
HIV, hepatitis B & C, andsexually transmitted infections ...
274
UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl) UvA-DARE (Digital Academic Repository) HIV, hepatitis B & C, and sexually transmitted infections Innovations in prevention and testing Bil, J.P. Publication date 2019 Document Version Final published version License Other Link to publication Citation for published version (APA): Bil, J. P. (2019). HIV, hepatitis B & C, and sexually transmitted infections: Innovations in prevention and testing. General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. Download date:30 Mar 2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of HIV, hepatitis B & C, andsexually transmitted infections ...

UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
HIV, hepatitis B & C, and sexually transmitted infectionsInnovations in prevention and testingBil, J.P.
Publication date2019Document VersionFinal published versionLicenseOther
Link to publication
Citation for published version (APA):Bil, J. P. (2019). HIV, hepatitis B & C, and sexually transmitted infections: Innovations inprevention and testing.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s)and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an opencontent license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, pleaselet the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the materialinaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letterto: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. Youwill be contacted as soon as possible.
Download date:30 Mar 2022



HIV, hepatitis B & C, andsexually transmitted infections:
Innovations in prevention and testing
Janneke Bil

HIV, hepatitis B & C, and sexually transmitted infections:Innovations in prevention and testing
Janneke Bil
http://dare.uva.nl/dissertaties
ISBN: 978-94-6361-335-4
The printing of this thesis was financially supported by: Virology Education, GGD Amsterdam and the Academic Medical Center/University of Amsterdam.
Layout and printing: Optima Grafische Communicatie, Rotterdam, the NetherlandsCover design: Remi Steenbakkers, Studio Smaak
© 2019 Joanna Ploontje Bil, Naarden, the Netherlands
All rights reserved. No part of this thesis may be reproduced, stored or shared without the prior permissions of the author or, when appropriate, the publishers of the articles. Published articles were reprinted with permission from the publishers.

HIV, hepatitis B & C, and sexually transmitted infections:Innovations in prevention and testing
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad van doctoraan de Universiteit van Amsterdamop gezag van de Rector Magnificus
prof. dr. ir. K.I.J. Maexten overstaan van een door het College voor Promoties ingestelde commissie,
in het openbaar te verdedigen in de Agnietenkapelop maandag 25 november 2019, te 14.00 uur
door Joanna Ploontje Bilgeboren te Zaanstad

PromotIeCommIssIe:
Promotor: Prof. dr. M. Prins AMC-UvACopromotores: Dr. F.R. Zuure GGD Amsterdam Dr. E. Davidovich GGD Amsterdam
Overige leden: Prof. dr. F.G.J. Cobelens AMC-UvA Prof. dr. J.E.A.M. van Bergen AMC-UvA Prof. dr. S.E. Geerlings AMC-UvA Prof. dr. J.B.F. de Wit Universiteit Utrecht Prof. dr. J.H. Richardus Erasmus Universiteit Rotterdam Prof. dr. J. del Amo Institute of Health Carlos III, Madrid
Faculteit der Geneeskunde

LIst of aBBreVIatIons
(a)OR (adjusted) odds ratio(c)ART (combination) antiretroviral
therapyACS Amsterdam Cohort StudyAIDS Acquired immunodeficiency
syndromeALT Elevated alanine aminotransfer-
aseaMASE advancing Migrant Access to
health Services in EuropeAnti-HBc Antibodies to hepatitis B core
antigenAnti-HBe Antibodies to HBeAnti-HBs Antibodies to HBsAgAnti-HCV Antibodies to HCVCAS Condomless anal sexCDC Centers for Disease Control and
PreventionCI Confidence intervalCrl Credible intervalsDAAs Direct-acting antiviralsEMA European Medicines AgencyEU European UnionFDA Food and Drug AdministrationFTC EmtricitabineGP General practitionerHBeAg Hepatitis B-e-antigenHBsAg Hepatitis B surface antigen
HBV Hepatitis B virusHCC Hepatocellular carcinomaHCV Hepatitis C virusHELIUS HEalthy Life in an Urban SettingHIV Human immunodeficiency virusHIVST HIV self-testsIQR Interquartile rangeMSM Men who have sex with menMSW Men who have sex with women
onlyNA Not applicableNGO Non-governmental organisationPEP Post-exposure prophylaxisPHSA Public Health Service of Amster-
damPrEP Pre-exposure prophylaxisRIVM National Institute for Public
Health and the Environment of the Ministry of Health, Welfare and Sport
SD Standard deviationSTI(s) Sexually transmitted infection(s)TasP Treatment as preventionTB TuberculosisTDF Tenofovir disoproxyl fumarateUK United KingdomUS/USA United States of AmericaWHO World Health Organization


taBLe of Contents
Chapter 1 General introduction 9
Chapter 2 Pre-exposure prophylaxis to prevent HIV infection 37Chapter 2.1 What do Dutch men who have sex with men think of pre-exposure
prophylaxis to prevent HIV infection? A cross-sectional study39
Chapter 2.2 Motives of Dutch men who have sex with men for daily and intermittent HIV pre-exposure prophylaxis usage and preferences for implementation: A qualitative study
59
Chapter 2.3 The acceptability of pre-exposure prophylaxis: Beliefs of healthcare professionals working in sexually transmitted infection clinics and HIV treatment centers
81
Chapter 3 Testing opportunities for HIV, hepatitis B, hepatitis C and sexually transmitted infections
111
Chapter 3.1 Disparities in access to and use of HIV-related health services in the Netherlands by migrant status and sexual orientation: A cross-sectional study among people recently diagnosed with HIV infection
113
Chapter 3.2 Hepatitis B and C screening needs among different ethnic groups: A population-based study in Amsterdam, the Netherlands
137
Chapter 3.3 Integrating hepatitis B, hepatitis C and HIV screening into tuberculosis entry screening for migrants in the Netherlands, 2013 to 2015
163
Chapter 3.4 Usage of purchased self-tests for HIV and sexually transmitted infections in Amsterdam, the Netherlands: Results of population-based and serial cross-sectional studies among the general population and sexual risk groups
181
Chapter 3.5 Usage of purchased self-tests for HIV infections among migrants living in the UK, France and the Netherlands: A cross-sectional study
205
Chapter 4 General discussion 215
appendix 241Summary 243Nederlandse samenvatting 249About the author 255Portfolio 257List of publications 261List of contributing authors 263Authors’ contributions per chapter 265Dankwoord 269


Chapter 1General introduction


11
General introduction
1This thesis focuses on the development and the use of innovative interventions for the prevention of human immunodeficiency virus (HIV), hepatitis B virus (HBV) infections, hepatitis C virus (HCV) infections and bacterial sexually transmitted infections (STIs). Three levels of prevention can be distinguished: primary, secondary and tertiary prevention.1 In infectious-diseases control, primary prevention focuses on the prevention of transmission; secondary prevention focuses on reducing the impact of an infection that has already been established by early testing and diagnosis while tertiary prevention focuses on managing (chronic) disease after diagnosis to prevent or reduce more severe outcomes of a disease by slowing or blocking the progression of a disease. The main focus of the thesis is on primary and secondary prevention. Chapter 2 will concentrate on pre-exposure prophylaxis (PrEP) to prevent HIV infections and chapter 3 on opportunities for improving testing for HIV, HBV, HCV and STIs.
The introduction of this thesis starts with a brief description of the epidemiology, the clinical course of infection and the current prevention strategies of the infections in focus. In sec-tion 1.2, the outline of this thesis is described, giving the aims, a description of the studied interventions and the data sources used in the thesis.
1.1 HIV, HBV, HCV and BaCTerIal STIs
1.1.1 HIV infection
In 1981 the first cases of acquired immunodeficiency syndrome (AIDS) were described and in 1983 the causative retrovirus was discovered, nowadays called HIV.2,3 HIV is transmitted through blood-blood contact (blood products and contaminated equipment), sexual contact and mother-to-child transmission (during pregnancy, birth or breastfeeding).4 HIV infec-tion reduces the function of the immune system by attacking the CD4 T cells in the human body.5,6 Infection occurs in three phases: an acute phase (primary infection), an asymptom-atic (latent) phase and a symptomatic phase (AIDS).4,6 AIDS refers to the development of opportunistic infections and tumours caused by the replication of the virus and the impaired function of the immune system. AIDS develops in approximately 8–11 years after antibody seroconversion in an untreated person and leads to death in a median of 8–13 years.7,8 In 1996, effective antiretroviral therapy (ART) became generally available for HIV. This aims at reaching viral suppression and hereby significantly reduces morbidity and mortality.9,10
HIV remains a major burden of disease globally with approximately 36.9 million people living with HIV at the end of 2017.11 In the Netherlands, approximately 1,000 HIV infections were acquired each year between 2000 and 2010.12 From 2010 onwards, the number of newly-acquired HIV infections declined steadily to about 450 new cases in 2017. It is estimated

Chapter 1
12
that by the end of 2017, 23,100 individuals were living with HIV in the Netherlands. Of those, 10% (approximately 2,256) were still undiagnosed or not linked to care.12 The main risk groups for HIV in the Netherlands are men who have sex with men (MSM) and first-generation migrants from HIV endemic countries. Of all individuals living with HIV in clinical care in the Netherlands by the end 0f 2017, 63% were MSM and 37% were heterosexual.12 Of HIV-positive MSM who were in care, 69% originated from the Netherlands, 11% from other European countries, 7% from South America, 5% from the Caribbean and 8% from other countries. Of women and heterosexual men in care, 37% originated from the Netherlands, 33% from sub-Saharan Africa, 8% from South America, 5% from the Caribbean, 4% from south or South-East Asia and 13% from other countries.12 The estimated HIV prevalence in 2012 in the Netherlands was 0.20% (95% credible intervals [CrI] 0.17–0.26%) in the general population, 8.3% (95% CrI 6.1–11.3%) among MSM, 2.3% (95% CrI 1.9–2.9) among migrants from sub-Saharan Africa and 0.3% (95% CrI 0.2–0.4%) among migrants from the Caribbean.13 Other key populations are people who inject drugs and female sex workers.13,14
Treatment with ARTs is currently recommended for all individuals with HIV, regardless of CD4 cell count, and consists of a combination of integrase strand transfer inhibitors, reverse transcriptase inhibitors (non-nucleoside and nucleoside) and protease inhibitors.15,16 Since the introduction of ART, the life expectancy of people living with HIV in high-income coun-tries has significantly improved; in some groups life expectancy is approaching that of the general population.10
As there is no vaccine available for HIV, important primary HIV prevention strategies in the Netherlands include behavioural interventions to prevent transmission to (sexual) partners (e.g., the promotion of condom use).4 Some MSM also reduce their risk of HIV infection by serosorting (i.e., having condomless sex with a partner with concordant HIV status), although the effectiveness of this strategy is limited.17-21 Other primary HIV prevention strat-egies include the screening of blood products, the implementation of safety and hygiene interventions in medical settings to prevent transmission and harm-reduction strategies among people who inject drugs (i.e., needle-and-syringe-exchange programme and opioid substitution therapy).4 There are also biomedical interventions that can prevent HIV infec-tions. HIV treatment not only reduces morbidity and mortality at the individual level but also prevents HIV transmission to others (treatment as prevention - TasP) by reducing the viral load of the person with HIV.22-27 For this reason, the early diagnosis and treatment of those identified with HIV can have a major impact on the transmission of HIV.28,29 A second biomedical intervention is pre-exposure prophylaxis (PEP). PEP aims to prevent an HIV infec-tion after high-risk exposure to the HIV virus. It consists of a treatment of 28 days with a combination of three antiretroviral drugs that should be ideally be started as early as possible but not later than 72 hours after high-risk exposure.30 In the Netherlands, PEP has

13
General introduction
1been available for individuals after high-risk exposure since 2000.31 The third biomedical in-tervention, pre-exposure prophylaxis (PrEP), aims to prevent HIV infection prior to exposure among HIV-negative individuals who are at increased risk of HIV infection. It consists of a daily or event-driven (intermittent, PrEP use before and after sex) regimen of lower-intensity ART (for detailed information, see section 1.2.2).32,33
Guidelines recommend HIV testing based on risk factors or signs, symptoms or medical conditions that can indicate an infection (in primary (e.g., general practitioner - GP) and secondary care (e.g., hospitals). European guidelines recommend the routine offering of HIV testing to patients who present HIV-indicator conditions, i.e., conditions that are AIDS defin-ing or are associated with an undiagnosed HIV prevalence of >0.1% and conditions where not identifying the presence of HIV infection may have significant adverse implications for the individual’s clinical management.34,35A selective HIV screening programme exists in the Netherlands for all pregnant women to prevent mother-to-child transmission, and all blood products are screened for HIV.4,36,37 Furthermore, STI clinics in the Netherlands provide HIV and STI testing to HIV risk groups at no cost according to the opting-out principle (i.e., every person is tested unless there is explicit refusal).38 In addition, HIV, HBV and HCV screening of people who inject drugs is recommended at drug treatment centres,4,39,40 although this is not routinely implemented.41 The World Health Organization (WHO) recommends the use of HIV self-tests as an additional approach to HIV testing services, as it could increase HIV testing rates.42,43 Self-tests can be performed and interpreted autonomously by lay-persons without involving healthcare professionals or certified laboratories.42 The use of HIV self-tests is not implemented in the Netherlands (for detailed information, see section 1.2.3). HIV is not a notifiable disease under the Dutch Public Health Act.
1.1.2 HBV and HCV infections
HBV and HCV were first identified in 1967 and 1989, respectively.44,45 HBV is transmitted through blood-to-blood and sexual contact, and from mother to child.39,46 HCV is transmitted by blood and from mother-to-child. Since 2000, HCV has emerged as an STI primarily among MSM living with HIV.47 More recently, data has indicated a relatively high number of HCV infections among HIV-negative MSM who apply for or use PrEP.48-51
HBV and HCV infections cause inflammation of the liver. Following HBV or HCV infection, the majority of cases remain asymptomatic during the acute phase. Among those infected with HBV during adulthood, approximately 5% to 10% develop chronic HBV infection.52-54 How-ever, up to 90% of children infected with HBV during the perinatal period and approximately 30% of children infected before the age of six years develop chronic HBV infection.54 Among those infected with HCV, approximately 75% develop chronic HCV infection.55 People with untreated chronic HBV or HCV infections can develop an end-stage liver disease such as liver

Chapter 1
14
cirrhosis or hepatocellular carcinoma (HCC, i.e., liver cancer). The progression rate of chronic infection to liver cirrhosis or HCC is highly dependent on several viral, host and extraneous factors.56-58 For untreated chronic HBV, the 5-year cumulative incidence of developing liver cirrhosis is 8–20%.54 Among those with liver cirrhosis, the 5-year cumulative risk of develop-ing hepatic compensation is approximately20% and 10–16% for the development of HCC among those with compensated cirrhosis.54,59 For HCV, an estimated 15–35% of people with HCV infection will develop liver cirrhosis after 25–30 years.60 Among those with HCV-related liver cirrhosis, an average of 2–3% develop HCC annually.60
Globally, an estimated 257 million people were living with chronic HBV infection and 71 million people with chronic HCV infection in 2015.61 The estimated chronic HBV and ever-chronic HCV prevalence among individuals aged 15 years and older in the Netherlands is 0.34% (ranging from 0.22% to 0.47%) and 0.16% (ranging from 0.06% to 0.27%), respec-tively.62-64 For both chronic HBV and HCV infections, first-generation migrants account for most infections in the Netherlands (81% and 60% of all chronic HBV and ever-chronic HCV infections, respectively).64 Other important key populations are people who inject drugs, MSM (for HCV mainly HIV-positive MSM and HIV-negative MSM who start or use PrEP), sex workers (HBV only), healthcare providers, people on haemodialysis, children of HBV/HCV-infected mothers, sexual or household contacts of infected persons, persons (including those with haemophilia) who received blood products before 1992 in the Netherlands and in countries where blood products are not screened for HCV, and long-term travellers to HBV endemic countries.39,40,65
For both HBV and HCV infection, effective treatment options are available. HBV treatment aims to induce long-term suppression of HBV replication and thus improve survival and qual-ity of life by preventing disease progression. Treatment of chronic HBV infection consists of the long-term administration of a potent nucleos(t)ide analogue with a high barrier to resistance or pegylated interferon-alfa.58 Treatment is indicated if HBV DNA >2,000 IU/ml, in case of elevated alanine aminotransferase (ALT), and/or at least moderate histological lesions, while all cirrhotic patients with detectable HBV DNA have an indication for treat-ment. HCV treatment aims to reach a sustained virological response (e.g., elimination of the virus). In 2014, direct-acting antivirals (DAAs) became available in the Netherlands for the treatment of chronic HCV infection.66 Initially, the costs of treatment with DAAs was only reimbursed for patients with advanced liver fibrosis but since 2015 costs have been reimbursed to all patients with chronic HCV infection irrespective of the stage of fibrosis. DAAs are not registered for the treatment of acute HCV infection. With cure rates of up to 95%,67 the availability of DAAs has significantly increased the effectiveness) and appreciably reduced the side effects of HCV treatment compared to previously recommended treat-ments, namely pegylated-interferon in combination with ribavirin.68

15
General introduction
1Although there is an effective vaccine available for HBV, this is not the case for HCV. In the Netherlands, HBV vaccination is offered free of charge to risk groups, such as MSM, sex workers, healthcare workers and asylum-seeking children. Since 2011, HBV vaccination is part of the national immunisation programme for children.39 Other primary prevention programmes for HBV and HCV focus on the HBV/HCV screening of blood products, the implementation of safety and hygienic interventions in medical settings to prevent transmis-sion, harm reduction strategies among people who inject drugs (i.e., a needle and syringe exchange programme and opioid substitution therapy), behavioural interventions to prevent the transmission to (sexual) partners (e.g., the promotion of condom use) and travel advice (including vaccination) for long-term travellers to an HBV endemic country.39,40
Besides HBV and HCV testing based on risk factors or signs, symptoms or medical conditions that can indicate an infection in primary (i.e., at GPs) and secondary care (e.g., at hospitals),69 several selective screening programmes exist in the Netherlands, including the screening of all pregnant women for HBV to prevent mother-to-child transmission,36 the screening at STI clinics of all clients belonging to HBV risk groups,38 the active screening of individuals with HIV in clinical care for HBV and HCV at their first consultation, and the annual screening of MSM with HIV at risk to HCV during follow-up in clinical care.15 As mentioned earlier, the screening for HIV, HBV and HCV of people who have ever inject drugs at drug treatment centres is also recommended,4 although has not been implemented fully.39-41,70 For migrants, no structural HBV and HCV screening programmes exist in the Netherlands. However, in 2016 the Dutch Health Council recommended that first-generation migrants from countries with an HBsAg or HCV-RNA prevalence of >2% should be offered HBV and HCV screening trough individual case-finding by GPs.71 Also, the Dutch Health Council recommended set-ting up local or regional HBV screening programmes in cities or regions that have relatively large numbers of first-generation migrants from HBV-endemic countries. For asylum seekers from HBV and HCV endemic countries, the Dutch Health Council recommends offering HBV and HCV screening during the admission procedure in the Netherlands, provided that care and treatment can be offered for those that are tested positive, but this measure has not yet been implemented. Furthermore, in accordance with the Dutch Public Health Act, all acute and chronic HBV and HCV infections must be reported to the department of infectious diseases of the Public Health Service in each patient’s hometown to enable contact tracing and vaccinate contacts susceptible to HBV.39,40 The number of acute HBV and chronic HBV infections reported to the Public Health Services in the Netherlands declined from 175 and 1,320 in 2012 to 100 and 1,320 cases per year in 2018, respectively. The number of reported acute HCV infections was relatively stable between 2012 and 2018 at around 60 cases per year.72

Chapter 1
16
1.1.3 Bacterial STIs
Globally, over one million STIs are acquired each day.73 In 2017, the most commonly di-agnosed bacterial STIs in the Netherlands were chlamydia (including lymphogranuloma venereum) with 58,004 diagnoses at STI clinics and by GPs, gonorrhoea (15,764 diagnoses at STI clinics and by GPs) and syphilis (1,228 diagnoses at STI clinics with no data reported by GPs).38 Chlamydia, gonorrhoea and syphilis infections are caused by the bacteria Chlamydia trachomatis, Neisseria gonorrhoeae and Treponema pallidum, which were discovered in 1907, 1879 and 1906, respectively.74-76 The main causes of transmission of these bacteria are through oral, vaginal and anal sexual contact, although mother-to-child transmission is also possible.77-79
Most chlamydia infections in the Netherlands are diagnosed in people younger than 25 years of age (64%), whereas most gonorrhoea and syphilis infections are diagnosed among MSM (74% and 95%, respectively).38 The number of STI consultations have continued to increase over time in the Netherlands with 150,593 consultation at STI clinics in 2017, but the number of positive tests remains relatively stable.38
Although a large proportion of chlamydia and gonorrhoea infections are asymptomatic, they can cause symptoms such as urethritis, proctitis, dysuria and increased vaginal or urethral discharge, while also being able to lead to complications such as pelvic inflammatory disease and infertility.80 Symptoms of syphilis depend on the stage of infection (primary, secondary, latent or tertiary) and can vary from skin ulcerations, sores and rash to gummas (soft non-cancerous growths) and neurological and cardiovascular symptoms.80
Although no vaccine is available for chlamydia, gonorrhoea and syphilis, infections can be ef-fectively treated with a short course of antibiotics.80 Primary prevention interventions focus on counselling with regard to safe sexual behaviour. Secondary prevention focuses on the early and more frequent testing of key populations, contact tracing and partner notification, as well as the early treatment of sexual partners of infected individuals.77-79 Besides testing based on risk factors or signs, symptoms or medical conditions that can indicate an infection by GPs,37 in the Netherlands STI screening for chlamydia, gonorrhoea, syphilis, HIV and HBV is offered free of charge at STI clinics to MSM, persons originating from regions with an increased HIV/STI prevalence (Eastern Europe, Africa, Latin America and Asia), commercial sex workers, persons notified by a sexual partner for HIV or STI, persons with HIV/STI-related symptoms, victims of sexual violence and partners of people from a risk group.38 Men and women below the age of 25 years who have none of the above-mentioned indications are also offered STI testing at STI clinics free of charge, although they are initially only tested for chlamydia and gonorrhoea. Furthermore, all blood products and all pregnant women

17
General introduction
1are screened for syphilis.36,77 Chlamydia, gonorrhoea and syphilis are not notifiable diseases under the Dutch Public Health Act.
1.1.4 Global and national targets
Global and national targets are set to reduce new infections and the burden of disease caused by HIV, HBV and HCV infections, and by bacterial STIs.
UNAIDS has set the following global target for HIV: by 2020, 90% of all people living with HIV know their HIV status, 90% of all people with diagnosed HIV infection receive ART and 90% of all people receiving ART have reached viral suppression (the 90–90–90 targets).81,82 In addition, by 2020 the number of new HIV infections among adults need to decline to fewer than 500,000 cases per year and there should be zero discrimination. By 2030, the aim is to achieve the 95–95–95 targets, with fewer than 200,000 new infections per year. In the Netherlands, the National Institute for Public Health and the Environment of the Ministry of Health, Welfare and Sport (RIVM) has set the goal to achieve the 95-95-95 targets for HIV by 2022 in the Netherlands and to reduce the annual number of new HIV diagnoses by <450, and 90% of people living with HIV experience a good quality of life (reduction of HIV stigma and discrimination).83 In 2017, 750 people were diagnosed with HIV in the Netherlands,12 and had already reached the 90–90–90 targets by the end of that year, with an estimated 90% of all people living with HIV in the Netherlands diagnosed and in care, 93% of those in care receiving ART and 95% of all people on ART having reached viral suppression.12
Already in 2015, Amsterdam was one of the first cities in the world to reach and exceed the 90–90–90 targets with 94% of people living with HIV knowing their HIV status, 90% of all people with diagnosed HIV infection receiving ART and 94% of all people receiving ART having viral suppression.84 In Amsterdam, a city-focused approach was launched in 2014 that combined various interventions to prevent transmission of HIV, including the promotion of prevention, earlier testing and the immediate treatment of infections with the ultimate goal of achieving no new HIV infections (H-TEAM; Hiv-Transmissie Eliminatie Amsterdam).85 The primary focus of the H-TEAM strategy had five key points: (1) the scaling up of PrEP use, (2) early and more frequent HIV testing, (3) awareness-raising for acute infection, including early detection and treatment, (4) starting HIV treatment early and (5) research into “post treatment control” (i.e., the effect of early treatment on the characteristics of the immune system and HIV).
For HBV and HCV infections, the WHO set the following global targets to eliminate viral hepatitis as a public health threat: by 2030, the incidence of chronic HBV and HCV should be reduced by 90% and there should be a 65% reduction in HBV and HCV related mortal-ity.86 To achieve these targets childhood HBV vaccination should achieve 90% coverage, 90%

Chapter 1
18
of mother-to-child transmissions should be prevented, 100% of blood donations should be screened in a quality-assured manner, 90% of injections should be administrated with safety-engineered devices in and out of health facilities, 300 sterile needles and syringes should be provided per year per person injecting drugs, 90% of viral HBV and HCV infec-tions should be diagnosed, and 80% of eligible persons with chronic HBV and chronic HCV should be treated. In the Netherlands, an estimated 49,000 (range 31,000–66,000) and 23,000 (range 8,000–38,000) people had chronic HBV and had a chronic HCV infection in 2016, respectively.64 Data from the Netherlands and other Western countries indicates that approximately 20–60% and 40–50% of people with HBV or HCV infections, respectively, are unaware of their infection.87-91 In the Netherlands, an estimated 500 deaths per year are attributed to HBV and HCV infections.92
In 2016, a national Dutch hepatitis action plan was launched to focus on five key elements: (1) the prevention of transmission by improving awareness and vaccination, (2) the identi-fication of HBV and HCV infections, (3) diagnostics and treatment, (4) the improvement of hepatitis care and (5) the improvement of surveillance data.93 In the same year, Amsterdam drafted a specific HBV and HCV action plan to increase awareness, prevent new infections, detect infections in risk groups, provide treatment to those diagnosed but not yet treated, and improve the treatment, care and positive health of those diagnosed with HBV and HCV.94
For bacterial STI, the Dutch aims for the 2017 to 2022 period are to develop effective strate-gies to reduce the burden of disease of chlamydia and to halve the number of new cases of gonorrhoea and syphilis infections per year, compared to those in 2016, to less than 7,000 diagnosis of gonorrhoea and less than 500 diagnosis of syphilis in 2022.83 In 2017, the num-ber of gonorrhoea cases diagnosed increased compared to 2016, whereas the number of syphilis diagnoses remained relatively stable.38 With regard to global targets on STI control, the WHO has drafted a global health sector strategy on STIs. One of its aims is to reduce the incidence of gonorrhoea by 90% by 2021 compared to 2018.95
1.2 THeSIS ouTlIne
1.2.1 aim
To reach the global, national and regional targets described in section 1.1.4, scaling up of effective interventions for the prevention of HIV, HBV and HCV infections and bacterial STIs are needed urgently. The overall aim of this thesis is to assess the acceptability and use of innovative interventions and explore new opportunities for the prevention of HIV, HBV and HCV infections and STIs among key populations. Chapter 2 of this thesis focuses on current aspects of acceptability, attitudes, beliefs and behavioural intentions towards the use of

19
General introduction
1PrEP among MSM and healthcare professionals. Chapter 3 discusses opportunities for HIV, HBV, HCV and STI testing, especially among migrant populations.
1.2.2 PreP to prevent HIV infection (chapter 2)
As mentioned in section 1.1.1, PrEP entails offering a regime of lower-intensity ART to HIV-negative individuals to reduce their risk of HIV infection. PrEP is offered in combination with interventions such as the promotion of condom use and counselling with regard to sexual-risk behaviour, frequent HIV and STI testing, and links to other HIV prevention services.32,33,96
As several studies demonstrated that PrEP is highly effective and safe,97,98 the Food and Drug Administration (FDA) of the United States (US) approved Truvada (emtricitabine/tenofovir disoproxil) for the use of PrEP in 2012.99 This was followed by the approval of the Euro-pean Medicines Agency (EMA) in the European Union (EU) in 2016.100 In 2015, the results of the PROUD and IPERGAY studies were published, which confirmed that both daily and event-driven PrEP regimens are highly effective and safe.101,102 In Amsterdam, a prospective, longitudinal, open-label demonstration study (The Amsterdam PrEP project - AMPrEP) was launched in 2015 to assess the uptake and acceptability of daily versus event-driven PrEP, which is ongoing.103 In 2016, Dutch PrEP guidelines were released33 and in 2018 the Dutch Minister of Health decided, upon advice of the Dutch Health Council,104 to reimburse the greatest part of the costs of PrEP use for a five year period to persons at high risk to HIV infection (i.e., high-risk MSM and, in some cases migrants from HIV endemic countries), including the costs of three-monthly check-ups by STI clinics of public health services.105 This national PrEP programme is starting in august 2019. After five years the long-term ef-fects of PrEP (reaching at-risk populations, the decrease of HIV incidence and the effect on STIs) will be evaluated and a decision will be taken as regards the continuation of PrEP state reimbursement in the Netherlands. Some STI clinics are already now offering three-monthly check-ups for informal PrEP users (i.e., people who have acquired PrEP online, from abroad or from friends).
There are still concerns about the costs of PrEP and potential risk compensation (i.e., increases in sexual risk behaviour and STIs).106 Other challenges in countries that have imple-mented PrEP are the suboptimal awareness of and use in communities that might benefit most from PrEP, and the limited engagement with PrEP care by providers.106 For the effective implementation of PrEP in the Netherlands, it is important to understand the acceptability of PrEP use among those at increased risk of HIV infection, such as MSM, and among those who play a critical role in its implementation, i.e., healthcare professionals. In chapter 2, the acceptability of PrEP among MSM and healthcare professionals prior to the launch of a PrEP implementation project in the Netherlands was assessed. In chapter 2.1, we studied PrEP awareness, the intention to use PrEP, and sociodemographic and psychosocial determinants

Chapter 1
20
associated with a higher intention to use PrEP among Dutch MSM in 2012–2013. In addition, anticipated condom use should men decide to use PrEP is explored, as is the influence of PrEP characteristics (cost, duration and efficacy) on the willingness to use PrEP. In chapter 2.2 explored more thoroughly the motives for wanting or not wanting to use PrEP should it become available, the motives for choosing between daily versus event-driven (intermittent) PrEP use, the anticipated motives for condom use when using PrEP and preferences for PrEP implementation (e.g., service characteristics) in a qualitative study utilising in-depth interviews. In chapter 2.3, we studied the acceptability of PrEP among professionals working at STI clinics (STI professionals) and at HIV treatment centres (HIV specialists).
1.2.3 Testing opportunities for HIV, HBV, HCV and STIs (Chapter 3)
HIV, HBV and HCV testing among migrants
As described in sections 1.1.1 and 1.1.2, migrants represent a significant group in the HIV, HBV and HCV epidemic in the Netherlands and across Europe. For HIV, estimates show that a large proportion of migrants are still unaware of their infection or diagnosed in a late stage.13,107 Furthermore, among people living with HIV in care in the Netherlands, migrants have lower rates of engagement in the various stages of the care continuum (i.e., retainment in care, on ART and virally suppressed),12 which suggests that migrants face specific barriers in accessing and utilising HIV health services. Such barriers exist at several levels, includ-ing structural, healthcare provider, and at individual and community levels.108-116 Structural barriers may include a lack of entitlement to healthcare (e.g., in the case of undocumented migrants). Barriers for migrants at the healthcare provider level include migrant insensitive services and language barriers, while individual barriers may include low-risk perception, fear of stigma or disease-related consequences, limited knowledge, differences in percep-tions about utilising (preventative) healthcare and a lack of financial resources. Barriers at the community level include discrimination and stigma, fear of loss of status and lack of community support.
To guide the development of strategies aimed at reducing barriers experienced by migrants and improve access to and the use of HIV health services in the Netherlands, more data is needed on the specific barriers experienced by migrants. Data as regards the differences in access to HIV-related health services between heterosexual migrants and non-migrants, and migrant and non-migrant MSM is limited as well. In chapter 3.1 we therefore studied access to and use of HIV services pre-and post diagnosis among non-migrants and migrant MSM and heterosexual men/women recently diagnosed with HIV in the Netherlands. These data will help determine the potential opportunities for improving HIV-related prevention and care for migrants. We also examined differences in experiences in living with HIV between these groups.

21
General introduction
1Screening programmes are needed to diagnose those migrants unaware of their HBV, HCV or HIV infection at an early stage. This can lead to the timelier initiation of treatment, resulting in the limitation of complications and the prevention of onwards transmission. In chapter 3.2 we studied the prevalence of HBV and HCV infection markers, along with their risk fac-tors, using data from a large, population-based study that included five large ethnic minority groups and persons of Dutch origin living in Amsterdam. We also studied the proportion of infected persons who were aware of their HBV and HCV infection since these data are not well known. The data will inform the development of screening and preventive interventions for specific migrant groups in Amsterdam.
In chapter 3.3 explored the feasibility of integrating HIV, HBV and HCV screening into an ex-isting healthcare service. We initiated a pilot screening project offering additional voluntary HIV, HBV and HCV screening to newly arrived migrants undergoing compulsory tuberculosis (TB) screening and evaluated uptake and diagnostic outcomes.
Self-testing for HIV and STIs
As referred to in section 1.1.1, self-tests can be performed and interpreted autonomously by lay persons without involving healthcare professionals or certified laboratories.42 Previous studies have shown that HIV self-tests can increase testing rates and lower the barriers to HIV testing since it raises feelings of confidentiality, convenience, autonomy and empower-ment. 42,43,117-119 Studies also reported good accuracy when it comes to unsupervised HIV self-tests , as well as high user acceptability.42,120-123 A growing number of countries, also in Europe, have in recent years or are currently developing policies to support HIV self-testing, with some countries actually having started to implemented HIV self-testing.124 In the Netherlands, legal restrictions limit the implementation of HIV self-testing as test kits can only be distributed by a medical doctor or pharmacist.125 Self-tests for STIs also have the potential of increasing STI testing rates but few studies have evaluated their accuracy and the limited data available reports alarmingly poor results.126-129 Additional concerns centre on the lack of a linkage to counselling and the treatment and care for HIV/ STI self-test users who test positive, 117,118,129 as well as the lack of clear information on and/or instructions that accompany some self-tests that are currently available.127,129-131 Despite these concerns and legal restrictions ,125 HIV/STI self-test kits have been readily available through the Internet in the past few years.130
Because of the anonymous nature of self-testing, the extent to which commercially sold HIV/STI self-tests are used and the determinants of usage are not well known. Therefore, in chapter 3.4 and 3.5, we explored the extent of HIV/STI self-test usage and its determinants among the general population, sexual risk groups and migrants.

Chapter 1
22
1.2.4 data sources
To achieve the aims of this thesis, a variety of study methods and designs (including quantitative, qualitative, pilot screenings studies), and data sources, were used. These are summarised in Table 1. A short description of the different data sources used for this thesis is given below.
Amsterdam Cohort Study (ACS) on HIV among MSM
The ACS on HIV among MSM living with and without HIV is an open, prospective cohort study initiated in 1984 that has the aim to investigate the epidemiology, sexual risk behaviour and predictors, natural history and pathogenesis of HIV, and to evaluate the effect of interven-tions.132,133 Participants visit the Public Health Service of Amsterdam every six months to complete self-administered questionnaires on sexual and psychosocial determinants of behaviour, to give blood for HIV testing (some of which is stored) and, since 2008, to undergo sexually transmitted infection testing. Data collected in 2012 and 2013 is used in chapter 2.1, and data collected in 2008 and 2013 in chapter 3.4.
advancing Migrant Access to health Services in Europe (aMASE) study
The aMASE study is a cross-sectional study that has the aim of identifying the structural, cultural and financial barriers to HIV prevention, diagnosis and treatment, and to determine the likely country of HIV acquisition in migrant populations living with HIV.116,134-136 aMASE comprises two cross-sectional, electronic surveys, one among migrant adults living with HIV and attending HIV services (the clinic survey) and one among migrant adults, independent of HIV status, living in Europe (the community survey). The clinic survey was conducted be-tween 2013 and 2015 in 57 HIV clinics in Belgium, Germany, Greece, Italy, the Netherlands, Portugal, Spain, Switzerland and the United Kingdom (UK). The community survey was pro-moted between 2014 and 2015 via social marketing and community participatory methods in Belgium, France, Germany, Greece, Italy, the Netherlands, Portugal, Spain and the UK, although migrants aged 18 or older living in all countries of the WHO European area were eligible. Participants of the clinic and community survey completed a questionnaire that addressed (1) detailed sociodemographic and extensive migration history data, (2) sexual and HIV-risk behaviour, (3) the use of health services and (4) the experience of living with HIV, including stigma and discrimination. The clinic survey data obtained was augmented with clinical data from patient records. In addition to the clinic survey data collected as part of aMASE, in the Netherlands non-migrants who visited one of the three participating HIV outpatient treatment clinics during the study period were asked to participate in the survey to provide comparative data for migrants and non-migrants. In chapter 3.1, the clinic survey data collected among migrants and non-migrants living in the Netherlands are used, while the community survey data collected among migrants living in the UK, France and the Netherlands is used in chapter 3.5.

23
General introduction
1Tabel 1. Data sources and study characteristics of studies described in this thesis
Chapter
study method (design)
data source / recruitment site Study population topic
Geographical location
Period of data collection
2.1 Quantitative(cross-sectional)
ACS on HIV HIV-negative MSM PrEP Amsterdam, the Netherlands
2012–2013
2.2 Qualitative(in-depth interviews)
ACS on HIV & online recruitment
HIV-negative MSM PrEP Amsterdam, the Netherlands
2013
2.3 Qualitative & quantitative(cross-sectional)
Public health services, HIV treatment centers
Healthcare professionals working at STI clinics and HIV treatment centers
PrEP The Netherlands 2014–2015
3.1 Quantitative (cross-sectional)
aMASE study: clinic survey (HIV treatment centers)
First-generation migrants and non-migrants living with HIV
HIV testing Amsterdam and the Hague, the Netherlands
2013–2015
3.2 Quantitative(cross-sectional)
HELIUS study First-generation migrants
HBV/HCV testing
Amsterdam, the Netherlands
2011–2014
3.3 Quantitative(cross-sectional)
Pilot screening project at five TB departments of public health services
First-generation migrants
HBV/HCV/HIV testing
Amsterdam & Gelderland, the Netherlands
2013–2015
3.4 Quantitative(cross-sectional)
Health Monitoring Survey
Representative sample of Amsterdam residents
HIV/STI self-testing
Amsterdam, the Netherlands
2008 & 2012
HELIUS study Random sample of Amsterdam residents from Surinamese, Turkish, Moroccan, Ghanaian and Dutch ethnic origin
2011–2015
ACS on HIV HIV-negative MSM 2008 & 2013
STI clinic HIV survey
HIV-negative STI clients 2007–2009 & 2012
3.5 Quantitative(cross-sectional)
aMASE study: community survey
First-generation migrants
HIV/STI self-testing
The Netherlands, France and the United Kingdom
2014–2015
ACS, Amsterdam Cohort Studies on HIV; aMASE study, advancing Migrant Access to health Services in Europe study; HBV, hepatitis B virus; HCV, hepatitis C virus; HELIUS study, Healthy Life In an Urban Setting study; HIV, human immunodeficiency virus; MSM, men who have sex with men; PrEP, pre-exposure prophylaxis; STI, sexually transmitted infections; TB, tuberculosis.
Chapter 1
24
Healthy Life in an Urban Setting (HELIUS) study
The HELIUS study is a multi-ethnic, population-based cohort study investigating mechanisms underlying ethnic differences in communicable and non-communicable diseases.137,138 A random sample of individuals aged from 18 to 70 years old was drawn from the municipality register of Amsterdam, stratified by ethnicity according to Surinamese (African Surinamese and South-Asian Surinamese are the main ethnic groups living in Amsterdam), Turkish, Moroccan, Ghanaian and Dutch origins. Participants underwent a physical examination and completed a self-administered questionnaire on paper or online. Participants unable to fill in the questionnaire themselves were assisted by an ethnically matched and trained interviewer. The baseline data that was collected between 2011 and 2015 is used in chapter 3.2 and 3.4. Follow-up visits to the study participants will start in 2019.
Amsterdam Health Monitoring Survey
Since 1999/2000, a random sample of Amsterdam residents is drawn from the municipality register every 4 years and asked to participate in a population-based cross-sectional health monitoring survey conducted by the public health service of Amsterdam.139,140 Participants complete questionnaires on paper or online with regard to physical, mental and sexual health. Participants unable to fill in a questionnaire are assisted by a trained interviewer. The data collected in 2008 and 2012 are used in chapter 3.4.
Biannual HIV survey among Amsterdam STI clinic clients
Biannually between 1991 and 2012, approximately 1,000 visitors of the Amsterdam STI outpatient clinic of the public health service were asked to participate in a cross-sectional survey that was initially started to measure HIV prevalence and later also other (blood-borne) infections.141,142 Participants were interviewed using standard questionnaires that included questions about risk factors for HIV and other infections, and HIV/STI testing behaviour. Participants received routine STI testing and were screened anonymously for HIV and, from 2007 onwards, for other infections (e.g., HCV, human papilloma virus, herpes simplex virus) as well. The data collected during several waves from 2007 through 2009 and in 2012 is used in chapter 3.1.
Additional data sources
In chapter 2.2 we conducted in-depth interviews with HIV-negative MSM recruited from the ACS and as well as online to assess motives concerning future PrEP use. In chapter 2.3 we conducted focus groups discussions with healthcare professionals working at the STI clinic in Amsterdam. The information obtained in these discussions was used to develop a questionnaire to measure the acceptability of PrEP in the Netherlands among professionals working at STI clinics and HIV treatment centres. In chapter 3.3 we initiated a screening project in which voluntary HIV, HBV and HCV screening was offered to migrants undergoing

25
General introduction
1compulsory TB screening in five TB departments of public health services in the Netherlands between 2013 and 2015. For this project we used routine data collected during the TB screening visit, data from immigration forms and additional data specifically collected for this project.
1.2.5 General discussion (chapter 4) and appendix
In chapter 4 the relevance of these studies together with the recent developments and chal-lenges are discussed. The appendix contains the English and Dutch summary of this thesis, a brief description of the author, the author’s portfolio and list of publications, and a list of all authors of the articles included in this thesis and their contributions.

Chapter 1
26
referenCes
1. Aschengrau A, Seage III GR. Chapter 16: Screening in Public Health Practice. In: Learning JB, ed. Es-sentials of Epidemiology in Public Health. Burlington, MA, USA: Jones & Bartlett Learning,, 2013.
2. Centers for Disease Control and Prevention (CDC). Pneumocystis pneumonia--los angeles. MMWR Morb Mortal Wkly Rep. 1981;30(21):250-252.
3. Barre-Sinoussi F, Chermann JC, Rey F, Nugeyre MT, Chamaret S, Gruest J, et al. Isolation of a T-lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (aIdS). Science. 1983;220(4599):868-871. doi:10.1126/science.6189183.
4. Rijksinstituut voor Volksgezondheid en Milieu (RIVM), Ministerie van Volksgezondheid, Welzijn en Sport. Hivinfectie richtlijn: humaan immunodeficiëntievirus. Bilthoven: RIVM, 2017.
5. Munier ML, Kelleher AD. acutely dysregulated, chronically disabled by the enemy within: T-cell responses to HIV-1 infection. Immunol Cell Biol. 2007;85(1):6-15. doi:10.1038/sj.icb.7100015.
6. Feinberg MB. Changing the natural history of HIV disease. Lancet. 1996;348(9022):239-246. doi:10.1016/S0140-6736(96)06231-9.
7. Collaborative Group on AIDS Incubation and HIV Survival including the CASCADE EU (Concerted Action on SeroConversion to AIDS and Death in Europe) Concerted Action. time from HIV-1 seroconversion to aIdS and death before widespread use of highly-active antiretroviral therapy: a collaborative re-analysis. The Lancet. 2000;355(9210):1131-1137. doi:10.1016/s0140-6736(00)02061-4.
8. Bacchetti P, Moss AR. Incubation period of aIdS in San Francisco. Nature. 1989;338(6212):251-253. doi:10.1038/338251a0.
9. Antiretroviral Therapy Cohort Collaboration. life expectancy of individuals on combination anti-retroviral therapy in high-income countries: a collaborative analysis of 14 cohort studies. Lancet. 2008;372(9635):293-299. doi:10.1016/S0140-6736(08)61113-7.
10. Antiretroviral Therapy Cohort Collaboration. Survival of HIV-positive patients starting antiret-roviral therapy between 1996 and 2013: a collaborative analysis of cohort studies. Lancet HIV. 2017;4(8):e349-e356. doi:10.1016/S2352-3018(17)30066-8.
11. World Health Organization (WHO). Factsheets HIV/aIdS. Available at: http://www.who.int/news-room/fact-sheets/detail/hiv-aids (accessed on 7 November 2018).
12. van Sighem AI, Boender TS, Wit FWNM, Smit C, Matser A, Reiss P. Monitoring report 2018. Human Immunodeficiency Virus (HIV) in the netherlands. Amsterdam: Stichting HIV Monitoring, 2018.
13. Op de Coul EL, Schreuder I, Conti S, van SA, Xiridou M, Van Veen MG, et al. Changing Patterns of undiagnosed HIV Infection in the netherlands: Who Benefits Most from Intensified HIV Test and treat Policies? PLoS One. 2015;10(7):e0133232. doi:10.1371/journal.pone.0133232.
14. van Veen MG, Presanis AM, Conti S, Xiridou M, Stengaard AR, Donoghoe MC, et al. national estimate of HIV prevalence in the netherlands: comparison and applicability of different estimation tools. AIDS. 2011;25(2):229-237. doi:10.1097/QAD.0b013e32834171bc.
15. Nederlandse Vereniging van HIV behandelaren (NVHB). richtlijn HIV. NVHB, 2018. 16. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral
agents in adults and adolescents living with HIV. department of Health and Human Services. Available at: http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf (accessed on 14 November 2018).
17. van den Boom W, Davidovich U, Heuker J, Lambers F, Prins M, Sandfort T, et al. Is Group sex a Higher-risk Setting for HIV and other Sexually Transmitted Infections Compared With dyadic Sex among Men Who Have Sex With Men? Sex Transm Dis. 2016;43(2):99-104. doi:10.1097/OLQ.0000000000000389.

27
General introduction
1 18. van den Boom W, Konings R, Davidovich U, Sandfort T, Prins M, Stolte IG. Is serosorting effective in
reducing the risk of HIV infection among men who have sex with men with casual sex partners? J Acquir Immune Defic Syndr. 2014;65(3):375-379. doi:10.1097/QAI.0000000000000051.
19. van den Boom W, Stolte I, Sandfort T, Davidovich U. Serosorting and sexual risk behaviour according to different casual partnership types among MSM: the study of one-night stands and sex buddies. AIDS Care. 2012;24(2):167-173. doi:10.1080/09540121.2011.603285.
20. van den Boom W, Stolte IG, Roggen A, Sandfort T, Prins M, Davidovich U. Is anyone around me using condoms? Site-specific condom-use norms and their potential impact on condomless sex across various gay venues and websites in The netherlands. Health Psychol. 2015;34(8):857-864. doi:10.1037/hea0000230.
21. Van Den Boom W, Stolte IG, Witlox R, Sandfort T, Prins M, Davidovich U. undetectable viral load and the decision to engage in unprotected anal intercourse among HIV-positive MSM. AIDS Behav. 2013;17(6):2136-2142. doi:10.1007/s10461-013-0453-9.
22. Townsend CL, Cortina-Borja M, Peckham CS, de Ruiter A, Lyall H, Tookey PA. low rates of mother-to-child transmission of HIV following effective pregnancy interventions in the united Kingdom and Ireland, 2000-2006. AIDS. 2008;22(8):973-981. doi:10.1097/QAD.0b013e3282f9b67a.
23. Tubiana R, Le CJ, Rouzioux C, Mandelbrot L, Hamrene K, Dollfus C, et al. Factors associated with mother-to-child transmission of HIV-1 despite a maternal viral load <500 copies/ml at delivery: a case-control study nested in the French perinatal cohort (ePF-anrS Co1). Clin Infect Dis. 2010;50(4):585-596. doi:10.1086/650005.
24. Quinn TC, Wawer MJ, Sewankambo N, Serwadda D, Li C, Wabwire-Mangen F, et al. Viral load and heterosexual transmission of human immunodeficiency virus type 1. rakai Project Study Group. N Engl J Med. 2000;342(13):921-929. doi:10.1056/NEJM200003303421303.
25. Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493-505. doi:10.1056/NEJMoa1105243.
26. Rodger AJ, Cambiano V, Bruun T, Vernazza P, Collins S, van Lunzen J, et al. Sexual activity Without Con-doms and risk of HIV Transmission in Serodifferent Couples When the HIV-Positive Partner Is using Suppressive antiretroviral Therapy. JAMA. 2016;316(2):171-181. doi:10.1001/jama.2016.5148.
27. Rodger AJ, Cambiano V, Bruun T, Vernazza P, Collins S, Degen O, et al. risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (ParTner): final results of a multicentre, prospective, observational study. Lancet. 2019 doi:10.1016/S0140-6736(19)30418-0.
28. Granich RM, Gilks CF, Dye C, De Cock KM, Williams BG. universal voluntary HIV testing with immedi-ate antiretroviral therapy as a strategy for elimination of HIV transmission: a mathematical model. Lancet. 2009;373(9657):48-57. doi:10.1016/S0140-6736(08)61697-9.
29. Ratmann O, van Sighem A, Bezemer D, Gavryushkina A, Jurriaans S, Wensing A, et al. sources of HIV infection among men having sex with men and implications for prevention. Sci Transl Med. 2016;8(320):320ra322. doi:10.1126/scitranslmed.aad1863.
30. World Health Organization (WHO). Post-exposure prophylaxis for HIV. Supplementary section to the 2013 WHo consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection, Chapter 5 – Clinical guidelines across the continuum of care: HIV diagnosis and arV drugs for HIV prevention. Geneva: WHO, 2014.
31. Sonder GJ, van den Hoek A, Regez RM, Brinkman K, Prins JM, Mulder JW, et al. trends in HIV postex-posure prophylaxis prescription and compliance after sexual exposure in amsterdam, 2000-2004. Sex Transm Dis. 2007;34(5):288-293. doi:10.1097/01.olq.0000237838.43716.ee.

Chapter 1
28
32. World Health Organization (WHO). Guideline on when to start antiretroviral therapy and on pre-exposure prohylaxis for HIV. Geneva: WHO, 2015.
33. Nederlandse Vereniging van HIV behandelaren (NVHB). HIV Pre-expositie profylaxe (PreP) richtlijn nederland. NVHB, 2019.
34. HIV in Europe. HIV indicator conditions: Guidance for implementing HIV testing in adults in health care setting. Copenhagen: HIV in Europe, 2012.
35. European Centre for Disease Prevention and control (ECDC). Public health guidance on HIV, hepatitis B and C testing in the eu/eea: an integrated approach. Stockholm: ECDC, 2018.
36. Op de Coul EL, Hahne S, van Weert YW, Oomen P, Smit C, van der Ploeg KP, et al. antenatal screen-ing for HIV, hepatitis B and syphilis in the netherlands is effective. BMC Infect Dis. 2011;11:185. doi:10.1186/1471-2334-11-185.
37. Nederlands Huisartsen Genootschap (NHG). nHG Standaard: Het soa-consult. Utrecht: NHG, 2013. 38. Visser M, van Aar F, Op de Coul ELM, Slurink IAL, van Wees DA, Hoenderboom BM, et al. sexually
transmitted infections in the netherlands in 2017. Bilthoven: RIVM, 2018. 39. Rijksinstituut voor Volksgezondheid en Milieu (RIVM), Ministerie van Volksgezondheid, Welzijn en
Sport. Hepatitis B richtlijn. Bilthoven, 2017. 40. Rijksinstituut voor Volksgezondheid en Milieu (RIVM), Ministerie van Volksgezondheid, Welzijn en
Sport. Hepatitis C richtlijn. Bilthoven: RIVM, 2013. 41. Laghaei F, van der Poel A. Wel of niet getest, en wat was de uitslag? Zelfgerapporteerde vs. gereg-
istreerde infectieziektestatus van harddrugsgebruikers in de verslavingszorg. Utrecht: Netherlands Institute of Mental Health and Addiction (Trimbos Instituut), 2014.
42. World Health Organization (WHO). Guidelines on HIV Self-Testing and Partner notification: Supple-ment to Consolidated Guidelines on HIV Testing Services. Geneva: WHO, 2016.
43. Johnson CC, Kennedy C, Fonner V, Siegfried N, Figueroa C, Dalal S, et al. examining the effects of HIV self-testing compared to standard HIV testing services: a systematic review and meta-analysis. J Int AIDS Soc. 2017;20(1):21594. doi:10.7448/IAS.20.1.21594.
44. Gerlich WH. Medical virology of hepatitis B: how it began and where we are now. Virol J. 2013;10:239. doi:10.1186/1743-422X-10-239.
45. Choo QL, Kuo G, Weiner AJ, Overby LR, Bradley DW, Houghton M. Isolation of a cdna clone de-rived from a blood-borne non-a, non-B viral hepatitis genome. Science. 1989;244(4902):359-362. doi:10.1126/science.2523562.
46. World Health Organization (WHO). Hepatitis B Fact sheet. Available at: https://www.who.int/en/news-room/fact-sheets/detail/hepatitis-b (accessed on 16 November 2018).
47. van de Laar TJ, Matthews GV, Prins M, Danta M. acute hepatitis C in HIV-infected men who have sex with men: an emerging sexually transmitted infection. AIDS. 2010;24(12):1799-1812. doi:10.1097/QAD.0b013e32833c11a5.
48. Hoornenborg E, Achterbergh RCA, Schim van der Loeff MF, Davidovich U, Hogewoning A, de Vries HJC, et al. MSM starting preexposure prophylaxis are at risk of hepatitis C virus infection. AIDS. 2017;31(11):1603-1610. doi:10.1097/QAD.0000000000001522.
49. Cotte L, Cua E, Reynes J, Raffi F, Rey D, Delobel P, et al. Hepatitis C virus incidence in HIV-infected and in preexposure prophylaxis (PreP)-using men having sex with men. Liver Int. 2018 doi:10.1111/liv.13922.
50. Hoornenborg E, Coyer LN, Achterbergh RCA, Schim van der Loeff MF, Bruisten S, de Vries HJC, et al. High incidence of hepatitis C virus (re-)infections among PreP users in the netherlands: Implications for prevention, monitoring and treatment [abstract TuPdX0104]. 22nd International AIDS confer-ence: Amsterdam, the Netherlands, 23-27 July 2018.

29
General introduction
1 51. Ramiere C, Charre C, Miailhes P, Bailly F, Radenne S, Uhres AC, et al. Patterns of HCV transmission
in HIV-infected and HIV-negative men having sex with men. Clin Infect Dis. 2019 doi:10.1093/cid/ciz160.
52. Edmunds WJ, Medley GF, Nokes DJ, Hall AJ, Whittle HC. The influence of age on the development of the hepatitis B carrier state. Proc Biol Sci. 1993;253(1337):197-201. doi:10.1098/rspb.1993.0102.
53. Hyams KC. risks of chronicity following acute hepatitis B virus infection: a review. Clin Infect Dis. 1995;20(4):992-1000. doi:10.1093/clinids/20.4.992.
54. Fattovich G. natural history and prognosis of hepatitis B. Semin Liver Dis. 2003;23(1):47-58. doi:10.1055/s-2003-37590.
55. Micallef JM, Kaldor JM, Dore GJ. Spontaneous viral clearance following acute hepatitis C infection: a systematic review of longitudinal studies. J Viral Hepat. 2006;13(1):34-41. doi:10.1111/j.1365-2893.2005.00651.x.
56. Seeff LB. natural history of chronic hepatitis C. Hepatology. 2002;36(5 Suppl 1):S35-46. doi:10.1053/jhep.2002.36806.
57. Fattovich G, Stroffolini T, Zagni I, Donato F. Hepatocellular carcinoma in cirrhosis: incidence and risk factors. Gastroenterology. 2004;127(5 Suppl 1):S35-50. doi:10.1053/j.gastro.2004.09.014.
58. European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. eaSl 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67(2):370-398. doi:10.1016/j.jhep.2017.03.021.
59. Raffetti E, Fattovich G, Donato F. Incidence of hepatocellular carcinoma in untreated subjects with chronic hepatitis B: a systematic review and meta-analysis. Liver Int. 2016;36(9):1239-1251. doi:10.1111/liv.13142.
60. Thrift AP, El-Serag HB, Kanwal F. Global epidemiology and burden of HCV infection and HCV-related disease. Nat Rev Gastroenterol Hepatol. 2017;14(2):122-132. doi:10.1038/nrgastro.2016.176.
61. World Health Organization (WHO). Global Hepatitis report, 2017. Geneva: WHO, 2017. 62. Hahne SJ, De Melker HE, Kretzschmar M, Mollema L, Van Der Klis FR, Van Der Sande MA, et al.
Prevalence of hepatitis B virus infection in The netherlands in 1996 and 2007. Epidemiol Infect. 2012;140(8):1469-1480. doi:10.1017/S095026881100224X.
63. Vriend HJ, Van Veen MG, Prins M, Urbanus AT, Boot HJ, Op De Coul EL. Hepatitis C virus prevalence in The netherlands: migrants account for most infections. Epidemiol Infect. 2013;141(6):1310-1317. doi:10.1017/S0950268812001884.
64. Koopsen J, van Steenbergen JE, Richardus JH, Prins M, Op de Coul ELM, Croes EA, et al. Chronic hepatitis B and C infections in the netherlands: estimated prevalence in risk groups and the general population. Epidemiol Infect. 2019;147:e147. doi:10.1017/S0950268819000359.
65. Koedijk FD, Op de Coul EL, Boot HJ, van de Laar MJ. Surveillance van hepatitis B in nederland, 2002-2005: acute infectie vooral via seksueel contact, chronische via verticale transmissie door moeders uit endemische gebieden. Ned Tijdschr Geneeskd. 2007;151(43):2389-2394.
66. Nederlandse Internisten Vereniging (NIV), Nederlandse Vereniging van HIV behandelaren (NVHB), Nederlandse Vereniging voor Maag-Darm-Leverziekten (NVMDL), Nederlandse Vereniging voor Hepatologie (NVH), Nederlandse Vereniging voor Ziekenhuis Apothekers (NVZA). HCV richtsnoer. Available at: https://hcvrichtsnoer.nl/ (accessed on 24 April 2019).
67. Banerjee D, Reddy KR. review article: safety and tolerability of direct-acting anti-viral agents in the new era of hepatitis C therapy. Aliment Pharmacol Ther. 2016;43(6):674-696. doi:10.1111/apt.13514.
68. European Association for the Study of the Liver (EASL). eaSl recommendations on Treatment of Hepatitis C 2018. J Hepatol. 2018;69(2):461-511. doi:10.1016/j.jhep.2018.03.026.
Chapter 1
30
69. Nederlands Huisartsen Genootschap (NHG). nHG-Standaard Virushepatitis en andere leveraan-doeningen. Utrecht: NHG, 2016.
70. van den Brink W, van de Glind G, Schippers G. Multidisciplinaire richtlijn opiaatverslaving. Utrecht: Tijdstroom D, 2013.
71. Gezondheidsraad. Screening van risicogroepen op hepatitis B en C. Den Haag: Gezondheidsraad, 2016.
72. Rijksinstituut voor Volksgezondheid en Milieu (RIVM). Meldingsplicht infectieziekten: Jaarlijkse meldingen per infectieziekte. Available at: https://www.rivm.nl/meldingsplicht-infectieziekten/overzicht-meldingen (accessed on 22 May 2019).
73. World Health Organization (WHO). Fact sheet sexually transmitted infections (STIs). Available at: http://www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis) (accessed on 24 November 2018).
74. Taylor-Robinson D. The discovery of Chlamydia trachomatis. Sex Transm Infect. 2017;93(1):10. doi:10.1136/sextrans-2016-053011.
75. Elbert NJ, van Gijn J, Gijselhart JP. neisser en de druiper [dutch]. Ned Tijdschr Geneeskd. 2013;157(23):A6252.
76. Tampa M, Sarbu I, Matei C, Benea V, Georgescu SR. Brief history of syphilis. J Med Life. 2014;7(1):4-10.
77. Rijksinstituut voor Volksgezondheid en Milieu (RIVM), Ministerie van Volksgezondheid, Welzijn en Sport. Syfilis richtlijn. Bilthoven: RIVM, 2016.
78. Rijksinstituut voor Volksgezondheid en Milieu (RIVM), Ministerie van Volksgezondheid, Welzijn en Sport. Chlamydia trachomatis en lymfogranuloma venereum richtlijn. Bilthoven: RIVM, 2013.
79. Rijksinstituut voor Volksgezondheid en Milieu (RIVM), Ministerie van Volksgezondheid, Welzijn en Sport. Gonorroe richtlijn. Bilthoven: RIVM, 2015.
80. Nederlandse Vereniging voor Dermatologie en Venereologie (NVDV). Multidisciplinaire richtlijn Seksueel overdraagbare aandoeningen (Herziening 2018). Utrecht: NVDV, 2018.
81. Joint United Nations Programme on HIV/AIDS (UNAIDS). 90-90-90: an ambitious treatment target to help end the aIdS epidemic. Geneva: UNAIDS, 2014.
82. Joint United Nations Programme on HIV/AIDS (UNAIDS). Fast-track: ending the aIdS epidemic by 2030. Geneva, UNAIDS, 2014.
83. David S, van Benthem B, Deug F, van Haastrecht P. nationaal actieplan soa, hiv en seksuele gezond-heid: 2017-2022. Bilthoven: RIVM, 2018.
84. Joint United Nations Programme on HIV/AIDS (UNAIDS). ending aIdS, Progress towards the 90-90-90 targets. Geneva: UNAIDS, 2017.
85. H-team. Available at: www.hteam.nl (accessed on 13 November 2018). 86. World Health Organization (WHO). Global Health Sector Strategy on viral hepatitis 2016-2021,
towards ending viral hepatitis. Geneva: WHO, 2016. 87. Spradling PR, Rupp L, Moorman AC, Lu M, Teshale EH, Gordon SC, et al. Hepatitis B and C virus infec-
tion among 1.2 million persons with access to care: factors associated with testing and infection prevalence. Clin Infect Dis. 2012;55(8):1047-1055. doi:10.1093/cid/cis616.
88. Denniston MM, Klevens RM, McQuillan GM, Jiles RB. awareness of infection, knowledge of hepatitis C, and medical follow-up among individuals testing positive for hepatitis C: national Health and nu-trition examination Survey 2001-2008. Hepatology. 2012;55(6):1652-1661. doi:10.1002/hep.25556.
89. Meffre C, Le Strat Y, Delarocque-Astagneau E, Dubois F, Antona D, Lemasson JM, et al. Prevalence of hepatitis B and hepatitis C virus infections in France in 2004: social factors are important predictors after adjusting for known risk factors. J Med Virol. 2010;82(4):546-555. doi:10.1002/jmv.21734.

31
General introduction
1 90. van der Ploeg C, Schönbeck Y, Hirschberg H. Prenatal screening for infectious diseases and erythro-
cytes immunisation [in dutch]. Leiden: TNO, 2015. 91. Willemse SB, Razavi-Shearer D, Zuure FR, Veldhuijzen IK, Croes EA, van der Meer AJ, et al. the
estimated future disease burden of hepatitis C virus in the netherlands with different treatment paradigms. Neth J Med. 2015;73(9):417-431.
92. Hofman R, Nusselder WJ, Veldhuijzen IK, Richardus JH. Mortality due to chronic viral hepatitis B and C infections in the netherlands [in dutch]. Ned Tijdschr Geneeskd. 2016;160(0):D511.
93. David S, Hogenbirk R, van Steenbergen J, Urbanus A. Meer dan opsporen. nationaal hepatitisplan: een strategie voor actie. Bilthoven: RIVM, 2016.
94. GGD Amsterdam. actieplan hepatitis B en C preventie en zorg in amsterdam. Available at: https://www.ggd.amsterdam.nl/beleid-onderzoek/onderzoek-infectiezi/actieplan-hepatitis/ (accessed on 13 November 2018).
95. World Health Organization (WHO). Global health sector strategy on sexually transmitted infections 2016–2021: towards ending STIs. Geneva: WHO, 2016.
96. European AIDS Clinical Society (EACS). Guidelines, Version 9.1. Brussels: EACS, 2018. 97. Grant RM, Lama JR, Anderson PL, McMahan V, Liu AY, Vargas L, et al. Preexposure chemoprophy-
laxis for HIV prevention in men who have sex with men. N Engl J Med. 2010;363(27):2587-2599. doi:10.1056/NEJMoa1011205.
98. Fonner VA, Dalglish SL, Kennedy CE, Baggaley R, O’Reilly KR, Koechlin FM, et al. effectiveness and safety of oral HIV preexposure prophylaxis for all populations. AIDS. 2016;30(12):1973-1983. doi:10.1097/QAD.0000000000001145.
99. U.S. Department of Health & Human Services, U.S. Food and Drug Administration (FDA),. truvada for PreP fact sheet: ensuring safe and proper use. Available at: https://www.fda.gov/downloads/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/UCM312290.pdf (accessed on 16 November 2018).
100. European Medicines Agency (EMA). Press release: first medicine for HIV pre-exposure prophylaxis recommended for approval in the eu. Turvada to enhance existing HIV prevention strategies. Avail-able at: https://www.ema.europa.eu/documents/press-release/first-medicine-hiv-pre-exposure-prophylaxis-recommended-approval-eu_en.pdf (accessed on 14 November 2018).
101. McCormack S, Dunn DT, Desai M, Dolling DI, Gafos M, Gilson R, et al. Pre-exposure prophylaxis to prevent the acquisition of HIV-1 infection (Proud): effectiveness results from the pilot phase of a pragmatic open-label randomised trial. Lancet. 2016;387(10013):53-60. doi:10.1016/S0140-6736(15)00056-2.
102. Molina JM, Capitant C, Spire B, Pialoux G, Cotte L, Charreau I, et al. on-demand Preexposure Prophy-laxis in Men at High risk for HIV-1 Infection. N Engl J Med. 2015;373(23):2237-2246. doi:10.1056/NEJMoa1506273.
103. Hoornenborg E, Achterbergh RC, van der Loeff MFS, Davidovich U, van der Helm JJ, Hogewon-ing A, et al. Men who have sex with men more often chose daily than event-driven use of pre-exposure prophylaxis: baseline analysis of a demonstration study in amsterdam. J Int AIDS Soc. 2018;21(3):e25105. doi:10.1002/jia2.25105.
104. Gezondheidsraad. Preventief gebruik van hiv-remmers. Den Haag: Gezondheidsraad, 2018. 105. Bruins B. Beleidsreactie preventief gebruik van hiv-remmers (PreP) [dutch]. Available at: https://
www.rijksoverheid.nl/regering/bewindspersonen/bruno-bruins/documenten/kamerstuk-ken/2018/07/10/kamerbrief-met-beleidsreactie-preventief-gebruik-van-hiv-remmers-prep (accessed on 17 September 2018).

Chapter 1
32
106. Hoornenborg E, Krakower DS, Prins M, Mayer KH. Pre-exposure prophylaxis for msm and transgender persons in early adopting countries. AIDS. 2017;31(16):2179-2191. doi:10.1097/QAD.0000000000001627.
107. Op de Coul EL, van Sighem A, Brinkman K, van Benthem BH, van der Ende ME, Geerlings S, et al. Factors associated with presenting late or with advanced HIV disease in the netherlands, 1996-2014: results from a national observational cohort. BMJ Open. 2016;6(1):e009688. doi:10.1136/bmjopen-2015-009688.
108. Alvarez-del Arco D, Monge S, Azcoaga A, Rio I, Hernando V, Gonzalez C, et al. HIV testing and counsel-ling for migrant populations living in high-income countries: a systematic review. Eur J Public Health. 2013;23(6):1039-1045. doi:10.1093/eurpub/cks130.
109. Seedat F, Hargreaves S, Nellums LB, Ouyang J, Brown M, Friedland JS. How effective are approaches to migrant screening for infectious diseases in europe? a systematic review. Lancet Infect Dis. 2018;18(9):e259-e271. doi:10.1016/S1473-3099(18)30117-8.
110. Deblonde J, De Koker P, Hamers FF, Fontaine J, Luchters S, Temmerman M. Barriers to HIV testing in europe: a systematic review. Eur J Public Health. 2010;20(4):422-432. doi:10.1093/eurpub/ckp231.
111. Hamdiui N, Stein ML, Timen A, Timmermans D, Wong A, van den Muijsenbergh M, et al. Hepatitis B in Moroccan-dutch: a quantitative study into determinants of screening participation. BMC Med. 2018;16(1):47. doi:10.1186/s12916-018-1034-6.
112. Hamdiui N, Stein ML, van der Veen YJJ, van den Muijsenbergh M, van Steenbergen JE. Hepatitis B in Moroccan-dutch: a qualitative study into determinants of screening participation. Eur J Public Health. 2018;28(5):916-922. doi:10.1093/eurpub/cky003.
113. Kuehne A, Koschollek C, Santos-Hovener C, Thorlie A, Mullerschon J, Mputu Tshibadi C, et al. Impact of HIV knowledge and stigma on the uptake of HIV testing - results from a community-based participatory research survey among migrants from sub-Saharan africa in Germany. PLoS One. 2018;13(4):e0194244. doi:10.1371/journal.pone.0194244.
114. Rade DA, Crawford G, Lobo R, Gray C, Brown G. sexual Health Help-seeking Behavior among mi-grants from Sub-Saharan africa and South east asia living in High Income Countries: a Systematic review. Int J Environ Res Public Health. 2018;15(7) doi:10.3390/ijerph15071311.
115. Tiittala P, Kivela P, Liitsola K, Ollgren J, Pasanen S, Vasankari T, et al. Important Gaps in HIV Knowledge, attitudes and Practices among Young asylum Seekers in Comparison to the General Population. J Immigr Minor Health. 2018;20(6):1415-1423. doi:10.1007/s10903-018-0707-8.
116. Fakoya I, Alvarez-Del Arco D, Copas AJ, Teixeira B, Block K, Gennotte AF, et al. Factors associated With access to HIV Testing and Primary Care among Migrants living in europe: Cross-Sectional Survey. JMIR Public Health Surveill. 2017;3(4):e84. doi:10.2196/publichealth.7741.
117. Joint United Nations Programme on HIV/AIDS (UNAIDS), World Health Organization (WHO). a short technical update on self-testing for HIV. Geneva: UNAIDS, 2013.
118. Napierala Mavedzenge S, Baggaley R, Corbett EL. a review of self-testing for HIV: research and policy priorities in a new era of HIV prevention. Clin Infect Dis. 2013;57(1):126-138. doi:10.1093/cid/cit156.
119. World Health Organization (WHO). report on the first international symposium on self-testing for HIV: The legal, ethical, gender, human rights and public health implications of HIV self-testing scale-up: Geneva, Switzerland, 8-9 april 2013. Geneva: WHO, 2013.
120. Krause J, Subklew-Sehume F, Kenyon C, Colebunders R. acceptability of HIV self-testing: a systematic literature review. BMC Public Health. 2013;13:735. doi:10.1186/1471-2458-13-735.
121. Pant Pai N, Sharma J, Shivkumar S, Pillay S, Vadnais C, Joseph L, et al. supervised and unsuper-vised self-testing for HIV in high- and low-risk populations: a systematic review. PLoS Med. 2013;10(4):e1001414. doi:10.1371/journal.pmed.1001414.

33
General introduction
1 122. Figueroa C, Johnson C, Verster A, Baggaley R. attitudes and acceptability on HIV Self-testing among
Key Populations: a literature review. AIDS Behav. 2015;19(11):1949-1965. doi:10.1007/s10461-015-1097-8.
123. Stevens DR, Vrana CJ, Dlin RE, Korte JE. a Global review of HIV Self-testing: Themes and Implications. AIDS Behav. 2017 doi:10.1007/s10461-017-1707-8.
124. Unitaid, World Health Organization (WHO). Market and technology landscape: HIV rapid diagnostic tests for self-testing. Geneva: Unitaid, 2018.
125. Besluit in-vitro diagnostica [dutch]. Available at: https://wetten.overheid.nl/jci1.3:c:BWBR0012610&z=2016-01-01&g=2016-01-01 (accessed on 30 January 2019).
126. van Dommelen L, van Tiel FH, Ouburg S, Brouwers EE, Terporten PH, Savelkoul PH, et al. alarmingly poor performance in Chlamydia trachomatis point-of-care testing. Sex Transm Infect. 2010;86(5):355-359. doi:10.1136/sti.2010.042598.
127. Owens SL, Arora N, Quinn N, Peeling RW, Holmes KK, Gaydos CA. utilising the internet to test for sexually transmitted infections: results of a survey and accuracy testing. Sex Transm Infect. 2010;86(2):112-116. doi:10.1136/sti.2009.037226.
128. Peterman TA, Kreisel K, Habel MA, Pearson WS, Dittus PJ, Papp JR. Preparing for the Chlamydia and Gonorrhea self-test. Sex Transm Dis. 2018;45(3):e7-e9. doi:10.1097/OLQ.0000000000000737.
129. Van den Broek IVF, Sukel B, Bos H, Den Baas C. evaluatie van het aanbod van online-aanbieders van soa-zelftesten in nederland [dutch]. Bilthoven: RIVM, 2016.
130. Pars L, van Bergen J. Soa-testen, zelf doen of laten (doen)? [dutch]. Amsterdam: SOA AIDS Nederland, 2013.
131. Bustamante MJ, Konda KA, Joseph DD, Leon SR, Calvo GM, Salvatierra J, et al. HIV self-testing in Peru: questionable availability, high acceptability but potential low linkage to care among men who have sex with men and transgender women. Int J STD AIDS. 2016 doi:10.1177/0956462416630674.
132. van Griensven GJ, de Vroome EM, Goudsmit J, Coutinho RA. Changes in sexual behaviour and the fall in incidence of HIV infection among homosexual men. BMJ. 1989;298(6668):218-221. doi: 10.1136/bmj.298.6668.218.
133. Matser A, Van Bilsen W, Prins M. The amsterdam Cohort Studies on HIV infection: annual report 2017. In: van Sighem AI, Boender TS, Wit FWNM, Smit C, Matser A, Reiss P, eds. Monitoring Report 2018 Human Immunodeficiency Virus (HIV) in the Netherlands. Amsterdam: Stichting HIV Monitoring, 2018.
134. Fakoya I, Alvarez-Del Arco D, Monge S, Copas AJ, Gennotte AF, Volny-Anne A, et al. advancing migrant access to Health Services in europe (aMaSe): Protocol for a Cross-sectional Study. JMIR Res Protoc. 2016;5(2):e74. doi:10.2196/resprot.5085.
135. Fakoya I, Alvarez-Del Arco D, Monge S, Copas AJ, Gennotte AF, Volny-Anne A, et al. HIV testing history and access to treatment among migrants living with HIV in europe. J Int AIDS Soc. 2018;21 Suppl 4:e25123. doi:10.1002/jia2.25123.
136. Alvarez-Del Arco D, Fakoya I, Thomadakis C, Pantazis N, Touloumi G, Gennotte AF, et al. High levels of postmigration HIV acquisition within nine european countries. AIDS. 2017;31(14):1979-1988. doi:10.1097/QAD.0000000000001571.
137. Stronks K, Snijder MB, Peters RJ, Prins M, Schene AH, Zwinderman AH. unravelling the impact of ethnicity on health in europe: the HelIuS study. BMC Public Health. 2013;13:402. doi:10.1186/1471-2458-13-402.
138. Snijder MB, Galenkamp H, Prins M, Derks EM, Peters RJG, Zwinderman AH, et al. Cohort profile: the Healthy life in an urban Setting (HelIuS) study in amsterdam, The netherlands. BMJ Open. 2017;7(12):e017873. doi:10.1136/bmjopen-2017-017873.

Chapter 1
34
139. Geneeskundige en Gezondheidsdienst (GGD) Amsterdam. amsterdammers gezond en wel? amster-damse Gezondheidsmonitor 2012 [dutch]. Amsterdam: GGD Amsterdam, 2013.
140. Dijkshoorn H, van Dijk TK, Janssen AP. Zo gezond is amsterdam! eindrapport amsterdamse Gezond-heidsmonitor 2008 [dutch]. Amsterdam: GGD Amsterdam, 2009.
141. van den Hoek JA, Fennema JS, van Haastrecht HJ, van Doornum GJ, Henquet CJ, Coutinho RA. HIV-prevalentie bij bezoekers van een polikliniek voor seksueel overdraagbare aandoeningen en bij een groep prostituées en prostituanten [dutch]. Ned Tijdschr Geneeskd. 1992;136(37):1813-1818.
142. Urbanus AT, Van De Laar TJ, Geskus R, Vanhommerig JW, Van Rooijen MS, Schinkel J, et al. trends in hepatitis C virus infections among MSM attending a sexually transmitted infection clinic; 1995-2010. AIDS. 2014;28(5):781-790. doi:10.1097/QAD.0000000000000126.



Chapter 2Pre-exposure prophylaxis to prevent
HIV infection


Chapter 2.1What do dutch men who have sex with
men think of pre-exposure prophylaxis to prevent HIV infection? A cross-sectional study
Janneke P. Bil, Udi Davidovich, Wendy M. van der Veldt, Maria Prins, Henry J.C. de Vries, Gerard J.B. Sonder, Ineke G. Stolte
Published in AIDS, 2015; 29(8):955-964

Chapter 2.1
40
aBstraCt
objectives
Although pre-exposure prophylaxis (PrEP) is not registered in Europe, including the Nether-lands, its approval and implementation are expected in the near future. We aimed to gain insight into PrEP awareness and the intention to use PrEP among men who have sex with men (MSM).
design
Cross-sectional study among 448 HIV-negative participants of the Amsterdam Cohort Study who completed a questionnaire concerning behaviour and PrEP between 2012 and 2013.
methods
Characteristics, PrEP awareness, and intention to use PrEP were described and multinomial logistic regression was used to identify determinants of a medium and high intention to use PrEP.
results
PrEP awareness was 54%, but only 13% reported a high intention to use PrEP. High-risk MSM were more likely to have a medium (adjusted odds ratio [aOR] 1.78, 95% confidence interval [CI] 1.07– 2.97) or high (aOR 3.92, 95% CI 1.68– 9.15) intention to use PrEP than low-risk MSM, as were MSM with higher perceptions of self-efficacy to use PrEP (high intention: aOR 6.15, 95% CI 2.50–15.09) and higher perceptions of relief due to PrEP (medium intention: aOR 2.67, 95% CI 1.32–5.40; high intention: aOR 14.87, 95% CI 5.98– 37.01) than MSM with lower perceptions. MSM with higher perceptions of shame about using PrEP (medium inten-tion: aOR 0.35, 95% CI 0.19–0.62; high intention: aOR 0.22, 95% CI 0.07–0.71) or with more worries about side-effects were less likely to have a high (aOR 0.18, 95% CI 0.06–0.54) or medium (aOR 0.29, 95% CI 0.12– 0.72) intention to use PrEP.
Conclusion
The overall intention to use PrEP was relatively low, but higher among high-risk MSM. If PrEP implementation among high-risk MSM in the Netherlands becomes reality, PrEP awareness should be increased and psychosocial determinants that will influence uptake should be addressed.

