High-resolution magnetic resonance imaging for the assessment of hand osteoarthritis
11
ARTHRITIS & RHEUMATISM Vol. 52, No. 8, August 2005, pp 2355–2365 DOI 10.1002/art.21210 © 2005, American College of Rheumatology High-Resolution Magnetic Resonance Imaging for the Assessment of Hand Osteoarthritis Ai Lyn Tan, 1 Andrew J. Grainger, 1 Steven F. Tanner, 1 David M. Shelley, 1 Colin Pease, 1 Paul Emery, 1 and Dennis McGonagle 2 Objective. To investigate the use of a novel surface coil for clinically utilized magnetic resonance imaging (MRI) scanners, in order to describe the microanatomic basis for hand osteoarthritis (OA) at all stages of disease. Methods. MRI of proximal or distal interphalan- geal joints was performed in 58 subjects: 16 patients with early OA (symptom duration <12 months), 14 patients with chronic OA, 10 patients with clinically normal asymptomatic joints adjacent to arthritic joints, and 18 normal controls. High-resolution images were obtained with displayed pixel dimensions of 80–100 m using a 1.5T scanner and a 23-mm–diameter surface coil. All joint structures were evaluated. Results. The high-resolution images of every joint structure showed comparable abnormalities in both early and chronic OA, including cartilage loss, bone edema, synovial enhancement, osteophytosis, and ero- sions. Heberden’s and Bouchard’s node formation oc- curred at regions where soft tissue bulged through the capsule between the dorsal tendons and collateral liga- ments (CLs). Prominent CL thickening or disruption (100% of OA patients) was evident even in joints where cartilage was partially preserved. Clinically normal joints adjacent to OA hand joints showed thickening and enhancement of CLs which was the most common abnormality seen (80% of OA patients). Older normal subjects showed subtle changes within the CLs. Conclusion. Obtaining high-resolution MR im- ages from clinically utilized scanners represents a novel way for exploring the microanatomic basis of hand arthritis and may have considerable potential in the clinical setting. In the present evaluation in nodal OA, previously unappreciated CL abnormalities were espe- cially common. The hand is commonly involved in both inflam- matory arthritis and osteoarthritis (OA), but the micro- anatomic basis for hand disease damage and localization is unclear. While synovitis is the primary abnormality in rheumatoid arthritis (RA), and enthesitis/osteitis and synovitis are central to the pathogenesis of spondylar- thropathy (SpA), the microanatomic basis for hand OA, especially at the earliest stages of disease, is less apparent. Osteoarthritis has been viewed primarily in rela- tion to cartilage loss, but the importance of bone abnor- malities and joint inflammation in OA has also been well documented (1,2), as has the need to consider the whole joint organ in disease pathogenesis (3). Conventional magnetic resonance imaging (MRI) has been used to explore the anatomic sites of abnormality in large joint OA, and has enhanced our understanding of disease mechanisms in the knee and hip, where both subchon- dral bone edema and synovitis are associated with pain, and bone edema itself is associated with progressive disease (4–6). Knee OA may be difficult to recognize at clinical presentation and patients with knee pain but normal radiographic findings would not normally be referred to a rheumatologist. The clinical pattern of the early stages of distal interphalangeal joint (DIP) and proximal inter- phalangeal joint (PIP) involvement in OA is often diagnostic, and does not rely on radiographic criteria, Supported by the Medical Research Council, UK and the Arthritis Research Campaign, UK. 1 Ai Lyn Tan, MRCP, Andrew J. Grainger, MRCP, FRCR, Steven F. Tanner, PhD, David M. Shelley, BSc, Colin Pease, FRCP, Paul Emery, MA, MD, FRCP: Leeds General Infirmary, Leeds, UK; 2 Dennis McGonagle, PhD, FRCPI: Leeds General Infirmary, Leeds, and Calderdale Royal Hospital, Halifax, UK. Address correspondence and reprint requests to Dennis McGonagle, PhD, FRCPI, Academic Unit of Musculoskeletal Disease, 2nd Floor, Chapel Allerton Hospital, Chapeltown Road, Leeds LS7 4SA, UK. E-mail: [email protected]. Submitted for publication February 7, 2005; accepted in revised form May 3, 2005. 2355
Transcript of High-resolution magnetic resonance imaging for the assessment of hand osteoarthritis

ARTHRITIS & RHEUMATISMVol. 52, No. 8, August 2005, pp 2355–2365DOI 10.1002/art.21210© 2005, American College of Rheumatology
High-Resolution Magnetic Resonance Imaging for theAssessment of Hand Osteoarthritis
Ai Lyn Tan,1 Andrew J. Grainger,1 Steven F. Tanner,1 David M. Shelley,1 Colin Pease,1
Paul Emery,1 and Dennis McGonagle2
Objective. To investigate the use of a novel surfacecoil for clinically utilized magnetic resonance imaging(MRI) scanners, in order to describe the microanatomicbasis for hand osteoarthritis (OA) at all stages ofdisease.
Methods. MRI of proximal or distal interphalan-geal joints was performed in 58 subjects: 16 patientswith early OA (symptom duration <12 months), 14patients with chronic OA, 10 patients with clinicallynormal asymptomatic joints adjacent to arthritic joints,and 18 normal controls. High-resolution images wereobtained with displayed pixel dimensions of 80–100 �musing a 1.5T scanner and a 23-mm–diameter surfacecoil. All joint structures were evaluated.
