I, Vela E, Frutiger Y, Richter L, Grogan TM: Plasma cells in multiple myeloma express a natural killer cell-associated antigen: CD56 (NKH-l; Leu-19). Blood 76:377, 1990
53. Ikushima S, Yoshihara T, Matsumura T, Misawa S-I, Morioka Y, Hibi S, Imashuku S: Expression of CD56/NCAM on hematopoi- etic malignant cells. A useful marker for acute monocytic and mega- karyocytic leukemias. Int J Hematol 54:395, 1991
54. Scott AA, Kopecky KJ, Grogan T M , Head DR, Richter LC, Troy FA, Mullen J, Ye J, Appelbaum FR, Theil K, Willman C L CD56 A determinant of extramedullary involvement in acute myeloid leukemia with t(8;21) and/or monocytic differentiation. (in preparation)
55. Kern WF, Spier CM, Miller TP, Grogan TM: NCAM (CD56)- positive malignant lymphoma. Leuk Lymphoma l2:l, 1993
Copyright © 2022 FDOKUMEN




