41
PrEP awareness and the intention to use PrEP among MSM
2.1
InTroduCTIon
Despite widespread implementation of behavioural interventions to prevent transmission of HIV and high coverage of antiretroviral therapy (ART) among HIV-infected men who have sex with men (MSM), HIV continues to spread among this group in the Netherlands and other countries.1 Annually, about 1100 newly diagnosed HIV infections are registered in the Netherlands, of which 700–750 are among MSM, whose HIV incidence has fluctuated between 2.0 and 0.6 per 100 person-years from 2009 through 2012.2,3
Pre-exposure prophylaxis (PrEP) is a new biomedical approach that offers HIV-negative individuals a regime of lower-intensity ART to reduce their risk of HIV infection. In 2010, the multinational pre-exposure prophylaxis initiative (iPrEX) study showed a 44% reduction in HIV acquisition in MSM receiving daily PrEP (tenofovir disoproxyl fumarate - TDF - and emtricitabine - FTC) compared with placebo controls, and a 92% reduction among adherent MSM (i.e., with detectable drug levels).4 Although drug adherence, side-effects, and pos-sible drug-resistance are serious challenges, the Food and Drug Administration in the United States approved PrEP in May 2012 for uninfected individuals who are at high risk of HIV infection and who engage in sexual activity with HIV-infected partners.5
Although PrEP is not yet registered in Europe, including the Netherlands, its approval and implementation are expected in the near future. Knowledge and willingness to use PrEP among those at increased risk for HIV infection, such as MSM, are necessary for PrEP uptake and will determine the success of PrEP implementation. However, knowledge and willing-ness to use PrEP have not been studied yet in the Netherlands.
This study aims to gain insight into PrEP awareness, the intention to use PrEP and to identify sociodemographic and psychosocial determinants of a higher intention to use PrEP among Dutch MSM. We hypothesized that MSM at higher risk for HIV infection will be more aware of PrEP and will have a higher intention to use PrEP than MSM at lower risk. Although behavioural intentions do not absolutely predict actual PrEP uptake, they provide a good indication of the general willingness to use PrEP.6,7
In this study, we additionally explored the anticipated condom use if men would decide to use PrEP because PrEP use might affect sexual behaviour. Finally, we explored the influence of PrEP characteristics (cost, duration, and efficacy) on the willingness to use PrEP.

Chapter 2.1
42
MeTHodS
study population and procedures
The Amsterdam Cohort Study (ACS) among MSM is an open, prospective cohort study initi-ated in 1984 aiming to investigate the epidemiology, natural history, and pathogenesis of HIV, and to evaluate the effect of interventions.8,9 Participants visit the Public Health Service Amsterdam every 6 months to complete self-administrated questionnaires on sexual be-haviour, give blood for HIV testing (two ELISAs: AxSYM; Abbot Laboratories, North Chicago, Illinois, USA; Vironostika, Organon Teknika, Boxtel, The Netherlands), storage and since 2008 also sexually transmitted infection (STI) screening (gonorrhoea: nucleic acid amplification test on pharyngeal/anal swabs and urine: Gen-Probe Aptima Combo 2 Assay, Gen-Probe Incorporated, San Diego, California, USA). The ACS was approved by the Medical Ethical Committee of the Amsterdam Medical Center of Amsterdam, the Netherlands.
For our cross-sectional study, data were collected during one 6-monthly data wave (June 2012–January 2013), when the ACS questionnaire was augmented with items about PrEP awareness and intention to use PrEP. Before answering questions about PrEP, participants were given the following written information: ‘Pre-exposure prophylaxis (PrEP) refers to the possibility for HIV-negative individuals to take anti-HIV drugs daily for an extended period of time to reduce the risk of HIV infection. The efficacy of PrEP is still being tested and therefore PrEP is not (yet) available in the Netherlands’. Participants were given no information about PrEP efficacy, side-effects, costs or duration. We included HIV-negative MSM who completed questions related to PrEP awareness and the intention to use PrEP.
Variables
Sociodemographic characteristics
Characteristics included age, nationality (Dutch/non–Dutch), educational level (no college degree/at least college degree), and net monthly income level (low: ≤1700 Euro/medium: 1701–2950 Euro/high: ≥2951 Euro).
Sexual behaviour
Men were categorized into HIV-risk infection group based on three risk factors for HIV sero-conversion identified in previous research within the ACS: having receptive condomless anal sex (CAS) with casual partners; having more than five casual partners in the preceding six months; diagnosed gonorrhoea (urethral or rectal) at ACS visit.3 Men reporting at least one of these factors were defined as high-risk (Hr-MSM). Those reporting none of these factors were defined as low-risk (Lr-MSM).

43
PrEP awareness and the intention to use PrEP among MSM
2.1
CAS was defined as not or not always using a condom during anal sex; condom use was mea-sured on a 5-point scale ranging from ‘always’ to ‘never’. Two questions concerning steady partners were combined and categorized into having no steady partner, an HIV-negative steady partner, and a steady partner with positive or unknown HIV status.
Awareness of and beliefs about PrEP
We asked participants if they had ever heard of PrEP. Those aware of PrEP were asked about their chief source of knowledge (multiple-choice question). All participants (aware or un-aware of PrEP) were asked about their beliefs about PrEP; efficacy (measured on a 4-point scale ranging from ‘PrEP can reduce the risk of HIV by 100%’ to ‘PrEP does not reduce the risk of HIV’); efficacy in combination with always, sometimes or never using condoms (measured in three questions, all on a 7-point scale ranging from ‘no protection’ to ‘100% protection’); and side-effects (‘rare’, ‘sometimes reported’, ‘appear frequently’, ‘knowledge is still scarce’).
Intention to use PrEP
The intention to use PrEP was assessed in all MSM (aware or unaware of PrEP) by two ques-tions: ‘How likely are you to use PrEP if it becomes available in the Netherlands?’ and ‘Are you planning on using PrEP if it becomes available in the Netherlands?’ (both measured on a 7-point scale from ‘very unlikely’ to ‘very likely’). Given their acceptable correlation (Spear-man rho 0.7; p<0.001), the mean score of these items was used to represent the ‘intention to use PrEP’. Intention to use PrEP was categorized based on tertiles, into low (score <2), medium (score 2–4), and high intention (score >4).
Psychosocial determinants concerning PrEP
The questionnaire included 13 items measuring psychosocial determinants concerning PrEP. For analyses, items were combined if they measured the same psychosocial determinant and had acceptable reliability (>3 items: Cronbach’s alpha >0.6). This resulted in eight deter-minants. Three concerned perceived self-efficacy; to use PrEP, to use PrEP every day on time, and to pay for PrEP (four items: €50, €100, €500, or €1000 per month, Cronbach’s alpha 0.9). The other five concerned perceived emotional impact of PrEP: whether men would feel worried about PrEP side-effects, worried about PrEP efficacy, less worried about getting HIV-infected when using PrEP, ashamed about using PrEP, and relieved when using PrEP (three items: feeling liberated, relieved, and hopeful, Cronbach’s alpha 0.9). All items were measured on a 7-point scale (ranging from ‘very difficult’ to ‘very easy’ or ‘totally disagree’ to ‘totally agree’).
As determinants were not normally distributed and a linear association was absent, they were dichotomized at the logical mid-point of a 7-point scale, with scores 4 or less represent-ing low perceptions and scores more than 4 representing higher perceptions.

Chapter 2.1
44
Anticipated condom use
Anticipated condom use was measured by the item: ‘I would be less likely to use condoms when using PrEP’ (7-point scale ranging from ‘totally disagree’ to ‘totally agree’). As earlier, responses were dichotomized into ‘no anticipated decrease in condom use while using PrEP’ (score <4) or ‘anticipated decrease in condom use while using PrEP’ (score >4). Perceived self-efficacy to use condoms while using PrEP was measured with one item: ‘How easy would it be to continue using condoms while using PrEP?’ (7-point scale ranging from ‘very easy’ to ‘very difficult’), which was dichotomized into ‘high perceived self-efficacy’ (score <4) and ‘low perceived self-efficacy’ (score >4).
Influence of PrEP characteristics among MSM with high intention to use PrEP
We assessed willingness to use PrEP at various levels of monthly cost (€50, €100, €500, €1000), for different duration of usage (3, 6 months, 1, 5, and 10 years), and when less than 100% efficacy (two combined items because they had acceptable correlation: Spearman rho 0.6; p<0.001). Willingness was analysed for participants with a high intention to use PrEP only. Items were measured on a 7-point scale ranging from ‘definitely not willing’ to ‘very willing’. Responses were dichotomized at mid-point into ‘unwilling’ (score <4) and ‘willing’ (score >4).
statistical analyses
First, we described sociodemographic characteristics, sexual (risk) behaviour, and PrEP awareness. We compared distributions of characteristics and potential determinants between Hr-MSM and Lr-MSM, using chi-square tests for categorical variables and Mann-Whitney U tests for all, not normally distributed, continuous variables.
Second, we performed multinomial logistic regression analyses to explore whether sociode-mographic characteristics, sexual (risk) behaviour, and psychosocial determinants were associated with a medium or high intention (reference is low intention) to use PrEP. Due to the many variables, the multivariate model was built in three steps: sociodemographic characteristics and sexual (risk) behaviour associated with a higher intention (overall p<0.10) in univariate analysis were included in a multivariate model; psychosocial determinants as-sociated with a higher intention (overall p<0.10) in univariate analyses were included in a separate multivariate model; variables associated with a higher intention to use PrEP (overall p<0.10) in one of the two multivariate models were included in a final multivariate model, and considered statistically significant if the overall p-value <0.05. In sensitivity analyses, the three HIV risk factors defining Hr-MSM (number of casual partners, receptive CAS with casual partners, gonorrhoea diagnosis) were included separately in the final model.

45
PrEP awareness and the intention to use PrEP among MSM
2.1
Third, we described anticipated condom use when using PrEP and employed chi-square tests to evaluate whether results differed among subgroups (MSM currently vs. not currently engaging in CAS and MSM with a low vs. medium vs. high intention to use PrEP).
Fourth, we described the influence of PrEP characteristics on the willingness to use PrEP among MSM with initially high intention to use PrEP.
Analyses were performed using STATA Intercooled 13.1 (STATA Corporation, College Station, Texas, USA).
reSulTS
Participant characteristics
From June 2012 to January 2013, 466 HIV-negative MSM had a 6-monthly ACS visit, of whom 448 (96%) completed PrEP questions and were included in this study. Their median age was 40 years (interquartile range [IQR] 35–45] (Table 1), most were Dutch (92%; 404/440), col-lege graduates (90%; 404/447), and had a medium income (41%; 163/397). In the preceding six months, men reported a median of 4 (IQR 0–11) casual partners and 64% (276/433) had a steady partner. Over half of participants (59%; 261/444) reported CAS in the preceding 6 months and 3% (11/434) were diagnosed with gonorrhoea at their ACS visit. Overall, 47% (202/430) were defined as Hr-MSM, of whom 89% (179/201) had more than five casual part-ners; 30% (61/202) had receptive CAS with casual partners, and 6% (11/198) were diagnosed with gonorrhoea. Hr-MSM were significantly older (median age 41, IQR 36–45 vs. 39 years, IQR 34–43) and less likely to have a steady partner (51 vs. 24%) than Lr-MSM.
awareness of and beliefs about PreP
Of the 448 participants, 54% (n=242) were aware of PrEP (Table 1). Hr-MSM were more likely to be aware of PrEP than Lr-MSM (60 vs. 50%, respectively; p=0.031). Almost half of MSM aware of PrEP (42%; 102/241) reported the ACS as their chief source of knowledge followed by the internet and a professional healthcare provider (both 10%).
About one-third believed PrEP could significantly reduce the risk of HIV (38%; 168/448) and a comparable proportion was unaware of PrEP efficacy (38%; 169/448). A majority was unaware of PrEP side-effects (66%; 294/448), but of 154 men that were aware 58% believed that side-effects appeared frequently. Beliefs about side-effects did not differ between Hr-MSM and Lr-MSM. MSM believed that PrEP had a high protective effect if always combined with condoms (mean 5.5, standard deviation [SD] 1.7), but only medium effective if some-

Chapter 2.1
46
Table 1. Characteristics, PrEP awareness and beliefs about PrEP according to sexual risk behaviour among 448 HIV-negative MSM participating in the Amsterdam Cohort Studies from June 2012 through January 2013, Amsterdam, the Netherlands
total (N=448)
risk of HIV infectiona
p-value
Lr-msm (n=228)
Hr-msm (n=202)
n % n % n %
age (years)
(Median [IQR]) 40 [34–35] 39 [34–43] 41 [36–45] 0.006b
nationality
Non-Dutch 36 8.2 21 9.3 15 7.6 0.518c
Dutch 404 91.8 204 90.7 183 92.4
educational level
No college degree 43 9.6 23 10.1 18 8.9 0.678c
At least college degree 404 90.4 205 89.9 184 91.1
monthly income level
Low (<1700 Euro) 114 28.7 53 26.0 57 32.2 0.274c
Medium (1701–2950 Euro) 163 41.1 90 44.1 65 36.7
High (>2950 Euro) 120 30.2 61 29.9 55 31.1
steady partner
None 157 36.3 53 24.4 101 51.0 <0.001c
HIV-negative 214 49.4 132 60.8 72 36.4
Positive or unknown HIV status 62 14.3 32 14.7 25 12.6
number of casual sexual partners in the preceding 6 months
(Median [IQR]) 4 [0–11] 0 [0–2] 12 [7–21] NAd
CaS in the preceding 6 months (insertive and/or receptive)
Currently not engaging in CAS 183 41.2 104 45.6 71 35.3 NAd
CAS with steady partner 151 34.0 112 49.1 32 15.9
CAS with casual partner 82 18.5 11 4.8 71 35.3
CAS with steady and casual partner 28 6.3 1 0.4 27 13.4
Gonorrhea at aCs visit
No 423 97.5 228 100.0 187 94.4 NAd
Yes 11 2.5 0 0.0 11 5.6
awareness of PreP
Never heard of PrEP 206 46.0 114 50.0 80 39.6 0.031c
Ever heard of PrEP 242 54.0 114 50.0 123 60.4

47
PrEP awareness and the intention to use PrEP among MSM
2.1
Table 1. (continued)
total (N=448)
risk of HIV infectiona
p-value
Lr-msm (n=228)
Hr-msm (n=202)
n % n % n %
Chief source of knowledge about PrePe
Internet 23 9.5 6 5.3 15 12.3 0.251c
HIV-patient organization 8 3.3 3 2.7 5 4.1
Professional healthcare provider 23 9.5 9 8.0 13 10.7
ACS 102 42.3 54 47.8 46 37.7
Newspaper/TV 17 7.1 8 7.1 9 7.4
Friends/family 21 8.7 8 7.1 13 10.7
Other 16 6.6 11 9.7 5 4.1
Unknown 31 12.9 14 12.4 16 13.1
Beliefs about efficacy of PreP
PrEP can reduce the risk of HIV by 100% 1 0.2 0 0.0 1 0.5 0.100c
PrEP can significantly reduce the risk of HIV 168 37.5 76 33.3 85 42.1
PrEP could slightly reduce the risk of HIV 103 22.9 60 26.3 42 20.8
PrEP does not reduce the risk of HIV 7 1.6 6 2.6 1 0.5
I do not know 169 37.7 86 37.7 73 36.1
Beliefs about side-effects of PreP
Side-effects are rare 2 0.5 1 0.4 1 0.5 0.096c
Side-effects are sometimes reported 46 10.3 20 8.8 23 11.4
Side-effects appear frequently 70 15.6 30 13.2 38 18.8
Knowledge about side-effects is still scarce 36 8.0 14 6.1 21 10.4
I do not know 294 65.6 163 71.5 119 58.9
Beliefs about efficacy of PreP (mean [Sd]) (1. no protection - 7. 100% protection for HIV)
Efficacy when you always use condoms during anal sex 5.5 [1.7] 5.4 [1.8] 5.6 [1.6] 0.114b
Efficacy when you sometimes use condoms during anal sex 3.8 [1.4] 3.5 [1.5] 4.1 [1.3] <0.001b
Efficacy when you never use condoms during anal sex 3.2 [1.5] 3.0 [1.5] 3.4 [1.4] 0.001b
ACS, Amsterdam Cohort Studies; CAS, condomless anal sex; Hr-MSM, MSM at high risk of HIV infection; IQR, interquartile range; Lr-MSM, MSM at low risk of HIV infection; NA, not applicable; PrEP, pre-exposure prophy-laxis; SD, standard deviation.a 18 missing on HIV risk group.b Mann–Whitney U test.c Chi-square test.d We did not test differences for these determinants because they were used to categorize Hr/Lr-MSM.e Measured among MSM aware of PrEP.

Chapter 2.1
48 49
PrEP awareness and the intention to use PrEP among MSM
2.1
times (mean 3.8, SD 1.4) or never (mean 3.2, SD 1.5) combined with condoms. For the last two items, Hr-MSM perceived PrEP to more effective than Lr-MSM (p<0.001).
determinants of intention to use PreP
Of all participants, 27% (n=120) had a low intention, 60% (n=270) a medium intention and 13% (n=58) a high intention to use PrEP. Multivariate multinomial regression analyses includ-ing sociodemographics and sexual (risk) behaviour variables with a univariate p-value <0.10 (Table 2) showed that Hr-MSM and MSM with no steady partner or with a steady partner with a positive or unknown HIV status were more likely to have higher intentions to use PrEP. Educational level became non-significant.
In multivariate analyses including psychosocial determinants with a univariate p-value <0.10 (Table 3), all perceptions, except those concerning worries about PrEP efficacy and about getting HIV-infected when using PrEP, were associated with higher intentions to use PrEP.
In the final combined multivariate model (Table 4), including all variables with a p-value <0.10 from Tables 2 and 3, Hr-MSM were more likely to have a medium (adjusted odds ratio [aOR] 1.78, 95% confidence interval [CI] 1.07–2.97) or high intention to use PrEP (aOR 3.92, 95% CI 1.68–9.15) than Lr-MSM. Sensitivity analyses found that all three separate HIV risk factors defining Hr-MSM (number of casual partners, receptive CAS with casual partners, gonorrhoea diagnosis) were associated with higher intention to use PrEP, but only the number of casual partners was statistically significant (p=0.020, data not shown). The effect of steady partner de-creased and became statistically non-significant. MSM that were aware of PrEP were also more likely to have a high intention to use PrEP (aOR 2.41, 95% CI 1.07–5.45) than those unaware, but the overall effect on intention was not statistically significant (p=0.105). MSM with high per-ceived self-efficacy to use PrEP were more likely to have a high intention to use PrEP (aOR 6.15, 95% CI 2.50–15.09) than MSM with low perceived self-efficacy (overall p<0.001). Furthermore, having higher perceptions of relief when using PrEP was associated with a medium (aOR 2.67, 95% CI 1.32–5.40) and high intention to use PrEP (aOR 14.87, 95% CI 5.98–37.01). Feelings of shame about using PrEP decreased the intention to use PrEP (aOR 0.35, 95% CI 0.19–0.62) for medium and aOR 0.22 (95% CI 0.07–0.71) for high intention], as did worries about side-effects of PrEP (aOR 0.29, 95% CI 0.12–0.72) and aOR 0.18 (95% CI 0.06–0.54), respectively].
anticipated condom use
About one-third of participants (39%; 174/447) anticipated a decrease in their condom use during anal sex while using PrEP (Table 5). In addition, about one-quarter (26%; 115/446) had low perceived self-efficacy to use condoms in combination with PrEP. These proportions were higher among MSM currently having CAS than those currently not having CAS (respec-tively 43 vs. 33%, p=0.038; and 30 vs. 20%, p=0.017). Likewise, proportions of MSM that

Chapter 2.1
48 49
PrEP awareness and the intention to use PrEP among MSM
2.1
Tabl
e 2.
Mul
tinom
ial l
ogisti
c reg
ress
ion
anal
ysis
of d
emog
raph
ic d
eter
min
ants
and
sexu
al b
ehav
iour
ass
ocia
ted
with
the
inte
ntion
to u
se P
rEP
amon
g 44
8 HI
V-ne
gativ
e M
SM
parti
cipa
ting
in th
e Am
ster
dam
Coh
ort S
tudi
es fr
om Ju
ne 2
012
thro
ugh
Janu
ary
2013
, Am
ster
dam
, The
Net
herla
nds
low
inte
ntion
to
use
PreP
(ref
.)
Med
ium
inte
ntion
to u
se P
reP
High
inte
ntion
to u
se P
reP
ove
rall
p-va
luea
n=12
0(n
=270
)(n
=58)
n%
n%
or
(95%
CI)
or
(95%
CI)
n%
or
(95%
CI)
aor
(95%
CI)
age
(yea
rs)
18–3
741
27.3
9462
.71
1510
.0%
1
37–4
339
26.2
8859
.10.
98 (0
.58–
1.67
)22
14.8
%1.
54 (0
.70—
3.40
)
>43
4026
.888
59.1
0.96
(0.5
7–1.
62)
2114
.1%
1.44
(0.6
5–3.
17)
nati
onal
ity
Non
-Dut
ch9
25.0
1952
.81
822
.2%
1
Dutc
h10
826
.724
861
.41.
09 (0
.48–
2.48
)48
11.9
%0.
50 (0
.18–
1.38
)
educ
ation
al l
evel
No
colle
ge d
egre
e7
16.3
2558
.11
111
25.6
%1b
1b
At le
ast c
olle
ge d
egre
e11
227
.724
560
.60.
61 (0
.26–
1.46
)0.
75 (0
.30–
1.83
)47
11.6
%0.
27 (0
.10–
0.73
)0.
35 (0
.12–
1.00
)0.
100
net
mon
thly
inco
me
leve
l
Low
(<17
00 E
uro)
2723
.765
57.0
122
19.3
%1b
Med
ium
(170
1–29
50 E
uro)
4427
.095
58.3
0.90
(0.5
1–1.
59)
2414
.7%
0.67
(0.3
2–1.
42)
High
(>29
50 E
uro)
3428
.378
65.0
0.95
(0.5
2–1.
74)
86.
7%0.
29 (0
.11–
0.75
)
stea
dy p
artn
er
Non
e30
19.1
100
63.7
1.82
(1.1
0–3.
01)
1.50
(0.8
8–2.
55)
2717
.2%
3.94
(1.8
6–8.
35)
2.22
(0.9
9–4.
95)
HIV-
nega
tive
7032
.712
859
.81b
116
7.5%
1d1b
0.04
4
Positi
ve o
r unk
now
n HI
V st
atus
1422
.634
54.8
1.33
(0.6
7–2.
64)
1.29
(0.6
1–2.
70)
1422
.6%
4.38
(1.7
5–10
.96)
3.74
(1.4
0–9.
96)
HIV
risk
beha
viou
r gro
up
Lr-M
SM73
32.3
133
58.8
1b1b
208.
8%1c
1c0.
016
Hr
-MSM
4019
.6
129
63.2
1.72
(1.0
9–2.
71)
1.63
(1.0
1–2.
66)
35
17.2
%3.
19 (1
.63–
6.25
)2.
78 (1
.36–
5.70
)
aOR,
adj
uste
d od
ds ra
tio; C
I, co
nfide
nce
inte
rval
; Hr-M
SM, m
en h
avin
g se
x w
ith m
en a
t hig
h ris
k of
HIV
infe
ction
; Lr-M
SM, m
en h
avin
g se
x w
ith m
en a
t low
risk
of H
IV in
fec-
tion;
OR,
odd
s rati
o; P
rEP,
pre
-exp
osur
e pr
ophy
laxi
s.a O
vera
ll p-
valu
e of
hig
her i
nten
tion
in a
djus
ted
anal
yses
, b p<0.
05, c p<
0.01
, d p<0.
001

Chapter 2.1
50
Tabl
e 3.
Mul
tinom
ial l
ogisti
c re
gres
sion
anal
ysis
of p
sych
osoc
ial d
eter
min
ants
ass
ocia
ted
with
the
inte
ntion
to u
se P
rEP
amon
g 44
8 HI
V-ne
gativ
e M
SM p
artic
ipati
ng in
the
Amst
erda
m C
ohor
t Stu
dies
from
June
201
2 th
roug
h Ja
nuar
y 20
13, A
mst
erda
m, T
he N
ethe
rland
slo
w in
tenti
on to
us
e Pr
eP (r
ef.)
Med
ium
inte
ntion
to u
se P
reP
High
inte
ntion
to u
se P
reP
n=12
0n=
270
n=58
ove
rall
p-va
luec
n%
n%
or
(95%
CI)
aor
(95%
CI)
n%
or
(95%
CI)
aor
(95%
CI)
PreP
aw
aren
ess (
awar
e vs
. una
war
e)
Awar
e of
PrE
P55
22.7
147
60.7
1.41
(0.9
2–2.
17)
1.39
(0.8
8–2.
18)
4016
.52.
63 (1
.36–
5.09
)e2.
71 (1
.27–
5.77
)d0.
035
Perc
eive
d se
lf-effi
cacy
(hig
h vs
. low
)
High
per
ceiv
ed se
lf-effi
cacy
to u
se P
rEP
1718
.746
50.5
b1.
27 (0
.69–
2.32
)1.
06 (0
.57–
1.99
)28
30.8
5.66
(2.7
3–11
.70)
f3.
94 (1
.74–
8.90
)e<0
.001
High
per
ceiv
ed se
lf-effi
cacy
to u
se P
rEP
ev
ery
day
on ti
me
3423
.9a
8761
.3a
1.20
(0.7
5–1.
92)
2114
.81.
42 (0
.73–
2.77
)
High
per
ceiv
ed se
lf-effi
cacy
to p
ay fo
r PrE
P (5
0–10
00eu
ro/m
onth
)18
24.0
a47
62.7
a1.
19 (0
.66–
2.15
)10
13.3
1.17
(0.5
0–2.
72)
Perc
eive
d em
otion
al im
pact
of P
reP
(hig
h vs
. low
)
High
per
cepti
on o
f wor
ry a
bout
PrE
P sid
e-eff
ects
112
30.3
a21
959
.20.
27 (0
.12–
0.61
)e0.
40 (0
.15–
1.07
)39
10.5
0.13
(0.0
5–0.
33)f
0.22
(0.0
7–0.
74)d
0.05
1
High
per
cepti
on o
f wor
ry a
bout
PrE
P effi
cacy
107
30.0
a20
958
.50.
38 (0
.20–
0.74
)e0.
64 (0
.29–
1.41
)41
11.5
0.27
(0.1
2–0.
62)e
0.70
(0.2
3–2.
09)
0.53
8
High
per
cepti
on o
f dec
reas
ed w
orry
abo
ut
getti
ng H
IV in
fect
ed w
hen
usin
g Pr
EP46
25.0
a10
557
.11.
01 (0
.65–
1.57
)1.
05 (0
.66–
1.68
)33
17.9
2.09
(1.1
1–3.
96)d
1.70
(0.8
1–3.
58)
0.33
0
High
per
cepti
on o
f sha
me
abou
t usin
g Pr
EP35
44.3
a38
48.1
0.39
(0.2
3–0.
66)f
0.40
(0.2
3–0.
68)e
67.
60.
28 (0
.11–
0.70
)e0.
27 (0
.09–
0.76
)d0.
002
Hi
gh p
erce
ption
of r
elie
f whe
n us
ing
PrEP
1513
.3a
61
54.0
a2.
03 (1
.10–
3.75
)d2.
11 (1
.11–
4.00
)d
3732
.7a
12.8
3 (5
.95–
27.6
3)f
11.1
0 (4
.83–
25.5
0)f
<0.0
01
aOR,
adj
uste
d od
ds ra
tio; C
I, co
nfide
nce
inte
rval
; MSM
, men
who
hav
e se
x w
ith m
en; O
R, o
dds r
atio;
PrE
P, p
re-e
xpos
ure
prop
hyla
xis.
a 1
miss
ing
excl
uded
.b
4 m
issin
gs e
xclu
ded.
c O
vera
ll p-
valu
e ad
just
ed a
naly
ses.
d p<
0.05
.e
p<0.
01.
f p<
0.00
1.

51
PrEP awareness and the intention to use PrEP among MSM
2.1
anticipated less condom use while using PrEP and that perceived a low self-efficacy to use condoms increased with increasing intention to use PrEP (35–52%, p=0.090 and 21–45%, p=0.002, respectively).
Influence of PreP characteristics among MSM with a high intention to use PreP
In total, 58 men had a high intention to use PrEP, of whom a majority was willing to take PrEP daily for 3 (88%), 6 months (85%), or 1 year (74%), and about half even for 5 (59%) or 10 years (52%). There were 32 MSM (55%) who were willing to use PrEP when having to pay. Willingness to use PrEP decreased with increasing costs: 55% would take PrEP at €50 per month, but only 3% remained willing at €1000 per month. Finally, 23 MSM (40%) remained willing to take PrEP even if it were less than 100% effective.
Table 4. Multinomial logistic regression analysis of sexual behaviour and psychosocial determinants associ-ated with the intention to use PrEP among 448 HIV-negative MSM participating in the Amsterdam Cohort Studies from June 2012 through January 2013, Amsterdam, The Netherlands
Medium intention to use PrePa
High intention to use PrePa
aor (95% CI) aor (95% CI) overall p-valueb
Sexual behaviour
steady partner
None 1.38 (0.80–2.39) 2.19 (0.87–5.47)
HIV-negative 1 1 0.260
Positive or unknown HIV status 0.86 (0.39–1.89) 2.06 (0.68–6.28)
HIV risk behaviour group
Lr-MSM 1c 1d
Hr-MSM 1.78 (1.07–2.97) 3.92 (1.68–9.15) 0.005
Psychosocial determinants
PreP awareness (aware vs. unaware)
Aware of PrEP 1.27 (0.78–2.06) 2.41 (1.07–5.45)c 0.105
Perceived self-efficacy (high vs. low)
High perceived self-efficacy to use PrEP 1.25 (0.64–2.45) 6.15 (2.50–15.09)e <0.001
Perceived emotional impact of PreP (high vs. low)
High perception of worry about PrEP side-effects 0.29 (0.12–0.72)d 0.18 (0.06–0.54)d 0.008
High perception of shame about using PrEP 0.35 (0.19–0.62)e 0.22 (0.07–0.71)c <0.001
High perception of relief when using PrEP 2.67 (1.32–5.40)d 14.87 (5.98–37.01)e <0.001
aOR, adjusted odds ratio; CI, confidence interval; Hr-MSM, men having sex with men at high risk of HIV infec-tion; Lr-MSM, men having sex with men at low risk of HIV infection; PrEP, pre-exposure prophylaxis.a Ref. low intention to use PrEP.b Overall p-value adjusted analyses.c p<0.05.d p<0.01.e p<0.001.

Chapter 2.1
52
dISCuSSIon
This is the first study focusing on awareness of PrEP and intention to use PrEP among Dutch MSM. About half of the MSM in the ACS were aware of PrEP; most MSM were unaware of PrEP side-effects, and only 13% had a high intention to use PrEP. High-risk sexual behaviour was independently associated with a higher intention, as were psychosocial determinants such as high perceived self-efficacy and high perceptions of relief when using PrEP. Feel-ings of shame about using PrEP, worries about side-effects and PrEP characteristics, such as increasing costs and perceived insufficient efficacy were found to decrease the intention to use PrEP.
Compared with other studies from high-income countries, where proportions of a high intention to use PrEP ranged between 28 and 74%,10-18 our proportion of 13% was relatively low. These differences are unlikely to be explained by differences in behavioural characteris-tics as study populations seem similar. This finding suggests that acceptability of PrEP might currently be lower in the Netherlands than elsewhere, possibly explained by differences in PrEP knowledge.
Previous cost-effectiveness studies show that PrEP is most likely to be beneficial when target-ing Hr-MSM, but the effect depends highly on uptake, adherence, frequency of monitoring and duration of PrEP use.19-23 We found Hr-MSM more often aware and more likely to have a higher intention to use PrEP, which implies that PrEP acceptability is higher among those who could benefit most from PrEP. MSM with an HIV-positive steady partner likewise had higher intentions to use PrEP, but this association became statistically non-significant in the
Table 5. Anticipated condom use while using PrEP based on current condom use and the intention to use PrEP among 448 HIV-negative MSM participating in the Amsterdam Cohort Studies from June 2012 through Janu-ary 2013, Amsterdam, The Netherlands
anticipated decrease incondom use while using PreP
low perceived self-efficacy to use condoms while using PreP
n/N % p-value n/N % p-value
total 174/447 38.9 115/446 25.8
Cas in the preceding 6 months
Currently not engaging in CAS 61/183 33.3 0.038 36/183 19.7 0.017
Currently engaging in CAS 112/260 43.1 77/259 29.7
Intention to use PreP
Low 42/119 35.3 0.09 25/119 21.0 0.002
Medium 102/270 37.8 64/269 23.8
High 30/58 51.7 26/58 44.8
CAS, condomless anal sex; MSM, men who have sex with men; PrEP, pre-exposure prophylaxis.

53
PrEP awareness and the intention to use PrEP among MSM
2.1
final model. Interestingly, additional analyses (based on Baron and Kenny’s steps of media-tion, 1986)24 found that higher perceptions of relief when using PrEP partially mediated the effect of having an HIV-positive partner on the intention to use PrEP, suggesting that relief provided by PrEP is key in making PrEP attractive for serodiscordant couples. Whether it is relief from fear of HIV infection or relief of not having to use condoms should be further explored. The relevance of PrEP in the context of serodiscordant relationships might change in the near future as growing evidence, also among MSM, suggests that successful treatment of HIV-positive persons can significantly reduce the risk of HIV transmission to HIV-negative partners (i.e. treatment as prevention).25-27 This could make the future need of using PrEP in serodiscordant relationships redundant when the HIV-positive partner is successfully treated.
A concern with the introduction of PrEP is that its use could lead to a decrease in condom use, which could counteract the impact of PrEP on HIV incidence.19-23 Similar effects were found with the introduction of ART, when strong increases in sexual risk behaviour and STI were seen.28 This study indeed found indications that MSM would not use PrEP and condoms si-multaneously. Overall, about one-third of our participants would decrease condom use while using PrEP, and this proportion was higher among those with higher intentions to use PrEP and those currently engaging in CAS. An anticipated decrease in condom use was observed, to various degrees, in previous studies among MSM in New York City, Australia, and Beijing.10,14,29 These findings emphasize the importance of integrating PrEP into routine STI screening and counselling consults, with an additional focus on PrEP adherence and continued condom use to prevent STI. Also, PrEP should be prioritized for Hr-MSM who are currently using condoms inconsistently, as PrEP could be their first workable HIV prevention method.30
In this study, we found psychosocial determinants and PrEP characteristics to be barriers for the intention to use PrEP. Therefore, if PrEP use in the Netherlands becomes a reality, successful uptake will depend on successfully addressing feelings of shame about using PrEP among those eligible for PrEP, the provision of clear information on PrEP efficacy and side-effects and the extent of PrEP cost coverage by insurance companies or other sources of cost coverage. As actual uptake of PrEP will most likely also be influenced by a variety of other factors, such as healthcare provider attitudes and the accessibility of PrEP resources, these factors should also be addressed alongside implementing cues to action.6,7
Some limitations need to be addressed. First, our study population consisted mainly of highly educated, native Dutch MSM who might not represent the nationwide MSM popu-lation. However, sexual risk behaviour, age, and origin among ACS participants have been similar to MSM participants in nationwide monitoring studies on homosexuality, health and well being.31 Second, our study population was most likely more informed about PrEP than the general MSM population, as participants aware of PrEP reported the ACS as their

Chapter 2.1
54
chief knowledge source. On the contrary, we gave participants little information about PrEP before asking about PrEP. Although half of them had heard of PrEP, the rest had to speculate about its efficacy and potential side-effects that might have influenced their responses.
In conclusion, although about half of the HIV-negative MSM in this Amsterdam Cohort was aware of PrEP, the intention to use PrEP was relatively low. Interestingly, both were significantly higher among the potential target group of PrEP: MSM at higher risk of HIV infection. When PrEP implementation starts in the Netherlands, PrEP costs and psychosocial determinants will influence acceptability and uptake of PrEP and should therefore be ad-dressed in targeted information campaigns. Importantly, PrEP implementation should be combined with other HIV and STI prevention strategies such as condom use, increasing HIV testing and applying treatment as prevention as only a combined approach would most likely be effective in further decreasing HIV incidence and preventing an attendant rise in STI transmission.32,33
acknowledgements
The authors acknowledge all participants of the ACS for their contribution, research nurses of the ACS Marc van Wijk and Marjolein Martens for data collection and cohort manage-ment, Gerben-Rienk Visser and Linda May for data management, Ronald Geskus for statisti-cal advice and Lucy Phillips for editing the final article.
funding
Fund for the present study was received from the Research and Development Funds of the Public Health Service Amsterdam (project number KP2657). The Amsterdam Cohort Studies (ACS) on HIV Infection and AIDS are part of the Netherlands HIV Monitoring Foundation and are financially supported by the Netherlands National Institute for Public Health and the Environment. The ACS are a collaboration of the Public Health Service Amsterdam, the Aca-demic Medical Center of the University of Amsterdam, Sanquin Blood Supply Foundation, and the University Medical Center of Utrecht. The funders of the present study had no role in its design, data collection and analysis, decision to publish, or preparation of the article.
Conflicts of interest
There are no conflicts of interest.

55
PrEP awareness and the intention to use PrEP among MSM
2.1
referenCes
1. European Centre for Disease Prevention and Control (ECDC), World Health Organization (WHO) Regional Office for Europe. HIV/aIdS surveillance in europe 2012. Stockholm: ECDC, 2013.
2. van Sighem A, Gras L, Kesselring A, Smit C, Engelhard E, Stolte IG, et al. Monitoring report 2013: Human Immunodeficiency Virus (HIV) infection in the netherlands. Amsterdam: Stichting HIV moni-toring, 2013.
3. Jansen IA, Geskus RB, Davidovich U, Jurriaans S, Coutinho RA, Prins M, et al. ongoing HIV-1 transmis-sion among men who have sex with men in amsterdam: a 25-year prospective cohort study. AIDS. 2011;25(4):493-501. doi:10.1097/QAD.0b013e328342fbe9.
4. Grant RM, Lama JR, Anderson PL, McMahan V, Liu AY, Vargas L, et al. Preexposure chemoprophy-laxis for HIV prevention in men who have sex with men. N Engl J Med. 2010;363(27):2587-2599. doi:10.1056/NEJMoa1011205.
5. Smith DK, Grant RM, Weidle PJ, Lansky A, Mermin J, Fenton KA. Interim Guidance: Preexposure Prophylaxis for the Prevention of HIV infection in Men Who Have Sex with Men. CDC Morbidity and Mortality Weekly Report (MMWR). 2011;60(03):65-68.
6. Bartholomw LK, Parcel GS, Kok G, Gottlieb NH, Fernandez ME. Planning health promotion programs, an intervention mapping approach. San Francisco: Jossey-Bass, 2011.
7. Glanz K, Rimer BK, Viswanath K. Health Behavior and Health education: Theory, research, and prac-tice. San Francisco, CA: Jossey-Bass, 2008.
8. Stolte IG, Prins M. The amsterdam Cohort Studies on HIV infection - annual report 2012. In: van Sighem A, Gras L, Kesselring A, Smit C, Engelhard E, Stolte I, et al., eds. Monitoring Report 2013: Human Immunodeficiency Virus (HIV) Infection in the Netherlands. Amsterdam: Stichting HIV moni-toring, 2013.
9. van Griensven GJ, de Vroome EM, Goudsmit J, Coutinho RA. Changes in sexual behaviour and the fall in incidence of HIV infection among homosexual men. BMJ. 1989;298(6668):218-221. doi: 10.1136/bmj.298.6668.218.
10. Golub SA, Kowalczyk W, Weinberger CL, Parsons JT. Preexposure prophylaxis and predicted condom use among high-risk men who have sex with men. J Acquir Immune Defic Syndr. 2010;54(5):548-555. doi:10.1097/QAI.0b013e3181e19a54.
11. Mimiaga MJ, Case P, Johnson CV, Safren SA, Mayer KH. Preexposure antiretroviral prophylaxis attitudes in high-risk Boston area men who report having sex with men: limited knowledge and experience but potential for increased utilization after education. J Acquir Immune Defic Syndr. 2009;50(1):77-83. doi:10.1097/QAI.0b013e31818d5a27.
12. Krakower DS, Mimiaga MJ, Rosenberger JG, Novak DS, Mitty JA, White JM, et al. limited awareness and low Immediate uptake of Pre-exposure Prophylaxis among Men Who Have Sex with Men using an Internet Social networking Site. PLoS One. 2012;7(3):e33119. doi:10.1371/journal.pone.0033119.
13. Barash EA, Golden M. awareness and use of HIV pre-exposure prophylaxis among attendees of a Seattle gay pride event and sexually transmitted disease clinic. AIDS Patient Care STDS. 2010;24(11):689-691. doi:10.1089/apc.2010.0173.
14. Holt M, Murphy DA, Callander D, Ellard J, Rosengarten M, Kippax SC, et al. Willingness to use HIV pre-exposure prophylaxis and the likelihood of decreased condom use are both associated with un-protected anal intercourse and the perceived likelihood of becoming HIV positive among australian gay and bisexual men. Sex Transm Infect. 2012;88(4):258-263. doi:10.1136/sextrans-2011-050312.

Chapter 2.1
56
15. Leonardi M, Lee E, Tan DH. awareness of, usage of and willingness to use HIV pre-exposure prophy-laxis among men in downtown Toronto, Canada. Int J STD AIDS. 2011;22(12):738-741. doi:10.1258/ijsa.2011.011057.
16. Golub SA, Gamarel KE, Rendina HJ, Surace A, Lelutiu-Weinberger CL. From efficacy to effectiveness: facilitators and barriers to PreP acceptability and motivations for adherence among MSM and transgender women in new York City. AIDS Patient Care STDS. 2013;27(4):248-254. doi:10.1089/apc.2012.0419.
17. Mustanski B, Johnson AK, Garofalo R, Ryan D, Birkett M. Perceived likelihood of using HIV pre-exposure prophylaxis medications among young men who have sex with men. AIDS Behav. 2013;17(6):2173-2179. doi:10.1007/s10461-012-0359-y.
18. Young I, McDaid L. How acceptable are antiretrovirals for the Prevention of Sexually Transmitted HIV?: a review of research on the acceptability of oral Pre-exposure Prophylaxis and Treatment as Prevention. AIDS Behav. 2013 doi:10.1007/s10461-013-0560-7.
19. Gomez GB, Borquez A, Case KK, Wheelock A, Vassall A, Hankins C. the cost and impact of scaling up pre-exposure prophylaxis for HIV prevention: a systematic review of cost-effectiveness modelling studies. PLoS Med. 2013;10(3):e1001401. doi:10.1371/journal.pmed.1001401.
20. Paltiel AD, Freedberg KA, Scott CA, Schackman BR, Losina E, Wang B, et al. HIV preexposure prophy-laxis in the united States: impact on lifetime infection risk, clinical outcomes, and cost-effectiveness. Clin Infect Dis. 2009;48(6):806-815. doi:10.1086/597095.
21. Schackman BR, Eggman AA. Cost-effectiveness of pre-exposure prophylaxis for HIV: a review. Curr Opin HIV AIDS. 2012;7(6):587-592. doi:10.1097/COH.0b013e3283582c8b.
22. Juusola JL, Brandeau ML, Owens DK, Bendavid E. The cost-effectiveness of preexposure prophy-laxis for HIV prevention in the united States in men who have sex with men. Ann Intern Med. 2012;156(8):541-550. doi:10.7326/0003-4819-156-8-201204170-00001.
23. Desai K, Sansom SL, Ackers ML, Stewart SR, Hall HI, Hu DJ, et al. modeling the impact of HIV chemo-prophylaxis strategies among men who have sex with men in the united States: HIV infections pre-vented and cost-effectiveness. AIDS. 2008;22(14):1829-1839. doi:10.1097/QAD.0b013e32830e00f5.
24. Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173-1182. doi:10.1037/0022-3514.51.6.1173.
25. Quinn TC, Wawer MJ, Sewankambo N, Serwadda D, Li C, Wabwire-Mangen F, et al. Viral load and heterosexual transmission of human immunodeficiency virus type 1. rakai Project Study Group. N Engl J Med. 2000;342(13):921-929. doi:10.1056/NEJM200003303421303.
26. Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493-505. doi:10.1056/NEJMoa1105243.
27. Rodger A, Bruun T, Cambiano V, Vernazza P, strada V, Van Lunzen J, et al. HIV transmission risk Through Condomless Sex If HIV+ Partner on Suppressive arT: ParTner Study [abstract 153lB]. 21ste Conference on Retroviruses and Oppotunistic Infections: Boston, USA, 3-6 March 2014.
28. Stolte IG, Dukers NH, Geskus RB, Coutinho RA, de Wit JB. Homosexual men change to risky sex when perceiving less threat of HIV/aIdS since availability of highly active antiretroviral therapy: a longitu-dinal study. AIDS. 2004;18(2):303-309. doi:10.1097/00002030-200401230-00021.
29. Zhou F, Gao L, Li S, Li D, Zhang L, Fan W, et al. Willingness to accept HIV pre-exposure prophy-laxis among Chinese men who have sex with men. PLoS One. 2012;7(3):e32329. doi:10.1371/annotation/8d587ce6-3695-4028-8f2d-3a3c10d489b6.

57
PrEP awareness and the intention to use PrEP among MSM
2.1
30. Grant RM, Anderson PL, McMahan V, Liu A, Amico KR, Mehrotra M, et al. uptake of pre-exposure prophylaxis, sexual practices, and HIV incidence in men and transgender women who have sex with men: a cohort study. Lancet Infect Dis. 2014;14(9):820-829. doi:10.1016/S1473-3099(14)70847-3.
31. van Empelen P, van Berkel M, Roos E, Zuilhof W. Schorer Monitor 2011. Amsterdam: Schorer, 2011. 32. Cremin I, Alsallaq R, Dybul M, Piot P, Garnett G, Hallett TB. The new role of antiretrovirals in combina-
tion HIV prevention: a mathematical modelling analysis. AIDS. 2013;27(3):447-458. doi:10.1097/QAD.0b013e32835ca2dd.
33. van Sighem A, van den Hengel R, Bezemer D, de Wolf F. Pre-exposure prophylaxis versus ‘test and treat’ amongst men who have sex with men in the netherlands [abstract]. 3rd International HIV Workshop on Treatment as Prevention: Vancouver, BC, Canada, 22-25 April 2013.


Chapter 2.2Motives of dutch men who have sex
with men for daily and intermittent HIV pre-exposure prophylaxis usage and
preferences for implementation: A qualitative study
Janneke P. Bil, Wendy M. van der Veldt, Maria Prins, Ineke G. Stolte*, Udi Davidovich*
* Both authors contributed equally to this article
Published in Medicine, 2016; 95(39):e4910

Chapter 2.2
60
aBstraCt
Although PrEP is not yet registered in Europe, including the Netherlands, its approval and implementation are expected in the near future. To inform future pre-exposure prophylaxis (PrEP) implementation, this study aimed to gain insight into motives and preferences for daily or intermittent PrEP use among Dutch HIV-negative men who have sex with men (MSM).
Between February and December 2013, semistructured interviews were conducted until data saturation was reached (N=20). Interviews were analysed using the Grounded Theory approach.
Motives for (not) using daily PrEP were based on beliefs about PrEP efficacy and side effects, preferences for other prevention strategies, self-perceived HIV risk, self-perceived efficacy of PrEP adherence, beliefs about possible benefits (e.g., anxiety reduction, sex life improve-ment) and barriers of PrEP use (e.g., costs, monitoring procedures). The perceived benefits of intermittent versus daily PrEP use were the lower costs and side effects and the lower threshold to decision to start using intermittent PrEP. Barriers of intermittent PrEP versus daily PrEP use were the perceived need to plan their sex life and adhere to multiple preven-tion strategies. Although some perceived PrEP as a condom substitute, others were likely to combine PrEP and condoms for sexually transmitted infections (STI) prevention and increased HIV protection. Participants preferred PrEP service locations to have specialized knowledge of HIV, antiretroviral therapy, sexual behaviour, STIs, patients’ medical background, be easily approachable, be able to perform PrEP follow-up monitoring, and provide support.
To maximize the public health impact of PrEP, ensuring high uptake among MSM at highest risk is important. Therefore, targeted information about PrEP efficacy and side effects need to be developed, barriers for accessing PrEP services should be minimized, and perceived self-efficacy to use PrEP should be addressed and improved. To prevent increases in STIs, condom use should be monitored and PrEP should be integrated into routine STI screening and counselling.

61
Motives for PrEP usage among MSM
2.2
InTroduCTIon
HIV transmission among men who have sex with men (MSM) continues, despite widespread implementation of behavioural interventions and high coverage of antiretroviral therapy (ART).1-4 Recent studies have shown that pre-exposure prophylaxis (PrEP), that is, offering HIV-negative MSM a daily or intermittent regime of lower-intensity ART, can significantly reduce risk of HIV infection.5-7 The US Food and Drug Administration approved PrEP, and the Centers for Disease Control and Prevention (CDC) and the World Health Organization implemented daily PrEP for high-risk MSM in their HIV guidelines.8 Although PrEP is not yet registered in Europe, including the Netherlands, its approval and implementation are expected in the near future.
The cost-effectiveness of PrEP and its impact on HIV incidence will highly depend on PrEP uptake among MSM at increased risk of HIV infection, PrEP costs, epidemic context, and adherence.9-14 Regarding uptake, it is important to understand why MSM would choose to use or not use PrEP. Though several qualitative and quantitative studies have been conducted out-side Europe regarding possible motives for PrEP use among MSM,15-21 only one (quantitative) study included European MSM. In this study the intention to use PrEP was relatively low, but higher among high-risk MSM, those with a high perceived self-efficacy to use PrEP, and high perceptions of anticipated relief when using PrEP.22 To inform future PrEP implementation in the Netherlands, in-depth understanding of motives behind PrEP use among Dutch MSM is needed. In particular, knowledge regarding specific motives for intermittent versus daily PrEP use and preferred PrEP service characteristics. These results can guide future implementation strategies to ensure high uptake of PrEP and maximize PrEP’s public health impact.
This qualitative study aims to explore more thoroughly the motives for wanting or not want-ing to use PrEP if it becomes available, motives for daily versus intermittent PrEP use, the anticipated motives for condom use when using PrEP, and preferences for PrEP implementa-tion (e.g., service characteristics).
MeTHodS
recruitment
Participants were recruited through the Amsterdam Cohort Studies (ACS). The ACS is an open, prospective cohort study initiated in 1984 aiming to investigate HIV epidemiology, natural history, pathogenesis, and evaluate the effect of interventions among MSM.23,24 Participants visit the Pub-lic Health Service Amsterdam biannually to complete self-administrated questionnaires on sexual behaviour and give blood for HIV and sexually transmitted infection (STI) testing and storage.

Chapter 2.2
62
To identify eligible participants, we used quantitative data regarding awareness, beliefs, and intention to use PrEP obtained among HIV-negative participants during one wave (June 2012–January 2013).22 For the present study we included: MSM with a high intention to use PrEP (irrespective of HIV risk and type of steady partner); and MSM with a low intention to use PrEP who have been defined as eligible candidates for PrEP,8,9 that is, MSM at increased risk for HIV (having >5 casual partners and/or reporting condomless anal sex with casual partners in the preceding six months) and HIV-negative MSM in serodiscordant relation-ships. To increase the group of MSM with a high intention to use PrEP, we placed online advertisements on the Public Health Service of Amsterdam website and on two HIV informa-tion websites to find men interested in using PrEP in the future. Recruitment continued until data saturation was reached.
The ACS research nurse contacted eligible ACS participants by phone, email, or person-ally during their biannual ACS visit for participation in this study. Those who accepted to participate in the study where then contacted by the researcher. The researcher contacted participants recruited through websites directly.
Procedure
Semistructured interviews of approximately 60 minutes each were conducted between February and December 2013 by one female interviewer (JPB, PhD-student) in Dutch or English at the Public Health Service of Amsterdam or at the participants’ homes. Before the interviews, participants received study information, including study purpose, a short de-scription of daily PrEP, the iPrEX study results on effectiveness and side effects,5 CDC recom-mendations on PrEP follow-up check-ups,8 and the estimated Dutch costs of PrEP (tenofovir disoproxyl fumarate/emtricitabine: approximately €580 monthly). During one interview, the participant’s steady partner was present.
As this study was conducted before the IPERGAY trial indicated PrEP can be effectively taken up to two hours before a risk episode,7 we defined intermittent PrEP as using PrEP three days before until three days after a high-risk period of sexual behaviour, which was explained during the interview. Before the start of the interview, the interviewer introduced herself, the study purpose and interview procedure were explained, and oral informed consent was obtained. Information regarding level of education, income, age, most recent HIV-test result and test location, and relationship status (having a steady partner and HIV-status of steady partner) were obtained at the start of the interview and recorded on tape.
The central interview topics were: intention to use PrEP in the future, reasons for wanting or not wanting to use daily PrEP, and perceived benefits and barriers of using PrEP. The following topics were also addressed: motives for wanting or not wanting to use intermittent

63
Motives for PrEP usage among MSM
2.2
PrEP, perceived motives for using or not using condoms when using PrEP, and opinions about preferred PrEP services (location of PrEP prescription and service characteristics).
All interviews were audiotaped and transcribed verbatim (quotes are translated) and short-field notes were made during and shortly after the interviews. Person identifiers were deleted from the transcripts and only the involved interviewer had access to the audiotapes. Participants received a gift certificate of €20 for participating.
Ethical approval by an ethics committee or institutional review board was not necessary for this study according to Dutch legislation as participants were not subjected to procedures or rules of behaviour which resulted in an infringement of the physical and/or psychological integrity of the participant.25
analyses
The data analysis team consisted of four researchers from different disciplines (health sci-ences [JPB, IGS], medical anthropology [WMvdV], epidemiology [IGS], and psychology [UD]). Data analysis was done in accordance with the Grounded Theory approach and consisted of three phases.26-28 First, JPB and WMvdV independently read and coded (open and inductive) each transcript. Labelling was concise and self-explanatory and discussed until consensus was reached. Second, after developing the provisional coding scheme, codes were com-bined into categories. Third, core themes were defined in which categories could be placed. Core themes consisted of at least one category. Categories and core themes emerged from discussions with the complete data analysis team. Analyses were performed using MAXQDA 11.0.6 (Verbi GmbH, Berlin).
reSulTS
sample characteristics
A total of 20 interviews were conducted after which data saturation was reached. Seven-teen MSM were recruited through the ACS. Response rate among ACS participants was 44% (17/39). Three MSM were recruited online. Participants had a median age of 41 years (interquartile range 38–46), 80% lived in Amsterdam, 65% were college graduates, and 45% had a high annual income level (>€33,000) according to Dutch standards.29 Regarding steady relationships, 45% had no steady partner, 35% had an HIV-positive partner, and 15% had an HIV-negative steady partner. The HIV status of one participant’s steady partner was not asked. Eight MSM expressed a high intention to use daily PrEP if it becomes available, 10 expressed a low intention, and two were in doubt about their future PrEP use.

Chapter 2.2
64
daily PreP
We identified eight motives for wanting to use daily PrEP if it becomes available (Table 1):1. Daily PrEP can protect against possible HIV infection: Some participants believed that
PrEP could give them the desired (additional) protection to prevent HIV infection (quote 1A, 1B). Also, some participants stated that PrEP would provide the opportunity to pre-vent the spread of HIV to others (quote 1C).
2. Daily PrEP in combination with other protection strategies offers complete coverage against HIV infection: Some participants believed that HIV protection of other prevention strategies was insufficient because of their self-perceived high HIV risk (quote 2A), they thought condoms could break or HIV could be transmitted in ways other than anal sex (quote 2B, 2C). Adding PrEP to their prevention strategies would provide the feeling of complete coverage.
3. Daily PrEP offers additional protection for discordant couples: Participants in serodiscor-dant steady relationships stated being worried about getting HIV from their HIV-positive steady partner. PrEP use, in combination with an undetectable viral load from their partner, would increase their perceived protection against HIV infection (quote 3A, 3B).
4. Daily PrEP reduces anxiety about HIV transmission: Because participants believed that PrEP could offer them (additional) protection against HIV infection, they believed that PrEP could increase their feeling of safety and reduce their anxiety of contracting HIV (quote 2A, 2B, 3A, 3B).
5. Daily PrEP is easier to use than condoms: Some participants stated different reasons why using condoms was difficult for them (quote 5A, 5B). The perceived advantage of daily PrEP is its continuous protection against HIV and the increase of participants’ self-perceived efficacy to adhere to PrEP.
6. Daily PrEP can improve quality of sex life: Some participants felt PrEP would facilitate condomless sex or decrease HIV anxiety, which would increase the potential to experi-ment with sex (quote 6A), increase their own or their partners’ sexual pleasure (quote 6B), and improve the quality of their sex life (quote 6C).
7. Daily PrEP makes engaging in (sexual) relationships with a potential HIV-positive partner easier: For some participants, a barrier for engaging in a steady relationship with an HIV-positive person is the necessity to use condoms during sex as this reduces the feeling of intimacy (quote 7A). As PrEP would reduce the need for condoms, they would feel free to engage in a serodiscordant relationship (quote 7B).
8. Daily PrEP provides solidarity with HIV-positive partner: Some participants stated that PrEP would offer them the opportunity to support their HIV-positive partner in taking daily ART (quote 8A).
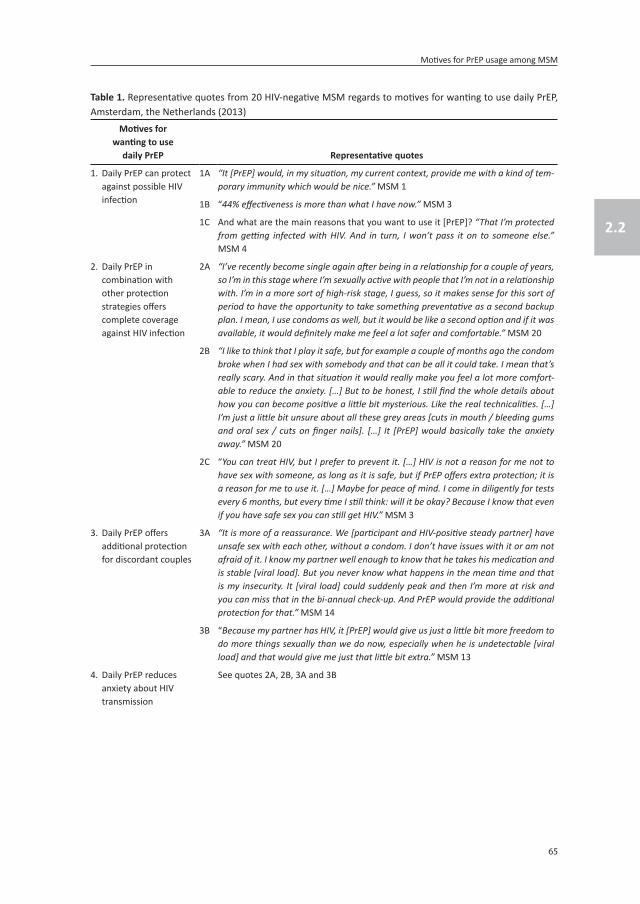
65
Motives for PrEP usage among MSM
2.2
Table 1. Representative quotes from 20 HIV-negative MSM regards to motives for wanting to use daily PrEP, Amsterdam, the Netherlands (2013)
Motives for wanting to use
daily PreP representative quotes
1. Daily PrEP can protect against possible HIV infection
1A “It [PrEP] would, in my situation, my current context, provide me with a kind of tem-porary immunity which would be nice.” MSM 1
1B “44% effectiveness is more than what I have now.” MSM 3
1C And what are the main reasons that you want to use it [PrEP]? “That I’m protected from getting infected with HIV. And in turn, I won’t pass it on to someone else.” MSM 4
2. Daily PrEP in combination with other protection strategies offers complete coverage against HIV infection
2A “I’ve recently become single again after being in a relationship for a couple of years, so I’m in this stage where I’m sexually active with people that I’m not in a relationship with. I’m in a more sort of high-risk stage, I guess, so it makes sense for this sort of period to have the opportunity to take something preventative as a second backup plan. I mean, I use condoms as well, but it would be like a second option and if it was available, it would definitely make me feel a lot safer and comfortable.” MSM 20
2B “I like to think that I play it safe, but for example a couple of months ago the condom broke when I had sex with somebody and that can be all it could take. I mean that’s really scary. And in that situation it would really make you feel a lot more comfort-able to reduce the anxiety. […] But to be honest, I still find the whole details about how you can become positive a little bit mysterious. Like the real technicalities. […] I’m just a little bit unsure about all these grey areas [cuts in mouth / bleeding gums and oral sex / cuts on finger nails]. […] It [PrEP] would basically take the anxiety away.” MSM 20
2C “You can treat HIV, but I prefer to prevent it. […] HIV is not a reason for me not to have sex with someone, as long as it is safe, but if PrEP offers extra protection; it is a reason for me to use it. […] Maybe for peace of mind. I come in diligently for tests every 6 months, but every time I still think: will it be okay? Because I know that even if you have safe sex you can still get HIV.” MSM 3
3. Daily PrEP offers additional protection for discordant couples
3A “It is more of a reassurance. We [participant and HIV-positive steady partner] have unsafe sex with each other, without a condom. I don’t have issues with it or am not afraid of it. I know my partner well enough to know that he takes his medication and is stable [viral load]. But you never know what happens in the mean time and that is my insecurity. It [viral load] could suddenly peak and then I’m more at risk and you can miss that in the bi-annual check-up. And PrEP would provide the additional protection for that.” MSM 14
3B “Because my partner has HIV, it [PrEP] would give us just a little bit more freedom to do more things sexually than we do now, especially when he is undetectable [viral load] and that would give me just that little bit extra.” MSM 13
4. Daily PrEP reduces anxiety about HIV transmission
See quotes 2A, 2B, 3A and 3B

Chapter 2.2
66
We identified 10 motives for not wanting to use daily PrEP in the future (Table 2):1. Daily PrEP is not sufficiently effective as an HIV risk reduction strategy: Some participants
perceived the efficacy of daily PrEP as too low. Perceptions of insufficient efficacy differed between participants, for example, some participants felt less than 100% efficacy was insufficient (quote 1A), whereas others perceived efficacy less than 50% as insufficient (quote 1B).
2. Non-belief in present research and data: Some participants stated distrusting the results of the published PrEP efficacy trials and were therefore not willing to consider taking PrEP (quote 2A).
3. Daily PrEP is not needed because of a low self-perceived HIV risk: Some participants stated not needing PrEP because of their sexual lifestyle (e.g., number of partners [quote
Table 1. (continued)
Motives for wanting to use
daily PreP representative quotes
5. Daily PrEP is easier to use than condoms
5A “Yes, I think it is easier than using condoms. You use a condom at the heat of the moment, so then you have to get the condom out. And PrEP, that is something you use every day. So you lay a foundation for 24 hours. And a condom doesn’t do that […]. It [PrEP] works much better than a condom. It is continually present.” MSM 20
5B Is PrEP something for you personally? “I think so, yes. Because I always try to have sex as safely as possible, but yes, there are times that you just had too much to drink or the passion is so overwhelming that you forget. […] It would offer me a little bit more freedom. I would worry a little bit less.” MSM 17
6. Daily PrEP can improve quality of sex life
6A “I would just take it [PrEP] to have unsafe sex and then also under the influence of drugs. I would like to experiment with that.” MSM 1
6B What would be the reason for you to want to use it [PrEP]? “Yes, first of all to protect myself and second of all, to please a bed partner because they prefer to have sex without a condom.” MSM 19
6C “Because my partner has HIV and I think for us it would be easier to also love each other more in a sexual sense. Because it lowers that barrier. […] His HIV-status sepa-rates us sexually, in other words, we don’t have sex. This is mainly due to his fear of infecting me. If I use it [PrEP] I’m better protected which will make it easier for him, and eventually also for me, to just have sex with each other.” MSM 13
7. Daily PrEP makes engaging in (sexual) relationships with a potential HIV-positive partner easier
7A “I can imagine that at a certain stage in your relationship [with an HIV-positive part-ner] you want unprotected [condomless] sex, because it is more intimate.” MSM 15
7B “I never want to have an HIV-positive boyfriend again, that limits me sexually, but if PrEP would be there, there wouldn’t be a barrier to engage in a relationship with someone.” MSM 11
8. Daily PrEP provides solidarity with HIV-positive partner
8A “Yes […] I would want to use the medication [ART] so that he [HIV-positive partner] isn’t alone in it, so from a social point of view I would take them, so that we can do it together. Now I don’t need medication but in this case [if PrEP were to be available] there would be a reason for me to take them.” MSM 13
ART, combination antiretroviral therapy; MSM, Men who have sex with men; PrEP, pre-exposure prophylaxis.
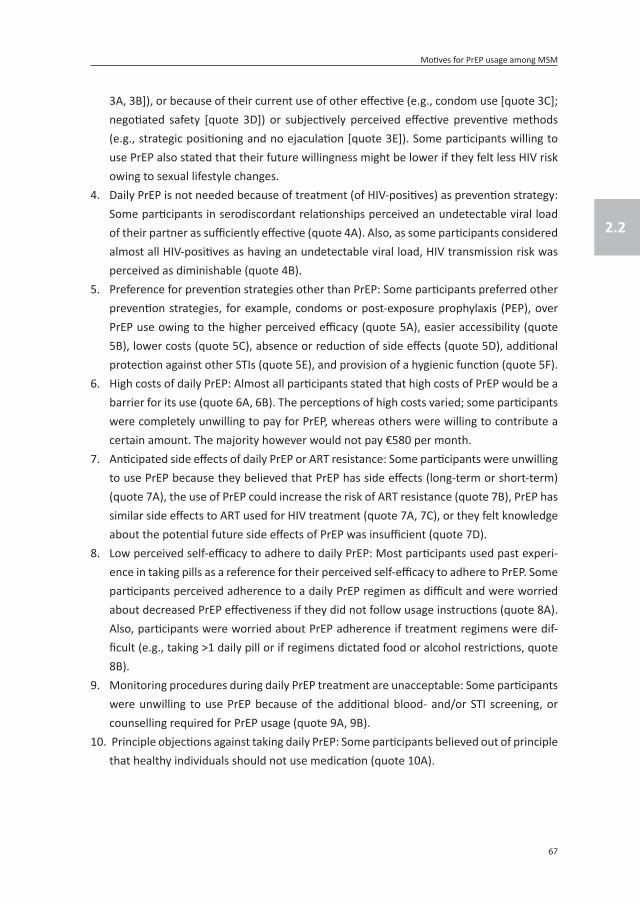
67
Motives for PrEP usage among MSM
2.2
3A, 3B]), or because of their current use of other effective (e.g., condom use [quote 3C]; negotiated safety [quote 3D]) or subjectively perceived effective preventive methods (e.g., strategic positioning and no ejaculation [quote 3E]). Some participants willing to use PrEP also stated that their future willingness might be lower if they felt less HIV risk owing to sexual lifestyle changes.
4. Daily PrEP is not needed because of treatment (of HIV-positives) as prevention strategy: Some participants in serodiscordant relationships perceived an undetectable viral load of their partner as sufficiently effective (quote 4A). Also, as some participants considered almost all HIV-positives as having an undetectable viral load, HIV transmission risk was perceived as diminishable (quote 4B).
5. Preference for prevention strategies other than PrEP: Some participants preferred other prevention strategies, for example, condoms or post-exposure prophylaxis (PEP), over PrEP use owing to the higher perceived efficacy (quote 5A), easier accessibility (quote 5B), lower costs (quote 5C), absence or reduction of side effects (quote 5D), additional protection against other STIs (quote 5E), and provision of a hygienic function (quote 5F).
6. High costs of daily PrEP: Almost all participants stated that high costs of PrEP would be a barrier for its use (quote 6A, 6B). The perceptions of high costs varied; some participants were completely unwilling to pay for PrEP, whereas others were willing to contribute a certain amount. The majority however would not pay €580 per month.
7. Anticipated side effects of daily PrEP or ART resistance: Some participants were unwilling to use PrEP because they believed that PrEP has side effects (long-term or short-term) (quote 7A), the use of PrEP could increase the risk of ART resistance (quote 7B), PrEP has similar side effects to ART used for HIV treatment (quote 7A, 7C), or they felt knowledge about the potential future side effects of PrEP was insufficient (quote 7D).
8. Low perceived self-efficacy to adhere to daily PrEP: Most participants used past experi-ence in taking pills as a reference for their perceived self-efficacy to adhere to PrEP. Some participants perceived adherence to a daily PrEP regimen as difficult and were worried about decreased PrEP effectiveness if they did not follow usage instructions (quote 8A). Also, participants were worried about PrEP adherence if treatment regimens were dif-ficult (e.g., taking >1 daily pill or if regimens dictated food or alcohol restrictions, quote 8B).
9. Monitoring procedures during daily PrEP treatment are unacceptable: Some participants were unwilling to use PrEP because of the additional blood- and/or STI screening, or counselling required for PrEP usage (quote 9A, 9B).
10. Principle objections against taking daily PrEP: Some participants believed out of principle that healthy individuals should not use medication (quote 10A).

Chapter 2.2
68
Table 2. Representative quotes from 20 HIV-negative MSM in regards to motives for not wanting to use daily PrEP, Amsterdam, the Netherlands (2013)
Motives for not wanting
to use daily PreP representative quotes
1. Daily PrEP is not sufficiently effective as an HIV risk reduction strategy
1A “I want it [PrEP] to be 100% effective. Otherwise you still take a risk.” MSM 15
1B “I wouldn’t consider it if the effectiveness is really low and there are a lot of side effects. If the additional protection is only 10%, it is too low to contribute a lot in our relationship. Then I would take a pill and I don’t really know why I’m doing it. Look, if the effectiveness is high or at least above 50% or 70% then it would be the perfect addition.” MSM 14
2. Non-belief in present research and data
2A “To be honest, I don’t think the study is very reliable. How can you test if someone is in-fected with HIV or not […].” MSM 9
3. Daily PrEP is not needed due to a low self-perceived HIV risk
3A “I don’t know, I find it difficult, because first of all, I really don’t have that much sex outside of my relationship that I think I constantly have to take pills for that one time I have sex […]. If I were to possibly enter a phase that I have a lot of sex outside of my relationship then at some point I might consider it [PrEP].” MSM 16
3B “Basically, I am in a monogamous relationship and I am not really at risk of HIV, or not at great risk. If something were to happen, then I would prefer to take the morning after pill [PEP] […].” MSM 12
3C “If you just have safe sex with condoms, I think that is the best protection, and if you use them well, make sure it doesn’t brake and you follow the normal guidelines or rules for safe sex, then I don’t think you need it [PrEP].” MSM 8
3D “If I have sex outside of my steady relationship then I’m having safe sex. But with my boy-friend, my steady partner, we have unsafe sex. So actually I don’t really need PrEP.” MSM 9
3E “Well the consideration also has to do with the number of times I have sex, maybe also with me having more passive sex, so getting fucked. Usually I am more active, that also has something to do with it. One of the considerations is being active, so the risk is lower. Actu-ally you’re reducing your risk, by not ejaculating and mainly being the active one.” MSM 16
4. Daily PrEP is not needed due to treatment (of HIV-positives) as prevention strategy
4A “I wouldn’t use it, for example, because of my [HIV-positive] partner. Because I think, his viral load is undetectable, so if I only have sex with him, I will not take in into consideration […].” MSM 16
4B “[…] As I understand now, almost no one has a detectable viral load, so the chance is low that you will get infected. So, I don’t really see the advantage of taking PrEP.” MSM 11
5. Preference for prevention strategies other than PrEP
5A “If you just have safe sex with condoms, I think that is the best protection, and if you use them well, make sure it doesn’t break and you follow the normal guidelines or rules for safe sex, then I don’t think you need it [PrEP]”. MSM 8
5B “Well, you can get them [condoms] on every street corner, they are for sale everywhere. And well, with PrEP you could forget to order it, or prescriptions don’t arrive at the doctor or pharmacy, or that they have run out.” MSM 8
5C Do you have more reasons why you don’t want to use it [PrEP]? “Because it is really expen-sive, a condom is so much cheaper, that is also one of the reasons.” MSM 9
5D “I see what those pills do and I see what happens if you have HIV. You really don’t want that. So for me I just go for what I know are the safest options and those are condoms. Always.” MSM 7
5E So if it [PrEP] would be available in the Netherlands, would you use it? “No, because of the thing about condoms. I just notice that without condoms you can contract so much more [STIs] than without. So condoms protect against HIV, but they also protect against so much more and therefore remain a necessity.” MSM 5

69
Motives for PrEP usage among MSM
2.2
Table 2. (continued)
Motives for not wanting
to use daily PreP representative quotes
5F “Well, safe sex [with condoms]: that is safe and it is clean. Then I don’t have all that fuss. It is not difficult for me now so it is not even a question.” MSM 6
6. High costs of daily PrEP
6A “At the moment I’m on benefits so every Euro is one too many. At the moment I don’t have money for it [PrEP]. So that means I have to make a different choice. But 25 Euro I would find acceptable considering my income.” MSM 1
6B “Would there be any reason why you would not want to start using PrEP? […] and the price of PrEP. I mean, I don’t mind contributing but I’m not paying 500, almost 600 Euro per month. That means almost 7000 Euro annually. […] If there are few side effects and the health insurance funds are willing to cover most or all of the costs, or I have to contribute a little bit, nothing would stop me.” MSM 17
7. Anticipated side effects of daily PrEP or ART resistance
7A “If it has similar side effects as other HIV medication, of what I know about them, it makes it [PrEP] a non option. In that case I would pretty much poison my body now and in 20 years face all kinds of problems. In that case I most definitely don’t want to use it and I would rather sleep less soundly for a night. No, if they say that there are few side effects, I wouldn’t trust that. […] It should be as safe as a vitamin pill.” MSM 2
7B “And if I got it [HIV] after all the precautions, then you’re stuck taking all sorts of antiretro-virals […] and then I think Truvuda would be more effective than if you have already been using it [Truvada as PrEP] for who knows how long.” MSM 8
7C “I associate HIV medication with heavy medication that is harmful in a different way.” MSM 2
7D “But yes, I don’t know if I would use it so easily because it is kind of new. It is not clear what the effect is because they have tested it on a number of people but they don’t yet know what the future complaints could be. […] If the research is a bit further along, then I would think about it because of course there is nothing better than not using anything.” MSM 18
8. Low perceived self-efficacy to adhere to daily PrEP
8A “The most important thing from daily use is that I have no doubt that I will forget it and this will decrease the effectiveness, so it is not for me, I’m very sure about my habits when it comes to condom use. I can trust myself in that. […] But a daily pill, I’m not sure if I can trust myself in that. As a result I would feel guilty and I would think: I forgot it again, twice, will it be effective?” MSM 5.
8B What would make it more difficult to use PrEP daily? “For example, If you have to take it two hours before dinner, or not in combination with alcohol. If the treatment regimen is difficult.” MSM2
9. Monitoring procedures during daily PrEP treatment are unacceptable
9A “If I have to get my blood drawn every time, I would think, what a fuss, just use a condom, you can buy them everywhere, you can even pull one out of a wall (vending machine).” MSM 11
9B How would you feel about that [counselling on safe sex and additional test in combina-tion with PrEP]? “You almost sign up for a social check up pill. Counselling etc. is a bit too extreme. […] As a quite free-spirited person I don’t think I would want that attached to it.” MSM 12
10. Principle objections against taking daily PrEP
10A “For me it would feel like a burden to take a pill every day. If I had HIV then I would take the medication because I want to live a healthy life for as long as possible. I want to prevent that the virus emerges but if I don’t have the virus why should I burden my body with it? That would feel unnatural to me; that I would get side effects, that I have to go to the laboratory to get blood drawn because I’m taking medication while I’m not sick but do have to get my kidney and liver function tested twice a year. Well I wouldn’t want that. I would not do it.” MSM 6
MSM, Men who have sex with men; PrEP, pre-exposure prophylaxis; STIs, sexually transmitted infections.

Chapter 2.2
70
Intermittent PreP
After discussing motives regarding daily use of PrEP, we asked participants about percep-tions regarding intermittent PrEP usage. Of 19 participants, 12 had a low intention of using intermittent PrEP, five had a high intention, and two participants were in doubt about using intermittent PrEP. For the first participant, the intention to use intermittent PrEP was not explored as it was added as an interview topic after the first interview.
We identified three motives for preferring intermittent PrEP over daily PrEP (Table 3):1. The decision to start intermittent PrEP is easier compared to daily PrEP: Some partici-
pants thought it would be less hard to make the decision to use intermittent PrEP than the decision to use daily PrEP (quote 1A).
2. Intermittent PrEP has less side effects compared to daily PrEP: Some participants be-lieved taking PrEP less frequently or for a short period (as in intermittent PrEP) reduces side effects and potentially harmful effects (quote 2A).
3. Intermittent PrEP reduces financial costs compared to daily PrEP: Some participants stated that intermittent PrEP would increase their control over the financial costs as they could choose the period and duration of PrEP use (quote 3A).
We identified two motives for preferring daily PrEP over intermittent PrEP (Table 3):1. Intermittent PrEP requires unwanted planning of sex life: Most participants stated they
did not plan their sex life and that sex usually happened spontaneously. As intermittent PrEP entails planning when to start taking PrEP, participants argued that intermittent PrEP would not work for them (quote 1B).
2. Using intermittent PrEP makes adherence to other HIV prevention strategies more dif-ficult: Some participants believed using intermittent PrEP would necessitate different prevention strategies in different situations, when on or off PrEP, which makes adher-ence difficult (quote 2B).
anticipated condom use when using daily PreP
We identified two motives for combining PrEP with condom use (Table 4):1. Condoms are needed to prevent other STIs (quote 1A).2. Combining the two strategies increases protection against HIV (quote 2A).
We identified one motive for solely using PrEP, that is, using PrEP solely is sufficiently effec-tive to prevent an HIV infection (quote 1B, 1C). Furthermore, some participants in serodis-cordant relationships stated they would only use condoms in combination with PrEP if their HIV-positive partner’s viral load was detectable.

71
Motives for PrEP usage among MSM
2.2
Location of PreP prescription
Participants preferred the following locations for PrEP prescription if it were to become available in the Netherlands: Public Health Service (i.e., STI clinic), general practitioner, and the hospital (i.e., HIV-specialist). Preference for locations was based on the following characteristics of healthcare providers (Table 5): having specialized knowledge of HIV (and ART) (quote 1); having specialized knowledge of sexual behaviour and other STIs (quote 2); possibility of performing medical check-up and/or counselling (quote 3); having specialized knowledge of personal medical background and the use of current (medical) drugs (quote 4); easily accessible (quote 2); and having time to counsel men and provide support for PrEP users (quote 6). The perceived pros and cons for the distribution of PrEP services by different healthcare provider are presented in Table 5.
Table 3. Representative quotes from 19 HIV-negative MSM in regards to motives for wanting and not wanting to use intermittent PrEP, Amsterdam, the Netherlands (2013)Motives for preferring intermittent PreP over
daily PreP representative quotes
1. The decision to start intermittent PrEP is easier compared to daily PrEP
1A “[…] It also sounds less hard to make the decision.” MSM 10
2. Intermittent PrEP has less side effects compared to daily PrEP
2A “I still feel like I would be putting poison into my body, but it is limited and not for a long time so I would expect it to be less harmful than if you use the medication for a longer period of time.” MSM 2
3. Intermitted PrEP reduces financial costs compared to daily PrEP
3A “Well, I can imagine myself doing it, that after a quiet period that you feel the need to do something crazy and go on a holiday. And that you take it in that way. And then you don’t have all the costs, you take it for a shorter period of time so it will be cheaper and you can control it. You can say, for example: I want to pay this much and that means I can use it four times a year for a week.” MSM 12
Motives for preferring daily PreP over
intermittent PreP representative quotes
1. Intermittent PrEP requires unwanted planning of sex life
1B “Yes, a little bit stupid. For me sex is something spontaneous and not something you plan, okay I’m having sex in three days and I’ll start taking PrEP. No, I think that is nonsense.” MSM 9
2. Using intermittent PrEP makes adherence to other HIV prevention strategies more difficult
2B “That sounds even more complicated behaviour-wise. But it is also less hard to make the decision.” What do you mean by more complicated behaviour? “Well the last de-cennium my theory was that you have to have continuous behaviour and not think: now I can do whatever I want and after that it stops. […] I don’t believe in having two sex lives. Maybe I’m still negative [HIV] after all those year because I had one policy. Not like: here I can do this, and there I can do that. That has been my safety. […] So, no, I never had a double approach.” MSM 10
MSM, Men who have sex with men; PrEP, pre-exposure prophylaxis.