Results. The high-resolution images of every jointstructure showed comparable abnormalities in bothearly and chronic OA, including cartilage loss, boneedema, synovial enhancement, osteophytosis, and ero-sions. Heberden’s and Bouchard’s node formation oc-curred at regions where soft tissue bulged through thecapsule between the dorsal tendons and collateral liga-ments (CLs). Prominent CL thickening or disruption(100% of OA patients) was evident even in joints wherecartilage was partially preserved. Clinically normaljoints adjacent to OA hand joints showed thickeningand enhancement of CLs which was the most common
abnormality seen (80% of OA patients). Older normalsubjects showed subtle changes within the CLs.
Conclusion. Obtaining high-resolution MR im-ages from clinically utilized scanners represents a novelway for exploring the microanatomic basis of handarthritis and may have considerable potential in theclinical setting. In the present evaluation in nodal OA,previously unappreciated CL abnormalities were espe-cially common.
The hand is commonly involved in both inflam-matory arthritis and osteoarthritis (OA), but the micro-anatomic basis for hand disease damage and localizationis unclear. While synovitis is the primary abnormalityin rheumatoid arthritis (RA), and enthesitis/osteitis andsynovitis are central to the pathogenesis of spondylar-thropathy (SpA), the microanatomic basis for handOA, especially at the earliest stages of disease, is lessapparent.
Osteoarthritis has been viewed primarily in rela-tion to cartilage loss, but the importance of bone abnor-malities and joint inflammation in OA has also been welldocumented (1,2), as has the need to consider the wholejoint organ in disease pathogenesis (3). Conventionalmagnetic resonance imaging (MRI) has been used toexplore the anatomic sites of abnormality in large jointOA, and has enhanced our understanding of diseasemechanisms in the knee and hip, where both subchon-dral bone edema and synovitis are associated with pain,and bone edema itself is associated with progressivedisease (4–6).
Knee OA may be difficult to recognize at clinicalpresentation and patients with knee pain but normalradiographic findings would not normally be referred toa rheumatologist. The clinical pattern of the early stagesof distal interphalangeal joint (DIP) and proximal inter-phalangeal joint (PIP) involvement in OA is oftendiagnostic, and does not rely on radiographic criteria,
Supported by the Medical Research Council, UK and theArthritis Research Campaign, UK.
1Ai Lyn Tan, MRCP, Andrew J. Grainger, MRCP, FRCR,Steven F. Tanner, PhD, David M. Shelley, BSc, Colin Pease, FRCP,Paul Emery, MA, MD, FRCP: Leeds General Infirmary, Leeds, UK;2Dennis McGonagle, PhD, FRCPI: Leeds General Infirmary, Leeds,and Calderdale Royal Hospital, Halifax, UK.
Address correspondence and reprint requests to DennisMcGonagle, PhD, FRCPI, Academic Unit of Musculoskeletal Disease,2nd Floor, Chapel Allerton Hospital, Chapeltown Road, Leeds LS74SA, UK. E-mail: [email protected].
Submitted for publication February 7, 2005; accepted inrevised form May 3, 2005.
2355

which are of limited use in diagnosis of early handdisease and disease at other sites prone to OA, includingthe knee (7,8). Furthermore, patients with hand OA aremore likely to present to the early arthritis clinic thanare those with early knee symptoms; hence, there is thepotential to recognize and evaluate OA soon aftersymptom onset. The spatial resolution limitation ofcurrently available MRI has precluded detailed high-resolution imaging assessment of hand OA. However,previous small pilot studies using custom-built high-resolution MRI equipment showed that MRI was a validmethod for the assessment of small joint structures,including the bone trabeculae, cartilage, ligaments, andtendons (9,10). Dedicated high-resolution MRI scannershave also been developed for animal research, wherethey show considerable potential in the evaluation oftherapy for joint inflammation (11).
An anatomic understanding of the earliest stagesof hand OA may have important implications for eluci-dating its pathogenesis, and high-resolution MRI repre-sents a potentially useful way for such a detailed assess-ment. This study optimized recently developed high-resolution MRI coils, that can be fitted to existingcommercially available scanners routinely used in theclinical setting, to explore the microanatomic basis forhand OA.
PATIENTS AND METHODS
Patients. Fifty-eight subjects provided informed con-sent and participated in the study. The study was approved bythe local ethics committee at the Leeds Teaching HospitalsNational Health Service Trust. In total, images from 40patients with hand OA and 18 normal control subjects werescanned. All subjects were invited to participate in the studyeither from rheumatology outpatient clinics or via leaflets andposters about the study distributed in the clinics. Either a DIPor a PIP joint was scanned. Sixteen female patients with amean age of 56 years (range 49–69 years) had early OA (8 DIPjoints, 8 PIP joints) defined by disease duration of �12 months(mean 8 months). The disease duration was determined fromthe onset of symptoms (pain, swelling, or tenderness) in any ofthe finger joints with clinical OA. Fourteen patients (11women, 3 men) with a mean age of 60 years (range 51–68years) and OA symptoms termed chronic (duration �12months [mean 75 months]) were also imaged (9 DIP joints, 5PIP joints). Findings on radiography of the hands can appearnormal at clinical presentation of OA, and therefore, radio-graphic depiction of OA was not mandatory for the diagnosisof OA in this study. The patients with OA were diagnosed onclinical grounds with DIP or PIP joint soft tissue swelling orbony thickening and the absence of other arthropathies, in-cluding RA, psoriatic arthritis, and gout, or any traumaticinjury to the joint selected for imaging.
Ten patients (8 women, 2 men; mean age of 60 years[range 46–72 years]) with hand OA (mean disease duration120 months; 5 DIP joints, 5 PIP joints) and at least 1 clinicallynormal joint were randomly selected from the OA cohort, forMRI of the clinically normal joint that had never beensymptomatic. This group may represent the earliest stages ofOA, since disease tends to progress to affect the uninvolvedfinger joints over time (7). This group of patients are hence-forth referred to as the “latent OA” group.
Eighteen healthy volunteers who had no known OAwith asymptomatic finger joints also had 1 finger joint scanned(10 DIP joints, 8 PIP joints). The healthy volunteer group wasdivided into those �40 years old (mean 34 years [range 30–37years]; 4 women, 4 men) and those �40 years old (mean 55years [range 42–72 years]; 5 women, 5 men). This group wasdivided at age 40 years arbitrarily because clinical hand OAusually presents at �50 years of age.
MRI data acquisition. MR images were acquired usinga 1.5T Gyroscan ACS-NT scanner (Philips, Best, The Nether-lands). Subjects were placed in the prone position with thehand extended in front of the body. The surface coil was placedon top of the relevant joint and held in place using sandbags.The DIP and PIP joints are small in relation to most otherjoints that are routinely studied using MRI. Examination ofthese joints therefore required methods that measured the MRdata at adequate resolution to distinguish the relevant jointfeatures. In previous investigations this was achieved by study-ing fingers from cadavers, with long imaging times and/or useof specialized imaging coils to obtain the required signal-to-noise levels (9,10,12,13). In the present study, a Philips 23-mm–diameter surface “microscopy” coil was used to acquireadequate signal levels from the small voxels required forhigh-resolution study of the DIP and PIP joints.
The examination protocol was designed to visualize thedifferent joint structures. This protocol included the acquisi-tion of T1-weighted axial and coronal spin-echo (SE) imagesfor the assessment of the anatomy of most of the structures,T2-weighted fat-suppressed SE images to identify areas ofedema and fluid in the joint space and cystic lesions, andproton-density–weighted 2-dimensional SE images to study thecollateral ligaments (CLs). In addition, 3-dimensionalgradient-echo sagittal images were acquired using a water-selective radiofrequency excitation pulse to assess the cartilageand tendons. After intravenous injection of 10 ml of thecontrast agent gadolinium diethylene tetrapentaacetic acid(Gd-DTPA), axial and coronal T1-weighted fat-suppressed SEimages were also obtained, highlighting areas of inflammationin the soft tissue and bone. The imaging sequences employeda field of view of either 40 or 45 mm and a data acquisitionmatrix of 256 � 204 with 512 � 512 Fourier transformed datapoints. The measured slices were 1 mm thick, and the acquiredin-plane pixel dimension was therefore 160–200 �m with adisplayed pixel dimension of 80–100 �m. The T1-weightedmeasurements were made with repetition time (TR) and echotime (TE) values of 475 msec and 18 msec, respectively, and 2signal averages, while T2-weighted images were acquired usinga turbo spin-echo (TSE) sequence and 3 signal averages with aTR value of at least 3,500 msec and a TE of 100 msec. Theproton-density–weighted data were obtained using a TSEsequence with centric data acquisition, 2 signal averages, andTR/TE values of 2,000 msec/15 msec. A flip angle of 45° and
2356 TAN ET AL

TR/TE values of 3,000 msec/12 msec were used to obtain thegradient-echo images. The total examination time was �50minutes.
MRI analysis. MR images were read at a workstation(Philips Easy Vision) by 2 readers, including an experiencedmusculoskeletal radiologist. All groups (early OA, chronic OA,latent OA, and normal control) were analyzed in a randomorder. The observers were blinded to the clinical status and thecategory of the subjects. The scoring was performed by con-sensus between the 2 readers. The features of the followinganatomic structures were described and evaluated in a dichot-omous manner: cartilage, bone cortex, CL, extensor expansion,bone edema, cysts, erosions, osteophytes/nodes (Heberden’s orBouchard’s), joint fluid, and capsule/synovium. Where deter-mination of the location of the abnormality (such as boneedema, cysts, erosions, or osteophytes) was possible, this wasalso recorded.
MRI-determined joint erosions were recorded when a
cortical break was evident on T1-weighted images on bothcoronal and axial images. In contrast, a well-circumscribedarea of trabecular absence within the bone was termed a cyst.Osteophytes at either ligament origins or insertions or attendon insertions were termed enthesophytes.
Regions of synovitis or capsulitis were defined onimages acquired after the injection of the contrast agent. TheT2-weighted fat-suppressed SE images were used to identifybone marrow edema–like lesions, henceforth referred to asbone edema, and the images were compared with the Gd-DTPA–enhanced images to distinguish between bone edema (showingenhancement) and cysts filled with fluid (nonenhancing).
Statistical analysis. Fisher’s exact test was used tocompare the proportion of abnormalities between the groups.Because this was a pilot study, no correction for multipletesting was performed, and the results of significance tests arepresented as a guideline only. All analyses were performedwith SPSS version 11.0 (Chicago, IL).