Chapter 2.2
72
dISCuSSIon
This qualitative study revealed several motives for wanting or not wanting to use PrEP and preferences with respect to PrEP implementation among HIV-negative Dutch MSM if PrEP becomes available in the Netherlands. These results can guide future implementation strat-egies to ensure high uptake of PrEP and maximize PrEP’s public health impact.
First, we found the motives for PrEP use were based on beliefs regarding PrEP efficacy, PrEP side effects, and trust regarding published research data. Recent trial results have corrobo-rated that PrEP is highly effective, has minimum side effects, and risk of ART resistance is low when PrEP is taken correctly.5-7 To correct wrong beliefs about PrEP and increase positive attitudes toward PrEP, knowledge about current and possible future data on PrEP efficacy and side effects should be increased.
Second, we found perceived self-efficacy to be an important motive for wanting or not wanting to use daily and or intermittent PrEP. To improve the perceived self-efficacy, it is important to carefully look at individual skills regarding PrEP use and adherence, and decide, based on the type of skill problems, whether daily or intermittent PrEP is most suited and which skill enhancing interventions is needed.
Table 4. Representative quotes from 20 HIV-negative MSM in regards to anticipated condom use when using daily PrEP, Amsterdam, the Netherlands (2013)
Motives for combining daily PreP
with condom use representative quotes
1. Condoms are needed to prevent other STIs
1A “And if you leave out condoms, you’re still at risk for other STIs. Do you want them? I don’t. I just see PrEP as an additional safety measure.” MSM 4
2. Combining the two strategies increases protection against HIV
2A “I’m in a sort of high risk stage, so it makes sense for this sort of period to take some-thing preventative as a second backup plan. I mean, I use condoms as well, but it would be like a second option.” MSM 20
Motives for solely using daily PreP (without condom use) representative quotes
1. Using PrEP solely is sufficiently effective to prevent an HIV infection
1B So for you it doesn’t seem useful to use them [PrEP and condoms] together? “No, just because I see it [PrEP] as something to prevent getting HIV and therefore it allows you to bareback.” MSM 1
1C Would anything change in your behaviour or feelings [when using PrEP]? “Not in the beginning but if I would use it for a long time probably it will. If I see every time that I don’t have HIV, I think at one point I will start taking risks.” What do you mean by taking risks? “That I would be less worried about condom use. And that would be a negative side. If I were to look at myself I can see that happening.” MSM 17
MSM, Men who have sex with men; PrEP, pre-exposure prophylaxis; STIs, sexually transmitted infections.
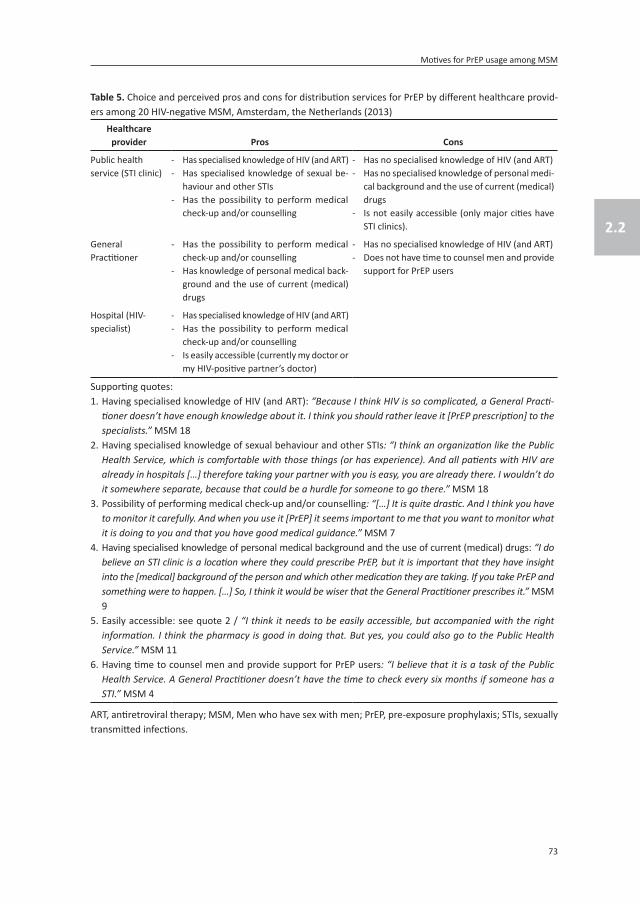
73
Motives for PrEP usage among MSM
2.2
Table 5. Choice and perceived pros and cons for distribution services for PrEP by different healthcare provid-ers among 20 HIV-negative MSM, Amsterdam, the Netherlands (2013)
Healthcare provider Pros Cons
Public health service (STI clinic)
- Has specialised knowledge of HIV (and ART)- Has specialised knowledge of sexual be-
haviour and other STIs- Has the possibility to perform medical
check-up and/or counselling
- Has no specialised knowledge of HIV (and ART)- Has no specialised knowledge of personal medi-
cal background and the use of current (medical) drugs
- Is not easily accessible (only major cities have STI clinics).
General Practitioner
- Has the possibility to perform medical check-up and/or counselling
- Has knowledge of personal medical back-ground and the use of current (medical) drugs
- Has no specialised knowledge of HIV (and ART)- Does not have time to counsel men and provide
support for PrEP users
Hospital (HIV-specialist)
- Has specialised knowledge of HIV (and ART)- Has the possibility to perform medical
check-up and/or counselling- Is easily accessible (currently my doctor or
my HIV-positive partner’s doctor)
Supporting quotes:1. Having specialised knowledge of HIV (and ART): “Because I think HIV is so complicated, a General Practi-
tioner doesn’t have enough knowledge about it. I think you should rather leave it [PrEP prescription] to the specialists.” MSM 18
2. Having specialised knowledge of sexual behaviour and other STIs: “I think an organization like the Public Health Service, which is comfortable with those things (or has experience). And all patients with HIV are already in hospitals […] therefore taking your partner with you is easy, you are already there. I wouldn’t do it somewhere separate, because that could be a hurdle for someone to go there.” MSM 18
3. Possibility of performing medical check-up and/or counselling: “[…] It is quite drastic. And I think you have to monitor it carefully. And when you use it [PrEP] it seems important to me that you want to monitor what it is doing to you and that you have good medical guidance.” MSM 7
4. Having specialised knowledge of personal medical background and the use of current (medical) drugs: “I do believe an STI clinic is a location where they could prescribe PrEP, but it is important that they have insight into the [medical] background of the person and which other medication they are taking. If you take PrEP and something were to happen. […] So, I think it would be wiser that the General Practitioner prescribes it.” MSM 9
5. Easily accessible: see quote 2 / “I think it needs to be easily accessible, but accompanied with the right information. I think the pharmacy is good in doing that. But yes, you could also go to the Public Health Service.” MSM 11
6. Having time to counsel men and provide support for PrEP users: “I believe that it is a task of the Public Health Service. A General Practitioner doesn’t have the time to check every six months if someone has a STI.” MSM 4
ART, antiretroviral therapy; MSM, Men who have sex with men; PrEP, pre-exposure prophylaxis; STIs, sexually transmitted infections.

Chapter 2.2
74
Third, we found environmental factors, for example, perceived difficulties in accessing PrEP services, frequent monitoring procedures, and high costs of PrEP, were potential barriers for PrEP uptake. To reduce these barriers, PrEP services should be set up in line with MSM preferences by offering PrEP in easily accessible facilities (e.g., involve efficient health moni-toring procedures, offer services at convenient times and locations) with sufficient experi-ence and specialized knowledge regarding PrEP prescription. Furthermore, it is important to advocate for the (partial) coverage of PrEP costs by insurance companies or other sources of cost coverage.
Regarding motives for PrEP use among men in serodiscordant relationships, results showed that some men perceived PrEP as a good addition to current prevention methods since it could increase their protection, reduce their anxiety, and improve sexual satisfaction in their relationships. However, some men perceived PrEP as unnecessary in discordant relation-ships where the HIV-positive partner had an undetectable viral load because of the low transmission risk. As growing evidence supports the latter, also among MSM,30-32 using PrEP in serodiscordant relationships might become redundant.
Our results regarding intermittent PrEP show that most men were sceptical about its use as it requires planning of their sex life and this would not fit in with their sex life habits. However, our study was conducted before the IPERGAY trial results indicated PrEP could be effectively taken up to two hours before a risk episode.7 We defined intermittent PrEP as using PrEP three days before high-risk sexual behaviour. The shorter time frame of plan-ning sex in advance might increase its acceptability. Furthermore, as men perceived using intermittent PrEP as having reduced costs and fewer side effects compared to daily PrEP, intermittent PrEP options could increase general PrEP acceptability.
Our results indicate that some men perceived PrEP as a substitute for condom use. Although a decrease in condom use was not observed in study settings,6,33 a decrease was seen among PrEP users in a clinical practice settings.34 To deal with possible decreases in condom use or increases in STIs when PrEP is implemented in real-life settings, STI prevalence should be monitored after PrEP initiation, PrEP programs should include routine STI screening, and address risk and severity perceptions in regard to other STIs.
The motives for daily PrEP use found in this study are comparable to those found in other studies among MSM.15-22 However, the following motives found in other studies were not considered important by our study population: PrEP will help link individuals to the health-care system,19 fear that others will think users of PrEP have HIV,33 others will identify PrEP users as MSM,33 and generally feeling ashamed about using PrEP.22 These differences are probably explained by our study population and its context, as we included mainly older, na-

75
Motives for PrEP usage among MSM
2.2
tive Dutch MSM participating in a cohort study and hence accustomed to disclosure, having overcome barriers for engaging with healthcare systems, and living in a country with well organized health provision and an open gay culture. Furthermore, participants of a qualita-tive study might be more open to discuss PrEP and feel less shame to use PrEP. As motives might differ in other countries, interventions for PrEP implementation should be adapted to the countries’ healthcare system, social norms, and risk population.
Regarding limitations, although MSM are likely to be the most important target group for PrEP in the Netherlands, other groups, for example, transgenders, high-risk heterosexuals, bisexual men, and sex workers might also be considered eligible for PrEP. If PrEP also be-comes available for those groups, their specific motives and preferences should be further explored as they might differ among those groups. Furthermore, as mentioned earlier, the selection of MSM participating in a cohort study might have influenced our results. Our find-ings may therefore not be generalized to the broader range of MSM living in the Netherlands or outside of it. We recommend that motives to use PrEP among high risk, for example, younger MSM and those not yet readily engaged with healthcare systems, should be further explored. Finally, we measured behavioural intentions and motives to use PrEP. Although behavioural intentions provide a good indication of the general willingness to use PrEP on the individual level, they do not absolutely predict actual PrEP uptake. Actual uptake of PrEP will most likely also be influenced by a variety of other external factors, such as social, organizational or environmental factors, and these factors should also be addressed.35,36
In conclusion, the future use of daily PrEP among HIV-negative MSM depends on the personal evaluation of benefits, barriers related to PrEP, and the perceived self-efficacy to adhere to PrEP. To maximize the public health impact of PrEP, ensuring high uptake among MSM at highest risk is important. Therefore, targeted information aimed at improving knowledge about PrEP efficacy and side effects needs to be developed. Furthermore, barri-ers for accessing PrEP services should be minimized according to the indicated needs of the target population. Perceived self-efficacy to use PrEP should be improved and addressed differently based on individual assessments of skill problems and of preferences for daily or intermittent PrEP. Finally, as this study shows that some men perceived PrEP as a substitute for condom use, it is important to discuss, monitor, and study condom use change and its consequences, and work toward integrating routine STI screening and counselling in PrEP prescription programs.
acknowledgements
The authors acknowledge all participants for their valuable contribution, research nurses of the ACS Marc van Wijk and Marjolein Martens for helping with the recruitment of par-

Chapter 2.2
76
ticipants, Broek Tekst- & Dataverwerking and Lisanne Möller for transcribing the interviews, and Claire Buswell for editing the final manuscript.
funding
Funding for the present study was received from the Public Health Service Amsterdam Research and Development Fund (project number 12–8). The Amsterdam Cohort Studies (ACS) on HIV infection and AIDS, which is a collaboration between the Public Health Service of Amsterdam, the Academic Medical Center of the University of Amsterdam, Sanquin Blood Supply Foundation, Medical Center Jan van Goyen, and the HIV Focus Center of the DC-Clinics, is part of the Netherlands HIV Monitoring Foundation and financially supported by the Center for Infectious Disease Control of the Netherlands National Institute for Public Health and the Environment.
Conflicts of interest
Maria Prins and Udi Davidovich have received a research grant (under fully unrestricted terms) from Gilead Sciences for other studies concerning PrEP.

77
Motives for PrEP usage among MSM
2.2
referenCes
1. European Centre for Disease Prevention and Control (ECDC), World Health Organization (WHO) Regional Office for Europe. HIV/aIdS surveillance in europe 2012. Stockholm: ECDC, 2013.
2. van Sighem A, Gras L, Smit C, Stolte I, Reiss P. Human Immunodeficiency Virus (HIV) infection in the netherlands: HIV Monitoring report 2015. Amsterdam: Stichting HIV Monitoring, 2015.
3. Jansen IA, Geskus RB, Davidovich U, Jurriaans S, Coutinho RA, Prins M, et al. ongoing HIV-1 transmis-sion among men who have sex with men in amsterdam: a 25-year prospective cohort study. AIDS. 2011;25(4):493-501. doi:10.1097/QAD.0b013e328342fbe9.
4. Beyrer C, Baral SD, F. vG, oodreau SM, hariyalertsak S, irtz AL, et al. Global epidemiology of HIV infection in men who have sex with men. Lancet. 2012;380(9839):367-377. doi:10.1016/S0140-6736(12)60821-6.
5. Grant RM, Lama JR, Anderson PL, McMahan V, Liu AY, Vargas L, et al. Preexposure chemoprophy-laxis for HIV prevention in men who have sex with men. N Engl J Med. 2010;363(27):2587-2599. doi:10.1056/NEJMoa1011205.
6. McCormack S, Dunn DT, Desai M, Dolling DI, Gafos M, Gilson R, et al. Pre-exposure prophylaxis to prevent the acquisition of HIV-1 infection (Proud): effectiveness results from the pilot phase of a pragmatic open-label randomised trial. Lancet. 2016;387(10013):53-60. doi:10.1016/S0140-6736(15)00056-2.
7. Molina JM, Capitant C, Spire B, Pialoux G, Cotte L, Charreau I, et al. on-demand Preexposure Prophy-laxis in Men at High risk for HIV-1 Infection. N Engl J Med. 2015;373(23):2237-2246. doi:10.1056/NEJMoa1506273.
8. Centers for Disease Control and Prevention (CDC). Pre-exposure Prophylaxis for the prevention of HIV infection in the united States, 2014: a clinical Practice Guideline. CDC, 2014.
9. World Health Organization (WHO). Guideline on when to start antiretroviral therapy and on pre-exposure prohylaxis for HIV. Geneva: WHO, 2015.
10. Gomez GB, Borquez A, Case KK, Wheelock A, Vassall A, Hankins C. the cost and impact of scaling up pre-exposure prophylaxis for HIV prevention: a systematic review of cost-effectiveness modelling studies. PLoS Med. 2013;10(3):e1001401. doi:10.1371/journal.pmed.1001401.
11. Cambiano V, Miners A, Phillips A. What do we know about the cost-effectiveness of HIV pre-exposure prophylaxis, and is it affordable? Curr Opin HIV AIDS. 2015;11(1):56-66. doi:10.1097/COH.0000000000000217.
12. Desai K, Sansom SL, Ackers ML, Stewart SR, Hall HI, Hu DJ, et al. modeling the impact of HIV chemo-prophylaxis strategies among men who have sex with men in the united States: HIV infections pre-vented and cost-effectiveness. AIDS. 2008;22(14):1829-1839. doi:10.1097/QAD.0b013e32830e00f5.
13. Juusola JL, Brandeau ML, Owens DK, Bendavid E. The cost-effectiveness of preexposure prophy-laxis for HIV prevention in the united States in men who have sex with men. Ann Intern Med. 2012;156(8):541-550. doi:10.7326/0003-4819-156-8-201204170-00001.
14. Schneider K, Gray RT, Wilson DP. a cost-effectiveness analysis of HIV preexposure prophylaxis for men who have sex with men in australia. Clin Infect Dis. 2014;58(7):1027-1034. doi:10.1093/cid/cit946.
15. Golub SA, Gamarel KE, Rendina HJ, Surace A, Lelutiu-Weinberger CL. From efficacy to effectiveness: facilitators and barriers to PreP acceptability and motivations for adherence among MSM and transgender women in new York City. AIDS Patient Care STDS. 2013;27(4):248-254. doi:10.1089/apc.2012.0419.

Chapter 2.2
78
16. Brooks RA, Kaplan RL, Lieber E, Landovitz RJ, Lee SJ, Leibowitz AA. Motivators, concerns, and barriers to adoption of preexposure prophylaxis for HIV prevention among gay and bisexual men in HIV-serodiscordant male relationships. AIDS Care. 2011;23(9):1136-1145. doi:10.1080/09540121.2011.554528.
17. Brooks RA, Landovitz RJ, Kaplan RL, Lieber E, Lee SJ, Barkley TW. Sexual risk behaviors and accept-ability of HIV pre-exposure prophylaxis among HIV-negative gay and bisexual men in serodiscordant relationships: a mixed methods study. AIDS Patient Care STDS. 2012;26(2):87-94. doi:10.1089/apc.2011.0283.
18. Galea JT, Kinsler JJ, Salazar X, Lee SJ, Giron M, Sayles JN, et al. acceptability of pre-exposure prophylaxis as an HIV prevention strategy: barriers and facilitators to pre-exposure prophylaxis uptake among at-risk Peruvian populations. Int J STD AIDS. 2011;22(5):256-262. doi:10.1258/ijsa.2009.009255.
19. Galindo GR, Walker JN, Hazelton P, Lane T, Steward WT, Morin SF, et al. Community member per-spectives from transgender women and men who have sex with men on pre-exposure prophy-laxis as an HIV prevention strategy: implications for implementation. Implement Sci. 2012;7(1):116. doi:10.1186/1748-5908-7-116.
20. Wheelock A, Eisingerich AB, Ananworanich J, Gomez GB, Hallett TB, Dybul MR, et al. are thai msm willing to take PreP for HIV prevention? an analysis of attitudes, preferences and acceptance. PLoS One. 2013;8(1):e54288. doi:10.1371/journal.pone.0054288.
21. Gamarel KE, Golub SA. Intimacy Motivations and Pre-exposure Prophylaxis (PreP) adoption Inten-tions among HIV-negative Men Who Have Sex with Men (MSM) in romantic relationships. Ann Behav Med. 2014;49(2):177-186. doi:10.1007/s12160-014-9646-3.
22. Bil JP, Davidovich U, van der Veldt WM, Prins M, de Vries HJ, Sonder GJ, et al. What do dutch MSM think of preexposure prophylaxis to prevent HIV-infection? a cross-sectional study. AIDS. 2015;29(8):955-964. doi:10.1097/QAD.0000000000000639.
23. Stolte IG, Prins M. The amsterdam Cohort Studies on HIV infection: annual report 2014. In: van Sighem AI, Gras L, Smit C, al e, eds. Human Immunodeficiency Virus (HIV) Infection in the Netherlands: HIV Monitoring Report 2015. Amsterdam: Stichting HIV monitoring, 2015.
24. van Griensven GJ, de Vroome EM, Goudsmit J, Coutinho RA. Changes in sexual behaviour and the fall in incidence of HIV infection among homosexual men. BMJ. 1989;298(6668):218-221. doi: 10.1136/bmj.298.6668.218.
25. Central Committee on Research Involving Human Subjects. Your research: does it fall under the WMo? Available at: http://www.ccmo.nl/ (accessed on 21 July 2016).
26. Glaser B, Strauss A. The discovery of grounded theory: strategies for qualitative research. Chicago: Aldine, 1967.
27. Strauss A. Qualitative analysis for social scientists. Newbury Park, CA: Sage, 1987. 28. Green J, Thorogood N. analysing Qualitative data. Qualitative methods for health research. London:
SAGE, 2004. 29. CPB Netherlands Bureau for Economic Policy Analyses. CPBs short-term forecasts September 2014.
Available at: http://www.cpb.nl/cijfer/kortetermijnraming-september-2014 (accessed on 3 December 2014).
30. Quinn TC, Wawer MJ, Sewankambo N, Serwadda D, Li C, Wabwire-Mangen F, et al. Viral load and heterosexual transmission of human immunodeficiency virus type 1. rakai Project Study Group. N Engl J Med. 2000;342(13):921-929. doi:10.1056/NEJM200003303421303.
31. Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493-505. doi:10.1056/NEJMoa1105243.

79
Motives for PrEP usage among MSM
2.2
32. Rodger A, Bruun T, Cambiano V, Vernazza P, strada V, Van Lunzen J, et al. HIV transmission risk Through Condomless Sex If HIV+ Partner on Suppressive arT: ParTner Study [abstract 153lB]. 21ste Conference on Retroviruses and Oppotunistic Infections: Boston, USA, 3-6 March 2014.
33. Grant RM, Anderson PL, McMahan V, Liu A, Amico KR, Mehrotra M, et al. uptake of pre-exposure prophylaxis, sexual practices, and HIV incidence in men and transgender women who have sex with men: a cohort study. Lancet Infect Dis. 2014;14(9):820-829. doi:10.1016/S1473-3099(14)70847-3.
34. Volk JE, Marcus JL, Phengrasamy T, Blechinger D, Nguyen DP, Follansbee S, et al. no new HIV Infec-tions With Increasing use of HIV Preexposure Prophylaxis in a Clinical Practice Setting. Clin Infect Dis. 2015;61(10):1601-1603. doi:10.1093/cid/civ778.
35. Bartholomw LK, Parcel GS, Kok G, Gottlieb NH, Fernandez ME. Planning health promotion programs, an intervention mapping approach. San Francisco: Jossey-Bass, 2011.
36. Glanz K, Rimer BK, Viswanath K. Health Behavior and Health education: Theory, research, and prac-tice. San Francisco, CA: Jossey-Bass, 2008.

Chapter 2.3The acceptability of
pre-exposure prophylaxis: Beliefs of healthcare professionals working in sexually transmitted infection clinics and
HIV treatment centers
Janneke P. Bil*, Elske Hoornenborg*, Maria Prins, Arjan Hogewoning, Fernando Dias Goncalves Lima, Henry J. C. de Vries, Udi Davidovich
* Both authors contributed equally to this article
Published in Frontiers in Public Health, 2018; 6:5

Chapter 2.3
82
aBstraCt
Background
Pre-exposure prophylaxis (PrEP) is highly effective for preventing HIV infections, but is not yet implemented in the Netherlands. As the attitudes of healthcare professionals toward PrEP can influence future PrEP implementation, we studied PrEP knowledge and beliefs and their association with PrEP acceptability among professionals in clinics for sexually transmit-ted infection (STI professionals) and HIV treatment centers (HIV specialists). In addition, we examined preferred regimens, attitudes toward providing PrEP to key populations and to reimbursement of PrEP costs.
methods
An online questionnaire was distributed among 24 public health STI clinics and 27 HIV treatment centers nationwide in the Netherlands between January and August 2015. The acceptability of PrEP was measured on a 7-point Likert scale ranging from 1=low to 7=high acceptability. Univariable and multivariable linear regression analyses were used to explore associations between demographic characteristics, PrEP knowledge, beliefs about PrEP, and PrEP acceptability.
results
In total, 209 people (143 STI professionals and 66 HIV specialists) completed the question-naire. The mean acceptability of PrEP implementation was 4.28 (SD 1.68) among STI profes-sionals and 4.42 (SD 1.67) among HIV specialists. The mean score on self-perceived knowl-edge related to PrEP efficacy was 3.90 (SD 1.57) among STI professionals and 5.68 (SD 1.08) among HIV specialists (p-value of <0.001). Beliefs associated with lower PrEP acceptability among both groups were the fear that PrEP use will lead to a decrease in condom use and an increase in STI, the high costs of PrEP and ethical issues regarding prescribing antiretroviral medication to healthy individuals. No preference for a daily or an event-driven regimen was detected. Most participants deemed the following groups to be eligible for PrEP: men who have sex with men (MSM) who regularly get post-exposure prophylaxis, MSM who never used condoms with casual partners and MSM with an HIV-positive partner with a detectable viral load. Over half of the participants indicated that PrEP users should partly (54.1%) or fully (35.4%) pay the costs of PrEP.
Conclusion
In 2015, PrEP acceptability was only moderate among Dutch STI professionals and HIV specialists, which is far from an optimal setting. Addressing barriers to PrEP acceptability in educational programs for various types of healthcare professionals is needed to successfully implement PrEP in the Netherlands.
83
Beliefs of healthcare professionals on PrEP
2.3
InTroduCTIon
Pre-exposure prophylaxis (PrEP) entails offering a regime of lower-intensity antiretroviral therapy (ART) to HIV-negative individuals to reduce their risk of HIV infection. PrEP is offered in combination with other behavioural interventions such as condom use, counselling on sexual-risk behaviour, frequent HIV testing, and linkage to other HIV prevention services.1-3 Several studies have demonstrated that both daily and event-driven PrEP regimens are highly effective,4-7 and the current guidelines of a number of international organizations include PrEP as a prevention strategy for key populations. In the developed world, HIV spreads most rapidly in men who have sex with men (MSM).1,8 A modelling study based on Dutch data estimated that 30% (range: 22–39%) of new HIV infections could have been averted if half of all MSM under 30 had received PrEP in combination with immediate ART for those who test positive.9 In addition, PrEP implementation was estimated to be cost-effective in the Netherlands over a 40-year time frame if PrEP was provided to the 10% most sexually active MSM.10 Despite these results and the July 2016 approval of Truvada (emtricitabine/tenofovir disoproxil) for PrEP in the European Union, PrEP is not yet routinely available or reimbursed in the Netherlands.
For the effective implementation of PrEP, it is important to understand healthcare profes-sionals’ level of knowledge and beliefs or concerns about PrEP, as they will play a critical role in its implementation. The acceptability of PrEP among healthcare professionals at clinics for sexually transmitted infections (STIs) and HIV treatment centers is of particular importance as PrEP is most likely to be implemented at these facilities, due to their experience in offering prevention services to individuals at risk for HIV and experience in providing HIV treatment, respectively.
In this cross-sectional study among professionals working at STI clinics (STI professionals) and at HIV treatment centers (HIV specialists) in the Netherlands, we aimed to gain insight into the acceptability of PrEP, prescription setting, potential determinants of PrEP accept-ability (such as knowledge and beliefs about PrEP), and preferred PrEP regimens. We exam-ined attitudes toward providing PrEP to key populations and toward the reimbursement of PrEP costs. The resulting insights will guide future PrEP implementation strategies and help design PrEP educational programs for professionals.

Chapter 2.3
84
MaTerIalS and MeTHodS
Procedures and recruitment
First, we conducted two focus group discussions with a total of 16 STI professionals from the Public Health Service of Amsterdam (three physicians, 12 nurses, and one doctor’s assistant) in October 2014. The central topics were PrEP acceptability and underlying PrEP beliefs. Each participant was asked about his/her opinion regarding PrEP implementation and was asked to shortly explain their most important argument(s) to support their opinion. All arguments where thereafter discussed within the group. The results of the focus group discussions were analysed by three researchers from diverse disciplines: health sciences (JPB), medicine (EH), and psychol-ogy (UD). In the qualitative analyses, PrEP beliefs measured in the focus group discussions were categorized into major themes using thematic content analysis. Second, based on focus group discussions, we developed two questionnaires. The first was aimed at STI professionals and included all PrEP beliefs measured in the focus group discussions. The second, aimed at HIV specialists, was condensed to encourage maximum response from this group. It included only the major themes derived from the qualitative analyses (Table S1 in Supplementary Material).
The questionnaire for STI professionals was distributed from January through May 2015 via email invitations to key contacts at all official public health STI clinics (n=24) in the Netherlands. The contacts were asked to further distribute the questionnaire within their organization. The invitation and questionnaire for HIV specialists were emailed from June through August 2015 directly to physicians at all HIV treatment centers (n=27) and to the nurse practitioners through their professional organization. In the email invitation for the questionnaire, participants were informed about PrEP, the aim of the study, and the spon-sor of the study. One follow-up email was sent to increase the response rate. Participation was voluntary, and no financial incentive was offered. As the questionnaire was anonymous and did not request personal or sensitive data, approval by an ethics committee was not required, according to Dutch legislation.
measurements
Demographics, characteristics, and PrEP experience
Characteristics included age, gender, the type of professional (nurse, physician, or other, e.g., managers, doctors’ assistants, and administrative workers), the location of STI clinic (large urban area/outside of large urban area) or the type of hospital (academic or general), and the length of employment in STI clinic/hospital. HIV specialists were additionally asked for the number of HIV-positive patients at their clinic. Experience with PrEP was measured by asking whether participants had received questions about PrEP from clients/patients in the previous six months. HIV specialists were additionally asked whether they had ever prescribed PrEP.

85
Beliefs of healthcare professionals on PrEP
2.3
PrEP acceptability
PrEP acceptability was measured via several items on a 7-point scale ranging from 1 “completely disagree” to 7 “completely agree.” The acceptability of PrEP implementation in the Netherlands was measured by one central item: “If PrEP is registered (i.e., granted market authorization), it should be implemented in the Netherlands as a new HIV interven-tion strategy.” In addition, among STI professionals, we also measured the acceptability of implementation at STI clinics by the item: ”If PrEP is registered, it should be prescribed at STI clinics.” Among HIV specialists, we additionally measured acceptability toward implementa-tion at HIV treatment centers and at general practitioners’ offices by the items: “If PrEP is registered, it should be prescribed by HIV specialists,” and “If PrEP is registered, it should be prescribed by general practitioners.” Moreover, we queried their willingness to prescribe through the item: “If PrEP is registered, I would be willing to prescribe PrEP.”
Self-perceived knowledge of PrEP
For all participants (except where indicated in parentheses), the following self-perceived items were measured on a 7-point Likert scale ranging from 1 “very poor” to 7 “very good”: knowledge of PrEP efficacy and the frequency/severity of side effects, the efficacy to inform patients about PrEP (only among STI professionals), the ability to identify key populations for PrEP use (only among HIV specialists), and the capability of deciding to prescribe PrEP (only among HIV specialists). Self-perceived knowledge about the frequency and severity of side effects was combined in one item in the analysis (self-perceived knowledge about side effects) as it was highly correlated (Spearman’s rho >0.9; p<0.001).
Beliefs about PrEP
Based on the focus group discussions, general beliefs about PrEP were measured with 50 items among STI professionals and 15 items among HIV specialists (Table S1 in Supplemen-tary Material). For analyses, items were combined if they measured the same belief and had acceptable correlation (two items: Spearman’s rho >0.6 and p<0.05; more than two items: Cronbach’s alpha >0.7). As the data collection of general beliefs differed between STI professionals (where all beliefs from the focus group discussions were measured) and HIV specialists (where only the selected major themes from the focus group discussions were measured), these correlation analyses were done separately for STI professionals and HIV specialists, and no comparisons were performed between the groups regarding beliefs. This resulted in 16 general beliefs about PrEP in the questionnaire for STI professionals and eight in the questionnaire for HIV specialists. All general beliefs were measured on a 7-point scale ranging from 1 “completely disagree” to 7 “completely agree.”
Among STI professionals, we additionally measured one belief about PrEP efficacy (ranging from “PrEP can reduce the risk of HIV by 100%” to “Although PrEP reduces the risk of HIV,

Chapter 2.3
86
there is still a great risk of HIV transmission”): one belief about the frequency of side effects (side effects are rare/are sometimes reported/appear frequently/knowledge is still scarce/I don’t know) and one belief about the severity of side effects (side effects are often severe/are often mild or non-severe/knowledge is still scarce/I don’t know).
Daily versus event-driven PrEP use
Beliefs about daily versus event-driven PrEP were measured with seven items in both questionnaires, using a 7-point scale ranging from 1 “completely disagree” to 7 “completely agree” (see Table S2 in Supplementary Material for more details). Given the good correlation between items (Cronbach’s alpha of 0.81 for STI professionals and 0.77 for HIV specialists), all seven items were combined.
Key populations, reimbursement of PrEP costs and serodiscordant couples
Questions were asked about the perceived PrEP eligibility of key groups (MSM, heterosexu-als, and commercial sex workers) within different behavioural scenarios (e.g., condom use, repeatedly having an STI, having an HIV-positive partner, repeatedly using post-exposure prophylaxis). For each scenario, participants were asked to assess eligibility by choosing one of the following options: not eligible/possibly eligible/eligible.
Participants were also asked who should pay for PrEP (PrEP user/health insurance/govern-ment/partially PrEP users and partially health insurance or government/neutral).
HIV specialists were asked what intervention they prefer to prevent HIV transmission in serodiscordant couples (only ART for the HIV-positive partner/only PrEP for the HIV-negative partner/ART for the HIV-positive partner and PrEP for HIV-negative partner as a transition phase until the HIV-positive partner has an undetectable viral load/only counselling).
statistical analyses
We described demographic characteristics, PrEP experience and knowledge, general beliefs about PrEP and about event-driven versus daily use, key populations, reimbursement of costs, and preferred interventions for serodiscordant couples. We compared distributions of acceptability and knowledge by the type of healthcare provider (nurse/physician/other profession) and between STI professionals and HIV specialists, using Student’s t-tests and one-way ANOVA for normally distributed continuous variables and Mann-Whitney U-tests and Kruskal-Wallis tests for not-normally distributed continuous variables. Because of the differences in how the general beliefs were constructed among STI professionals and HIV specialists, a direct comparison between the general beliefs between STI clinic professionals and HIV specialists was not possible.

87
Beliefs of healthcare professionals on PrEP
2.3
We performed univariable and multivariable linear regression analyses to explore associa-tions between demographic characteristics, PrEP knowledge, PrEP beliefs, and the accept-ability of PrEP implementation in the Netherlands. A multivariable model was built using backward techniques. First, variables on PrEP knowledge and beliefs with a p-value <0.10 in univariable analyses were entered into the model. Second, also demographic determinants with a p<0.10 in univariable analyses were entered into the model. A p-value <0.05 was considered to be statistically significant. Interactions between the variables in the final model were checked. As the data collection differed between STI professionals and HIV specialists, analyses were done separately for STI professionals and HIV specialists. Analyses were performed using STATA Intercooled 13.1 (STATA Corporation, College Station, TX, USA).
reSulTS
demographic characteristics and PreP experience
All of the 24 STI clinics we contacted agreed to participate in the study (Figure 1). In the nine STI clinics that provided data on the number of questionnaires distributed, the response rate was 54.4% (104/191). In total, 143 STI professionals completed the questionnaire (Table 1): 93 nurses, 37 physicians, and 13 other professionals. A majority of respondents (113/143; 79.0%) were female; about half worked in an STI clinic in a large urban area (65/143; 45.5%) and most (95/143; 66.4%) had worked for more than four years in an STI clinic. About half
Contact persons of 24 STI clinics were approached who further distributed the questionnaire within their organisation a
170 HIV specialists of 27 centers were invited to participate
143 STI professionals participated b 66 HIV specialists participated(response rate 39%)
Nursesn=93
STI professionals HIV specialists
Othern=13
Physiciansn=37
Nursesn=40
Physiciansn=26
Figure 1. Flowchart of recruitment procedures of STI professionals working at STI clinics of the Public Health Service and HIV specialists working at HIV treatment centers, the Netherlands, 2015STI, sexually transmitted infection.a Total number of persons invited by contact persons is unknown.b Response rate was 54% (104/191) among nine clinics that provided data on the number of questionnaires
distributed.

Chapter 2.3
88
(69/143; 48.3%) had received questions about PrEP from clients in the preceding six months but only 4.3% (3/69) were queried at least once a week.
Of 170 HIV specialists invited to participate, 66 (38.8%) completed the questionnaire, includ-ing 40 nurses and 26 physicians (Table 1). Most HIV specialists were female (39/66; 59.1%); half (34/66; 51.5%) worked in an academic hospital and 84.8% (56/66) had more than four years of experience. Of these specialists, 83.3% (55/66) had received patient questions about PrEP in the preceding six months and 7.6% (5/66) had ever prescribed PrEP.
PreP acceptability
Among STI professionals and HIV specialists, the mean score on the acceptability of PrEP implementation in the Netherlands was 4.28 (SD 1.68) and 4.42 (SD 1.67), respectively (Table 2). The mean acceptability score of PrEP implementation at STI clinics was 4.16 (SD 1.86) among STI professionals and 4.48 (SD 1.83) among HIV specialists. Among the latter, the mean acceptability score for implementation at HIV treatment centers was 3.91 (SD 1.97) and 2.45 (SD 1.82) for implementation at general practitioners’ offices. Their mean score for the willingness to prescribe PrEP was 4.39 (SD 1.89).
Self-perceived knowledge of PreP
Among STI professionals, the mean score on self-perceived knowledge was 3.90 (SD 1.57) for PrEP efficacy and 2.84 (SD 1.39) for PrEP side effects; the mean score on self-perceived efficacy to inform clients about PrEP was 2.89 (SD 1.44) (Table 2). The mean score on self-perceived knowledge among HIV specialists was 5.68 (SD 1.08) for PrEP efficacy and 5.61 (SD 1.34) for side effects; it was 5.02 (SD 1.33) for self-perceived efficacy to identify key groups and 4.61 (SD 1.40) for the decision to prescribe PrEP. Self-perceived knowledge of efficacy (z=-7.46, p<0.001) and side effects (z=-9.60, p<0.001) was significantly higher among HIV specialists compared to that among STI professionals.
Beliefs about PreP
Among STI professionals, the three general beliefs with the strongest agreement scores were (Table 2): “it is unclear who will have to pay for PrEP” (mean 5.52, SD 1.51), “tak-ing PrEP is better than getting HIV” (mean 5.27, SD 1.49), and “adherence to PrEP will be insufficient” (mean 5.25, SD 1.41). Among HIV specialists, the three general beliefs with the highest agreement scores were “the use of PrEP will lead to a decrease in condom use and an increase in STI” (mean 5.13, SD 1.34), “I’m worried about long-term side effects of PrEP” (mean 4.89, SD 1.51), and “it is unethical to prescribe ART to healthy individuals” (mean 4.64, SD 1.72).

89
Beliefs of healthcare professionals on PrEP
2.3
Table 1. Demographic characteristics and PrEP experience of 209 healthcare professionals, the Netherlands (2015)stI professionals HIV specialists
total(N=143)
nurse(n=93)
Physician(n=37)
other(n=13)
total(N=66)
nurse(n=40)
Physician(n=26)
n % n % n % n % n % n % n %
age
<40 years 57 39.9 29 31.2 20 54.1 8 61.5 11 16.7 7 17.5 4 15.4
40–49 years 41 28.7 33 35.5 6 16.2 2 15.4 27 40.9 16 40.0 11 42.3
50–59 years 34 23.8 25 26.9 6 16.2 3 23.1 19 28.8 14 35.0 5 19.2
> 60 years 11 7.7 6 6.5 5 13.5 0 0.0 9 13.6 3 7.5 6 23.1
Gender
Male 30 21.0 13 14.0 14 37.8 3 23.1 27 40.9 12 30.0 15 57.7
Female 113 79.0 80 86.0 23 62.2 10 76.9 39 59.1 28 70.0 11 42.3
location of STI clinic
Large urban area (Amsterdam, The Hague, Rotterdam, Utrecht)
65 45.5 42 45.2 15 40.5 8 61.5 NA
Outside large urban area 75 52.5 50 53.8 20 54.1 5 38.5 NA
Missing data 3 2.1 1 1.1 2 5.4 0 0.0
type of hospital
Academic NA 32 48.5 18 45.0 14 53.8
General NA 34 51.5 22 55.0 12 46.2
length of employment in STI clinic/hospital
0–4 years 48 33.6 24 25.8 18 48.7 6 46.2 10 15.2 7 17.5 3 11.5
5–9 years 45 31.5 33 35.5 11 29.7 1 7.7 18 27.3 10 25.0 8 30.8
10–14 years 31 21.7 26 28.0 4 10.8 1 7.7 21 31.8 17 42.5 4 15.4
>15 years 19 13.3 10 10.8 4 10.8 5 38.5 17 25.8 6 15.0 11 42.3
number of HIV-positive patients in care
<250 NA 25 37.9 10 25.0 15 57.7
>250 NA 41 62.1 30 75.0 11 42.3
Questions about PreP from clients in the previous 6 months
No questions 65 45.5 40 43.0 22 59.5 3 23.1 11 16.7 5 12.5 6 23.0
Very rarely (one to two in the preceding 6 months)
51 35.7 41 44.1 7 18.9 3 23.1 28 42.4 16 40.0 12 46.2
Sometimes (one to two per month)
15 10.5 10 10.8 3 8.1 2 15.4 24 36.4 16 40.0 8 30.8
Regularly (at least once a week) 3 2.1 2 2.2 1 2.7 0 0.0 3 4.5 3 7.5 0 0.0
NA (no contact with clients) 9 6.3 0 0.0 4 10.8 5 38.5 0 0.0 0 0.0 0 0.0
ever prescribed PreP
No NA 56 84.9 31 77.5 25 96.2
Yes NA 5 7.6 4 10.0 1 3.9
NA NA 5 7.6 5 12.5 0 0.0
NA, not applicable (item not included in the questionnaire for the indicated practice setting); PrEP, pre-expo-sure prophylaxis; STI, sexually transmitted infection.

Chapter 2.3
90 91
Beliefs of healthcare professionals on PrEP
2.3
Tabl
e 2.
Kno
wle
dge
and
belie
fs a
bout
PrE
P am
ong
209
heal
thca
re p
rofe
ssio
nals,
the
Net
herla
nds (
2015
)st
I pro
fess
iona
ls
HIV
spec
ialis
tsst
I pr
ofes
siona
ls vs
. HIV
sp
ecia
lists
tota
ln
urse
Phys
ician
oth
erST
I nur
se v
s.
stI p
hysic
ian
vs. S
TI o
ther
tota
ln
urse
Phys
ician
HIV
nurs
e vs
. HI
V ph
ysici
an(N
=143
)(n
=93)
(n=3
7)(n
=13)
(N=6
6)(n
=40)
(n=2
6)
Mea
n (S
d)M
ean
(Sd)
Mea
n (S
d)M
ean
(Sd)
Mea
n (S
d)M
ean
(Sd)
Mea
n (S
d)
PreP
acc
epta
bilit
y (7
-poi
nt sc
ale:
1” c
ompl
etel
y di
sagr
ee” t
o 7”
com
plet
ely
agre
e”)
If Pr
EP is
regi
ster
ed, i
t sho
uld
be im
plem
ente
d in
the
Neth
erla
nds a
s a
new
HIV
inte
rven
tion
stra
tegy
4.28
(1.6
8)4.
20 (1
.56)
4.00
(1.8
4)5.
62 (1
.56)
F(2,
140)
=4.9
8,
p=0.
008
4.42
(1.6
7)4.
73 (1
.47)
3.96
(1.8
9)t(6
4)=-
1.84
, p=
0.07
0t(2
07)=
-0.5
8,
p=0.
563
If Pr
EP is
regi
ster
ed, i
t sho
uld
be p
resc
ribed
at S
TI cl
inics
4.16
(4.0
1)4.
01 (1
.75)
4.14
(2.0
7)5.
31 (1
.70)
F(2,
140)
=2.8
6,
p=0.
061
4.48
(1.8
3)4.
53 (1
.85)
4.42
(1.8
4)t(6
4)=-
0.22
, p=
0.82
7z=
-1.2
2.
p=0.
224
If Pr
EP is
regi
ster
ed, i
t sho
uld
be p
resc
ribed
by
HIV
spec
ialis
tsNA
3.91
(1.9
7)4.
03 (2
.06)
3.73
(1.8
7)z=
-0.6
6,
p=0.
510
If Pr
EP is
regi
ster
ed, i
t sho
uld
be p
resc
ribed
by
gene
ral p
racti
tione
rsNA
2.45
(1.8
2)2.
65 (1
.94)
2.15
(1.6
2)z=
-0.9
7,
p=0.
333
If Pr
EP is
regi
ster
ed, I
wou
ld b
e w
illin
g to
pre
scrib
e Pr
EPNA
4.39
(1.8
9)4.
55 (1
.72)
4.15
(2.1
3)z=
-0.6
9,
p=0.
489
Self-
perc
eive
d kn
owle
dge
of P
reP
(7-p
oint
scal
e: 1
“ver
y po
or” t
o 7
“ver
y go
od”)
Self-
perc
eive
d kn
owle
dge
of P
rEP
effica
cy3.
90 (1
.57)
3.67
(1.4
9)4.
35 (1
.64)
4.23
(1.7
4)F(
2,14
0)=2
.91,
p=
0.05
85.
68 (1
.08)
5.48
(1.1
1)6.
00 (0
.98)
z=1.
89,
p=0.
059
z=-7
.45,
p<
0.00
1
Self-
perc
eive
d kn
owle
dge
of P
rEP
side
effec
ts2.
84 (1
.39)
2.68
(1.2
6)3.
36 (1
.53)
2.46
(1.6
3)H(
2)=6
.21,
p=
0.04
55.
61 (1
.34)
5.28
(1.3
6)6.
12 (1
.15)
z=2.
80,
p=0.
005
z=-9
.60,
p<
0.00
1
Self-
perc
eive
d effi
cacy
to in
form
clie
nts a
bout
PrE
P2.
89 (1
.44)
2.69
(1.2
2)3.
41 (1
.72)
2.85
(1.7
7)H(
2)=
4.35
, p=
0.11
4NA
Self-
perc
eive
d ab
ility
to id
entif
y ke
y po
pula
tions
for P
rEP
NA5.
02 (1
.33)
4.95
(1.3
8)5.
12 (1
.28)
t(64)
=0.4
9,
p=0.
625
Self-
perc
eive
d ca
pabi
lity
of d
ecid
ing
to p
resc
ribe
PrEP
NA4.
61 (1
.40)
4.33
(1.3
7)5.
04 (1
.37)
t(64)
=2.0
7,
p=0.
042

Chapter 2.3
90 91
Beliefs of healthcare professionals on PrEP
2.3
Tabl
e 2.
(con
tinue
d)st
I pro
fess
iona
ls
HIV
spec
ialis
tsst
I pr
ofes
siona
ls vs
. HIV
sp
ecia
lists
tota
ln
urse
Phys
ician
oth
erST
I nur
se v
s.
stI p
hysic
ian
vs. S
TI o
ther
tota
ln
urse
Phys
ician
HIV
nurs
e vs
. HI
V ph
ysici
an(N
=143
)(n
=93)
(n=3
7)(n
=13)
(N=6
6)(n
=40)
(n=2
6)
Mea
n (S
d)M
ean
(Sd)
Mea
n (S
d)M
ean
(Sd)
Mea
n (S
d)M
ean
(Sd)
Mea
n (S
d)
Gene
ral b
elie
fs a
bout
Pre
P (7
-poi
nt sc
ale:
1 “c
ompl
etel
y di
sagr
ee” t
o 7
“com
plet
ely
agre
e”)
It is
uncle
ar w
ho h
as to
pay
for P
rEP
5.52
(1.5
1)5.
58 (1
.46)
5.57
(1.6
6)5.
00 (1
.41)
H(2)
=2.4
1,
p=0.
300
NA
Taki
ng P
rEP
is be
tter t
han
getti
ng H
IV5.
27 (1
.49)
5.09
(1.5
9)5.
51 (1
.26)
5.85
(1.1
4)H(
2)=3
.53,
p=
0.17
1NA
Adhe
renc
e to
PrE
P w
ill b
e in
suffi
cient
5.25
(1.4
1)5.
21 (1
.44)
5.46
(1.4
0)4.
92 (1
.20)
H(2)
=2.5
46,
p=0.
280
NA
The
role
of t
he p
harm
aceu
tical
com
pani
es in
rega
rd to
PrE
P is
uncle
ar4.
97 (1
.43)
5.06
(1.4
7)4.
65 (1
.25)
5.23
(1.5
9)H(
2)=4
.15,
p=
0.12
6NA
The
use
of P
rEP
will
lead
to a
dec
reas
e in
cond
om u
se a
nd in
crea
se in
ST
I4.
87 (1
.21)
5.07
(1.0
8)4.
66 (1
.34)
4.02
(1.3
2)F(
2,14
0)=5
.42,
p=
0.00
55.
13 (1
.34)
5.10
(1.3
7)5.
17 (1
.32)
z=0.
27,
p=0.
785
PrEP
is ch
eape
r tha
n lif
elon
g HI
V tr
eatm
ent
4.86
(1.4
9)4.
72 (1
.48)
5.05
(1.5
4)5.
31 (1
.38)
F(2,
140)
=1.3
1,
p=0.
274
NA
PrEP
is a
n eff
ectiv
e in
terv
entio
n to
pre
vent
HIV
4.74
(1.3
6)4.
68 (1
.33)
4.65
(1.5
2)5.
46 (0
.97)
H(2)
=3.6
7,
p=0.
160
3.88
(0.8
9)3.
87 (0
.91)
3.88
(0.8
9)t(6
4)=0
.06,
p=
0.95
4
PrEP
pre
scrip
tion
shou
ld b
e pa
rt o
f rou
tine
care
at S
TI cl
inics
4.67
(1.6
6)4.
74 (1
.62)
4.20
(1.7
6)5.
54 (1
.38)
H(2)
=6.9
9,
p=0.
030
NA
Ther
e is
not e
noug
h kn
owle
dge
yet a
bout
PrE
P4.
67 (1
.23)
4.84
(1.1
8)4.
48 (1
.31)
3.98
(1.0
9)F(
2,14
0)=3
.45,
p=
0.03
4NA
Cost
s of P
rEP
are
a pr
oble
m4.
66 (1
.16)
4.65
(1.0
9)4.
87 (1
.24)
4.12
(1.2
9)F(
2,14
0),
p=0.
134
NA
I wou
ld w
orry
that
som
e pe
ople
hav
e to
use
PrE
P lif
elon
g4.
56 (1
.76)
4.74
(1.7
1)4.
43 (1
.68)
3.62
(2.1
0)H(
2)=4
.08,
p=
0.13
0NA
It is
unet
hica
l to
pres
crib
e AR
T to
hea
lthy
indi
vidu
als
4.31
(1.4
9)4.
44 (1
.48)
4.24
(1.4
2)3.
62 (1
.69)
F(2,
140)
=1.7
9,
p=0.
170
4.64
(1.7
2)4.
85 (1
.41)
4.31
(2.0
9)z=
-0.9
1,
p=0.
364
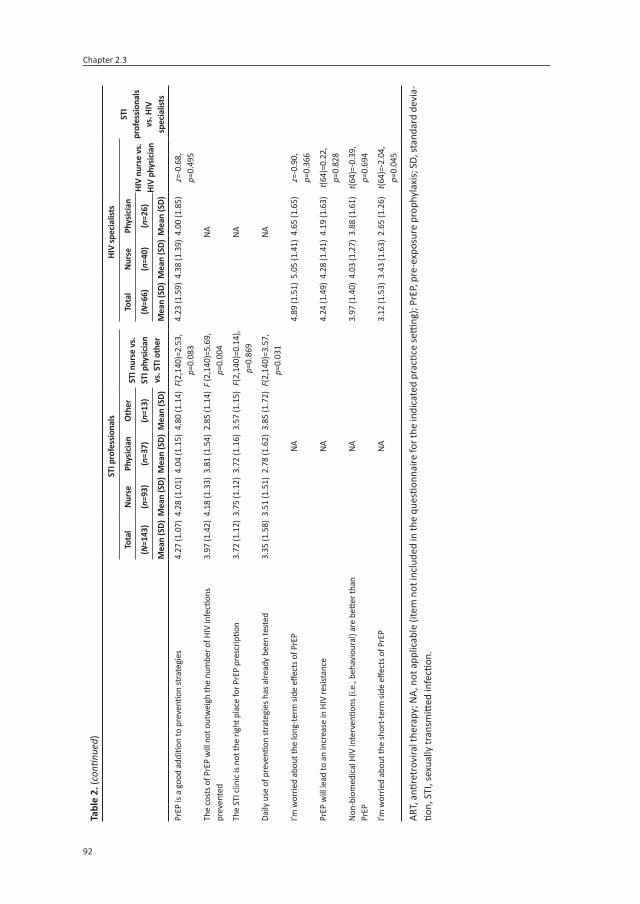
Chapter 2.3
92 93
Beliefs of healthcare professionals on PrEP
2.3
Tabl
e 2.
(con
tinue
d)st
I pro
fess
iona
ls
HIV
spec
ialis
tsst
I pr
ofes
siona
ls vs
. HIV
sp
ecia
lists
tota
ln
urse
Phys
ician
oth
erST
I nur
se v
s.
stI p
hysic
ian
vs. S
TI o
ther
tota
ln
urse
Phys
ician
HIV
nurs
e vs
. HI
V ph
ysici
an(N
=143
)(n
=93)
(n=3
7)(n
=13)
(N=6
6)(n
=40)
(n=2
6)
Mea
n (S
d)M
ean
(Sd)
Mea
n (S
d)M
ean
(Sd)
Mea
n (S
d)M
ean
(Sd)
Mea
n (S
d)
PrEP
is a
goo
d ad
ditio
n to
pre
venti
on st
rate
gies
4.27
(1.0
7)4.
28 (1
.01)
4.04
(1.1
5)4.
80 (1
.14)
F(2,
140)
=2.5
3,
p=0.
083
4.23
(1.5
9)4.
38 (1
.39)
4.00
(1.8
5)z=
-0.6
8,
p=0.
495
The
cost
s of P
rEP
will
not
out
wei
gh th
e nu
mbe
r of H
IV in
fecti
ons
prev
ente
d3.
97 (1
.42)
4.18
(1.3
3)3.
81 (1
.54)
2.85
(1.1
4)F
(2,1
40)=
5.69
, p=
0.00
4NA
The
STI c
linic
is no
t the
righ
t pla
ce fo
r PrE
P pr
escr
iptio
n3.
72 (1
.12)
3.75
(1.1
2)3.
72 (1
.16)
3.57
(1.1
5)F(
2,14
0)=0
.14)
, p=
0.86
9NA
Daily
use
of p
reve
ntion
stra
tegi
es h
as a
lread
y be
en te
sted
3.35
(1.5
8)3.
51 (1
.51)
2.78
(1.6
2)3.
85 (1
.72)
F(2,
140)
=3.5
7,
p=0.
031
NA
I’m w
orrie
d ab
out t
he lo
ng-te
rm si
de e
ffect
s of P
rEP
NA4.
89 (1
.51)
5.05
(1.4
1)4.
65 (1
.65)
z=-0
.90,
p=
0.36
6
PrEP
will
lead
to a
n in
crea
se in
HIV
resis
tanc
eNA
4.24
(1.4
9)4.
28 (1
.41)
4.19
(1.6
3)t(6
4)=0
.22,
p=
0.82
8
Non-
biom
edica
l HIV
inte
rven
tions
(i.e
., be
havi
oura
l) ar
e be
tter t
han
PrEP
NA3.
97 (1
.40)
4.03
(1.2
7)3.
88 (1
.61)
t(64)
=-0.
39,
p=0.
694
I’m w
orrie
d ab
out t
he sh
ort-t
erm
side
effe
cts o
f PrE
PNA
3.12
(1.5
3)3.
43 (1
.63)
2.65
(1.2
6)t(6
4)=-
2.04
, p=
0.04
5
ART,
anti
retr
ovira
l the
rapy
; NA,
not
app
licab
le (i
tem
not
incl
uded
in th
e qu
estio
nnai
re fo
r the
indi
cate
d pr
actic
e se
tting
); Pr
EP, p
re-e
xpos
ure
prop
hyla
xis;
SD,
stan
dard
dev
ia-
tion,
STI
, sex
ually
tran
smitt
ed in
fecti
on.

Chapter 2.3
92 93
Beliefs of healthcare professionals on PrEP
2.3
determinants of PreP acceptability
In the final multivariable analyses among STI professionals (Table 3), the following beliefs were associated with a higher acceptability of PrEP implementation in the Netherlands: “taking PrEP is better than getting HIV” (β=0.15, p=0.020), “PrEP is an effective intervention to prevent HIV” (β=0.45, p<0.001), and “PrEP prescription should be part of routine care at STI clinics” (β=0.17, p=0.013). Beliefs associated with a lower PrEP acceptability among STI professionals were “the use of PrEP will lead to a decrease in condom use and increase in STI” (β=-0.21, p=0.034) and “the costs of PrEP are a problem” (β=-0.28, p=0.019).
Table 3. Determinants of acceptability of PrEP implementation in the Netherlands among 143 STI profession-als in the Netherlands (2015)
univariable analyses Multivariable analyses
β (95% CI) p-value β (95% CI) p-value
age
<40 years Ref. 0.101
40–49 years 0.20 (-0.47: 0.88)
50–59 years 0.38 (-0.33: 1.09)
> 60 years -0.03 (-2.11: 0.05)
Gender
Male Ref. 0.031
Female -0.74 (-1.42: -0.07)
Profession
Nurse Ref.
Physician -0.20 (-0.83: 0.42) 0.008
Other 1.41 (0.45: 2.37)
location of STI clinic
Large urban area (Amsterdam, The Hague, Rotterdam, Utrecht)
Ref. 0.027
Outside large urban area 0.63 (0.07: 1.19)
length of employment within STI clinic
0–4 years Ref. 0.069
5–9 years 0.14 (-0.54: 0.82)
10–14 years -0.07 (-0.83: 0.68)
>15 years 1.11 (0.22: 1.99)
Questions about PreP from clients in the previous 6 months
No Ref. 0.201
Yes 0.36 (-0.19: 0.92)
Self-perceived knowledge of PreP (7-point scale: 1 “very poor” to 7 “very good”)
Self-perceived knowledge of PrEP efficacy 0.31 (0.14: 0.48) <0.001
Self-perceived knowledge of PrEP side effects 0.31 (0.11: 0.50) 0.002
Self-perceived efficacy to inform clients about PrEP 0.31 (0.13: 0.50) 0.001
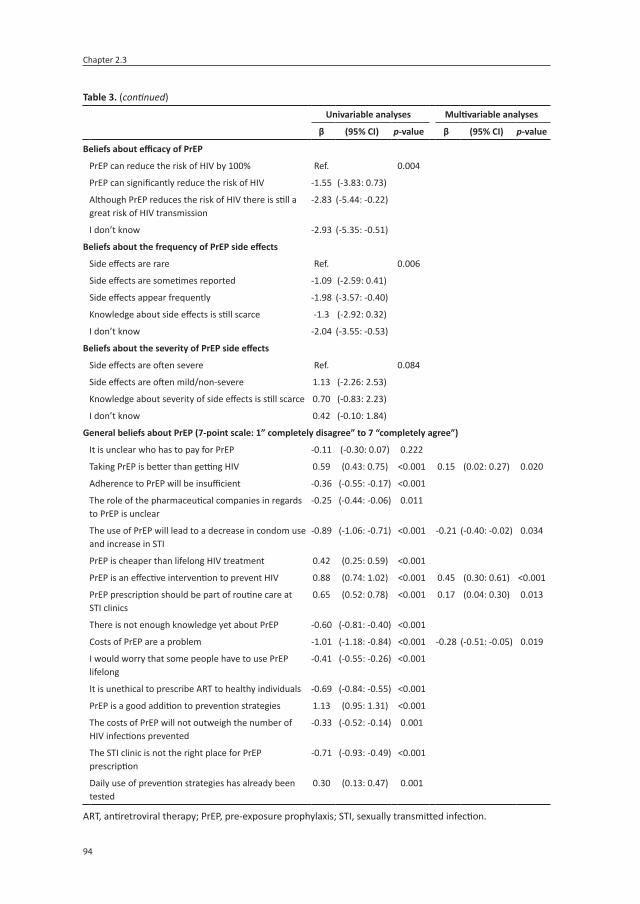
Chapter 2.3
94
Table 3. (continued)
univariable analyses Multivariable analyses
β (95% CI) p-value β (95% CI) p-value
Beliefs about efficacy of PreP
PrEP can reduce the risk of HIV by 100% Ref. 0.004
PrEP can significantly reduce the risk of HIV -1.55 (-3.83: 0.73)
Although PrEP reduces the risk of HIV there is still a great risk of HIV transmission
-2.83 (-5.44: -0.22)
I don’t know -2.93 (-5.35: -0.51)
Beliefs about the frequency of PreP side effects
Side effects are rare Ref. 0.006
Side effects are sometimes reported -1.09 (-2.59: 0.41)
Side effects appear frequently -1.98 (-3.57: -0.40)
Knowledge about side effects is still scarce -1.3 (-2.92: 0.32)
I don’t know -2.04 (-3.55: -0.53)
Beliefs about the severity of PreP side effects
Side effects are often severe Ref. 0.084
Side effects are often mild/non-severe 1.13 (-2.26: 2.53)
Knowledge about severity of side effects is still scarce 0.70 (-0.83: 2.23)
I don’t know 0.42 (-0.10: 1.84)
General beliefs about PreP (7-point scale: 1” completely disagree” to 7 “completely agree”)
It is unclear who has to pay for PrEP -0.11 (-0.30: 0.07) 0.222
Taking PrEP is better than getting HIV 0.59 (0.43: 0.75) <0.001 0.15 (0.02: 0.27) 0.020
Adherence to PrEP will be insufficient -0.36 (-0.55: -0.17) <0.001
The role of the pharmaceutical companies in regards to PrEP is unclear
-0.25 (-0.44: -0.06) 0.011
The use of PrEP will lead to a decrease in condom use and increase in STI
-0.89 (-1.06: -0.71) <0.001 -0.21 (-0.40: -0.02) 0.034
PrEP is cheaper than lifelong HIV treatment 0.42 (0.25: 0.59) <0.001
PrEP is an effective intervention to prevent HIV 0.88 (0.74: 1.02) <0.001 0.45 (0.30: 0.61) <0.001
PrEP prescription should be part of routine care at STI clinics
0.65 (0.52: 0.78) <0.001 0.17 (0.04: 0.30) 0.013
There is not enough knowledge yet about PrEP -0.60 (-0.81: -0.40) <0.001
Costs of PrEP are a problem -1.01 (-1.18: -0.84) <0.001 -0.28 (-0.51: -0.05) 0.019
I would worry that some people have to use PrEP lifelong
-0.41 (-0.55: -0.26) <0.001
It is unethical to prescribe ART to healthy individuals -0.69 (-0.84: -0.55) <0.001
PrEP is a good addition to prevention strategies 1.13 (0.95: 1.31) <0.001
The costs of PrEP will not outweigh the number of HIV infections prevented
-0.33 (-0.52: -0.14) 0.001
The STI clinic is not the right place for PrEP prescription
-0.71 (-0.93: -0.49) <0.001
Daily use of prevention strategies has already been tested
0.30 (0.13: 0.47) 0.001
ART, antiretroviral therapy; PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection.

95
Beliefs of healthcare professionals on PrEP
2.3
In the final multivariable analyses among HIV specialists (Table 4), physicians were less likely to have a positive attitude toward PrEP implementation than nurses (β=-0.83, p=0.008). Beliefs associated with a higher PrEP acceptability among all HIV specialists were “PrEP is an effective intervention to prevent HIV” (β=0.49, p=0.023) and “PrEP is a good addition to prevention strategies” (β=0.28, p=0.040). The belief associated with a lower PrEP accept-ability was “it is unethical to prescribe ART to healthy individuals” (β=-0.31, p=0.005).
Table 4. Determinants of acceptability of PrEP implementation in the Netherlands among 66 HIV specialists in the Netherlands (2015)
univariable analyses Multivariable analyses
β (95% CI) p-value β (95% CI) p-value
age
<40 years Ref. 0.447
40–49 years -0.27 (-1.47: 0.93)
50–59 years 0.10 (-1.17: 1.37)
> 60 years -0.97 (-2.48: 0.54)
Gender
Male Ref.
Female -0.10 (-0.94: 0.75) 0.819
Profession
Nurse Ref. 0.070 Ref.
Physician -0.76 (-1.59: 0.06) -0.83 (-1.44: -0.22) 0.008
type of hospital
Academic Ref.
General 0.22 (-0.61: 1.05) 0.603
length of employment within hospital
0–4 years Ref. 0.503
5–9 years 0.01 (-1.31: 1.34)
10–14 years 0.02 (-1.27: 1.31)
>15 years -0.72 (2.06: 0.62)
number of HIV-positive patients in care
<250 Ref.
>250 0.23 (-0.62: 1.09) 0.589
Questions about PreP from patients in the previous 6 months
No Ref. 0.651
Yes 0.12 (-0.40: 0.64)
ever prescribed PreP
No Ref.
Yes 0.61 (-0.94: 2.15) 0.435

Chapter 2.3
96
daily versus event-driven PreP use
There was no preference for daily or event-driven PrEP, given the mean score of the com-bined beliefs about event-driven versus daily PrEP of 3.99 (SD 1.00) among STI professionals and 4.14 (SD 1.01) among HIV specialists (Table S2 in Supplementary Material).
Key populations, serodiscordant couples, and reimbursement of PreP costs
As shown in Figure 2, most participants believed the following groups to be eligible for PrEP: MSM who regularly get post-exposure prophylaxis after a sexual exposure (136/209; 65.1%), MSM who never use condoms with casual partners (134/209; 64.1%), and MSM or het-erosexuals who have an HIV-positive steady partner with a detectable viral load (132/209; 63.2% and 112/209; 53.6%, respectively).
To prevent HIV transmission within serodiscordant couples, most HIV specialists preferred to treat only the HIV-positive partner (34/66; 51.5%) or to treat the HIV-positive partner while providing PrEP to the HIV-negative partner as long as the HIV-positive partner has a detectable viral load (26/66; 39.4%). A minority preferred only prescribing PrEP for the HIV-negative partner (2/66; 3.0%) or prescribing ART for the HIV-positive partner and PrEP for the HIV-negative partner without limited timeframe (2/66; 3.0%), or just counselling (2/66;
Table 4. (continued)
univariable analyses Multivariable analyses
β (95% CI) p-value β (95% CI) p-value
Self-perceived knowledge of PreP (7-point scale: 1 “very poor” to 7 “very good”)
Self-perceived knowledge of PrEP efficacy 0.26 (-0.12: 0.64) 0.175
Self-perceived knowledge of PrEP side effects 0.05 (-0.26: 0.36) 0.742
Self-perceived efficacy to identify target groups of PrEP
0.17 (-0.14: 0.48) 0.279
Self-perceived capability of deciding to prescribe PrEP 0.12 (-0.18: 0.41) 0.431
General beliefs about PreP (7-point scale: 1 “completely disagree” to 7 “completely agree”)
The use of PrEP will lead to a decrease in condom use and increase in STI
-0.69 (-0.95: 0.43) <0.001
PrEP is an effective intervention to prevent HIV 1.09 (0.71: 1.47) <0.001 0.49 (0.07: 0.92) 0.023
It is unethical to prescribe ART to healthy individuals -0.54 (-0.75: -0.34) <0.001 -0.31 (-0.53: -0.10) 0.005
PrEP is a good addition to prevention strategies 0.68 (0.47: 0.88) <0.001 0.28 (0.01: 0.54) 0.040
I’m worried about the long-term side effects of PrEP -0.18 (-0.46: 0.09) 0.187
PrEP will lead to an increase in HIV resistance -0.30 (-0.57: -0.03) 0.032
Non-biomedical HIV interventions (i.e. behavioural) are better than PrEP
-0.23 (-0.52: 0.06) 0.125
I’m worried about the short-term side effects of PrEP 0.04 (-0.24: 0.31) 0.789
ART, antiretroviral therapy; PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection.

97
Beliefs of healthcare professionals on PrEP
2.3
3.0%). HIV physicians and nurses did not differ significantly in their preferences to prevent HIV transmission within serodiscordant couples.
As to PrEP costs, over half of STI professionals and HIV specialists (113/209; 54.1%) indicated that PrEP users should partially contribute, whereas 35.4% (74/209) indicated that PrEP us-ers should pay all the costs; 5.7% (12/209) favoured complete coverage by health insurance, 4.3% (9/209) were neutral, and 0.5% (1/209) indicated that the government should pay all the costs.
Figure 2: Beliefs about eligble key populations (A: men having sex with men, B: heterosexual men and women, C: commercial sexworkers) for pre-exposure prophylaxis (PrEP) among health care providers, the Netherlands (2015).
PrEP: pre-exposure prophylaxis, STI: sexually transmitted infection, PEP: post-exposure prophylaxis
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
….never use condoms with
casual partners
….sometimes use condoms with casual
partners
….always use condoms with
casual partners
….regularly have an STI (other
than HIV)
….regularly get PEP after a sex
incident
….have a high number of casual
partners
….have a sex addiction
….have erectile dysfunction while using condoms
….have a high level of anxiety
for HIV
….have an HIV-positive steady
partner with detectable viral
load
….have an HIV-positive steady
partner with undetectable viral
load
Prop
ortio
n pe
rcei
ved
by
parti
cipa
nts
as
elig
ble
for P
rEP
A. Men having sex with men
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
….never use condoms with
casual partners
….sometimes use condoms with
casual partners
….always use condoms with
casual partners
….regularly have an STI (other
than HIV)
….regularly get PEP after a sex
incident
….have a high number of casual
partners
….have a sex addiction
….have erectile dysfunction while using condoms
(for men)
….have a high level of anxiety
for HIV
….have an HIV-positive steady
partner with detectable viral
load
….have an HIV-positive steady
partner with undetectable viral
load
….have an HIV-positive partner and want to get
pregnant
Prop
ortio
n pe
rcei
ved
by
part
icip
ants
as
elig
ble
for P
rEP
B. Heterosexual men and women
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
….never use condoms with
casual partners/clients
….sometimes use condoms with casual
partners/clients
….always use condoms with
casual partners/clients
….regularly have an STI (other
than HIV)
Prop
ortio
n pe
rcei
ved
by
parti
cipa
nts
as
elig
ble
for P
rEP
C. Commercial sexworkers
STI nurse
STI physician
STI other profession
HIV nurse
HIV physician
Figure 2. Beliefs among healthcare professionals as to which key populations are eligible for PrEP in the Neth-erlands: (a) men having sex with men, (B) heterosexual men and women, and (C) commercial sex workersSTI, sexually transmitted infection; PEP, post-exposure prophylaxis; PrEP, pre-exposure prophylaxis.

Chapter 2.3
98
dISCuSSIon
This cross-sectional study on PrEP acceptability and its determinants found only moderate PrEP acceptability among STI professionals and HIV specialists. These moderate levels of acceptability are worrisome as they may impede smooth implementation of PrEP in the Netherlands. Facilitating factors toward PrEP acceptability in the Netherlands were the beliefs that PrEP is an effective intervention to prevent HIV, PrEP prescription should be a part of routine care at STI clinics, PrEP is a good addition to prevention strategies, and that taking PrEP is better than getting HIV. Beliefs forming barriers to PrEP implementation were the perceived potential decrease in condom use and the increase in STI prevalence, the high costs of PrEP, and the belief that it is unethical to prescribe ART to healthy individuals. Previous studies on PrEP-related beliefs of healthcare professionals in developed countries have identified concerns regarding drug resistance, low adherence, a rise in STI, long-term toxicity, and lack of country-specific guidance.11-15 Some of these findings are now corrobo-rated by our data for the Dutch context.
In order to increase the acceptability of PrEP implementation among healthcare profession-als in the Netherlands, the beliefs that may form barriers for PrEP implementation need to be addressed and beliefs that could facilitate PrEP implementation need to be more broadly communicated. Regarding the concerns around the anticipated decrease in condom use and the increase in STI in PrEP users, open-label studies showed mixed results.16-21 If PrEP is implemented in the Netherlands, structured sexual-risk behaviour counselling should be offered as the standard component of consultations.22 Addressing such concerns among healthcare professionals and offering them tools to intervene on such topics among their clients may increase PrEP acceptability.
In our study and others across Europe,23 beliefs regarding the high costs of PrEP were likewise found to be a potential barrier for PrEP implementation. The costs of PrEP are indeed high and the implementation of PrEP therefore costly, but this barrier may be partly overcome if the study results that PrEP is most likely to be cost-effective and potentially even cost-saving are highlighted.10,24,25 In our study, over half of participants had the opinion that PrEP users need to contribute to the costs of PrEP. However, this was not further explored in relation to the amount that would need to be contributed and to the income. For those who cannot otherwise afford PrEP, the acceptability of public funding of costs was high in a study from the USA.26 The high costs have also shown to be a potential barrier for the use of PrEP by potentially eligible candidates in the Netherlands.27,28 The problem of cost combined with the lack of a reimbursement system clearly requires a solution to enable successful PrEP implementation in the Netherlands and probably in other countries lacking PrEP reimburse-ment programs. The recent introduction of significantly cheaper generic PrEP, also in the

99
Beliefs of healthcare professionals on PrEP
2.3
Netherlands,29 could provide a partial answer to the growing demand from PrEP in countries that lack a reimbursement system.
Although adherence to PrEP and long-term side effects were important concerns for partici-pants, they were in our analysis not associated with the acceptability of PrEP implementa-tion in the Netherlands. This finding could reflect current professional knowledge that (1) even with suboptimal levels of adherence, PrEP still yields a high level of protection and does not lead to drug resistance;16 and (2) possible long-term side are likely to be non-severe.7,30,31
Among STI professionals, self-perceived knowledge of PrEP efficacy and side effects was significantly lower compared to HIV specialists, perhaps a result of their different educa-tional and professional background. An alternative explanation is that data were collected earlier among STI professionals than among HIV specialists, and the interim period saw new research outcomes of PrEP studies,5-7 publication of the World Health Organization PrEP guidelines,1 and publicity for the start of the Amsterdam PrEP project.32 These developments could explain differences in knowledge between the two professional groups. It is important to improve PrEP knowledge among STI professionals, particularly as future PrEP programs are likely to be implemented at STI clinics. Many MSM at risk for HIV and STI make use of free STI testing and treatment at Dutch STI clinics,33 and therefore PrEP counselling and provision could easily be incorporated into this setting. Our results also show that among HIV specialists, the implementation of PrEP is more acceptable at STI clinics than at HIV treatment centers. Although HIV specialists have more knowledge regarding ART, people wanting PrEP are not normally in need of such expensive and specialized hospital-based knowledge or care.
In regard to use of daily or event-driven PrEP, our study showed no clear preference among the respondents. This may reflect the timing of the survey, which was taken just after the early interruption of two large European PrEP studies (one among daily and one among event-driven PrEP users) that both showed 86% reduction in the number of new HIV infec-tions.5,6
As for key eligible populations, healthcare professionals focused on MSM at a high risk of sexual acquisition of HIV and heterosexuals with an HIV-positive partner with a detectable viral load. These findings align with other studies34,35 and with recommendations for PrEP use in guidelines,1-3 indicating that healthcare professionals in STI clinics and HIV treatment centers can correctly identify individuals eligible for PrEP.
Strengths of this study are its nationwide character, its use of both nurses and medical doc-tors from two different settings, and its application of measurement tools that were empiri-

Chapter 2.3
100
cally generated through a qualitative elicitation process. However, some limitations need to be addressed. First, the number of completed questionnaires and the response rate were relatively low, as is common in survey-based research.36 Nevertheless, people from almost all invited STI clinics responded, as did more than one-third of HIV specialists. Second, to increase the response rate in the latter group, they were provided with a shorter question-naire than was given to STI professionals, which made the comparison between the two groups more limited. Third, we did not include general practitioners in our study. As it may be likely that PrEP is implemented at general practitioners, PrEP acceptability should also be explored among this group of healthcare professionals.
In conclusion, healthcare professionals in STI clinics and HIV treatment centers in the Neth-erlands have only a moderate level of acceptability toward PrEP implementation, and PrEP knowledge among STI professionals is suboptimal. This may impede the smooth implemen-tation of PrEP in the Netherlands. The high costs of PrEP, worries about a possible decrease in condom use and an increase in STI, and the belief that it is unethical to prescribe ART to healthy individuals were identified as influential barriers for PrEP implementation and need to be addressed in order to successfully implement PrEP in the future. Furthermore, it is important to increase PrEP knowledge in educational programs for STI professionals.
acknowledgements
The authors wish to thank the following persons for their invaluable support: all participants of the study, Annebel Tahey for dissemination of the survey at the STI outpatient clinic of the Public Health Service of Amsterdam, Ineke Stolte for help with designing the questionnaire, and Lucy Phillips for editing this manuscript.
funding
This project received funding from the Public Health Service of Amsterdam Research and Development Funds (grant number 16–11).
Conflicts of interest
The institute received financial reimbursement for time served by Elske Hoornenborg on advisory boards of Gilead Sciences. For Maria Prins, the institute received independent re-search support and speaker’s fees from Gilead, AbbVie, MSD, and Roche. For Udi Davidovich, the institute received independent research support from Gilead, AbbVie, MSD, and ViiV. The Public Health Service of Amsterdam receives PrEP medication from Gilead Sciences for the Amsterdam PrEP project, and participates in a Gilead-sponsored study. All other authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.

101
Beliefs of healthcare professionals on PrEP
2.3
referenCes
1. World Health Organization (WHO). Guideline on when to start antiretroviral therapy and on pre-exposure prohylaxis for HIV. Geneva: WHO, 2015.
2. European AIDS Clinincal Society (EACS). european Guidelines for treatment of HIV-positive adults in europe; Guidelines 9.0. Brussels: EACS, 2015.
3. Centers for Disease Control and Prevention (CDC). Pre-exposure Prophylaxis for the prevention of HIV infection in the united States, 2014: a clinical Practice Guideline. CDC, 2014.
4. Grant RM, Lama JR, Anderson PL, McMahan V, Liu AY, Vargas L, et al. Preexposure chemoprophy-laxis for HIV prevention in men who have sex with men. N Engl J Med. 2010;363(27):2587-2599. doi:10.1056/NEJMoa1011205.
5. McCormack S, Dunn DT, Desai M, Dolling DI, Gafos M, Gilson R, et al. Pre-exposure prophylaxis to prevent the acquisition of HIV-1 infection (Proud): effectiveness results from the pilot phase of a pragmatic open-label randomised trial. Lancet. 2016;387(10013):53-60. doi:10.1016/S0140-6736(15)00056-2.
6. Molina JM, Capitant C, Spire B, Pialoux G, Cotte L, Charreau I, et al. on-demand Preexposure Prophy-laxis in Men at High risk for HIV-1 Infection. N Engl J Med. 2015;373(23):2237-2246. doi:10.1056/NEJMoa1506273.
7. Fonner VA, Dalglish SL, Kennedy CE, Baggaley R, O’Reilly KR, Koechlin FM, et al. effectiveness and safety of oral HIV preexposure prophylaxis for all populations. AIDS. 2016;30(12):1973-1983. doi:10.1097/QAD.0000000000001145.
8. UNAIDS. aIdS by the numbers. Available at: http://www.unaids.org/sites/default/files/media_asset/AIDS-by-the-numbers-2016_en.pdf (accessed on 6 November 2017).
9. Ratmann O, van Sighem A, Bezemer D, Gavryushkina A, Jurriaans S, Wensing A, et al. sources of HIV infection among men having sex with men and implications for prevention. Sci Transl Med. 2016;8(320):320ra322. doi:10.1126/scitranslmed.aad1863.
10. Nichols BE, Boucher CAB, van der Valk M, Rijnders BJA, van de Vijver D. Cost-effectiveness analysis of pre-exposure prophylaxis for HIV-1 prevention in the netherlands: a mathematical modelling study. Lancet Infect Dis. 2016;16(12):1423-1429. doi:10.1016/S1473-3099(16)30311-5.
11. Tellalian D, Maznavi K, Bredeek UF, Hardy WD. Pre-exposure prophylaxis (PreP) for HIV infection: results of a survey of HIV healthcare providers evaluating their knowledge, attitudes, and prescrib-ing practices. AIDS Patient Care STDS. 2013;27(10):553-559. doi:10.1089/apc.2013.0173.
12. Krakower D, Ware N, Mitty JA, Maloney K, Mayer KH. HIV providers’ perceived barriers and facilita-tors to implementing pre-exposure prophylaxis in care settings: a qualitative study. AIDS Behav. 2014;18(9):1712-1721. doi:10.1007/s10461-014-0839-3.
13. Puro V, Palummieri A, De Carli G, Piselli P, Ippolito G. attitude towards antiretroviral Pre-exposure Pro-phylaxis (PreP) prescription among HIV specialists. BMC Infect Dis. 2013;13:217. doi:10.1186/1471-2334-13-217.
14. Krakower DS, Mayer KH. the role of healthcare providers in the roll out of preexposure prophylaxis. Curr Opin HIV AIDS. 2016;11(1):41-48. doi:10.1097/COH.0000000000000206.
15. Desai M, Gafos M, Dolling D, McCormack S, Nardone A, study P. Healthcare providers’ knowledge of, attitudes to and practice of pre-exposure prophylaxis for HIV infection. HIV Med. 2016;17(2):133-142. doi:10.1111/hiv.12285.
16. Grant RM, Anderson PL, McMahan V, Liu A, Amico KR, Mehrotra M, et al. uptake of pre-exposure prophylaxis, sexual practices, and HIV incidence in men and transgender women who have sex with men: a cohort study. Lancet Infect Dis. 2014;14(9):820-829. doi:10.1016/S1473-3099(14)70847-3.