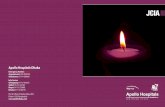
Figure 1. a and b, Percentage of subjects with abnormalities in soft tissue structures (a) and bone (b) in the groups studied. Although virtually everyjoint structure was affected in both chronic and early osteoarthritis (OA), the abnormalities observed in early OA tended to be relatively milder. Thejoints scanned in the “latent OA” group were asymptomatic with no history of pain or swelling, as were the joints of the “normal” group, butabnormalities were more frequent in the latent OA group, particularly abnormalities in the collateral ligaments and the extensor tendons, andosteophyte formations. Additionally, cartilage abnormalities were less frequent than ligamentous or tendon abnormalities in the latent OA group.This demonstrates that in OA, every joint structure is affected, consistent with the idea that OA is ultimately a failure of the joint. � � P � 0.05,�� � P � 0.001, compared with the normal group. c, Percentage of subjects in the latent OA group, normal �40 years old group, and normal �40years old group with abnormalities in the various structures. The younger normal group had virtually no abnormality detected in the joints, but subtleabnormality of the ligaments, the extensor tendon, and bone edema were observed in the normal �40 years old group. † � P � 0.05 compared withthe normal �40 years old group.
HIGH-RESOLUTION MRI OF HAND OA 2357

RESULTS
Early and chronic OA. All MR studies weresatisfactory, with no subject having to be excluded on thebasis of technical failure. Virtually every joint structureevaluated showed abnormalities in all patients witheither early or chronic OA, reflecting the known factthat OA is a whole organ disease and ultimately adisease of joint failure (Figure 1). The findings in earlyand chronic OA are compared before presenting thefeatures of latent OA and the normal group.
Articular cartilage. On coronal and sagittal imag-ing, generalized full-thickness loss of articular cartilagewas evident in 4 of the 30 subjects, occurring in both theearly (3 of 16) and chronic OA (1 of 14) groups,indicating marked cartilage loss at clinical presentation.A further 5 subjects had generalized full-thickness lossvisible only on the coronal plane (2 with early OA and 3with chronic OA). In the remaining 21 subjects in whomcartilage loss was incomplete and variable, an ulnarpredilection for cartilage loss was observed, with 10 of 21patients (48%) experiencing ulnar loss, as comparedwith 5 of 21 (24%) experiencing radial loss and 6 of 21
(29%) patients experiencing symmetric but not full-thickness loss. On sagittal imaging, cartilage loss wasmost pronounced on the volar joint surfaces (Figure 2).
MRI-determined subchondral bone sclerosis,seen as low signal change in the subchondral bone on allsequences, was evident on the distal side of the PIP andDIP joints in 9 of 16 patients with early OA (56%) andin 13 of 14 with chronic OA (93%) (P � 0.04). Thetrabecular architecture appeared normal and discretebreaks in the subchondral bone, suggestive of microfrac-tures, could not be identified with the imaging resolutionobtained in this study.
Collateral ligaments. Ligament abnormalitieswere universal in both chronic and early disease.Changes seen ranged from thickening and increasedsignal within the ligament to complete disruption (Fig-ure 3), with Gd-DTPA enhancement evident in theabnormal ligaments (Figure 4). Complete disruption ofboth CLs was evident in 16 of 30 patients (9 of 16 withearly OA and 7 of 14 with chronic OA). While ligamentdisruption was common in the ligament midsubstance,increased signal was evident throughout the abnormal
Figure 2. Sagittal gradient-echo water-selective excitation imaging. a, The articular cartilage (arrows) in the proximal interphalangeal (PIP) jointand the normal extensor tendon (arrowhead) of a normal subject. b, The PIP joint of a patient with severe chronic osteoarthritis, demonstratingcomplete loss of the articular cartilage. Note the thickening and high signal change in the extensor tendon close to its insertion (arrow). Note alsothe high signal in the bone marrow representing edema at the tendon enthesis site (arrowhead) and the large dorsal osteophyte (�). c, A commonlyseen pattern of cartilage loss predominantly affecting the volar aspect articular surfaces, with more dorsal cartilage preservation. Severe soft tissueswelling around the dorsum of the joint is also present along with prominent dorsal osteophytes (arrowheads). V � volar aspect of joint.
2358 TAN ET AL

Figure 3. Coronal proton-density–weighted images showing the collateral ligaments. a, The proximal interphalangeal (PIP) joint in a 37-year-oldnormal volunteer. The collateral ligaments are seen as thin low-signal bands identified at either side of the joint (arrowheads). b, An asymptomaticdistal interphalangeal (DIP) joint in a patient with clinical and symptomatic osteoarthritis (OA) in adjacent joints. There is subtle collateral ligamentthickening with increased signal within the ligaments (arrows). This was the sole abnormality. c, Involved DIP joint in a patient with early OA. Thereis thickening and some increase in signal in the collateral ligaments on both sides of the joint (arrowheads). The changes are seen centered closeto the proximal ligament enthesis sites. An erosion is also seen close to the proximal origin of the radial collateral ligament (arrow). d, The PIP jointof a patient with severe chronic OA. The ligaments show severe disruption particularly on the radial side (arrowhead), and there is associated ulnardeviation of the intermediate phalanx.
HIGH-RESOLUTION MRI OF HAND OA 2359

ligaments, being seen at their origin, midregion, andinsertions. This increased signal was seen on both T1-and T2-weighted imaging and would be consistent withmyxoid degeneration of the ligament, such as that seenin other ligamentous and tendinous structures. Edemawas seen in the adjacent extracapsular tissues.