Chapter 2.3
102
17. Liu AY, Cohen SE, Vittinghoff E, Anderson PL, Doblecki-Lewis S, Bacon O, et al. Preexposure Prophy-laxis for HIV Infection Integrated With Municipal- and Community-Based Sexual Health Services. JAMA Intern Med. 2016;176(1):75-84. doi:10.1001/jamainternmed.2015.4683.
18. Marcus JL, Hurley LB, Hare CB, Nguyen DP, Phengrasamy T, Silverberg MJ, et al. Preexposure Prophylaxis for HIV Prevention in a large Integrated Health Care System: adherence, renal Safety, and discon-tinuation. J Acquir Immune Defic Syndr. 2016;73(5):540-546. doi:10.1097/QAI.0000000000001129.
19. Volk JE, Marcus JL, Phengrasamy T, Blechinger D, Nguyen DP, Follansbee S, et al. no new HIV Infec-tions With Increasing use of HIV Preexposure Prophylaxis in a Clinical Practice Setting. Clin Infect Dis. 2015;61(10):1601-1603. doi:10.1093/cid/civ778.
20. Montano M, Dombrowsk, J, Barbee, A, Golden, M, Khosropour, C. Changes in sexual behavior and STI diagnoses among MSM using PreP in Seattle, Wa [abstract 979]. Conference on Retroviruses and Opportunistic Infections: Seattle, Washington, USA, 13-16 February 2017.
21. Lal L, Audsley J, Murphy DA, Fairley CK, Stoove M, Roth N, et al. Medication adherence, condom use and sexually transmitted infections in australian preexposure prophylaxis users. AIDS. 2017;31(12):1709-1714. doi:10.1097/QAD.0000000000001519.
22. Nederlandse vereniging van hiv behandelaren (NVHB). HIV Pre-expositie profylaxe (PreP) richtlijn nederland. Amsterdam: NVHB, 2016.
23. Noori T, Pharris A. Meeting report: Pre-exposure Human Immunodeficiency Virus Prophylaxis in the eu/eea: Challenges and opportunities, Stockholm april 2016. Euro Surveill. 2016;21(25) doi:10.2807/1560-7917.ES.2016.21.25.30263.
24. Cambiano V, Miners A, Dunn D, McCormack S, Ong KJ, Gill ON, et al. Cost-effectiveness of pre-exposure prophylaxis for HIV prevention in men who have sex with men in the uK: a modelling study and health economic evaluation. Lancet Infect Dis. 2018;18(1):85-94. doi:10.1016/S1473-3099(17)30540-6.
25. Ong KJ, Desai S, Field N, Desai M, Nardone A, van Hoek AJ, et al. economic evaluation of HIV pre-exposure prophylaxis among men-who-have-sex-with-men in england in 2016. Euro Surveill. 2017;22(42) doi:10.2807/1560-7917.ES.2017.22.42.17-00192.
26. Smith DK, Mendoza MC, Stryker JE, Rose CE. PreP awareness and attitudes in a national Survey of Primary Care Clinicians in the united States, 2009-2015. PLoS One. 2016;11(6):e0156592. doi:10.1371/journal.pone.0156592.
27. Bil JP, Davidovich U, van der Veldt WM, Prins M, de Vries HJ, Sonder GJ, et al. What do dutch MSM think of preexposure prophylaxis to prevent HIV-infection? a cross-sectional study. AIDS. 2015;29(8):955-964. doi:10.1097/QAD.0000000000000639.
28. Bil JP, van der Veldt WM, Prins M, Stolte IG, Davidovich U. Motives of dutch men who have sex with men for daily and intermittent HIV pre-exposure prophylaxis usage and preferences for implementation: a qualitative study. Medicine (Baltimore). 2016;95(39):e4910. doi:10.1097/MD.0000000000004910.
29. Nu.nl. PreP available in the netherlands at 80% lower price. Available at: https://www.nu.nl/gezondheid/4982345/hiv-preventiepil-prep-wordt-ruim-80-procent-goedkoper.html (accessed on 6 November 2017).
30. Winston J, Chonchol M, Gallant J, Durr J, Canada RB, Liu H, et al. discontinuation of tenofovir diso-proxil fumarate for presumed renal adverse events in treatment-naive HIV-1 patients: meta-analysis of randomized clinical studies. HIV Clin Trials. 2014;15(6):231-245. doi:10.1310/hct1506-231.
31. Tinago W, Cotter AG, Sabin CA, Macken A, Kavanagh E, Brady JJ, et al. Predictors of longitudinal change in bone mineral density in a cohort of HIV-positive and negative patients. AIDS. 2017;31(5):643-652. doi:10.1097/QAD.0000000000001372.

103
Beliefs of healthcare professionals on PrEP
2.3
32. AMPrEP study group. study protocol amPreP. Available at: http://www.trialregister.nl/trialreg/admin/rctsearch.asp?Term=amprep (accessed on 14 June 2017).
33. Rijksinstituut voor Volksgezondheid en Milieu (RIVM). Sexually transmitted infections including HIV, in the netherlands in 2016. Bilthoven: RIVM, 2017.
34. Adams LM, Balderson BH. HIV providers’ likelihood to prescribe pre-exposure prophylaxis (PreP) for HIV prevention differs by patient type: a short report. AIDS Care. 2016;28(9):1154-1158. doi:10.1080/09540121.2016.1153595.
35. Krakower DS, Beekmann SE, Polgreen PM, Mayer KH. diffusion of newer HIV Prevention Innovations: Variable Practices of Frontline Infectious diseases Physicians. Clin Infect Dis. 2016;62(1):99-105. doi:10.1093/cid/civ736.
36. BMJ. Planning and conducting a survey. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/epidemiology-uninitiated/5-planning-and-conducting-survey (accessed on 14 June 2017).

Chapter 2.3
104
SuPP
leM
enTa
rY T
aBl
eS
Tabl
e S1
. Ove
rvie
w o
f PrE
P be
liefs
, mea
sure
d ite
ms a
nd re
liabi
lity
of it
ems m
easu
red
amon
g ST
I pro
fess
iona
ls an
d HI
V sp
ecia
lists
, the
Net
herla
nds (
2015
)Be
liefs
and
item
s mea
sure
d am
ong
stI p
rofe
ssio
nals
Belie
fsIte
ms
Corr
elati
ona
It is
uncl
ear w
ho h
as to
pay
for P
rEP
I bel
ief i
t is t
o un
clea
r who
shou
ld p
ay fo
r PrE
PN
A
Taki
ng P
rEP
is be
tter t
han
getti
ng H
IVI b
elie
f tha
t tak
ing
PrEP
is b
etter
than
getti
ng H
IVN
A
Adhe
renc
e to
PrE
P w
ill b
e in
suffi
cien
tI w
ould
wor
ry a
bout
adh
eren
ce to
PrE
P w
hen
prov
idin
g Pr
EP0.
72
I wou
ld w
orry
abo
ut th
e m
isuse
of P
rEP
The
role
of t
he p
harm
aceu
tical
co
mpa
nies
in re
gard
s to
PrEP
is u
ncle
arI w
ould
wor
ry a
bout
the
role
of t
he p
harm
aceu
tical
com
pani
es w
hen
prov
idin
g Pr
EPN
A
The
use
of P
rEP
will
lead
to a
dec
reas
e in
con
dom
use
and
incr
ease
in S
TIs
I bel
ief t
hat p
rovi
ding
PrE
P sti
mul
ates
risk
beh
avio
ur0.
90
I bel
ief t
hat p
rovi
ding
PrE
P de
crea
ses p
erso
nal r
espo
nsib
ility
to p
reve
nt H
IV
I bel
ief t
he u
se o
f PrE
P w
ill le
ad to
a d
ecre
ase
in c
ondo
m u
se
I bel
ief P
rEP
is a
cart
e bl
anch
e to
stop
usin
g co
ndom
s
I bel
ief P
rEP
will
cha
nge
the
norm
in re
gard
s to
cond
om u
se
I bel
ief t
hat i
s mor
e di
fficu
lt to
use
con
dom
s afte
r som
eone
has
stop
ped
usin
g Pr
EP
I bel
ief t
hat t
he u
se o
f PrE
P w
ill le
ad to
an
incr
ease
in th
e nu
mbe
r of S
TIs
As th
ere
will
be
an in
crea
se in
STI
s due
to P
rEP,
I be
lief t
hat t
here
is a
n in
crea
sed
HIV
tran
smiss
ion
risk
inst
ead
of d
ecre
ased
PrEP
is c
heap
er th
an li
fe lo
ng H
IV
trea
tmen
tI b
elie
f PrE
P us
ing
PrEP
is c
heap
er th
an u
sing
life
long
HIV
trea
tmen
tN
A
PrEP
is a
n eff
ectiv
e in
terv
entio
n to
pr
even
t HIV
I bel
ief t
hat P
rEP
is an
effe
ctive
inte
rven
tion
for i
ndiv
idua
ls to
pre
vent
HIV
0.67
I bel
ief P
rEP
is an
effe
ctive
inte
rven
tion
to re
duce
the
num
ber o
f new
HIV
infe
ction
s in
the
Net
herla
nds
PrEP
pre
scrip
tion
shou
ld b
e pa
rt o
f ro
utine
car
e of
STI
clin
ics
I bel
ief i
t is i
mpo
rtan
t tha
t the
STI
clin
ic su
ppor
ts n
ew d
evel
opm
ents
, suc
h as
PrE
P0.
82
I bel
ief t
hat P
rEP
pres
crip
tion
shou
ld b
e pa
rt o
f rou
tine
care
of S
TI c
linic
s

105
Beliefs of healthcare professionals on PrEP
2.3
Tabl
e S1
. (co
ntinu
ed)
Belie
fs a
nd it
ems m
easu
red
amon
g st
I pro
fess
iona
ls
Belie
fsIte
ms
Corr
elati
ona
Ther
e is
not e
noug
h kn
owle
dge
yet
abou
t PrE
PI b
elie
f tha
t the
re is
not
eno
ugh
know
ledg
e ye
t abo
ut th
e lo
ng te
rm e
ffect
s of P
rEP
to st
art p
rovi
ding
PrE
P at
the
STI c
linic
0.82
I bel
ief t
hat t
hey
key
popu
latio
ns fo
r PrE
P is
to u
ncle
ar y
et
I wou
ld w
orry
abo
ut th
e effi
cacy
of P
rEP
I wou
ld w
orry
abo
ut th
e lo
ng te
rm si
de e
ffect
s of P
rEP
whe
n pr
ovid
ing
PrEP
I wou
ld w
orry
abo
ut A
RT re
sista
nce
whe
n pr
ovid
ing
PrEP
Cost
s of P
rEP
are
a pr
oble
mI b
elie
f the
re is
not
eno
ugh
publ
ic su
ppor
t to
prov
ide
PrEP
0.80
I bel
ief t
here
is n
ot e
noug
h pu
blic
supp
ort f
or th
e co
vera
ge o
f PrE
P co
sts
I bel
ief i
t is b
etter
to sp
ent m
oney
and
reso
urce
s on
othe
r int
erve
ntion
s tha
n Pr
EP
I bel
ief t
he c
osts
of t
reati
ng o
ther
STI
s will
incr
ease
due
to th
e us
e of
PrE
P
I bel
ief t
hat y
ou sh
ould
not
pro
vide
exp
ensiv
e dr
ugs t
o in
divi
dual
s tha
t are
not
will
ing
to h
ave
safe
sex
I wou
ld w
orry
that
som
e pe
ople
hav
e to
use
PrE
P lif
e lo
ngI w
ould
wor
ry th
at so
me
indi
vidu
als w
ould
use
PrE
P lif
e lo
ng w
hen
prov
idin
g Pr
EPN
A
It is
unet
hica
l to
pres
crib
e an
tiret
rovi
ral
ther
apy
to h
ealth
y in
divi
dual
sI b
elie
f it i
s une
thic
al to
pre
scrib
e he
alth
y in
divi
dual
s dai
ly p
ills t
o pr
even
t HIV
0.91
I bel
ief t
hat b
y pr
ovid
ing
PrEP
we
incr
ease
med
ical
izatio
n
I bel
ief t
akin
g m
edic
ation
to su
ppor
t sex
ual c
hoic
es is
unw
ante
d
I bel
ief t
akin
g Pr
EP li
felo
ng b
y he
alth
y in
divi
dual
s is w
orris
ome
I bel
ief t
akin
g Pr
EP te
mpo
raril
y by
hea
lthy
indi
vidu
als i
s wor
risom
e

Chapter 2.3
106
Tabl
e S1
. (co
ntinu
ed)
Belie
fs a
nd it
ems m
easu
red
amon
g st
I pro
fess
iona
ls
Belie
fsIte
ms
Corr
elati
ona
PrEP
is a
goo
d ad
ditio
n to
pre
venti
on
stra
tegi
esI b
elie
f PrE
P is
a go
od a
dditi
on fo
r ind
ivid
uals
that
are
not
abl
e to
use
con
dom
s con
siste
ntly
0.81
I bel
ief P
rEP
is a
good
add
ition
for i
ndiv
idua
ls in
a se
rodi
scor
dant
rela
tions
hip
I bel
ief P
rEP
is a
good
add
ition
for i
ndiv
idua
ls w
ith h
igh
HIV
anxi
ety
I bel
ief P
rEP
is a
good
add
ition
to in
crea
se th
e qu
ality
of s
ex li
fe
I bel
ief P
rEP
is un
nece
ssar
y as
ther
e ar
e be
tter a
ltern
ative
s to
prev
ent H
IVb
I bel
ief t
hat p
rovi
ding
PrE
P w
ill in
terfe
re w
ith c
urre
nt c
ouns
ellin
g st
rate
gies
b
I bel
ief t
hat P
rEP
has t
he a
dvan
tage
to p
rovi
de e
xtra
cou
nsel
ling
to th
ose
at h
igh
risk
of H
IV
I bel
ief t
hat i
ndiv
idua
ls w
ho a
re n
ot a
ble
to u
se c
ondo
ms c
onsis
tent
ly a
re a
lso n
ot a
ble
to c
onsis
tent
ly u
se d
aily
dru
gsb
We
shou
ld p
rovi
de b
oth
daily
and
eve
nt-d
riven
PrE
P as
I be
lief t
hat t
his i
ncre
ases
the
choi
ce o
f HIV
pre
venti
on o
ption
s
The
cost
s of P
rEP
will
not
out
wei
gh th
e nu
mbe
r of H
IV in
fecti
ons p
reve
nted
I bel
ief t
he c
osts
of P
rEP
will
not
out
wei
gh th
e nu
mbe
r of H
IV in
fecti
ons p
reve
nted
NA
The
STI-c
linic
is n
ot th
e rig
ht p
lace
for
PrEP
pre
scrip
tion
I bel
ief t
he S
TI c
linic
has
the
mor
al o
blig
ation
to d
o re
sear
ch o
n Pr
EPb
0.72
I bel
ief p
rovi
ding
PrE
P co
mpl
icat
es c
urre
nt g
uide
lines
I bel
ief t
he S
TI c
linic
lack
s cap
acity
to p
resc
ribe
PrEP
I bel
ief t
he S
TI c
linic
lack
s the
kno
wle
dge
and
abili
ty to
pro
vide
cou
nsel
ling
for P
rEP
adhe
renc
e
I bel
ief t
he S
TI c
linic
is th
e rig
ht p
lace
to re
ach
the
key
popu
latio
ns fo
r PrE
Pb
Daily
use
of p
reve
ntion
stra
tegi
es h
as
alre
ady
been
test
ed b
efor
eI w
ould
not
wor
ry a
bout
adh
eren
ce b
ecau
se d
aily
use
of d
rugs
for t
he p
reve
ntion
of c
ondi
tions
has
alre
ady
been
pro
ven
to
wor
kN
A
Belie
fs a
nd it
ems m
easu
red
amon
g HI
V sp
ecia
lists
Belie
fsIte
ms
Corr
elati
on1
The
use
of P
rEP
will
lead
to a
dec
reas
e in
con
dom
use
and
incr
ease
in S
TIs
I bel
ief t
he u
se o
f PrE
P w
ill le
ad to
a d
ecre
ase
in c
ondo
m u
se0.
83
I bel
ief t
hat t
he u
se o
f PrE
P w
ill le
ad to
an
incr
ease
in th
e nu
mbe
r of S
TIs

107
Beliefs of healthcare professionals on PrEP
2.3
Tabl
e S1
. (co
ntinu
ed)
Belie
fs a
nd it
ems m
easu
red
amon
g st
I pro
fess
iona
ls
Belie
fsIte
ms
Corr
elati
ona
PrEP
is a
n eff
ectiv
e in
terv
entio
n to
pr
even
t HIV
I bel
ief t
hat P
rEP
is an
effe
ctive
inte
rven
tion
for i
ndiv
idua
ls to
pre
vent
HIV
0.73
I bel
ief P
rEP
is an
effe
ctive
inte
rven
tion
to re
duce
the
num
ber o
f new
HIV
infe
ction
s in
the
Net
herla
nds
As th
ere
will
be
an in
crea
se in
STI
s due
to P
rEP,
I be
lief t
hat t
here
is a
n in
crea
sed
HIV
tran
smiss
ion
risk
inst
ead
of d
ecre
ased
b
I bel
ief P
rEP
will
be
cost
effe
ctive
.
I’m b
elie
f tha
t the
re is
not
eno
ugh
know
ledg
e ye
t abo
ut P
rEP
in a
real
-life
setti
ngb
I’m w
orrie
d th
at P
rEP
is no
t 100
% e
ffecti
veb
I’m w
orrie
d ab
out P
rEP
adhe
renc
eb
It is
unet
hica
l to
pres
crib
e an
tiret
rovi
ral
ther
apy
to h
ealth
y in
divi
dual
sI b
elie
f it i
s une
thic
al to
pre
scrib
e he
alth
y in
divi
dual
s dai
ly p
ills t
o pr
even
t HIV
NA
PrEP
is a
goo
d ad
ditio
n to
pre
venti
on
stra
tegi
esI b
elie
f PrE
P is
unne
cess
ary
as th
ere
are
bette
r alte
rnati
ve to
pre
vent
HIV
bN
A
I’m w
orrie
d ab
out t
he lo
ng te
rm si
de
effec
ts o
f PrE
PI’m
wor
ried
abou
t the
long
term
side
effe
cts o
f PrE
PN
A
PrEP
will
lead
to a
n in
crea
se in
HIV
re
sista
nce
I bel
ief t
hat t
he u
se o
f ART
for p
reve
ntion
will
lead
to a
n in
crea
se in
HIV
resis
tanc
eN
A
Non
-bio
med
ical
HIV
inte
rven
tions
(i.e
., be
havi
oura
l int
erve
ntion
s) a
re b
etter
I thi
nk n
on-b
iom
edic
al H
IV in
terv
entio
n lik
e be
havi
oura
l int
erve
ntion
are
bett
er th
an P
rEP
NA
I’m w
orrie
d ab
out t
he sh
ort t
erm
side
eff
ects
of P
rEP
I’m w
orrie
d ab
out t
he sh
ort t
erm
side
effe
cts o
f PrE
PN
A
PrEP
, pre
-exp
osur
e pr
ophy
laxi
s; S
TI, s
exua
lly tr
ansm
itted
infe
ction
.Al
l ite
ms a
nd b
elie
fs w
ere
mea
sure
d on
a 7
-poi
nt sc
ale
rang
ing
from
1”C
ompl
etel
y di
sagr
ee”
to 7
”Com
plet
ely
agre
e”.
The
ques
tionn
aire
am
ong
STI c
linic
pro
fess
iona
ls in
clud
ed a
ll Pr
EP b
elie
fs m
easu
red
in th
e fo
cus
grou
p di
scus
sions
. The
que
stion
naire
am
ong
HIV
trea
ting
spec
ialis
ts o
nly
incl
uded
maj
or th
emes
that
wer
e de
rived
from
the
anal
yses
from
the
focu
s gro
up d
iscus
sions
.a I
tem
s wer
e co
mbi
ned
if th
ey m
easu
red
the
sam
e be
lief a
nd h
ad a
ccep
tabl
e co
rrel
ation
(2 it
ems:
Spe
arm
an rh
o >0
.6 a
nd p
<0.0
5; >
2 ite
ms:
Cro
nbac
h’s a
lpha
>0.
7)b T
he re
vers
ed sc
ale
was
use
d to
com
bine
this
item
with
the
othe
r ite
ms i
n th
e as
soci
ated
bel
ief

Chapter 2.3
108
Tabl
e S2
. Bel
iefs
abo
ut e
vent
-driv
en v
ersu
s dai
ly P
rEP
amon
g 20
9 he
alth
care
pro
vide
rs, t
he N
ethe
rland
s (20
15)
Item
s
stI p
rofe
ssio
nals
HIV
spec
ialis
ts
STI p
rofe
ssio
nals
vs.
HI
V sp
ecia
lists
tota
ln
urse
Phys
icia
no
ther
STI n
urse
vs.
st
I phy
sici
an
vs. S
TI o
ther
tota
ln
urse
Phys
icia
nHI
V nu
rse
vs.
HIV
phys
icia
n(N
=143
)(n
=93)
(n=3
7)(n
=13)
(N=6
6)(n
=40)
(n=2
6)
mea
nSd
mea
nSd
mea
nSd
mea
nSd
mea
nSd
mea
nSd
mea
nSd
Even
t-driv
en P
rEP
is a
bette
r opti
on
than
dai
ly P
rEP
4.14
1.48
4.08
1.56
4.35
1.42
4.00
1.00
F(2,
140)
=0.5
2,p=
0.59
34.
261.
434.
231.
194.
311.
76t(
64)=
0.23
,p=
0.82
0t(
207)
=-0.
54,
p=0.
589
Even
t-driv
en P
rEP
is ea
sier t
o m
aint
ain
than
dai
ly P
rEP
4.38
1.47
4.35
1.49
4.54
1.48
4.15
1.34
F(2,
140)
=0.3
8,p=
0.68
34.
771.
614.
831.
484.
691.
81t(
207)
=-0.
33,
p=0.
746
t(20
7)=-
1.72
,p=
0.08
7
Daily
PrE
P is
mor
e eff
ectiv
e th
an e
vent
-dr
iven
PrE
P14.
391.
274.
241.
144.
781.
474.
381.
45F(
2,14
0)=2
.50,
p=0.
086
4.18
1.49
4.50
1.32
3.69
1.62
t(20
7)=-
2.22
,p=
0.03
0t(
207)
=1.0
5,p=
0.29
5
Even
t-driv
en P
rEP
will
be
pref
erre
d ov
er
daily
PrE
P be
caus
e it
will
be
chea
per
4.52
1.31
4.43
1.38
4.54
1.17
5.08
1.11
F(2,
140)
=1.4
1,p=
0.24
94.
411.
604.
351.
564.
501.
68t(
207)
=0.3
7,p=
0.71
3t(
207)
=0.5
2,p=
0.60
5
Even
t-driv
en P
rEP
will
be
less
of a
bu
rden
than
dai
ly P
rEP
4.59
1.42
4.48
1.38
4.92
1.38
4.38
1.71
F(2,
140)
=1.4
0,p=
0.24
94.
731.
334.
781.
354.
651.
32t(
207)
=-0.
36,
p=0.
721
t(20
7)=-
0.68
,p=
0.49
7
I hav
e le
ss o
bjec
tions
aga
inst
pro
vidi
ng
even
t-driv
en P
rEP
than
aga
inst
pr
ovid
ing
daily
PrE
P
3.55
1.72
3.53
1.69
3.57
1.80
3.62
1.80
F(2,
140)
=0.0
2,p=
0.98
13.
521.
823.
751.
583.
152.
11t(
207)
=-1.
31,
p=0.
195
t(20
7)=0
.12,
p=0.
908
Even
t-driv
en P
rEP
is m
ore
com
plic
ated
to
use
cor
rect
ly th
an d
aily
PrE
Pa4.
871.
454.
841.
424.
971.
484.
851.
72F(
2,14
0)=0
.11,
p=0.
892
4.50
1.63
4.73
1.52
4.15
1.76
t(20
7)=-
1.40
,p=
0.16
6t(
207)
=1.6
6,p=
0.09
8
ove
rall:
eve
nt-d
riven
Pre
P is
pre
ferr
ed
over
dai
ly P
rePb
3.99
1.00
3.97
1.03
4.02
0.95
4.00
0.99
F(2,
140)
=0.0
4,p=
0.96
44.
141.
014.
100.
914.
211.
17t(
64)=
-0.4
2,p=
0.67
3t(
207)
=-1.
05,
p=0.
297
PrEP
, pre
-exp
osur
e pr
ophy
laxi
s; S
TI, s
exua
lly tr
ansm
itted
infe
ction
; SD,
stan
dard
dev
iatio
n.Al
l ite
ms a
nd b
elie
fs w
ere
mea
sure
d on
a 7
-poi
nt sc
ale
rang
ing
from
1”C
ompl
etel
y di
sagr
ee”
to 7
”Com
plet
ely
agre
e”.
a The
reve
rsed
scal
e w
as u
sed
to c
ombi
ne th
is ite
m w
ith th
e ot
her i
tem
s in
the
over
all b
elie
f “ev
ent-d
riven
PrE
P is
pref
erre
d ov
er d
aily
PrE
P”b I
nclu
des a
ll ite
ms m
easu
red
amon
g ST
I clin
ic p
rofe
ssio
nals
and
HIV
trea
ting
spec
ialis
ts (S
TI c
linic
pro
fess
iona
ls: C
ronb
ach’
s alp
ha=0
.81;
HIV
trea
ting
spec
ialis
ts: C
ronb
ach’
s al
pha=
0.77
).



Chapter 3testing opportunities for HIV, hepatitis B,
hepatitis C and sexually transmitted infections


Chapter 3.1disparities in access to and use of HIV-
related health services in the netherlands by migrant status and sexual orientation:
A cross-sectional study among people recently diagnosed with HIV infection
Janneke P. Bil, Freke R. Zuure, Debora Alvarez-del Arco, Jan M.Prins, Kees Brinkman, Eliane Leyten, Ard van Sighem, Fiona Burns, Maria Prins
Submitted

Chapter 3.1
114
aBstraCt
Background
Migrants often face barriers to accessing healthcare. We examined disparities in access to and use of HIV-related health services between migrant and non-migrant people recently diagnosed with HIV living in the Netherlands, taken into account sexual orientation. Also, we examined differences in experiences in living with HIV between these groups.
methods
We used a questionnaire and clinical data collected between July 2013 and June 2015 among migrant and non-migrant participants of the European cross-sectional aMASE (Advancing Migrant Access to health Services in Europe) study in the Netherlands. Using univariable lo-gistic regression analyses, we compared outcomes on between migrants and non-migrants, stratified by sexual orientation (with non-migrant men having sex with men - MSM - as the reference group).
results
We included 77 migrant MSM, 115 non-migrant MSM, 21 migrant heterosexual men, 14 non-migrant heterosexual men and 20 migrant women. In univariable analyses, all heterosexual groups were less likely to ever have had an HIV-negative test before their diagnosis and were more likely to be diagnosed late than non-migrant MSM. All migrant groups were more likely to have experienced difficulties accessing general healthcare in the Netherlands and were less likely to have heard of post-exposure prophylaxis than non-migrant MSM. Migrants frequently reported uncertainty about their rights to healthcare and language barriers. Most (93%) participants visited a healthcare facility in the two years before HIV diagnosis but only in 41% an HIV test was discussed during that visit (no statistical difference between groups). Migrant heterosexuals were more likely to have missed appointments at their HIV clinic due to the travel costs than non-migrant MSM. Migrant MSM and women were more likely to have experienced HIV discrimination in the Netherlands than non-migrant MSM.
Conclusion
Disparities in access to and use of HIV-related health services and experiences exist by mi-grant status but also by sexual orientation. Our data suggests heterosexual men and women may particularly benefit from improved access to HIV testing (e.g., through provider-initiated testing), while migrant MSM may benefit from improved access to HIV prevention interven-tions (e.g., pre-exposure prophylaxis).

115
Access to and use of HIV-related healthcare services
3.1
BaCKGround
Migrants represent a significant group in the HIV epidemic across Europe, including in the Netherlands.1-3 An estimated 22,900 people were living with HIV in the Netherlands in 2017, with 89% diagnosed and linked to care, 92% of those in care were on combination antiretro-viral therapy (cART) and of those on ART 95% were virally supressed.4 Almost half (43%) of all HIV-positive people in care in the Netherlands in 2017 were born outside of the Nether-lands4 and data suggest that migrants are doing less well in the cascade of care. HIV-positive people originating from South-East Asia, sub-Saharan Africa, Surinam, the Caribbean or Latin America were more likely to enter clinical care with late-stage infection (clinical AIDS event or a CD4-count <350 cells/mm3) or an advanced HIV infection (AIDS or CD4-count <200 cells/mm3) than those of Dutch origin.5 In the Netherlands, migrants are also more likely to have higher rates of lost to follow-up from HIV care,6 a longer time to virological suppression after combination antiretroviral therapy (cART) initiation, and higher risk of treatment failure4 than those of Dutch origin. These data are in line with findings across the European Union/Economic Area3 and suggest migrants face barriers in accessing and utilizing HIV health services. Hence, we need to better understand the specific barriers migrants face. Such data guide the development of strategies aimed at improving HIV prevention measures as well as optimising individual and public health outcomes.
The advancing Migrant Access to health Services in Europe (aMASE) study was set up to examine access to and use of HIV-related health services and identify structural, cultural and financial barriers to HIV prevention, diagnosis and treatment among several migrant groups living in Europe.7 Results of the aMASE study suggest opportunities for HIV testing and prevention are still being missed among migrants living in Europe.8-10 However, the extent to which this differs between migrants and non-migrants and according to their sexual orienta-tion is not well known. Therefore, this study aims to examine differences in access to and use of HIV-related health services between migrants and non-migrants recently diagnosed in the Netherlands, taken into account their sexual orientation. In addition, we examined differences in experiences in living with HIV between these groups.
MeTHodS
study design and procedures
A cross-sectional study was conducted among migrant and non-migrant individuals living with HIV in the Netherlands. Migrants were included in the clinic survey of the aMASE study, as described in detail elsewhere.7 In summary, the aMASE study was conducted between July 2013 and June 2015 in nine European countries. Migrants were included if they were

Chapter 3.1
116
diagnosed with HIV within five years of recruitment, aged >18 years, foreign-born and resident in the country of recruitment for >6 months, and able to complete, either alone or supported, a computer-assisted self or personal interview in any one of the 15 languages available. For the present study, we used data collected at all participating HIV outpatient treatment clinics in the Netherlands (Amsterdam UMC [location AMC], OLVG in Amsterdam and Haaglanden Medisch Centrum, in The Hague). In addition to the aMASE data collection among migrants, in the Netherlands all non-migrants (i.e., those born in the Netherlands) who attended any of the three HIV outpatient treatment clinics during the same study period and were diagnosed with HIV within five years and aged > 18 years were also asked to participate.
Participants completed a questionnaire on HIV-related services (which included access to HIV testing and healthcare pre-diagnosis and access to treatment and ongoing care after HIV diag-nosis) and experiences. Clinical data were obtained from the national ATHENA (AIDS Therapy Evaluation in the Netherlands) HIV cohort database.4 For people who declined to participate, we collected data on age, country of birth, sexual orientation and reason for decline.
Variables
Socio-demographic characteristics and migration history
Characteristics included self-reported sexual orientation, self-defined ethnicity, educational level, current work status, income level, age, household hunger in the past four weeks and attending religious services. Migration history included years since migration, age at migra-tion, region of birth and immigration status.
Access to HIV testing and healthcare pre-diagnosis
We measured factors related to HIV diagnosis, HIV testing behaviour, access to care and awareness of post-exposure prophylaxis (PEP). Factors related to HIV diagnosis included: age at HIV diagnosis, years since HIV diagnosis, location of HIV diagnosis, reason for HIV test, CD4 count and late stage HIV infection at HIV diagnosis. Among migrants we also collected data on the years between migration to the Netherlands and HIV diagnosis, country of HIV diagnosis and country of previous HIV negative test. Factors related to HIV test behaviour included: ever had an HIV test before HIV diagnosis and years between previous negative HIV test and HIV diagnosis. Variables measuring access to care included registration at a general practitioner (GP) in the Netherlands (GPs are the first point of access to healthcare in the Netherlands), healthcare usage in the Netherlands in the two years before HIV diagnosis and experienced difficulties accessing healthcare in the Netherlands. Among those who used healthcare in the Netherlands, we asked which healthcare professionals were visited and whether or not an HIV test was discussed during these visits.

117
Access to and use of HIV-related healthcare services
3.1
Access to treatment and ongoing care
We measured use of cART, time between HIV diagnosis and starting cART, self-reported cART adherence and self-reported difficulty to take HIV medication on a regular basis. Further-more, participants were asked if they ever missed an appointment at the HIV clinic due to the travel costs.
Experiences in living with HIV
Participants were asked if they had disclosed their HIV status to their steady partner or to friends and family, if they received HIV support through any non-governmental organisa-tions (NGOs), and if they ever felt discriminated in the Netherlands because of their HIV status, ethnicity, race or origin, or sexuality.
statistical analyses
As previous studies have shown outcomes are influenced by sexual orientation,8,9 partici-pants were grouped into: migrant MSM, non-migrant MSM, migrant heterosexual men, non-migrant heterosexual men, migrant women and non-migrant women. Socio-demographic characteristics and non-dichotomous outcomes were compared between groups using chi-square tests and Fisher’s exact tests for categorical variables and one-way ANOVA (normally distributed) and Kruskal Wallis tests (not normally distributed) for continuous variables. Di-chotomous outcomes related to access to HIV prevention, testing, care pre-diagnosis, treat-ment, ongoing care and experiences in living with HIV were used as separate end-points. The univariable odds ratios (ORs) were calculated using logistic regression or penalized logistic regression in a table with a zero cell count.11
In additional analyses, we adjusted outcomes for participants’ age by constructing multivari-able models as age is a potential confounder. We also compared all outcomes by region of birth in MSM only, due to the low numbers of migrant heterosexual men and women.
In the analyses, participants with unknown or missing data were excluded. Analyses were performed using STATA Intercooled 13.1 (STATA Corporation, College Station, Texas, USA). A p value of <0.05 was considered statistically significant.
reSulTS
Of 417 invited HIV-positive patients, 60% (n=252) participated. The response rate was lower among migrants from Latin America/Caribbean and women and heterosexual men than non-migrants and MSM, respectively. Also, participants recruited at the Amsterdam UMC were less likely to participate than those recruited elsewhere.

Chapter 3.1
118
In total 247 participants were included in the analyses (Table 1): 77 migrant MSM, 115 non-migrant MSM, 21 migrant heterosexual men, 14 non-migrant heterosexual men and 20 migrant women. Five non-migrant women were excluded from the analyses because of their low number. Groups differed with regard to variables reflecting socio-economic status (all p-values <0.01), current age (p=0.002), age at migration (p=0.003), self-defined ethnicity (p<0.001), immigration status (p<0.001), attendance of religious services (p<0.001) and recruitment site (p=0.012) (Table 1). There was a difference in region of birth between MSM and heterosexual migrants (p<0.001); with 40% of the MSM migrants originating from Europe and more than half of the heterosexual migrants originate from sub-Saharan Africa.
access to HIV testing and healthcare pre-diagnosis
The median age at HIV diagnosis was 39 years (IQR 31–47) and median time since HIV diag-nosis was 2 years (IQR 1–4) (Table 2a). Migrants were a median of 8 years (IQR 2–21) in the Netherlands before HIV diagnosis.
While MSM were most frequently diagnosed at a sexual health or HIV testing clinic and most commonly tested for HIV because it was part of a routine health check-up, most heterosexu-als men and women (both migrants and non-migrants) were diagnosed in a hospital and stated a doctor advised the HIV test due to health problems.
Overall, 78% had a previous negative HIV test before HIV diagnosis and 42% were diagnosed with a late-stage HIV infection. Most (93%) participants visited a healthcare facility in the two years prior to diagnosis, with 41% reporting that HIV testing was discussed (Table 2a). Most participants who used a healthcare facility visited a GP and/or dentist; 26% of those who visited a GP, recalled that an HIV test was discussed (Figure 1). The proportion visiting a GP was lower among migrant groups (range 53–65%) than among the non-migrant groups (range 74–84%) (p=0.009).
In univariable analyses (Figure 2A), having had a previous HIV-negative test was less likely in migrant heterosexual men (OR 0.22, 95% CI 0.08–0.58), non-migrant heterosexual men (OR 0.09, 95% CI 0.03–0.29) and migrant women (OR 0.30, 95% CI 0.11–0.81) than in non-migrant MSM, whereas the difference between migrant (OR 1.65, 95% CI 0.70–3.91) and non-migrant MSM was not statistically significant. Also, among those who had an HIV-negative test, the median time between the previous HIV-negative test and HIV diagnosis was significantly longer among all heterosexual men and women than migrant and non-migrant MSM (p=0.002, Table 2a). Being diagnosed with a late-stage HIV infection was more likely in migrant heterosexual men (OR 11.49, 95% CI 3.17–41.69), non-migrant heterosexual men (OR 5.07, 95% CI 1.49–17.24) and migrant women (OR 2.79, 95% CI 1.03–7.52) than non-migrant MSM, whereas this did not differ between migrant (OR 1.10, 95% CI 0.59–2.04)

119
Access to and use of HIV-related healthcare services
3.1
Tabl
e 1.
Soc
iode
mog
raph
ic c
hara
cter
istics
and
mig
ratio
n hi
stor
y of
Dut
ch a
MAS
E-st
udy
parti
cipa
nts (
N=2
47),
2013
–201
5
tota
lm
igra
nt m
smn
on-m
igra
nt
msm
mig
rant
he
tero
sexu
al
men
non
-mig
rant
he
tero
sexu
al
men
mig
rant
w
omen
(N=2
47)
(n=7
7)(n
=115
)(n
=21)
(n=1
4)(n
=20)
n/N
%n/
N%
n/N
%n/
N%
n/N
%n/
N%
p-va
lue
High
er e
duca
tiona
l lev
el (c
olle
ge d
egre
e or
hig
her)
107/
247
43.3
33/7
742
.961
/115
53.0
4/21
19.0
6/14
42.9
3/20
15.0
0.00
3
Curr
ently
wor
king
185/
246
75.2
58/7
775
.399
/115
86.1
10/2
147
.69/
1464
.39/
1947
.4<0
.001
low
er in
com
e le
vel (
less
than
min
imum
wag
e)91
/231
39.4
36/6
852
.916
/113
14.2
18/1
994
.76/
1442
.915
/17
88.2
<0.0
01
Mod
erat
e/se
vere
hou
seho
ld h
unge
r in
the
past
4 w
eeks
49/2
4420
.115
/74
20.3
15/1
1513
.09/
2142
.92/
1414
.38/
2040
.00.
004
age
(Med
ian,
IQr)
4133
–49
3628
–46
4336
–51
4540
–48
4133
–55
3933
–48
0.00
2
Year
s sin
ce m
igra
tion
to th
e n
ethe
rland
s (M
edia
n, IQ
r)10
4–23
84–
25N
A11
7–15
NA
114–
220.
965
age
at m
igra
tion
to th
e n
ethe
rland
s (M
edia
n, IQ
r)25
21–3
324
21–2
9N
A34
26–3
8N
A24
19–3
90.
003
regi
on o
f birt
h<0
.001
Sub-
Saha
ran
Afric
a30
/118
25.4
4/77
5.2
NA
16/2
176
.2N
A10
/20
50.0
Latin
Am
eric
a / C
arib
bean
27/1
1822
.919
/77
24.7
3/21
14.3
5/20
25.0
Euro
pe33
/118
28.0
31/7
740
.30/
210.
02/
2010
.0
Oth
er28
/118
23.7
23/7
729
.92/
219.
53/
2015
.0
Self-
defin
ed e
thni
city
<0.0
01a
Euro
pean
149/
245
60.8
035
/76
46.1
99/1
1486
.80/
210.
012
/14
85.7
3/20
15.0
Oth
er96
/245
39.2
041
/76
54.0
15/1
1413
.221
/21
100.
02/
1414
.317
/20
85.0
Afr
ican
32/2
4513
.10
4/76
5.3
1/11
40.
917
/21
81.0
0/14
0.0
10/2
050
.0
Am
eric
an6/
245
2.40
3/76
3.9
0/11
40.
00/
210.
00/
140.
03/
2015
.0
Asia
n17
/245
6.90
10/7
613
.23/
114
2.6
1/21
4.8
1/14
7.1
2/20
10.0
Mix
ed20
/245
8.20
10/7
613
.27/
114
6.1
1/21
4.8
0/14
0.0
2/20
10.0
Lati
n Am
eric
a / C
arib
bean
13/2
455.
309/
7611
.83/
114
2.6
0/21
0.0
1/14
7.1
0/20
0.0

Chapter 3.1
120 121
Access to and use of HIV-related healthcare services
3.1
Tabl
e 1.
(con
tinue
d)
tota
lm
igra
nt m
smn
on-m
igra
nt
msm
mig
rant
he
tero
sexu
al
men
non
-mig
rant
he
tero
sexu
al
men
mig
rant
w
omen
(N=2
47)
(n=7
7)(n
=115
)(n
=21)
(n=1
4)(n
=20)
n/N
%n/
N%
n/N
%n/
N%
n/N
%n/
N%
p-va
lue
Mid
dle
East
ern
8/24
53.
305/
766.
61/
114
0.9
2/21
9.5
0/14
0.0
0/20
0.0
Imm
igra
tion
stat
us<0
.001
Perm
anen
t res
iden
cy p
erm
it84
/108
77.8
63/7
287
.5N
A9/
1947
.4N
A12
/17
70.6
Tem
pora
ry re
siden
cy p
erm
it16
/108
14.8
8/72
11.1
4/19
21.1
4/17
23.5
Refu
gee
stat
us /
unkn
own
8/10
87.
41/
721.
46/
1931
.61/
175.
9
atten
ding
relig
ious
serv
ices
at l
east
onc
e a
year
74/2
3931
.023
/72
31.9
20/1
1517
.414
/18
77.8
2/14
14.3
15 /2
075
.0<0
.001
recr
uitm
ent s
ite0.
012
Amst
erda
m U
MC
(loca
tion
AMC)
, Am
ster
dam
76/2
4730
.826
/77
33.8
30/1
1526
.18/
2138
.16/
1442
.96/
2030
.0
OLV
G, A
mst
erda
m12
1/24
749
.035
/77
45.5
68/1
1559
.110
/21
47.6
2/14
14.3
6/20
30.0
Ha
agla
nden
Med
isch
Cent
rum
, The
Hag
ue50
/247
20.2
16/7
720
.817
/115
14.8
3/21
14.3
6/14
42.9
8/20
40.0
MSM
, men
who
hav
e se
x w
ith m
en; I
QR,
inte
rqua
rtile
rang
e; N
A, N
ot a
pplic
able
.a p
-val
ue fo
r diff
eren
ce b
etw
een
Euro
pean
and
Oth
er.

Chapter 3.1
120 121
Access to and use of HIV-related healthcare services
3.1
and non-migrant MSM. All three migrant groups (MSM: OR 8.62, 95% CI 2.61–28.48; heterosexual men: OR 6.43, 95% CI 1.34–30.74; and women: OR 8.77, 95% CI 1.98–38.97) were more likely to have experienced difficulties accessing healthcare in the Netherlands than non-migrant MSM. Most frequently reported difficulties accessing healthcare in the Netherlands among migrants were uncertainty regarding their right to access healthcare and language barriers (Table 2a). Overall, 66% had ever heard of PEP. Migrant MSM (OR 0.18, 95% CI 0.08–0.37), migrant heterosexual men (OR 0.02, 95% CI 0.01–0.08), non-migrant het-erosexual men (OR 0.16, 95% CI 0.05–0.53) and migrant women (OR 0.03, 95% CI 0.01–0.10) were less likely to have heard of PEP than non-migrant MSM. Healthcare usage in the two years before HIV diagnosis and the proportion in which an HIV test was discussed during healthcare attendance did not differ significantly between groups.
Antenata
l care
Dentis
t
Drug tr
eatm
ent c
enter
Genera
l Prac
titioner
Hospita
l: Emerg
ency
Room
Hospita
l: Inpati
ent a
dmission
Hospita
l: Outpati
ent c
linic
Medica
l care
at re
fugee ce
nter
Mental
health
facil
ity
Sexual
health
clinic
or HIV te
sting cl
inic0
10
20
30
40
50
60
70
80
90
100Pe
rcen
tage
(%
)
Non-migrant MSM (n=110)
Migrant MSM (n=52)
Non-migrant heterosexual men (n=12)
Migrant heterosexual men (n=15)
Migrant heterosexual women (n=13)
Figure 1. Healthcare attendance in the two years before HIV diagnosis and the proportion in which HIV testing was discussed among Dutch aMASE-study participants, 2013–2015MSM, Men who have sex with men.Note: dashed lines represent the proportion of cases in which an HIV test was discussed during healthcare attendance.

Chapter 3.1
122 123
Access to and use of HIV-related healthcare services
3.1
Tabl
e 2a
. Acc
ess t
o HI
V te
sting
and
hea
lthca
re p
re-d
iagn
osis
amon
g Du
tch
aMAS
E-st
udy
parti
cipa
nts (
N=2
47),
2013
–201
5
tota
l m
igra
ntm
smn
on-m
igra
ntm
sm
mig
rant
hete
rose
xual
men
non
-mig
rant
hete
rose
xual
men
mig
rant
wom
en
(N=2
47)
(n=7
7)(n
=115
)(n
=21)
(n=1
4)(n
=20)
n%
n%
n%
n%
n%
p-va
luea
age
(yea
rs) a
t HIV
dia
gnos
is (M
edia
n, IQ
r)b
3931
–47
3426
–44
4133
–49
4238
–47
3832
–50
3730
–46
0.00
6Ye
ars s
ince
HIV
dia
gnos
is (M
edia
n, IQ
r)2
1–4
21–
33
1–4
21–
33
1–4
21–
40.
046
loca
tion
of H
IV d
iagn
osis
<0.0
01c
Sexu
al h
ealth
clin
ic /
HIV
testi
ng c
linic
103/
238
43.3
42/7
060
.052
/115
45.2
2/19
10.5
3/14
21.4
4/20
20.0
Hosp
ital
66/2
3827
.713
/70
18.6
25/1
1521
.710
/19
52.6
9/14
64.3
9/20
45.0
GP57
/238
23.9
12/7
017
.134
/115
29.6
4/19
21.1
1/14
7.1
6/20
30.0
Oth
erd
12/2
385.
03/
704.
34/
115
3.5
3/19
15.8
1/14
7.1
1/20
5.0
reas
on fo
r HIV
test
e
It w
as p
art o
f a ro
utine
hea
lth c
heck
up89
/245
36.3
30/7
739
.051
/114
44.7
4/21
19.1
3/13
23.1
1/20
5.0
A do
ctor
adv
ised
me
to te
st d
ue to
hea
lth p
robl
ems
86/2
4535
.118
/77
23.4
36/1
1431
.613
/21
61.9
5/13
38.5
14/2
070
.0I f
elt I
was
at r
isk48
/245
19.6
22/7
728
.621
/114
18.4
3/21
14.3
1/13
7.7
1/20
5.0
I had
sexu
al c
onta
ct w
ith so
meo
ne I
knew
/tho
ught
had
HIV
37/2
4515
.119
/77
24.7
13/1
1411
.40/
210.
03/
1323
.12/
2010
.0O
ther
f16
/245
6.5
3/77
3.9
5/11
44.
43/
2114
.32/
1315
.43/
2015
.0Ye
ars b
etw
een
mig
ratio
n to
the
net
herla
nds a
nd H
IV d
iagn
osis
82–
216
1–22
NA
94–
15N
A10
2–19
0.91
1Co
untr
y of
HIV
dia
gnos
is0.
696
The
Net
herla
nds
109/
118
92.4
70/7
790
.9N
A19
/21
90.5
NA
20/2
010
0.0
Coun
try
of b
irth
7/11
85.
95/
776.
52/
219.
50/
200.
0O
ther
cou
ntry
2/11
81.
72/
772.
60/
210.
00/
200.
0Cd
4 ce
ll co
unt (
cells
/mm
3 ) at H
IV d
iagn
osis
(Med
ian,
IQr)
g40
022
0–57
043
028
0–58
047
532
0–64
712
540
–230
225
20–5
7026
050
–430
<0.0
01la
te-s
tage
HIV
infe
ction
at H
IV d
iagn
osis
(aId
S or
a C
d4 c
ount
<35
0 ce
lls/m
m3)
101/
239
42.3
26/7
435
.137
/112
33.0
17/2
085
.010
/14
71.4
11/1
957
.9
ever
had
a n
egati
ve H
IV te
st b
efor
e HI
V di
agno
sis
192/
247
77.7
69/7
789
.696
/115
83.5
11/2
152
.44/
1428
.612
/20
60.0
Year
s bet
wee
n pr
evio
us n
egati
ve H
IV te
st a
nd H
IV d
iagn
osis
(Med
ian,
IQ
r)h,
i2
1–4
21–
41
0–3
61–
96
2–11
53–
120.
002
Coun
try
of p
revi
ous H
IV n
egati
ve te
sti
The
Net
herla
nds
52/8
660
.541
/66
62.1
NA
5/10
50.0
NA
6/10
60.0
Anot
her c
ount
ry34
/86
39.5
25/6
637
.95/
1050
.04/
1040
.0
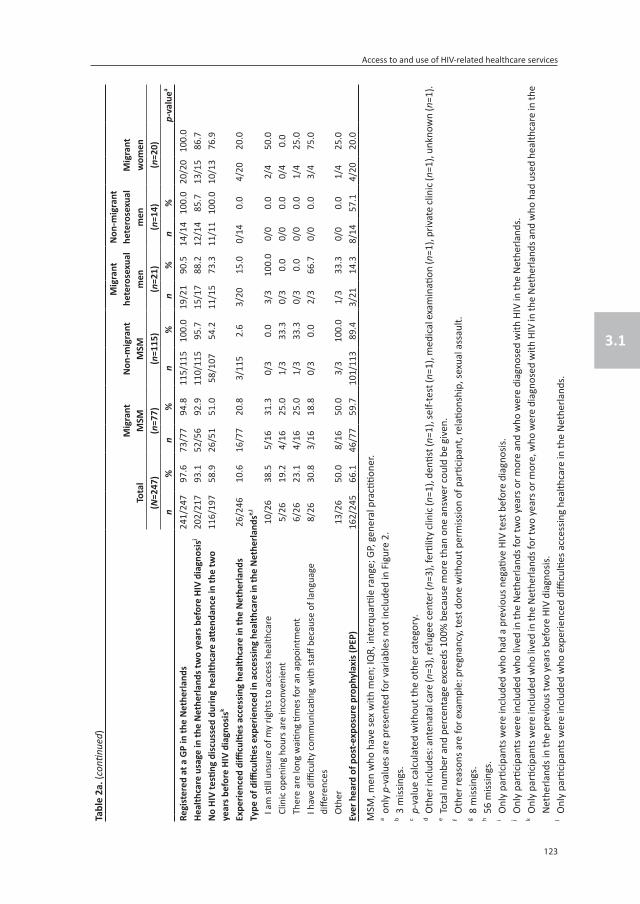
Chapter 3.1
122 123
Access to and use of HIV-related healthcare services
3.1
Tabl
e 2a
. (co
ntinu
ed)
tota
l m
igra
ntm
smn
on-m
igra
ntm
sm
mig
rant
hete
rose
xual
men
non
-mig
rant
hete
rose
xual
men
mig
rant
wom
en
(N=2
47)
(n=7
7)(n
=115
)(n
=21)
(n=1
4)(n
=20)
n%
n%
n%
n%
n%
p-va
luea
regi
ster
ed a
t a G
P in
the
net
herla
nds
241/
247
97.6
73/7
794
.811
5/11
510
0.0
19/2
190
.514
/14
100.
020
/20
100.
0He
alth
care
usa
ge in
the
net
herla
nds t
wo
year
s bef
ore
HIV
diag
nosi
sj20
2/21
793
.152
/56
92.9
110/
115
95.7
15/1
788
.212
/14
85.7
13/1
586
.7n
o HI
V te
sting
dis
cuss
ed d
urin
g he
alth
care
att
enda
nce
in th
e tw
o ye
ars b
efor
e HI
V di
agno
sisk
116/
197
58.9
26/5
151
.058
/107
54.2
11/1
573
.311
/11
100.
010
/13
76.9
expe
rienc
ed d
ifficu
lties
acc
essi
ng h
ealth
care
in th
e n
ethe
rland
s26
/246
10.6
16/7
720
.83/
115
2.6
3/20
15.0
0/14
0.0
4/20
20.0
Type
of d
ifficu
lties
exp
erie
nced
in a
cces
sing
hea
lthca
re in
the
net
herla
ndse,
l
I am
still
unsu
re o
f my
right
s to
acce
ss h
ealth
care
10/2
638
.55/
1631
.30/
30.
03/
310
0.0
0/0
0.0
2/4
50.0
Clin
ic o
peni
ng h
ours
are
inco
nven
ient
5/26
19.2
4/16
25.0
1/3
33.3
0/3
0.0
0/0
0.0
0/4
0.0
Ther
e ar
e lo
ng w
aitin
g tim
es fo
r an
appo
intm
ent
6/26
23.1
4/16
25.0
1/3
33.3
0/3
0.0
0/0
0.0
1/4
25.0
I hav
e di
fficu
lty c
omm
unic
ating
with
staff
bec
ause
of l
angu
age
diffe
renc
es8/
2630
.83/
1618
.80/
30.
02/
366
.70/
00.
03/
475
.0
Oth
er13
/26
50.0
8/16
50.0
3/3
100.
01/
333
.30/
00.
01/
425
.0ev
er h
eard
of p
ost-e
xpos
ure
prop
hyla
xis (
PeP)
162/
245
66.1
46/7
759
.710
1/11
389
.43/
2114
.38/
1457
.14/
2020
.0
MSM
, men
who
hav
e se
x w
ith m
en; I
QR,
inte
rqua
rtile
rang
e; G
P, g
ener
al p
racti
tione
r.a o
nly
p-va
lues
are
pre
sent
ed fo
r var
iabl
es n
ot in
clud
ed in
Fig
ure
2.b 3
miss
ings
.c p
-val
ue c
alcu
late
d w
ithou
t the
oth
er c
ateg
ory.
d Oth
er in
clud
es: a
nten
atal
care
(n=3
), re
fuge
e ce
nter
(n=3
), fe
rtilit
y cl
inic
(n=1
), de
ntist
(n=1
), se
lf-te
st (n
=1),
med
ical
exa
min
ation
(n=1
), pr
ivat
e cl
inic
(n=1
), un
know
n (n
=1).
e Tot
al n
umbe
r and
per
cent
age
exce
eds 1
00%
bec
ause
mor
e th
an o
ne a
nsw
er c
ould
be
give
n.f O
ther
reas
ons a
re fo
r exa
mpl
e: p
regn
ancy
, tes
t don
e w
ithou
t per
miss
ion
of p
artic
ipan
t, re
latio
nshi
p, se
xual
ass
ault.
g 8 m
issin
gs.
h 56
miss
ings
.i O
nly
parti
cipa
nts w
ere
incl
uded
who
had
a p
revi
ous n
egati
ve H
IV te
st b
efor
e di
agno
sis.
j Onl
y pa
rtici
pant
s wer
e in
clud
ed w
ho li
ved
in th
e N
ethe
rland
s for
two
year
s or m
ore
and
who
wer
e di
agno
sed
with
HIV
in th
e N
ethe
rland
s.k O
nly
parti
cipa
nts w
ere
incl
uded
who
live
d in
the
Net
herla
nds f
or tw
o ye
ars o
r mor
e, w
ho w
ere
diag
nose
d w
ith H
IV in
the
Net
herla
nds a
nd w
ho h
ad u
sed
heal
thca
re in
the
Net
herla
nds i
n th
e pr
evio
us tw
o ye
ars b
efor
e HI
V di
agno
sis.
l Onl
y pa
rtici
pant
s wer
e in
clud
ed w
ho e
xper
ienc
ed d
ifficu
lties
acc
essin
g he
alth
care
in th
e N
ethe
rland
s.

Chapter 3.1
124 125
Access to and use of HIV-related healthcare services
3.1
Tabl
e 2b
. Acc
ess t
o tr
eatm
ent a
nd o
ngoi
ng H
IV c
are
amon
g Du
tch
aMAS
E-st
udy
parti
cipa
nts (
N=2
47),
2013
–201
5
tota
lm
igra
ntm
smn
on-m
igra
nt
msm
mig
rant
he
tero
sexu
al
men
non
-mig
rant
he
tero
sexu
al
men
mig
rant
wom
en
(N=2
47)
(n=7
7)(n
=115
)(n
=21)
(n=1
4)(n
=20)
n%
n%
n%
n%
n%
p-va
luea
Curr
ently
taki
ng c
art
212/
247
85.8
67/7
787
.096
/115
83.5
19/2
190
.513
/14
92.9
17/2
085
.0
Wee
ks b
etw
een
star
t car
T an
d HI
V di
agno
sis (
Med
ian,
IQr)
b,c
63–
439
3–31
74–
593
1–7
32–
73
2–34
0.00
2
reas
on fo
r no
cart
use
d
My
doct
or sa
ys I
do n
ot n
eed
them
yet
21/3
560
.06/
1060
.012
/19
63.2
0/2
0.0
1/1
100.
02/
366
.7
I’m a
frai
d of
the
side
effec
ts3/
358.
60/
100.
02/
1910
.50/
20.
00/
10.
01/
333
.3
I’m o
n a
trea
tmen
t bre
ak I
agre
ed w
ith m
y do
ctor
5/35
14.3
1/10
10.0
4/19
21.1
0/2
0.0
0/1
0.0
0/3
0.0
I will
star
t soo
n/to
day
8/35
22.9
3/10
30.0
3/19
15.8
2/2
100.
00/
10.
00/
30.
0
I am
wai
ting
for a
ppro
val
1/35
2.9
0/10
0.0
1/19
5.3
0/2
0.0
0/1
0.0
0/3
0.0
High
self-
repo
rted
car
t ad
here
nceb,
e20
5/20
998
.165
/66
98.5
93/9
597
.918
/18
100.
013
/13
100.
016
/17
94.1
Find
ing
it di
fficu
lt to
take
HIV
med
icati
on o
n a
regu
lar b
asis
b,f
27/1
9114
.17/
5313
.210
/92
10.9
4/17
23.5
1/13
7.7
5/16
31.3
mis
sed
appo
intm
ents
at H
IV c
linic
due
to th
e tr
avel
cos
ts10
/246
4.1
3/76
3.9
1/11
50.
93/
2114
.30/
140.
03/
2015
.0
MSM
, men
who
hav
e se
x w
ith m
en; c
ART,
com
bina
tion
antir
etro
vira
l the
rapy
; IQ
R, in
terq
uarti
le ra
nge.
a onl
y p-
valu
es a
re p
rese
nted
for v
aria
bles
not
incl
uded
in F
igur
e 2.
b Onl
y pa
rtici
pant
s wer
e in
clud
ed w
ho w
ere
curr
ently
usin
g cA
RT.
c 16
miss
ings
.d O
nly
parti
cipa
nts w
ere
incl
uded
who
wer
e no
t cur
rent
ly u
sing
cART
. Tot
al n
umbe
r and
per
cent
age
exce
eds 1
00%
bec
ause
par
ticip
ants
cou
ld in
dica
te m
ore
than
one
rea-
son.
e Mea
sure
d on
a 4
-poi
nt Li
kert
scal
e an
d di
chot
omize
d fo
r ana
lyse
s whe
reas
the
answ
ers s
tron
gly
agre
e an
d ag
ree
on th
e st
atem
ent “
I alw
ays f
ollo
w m
y do
ctor
’s in
stru
ction
s ab
out t
akin
g m
y HI
V m
edic
ation
” re
pres
ent h
igh
self-
repo
rted
cAR
T ad
here
nce
and
stro
ngly
disa
gree
and
disa
gree
repr
esen
ts lo
w se
lf-re
port
ed a
dher
ence
.f M
easu
red
on a
4-p
oint
Like
rt sc
ale
and
dich
otom
ized
for a
naly
ses w
here
as th
e an
swer
s str
ongl
y ag
ree
and
agre
e on
the
stat
emen
t “I fi
nd it
diffi
cult
to ta
ke m
y HI
V m
edic
a-tio
n on
a re
gula
r bas
is” re
pres
ent fi
ndin
g it
diffi
cult
to ta
ke H
IV m
edic
ation
on
a re
gula
r bas
is an
d st
rong
ly d
isagr
ee a
nd d
isagr
ee re
pres
ents
not
find
ing
it di
fficu
lt to
take
HI
V m
edic
ation
on
a re
gula
r bas
is.

Chapter 3.1
124 125
Access to and use of HIV-related healthcare services
3.1
Tabl
e 2c
. Exp
erie
nces
in li
ving
with
HIV
am
ong
Dutc
h aM
ASE-
stud
y pa
rtici
pant
s (N
=247
), 20
13–2
015
tota
lm
igra
ntm
smn
on-m
igra
nt
msm
mig
rant
he
tero
sexu
al
men
non
-mig
rant
he
tero
sexu
al
men
mig
rant
wom
en
(N=2
47)
(n=7
7)(n
=115
)(n
=21)
(n=1
4)(n
=20)
n%
n%
n%
n%
n%
disc
losu
re o
f HIV
stat
us to
stea
dy p
artn
era
118/
126
93.7
32/3
688
.960
/62
96.8
9/10
90.0
8/8
100.
09/
1090
.0
disc
losu
re o
f HIV
stat
us to
frie
nds o
r fam
ily20
4/24
682
.963
/77
81.8
97/1
1584
.316
/21
76.2
12/1
485
.716
/19
84.2
In c
onta
ct w
ith a
ny n
Go
’s fo
r HIV
supp
ort
56/2
4622
.714
/77
18.2
34/1
1529
.63/
2114
.32/
1414
.33/
2015
.0
ever
bee
n di
scrim
inat
ed in
the
net
herla
nds b
ecau
se o
f HIV
stat
us40
/246
16.3
19/7
625
.010
/115
8.7
3/21
14.3
2/14
14.3
6/20
30.0
ever
bee
n di
scrim
inat
ed in
the
net
herla
nds b
ecau
se o
f eth
nici
ty, r
ace
or o
rigin
50/1
1643
.130
/76
39.5
NA
9/21
42.9
NA
11/1
957
.9
ever
bee
n di
scrim
inat
ed in
the
net
herla
nds b
ecau
se o
f sex
ualit
y88
/191
46.1
31/7
640
.857
/115
49.6
NA
NA
NA
MSM
, men
who
hav
e se
x w
ith m
en; N
GO, n
on-g
over
nmen
tal o
rgan
izatio
n; N
A, N
ot a
pplic
able
.a O
nly
parti
cipa
nts w
ere
incl
uded
who
had
a st
eady
par
tner
.

Chapter 3.1
126
Comparing outcomes by region of birth and restricting the analyses to MSM, MSM born in sub-Saharan Africa (OR 12.44, 95% CI 0.98–157.33), another country in Europe (OR 8.96, 95% CI 2.10–38.28) or in another region (OR 19.91, 95% CI 4.75–83.38) were more likely to have difficulties accessing healthcare in the Netherlands than non-migrant MSM. Also, MSM born in sub-Saharan Africa (OR 0.12, 95% CI 0.02–0.92), Latin America/Caribbean (OR 0.13, 95% CI 0.04–0.39), another country in Europe (OR 0.29, 95% CI 0.11–0.77) or in another region (OR 0.13, 95% CI 0.05–0.36) were less likely to have heard of PEP than non-migrant MSM. No significant differences were found in the other outcomes on access to HIV testing and healthcare pre-diagnosis between region of birth among MSM.
access to treatment and ongoing HIV care
Overall, 86% of participants reported they were on cART, median time between HIV diagnosis and starting cART was 6 weeks (IQR 3–43). Almost all (98%) reported high cART adherence, 14% found it difficult to take HIV medication on a regular basis; 4% missed appointments at their HIV clinic due to the travel costs (Table 2b).
In univariable analyses (Figure 2B), migrant heterosexual men (OR 14.44, 95% CI 2.00–104.05) and migrant women (OR 15.27, 95% CI 2.11–110.33) were more likely to have missed appointments at their HIV clinic due to the travel costs than non-migrant MSM. All heterosexual groups were more likely to start cART earlier after their HIV diagnosis than non-migrant and migrant MSM (p=0.002, Table 2b). No significant differences were found in the other outcomes on access to treatment and ongoing HIV care and there were no significant differences between region of birth among MSM.
experiences in living with HIV
Most participants had disclosed their HIV status to their steady partner (94%) and to friends and family (83%) and 23% were in contact with an NGO for HIV support (Table 2c). 16% respondents reported experiencing discrimination because of their HIV status. Among migrants, 43% reported discrimination in the Netherlands because of their ethnicity, race or country of origin and 46% of migrant and non-migrant MSM reported discrimination because of their sexuality.
In univariable analyses (Figure 2C), migrant MSM (OR 3.50, 95% CI 1.52–8.03) and migrant women (OR 4.50, 95% CI 1.42–14.29) were more likely to report ever been discriminated in the Netherlands because of their HIV-status than non-migrant MSM. Other outcomes on experiences in living with HIV did not differ significantly between groups.
Comparing outcomes of experiences in living with HIV by region of birth, MSM born in a re-gion other than sub-Saharan Africa, Latin America/Caribbean or Europe were less likely to be

127
Access to and use of HIV-related healthcare services
3.1
in contact with an NGO for HIV support than non-migrant MSM (OR 0.11, 95% CI 0.39–3.13). MSM born in sub-Saharan Africa (OR 3.50, 95% CI 0.33–36.86), Latin-America/Caribbean (OR 1.97,95% CI 0.49–7.93), another country in Europe (OR 4.50, 95% CI 1.63–12.42) or another region (OR 3.71, 95% CI 1.19–11.52) were more likely to have experienced HIV discrimina-tion in the Netherlands than non-migrant MSM, although this effect was not statistically significant for MSM from sub-Saharan Africa and Latin-America/Caribbean. Other outcomes on experiences in living with HIV did not differ significantly between region of birth among MSM.
When adjusting for age, outcomes on access to testing and healthcare pre-diagnosis, access to treatment and ongoing HIV care and experiences in living with HIV yielded comparable results.
dISCuSSIon
This study, focusing on migrant and non-migrant persons recently diagnosed with HIV liv-ing in the Netherlands, found disparities in access to HIV prevention, testing and care and experience of HIV-related discrimination by migrant status but also by sexual orientation.
Previous HIV testing and late-stage HIV infection diagnosis did not differ between migrant and non-migrant MSM. However, migrant and non-migrant heterosexual participants were less likely to have had an HIV test before their HIV diagnosis and were more often diagnosed with a late-stage HIV infection than non-migrant MSM, indicating they are facing barriers in accessing HIV testing services. The finding that almost all participants visited a healthcare facility in the two years before HIV diagnosis but only in 40% an HIV test was discussed sug-gests that testing opportunities are being missed, as has been demonstrated at the European level.9 In line with our findings, another study in the Netherlands found that HIV testing was often not discussed during GP consultations prior to HIV diagnosis.12 These data suggest that increased provider-initiated testing, especially at the GP but also during hospital admissions, in dental or mental health facilities, is needed to increase earlier HIV diagnosis, especially among heterosexuals. Provider-initiated HIV testing in such settings is particularly important as data from the aMASE community survey showed that low risk perception is one of the main barriers to HIV testing among both heterosexual migrants and migrant MSM.8
Our data show that the majority of migrant (90%) and non-migrant (84%) MSM had a nega-tive HIV test before their HIV diagnosis. However, previous estimations of the aMASE study data showed that a considerable proportion of HIV-positive migrant MSM in Europe and the Netherlands acquired their HIV infection postmigration.10 Therefore, improving early access

Chapter 3.1
128
Ever had a negative HIV test before HIV diagnosis***
Late HIV diagnosis***
Healthcare usage in the Netherlands 2 years before HIV diagnosisa
No HIV test discussed during healthcare attendance in the 2 years before HIV diagnosisb
Experienced difficulties accessing healthcare in the Netherlands**
Ever heard of PEP***
id
.001 .01 .1 1 10 100 1000
Odds Ratio
A. Access to testing and healthcare pre HIV diagnosis
Currently taking cART
High self-reported cART adherencec
Finding it difficult to take HIV medication on a regular basisc
Missed apointments at HIV clinic due to travel costs*
id
.001 .01 .1 1 10 100 1000
Odds Ratio
B. Access to treatment and ongoing care
Disclosure of HIV status to steady partnerd
Disclosure of HIV status to friends or family
In contact with any NGO's for HIV support
Ever been discriminated in the Netherlands because of HIV status*
Ever been discriminated in the Netherlands because of sexualitye
id
.001 .01 .1 1 10 100 1000
Odds Ratio
C. Experiences in living with HIV
Non-migrant MSM (ref.) Migrant MSM Migrant heterosexual men Non-Migrant heterosexual men Migrant women
Figure 2. Univariable analyses of the relationship between migrant status and sexual orientation and (A) ac-cess to testing and healthcare pre HIV diagnosis, (B) access to treatment and ongoing care and (C) experiences in living with HIV among Dutch aMASE-study participants, 2013–2015MSM: men who have sex with men; PEP: post-exposure prophylaxis; cART: combination antiretroviral thera-py; NGO: non-governmental organisation.a Only participants were included who lived in the Netherlands for two years or more and who were diag-
nosed with HIV in the Netherlands.b Only participants were included who lived in the Netherlands for two years or more, who were diagnosed
with HIV in the Netherlands and who had used healthcare in the Netherlands in the previous two years before HIV diagnosis.
c Only participants were included who were currently using cART.d Only participants were included who had a steady partner.e Only MSM were included in this analysis.* p<0.05 ** p <0.01 *** p <0.001.

129
Access to and use of HIV-related healthcare services
3.1
to behavioural and biomedical HIV prevention interventions (i.e., pre- and post exposure prophylaxis - PEP and PrEP) among HIV-negative migrant MSM is important. As a first step increasing awareness of biomedical interventions among migrant MSM is necessary as we show that PEP awareness was significantly lower among migrant MSM than among non-migrant MSM. The latter might be indicative for lower levels of awareness of PrEP and other HIV prevention strategies, such use of (free) condoms, which we did not measure.
In our study approximately one-fifth of all migrants experienced difficulties accessing health-care in the Netherlands, which was significantly higher than among non-migrant MSM. Most reported difficulties were uncertainty about entitlement to healthcare and language barriers. These barriers are not specific to HIV-related healthcare services and have been described widely in other studies regarding access to healthcare among migrants.13 Although almost all participants were registered at a GP and migrants living with HIV in the Netherlands experience less difficulties accessing healthcare than migrants in some other countries in Europe,9,14 these structural barriers in the access to care for migrants need to be addressed. In the Netherlands, all residents (including asylum seekers and refugees) are entitled to a basic health insurance package which includes the bulk of essential healthcare (including care provided by a GP), medications and medical aids.15 For undocumented migrants who lack the resources to pay for healthcare, systems are in place to reimburse medical costs.16 Knowledge about these rights to care should be improved. Also, healthcare systems need to become more migrant-friendly, e.g., overcoming language and cultural barriers in service delivery, improving the culture competencies of health workers and organisations and improving health literacy (i.e., the degree to which an individual has the capacity to obtain, communicate, process, and understand basic health information and services to make ap-propriate health decisions).13,17,18 In order to decrease barriers for migrant communities, alternative options for HIV prevention, testing and care besides traditional healthcare set-tings should also be explored, for example through community outreach, expanding HIV support via NGO’s for groups currently not reached, and the use of HIV self-tests.19-21 As our data show about 75% of heterosexual migrant visited a religious service, partnerships with and community outreach through religious services could be utilized to increase HIV testing.
In regard to access to HIV treatment and care, overall cART usage was high (86%) and, al-though 14% reported difficulties taking HIV medication on a regular basis, it was encouraging that self-reported cART adherence was high, with no significant differences between groups. However, we found that migrant heterosexual men and women more often reported missing an appointment at their HIV clinic because of travel expenses than non-migrant MSM. This difference is most likely related to a lower socioeconomic status and these results are con-sistent with European data.8,9 As missing clinical appointments might lead to suboptimal HIV care and treatment, efforts should be made to discuss the costs of travel with HIV-positive

Chapter 3.1
130
patients not showing up for their appointments and opportunities to overcome such barriers should be explored. Furthermore, we found a high proportion of migrant heterosexual men and migrant women were earning less than minimum wage and experienced moderate/severe household hunger. The potential impact of poverty in this group on access to care and quality of life should be further explored.
Furthermore, our study shows that about a quarter of migrant MSM and migrant women had experienced HIV discrimination in the Netherlands. Previous studies have shown that HIV stigma and related HIV discrimination is a major barrier to accessing prevention, care, and treatment services and can negatively impact social relationships, the psychological wellbeing of people living with HIV/AIDS and labour participation.22-28 As we did not ask participants about the context of HIV discrimination, it is unclear if discrimination took place at the structural, individual or community level.22,27 As showed that the psychological impact of stigma varies by social setting26 and interventions to tackle HIV discrimination differ per setting,27 collecting data regarding the setting in which HIV discrimination took place in future studies is important in order to develop effective interventions. We also observed high levels of ethnic discrimination among migrants (43%) and, among MSM, high levels of discrimination due to sexuality (46%). These proportions are worrisome and interventions are urgently needed to limit the potential impact on quality of life and access to care.
The main strength of our study is the comparison of a rich set of data between HIV-positive migrants and non-migrants living in the same country, data not available in many studies evaluating access to services among migrants.8,9 However, some limitations need to be ad-dressed beside the limitations of the aMASE study described elsewere.7,9 First, due to low numbers, non-migrant women were not included in our analyses and therefore we were not able to compare outcomes between migrant and non-migrant women. Second, due to small numbers we were unable to perform multivariable analyses in which variables other than age were included. Third, although the survey was comprehensive, detailed information to assess determinants of underlying barriers that limit access to HIV related health services was not possible. Fourth, our results might not be generalizable to other countries/settings as they might serve different populations and migrant groups, and have different health systems. Also, the response rate of a study might affect the generalizability. The response rate in our study was 60%, which is relatively high for a study covering sensitive topics such as HIV, sexuality and discrimination and focussing on migrants. However, there might be selection bias as non-respondent analyses showed that migrants from Latin America/Carib-bean and women and heterosexual men were less likely to participate.

131
Access to and use of HIV-related healthcare services
3.1
ConCluSIonS
In conclusion, we observed disparities in access to and use of HIV-related health services and experiences in living with HIV by migrant status but also by sexual orientation. To make services more accessible and to ensure timely HIV prevention, diagnosis and care, inter-ventions need to be tailored according to the individual. Our data suggests heterosexual men and women may particularly benefit from improved access to HIV testing (e.g. through provider-initiated testing), while migrant MSM may benefit from improved access to HIV prevention interventions (e.g., PrEP).
acknowledgements
The authors acknowledge all participants of the aMASE study for their contribution; par-ticipating HIV treatment centers (Amsterdam UMC [location AMC], OLVG and Haaglanden Medisch Centrum), Saskia Bogers, Emilia Ric-Doe and Darshni Jhagroe for their help with the recruitment of participants during their research internship at the department of Infectious Diseases Research and Prevention of the Public Health Service of Amsterdam; the ATHENA/SHM Cohort Study for providing participants’ HIV clinic data; Anders Boyd for statistical advice and the funders for the financial support.
This study would not be possible without the entire Work Package 14 collaboration. The aMASE study team are: Aerssens A, Aguado M, Alimi B, Álvarez.D, Anagnostou O, Anderson J, Antoniadou A, Arando M, Barberà MJ, Barros H, Barthélemy A,Belda-Ibáñez J, Bertisch B, Bil J, Blanco JR, Block K, Boesecke C, Boura M, Burgos J, Burns FM, Cabo J, Calabuig E, Campbell L, Cardoso O, Claudia W, Clumeck N, Colucci A, Corrao S, Cuellar S, Cunha J, Daikos G, Darling K, del Amo J, del Romero J, Dellot P, Dixneuf M, Domingo P, Dronda F, Ebeling F, Engelhardt A, Engler B, Fakoya I, Farrell J, Fehr J, Feijó M, Fernández E, Fernández García E, Fernandez T, Fortes AL, Fox J, Garcia de Olalla P, García F, Gargalianos-Kakolyris P, Gennotte AF, Germano I, Gilleran G, Gilson R, Goepel S, Gogos HA, Gómez Sirvent JL, Gountas I, Gregg A, Gutiérrez F, Gutierrez MM, Hermans I, Hoeksma K, Iribarren JA, Knobel H, Koulai L, Kourkounti S, La Morté C, LeCompte T, Ledergerber B, Leonidou L, Leyten E, Ligero MC, Lindergard G, Lino S, Lopes MJ, Lopez Lirola A, Louhenapessy M, Lourida G, Luzi AM, Maltez F, Manirankunda L, Martín-Pérez A, Martins L, Masía M, Mateu MG, Meireles P, Mendes A, Metallidis S, Mguni S, Milinkovic A, Miró JM, Mohrmann K, Monge S, Montero M, Mouhebati T, Moutschen M, Müller M, Murphy C, Nöstlinger C, Ocaña I, Okumu-Fransche S, Onwuchekwa G, Ospina JE, Otiko D, Pacheco P, Palacios R, Paparizos V, Papastamopoulos V, Paredes V, Patel N, Pellicer T, Peña A, Petrosillo N, Pinheiro A, Poças J, Portillo A, Post F, Prestileo F, Prestileo T, Prins M, Prins J, Protopapas K, Psichogiou M, Pulido F, Rebollo J, Reiss P, Ribeirinho A, Río I, Robau M, Rockstroh JK, Rodrigues E, Rodríguez M, Sajani C, Salavert M, Salman R, Sanz N, Schuettfort G, Schüttfort G, Schwarze- Zander C, Serrão R, Silva D, Silva V, Silverio P, Skoutelis A, Staehelin

Chapter 3.1
132
C, Stephan C, Stretton C, Styles F, Sutre AF, Taylor S, Teixeira B, Thierfelder C, Touloumi G, Tsachouridou O, Tudor K, Valadas E, van Frankenhuijsen M, Vázquez M, Velasco Arribas M, Vera M, Vinciana P, Volny-Anne A, Voudouri N, Wasmuth JC, Wengenroth C, Wilkins E, Young L, Yurdakul S, Zafra Espinosa T, Zuilhof W, Zuure F.
funding
The aMASE study is part of Work Package 14 of EuroCoord, which is funded by the EU’s Sev-enth Framework Programme for research, technological development, and demonstration (under grant no. 260694). Additional funding for the data collection of non-migrants and the analyses of the present study was received from the Public Health Service of Amsterdam’s Research and Development Fund (project number 12-29).
The ATHENA database is maintained by Stichting HIV Monitoring and supported by a grant from the Dutch Ministry of Health, Welfare and Sport through the Centre for Infectious Disease Control of the National Institute for Public Health and the Environment.
Conflicts of interest
F.R. Zuure worked on projects (partly) funded or sponsored by non-restricted grants from Abbvie, Gilead Sciences, Janssen-Cilag, MSD, Orasure Technologies and Roche Diagnostics. All other authors have no conflicts of interest related to this study.
ethics approval and consent to participate
The study was submitted to the Ethics Committee of Academic Medical Center in Amster-dam who confirmed that the Medical Research Involving Human Subjects Act (WMO) does not apply to this study and therefore official approval by an Ethics Committee is not required (2013_137#20131038). All participants consented to take part in the study.