In 14 of 30 patients in whom complete CLdisruption was not a feature, the CLs were abnormal,appearing thickened or with an indistinct appearance,particularly at the proximal attachment. Furthermore, 6of 14 patients showed Gd-DTPA enhancement of bothCLs, with only 1 of the CLs enhanced in 5 of 14. Threepatients with chronic OA had no enhancement in theabnormally thickened CLs. In general, all patients withearly and chronic OA had some degree of ligamentabnormality, and all those with early OA showed Gd-DTPA enhancement (16 of 16), whereas 11 of 14 withchronic OA had signs of enhancement (P � 0.09).
When the pattern of ligament abnormality wascompared with the articular cartilage damage in thejoint, it was noted that among the 21 of 30 subjects whohad cartilage that was partially preserved, 10 of 21subjects had complete bilateral CL destruction, indicat-
ing end-stage ligament disease despite reasonable carti-lage preservation. Two of the 4 subjects with completecartilage loss had complete bilateral ligament disruption.Along with the ligament disruption, joint subluxationwas seen in 14 of 30 patients with OA. When present,subluxation was more commonly seen toward the ulnarside (varus subluxation); 11 of 14 patients (79%) hadulnar subluxation, compared with 3 of 14 (21%) withradial subluxation (Figure 3d).
Tendons. Thickening of the extensor tendons wasnoted close to their enthesis site in almost all of the OApatients (14 of 16 with early OA, 11 of 14 with chronicOA) (Figure 2). All affected tendons had signs of enhance-ment. In the absence of severe cartilage loss (n � 21), only16 of 21 subjects had extensor tendon abnormalities,despite the CLs being universally abnormal.
Bone edema. Four major patterns of bone edemawere noted. The most common pattern was focal sub-chondral edema in 8 of 16 patients with early OA and 5of 14 with chronic OA. Most of these subchondralregions of bone edema (10 lesions in 9 subjects) were onthe proximal side of the joints, directly adjacent to siteswhere the CLs exert pressure on the proximal phalanx.
Figure 4. a, Coronal gadolinium-enhanced T1-weighted image with fat suppression, showing the distal interphalangeal (DIP) joint of a normalsubject. No enhancement of either the ligaments (arrowheads) or the adjacent structures is shown. This is in contrast to the findings in b, in whichflorid enhancement and thickening is seen within the ligaments and surrounding soft tissues (arrows) in a patient with severe chronic osteoarthritis.c, Clinically normal and asymptomatic DIP joint adjacent to an osteoarthritic joint. There is subtle enhancement and mild thickening in the ligamentsof this joint (arrows), which otherwise appeared normal.
2360 TAN ET AL

The second pattern occurred at the CL attach-ment (14 lesions in 9 patients) (Figure 5a). Bone edemaat the CL entheses was seen in 4 of 16 patients with earlyOA and 5 of 14 with chronic OA patients. In these 14regions of bone edema at the CL entheses, all except 1were at the CL insertion on the distal phalanges of eitherthe PIP or DIP joints. Enthesophytes were present in 8of 14 sites of CL enthesis bone edema. Only 2 of 14 boneedema lesions at the CL entheses (14%) were related to
bone erosions, while 7 of 10 of the subchondral boneedema lesions (70%) were associated with bone erosions(P � 0.01).
Diffuse edema on both sides of the joint, wherecartilage was lost (representing a “kissing edema” pat-tern as described for large joints), was seen in 5 of 16patients with early OA and 4 of 14 with chronic OA.Lastly, small regions of focal edema present elsewhereand not related to subchondral bone or enthesis were
Figure 5. Images illustrating how the expression of small joint osteoarthritis (OA) is influenced by the collateral ligaments. a, Perientheseal boneedema on a T2-weighted fat-suppressed coronal image, appearing as high signal adjacent to the ligament insertion (arrow). b, An erosion seen atthe proximal origin of the radial collateral ligament (�). Both of the collateral ligaments are abnormally thickened and show high-signalintrasubstance change. c, The appearance of acute Heberden’s nodes, seen as bulging enhanced soft tissue (arrowheads) on this axialgadolinium-enhanced T1-weighted image through the distal intermediate phalanx close to the distal interphalangeal joint. The bulging soft tissueappears to occur at points of “weakness” between the extensor tendon (black arrow) and ligaments (white arrows). d, Osteophyte formation inchronic OA occurring on the dorsum of the phalanx (arrows) at a site corresponding to that where acute Heberden’s nodes are evident in c.
HIGH-RESOLUTION MRI OF HAND OA 2361

seen in 1 of 16 patients with early OA and 1 of 14 withchronic OA.
Erosions and cysts. Erosions, as defined by bonecortex disruption in 2 planes, were evident in 11 of 16patients with early OA (22 erosions) and 7 of 14 withchronic OA (10 erosions). Two patterns of erosion wereevident. The most common type of erosion occurredadjacent to the CLs, and was evident in 17 subjects (24erosions) (Figure 5b). Less common were central jointerosions, which were evident at sites of cartilage lossin 6 patients with OA (8 erosions). Bone cysts werealso visible in a smaller proportion of patients, beingpresent in 3 of 16 patients with early OA and 4 of 14 withchronic OA.
Osteophytes. The most common site for osteo-phyte development is at the bone–cartilage interface ofthe more proximal phalanx in both PIP and DIP joints,predominantly on the dorsal proximal side of the joint.These generally appeared hook-like and pointed proxi-mally (Figure 2c). The sites of osteophytes in chronicdisease also corresponded with the enhancing soft tissuethat was bulging through the joint at areas of leastresistance in early disease (Figures 5c and d). Someosteophytes were associated with adjacent bone en-
hancement following Gd-DTPA administration; thesetended to occur in the early OA group.
Enthesophytes. New bone formation at ligamentorigins or insertions (enthesophytes) was more commonin longer standing OA than in early disease, as evi-denced by examples in 3 of 16 of patients with early OA(19%) (5 enthesophytes), versus examples in 6 of 14patients with chronic OA (43%) (9 enthesophytes), andwas invariably evident at ligament insertions but notorigins. Furthermore, all of the enthesophytes in thepatients with early OA (5 of 5) showed Gd-DTPAenhancement in the CLs, while only 4 of 9 enthesophytesin patients with chronic OA (44%) showed enhancement(P � 0.09). Similarly, bone edema adjacent to or withinenthesophytes was more common in the early OA group,with 4 of 5 cases (80%) in the early OA group, versus 4of 9 cases (44%) in the chronic OA group (P � 0.30).
Synovium and joint capsule. Excess joint fluidvisible on the T2-weighted fat-suppressed SE sequencewas evident in the joint space in a majority of the OApatients (n � 22 [73%]). Fluid and synovial enhance-ment was especially common in the dorsal recess of thejoint in OA. In the axial sequences the central extensortendon slip and the adjacent lateral bands appear to
Figure 6. Coronal T1-weighted (a) and gadolinium-enhanced T1-weighted (b) images through the distal interphalangeal joint of an asymptomaticnormal control subject 64 years of age. The only abnormal finding is thickening of the collateral ligaments, which show increased signal within theirsubstance on unenhanced T1 imaging (arrows) and intrasubstance enhancement following intravenous gadolinium administration (arrowheads).
2362 TAN ET AL

have been pushed outwards and apart by soft tissueswelling in the PIP joints, and outward in the DIP joints(12 of 16 patients with early OA, 12 of 14 with chronicOA). The bulging of the soft tissue tended to occurthrough areas of least resistance at sites of anatomicweakness in the joint capsule, between the extensortendons and CLs, and the flexor tendons and CLs(Figure 5c).
Asymptomatic joint in an OA-affected hand (la-tent OA). Although the joints scanned in the group of 10OA patients were apparently unaffected and completelyasymptomatic, with no history of pain or swelling, andwere clinically normal, these joints showed abnormali-ties on MRI (Figure 1c). The CLs were the most affectedstructure (n � 7 [70%]), although abnormalities wereoften mild with only thickening of the ligament, partic-ularly at the proximal attachment (associated with intra-substance increased signal and Gd-DTPA enhancementin all cases) (Figures 3b and 4c). Similarly, the extensortendon was also often affected to some degree, withthickening at the distal attachment (n � 6 [60%]). Threeof the 7 patients with ligament abnormalities also hadassociated bone edema. Four patients with ligamentabnormalities had subtle cartilage loss, 1 of whom alsohad a bone erosion at the site of cartilage loss. Smallosteophytes were observed in 5 patients with ligamentabnormalities, located mainly on the dorsal phalanxproximal to the joint. Cartilage damage without ligamentchange was not seen.
Normal subjects. All of the younger controlsubjects had completely normal joints including liga-ments, cartilage, and bone, with a small region of normalsynovial fluid evident at the articular margins. However,5 of 10 older control subjects had subtle abnormality ofthe CLs, with thickening, and 3 of the 5 had Gd-DTPAenhancement (Figures 1c and 6). Two subjects also hadsmall regions of bone edema, with 1 showing edemaadjacent to the abnormal CL. The tendons appeareduniform, and the insertions did not show changes orheterogeneity in signal intensity (Figure 2a). No cysts,erosions, or soft tissue swelling were seen in any of thenormal finger joints. Consistent with reports of occa-sional osteophytes found on radiographs of older asymp-tomatic subjects, osteophytes were observed in 2 oldernormal subjects in this study with preservation of jointcartilage.
DISCUSSION
In this study we used a novel high-resolutionMRI coil that can be utilized in clinically available
scanners to investigate the microanatomic basis for handOA. Hand OA was chosen for study because its micro-anatomic basis is less well defined compared with that ofRA and SpA. Consistent with the known features of OA,every joint structure showed variable abnormalities.Severe destructive and inflammatory changes, as sug-gested by Gd-DTPA enhancement, were evident inevery joint structure in early hand OA. Joint collateralligament abnormalities were especially common, andsubtle ligament changes were the most common changesin normal joints adjacent to OA joints.
This study confirmed a number of interestingobservations in relation to hand OA and raised anumber of new issues. For example, subchondral bonesclerosis was especially common in chronic OA, whichmay support the recent assertion that subchondral bonesclerosis represents secondary remodeling and is notprimarily responsible for cartilage damage as originallysuggested (14). The mechanism of bone edema in OA isunknown but is considered to be related to bone micro-fracture or microcracks. The resolution of the images inthis study was not adequate for showing trabecularmicrocracks or microfractures, but subchondral edemawithout obvious trabecular fracture or damage to re-gions of adjacent cartilage was evident. Also, unlikefindings in RA, erosions were more commonly seen onMRI in early OA, supporting the concept of the signif-icant healing and remodeling that is known to occur inOA as compared with RA. Joint inflammation as deter-mined by Gd-DTPA uptake was common not only in thesynovium in OA but also in most other joint structures,including ligaments, tendons, extracapsular tissues, andbone marrow, and was comparable in degree and loca-tion in both patients with early disease and those withpainful chronic joint involvement.