133
Access to and use of HIV-related healthcare services
3.1
referenCes
1. European Centre for Disease Prevention and Control (ECDC). migrant health: epidemiology of HIV and aIdS in migrant communities and ethnic minorities in eu/eea countries. Stockholm: ECDC, 2010.
2. European Centre for Disease Prevention and Control (ECDC). HIV and migrants: monitoring imple-mentation of the dublin declaration on Partnership to Fight HIV/aIdS in europe and Central asia: 2017 progress report. Stockholm: ECDC, 2017.
3. Hernando V, Alvarez-del Arco D, Alejos B, Monge S, Amato-Gauci AJ, Noori T, et al. HIV Infection in Mi-grant Populations in the european union and european economic area in 2007-2012: an epidemic on the move. J Acquir Immune Defic Syndr. 2015;70(2):204-211. doi:10.1097/QAI.0000000000000717.
4. Van Sighem AI, Boender TS, Wit FWNM, Smit C, Matser A, Reiss P. Monitoring report 2018. Human Immunodeficiency Virus (HIV) Infection in the netherlands. Amsterdam: Stichting HIV Monitoring, 2018.
5. Op de Coul EL, van Sighem A, Brinkman K, van Benthem BH, van der Ende ME, Geerlings S, et al. Factors associated with presenting late or with advanced HIV disease in the netherlands, 1996-2014: results from a national observational cohort. BMJ Open. 2016;6(1):e009688. doi:10.1136/bmjopen-2015-009688.
6. Van Andel E, Been SK, Rokx C, van der Ende ME. risk factors in an HIV-infected population for refrain-ing from specialist care. AIDS Care. 2016;28(10):1255-1260. doi:10.1080/09540121.2016.1168914.
7. Fakoya I, Alvarez-Del Arco D, Monge S, Copas AJ, Gennotte AF, Volny-Anne A, et al. advancing migrant access to Health Services in europe (aMaSe): Protocol for a Cross-sectional Study. JMIR Res Protoc. 2016;5(2):e74. doi:10.2196/resprot.5085.
8. Fakoya I, Alvarez-Del Arco D, Copas AJ, Teixeira B, Block K, Gennotte AF, et al. Factors associated With access to HIV Testing and Primary Care among Migrants living in europe: Cross-Sectional Survey. JMIR Public Health Surveill. 2017;3(4):e84. doi:10.2196/publichealth.7741.
9. Fakoya I, Alvarez-Del Arco D, Monge S, Copas AJ, Gennotte AF, Volny-Anne A, et al. HIV testing history and access to treatment among migrants living with HIV in europe. J Int AIDS Soc. 2018;21 Suppl 4:e25123. doi:10.1002/jia2.25123.
10. Alvarez-Del Arco D, Fakoya I, Thomadakis C, Pantazis N, Touloumi G, Gennotte AF, et al. High lev-els of post-migration HIV acquisition within nine european countries. AIDS. 2017 doi:10.1097/QAD.0000000000001571.
11. Heinze G, Schemper M. a solution to the problem of separation in logistic regression. Stat Med. 2002;21(16):2409-2419. doi:10.1002/sim.1047.
12. Joore IK, Geerlings SE, Brinkman K, van Bergen JE, Prins JM. The importance of registration of sexual orientation and recognition of indicator conditions for an adequate HIV risk-assessment. BMC Infect Dis. 2017;17(1):178. doi:10.1186/s12879-017-2279-y.
13. Rechel B, Mladovsky P, Ingleby D, Mackenbach JP, McKee M. Migration and health in an increasingly diverse europe. Lancet. 2013;381(9873):1235-1245. doi:10.1016/S0140-6736(12)62086-8.
14. Ndumbi P, Del Romero J, Pulido F, Velasco Arribas M, Dronda F, Blanco Ramos JR, et al. Barriers to health care services for migrants living with HIV in Spain. Eur J Public Health. 2018;28(3):451-457. doi:10.1093/eurpub/ckx225.
15. Dutch Ministry of Health, Welfare and Sport. Healthcare in the netherlands. Available at: https://www.government.nl/documents/leaflets/2016/02/09/healthcare-in-the-netherlands (accessed on 16 August 2018).

Chapter 3.1
134
16. CAK regelingen. regeling onverzekerbare vreemdelingen [dutch]. Available at: https://www.hetcak.nl/zakelijk/regelingen/onverzekerbare-vreemdelingen (accessed on 16 August 2018).
17. Centers for Disease Control and Prevention (CDC). Health Literacy. Available at: http://www.cdc.gov/healthliteracy/learn/ (accessed on 16 August 2018).
18. Perazzo J, Reyes D, Webel A. a Systematic review of Health literacy Interventions for People living with HIV. AIDS Behav. 2017;21(3):812-821. doi:10.1007/s10461-016-1329-6.
19. World Health Organization (WHO). Guidelines on HIV Self-Testing and Partner notification: Supple-ment to Consolidated Guidelines on HIV Testing Services. Geneva: WHO, 2016.
20. Bil JP, Prins M, Fakoya I, Volny-Anne A, Burns F, Zuure FR. usage of purchased self-tests for HIV infec-tions among migrants living in the uK, France and the netherlands: a cross-sectional study. Sex Transm Infect. 2018 doi:10.1136/sextrans-2018-053583.
21. Bil JP, Prins M, Stolte IG, Dijkshoorn H, Heijman T, Snijder MB, et al. usage of purchased self-tests for HIV and sexually transmitted infections in amsterdam, the netherlands: results of population-based and serial cross-sectional studies among the general population and sexual risk groups. BMJ Open. 2017;7(9):e016609. doi:10.1136/bmjopen-2017-016609.
22. Alvarez-del Arco D, Monge S, Azcoaga A, Rio I, Hernando V, Gonzalez C, et al. HIV testing and counsel-ling for migrant populations living in high-income countries: a systematic review. Eur J Public Health. 2013;23(6):1039-1045. doi:10.1093/eurpub/cks130.
23. Fakoya I, Reynolds R, Caswell G, Shiripinda I. Barriers to HIV testing for migrant black africans in Western europe. HIV Med. 2008;9 Suppl 2:23-25. doi:10.1111/j.1468-1293.2008.00587.x.
24. Sumari-de Boer IM, Sprangers MA, Prins JM, Nieuwkerk PT. HIV stigma and depressive symptoms are related to adherence and virological response to antiretroviral treatment among immigrant and indigenous HIV infected patients. AIDS Behav. 2012;16(6):1681-1689. doi:10.1007/s10461-011-0112-y.
25. Chinouya M, Hildreth A, Goodall D, Aspinall P, Hudson A. Migrants and HIV stigma: findings from the Stigma Index Study (uK). Health Soc Care Community. 2017;25(1):35-42. doi:10.1111/hsc.12179.
26. Stutterheim SE, Pryor JB, Bos AE, Hoogendijk R, Muris P, Schaalma HP. HIV-related stigma and psycho-logical distress: the harmful effects of specific stigma manifestations in various social settings. AIDS. 2009;23(17):2353-2357. doi:10.1097/QAD.0b013e3283320dce.
27. Mahajan AP, Sayles JN, Patel VA, Remien RH, Sawires SR, Ortiz DJ, et al. Stigma in the HIV/aIdS epi-demic: a review of the literature and recommendations for the way forward. AIDS. 2008;22 Suppl 2:S67-79. doi:10.1097/01.aids.0000327438.13291.62.
28. Stutterheim SE, Brands R, Baas I, Lechner L, Kok G, Bos AER. HIV Status disclosure in the Workplace: Positive and Stigmatizing experiences of Health Care Workers living with HIV. J Assoc Nurses AIDS Care. 2017;28(6):923-937. doi:10.1016/j.jana.2017.06.014.



Chapter 3.2Hepatitis B and C screening needs among
different ethnic groups: A population-based study in Amsterdam,
the Netherlands
Janneke P. Bil*, Freke R. Zuure*, Maartje Visser, Marieke B. Snijder, Anders Boyd, Petra Blom, Gerard J.B. Sonder, Janke Schinkel, Maria Prins
* Both authors contributed equally to this article
Published in JHEP Reports, 2019

Chapter 3.2
138
aBstraCt
Background & aims
Data on the prevalence of chronic hepatitis B (HBV) and hepatitis C (HCV) virus infections, including the proportion of individuals aware of infection, are scarce among migrants living in Europe. We estimated the prevalence of past and present HBV and HCV infection, along with their determinants and peoples’ awareness of infection status, among different groups of first-generation migrants and Dutch-origin residents of Amsterdam.
methods
Cross-sectional data of 998 Surinamese (mostly South-Asian and African-Surinamese), 500 Ghanaian, 497 Turkish, 498 Moroccan and 500 Dutch-origin participants from the obser-vational population-based HELIUS study were used. Blood samples of participants were tested for HBV and HCV infection. Infection awareness was determined using records from participants’ general practitioners.
results
Age- and gender-adjusted chronic HBV prevalence was highest among Ghanaian participants (5.4%), followed by Turkish (4.1%), African-Surinamese (1.9%), Moroccan (1.2%), South-Asian Surinamese (0.9%) and Dutch (0.4%) participants. A total of 58.1% of the cases were aware of their infection. In multinomial logistic regression analyses, Ghanaian (adjusted odds ratio [aOR] 42.23; 95% confidence interval [CI] 9.29–192.01), African-Surinamese (aOR 6.16; 95%CI 1.27–29.79), and Turkish (aOR 13.44; 95% CI 2.94–61.39) participants were at increased risk of chronic HBV infection compared with those of Dutch origin. Older participants were also at increased risk (aOR 1.02 per year; 95% CI 1.00–1.05), whereas women were at lower risk (aOR 0.49; 95% CI 0.29–0.83). HCV prevalence was 0.4% (95% CI 0.1–1.3%) among Dutch and African-Surinamese and 0% (95% CI 0.0–0.5%) for each of the other groups; all cases with follow-up data were aware of their infection.
Conclusions
Ghanaian, Turkish and African-Surinamese first-generation migrants are at increased risk of chronic HBV infection and many are unaware of their infection, whereas HCV prevalence was low among all ethnic groups. Screening campaigns are urgently warranted and need to consider specific ethnic groups.

139
HBV and HCV screening needs among ethnic groups
3.2
InTroduCTIon
Chronic hepatitis B virus (HBV) and hepatitis C virus (HCV) infections are estimated to affect 4.7 million and 5.6 million people living in Europe, respectively.1 In the Netherlands, it is esti-mated that 49,000 people were living with chronic HBV infection in 2016 and 23,000 people had ever been chronically infected with HCV (0.34% and 0.16% of the adult population, respectively), with an estimated 500 deaths each year attributed to infection.2,3 Currently, effective treatment options to suppress HBV and cure HCV infection are available4,5 without restricted access in the Netherlands. Furthermore, the contacts of newly diagnosed HBV-infected individuals are notified and if still susceptible, are offered vaccination. However, the onset of HBV and HCV infection and initial development of liver damage in chronically in-fected patients is often asymptomatic,6-8 which leaves many infected individuals unaware of their infection, delaying diagnosis and therefore treatment initiation. Reports from Western countries show that 21–55% and 43–50% of HBV and HCV-infected individuals, respectively, do not know their infection status.9-11 However, data from the Netherlands is scarce. Data from the Dutch antenatal screening program suggest that up to 58% of HBV-infected indi-viduals may be unaware of their infection12 and for HCV, it was estimated at 51% based on notification and laboratory data.13
Screening for HBV and HCV infections facilitates identifying undiagnosed infections, improv-ing individual prognosis and limiting further transmission. For some risk groups in the Neth-erlands screening is part of existing health care programs (i.e., HIV care; HBV vaccination program and HIV pre-exposure prophylaxis - PrEP - for men who have sex with men – MSM - and sex workers; harm reduction programs for people who inject drugs14-17). Furthermore, routine HBV screening is integrated into antenatal care in the Netherlands.12 Since 1989, new-borns from HBV surface antigen (HBsAg)-positive mothers have been vaccinated im-mediately after birth and in 2011 universal HBV vaccination was introduced for all children regardless of ethnic origin.
First-generation migrants are estimated to account for a relatively large proportion of chronic HBV and HCV infections in the Netherlands (81% and 60% respectively) and many other Northern and Western European countries.18 The Health Council of the Netherlands and Dutch guidelines for general practitioners (GPs) advise to offer screening to migrants from HBV and/or HCV-endemic countries,19,20 but this is still not common practice. This may partly be due to the ethnic heterogeneity of migrant populations, each with an accompanying risk for infection and degree of infection status awareness.
Evaluating infection prevalence, associated risk factors and awareness of infection status across specific migrant groups is thus critical if screening and prevention programs are to ef-

Chapter 3.2
140
fectively target individuals in need of screening. However, population-based studies on HBV and HCV prevalence among migrant subpopulations are limited, and those that have been conducted generally lack data regarding awareness of infection status.21 In order to inform the development of screening and preventive interventions for migrants, we studied the prevalence of HBV and HCV infection markers, along with their risk factors, using data from a large, population-based study including five large ethnic minority groups and individuals of Dutch origin living in Amsterdam, the Netherlands. We also evaluated infection status awareness among individuals identified with chronic infection.
MaTerIalS and MeTHodS
study population and design
Participants were recruited from the HELIUS (HEalthy LIfe in an Urban Setting) study, a multi-ethnic population-based cohort study in Amsterdam. The design, methodology and response rate of the HELIUS study are described in detail elsewhere.22,23 In brief, the HELIUS study aimed to investigate mechanisms underlying the impact of ethnicity on communicable and non-communicable diseases. An invitation for HELIUS study participation was sent to individuals aged 18– 70 years old, randomly sampled, stratified by ethnicity, from the mu-nicipality register of Amsterdam. People of Surinamese, Turkish, Moroccan, Ghanaian, and Dutch ethnic origin were included. Of the Surinamese living in the Netherlands, most are either of African or South-Asian origin. Participants underwent a physical examination during which biological samples were collected. Furthermore, a detailed questionnaire was admin-istered in which questions were asked on sexual orientation, level of education, risk factors for HBV and/or HCV infection (having surgery in a non-Western country [i.e., all forms of surgery including dental surgery, caesarean section, cosmetic and keyhole surgery involving skin incisions, etc.], having a blood transfusion in a non-Western country or before 1990 in a Western country, ever-injecting drug use and lifetime number of sexual partners) and, except for those of Dutch origin, migration history (age at migration and reason for migration).
All participants provided written informed consent for participation in the study. In the writ-ten consent form, participants could opt out of having their biological samples stored and/or medical data obtained from patient records. Baseline data collection of the HELIUS study took place from 2011 to 2015. The HELIUS study conforms to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the AMC Ethical Review Board.
For the current study, HELIUS participants recruited between January 2011 and June 2014 were eligible for selection if they had completed the questionnaire, participated in the physical examination and had at least four stored tubes of EDTA plasma. We only included

141
HBV and HCV screening needs among ethnic groups
3.2
first-generation migrants for non-Dutch ethnic groups. We selected a random sample of 500 eligible participants for each ethnic group, while oversampling for Surinamese (n=1,000) in order to include sufficient numbers of African and South-Asian Surinamese participants. This resulted in a total sample size of 3,000 people.
ethnicity
Ethnicity was based on the country of birth of the participant and the country of birth of both parents, which is a widely accepted indicator of ethnic origin in the Netherlands.24 More specifically, a participant was considered of non-Dutch ethnic origin if he or she was (A) born outside the Netherlands and had at least one parent who was born outside the Netherlands (first-generation migrant) or (B) the participant was born in the Netherlands and both her/his parents were born outside the Netherlands (second-generation migrant). For the Dutch sample, we invited people who were born in the Netherlands and whose parents were born in the Netherlands. A limitation of the country-of-birth indicator for ethnicity is that people who are born in the same country might have a different ethnic background, which, in the Dutch context, is applicable to the Surinamese population.24 Therefore, participants of Surinamese ethnic origin were further classified according to self-reported ethnic origin (obtained by questionnaire) into ‘African’, ‘South-Asian’, ‘Javanese’ or ‘other/unknown’ Surinamese ethnic origin.23
laboratory testing
Blood samples were centrifuged and stored at -20°C within two hours of collection and transported to -80°C storage on the same day. Stored blood samples of the 3,000 selected participants obtained at HELIUS baseline data collection were tested for markers of past and present HBV and HCV infection in 2015 and 2016. For HBV, samples were first tested for anti-bodies to hepatitis B core antigen (anti-HBc total) using microparticle enzyme immunoassay (LIAISON® Anti-HBc, Diasorin, Italy). When positive or indeterminate, HBsAg and antibodies to HBsAg (anti-HBs) were determined (LIAISON® XL Murex HBsAg Quant Assay, Diasorin, Italy). Samples positive for HBsAg (>0.05 IU/ml) were tested for hepatitis B-e-antigen (HBeAg) and antibodies to HBeAg (anti-HBe) (LIAISON® HBeAg and LIAISON® Anti-HBe respectively), and for the presence of HBV-DNA (COBAS® AmpliPrep/COBAS® TaqMan® HBV Test, v2.0, Roche Molecular Diagnostics, Pleasanton, USA). For HBV-DNA measurements, sera were diluted 1:10 with HBV-DNA negative serum, resulting in a quantitative detection limit of 165 IU/ml. HCV serological testing was done by third-generation commercial microparticle EIA system (AxSym HCV version 3.0; Abbott Laboratories, North Chicago, IL, USA). Samples with HCV antibody (anti-HCV) reactivity ≥1.0 were further tested for HCV-RNA using COBAS Ampliprep/COBAS TaqMan (CAP-CTM HCV test v2.0; Roche Diagnostics, Mannheim, Ger-many). Participants with low-reactive anti-HCV test results (reactivity between 1.0–1.8) who tested HCV-RNA negative were considered anti-HCV negative (non-exposed). From these

Chapter 3.2
142
results, we defined three infection groups for HBV: non-exposed, past-HBV infection (further differentiated as resolved infection and isolated anti-HBc) and chronic HBV infection); and three infection groups for HCV: non-exposed, past (resolved) HCV infection and chronic HCV infection (Table 1).
awareness of infection status
According to HELIUS study procedures, we informed GPs of participants with a chronic HBV or HCV infection by letter asking them to verify whether their patient was aware of his/her infection and if not, to inform their patient and to perform confirmatory testing. We collected data on the number of previously diagnosed infections and confirmatory results by sending a data collection form to GPs six weeks after the initial letter. GPs who did not respond were re-contacted and data were collected over telephone. Participants with no declared GP were sent a letter asking to contact the Public Health Service of Amsterdam for further information on their test results and repeat testing.
statistical analyses
Demographic characteristics were compared between ethnic groups using Pearson’s χ² or Fisher’s exact tests for categorical variables and Kruskal-Wallis tests for continuous variables. For each ethnic group, crude prevalences of HBV and HCV infection groups were estimated along with their 95% confidence interval (CI) using the Jeffreys method. For HBV, adjusted
Table 1. Definition of HBV and HCV infection groupsHBV infection groups
anti-HBc HBsag anti-HBs
Non-exposed a negative negative b NA
Past infection: Resolved-HBV infection positive or indeterminate negative positive
Past infection: Isolated anti-HBc positive or indeterminate negative negative
Chronic HBV infection positive or indeterminate positive negative
HCV infection groups
anti-HCV HCV-rna
Non-exposed negative negative c
low-reactive d negative
Past infection: Resolved-HCV infection positive negative
Chronic HCV infection positive positive
Anti-HBc, antibodies to hepatitis B core antigen; anti-HBs, antibodies to HBsAg; anti-HCV, antibodies to HCV; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus, HCV, hepatitis C virus; NA, not applicablea Vaccination status unknown.b Not tested but assumed negative when anti-HBc was negative.c Not tested but assumed negative when anti-HCV was negative.d Reactivity between 1.0–1.8.

143
HBV and HCV screening needs among ethnic groups
3.2
prevalence was also presented as average marginal predicted probabilities from a logistic regression model correcting for age and sex. Univariable and multivariable multinominal logistic regression models were used to assess determinants of past-HBV infection or chronic HBV infection when compared to HBV non-exposed. Variables associated with an overall p-value ≤0.1 in univariable analyses were considered in a full multivariable model. A stepwise backward selection procedure was used whereby covariables with associated p-values >0.05 were removed to reach a final multivariable model. We evaluated the following variables: ethnicity, age, sex, level of education (i.e., less than higher vocational schooling or university versus vocational schooling or university), having surgery in a non-Western country, having a blood transfusion in a non-Western country or before 1990 in a Western country, and lifetime number of sexual partners. Interactions between ethnicity and other variables in the final model were tested. We also added age at migration and reason for migration separately to the final multivariable model while only including first-generation migrants. SPSS for Win-dows (version 21, Chicago, IL) and STATA Intercooled (version 13.1, College Station, TX) were used for statistical analyses and a p-value of ≤0.05 was considered statistically significant.
reSulTS
study population
Of 10,572 HELIUS participants, 8,621 were eligible for selection in the current study (Figure 1). Five hundred people of Dutch origin and 2,500 first-generation migrants (500 Turkish, 500 Moroccan, 500 Ghanaian and 1,000 Surinamese) were randomly selected, of whom 2,993 were tested for anti-HCV and 2,987 for anti-HBc. Table 2 summarizes demographic characteristics, migration history and presence of risk factors for HBV and/or HCV infection in the study population stratified by ethnic group. We found significant differences across ethnic groups regarding age (p<0.001), sex (p=0.003), educational level (p<0.001), age at migration (p<0.001), reason for migration (p<0.001), having had surgery in a non-Western country (p<0.001), having had a blood transfusion (p=0.003), and number of lifetime sexual partners (p<0.001).
Chronic HBV and HCV infection
The age- and sex-adjusted prevalence of past and chronic HBV infection ranged from 2.6% (95% CI 1.2–4.0%) and 0.4% (95% CI <0.1–0.9%) among individuals of Dutch origin to 61.5% (95% CI 57.5–65.6%) and 5.4% (95% CI 3.5–7.4%) among Ghanaians, respectively (Figure 2; Table S1). Results were comparable to crude estimates. Age- and sex-adjusted prevalence of past and chronic HBV infection significantly differed between ethnic groups (overall p <0.001). The three Surinamese ethnic groups differed significantly from each other regard-ing past-HBV infection (p<0.001) but not regarding chronic HBV infection (p=0.19).

Chapter 3.2
144
The prevalence of chronic HCV infection per ethnic group ranged from 0% (95% CI 0.0–0.5%) among South-Asian Surinamese, Ghanaian, Turks and Moroccan to 0.4% (95% CI 0.1–1.3%) among people of Dutch and African-Surinamese origin (Figure 3, Table S1).
awareness of HBV and HCV infection status
Data regarding awareness of infection status and follow-up test results were obtained for 41/64 (64.1%) people with chronic HBV infection. For 23 people these data were not ob-tained for the following reasons: no consent for retrieval of medical information (n=7), did not show-up for re-testing at the GP (n=5), no registration at a GP and did not show-up for re-testing at the Public Health Service (n=5), no data obtained from GP (n=4), person moved abroad and went to foreign GP for re-testing (n=1); person was deceased (n=1). In total, 75.6% (31/41) had a confirmed chronic HBV infection either from re-testing or by their GP. Of 31 confirmed chronically infected individuals, 18 (58.1%; 95% CI 40.6–74.1%) were al-ready aware of their infection status. We found differences between ethnic groups and men and women regarding awareness of infection status, although not statistically significant.
Figure 1. Flowchart depicting the selection of participants and laboratory testing algorithm of the study on HBV and HCV prevalence and awareness of infection status within the HELIUS study, Amsterdam, the Neth-erlands, 2011–2014Anti-HBc, antibodies to hepatitis B core antigen; anti-HBe, antibodies to HBe; anti-HBs, antibodies to HBsAg; anti-HCV, antibodies to HCV; HBeAg, hepatitis B-e-antigen; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus, HCV, hepatitis C virus.* 1 individual was not tested for HBeAg due to insufficient blood

145
HBV and HCV screening needs among ethnic groups
3.2
Tabl
e 2.
Dem
ogra
phic
cha
ract
eristi
cs, m
igra
tion
hist
ory
and
HBV/
HCV
risk
fact
ors a
mon
g 2,
993
Dutc
h an
d fir
st-g
ener
ation
mig
rant
par
ticip
ants
of t
he H
ELIU
S st
udy,
Am
ster
-da
m, t
he N
ethe
rland
s, 2
011–
2014
dutc
h (n
=500
)
Surin
ames
e (n
=998
)
Gha
naia
n(n
=500
)tu
rkis
h(n
=497
)m
oroc
can
(n=4
98)
p-va
lue
sout
h-as
ian
surin
ames
e
(n=4
63)
afric
an
surin
ames
e (n
=475
)
oth
er/
unk
now
n a
(n=6
0)
n%
n%
n%
n%
n%
n%
n%
age
(yea
rs)
M
edia
n [IQ
R]46
[35–
57]
51[4
4–58
]53
[45–
58]
52[4
5–57
]48
[41–
54]
46[3
9–51
]47
[39–
53]
<0.0
01b
M
issin
g0
00
00
00
00
00
00
0
Sex
& m
ale
sexu
al b
ehav
iour
stat
us
W
omen
261
52.2
262
56.6
295
62.1
3660
.028
857
.624
749
.728
857
.80.
003c,
d
M
en23
947
.820
143
.418
037
.924
40.0
212
42.4
250
50.3
210
42.2
M
SW20
040
.016
134
.815
532
.616
26.7
177
35.4
180
36.2
151
30.3
M
SM27
5.4
91.
97
1.5
00.
05
1.0
71.
45
1.0
M
en w
ho n
ever
had
sex
71.
412
2.6
61.
35
8.3
81.
619
3.8
285.
6
M
issin
g da
ta o
n se
xual
par
tner
s’ g
ende
r5
1.0
194.
112
2.5
35.
022
4.4
448.
926
5.2
High
est l
evel
of e
duca
tion
Le
ss th
an h
ighe
r voc
ation
al sc
hool
ing
or u
nive
rsity
177
35.4
370
79.9
381
80.2
4473
.345
991
.844
188
.744
088
.4<0
.001
c
Hi
gher
voc
ation
al sc
hool
ing
or u
nive
rsity
321
64.2
9019
.490
18.9
1321
.729
5.8
5410
.953
10.6
M
issin
g2
0.4
30.
64
0.8
35.
012
2.4
20.
45
1.0
age
at m
igra
tion
M
edia
n [IQ
R]-
-18
[11–
23]
20[1
2–27
]23
[16–
29]
28[2
3–33
]17
[11–
22]
18[1
0–24
]<0
.001
b,e
M
issin
g-
-8
1.7
112.
38
13.3
112.
212
2.4
255.
0
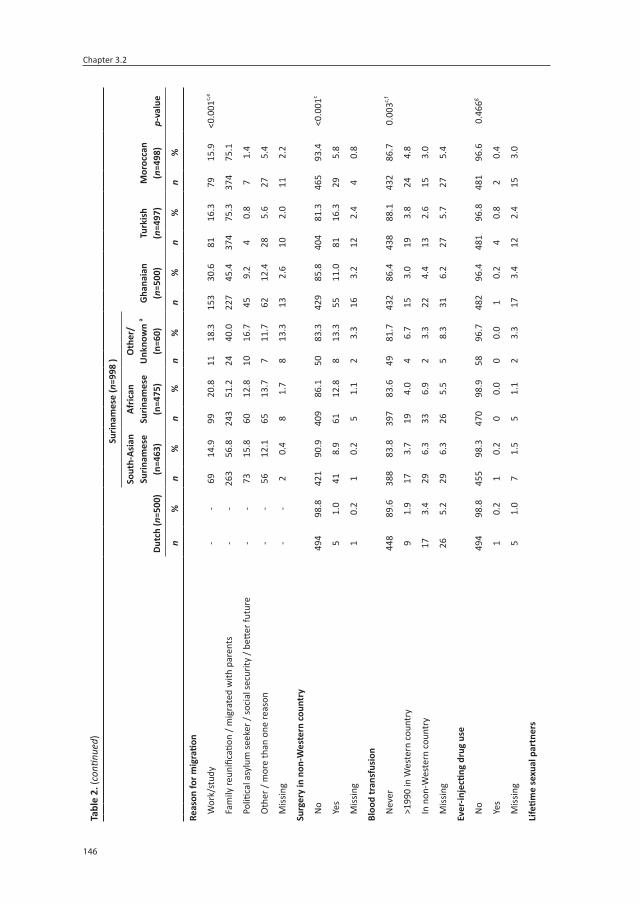
Chapter 3.2
146
Tabl
e 2.
(con
tinue
d)
dutc
h (n
=500
)
Surin
ames
e (n
=998
)
Gha
naia
n(n
=500
)tu
rkis
h(n
=497
)m
oroc
can
(n=4
98)
p-va
lue
sout
h-as
ian
surin
ames
e
(n=4
63)
afric
an
surin
ames
e (n
=475
)
oth
er/
unk
now
n a
(n=6
0)
n%
n%
n%
n%
n%
n%
n%
reas
on fo
r mig
ratio
n
W
ork/
stud
y-
-69
14.9
9920
.811
18.3
153
30.6
8116
.379
15.9
<0.0
01c,
e
Fa
mily
reun
ifica
tion
/ mig
rate
d w
ith p
aren
ts-
-26
356
.824
351
.224
40.0
227
45.4
374
75.3
374
75.1
Po
litica
l asy
lum
seek
er /
soci
al se
curit
y / b
etter
futu
re-
-73
15.8
6012
.810
16.7
459.
24
0.8
71.
4
O
ther
/ m
ore
than
one
reas
on-
-56
12.1
6513
.77
11.7
6212
.428
5.6
275.
4
M
issin
g-
-2
0.4
81.
78
13.3
132.
610
2.0
112.
2
Surg
ery
in n
on-W
este
rn c
ount
ry
N
o49
498
.842
190
.940
986
.150
83.3
429
85.8
404
81.3
465
93.4
<0.0
01c
Ye
s5
1.0
418.
961
12.8
813
.355
11.0
8116
.329
5.8
M
issin
g1
0.2
10.
25
1.1
23.
316
3.2
122.
44
0.8
Bloo
d tr
ansf
usio
n
N
ever
448
89.6
388
83.8
397
83.6
4981
.743
286
.443
888
.143
286
.70.
003c,
f
>1
990
in W
este
rn c
ount
ry9
1.9
173.
719
4.0
46.
715
3.0
193.
824
4.8
In
non
-Wes
tern
cou
ntry
173.
429
6.3
336.
92
3.3
224.
413
2.6
153.
0
M
issin
g26
5.2
296.
326
5.5
58.
331
6.2
275.
727
5.4
ever
-inje
cting
dru
g us
e
N
o49
498
.845
598
.347
098
.958
96.7
482
96.4
481
96.8
481
96.6
0.46
6g
Ye
s1
0.2
10.
20
0.0
00.
01
0.2
40.
82
0.4
M
issin
g5
1.0
71.
55
1.1
23.
317
3.4
122.
415
3.0
life
time
sexu
al p
artn
ers

147
HBV and HCV screening needs among ethnic groups
3.2
Tabl
e 2.
(con
tinue
d)
dutc
h (n
=500
)
Surin
ames
e (n
=998
)
Gha
naia
n(n
=500
)tu
rkis
h(n
=497
)m
oroc
can
(n=4
98)
p-va
lue
sout
h-as
ian
surin
ames
e
(n=4
63)
afric
an
surin
ames
e (n
=475
)
oth
er/
unk
now
n a
(n=6
0)
n%
n%
n%
n%
n%
n%
n%
0–
165
13.0
196
42.3
5712
.013
21.7
7214
.431
062
.434
569
.3<0
.001
c
2
346.
872
15.6
388.
011
18.3
7615
.230
6.0
336.
6
3–
614
729
.481
17.5
177
37.3
1830
.017
735
.434
6.8
499.
8
>7
247
49.4
8317
.916
434
.513
21.7
108
21.6
6312
.739
7.8
M
issin
g7
1.4
316.
739
8.2
58.
367
13.4
6012
.132
6.4
HBV,
hep
atitis
B v
irus;
HCV
, hep
atitis
C v
irus;
IQR,
inte
rqua
rtile
rang
e; M
SM, m
en w
ho h
ave
sex
with
men
; MSW
, men
who
hav
e se
x w
ith w
omen
onl
y.a I
nclu
ding
29
Java
nese
, 13
of m
ixed
eth
nici
ty, 4
oth
er, 1
4 un
know
n.b K
rusk
al-W
allis
test
.c P
ears
on’s
χ² te
st.
d p-v
alue
for t
he d
iffer
ence
in g
ende
r.e D
utch
par
ticip
ants
wer
e ex
clud
ed fo
r the
cal
cula
tion
of th
e p-
valu
e an
d th
e m
edia
n an
d IQ
R fo
r the
tota
l gro
up (i
f app
licab
le).
f Sur
inam
ese
othe
r/un
know
n w
ere
excl
uded
for t
he c
alcu
latio
n of
the
p-va
lue
due
to th
e lo
w n
umbe
rs o
f par
ticip
ants
in th
is gr
oup.
g Fish
er’s
exac
t tes
t.

Chapter 3.2
148
When stratified by ethnicity, the proportion of people aware of their chronic HBV infection status were 33.3% (4/12 Ghanaian), 50.0% (1/2 Moroccan), 63.6% (7/11 Turkish), and 100% (1/1 Dutch; 4/4 African-Surinamese; 1/1 South-Asian Surinamese) (p=0.13). When strati-fied by gender, women were more likely to be aware of their chronic HBV infection status than men (75% [9/12] versus 47.4% [9/19]), although the difference was not statistically significant (p=0.16).
Data regarding awareness of HCV infection status were available for three of four people chronically infected with HCV. All three had been previously diagnosed and were in spe-cialized care. The GP of the fourth chronically infected person was uncertain whether the patient had been previously diagnosed; however, this person was referred to specialized care after our notification letter was received.
markers of HBV infection and immunity
Among all people with past-HBV infection for whom an anti-HBs test result (positive/negative) was available, 71.4% (503/704; 95% CI 68.0–74.7%) tested anti-HBs positive while 28.6% (201/704; 95% CI 25.3–32.0%) had no anti-HBs. The prevalence of isolated anti-HBc positivity differed significantly between ethnic groups (Dutch: 23.1%, 3/13; South-Asian
Figure 2. Prevalence of HBV infection among participants of the HELIUS study, 2011–2014Prevalence of HBV status is given for each ethnic group recruited in the HELIUS study. Past-HBV infection (a) is separated into either resolved-HBV infection (B) or isolated anti-HBc positive infection (C). Chronic HBV infec-tion is given in (d). Point estimates are represented by boxes and 95% confidence intervals by bars. Estimates in colored boxes are unadjusted whereas those in hollow boxes are adjusted for age and sex.Anti-HBc, antibodies to hepatitis B core antigen; HBV, hepatitis B virus.* p<0.05 compared with participants of Dutch origin

149
HBV and HCV screening needs among ethnic groups
3.2Surinamese: 23.3%, 14/60; African-Surinamese: 11.3%, 13/115; Ghanaian: 42.5%, 125/294; Turkish: 15.9%, 20/126; Moroccan: 28.6%, 24/85; p<0.001).
Among people with chronic HBV infection, 3.2% (2/63; 95% CI 0.7–9.8%) were HBeAg positive and 91.9% (57/62; 95% CI 83.2–96.9%) were anti-HBe positive (1/64 had insufficient blood available for HBeAg testing and 2/64 had indeterminate anti-HBe test results). In total, 3.1% (2/64; 95% CI 0.7–9.6%) of chronically infected participants had HBV-DNA levels of 20,000 IU/ml or higher; 12.5% (8/64; 95% CI 6.1–22.2%) had HBV-DNA levels between 2,000–19,999 IU/ml; 25% (16/64; 95% CI 15.7–36.5%) had HBV-DNA levels between 220–1,999 IU/ml; whereas in 59.4% (38/64; 95% CI 47.1–70.8%) of participants HBV-DNA was below 220 IU/ml or not detected.
All individuals newly diagnosed with chronic HBV infection as a result of our study (n=13) were HBeAg negative and anti-HBe positive. Of those, 15.4% (2/13; 95% CI 3.34–40.90%) had HBV-DNA levels between 2,000–19,999 IU/ml; 46.2% (6/13; 95% CI 22.11–71.71%) between 220–2,000 IU/ml and in 38.5% (5/13; 95% CI 16.5–65.0%) HBV-DNA was below 220 IU/ml or not detected.
determinants of infection
In multivariable analyses, ethnicity, age, sex and educational level were significantly associ-ated with HBV infection status (Table 3). Participants of South-Asian Surinamese (adjusted odds ratio [aOR] 4.12; 95% CI 2.19–7.75), African-Surinamese (aOR 9.28; 95% CI 5.06–17.03), Ghanaian (aOR 66.10; 95% CI 35.76–122.17), Turkish (aOR 13.19; 95% CI 7.13–24.39) and Moroccan (aOR 7.06; 95% CI 3.79–13.18) origin were at increased risk of past-HBV infection
Figure 3. Prevalence of HCV infection among partici-pants of the HELIUS study, 2011–2014Prevalence of HCV status is given for each ethnic group recruited in the HELIUS study. Point estimates of unadjusted past-HCV infection (a) and chronic HCV infection (B) are represented by boxes and 95% confidence intervals by bars.HCV, hepatitis C virus.

Chapter 3.2
150 151
HBV and HCV screening needs among ethnic groups
3.2
Tabl
e 3.
Mul
tinom
inal
uni
varia
ble
and
mul
tivar
iabl
e lo
gisti
c re
gres
sion
anal
yses
of d
eter
min
ants
ass
ocia
ted
with
pas
t-HBV
infe
ction
and
chr
onic
HBV
infe
ction
(ver
sus n
on-
expo
sed)
am
ong
2,98
7 Du
tch
and
first
gen
erati
on m
igra
nt p
artic
ipan
ts o
f the
HEL
IUS
stud
y, Am
ster
dam
, the
Net
herla
nds,
201
1–20
14Pa
st-H
BV in
fecti
onCh
roni
c HB
V in
fecti
on
or
(95%
CI)
aor
(95%
CI)
or
(95%
CI)
aor
(95%
CI)
p-va
lue
a
ethn
icity
b<0
.001
Dutc
h1
11
1
Sout
h-As
ian
Surin
ames
e5.
72(3
.10–
10.5
6)4.
12(2
.19–
7.75
)1.
83(0
.30–
10.9
9)1.
70(0
.27–
10.5
6)
Afric
an-S
urin
ames
e12
.36
(6.8
6–22
.29)
9.28
(5.0
6–17
.03)
6.24
(1.3
4–29
.04)
6.16
(1.2
7–29
.79)
Ghan
aian
68.3
6(3
8.19
–122
.36)
66.1
0(3
5.76
–122
.17)
37.7
5(8
.87–
160.
78)
42.2
3(9
.29–
192.
01)
Turk
ish13
.43
(7.4
7–24
.16)
13.1
9(7
.13–
24.3
9)13
.16
(3.0
5–56
.88)
13.4
4(2
.94–
61.3
9)
Mor
occa
n7.
79(4
.28–
14.1
7)7.
06(3
.79–
13.1
8)2.
38(0
.43–
13.0
8)2.
50(0
.43–
14.3
5)
age
(per
yea
r)1.
04(1
.03–
1.05
)1.
06(1
.05–
1.07
)1.
01(0
.99–
1.04
)1.
02(1
.00–
1.05
)<0
.001
sex
0.00
9
Men
11
11
Wom
en0.
86(0
.73–
1.02
)0.
83(0
.68–
1.01
)0.
54(0
.33–
0.90
)0.
49(0
.29–
0.83
)
High
est l
evel
of e
duca
tion
0.00
5
Less
than
hig
her v
ocati
onal
scho
olin
g or
uni
vers
ity1
11
1
High
er v
ocati
onal
scho
olin
g or
uni
vers
ity0.
24(0
.18–
0.32
)0.
59(0
.42–
0.82
)0.
39(0
.19–
0.82
)0.
92(0
.42–
2.05
)
Surg
ery
in n
on-W
este
rn c
ount
ry
No
11
Yes
1.40
(1.0
6–1.
84)
1.29
(0.5
8–2.
87)
Bloo
d tr
ansf
usio
n
Nev
er o
r >19
90 in
Wes
tern
cou
ntry
11
Befo
re 1
990
or >
1990
in n
on-W
este
rn c
ount
ry1.
08(0
.72–
1.61
)1.
10(0
.34–
3.58
)

Chapter 3.2
150 151
HBV and HCV screening needs among ethnic groups
3.2
Tabl
e 3.
(con
tinue
d)
Past
-HBV
infe
ction
Chro
nic
HBV
infe
ction
or
(95%
CI)
aor
(95%
CI)
or
(95%
CI)
aor
(95%
CI)
p-va
lue
a
life
time
sexu
al p
artn
ers
0–1
11
21.
34(0
.99–
1.81
)1.
29(0
.57–
2.92
)
3–6
1.51
(1.2
0–1.
88)
1.29
(0.6
9–2.
40)
>7
0.91
(0.7
2–1.
16)
0.72
(0.3
6–1.
45)
(a)O
R, (a
djus
ted)
odd
s rati
o; C
I, co
nfide
nce
inte
rval
; HBV
, hep
atitis
B v
irus.
In m
ultiv
aria
ble
anal
ysis,
the
follo
win
g va
riabl
es w
ere
excl
uded
bec
ause
thei
r ove
rall
p-va
lues
wer
e no
long
er b
elow
the
pre-
spec
ified
thre
shol
d: s
urge
ry in
non
-Wes
tern
co
untr
y (p
=0.5
45) a
nd li
fetim
e se
xual
par
tner
s (p=
0.49
5).
a Ove
rall
p-va
lue
of a
log-
likel
ihoo
d ra
tio te
st c
ompa
ring
full
mod
el to
a m
odel
with
indi
vidu
al c
ovar
iabl
e ex
clud
ed.
b Sur
inam
ese
of o
ther
/unk
now
n et
hnic
ity w
ere
not i
nclu
ded
in th
e an
alys
es b
ecau
se o
f a lo
w n
umbe
r of p
artic
ipan
ts.
Chapter 3.2
152
compared with those of Dutch ethnicity. Participants of African-Surinamese (aOR 6.16; 95% CI 1.27–29.79), Ghanaian (aOR 42.23, 95%CI 9.29–291.01) and Turkish (aOR 13.44; 95% CI 2.94–61.39) origin were at increased risk of chronic HBV infection compared with those of Dutch origin, whereas those of South-Asian Surinamese (aOR 1.70; 95% CI=0.27–10.56) and Moroccan (aOR 2.50; 95% CI 0.43–14.35) origin were not.
Older age was significantly associated with past-HBV infection (aOR 1.06 per year; 95% CI 1.05–1.07) and tended to be associated with chronic HBV infection (aOR 1.02 per year; 95% CI 1.00–1.05). Women were at significantly lower risk of chronic HBV infection (aOR 0.49; 95% CI 0.29–0.83) compared with men, and a similar, but non-significant, sex difference was observed for past-HBV infection (aOR 0.83; 95% CI 0.68–1.01). Those with higher educational level (aOR 0.59; 95% CI 0.42–0.82) were less likely to have past-HBV infection compared to less well educated participants.
Among non-Dutch participants, higher age at migration was significantly associated with past-HBV infection (aOR 1.02 per year; 95% CI 1.00–1.03; p=0.01) but not with chronic HBV infection (aOR 1.02 per year; 95% CI 0.99–1.06; p=0.20)(overall p=0.02). The reason for migration was not significantly associated with HBV infection status (p=0.9; data not shown).
The few participants infected with HCV precluded multivariable analysis. All four HCV-RNA-positive people were aged ≥50 years; two were of Dutch origin and two of African-Surinamese origin; three were men. Two individuals reported to be HIV-positive, one person reported ever-injecting drug use, and one person of African-Surinamese origin did not report any risk factors for HCV infection. None of the four participants were co-infected with HBV.
dISCuSSIon
In this population-based cross-sectional study, conducted in a country with low prevalence of HBV and HCV infection in the general population, we found a higher prevalence of chronic HBV infection among first-generation migrants of Ghanaian, Turkish and African-Surinamese ethnicity compared to the host population, whereas the prevalence of chronic HCV infection was low among all ethnic groups. All HCV-infected individuals for whom this information was available were aware of their infections, whereas a substantial proportion of people with chronic HBV infection were in fact unaware.
The age- and sex-adjusted chronic HBV infection prevalence in our study among first-gener-ation migrants from Turkey (4.1%) and Morocco (1.2%) is comparable to previous estimates among first-generation migrants from these countries25 including those of an Amsterdam

153
HBV and HCV screening needs among ethnic groups
3.2
study among a small group of first-generation migrants,26 as well as others reporting country-of-origin estimates.25,27 Slightly lower chronic HBV infection prevalence was found in several screening pilot programs for first-generation migrants of Turkish origin in the Netherlands, ranging from 1.7% to 3.1%.28-30 These programs, however, most likely do not attract individu-als who are already aware of their infection, which may explain their lower prevalence.
For first-generation migrants from Suriname, we found a higher prevalence of past and chronic HBV infection among the African-Surinamese than among the South-Asian Surinam-ese, although the latter difference was not statistically significant. The difference in HBV infection prevalence between Surinamese ethnic groups has also been demonstrated in a study conducted in Suriname, where prevalence among the South-Asian Surinamese was similar to our findings and prevalence among the African-Surinamese was somewhat higher.31 Interestingly, as the African-Surinamese are mostly descendants of enslaved people from Western Africa (a high-prevalence region for HBV), whereas the South-Asian Surinamese are descendants of contract workers from India (a country of much lower HBV prevalence),27 the difference in prevalence could be explained by confined interactions within sub-ethnicities over centuries, which then carried over when immigrating to the Netherlands. Nevertheless, our findings illustrate the need to consider ethnic subgroups within countries of origin when studying prevalence and identifying people in need of HBV screening.
The prevalence of chronic HBV infection among first-generation migrants of Ghanaian origin (5.4%) was much lower compared with estimates in Ghana derived from two large meta-analyses (12.9%; 95% CI 12.4–13.4%27 and 12.3%; 95% CI 11.3–13.4%32) and a study among recent (<5 years) migrants of Ghanaian ethnicity in Spain (15/92; 16.3%; 95% CI 9.8–24.8%).33 The lower prevalence in our study may be explained by shorter exposure time to HBV in their home country compared to those who did not migrate, the salmon bias (i.e., severely ill migrants with HBV infection tend to return to die in their home country) and/or the healthy migrant hypothesis (i.e., a selection of healthier individuals opt for migration).
It is of concern that over 40% of the participants chronically infected with HBV were not aware of their infection status. Unawareness of infection status was much lower for those identified with HCV infection. Men, who are at higher risk of chronic HBV infection, were less likely to be aware of their HBV infection status than women (although not statistically significant). Women may be more likely to be aware of their infection as a result of routine HBV screening in prenatal care programs in the Netherlands to prevent mother-to-child transmission, which was implemented in 1989. Our findings indicate that additional screen-ing programs are needed to identify undiagnosed HBV infections among both men and women of Ghanaian and Turkish origin in order to prevent liver-related disease and onward transmission.

Chapter 3.2
154
A large proportion of those of non-Dutch ethnicity had past-HBV infection, with the propor-tions per ethnic group reflecting endemic patterns of their countries of origin. This indicates that many migrants acquired immunity to HBV infection. We did, however, find relatively high levels of isolated-anti-HBc serologic status, especially among those of Ghanaian origin. Isolated-anti-HBc may result from different scenarios: resolved infection acquired many years ago where detectable anti-HBs has been lost, acute HBV infection, false-positive anti-HBc test, or occult HBV infection where patients with undetectable HBsAg have detectable HBV-DNA. Patients originating from high HBV-endemic countries are known to be more likely to develop occult HBV infection compared with those from low-endemic countries.34 However, even in high-endemic regions for HBV, occult HBV infection usually is not very common, and estimated at around 6% in anti-HBc positive, HBsAg negative blood donors.35 Hence, we believe that the high levels of isolated anti-HBc among non-Dutch ethnic groups are more likely to result from resolved infections that were acquired during early childhood and adolescence. As a large proportion of first-generation migrants are immune to HBV, the primary requirement for HBV prevention is screening to identify chronic infections.
Although migrants are estimated to account for many chronic HCV infections in the Neth-erlands,3 as well as in many other European countries,18,21 we found only four chronic HCV infections among 2,993 people tested. For first-generation migrants of Turkish and Moroc-can ethnicity, we did not expect an anti-HCV antibody prevalence higher than among those of Dutch origin, since country-of-origin estimates are low36 and the prevalence among these groups in previous studies in the Netherlands was also low.37 For migrants from Ghana and Suriname, we expected a higher prevalence based on previous studies in the country of origin and/or the Netherlands.37-40 The low HCV infection prevalence found in our study may be due to the same reasons as mentioned for HBV infection. Alternatively, for some countries of origin, there are vast differences in HCV prevalence across regions (Ghana38) and in sub-ethnicities (Javanese Surinamese40), which might not be reflected in our study.
Although HCV screening for the ethnic groups in our study does not seem justified, combined screening for HBV and HCV may still be cost-effective as the additional costs of simultane-ous screening for HCV are small, especially when considering the cost-effectiveness of this strategy for countries of origin with chronic HBV and HCV prevalence ≥0.41% and ≥0.22%, respectively.41 This suggests that combined HBV and HCV screening of first-generation migrants of Ghanaian and Surinamese origin may be cost-effective despite the low HCV prevalence found in our study.
This study has several limitations. First, although HELIUS participants aged 18-70 years were recruited via an ethnicity stratified random selection of the municipal registry of Amsterdam and our study includes a random selection of HELIUS participants, there may

155
HBV and HCV screening needs among ethnic groups
3.2
be selection bias. Undocumented people and those aged >70 years who may be at higher risk of infection are not included. Furthermore, HELIUS participants may be more concerned about their health compared with non-participants. Notwithstanding the low response rate in the HELIUS study (28%),23 non-response was not linked to socioeconomic differences. Second, with 500 participants per ethnic group, comparisons in HBsAg and HCV prevalence could be underpowered. A posteriori sample size calculation revealed that based on the unadjusted HBsAg prevalence of 0.4% in Dutch-origin participants as reference group, a minimum HBsAg prevalence of 1.6% would have been required in another ethnic group to find a significant difference with 80% power.42 In particular, we did observe a notably higher prevalence of chronic HBV infection for participants of South-Asian Surinamese, Surinamese other/unknown and Moroccan origin than those of Dutch origin, but the aORs were likely not significant because of insufficient power. Third, because the numbers of MSM were small in the non-Dutch ethnic origin groups, sexual behaviour status was not included in the multivariable regression analyses assessing factors associated with HBV infection. Fourth, 10 HBsAg-positive individuals tested HBsAg negative after re-testing at their GP. We found that eight of those had low levels of HBsAg (<0.1) in the initial test and undetectable or low levels (<220 IU/ml) of HBV-DNA. This suggests the presence of low-level HBsAg, a false-positive primary test result, or clearance of HBsAg between HELIUS data collection and re-testing. Finally, we did not determine anti-HBs among those who tested anti-HBc negative, hence we were unable to assess the proportion of our population vaccinated against HBV infection.
In conclusion, the prevalence of chronic HBV infection among first-generation migrants of Ghanaian, Turkish and African-Surinamese origin living in Amsterdam is relatively high compared with the Dutch-origin population, and many are unaware of their infection status. Increased case-finding efforts by GPs and HBV screening programs targeting these migrant groups, as recommended by the Dutch Health Council,20 are needed to identify undiagnosed infections and link infected people to care to decrease HBV-related morbidity and mortality. Importantly, as emphasized by the World Health Organization,43 screening and treatment programs for migrant populations should provide accessible options for timely screening and treatment, as there are a number of barriers to detection and treatment of infectious diseases among migrants,44 Programs should address factors influencing participation in HBV screening, such as stigma and fatalism45-47 and integrate strategies to facilitate access, such as outreach awareness raising.44 HCV screening for the large ethnic groups in Amster-dam seems unjustified, but combined HBV and HCV screening might still be cost-effective if offered to first-generation migrants of Ghanaian and Surinamese origin.
acknowledgements
The authors would like to acknowledge the HELIUS participants for their contribution; the HELIUS team for data collection and management; Annemarie Teitsma-Jansen for sending

Chapter 3.2
156
notification letters and data collection forms to GPs; Sylvia Bruisten and Nienke Alberts for coordinating the sample selection and transportation; Gini van Rijckevorsel for advice on the algorithm for HBV testing; and the funders for financial support.
funding
The HELIUS study is conducted by the Academic Medical Center Amsterdam and the Public Health Service of Amsterdam. Both organizations provided core support for HELIUS. The HELIUS study is also funded by the Dutch Heart Foundation (2010T084), the Netherlands Organization for Health Research and Development (ZonMw) (200500003), the European Union (FP-7) (278901), and the European Fund for the Integration of non-EU immigrants (EIF) (2013EIF013). The current study was additionally funded by the R&D Fund of the Public Health Service of Amsterdam, the Regional Support Programme of the RIVM Centre for Infectious Disease Control, and via an unrestricted grant from Gilead Sciences. In addi-tion, Roche Diagnostics provided test kits for HBV-DNA testing (unrestricted grant). Gilead Sciences and Roche Diagnostics did not have involvement in study design, data collection, analysis and interpretation, nor in the writing and publication of this article.
Conflicts of interest
Freke Zuure worked on projects (partly) funded or sponsored by non-restricted grants from Abbvie, Gilead Sciences, Janssen-Cilag, MSD, Orasure Technologies and Roche Diagnos-tics. Janneke Bil has worked on several research projects for which her institute received (restricted and unrestricted) grants from Gilead Sciences. Maartje Visser: no conflicts of interest. Marieke Snijder: no conflicts of interest. Anders Boyd: no conflicts of interest. Petra Blom: no conflicts of interest. Gerard Sonder: no conflicts of interest. Janke Schinkel serves as a scientific advisor for Gilead Sciences, and received non-restricted research grants from Gilead Sciences, Abbvie, MSD, Roche Diagnostics, paid to her institute. Maria Prins obtained unrestricted research grants and speaker’s fees from Gilead Sciences, Roche, Abbvie and MSD, paid to her institute.

157
HBV and HCV screening needs among ethnic groups
3.2
SuPP
leM
enTa
rY T
aBl
eS
Tabl
e S1
. HBV
and
HCV
pre
vale
nce
amon
g Du
tch
and
first
-gen
erati
on m
igra
nt p
artic
ipan
ts o
f the
HEL
IUS
stud
y, Am
ster
dam
, the
Net
herla
nds,
201
1-20
14
dutc
h
surin
ames
e
sout
h-as
ian
surin
ames
eaf
rican
-sur
inam
ese
oth
er/u
nkno
wn
ethn
icity
a
n/N
Crud
epr
eval
ence
(95%
CI)
age-
en
gend
er
adju
sted
prev
alen
ce(9
5% C
I)n/
N
Crud
epr
eval
ence
(95%
CI)
age-
en
gend
er
adju
sted
prev
alen
ce(9
5% C
I)n/
N
Crud
epr
eval
ence
(9
5% C
I)
age-
en
gend
er
adju
sted
prev
alen
ce(9
5% C
I)n/
N
Crud
epr
eval
ence
(9
5% C
I)
age-
en
gend
er
adju
sted
prev
alen
ce(9
5% C
I)
HBV
(Nto
tal=
2,98
7)
Non
-exp
osed
485/
500
97.0
%(9
5.2-
98.2
%)
97.0
%(9
5.5-
98.5
%)
398/
462
86.1
%(8
2.8-
89.1
%)
87.6
%(8
4.8-
90.5
%)
350/
475
73.7
%(6
9.6-
77.5
%)
76.4
%(7
2.8-
80.0
%)
47/6
078
.3%
(66.
7-87
.3%
)80
.6%
(71.
3-89
.9%
)
Past
infe
ction
13/5
002.
6%(1
.5-4
.3%
)2.
6%(1
.2-4
.0%
)61
/462
13.2
%(1
0.3-
16.5
%)
11.7
%(9
.0-1
4.5%
)11
6/47
524
.4%
(20.
7-28
.4%
)21
.7%
(18.
2-25
.1%
)12
/60
20.0
%(1
1.4-
31.4
%)
17.8
%(8
.8-2
6.8%
)
Re
solv
ed in
fecti
on10
/500
2.0%
(1.0
-3.5
%)
2.0%
(0.8
-3.3
%)
46/4
6110
.0%
(7.5
-13.
0%)
9.3%
(6.8
-11.
9%)
102/
474
21.5
%(1
8.0-
25.4
%)
19.5
%(1
6.1-
22.9
%)
10/6
016
.7%
(8.9
-27.
6%)
15.0
%(6
.5-2
3.5%
)
Is
olat
ed a
nti-H
Bc3/
500
0.6%
(0.2
-1.6
%)
0.6%
(<0.
1-1.
3%)
14/4
613.
0%(1
.8-4
.9%
)3.
1%(1
.6-4
.7%
)13
/474
2.7%
(1.5
-4.5
%)
2.7%
(1.3
-4.1
%)
2/60
3.3%
(0.7
-10.
3%)
3.0%
(<0.
1-7.
2%)
Chro
nic
HBV
infe
ction
2/50
00.
4%(0
.1-1
.3%
)0.
4%(<
0.1-
0.9%
)3/
462
0.6%
(0.2
-1.7
%)
0.9%
(<0.
1-1.
7%)
9/47
51.
9%(0
.9-3
.4%
)1.
9%(0
.7-3
.2%
)1/
601.
7%(0
.2-7
.5%
)1.
7%(<
0.1-
4.9%
)
HCV
(Nto
tal=
2,99
3)
Non
-exp
osed
497/
500
99.4
% (9
8.4-
99.8
%)
NA
463/
463
100.
0%(9
9.5-
100.
0%)
NA
473/
475
99.6
%(9
8.7-
99.9
%)
NA
60/6
010
0.0%
(95.
9-10
0.0%
)N
A
Past
(res
olve
d) in
fecti
on1/
500
0.2%
(<0.
1-0.
9%)
NA
0/46
30.
0%(0
.0-0
.5%
)N
A0/
475
0.0%
(0.0
-0.5
%)
NA
0/60
0.0%
(0.0
-4.1
%)
NA
Chro
nic
HCV
infe
ction
2/50
00.
4%(0
.1-1
.3%
)N
A0/
463
0.0%
(0.0
-0.5
%)
NA
2/47
50.
4%(0
.1-1
.3%
)N
A0/
600.
0%(0
.0-4
.1%
)N
A

Chapter 3.2
158 159
HBV and HCV screening needs among ethnic groups
3.2
Tabl
e S1
. (co
ntinu
ed)
Gha
naia
ntu
rkis
hm
oroc
can
n/N
Crud
epr
eval
ence
(95%
CI)
age-
en
gend
er
adju
sted
prev
alen
ce(9
5% C
I)n/
N
Crud
epr
eval
ence
(95%
CI)
age-
en
gend
er
adju
sted
prev
alen
ce (9
5% C
I)n/
N
Crud
epr
eval
ence
(95%
CI)
age-
en
gend
er
adju
sted
prev
alen
ce (9
5% C
I)
HBV
(Nto
tal=
2,98
7)
Non
-exp
osed
167/
499
33.5
%(2
9.4-
37.7
%)
33.3
%(2
9.4-
37.2
2%)
350/
495
70.7
%(6
6.6-
74.6
%)
67.8
%(6
3.7-
71.9
%)
407/
496
82.1
%(7
8.5-
85.2
%)
80.7
%(7
7.2-
84.2
%)
Past
infe
ction
306/
499
61.3
%(5
7.0-
65.5
%)
61.5
%(5
7.5-
65.6
%)
126/
495
25.5
%(2
1.8-
29.4
%)
28.4
%(2
4.4-
32.4
%)
85/4
9617
.1%
(14.
0-20
.6%
)18
.5%
(15.
1-21
.9%
)
Re
solv
ed in
fecti
on16
9/48
734
.7%
(30.
6-39
.0%
)36
.8%
(32.
7-40
.9%
)10
6/49
521
.4%
(18.
0-25
.2%
)24
.0%
(20.
2-27
.9%
)60
/495
12.1
%(9
.5-1
5.2%
)13
.5%
(10.
5-16
.6%
)
Is
olat
ed a
nti-H
Bc12
5/48
725
.7%
(21.
9-29
.7%
)28
.0%
(24.
1-31
.9%
)20
/495
4.0%
(2.6
-6.1
%)
4.9%
(2.9
-6.9
%)
24/4
954.
8%(3
.2-7
.0%
)5.
8%(2
.9-6
.9%
)
Chro
nic
HBV
infe
ction
26/4
995.
2%(3
.5-7
.4%
)5.
4%(3
.5-7
.4%
)19
/495
3.8%
(2.4
-5.8
%)
4.1%
(2.4
-5.9
%)
4/49
60.
8%(0
.3-1
.9%
)1.
2%(0
.2-2
.2%
)
HCV
(Nto
tal=
2,99
3)
Non
-exp
osed
500/
500
100.
0%(9
9.5-
100.
0%)
NA
497/
497
100.
0%(9
9.5-
100.
0%)
NA
498/
498
100.
0%(9
9.5-
100.
0%)
NA
Past
(res
olve
d) in
fecti
on0/
500
0.0%
(0.0
-0.5
%)
NA
0/49
70.
0%(0
.0-0
.5%
)N
A0/
498
0.0%
(0.0
-0.5
%)
NA
Chro
nic
HCV
infe
ction
0/50
00.
0%(0
.0-0
.5%
)N
A0/
497
0.0%
(0.0
-0.5
%)
NA
0/49
80.
0%(0
.0-0
.5%
)N
A
Anti-
HBc,
anti
bodi
es to
HBV
cor
e an
tigen
; HBV
, hep
atitis
B v
irus;
HCV
, hep
atitis
C v
irus;
NA,
not
ava
ilabl
e.a I
nclu
ding
29
Java
nese
, 13
of m
ixed
eth
nici
ty, 4
oth
er, 1
4 un
know
n

Chapter 3.2
158 159
HBV and HCV screening needs among ethnic groups
3.2
referenCes
1. European Centre for Disease Prevention and Control (ECDC). Systematic review on hepatitis B and C prevalence in the eu/eea. Stockholm: ECDC, 2016.
2. Hofman R, Nusselder WJ, Veldhuijzen IK, Richardus JH. Mortality due to chronic viral hepatitis B and C infections in the netherlands [in dutch]. Ned Tijdschr Geneeskd. 2016;160(0):D511.
3. Koopsen J, van Steenbergen JE, Richardus JH, Prins M, Op de Coul ELM, Croes EA, et al. Chronic hepatitis B and C infections in the netherlands: estimated prevalence in risk groups and the general population. Epidemiol Infect. 2019;147:e147. doi:10.1017/S0950268819000359.
4. Webster DP, Klenerman P, Dusheiko GM. Hepatitis C. Lancet. 2015;385(9973):1124-1135. doi:10.1016/S0140-6736(14)62401-6.
5. Hadziyannis SJ. update on Hepatitis B Virus Infection: Focus on Treatment. J Clin Transl Hepatol. 2014;2(4):285-291. doi:10.14218/JCTH.2014.00026.
6. Memon MI, Memon MA. Hepatitis C: an epidemiological review. J Viral Hepat. 2002;9(2):84-100. 7. Seeff LB. natural history of chronic hepatitis C. Hepatology. 2002;36(5 Suppl 1):S35-46. doi:10.1053/
jhep.2002.36806. 8. Shepard CW, Simard EP, Finelli L, Fiore AE, Bell BP. Hepatitis B virus infection: epidemiology and
vaccination. Epidemiol Rev. 2006;28:112-125. doi:10.1093/epirev/mxj009. 9. Spradling PR, Rupp L, Moorman AC, Lu M, Teshale EH, Gordon SC, et al. Hepatitis B and C virus infec-
tion among 1.2 million persons with access to care: factors associated with testing and infection prevalence. Clin Infect Dis. 2012;55(8):1047-1055. doi:10.1093/cid/cis616.
10. Denniston MM, Klevens RM, McQuillan GM, Jiles RB. awareness of infection, knowledge of hepatitis C, and medical follow-up among individuals testing positive for hepatitis C: national Health and nu-trition examination Survey 2001-2008. Hepatology. 2012;55(6):1652-1661. doi:10.1002/hep.25556.
11. Meffre C, Le Strat Y, Delarocque-Astagneau E, Dubois F, Antona D, Lemasson JM, et al. Prevalence of hepatitis B and hepatitis C virus infections in France in 2004: social factors are important predictors after adjusting for known risk factors. J Med Virol. 2010;82(4):546-555. doi:10.1002/jmv.21734.
12. van der Ploeg C, Schönbeck Y, Hirschberg H. Prenatal screening for infectious diseases and erythro-cytes immunisation [in dutch]. Leiden: TNO, 2015.
13. Willemse SB, Razavi-Shearer D, Zuure FR, Veldhuijzen IK, Croes EA, van der Meer AJ, et al. the estimated future disease burden of hepatitis C virus in the netherlands with different treatment paradigms. Neth J Med. 2015;73(9):417-431.
14. Dutch Association of HIV-Treating Physicians (NVHB). HIV treatment guidelines for the netherlands [in dutch]. Available at: http://richtlijnhiv.nvhb.nl/index.php/Inhoud (accessed on August 2018).
15. Loth C, Wits E, de Jong C, van de Mheen D. Guideline for opiate maintenance treatment, revised version [in dutch]. Amersfoort: Resultaat Scoren, 2012.
16. van Rijckevorsel G. WJ, Kretzschmar M., Siedenburg E., Sonder G., Geskus R., Coutinho R, van den Hoek A. Targeted vaccination programme successvul in reducing acute hepatitis B in men having sex with men in amsterdam, The netherlands. Journal of Hepatology. 2013;59:1177-1183. doi: 10.1016/j.jhep.2013.08.002.
17. Hoornenborg E, Rijnders B. HIV Pre-expositie profylaxe (PreP) guidelines netherlands [in dutch]. Dutch Association of HIV-Treating Physicians (NVHB), 2016.
18. European Centre for Disease Prevention and Control (ECDC). epidemiological assessment of hepatitis B and C among migrants in the eu/eea. Stockholm: ECDC, 2016.
19. Dutch College of General Practitioners (NHG). nHG Guideline Viral Hepatitis and other liver diseases (third revision) [in dutch]. NHG, 2016.

Chapter 3.2
160
20. Health Council of the Netherlands. Screening risk groups for hepatitis B and C. The Hague: Health Council of the Netherlands, 2016.
21. Hahne SJ, Veldhuijzen IK, Wiessing L, Lim TA, Salminen M, Laar M. Infection with hepatitis B and C virus in europe: a systematic review of prevalence and cost-effectiveness of screening. BMC Infect Dis. 2013;13:181. doi:10.1186/1471-2334-13-181.
22. Stronks K, Snijder MB, Peters RJ, Prins M, Schene AH, Zwinderman AH. unravelling the impact of ethnicity on health in europe: the HelIuS study. BMC Public Health. 2013;13:402. doi:10.1186/1471-2458-13-402.
23. Snijder MB, Galenkamp H, Prins M, Derks EM, Peters RJG, Zwinderman AH, et al. Cohort profile: the Healthy life in an urban Setting (HelIuS) study in amsterdam, The netherlands. BMJ Open. 2017;7(12):e017873. doi:10.1136/bmjopen-2017-017873.
24. Stronks K, Kulu-Glasgow I, Agyemang C. The utility of ‘country of birth’ for the classification of ethnic groups in health research: the dutch experience. Ethn Health. 2009;14(3):255-269. doi:10.1080/13557850802509206.
25. Kowdley KV, Wang CC, Welch S, Roberts H, Brosgart CL. Prevalence of chronic hepatitis B among foreign-born persons living in the united States by country of origin. Hepatology. 2012;56(2):422-433. doi:10.1002/hep.24804.
26. Baaten GG, Sonder GJ, Dukers NH, Coutinho RA, Van den Hoek JA. Population-based study on the seroprevalence of hepatitis a, B, and C virus infection in amsterdam, 2004. J Med Virol. 2007;79(12):1802-1810. doi:10.1002/jmv.21009.
27. Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ. estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet. 2015;386(10003):1546-1555. doi:10.1016/S0140-6736(15)61412-X.
28. van der Veen YJ, van Empelen P, de Zwart O, Visser H, Mackenbach JP, Richardus JH. Cultural tailoring to promote hepatitis B screening in Turkish dutch: a randomized control study. Health Promot Int. 2014;29(4):692-704. doi:10.1093/heapro/dat020.
29. Richter C, Beest GT, Sancak I, Aydinly R, Bulbul K, Laetemia-Tomata F, et al. Hepatitis B prevalence in the Turkish population of arnhem: implications for national screening policy? Epidemiol Infect. 2012;140(4):724-730. doi:10.1017/S0950268811001270.
30. Niessen W, Benne R, van Zeijl J, van der Have J, Broer J. Inviting migrants for hepatitis B testing by letter. Is it effective? [dutch]. Inf Bulletin. 2013;24(4):107-112.
31. Mac Donald-Ottevanger MS, van de Laar T, Zijlmans W, Prins M, Brinkman K, Roosblad J, et al. Preva-lence, determinants of chronic hepatitis B infection and hepatitis B genotypes in multi-ethnic Suri-name. abstracts of The International liver Congress 2017. Journal of Hepatology. 2017;66(1):S252–S253.
32. Ofori-Asenso R, Agyeman AA. Hepatitis B in Ghana: a systematic review & meta-analysis of preva-lence studies (1995-2015). BMC Infect Dis. 2016;16:130. doi:10.1186/s12879-016-1467-5.
33. Manzardo C, Trevino B, Gomez i Prat J, Cabezos J, Mongui E, Claveria I, et al. Communicable diseases in the immigrant population attended to in a tropical medicine unit: epidemiological aspects and public health issues. Travel Med Infect Dis. 2008;6(1-2):4-11. doi:10.1016/j.tmaid.2007.11.002.
34. Chemin I, Trepo C. Clinical impact of occult HBV infections. J Clin Virol. 2005;34 Suppl 1:S15-21. 35. Said ZN. an overview of occult hepatitis B virus infection. World J Gastroenterol. 2011;17(15):1927-
1938. doi:10.3748/wjg.v17.i15.1927. 36. Polaris Observatory, HCV Collaborators. Global prevalence and genotype distribution of hepatitis
C virus infection in 2015: a modelling study. Lancet Gastroenterol Hepatol. 2017;2(3):161-176. doi:10.1016/S2468-1253(16)30181-9.

161
HBV and HCV screening needs among ethnic groups
3.2
37. Urbanus AT, van de Laar TJ, van den Hoek A, Zuure FR, Speksnijder AG, Baaten GG, et al. Hepatitis C in the general population of various ethnic origins living in the netherlands: should non-Western migrants be screened? J Hepatol. 2011;55(6):1207-1214. doi:10.1016/j.jhep.2011.02.028.
38. Agyeman AA, Ofori-Asenso R, Mprah A, Ashiagbor G. epidemiology of hepatitis C virus in Ghana: a systematic review and meta-analysis. BMC Infect Dis. 2016;16:391. doi:10.1186/s12879-016-1708-7.
39. Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infec-tion: new estimates of age-specific antibody to HCV seroprevalence. Hepatology. 2013;57(4):1333-1342. doi:10.1002/hep.26141.
40. Mac Donald-Ottevanger MS, Vreden S, van der Helm JJ, van de Laar T, Molenkamp R, Dams E, et al. Prevalence, determinants and genetic diversity of hepatitis C virus in the multi-ethnic population living in suriname. Virology. 2016;499:114-120. doi:10.1016/j.virol.2016.07.001.
41. Suijkerbuijk AWM, van Hoek AJ, Koopsen J, de Man RA, Mangen MJ, de Melker HE, et al. Cost-effec-tiveness of screening for chronic hepatitis B and C among migrant populations in a low endemic country. PLoS One. 2018;13(11):e0207037. doi:10.1371/journal.pone.0207037.
42. Demidenko E. Sample size determination for logistic regression revisited. Stat Med. 2007;26(18):3385-3397. doi:10.1002/sim.2771.
43. World Health Organization (WHO). Global Hepatitis report 2017. Geneva: WHO, 2017. 44. Seedat F, Hargreaves S, Nellums LB, Ouyang J, Brown M, Friedland JS. How effective are approaches
to migrant screening for infectious diseases in europe? a systematic review. Lancet Infect Dis. 2018;18(9):e259-e271. doi:10.1016/S1473-3099(18)30117-8.
45. Hamdiui N, Stein ML, Timen A, Timmermans D, Wong A, van den Muijsenbergh M, et al. Hepatitis B in Moroccan-dutch: a quantitative study into determinants of screening participation. BMC Med. 2018;16(1):47. doi:10.1186/s12916-018-1034-6.
46. van der Veen YJ, van Empelen P, Looman CW, Richardus JH. Social-cognitive and socio-cultural pre-dictors of hepatitis B virus-screening in Turkish migrants, the netherlands. J Immigr Minor Health. 2014;16(5):811-821. doi:10.1007/s10903-013-9872-y.
47. Blanas DA, Nichols K, Bekele M, Shankar H, Bekele S, Jandorf L, et al. adapting the andersen model to a francophone West african immigrant population: hepatitis B screening and linkage to care in new York City. J Community Health. 2015;40(1):175-184. doi:10.1007/s10900-014-9916-9.


Chapter 3.3Integrating hepatitis B, hepatitis C and HIV screening into tuberculosis entry
screening for migrants in the netherlands, 2013 to 2015
Janneke P. Bil, Peter A.G. Schrooders, Maria Prins, Peter M. Kouw, Judith H.E. Klomp, Maarten Scholing, Lutje PHM Huijbregts, Gerard J.B. Sonder,
Toos C.H.F.M. Waegemaekers, Henry J.C. de Vries, Wieneke Meijer, Freke R. Zuure*, Alma Tostmann*
* Both authors contributed equally to this article
Published in Euro surveillance, 2018; 23(11)

Chapter 3.3
164
aBstraCt
We evaluated uptake and diagnostic outcomes of voluntary hepatitis B (HBV) and C virus (HCV) screening offered during routine tuberculosis entry screening to migrants in Gelder-land and Amsterdam, the Netherlands, between 2013 and 2015. In Amsterdam, HIV screen-ing was also offered. Overall, 54% (461/859) accepted screening. Prevalence of chronic HBV infection (HBsAg-positive) and HCV exposure (anti-HCV-positive) in Gelderland was 4.48% (9/201; 95% confidence interval (CI) 2.37–8.29) and 0.99% (2/203; 95% CI 0.27–3.52), re-spectively, all infections were newly diagnosed. Prevalence of chronic HBV infection, HCV exposure and chronic HCV infection (HCV RNA-positive) in Amsterdam was 0.39% (1/256; 95% CI 0.07–2.18), 1.17% (3/256; 95% CI 0.40–3.39) and 0.39% (1/256; 95% CI 0.07–2.18), respectively, with all chronic HBV/HCV infections previously diagnosed. No HIV infections were found. In univariate analyses, newly diagnosed chronic HBV infection was more likely in participants migrating for reasons other than work or study (4.35% vs. 0.83%; odds ratio (OR) 5.45; 95% CI 1.12–26.60) and was less likely in participants in Amsterdam than Gelderland (0.00% vs. 4.48%; OR=0.04; 95% CI 0.00–0.69). Regional differences in HBV prevalence might be explained by differences in the populations entering compulsory tuberculosis screening. Pre-screening selection of migrants based on risk factors merits further exploration.

165
HBV, HCV and HIV screening during TB entry screening
3.3
InTroduCTIon
In the Netherlands, it is estimated that 39,000 individuals have a chronic hepatitis B virus (HBV) infection (HBsAg-positive),1 19,000 have a chronic hepatitis C virus (HCV) infection (HCV RNA-positive)2 and 23,000 have a human immunodeficiency virus (HIV) infection.3 A large proportion of chronic HBV infections (ca. 50%) and past/chronic HCV infections (ca. 40%; anti-HCV positive) are estimated to be found among migrants coming from countries endemic for HBV or HCV, respectively, and ca. 40% of HIV patients in clinical care are mi-grants.1,3,4
Currently, effective treatment options are available for HBV, HCV and HIV infections. How-ever, the often asymptomatic onset of these infections and disease development of HBV and HCV infections may delay diagnosis and therefore treatment. Screening for HBV, HCV and HIV can identify undiagnosed infections, improving the prognosis and limiting transmis-sion to others by linking infected persons to treatment and care at an early stage.5-8 To find undiagnosed cases, several HBV and HCV screening programmes, mostly community-based, have targeted specific groups of migrants in the Netherlands in recent years.9 The prevalence found in those programmes ranged from 0% to 9.5% for chronic HBV infection (HBsAg-positive) and from 0% to 6.5% for HCV exposure (anti-HCV positive), depending on the target group and the recruitment strategy.9-18 However, these programmes were not sustainable, because they were done only once, highly labour-intensive and tailored to particular migrant groups and residential areas.9 The integration of screening into existing healthcare services could increase long-term sustainability and continuity in reaching and screening key popula-tions. In addition, integration would most probably make such screening programmes more cost-effective because fewer additional resources would be required. As countries with high endemicity for tuberculosis (TB) largely overlap with countries with a high HBV, HCV or HIV prevalence, screening for these viruses could be integrated into the existing TB entry screen-ing performed by TB departments of the Public Health Services in the Netherlands. TB entry screening is compulsory for migrants from outside the European Union (EU) who intend to stay in the Netherlands for more than three months.19 Since January 2015, the compulsory screening has been further restricted to non-EU migrants originating from countries with TB incidence of more than 50 per 100,000 inhabitants per year.
To evaluate whether integrated TB, HBV, HCV and HIV screening is effective and acceptable among migrants, we initiated a screening project offering additional voluntary HBV, HCV and HIV screening to migrants undergoing compulsory TB screening. We studied the uptake of screening and the prevalence and determinants of newly diagnosed HBV, HCV and HIV infec-tions. The resulting data can be used to support policy-makers in the decision on integrating screening for these infections into the existing TB entry screening for migrants.

Chapter 3.3
166
MeTHodS
study population
This screening project was performed at five TB departments of the Public Health Services in the Netherlands (a convenience sample: four in the province of Gelderland, one in the city of Amsterdam). In Gelderland, recruitment continued until at least 352 TB department visitors had been asked to participate (October 2013 to February 2015). The sample size was based on an expected prevalence of 4.5% HBsAg-positive samples, with a 2.5% margin of error at an alpha of 0.05 in order to detect a minimum HBsAg positivity rate of at least 2%. In Amsterdam, we used a convenience sample of 250 participants, and recruitment took place from July 2015 through August 2015. Migrants visiting these TB departments have migrated primarily for work, study or family reunification. Asylum seekers are usually screened at TB departments in refugee centres and were therefore not included in this project. HBV and HCV screening was offered to all migrants attending the five TB departments for their compulsory TB entry screening. In Amsterdam, HIV screening was also offered.
recruitment
Migrants 18 years or older who were able to read the project information were eligible for HBV, HCV and HIV screening. In Gelderland, migrants were excluded if they had been vaccinated against HBV, whereas in Amsterdam, HBV vaccination history was not recorded. In Amsterdam, migrants were excluded if they intended to stay less than six months in the Netherlands, in order to ensure that those testing positive could be linked to care in the Netherlands.
All participants provided written informed consent. The project was conducted according to the ethical guidelines of the 1975 Declaration of Helsinki. The local medical ethics com-mittee of the region Arnhem-Nijmegen (Radboud University Medical Center) approved the screening project (2013/172).
screening procedure
In Gelderland, migrants received information about HBV and HCV screening before their appointment for TB screening by post. In Amsterdam, where only walk-in TB consultations are provided, migrants received information about HBV, HCV and HIV screening on arrival for TB screening. Project information was available in Dutch and English and, in Amsterdam, also in Arabic, Chinese, French, Portuguese, Russian and Spanish. After eligible migrants had completed their routine TB screening, they were asked to participate in this screening proj-ect and the informed consent form was signed. Blood was drawn from those who accepted HBV, HCV and HIV screening. In Amsterdam, participants could opt out of testing for any of the three infections individually.

167
HBV, HCV and HIV screening during TB entry screening
3.3
From all eligible migrants, the following data were collected during their TB screening visit: age, sex, country of origin and intended length of stay in the Netherlands. In Gelderland, reason for migration was included as an open-ended question. In Amsterdam, data on the reason for migration were derived from migration forms that categorised answers as work/study or other (e.g., partner or family reunification, but not further specified). In Amster-dam, participants were also asked whether they were currently registered with a general practitioner (GP) in the Netherlands and whether they had health insurance. In both regions, all persons who declined HBV, HCV and HIV screening were asked for the reason for non-participation, using an open-ended question.
laboratory testing
In Gelderland, blood samples were tested for anti-HBc and anti-HCV at the laboratory of the Gelre Hospital in Apeldoorn (ADVIA Centaur, Siemens, Germany), Meander Medical Center in Amersfoort (ARCHITECT, Abbott, United States) or Slingeland Hospital in Doetinchem (Co-bas 6000, Roche, Switzerland). Samples positive for anti-HBc were further tested for HBsAg, anti-HBs, anti-HBe and HBeAg.
In Amsterdam, blood samples were first tested for HBsAg, anti-HCV, and HIV antigen or anti-bodies (LIAISON XL MUREX, DiaSorin, Italy) at the laboratory of the Public Health Service of Amsterdam. Samples positive for HBsAg were further tested for anti-HBc, anti-HBs, anti-HBe and HBeAg. Samples positive for anti-HCV were further tested for HCV RNA (HCV Quan-titative test, version 2.0, Cobas AmpliPrep/Cobas TaqMan, Roche, Switzerland). Samples positive for HIV antigen or antibodies were confirmed with Western blot (INNO-LIA HIV I/II Score, Innogenetics, Belgium), HIV-1 p24 antigen test (Vidas HIV P24, Bio Merieux) and HIV viral-load testing (HI2CAP, Roche, Switzerland).
Persons found HBsAg-positive were considered to have a chronic HBV infection. As the incidence of acute HBV infection in the Netherlands is very low, also among migrants, we assumed all HBsAg-positive persons to be chronically infected. Persons found positive for anti-HCV were considered exposed to HCV, persons positive for HCV RNA were considered to have a chronic HCV infection, and persons with confirmed HIV antigen- or antibody-positive tests were considered HIV-positive.
Follow-up procedure
Participants who did not have a chronic HBV infection, an HCV infection or HIV infection received a letter with their test results. Participants with an infection were verbally informed of their test results by a nurse or doctor at the Public Health Service and referred to their GP, the first point of care in the Netherlands. At the TB clinics in Gelderland, HCV RNA testing for those who tested anti-HCV positive was not included. These participants were referred to

Chapter 3.3
168
their GP for further testing. In accordance with the Dutch Public Health Act, chronic HBV in-fections were reported to the department of infectious diseases of the Public Health Service in each patient’s hometown, to enable contact tracing.
In Amsterdam, participants with a chronic HBV, chronic HCV or HIV infection were contacted three and six months after they had received their results to ask if they had received follow-up care. We collected data on whether they had started treatment and whether they had visited their GP or a specialist.
statistical analyses
We described the following characteristics for all eligible migrants: age, sex, reason for migra-tion, intended length of stay, region of origin, registration at GP, health insurance coverage, and HBV, HCV and HCV prevalence in the country of origin. Countries of origin were grouped into regions of origin according to the World Health Organization classification.20 We also created three dichotomous variables (low-endemic vs intermediate/high-endemic) related to the HBV, HCV and HIV prevalence in the country of origin, using estimates by Schweitzer et al.,21 Gower et al.22 and the Global Burden of Disease Study,23 respectively. Based on the categorisation of the reported estimates in the literature cut-off points of 2.0%, 2.5% and 2.12% were used to dichotomise HBV, HCV and HIV prevalence, respectively.
We compared the characteristics between those who refused and those who accepted the additional HBV, HCV and HIV screening, and also between participants recruited in Gelder-land and those recruited in Amsterdam, using chi-squared tests for categorical variables and Mann-Whitney U-tests for continuous variables. We calculated the screening uptake (defined as the number of migrants who accepted screening among all the eligible persons) and described reasons for declining screening. In all analyses, the four sites in Gelderland were treated as one, as all used the same recruitment strategy and served comparable populations.
HBsAg, anti-HCV, HCV RNA and HIV prevalence and corresponding 95% confidence intervals (CI) were calculated using Wilson intervals. Using univariate logistic regression analyses, we examined determinants of a newly diagnosed chronic HBV infection, excluding persons with a previously diagnosed HBV infection. Penalised logistic regression was used to calculate odds ratios (OR) and 95% CI in a table with a zero cell count.
In all analyses, cases with unknown or missing data were excluded. Analyses were performed using STATA Intercooled 13.1 (STATA Corporation, College Station, United States). Statistical significance was set at p<0.05.

169
HBV, HCV and HIV screening during TB entry screening
3.3
reSulTS
Characteristics of participants
A total of 968 migrants, aged 18 years or older, attended the five TB departments for their TB entry screening (Figure).
In Gelderland, 35 migrants were excluded because of prior HBV vaccination. In Amsterdam, 58 migrants were excluded because they intended to stay less than six months in the Netherlands. Furthermore, 16 migrants were excluded because they were unable to read the project information. Of 859 eligible migrants who were asked to participate, 461 (54%) accepted HBV or HCV (and in Amsterdam, HIV) screening. There was no significant differ-ence between response rates in Gelderland vs. Amsterdam (57% vs. 51%; p=0.113). Sex, age, region of origin, reason for migration, intended length of stay in the Netherlands and HBV and HCV prevalence in the country of origin did not significantly differ between those
968 migrants aged 18 years or older attended thetuberculosis clinic of the Public Health Service ofGelderland or Amsterdam during the study period
859 migrants were offered voluntary HBV, HCV andHIVa screening
461 migrants (54%) accepted screening
457 were screened for chronic HBV Infection (HBsAg)459 were screened for HCV exposure (anti-HCV)
256 were screened for chronic HCV infection (HCV-RNA)c
255 were screened for HIV infectiona
HBV infection10/457 (2.19%; 95% CI: 1.19-3.98) HBsAg-positive
HCV infection- 5/459 (1.09%; 95% CI 0.47-2.52) anti-HCV-positive
- 2/459 (0.44%; 95% CI 0.12-1.57) HCV RNA-positivec
- 9 HBsAg-positive cases were previously undiagnosed- 1 HBsAg-positive case was previously diagnosed and
treated
- In Gelderland, all anti-HCV positive cases (n=2) werepreviously diagnosed
- In Amsterdam, all HCV RNA-positive cases (n=1) werepreviously diagnosed but had discontinued treatment and
were not in clinical care
HIV infectiona
0/255 HIV-positive
109 migrants were excluded:- 58 were planning to stay <6 months in theNetherlands (Amsterdam)- 35 were vaccinated against HBV infection(Gelderland)- 16 were not able to read the project information
Reasons for declining screeningb (n=398):- Already been tested (35%; n=141)- Time constraints (18%; n=70)- Fear of blood-drawing (14%; n=54)- Does not want to be tested (12%; n=46)- No specific reason for decline (7%; n=29)- Doesn’t feel at risk (4%; n=17)- Afraid (reason not specified) (4%; n=17)- Needs more time to decide (3%; n=13)- Other reasons (8%; n=33)- Missing (3%; n=11)
In 2 persons, we were unable to draw blood
In 2 persons, HBsAg was not determined1 person opted out of HIV screeninga
Figure. Recruitment strategy and clinical outcomes of hepatitis B, hepatitis C and HIV screening offered to migrants attending compulsory tuberculosis entry screening at the Public Health Services, the Netherlands, 2013–2015 (n=859)HBV, hepatitis B virus; HCV, hepatitis C virus; HIV, human immunodeficiency virus.a HIV screening was only offered at the Public Health Service of Amsterdam.b The percentages add up to >100% as participants could have mentioned more than one reason for declining
screening.c HCV RNA was only tested in Amsterdam.

Chapter 3.3
170
Table 1. Characteristics of migrants who accepted HBV, HCV and HIVa screening during compulsory TB screen-ing at Public Health Services, the Netherlands 2013–2015 (n=459)
total Gelderland amsterdam
(n=459) (n=203) (n=256)
n % n % n % p-value
age (years), median [IQr] 29 [26–35] 28 [25–34] 30 [27–36] <0.001
sex 0.804
Male 211 45.97 92 45.32 119 46.48
Female 248 54.03 111 54.68 137 53.52
reason for immigration <0.001
Work or study 244 53.16 93 45.81 151 58.98
Other (e.g., family reunification) 162 35.29 110 54.19 52 20.31
Missing 53 11.55 0 0.00 53 20.70
Intended length of stay in the netherlandsb
<1 year NA 19 9.36 NA NA
1–2 years 28 13.79
>2 years 116 57.14
Missing 40 19.70
region of origin (categorised according to WHo regions) <0.001
South-East Asia 154 33.55 47 23.15 107 41.80
Europe (southern/eastern) 95 20.70 42 20.69 53 20.70
Western Pacific 86 18.74 42 20.69 44 17.19
Africa 61 13.29 32 15.76 29 11.33
Eastern Mediterranean 39 8.50 22 10.84 17 6.64
Americas (Latin America/Caribbean) 23 5.01 18 8.87 5 1.95
Missing 1 0.22 0 0.00 1 0.39
estimated HBV prevalence (HBsag-positive) in the country of originc <0.001
<2% 204 44.44 66 32.51 138 53.91
>2% 252 54.90 136 67.00 116 45.31
Missing 3 0.65 1 0.49 2 0.78
estimated HCV prevalence (HCV-rna positive) in the country of originc 0.470
<2.5% 398 86.71 179 88.18 219 85.55
>2.5% 60 13.07 24 11.82 36 14.06
Missing 1 0.22 0 0.00 1 0.39
estimated HIV prevalence in the country of originc 0.104
<2.12% 403 87.80 173 85.22 230 89.84
>2.12% 55 11.98 30 14.78 25 9.77
Missing 1 0.22 0 0.00 1 0.39

171
HBV, HCV and HIV screening during TB entry screening
3.3
who refused and those who accepted screening. Participants who originated from a country with an estimated HIV prevalence of >2.12% were more likely to accept screening compared with participants from a country with an estimated HIV prevalence of <2.12% (65% vs. 52%; p=0.022). The most commonly mentioned reasons for declining screening were: already been tested (35%; 141/398), time constraints (18%; 70/398) and fear of blood-drawing (14%; 54/398). Already been tested as a reason for declining was more likely to be reported by migrants from South-East Asia compared with other regions (50% vs. 10-36%; p<0.001) and by migrants visiting the TB clinic in Amsterdam compared with Gelderland (42% vs. 25%; p<0.001).
Two of the 461 migrants who accepted screening were ultimately not screened because blood-drawing failed. For 459 screened participants (203 in Gelderland and 256 in Amster-dam), median age was 29 years (interquartile range (IQR): 26-35 years) and 46% were male (Table 1). About half of the participants migrated for work/study (53%), and a third (34%) of all participants originated from South-East Asia. Only one person (1/256; 0.39%) in Amster-dam opted out of HIV testing, citing a low risk perception.
Table 1. (continued)
total Gelderland amsterdam
(n=459) (n=203) (n=256)
n % n % n % p-value
registered at a general practitioner in the netherlandsd
No NA NA 174 67.97 NA
Yes 78 30.47
Missing 4 1.56
registered for health insurance coverage in the netherlandsd
No NA NA 72 28.13 NA
Yes, Dutch health insurance 122 47.66
Yes, foreign health insurance 27 10.55
Yes, student health insurance 10 3.91
Yes, but unknown which one 21 8.20
Missing 4 1.56
HBV, hepatitis B virus; HCV, hepatitis C virus; HIV, human immunodeficiency virus; IQR, Interquartile range; NA, not applicable (not measured); TB, tuberculosis; WHO, World Health Organization.This table excludes migrants who accepted screening but in whom blood-drawing failed (n=2).a HIV screening was included only in Amsterdam.b Measured only among participants from Gelderland.c Participants were grouped and categorised according to the estimated HBV, HCV and HIV prevalence re-
ported by Schweitzer et al.,21 Gower et al.22 and the Global Burden of Disease Study,23 respectively.d Measured only among participants from Amsterdam.

Chapter 3.3
172
Table 2. Univariate analysis of potential determinants of newly diagnosed chronic HBV infection among mi-grants who accepted HBV, HCV and HIVa screening during compulsory tuberculosis entry screening at Public Health Services, the Netherlands, 2013–2015 (n=456)
newly diagnosed chronic HBV infection univariate analyses
n/N % or (95% CI) p-value
sex
Male 3/210 1.43 1 0.433
Female 6/246 2.44 1.72 (0.43–6.98)
age
18–26 year 2/125 1.60 1 0.165
27–32 year 6/175 3.43 2.18 (0.43–11.00)
>32 year 1/156 0.64 0.40 (0.04–4.43)
reason for immigration
Work or study 2/242 0.83 1 0.019
Other (e.g., family reunification) 7/161 4.35 5.45 (1.12–26.60)
Missing 0/53 0.00 b b
Intended length of stay in the netherlandsc
<1 year 0/19 0.00 1 0.399
1–2 years 2/28 7.14 3.68 (0.17–81.03)
>2 years 3/114 2.63 1.22 (0.06–24.64)
Missing 4/40 10.00 b b
region of origin (categorised according to WHo regions)
South-East Asia 3/154 1.95 1 0.976
Europe (southern/eastern) 3/95 3.16 1.64 (0.36–7.37)
Western Pacific 2/84 2.38 1.31 (0.25–6.80)
Africa 1/60 1.67 1.09 (0.16–7.56)
Eastern Mediterranean 0/39 0.00 0.55 (0.28–10.83)
Americas (Latin America/Caribbean) 0/23 0.00 0.92 (0.05–18.40)
Missing 0/1 0.00 b b
estimated HBV prevalence (HBsag-positive) in the country of origind
<2% 3/204 1.47 1 0.664
>2% 5/249 2.01 1.37 (0.32–5.82)
Missing 1/3 33.33 b b
location of screening
Gelderland 9/201 4.48 25.22 (1.46–435.95)
Amsterdam 0/255 0.00 1 0.026
CI, confidence interval; HBV, hepatitis B virus; OR, odds ratio; WHO, World Health Organization.This table excludes migrants who accepted screening but in whom blood drawing failed (n=2), participants in which HBsAg was not determined (n=2), and the previously diagnosed HBV-infected participant (n=1).a HIV screening was included only in Amsterdam.b Missing categories were excluded from the analysis.c Measured only among participants from Gelderland.d Participants were grouped and categorised according to the estimated HBV prevalence reported by Sch-
weitzer et al.21

173
HBV, HCV and HIV screening during TB entry screening
3.3
Participants in Gelderland were younger and more often had migrated for reasons other than work/study (e.g., family reunification) compared with Amsterdam, where most participants had migrated because of work/study. The region of origin also differed significantly between the participants from Gelderland and Amsterdam (p<0.001). Furthermore, participants in Gelderland more often originated from a country with an HBV prevalence of >2% compared with Amsterdam participants.
Prevalence and determinants of newly diagnosed HBV, HCV and HIV infections
In Gelderland, 29 of the 203 participants were anti-HBc-positive (14.3%; 95% CI 10.1-19.8%) and the prevalence of chronic HBV infections was 4.48% (9/201; 95% CI 2.37-8.29%). In two cases, HBsAg was not determined. Two of the 203 participants were anti-HCV-positive (0.99%; 95% CI 0.27-3.52%). All HBV and HCV infections in Gelderland were newly diagnosed.
In Amsterdam, one of the 256 participants had a chronic HBV infection (0.39% (1/256; 95% CI 0.07-2.18%). Three of 256 participants were anti-HCV-positive (1.17%; 95% CI 0.40-3.39%) of whom one had a chronic HCV infection (0.39% (1/256; 95% CI 0.07-2.18%). Both partici-pants in Amsterdam with a chronic HBV and HCV infection were previously diagnosed. The participant with chronic HBV infection reported that they had been successfully treated and were being monitored in their country of origin. The participant with chronic HCV infection had started treatment in the country of origin, but discontinued it there because of side effects. This patient was referred to a Dutch hepatitis treatment centre and successfully completed HCV treatment approximately six months after screening. No HIV infections were found in Amsterdam.
Characteristics of all participants with a newly diagnosed chronic HBV infection (9/457; 1.97%; 95% CI 1.04-3.70%) are shown in Table 2. In univariate analyses, participants who migrated to the Netherlands for reasons other than work/study were more likely to have a newly diagnosed chronic HBV infection than those who migrated for work/study (4.3% vs. 0.8%; OR=5.45; 95% CI 1.12-26.60). Participants in Amsterdam were less likely to have a newly diagnosed chronic HBV infection than those in Gelderland (0% vs. 4.5%; OR=0.04; 95% CI 0.00–0.69). No other variables were statistically significantly associated with having a newly diagnosed chronic HBV infection.
dISCuSSIon
In this project, about half (54%) of the migrants attending the existing compulsory TB entry screening at Public Health Services accepted additional HBV, HCV and HIV screening. The prevalence of chronic HBV infection (HBsAg-positive) and HCV exposure (anti-HCV-positive)

Chapter 3.3
174
in Gelderland was 4.48% and 0.99%, respectively, and all were newly diagnosed. The preva-lence of chronic HBV infection in Amsterdam was 0.39%. The prevalence of HCV exposure (anti-HCV-positive) and chronic HCV infection (HCV RNA-positive) in Amsterdam was 1.17% and 0.39%, respectively. All chronic HBV and HCV infections in Amsterdam were previously diagnosed. No HIV infections were found.
Surprisingly, we found a significant difference in the prevalence of newly diagnosed chronic HBV infections between Gelderland (4.48%) and Amsterdam (0%). There are several poten-tial explanations. The background HBV prevalence in the countries of origin of Gelderland participants was higher compared with Amsterdam participants. However, in univariate analyses, background HBV prevalence was not associated with newly diagnosed chronic HBV infection. In addition, those who migrated to the Netherlands for reasons other than work/study were more likely to have a newly diagnosed HBV infection, perhaps reflecting an in-creased risk among those with a lower socioeconomic status. The fact that more Gelderland participants migrated to the Netherlands for reasons other than work/study might therefore help explain the higher prevalence found among Gelderland participants. The differences in country of origin and reason for migration between participants in Gelderland and Amster-dam indicate that different areas in the Netherlands attract different groups of migrants, which is most probably due to work, study or housing opportunities in a given area or due to the migration history of family members. Another explanation for the varying prevalence of newly diagnosed chronic HBV infections might be differences in unmeasured HBV risk factors between participants from Gelderland and Amsterdam. Prior HBV vaccination was not among the exclusion criteria in Amsterdam, but it was in Gelderland.
In a comparable study from Scotland, where an integrated TB, HBV, HCV and HIV screening was only offered to international students, the prevalence of newly diagnosed HBV infec-tions was also low (HBsAg prevalence: 2.6%, prevalence of newly diagnosed HBV infections: 1.3%, no HCV or HIV infections were found).24 The screening uptake found in both regions of our project was higher compared with the project in Scotland (35%) and compared with previous non-integrated HBV and HCV screening projects targeting migrants in the Nether-lands (range: 7–42%).9-18,24 Uptake was lower compared with response rates for antenatal HBV and HIV screening of migrants in the Netherlands (HBV: 99.99%, HIV: 99.8%),25 however, pregnant women could be generally more interested in screening if its primary aim is to prevent transmission to the unborn child. Furthermore, antenatal HBV and HIV testing in the Netherlands are offered according to the opt-out principle (everyone gets tested unless they explicitly refuse). The opt-out approach substantially improves HIV testing rates not only among pregnant women but also among clients of outpatient clinics focussed on sexu-ally transmitted infections.26,27 Similarly, an opt-out testing strategy might improve response rates to integrated HBV, HCV and HIV screening at the TB departments.

175
HBV, HCV and HIV screening during TB entry screening
3.3
We found that the most common reason for declining screening was having already been tested. This might be indicative of a group with adequate access to care in their country of origin, in which HBV, HCV and HIV screening might therefore yield fewer newly diagnosed infections. Our results suggest that adding HIV screening is acceptable to migrants, as we saw no statistically significant difference in uptake between Amsterdam, where HIV screen-ing was included, and Gelderland, where it was not. Only one person opted out of the HIV testing.
Unfortunately, the resources needed to add HBV, HCV and HIV screening to the compulsory TB entry screening were not measured. Whether adding HBV, HCV and HIV screening to the compulsory TB entry screening in the Netherlands will be cost-effective needs to be further explored. A previous study from the Netherlands estimated that one-time-only, non-integrated HBV screening of all migrants from HBV-endemic countries (estimated back-ground HBsAg prevalence: 3.35%), with a participation rate of 35%, was most probably cost-effective.28 Although the overall HBV prevalence in our project was lower than 3.35%, overall HCV prevalence was low and no HIV infections were found, integrating HBV, HCV and HIV screening into the TB entry screening might also be cost-effective, as the programme costs of integrated screening programmes are expected to be lower compared with non-integrated screening. To further increase effectiveness, a pre-screening selection of migrants based on risk factors deserves exploration, e.g., reason for migration, country of origin, or HBV, HCV and HIV risk factors such as blood transfusion history and injecting drug use.29
If HBV, HCV and HIV screening were to be integrated into the TB entry screening, it should be taken into account that not all migrants are registered with a GP or have a Dutch health insurance at the time of screening. Although registering with a GP is easy and all Dutch citizens (including legal migrants and regardless of health status) are entitled to Dutch health insurance, extra guidance is needed to make sure that HBV, HCV and HIV-diagnosed migrants register with a GP and get a Dutch health insurance, and that they will be successfully re-ferred and linked to specialised care.30,31 Also, additional screening for migrants is needed to reach HBV, HCV and HIV risk groups who are not required to have TB entry screening (e.g., migrants from countries with high endemicity for HBV, HCV or HIV but with low endemicity for TB). Alternatives such as case finding through GPs should be explored for effectiveness and acceptability.
Our project has several limitations. Firstly, as our objective was to study the acceptability and effectiveness of HBV, HCV and HIV screening within the normal TB screening procedures, we decided not to measure HBV, HCV and HIV risk factors. Measuring HBV, HCV and HIV risk factors would have provided more insight into the usefulness of risk-based screening and could potentially have provided more insight into the differences between the prevalence of

Chapter 3.3
176
newly diagnosed chronic HBV infections between Gelderland and Amsterdam. Also, due to a low number of HBV infections, the analyses of demographic and migration characteristics as potential determinants of HBV were limited. Secondly, results of this project may not be generalizable to all migrants attending TB screening in the Netherlands, especially as we found regional differences in the characteristics and HBV prevalence of our populations and as migration flow changes over time. Finally, the inclusion criteria, recruitment procedures (the available translations and the timing of receipt of the project information) and screen-ing procedure (in- or exclusion of HIV testing) differed slightly between the two regions. However, despite these small differences, uptake of screening between Gelderland and Amsterdam was similar.
ConCluSIon
About half of the migrants visiting the five TB departments accepted HBV, HCV and HIV screening. The prevalence of newly diagnosed HBV infections was lower intermediate (2–4.99%)21 in migrants screened in Gelderland, but no newly diagnosed HBV infections were found in Amsterdam. This regional difference probably reflects the differences in countries of origin and reasons for migration (which may be related to differences in social economic status) between participants in Gelderland and Amsterdam. The prevalence of newly diagnosed HCV infections was low in both regions, and no HIV infections were found. A more effective strategy might be targeted, integrated TB, HBV, HCV and HIV screening for migrants, which includes pre-screening selection based on risk factors and an opt-out testing approach. Data and cost-effectiveness studies are needed for decision-making regarding the implementation of HBV, HCV and HIV screening that is integrated into entry screening at TB departments.
acknowledgements
The authors acknowledge all participants for their contribution, all colleagues from the Public Health Service of Gelderland and Amsterdam for their help with execution of this screening project, Lucy Phillips for editing the final manuscript, and the funders for the financial support.
funding
Funding for the current screening project was received from the research and development fund of the Public Health Service of Amsterdam (project number 13–17), the regional sup-port fund of the Center for Infectious Disease Control of the Netherlands National Institute for Public Health and the Environment (Letter CIB/RC/10–13), and from Gilead Sciences, Inc.

177
HBV, HCV and HIV screening during TB entry screening
3.3
Those funding this project had no role in its design, data collection and analysis, interpreta-tion, decision to publish, or preparation of the manuscript.
Conflicts of interest
Maria Prins and Freke R Zuure report that their institute received grants from Gilead Sci-ences, Inc., Roche, MSD and AbbVie and non-financial support from OraSure Technologies, all not related to this project.

Chapter 3.3
178
referenCes
1. Hahne SJ, De Melker HE, Kretzschmar M, Mollema L, Van Der Klis FR, Van Der Sande MA, et al. Prevalence of hepatitis B virus infection in The netherlands in 1996 and 2007. Epidemiol Infect. 2012;140(8):1469-1480. doi:10.1017/S095026881100224X.
2. Willemse SB, Razavi-Shearer D, Zuure FR, Veldhuijzen IK, Croes EA, van der Meer AJ, et al. the estimated future disease burden of hepatitis C virus in the netherlands with different treatment paradigms. Neth J Med. 2015;73(9):417-431.
3. van Sighem AI, Boender TS, Wit FWNM, Smit C, Matser A, Reiss P. Monitoring report 2017. Human Immunodeficiency Virus (HIV) Infection in the netherlands. Amsterdam: Stichting HIV Monitoring, 2017.
4. Vriend HJ, Van Veen MG, Prins M, Urbanus AT, Boot HJ, Op De Coul EL. Hepatitis C virus prevalence in The netherlands: migrants account for most infections. Epidemiol Infect. 2013;141(6):1310-1317. doi:10.1017/S0950268812001884.
5. van Zonneveld M, Honkoop P, Hansen BE, Niesters HG, Darwish Murad S, de Man RA, et al. Long-term follow-up of alpha-interferon treatment of patients with chronic hepatitis B. Hepatology. 2004;39(3):804-810. doi:10.1002/hep.20128.
6. van der Meer AJ, Veldt BJ, Feld JJ, Wedemeyer H, Dufour JF, Lammert F, et al. association between sustained virological response and all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. JAMA. 2012;308(24):2584-2593. doi:10.1001/jama.2012.144878.
7. Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493-505. doi:10.1056/NEJMoa1105243.
8. Insight Start Study Group, Lundgren JD, Babiker AG, Gordin F, Emery S, Grund B, et al. Initiation of antiretroviral Therapy in early asymptomatic HIV Infection. N Engl J Med. 2015;373(9):795-807. doi:10.1056/NEJMoa1506816.
9. Urbanus AT, Steenbergen JE. Hepatitis B-virus en hepatitis C-virus screeningsprojecten voor migrant-en in nederland: stand van zaken 2014 [dutch]. Tijdschrift voor Infectieziekten. 2015;10(2):31-36.
10. Zuure FR, Bouman J, Martens M, Vanhommerig JW, Urbanus AT, Davidovich U, et al. screening for hepatitis B and C in first-generation egyptian migrants living in the netherlands. Liver Int. 2013;33(5):727-738. doi:10.1111/liv.12131.
11. Veldhuijzen IK, Wolter R, Rijckborst V, Mostert M, Voeten HA, Cheung Y, et al. Identification and treatment of chronic hepatitis B in Chinese migrants: results of a project offering on-site testing in rotterdam, The netherlands. J Hepatol. 2012;57(6):1171-1176. doi:10.1016/j.jhep.2012.07.036.
12. Richter C, Ter Beest G, Gisolf EH, van Bentum P, Waegemaekers C, Swanink C, et al. screening for chronic hepatitis B and C in migrants from afghanistan, Iran, Iraq, the former Soviet republics, and Vietnam in the arnhem region, the netherlands. Epidemiol Infect. 2014:1-7. doi:10.1017/S0950268813003415.
13. Richter C, Beest GT, Sancak I, Aydinly R, Bulbul K, Laetemia-Tomata F, et al. Hepatitis B prevalence in the Turkish population of arnhem: implications for national screening policy? Epidemiol Infect. 2012;140(4):724-730. doi:10.1017/S0950268811001270.
14. van der Veen YJ, van Empelen P, de Zwart O, Visser H, Mackenbach JP, Richardus JH. Cultural tailoring to promote hepatitis B screening in Turkish dutch: a randomized control study. Health Promot Int. 2014;29(4):692-704. doi:10.1093/heapro/dat020.
15. Niessen W, Benne R, van Zeijl J, van der Have J, Broer J. Is het schriftelijk oproepen van immigranten voor hepatitis B-onderzoek effectief? [dutch]. Infectieziekten Bulletin. 2013;24(4):107-112.
179
HBV, HCV and HIV screening during TB entry screening
3.3
16. Coenen S, van Meer S, Vrolijk JM, Richter C, van Erpecum KJ, Mostert MC, et al. Clinical impact of five large-scale screening projects for chronic hepatitis B in Chinese migrants in the netherlands. Liver Int. 2016;36(10):1425-1432. doi:10.1111/liv.13125.
17. Menger H, Neve G. ‘Vietnam tussen de tulpen’ Screening op hepatitis B van Vietnamese inwoners van noord-Holland [dutch]. Infectieziekten Bulletin. 2013;24(2):45-47.
18. Grintjes MANP, Dofferhoff ASM, Stelma F, Koene RPM, van Crevel R, van den Muijsenbergh M, et al. Hepatitis C-opsporing onder migranten in nijmegen (HeCoM) [dutch]. Tijdschrift voor Infectieziek-ten. 2014;9(5).
19. de Vries G, Riesmeijer R. national Tuberculosis Control Plan 2016-2020: Towards elimination. Bilthoven: National Institute for Public Health and the Environment, Ministry of Health, Welfare and Sport, 2016.
20. World Health Organization. WHo regional offices. Available at: http://www.who.int/about/regions/en/ (accessed on 30 September 2016).
21. Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ. estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet. 2015;386(10003):1546-1555. doi:10.1016/S0140-6736(15)61412-X.
22. Gower E, Estes C, Blach S, Razavi-Shearer K, Razavi H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J Hepatol. 2014;61(1 Suppl):S45-57. doi:10.1016/j.jhep.2014.07.027.
23. Wang H, Wolock TM, Carter A, Nguyen G, Kyu HH, Gakidou E, et al. estimates of global, regional, and national incidence, prevalence, and mortality of HIV, 1980-2015: the Global Burden of disease Study 2015. Lancet HIV. 2016;3(8):e361-e387. doi:10.1016/S2352-3018(16)30087-X.
24. Fernandez M, Manzanares S, Jacques C, Caylá J, Rossi M, Thomson R, et al. screening for chronic viral hepatitis in migrant populations: report on four HePscreen pilot studies. HEPscreen, 2014.
25. Op de Coul EL, Hahne S, van Weert YW, Oomen P, Smit C, van der Ploeg KP, et al. antenatal screen-ing for HIV, hepatitis B and syphilis in the netherlands is effective. BMC Infect Dis. 2011;11:185. doi:10.1186/1471-2334-11-185.
26. Heijman RL, Stolte IG, Thiesbrummel HF, van Leent E, Coutinho RA, Fennema JS, et al. opting out increases HIV testing in a large sexually transmitted infections outpatient clinic. Sex Transm Infect. 2009;85(4):249-255. doi:10.1136/sti.2008.033258.
27. Mulder-Folkerts DK, van den Hoek JA, van der Bij AK, Boer K, Schutte MF, Coutinho RA. Less refusal to participate in HIV screening among pregnant women in the amsterdam region since the intro-duction of standard HIV screening using the opting-out method [article in dutch]. Ned Tijdschr Geneeskd. 2004;148(41):2035-2037.
28. Veldhuijzen IK, Toy M, Hahne SJ, De Wit GA, Schalm SW, de Man RA, et al. screening and early treatment of migrants for chronic hepatitis B virus infection is cost-effective. Gastroenterology. 2010;138(2):522-530. doi:10.1053/j.gastro.2009.10.039.
29. Zuure FR, Urbanus AT, Langendam MW, Helsper CW, van den Berg CH, Davidovich U, et al. outcomes of hepatitis C screening programs targeted at risk groups hidden in the general population: a sys-tematic review. BMC Public Health. 2014;14:66. doi:10.1186/1471-2458-14-66.
30. van Veen MG, Trienekens SC, Heijman T, Gotz HM, Zaheri S, Ladbury G, et al. delayed linkage to care in one-third of HIV-positive individuals in the netherlands. Sex Transm Infect. 2015;91(8):603-609. doi:10.1136/sextrans-2014-051980.
31. Scheppers E, van Dongen E, Dekker J, Geertzen J, Dekker J. Potential barriers to the use of health services among ethnic minorities: a review. Fam Pract. 2006;23(3):325-348. doi:10.1093/fampra/cmi113.


Chapter 3.4usage of purchased self-tests for HIV and sexually transmitted infections in
amsterdam, the netherlands: Results of population-based and serial
cross-sectional studies among the general population and sexual risk groups
Janneke P. Bil, Maria Prins, Ineke G. Stolte, Henriëtte Dijkshoorn, Titia Heijman, Marieke B. Snijder, Udi Davidovich, Freke R. Zuure
Published in BMJ Open, 2017; 7(9):e016609

Chapter 3.4
182
aBstraCt
objectives
There are limited data on the usage of commercially bought self-tests for HIV and other sexually transmitted infections (STIs). Therefore, we studied HIV/STI self-test usage and its determinants among the general population and sexual risk groups between 2007 and 2015 in Amsterdam, the Netherlands.
setting
Data were collected in four different studies among the general population (S1–2) and sexual risk groups (S3–4).
Participants
S1-Amsterdam residents participating in representative population-based surveys (2008 and 2012; n=6044) drawn from the municipality register; S2-Participants of a population-based study stratified by ethnicity drawn from the municipality register of Amsterdam (2011–2015; n=17603); S3-Men having sex with men (MSM) participating in an HIV observational cohort study (2008 and 2013; n=597); and S4-STI clinic clients participating in a cross-sectional survey (2007–2012; n=5655).
Primary and secondary outcome measures
Prevalence of HIV/STI self-test usage and its determinants.
results
The prevalence of HIV/STI self-test usage in the preceding 6-12 months varied between 1% and 2% across studies. Chlamydia self-tests were most commonly used, except among MSM in S3. Chlamydia and syphilis self-test usage increased over time among the representa-tive sample of Amsterdam residents (S1) and chlamydia self-test usage increased over time among STI clinic clients (S4). Self-test usage was associated with African Surinamese or Gha-naian ethnic origin (S2), being woman or MSM (S1 and 4) and having had a higher number of sexual partners (S1–2). Among those in the general population who tested for HIV/STI in the preceding 12 months, 5–9% used a self-test.
Conclusions
Despite low HIV/STI self-test usage, we observed increases over time in chlamydia and syphi-lis self-test usage. Furthermore, self-test usage was higher among high-risk individuals in the general population. It is important to continue monitoring self-test usage and informing the public about the unknown quality of available self-tests in the Netherlands and about the pros and cons of self-testing.

183
HIV/STI self-test usage in the Netherlands
3.4
InTroduCTIon
Self-tests for HIV and other sexually transmitted infections (STIs) are tests that are collected, performed and interpreted autonomously by individuals wanting to know their HIV/STI status.1,2 Self-sampling tests differ from self-tests as they involve a laboratory for the analysis of self-collected specimens.
HIV self-tests may be a promising prevention strategy as they can lead to increased testing rates,1,3-5 and safer sex practices.6,7 Studies report good accuracy of unsupervised HIV self-testing and high user acceptability.1,3,4,8,9 Despite legislation that prohibits over-the-counter sold HIV tests (including HIV self-tests), HIV self-tests are easily available through the internet in the Netherlands.10
Unlike self-sampling, where accuracy is shown to be high,11 few studies have evaluated the accuracy of STI self-tests other than HIV and the limited data available report alarmingly poor results.12,13 Also, there are concerns about the lack of linkage to counselling, treatment and care for HIV/STI self-test users who test positive2,14 and the lack of clear information and/or instructions for self-tests that are currently available.10,13,15 Due to these concerns, the National Institute for STI and AIDS Control in the Netherlands (STI AIDS Netherlands) cur-rently recommends against the use of STI self-tests.10 However, like HIV tests, STI self-tests have already been easily available through the internet, at the pharmacy and drugstore for a number of years.
Due to the anonymous nature of self-testing, the extent to which commercially sold HIV/STI self-tests are used and determinants of usage are not well known. Studies among men having sex with men (MSM) in France in 200916 and among attendees of a street-based HIV testing programme in Spain in 2010–201217 found that 0.6–0.8% of participants had ever used an HIV self-test. A study among an internet panel in the Netherlands in 2006 found that 0.1%, 0.08% and 0.03% of participants had ever used a self-test for HIV, chlamydia and syphi-lis, respectively.18 In a study among online recruited MSM in China in 2013, 20% reported HIV self-test usage.19 However, these studies were not designed to study the population-based prevalence of HIV/STI self-test usage or study trends over time. Furthermore, analyses of determinants of usage16-18 were restricted to HIV self-test or overall self-test usage, including non-HIV/STI self-tests, for example, for diabetes or cholesterol.
To gain insight into HIV and STI (i.e., chlamydia and syphilis) self- test usage in the Nether-lands, we studied (temporal trends in) HIV/STI self-test usage and its determinants among the general population and high-risk groups in Amsterdam, the Netherlands.

Chapter 3.4
184
MeTHodS
study populations
Between 2007 and 2015, data regarding HIV/STI self-test usage were collected in four dif-ferent studies (S1–4) in Amsterdam, the Netherlands, among the general population (S1–2) and HIV-negative high-risk groups (S3–4) (Table 1):
S1: Representative sample of Amsterdam residents participating in a serial cross-sectional Health Monitoring Survey
Every four years, a random sample of Amsterdam residents is drawn from the municipality register and asked to participate in a representative population-based cross-sectional Health Monitoring Survey conducted by the Public Health Service of Amsterdam.20,21 Participants complete questionnaires (paper/online) on physical, mental and sexual health. Participants unable to fill in a questionnaire on paper or online and hard to reach groups are assisted by a trained interviewer. Participation rates in the Health Monitor Survey were 50% in 2008 and 38% in 2012. Questions on HIV/STI self-tests usage were answered in the 2008 and 2012 surveys by participants aged 16–54 years and 19–64 years, respectively. To compare both waves, only participants aged between 19 and 54 years were included.
Table 1. Descriptive of the contributing studies for this manuscript
studystudy design Study population
Period of data collection N
S1: The Health Monitoring Survey
Serial cross-
sectional
Representative sample of Amsterdam residents
2008 and 2012 Total: 6,0442008: 2,5472012: 3,497
S2: The HEalthy Life in an Urban Setting (HELIUS) Study
Cohort study
Random sample of Amsterdam residents
from Surinamese, Turkish, Moroccan, Ghanaian and
Dutch ethnic origin
2011–2015 (baseline data)
Total: 17,603
S3: The Amsterdam Cohort Studies (ACS)
Cohort study
HIV-negative MSM 2008 and 2013 Total: 5972008: 4472013: 469
S4: STI Clinic HIV Survey Serial cross-
sectional
HIV-negative STI clients of the Public Health Service of
Amsterdam
2007–2009 and 2012
Total: 5,655Autumn 2007: 949Spring 2008: 935
Autumn 2008: 924Spring 2009: 935
Autumn 2009: 911Spring 2012: 1,001
MSM, men having sex with men; STI, sexually transmitted infection.

185
HIV/STI self-test usage in the Netherlands
3.4
S2: Participants of the multiethnic HELIUS Study
The HEalthy LIfe in an Urban Setting (HELIUS) Study is a multiethnic population-based cohort study investigating mechanisms underlying ethnic differences in communicable and non-communicable diseases22. A random sample of individuals aged 18–70 years old was drawn from the municipality register of Amsterdam, stratified by ethnicity, including those of Surinamese (with African Surinamese and South-Asian Surinamese as the main ethnic groups), Turkish, Moroccan, Ghanaian and Dutch ethnic origin. Response rate (number participated/number invited) in the HELIUS Study was 28%. Baseline data collection took place in 2011–2015. Participants underwent a physical examination and completed a self-administered questionnaire (paper/online), including questions on sexual health and HIV/STI self-test usage. Participants unable to fill in the questionnaire themselves were assisted by an ethnically matched trained interviewer. To compare results with the results of study 1 (representative sample of Amsterdam residents), only participants aged between 19 and 54 years were included in the analyses.
S3: MSM participating in the Amsterdam Cohort Studies (ACS)
The Amsterdam Cohort Studies (ACS) among MSM started in 1984 and is an open, prospec-tive cohort study that investigates the epidemiology, pathogenesis, risk factors and effect of interventions concerning HIV/AIDS and other bloodborne infections and STIs in the Neth-erlands.23,24 Biannually, HIV-positive and HIV-negative participants complete questionnaires (paper/online) on sexual behaviour, give blood for HIV testing and storage and, since 2008, are tested for STI. HIV/STI self-test usage was measured in two waves (early 2008 and late 2013). For the present study, HIV-positive MSM were excluded (2008: n=88; 2013: n=61).
S4: STI clinic clients participating in a serial cross-sectional survey
Biannually between 1991 and 2012, approximately 1000 visitors of the Amsterdam STI outpatient clinic of the Public Health Service were asked to participate in a cross-sectional survey, initially started to measure HIV prevalence and later also other (bloodborne) infec-tions.25,26 Participants were interviewed using standard questionnaires which included ques-tions about risk factors for HIV and other infections and HIV/STI test behaviour. Participants received routine STI testing and were anonymously screened for HIV and from 2007 onwards also for other infections (e.g., hepatitis C virus, human papilloma virus, herpes simplex vi-rus). Participation rate varied between 65% and 96% over the years. Data on HIV/STI self-test usage were collected in six waves: Autumn 2007, Spring 2008, Autumn 2008, Spring 2009, Autumn 2009 and Spring 2012. For the present study, HIV-positive STI clinic clients were excluded (n=408).
We included only participants with available HIV/STI self-test data. S2–4 received institu-tional review board approval by the medical ethics committee of the Academic Medical

Chapter 3.4
186
Center of Amsterdam (S2: project number 10/100; S3: project number 07/182; S4: project number 06/257). For S1, approval by an ethics committee or institutional review board was not necessary according to Dutch legislation on medical research involving human subjects. Detailed information about the studies can be found elsewhere.20-26
Variables
Sociodemographics, sexual (risk) behaviour and self-test usage
Age, ethnic origin, education level and sexual behaviour (testing behaviour, condomless inter-course, number of sexual partners, STI diagnosis) were obtained according to the individual study protocols. Non-Dutch ethnic origin was defined as being born outside the Netherlands with at least one parent who was also born outside the Netherlands (first-generation mi-grant) or being born in the Netherlands but with both parents born outside the Netherlands (second-generation migrant).27 In the HELIUS Study (S2), participants’ ethnicity was based on their and their parents’ country of birth. Surinamese subgroups (South-Asian Surinamese, African Surinamese, Javanese Surinamese and Surinamese other/unknown) were classified according to self-reported ethnic origin. Due to small numbers, Javanese Surinamese were included in the Surinamese other/unknown group. Age was grouped into four categories (16–24 years/25–29 years/30–34years/>35years). Number of (lifetime) sexual partners was categorised based on tertiles. Condomless intercourse was defined as not always or never using a condom while practising vaginal and/or anal sex with casual partners. Among STI clinic clients (S4), this variable included both steady and casual partners since partner type was not measured.
HIV/STI self-test usage was defined as having used a HIV, chlamydia and/or syphilis self-test in the preceding 6 (S3: MSM participating in the ACS) or 12 months (S1–2: the general population and S4: STI clinic clients). We focussed on HIV, chlamydia and syphilis self-tests as at the start of the study these were the main HIV/STI self-tests available through the internet and/or pharmacies. In each study, self-tests were explained to participants as home tests that they had bought (e.g., through the internet, at the pharmacy and/or at a drugstore) for self-use at home.
Additionally, general HIV/STI testing behaviour in the previous 12 and 6 months, including self-testing, was measured among the general population (S1–2), respectively. As our sexual risk groups (S3–4) received HIV/STI testing at the time and location of recruitment, general HIV/STI testing behaviour was not measured in these groups.

187
HIV/STI self-test usage in the Netherlands
3.4
statistical analyses
Within each study, we described study population characteristics and prevalence of self-test usage. Prevalence of self-test usage and 95% CIs among the representative sample of Amsterdam residents (S1) were weighted by sex, age, district and in 2012 also for income, marital status, household size and ethnic origin to calculate the Amsterdam population-based prevalence of self-test usage. Time trend in HIV/STI self-test usage among the rep-resentative sample of Amsterdam residents (S1) was assessed by using chi-square tests. In S2–4, Wilson intervals28 were used to determine 95% CIs as self-test usage prevalence was low. Time trend in HIV/STI self-test usage among STI clinic clients (S4) was assessed by logis-tic regression analyses using restricted cubic splines to take the non-linear time trend into account. For all analyses among MSM participating in the ACS (S3), we performed logistic regression analyses using generalised estimating equations to correct for repeated measure-ments. For participants of the multiethnic HELIUS Study (S2), no time trend was assessed. Among the general population (S1–2), we additionally calculated the proportion of self-test usage among participants who reported to have had an HIV/STI test in the previous 12 and 6 months, respectively.
Using univariable and multivariable logistic regression analyses, we assessed determinants of HIV/STI self-test usage. Despite our large sample sizes, we were unable to identify deter-minants for HIV and STI self-test usage separately because of the small numbers of HIV/STI self-test users. Determinants in the analyses included age, ethnic origin, education level, sexual risk behaviour and calendar year of data collection. For univariable and multivariable analyses, among the representative sample of Amsterdam residents (S1), no weighting was used. Determinants of self-test usage among participants of the multiethnic HELIUS Study (S2) were only assessed among those aged 18–34 years, because questions on sexual risk behaviour were optional for participants aged 35 years or older. Variables with a p-value <0.10 in univariable analyses were included in the final multivariable models. We checked for interactions between the independent variables in the final models.
A p-value of <0.05 level was considered statistically significant. Analyses were performed using STATA Intercooled 13.1 (STATA Corporation, College Station, Texas, USA) and SPSS V.21 (SPSS, Chicago, USA).

Chapter 3.4
188 189
HIV/STI self-test usage in the Netherlands
3.4
reSulTS
Characteristics
In total, 29,899 individuals were included in this study: 6,044 inhabitants of Amsterdam (S1), 17,603 participants of the multiethnic HELIUS Study (S2), 597 MSM participating in the ACS (S3) and 5,655 STI clinic clients (S4) (Table 1).
Of 6,044 inhabitants of Amsterdam participating in the Health Monitoring Survey (S1), 2,547 participated in 2008 and 3,497 in 2012. Participants had a median age of 35 years (IQR 28–45), 60% (3621/6,044) were women, 77% (4,660/6,044) had a college degree or higher, 58% (3,486/6,044) were of Dutch origin and 21% (1,288/6,044) had been tested for HIV and/or STI in the previous 12 months.
Of 17,603 participants of the multiethnic HELIUS Study (S2), the median age was 40 years (IQR 30–48), 59% (10,339/17,603) were women, 27% (4,822/17,603) had a college degree or higher and 10% (1,794/17,603) were tested for HIV and/or STI in the previous 6 months. Seventeen per cent (3,051/17,603) were of Dutch origin, 13% (2,353/17,603) of South-Asian Surinamese, 16% (2,875/17,603) of African Surinamese, 2.0% (352/17,603) of other or un-known Surinamese origin, 20% (3,470/17,603) of Turkish, 20% (3,566/17,603) of Moroccan and 11% (1,,905/17,603) of Ghanaian origin.
Of 597 MSM participating in the ACS (S3), 447 participated in early 2008 and 469 partici-pated in late 2013 (319 MSM participated in both waves). Participants had a median age of 38 years (IQR 33–43), 91% (543/597) had a college degree or higher and 79% (469/597) were of Dutch origin.
Of 5,655 STI clinic clients participating in the cross-sectional survey STI Clinic HIV Survey (S4), 949 participated in Autumn 2007, 935 in Spring 2008, 924 in Autumn 2008, 935 in Spring 2009, 911 in Autumn 2009 and 1001 in Spring 2012. Participants had a median age of 26 years (IQR 22–34), 46% (2,571/5,655) were women, 50% (2,852/5,655) had a college degree or higher, 57% (3,199/5,655) were of Dutch origin and 13% (762/5,655) were diagnosed with an STI at their visit.
Prevalence of HIV/STI self-test usage
Among the representative sample of Amsterdam residents (S1; Table 2), HIV/STI self-test usage in the preceding 12 months increased from 0.9% (22/2,547; 95% CI 0.6%–1.4%) in 2008 to 1.3% (57/3,497; 95% CI 1.0%–1.8%) in 2012, respectively (p<0.001). This increase was primarily due to increases in chlamydia (2008: 0.7%, 2012: 1.2%, p<0.001) and syphilis self-test usage (2008: 0.1%, 2012: 0.4%, p<0.001). Among those who were tested for HIV/
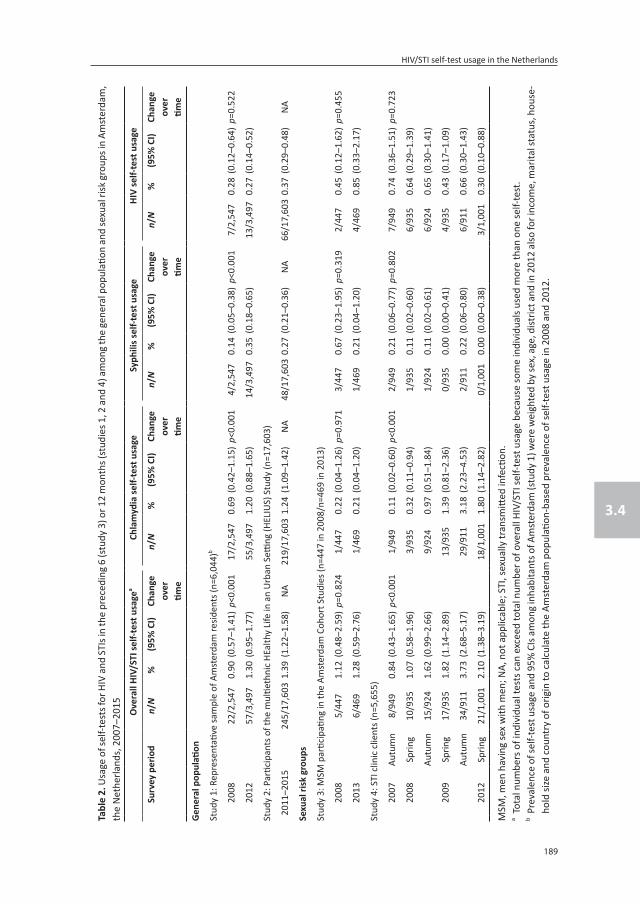
Chapter 3.4
188 189
HIV/STI self-test usage in the Netherlands
3.4
Tabl
e 2.
Usa
ge o
f sel
f-tes
ts fo
r HIV
and
STI
s in
the
prec
edin
g 6
(stu
dy 3
) or 1
2 m
onth
s (st
udie
s 1, 2
and
4) a
mon
g th
e ge
nera
l pop
ulati
on a
nd se
xual
risk
gro
ups i
n Am
ster
dam
, th
e N
ethe
rland
s, 2
007–
2015
o
vera
ll HI
V/ST
I sel
f-tes
t usa
gea
Ch
lam
ydia
self-
test
usa
ge
syph
ilis s
elf-t
est u
sage
HI
V se
lf-te
st u
sage
surv
ey p
erio
dn/
N%
(95%
CI)
Chan
geov
ertim
e
n/N
%(9
5% C
I)Ch
ange
over
time
n/N
%(9
5% C
I)Ch
ange
over
time
n/N
%(9
5% C
I)Ch
ange
over
time
Gen
eral
pop
ulati
on
Stud
y 1:
Rep
rese
ntati
ve sa
mpl
e of
Am
ster
dam
resid
ents
(n=6
,044
)b
2008
22/2
,547
0.90
(0.5
7–1.
41)
p<0.
001
17/2
,547
0.69
(0.4
2–1.
15)
p<0.
001
4/2,
547
0.14
(0.0
5–0.
38)
p<0.
001
7/2,
547
0.28
(0.1
2–0.
64)
p=0.
522
2012
57/3
,497
1.30
(0.9
5–1.
77)
55/3
,497
1.20
(0.8
8–1.
65)
14/3
,497
0.35
(0.1
8–0.
65)
13/3
,497
0.27
(0.1
4–0.
52)
Stud
y 2:
Par
ticip
ants
of t
he m
ultie
thni
c HE
alth
y Li
fe in
an
Urb
an S
etting
(HEL
IUS)
Stu
dy (n
=17,
603)
2011
–201
524
5/17
,603
1.39
(1.2
2–1.
58)
NA
219/
17,6
031.
24(1
.09–
1.42
)N
A48
/17,
603
0.27
(0.2
1–0.
36)
NA
66/1
7,60
30.
37(0
.29–
0.48
)N
A
sexu
al ri
sk g
roup
s
Stud
y 3:
MSM
par
ticip
ating
in th
e Am
ster
dam
Coh
ort S
tudi
es (n
=447
in 2
008/
n=46
9 in
201
3)
2008
5/44
71.
12(0
.48–
2.59
)p=
0.82
41/
447
0.22
(0.0
4–1.
26)
p=0.
971
3/44
70.
67(0
.23–
1.95
)p=
0.31
92/
447
0.45
(0.1
2–1.
62)
p=0.
455
2013
6/46
91.
28(0
.59–
2.76
)1/
469
0.21
(0.0
4–1.
20)
1/46
90.
21(0
.04–
1.20
)4/
469
0.85
(0.3
3–2.
17)
Stud
y 4:
STI
clin
ic c
lient
s (n=
5,65
5)
2007
Autu
mn
8/94
90.
84(0
.43–
1.65
)p<
0.00
11/
949
0.11
(0.0
2–0.
60)
p<0.
001
2/94
90.
21(0
.06–
0.77
)p=
0.80
27/
949
0.74
(0.3
6–1.
51)
p=0.
723
2008
Sprin
g10
/935
1.07
(0.5
8–1.
96)
3/93
50.
32(0
.11–
0.94
)1/
935
0.11
(0.0
2–0.
60)
6/93
50.
64(0
.29–
1.39
)
Autu
mn
15/9
241.
62(0
.99–
2.66
)9/
924
0.97
(0.5
1–1.
84)
1/92
40.
11(0
.02–
0.61
)6/
924
0.65
(0.3
0–1.
41)
2009
Sprin
g17
/935
1.82
(1.1
4–2.
89)
13/9
351.
39(0
.81–
2.36
)0/
935
0.00
(0.0
0–0.
41)
4/93
50.
43(0
.17–
1.09
)
Autu
mn
34/9
113.
73(2
.68–
5.17
)29
/911
3.18
(2.2
3–4.
53)
2/91
10.
22(0
.06–
0.80
)6/
911
0.66
(0.3
0–1.
43)
2012
Sprin
g21
/1,0
012.
10(1
.38–
3.19
)18
/1,0
011.
80(1
.14–
2.82
)0/
1,00
10.
00(0
.00–
0.38
)3/
1,00
10.
30(0
.10–
0.88
)
MSM
, men
hav
ing
sex
with
men
; NA,
not
app
licab
le; S
TI, s
exua
lly tr
ansm
itted
infe
ction
.a T
otal
num
bers
of i
ndiv
idua
l tes
ts c
an e
xcee
d to
tal n
umbe
r of o
vera
ll HI
V/ST
I sel
f-tes
t usa
ge b
ecau
se so
me
indi
vidu
als u
sed
mor
e th
an o
ne se
lf-te
st.
b Pre
vale
nce
of se
lf-te
st u
sage
and
95%
CIs
am
ong
inha
bita
nts o
f Am
ster
dam
(stu
dy 1
) wer
e w
eigh
ted
by se
x, a
ge, d
istric
t and
in 2
012
also
for i
ncom
e, m
arita
l sta
tus,
hou
se-
hold
size
and
cou
ntry
of o
rigin
to c
alcu
late
the
Amst
erda
m p
opul
ation
-bas
ed p
reva
lenc
e of
self-
test
usa
ge in
200
8 an
d 20
12.

Chapter 3.4
190
STIs in the preceding 12 months, 5.4% (70/1,288; 95% CI 4.3%–6.8%) used a self-test. This proportion significantly increased over time (2008: 3.7%, 2012: 6.8%, p=0.014) and was higher among those of non-Dutch ethnicity, although borderline significant (Dutch: 4.4%, non-Dutch: 6.9%, p=0.056).
Among participants of the multiethnic HELIUS Study (S2), 1.4% (245/17,603; 95% CI 1.2%–1.6%) used an HIV/STI self-test in the preceding 12 months. Among those tested for HIV/STIs in the preceding 6 months, 8.8% (158/1,794; 95% CI 7.6%–10%) used a self-test. The latter was significantly different between ethnic groups (Surinamese other/unknown 13%, South-Asian Surinamese 12%, African Surinamese 12%, Dutch 8.4%, Ghanaian 5.6%, Moroccan 5.0% and Turkish 4.6%, p<0.001).
Among MSM participating in the ACS (S3), HIV/STI self-test usage in the preceding 6 months remained stable over time, 1.1% (5/447; 95% CI 0.5%–2.6%) in 2008 and 1.3% (6/469; 95% CI 0.6%–2.8%) in 2013 (p=0.824).
Among STI clinic clients (S4), HIV/STI self-test usage in the preceding 12 months increased from 0.8% (8/949; 95% CI 0.4%–1.7%) in 2007 to 2.1% (21/1,001; 95% CI 1.4%–3.2%) in 2012 (p<0.001). This increase was primarily due to an increase in chlamydia self-test usage (2007: 0.1%, 2012: 1.8%, p<0.001).
Overall, chlamydia self-tests were most used, except among MSM participating in the ACS where HIV self-tests were most used.
determinants of HIV/STI self-test usage
In multivariable analyses among the representative sample of Amsterdam residents (S1; Table 3), only participants aged between 30 and 34 years (adjusted OR (aOR) 2.14, 95% CI 1.01–4.55) were significantly more likely to have used self-tests compared with those aged between 19 and 24 years, whereas the aOR was 1.81 (95% CI 0.85–3.89) and 0.84 (95% CI 0.39–1.84) for those aged between 25–29 years and ≥35 years, respectively (overall p=0.013). Also, MSM (aOR 3.43, 95% CI 1.24–9.48) and women (aOR 3.63 (95% CI 1.83–7.21)) were more likely to have used self-tests compared with heterosexual men. Those reporting one or more sexual partners in the preceding 12 months (one partner: aOR 0.86 (95% CI 0.37–1.97); >2 partners: aOR 5.77 (95% CI 2.15–15.46) were more likely to have used self-tests compared with participants reporting no partners. As described above, self-test usage was higher in 2012 compared with 2008 (aOR 1.16, 95% CI 1.01–1.32).
Among participants of the multiethnic HELIUS Study (S2; Table 4), participants aged between 30 and 34 years (aOR 0.59, 95% CI 0.39–0.90) were less likely to have used self-tests com-

191
HIV/STI self-test usage in the Netherlands
3.4
pared with participants aged 19–24 years, whereas the aOR was 0.91 (95% CI 0.63–1.32) for those aged between 25 and 29 years (overall p=0.032). African Surinamese (aOR 2.54, 95% CI 1.69–3.82) and Ghanaian participants (aOR 1.89, 95% CI 1.04–3.44) were more likely
Table 3. Determinants associated with the usage of self-tests for HIV and STIs in the previous 12 months among a representative sample of Amsterdam residents, 2008 and 2012, the Netherlands
HIV/STI self-test usage univariable analyses Multivariable analyses
n N %or
(95% CI)p-value aor (95% CI) p-value
age (years)
19–24 11 802 1.37 1 0.001 1 0.013
25–29 21 950 2.21 1.63 (0.78–3.39) 1.81 (0.85–3.89)
30–34 23 1,101 2.09 1.53 (0.74–3.17) 2.14 (1.01–4.55)
>35 24 3,191 0.75 0.55 (0.27–1.12) 0.84 (0.39–1.84)
Sexual orientation
Heterosexual men 15 2,115 0.71 1 0.004 1 0.001
MSM 7 249 2.81 4.05 (1.64–10.03) 3.43 (1.24–9.48)
Women 57 3,621 1.57 2.24 (1.27–3.96) 3.63 (1.83–7.21)
Missing 0 59 0.00
education level
No college degree 16 1,290 1.24 1 0.801
At least college degree 62 4,660 1.33 1.07 (0.62–1.87)
Missing 1 94 1.06
ethnic origin
Dutch 40 3,486 1.15 1 0.204
Non-Dutch 39 2,558 1.52 1.33 (0.86–2.08)
Condomless intercourse with casual partner in the previous 12 months
No 49 5,273 0.93 1 <0.001 1 0.934
Yes 24 546 4.40 4.90 (2.98–8.05) 1.03 (0.50–2.13)
Missing 6 225 2.67
number partners in the previous 12 months
0 7 967 0.72 1 <0.001 1 <0.001
1 30 4,090 0.73 1.01 (0.44–2.31) 0.86 (0.37–1.97)
>2 35 747 4.69 6.74 (2.98–15.27) 5.77 (2.15–15.46)
Missing 7 240 2.92
survey perioda
2008 22 2,547 0.86 1 0.011 1 0.031
2012 57 3,497 1.63 1.17 (1.04–1.33) 1.16 (1.01–1.32)
(a)OR, (adjusted) Odds Ratio; MSM, men having sex with men; STI, sexually transmitted infection.a The calculated prevalence and 95% CI were calculated based on unweighted numbers and therefore differ
from the estimated prevalence and 95% CI presented in Table 2.

Chapter 3.4
192
Table 4. Determinants associated with the usage of self-tests for HIV and STIs in the previous 12 months among participants of the multiethnic HELIUS study between 2011 and 2015, Amsterdam, the Netherlands
HIV/STI self-test usage univariable analyses Multivariable analyses
n N % or (95% CI) p-value aor (95% CI) p-value
age (years)
19–24 65 2,259 2.88 1 0.064 1 0.032
25–29 71 2,028 3.50 1.22 (0.87–1.72) 0.91 (0.63–1.32)
30–34 47 2,072 2.27 0.78 (0.54–1.15) 0.59 (0.39–0.90)
Gender
Men 70 2,602 2.69 1 0.457
Women 113 3,757 3.01 1.12 (0.83–1.52)
education level
No college degree 123 4,119 2.99 1 0.462
At least college degree 59 2,216 2.66 0.89 (0.65–1.22)
Missing 1 26 4.17
ethnic origin
Dutch 42 1,184 3.55 1 <0.001 1 <0.001
Surinamese
South-Asian Surinamese 25 832 3.00 0.84 (0.51–1.39) 1.29 (0.77–2.17)
African Surinamese 69 822 8.39 2.49 (1.68–3.70) 2.54 (1.69–3.82)
Other/unknown 5 100 5.00 1.43 (0.55–3.70) 1.77 (0.68–4.64)
Ghanaian 19 438 4.34 1.23 (0.71–2.14) 1.89 (1.04–3.44)
Turkish 11 1,375 0.80 0.22 (0.11–0.43) 0.52 (0.26–1.03)
Moroccan 12 1,592 0.75 0.21 (0.11–0.39) 0.44 (0.22–0.89)
Missing 0 16 0.00
Migration status
NA (Dutch) 42 1,184 3.55 1 0.313
First-generation migrant 46 1,671 2.75 0.77 (0.50–1.18)
Second-generation migrant 95 3,504 2.71 0.76 (0.52–1.10)
number of lifetime sexual partners
0–1 18 2,887 0.62 1 <0.001 1 <0.001
2–5 57 1,433 3.98 6.60 (3.87–11.26) 4.11 (2.33–7.23)
>5 105 1,842 5.70 9.63 (5.82–15.94) 5.65 (3.22–9.93)
Missing 3 197 1.52
Condomless intercourse with casual partners in the preceding 6 months
No 140 5,617 2.50 1 <0.001 1 0.073
Yes 37 513 7.20 2.99 (2.05–4.37) 1.45 (0.97–2.18)
Missing 10 409 2.40
(a)OR, (adjusted) Odds Ratio; HELIUS, HEalthy Life in an Urban Setting study; NA, not applicable; STI, sexually transmitted infection.

193
HIV/STI self-test usage in the Netherlands
3.4
to have used self-tests compared with Dutch participants, whereas Moroccan participants (aOR 0.44, 95% CI 0.22–0.89) were less likely to have used self-tests (overall p<0.001). Also, those reporting >2 lifetime sexual partners (2–5 partners: aOR 4.11, 95% CI 2.33–7.23; >5 partners: aOR 5.65, 95% CI 3.22–9.93) were more likely to have used self-tests compared with participants reporting <2 sexual partners.
Among MSM participating in the ACS (S3; Table 5), those reporting 3–8 casual partners in the preceding 6 months (unadjusted OR 9.86, 95% CI 1.21–80.55) were more likely to have used self-tests compared with participants reporting <3 casual partners, whereas the OR 1.32 (95% CI 0.08–21.18) was for those reporting >8 casual partners (overall p=0.028).
Table 5. Determinants associated with the usage of self-tests for HIV and STIs in the previous 6 months among HIV-negative MSM participating in the Amsterdam Cohort Studies in 2008 and 2013, Amsterdam, the Neth-erlands
HIV/STI self-test usage univariable analyses
n N % or (95% CI) p-value
age (years)
18–29 3 124 2.42 1 0.334
30–34 3 198 1.52 0.62 (0.12–3.14)
>35 5 194 2.58 0.34 (0.08–1.45)
education level
No college degree 2 93 2.15 1 0.384
At least college degree 9 823 1.09 0.5 (0.11–2.36)
ethnic origin
Dutch 9 731 1.23 1 0.821
Non-Dutch 2 136 1.47 1.20 (0.26–5.59)
Missing 0 49 0.00
number of sexual partners in the previous 6 months
0–2 1 672 0.15 1 <0.001
3–8 7 206 3.40 6.60 (3.87–11.26)
>8 1 38 2.63 9.63 (5.82–15.94)
Missing 2 916 0.22
Condomless intercourse with casual partners in the preceding 6 months
No 6 672 0.89 1 0.028
Yes 4 206 1.94 9.86 (1.21–80.55)
Missing 1 38 2.63 1.32 (0.08–21.18)
survey period
2008 5 447 1.12 1 0.824
2013 6 469 1.28 1.03 (0.81–1.31)
MSM, men having sex with men; STI, sexually transmitted infection.

Chapter 3.4
194 195
HIV/STI self-test usage in the Netherlands
3.4
Tabl
e 6.
Det
erm
inan
ts a
ssoc
iate
d w
ith th
e us
age
of se
lf-te
sts f
or H
IV a
nd S
TIs i
n th
e pr
evio
us 1
2 m
onth
s am
ong
clie
nts o
f the
STI
clin
ic o
f the
Pub
lic H
ealth
Ser
vice
Am
ster
-da
m, t
he N
ethe
rland
s (20
07–2
012)
HIV/
STI s
elf-t
est
usag
eu
niva
riabl
e an
alys
es
HIV/
STI s
elf-t
est u
sage
Mul
tivar
iabl
e an
alys
es
nN
%o
r (9
5% C
I)p-
valu
e
nN
%o
r (9
5% C
I)p-
valu
e
age
(yea
rs)
16–2
441
2,19
21.
871
0.52
7
25–2
930
1,33
12.
251.
21(0
.75–
1.95
)
30–3
410
727
1.38
0.73
(0.3
7–1.
47)
Sexu
al o
rient
ation
* S
urve
y pe
riod
>35
241,
405
1.71
0.91
(0.5
5–1.
52)
Hete
rose
xual
men
Sexu
al o
rient
ation
2007
235
80.
561
0.53
6
Hete
rose
xual
men
201,
994
1.00
10.
003
2008
566
40.
751.
35(0
.26–
7.00
)
MSM
251,
065
2.35
2.37
(1.3
1–4.
29)
2009
964
81.
392.
51(0
.54–
11.6
7)
Wom
en59
2,57
12.
292.
32(1
.39–
3.86
)20
124
324
1.23
2.23
(0.4
1–12
.23)
Miss
ing
125
4.00
msm
surv
ey p
erio
d20
074
140
2.86
10.
553
2007
894
90.
841
0.00
120
0810
337
2.97
1.04
(0.3
2–3.
37)
2008
251,
859
1.34
1.60
(0.7
2–3.
57)
2009
939
12.
300.
80(0
.24–
2.64
)
2009
511,
846
2.76
3.34
(1.5
8–7.
07)
2012
219
71.
020.
35(0
.06–
1.93
)
2012
211,
001
2.10
2.52
(1.1
1–5.
72)
Wom
en
educ
ation
leve
l20
072
451
0.44
1<0
.001
No
colle
ge d
egre
e26
1,78
61.
461
0.17
720
0810
858
1.17
2.65
(0.5
8–12
.14)
At le
ast c
olle
ge d
egre
e57
2,85
22.
001.
38 (0
.87–
2.20
)20
0933
807
4.09
9.57
(2.2
9–40
.08)
Miss
ing
221,
017
2.16
2012
1445
53.
087.
13(1
.61–
31.5
4)

Chapter 3.4
194 195
HIV/STI self-test usage in the Netherlands
3.4
Tabl
e 6.
(con
tinue
d)
HIV/
STI s
elf-t
est
usag
eu
niva
riabl
e an
alys
es
HIV/
STI s
elf-t
est u
sage
Mul
tivar
iabl
e an
alys
es
nN
%o
r (9
5% C
I)p-
valu
e
nN
%o
r (9
5% C
I)p-
valu
e
ethn
ic o
rigin
Dutc
h67
3,19
92.
091
0.25
5
Firs
t-gen
erati
on m
igra
nt15
1,10
61.
360.
64(0
.37–
1.13
)
Seco
nd-g
ener
ation
mig
rant
211,
259
1.67
0.79
(0.4
8–1.
30)
Miss
ing
291
2.20
Cond
omle
ss in
terc
ours
e in
the
prec
edin
g 6
mon
ths (
vagi
nal o
r ana
l)
No
cond
omle
ss in
terc
ours
e13
974
1.33
10.
215
Cond
omle
ss in
terc
ours
e71
3,67
11.
931.
46(0
.80–
2.65
)
Miss
ing
211,
010
2.08
num
ber o
f life
time
sexu
al p
artn
ers
0–8
351,
944
1.80
10.
297
9–20
291,
873
1.55
0.86
(0.5
2–1.
41)
>21
411,
835
2.23
1.25
(0.7
9–1.
97)
Miss
ing
03
0.00
STI d
iagn
osis
at v
isit
(chl
amyd
ia/s
yphi
lis/g
onor
rhoe
a/HI
V)
No
STI
914,
840
1.88
10.
741
STI
1376
21.
710.
91(0
.50–
1.63
)
Miss
ing
153
1.89
MSM
, men
hav
ing
sex
with
men
; STI
, sex
ually
tran
smitt
ed in
fecti
on.

Chapter 3.4
196
Among STI clinic clients (S4; Table 6), MSM (unadjusted OR 2.37, 95% CI 1.31–4.29) and women (unadjusted OR 2.32, 95% CI 1.39–3.86) were more likely to have used self-tests compared with heterosexual men. In multivariable analyses among STI clinic clients, a sta-tistically significant interaction between sexual orientation and calendar period was found (p=0.032). Self-test usage significantly increased over time among women (2007: 0.4%, 2012: 3.1%, p<0.001), whereas the increase among heterosexual men and decrease among MSM were not statistically significant.
dISCuSSIon
This study shows that the prevalence of HIV/STI self-test usage in the preceding 6–12 months among both the general population and high-risk groups in Amsterdam, the Netherlands, is relatively low (1–2%). However, chlamydia and syphilis self-test usage increased over time among a representative sample of Amsterdam residents (S1) and chlamydia self-test usage increased over time among STI clinic clients (S4).
The overall low HIV/STI self-test usage among the general population and sexual risk groups is in line with findings from other European studies on HIV self-testing (France; Spain)16,17 and on HIV/STI self-testing (the Netherlands).18 However, in a study from China, 20% of MSM reported prior HIV self-testing19. The difference between Europe and China on HIV self-test usage can be explained by legal restrictions on selling HIV self-tests. In China HIV self-test can be legally sold, whereas in France, Spain and the Netherlands, there were legal restrictions on HIV self-tests at the time the studies were conducted. In France, HIV self-tests became legally available in 2015, after the study on HIV self-test usage was conducted.1
Although we found an overall low HIV/STI self-test usage in the general population 5–9% of the individuals who tested for HIV/STI in the preceding 6 or 12 months used a self-test. This finding indicates that although self-testing is currently not recommended by the National Institute for STI and AIDS control in the Netherlands (STI AIDS Netherlands),10 a substantial proportion opt for self-testing as their method of testing. Furthermore, our study shows HIV/STI self-test usage was higher among women and MSM compared with heterosexual men in the representative sample of Amsterdam residents and among STI clinic clients. These results are consistent with results that women and MSM are in general more likely to test for HIV and STI compared with heterosexual men.20 Heterosexual men might perceive themselves at lower risk for HIV/STI than women and MSM and therefore less often test for HIV/STI. It might also be that heterosexual men experience greater barriers to test for HIV/STI. Among the general population and MSM participating in the ACS, also a higher number of sexual partners were associated with higher self-test usage, suggesting self-tests might

197
HIV/STI self-test usage in the Netherlands
3.4
be used by individuals at higher risk of HIV/STI and therefore may be reaching the relevant populations.29 Among participants of the multiethnic HELIUS Study, we found that individu-als of African Surinamese or Ghanaian origin were more likely to use self-tests. In addition, among HELIUS Study participants who have tested for HIV/STI in the preceding 12 months, individuals of Surinamese origin (all subgroups: South-Asian, African and other/unknown Suriname origin) more often opted for the use of a self-test compared with other ethnic groups. It might be that individuals of Surinamese or Ghanaian origin more often experience barriers to test at regular facilities than the other groups and therefore more often opt for self-testing. This might suggest that self-testing could increase HIV/STI test uptake among these groups, but this should be further explored in future studies. Also, it might be that individuals of Surinamese or Ghanaian origin are more aware of the availability of HIV/ST self-tests. This association between self-testing and ethnic origin was not found among the representative sample of Amsterdam residents (S1) and our sexual risk groups (S3–4). This is most likely because in these studies we grouped all non-Dutch origin ethnicities together because of small numbers.
Although we found an association between age and self-test usage in the two studies among the general population, this association was not found among the sexual risk groups. However, the results with regard to age and self-testing among the representative sample of Amsterdam residents and among the participants of the multiethnic HELIUS Study were inconsistent.
The low HIV/ST self-test usage among our high-risk groups can be explained by our data sources, since we included individuals who attended the Public Health Service’s HIV/STI test-ing facilities and MSM participating in the ACS who were offered structural biannual HIV/STI testing. These individuals may have overcome testing barriers related to these facilities and therefore be less likely to opt for self-testing.
Our study shows that in recent years chlamydia self-tests are most commonly used in all study groups except for MSM participating in the ACS. This could be due to higher self-perceived risk of chlamydia; one of the most prevalent and well-known STIs among heterosexuals.29 Furthermore, we found that increases in chlamydia self-test usage are primarily responsible for the observed overall increases of HIV/STI self-test usage among Amsterdam inhabitants and STI clinic clients. Our data cannot ascertain whether increased availability of chlamydia self-tests led to their increased usage. However, an increase in awareness of chlamydia self-testing is another plausible explanation, especially considering a chlamydia screening imple-mentation programme that was conducted between 2008 and 2010, in which all 16-year old to 29-year-old residents in Amsterdam and other cities were informed about chlamydia and invited to apply for a free self-sampling test kit.30,31 Although the participation rate in this

Chapter 3.4
198
screening programme was low (16%)30,31 and self-sampling tests differ from self-tests, this may have increased general awareness about availability of self-tests and therefore explain the peak of self-test usage seen in 2009 among STI clinic clients.
HIV self-testing may be a valuable (additional) strategy to reach risk groups for testing, as highly accurate self-tests are available and acceptability is high among key groups.1,9,32 Some countries, for example, France, UK and USA have already approved an HIV self-test for sale.1,33,34 The Netherlands has not authorised HIV self-tests for sale, but from 2014 to 2015 HIV self-tests were offered in combination with online counselling in a pilot study targeting MSM and migrants from HIV endemic countries.35 Preliminary results of this pilot study and other studies show that a large proportion of HIV self-test users have never or not recently been tested for HIV.3,16,35 This suggests HIV self-testing programmes can be of additional value to increase testing rates among individuals not reached at regular testing facilities. However, this might only be true for individuals who are aware of their HIV risk. Additional interventions are needed to promote HIV testing among those individuals at risk for an HIV infection who are unaware of their risk.36 Also, it is important when implementing HIV self-testing programmes that highly accurate HIV self-tests and counselling and linkage to care are offered.1,37
For STIs other than HIV, the accuracy of currently available self-tests is less clear. Previous studies have shown that the accuracy of chlamydia self-tests is low and tests have been sold without proper instructions and information.10,12,13 The observed increase in chlamydia self-test usage is concerning. Therefore, it is important to gain insight into the accuracy of currently available STI self-tests. Furthermore, it is important to continue monitoring self-test usage and informing the public about the unknown accuracy and the pros and cons of self-testing.
The strengths of this study are the large sample size and that we were able to assess HIV/STI self-test usage in both the general population and sexual risk groups. However, some limita-tions need to be addressed. First, the results are limited to the population of Amsterdam, an urban population with nearby access to a free-of-cost HIV/STI testing service for HIV/STI risk groups at the Public Health Service and therefore less generalizable to other, for example, more rural settings. Second, individuals participating in health-related research might not be representative of the general population. However, we were able to calculate population-based estimates by applying weighting among the sample of Amsterdam inhabitants (S1) and were able to estimate self-test usage among a multiethnic population in Amsterdam (S2), a group that is often under-represented in health-related research. Third, we were un-able to identify determinants for HIV, chlamydia and syphilis self-test usage separately due to small numbers. Determinants may differ across different STIs, for example, MSM might

199
HIV/STI self-test usage in the Netherlands
3.4
be more likely to use HIV self-tests, whereas women might be more likely to use chlamydia self-tests. Fourth, we only focussed on HIV, chlamydia and syphilis self-tests. Currently, other STI self-tests are available (e.g., gonorrhoea self-test). Although this study gives an indication of the overall self-test usage, future studies should include other self-tests available.
In conclusion, overall HIV/STI self-test usage in Amsterdam, the Netherlands, is relatively low. However, chlamydia and syphilis self-test usage increased over time among the repre-sentative sample of Amsterdam residents and chlamydia self-test usage increased over time among STI clinic clients. Furthermore, a substantial proportion of persons in the general population who had been tested for HIV/STI reported the use of a self-test and we found higher self-test usage among participants of Surinamese or Ghanaian origin. It is important to continue monitoring self-test usage and informing the public about the unknown quality of current self-tests available and regarding pros and cons of self-testing. Also, motives for self-test usage among different ethnic groups should be further explored in future studies. Self-testing programmes can be a valuable additional strategy for public health professionals to address the needs of certain risk groups and increase testing rates and the higher HIV/STI self-test usage among those at higher risk for HIV/STI in the general population sug-gests that self-test programmes might have an appeal to these groups. When implementing such programmes, it is however imperative that high-quality tests are used and alternative counselling (e.g., online) and linkage to care are offered.
acknowledgements
The authors acknowledge all participants of the different studies for their contribution, research teams for data collection and data management, Darshni Jhagroe for helping with the analyses of the study 4, Ronald Geskus for statistical advice, Claire Buswell for editing the final manuscript and the funders for the financial support.
funding
Funding for the present study was received from the Public Health Service of Amsterdam’s (PHSA) Research and Development Fund (project number 07–13).
The population-based cross-sectional Health Monitoring Survey is financially supported and conducted by the PHSA.
The HEalthy Life in an Urban Setting (HELIUS) Study is conducted by the Academic Medical Center (AMC) in Amsterdam and the PHSA. Both organisations provide core support for HELIUS. The HELIUS Study is also funded by the Dutch Heart Foundation (grant number 2010T084), the Netherlands Organisation for Health Research and Development (ZonMw; grant number 200500003) and the European Union (FP-7; grant number 278901).