The formation of Heberden’s and Bouchard’snodes is a characteristic clinical feature of OA. Softtissue was observed to bulge through the sites of relativeweakness of the joint capsule at the 4 locations boundedby the medial and lateral CLs and the flexor andextensor tendons, especially on the dorsal aspect of thejoint in early OA. In late OA, Heberden’s and Bou-chard’s node formation was evident at the same sites,suggesting that ossification of tissue at these sites wasrelated to prior inflammation and CL position as previ-ously hypothesized (15), and further suggesting that thephenotype of hand OA is related to the functionalanatomy of the joint. Longitudinal studies are needed toconfirm this theory.
Perhaps the most interesting result of this studywas the common occurrence of ligament abnormalities.
HIGH-RESOLUTION MRI OF HAND OA 2363

To the best of our knowledge, there are no previousstudies implicating ligament diseases in hand OA. It is,however, well recognized that trauma or disruption ofthe ligament of large joints is associated with the subse-quent development of OA in experimental and clinicalsettings. Knee cruciate ligament disruption is associatedwith subsequent canine OA (16). In humans, chronicknee joint ligament instability is associated with OAdevelopment (17–19). Therefore, large joint OA couldbe seen as an inevitable consequence of ligament failure(14). In the case of small joints it has been shown thatthe PIP CLs are the primary restraint to varus and valgusjoint angulation (20), and that reconstruction of theligaments as opposed to other joint structures has thegreatest benefit in the amelioration of carpometacarpaljoint OA (19). While ligament laxity may be important inknee OA, the relationship between joint laxity in thesmall joints and associated OA remains controversial(21–23). In this study we also noted that other MRI-determined joint abnormalities, including erosion, boneedema, and new bone formation, bore a close anatomicrelationship to the abnormal ligaments. Furthermore,older normal subjects had subtle ligament abnormalities,generally showing a lesser degree of enhancement with-out frank disruption compared with patients who hadclinically evident OA. The question arises, therefore,whether the ligament changes are age related or if theyare in some way implicated in the pathogenesis of handOA. Further longitudinal studies specifically examiningligaments in the early stages of hand OA are planned.
Based on the observation that enthesophytes(new bone formation at ligament attachments) werecommon in OA, it has been suggested that this supportsthe importance of bone in the pathogenesis of OA (2).However, hand OA is characterized by enthesopathicchanges especially in the soft tissue side of ligamententhesis, and also with bone edema at ligament attach-ments. Therefore, entheseal new bone in OA couldsimply reflect a reactive bone-forming process at theenthesis, in a manner reminiscent of diseases such asankylosing spondylitis and psoriatic arthritis, rather thanan intrinsic bone disorder (1).
There were a number of limitations to this study.Although we identified the ligament as a prominent siteof abnormality in hand OA, we could not obtain histo-logic proof of ligament disease, since an in vivo study ofligaments precludes the comparison with equivalentsections obtained for histopathologic study. Identifica-tion of image features is possible, however, due to goodanatomical detail and analogy to findings described inprevious reports involving cadaver specimens and ani-
mal models (9,10,12,13,24). Although we studied theearly symptomatic phases of OA, it is clear that it isvirtually impossible to study the early pathologic phasesof hand OA, since patients with symptoms of a fewmonths’ duration often had joint abnormalities compa-rable with those in patients who had chronic disease.This is well described for other sites of OA presentation,including the hip joint (25). However, we referred tothese patients as having early OA, because they wereassessed following a first symptomatic episode, and wealso assessed uninvolved joints that may develop clinicalOA at a later stage. Furthermore, we divided the normalsubjects into a younger group and an older group, moreclosely age-matched with the patients.
Because OA is a disease of aging, it is possiblethat it represents an aberrant age-related process. It wasclear that older normal subjects had ligament abnormal-ities that younger normal subjects did not have. Al-though the sample sizes of the groups were compara-tively small in this pilot study, and multiple tests wereperformed, the findings consistently indicated promi-nent ligament damage, particularly in early and chronicOA. Finally, the demonstration of ligament abnormali-ties in the small joints could reflect the unique anatomyand biomechanics of these joints, and it remains to beproven whether ligament changes are common in othergeneralized OA-prone sites, including the spine, hip, andknee.
In conclusion, this study used high-resolutionMRI in patients with OA to better define the microana-tomic basis for early hand joint involvement. The resultsof the study reaffirm some longstanding concepts relat-ing to OA, in particular the concept of whole joint organinvolvement, even at disease onset. The findings alsoraise important questions about the role of ligaments inhand OA. This MRI technique should become widelyavailable to rheumatologists to investigate the microana-tomic basis for OA and other diseases in the clinicalsetting. In particular, the findings of this study highlightthe need for more research into ligament abnormalitiesin the early stages of OA.
ACKNOWLEDGMENTSWe would like to thank all who volunteered or referred
patients for the study. We would also like to thank all the staffat the Leeds General Infirmary MRI Unit for their serviceswith regard to the study, and Dr. Elizabeth Hensor for adviceon statistical analysis.
REFERENCES1. Felson DT, Neogi T. Osteoarthritis: is it a disease of cartilage or of
bone? [editorial]. Arthritis Rheum 2004;50:341–4.