Chapter 3.4
200
The Amsterdam Cohort Studies (ACS) on HIV infection and AIDS, which is a collaboration between the PHSA, the AMC/the University of Amsterdam, Sanquin Blood Supply Founda-tion, Medical Center Jan van Goyen and the HIV Focus Center of the DC-Clinics, is part of the Netherlands HIV Monitoring Foundation and financially supported by the Center for Infectious Disease Control of the Netherlands National Institute for Public Health and the Environment.
The cross-sectional survey among clients of the PHSA’s sexually transmitted infection out-patient clinic was funded by the Center for Infectious Disease Control of the Netherlands National Institute for Public Health and the Environment’s and the PHSA’s Research and Development Fund.
The funders of the present study had no role in its design, data collection and analysis, deci-sion to publish or preparation of the manuscript.
Conflicts of interest
Maria Prins, Udi Davidovich and Freke R. Zuure have received non-financial support (i.e., HIV self-test kits) from OraSure Technologies, Inc. for another (investigator initiated) study concerning HIV self-testing.

201
HIV/STI self-test usage in the Netherlands
3.4
referenCes
1. World Health Organization (WHO). Guidelines on HIV Self-Testing and Partner notification: Supple-ment to Consolidated Guidelines on HIV Testing Services. Geneva: WHO, 2016.
2. Joint United Nations Programme on HIV/AIDS (UNAIDS), World Health Organization (WHO). a short technical update on self-testing for HIV. Geneva: UNAIDS, 2013.
3. Krause J, Subklew-Sehume F, Kenyon C, Colebunders R. acceptability of HIV self-testing: a systematic literature review. BMC Public Health. 2013;13:735. doi:10.1186/1471-2458-13-735.
4. Pant Pai N, Sharma J, Shivkumar S, Pillay S, Vadnais C, Joseph L, et al. supervised and unsuper-vised self-testing for HIV in high- and low-risk populations: a systematic review. PLoS Med. 2013;10(4):e1001414. doi:10.1371/journal.pmed.1001414.
5. Johnson CC, Kennedy C, Fonner V, Siegfried N, Figueroa C, Dalal S, et al. examining the effects of HIV self-testing compared to standard HIV testing services: a systematic review and meta-analysis. J Int AIDS Soc. 2017;20(1):21594. doi:10.7448/IAS.20.1.21594.
6. Balan IC, Carballo-Dieguez A, Frasca T, Dolezal C, Ibitoye M. the impact of rapid HIV home test use with sexual partners on subsequent sexual behavior among men who have sex with men. AIDS Behav. 2014;18(2):254-262. doi:10.1007/s10461-013-0497-x.
7. Martinez O, Carballo-Dieguez A, Ibitoye M, Frasca T, Brown W, Balan I. anticipated and actual reac-tions to receiving HIV positive results through self-testing among gay and bisexual men. AIDS Behav. 2014;18(12):2485-2495.
8. Figueroa C, Johnson C, Verster A, Baggaley R. attitudes and acceptability on HIV Self-testing among Key Populations: a literature review. AIDS Behav. 2015;19(11):1949-1965. doi:10.1007/s10461-015-1097-8.
9. Stevens DR, Vrana CJ, Dlin RE, Korte JE. a Global review of HIV Self-testing: Themes and Implications. AIDS Behav. 2017 doi:10.1007/s10461-017-1707-8.
10. Pars L, van Bergen J. Soa-testen, zelf doen of laten (doen)? [dutch]. Amsterdam: SOA AIDS Nederland, 2013.
11. Lunny C, Taylor D, Hoang L, Wong T, Gilbert M, Lester R, et al. self-Collected versus Clinician-Collected Sampling for Chlamydia and Gonorrhea Screening: a Systemic review and Meta-analysis. PLoS One. 2015;10(7):e0132776. doi:10.1371/journal.pone.0132776.
12. van Dommelen L, van Tiel FH, Ouburg S, Brouwers EE, Terporten PH, Savelkoul PH, et al. alarmingly poor performance in Chlamydia trachomatis point-of-care testing. Sex Transm Infect. 2010;86(5):355-359. doi:10.1136/sti.2010.042598.
13. Owens SL, Arora N, Quinn N, Peeling RW, Holmes KK, Gaydos CA. utilising the internet to test for sexually transmitted infections: results of a survey and accuracy testing. Sex Transm Infect. 2010;86(2):112-116. doi:10.1136/sti.2009.037226.
14. Napierala Mavedzenge S, Baggaley R, Corbett EL. a review of self-testing for HIV: research and policy priorities in a new era of HIV prevention. Clin Infect Dis. 2013;57(1):126-138. doi:10.1093/cid/cit156.
15. Bustamante MJ, Konda KA, Joseph DD, Leon SR, Calvo GM, Salvatierra J, et al. HIV self-testing in Peru: questionable availability, high acceptability but potential low linkage to care among men who have sex with men and transgender women. Int J STD AIDS. 2016 doi:10.1177/0956462416630674.
16. Greacen T, Friboulet D, Fugon L, Hefez S, Lorente N, Spire B. access to and use of unauthorised online HIV self-tests by internet-using French-speaking men who have sex with men. Sex Transm Infect. 2012;88(5):368-374. doi:10.1136/sextrans-2011-050405.

Chapter 3.4
202
17. Belza MJ, Figueroa C, Rosales-Statkus ME, Ruiz M, Vallejo F, de la Fuente L, et al. low knowledge and anecdotal use of unauthorized online HIV self-test kits among attendees at a street-based HIV rapid testing programme in Spain. Int J Infect Dis. 2014;25:196-200. doi:10.1016/j.ijid.2014.03.1379.
18. Ronda G, Portegijs P, Dinant GJ, Buntinx F, Norg R, van der Weijden T. use of diagnostic self-tests on body materials among Internet users in the netherlands: prevalence and correlates of use. BMC Public Health. 2009;9:100. doi:10.1186/1471-2458-9-100.
19. Han L, Bien CH, Wei C, Muessig KE, Yang M, Liu F, et al. HIV self-testing among online MSM in China: implications for expanding HIV testing among key populations. J Acquir Immune Defic Syndr. 2014;67(2):216-221. doi:10.1097/QAI.0000000000000278.
20. Geneeskundige en Gezondheidsdienst (GGD) Amsterdam. amsterdammers gezond en wel? amster-damse Gezondheidsmonitor 2012 [dutch]. Amsterdam: GGD Amsterdam, 2013.
21. Dijkshoorn H, van Dijk TK, Janssen AP. Zo gezond is amsterdam! eindrapport amsterdamse Gezond-heidsmonitor 2008 [dutch]. Amsterdam: GGD Amsterdam, 2009.
22. Stronks K, Snijder MB, Peters RJ, Prins M, Schene AH, Zwinderman AH. unravelling the impact of ethnicity on health in europe: the HelIuS study. BMC Public Health. 2013;13:402. doi:10.1186/1471-2458-13-402.
23. van Griensven GJ, de Vroome EM, Goudsmit J, Coutinho RA. Changes in sexual behaviour and the fall in incidence of HIV infection among homosexual men. BMJ. 1989;298(6668):218-221. doi: 10.1136/bmj.298.6668.218.
24. Matser A, Prins M. The amsterdam Cohort Studies on HIV infection: annual report 2015. In: Van Sighem AI, Boender TS, Wit FWNM, Smit C, Matser A, Reiss P, eds. Human Immunodeficiency Virus (HIV) Infection in the Netherlands: HIV Monitoring Report 2016. Amsterdam: Stichting HIV monitor-ing, 2016.
25. van den Hoek JA, Fennema JS, van Haastrecht HJ, van Doornum GJ, Henquet CJ, Coutinho RA. HIV-prevalentie bij bezoekers van een polikliniek voor seksueel overdraagbare aandoeningen en bij een groep prostituées en prostituanten [dutch]. Ned Tijdschr Geneeskd. 1992;136(37):1813-1818.
26. Urbanus AT, Van De Laar TJ, Geskus R, Vanhommerig JW, Van Rooijen MS, Schinkel J, et al. trends in hepatitis C virus infections among MSM attending a sexually transmitted infection clinic; 1995-2010. AIDS. 2014;28(5):781-790. doi:10.1097/QAD.0000000000000126.
27. Statistics Netherlands. definitions: People with a foreign background. Available at: http://www.cbs.nl/en-GB/menu/themas/dossiers/allochtonen/methoden/begrippen/default.htm?Languageswitch=on&ConceptID=315 (accessed on 5 November 2015).
28. Brown LD, Cai TT, DasGupta A. Interval estimation for a binomial proportion. Statistical Science. 2001;16(2):101-117.
29. van den Broek IVF, van Aar F, van Oeffelen AAM, Op de Coul ELM, Woestenberg PJ, Heijne JCM, et al. Sexually transmitted infections in the netherlands in 2015. Bilthoven: National Institute for Public Health and the Environment, 2016.
30. van Bergen JE, Fennema JS, van den Broek IV, Brouwers EE, de Feijter EM, Hoebe CJ, et al. ratio-nale, design, and results of the first screening round of a comprehensive, register-based, Chla-mydia screening implementation programme in the netherlands. BMC Infect Dis. 2010;10:293. doi:10.1186/1471-2334-10-293.
31. van den Broek IV, Hoebe CJ, van Bergen JE, Brouwers EE, de Feijter EM, Fennema JS, et al. evalua-tion design of a systematic, selective, internet-based, Chlamydia screening implementation in the netherlands, 2008-2010: implications of first results for the analysis. BMC Infect Dis. 2010;10:89. doi:10.1186/1471-2334-10-89.

203
HIV/STI self-test usage in the Netherlands
3.4
32. Flowers P, Riddell J, Park C, Ahmed B, Young I, Frankis J, et al. Preparedness for use of the rapid result HIV self-test by gay men and other men who have sex with men (MSM): a mixed methods explor-atory study among MSM and those involved in HIV prevention and care. HIV Med. 2017;18(4):245-255. doi:10.1111/hiv.12420.
33. The Guardian. HIV self-testing kit goes on sale in uK. Available at: http://www.theguardian.com/society/2015/apr/27/hiv-self-testing-kit-on-sale-uk-biosure (accessed on 1 November 2016).
34. U.S.Food and Drug Administration (FDA). oraQuick® In-Home HIV Test: Summary of Safety and effec-tiveness. Available at: http://www.fda.gov/downloads/BiologicsBloodVaccines/BloodBloodProducts/ApprovedProducts /PremarketApprovalsPMAs/UCM312534.pdf (accessed on 25 February 2015).
35. Zuure FR, van der Helm J, van Bergen JEAM, Coutinho RA, Geerlings SE, Götz HM, et al. Home testing for HIV succeeds in reaching first-time and infrequent testers in the netherlands: results of the HIVTest@Home trial [abstract]. The international AIDS conference: Durban, South Africa, 18-22 July 2016.
36. Flowers P, Estcourt C, Sonnenberg P, Burns F. HIV testing intervention development among men who have sex with men in the developed world. Sex Health. 2017 doi:10.1071/SH16081.
37. Greacen T, Kersaudy-Rahib D, Le Gall JM, Lydie N, Ghosn J, Champenois K. Comparing the Information and Support needs of different Population Groups in Preparation for 2015 Government approval for HIV Self-testing in France. PLoS One. 2016;11(3):e0152567. doi:10.1371/journal.pone.0152567.


Chapter 3.5usage of purchased self-tests for HIV
infections among migrants living in the uK, France and the netherlands:
A cross-sectional study
Janneke P. Bil, Maria Prins, Ibidun Fakoya, Alain Volny-Anne, Fiona Burns, Freke R. Zuure
Published in Sexually Transmitted Infections, 2018

Chapter 3.5
206
aBstraCt
objectives
Self-tests are performed and interpreted autonomously by a person without involving a healthcare professional or a certified laboratory. To gain insight into the usage of purchased HIV self-tests (HIVST) among migrants living in high-income countries, we studied the preva-lence and determinants of HIVST usage among migrants living in the UK, France and the Netherlands.
methods
We used web-based questionnaire data collected between April 2014 and July 2015 among migrants living in the UK, France and the Netherlands who participated in the cross-sectional community survey of the aMASE (advancing Migrant Access to health Services in Europe) study. HIVST usage in the preceding 12 months and the corresponding 95% CIs were cal-culated. Using univariate logistic regression analyses, determinants of HIVST usage were evaluated.
results
Among 477 migrants living in the UK (n=235), France (n=98) and the Netherlands (n=144) HIVST usage in the preceding 12 months was 1.89% (9/477, 95% CI 0.66% to 3.11%). As all nine HIVST users were men who have sex with men (MSM), we restricted our univariate analyses to MSM (n=240). HIVST usage was borderline significantly lower among MSM living in France and the Netherlands compared with those living in the UK (UK: reference; France: OR 0.20, 95% CI 0.03 to 1.14; the Netherlands: OR 0.06, 95% CI 0.00 to 1.05). Age, region of birth, educational level, registration at a general practitioner, recent number of male sexual partners and hard drug use were not associated with HIVST usage among MSM.
Conclusions
HIVST usage among migrants from the UK, France and the Netherlands was relatively low between 2014 and 2015 but higher among migrant MSM. To increase HIV testing rates among migrants, programmes need to be developed to promote HIVST among this group. Also, as more countries approve usage of HIVST, systems need to be established to ensure linkage to confirmatory testing and care following a positive test.

207
HIV self-test usage among migrants
3.5
InTroduCTIon
Self-tests are tests that can be performed and interpreted autonomously by laypersons without involving healthcare professionals or certified laboratories.1 The WHO currently recommends the usage of self-tests for HIV infections (HIVST) as an additional approach to HIV testing services, as it could increase HIV testing rates.1,2 However, ensuring linkage to confirmatory testing and specialist care for those with a positive HIVST result remains a concern.
Within Europe, migrants represent a significant group in the HIV epidemic, and migrants are more likely to be undiagnosed or diagnosed late compared with non-migrants.3 HIVST may help overcome the barriers migrants encounter in accessing traditional testing services and therefore increase HIV testing rates among this group.1,4
To gain more insight into the recent usage of purchased HIVST by migrants living in Europe, we studied its prevalence and determinants among migrants living in the UK, France and the Netherlands. Furthermore, we studied the HIVST positivity rate and the extent to which users attend professional healthcare providers for confirmation testing to gain insight into linkage to care among HIVST users.
MeTHodS
We included participants of the web-based community survey of the aMASE (advancing Migrant Access to health Services in Europe) study. Detailed information on the aMASE study is provided elsewhere.5,6 Briefly, the cross-sectional aMASE community survey aimed to identify the structural, cultural and financial barriers to HIV prevention, diagnosis and treatment in migrant populations. The community survey was promoted between April 2014 and July 2015 via social marketing and community participatory methods in nine coun-tries (Belgium, France, Germany, Greece, Italy, the Netherlands, Portugal, Spain and the UK), although migrants aged 18 or older living in all countries of the WHO European area were eligible. Migrants were defined as foreign-born individuals intending to live in their current country of residence for ≥6 months. Participants completed a questionnaire (available in 14 languages) which included (1) detailed socio-demographic data and extensive migration history data, (2) sexual and HIV risk behaviour, (3) use of health services and (4) experiences of living with HIV, including stigma and discrimination. HIVST questions were only included in the survey of people who reported living in the UK, France and the Netherlands. Hence, our study only includes aMASE participants living in the UK, France and the Netherlands. Ques-tions addressed HIVST usage in the preceding 12 months, the HIVST result, whether persons

Chapter 3.5
208
went to a professional healthcare provider for confirmatory testing and the confirmation test results. HIV-positive participants diagnosed more than one year prior to survey completion were excluded, as were participants who did not answer the question regarding HIVST use.
Participant characteristics (age, sexual orientation, educational level, country of residence, years since migration and region of birth) and the percentage and corresponding 95% CIs of HIVST usage were calculated. Among HIVST users, HIVST results and follow-up testing behav-iour were described. To evaluate determinants of HIVST usage, we calculated ORs and 95% CI by a univariate logistic regression model adapted for rare events and fit using penalized maximum likelihood estimation. Potential determinants include country of residence, age (<27 years, 27–35 years, >35 years), region of birth (developing/developed region based on the United Nations classification), educational level (lower secondary level, upper secondary level or higher), registration at a general practitioner (no, yes), number of sexual partners in the preceding 12 months (0–5, 6–20, >21) and hard drug use in the preceding five years (no, yes). A p value <0.05 was considered statistically significant. Analyses were performed using STATA Intercooled V.13.1.
reSulTS
In total, 552 migrants participated in the aMASE community survey in the UK (n=265), France (n=126) and the Netherlands (n=161). Of these, 70 HIV-positive participants were diagnosed more than one year before survey completion and five participants with missing HIVST usage data were excluded from the analyses. Of the 477 included participants, the median age was 34 (IQR 27–43) years, 91% (n=435) had finished at least upper secondary educational level, and 36% (n=171) were women, 13% (n=64) were heterosexual men, 50% (n=240) were men having sex with men (MSM) and 0.42% (n=2) transgender people. The median year since migration was 7 (IQR 3–13), and 50% (n=236) were born in another European country, 21% (n=102) in Latin America/Caribbean, 14% (n=67) in Africa, 7% (n=33) in Asia and 8% (n=39) in the rest of the world.
HIVST usage in the preceding 12 months was 1.89% (9/477, 95% CI 0.66%–3.11%). Eight HIVST users reported their HIVST result was negative and one reported a failed/indeter-minate result. Of those with a negative HIVST result, four (50%) went to a professional healthcare provider for confirmation testing, and all confirmation HIV tests were negative. Participants whose test failed or was indeterminate did not seek confirmation testing.
All nine HIVST users were MSM, corresponding to an HIVST usage of 3.75% (9/240, 95% CI 1.33%–6.17%) among MSM. Of all HIVST users, five went to a sexual health clinic or HIV

209
HIV self-test usage among migrants
3.5
testing clinic for their last HIV test, while one went to a private clinic, and three used a self-test for their last HIV test. As these HIVST users were all MSM, we included only MSM in our univariate analyses (Table 1). HIVST usage was borderline significantly lower among MSM living in France and the Netherlands compared with those living in the UK (UK: reference; France: OR 0.20, 95% CI 0.03–1.14; the Netherlands: OR 0.06, 95% CI 0.00–1.05). No other variables were significantly associated with HIVST usage among MSM.
Table 1. Potential determinants of HIV self-test usage among 240 migrant MSM living in the UK, France and the Netherlands, 2014–2015
HIVST users/ total population(n/N)
HIVst usage(%) or 95% CI p-value
Current country of residence
UK 8/88 9.09 1 0.042
France 1/73 1.37 0.20 0.03–1.14
The Netherlands 0/79 0.00 0.06 0.00–1.05
age (years)
<27 1/70 1.43 1 0.394
27–35 3/89 3.37 1.87 0.27–13.03
>35 5/81 6.17 3.33 0.53–20.86
region of birth
Developing regions 1/108 0.93 1 0.076
Developed regions 8/132 6.06 4.89 0.85–28.29
educational level
Upper secondary or higher 9/221 4.07 1 0.705
Lower secondary or lower 0/19 0.00 0.57 0.03–10.23
registered at a general practitioner
No 1/59 1.69 1 0.471
Yes 8/181 4.42 1.91 0.33–11.12
number of male sexual partners in the preceding 12 months
0–5 2/72 2.78 1 0.939
6–20 4/99 4.04 1.33 0.27–6.43
>21 2/61 3.28 1.18 0.19–7.07
Missing 1/8 0.13
Hard drug use in the preceding 5 years
No 3/129 2.33 1 0.231
Yes 6/110 5.45 2.25 0.60–8.46
Missing 0/1 0.00
HIVST, HIV self-test; MSM, men who have sex with men.

Chapter 3.5
210
dISCuSSIon
This study shows that the overall HIVST usage in the preceding 12 months among migrants living in the UK, France and the Netherlands is low (2%), but higher among MSM (4%). Among MSM, HIVST usage was higher in those living in the UK compared with those living in France and the Netherlands.
The low overall HIVST usage is in line with findings from previous European studies conducted among French MSM (2009),7 Spanish attendees of a street-based HIV testing programme (2010–2012)8 and a Dutch study among the general population and sexual risk groups (2007–2015).9 However, a Chinese study showed that 20% of Chinese MSM reported prior HIVST usage.10 The differences between the HIVST usage prevalence between Europe and China might be explained by Europe’s legal restrictions on selling HIVST, whereas China has a national policy supporting HIVST. In Europe, only the UK and France have recently approved HIVST for sale (UK: April 2015; France: September 2015).11 Although UK approval of HIVST took place during recruitment for this study, five out of eight UK self-test users participated in this study prior to the HIVST approval. Hence the approval may only partially explain the lower number of HIVST users in France and the Netherlands compared with the UK. Data from the UK showed that in the first 9 months after HIVST approval, approximately 25,000 tests were sold, indicating that usage is likely to increase as more countries approve HIVST usage and the tests become more easily available.12 It is therefore important to remove legislative barriers to and promote HIVST access and establish systems to provide linkage of users to confirmatory testing and care following a positive test.
In our study, HIVST usage was reported only by migrant MSM, not by heterosexual migrants. To successfully implement HIVST as an additional approach to increase HIV testing rates among migrants, HIVST awareness and potential motives and barriers to usage should be further explored especially among heterosexual migrants.
Our results further show that most HIVST users had a negative self-test result, and 50% went for confirmation testing. When questioned about the location of their last HIV test, the majority of self-test users reported a professional sexual health clinic or HIV testing clinic. These results suggest that some HIVST users might not experience barriers in accessing regular HIV healthcare services but rather use HIVST alongside regular services. A previous qualitative study among UK MSM also described self-testing as an opportunity to ‘top-up’ between other tests.13
Regarding study strengths, we were able to assess HIVST usage among a diverse sample of heterosexual and MSM migrants living in three European countries. Limitations include

211
HIV self-test usage among migrants
3.5
the representativeness of our study population. Since we used convenience sampling and a web-based questionnaire which generally attracts persons with higher (digital) literacy, our population is unlikely to represent the whole migrant population in the UK, France and the Netherlands. Also, due to the small number of HIVST users, we had low statistical power to assess determinants of HIVST usage.
In conclusion, HIVST usage among migrants from the UK, France and the Netherlands par-ticipating in an HIV community survey was relatively low between 2014 and 2015, but higher among migrant MSM. As HIVST has the potential to increase testing rates and decrease late diagnoses, programmes should be developed to promote and facilitate HIVST among mi-grants, especially among heterosexual migrants. To evaluate such programmes, HIVST usage should be closely monitored. In addition, as more countries approve HIVST, systems should be established to ensure linkage to confirmatory testing and care following a positive test.
acknowledgements
The authors acknowledge all participants of the aMASE study for their contribution; Emilia Ric-Doe for her help with the recruitment of participants in the Netherlands, Lucy Philips for editing the final manuscript and the funders for the financial support.
This study would not be possible without the entire Work Package 14 collaboration. The aMASE study team includes: Aerssens A, Aguado M, Alimi B, Álvarez D, Anagnostou O, ander-son J, Antoniadou A, Arando M, Barberà MJ, Barros H, Barthélemy A, Belda-Ibáñez J, Bertisch B, Bil J, Blanco JR, Block K, Boesecke C, Boura M, Burgos J, Burns FM, Cabo J, Calabuig E, Campbell L, Cardoso O, Claudia W, Clumeck N, Colucci A, Corrao S, Cuellar S, Cunha J, Daikos G, Darling K, del Amo J, del Romero J, Dellot P, Dixneuf M, Domingo P, Dronda F, Ebeling F, Engelhardt A, Engler B, Fakoya I, Farrell J, Fehr J, Feijó M, Fernández E, Fernández García E, Fernandez T, Fortes AL, Fox J, Garcia de Olalla P, García F, Gargalianos-Kakolyris P, Gennotte AF, Germano I, Gilleran G, Gilson R, Goepel S, Gogos HA, Gómez Sirvent JL, Gountas I, Gregg A, Gutiérrez F, Gutierrez MM, Hermans I, Iribarren JA, Knobel H, Koulai L, Kourkounti S, La Morté C, LeCompte T, Ledergerber B, Leonidou L, Ligero MC, Lindergard G, Lino S, Lopes MJ, Lopez Lirola A, Louhenapessy M, Lourida G, Luzi AM, Maltez F, Manirankunda L, Martín-Pérez A, Martins L, Masía M, Mateu MG, Meireles P, Mendes A, Metallidis S, Mguni S, Milinkovic A, Miró JM, Mohrmann K, Monge S, Montero M, Mouhebati T, Moutschen M, Müller M, Murphy C, Nöstlinger C, Ocaña I, Okumu-Fransche S, Onwuchekwa G, Ospina JE, Otiko D, Pacheco P, Palacios R, Paparizos V, Papastamopoulos V, Paredes V, Patel N, Pellicer T, Peña A, Petrosillo N, Pinheiro A, Poças J, Portillo A, Post F, Prestileo F, Prestileo T, Prins M, Prins P, Protopapas K, Psichogiou M, Pulido F, Rebollo J, Ribeirinho A, Río I, Robau M, Rockstroh JK, Rodrigues E, Rodríguez M, Sajani C, Salavert M, Salman R, Sanz N, Schuettfort G, Schüttfort G, Schwarze- Zander C, Serrão R, Silva D, Silva V, Silverio P, Skoutelis A, Staehelin C, Stephan C,

Chapter 3.5
212
Stretton C, Styles F, Sutre AF, Taylor S, Teixeira B, Thierfelder C, Touloumi G, Tsachouridou O, Tudor K, Valadas E, van Frankenhuijsen M, Vázquez M, Velasco Arribas M, Vera M, Vinciana P, Volny-Anne A, Voudouri N, Wasmuth JC, Wengenroth C, Wilkins E, Young L, Yurdakul S, Zafra Espinosa T, Zuilhof W, Zuure F.
funding
The aMASE study is part of Work Package 14 of EuroCoord, which is funded by the EU’s Seventh Framework Programme for research, technological development and demonstra-tion (EuroCoord grant no. 260694). Additional funding for the analyses of the present study was received from the Public Health Service of Amsterdam’s Research and Development Fund (project n0. 12–29).
Conflicts of interest
Maria Prins and Freke Zuure have received non-financial support (i.e., HIVST kits) from OraSure Technologies for another investigator-initiated study concerning HIV self-testing. Fiona Burns has received conference support and consultancy fees from Gilead Sciences Ltd.

213
HIV self-test usage among migrants
3.5
referenCes
1. World Health Organization (WHO). Guidelines on HIV Self-Testing and Partner notification: Supple-ment to Consolidated Guidelines on HIV Testing Services. Geneva: WHO, 2016.
2. Johnson CC, Kennedy C, Fonner V, Siegfried N, Figueroa C, Dalal S, et al. examining the effects of HIV self-testing compared to standard HIV testing services: a systematic review and meta-analysis. J Int AIDS Soc. 2017;20(1):21594. doi:10.7448/IAS.20.1.21594.
3. Hernando V, Alvarez-del Arco D, Alejos B, Monge S, Amato-Gauci AJ, Noori T, et al. HIV Infection in Mi-grant Populations in the european union and european economic area in 2007-2012: an epidemic on the move. J Acquir Immune Defic Syndr. 2015;70(2):204-211. doi:10.1097/QAI.0000000000000717.
4. Alvarez-del Arco D, Monge S, Azcoaga A, Rio I, Hernando V, Gonzalez C, et al. HIV testing and counsel-ling for migrant populations living in high-income countries: a systematic review. Eur J Public Health. 2013;23(6):1039-1045. doi:10.1093/eurpub/cks130.
5. Fakoya I, Alvarez-Del Arco D, Monge S, Copas AJ, Gennotte AF, Volny-Anne A, et al. advancing migrant access to Health Services in europe (aMaSe): Protocol for a Cross-sectional Study. JMIR Res Protoc. 2016;5(2):e74. doi:10.2196/resprot.5085.
6. Fakoya I, Alvarez-Del Arco D, Copas AJ, Teixeira B, Block K, Gennotte AF, et al. Factors associated With access to HIV Testing and Primary Care among Migrants living in europe: Cross-Sectional Survey. JMIR Public Health Surveill. 2017;3(4):e84. doi:10.2196/publichealth.7741.
7. Greacen T, Friboulet D, Fugon L, Hefez S, Lorente N, Spire B. access to and use of unauthorised online HIV self-tests by internet-using French-speaking men who have sex with men. Sex Transm Infect. 2012;88(5):368-374. doi:10.1136/sextrans-2011-050405.
8. Belza MJ, Figueroa C, Rosales-Statkus ME, Ruiz M, Vallejo F, de la Fuente L, et al. low knowledge and anecdotal use of unauthorized online HIV self-test kits among attendees at a street-based HIV rapid testing programme in Spain. Int J Infect Dis. 2014;25:196-200. doi:10.1016/j.ijid.2014.03.1379.
9. Bil JP, Prins M, Stolte IG, Dijkshoorn H, Heijman T, Snijder MB, et al. usage of purchased self-tests for HIV and sexually transmitted infections in amsterdam, the netherlands: results of population-based and serial cross-sectional studies among the general population and sexual risk groups. BMJ Open. 2017;7(9):e016609. doi:10.1136/bmjopen-2017-016609.
10. Han L, Bien CH, Wei C, Muessig KE, Yang M, Liu F, et al. HIV self-testing among online MSM in China: implications for expanding HIV testing among key populations. J Acquir Immune Defic Syndr. 2014;67(2):216-221. doi:10.1097/QAI.0000000000000278.
11. UNITAID. HIV rapid diagnostic tests for self-testing. Vernier: UNITAID, 2016. 12. Brady M, Carpenter G, Bard B. Self-testing for HIV: initial experience of the uK’s first kit [abstract].
22nd Annual Conference of the British HIV Association: Manchester, UK, 19-22 April 2016. 13. Witzel TC, Weatherburn P, Rodger AJ, Bourne AH, Burns FM. risk, reassurance and routine: a qualita-
tive study of narrative understandings of the potential for HIV self-testing among men who have sex with men in england. BMC Public Health. 2017;17(1):491. doi:10.1186/s12889-017-4370-0.


Chapter 4General discussion


217
General discussion
4
The overarching aim of this thesis is to assess the acceptability and use of innovative inter-ventions and explore new opportunities for the prevention of the human immunodeficiency virus (HIV), the hepatitis B virus (HBV), the hepatitis C virus (HCV) and sexually transmitted infections (STIs) among key populations. In chapter 2 of this thesis we focussed on the cur-rent aspects of acceptability, attitudes, beliefs and behavioural intentions towards the use of pre-exposure prophylaxis (PrEP) to prevent HIV infection among men who have sex with men (MSM) and healthcare professionals. In chapter 3 we focussed on testing opportunities for HIV, HBV, HCV and STIs, especially among migrants.
4.1 PreP to PreVent HIV InfeCtIon
4.1.1 Intention and motives to use PreP among MSM
For the implementation of PrEP, it is important to gain an insight into the acceptability and potential uptake of PrEP among MSM, the most important target group with regard to PrEP in the Netherlands and many high-income countries. Our study in chapter 2.1, conducted in 2012-2013, is the first to describe the intention to use PrEP among MSM before any study or project offering PrEP was initiated in the Netherlands. We found that about half of the HIV-negative MSM participating in the Amsterdam Cohort Studies (ACS) on HIV were aware of PrEP but only 13% had the intention to use PrEP on a daily basis. The intention to use PrEP was significantly higher among MSM at a high risk of HIV infection than among those at low risk. More recent data from the same cohort has indicated an increase in the proportion of MSM with a high intention to use PrEP to 30% between 2015 and 2017.1 This trend indicates that PrEP is becoming more widely accepted as an HIV prevention method. Most likely, this is due to (1) an increased PrEP awareness, an assumption supported by the results of a 2018 survey among MSM living with and without HIV in the Netherlands, which showed that 79% MSM were aware of PrEP,2 and (2) new evidence from two landmark PrEP studies, the PROUD study,3 which confirms the efficacy of daily PrEP, and the IPERGAY study,4 which indicates the efficacy of event-driven PrEP.
The shown efficacy of event-driven PrEP, and therefore the added option for a PrEP regimen next to daily PrEP, could also have resulted in an increase in the intention to use PrEP since 17% of the HIV-negative MSM participating in the ACS had a high intention to use PrEP daily and 21% a high intention to use event-driven PrEP between 2015 and 2017.1 Data from the Dutch Amsterdam PrEP (AMPrEP) project and the Belgium PrEP Demonstration Project (Be-PrEP-ared), where participants were offered a choice between a daily or event-driven PrEP regimen, showed that a majority of eligible MSM preferred a daily over event-driven PrEP regimen (73–77% versus 24–27%).5-7 In contrast, in an open-label extension PrEP study in Paris, France, where participants were also offered a choice between daily and event-

Chapter 4
218
driven PrEP, the majority (76%) opted for event-driven PrEP.8 We showed in chapter 2.2 that, among MSM, the perceived motives for preferring event-driven PrEP over daily PrEP were the perceived lower threshold to initiating PrEP, the expected reduction of side effects and the lower costs. The barriers to using event-driven PrEP were the need to plan one’s sex life and the difficulty of switching and adhering to multiple prevention strategies in different situations when using or not using PrEP. These motives and barriers are comparable with the results on motives demonstrated by the Dutch and Belgian demonstration projects.5-7 In conclusion, it is clear that many MSM have a high intention to use PrEP and that offering a choice of two dosing regimens could further personalise HIV prevention, thereby enhancing the uptake and adherence to PrEP. When the national PrEP program is implemented at STI clinics in the Netherlands, which starts in August 2019, it is important to monitor the choice of a PrEP regimen and actual PrEP use since this will have an impact of the cost-effectiveness of the programme.9
For the development of PrEP programmes, it is helpful to understand the motives for want-ing or not wanting to use PrEP. Prior to our study in chapter 2.2 no such data was available in the Netherlands. Our results in chapter 2.2 indicating the motives by HIV-negative MSM for wanting to use daily PrEP in the future were based on beliefs about PrEP efficacy to prevent HIV, expectations of a high self-efficacy of PrEP adherence and beliefs about pos-sible benefits (e.g., anxiety reduction, sex-life improvement). Motives for not wanting to use PrEP were based on beliefs about PrEP having insufficient efficacy to prevent HIV infection, non-belief in current research and data, a low self-perceived HIV risk, a preferences for other prevention strategies, such as condoms and treatment as prevention (TasP), the anticipated side effects or antiretroviral (ART) resistance, concern about being able to adhere to the PrEP regime, perceived barriers to accessing PrEP services (e.g., costs, monitoring procedures) and a principle objection to PrEP use. In chapter 2.1 we also found that feelings of shame about the use of PrEP were a barrier for future use. Several modelling studies have shown that the public health impact of PrEP also depends, apart from adherence, the frequency of monitoring and the duration of PrEP use, on the uptake of PrEP amongst those at the highest risk of HIV infection.10,11
According to psychosocial health behaviour theories, such as the Health Belief Model,12 the intention to use PrEP can be enhanced by lowering the perceived barriers and increasing the perceived benefits and the self-efficacy of adhering to the PrEP regime. In the Health Belief Model these elements are balanced against the perceived susceptibility to and the severity of the disease. In addition, cues to action (e.g., information about PrEP from others, the media or healthcare providers) can trigger actual PrEP uptake. The results of our studies reported in chapters 2.1 and 2.2 show that before and during the implementation of PrEP programmes it is necessary to provide clear information on the efficacy and side-effects

219
General discussion
4
of PrEP, to improve perceptions about the self-efficacy of using PrEP, to address feelings of shame about using PrEP, and to enhance access to PrEP and PrEP services. Perceived self-efficacy can, for example, be improved by assessing individual skills with regard to the use of and adherence to PrEP. The choice of a PrEP regimen can be discussed and specific interventions can be offered based on these skills. Feelings of shame about using PrEP and its stigma can, for example, be reduced by implementing specific campaigns. Access to PrEP and PrEP services are discussed further in section 4.1.2.
4.1.2 access to PreP and PreP service delivery
Despite the growing intention to use PrEP indicated by the ACS, only a small fraction of MSM (7%) was actually using PrEP in 2017.1 The results of a survey among MSM in the Netherlands conducted in 2018 indicated that of those aware of PrEP, 5% were currently using PrEP.2 The low PrEP use is most likely due to the fact that PrEP had not yet been imple-mented in the Netherlands and that PrEP was only available trough the participation in study settings with limited capacity. More recently it has been prescribed by a limited number of general practitioners (GPs), STI and HIV clinics. It is expected that the implementation of the national PrEP programme will lead to a large increase in PrEP users. However, the ACS also showed that the proportion of MSM with a high intention to use PrEP among those potentially eligible for PrEP (based on national guidelines) was still only 51%.1 This indicates that a large proportion of the men who might benefit from PrEP might still not use PrEP when the national PrEP programme is in operation. It is thus very important to monitor whether the groups at high risk to HIV infection are reached by the national PrEP programme and to engage in promotional activities to increase awareness and remove barriers to the use of PrEP, if necessary. Data from the United States (US), the first nation where PrEP was approved in 2012, have indicated a disproportionate low PrEP uptake and PrEP awareness among Afro-American MSM.13-15 Groups that might be less involved in PrEP programmes in the Netherlands are migrants, young MSM and transgender people.6,16 Exploring their specific motives and preferences for PrEP use and services could help to develop interven-tions specifically targeting PrEP uptake in these groups.
The data in chapters 2.1 and 2.2 suggest that the anticipated costs of PrEP was a major bar-rier for the uptake of PrEP among MSM prior to 2017. When generic PrEP became available in the Netherlands in 2017 this significantly reduced the price of PrEP from €580.00 to ap-proximately €25.00 for a month’s supply if taken daily.17 Implementation of the national PrEP programme in 2019 for those persons at high risk of HIV infection (i.e., high-risk MSM) will further reduce the costs of PrEP since PrEP will be made available at significantly lower costs to the participants of the program.18 This large cost reduction should improve the uptake of PrEP. In addition, the availability of cheaper, generic PrEP will have a positive effect on its costs-effectiveness.9-11,19-22

Chapter 4
220
When PrEP is implemented nationwide, it is important that PrEP services are easily acces-sible and are equipped to provide adequate PrEP support. The results in chapter 2.2 indicate that MSM prefer the public health service (i.e., a STI clinic), a GP, and a hospital (i.e., an HIV-specialist) as PrEP service locations. It is also shown that potential users of PrEP prefer PrEP service locations to have specialised knowledge of HIV, antiretroviral therapy (ART), sexual behaviour, STIs and a patient’s medical background; to be easily approachable; and to be able to perform PrEP follow-up monitoring and provide support. The implementation of the national PrEP programme, which will take place at STI clinics, will increase access to PrEP care. STI clinics already have specialised knowledge of HIV, sexual behaviour, STIs and are able to provide care for potential future PrEP users (i.e., HIV-negative MSM). The prescription of PrEP through GPs and HIV specialists will not be imbedded in the PrEP pro-gramme, although some GPs and HIV specialist already prescribe PrEP and could continue to do so. Possibly, some people will still need to be referred to their GP for PrEP care as there will be a restriction on the total number of people who can be enrolled in the national programme. Also, some people might prefer a GP over a STI clinic for PrEP care, although in this case a barrier for potential users of PrEP care may be cost since they will have to pay the full amount of PrEP costs and for (some of the) costs of medical follow-up and counselling. The restriction on the number of people who can be enrolled in the national programme might also lead a continuation of unsupervised PrEP use without monitoring by a healthcare professional.
Since we also found that frequent monitoring procedures (chapter 2.2) are a barrier to PrEP usage, alternative PrEP service delivery options or a reduced PrEP monitoring frequency could be explored to lower the barrier, as well as the anticipated increased workload at ST clinics when the national programme is rolled out. Reduced PrEP monitoring might be an option for event-driven PrEP users as it has been shown that they engage in lower-risk behaviour than daily PrEP users.5,6,8 Risk behaviour and PrEP use of PrEP users may vary over time and the PrEP monitoring frequency could be altered accordingly. The Public Health Service of Amsterdam is currently embarking on a study in which PrEP is offered online (EZI-PrEP) to provide a low-threshold alternative to a standard in-clinic PrEP service. Within this study a randomised controlled trial will examine a reduced intensity monitoring schedule (six-monthly versus three-monthly).
4.1.3 risk compensation
The results discussed in chapter 2.2 show that some MSM perceive PrEP as a condom substi-tute, while others are likely to combine PrEP and condoms for the prevention of HIV and STIs. In chapter 2.1 about one-third of the participants stated that they would decrease condom use while using PrEP. This proportion was higher among those with higher intentions to use PrEP and those currently engaging in condomless anal sex when compared to their coun-

221
General discussion
4
terparts. Studies regarding risk compensation after starting PrEP vary in their results. The findings of several open-label PrEP trials and observational PrEP studies suggest an increase of STIs after PrEP use and a decline in condom use for anal sex, especially among MSM already using condoms inconsistently.23 An open-label PrEP study in Australia also found that STIs had increased.24 However, the results of the first two years of the AMPrEP project indicated that the number of condomless anal sex acts with casual partners increased, whereas the number of partners, the number sex acts and the incidence of STIs remained stable.25 In addition, the baseline data from the AMPrEP project shows a relatively high HCV prevalence among MSM who start PrEP.26 This might be the result of an increasing overlap between the sexual networks of HIV-positive and HIV-negative MSM. It should be noted that the interpretation of studies on risk compensation after PrEP initiation is difficult because often no data on STIs before PrEP initiation is available and the incidence of STIs and the fact that condomless sex was already increasing over time before PrEP implementation.27 Furthermore, the observed increase in STIs could also reflect the increased STI testing during follow-up monitoring of PrEP users. Results of the systematic review of risk compensation also indicated a bigger increase in STI diagnosis in more recent studies and in studies with longer follow-up times.23 This suggests that condom use could decrease over time because of growing trust in the efficacy of PrEP in the prevention of HIV infection. For this reason, the long-term monitoring of STI incidence and condom use is required. It is also important to offer PrEP in combination with counselling on condom use as an STI reduction strategy, other risk reduction strategies and regular STI testing (including the testing for HCV). Knowledge of STIs and their potential risk, as well as ways to avoid this should continue to be discussed.
4.1.4 acceptability of PreP among healthcare providers
It is important to know and understand the attitudes towards PrEP among healthcare pro-viders as it could influence the implementation and uptake of PrEP. Healthcare professionals can initiate discussions on and provide evidence-based information about PrEP so that well-informed decisions can be made about PrEP initiation by those at high risk of HIV infection. Because no data was yet available in the Netherlands, we explored the acceptability of PrEP among professionals working at STI clinics (STI professionals) and at HIV treatment centres (HIV specialists) (chapter 2.3). Our results showed that in 2015, the acceptability of PrEP among these groups was only moderate, while knowledge about PrEP among STI profes-sionals was suboptimal. Facilitating factors toward implementation were the belief that PrEP was an effective intervention to prevent HIV infection, PrEP prescription was part of routine care at STI clinics, PrEP was a good addition to prevention strategies, and that any possible negative impact of PrEP was still preferable to the impact of contracting HIV. Barriers to PrEP implementation were a perceived potential decrease in condom use and an increase in STIs, the high costs of PrEP and the belief that it is unethical to prescribe ART to healthy individuals.

Chapter 4
222
To increase the acceptability of PrEP implementation among healthcare professionals in the Netherlands, their beliefs that may form barriers to PrEP implementation need to be addressed and motives that could facilitate PrEP implementation need to be more broadly communicated. As indicated in chapter 2.3, it is especially important to improve knowledge about PrEP among STI professionals since their PrEP knowledge was significantly lower compared to that of HIV specialists. This situation is often referred to in the literature as the “purview paradox”, where providers who are best trained to provide PrEP (i.e., HIV specialist) often do not see HIV-negative people who would benefit from PrEP, while STI professionals and GPs who regularly care for HIV-negative patients are often not trained to provide PrEP.28
Also, as one of the main barriers among professionals regarding PrEP implementation was the concern about risk compensation (chapter 2.3), it is imperative that healthcare profes-sionals are adequately trained in counselling and provided with the tools and skills to discuss condom use and the prevention of STIs among PrEP users. It is also important that the train-ing of healthcare professionals should include the ability to discuss substance use, including chemsex, sexual compulsivity and mental health issues, since data from PrEP studies shows that a high proportion of PrEP users are experiencing problems in this regard.3,4,6 It is likely that PrEP knowledge and acceptability have already increased among STI professionals since 2015 as more data on PrEP efficacy, the cost-effectiveness of PrEP and PrEP implementation in the Netherlands has become available. In addition, a growing number of professionals at STI clinics have been trained to provide PrEP, some as part of the We Are PrEPared initiative, which was initiated in 2017 with the aim of creating the infrastructure for PrEP implementa-tion in the Netherlands, train professionals and inform key populations about PrEP.29 In a unpublished survey conducted in 2018 among STI clinic nurses in Amsterdam we indeed found a significant increase in the acceptability of PrEP compared to 2015.30 However, it is important that other professionals are informed and trained with regard to PrEP and those already trained are updated about new PrEP results.
In this thesis we did not explore the attitudes of GPs towards PrEP in the Netherlands. Data from a Dutch study from 2016 showed that although PrEP knowledge was still low among GPs, most of them were relatively positive about PrEP implementation and would discuss PrEP with their patients.31 Like STI professionals and HIV specialists, GPs were nevertheless still concerned about PrEP adherence and risk compensation. As GPs are typically the first point of access to healthcare in the Netherlands, including sexual health care, they are cru-cial agents with regard to identifying eligible candidates for PrEP and initiating discussions about PrEP. It is therefore important that GPs are well-informed about PrEP treatment and monitoring, and trained in discussing PrEP initiation and use with their patients. Besides monitoring PrEP implementation at STI clinics (which is part of the national programme), the close monitoring of PrEP implementation in GP practices is vital.

223
General discussion
4
4.1.5 Conclusion
To implement PrEP in the Netherlands successfully, it is important to address barriers to PrEP use among those at high risk of HIV infection by providing adequate information as regards to PrEP efficacy and side-effects, to improve the perceived self-efficacy of using PrEP, to prevent PrEP-related stigma, and to ensure adequate access to PrEP and PrEP services. Since healthcare providers will play a critical role in the implementation of PrEP, it is vital to improve acceptability of PrEP among healthcare professionals by reducing gaps in their PrEP knowledge and providing them training regarding PrEP. For those who decide to use PrEP, healthcare providers should provide high-quality, evidence-based PrEP counselling and care that includes medical follow-up, regular STI testing and the discussion of topics such as adherence to PrEP, concurrent condom use and other (STI) prevention strategies. For those not using PrEP, either because they are not eligible or do not want to use PrEP, the standard prevention strategies such as condom use should remain a viable, normative and socially accepted option and should be facilitated by health providers.
Future research should focus on long-term PrEP uptake, especially among difficult-to-serve groups, risk compensation and adherence to PrEP, as well as the psychosocial influence of PrEP (e.g., sexual well-being and stigma-related experiences with regard to PrEP). Finally, to ensure adequate access, also to difficult-to-serve groups, innovative PrEP service delivery options and reduced PrEP monitoring should be explored.
4.2 TeSTInG oPPorTunITIeS For HIV, HBV, HCV and STIs
4.2.1 Barriers to testing among migrants
Migrants living in Europe and other high-income countries face specific barriers to HIV, HBV and HCV testing, and sexual health-seeking behaviour at the structural, healthcare provider, individual and community level, as outlined in chapter 1.2.3. Concerning access to HIV testing and the use of HIV-related health services, the extent to which barriers differ between migrants and non-migrants by sexual orientation is not well known. In chapter 3.1 we therefore examined the differences in the use of HIV-related health services between migrant and non-migrants, stratified by sexual orientation. The inclusion of non-migrants differed from previous studies to be able to compare access to care between migrants and non-migrants.32,33 We showed that disparities in access to and the use of HIV-related health services and experiences exist between migrants and non-migrants, with sexual orientation being a factor. Our data suggest that heterosexual men and women may particularly benefit from improved access to HIV testing (e.g., through provider-initiated testing). Migrant MSM may benefit from improved access to HIV prevention interventions (e.g., PrEP) as our data in chapter 3.1 showed that most (96%) migrant MSM recently diagnosed with HIV had tested

Chapter 4
224
negatively before diagnosis but might be less aware of HIV prevention measures than non-migrant MSM. Our results also indicate that monitoring the cascade of care and progress to the UNAIDS 90-90-90 targets (see chapter 1.1.4) by subgroups (e.g., migrants status in combination with sexual orientation) might assist to determine on which part of the cascade interventions are needed for specific groups to close gaps.
To increase HIV testing, especially among heterosexual migrants, the removal of barriers to testing is crucial. Several studies describe the interventions needed to overcome such barriers, such as community involvement and collaboration, tailored outreach, healthcare provider endorsement of testing, culturally sensitive communication about testing and counselling, having well-trained and dedicated staff, improving health literacy, and reducing stigma and discrimination.34-44 Our data (chapter 3.1) shows a large proportion (76%) of het-erosexual migrants regularly visits a religious service. These services might thus be a way to establish community involvement. Reducing stigma and discrimination with respect to HIV remains very important since we showed in chapter 3.1 that about a quarter of migrant MSM and migrant women recently diagnosed with HIV had experienced HIV-related discrimina-tion in the Netherlands versus 17% in non-migrant MSM. Previous studies have shown that the stigma of HIV and the resultant discrimination is a major barrier to accessing prevention, care and treatment services, and can negatively impact social relationships, the psychological wellbeing of people living with HIV/AIDS and labour participation.34,45-50 Although stigma and discrimination are very difficult to change, there are approaches that could be successful, such as providing stereotype-inconsistent information in media campaigns and promoting interpersonal contact between stigmatised persons and communities.51
4.2.2 Testing strategies and screening programmes
Several strategies exist for HIV, HBV and HCV testing, depending on the population group tar-geted, the local epidemiology and healthcare infrastructure.52 Testing can, for example, take place through individual case-finding (e.g., opportunistic testing) or screening programmes.
The Dutch Health Council recommend HBV and HCV testing for first-generation migrants originating from countries with an estimated chronic HBV or chronic HCV infection preva-lence of >2%,53 and testing can be best carried out as individual-case finding by GPs. The Dutch Health Council also recommends setting up local or regional HBV screening pro-grammes in cities or regions that have relatively large numbers of first-generation migrants from HBV-endemic countries.
However, the prevalence among migrants in host countries may differ from prevalence in their countries of origin. To inform the development of a local screening programme for mi-grants in Amsterdam, we assessed the prevalence of HBV and HCV among different groups

225
General discussion
4
of first-generation migrants living in Amsterdam (chapter 3.2). Our results show chronic HBV prevalence was highest among first-generation migrants of Ghanaian (5.4%) and Turkish (4.1%) origin. Based on the prevalence in the country of origin (13% and 4%, respectively54) individual case-finding and screening for HBV would have also been recommended for these two groups. The chronic HBV prevalence of people of Surinamese origin in our study was under the 2% threshold, but based on the prevalence in the country of origin (3.91%) screen-ing would have been recommended.54 For those of Moroccan origin, HBV prevalence in the country of origin and the prevalence found in our study were comparable and under the 2% prevalence threshold. HCV prevalence in our study was low among all groups.
4.2.2.1 Individual case-finding for HIV, HBV and HCV
As mentioned earlier, GPs are the first points of access to healthcare in the Netherlands. In 2018, GPs registered an average of 4.5 contacts per patient,55 and the GP clinic is therefore an important setting for testing being initiated. Our results in chapter 3.1 indicate that a large (93%) proportion of individuals recently diagnosed with HIV in the Netherlands had visited a GP in the two years before diagnosis. However, only in a small proportion of these visits was an HIV test discussed. Another Dutch study found similar results also in that only 40% of patients with an HIV-indicator condition were offered an HIV test.56 This is in line with other studies in European countries showing many missed opportunities for HIV, HBV and HCV testing in primary healthcare settings.33,57,58 These data indicate that case-finding at GPs has the potential to increase earlier HIV, HBV and HCV diagnosis among groups at risk of infection if these groups are being correctly identified and are offered a test.
Several studies found that when HIV, HBV and HCV testing was offered in a primary care setting this was highly acceptable to patients, but it was less acceptable to GPs.57 Barriers to HIV, HBV and HCV testing identified by GPs include competing priorities and lack of time; complexity of and concerns about guidelines (e.g., doubts about the correct target group for testing, lack of clarity on when to repeat tests, overlong lists of indicator conditions or risk factors); lack of specific HIV, HBV and HCV knowledge and screening recommendations; lack of training and experience in communicating about sexual health and the communication of test results; language barriers when it comes to migrant populations; the additional testing costs for patients; and concerns about the impact on patients and the patient-provider rela-tionship of offering tests (e.g., stigmatization).57,59-65 Other barriers are the non-registration in patient files of risk factors for infection, such as sexual orientation and country of origin.56 The solutions proposed by GPs to overcome some of the barriers are to increase their knowledge about HIV, HBV and HCV and the screening guidelines, introducing sexual risk assessments for all patients, (facilitating) the registration of countries of birth and sexual orientation, testing reminders, implementing HIV indicator condition-guided testing only in high HIV prevalence areas and combining HIV tests with other blood tests.56,59,64 Indicator

Chapter 4
226
condition-guided testing has also been proposed to help normalise testing and reduce bar-riers such as stigma among healthcare providers and patients since it can provide a clinical rationale for testing.57,66 To scale up individual case-finding at GPs, additional resources (e.g., financial support, supporting registration systems, clear guidelines and/or training) are needed.
Besides GPs, individual case-finding for HIV, HBV and HCV could also take place in other healthcare settings (e.g., hospitals, drug treatment centres and prisons) that also deliver care to people at risk to HIV, HBV and HCV. Individual case-finding at dentists and mental healthcare facilities could be proposed as well, as our results (chapter 3.1) indicate that a substantial proportion of individuals recently diagnosed with HIV infection had visited such facilities before diagnosis. The results of a systematic review suggests that HCV screening at psychiatric clinics is effective.67 However, it is important to first assess the acceptability to patients and healthcare providers of implementing screenings at such locations and to create preconditions for the effective implementation of screening (including a linkage to care after a positive test).
4.2.2.2 HIV, HBV and HCV screening programmes for migrants
A recent cost-effectiveness study in the Netherlands estimated that chronic HBV and HCV screening was even cost-effective for migrants from countries with chronic HBV or HCV prevalence as low as >0.41% and >0.22%, respectively, and that for most countries of origin a combined HBV and HCV screening is the most cost-effective.68 In the case of some migrants groups, e.g., migrants from Turkey, a single HBV screening was estimated to be more cost-effective than a combined HBV and HCV screening since HCV prevalence is low in these groups. In chapter 3.2 we showed that the prevalence of chronic HCV infection was low among the large ethnic groups living in Amsterdam (<0.4%), although HCV prevalence for those of Dutch origin and first-generation migrants of African-Surinamese origin (both 0.4%) was above the cost-effectiveness threshold of >0.22%.
In the previously mentioned cost-effectiveness study, HIV screening was not included. Since the key populations for HIV, HBV and HCV overlap, future studies should establish the cost-effectiveness of combined screening. Our results in chapter 3.3 suggest that the combina-tion of HIV, HBV and HCV screening is acceptable, since there was no statistically significant difference in screening uptake among migrants visiting the tuberculosis (TB) entry screening in Amsterdam, where HIV, HBV and HCV screening was offered, and in Gelderland, where only HBV and HCV screening was offered. In Amsterdam, only one person (1/256; 0.39%) opted out of HIV testing.

227
General discussion
4
Screening programmes can be integrated into existing healthcare services or can take place in community settings (i.e., in community centres, outreach testing and social network testing).52 Furthermore, screening programmes could follow a mass or selective screening approach.69 In the Netherlands, several selective HBV and HCV screening programmes, mostly community-based, have targeted specific groups of migrants in the past decade.70 Community-based testing could reach individuals at risk who are not in contact with formal health services. Evidence has shown that such testing could result in a high uptake and high positivity rates.52 However, the community-based HBV and HCV screening programmes done in the Netherlands were not sustainable since they were set up to be done only once and were typically highly labour-intensive. In addition, the programmes were tailored to particular migrant groups and residential areas. The integration of screening into existing healthcare services could increase long-term sustainability and continuity in reaching and screening key populations.67 A systematic review on HCV testing interventions showed that practitioner-based interventions were more effective than media/information-based inter-ventions with regard to increasing test uptake and cases detected.71 Another review found that integrated screening programmes in general screened a larger number of individuals than did non-integrated screening programmes in countries with a low HCV prevalence.67 In addition, integration would most probably make such screening programmes more cost-effective as fewer additional resources would be required. However, this should be explored in future research.
In chapter 3.3 we initiated a screening project integrating voluntary HIV, HBV and HCV screening into the compulsory TB screening for migrants from TB-endemic countries migrat-ing from outside the European Union (EU). In this project about half the migrants accepted integrated screening. The effectiveness of finding newly diagnosed infections differed by region. The prevalence of newly diagnosed HBV infections was 4.48% in Gelderland while no newly diagnosed HBV infections were found in Amsterdam. The prevalence of newly diagnosed HCV infections was low in both regions and no HIV infections were found. In another study in Amsterdam and Rotterdam, a non-targeted HIV-testing programme was initiated at hospital emergency departments. In this study, 43% accepted screening but the screening was not cost-effective because of the low HIV prevalence (0.03%) found.72 In a non-targeted HCV screening project at hospital emergency departments in Belgium, 80% of migrants accepted screening. Here also, a low HCV prevalence (0.9% with 0.2% being newly diagnosed) was found.73 The results of these studies indicate that integrated screening for migrants, which includes pre-screening selection based on risk factors,74-76 might be more effective, as was demonstrated in a systemic review on HCV screening.67 When using a pre-screening, it is important that applied risk factors and cut-off points are evidence-based. Another important subgroup of migrants are asylum seekers and undocumented migrants, which were not included in our screening project. Entry screening of asylum seekers might

Chapter 4
228
be an effective way to reach and test this group, and this approach was also recommended by the Dutch Health Council.53 It might be organised within the TB screening programme in asylum-seeker centres. Prevalence data among asylum seekers in the Netherlands and Germany indicates that the prevalence of HIV and HBV is relatively high among some groups of asylum seekers.77,78 It is recommended that future studies focus on the acceptability and feasibility of integrated entry screening for asylum seekers. For undocumented migrants, who are not registered and targeted by regular screening programmes, little is known about the prevalence of HBV, HCV and HIV and effective screening strategies. To determine the prevalence within this group, a current pilot project offers HBV and HCV screening to un-documented migrants visiting a charity-based organisation providing primary healthcare in Amsterdam free-of-charge.
Besides a targeted screening for key populations (e.g., migrants), another type of screening that could be considered is a generalised testing approach in areas of intermediate or high HIV/HBV/HCV prevalence (“hot spots”).57 Another strategy is birth-cohort testing. Studies have shown birth-cohort testing for HCV can be an effective testing strategy when prevalence rates are markedly higher among people of a given birth cohort.57 However, a Dutch study assessing HBV and HCV birth-cohort testing in two hot spots in the south of the Netherlands found a chronic HBV prevalence of 0.26% and no chronic HCV infections, suggesting that this testing method might not be effective in the Netherlands.79 An alternative approach might be a generalised testing approach in areas with a high number of migrants originating from HIV, HBV or HCV endemic countries (e.g., by GPs). Future studies should investigate which testing approach (a selective or a generalised one, or a combination of both) and in which settings, screening would be most effective.
4.2.2.3 Self-testing for HIV and STIs
As outlined in chapter 1.2.3, HIV/STI self-tests (i.e., tests that are performed and interpreted autonomously by lay persons without involving healthcare professionals or certified labora-tories) could lower testing barriers since it raises feelings of confidentiality, autonomy and empowerment and convenience. It can significantly increase the uptake and frequency of testing among key populations.80-85 In chapter 3.4 we showed that the use of HIV/STI self-tests is relatively low among the general population and sexual risk groups (1–2%) in Amsterdam. In chapter 3.5 we showed that the use of HIV self-tests among migrant MSM living in Europe was 4% but that no heterosexual migrants had used an HIV self-test in the preceding 12 months.
The reason for relatively low HIV/STI self-test usage in the Netherlands may be that HIV/STI-related healthcare is relatively well organised and easily accessible in the Netherlands. High-risk groups are offered HIV/STI testing and counselling at STI clinics free of charge. HIV/STI
229
General discussion
4
testing and counselling is also offered by GPs, although HIV/STI tests are not free of charge. The low use of HIV self-tests might also be because of legal restrictions with regard to the sale of HIV self-tests in the Netherlands (see chapter 1.2.3). Currently, only a few pharmacies in the Netherlands are offering HIV self-tests,86 although a number of commercial providers also offer HIV/STI self-tests, mainly through the Internet. For STI self-tests, low usage may be explained by the low accuracy of STI self-tests. Because of this, the National Institute for STI and AIDS Control in the Netherlands (STI AIDS Netherlands) and the Public Health Service in the Netherlands do not recommend the use of STI self-tests.87,88 Other concerns about self-testing are the lack of clear information and instructions offered by the current commercial providers of self-tests and the fact that there is no direct linkage to counselling and care for those who test positive.82,83,89-92
In chapter 3.4 we showed that the use of chlamydia and syphilis self-tests increased over time among a representative sample of Amsterdam residents. Among STI clinic clients, only chlamydia self-test usage increased over time. Although we found overall low HIV/STI self-test usage in the general population (chapter 3.4), 5–9% of the individuals who tested for HIV/STI in the preceding 6 or 12 months opted to self-test. It is likely that HIV/STI self-testing will increase over time for a number of reasons. First, it is expected that more (accurate or innovative) self-tests will become available.93,94 Second, legal restrictions to HIV self-testing will be lifted when the new EU regulations on in-vitro diagnostic medical devices are implemented in the Netherlands in 2022.95 As a result commercial providers will probably promote HIV/STI self-tests more actively. In addition, HIV/STI self-test programmes could then be developed further and implemented by healthcare professionals. For suc-cessful implementation, it is important that quality procedures, adequate information and instructions, counselling and linkage to care are established. The need by individuals for HIV/STI testing services to be quick and easy, which will increase a feeling of autonomy and confidentiality, will most likely become more important in the future. The expected increase in HIV/STI self-test usage requires a more systematic monitoring, which will help to measure the potential contribution of self-testing on HIV/STI testing rates. It will be important to inform the public about quality issues and the pros and cons of self-testing.
Unlike self-testing for STIs, STI self-sampling tests available via the Internet in the Netherlands (i.e., self-collected specimens that are sent to a laboratory for analysis) seem to perform well. A study of the available STI self-sampling tests in 2016 showed that the tests had sensitivity and specificity above 95%.89 Several studies also indicate that self-sampling is highly accept-able among key populations.96,97 However, data on the current use of self-sampling tests is not readily available in the Netherlands. For this reason, besides monitoring self-tests usage, it would be useful to monitor systematically the use of self-sampling tests and to collect data on the acceptability of self-sampling. Despite the superior accuracy of self-sampling over

Chapter 4
230
self-testing, some individuals may, however, still prefer self-testing because of the perceived convenience and ease of obtaining results quickly and anonymously. When healthcare professionals or health programmes embark on the self-testing or self-sampling initiatives, they must bear in mind that many individuals may be unaware of the difference between self-sampling and self-testing, and their varying accuracy.
Novel testing approaches, including rapid point-of-care testing and the use of self-sampling tests, can also be considered to increase the testing coverage in HIV, HBV and HCV screening programmes.52,57 Point-of-care tests are performed near or at the point of patient care. Point-of-care testing can also help to optimise treatment decision-making, avoid referrals, improve the efficiency of care and facilitate testing in settings were no laboratory is available.98
4.3.3 Conclusion
The work presented in this thesis demonstrates that migrants face barriers to accessing prevention and care. To eliminate HIV, HBV, HCV and STIs as public health threats and re-duce morbidity and mortality, the earlier testing of migrants by individual case-finding and screening programmes is important.
Individual case-finding seems to be most useful when done by GPs, but it is important to address the barriers to testing for HIV, HBV and HCV among GPs. Screening programmes for HBV, HCV and potentially HIV are needed for specific migrant groups. To ensure the sustain-ability of a screening programme, the integration of screening under existing healthcare services is recommended. The results reported in chapter 3.3 indicate that HIV, HBV and HCV screening integrated with TB entry-screening is feasible and acceptable, although the (cost-)effectiveness could vary depending on the population group targeted. Innovative test-ing strategies, such as self-testing, may provide opportunities for increased testing among groups that have an increased risk to infection by overcoming some barriers for testing. However, the use of self-tests for STIs (excluding HIV) is not recommended because of the low accuracy these tests.
Future research should focus on establishing effective testing or screening programmes for migrants in which feasibility, acceptability and effectiveness is measured. In addition, it is recommended that future studies compare the effectiveness of different programmes. With regard to self-testing and self-sampling, it is important to monitor usage systematically since self-testing and self-sampling may increase over time. The quality of the available testing options offered also requires attention.

231
General discussion
4
4.3 ConCludInG reMarKS
To reach the global and national targets of reducing the burden of disease caused by HIV, HBV and HCV infections and bacterial STIs, a single, one-fits-all intervention is unlikely to be effective. A combination of interventions will be needed. A range of intervention possibilities could further personalise prevention, reduce barriers to usage and increase actual uptake, thereby increasing the public health impact. In the case of primary prevention against HIV infection, for example, offering a choice between condoms, daily and event-driven PrEP next to applying treatment as prevention principles could increase the uptake of preven-tion interventions. PrEP should be offered in combination with HIV and STI testing, which also includes HCV, as well as interventions to prevent an increase in STIs. At the secondary prevention level, the availability of choice between testing by means of a self-test, a self-sampling test, participation in a screening programme or tests integrated within existing healthcare facilities (e.g., GPs, hospitals, dentists, drug treatment centres, prisons, mental healthcare centres and TB departments) could increase testing uptake. It is important for people who test negative to be offered interventions to prevent infection at a later stage, and for those who test positive to be linked to treatment and care.
Monitoring the cascade of care will help to assess the progress being made towards achiev-ing global and national targets. For HIV, the cascade of care in the Netherlands is relatively well known as data from HIV patients in clinical care are monitored systematically. For HBV, HCV and STIs, the cascades of care are less readily used despite acute and chronic HBV and HCV being compulsory notifiable diseases. The efforts being made to implement a similar systematic monitoring system for HBV and HCV as for HIV99 will help determine current progress and will inform on which parts of the care cascade interventions are needed. As mentioned in section 4.2.1, monitoring the cascade by subgroups (e.g., migrant status in combination with sexual orientation) could provide more insight into the interventions needed by specific groups. It is recommended that the cascade of care for those living with an infection is extended by prevention indicators for the population at risk of infection.100
It is very important that new effective interventions are implemented rapidly so that proper implementation is not impeded. Currently, the slow implementation of PrEP in the Nether-lands has motivated/forced some MSM to acquire PrEP informally, e.g., online, from abroad or from friends.1,2 Such PrEP users are typically not optimally monitored by medical profes-sionals and may use non-evidence-based PrEP regimens.101 With regard to HIV self-tests, the outdated legal restrictions on the sale of HIV self-tests limits the implementation of HIV self-test programmes by public health organisations and hampers the uptake of testing in the Netherlands. This may have encouraged some individuals to purchase low quality HIV

Chapter 4
232
or STI self-tests via the Internet. Often such persons are not adequately informed about the proper use of these tests or are not properly linked to care when needed.
The studies presented in this thesis have provided insight into the processes of PrEP use ac-ceptance among MSM and healthcare professionals in the Netherlands. The insights should help to determine which interventions are needed to effectively implement PrEP nation-ally. This thesis has also provided evidence on HIV, HBV, HCV and STI testing opportunities, especially in the case of migrants. This information can be used to develop and implement effective testing and screening programmes in the future. This thesis also points to chal-lenges and areas of future research. Challenges specifically related to increased PrEP use are potential increases in STIs, PrEP adherence and sexual well-being while on PrEP. As regards the testing and screening of migrants, effective, sustainable programmes to reach migrants having undiagnosed HIV, HBV and HCV infections are yet to be evaluated in demonstration projects. For HIV and STIs self-testing and self-sampling tests, important focus areas are the provision of adequate information, counselling and linkage to care.

233
General discussion
4
referenCes
1. Coyer L, van Bilsen W, Bil J, Davidovich U, Hoornenborg E, Prins M, et al. Pre-exposure prophylaxis among men who have sex with men in the amsterdam Cohort Studies: use, eligibility, and intention to use. PLoS One. 2018;13(10):e0205663. doi:10.1371/journal.pone.0205663.
2. den Daas C, Zuilhof W, van Bijnen A, Vermey K, Dörfler T, de Wit J. rapport survey mannen & sek-sualiteit 2018. Seks en gezondheid: het handelen en denken van MSM in nederland. Universiteit Utrecht, RIVM, SOA AIDS Nederland, 2018.
3. Molina JM, Capitant C, Spire B, Pialoux G, Cotte L, Charreau I, et al. on-demand Preexposure Prophy-laxis in Men at High risk for HIV-1 Infection. N Engl J Med. 2015;373(23):2237-2246. doi:10.1056/NEJMoa1506273.
4. McCormack S, Dunn DT, Desai M, Dolling DI, Gafos M, Gilson R, et al. Pre-exposure prophylaxis to prevent the acquisition of HIV-1 infection (Proud): effectiveness results from the pilot phase of a pragmatic open-label randomised trial. Lancet. 2016;387(10013):53-60. doi:10.1016/S0140-6736(15)00056-2.
5. Reyniers T, Nostlinger C, Laga M, De Baetselier I, Crucitti T, Wouters K, et al. Choosing Between daily and event-driven Pre-exposure Prophylaxis: results of a Belgian PreP demonstration Project. J Acquir Immune Defic Syndr. 2018;79(2):186-194. doi:10.1097/QAI.0000000000001791.
6. Hoornenborg E, Achterbergh RC, van der Loeff MFS, Davidovich U, van der Helm JJ, Hogewon-ing A, et al. Men who have sex with men more often chose daily than event-driven use of pre-exposure prophylaxis: baseline analysis of a demonstration study in amsterdam. J Int AIDS Soc. 2018;21(3):e25105. doi:10.1002/jia2.25105.
7. Zimmermann HML, Eekman SW, Achterbergh RCA, Prins M, Schim van der Loeff MF, de Vries HJC, et al. Pre-exposure prophylaxis (PreP) among men who have sex with men (MSM) in the netherlands: motives for starting, choosing for, switching to, or stopping with daily or event-driven PreP [ab-stract]. AIDSImpact: Cape Town, 13-15 November 2017.
8. Noret M, Balavoine S, Pintado C, Siguier M, Brun A, Bauer R, et al. daily or on-demand oral tenofovir disoproxil fumarate/emtricitabine for HIV pre-exposure prophylaxis: experience from a hospital-based clinic in France. AIDS. 2018;32(15):2161-2169. doi:10.1097/QAD.0000000000001939.
9. Nichols BE, Boucher CAB, van der Valk M, Rijnders BJA, van de Vijver D. Cost-effectiveness analysis of pre-exposure prophylaxis for HIV-1 prevention in the netherlands: a mathematical modelling study. Lancet Infect Dis. 2016;16(12):1423-1429. doi:10.1016/S1473-3099(16)30311-5.
10. Gomez GB, Borquez A, Case KK, Wheelock A, Vassall A, Hankins C. the cost and impact of scaling up pre-exposure prophylaxis for HIV prevention: a systematic review of cost-effectiveness modelling studies. PLoS Med. 2013;10(3):e1001401. doi:10.1371/journal.pmed.1001401.
11. van de Vijver D, Richter AK, Boucher CAB, Gunsenheimer-Bartmeyer B, Kollan C, Nichols BE, et al. Cost-effectiveness and budget effect of pre-exposure prophylaxis for HIV-1 prevention in Germany from 2018 to 2058. Euro Surveill. 2019;24(7) doi:10.2807/1560-7917.ES.2019.24.7.1800398.
12. Janz NK, Becker MH. the Health Belief model: a decade later. Health Educ Q. 1984;11(1):1-47. doi:10.1177/109019818401100101.
13. Eaton LA, Driffin DD, Bauermeister J, Smith H, Conway-Washington C. Minimal awareness and Stalled uptake of Pre-exposure Prophylaxis (PreP) among at risk, HIV-negative, Black Men Who Have Sex with Men. AIDS Patient Care STDS. 2015;29(8):423-429. doi:10.1089/apc.2014.0303.
14. Eaton LA, Matthews DD, Driffin DD, Bukowski L, Wilson PA, Stall RD, et al. a Multi-uS City assess-ment of awareness and uptake of Pre-exposure Prophylaxis (PreP) for HIV Prevention among Black

Chapter 4
234
Men and Transgender Women Who Have Sex with Men. Prev Sci. 2017;18(5):505-516. doi:10.1007/s11121-017-0756-6.
15. Kuhns LM, Hotton AL, Schneider J, Garofalo R, Fujimoto K. use of Pre-exposure Prophylaxis (PreP) in Young Men Who Have Sex with Men is associated with race, Sexual risk Behavior and Peer network Size. AIDS Behav. 2017;21(5):1376-1382. doi:10.1007/s10461-017-1739-0.
16. Chapin-Bardales J, Schmidt AJ, Guy RJ, Kaldor JM, McGregor S, Sasse A, et al. trends in human im-munodeficiency virus diagnoses among men who have sex with men in north america, Western europe, and australia, 2000-2014. Ann Epidemiol. 2018;28(12):874-880. doi:10.1016/j.annepi-dem.2018.09.006.
17. PrEPnu. PreP Prijslijst. Available at: https://www.prepnu.nl/prijs/ (accessed on 23 May 2019). 18. Bruins B. Beleidsreactie preventief gebruik van hiv-remmers (PreP) [dutch]. Available at: https://
www.rijksoverheid.nl/regering/bewindspersonen/bruno-bruins/documenten/kamerstuk-ken/2018/07/10/kamerbrief-met-beleidsreactie-preventief-gebruik-van-hiv-remmers-prep (accessed on 17 September 2018).
19. Cambiano V, Miners A, Phillips A. What do we know about the cost-effectiveness of HIV pre-exposure prophylaxis, and is it affordable? Curr Opin HIV AIDS. 2015;11(1):56-66. doi:10.1097/COH.0000000000000217.
20. Schneider K, Gray RT, Wilson DP. a cost-effectiveness analysis of HIV preexposure prophylaxis for men who have sex with men in australia. Clin Infect Dis. 2014;58(7):1027-1034. doi:10.1093/cid/cit946.
21. Ong KJ, Desai S, Field N, Desai M, Nardone A, van Hoek AJ, et al. economic evaluation of HIV pre-exposure prophylaxis among men-who-have-sex-with-men in england in 2016. Euro Surveill. 2017;22(42) doi:10.2807/1560-7917.ES.2017.22.42.17-00192.
22. Cambiano V, Miners A, Dunn D, McCormack S, Ong KJ, Gill ON, et al. Cost-effectiveness of pre-exposure prophylaxis for HIV prevention in men who have sex with men in the uK: a modelling study and health economic evaluation. Lancet Infect Dis. 2018;18(1):85-94. doi:10.1016/S1473-3099(17)30540-6.
23. Traeger MW, Schroeder SE, Wright EJ, Hellard ME, Cornelisse VJ, Doyle JS, et al. effects of Pre-exposure Prophylaxis for the Prevention of Human Immunodeficiency Virus Infection on Sexual risk Behavior in Men Who Have Sex With Men: a Systematic review and Meta-analysis. Clin Infect Dis. 2018;67(5):676-686. doi:10.1093/cid/ciy182.
24. Traeger MW, Cornelisse VJ, Asselin J, Price B, Roth NJ, Willcox J, et al. association of HIV Preexposure Prophylaxis With Incidence of Sexually Transmitted Infections among Individuals at High risk of HIV Infection. JAMA. 2019;321(14):1380-1390. doi:10.1001/jama.2019.2947.
25. Hoornenborg E, Coyer L, Achterbergh RCA, Matser A, Schim van der Loeff MF, Boyd A, et al. sexual behaviour and incidence of HIV and sexually transmitted infections among men who have sex with men using daily and event-driven pre-exposure prophylaxis in aMPreP: 2 year results from a demonstration study. Lancet HIV. 2019 doi:10.1016/S2352-3018(19)30136-5.
26. Hoornenborg E, Achterbergh RCA, Schim van der Loeff MF, Davidovich U, Hogewoning A, de Vries HJC, et al. MSM starting preexposure prophylaxis are at risk of hepatitis C virus infection. AIDS. 2017;31(11):1603-1610. doi:10.1097/QAD.0000000000001522.
27. Hoornenborg E, Krakower DS, Prins M, Mayer KH. Pre-exposure prophylaxis for msm and transgender persons in early adopting countries. AIDS. 2017;31(16):2179-2191. doi:10.1097/QAD.0000000000001627.

235
General discussion
4
28. Pinto RM, Berringer KR, Melendez R, Mmeje O. Improving PreP Implementation Through Multi-level Interventions: a Synthesis of the literature. AIDS Behav. 2018;22(11):3681-3691. doi:10.1007/s10461-018-2184-4.
29. GGD Gelderland. PreP-zorg in nederland. Available at: https://ggdgelderlandzuid.nl/nieuwsbrief/relaties-sense-oost/prep-zorg-in-nederland/ (accessed on 27 May 2019).
30. Neervoort L. let’s talk about PreP: een onderzoek naar attitudes en behoeften t.a.v. PreP en PreP zorg onder de verpleegkundigen werkzaam op de soa polikliniek GGd amsterdam [dutch, unpub-lished Bachelor thesis]. Amsterdam: GGD Amsterdam, 2019.
31. Vanbellinghen MC, Poelakker RF, Joosten SCM. nederlandse huisartsen en PreP. een onderzoek naar de kennis, mening en verwachtingen van huisartsen over PreP. Available at: https://www.soaaids.nl/nl/item/seksoa-article/nederlandse-huisartsen-en-prep (accessed on 5 December 2018).
32. Fakoya I, Alvarez-Del Arco D, Copas AJ, Teixeira B, Block K, Gennotte AF, et al. Factors associated With access to HIV Testing and Primary Care among Migrants living in europe: Cross-Sectional Survey. JMIR Public Health Surveill. 2017;3(4):e84. doi:10.2196/publichealth.7741.
33. Fakoya I, Alvarez-Del Arco D, Monge S, Copas AJ, Gennotte AF, Volny-Anne A, et al. HIV testing history and access to treatment among migrants living with HIV in europe. J Int AIDS Soc. 2018;21 Suppl 4:e25123. doi:10.1002/jia2.25123.
34. Alvarez-del Arco D, Monge S, Azcoaga A, Rio I, Hernando V, Gonzalez C, et al. HIV testing and counsel-ling for migrant populations living in high-income countries: a systematic review. Eur J Public Health. 2013;23(6):1039-1045. doi:10.1093/eurpub/cks130.
35. Seedat F, Hargreaves S, Nellums LB, Ouyang J, Brown M, Friedland JS. How effective are approaches to migrant screening for infectious diseases in europe? a systematic review. Lancet Infect Dis. 2018;18(9):e259-e271. doi:10.1016/S1473-3099(18)30117-8.
36. Deblonde J, De Koker P, Hamers FF, Fontaine J, Luchters S, Temmerman M. Barriers to HIV testing in europe: a systematic review. Eur J Public Health. 2010;20(4):422-432. doi:10.1093/eurpub/ckp231.
37. Hamdiui N, Stein ML, Timen A, Timmermans D, Wong A, van den Muijsenbergh M, et al. Hepatitis B in Moroccan-dutch: a quantitative study into determinants of screening participation. BMC Med. 2018;16(1):47. doi:10.1186/s12916-018-1034-6.
38. Hamdiui N, Stein ML, van der Veen YJJ, van den Muijsenbergh M, van Steenbergen JE. Hepatitis B in Moroccan-dutch: a qualitative study into determinants of screening participation. Eur J Public Health. 2018;28(5):916-922. doi:10.1093/eurpub/cky003.
39. Kuehne A, Koschollek C, Santos-Hovener C, Thorlie A, Mullerschon J, Mputu Tshibadi C, et al. Impact of HIV knowledge and stigma on the uptake of HIV testing - results from a community-based participatory research survey among migrants from sub-Saharan africa in Germany. PLoS One. 2018;13(4):e0194244. doi:10.1371/journal.pone.0194244.
40. Rade DA, Crawford G, Lobo R, Gray C, Brown G. sexual Health Help-seeking Behavior among mi-grants from Sub-Saharan africa and South east asia living in High Income Countries: a Systematic review. Int J Environ Res Public Health. 2018;15(7) doi:10.3390/ijerph15071311.
41. Tiittala P, Kivela P, Liitsola K, Ollgren J, Pasanen S, Vasankari T, et al. Important Gaps in HIV Knowledge, attitudes and Practices among Young asylum Seekers in Comparison to the General Population. J Immigr Minor Health. 2018;20(6):1415-1423. doi:10.1007/s10903-018-0707-8.
42. Rechel B, Mladovsky P, Ingleby D, Mackenbach JP, McKee M. Migration and health in an increasingly diverse europe. Lancet. 2013;381(9873):1235-1245. doi:10.1016/S0140-6736(12)62086-8.
43. Centers for Disease Control and Prevention (CDC). Health Literacy. Available at: http://www.cdc.gov/healthliteracy/learn/ (accessed on 16 August 2018).

Chapter 4
236
44. Perazzo J, Reyes D, Webel A. a Systematic review of Health literacy Interventions for People living with HIV. AIDS Behav. 2017;21(3):812-821. doi:10.1007/s10461-016-1329-6.
45. Fakoya I, Reynolds R, Caswell G, Shiripinda I. Barriers to HIV testing for migrant black africans in Western europe. HIV Med. 2008;9 Suppl 2:23-25. doi:10.1111/j.1468-1293.2008.00587.x.
46. Sumari-de Boer IM, Sprangers MA, Prins JM, Nieuwkerk PT. HIV stigma and depressive symptoms are related to adherence and virological response to antiretroviral treatment among immigrant and indigenous HIV infected patients. AIDS Behav. 2012;16(6):1681-1689. doi:10.1007/s10461-011-0112-y.
47. Chinouya M, Hildreth A, Goodall D, Aspinall P, Hudson A. Migrants and HIV stigma: findings from the Stigma Index Study (uK). Health Soc Care Community. 2017;25(1):35-42. doi:10.1111/hsc.12179.
48. Stutterheim SE, Pryor JB, Bos AE, Hoogendijk R, Muris P, Schaalma HP. HIV-related stigma and psycho-logical distress: the harmful effects of specific stigma manifestations in various social settings. AIDS. 2009;23(17):2353-2357. doi:10.1097/QAD.0b013e3283320dce.
49. Mahajan AP, Sayles JN, Patel VA, Remien RH, Sawires SR, Ortiz DJ, et al. Stigma in the HIV/aIdS epi-demic: a review of the literature and recommendations for the way forward. AIDS. 2008;22 Suppl 2:S67-79. doi:10.1097/01.aids.0000327438.13291.62.
50. Stutterheim SE, Brands R, Baas I, Lechner L, Kok G, Bos AER. HIV Status disclosure in the Workplace: Positive and Stigmatizing experiences of Health Care Workers living with HIV. J Assoc Nurses AIDS Care. 2017;28(6):923-937. doi:10.1016/j.jana.2017.06.014.
51. Bartholomw LK, Parcel GS, Kok G, Gottlieb NH, Fernandez ME. Planning health promotion programs, an intervention mapping approach. San Francisco: Jossey-Bass, 2011.
52. European Centre for Disease Prevention and Control (ECDC). Hepatitis B and C testing strategies in healthcare and community settings in the eu/eea: a systematic review. Stockholm: ECDC, 2018.
53. Gezondheidsraad. Screening van risicogroepen op hepatitis B en C. Den Haag: Gezondheidsraad, 2016.
54. Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ. estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet. 2015;386(10003):1546-1555. doi:10.1016/S0140-6736(15)61412-X.
55. Meijer WM, Verberne LDM, Weesie YM, Davids RN, Winckers MLJJ, Korteweg L, et al. nivel zorgreg-istraties eerste lijn: contacten huisartsenpraktijk [dutch]. Available at: https://www.nivel.nl/nl/nivel-zorgregistraties-eerste-lijn/contacten-huisartsenpraktijk (accessed on 16 July 2019).
56. Joore IK, Geerlings SE, Brinkman K, van Bergen JE, Prins JM. The importance of registration of sexual orientation and recognition of indicator conditions for an adequate HIV risk-assessment. BMC Infect Dis. 2017;17(1):178. doi:10.1186/s12879-017-2279-y.
57. European Centre for Disease Prevention and control (ECDC). Public health guidance on HIV, hepatitis B and C testing in the eu/eea: an integrated approach. Stockholm: ECDC, 2018.
58. Bielen R, Koc OM, Busschots D, Robaeys G, Aertgeerts B, Vaes B, et al. assessing testing rates for viral hepatitis B and C by general practitioners in Flanders, Belgium: a registry-based study. BMJ Open. 2019;9(5):e026464. doi:10.1136/bmjopen-2018-026464.
59. Joore IK, van Roosmalen SL, van Bergen JE, van Dijk N. General practitioners’ barriers and fa-cilitators towards new provider-initiated HIV testing strategies: a qualitative study. Int J STD AIDS. 2017;28(5):459-466. doi:10.1177/0956462416652274.
60. Jewett A, Garg A, Meyer K, Wagner LD, Krauskopf K, Brown KA, et al. Hepatitis C virus testing per-spectives among primary care physicians in four large primary care settings. Health Promot Pract. 2015;16(2):256-263. doi:10.1177/1524839914532291.

237
General discussion
4
61. Deblonde J, Van Beckhoven D, Loos J, Boffin N, Sasse A, Nostlinger C, et al. HIV testing within gen-eral practices in europe: a mixed-methods systematic review. BMC Public Health. 2018;18(1):1191. doi:10.1186/s12889-018-6107-0.
62. Kallman JB, Arsalla A, Park V, Dhungel S, Bhatia P, Haddad D, et al. Screening for hepatitis B, C and non-alcoholic fatty liver disease: a survey of community-based physicians. Aliment Pharmacol Ther. 2009;29(9):1019-1024. doi:10.1111/j.1365-2036.2009.03961.x.
63. Guirgis M, Yan K, Bu YM, Zekry A. General practitioners’ knowledge and management of viral hepatitis in the migrant population. Intern Med J. 2012;42(5):497-504. doi:10.1111/j.1445-5994.2011.02440.x.
64. Shehata N, Austin T, Ha S, Timmerman K. Barriers to and facilitators of hepatitis C virus screening and testing: a scoping review. Can Commun Dis Rep. 2018;44(7-8):166-172.
65. Falla AM, Veldhuijzen IK, Ahmad AA, Levi M, Richardus JH. language support for linguistic minority chronic hepatitis B/C patients: an exploratory study of availability and clinicians’ perceptions of language barriers in six european countries. BMC Health Serv Res. 2017;17(1):150. doi:10.1186/s12913-017-2095-5.
66. Lazarus JV, Hoekstra M, Raben D, Delpech V, Coenen T, Lundgren JD, et al. the case for indicator condition-guided HIV screening. HIV Med. 2013;14(7):445-448. doi:10.1111/hiv.12022.
67. Zuure FR, Urbanus AT, Langendam MW, Helsper CW, van den Berg CH, Davidovich U, et al. outcomes of hepatitis C screening programs targeted at risk groups hidden in the general population: a sys-tematic review. BMC Public Health. 2014;14:66. doi:10.1186/1471-2458-14-66.
68. Suijkerbuijk AWM, van Hoek AJ, Koopsen J, de Man RA, Mangen MJ, de Melker HE, et al. Cost-effec-tiveness of screening for chronic hepatitis B and C among migrant populations in a low endemic country. PLoS One. 2018;13(11):e0207037. doi:10.1371/journal.pone.0207037.
69. Wilson JMG, Jungner G. Principles and practice of screening for disease. Geneva: World Health Organization, 1968.
70. Urbanus AT, Steenbergen JE. Hepatitis B-virus en hepatitis C-virus screeningsprojecten voor migrant-en in nederland: stand van zaken 2014 [dutch]. Tijdschrift voor Infectieziekten. 2015;10(2):31-36.
71. Aspinall EJ, Doyle JS, Corson S, Hellard ME, Hunt D, Goldberg D, et al. Targeted hepatitis C antibody testing interventions: a systematic review and meta-analysis. Eur J Epidemiol. 2015;30(2):115-129. doi:10.1007/s10654-014-9958-4.
72. Luiken GPM, Joore IK, Taselaar A, Schuit SCE, Geerlings SE, Govers A, et al. non-targeted HIV screen-ing in emergency departments in the netherlands. Neth J Med. 2017;75(9):386-393.
73. Bielen R, Kremer C, Koc OM, Busschots D, Hendrickx DM, Vanelderen P, et al. Screening for hepatitis C at the emergency department: Should babyboomers also be screened in Belgium? Liver Int. 2019;39(4):667-675. doi:10.1111/liv.14016.
74. Zuure F, Davidovich U, Kok G, Depla AC, Hoebe C, van den Hoek A, et al. evaluation of a risk as-sessment questionnaire to assist hepatitis C screening in the general population. Euro Surveill. 2010;15(15):19539. doi:10.2807/ese.15.15.19539-en.
75. Newsum AM, Stolte IG, van der Meer JT, Schinkel J, van der Valk M, Vanhommerig JW, et al. devel-opment and validation of the HCV-MoSaIC risk score to assist testing for acute hepatitis C virus (HCV) infection in HIV-infected men who have sex with men (MSM). Euro Surveill. 2017;22(21) doi:10.2807/1560-7917.ES.2017.22.21.30540.
76. Dijkstra M, de Bree GJ, Stolte IG, Davidovich U, Sanders EJ, Prins M, et al. development and validation of a risk score to assist screening for acute HIV-1 infection among men who have sex with men. BMC Infect Dis. 2017;17(1):425. doi:10.1186/s12879-017-2508-4.
77. Freidl GS, Tostmann A, Curvers M, Ruijs WLM, Smits G, Schepp R, et al. Immunity against measles, mumps, rubella, varicella, diphtheria, tetanus, polio, hepatitis a and hepatitis B among adult

Chapter 4
238
asylum seekers in the netherlands, 2016. Vaccine. 2018;36(12):1664-1672. doi:10.1016/j.vac-cine.2018.01.079.
78. Ackermann N, Marosevic D, Hormansdorfer S, Eberle U, Rieder G, Treis B, et al. Screening for infectious diseases among newly arrived asylum seekers, Bavaria, Germany, 2015. Euro Surveill. 2018;23(10) doi:10.2807/1560-7917.ES.2018.23.10.17-00176.
79. Heil J, Hoebe C, Cals JWL, Ter Waarbeek HLG, van Loo IHM, Dukers-Muijrers N. detecting Hepati-tis B and C by Combined Public Health and Primary Care Birth Cohort Testing. Ann Fam Med. 2018;16(1):21-27. doi:10.1370/afm.2166.
80. World Health Organization (WHO). Guidelines on HIV Self-Testing and Partner notification: Supple-ment to Consolidated Guidelines on HIV Testing Services. Geneva: WHO, 2016.
81. Johnson CC, Kennedy C, Fonner V, Siegfried N, Figueroa C, Dalal S, et al. examining the effects of HIV self-testing compared to standard HIV testing services: a systematic review and meta-analysis. J Int AIDS Soc. 2017;20(1):21594. doi:10.7448/IAS.20.1.21594.
82. Joint United Nations Programme on HIV/AIDS (UNAIDS), World Health Organization (WHO). a short technical update on self-testing for HIV. Geneva: UNAIDS, 2013.
83. Napierala Mavedzenge S, Baggaley R, Corbett EL. a review of self-testing for HIV: research and policy priorities in a new era of HIV prevention. Clin Infect Dis. 2013;57(1):126-138. doi:10.1093/cid/cit156.
84. World Health Organization (WHO). report on the first international symposium on self-testing for HIV: The legal, ethical, gender, human rights and public health implications of HIV self-testing scale-up: Geneva, Switzerland, 8-9 april 2013. Geneva: WHO, 2013.
85. Zuure FR, van der Helm J, van Bergen JEAM, Coutinho RA, Geerlings SE, Götz HM, et al. Home testing for HIV succeeds in reaching first-time and infrequent testers in the netherlands: results of the HIVTest@Home trial [abstract]. The international AIDS conference: Durban, South Africa, 18-22 July 2016.
86. Pharmaceutisch Weekblad. rotterdamse apotheek biedt ook soa-testen uit de muur. Available at: https://www.pw.nl/nieuws/2017/rotterdamse-apotheek-biedt-ook-soa-testen-uit-de-muur (ac-cessed on 30 April 2019).
87. GGD Amsterdam. Zelfafnametest [dutch]. Available at: https://www.ggd.amsterdam.nl/infectieziek-ten/soa-hiv-sense/zelfafnametest/ (accessed on 19 February 2019).
88. SOA AIDS Nederland. Soa-zelftest. Available at: https://www.soaaids.nl/nl/soas/de-soa-test/hoe-werkt-het/soa-zelftest (accessed on 10 April 2019).
89. Van den Broek IVF, Sukel B, Bos H, Den Baas C. evaluatie van het aanbod van online-aanbieders van soa-zelftesten in nederland [dutch]. Bilthoven: RIVM, 2016.
90. Owens SL, Arora N, Quinn N, Peeling RW, Holmes KK, Gaydos CA. utilising the internet to test for sexually transmitted infections: results of a survey and accuracy testing. Sex Transm Infect. 2010;86(2):112-116. doi:10.1136/sti.2009.037226.
91. Pars L, van Bergen J. Soa-testen, zelf doen of laten (doen)? [dutch]. Amsterdam: SOA AIDS Nederland, 2013.
92. Bustamante MJ, Konda KA, Joseph DD, Leon SR, Calvo GM, Salvatierra J, et al. HIV self-testing in Peru: questionable availability, high acceptability but potential low linkage to care among men who have sex with men and transgender women. Int J STD AIDS. 2016 doi:10.1177/0956462416630674.
93. Unitaid, World Health Organization (WHO). Market and technology landscape: HIV rapid diagnostic tests for self-testing. Geneva: Unitaid, 2018.
94. Brady M, Carpenter G, Bard B. Self-testing for HIV: initial experience of the uK’s first kit [abstract]. 22nd Annual Conference of the British HIV Association: Manchester, UK, 19-22 April 2016.

239
General discussion
4
95. European Commission. The new regulations on medical devices. Available at: https://ec.europa.eu/growth/sectors/medical-devices/regulatory-framework_en (accessed on 7 February 2019).
96. Graseck AS, Shih SL, Peipert JF. Home versus clinic-based specimen collection for Chlamydia tra-chomatis and neisseria gonorrhoeae. Expert Rev Anti Infect Ther. 2011;9(2):183-194. doi:10.1586/eri.10.164.
97. Shih SL, Graseck AS, Secura GM, Peipert JF. Screening for sexually transmitted infections at home or in the clinic? Curr Opin Infect Dis. 2011;24(1):78-84. doi:10.1097/QCO.0b013e32834204a8.
98. Kosack CS, Page AL, Klatser PR. a guide to aid the selection of diagnostic tests. Bull World Health Organ. 2017;95(9):639-645. doi:10.2471/BLT.16.187468.
99. ZonMw. Project “development of a registry for improving rational use of pharmacotherapy for chronic hepatitis B and C patients”. Available at: https://www.zonmw.nl/nl/onderzoek-resultaten/doelmatigheidsonderzoek/programmas/project-detail/goed-gebruik-geneesmiddelen/development-of-a-registry-for-improving-rational-use-of-pharmacotherapy-for-chronic-hepatitis-b-and/ (accessed on 7 July 2019).
100. Schaefer R, Gregson S, Fearon E, Hensen B, Hallett TB, Hargreaves JR. HIV prevention cascades: a unifying framework to replicate the successes of treatment cascades. Lancet HIV. 2019;6(1):PE60-E66. doi:10.1016/S2352-3018(18)30327-8.
101. Hulstein SH, Hoornenborg E, Matser A, Hogewoning A, van Duijnhoven YT, Prins M, et al. rapid uptake of care by men who have sex with men who use informal and self-obtained PreP in amsterdam - The InPreP Project [WePeC218: Poster Presentation]. 22nd International AIDS conference: Amsterdam, the Netherlands, 23-27 July 2018.


appendixsummary
nederlandse samenvattingabout the author
Portfoliolist of publications
list of contributing authorsauthors’ contributions per chapter
dankwoord


243
Summary
a
SuMMarY
The studies described in this thesis aimed to assess the acceptability and use of innovative interventions and to explore new opportunities for the prevention of HIV, hepatitis B virus (HBV), hepatitis C virus (HCV) infections and sexually transmitted infections (STIs) among key populations. Chapter 1 (general introduction) provides a brief description of the epidemiol-ogy, the clinical course of infections and the current prevention strategies for each infection. Chapter 1 also describes the outline of this thesis; including the aims, a description of the studied interventions and the studies and their design used in this thesis.
Chapter 2: Pre-exposure prophylaxis to prevent HIV infection
Pre-exposure prophylaxis (PrEP) is a biomedical intervention that aims to prevent HIV infec-tion prior to exposure among HIV-negative individuals who are at increased risk of HIV infec-tion. For effective implementation of PrEP, it is important to understand the acceptability of PrEP among those at increased risk for HIV infection and among professionals who play a critical role in PrEP implementation. Therefore, in chapter 2 we assessed the current aspects of acceptability, attitudes, beliefs and behavioural intentions towards the use of PrEP among men who have sex with men (MSM) and healthcare professionals in the Netherlands, prior to any implementation of PrEP programs or studies started in the Netherlands.
In chapter 2.1, we studied PrEP awareness, the intention to use PrEP, and socio-demographic and psychosocial determinants associated with a higher intention to use PrEP among Dutch MSM participating in the Amsterdam Cohort Studies in 2012–2013. We found that about half of the MSM were aware of PrEP; most MSM were unaware of PrEP side-effects, and only 13% had a high intention to use PrEP. High-risk sexual behaviour was independently as-sociated with a higher intention, as were psychosocial determinants such as high perceived self-efficacy and high perceptions of relief when using PrEP. Feelings of shame about using PrEP, worries about side-effects and PrEP characteristics, such as high costs and perceived insufficient efficacy were found to decrease the intention to use PrEP. In chapter 2.1 we ad-ditionally explored anticipated condom use if men would decide to use PrEP. We found that about one-third of our participants would decrease condom use while using PrEP, and this proportion was higher among those with higher intentions to use PrEP and those currently engaging in condomless anal sex.
In chapter 2.2, motives for wanting or not wanting to use PrEP if it becomes available, motives for daily versus event-driven (intermittent) PrEP use, the anticipated motives for condom use when using PrEP, and preferences for PrEP implementation (e.g., service char-acteristics) were more thoroughly explored among MSM in a qualitative study conducted in 2013, utilizing in-depth interviews. Our results showed that motives for (not) using daily PrEP

Appendix
244
were based on beliefs about PrEP efficacy and side effects, preferences for other prevention strategies, self-perceived HIV risk, self-perceived efficacy of PrEP adherence, beliefs about possible benefits (e.g., anxiety reduction, sex life improvement) and barriers of PrEP use (e.g., costs, monitoring procedures). The perceived benefits of intermittent over daily PrEP use were the lower costs and side effects and the lower threshold to decision to start using intermittent PrEP. Barriers specific for intermittent PrEP use were the perceived need to plan their sex life and anticipated difficulty to adhere to alternating prevention strategies (when on and off PrEP). Although some perceived PrEP as a condom substitute, others were likely to combine PrEP and condoms for STI prevention and increased HIV protection. Participants preferred PrEP service locations to have specialized knowledge of HIV, antiretroviral therapy, sexual behavior, STIs, patients’ medical background, be easily approachable, be able to perform PrEP follow-up monitoring, and provide support.
In chapter 2.3, we aimed to gain insight into the acceptability of PrEP, prescription setting, potential determinants of PrEP acceptability (such as knowledge and beliefs about PrEP) among professionals working at STI clinics (STI professionals) and at HIV treatment centers (HIV specialists) in 2014–2015. We found that STI professionals and HIV specialists had only a moderate level of acceptability toward PrEP implementation, and PrEP knowledge among STI professionals was suboptimal. The high costs of PrEP, worries about a possible decrease in condom use and an increase in STI, and the belief that it is unethical to prescribe ART to healthy individuals were identified as influential barriers for PrEP implementation. We also examined attitudes of healthcare professionals toward providing PrEP to key popula-tions and toward the reimbursement of PrEP costs. Most participants deemed the following groups to be eligible for PrEP: MSM who regularly get post-exposure prophylaxis, MSM who never used condoms with casual partners and MSM with an HIV-positive partner with a detectable viral load. Over half of the participants indicated that PrEP users should partly or fully pay the costs of PrEP.
Our results from chapter 2 showed it is important to address barriers to PrEP use among those at high risk of HIV infection by providing adequate information as regards to PrEP efficacy and side-effects, to improve the perceived self-efficacy of using PrEP, to prevent PrEP-related stigma, and to ensure adequate access to PrEP and PrEP services. Since health-care providers will play a critical role in the implementation of PrEP, it is vital to improve ac-ceptability of PrEP among healthcare professionals by reducing gaps in their PrEP knowledge and providing them training regarding PrEP. For those who decide to use PrEP, healthcare providers should provide high-quality, evidence-based PrEP counselling and care that in-cludes medical follow-up, regular STI testing and the discussion of topics such as adherence to PrEP, concurrent condom use and other (STI) prevention strategies. For those not using PrEP, either because they are not eligible or do not want to use PrEP, the standard preven-

245
Summary
a
tion strategies such as condom use should remain a viable, normative and socially accepted option and should be facilitated by health providers.
Chapter 3: testing opportunities for HIV, hepatitis B, hepatitis C and sexually transmitted infections
In chapter 3 we focused opportunities for HIV, HBV, HCV and STI testing, especially among migrant populations. Migrants represent a significant group in the HIV, HBV and HCV epi-demic in the Netherlands and across Europe and many face specific barriers in accessing HIV, HBV and HCV testing and care.
In chapter 3.1 we studied access to and use of HIV services pre-and post diagnosis among non-migrants and migrant MSM and heterosexual men/women living in the Netherlands who were diagnosed with HIV in the previous five years before study participation (2013–2015). Our results show disparities in access to HIV prevention, testing and care and experience of HIV-related discrimination by migrant status but also by sexual orientation. Also, our data also showed testing opportunities are being missed by healthcare professionals as almost all participants visited a healthcare facility in the two years before HIV diagnosis, but HIV testing was discussed or offered in only 40% of those visits. Our data suggests heterosexual men and women, who are less likely to have ever tested for HIV and are more like to be diagnosed late with HIV, may particularly benefit from improved access to HIV testing (e.g., through provider-initiated testing), while migrant MSM, who are most likely to be less aware of HIV prevention options than non-migrant MSM, may benefit from improved access to HIV prevention interventions (e.g., PrEP).
Data on the prevalence of chronic HBV and HCV infections, including the proportion of those aware of infection, is scarce among migrants living in Europe. In chapter 3.2 we therefore estimated the prevalence of past and present HBV and HCV infection, along with their determinants and awareness of infection status, among different groups of first-generation migrants and Dutch-origin residents of Amsterdam between 2011 and 2014. Our results showed the prevalence of chronic HBV infection was highest among first-generation mi-grants of Ghanaian origin (5.4%), followed by those Turkish (4.1%), African-Surinamese (1.9%), Moroccan (1.2%), South-Asian Surinamese (0.9%) and Dutch (0.4%) origin. Of those with a chronic infection 42% were unaware of their infection. The HCV prevalence was low among all ethnic groups.
In chapter 3.3 we evaluated whether integrated tuberculosis (TB), HIV, HBV and HCV screen-ing is effective and acceptable among migrant. We initiated a screening project offering additional voluntary HIV, HBV and HCV screening to migrants undergoing compulsory TB screening in Gelderland and Amsterdam in the Netherlands in 2013–2015. We studied the

Appendix
246
uptake of screening and the prevalence and determinants of newly diagnosed HIV, HBV and HCV infections. Our results showed about half of the migrants accepted HIV, HBV and HCV screening. Also, adding HIV screening seemed to be acceptable as only one person opted out of HIV testing. The prevalence of newly diagnosed HBV infections was 4.48% in migrants screened in Gelderland, but no newly diagnosed HBV infections were found in Amsterdam. This regional difference probably reflects the differences in countries of origin and reasons for migration (which may be related to differences in social economic status) between par-ticipants in Gelderland and Amsterdam. The prevalence of newly diagnosed HCV infections was low in both regions and no HIV infections were found.
Due to the anonymous nature of self-testing (i.e., tests that can be performed and inter-preted autonomously by lay persons without involving healthcare professionals or certified laboratories) the extent to which commercially sold HIV/STI self-tests are used and determi-nants of usage are not well known. Therefore, in chapter 3.4 and 3.5 we explored the extent of HIV/STI self-test usage and its determinants.
In chapter 3.4 we studied (temporal trends in) HIV/STI self-test usage and its determinants among the general population and high-risk groups between 2007 and 2015 in Amsterdam, the Netherlands. Our results showed the prevalence of HIV/STI self-test usage in the preced-ing 6–12 months varied between 1% and 2%. Chlamydia self-tests were most commonly used, except among MSM. We observed increases over time in chlamydia among Amsterdam residents and STI clinic clients and syphilis self-test usage among Amsterdam residents. Fur-thermore, self-test usage was higher among participants of African Surinamese or Ghanaian origin, woman or MSM and among those with a higher number of sexual partners compared to those of Dutch origin, heterosexual men and those with a lower number of partners, respectively. Among those in the general population who tested for HIV/STI in the preceding 12 months, 5–9% used a self-test.
In chapter 3.5, we studied the prevalence and determinants of HIV self-test usage among migrants living in the United Kingdom (UK), France and the Netherlands in 2014–2015. Fur-thermore, we studied the HIV self-test positivity rate and the extent to which users attend professional healthcare providers for confirmation testing to gain insight into linkage to care among HIV self-test users. This study shows that the overall HIV self-test usage in the preced-ing 12 months among migrants living in the UK, France and the Netherlands is low (2%), but higher among MSM (4%). Among MSM, HIV self-test usage was higher in those living in the UK compared with those living in France and the Netherlands. Eight HIVST users reported their HIV self-test result was negative and one reported a failed/indeterminate result. Of the users with a negative HIV self-test result, half of them went to a professional healthcare provider for confirmation testing and all confirmation HIV tests were negative.

247
Summary
a
Our results from chapter 4 demonstrate that migrants face barriers in accessing prevention and care. To eliminate HIV, HBV, HCV and STIs as public health threats and reduce morbid-ity and mortality, the earlier testing of migrants by individual case-finding and screening programmes is important. Individual case-finding seems to be most useful when done by GPs, but it is important to address the barriers to testing for HIV, HBV and HCV among GPs. Screening programmes for HBV, HCV and potentially HIV are needed for specific migrant groups. To ensure the sustainability of a screening programme, the integration of screening under existing healthcare services is recommended. The results reported in chapter 3.3 indicate that HIV, HBV and HCV screening integrated with TB entry-screening is feasible and acceptable, although the (cost-)effectiveness could vary depending on the population group targeted. Innovative testing strategies, such as self-testing, may provide opportunities for increased testing among groups that at increased risk of infection by overcoming some bar-riers for testing. However, the use of self-tests for STIs (excluding HIV) is not recommended because of the low accuracy these tests.
Chapter 4: General discussion
In chapter 4 the relevance of these studies together with the recent development are discussed. In conclusion, to reach the global and national targets of reducing the burden of disease caused by HIV, HBV, HCV infections and STIs a combination of innovative inter-ventions are required and need to be implemented rapidly. Furthermore, monitoring the progress made towards global and national targets by subgroups might help determine which interventions are needed for specific groups. This thesis also points to challenges and areas of future research. Challenges specifically related to increased PrEP use are the potential increases in STIs, PrEP adherence and sexual well-being while on PrEP. As regards the testing and screening of migrants, effective, sustainable programs to reach migrants with undiagnosed HIV, HBV and HCV infections are yet to be evaluated in demonstration projects. For HIV and STI self-testing and self-sampling tests, important focus points are the provision of adequate information, counselling and linkage to care.


249
Nederlandse samenvatting
a
nederlandSe SaMenVaTTInG
Infecties met het humaan immunodeficiëntie virus (hiv), hepatitis B virus, hepatitis C virus en seksueel overdraagbare aandoeningen (soa’s) zijn belangrijke gezondheidsproblemen, zowel wereldwijd als in Nederland. Zonder behandeling kunnen deze infecties ernstige gevolgen voor de gezondheid hebben. De overdracht van infecties kan voorkomen worden door het voorkomen van contact met lichaamsproducten die infecties kunnen overdragen, bijvoorbeeld door condoomgebruik, harm reduction programma’s voor personen die drugs injecteren (spuit omruil programma’s, methadon verstrekking) (hiv, hepatitis B en C) en hy-giënemaatregelen in medische instellingen (hiv, hepatitis B en C). Hiernaast kan overdracht voorkomen worden door vaccinatie (hepatitis B), biomedisch interventies zoals pre-expositie profylaxe (PrEP) voor hiv en het tijdig testen en behandelen van personen met een infectie. Voor deze infecties zijn goede diagnostische testen en behandeling beschikbaar. Echter er zijn nog veel personen die een hiv, hepatitis B, hepatitis C infectie of een soa hebben maar hiervan nog niet op de hoogte zijn. Nieuwe innovatieve interventies zijn daarom nodig om infecties te voorkomen, tijdig op te sporen en vroeg te behandelen. In dit proefschrift wordt ingegaan op studies naar de acceptatie en het gebruik van innovatieve interventies, en wordt gezocht naar nieuwe mogelijkheden voor de preventie van hiv, hepatitis B, hepatitis C en soa’s onder de belangrijkste doelgroepen.
Hoofdstuk 1 (introductie) van dit proefschrift beschrijft de epidemiologie, het natuurlijk beloop en de huidige preventie strategieën van hiv, hepatitis B, hepatitis C en soa. Hiernaast wordt de inhoud van dit proefschrift ingeleid.
Hoofdstuk 2: Pre-expositie profylaxe om hiv te voorkomen
PrEP voor hiv betekent het slikken van medicatie om een hiv infectie te voorkomen. PrEP is bedoeld voor personen die geen hiv hebben, maar die wel een verhoogd risico lopen om hiv op te lopen. PrEP kan dagelijks geslikt worden of rondom de seks (intermitterende PrEP gebruik). PrEP is in Nederland sinds 2016 geregistreerd. Vanaf augustus 2019 zal PrEP in een landelijk project uitgerold gaan worden. Voor een effectieve implementatie van PrEP is het belangrijk de acceptatie van PrEP te onderzoeken onder personen met een verhoogd risico op hiv en onder de professionals die een belangrijke rol spelen bij de PrEP verstrekking. In hoofdstuk 2 hebben we daarom voordat PrEP beschikbaar was in Nederland de kennis en acceptatie van PrEP onderzocht onder mannen die seks hebben met mannen (MSM) en zorgverleners.
In hoofdstuk 2.1 vonden we dat in 2012–2013 ongeveer de helft van de MSM had gehoord van PrEP. De meeste mannen waren nog onbekend met de bijwerkingen van het gebruik. Ook vonden we dat 13% van de MSM een hoge intentie had om PrEP in de toekomst te

Appendix
250
gaan gebruiken. MSM die meer risicovol seksueel gedrag rapporteerden hadden een hogere intentie om PrEP te gaan gebruiken. Ook MSM die van zichzelf dachten dat ze PrEP trouw konden slikken en die dachten dat PrEP opgelucht gevoel zou geven, hadden een hogere intentie om PrEP te gaan gebruiken. MSM die bezorgd waren over bijwerkingen, de effecti-viteit van PrEP of de kosten van PrEP hadden een lagere intentie om PrEP te gaan gebruiken. Ook MSM die zich zouden schamen voor het gebruik van PrEP hadden een lagere intentie. Onze resultaten lieten verder zien dat ongeveer één derde van de MSM verwachtte dat als ze PrEP zouden gebruiken hun condoomgebruik zou afnemen.
In hoofdstuk 2.2 hebben we in 2013 door middel van diepte interviews onderzocht welke motieven MSM hebben om PrEP wel of niet te gaan gebruiken in de toekomst. We vonden dat hun motieven gebaseerd waren op overtuigingen over de effectiviteit en bijwerkingen, de voorkeur voor andere preventie strategieën (zoals condooms), hun ingeschatte risico op hiv en therapietrouw. Ook waren motieven gebaseerd op de verwachte voor- en nadelen van PrEP gebruik. Voordelen waren bijvoorbeeld de vermindering van angst voor hiv en de verbetering van de kwaliteit van het seks leven, nadelen waren de kosten van PrEP en de medische controles tijdens het PrEP gebruik. Sommige MSM gaven aan PrEP te willen gaan gebruiken als een vervanging van het condoom, terwijl anderen PrEP en condooms wilden gaan combineren voor extra bescherming. Deelnemers gaven aan dat professionals die PrEP gaan verstrekken gespecialiseerde kennis over hiv, gebruik van antivirale medicatie, seksueel gedrag, soa’s en de medische voorgeschiedenis van PrEP gebruikers zouden moeten hebben. Daarnaast moeten locaties goed toegankelijk zijn en mogelijkheden bieden voor medische begeleiding en ondersteuning bij PrEP gebruik.
In hoofdstuk 2.3 hebben we de kennis en acceptatie van PrEP onder soa-polikliniek mede-werkers en behandelaren/consulenten in hiv centra onderzocht in 2014–2015. We vonden dat de acceptatie matig was en de kennis van PrEP onder soa-polikliniek medewerkers suboptimaal. Zorgverleners maakten zich het meest zorgen over een mogelijk afname van condoomgebruik en een toename van andere soa’s. Daarnaast vonden sommige zorgverle-ners het onethisch om antivirale middelen voor te schrijven aan gezonde personen. Zorgver-leners vonden de volgende groepen geschikt waren om PrEP te gaan gebruiken: MSM die regelmatig post-exposure profylaxe krijgen (behandeling na een risicovol seksueel contact om de kans op een hiv infectie te verkleinen), MSM die nooit een condoom gebruiken met losse partners en MSM met een partner met hiv waarbij het virus niet onderdrukt is. Meer dan de helft van de zorgverleners vond dat PrEP gebruikers zelf een deel of alle kosten van PrEP zouden moeten betalen.
Voor de effectiviteit van een PrEP programma is het belangrijk dat het gebruik van PrEP hoog is onder MSM met het hoogste risico op hiv. De resultaten van hoofdstuk 2 laten zien dat het

251
Nederlandse samenvatting
a
belangrijk is dat barrières voor het gebruik van PrEP geminimaliseerd worden, bijvoorbeeld door het ontwikkelen van campagnes over de effectiviteit van PrEP en de bijwerkingen. Ook zouden er interventies moeten worden aangeboden of ontwikkeld om de therapietrouw te bevorderen en om PrEP-gerelateerde stigma te voorkomen. Verder is het belangrijk dat er goede toegang is tot PrEP en PrEP zorg. Zorgverleners spelen een belangrijke rol bij het aanbieden van PrEP. Daarom wordt aanbevolen zorgverleners adequaat te trainen en te in-formeren over PrEP. Het is belangrijk dat PrEP gebruikers counseling, medische begeleiding en soa screening aanboden wordt. Verder is het belangrijk dat therapietrouw, condoomge-bruik en andere preventie strategieën besproken wordt met PrEP gebruikers. Voor personen die geen PrEP (gaan) gebruiken, omdat ze niet in aanmerking komen of omdat ze geen PrEP willen gebruiken, zou condoomgebruik een normatieve en sociaal geaccepteerde optie moeten blijven.
Hoofdstuk 3: testen op hiv, hepatitis B en hepatitis C en soa’s
In hoofdstuk 3 onderzochten we nieuwe mogelijkheden om te testen op hiv, hepatitis B en hepatitis C. Personen die geboren zijn in een land waar hiv, hepatitis B en C nog veel voorkomt vormen een belangrijke groep in de epidemie van deze infecties in Nederland en in Europa. Zij ervaren echter specifieke barrières om zich op hiv, hepatitis B en hepatitis C te laten testen. Daarom richt dit hoofdstuk zich vooral op het testen van personen die niet geboren zijn in Nederland.
In hoofdstuk 3.1 onderzochten we allereerst of er verschillen zijn in de toegang tot en gebruik van hiv preventie en zorg voor en na hiv diagnose onder mannen en vrouwen die wel en niet geboren zijn in Nederland. Onze resultaten laten zien dat er verschillen zijn er in de toegang tot hiv preventie en zorg en in de mate van hiv discriminatie, maar dat naast geboorteland seksuele oriëntatie ook een belangrijke rol speelt. We toonden aan dat er gemiste kansen zijn om personen vroegtijdig te testen op hiv omdat bijna alle deelnemers in de studie in de twee jaar voor de hiv diagnose een zorginstelling bezochten waarbij slechts in 40% van die bezoeken een hiv test werd besproken. Omdat onze data laten zien dat hete-roseksuele mannen en vrouwen zich minder vaak laten testen op hiv en zij vaak in een laat stadium van een hiv infectie gediagnosticeerd worden is het belangrijk om de mogelijkheden voor deze groep om zich te laten testen te vergroten. Voor MSM die niet geboren zijn in Nederland is het belangrijk is om toegang tot hiv preventie (zoals PrEP) te vergroten omdat zij hoogstwaarschijnlijk minder op de hoogte zijn van de opties om hiv te voorkomen dan MSM die wel in Nederland geboren zijn.
In hoofdstuk 3.2 onderzochten we hoe vaak hepatitis B en C voorkomen onder verschillende groepen Amsterdammers. We onderzochten ook hoeveel personen met een hepatitis B of hepatitis C infectie al op de hoogte waren dat zij een infectie hadden. Onze resultaten laten

Appendix
252
zien dat een chronische hepatitis B infectie het vaakst voorkwam onder Amsterdammers geboren in Ghana, gevolgd door Amsterdammers met een Turkse, Creools-Surinaamse, Marokkaanse, Hindoestaans-Surinaamse en Nederlandse migratieachtergrond. Ruim veertig procent van de personen met een chronische hepatitis B infectie was hiervan nog niet op de hoogte. Een chronische hepatitis C infectie kwam weinig voor onder alle groepen.
In hoofdstuk 3.3 hebben we in 2013–2015 onderzocht wat de effectiviteit en haalbaarheid was van vrijwillige hiv, hepatitis B en hepatitis C screening geïntegreerd in de tuberculose screening kort na aankomst in Nederland. Deze screening is verplicht voor personen gebo-ren in landen waar tuberculose vaak voorkomt. In dit screeningsproject gaf ongeveer de helft van de personen die de tuberculose afdelingen in Gelderland en Amsterdam bezochten toestemming voor het testen op hiv, hepatitis B en hepatitis C. In Gelderland had ruim 4% van de geteste personen een niet eerder gediagnosticeerde chronische hepatitis B infectie, terwijl er in Amsterdam geen nieuwe hepatitis B infecties werden gevonden. Dit verschil zou mogelijk verklaard kunnen worden door verschillen in de landen van herkomst en de redenen van migratie tussen deelnemers uit beide regio’s. Nieuw gediagnosticeerd hepatitis C infecties kwamen weinig voor in beide regio’s en er werden geen hiv infecties gevonden.
Zelftesten zijn testen die zelfstandig afgenomen en afgelezen worden door personen zonder tussenkomst van een zorgverlener of gecertificeerd laboratorium. Omdat er nog weinig gegevens bekend zijn of personen zelftesten voor hiv en soa gebruiken en wat de karakte-ristieken zijn van hiv/soa zelftest gebruikers, hebben we dit onderzocht in hoofdstuk 3.4 en 3.5.
In hoofdstuk 3.4 onderzochten we het gebruik van hiv en soa zelftesten tussen 2007 en 2015 onder de algemene bevolking en onder hoog-risico groepen in Amsterdam. Onze resultaten laten zien dat het gebruik van hiv/soa zelftesten in de laatste 6-12 maanden laag was (1–2%) onder alle groepen. Zelftesten voor chlamydia werden het meest gebruikt, behalve onder MSM. Het gebruik van zelftesten voor chlamydia (onder de Amsterdamse bevolking en soa polikliniek bezoekers) en syfilis (onder de Amsterdamse bevolking) nam toe over de tijd. Zelftest gebruik was hoger onder personen met een Creools-Surinaamse en Ghanese migratieachtergrond, onder vrouwen en MSM en onder personen met een hoger aantal seksuele partners dan onder personen zonder migratieachtergrond, heteroseksuele man-nen en personen met een lager aantal partners.
In hoofdstuk 3.5 onderzochten we het gebruik van hiv zelftesten onder personen met een migratieachtergrond wonende in het Verenigd Koninkrijk, Frankrijk en Nederland in 2014-2015. In deze studie was het gebruik van hiv zelftesten in de laatste 12 maanden laag (2%), maar hoger onder MSM (4%). Het gebruik van hiv zelftesten was hoger onder MSM met

253
Nederlandse samenvatting
a
een migratieachtergrond die in het Verenigd Koninkrijk woonden dan onder MSM met een migratieachtergrond die in Frankrijk of Nederland woonden. Bij één gebruiker gaf de hiv zelftest geen testresultaat, bij de rest was de gebruikers was de test negatief (de test had geen hiv gedetecteerd). Van de personen met een negatief zelftest resultaat ging de helft naar een zorgverlener voor het herhalen van de test.
De resultaten van hoofdstuk 3 laten zien dat personen die niet geboren zijn in Nederland barrières ervaren in de toegang tot zorg (inclusief testen). Om de ziektelast door hiv, hepatitis B, hepatitis C en soa’s te laten afnemen is het belangrijk dat zorgverleners testen aanbieden aan specifieke groepen die niet geboren zijn in Nederland en waar deze infecties nog vaak voorkomen en dat er screeningsprogramma opgezet worden. Huisartsen zouden het best testen kunnen aanbieden aan individuele personen. Het is echter van belang dat barrières die huisartsen ervaren om op hiv, hepatitis B en C te testen geminimaliseerd worden. Bij het opzetten van screeningsprogramma’s is het aanbevolen om een screeningsprogramma te in-tegreren in bestaande zorgverlening. Geïntegreerde hiv, hepatitis B, hepatitis C screening in de bestaande tuberculose binnenkomst screening voor nieuwe Nederlanders lijkt haalbaar, maar de (kosten-)effectiviteit zal afhangen van de specifieke groep die getest wordt. Zelf-testen kunnen barrières die sommige personen ervaren om zich te laten testen wegnemen. Echter voor soa’s (exclusief hiv) wordt het gebruik van zelftesten nog afgeraden omdat de nauwkeurigheid van de testen laag is.
Hoofdstuk 4: algemene discussie
In hoofdstuk 4 worden de relevantie van deze studies en de recente ontwikkelingen en de uitdagingen bediscussieerd. Om de ziektelast veroorzaakt door hiv, hepatitis B, hepatitis C en soa te verminderen zijn innovatieve preventieve interventies hard nodig en is het belangrijk dat deze snel geïmplementeerd worden. Om te bepalen welke interventies nodig zijn voor specifieke doelgroepen is het belangrijk de voortgang in het bereiken van internationale en nationale doelen te monitoren per subgroep. Specifieke uitdagingen ten aanzien van de toename van PrEP gebruik zijn het tegengaan van de mogelijke toename van soa’s, het be-vorderen van de therapietrouw en het seksueel welbevinden tijdens PrEP gebruik. Voor het testen en screening van personen niet geboren in Nederland is het belangrijk dat effectieve programma’s geëvalueerd worden in demonstratieprojecten. Voor zelftesten zijn de uitda-gingen het adequaat aanbieden van informatie en counseling, en een goede doorverwijzing bij een positieve testuitslag.


255
About the author
a
aBouT THe auTHor
Janneke Bil was born on the 21st of September 1983 in Zaanstad, the Netherlands. Following high school, she enrolled in a bachelor’s degree program in Social Work (Sociaal Pedago-gische Hulpverlening). After one year, she switched to a bachelor’s degree in Nursing at the Hogeschool van Amsterdam (HvA) from which she graduated in 2006. Her final thesis which was on the topic of patient safety in the internal medicine ward won the prize for best thesis of the year (internal competition within the bachelor’s degree of Nursing).
From 2006 to 2010 she worked as a clinical nurse, and later as a senior nurse focusing on quality and innovation, in the department of Gastrointestinal, Hepatology and Internal Medicine of the Amsterdam UMC, location AMC.
In 2008 she began a master’s degree programme in Health Sciences at the Vrije University (VU) of Amsterdam, specializing in Infectious Diseases. During her master’s programme she continued to work part-time as a clinical nurse in the department of Hematology and Oncol-ogy of the AMC. Between 2011 and 2012 she carried out her master’s thesis at the Public Health Service of Amsterdam (GGD Amsterdam) on risk factors for a tuberculosis infection among close contacts of pulmonary tuberculosis cases. In 2012 she graduated from her master’s degree in Health Sciences receiving a Cum Laude.
After obtaining her master’s degree she started working as a junior consultant of epidemiol-ogy for the Amsterdam Institute for Global Health and Development (AIGHD) and KNCV Tuberculosis Foundation. Here she worked on a project on the cost-effectiveness of new diagnostic tools for (multi-resistant) tuberculosis in China. After finishing this project, she returned to the department of Infectious Diseases, Research and Prevention of the Public Health Service of Amsterdam in December 2012 where she began work on a doctoral de-gree. Her PhD incorporated projects focusing on current aspects of acceptability, attitudes, beliefs and behavioural intentions towards the use of pre-exposure prophylaxis (PrEP) to prevent HIV infection among men who have sex with men and healthcare professionals. Her thesis also focussed on testing opportunities for HIV, hepatitis B, hepatitis C and sexually transmitted infections (STIs), especially among migrants.
Currently, Janneke is working at the Public Health Service of Amsterdam as a research co-ordinator for a pharmaceutical-sponsored, phase 3, randomized, double-blind clinical trial on PrEP.


257
Portfolio
a
PortfoLIo
Phd training
Year eCts
General courses
- Scientific Writing in English for Publication, AMC Graduate School, the Netherlands 2015 1.5
- Oral Presentation, AMC Graduate School, the Netherlands 2015 0.8
- Project Management, AMC Graduate School, the Netherlands 2015 0.6
- eBROK, NFU Brokacademie, the Netherlands 2015 1.0
- Advanced Topics in Biostatistics 2016 2.1
Specific courses
- Infectious Diseases, AMC Graduate School, the Netherlands 2013 1.3
- Epidemiology of Infectious Diseases, NIHES, Erasmus Medical Center, the Netherlands
2014 0.5
- Qualitative Research, AMC Graduate School, the Netherlands 2015 1.9
- Planning and Evaluation of Screening, NIHES, Erasmus Medical Center, the Netherlands
2016 1.4
- Weekly PhD educational hour (Seminars, Journal Club, Peer Education, Epidemiology class), Department of Infectious Diseases, Public Health Service of Amsterdam, the Netherlands
2012–2016 14.0
- Motivational Interviewing, STI clinic, Public Health Service of Amsterdam, the Netherlands
2017–2018 1.0
- Intervention Mapping, Maastricht University, the Netherlands 2019 1.2
Seminars, workshops, master classes
- Lecture “Treatment as Prevention: The key to an AIDS-free generation”, Amsterdam Institute for Global Health and Development, Amsterdam, the Netherlands
2013 0.1
- Symposium: Hiv-zorg als rolmodel, Virology Education, The Hague, the Netherlands 2013 0.1
- Symposium: “Gevluchte gezinnen, gezonde gezinnen?”, GGD GHOR Nederland, Amsterdam, the Netherlands
2014 0.1
- Online workshop: Chemsex: an introduction, National Institute for STI and AIDS Control in the Netherlands
2017 0.1
- Symposium: HBV en HCV: stand van kennis 2014, National Institute for Public Health and the Environment, Bilthoven, the Netherlands
2014 0.1
- Online workshop: Basic knowledge of STI and HIV, National Institute for STI and AIDS Control in the Netherlands
2017 0.1
Oral abstract presentations
- “Perceived motives for the future daily and intermittent use of pre-exposure prophylaxis to prevent HIV-infection among men having sex with men in the Netherlands: a qualitative study”, International AIDSImpact Conference, Amsterdam, the Netherlands
2015 0.5

Appendix
258
- “Beliefs and attitudes towards pre-exposure prophylaxis prescription among health care providers: a qualitative study”, International AIDSImpact Conference, Amsterdam, the Netherlands (presented by Elske Hoornenborg)
2015 0.5
- “Low knowledge and moderate acceptability towards the prescription of pre-exposure prophylaxis among Dutch healthcare providers of sexual health clinics: a mixed-methods study”, Netherlands conference on HIV pathogenesis, epidemiology, prevention and treatment (NCHIV), Amsterdam, the Netherlands (oral poster presentation)
2015 0.5
- “Usage of self-tests for HIV and STIs among the general population and sexual risk groups in Amsterdam, the Netherlands”, International AIDSImpact Conference, Amsterdam, the Netherlands
2015 0.5
- “Differences in access to HIV testing, treatment and healthcare among non-migrants and migrants living with HIV in the Netherlands: a cross-sectional study”, International AIDSImpact Conference, Cape Town, South Africa (oral poster presentation)
2017 0.5
- “Differences in access to HIV testing, treatment and healthcare among non-migrants and migrants living with HIV in the Netherlands: a cross-sectional study”, Netherlands conference on HIV pathogenesis, epidemiology, prevention and treatment (NCHIV), Amsterdam, the Netherlands
2017 0.5
Poster abstract presentations
- “Low intention to use Pre-Exposure Prophylaxis (PrEP) to prevent HIV-infection among men having sex with men (MSM) in the Netherlands”, Dutch Epidemiology conference (WEON), Utrecht, the Netherlands
2013 0.5
- “The intention to use Pre-Exposure Prophylaxis (PrEP) to prevent HIV infection among men having sex with men in the Netherlands”, Netherlands conference on HIV pathogenesis, epidemiology, prevention and treatment (NCHIV), Amsterdam, the Netherlands
2013 0.5
- “The intention to use Pre-Exposure Prophylaxis (PrEP) to prevent HIV infection among men having sex with men in the Netherlands”, International AIDSImpact Conference, Barcelona, Spain (presented by Ineke Stolte)
2013 0.5
- “Motives and barriers to use Pre-Exposure Prophylaxis (PrEP) to prevent HIV-infection among men having sex with men (MSM): a qualitative study”, Netherlands conference on HIV pathogenesis, epidemiology, prevention and treatment (NCHIV), Amsterdam, the Netherlands
2014 0.5
- “The intention to use Pre-Exposure Prophylaxis (PrEP) to prevent HIV-infection among men having sex with men (MSM) in Amsterdam, the Netherlands”, 20th International AIDS Conference, Melbourne, Australia
2014 0.5
- “Motives and barriers to use Pre-Exposure Prophylaxis (PrEP) to prevent HIV-infection among men having sex with men (MSM): a qualitative study”, 20th International AIDS Conference, Melbourne, Australia
2014 0.5
- “Usage of self-tests for HIV and STIs among the general population and sexual risk groups in Amsterdam, the Netherlands”, 20th International AIDS Conference, Melbourne, Australia
2014 0.5
- “Usage of self-tests for HIV and STIs among the general population and sexual risk groups in Amsterdam, the Netherlands”, Netherlands conference on HIV pathogenesis, epidemiology, prevention and treatment (NCHIV), Amsterdam, the Netherlands
2014 0.5

259
Portfolio
a
- “Acceptability and effectiveness of integrating voluntary hepatitis B, C and HIV screening in the compulsory tuberculosis entry screening for migrants in Amsterdam, The Netherlands”, 26th Transmissiedag Infectieziekten, Amersfoort, the Netherlands (presented by Freke Zuure)
2016 0.5
- “Integrating voluntary hepatitis B, C and HIV screening in the compulsory tuberculosis entry screening for immigrants, The Netherlands: a pilot project”, European Association for the Study of the Liver (EASL), Amsterdam, the Netherlands
2017 0.5
(Inter)national conferences visited
- Dutch epidemiology conference (WEON), Utrecht, the Netherlands 2013 0.2
- Netherlands conference on HIV pathogenesis, epidemiology, prevention and treatment (NCHIV), Amsterdam, the Netherlands
2013, 2014, 2015, 2016, 2017
1.0
- Dutch National STI, HIV and sex conference, Amsterdam, the Netherlands 2013,2014, 2015, 2017, 2018
0.8
- 20th International AIDS Conference, Melbourne, Australia 2014 1.0
- Dutch National Hepatitis conference, Amsterdam/Rotterdam, the Netherlands 2014, 2015, 2016, 2018
0.6
- 12th International AIDSImpact Conference, Amsterdam, the Netherlands 2015 0.6
- 3rd International Meeting on Elimination of Viral Hepatitis, Amsterdam, the Netherlands
2016 0.2
- 13th International AIDSImpact Conference, Cape Town, the Netherlands 2017 0.6
Other academic activities
- Coordinator of the bi-annual newsletter for the participants (men who have sex with men) of the Amsterdam Cohort Studies on HIV
2013-2014 2.0
- Member of the organizing committee of the dissemination meeting for participants (men who have sex with men) of the Amsterdam Cohort Studies on HIV/AIDS
2014 0.5
- Organizer of a community dissemination meeting for sexual health, HIV and STI to various migrant groups in the Netherlands
2016 0.5
- Dissemination of the results of conducted research to the involved migrant communities and participating clinics/organizations during various meetings and through newsletter items
2013-2018 2.0
- Peer-reviewer for International Journal of Drug Policy (n=1); AIDS and Behavior (n=1); International Journal of STD & AIDS (n=1); JMIR (n=1); Eurosurveillance (n=1); Sexually Transmitted Infections (n=1); BMJ Open (n=1)
2012-2018 1.4
- Coordinator Workshop “PrEP in de spreekkamer” during the national STI, HIV and sex conference, Amsterdam, the Netherlands
2017 0.5
total 47.8
teaching
Supervising
- Darshni Jhagroe, Master student Biomedical Sciences (VU university Amsterdam), “The usage of self-tests for STI and/or HIV among visitors of the STI clinic in Amsterdam, the Netherlands”
2013-2014 3.0

Appendix
260
- Saskia Bogers, Medical Master student (University of Amsterdam), “Barriers for access to healthcare and HIV prevention, testing, and treatment among migrants and native Dutch HIV-positive patients in the Netherlands: an explorative study”
2014 2.0
- Emilia Ric-Doe, Master student International Public Health (VU university Amsterdam), “Determinants of a late HIV diagnosis: the role of country of origin”
2015 3.0
- Fernando Dias Gonçalves Lima, Medical Master student (University of Amsterdam), “Knowledge, attitudes and beliefs of HIV specialists and HIV nurse practitioners about pre-exposure prophylaxis for HIV prevention”
2015–2016 2.0
Lecturing
- Co-mentor during the Epidemiology course for new PhD-students, Department of Infectious Diseases, Public Health Service of Amsterdam
2015–2017 0.3
- Guest lecturer during the career day for bachelor students Health Sciences of the Vrije University of Amsterdam
2017 0.1
total 10.4
scholarships
- Young Investigator bursary, European Association for the Study of the Liver (EASL), Amsterdam, the Netherlands
2017

261
List of publications
a
lIST oF PuBlICaTIonS
Peer reviewed publications
- Bil JP, Davidovich U, van der Veldt WM, Prins M, de Vries HJC, Sonder GJB, Stolte IG. What do dutch MSM think of preexposure prophylaxis to prevent HIV-infection? a cross-sectional study. AIDS 2015;29(8):955-964. doi: 10.1097/QAD.0000000000000639.
- Bil JP, van der Veldt WM, Prins M, Stolte IG, Davidovich U. Motives of dutch men who have sex with men for daily and intermittent HIV pre-exposure prophylaxis us-age and preferences for implementation: a qualitative study. Medicine (Baltimore) 2016;95(39):e4910. doi: 10.1097/MD.0000000000004910.
- Bil JP, Prins M, Stolte IG, Dijkshoorn H, Heijman T, Snijder MB, Davidovich U, Zuure FR. usage of purchased self-tests for HIV and sexually transmitted infections in amster-dam, the netherlands: results of population-based and serial cross-sectional studies among the general population and sexual risk groups. BMJ Open 2017;7(9):e016609. doi: 10.1136/bmjopen-2017-016609.
- Fakoya I, Álvarez-Del Arco D, Copas AJ, Teixeira B, Block K, Gennotte AF, Volny-Anne A, Bil JP, Touloumi G, Del Amo J, Burns FM. Factors associated With access to HIV Testing and Primary Care among Migrants living in europe: Cross-Sectional Survey. JMIR Public Health Surveill.2017;3(4):e84. doi:10.2196/publichealth.7741.
- Bil JP*, Hoornenborg E*, Prins M, Hogewoning A, Dias Goncalves Lima F, de Vries HJC, Davidovich U. The acceptability of Pre-exposure Prophylaxis: Beliefs of Health-Care Professionals Working in Sexually Transmitted Infections Clinics and HIV Treatment Centers. Front Public Health 2018;6:5. doi: 10.3389/fpubh.2018.00005.
* Both authors contributed equally to this article- Bil JP, Prins M, Fakoya I, Volny-Anne A, Burns F, Zuure FR. usage of purchased self-tests
for HIV infections among migrants living in the uK, France and the netherlands: a cross-sectional study. Sex Transm Infect 2018 doi: 10.1136/sextrans-2018-053583.
- Bil JP, Schrooders PAG, Prins M, Kouw PM, Klomp JHE, Scholing M, Huijbregts LPHM, Sonder GJB, Waegemaekers TCHFM, de Vries HJC, Meijer W, Zuure FR, Tostmann A. Inte-grating hepatitis B, hepatitis C and HIV screening into tuberculosis entry screening for migrants in the netherlands, 2013 to 2015. Euro Surveill 2018;23(11) doi: 10.2807/1560-7917.ES.2018.23.11.17-00491.
- Coyer L, van Bilsen W, Bil JP, Davidovich U, Hoornenborg E, Prins M, Matser A. Pre-exposure prophylaxis among men who have sex with men in the amsterdam Cohort Studies: use, eligibility, and intention to use. PLoS One 2018;13(10):e0205663. doi: 10.1371/journal.pone.0205663.
- Reyniers T, Vuylsteke B, Pirotte B, Hoornenborg E, Bil JP, Wouters K, Laga M, Nöstlinger C. Physicians’ preparedness for pre-exposure prophylaxis: results of an online survey in Belgium. Sex Health 2018;15(6):606-11 doi: 10.1071/SH18072.

Appendix
262
- Zuure FR*, Bil JP*, Visser M, Snijder MB, Boyd A, Blom P, Sonder GJB, Schinkel J, Prins M. Hepatitis B and C screening needs among different ethnic groups: a population-based study in amsterdam, the netherlands. JHEP Reports 2019. Advance online publication. doi:10.1016/j.jhepr.2019.04.003.
* Both authors contributed equally to this article
Submitted publications
- Bil JP, Zuure FR, Alvarez-del Arco D, Prins JM, Brinkman K, Leyten E, van Sighem A, Burns F, Prins M. disparities in access to and use of HIV-related health services in the nether-lands by migrant status and sexual orientation: a cross-sectional study among people recently diagnosed with HIV infection.
non-peer reviewed publications
- Hoornenborg E, de Vries HJC, Schim van der Loeff MF, Davidovich U, Bil JP, Achterbergh RA, Fennema JS, Prins M. Pre-expositieprofylaxe voor preventie van hiv-transmissie: stand van zaken en amsterdam PreP-project. HIV Bulletin 2015;4.
Publications about my research
- Van Venrooij T. lage bereidheid tot pre-expositieprofylaxe. Ned Tijdschr Geneeskd. 2015;159:C2611.
- Van Heest F. Soa-zelftesten niet populair in amsterdam. Ned Tijdschr Geneeskd. 2017;161:C3676.

263
List of contributing authors
a
lIST oF ConTrIBuTInG auTHorS
Débora Alvarez-del Arco National Centre for Epidemiology. Instituto de Salud Carlos III, Universidad Complutense de Madrid, Spain
Petra Blom Department of Medical Microbiology, Amsterdam UMC (location AMC), University of Amsterdam, the Netherlands
Anders Boyd Department of Infectious Diseases, Research and Prevention, Public Health Service of Amsterdam, The NetherlandsINSERM, Institut Pierre Louis d’Epidémiologie et de Santé Publique, Saint Antoine Hospital, AP-HP, Sorbonne Université, Paris, France
Kees Brinkman Department of Internal Medicine, Onze Lieve Vrouwe Gasthuis (OLVG), Amsterdam, the Netherlands
Fiona Burns Institute for Global health, University College London, United Kingdom
Udi Davidovich Department of Infectious Diseases, Research and Prevention, Public Health Service of Amsterdam, The NetherlandsDepartment of Internal Medicine, Amsterdam Infection and Immunity Institute (AI&II), Amsterdam UMC (location AMC), University of Amsterdam, the Netherlands
Fernando Dias Goncalves Lima Department of Infectious Diseases, Research and Prevention, Public Health Service of Amsterdam, The Netherlands
Henriëtte Dijkshoorn Department of Epidemiology and Health Promotion, Public Health Service ofAmsterdam, The Netherlands
Ibidun Fakoya Institute of Global Health, University College London, United Kingdom
Titia Heijman Sexually Transmitted Infections Outpatient Clinic, Public Health Service ofAmsterdam, The Netherlands
Arjan Hogewoning Sexually Transmitted Infections Outpatient Clinic, Public Health Service ofAmsterdam, The NetherlandsDepartment of Dermatology, Amsterdam UMC (location AMC), University of Amsterdam, the Netherlands
Elske Hoornenborg Department of Infectious Diseases Research and Prevention, Public Health Service of Amsterdam, The NetherlandsSexually Transmitted Infections Outpatient Clinic, Public Health Service ofAmsterdam, the Netherlands
Lutje P.H.M. Huijbregts Department of Infectious Diseases, Public Health Service of Noord- en Oost-Gelderland, Warnsveld, the Netherlands
Judith H.E. Klomp Department of Infectious Diseases, Public Health Service of Gelderland Zuid, Nijmegen, the Netherlands
Peter M. Kouw Department of Infectious Diseases, Tuberculosis clinic, Public Health Service of Amsterdam, Amsterdam, the Netherlands
Eliane Leyten Department of Internal Medicine, Medical Center Haaglanden-Bronovo, The Hague, the Netherlands
Wieneke Meijer Department of Infectious Diseases, Tuberculosis clinic, Public Health Service of Amsterdam, Amsterdam, the Netherlands
Jan M. Prins Department of Internal Medicine, Amsterdam UMC (location AMC), University of Amsterdam, the Netherlands
Maria Prins Department of Infectious Diseases, Research and Prevention, Public Health Service of Amsterdam, The NetherlandsDepartment of Internal Medicine, Amsterdam Infection and Immunity Institute (AI&II), Amsterdam UMC (location AMC), University of Amsterdam, the Netherlands

Appendix
264
Janke Schinkel Department of Medical Microbiology, Amsterdam UMC (location AMC), University of Amsterdam, the Netherlands
Maarten Scholing Department of Infectious Diseases, Public Health Laboratory, Public Health Service of Amsterdam, Amsterdam, the NetherlandsDepartment of Medical Microbiology, Onze Lieve Vrouwe Gasthuis (OLVG), Amsterdam, the Netherlands
Peter A.G. Schrooders Department of Infectious Diseases, Public Health Service of Noord- en Oost-Gelderland, Warnsveld, the Netherlands
Ard van Sighem Stichting HIV Monitoring, Amsterdam, The Netherlands
Marieke B. Snijder Department of Public Health, Amsterdam UMC (location AMC), University of Amsterdam, the NetherlandsDepartment of Clinical Epidemiology, Biostatistics and Bioinformatics, Amsterdam UMC (location AMC), University of Amsterdam, the Netherlands
Gerard J.B. Sonder Department of Infectious Diseases, Public Health Service of AmsterdamDepartment of Internal Medicine, Amsterdam Infection and Immunity Institute (AI&II), Amsterdam UMC (location AMC), University of Amsterdam, the Netherlands
Ineke G. Stolte Department of Infectious Diseases, Research and Prevention, Public Health Service of Amsterdam, The NetherlandsDepartment of Internal Medicine, Amsterdam Infection and Immunity Institute (AI&II), Amsterdam UMC (location AMC), University of Amsterdam, the Netherlands
Alma Tostmann Department of Primary and Community Care, Radboud University Medical Center, Nijmegen, the Netherlands
Wendy M. van der Veldt Department of Infectious Diseases, Research and Prevention, Public Health Service of Amsterdam, the Netherlands
Alain Volny-Anne European AIDS Treatment Group, Brussels, Belgium
Maartje Visser The national Institute for Public Health and the Environment, Bilthoven, the Netherlands
Henry J.C. de Vries Department of Internal Medicine, Amsterdam Infection and Immunity Institute (AI&II), Amsterdam UMC (location AMC), University of Amsterdam, the NetherlandsSexually Transmitted Infections Outpatient Clinic, Public Health Service ofAmsterdam, The NetherlandsDepartment of Dermatology, Amsterdam UMC (location AMC), University of Amsterdam, the NetherlandsDepartment of Infectious Diseases, Public Health Service of AmsterdamCenter for Infectious Disease Control, National Institute of Public Health and the Environment, Bilthoven, Netherlands
Toos C.H.F.M. Waegemaekers National Coordination Centre for Communicable Disease Control, National Institute for Public Health and the Environment, Bilthoven, the Netherlands
Freke R. Zuure Department of Infectious Diseases, Research and Prevention, Public Health Service of Amsterdam, The NetherlandsDepartment of Internal Medicine, Amsterdam Infection and Immunity Institute (AI&II), Amsterdam UMC (location AMC), University of Amsterdam, the Netherlands

265
Authors’ contributions per chapter
a
auTHorS’ ConTrIBuTIonS Per CHaPTer
Chapter 2.1: What do dutch men who have sex with men think of pre-exposure prophylaxis to prevent HIV-infection? a cross-sectional study
Janneke P. Bil interpreted the data, and wrote the draft article. Ineke G. Stolte and Udi Davidovich designed and supervised the overall study, and contributed to the analyses and interpretation of the data. Wendy M. van der Veldt, Maria Prins, Henry J.C.de Vries, and Gerard J.B. Sonder provided substantial contributions to the interpretation of the data. All authors contributed to subsequent drafts and approved the final version of the article.
Chapter 2.2: Motives of dutch men who have sex with men for daily and intermittent HIV pre-exposure prophylaxis usage and preferences for implementation: a qualitative study
Janneke P. Bil conducted the semi structured interviews and wrote the draft manuscript. Janneke P. Bil and Wendy M. van der Veldt read and coded the interview transcripts. Jan-neke P. Bil, Wendy M. van der Veldt, Ineke G. Stolte and Udi Davidovich analyzed the data. Ineke G. Stolte and Udi Davidovich designed and supervised the overall study. Maria Prins provided substantial contributions to the interpretation of the data. All authors contributed to subsequent drafts and approved the final version of the article.
Chapter 2.3: The acceptability of pre-exposure prophylaxis: Beliefs of health-care professionals working in sexually transmitted infections clinics and HIV treatment centers
Janneke P. Bil, Elske Hoornenborg, and Udi Davidovich designed the study. Janneke P. Bil, Elske Hoornenborg, Fernando Dias Goncalves Lima and Udi Davidovich collected the data. Janneke P. Bil and Udi Davidovich analyzed the data. Janneke P. Bil and Elske Hoornenborg wrote the draft manuscript. All authors contributed to the interpretation of the data and contributed to subsequent drafts of the article. Udi Davidovich supervised the overall study.
Chapter 3.1: disparities in access to and use of HIV-related health services between migrant and non-migrant people living in the netherlands: a cross-sectional study
Janneke P. Bil interpreted the data, and wrote the draft manuscript. Janneke P. Bil, Freke R. Zuure and Maria Prins designed this study in the Netherlands, and Freke R. Zuure en Maria Prins supervised the analyses and interpretation of the data. Julia de Amo and Fiona Burns led the design and implementation of the European aMASE study. Debora Alvarez-del Arco coordinated the European aMASE study. Jan M. Prins, Kees Brinkman, Eliane Leyten were the responsible investigators in the three participating HIV outpatient clinics in the Neth-erlands. Ard van Sighem provided clinic indicator data from the HIV ATHENA (AIDS Therapy Evaluation in the Netherlands) HIV cohort database.

Appendix
266
All authors provided substantial contributions to the interpretation of the data and to subse-quent drafts and approved the final version of the manuscript.
Chapter 3.2: Hepatitis B and C screening needs among different ethnic groups: a population-based study in amsterdam, the netherlands
Freke R. Zuure coordinated the current study and drafted the manuscript; Janneke P. Bil performed data management and the statistical analyses and coordinated the collection of clinical follow-up data; Maartje Visser performed data management and analyses during her internship; Marieke B. Snijder coordinated the HELIUS study (data collection and data management) and contributed to the study design of the current study; Anders Boyd con-tributed to the statistical analyses; Petra Blom and Janke Schinkel coordinated the laboratory testing; Janke Schinkel and Gerard J.B. Sonder contributed to the study design; Maria Prins conceived and supervised the current study. All authors contributed to the interpretation of the results and the writing of the manuscript.
Chapter 3.3: Integrating hepatitis B, hepatitis C and HIV screening into tuberculosis entry screening for migrants in the netherlands, 2013 to 2015
Janneke P. Bil wrote the draft manuscript. Peter Schrooders, Judith Klomp, Lutje Huijbregts, Toos Weagemaekers and Alma Tostmann designed and coordinated the project in Gelder-land. Janneke Bil, Maria Prins, and Freke Zuure designed and coordinated the project in Am-sterdam. Peter Kouw, Gerard Sonder, Henry de Vries, Maarten Scholing and Wieneke Meijer contributed to project design and logistics in Amsterdam. All authors provided substantial contributions to the interpretation of the data and to subsequent drafts, and all approved the final version of the manuscript.
Chapter 3.4: usage of purchased self-tests for HIV and sexually transmitted infections in amsterdam, the netherlands: results of population-based and serial cross-sectional studies among the general population and sexual risk groups
Janneke P. Bil interpreted the data and wrote the draft manuscript. Freke R. Zuure designed and supervised the overall study and contributed to the analyses and interpretation of the data. Maria Prins, Ineke G. Stolte, Henriëtte Dijkshoorn, Titia Heijman, Marieke B. Snijder and Udi Davidovich provided contributions to the data collection and management in the different studies. All authors provided substantial contributions to the interpretation of the data and to subsequent drafts and approved the final version of the manuscript.
Chapter 3.5: usage of purchased self-tests for HIV infections among migrants living in the uK, France and the netherlands: a cross-sectional study
Janneke P. Bil interpreted the data and wrote the draft of the manuscript. Janneke P. Bil, Freke R. Zuure and Maria Prins designed this study on self-testing, and Freke R. Zuure and

267
Authors’ contributions per chapter
a
Maria Prins supervised the analyses and interpretation of the data. Fiona Burns led the design and implementation of the European aMASE study. Ibidun Fakoya coordinated the European aMASE study. Alain Volny-Anne was responsible for the data collection in France. All authors provided substantial contributions to the interpretation of the data and to subse-quent drafts, and approved the final version of the manuscript.


269
Dankwoord
a
danKWoord
Allereerst wik ik mijn promotor en copromotors bedanken. Maria, wat heb ik veel van jou geleerd! Dank voor het delen van al je kennis en ervaring, en voor al je wijze adviezen en je geduld als ik het even niet meer zag zitten. Freke, wat was het fijn om met jou samen te werken! Dank voor je praktische insteek op zaken en dat ik altijd bij je binnen kon lopen als dat nodig was. Udi, bij jou weet je nooit wat je kunt verwachten maar dat maakt het promoveren zeker niet saai! Dank voor je psychologische inzichten en hopelijk kan ik de toekomst nog vaak bij je terecht als ik bij Martijn geen verlaten snoepgoed kan vinden of als ik om een mooie filosofische zin verlegen zit. Ineke, dankzij jou ben ik uiteindelijk echt begonnen met werken bij de GGD en later werd je mijn copromotor. Maar door de nieuwe uitdaging die je aanging heb je het stokje overgedragen aan Udi. Dank voor al je begeleiding tijdens het begin van mijn carrière als onderzoekster.
Lieve paranimfen Sil en Suus, dank dat jullie naast mij willen staan tijdens de verdediging. Sil, dank je wel voor de ontelbare keren dat je vroeg hoe het met mijn promotie ging, je be-moedigende woorden en je enthousiasme toen ik (meerdere keren) vertelde dat het boekje (bijna) af was. Je vrolijkheid, enthousiasme, de reizen die je maakt en je sociale karakter zijn inspirerend! Suus, dank voor je luisterende oor tijdens het laatste stukje van mijn promotie, de gezellige koffies en de baby klets. Wat fijn dat ik jou als mijn collega heb en dat we dat voorlopig nog even blijven. Op veel meer gezelligheid in de toekomst!
Niks maakt het werk zo leuk als je collega’s! Dank lieve kamergenootjes, met elkaar deelden we lief en leed: Dani (mijn steun en toeverlaat tijdens mijn hele promotie! Ik mis je!) & Wijnand (geniet nog heerlijk samen van het mooie Australië, als jullie ooit terugkomen, gaan we zeker weer biertjes drinken), Martijn (heerlijk hoe nuchter je bent en jij, en je boekje, zijn natuurlijk mijn grote voorbeeld voor mijn promotie), Astrid (mijn voorbeeld om alles altijd op orde te hebben maar nog steeds tijd te hebben voor gezelligheid), Titia (gezellig om een kamer met elkaar te delen). Een speciale dank aan mijn lieve DISCOVER collega’s: Marc (dank voor alle gezelligheid en op veel meer gedeelde cappuccino’s), Mark (je passie is inspirerend), Elske (met jou is samenwerken altijd fijn!), Iris, Dewi, Esther, Margreet, Sandra, Gera, Amber, Ruth, Corinne en Jean-Paul (nu hopelijk in je auto naar je patiënten in de huisartsenpraktijk). Mijn andere lieve (oud) collega’s, dank voor alle gezelligheid: Rosa, Nienke, Carolien, Joost, Bart, Elske Marra, Sofie, Jannie, Gerben Rienk, Sandra, Christiaan, Linda, Ronald, Lisanne, Marjolein, Will, Nora, Robert, Maria Oud, Ai-Hsiang, Roel, Maartje Dijkstra, Maartje Basten, Amy, Maarten Schim van der Loeff, Maarten Bedert, Myrthe, Wendy, Laura, Ivette, Leeann, Samantha, Bas, Ward, Tamara, Eline, Michelle, Liza, Silvia, Yvonne, Ellen, Anders, Ceranza, Ertan, Dominque, Marije, Vita, Marita, Roel, Hanne, Arjan, Bart-Jan, Elisabeth, Adriaan,

Appendix
270
Kees, Frank, Michelle, Kenneth, alle andere collega’s van de soa poli, het lab, alle andere afdelingen binnen de GGD en iedereen die ik vergeten ben!
Graag wil ik nogmaals alle deelnemers van de studies bedanken voor hun deelname. The work in this thesis would also not have been possible without the co-authors. Thank you for all your contributions and help with the different studies. Lucy and Clair, thank you for editing my manuscripts. Saskia, Emilia, Darshni en Fernando, bedankt voor jullie hulp met de data verzameling van mijn studies tijdens jullie stages.
Dear members of my PhD thesis committee, thank you for taking the time to read and eva-luate my thesis. I’m looking forward to the discussions about my thesis during my defense.
Lieve Aukje, Bauke, Sil, Erik, Marjolijn, Roel, Thessa, Mark, Sietske, Dirk, Maud, Rob, Klari en Theo; jullie zijn echte toppertjes! Het begon met de meiden maar de mannen zijn nu ook onmisbaar geworden. Wat we ook doen het is altijd gezellig! Dank voor al jullie steun tijdens mijn promotietraject. Ik hoop dat de toekomst nog veel meer etentjes, festivals, spel-letjesavonden, borrels, weekendjes weg en veel meer leuks voor ons in petto heeft!
Leerwerkplaats groepje: Daniëlle, Sanne, Fleur, Kirby, Sil. Wat een gezelligheid altijd! Leuk om jullie wilde avonturen uit het ziekenhuis, I.C., ambulance en van de supplementen indus-trie te horen en met weemoed terug te denken aan onze tijd samen op de afdeling!
Anne, Rasjna, Rajni, Maud en Sil, mijn andere verpleegkundige clubje. Ondanks dat ik toch echt voldoende vrienden had (:-0) hebben jullie mijn hart gestolen! Wanneer gaan we weer met z’n allen daten?
Suzanne, mijn alleroudste vriendinnetje die nu een echte Hagenees is geworden! Onafschei-delijk waren we op de basisschool, de goede oude tijd! Wat leuk dat we nog steeds contact hebben.
Kim, de havo, samenwonen, vakanties, biertjes… wat hebben we niet beleefd samen? Nog belangrijker; wat gaan we nog beleven? Nu samen met de altijd kletsgrage Remi! Remi, dank dat je jouw creatieve geest hebt los willen laten op de cover van mijn boekje!
Martine en Mariska, lachen, gieren, brullen op z’n Zaans! Als ik jullie zie dan is het of we gewoon nog in de klas op de havo zitten. Gelukkig alleen geen gym meer :-).
Roos en Karin, natuurlijk was dit proefschrift bij lange na niet zo leuk als ons Bijlmer brand-weerproject. Ik kan niet wachten tot we weer een fles wijn kunnen opentrekken!

271
Dankwoord
a
Sarah, het congres samen met Maria naar Japan was het begin van onze vriendschap. Nu helaas geen AMC collega’s meer maar wat gezellig dat we elkaar nog steeds blijven zien en dat de mannen en kinderen nu ook vaak aanhaken!
Hockey chicks; van Dames 7 naar Dames 16 maar wat was het heerlijk om soms de frustratie van mijn PhD te kunnen botvieren op de hockeybal! Jammer dat het team nu niet meer bestaat maar wie weet een reünie in de toekomst?
Lieve papa en mama, aan jullie de allergrootste dank! Jullie hebben mij alle kansen gegeven die hebben geleid tot het maken van dit boekje. Dank voor jullie onvoorwaardelijke steun en liefde. Ik hou van jullie!
Natuurlijk ook alle lieve opa’s en oma’s bedankt voor alle kansen die jullie voor mij gecre-eerd hebben. Jullie hebben mij, samen met papa en mama, geleerd dat hard werken loont maar dat familietijd en gezelligheid nog belangrijker zijn. Marjolein, lief zusje, wat ben ik super trots op jou dat je hebt gekozen voor je passie, de sport en je hondjes! Nu woon je met de altijd gezellige Edward in jullie berghutje in Zwitserland. Dank dat jullie vaak de reis naar Nederland maken voor wat familietijd! De rest van de familie, ooms, tantes, neefjes, nichtjes, achterneefjes, altijd heerlijk om weer in Zeeland te zijn. Met jullie voelt het echt als een tweede thuis.
Lieve Reinoud, allereerst dank voor je hulp bij het redigeren van mijn proefschrift! Dear Marion, although sadly no longer with us, still lots on my mind. So happy that I had the chance to get to know your loving spirit. Thank your both for all the lovely times together, and Reinoud, hopelijk in de toekomst nog veel meer vakanties samen om te kijken wie de meeste spelletjes kan winnen. Claudia, James, Liam, Raff, Steven, Denise, Rob, Liane and rest of the family Boers and Rademeyer, thank you for welcoming me into the family.
Last but definitely not least, my family: Alex, Emily and the new monkey on the way. Xan, you are the best! Thank you for all your support, love and all your suggestions for solutions (which have probably not all been used otherwise this PhD would have been completed years ago). The time of my PhD thesis being finished now now or just now is over but it is actually finished NOW! I’m looking forward to a lot of new adventures together in the future.




