2364 TAN ET AL

2. Rogers J, Shepstone L, Dieppe P. Is osteoarthritis a systemicdisorder of bone? Arthritis Rheum 2004;50:452–7.
3. Dieppe P. Osteoarthritis: time to shift the paradigm: this includesdistinguishing between severe disease and common minor disabil-ity. BMJ 1999;318:1299–300.
4. Felson DT, Chaisson CE, Hill CL, Totterman SM, Gale ME,Skinner KM, et al. The association of bone marrow lesions withpain in knee osteoarthritis. Ann Intern Med 2001;134:541–9.
5. Hill CL, Gale DG, Chaisson CE, Skinner K, Kazis L, Gale ME, etal. Knee effusions, popliteal cysts, and synovial thickening: associ-ation with knee pain in osteoarthritis. J Rheumatol 2001;28:1330–7.
6. Boutry N, Paul C, Leroy X, Fredoux D, Migaud H, Cotten A.Rapidly destructive osteoarthritis of the hip: MR imaging findings.AJR Am J Roentgenol 2002;179:657–63.
7. Niu J, Zhang Y, LaValley M, Chaisson CE, Aliabadi P. Symmetryand clustering of symptomatic hand osteoarthritis in elderly menand women: the Framingham Study. Rheumatology (Oxford)2003;42:343–8.
8. Bagge E, Bjelle A, Eden S, Svanborg A. Osteoarthritis in theelderly: clinical and radiological findings in 79 and 85 year olds.Ann Rheum Dis 1991;50:535–9.
9. Lewis AR, Nolan MJ, Hodgson RJ, Benjamin M, Ralphs JR,Archer CW, et al. High resolution magnetic resonance imaging ofthe proximal interphalangeal joints: correlation with histology andproduction of a three-dimensional data set. J Hand Surg [Br]1996;21:488–95.
10. Erickson SJ, Kneeland JB, Middleton WD, Jesmanowicz A, HydeJ, Lawson TL, et al. MR imaging of the finger: correlation withnormal anatomic sections. AJR Am J Roentgenol 1989;152:1013–9.
11. Dawson J, Gustard S, Beckmann N. High-resolution three-dimen-sional magnetic resonance imaging for the investigation of kneejoint damage during the time course of antigen-induced arthritis inrabbits. Arthritis Rheum 1999;42:119–28.
12. Clavero JA, Alomar X, Monill JM, Esplugas M, Golano P,Mendoza M, et al. MR imaging of ligament and tendon injuries ofthe fingers. Radiographics 2002;22:237–56.
13. Rumpel H, Peh WC. Imaging of finger joints in a whole-body MR
system using a simple and low-cost solenoidal coil. J Magn ResonImaging 2001;14:800–2.
14. Burr DB. The importance of subchondral bone in the progressionof osteoarthritis. J Rheumatol Suppl 2004;70:77–80.
15. Alexander CJ. Heberden’s and Bouchard’s nodes. Ann Rheum Dis1999;58:675–8.
16. Brandt KD, Braunstein EM, Visco DM, O’Connor B, Heck D,Albrecht M. Anterior (cranial) cruciate ligament transection in thedog: a bona fide model of osteoarthritis, not merely of cartilageinjury and repair. J Rheumatol 1991;18:436–46.
17. Kannus P, Jarvinen M. Posttraumatic anterior cruciate ligamentinsufficiency as a cause of osteoarthritis in a knee joint. ClinRheumatol 1989;8:251–60.
18. Von Porat A, Roos EM, Roos H. High prevalence of osteoarthritis14 years after an anterior cruciate ligament tear in male soccerplayers: a study of radiographic and patient relevant outcomes.Ann Rheum Dis 2004;63:269–73.
19. Kriegs-Au G, Petje G, Fojtl E, Ganger R, Zachs I. Ligamentreconstruction with or without tendon interposition to treat pri-mary thumb carpometacarpal osteoarthritis: a prospective ran-domized study. J Bone Joint Surg Am 2004;86:209–18.
20. Kiefhaber TR, Stern PJ, Grood ES. Lateral stability of theproximal interphalangeal joint. J Hand Surg [Am] 1986;11:661–9.
21. Kraus VB, Li YJ, Martin ER, Jordan JM, Renner JB, Doherty M,et al. Articular hypermobility is a protective factor for handosteoarthritis. Arthritis Rheum 2004;50:2178–83.
22. Dolan AL, Hart DJ, Doyle DV, Grahame R, Spector TD. Therelationship of joint hypermobility, bone mineral density, andosteoarthritis in the general population: the Chingford Study.J Rheumatol 2003;30:799–803.
23. Jonsson H, Valtysdottir ST, Kjartansson O, Brekkan A. Hypermo-bility associated with osteoarthritis of the thumb base: a clinicaland radiological subset of hand osteoarthritis. Ann Rheum Dis1996;55:540–3.
24. Weber MH, Sharp JC, Latta P, Sramek M, Hassard HT, Orr FW.Magnetic resonance imaging of trabecular and cortical bone inmice: comparison of high resolution in vivo and ex vivo MR imageswith corresponding histology. Eur J Radiol 2005;53:96–102.
25. Birrell FN. Patterns of joint pain: lessons from epidemiology.Rheumatology (Oxford) 2004;43:408–9.
HIGH-RESOLUTION MRI OF HAND OA 2365